User login
-
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Pig heart transplants and the ethical challenges that lie ahead
The long-struggling field of cardiac xenotransplantation has had a very good year.
In January, the University of Maryland made history by keeping a 57-year-old man deemed too sick for a human heart transplant alive for 2 months with a genetically engineered pig heart. On July 12, New York University surgeons reported that heart function was “completely normal with excellent contractility” in two brain-dead patients with pig hearts beating in their chests for 72 hours.

The NYU team approached the project with a decedent model in mind and, after discussions with their IRB equivalent, settled on a 72-hour window because that’s the time they typically keep people ventilated when trying to place their organs, explained Robert A. Montgomery, MD, DPhil, director of the NYU Langone Transplant Institute.
“There’s no real ethical argument for that,” he said in an interview. The consideration is what the family is willing to do when trying to balance doing “something very altruistic and good versus having closure.”
Some families have religious beliefs that burial or interment has to occur very rapidly, whereas others, including one of the family donors, were willing to have the research go on much longer, Dr. Montgomery said. Indeed, the next protocol is being written to consider maintaining the bodies for 2-4 weeks.
“People do vary and you have to kind of accommodate that variation,” he said. “For some people, this isn’t going to be what they’re going to want and that’s why you have to go through the consent process.”
Informed authorization
Arthur L. Caplan, PhD, director of medical ethics at the NYU Langone Medical Center, said the Uniform Anatomical Gift Act recognizes an individual’s right to be an organ donor for transplant and research, but it “mentions nothing about maintaining you in a dead state artificially for research purposes.”
“It’s a major shift in what people are thinking about doing when they die or their relatives die,” he said.
Because organ donation is controlled at the state, not federal, level, the possibility of donating organs for xenotransplantation, like medical aid in dying, will vary between states, observed Dr. Caplan. The best way to ensure that patients whose organs are found to be unsuitable for transplantation have the option is to change state laws.
He noted that cases are already springing up where people are requesting postmortem sperm or egg donations without direct consents from the person who died. “So we have this new area opening up of handling the use of the dead body and we need to bring the law into sync with the possibilities that are out there.”
In terms of informed authorization (informed consent is reserved for the living), Dr. Caplan said there should be written evidence the person wanted to be a donor and, while not required by law, all survivors should give their permission and understand what’s going to be done in terms of the experiment, such as the use of animal parts, when the body will be returned, and the possibility of zoonotic viral infection.
“They have to fully accept that the person is dead and we’re just maintaining them artificially,” he said. “There’s no maintaining anyone who’s alive. That’s a source of a lot of confusion.”
Special committees also need to be appointed with voices from people in organ procurement, law, theology, and patient groups to monitor practice to ensure people who have given permission understood the process, that families have their questions answered independent of the research team, and that clear limits are set on how long experiments will last.
As to what those limits should be: “I think in terms of a week or 2,” Dr. Caplan said. “Obviously we could maintain bodies longer and people have. But I think, culturally in our society, going much past that starts to perhaps stress emotionally, psychologically, family and friends about getting closure.”
“I’m not as comfortable when people say things like, ‘How about 2 months?’ ” he said. “That’s a long time to sort of accept the fact that somebody has died but you can’t complete all the things that go along with the death.”
Dr. Caplan is also uncomfortable with the use of one-off emergency authorizations, as used for Maryland resident David Bennett Sr., who was rejected for standard heart transplantation and required mechanical circulatory support to stay alive.
“It’s too premature, I believe, even to try and rescue someone,” he said. “We need to learn more from the deceased models.”
A better model
Dr. Montgomery noted that primates are very imperfect models for predicting what’s going to happen in humans, and that in order to do xenotransplantation in living humans, there are only two pathways – the one-off emergency authorization or a clinical phase 1 trial.
The decedent model, he said, “will make human trials safer because it’s an intermediate step. You don’t have a living human’s life on the line when you’re trying to do iterative changes and improve the procedure.”
The team, for example, omitted a perfusion pump that was used in the Maryland case and would likely have made its way into phase 1 trials based on baboon data that suggested it was important to have the heart on the pump for hours before it was transplanted, he said. “We didn’t do any of that. We just did it like we would do a regular heart transplant and it started right up, immediately, and started to work.”
The researchers did not release details on the immunosuppression regimen, but noted that, unlike Maryland, they also did not use the experimental anti-CD40 antibody to tamp down the recipients’ immune system.
Although Mr. Bennett’s autopsy did not show any conventional sign of graft rejection, the transplanted pig heart was infected with porcine cytomegalovirus (PCMV) and Mr. Bennett showed traces of DNA from PCMV in his circulation.
Nailing down safety
Dr. Montgomery said he wouldn’t rule out xenotransplantation in a living human, but that the safety issues need to be nailed down. “I think that the tests used on the pig that was the donor for the Bennett case were not sensitive enough for latent virus, and that’s how it slipped through. So there was a bit of going back to the drawing board, really looking at each of the tests, and being sure we had the sensitivity to pick up a latent virus.”
He noted that United Therapeutics, which funded the research and provided the engineered pigs through its subsidiary Revivicor, has created and validated a more sensitive polymerase chain reaction test that covers some 35 different pathogens, microbes, and parasites. NYU has also developed its own platform to repeat the testing and for monitoring after the transplant. “The ones that we’re currently using would have picked up the virus.”
Stuart Russell, MD, a professor of medicine who specializes in advanced HF at Duke University, Durham, N.C., said “the biggest thing from my perspective is those two amazing families that were willing let this happen. ... If 20 years from now, this is what we’re doing, it’s related to these families being this generous at a really tough time in their lives.”
Dr. Russell said he awaits publication of the data on what the pathology of the heart looks like, but that the experiments “help to give us a lot of reassurance that we don’t need to worry about hyperacute rejection,” which by definition is going to happen in the first 24-48 hours.
That said, longer-term data is essential to potential safety issues. Notably, among the 10 genetic modifications made to the pigs, four were porcine gene knockouts, including a growth hormone receptor knockout to prevent abnormal organ growth inside the recipient’s chest. As a result, the organs seem to be small for the age of the pig and just don’t grow that well, admitted Dr. Montgomery, who said they are currently analyzing this with echocardiography.
Dr. Russell said this may create a sizing issue, but also “if you have a heart that’s more stressed in the pig, from the point of being a donor, maybe it’s not as good a heart as if it was growing normally. But that kind of stuff, I think, is going to take more than two cases and longer-term data to sort out.”
Sharon Hunt, MD, professor emerita, Stanford (Calif.) University Medical Center, and past president of the International Society for Heart Lung Transplantation, said it’s not the technical aspects, but the biology of xenotransplantation that’s really daunting.
“It’s not the physical act of doing it, like they needed a bigger heart or a smaller heart. Those are technical problems but they’ll manage them,” she said. “The big problem is biological – and the bottom line is we don’t really know. We may have overcome hyperacute rejection, which is great, but the rest remains to be seen.”
Dr. Hunt, who worked with heart transplantation pioneer Norman Shumway, MD, and spent decades caring for patients after transplantation, said most families will consent to 24 or 48 hours or even a week of experimentation on a brain-dead loved one, but what the transplant community wants to know is whether this is workable for many months.
“So the fact that the xenotransplant works for 72 hours, yeah, that’s groovy. But, you know, the answer is kind of ‘so what,’ ” she said. “I’d like to see this go for months, like they were trying to do in the human in Maryland.”
For phase 1 trials, even longer-term survival with or without rejection or with rejection that’s treatable is needed, Dr. Hunt suggested.
“We haven’t seen that yet. The Maryland people were very valiant but they lost the cause,” she said. “There’s just so much more to do before we have a viable model to start anything like a phase 1 trial. I’d love it if that happens in my lifetime, but I’m not sure it’s going to.”
Dr. Russell and Dr. Hunt reported no relevant financial relationships. Dr. Caplan reported serving as a director, officer, partner, employee, advisor, consultant, or trustee for Johnson & Johnson’s Panel for Compassionate Drug Use (unpaid position) and is a contributing author and adviser for Medscape.
A version of this article first appeared on Medscape.com.
The long-struggling field of cardiac xenotransplantation has had a very good year.
In January, the University of Maryland made history by keeping a 57-year-old man deemed too sick for a human heart transplant alive for 2 months with a genetically engineered pig heart. On July 12, New York University surgeons reported that heart function was “completely normal with excellent contractility” in two brain-dead patients with pig hearts beating in their chests for 72 hours.
The NYU team approached the project with a decedent model in mind and, after discussions with their IRB equivalent, settled on a 72-hour window because that’s the time they typically keep people ventilated when trying to place their organs, explained Robert A. Montgomery, MD, DPhil, director of the NYU Langone Transplant Institute.
“There’s no real ethical argument for that,” he said in an interview. The consideration is what the family is willing to do when trying to balance doing “something very altruistic and good versus having closure.”
Some families have religious beliefs that burial or interment has to occur very rapidly, whereas others, including one of the family donors, were willing to have the research go on much longer, Dr. Montgomery said. Indeed, the next protocol is being written to consider maintaining the bodies for 2-4 weeks.
“People do vary and you have to kind of accommodate that variation,” he said. “For some people, this isn’t going to be what they’re going to want and that’s why you have to go through the consent process.”
Informed authorization
Arthur L. Caplan, PhD, director of medical ethics at the NYU Langone Medical Center, said the Uniform Anatomical Gift Act recognizes an individual’s right to be an organ donor for transplant and research, but it “mentions nothing about maintaining you in a dead state artificially for research purposes.”
“It’s a major shift in what people are thinking about doing when they die or their relatives die,” he said.
Because organ donation is controlled at the state, not federal, level, the possibility of donating organs for xenotransplantation, like medical aid in dying, will vary between states, observed Dr. Caplan. The best way to ensure that patients whose organs are found to be unsuitable for transplantation have the option is to change state laws.
He noted that cases are already springing up where people are requesting postmortem sperm or egg donations without direct consents from the person who died. “So we have this new area opening up of handling the use of the dead body and we need to bring the law into sync with the possibilities that are out there.”
In terms of informed authorization (informed consent is reserved for the living), Dr. Caplan said there should be written evidence the person wanted to be a donor and, while not required by law, all survivors should give their permission and understand what’s going to be done in terms of the experiment, such as the use of animal parts, when the body will be returned, and the possibility of zoonotic viral infection.
“They have to fully accept that the person is dead and we’re just maintaining them artificially,” he said. “There’s no maintaining anyone who’s alive. That’s a source of a lot of confusion.”
Special committees also need to be appointed with voices from people in organ procurement, law, theology, and patient groups to monitor practice to ensure people who have given permission understood the process, that families have their questions answered independent of the research team, and that clear limits are set on how long experiments will last.
As to what those limits should be: “I think in terms of a week or 2,” Dr. Caplan said. “Obviously we could maintain bodies longer and people have. But I think, culturally in our society, going much past that starts to perhaps stress emotionally, psychologically, family and friends about getting closure.”
“I’m not as comfortable when people say things like, ‘How about 2 months?’ ” he said. “That’s a long time to sort of accept the fact that somebody has died but you can’t complete all the things that go along with the death.”
Dr. Caplan is also uncomfortable with the use of one-off emergency authorizations, as used for Maryland resident David Bennett Sr., who was rejected for standard heart transplantation and required mechanical circulatory support to stay alive.
“It’s too premature, I believe, even to try and rescue someone,” he said. “We need to learn more from the deceased models.”
A better model
Dr. Montgomery noted that primates are very imperfect models for predicting what’s going to happen in humans, and that in order to do xenotransplantation in living humans, there are only two pathways – the one-off emergency authorization or a clinical phase 1 trial.
The decedent model, he said, “will make human trials safer because it’s an intermediate step. You don’t have a living human’s life on the line when you’re trying to do iterative changes and improve the procedure.”
The team, for example, omitted a perfusion pump that was used in the Maryland case and would likely have made its way into phase 1 trials based on baboon data that suggested it was important to have the heart on the pump for hours before it was transplanted, he said. “We didn’t do any of that. We just did it like we would do a regular heart transplant and it started right up, immediately, and started to work.”
The researchers did not release details on the immunosuppression regimen, but noted that, unlike Maryland, they also did not use the experimental anti-CD40 antibody to tamp down the recipients’ immune system.
Although Mr. Bennett’s autopsy did not show any conventional sign of graft rejection, the transplanted pig heart was infected with porcine cytomegalovirus (PCMV) and Mr. Bennett showed traces of DNA from PCMV in his circulation.
Nailing down safety
Dr. Montgomery said he wouldn’t rule out xenotransplantation in a living human, but that the safety issues need to be nailed down. “I think that the tests used on the pig that was the donor for the Bennett case were not sensitive enough for latent virus, and that’s how it slipped through. So there was a bit of going back to the drawing board, really looking at each of the tests, and being sure we had the sensitivity to pick up a latent virus.”
He noted that United Therapeutics, which funded the research and provided the engineered pigs through its subsidiary Revivicor, has created and validated a more sensitive polymerase chain reaction test that covers some 35 different pathogens, microbes, and parasites. NYU has also developed its own platform to repeat the testing and for monitoring after the transplant. “The ones that we’re currently using would have picked up the virus.”
Stuart Russell, MD, a professor of medicine who specializes in advanced HF at Duke University, Durham, N.C., said “the biggest thing from my perspective is those two amazing families that were willing let this happen. ... If 20 years from now, this is what we’re doing, it’s related to these families being this generous at a really tough time in their lives.”
Dr. Russell said he awaits publication of the data on what the pathology of the heart looks like, but that the experiments “help to give us a lot of reassurance that we don’t need to worry about hyperacute rejection,” which by definition is going to happen in the first 24-48 hours.
That said, longer-term data is essential to potential safety issues. Notably, among the 10 genetic modifications made to the pigs, four were porcine gene knockouts, including a growth hormone receptor knockout to prevent abnormal organ growth inside the recipient’s chest. As a result, the organs seem to be small for the age of the pig and just don’t grow that well, admitted Dr. Montgomery, who said they are currently analyzing this with echocardiography.
Dr. Russell said this may create a sizing issue, but also “if you have a heart that’s more stressed in the pig, from the point of being a donor, maybe it’s not as good a heart as if it was growing normally. But that kind of stuff, I think, is going to take more than two cases and longer-term data to sort out.”
Sharon Hunt, MD, professor emerita, Stanford (Calif.) University Medical Center, and past president of the International Society for Heart Lung Transplantation, said it’s not the technical aspects, but the biology of xenotransplantation that’s really daunting.
“It’s not the physical act of doing it, like they needed a bigger heart or a smaller heart. Those are technical problems but they’ll manage them,” she said. “The big problem is biological – and the bottom line is we don’t really know. We may have overcome hyperacute rejection, which is great, but the rest remains to be seen.”
Dr. Hunt, who worked with heart transplantation pioneer Norman Shumway, MD, and spent decades caring for patients after transplantation, said most families will consent to 24 or 48 hours or even a week of experimentation on a brain-dead loved one, but what the transplant community wants to know is whether this is workable for many months.
“So the fact that the xenotransplant works for 72 hours, yeah, that’s groovy. But, you know, the answer is kind of ‘so what,’ ” she said. “I’d like to see this go for months, like they were trying to do in the human in Maryland.”
For phase 1 trials, even longer-term survival with or without rejection or with rejection that’s treatable is needed, Dr. Hunt suggested.
“We haven’t seen that yet. The Maryland people were very valiant but they lost the cause,” she said. “There’s just so much more to do before we have a viable model to start anything like a phase 1 trial. I’d love it if that happens in my lifetime, but I’m not sure it’s going to.”
Dr. Russell and Dr. Hunt reported no relevant financial relationships. Dr. Caplan reported serving as a director, officer, partner, employee, advisor, consultant, or trustee for Johnson & Johnson’s Panel for Compassionate Drug Use (unpaid position) and is a contributing author and adviser for Medscape.
A version of this article first appeared on Medscape.com.
The long-struggling field of cardiac xenotransplantation has had a very good year.
In January, the University of Maryland made history by keeping a 57-year-old man deemed too sick for a human heart transplant alive for 2 months with a genetically engineered pig heart. On July 12, New York University surgeons reported that heart function was “completely normal with excellent contractility” in two brain-dead patients with pig hearts beating in their chests for 72 hours.
The NYU team approached the project with a decedent model in mind and, after discussions with their IRB equivalent, settled on a 72-hour window because that’s the time they typically keep people ventilated when trying to place their organs, explained Robert A. Montgomery, MD, DPhil, director of the NYU Langone Transplant Institute.
“There’s no real ethical argument for that,” he said in an interview. The consideration is what the family is willing to do when trying to balance doing “something very altruistic and good versus having closure.”
Some families have religious beliefs that burial or interment has to occur very rapidly, whereas others, including one of the family donors, were willing to have the research go on much longer, Dr. Montgomery said. Indeed, the next protocol is being written to consider maintaining the bodies for 2-4 weeks.
“People do vary and you have to kind of accommodate that variation,” he said. “For some people, this isn’t going to be what they’re going to want and that’s why you have to go through the consent process.”
Informed authorization
Arthur L. Caplan, PhD, director of medical ethics at the NYU Langone Medical Center, said the Uniform Anatomical Gift Act recognizes an individual’s right to be an organ donor for transplant and research, but it “mentions nothing about maintaining you in a dead state artificially for research purposes.”
“It’s a major shift in what people are thinking about doing when they die or their relatives die,” he said.
Because organ donation is controlled at the state, not federal, level, the possibility of donating organs for xenotransplantation, like medical aid in dying, will vary between states, observed Dr. Caplan. The best way to ensure that patients whose organs are found to be unsuitable for transplantation have the option is to change state laws.
He noted that cases are already springing up where people are requesting postmortem sperm or egg donations without direct consents from the person who died. “So we have this new area opening up of handling the use of the dead body and we need to bring the law into sync with the possibilities that are out there.”
In terms of informed authorization (informed consent is reserved for the living), Dr. Caplan said there should be written evidence the person wanted to be a donor and, while not required by law, all survivors should give their permission and understand what’s going to be done in terms of the experiment, such as the use of animal parts, when the body will be returned, and the possibility of zoonotic viral infection.
“They have to fully accept that the person is dead and we’re just maintaining them artificially,” he said. “There’s no maintaining anyone who’s alive. That’s a source of a lot of confusion.”
Special committees also need to be appointed with voices from people in organ procurement, law, theology, and patient groups to monitor practice to ensure people who have given permission understood the process, that families have their questions answered independent of the research team, and that clear limits are set on how long experiments will last.
As to what those limits should be: “I think in terms of a week or 2,” Dr. Caplan said. “Obviously we could maintain bodies longer and people have. But I think, culturally in our society, going much past that starts to perhaps stress emotionally, psychologically, family and friends about getting closure.”
“I’m not as comfortable when people say things like, ‘How about 2 months?’ ” he said. “That’s a long time to sort of accept the fact that somebody has died but you can’t complete all the things that go along with the death.”
Dr. Caplan is also uncomfortable with the use of one-off emergency authorizations, as used for Maryland resident David Bennett Sr., who was rejected for standard heart transplantation and required mechanical circulatory support to stay alive.
“It’s too premature, I believe, even to try and rescue someone,” he said. “We need to learn more from the deceased models.”
A better model
Dr. Montgomery noted that primates are very imperfect models for predicting what’s going to happen in humans, and that in order to do xenotransplantation in living humans, there are only two pathways – the one-off emergency authorization or a clinical phase 1 trial.
The decedent model, he said, “will make human trials safer because it’s an intermediate step. You don’t have a living human’s life on the line when you’re trying to do iterative changes and improve the procedure.”
The team, for example, omitted a perfusion pump that was used in the Maryland case and would likely have made its way into phase 1 trials based on baboon data that suggested it was important to have the heart on the pump for hours before it was transplanted, he said. “We didn’t do any of that. We just did it like we would do a regular heart transplant and it started right up, immediately, and started to work.”
The researchers did not release details on the immunosuppression regimen, but noted that, unlike Maryland, they also did not use the experimental anti-CD40 antibody to tamp down the recipients’ immune system.
Although Mr. Bennett’s autopsy did not show any conventional sign of graft rejection, the transplanted pig heart was infected with porcine cytomegalovirus (PCMV) and Mr. Bennett showed traces of DNA from PCMV in his circulation.
Nailing down safety
Dr. Montgomery said he wouldn’t rule out xenotransplantation in a living human, but that the safety issues need to be nailed down. “I think that the tests used on the pig that was the donor for the Bennett case were not sensitive enough for latent virus, and that’s how it slipped through. So there was a bit of going back to the drawing board, really looking at each of the tests, and being sure we had the sensitivity to pick up a latent virus.”
He noted that United Therapeutics, which funded the research and provided the engineered pigs through its subsidiary Revivicor, has created and validated a more sensitive polymerase chain reaction test that covers some 35 different pathogens, microbes, and parasites. NYU has also developed its own platform to repeat the testing and for monitoring after the transplant. “The ones that we’re currently using would have picked up the virus.”
Stuart Russell, MD, a professor of medicine who specializes in advanced HF at Duke University, Durham, N.C., said “the biggest thing from my perspective is those two amazing families that were willing let this happen. ... If 20 years from now, this is what we’re doing, it’s related to these families being this generous at a really tough time in their lives.”
Dr. Russell said he awaits publication of the data on what the pathology of the heart looks like, but that the experiments “help to give us a lot of reassurance that we don’t need to worry about hyperacute rejection,” which by definition is going to happen in the first 24-48 hours.
That said, longer-term data is essential to potential safety issues. Notably, among the 10 genetic modifications made to the pigs, four were porcine gene knockouts, including a growth hormone receptor knockout to prevent abnormal organ growth inside the recipient’s chest. As a result, the organs seem to be small for the age of the pig and just don’t grow that well, admitted Dr. Montgomery, who said they are currently analyzing this with echocardiography.
Dr. Russell said this may create a sizing issue, but also “if you have a heart that’s more stressed in the pig, from the point of being a donor, maybe it’s not as good a heart as if it was growing normally. But that kind of stuff, I think, is going to take more than two cases and longer-term data to sort out.”
Sharon Hunt, MD, professor emerita, Stanford (Calif.) University Medical Center, and past president of the International Society for Heart Lung Transplantation, said it’s not the technical aspects, but the biology of xenotransplantation that’s really daunting.
“It’s not the physical act of doing it, like they needed a bigger heart or a smaller heart. Those are technical problems but they’ll manage them,” she said. “The big problem is biological – and the bottom line is we don’t really know. We may have overcome hyperacute rejection, which is great, but the rest remains to be seen.”
Dr. Hunt, who worked with heart transplantation pioneer Norman Shumway, MD, and spent decades caring for patients after transplantation, said most families will consent to 24 or 48 hours or even a week of experimentation on a brain-dead loved one, but what the transplant community wants to know is whether this is workable for many months.
“So the fact that the xenotransplant works for 72 hours, yeah, that’s groovy. But, you know, the answer is kind of ‘so what,’ ” she said. “I’d like to see this go for months, like they were trying to do in the human in Maryland.”
For phase 1 trials, even longer-term survival with or without rejection or with rejection that’s treatable is needed, Dr. Hunt suggested.
“We haven’t seen that yet. The Maryland people were very valiant but they lost the cause,” she said. “There’s just so much more to do before we have a viable model to start anything like a phase 1 trial. I’d love it if that happens in my lifetime, but I’m not sure it’s going to.”
Dr. Russell and Dr. Hunt reported no relevant financial relationships. Dr. Caplan reported serving as a director, officer, partner, employee, advisor, consultant, or trustee for Johnson & Johnson’s Panel for Compassionate Drug Use (unpaid position) and is a contributing author and adviser for Medscape.
A version of this article first appeared on Medscape.com.
Lung cancer treatment combo may be effective after ICI failure
In a phase 2 clinical trial, the combination of an immune checkpoint inhibitor (ICI) and a vascular endothelial growth factor (VEGF) inhibitor led to improved overall survival versus standard of care in patients with non–small cell lung cancer (NSCLC) who had failed previous ICI therapy.
NSCLC patients usually receive immune checkpoint inhibitor therapy at some point, whether in the adjuvant or neoadjuvant setting, or among stage 3 patients after radiation. “The majority of patients who get diagnosed with lung cancer will get some sort of immunotherapy, and we know that at least from the advanced setting, about 15% of those will have long-term responses, which means the majority of patients will develop tumor resistance to immune checkpoint inhibitor therapy,” said Karen L. Reckamp, MD, who is the lead author of the study published online in Journal of Clinical Oncology.
That clinical need has led to the combination of ICIs with VEGF inhibitors. This approach is approved for first-line therapy of renal cell cancer, endometrial, and hepatocellular cancer. Along with its effect on tumor vasculature, VEGF inhibition assists in the activation and maturation of dendritic cells, as well as to attract cytotoxic T cells to the tumor. “By both changing the vasculature and changing the tumor milieu, there’s a potential to overcome that immune suppression and potentially overcome that (ICI) resistance,” said Dr. Reckamp, who is associate director of clinical research at Cedars Sinai Medical Center, Los Angeles. “The results of the study were encouraging. . We would like to confirm this finding in a phase 3 trial and potentially provide to patients an option that does not include chemotherapy and can potentially overcome resistance to their prior immune checkpoint inhibitor therapy,” Dr. Reckamp said.
The study included 136 patients. The median patient age was 66 years and 61% were male. The ICI/VEGF arm had better overall survival (hazard ratio, 0.69; SLR one-sided P = .05). The median overall survival was 14.5 months in the ICI/VEGF arm, versus 11.6 months in the standard care arm. Both arms had similar response rates, and grade 3 or higher treatment-related adverse events were more common in the chemotherapy arm (60% versus 42%).
The next step is a phase 3 trial and Dr. Reckamp hopes to improve patient selection for VEGF inhibitor and VEGF receptor inhibitor therapy. “The precision medicine that’s associated with other tumor alterations has kind of been elusive for VEGF therapies, but I would hope with potentially a larger trial and understanding of some of the biomarkers that we might find a more select patient population who will benefit the most,” Dr. Reckamp said.
She also noted that the comparative arm in the phase 2 study was a combination of docetaxel and ramucirumab. “That combination has shown to be more effective than single agent docetaxel alone so [the new study] was really improved overall survival over the best standard of care therapy we have,” Dr. Reckamp said.
The study was funded, in part, by Eli Lilly and Company and Merck Sharp & Dohme Corp. Dr. Reckamp disclosed ties to Amgen, Tesaro, Takeda, AstraZeneca, Seattle Genetics, Genentech, Blueprint Medicines, Daiichi Sankyo/Lilly, EMD Serono, Janssen Oncology, Merck KGaA, GlaxoSmithKline, and Mirati Therapeutics.
In a phase 2 clinical trial, the combination of an immune checkpoint inhibitor (ICI) and a vascular endothelial growth factor (VEGF) inhibitor led to improved overall survival versus standard of care in patients with non–small cell lung cancer (NSCLC) who had failed previous ICI therapy.
NSCLC patients usually receive immune checkpoint inhibitor therapy at some point, whether in the adjuvant or neoadjuvant setting, or among stage 3 patients after radiation. “The majority of patients who get diagnosed with lung cancer will get some sort of immunotherapy, and we know that at least from the advanced setting, about 15% of those will have long-term responses, which means the majority of patients will develop tumor resistance to immune checkpoint inhibitor therapy,” said Karen L. Reckamp, MD, who is the lead author of the study published online in Journal of Clinical Oncology.
That clinical need has led to the combination of ICIs with VEGF inhibitors. This approach is approved for first-line therapy of renal cell cancer, endometrial, and hepatocellular cancer. Along with its effect on tumor vasculature, VEGF inhibition assists in the activation and maturation of dendritic cells, as well as to attract cytotoxic T cells to the tumor. “By both changing the vasculature and changing the tumor milieu, there’s a potential to overcome that immune suppression and potentially overcome that (ICI) resistance,” said Dr. Reckamp, who is associate director of clinical research at Cedars Sinai Medical Center, Los Angeles. “The results of the study were encouraging. . We would like to confirm this finding in a phase 3 trial and potentially provide to patients an option that does not include chemotherapy and can potentially overcome resistance to their prior immune checkpoint inhibitor therapy,” Dr. Reckamp said.
The study included 136 patients. The median patient age was 66 years and 61% were male. The ICI/VEGF arm had better overall survival (hazard ratio, 0.69; SLR one-sided P = .05). The median overall survival was 14.5 months in the ICI/VEGF arm, versus 11.6 months in the standard care arm. Both arms had similar response rates, and grade 3 or higher treatment-related adverse events were more common in the chemotherapy arm (60% versus 42%).
The next step is a phase 3 trial and Dr. Reckamp hopes to improve patient selection for VEGF inhibitor and VEGF receptor inhibitor therapy. “The precision medicine that’s associated with other tumor alterations has kind of been elusive for VEGF therapies, but I would hope with potentially a larger trial and understanding of some of the biomarkers that we might find a more select patient population who will benefit the most,” Dr. Reckamp said.
She also noted that the comparative arm in the phase 2 study was a combination of docetaxel and ramucirumab. “That combination has shown to be more effective than single agent docetaxel alone so [the new study] was really improved overall survival over the best standard of care therapy we have,” Dr. Reckamp said.
The study was funded, in part, by Eli Lilly and Company and Merck Sharp & Dohme Corp. Dr. Reckamp disclosed ties to Amgen, Tesaro, Takeda, AstraZeneca, Seattle Genetics, Genentech, Blueprint Medicines, Daiichi Sankyo/Lilly, EMD Serono, Janssen Oncology, Merck KGaA, GlaxoSmithKline, and Mirati Therapeutics.
In a phase 2 clinical trial, the combination of an immune checkpoint inhibitor (ICI) and a vascular endothelial growth factor (VEGF) inhibitor led to improved overall survival versus standard of care in patients with non–small cell lung cancer (NSCLC) who had failed previous ICI therapy.
NSCLC patients usually receive immune checkpoint inhibitor therapy at some point, whether in the adjuvant or neoadjuvant setting, or among stage 3 patients after radiation. “The majority of patients who get diagnosed with lung cancer will get some sort of immunotherapy, and we know that at least from the advanced setting, about 15% of those will have long-term responses, which means the majority of patients will develop tumor resistance to immune checkpoint inhibitor therapy,” said Karen L. Reckamp, MD, who is the lead author of the study published online in Journal of Clinical Oncology.
That clinical need has led to the combination of ICIs with VEGF inhibitors. This approach is approved for first-line therapy of renal cell cancer, endometrial, and hepatocellular cancer. Along with its effect on tumor vasculature, VEGF inhibition assists in the activation and maturation of dendritic cells, as well as to attract cytotoxic T cells to the tumor. “By both changing the vasculature and changing the tumor milieu, there’s a potential to overcome that immune suppression and potentially overcome that (ICI) resistance,” said Dr. Reckamp, who is associate director of clinical research at Cedars Sinai Medical Center, Los Angeles. “The results of the study were encouraging. . We would like to confirm this finding in a phase 3 trial and potentially provide to patients an option that does not include chemotherapy and can potentially overcome resistance to their prior immune checkpoint inhibitor therapy,” Dr. Reckamp said.
The study included 136 patients. The median patient age was 66 years and 61% were male. The ICI/VEGF arm had better overall survival (hazard ratio, 0.69; SLR one-sided P = .05). The median overall survival was 14.5 months in the ICI/VEGF arm, versus 11.6 months in the standard care arm. Both arms had similar response rates, and grade 3 or higher treatment-related adverse events were more common in the chemotherapy arm (60% versus 42%).
The next step is a phase 3 trial and Dr. Reckamp hopes to improve patient selection for VEGF inhibitor and VEGF receptor inhibitor therapy. “The precision medicine that’s associated with other tumor alterations has kind of been elusive for VEGF therapies, but I would hope with potentially a larger trial and understanding of some of the biomarkers that we might find a more select patient population who will benefit the most,” Dr. Reckamp said.
She also noted that the comparative arm in the phase 2 study was a combination of docetaxel and ramucirumab. “That combination has shown to be more effective than single agent docetaxel alone so [the new study] was really improved overall survival over the best standard of care therapy we have,” Dr. Reckamp said.
The study was funded, in part, by Eli Lilly and Company and Merck Sharp & Dohme Corp. Dr. Reckamp disclosed ties to Amgen, Tesaro, Takeda, AstraZeneca, Seattle Genetics, Genentech, Blueprint Medicines, Daiichi Sankyo/Lilly, EMD Serono, Janssen Oncology, Merck KGaA, GlaxoSmithKline, and Mirati Therapeutics.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Does your patient have long COVID? Some clues on what to look for
New Yorker Lyss Stern came down with COVID-19 at the beginning of the pandemic, in March 2020. She ran a 103° F fever for 5 days straight and was bedridden for several weeks. Yet symptoms such as a persistent headache and tinnitus, or ringing in her ears, lingered.
“Four months later, I still couldn’t walk four blocks without becoming winded,” says Ms. Stern, 48. Five months after her diagnosis, her doctors finally gave a name to her condition: long COVID.
Long COVID is known by many different names: long-haul COVID, postacute COVID-19, or even chronic COVID. It’s a general term used to describe the range of ongoing health problems people can have after their infection.
Another earlier report found that one in five COVID-19 survivors between the ages of 18 and 64, and one in four survivors aged at least 65, have a health condition that may be related to their previous bout with the virus.
Unfortunately, there’s no easy way to screen for long COVID.
“There’s no definite laboratory test to give us a diagnosis,” says Daniel Sterman, MD, director of the division of pulmonary, critical care and sleep medicine at NYU Langone Health in New York. “We’re also still working on a definition, since there’s a whole slew of symptoms associated with the condition.”
It’s a challenge that Ms. Stern is personally acquainted with after she bounced from doctor to doctor for several months before she found her way to the Center for Post-COVID Care at Mount Sinai Hospital in New York. “It was a relief to have an official diagnosis, even if it didn’t bring immediate answers,” she says.
What to look for
Many people who become infected with COVID-19 get symptoms that linger for 2-3 weeks after their infection has cleared, says Brittany Baloun, a certified nurse practitioner at the Cleveland Clinic. “It’s not unusual to feel some residual shortness of breath or heart palpitations, especially if you are exerting yourself,” she says. “The acute phase of COVID itself can last for up to 14 days. But if it’s been 30 days since you came down with the virus, and your symptoms are still there and not improving, it indicates some level of long COVID.”
More than 200 symptoms can be linked to long COVID. But perhaps the one that stands out the most is constant fatigue that interferes with daily life.
“We often hear that these patients can’t fold the laundry or take a short walk with their dog without feeling exhausted,” Ms. Baloun says.
This exhaustion may get worse after patients exercise or do something mentally taxing, a condition known as postexertional malaise.
“It can be crushing fatigue; I may clean my room for an hour and talk to a friend, and the next day feel like I can’t get out of bed,” says Allison Guy, 36, who was diagnosed with COVID in February 2021. She’s now a long-COVID advocate in Washington.
Other symptoms can be divided into different categories, which include cardiac/lung symptoms such as shortness of breath, coughing, chest pain, and heart palpitations, as well as neurologic symptoms.
One of the most common neurologic symptoms is brain fog, says Andrew Schamess, MD, a professor of internal medicine at Ohio State University Wexner Medical Center, Columbus, who runs its post-COVID recovery program. “Patients describe feeling ‘fuzzy’ or ‘spacey,’ and often report that they are forgetful or have memory problems,” he says. Others include:
- Headache.
- Sleep problems. One 2022 study from the Cleveland Clinic found that more than 40% of patients with long COVID reported sleep disturbances.
- Dizziness when standing.
- Pins-and-needles feelings.
- Changes in smell or taste.
- Depression or anxiety.
You could also have digestive symptoms such as diarrhea or stomach pain. Other symptoms include joint or muscle pain, rashes, or changes in menstrual cycles.
Risk of having other health conditions
People who have had COVID-19, particularly a severe case, may be more at risk of getting other health conditions, such as:
- Type 2 diabetes.
- Kidney failure.
- Pulmonary embolism, or a blood clot in the lung.
- Myocarditis, an inflamed heart.
While it’s hard to say precisely whether these conditions were caused by COVID, they are most likely linked to it, says Dr. Schamess. A March 2022 study published in The Lancet Diabetes & Endocrinology, for example, found that people who had recovered from COVID-19 had a 40% higher risk of being diagnosed with type 2 diabetes over the next year.
“We don’t know for sure that infection with COVID-19 triggered someone’s diabetes – it may have been that they already had risk factors and the virus pushed them over the edge,” he says.
COVID-19 itself may also worsen conditions you already have, such as asthma, sleep apnea, or fibromyalgia. “We see patients with previously mild asthma who come in constantly coughing and wheezing, for example,” says Dr. Schamess. “They usually respond well once we start aggressive treatment.” That might include a continuous positive airway pressure, or CPAP, setup to help treat sleep apnea, or gabapentin to treat fibromyalgia symptoms.
Is it long COVID or something else?
Long COVID can cause a long list of symptoms, and they can easily mean other ailments. That’s one reason why, if your symptoms last for more than a month, it’s important to see a doctor, Ms. Baloun says. They can run a wide variety of tests to check for other conditions, such as a thyroid disorder or vitamin deficiency, that could be confused with long COVID.
They should also run blood tests such as D-dimer. This helps rule out a pulmonary embolism, which can be a complication of COVID-19 and also causes symptoms that may mimic long COVID, such as breathlessness and anxiety. They will also run tests to look for inflammation, Ms. Baloun says.
“These tests can’t provide definitive answers, but they can help provide clues as to what’s causing symptoms and whether they are related to long COVID,” she says.
What’s just as important, says Dr. Schamess, is a careful medical history. This can help pinpoint exactly when symptoms started, when they worsened, and whether anything else could have triggered them.
“I saw a patient recently who presented with symptoms of brain fog, memory loss, fatigue, headache, and sleep disturbance 5 months after she had COVID-19,” says Dr. Schamess. “After we talked, we realized that her symptoms were due to a fainting spell a couple of months earlier where she whacked her head very hard. She didn’t have long COVID – she had a concussion. But I wouldn’t have picked that up if I had just run a whole battery of tests.”
Ms. Stern agrees. “If you have long COVID, you may come across doctors who dismiss your symptoms, especially if your workups don’t show an obvious problem,” she says. “But you know your body. If it still seems like something is wrong, then you need to continue to push until you find answers.”
A version of this article first appeared on WebMD.com.
New Yorker Lyss Stern came down with COVID-19 at the beginning of the pandemic, in March 2020. She ran a 103° F fever for 5 days straight and was bedridden for several weeks. Yet symptoms such as a persistent headache and tinnitus, or ringing in her ears, lingered.
“Four months later, I still couldn’t walk four blocks without becoming winded,” says Ms. Stern, 48. Five months after her diagnosis, her doctors finally gave a name to her condition: long COVID.
Long COVID is known by many different names: long-haul COVID, postacute COVID-19, or even chronic COVID. It’s a general term used to describe the range of ongoing health problems people can have after their infection.
Another earlier report found that one in five COVID-19 survivors between the ages of 18 and 64, and one in four survivors aged at least 65, have a health condition that may be related to their previous bout with the virus.
Unfortunately, there’s no easy way to screen for long COVID.
“There’s no definite laboratory test to give us a diagnosis,” says Daniel Sterman, MD, director of the division of pulmonary, critical care and sleep medicine at NYU Langone Health in New York. “We’re also still working on a definition, since there’s a whole slew of symptoms associated with the condition.”
It’s a challenge that Ms. Stern is personally acquainted with after she bounced from doctor to doctor for several months before she found her way to the Center for Post-COVID Care at Mount Sinai Hospital in New York. “It was a relief to have an official diagnosis, even if it didn’t bring immediate answers,” she says.
What to look for
Many people who become infected with COVID-19 get symptoms that linger for 2-3 weeks after their infection has cleared, says Brittany Baloun, a certified nurse practitioner at the Cleveland Clinic. “It’s not unusual to feel some residual shortness of breath or heart palpitations, especially if you are exerting yourself,” she says. “The acute phase of COVID itself can last for up to 14 days. But if it’s been 30 days since you came down with the virus, and your symptoms are still there and not improving, it indicates some level of long COVID.”
More than 200 symptoms can be linked to long COVID. But perhaps the one that stands out the most is constant fatigue that interferes with daily life.
“We often hear that these patients can’t fold the laundry or take a short walk with their dog without feeling exhausted,” Ms. Baloun says.
This exhaustion may get worse after patients exercise or do something mentally taxing, a condition known as postexertional malaise.
“It can be crushing fatigue; I may clean my room for an hour and talk to a friend, and the next day feel like I can’t get out of bed,” says Allison Guy, 36, who was diagnosed with COVID in February 2021. She’s now a long-COVID advocate in Washington.
Other symptoms can be divided into different categories, which include cardiac/lung symptoms such as shortness of breath, coughing, chest pain, and heart palpitations, as well as neurologic symptoms.
One of the most common neurologic symptoms is brain fog, says Andrew Schamess, MD, a professor of internal medicine at Ohio State University Wexner Medical Center, Columbus, who runs its post-COVID recovery program. “Patients describe feeling ‘fuzzy’ or ‘spacey,’ and often report that they are forgetful or have memory problems,” he says. Others include:
- Headache.
- Sleep problems. One 2022 study from the Cleveland Clinic found that more than 40% of patients with long COVID reported sleep disturbances.
- Dizziness when standing.
- Pins-and-needles feelings.
- Changes in smell or taste.
- Depression or anxiety.
You could also have digestive symptoms such as diarrhea or stomach pain. Other symptoms include joint or muscle pain, rashes, or changes in menstrual cycles.
Risk of having other health conditions
People who have had COVID-19, particularly a severe case, may be more at risk of getting other health conditions, such as:
- Type 2 diabetes.
- Kidney failure.
- Pulmonary embolism, or a blood clot in the lung.
- Myocarditis, an inflamed heart.
While it’s hard to say precisely whether these conditions were caused by COVID, they are most likely linked to it, says Dr. Schamess. A March 2022 study published in The Lancet Diabetes & Endocrinology, for example, found that people who had recovered from COVID-19 had a 40% higher risk of being diagnosed with type 2 diabetes over the next year.
“We don’t know for sure that infection with COVID-19 triggered someone’s diabetes – it may have been that they already had risk factors and the virus pushed them over the edge,” he says.
COVID-19 itself may also worsen conditions you already have, such as asthma, sleep apnea, or fibromyalgia. “We see patients with previously mild asthma who come in constantly coughing and wheezing, for example,” says Dr. Schamess. “They usually respond well once we start aggressive treatment.” That might include a continuous positive airway pressure, or CPAP, setup to help treat sleep apnea, or gabapentin to treat fibromyalgia symptoms.
Is it long COVID or something else?
Long COVID can cause a long list of symptoms, and they can easily mean other ailments. That’s one reason why, if your symptoms last for more than a month, it’s important to see a doctor, Ms. Baloun says. They can run a wide variety of tests to check for other conditions, such as a thyroid disorder or vitamin deficiency, that could be confused with long COVID.
They should also run blood tests such as D-dimer. This helps rule out a pulmonary embolism, which can be a complication of COVID-19 and also causes symptoms that may mimic long COVID, such as breathlessness and anxiety. They will also run tests to look for inflammation, Ms. Baloun says.
“These tests can’t provide definitive answers, but they can help provide clues as to what’s causing symptoms and whether they are related to long COVID,” she says.
What’s just as important, says Dr. Schamess, is a careful medical history. This can help pinpoint exactly when symptoms started, when they worsened, and whether anything else could have triggered them.
“I saw a patient recently who presented with symptoms of brain fog, memory loss, fatigue, headache, and sleep disturbance 5 months after she had COVID-19,” says Dr. Schamess. “After we talked, we realized that her symptoms were due to a fainting spell a couple of months earlier where she whacked her head very hard. She didn’t have long COVID – she had a concussion. But I wouldn’t have picked that up if I had just run a whole battery of tests.”
Ms. Stern agrees. “If you have long COVID, you may come across doctors who dismiss your symptoms, especially if your workups don’t show an obvious problem,” she says. “But you know your body. If it still seems like something is wrong, then you need to continue to push until you find answers.”
A version of this article first appeared on WebMD.com.
New Yorker Lyss Stern came down with COVID-19 at the beginning of the pandemic, in March 2020. She ran a 103° F fever for 5 days straight and was bedridden for several weeks. Yet symptoms such as a persistent headache and tinnitus, or ringing in her ears, lingered.
“Four months later, I still couldn’t walk four blocks without becoming winded,” says Ms. Stern, 48. Five months after her diagnosis, her doctors finally gave a name to her condition: long COVID.
Long COVID is known by many different names: long-haul COVID, postacute COVID-19, or even chronic COVID. It’s a general term used to describe the range of ongoing health problems people can have after their infection.
Another earlier report found that one in five COVID-19 survivors between the ages of 18 and 64, and one in four survivors aged at least 65, have a health condition that may be related to their previous bout with the virus.
Unfortunately, there’s no easy way to screen for long COVID.
“There’s no definite laboratory test to give us a diagnosis,” says Daniel Sterman, MD, director of the division of pulmonary, critical care and sleep medicine at NYU Langone Health in New York. “We’re also still working on a definition, since there’s a whole slew of symptoms associated with the condition.”
It’s a challenge that Ms. Stern is personally acquainted with after she bounced from doctor to doctor for several months before she found her way to the Center for Post-COVID Care at Mount Sinai Hospital in New York. “It was a relief to have an official diagnosis, even if it didn’t bring immediate answers,” she says.
What to look for
Many people who become infected with COVID-19 get symptoms that linger for 2-3 weeks after their infection has cleared, says Brittany Baloun, a certified nurse practitioner at the Cleveland Clinic. “It’s not unusual to feel some residual shortness of breath or heart palpitations, especially if you are exerting yourself,” she says. “The acute phase of COVID itself can last for up to 14 days. But if it’s been 30 days since you came down with the virus, and your symptoms are still there and not improving, it indicates some level of long COVID.”
More than 200 symptoms can be linked to long COVID. But perhaps the one that stands out the most is constant fatigue that interferes with daily life.
“We often hear that these patients can’t fold the laundry or take a short walk with their dog without feeling exhausted,” Ms. Baloun says.
This exhaustion may get worse after patients exercise or do something mentally taxing, a condition known as postexertional malaise.
“It can be crushing fatigue; I may clean my room for an hour and talk to a friend, and the next day feel like I can’t get out of bed,” says Allison Guy, 36, who was diagnosed with COVID in February 2021. She’s now a long-COVID advocate in Washington.
Other symptoms can be divided into different categories, which include cardiac/lung symptoms such as shortness of breath, coughing, chest pain, and heart palpitations, as well as neurologic symptoms.
One of the most common neurologic symptoms is brain fog, says Andrew Schamess, MD, a professor of internal medicine at Ohio State University Wexner Medical Center, Columbus, who runs its post-COVID recovery program. “Patients describe feeling ‘fuzzy’ or ‘spacey,’ and often report that they are forgetful or have memory problems,” he says. Others include:
- Headache.
- Sleep problems. One 2022 study from the Cleveland Clinic found that more than 40% of patients with long COVID reported sleep disturbances.
- Dizziness when standing.
- Pins-and-needles feelings.
- Changes in smell or taste.
- Depression or anxiety.
You could also have digestive symptoms such as diarrhea or stomach pain. Other symptoms include joint or muscle pain, rashes, or changes in menstrual cycles.
Risk of having other health conditions
People who have had COVID-19, particularly a severe case, may be more at risk of getting other health conditions, such as:
- Type 2 diabetes.
- Kidney failure.
- Pulmonary embolism, or a blood clot in the lung.
- Myocarditis, an inflamed heart.
While it’s hard to say precisely whether these conditions were caused by COVID, they are most likely linked to it, says Dr. Schamess. A March 2022 study published in The Lancet Diabetes & Endocrinology, for example, found that people who had recovered from COVID-19 had a 40% higher risk of being diagnosed with type 2 diabetes over the next year.
“We don’t know for sure that infection with COVID-19 triggered someone’s diabetes – it may have been that they already had risk factors and the virus pushed them over the edge,” he says.
COVID-19 itself may also worsen conditions you already have, such as asthma, sleep apnea, or fibromyalgia. “We see patients with previously mild asthma who come in constantly coughing and wheezing, for example,” says Dr. Schamess. “They usually respond well once we start aggressive treatment.” That might include a continuous positive airway pressure, or CPAP, setup to help treat sleep apnea, or gabapentin to treat fibromyalgia symptoms.
Is it long COVID or something else?
Long COVID can cause a long list of symptoms, and they can easily mean other ailments. That’s one reason why, if your symptoms last for more than a month, it’s important to see a doctor, Ms. Baloun says. They can run a wide variety of tests to check for other conditions, such as a thyroid disorder or vitamin deficiency, that could be confused with long COVID.
They should also run blood tests such as D-dimer. This helps rule out a pulmonary embolism, which can be a complication of COVID-19 and also causes symptoms that may mimic long COVID, such as breathlessness and anxiety. They will also run tests to look for inflammation, Ms. Baloun says.
“These tests can’t provide definitive answers, but they can help provide clues as to what’s causing symptoms and whether they are related to long COVID,” she says.
What’s just as important, says Dr. Schamess, is a careful medical history. This can help pinpoint exactly when symptoms started, when they worsened, and whether anything else could have triggered them.
“I saw a patient recently who presented with symptoms of brain fog, memory loss, fatigue, headache, and sleep disturbance 5 months after she had COVID-19,” says Dr. Schamess. “After we talked, we realized that her symptoms were due to a fainting spell a couple of months earlier where she whacked her head very hard. She didn’t have long COVID – she had a concussion. But I wouldn’t have picked that up if I had just run a whole battery of tests.”
Ms. Stern agrees. “If you have long COVID, you may come across doctors who dismiss your symptoms, especially if your workups don’t show an obvious problem,” she says. “But you know your body. If it still seems like something is wrong, then you need to continue to push until you find answers.”
A version of this article first appeared on WebMD.com.
Race-specific spirometry may miss emphysema diagnoses
An overreliance on spirometry to identify emphysema led to missed cases in Black individuals, particularly men, based on a secondary data analysis of 2,674 people.
“Over the last few years, there has been growing debate around the use of race adjustment in diagnostic algorithms and equations commonly used in medicine,” lead author Gabrielle Yi-Hui Liu, MD, said in an interview. “Whereas, previously it was common to accept racial or ethnic differences in clinical measures and outcomes as inherent differences among populations, there is now more recognition of how racism, socioeconomic status, and environmental exposures can cause these racial differences. Our initial interest in this study was to examine how the use of race-specific spirometry reference equations, and the use of spirometry in general, may be contributing to racial disparities.”
“Previous studies have suggested that the use of race-specific equations in spirometry can exacerbate racial inequities in healthcare outcomes by under-recognition of early disease in Black adults, and this study adds to that evidence,” said Suman Pal, MBBS, of the University of New Mexico, Albuquerque, in an interview.
“By examining the crucial ways in which systemic factors in medicine, such as race-specific equations, exacerbate racial inequities in healthcare, this study is a timely analysis in a moment of national reckoning of structural racism,” said Dr. Pal, who was not involved in the study.
In a study published in Annals of Internal Medicine, Dr. Liu and colleagues at Northwestern University, Chicago, conducted a secondary analysis of data from the CARDIA Lung study (Coronary Artery Risk Development In Young Adults).
The primary outcome of the study was the prevalence of emphysema among participants with various measures of normal spirometry results, stratified by sex and race. The normal results included an forced expiratory volume in 1 second (FEV1)–forced vital capacity (FVC) ratio greater than or equal to 0.7 or greater than or equal to the lower limit of normal. The participants also were stratified by FEV1 percent predicted, using race-specific reference equations, for FEV1 between 80% and 99% of predicted, or an FEV1 between 100% and 120% of predicted.
The study population included 485 Black men, 762 Black women, 659 White men, and 768 White women who received both a CT scan (in 2010-2011) and spirometry (obtained in 2015-2016) in the CARDIA study. The mean age of the participants at the spirometry exam was 55 years.
A total of 5.3% of the participants had emphysema after stratifying by FEV1-FVC ratio. The prevalence was significantly higher for Black men, compared with White men (12.3% vs. 4.0%; relative risk, 3.0), and for Black women, compared with White women (5.0% vs. 2.6%; RR, 1.9).
The association between Black race and emphysema risk persisted but decreased when the researchers used a race-neutral estimate.
When the participants were stratified by race-specific FEV1 percent predicted, 6.5% of individuals with a race-specific FEV1 between 80% and 99% had emphysema. After controlling for factors including age and smoking, emphysema was significantly more prevalent in Black men versus White men (15.5% vs. 4.0%) and in Black women, compared with White women (6.6% vs. 3.4%).
The racial difference persisted in men with a race-specific FEV1 between 100% and 120% of predicted. Of these, 4.0% had emphysema. The prevalence was significantly higher in Black men, compared with White men (13.9% vs. 2.2%), but similar between Black women and White women (2.6% vs. 2.0%).
The use of race-neutral equations reduced, but did not eliminate, these disparities, the researchers said.
The findings were limited by the lack of CT imaging data from the same visit as the final spirometry collection, the researchers noted. “Given that imaging was obtained 5 years before spirometry and emphysema is an irreversible finding, this may have led to an overall underestimation of the prevalence of emphysema.”
Spirometry alone misses cases
“We were surprised by the substantial rates of emphysema we saw among Black men in our cohort with normal spirometry,” Dr. Liu said in an interview. “We did not expect to find than more than one in eight Black men with an FEV1 between 100% and 120% predicted would have emphysema – a rate more than six times higher than White men with the same range of FEV1.”
“One takeaway is that we are likely missing a lot of people with impaired respiratory health or true lung disease by only using spirometry to diagnose COPD,” said Dr. Liu. In clinical practice, “physicians should consider ordering CT scans on patients with normal spirometry who have respiratory symptoms such as cough or shortness of breath. If emphysema is found, physicians should discuss mitigating any potential risk factors and consider the use of COPD medications such as inhalers.
“Our findings also support using race-neutral reference equations to interpret spirometry instead of race-specific equations. Racial disparities in rates of emphysema among those with ‘normal’ FEV1 [between 80% and 120% predicted], were attenuated or eliminated when race-neutral equations were used to calculate FEV1. This suggests that race-specific equations are normalizing worse lung health in Black adults,” Dr. Liu explained.
“We need to continue research into additional tools that can be used to assess respiratory health and diagnose COPD, while keeping in mind how these tools may affect racial disparities,” said Dr. Liu. “Our study suggests that our reliance on spirometry measures such as FEV1/FVC ratio and FEV1 is missing a number of people with respiratory symptoms and CT evidence of lung disease, and that this is disproportionately affecting Black adults in the United States.” Looking ahead, “it is important to find better tools to identify people with impaired respiratory health or early manifestations of disease so we can intercept chronic lung disease before it becomes clinically apparent and patients have sustained significant lung damage.”
The CARDIA study was supported by the National Heart, Lung, and Blood Institute in collaboration with the University of Alabama at Birmingham, Northwestern University, the University of Minnesota, and the Kaiser Foundation Research Institute. Dr. Liu was supported by a grant from the National Institutes of Health. The researchers had no financial conflicts to disclose. Dr. Pal had no financial conflicts to disclose.
*This article was updated 7/22/2022.
An overreliance on spirometry to identify emphysema led to missed cases in Black individuals, particularly men, based on a secondary data analysis of 2,674 people.
“Over the last few years, there has been growing debate around the use of race adjustment in diagnostic algorithms and equations commonly used in medicine,” lead author Gabrielle Yi-Hui Liu, MD, said in an interview. “Whereas, previously it was common to accept racial or ethnic differences in clinical measures and outcomes as inherent differences among populations, there is now more recognition of how racism, socioeconomic status, and environmental exposures can cause these racial differences. Our initial interest in this study was to examine how the use of race-specific spirometry reference equations, and the use of spirometry in general, may be contributing to racial disparities.”
“Previous studies have suggested that the use of race-specific equations in spirometry can exacerbate racial inequities in healthcare outcomes by under-recognition of early disease in Black adults, and this study adds to that evidence,” said Suman Pal, MBBS, of the University of New Mexico, Albuquerque, in an interview.
“By examining the crucial ways in which systemic factors in medicine, such as race-specific equations, exacerbate racial inequities in healthcare, this study is a timely analysis in a moment of national reckoning of structural racism,” said Dr. Pal, who was not involved in the study.
In a study published in Annals of Internal Medicine, Dr. Liu and colleagues at Northwestern University, Chicago, conducted a secondary analysis of data from the CARDIA Lung study (Coronary Artery Risk Development In Young Adults).
The primary outcome of the study was the prevalence of emphysema among participants with various measures of normal spirometry results, stratified by sex and race. The normal results included an forced expiratory volume in 1 second (FEV1)–forced vital capacity (FVC) ratio greater than or equal to 0.7 or greater than or equal to the lower limit of normal. The participants also were stratified by FEV1 percent predicted, using race-specific reference equations, for FEV1 between 80% and 99% of predicted, or an FEV1 between 100% and 120% of predicted.
The study population included 485 Black men, 762 Black women, 659 White men, and 768 White women who received both a CT scan (in 2010-2011) and spirometry (obtained in 2015-2016) in the CARDIA study. The mean age of the participants at the spirometry exam was 55 years.
A total of 5.3% of the participants had emphysema after stratifying by FEV1-FVC ratio. The prevalence was significantly higher for Black men, compared with White men (12.3% vs. 4.0%; relative risk, 3.0), and for Black women, compared with White women (5.0% vs. 2.6%; RR, 1.9).
The association between Black race and emphysema risk persisted but decreased when the researchers used a race-neutral estimate.
When the participants were stratified by race-specific FEV1 percent predicted, 6.5% of individuals with a race-specific FEV1 between 80% and 99% had emphysema. After controlling for factors including age and smoking, emphysema was significantly more prevalent in Black men versus White men (15.5% vs. 4.0%) and in Black women, compared with White women (6.6% vs. 3.4%).
The racial difference persisted in men with a race-specific FEV1 between 100% and 120% of predicted. Of these, 4.0% had emphysema. The prevalence was significantly higher in Black men, compared with White men (13.9% vs. 2.2%), but similar between Black women and White women (2.6% vs. 2.0%).
The use of race-neutral equations reduced, but did not eliminate, these disparities, the researchers said.
The findings were limited by the lack of CT imaging data from the same visit as the final spirometry collection, the researchers noted. “Given that imaging was obtained 5 years before spirometry and emphysema is an irreversible finding, this may have led to an overall underestimation of the prevalence of emphysema.”
Spirometry alone misses cases
“We were surprised by the substantial rates of emphysema we saw among Black men in our cohort with normal spirometry,” Dr. Liu said in an interview. “We did not expect to find than more than one in eight Black men with an FEV1 between 100% and 120% predicted would have emphysema – a rate more than six times higher than White men with the same range of FEV1.”
“One takeaway is that we are likely missing a lot of people with impaired respiratory health or true lung disease by only using spirometry to diagnose COPD,” said Dr. Liu. In clinical practice, “physicians should consider ordering CT scans on patients with normal spirometry who have respiratory symptoms such as cough or shortness of breath. If emphysema is found, physicians should discuss mitigating any potential risk factors and consider the use of COPD medications such as inhalers.
“Our findings also support using race-neutral reference equations to interpret spirometry instead of race-specific equations. Racial disparities in rates of emphysema among those with ‘normal’ FEV1 [between 80% and 120% predicted], were attenuated or eliminated when race-neutral equations were used to calculate FEV1. This suggests that race-specific equations are normalizing worse lung health in Black adults,” Dr. Liu explained.
“We need to continue research into additional tools that can be used to assess respiratory health and diagnose COPD, while keeping in mind how these tools may affect racial disparities,” said Dr. Liu. “Our study suggests that our reliance on spirometry measures such as FEV1/FVC ratio and FEV1 is missing a number of people with respiratory symptoms and CT evidence of lung disease, and that this is disproportionately affecting Black adults in the United States.” Looking ahead, “it is important to find better tools to identify people with impaired respiratory health or early manifestations of disease so we can intercept chronic lung disease before it becomes clinically apparent and patients have sustained significant lung damage.”
The CARDIA study was supported by the National Heart, Lung, and Blood Institute in collaboration with the University of Alabama at Birmingham, Northwestern University, the University of Minnesota, and the Kaiser Foundation Research Institute. Dr. Liu was supported by a grant from the National Institutes of Health. The researchers had no financial conflicts to disclose. Dr. Pal had no financial conflicts to disclose.
*This article was updated 7/22/2022.
An overreliance on spirometry to identify emphysema led to missed cases in Black individuals, particularly men, based on a secondary data analysis of 2,674 people.
“Over the last few years, there has been growing debate around the use of race adjustment in diagnostic algorithms and equations commonly used in medicine,” lead author Gabrielle Yi-Hui Liu, MD, said in an interview. “Whereas, previously it was common to accept racial or ethnic differences in clinical measures and outcomes as inherent differences among populations, there is now more recognition of how racism, socioeconomic status, and environmental exposures can cause these racial differences. Our initial interest in this study was to examine how the use of race-specific spirometry reference equations, and the use of spirometry in general, may be contributing to racial disparities.”
“Previous studies have suggested that the use of race-specific equations in spirometry can exacerbate racial inequities in healthcare outcomes by under-recognition of early disease in Black adults, and this study adds to that evidence,” said Suman Pal, MBBS, of the University of New Mexico, Albuquerque, in an interview.
“By examining the crucial ways in which systemic factors in medicine, such as race-specific equations, exacerbate racial inequities in healthcare, this study is a timely analysis in a moment of national reckoning of structural racism,” said Dr. Pal, who was not involved in the study.
In a study published in Annals of Internal Medicine, Dr. Liu and colleagues at Northwestern University, Chicago, conducted a secondary analysis of data from the CARDIA Lung study (Coronary Artery Risk Development In Young Adults).
The primary outcome of the study was the prevalence of emphysema among participants with various measures of normal spirometry results, stratified by sex and race. The normal results included an forced expiratory volume in 1 second (FEV1)–forced vital capacity (FVC) ratio greater than or equal to 0.7 or greater than or equal to the lower limit of normal. The participants also were stratified by FEV1 percent predicted, using race-specific reference equations, for FEV1 between 80% and 99% of predicted, or an FEV1 between 100% and 120% of predicted.
The study population included 485 Black men, 762 Black women, 659 White men, and 768 White women who received both a CT scan (in 2010-2011) and spirometry (obtained in 2015-2016) in the CARDIA study. The mean age of the participants at the spirometry exam was 55 years.
A total of 5.3% of the participants had emphysema after stratifying by FEV1-FVC ratio. The prevalence was significantly higher for Black men, compared with White men (12.3% vs. 4.0%; relative risk, 3.0), and for Black women, compared with White women (5.0% vs. 2.6%; RR, 1.9).
The association between Black race and emphysema risk persisted but decreased when the researchers used a race-neutral estimate.
When the participants were stratified by race-specific FEV1 percent predicted, 6.5% of individuals with a race-specific FEV1 between 80% and 99% had emphysema. After controlling for factors including age and smoking, emphysema was significantly more prevalent in Black men versus White men (15.5% vs. 4.0%) and in Black women, compared with White women (6.6% vs. 3.4%).
The racial difference persisted in men with a race-specific FEV1 between 100% and 120% of predicted. Of these, 4.0% had emphysema. The prevalence was significantly higher in Black men, compared with White men (13.9% vs. 2.2%), but similar between Black women and White women (2.6% vs. 2.0%).
The use of race-neutral equations reduced, but did not eliminate, these disparities, the researchers said.
The findings were limited by the lack of CT imaging data from the same visit as the final spirometry collection, the researchers noted. “Given that imaging was obtained 5 years before spirometry and emphysema is an irreversible finding, this may have led to an overall underestimation of the prevalence of emphysema.”
Spirometry alone misses cases
“We were surprised by the substantial rates of emphysema we saw among Black men in our cohort with normal spirometry,” Dr. Liu said in an interview. “We did not expect to find than more than one in eight Black men with an FEV1 between 100% and 120% predicted would have emphysema – a rate more than six times higher than White men with the same range of FEV1.”
“One takeaway is that we are likely missing a lot of people with impaired respiratory health or true lung disease by only using spirometry to diagnose COPD,” said Dr. Liu. In clinical practice, “physicians should consider ordering CT scans on patients with normal spirometry who have respiratory symptoms such as cough or shortness of breath. If emphysema is found, physicians should discuss mitigating any potential risk factors and consider the use of COPD medications such as inhalers.
“Our findings also support using race-neutral reference equations to interpret spirometry instead of race-specific equations. Racial disparities in rates of emphysema among those with ‘normal’ FEV1 [between 80% and 120% predicted], were attenuated or eliminated when race-neutral equations were used to calculate FEV1. This suggests that race-specific equations are normalizing worse lung health in Black adults,” Dr. Liu explained.
“We need to continue research into additional tools that can be used to assess respiratory health and diagnose COPD, while keeping in mind how these tools may affect racial disparities,” said Dr. Liu. “Our study suggests that our reliance on spirometry measures such as FEV1/FVC ratio and FEV1 is missing a number of people with respiratory symptoms and CT evidence of lung disease, and that this is disproportionately affecting Black adults in the United States.” Looking ahead, “it is important to find better tools to identify people with impaired respiratory health or early manifestations of disease so we can intercept chronic lung disease before it becomes clinically apparent and patients have sustained significant lung damage.”
The CARDIA study was supported by the National Heart, Lung, and Blood Institute in collaboration with the University of Alabama at Birmingham, Northwestern University, the University of Minnesota, and the Kaiser Foundation Research Institute. Dr. Liu was supported by a grant from the National Institutes of Health. The researchers had no financial conflicts to disclose. Dr. Pal had no financial conflicts to disclose.
*This article was updated 7/22/2022.
FROM ANNALS OF INTERNAL MEDICINE
Biden tests positive for COVID-19: White House
Biden, 79, is experiencing “very mild” symptoms, White House Press Secretary Karine Jean-Pierre said in a statement. The president is fully vaccinated and has been boosted twice and has started taking the antiviral Paxlovid since testing positive, Ms. Jean-Pierre said.
President Biden plans to isolate at the White House and “will continue to carry out all of his duties fully during that time,” the statement said.
“He has been in contact with members of the White House staff by phone this morning, and will participate in his planned meetings at the White House this morning via phone and Zoom from the residence.”
President Biden will return to in-person work after he tests negative.
This is a developing story. Please check back for updates. A version of this article first appeared on WebMD.com .
Biden, 79, is experiencing “very mild” symptoms, White House Press Secretary Karine Jean-Pierre said in a statement. The president is fully vaccinated and has been boosted twice and has started taking the antiviral Paxlovid since testing positive, Ms. Jean-Pierre said.
President Biden plans to isolate at the White House and “will continue to carry out all of his duties fully during that time,” the statement said.
“He has been in contact with members of the White House staff by phone this morning, and will participate in his planned meetings at the White House this morning via phone and Zoom from the residence.”
President Biden will return to in-person work after he tests negative.
This is a developing story. Please check back for updates. A version of this article first appeared on WebMD.com .
Biden, 79, is experiencing “very mild” symptoms, White House Press Secretary Karine Jean-Pierre said in a statement. The president is fully vaccinated and has been boosted twice and has started taking the antiviral Paxlovid since testing positive, Ms. Jean-Pierre said.
President Biden plans to isolate at the White House and “will continue to carry out all of his duties fully during that time,” the statement said.
“He has been in contact with members of the White House staff by phone this morning, and will participate in his planned meetings at the White House this morning via phone and Zoom from the residence.”
President Biden will return to in-person work after he tests negative.
This is a developing story. Please check back for updates. A version of this article first appeared on WebMD.com .
Job market for physicians, advanced practitioners rebounds after COVID-19 slump: Report
After a year of uncertainty and decline because of the COVID-19 pandemic, according to a recently released report from Merritt Hawkins, the physician search division of AMN Healthcare.
The study is based on an analysis of job search and consulting assignments that the firm conducted on behalf of its health care organization clients from April 1, 2021, to March 31, 2022.
“Search engagements were down a little over 30% in 2020, but by the end of 2021, everything started spiking dramatically to the point of where we were at a 34-year high,” Michael Belkin, divisional vice president with Merritt Hawkins, told this news organization. “The pendulum has gone all the way back. People are more interested in going out and seeing their physicians.”
Demand for physicians was suppressed during the peak of the pandemic, as many hospitals curtailed elective procedures and many patients refrained from entering a medical facility. A large backlog of patients needing care subsequently developed.
This, combined with an aging population and widespread chronic medical conditions, has caused a strong surge in demand for physicians and advanced practitioners, according to the report.
In addition to the volume of searches increasing, physician starting salaries have rebounded from the COVID-19 downturn.
Average starting salaries of 14 physician specialties tracked in 2021/2022 increased, while only 3 decreased. Orthopedic surgeons were offered an average of $565,000 to start, exclusive of signing bonuses and other incentives, up from $546,000 the previous year. Urologists were offered an average of $510,000 to start, up from $497,000; gastroenterologists were offered $474,000, up from $453,000; while radiologists were offered $455,000, up from $401,000.
Similarly, a recent Medscape study based on responses from more than 13,000 U.S. physicians across 29 specialties found that income for all physician specialists increased, with otolaryngologists, gastroenterologists, and dermatologists experiencing the greatest gains.
A new reality
While the job market for physicians and advanced practitioners has seemingly recovered, there are many differences between today’s working environment for clinicians and what existed during the pandemic.
First, specialists are now stepping into the spotlight, a position that primary care clinicians previously held. The majority of Merritt Hawkins’ search engagements (64%) in 2021/2022 were for physician specialists, including cardiologists, gastroenterologists, orthopedic surgeons, neurologists, oncologists, and others. Only 17% of the search engagements were for primary care physicians, down from 18% in 2020/2021 and 20% in 2019/2020.
“We’ve seen specialties bounce back faster. Of course, you’ve got the aging population; you’ve got people that want that specialized care,” Mr. Belkin said.
Advanced practitioners also are playing a more significant role in the postpandemic word. In fact, 19% of Merritt Hawkins’ search engagements were for advanced practitioners, including nurse practitioners (NPs), physician assistants, and certified registered nurse anesthetists, up from 18% the previous year and just 13% the year prior to that, indicating growing demand for nonphysician providers.
NPs, in fact, topped the list of most requested search engagements, underscoring a shift from traditional physician office-based primary care delivery settings toward “convenient care” settings such as urgent care centers and retail clinics that are largely staffed by NPs and other advanced practitioners.
Advanced practitioners are taking on more responsibility for primary care simply because there is a large number of these professionals ready to take on the challenge.
The health care industry was “not able to produce enough primary care physicians over the last decade. So advanced practitioners, I believe, have slowly started to work alongside those primary care physicians. In a lot of areas such as your retail space, your CVS, your Walmart, your Walgreens, your standalone urgent cares, they’ve stepped up,” Mr. Belkin said.
Advanced practitioners also are providing the convenience that consumers are increasingly demanding.
“We are a society that wants things immediately ... but it’s still a challenge to schedule an appointment with a physician. However, it’s less of a challenge to get into a retail clinic or an urgent care center or to schedule something through telehealth,” Mr. Belkin noted.
More than just money
With the job market strong, the challenge for health care organizations is to create competitive recruiting packages. Sure enough, 92% of candidates were offered signing bonuses in 2021/2022 compared with just 61% in 2020/2021.
The financial incentives, however, might not be enough. In this environment, health care organizations need to go beyond simply offering competitive salaries to new recruits. For example, clinicians are seeking flexibility, as many potential hires are seeking remote positions. In fact, 18% of radiology search engagements were for teleradiologists, while 15% of its search engagements for psychiatrists were for telepsychiatrists in 2021/2022.
“Right now, quality of life is a very important factor. It’s work-life balance. It’s sensitivity to the stresses that we just experienced over the last 2.5 years,” Mr. Belkin concluded. “There’s more sensitivity around the culture of the organizations. What’s the leadership like? How did the organization handle the pandemic? How do they respond?”
A version of this article first appeared on Medscape.com.
After a year of uncertainty and decline because of the COVID-19 pandemic, according to a recently released report from Merritt Hawkins, the physician search division of AMN Healthcare.
The study is based on an analysis of job search and consulting assignments that the firm conducted on behalf of its health care organization clients from April 1, 2021, to March 31, 2022.
“Search engagements were down a little over 30% in 2020, but by the end of 2021, everything started spiking dramatically to the point of where we were at a 34-year high,” Michael Belkin, divisional vice president with Merritt Hawkins, told this news organization. “The pendulum has gone all the way back. People are more interested in going out and seeing their physicians.”
Demand for physicians was suppressed during the peak of the pandemic, as many hospitals curtailed elective procedures and many patients refrained from entering a medical facility. A large backlog of patients needing care subsequently developed.
This, combined with an aging population and widespread chronic medical conditions, has caused a strong surge in demand for physicians and advanced practitioners, according to the report.
In addition to the volume of searches increasing, physician starting salaries have rebounded from the COVID-19 downturn.
Average starting salaries of 14 physician specialties tracked in 2021/2022 increased, while only 3 decreased. Orthopedic surgeons were offered an average of $565,000 to start, exclusive of signing bonuses and other incentives, up from $546,000 the previous year. Urologists were offered an average of $510,000 to start, up from $497,000; gastroenterologists were offered $474,000, up from $453,000; while radiologists were offered $455,000, up from $401,000.
Similarly, a recent Medscape study based on responses from more than 13,000 U.S. physicians across 29 specialties found that income for all physician specialists increased, with otolaryngologists, gastroenterologists, and dermatologists experiencing the greatest gains.
A new reality
While the job market for physicians and advanced practitioners has seemingly recovered, there are many differences between today’s working environment for clinicians and what existed during the pandemic.
First, specialists are now stepping into the spotlight, a position that primary care clinicians previously held. The majority of Merritt Hawkins’ search engagements (64%) in 2021/2022 were for physician specialists, including cardiologists, gastroenterologists, orthopedic surgeons, neurologists, oncologists, and others. Only 17% of the search engagements were for primary care physicians, down from 18% in 2020/2021 and 20% in 2019/2020.
“We’ve seen specialties bounce back faster. Of course, you’ve got the aging population; you’ve got people that want that specialized care,” Mr. Belkin said.
Advanced practitioners also are playing a more significant role in the postpandemic word. In fact, 19% of Merritt Hawkins’ search engagements were for advanced practitioners, including nurse practitioners (NPs), physician assistants, and certified registered nurse anesthetists, up from 18% the previous year and just 13% the year prior to that, indicating growing demand for nonphysician providers.
NPs, in fact, topped the list of most requested search engagements, underscoring a shift from traditional physician office-based primary care delivery settings toward “convenient care” settings such as urgent care centers and retail clinics that are largely staffed by NPs and other advanced practitioners.
Advanced practitioners are taking on more responsibility for primary care simply because there is a large number of these professionals ready to take on the challenge.
The health care industry was “not able to produce enough primary care physicians over the last decade. So advanced practitioners, I believe, have slowly started to work alongside those primary care physicians. In a lot of areas such as your retail space, your CVS, your Walmart, your Walgreens, your standalone urgent cares, they’ve stepped up,” Mr. Belkin said.
Advanced practitioners also are providing the convenience that consumers are increasingly demanding.
“We are a society that wants things immediately ... but it’s still a challenge to schedule an appointment with a physician. However, it’s less of a challenge to get into a retail clinic or an urgent care center or to schedule something through telehealth,” Mr. Belkin noted.
More than just money
With the job market strong, the challenge for health care organizations is to create competitive recruiting packages. Sure enough, 92% of candidates were offered signing bonuses in 2021/2022 compared with just 61% in 2020/2021.
The financial incentives, however, might not be enough. In this environment, health care organizations need to go beyond simply offering competitive salaries to new recruits. For example, clinicians are seeking flexibility, as many potential hires are seeking remote positions. In fact, 18% of radiology search engagements were for teleradiologists, while 15% of its search engagements for psychiatrists were for telepsychiatrists in 2021/2022.
“Right now, quality of life is a very important factor. It’s work-life balance. It’s sensitivity to the stresses that we just experienced over the last 2.5 years,” Mr. Belkin concluded. “There’s more sensitivity around the culture of the organizations. What’s the leadership like? How did the organization handle the pandemic? How do they respond?”
A version of this article first appeared on Medscape.com.
After a year of uncertainty and decline because of the COVID-19 pandemic, according to a recently released report from Merritt Hawkins, the physician search division of AMN Healthcare.
The study is based on an analysis of job search and consulting assignments that the firm conducted on behalf of its health care organization clients from April 1, 2021, to March 31, 2022.
“Search engagements were down a little over 30% in 2020, but by the end of 2021, everything started spiking dramatically to the point of where we were at a 34-year high,” Michael Belkin, divisional vice president with Merritt Hawkins, told this news organization. “The pendulum has gone all the way back. People are more interested in going out and seeing their physicians.”
Demand for physicians was suppressed during the peak of the pandemic, as many hospitals curtailed elective procedures and many patients refrained from entering a medical facility. A large backlog of patients needing care subsequently developed.
This, combined with an aging population and widespread chronic medical conditions, has caused a strong surge in demand for physicians and advanced practitioners, according to the report.
In addition to the volume of searches increasing, physician starting salaries have rebounded from the COVID-19 downturn.
Average starting salaries of 14 physician specialties tracked in 2021/2022 increased, while only 3 decreased. Orthopedic surgeons were offered an average of $565,000 to start, exclusive of signing bonuses and other incentives, up from $546,000 the previous year. Urologists were offered an average of $510,000 to start, up from $497,000; gastroenterologists were offered $474,000, up from $453,000; while radiologists were offered $455,000, up from $401,000.
Similarly, a recent Medscape study based on responses from more than 13,000 U.S. physicians across 29 specialties found that income for all physician specialists increased, with otolaryngologists, gastroenterologists, and dermatologists experiencing the greatest gains.
A new reality
While the job market for physicians and advanced practitioners has seemingly recovered, there are many differences between today’s working environment for clinicians and what existed during the pandemic.
First, specialists are now stepping into the spotlight, a position that primary care clinicians previously held. The majority of Merritt Hawkins’ search engagements (64%) in 2021/2022 were for physician specialists, including cardiologists, gastroenterologists, orthopedic surgeons, neurologists, oncologists, and others. Only 17% of the search engagements were for primary care physicians, down from 18% in 2020/2021 and 20% in 2019/2020.
“We’ve seen specialties bounce back faster. Of course, you’ve got the aging population; you’ve got people that want that specialized care,” Mr. Belkin said.
Advanced practitioners also are playing a more significant role in the postpandemic word. In fact, 19% of Merritt Hawkins’ search engagements were for advanced practitioners, including nurse practitioners (NPs), physician assistants, and certified registered nurse anesthetists, up from 18% the previous year and just 13% the year prior to that, indicating growing demand for nonphysician providers.
NPs, in fact, topped the list of most requested search engagements, underscoring a shift from traditional physician office-based primary care delivery settings toward “convenient care” settings such as urgent care centers and retail clinics that are largely staffed by NPs and other advanced practitioners.
Advanced practitioners are taking on more responsibility for primary care simply because there is a large number of these professionals ready to take on the challenge.
The health care industry was “not able to produce enough primary care physicians over the last decade. So advanced practitioners, I believe, have slowly started to work alongside those primary care physicians. In a lot of areas such as your retail space, your CVS, your Walmart, your Walgreens, your standalone urgent cares, they’ve stepped up,” Mr. Belkin said.
Advanced practitioners also are providing the convenience that consumers are increasingly demanding.
“We are a society that wants things immediately ... but it’s still a challenge to schedule an appointment with a physician. However, it’s less of a challenge to get into a retail clinic or an urgent care center or to schedule something through telehealth,” Mr. Belkin noted.
More than just money
With the job market strong, the challenge for health care organizations is to create competitive recruiting packages. Sure enough, 92% of candidates were offered signing bonuses in 2021/2022 compared with just 61% in 2020/2021.
The financial incentives, however, might not be enough. In this environment, health care organizations need to go beyond simply offering competitive salaries to new recruits. For example, clinicians are seeking flexibility, as many potential hires are seeking remote positions. In fact, 18% of radiology search engagements were for teleradiologists, while 15% of its search engagements for psychiatrists were for telepsychiatrists in 2021/2022.
“Right now, quality of life is a very important factor. It’s work-life balance. It’s sensitivity to the stresses that we just experienced over the last 2.5 years,” Mr. Belkin concluded. “There’s more sensitivity around the culture of the organizations. What’s the leadership like? How did the organization handle the pandemic? How do they respond?”
A version of this article first appeared on Medscape.com.
What are your weaknesses?
In a video posted to TikTok by the comedian Will Flanary, MD, better known to his followers as Dr. Glaucomflecken, he imitates a neurosurgical residency interview. With glasses perched on the bridge of his nose, Dr. Glaucomflecken poses as the attending, asking: “What are your weaknesses?”
The residency applicant answers without hesitation: “My physiological need for sleep.” “What are your strengths?” The resident replies with the hard, steely stare of the determined and uninitiated: “My desire to eliminate my physiological need for sleep.”
If you follow Dr. Glaucomflecken on Twitter, you might know the skit I’m referencing. For many physicians and physicians-in-training, what makes the satire successful is its reflection of reality.
Many things have changed in medicine since his time, but the tired trope of the sleepless surgeon hangs on. Undaunted, I spent my second and third year of medical school accumulating accolades, conducting research, and connecting with mentors with the singular goal of joining the surgical ranks.
Midway through my third year, I completed a month-long surgical subinternship designed to give students a taste of what life would look like as an intern. I loved the operating room; it felt like the difference between being on dry land and being underwater. There were fewer distractions – your patient in the spotlight while everything else receded to the shadows.
However, as the month wore on, something stronger took hold. I couldn’t keep my eyes open in the darkened operating rooms and had to decline stools, fearing that I would fall asleep if I sat down.
On early morning prerounds, it’s 4:50 a.m. when I glance at the clock and pull back the curtain, already apologizing. My patient rolls over, flashing a wry smile. “Do you ever go home?” I’ve seen residents respond to this exact question in various ways. I live here. Yes. No. Soon. Not enough. My partner doesn’t think so.
There are days and, yes, years when we are led to believe this is what we live for: to be constantly available to our patients. It feels like a hollow victory when the patient, 2 days out from a total colectomy, begins to worry about your personal life. I ask her how she slept (not enough), any fevers (no), vomiting (no), urinating (I pause – she has a catheter).
My favorite part of these early morning rounds is the pause in my scripted litany of questions to listen to heart and lungs. It never fails to feel sacred: Patients become so quiet and still that I can’t help but think they have faith in me. Without prompting, she slides the back of her hospital gown forward like a curtain, already taking deep breaths so I can hear her lungs.
I look outside. The streetlights are still on, and from the seventh-floor window, I can watch staff making their way through the sliding double-doors, just beyond the yellowed pools of streetlight. I smile. I love medicine. I’m so tired.
For many in medicine, we are treated, and thus behave, as though our ability to manipulate physiology should also apply within the borders of our bodies: commanding less sleep, food, or bathroom breaks.
It places health care workers solidly in the realm of superhuman, living beyond one’s corporeal needs. The pandemic only heightened this misappropriation – adding hero and setting out a pedestal for health care workers to make their ungainly ascent. This kind of unsolicited admiration implicitly implies inhumanness, an otherness.
What would it look like if we started treating ourselves less like physicians and more like patients? I wish I was offering a solution, but really this is just a story.
To students rising through the ranks of medical training, identify what it is you need early and often. I can count on one hand how many physicians I’ve seen take a lunch break – even 10 minutes. Embrace hard work and self-preservation equally. My hope is that if enough of us take this path, it just might become a matter of course.
Dr. Meffert is a resident in the department of emergency medicine, MedStar Georgetown University Hospital, Washington Hospital Center, Washington. Dr. Meffert disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a video posted to TikTok by the comedian Will Flanary, MD, better known to his followers as Dr. Glaucomflecken, he imitates a neurosurgical residency interview. With glasses perched on the bridge of his nose, Dr. Glaucomflecken poses as the attending, asking: “What are your weaknesses?”
The residency applicant answers without hesitation: “My physiological need for sleep.” “What are your strengths?” The resident replies with the hard, steely stare of the determined and uninitiated: “My desire to eliminate my physiological need for sleep.”
If you follow Dr. Glaucomflecken on Twitter, you might know the skit I’m referencing. For many physicians and physicians-in-training, what makes the satire successful is its reflection of reality.
Many things have changed in medicine since his time, but the tired trope of the sleepless surgeon hangs on. Undaunted, I spent my second and third year of medical school accumulating accolades, conducting research, and connecting with mentors with the singular goal of joining the surgical ranks.
Midway through my third year, I completed a month-long surgical subinternship designed to give students a taste of what life would look like as an intern. I loved the operating room; it felt like the difference between being on dry land and being underwater. There were fewer distractions – your patient in the spotlight while everything else receded to the shadows.
However, as the month wore on, something stronger took hold. I couldn’t keep my eyes open in the darkened operating rooms and had to decline stools, fearing that I would fall asleep if I sat down.
On early morning prerounds, it’s 4:50 a.m. when I glance at the clock and pull back the curtain, already apologizing. My patient rolls over, flashing a wry smile. “Do you ever go home?” I’ve seen residents respond to this exact question in various ways. I live here. Yes. No. Soon. Not enough. My partner doesn’t think so.
There are days and, yes, years when we are led to believe this is what we live for: to be constantly available to our patients. It feels like a hollow victory when the patient, 2 days out from a total colectomy, begins to worry about your personal life. I ask her how she slept (not enough), any fevers (no), vomiting (no), urinating (I pause – she has a catheter).
My favorite part of these early morning rounds is the pause in my scripted litany of questions to listen to heart and lungs. It never fails to feel sacred: Patients become so quiet and still that I can’t help but think they have faith in me. Without prompting, she slides the back of her hospital gown forward like a curtain, already taking deep breaths so I can hear her lungs.
I look outside. The streetlights are still on, and from the seventh-floor window, I can watch staff making their way through the sliding double-doors, just beyond the yellowed pools of streetlight. I smile. I love medicine. I’m so tired.
For many in medicine, we are treated, and thus behave, as though our ability to manipulate physiology should also apply within the borders of our bodies: commanding less sleep, food, or bathroom breaks.
It places health care workers solidly in the realm of superhuman, living beyond one’s corporeal needs. The pandemic only heightened this misappropriation – adding hero and setting out a pedestal for health care workers to make their ungainly ascent. This kind of unsolicited admiration implicitly implies inhumanness, an otherness.
What would it look like if we started treating ourselves less like physicians and more like patients? I wish I was offering a solution, but really this is just a story.
To students rising through the ranks of medical training, identify what it is you need early and often. I can count on one hand how many physicians I’ve seen take a lunch break – even 10 minutes. Embrace hard work and self-preservation equally. My hope is that if enough of us take this path, it just might become a matter of course.
Dr. Meffert is a resident in the department of emergency medicine, MedStar Georgetown University Hospital, Washington Hospital Center, Washington. Dr. Meffert disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a video posted to TikTok by the comedian Will Flanary, MD, better known to his followers as Dr. Glaucomflecken, he imitates a neurosurgical residency interview. With glasses perched on the bridge of his nose, Dr. Glaucomflecken poses as the attending, asking: “What are your weaknesses?”
The residency applicant answers without hesitation: “My physiological need for sleep.” “What are your strengths?” The resident replies with the hard, steely stare of the determined and uninitiated: “My desire to eliminate my physiological need for sleep.”
If you follow Dr. Glaucomflecken on Twitter, you might know the skit I’m referencing. For many physicians and physicians-in-training, what makes the satire successful is its reflection of reality.
Many things have changed in medicine since his time, but the tired trope of the sleepless surgeon hangs on. Undaunted, I spent my second and third year of medical school accumulating accolades, conducting research, and connecting with mentors with the singular goal of joining the surgical ranks.
Midway through my third year, I completed a month-long surgical subinternship designed to give students a taste of what life would look like as an intern. I loved the operating room; it felt like the difference between being on dry land and being underwater. There were fewer distractions – your patient in the spotlight while everything else receded to the shadows.
However, as the month wore on, something stronger took hold. I couldn’t keep my eyes open in the darkened operating rooms and had to decline stools, fearing that I would fall asleep if I sat down.
On early morning prerounds, it’s 4:50 a.m. when I glance at the clock and pull back the curtain, already apologizing. My patient rolls over, flashing a wry smile. “Do you ever go home?” I’ve seen residents respond to this exact question in various ways. I live here. Yes. No. Soon. Not enough. My partner doesn’t think so.
There are days and, yes, years when we are led to believe this is what we live for: to be constantly available to our patients. It feels like a hollow victory when the patient, 2 days out from a total colectomy, begins to worry about your personal life. I ask her how she slept (not enough), any fevers (no), vomiting (no), urinating (I pause – she has a catheter).
My favorite part of these early morning rounds is the pause in my scripted litany of questions to listen to heart and lungs. It never fails to feel sacred: Patients become so quiet and still that I can’t help but think they have faith in me. Without prompting, she slides the back of her hospital gown forward like a curtain, already taking deep breaths so I can hear her lungs.
I look outside. The streetlights are still on, and from the seventh-floor window, I can watch staff making their way through the sliding double-doors, just beyond the yellowed pools of streetlight. I smile. I love medicine. I’m so tired.
For many in medicine, we are treated, and thus behave, as though our ability to manipulate physiology should also apply within the borders of our bodies: commanding less sleep, food, or bathroom breaks.
It places health care workers solidly in the realm of superhuman, living beyond one’s corporeal needs. The pandemic only heightened this misappropriation – adding hero and setting out a pedestal for health care workers to make their ungainly ascent. This kind of unsolicited admiration implicitly implies inhumanness, an otherness.
What would it look like if we started treating ourselves less like physicians and more like patients? I wish I was offering a solution, but really this is just a story.
To students rising through the ranks of medical training, identify what it is you need early and often. I can count on one hand how many physicians I’ve seen take a lunch break – even 10 minutes. Embrace hard work and self-preservation equally. My hope is that if enough of us take this path, it just might become a matter of course.
Dr. Meffert is a resident in the department of emergency medicine, MedStar Georgetown University Hospital, Washington Hospital Center, Washington. Dr. Meffert disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Charcoal could be the cure for the common high-fat diet
Charcoal won’t let high-fat diet weigh you down
Do you want to be the funniest person alive? Of course you do. It’s really simple too, just one joke can make you the greatest comedian of all time. All you have to do is go camping and cook food over a roaring campfire. When someone drops food into the fire (which they always will), get ready. Once they fish out the offending food, which is almost certainly coated in hot coals, tell them: “Ah, eat it anyway. A little texture never hurt!” Trust us, most hilarious and original gag of all time.
But before your hapless friend brushes off his hot dog and forces a laugh, consider this: Japanese researchers have found that a charcoal supplement can prevent weight gain in mice consuming a high-fat diet. Charcoal is actually quite the helpful substance, and not just for grilling. It’s been used as medicine for hundreds of years and even today is used as a treatment for drug overdose and excess gas and flatulence.
The study involved two groups of mice: One was fed a normal diet, the other a high-fat diet. After 12 weeks, the high-fat diet mice had gained weight. At that point, edible activated charcoal was added to their diet. From that point, weight gain was similar between the two groups, and the amount of bile acid, cholesterol, triglyceride, and fatty acid excreted by the high-fat mice increased by two to four times.
The researchers supported the notion that consuming an activated charcoal supplement before or while eating fatty food could prevent weight gain from said fatty food. Which works out well for the classic American barbecue, which is traditionally both high in fat and charcoal. All you have to do is buy some extra charcoal briquettes to pass around and munch on with your friends. Now that’s a party we can get behind.
There’s awake, and then there’s neurologically awake
Time to toss another urban legend onto the trash heap of history. Say goodbye to the benefits of uninterrupted sleep. It’s a fraud, a fake, a myth, a hit or myth, a swing and a myth, an old wives’ tale. You can stuff it and put it on a shelf next to Bigfoot, the Slender Man, and Twinkies.

We all thought we needed 8 hours of uninterrupted sleep every night, but guess who we forgot to tell? Our brains. They’ve been doing exactly the opposite all along, laughing at us the whole time. Smug SOBs.
To straighten out this mess, let’s bring in a scientist, Celia Kjaerby of the Center for Translational Neuromedicine at the University of Copenhagen: “You may think that sleep is a constant state that you are in, and then you wake up. But there is a lot more to sleep than meets the eye. We have learned that noradrenaline causes you to wake up more than 100 times a night. And that is during perfectly normal sleep.”
Those 100 or so sleep interruptions are so brief that we don’t even notice, but they are very important, according to a study conducted at the university. Those tiny little wake-up calls are “the essence for the part of sleep that makes us wake up rested and which enables us to remember what we learned the day before. ... The very short awakenings are created by waves of norepinephrine [and they] reset the brain so that it is ready to store memory when you dive back into sleep,” lead author Maiken Nedergaard, MD, explained.
The investigators compared the level of noradrenaline in sleeping mice with their electrical activity and found that the hormone constantly increased and decreased in a wavelike pattern. A high level meant that the animal was neurologically awake. Deeper valleys between the high points meant better sleep, and the mice with the “highest number of deep noradrenaline valleys were also the ones with the best memory,” the team said in their written statement.
Not just the best memory, they said, but “super memory.” That, of course, was enough to get the attention of Marvel Comics, so the next Disney superhero blockbuster will feature Nocturna, the queen of the night. Her power? Never forgets. Her archnemesis? The Insomniac. Her catchphrase? “Let me sleep on it.”
Words can hurt, literally
Growing up, we’re sure you heard the “sticks and stones” rhyme. Maybe you’ve even recited it once or twice to defend yourself. Well, forget it, because words can hurt and your brain knows it.

In a new study published in Frontiers in Communication, Marijn Struiksma, PhD, of Utrecht University, and colleagues incorporated the use of electroencephalography (EEG) and skin conductance on 79 women to see how words (specifically insults) actually affect the human body.
Each subject was asked to read three different types of statements: an insult, a compliment, and something factual but neutral. Half of the statements contained the subject’s name and half used somebody else’s. The participants were told that these statements were collected from three men.
Nobody interacted with each other, and the setting was completely clinical, yet the results were unmistakable. The EEG showed an effect in P2 amplitude with repetitive insults, no matter who it was about. Even though the insults weren’t real and the participants were aware of it, the brain still recognized them as hurtful, coming across as “mini slaps in the face,” Dr. Struiksma noted in a written statement.
The researchers noted that more needs to be done to better understand the long-term effects that insults can have and create a deeper understanding between words and emotion, but studying the effects of insults in a real-life setting is ethically tricky. This study is a start.
So, yeah, sticks and stones can break your bones, but words will actually hurt you.
This article was updated 7/21/22.
Charcoal won’t let high-fat diet weigh you down
Do you want to be the funniest person alive? Of course you do. It’s really simple too, just one joke can make you the greatest comedian of all time. All you have to do is go camping and cook food over a roaring campfire. When someone drops food into the fire (which they always will), get ready. Once they fish out the offending food, which is almost certainly coated in hot coals, tell them: “Ah, eat it anyway. A little texture never hurt!” Trust us, most hilarious and original gag of all time.
But before your hapless friend brushes off his hot dog and forces a laugh, consider this: Japanese researchers have found that a charcoal supplement can prevent weight gain in mice consuming a high-fat diet. Charcoal is actually quite the helpful substance, and not just for grilling. It’s been used as medicine for hundreds of years and even today is used as a treatment for drug overdose and excess gas and flatulence.
The study involved two groups of mice: One was fed a normal diet, the other a high-fat diet. After 12 weeks, the high-fat diet mice had gained weight. At that point, edible activated charcoal was added to their diet. From that point, weight gain was similar between the two groups, and the amount of bile acid, cholesterol, triglyceride, and fatty acid excreted by the high-fat mice increased by two to four times.
The researchers supported the notion that consuming an activated charcoal supplement before or while eating fatty food could prevent weight gain from said fatty food. Which works out well for the classic American barbecue, which is traditionally both high in fat and charcoal. All you have to do is buy some extra charcoal briquettes to pass around and munch on with your friends. Now that’s a party we can get behind.
There’s awake, and then there’s neurologically awake
Time to toss another urban legend onto the trash heap of history. Say goodbye to the benefits of uninterrupted sleep. It’s a fraud, a fake, a myth, a hit or myth, a swing and a myth, an old wives’ tale. You can stuff it and put it on a shelf next to Bigfoot, the Slender Man, and Twinkies.
We all thought we needed 8 hours of uninterrupted sleep every night, but guess who we forgot to tell? Our brains. They’ve been doing exactly the opposite all along, laughing at us the whole time. Smug SOBs.
To straighten out this mess, let’s bring in a scientist, Celia Kjaerby of the Center for Translational Neuromedicine at the University of Copenhagen: “You may think that sleep is a constant state that you are in, and then you wake up. But there is a lot more to sleep than meets the eye. We have learned that noradrenaline causes you to wake up more than 100 times a night. And that is during perfectly normal sleep.”
Those 100 or so sleep interruptions are so brief that we don’t even notice, but they are very important, according to a study conducted at the university. Those tiny little wake-up calls are “the essence for the part of sleep that makes us wake up rested and which enables us to remember what we learned the day before. ... The very short awakenings are created by waves of norepinephrine [and they] reset the brain so that it is ready to store memory when you dive back into sleep,” lead author Maiken Nedergaard, MD, explained.
The investigators compared the level of noradrenaline in sleeping mice with their electrical activity and found that the hormone constantly increased and decreased in a wavelike pattern. A high level meant that the animal was neurologically awake. Deeper valleys between the high points meant better sleep, and the mice with the “highest number of deep noradrenaline valleys were also the ones with the best memory,” the team said in their written statement.
Not just the best memory, they said, but “super memory.” That, of course, was enough to get the attention of Marvel Comics, so the next Disney superhero blockbuster will feature Nocturna, the queen of the night. Her power? Never forgets. Her archnemesis? The Insomniac. Her catchphrase? “Let me sleep on it.”
Words can hurt, literally
Growing up, we’re sure you heard the “sticks and stones” rhyme. Maybe you’ve even recited it once or twice to defend yourself. Well, forget it, because words can hurt and your brain knows it.
In a new study published in Frontiers in Communication, Marijn Struiksma, PhD, of Utrecht University, and colleagues incorporated the use of electroencephalography (EEG) and skin conductance on 79 women to see how words (specifically insults) actually affect the human body.
Each subject was asked to read three different types of statements: an insult, a compliment, and something factual but neutral. Half of the statements contained the subject’s name and half used somebody else’s. The participants were told that these statements were collected from three men.
Nobody interacted with each other, and the setting was completely clinical, yet the results were unmistakable. The EEG showed an effect in P2 amplitude with repetitive insults, no matter who it was about. Even though the insults weren’t real and the participants were aware of it, the brain still recognized them as hurtful, coming across as “mini slaps in the face,” Dr. Struiksma noted in a written statement.
The researchers noted that more needs to be done to better understand the long-term effects that insults can have and create a deeper understanding between words and emotion, but studying the effects of insults in a real-life setting is ethically tricky. This study is a start.
So, yeah, sticks and stones can break your bones, but words will actually hurt you.
This article was updated 7/21/22.
Charcoal won’t let high-fat diet weigh you down
Do you want to be the funniest person alive? Of course you do. It’s really simple too, just one joke can make you the greatest comedian of all time. All you have to do is go camping and cook food over a roaring campfire. When someone drops food into the fire (which they always will), get ready. Once they fish out the offending food, which is almost certainly coated in hot coals, tell them: “Ah, eat it anyway. A little texture never hurt!” Trust us, most hilarious and original gag of all time.
But before your hapless friend brushes off his hot dog and forces a laugh, consider this: Japanese researchers have found that a charcoal supplement can prevent weight gain in mice consuming a high-fat diet. Charcoal is actually quite the helpful substance, and not just for grilling. It’s been used as medicine for hundreds of years and even today is used as a treatment for drug overdose and excess gas and flatulence.
The study involved two groups of mice: One was fed a normal diet, the other a high-fat diet. After 12 weeks, the high-fat diet mice had gained weight. At that point, edible activated charcoal was added to their diet. From that point, weight gain was similar between the two groups, and the amount of bile acid, cholesterol, triglyceride, and fatty acid excreted by the high-fat mice increased by two to four times.
The researchers supported the notion that consuming an activated charcoal supplement before or while eating fatty food could prevent weight gain from said fatty food. Which works out well for the classic American barbecue, which is traditionally both high in fat and charcoal. All you have to do is buy some extra charcoal briquettes to pass around and munch on with your friends. Now that’s a party we can get behind.
There’s awake, and then there’s neurologically awake
Time to toss another urban legend onto the trash heap of history. Say goodbye to the benefits of uninterrupted sleep. It’s a fraud, a fake, a myth, a hit or myth, a swing and a myth, an old wives’ tale. You can stuff it and put it on a shelf next to Bigfoot, the Slender Man, and Twinkies.
We all thought we needed 8 hours of uninterrupted sleep every night, but guess who we forgot to tell? Our brains. They’ve been doing exactly the opposite all along, laughing at us the whole time. Smug SOBs.
To straighten out this mess, let’s bring in a scientist, Celia Kjaerby of the Center for Translational Neuromedicine at the University of Copenhagen: “You may think that sleep is a constant state that you are in, and then you wake up. But there is a lot more to sleep than meets the eye. We have learned that noradrenaline causes you to wake up more than 100 times a night. And that is during perfectly normal sleep.”
Those 100 or so sleep interruptions are so brief that we don’t even notice, but they are very important, according to a study conducted at the university. Those tiny little wake-up calls are “the essence for the part of sleep that makes us wake up rested and which enables us to remember what we learned the day before. ... The very short awakenings are created by waves of norepinephrine [and they] reset the brain so that it is ready to store memory when you dive back into sleep,” lead author Maiken Nedergaard, MD, explained.
The investigators compared the level of noradrenaline in sleeping mice with their electrical activity and found that the hormone constantly increased and decreased in a wavelike pattern. A high level meant that the animal was neurologically awake. Deeper valleys between the high points meant better sleep, and the mice with the “highest number of deep noradrenaline valleys were also the ones with the best memory,” the team said in their written statement.
Not just the best memory, they said, but “super memory.” That, of course, was enough to get the attention of Marvel Comics, so the next Disney superhero blockbuster will feature Nocturna, the queen of the night. Her power? Never forgets. Her archnemesis? The Insomniac. Her catchphrase? “Let me sleep on it.”
Words can hurt, literally
Growing up, we’re sure you heard the “sticks and stones” rhyme. Maybe you’ve even recited it once or twice to defend yourself. Well, forget it, because words can hurt and your brain knows it.
In a new study published in Frontiers in Communication, Marijn Struiksma, PhD, of Utrecht University, and colleagues incorporated the use of electroencephalography (EEG) and skin conductance on 79 women to see how words (specifically insults) actually affect the human body.
Each subject was asked to read three different types of statements: an insult, a compliment, and something factual but neutral. Half of the statements contained the subject’s name and half used somebody else’s. The participants were told that these statements were collected from three men.
Nobody interacted with each other, and the setting was completely clinical, yet the results were unmistakable. The EEG showed an effect in P2 amplitude with repetitive insults, no matter who it was about. Even though the insults weren’t real and the participants were aware of it, the brain still recognized them as hurtful, coming across as “mini slaps in the face,” Dr. Struiksma noted in a written statement.
The researchers noted that more needs to be done to better understand the long-term effects that insults can have and create a deeper understanding between words and emotion, but studying the effects of insults in a real-life setting is ethically tricky. This study is a start.
So, yeah, sticks and stones can break your bones, but words will actually hurt you.
This article was updated 7/21/22.
Steroids no cure for obstructive sleep apnea in children
Children with obstructive sleep apnea syndrome (OSAS) who undergo treatment with intranasal corticosteroids (INCS) did not experience significant improvement in polysomnographic, neurobehavioral, and other symptoms at 3 and 12 months of treatment. At 12 months of INCS treatment, there was a statistically significant but not clinically relevant reduction in the obstructive apnea hypopnea index (OHAI).
“Previous studies were done in children with OSA with an obstructive apnea hypopnea index of less than 5, so they had very mild OSA,” Ignacio Tapia, MD, associate professor of pediatrics, University of Pennsylvania, Philadelphia, said in an interview.
“But then people started using the INCS for a whole range of OSA, so this is why we wanted to do the trial, to make sure that these drugs were being used correctly,” he added.
“The main message from this paper is that I think INCS may still have a role to play in OSA to treat some of the symptoms, like snoring, and in our study, quality of life indices also improved, ,” Dr. Tapia emphasized.
The study was published online in the journal Chest.
3 months of INCS
A total of 134 children between 5 and 12 years of age were randomly assigned to receive INCS for 3 months or placebo. Children in the original INCS arm were then reassigned to receive 9 more months of the same treatment or placebo. Symptoms as well as polysomnographic and neurobehavioral findings were measured at baseline, at 3 months, and again at 12 months.
“The primary outcome was OAHI change at 3 months, available for 122 children,” the authors explained. The OSAS was defined as an OAHI of between two and three events per hour. The median age of the children at baseline was 7.9 years, and the median OAHI baseline score was 5.8/hr (95% confidence interval, 3.6-9.7/hr). The total daily dose of the INCS used was 110 mcg.
At 3 months, the mean change in the OAHI from baseline was –1.73/hr (95% CI, –3.91 to 1.92/hr), while at 12 months, the mean change in the same index was –1.21 (–4.22 to 1.71/hr). These changes were not significantly different from OAHI changes observed among control participants. “OSAS symptoms and neurobehavioral results were not different [either] between the INCS and placebo groups at 3 and12 months,” the authors added.
However, among those children who received INCS treatment for the entire 12 months, the OAHI decreased significantly from 7.2/hr (95% CI, 3.62-9.88/hr) at baseline to 3.71/hr (95% CI, 1.56-6.4/hr; P = .039), although the OAHI did not normalize, the authors noted. Asked to clarify whether this change was not significant, Dr. Tapia said that it did meet statistical significance, but clinically, it meant that the children still needed some form of treatment, because they still had OSA in the range needing treatment.
The placebo group had more asthma exacerbations, upper respiratory tract infections, and exacerbations of OSAS symptoms, compared with children in the INCS group. It is possible that INCS provided a certain degree of protection from asthma exacerbation, the authors suggested.
However, recent guidelines from the American Academy of Pediatrics suggest that clinicians may prescribe these agents for children with mild OSAS in whom adenotonsillectomy is contraindicated; for those with mild postoperative OSAS, adenotonsillectomy remains the treatment of choice for childhood OSA. “The low level of enthusiasm for INCS in these guidelines is based on results from studies of INCS treatment of OSAS that had been limited by small sample size, lack of placebo control, limited duration, and variability in baseline data,” the authors wrote.
“The results of the current larger and more rigorous study of children with a wider range of OSAS also do not support the currently liberal use of INCS for the treatment of OSAS,” they wrote.
Complex issue
In a comment, Rakesh Bhattacharjee, MD, associate professor of pediatrics, University of California, San Diego, noted that he does prescribe INCS for children with mild OSA but not for all children. “We based our decisions on polysomnography, which we use to categorize OSA as mild, moderate, or severe.
“But we certainly do offer this treatment for children with mild sleep apnea as a way to avoid surgical treatment,” Dr. Bhattacharjee added. He also uses INCS for residual sleep apnea that some children experience following adenotonsillectomy. As the current study suggests, many people are treating sleep apnea empirically without confirming the severity of the disorder by a sleep study.
“If a sleep study is not done, we don’t know how severe it is, so this would advocate for the utility of a sleep study so that you can quantify the severity of symptoms and target your therapy to children who might be appropriate for INCS therapy,” Dr. Bhattacharjee said.
On the other hand, surgery is not always relevant even if a child has enlarged adenoids and tonsils, as, for example, a child with obesity. In these children, physicians need to think about other treatments, such as continuous positive airways pressure. “CPAP is not perfect,” Dr. Bhattacharjee observed. “And as pediatricians, we need to do a lot of work to improve the use of CPAP, but, that said, there are children for whom INCS and surgery might be a waste of time, and this is where CPAP might be an alternative.”
Dr. Bhattacharjee previously was the lead author of a large study of children who underwent treatment with CPAP. While findings suggested that adherence to treatment is lower in children than it is for adults, the authors also showed that numerous actionable factors could used to improve adherence to CPAP among children who might otherwise benefit from it.
The authors disclosed no relevant financial relationships. Dr. Bhattacharjee has served as a scientific adviser for Jazz Pharmaceuticals.
A version of this article first appeared on Medscape.com.
Children with obstructive sleep apnea syndrome (OSAS) who undergo treatment with intranasal corticosteroids (INCS) did not experience significant improvement in polysomnographic, neurobehavioral, and other symptoms at 3 and 12 months of treatment. At 12 months of INCS treatment, there was a statistically significant but not clinically relevant reduction in the obstructive apnea hypopnea index (OHAI).
“Previous studies were done in children with OSA with an obstructive apnea hypopnea index of less than 5, so they had very mild OSA,” Ignacio Tapia, MD, associate professor of pediatrics, University of Pennsylvania, Philadelphia, said in an interview.
“But then people started using the INCS for a whole range of OSA, so this is why we wanted to do the trial, to make sure that these drugs were being used correctly,” he added.
“The main message from this paper is that I think INCS may still have a role to play in OSA to treat some of the symptoms, like snoring, and in our study, quality of life indices also improved, ,” Dr. Tapia emphasized.
The study was published online in the journal Chest.
3 months of INCS
A total of 134 children between 5 and 12 years of age were randomly assigned to receive INCS for 3 months or placebo. Children in the original INCS arm were then reassigned to receive 9 more months of the same treatment or placebo. Symptoms as well as polysomnographic and neurobehavioral findings were measured at baseline, at 3 months, and again at 12 months.
“The primary outcome was OAHI change at 3 months, available for 122 children,” the authors explained. The OSAS was defined as an OAHI of between two and three events per hour. The median age of the children at baseline was 7.9 years, and the median OAHI baseline score was 5.8/hr (95% confidence interval, 3.6-9.7/hr). The total daily dose of the INCS used was 110 mcg.
At 3 months, the mean change in the OAHI from baseline was –1.73/hr (95% CI, –3.91 to 1.92/hr), while at 12 months, the mean change in the same index was –1.21 (–4.22 to 1.71/hr). These changes were not significantly different from OAHI changes observed among control participants. “OSAS symptoms and neurobehavioral results were not different [either] between the INCS and placebo groups at 3 and12 months,” the authors added.
However, among those children who received INCS treatment for the entire 12 months, the OAHI decreased significantly from 7.2/hr (95% CI, 3.62-9.88/hr) at baseline to 3.71/hr (95% CI, 1.56-6.4/hr; P = .039), although the OAHI did not normalize, the authors noted. Asked to clarify whether this change was not significant, Dr. Tapia said that it did meet statistical significance, but clinically, it meant that the children still needed some form of treatment, because they still had OSA in the range needing treatment.
The placebo group had more asthma exacerbations, upper respiratory tract infections, and exacerbations of OSAS symptoms, compared with children in the INCS group. It is possible that INCS provided a certain degree of protection from asthma exacerbation, the authors suggested.
However, recent guidelines from the American Academy of Pediatrics suggest that clinicians may prescribe these agents for children with mild OSAS in whom adenotonsillectomy is contraindicated; for those with mild postoperative OSAS, adenotonsillectomy remains the treatment of choice for childhood OSA. “The low level of enthusiasm for INCS in these guidelines is based on results from studies of INCS treatment of OSAS that had been limited by small sample size, lack of placebo control, limited duration, and variability in baseline data,” the authors wrote.
“The results of the current larger and more rigorous study of children with a wider range of OSAS also do not support the currently liberal use of INCS for the treatment of OSAS,” they wrote.
Complex issue
In a comment, Rakesh Bhattacharjee, MD, associate professor of pediatrics, University of California, San Diego, noted that he does prescribe INCS for children with mild OSA but not for all children. “We based our decisions on polysomnography, which we use to categorize OSA as mild, moderate, or severe.
“But we certainly do offer this treatment for children with mild sleep apnea as a way to avoid surgical treatment,” Dr. Bhattacharjee added. He also uses INCS for residual sleep apnea that some children experience following adenotonsillectomy. As the current study suggests, many people are treating sleep apnea empirically without confirming the severity of the disorder by a sleep study.
“If a sleep study is not done, we don’t know how severe it is, so this would advocate for the utility of a sleep study so that you can quantify the severity of symptoms and target your therapy to children who might be appropriate for INCS therapy,” Dr. Bhattacharjee said.
On the other hand, surgery is not always relevant even if a child has enlarged adenoids and tonsils, as, for example, a child with obesity. In these children, physicians need to think about other treatments, such as continuous positive airways pressure. “CPAP is not perfect,” Dr. Bhattacharjee observed. “And as pediatricians, we need to do a lot of work to improve the use of CPAP, but, that said, there are children for whom INCS and surgery might be a waste of time, and this is where CPAP might be an alternative.”
Dr. Bhattacharjee previously was the lead author of a large study of children who underwent treatment with CPAP. While findings suggested that adherence to treatment is lower in children than it is for adults, the authors also showed that numerous actionable factors could used to improve adherence to CPAP among children who might otherwise benefit from it.
The authors disclosed no relevant financial relationships. Dr. Bhattacharjee has served as a scientific adviser for Jazz Pharmaceuticals.
A version of this article first appeared on Medscape.com.
Children with obstructive sleep apnea syndrome (OSAS) who undergo treatment with intranasal corticosteroids (INCS) did not experience significant improvement in polysomnographic, neurobehavioral, and other symptoms at 3 and 12 months of treatment. At 12 months of INCS treatment, there was a statistically significant but not clinically relevant reduction in the obstructive apnea hypopnea index (OHAI).
“Previous studies were done in children with OSA with an obstructive apnea hypopnea index of less than 5, so they had very mild OSA,” Ignacio Tapia, MD, associate professor of pediatrics, University of Pennsylvania, Philadelphia, said in an interview.
“But then people started using the INCS for a whole range of OSA, so this is why we wanted to do the trial, to make sure that these drugs were being used correctly,” he added.
“The main message from this paper is that I think INCS may still have a role to play in OSA to treat some of the symptoms, like snoring, and in our study, quality of life indices also improved, ,” Dr. Tapia emphasized.
The study was published online in the journal Chest.
3 months of INCS
A total of 134 children between 5 and 12 years of age were randomly assigned to receive INCS for 3 months or placebo. Children in the original INCS arm were then reassigned to receive 9 more months of the same treatment or placebo. Symptoms as well as polysomnographic and neurobehavioral findings were measured at baseline, at 3 months, and again at 12 months.
“The primary outcome was OAHI change at 3 months, available for 122 children,” the authors explained. The OSAS was defined as an OAHI of between two and three events per hour. The median age of the children at baseline was 7.9 years, and the median OAHI baseline score was 5.8/hr (95% confidence interval, 3.6-9.7/hr). The total daily dose of the INCS used was 110 mcg.
At 3 months, the mean change in the OAHI from baseline was –1.73/hr (95% CI, –3.91 to 1.92/hr), while at 12 months, the mean change in the same index was –1.21 (–4.22 to 1.71/hr). These changes were not significantly different from OAHI changes observed among control participants. “OSAS symptoms and neurobehavioral results were not different [either] between the INCS and placebo groups at 3 and12 months,” the authors added.
However, among those children who received INCS treatment for the entire 12 months, the OAHI decreased significantly from 7.2/hr (95% CI, 3.62-9.88/hr) at baseline to 3.71/hr (95% CI, 1.56-6.4/hr; P = .039), although the OAHI did not normalize, the authors noted. Asked to clarify whether this change was not significant, Dr. Tapia said that it did meet statistical significance, but clinically, it meant that the children still needed some form of treatment, because they still had OSA in the range needing treatment.
The placebo group had more asthma exacerbations, upper respiratory tract infections, and exacerbations of OSAS symptoms, compared with children in the INCS group. It is possible that INCS provided a certain degree of protection from asthma exacerbation, the authors suggested.
However, recent guidelines from the American Academy of Pediatrics suggest that clinicians may prescribe these agents for children with mild OSAS in whom adenotonsillectomy is contraindicated; for those with mild postoperative OSAS, adenotonsillectomy remains the treatment of choice for childhood OSA. “The low level of enthusiasm for INCS in these guidelines is based on results from studies of INCS treatment of OSAS that had been limited by small sample size, lack of placebo control, limited duration, and variability in baseline data,” the authors wrote.
“The results of the current larger and more rigorous study of children with a wider range of OSAS also do not support the currently liberal use of INCS for the treatment of OSAS,” they wrote.
Complex issue
In a comment, Rakesh Bhattacharjee, MD, associate professor of pediatrics, University of California, San Diego, noted that he does prescribe INCS for children with mild OSA but not for all children. “We based our decisions on polysomnography, which we use to categorize OSA as mild, moderate, or severe.
“But we certainly do offer this treatment for children with mild sleep apnea as a way to avoid surgical treatment,” Dr. Bhattacharjee added. He also uses INCS for residual sleep apnea that some children experience following adenotonsillectomy. As the current study suggests, many people are treating sleep apnea empirically without confirming the severity of the disorder by a sleep study.
“If a sleep study is not done, we don’t know how severe it is, so this would advocate for the utility of a sleep study so that you can quantify the severity of symptoms and target your therapy to children who might be appropriate for INCS therapy,” Dr. Bhattacharjee said.
On the other hand, surgery is not always relevant even if a child has enlarged adenoids and tonsils, as, for example, a child with obesity. In these children, physicians need to think about other treatments, such as continuous positive airways pressure. “CPAP is not perfect,” Dr. Bhattacharjee observed. “And as pediatricians, we need to do a lot of work to improve the use of CPAP, but, that said, there are children for whom INCS and surgery might be a waste of time, and this is where CPAP might be an alternative.”
Dr. Bhattacharjee previously was the lead author of a large study of children who underwent treatment with CPAP. While findings suggested that adherence to treatment is lower in children than it is for adults, the authors also showed that numerous actionable factors could used to improve adherence to CPAP among children who might otherwise benefit from it.
The authors disclosed no relevant financial relationships. Dr. Bhattacharjee has served as a scientific adviser for Jazz Pharmaceuticals.
A version of this article first appeared on Medscape.com.
FROM CHEST
Children and COVID: Does latest rise in new cases point toward stabilization?
New COVID-19 cases rose for the second time in 3 weeks, as the effort to vaccinate the youngest children continued to slow after just 3 full weeks.
Nationally, over 75,000 children under age 5 years received their first dose of COVID-19 vaccine during the week of July 7-13. That number is down from the previous week – 118,000 from June 30 to July 6 – which, in turn, was lower than the 206,000 doses administered through the first 10 days after approval, based on data from the Centers for Disease Control and Prevention. That all adds up to just under 400,000 vaccinated children, or 2% of the eligible population under age 5, as of July 13.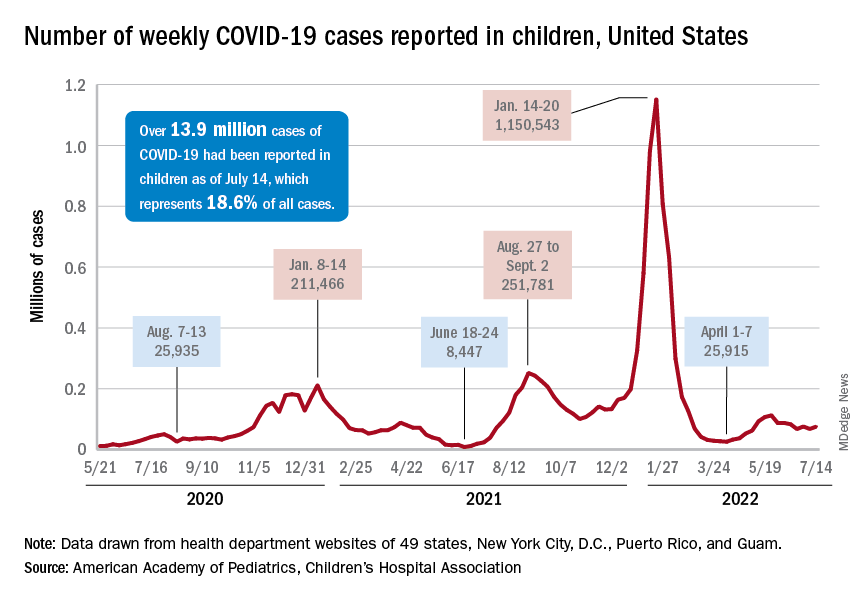
State-level data, meanwhile, show considerable variation, the American Academy of Pediatrics noted in its weekly analysis of the CDC vaccine data. Vermont has already vaccinated 10.0% of children under age 5 years, and Massachusetts is at 9.5%, while Mississippi (0.3%), Alabama (0.5%), and Louisiana (0.8%) are still below 1%, the AAP said.
New cases show signs of steadying
The national count was up by 11.1% for the week of July 8-14, rising to 75,000 new cases, compared with 68,000 the previous week, but the recent trend seems to be leaning toward steadiness. The overall number has been between 67,000 and 76,000 over the past 4 weeks, alternating between rising and falling in that time span, according to data gathered by the AAP and the Children’s Hospital Association from state and territorial health departments.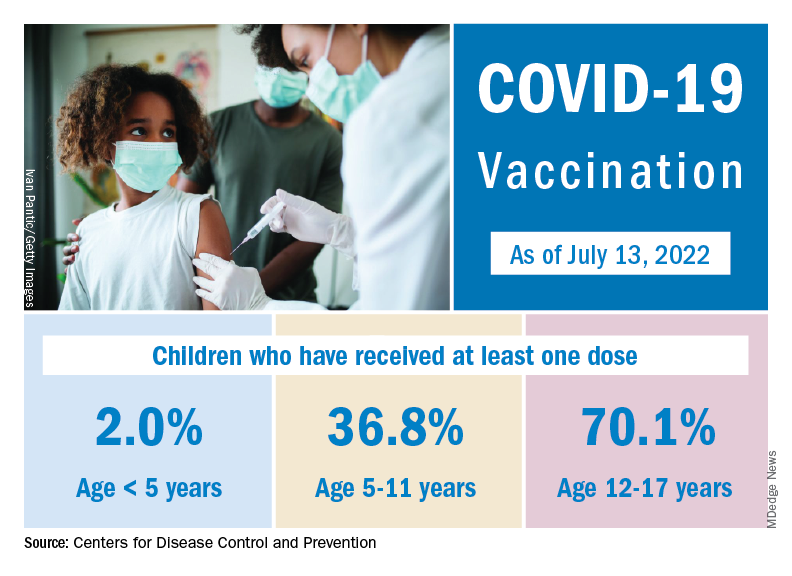
the two groups said, also noting that several states have stopped updating their online dashboards over the past year, making the current total artificially low in comparison.
Taken with that grain of salt, the cumulative number of child cases since the start of the pandemic is just over 13.9 million, which represents 18.6% of all cases in the United States. That proportion has been declining in recent weeks and was as high as 19.0% as late as mid-May. “While COVID-19 cases are likely increasingly underreported for all age groups, this decline indicates that children are disproportionately undercounted in reported COVID-19 cases,” the AAP and CHA said.
New COVID-19 cases rose for the second time in 3 weeks, as the effort to vaccinate the youngest children continued to slow after just 3 full weeks.
Nationally, over 75,000 children under age 5 years received their first dose of COVID-19 vaccine during the week of July 7-13. That number is down from the previous week – 118,000 from June 30 to July 6 – which, in turn, was lower than the 206,000 doses administered through the first 10 days after approval, based on data from the Centers for Disease Control and Prevention. That all adds up to just under 400,000 vaccinated children, or 2% of the eligible population under age 5, as of July 13.
State-level data, meanwhile, show considerable variation, the American Academy of Pediatrics noted in its weekly analysis of the CDC vaccine data. Vermont has already vaccinated 10.0% of children under age 5 years, and Massachusetts is at 9.5%, while Mississippi (0.3%), Alabama (0.5%), and Louisiana (0.8%) are still below 1%, the AAP said.
New cases show signs of steadying
The national count was up by 11.1% for the week of July 8-14, rising to 75,000 new cases, compared with 68,000 the previous week, but the recent trend seems to be leaning toward steadiness. The overall number has been between 67,000 and 76,000 over the past 4 weeks, alternating between rising and falling in that time span, according to data gathered by the AAP and the Children’s Hospital Association from state and territorial health departments.
the two groups said, also noting that several states have stopped updating their online dashboards over the past year, making the current total artificially low in comparison.
Taken with that grain of salt, the cumulative number of child cases since the start of the pandemic is just over 13.9 million, which represents 18.6% of all cases in the United States. That proportion has been declining in recent weeks and was as high as 19.0% as late as mid-May. “While COVID-19 cases are likely increasingly underreported for all age groups, this decline indicates that children are disproportionately undercounted in reported COVID-19 cases,” the AAP and CHA said.
New COVID-19 cases rose for the second time in 3 weeks, as the effort to vaccinate the youngest children continued to slow after just 3 full weeks.
Nationally, over 75,000 children under age 5 years received their first dose of COVID-19 vaccine during the week of July 7-13. That number is down from the previous week – 118,000 from June 30 to July 6 – which, in turn, was lower than the 206,000 doses administered through the first 10 days after approval, based on data from the Centers for Disease Control and Prevention. That all adds up to just under 400,000 vaccinated children, or 2% of the eligible population under age 5, as of July 13.
State-level data, meanwhile, show considerable variation, the American Academy of Pediatrics noted in its weekly analysis of the CDC vaccine data. Vermont has already vaccinated 10.0% of children under age 5 years, and Massachusetts is at 9.5%, while Mississippi (0.3%), Alabama (0.5%), and Louisiana (0.8%) are still below 1%, the AAP said.
New cases show signs of steadying
The national count was up by 11.1% for the week of July 8-14, rising to 75,000 new cases, compared with 68,000 the previous week, but the recent trend seems to be leaning toward steadiness. The overall number has been between 67,000 and 76,000 over the past 4 weeks, alternating between rising and falling in that time span, according to data gathered by the AAP and the Children’s Hospital Association from state and territorial health departments.
the two groups said, also noting that several states have stopped updating their online dashboards over the past year, making the current total artificially low in comparison.
Taken with that grain of salt, the cumulative number of child cases since the start of the pandemic is just over 13.9 million, which represents 18.6% of all cases in the United States. That proportion has been declining in recent weeks and was as high as 19.0% as late as mid-May. “While COVID-19 cases are likely increasingly underreported for all age groups, this decline indicates that children are disproportionately undercounted in reported COVID-19 cases,” the AAP and CHA said.