User login
-
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Obesity and lung disease: Much more than BMI
The diverse effects of obesity on lung health and disease are increasingly being teased apart, with researchers honing in on the impact of metabolic dysfunction, circulating inflammatory factors produced by adipose tissue, lipid handling, and other factors – in addition to body mass index – that are associated with the obese state.
“The bird’s eye view is that obesity completely changes lung health. It’s something we’ve only recently begun to appreciate,” said Anne E. Dixon, MA, BM, BCh, director of the Vermont Lung Center at the University of Vermont, Burlington, who is focused on the research field of obesity and lung disease.

Structural, mechanical effects of obesity on lung function are better known and appreciated. Accumulation of fat in the mediastinum and abdominal and thoracic cavities causes reductions in lung volume, in functional residual capacity, and in the compliance of the lungs, chest wall, and entire respiratory system, for instance.
Yet obesity is more than a state of increased BMI, and “what we’ve begun to understand is that [its impact on the lungs and respiratory health] is much more complicated than just a mechanical problem,” said Dr. Dixon, also director of pulmonary and critical care medicine at the University of Vermont Medical Center and professor of medicine at the medical college.
With obesity, adipose tissue changes not only in quantity, but in function, producing proinflammatory cytokines and hormones – such as leptin, tumor necrosis factor-alpha (TNF-alpha), and interleukin-6 – that can have direct effects on the lung. Insulin resistance, which is common with obesity, is also seemingly deleterious. And obesity-associated changes in immune function, lipid handling, diet, and the gut microbiome may also impact lung health and disease, she said.
Dr. Dixon, who wrote about these changes in a 2018 review article in the journal CHEST and another 2019 piece in Expert Review of Respiratory Medicine, has developed a research program focused on obesity and lung disease and has edited a book and organized international conferences on the topic. (CHEST 2018;153[3]:702-9 and Exper Rev Respir Med. 2018;12[9]:755-67.)
“The more I do, the more I realize that there are multiple obesity-associated changes involved, and that [our current high level of] obesity is like a huge population-level natural experiment ... on lung health,” she told this news organization.
Associations between lung disease and the metabolic and other disturbances of obesity are most established in asthma research and have taken hold in the realm of sleep-disordered breathing. But as the prevalence of obesity continues to grow, its role in other lung diseases such as chronic obstructive pulmonary disorder (COPD) and, most recently, pulmonary arterial hypertension (PAH), is getting attention in academia.
And certainly, COVID-19 has highlighted an “urgent need” to better understand how obesity increases susceptibility to severe viral infections, Dr. Dixon added.
Here are some glimpses into current thinking and some examples of research that may have preventive and therapeutic implications in the future:
OSA and OHS
“With sleep apnea we tend to focus on anatomic considerations, but there may be relationships or interactions between obesity and neuromuscular function and neuroventilatory control,” Susheel P. Patil, MD, PhD, director of the sleep medicine program for University Hospitals and assistant professor at Case Western Reserve University, Cleveland, said in an interview.

Some studies suggest, for instance, that TNF-alpha can increase obstructive sleep apnea (OSA) susceptibility and severity through its neuroventilatory modulating properties during sleep. And the potential for additional proinflammatory cytokines produced by adipose tissue to similarly affect upper airway neuroventilatory control is an “intriguing line” of inquiry for researchers in the sleep apnea space, he said.
Leptin is of interest particularly in obesity hypoventilation syndrome (OHS), which is characterized by chronic daytime hypercapnia. Best known as a satiety hormone, leptin is produced by adipose tissue and suppresses appetite at the central nervous system level. But it has long been known that leptin also affects ventilation and the control of breathing.
When transported across the blood-brain barrier, leptin increases the hypercapnic ventilatory response, Babak Mokhlesi, MD, MSc, codirector of the Rush Lung Center and chief of pulmonary, critical care, and sleep medicine at Rush University Medical Center in Chicago, said in an interview.
Research suggests that patients with OHS may have resistance to leptin at the central nervous system level – with leptin not reaching the sites of ventilatory control. This is a “prevailing theory” and could explain why these patients “do not augment their ventilation to maintain homeostasis, normal levels of CO2,” Dr. Mokhlesi said.

“Why some patients with severe obesity develop CO2 retention while others do not is not fully understood,” he said, noting that patients with OHS can normalize their CO2 quickly when instructed to take deep breaths. “What we know is that the centers in the brain responsible for augmenting ventilation when CO2 goes up are somehow blunted.”
In a study of obese mice led by Vsevolod Y. Polotsky, MD, PhD, of Johns Hopkins University, Baltimore – and highlighted by Dr. Mokhlesi as an example of important, recent research – leptin delivered intranasally alleviated hypoventilation (and upper-airway obstruction), while intraperitoneally administered leptin did not, seemingly overcoming “central leptin deficiency.” (Am J Respir Crit Care Med. 2019;199[6]:773-83).
“This proved that there is some level of resistance in this animal model ... and has potential for therapeutics in the future,” Dr. Mokhlesi said.
Understanding the role of insulin resistance in OSA is another research focus. Some data suggest that insulin resistance, which is more common in obesity, is more prevalent in populations with OSA, Dr. Patil said. Researchers have discussed a bidirectional relationship for years, but it’s likely that insulin resistance is a precursor, he said.
In a mechanistic study published in 2016, Dr. Patil and his coinvestigators found that obese individuals with insulin resistance but without frank diabetes or sleep apnea demonstrated preclinical elevations in pharyngeal collapsibility during sleep. The findings suggest that insulin resistance could play a causal role in OSA pathogenesis by “generating requisite elevations in pharyngeal collapsibility,” they wrote (Eur. Respir J. 2016;47[6]:1718-26).
More recently, Dr. Patil noted in the interview, there is increasing appreciation in academia that the type of fat may be important to predicting OSA. “Visceral fat has a completely different cytokine-secretion profile than subcutaneous fat ... it is the more metabolically active fat that may secondarily impact upper airway function though a neuroinflammatory mechanism,” he said. “That is one of the working hypotheses today.”
Asthma
Research has so roundly suggested that metabolic dysfunction contributes to severe, poorly controlled asthma that there’s recent and growing interest in targeting metabolic dysfunction as part of the treatment of obese asthma, said Dr. Dixon, whose own research in obesity and lung disease has focused on asthma.
Data from animal models and some epidemiologic studies have suggested that drugs used to treat type 2 diabetes mellitus, such as glucagon-like peptide receptor-1 (GLPR-1) agonists and metformin, may help control asthma. In one recent study – cited by Dr. Dixon in a 2022 review of obesity and asthma – people with obesity and asthma who were prescribed GLPR-1 agonists for diabetes had fewer asthma exacerbations compared with those who took other medications for diabetes (Semin Respir Crit Care Med. 2022 Feb 17. doi: 10.1055/s-0042-1742384).
There is also research interest in targeting the pro-inflammatory adipokine interleukin 6 (IL-6), since increased circulating levels of IL-6 correlate with asthma severity, and in addressing oxidative stress in asthma through treatment with a mitochondrially targeted antioxidant, she said. Oxidative stress is increased in the airways of people with obesity, and researchers believe it may contribute to the pathophysiology of obese asthma through effects on airway nitric oxide levels.
(Her own research work at the University of Vermont has found associations between poor asthma control and high levels of leptin, and similar associations involving low levels of adiponectin, an anti-inflammatory adipokine that has been shown to downregulate eosinophil recruitment in the airways.)
Weight loss has been shown in mostly small, single-center studies to improve asthma control, but short of weight loss, researchers are also investigating the role of poor dietary quality. Thus far, data suggest that it’s the composition of the diet, and not just its contribution to weight gain, that could be impactful, Dr. Dixon said.
More basic research questions cited by Dr. Dixon include the extent to which adipose tissue inflammation causes inflammation in the lungs. “It’s a little unclear whether all the metabolic dysfunction associated with poor asthma control is causing inflammation in the lungs,” she said, though “we’ve done some work here that shows mediators produced by the adipose tissue could be impacting production of inflammatory mediators by the airway epithelium.”
Overall, she said, “the big questions [in asthma] are, how does adipose tissue affect the airway? Is it through direct effects? Through effects on the immune system? And obesity is affected by diet and the gut microbiome – how can these be [impacting] the airway?”
Obesity “is associated with so many changes – the gut, the immune system, and metabolic dysfunction, in addition to airway mechanics,” she said, “that I no longer think, as I did when I came to this, that it’s just one thing. It’s probably all of these things together.”
In the meantime, questions about potential shared pathways for the development of obesity and asthma remain. “Obesity is a risk factor for developing asthma, but it’s also entirely possible that asthma is a risk factor for developing obesity,” she said. (Some data from pediatric populations, she noted, suggest that nonobese children with asthma are at increased risk of developing obesity.)
Also important, Dr. Dixon said, is “emerging literature in the last 5-10 years” that suggests that people with obesity are more susceptible to the effects of air pollution. Research involving inner-city schoolchildren with asthma, for instance, has shown that those with obesity had worse symptoms with air pollution exposure than did those who were not obese.
Pulmonary arterial hypertension
Some research has looked at adipose tissue–produced substances in PAH, but the most well-established association in obesity and PAH involves insulin resistance.
“I don’t think we’re certain as a community that obesity [in general] is the problem – it’s not itself considered a risk factor for PAH,” Anna R. Hemnes, MD, associate professor of medicine at Vanderbilt University Medical Center in Nashville, Tenn., said in an interview. She noted that it’s “hard to dissect obesity” apart.
Researchers are “more confident,” she said, “that insulin resistance – one feature of obesity [in some people] – is associated with worse outcomes in PAH.” Metabolic disease resembling insulin resistance is common in PAH and is believed to contribute to pulmonary vascular disease and right ventricular (RV) failure – the main cause of mortality in PAH – at least in part because of increased oxidative stress.
Dr. Hemnes led a mechanistic phase II clinical trial of metformin in PAH in which the drug was associated with improved RV fractional area change and reduced RV lipid deposition (J Am Heart Assoc. 2020;9[22]:e018349), and she’s now leading a National Institutes of Health–funded multicenter trial looking at the impact of metformin and an exercise intervention on 6-minute walk distance and World Health Organization functional class in PAH.
At the Rush Lung Center, in the meantime, Dr. Mokhlesi is utilizing animal models of OSA and OHS to explore the effect of hypoxia and nighttime hypercapnia on the development of PAH. “I think the jury is still out as to whether obesity itself is a major risk factor, but if so, by what mechanism?” he said. “Is it worsening [sleep-disordered breathing], which then worsens PAH?”
COPD
The focus in COPD has traditionally been on underweight, but the relationship between obesity and COPD has increasingly been recognized in the last 10-15 years, said Frits M. E. Franssen, MD, PhD, of CIRO, a research institute in Horn, the Netherlands, that treats COPD and other chronic lung diseases, and of the department of respiratory medicine at Maastricht University.
Researchers like Dr. Franssen are trying, for one, to understand obesity’s impact on COPD pathophysiology and to tease apart the impact of both conditions on disease severity and patient-related outcomes such as exercise capacity and exercise-related symptoms.
When Dr. Franssen’s group compared responses to weight-bearing exercise (6-min. walk test) and weight-supported exercise (cycling) in obese and normal weight COPD patients matched for age, gender, and degree of airflow limitation, the researchers found that walking capacity was significantly reduced while cycling capacity was preserved in the obese group (Respirology. 2016;21[3]:483-8).
Exercise-related symptoms (dyspnea and leg fatigue) were largely comparable between the obese and normal-weight COPD patients in both exercise modalities. However, in other studies, dyspnea ratings during cycling – at any given level of ventilation – have been lower in obese patients, indicating that “additional fat mass may have a beneficial effect on lung functioning [in non–weight-bearing exercise],” he said in an interview.
Dr. Franssen’s group also has assessed body composition in overweight and obese patients with COPD and found that a significant number have low muscle mass. These patients had worse lung function, exercise tolerance, and muscle strength compared to patients with comparable BMI and normal muscle mass (Respir Res. 2021 Mar 25. doi: 10.1186/s12931-021-01689-w).
“We’d always thought that obese patients have normal muscle mass ... but now we know it can be dramatically low,” he said. In assessing obesity and formulating any weight loss plans, “we’re now interested not only in weight but in the distribution of fat mass and fat-free mass ... and in maintaining muscle mass in patients who are [prescribed dietary interventions].”
Paradoxically, in patients with severe COPD, obesity is associated with prolonged survival, while in patients with mild to moderate COPD, obesity is associated with increased mortality risk, he noted.
The impact of adipose tissue and the chronic inflammation and metabolic disturbances that characterize obesity are currently largely unexplored, he said. Researchers have not yet studied what optimal weights may be for patients with COPD. “And we’re interested in the questions, are body weight and body composition the result of the disease, or [are they] determining the type of COPD one will get?” Dr. Franssen said.
Patients with COPD who are obese have “more of the phenotype of chronic bronchitis,” he noted, “while typical emphysema patients are normally underweight.”
The diverse effects of obesity on lung health and disease are increasingly being teased apart, with researchers honing in on the impact of metabolic dysfunction, circulating inflammatory factors produced by adipose tissue, lipid handling, and other factors – in addition to body mass index – that are associated with the obese state.
“The bird’s eye view is that obesity completely changes lung health. It’s something we’ve only recently begun to appreciate,” said Anne E. Dixon, MA, BM, BCh, director of the Vermont Lung Center at the University of Vermont, Burlington, who is focused on the research field of obesity and lung disease.
Structural, mechanical effects of obesity on lung function are better known and appreciated. Accumulation of fat in the mediastinum and abdominal and thoracic cavities causes reductions in lung volume, in functional residual capacity, and in the compliance of the lungs, chest wall, and entire respiratory system, for instance.
Yet obesity is more than a state of increased BMI, and “what we’ve begun to understand is that [its impact on the lungs and respiratory health] is much more complicated than just a mechanical problem,” said Dr. Dixon, also director of pulmonary and critical care medicine at the University of Vermont Medical Center and professor of medicine at the medical college.
With obesity, adipose tissue changes not only in quantity, but in function, producing proinflammatory cytokines and hormones – such as leptin, tumor necrosis factor-alpha (TNF-alpha), and interleukin-6 – that can have direct effects on the lung. Insulin resistance, which is common with obesity, is also seemingly deleterious. And obesity-associated changes in immune function, lipid handling, diet, and the gut microbiome may also impact lung health and disease, she said.
Dr. Dixon, who wrote about these changes in a 2018 review article in the journal CHEST and another 2019 piece in Expert Review of Respiratory Medicine, has developed a research program focused on obesity and lung disease and has edited a book and organized international conferences on the topic. (CHEST 2018;153[3]:702-9 and Exper Rev Respir Med. 2018;12[9]:755-67.)
“The more I do, the more I realize that there are multiple obesity-associated changes involved, and that [our current high level of] obesity is like a huge population-level natural experiment ... on lung health,” she told this news organization.
Associations between lung disease and the metabolic and other disturbances of obesity are most established in asthma research and have taken hold in the realm of sleep-disordered breathing. But as the prevalence of obesity continues to grow, its role in other lung diseases such as chronic obstructive pulmonary disorder (COPD) and, most recently, pulmonary arterial hypertension (PAH), is getting attention in academia.
And certainly, COVID-19 has highlighted an “urgent need” to better understand how obesity increases susceptibility to severe viral infections, Dr. Dixon added.
Here are some glimpses into current thinking and some examples of research that may have preventive and therapeutic implications in the future:
OSA and OHS
“With sleep apnea we tend to focus on anatomic considerations, but there may be relationships or interactions between obesity and neuromuscular function and neuroventilatory control,” Susheel P. Patil, MD, PhD, director of the sleep medicine program for University Hospitals and assistant professor at Case Western Reserve University, Cleveland, said in an interview.
Some studies suggest, for instance, that TNF-alpha can increase obstructive sleep apnea (OSA) susceptibility and severity through its neuroventilatory modulating properties during sleep. And the potential for additional proinflammatory cytokines produced by adipose tissue to similarly affect upper airway neuroventilatory control is an “intriguing line” of inquiry for researchers in the sleep apnea space, he said.
Leptin is of interest particularly in obesity hypoventilation syndrome (OHS), which is characterized by chronic daytime hypercapnia. Best known as a satiety hormone, leptin is produced by adipose tissue and suppresses appetite at the central nervous system level. But it has long been known that leptin also affects ventilation and the control of breathing.
When transported across the blood-brain barrier, leptin increases the hypercapnic ventilatory response, Babak Mokhlesi, MD, MSc, codirector of the Rush Lung Center and chief of pulmonary, critical care, and sleep medicine at Rush University Medical Center in Chicago, said in an interview.
Research suggests that patients with OHS may have resistance to leptin at the central nervous system level – with leptin not reaching the sites of ventilatory control. This is a “prevailing theory” and could explain why these patients “do not augment their ventilation to maintain homeostasis, normal levels of CO2,” Dr. Mokhlesi said.
“Why some patients with severe obesity develop CO2 retention while others do not is not fully understood,” he said, noting that patients with OHS can normalize their CO2 quickly when instructed to take deep breaths. “What we know is that the centers in the brain responsible for augmenting ventilation when CO2 goes up are somehow blunted.”
In a study of obese mice led by Vsevolod Y. Polotsky, MD, PhD, of Johns Hopkins University, Baltimore – and highlighted by Dr. Mokhlesi as an example of important, recent research – leptin delivered intranasally alleviated hypoventilation (and upper-airway obstruction), while intraperitoneally administered leptin did not, seemingly overcoming “central leptin deficiency.” (Am J Respir Crit Care Med. 2019;199[6]:773-83).
“This proved that there is some level of resistance in this animal model ... and has potential for therapeutics in the future,” Dr. Mokhlesi said.
Understanding the role of insulin resistance in OSA is another research focus. Some data suggest that insulin resistance, which is more common in obesity, is more prevalent in populations with OSA, Dr. Patil said. Researchers have discussed a bidirectional relationship for years, but it’s likely that insulin resistance is a precursor, he said.
In a mechanistic study published in 2016, Dr. Patil and his coinvestigators found that obese individuals with insulin resistance but without frank diabetes or sleep apnea demonstrated preclinical elevations in pharyngeal collapsibility during sleep. The findings suggest that insulin resistance could play a causal role in OSA pathogenesis by “generating requisite elevations in pharyngeal collapsibility,” they wrote (Eur. Respir J. 2016;47[6]:1718-26).
More recently, Dr. Patil noted in the interview, there is increasing appreciation in academia that the type of fat may be important to predicting OSA. “Visceral fat has a completely different cytokine-secretion profile than subcutaneous fat ... it is the more metabolically active fat that may secondarily impact upper airway function though a neuroinflammatory mechanism,” he said. “That is one of the working hypotheses today.”
Asthma
Research has so roundly suggested that metabolic dysfunction contributes to severe, poorly controlled asthma that there’s recent and growing interest in targeting metabolic dysfunction as part of the treatment of obese asthma, said Dr. Dixon, whose own research in obesity and lung disease has focused on asthma.
Data from animal models and some epidemiologic studies have suggested that drugs used to treat type 2 diabetes mellitus, such as glucagon-like peptide receptor-1 (GLPR-1) agonists and metformin, may help control asthma. In one recent study – cited by Dr. Dixon in a 2022 review of obesity and asthma – people with obesity and asthma who were prescribed GLPR-1 agonists for diabetes had fewer asthma exacerbations compared with those who took other medications for diabetes (Semin Respir Crit Care Med. 2022 Feb 17. doi: 10.1055/s-0042-1742384).
There is also research interest in targeting the pro-inflammatory adipokine interleukin 6 (IL-6), since increased circulating levels of IL-6 correlate with asthma severity, and in addressing oxidative stress in asthma through treatment with a mitochondrially targeted antioxidant, she said. Oxidative stress is increased in the airways of people with obesity, and researchers believe it may contribute to the pathophysiology of obese asthma through effects on airway nitric oxide levels.
(Her own research work at the University of Vermont has found associations between poor asthma control and high levels of leptin, and similar associations involving low levels of adiponectin, an anti-inflammatory adipokine that has been shown to downregulate eosinophil recruitment in the airways.)
Weight loss has been shown in mostly small, single-center studies to improve asthma control, but short of weight loss, researchers are also investigating the role of poor dietary quality. Thus far, data suggest that it’s the composition of the diet, and not just its contribution to weight gain, that could be impactful, Dr. Dixon said.
More basic research questions cited by Dr. Dixon include the extent to which adipose tissue inflammation causes inflammation in the lungs. “It’s a little unclear whether all the metabolic dysfunction associated with poor asthma control is causing inflammation in the lungs,” she said, though “we’ve done some work here that shows mediators produced by the adipose tissue could be impacting production of inflammatory mediators by the airway epithelium.”
Overall, she said, “the big questions [in asthma] are, how does adipose tissue affect the airway? Is it through direct effects? Through effects on the immune system? And obesity is affected by diet and the gut microbiome – how can these be [impacting] the airway?”
Obesity “is associated with so many changes – the gut, the immune system, and metabolic dysfunction, in addition to airway mechanics,” she said, “that I no longer think, as I did when I came to this, that it’s just one thing. It’s probably all of these things together.”
In the meantime, questions about potential shared pathways for the development of obesity and asthma remain. “Obesity is a risk factor for developing asthma, but it’s also entirely possible that asthma is a risk factor for developing obesity,” she said. (Some data from pediatric populations, she noted, suggest that nonobese children with asthma are at increased risk of developing obesity.)
Also important, Dr. Dixon said, is “emerging literature in the last 5-10 years” that suggests that people with obesity are more susceptible to the effects of air pollution. Research involving inner-city schoolchildren with asthma, for instance, has shown that those with obesity had worse symptoms with air pollution exposure than did those who were not obese.
Pulmonary arterial hypertension
Some research has looked at adipose tissue–produced substances in PAH, but the most well-established association in obesity and PAH involves insulin resistance.
“I don’t think we’re certain as a community that obesity [in general] is the problem – it’s not itself considered a risk factor for PAH,” Anna R. Hemnes, MD, associate professor of medicine at Vanderbilt University Medical Center in Nashville, Tenn., said in an interview. She noted that it’s “hard to dissect obesity” apart.
Researchers are “more confident,” she said, “that insulin resistance – one feature of obesity [in some people] – is associated with worse outcomes in PAH.” Metabolic disease resembling insulin resistance is common in PAH and is believed to contribute to pulmonary vascular disease and right ventricular (RV) failure – the main cause of mortality in PAH – at least in part because of increased oxidative stress.
Dr. Hemnes led a mechanistic phase II clinical trial of metformin in PAH in which the drug was associated with improved RV fractional area change and reduced RV lipid deposition (J Am Heart Assoc. 2020;9[22]:e018349), and she’s now leading a National Institutes of Health–funded multicenter trial looking at the impact of metformin and an exercise intervention on 6-minute walk distance and World Health Organization functional class in PAH.
At the Rush Lung Center, in the meantime, Dr. Mokhlesi is utilizing animal models of OSA and OHS to explore the effect of hypoxia and nighttime hypercapnia on the development of PAH. “I think the jury is still out as to whether obesity itself is a major risk factor, but if so, by what mechanism?” he said. “Is it worsening [sleep-disordered breathing], which then worsens PAH?”
COPD
The focus in COPD has traditionally been on underweight, but the relationship between obesity and COPD has increasingly been recognized in the last 10-15 years, said Frits M. E. Franssen, MD, PhD, of CIRO, a research institute in Horn, the Netherlands, that treats COPD and other chronic lung diseases, and of the department of respiratory medicine at Maastricht University.
Researchers like Dr. Franssen are trying, for one, to understand obesity’s impact on COPD pathophysiology and to tease apart the impact of both conditions on disease severity and patient-related outcomes such as exercise capacity and exercise-related symptoms.
When Dr. Franssen’s group compared responses to weight-bearing exercise (6-min. walk test) and weight-supported exercise (cycling) in obese and normal weight COPD patients matched for age, gender, and degree of airflow limitation, the researchers found that walking capacity was significantly reduced while cycling capacity was preserved in the obese group (Respirology. 2016;21[3]:483-8).
Exercise-related symptoms (dyspnea and leg fatigue) were largely comparable between the obese and normal-weight COPD patients in both exercise modalities. However, in other studies, dyspnea ratings during cycling – at any given level of ventilation – have been lower in obese patients, indicating that “additional fat mass may have a beneficial effect on lung functioning [in non–weight-bearing exercise],” he said in an interview.
Dr. Franssen’s group also has assessed body composition in overweight and obese patients with COPD and found that a significant number have low muscle mass. These patients had worse lung function, exercise tolerance, and muscle strength compared to patients with comparable BMI and normal muscle mass (Respir Res. 2021 Mar 25. doi: 10.1186/s12931-021-01689-w).
“We’d always thought that obese patients have normal muscle mass ... but now we know it can be dramatically low,” he said. In assessing obesity and formulating any weight loss plans, “we’re now interested not only in weight but in the distribution of fat mass and fat-free mass ... and in maintaining muscle mass in patients who are [prescribed dietary interventions].”
Paradoxically, in patients with severe COPD, obesity is associated with prolonged survival, while in patients with mild to moderate COPD, obesity is associated with increased mortality risk, he noted.
The impact of adipose tissue and the chronic inflammation and metabolic disturbances that characterize obesity are currently largely unexplored, he said. Researchers have not yet studied what optimal weights may be for patients with COPD. “And we’re interested in the questions, are body weight and body composition the result of the disease, or [are they] determining the type of COPD one will get?” Dr. Franssen said.
Patients with COPD who are obese have “more of the phenotype of chronic bronchitis,” he noted, “while typical emphysema patients are normally underweight.”
The diverse effects of obesity on lung health and disease are increasingly being teased apart, with researchers honing in on the impact of metabolic dysfunction, circulating inflammatory factors produced by adipose tissue, lipid handling, and other factors – in addition to body mass index – that are associated with the obese state.
“The bird’s eye view is that obesity completely changes lung health. It’s something we’ve only recently begun to appreciate,” said Anne E. Dixon, MA, BM, BCh, director of the Vermont Lung Center at the University of Vermont, Burlington, who is focused on the research field of obesity and lung disease.
Structural, mechanical effects of obesity on lung function are better known and appreciated. Accumulation of fat in the mediastinum and abdominal and thoracic cavities causes reductions in lung volume, in functional residual capacity, and in the compliance of the lungs, chest wall, and entire respiratory system, for instance.
Yet obesity is more than a state of increased BMI, and “what we’ve begun to understand is that [its impact on the lungs and respiratory health] is much more complicated than just a mechanical problem,” said Dr. Dixon, also director of pulmonary and critical care medicine at the University of Vermont Medical Center and professor of medicine at the medical college.
With obesity, adipose tissue changes not only in quantity, but in function, producing proinflammatory cytokines and hormones – such as leptin, tumor necrosis factor-alpha (TNF-alpha), and interleukin-6 – that can have direct effects on the lung. Insulin resistance, which is common with obesity, is also seemingly deleterious. And obesity-associated changes in immune function, lipid handling, diet, and the gut microbiome may also impact lung health and disease, she said.
Dr. Dixon, who wrote about these changes in a 2018 review article in the journal CHEST and another 2019 piece in Expert Review of Respiratory Medicine, has developed a research program focused on obesity and lung disease and has edited a book and organized international conferences on the topic. (CHEST 2018;153[3]:702-9 and Exper Rev Respir Med. 2018;12[9]:755-67.)
“The more I do, the more I realize that there are multiple obesity-associated changes involved, and that [our current high level of] obesity is like a huge population-level natural experiment ... on lung health,” she told this news organization.
Associations between lung disease and the metabolic and other disturbances of obesity are most established in asthma research and have taken hold in the realm of sleep-disordered breathing. But as the prevalence of obesity continues to grow, its role in other lung diseases such as chronic obstructive pulmonary disorder (COPD) and, most recently, pulmonary arterial hypertension (PAH), is getting attention in academia.
And certainly, COVID-19 has highlighted an “urgent need” to better understand how obesity increases susceptibility to severe viral infections, Dr. Dixon added.
Here are some glimpses into current thinking and some examples of research that may have preventive and therapeutic implications in the future:
OSA and OHS
“With sleep apnea we tend to focus on anatomic considerations, but there may be relationships or interactions between obesity and neuromuscular function and neuroventilatory control,” Susheel P. Patil, MD, PhD, director of the sleep medicine program for University Hospitals and assistant professor at Case Western Reserve University, Cleveland, said in an interview.
Some studies suggest, for instance, that TNF-alpha can increase obstructive sleep apnea (OSA) susceptibility and severity through its neuroventilatory modulating properties during sleep. And the potential for additional proinflammatory cytokines produced by adipose tissue to similarly affect upper airway neuroventilatory control is an “intriguing line” of inquiry for researchers in the sleep apnea space, he said.
Leptin is of interest particularly in obesity hypoventilation syndrome (OHS), which is characterized by chronic daytime hypercapnia. Best known as a satiety hormone, leptin is produced by adipose tissue and suppresses appetite at the central nervous system level. But it has long been known that leptin also affects ventilation and the control of breathing.
When transported across the blood-brain barrier, leptin increases the hypercapnic ventilatory response, Babak Mokhlesi, MD, MSc, codirector of the Rush Lung Center and chief of pulmonary, critical care, and sleep medicine at Rush University Medical Center in Chicago, said in an interview.
Research suggests that patients with OHS may have resistance to leptin at the central nervous system level – with leptin not reaching the sites of ventilatory control. This is a “prevailing theory” and could explain why these patients “do not augment their ventilation to maintain homeostasis, normal levels of CO2,” Dr. Mokhlesi said.
“Why some patients with severe obesity develop CO2 retention while others do not is not fully understood,” he said, noting that patients with OHS can normalize their CO2 quickly when instructed to take deep breaths. “What we know is that the centers in the brain responsible for augmenting ventilation when CO2 goes up are somehow blunted.”
In a study of obese mice led by Vsevolod Y. Polotsky, MD, PhD, of Johns Hopkins University, Baltimore – and highlighted by Dr. Mokhlesi as an example of important, recent research – leptin delivered intranasally alleviated hypoventilation (and upper-airway obstruction), while intraperitoneally administered leptin did not, seemingly overcoming “central leptin deficiency.” (Am J Respir Crit Care Med. 2019;199[6]:773-83).
“This proved that there is some level of resistance in this animal model ... and has potential for therapeutics in the future,” Dr. Mokhlesi said.
Understanding the role of insulin resistance in OSA is another research focus. Some data suggest that insulin resistance, which is more common in obesity, is more prevalent in populations with OSA, Dr. Patil said. Researchers have discussed a bidirectional relationship for years, but it’s likely that insulin resistance is a precursor, he said.
In a mechanistic study published in 2016, Dr. Patil and his coinvestigators found that obese individuals with insulin resistance but without frank diabetes or sleep apnea demonstrated preclinical elevations in pharyngeal collapsibility during sleep. The findings suggest that insulin resistance could play a causal role in OSA pathogenesis by “generating requisite elevations in pharyngeal collapsibility,” they wrote (Eur. Respir J. 2016;47[6]:1718-26).
More recently, Dr. Patil noted in the interview, there is increasing appreciation in academia that the type of fat may be important to predicting OSA. “Visceral fat has a completely different cytokine-secretion profile than subcutaneous fat ... it is the more metabolically active fat that may secondarily impact upper airway function though a neuroinflammatory mechanism,” he said. “That is one of the working hypotheses today.”
Asthma
Research has so roundly suggested that metabolic dysfunction contributes to severe, poorly controlled asthma that there’s recent and growing interest in targeting metabolic dysfunction as part of the treatment of obese asthma, said Dr. Dixon, whose own research in obesity and lung disease has focused on asthma.
Data from animal models and some epidemiologic studies have suggested that drugs used to treat type 2 diabetes mellitus, such as glucagon-like peptide receptor-1 (GLPR-1) agonists and metformin, may help control asthma. In one recent study – cited by Dr. Dixon in a 2022 review of obesity and asthma – people with obesity and asthma who were prescribed GLPR-1 agonists for diabetes had fewer asthma exacerbations compared with those who took other medications for diabetes (Semin Respir Crit Care Med. 2022 Feb 17. doi: 10.1055/s-0042-1742384).
There is also research interest in targeting the pro-inflammatory adipokine interleukin 6 (IL-6), since increased circulating levels of IL-6 correlate with asthma severity, and in addressing oxidative stress in asthma through treatment with a mitochondrially targeted antioxidant, she said. Oxidative stress is increased in the airways of people with obesity, and researchers believe it may contribute to the pathophysiology of obese asthma through effects on airway nitric oxide levels.
(Her own research work at the University of Vermont has found associations between poor asthma control and high levels of leptin, and similar associations involving low levels of adiponectin, an anti-inflammatory adipokine that has been shown to downregulate eosinophil recruitment in the airways.)
Weight loss has been shown in mostly small, single-center studies to improve asthma control, but short of weight loss, researchers are also investigating the role of poor dietary quality. Thus far, data suggest that it’s the composition of the diet, and not just its contribution to weight gain, that could be impactful, Dr. Dixon said.
More basic research questions cited by Dr. Dixon include the extent to which adipose tissue inflammation causes inflammation in the lungs. “It’s a little unclear whether all the metabolic dysfunction associated with poor asthma control is causing inflammation in the lungs,” she said, though “we’ve done some work here that shows mediators produced by the adipose tissue could be impacting production of inflammatory mediators by the airway epithelium.”
Overall, she said, “the big questions [in asthma] are, how does adipose tissue affect the airway? Is it through direct effects? Through effects on the immune system? And obesity is affected by diet and the gut microbiome – how can these be [impacting] the airway?”
Obesity “is associated with so many changes – the gut, the immune system, and metabolic dysfunction, in addition to airway mechanics,” she said, “that I no longer think, as I did when I came to this, that it’s just one thing. It’s probably all of these things together.”
In the meantime, questions about potential shared pathways for the development of obesity and asthma remain. “Obesity is a risk factor for developing asthma, but it’s also entirely possible that asthma is a risk factor for developing obesity,” she said. (Some data from pediatric populations, she noted, suggest that nonobese children with asthma are at increased risk of developing obesity.)
Also important, Dr. Dixon said, is “emerging literature in the last 5-10 years” that suggests that people with obesity are more susceptible to the effects of air pollution. Research involving inner-city schoolchildren with asthma, for instance, has shown that those with obesity had worse symptoms with air pollution exposure than did those who were not obese.
Pulmonary arterial hypertension
Some research has looked at adipose tissue–produced substances in PAH, but the most well-established association in obesity and PAH involves insulin resistance.
“I don’t think we’re certain as a community that obesity [in general] is the problem – it’s not itself considered a risk factor for PAH,” Anna R. Hemnes, MD, associate professor of medicine at Vanderbilt University Medical Center in Nashville, Tenn., said in an interview. She noted that it’s “hard to dissect obesity” apart.
Researchers are “more confident,” she said, “that insulin resistance – one feature of obesity [in some people] – is associated with worse outcomes in PAH.” Metabolic disease resembling insulin resistance is common in PAH and is believed to contribute to pulmonary vascular disease and right ventricular (RV) failure – the main cause of mortality in PAH – at least in part because of increased oxidative stress.
Dr. Hemnes led a mechanistic phase II clinical trial of metformin in PAH in which the drug was associated with improved RV fractional area change and reduced RV lipid deposition (J Am Heart Assoc. 2020;9[22]:e018349), and she’s now leading a National Institutes of Health–funded multicenter trial looking at the impact of metformin and an exercise intervention on 6-minute walk distance and World Health Organization functional class in PAH.
At the Rush Lung Center, in the meantime, Dr. Mokhlesi is utilizing animal models of OSA and OHS to explore the effect of hypoxia and nighttime hypercapnia on the development of PAH. “I think the jury is still out as to whether obesity itself is a major risk factor, but if so, by what mechanism?” he said. “Is it worsening [sleep-disordered breathing], which then worsens PAH?”
COPD
The focus in COPD has traditionally been on underweight, but the relationship between obesity and COPD has increasingly been recognized in the last 10-15 years, said Frits M. E. Franssen, MD, PhD, of CIRO, a research institute in Horn, the Netherlands, that treats COPD and other chronic lung diseases, and of the department of respiratory medicine at Maastricht University.
Researchers like Dr. Franssen are trying, for one, to understand obesity’s impact on COPD pathophysiology and to tease apart the impact of both conditions on disease severity and patient-related outcomes such as exercise capacity and exercise-related symptoms.
When Dr. Franssen’s group compared responses to weight-bearing exercise (6-min. walk test) and weight-supported exercise (cycling) in obese and normal weight COPD patients matched for age, gender, and degree of airflow limitation, the researchers found that walking capacity was significantly reduced while cycling capacity was preserved in the obese group (Respirology. 2016;21[3]:483-8).
Exercise-related symptoms (dyspnea and leg fatigue) were largely comparable between the obese and normal-weight COPD patients in both exercise modalities. However, in other studies, dyspnea ratings during cycling – at any given level of ventilation – have been lower in obese patients, indicating that “additional fat mass may have a beneficial effect on lung functioning [in non–weight-bearing exercise],” he said in an interview.
Dr. Franssen’s group also has assessed body composition in overweight and obese patients with COPD and found that a significant number have low muscle mass. These patients had worse lung function, exercise tolerance, and muscle strength compared to patients with comparable BMI and normal muscle mass (Respir Res. 2021 Mar 25. doi: 10.1186/s12931-021-01689-w).
“We’d always thought that obese patients have normal muscle mass ... but now we know it can be dramatically low,” he said. In assessing obesity and formulating any weight loss plans, “we’re now interested not only in weight but in the distribution of fat mass and fat-free mass ... and in maintaining muscle mass in patients who are [prescribed dietary interventions].”
Paradoxically, in patients with severe COPD, obesity is associated with prolonged survival, while in patients with mild to moderate COPD, obesity is associated with increased mortality risk, he noted.
The impact of adipose tissue and the chronic inflammation and metabolic disturbances that characterize obesity are currently largely unexplored, he said. Researchers have not yet studied what optimal weights may be for patients with COPD. “And we’re interested in the questions, are body weight and body composition the result of the disease, or [are they] determining the type of COPD one will get?” Dr. Franssen said.
Patients with COPD who are obese have “more of the phenotype of chronic bronchitis,” he noted, “while typical emphysema patients are normally underweight.”
Some smokers don’t get lung cancer; genetics might explain it
These people have genes that help limit mutations to DNA that would turn cells malignant and make them grow into tumors, the researchers say.
Scientists have long suspected that smoking leads to lung cancer by triggering DNA mutations in healthy cells. But it was hard for them to identify the mutations in healthy cells that might help predict future cancer risk, Jan Vijg, PhD, a senior author of the study and researcher at the University School of Medicine, Shanghai, China, said in a statement.
His team used a process called single-cell whole genome sequencing to examine cells lining the lungs of 19 smokers and 14 nonsmokers ranging in age from their pre-teens to their mid-80s. The cells came from patients who had tissue samples collected from their lungs during diagnostic testing unrelated to cancer. The scientists reported their findings in Nature Genetics.
The researchers specifically looked at cells lining the lungs because these cells can survive for years and build up mutations over time that are linked to aging and smoking.
“Of all the lung’s cell types, these are among the most likely to become cancerous,” says Simon Spivack, MD, a senior author of the study and professor at the Albert Einstein College of Medicine, New York.
Smokers had far more gene mutations that can cause lung cancer than nonsmokers, the analysis found.
“This experimentally confirms that smoking increases lung cancer risk by increasing the frequency of mutations, as previously hypothesized,” says Dr. Spivack. “This is likely one reason why so few nonsmokers get lung cancer, while 10 to 20 percent of lifelong smokers do.”
Among the smokers, people had smoked a maximum of 116 pack-years. A pack-year is the equivalent of smoking one pack a day for a year. The number of mutations detected in smokers’ lung cells increased in direct proportion to the number of pack-years they smoked.
But after 23 pack-years, the lung cells in smokers didn’t appear to add more mutations, the researchers report, suggesting that some people’s genes might make them more likely to fight mutations.
“The heaviest smokers did not have the highest mutation burden,” says Dr. Spivack. “Our data suggest that these individuals may have survived for so long in spite of their heavy smoking because they managed to suppress further mutation accumulation.”
While it’s possible these findings could one day help doctors come up with better ways to screen for lung cancer and treat the disease, that’s still a long way off. Many more lab tests and larger studies will be needed to better pinpoint which smokers might be more prone to lung cancer and why.
A version of this article first appeared on WebMD.com.
These people have genes that help limit mutations to DNA that would turn cells malignant and make them grow into tumors, the researchers say.
Scientists have long suspected that smoking leads to lung cancer by triggering DNA mutations in healthy cells. But it was hard for them to identify the mutations in healthy cells that might help predict future cancer risk, Jan Vijg, PhD, a senior author of the study and researcher at the University School of Medicine, Shanghai, China, said in a statement.
His team used a process called single-cell whole genome sequencing to examine cells lining the lungs of 19 smokers and 14 nonsmokers ranging in age from their pre-teens to their mid-80s. The cells came from patients who had tissue samples collected from their lungs during diagnostic testing unrelated to cancer. The scientists reported their findings in Nature Genetics.
The researchers specifically looked at cells lining the lungs because these cells can survive for years and build up mutations over time that are linked to aging and smoking.
“Of all the lung’s cell types, these are among the most likely to become cancerous,” says Simon Spivack, MD, a senior author of the study and professor at the Albert Einstein College of Medicine, New York.
Smokers had far more gene mutations that can cause lung cancer than nonsmokers, the analysis found.
“This experimentally confirms that smoking increases lung cancer risk by increasing the frequency of mutations, as previously hypothesized,” says Dr. Spivack. “This is likely one reason why so few nonsmokers get lung cancer, while 10 to 20 percent of lifelong smokers do.”
Among the smokers, people had smoked a maximum of 116 pack-years. A pack-year is the equivalent of smoking one pack a day for a year. The number of mutations detected in smokers’ lung cells increased in direct proportion to the number of pack-years they smoked.
But after 23 pack-years, the lung cells in smokers didn’t appear to add more mutations, the researchers report, suggesting that some people’s genes might make them more likely to fight mutations.
“The heaviest smokers did not have the highest mutation burden,” says Dr. Spivack. “Our data suggest that these individuals may have survived for so long in spite of their heavy smoking because they managed to suppress further mutation accumulation.”
While it’s possible these findings could one day help doctors come up with better ways to screen for lung cancer and treat the disease, that’s still a long way off. Many more lab tests and larger studies will be needed to better pinpoint which smokers might be more prone to lung cancer and why.
A version of this article first appeared on WebMD.com.
These people have genes that help limit mutations to DNA that would turn cells malignant and make them grow into tumors, the researchers say.
Scientists have long suspected that smoking leads to lung cancer by triggering DNA mutations in healthy cells. But it was hard for them to identify the mutations in healthy cells that might help predict future cancer risk, Jan Vijg, PhD, a senior author of the study and researcher at the University School of Medicine, Shanghai, China, said in a statement.
His team used a process called single-cell whole genome sequencing to examine cells lining the lungs of 19 smokers and 14 nonsmokers ranging in age from their pre-teens to their mid-80s. The cells came from patients who had tissue samples collected from their lungs during diagnostic testing unrelated to cancer. The scientists reported their findings in Nature Genetics.
The researchers specifically looked at cells lining the lungs because these cells can survive for years and build up mutations over time that are linked to aging and smoking.
“Of all the lung’s cell types, these are among the most likely to become cancerous,” says Simon Spivack, MD, a senior author of the study and professor at the Albert Einstein College of Medicine, New York.
Smokers had far more gene mutations that can cause lung cancer than nonsmokers, the analysis found.
“This experimentally confirms that smoking increases lung cancer risk by increasing the frequency of mutations, as previously hypothesized,” says Dr. Spivack. “This is likely one reason why so few nonsmokers get lung cancer, while 10 to 20 percent of lifelong smokers do.”
Among the smokers, people had smoked a maximum of 116 pack-years. A pack-year is the equivalent of smoking one pack a day for a year. The number of mutations detected in smokers’ lung cells increased in direct proportion to the number of pack-years they smoked.
But after 23 pack-years, the lung cells in smokers didn’t appear to add more mutations, the researchers report, suggesting that some people’s genes might make them more likely to fight mutations.
“The heaviest smokers did not have the highest mutation burden,” says Dr. Spivack. “Our data suggest that these individuals may have survived for so long in spite of their heavy smoking because they managed to suppress further mutation accumulation.”
While it’s possible these findings could one day help doctors come up with better ways to screen for lung cancer and treat the disease, that’s still a long way off. Many more lab tests and larger studies will be needed to better pinpoint which smokers might be more prone to lung cancer and why.
A version of this article first appeared on WebMD.com.
FROM NATURE GENETICS
Cannabis vaping continues its rise in teens
More teenagers in the United States reported cannabis use with vaping in 2019, compared with 2017, while cannabis use without vaping declined, based on annual survey data from more than 50,000 teens.
“With vaping prevalence rising so quickly among teens, getting a clearer picture of how cannabis use is shifting helps inform prevention and cessation efforts,” corresponding author Noah T. Kreski, MPH, of Columbia University, New York, said in an interview.
“In just 2 years, the most common cannabis use pattern changed from ‘occasional use without vaping’ to ‘frequent use with vaping,’ said Mx. Kreski, who uses the honorific Mx. and the pronouns they/them. “Knowing that, as well as the high overlap of cannabis vaping with nicotine use and binge drinking, adds to the urgency of reducing adolescent vaping.”
To quantify the trends in cannabis vaping, the researchers reviewed data from Monitoring the Future, an annual survey of high school students across the United States. The study population included 51,052 individuals; approximately 49% were male and 49% were non-Hispanic White. The researchers examined frequency of cannabis use, trends across demographic groups, and concurrent use of cannabis and other substances such as alcohol and tobacco. The findings were published in the journal Addiction.
Frequent cannabis use was defined as six or more times in the past 30 days; occasional use was defined as one to five times in the past 30 days.
Frequent cannabis use with vaping increased from 2.1% in 2017 to 5.4% in 2019. Occasional cannabis use with vaping also increased, though less dramatically, from less than 2% in 2017 to approximately 3.5% in 2019.
By contrast, both frequent and occasional cannabis use without vaping declined from 2017 to 2019 (from 3.8% to 2.1% and from 6.9% to 4.4%, respectively).
Overall, the prevalence of any level of cannabis use increased from 13.9% in 2017 to 15.4% in 2019. Both males and females showed a similar increase in reported frequent cannabis use with vaping of approximately 3%.
The results document that vaping cannabis has become more common than smoking alone among U.S. teens across almost all demographic groups, and across sex, race, urbanicity, and level of parent education; however, the increased was especially marked among Hispanic/Latinx teens and those of lower socioeconomic status, the researchers wrote.
The researchers also examined the associations between cannabis use with and without vaping and concurrent nicotine and alcohol use. Overall, the strongest association was between smoking or vaping nicotine and vaping cannabis; teens who smoked or vaped nicotine were 42 times more likely than nonnicotine users to report vaping cannabis in the past 30 days (adjusted odds ratio, 42.28). In addition, more occasions of binge drinking were more strongly associated with cannabis use with vaping (up to 10 times more likely), compared with cannabis use without vaping, (aORs, 4.48-10.09).
The study findings were limited by several factors, including the lack of questions on tetrahydrocannabinol (THC) or cannabidiol content of the cannabis products used, although evidence suggests that the potency of cannabis products in the United States is increasing, the researchers noted. Other limitations included the cross-sectional design, which prevents making associations about causality, and lack of data on the quantity of cannabis used; only data on frequency of use were recorded.
However, the results reflect a rise in cannabis use with vaping among teens in the United States, along with an increased risk of tobacco use, e-cigarette use, and binge drinking, the researchers said.
As cannabis legalization expands across the United States, policies are needed to deter use among adolescents, the researchers wrote. “These policies should be crafted to reduce an emphasis on criminalization in preference for public health promotion given the history of unequal application of punitive consequences of drug use for racialized minorities in the United States. As products, delivery systems, potency, and marketing proliferate within a for-profit industry, increased attention to youth trends, including investment in sustained and evidence-based prevention and intervention, is increasingly necessary.”
The take-home message for clinicians is to ask whether your patients are vaping, because the prevalence is not only up, but fairly universal, Mx. Kreski said. “Have a discussion that covers a broad range of substance use topics and informs teens of the potential risks of vaping, while avoiding stigma.”
The message for parents is “to talk to your kids about the risks of vaping,” said Mx. Kreski. “Prioritize open communication rather than punishment, and work together with your teens to prevent or reduce vaping.” The message for teens: “Understand that vaping has risks. You should feel empowered to talk to your parents or doctor about those risks. While it may seem like everyone’s vaping, the majority don’t. Keeping communication open between parents/caregivers, teens, and health care providers is one of the best ways to address these trends in vaping.”
Beware more powerful cannabis products
“While drug use in general is declining in adolescents, marijuana use remains very common,” Kelly A. Curran, MD, of the University of Oklahoma Health Sciences Center, Oklahoma City, said in an interview.
“There is growing evidence that marijuana is now the first drug used by adolescents – replacing alcohol and nicotine – and frequent use can lead to substance abuse,” said Dr. Curran, who specializes in adolescent medicine but was involved in the study. “Cannabis use patterns have evolved over time. As I frequently tell my patients and their families, new strains and hybrids of marijuana have higher potencies of THC. Many adolescents are eschewing smoking and in its place using marijuana concentrates (wax, oil, shatter) via vape, dab pen, or rig. Use of these methods puts adolescents at high risk of social and health complications such as [e-cigarette or vaping use-associated lung injury], cannabis hyperemesis syndrome, and psychosis – and understanding these patterns and associated drug use helps health care professionals and parents keep adolescents safe.”
The take-home message for clinicians is that marijuana use via vaping continues to rise and to become more common than “traditional” marijuana smoking, Dr. Curran said. “This increase is across genders, in nearly all race/ethnicities (especially in Latinx youth), and in youth from lower socioeconomic status.” Vaping marijuana is associated with other substance abuse, so health care professionals should include questions about different forms of marijuana use, such as vape, dab pen, or rig, when working with patients, and counsel patients and families about the risks associated with use of any of these products.
The study was supported by the National Center for Injury Prevention and Control and by the National Institute on Drug Abuse. The researchers had no financial conflicts to disclose. Dr. Curran had no financial conflicts to disclose and serves on the editorial advisory board of Pediatric News.
More teenagers in the United States reported cannabis use with vaping in 2019, compared with 2017, while cannabis use without vaping declined, based on annual survey data from more than 50,000 teens.
“With vaping prevalence rising so quickly among teens, getting a clearer picture of how cannabis use is shifting helps inform prevention and cessation efforts,” corresponding author Noah T. Kreski, MPH, of Columbia University, New York, said in an interview.
“In just 2 years, the most common cannabis use pattern changed from ‘occasional use without vaping’ to ‘frequent use with vaping,’ said Mx. Kreski, who uses the honorific Mx. and the pronouns they/them. “Knowing that, as well as the high overlap of cannabis vaping with nicotine use and binge drinking, adds to the urgency of reducing adolescent vaping.”
To quantify the trends in cannabis vaping, the researchers reviewed data from Monitoring the Future, an annual survey of high school students across the United States. The study population included 51,052 individuals; approximately 49% were male and 49% were non-Hispanic White. The researchers examined frequency of cannabis use, trends across demographic groups, and concurrent use of cannabis and other substances such as alcohol and tobacco. The findings were published in the journal Addiction.
Frequent cannabis use was defined as six or more times in the past 30 days; occasional use was defined as one to five times in the past 30 days.
Frequent cannabis use with vaping increased from 2.1% in 2017 to 5.4% in 2019. Occasional cannabis use with vaping also increased, though less dramatically, from less than 2% in 2017 to approximately 3.5% in 2019.
By contrast, both frequent and occasional cannabis use without vaping declined from 2017 to 2019 (from 3.8% to 2.1% and from 6.9% to 4.4%, respectively).
Overall, the prevalence of any level of cannabis use increased from 13.9% in 2017 to 15.4% in 2019. Both males and females showed a similar increase in reported frequent cannabis use with vaping of approximately 3%.
The results document that vaping cannabis has become more common than smoking alone among U.S. teens across almost all demographic groups, and across sex, race, urbanicity, and level of parent education; however, the increased was especially marked among Hispanic/Latinx teens and those of lower socioeconomic status, the researchers wrote.
The researchers also examined the associations between cannabis use with and without vaping and concurrent nicotine and alcohol use. Overall, the strongest association was between smoking or vaping nicotine and vaping cannabis; teens who smoked or vaped nicotine were 42 times more likely than nonnicotine users to report vaping cannabis in the past 30 days (adjusted odds ratio, 42.28). In addition, more occasions of binge drinking were more strongly associated with cannabis use with vaping (up to 10 times more likely), compared with cannabis use without vaping, (aORs, 4.48-10.09).
The study findings were limited by several factors, including the lack of questions on tetrahydrocannabinol (THC) or cannabidiol content of the cannabis products used, although evidence suggests that the potency of cannabis products in the United States is increasing, the researchers noted. Other limitations included the cross-sectional design, which prevents making associations about causality, and lack of data on the quantity of cannabis used; only data on frequency of use were recorded.
However, the results reflect a rise in cannabis use with vaping among teens in the United States, along with an increased risk of tobacco use, e-cigarette use, and binge drinking, the researchers said.
As cannabis legalization expands across the United States, policies are needed to deter use among adolescents, the researchers wrote. “These policies should be crafted to reduce an emphasis on criminalization in preference for public health promotion given the history of unequal application of punitive consequences of drug use for racialized minorities in the United States. As products, delivery systems, potency, and marketing proliferate within a for-profit industry, increased attention to youth trends, including investment in sustained and evidence-based prevention and intervention, is increasingly necessary.”
The take-home message for clinicians is to ask whether your patients are vaping, because the prevalence is not only up, but fairly universal, Mx. Kreski said. “Have a discussion that covers a broad range of substance use topics and informs teens of the potential risks of vaping, while avoiding stigma.”
The message for parents is “to talk to your kids about the risks of vaping,” said Mx. Kreski. “Prioritize open communication rather than punishment, and work together with your teens to prevent or reduce vaping.” The message for teens: “Understand that vaping has risks. You should feel empowered to talk to your parents or doctor about those risks. While it may seem like everyone’s vaping, the majority don’t. Keeping communication open between parents/caregivers, teens, and health care providers is one of the best ways to address these trends in vaping.”
Beware more powerful cannabis products
“While drug use in general is declining in adolescents, marijuana use remains very common,” Kelly A. Curran, MD, of the University of Oklahoma Health Sciences Center, Oklahoma City, said in an interview.
“There is growing evidence that marijuana is now the first drug used by adolescents – replacing alcohol and nicotine – and frequent use can lead to substance abuse,” said Dr. Curran, who specializes in adolescent medicine but was involved in the study. “Cannabis use patterns have evolved over time. As I frequently tell my patients and their families, new strains and hybrids of marijuana have higher potencies of THC. Many adolescents are eschewing smoking and in its place using marijuana concentrates (wax, oil, shatter) via vape, dab pen, or rig. Use of these methods puts adolescents at high risk of social and health complications such as [e-cigarette or vaping use-associated lung injury], cannabis hyperemesis syndrome, and psychosis – and understanding these patterns and associated drug use helps health care professionals and parents keep adolescents safe.”
The take-home message for clinicians is that marijuana use via vaping continues to rise and to become more common than “traditional” marijuana smoking, Dr. Curran said. “This increase is across genders, in nearly all race/ethnicities (especially in Latinx youth), and in youth from lower socioeconomic status.” Vaping marijuana is associated with other substance abuse, so health care professionals should include questions about different forms of marijuana use, such as vape, dab pen, or rig, when working with patients, and counsel patients and families about the risks associated with use of any of these products.
The study was supported by the National Center for Injury Prevention and Control and by the National Institute on Drug Abuse. The researchers had no financial conflicts to disclose. Dr. Curran had no financial conflicts to disclose and serves on the editorial advisory board of Pediatric News.
More teenagers in the United States reported cannabis use with vaping in 2019, compared with 2017, while cannabis use without vaping declined, based on annual survey data from more than 50,000 teens.
“With vaping prevalence rising so quickly among teens, getting a clearer picture of how cannabis use is shifting helps inform prevention and cessation efforts,” corresponding author Noah T. Kreski, MPH, of Columbia University, New York, said in an interview.
“In just 2 years, the most common cannabis use pattern changed from ‘occasional use without vaping’ to ‘frequent use with vaping,’ said Mx. Kreski, who uses the honorific Mx. and the pronouns they/them. “Knowing that, as well as the high overlap of cannabis vaping with nicotine use and binge drinking, adds to the urgency of reducing adolescent vaping.”
To quantify the trends in cannabis vaping, the researchers reviewed data from Monitoring the Future, an annual survey of high school students across the United States. The study population included 51,052 individuals; approximately 49% were male and 49% were non-Hispanic White. The researchers examined frequency of cannabis use, trends across demographic groups, and concurrent use of cannabis and other substances such as alcohol and tobacco. The findings were published in the journal Addiction.
Frequent cannabis use was defined as six or more times in the past 30 days; occasional use was defined as one to five times in the past 30 days.
Frequent cannabis use with vaping increased from 2.1% in 2017 to 5.4% in 2019. Occasional cannabis use with vaping also increased, though less dramatically, from less than 2% in 2017 to approximately 3.5% in 2019.
By contrast, both frequent and occasional cannabis use without vaping declined from 2017 to 2019 (from 3.8% to 2.1% and from 6.9% to 4.4%, respectively).
Overall, the prevalence of any level of cannabis use increased from 13.9% in 2017 to 15.4% in 2019. Both males and females showed a similar increase in reported frequent cannabis use with vaping of approximately 3%.
The results document that vaping cannabis has become more common than smoking alone among U.S. teens across almost all demographic groups, and across sex, race, urbanicity, and level of parent education; however, the increased was especially marked among Hispanic/Latinx teens and those of lower socioeconomic status, the researchers wrote.
The researchers also examined the associations between cannabis use with and without vaping and concurrent nicotine and alcohol use. Overall, the strongest association was between smoking or vaping nicotine and vaping cannabis; teens who smoked or vaped nicotine were 42 times more likely than nonnicotine users to report vaping cannabis in the past 30 days (adjusted odds ratio, 42.28). In addition, more occasions of binge drinking were more strongly associated with cannabis use with vaping (up to 10 times more likely), compared with cannabis use without vaping, (aORs, 4.48-10.09).
The study findings were limited by several factors, including the lack of questions on tetrahydrocannabinol (THC) or cannabidiol content of the cannabis products used, although evidence suggests that the potency of cannabis products in the United States is increasing, the researchers noted. Other limitations included the cross-sectional design, which prevents making associations about causality, and lack of data on the quantity of cannabis used; only data on frequency of use were recorded.
However, the results reflect a rise in cannabis use with vaping among teens in the United States, along with an increased risk of tobacco use, e-cigarette use, and binge drinking, the researchers said.
As cannabis legalization expands across the United States, policies are needed to deter use among adolescents, the researchers wrote. “These policies should be crafted to reduce an emphasis on criminalization in preference for public health promotion given the history of unequal application of punitive consequences of drug use for racialized minorities in the United States. As products, delivery systems, potency, and marketing proliferate within a for-profit industry, increased attention to youth trends, including investment in sustained and evidence-based prevention and intervention, is increasingly necessary.”
The take-home message for clinicians is to ask whether your patients are vaping, because the prevalence is not only up, but fairly universal, Mx. Kreski said. “Have a discussion that covers a broad range of substance use topics and informs teens of the potential risks of vaping, while avoiding stigma.”
The message for parents is “to talk to your kids about the risks of vaping,” said Mx. Kreski. “Prioritize open communication rather than punishment, and work together with your teens to prevent or reduce vaping.” The message for teens: “Understand that vaping has risks. You should feel empowered to talk to your parents or doctor about those risks. While it may seem like everyone’s vaping, the majority don’t. Keeping communication open between parents/caregivers, teens, and health care providers is one of the best ways to address these trends in vaping.”
Beware more powerful cannabis products
“While drug use in general is declining in adolescents, marijuana use remains very common,” Kelly A. Curran, MD, of the University of Oklahoma Health Sciences Center, Oklahoma City, said in an interview.
“There is growing evidence that marijuana is now the first drug used by adolescents – replacing alcohol and nicotine – and frequent use can lead to substance abuse,” said Dr. Curran, who specializes in adolescent medicine but was involved in the study. “Cannabis use patterns have evolved over time. As I frequently tell my patients and their families, new strains and hybrids of marijuana have higher potencies of THC. Many adolescents are eschewing smoking and in its place using marijuana concentrates (wax, oil, shatter) via vape, dab pen, or rig. Use of these methods puts adolescents at high risk of social and health complications such as [e-cigarette or vaping use-associated lung injury], cannabis hyperemesis syndrome, and psychosis – and understanding these patterns and associated drug use helps health care professionals and parents keep adolescents safe.”
The take-home message for clinicians is that marijuana use via vaping continues to rise and to become more common than “traditional” marijuana smoking, Dr. Curran said. “This increase is across genders, in nearly all race/ethnicities (especially in Latinx youth), and in youth from lower socioeconomic status.” Vaping marijuana is associated with other substance abuse, so health care professionals should include questions about different forms of marijuana use, such as vape, dab pen, or rig, when working with patients, and counsel patients and families about the risks associated with use of any of these products.
The study was supported by the National Center for Injury Prevention and Control and by the National Institute on Drug Abuse. The researchers had no financial conflicts to disclose. Dr. Curran had no financial conflicts to disclose and serves on the editorial advisory board of Pediatric News.
FROM ADDICTION
Improved cancer survival in states with ACA Medicaid expansion
compared with patients in states that did not adopt the expansion.
The finding comes from an American Cancer Society study of more than 2 million patients with newly diagnosed cancer, published online in the Journal of the National Cancer Institute.
The analysis also showed that the evidence was strongest for malignancies with poor prognosis such as lung, pancreatic, and liver cancer, and also for colorectal cancer.
Importantly, improvements in survival were larger in non-Hispanic Black patients and individuals residing in rural areas, suggesting there was a narrowing of disparities in cancer survival by race and rurality.
“Our findings provide further evidence of the importance of expanding Medicaid eligibility in all states, particularly considering the economic crisis and health care disruptions caused by the COVID-19 pandemic,” said lead author Xuesong Han, PhD, scientific director of health services research at the American Cancer Society, in a statement. “What’s encouraging is the American Rescue Plan Act of 2021 provides new incentives for Medicaid expansion in states that have yet to increase eligibility.”
The ACA provided states with incentives to expand Medicaid eligibility to all low-income adults under 138% federal poverty level, regardless of parental status.
As of last month, just 12 states have not yet opted for Medicaid expansion, even though the American Rescue Plan Act of 2021 provides new incentives for those remaining jurisdictions. But to date, none of the remaining states have taken advantage of these new incentives.
An interactive map showing the status of Medicare expansion by state is available here. The 12 states that have not adopted Medicare expansion (as of April) are Alabama, Florida, Georgia, Kansas, Mississippi, North Carolina, South Carolina, South Dakota, Tennessee, Texas, Wisconsin, and Wyoming.
The benefit of Medicaid expansion on cancer outcomes has already been observed in other studies. The first study to show a survival benefit was presented at the 2020 American Society of Clinical Oncology annual meeting. That analysis showed that cancer mortality declined by 29% in states that expanded Medicaid and by 25% in those that did not. The authors also noted that the greatest mortality benefit was observed in Hispanic patients.
Improved survival with expansion
In the current paper, Dr. Han and colleagues used population-based cancer registries from 42 states and compared data on patients aged 18-62 years who were diagnosed with cancer in a period of 2 years before (2010-2012) and after (2014-2016) ACA Medicaid expansion. They were followed through Sept. 30, 2013, and Dec. 31, 2017, respectively.
The analysis involved a total of 2.5 million patients, of whom 1.52 million lived in states that adopted Medicaid expansion and compared with 1 million patients were in states that did not.
Patients with grouped by sex, race and ethnicity, census tract-level poverty, and rurality. The authors note that non-Hispanic Black patients and those from high poverty areas and nonmetropolitan areas were disproportionately represented in nonexpansion states.
During the 2-year follow-up period, a total of 453,487 deaths occurred (257,950 in expansion states and 195,537 in nonexpansion states).
Overall, patients in expansion states generally had better survival versus those in nonexpansion states, the authors comment. However, for most cancer types, overall survival improved after the ACA for both groups of states.
The 2-year overall survival increased from 80.6% before the ACA to 82.2% post ACA in expansion states and from 78.7% to 80% in nonexpansion states.
This extrapolated to net increase of 0.44 percentage points in expansion states after adjusting for sociodemographic factors. By cancer site, the net increase was greater for colorectal cancer, lung cancer, non-Hodgkin’s lymphoma, pancreatic cancer, and liver cancer.
For Hispanic patients, 2-year survival also increased but was similar in expansion and nonexpansion states, and little net change was associated with Medicaid expansion.
“Our study shows that the increase was largely driven by improvements in survival for cancer types with poor prognosis, suggesting improved access to timely and effective treatments,” said Dr. Han. “It adds to accumulating evidence of the multiple benefits of Medicaid expansion.”
A version of this article first appeared on Medscape.com.
compared with patients in states that did not adopt the expansion.
The finding comes from an American Cancer Society study of more than 2 million patients with newly diagnosed cancer, published online in the Journal of the National Cancer Institute.
The analysis also showed that the evidence was strongest for malignancies with poor prognosis such as lung, pancreatic, and liver cancer, and also for colorectal cancer.
Importantly, improvements in survival were larger in non-Hispanic Black patients and individuals residing in rural areas, suggesting there was a narrowing of disparities in cancer survival by race and rurality.
“Our findings provide further evidence of the importance of expanding Medicaid eligibility in all states, particularly considering the economic crisis and health care disruptions caused by the COVID-19 pandemic,” said lead author Xuesong Han, PhD, scientific director of health services research at the American Cancer Society, in a statement. “What’s encouraging is the American Rescue Plan Act of 2021 provides new incentives for Medicaid expansion in states that have yet to increase eligibility.”
The ACA provided states with incentives to expand Medicaid eligibility to all low-income adults under 138% federal poverty level, regardless of parental status.
As of last month, just 12 states have not yet opted for Medicaid expansion, even though the American Rescue Plan Act of 2021 provides new incentives for those remaining jurisdictions. But to date, none of the remaining states have taken advantage of these new incentives.
An interactive map showing the status of Medicare expansion by state is available here. The 12 states that have not adopted Medicare expansion (as of April) are Alabama, Florida, Georgia, Kansas, Mississippi, North Carolina, South Carolina, South Dakota, Tennessee, Texas, Wisconsin, and Wyoming.
The benefit of Medicaid expansion on cancer outcomes has already been observed in other studies. The first study to show a survival benefit was presented at the 2020 American Society of Clinical Oncology annual meeting. That analysis showed that cancer mortality declined by 29% in states that expanded Medicaid and by 25% in those that did not. The authors also noted that the greatest mortality benefit was observed in Hispanic patients.
Improved survival with expansion
In the current paper, Dr. Han and colleagues used population-based cancer registries from 42 states and compared data on patients aged 18-62 years who were diagnosed with cancer in a period of 2 years before (2010-2012) and after (2014-2016) ACA Medicaid expansion. They were followed through Sept. 30, 2013, and Dec. 31, 2017, respectively.
The analysis involved a total of 2.5 million patients, of whom 1.52 million lived in states that adopted Medicaid expansion and compared with 1 million patients were in states that did not.
Patients with grouped by sex, race and ethnicity, census tract-level poverty, and rurality. The authors note that non-Hispanic Black patients and those from high poverty areas and nonmetropolitan areas were disproportionately represented in nonexpansion states.
During the 2-year follow-up period, a total of 453,487 deaths occurred (257,950 in expansion states and 195,537 in nonexpansion states).
Overall, patients in expansion states generally had better survival versus those in nonexpansion states, the authors comment. However, for most cancer types, overall survival improved after the ACA for both groups of states.
The 2-year overall survival increased from 80.6% before the ACA to 82.2% post ACA in expansion states and from 78.7% to 80% in nonexpansion states.
This extrapolated to net increase of 0.44 percentage points in expansion states after adjusting for sociodemographic factors. By cancer site, the net increase was greater for colorectal cancer, lung cancer, non-Hodgkin’s lymphoma, pancreatic cancer, and liver cancer.
For Hispanic patients, 2-year survival also increased but was similar in expansion and nonexpansion states, and little net change was associated with Medicaid expansion.
“Our study shows that the increase was largely driven by improvements in survival for cancer types with poor prognosis, suggesting improved access to timely and effective treatments,” said Dr. Han. “It adds to accumulating evidence of the multiple benefits of Medicaid expansion.”
A version of this article first appeared on Medscape.com.
compared with patients in states that did not adopt the expansion.
The finding comes from an American Cancer Society study of more than 2 million patients with newly diagnosed cancer, published online in the Journal of the National Cancer Institute.
The analysis also showed that the evidence was strongest for malignancies with poor prognosis such as lung, pancreatic, and liver cancer, and also for colorectal cancer.
Importantly, improvements in survival were larger in non-Hispanic Black patients and individuals residing in rural areas, suggesting there was a narrowing of disparities in cancer survival by race and rurality.
“Our findings provide further evidence of the importance of expanding Medicaid eligibility in all states, particularly considering the economic crisis and health care disruptions caused by the COVID-19 pandemic,” said lead author Xuesong Han, PhD, scientific director of health services research at the American Cancer Society, in a statement. “What’s encouraging is the American Rescue Plan Act of 2021 provides new incentives for Medicaid expansion in states that have yet to increase eligibility.”
The ACA provided states with incentives to expand Medicaid eligibility to all low-income adults under 138% federal poverty level, regardless of parental status.
As of last month, just 12 states have not yet opted for Medicaid expansion, even though the American Rescue Plan Act of 2021 provides new incentives for those remaining jurisdictions. But to date, none of the remaining states have taken advantage of these new incentives.
An interactive map showing the status of Medicare expansion by state is available here. The 12 states that have not adopted Medicare expansion (as of April) are Alabama, Florida, Georgia, Kansas, Mississippi, North Carolina, South Carolina, South Dakota, Tennessee, Texas, Wisconsin, and Wyoming.
The benefit of Medicaid expansion on cancer outcomes has already been observed in other studies. The first study to show a survival benefit was presented at the 2020 American Society of Clinical Oncology annual meeting. That analysis showed that cancer mortality declined by 29% in states that expanded Medicaid and by 25% in those that did not. The authors also noted that the greatest mortality benefit was observed in Hispanic patients.
Improved survival with expansion
In the current paper, Dr. Han and colleagues used population-based cancer registries from 42 states and compared data on patients aged 18-62 years who were diagnosed with cancer in a period of 2 years before (2010-2012) and after (2014-2016) ACA Medicaid expansion. They were followed through Sept. 30, 2013, and Dec. 31, 2017, respectively.
The analysis involved a total of 2.5 million patients, of whom 1.52 million lived in states that adopted Medicaid expansion and compared with 1 million patients were in states that did not.
Patients with grouped by sex, race and ethnicity, census tract-level poverty, and rurality. The authors note that non-Hispanic Black patients and those from high poverty areas and nonmetropolitan areas were disproportionately represented in nonexpansion states.
During the 2-year follow-up period, a total of 453,487 deaths occurred (257,950 in expansion states and 195,537 in nonexpansion states).
Overall, patients in expansion states generally had better survival versus those in nonexpansion states, the authors comment. However, for most cancer types, overall survival improved after the ACA for both groups of states.
The 2-year overall survival increased from 80.6% before the ACA to 82.2% post ACA in expansion states and from 78.7% to 80% in nonexpansion states.
This extrapolated to net increase of 0.44 percentage points in expansion states after adjusting for sociodemographic factors. By cancer site, the net increase was greater for colorectal cancer, lung cancer, non-Hodgkin’s lymphoma, pancreatic cancer, and liver cancer.
For Hispanic patients, 2-year survival also increased but was similar in expansion and nonexpansion states, and little net change was associated with Medicaid expansion.
“Our study shows that the increase was largely driven by improvements in survival for cancer types with poor prognosis, suggesting improved access to timely and effective treatments,” said Dr. Han. “It adds to accumulating evidence of the multiple benefits of Medicaid expansion.”
A version of this article first appeared on Medscape.com.
NAVIGATOR steers uncontrolled asthma toward calmer seas
SAN FRANCISCO – Nearly half of all patients with severe, uncontrolled asthma who received a full course of the biologic agent tezepelumab (Tezspire) in the NAVIGATOR trial had a complete response to treatment at 1 year, results of a prespecified exploratory analysis indicated.
Among 471 patients assigned to tezepelumab who completed the on-treatment period of the phase 3 randomized trial, 46% had a complete response at 52 weeks, compared with 24% of patients assigned to placebo.
Complete response was defined as reduction in exacerbations of at least 50% over the previous year, improvement from baseline in Asthma Control Questionnaire 6 (ACQ-6) total score of at least 0.5 points, improvement in prebronchodilator forced expiratory volume in 1 second (pre-BD FEV1), and physician-assessed Clinical Global Impression measure of clinical change (CGI-C) score.
“These data further support the efficacy of tezepelumab in a broad population of patients with severe, uncontrolled asthma,” said Njira Lugogo, MD, of the division of pulmonary and critical care medicine at the University of Michigan, Ann Arbor.
Dr. Lugogo presented results of the exploratory analysis at the American Thoracic Society’s international conference.
Exacerbations reduced, lung function improved
Primary results from NAVIGATOR, published in The New England Journal of Medicine, showed that patients with severe, uncontrolled asthma randomly assigned to tezepelumab had fewer exacerbations and better lung function, asthma control, and health-related quality of life compared with patients assigned to placebo.
The investigators noted that approximately 10% of patients with asthma have symptoms and exacerbations despite maximal standard-of-care controller therapy.
Tezepelumab is a human monoclonal antibody that inhibits action of thymic stromal lymphopoietin (TSLP), an epithelial cytokine that is released in response to airborne triggers of asthma. TSLP is a major contributor to initiation and persistence of airway inflammation, Dr. Lugogo said.
The on-treatment analysis looked at all patients in the trial who completed 52 weeks of treatment and had complete data for all criteria studied.
The odds ratios (OR) for patients on tezepelumab achieving each of the response criteria are shown in the table.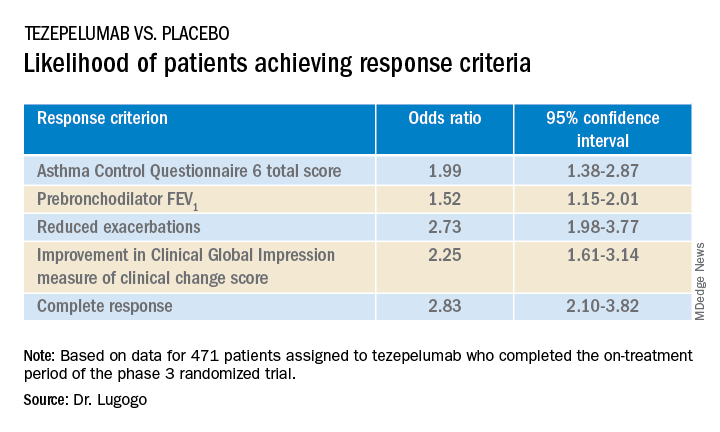
Exacerbations explored
In a separate presentation, Christopher S. Ambrose, MD, MBA, of AstraZeneca in Gaithersburg, Md., presented information from investigator-narrative descriptions of all hospitalization events related to asthma exacerbations (mild, moderate, or severe) that occurred while the investigator was blinded to each patient’s treatment assignment in NAVIGATOR.
In all, 39 of 531 patients (7.3%) assigned to placebo had a total of 78 exacerbations requiring hospitalization, compared with 13 of 528 patients (2.5%) assigned to tezepelumab. The latter group had a total of 14 exacerbations requiring hospitalization during the study.
Among hospitalized patients, 32 of the 39 assigned to placebo had severe, incapacitating exacerbations, compared with 5 of 13 assigned to tezepelumab.
Reported symptoms were generally similar between hospitalized patients in the two treatment groups, although there appeared to be trends toward lower incidence of dyspnea, fever, and tachycardia with tezepelumab.
Health care resource utilization, a surrogate marker for disease burden, was substantially lower for patients assigned to tezepelumab.
Infections were the most common triggers of exacerbations in both groups.
“These data provide further evidence that tezepelumab can reduce the burden of disease of severe uncontrolled asthma, both to patients and to health care systems,” Dr. Ambrose said.
Head-to-head studies needed
Although there have been no head-to-head comparisons of biologic agents for asthma to date, results of these studies suggest that tezepelumab has efficacy similar to that of other agents for reducing exacerbation, said Fernando Holguin, MD, MPH, from the University of Colorado at Denver, Aurora, who comoderated the oral session where the data were presented but was not involved in the study.
Biologic agents appear to be slightly more effective against type 2 inflammation in asthma, “but in general I think we give it to a broader severe population, so that’s exciting,” he told this news organization.
Comoderator Amisha Barochia, MBBS, MHS, of the National Institutes of Health, Bethesda, Md., told this news organization that head-to-head trials of biologic agents would provide important clinical information going forward.
“Should we switch to a different biologic or add a second biologic? Those are questions we need answers for,” she said.
The NAVIGATOR trial is funded by AstraZeneca and Amgen. Dr. Lugogo disclosed financial relationships with both companies. Dr. Holguin and Dr. Barochia have disclosed no financial relationships relevant to the studies presented.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO – Nearly half of all patients with severe, uncontrolled asthma who received a full course of the biologic agent tezepelumab (Tezspire) in the NAVIGATOR trial had a complete response to treatment at 1 year, results of a prespecified exploratory analysis indicated.
Among 471 patients assigned to tezepelumab who completed the on-treatment period of the phase 3 randomized trial, 46% had a complete response at 52 weeks, compared with 24% of patients assigned to placebo.
Complete response was defined as reduction in exacerbations of at least 50% over the previous year, improvement from baseline in Asthma Control Questionnaire 6 (ACQ-6) total score of at least 0.5 points, improvement in prebronchodilator forced expiratory volume in 1 second (pre-BD FEV1), and physician-assessed Clinical Global Impression measure of clinical change (CGI-C) score.
“These data further support the efficacy of tezepelumab in a broad population of patients with severe, uncontrolled asthma,” said Njira Lugogo, MD, of the division of pulmonary and critical care medicine at the University of Michigan, Ann Arbor.
Dr. Lugogo presented results of the exploratory analysis at the American Thoracic Society’s international conference.
Exacerbations reduced, lung function improved
Primary results from NAVIGATOR, published in The New England Journal of Medicine, showed that patients with severe, uncontrolled asthma randomly assigned to tezepelumab had fewer exacerbations and better lung function, asthma control, and health-related quality of life compared with patients assigned to placebo.
The investigators noted that approximately 10% of patients with asthma have symptoms and exacerbations despite maximal standard-of-care controller therapy.
Tezepelumab is a human monoclonal antibody that inhibits action of thymic stromal lymphopoietin (TSLP), an epithelial cytokine that is released in response to airborne triggers of asthma. TSLP is a major contributor to initiation and persistence of airway inflammation, Dr. Lugogo said.
The on-treatment analysis looked at all patients in the trial who completed 52 weeks of treatment and had complete data for all criteria studied.
The odds ratios (OR) for patients on tezepelumab achieving each of the response criteria are shown in the table.
Exacerbations explored
In a separate presentation, Christopher S. Ambrose, MD, MBA, of AstraZeneca in Gaithersburg, Md., presented information from investigator-narrative descriptions of all hospitalization events related to asthma exacerbations (mild, moderate, or severe) that occurred while the investigator was blinded to each patient’s treatment assignment in NAVIGATOR.
In all, 39 of 531 patients (7.3%) assigned to placebo had a total of 78 exacerbations requiring hospitalization, compared with 13 of 528 patients (2.5%) assigned to tezepelumab. The latter group had a total of 14 exacerbations requiring hospitalization during the study.
Among hospitalized patients, 32 of the 39 assigned to placebo had severe, incapacitating exacerbations, compared with 5 of 13 assigned to tezepelumab.
Reported symptoms were generally similar between hospitalized patients in the two treatment groups, although there appeared to be trends toward lower incidence of dyspnea, fever, and tachycardia with tezepelumab.
Health care resource utilization, a surrogate marker for disease burden, was substantially lower for patients assigned to tezepelumab.
Infections were the most common triggers of exacerbations in both groups.
“These data provide further evidence that tezepelumab can reduce the burden of disease of severe uncontrolled asthma, both to patients and to health care systems,” Dr. Ambrose said.
Head-to-head studies needed
Although there have been no head-to-head comparisons of biologic agents for asthma to date, results of these studies suggest that tezepelumab has efficacy similar to that of other agents for reducing exacerbation, said Fernando Holguin, MD, MPH, from the University of Colorado at Denver, Aurora, who comoderated the oral session where the data were presented but was not involved in the study.
Biologic agents appear to be slightly more effective against type 2 inflammation in asthma, “but in general I think we give it to a broader severe population, so that’s exciting,” he told this news organization.
Comoderator Amisha Barochia, MBBS, MHS, of the National Institutes of Health, Bethesda, Md., told this news organization that head-to-head trials of biologic agents would provide important clinical information going forward.
“Should we switch to a different biologic or add a second biologic? Those are questions we need answers for,” she said.
The NAVIGATOR trial is funded by AstraZeneca and Amgen. Dr. Lugogo disclosed financial relationships with both companies. Dr. Holguin and Dr. Barochia have disclosed no financial relationships relevant to the studies presented.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO – Nearly half of all patients with severe, uncontrolled asthma who received a full course of the biologic agent tezepelumab (Tezspire) in the NAVIGATOR trial had a complete response to treatment at 1 year, results of a prespecified exploratory analysis indicated.
Among 471 patients assigned to tezepelumab who completed the on-treatment period of the phase 3 randomized trial, 46% had a complete response at 52 weeks, compared with 24% of patients assigned to placebo.
Complete response was defined as reduction in exacerbations of at least 50% over the previous year, improvement from baseline in Asthma Control Questionnaire 6 (ACQ-6) total score of at least 0.5 points, improvement in prebronchodilator forced expiratory volume in 1 second (pre-BD FEV1), and physician-assessed Clinical Global Impression measure of clinical change (CGI-C) score.
“These data further support the efficacy of tezepelumab in a broad population of patients with severe, uncontrolled asthma,” said Njira Lugogo, MD, of the division of pulmonary and critical care medicine at the University of Michigan, Ann Arbor.
Dr. Lugogo presented results of the exploratory analysis at the American Thoracic Society’s international conference.
Exacerbations reduced, lung function improved
Primary results from NAVIGATOR, published in The New England Journal of Medicine, showed that patients with severe, uncontrolled asthma randomly assigned to tezepelumab had fewer exacerbations and better lung function, asthma control, and health-related quality of life compared with patients assigned to placebo.
The investigators noted that approximately 10% of patients with asthma have symptoms and exacerbations despite maximal standard-of-care controller therapy.
Tezepelumab is a human monoclonal antibody that inhibits action of thymic stromal lymphopoietin (TSLP), an epithelial cytokine that is released in response to airborne triggers of asthma. TSLP is a major contributor to initiation and persistence of airway inflammation, Dr. Lugogo said.
The on-treatment analysis looked at all patients in the trial who completed 52 weeks of treatment and had complete data for all criteria studied.
The odds ratios (OR) for patients on tezepelumab achieving each of the response criteria are shown in the table.
Exacerbations explored
In a separate presentation, Christopher S. Ambrose, MD, MBA, of AstraZeneca in Gaithersburg, Md., presented information from investigator-narrative descriptions of all hospitalization events related to asthma exacerbations (mild, moderate, or severe) that occurred while the investigator was blinded to each patient’s treatment assignment in NAVIGATOR.
In all, 39 of 531 patients (7.3%) assigned to placebo had a total of 78 exacerbations requiring hospitalization, compared with 13 of 528 patients (2.5%) assigned to tezepelumab. The latter group had a total of 14 exacerbations requiring hospitalization during the study.
Among hospitalized patients, 32 of the 39 assigned to placebo had severe, incapacitating exacerbations, compared with 5 of 13 assigned to tezepelumab.
Reported symptoms were generally similar between hospitalized patients in the two treatment groups, although there appeared to be trends toward lower incidence of dyspnea, fever, and tachycardia with tezepelumab.
Health care resource utilization, a surrogate marker for disease burden, was substantially lower for patients assigned to tezepelumab.
Infections were the most common triggers of exacerbations in both groups.
“These data provide further evidence that tezepelumab can reduce the burden of disease of severe uncontrolled asthma, both to patients and to health care systems,” Dr. Ambrose said.
Head-to-head studies needed
Although there have been no head-to-head comparisons of biologic agents for asthma to date, results of these studies suggest that tezepelumab has efficacy similar to that of other agents for reducing exacerbation, said Fernando Holguin, MD, MPH, from the University of Colorado at Denver, Aurora, who comoderated the oral session where the data were presented but was not involved in the study.
Biologic agents appear to be slightly more effective against type 2 inflammation in asthma, “but in general I think we give it to a broader severe population, so that’s exciting,” he told this news organization.
Comoderator Amisha Barochia, MBBS, MHS, of the National Institutes of Health, Bethesda, Md., told this news organization that head-to-head trials of biologic agents would provide important clinical information going forward.
“Should we switch to a different biologic or add a second biologic? Those are questions we need answers for,” she said.
The NAVIGATOR trial is funded by AstraZeneca and Amgen. Dr. Lugogo disclosed financial relationships with both companies. Dr. Holguin and Dr. Barochia have disclosed no financial relationships relevant to the studies presented.
A version of this article first appeared on Medscape.com.
AT ATS 2022
Cancer patients unaware of their increased thrombosis risk
It is up to their physician to discuss this with them.
This link is explained by the authors of an article in Cancer Treatment and Research Communications that reports results of a survey carried out by the European Cancer Patient Coalition (ECPC). “The aim of this pan-European patient survey was to assess patient awareness and knowledge about cancer-associated thrombosis (CAT), including risk factors, signs and symptoms, and interventions, to better prevent and treat CAT,” write the authors. “The idea was to create a sort of starting point for subsequent communication and information strategies and for comparing the results of any action taken in this area,” they add.
A roundtable discussion that included oncology healthcare professionals, policymakers, and patient advocates was convened to discuss and review the evidence regarding their ongoing concerns of excessive CAT-associated morbidity and mortality, as well as patients’ desire for greater CAT awareness.
“These discussions demonstrated that very little change had occurred over the years and that greater knowledge about CAT was still needed across the spectrum of healthcare practitioners and patients, particularly regarding primary and secondary prevention of thrombosis,” the authors write.
It was from this starting point that the idea for the pan-European survey was born. The ECPC, widely viewed as the “unified voice of cancer patients across Europe,” led the survey. This survey spanned six countries (France, Germany, Greece, Italy, United Kingdom, and Spain) and involved 1,365 patients and caregivers. The ECPC survey result was originally released at World Thrombosis Day in late 2018.
In an interview, Anna Falanga, MD, the main author of the article and professor of hematology at the University of Milan-Bicocca, Italy, reviewed the results and explained how to improve knowledge of CAT among patients with cancer.
“Data support that up to 20% of patients with cancer will experience venous thromboembolism (VTE), which is approximately 4–5 times higher than the general population,” said Dr. Falanga, who is also chief of the department of immunohematology and transfusion medicine and the Thrombosis and Hemostasis Center at the Hospital Papa Giovanni XXIII, in Bergamo, Italy.
“We have known about the link between thrombosis and cancer since the 19th century, but it has taken until midway through the last century for our level of understanding and awareness of the problem to reach its current level. Initially, this was limited to fundamental research, with large advances in our understanding of the mechanisms of the link between the two; it has only been more recently that we have had clinical studies that have piqued the interest of healthcare professionals, who were previously uninterested in the topic,” she said.
Poor understanding
One piece of data stands out from the European survey: Nearly three quarters of respondents (72%) said that before taking part in the survey, they were not aware that people with cancer have a higher-than-normal risk of developing thrombosis. “We asked participants to rate their overall understanding of CAT on a scale of 1 (low) to 10 (high), with the average (mean) score obtained being 4.1. Only 21% of patients gave a rating of 7 or above (high understanding). The average rating was very similar in the different countries surveyed,” write the authors. They note that the survey also assessed how much participants had learned about the topic from their physicians.
Approximately 35% of patients were made aware of CAT either immediately before or at the time of their cancer diagnosis. Of particular concern, one quarter (26%) of respondents (the largest proportion) noted that they first became aware of CAT when they suffered a blood clot. The average rating was very similar in the different countries surveyed. “Let us not forget that cancer and cancer treatments themselves cause a number of side effects, some of which can be very serious, so in some ways, a clot might be seen as a minor problem. Yet, in reality, it isn’t. It is a significant cause of death and disease in cancer patients,” said Dr. Falanga.
When discussing prevention, most respondents (87%) said they were aware that taking a walk could reduce their risk. Slightly fewer were aware that stopping smoking could reduce their risk (75%), and even fewer were aware that keeping hydrated (63%) and stretching their legs (55%) could reduce their risk.
Symptoms of CAT appeared to be relatively well known; 73% of survey participants indicated that they were aware that swelling in the foot, ankle, or leg could be a sign of DVT, and 71% indicated that shortness of breath could be a sign of pulmonary embolism (PE). “Other symptoms, however, were less well known, with just over half (57%) of participants being aware that pain, cramping, and tenderness could be a sign of DVT. About one third (33%) knew that irregular heartbeat could be a sign of PE. These results varied between countries,” according to the authors.
The survey highlighted that just over a third of respondents said that they were currently using anticoagulants, although almost all (96%) knew that anticoagulants could be used to effectively treat thrombosis. Only 41% of those using anticoagulants said they had been told about any possible side effects.
The Italian situation
The report containing the full results of the European survey goes even further, since, in addition to its overall results, it also gives information about individual countries.
The data from Italy, which are based on 246 persons, show that only 27% of patients and caregivers were aware of the increased risk of thrombosis after a cancer diagnosis. This figure is in line with the overall results of the survey, although the average score of the 10-point scale was lower for the Italy cohort (3.3/10 vs 4.1/10).
The results are more variable in terms of knowledge of risk factors. Most respondents (89%) said that they were aware of the risks related to inactivity. Just over half (52%), however, said that they were aware of the risks related to radiotherapy. Nevertheless, 75% of participants knew about the risks relating to cancer surgery and chemotherapy. “To all intents and purposes, all types of cancer drug can significantly affect the risk of developing a clot. And this is also the case for more modern types of treatment, such as immunotherapy,” said Dr. Falanga.
Most respondents reported that they got information about cancer-associated thrombosis verbally, usually from their hospital doctor (11%). Some respondents (6%) said that they found out about it from their own research, usually online. Almost 1 in 4 patients (24%) in Italy said that they first became aware of CAT when they suffered a blood clot. Answers to questions about knowledge of symptoms show that 58% of Italian patients and caregivers know that swelling of the lower limbs can be a symptom of DVT, and the same percentage knows that shortness of breath might indicate PE.
In terms of preventive action, the picture in Italy is somewhat variable: 74% of participants were aware of the importance of walking, but far fewer knew about the need to stop smoking (57%) and stretch the legs (35%). Of the 41% of Italians who were also taking an anticoagulant drug, 53% said that they knew about the possible side effects of such medication.
Which way forward?
“The high rate of CAT suggests that, despite the clinical evidence and clear guideline recommendations for patients with cancer, CAT prevention and recognition remain low among healthcare professionals,” the authors write.
The results of the ECPC survey further confirm those of previous studies, highlighting patients’ lack of knowledge about CAT and the need for more in-depth discussions between physician and patient.
So, what can be done? As highlighted by previous studies, “patients’ experiences are an education in themselves, particularly for the oncology care team,” the authors write. “Once the patient has a thrombosis, the opportunity for thrombosis prevention, which should be the most crucial focus of the care clinics (surgical, oncology, and palliative care), is gone,” they add.
“Oncology professionals, as well as other members of the patient’s care team (eg, internists, surgeons, nurses), need to perform better, at every stage of the patient’s cancer pathway, to ensure patients are aware of CAT and their individual risk to develop a blood clot,” said Dr. Falanga. She explained that in this group, it is the general practitioner who is the first contact. “These professionals are on the front line of the battle; they are among the first healthcare workers given the chance to suspect a clot and should, therefore, be fully aware of the increased risk in oncology patients,” she reiterated.
Experts agree on the fact that a multidisciplinary approach is of utmost importance in this context: the different roles in the team must be clear. “It is also fundamental to establish who does what in terms of educating and informing the patient,” said Dr. Falanga.
The researchers also put forward an example of a successful initiative: the Venous Thromboembolism Prevention in the Ambulatory Cancer Clinic (VTE-PACC) program. The initiative was developed by experts from the University of Vermont and was described in a recent article in JCO Oncology Practice.
Numerous resources are available online to help physicians talk to their patients and explain the risks linked to CAT along the continuum of cancer care. Among them is a resource titled, “Cancer Associated Thrombosis (CAT): Be Clot Conscious,” which can be found on the ECPC’s website.
“We have a collective responsibility using the ECPC patient survey as a baseline to inform patients with cancer on how to identify signs and symptoms of CAT to enable faster diagnosis and treatment,” the authors conclude.
This article was translated from Univadis Italy.
It is up to their physician to discuss this with them.
This link is explained by the authors of an article in Cancer Treatment and Research Communications that reports results of a survey carried out by the European Cancer Patient Coalition (ECPC). “The aim of this pan-European patient survey was to assess patient awareness and knowledge about cancer-associated thrombosis (CAT), including risk factors, signs and symptoms, and interventions, to better prevent and treat CAT,” write the authors. “The idea was to create a sort of starting point for subsequent communication and information strategies and for comparing the results of any action taken in this area,” they add.
A roundtable discussion that included oncology healthcare professionals, policymakers, and patient advocates was convened to discuss and review the evidence regarding their ongoing concerns of excessive CAT-associated morbidity and mortality, as well as patients’ desire for greater CAT awareness.
“These discussions demonstrated that very little change had occurred over the years and that greater knowledge about CAT was still needed across the spectrum of healthcare practitioners and patients, particularly regarding primary and secondary prevention of thrombosis,” the authors write.
It was from this starting point that the idea for the pan-European survey was born. The ECPC, widely viewed as the “unified voice of cancer patients across Europe,” led the survey. This survey spanned six countries (France, Germany, Greece, Italy, United Kingdom, and Spain) and involved 1,365 patients and caregivers. The ECPC survey result was originally released at World Thrombosis Day in late 2018.
In an interview, Anna Falanga, MD, the main author of the article and professor of hematology at the University of Milan-Bicocca, Italy, reviewed the results and explained how to improve knowledge of CAT among patients with cancer.
“Data support that up to 20% of patients with cancer will experience venous thromboembolism (VTE), which is approximately 4–5 times higher than the general population,” said Dr. Falanga, who is also chief of the department of immunohematology and transfusion medicine and the Thrombosis and Hemostasis Center at the Hospital Papa Giovanni XXIII, in Bergamo, Italy.
“We have known about the link between thrombosis and cancer since the 19th century, but it has taken until midway through the last century for our level of understanding and awareness of the problem to reach its current level. Initially, this was limited to fundamental research, with large advances in our understanding of the mechanisms of the link between the two; it has only been more recently that we have had clinical studies that have piqued the interest of healthcare professionals, who were previously uninterested in the topic,” she said.
Poor understanding
One piece of data stands out from the European survey: Nearly three quarters of respondents (72%) said that before taking part in the survey, they were not aware that people with cancer have a higher-than-normal risk of developing thrombosis. “We asked participants to rate their overall understanding of CAT on a scale of 1 (low) to 10 (high), with the average (mean) score obtained being 4.1. Only 21% of patients gave a rating of 7 or above (high understanding). The average rating was very similar in the different countries surveyed,” write the authors. They note that the survey also assessed how much participants had learned about the topic from their physicians.
Approximately 35% of patients were made aware of CAT either immediately before or at the time of their cancer diagnosis. Of particular concern, one quarter (26%) of respondents (the largest proportion) noted that they first became aware of CAT when they suffered a blood clot. The average rating was very similar in the different countries surveyed. “Let us not forget that cancer and cancer treatments themselves cause a number of side effects, some of which can be very serious, so in some ways, a clot might be seen as a minor problem. Yet, in reality, it isn’t. It is a significant cause of death and disease in cancer patients,” said Dr. Falanga.
When discussing prevention, most respondents (87%) said they were aware that taking a walk could reduce their risk. Slightly fewer were aware that stopping smoking could reduce their risk (75%), and even fewer were aware that keeping hydrated (63%) and stretching their legs (55%) could reduce their risk.
Symptoms of CAT appeared to be relatively well known; 73% of survey participants indicated that they were aware that swelling in the foot, ankle, or leg could be a sign of DVT, and 71% indicated that shortness of breath could be a sign of pulmonary embolism (PE). “Other symptoms, however, were less well known, with just over half (57%) of participants being aware that pain, cramping, and tenderness could be a sign of DVT. About one third (33%) knew that irregular heartbeat could be a sign of PE. These results varied between countries,” according to the authors.
The survey highlighted that just over a third of respondents said that they were currently using anticoagulants, although almost all (96%) knew that anticoagulants could be used to effectively treat thrombosis. Only 41% of those using anticoagulants said they had been told about any possible side effects.
The Italian situation
The report containing the full results of the European survey goes even further, since, in addition to its overall results, it also gives information about individual countries.
The data from Italy, which are based on 246 persons, show that only 27% of patients and caregivers were aware of the increased risk of thrombosis after a cancer diagnosis. This figure is in line with the overall results of the survey, although the average score of the 10-point scale was lower for the Italy cohort (3.3/10 vs 4.1/10).
The results are more variable in terms of knowledge of risk factors. Most respondents (89%) said that they were aware of the risks related to inactivity. Just over half (52%), however, said that they were aware of the risks related to radiotherapy. Nevertheless, 75% of participants knew about the risks relating to cancer surgery and chemotherapy. “To all intents and purposes, all types of cancer drug can significantly affect the risk of developing a clot. And this is also the case for more modern types of treatment, such as immunotherapy,” said Dr. Falanga.
Most respondents reported that they got information about cancer-associated thrombosis verbally, usually from their hospital doctor (11%). Some respondents (6%) said that they found out about it from their own research, usually online. Almost 1 in 4 patients (24%) in Italy said that they first became aware of CAT when they suffered a blood clot. Answers to questions about knowledge of symptoms show that 58% of Italian patients and caregivers know that swelling of the lower limbs can be a symptom of DVT, and the same percentage knows that shortness of breath might indicate PE.
In terms of preventive action, the picture in Italy is somewhat variable: 74% of participants were aware of the importance of walking, but far fewer knew about the need to stop smoking (57%) and stretch the legs (35%). Of the 41% of Italians who were also taking an anticoagulant drug, 53% said that they knew about the possible side effects of such medication.
Which way forward?
“The high rate of CAT suggests that, despite the clinical evidence and clear guideline recommendations for patients with cancer, CAT prevention and recognition remain low among healthcare professionals,” the authors write.
The results of the ECPC survey further confirm those of previous studies, highlighting patients’ lack of knowledge about CAT and the need for more in-depth discussions between physician and patient.
So, what can be done? As highlighted by previous studies, “patients’ experiences are an education in themselves, particularly for the oncology care team,” the authors write. “Once the patient has a thrombosis, the opportunity for thrombosis prevention, which should be the most crucial focus of the care clinics (surgical, oncology, and palliative care), is gone,” they add.
“Oncology professionals, as well as other members of the patient’s care team (eg, internists, surgeons, nurses), need to perform better, at every stage of the patient’s cancer pathway, to ensure patients are aware of CAT and their individual risk to develop a blood clot,” said Dr. Falanga. She explained that in this group, it is the general practitioner who is the first contact. “These professionals are on the front line of the battle; they are among the first healthcare workers given the chance to suspect a clot and should, therefore, be fully aware of the increased risk in oncology patients,” she reiterated.
Experts agree on the fact that a multidisciplinary approach is of utmost importance in this context: the different roles in the team must be clear. “It is also fundamental to establish who does what in terms of educating and informing the patient,” said Dr. Falanga.
The researchers also put forward an example of a successful initiative: the Venous Thromboembolism Prevention in the Ambulatory Cancer Clinic (VTE-PACC) program. The initiative was developed by experts from the University of Vermont and was described in a recent article in JCO Oncology Practice.
Numerous resources are available online to help physicians talk to their patients and explain the risks linked to CAT along the continuum of cancer care. Among them is a resource titled, “Cancer Associated Thrombosis (CAT): Be Clot Conscious,” which can be found on the ECPC’s website.
“We have a collective responsibility using the ECPC patient survey as a baseline to inform patients with cancer on how to identify signs and symptoms of CAT to enable faster diagnosis and treatment,” the authors conclude.
This article was translated from Univadis Italy.
It is up to their physician to discuss this with them.
This link is explained by the authors of an article in Cancer Treatment and Research Communications that reports results of a survey carried out by the European Cancer Patient Coalition (ECPC). “The aim of this pan-European patient survey was to assess patient awareness and knowledge about cancer-associated thrombosis (CAT), including risk factors, signs and symptoms, and interventions, to better prevent and treat CAT,” write the authors. “The idea was to create a sort of starting point for subsequent communication and information strategies and for comparing the results of any action taken in this area,” they add.
A roundtable discussion that included oncology healthcare professionals, policymakers, and patient advocates was convened to discuss and review the evidence regarding their ongoing concerns of excessive CAT-associated morbidity and mortality, as well as patients’ desire for greater CAT awareness.
“These discussions demonstrated that very little change had occurred over the years and that greater knowledge about CAT was still needed across the spectrum of healthcare practitioners and patients, particularly regarding primary and secondary prevention of thrombosis,” the authors write.
It was from this starting point that the idea for the pan-European survey was born. The ECPC, widely viewed as the “unified voice of cancer patients across Europe,” led the survey. This survey spanned six countries (France, Germany, Greece, Italy, United Kingdom, and Spain) and involved 1,365 patients and caregivers. The ECPC survey result was originally released at World Thrombosis Day in late 2018.
In an interview, Anna Falanga, MD, the main author of the article and professor of hematology at the University of Milan-Bicocca, Italy, reviewed the results and explained how to improve knowledge of CAT among patients with cancer.
“Data support that up to 20% of patients with cancer will experience venous thromboembolism (VTE), which is approximately 4–5 times higher than the general population,” said Dr. Falanga, who is also chief of the department of immunohematology and transfusion medicine and the Thrombosis and Hemostasis Center at the Hospital Papa Giovanni XXIII, in Bergamo, Italy.
“We have known about the link between thrombosis and cancer since the 19th century, but it has taken until midway through the last century for our level of understanding and awareness of the problem to reach its current level. Initially, this was limited to fundamental research, with large advances in our understanding of the mechanisms of the link between the two; it has only been more recently that we have had clinical studies that have piqued the interest of healthcare professionals, who were previously uninterested in the topic,” she said.
Poor understanding
One piece of data stands out from the European survey: Nearly three quarters of respondents (72%) said that before taking part in the survey, they were not aware that people with cancer have a higher-than-normal risk of developing thrombosis. “We asked participants to rate their overall understanding of CAT on a scale of 1 (low) to 10 (high), with the average (mean) score obtained being 4.1. Only 21% of patients gave a rating of 7 or above (high understanding). The average rating was very similar in the different countries surveyed,” write the authors. They note that the survey also assessed how much participants had learned about the topic from their physicians.
Approximately 35% of patients were made aware of CAT either immediately before or at the time of their cancer diagnosis. Of particular concern, one quarter (26%) of respondents (the largest proportion) noted that they first became aware of CAT when they suffered a blood clot. The average rating was very similar in the different countries surveyed. “Let us not forget that cancer and cancer treatments themselves cause a number of side effects, some of which can be very serious, so in some ways, a clot might be seen as a minor problem. Yet, in reality, it isn’t. It is a significant cause of death and disease in cancer patients,” said Dr. Falanga.
When discussing prevention, most respondents (87%) said they were aware that taking a walk could reduce their risk. Slightly fewer were aware that stopping smoking could reduce their risk (75%), and even fewer were aware that keeping hydrated (63%) and stretching their legs (55%) could reduce their risk.
Symptoms of CAT appeared to be relatively well known; 73% of survey participants indicated that they were aware that swelling in the foot, ankle, or leg could be a sign of DVT, and 71% indicated that shortness of breath could be a sign of pulmonary embolism (PE). “Other symptoms, however, were less well known, with just over half (57%) of participants being aware that pain, cramping, and tenderness could be a sign of DVT. About one third (33%) knew that irregular heartbeat could be a sign of PE. These results varied between countries,” according to the authors.
The survey highlighted that just over a third of respondents said that they were currently using anticoagulants, although almost all (96%) knew that anticoagulants could be used to effectively treat thrombosis. Only 41% of those using anticoagulants said they had been told about any possible side effects.
The Italian situation
The report containing the full results of the European survey goes even further, since, in addition to its overall results, it also gives information about individual countries.
The data from Italy, which are based on 246 persons, show that only 27% of patients and caregivers were aware of the increased risk of thrombosis after a cancer diagnosis. This figure is in line with the overall results of the survey, although the average score of the 10-point scale was lower for the Italy cohort (3.3/10 vs 4.1/10).
The results are more variable in terms of knowledge of risk factors. Most respondents (89%) said that they were aware of the risks related to inactivity. Just over half (52%), however, said that they were aware of the risks related to radiotherapy. Nevertheless, 75% of participants knew about the risks relating to cancer surgery and chemotherapy. “To all intents and purposes, all types of cancer drug can significantly affect the risk of developing a clot. And this is also the case for more modern types of treatment, such as immunotherapy,” said Dr. Falanga.
Most respondents reported that they got information about cancer-associated thrombosis verbally, usually from their hospital doctor (11%). Some respondents (6%) said that they found out about it from their own research, usually online. Almost 1 in 4 patients (24%) in Italy said that they first became aware of CAT when they suffered a blood clot. Answers to questions about knowledge of symptoms show that 58% of Italian patients and caregivers know that swelling of the lower limbs can be a symptom of DVT, and the same percentage knows that shortness of breath might indicate PE.
In terms of preventive action, the picture in Italy is somewhat variable: 74% of participants were aware of the importance of walking, but far fewer knew about the need to stop smoking (57%) and stretch the legs (35%). Of the 41% of Italians who were also taking an anticoagulant drug, 53% said that they knew about the possible side effects of such medication.
Which way forward?
“The high rate of CAT suggests that, despite the clinical evidence and clear guideline recommendations for patients with cancer, CAT prevention and recognition remain low among healthcare professionals,” the authors write.
The results of the ECPC survey further confirm those of previous studies, highlighting patients’ lack of knowledge about CAT and the need for more in-depth discussions between physician and patient.
So, what can be done? As highlighted by previous studies, “patients’ experiences are an education in themselves, particularly for the oncology care team,” the authors write. “Once the patient has a thrombosis, the opportunity for thrombosis prevention, which should be the most crucial focus of the care clinics (surgical, oncology, and palliative care), is gone,” they add.
“Oncology professionals, as well as other members of the patient’s care team (eg, internists, surgeons, nurses), need to perform better, at every stage of the patient’s cancer pathway, to ensure patients are aware of CAT and their individual risk to develop a blood clot,” said Dr. Falanga. She explained that in this group, it is the general practitioner who is the first contact. “These professionals are on the front line of the battle; they are among the first healthcare workers given the chance to suspect a clot and should, therefore, be fully aware of the increased risk in oncology patients,” she reiterated.
Experts agree on the fact that a multidisciplinary approach is of utmost importance in this context: the different roles in the team must be clear. “It is also fundamental to establish who does what in terms of educating and informing the patient,” said Dr. Falanga.
The researchers also put forward an example of a successful initiative: the Venous Thromboembolism Prevention in the Ambulatory Cancer Clinic (VTE-PACC) program. The initiative was developed by experts from the University of Vermont and was described in a recent article in JCO Oncology Practice.
Numerous resources are available online to help physicians talk to their patients and explain the risks linked to CAT along the continuum of cancer care. Among them is a resource titled, “Cancer Associated Thrombosis (CAT): Be Clot Conscious,” which can be found on the ECPC’s website.
“We have a collective responsibility using the ECPC patient survey as a baseline to inform patients with cancer on how to identify signs and symptoms of CAT to enable faster diagnosis and treatment,” the authors conclude.
This article was translated from Univadis Italy.
FROM CANCER TREATMENT AND RESEARCH COMMUNICATIONS
Common brain parasite linked to attractiveness, new study
That Toxoplasma gondii looks good on you
Parasite and attractiveness don’t usually go together, but it appears that nobody told Toxoplasma gondii. The world’s most successful parasite affects 30%-50% of the world’s population, and it’s mainly thought to go after the brain in humans, possibly changing behavior and leading to neurological disorders and mental illness.
Now, are you ready to be super confused? According to a recent study, those affected with T. gondii were seen as more attractive and healthy looking, compared with noninfected people. It doesn’t make much sense to us, but it could be an evolutionary thing: The more attractive the parasite makes a person or animal, the more likely it is to spread.![]()
“Some sexually transmitted parasites, such as T. gondii, may produce changes in the appearance and behavior of the human host, either as a by-product of the infection or as the result of the manipulation of the parasite to increase its spread to new hosts,” Javier Borráz-León, PhD, of the University of Turku (Finland), and associates wrote in PeerJ.
Previous research has suggested that men with more testosterone are more likely to become infected because of their behavior with the extra hormones. It’s also been noted that the parasite may manipulate hormones for its own gain, but that’s not proven. Infected women were found to have a lower BMI, more confidence in their appearance, and more partners. Dr. Borráz-León and associates also found that “Toxoplasma-infected subjects had significantly lower facial fluctuating asymmetry than the noninfected people,” ScienceAlert said.
We usually perceive parasites as a bad thing, but honestly this one isn’t sounding too bad. It seems to help with some confidence boosters, and who doesn’t want that? We’re thinking that T. gondii could be the Next Big Thing. All it needs is some marketing and … what if it was covered with nonpareils?
Give it to me straight, Doc. Don’t sugar coat it.
Okay, so he’s not a doctor – not a medical doctor, anyway – but that’s exactly what he did. William H. Grover, PhD, has sugar coated drugs in the name of fraud prevention. We will explain.
The sugar coating comes in the form of nonpareils, the tiny and colorful round sprinkles often found covering small discs of chocolate. Dr. Grover, a bioengineering professor at the University of California, Riverside, who has been working on ways to ensure the authenticity of pharmaceuticals, “started wondering how many different patterns of colored nonpareils were possible on these candies,” he said in a statement from the university.
With just eight colors and an average of 92 individual nonpareils on each candy, the combinations, he found out, are almost endless. Could the same thing be done with a pill? Could the nonpareils be applied as a coating to a pill, giving it a unique pattern that could be stored by the manufacturer and used later as identification?
After much time and effort involving edible cake-decorating glue, Tylenol capsules, smartphones, and computer simulations, he produced CandyCode, an algorithm that converts a photo of a nonpareil-covered pill “into a set of text strings suitable for storing in a computer database and querying by consumers,” the statement explained.
Dr. Grover also mentioned a side benefit: “Anecdotally, I found that CandyCoded caplets were more pleasant to swallow than plain caplets, confirming Mary Poppins’ classic observation about the relationship between sugar and medicine.”
First of all, we can’t believe we just used a Mary Poppins reference. Not exactly what you’d call MDedgey, is it? Second of all, what about the children? We’re talking about drugs that, literally, have been turned into candy. Are the kids going to love them, too? Sounds more like a job for Mr. Yuk.
So you want to be a superhero?
Be honest, who didn’t want to be a superhero when they were a kid? There’s a reason every other movie released in the past decade has been a superhero movie. That’s how we’ve ended up with the millionth Batman reboot and Marvel scraping the bottom of the C-list hero barrel. (Seriously, who’d actually heard of Moon Knight before now?)

Point is, we all like to fantasize, and now a meta-analysis from researchers in Germany and the United States has given us all a reason to strike those dashing superhero poses. Through evaluation of 130 studies and over 10,000 people, the researchers found that power posing (and perfect posture) was strongly associated with increased confidence and self-worth. It was also associated with improved behavior, though the connection was less strong.
Sadly though, the research found no connection with power posing and changes in testosterone or cortisol levels. Standing like a superhero may make you feel good, but it won’t give your body any cool powers or superhuman abilities. But don’t despair, because we’re not finished yet. In fact, it may be the biggest news we’ve ever reported for LOTME: A group of scientists from the University of Kentucky has assembled the full genome of a salamander.
Wait, we have more! Beyond having a genome ten times bigger than a human, this salamander, the axolotl from Mexico, is the model of natural regeneration. Name a body part, and the axolotl can grow it back. It can even regenerate portions of its brain. And now that we have access to the complete genome, it’s possible that one day we could use the axolotl’s regeneration for ourselves. Growing back limbs, regenerating spinal cords, the sky’s the limit. And if Wolverine and Deadpool are anything to go by, it’s all you need to get that superhero career off the ground. Salamander powers may not have the cachet of a radioactive spider, but we’ll take what we can get.
Post your way to financial hardship
After you pump your gas at the gas station, how do you pay? At the pump or inside? How frequently do you post to your social media pages? What kind of content are you posting?
That kind of nontraditional credit data hasn’t been considered by lenders and credit agencies, but that is changing. The reasoning? It’s opening more opportunities for those without much credit history. But according to a paper published by Janine S. Hiller of Virginia Tech and Lindsay Sain Jones, a financial regulation researcher at the University of Georgia, this just opens a can of worms.
Why is this so dangerous? Well, alternative credit scoring isn’t covered by the Fair Credit Reporting Act or Equal Opportunity Act, so the consumer doesn’t have the ability to dispute any data the credit agencies or lenders receive. Then there’s the “credit boost,” which some companies offer to gain access to the consumer’s data. Often there are no limitations on how long it’s kept. That purchase you made 2 years ago can come back to haunt you.
It also creates a cause for the possibility of discrimination based on “lifestyle-related data points,” which some lenders use to determine creditworthiness: zip code, age, gender, race, socioeconomic status. Even where the consumer went to college is a factor taken under consideration.
“There are all kinds of factors that can be correlated with creditworthiness, but that doesn’t mean they should be used,” Ms. Jones said in the EurekAlert statement.
Let’s say someone applies for a loan needed for a medical procedure. They could be denied because the lender or a credit-reporting agency didn’t like the data they received (most times without the consumer’s consent). Talk about a broken system.
That Toxoplasma gondii looks good on you
Parasite and attractiveness don’t usually go together, but it appears that nobody told Toxoplasma gondii. The world’s most successful parasite affects 30%-50% of the world’s population, and it’s mainly thought to go after the brain in humans, possibly changing behavior and leading to neurological disorders and mental illness.
Now, are you ready to be super confused? According to a recent study, those affected with T. gondii were seen as more attractive and healthy looking, compared with noninfected people. It doesn’t make much sense to us, but it could be an evolutionary thing: The more attractive the parasite makes a person or animal, the more likely it is to spread.![]()
“Some sexually transmitted parasites, such as T. gondii, may produce changes in the appearance and behavior of the human host, either as a by-product of the infection or as the result of the manipulation of the parasite to increase its spread to new hosts,” Javier Borráz-León, PhD, of the University of Turku (Finland), and associates wrote in PeerJ.
Previous research has suggested that men with more testosterone are more likely to become infected because of their behavior with the extra hormones. It’s also been noted that the parasite may manipulate hormones for its own gain, but that’s not proven. Infected women were found to have a lower BMI, more confidence in their appearance, and more partners. Dr. Borráz-León and associates also found that “Toxoplasma-infected subjects had significantly lower facial fluctuating asymmetry than the noninfected people,” ScienceAlert said.
We usually perceive parasites as a bad thing, but honestly this one isn’t sounding too bad. It seems to help with some confidence boosters, and who doesn’t want that? We’re thinking that T. gondii could be the Next Big Thing. All it needs is some marketing and … what if it was covered with nonpareils?
Give it to me straight, Doc. Don’t sugar coat it.
Okay, so he’s not a doctor – not a medical doctor, anyway – but that’s exactly what he did. William H. Grover, PhD, has sugar coated drugs in the name of fraud prevention. We will explain.
The sugar coating comes in the form of nonpareils, the tiny and colorful round sprinkles often found covering small discs of chocolate. Dr. Grover, a bioengineering professor at the University of California, Riverside, who has been working on ways to ensure the authenticity of pharmaceuticals, “started wondering how many different patterns of colored nonpareils were possible on these candies,” he said in a statement from the university.
With just eight colors and an average of 92 individual nonpareils on each candy, the combinations, he found out, are almost endless. Could the same thing be done with a pill? Could the nonpareils be applied as a coating to a pill, giving it a unique pattern that could be stored by the manufacturer and used later as identification?
After much time and effort involving edible cake-decorating glue, Tylenol capsules, smartphones, and computer simulations, he produced CandyCode, an algorithm that converts a photo of a nonpareil-covered pill “into a set of text strings suitable for storing in a computer database and querying by consumers,” the statement explained.
Dr. Grover also mentioned a side benefit: “Anecdotally, I found that CandyCoded caplets were more pleasant to swallow than plain caplets, confirming Mary Poppins’ classic observation about the relationship between sugar and medicine.”
First of all, we can’t believe we just used a Mary Poppins reference. Not exactly what you’d call MDedgey, is it? Second of all, what about the children? We’re talking about drugs that, literally, have been turned into candy. Are the kids going to love them, too? Sounds more like a job for Mr. Yuk.
So you want to be a superhero?
Be honest, who didn’t want to be a superhero when they were a kid? There’s a reason every other movie released in the past decade has been a superhero movie. That’s how we’ve ended up with the millionth Batman reboot and Marvel scraping the bottom of the C-list hero barrel. (Seriously, who’d actually heard of Moon Knight before now?)
Point is, we all like to fantasize, and now a meta-analysis from researchers in Germany and the United States has given us all a reason to strike those dashing superhero poses. Through evaluation of 130 studies and over 10,000 people, the researchers found that power posing (and perfect posture) was strongly associated with increased confidence and self-worth. It was also associated with improved behavior, though the connection was less strong.
Sadly though, the research found no connection with power posing and changes in testosterone or cortisol levels. Standing like a superhero may make you feel good, but it won’t give your body any cool powers or superhuman abilities. But don’t despair, because we’re not finished yet. In fact, it may be the biggest news we’ve ever reported for LOTME: A group of scientists from the University of Kentucky has assembled the full genome of a salamander.
Wait, we have more! Beyond having a genome ten times bigger than a human, this salamander, the axolotl from Mexico, is the model of natural regeneration. Name a body part, and the axolotl can grow it back. It can even regenerate portions of its brain. And now that we have access to the complete genome, it’s possible that one day we could use the axolotl’s regeneration for ourselves. Growing back limbs, regenerating spinal cords, the sky’s the limit. And if Wolverine and Deadpool are anything to go by, it’s all you need to get that superhero career off the ground. Salamander powers may not have the cachet of a radioactive spider, but we’ll take what we can get.
Post your way to financial hardship
After you pump your gas at the gas station, how do you pay? At the pump or inside? How frequently do you post to your social media pages? What kind of content are you posting?
That kind of nontraditional credit data hasn’t been considered by lenders and credit agencies, but that is changing. The reasoning? It’s opening more opportunities for those without much credit history. But according to a paper published by Janine S. Hiller of Virginia Tech and Lindsay Sain Jones, a financial regulation researcher at the University of Georgia, this just opens a can of worms.
Why is this so dangerous? Well, alternative credit scoring isn’t covered by the Fair Credit Reporting Act or Equal Opportunity Act, so the consumer doesn’t have the ability to dispute any data the credit agencies or lenders receive. Then there’s the “credit boost,” which some companies offer to gain access to the consumer’s data. Often there are no limitations on how long it’s kept. That purchase you made 2 years ago can come back to haunt you.
It also creates a cause for the possibility of discrimination based on “lifestyle-related data points,” which some lenders use to determine creditworthiness: zip code, age, gender, race, socioeconomic status. Even where the consumer went to college is a factor taken under consideration.
“There are all kinds of factors that can be correlated with creditworthiness, but that doesn’t mean they should be used,” Ms. Jones said in the EurekAlert statement.
Let’s say someone applies for a loan needed for a medical procedure. They could be denied because the lender or a credit-reporting agency didn’t like the data they received (most times without the consumer’s consent). Talk about a broken system.
That Toxoplasma gondii looks good on you
Parasite and attractiveness don’t usually go together, but it appears that nobody told Toxoplasma gondii. The world’s most successful parasite affects 30%-50% of the world’s population, and it’s mainly thought to go after the brain in humans, possibly changing behavior and leading to neurological disorders and mental illness.
Now, are you ready to be super confused? According to a recent study, those affected with T. gondii were seen as more attractive and healthy looking, compared with noninfected people. It doesn’t make much sense to us, but it could be an evolutionary thing: The more attractive the parasite makes a person or animal, the more likely it is to spread.![]()
“Some sexually transmitted parasites, such as T. gondii, may produce changes in the appearance and behavior of the human host, either as a by-product of the infection or as the result of the manipulation of the parasite to increase its spread to new hosts,” Javier Borráz-León, PhD, of the University of Turku (Finland), and associates wrote in PeerJ.
Previous research has suggested that men with more testosterone are more likely to become infected because of their behavior with the extra hormones. It’s also been noted that the parasite may manipulate hormones for its own gain, but that’s not proven. Infected women were found to have a lower BMI, more confidence in their appearance, and more partners. Dr. Borráz-León and associates also found that “Toxoplasma-infected subjects had significantly lower facial fluctuating asymmetry than the noninfected people,” ScienceAlert said.
We usually perceive parasites as a bad thing, but honestly this one isn’t sounding too bad. It seems to help with some confidence boosters, and who doesn’t want that? We’re thinking that T. gondii could be the Next Big Thing. All it needs is some marketing and … what if it was covered with nonpareils?
Give it to me straight, Doc. Don’t sugar coat it.
Okay, so he’s not a doctor – not a medical doctor, anyway – but that’s exactly what he did. William H. Grover, PhD, has sugar coated drugs in the name of fraud prevention. We will explain.
The sugar coating comes in the form of nonpareils, the tiny and colorful round sprinkles often found covering small discs of chocolate. Dr. Grover, a bioengineering professor at the University of California, Riverside, who has been working on ways to ensure the authenticity of pharmaceuticals, “started wondering how many different patterns of colored nonpareils were possible on these candies,” he said in a statement from the university.
With just eight colors and an average of 92 individual nonpareils on each candy, the combinations, he found out, are almost endless. Could the same thing be done with a pill? Could the nonpareils be applied as a coating to a pill, giving it a unique pattern that could be stored by the manufacturer and used later as identification?
After much time and effort involving edible cake-decorating glue, Tylenol capsules, smartphones, and computer simulations, he produced CandyCode, an algorithm that converts a photo of a nonpareil-covered pill “into a set of text strings suitable for storing in a computer database and querying by consumers,” the statement explained.
Dr. Grover also mentioned a side benefit: “Anecdotally, I found that CandyCoded caplets were more pleasant to swallow than plain caplets, confirming Mary Poppins’ classic observation about the relationship between sugar and medicine.”
First of all, we can’t believe we just used a Mary Poppins reference. Not exactly what you’d call MDedgey, is it? Second of all, what about the children? We’re talking about drugs that, literally, have been turned into candy. Are the kids going to love them, too? Sounds more like a job for Mr. Yuk.
So you want to be a superhero?
Be honest, who didn’t want to be a superhero when they were a kid? There’s a reason every other movie released in the past decade has been a superhero movie. That’s how we’ve ended up with the millionth Batman reboot and Marvel scraping the bottom of the C-list hero barrel. (Seriously, who’d actually heard of Moon Knight before now?)
Point is, we all like to fantasize, and now a meta-analysis from researchers in Germany and the United States has given us all a reason to strike those dashing superhero poses. Through evaluation of 130 studies and over 10,000 people, the researchers found that power posing (and perfect posture) was strongly associated with increased confidence and self-worth. It was also associated with improved behavior, though the connection was less strong.
Sadly though, the research found no connection with power posing and changes in testosterone or cortisol levels. Standing like a superhero may make you feel good, but it won’t give your body any cool powers or superhuman abilities. But don’t despair, because we’re not finished yet. In fact, it may be the biggest news we’ve ever reported for LOTME: A group of scientists from the University of Kentucky has assembled the full genome of a salamander.
Wait, we have more! Beyond having a genome ten times bigger than a human, this salamander, the axolotl from Mexico, is the model of natural regeneration. Name a body part, and the axolotl can grow it back. It can even regenerate portions of its brain. And now that we have access to the complete genome, it’s possible that one day we could use the axolotl’s regeneration for ourselves. Growing back limbs, regenerating spinal cords, the sky’s the limit. And if Wolverine and Deadpool are anything to go by, it’s all you need to get that superhero career off the ground. Salamander powers may not have the cachet of a radioactive spider, but we’ll take what we can get.
Post your way to financial hardship
After you pump your gas at the gas station, how do you pay? At the pump or inside? How frequently do you post to your social media pages? What kind of content are you posting?
That kind of nontraditional credit data hasn’t been considered by lenders and credit agencies, but that is changing. The reasoning? It’s opening more opportunities for those without much credit history. But according to a paper published by Janine S. Hiller of Virginia Tech and Lindsay Sain Jones, a financial regulation researcher at the University of Georgia, this just opens a can of worms.
Why is this so dangerous? Well, alternative credit scoring isn’t covered by the Fair Credit Reporting Act or Equal Opportunity Act, so the consumer doesn’t have the ability to dispute any data the credit agencies or lenders receive. Then there’s the “credit boost,” which some companies offer to gain access to the consumer’s data. Often there are no limitations on how long it’s kept. That purchase you made 2 years ago can come back to haunt you.
It also creates a cause for the possibility of discrimination based on “lifestyle-related data points,” which some lenders use to determine creditworthiness: zip code, age, gender, race, socioeconomic status. Even where the consumer went to college is a factor taken under consideration.
“There are all kinds of factors that can be correlated with creditworthiness, but that doesn’t mean they should be used,” Ms. Jones said in the EurekAlert statement.
Let’s say someone applies for a loan needed for a medical procedure. They could be denied because the lender or a credit-reporting agency didn’t like the data they received (most times without the consumer’s consent). Talk about a broken system.
Omicron breakthrough cases boost protection, studies say
two preprint studies show.
The University of Washington, Seattle, working with Vir Biotechnology of San Francisco, looked at blood samples of vaccinated people who had breakthrough cases of Delta or Omicron and compared the samples with three other groups: people who caught COVID and were later vaccinated, vaccinated people who were never infected, and people who were infected and never vaccinated.
The vaccinated people who had a breakthrough case of Omicron produced antibodies that helped protect against coronavirus variants, whereas unvaccinated people who caught Omicron didn’t produce as many antibodies, the study showed.
BioNTech, the German biotechnology company, found that people who’d been double and triple vaccinated and then became infected with Omicron had a better B-cell response than people who’d gotten a booster shot but had not been infected.
The University of Washington research team also came up with similar findings about B cells.
The findings don’t mean people should deliberately try to become infected with COVID, said Alexandra Walls, PhD, one of the University of Washington scientists, according to Business Standard.
But the study does indicate “that we are at the point where we may want to consider having a different vaccine to boost people,” said David Veesler, PhD, of the University of Washington team.
“We should think about breakthrough infections as essentially equivalent to another dose of vaccine,” John Wherry, PhD, a professor and director of the Institute for Immunology at the University of Pennsylvania, Philadelphia, told Business Standard. Dr. Wherry was not involved in the studies but reviewed the BioNTech study.
A version of this article first appeared on WebMD.com.
two preprint studies show.
The University of Washington, Seattle, working with Vir Biotechnology of San Francisco, looked at blood samples of vaccinated people who had breakthrough cases of Delta or Omicron and compared the samples with three other groups: people who caught COVID and were later vaccinated, vaccinated people who were never infected, and people who were infected and never vaccinated.
The vaccinated people who had a breakthrough case of Omicron produced antibodies that helped protect against coronavirus variants, whereas unvaccinated people who caught Omicron didn’t produce as many antibodies, the study showed.
BioNTech, the German biotechnology company, found that people who’d been double and triple vaccinated and then became infected with Omicron had a better B-cell response than people who’d gotten a booster shot but had not been infected.
The University of Washington research team also came up with similar findings about B cells.
The findings don’t mean people should deliberately try to become infected with COVID, said Alexandra Walls, PhD, one of the University of Washington scientists, according to Business Standard.
But the study does indicate “that we are at the point where we may want to consider having a different vaccine to boost people,” said David Veesler, PhD, of the University of Washington team.
“We should think about breakthrough infections as essentially equivalent to another dose of vaccine,” John Wherry, PhD, a professor and director of the Institute for Immunology at the University of Pennsylvania, Philadelphia, told Business Standard. Dr. Wherry was not involved in the studies but reviewed the BioNTech study.
A version of this article first appeared on WebMD.com.
two preprint studies show.
The University of Washington, Seattle, working with Vir Biotechnology of San Francisco, looked at blood samples of vaccinated people who had breakthrough cases of Delta or Omicron and compared the samples with three other groups: people who caught COVID and were later vaccinated, vaccinated people who were never infected, and people who were infected and never vaccinated.
The vaccinated people who had a breakthrough case of Omicron produced antibodies that helped protect against coronavirus variants, whereas unvaccinated people who caught Omicron didn’t produce as many antibodies, the study showed.
BioNTech, the German biotechnology company, found that people who’d been double and triple vaccinated and then became infected with Omicron had a better B-cell response than people who’d gotten a booster shot but had not been infected.
The University of Washington research team also came up with similar findings about B cells.
The findings don’t mean people should deliberately try to become infected with COVID, said Alexandra Walls, PhD, one of the University of Washington scientists, according to Business Standard.
But the study does indicate “that we are at the point where we may want to consider having a different vaccine to boost people,” said David Veesler, PhD, of the University of Washington team.
“We should think about breakthrough infections as essentially equivalent to another dose of vaccine,” John Wherry, PhD, a professor and director of the Institute for Immunology at the University of Pennsylvania, Philadelphia, told Business Standard. Dr. Wherry was not involved in the studies but reviewed the BioNTech study.
A version of this article first appeared on WebMD.com.
FDA authorizes Pfizer’s COVID booster for kids ages 5 to 11
emergency use authorization (EUA), allowing the Pfizer-BioNTech COVID-19 booster shot for children ages 5 to 11 who are at least 5 months out from their first vaccine series.

According to the most recent data from the Centers for Disease Control and Prevention, 28.6% of children in this age group have received both initial doses of Pfizer’s COVID-19 vaccine, and 35.3% have received their first dose.
Pfizer’s vaccine trial involving 4,500 children showed few side effects among children younger than 12 who received a booster, or third dose, according to a company statement.
Pfizer asked the FDA for an amended authorization in April, after submitting data showing that a third dose in children between 5 and 11 raised antibodies targeting the Omicron variant by 36 times.
“While it has largely been the case that COVID-19 tends to be less severe in children than adults, the omicron wave has seen more kids getting sick with the disease and being hospitalized, and children may also experience longer-term effects, even following initially mild disease,” FDA Commissioner Robert M. Califf, MD, said in a news release.
A study done by the New York State Department of Health showed the effectiveness of Pfizer’s two-dose vaccine series fell from 68% to 12% 4-5 months after the second dose was given to children 5 to 11 during the Omicron surge. A CDC study published in March also showed that the Pfizer shot reduced the risk of Omicron by 31% in children 5 to 11, a significantly lower rate than for kids 12 to 15, who had a 59% risk reduction after receiving two doses.
To some experts, this data suggest an even greater need for children under 12 to be eligible for a third dose.
“Since authorizing the vaccine for children down to 5 years of age in October 2021, emerging data suggest that vaccine effectiveness against COVID-19 wanes after the second dose of the vaccine in all authorized populations,” says Peter Marks, MD, PhD, the director of the FDA’s Center for Biologics Evaluation and Research.
The CDC still needs to sign off on the shots before they can be allowed. The agency’s Advisory Committee on Immunization Practices is set to meet on May 19 to discuss boosters in this age group.
FDA advisory panels plan to meet next month to discuss allowing Pfizer’s and Moderna’s COVID-19 vaccines for children under 6 years old.
A version of this article first appeared on WebMD.com.
emergency use authorization (EUA), allowing the Pfizer-BioNTech COVID-19 booster shot for children ages 5 to 11 who are at least 5 months out from their first vaccine series.
According to the most recent data from the Centers for Disease Control and Prevention, 28.6% of children in this age group have received both initial doses of Pfizer’s COVID-19 vaccine, and 35.3% have received their first dose.
Pfizer’s vaccine trial involving 4,500 children showed few side effects among children younger than 12 who received a booster, or third dose, according to a company statement.
Pfizer asked the FDA for an amended authorization in April, after submitting data showing that a third dose in children between 5 and 11 raised antibodies targeting the Omicron variant by 36 times.
“While it has largely been the case that COVID-19 tends to be less severe in children than adults, the omicron wave has seen more kids getting sick with the disease and being hospitalized, and children may also experience longer-term effects, even following initially mild disease,” FDA Commissioner Robert M. Califf, MD, said in a news release.
A study done by the New York State Department of Health showed the effectiveness of Pfizer’s two-dose vaccine series fell from 68% to 12% 4-5 months after the second dose was given to children 5 to 11 during the Omicron surge. A CDC study published in March also showed that the Pfizer shot reduced the risk of Omicron by 31% in children 5 to 11, a significantly lower rate than for kids 12 to 15, who had a 59% risk reduction after receiving two doses.
To some experts, this data suggest an even greater need for children under 12 to be eligible for a third dose.
“Since authorizing the vaccine for children down to 5 years of age in October 2021, emerging data suggest that vaccine effectiveness against COVID-19 wanes after the second dose of the vaccine in all authorized populations,” says Peter Marks, MD, PhD, the director of the FDA’s Center for Biologics Evaluation and Research.
The CDC still needs to sign off on the shots before they can be allowed. The agency’s Advisory Committee on Immunization Practices is set to meet on May 19 to discuss boosters in this age group.
FDA advisory panels plan to meet next month to discuss allowing Pfizer’s and Moderna’s COVID-19 vaccines for children under 6 years old.
A version of this article first appeared on WebMD.com.
emergency use authorization (EUA), allowing the Pfizer-BioNTech COVID-19 booster shot for children ages 5 to 11 who are at least 5 months out from their first vaccine series.
According to the most recent data from the Centers for Disease Control and Prevention, 28.6% of children in this age group have received both initial doses of Pfizer’s COVID-19 vaccine, and 35.3% have received their first dose.
Pfizer’s vaccine trial involving 4,500 children showed few side effects among children younger than 12 who received a booster, or third dose, according to a company statement.
Pfizer asked the FDA for an amended authorization in April, after submitting data showing that a third dose in children between 5 and 11 raised antibodies targeting the Omicron variant by 36 times.
“While it has largely been the case that COVID-19 tends to be less severe in children than adults, the omicron wave has seen more kids getting sick with the disease and being hospitalized, and children may also experience longer-term effects, even following initially mild disease,” FDA Commissioner Robert M. Califf, MD, said in a news release.
A study done by the New York State Department of Health showed the effectiveness of Pfizer’s two-dose vaccine series fell from 68% to 12% 4-5 months after the second dose was given to children 5 to 11 during the Omicron surge. A CDC study published in March also showed that the Pfizer shot reduced the risk of Omicron by 31% in children 5 to 11, a significantly lower rate than for kids 12 to 15, who had a 59% risk reduction after receiving two doses.
To some experts, this data suggest an even greater need for children under 12 to be eligible for a third dose.
“Since authorizing the vaccine for children down to 5 years of age in October 2021, emerging data suggest that vaccine effectiveness against COVID-19 wanes after the second dose of the vaccine in all authorized populations,” says Peter Marks, MD, PhD, the director of the FDA’s Center for Biologics Evaluation and Research.
The CDC still needs to sign off on the shots before they can be allowed. The agency’s Advisory Committee on Immunization Practices is set to meet on May 19 to discuss boosters in this age group.
FDA advisory panels plan to meet next month to discuss allowing Pfizer’s and Moderna’s COVID-19 vaccines for children under 6 years old.
A version of this article first appeared on WebMD.com.
Why do clinical trials still underrepresent minority groups?
It’s no secret that, for decades, the participants in clinical trials for new drugs and medical devices haven’t accurately represented the diverse groups of patients the drugs and devices were designed for.
In a recently published draft guidance, the Food and Drug Administration recommended that companies in charge of running these trials should submit a proposal to the agency that would address how they plan to enroll more “clinically relevant populations” and historically underrepresented racial and ethnic groups.
It’s an issue that the U.S. has been trying to fix for years. In 1993, the NIH Revitalization Act was passed into law. It mandated the appropriate inclusion of women and racial minorities in all National Institutes of Health–funded research.
Since then, the FDA has put out plans that encourage trial sponsors to recruit more diverse enrollees, offering strategies and best practices rather than establishing requirements or quotas that companies would be forced to meet. Despite its efforts to encourage inclusion, people of color continue to be largely underrepresented in clinical trials.
Experts aren’t just calling for trial cohorts to reflect U.S. census data. Rather, the demographics of participants should match those of the diagnosis being studied. An analysis of 24 clinical trials of cardiovascular drugs, for example, found that Black Americans made up 2.9% of trial participants, compared with 83.1% for White people. Given that cardiovascular diseases affect Black Americans at almost the same rate as Whites (23.5% and 23.7%, respectively) – and keeping in mind that Black Americans make up 13.4% of the population and White people represent 76.3% – the degree of underrepresentation is glaring.
One commonly cited reason for this lack of representation is that people of color, especially Black Americans, have lingering feelings of mistrust toward the medical field. The U.S.-run Tuskegee study – during which researchers documented the natural progression of syphilis in hundreds of Black men who were kept from life-saving treatment – is, justifiably, often named as a notable source of that suspicion.
But blaming the disproportionately low numbers of Black participants in clinical trials on medical mistrust is an easy answer to a much more complicated issue, said cardiologist Clyde Yancy, MD, who also serves as the vice dean for diversity and inclusion at Northwestern University’s Feinberg School of Medicine, Chicago.
“We need to not put the onus on the back of the patient cohort, and say they are the problem,” Dr. Yancy said, adding that many trials add financial barriers and don’t provide proper transportation for participants who may live farther away.
The diversity of the study team itself – the institutions, researchers, and recruiters – also contributes to a lack of diversity in the participant pool. When considering all of these factors, “you begin to understand the complexity and the multidimensionality of why we have underrepresentation,” said Dr. Yancy. “So I would not promulgate the notion that this is simply because patients don’t trust the system.”
Soumya Niranjan, PhD, worked as a study coordinator at the Tulane Cancer Center in New Orleans, La., where she recruited patients for a prostate cancer study. After researching the impact of clinicians’ biases on the recruitment of racial and ethnic minorities in oncology trials, she found that some recruiters view patients of color as less promising participants.
“Who ends up being approached for a clinical trial is based on a preset rubric that one has in mind about a patient who may be eligible for a cancer study,” said Dr. Niranjan. “There is a characterization of, ‘we want to make sure this patient is compliant, that they will be a good historian and seem responsible.’ ... Our study showed that it kind of fell along racial lines.”
In her study, published in the journal Cancer in 2020, Dr. Niranjan wrote that researchers sometimes “perceived racial minority groups to have low knowledge of cancer clinical trials. This was considered to be a hindrance while explaining cancer clinical trials in the face of limited provider time during a clinical encounter.”
Some researchers believed minority participants, especially Black women, would be less likely to file study protocols. Others said people of color are more likely to be selfish.
She quoted one research investigator as saying Black people are less knowledgeable.
“African Americans I think have less knowledge,” the unnamed researcher said. “We take a little bit more time to explain to African American [sic]. I think ... they have more questions because we know they are not more knowledgeable so I think it takes time. They have a lot of questions.”
Progress over the years
The FDA’s recent draft builds upon a guidance from 2016, which already recommended that trial teams submit an inclusion plan to the agency at the earliest phase of development. While the recent announcement is another step in the right direction, it may not be substantial enough.
“There’s always an enrollment plan,” Dr. Niranjan said. “But those enrollment plans are not enforced. So if it’s not enforced, what does that look like?”
In an emailed statement to this news organization, Lola Fashoyin-Aje, MD, the deputy director of the FDA Oncology Center of Excellence’s division to expand diversity, emphasized that the draft guidance does not require anything, but that the agency “expect[s] sponsors will follow FDA’s recommendations as described in the draft guidance.”
Without requirements, it’s up to the sponsor to make the effort to enroll people with varied racial and ethnic backgrounds. During the development of the COVID-19 vaccine, Moderna announced that the company would slow the trial’s enrollment to ensure minority groups were properly represented.
Not every sponsor is as motivated to make this a concerted effort, and some simply don’t have the funds to allocate to strengthening the enrollment process.
“There’s so much red tape and paperwork to get the funding for a clinical trial,” said Julie Silver, MD, professor of physical medicine and rehabilitation at Harvard Medical School, Boston, who studies workforce diversity and inclusion. “Even when people are equitably included, the amount of funding they have to do the trial might not be enough to do an analysis that shows potential differences.”
Whether the FDA will enforce enrollment plans in the future remains an open question; however, Dr. Yancy said the most effective way to do this would be through incentives, rather than penalties.
According to Dr. Fashoyin-Aje, the FDA and sponsors “will learn from these submissions and over time, whether and how these diversity plans lead to meaningful changes in clinical trial representation will need to be assessed, including whether additional steps need to be taken.”
A version of this article first appeared on Medscape.com.
It’s no secret that, for decades, the participants in clinical trials for new drugs and medical devices haven’t accurately represented the diverse groups of patients the drugs and devices were designed for.
In a recently published draft guidance, the Food and Drug Administration recommended that companies in charge of running these trials should submit a proposal to the agency that would address how they plan to enroll more “clinically relevant populations” and historically underrepresented racial and ethnic groups.
It’s an issue that the U.S. has been trying to fix for years. In 1993, the NIH Revitalization Act was passed into law. It mandated the appropriate inclusion of women and racial minorities in all National Institutes of Health–funded research.
Since then, the FDA has put out plans that encourage trial sponsors to recruit more diverse enrollees, offering strategies and best practices rather than establishing requirements or quotas that companies would be forced to meet. Despite its efforts to encourage inclusion, people of color continue to be largely underrepresented in clinical trials.
Experts aren’t just calling for trial cohorts to reflect U.S. census data. Rather, the demographics of participants should match those of the diagnosis being studied. An analysis of 24 clinical trials of cardiovascular drugs, for example, found that Black Americans made up 2.9% of trial participants, compared with 83.1% for White people. Given that cardiovascular diseases affect Black Americans at almost the same rate as Whites (23.5% and 23.7%, respectively) – and keeping in mind that Black Americans make up 13.4% of the population and White people represent 76.3% – the degree of underrepresentation is glaring.
One commonly cited reason for this lack of representation is that people of color, especially Black Americans, have lingering feelings of mistrust toward the medical field. The U.S.-run Tuskegee study – during which researchers documented the natural progression of syphilis in hundreds of Black men who were kept from life-saving treatment – is, justifiably, often named as a notable source of that suspicion.
But blaming the disproportionately low numbers of Black participants in clinical trials on medical mistrust is an easy answer to a much more complicated issue, said cardiologist Clyde Yancy, MD, who also serves as the vice dean for diversity and inclusion at Northwestern University’s Feinberg School of Medicine, Chicago.
“We need to not put the onus on the back of the patient cohort, and say they are the problem,” Dr. Yancy said, adding that many trials add financial barriers and don’t provide proper transportation for participants who may live farther away.
The diversity of the study team itself – the institutions, researchers, and recruiters – also contributes to a lack of diversity in the participant pool. When considering all of these factors, “you begin to understand the complexity and the multidimensionality of why we have underrepresentation,” said Dr. Yancy. “So I would not promulgate the notion that this is simply because patients don’t trust the system.”
Soumya Niranjan, PhD, worked as a study coordinator at the Tulane Cancer Center in New Orleans, La., where she recruited patients for a prostate cancer study. After researching the impact of clinicians’ biases on the recruitment of racial and ethnic minorities in oncology trials, she found that some recruiters view patients of color as less promising participants.
“Who ends up being approached for a clinical trial is based on a preset rubric that one has in mind about a patient who may be eligible for a cancer study,” said Dr. Niranjan. “There is a characterization of, ‘we want to make sure this patient is compliant, that they will be a good historian and seem responsible.’ ... Our study showed that it kind of fell along racial lines.”
In her study, published in the journal Cancer in 2020, Dr. Niranjan wrote that researchers sometimes “perceived racial minority groups to have low knowledge of cancer clinical trials. This was considered to be a hindrance while explaining cancer clinical trials in the face of limited provider time during a clinical encounter.”
Some researchers believed minority participants, especially Black women, would be less likely to file study protocols. Others said people of color are more likely to be selfish.
She quoted one research investigator as saying Black people are less knowledgeable.
“African Americans I think have less knowledge,” the unnamed researcher said. “We take a little bit more time to explain to African American [sic]. I think ... they have more questions because we know they are not more knowledgeable so I think it takes time. They have a lot of questions.”
Progress over the years
The FDA’s recent draft builds upon a guidance from 2016, which already recommended that trial teams submit an inclusion plan to the agency at the earliest phase of development. While the recent announcement is another step in the right direction, it may not be substantial enough.
“There’s always an enrollment plan,” Dr. Niranjan said. “But those enrollment plans are not enforced. So if it’s not enforced, what does that look like?”
In an emailed statement to this news organization, Lola Fashoyin-Aje, MD, the deputy director of the FDA Oncology Center of Excellence’s division to expand diversity, emphasized that the draft guidance does not require anything, but that the agency “expect[s] sponsors will follow FDA’s recommendations as described in the draft guidance.”
Without requirements, it’s up to the sponsor to make the effort to enroll people with varied racial and ethnic backgrounds. During the development of the COVID-19 vaccine, Moderna announced that the company would slow the trial’s enrollment to ensure minority groups were properly represented.
Not every sponsor is as motivated to make this a concerted effort, and some simply don’t have the funds to allocate to strengthening the enrollment process.
“There’s so much red tape and paperwork to get the funding for a clinical trial,” said Julie Silver, MD, professor of physical medicine and rehabilitation at Harvard Medical School, Boston, who studies workforce diversity and inclusion. “Even when people are equitably included, the amount of funding they have to do the trial might not be enough to do an analysis that shows potential differences.”
Whether the FDA will enforce enrollment plans in the future remains an open question; however, Dr. Yancy said the most effective way to do this would be through incentives, rather than penalties.
According to Dr. Fashoyin-Aje, the FDA and sponsors “will learn from these submissions and over time, whether and how these diversity plans lead to meaningful changes in clinical trial representation will need to be assessed, including whether additional steps need to be taken.”
A version of this article first appeared on Medscape.com.
It’s no secret that, for decades, the participants in clinical trials for new drugs and medical devices haven’t accurately represented the diverse groups of patients the drugs and devices were designed for.
In a recently published draft guidance, the Food and Drug Administration recommended that companies in charge of running these trials should submit a proposal to the agency that would address how they plan to enroll more “clinically relevant populations” and historically underrepresented racial and ethnic groups.
It’s an issue that the U.S. has been trying to fix for years. In 1993, the NIH Revitalization Act was passed into law. It mandated the appropriate inclusion of women and racial minorities in all National Institutes of Health–funded research.
Since then, the FDA has put out plans that encourage trial sponsors to recruit more diverse enrollees, offering strategies and best practices rather than establishing requirements or quotas that companies would be forced to meet. Despite its efforts to encourage inclusion, people of color continue to be largely underrepresented in clinical trials.
Experts aren’t just calling for trial cohorts to reflect U.S. census data. Rather, the demographics of participants should match those of the diagnosis being studied. An analysis of 24 clinical trials of cardiovascular drugs, for example, found that Black Americans made up 2.9% of trial participants, compared with 83.1% for White people. Given that cardiovascular diseases affect Black Americans at almost the same rate as Whites (23.5% and 23.7%, respectively) – and keeping in mind that Black Americans make up 13.4% of the population and White people represent 76.3% – the degree of underrepresentation is glaring.
One commonly cited reason for this lack of representation is that people of color, especially Black Americans, have lingering feelings of mistrust toward the medical field. The U.S.-run Tuskegee study – during which researchers documented the natural progression of syphilis in hundreds of Black men who were kept from life-saving treatment – is, justifiably, often named as a notable source of that suspicion.
But blaming the disproportionately low numbers of Black participants in clinical trials on medical mistrust is an easy answer to a much more complicated issue, said cardiologist Clyde Yancy, MD, who also serves as the vice dean for diversity and inclusion at Northwestern University’s Feinberg School of Medicine, Chicago.
“We need to not put the onus on the back of the patient cohort, and say they are the problem,” Dr. Yancy said, adding that many trials add financial barriers and don’t provide proper transportation for participants who may live farther away.
The diversity of the study team itself – the institutions, researchers, and recruiters – also contributes to a lack of diversity in the participant pool. When considering all of these factors, “you begin to understand the complexity and the multidimensionality of why we have underrepresentation,” said Dr. Yancy. “So I would not promulgate the notion that this is simply because patients don’t trust the system.”
Soumya Niranjan, PhD, worked as a study coordinator at the Tulane Cancer Center in New Orleans, La., where she recruited patients for a prostate cancer study. After researching the impact of clinicians’ biases on the recruitment of racial and ethnic minorities in oncology trials, she found that some recruiters view patients of color as less promising participants.
“Who ends up being approached for a clinical trial is based on a preset rubric that one has in mind about a patient who may be eligible for a cancer study,” said Dr. Niranjan. “There is a characterization of, ‘we want to make sure this patient is compliant, that they will be a good historian and seem responsible.’ ... Our study showed that it kind of fell along racial lines.”
In her study, published in the journal Cancer in 2020, Dr. Niranjan wrote that researchers sometimes “perceived racial minority groups to have low knowledge of cancer clinical trials. This was considered to be a hindrance while explaining cancer clinical trials in the face of limited provider time during a clinical encounter.”
Some researchers believed minority participants, especially Black women, would be less likely to file study protocols. Others said people of color are more likely to be selfish.
She quoted one research investigator as saying Black people are less knowledgeable.
“African Americans I think have less knowledge,” the unnamed researcher said. “We take a little bit more time to explain to African American [sic]. I think ... they have more questions because we know they are not more knowledgeable so I think it takes time. They have a lot of questions.”
Progress over the years
The FDA’s recent draft builds upon a guidance from 2016, which already recommended that trial teams submit an inclusion plan to the agency at the earliest phase of development. While the recent announcement is another step in the right direction, it may not be substantial enough.
“There’s always an enrollment plan,” Dr. Niranjan said. “But those enrollment plans are not enforced. So if it’s not enforced, what does that look like?”
In an emailed statement to this news organization, Lola Fashoyin-Aje, MD, the deputy director of the FDA Oncology Center of Excellence’s division to expand diversity, emphasized that the draft guidance does not require anything, but that the agency “expect[s] sponsors will follow FDA’s recommendations as described in the draft guidance.”
Without requirements, it’s up to the sponsor to make the effort to enroll people with varied racial and ethnic backgrounds. During the development of the COVID-19 vaccine, Moderna announced that the company would slow the trial’s enrollment to ensure minority groups were properly represented.
Not every sponsor is as motivated to make this a concerted effort, and some simply don’t have the funds to allocate to strengthening the enrollment process.
“There’s so much red tape and paperwork to get the funding for a clinical trial,” said Julie Silver, MD, professor of physical medicine and rehabilitation at Harvard Medical School, Boston, who studies workforce diversity and inclusion. “Even when people are equitably included, the amount of funding they have to do the trial might not be enough to do an analysis that shows potential differences.”
Whether the FDA will enforce enrollment plans in the future remains an open question; however, Dr. Yancy said the most effective way to do this would be through incentives, rather than penalties.
According to Dr. Fashoyin-Aje, the FDA and sponsors “will learn from these submissions and over time, whether and how these diversity plans lead to meaningful changes in clinical trial representation will need to be assessed, including whether additional steps need to be taken.”
A version of this article first appeared on Medscape.com.