User login
-
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Two rare neurologic conditions linked to COVID-19
A 50-year-old man developed Miller Fisher syndrome and a 39-year-old man developed polyneuritis cranialis. Both are variants of Guillain-Barré syndrome (GBS), which physicians in China and Italy also linked to COVID-19 infection, as previously reported by Medscape Medical News.
In both cases, physicians made the diagnoses based on abnormal eye examinations. The two patients responded to treatment and improved over 2 weeks, with only the 50-year-old featuring residual symptoms of anosmia and ageusia.
The report was published online April 17 in Neurology.
The 50-year-old man was admitted to an emergency room with a temperature of 99.9°F (37.7°C). He reported 2 days of vertical diplopia, perioral paresthesias, and gait instability. His neurologic examination showed intact cognitive function and language.
Five days earlier he developed a cough, malaise, headache, low back pain, fever, anosmia, and ageusia.
His neuro-ophthalmologic examination showed right hypertropia in all fields of gaze, severe limitations to the adduction and downgaze movements of his right eye, and left eye nystagmus on left gaze. These findings were consistent with right internuclear ophthalmoparesis and right fascicular oculomotor palsy.
He responded to intravenous (IV) immunoglobulin therapy and was discharged home 2 weeks after admission.
The 39-year-old man was admitted to the emergency room with acute onset diplopia and ageusia. Three days earlier he had presented with diarrhea, a low-grade fever and in generally poor condition, without any headache, respiratory symptoms, or dyspnea.
He showed esotropia of 10 prism diopters at distance and 4 prism diopters at near, severe abduction deficits in both eyes, and fixation nystagmus, with the upper gaze more impaired, all consistent with bilateral abducens palsy.
The patient was discharged home and treated symptomatically with acetaminophen and telemedicine monitoring “due to a complete hospital saturation with COVID-19 patients,” wrote the researchers, led by Consuelo Gutiérrez-Ortiz, MD, PhD, Hospital Universitario Príncipe de Asturias, Madrid, Spain.
Two weeks later, he had made a complete neurologic recovery with no ageusia, complete eye movements, and normal deep tendon reflexes.
“Fisher syndrome and polyneuritis cranialis in these two patients with the SARS-CoV-2 infection could be simply coincidental. However, taking into account the temporal relationship, we feel that COVID-19 might have been responsible for the development of these two neurological pictures,” the authors noted.
European Regional Development Funds (FEDER) supported this research.
This article first appeared on Medscape.com.
A 50-year-old man developed Miller Fisher syndrome and a 39-year-old man developed polyneuritis cranialis. Both are variants of Guillain-Barré syndrome (GBS), which physicians in China and Italy also linked to COVID-19 infection, as previously reported by Medscape Medical News.
In both cases, physicians made the diagnoses based on abnormal eye examinations. The two patients responded to treatment and improved over 2 weeks, with only the 50-year-old featuring residual symptoms of anosmia and ageusia.
The report was published online April 17 in Neurology.
The 50-year-old man was admitted to an emergency room with a temperature of 99.9°F (37.7°C). He reported 2 days of vertical diplopia, perioral paresthesias, and gait instability. His neurologic examination showed intact cognitive function and language.
Five days earlier he developed a cough, malaise, headache, low back pain, fever, anosmia, and ageusia.
His neuro-ophthalmologic examination showed right hypertropia in all fields of gaze, severe limitations to the adduction and downgaze movements of his right eye, and left eye nystagmus on left gaze. These findings were consistent with right internuclear ophthalmoparesis and right fascicular oculomotor palsy.
He responded to intravenous (IV) immunoglobulin therapy and was discharged home 2 weeks after admission.
The 39-year-old man was admitted to the emergency room with acute onset diplopia and ageusia. Three days earlier he had presented with diarrhea, a low-grade fever and in generally poor condition, without any headache, respiratory symptoms, or dyspnea.
He showed esotropia of 10 prism diopters at distance and 4 prism diopters at near, severe abduction deficits in both eyes, and fixation nystagmus, with the upper gaze more impaired, all consistent with bilateral abducens palsy.
The patient was discharged home and treated symptomatically with acetaminophen and telemedicine monitoring “due to a complete hospital saturation with COVID-19 patients,” wrote the researchers, led by Consuelo Gutiérrez-Ortiz, MD, PhD, Hospital Universitario Príncipe de Asturias, Madrid, Spain.
Two weeks later, he had made a complete neurologic recovery with no ageusia, complete eye movements, and normal deep tendon reflexes.
“Fisher syndrome and polyneuritis cranialis in these two patients with the SARS-CoV-2 infection could be simply coincidental. However, taking into account the temporal relationship, we feel that COVID-19 might have been responsible for the development of these two neurological pictures,” the authors noted.
European Regional Development Funds (FEDER) supported this research.
This article first appeared on Medscape.com.
A 50-year-old man developed Miller Fisher syndrome and a 39-year-old man developed polyneuritis cranialis. Both are variants of Guillain-Barré syndrome (GBS), which physicians in China and Italy also linked to COVID-19 infection, as previously reported by Medscape Medical News.
In both cases, physicians made the diagnoses based on abnormal eye examinations. The two patients responded to treatment and improved over 2 weeks, with only the 50-year-old featuring residual symptoms of anosmia and ageusia.
The report was published online April 17 in Neurology.
The 50-year-old man was admitted to an emergency room with a temperature of 99.9°F (37.7°C). He reported 2 days of vertical diplopia, perioral paresthesias, and gait instability. His neurologic examination showed intact cognitive function and language.
Five days earlier he developed a cough, malaise, headache, low back pain, fever, anosmia, and ageusia.
His neuro-ophthalmologic examination showed right hypertropia in all fields of gaze, severe limitations to the adduction and downgaze movements of his right eye, and left eye nystagmus on left gaze. These findings were consistent with right internuclear ophthalmoparesis and right fascicular oculomotor palsy.
He responded to intravenous (IV) immunoglobulin therapy and was discharged home 2 weeks after admission.
The 39-year-old man was admitted to the emergency room with acute onset diplopia and ageusia. Three days earlier he had presented with diarrhea, a low-grade fever and in generally poor condition, without any headache, respiratory symptoms, or dyspnea.
He showed esotropia of 10 prism diopters at distance and 4 prism diopters at near, severe abduction deficits in both eyes, and fixation nystagmus, with the upper gaze more impaired, all consistent with bilateral abducens palsy.
The patient was discharged home and treated symptomatically with acetaminophen and telemedicine monitoring “due to a complete hospital saturation with COVID-19 patients,” wrote the researchers, led by Consuelo Gutiérrez-Ortiz, MD, PhD, Hospital Universitario Príncipe de Asturias, Madrid, Spain.
Two weeks later, he had made a complete neurologic recovery with no ageusia, complete eye movements, and normal deep tendon reflexes.
“Fisher syndrome and polyneuritis cranialis in these two patients with the SARS-CoV-2 infection could be simply coincidental. However, taking into account the temporal relationship, we feel that COVID-19 might have been responsible for the development of these two neurological pictures,” the authors noted.
European Regional Development Funds (FEDER) supported this research.
This article first appeared on Medscape.com.
Survey: Hydroxychloroquine use fairly common in COVID-19
One of five physicians in front-line treatment roles has prescribed hydroxychloroquine for COVID-19, according to a new survey from health care market research company InCrowd.
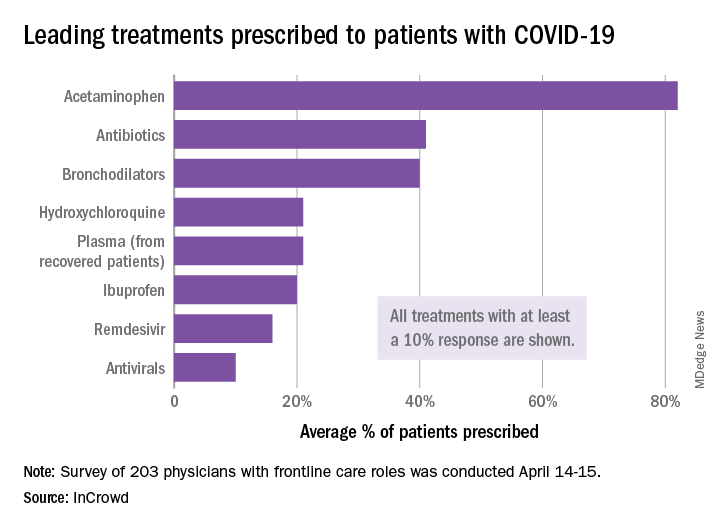
The most common treatments were acetaminophen, prescribed to 82% of patients, antibiotics (41%), and bronchodilators (40%), InCrowd said after surveying 203 primary care physicians, pediatricians, and emergency medicine or critical care physicians who are treating at least 20 patients with flulike symptoms.
On April 24, the Food and Drug Administration warned against the use of hydroxychloroquine or chloroquine outside of hospitals and clinical trials.
The InCrowd survey, which took place April 14-15 and is the fourth in a series investigating COVID-19’s impact on physicians, showed that access to testing was up to 82% in mid-April, compared with 67% in March and 20% in late February. The April respondents also were twice as likely (59% vs. 24% in March) to say that their facilities were prepared to treat patients, InCrowd reported.
“U.S. physicians report sluggish optimism around preparedness, safety, and institutional efforts, while many worry about the future, including a second outbreak and job security,” the company said in a separate written statement.
The average estimate for a return to normal was just over 6 months among respondents, and only 28% believed that their facility was prepared for a second outbreak later in the year, InCrowd noted.
On a personal level, 45% of the respondents were concerned about the safety of their job. An emergency/critical care physician from Tennessee said, “We’ve been cutting back on staff due to overall revenue reductions, but have increased acuity and complexity which requires more staffing. This puts even more of a burden on those of us still here.”
Support for institutional responses to slow the pandemic was strongest for state governments, which gained approval from 54% of front-line physicians, up from 33% in March. Actions taken by the federal government were supported by 21% of respondents, compared with 38% for the World Health Organization and 46% for governments outside the United States, InCrowd reported.
Suggestions for further actions by state and local authorities included this comment from an emergency/critical care physician in Florida: “Continued, broad and properly enforced stay at home and social distancing measures MUST remain in place to keep citizens and healthcare workers safe, and the latter alive and in adequate supply.”
One of five physicians in front-line treatment roles has prescribed hydroxychloroquine for COVID-19, according to a new survey from health care market research company InCrowd.
The most common treatments were acetaminophen, prescribed to 82% of patients, antibiotics (41%), and bronchodilators (40%), InCrowd said after surveying 203 primary care physicians, pediatricians, and emergency medicine or critical care physicians who are treating at least 20 patients with flulike symptoms.
On April 24, the Food and Drug Administration warned against the use of hydroxychloroquine or chloroquine outside of hospitals and clinical trials.
The InCrowd survey, which took place April 14-15 and is the fourth in a series investigating COVID-19’s impact on physicians, showed that access to testing was up to 82% in mid-April, compared with 67% in March and 20% in late February. The April respondents also were twice as likely (59% vs. 24% in March) to say that their facilities were prepared to treat patients, InCrowd reported.
“U.S. physicians report sluggish optimism around preparedness, safety, and institutional efforts, while many worry about the future, including a second outbreak and job security,” the company said in a separate written statement.
The average estimate for a return to normal was just over 6 months among respondents, and only 28% believed that their facility was prepared for a second outbreak later in the year, InCrowd noted.
On a personal level, 45% of the respondents were concerned about the safety of their job. An emergency/critical care physician from Tennessee said, “We’ve been cutting back on staff due to overall revenue reductions, but have increased acuity and complexity which requires more staffing. This puts even more of a burden on those of us still here.”
Support for institutional responses to slow the pandemic was strongest for state governments, which gained approval from 54% of front-line physicians, up from 33% in March. Actions taken by the federal government were supported by 21% of respondents, compared with 38% for the World Health Organization and 46% for governments outside the United States, InCrowd reported.
Suggestions for further actions by state and local authorities included this comment from an emergency/critical care physician in Florida: “Continued, broad and properly enforced stay at home and social distancing measures MUST remain in place to keep citizens and healthcare workers safe, and the latter alive and in adequate supply.”
One of five physicians in front-line treatment roles has prescribed hydroxychloroquine for COVID-19, according to a new survey from health care market research company InCrowd.
The most common treatments were acetaminophen, prescribed to 82% of patients, antibiotics (41%), and bronchodilators (40%), InCrowd said after surveying 203 primary care physicians, pediatricians, and emergency medicine or critical care physicians who are treating at least 20 patients with flulike symptoms.
On April 24, the Food and Drug Administration warned against the use of hydroxychloroquine or chloroquine outside of hospitals and clinical trials.
The InCrowd survey, which took place April 14-15 and is the fourth in a series investigating COVID-19’s impact on physicians, showed that access to testing was up to 82% in mid-April, compared with 67% in March and 20% in late February. The April respondents also were twice as likely (59% vs. 24% in March) to say that their facilities were prepared to treat patients, InCrowd reported.
“U.S. physicians report sluggish optimism around preparedness, safety, and institutional efforts, while many worry about the future, including a second outbreak and job security,” the company said in a separate written statement.
The average estimate for a return to normal was just over 6 months among respondents, and only 28% believed that their facility was prepared for a second outbreak later in the year, InCrowd noted.
On a personal level, 45% of the respondents were concerned about the safety of their job. An emergency/critical care physician from Tennessee said, “We’ve been cutting back on staff due to overall revenue reductions, but have increased acuity and complexity which requires more staffing. This puts even more of a burden on those of us still here.”
Support for institutional responses to slow the pandemic was strongest for state governments, which gained approval from 54% of front-line physicians, up from 33% in March. Actions taken by the federal government were supported by 21% of respondents, compared with 38% for the World Health Organization and 46% for governments outside the United States, InCrowd reported.
Suggestions for further actions by state and local authorities included this comment from an emergency/critical care physician in Florida: “Continued, broad and properly enforced stay at home and social distancing measures MUST remain in place to keep citizens and healthcare workers safe, and the latter alive and in adequate supply.”
COVID-19: No U.S. spike expected in pandemic-related suicidal ideation
Americans are not feeling more suicidal even in the depths of the COVID-19 pandemic of spring 2020, according to analysis of real-time national data accrued through the Crisis Text Line.
But that’s not to say Americans are feeling less distressed. Quite the contrary, Nancy Lublin, CEO and cofounder of Crisis Text Line, noted at the virtual annual meeting of the American Association of Suicidology.
“We’ve seen a 40% increase in volume since early March. Seventy-eight percent of our conversations are now including words like ‘freaked out,’ ‘panicked,’ ‘scared.’ People are worried about COVID-19. They’re nervous about symptoms; they’re concerned for family on the front lines,” she said.
And yet, from mid-March through mid-April, only 22% of texters to the crisis line expressed suicidal ideation, down from a usual background rate of 28%. Moreover, just 13% of texters who mentioned ‘COVID,’ ‘quarantine,’ or ‘virus’ expressed suicidal ideation, compared with 25% of other texters.
Ms. Lublin and her data crunchers are tracking not only the impact of the disease, but they’re also monitoring the mental health effects of the quarantine and social distancing.
“People are away from their routines, and perhaps [are] quarantined with abusive people. We’ve seen a 48% increase in texts involving sexual abuse and a 74% increase in domestic violence,” she said.
Texts focused on eating disorders or body image issues have jumped by 45%. And roughly two-thirds of texters now describe feelings of depression.
One of the biggest mental health impacts she and colleagues have seen stem from the economic recession triggered by the pandemic.
“We’ve seen more people reach out with fears of bankruptcy, fears of homelessness, fears of financial ruin. Thirty-two percent of our texters now report household incomes under $20,000 per year. That’s up from 19% before,” according to Ms. Lublin.
The Crisis Text Line (text HOME to 741741) uses machine-learning algorithms that sift through incoming text messages from people in crisis for key words, then ranks the messages by severity. Since its launch in 2013, this service, available 24/7, has processed roughly 150 million text messages. The high-risk texters – for example, someone who’s swallowed a bottle of pills or is texting from the San Francisco’s Golden Gate Bridge, as has occurred some 500 times – are connected in an average of 24 seconds with a thoroughly trained volunteer crisis counselor. And there is a third party in these texting conversations: a paid staff supervisor with a master’s degree in a relevant discipline who follows the encounter in real time and can step in if needed.
“Active rescues are involved in less than 1% of our conversations, but still we do them on average 26 times per day. Over the years, we’ve completed more than 32,000 active rescues,” she said.
The Crisis Text Line is not exclusively a suicide prevention hotline. The top five issues people text about involve relationship concerns, depression, anxiety, self-harm, and suicidal ideation. Over time, Ms. Lublin and staff have used Big Data to tweak the screening algorithm as they’ve identified even higher red flag texting words than “suicide.”
“The word ‘military’ makes it twice as likely that we’ll have to call 9-1-1 than the word ‘suicide.’ ‘Gun,’ ‘rope’ – four times as likely. In the [United KIngdom], where we’re also operating, we see the word ‘cliff’ is a more lethal word than the word ‘suicide.’ But the most dangerous words that we see are any named pill,” she said.
The Crisis Text Line was recently awarded a 2020 TED Audacious Project grant to expand their services from English to also be offered in Spanish, French, Portuguese, and Arabic worldwide within the next two and a half years. This will provide coverage to one-third of the world’s population, including people with cell phones living in countries with very limited mental health services.
Will COVID-19 trigger a spike in deaths by suicide?
Whether the COVID-19 pandemic will result in a bump in suicide rates is unclear and will remain so for quite a while, according to David Gunnell, MD, PhD, a suicidologist and professor of epidemiology at the University of Bristol (England).
In the United Kingdom, investigation of a suspicious death typically takes more than 6 months before an official declaration of suicide is recorded by the medical examiner. The lag time is even longer in the United States: The latest national suicide rate data are for 2018 because state-by-state reporting practices vary widely, he noted at a National Press Foundation briefing on COVID-19 and mental health.
Although suicide is consistently the 10th-leading cause of death in the United States, it’s important to put it in perspective, he added. In 2018, there were an average of 4,000 deaths by suicide per month nationally, whereas in March and April of 2020, there were 28,400 deaths per month attributable to COVID-19.
A classic study of the Spanish influenza pandemic in the United States during 1918-1919 concluded that there was “a slight upturn” in the rate of suicide in the months following the pandemic’s peak. More recently, a study of the 2003 SARS (severe acute respiratory syndrome) epidemic in Hong Kong found roughly a 30% increase in the rate of suicide among the elderly during that time frame, Dr. Gunnell noted.
“What limited evidence there is provides an indication of a small rise in suicides, but the number of deaths is far outweighed by the number of deaths associated with these big pandemics,” according to the epidemiologist.
Pandemics aside, there is far more compelling evidence that periods of economic recession are associated with an increase in the suicide rate, he added.
Another speaker, Holly C. Wilcox, PhD, a psychiatric epidemiologist at Johns Hopkins University, Baltimore, commented: “It’s not surprising that, during times of disaster the suicide rates decrease a bit. It could be because of people coming toghether. It could be one silver lining of COVID-19. But if there’s prolonged stress economically and socially and we can’t work towards reducing stress for people, we could see an increase. I don’t know if we will.”
In a recent article, Dr. Gunnell and coauthors offered a series of recommendations aimed at blunting the mental health consequences of COVID-19 and the related economic fallout (Lancet Psychiatry. 2020 Apr 21. doi: 10.1016/S2215-0366[20]30171-1).
The authors highlighted the need for interventions aimed at defusing the adverse impact of self-isolation, social distancing, fear, an anticipated rise in alcohol misuse, joblessness, interrupted education, bereavement, and complicated grief. Governments can blunt the well-established effect of financial distress as a risk factor for suicide by providing safety nets in the form of supports for housing, food, and unemployment benefits. And it will be important that those mental health services that develop expertise in performing psychiatric assessments and interventions remotely via telemedicine share their insights, Dr. Gunnell said.
Americans are not feeling more suicidal even in the depths of the COVID-19 pandemic of spring 2020, according to analysis of real-time national data accrued through the Crisis Text Line.
But that’s not to say Americans are feeling less distressed. Quite the contrary, Nancy Lublin, CEO and cofounder of Crisis Text Line, noted at the virtual annual meeting of the American Association of Suicidology.
“We’ve seen a 40% increase in volume since early March. Seventy-eight percent of our conversations are now including words like ‘freaked out,’ ‘panicked,’ ‘scared.’ People are worried about COVID-19. They’re nervous about symptoms; they’re concerned for family on the front lines,” she said.
And yet, from mid-March through mid-April, only 22% of texters to the crisis line expressed suicidal ideation, down from a usual background rate of 28%. Moreover, just 13% of texters who mentioned ‘COVID,’ ‘quarantine,’ or ‘virus’ expressed suicidal ideation, compared with 25% of other texters.
Ms. Lublin and her data crunchers are tracking not only the impact of the disease, but they’re also monitoring the mental health effects of the quarantine and social distancing.
“People are away from their routines, and perhaps [are] quarantined with abusive people. We’ve seen a 48% increase in texts involving sexual abuse and a 74% increase in domestic violence,” she said.
Texts focused on eating disorders or body image issues have jumped by 45%. And roughly two-thirds of texters now describe feelings of depression.
One of the biggest mental health impacts she and colleagues have seen stem from the economic recession triggered by the pandemic.
“We’ve seen more people reach out with fears of bankruptcy, fears of homelessness, fears of financial ruin. Thirty-two percent of our texters now report household incomes under $20,000 per year. That’s up from 19% before,” according to Ms. Lublin.
The Crisis Text Line (text HOME to 741741) uses machine-learning algorithms that sift through incoming text messages from people in crisis for key words, then ranks the messages by severity. Since its launch in 2013, this service, available 24/7, has processed roughly 150 million text messages. The high-risk texters – for example, someone who’s swallowed a bottle of pills or is texting from the San Francisco’s Golden Gate Bridge, as has occurred some 500 times – are connected in an average of 24 seconds with a thoroughly trained volunteer crisis counselor. And there is a third party in these texting conversations: a paid staff supervisor with a master’s degree in a relevant discipline who follows the encounter in real time and can step in if needed.
“Active rescues are involved in less than 1% of our conversations, but still we do them on average 26 times per day. Over the years, we’ve completed more than 32,000 active rescues,” she said.
The Crisis Text Line is not exclusively a suicide prevention hotline. The top five issues people text about involve relationship concerns, depression, anxiety, self-harm, and suicidal ideation. Over time, Ms. Lublin and staff have used Big Data to tweak the screening algorithm as they’ve identified even higher red flag texting words than “suicide.”
“The word ‘military’ makes it twice as likely that we’ll have to call 9-1-1 than the word ‘suicide.’ ‘Gun,’ ‘rope’ – four times as likely. In the [United KIngdom], where we’re also operating, we see the word ‘cliff’ is a more lethal word than the word ‘suicide.’ But the most dangerous words that we see are any named pill,” she said.
The Crisis Text Line was recently awarded a 2020 TED Audacious Project grant to expand their services from English to also be offered in Spanish, French, Portuguese, and Arabic worldwide within the next two and a half years. This will provide coverage to one-third of the world’s population, including people with cell phones living in countries with very limited mental health services.
Will COVID-19 trigger a spike in deaths by suicide?
Whether the COVID-19 pandemic will result in a bump in suicide rates is unclear and will remain so for quite a while, according to David Gunnell, MD, PhD, a suicidologist and professor of epidemiology at the University of Bristol (England).
In the United Kingdom, investigation of a suspicious death typically takes more than 6 months before an official declaration of suicide is recorded by the medical examiner. The lag time is even longer in the United States: The latest national suicide rate data are for 2018 because state-by-state reporting practices vary widely, he noted at a National Press Foundation briefing on COVID-19 and mental health.
Although suicide is consistently the 10th-leading cause of death in the United States, it’s important to put it in perspective, he added. In 2018, there were an average of 4,000 deaths by suicide per month nationally, whereas in March and April of 2020, there were 28,400 deaths per month attributable to COVID-19.
A classic study of the Spanish influenza pandemic in the United States during 1918-1919 concluded that there was “a slight upturn” in the rate of suicide in the months following the pandemic’s peak. More recently, a study of the 2003 SARS (severe acute respiratory syndrome) epidemic in Hong Kong found roughly a 30% increase in the rate of suicide among the elderly during that time frame, Dr. Gunnell noted.
“What limited evidence there is provides an indication of a small rise in suicides, but the number of deaths is far outweighed by the number of deaths associated with these big pandemics,” according to the epidemiologist.
Pandemics aside, there is far more compelling evidence that periods of economic recession are associated with an increase in the suicide rate, he added.
Another speaker, Holly C. Wilcox, PhD, a psychiatric epidemiologist at Johns Hopkins University, Baltimore, commented: “It’s not surprising that, during times of disaster the suicide rates decrease a bit. It could be because of people coming toghether. It could be one silver lining of COVID-19. But if there’s prolonged stress economically and socially and we can’t work towards reducing stress for people, we could see an increase. I don’t know if we will.”
In a recent article, Dr. Gunnell and coauthors offered a series of recommendations aimed at blunting the mental health consequences of COVID-19 and the related economic fallout (Lancet Psychiatry. 2020 Apr 21. doi: 10.1016/S2215-0366[20]30171-1).
The authors highlighted the need for interventions aimed at defusing the adverse impact of self-isolation, social distancing, fear, an anticipated rise in alcohol misuse, joblessness, interrupted education, bereavement, and complicated grief. Governments can blunt the well-established effect of financial distress as a risk factor for suicide by providing safety nets in the form of supports for housing, food, and unemployment benefits. And it will be important that those mental health services that develop expertise in performing psychiatric assessments and interventions remotely via telemedicine share their insights, Dr. Gunnell said.
Americans are not feeling more suicidal even in the depths of the COVID-19 pandemic of spring 2020, according to analysis of real-time national data accrued through the Crisis Text Line.
But that’s not to say Americans are feeling less distressed. Quite the contrary, Nancy Lublin, CEO and cofounder of Crisis Text Line, noted at the virtual annual meeting of the American Association of Suicidology.
“We’ve seen a 40% increase in volume since early March. Seventy-eight percent of our conversations are now including words like ‘freaked out,’ ‘panicked,’ ‘scared.’ People are worried about COVID-19. They’re nervous about symptoms; they’re concerned for family on the front lines,” she said.
And yet, from mid-March through mid-April, only 22% of texters to the crisis line expressed suicidal ideation, down from a usual background rate of 28%. Moreover, just 13% of texters who mentioned ‘COVID,’ ‘quarantine,’ or ‘virus’ expressed suicidal ideation, compared with 25% of other texters.
Ms. Lublin and her data crunchers are tracking not only the impact of the disease, but they’re also monitoring the mental health effects of the quarantine and social distancing.
“People are away from their routines, and perhaps [are] quarantined with abusive people. We’ve seen a 48% increase in texts involving sexual abuse and a 74% increase in domestic violence,” she said.
Texts focused on eating disorders or body image issues have jumped by 45%. And roughly two-thirds of texters now describe feelings of depression.
One of the biggest mental health impacts she and colleagues have seen stem from the economic recession triggered by the pandemic.
“We’ve seen more people reach out with fears of bankruptcy, fears of homelessness, fears of financial ruin. Thirty-two percent of our texters now report household incomes under $20,000 per year. That’s up from 19% before,” according to Ms. Lublin.
The Crisis Text Line (text HOME to 741741) uses machine-learning algorithms that sift through incoming text messages from people in crisis for key words, then ranks the messages by severity. Since its launch in 2013, this service, available 24/7, has processed roughly 150 million text messages. The high-risk texters – for example, someone who’s swallowed a bottle of pills or is texting from the San Francisco’s Golden Gate Bridge, as has occurred some 500 times – are connected in an average of 24 seconds with a thoroughly trained volunteer crisis counselor. And there is a third party in these texting conversations: a paid staff supervisor with a master’s degree in a relevant discipline who follows the encounter in real time and can step in if needed.
“Active rescues are involved in less than 1% of our conversations, but still we do them on average 26 times per day. Over the years, we’ve completed more than 32,000 active rescues,” she said.
The Crisis Text Line is not exclusively a suicide prevention hotline. The top five issues people text about involve relationship concerns, depression, anxiety, self-harm, and suicidal ideation. Over time, Ms. Lublin and staff have used Big Data to tweak the screening algorithm as they’ve identified even higher red flag texting words than “suicide.”
“The word ‘military’ makes it twice as likely that we’ll have to call 9-1-1 than the word ‘suicide.’ ‘Gun,’ ‘rope’ – four times as likely. In the [United KIngdom], where we’re also operating, we see the word ‘cliff’ is a more lethal word than the word ‘suicide.’ But the most dangerous words that we see are any named pill,” she said.
The Crisis Text Line was recently awarded a 2020 TED Audacious Project grant to expand their services from English to also be offered in Spanish, French, Portuguese, and Arabic worldwide within the next two and a half years. This will provide coverage to one-third of the world’s population, including people with cell phones living in countries with very limited mental health services.
Will COVID-19 trigger a spike in deaths by suicide?
Whether the COVID-19 pandemic will result in a bump in suicide rates is unclear and will remain so for quite a while, according to David Gunnell, MD, PhD, a suicidologist and professor of epidemiology at the University of Bristol (England).
In the United Kingdom, investigation of a suspicious death typically takes more than 6 months before an official declaration of suicide is recorded by the medical examiner. The lag time is even longer in the United States: The latest national suicide rate data are for 2018 because state-by-state reporting practices vary widely, he noted at a National Press Foundation briefing on COVID-19 and mental health.
Although suicide is consistently the 10th-leading cause of death in the United States, it’s important to put it in perspective, he added. In 2018, there were an average of 4,000 deaths by suicide per month nationally, whereas in March and April of 2020, there were 28,400 deaths per month attributable to COVID-19.
A classic study of the Spanish influenza pandemic in the United States during 1918-1919 concluded that there was “a slight upturn” in the rate of suicide in the months following the pandemic’s peak. More recently, a study of the 2003 SARS (severe acute respiratory syndrome) epidemic in Hong Kong found roughly a 30% increase in the rate of suicide among the elderly during that time frame, Dr. Gunnell noted.
“What limited evidence there is provides an indication of a small rise in suicides, but the number of deaths is far outweighed by the number of deaths associated with these big pandemics,” according to the epidemiologist.
Pandemics aside, there is far more compelling evidence that periods of economic recession are associated with an increase in the suicide rate, he added.
Another speaker, Holly C. Wilcox, PhD, a psychiatric epidemiologist at Johns Hopkins University, Baltimore, commented: “It’s not surprising that, during times of disaster the suicide rates decrease a bit. It could be because of people coming toghether. It could be one silver lining of COVID-19. But if there’s prolonged stress economically and socially and we can’t work towards reducing stress for people, we could see an increase. I don’t know if we will.”
In a recent article, Dr. Gunnell and coauthors offered a series of recommendations aimed at blunting the mental health consequences of COVID-19 and the related economic fallout (Lancet Psychiatry. 2020 Apr 21. doi: 10.1016/S2215-0366[20]30171-1).
The authors highlighted the need for interventions aimed at defusing the adverse impact of self-isolation, social distancing, fear, an anticipated rise in alcohol misuse, joblessness, interrupted education, bereavement, and complicated grief. Governments can blunt the well-established effect of financial distress as a risk factor for suicide by providing safety nets in the form of supports for housing, food, and unemployment benefits. And it will be important that those mental health services that develop expertise in performing psychiatric assessments and interventions remotely via telemedicine share their insights, Dr. Gunnell said.
FROM AAS 2020
COVID-19: Calls to NYC crisis hotline soar
Calls to a mental health crisis hotline in New York City have soared during the COVID-19 pandemic, which has closed schools and businesses, put millions out of work, and ushered in stay-at-home orders.
ensuring that care is available when and where needed during a crisis, whether that be an individual crisis, a local community crisis, or a national mental health crisis like we are facing right now,” said Kimberly Williams, president and CEO of Vibrant Emotional Health.
Vibrant Emotional Health, formerly the Mental Health Association of New York City, provides crisis line services across the United States in partnership with local and federal governments and corporations. NYC Well is one of them.
Ms. Williams and two of her colleagues spoke about crisis hotlines April 25 during the American Psychiatric Association’s Virtual Spring Highlights Meeting.
Rapid crisis intervention
Crisis hotlines provide “rapid crisis intervention, delivering help immediately from trained crisis counselors who respond to unique needs, actively engage in collaborative problem solving, and assess risk for suicide,” Ms. Williams said.
They have a proven track record, she noted. Research shows that they are able to decrease emotional distress and reduce suicidality in crisis situations.
Kelly Clarke, program director of NYC Well, noted that inbound call volume has increased roughly 50% since the COVID-19 pandemic hit.
Callers to NYC Well most commonly report mood/anxiety concerns, stressful life events, and interpersonal problems. “Many people are reaching out to seek support in how to manage their own emotional well-being in light of the pandemic and the restrictions put in place,” said Ms. Clarke.
Multilingual peer support specialists and counselors with NYC Well provide free, confidential support by talk, text, or chat 24 hours per day, 7 days per week, 365 days a year. The service also provides mobile crisis teams and follow-up services. NYC Well has set up a landing page of resources specifically geared toward COVID-19.
How to cope with the rapid growth and at the same time ensure high quality of services are two key challenges for NYC Well, Ms. Clarke said.
“Absolutely essential” service
For John Draper, PhD, the experience early in his career of working on a mobile mental health crisis team in Brooklyn “changed his life.”
First, it showed him that, for people who are severely psychiatrically ill, “care has to come to them,” said Dr. Draper, executive vice president of national networks for Vibrant Emotional Health.
“So many of the people we were seeing were too depressed to get out of bed, much less get to a clinic, and I realized our system was not set up to serve its customers. It was like putting a spinal cord injury clinic at the top of a stairs,” he said.
Crisis hotlines are “absolutely essential.” Their value for communities and individuals “can’t be overestimated,” said Dr. Draper.
This was revealed after the terrorist attacks of 9/11 and now with COVID-19, said Dr. Draper. He noted, that following the attacks of 9/11, a federal report referred to crisis hotlines as “the single most important asset in the response.”
A version of this article originally appeared on Medscape.com.
Calls to a mental health crisis hotline in New York City have soared during the COVID-19 pandemic, which has closed schools and businesses, put millions out of work, and ushered in stay-at-home orders.
ensuring that care is available when and where needed during a crisis, whether that be an individual crisis, a local community crisis, or a national mental health crisis like we are facing right now,” said Kimberly Williams, president and CEO of Vibrant Emotional Health.
Vibrant Emotional Health, formerly the Mental Health Association of New York City, provides crisis line services across the United States in partnership with local and federal governments and corporations. NYC Well is one of them.
Ms. Williams and two of her colleagues spoke about crisis hotlines April 25 during the American Psychiatric Association’s Virtual Spring Highlights Meeting.
Rapid crisis intervention
Crisis hotlines provide “rapid crisis intervention, delivering help immediately from trained crisis counselors who respond to unique needs, actively engage in collaborative problem solving, and assess risk for suicide,” Ms. Williams said.
They have a proven track record, she noted. Research shows that they are able to decrease emotional distress and reduce suicidality in crisis situations.
Kelly Clarke, program director of NYC Well, noted that inbound call volume has increased roughly 50% since the COVID-19 pandemic hit.
Callers to NYC Well most commonly report mood/anxiety concerns, stressful life events, and interpersonal problems. “Many people are reaching out to seek support in how to manage their own emotional well-being in light of the pandemic and the restrictions put in place,” said Ms. Clarke.
Multilingual peer support specialists and counselors with NYC Well provide free, confidential support by talk, text, or chat 24 hours per day, 7 days per week, 365 days a year. The service also provides mobile crisis teams and follow-up services. NYC Well has set up a landing page of resources specifically geared toward COVID-19.
How to cope with the rapid growth and at the same time ensure high quality of services are two key challenges for NYC Well, Ms. Clarke said.
“Absolutely essential” service
For John Draper, PhD, the experience early in his career of working on a mobile mental health crisis team in Brooklyn “changed his life.”
First, it showed him that, for people who are severely psychiatrically ill, “care has to come to them,” said Dr. Draper, executive vice president of national networks for Vibrant Emotional Health.
“So many of the people we were seeing were too depressed to get out of bed, much less get to a clinic, and I realized our system was not set up to serve its customers. It was like putting a spinal cord injury clinic at the top of a stairs,” he said.
Crisis hotlines are “absolutely essential.” Their value for communities and individuals “can’t be overestimated,” said Dr. Draper.
This was revealed after the terrorist attacks of 9/11 and now with COVID-19, said Dr. Draper. He noted, that following the attacks of 9/11, a federal report referred to crisis hotlines as “the single most important asset in the response.”
A version of this article originally appeared on Medscape.com.
Calls to a mental health crisis hotline in New York City have soared during the COVID-19 pandemic, which has closed schools and businesses, put millions out of work, and ushered in stay-at-home orders.
ensuring that care is available when and where needed during a crisis, whether that be an individual crisis, a local community crisis, or a national mental health crisis like we are facing right now,” said Kimberly Williams, president and CEO of Vibrant Emotional Health.
Vibrant Emotional Health, formerly the Mental Health Association of New York City, provides crisis line services across the United States in partnership with local and federal governments and corporations. NYC Well is one of them.
Ms. Williams and two of her colleagues spoke about crisis hotlines April 25 during the American Psychiatric Association’s Virtual Spring Highlights Meeting.
Rapid crisis intervention
Crisis hotlines provide “rapid crisis intervention, delivering help immediately from trained crisis counselors who respond to unique needs, actively engage in collaborative problem solving, and assess risk for suicide,” Ms. Williams said.
They have a proven track record, she noted. Research shows that they are able to decrease emotional distress and reduce suicidality in crisis situations.
Kelly Clarke, program director of NYC Well, noted that inbound call volume has increased roughly 50% since the COVID-19 pandemic hit.
Callers to NYC Well most commonly report mood/anxiety concerns, stressful life events, and interpersonal problems. “Many people are reaching out to seek support in how to manage their own emotional well-being in light of the pandemic and the restrictions put in place,” said Ms. Clarke.
Multilingual peer support specialists and counselors with NYC Well provide free, confidential support by talk, text, or chat 24 hours per day, 7 days per week, 365 days a year. The service also provides mobile crisis teams and follow-up services. NYC Well has set up a landing page of resources specifically geared toward COVID-19.
How to cope with the rapid growth and at the same time ensure high quality of services are two key challenges for NYC Well, Ms. Clarke said.
“Absolutely essential” service
For John Draper, PhD, the experience early in his career of working on a mobile mental health crisis team in Brooklyn “changed his life.”
First, it showed him that, for people who are severely psychiatrically ill, “care has to come to them,” said Dr. Draper, executive vice president of national networks for Vibrant Emotional Health.
“So many of the people we were seeing were too depressed to get out of bed, much less get to a clinic, and I realized our system was not set up to serve its customers. It was like putting a spinal cord injury clinic at the top of a stairs,” he said.
Crisis hotlines are “absolutely essential.” Their value for communities and individuals “can’t be overestimated,” said Dr. Draper.
This was revealed after the terrorist attacks of 9/11 and now with COVID-19, said Dr. Draper. He noted, that following the attacks of 9/11, a federal report referred to crisis hotlines as “the single most important asset in the response.”
A version of this article originally appeared on Medscape.com.
Volunteer surgeon describes working at a New York hospital

In an April 18 Twitter post, Dr. Salles wrote that her unit had experienced three code blues and two deaths in a single night.
“I don’t know how many times I’ve called to tell someone their loved one has died,” she wrote in the post. “I had to do it again last night. ... Of the five patients I’ve personally been responsible for in the past two nights, two have come so close to dying that we called a code blue. That means 40% of my patients have coded. Never in my life has anything close to that happened,” she continued in the thread.
Dr. Salles, a minimally invasive and bariatric surgeon and scholar in residence at Stanford (Calif.) University, headed to New York in mid-April to assist with COVID-19 treatment efforts. Before the trip, she collected as many supplies and as much personal protective equipment as she could acquire, some of which were donated by Good Samaritans. On her first day as a volunteer, Dr. Salles recounted the stark differences between what she is used to seeing and her new environment and the novel challenges she has encountered in New York.
“Things that were not normal now seem normal,” she wrote in an April 15 Twitter post. “ICU patients in [a postanesthesia care unit] and Preop is the new normal. Patients satting in the 70s and 80s seems normal. ICU docs managing [continuous veno-venous hemodialysis] seems normal. Working with strangers seems normal. ... Obviously everyone walking around with barely any skin exposed is also the new normal.”
Similar to a “normal” ICU, new patients are admitted daily, Dr. Salles noted. However, the majority of those who leave the ICU do not go home, she wrote.
“Almost all of the ones who leave are doing so because they’ve died rather than getting better,” she wrote in the same April 19 Twitter thread. “There is a pervasive feeling of helplessness. ... The tools we are working with seem insufficient. For the sickest patients, there are no ventilator settings that seem to work, there are no medications that seem to help. I am not used to this.”
When patients are close to dying, health care workers do their best to connect the patient to loved ones through video calls, watching as family members say their last goodbyes through a screen, Dr. Salles detailed in a later post.
“Their voices cracked, and though they weren’t speaking English, I could hear their pain,” she wrote in an April 20 Twitter post. “For a moment, I imagined having to say goodbye to my mother this way. To not be able to be there, to not be able to hold her hand, to not be able to hug her. And I watched my colleague, who amazingly kept her composure until they had said everything they wanted to say. It was only after they hung up that I saw the tears well up in her eyes.”
But amid the dark days and bleak outcomes, Dr. Salles has found silver linings, humor, and gifts for which to be thankful.
“People are really generous,” she wrote in an April 15 post. “So many have offered to pay for transportation. Other docs in NY have offered to help me with supplies (and I am paying it forward). Grateful to you all!”
In another post, Dr. Salles joked that her “small head” makes it difficult to wear PPE.
“Wearing an N95 for hours really sucks,” she wrote. “It rides up, I pull it down. It digs into my cheeks, I pull it up. Repeat.”
The volunteer experience thus far has also made Dr. Salles question the future and worry about the mental health of her fellow health care professionals.
“The people who have been in NYC since the beginning of this, and those who work in Lombardy, Italy, and in Wuhan, China have faced loss for weeks to months,” she wrote in an April 18 Twitter post. “Not only do we not know when this will end, but it is likely that after it fades, it will come back in a second wave. I am lucky. I’m just a visitor here. I have the privilege to observe and learn and hopefully help, knowing I will be able to walk away. But what about those who can’t walk away? Social distancing is starting to work. But for healthcare workers, the ongoing devastation is very real. What is our long term plan?”
Dr. Salles expressed concern for health care workers who are witnessing “horrible things” with little time to process the experiences.
“It may be especially hard for those who are now working in specialties they are not used to, having to provide care they are not familiar with. They are all doing their best, but inevitably mistakes will be made, and they will likely blame themselves,” she wrote. “How do we best support them?”
Stay tuned for upcoming commentaries from Dr. Salles on her COVID-19 volunteer experience in New York City.
In an April 18 Twitter post, Dr. Salles wrote that her unit had experienced three code blues and two deaths in a single night.
“I don’t know how many times I’ve called to tell someone their loved one has died,” she wrote in the post. “I had to do it again last night. ... Of the five patients I’ve personally been responsible for in the past two nights, two have come so close to dying that we called a code blue. That means 40% of my patients have coded. Never in my life has anything close to that happened,” she continued in the thread.
Dr. Salles, a minimally invasive and bariatric surgeon and scholar in residence at Stanford (Calif.) University, headed to New York in mid-April to assist with COVID-19 treatment efforts. Before the trip, she collected as many supplies and as much personal protective equipment as she could acquire, some of which were donated by Good Samaritans. On her first day as a volunteer, Dr. Salles recounted the stark differences between what she is used to seeing and her new environment and the novel challenges she has encountered in New York.
“Things that were not normal now seem normal,” she wrote in an April 15 Twitter post. “ICU patients in [a postanesthesia care unit] and Preop is the new normal. Patients satting in the 70s and 80s seems normal. ICU docs managing [continuous veno-venous hemodialysis] seems normal. Working with strangers seems normal. ... Obviously everyone walking around with barely any skin exposed is also the new normal.”
Similar to a “normal” ICU, new patients are admitted daily, Dr. Salles noted. However, the majority of those who leave the ICU do not go home, she wrote.
“Almost all of the ones who leave are doing so because they’ve died rather than getting better,” she wrote in the same April 19 Twitter thread. “There is a pervasive feeling of helplessness. ... The tools we are working with seem insufficient. For the sickest patients, there are no ventilator settings that seem to work, there are no medications that seem to help. I am not used to this.”
When patients are close to dying, health care workers do their best to connect the patient to loved ones through video calls, watching as family members say their last goodbyes through a screen, Dr. Salles detailed in a later post.
“Their voices cracked, and though they weren’t speaking English, I could hear their pain,” she wrote in an April 20 Twitter post. “For a moment, I imagined having to say goodbye to my mother this way. To not be able to be there, to not be able to hold her hand, to not be able to hug her. And I watched my colleague, who amazingly kept her composure until they had said everything they wanted to say. It was only after they hung up that I saw the tears well up in her eyes.”
But amid the dark days and bleak outcomes, Dr. Salles has found silver linings, humor, and gifts for which to be thankful.
“People are really generous,” she wrote in an April 15 post. “So many have offered to pay for transportation. Other docs in NY have offered to help me with supplies (and I am paying it forward). Grateful to you all!”
In another post, Dr. Salles joked that her “small head” makes it difficult to wear PPE.
“Wearing an N95 for hours really sucks,” she wrote. “It rides up, I pull it down. It digs into my cheeks, I pull it up. Repeat.”
The volunteer experience thus far has also made Dr. Salles question the future and worry about the mental health of her fellow health care professionals.
“The people who have been in NYC since the beginning of this, and those who work in Lombardy, Italy, and in Wuhan, China have faced loss for weeks to months,” she wrote in an April 18 Twitter post. “Not only do we not know when this will end, but it is likely that after it fades, it will come back in a second wave. I am lucky. I’m just a visitor here. I have the privilege to observe and learn and hopefully help, knowing I will be able to walk away. But what about those who can’t walk away? Social distancing is starting to work. But for healthcare workers, the ongoing devastation is very real. What is our long term plan?”
Dr. Salles expressed concern for health care workers who are witnessing “horrible things” with little time to process the experiences.
“It may be especially hard for those who are now working in specialties they are not used to, having to provide care they are not familiar with. They are all doing their best, but inevitably mistakes will be made, and they will likely blame themselves,” she wrote. “How do we best support them?”
Stay tuned for upcoming commentaries from Dr. Salles on her COVID-19 volunteer experience in New York City.
In an April 18 Twitter post, Dr. Salles wrote that her unit had experienced three code blues and two deaths in a single night.
“I don’t know how many times I’ve called to tell someone their loved one has died,” she wrote in the post. “I had to do it again last night. ... Of the five patients I’ve personally been responsible for in the past two nights, two have come so close to dying that we called a code blue. That means 40% of my patients have coded. Never in my life has anything close to that happened,” she continued in the thread.
Dr. Salles, a minimally invasive and bariatric surgeon and scholar in residence at Stanford (Calif.) University, headed to New York in mid-April to assist with COVID-19 treatment efforts. Before the trip, she collected as many supplies and as much personal protective equipment as she could acquire, some of which were donated by Good Samaritans. On her first day as a volunteer, Dr. Salles recounted the stark differences between what she is used to seeing and her new environment and the novel challenges she has encountered in New York.
“Things that were not normal now seem normal,” she wrote in an April 15 Twitter post. “ICU patients in [a postanesthesia care unit] and Preop is the new normal. Patients satting in the 70s and 80s seems normal. ICU docs managing [continuous veno-venous hemodialysis] seems normal. Working with strangers seems normal. ... Obviously everyone walking around with barely any skin exposed is also the new normal.”
Similar to a “normal” ICU, new patients are admitted daily, Dr. Salles noted. However, the majority of those who leave the ICU do not go home, she wrote.
“Almost all of the ones who leave are doing so because they’ve died rather than getting better,” she wrote in the same April 19 Twitter thread. “There is a pervasive feeling of helplessness. ... The tools we are working with seem insufficient. For the sickest patients, there are no ventilator settings that seem to work, there are no medications that seem to help. I am not used to this.”
When patients are close to dying, health care workers do their best to connect the patient to loved ones through video calls, watching as family members say their last goodbyes through a screen, Dr. Salles detailed in a later post.
“Their voices cracked, and though they weren’t speaking English, I could hear their pain,” she wrote in an April 20 Twitter post. “For a moment, I imagined having to say goodbye to my mother this way. To not be able to be there, to not be able to hold her hand, to not be able to hug her. And I watched my colleague, who amazingly kept her composure until they had said everything they wanted to say. It was only after they hung up that I saw the tears well up in her eyes.”
But amid the dark days and bleak outcomes, Dr. Salles has found silver linings, humor, and gifts for which to be thankful.
“People are really generous,” she wrote in an April 15 post. “So many have offered to pay for transportation. Other docs in NY have offered to help me with supplies (and I am paying it forward). Grateful to you all!”
In another post, Dr. Salles joked that her “small head” makes it difficult to wear PPE.
“Wearing an N95 for hours really sucks,” she wrote. “It rides up, I pull it down. It digs into my cheeks, I pull it up. Repeat.”
The volunteer experience thus far has also made Dr. Salles question the future and worry about the mental health of her fellow health care professionals.
“The people who have been in NYC since the beginning of this, and those who work in Lombardy, Italy, and in Wuhan, China have faced loss for weeks to months,” she wrote in an April 18 Twitter post. “Not only do we not know when this will end, but it is likely that after it fades, it will come back in a second wave. I am lucky. I’m just a visitor here. I have the privilege to observe and learn and hopefully help, knowing I will be able to walk away. But what about those who can’t walk away? Social distancing is starting to work. But for healthcare workers, the ongoing devastation is very real. What is our long term plan?”
Dr. Salles expressed concern for health care workers who are witnessing “horrible things” with little time to process the experiences.
“It may be especially hard for those who are now working in specialties they are not used to, having to provide care they are not familiar with. They are all doing their best, but inevitably mistakes will be made, and they will likely blame themselves,” she wrote. “How do we best support them?”
Stay tuned for upcoming commentaries from Dr. Salles on her COVID-19 volunteer experience in New York City.
Large study of COVID-19 N.Y.C. hospital cases shows high mortality
according to a report published in JAMA (2020 Apr 22. doi: 10.1001/jama.2020.6775).
The study, which represents the largest cohort of hospitalized patients with COVID-19 in the United States thus far, confirmed that the highest-risk groups are older, male, and those with preexisting hypertension, diabetes, or obesity.
Mortality rates are difficult to compare between studies, emphasizes corresponding author Karina W. Davidson, PhD. Health care systems and resources can affect outcomes as well as patient demographics and the prevalence of comorbidities. In addition, “the speed with which people present with symptoms and where they are in the course of disease” differ between patient series, said Dr. Davidson, professor and senior vice president at the Feinstein Institutes for Medical Research and senior vice president of research, Northwell Health, Manhasset, N.Y.
“But given all of those, we know that our study represents a fairly large sample of consecutive patients. This is what the mortality rate looks like among those requiring hospitalization at the early stage of the pandemic,” Dr. Davidson said.
The large patient sample reflects the diversity of the city and its environs. “It’s a large representative sample of very diverse patients ranging in age from zero (under a year) to 107, from all walks of life and socioeconomic levels,” Dr. Davidson continued. Eight of the 12 participating N.Y.C.–area hospitals are on Long Island, one each in Manhattan and Staten Island, and two in Queens.
For the study, first author Safiya Richardson, MD, MPH, and colleagues in the Northwell COVID-19 Research Consortium analyzed EHRs of 5,700 patients hospitalized with confirmed COVID-19 during March 1, 2020–April 4, 2020.
Overall, 1,151 (20.2%) of the 5,700 patients required mechanical ventilation. As of April 4, 831 (72.2%) of these patients remained in the hospital, 38 (3.3%) were discharged, and 282 (24.5%) had died.
When the authors restricted their analysis to the 2,634 patients whose outcomes (discharge or death) were known at the end of the study, 373 (14.2%) had been treated in the intensive care unit, 320 (12.2%) received invasive mechanical ventilation, 81 (3.2%) received dialysis, and 553 (21%) died.
As seen in other COVID-19 studies, increasing age was associated with a higher risk of death. Of patients receiving mechanical ventilation and whose outcomes (discharge or death) were known, 88.1% died. When stratified by age, the mortality rates for ventilated patients were 76.4% for those aged 18-65 years and 97.2% for those older than 65 years.
Among those who did not require mechanical ventilation and whose outcomes (discharge or death) were known, 19.8% of patients aged 18-65 years died, as did 26.6% of those older than 65 years. No patient under 18 years died during the study period.
“There can be risks with mechanical ventilation, like the development of ventilator-associated pneumonia (VAP), which occurs in 10%-25% of ventilated patients and tends to occur within 5 days. The authors didn’t report data on VAP, but it seems that the mortality for ventilated patients would most likely be attributable to disease severity rather than the ventilation itself,” said Cindy Prins, PhD, director of the Master of Public Health program and clinical associate professor of epidemiology at the University of Florida, Gainesville.
The median follow-up time after discharge was 4.4 days. During the study period, 45 (2.2%) patients were readmitted, with median time to readmission of 3 days.
The most common comorbidities among all 5,700 patients were hypertension (57%), obesity (41%), and diabetes (34%). As has been seen in other patient series, male sex and increasing age were associated with a higher risk for death.
The most surprising finding, Dr. Davidson said, was that fever was uncommon. “Of 5,700 patients requiring admission because of respiratory distress, only a third had fever. So fever should not be a single symptom upon which people make a decision to seek help.”
Dr. Prins was intrigued by the observation that 2% of the patients tested positive for a respiratory virus panel as well as for COVID-19. “Because of a shortage of COVID-19 testing supplies, some hospitals have been running respiratory panels before testing for COVID-19. But this study provides more evidence that a positive result on a respiratory panel does not rule out COVID-19 infection.”
The clinical situation is constantly in flux. “We’ve been seeing since March 8 that the severity of patients has lessened dramatically, and they are coming in later in the disease. Many things are changing, we hope for the better,” Dr. Davidson said.
This article was first published on Medscape.com.
according to a report published in JAMA (2020 Apr 22. doi: 10.1001/jama.2020.6775).
The study, which represents the largest cohort of hospitalized patients with COVID-19 in the United States thus far, confirmed that the highest-risk groups are older, male, and those with preexisting hypertension, diabetes, or obesity.
Mortality rates are difficult to compare between studies, emphasizes corresponding author Karina W. Davidson, PhD. Health care systems and resources can affect outcomes as well as patient demographics and the prevalence of comorbidities. In addition, “the speed with which people present with symptoms and where they are in the course of disease” differ between patient series, said Dr. Davidson, professor and senior vice president at the Feinstein Institutes for Medical Research and senior vice president of research, Northwell Health, Manhasset, N.Y.
“But given all of those, we know that our study represents a fairly large sample of consecutive patients. This is what the mortality rate looks like among those requiring hospitalization at the early stage of the pandemic,” Dr. Davidson said.
The large patient sample reflects the diversity of the city and its environs. “It’s a large representative sample of very diverse patients ranging in age from zero (under a year) to 107, from all walks of life and socioeconomic levels,” Dr. Davidson continued. Eight of the 12 participating N.Y.C.–area hospitals are on Long Island, one each in Manhattan and Staten Island, and two in Queens.
For the study, first author Safiya Richardson, MD, MPH, and colleagues in the Northwell COVID-19 Research Consortium analyzed EHRs of 5,700 patients hospitalized with confirmed COVID-19 during March 1, 2020–April 4, 2020.
Overall, 1,151 (20.2%) of the 5,700 patients required mechanical ventilation. As of April 4, 831 (72.2%) of these patients remained in the hospital, 38 (3.3%) were discharged, and 282 (24.5%) had died.
When the authors restricted their analysis to the 2,634 patients whose outcomes (discharge or death) were known at the end of the study, 373 (14.2%) had been treated in the intensive care unit, 320 (12.2%) received invasive mechanical ventilation, 81 (3.2%) received dialysis, and 553 (21%) died.
As seen in other COVID-19 studies, increasing age was associated with a higher risk of death. Of patients receiving mechanical ventilation and whose outcomes (discharge or death) were known, 88.1% died. When stratified by age, the mortality rates for ventilated patients were 76.4% for those aged 18-65 years and 97.2% for those older than 65 years.
Among those who did not require mechanical ventilation and whose outcomes (discharge or death) were known, 19.8% of patients aged 18-65 years died, as did 26.6% of those older than 65 years. No patient under 18 years died during the study period.
“There can be risks with mechanical ventilation, like the development of ventilator-associated pneumonia (VAP), which occurs in 10%-25% of ventilated patients and tends to occur within 5 days. The authors didn’t report data on VAP, but it seems that the mortality for ventilated patients would most likely be attributable to disease severity rather than the ventilation itself,” said Cindy Prins, PhD, director of the Master of Public Health program and clinical associate professor of epidemiology at the University of Florida, Gainesville.
The median follow-up time after discharge was 4.4 days. During the study period, 45 (2.2%) patients were readmitted, with median time to readmission of 3 days.
The most common comorbidities among all 5,700 patients were hypertension (57%), obesity (41%), and diabetes (34%). As has been seen in other patient series, male sex and increasing age were associated with a higher risk for death.
The most surprising finding, Dr. Davidson said, was that fever was uncommon. “Of 5,700 patients requiring admission because of respiratory distress, only a third had fever. So fever should not be a single symptom upon which people make a decision to seek help.”
Dr. Prins was intrigued by the observation that 2% of the patients tested positive for a respiratory virus panel as well as for COVID-19. “Because of a shortage of COVID-19 testing supplies, some hospitals have been running respiratory panels before testing for COVID-19. But this study provides more evidence that a positive result on a respiratory panel does not rule out COVID-19 infection.”
The clinical situation is constantly in flux. “We’ve been seeing since March 8 that the severity of patients has lessened dramatically, and they are coming in later in the disease. Many things are changing, we hope for the better,” Dr. Davidson said.
This article was first published on Medscape.com.
according to a report published in JAMA (2020 Apr 22. doi: 10.1001/jama.2020.6775).
The study, which represents the largest cohort of hospitalized patients with COVID-19 in the United States thus far, confirmed that the highest-risk groups are older, male, and those with preexisting hypertension, diabetes, or obesity.
Mortality rates are difficult to compare between studies, emphasizes corresponding author Karina W. Davidson, PhD. Health care systems and resources can affect outcomes as well as patient demographics and the prevalence of comorbidities. In addition, “the speed with which people present with symptoms and where they are in the course of disease” differ between patient series, said Dr. Davidson, professor and senior vice president at the Feinstein Institutes for Medical Research and senior vice president of research, Northwell Health, Manhasset, N.Y.
“But given all of those, we know that our study represents a fairly large sample of consecutive patients. This is what the mortality rate looks like among those requiring hospitalization at the early stage of the pandemic,” Dr. Davidson said.
The large patient sample reflects the diversity of the city and its environs. “It’s a large representative sample of very diverse patients ranging in age from zero (under a year) to 107, from all walks of life and socioeconomic levels,” Dr. Davidson continued. Eight of the 12 participating N.Y.C.–area hospitals are on Long Island, one each in Manhattan and Staten Island, and two in Queens.
For the study, first author Safiya Richardson, MD, MPH, and colleagues in the Northwell COVID-19 Research Consortium analyzed EHRs of 5,700 patients hospitalized with confirmed COVID-19 during March 1, 2020–April 4, 2020.
Overall, 1,151 (20.2%) of the 5,700 patients required mechanical ventilation. As of April 4, 831 (72.2%) of these patients remained in the hospital, 38 (3.3%) were discharged, and 282 (24.5%) had died.
When the authors restricted their analysis to the 2,634 patients whose outcomes (discharge or death) were known at the end of the study, 373 (14.2%) had been treated in the intensive care unit, 320 (12.2%) received invasive mechanical ventilation, 81 (3.2%) received dialysis, and 553 (21%) died.
As seen in other COVID-19 studies, increasing age was associated with a higher risk of death. Of patients receiving mechanical ventilation and whose outcomes (discharge or death) were known, 88.1% died. When stratified by age, the mortality rates for ventilated patients were 76.4% for those aged 18-65 years and 97.2% for those older than 65 years.
Among those who did not require mechanical ventilation and whose outcomes (discharge or death) were known, 19.8% of patients aged 18-65 years died, as did 26.6% of those older than 65 years. No patient under 18 years died during the study period.
“There can be risks with mechanical ventilation, like the development of ventilator-associated pneumonia (VAP), which occurs in 10%-25% of ventilated patients and tends to occur within 5 days. The authors didn’t report data on VAP, but it seems that the mortality for ventilated patients would most likely be attributable to disease severity rather than the ventilation itself,” said Cindy Prins, PhD, director of the Master of Public Health program and clinical associate professor of epidemiology at the University of Florida, Gainesville.
The median follow-up time after discharge was 4.4 days. During the study period, 45 (2.2%) patients were readmitted, with median time to readmission of 3 days.
The most common comorbidities among all 5,700 patients were hypertension (57%), obesity (41%), and diabetes (34%). As has been seen in other patient series, male sex and increasing age were associated with a higher risk for death.
The most surprising finding, Dr. Davidson said, was that fever was uncommon. “Of 5,700 patients requiring admission because of respiratory distress, only a third had fever. So fever should not be a single symptom upon which people make a decision to seek help.”
Dr. Prins was intrigued by the observation that 2% of the patients tested positive for a respiratory virus panel as well as for COVID-19. “Because of a shortage of COVID-19 testing supplies, some hospitals have been running respiratory panels before testing for COVID-19. But this study provides more evidence that a positive result on a respiratory panel does not rule out COVID-19 infection.”
The clinical situation is constantly in flux. “We’ve been seeing since March 8 that the severity of patients has lessened dramatically, and they are coming in later in the disease. Many things are changing, we hope for the better,” Dr. Davidson said.
This article was first published on Medscape.com.
Chest imaging guidelines released for pediatric COVID-19
Differences are emerging between chest imaging findings in adults and children with COVID-19 pneumonia, according to a new international consensus statement published online April 23 in Radiology: Cardiothoracic Imaging.
“Chest imaging plays an important role in evaluation of pediatric patients with COVID-19, however there is currently little information available describing imaging manifestations of pediatric COVID-19 and even less discussing utilization of imaging studies in pediatric patients,” write Alexandra M. Foust, DO, from the Department of Radiology, Boston Children’s Hospital and Harvard Medical School, Massachusetts, and colleagues.
The authors wrote the consensus statement to help clinicians evaluate children with potential COVID-19, interpret chest imaging findings, and determine the best treatment for these patients.
As a dedicated pediatric radiologist in tertiary care, senior author Edward Y. Lee, MD, MPH, also from Boston Children’s Hospital, said he works with many international pediatric chest radiologists, and the document provides an international perspective. Information on chest imaging for pediatric patients with COVID-19 is scarce, and clinicians are clamoring for information to inform clinical decisions, he said. He noted that the recommendations are practical and easy to use.
The first step in evaluating a child with suspected COVID-19 is to consider the larger clinical picture. “You really have to look at the patient as a person, and when you look at them, [consider] their underlying risk factors – some people we know are prone to have more serious infection from COVID-19 because they have underlying medical problems,” Lee said.
Certain findings on chest x-ray (CXR) are more specific for COVID-19 pneumonia, whereas CT is better for characterizing and confirming and for differentiating one lung infection from another, Lee explained.
Structured reporting
Toward this end, the authors developed tables that provide standardized language to describe imaging findings in patients with suspected COVID-19 pneumonia. Advantages of this type of “structured reporting” include improved understanding and clarity between the radiologist and the ordering provider.
The authors note that structured reporting is likely to be most useful in regions where COVID-19 is highly prevalent. The COVID-19 imaging presentation in children overlaps with some other ailments, including influenza, e-cigarette vaping–associated lung injury, and eosinophilic lung disease. Thus, the use of structured reporting in low-incidence settings could lead to false positive findings.
Commonly seen CXR findings in children with COVID-19 pneumonia include bilaterally distributed peripheral and/or subpleural ground-glass opacities (GGOs) and/or consolidation. Nonspecific findings include “unilateral peripheral or peripheral and central ground-glass opacities and/or consolidation; bilateral peribronchial thickening and/or peribronchial opacities; and multifocal or diffuse GGOs and/or consolidation without specific distribution.”
On CT, commonly seen findings in pediatric COVID-19 pneumonia include “bilateral, peripheral and/or subpleural GGOs and/or consolidation in lower lobe predominant pattern; and ‘halo’ sign early” in the disease course. Indeterminate CT findings include “unilateral peripheral or peripheral and central GGOs and/or consolidation; bilateral peribronchial thickening and/or peribronchial opacities; multivocal or diffuse GGOs and/or consolidation without specific distribution; and ‘crazy paving’ sign.”
Imaging recommendations
Initial chest imaging is not generally recommended for screening of symptomatic or asymptomatic children with suspected COVID-19, nor for children with mild clinical symptoms unless the child is at risk for disease progression or worsens clinically.
An initial CXR may be appropriate for children with moderate to severe clinical symptoms – regardless of whether they have COVID-19 – and the patient may undergo a chest CT if the results could influence clinical management.
A repeat reverse transcription polymerase chain reaction (RT-PCR) test for COVID-19 should be considered for children with moderate to severe symptoms whose initial laboratory result was negative but whose chest imaging findings are consistent with COVID-19.
Chest imaging may be used as a first step in the workup for suspected COVID-19 patients in resource-constrained environments where rapid triage may be needed to spare other resources, such as hospital beds and staffing.
It may be appropriate to conduct sequential CXR examinations for pediatric patients with COVID-19 to assess therapeutic response, evaluate clinical worsening, or determine positioning of life support devices, according to the authors.
Post-recovery follow-up chest imaging is not recommended for asymptomatic pediatric patients after recovery from disease that followed a mild course. Post-recovery imaging may be appropriate for asymptomatic children who initially had moderate to severe illness; the decision should be based on clinical concern that the patient may develop long-term lung injury.
Post-recovery follow-up imaging may be appropriate for children whose symptoms persist or worsen regardless of initial illness severity.
Lee and coauthors have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Differences are emerging between chest imaging findings in adults and children with COVID-19 pneumonia, according to a new international consensus statement published online April 23 in Radiology: Cardiothoracic Imaging.
“Chest imaging plays an important role in evaluation of pediatric patients with COVID-19, however there is currently little information available describing imaging manifestations of pediatric COVID-19 and even less discussing utilization of imaging studies in pediatric patients,” write Alexandra M. Foust, DO, from the Department of Radiology, Boston Children’s Hospital and Harvard Medical School, Massachusetts, and colleagues.
The authors wrote the consensus statement to help clinicians evaluate children with potential COVID-19, interpret chest imaging findings, and determine the best treatment for these patients.
As a dedicated pediatric radiologist in tertiary care, senior author Edward Y. Lee, MD, MPH, also from Boston Children’s Hospital, said he works with many international pediatric chest radiologists, and the document provides an international perspective. Information on chest imaging for pediatric patients with COVID-19 is scarce, and clinicians are clamoring for information to inform clinical decisions, he said. He noted that the recommendations are practical and easy to use.
The first step in evaluating a child with suspected COVID-19 is to consider the larger clinical picture. “You really have to look at the patient as a person, and when you look at them, [consider] their underlying risk factors – some people we know are prone to have more serious infection from COVID-19 because they have underlying medical problems,” Lee said.
Certain findings on chest x-ray (CXR) are more specific for COVID-19 pneumonia, whereas CT is better for characterizing and confirming and for differentiating one lung infection from another, Lee explained.
Structured reporting
Toward this end, the authors developed tables that provide standardized language to describe imaging findings in patients with suspected COVID-19 pneumonia. Advantages of this type of “structured reporting” include improved understanding and clarity between the radiologist and the ordering provider.
The authors note that structured reporting is likely to be most useful in regions where COVID-19 is highly prevalent. The COVID-19 imaging presentation in children overlaps with some other ailments, including influenza, e-cigarette vaping–associated lung injury, and eosinophilic lung disease. Thus, the use of structured reporting in low-incidence settings could lead to false positive findings.
Commonly seen CXR findings in children with COVID-19 pneumonia include bilaterally distributed peripheral and/or subpleural ground-glass opacities (GGOs) and/or consolidation. Nonspecific findings include “unilateral peripheral or peripheral and central ground-glass opacities and/or consolidation; bilateral peribronchial thickening and/or peribronchial opacities; and multifocal or diffuse GGOs and/or consolidation without specific distribution.”
On CT, commonly seen findings in pediatric COVID-19 pneumonia include “bilateral, peripheral and/or subpleural GGOs and/or consolidation in lower lobe predominant pattern; and ‘halo’ sign early” in the disease course. Indeterminate CT findings include “unilateral peripheral or peripheral and central GGOs and/or consolidation; bilateral peribronchial thickening and/or peribronchial opacities; multivocal or diffuse GGOs and/or consolidation without specific distribution; and ‘crazy paving’ sign.”
Imaging recommendations
Initial chest imaging is not generally recommended for screening of symptomatic or asymptomatic children with suspected COVID-19, nor for children with mild clinical symptoms unless the child is at risk for disease progression or worsens clinically.
An initial CXR may be appropriate for children with moderate to severe clinical symptoms – regardless of whether they have COVID-19 – and the patient may undergo a chest CT if the results could influence clinical management.
A repeat reverse transcription polymerase chain reaction (RT-PCR) test for COVID-19 should be considered for children with moderate to severe symptoms whose initial laboratory result was negative but whose chest imaging findings are consistent with COVID-19.
Chest imaging may be used as a first step in the workup for suspected COVID-19 patients in resource-constrained environments where rapid triage may be needed to spare other resources, such as hospital beds and staffing.
It may be appropriate to conduct sequential CXR examinations for pediatric patients with COVID-19 to assess therapeutic response, evaluate clinical worsening, or determine positioning of life support devices, according to the authors.
Post-recovery follow-up chest imaging is not recommended for asymptomatic pediatric patients after recovery from disease that followed a mild course. Post-recovery imaging may be appropriate for asymptomatic children who initially had moderate to severe illness; the decision should be based on clinical concern that the patient may develop long-term lung injury.
Post-recovery follow-up imaging may be appropriate for children whose symptoms persist or worsen regardless of initial illness severity.
Lee and coauthors have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Differences are emerging between chest imaging findings in adults and children with COVID-19 pneumonia, according to a new international consensus statement published online April 23 in Radiology: Cardiothoracic Imaging.
“Chest imaging plays an important role in evaluation of pediatric patients with COVID-19, however there is currently little information available describing imaging manifestations of pediatric COVID-19 and even less discussing utilization of imaging studies in pediatric patients,” write Alexandra M. Foust, DO, from the Department of Radiology, Boston Children’s Hospital and Harvard Medical School, Massachusetts, and colleagues.
The authors wrote the consensus statement to help clinicians evaluate children with potential COVID-19, interpret chest imaging findings, and determine the best treatment for these patients.
As a dedicated pediatric radiologist in tertiary care, senior author Edward Y. Lee, MD, MPH, also from Boston Children’s Hospital, said he works with many international pediatric chest radiologists, and the document provides an international perspective. Information on chest imaging for pediatric patients with COVID-19 is scarce, and clinicians are clamoring for information to inform clinical decisions, he said. He noted that the recommendations are practical and easy to use.
The first step in evaluating a child with suspected COVID-19 is to consider the larger clinical picture. “You really have to look at the patient as a person, and when you look at them, [consider] their underlying risk factors – some people we know are prone to have more serious infection from COVID-19 because they have underlying medical problems,” Lee said.
Certain findings on chest x-ray (CXR) are more specific for COVID-19 pneumonia, whereas CT is better for characterizing and confirming and for differentiating one lung infection from another, Lee explained.
Structured reporting
Toward this end, the authors developed tables that provide standardized language to describe imaging findings in patients with suspected COVID-19 pneumonia. Advantages of this type of “structured reporting” include improved understanding and clarity between the radiologist and the ordering provider.
The authors note that structured reporting is likely to be most useful in regions where COVID-19 is highly prevalent. The COVID-19 imaging presentation in children overlaps with some other ailments, including influenza, e-cigarette vaping–associated lung injury, and eosinophilic lung disease. Thus, the use of structured reporting in low-incidence settings could lead to false positive findings.
Commonly seen CXR findings in children with COVID-19 pneumonia include bilaterally distributed peripheral and/or subpleural ground-glass opacities (GGOs) and/or consolidation. Nonspecific findings include “unilateral peripheral or peripheral and central ground-glass opacities and/or consolidation; bilateral peribronchial thickening and/or peribronchial opacities; and multifocal or diffuse GGOs and/or consolidation without specific distribution.”
On CT, commonly seen findings in pediatric COVID-19 pneumonia include “bilateral, peripheral and/or subpleural GGOs and/or consolidation in lower lobe predominant pattern; and ‘halo’ sign early” in the disease course. Indeterminate CT findings include “unilateral peripheral or peripheral and central GGOs and/or consolidation; bilateral peribronchial thickening and/or peribronchial opacities; multivocal or diffuse GGOs and/or consolidation without specific distribution; and ‘crazy paving’ sign.”
Imaging recommendations
Initial chest imaging is not generally recommended for screening of symptomatic or asymptomatic children with suspected COVID-19, nor for children with mild clinical symptoms unless the child is at risk for disease progression or worsens clinically.
An initial CXR may be appropriate for children with moderate to severe clinical symptoms – regardless of whether they have COVID-19 – and the patient may undergo a chest CT if the results could influence clinical management.
A repeat reverse transcription polymerase chain reaction (RT-PCR) test for COVID-19 should be considered for children with moderate to severe symptoms whose initial laboratory result was negative but whose chest imaging findings are consistent with COVID-19.
Chest imaging may be used as a first step in the workup for suspected COVID-19 patients in resource-constrained environments where rapid triage may be needed to spare other resources, such as hospital beds and staffing.
It may be appropriate to conduct sequential CXR examinations for pediatric patients with COVID-19 to assess therapeutic response, evaluate clinical worsening, or determine positioning of life support devices, according to the authors.
Post-recovery follow-up chest imaging is not recommended for asymptomatic pediatric patients after recovery from disease that followed a mild course. Post-recovery imaging may be appropriate for asymptomatic children who initially had moderate to severe illness; the decision should be based on clinical concern that the patient may develop long-term lung injury.
Post-recovery follow-up imaging may be appropriate for children whose symptoms persist or worsen regardless of initial illness severity.
Lee and coauthors have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
COVID-19: Employers cut doc pay and bonuses: What’s your recourse?
Employed physicians have had to take large pay cuts, give up bonuses, go on leave, or have even been terminated. In many cases, these actions violate their contract. How can they fight them?
Michael D., MD, a colorectal surgeon employed in a large surgical practice in Georgia, is still trying to make sense of a late-night directive from the practice, received in late March.
The practice had just started seeing a steep decline in appointments because of the COVID-19 pandemic. In a hastily arranged group phone call at 11:00 p.m., the CEO told the group what would have to be done.
They would be taking a 50% reduction in salaries, their bonuses for work already done were being withheld, and they would have to use their paid time off (PTO) in order to get their full March salary.
“It’s been over 2 weeks now, and still we’ve seen nothing formalized in writing,” said Dr. D., who asked that his name not be used because he was told that, under no circumstances, should anyone talk to the media.
“They have not told us anything more since then,” he said. “There’s just been a lot of hearsay and speculation.”
Dr. D. has been in touch with employed physicians at other practices, and their experiences run the gamut. One doctor at a large multispecialty group said his salary hadn’t been reduced at all, but a cardiologist was just told he will be laid off in 60 days.
Asking for big sacrifices
As the pandemic has intensified, employed physicians have started to see massive changes in their payment arrangements. They have had to take large pay cuts, give up bonuses, go on leave, and have even been terminated.
“In my 11 years of work on physician contracts, I have never seen changes as drastic as these,” said Kyle Claussen, a physician contract attorney and CEO of Resolve, a company that advises physicians on their careers. The company is based in Columbia, Mo.
He has heard from more than 100 doctors about these proposed changes in their contracts and related matters. Even graduating residents, he said, are being told that the start dates for their new jobs will be delayed.
In many cases, these actions violate the employed physicians’ contracts, said Ericka Adler, a physician contract attorney at Roetzel & Andress in Chicago.
“Some employers are acting out of desperation and are not making legally sound decisions,” Ms. Adler said. “It’s especially upsetting when they do not try to even talk to or work with the doctor first.”
Employers making unfounded unilateral changes
Ms. Adler said some employers are simply issuing a letter to all doctors. “It goes something like, ‘Just to let you know, we are cutting compensation effective immediately,’ and this may apply across the board to all doctors,” she said.
“But the problem with letters is that this is a contractual matter,” she said. “The employer needs to renegotiate each doctor’s contract.”
Employers might insist that the unilateral changes are based on terms in the contract, but this is usually unfounded, both lawyers said. A “force majeure” clause in contracts would allow the employer to set aside terms under certain specified emergencies, and the pandemic might be one of them. But Mr. Claussen said force majeure clauses are rare in physician contracts, and Ms. Adler said she has never seen one.
Lacking a force majeure clause, employers may try to turn to a common law doctrine that allows employers to set aside a contract when it is impossible to perform its terms, owing, for example, to “an unexpected intervening event.” But this tactic is also questionable, says Ms. Adler, who also represents the employer’s side of the contract. “This is a very high standard and unlikely to be satisfied,” she said.
Employers are desperate to amend contracts
Lacking a cause to take unilateral action, many employers are desperately trying to amend their physician contracts – the subject of the plaintive emails that employed physicians started receiving in mid-March.
“Doctors are trying to decide how they will react to these documents,” Mr. Claussen said. “If they don’t sign, they run the risk of being terminated.” He is expecting termination letters for some of these doctors to start coming in 2-3 weeks.
In response to these amendments, “doctors want to reach out to their employers and see if something can be negotiated,” he said. “Some employers have been amenable, but others have so far not been.”
Ms. Adler said the amendments typically offer open-ended arrangements favoring the employer. “The document might call for a temporary pay cut until the employer thinks they can restore the old salary, but it is up to the employer to decide when that would be,” she said.
Also, when the employer owes the physician for services already performed, the amendments don’t promise to pay them the full amount owed, she said.
Ms. Adler advises doctors to ask for a provision that restoration of their original salary will occur at a definite point in time, such as 30 days after the organization is back at previous volume. And if the doctor is owed money, the doctor should ask for full payment – and to sweeten that offer, allow the employer to pay the doctor back over a period, she says.
Just in the past month, employers have been pushing for several specific changes in doctors’ employment status. Here are some changes that Mr. Claussen and Ms. Adler have been seeing.
Withholding quarterly bonuses
In March, just before quarterly bonus payments were due, employed physicians started getting notices that they would not get the bonus, Mr. Claussen said. This covered work already done, and it amounted to a lot of money because practices were busy then.
“Not paying bonuses is a very big deal because they can make up to 50% of a physician’s total compensation,” Mr. Claussen said. He added that unilaterally withholding those funds, without a change in the contract, is legally questionable.
In addition to these changes on past bonuses, he said employers are now trying to temporarily end bonuses going forward through the contract amendments. “It’s not a good idea to sign this,” he said.
Doctors paid on pure production are left in the lurch
As volume falls, some hospitals and practices are shutting down doctors’ offices for all but emergencies, leaving their employed doctors with practically nothing to do. Doctors paid purely on their productivity are devastated by this change because their income virtually goes to zero, Mr. Claussen said.
He said office shutdowns are particularly common for specialists because hospitals have been stopping elective procedures during the pandemic, but they can also happen in primary care, which has seen steep declines in patient volume, too.
Having doctors on pure production means that employers can keep doctors hired without having to pay them, Mr. Claussen said. He has seen some employers try to shift more doctors into pure production through the amended contracts.
But Ms. Adler said having doctors on pure production is actually disadvantageous for employers in the current climate. The employer may end up being owed money because of advance payments they have already made to these doctors, she said.
In any case, both lawyers agreed that doctors on a pure production model are in an untenable situation right now. Ms. Adler said they are not earning money but are still technically at work, so they cannot collect unemployment compensation, which would give them some income.
Forcing doctors to use paid time off
To provide some pay for doctors who have no volume, many employers are forcing these doctors to use up their PTO days, which typically amount to about 4 weeks, Mr. Claussen said. “These doctors have no choice in the matter,” he said.
Furthermore, while on PTO, they are being required to take call. Employers are still obligated to cover call, and there may not be enough doctors still working to fill the call schedule. But making doctors do this work on their time off may be a violation of the contract, Mr. Claussen said.
Terminating physicians
Doctors who have little to do are often put on furlough. This means they don’t get paid but they keep their benefits, Ms. Adler said. The next step, she said, is to lay them off, with the stated intention of rehiring them.
Once laid off, she said, they can get unemployment payments. “Unemployment payments may not be anywhere near what they were earning before, but they are better than not earning anything,” Ms. Adler said.
In some cases, employers are just terminating them and are offering no prospect of rehiring them, she said. Ms. Adler said terminations can be a big problem for doctors. Physicians might have to repay a signing bonus or they might lose their malpractice coverage, forcing them to buy a tail. They could also be subject to a noncompete clause, which would not allow them to practice in the area, she said.
Terminating without cause typically requires 60-90 days’ notice, which both sides might use to negotiate some changes in the contract. But Ms. Adler said some employers are firing doctors with cause, and are using legally questionable reasons to do so.
“In most cases, these employers are grasping at straws,” she said. As a result, she expects many fired doctors will file wrongful termination lawsuits. She thinks employers are better advised to negotiate with the physicians.
Delaying start dates for new physicians
Typically, graduating residents and fellows signed with their new employers months ago and are ready to start working on July 1. But some employers are pushing back the start date for several months, Mr. Claussen said.
Mr. Claussen has been helping several clients in this situation. He said these delays are often a clear violation of the employment contract. Most contracts require an amendment to change the start date, he said.
Mr. Claussen said some employers have agreed to a new start date in an amended contract, giving the new physicians a solid date to work with. Not having work can be a real problem for graduating residents, who typically have to start paying off loans.
Now physicians won’t become a new partner
Mr. Claussen said physicians who are up for becoming partner are now being told that the deal is off. With less money coming in, existing partners are not willing to share it with a new partner, and there is no work for a new partner.
“The promise to make them partner is usually a verbal promise, so it is much less likely to be a breach of contract,” he said. “It is frustrating for physicians who were expecting to become partner.”
What can physicians do?
When employers present changes to them, physicians often feel their hands are tied, Ms. Adler said. In these dangerous times, they are expected to make sacrifices to keep the organization from going out of business.
Even if they wanted to file suits against their employer, “they can’t go to court right now because the courts are closed,” Ms. Adler said. “Employers are banking on doctors not doing anything.”
In most cases, however, doctors don’t have to act right away, she said. “Just because you have not reacted to the new situation does not mean you accepted it,” she said. “You can wait months, even years to file a lawsuit, depending on the state and the cause of action.”
Ms. Adler recommended that doctors make it clear that they don’t agree with the changes. An attorney experienced in physician contracts can review the changes being made and the amended contracts being offered.
Thanks to recent federal changes, employers have to have some ways to continue paying physicians, Ms. Adler said. Medical practices with fewer than 500 employees can get loans from the federal government that would not have to be repaid if they met certain stipulations, such as hiring back all the employees they terminate, she said.
Mr. Claussen said physicians should resist the obvious dangers, such as a shift to a pure production salary, denying bonus payments for work already done, and forcing physicians you use up PTO days.
He also suggested persuading employers to postpone rather than eliminate payments. “Some employers have agreed to postpone payments until a date later in 2020 rather than eliminate them,” he said. “The aim is that the organization will be back on its feet at that time.”
Mr. Claussen said he is trying to limit the contract amendments to 1 or 2 months. Because the situation caused by the pandemic is so fluid, “this allows for flexibility,” he said. “We can revisit the situation and come up with different changes.”
Ms. Adler doubts employers would accept short-term changes with a definite end date because such changes would not be in the employer’s interest. But Mr. Claussen said one employer has agreed to reevaluate its contracts in June.
Both lawyers agreed that many employers are trying to work with their physicians. “In 90% of the cases I have seen, both sides cooperate,” Ms. Adler said. “Because of the situation, people are being much more conciliatory than they would have been.”
A version of this article originally appeared on Medscape.com.
Employed physicians have had to take large pay cuts, give up bonuses, go on leave, or have even been terminated. In many cases, these actions violate their contract. How can they fight them?
Michael D., MD, a colorectal surgeon employed in a large surgical practice in Georgia, is still trying to make sense of a late-night directive from the practice, received in late March.
The practice had just started seeing a steep decline in appointments because of the COVID-19 pandemic. In a hastily arranged group phone call at 11:00 p.m., the CEO told the group what would have to be done.
They would be taking a 50% reduction in salaries, their bonuses for work already done were being withheld, and they would have to use their paid time off (PTO) in order to get their full March salary.
“It’s been over 2 weeks now, and still we’ve seen nothing formalized in writing,” said Dr. D., who asked that his name not be used because he was told that, under no circumstances, should anyone talk to the media.
“They have not told us anything more since then,” he said. “There’s just been a lot of hearsay and speculation.”
Dr. D. has been in touch with employed physicians at other practices, and their experiences run the gamut. One doctor at a large multispecialty group said his salary hadn’t been reduced at all, but a cardiologist was just told he will be laid off in 60 days.
Asking for big sacrifices
As the pandemic has intensified, employed physicians have started to see massive changes in their payment arrangements. They have had to take large pay cuts, give up bonuses, go on leave, and have even been terminated.
“In my 11 years of work on physician contracts, I have never seen changes as drastic as these,” said Kyle Claussen, a physician contract attorney and CEO of Resolve, a company that advises physicians on their careers. The company is based in Columbia, Mo.
He has heard from more than 100 doctors about these proposed changes in their contracts and related matters. Even graduating residents, he said, are being told that the start dates for their new jobs will be delayed.
In many cases, these actions violate the employed physicians’ contracts, said Ericka Adler, a physician contract attorney at Roetzel & Andress in Chicago.
“Some employers are acting out of desperation and are not making legally sound decisions,” Ms. Adler said. “It’s especially upsetting when they do not try to even talk to or work with the doctor first.”
Employers making unfounded unilateral changes
Ms. Adler said some employers are simply issuing a letter to all doctors. “It goes something like, ‘Just to let you know, we are cutting compensation effective immediately,’ and this may apply across the board to all doctors,” she said.
“But the problem with letters is that this is a contractual matter,” she said. “The employer needs to renegotiate each doctor’s contract.”
Employers might insist that the unilateral changes are based on terms in the contract, but this is usually unfounded, both lawyers said. A “force majeure” clause in contracts would allow the employer to set aside terms under certain specified emergencies, and the pandemic might be one of them. But Mr. Claussen said force majeure clauses are rare in physician contracts, and Ms. Adler said she has never seen one.
Lacking a force majeure clause, employers may try to turn to a common law doctrine that allows employers to set aside a contract when it is impossible to perform its terms, owing, for example, to “an unexpected intervening event.” But this tactic is also questionable, says Ms. Adler, who also represents the employer’s side of the contract. “This is a very high standard and unlikely to be satisfied,” she said.
Employers are desperate to amend contracts
Lacking a cause to take unilateral action, many employers are desperately trying to amend their physician contracts – the subject of the plaintive emails that employed physicians started receiving in mid-March.
“Doctors are trying to decide how they will react to these documents,” Mr. Claussen said. “If they don’t sign, they run the risk of being terminated.” He is expecting termination letters for some of these doctors to start coming in 2-3 weeks.
In response to these amendments, “doctors want to reach out to their employers and see if something can be negotiated,” he said. “Some employers have been amenable, but others have so far not been.”
Ms. Adler said the amendments typically offer open-ended arrangements favoring the employer. “The document might call for a temporary pay cut until the employer thinks they can restore the old salary, but it is up to the employer to decide when that would be,” she said.
Also, when the employer owes the physician for services already performed, the amendments don’t promise to pay them the full amount owed, she said.
Ms. Adler advises doctors to ask for a provision that restoration of their original salary will occur at a definite point in time, such as 30 days after the organization is back at previous volume. And if the doctor is owed money, the doctor should ask for full payment – and to sweeten that offer, allow the employer to pay the doctor back over a period, she says.
Just in the past month, employers have been pushing for several specific changes in doctors’ employment status. Here are some changes that Mr. Claussen and Ms. Adler have been seeing.
Withholding quarterly bonuses
In March, just before quarterly bonus payments were due, employed physicians started getting notices that they would not get the bonus, Mr. Claussen said. This covered work already done, and it amounted to a lot of money because practices were busy then.
“Not paying bonuses is a very big deal because they can make up to 50% of a physician’s total compensation,” Mr. Claussen said. He added that unilaterally withholding those funds, without a change in the contract, is legally questionable.
In addition to these changes on past bonuses, he said employers are now trying to temporarily end bonuses going forward through the contract amendments. “It’s not a good idea to sign this,” he said.
Doctors paid on pure production are left in the lurch
As volume falls, some hospitals and practices are shutting down doctors’ offices for all but emergencies, leaving their employed doctors with practically nothing to do. Doctors paid purely on their productivity are devastated by this change because their income virtually goes to zero, Mr. Claussen said.
He said office shutdowns are particularly common for specialists because hospitals have been stopping elective procedures during the pandemic, but they can also happen in primary care, which has seen steep declines in patient volume, too.
Having doctors on pure production means that employers can keep doctors hired without having to pay them, Mr. Claussen said. He has seen some employers try to shift more doctors into pure production through the amended contracts.
But Ms. Adler said having doctors on pure production is actually disadvantageous for employers in the current climate. The employer may end up being owed money because of advance payments they have already made to these doctors, she said.
In any case, both lawyers agreed that doctors on a pure production model are in an untenable situation right now. Ms. Adler said they are not earning money but are still technically at work, so they cannot collect unemployment compensation, which would give them some income.
Forcing doctors to use paid time off
To provide some pay for doctors who have no volume, many employers are forcing these doctors to use up their PTO days, which typically amount to about 4 weeks, Mr. Claussen said. “These doctors have no choice in the matter,” he said.
Furthermore, while on PTO, they are being required to take call. Employers are still obligated to cover call, and there may not be enough doctors still working to fill the call schedule. But making doctors do this work on their time off may be a violation of the contract, Mr. Claussen said.
Terminating physicians
Doctors who have little to do are often put on furlough. This means they don’t get paid but they keep their benefits, Ms. Adler said. The next step, she said, is to lay them off, with the stated intention of rehiring them.
Once laid off, she said, they can get unemployment payments. “Unemployment payments may not be anywhere near what they were earning before, but they are better than not earning anything,” Ms. Adler said.
In some cases, employers are just terminating them and are offering no prospect of rehiring them, she said. Ms. Adler said terminations can be a big problem for doctors. Physicians might have to repay a signing bonus or they might lose their malpractice coverage, forcing them to buy a tail. They could also be subject to a noncompete clause, which would not allow them to practice in the area, she said.
Terminating without cause typically requires 60-90 days’ notice, which both sides might use to negotiate some changes in the contract. But Ms. Adler said some employers are firing doctors with cause, and are using legally questionable reasons to do so.
“In most cases, these employers are grasping at straws,” she said. As a result, she expects many fired doctors will file wrongful termination lawsuits. She thinks employers are better advised to negotiate with the physicians.
Delaying start dates for new physicians
Typically, graduating residents and fellows signed with their new employers months ago and are ready to start working on July 1. But some employers are pushing back the start date for several months, Mr. Claussen said.
Mr. Claussen has been helping several clients in this situation. He said these delays are often a clear violation of the employment contract. Most contracts require an amendment to change the start date, he said.
Mr. Claussen said some employers have agreed to a new start date in an amended contract, giving the new physicians a solid date to work with. Not having work can be a real problem for graduating residents, who typically have to start paying off loans.
Now physicians won’t become a new partner
Mr. Claussen said physicians who are up for becoming partner are now being told that the deal is off. With less money coming in, existing partners are not willing to share it with a new partner, and there is no work for a new partner.
“The promise to make them partner is usually a verbal promise, so it is much less likely to be a breach of contract,” he said. “It is frustrating for physicians who were expecting to become partner.”
What can physicians do?
When employers present changes to them, physicians often feel their hands are tied, Ms. Adler said. In these dangerous times, they are expected to make sacrifices to keep the organization from going out of business.
Even if they wanted to file suits against their employer, “they can’t go to court right now because the courts are closed,” Ms. Adler said. “Employers are banking on doctors not doing anything.”
In most cases, however, doctors don’t have to act right away, she said. “Just because you have not reacted to the new situation does not mean you accepted it,” she said. “You can wait months, even years to file a lawsuit, depending on the state and the cause of action.”
Ms. Adler recommended that doctors make it clear that they don’t agree with the changes. An attorney experienced in physician contracts can review the changes being made and the amended contracts being offered.
Thanks to recent federal changes, employers have to have some ways to continue paying physicians, Ms. Adler said. Medical practices with fewer than 500 employees can get loans from the federal government that would not have to be repaid if they met certain stipulations, such as hiring back all the employees they terminate, she said.
Mr. Claussen said physicians should resist the obvious dangers, such as a shift to a pure production salary, denying bonus payments for work already done, and forcing physicians you use up PTO days.
He also suggested persuading employers to postpone rather than eliminate payments. “Some employers have agreed to postpone payments until a date later in 2020 rather than eliminate them,” he said. “The aim is that the organization will be back on its feet at that time.”
Mr. Claussen said he is trying to limit the contract amendments to 1 or 2 months. Because the situation caused by the pandemic is so fluid, “this allows for flexibility,” he said. “We can revisit the situation and come up with different changes.”
Ms. Adler doubts employers would accept short-term changes with a definite end date because such changes would not be in the employer’s interest. But Mr. Claussen said one employer has agreed to reevaluate its contracts in June.
Both lawyers agreed that many employers are trying to work with their physicians. “In 90% of the cases I have seen, both sides cooperate,” Ms. Adler said. “Because of the situation, people are being much more conciliatory than they would have been.”
A version of this article originally appeared on Medscape.com.
Employed physicians have had to take large pay cuts, give up bonuses, go on leave, or have even been terminated. In many cases, these actions violate their contract. How can they fight them?
Michael D., MD, a colorectal surgeon employed in a large surgical practice in Georgia, is still trying to make sense of a late-night directive from the practice, received in late March.
The practice had just started seeing a steep decline in appointments because of the COVID-19 pandemic. In a hastily arranged group phone call at 11:00 p.m., the CEO told the group what would have to be done.
They would be taking a 50% reduction in salaries, their bonuses for work already done were being withheld, and they would have to use their paid time off (PTO) in order to get their full March salary.
“It’s been over 2 weeks now, and still we’ve seen nothing formalized in writing,” said Dr. D., who asked that his name not be used because he was told that, under no circumstances, should anyone talk to the media.
“They have not told us anything more since then,” he said. “There’s just been a lot of hearsay and speculation.”
Dr. D. has been in touch with employed physicians at other practices, and their experiences run the gamut. One doctor at a large multispecialty group said his salary hadn’t been reduced at all, but a cardiologist was just told he will be laid off in 60 days.
Asking for big sacrifices
As the pandemic has intensified, employed physicians have started to see massive changes in their payment arrangements. They have had to take large pay cuts, give up bonuses, go on leave, and have even been terminated.
“In my 11 years of work on physician contracts, I have never seen changes as drastic as these,” said Kyle Claussen, a physician contract attorney and CEO of Resolve, a company that advises physicians on their careers. The company is based in Columbia, Mo.
He has heard from more than 100 doctors about these proposed changes in their contracts and related matters. Even graduating residents, he said, are being told that the start dates for their new jobs will be delayed.
In many cases, these actions violate the employed physicians’ contracts, said Ericka Adler, a physician contract attorney at Roetzel & Andress in Chicago.
“Some employers are acting out of desperation and are not making legally sound decisions,” Ms. Adler said. “It’s especially upsetting when they do not try to even talk to or work with the doctor first.”
Employers making unfounded unilateral changes
Ms. Adler said some employers are simply issuing a letter to all doctors. “It goes something like, ‘Just to let you know, we are cutting compensation effective immediately,’ and this may apply across the board to all doctors,” she said.
“But the problem with letters is that this is a contractual matter,” she said. “The employer needs to renegotiate each doctor’s contract.”
Employers might insist that the unilateral changes are based on terms in the contract, but this is usually unfounded, both lawyers said. A “force majeure” clause in contracts would allow the employer to set aside terms under certain specified emergencies, and the pandemic might be one of them. But Mr. Claussen said force majeure clauses are rare in physician contracts, and Ms. Adler said she has never seen one.
Lacking a force majeure clause, employers may try to turn to a common law doctrine that allows employers to set aside a contract when it is impossible to perform its terms, owing, for example, to “an unexpected intervening event.” But this tactic is also questionable, says Ms. Adler, who also represents the employer’s side of the contract. “This is a very high standard and unlikely to be satisfied,” she said.
Employers are desperate to amend contracts
Lacking a cause to take unilateral action, many employers are desperately trying to amend their physician contracts – the subject of the plaintive emails that employed physicians started receiving in mid-March.
“Doctors are trying to decide how they will react to these documents,” Mr. Claussen said. “If they don’t sign, they run the risk of being terminated.” He is expecting termination letters for some of these doctors to start coming in 2-3 weeks.
In response to these amendments, “doctors want to reach out to their employers and see if something can be negotiated,” he said. “Some employers have been amenable, but others have so far not been.”
Ms. Adler said the amendments typically offer open-ended arrangements favoring the employer. “The document might call for a temporary pay cut until the employer thinks they can restore the old salary, but it is up to the employer to decide when that would be,” she said.
Also, when the employer owes the physician for services already performed, the amendments don’t promise to pay them the full amount owed, she said.
Ms. Adler advises doctors to ask for a provision that restoration of their original salary will occur at a definite point in time, such as 30 days after the organization is back at previous volume. And if the doctor is owed money, the doctor should ask for full payment – and to sweeten that offer, allow the employer to pay the doctor back over a period, she says.
Just in the past month, employers have been pushing for several specific changes in doctors’ employment status. Here are some changes that Mr. Claussen and Ms. Adler have been seeing.
Withholding quarterly bonuses
In March, just before quarterly bonus payments were due, employed physicians started getting notices that they would not get the bonus, Mr. Claussen said. This covered work already done, and it amounted to a lot of money because practices were busy then.
“Not paying bonuses is a very big deal because they can make up to 50% of a physician’s total compensation,” Mr. Claussen said. He added that unilaterally withholding those funds, without a change in the contract, is legally questionable.
In addition to these changes on past bonuses, he said employers are now trying to temporarily end bonuses going forward through the contract amendments. “It’s not a good idea to sign this,” he said.
Doctors paid on pure production are left in the lurch
As volume falls, some hospitals and practices are shutting down doctors’ offices for all but emergencies, leaving their employed doctors with practically nothing to do. Doctors paid purely on their productivity are devastated by this change because their income virtually goes to zero, Mr. Claussen said.
He said office shutdowns are particularly common for specialists because hospitals have been stopping elective procedures during the pandemic, but they can also happen in primary care, which has seen steep declines in patient volume, too.
Having doctors on pure production means that employers can keep doctors hired without having to pay them, Mr. Claussen said. He has seen some employers try to shift more doctors into pure production through the amended contracts.
But Ms. Adler said having doctors on pure production is actually disadvantageous for employers in the current climate. The employer may end up being owed money because of advance payments they have already made to these doctors, she said.
In any case, both lawyers agreed that doctors on a pure production model are in an untenable situation right now. Ms. Adler said they are not earning money but are still technically at work, so they cannot collect unemployment compensation, which would give them some income.
Forcing doctors to use paid time off
To provide some pay for doctors who have no volume, many employers are forcing these doctors to use up their PTO days, which typically amount to about 4 weeks, Mr. Claussen said. “These doctors have no choice in the matter,” he said.
Furthermore, while on PTO, they are being required to take call. Employers are still obligated to cover call, and there may not be enough doctors still working to fill the call schedule. But making doctors do this work on their time off may be a violation of the contract, Mr. Claussen said.
Terminating physicians
Doctors who have little to do are often put on furlough. This means they don’t get paid but they keep their benefits, Ms. Adler said. The next step, she said, is to lay them off, with the stated intention of rehiring them.
Once laid off, she said, they can get unemployment payments. “Unemployment payments may not be anywhere near what they were earning before, but they are better than not earning anything,” Ms. Adler said.
In some cases, employers are just terminating them and are offering no prospect of rehiring them, she said. Ms. Adler said terminations can be a big problem for doctors. Physicians might have to repay a signing bonus or they might lose their malpractice coverage, forcing them to buy a tail. They could also be subject to a noncompete clause, which would not allow them to practice in the area, she said.
Terminating without cause typically requires 60-90 days’ notice, which both sides might use to negotiate some changes in the contract. But Ms. Adler said some employers are firing doctors with cause, and are using legally questionable reasons to do so.
“In most cases, these employers are grasping at straws,” she said. As a result, she expects many fired doctors will file wrongful termination lawsuits. She thinks employers are better advised to negotiate with the physicians.
Delaying start dates for new physicians
Typically, graduating residents and fellows signed with their new employers months ago and are ready to start working on July 1. But some employers are pushing back the start date for several months, Mr. Claussen said.
Mr. Claussen has been helping several clients in this situation. He said these delays are often a clear violation of the employment contract. Most contracts require an amendment to change the start date, he said.
Mr. Claussen said some employers have agreed to a new start date in an amended contract, giving the new physicians a solid date to work with. Not having work can be a real problem for graduating residents, who typically have to start paying off loans.
Now physicians won’t become a new partner
Mr. Claussen said physicians who are up for becoming partner are now being told that the deal is off. With less money coming in, existing partners are not willing to share it with a new partner, and there is no work for a new partner.
“The promise to make them partner is usually a verbal promise, so it is much less likely to be a breach of contract,” he said. “It is frustrating for physicians who were expecting to become partner.”
What can physicians do?
When employers present changes to them, physicians often feel their hands are tied, Ms. Adler said. In these dangerous times, they are expected to make sacrifices to keep the organization from going out of business.
Even if they wanted to file suits against their employer, “they can’t go to court right now because the courts are closed,” Ms. Adler said. “Employers are banking on doctors not doing anything.”
In most cases, however, doctors don’t have to act right away, she said. “Just because you have not reacted to the new situation does not mean you accepted it,” she said. “You can wait months, even years to file a lawsuit, depending on the state and the cause of action.”
Ms. Adler recommended that doctors make it clear that they don’t agree with the changes. An attorney experienced in physician contracts can review the changes being made and the amended contracts being offered.
Thanks to recent federal changes, employers have to have some ways to continue paying physicians, Ms. Adler said. Medical practices with fewer than 500 employees can get loans from the federal government that would not have to be repaid if they met certain stipulations, such as hiring back all the employees they terminate, she said.
Mr. Claussen said physicians should resist the obvious dangers, such as a shift to a pure production salary, denying bonus payments for work already done, and forcing physicians you use up PTO days.
He also suggested persuading employers to postpone rather than eliminate payments. “Some employers have agreed to postpone payments until a date later in 2020 rather than eliminate them,” he said. “The aim is that the organization will be back on its feet at that time.”
Mr. Claussen said he is trying to limit the contract amendments to 1 or 2 months. Because the situation caused by the pandemic is so fluid, “this allows for flexibility,” he said. “We can revisit the situation and come up with different changes.”
Ms. Adler doubts employers would accept short-term changes with a definite end date because such changes would not be in the employer’s interest. But Mr. Claussen said one employer has agreed to reevaluate its contracts in June.
Both lawyers agreed that many employers are trying to work with their physicians. “In 90% of the cases I have seen, both sides cooperate,” Ms. Adler said. “Because of the situation, people are being much more conciliatory than they would have been.”
A version of this article originally appeared on Medscape.com.
Sleep quality may affect COPD risk in African American smokers
African American smokers who logged more total sleep time and greater sleep efficacy performed better on a functional walk test than did those with poorer sleep, based on data from 209 adults.

African American smokers tend to develop COPD sooner and also report more sleep problems, compared with white smokers, wrote Andrew J. Gangemi, MD, of Temple University Hospital, Philadelphia, and colleagues.
In addition, African Americans tend to develop COPD at a younger age and with lower levels of smoking than do non-Hispanic whites, they said. “Sleep health may be a contributing factor to the lung and cardiovascular health disparity experienced by AA smokers,” in part because data suggest that insufficient sleep may be associated with increased risk of COPD exacerbation in smokers in general, they said.
In a study published in Chest, the researchers reviewed data from 209 African American adults aged 40-65 years who had smoked at least one cigarette in the past month. The average age of the participants was 55 years, 59% were women, and the average smoking habit was nine cigarettes per day.
The researchers measured functional exercise capacity of the participants using the 6-minute walk test (6MWT). Total sleep time (TST) and sleep efficacy (SE) were measured by way of a finger-based device.
Smokers of at least 10 cigarettes per day gained an additional 0.05-0.58 meters in distance covered on the 6MWT for every added minute of total sleep time in a multivariable regression analysis. Similarly, smokers of at least 10 cigarettes per day gained an additional 0.84-6.17–meter increase in distance covered on the 6MWT for every added percentage of sleep efficacy.
The reasons for the impact of SE and TST on functional exercise capacity in smokers remain unclear, the researchers said. “Heavier smokers have higher levels of autonomic imbalance, including higher resting heart rate and heart rate variability, impaired 24-hour cardiovascular sympathetic tone, and blunted cerebrovascular autonomic regulation and baroreflex response to hypercapnia,” they said.
Also unclear is the reason for the large magnitude of the association between SE and smoking vs. the lesser association between TST and smoking on 6MWT results, the researchers wrote. “Poor sleep efficiency, outside of traditional OSA scoring, is predictive of myocardial infarction, stroke, and cardiovascular-related mortality risk. Moreover, deficits in sleep efficiency have been consistently demonstrated in smokers versus nonsmokers,” they said.
The study findings were limited by several factors including inability to extrapolate data to other demographic groups and the cross-sectional design, the researchers noted. In addition, they did not address how TST and SE may relate to lung function.
However, the results “extend current knowledge about the potential role of improved sleep health to functional exercise capacity in AA smokers,” and set the stage for future studies of how changes in sleep health may affect lung and functional exercise capacity in smokers over time, as well as effects on inflammation and autonomic imbalance, the researchers concluded.
The study was supported by the National Institute on Minority Health and Health Disparities and by the National Institute of General Medical Sciences, both part of the National Institutes Health. The researchers had no financial conflicts to disclose.
SOURCE: Gangemi A et al. Chest 2020 Apr 23. doi: 10.1016/j.chest.2020.03.070.
African American smokers who logged more total sleep time and greater sleep efficacy performed better on a functional walk test than did those with poorer sleep, based on data from 209 adults.
African American smokers tend to develop COPD sooner and also report more sleep problems, compared with white smokers, wrote Andrew J. Gangemi, MD, of Temple University Hospital, Philadelphia, and colleagues.
In addition, African Americans tend to develop COPD at a younger age and with lower levels of smoking than do non-Hispanic whites, they said. “Sleep health may be a contributing factor to the lung and cardiovascular health disparity experienced by AA smokers,” in part because data suggest that insufficient sleep may be associated with increased risk of COPD exacerbation in smokers in general, they said.
In a study published in Chest, the researchers reviewed data from 209 African American adults aged 40-65 years who had smoked at least one cigarette in the past month. The average age of the participants was 55 years, 59% were women, and the average smoking habit was nine cigarettes per day.
The researchers measured functional exercise capacity of the participants using the 6-minute walk test (6MWT). Total sleep time (TST) and sleep efficacy (SE) were measured by way of a finger-based device.
Smokers of at least 10 cigarettes per day gained an additional 0.05-0.58 meters in distance covered on the 6MWT for every added minute of total sleep time in a multivariable regression analysis. Similarly, smokers of at least 10 cigarettes per day gained an additional 0.84-6.17–meter increase in distance covered on the 6MWT for every added percentage of sleep efficacy.
The reasons for the impact of SE and TST on functional exercise capacity in smokers remain unclear, the researchers said. “Heavier smokers have higher levels of autonomic imbalance, including higher resting heart rate and heart rate variability, impaired 24-hour cardiovascular sympathetic tone, and blunted cerebrovascular autonomic regulation and baroreflex response to hypercapnia,” they said.
Also unclear is the reason for the large magnitude of the association between SE and smoking vs. the lesser association between TST and smoking on 6MWT results, the researchers wrote. “Poor sleep efficiency, outside of traditional OSA scoring, is predictive of myocardial infarction, stroke, and cardiovascular-related mortality risk. Moreover, deficits in sleep efficiency have been consistently demonstrated in smokers versus nonsmokers,” they said.
The study findings were limited by several factors including inability to extrapolate data to other demographic groups and the cross-sectional design, the researchers noted. In addition, they did not address how TST and SE may relate to lung function.
However, the results “extend current knowledge about the potential role of improved sleep health to functional exercise capacity in AA smokers,” and set the stage for future studies of how changes in sleep health may affect lung and functional exercise capacity in smokers over time, as well as effects on inflammation and autonomic imbalance, the researchers concluded.
The study was supported by the National Institute on Minority Health and Health Disparities and by the National Institute of General Medical Sciences, both part of the National Institutes Health. The researchers had no financial conflicts to disclose.
SOURCE: Gangemi A et al. Chest 2020 Apr 23. doi: 10.1016/j.chest.2020.03.070.
African American smokers who logged more total sleep time and greater sleep efficacy performed better on a functional walk test than did those with poorer sleep, based on data from 209 adults.
African American smokers tend to develop COPD sooner and also report more sleep problems, compared with white smokers, wrote Andrew J. Gangemi, MD, of Temple University Hospital, Philadelphia, and colleagues.
In addition, African Americans tend to develop COPD at a younger age and with lower levels of smoking than do non-Hispanic whites, they said. “Sleep health may be a contributing factor to the lung and cardiovascular health disparity experienced by AA smokers,” in part because data suggest that insufficient sleep may be associated with increased risk of COPD exacerbation in smokers in general, they said.
In a study published in Chest, the researchers reviewed data from 209 African American adults aged 40-65 years who had smoked at least one cigarette in the past month. The average age of the participants was 55 years, 59% were women, and the average smoking habit was nine cigarettes per day.
The researchers measured functional exercise capacity of the participants using the 6-minute walk test (6MWT). Total sleep time (TST) and sleep efficacy (SE) were measured by way of a finger-based device.
Smokers of at least 10 cigarettes per day gained an additional 0.05-0.58 meters in distance covered on the 6MWT for every added minute of total sleep time in a multivariable regression analysis. Similarly, smokers of at least 10 cigarettes per day gained an additional 0.84-6.17–meter increase in distance covered on the 6MWT for every added percentage of sleep efficacy.
The reasons for the impact of SE and TST on functional exercise capacity in smokers remain unclear, the researchers said. “Heavier smokers have higher levels of autonomic imbalance, including higher resting heart rate and heart rate variability, impaired 24-hour cardiovascular sympathetic tone, and blunted cerebrovascular autonomic regulation and baroreflex response to hypercapnia,” they said.
Also unclear is the reason for the large magnitude of the association between SE and smoking vs. the lesser association between TST and smoking on 6MWT results, the researchers wrote. “Poor sleep efficiency, outside of traditional OSA scoring, is predictive of myocardial infarction, stroke, and cardiovascular-related mortality risk. Moreover, deficits in sleep efficiency have been consistently demonstrated in smokers versus nonsmokers,” they said.
The study findings were limited by several factors including inability to extrapolate data to other demographic groups and the cross-sectional design, the researchers noted. In addition, they did not address how TST and SE may relate to lung function.
However, the results “extend current knowledge about the potential role of improved sleep health to functional exercise capacity in AA smokers,” and set the stage for future studies of how changes in sleep health may affect lung and functional exercise capacity in smokers over time, as well as effects on inflammation and autonomic imbalance, the researchers concluded.
The study was supported by the National Institute on Minority Health and Health Disparities and by the National Institute of General Medical Sciences, both part of the National Institutes Health. The researchers had no financial conflicts to disclose.
SOURCE: Gangemi A et al. Chest 2020 Apr 23. doi: 10.1016/j.chest.2020.03.070.
FROM CHEST
Hospitals update hydroxychloroquine protocols after FDA warning
Across the country, hospitals are incorporating Friday’s warning from the US Food and Drug Administration (FDA) about the risks of prescribing hydroxychloroquine and chloroquine for COVID-19 into their treatment protocols.
For some hospitals, the message affirmed the cautious approach they were already taking with hydroxychloroquine. “From a New York state or Northwell perspective, there is no major change,” said Onisis Stefas, PharmD, vice president of pharmacy at Northwell Health in New York. “We were not prescribing it out in the community very early on because of the concerns associated with the heart arrhythmias.”
Brigham and Women’s Hospital in Boston, Massachusetts, is currently in the process of updating its publicly available COVID-19 protocols website “to incorporate the FDA’s updated safety assessment and ongoing clinical trials,” a hospital spokesperson told Medscape Medical News. Prior to the updates, the treatment protocols indicated that hydroxychloroquine should only be considered after weighing the risks and benefits for patients who are not candidates for other clinical trials and meet a specific set of health criteria.
The warning is a timely and important synthesis of what physicians know about the drugs so far and how cautiously clinicians across the country should be using them, said Rajesh T. Gandhi, MD, infectious diseases physician at Massachusetts General Hospital (MGH), Boston, professor of medicine at Harvard Medical School, member of the Infectious Diseases Society of America (IDSA), and chair-elect of the HIV Medicine Association.
“I think to be honest it’s a really important message to the public and clinicians across the country,” said Gandhi. “Because we all know there is just a ton of discussion around this drug ... and it came out fairly and said what we know right now.”
The two antimalarial drugs have been at the center of much political debate and scientific scrutiny in recent weeks, following President Trump’s endorsement and the FDA’s emergency use authorization for the two medications in March. Hospitals across the country had incorporated hydroxychloroquine and chloroquine into their constantly evolving treatment protocols for patients with COVID-19.
But the evidence that these drugs actually help treat COVID-19 remains scant. Some small studies suggest the therapies help patients with COVID-19, while others conclude the drugs have no effect or even harm patients. In the United States, medical societies including the American Heart Association have also warned about the serious cardiac issues that can accompany these drugs for some patients.
In the new warning, the FDA said it “cautions against use of hydroxychloroquine or chloroquine for COVID-19 patients outside of the hospital setting or a clinical trial” and urged “close supervision” of patients treated with these therapies, citing cardiac side effects.
The FDA also said it is aware that the outpatient prescription of these medications has increased since its March authorization, but the drugs still have not been shown to be safe or effective in treating or preventing COVID-19.
The FDA announcement is consistent with protocols established by the National Institutes of Health and IDSA earlier this month that recommend against using hydroxychloroquine or chloroquine, except when these drugs are administered as part of a clinical trial.
“We agree wholeheartedly with the FDA and have been hoping that the FDA would in fact issue that kind of clarification,” said Samuel Brown, MD, study committee cochair of the ORCHID clinical trial, a multicenter, blinded study investigating the safety and efficacy of hydroxychloroquine. These medications need to be tested in clinical trials that are able to focus closely on safety monitoring, he said. Experts at Vanderbilt University, one of the medical centers participating in the ORCHID clinical trial, decided before Tennessee had any cases of COVID-19 that unproven therapies like hydroxychloroquine would only be available through clinical trials, said Wesley Self, MD, associate professor of emergency medicine at Vanderbilt University, Nashville, Tennessee, and chair of the ORCHID study committee.
Northwell Health, like other hospitals in New York, has been following a March executive order issued by Governor Andrew Cuomo limiting the use of these drugs for COVID-19 outside of clinical trials, said Stefas. At Northwell Health, patients with COVID-19 only receive hydroxychloroquine or chloroquine when treated in hospital, where they can be closely monitored, or as part of a clinical trial. The hospital system’s protocols currently do not recommend pairing hydroxychloroquine with azithromycin, said Stefas. The new FDA announcement is “very similar” to New York’s existing executive order, he said. “Reading through this reinforces a lot of what we originally thought.”
At MGH in Boston, the FDA safety warning is in line with and “solidifies” the hospital’s evolving protocols, said Gandhi. Clinicians at MGH have been steadily moving away from prescribing hydroxychloroquine outside of clinical trials as the efficacy has remained murky, the serious side effects have become more evident, and clinical trials to assess the drug have gotten underway in recent weeks, he said. Given the conflicting evidence, Gandhi feels the use of these drugs needs to be focused in clinical trials, where scientists can truly evaluate how much they help or harm.
“We know fundamentally that’s the way to do this,” Gandhi said. “We also don’t know that it doesn’t work, so it is ethical and incumbent upon us to do a study,” Gandhi said.
Other hospitals are already heeding the FDA’s warning. At UW Medicine in Washington state, for example, hydroxychloroquine was considered a possible treatment for COVID-19 prior to the FDA’s recent announcement. “Based on FDA guidance, hydroxychloroquine is no longer recommended as therapy for COVID-19 unless done through a clinical trial,” said Tim Dellit, MD, chief medical officer for UW Medicine.
Michigan Medicine stopped using hydroxychloroquine and azithromycin (both separately and in combination) about a month ago, said Daniel Kaul, MD, a professor of infectious disease at the University of Michigan. “When we reviewed the data that was available in more detail, we realized that it was essentially uninterpretable,” he said. As of Monday, the only patients receiving this drug at Michigan Medicine are those enrolled in the ORCHID clinical trial.
But that does not seem to be the case everywhere. Most patients transferred to Michigan Medicine from other hospitals have received these drugs, indicating they are still being widely used, said Kaul. “I think this FDA guidance is appropriate and may reduce usage of this drug and make people more aware of the potential side effects both in inpatient and outpatient settings.”
Hopefully, the FDA guidance will help slow the use of these drugs outside the appropriate clinical trial setting, said Kaul. “I think that the kind of politicization of this drug, which is pretty much unprecedented in my experience, created a really harmful environment where calm decision making and assessment of the relative risks and benefits became somewhat impossible,” said Kaul.
This article first appeared on Medscape.com.
Across the country, hospitals are incorporating Friday’s warning from the US Food and Drug Administration (FDA) about the risks of prescribing hydroxychloroquine and chloroquine for COVID-19 into their treatment protocols.
For some hospitals, the message affirmed the cautious approach they were already taking with hydroxychloroquine. “From a New York state or Northwell perspective, there is no major change,” said Onisis Stefas, PharmD, vice president of pharmacy at Northwell Health in New York. “We were not prescribing it out in the community very early on because of the concerns associated with the heart arrhythmias.”
Brigham and Women’s Hospital in Boston, Massachusetts, is currently in the process of updating its publicly available COVID-19 protocols website “to incorporate the FDA’s updated safety assessment and ongoing clinical trials,” a hospital spokesperson told Medscape Medical News. Prior to the updates, the treatment protocols indicated that hydroxychloroquine should only be considered after weighing the risks and benefits for patients who are not candidates for other clinical trials and meet a specific set of health criteria.
The warning is a timely and important synthesis of what physicians know about the drugs so far and how cautiously clinicians across the country should be using them, said Rajesh T. Gandhi, MD, infectious diseases physician at Massachusetts General Hospital (MGH), Boston, professor of medicine at Harvard Medical School, member of the Infectious Diseases Society of America (IDSA), and chair-elect of the HIV Medicine Association.
“I think to be honest it’s a really important message to the public and clinicians across the country,” said Gandhi. “Because we all know there is just a ton of discussion around this drug ... and it came out fairly and said what we know right now.”
The two antimalarial drugs have been at the center of much political debate and scientific scrutiny in recent weeks, following President Trump’s endorsement and the FDA’s emergency use authorization for the two medications in March. Hospitals across the country had incorporated hydroxychloroquine and chloroquine into their constantly evolving treatment protocols for patients with COVID-19.
But the evidence that these drugs actually help treat COVID-19 remains scant. Some small studies suggest the therapies help patients with COVID-19, while others conclude the drugs have no effect or even harm patients. In the United States, medical societies including the American Heart Association have also warned about the serious cardiac issues that can accompany these drugs for some patients.
In the new warning, the FDA said it “cautions against use of hydroxychloroquine or chloroquine for COVID-19 patients outside of the hospital setting or a clinical trial” and urged “close supervision” of patients treated with these therapies, citing cardiac side effects.
The FDA also said it is aware that the outpatient prescription of these medications has increased since its March authorization, but the drugs still have not been shown to be safe or effective in treating or preventing COVID-19.
The FDA announcement is consistent with protocols established by the National Institutes of Health and IDSA earlier this month that recommend against using hydroxychloroquine or chloroquine, except when these drugs are administered as part of a clinical trial.
“We agree wholeheartedly with the FDA and have been hoping that the FDA would in fact issue that kind of clarification,” said Samuel Brown, MD, study committee cochair of the ORCHID clinical trial, a multicenter, blinded study investigating the safety and efficacy of hydroxychloroquine. These medications need to be tested in clinical trials that are able to focus closely on safety monitoring, he said. Experts at Vanderbilt University, one of the medical centers participating in the ORCHID clinical trial, decided before Tennessee had any cases of COVID-19 that unproven therapies like hydroxychloroquine would only be available through clinical trials, said Wesley Self, MD, associate professor of emergency medicine at Vanderbilt University, Nashville, Tennessee, and chair of the ORCHID study committee.
Northwell Health, like other hospitals in New York, has been following a March executive order issued by Governor Andrew Cuomo limiting the use of these drugs for COVID-19 outside of clinical trials, said Stefas. At Northwell Health, patients with COVID-19 only receive hydroxychloroquine or chloroquine when treated in hospital, where they can be closely monitored, or as part of a clinical trial. The hospital system’s protocols currently do not recommend pairing hydroxychloroquine with azithromycin, said Stefas. The new FDA announcement is “very similar” to New York’s existing executive order, he said. “Reading through this reinforces a lot of what we originally thought.”
At MGH in Boston, the FDA safety warning is in line with and “solidifies” the hospital’s evolving protocols, said Gandhi. Clinicians at MGH have been steadily moving away from prescribing hydroxychloroquine outside of clinical trials as the efficacy has remained murky, the serious side effects have become more evident, and clinical trials to assess the drug have gotten underway in recent weeks, he said. Given the conflicting evidence, Gandhi feels the use of these drugs needs to be focused in clinical trials, where scientists can truly evaluate how much they help or harm.
“We know fundamentally that’s the way to do this,” Gandhi said. “We also don’t know that it doesn’t work, so it is ethical and incumbent upon us to do a study,” Gandhi said.
Other hospitals are already heeding the FDA’s warning. At UW Medicine in Washington state, for example, hydroxychloroquine was considered a possible treatment for COVID-19 prior to the FDA’s recent announcement. “Based on FDA guidance, hydroxychloroquine is no longer recommended as therapy for COVID-19 unless done through a clinical trial,” said Tim Dellit, MD, chief medical officer for UW Medicine.
Michigan Medicine stopped using hydroxychloroquine and azithromycin (both separately and in combination) about a month ago, said Daniel Kaul, MD, a professor of infectious disease at the University of Michigan. “When we reviewed the data that was available in more detail, we realized that it was essentially uninterpretable,” he said. As of Monday, the only patients receiving this drug at Michigan Medicine are those enrolled in the ORCHID clinical trial.
But that does not seem to be the case everywhere. Most patients transferred to Michigan Medicine from other hospitals have received these drugs, indicating they are still being widely used, said Kaul. “I think this FDA guidance is appropriate and may reduce usage of this drug and make people more aware of the potential side effects both in inpatient and outpatient settings.”
Hopefully, the FDA guidance will help slow the use of these drugs outside the appropriate clinical trial setting, said Kaul. “I think that the kind of politicization of this drug, which is pretty much unprecedented in my experience, created a really harmful environment where calm decision making and assessment of the relative risks and benefits became somewhat impossible,” said Kaul.
This article first appeared on Medscape.com.
Across the country, hospitals are incorporating Friday’s warning from the US Food and Drug Administration (FDA) about the risks of prescribing hydroxychloroquine and chloroquine for COVID-19 into their treatment protocols.
For some hospitals, the message affirmed the cautious approach they were already taking with hydroxychloroquine. “From a New York state or Northwell perspective, there is no major change,” said Onisis Stefas, PharmD, vice president of pharmacy at Northwell Health in New York. “We were not prescribing it out in the community very early on because of the concerns associated with the heart arrhythmias.”
Brigham and Women’s Hospital in Boston, Massachusetts, is currently in the process of updating its publicly available COVID-19 protocols website “to incorporate the FDA’s updated safety assessment and ongoing clinical trials,” a hospital spokesperson told Medscape Medical News. Prior to the updates, the treatment protocols indicated that hydroxychloroquine should only be considered after weighing the risks and benefits for patients who are not candidates for other clinical trials and meet a specific set of health criteria.
The warning is a timely and important synthesis of what physicians know about the drugs so far and how cautiously clinicians across the country should be using them, said Rajesh T. Gandhi, MD, infectious diseases physician at Massachusetts General Hospital (MGH), Boston, professor of medicine at Harvard Medical School, member of the Infectious Diseases Society of America (IDSA), and chair-elect of the HIV Medicine Association.
“I think to be honest it’s a really important message to the public and clinicians across the country,” said Gandhi. “Because we all know there is just a ton of discussion around this drug ... and it came out fairly and said what we know right now.”
The two antimalarial drugs have been at the center of much political debate and scientific scrutiny in recent weeks, following President Trump’s endorsement and the FDA’s emergency use authorization for the two medications in March. Hospitals across the country had incorporated hydroxychloroquine and chloroquine into their constantly evolving treatment protocols for patients with COVID-19.
But the evidence that these drugs actually help treat COVID-19 remains scant. Some small studies suggest the therapies help patients with COVID-19, while others conclude the drugs have no effect or even harm patients. In the United States, medical societies including the American Heart Association have also warned about the serious cardiac issues that can accompany these drugs for some patients.
In the new warning, the FDA said it “cautions against use of hydroxychloroquine or chloroquine for COVID-19 patients outside of the hospital setting or a clinical trial” and urged “close supervision” of patients treated with these therapies, citing cardiac side effects.
The FDA also said it is aware that the outpatient prescription of these medications has increased since its March authorization, but the drugs still have not been shown to be safe or effective in treating or preventing COVID-19.
The FDA announcement is consistent with protocols established by the National Institutes of Health and IDSA earlier this month that recommend against using hydroxychloroquine or chloroquine, except when these drugs are administered as part of a clinical trial.
“We agree wholeheartedly with the FDA and have been hoping that the FDA would in fact issue that kind of clarification,” said Samuel Brown, MD, study committee cochair of the ORCHID clinical trial, a multicenter, blinded study investigating the safety and efficacy of hydroxychloroquine. These medications need to be tested in clinical trials that are able to focus closely on safety monitoring, he said. Experts at Vanderbilt University, one of the medical centers participating in the ORCHID clinical trial, decided before Tennessee had any cases of COVID-19 that unproven therapies like hydroxychloroquine would only be available through clinical trials, said Wesley Self, MD, associate professor of emergency medicine at Vanderbilt University, Nashville, Tennessee, and chair of the ORCHID study committee.
Northwell Health, like other hospitals in New York, has been following a March executive order issued by Governor Andrew Cuomo limiting the use of these drugs for COVID-19 outside of clinical trials, said Stefas. At Northwell Health, patients with COVID-19 only receive hydroxychloroquine or chloroquine when treated in hospital, where they can be closely monitored, or as part of a clinical trial. The hospital system’s protocols currently do not recommend pairing hydroxychloroquine with azithromycin, said Stefas. The new FDA announcement is “very similar” to New York’s existing executive order, he said. “Reading through this reinforces a lot of what we originally thought.”
At MGH in Boston, the FDA safety warning is in line with and “solidifies” the hospital’s evolving protocols, said Gandhi. Clinicians at MGH have been steadily moving away from prescribing hydroxychloroquine outside of clinical trials as the efficacy has remained murky, the serious side effects have become more evident, and clinical trials to assess the drug have gotten underway in recent weeks, he said. Given the conflicting evidence, Gandhi feels the use of these drugs needs to be focused in clinical trials, where scientists can truly evaluate how much they help or harm.
“We know fundamentally that’s the way to do this,” Gandhi said. “We also don’t know that it doesn’t work, so it is ethical and incumbent upon us to do a study,” Gandhi said.
Other hospitals are already heeding the FDA’s warning. At UW Medicine in Washington state, for example, hydroxychloroquine was considered a possible treatment for COVID-19 prior to the FDA’s recent announcement. “Based on FDA guidance, hydroxychloroquine is no longer recommended as therapy for COVID-19 unless done through a clinical trial,” said Tim Dellit, MD, chief medical officer for UW Medicine.
Michigan Medicine stopped using hydroxychloroquine and azithromycin (both separately and in combination) about a month ago, said Daniel Kaul, MD, a professor of infectious disease at the University of Michigan. “When we reviewed the data that was available in more detail, we realized that it was essentially uninterpretable,” he said. As of Monday, the only patients receiving this drug at Michigan Medicine are those enrolled in the ORCHID clinical trial.
But that does not seem to be the case everywhere. Most patients transferred to Michigan Medicine from other hospitals have received these drugs, indicating they are still being widely used, said Kaul. “I think this FDA guidance is appropriate and may reduce usage of this drug and make people more aware of the potential side effects both in inpatient and outpatient settings.”
Hopefully, the FDA guidance will help slow the use of these drugs outside the appropriate clinical trial setting, said Kaul. “I think that the kind of politicization of this drug, which is pretty much unprecedented in my experience, created a really harmful environment where calm decision making and assessment of the relative risks and benefits became somewhat impossible,” said Kaul.
This article first appeared on Medscape.com.