User login
-
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
In those with obesity, will losing weight cut COVID-19 severity?
As study after study piles up showing that those with obesity who become infected with SARS-CoV-2 are more likely to have severe disease, several experts gave advice for clinicians and patients during the virtual ObesityWeek Interactive 2020 meeting.
Pichamol Jirapinyo, MD, MPH, associate director of bariatric endoscopy at Brigham and Women’s Hospital, Boston, presented a study on those with obesity from New England hospitals which adds to the evidence that this is “a vulnerable population for COVID-19, like elderly or immunocompromised people,” Dr. Jirapinyo said in an interview.
These findings reinforce the need for clinicians to be “more aware of complications of obesity and refer earlier for treatment,” she added.
One audience member wanted to know if there are data showing whether people with a body mass index (BMI) above 35 kg/m2 who successfully lose weight subsequently have lower rates of hospitalization, ICU admission, and death if they become infected with SARS-CoV-2.
Dr. Jirapinyo said she is not aware of any such studies, but anecdotally, two of her patients who had endoscopic sleeve gastroplasty last fall (whose BMI dropped from about 38 to 30) and later became infected with COVID-19 had mild symptoms.
But David A. Kass, MD, director, Institute of CardioScience at Johns Hopkins University, Baltimore, cautioned that
“Whether this gets reversed by weight loss is an attractive hypothesis, but at this point, it’s still a hypothesis,” he stressed.
Changes to immunity, inflammatory signaling in obesity
“There must be north of 600 or more studies by now with this message that obesity – particularly severe obesity with a BMI of 35 and higher – is a strong independent risk factor for worse COVID-19 outcome,” Dr. Kass emphasized.
“[COVID-19] revealed to the public in a somewhat dramatic fashion that being very obese does put one at higher risk of this disease being more debilitating and even fatal,” he added.
“Before this pandemic, many viewed obesity as only a problem if you have the other associated diseases – hypertension, diabetes, heart disease, atherosclerosis, obstructive sleep apnea, etc.”
“What was not as appreciated is that marked obesity changes the body in various ways all by itself – altering metabolism, inflammatory signaling, immune surveillance, and responsiveness (including a less robust response to vaccines that has been written about as well).”
“This is a bit like having a genetic abnormality that makes you at higher risk for getting, say, cancer,” he explained.
“It is there, it is real, it has an impact – but it still does take other stresses to reveal the risk potential. COVID-19 did that with obesity,” he said.
Latest study on effect of obesity, diabetes on COVID-19 severity
The study presented by Dr. Jirapinyo and colleagues identified 1,680 patients with COVID-19 at six hospitals in March 2020. Patients were a mean age of 51 years, had a mean BMI of 29.4, and 39% had obesity. Patients who required hospitalization were more likely to have obesity (46% vs. 35%; P < .0001).
Obesity was a significant risk factor for hospitalization (odds ratio, 1.7), ICU admission (OR, 1.8), and intubation (OR, 1.8; all P < .001), after controlling for age, sex, cardiovascular, pulmonary, liver, and kidney disease, and cancer.
Compared with having a normal weight, having severe obesity was also associated with roughly threefold higher risks of ICU admission and intubation – after controlling for major comorbidities.
Pandemic focuses minds on obesity prevention, treatment
Naveed Sattar, MD, PhD, said in an interview that these latest findings are “highly consistent with other studies that point to excess adiposity as a potential modifiable risk factor for more severe COVID-19.”
It “also strongly suggests that if people are worried about their risk for COVID-19 and want to improve their chances of a milder outcome, then it is reasonable to encourage them to make sustainable lifestyle changes that may lessen weight and improve their fitness levels,” said Dr. Sattar, professor of metabolic medicine, University of Glasgow.
“But of course, the big worry,” he added, “is that many are putting on weight due to lockdowns, less commuting to work, anxiety, and overeating and drinking, etc., so that many are struggling, and especially those at highest risk, such as those living in more overcrowded housing, etc. By contrast, more advantaged folk may have an easier time to improve lifestyles.”
The pandemic highlights that “we need a concerted effort on obesity prevention and treatment,” according to Dr. Sattar.
“For years we have realized links between obesity and chronic cardiometabolic conditions,” he said, “but to think excess weight may also be detrimental to acute effects of a novel virus running amok in the world has focused minds on obesity in a manner not seen before.
“Whether these new painful learnings lead to a more determined effort in countries to improve the obesogenic environment or to place more resources into prevention and management of obesity remains to be seen,” he said.
Increased inquiries about bariatric surgery following COVID-19
Meanwhile, Matthew M. Hutter, MD, MPH, president, American Society for Metabolic and Bariatric Surgery, said in an interview that “COVID-19 and studies like this are now making many aware that obesity is not just a lifestyle choice or a cosmetic issue, but “a disease that needs to be taken seriously” and treated.
“Metabolic and bariatric surgery is a very safe and effective treatment for persons with obesity with a BMI >40 kg/m2 or BMI >35 kg/m2 and related diseases like diabetes, hypertension, sleep apnea, reflux, back pain, and many others,” added Dr. Hutter, who is also professor of surgery, Harvard Medical School, Boston.
“Recently, some metabolic and bariatric centers have seen an increase in patients considering surgery,” he said. “Some say that COVID-19 has made them realize they need to do something to be healthier.”
“Currently, less than 1% of those who could benefit from surgery are actually having” it each year, Dr. Hutter noted, “and I think there are many who should seriously consider surgery to be healthier, live longer, and live better.”
This article first appeared on Medscape.com.
As study after study piles up showing that those with obesity who become infected with SARS-CoV-2 are more likely to have severe disease, several experts gave advice for clinicians and patients during the virtual ObesityWeek Interactive 2020 meeting.
Pichamol Jirapinyo, MD, MPH, associate director of bariatric endoscopy at Brigham and Women’s Hospital, Boston, presented a study on those with obesity from New England hospitals which adds to the evidence that this is “a vulnerable population for COVID-19, like elderly or immunocompromised people,” Dr. Jirapinyo said in an interview.
These findings reinforce the need for clinicians to be “more aware of complications of obesity and refer earlier for treatment,” she added.
One audience member wanted to know if there are data showing whether people with a body mass index (BMI) above 35 kg/m2 who successfully lose weight subsequently have lower rates of hospitalization, ICU admission, and death if they become infected with SARS-CoV-2.
Dr. Jirapinyo said she is not aware of any such studies, but anecdotally, two of her patients who had endoscopic sleeve gastroplasty last fall (whose BMI dropped from about 38 to 30) and later became infected with COVID-19 had mild symptoms.
But David A. Kass, MD, director, Institute of CardioScience at Johns Hopkins University, Baltimore, cautioned that
“Whether this gets reversed by weight loss is an attractive hypothesis, but at this point, it’s still a hypothesis,” he stressed.
Changes to immunity, inflammatory signaling in obesity
“There must be north of 600 or more studies by now with this message that obesity – particularly severe obesity with a BMI of 35 and higher – is a strong independent risk factor for worse COVID-19 outcome,” Dr. Kass emphasized.
“[COVID-19] revealed to the public in a somewhat dramatic fashion that being very obese does put one at higher risk of this disease being more debilitating and even fatal,” he added.
“Before this pandemic, many viewed obesity as only a problem if you have the other associated diseases – hypertension, diabetes, heart disease, atherosclerosis, obstructive sleep apnea, etc.”
“What was not as appreciated is that marked obesity changes the body in various ways all by itself – altering metabolism, inflammatory signaling, immune surveillance, and responsiveness (including a less robust response to vaccines that has been written about as well).”
“This is a bit like having a genetic abnormality that makes you at higher risk for getting, say, cancer,” he explained.
“It is there, it is real, it has an impact – but it still does take other stresses to reveal the risk potential. COVID-19 did that with obesity,” he said.
Latest study on effect of obesity, diabetes on COVID-19 severity
The study presented by Dr. Jirapinyo and colleagues identified 1,680 patients with COVID-19 at six hospitals in March 2020. Patients were a mean age of 51 years, had a mean BMI of 29.4, and 39% had obesity. Patients who required hospitalization were more likely to have obesity (46% vs. 35%; P < .0001).
Obesity was a significant risk factor for hospitalization (odds ratio, 1.7), ICU admission (OR, 1.8), and intubation (OR, 1.8; all P < .001), after controlling for age, sex, cardiovascular, pulmonary, liver, and kidney disease, and cancer.
Compared with having a normal weight, having severe obesity was also associated with roughly threefold higher risks of ICU admission and intubation – after controlling for major comorbidities.
Pandemic focuses minds on obesity prevention, treatment
Naveed Sattar, MD, PhD, said in an interview that these latest findings are “highly consistent with other studies that point to excess adiposity as a potential modifiable risk factor for more severe COVID-19.”
It “also strongly suggests that if people are worried about their risk for COVID-19 and want to improve their chances of a milder outcome, then it is reasonable to encourage them to make sustainable lifestyle changes that may lessen weight and improve their fitness levels,” said Dr. Sattar, professor of metabolic medicine, University of Glasgow.
“But of course, the big worry,” he added, “is that many are putting on weight due to lockdowns, less commuting to work, anxiety, and overeating and drinking, etc., so that many are struggling, and especially those at highest risk, such as those living in more overcrowded housing, etc. By contrast, more advantaged folk may have an easier time to improve lifestyles.”
The pandemic highlights that “we need a concerted effort on obesity prevention and treatment,” according to Dr. Sattar.
“For years we have realized links between obesity and chronic cardiometabolic conditions,” he said, “but to think excess weight may also be detrimental to acute effects of a novel virus running amok in the world has focused minds on obesity in a manner not seen before.
“Whether these new painful learnings lead to a more determined effort in countries to improve the obesogenic environment or to place more resources into prevention and management of obesity remains to be seen,” he said.
Increased inquiries about bariatric surgery following COVID-19
Meanwhile, Matthew M. Hutter, MD, MPH, president, American Society for Metabolic and Bariatric Surgery, said in an interview that “COVID-19 and studies like this are now making many aware that obesity is not just a lifestyle choice or a cosmetic issue, but “a disease that needs to be taken seriously” and treated.
“Metabolic and bariatric surgery is a very safe and effective treatment for persons with obesity with a BMI >40 kg/m2 or BMI >35 kg/m2 and related diseases like diabetes, hypertension, sleep apnea, reflux, back pain, and many others,” added Dr. Hutter, who is also professor of surgery, Harvard Medical School, Boston.
“Recently, some metabolic and bariatric centers have seen an increase in patients considering surgery,” he said. “Some say that COVID-19 has made them realize they need to do something to be healthier.”
“Currently, less than 1% of those who could benefit from surgery are actually having” it each year, Dr. Hutter noted, “and I think there are many who should seriously consider surgery to be healthier, live longer, and live better.”
This article first appeared on Medscape.com.
As study after study piles up showing that those with obesity who become infected with SARS-CoV-2 are more likely to have severe disease, several experts gave advice for clinicians and patients during the virtual ObesityWeek Interactive 2020 meeting.
Pichamol Jirapinyo, MD, MPH, associate director of bariatric endoscopy at Brigham and Women’s Hospital, Boston, presented a study on those with obesity from New England hospitals which adds to the evidence that this is “a vulnerable population for COVID-19, like elderly or immunocompromised people,” Dr. Jirapinyo said in an interview.
These findings reinforce the need for clinicians to be “more aware of complications of obesity and refer earlier for treatment,” she added.
One audience member wanted to know if there are data showing whether people with a body mass index (BMI) above 35 kg/m2 who successfully lose weight subsequently have lower rates of hospitalization, ICU admission, and death if they become infected with SARS-CoV-2.
Dr. Jirapinyo said she is not aware of any such studies, but anecdotally, two of her patients who had endoscopic sleeve gastroplasty last fall (whose BMI dropped from about 38 to 30) and later became infected with COVID-19 had mild symptoms.
But David A. Kass, MD, director, Institute of CardioScience at Johns Hopkins University, Baltimore, cautioned that
“Whether this gets reversed by weight loss is an attractive hypothesis, but at this point, it’s still a hypothesis,” he stressed.
Changes to immunity, inflammatory signaling in obesity
“There must be north of 600 or more studies by now with this message that obesity – particularly severe obesity with a BMI of 35 and higher – is a strong independent risk factor for worse COVID-19 outcome,” Dr. Kass emphasized.
“[COVID-19] revealed to the public in a somewhat dramatic fashion that being very obese does put one at higher risk of this disease being more debilitating and even fatal,” he added.
“Before this pandemic, many viewed obesity as only a problem if you have the other associated diseases – hypertension, diabetes, heart disease, atherosclerosis, obstructive sleep apnea, etc.”
“What was not as appreciated is that marked obesity changes the body in various ways all by itself – altering metabolism, inflammatory signaling, immune surveillance, and responsiveness (including a less robust response to vaccines that has been written about as well).”
“This is a bit like having a genetic abnormality that makes you at higher risk for getting, say, cancer,” he explained.
“It is there, it is real, it has an impact – but it still does take other stresses to reveal the risk potential. COVID-19 did that with obesity,” he said.
Latest study on effect of obesity, diabetes on COVID-19 severity
The study presented by Dr. Jirapinyo and colleagues identified 1,680 patients with COVID-19 at six hospitals in March 2020. Patients were a mean age of 51 years, had a mean BMI of 29.4, and 39% had obesity. Patients who required hospitalization were more likely to have obesity (46% vs. 35%; P < .0001).
Obesity was a significant risk factor for hospitalization (odds ratio, 1.7), ICU admission (OR, 1.8), and intubation (OR, 1.8; all P < .001), after controlling for age, sex, cardiovascular, pulmonary, liver, and kidney disease, and cancer.
Compared with having a normal weight, having severe obesity was also associated with roughly threefold higher risks of ICU admission and intubation – after controlling for major comorbidities.
Pandemic focuses minds on obesity prevention, treatment
Naveed Sattar, MD, PhD, said in an interview that these latest findings are “highly consistent with other studies that point to excess adiposity as a potential modifiable risk factor for more severe COVID-19.”
It “also strongly suggests that if people are worried about their risk for COVID-19 and want to improve their chances of a milder outcome, then it is reasonable to encourage them to make sustainable lifestyle changes that may lessen weight and improve their fitness levels,” said Dr. Sattar, professor of metabolic medicine, University of Glasgow.
“But of course, the big worry,” he added, “is that many are putting on weight due to lockdowns, less commuting to work, anxiety, and overeating and drinking, etc., so that many are struggling, and especially those at highest risk, such as those living in more overcrowded housing, etc. By contrast, more advantaged folk may have an easier time to improve lifestyles.”
The pandemic highlights that “we need a concerted effort on obesity prevention and treatment,” according to Dr. Sattar.
“For years we have realized links between obesity and chronic cardiometabolic conditions,” he said, “but to think excess weight may also be detrimental to acute effects of a novel virus running amok in the world has focused minds on obesity in a manner not seen before.
“Whether these new painful learnings lead to a more determined effort in countries to improve the obesogenic environment or to place more resources into prevention and management of obesity remains to be seen,” he said.
Increased inquiries about bariatric surgery following COVID-19
Meanwhile, Matthew M. Hutter, MD, MPH, president, American Society for Metabolic and Bariatric Surgery, said in an interview that “COVID-19 and studies like this are now making many aware that obesity is not just a lifestyle choice or a cosmetic issue, but “a disease that needs to be taken seriously” and treated.
“Metabolic and bariatric surgery is a very safe and effective treatment for persons with obesity with a BMI >40 kg/m2 or BMI >35 kg/m2 and related diseases like diabetes, hypertension, sleep apnea, reflux, back pain, and many others,” added Dr. Hutter, who is also professor of surgery, Harvard Medical School, Boston.
“Recently, some metabolic and bariatric centers have seen an increase in patients considering surgery,” he said. “Some say that COVID-19 has made them realize they need to do something to be healthier.”
“Currently, less than 1% of those who could benefit from surgery are actually having” it each year, Dr. Hutter noted, “and I think there are many who should seriously consider surgery to be healthier, live longer, and live better.”
This article first appeared on Medscape.com.
'Tragic' milestone: 1 million children with COVID-19
The number of new cases soared in the past week as the United States exceeded 1 million children infected with the coronavirus, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.

For the first time, the number of cases in children for the week ending Nov. 12 passed 100,000, and it didn’t stop until it reached 111,946, bringing the total for the pandemic to 1,039,464 reported cases in 49 states (New York is not reporting ages), the District of Columbia, New York City, and Guam, the AAP and the CHA said in their weekly COVID-19 update.
“As a pediatrician who has practiced medicine for over 3 decades, I find this number staggering and tragic. We haven’t seen a virus flash through our communities in this way since before we had vaccines for measles and polio,” AAP President Sally Goza, MD, said in a written statement.
The previous 1-week high of almost 74,000 cases came just last week, and that number had surpassed the previous week’s new high of 61,000. The number of cumulative child cases, meanwhile, has doubled since Sept. 3, when it was just over 513,000. Children now represent 11.5% of all COVID-19 cases since the start of the pandemic in the jurisdictions reporting age distribution, the AAP and CHA said.
For the week ending Nov. 12, COVID-19 cases children made up 14% of cases nationally, rising from 13% the week before and reversing a decline that started in mid-October, the AAP/CHA data show.
The two groups continue to note the rarity of severe illness in children, but the number of deaths nationally had its biggest 1-week increase since late July, as the total rose from 123 to 133 in the 42 states reporting such data by age, as well as New York City. The cumulative hospitalization rate for children decreased slightly in the past week and is now down to 1.6% in the 23 states (and NYC) with available data, the AAP and CHA said.
The AAP called on elected leaders to enact a national strategy to combat the spread of the virus and urged health authorities to do more to collect data on longer-term impacts on children.
We’re very concerned about how this will impact all children, including toddlers who are missing key educational opportunities, as well as adolescents who may be at higher risk for anxiety and depression,” Dr. Goza said.
The number of new cases soared in the past week as the United States exceeded 1 million children infected with the coronavirus, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
For the first time, the number of cases in children for the week ending Nov. 12 passed 100,000, and it didn’t stop until it reached 111,946, bringing the total for the pandemic to 1,039,464 reported cases in 49 states (New York is not reporting ages), the District of Columbia, New York City, and Guam, the AAP and the CHA said in their weekly COVID-19 update.
“As a pediatrician who has practiced medicine for over 3 decades, I find this number staggering and tragic. We haven’t seen a virus flash through our communities in this way since before we had vaccines for measles and polio,” AAP President Sally Goza, MD, said in a written statement.
The previous 1-week high of almost 74,000 cases came just last week, and that number had surpassed the previous week’s new high of 61,000. The number of cumulative child cases, meanwhile, has doubled since Sept. 3, when it was just over 513,000. Children now represent 11.5% of all COVID-19 cases since the start of the pandemic in the jurisdictions reporting age distribution, the AAP and CHA said.
For the week ending Nov. 12, COVID-19 cases children made up 14% of cases nationally, rising from 13% the week before and reversing a decline that started in mid-October, the AAP/CHA data show.
The two groups continue to note the rarity of severe illness in children, but the number of deaths nationally had its biggest 1-week increase since late July, as the total rose from 123 to 133 in the 42 states reporting such data by age, as well as New York City. The cumulative hospitalization rate for children decreased slightly in the past week and is now down to 1.6% in the 23 states (and NYC) with available data, the AAP and CHA said.
The AAP called on elected leaders to enact a national strategy to combat the spread of the virus and urged health authorities to do more to collect data on longer-term impacts on children.
We’re very concerned about how this will impact all children, including toddlers who are missing key educational opportunities, as well as adolescents who may be at higher risk for anxiety and depression,” Dr. Goza said.
The number of new cases soared in the past week as the United States exceeded 1 million children infected with the coronavirus, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
For the first time, the number of cases in children for the week ending Nov. 12 passed 100,000, and it didn’t stop until it reached 111,946, bringing the total for the pandemic to 1,039,464 reported cases in 49 states (New York is not reporting ages), the District of Columbia, New York City, and Guam, the AAP and the CHA said in their weekly COVID-19 update.
“As a pediatrician who has practiced medicine for over 3 decades, I find this number staggering and tragic. We haven’t seen a virus flash through our communities in this way since before we had vaccines for measles and polio,” AAP President Sally Goza, MD, said in a written statement.
The previous 1-week high of almost 74,000 cases came just last week, and that number had surpassed the previous week’s new high of 61,000. The number of cumulative child cases, meanwhile, has doubled since Sept. 3, when it was just over 513,000. Children now represent 11.5% of all COVID-19 cases since the start of the pandemic in the jurisdictions reporting age distribution, the AAP and CHA said.
For the week ending Nov. 12, COVID-19 cases children made up 14% of cases nationally, rising from 13% the week before and reversing a decline that started in mid-October, the AAP/CHA data show.
The two groups continue to note the rarity of severe illness in children, but the number of deaths nationally had its biggest 1-week increase since late July, as the total rose from 123 to 133 in the 42 states reporting such data by age, as well as New York City. The cumulative hospitalization rate for children decreased slightly in the past week and is now down to 1.6% in the 23 states (and NYC) with available data, the AAP and CHA said.
The AAP called on elected leaders to enact a national strategy to combat the spread of the virus and urged health authorities to do more to collect data on longer-term impacts on children.
We’re very concerned about how this will impact all children, including toddlers who are missing key educational opportunities, as well as adolescents who may be at higher risk for anxiety and depression,” Dr. Goza said.
New-onset AFib common but unrecognized in the month after cardiac surgery
One in five patients at elevated stroke risk who underwent cardiac surgery with no history of atrial fibrillation preoperatively or at discharge developed postoperative AFib documented on a continuous cardiac rhythm monitoring device within the first 30 days after leaving the hospital in the randomized SEARCH-AF trial.

“Postoperative atrial fibrillation after cardiac surgery is not confined to the hospitalization period per se. We believe that these data should help inform on clinical practice guidelines on monitoring for postoperative atrial fibrillation in such patients,” said Subodh Verma, MD, PhD, reporting the results at the virtual American Heart Association scientific sessions.
“Guidelines provide little or no direction on optimal monitoring post cardiac surgery, particularly if patients are in sinus rhythm at discharge,” the surgeon noted.
SEARCH-AF was an open-label, multicenter study that included 336 patients at elevated stroke risk with an average CHA2DS2-VASc score of 4, no history of preoperative AFib, and none more than briefly with resolution during hospitalization. They were randomized to 30 days of postdischarge continuous cardiac rhythm monitoring with Medtronic’s SEEQ device, to Icentia’s CardioSTAT device, or to usual care, with Holter monitoring at the discretion of the treating physicians.
The primary result was a cumulative duration of AFib or atrial flutter of 6 minutes or longer during that 30-day period. This outcome occurred in 19.6% of the enhanced cardiac monitoring group and 1.7% of usual-care controls. Thus, there is an ongoing persistent occult risk of AFib that typically goes unrecognized. This 10-fold difference in the incidence of postoperative AFib translated into an absolute 17.9% between-group difference and a number-needed-to-treat of 6.
The secondary outcome of a cumulative atrial fib/flutter burden of 6 hours or more during 30 days occurred in 8.6% of the continuously monitored group and none of the controls. A cumulative AFib/flutter burden of 24 hours or greater occurred in 3.1% of the enhanced cardiac monitoring group and zero controls. These are AFib burdens that in other studies have been linked to increased risks of stroke and death, said Dr. Verma, professor of cardiovascular surgery at the University of Toronto.
“From a clinical standpoint, what this trial tells me is for my patients being discharged home tomorrow from the hospital, where they haven’t had AFib and I haven’t initiated anticoagulation, I have a low threshold to monitor these patients and to watch for periods of sustained unrecognized atrial fibrillation,” the surgeon added.
Experts: Results won’t change guidelines
Discussant Ben Freedman, MBBS, PhD, noted that the U.S. Preventive Services Task Force has stated that there are insufficient data available to recommend ECG screening for AFib to prevent stroke. Before the task force can be convinced to recommend it and for payers to cover it, a number of key questions need to be answered. And the SEARCH-AF trial doesn’t provide those answers, said Dr. Freedman, professor of cardiology and deputy director of the Heart Research Institute at the University of Sydney.
First off, it’ll be necessary to know if the risk posed by screen-detected AFib, including postoperative AFib, is similar to that of clinical AFib. Next, it must be shown that this screen-detected postoperative AFib is actionable; that is, that a screening strategy to detect postoperative AFib arising after discharge and then treat with oral anticoagulants will actually prevent more strokes than with usual care. There are large studies underway addressing that question, including HEARTLINE, STROKESTOP, and SAFERGUARD-AF, he observed.
In an interview, Rod S. Passman, MD, who gave a state-of-the-art talk on AFib detection at the meeting and wasn’t involved in SEARCH-AF, said he doesn’t consider the results practice-changing.
“It’s not guideline-changing because you’ve only shown that more intensive monitoring finds more AFib. Guideline-changing would be that finding that AFib and doing something about it impacts hard outcomes, and we don’t have that data yet,” said Dr. Passman, an electrophysiologist who is director of the Center for Arrhythmia Research and professor of medicine and preventive medicine at Northwestern University, Chicago.
The SEARCH-AF trial was funded by the Heart and Stroke Foundation of Canada, Bristol Myers Squibb, Pfizer, and Boehringer Ingelheim. Dr. Verma reported having received speaker’s fees and/or research support from those and other pharmaceutical companies. Dr. Freedman disclosed having no financial conflicts.
One in five patients at elevated stroke risk who underwent cardiac surgery with no history of atrial fibrillation preoperatively or at discharge developed postoperative AFib documented on a continuous cardiac rhythm monitoring device within the first 30 days after leaving the hospital in the randomized SEARCH-AF trial.
“Postoperative atrial fibrillation after cardiac surgery is not confined to the hospitalization period per se. We believe that these data should help inform on clinical practice guidelines on monitoring for postoperative atrial fibrillation in such patients,” said Subodh Verma, MD, PhD, reporting the results at the virtual American Heart Association scientific sessions.
“Guidelines provide little or no direction on optimal monitoring post cardiac surgery, particularly if patients are in sinus rhythm at discharge,” the surgeon noted.
SEARCH-AF was an open-label, multicenter study that included 336 patients at elevated stroke risk with an average CHA2DS2-VASc score of 4, no history of preoperative AFib, and none more than briefly with resolution during hospitalization. They were randomized to 30 days of postdischarge continuous cardiac rhythm monitoring with Medtronic’s SEEQ device, to Icentia’s CardioSTAT device, or to usual care, with Holter monitoring at the discretion of the treating physicians.
The primary result was a cumulative duration of AFib or atrial flutter of 6 minutes or longer during that 30-day period. This outcome occurred in 19.6% of the enhanced cardiac monitoring group and 1.7% of usual-care controls. Thus, there is an ongoing persistent occult risk of AFib that typically goes unrecognized. This 10-fold difference in the incidence of postoperative AFib translated into an absolute 17.9% between-group difference and a number-needed-to-treat of 6.
The secondary outcome of a cumulative atrial fib/flutter burden of 6 hours or more during 30 days occurred in 8.6% of the continuously monitored group and none of the controls. A cumulative AFib/flutter burden of 24 hours or greater occurred in 3.1% of the enhanced cardiac monitoring group and zero controls. These are AFib burdens that in other studies have been linked to increased risks of stroke and death, said Dr. Verma, professor of cardiovascular surgery at the University of Toronto.
“From a clinical standpoint, what this trial tells me is for my patients being discharged home tomorrow from the hospital, where they haven’t had AFib and I haven’t initiated anticoagulation, I have a low threshold to monitor these patients and to watch for periods of sustained unrecognized atrial fibrillation,” the surgeon added.
Experts: Results won’t change guidelines
Discussant Ben Freedman, MBBS, PhD, noted that the U.S. Preventive Services Task Force has stated that there are insufficient data available to recommend ECG screening for AFib to prevent stroke. Before the task force can be convinced to recommend it and for payers to cover it, a number of key questions need to be answered. And the SEARCH-AF trial doesn’t provide those answers, said Dr. Freedman, professor of cardiology and deputy director of the Heart Research Institute at the University of Sydney.
First off, it’ll be necessary to know if the risk posed by screen-detected AFib, including postoperative AFib, is similar to that of clinical AFib. Next, it must be shown that this screen-detected postoperative AFib is actionable; that is, that a screening strategy to detect postoperative AFib arising after discharge and then treat with oral anticoagulants will actually prevent more strokes than with usual care. There are large studies underway addressing that question, including HEARTLINE, STROKESTOP, and SAFERGUARD-AF, he observed.
In an interview, Rod S. Passman, MD, who gave a state-of-the-art talk on AFib detection at the meeting and wasn’t involved in SEARCH-AF, said he doesn’t consider the results practice-changing.
“It’s not guideline-changing because you’ve only shown that more intensive monitoring finds more AFib. Guideline-changing would be that finding that AFib and doing something about it impacts hard outcomes, and we don’t have that data yet,” said Dr. Passman, an electrophysiologist who is director of the Center for Arrhythmia Research and professor of medicine and preventive medicine at Northwestern University, Chicago.
The SEARCH-AF trial was funded by the Heart and Stroke Foundation of Canada, Bristol Myers Squibb, Pfizer, and Boehringer Ingelheim. Dr. Verma reported having received speaker’s fees and/or research support from those and other pharmaceutical companies. Dr. Freedman disclosed having no financial conflicts.
One in five patients at elevated stroke risk who underwent cardiac surgery with no history of atrial fibrillation preoperatively or at discharge developed postoperative AFib documented on a continuous cardiac rhythm monitoring device within the first 30 days after leaving the hospital in the randomized SEARCH-AF trial.
“Postoperative atrial fibrillation after cardiac surgery is not confined to the hospitalization period per se. We believe that these data should help inform on clinical practice guidelines on monitoring for postoperative atrial fibrillation in such patients,” said Subodh Verma, MD, PhD, reporting the results at the virtual American Heart Association scientific sessions.
“Guidelines provide little or no direction on optimal monitoring post cardiac surgery, particularly if patients are in sinus rhythm at discharge,” the surgeon noted.
SEARCH-AF was an open-label, multicenter study that included 336 patients at elevated stroke risk with an average CHA2DS2-VASc score of 4, no history of preoperative AFib, and none more than briefly with resolution during hospitalization. They were randomized to 30 days of postdischarge continuous cardiac rhythm monitoring with Medtronic’s SEEQ device, to Icentia’s CardioSTAT device, or to usual care, with Holter monitoring at the discretion of the treating physicians.
The primary result was a cumulative duration of AFib or atrial flutter of 6 minutes or longer during that 30-day period. This outcome occurred in 19.6% of the enhanced cardiac monitoring group and 1.7% of usual-care controls. Thus, there is an ongoing persistent occult risk of AFib that typically goes unrecognized. This 10-fold difference in the incidence of postoperative AFib translated into an absolute 17.9% between-group difference and a number-needed-to-treat of 6.
The secondary outcome of a cumulative atrial fib/flutter burden of 6 hours or more during 30 days occurred in 8.6% of the continuously monitored group and none of the controls. A cumulative AFib/flutter burden of 24 hours or greater occurred in 3.1% of the enhanced cardiac monitoring group and zero controls. These are AFib burdens that in other studies have been linked to increased risks of stroke and death, said Dr. Verma, professor of cardiovascular surgery at the University of Toronto.
“From a clinical standpoint, what this trial tells me is for my patients being discharged home tomorrow from the hospital, where they haven’t had AFib and I haven’t initiated anticoagulation, I have a low threshold to monitor these patients and to watch for periods of sustained unrecognized atrial fibrillation,” the surgeon added.
Experts: Results won’t change guidelines
Discussant Ben Freedman, MBBS, PhD, noted that the U.S. Preventive Services Task Force has stated that there are insufficient data available to recommend ECG screening for AFib to prevent stroke. Before the task force can be convinced to recommend it and for payers to cover it, a number of key questions need to be answered. And the SEARCH-AF trial doesn’t provide those answers, said Dr. Freedman, professor of cardiology and deputy director of the Heart Research Institute at the University of Sydney.
First off, it’ll be necessary to know if the risk posed by screen-detected AFib, including postoperative AFib, is similar to that of clinical AFib. Next, it must be shown that this screen-detected postoperative AFib is actionable; that is, that a screening strategy to detect postoperative AFib arising after discharge and then treat with oral anticoagulants will actually prevent more strokes than with usual care. There are large studies underway addressing that question, including HEARTLINE, STROKESTOP, and SAFERGUARD-AF, he observed.
In an interview, Rod S. Passman, MD, who gave a state-of-the-art talk on AFib detection at the meeting and wasn’t involved in SEARCH-AF, said he doesn’t consider the results practice-changing.
“It’s not guideline-changing because you’ve only shown that more intensive monitoring finds more AFib. Guideline-changing would be that finding that AFib and doing something about it impacts hard outcomes, and we don’t have that data yet,” said Dr. Passman, an electrophysiologist who is director of the Center for Arrhythmia Research and professor of medicine and preventive medicine at Northwestern University, Chicago.
The SEARCH-AF trial was funded by the Heart and Stroke Foundation of Canada, Bristol Myers Squibb, Pfizer, and Boehringer Ingelheim. Dr. Verma reported having received speaker’s fees and/or research support from those and other pharmaceutical companies. Dr. Freedman disclosed having no financial conflicts.
FROM AHA 2020
COVID-19: Choosing the proper treatment at the proper time
Coronavirus disease 2019 (COVID-19), the disease caused by the highly contagious virus SARS-CoV-2, has affected over 45 million people worldwide and caused over 1.2 million deaths. Preventative strategies, including social distancing and facial coverings, have proven to be effective to decrease the risk of transmission. Unfortunately, despite these measures, a large number of individuals continue to get infected throughout the world. While most patients typically stay asymptomatic or develop mild forms of the disease, a fraction of them will progress to more severe forms that would necessitate hospital care. Since this is a novel virus, we do not have an effective antimicrobial agent and the care we provide is mostly supportive, aiming to prevent and treat the systemic complications produced by the virus and the inflammatory response that ensues.
The phases of COVID 19
COVID-19 can be clinically divided into three phases (Mason RJ, et al. Eur Respir J. 2020 Apr;55[4]).
The asymptomatic phase: Also known as incubation period. During this stage, the SARS-CoV-2 virus binds to the epithelial cells of the upper respiratory tract and starts replicating.
The viral phase: Associated with the classic constitutional symptoms such as fever, chills, headache, cough, fatigue, and diarrhea. This phase typically begins 4-6 days after exposure to SARS-CoV-2 and is characterized by high levels of viral replication and migration to the conducting airways, triggering the innate immune response.
The pulmonary phase: Characterized by hypoxia and ground glass infiltrates on computed tomography of the chest. By now, the virus has reached the respiratory bronchioles and the alveoli. During this phase (about 8-10 days after exposure) the virus begins to die, and the host immune response ensues. By now the number of viral units is very small, but the host immune reaction against the virus has begun to mount.

The virus is actively replicating during the asymptomatic and at the beginning of the viral phase. The severity of symptoms varies according to the viral load and patient comorbidities [mild-moderate (81%), severe (14%), and critical (5%)]. The disease course is characterized by dysregulated immunity, profound inflammatory response, and dysregulated coagulation. By distinguishing these phases, clinicians can start interventions that would aim at the main cause of the derangement at each specific phase. For example, antiviral agents seem more appropriate in the early phases of the disease, while anti-inflammatory medications could target the inflammatory response that occurs in the pulmonary phase (Figure 1).
The tools in our toolbox: Timing is paramount
Remdesivir
The preliminary results from a recent trial that compared remdesivir with placebo, given 6-12 days from the onset of symptoms, revealed a shorter time to recovery with Remdesivir (Beigel JH, et al. N Engl J Med. 2020 Oct;8. NEJMoa2007764). The patients who received remdesivir within 10 days of the onset of symptoms had a shorter recovery time compared with those who received it after 10 days from the onset of symptoms. Moreover, remdesivir did not alter the disease course in patients who received the drug after the onset of hypoxia. These results are consistent with those of Wang and colleagues who reported no effect in time to clinical improvement in most patients who received the drug 10 days after the onset of symptoms (Wang Y, et al. Lancet. 2020 May;395[10236]:1569-78). In most antiviral trials, the agent was potentially given when the immune response had already begun, stage in which the number of viral units is not as large as in the earlier phases, possibly explaining the lack effect in time of clinical improvement or mortality.
Convalescent plasma
Piechotta and colleagues recently showed that convalescent plasma, when given to patients more than 14 days from the onset of symptoms, provided no benefit in time to clinical improvement or 28-day mortality. At 14 days or later, the pulmonary phase (characterized by systemic inflammation) had started in nearly all patients. As it seems apparent, any intervention not targeted to modulate the inflammatory response is unlikely to make a difference in this stage. (Piechotta V, et al. Cochrane Database Syst Rev. 2020 Jul;7[7]:CD013600).
The negative results of these studies (antivirals and convalescent plasma) highlight the importance of timing. In most of these trials, the intervention was started at the end of the viral phase or in the pulmonary phase, when the virus was nearly or completely dead, but the host immune response has begun to mount.
Corticosteroids
Corticosteroids (methylprednisolone and dexamethasone) have shown positive effects when given at the proper time (beginning of the pulmonary phase). A recent study revealed a lower 28-day mortality when compared with placebo in hospitalized patients with COVID-19. However, a prespecified subgroup analysis showed no benefit and a signal of possible harm among those who received dexamethasone in the absence of hypoxia (viral phase) (Lim WS, et al. N Engl J Med. 2020 Jul;[NEJMoa2021436]). A meta-analysis of seven randomized trials that used different doses and types of corticosteroids (dexamethasone, methylprednisolone, and hydrocortisone) reported a lower 28-day mortality in the corticosteroids group. The benefit was more pronounced when the corticosteroids was used in critically ill patients who were not receiving invasive mechanical ventilation.
Self-proning
Self-proning is also thought to be beneficial during the pulmonary phase. Prone positioning for at least 3 hours improved oxygenation but the result was not sustained (Coppo A, et al. Lancet Respir Med. 2020 Aug;8[8]:765-74). A retrospective analysis of 199 patients with COVID-19 in the pulmonary phase who were being supported by high-flow nasal cannula showed that awake proning for more than 16 hours had no effect in the risk of intubation or mortality (Ferrando C, et al. reduce the use of critical care resources, and improve survival. We aimed to examine whether the combination of high-flow nasal oxygen therapy (HFNOCrit Care. 2020 [Oct];24[1]:597). There is concern that this intervention might produce a delay in intubation in patients who have worsening oxygenation; this is especially important as delayed intubation can be associated with worse outcomes. Despite the conflicting data, awake self-proning is a reasonable intervention that should be considered provided that it does not interfere with treatments that have been proven beneficial. As prospective evidence becomes available, recommendations may possibly change.
What about thromboembolic events?
Data on arterial and venous thromboembolic events (VTE) in the disease course of COVID-19 are largely variable. The prevalence of VTE in COVID-19 seems to be higher than other in causes of sepsis especially in critically ill patients. (Bilaloglu S, et al. JAMA. 2020 Aug;324(8):799-801). Despite the use of pharmacological prophylaxis, VTE was seen in 13.6% of critically ill patients and 3.6% of medical ward patients and associated with a higher mortality. Therefore, more trials are needed to understand the most effective way to prevent VTE. At the current time, clinicians need to be vigilant to detect VTE as early as possible. Some options to consider include performing a daily evaluation of the possible risks (emphasizing prevention), routine bedside point of care ultrasound, early diagnostic imaging studies for clinically suspected VTE, early mobilization and delirium prevention. Prophylactic doses of LMWH or UH for all hospitalized patients with no or low risk of bleeding or non-hospitalized patient with high risk for VTE can be entertained (Bikdeli B, et al. J Am Coll Cardiol 2020 Apr;75[23]:2950-73). Therapeutic dose anticoagulation should be only used in confirmed VTE or in highly suspected VTE with difficulties to obtain standard confirmatory imaging. A therapeutic approach based solely on D-dimer should be avoided, because the evidence is insufficient and the risk of bleeding in critically ill patients is not insignificant.

The available evidence is helpful but not definitive making it difficult to have a clear pathway to effectively treat the systemic effects of COVID-19. One should consider remdesivir and convalescent plasma during the viral phase before hypoxia ensue. Anti-inflammatory interventions (dexamethasone or methylprednisolone) should be given as soon as the pulmonary manifestations start (hypoxia). The type, optimal dose, and duration of corticosteroids vary from trial to trial and no evidence suggests that higher doses are associated with more benefit. It is not only important to choose the right treatment but also the phase when such treatment is most likely to be effective!
Dr. Megri is a Pulmonary and Critical Care Fellow at the University of Kentucky. Dr. Coz is Associate Professor of Medicine, University of Kentucky.
Coronavirus disease 2019 (COVID-19), the disease caused by the highly contagious virus SARS-CoV-2, has affected over 45 million people worldwide and caused over 1.2 million deaths. Preventative strategies, including social distancing and facial coverings, have proven to be effective to decrease the risk of transmission. Unfortunately, despite these measures, a large number of individuals continue to get infected throughout the world. While most patients typically stay asymptomatic or develop mild forms of the disease, a fraction of them will progress to more severe forms that would necessitate hospital care. Since this is a novel virus, we do not have an effective antimicrobial agent and the care we provide is mostly supportive, aiming to prevent and treat the systemic complications produced by the virus and the inflammatory response that ensues.
The phases of COVID 19
COVID-19 can be clinically divided into three phases (Mason RJ, et al. Eur Respir J. 2020 Apr;55[4]).
The asymptomatic phase: Also known as incubation period. During this stage, the SARS-CoV-2 virus binds to the epithelial cells of the upper respiratory tract and starts replicating.
The viral phase: Associated with the classic constitutional symptoms such as fever, chills, headache, cough, fatigue, and diarrhea. This phase typically begins 4-6 days after exposure to SARS-CoV-2 and is characterized by high levels of viral replication and migration to the conducting airways, triggering the innate immune response.
The pulmonary phase: Characterized by hypoxia and ground glass infiltrates on computed tomography of the chest. By now, the virus has reached the respiratory bronchioles and the alveoli. During this phase (about 8-10 days after exposure) the virus begins to die, and the host immune response ensues. By now the number of viral units is very small, but the host immune reaction against the virus has begun to mount.
The virus is actively replicating during the asymptomatic and at the beginning of the viral phase. The severity of symptoms varies according to the viral load and patient comorbidities [mild-moderate (81%), severe (14%), and critical (5%)]. The disease course is characterized by dysregulated immunity, profound inflammatory response, and dysregulated coagulation. By distinguishing these phases, clinicians can start interventions that would aim at the main cause of the derangement at each specific phase. For example, antiviral agents seem more appropriate in the early phases of the disease, while anti-inflammatory medications could target the inflammatory response that occurs in the pulmonary phase (Figure 1).
The tools in our toolbox: Timing is paramount
Remdesivir
The preliminary results from a recent trial that compared remdesivir with placebo, given 6-12 days from the onset of symptoms, revealed a shorter time to recovery with Remdesivir (Beigel JH, et al. N Engl J Med. 2020 Oct;8. NEJMoa2007764). The patients who received remdesivir within 10 days of the onset of symptoms had a shorter recovery time compared with those who received it after 10 days from the onset of symptoms. Moreover, remdesivir did not alter the disease course in patients who received the drug after the onset of hypoxia. These results are consistent with those of Wang and colleagues who reported no effect in time to clinical improvement in most patients who received the drug 10 days after the onset of symptoms (Wang Y, et al. Lancet. 2020 May;395[10236]:1569-78). In most antiviral trials, the agent was potentially given when the immune response had already begun, stage in which the number of viral units is not as large as in the earlier phases, possibly explaining the lack effect in time of clinical improvement or mortality.
Convalescent plasma
Piechotta and colleagues recently showed that convalescent plasma, when given to patients more than 14 days from the onset of symptoms, provided no benefit in time to clinical improvement or 28-day mortality. At 14 days or later, the pulmonary phase (characterized by systemic inflammation) had started in nearly all patients. As it seems apparent, any intervention not targeted to modulate the inflammatory response is unlikely to make a difference in this stage. (Piechotta V, et al. Cochrane Database Syst Rev. 2020 Jul;7[7]:CD013600).
The negative results of these studies (antivirals and convalescent plasma) highlight the importance of timing. In most of these trials, the intervention was started at the end of the viral phase or in the pulmonary phase, when the virus was nearly or completely dead, but the host immune response has begun to mount.
Corticosteroids
Corticosteroids (methylprednisolone and dexamethasone) have shown positive effects when given at the proper time (beginning of the pulmonary phase). A recent study revealed a lower 28-day mortality when compared with placebo in hospitalized patients with COVID-19. However, a prespecified subgroup analysis showed no benefit and a signal of possible harm among those who received dexamethasone in the absence of hypoxia (viral phase) (Lim WS, et al. N Engl J Med. 2020 Jul;[NEJMoa2021436]). A meta-analysis of seven randomized trials that used different doses and types of corticosteroids (dexamethasone, methylprednisolone, and hydrocortisone) reported a lower 28-day mortality in the corticosteroids group. The benefit was more pronounced when the corticosteroids was used in critically ill patients who were not receiving invasive mechanical ventilation.
Self-proning
Self-proning is also thought to be beneficial during the pulmonary phase. Prone positioning for at least 3 hours improved oxygenation but the result was not sustained (Coppo A, et al. Lancet Respir Med. 2020 Aug;8[8]:765-74). A retrospective analysis of 199 patients with COVID-19 in the pulmonary phase who were being supported by high-flow nasal cannula showed that awake proning for more than 16 hours had no effect in the risk of intubation or mortality (Ferrando C, et al. reduce the use of critical care resources, and improve survival. We aimed to examine whether the combination of high-flow nasal oxygen therapy (HFNOCrit Care. 2020 [Oct];24[1]:597). There is concern that this intervention might produce a delay in intubation in patients who have worsening oxygenation; this is especially important as delayed intubation can be associated with worse outcomes. Despite the conflicting data, awake self-proning is a reasonable intervention that should be considered provided that it does not interfere with treatments that have been proven beneficial. As prospective evidence becomes available, recommendations may possibly change.
What about thromboembolic events?
Data on arterial and venous thromboembolic events (VTE) in the disease course of COVID-19 are largely variable. The prevalence of VTE in COVID-19 seems to be higher than other in causes of sepsis especially in critically ill patients. (Bilaloglu S, et al. JAMA. 2020 Aug;324(8):799-801). Despite the use of pharmacological prophylaxis, VTE was seen in 13.6% of critically ill patients and 3.6% of medical ward patients and associated with a higher mortality. Therefore, more trials are needed to understand the most effective way to prevent VTE. At the current time, clinicians need to be vigilant to detect VTE as early as possible. Some options to consider include performing a daily evaluation of the possible risks (emphasizing prevention), routine bedside point of care ultrasound, early diagnostic imaging studies for clinically suspected VTE, early mobilization and delirium prevention. Prophylactic doses of LMWH or UH for all hospitalized patients with no or low risk of bleeding or non-hospitalized patient with high risk for VTE can be entertained (Bikdeli B, et al. J Am Coll Cardiol 2020 Apr;75[23]:2950-73). Therapeutic dose anticoagulation should be only used in confirmed VTE or in highly suspected VTE with difficulties to obtain standard confirmatory imaging. A therapeutic approach based solely on D-dimer should be avoided, because the evidence is insufficient and the risk of bleeding in critically ill patients is not insignificant.
The available evidence is helpful but not definitive making it difficult to have a clear pathway to effectively treat the systemic effects of COVID-19. One should consider remdesivir and convalescent plasma during the viral phase before hypoxia ensue. Anti-inflammatory interventions (dexamethasone or methylprednisolone) should be given as soon as the pulmonary manifestations start (hypoxia). The type, optimal dose, and duration of corticosteroids vary from trial to trial and no evidence suggests that higher doses are associated with more benefit. It is not only important to choose the right treatment but also the phase when such treatment is most likely to be effective!
Dr. Megri is a Pulmonary and Critical Care Fellow at the University of Kentucky. Dr. Coz is Associate Professor of Medicine, University of Kentucky.
Coronavirus disease 2019 (COVID-19), the disease caused by the highly contagious virus SARS-CoV-2, has affected over 45 million people worldwide and caused over 1.2 million deaths. Preventative strategies, including social distancing and facial coverings, have proven to be effective to decrease the risk of transmission. Unfortunately, despite these measures, a large number of individuals continue to get infected throughout the world. While most patients typically stay asymptomatic or develop mild forms of the disease, a fraction of them will progress to more severe forms that would necessitate hospital care. Since this is a novel virus, we do not have an effective antimicrobial agent and the care we provide is mostly supportive, aiming to prevent and treat the systemic complications produced by the virus and the inflammatory response that ensues.
The phases of COVID 19
COVID-19 can be clinically divided into three phases (Mason RJ, et al. Eur Respir J. 2020 Apr;55[4]).
The asymptomatic phase: Also known as incubation period. During this stage, the SARS-CoV-2 virus binds to the epithelial cells of the upper respiratory tract and starts replicating.
The viral phase: Associated with the classic constitutional symptoms such as fever, chills, headache, cough, fatigue, and diarrhea. This phase typically begins 4-6 days after exposure to SARS-CoV-2 and is characterized by high levels of viral replication and migration to the conducting airways, triggering the innate immune response.
The pulmonary phase: Characterized by hypoxia and ground glass infiltrates on computed tomography of the chest. By now, the virus has reached the respiratory bronchioles and the alveoli. During this phase (about 8-10 days after exposure) the virus begins to die, and the host immune response ensues. By now the number of viral units is very small, but the host immune reaction against the virus has begun to mount.
The virus is actively replicating during the asymptomatic and at the beginning of the viral phase. The severity of symptoms varies according to the viral load and patient comorbidities [mild-moderate (81%), severe (14%), and critical (5%)]. The disease course is characterized by dysregulated immunity, profound inflammatory response, and dysregulated coagulation. By distinguishing these phases, clinicians can start interventions that would aim at the main cause of the derangement at each specific phase. For example, antiviral agents seem more appropriate in the early phases of the disease, while anti-inflammatory medications could target the inflammatory response that occurs in the pulmonary phase (Figure 1).
The tools in our toolbox: Timing is paramount
Remdesivir
The preliminary results from a recent trial that compared remdesivir with placebo, given 6-12 days from the onset of symptoms, revealed a shorter time to recovery with Remdesivir (Beigel JH, et al. N Engl J Med. 2020 Oct;8. NEJMoa2007764). The patients who received remdesivir within 10 days of the onset of symptoms had a shorter recovery time compared with those who received it after 10 days from the onset of symptoms. Moreover, remdesivir did not alter the disease course in patients who received the drug after the onset of hypoxia. These results are consistent with those of Wang and colleagues who reported no effect in time to clinical improvement in most patients who received the drug 10 days after the onset of symptoms (Wang Y, et al. Lancet. 2020 May;395[10236]:1569-78). In most antiviral trials, the agent was potentially given when the immune response had already begun, stage in which the number of viral units is not as large as in the earlier phases, possibly explaining the lack effect in time of clinical improvement or mortality.
Convalescent plasma
Piechotta and colleagues recently showed that convalescent plasma, when given to patients more than 14 days from the onset of symptoms, provided no benefit in time to clinical improvement or 28-day mortality. At 14 days or later, the pulmonary phase (characterized by systemic inflammation) had started in nearly all patients. As it seems apparent, any intervention not targeted to modulate the inflammatory response is unlikely to make a difference in this stage. (Piechotta V, et al. Cochrane Database Syst Rev. 2020 Jul;7[7]:CD013600).
The negative results of these studies (antivirals and convalescent plasma) highlight the importance of timing. In most of these trials, the intervention was started at the end of the viral phase or in the pulmonary phase, when the virus was nearly or completely dead, but the host immune response has begun to mount.
Corticosteroids
Corticosteroids (methylprednisolone and dexamethasone) have shown positive effects when given at the proper time (beginning of the pulmonary phase). A recent study revealed a lower 28-day mortality when compared with placebo in hospitalized patients with COVID-19. However, a prespecified subgroup analysis showed no benefit and a signal of possible harm among those who received dexamethasone in the absence of hypoxia (viral phase) (Lim WS, et al. N Engl J Med. 2020 Jul;[NEJMoa2021436]). A meta-analysis of seven randomized trials that used different doses and types of corticosteroids (dexamethasone, methylprednisolone, and hydrocortisone) reported a lower 28-day mortality in the corticosteroids group. The benefit was more pronounced when the corticosteroids was used in critically ill patients who were not receiving invasive mechanical ventilation.
Self-proning
Self-proning is also thought to be beneficial during the pulmonary phase. Prone positioning for at least 3 hours improved oxygenation but the result was not sustained (Coppo A, et al. Lancet Respir Med. 2020 Aug;8[8]:765-74). A retrospective analysis of 199 patients with COVID-19 in the pulmonary phase who were being supported by high-flow nasal cannula showed that awake proning for more than 16 hours had no effect in the risk of intubation or mortality (Ferrando C, et al. reduce the use of critical care resources, and improve survival. We aimed to examine whether the combination of high-flow nasal oxygen therapy (HFNOCrit Care. 2020 [Oct];24[1]:597). There is concern that this intervention might produce a delay in intubation in patients who have worsening oxygenation; this is especially important as delayed intubation can be associated with worse outcomes. Despite the conflicting data, awake self-proning is a reasonable intervention that should be considered provided that it does not interfere with treatments that have been proven beneficial. As prospective evidence becomes available, recommendations may possibly change.
What about thromboembolic events?
Data on arterial and venous thromboembolic events (VTE) in the disease course of COVID-19 are largely variable. The prevalence of VTE in COVID-19 seems to be higher than other in causes of sepsis especially in critically ill patients. (Bilaloglu S, et al. JAMA. 2020 Aug;324(8):799-801). Despite the use of pharmacological prophylaxis, VTE was seen in 13.6% of critically ill patients and 3.6% of medical ward patients and associated with a higher mortality. Therefore, more trials are needed to understand the most effective way to prevent VTE. At the current time, clinicians need to be vigilant to detect VTE as early as possible. Some options to consider include performing a daily evaluation of the possible risks (emphasizing prevention), routine bedside point of care ultrasound, early diagnostic imaging studies for clinically suspected VTE, early mobilization and delirium prevention. Prophylactic doses of LMWH or UH for all hospitalized patients with no or low risk of bleeding or non-hospitalized patient with high risk for VTE can be entertained (Bikdeli B, et al. J Am Coll Cardiol 2020 Apr;75[23]:2950-73). Therapeutic dose anticoagulation should be only used in confirmed VTE or in highly suspected VTE with difficulties to obtain standard confirmatory imaging. A therapeutic approach based solely on D-dimer should be avoided, because the evidence is insufficient and the risk of bleeding in critically ill patients is not insignificant.
The available evidence is helpful but not definitive making it difficult to have a clear pathway to effectively treat the systemic effects of COVID-19. One should consider remdesivir and convalescent plasma during the viral phase before hypoxia ensue. Anti-inflammatory interventions (dexamethasone or methylprednisolone) should be given as soon as the pulmonary manifestations start (hypoxia). The type, optimal dose, and duration of corticosteroids vary from trial to trial and no evidence suggests that higher doses are associated with more benefit. It is not only important to choose the right treatment but also the phase when such treatment is most likely to be effective!
Dr. Megri is a Pulmonary and Critical Care Fellow at the University of Kentucky. Dr. Coz is Associate Professor of Medicine, University of Kentucky.
VTEs tied to immune checkpoint inhibitor cancer treatment
Cancer patients who receive an immune checkpoint inhibitor have more than a doubled rate of venous thromboembolism during the subsequent 2 years, compared with their rate during the 2 years before treatment, according to a retrospective analysis of more than 2,800 patients treated at a single U.S. center.
The study focused on cancer patients treated with an immune checkpoint inhibitor (ICI) at Massachusetts General Hospital in Boston. It showed that during the 2 years prior to treatment with any type of ICI, the incidence of venous thromboembolic events (VTE) was 4.85/100 patient-years that then jumped to 11.75/100 patient-years during the 2 years following treatment. This translated into an incidence rate ratio of 2.43 during posttreatment follow-up, compared with pretreatment, Jingyi Gong, MD, said at the virtual American Heart Association scientific sessions.
The increased VTE rate resulted from rises in both the rate of deep vein thrombosis, which had an IRR of 3.23 during the posttreatment period, and for pulmonary embolism, which showed an IRR of 2.24, said Dr. Gong, a physician at Brigham and Women’s Hospital in Boston. She hypothesized that this effect may result from a procoagulant effect of the immune activation and inflammation triggered by ICIs.
Hypothesis-generating results
Cardiologists cautioned that these findings should only be considered hypothesis generating, but raise an important alert for clinicians to have heightened awareness of the potential for VTE following ICI treatment.
“A clear message is to be aware that there is this signal, and be vigilant for patients who might present with VTE following ICI treatment,” commented Richard J. Kovacs, MD, a cardiologist and professor at Indiana University, Indianapolis. The data that Dr. Gong reported are “moderately convincing,” he added in an interview.

“Awareness that patients who receive ICI may be at increased VTE risk is very important,” agreed Umberto Campia, MD, a cardiologist, vascular specialist, and member of the cardio-oncology group at Brigham and Women’s Hospital, who was not involved in the new study.
The potential impact of ICI treatment on VTE risk is slowly emerging, added Dr. Campia. Until recently, the literature primarily was case reports, but recently another retrospective, single-center study came out that reported a 13% incidence of VTE in cancer patients following ICI treatment. On the other hand, a recently published meta-analysis of more than 20,000 patients from 68 ICI studies failed to find a suggestion of increased VTE incidence following ICI interventions.
Attempting to assess the impact of treatment on VTE risk in cancer patients is challenging because cancer itself boosts the risk. Recommendations on the use of VTE prophylaxis in cancer patients most recently came out in 2014 from the American Society of Clinical Oncology, which said that VTE prophylaxis for ambulatory cancer patients “may be considered for highly select high-risk patients.” The impact of cancer therapy on VTE risk and the need for prophylaxis is usually assessed by applying the Khorana score, Dr. Campia said in an interview.
VTE spikes acutely after ICI treatment
Dr. Gong analyzed VTE incidence rates by time during the total 4-year period studied, and found that the rate gradually and steadily rose with time throughout the 2 years preceding treatment, spiked immediately following ICI treatment, and then gradually and steadily fell back to roughly the rate seen just before treatment, reaching that level about a year after treatment. She ran a sensitivity analysis that excluded patients who died during the first year following their ICI treatment, and in this calculation an acute spike in VTE following ICI treatment still occurred but with reduced magnitude.
She also reported the results of several subgroup analyses. The IRRs remained consistent among women and men, among patients who were aged over or under 65 years, and regardless of cancer type or treatment with corticosteroids. But the subgroup analyses identified two parameters that seemed to clearly split VTE rates.
Among patients on treatment with an anticoagulant agent at the time of their ICI treatment, roughly 10% of the patients, the IRR was 0.56, compared with a ratio of 3.86 among the other patients, suggesting possible protection. A second factor that seemed linked with VTE incidence was the number of ICI treatment cycles a patient received. Those who received more than five cycles had a risk ratio of 3.95, while those who received five or fewer cycles had a RR of 1.66.
Her analysis included 2,842 cancer patients who received treatment with an ICI at Massachusetts General Hospital. Patients averaged 64 years of age, slightly more than half were men, and 13% had a prior history of VTE. Patients received an average of 5 ICI treatment cycles, but a quarter of the patients received more than 10 cycles.
During the 2-year follow-up, 244 patients (9%) developed VTE. The patients who developed VTE were significantly younger than those who did not, with an average age of 63 years, compared with 65. And the patients who eventually developed VTE had a significantly higher prevalence of prior VTE at 18%, compared with 12% among the patients who stayed VTE free.
The cancer types patients had were non–small cell lung, 29%; melanoma, 28%; head and neck, 12%; renal genitourinary, 6%; and other, 25%. ICIs have been available for routine U.S. practice since 2011. The class includes agents such as pembrolizumab (Keytruda) and durvalumab (Imfinzi).
Researchers would need to perform a prospective, randomized study to determine whether anticoagulant prophylaxis is clearly beneficial for patients receiving ICI treatment, Dr. Gong said. But both Dr. Kovacs and Dr. Campia said that more data on this topic are first needed.
“We need to confirm that treatment with ICI is associated with VTEs. Retrospective data are not definitive,” said Dr. Campia. “We would need to prospectively assess the impact of ICI,” which will not be easy, as it’s quickly become a cornerstone for treating many cancers. “We need to become more familiar with the adverse effects of these drugs. We are still learning about their toxicities.”
The study had no commercial funding. Dr. Gong, Dr. Kovacs, and Dr. Campia had no disclosures.
Cancer patients who receive an immune checkpoint inhibitor have more than a doubled rate of venous thromboembolism during the subsequent 2 years, compared with their rate during the 2 years before treatment, according to a retrospective analysis of more than 2,800 patients treated at a single U.S. center.
The study focused on cancer patients treated with an immune checkpoint inhibitor (ICI) at Massachusetts General Hospital in Boston. It showed that during the 2 years prior to treatment with any type of ICI, the incidence of venous thromboembolic events (VTE) was 4.85/100 patient-years that then jumped to 11.75/100 patient-years during the 2 years following treatment. This translated into an incidence rate ratio of 2.43 during posttreatment follow-up, compared with pretreatment, Jingyi Gong, MD, said at the virtual American Heart Association scientific sessions.
The increased VTE rate resulted from rises in both the rate of deep vein thrombosis, which had an IRR of 3.23 during the posttreatment period, and for pulmonary embolism, which showed an IRR of 2.24, said Dr. Gong, a physician at Brigham and Women’s Hospital in Boston. She hypothesized that this effect may result from a procoagulant effect of the immune activation and inflammation triggered by ICIs.
Hypothesis-generating results
Cardiologists cautioned that these findings should only be considered hypothesis generating, but raise an important alert for clinicians to have heightened awareness of the potential for VTE following ICI treatment.
“A clear message is to be aware that there is this signal, and be vigilant for patients who might present with VTE following ICI treatment,” commented Richard J. Kovacs, MD, a cardiologist and professor at Indiana University, Indianapolis. The data that Dr. Gong reported are “moderately convincing,” he added in an interview.
“Awareness that patients who receive ICI may be at increased VTE risk is very important,” agreed Umberto Campia, MD, a cardiologist, vascular specialist, and member of the cardio-oncology group at Brigham and Women’s Hospital, who was not involved in the new study.
The potential impact of ICI treatment on VTE risk is slowly emerging, added Dr. Campia. Until recently, the literature primarily was case reports, but recently another retrospective, single-center study came out that reported a 13% incidence of VTE in cancer patients following ICI treatment. On the other hand, a recently published meta-analysis of more than 20,000 patients from 68 ICI studies failed to find a suggestion of increased VTE incidence following ICI interventions.
Attempting to assess the impact of treatment on VTE risk in cancer patients is challenging because cancer itself boosts the risk. Recommendations on the use of VTE prophylaxis in cancer patients most recently came out in 2014 from the American Society of Clinical Oncology, which said that VTE prophylaxis for ambulatory cancer patients “may be considered for highly select high-risk patients.” The impact of cancer therapy on VTE risk and the need for prophylaxis is usually assessed by applying the Khorana score, Dr. Campia said in an interview.
VTE spikes acutely after ICI treatment
Dr. Gong analyzed VTE incidence rates by time during the total 4-year period studied, and found that the rate gradually and steadily rose with time throughout the 2 years preceding treatment, spiked immediately following ICI treatment, and then gradually and steadily fell back to roughly the rate seen just before treatment, reaching that level about a year after treatment. She ran a sensitivity analysis that excluded patients who died during the first year following their ICI treatment, and in this calculation an acute spike in VTE following ICI treatment still occurred but with reduced magnitude.
She also reported the results of several subgroup analyses. The IRRs remained consistent among women and men, among patients who were aged over or under 65 years, and regardless of cancer type or treatment with corticosteroids. But the subgroup analyses identified two parameters that seemed to clearly split VTE rates.
Among patients on treatment with an anticoagulant agent at the time of their ICI treatment, roughly 10% of the patients, the IRR was 0.56, compared with a ratio of 3.86 among the other patients, suggesting possible protection. A second factor that seemed linked with VTE incidence was the number of ICI treatment cycles a patient received. Those who received more than five cycles had a risk ratio of 3.95, while those who received five or fewer cycles had a RR of 1.66.
Her analysis included 2,842 cancer patients who received treatment with an ICI at Massachusetts General Hospital. Patients averaged 64 years of age, slightly more than half were men, and 13% had a prior history of VTE. Patients received an average of 5 ICI treatment cycles, but a quarter of the patients received more than 10 cycles.
During the 2-year follow-up, 244 patients (9%) developed VTE. The patients who developed VTE were significantly younger than those who did not, with an average age of 63 years, compared with 65. And the patients who eventually developed VTE had a significantly higher prevalence of prior VTE at 18%, compared with 12% among the patients who stayed VTE free.
The cancer types patients had were non–small cell lung, 29%; melanoma, 28%; head and neck, 12%; renal genitourinary, 6%; and other, 25%. ICIs have been available for routine U.S. practice since 2011. The class includes agents such as pembrolizumab (Keytruda) and durvalumab (Imfinzi).
Researchers would need to perform a prospective, randomized study to determine whether anticoagulant prophylaxis is clearly beneficial for patients receiving ICI treatment, Dr. Gong said. But both Dr. Kovacs and Dr. Campia said that more data on this topic are first needed.
“We need to confirm that treatment with ICI is associated with VTEs. Retrospective data are not definitive,” said Dr. Campia. “We would need to prospectively assess the impact of ICI,” which will not be easy, as it’s quickly become a cornerstone for treating many cancers. “We need to become more familiar with the adverse effects of these drugs. We are still learning about their toxicities.”
The study had no commercial funding. Dr. Gong, Dr. Kovacs, and Dr. Campia had no disclosures.
Cancer patients who receive an immune checkpoint inhibitor have more than a doubled rate of venous thromboembolism during the subsequent 2 years, compared with their rate during the 2 years before treatment, according to a retrospective analysis of more than 2,800 patients treated at a single U.S. center.
The study focused on cancer patients treated with an immune checkpoint inhibitor (ICI) at Massachusetts General Hospital in Boston. It showed that during the 2 years prior to treatment with any type of ICI, the incidence of venous thromboembolic events (VTE) was 4.85/100 patient-years that then jumped to 11.75/100 patient-years during the 2 years following treatment. This translated into an incidence rate ratio of 2.43 during posttreatment follow-up, compared with pretreatment, Jingyi Gong, MD, said at the virtual American Heart Association scientific sessions.
The increased VTE rate resulted from rises in both the rate of deep vein thrombosis, which had an IRR of 3.23 during the posttreatment period, and for pulmonary embolism, which showed an IRR of 2.24, said Dr. Gong, a physician at Brigham and Women’s Hospital in Boston. She hypothesized that this effect may result from a procoagulant effect of the immune activation and inflammation triggered by ICIs.
Hypothesis-generating results
Cardiologists cautioned that these findings should only be considered hypothesis generating, but raise an important alert for clinicians to have heightened awareness of the potential for VTE following ICI treatment.
“A clear message is to be aware that there is this signal, and be vigilant for patients who might present with VTE following ICI treatment,” commented Richard J. Kovacs, MD, a cardiologist and professor at Indiana University, Indianapolis. The data that Dr. Gong reported are “moderately convincing,” he added in an interview.
“Awareness that patients who receive ICI may be at increased VTE risk is very important,” agreed Umberto Campia, MD, a cardiologist, vascular specialist, and member of the cardio-oncology group at Brigham and Women’s Hospital, who was not involved in the new study.
The potential impact of ICI treatment on VTE risk is slowly emerging, added Dr. Campia. Until recently, the literature primarily was case reports, but recently another retrospective, single-center study came out that reported a 13% incidence of VTE in cancer patients following ICI treatment. On the other hand, a recently published meta-analysis of more than 20,000 patients from 68 ICI studies failed to find a suggestion of increased VTE incidence following ICI interventions.
Attempting to assess the impact of treatment on VTE risk in cancer patients is challenging because cancer itself boosts the risk. Recommendations on the use of VTE prophylaxis in cancer patients most recently came out in 2014 from the American Society of Clinical Oncology, which said that VTE prophylaxis for ambulatory cancer patients “may be considered for highly select high-risk patients.” The impact of cancer therapy on VTE risk and the need for prophylaxis is usually assessed by applying the Khorana score, Dr. Campia said in an interview.
VTE spikes acutely after ICI treatment
Dr. Gong analyzed VTE incidence rates by time during the total 4-year period studied, and found that the rate gradually and steadily rose with time throughout the 2 years preceding treatment, spiked immediately following ICI treatment, and then gradually and steadily fell back to roughly the rate seen just before treatment, reaching that level about a year after treatment. She ran a sensitivity analysis that excluded patients who died during the first year following their ICI treatment, and in this calculation an acute spike in VTE following ICI treatment still occurred but with reduced magnitude.
She also reported the results of several subgroup analyses. The IRRs remained consistent among women and men, among patients who were aged over or under 65 years, and regardless of cancer type or treatment with corticosteroids. But the subgroup analyses identified two parameters that seemed to clearly split VTE rates.
Among patients on treatment with an anticoagulant agent at the time of their ICI treatment, roughly 10% of the patients, the IRR was 0.56, compared with a ratio of 3.86 among the other patients, suggesting possible protection. A second factor that seemed linked with VTE incidence was the number of ICI treatment cycles a patient received. Those who received more than five cycles had a risk ratio of 3.95, while those who received five or fewer cycles had a RR of 1.66.
Her analysis included 2,842 cancer patients who received treatment with an ICI at Massachusetts General Hospital. Patients averaged 64 years of age, slightly more than half were men, and 13% had a prior history of VTE. Patients received an average of 5 ICI treatment cycles, but a quarter of the patients received more than 10 cycles.
During the 2-year follow-up, 244 patients (9%) developed VTE. The patients who developed VTE were significantly younger than those who did not, with an average age of 63 years, compared with 65. And the patients who eventually developed VTE had a significantly higher prevalence of prior VTE at 18%, compared with 12% among the patients who stayed VTE free.
The cancer types patients had were non–small cell lung, 29%; melanoma, 28%; head and neck, 12%; renal genitourinary, 6%; and other, 25%. ICIs have been available for routine U.S. practice since 2011. The class includes agents such as pembrolizumab (Keytruda) and durvalumab (Imfinzi).
Researchers would need to perform a prospective, randomized study to determine whether anticoagulant prophylaxis is clearly beneficial for patients receiving ICI treatment, Dr. Gong said. But both Dr. Kovacs and Dr. Campia said that more data on this topic are first needed.
“We need to confirm that treatment with ICI is associated with VTEs. Retrospective data are not definitive,” said Dr. Campia. “We would need to prospectively assess the impact of ICI,” which will not be easy, as it’s quickly become a cornerstone for treating many cancers. “We need to become more familiar with the adverse effects of these drugs. We are still learning about their toxicities.”
The study had no commercial funding. Dr. Gong, Dr. Kovacs, and Dr. Campia had no disclosures.
FROM AHA 2020
Options grow for interstitial lung disease other than idiopathic pulmonary fibrosis
Care of the patient with a fibrosing interstitial lung disease (ILD) presents constant challenges not just in the diagnosis of ILD but in the choice of treatment. Since the FDA approval of both nintedanib and pirfenidone for the treatment of idiopathic pulmonary fibrosis (IPF) in 2014, interest has grown for their employ in treating other non-IPF ILDs. This is especially true in cases with the pattern of radiographic or histopathological disease is similar to IPF – a usual interstitial pneumonia (UIP) pattern – despite not meeting criteria for an IPF diagnosis due to the identification of a predisposing etiology. As research evolves, clinicians may have more options to fight the vast variety of fibrosing ILDs encountered in practice.

In 2014, the publication of separate clinical trials of nintedanib and pirfenidone in patients with IPF marked a new beginning in the treatment of this disease. Nintedanib, a tyrosine kinase inhibitor with multiple targets, was shown to decrease progression of disease as measured by the annual rate of decline in forced vital capacity (FVC) (Richeldi L, et al. N Engl J Med. 2014 May;370[22]:2071-82). Pirfenidone, whose antifibrotic mechanisms are not completely understood, similarly slowed disease progression via a decrease in the percent change of predicted FVC (Lederer DJ, et al. N Engl J Med. 2014 May;370[19]:2083-92). Clinicians were now armed with two therapeutic options following the subsequent FDA approval of both drugs for the treatment of IPF. This represented a giant leap forward in the management of the disease, as prior to 2014 the only available options were supportive care and lung transplant for appropriate candidates.
As IPF represents but 20% of ILDs in the United States, a significant proportion of diseases were left without an antifibrotic option after the arrival of nintedanib and pirfenidone. (Lederer DJ. N Engl J Med. 2018 May;378:1811-23). For the others, such as chronic hypersensitivity pneumonitis and the many connective tissue disease-associated ILDs, treatment revolved around a variety of anti-inflammatory pharmaceuticals. Common treatment choices include corticosteroids, mycophenolate, and azathioprine. The data in support of these treatments for non-IPF ILD is comparatively lean in contrast to the more robust pirfenidone and nintedanib IPF trials.
One notable exception includes the Scleroderma Lung Studies. In Scleroderma Lung Study II (SLS II), 142 patients with scleroderma-related interstitial lung disease were randomized to oral mycophenolate for 24 months vs oral cyclophosphamide for 12 months plus placebo for 12 months (Tashkin DP, et al. Lancet Respir Med. 2016 Sep;4(9):708-19). The 2006 Scleroderma Lung Study established oral cyclophosphamide in scleroderma lung disease as a reasonable standard of care after demonstrating a slowing of disease progression after 12 months of therapy (Tashkin DP, et al. N Engl J Med. 2006 Jun;354[25]:2655-66). In SLS II, both cyclophosphamide and mycophenolate improved lung function at 24 months, but mycophenolate was better tolerated with less toxicity.
Other supportive data for immunosuppressive treatments for non-IPF ILD rely heavily on smaller studies, case reports, and retrospective reviews. Choices of who and when to treat are often unclear and typically come from physician preferences and patient values discussions. In the cases of connective tissue disease-associated ILD, patients may already require treatment for the underlying condition. And, while some therapies could be beneficial in a concurrent manner for a patient’s lung disease, many others are not (TNF-alpha antibody therapy, for example).
A major step forward for patients with scleroderma lung disease came with the publication of the SENSCIS trial (Oliver D, et al. N Engl J Med. 2019 Jun;380:2518-28). A total of 576 patients with scleroderma of recent onset (< 7 years) and at least 10% fibrosis on chest CT were randomized to receive either nintedanib or placebo. Patients were allowed to be supported by other therapies at stable doses prior to enrollment, and as such almost half of the patients were receiving mycophenolate. A significant improvement in annual FVC decline was reported in the treatment group, although the effect was tempered in the subgroup analysis when considering patients already on mycophenolate. Thus, the role of nintedanib in patients taking mycophenolate is less clear.
An ongoing study may clarify the role of mycophenolate and antifibrotic therapy in these patients. The phase 2 Scleroderma Lung Study III has a planned enrollment of 150 patients who are either treatment-naïve or only recently started on therapy (www.clinicaltrials.gov; NCT03221257). Patients are randomized to mycophenolate plus pirfenidone vs mycophenolate plus placebo, and the treatment phase will last 18 months. The primary outcome is change in baseline FVC. This trial design will hopefully answer whether the combination of an antifibrotic with an anti-inflammatory medication is superior to the anti-inflammatory therapy alone, in patients with at least some evidence of inflammation (ground-glass opacifications) on high-resolution CT scan (HRCT).
In ILD other than that associated with scleroderma, nintedanib was again explored in a large randomized controlled clinical trial. In INBUILD, 663 patients with progressive ILD not caused by IPF or scleroderma were randomized to nintedanib vs placebo for one year (Flaherty KR. N Engl J Med. 2019 Sep;381:1718-27). A majority of the patients (62%) had a UIP pattern on CT scan. There was overall improvement in the annual rate of decline in FVC in the treatment group, especially in the pr-determined subgroup of patients with a UIP pattern. The most common ILDs in the study were chronic hypersensitivity pneumonitis and that associated with connective tissue disease.
Pirfenidone is also being studied in multiple trials for various types of non-IPF ILD. Studies are either completed and nearing publication, or are ongoing. Some examples include the TRAIL1 study examining pirfenidone vs placebo in patients with rheumatoid arthritis (www.clinicaltrials.gov; NCT02808871), and the phase 2 RELIEF study that explores pirfenidone vs placebo in patients with progressive ILD from a variety of etiologies.
As more clinical trials are published, clinicians are now facing a different dilemma. Whereas the options for treatment were limited to only various anti-inflammatory medications in past years for patients with non-IPF ILDs, the growing body of literature supporting antifibrotics present a new therapeutic avenue to explore. Which patients should be started on anti-inflammatory medications, and which should start antifibrotics? Those questions may never be answered satisfactorily in clinical trials. Mycophenolate has become so entrenched in many treatment plans, enrollment into such a study comparing the two therapeutic classes head-to-head would be challenging.
However, a consideration of the specific phenotype of the patient’s ILD is a suggested approach that comes from clinical experience. Patients with more inflammatory changes on CT scan, such as more ground glass opacifications or a non-UIP pattern, might benefit from initiation of anti-inflammatory therapies such as a combination of corticosteroids and mycophenolate. Conversely, initiating antifibrotic therapy upfront, with or without concomitant mycophenolate, is a consideration if the pattern of disease is consistent with UIP on CT scan.
Ultimately, referral to a dedicated interstitial lung disease center for expert evaluation and multidisciplinary discussion may be warranted to sift through these difficult situations, especially as the field of research grows more robust. In any event, the future for patients with these diseases, though still challenged, is brighter than before.
Dr. Kershaw is Associate Professor of Medicine, Division of Pulmonary & Critical Care Medicine, University of Texas Southwestern Medical Center. He is the current section editor for Pulmonary
Perpsectives®and Vice Chair of the Interstitial and Diffuse Lung Disease NetWork at CHEST.
Care of the patient with a fibrosing interstitial lung disease (ILD) presents constant challenges not just in the diagnosis of ILD but in the choice of treatment. Since the FDA approval of both nintedanib and pirfenidone for the treatment of idiopathic pulmonary fibrosis (IPF) in 2014, interest has grown for their employ in treating other non-IPF ILDs. This is especially true in cases with the pattern of radiographic or histopathological disease is similar to IPF – a usual interstitial pneumonia (UIP) pattern – despite not meeting criteria for an IPF diagnosis due to the identification of a predisposing etiology. As research evolves, clinicians may have more options to fight the vast variety of fibrosing ILDs encountered in practice.
In 2014, the publication of separate clinical trials of nintedanib and pirfenidone in patients with IPF marked a new beginning in the treatment of this disease. Nintedanib, a tyrosine kinase inhibitor with multiple targets, was shown to decrease progression of disease as measured by the annual rate of decline in forced vital capacity (FVC) (Richeldi L, et al. N Engl J Med. 2014 May;370[22]:2071-82). Pirfenidone, whose antifibrotic mechanisms are not completely understood, similarly slowed disease progression via a decrease in the percent change of predicted FVC (Lederer DJ, et al. N Engl J Med. 2014 May;370[19]:2083-92). Clinicians were now armed with two therapeutic options following the subsequent FDA approval of both drugs for the treatment of IPF. This represented a giant leap forward in the management of the disease, as prior to 2014 the only available options were supportive care and lung transplant for appropriate candidates.
As IPF represents but 20% of ILDs in the United States, a significant proportion of diseases were left without an antifibrotic option after the arrival of nintedanib and pirfenidone. (Lederer DJ. N Engl J Med. 2018 May;378:1811-23). For the others, such as chronic hypersensitivity pneumonitis and the many connective tissue disease-associated ILDs, treatment revolved around a variety of anti-inflammatory pharmaceuticals. Common treatment choices include corticosteroids, mycophenolate, and azathioprine. The data in support of these treatments for non-IPF ILD is comparatively lean in contrast to the more robust pirfenidone and nintedanib IPF trials.
One notable exception includes the Scleroderma Lung Studies. In Scleroderma Lung Study II (SLS II), 142 patients with scleroderma-related interstitial lung disease were randomized to oral mycophenolate for 24 months vs oral cyclophosphamide for 12 months plus placebo for 12 months (Tashkin DP, et al. Lancet Respir Med. 2016 Sep;4(9):708-19). The 2006 Scleroderma Lung Study established oral cyclophosphamide in scleroderma lung disease as a reasonable standard of care after demonstrating a slowing of disease progression after 12 months of therapy (Tashkin DP, et al. N Engl J Med. 2006 Jun;354[25]:2655-66). In SLS II, both cyclophosphamide and mycophenolate improved lung function at 24 months, but mycophenolate was better tolerated with less toxicity.
Other supportive data for immunosuppressive treatments for non-IPF ILD rely heavily on smaller studies, case reports, and retrospective reviews. Choices of who and when to treat are often unclear and typically come from physician preferences and patient values discussions. In the cases of connective tissue disease-associated ILD, patients may already require treatment for the underlying condition. And, while some therapies could be beneficial in a concurrent manner for a patient’s lung disease, many others are not (TNF-alpha antibody therapy, for example).
A major step forward for patients with scleroderma lung disease came with the publication of the SENSCIS trial (Oliver D, et al. N Engl J Med. 2019 Jun;380:2518-28). A total of 576 patients with scleroderma of recent onset (< 7 years) and at least 10% fibrosis on chest CT were randomized to receive either nintedanib or placebo. Patients were allowed to be supported by other therapies at stable doses prior to enrollment, and as such almost half of the patients were receiving mycophenolate. A significant improvement in annual FVC decline was reported in the treatment group, although the effect was tempered in the subgroup analysis when considering patients already on mycophenolate. Thus, the role of nintedanib in patients taking mycophenolate is less clear.
An ongoing study may clarify the role of mycophenolate and antifibrotic therapy in these patients. The phase 2 Scleroderma Lung Study III has a planned enrollment of 150 patients who are either treatment-naïve or only recently started on therapy (www.clinicaltrials.gov; NCT03221257). Patients are randomized to mycophenolate plus pirfenidone vs mycophenolate plus placebo, and the treatment phase will last 18 months. The primary outcome is change in baseline FVC. This trial design will hopefully answer whether the combination of an antifibrotic with an anti-inflammatory medication is superior to the anti-inflammatory therapy alone, in patients with at least some evidence of inflammation (ground-glass opacifications) on high-resolution CT scan (HRCT).
In ILD other than that associated with scleroderma, nintedanib was again explored in a large randomized controlled clinical trial. In INBUILD, 663 patients with progressive ILD not caused by IPF or scleroderma were randomized to nintedanib vs placebo for one year (Flaherty KR. N Engl J Med. 2019 Sep;381:1718-27). A majority of the patients (62%) had a UIP pattern on CT scan. There was overall improvement in the annual rate of decline in FVC in the treatment group, especially in the pr-determined subgroup of patients with a UIP pattern. The most common ILDs in the study were chronic hypersensitivity pneumonitis and that associated with connective tissue disease.
Pirfenidone is also being studied in multiple trials for various types of non-IPF ILD. Studies are either completed and nearing publication, or are ongoing. Some examples include the TRAIL1 study examining pirfenidone vs placebo in patients with rheumatoid arthritis (www.clinicaltrials.gov; NCT02808871), and the phase 2 RELIEF study that explores pirfenidone vs placebo in patients with progressive ILD from a variety of etiologies.
As more clinical trials are published, clinicians are now facing a different dilemma. Whereas the options for treatment were limited to only various anti-inflammatory medications in past years for patients with non-IPF ILDs, the growing body of literature supporting antifibrotics present a new therapeutic avenue to explore. Which patients should be started on anti-inflammatory medications, and which should start antifibrotics? Those questions may never be answered satisfactorily in clinical trials. Mycophenolate has become so entrenched in many treatment plans, enrollment into such a study comparing the two therapeutic classes head-to-head would be challenging.
However, a consideration of the specific phenotype of the patient’s ILD is a suggested approach that comes from clinical experience. Patients with more inflammatory changes on CT scan, such as more ground glass opacifications or a non-UIP pattern, might benefit from initiation of anti-inflammatory therapies such as a combination of corticosteroids and mycophenolate. Conversely, initiating antifibrotic therapy upfront, with or without concomitant mycophenolate, is a consideration if the pattern of disease is consistent with UIP on CT scan.
Ultimately, referral to a dedicated interstitial lung disease center for expert evaluation and multidisciplinary discussion may be warranted to sift through these difficult situations, especially as the field of research grows more robust. In any event, the future for patients with these diseases, though still challenged, is brighter than before.
Dr. Kershaw is Associate Professor of Medicine, Division of Pulmonary & Critical Care Medicine, University of Texas Southwestern Medical Center. He is the current section editor for Pulmonary
Perpsectives®and Vice Chair of the Interstitial and Diffuse Lung Disease NetWork at CHEST.
Care of the patient with a fibrosing interstitial lung disease (ILD) presents constant challenges not just in the diagnosis of ILD but in the choice of treatment. Since the FDA approval of both nintedanib and pirfenidone for the treatment of idiopathic pulmonary fibrosis (IPF) in 2014, interest has grown for their employ in treating other non-IPF ILDs. This is especially true in cases with the pattern of radiographic or histopathological disease is similar to IPF – a usual interstitial pneumonia (UIP) pattern – despite not meeting criteria for an IPF diagnosis due to the identification of a predisposing etiology. As research evolves, clinicians may have more options to fight the vast variety of fibrosing ILDs encountered in practice.
In 2014, the publication of separate clinical trials of nintedanib and pirfenidone in patients with IPF marked a new beginning in the treatment of this disease. Nintedanib, a tyrosine kinase inhibitor with multiple targets, was shown to decrease progression of disease as measured by the annual rate of decline in forced vital capacity (FVC) (Richeldi L, et al. N Engl J Med. 2014 May;370[22]:2071-82). Pirfenidone, whose antifibrotic mechanisms are not completely understood, similarly slowed disease progression via a decrease in the percent change of predicted FVC (Lederer DJ, et al. N Engl J Med. 2014 May;370[19]:2083-92). Clinicians were now armed with two therapeutic options following the subsequent FDA approval of both drugs for the treatment of IPF. This represented a giant leap forward in the management of the disease, as prior to 2014 the only available options were supportive care and lung transplant for appropriate candidates.
As IPF represents but 20% of ILDs in the United States, a significant proportion of diseases were left without an antifibrotic option after the arrival of nintedanib and pirfenidone. (Lederer DJ. N Engl J Med. 2018 May;378:1811-23). For the others, such as chronic hypersensitivity pneumonitis and the many connective tissue disease-associated ILDs, treatment revolved around a variety of anti-inflammatory pharmaceuticals. Common treatment choices include corticosteroids, mycophenolate, and azathioprine. The data in support of these treatments for non-IPF ILD is comparatively lean in contrast to the more robust pirfenidone and nintedanib IPF trials.
One notable exception includes the Scleroderma Lung Studies. In Scleroderma Lung Study II (SLS II), 142 patients with scleroderma-related interstitial lung disease were randomized to oral mycophenolate for 24 months vs oral cyclophosphamide for 12 months plus placebo for 12 months (Tashkin DP, et al. Lancet Respir Med. 2016 Sep;4(9):708-19). The 2006 Scleroderma Lung Study established oral cyclophosphamide in scleroderma lung disease as a reasonable standard of care after demonstrating a slowing of disease progression after 12 months of therapy (Tashkin DP, et al. N Engl J Med. 2006 Jun;354[25]:2655-66). In SLS II, both cyclophosphamide and mycophenolate improved lung function at 24 months, but mycophenolate was better tolerated with less toxicity.
Other supportive data for immunosuppressive treatments for non-IPF ILD rely heavily on smaller studies, case reports, and retrospective reviews. Choices of who and when to treat are often unclear and typically come from physician preferences and patient values discussions. In the cases of connective tissue disease-associated ILD, patients may already require treatment for the underlying condition. And, while some therapies could be beneficial in a concurrent manner for a patient’s lung disease, many others are not (TNF-alpha antibody therapy, for example).
A major step forward for patients with scleroderma lung disease came with the publication of the SENSCIS trial (Oliver D, et al. N Engl J Med. 2019 Jun;380:2518-28). A total of 576 patients with scleroderma of recent onset (< 7 years) and at least 10% fibrosis on chest CT were randomized to receive either nintedanib or placebo. Patients were allowed to be supported by other therapies at stable doses prior to enrollment, and as such almost half of the patients were receiving mycophenolate. A significant improvement in annual FVC decline was reported in the treatment group, although the effect was tempered in the subgroup analysis when considering patients already on mycophenolate. Thus, the role of nintedanib in patients taking mycophenolate is less clear.
An ongoing study may clarify the role of mycophenolate and antifibrotic therapy in these patients. The phase 2 Scleroderma Lung Study III has a planned enrollment of 150 patients who are either treatment-naïve or only recently started on therapy (www.clinicaltrials.gov; NCT03221257). Patients are randomized to mycophenolate plus pirfenidone vs mycophenolate plus placebo, and the treatment phase will last 18 months. The primary outcome is change in baseline FVC. This trial design will hopefully answer whether the combination of an antifibrotic with an anti-inflammatory medication is superior to the anti-inflammatory therapy alone, in patients with at least some evidence of inflammation (ground-glass opacifications) on high-resolution CT scan (HRCT).
In ILD other than that associated with scleroderma, nintedanib was again explored in a large randomized controlled clinical trial. In INBUILD, 663 patients with progressive ILD not caused by IPF or scleroderma were randomized to nintedanib vs placebo for one year (Flaherty KR. N Engl J Med. 2019 Sep;381:1718-27). A majority of the patients (62%) had a UIP pattern on CT scan. There was overall improvement in the annual rate of decline in FVC in the treatment group, especially in the pr-determined subgroup of patients with a UIP pattern. The most common ILDs in the study were chronic hypersensitivity pneumonitis and that associated with connective tissue disease.
Pirfenidone is also being studied in multiple trials for various types of non-IPF ILD. Studies are either completed and nearing publication, or are ongoing. Some examples include the TRAIL1 study examining pirfenidone vs placebo in patients with rheumatoid arthritis (www.clinicaltrials.gov; NCT02808871), and the phase 2 RELIEF study that explores pirfenidone vs placebo in patients with progressive ILD from a variety of etiologies.
As more clinical trials are published, clinicians are now facing a different dilemma. Whereas the options for treatment were limited to only various anti-inflammatory medications in past years for patients with non-IPF ILDs, the growing body of literature supporting antifibrotics present a new therapeutic avenue to explore. Which patients should be started on anti-inflammatory medications, and which should start antifibrotics? Those questions may never be answered satisfactorily in clinical trials. Mycophenolate has become so entrenched in many treatment plans, enrollment into such a study comparing the two therapeutic classes head-to-head would be challenging.
However, a consideration of the specific phenotype of the patient’s ILD is a suggested approach that comes from clinical experience. Patients with more inflammatory changes on CT scan, such as more ground glass opacifications or a non-UIP pattern, might benefit from initiation of anti-inflammatory therapies such as a combination of corticosteroids and mycophenolate. Conversely, initiating antifibrotic therapy upfront, with or without concomitant mycophenolate, is a consideration if the pattern of disease is consistent with UIP on CT scan.
Ultimately, referral to a dedicated interstitial lung disease center for expert evaluation and multidisciplinary discussion may be warranted to sift through these difficult situations, especially as the field of research grows more robust. In any event, the future for patients with these diseases, though still challenged, is brighter than before.
Dr. Kershaw is Associate Professor of Medicine, Division of Pulmonary & Critical Care Medicine, University of Texas Southwestern Medical Center. He is the current section editor for Pulmonary
Perpsectives®and Vice Chair of the Interstitial and Diffuse Lung Disease NetWork at CHEST.
Open enrollment 2021: A big start for HealthCare.gov
Over 818,000 plans were selected for the 2021 coverage year during the first week, Nov.1-7, of this year’s open enrollment on the federal health insurance exchange, according to the Centers for Medicare & Medicaid Services.
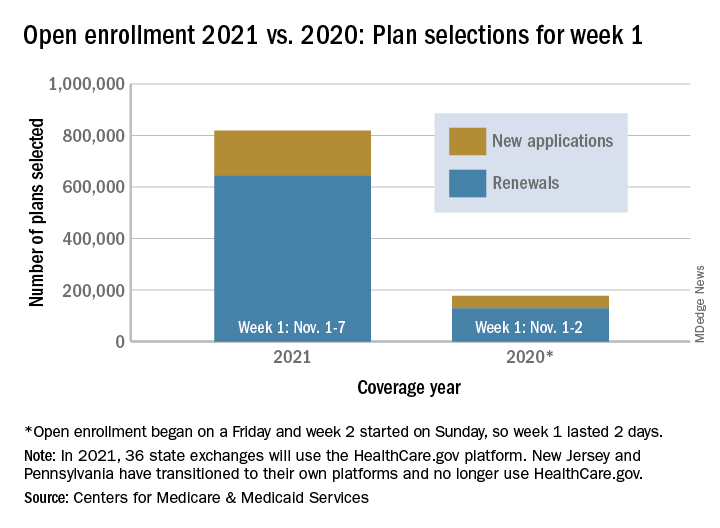
The bulk of those plans, nearly 79%, were renewals by consumers who had coverage through the federal exchange this year. The balance covers new plans selected by individuals who were not covered through HealthCare.gov this year, the CMS noted in a written statement.
The total enrollment for week 1 marks a considerable increase over last year’s first week of open enrollment, which saw approximately 177,000 plans selected, but Nov. 1 fell on a Friday in 2019, so that total represents only 2 days since weeks are tracked as running from Sunday to Saturday, the CMS explained.
For the 2021 benefit year, the HealthCare.gov platform covers 36 states, down from 38 for the 2020 benefit year, because New Jersey and Pennsylvania have “transitioned to their own state-based exchange platforms,” the CMS noted, adding that the two accounted for 7% of all plans selected last year.
“The final number of plan selections associated with enrollment activity during a reporting period may change due to plan modifications or cancellations,” CMS said, and its weekly snapshot “does not report the number of consumers who have paid premiums to effectuate their enrollment.”
This year’s open-enrollment period on HealthCare.gov is scheduled to conclude Dec. 15.
Over 818,000 plans were selected for the 2021 coverage year during the first week, Nov.1-7, of this year’s open enrollment on the federal health insurance exchange, according to the Centers for Medicare & Medicaid Services.
The bulk of those plans, nearly 79%, were renewals by consumers who had coverage through the federal exchange this year. The balance covers new plans selected by individuals who were not covered through HealthCare.gov this year, the CMS noted in a written statement.
The total enrollment for week 1 marks a considerable increase over last year’s first week of open enrollment, which saw approximately 177,000 plans selected, but Nov. 1 fell on a Friday in 2019, so that total represents only 2 days since weeks are tracked as running from Sunday to Saturday, the CMS explained.
For the 2021 benefit year, the HealthCare.gov platform covers 36 states, down from 38 for the 2020 benefit year, because New Jersey and Pennsylvania have “transitioned to their own state-based exchange platforms,” the CMS noted, adding that the two accounted for 7% of all plans selected last year.
“The final number of plan selections associated with enrollment activity during a reporting period may change due to plan modifications or cancellations,” CMS said, and its weekly snapshot “does not report the number of consumers who have paid premiums to effectuate their enrollment.”
This year’s open-enrollment period on HealthCare.gov is scheduled to conclude Dec. 15.
Over 818,000 plans were selected for the 2021 coverage year during the first week, Nov.1-7, of this year’s open enrollment on the federal health insurance exchange, according to the Centers for Medicare & Medicaid Services.
The bulk of those plans, nearly 79%, were renewals by consumers who had coverage through the federal exchange this year. The balance covers new plans selected by individuals who were not covered through HealthCare.gov this year, the CMS noted in a written statement.
The total enrollment for week 1 marks a considerable increase over last year’s first week of open enrollment, which saw approximately 177,000 plans selected, but Nov. 1 fell on a Friday in 2019, so that total represents only 2 days since weeks are tracked as running from Sunday to Saturday, the CMS explained.
For the 2021 benefit year, the HealthCare.gov platform covers 36 states, down from 38 for the 2020 benefit year, because New Jersey and Pennsylvania have “transitioned to their own state-based exchange platforms,” the CMS noted, adding that the two accounted for 7% of all plans selected last year.
“The final number of plan selections associated with enrollment activity during a reporting period may change due to plan modifications or cancellations,” CMS said, and its weekly snapshot “does not report the number of consumers who have paid premiums to effectuate their enrollment.”
This year’s open-enrollment period on HealthCare.gov is scheduled to conclude Dec. 15.
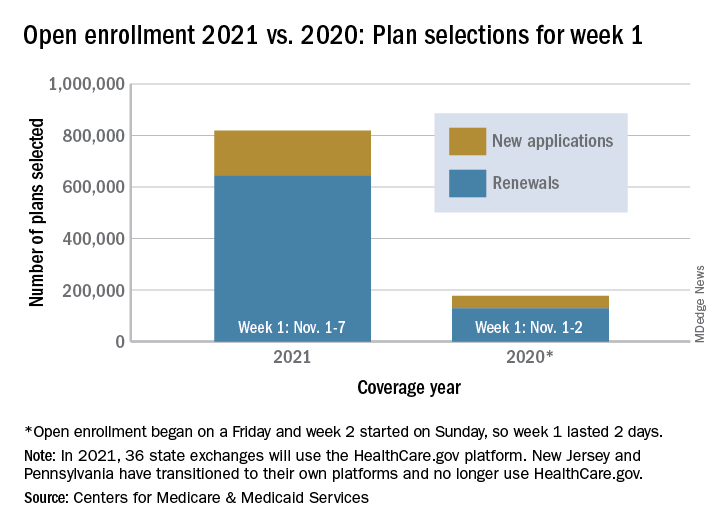
FDA-approved peanut immunotherapy protocol comes with a cost
Peanut allergy immunotherapy now comes with approval from the US Food and Drug Administration (FDA), but it also comes with protocols, standards, and paperwork. Whether it will be widely adopted has yet to be determined.
A few dozen allergists around the world have been offering food allergy immunotherapy for many years, having developed their own measuring techniques using store-bought food.
But the vast majority of allergists are not interested in developing home-grown treatments, not only because it involves research and development, but also because it comes with legal risks.
“Finally we have another treatment option,” said Edwin Kim, MD, from the UNC Allergy and Immunology Clinic in Chapel Hill, N.C. “This is what we were waiting for. It’s not cowboy stuff; this works.”
In January, the FDA approved peanut allergen powder (Palforzia) for patients 4-17 years of age, as reported by Medscape Medical News.
The pill contains measured doses of peanut flour and comes with a protocol that will allow allergists to bring patients to a peanut tolerance of 300 mg (about one peanut) and a black-box warning about anaphylaxis risk.
And before allergists can prescribe it, they must take a Risk Evaluation and Mitigation Strategy course to learn about dosing and the allergic reaction protocol.
“That may scare some away,” said Dr. Kim, who discussed the FDA-approved option during his presentation at the American College of Allergy, Asthma & Immunology 2020 Annual Scientific Meeting.
Allergic reaction, including the potential for anaphylaxis, has always been an issue with immunotherapy.
“People make the argument that there is a difference” between an expected allergic reaction – such as one that occurs after the administration of immunotherapy – and an unexpected reaction, he said. Because an expected reaction can be treated quickly, “some feel these expected reactions don’t matter so much.”
“Others say a reaction is a reaction” and argue that if, a treatment causes reaction, then it doesn’t make sense, he explained.
It comes down to patients – they must be willing to take a risk to develop tolerance and improve their quality of life – and the allergists willing to treat them.
The peanut powder involves paperwork, preauthorization forms, denials of care, a higher price tag, regimented procedures, and a prerequisite number of visits with patients. “Not everyone will want to do this,” said Dr. Kim.
The regimen involves three phases. During initial dose escalation, five doses are administered in the office on day 1. Then, over the next 6 months, updoses are administered during 11 in-office sessions and a 300-mg tolerance is achieved. Finally, to maintain tolerance to one peanut, daily doses are administered at home.
The drug cost alone is about $4,200 a year, according to Institute for Clinical and Economic Review. Peanut flour from the grocery store is cheaper, but comes with the risk of bacteria or other contamination.
“This product offers some reassurance, and that matters,” Dr. Kim said.
It’s good to have more options for food allergy treatment. “We need a more proactive way to treat food allergy; avoidance is not good enough,” he explained. “And presumably, at some point, the patient will be able to eat a grocery-store peanut instead of buying the pills.”
The art of medicine
But not all allergists will be able to make the protocol work. And it’s not clear whether there is room to alter treatment and offer patients with a higher tolerance a higher starting dose. What we do know, though, is that “the product leaves little room for ‘the art of medicine,’ ” Kim said.
That art is practiced by Arnon Elizur, MD, from the Shamir Medical Center in Tzrifin, Israel, but it’s backed by a rigid home-grown protocol.
Since 2010, he has treated 1,800 patients for peanut allergy, updosing slowly to a tolerance of 3,000 mg of peanut, the equivalent of 10 peanuts. He keeps the maintenance dose at four peanuts (1,200 mg). His center takes a personalized approach, starting patients on the highest dose they can tolerate and working up, with daily patient check-ins from home and a staff available around the clock to answer questions and deal with reactions.
“We aim for full sensitization,” Dr. Elizur said in an interview.
The peanut pill is “a big step forward” for immunotherapy, he said. It is “a standardized product, checked for bacteria and allergen content, which is available to a wide community of physicians.”
But, he pointed out, “it’s expensive.” And it’s only for peanut. “There are millions of food-allergic patients around the world dying from adverse reactions to many different kinds of food. We don’t want to wait for years for a product for all of them. We can use the actual food.”
He questions the lifelong maintenance protocol with a daily 300-mg pill. “If you can’t eat a peanut, why would you buy a drug that’s a peanut?” he asked.
He also said he’s disappointed that the product is not indicated for adults.
At the Shamir clinic, reactions are closely monitored. “Some are mild, others we treat with autoinjectors, epinephrine,” he reported. “Those are the most undesirable.”
Data from his center show that reactions occur in about 15% of patients. But his treatment success rates are good. In an average of 8 months, he is able to get 80% of his adult patients to full sensitization.
But it’s not for all patients or for all clinics, he acknowledged. “We continue to look at this balance in quality of life throughout the process. Our goal is to improve the quality of life threshold.”
Treatment that involves “native food” is “a lot of work” and requires “a lot of investment,” Dr. Elizur said. His center uses a web reporting system to maintain a 24/7 dialogue with patients, “and we look at the reports every day.” They also have a physician on call at all times. “Not everyone can commit to providing care throughout the day and night.”
His center charges the equivalent of $US3,000 per food allergy treated. “That’s whether it takes 6 months or 2 years,” he said.
There are more than 1,000 people on his 3-year waiting list.
“This is the first year that the American College of Allergy, Asthma, and Immunology is not hosting a pro–con debate on oral immunotherapy,” Dr. Kim pointed out. “We have a therapy now.”
However, the pandemic has slowed treatment uptake. “Immunotherapy is not easy to do, whether it’s FDA approved or not,” he explained. With at least 11 doctor visits in the first 6 months – each visit is between 30 minutes and 2-3 hours long – it hasn’t been possible to set up this year. “It’s not ideal.”
It will be interesting to see “how this will roll out and how it will be adopted,” Dr. Kim said. “From a food allergy point of view, the next 12 months are going to be very interesting.”
Dr. Kim reports receiving consulting honorarium from Aimmune, the maker of Palforzia; being on the clinical medical advisory board for DBV Technologies; and consulting for Aimmune, Allakos, Allergenis, DBV, Duke Clinical Research Institute, Ukko Incorporated, Vibrant America, and Kenota Health. Dr. Elizur has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Peanut allergy immunotherapy now comes with approval from the US Food and Drug Administration (FDA), but it also comes with protocols, standards, and paperwork. Whether it will be widely adopted has yet to be determined.
A few dozen allergists around the world have been offering food allergy immunotherapy for many years, having developed their own measuring techniques using store-bought food.
But the vast majority of allergists are not interested in developing home-grown treatments, not only because it involves research and development, but also because it comes with legal risks.
“Finally we have another treatment option,” said Edwin Kim, MD, from the UNC Allergy and Immunology Clinic in Chapel Hill, N.C. “This is what we were waiting for. It’s not cowboy stuff; this works.”
In January, the FDA approved peanut allergen powder (Palforzia) for patients 4-17 years of age, as reported by Medscape Medical News.
The pill contains measured doses of peanut flour and comes with a protocol that will allow allergists to bring patients to a peanut tolerance of 300 mg (about one peanut) and a black-box warning about anaphylaxis risk.
And before allergists can prescribe it, they must take a Risk Evaluation and Mitigation Strategy course to learn about dosing and the allergic reaction protocol.
“That may scare some away,” said Dr. Kim, who discussed the FDA-approved option during his presentation at the American College of Allergy, Asthma & Immunology 2020 Annual Scientific Meeting.
Allergic reaction, including the potential for anaphylaxis, has always been an issue with immunotherapy.
“People make the argument that there is a difference” between an expected allergic reaction – such as one that occurs after the administration of immunotherapy – and an unexpected reaction, he said. Because an expected reaction can be treated quickly, “some feel these expected reactions don’t matter so much.”
“Others say a reaction is a reaction” and argue that if, a treatment causes reaction, then it doesn’t make sense, he explained.
It comes down to patients – they must be willing to take a risk to develop tolerance and improve their quality of life – and the allergists willing to treat them.
The peanut powder involves paperwork, preauthorization forms, denials of care, a higher price tag, regimented procedures, and a prerequisite number of visits with patients. “Not everyone will want to do this,” said Dr. Kim.
The regimen involves three phases. During initial dose escalation, five doses are administered in the office on day 1. Then, over the next 6 months, updoses are administered during 11 in-office sessions and a 300-mg tolerance is achieved. Finally, to maintain tolerance to one peanut, daily doses are administered at home.
The drug cost alone is about $4,200 a year, according to Institute for Clinical and Economic Review. Peanut flour from the grocery store is cheaper, but comes with the risk of bacteria or other contamination.
“This product offers some reassurance, and that matters,” Dr. Kim said.
It’s good to have more options for food allergy treatment. “We need a more proactive way to treat food allergy; avoidance is not good enough,” he explained. “And presumably, at some point, the patient will be able to eat a grocery-store peanut instead of buying the pills.”
The art of medicine
But not all allergists will be able to make the protocol work. And it’s not clear whether there is room to alter treatment and offer patients with a higher tolerance a higher starting dose. What we do know, though, is that “the product leaves little room for ‘the art of medicine,’ ” Kim said.
That art is practiced by Arnon Elizur, MD, from the Shamir Medical Center in Tzrifin, Israel, but it’s backed by a rigid home-grown protocol.
Since 2010, he has treated 1,800 patients for peanut allergy, updosing slowly to a tolerance of 3,000 mg of peanut, the equivalent of 10 peanuts. He keeps the maintenance dose at four peanuts (1,200 mg). His center takes a personalized approach, starting patients on the highest dose they can tolerate and working up, with daily patient check-ins from home and a staff available around the clock to answer questions and deal with reactions.
“We aim for full sensitization,” Dr. Elizur said in an interview.
The peanut pill is “a big step forward” for immunotherapy, he said. It is “a standardized product, checked for bacteria and allergen content, which is available to a wide community of physicians.”
But, he pointed out, “it’s expensive.” And it’s only for peanut. “There are millions of food-allergic patients around the world dying from adverse reactions to many different kinds of food. We don’t want to wait for years for a product for all of them. We can use the actual food.”
He questions the lifelong maintenance protocol with a daily 300-mg pill. “If you can’t eat a peanut, why would you buy a drug that’s a peanut?” he asked.
He also said he’s disappointed that the product is not indicated for adults.
At the Shamir clinic, reactions are closely monitored. “Some are mild, others we treat with autoinjectors, epinephrine,” he reported. “Those are the most undesirable.”
Data from his center show that reactions occur in about 15% of patients. But his treatment success rates are good. In an average of 8 months, he is able to get 80% of his adult patients to full sensitization.
But it’s not for all patients or for all clinics, he acknowledged. “We continue to look at this balance in quality of life throughout the process. Our goal is to improve the quality of life threshold.”
Treatment that involves “native food” is “a lot of work” and requires “a lot of investment,” Dr. Elizur said. His center uses a web reporting system to maintain a 24/7 dialogue with patients, “and we look at the reports every day.” They also have a physician on call at all times. “Not everyone can commit to providing care throughout the day and night.”
His center charges the equivalent of $US3,000 per food allergy treated. “That’s whether it takes 6 months or 2 years,” he said.
There are more than 1,000 people on his 3-year waiting list.
“This is the first year that the American College of Allergy, Asthma, and Immunology is not hosting a pro–con debate on oral immunotherapy,” Dr. Kim pointed out. “We have a therapy now.”
However, the pandemic has slowed treatment uptake. “Immunotherapy is not easy to do, whether it’s FDA approved or not,” he explained. With at least 11 doctor visits in the first 6 months – each visit is between 30 minutes and 2-3 hours long – it hasn’t been possible to set up this year. “It’s not ideal.”
It will be interesting to see “how this will roll out and how it will be adopted,” Dr. Kim said. “From a food allergy point of view, the next 12 months are going to be very interesting.”
Dr. Kim reports receiving consulting honorarium from Aimmune, the maker of Palforzia; being on the clinical medical advisory board for DBV Technologies; and consulting for Aimmune, Allakos, Allergenis, DBV, Duke Clinical Research Institute, Ukko Incorporated, Vibrant America, and Kenota Health. Dr. Elizur has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Peanut allergy immunotherapy now comes with approval from the US Food and Drug Administration (FDA), but it also comes with protocols, standards, and paperwork. Whether it will be widely adopted has yet to be determined.
A few dozen allergists around the world have been offering food allergy immunotherapy for many years, having developed their own measuring techniques using store-bought food.
But the vast majority of allergists are not interested in developing home-grown treatments, not only because it involves research and development, but also because it comes with legal risks.
“Finally we have another treatment option,” said Edwin Kim, MD, from the UNC Allergy and Immunology Clinic in Chapel Hill, N.C. “This is what we were waiting for. It’s not cowboy stuff; this works.”
In January, the FDA approved peanut allergen powder (Palforzia) for patients 4-17 years of age, as reported by Medscape Medical News.
The pill contains measured doses of peanut flour and comes with a protocol that will allow allergists to bring patients to a peanut tolerance of 300 mg (about one peanut) and a black-box warning about anaphylaxis risk.
And before allergists can prescribe it, they must take a Risk Evaluation and Mitigation Strategy course to learn about dosing and the allergic reaction protocol.
“That may scare some away,” said Dr. Kim, who discussed the FDA-approved option during his presentation at the American College of Allergy, Asthma & Immunology 2020 Annual Scientific Meeting.
Allergic reaction, including the potential for anaphylaxis, has always been an issue with immunotherapy.
“People make the argument that there is a difference” between an expected allergic reaction – such as one that occurs after the administration of immunotherapy – and an unexpected reaction, he said. Because an expected reaction can be treated quickly, “some feel these expected reactions don’t matter so much.”
“Others say a reaction is a reaction” and argue that if, a treatment causes reaction, then it doesn’t make sense, he explained.
It comes down to patients – they must be willing to take a risk to develop tolerance and improve their quality of life – and the allergists willing to treat them.
The peanut powder involves paperwork, preauthorization forms, denials of care, a higher price tag, regimented procedures, and a prerequisite number of visits with patients. “Not everyone will want to do this,” said Dr. Kim.
The regimen involves three phases. During initial dose escalation, five doses are administered in the office on day 1. Then, over the next 6 months, updoses are administered during 11 in-office sessions and a 300-mg tolerance is achieved. Finally, to maintain tolerance to one peanut, daily doses are administered at home.
The drug cost alone is about $4,200 a year, according to Institute for Clinical and Economic Review. Peanut flour from the grocery store is cheaper, but comes with the risk of bacteria or other contamination.
“This product offers some reassurance, and that matters,” Dr. Kim said.
It’s good to have more options for food allergy treatment. “We need a more proactive way to treat food allergy; avoidance is not good enough,” he explained. “And presumably, at some point, the patient will be able to eat a grocery-store peanut instead of buying the pills.”
The art of medicine
But not all allergists will be able to make the protocol work. And it’s not clear whether there is room to alter treatment and offer patients with a higher tolerance a higher starting dose. What we do know, though, is that “the product leaves little room for ‘the art of medicine,’ ” Kim said.
That art is practiced by Arnon Elizur, MD, from the Shamir Medical Center in Tzrifin, Israel, but it’s backed by a rigid home-grown protocol.
Since 2010, he has treated 1,800 patients for peanut allergy, updosing slowly to a tolerance of 3,000 mg of peanut, the equivalent of 10 peanuts. He keeps the maintenance dose at four peanuts (1,200 mg). His center takes a personalized approach, starting patients on the highest dose they can tolerate and working up, with daily patient check-ins from home and a staff available around the clock to answer questions and deal with reactions.
“We aim for full sensitization,” Dr. Elizur said in an interview.
The peanut pill is “a big step forward” for immunotherapy, he said. It is “a standardized product, checked for bacteria and allergen content, which is available to a wide community of physicians.”
But, he pointed out, “it’s expensive.” And it’s only for peanut. “There are millions of food-allergic patients around the world dying from adverse reactions to many different kinds of food. We don’t want to wait for years for a product for all of them. We can use the actual food.”
He questions the lifelong maintenance protocol with a daily 300-mg pill. “If you can’t eat a peanut, why would you buy a drug that’s a peanut?” he asked.
He also said he’s disappointed that the product is not indicated for adults.
At the Shamir clinic, reactions are closely monitored. “Some are mild, others we treat with autoinjectors, epinephrine,” he reported. “Those are the most undesirable.”
Data from his center show that reactions occur in about 15% of patients. But his treatment success rates are good. In an average of 8 months, he is able to get 80% of his adult patients to full sensitization.
But it’s not for all patients or for all clinics, he acknowledged. “We continue to look at this balance in quality of life throughout the process. Our goal is to improve the quality of life threshold.”
Treatment that involves “native food” is “a lot of work” and requires “a lot of investment,” Dr. Elizur said. His center uses a web reporting system to maintain a 24/7 dialogue with patients, “and we look at the reports every day.” They also have a physician on call at all times. “Not everyone can commit to providing care throughout the day and night.”
His center charges the equivalent of $US3,000 per food allergy treated. “That’s whether it takes 6 months or 2 years,” he said.
There are more than 1,000 people on his 3-year waiting list.
“This is the first year that the American College of Allergy, Asthma, and Immunology is not hosting a pro–con debate on oral immunotherapy,” Dr. Kim pointed out. “We have a therapy now.”
However, the pandemic has slowed treatment uptake. “Immunotherapy is not easy to do, whether it’s FDA approved or not,” he explained. With at least 11 doctor visits in the first 6 months – each visit is between 30 minutes and 2-3 hours long – it hasn’t been possible to set up this year. “It’s not ideal.”
It will be interesting to see “how this will roll out and how it will be adopted,” Dr. Kim said. “From a food allergy point of view, the next 12 months are going to be very interesting.”
Dr. Kim reports receiving consulting honorarium from Aimmune, the maker of Palforzia; being on the clinical medical advisory board for DBV Technologies; and consulting for Aimmune, Allakos, Allergenis, DBV, Duke Clinical Research Institute, Ukko Incorporated, Vibrant America, and Kenota Health. Dr. Elizur has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Moderna: Interim data show 94.5% efficacy for COVID-19 vaccine, will seek FDA EUA
The Moderna mRNA-1273 vaccine, in development to prevent COVID-19, yielded 94.5% efficacy in early results and is generally well tolerated, the company announced early Monday. The product can be stored at refrigeration temperatures common to many physician offices, pharmacies, and hospitals.
The first interim results of the phase 3 COVE trial included 95 participants with confirmed COVID-19. An independent data safety monitoring board, which was appointed by the National Institutes of Health, informed Moderna that 90 of the patients who were positive for COVID-19 were in a placebo group and that 5 patients were in the mRNA-1273 vaccine group, resulting in a vaccine efficacy of 94.5% (P < .0001).
Interim data included 11 patients with severe COVID-19, all of whom were in the placebo group.
“This positive interim analysis from our phase 3 study has given us the first clinical validation that our vaccine can prevent COVID-19 disease, including severe disease,” said Stéphane Bancel, CEO of Moderna, said in a statement.
The vaccine met its primary study endpoint, which was based on adjudicated data that were collected starting 2 weeks after the second dose of mRNA-1273. The interim study population included people who could be at higher risk for COVID-19, including 15 adults aged 65 years and older and 20 participants from diverse communities.
Safety data
The DSMB also reviewed safety data for the COVE study interim results. The vaccine was generally safe and well tolerated, as determined on the basis of solicited adverse events. Most adverse events were mild to moderate and were generally short-lived, according to a company news release.
Injection-site pain was reported in 2.7% of participants after the first dose. After the second dose, 9.7% of participants reported fatigue, 8.9% reported myalgia, 5.2% reported arthralgia, 4.5% reported headache, 4.1% reported pain, and 2.0% reported erythema or redness at the injection site.
Moderna plans to request emergency-use authorization (EUA) from the Food and Drug Administration in the coming weeks. The company expects that the EUA will be based on more data from the COVE study, including a final analysis of 151 patients with a median follow-up of more than 2 months. Moderna also plans to seek authorizations from global regulatory agencies.
The company expects to have approximately 20 million doses of mRNA-1273 ready to ship in the United States by the end of the year. In addition, the company says it remains on track to manufacture between 500 million and 1 billion doses globally in 2021.
Moderna is developing distribution plans in conjunction with the Centers for Disease Control and Prevention, the federal government’s Operation Warp Speed, and McKesson, a COVID-19 vaccine distributor contracted by the U.S. government.
Refrigeration requirements
The mRNA-1273 vaccine can be shipped and stored for up to 6 months at –20° C (about –4° F), a temperature maintained in most home or medical freezers, according to Moderna. The company expects that, after the product thaws, it will remain stable at standard refrigerator temperatures of 2°-8° C (36°-46° F) for up to 30 days within the 6-month shelf life.
Because the mRNA-1273 vaccine is stable at these refrigerator temperatures, it can be stored at most physicians’ offices, pharmacies, and hospitals, the company noted. In contrast, the similar Pfizer BTN162b2 vaccine – early results for which showed a 90% efficacy rate – requires shipment and storage at “deep-freeze” conditions of –70° C or –80° C, which is more challenging from a logistic point of view.
Moderna’s mRNA-1273 can be kept at room temperature for up to 12 hours after removal from a refrigerator for patient administration. The vaccine will not require dilution prior to use.
More than 30,000 people aged older than 18 years in the United States are enrolled in the COVE study. The research is being conducted in collaboration with the National Institute of Allergy and Infectious Diseases and the Biomedical Advanced Research and Development Authority, part of the Office of the Assistant Secretary for Preparedness and Response at the Department of Health & Human Services.
A version of this article originally appeared on Medscape.com.
The Moderna mRNA-1273 vaccine, in development to prevent COVID-19, yielded 94.5% efficacy in early results and is generally well tolerated, the company announced early Monday. The product can be stored at refrigeration temperatures common to many physician offices, pharmacies, and hospitals.
The first interim results of the phase 3 COVE trial included 95 participants with confirmed COVID-19. An independent data safety monitoring board, which was appointed by the National Institutes of Health, informed Moderna that 90 of the patients who were positive for COVID-19 were in a placebo group and that 5 patients were in the mRNA-1273 vaccine group, resulting in a vaccine efficacy of 94.5% (P < .0001).
Interim data included 11 patients with severe COVID-19, all of whom were in the placebo group.
“This positive interim analysis from our phase 3 study has given us the first clinical validation that our vaccine can prevent COVID-19 disease, including severe disease,” said Stéphane Bancel, CEO of Moderna, said in a statement.
The vaccine met its primary study endpoint, which was based on adjudicated data that were collected starting 2 weeks after the second dose of mRNA-1273. The interim study population included people who could be at higher risk for COVID-19, including 15 adults aged 65 years and older and 20 participants from diverse communities.
Safety data
The DSMB also reviewed safety data for the COVE study interim results. The vaccine was generally safe and well tolerated, as determined on the basis of solicited adverse events. Most adverse events were mild to moderate and were generally short-lived, according to a company news release.
Injection-site pain was reported in 2.7% of participants after the first dose. After the second dose, 9.7% of participants reported fatigue, 8.9% reported myalgia, 5.2% reported arthralgia, 4.5% reported headache, 4.1% reported pain, and 2.0% reported erythema or redness at the injection site.
Moderna plans to request emergency-use authorization (EUA) from the Food and Drug Administration in the coming weeks. The company expects that the EUA will be based on more data from the COVE study, including a final analysis of 151 patients with a median follow-up of more than 2 months. Moderna also plans to seek authorizations from global regulatory agencies.
The company expects to have approximately 20 million doses of mRNA-1273 ready to ship in the United States by the end of the year. In addition, the company says it remains on track to manufacture between 500 million and 1 billion doses globally in 2021.
Moderna is developing distribution plans in conjunction with the Centers for Disease Control and Prevention, the federal government’s Operation Warp Speed, and McKesson, a COVID-19 vaccine distributor contracted by the U.S. government.
Refrigeration requirements
The mRNA-1273 vaccine can be shipped and stored for up to 6 months at –20° C (about –4° F), a temperature maintained in most home or medical freezers, according to Moderna. The company expects that, after the product thaws, it will remain stable at standard refrigerator temperatures of 2°-8° C (36°-46° F) for up to 30 days within the 6-month shelf life.
Because the mRNA-1273 vaccine is stable at these refrigerator temperatures, it can be stored at most physicians’ offices, pharmacies, and hospitals, the company noted. In contrast, the similar Pfizer BTN162b2 vaccine – early results for which showed a 90% efficacy rate – requires shipment and storage at “deep-freeze” conditions of –70° C or –80° C, which is more challenging from a logistic point of view.
Moderna’s mRNA-1273 can be kept at room temperature for up to 12 hours after removal from a refrigerator for patient administration. The vaccine will not require dilution prior to use.
More than 30,000 people aged older than 18 years in the United States are enrolled in the COVE study. The research is being conducted in collaboration with the National Institute of Allergy and Infectious Diseases and the Biomedical Advanced Research and Development Authority, part of the Office of the Assistant Secretary for Preparedness and Response at the Department of Health & Human Services.
A version of this article originally appeared on Medscape.com.
The Moderna mRNA-1273 vaccine, in development to prevent COVID-19, yielded 94.5% efficacy in early results and is generally well tolerated, the company announced early Monday. The product can be stored at refrigeration temperatures common to many physician offices, pharmacies, and hospitals.
The first interim results of the phase 3 COVE trial included 95 participants with confirmed COVID-19. An independent data safety monitoring board, which was appointed by the National Institutes of Health, informed Moderna that 90 of the patients who were positive for COVID-19 were in a placebo group and that 5 patients were in the mRNA-1273 vaccine group, resulting in a vaccine efficacy of 94.5% (P < .0001).
Interim data included 11 patients with severe COVID-19, all of whom were in the placebo group.
“This positive interim analysis from our phase 3 study has given us the first clinical validation that our vaccine can prevent COVID-19 disease, including severe disease,” said Stéphane Bancel, CEO of Moderna, said in a statement.
The vaccine met its primary study endpoint, which was based on adjudicated data that were collected starting 2 weeks after the second dose of mRNA-1273. The interim study population included people who could be at higher risk for COVID-19, including 15 adults aged 65 years and older and 20 participants from diverse communities.
Safety data
The DSMB also reviewed safety data for the COVE study interim results. The vaccine was generally safe and well tolerated, as determined on the basis of solicited adverse events. Most adverse events were mild to moderate and were generally short-lived, according to a company news release.
Injection-site pain was reported in 2.7% of participants after the first dose. After the second dose, 9.7% of participants reported fatigue, 8.9% reported myalgia, 5.2% reported arthralgia, 4.5% reported headache, 4.1% reported pain, and 2.0% reported erythema or redness at the injection site.
Moderna plans to request emergency-use authorization (EUA) from the Food and Drug Administration in the coming weeks. The company expects that the EUA will be based on more data from the COVE study, including a final analysis of 151 patients with a median follow-up of more than 2 months. Moderna also plans to seek authorizations from global regulatory agencies.
The company expects to have approximately 20 million doses of mRNA-1273 ready to ship in the United States by the end of the year. In addition, the company says it remains on track to manufacture between 500 million and 1 billion doses globally in 2021.
Moderna is developing distribution plans in conjunction with the Centers for Disease Control and Prevention, the federal government’s Operation Warp Speed, and McKesson, a COVID-19 vaccine distributor contracted by the U.S. government.
Refrigeration requirements
The mRNA-1273 vaccine can be shipped and stored for up to 6 months at –20° C (about –4° F), a temperature maintained in most home or medical freezers, according to Moderna. The company expects that, after the product thaws, it will remain stable at standard refrigerator temperatures of 2°-8° C (36°-46° F) for up to 30 days within the 6-month shelf life.
Because the mRNA-1273 vaccine is stable at these refrigerator temperatures, it can be stored at most physicians’ offices, pharmacies, and hospitals, the company noted. In contrast, the similar Pfizer BTN162b2 vaccine – early results for which showed a 90% efficacy rate – requires shipment and storage at “deep-freeze” conditions of –70° C or –80° C, which is more challenging from a logistic point of view.
Moderna’s mRNA-1273 can be kept at room temperature for up to 12 hours after removal from a refrigerator for patient administration. The vaccine will not require dilution prior to use.
More than 30,000 people aged older than 18 years in the United States are enrolled in the COVE study. The research is being conducted in collaboration with the National Institute of Allergy and Infectious Diseases and the Biomedical Advanced Research and Development Authority, part of the Office of the Assistant Secretary for Preparedness and Response at the Department of Health & Human Services.
A version of this article originally appeared on Medscape.com.
Combined OCT, cardiac MRI unravels root cause in most MINOCA
Optical CT (OCT) plus cardiac MRI (CMR) provides a more specific diagnosis in the majority of women presenting with myocardial infarction with nonobstructive coronary arteries (MINOCA).
The multimodal imaging strategy identified the underlying cause of MINOCA in 85% of women in the HARP-MINOCA study. Overall, 64% of women had a true MI and 21% had an alternate nonischemic diagnosis, most commonly myocarditis.

“OCTCMR findings correlated well with OCT culprit lesions, demonstrating that nonobstructive culprit lesions frequently cause MINOCA,” said study author Harmony Reynolds, MD, director of New York University Langone’s Sarah Ross Soter Center for Women’s Cardiovascular Research.
The results were presented at the virtual American Heart Association (AHA) Scientific Sessions 2020 and published simultaneously in Circulation.
MINOCA occurs in up to 15% of patients with MI and is defined as MI meeting the universal definition but with less than 50% stenosis in all major epicardial arteries on angiography and no specific alternate diagnosis to explain the presentation.
It is three times more common in women than in men and also disproportionately affects Black, Hispanic, Maori, and Pacific persons. MINOCA has several causes, leading to uncertainty in diagnostic testing and treatment.
“Different doctors tell patients different messages about MINOCA and may incorrectly say the event wasn’t a heart attack,” Dr. Reynolds said in an earlier press briefing. “I had a patient who was told ‘your arteries are open,’ and they gave her Xanax.”
As part of the Women’s Heart Attack Research Program (HARP), researchers enrolled 301 women with a clinical diagnosis of MI, of whom 170 were diagnosed with MINOCA during angiography and underwent OCT at that time, followed by CMR within 1 week of the acute presentation.
All images were interpreted by an independent core laboratory blinded to results of the other tests and clinical information. The final cohort included 145 women with interpretable OCT images.
Their median age was 60 years, 49.7% were white non-Hispanic, and 97% presented with a provisional diagnosis of non–ST-segment MI. Their median peak troponin level was 0.94 ng/mL.
OCT identified a definite or probable culprit lesion in 46% of women, most commonly atherosclerosis or thrombosis. On multivariable analysis, having a culprit lesion was associated with older age, abnormal angiography findings at the site, and diabetes, but not peak troponin level or severity of angiographic stenosis.
CMR available in 116 women showed evidence of infarction or regional injury in 69%. Multivariate predictors of an abnormal CMR were higher peak troponin and diastolic blood pressure but not an OCT culprit lesion or angiographic stenosis severity.
When the OCT and CMR results were combined, a cause of MINOCA was identified in 84.5% of women. Three-fourths of the causes were ischemic (64% MI) and one-quarter were nonischemic (15% myocarditis, 3% Takotsubo syndrome, and 3% nonischemic cardiomyopathy). In the remaining 15%, no cause of MINOCA was identified.
To emphasize the effect multimodal imaging can have on treatment, Dr. Reynolds highlighted a 44-year-old woman with no risk factors for coronary artery disease who had chest pain in the context of heavy menstrual bleeding, a low hemoglobin level, and peak troponin level of 3.25 ng/mL.
Unexpectedly, imaging revealed a left anterior descending (LAD) plaque rupture in a thin-cap fibroatheroma, causing a small transmural infarction at the terminus of the LAD.
“Without this diagnosis, it’s unlikely she would have received antiplatelet therapy or statins and might have been given a diagnosis of supply/demand mismatch, when the real diagnosis was MI,” Dr. Reynolds observed.
“Finally we can say this is not just crazy women. There is really something going on,” said panelist Roxana Mehran, MD, of the Icahn School of Medicine at Mount Sinai in New York. “You have now told us this is most likely atherosclerosis for pretty much 85% of the cases. So make the diagnosis and, of course, make sure you treat these patients accordingly for risk factor modification, really thinking about a ruptured plaque.”
Combining OCT and MRI may result in a more specific diagnosis and better treatment but also raises costs and logistical considerations.
“Implementation challenges are that not every form of testing is available in every medical center,” Dr. Reynolds said in an interview. “Many centers have cardiac MRI,” whereas “OCT is not currently available at most medical centers where heart attack patients are treated but is available at specialized centers.”
Asked during the session about the use of CT angiography, invited discussant Martha Gulati, MD, president-elect of the American Society for Preventive Cardiology, said, “For me, CT is helpful when I’m not sure if there’s any plaque because the angiogram looked really normal and there was no opportunity to do intracoronary imaging. And sometimes that will help me, in particular, if a patient doesn’t want to take a statin.”
Dr. Gulati pointed out that the European Society of Cardiology MINOCA guidelines recommend OCT and CMR, whereas the 2019 AHA statement on MINOCA, which she coauthored, also recommends OCT and CMR, but almost as one or the other.
“We already said that you should do cardiac MR to try to make a diagnosis, but I think the combination of the two needs to be emphasized when we next draft these guidelines. It really will help,” Dr. Gulati said in an interview.
“But using OCT, particularly, needs to be in the setting of the MI. I don’t think you want to do a procedure again,” she said. “So we really need it to become more widely available because at the time of an MI, you won’t necessarily know that you’re not going to find an obstructive lesion.”
Dr. Gulati pointed out several unanswered questions, including whether the diagnosis was missed in some patients, because OCT of all three vessels was available in only 59%, and how the use of high-sensitivity troponin, which was left up to the individual institution, might affect the usefulness of OCT and CMR.
It’s also unknown whether the mechanism is different for ST-segment elevation MI, as the trial included very few cases, although MINOCA often occurs in this setting. Future OCT/CMR studies will also need to enroll men to determine potential sex differences, if any.
Commenting on the study, B. Hadley Wilson, MD, Sanger Heart & Vascular Institute in Charlotte, N.C., said, “There would need to be further justification of this invasive interventional procedure to be sure that the benefit outweighed the risk of putting a wire and an OCT catheter down patients without any significant angiographic blockage and to assure interventional cardiologists of its value here.”
He pointed out that noninvasive CMR appears helpful in the diagnosis of nearly three-quarters of these patients and perhaps could be done first to direct which of those with an ischemic cause might benefit from invasive OCT at catheterization. This seems most pertinent in patients with a high suspicion of coronary artery disease or recurrent MINOCA.
“Overall, we need to consider the expense, logistics, and small risk of these combined modalities, particularly in everyday practice, before making recommendations,” Dr. Wilson said. “ Since OCT is much less available than intravascular ultrasound, it would require a challenging marketplace paradigm shift to implement this multimodality imaging strategy regionally and locally in the U.S., including the added costs. However, further study to direct the more judicious use of either CMR and/or combined with OCT is warranted in these patients.”
The study was funded by the AHA through a grant from the Go Red for Women Strategically Focused Research Network. Dr. Reynolds reported in-kind donations from Abbott Vascular and Siemens related to the study and nonfinancial support from BioTelemetry outside the study. Dr. Gulati and Dr. Wilson reported having no relevant disclosures.
A version of this article originally appeared on Medscape.com.
Optical CT (OCT) plus cardiac MRI (CMR) provides a more specific diagnosis in the majority of women presenting with myocardial infarction with nonobstructive coronary arteries (MINOCA).
The multimodal imaging strategy identified the underlying cause of MINOCA in 85% of women in the HARP-MINOCA study. Overall, 64% of women had a true MI and 21% had an alternate nonischemic diagnosis, most commonly myocarditis.
“OCTCMR findings correlated well with OCT culprit lesions, demonstrating that nonobstructive culprit lesions frequently cause MINOCA,” said study author Harmony Reynolds, MD, director of New York University Langone’s Sarah Ross Soter Center for Women’s Cardiovascular Research.
The results were presented at the virtual American Heart Association (AHA) Scientific Sessions 2020 and published simultaneously in Circulation.
MINOCA occurs in up to 15% of patients with MI and is defined as MI meeting the universal definition but with less than 50% stenosis in all major epicardial arteries on angiography and no specific alternate diagnosis to explain the presentation.
It is three times more common in women than in men and also disproportionately affects Black, Hispanic, Maori, and Pacific persons. MINOCA has several causes, leading to uncertainty in diagnostic testing and treatment.
“Different doctors tell patients different messages about MINOCA and may incorrectly say the event wasn’t a heart attack,” Dr. Reynolds said in an earlier press briefing. “I had a patient who was told ‘your arteries are open,’ and they gave her Xanax.”
As part of the Women’s Heart Attack Research Program (HARP), researchers enrolled 301 women with a clinical diagnosis of MI, of whom 170 were diagnosed with MINOCA during angiography and underwent OCT at that time, followed by CMR within 1 week of the acute presentation.
All images were interpreted by an independent core laboratory blinded to results of the other tests and clinical information. The final cohort included 145 women with interpretable OCT images.
Their median age was 60 years, 49.7% were white non-Hispanic, and 97% presented with a provisional diagnosis of non–ST-segment MI. Their median peak troponin level was 0.94 ng/mL.
OCT identified a definite or probable culprit lesion in 46% of women, most commonly atherosclerosis or thrombosis. On multivariable analysis, having a culprit lesion was associated with older age, abnormal angiography findings at the site, and diabetes, but not peak troponin level or severity of angiographic stenosis.
CMR available in 116 women showed evidence of infarction or regional injury in 69%. Multivariate predictors of an abnormal CMR were higher peak troponin and diastolic blood pressure but not an OCT culprit lesion or angiographic stenosis severity.
When the OCT and CMR results were combined, a cause of MINOCA was identified in 84.5% of women. Three-fourths of the causes were ischemic (64% MI) and one-quarter were nonischemic (15% myocarditis, 3% Takotsubo syndrome, and 3% nonischemic cardiomyopathy). In the remaining 15%, no cause of MINOCA was identified.
To emphasize the effect multimodal imaging can have on treatment, Dr. Reynolds highlighted a 44-year-old woman with no risk factors for coronary artery disease who had chest pain in the context of heavy menstrual bleeding, a low hemoglobin level, and peak troponin level of 3.25 ng/mL.
Unexpectedly, imaging revealed a left anterior descending (LAD) plaque rupture in a thin-cap fibroatheroma, causing a small transmural infarction at the terminus of the LAD.
“Without this diagnosis, it’s unlikely she would have received antiplatelet therapy or statins and might have been given a diagnosis of supply/demand mismatch, when the real diagnosis was MI,” Dr. Reynolds observed.
“Finally we can say this is not just crazy women. There is really something going on,” said panelist Roxana Mehran, MD, of the Icahn School of Medicine at Mount Sinai in New York. “You have now told us this is most likely atherosclerosis for pretty much 85% of the cases. So make the diagnosis and, of course, make sure you treat these patients accordingly for risk factor modification, really thinking about a ruptured plaque.”
Combining OCT and MRI may result in a more specific diagnosis and better treatment but also raises costs and logistical considerations.
“Implementation challenges are that not every form of testing is available in every medical center,” Dr. Reynolds said in an interview. “Many centers have cardiac MRI,” whereas “OCT is not currently available at most medical centers where heart attack patients are treated but is available at specialized centers.”
Asked during the session about the use of CT angiography, invited discussant Martha Gulati, MD, president-elect of the American Society for Preventive Cardiology, said, “For me, CT is helpful when I’m not sure if there’s any plaque because the angiogram looked really normal and there was no opportunity to do intracoronary imaging. And sometimes that will help me, in particular, if a patient doesn’t want to take a statin.”
Dr. Gulati pointed out that the European Society of Cardiology MINOCA guidelines recommend OCT and CMR, whereas the 2019 AHA statement on MINOCA, which she coauthored, also recommends OCT and CMR, but almost as one or the other.
“We already said that you should do cardiac MR to try to make a diagnosis, but I think the combination of the two needs to be emphasized when we next draft these guidelines. It really will help,” Dr. Gulati said in an interview.
“But using OCT, particularly, needs to be in the setting of the MI. I don’t think you want to do a procedure again,” she said. “So we really need it to become more widely available because at the time of an MI, you won’t necessarily know that you’re not going to find an obstructive lesion.”
Dr. Gulati pointed out several unanswered questions, including whether the diagnosis was missed in some patients, because OCT of all three vessels was available in only 59%, and how the use of high-sensitivity troponin, which was left up to the individual institution, might affect the usefulness of OCT and CMR.
It’s also unknown whether the mechanism is different for ST-segment elevation MI, as the trial included very few cases, although MINOCA often occurs in this setting. Future OCT/CMR studies will also need to enroll men to determine potential sex differences, if any.
Commenting on the study, B. Hadley Wilson, MD, Sanger Heart & Vascular Institute in Charlotte, N.C., said, “There would need to be further justification of this invasive interventional procedure to be sure that the benefit outweighed the risk of putting a wire and an OCT catheter down patients without any significant angiographic blockage and to assure interventional cardiologists of its value here.”
He pointed out that noninvasive CMR appears helpful in the diagnosis of nearly three-quarters of these patients and perhaps could be done first to direct which of those with an ischemic cause might benefit from invasive OCT at catheterization. This seems most pertinent in patients with a high suspicion of coronary artery disease or recurrent MINOCA.
“Overall, we need to consider the expense, logistics, and small risk of these combined modalities, particularly in everyday practice, before making recommendations,” Dr. Wilson said. “ Since OCT is much less available than intravascular ultrasound, it would require a challenging marketplace paradigm shift to implement this multimodality imaging strategy regionally and locally in the U.S., including the added costs. However, further study to direct the more judicious use of either CMR and/or combined with OCT is warranted in these patients.”
The study was funded by the AHA through a grant from the Go Red for Women Strategically Focused Research Network. Dr. Reynolds reported in-kind donations from Abbott Vascular and Siemens related to the study and nonfinancial support from BioTelemetry outside the study. Dr. Gulati and Dr. Wilson reported having no relevant disclosures.
A version of this article originally appeared on Medscape.com.
Optical CT (OCT) plus cardiac MRI (CMR) provides a more specific diagnosis in the majority of women presenting with myocardial infarction with nonobstructive coronary arteries (MINOCA).
The multimodal imaging strategy identified the underlying cause of MINOCA in 85% of women in the HARP-MINOCA study. Overall, 64% of women had a true MI and 21% had an alternate nonischemic diagnosis, most commonly myocarditis.
“OCTCMR findings correlated well with OCT culprit lesions, demonstrating that nonobstructive culprit lesions frequently cause MINOCA,” said study author Harmony Reynolds, MD, director of New York University Langone’s Sarah Ross Soter Center for Women’s Cardiovascular Research.
The results were presented at the virtual American Heart Association (AHA) Scientific Sessions 2020 and published simultaneously in Circulation.
MINOCA occurs in up to 15% of patients with MI and is defined as MI meeting the universal definition but with less than 50% stenosis in all major epicardial arteries on angiography and no specific alternate diagnosis to explain the presentation.
It is three times more common in women than in men and also disproportionately affects Black, Hispanic, Maori, and Pacific persons. MINOCA has several causes, leading to uncertainty in diagnostic testing and treatment.
“Different doctors tell patients different messages about MINOCA and may incorrectly say the event wasn’t a heart attack,” Dr. Reynolds said in an earlier press briefing. “I had a patient who was told ‘your arteries are open,’ and they gave her Xanax.”
As part of the Women’s Heart Attack Research Program (HARP), researchers enrolled 301 women with a clinical diagnosis of MI, of whom 170 were diagnosed with MINOCA during angiography and underwent OCT at that time, followed by CMR within 1 week of the acute presentation.
All images were interpreted by an independent core laboratory blinded to results of the other tests and clinical information. The final cohort included 145 women with interpretable OCT images.
Their median age was 60 years, 49.7% were white non-Hispanic, and 97% presented with a provisional diagnosis of non–ST-segment MI. Their median peak troponin level was 0.94 ng/mL.
OCT identified a definite or probable culprit lesion in 46% of women, most commonly atherosclerosis or thrombosis. On multivariable analysis, having a culprit lesion was associated with older age, abnormal angiography findings at the site, and diabetes, but not peak troponin level or severity of angiographic stenosis.
CMR available in 116 women showed evidence of infarction or regional injury in 69%. Multivariate predictors of an abnormal CMR were higher peak troponin and diastolic blood pressure but not an OCT culprit lesion or angiographic stenosis severity.
When the OCT and CMR results were combined, a cause of MINOCA was identified in 84.5% of women. Three-fourths of the causes were ischemic (64% MI) and one-quarter were nonischemic (15% myocarditis, 3% Takotsubo syndrome, and 3% nonischemic cardiomyopathy). In the remaining 15%, no cause of MINOCA was identified.
To emphasize the effect multimodal imaging can have on treatment, Dr. Reynolds highlighted a 44-year-old woman with no risk factors for coronary artery disease who had chest pain in the context of heavy menstrual bleeding, a low hemoglobin level, and peak troponin level of 3.25 ng/mL.
Unexpectedly, imaging revealed a left anterior descending (LAD) plaque rupture in a thin-cap fibroatheroma, causing a small transmural infarction at the terminus of the LAD.
“Without this diagnosis, it’s unlikely she would have received antiplatelet therapy or statins and might have been given a diagnosis of supply/demand mismatch, when the real diagnosis was MI,” Dr. Reynolds observed.
“Finally we can say this is not just crazy women. There is really something going on,” said panelist Roxana Mehran, MD, of the Icahn School of Medicine at Mount Sinai in New York. “You have now told us this is most likely atherosclerosis for pretty much 85% of the cases. So make the diagnosis and, of course, make sure you treat these patients accordingly for risk factor modification, really thinking about a ruptured plaque.”
Combining OCT and MRI may result in a more specific diagnosis and better treatment but also raises costs and logistical considerations.
“Implementation challenges are that not every form of testing is available in every medical center,” Dr. Reynolds said in an interview. “Many centers have cardiac MRI,” whereas “OCT is not currently available at most medical centers where heart attack patients are treated but is available at specialized centers.”
Asked during the session about the use of CT angiography, invited discussant Martha Gulati, MD, president-elect of the American Society for Preventive Cardiology, said, “For me, CT is helpful when I’m not sure if there’s any plaque because the angiogram looked really normal and there was no opportunity to do intracoronary imaging. And sometimes that will help me, in particular, if a patient doesn’t want to take a statin.”
Dr. Gulati pointed out that the European Society of Cardiology MINOCA guidelines recommend OCT and CMR, whereas the 2019 AHA statement on MINOCA, which she coauthored, also recommends OCT and CMR, but almost as one or the other.
“We already said that you should do cardiac MR to try to make a diagnosis, but I think the combination of the two needs to be emphasized when we next draft these guidelines. It really will help,” Dr. Gulati said in an interview.
“But using OCT, particularly, needs to be in the setting of the MI. I don’t think you want to do a procedure again,” she said. “So we really need it to become more widely available because at the time of an MI, you won’t necessarily know that you’re not going to find an obstructive lesion.”
Dr. Gulati pointed out several unanswered questions, including whether the diagnosis was missed in some patients, because OCT of all three vessels was available in only 59%, and how the use of high-sensitivity troponin, which was left up to the individual institution, might affect the usefulness of OCT and CMR.
It’s also unknown whether the mechanism is different for ST-segment elevation MI, as the trial included very few cases, although MINOCA often occurs in this setting. Future OCT/CMR studies will also need to enroll men to determine potential sex differences, if any.
Commenting on the study, B. Hadley Wilson, MD, Sanger Heart & Vascular Institute in Charlotte, N.C., said, “There would need to be further justification of this invasive interventional procedure to be sure that the benefit outweighed the risk of putting a wire and an OCT catheter down patients without any significant angiographic blockage and to assure interventional cardiologists of its value here.”
He pointed out that noninvasive CMR appears helpful in the diagnosis of nearly three-quarters of these patients and perhaps could be done first to direct which of those with an ischemic cause might benefit from invasive OCT at catheterization. This seems most pertinent in patients with a high suspicion of coronary artery disease or recurrent MINOCA.
“Overall, we need to consider the expense, logistics, and small risk of these combined modalities, particularly in everyday practice, before making recommendations,” Dr. Wilson said. “ Since OCT is much less available than intravascular ultrasound, it would require a challenging marketplace paradigm shift to implement this multimodality imaging strategy regionally and locally in the U.S., including the added costs. However, further study to direct the more judicious use of either CMR and/or combined with OCT is warranted in these patients.”
The study was funded by the AHA through a grant from the Go Red for Women Strategically Focused Research Network. Dr. Reynolds reported in-kind donations from Abbott Vascular and Siemens related to the study and nonfinancial support from BioTelemetry outside the study. Dr. Gulati and Dr. Wilson reported having no relevant disclosures.
A version of this article originally appeared on Medscape.com.