User login
-
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Exceeding exercise guidelines boosts survival, to a point
A new study suggests that going beyond current guidance on moderate and vigorous physical activity levels may add years to one’s life.
Americans are advised to do a minimum of 150-300 minutes a week of moderate exercise or 75-150 minutes a week of vigorous exercise, or an equivalent combination of both, according to U.S. Department of Health and Human Services Physical Activity Guidelines.
Results from more than 100,000 U.S. adults followed for 30 years showed that .
Adults who reported completing four times the minimum recommended activity levels saw no clear incremental mortality benefit but also no harm, according to the study, published in the journal Circulation.
“I think we’re worried more about the lower end and people that are not even doing the minimum, but this should be reassuring to people who like to do a lot of exercise,” senior author Edward Giovannucci, MD, ScD, with the Harvard T.H. Chan School of Public Health, Boston, told this news organization.
Some studies have suggested that long-term, high-intensity exercise (e.g., marathons, triathlons, and long-distance cycling) may be associated with increased risks of atrial fibrillation, coronary artery calcification, and sudden cardiac death.
A recent analysis from the Copenhagen City Heart Study showed a U-shaped association between long-term all-cause mortality and 0 to 2.5 hours and more than 10 hours of weekly, leisure-time sports activities.
Most studies suggesting harm, however, have used only one measurement of physical activity capturing a mix of people who chronically exercise at high levels and those who do it sporadically, which possibly can be harmful, Dr. Giovannucci said. “We were better able to look at consistent long-term activity and saw there was no harm.”
The study included 116,221 participants in the Nurses’ Health Study and the Health Professionals Follow-up Study between 1988 and 2018, who completed up to 15 (median, 11) questionnaires on their health and leisure-time physical activity that were updated every 2 years.
Most were White (96%), 63% were female, and the average age and body mass index over follow-up was 66 years and 26 kg/m2. During 30 years of follow-up, there were 47,596 deaths.
‘Any effort is worthwhile’
The analysis found that individuals who met the guideline for long-term vigorous physical activity (75-150 min/week) cut their adjusted risk of death from cardiovascular disease (CVD) by a whopping 31%, from non-CVD causes by 15%, and all-causes by 19%, compared with those with no long-term vigorous activity.
Those completing two to four times the recommended minimum (150-299 min/week) had a 27%-33% lower risk of CVD mortality, 19% lower risk of non-CVD mortality, and 21%-23% lower risk of all-cause mortality.
Higher levels did not appear to further lower mortality risk. For example, 300-374 min/week of vigorous physical activity was associated with a 32% lower risk of CVD death, 18% lower risk of non-CVD death, and 22% lower risk of dying from any cause.
The analysis also found that individuals who met the guidelines for moderate physical activity had lower CVD, non-CVD, and all-cause mortality risks whether they were active 150-244 min/week (22%, 19%, and 20%, respectively) or 225-299 min/week (21%, 25%, and 20%, respectively), compared with those with almost no long-term moderate activity.
Those fitting in two to four times the recommended minimum (300-599 min/week) had a 28%-38% lower risk of CVD mortality, 25%-27% lower risk of non-CVD mortality, and 26%-31% lower risk of all-cause mortality.
The mortality benefit appeared to plateau, with 600 min/week of moderate physical activity showing associations similar to 300-599 min/week.
“The sweet spot seems to be two to four times the recommended levels but for people who are sedentary, I think one of the key messages that I give my patients is that any effort is worthwhile; that any physical activity, even less than the recommended, has some mortality reduction,” Erin Michos, MD, MHS, associate director of preventive cardiology at Johns Hopkins University, Baltimore, said in an interview.
Indeed, individuals who reported doing just 20-74 minutes of moderate exercise per week had a 19% lower risk of dying from any cause and a 13% lower risk of dying from CVD compared with those doing less.
Current American Heart Association (AHA) recommendations are for at least 150 minutes per week of moderate-intensity aerobic exercise or 75 minutes per week of vigorous aerobic exercise, or a combination of both.
“This suggests that even more is probably better, in the range of two to four times that, so maybe we should move our targets a little bit higher, which is kind of what the Department of Health and Human Services has already done,” said Dr. Michos, who was not involved in the study.
Former AHA president Donna K. Arnett, PhD, who was not involved in the study, said in a statement that “we’ve known for a long time that moderate or intense levels of physical exercise can reduce a person’s risk of both atherosclerotic cardiovascular disease and mortality.
“We have also seen that getting more than 300 minutes of moderate-intensity aerobic physical activity or more than 150 minutes of vigorous-intensity aerobic physical exercise each week may reduce a person’s risk of atherosclerotic cardiovascular disease even further, so it makes sense that getting those extra minutes of exercise may also decrease mortality,” she added.
Mix and match
Dr. Giovannucci noted that the joint effects of the two types of exercise on mortality have not been studied and “there are some questions, for example, about whether doing a lot of moderate activity is sufficient or can you get more benefits by doing vigorous activity also.”
Joint analyses of both exercise intensities found that additional vigorous physical activity was associated with lower mortality among participants with insufficient (less than 300 min/week) levels of moderate exercise but not among those with at least 300 min/week of moderate exercise.
“The main message is that you can get essentially all of the benefit by just doing moderate exercise,” Dr. Giovannucci said. “There’s no magic benefit of doing vigorous [exercise]. But if someone wants to do vigorous, they can get the benefit in about half the time. So if you only have 2-3 hours a week to exercise and can do, say 2 or 3 hours of running, you can get pretty much the maximum benefit.”
Sensitivity analyses showed a consistent association between long-term leisure physical activity and mortality without adjustment for body mass index/calorie intake.
“Some people think the effect of exercise is to lower your body weight or keep it down, which could be one of the benefits, but even independent of that, you get benefits even if it has no effect on your weight,” he said. “So, definitely, that’s important.”
Dr. Michos pointed out that vigorous physical activity may seem daunting for many individuals but that moderate exercise can include activities such as brisk walking, ballroom dancing, active yoga, and recreational swimming.
“The nice thing is that you can really combine or substitute both and get just as similar mortality reductions with moderate physical activity, because a lot of patients may not want to do vigorous activity,” she said. “They don’t want to get on the treadmill; that’s too intimidating or stressful.”
The study was supported by the National Institutes of Health. The authors and Dr. Michos report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new study suggests that going beyond current guidance on moderate and vigorous physical activity levels may add years to one’s life.
Americans are advised to do a minimum of 150-300 minutes a week of moderate exercise or 75-150 minutes a week of vigorous exercise, or an equivalent combination of both, according to U.S. Department of Health and Human Services Physical Activity Guidelines.
Results from more than 100,000 U.S. adults followed for 30 years showed that .
Adults who reported completing four times the minimum recommended activity levels saw no clear incremental mortality benefit but also no harm, according to the study, published in the journal Circulation.
“I think we’re worried more about the lower end and people that are not even doing the minimum, but this should be reassuring to people who like to do a lot of exercise,” senior author Edward Giovannucci, MD, ScD, with the Harvard T.H. Chan School of Public Health, Boston, told this news organization.
Some studies have suggested that long-term, high-intensity exercise (e.g., marathons, triathlons, and long-distance cycling) may be associated with increased risks of atrial fibrillation, coronary artery calcification, and sudden cardiac death.
A recent analysis from the Copenhagen City Heart Study showed a U-shaped association between long-term all-cause mortality and 0 to 2.5 hours and more than 10 hours of weekly, leisure-time sports activities.
Most studies suggesting harm, however, have used only one measurement of physical activity capturing a mix of people who chronically exercise at high levels and those who do it sporadically, which possibly can be harmful, Dr. Giovannucci said. “We were better able to look at consistent long-term activity and saw there was no harm.”
The study included 116,221 participants in the Nurses’ Health Study and the Health Professionals Follow-up Study between 1988 and 2018, who completed up to 15 (median, 11) questionnaires on their health and leisure-time physical activity that were updated every 2 years.
Most were White (96%), 63% were female, and the average age and body mass index over follow-up was 66 years and 26 kg/m2. During 30 years of follow-up, there were 47,596 deaths.
‘Any effort is worthwhile’
The analysis found that individuals who met the guideline for long-term vigorous physical activity (75-150 min/week) cut their adjusted risk of death from cardiovascular disease (CVD) by a whopping 31%, from non-CVD causes by 15%, and all-causes by 19%, compared with those with no long-term vigorous activity.
Those completing two to four times the recommended minimum (150-299 min/week) had a 27%-33% lower risk of CVD mortality, 19% lower risk of non-CVD mortality, and 21%-23% lower risk of all-cause mortality.
Higher levels did not appear to further lower mortality risk. For example, 300-374 min/week of vigorous physical activity was associated with a 32% lower risk of CVD death, 18% lower risk of non-CVD death, and 22% lower risk of dying from any cause.
The analysis also found that individuals who met the guidelines for moderate physical activity had lower CVD, non-CVD, and all-cause mortality risks whether they were active 150-244 min/week (22%, 19%, and 20%, respectively) or 225-299 min/week (21%, 25%, and 20%, respectively), compared with those with almost no long-term moderate activity.
Those fitting in two to four times the recommended minimum (300-599 min/week) had a 28%-38% lower risk of CVD mortality, 25%-27% lower risk of non-CVD mortality, and 26%-31% lower risk of all-cause mortality.
The mortality benefit appeared to plateau, with 600 min/week of moderate physical activity showing associations similar to 300-599 min/week.
“The sweet spot seems to be two to four times the recommended levels but for people who are sedentary, I think one of the key messages that I give my patients is that any effort is worthwhile; that any physical activity, even less than the recommended, has some mortality reduction,” Erin Michos, MD, MHS, associate director of preventive cardiology at Johns Hopkins University, Baltimore, said in an interview.
Indeed, individuals who reported doing just 20-74 minutes of moderate exercise per week had a 19% lower risk of dying from any cause and a 13% lower risk of dying from CVD compared with those doing less.
Current American Heart Association (AHA) recommendations are for at least 150 minutes per week of moderate-intensity aerobic exercise or 75 minutes per week of vigorous aerobic exercise, or a combination of both.
“This suggests that even more is probably better, in the range of two to four times that, so maybe we should move our targets a little bit higher, which is kind of what the Department of Health and Human Services has already done,” said Dr. Michos, who was not involved in the study.
Former AHA president Donna K. Arnett, PhD, who was not involved in the study, said in a statement that “we’ve known for a long time that moderate or intense levels of physical exercise can reduce a person’s risk of both atherosclerotic cardiovascular disease and mortality.
“We have also seen that getting more than 300 minutes of moderate-intensity aerobic physical activity or more than 150 minutes of vigorous-intensity aerobic physical exercise each week may reduce a person’s risk of atherosclerotic cardiovascular disease even further, so it makes sense that getting those extra minutes of exercise may also decrease mortality,” she added.
Mix and match
Dr. Giovannucci noted that the joint effects of the two types of exercise on mortality have not been studied and “there are some questions, for example, about whether doing a lot of moderate activity is sufficient or can you get more benefits by doing vigorous activity also.”
Joint analyses of both exercise intensities found that additional vigorous physical activity was associated with lower mortality among participants with insufficient (less than 300 min/week) levels of moderate exercise but not among those with at least 300 min/week of moderate exercise.
“The main message is that you can get essentially all of the benefit by just doing moderate exercise,” Dr. Giovannucci said. “There’s no magic benefit of doing vigorous [exercise]. But if someone wants to do vigorous, they can get the benefit in about half the time. So if you only have 2-3 hours a week to exercise and can do, say 2 or 3 hours of running, you can get pretty much the maximum benefit.”
Sensitivity analyses showed a consistent association between long-term leisure physical activity and mortality without adjustment for body mass index/calorie intake.
“Some people think the effect of exercise is to lower your body weight or keep it down, which could be one of the benefits, but even independent of that, you get benefits even if it has no effect on your weight,” he said. “So, definitely, that’s important.”
Dr. Michos pointed out that vigorous physical activity may seem daunting for many individuals but that moderate exercise can include activities such as brisk walking, ballroom dancing, active yoga, and recreational swimming.
“The nice thing is that you can really combine or substitute both and get just as similar mortality reductions with moderate physical activity, because a lot of patients may not want to do vigorous activity,” she said. “They don’t want to get on the treadmill; that’s too intimidating or stressful.”
The study was supported by the National Institutes of Health. The authors and Dr. Michos report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new study suggests that going beyond current guidance on moderate and vigorous physical activity levels may add years to one’s life.
Americans are advised to do a minimum of 150-300 minutes a week of moderate exercise or 75-150 minutes a week of vigorous exercise, or an equivalent combination of both, according to U.S. Department of Health and Human Services Physical Activity Guidelines.
Results from more than 100,000 U.S. adults followed for 30 years showed that .
Adults who reported completing four times the minimum recommended activity levels saw no clear incremental mortality benefit but also no harm, according to the study, published in the journal Circulation.
“I think we’re worried more about the lower end and people that are not even doing the minimum, but this should be reassuring to people who like to do a lot of exercise,” senior author Edward Giovannucci, MD, ScD, with the Harvard T.H. Chan School of Public Health, Boston, told this news organization.
Some studies have suggested that long-term, high-intensity exercise (e.g., marathons, triathlons, and long-distance cycling) may be associated with increased risks of atrial fibrillation, coronary artery calcification, and sudden cardiac death.
A recent analysis from the Copenhagen City Heart Study showed a U-shaped association between long-term all-cause mortality and 0 to 2.5 hours and more than 10 hours of weekly, leisure-time sports activities.
Most studies suggesting harm, however, have used only one measurement of physical activity capturing a mix of people who chronically exercise at high levels and those who do it sporadically, which possibly can be harmful, Dr. Giovannucci said. “We were better able to look at consistent long-term activity and saw there was no harm.”
The study included 116,221 participants in the Nurses’ Health Study and the Health Professionals Follow-up Study between 1988 and 2018, who completed up to 15 (median, 11) questionnaires on their health and leisure-time physical activity that were updated every 2 years.
Most were White (96%), 63% were female, and the average age and body mass index over follow-up was 66 years and 26 kg/m2. During 30 years of follow-up, there were 47,596 deaths.
‘Any effort is worthwhile’
The analysis found that individuals who met the guideline for long-term vigorous physical activity (75-150 min/week) cut their adjusted risk of death from cardiovascular disease (CVD) by a whopping 31%, from non-CVD causes by 15%, and all-causes by 19%, compared with those with no long-term vigorous activity.
Those completing two to four times the recommended minimum (150-299 min/week) had a 27%-33% lower risk of CVD mortality, 19% lower risk of non-CVD mortality, and 21%-23% lower risk of all-cause mortality.
Higher levels did not appear to further lower mortality risk. For example, 300-374 min/week of vigorous physical activity was associated with a 32% lower risk of CVD death, 18% lower risk of non-CVD death, and 22% lower risk of dying from any cause.
The analysis also found that individuals who met the guidelines for moderate physical activity had lower CVD, non-CVD, and all-cause mortality risks whether they were active 150-244 min/week (22%, 19%, and 20%, respectively) or 225-299 min/week (21%, 25%, and 20%, respectively), compared with those with almost no long-term moderate activity.
Those fitting in two to four times the recommended minimum (300-599 min/week) had a 28%-38% lower risk of CVD mortality, 25%-27% lower risk of non-CVD mortality, and 26%-31% lower risk of all-cause mortality.
The mortality benefit appeared to plateau, with 600 min/week of moderate physical activity showing associations similar to 300-599 min/week.
“The sweet spot seems to be two to four times the recommended levels but for people who are sedentary, I think one of the key messages that I give my patients is that any effort is worthwhile; that any physical activity, even less than the recommended, has some mortality reduction,” Erin Michos, MD, MHS, associate director of preventive cardiology at Johns Hopkins University, Baltimore, said in an interview.
Indeed, individuals who reported doing just 20-74 minutes of moderate exercise per week had a 19% lower risk of dying from any cause and a 13% lower risk of dying from CVD compared with those doing less.
Current American Heart Association (AHA) recommendations are for at least 150 minutes per week of moderate-intensity aerobic exercise or 75 minutes per week of vigorous aerobic exercise, or a combination of both.
“This suggests that even more is probably better, in the range of two to four times that, so maybe we should move our targets a little bit higher, which is kind of what the Department of Health and Human Services has already done,” said Dr. Michos, who was not involved in the study.
Former AHA president Donna K. Arnett, PhD, who was not involved in the study, said in a statement that “we’ve known for a long time that moderate or intense levels of physical exercise can reduce a person’s risk of both atherosclerotic cardiovascular disease and mortality.
“We have also seen that getting more than 300 minutes of moderate-intensity aerobic physical activity or more than 150 minutes of vigorous-intensity aerobic physical exercise each week may reduce a person’s risk of atherosclerotic cardiovascular disease even further, so it makes sense that getting those extra minutes of exercise may also decrease mortality,” she added.
Mix and match
Dr. Giovannucci noted that the joint effects of the two types of exercise on mortality have not been studied and “there are some questions, for example, about whether doing a lot of moderate activity is sufficient or can you get more benefits by doing vigorous activity also.”
Joint analyses of both exercise intensities found that additional vigorous physical activity was associated with lower mortality among participants with insufficient (less than 300 min/week) levels of moderate exercise but not among those with at least 300 min/week of moderate exercise.
“The main message is that you can get essentially all of the benefit by just doing moderate exercise,” Dr. Giovannucci said. “There’s no magic benefit of doing vigorous [exercise]. But if someone wants to do vigorous, they can get the benefit in about half the time. So if you only have 2-3 hours a week to exercise and can do, say 2 or 3 hours of running, you can get pretty much the maximum benefit.”
Sensitivity analyses showed a consistent association between long-term leisure physical activity and mortality without adjustment for body mass index/calorie intake.
“Some people think the effect of exercise is to lower your body weight or keep it down, which could be one of the benefits, but even independent of that, you get benefits even if it has no effect on your weight,” he said. “So, definitely, that’s important.”
Dr. Michos pointed out that vigorous physical activity may seem daunting for many individuals but that moderate exercise can include activities such as brisk walking, ballroom dancing, active yoga, and recreational swimming.
“The nice thing is that you can really combine or substitute both and get just as similar mortality reductions with moderate physical activity, because a lot of patients may not want to do vigorous activity,” she said. “They don’t want to get on the treadmill; that’s too intimidating or stressful.”
The study was supported by the National Institutes of Health. The authors and Dr. Michos report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM CIRCULATION
High plasma IgE predicts COPD exacerbation, mortality
COPD patients with high plasma immunoglobulin E are more likely to have exacerbations and die from any cause, based on a Danish population-cohort study.
hinting at different subsets of patients with COPD, lead author Yunus Çolak MD, PhD, of Copenhagen University Hospital, and colleagues reported.
“Additional biomarkers are necessary as blood eosinophils alone seem insufficient for risk stratification in COPD,” the investigators wrote in Annals of Allergy, Asthma & Immunology. “Since asthma and COPD share some pathophysiological mechanisms, a logical approach would be to investigate well-known biomarkers for asthma in COPD and vice versa.”
Dr. Çolak and colleagues cited previous research supporting this perspective. Specifically, IgE-targeting monoclonal antibodies have shown promise in patients with severe asthma and asthma-COPD overlap, whereas COPD with high IgE has been associated with a history of lung function decline and previous exacerbations.
The present study drew from a database of 46,598 adults enrolled in the Copenhagen General Population study. All participants underwent physical examination, completed a questionnaire, and provided blood for analysis. From this population, 1,559 individuals had COPD, among whom 446 had high plasma IgE (at least 76 IU/mL).
Over a median follow-up of 6.9 years in the COPD group, 224 severe exacerbations and 434 deaths of any cause occurred. Compared with COPD patients who had normal plasma IgE, those with high IgE were 43% more likely to have severe exacerbation (hazard ratio, 1.43; 95% confidence interval, 1.07-1.89) and 30% more likely to die of any cause (HR, 1.30; 95% CI, 1.06-1.62). These risks were similar when excluding patients with IgE of 700 IU/mL or higher.
“These findings suggest that plasma IgE concentration may be a potential prognostic biomarker and treatment target for a subset of COPD patient,” wrote Dr. Çolak and colleagues.
The above risks increased moderately when the high IgE group was trimmed to include only those with low eosinophils (less than 300 cells/mcL); in this subgroup, risk of exacerbation was increased 62% (HR, 1.62; 95% CI, 1.17-2.24), while risk of all-cause mortality was increased 47% (HR, 1.47; 95% CI, 1.14-1.88).
“We were not able to show that individuals with higher blood eosinophils further stratified by IgE had higher risk of severe exacerbation or all-cause mortality,” the investigators wrote, although they noted “the relatively low statistical power in stratified analysis,” considering the wide confidence intervals observed.
“Thus, we should be careful with interpreting the results in relation to blood eosinophils and IgE combined,” they suggested. “However, we believe that the mechanisms driving exacerbations through plasma IgE are different from those driving blood eosinophils, and we believe that plasma IgE may be a marker for a subset of COPD patients similar to blood eosinophils, which is compatible with the heterogeneity of patients with COPD.”

According to principal author Shoaib Afzal, MD, PhD, of Copenhagen University Hospital, the findings are “probably no surprise for practitioners that often observe overlap between asthma and COPD pathology.”
As smoking prevalence goes down in many countries, relatively more never-smokers are being diagnosed with COPD, Dr. Afzal said in a written comment, “which means that asthma as a risk factor for COPD is gaining importance.”
While patients with asthma can be treated with IgE-targeting omalizumab, a trial evaluating the same biologic for COPD patients with high IgE was withdrawn because of a lack of recruitment; however, Dr. Afzal suggested that this should not be the end of the story, since these new data imply that more patients could benefit than previously recognized.
“Our observational study has generated a hypothesis that needs to be tested by pulmonologists in randomized interventions trials designed with updated inclusion criteria,” he said.
Such trials are needed, Dr. Afzal went on, because they could help unlock the “huge” potential benefit that may come from characterizing COPD patients beyond “exposures, symptoms, and spirometry.”
“Sadly, the progress in establishing biomarkers in COPD for improving risk stratification and treatment allocation have been rather disappointing in the last decades, with the exception of small successes with eosinophils and perhaps FeNO,” Dr. Afzal said.

Nathaniel Marchetti, DO, professor of thoracic medicine and surgery at Temple University and medical director of the respiratory ICU at Temple University Hospital, both in Philadelphia, said the study by Dr. Afzal and colleagues is noteworthy because “biomarkers for COPD are desperately needed to help risk stratify patients for exacerbation risk and risk of disease progression and even mortality.”
In a written comment, Dr. Marchetti agreed with Dr. Afzal that the findings “open the possibility for interventional trials targeting IgE,” which could one day reshape the way patients with COPD are treated.
“I think that biomarkers will become vital in caring for patients with COPD in the future,” Dr. Marchetti said. “There will be medications that will be used to target different pathways of inflammation that drive disease progression and exacerbations. Biomarkers will be important in driving personalized medicine in COPD. We already know the disease seems to vary greatly from patient to patient.”
The study was supported by The Capital Region of Copenhagen, The Danish Lung Foundation, The Velux Foundation, and others. The investigators disclosed relationships with Boehringer Ingelheim, AstraZeneca, Sanofi Genzyme, and others. Dr. Marchetti disclosed no conflicts of interest.
COPD patients with high plasma immunoglobulin E are more likely to have exacerbations and die from any cause, based on a Danish population-cohort study.
hinting at different subsets of patients with COPD, lead author Yunus Çolak MD, PhD, of Copenhagen University Hospital, and colleagues reported.
“Additional biomarkers are necessary as blood eosinophils alone seem insufficient for risk stratification in COPD,” the investigators wrote in Annals of Allergy, Asthma & Immunology. “Since asthma and COPD share some pathophysiological mechanisms, a logical approach would be to investigate well-known biomarkers for asthma in COPD and vice versa.”
Dr. Çolak and colleagues cited previous research supporting this perspective. Specifically, IgE-targeting monoclonal antibodies have shown promise in patients with severe asthma and asthma-COPD overlap, whereas COPD with high IgE has been associated with a history of lung function decline and previous exacerbations.
The present study drew from a database of 46,598 adults enrolled in the Copenhagen General Population study. All participants underwent physical examination, completed a questionnaire, and provided blood for analysis. From this population, 1,559 individuals had COPD, among whom 446 had high plasma IgE (at least 76 IU/mL).
Over a median follow-up of 6.9 years in the COPD group, 224 severe exacerbations and 434 deaths of any cause occurred. Compared with COPD patients who had normal plasma IgE, those with high IgE were 43% more likely to have severe exacerbation (hazard ratio, 1.43; 95% confidence interval, 1.07-1.89) and 30% more likely to die of any cause (HR, 1.30; 95% CI, 1.06-1.62). These risks were similar when excluding patients with IgE of 700 IU/mL or higher.
“These findings suggest that plasma IgE concentration may be a potential prognostic biomarker and treatment target for a subset of COPD patient,” wrote Dr. Çolak and colleagues.
The above risks increased moderately when the high IgE group was trimmed to include only those with low eosinophils (less than 300 cells/mcL); in this subgroup, risk of exacerbation was increased 62% (HR, 1.62; 95% CI, 1.17-2.24), while risk of all-cause mortality was increased 47% (HR, 1.47; 95% CI, 1.14-1.88).
“We were not able to show that individuals with higher blood eosinophils further stratified by IgE had higher risk of severe exacerbation or all-cause mortality,” the investigators wrote, although they noted “the relatively low statistical power in stratified analysis,” considering the wide confidence intervals observed.
“Thus, we should be careful with interpreting the results in relation to blood eosinophils and IgE combined,” they suggested. “However, we believe that the mechanisms driving exacerbations through plasma IgE are different from those driving blood eosinophils, and we believe that plasma IgE may be a marker for a subset of COPD patients similar to blood eosinophils, which is compatible with the heterogeneity of patients with COPD.”
According to principal author Shoaib Afzal, MD, PhD, of Copenhagen University Hospital, the findings are “probably no surprise for practitioners that often observe overlap between asthma and COPD pathology.”
As smoking prevalence goes down in many countries, relatively more never-smokers are being diagnosed with COPD, Dr. Afzal said in a written comment, “which means that asthma as a risk factor for COPD is gaining importance.”
While patients with asthma can be treated with IgE-targeting omalizumab, a trial evaluating the same biologic for COPD patients with high IgE was withdrawn because of a lack of recruitment; however, Dr. Afzal suggested that this should not be the end of the story, since these new data imply that more patients could benefit than previously recognized.
“Our observational study has generated a hypothesis that needs to be tested by pulmonologists in randomized interventions trials designed with updated inclusion criteria,” he said.
Such trials are needed, Dr. Afzal went on, because they could help unlock the “huge” potential benefit that may come from characterizing COPD patients beyond “exposures, symptoms, and spirometry.”
“Sadly, the progress in establishing biomarkers in COPD for improving risk stratification and treatment allocation have been rather disappointing in the last decades, with the exception of small successes with eosinophils and perhaps FeNO,” Dr. Afzal said.
Nathaniel Marchetti, DO, professor of thoracic medicine and surgery at Temple University and medical director of the respiratory ICU at Temple University Hospital, both in Philadelphia, said the study by Dr. Afzal and colleagues is noteworthy because “biomarkers for COPD are desperately needed to help risk stratify patients for exacerbation risk and risk of disease progression and even mortality.”
In a written comment, Dr. Marchetti agreed with Dr. Afzal that the findings “open the possibility for interventional trials targeting IgE,” which could one day reshape the way patients with COPD are treated.
“I think that biomarkers will become vital in caring for patients with COPD in the future,” Dr. Marchetti said. “There will be medications that will be used to target different pathways of inflammation that drive disease progression and exacerbations. Biomarkers will be important in driving personalized medicine in COPD. We already know the disease seems to vary greatly from patient to patient.”
The study was supported by The Capital Region of Copenhagen, The Danish Lung Foundation, The Velux Foundation, and others. The investigators disclosed relationships with Boehringer Ingelheim, AstraZeneca, Sanofi Genzyme, and others. Dr. Marchetti disclosed no conflicts of interest.
COPD patients with high plasma immunoglobulin E are more likely to have exacerbations and die from any cause, based on a Danish population-cohort study.
hinting at different subsets of patients with COPD, lead author Yunus Çolak MD, PhD, of Copenhagen University Hospital, and colleagues reported.
“Additional biomarkers are necessary as blood eosinophils alone seem insufficient for risk stratification in COPD,” the investigators wrote in Annals of Allergy, Asthma & Immunology. “Since asthma and COPD share some pathophysiological mechanisms, a logical approach would be to investigate well-known biomarkers for asthma in COPD and vice versa.”
Dr. Çolak and colleagues cited previous research supporting this perspective. Specifically, IgE-targeting monoclonal antibodies have shown promise in patients with severe asthma and asthma-COPD overlap, whereas COPD with high IgE has been associated with a history of lung function decline and previous exacerbations.
The present study drew from a database of 46,598 adults enrolled in the Copenhagen General Population study. All participants underwent physical examination, completed a questionnaire, and provided blood for analysis. From this population, 1,559 individuals had COPD, among whom 446 had high plasma IgE (at least 76 IU/mL).
Over a median follow-up of 6.9 years in the COPD group, 224 severe exacerbations and 434 deaths of any cause occurred. Compared with COPD patients who had normal plasma IgE, those with high IgE were 43% more likely to have severe exacerbation (hazard ratio, 1.43; 95% confidence interval, 1.07-1.89) and 30% more likely to die of any cause (HR, 1.30; 95% CI, 1.06-1.62). These risks were similar when excluding patients with IgE of 700 IU/mL or higher.
“These findings suggest that plasma IgE concentration may be a potential prognostic biomarker and treatment target for a subset of COPD patient,” wrote Dr. Çolak and colleagues.
The above risks increased moderately when the high IgE group was trimmed to include only those with low eosinophils (less than 300 cells/mcL); in this subgroup, risk of exacerbation was increased 62% (HR, 1.62; 95% CI, 1.17-2.24), while risk of all-cause mortality was increased 47% (HR, 1.47; 95% CI, 1.14-1.88).
“We were not able to show that individuals with higher blood eosinophils further stratified by IgE had higher risk of severe exacerbation or all-cause mortality,” the investigators wrote, although they noted “the relatively low statistical power in stratified analysis,” considering the wide confidence intervals observed.
“Thus, we should be careful with interpreting the results in relation to blood eosinophils and IgE combined,” they suggested. “However, we believe that the mechanisms driving exacerbations through plasma IgE are different from those driving blood eosinophils, and we believe that plasma IgE may be a marker for a subset of COPD patients similar to blood eosinophils, which is compatible with the heterogeneity of patients with COPD.”
According to principal author Shoaib Afzal, MD, PhD, of Copenhagen University Hospital, the findings are “probably no surprise for practitioners that often observe overlap between asthma and COPD pathology.”
As smoking prevalence goes down in many countries, relatively more never-smokers are being diagnosed with COPD, Dr. Afzal said in a written comment, “which means that asthma as a risk factor for COPD is gaining importance.”
While patients with asthma can be treated with IgE-targeting omalizumab, a trial evaluating the same biologic for COPD patients with high IgE was withdrawn because of a lack of recruitment; however, Dr. Afzal suggested that this should not be the end of the story, since these new data imply that more patients could benefit than previously recognized.
“Our observational study has generated a hypothesis that needs to be tested by pulmonologists in randomized interventions trials designed with updated inclusion criteria,” he said.
Such trials are needed, Dr. Afzal went on, because they could help unlock the “huge” potential benefit that may come from characterizing COPD patients beyond “exposures, symptoms, and spirometry.”
“Sadly, the progress in establishing biomarkers in COPD for improving risk stratification and treatment allocation have been rather disappointing in the last decades, with the exception of small successes with eosinophils and perhaps FeNO,” Dr. Afzal said.
Nathaniel Marchetti, DO, professor of thoracic medicine and surgery at Temple University and medical director of the respiratory ICU at Temple University Hospital, both in Philadelphia, said the study by Dr. Afzal and colleagues is noteworthy because “biomarkers for COPD are desperately needed to help risk stratify patients for exacerbation risk and risk of disease progression and even mortality.”
In a written comment, Dr. Marchetti agreed with Dr. Afzal that the findings “open the possibility for interventional trials targeting IgE,” which could one day reshape the way patients with COPD are treated.
“I think that biomarkers will become vital in caring for patients with COPD in the future,” Dr. Marchetti said. “There will be medications that will be used to target different pathways of inflammation that drive disease progression and exacerbations. Biomarkers will be important in driving personalized medicine in COPD. We already know the disease seems to vary greatly from patient to patient.”
The study was supported by The Capital Region of Copenhagen, The Danish Lung Foundation, The Velux Foundation, and others. The investigators disclosed relationships with Boehringer Ingelheim, AstraZeneca, Sanofi Genzyme, and others. Dr. Marchetti disclosed no conflicts of interest.
FROM ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY
Children and COVID: Many parents see vaccine as the greater risk
New COVID-19 cases rose for the second week in a row as cumulative cases among U.S. children passed the 14-million mark, but a recent survey shows that more than half of parents believe that the vaccine is a greater risk to children under age 5 years than the virus.
In a Kaiser Family Foundation survey conducted July 7-17, 53% of parents with children aged 6 months to 5 years said that the vaccine is “a bigger risk to their child’s health than getting infected with COVID-19, compared to 44% who say getting infected is the bigger risk,” KFF reported July 26.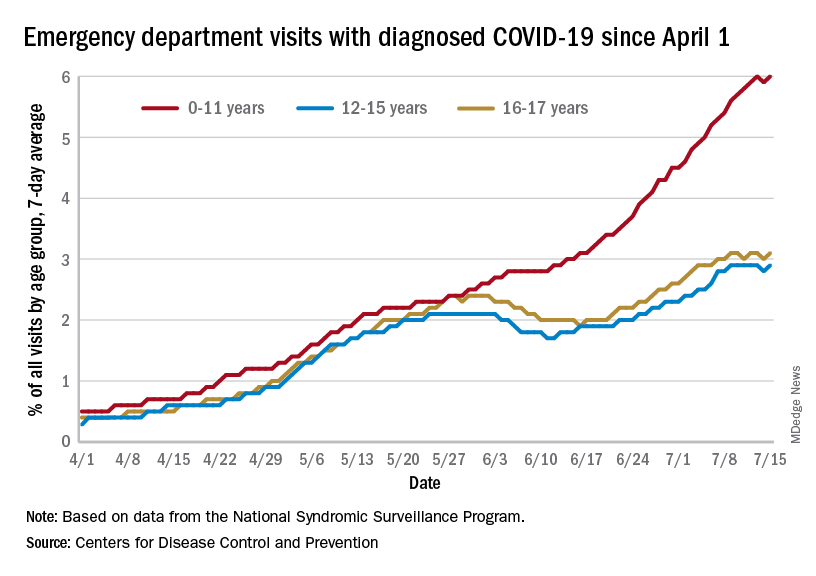
More than 4 out of 10 of respondents (43%) said that they will “definitely not” get their eligible children vaccinated, while only 7% said that their children had already received it and 10% said their children would get it as soon as possible, according to the KFF survey, which had an overall sample size of 1,847 adults, including an oversample of 471 parents of children under age 5.
Vaccine initiation has been slow in the first month since it was approved for the youngest children. Just 2.8% of all eligible children under age 5 had received an initial dose as of July 19, compared with first-month uptake figures of more than 18% for the 5- to 11-year-olds and 27% for those aged 12-15, based on data from the Centers for Disease Control and Prevention.
The current rates for vaccination in those aged 5 and older look like this: 70.2% of 12- to 17-year-olds have received at least one dose, versus 37.1% of those aged 5-11. Just over 60% of the older children were fully vaccinated as of July 19, as were 30.2% of the 5- to 11-year-olds, the CDC reported on its COVID Data Tracker.
Number of new cases hits 2-month high
Despite the vaccine, SARS-CoV-2 and its various mutations have continued with their summer travels. With 92,000 newly infected children added for the week of July 15-21, there have now been a total of 14,003,497 pediatric cases reported since the start of the pandemic, which works out to 18.6% of cases in all ages, the American Academy of Pediatrics and the Children’s Hospital Association said in their weekly COVID-19 report.
The 92,000 new cases represent an increase of almost 22% over the previous week and mark the highest 1-week count since May, when the total passed 100,000 for 2 consecutive weeks. More recently the trend had seemed more stable as weekly cases dropped twice and rose twice as the total hovered around 70,000, based on the data collected by the AAP and CHA from state and territorial health departments.
A different scenario has played out for emergency department visits and hospital admissions, which have risen steadily since the beginning of April. The admission rate for children aged 0-17, which was just 0.13 new patients per 100,000 population on April 11, was up to 0.44 per 100,000 on July 21. By comparison, the highest rate reached last year during the Delta surge was 0.47 per 100,000, based on CDC data.
The 7-day average of emergency dept. visits among the youngest age group, 0-11 years, shows the same general increase as hospital admissions, but the older children have diverged form that path (see graph). For those aged 12-15 and 16-17, hospitalizations started dropping in late May and into mid-June before climbing again, although more slowly than for the youngest group, the CDC data show.
The ED visit rate with diagnosed COVID among those aged 0-11, measured at 6.1% of all visits on July 19, is, in fact, considerably higher than at any time during the Delta surge last year, when it never passed 4.0%, although much lower than peak Omicron (14.1%). That 6.1% was also higher than any other age group on that day, adults included, the CDC said.
New COVID-19 cases rose for the second week in a row as cumulative cases among U.S. children passed the 14-million mark, but a recent survey shows that more than half of parents believe that the vaccine is a greater risk to children under age 5 years than the virus.
In a Kaiser Family Foundation survey conducted July 7-17, 53% of parents with children aged 6 months to 5 years said that the vaccine is “a bigger risk to their child’s health than getting infected with COVID-19, compared to 44% who say getting infected is the bigger risk,” KFF reported July 26.
More than 4 out of 10 of respondents (43%) said that they will “definitely not” get their eligible children vaccinated, while only 7% said that their children had already received it and 10% said their children would get it as soon as possible, according to the KFF survey, which had an overall sample size of 1,847 adults, including an oversample of 471 parents of children under age 5.
Vaccine initiation has been slow in the first month since it was approved for the youngest children. Just 2.8% of all eligible children under age 5 had received an initial dose as of July 19, compared with first-month uptake figures of more than 18% for the 5- to 11-year-olds and 27% for those aged 12-15, based on data from the Centers for Disease Control and Prevention.
The current rates for vaccination in those aged 5 and older look like this: 70.2% of 12- to 17-year-olds have received at least one dose, versus 37.1% of those aged 5-11. Just over 60% of the older children were fully vaccinated as of July 19, as were 30.2% of the 5- to 11-year-olds, the CDC reported on its COVID Data Tracker.
Number of new cases hits 2-month high
Despite the vaccine, SARS-CoV-2 and its various mutations have continued with their summer travels. With 92,000 newly infected children added for the week of July 15-21, there have now been a total of 14,003,497 pediatric cases reported since the start of the pandemic, which works out to 18.6% of cases in all ages, the American Academy of Pediatrics and the Children’s Hospital Association said in their weekly COVID-19 report.
The 92,000 new cases represent an increase of almost 22% over the previous week and mark the highest 1-week count since May, when the total passed 100,000 for 2 consecutive weeks. More recently the trend had seemed more stable as weekly cases dropped twice and rose twice as the total hovered around 70,000, based on the data collected by the AAP and CHA from state and territorial health departments.
A different scenario has played out for emergency department visits and hospital admissions, which have risen steadily since the beginning of April. The admission rate for children aged 0-17, which was just 0.13 new patients per 100,000 population on April 11, was up to 0.44 per 100,000 on July 21. By comparison, the highest rate reached last year during the Delta surge was 0.47 per 100,000, based on CDC data.
The 7-day average of emergency dept. visits among the youngest age group, 0-11 years, shows the same general increase as hospital admissions, but the older children have diverged form that path (see graph). For those aged 12-15 and 16-17, hospitalizations started dropping in late May and into mid-June before climbing again, although more slowly than for the youngest group, the CDC data show.
The ED visit rate with diagnosed COVID among those aged 0-11, measured at 6.1% of all visits on July 19, is, in fact, considerably higher than at any time during the Delta surge last year, when it never passed 4.0%, although much lower than peak Omicron (14.1%). That 6.1% was also higher than any other age group on that day, adults included, the CDC said.
New COVID-19 cases rose for the second week in a row as cumulative cases among U.S. children passed the 14-million mark, but a recent survey shows that more than half of parents believe that the vaccine is a greater risk to children under age 5 years than the virus.
In a Kaiser Family Foundation survey conducted July 7-17, 53% of parents with children aged 6 months to 5 years said that the vaccine is “a bigger risk to their child’s health than getting infected with COVID-19, compared to 44% who say getting infected is the bigger risk,” KFF reported July 26.
More than 4 out of 10 of respondents (43%) said that they will “definitely not” get their eligible children vaccinated, while only 7% said that their children had already received it and 10% said their children would get it as soon as possible, according to the KFF survey, which had an overall sample size of 1,847 adults, including an oversample of 471 parents of children under age 5.
Vaccine initiation has been slow in the first month since it was approved for the youngest children. Just 2.8% of all eligible children under age 5 had received an initial dose as of July 19, compared with first-month uptake figures of more than 18% for the 5- to 11-year-olds and 27% for those aged 12-15, based on data from the Centers for Disease Control and Prevention.
The current rates for vaccination in those aged 5 and older look like this: 70.2% of 12- to 17-year-olds have received at least one dose, versus 37.1% of those aged 5-11. Just over 60% of the older children were fully vaccinated as of July 19, as were 30.2% of the 5- to 11-year-olds, the CDC reported on its COVID Data Tracker.
Number of new cases hits 2-month high
Despite the vaccine, SARS-CoV-2 and its various mutations have continued with their summer travels. With 92,000 newly infected children added for the week of July 15-21, there have now been a total of 14,003,497 pediatric cases reported since the start of the pandemic, which works out to 18.6% of cases in all ages, the American Academy of Pediatrics and the Children’s Hospital Association said in their weekly COVID-19 report.
The 92,000 new cases represent an increase of almost 22% over the previous week and mark the highest 1-week count since May, when the total passed 100,000 for 2 consecutive weeks. More recently the trend had seemed more stable as weekly cases dropped twice and rose twice as the total hovered around 70,000, based on the data collected by the AAP and CHA from state and territorial health departments.
A different scenario has played out for emergency department visits and hospital admissions, which have risen steadily since the beginning of April. The admission rate for children aged 0-17, which was just 0.13 new patients per 100,000 population on April 11, was up to 0.44 per 100,000 on July 21. By comparison, the highest rate reached last year during the Delta surge was 0.47 per 100,000, based on CDC data.
The 7-day average of emergency dept. visits among the youngest age group, 0-11 years, shows the same general increase as hospital admissions, but the older children have diverged form that path (see graph). For those aged 12-15 and 16-17, hospitalizations started dropping in late May and into mid-June before climbing again, although more slowly than for the youngest group, the CDC data show.
The ED visit rate with diagnosed COVID among those aged 0-11, measured at 6.1% of all visits on July 19, is, in fact, considerably higher than at any time during the Delta surge last year, when it never passed 4.0%, although much lower than peak Omicron (14.1%). That 6.1% was also higher than any other age group on that day, adults included, the CDC said.
U.S. News issues top hospitals list, now with expanded health equity measures
For the seventh consecutive year, the Mayo Clinic in Rochester, Minn., took the top spot in the annual honor roll of best hospitals, published July 26 by U.S. News & World Report.
The 2022 rankings, which marks the 33rd edition, showcase several methodology changes, including new ratings for ovarian, prostate, and uterine cancer surgeries that “provide patients ... with previously unavailable information to assist them in making a critical health care decision,” a news release from the publication explains.
said the release. Finally, a new metric called “home time” determines how successfully each hospital helps patients return home.
Mayo Clinic remains No. 1
For the 2022-2023 rankings and ratings, U.S. News compared more than 4,500 medical centers across the country in 15 specialties and 20 procedures and conditions. Of these, 493 were recognized as Best Regional Hospitals as a result of their overall strong performance.
The list was then narrowed to the top 20 hospitals, outlined in the honor roll below, that deliver “exceptional treatment across multiple areas of care.”
Following Mayo Clinic in the annual ranking’s top spot, Cedars-Sinai Medical Center in Los Angeles rises from No. 6 to No. 2, and New York University Langone Hospitals finish third, up from eighth in 2021.
Cleveland Clinic in Ohio holds the No. 4 spot, down two from 2021, while Johns Hopkins Hospital in Baltimore and UCLA Medical Center in Los Angeles tie for fifth place. Rounding out the top 10, in order, are: New York–Presbyterian Hospital–Columbia and Cornell, New York; Massachusetts General Hospital, Boston; Northwestern Memorial Hospital, Chicago; Stanford (Calif.) Health Care–Stanford Hospital.
The following hospitals complete the top 20 in the United States:
- 11. Barnes-Jewish Hospital, St. Louis
- 12. UCSF Medical Center, San Francisco
- 13. Hospitals of the University of Pennsylvania–Penn Presbyterian, Philadelphia
- 14. Brigham and Women’s Hospital, Boston
- 15. Houston Methodist Hospital
- 16. Mount Sinai Hospital, New York
- 17. University of Michigan Health–Michigan Medicine, Ann Arbor
- 18. Mayo Clinic–Phoenix
- 19. Vanderbilt University Medical Center, Nashville, Tenn.
- 20. Rush University Medical Center, Chicago
For the specialty rankings, the University of Texas MD Anderson Cancer Center, Houston, remains No. 1 in cancer care, the Cleveland Clinic is No. 1 in cardiology and heart surgery, and the Hospital for Special Surgery in New York is No. 1 in orthopedics.
Top five for cancer
- 1. University of Texas MD Anderson Cancer Center, Houston
- 2. Memorial Sloan Kettering Cancer Center, New York
- 3. Mayo Clinic, Rochester, Minn.
- 4. Dana-Farber/Brigham and Women’s Cancer Center, Boston
- 5. UCLA Medical Center, Los Angeles
Top five for cardiology and heart surgery
- 1. Cleveland Clinic
- 2. Mayo Clinic, Rochester, Minn.
- 3. Cedars-Sinai Medical Center, Los Angeles
- 4. New York–Presbyterian Hospital–Columbia and Cornell, New York
- 5. New York University Langone Hospitals
Top five for orthopedics
- 1. Hospital for Special Surgery, New York
- 2. Mayo Clinic, Rochester, Minn.
- 3. Cedars-Sinai Medical Center, Los Angeles
- 4. New York University Langone Hospitals
- 5. (tie) Rush University Medical Center, Chicago
- 5. (tie) UCLA Medical Center, Los Angeles
According to the news release, the procedures and conditions ratings are based entirely on objective patient care measures like survival rates, patient experience, home time, and level of nursing care. The Best Hospitals rankings consider a variety of data provided by the Centers for Medicare & Medicaid Services, American Hospital Association, professional organizations, and medical specialists.
The full report is available online.
A version of this article first appeared on Medscape.com.
For the seventh consecutive year, the Mayo Clinic in Rochester, Minn., took the top spot in the annual honor roll of best hospitals, published July 26 by U.S. News & World Report.
The 2022 rankings, which marks the 33rd edition, showcase several methodology changes, including new ratings for ovarian, prostate, and uterine cancer surgeries that “provide patients ... with previously unavailable information to assist them in making a critical health care decision,” a news release from the publication explains.
said the release. Finally, a new metric called “home time” determines how successfully each hospital helps patients return home.
Mayo Clinic remains No. 1
For the 2022-2023 rankings and ratings, U.S. News compared more than 4,500 medical centers across the country in 15 specialties and 20 procedures and conditions. Of these, 493 were recognized as Best Regional Hospitals as a result of their overall strong performance.
The list was then narrowed to the top 20 hospitals, outlined in the honor roll below, that deliver “exceptional treatment across multiple areas of care.”
Following Mayo Clinic in the annual ranking’s top spot, Cedars-Sinai Medical Center in Los Angeles rises from No. 6 to No. 2, and New York University Langone Hospitals finish third, up from eighth in 2021.
Cleveland Clinic in Ohio holds the No. 4 spot, down two from 2021, while Johns Hopkins Hospital in Baltimore and UCLA Medical Center in Los Angeles tie for fifth place. Rounding out the top 10, in order, are: New York–Presbyterian Hospital–Columbia and Cornell, New York; Massachusetts General Hospital, Boston; Northwestern Memorial Hospital, Chicago; Stanford (Calif.) Health Care–Stanford Hospital.
The following hospitals complete the top 20 in the United States:
- 11. Barnes-Jewish Hospital, St. Louis
- 12. UCSF Medical Center, San Francisco
- 13. Hospitals of the University of Pennsylvania–Penn Presbyterian, Philadelphia
- 14. Brigham and Women’s Hospital, Boston
- 15. Houston Methodist Hospital
- 16. Mount Sinai Hospital, New York
- 17. University of Michigan Health–Michigan Medicine, Ann Arbor
- 18. Mayo Clinic–Phoenix
- 19. Vanderbilt University Medical Center, Nashville, Tenn.
- 20. Rush University Medical Center, Chicago
For the specialty rankings, the University of Texas MD Anderson Cancer Center, Houston, remains No. 1 in cancer care, the Cleveland Clinic is No. 1 in cardiology and heart surgery, and the Hospital for Special Surgery in New York is No. 1 in orthopedics.
Top five for cancer
- 1. University of Texas MD Anderson Cancer Center, Houston
- 2. Memorial Sloan Kettering Cancer Center, New York
- 3. Mayo Clinic, Rochester, Minn.
- 4. Dana-Farber/Brigham and Women’s Cancer Center, Boston
- 5. UCLA Medical Center, Los Angeles
Top five for cardiology and heart surgery
- 1. Cleveland Clinic
- 2. Mayo Clinic, Rochester, Minn.
- 3. Cedars-Sinai Medical Center, Los Angeles
- 4. New York–Presbyterian Hospital–Columbia and Cornell, New York
- 5. New York University Langone Hospitals
Top five for orthopedics
- 1. Hospital for Special Surgery, New York
- 2. Mayo Clinic, Rochester, Minn.
- 3. Cedars-Sinai Medical Center, Los Angeles
- 4. New York University Langone Hospitals
- 5. (tie) Rush University Medical Center, Chicago
- 5. (tie) UCLA Medical Center, Los Angeles
According to the news release, the procedures and conditions ratings are based entirely on objective patient care measures like survival rates, patient experience, home time, and level of nursing care. The Best Hospitals rankings consider a variety of data provided by the Centers for Medicare & Medicaid Services, American Hospital Association, professional organizations, and medical specialists.
The full report is available online.
A version of this article first appeared on Medscape.com.
For the seventh consecutive year, the Mayo Clinic in Rochester, Minn., took the top spot in the annual honor roll of best hospitals, published July 26 by U.S. News & World Report.
The 2022 rankings, which marks the 33rd edition, showcase several methodology changes, including new ratings for ovarian, prostate, and uterine cancer surgeries that “provide patients ... with previously unavailable information to assist them in making a critical health care decision,” a news release from the publication explains.
said the release. Finally, a new metric called “home time” determines how successfully each hospital helps patients return home.
Mayo Clinic remains No. 1
For the 2022-2023 rankings and ratings, U.S. News compared more than 4,500 medical centers across the country in 15 specialties and 20 procedures and conditions. Of these, 493 were recognized as Best Regional Hospitals as a result of their overall strong performance.
The list was then narrowed to the top 20 hospitals, outlined in the honor roll below, that deliver “exceptional treatment across multiple areas of care.”
Following Mayo Clinic in the annual ranking’s top spot, Cedars-Sinai Medical Center in Los Angeles rises from No. 6 to No. 2, and New York University Langone Hospitals finish third, up from eighth in 2021.
Cleveland Clinic in Ohio holds the No. 4 spot, down two from 2021, while Johns Hopkins Hospital in Baltimore and UCLA Medical Center in Los Angeles tie for fifth place. Rounding out the top 10, in order, are: New York–Presbyterian Hospital–Columbia and Cornell, New York; Massachusetts General Hospital, Boston; Northwestern Memorial Hospital, Chicago; Stanford (Calif.) Health Care–Stanford Hospital.
The following hospitals complete the top 20 in the United States:
- 11. Barnes-Jewish Hospital, St. Louis
- 12. UCSF Medical Center, San Francisco
- 13. Hospitals of the University of Pennsylvania–Penn Presbyterian, Philadelphia
- 14. Brigham and Women’s Hospital, Boston
- 15. Houston Methodist Hospital
- 16. Mount Sinai Hospital, New York
- 17. University of Michigan Health–Michigan Medicine, Ann Arbor
- 18. Mayo Clinic–Phoenix
- 19. Vanderbilt University Medical Center, Nashville, Tenn.
- 20. Rush University Medical Center, Chicago
For the specialty rankings, the University of Texas MD Anderson Cancer Center, Houston, remains No. 1 in cancer care, the Cleveland Clinic is No. 1 in cardiology and heart surgery, and the Hospital for Special Surgery in New York is No. 1 in orthopedics.
Top five for cancer
- 1. University of Texas MD Anderson Cancer Center, Houston
- 2. Memorial Sloan Kettering Cancer Center, New York
- 3. Mayo Clinic, Rochester, Minn.
- 4. Dana-Farber/Brigham and Women’s Cancer Center, Boston
- 5. UCLA Medical Center, Los Angeles
Top five for cardiology and heart surgery
- 1. Cleveland Clinic
- 2. Mayo Clinic, Rochester, Minn.
- 3. Cedars-Sinai Medical Center, Los Angeles
- 4. New York–Presbyterian Hospital–Columbia and Cornell, New York
- 5. New York University Langone Hospitals
Top five for orthopedics
- 1. Hospital for Special Surgery, New York
- 2. Mayo Clinic, Rochester, Minn.
- 3. Cedars-Sinai Medical Center, Los Angeles
- 4. New York University Langone Hospitals
- 5. (tie) Rush University Medical Center, Chicago
- 5. (tie) UCLA Medical Center, Los Angeles
According to the news release, the procedures and conditions ratings are based entirely on objective patient care measures like survival rates, patient experience, home time, and level of nursing care. The Best Hospitals rankings consider a variety of data provided by the Centers for Medicare & Medicaid Services, American Hospital Association, professional organizations, and medical specialists.
The full report is available online.
A version of this article first appeared on Medscape.com.
Are head-to-head cancer drug trials rigged?
More than half of studies testing anticancer drugs against each other have rules with regard to dose modification and growth support that favor the experimental drug arm, a new analysis suggests.
“We found it sobering that this practice is so common,” Timothée Olivier, MD, with Geneva University Hospital and the University of California, San Francisco, said in an interview.
than if the trial would have been designed with fairer rules, he explained.
This leaves open the question of whether new drugs are truly superior to older ones or if instead different outcomes are caused by more aggressive dosing or growth factor support, the investigators said.
Dr. Olivier, with UCSF coinvestigators Alyson Haslam, PhD, and Vinay Prasad, MD, reported their findings online in the European Journal of Cancer.
‘Highly concerning’
Different drug modification rules or growth factor support guidance may affect the results of randomized controlled trials (RCTs) of testing new cancer agents.
For their study, Dr. Olivier and colleagues did a cross-sectional analysis of all 62 head-to-head registration RCTs that led to Food and Drug Administration approval between 2009 and 2021.
All of the trials examined anticancer drugs in the advanced or metastatic setting where a comparison was made between arms regarding either dose modification rules or myeloid growth factors recommendations.
The researchers assessed imbalance in drug modification rules, myeloid growth factor recommendations, or both, according to prespecified rules.
They discovered that 40 of the 62 trials (65%) had unequal rules for dose medication, granulocyte colony-stimulating factor (G-CSF) use, or both.
Six trials (10%) had rules favoring the control arm, while 34 (55%) had rules favoring the experimental arm. Among these, 50% had unequal drug modification rules, 41% had unequal G-CSF rules, and 9% had both.
Dr. Olivier said in an interview the results are “highly concerning because when you are investigating the effect of a new drug, you don’t want to have a false sense of a drug’s effect because of other factors not directly related to the drug’s efficacy.”
“If you introduce unfair rules about dose modification or supporting medication that favors the new drug, then you don’t know if a positive trial is due to the effect of the new drug or to the effect of differential dosing or supporting medication,” he added.
Blame industry?
Dr. Olivier said the fact that most registration trials are industry-sponsored is likely the primary explanation of the findings.
“Industry-sponsored trials may be designed so that the new drug has the best chance to get the largest ‘win,’ because this means more market share and more profit for the company that manufactures the drug. This is not a criticism of the industry, which runs on a business model that naturally aims to gain more market share and more profit,” Dr. Olivier said.
“However, it is the role and duty of regulators to reconcile industry incentives with the patients’ best interests, and there is accumulating data showing the regulators are failing to do so,” he added.
Addressing this problem will likely take buy-in from multiple stakeholders.
Awareness of the problem is a first step and understanding the influence of commercial incentives in drug development is also key, Dr. Olivier said.
Institutional review boards and drug regulators could also systematically evaluate drug dosing modification and supportive medication rules before a trial gets underway.
Regulators could also incentivize companies to implement balanced rules between arms by not granting drug approval based on trials suffering from such flaws.
“However, financial conflict of interest is present at many levels of drug development, including in drug regulation,” Dr. Olivier noted.
He pointed to a recent study that found when hematology-oncology medical reviewers working at the FDA leave the agency, more than half end up working or consulting for the pharmaceutical industry.
Dr. Olivier wondered: “How can one fairly and independently appraise a medical intervention if one’s current or future revenue depends on its source?”
The study was funded by Arnold Ventures, through a grant paid to UCSF. Dr. Olivier and Dr. Haslam had no relevant disclosures. Dr. Prasad reported receiving royalties from Arnold Ventures.
A version of this article first appeared on Medscape.com.
More than half of studies testing anticancer drugs against each other have rules with regard to dose modification and growth support that favor the experimental drug arm, a new analysis suggests.
“We found it sobering that this practice is so common,” Timothée Olivier, MD, with Geneva University Hospital and the University of California, San Francisco, said in an interview.
than if the trial would have been designed with fairer rules, he explained.
This leaves open the question of whether new drugs are truly superior to older ones or if instead different outcomes are caused by more aggressive dosing or growth factor support, the investigators said.
Dr. Olivier, with UCSF coinvestigators Alyson Haslam, PhD, and Vinay Prasad, MD, reported their findings online in the European Journal of Cancer.
‘Highly concerning’
Different drug modification rules or growth factor support guidance may affect the results of randomized controlled trials (RCTs) of testing new cancer agents.
For their study, Dr. Olivier and colleagues did a cross-sectional analysis of all 62 head-to-head registration RCTs that led to Food and Drug Administration approval between 2009 and 2021.
All of the trials examined anticancer drugs in the advanced or metastatic setting where a comparison was made between arms regarding either dose modification rules or myeloid growth factors recommendations.
The researchers assessed imbalance in drug modification rules, myeloid growth factor recommendations, or both, according to prespecified rules.
They discovered that 40 of the 62 trials (65%) had unequal rules for dose medication, granulocyte colony-stimulating factor (G-CSF) use, or both.
Six trials (10%) had rules favoring the control arm, while 34 (55%) had rules favoring the experimental arm. Among these, 50% had unequal drug modification rules, 41% had unequal G-CSF rules, and 9% had both.
Dr. Olivier said in an interview the results are “highly concerning because when you are investigating the effect of a new drug, you don’t want to have a false sense of a drug’s effect because of other factors not directly related to the drug’s efficacy.”
“If you introduce unfair rules about dose modification or supporting medication that favors the new drug, then you don’t know if a positive trial is due to the effect of the new drug or to the effect of differential dosing or supporting medication,” he added.
Blame industry?
Dr. Olivier said the fact that most registration trials are industry-sponsored is likely the primary explanation of the findings.
“Industry-sponsored trials may be designed so that the new drug has the best chance to get the largest ‘win,’ because this means more market share and more profit for the company that manufactures the drug. This is not a criticism of the industry, which runs on a business model that naturally aims to gain more market share and more profit,” Dr. Olivier said.
“However, it is the role and duty of regulators to reconcile industry incentives with the patients’ best interests, and there is accumulating data showing the regulators are failing to do so,” he added.
Addressing this problem will likely take buy-in from multiple stakeholders.
Awareness of the problem is a first step and understanding the influence of commercial incentives in drug development is also key, Dr. Olivier said.
Institutional review boards and drug regulators could also systematically evaluate drug dosing modification and supportive medication rules before a trial gets underway.
Regulators could also incentivize companies to implement balanced rules between arms by not granting drug approval based on trials suffering from such flaws.
“However, financial conflict of interest is present at many levels of drug development, including in drug regulation,” Dr. Olivier noted.
He pointed to a recent study that found when hematology-oncology medical reviewers working at the FDA leave the agency, more than half end up working or consulting for the pharmaceutical industry.
Dr. Olivier wondered: “How can one fairly and independently appraise a medical intervention if one’s current or future revenue depends on its source?”
The study was funded by Arnold Ventures, through a grant paid to UCSF. Dr. Olivier and Dr. Haslam had no relevant disclosures. Dr. Prasad reported receiving royalties from Arnold Ventures.
A version of this article first appeared on Medscape.com.
More than half of studies testing anticancer drugs against each other have rules with regard to dose modification and growth support that favor the experimental drug arm, a new analysis suggests.
“We found it sobering that this practice is so common,” Timothée Olivier, MD, with Geneva University Hospital and the University of California, San Francisco, said in an interview.
than if the trial would have been designed with fairer rules, he explained.
This leaves open the question of whether new drugs are truly superior to older ones or if instead different outcomes are caused by more aggressive dosing or growth factor support, the investigators said.
Dr. Olivier, with UCSF coinvestigators Alyson Haslam, PhD, and Vinay Prasad, MD, reported their findings online in the European Journal of Cancer.
‘Highly concerning’
Different drug modification rules or growth factor support guidance may affect the results of randomized controlled trials (RCTs) of testing new cancer agents.
For their study, Dr. Olivier and colleagues did a cross-sectional analysis of all 62 head-to-head registration RCTs that led to Food and Drug Administration approval between 2009 and 2021.
All of the trials examined anticancer drugs in the advanced or metastatic setting where a comparison was made between arms regarding either dose modification rules or myeloid growth factors recommendations.
The researchers assessed imbalance in drug modification rules, myeloid growth factor recommendations, or both, according to prespecified rules.
They discovered that 40 of the 62 trials (65%) had unequal rules for dose medication, granulocyte colony-stimulating factor (G-CSF) use, or both.
Six trials (10%) had rules favoring the control arm, while 34 (55%) had rules favoring the experimental arm. Among these, 50% had unequal drug modification rules, 41% had unequal G-CSF rules, and 9% had both.
Dr. Olivier said in an interview the results are “highly concerning because when you are investigating the effect of a new drug, you don’t want to have a false sense of a drug’s effect because of other factors not directly related to the drug’s efficacy.”
“If you introduce unfair rules about dose modification or supporting medication that favors the new drug, then you don’t know if a positive trial is due to the effect of the new drug or to the effect of differential dosing or supporting medication,” he added.
Blame industry?
Dr. Olivier said the fact that most registration trials are industry-sponsored is likely the primary explanation of the findings.
“Industry-sponsored trials may be designed so that the new drug has the best chance to get the largest ‘win,’ because this means more market share and more profit for the company that manufactures the drug. This is not a criticism of the industry, which runs on a business model that naturally aims to gain more market share and more profit,” Dr. Olivier said.
“However, it is the role and duty of regulators to reconcile industry incentives with the patients’ best interests, and there is accumulating data showing the regulators are failing to do so,” he added.
Addressing this problem will likely take buy-in from multiple stakeholders.
Awareness of the problem is a first step and understanding the influence of commercial incentives in drug development is also key, Dr. Olivier said.
Institutional review boards and drug regulators could also systematically evaluate drug dosing modification and supportive medication rules before a trial gets underway.
Regulators could also incentivize companies to implement balanced rules between arms by not granting drug approval based on trials suffering from such flaws.
“However, financial conflict of interest is present at many levels of drug development, including in drug regulation,” Dr. Olivier noted.
He pointed to a recent study that found when hematology-oncology medical reviewers working at the FDA leave the agency, more than half end up working or consulting for the pharmaceutical industry.
Dr. Olivier wondered: “How can one fairly and independently appraise a medical intervention if one’s current or future revenue depends on its source?”
The study was funded by Arnold Ventures, through a grant paid to UCSF. Dr. Olivier and Dr. Haslam had no relevant disclosures. Dr. Prasad reported receiving royalties from Arnold Ventures.
A version of this article first appeared on Medscape.com.
The next blood pressure breakthrough: temporary tattoos
As scientists work on wearable technology that promises to revolutionize health care, researchers from the University of Texas at Austin and Texas A&M University, College Station, are reporting a big win in the pursuit of one highly popular target: a noninvasive solution for continuous blood pressure monitoring at home.
Not only that, but this development comes in the surprising form of a temporary tattoo. That’s right: Just like the kind that children like to wear.
the researchers report in their new study.
“With this new technology, we are going to have an opportunity to understand how our blood pressure fluctuates during the day. We will be able to quantify how stress is impacting us,” says Roozbeh Jafari, PhD, a professor of biomedical engineering, electrical engineering, and computer science at Texas A&M, College Station, and a coauthor of the study.
Revealing the whole picture, not just dots
At-home blood pressure monitors have been around for many years now. They work just like the blood pressure machines doctors use at their office: You place your arm inside a cuff, press a button, feel a squeeze on your arm, and get a reading.
While results from this method are accurate, they are also just a moment in time. Our blood pressure can vary greatly throughout the day – especially among people who have labile hypertension, where blood pressure changes from one extreme to the other. So, looking at point-in-time readings is a bit like focusing on a few dots inside of a pointillism painting – one might miss the bigger picture.
Doctors may also find continuous monitoring useful for getting rid of false readings from “white coat syndrome.” Basically, this means a person’s blood pressure rises due to the anxiety of being in a doctor’s office but is not true hypertension.
Bottom line: The ability to monitor a person’s blood pressure continuously for hours or even days can provide clearer, and more accurate, insights into a person’s health.
How do health monitoring tattoos work?
Electronic tattoos for health monitoring are not completely new. John A. Rogers, PhD, of Northwestern University, Chicago, first put forth the idea of monitoring through temporary tattoos 12 years ago. Some concepts, such as UV monitoring tattoos, had already been adopted by scientists and put on the market. But the existing models weren’t suitable for monitoring blood pressure, according to Deji Akinwande, PhD, a professor of electrical and computer engineering at the University of Texas at Austin and another coauthor of the study.
“[UV monitoring tattoos] are very thick,” he says. “They create too much movement when used to measure blood pressure because they slide around.”
So, the Texas-based research team worked to develop an option that was slimmer and more stable.
“The key ingredient within e-tattoos is graphene,” says Dr. Akinwande.
Graphene is carbon that’s similar to what’s inside your graphite pencil. The material is conductive, meaning it can conduct small electrical currents through the skin. For blood pressure monitoring, graphene promotes bioelectrical impedance analysis (BIA), which is like the technology used in smart scales that measure body fat.
With e-tattoos, the thin layers of graphene stick to the skin and do not slide around, getting rid of “artifacts,” or bad data. The graphene e-tattoos can be worn on the skin for about a week – or roughly as long as the temporary tattoos kids love.
Once the graphene captures the raw data, a machine learning algorithm interprets the information and provides results in units used for measuring blood pressure: millimeters of mercury (mmHg), commonly referred to as blood pressure “points.”
How accurate are the results? The tests measured blood pressure within 0.2 ± 5.8 mmHg (systolic), 0.2 ± 4.5 mmHg (diastolic), and 0.1 ± 5.3 mmHg (mean arterial pressure). In other words: If this were a basketball player shooting baskets, the great majority of shots taken would be swishes and occasionally a few would hit the rim. That means good accuracy.
When will e-tattoos be available?
The teams of Dr. Jafari and Dr. Akinwande are working on a second generation of their e-tattoo that they expect to be available in the next 5 years.
The upgrade they envision will be smaller and compatible with smartwatches and phones that use Bluetooth technology and near-field communication (NFC) to transfer data and give it power. With these updates, e-tattoos for continuous blood pressure monitoring will be ready for clinical trials and mainstream use soon after.
“Everyone can benefit from knowing their blood pressure recordings,” Dr. Akinwande says. “It is not just for people at risk for hypertension but for others to proactively monitor their health, for stress and other factors.”
A version of this article first appeared on WebMD.com.
As scientists work on wearable technology that promises to revolutionize health care, researchers from the University of Texas at Austin and Texas A&M University, College Station, are reporting a big win in the pursuit of one highly popular target: a noninvasive solution for continuous blood pressure monitoring at home.
Not only that, but this development comes in the surprising form of a temporary tattoo. That’s right: Just like the kind that children like to wear.
the researchers report in their new study.
“With this new technology, we are going to have an opportunity to understand how our blood pressure fluctuates during the day. We will be able to quantify how stress is impacting us,” says Roozbeh Jafari, PhD, a professor of biomedical engineering, electrical engineering, and computer science at Texas A&M, College Station, and a coauthor of the study.
Revealing the whole picture, not just dots
At-home blood pressure monitors have been around for many years now. They work just like the blood pressure machines doctors use at their office: You place your arm inside a cuff, press a button, feel a squeeze on your arm, and get a reading.
While results from this method are accurate, they are also just a moment in time. Our blood pressure can vary greatly throughout the day – especially among people who have labile hypertension, where blood pressure changes from one extreme to the other. So, looking at point-in-time readings is a bit like focusing on a few dots inside of a pointillism painting – one might miss the bigger picture.
Doctors may also find continuous monitoring useful for getting rid of false readings from “white coat syndrome.” Basically, this means a person’s blood pressure rises due to the anxiety of being in a doctor’s office but is not true hypertension.
Bottom line: The ability to monitor a person’s blood pressure continuously for hours or even days can provide clearer, and more accurate, insights into a person’s health.
How do health monitoring tattoos work?
Electronic tattoos for health monitoring are not completely new. John A. Rogers, PhD, of Northwestern University, Chicago, first put forth the idea of monitoring through temporary tattoos 12 years ago. Some concepts, such as UV monitoring tattoos, had already been adopted by scientists and put on the market. But the existing models weren’t suitable for monitoring blood pressure, according to Deji Akinwande, PhD, a professor of electrical and computer engineering at the University of Texas at Austin and another coauthor of the study.
“[UV monitoring tattoos] are very thick,” he says. “They create too much movement when used to measure blood pressure because they slide around.”
So, the Texas-based research team worked to develop an option that was slimmer and more stable.
“The key ingredient within e-tattoos is graphene,” says Dr. Akinwande.
Graphene is carbon that’s similar to what’s inside your graphite pencil. The material is conductive, meaning it can conduct small electrical currents through the skin. For blood pressure monitoring, graphene promotes bioelectrical impedance analysis (BIA), which is like the technology used in smart scales that measure body fat.
With e-tattoos, the thin layers of graphene stick to the skin and do not slide around, getting rid of “artifacts,” or bad data. The graphene e-tattoos can be worn on the skin for about a week – or roughly as long as the temporary tattoos kids love.
Once the graphene captures the raw data, a machine learning algorithm interprets the information and provides results in units used for measuring blood pressure: millimeters of mercury (mmHg), commonly referred to as blood pressure “points.”
How accurate are the results? The tests measured blood pressure within 0.2 ± 5.8 mmHg (systolic), 0.2 ± 4.5 mmHg (diastolic), and 0.1 ± 5.3 mmHg (mean arterial pressure). In other words: If this were a basketball player shooting baskets, the great majority of shots taken would be swishes and occasionally a few would hit the rim. That means good accuracy.
When will e-tattoos be available?
The teams of Dr. Jafari and Dr. Akinwande are working on a second generation of their e-tattoo that they expect to be available in the next 5 years.
The upgrade they envision will be smaller and compatible with smartwatches and phones that use Bluetooth technology and near-field communication (NFC) to transfer data and give it power. With these updates, e-tattoos for continuous blood pressure monitoring will be ready for clinical trials and mainstream use soon after.
“Everyone can benefit from knowing their blood pressure recordings,” Dr. Akinwande says. “It is not just for people at risk for hypertension but for others to proactively monitor their health, for stress and other factors.”
A version of this article first appeared on WebMD.com.
As scientists work on wearable technology that promises to revolutionize health care, researchers from the University of Texas at Austin and Texas A&M University, College Station, are reporting a big win in the pursuit of one highly popular target: a noninvasive solution for continuous blood pressure monitoring at home.
Not only that, but this development comes in the surprising form of a temporary tattoo. That’s right: Just like the kind that children like to wear.
the researchers report in their new study.
“With this new technology, we are going to have an opportunity to understand how our blood pressure fluctuates during the day. We will be able to quantify how stress is impacting us,” says Roozbeh Jafari, PhD, a professor of biomedical engineering, electrical engineering, and computer science at Texas A&M, College Station, and a coauthor of the study.
Revealing the whole picture, not just dots
At-home blood pressure monitors have been around for many years now. They work just like the blood pressure machines doctors use at their office: You place your arm inside a cuff, press a button, feel a squeeze on your arm, and get a reading.
While results from this method are accurate, they are also just a moment in time. Our blood pressure can vary greatly throughout the day – especially among people who have labile hypertension, where blood pressure changes from one extreme to the other. So, looking at point-in-time readings is a bit like focusing on a few dots inside of a pointillism painting – one might miss the bigger picture.
Doctors may also find continuous monitoring useful for getting rid of false readings from “white coat syndrome.” Basically, this means a person’s blood pressure rises due to the anxiety of being in a doctor’s office but is not true hypertension.
Bottom line: The ability to monitor a person’s blood pressure continuously for hours or even days can provide clearer, and more accurate, insights into a person’s health.
How do health monitoring tattoos work?
Electronic tattoos for health monitoring are not completely new. John A. Rogers, PhD, of Northwestern University, Chicago, first put forth the idea of monitoring through temporary tattoos 12 years ago. Some concepts, such as UV monitoring tattoos, had already been adopted by scientists and put on the market. But the existing models weren’t suitable for monitoring blood pressure, according to Deji Akinwande, PhD, a professor of electrical and computer engineering at the University of Texas at Austin and another coauthor of the study.
“[UV monitoring tattoos] are very thick,” he says. “They create too much movement when used to measure blood pressure because they slide around.”
So, the Texas-based research team worked to develop an option that was slimmer and more stable.
“The key ingredient within e-tattoos is graphene,” says Dr. Akinwande.
Graphene is carbon that’s similar to what’s inside your graphite pencil. The material is conductive, meaning it can conduct small electrical currents through the skin. For blood pressure monitoring, graphene promotes bioelectrical impedance analysis (BIA), which is like the technology used in smart scales that measure body fat.
With e-tattoos, the thin layers of graphene stick to the skin and do not slide around, getting rid of “artifacts,” or bad data. The graphene e-tattoos can be worn on the skin for about a week – or roughly as long as the temporary tattoos kids love.
Once the graphene captures the raw data, a machine learning algorithm interprets the information and provides results in units used for measuring blood pressure: millimeters of mercury (mmHg), commonly referred to as blood pressure “points.”
How accurate are the results? The tests measured blood pressure within 0.2 ± 5.8 mmHg (systolic), 0.2 ± 4.5 mmHg (diastolic), and 0.1 ± 5.3 mmHg (mean arterial pressure). In other words: If this were a basketball player shooting baskets, the great majority of shots taken would be swishes and occasionally a few would hit the rim. That means good accuracy.
When will e-tattoos be available?
The teams of Dr. Jafari and Dr. Akinwande are working on a second generation of their e-tattoo that they expect to be available in the next 5 years.
The upgrade they envision will be smaller and compatible with smartwatches and phones that use Bluetooth technology and near-field communication (NFC) to transfer data and give it power. With these updates, e-tattoos for continuous blood pressure monitoring will be ready for clinical trials and mainstream use soon after.
“Everyone can benefit from knowing their blood pressure recordings,” Dr. Akinwande says. “It is not just for people at risk for hypertension but for others to proactively monitor their health, for stress and other factors.”
A version of this article first appeared on WebMD.com.
Two distinct phenotypes of COVID-related myocarditis emerge
Researchers from France have identified two distinct phenotypes of fulminant COVID-19–related myocarditis in adults, with different clinical presentations, immunologic profiles, and outcomes.
Differentiation between the two bioclinical entities is important to understand for patient management and further pathophysiological studies, they said.
The first phenotype occurs early (within a few days) in acute SARS-CoV-2 infection, with active viral replication (polymerase chain reaction positive) in adults who meet criteria for multisystem inflammatory syndrome (MIS-A+).
In this early phenotype, there is “limited systemic inflammation without skin and mucosal involvement, but myocardial dysfunction is fulminant and frequently associated with large pericardial effusions. These cases more often require extracorporeal membrane oxygenation [ECMO],” Guy Gorochov, MD, PhD, Sorbonne University, Paris, said in an interview.
The second is a delayed, postinfectious, immune-driven phenotype that occurs in adults who fail to meet the criteria for MIS-A (MIS-A–).
This phenotype occurs weeks after SARS-CoV-2 infection, usually beyond detectable active viral replication (PCR–) in the context of specific immune response and severe systemic inflammation with skin and mucosal involvement. Myocardial dysfunction is more progressive and rarely associated with large pericardial effusions, Dr. Gorochov explained.
The study was published in the Journal of the American College of Cardiology.
Evolving understanding
The findings are based on a retrospective analysis of 38 patients without a history of COVID-19 vaccination who were admitted to the intensive care unit from March 2020 to June 2021 for suspected fulminant COVID-19 myocarditis.
Patients were confirmed to have SARS-CoV-2 infection by PCR and/or by serologic testing. As noted in other studies, the patients were predominantly young men (66%; median age, 27.5 years). Twenty-five (66%) patients were MIS-A+ and 13 (34%) were MIS-A–.
In general, the MIS-A– patients were sicker and had worse outcomes.
Specifically, compared with the MIS-A+ patients, MIS-A– patients had a shorter time between the onset of COVID-19 symptoms and the development of myocarditis, a shorter time to ICU admission, and more severe presentations assessed using lower left ventricular ejection fraction and sequential organ failure assessment scores.
MIS-A– patients also had higher lactate levels, were more likely to need venoarterial ECMO (92% vs 16%), had higher ICU mortality (31% vs. 4%), and a had lower probability of survival at 3 months (68% vs. 96%), compared with their MIS-A+ peers.
Immunologic differences
The immunologic profiles of these two distinct clinical phenotypes also differed.
In MIS-A– early-type COVID-19 myocarditis, RNA polymerase III autoantibodies are frequently positive and serum levels of antiviral interferon-alpha and granulocyte-attracting interleukin-8 are elevated.
In contrast, in MIS-A+ delayed-type COVID-19 myocarditis, RNA polymerase III autoantibodies are negative and serum levels of IL-17 and IL-22 are highly elevated.
“We suggest that IL-17 and IL-22 are novel criteria that should help to assess in adults the recently recognized MIS-A,” Dr. Gorochov told this news organization. “It should be tested whether IL-17 and IL-22 are also elevated in children with MIS-C.”
The researchers also observed “extremely” high serum IL-10 levels in both patient groups. This has been previously associated with severe myocardial injury and an increase in the risk for death in severe COVID-19 patients.
The researchers said the phenotypic clustering of patients with fulminant COVID-19–related myocarditis “seems relevant” for their management.
MIS-A– cases, owing to the high risk for evolution toward refractory cardiogenic shock, should be “urgently” referred to a center with venoarterial ECMO and closely monitored to prevent a “too-late” cannulation, especially under cardiopulmonary resuscitation, known to be associated with poor outcomes, they advised.
They noted that the five patients who died in their series had late venoarterial ECMO implantation, while undergoing multiple organ failures or resuscitation.
Conversely, the risk for evolution to refractory cardiogenic shock is lower in MIS-A+ cases. However, identifying MIS-A+ cases is “all the more important given that numerous data support the efficacy of corticosteroids and/or intravenous immunoglobulins in MIS-C,” Dr. Gorochov and colleagues wrote.
The authors of a linked editorial said the French team should be “commended on their work in furthering our understanding of fulminant myocarditis related to COVID-19 infection.”
Ajith Nair, MD, Baylor College of Medicine, and Anita Deswal, MD, MPH, University of Texas M.D. Anderson Cancer Center, both in Houston, noted that fulminant myocarditis is rare and can result from either of two mechanisms: viral tropism or an immune-mediated mechanism.
“It remains to be seen whether using antiviral therapy versus immunomodulatory therapy on the basis of clinical and cytokine profiles will yield benefits,” they wrote.
“Fulminant myocarditis invariably requires hemodynamic support and carries a high mortality risk if it is recognized late. However, the long-term prognosis in patients who survive the critical period is favorable, with recovery of myocardial function,” they added.
“This study highlights the ever-shifting understanding of the pathophysiology and therapeutic approaches to fulminant myocarditis,” Dr. Nair and Dr. Deswal concluded.
This research was supported in part by the Foundation of France, French National Research Agency, Sorbonne University, and Clinical Research Hospital. The researchers have filed a patent application based on these results. Dr. Nair and Dr. Deswal have no relevant disclosures.
A version of this article first appeared on Medscape.com.
Researchers from France have identified two distinct phenotypes of fulminant COVID-19–related myocarditis in adults, with different clinical presentations, immunologic profiles, and outcomes.
Differentiation between the two bioclinical entities is important to understand for patient management and further pathophysiological studies, they said.
The first phenotype occurs early (within a few days) in acute SARS-CoV-2 infection, with active viral replication (polymerase chain reaction positive) in adults who meet criteria for multisystem inflammatory syndrome (MIS-A+).
In this early phenotype, there is “limited systemic inflammation without skin and mucosal involvement, but myocardial dysfunction is fulminant and frequently associated with large pericardial effusions. These cases more often require extracorporeal membrane oxygenation [ECMO],” Guy Gorochov, MD, PhD, Sorbonne University, Paris, said in an interview.
The second is a delayed, postinfectious, immune-driven phenotype that occurs in adults who fail to meet the criteria for MIS-A (MIS-A–).
This phenotype occurs weeks after SARS-CoV-2 infection, usually beyond detectable active viral replication (PCR–) in the context of specific immune response and severe systemic inflammation with skin and mucosal involvement. Myocardial dysfunction is more progressive and rarely associated with large pericardial effusions, Dr. Gorochov explained.
The study was published in the Journal of the American College of Cardiology.
Evolving understanding
The findings are based on a retrospective analysis of 38 patients without a history of COVID-19 vaccination who were admitted to the intensive care unit from March 2020 to June 2021 for suspected fulminant COVID-19 myocarditis.
Patients were confirmed to have SARS-CoV-2 infection by PCR and/or by serologic testing. As noted in other studies, the patients were predominantly young men (66%; median age, 27.5 years). Twenty-five (66%) patients were MIS-A+ and 13 (34%) were MIS-A–.
In general, the MIS-A– patients were sicker and had worse outcomes.
Specifically, compared with the MIS-A+ patients, MIS-A– patients had a shorter time between the onset of COVID-19 symptoms and the development of myocarditis, a shorter time to ICU admission, and more severe presentations assessed using lower left ventricular ejection fraction and sequential organ failure assessment scores.
MIS-A– patients also had higher lactate levels, were more likely to need venoarterial ECMO (92% vs 16%), had higher ICU mortality (31% vs. 4%), and a had lower probability of survival at 3 months (68% vs. 96%), compared with their MIS-A+ peers.
Immunologic differences
The immunologic profiles of these two distinct clinical phenotypes also differed.
In MIS-A– early-type COVID-19 myocarditis, RNA polymerase III autoantibodies are frequently positive and serum levels of antiviral interferon-alpha and granulocyte-attracting interleukin-8 are elevated.
In contrast, in MIS-A+ delayed-type COVID-19 myocarditis, RNA polymerase III autoantibodies are negative and serum levels of IL-17 and IL-22 are highly elevated.
“We suggest that IL-17 and IL-22 are novel criteria that should help to assess in adults the recently recognized MIS-A,” Dr. Gorochov told this news organization. “It should be tested whether IL-17 and IL-22 are also elevated in children with MIS-C.”
The researchers also observed “extremely” high serum IL-10 levels in both patient groups. This has been previously associated with severe myocardial injury and an increase in the risk for death in severe COVID-19 patients.
The researchers said the phenotypic clustering of patients with fulminant COVID-19–related myocarditis “seems relevant” for their management.
MIS-A– cases, owing to the high risk for evolution toward refractory cardiogenic shock, should be “urgently” referred to a center with venoarterial ECMO and closely monitored to prevent a “too-late” cannulation, especially under cardiopulmonary resuscitation, known to be associated with poor outcomes, they advised.
They noted that the five patients who died in their series had late venoarterial ECMO implantation, while undergoing multiple organ failures or resuscitation.
Conversely, the risk for evolution to refractory cardiogenic shock is lower in MIS-A+ cases. However, identifying MIS-A+ cases is “all the more important given that numerous data support the efficacy of corticosteroids and/or intravenous immunoglobulins in MIS-C,” Dr. Gorochov and colleagues wrote.
The authors of a linked editorial said the French team should be “commended on their work in furthering our understanding of fulminant myocarditis related to COVID-19 infection.”
Ajith Nair, MD, Baylor College of Medicine, and Anita Deswal, MD, MPH, University of Texas M.D. Anderson Cancer Center, both in Houston, noted that fulminant myocarditis is rare and can result from either of two mechanisms: viral tropism or an immune-mediated mechanism.
“It remains to be seen whether using antiviral therapy versus immunomodulatory therapy on the basis of clinical and cytokine profiles will yield benefits,” they wrote.
“Fulminant myocarditis invariably requires hemodynamic support and carries a high mortality risk if it is recognized late. However, the long-term prognosis in patients who survive the critical period is favorable, with recovery of myocardial function,” they added.
“This study highlights the ever-shifting understanding of the pathophysiology and therapeutic approaches to fulminant myocarditis,” Dr. Nair and Dr. Deswal concluded.
This research was supported in part by the Foundation of France, French National Research Agency, Sorbonne University, and Clinical Research Hospital. The researchers have filed a patent application based on these results. Dr. Nair and Dr. Deswal have no relevant disclosures.
A version of this article first appeared on Medscape.com.
Researchers from France have identified two distinct phenotypes of fulminant COVID-19–related myocarditis in adults, with different clinical presentations, immunologic profiles, and outcomes.
Differentiation between the two bioclinical entities is important to understand for patient management and further pathophysiological studies, they said.
The first phenotype occurs early (within a few days) in acute SARS-CoV-2 infection, with active viral replication (polymerase chain reaction positive) in adults who meet criteria for multisystem inflammatory syndrome (MIS-A+).
In this early phenotype, there is “limited systemic inflammation without skin and mucosal involvement, but myocardial dysfunction is fulminant and frequently associated with large pericardial effusions. These cases more often require extracorporeal membrane oxygenation [ECMO],” Guy Gorochov, MD, PhD, Sorbonne University, Paris, said in an interview.
The second is a delayed, postinfectious, immune-driven phenotype that occurs in adults who fail to meet the criteria for MIS-A (MIS-A–).
This phenotype occurs weeks after SARS-CoV-2 infection, usually beyond detectable active viral replication (PCR–) in the context of specific immune response and severe systemic inflammation with skin and mucosal involvement. Myocardial dysfunction is more progressive and rarely associated with large pericardial effusions, Dr. Gorochov explained.
The study was published in the Journal of the American College of Cardiology.
Evolving understanding
The findings are based on a retrospective analysis of 38 patients without a history of COVID-19 vaccination who were admitted to the intensive care unit from March 2020 to June 2021 for suspected fulminant COVID-19 myocarditis.
Patients were confirmed to have SARS-CoV-2 infection by PCR and/or by serologic testing. As noted in other studies, the patients were predominantly young men (66%; median age, 27.5 years). Twenty-five (66%) patients were MIS-A+ and 13 (34%) were MIS-A–.
In general, the MIS-A– patients were sicker and had worse outcomes.
Specifically, compared with the MIS-A+ patients, MIS-A– patients had a shorter time between the onset of COVID-19 symptoms and the development of myocarditis, a shorter time to ICU admission, and more severe presentations assessed using lower left ventricular ejection fraction and sequential organ failure assessment scores.
MIS-A– patients also had higher lactate levels, were more likely to need venoarterial ECMO (92% vs 16%), had higher ICU mortality (31% vs. 4%), and a had lower probability of survival at 3 months (68% vs. 96%), compared with their MIS-A+ peers.
Immunologic differences
The immunologic profiles of these two distinct clinical phenotypes also differed.
In MIS-A– early-type COVID-19 myocarditis, RNA polymerase III autoantibodies are frequently positive and serum levels of antiviral interferon-alpha and granulocyte-attracting interleukin-8 are elevated.
In contrast, in MIS-A+ delayed-type COVID-19 myocarditis, RNA polymerase III autoantibodies are negative and serum levels of IL-17 and IL-22 are highly elevated.
“We suggest that IL-17 and IL-22 are novel criteria that should help to assess in adults the recently recognized MIS-A,” Dr. Gorochov told this news organization. “It should be tested whether IL-17 and IL-22 are also elevated in children with MIS-C.”
The researchers also observed “extremely” high serum IL-10 levels in both patient groups. This has been previously associated with severe myocardial injury and an increase in the risk for death in severe COVID-19 patients.
The researchers said the phenotypic clustering of patients with fulminant COVID-19–related myocarditis “seems relevant” for their management.
MIS-A– cases, owing to the high risk for evolution toward refractory cardiogenic shock, should be “urgently” referred to a center with venoarterial ECMO and closely monitored to prevent a “too-late” cannulation, especially under cardiopulmonary resuscitation, known to be associated with poor outcomes, they advised.
They noted that the five patients who died in their series had late venoarterial ECMO implantation, while undergoing multiple organ failures or resuscitation.
Conversely, the risk for evolution to refractory cardiogenic shock is lower in MIS-A+ cases. However, identifying MIS-A+ cases is “all the more important given that numerous data support the efficacy of corticosteroids and/or intravenous immunoglobulins in MIS-C,” Dr. Gorochov and colleagues wrote.
The authors of a linked editorial said the French team should be “commended on their work in furthering our understanding of fulminant myocarditis related to COVID-19 infection.”
Ajith Nair, MD, Baylor College of Medicine, and Anita Deswal, MD, MPH, University of Texas M.D. Anderson Cancer Center, both in Houston, noted that fulminant myocarditis is rare and can result from either of two mechanisms: viral tropism or an immune-mediated mechanism.
“It remains to be seen whether using antiviral therapy versus immunomodulatory therapy on the basis of clinical and cytokine profiles will yield benefits,” they wrote.
“Fulminant myocarditis invariably requires hemodynamic support and carries a high mortality risk if it is recognized late. However, the long-term prognosis in patients who survive the critical period is favorable, with recovery of myocardial function,” they added.
“This study highlights the ever-shifting understanding of the pathophysiology and therapeutic approaches to fulminant myocarditis,” Dr. Nair and Dr. Deswal concluded.
This research was supported in part by the Foundation of France, French National Research Agency, Sorbonne University, and Clinical Research Hospital. The researchers have filed a patent application based on these results. Dr. Nair and Dr. Deswal have no relevant disclosures.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Hypertension heightens risk for severe COVID-19, even in the fully vaxxed
Adults with hypertension who were vaccinated for COVID-19 with at least one booster were more than twice as likely as vaccinated and boosted individuals without hypertension to be hospitalized for severe COVID-19, according to data from more than 900 individuals.
“We were surprised to learn that many people who were hospitalized with COVID-19 had hypertension and no other risk factors,” said Susan Cheng, MD, MPH, director of the Institute for Research on Healthy Aging in the department of cardiology at the Smidt Heart Institute, Los Angeles, and a senior author of the study. “This is concerning when you consider that almost half of American adults have high blood pressure.”
COVID-19 vaccines demonstrated ability to reduce death and some of the most severe side effects from the infection in the early stages of the pandemic. Although the Omicron surge prompted recommendations for a third mRNA vaccine dose, “a proportion of individuals who received three mRNA vaccine doses still required hospitalization for COVID-19 during the Omicron surge,” and the characteristics associated with severe illness in vaccinated and boosted patients have not been explored, Joseph Ebinger, MD, of Cedars-Sinai Medical Center, Los Angeles, and colleagues wrote.
Previous research has shown an association between high blood pressure an increased risk for developing severe COVID-19 compared to several other chronic health conditions, including kidney disease, type 2 diabetes, chronic obstructive pulmonary disease, and heart failure, the researchers noted.
In a study published in Hypertension, the researchers identified 912 adults who received at least three doses of mRNA COVID-19 vaccine and were later diagnosed with COVID-19 during the surge in infections from the Omicron variant between December 2021 and April 2022.
A total of 145 of the individuals were hospitalized (16%); of these, 125 (86%) had hypertension.
Patients with hypertension were the most likely to be hospitalized, with an odds ratio of 2.9. In addition to high blood pressure, factors including older age (OR, 1.3), chronic kidney disease (OR, 2.2), prior myocardial infarction or heart failure (OR, 2.2), and longer time since the last vaccination and COVID-19 infection were associated with increased risk of hospitalization in a multivariate analysis.
However, the increased risk of severe illness and hospitalization associated with high blood pressure persisted, with an OR of 2.6, in the absence of comorbid conditions such as type 2 diabetes, kidney disease, and heart failure, the researchers emphasized.
“Although the mechanism for hypertension-associated COVID-19 risk remains unclear, prior studies have identified delayed SARS-CoV-2 viral clearance and prolonged inflammatory response among hypertensive patients, which may contribute to greater disease severity,” they wrote.
The findings were limited by several factors, including the use of data from a single center and lack of information on which Omicron variants and subvariants were behind the infections, the researchers noted.
However, the results highlight the need for more research on how to reduce the risks of severe COVID-19 in vulnerable populations, and on the mechanism for a potential connection between high blood pressure and severe COVID-19, they said.
Given the high prevalence of hypertension worldwide, increased understanding of the hypertension-specific risks and identification of individual and population-level risk reduction strategies will be important to the transition of COVID-19 from pandemic to endemic, they concluded.
Omicron changes the game
“When the pandemic initially started, many conditions were seen to increase risk for more severe COVID illness, and hypertension was one of those factors – and then things changed,” lead author Dr. Ebinger said in an interview. “First, vaccines arrived on the scene and substantially reduced risk of severe COVID for everyone who received them. Second, Omicron arrived and, while more transmissible, this variant has been less likely to cause severe COVID. On the one hand, we have vaccines and boosters that we want to think of as ‘the great equalizer’ when it comes to preexisting conditions. On the other hand, we have a dominant set of SARS-CoV-2 subvariants that seem less virulent in most people.
“Taken together, we have been hoping and even assuming that we have been doing pretty well with minimizing risks. Unfortunately, our study results indicate this is not exactly the case,” he said.
“Although vaccines and boosters appear to have equalized or minimized the risks of severe COVID for some people, this has not happened for others – even in the setting of the milder Omicron variant. Of individuals who were fully vaccinated and boosted, having hypertension increased the odds of needing to be hospitalized after getting infected with Omicron by 2.6-fold, even when accounting for or in the absence of having any major chronic disease that might otherwise predispose to more severe COVID-19 illness,” Dr. Ebinger added.
“So, while the originally seen risks of having obesity or diabetes seem to have been minimized during this current era of pandemic, the risk of having hypertension has persisted. We found this both surprising and concerning, because hypertension is very common and present in over half of people over age 50.”
Surprisingly, “we found that a fair number of people, even after being fully vaccinated plus a having gotten a booster, will not only catch Omicron but get sick enough to need hospital care,” Dr. Ebinger emphasized. “Moreover, it is not just older adults with major comorbid conditions who are vulnerable. Our data show that this can happen to an adult of any age and especially if a person has only hypertension and otherwise no major chronic disease.”
The first takeaway message for clinicians at this time is to raise awareness, Dr. Ebinger stressed in the interview. “We need to raise understanding around the fact that receiving three doses of vaccine may not prevent severe COVID-19 illness in everyone, even when the circulating viral variant is presumed to be causing only mild disease in most people. Moreover, the people who are most at risk are not whom we might think they are. They are not the sickest of the sick. They include people who might not have major conditions such as heart disease or kidney disease, but they do have hypertension.”
Second, “we need more research to understand out why there is this link between hypertension and excess risk for the more severe forms of COVID-19, despite it arising from a supposedly milder variant,” said Dr. Ebinger.
“Third, we need to determine how to reduce these risks, whether through more tailored vaccine regimens or novel therapeutics or a combination approach,” he said.
Looking ahead, “the biological mechanism underpinning the association between hypertension and severe COVID-19 remains underexplored. Future work should focus on understanding the factors linking hypertension to severe COVID-19, as this may elucidate both information on how SARS-CoV-2 effects the body and potential targets for intervention,” Dr. Ebinger added.
The study was supported in part by Cedars-Sinai Medical Center, the Erika J. Glazer Family Foundation and the National Institutes of Health. The researchers had no financial conflicts to disclose.
Adults with hypertension who were vaccinated for COVID-19 with at least one booster were more than twice as likely as vaccinated and boosted individuals without hypertension to be hospitalized for severe COVID-19, according to data from more than 900 individuals.
“We were surprised to learn that many people who were hospitalized with COVID-19 had hypertension and no other risk factors,” said Susan Cheng, MD, MPH, director of the Institute for Research on Healthy Aging in the department of cardiology at the Smidt Heart Institute, Los Angeles, and a senior author of the study. “This is concerning when you consider that almost half of American adults have high blood pressure.”
COVID-19 vaccines demonstrated ability to reduce death and some of the most severe side effects from the infection in the early stages of the pandemic. Although the Omicron surge prompted recommendations for a third mRNA vaccine dose, “a proportion of individuals who received three mRNA vaccine doses still required hospitalization for COVID-19 during the Omicron surge,” and the characteristics associated with severe illness in vaccinated and boosted patients have not been explored, Joseph Ebinger, MD, of Cedars-Sinai Medical Center, Los Angeles, and colleagues wrote.
Previous research has shown an association between high blood pressure an increased risk for developing severe COVID-19 compared to several other chronic health conditions, including kidney disease, type 2 diabetes, chronic obstructive pulmonary disease, and heart failure, the researchers noted.
In a study published in Hypertension, the researchers identified 912 adults who received at least three doses of mRNA COVID-19 vaccine and were later diagnosed with COVID-19 during the surge in infections from the Omicron variant between December 2021 and April 2022.
A total of 145 of the individuals were hospitalized (16%); of these, 125 (86%) had hypertension.
Patients with hypertension were the most likely to be hospitalized, with an odds ratio of 2.9. In addition to high blood pressure, factors including older age (OR, 1.3), chronic kidney disease (OR, 2.2), prior myocardial infarction or heart failure (OR, 2.2), and longer time since the last vaccination and COVID-19 infection were associated with increased risk of hospitalization in a multivariate analysis.
However, the increased risk of severe illness and hospitalization associated with high blood pressure persisted, with an OR of 2.6, in the absence of comorbid conditions such as type 2 diabetes, kidney disease, and heart failure, the researchers emphasized.
“Although the mechanism for hypertension-associated COVID-19 risk remains unclear, prior studies have identified delayed SARS-CoV-2 viral clearance and prolonged inflammatory response among hypertensive patients, which may contribute to greater disease severity,” they wrote.
The findings were limited by several factors, including the use of data from a single center and lack of information on which Omicron variants and subvariants were behind the infections, the researchers noted.
However, the results highlight the need for more research on how to reduce the risks of severe COVID-19 in vulnerable populations, and on the mechanism for a potential connection between high blood pressure and severe COVID-19, they said.
Given the high prevalence of hypertension worldwide, increased understanding of the hypertension-specific risks and identification of individual and population-level risk reduction strategies will be important to the transition of COVID-19 from pandemic to endemic, they concluded.
Omicron changes the game
“When the pandemic initially started, many conditions were seen to increase risk for more severe COVID illness, and hypertension was one of those factors – and then things changed,” lead author Dr. Ebinger said in an interview. “First, vaccines arrived on the scene and substantially reduced risk of severe COVID for everyone who received them. Second, Omicron arrived and, while more transmissible, this variant has been less likely to cause severe COVID. On the one hand, we have vaccines and boosters that we want to think of as ‘the great equalizer’ when it comes to preexisting conditions. On the other hand, we have a dominant set of SARS-CoV-2 subvariants that seem less virulent in most people.
“Taken together, we have been hoping and even assuming that we have been doing pretty well with minimizing risks. Unfortunately, our study results indicate this is not exactly the case,” he said.
“Although vaccines and boosters appear to have equalized or minimized the risks of severe COVID for some people, this has not happened for others – even in the setting of the milder Omicron variant. Of individuals who were fully vaccinated and boosted, having hypertension increased the odds of needing to be hospitalized after getting infected with Omicron by 2.6-fold, even when accounting for or in the absence of having any major chronic disease that might otherwise predispose to more severe COVID-19 illness,” Dr. Ebinger added.
“So, while the originally seen risks of having obesity or diabetes seem to have been minimized during this current era of pandemic, the risk of having hypertension has persisted. We found this both surprising and concerning, because hypertension is very common and present in over half of people over age 50.”
Surprisingly, “we found that a fair number of people, even after being fully vaccinated plus a having gotten a booster, will not only catch Omicron but get sick enough to need hospital care,” Dr. Ebinger emphasized. “Moreover, it is not just older adults with major comorbid conditions who are vulnerable. Our data show that this can happen to an adult of any age and especially if a person has only hypertension and otherwise no major chronic disease.”
The first takeaway message for clinicians at this time is to raise awareness, Dr. Ebinger stressed in the interview. “We need to raise understanding around the fact that receiving three doses of vaccine may not prevent severe COVID-19 illness in everyone, even when the circulating viral variant is presumed to be causing only mild disease in most people. Moreover, the people who are most at risk are not whom we might think they are. They are not the sickest of the sick. They include people who might not have major conditions such as heart disease or kidney disease, but they do have hypertension.”
Second, “we need more research to understand out why there is this link between hypertension and excess risk for the more severe forms of COVID-19, despite it arising from a supposedly milder variant,” said Dr. Ebinger.
“Third, we need to determine how to reduce these risks, whether through more tailored vaccine regimens or novel therapeutics or a combination approach,” he said.
Looking ahead, “the biological mechanism underpinning the association between hypertension and severe COVID-19 remains underexplored. Future work should focus on understanding the factors linking hypertension to severe COVID-19, as this may elucidate both information on how SARS-CoV-2 effects the body and potential targets for intervention,” Dr. Ebinger added.
The study was supported in part by Cedars-Sinai Medical Center, the Erika J. Glazer Family Foundation and the National Institutes of Health. The researchers had no financial conflicts to disclose.
Adults with hypertension who were vaccinated for COVID-19 with at least one booster were more than twice as likely as vaccinated and boosted individuals without hypertension to be hospitalized for severe COVID-19, according to data from more than 900 individuals.
“We were surprised to learn that many people who were hospitalized with COVID-19 had hypertension and no other risk factors,” said Susan Cheng, MD, MPH, director of the Institute for Research on Healthy Aging in the department of cardiology at the Smidt Heart Institute, Los Angeles, and a senior author of the study. “This is concerning when you consider that almost half of American adults have high blood pressure.”
COVID-19 vaccines demonstrated ability to reduce death and some of the most severe side effects from the infection in the early stages of the pandemic. Although the Omicron surge prompted recommendations for a third mRNA vaccine dose, “a proportion of individuals who received three mRNA vaccine doses still required hospitalization for COVID-19 during the Omicron surge,” and the characteristics associated with severe illness in vaccinated and boosted patients have not been explored, Joseph Ebinger, MD, of Cedars-Sinai Medical Center, Los Angeles, and colleagues wrote.
Previous research has shown an association between high blood pressure an increased risk for developing severe COVID-19 compared to several other chronic health conditions, including kidney disease, type 2 diabetes, chronic obstructive pulmonary disease, and heart failure, the researchers noted.
In a study published in Hypertension, the researchers identified 912 adults who received at least three doses of mRNA COVID-19 vaccine and were later diagnosed with COVID-19 during the surge in infections from the Omicron variant between December 2021 and April 2022.
A total of 145 of the individuals were hospitalized (16%); of these, 125 (86%) had hypertension.
Patients with hypertension were the most likely to be hospitalized, with an odds ratio of 2.9. In addition to high blood pressure, factors including older age (OR, 1.3), chronic kidney disease (OR, 2.2), prior myocardial infarction or heart failure (OR, 2.2), and longer time since the last vaccination and COVID-19 infection were associated with increased risk of hospitalization in a multivariate analysis.
However, the increased risk of severe illness and hospitalization associated with high blood pressure persisted, with an OR of 2.6, in the absence of comorbid conditions such as type 2 diabetes, kidney disease, and heart failure, the researchers emphasized.
“Although the mechanism for hypertension-associated COVID-19 risk remains unclear, prior studies have identified delayed SARS-CoV-2 viral clearance and prolonged inflammatory response among hypertensive patients, which may contribute to greater disease severity,” they wrote.
The findings were limited by several factors, including the use of data from a single center and lack of information on which Omicron variants and subvariants were behind the infections, the researchers noted.
However, the results highlight the need for more research on how to reduce the risks of severe COVID-19 in vulnerable populations, and on the mechanism for a potential connection between high blood pressure and severe COVID-19, they said.
Given the high prevalence of hypertension worldwide, increased understanding of the hypertension-specific risks and identification of individual and population-level risk reduction strategies will be important to the transition of COVID-19 from pandemic to endemic, they concluded.
Omicron changes the game
“When the pandemic initially started, many conditions were seen to increase risk for more severe COVID illness, and hypertension was one of those factors – and then things changed,” lead author Dr. Ebinger said in an interview. “First, vaccines arrived on the scene and substantially reduced risk of severe COVID for everyone who received them. Second, Omicron arrived and, while more transmissible, this variant has been less likely to cause severe COVID. On the one hand, we have vaccines and boosters that we want to think of as ‘the great equalizer’ when it comes to preexisting conditions. On the other hand, we have a dominant set of SARS-CoV-2 subvariants that seem less virulent in most people.
“Taken together, we have been hoping and even assuming that we have been doing pretty well with minimizing risks. Unfortunately, our study results indicate this is not exactly the case,” he said.
“Although vaccines and boosters appear to have equalized or minimized the risks of severe COVID for some people, this has not happened for others – even in the setting of the milder Omicron variant. Of individuals who were fully vaccinated and boosted, having hypertension increased the odds of needing to be hospitalized after getting infected with Omicron by 2.6-fold, even when accounting for or in the absence of having any major chronic disease that might otherwise predispose to more severe COVID-19 illness,” Dr. Ebinger added.
“So, while the originally seen risks of having obesity or diabetes seem to have been minimized during this current era of pandemic, the risk of having hypertension has persisted. We found this both surprising and concerning, because hypertension is very common and present in over half of people over age 50.”
Surprisingly, “we found that a fair number of people, even after being fully vaccinated plus a having gotten a booster, will not only catch Omicron but get sick enough to need hospital care,” Dr. Ebinger emphasized. “Moreover, it is not just older adults with major comorbid conditions who are vulnerable. Our data show that this can happen to an adult of any age and especially if a person has only hypertension and otherwise no major chronic disease.”
The first takeaway message for clinicians at this time is to raise awareness, Dr. Ebinger stressed in the interview. “We need to raise understanding around the fact that receiving three doses of vaccine may not prevent severe COVID-19 illness in everyone, even when the circulating viral variant is presumed to be causing only mild disease in most people. Moreover, the people who are most at risk are not whom we might think they are. They are not the sickest of the sick. They include people who might not have major conditions such as heart disease or kidney disease, but they do have hypertension.”
Second, “we need more research to understand out why there is this link between hypertension and excess risk for the more severe forms of COVID-19, despite it arising from a supposedly milder variant,” said Dr. Ebinger.
“Third, we need to determine how to reduce these risks, whether through more tailored vaccine regimens or novel therapeutics or a combination approach,” he said.
Looking ahead, “the biological mechanism underpinning the association between hypertension and severe COVID-19 remains underexplored. Future work should focus on understanding the factors linking hypertension to severe COVID-19, as this may elucidate both information on how SARS-CoV-2 effects the body and potential targets for intervention,” Dr. Ebinger added.
The study was supported in part by Cedars-Sinai Medical Center, the Erika J. Glazer Family Foundation and the National Institutes of Health. The researchers had no financial conflicts to disclose.
FROM HYPERTENSION
Immune response may explain brain damage after COVID-19
It seems that the virus does not infect the brain directly. The scientists found evidence that antibodies – proteins produced by the immune system in response to viruses and other invaders – are involved in an attack on the cells lining the brain’s blood vessels, leading to inflammation and damage. The study was published in the journal Brain.
Brain tissue autopsy
“Patients often develop neurological complications with COVID-19, but the underlying pathophysiological process is not well understood,” Avindra Nath, MD, stated in a National Institutes of Health news release. Dr. Nath, who specializes in neuroimmunology, is the clinical director at the National Institute of Neurological Disorders and Stroke (NINDS) and the senior author of the study. “We had previously shown blood vessel damage and inflammation in patients’ brains at autopsy, but we didn’t understand the cause of the damage. I think in this paper we’ve gained important insight into the cascade of events.”
In this study, Dr. Nath and his team examined brain tissue from a subset of patients from their previous study. The nine individuals, ages 24-73 years, died shortly after contracting COVID-19. They were chosen because structural brain scans showed signs of blood vessel damage in the brain. The samples were compared with those from 10 controls. The team looked at neuroinflammation and immune responses using immunohistochemistry.
As in their earlier study, researchers found signs of leaky blood vessels based on the presence of blood proteins that normally do not cross the blood-brain barrier. This suggests that the tight junctions between the endothelial cells in the blood-brain barrier have been damaged.
Neurologic symptoms’ molecular basis
Dr. Nath and his colleagues discovered deposits of immune complexes on the surface of the cells. This finding is evidence that damage to endothelial cells was likely due to an immune response.
These observations suggest an antibody-mediated attack that activates endothelial cells. When endothelial cells are activated, they express proteins called adhesion molecules that cause platelets to stick together.
“Activation of the endothelial cells brings platelets that stick to the blood vessel walls, causing clots to form and leakage to occur. At the same time, the tight junctions between the endothelial cells get disrupted, causing them to leak,” Dr. Nath explained. “Once leakage occurs, immune cells such as macrophages may come to repair the damage, setting up inflammation. This, in turn, causes damage to neurons.”
Researchers found that in areas with damage to the endothelial cells, more than 300 genes showed decreased expression, whereas six genes were increased. These genes were associated with oxidative stress, DNA damage, and metabolic dysregulation. As the NIH news release notes, this may provide clues to the molecular basis of neurologic symptoms related to COVID-19 and offer potential therapeutic targets.
Together, these findings give insight into the immune response damaging the brain after COVID-19 infection. But it remains unclear what antigen the immune response is targeting, because the virus itself was not detected in the brain. It is possible that antibodies against the SARS-CoV-2 spike protein could bind to the angiotensin-converting enzyme 2 receptor used by the virus to enter cells. More research is needed to explore this hypothesis.
‘Brain fog’ explained?
The study may also have implications for understanding and treating long-term neurologic symptoms after COVID-19, which include headache, fatigue, loss of taste and smell, sleep problems, and “brain fog.” Had the patients in the study survived, the researchers believe they would likely have developed long COVID.
“It is quite possible that this same immune response persists in long COVID patients, resulting in neuronal injury,” said Dr. Nath. “There could be a small, indolent immune response that is continuing, which means that immune-modulating therapies might help these patients. So, these findings have very important therapeutic implications.”
The results suggest that treatments designed to prevent the development of the immune complexes observed in the study could be potential therapies for post-COVID neurologic symptoms.
This study was supported by the NINDS Division of Intramural Research (NS003130) and K23NS109284, the Roy J. Carver Foundation, and the Iowa Neuroscience Institute.
A version of this article first appeared on Medscape.com. This article was translated from Medscape French edition.
It seems that the virus does not infect the brain directly. The scientists found evidence that antibodies – proteins produced by the immune system in response to viruses and other invaders – are involved in an attack on the cells lining the brain’s blood vessels, leading to inflammation and damage. The study was published in the journal Brain.
Brain tissue autopsy
“Patients often develop neurological complications with COVID-19, but the underlying pathophysiological process is not well understood,” Avindra Nath, MD, stated in a National Institutes of Health news release. Dr. Nath, who specializes in neuroimmunology, is the clinical director at the National Institute of Neurological Disorders and Stroke (NINDS) and the senior author of the study. “We had previously shown blood vessel damage and inflammation in patients’ brains at autopsy, but we didn’t understand the cause of the damage. I think in this paper we’ve gained important insight into the cascade of events.”
In this study, Dr. Nath and his team examined brain tissue from a subset of patients from their previous study. The nine individuals, ages 24-73 years, died shortly after contracting COVID-19. They were chosen because structural brain scans showed signs of blood vessel damage in the brain. The samples were compared with those from 10 controls. The team looked at neuroinflammation and immune responses using immunohistochemistry.
As in their earlier study, researchers found signs of leaky blood vessels based on the presence of blood proteins that normally do not cross the blood-brain barrier. This suggests that the tight junctions between the endothelial cells in the blood-brain barrier have been damaged.
Neurologic symptoms’ molecular basis
Dr. Nath and his colleagues discovered deposits of immune complexes on the surface of the cells. This finding is evidence that damage to endothelial cells was likely due to an immune response.
These observations suggest an antibody-mediated attack that activates endothelial cells. When endothelial cells are activated, they express proteins called adhesion molecules that cause platelets to stick together.
“Activation of the endothelial cells brings platelets that stick to the blood vessel walls, causing clots to form and leakage to occur. At the same time, the tight junctions between the endothelial cells get disrupted, causing them to leak,” Dr. Nath explained. “Once leakage occurs, immune cells such as macrophages may come to repair the damage, setting up inflammation. This, in turn, causes damage to neurons.”
Researchers found that in areas with damage to the endothelial cells, more than 300 genes showed decreased expression, whereas six genes were increased. These genes were associated with oxidative stress, DNA damage, and metabolic dysregulation. As the NIH news release notes, this may provide clues to the molecular basis of neurologic symptoms related to COVID-19 and offer potential therapeutic targets.
Together, these findings give insight into the immune response damaging the brain after COVID-19 infection. But it remains unclear what antigen the immune response is targeting, because the virus itself was not detected in the brain. It is possible that antibodies against the SARS-CoV-2 spike protein could bind to the angiotensin-converting enzyme 2 receptor used by the virus to enter cells. More research is needed to explore this hypothesis.
‘Brain fog’ explained?
The study may also have implications for understanding and treating long-term neurologic symptoms after COVID-19, which include headache, fatigue, loss of taste and smell, sleep problems, and “brain fog.” Had the patients in the study survived, the researchers believe they would likely have developed long COVID.
“It is quite possible that this same immune response persists in long COVID patients, resulting in neuronal injury,” said Dr. Nath. “There could be a small, indolent immune response that is continuing, which means that immune-modulating therapies might help these patients. So, these findings have very important therapeutic implications.”
The results suggest that treatments designed to prevent the development of the immune complexes observed in the study could be potential therapies for post-COVID neurologic symptoms.
This study was supported by the NINDS Division of Intramural Research (NS003130) and K23NS109284, the Roy J. Carver Foundation, and the Iowa Neuroscience Institute.
A version of this article first appeared on Medscape.com. This article was translated from Medscape French edition.
It seems that the virus does not infect the brain directly. The scientists found evidence that antibodies – proteins produced by the immune system in response to viruses and other invaders – are involved in an attack on the cells lining the brain’s blood vessels, leading to inflammation and damage. The study was published in the journal Brain.
Brain tissue autopsy
“Patients often develop neurological complications with COVID-19, but the underlying pathophysiological process is not well understood,” Avindra Nath, MD, stated in a National Institutes of Health news release. Dr. Nath, who specializes in neuroimmunology, is the clinical director at the National Institute of Neurological Disorders and Stroke (NINDS) and the senior author of the study. “We had previously shown blood vessel damage and inflammation in patients’ brains at autopsy, but we didn’t understand the cause of the damage. I think in this paper we’ve gained important insight into the cascade of events.”
In this study, Dr. Nath and his team examined brain tissue from a subset of patients from their previous study. The nine individuals, ages 24-73 years, died shortly after contracting COVID-19. They were chosen because structural brain scans showed signs of blood vessel damage in the brain. The samples were compared with those from 10 controls. The team looked at neuroinflammation and immune responses using immunohistochemistry.
As in their earlier study, researchers found signs of leaky blood vessels based on the presence of blood proteins that normally do not cross the blood-brain barrier. This suggests that the tight junctions between the endothelial cells in the blood-brain barrier have been damaged.
Neurologic symptoms’ molecular basis
Dr. Nath and his colleagues discovered deposits of immune complexes on the surface of the cells. This finding is evidence that damage to endothelial cells was likely due to an immune response.
These observations suggest an antibody-mediated attack that activates endothelial cells. When endothelial cells are activated, they express proteins called adhesion molecules that cause platelets to stick together.
“Activation of the endothelial cells brings platelets that stick to the blood vessel walls, causing clots to form and leakage to occur. At the same time, the tight junctions between the endothelial cells get disrupted, causing them to leak,” Dr. Nath explained. “Once leakage occurs, immune cells such as macrophages may come to repair the damage, setting up inflammation. This, in turn, causes damage to neurons.”
Researchers found that in areas with damage to the endothelial cells, more than 300 genes showed decreased expression, whereas six genes were increased. These genes were associated with oxidative stress, DNA damage, and metabolic dysregulation. As the NIH news release notes, this may provide clues to the molecular basis of neurologic symptoms related to COVID-19 and offer potential therapeutic targets.
Together, these findings give insight into the immune response damaging the brain after COVID-19 infection. But it remains unclear what antigen the immune response is targeting, because the virus itself was not detected in the brain. It is possible that antibodies against the SARS-CoV-2 spike protein could bind to the angiotensin-converting enzyme 2 receptor used by the virus to enter cells. More research is needed to explore this hypothesis.
‘Brain fog’ explained?
The study may also have implications for understanding and treating long-term neurologic symptoms after COVID-19, which include headache, fatigue, loss of taste and smell, sleep problems, and “brain fog.” Had the patients in the study survived, the researchers believe they would likely have developed long COVID.
“It is quite possible that this same immune response persists in long COVID patients, resulting in neuronal injury,” said Dr. Nath. “There could be a small, indolent immune response that is continuing, which means that immune-modulating therapies might help these patients. So, these findings have very important therapeutic implications.”
The results suggest that treatments designed to prevent the development of the immune complexes observed in the study could be potential therapies for post-COVID neurologic symptoms.
This study was supported by the NINDS Division of Intramural Research (NS003130) and K23NS109284, the Roy J. Carver Foundation, and the Iowa Neuroscience Institute.
A version of this article first appeared on Medscape.com. This article was translated from Medscape French edition.
Anxiety in COPD: Consequential, but often overlooked
Anand S. Iyer, MD, MSPH, frequently hears his patients with chronic obstructive pulmonary disease (COPD) express fear and hopelessness and describe panic and other symptoms of anxiety. He sees anxiety affect the course of COPD, worsening symptoms and outcomes.
“I had questions about what we are doing [to help patients], so I began looking into the role of palliative care to help patients assess and manage these complex emotional and psychological symptoms,” said Dr. Iyer, assistant professor in the division of pulmonology, allergy, and critical care medicine at the University of Alabama at Birmingham.
His research is now focused on the integration of palliative care principles in COPD care. For Dr. Iyer and others engaged in research and/or patient care, finding ways of identifying and managing anxiety in patients with COPD – and other chronic lung diseases – is a calling of growing urgency.

More has been published about anxiety in patients with COPD than in other pulmonary conditions – and . Prevalence rates vary from about 1 in 4, to 1 in 2 or higher, depending on the instruments used and whether clinical DSM-based diagnoses are made, Dr. Iyer said.
A 2013 systematic review of 10 studies that utilized clinical interviews based on DSM criteria, for instance, found a prevalence of clinical anxiety of 10%-55% among inpatients and 13%-46% among outpatients with COPD. The results were similar, investigators said, to studies using self-report screening tools (Respiratory Care 2013;58[5]:858-66).
In the 16 years since an ACCP workshop panel on anxiety and depression in COPD reported higher prevalence rates than for other chronic diseases and detailed a host of problems and research needs (CHEST. 2008;134;43S-56), investigators have more fully documented links to COPD outcomes, showing, for instance, that anxiety predicts exacerbations, hospitalizations, poorer adherence to therapies, poorer quality of life and higher mortality.
Dr. Iyer and other experts say anxiety is still too often a neglected comorbidity. “It’s still underdiagnosed and therefore undertreated,” said Nick Hanania, MD, MS, professor of medicine and director of the Airways Clinical Research Center at Baylor College of Medicine, Houston.
The literature on optimal approaches for management remains limited, and the role of pharmacotherapy for anxiety (and depression) in the context of COPD has not been well investigated. But there have been some advances: Screening tools have been further studied, questionnaires specific to COPD have been developed, and pulmonary rehabilitation (PR) and cognitive behavioral therapy (CBT) have both been shown to be effective in decreasing anxiety.
Researchers and academic clinicians are talking, meanwhile, about how to have to important conversations about anxiety with patients who have COPD and other chronic lung conditions, and how improve care in the face of significant health system challenges.
Understanding anxiety in COPD
Anxiety is often intertwined with dyspnea in a bidirectional and complex relationship, but anxiety in COPD is not always acute or limited to times of acute exacerbations.
“There’s not only the acute experience of shortness of breath or a lung change episode, but there’s an anticipation that can occur, psychologically and socially,” said Lauren Garvin, PhD, of the department of psychiatry at the University of Iowa, Iowa City. Patients worry, “what if I’m short of breath in a particular situation? What if my devices fail when I’m out somewhere?”
Patients are often living “in a state of heightened surveillance of the body,” she noted, which can be exhausting and can impact functioning.
It’s also important to appreciate that anxiety is “a continuum of experience,” said Karin Hoth, PhD, associate professor of psychiatry at the medical school, whose research includes projects focusing on psychological adjustment in COPD.

“Research historically categorizes anxiety as ‘have or don’t have.’ But there’s a continuum of experience that we’re moving toward understanding and recognizing in research,” she said. “Anxiety is part of a patient’s whole experience, no matter where one falls on the continuum.”
Female sex, current smoking, greater airflow restrictions – and in some studies, younger age – have all been associated with a greater risk of anxiety in COPD. (It may well be that women receive more attention, leaving men with higher rates of undiagnosed anxiety, Dr. Hoth said.)
Dr. Iyer stresses the complex relationship between smoking – the No. 1 cause of COPD – and anxiety. Smoking has been associated in multiple studies with an increased risk of anxiety (Brain and Behavior. 2013;3[3]:302-26), he said. (A study led by Dr. Iyer found a similar frequency of anxiety symptoms in smokers with and without COPD [Journal of Psychosomatic Research. 2019;118:18-26].)
Some patients with COPD and anxiety may smoke in order to ease their anxiety, he said, making management of anxiety an important part of the smoking cessation desired for COPD improvement.
COPD medications such as bronchodilators may cause transient symptoms of anxiety, but these are rare and short-lived, Dr. Iyer said.
Screening tools and conversations
“It’s not just us not thinking about anxiety that’s the problem, it’s also patients thinking that it’s just the disease [causing their anxiety symptoms],” said Dr. Hanania, a member of the 2006 ACCP panel and an author of numerous papers on COPD and anxiety and depression. “There’s quite a bit of overlap between COPD symptoms and anxiety and depression symptoms, and unless you use structured questionnaires, you may not pick it up,” he said.
Screening tools include the Generalized Anxiety Disorder 7-item (GAD-7) scale, the PHQ-9 for depression and anxiety, and the longer Primary Care Evaluation of Mental Disorders (PRIME-MD). The Hospital Anxiety and Depression Scale (HADS), Dr. Iyer noted, has been well validated for use in ambulatory settings.
Validated screening tools specific to anxiety in COPD are also now an option. Abebaw M. Yohannes, PhD, MSc, FCCP, professor in the department of physical therapy at Azuza Pacific University in Orange, Calif., and the author of numerous studies on COPD and anxiety, developed one of these tools – the 10-item Anxiety Inventory for Respiratory Disease (AIR) scale – out of concern that other surveys contain overlapping somatic symptoms (Chest. 2013;144[5]:1587-96).

“We removed the physical symptoms [of anxiety] that often manifest in patients with COPD,” he said.
Dr. Iyer said screening tools can effectively “highlight which person might be dealing with high levels of anxiety symptoms that might meet a threshold of clinical significance and require collaborative or interprofessional management,” including with psychologists and psychiatrists.
They can also open the door to conversation with patients. “I’ll often bluntly ask, do you feel anxious? Do you feel scared, or hopeless about what the future holds for you?,” he said. “Anxiety about the future plays a big role, and helping patients navigate the illness and understand early how it might look … can ease the level of anxiety.”
Asking patients about their experiences in managing their symptoms and about their psychological and emotional well-being can help to normalize anxiety – and it can be therapeutic, said Dr. Hoth and Dr. Garvin. Asking “how it’s going with the things that really matter in [their] life” is often a good question, they said.
Patients “won’t be offended if you ask,” said Dr. Hoth. “They view their mood and [whole] well-being as part of their medical condition.”
Time is a challenge, she said, but “conversation can be done little by little, as part of a philosophy of engaging the patient around their whole functioning, even if there’s not [a need or] a route to refer just then.”
Such early and integrated conversation borrows from the palliative care model. “Palliative care is a specialty, but it can also be an approach to care,” Dr. Iyer said. He is leading a National Institutes of Health–funded study on nurse-coach–led early palliative care for older adults with COPD and wants to see training opportunities for pulmonologists to learn basic palliative care skills that would equip them to better guide management of mild-moderate anxiety and other complex symptoms.
Pulmonary rehabilitation
For many patients with COPD who have anxiety and/or depressive symptoms, referral for nonpharmacologic therapies such as psychotherapy, cognitive-behavioral therapy (CBT), and pulmonary rehabilitation (PR) is “one of the best things you can do,” Dr. Iyer said.
“If patients haven’t done pulmonary rehabilitation, get them in. And if they have done it before, get them back into it again,” he emphasized. “Accredited programs give a holistic approach to improving your strength, your breathlessness, your mindset and understanding of your breathlessness, and your own levels of security.”
Studies addressing the impact of PR and CBT on anxiety have been mostly small and observational but have yielded encouraging findings. A 2017 review reported that PR and CBT were effective in the treatment of anxiety and dyspnea, in the short term, in the majority of 47 studies (JAMA. 2017;18[12]:1096.e1-1096.e17). And a 2019 systematic review and meta-analysis focused on PR reported that, across 11 studies comprising 734 patients, PR conferred significant benefits for anxiety and depression compared with usual care (CHEST. 2019;156[1]:80-91).
Dr. Yohannes, Dr. Hanania, and colleagues recently reported on 734 patients with clinically stable COPD who completed a community-based 8-week PR program of 2 hours a week: 1 hour of exercise and 1 hour of education, the latter of which covered anxiety, panic management, and relaxation.
Patients who had severe dyspnea and comorbid anxiety and depression prior to PR – one-third of the group compared with 20% having anxiety alone and 5% having depression alone – had the most significant improvements in dyspnea scores and anxiety and depression scores (Respir Med. Apr 9. doi: 10.1016/j.rmed.2022.106850.)
The problem is, pulmonary rehabilitation is under-reimbursed and not widely accessible. It’s logistically challenging for patients to attend therapy 2-3 times a week. And according to a recently published study by Dr. Yohannes, Dr. Hanania, and colleagues, patients with more anxiety and dyspnea may be at higher risk of dropping out (Respir Med. 2022 Jan 20. doi: 10.1016/j.rmed.2022.10674). Moreover, Dr. Iyer said, there is a shortage of programs that are accredited.
Telehealth may help on some of these fronts. The efficacy of real-time video PR for COPD is being investigated in a randomized NIH trial (now in the recruitment phase) led by pulmonologist Surya P. Bhatt, MD, also at the University of Alabama at Birmingham.
Researchers also need to investigate issues of sustainability – to learn what “works best in the long run,” Dr. Iyer said.
Dr. Yohannes and Dr. Hanania are encouraged by a recent finding that patients with COPD who completed 8 weeks of PR maintained improvements in anxiety and quality-of-life scores at 2 years. (Improvements in dyspnea and other outcomes did not persist.) (CHEST. 2021;159[3]:967-74). Prospective studies contrasting maintenance programs with no maintenance following PR, are needed, they wrote.
Understanding psychological interventions
Dr. Hoth and Dr. Garvin advise their pulmonologist colleagues to feel as confident as possible in describing for patients what CBT and other psychological therapies entail.
“A person [with COPD] who is experiencing something on the continuum of anxiety might be really turning inward and [assessing] unwanted internal experiences” and accompanying thoughts, sensations, emotional impacts and behaviors, Dr. Garvin said.
Among the goals, she said, are to “make shifts around those internal experiences that might invoke some more tolerance or that might shift their relationship with the experiences, or even with the diagnosis itself and all the uncertainties it carries.”
Psychological therapies can involve social support, or “breath and grounding work,” she said. “There are lots of different approaches from different providers.”
Dr. Yohannes advocates incorporating principles of CBT into PR. “In the absence of one-on-one or group [stand-alone] CBT … the principles are worth incorporating as part of the education piece [of PR],” he said. “CBT helps patients to refocus their attention. … and gives them self-confidence to engage in exercise and to function a bit more in their daily activities.”
None of those interviewed for this story reported having any relevant conflicts of interest.
Anand S. Iyer, MD, MSPH, frequently hears his patients with chronic obstructive pulmonary disease (COPD) express fear and hopelessness and describe panic and other symptoms of anxiety. He sees anxiety affect the course of COPD, worsening symptoms and outcomes.
“I had questions about what we are doing [to help patients], so I began looking into the role of palliative care to help patients assess and manage these complex emotional and psychological symptoms,” said Dr. Iyer, assistant professor in the division of pulmonology, allergy, and critical care medicine at the University of Alabama at Birmingham.
His research is now focused on the integration of palliative care principles in COPD care. For Dr. Iyer and others engaged in research and/or patient care, finding ways of identifying and managing anxiety in patients with COPD – and other chronic lung diseases – is a calling of growing urgency.
More has been published about anxiety in patients with COPD than in other pulmonary conditions – and . Prevalence rates vary from about 1 in 4, to 1 in 2 or higher, depending on the instruments used and whether clinical DSM-based diagnoses are made, Dr. Iyer said.
A 2013 systematic review of 10 studies that utilized clinical interviews based on DSM criteria, for instance, found a prevalence of clinical anxiety of 10%-55% among inpatients and 13%-46% among outpatients with COPD. The results were similar, investigators said, to studies using self-report screening tools (Respiratory Care 2013;58[5]:858-66).
In the 16 years since an ACCP workshop panel on anxiety and depression in COPD reported higher prevalence rates than for other chronic diseases and detailed a host of problems and research needs (CHEST. 2008;134;43S-56), investigators have more fully documented links to COPD outcomes, showing, for instance, that anxiety predicts exacerbations, hospitalizations, poorer adherence to therapies, poorer quality of life and higher mortality.
Dr. Iyer and other experts say anxiety is still too often a neglected comorbidity. “It’s still underdiagnosed and therefore undertreated,” said Nick Hanania, MD, MS, professor of medicine and director of the Airways Clinical Research Center at Baylor College of Medicine, Houston.
The literature on optimal approaches for management remains limited, and the role of pharmacotherapy for anxiety (and depression) in the context of COPD has not been well investigated. But there have been some advances: Screening tools have been further studied, questionnaires specific to COPD have been developed, and pulmonary rehabilitation (PR) and cognitive behavioral therapy (CBT) have both been shown to be effective in decreasing anxiety.
Researchers and academic clinicians are talking, meanwhile, about how to have to important conversations about anxiety with patients who have COPD and other chronic lung conditions, and how improve care in the face of significant health system challenges.
Understanding anxiety in COPD
Anxiety is often intertwined with dyspnea in a bidirectional and complex relationship, but anxiety in COPD is not always acute or limited to times of acute exacerbations.
“There’s not only the acute experience of shortness of breath or a lung change episode, but there’s an anticipation that can occur, psychologically and socially,” said Lauren Garvin, PhD, of the department of psychiatry at the University of Iowa, Iowa City. Patients worry, “what if I’m short of breath in a particular situation? What if my devices fail when I’m out somewhere?”
Patients are often living “in a state of heightened surveillance of the body,” she noted, which can be exhausting and can impact functioning.
It’s also important to appreciate that anxiety is “a continuum of experience,” said Karin Hoth, PhD, associate professor of psychiatry at the medical school, whose research includes projects focusing on psychological adjustment in COPD.
“Research historically categorizes anxiety as ‘have or don’t have.’ But there’s a continuum of experience that we’re moving toward understanding and recognizing in research,” she said. “Anxiety is part of a patient’s whole experience, no matter where one falls on the continuum.”
Female sex, current smoking, greater airflow restrictions – and in some studies, younger age – have all been associated with a greater risk of anxiety in COPD. (It may well be that women receive more attention, leaving men with higher rates of undiagnosed anxiety, Dr. Hoth said.)
Dr. Iyer stresses the complex relationship between smoking – the No. 1 cause of COPD – and anxiety. Smoking has been associated in multiple studies with an increased risk of anxiety (Brain and Behavior. 2013;3[3]:302-26), he said. (A study led by Dr. Iyer found a similar frequency of anxiety symptoms in smokers with and without COPD [Journal of Psychosomatic Research. 2019;118:18-26].)
Some patients with COPD and anxiety may smoke in order to ease their anxiety, he said, making management of anxiety an important part of the smoking cessation desired for COPD improvement.
COPD medications such as bronchodilators may cause transient symptoms of anxiety, but these are rare and short-lived, Dr. Iyer said.
Screening tools and conversations
“It’s not just us not thinking about anxiety that’s the problem, it’s also patients thinking that it’s just the disease [causing their anxiety symptoms],” said Dr. Hanania, a member of the 2006 ACCP panel and an author of numerous papers on COPD and anxiety and depression. “There’s quite a bit of overlap between COPD symptoms and anxiety and depression symptoms, and unless you use structured questionnaires, you may not pick it up,” he said.
Screening tools include the Generalized Anxiety Disorder 7-item (GAD-7) scale, the PHQ-9 for depression and anxiety, and the longer Primary Care Evaluation of Mental Disorders (PRIME-MD). The Hospital Anxiety and Depression Scale (HADS), Dr. Iyer noted, has been well validated for use in ambulatory settings.
Validated screening tools specific to anxiety in COPD are also now an option. Abebaw M. Yohannes, PhD, MSc, FCCP, professor in the department of physical therapy at Azuza Pacific University in Orange, Calif., and the author of numerous studies on COPD and anxiety, developed one of these tools – the 10-item Anxiety Inventory for Respiratory Disease (AIR) scale – out of concern that other surveys contain overlapping somatic symptoms (Chest. 2013;144[5]:1587-96).
“We removed the physical symptoms [of anxiety] that often manifest in patients with COPD,” he said.
Dr. Iyer said screening tools can effectively “highlight which person might be dealing with high levels of anxiety symptoms that might meet a threshold of clinical significance and require collaborative or interprofessional management,” including with psychologists and psychiatrists.
They can also open the door to conversation with patients. “I’ll often bluntly ask, do you feel anxious? Do you feel scared, or hopeless about what the future holds for you?,” he said. “Anxiety about the future plays a big role, and helping patients navigate the illness and understand early how it might look … can ease the level of anxiety.”
Asking patients about their experiences in managing their symptoms and about their psychological and emotional well-being can help to normalize anxiety – and it can be therapeutic, said Dr. Hoth and Dr. Garvin. Asking “how it’s going with the things that really matter in [their] life” is often a good question, they said.
Patients “won’t be offended if you ask,” said Dr. Hoth. “They view their mood and [whole] well-being as part of their medical condition.”
Time is a challenge, she said, but “conversation can be done little by little, as part of a philosophy of engaging the patient around their whole functioning, even if there’s not [a need or] a route to refer just then.”
Such early and integrated conversation borrows from the palliative care model. “Palliative care is a specialty, but it can also be an approach to care,” Dr. Iyer said. He is leading a National Institutes of Health–funded study on nurse-coach–led early palliative care for older adults with COPD and wants to see training opportunities for pulmonologists to learn basic palliative care skills that would equip them to better guide management of mild-moderate anxiety and other complex symptoms.
Pulmonary rehabilitation
For many patients with COPD who have anxiety and/or depressive symptoms, referral for nonpharmacologic therapies such as psychotherapy, cognitive-behavioral therapy (CBT), and pulmonary rehabilitation (PR) is “one of the best things you can do,” Dr. Iyer said.
“If patients haven’t done pulmonary rehabilitation, get them in. And if they have done it before, get them back into it again,” he emphasized. “Accredited programs give a holistic approach to improving your strength, your breathlessness, your mindset and understanding of your breathlessness, and your own levels of security.”
Studies addressing the impact of PR and CBT on anxiety have been mostly small and observational but have yielded encouraging findings. A 2017 review reported that PR and CBT were effective in the treatment of anxiety and dyspnea, in the short term, in the majority of 47 studies (JAMA. 2017;18[12]:1096.e1-1096.e17). And a 2019 systematic review and meta-analysis focused on PR reported that, across 11 studies comprising 734 patients, PR conferred significant benefits for anxiety and depression compared with usual care (CHEST. 2019;156[1]:80-91).
Dr. Yohannes, Dr. Hanania, and colleagues recently reported on 734 patients with clinically stable COPD who completed a community-based 8-week PR program of 2 hours a week: 1 hour of exercise and 1 hour of education, the latter of which covered anxiety, panic management, and relaxation.
Patients who had severe dyspnea and comorbid anxiety and depression prior to PR – one-third of the group compared with 20% having anxiety alone and 5% having depression alone – had the most significant improvements in dyspnea scores and anxiety and depression scores (Respir Med. Apr 9. doi: 10.1016/j.rmed.2022.106850.)
The problem is, pulmonary rehabilitation is under-reimbursed and not widely accessible. It’s logistically challenging for patients to attend therapy 2-3 times a week. And according to a recently published study by Dr. Yohannes, Dr. Hanania, and colleagues, patients with more anxiety and dyspnea may be at higher risk of dropping out (Respir Med. 2022 Jan 20. doi: 10.1016/j.rmed.2022.10674). Moreover, Dr. Iyer said, there is a shortage of programs that are accredited.
Telehealth may help on some of these fronts. The efficacy of real-time video PR for COPD is being investigated in a randomized NIH trial (now in the recruitment phase) led by pulmonologist Surya P. Bhatt, MD, also at the University of Alabama at Birmingham.
Researchers also need to investigate issues of sustainability – to learn what “works best in the long run,” Dr. Iyer said.
Dr. Yohannes and Dr. Hanania are encouraged by a recent finding that patients with COPD who completed 8 weeks of PR maintained improvements in anxiety and quality-of-life scores at 2 years. (Improvements in dyspnea and other outcomes did not persist.) (CHEST. 2021;159[3]:967-74). Prospective studies contrasting maintenance programs with no maintenance following PR, are needed, they wrote.
Understanding psychological interventions
Dr. Hoth and Dr. Garvin advise their pulmonologist colleagues to feel as confident as possible in describing for patients what CBT and other psychological therapies entail.
“A person [with COPD] who is experiencing something on the continuum of anxiety might be really turning inward and [assessing] unwanted internal experiences” and accompanying thoughts, sensations, emotional impacts and behaviors, Dr. Garvin said.
Among the goals, she said, are to “make shifts around those internal experiences that might invoke some more tolerance or that might shift their relationship with the experiences, or even with the diagnosis itself and all the uncertainties it carries.”
Psychological therapies can involve social support, or “breath and grounding work,” she said. “There are lots of different approaches from different providers.”
Dr. Yohannes advocates incorporating principles of CBT into PR. “In the absence of one-on-one or group [stand-alone] CBT … the principles are worth incorporating as part of the education piece [of PR],” he said. “CBT helps patients to refocus their attention. … and gives them self-confidence to engage in exercise and to function a bit more in their daily activities.”
None of those interviewed for this story reported having any relevant conflicts of interest.
Anand S. Iyer, MD, MSPH, frequently hears his patients with chronic obstructive pulmonary disease (COPD) express fear and hopelessness and describe panic and other symptoms of anxiety. He sees anxiety affect the course of COPD, worsening symptoms and outcomes.
“I had questions about what we are doing [to help patients], so I began looking into the role of palliative care to help patients assess and manage these complex emotional and psychological symptoms,” said Dr. Iyer, assistant professor in the division of pulmonology, allergy, and critical care medicine at the University of Alabama at Birmingham.
His research is now focused on the integration of palliative care principles in COPD care. For Dr. Iyer and others engaged in research and/or patient care, finding ways of identifying and managing anxiety in patients with COPD – and other chronic lung diseases – is a calling of growing urgency.
More has been published about anxiety in patients with COPD than in other pulmonary conditions – and . Prevalence rates vary from about 1 in 4, to 1 in 2 or higher, depending on the instruments used and whether clinical DSM-based diagnoses are made, Dr. Iyer said.
A 2013 systematic review of 10 studies that utilized clinical interviews based on DSM criteria, for instance, found a prevalence of clinical anxiety of 10%-55% among inpatients and 13%-46% among outpatients with COPD. The results were similar, investigators said, to studies using self-report screening tools (Respiratory Care 2013;58[5]:858-66).
In the 16 years since an ACCP workshop panel on anxiety and depression in COPD reported higher prevalence rates than for other chronic diseases and detailed a host of problems and research needs (CHEST. 2008;134;43S-56), investigators have more fully documented links to COPD outcomes, showing, for instance, that anxiety predicts exacerbations, hospitalizations, poorer adherence to therapies, poorer quality of life and higher mortality.
Dr. Iyer and other experts say anxiety is still too often a neglected comorbidity. “It’s still underdiagnosed and therefore undertreated,” said Nick Hanania, MD, MS, professor of medicine and director of the Airways Clinical Research Center at Baylor College of Medicine, Houston.
The literature on optimal approaches for management remains limited, and the role of pharmacotherapy for anxiety (and depression) in the context of COPD has not been well investigated. But there have been some advances: Screening tools have been further studied, questionnaires specific to COPD have been developed, and pulmonary rehabilitation (PR) and cognitive behavioral therapy (CBT) have both been shown to be effective in decreasing anxiety.
Researchers and academic clinicians are talking, meanwhile, about how to have to important conversations about anxiety with patients who have COPD and other chronic lung conditions, and how improve care in the face of significant health system challenges.
Understanding anxiety in COPD
Anxiety is often intertwined with dyspnea in a bidirectional and complex relationship, but anxiety in COPD is not always acute or limited to times of acute exacerbations.
“There’s not only the acute experience of shortness of breath or a lung change episode, but there’s an anticipation that can occur, psychologically and socially,” said Lauren Garvin, PhD, of the department of psychiatry at the University of Iowa, Iowa City. Patients worry, “what if I’m short of breath in a particular situation? What if my devices fail when I’m out somewhere?”
Patients are often living “in a state of heightened surveillance of the body,” she noted, which can be exhausting and can impact functioning.
It’s also important to appreciate that anxiety is “a continuum of experience,” said Karin Hoth, PhD, associate professor of psychiatry at the medical school, whose research includes projects focusing on psychological adjustment in COPD.
“Research historically categorizes anxiety as ‘have or don’t have.’ But there’s a continuum of experience that we’re moving toward understanding and recognizing in research,” she said. “Anxiety is part of a patient’s whole experience, no matter where one falls on the continuum.”
Female sex, current smoking, greater airflow restrictions – and in some studies, younger age – have all been associated with a greater risk of anxiety in COPD. (It may well be that women receive more attention, leaving men with higher rates of undiagnosed anxiety, Dr. Hoth said.)
Dr. Iyer stresses the complex relationship between smoking – the No. 1 cause of COPD – and anxiety. Smoking has been associated in multiple studies with an increased risk of anxiety (Brain and Behavior. 2013;3[3]:302-26), he said. (A study led by Dr. Iyer found a similar frequency of anxiety symptoms in smokers with and without COPD [Journal of Psychosomatic Research. 2019;118:18-26].)
Some patients with COPD and anxiety may smoke in order to ease their anxiety, he said, making management of anxiety an important part of the smoking cessation desired for COPD improvement.
COPD medications such as bronchodilators may cause transient symptoms of anxiety, but these are rare and short-lived, Dr. Iyer said.
Screening tools and conversations
“It’s not just us not thinking about anxiety that’s the problem, it’s also patients thinking that it’s just the disease [causing their anxiety symptoms],” said Dr. Hanania, a member of the 2006 ACCP panel and an author of numerous papers on COPD and anxiety and depression. “There’s quite a bit of overlap between COPD symptoms and anxiety and depression symptoms, and unless you use structured questionnaires, you may not pick it up,” he said.
Screening tools include the Generalized Anxiety Disorder 7-item (GAD-7) scale, the PHQ-9 for depression and anxiety, and the longer Primary Care Evaluation of Mental Disorders (PRIME-MD). The Hospital Anxiety and Depression Scale (HADS), Dr. Iyer noted, has been well validated for use in ambulatory settings.
Validated screening tools specific to anxiety in COPD are also now an option. Abebaw M. Yohannes, PhD, MSc, FCCP, professor in the department of physical therapy at Azuza Pacific University in Orange, Calif., and the author of numerous studies on COPD and anxiety, developed one of these tools – the 10-item Anxiety Inventory for Respiratory Disease (AIR) scale – out of concern that other surveys contain overlapping somatic symptoms (Chest. 2013;144[5]:1587-96).
“We removed the physical symptoms [of anxiety] that often manifest in patients with COPD,” he said.
Dr. Iyer said screening tools can effectively “highlight which person might be dealing with high levels of anxiety symptoms that might meet a threshold of clinical significance and require collaborative or interprofessional management,” including with psychologists and psychiatrists.
They can also open the door to conversation with patients. “I’ll often bluntly ask, do you feel anxious? Do you feel scared, or hopeless about what the future holds for you?,” he said. “Anxiety about the future plays a big role, and helping patients navigate the illness and understand early how it might look … can ease the level of anxiety.”
Asking patients about their experiences in managing their symptoms and about their psychological and emotional well-being can help to normalize anxiety – and it can be therapeutic, said Dr. Hoth and Dr. Garvin. Asking “how it’s going with the things that really matter in [their] life” is often a good question, they said.
Patients “won’t be offended if you ask,” said Dr. Hoth. “They view their mood and [whole] well-being as part of their medical condition.”
Time is a challenge, she said, but “conversation can be done little by little, as part of a philosophy of engaging the patient around their whole functioning, even if there’s not [a need or] a route to refer just then.”
Such early and integrated conversation borrows from the palliative care model. “Palliative care is a specialty, but it can also be an approach to care,” Dr. Iyer said. He is leading a National Institutes of Health–funded study on nurse-coach–led early palliative care for older adults with COPD and wants to see training opportunities for pulmonologists to learn basic palliative care skills that would equip them to better guide management of mild-moderate anxiety and other complex symptoms.
Pulmonary rehabilitation
For many patients with COPD who have anxiety and/or depressive symptoms, referral for nonpharmacologic therapies such as psychotherapy, cognitive-behavioral therapy (CBT), and pulmonary rehabilitation (PR) is “one of the best things you can do,” Dr. Iyer said.
“If patients haven’t done pulmonary rehabilitation, get them in. And if they have done it before, get them back into it again,” he emphasized. “Accredited programs give a holistic approach to improving your strength, your breathlessness, your mindset and understanding of your breathlessness, and your own levels of security.”
Studies addressing the impact of PR and CBT on anxiety have been mostly small and observational but have yielded encouraging findings. A 2017 review reported that PR and CBT were effective in the treatment of anxiety and dyspnea, in the short term, in the majority of 47 studies (JAMA. 2017;18[12]:1096.e1-1096.e17). And a 2019 systematic review and meta-analysis focused on PR reported that, across 11 studies comprising 734 patients, PR conferred significant benefits for anxiety and depression compared with usual care (CHEST. 2019;156[1]:80-91).
Dr. Yohannes, Dr. Hanania, and colleagues recently reported on 734 patients with clinically stable COPD who completed a community-based 8-week PR program of 2 hours a week: 1 hour of exercise and 1 hour of education, the latter of which covered anxiety, panic management, and relaxation.
Patients who had severe dyspnea and comorbid anxiety and depression prior to PR – one-third of the group compared with 20% having anxiety alone and 5% having depression alone – had the most significant improvements in dyspnea scores and anxiety and depression scores (Respir Med. Apr 9. doi: 10.1016/j.rmed.2022.106850.)
The problem is, pulmonary rehabilitation is under-reimbursed and not widely accessible. It’s logistically challenging for patients to attend therapy 2-3 times a week. And according to a recently published study by Dr. Yohannes, Dr. Hanania, and colleagues, patients with more anxiety and dyspnea may be at higher risk of dropping out (Respir Med. 2022 Jan 20. doi: 10.1016/j.rmed.2022.10674). Moreover, Dr. Iyer said, there is a shortage of programs that are accredited.
Telehealth may help on some of these fronts. The efficacy of real-time video PR for COPD is being investigated in a randomized NIH trial (now in the recruitment phase) led by pulmonologist Surya P. Bhatt, MD, also at the University of Alabama at Birmingham.
Researchers also need to investigate issues of sustainability – to learn what “works best in the long run,” Dr. Iyer said.
Dr. Yohannes and Dr. Hanania are encouraged by a recent finding that patients with COPD who completed 8 weeks of PR maintained improvements in anxiety and quality-of-life scores at 2 years. (Improvements in dyspnea and other outcomes did not persist.) (CHEST. 2021;159[3]:967-74). Prospective studies contrasting maintenance programs with no maintenance following PR, are needed, they wrote.
Understanding psychological interventions
Dr. Hoth and Dr. Garvin advise their pulmonologist colleagues to feel as confident as possible in describing for patients what CBT and other psychological therapies entail.
“A person [with COPD] who is experiencing something on the continuum of anxiety might be really turning inward and [assessing] unwanted internal experiences” and accompanying thoughts, sensations, emotional impacts and behaviors, Dr. Garvin said.
Among the goals, she said, are to “make shifts around those internal experiences that might invoke some more tolerance or that might shift their relationship with the experiences, or even with the diagnosis itself and all the uncertainties it carries.”
Psychological therapies can involve social support, or “breath and grounding work,” she said. “There are lots of different approaches from different providers.”
Dr. Yohannes advocates incorporating principles of CBT into PR. “In the absence of one-on-one or group [stand-alone] CBT … the principles are worth incorporating as part of the education piece [of PR],” he said. “CBT helps patients to refocus their attention. … and gives them self-confidence to engage in exercise and to function a bit more in their daily activities.”
None of those interviewed for this story reported having any relevant conflicts of interest.