User login
-
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Pandemic hit Black children harder, study shows
Black children had almost three times as many COVID-related deaths as White children and about twice as many hospitalizations, according to a new study.
The study said that 1,556 children have died from the start of the pandemic until Nov. 30, 2022, with 593 of those children being 4 and under. Black children died of COVID-related causes 2.7 times more often than White children and were hospitalized 2.2 times more often than White children, the study said.
Lower vaccination rates for Black people may be a factor. The study said 43.6% of White children have received two or more vaccinations, compared with 40.2% of Black children.
“First and foremost, this study repudiates the misunderstanding that COVID-19 has not been of consequence to children who have had more than 15.5 million reported cases, representing 18 percent of all cases in the United States,” Reed Tuckson, MD, a member of the Black Coalition Against COVID board of directors and former District of Columbia public health commissioner, said in a news release.
“And second, our research shows that like their adult counterparts, Black and other children of color have shouldered more of the burden of COVID-19 than the White population.”
The study was commissioned by BCAC and conducted by the Satcher Health Leadership Institute of the Morehouse School of Medicine, Atlanta. It’s based on studies conducted by other agencies over 2 years.
Black and Hispanic children also had more severe COVID cases, the study said. Among 281 pediatric patients in New York, New Jersey, and Connecticut, 23.3% of severe cases were Black and 51% of severe cases were Hispanic.
The study says 1 in 310 Black children lost a parent or caregiver to COVID between April 2020 and June 2012, compared with 1 in 738 White children.
Economic and health-related hardships were experienced by 31% of Black households, 29% of Latino households, and 16% of White households, the study said.
“Children with COVID-19 in communities of color were sicker, [were] hospitalized and died at higher rates than White children,” Sandra Harris-Hooker, the interim executive director at the Satcher Health Leadership Institute of Morehouse School, said in the release. “We can now fully understand the devastating impact the virus had on communities of color across generations.”
The study recommends several changes, such as modifying eligibility requirements for the Children’s Health Insurance Program to help more children who fall into coverage gaps and expanding the Child Tax Credit.
A version of this article first appeared on WebMD.com.
Black children had almost three times as many COVID-related deaths as White children and about twice as many hospitalizations, according to a new study.
The study said that 1,556 children have died from the start of the pandemic until Nov. 30, 2022, with 593 of those children being 4 and under. Black children died of COVID-related causes 2.7 times more often than White children and were hospitalized 2.2 times more often than White children, the study said.
Lower vaccination rates for Black people may be a factor. The study said 43.6% of White children have received two or more vaccinations, compared with 40.2% of Black children.
“First and foremost, this study repudiates the misunderstanding that COVID-19 has not been of consequence to children who have had more than 15.5 million reported cases, representing 18 percent of all cases in the United States,” Reed Tuckson, MD, a member of the Black Coalition Against COVID board of directors and former District of Columbia public health commissioner, said in a news release.
“And second, our research shows that like their adult counterparts, Black and other children of color have shouldered more of the burden of COVID-19 than the White population.”
The study was commissioned by BCAC and conducted by the Satcher Health Leadership Institute of the Morehouse School of Medicine, Atlanta. It’s based on studies conducted by other agencies over 2 years.
Black and Hispanic children also had more severe COVID cases, the study said. Among 281 pediatric patients in New York, New Jersey, and Connecticut, 23.3% of severe cases were Black and 51% of severe cases were Hispanic.
The study says 1 in 310 Black children lost a parent or caregiver to COVID between April 2020 and June 2012, compared with 1 in 738 White children.
Economic and health-related hardships were experienced by 31% of Black households, 29% of Latino households, and 16% of White households, the study said.
“Children with COVID-19 in communities of color were sicker, [were] hospitalized and died at higher rates than White children,” Sandra Harris-Hooker, the interim executive director at the Satcher Health Leadership Institute of Morehouse School, said in the release. “We can now fully understand the devastating impact the virus had on communities of color across generations.”
The study recommends several changes, such as modifying eligibility requirements for the Children’s Health Insurance Program to help more children who fall into coverage gaps and expanding the Child Tax Credit.
A version of this article first appeared on WebMD.com.
Black children had almost three times as many COVID-related deaths as White children and about twice as many hospitalizations, according to a new study.
The study said that 1,556 children have died from the start of the pandemic until Nov. 30, 2022, with 593 of those children being 4 and under. Black children died of COVID-related causes 2.7 times more often than White children and were hospitalized 2.2 times more often than White children, the study said.
Lower vaccination rates for Black people may be a factor. The study said 43.6% of White children have received two or more vaccinations, compared with 40.2% of Black children.
“First and foremost, this study repudiates the misunderstanding that COVID-19 has not been of consequence to children who have had more than 15.5 million reported cases, representing 18 percent of all cases in the United States,” Reed Tuckson, MD, a member of the Black Coalition Against COVID board of directors and former District of Columbia public health commissioner, said in a news release.
“And second, our research shows that like their adult counterparts, Black and other children of color have shouldered more of the burden of COVID-19 than the White population.”
The study was commissioned by BCAC and conducted by the Satcher Health Leadership Institute of the Morehouse School of Medicine, Atlanta. It’s based on studies conducted by other agencies over 2 years.
Black and Hispanic children also had more severe COVID cases, the study said. Among 281 pediatric patients in New York, New Jersey, and Connecticut, 23.3% of severe cases were Black and 51% of severe cases were Hispanic.
The study says 1 in 310 Black children lost a parent or caregiver to COVID between April 2020 and June 2012, compared with 1 in 738 White children.
Economic and health-related hardships were experienced by 31% of Black households, 29% of Latino households, and 16% of White households, the study said.
“Children with COVID-19 in communities of color were sicker, [were] hospitalized and died at higher rates than White children,” Sandra Harris-Hooker, the interim executive director at the Satcher Health Leadership Institute of Morehouse School, said in the release. “We can now fully understand the devastating impact the virus had on communities of color across generations.”
The study recommends several changes, such as modifying eligibility requirements for the Children’s Health Insurance Program to help more children who fall into coverage gaps and expanding the Child Tax Credit.
A version of this article first appeared on WebMD.com.
Children and COVID: A look back as the fourth year begins
With 3 years of the COVID-19 experience now past, it’s safe to say that SARS-CoV-2 changed American society in ways that could not have been predicted when the first U.S. cases were reported in January of 2020.
Who would have guessed back then that not one but two vaccines would be developed, approved, and widely distributed before the end of the year? Or that those vaccines would be rejected by large segments of the population on ideological grounds? Could anyone have predicted in early 2020 that schools in 21 states would be forbidden by law to require COVID-19 vaccination in students?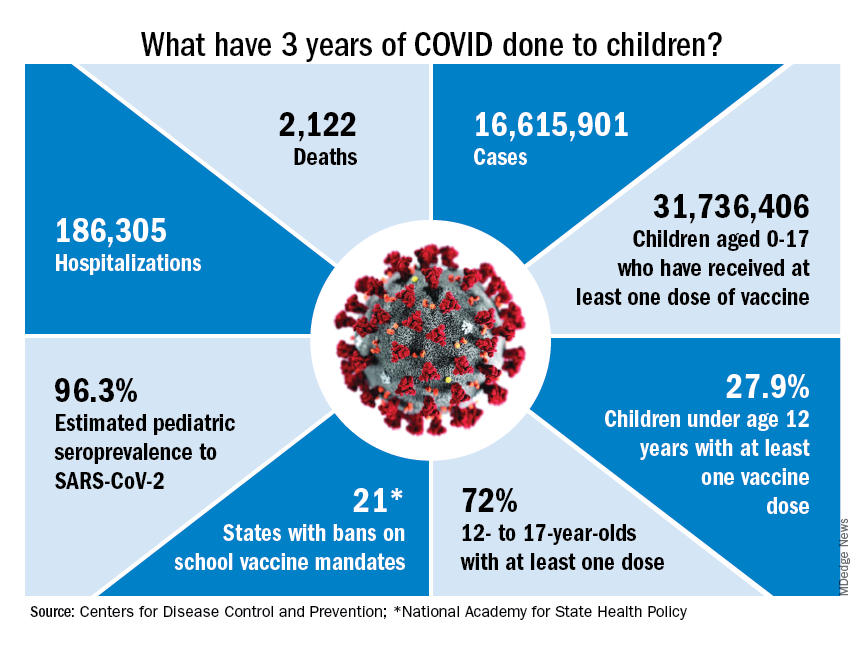
Vaccination is generally considered to be an activity of childhood, but that practice has been turned upside down with COVID-19. Among Americans aged 65 years and older, 95% have received at least one dose of vaccine, versus 27.9% of children younger than 12 years old, according to the Centers for Disease Control and Prevention.
The vaccine situation for children mirrors that of the population as a whole. The oldest children have the highest vaccination rates, and the rates decline along with age: 72.0% of those aged 12-17 years have received at least one dose, compared with 39.8% of 5- to 11-year-olds, 10.5% of 2- to 4-year-olds, and 8.0% of children under age 2, the CDC said on its COVID Data Tracker.
The youngest children were, of course, the last ones to be eligible for the vaccine, but their uptake has been much slower since emergency use was authorized in June of 2022. In the nearly 9 months since then, 9.5% of children aged 4 and under have received at least one dose, versus 66% of children aged 12-15 years in the first 9 months (May 2021 to March 2022).
Altogether, a total of 31.7 million, or 43%, of all children under age 18 had received at least one dose of COVID-19 vaccine as of March 8, 2023, according to the most recent CDC data.
Incidence: Counting COVID
Vaccination and other prevention efforts have tried to stem the tide, but what has COVID actually done to children since the Trump administration declared a nationwide emergency on March 13, 2020?
- 16.6 million cases.
- 186,035 new hospital admissions.
- 2,122 deaths.
Even the proportion of total COVID cases in children, 17.2%, is less than might be expected, given their relatively undervaccinated status.
Seroprevalence estimates seem to support the undercounting of pediatric cases. A survey of commercial laboratories working with the CDC put the seroprevalance of SARS-CoV-2 antibodies in children at 96.3% as of late 2022, based on tests of almost 27,000 specimens performed over an 8-week period from mid-October to mid-December. That would put the number of infected children at 65.7 million children.
Since Omicron
There has not been another major COVID-19 surge since the winter of 2021-2022, when the weekly rate of new cases reached 1,900 per 100,000 population in children aged 16-17 years in early January 2022 – the highest seen among children of any of the CDC’s age groups (0-4, 5-11, 12-15, 16-17) during the entire pandemic. Since the Omicron surge, the highest weekly rate was 221 per 100,000 during the week of May 15-21, again in 16- to 17-year-olds, the CDC reports.
The widely anticipated surge of COVID in the fall and winter of 2022 and 2023 – the so-called “tripledemic” involving influenza and respiratory syncytial virus – did not occur, possibly because so many Americans were vaccinated or previously infected, experts suggested. New-case rates, emergency room visits, and hospitalizations in children have continued to drop as winter comes to a close, CDC data show.
With 3 years of the COVID-19 experience now past, it’s safe to say that SARS-CoV-2 changed American society in ways that could not have been predicted when the first U.S. cases were reported in January of 2020.
Who would have guessed back then that not one but two vaccines would be developed, approved, and widely distributed before the end of the year? Or that those vaccines would be rejected by large segments of the population on ideological grounds? Could anyone have predicted in early 2020 that schools in 21 states would be forbidden by law to require COVID-19 vaccination in students?
Vaccination is generally considered to be an activity of childhood, but that practice has been turned upside down with COVID-19. Among Americans aged 65 years and older, 95% have received at least one dose of vaccine, versus 27.9% of children younger than 12 years old, according to the Centers for Disease Control and Prevention.
The vaccine situation for children mirrors that of the population as a whole. The oldest children have the highest vaccination rates, and the rates decline along with age: 72.0% of those aged 12-17 years have received at least one dose, compared with 39.8% of 5- to 11-year-olds, 10.5% of 2- to 4-year-olds, and 8.0% of children under age 2, the CDC said on its COVID Data Tracker.
The youngest children were, of course, the last ones to be eligible for the vaccine, but their uptake has been much slower since emergency use was authorized in June of 2022. In the nearly 9 months since then, 9.5% of children aged 4 and under have received at least one dose, versus 66% of children aged 12-15 years in the first 9 months (May 2021 to March 2022).
Altogether, a total of 31.7 million, or 43%, of all children under age 18 had received at least one dose of COVID-19 vaccine as of March 8, 2023, according to the most recent CDC data.
Incidence: Counting COVID
Vaccination and other prevention efforts have tried to stem the tide, but what has COVID actually done to children since the Trump administration declared a nationwide emergency on March 13, 2020?
- 16.6 million cases.
- 186,035 new hospital admissions.
- 2,122 deaths.
Even the proportion of total COVID cases in children, 17.2%, is less than might be expected, given their relatively undervaccinated status.
Seroprevalence estimates seem to support the undercounting of pediatric cases. A survey of commercial laboratories working with the CDC put the seroprevalance of SARS-CoV-2 antibodies in children at 96.3% as of late 2022, based on tests of almost 27,000 specimens performed over an 8-week period from mid-October to mid-December. That would put the number of infected children at 65.7 million children.
Since Omicron
There has not been another major COVID-19 surge since the winter of 2021-2022, when the weekly rate of new cases reached 1,900 per 100,000 population in children aged 16-17 years in early January 2022 – the highest seen among children of any of the CDC’s age groups (0-4, 5-11, 12-15, 16-17) during the entire pandemic. Since the Omicron surge, the highest weekly rate was 221 per 100,000 during the week of May 15-21, again in 16- to 17-year-olds, the CDC reports.
The widely anticipated surge of COVID in the fall and winter of 2022 and 2023 – the so-called “tripledemic” involving influenza and respiratory syncytial virus – did not occur, possibly because so many Americans were vaccinated or previously infected, experts suggested. New-case rates, emergency room visits, and hospitalizations in children have continued to drop as winter comes to a close, CDC data show.
With 3 years of the COVID-19 experience now past, it’s safe to say that SARS-CoV-2 changed American society in ways that could not have been predicted when the first U.S. cases were reported in January of 2020.
Who would have guessed back then that not one but two vaccines would be developed, approved, and widely distributed before the end of the year? Or that those vaccines would be rejected by large segments of the population on ideological grounds? Could anyone have predicted in early 2020 that schools in 21 states would be forbidden by law to require COVID-19 vaccination in students?
Vaccination is generally considered to be an activity of childhood, but that practice has been turned upside down with COVID-19. Among Americans aged 65 years and older, 95% have received at least one dose of vaccine, versus 27.9% of children younger than 12 years old, according to the Centers for Disease Control and Prevention.
The vaccine situation for children mirrors that of the population as a whole. The oldest children have the highest vaccination rates, and the rates decline along with age: 72.0% of those aged 12-17 years have received at least one dose, compared with 39.8% of 5- to 11-year-olds, 10.5% of 2- to 4-year-olds, and 8.0% of children under age 2, the CDC said on its COVID Data Tracker.
The youngest children were, of course, the last ones to be eligible for the vaccine, but their uptake has been much slower since emergency use was authorized in June of 2022. In the nearly 9 months since then, 9.5% of children aged 4 and under have received at least one dose, versus 66% of children aged 12-15 years in the first 9 months (May 2021 to March 2022).
Altogether, a total of 31.7 million, or 43%, of all children under age 18 had received at least one dose of COVID-19 vaccine as of March 8, 2023, according to the most recent CDC data.
Incidence: Counting COVID
Vaccination and other prevention efforts have tried to stem the tide, but what has COVID actually done to children since the Trump administration declared a nationwide emergency on March 13, 2020?
- 16.6 million cases.
- 186,035 new hospital admissions.
- 2,122 deaths.
Even the proportion of total COVID cases in children, 17.2%, is less than might be expected, given their relatively undervaccinated status.
Seroprevalence estimates seem to support the undercounting of pediatric cases. A survey of commercial laboratories working with the CDC put the seroprevalance of SARS-CoV-2 antibodies in children at 96.3% as of late 2022, based on tests of almost 27,000 specimens performed over an 8-week period from mid-October to mid-December. That would put the number of infected children at 65.7 million children.
Since Omicron
There has not been another major COVID-19 surge since the winter of 2021-2022, when the weekly rate of new cases reached 1,900 per 100,000 population in children aged 16-17 years in early January 2022 – the highest seen among children of any of the CDC’s age groups (0-4, 5-11, 12-15, 16-17) during the entire pandemic. Since the Omicron surge, the highest weekly rate was 221 per 100,000 during the week of May 15-21, again in 16- to 17-year-olds, the CDC reports.
The widely anticipated surge of COVID in the fall and winter of 2022 and 2023 – the so-called “tripledemic” involving influenza and respiratory syncytial virus – did not occur, possibly because so many Americans were vaccinated or previously infected, experts suggested. New-case rates, emergency room visits, and hospitalizations in children have continued to drop as winter comes to a close, CDC data show.
Factors linked with increased VTE risk in COVID outpatients
Though VTE risk is well studied and significant in those hospitalized with COVID, little is known about the risk in the outpatient setting, said the authors of the new research published online in JAMA Network Open.
The study was conducted at two integrated health care delivery systems in northern and southern California. Data were gathered from the Kaiser Permanente Virtual Data Warehouse and electronic health records.
Nearly 400,000 patients studied
Researchers, led by Margaret Fang, MD, with the division of hospital medicine, University of California, San Francisco, identified 398,530 outpatients with COVID-19 from Jan. 1, 2020, through Jan. 31, 2021.
VTE risk was low overall for ambulatory COVID patients.
“It is a reassuring study,” Dr. Fang said in an interview.
The researchers found that the risk is highest in the first 30 days after COVID-19 diagnosis (unadjusted rate, 0.58; 95% confidence interval, 0.51-0.67 per 100 person-years vs. 0.09; 95% CI, 0.08-0.11 per 100 person-years after 30 days).
Factors linked with high VTE risk
They also found that several factors were linked with a higher risk of blood clots in the study population, including being at least 55 years old; being male; having a history of blood clots or thrombophilia; and a body mass index (BMI) of at least 30 kg/m2.
The authors write, “These findings may help identify subsets of patients with COVID-19 who could benefit from VTE preventive strategies and more intensive short-term surveillance.”
Are routine anticoagulants justified?
Previously, randomized clinical trials have found that hospitalized patients with moderate COVID-19 may benefit from therapeutically dosed heparin anticoagulants but that therapeutic anticoagulation had no net benefit – and perhaps could even harm – patients who were critically ill with COVID.
“[M]uch less is known about the optimal thromboprophylaxis strategy for people with milder presentations of COVID-19 who do not require hospitalization,” they write.
Mild COVID VTE risk similar to general population
The authors note that rates of blood clots linked with COVID-19 are not much higher than the average blood clot rate in the general population, which is about 0.1-0.2 per 100 person-years.
Therefore, the results don’t justify routine administration of anticoagulation given the costs, inconvenience, and bleeding risks, they acknowledge.
Dr. Fang told this publication that it’s hard to know what to tell patients, given the overall low VTE risk. She said their study wasn’t designed to advise when to give prophylaxis.
Physicians should inform patients of their higher risk
“We should tell our patients who fall into these risk categories that blood clot is a concern after the development of COVID, especially in those first 30 days. And some people might benefit from increased surveillance,” Dr. Fang said.
”I think this study would support ongoing studies that look at whether selected patients benefit from VTE prophylaxis, for example low-dose anticoagulants,” she said.
Dr. Fang said the subgroup factors they found increased risk of blood clots for all patients, not just COVID-19 patients. It’s not clear why factors such as being male may increase blood clot risk, though that is consistent with previous literature, but higher risk with higher BMI might be related to a combination of inflammation or decreased mobility, she said.
Unanswered questions
Robert H. Hopkins Jr., MD, says the study helps answer a couple of important questions – that the VTE risk in nonhospitalized COVID-19 patients is low and when and for which patients risk may be highest.
However, there are several unanswered questions that argue against routine initiation of anticoagulants, notes the professor of internal medicine and pediatrics chief, division of general internal medicine, at University of Arkansas for Medical Sciences, Little Rock.
One is the change in the COVID variant landscape.
“We do not know whether rates of VTE are same or lower or higher with current circulating variants,” Dr. Hopkins said.
The authors acknowledge this as a limitation. Study data predate Omicron and subvariants, which appear to lower clinical severity, so it’s unclear whether VTE risk is different in this Omicron era.
Dr. Hopkins added another unknown: “We do not know whether vaccination affects rates of VTE in ambulatory breakthrough infection.”
Dr. Hopkins and the authors also note the lack of a control group in the study, to better compare risk.
Coauthor Dr. Prasad reports consultant fees from EpiExcellence LLC outside the submitted work. Coauthor Dr. Go reports grants paid to the division of research, Kaiser Permanente Northern California, from CSL Behring, Novartis, Bristol Meyers Squibb/Pfizer Alliance, and Janssen outside the submitted work.
The research was funded through Patient-Centered Outcomes Research Institute.
Dr. Hopkins reports no relevant financial relationships.
Though VTE risk is well studied and significant in those hospitalized with COVID, little is known about the risk in the outpatient setting, said the authors of the new research published online in JAMA Network Open.
The study was conducted at two integrated health care delivery systems in northern and southern California. Data were gathered from the Kaiser Permanente Virtual Data Warehouse and electronic health records.
Nearly 400,000 patients studied
Researchers, led by Margaret Fang, MD, with the division of hospital medicine, University of California, San Francisco, identified 398,530 outpatients with COVID-19 from Jan. 1, 2020, through Jan. 31, 2021.
VTE risk was low overall for ambulatory COVID patients.
“It is a reassuring study,” Dr. Fang said in an interview.
The researchers found that the risk is highest in the first 30 days after COVID-19 diagnosis (unadjusted rate, 0.58; 95% confidence interval, 0.51-0.67 per 100 person-years vs. 0.09; 95% CI, 0.08-0.11 per 100 person-years after 30 days).
Factors linked with high VTE risk
They also found that several factors were linked with a higher risk of blood clots in the study population, including being at least 55 years old; being male; having a history of blood clots or thrombophilia; and a body mass index (BMI) of at least 30 kg/m2.
The authors write, “These findings may help identify subsets of patients with COVID-19 who could benefit from VTE preventive strategies and more intensive short-term surveillance.”
Are routine anticoagulants justified?
Previously, randomized clinical trials have found that hospitalized patients with moderate COVID-19 may benefit from therapeutically dosed heparin anticoagulants but that therapeutic anticoagulation had no net benefit – and perhaps could even harm – patients who were critically ill with COVID.
“[M]uch less is known about the optimal thromboprophylaxis strategy for people with milder presentations of COVID-19 who do not require hospitalization,” they write.
Mild COVID VTE risk similar to general population
The authors note that rates of blood clots linked with COVID-19 are not much higher than the average blood clot rate in the general population, which is about 0.1-0.2 per 100 person-years.
Therefore, the results don’t justify routine administration of anticoagulation given the costs, inconvenience, and bleeding risks, they acknowledge.
Dr. Fang told this publication that it’s hard to know what to tell patients, given the overall low VTE risk. She said their study wasn’t designed to advise when to give prophylaxis.
Physicians should inform patients of their higher risk
“We should tell our patients who fall into these risk categories that blood clot is a concern after the development of COVID, especially in those first 30 days. And some people might benefit from increased surveillance,” Dr. Fang said.
”I think this study would support ongoing studies that look at whether selected patients benefit from VTE prophylaxis, for example low-dose anticoagulants,” she said.
Dr. Fang said the subgroup factors they found increased risk of blood clots for all patients, not just COVID-19 patients. It’s not clear why factors such as being male may increase blood clot risk, though that is consistent with previous literature, but higher risk with higher BMI might be related to a combination of inflammation or decreased mobility, she said.
Unanswered questions
Robert H. Hopkins Jr., MD, says the study helps answer a couple of important questions – that the VTE risk in nonhospitalized COVID-19 patients is low and when and for which patients risk may be highest.
However, there are several unanswered questions that argue against routine initiation of anticoagulants, notes the professor of internal medicine and pediatrics chief, division of general internal medicine, at University of Arkansas for Medical Sciences, Little Rock.
One is the change in the COVID variant landscape.
“We do not know whether rates of VTE are same or lower or higher with current circulating variants,” Dr. Hopkins said.
The authors acknowledge this as a limitation. Study data predate Omicron and subvariants, which appear to lower clinical severity, so it’s unclear whether VTE risk is different in this Omicron era.
Dr. Hopkins added another unknown: “We do not know whether vaccination affects rates of VTE in ambulatory breakthrough infection.”
Dr. Hopkins and the authors also note the lack of a control group in the study, to better compare risk.
Coauthor Dr. Prasad reports consultant fees from EpiExcellence LLC outside the submitted work. Coauthor Dr. Go reports grants paid to the division of research, Kaiser Permanente Northern California, from CSL Behring, Novartis, Bristol Meyers Squibb/Pfizer Alliance, and Janssen outside the submitted work.
The research was funded through Patient-Centered Outcomes Research Institute.
Dr. Hopkins reports no relevant financial relationships.
Though VTE risk is well studied and significant in those hospitalized with COVID, little is known about the risk in the outpatient setting, said the authors of the new research published online in JAMA Network Open.
The study was conducted at two integrated health care delivery systems in northern and southern California. Data were gathered from the Kaiser Permanente Virtual Data Warehouse and electronic health records.
Nearly 400,000 patients studied
Researchers, led by Margaret Fang, MD, with the division of hospital medicine, University of California, San Francisco, identified 398,530 outpatients with COVID-19 from Jan. 1, 2020, through Jan. 31, 2021.
VTE risk was low overall for ambulatory COVID patients.
“It is a reassuring study,” Dr. Fang said in an interview.
The researchers found that the risk is highest in the first 30 days after COVID-19 diagnosis (unadjusted rate, 0.58; 95% confidence interval, 0.51-0.67 per 100 person-years vs. 0.09; 95% CI, 0.08-0.11 per 100 person-years after 30 days).
Factors linked with high VTE risk
They also found that several factors were linked with a higher risk of blood clots in the study population, including being at least 55 years old; being male; having a history of blood clots or thrombophilia; and a body mass index (BMI) of at least 30 kg/m2.
The authors write, “These findings may help identify subsets of patients with COVID-19 who could benefit from VTE preventive strategies and more intensive short-term surveillance.”
Are routine anticoagulants justified?
Previously, randomized clinical trials have found that hospitalized patients with moderate COVID-19 may benefit from therapeutically dosed heparin anticoagulants but that therapeutic anticoagulation had no net benefit – and perhaps could even harm – patients who were critically ill with COVID.
“[M]uch less is known about the optimal thromboprophylaxis strategy for people with milder presentations of COVID-19 who do not require hospitalization,” they write.
Mild COVID VTE risk similar to general population
The authors note that rates of blood clots linked with COVID-19 are not much higher than the average blood clot rate in the general population, which is about 0.1-0.2 per 100 person-years.
Therefore, the results don’t justify routine administration of anticoagulation given the costs, inconvenience, and bleeding risks, they acknowledge.
Dr. Fang told this publication that it’s hard to know what to tell patients, given the overall low VTE risk. She said their study wasn’t designed to advise when to give prophylaxis.
Physicians should inform patients of their higher risk
“We should tell our patients who fall into these risk categories that blood clot is a concern after the development of COVID, especially in those first 30 days. And some people might benefit from increased surveillance,” Dr. Fang said.
”I think this study would support ongoing studies that look at whether selected patients benefit from VTE prophylaxis, for example low-dose anticoagulants,” she said.
Dr. Fang said the subgroup factors they found increased risk of blood clots for all patients, not just COVID-19 patients. It’s not clear why factors such as being male may increase blood clot risk, though that is consistent with previous literature, but higher risk with higher BMI might be related to a combination of inflammation or decreased mobility, she said.
Unanswered questions
Robert H. Hopkins Jr., MD, says the study helps answer a couple of important questions – that the VTE risk in nonhospitalized COVID-19 patients is low and when and for which patients risk may be highest.
However, there are several unanswered questions that argue against routine initiation of anticoagulants, notes the professor of internal medicine and pediatrics chief, division of general internal medicine, at University of Arkansas for Medical Sciences, Little Rock.
One is the change in the COVID variant landscape.
“We do not know whether rates of VTE are same or lower or higher with current circulating variants,” Dr. Hopkins said.
The authors acknowledge this as a limitation. Study data predate Omicron and subvariants, which appear to lower clinical severity, so it’s unclear whether VTE risk is different in this Omicron era.
Dr. Hopkins added another unknown: “We do not know whether vaccination affects rates of VTE in ambulatory breakthrough infection.”
Dr. Hopkins and the authors also note the lack of a control group in the study, to better compare risk.
Coauthor Dr. Prasad reports consultant fees from EpiExcellence LLC outside the submitted work. Coauthor Dr. Go reports grants paid to the division of research, Kaiser Permanente Northern California, from CSL Behring, Novartis, Bristol Meyers Squibb/Pfizer Alliance, and Janssen outside the submitted work.
The research was funded through Patient-Centered Outcomes Research Institute.
Dr. Hopkins reports no relevant financial relationships.
FROM JAMA NETWORK OPEN
Adherence to DASH diet reduced risk of COPD
Greater adherence to the Dietary Approaches to Stop Hypertension (DASH) diet was associated with a significantly reduced risk of chronic obstructive pulmonary disease (COPD) and improved lung function, based on data from more than 28,000 individuals in the United States.
but the effects of specific diet models such as the DASH diet and Mediterranean diet on COPD in particular has not been well studied, Jingli Wen, MD, of Nanjing Medical University, Jiangsu, China, and colleagues wrote.
In a study published in Frontiers in Nutrition, the researchers reviewed data from 28,605 adult participants in the National Health and Nutrition Examination Survey from 1999 to 2018.
The study population included 2,488 individuals with COPD participants and 25,607 individuals without COPD; the mean ages of the COPD and non-COPD groups were 60.2 years and 56.9 years, and the proportion of women was 63.7% and 51.4%, respectively. The primary outcome was the prevalence of COPD, defined as self-reports of a diagnosis of chronic bronchitis or emphysema. DASH diet scores were based on consumption of nine target nutrients: saturated fat, total fat, protein, cholesterol, fiber, magnesium, calcium, potassium, and sodium. Scores for compliance with the Mediterranean diet were based on intake of eight food categories: fruits, vegetables, legumes, fish, red meat, dairy products, alcohol, and olive oil.
Overall, a higher score for adherence to the DASH diet was significantly associated with a lower COPD risk (odds ratio, 0.83; P = .021). This association remained significant in subgroups of younger adults (OR, 0.74), men (OR, 0.73), and smokers (OR, 0.82).
By contrast, adherence to the Mediterranean diet was not significantly associated with COPD prevalence (OR, 1.03; P = .697).
The researchers also found a correlation between DASH diet adherence and improved lung function, especially among individuals without COPD. The risk of FEV1: forced vital capacity decrease, as well as dyspnea, cough, and expectoration, were negatively associated with greater adherence to the DASH diet, but greater adherence to the Mediterranean diet was only negatively associated with cough risk.
The relationship between the DASH diet and reduced COPD risk persisted after adjusting for occupational exposure and excluding participants with cardiovascular disease, cancer, or diabetes.
The current study is the first known to focus on the association between DASH diet and the risk of COPD among adults in the United States, the researchers wrote. The lack of effect of the Mediterranean diet on COPD, in contrast to some studies in other countries, “suggests that regional differences in diet may affect the role of diet in the development of COPD.”
The study findings were limited by several factors including the cross-sectional design that prevented conclusions of causality, the researchers noted. Other limitations included the lack of data of the impact of poor living habits, such as smoking, on food decisions, the use of short-term 24-hour dietary recall, and the reliance of self-reports for a diagnosis of COPD.
However, the results support the role of diet in COPD pathogenesis and expand the knowledge of relationships between the DASH diet and major chronic diseases, the researchers said. More prospective studies and clinical intervention studies are needed, but the findings should encourage clinicians to consider the potential role of a healthy diet in promoting lung health.
The study was supported by the Department of Health, Jiangsu Province, China. The researchers had no financial conflicts to disclose.
Greater adherence to the Dietary Approaches to Stop Hypertension (DASH) diet was associated with a significantly reduced risk of chronic obstructive pulmonary disease (COPD) and improved lung function, based on data from more than 28,000 individuals in the United States.
but the effects of specific diet models such as the DASH diet and Mediterranean diet on COPD in particular has not been well studied, Jingli Wen, MD, of Nanjing Medical University, Jiangsu, China, and colleagues wrote.
In a study published in Frontiers in Nutrition, the researchers reviewed data from 28,605 adult participants in the National Health and Nutrition Examination Survey from 1999 to 2018.
The study population included 2,488 individuals with COPD participants and 25,607 individuals without COPD; the mean ages of the COPD and non-COPD groups were 60.2 years and 56.9 years, and the proportion of women was 63.7% and 51.4%, respectively. The primary outcome was the prevalence of COPD, defined as self-reports of a diagnosis of chronic bronchitis or emphysema. DASH diet scores were based on consumption of nine target nutrients: saturated fat, total fat, protein, cholesterol, fiber, magnesium, calcium, potassium, and sodium. Scores for compliance with the Mediterranean diet were based on intake of eight food categories: fruits, vegetables, legumes, fish, red meat, dairy products, alcohol, and olive oil.
Overall, a higher score for adherence to the DASH diet was significantly associated with a lower COPD risk (odds ratio, 0.83; P = .021). This association remained significant in subgroups of younger adults (OR, 0.74), men (OR, 0.73), and smokers (OR, 0.82).
By contrast, adherence to the Mediterranean diet was not significantly associated with COPD prevalence (OR, 1.03; P = .697).
The researchers also found a correlation between DASH diet adherence and improved lung function, especially among individuals without COPD. The risk of FEV1: forced vital capacity decrease, as well as dyspnea, cough, and expectoration, were negatively associated with greater adherence to the DASH diet, but greater adherence to the Mediterranean diet was only negatively associated with cough risk.
The relationship between the DASH diet and reduced COPD risk persisted after adjusting for occupational exposure and excluding participants with cardiovascular disease, cancer, or diabetes.
The current study is the first known to focus on the association between DASH diet and the risk of COPD among adults in the United States, the researchers wrote. The lack of effect of the Mediterranean diet on COPD, in contrast to some studies in other countries, “suggests that regional differences in diet may affect the role of diet in the development of COPD.”
The study findings were limited by several factors including the cross-sectional design that prevented conclusions of causality, the researchers noted. Other limitations included the lack of data of the impact of poor living habits, such as smoking, on food decisions, the use of short-term 24-hour dietary recall, and the reliance of self-reports for a diagnosis of COPD.
However, the results support the role of diet in COPD pathogenesis and expand the knowledge of relationships between the DASH diet and major chronic diseases, the researchers said. More prospective studies and clinical intervention studies are needed, but the findings should encourage clinicians to consider the potential role of a healthy diet in promoting lung health.
The study was supported by the Department of Health, Jiangsu Province, China. The researchers had no financial conflicts to disclose.
Greater adherence to the Dietary Approaches to Stop Hypertension (DASH) diet was associated with a significantly reduced risk of chronic obstructive pulmonary disease (COPD) and improved lung function, based on data from more than 28,000 individuals in the United States.
but the effects of specific diet models such as the DASH diet and Mediterranean diet on COPD in particular has not been well studied, Jingli Wen, MD, of Nanjing Medical University, Jiangsu, China, and colleagues wrote.
In a study published in Frontiers in Nutrition, the researchers reviewed data from 28,605 adult participants in the National Health and Nutrition Examination Survey from 1999 to 2018.
The study population included 2,488 individuals with COPD participants and 25,607 individuals without COPD; the mean ages of the COPD and non-COPD groups were 60.2 years and 56.9 years, and the proportion of women was 63.7% and 51.4%, respectively. The primary outcome was the prevalence of COPD, defined as self-reports of a diagnosis of chronic bronchitis or emphysema. DASH diet scores were based on consumption of nine target nutrients: saturated fat, total fat, protein, cholesterol, fiber, magnesium, calcium, potassium, and sodium. Scores for compliance with the Mediterranean diet were based on intake of eight food categories: fruits, vegetables, legumes, fish, red meat, dairy products, alcohol, and olive oil.
Overall, a higher score for adherence to the DASH diet was significantly associated with a lower COPD risk (odds ratio, 0.83; P = .021). This association remained significant in subgroups of younger adults (OR, 0.74), men (OR, 0.73), and smokers (OR, 0.82).
By contrast, adherence to the Mediterranean diet was not significantly associated with COPD prevalence (OR, 1.03; P = .697).
The researchers also found a correlation between DASH diet adherence and improved lung function, especially among individuals without COPD. The risk of FEV1: forced vital capacity decrease, as well as dyspnea, cough, and expectoration, were negatively associated with greater adherence to the DASH diet, but greater adherence to the Mediterranean diet was only negatively associated with cough risk.
The relationship between the DASH diet and reduced COPD risk persisted after adjusting for occupational exposure and excluding participants with cardiovascular disease, cancer, or diabetes.
The current study is the first known to focus on the association between DASH diet and the risk of COPD among adults in the United States, the researchers wrote. The lack of effect of the Mediterranean diet on COPD, in contrast to some studies in other countries, “suggests that regional differences in diet may affect the role of diet in the development of COPD.”
The study findings were limited by several factors including the cross-sectional design that prevented conclusions of causality, the researchers noted. Other limitations included the lack of data of the impact of poor living habits, such as smoking, on food decisions, the use of short-term 24-hour dietary recall, and the reliance of self-reports for a diagnosis of COPD.
However, the results support the role of diet in COPD pathogenesis and expand the knowledge of relationships between the DASH diet and major chronic diseases, the researchers said. More prospective studies and clinical intervention studies are needed, but the findings should encourage clinicians to consider the potential role of a healthy diet in promoting lung health.
The study was supported by the Department of Health, Jiangsu Province, China. The researchers had no financial conflicts to disclose.
FROM FRONTIERS IN NUTRITION
Gestational diabetes affects fetal lung development
Lung development in the fetus may be adversely affected by a mother’s gestational diabetes, based on data from in vivo, in vitro, and ex vivo studies.
Gestational diabetes mellitus (GDM) has recently been associated with fetal lung underdevelopment (FLUD) and delayed lung maturation that may lead to immediate respiratory distress in newborns and later chronic lung disease, Pengzheng Chen, PhD, of Shandong University, Jinan, China, and colleagues wrote.
Antenatal corticosteroids are considered an effective treatment for gestational fetal lung underdevelopment, but recent studies have shown adverse effects of these medications, and therefore more research is needed to identify the etiology and pathogenesis of FLUD induced by GDM, they said.
In a study published in the International Journal of Nanomedicine, the researchers collected umbilical cord blood samples from patients with GDM and matched controls at a single hospital in China.
“Using an ex vivo exosome exposure model of fetal lung explants, we observed the morphological alteration of lung explants and evaluated the expression of molecules involved in lung development,” the researchers wrote.
Fetal lung underdevelopment was more common after exposure to exosomes from the umbilical cord plasma of individuals with gestational diabetes mellitus, compared with exosomes from healthy controls.
The researchers also used mouse models to examine the effects of exosomes on fetal lung development in vivo. They found that exosomes associated with GDM impeded the growth, branching morphogenesis, and maturation of fetal lungs in mouse models. In addition, the expression of the apoptotic biomarkers known as BAX, BIM, and cleaved CASPASE-3 was up-regulated in GDMUB-exosomes and HG-exos groups, but the antiapoptotic protein BCL-2 was down-regulated; this further supported the negative impact of GDM exomes on fetal lung development, the researchers said.
The researchers then conducted miRNA sequencing, which showed that the miRNA in placenta-derived exosomes from GDM pregnancies were distinct from the miRNA in exosomes from healthy control pregnancies.
The study findings were limited by several factors including the impurity of the isolated placenta-derived exosomes from the umbilical cord blood plasma, which were not placenta specific, the researchers noted. Other limitations included the lack of data on different stages of lung development, and more research is needed to validate miRNAs and to explore the signally pathways involved in fetal lung development.
However, the study is the first known to demonstrate an adverse effect of GDM on fetal lung development via in vitro, ex vivo, and in vitro models, they said.
“These data highlight an emerging role of placenta-derived exosomes in the pathogenesis of fetal lung underdevelopment in GDM pregnancies, and provide a novel strategy for maternal-fetal communication,” they concluded.
The study received no outside funding. The researchers had no financial conflicts to disclose.
Lung development in the fetus may be adversely affected by a mother’s gestational diabetes, based on data from in vivo, in vitro, and ex vivo studies.
Gestational diabetes mellitus (GDM) has recently been associated with fetal lung underdevelopment (FLUD) and delayed lung maturation that may lead to immediate respiratory distress in newborns and later chronic lung disease, Pengzheng Chen, PhD, of Shandong University, Jinan, China, and colleagues wrote.
Antenatal corticosteroids are considered an effective treatment for gestational fetal lung underdevelopment, but recent studies have shown adverse effects of these medications, and therefore more research is needed to identify the etiology and pathogenesis of FLUD induced by GDM, they said.
In a study published in the International Journal of Nanomedicine, the researchers collected umbilical cord blood samples from patients with GDM and matched controls at a single hospital in China.
“Using an ex vivo exosome exposure model of fetal lung explants, we observed the morphological alteration of lung explants and evaluated the expression of molecules involved in lung development,” the researchers wrote.
Fetal lung underdevelopment was more common after exposure to exosomes from the umbilical cord plasma of individuals with gestational diabetes mellitus, compared with exosomes from healthy controls.
The researchers also used mouse models to examine the effects of exosomes on fetal lung development in vivo. They found that exosomes associated with GDM impeded the growth, branching morphogenesis, and maturation of fetal lungs in mouse models. In addition, the expression of the apoptotic biomarkers known as BAX, BIM, and cleaved CASPASE-3 was up-regulated in GDMUB-exosomes and HG-exos groups, but the antiapoptotic protein BCL-2 was down-regulated; this further supported the negative impact of GDM exomes on fetal lung development, the researchers said.
The researchers then conducted miRNA sequencing, which showed that the miRNA in placenta-derived exosomes from GDM pregnancies were distinct from the miRNA in exosomes from healthy control pregnancies.
The study findings were limited by several factors including the impurity of the isolated placenta-derived exosomes from the umbilical cord blood plasma, which were not placenta specific, the researchers noted. Other limitations included the lack of data on different stages of lung development, and more research is needed to validate miRNAs and to explore the signally pathways involved in fetal lung development.
However, the study is the first known to demonstrate an adverse effect of GDM on fetal lung development via in vitro, ex vivo, and in vitro models, they said.
“These data highlight an emerging role of placenta-derived exosomes in the pathogenesis of fetal lung underdevelopment in GDM pregnancies, and provide a novel strategy for maternal-fetal communication,” they concluded.
The study received no outside funding. The researchers had no financial conflicts to disclose.
Lung development in the fetus may be adversely affected by a mother’s gestational diabetes, based on data from in vivo, in vitro, and ex vivo studies.
Gestational diabetes mellitus (GDM) has recently been associated with fetal lung underdevelopment (FLUD) and delayed lung maturation that may lead to immediate respiratory distress in newborns and later chronic lung disease, Pengzheng Chen, PhD, of Shandong University, Jinan, China, and colleagues wrote.
Antenatal corticosteroids are considered an effective treatment for gestational fetal lung underdevelopment, but recent studies have shown adverse effects of these medications, and therefore more research is needed to identify the etiology and pathogenesis of FLUD induced by GDM, they said.
In a study published in the International Journal of Nanomedicine, the researchers collected umbilical cord blood samples from patients with GDM and matched controls at a single hospital in China.
“Using an ex vivo exosome exposure model of fetal lung explants, we observed the morphological alteration of lung explants and evaluated the expression of molecules involved in lung development,” the researchers wrote.
Fetal lung underdevelopment was more common after exposure to exosomes from the umbilical cord plasma of individuals with gestational diabetes mellitus, compared with exosomes from healthy controls.
The researchers also used mouse models to examine the effects of exosomes on fetal lung development in vivo. They found that exosomes associated with GDM impeded the growth, branching morphogenesis, and maturation of fetal lungs in mouse models. In addition, the expression of the apoptotic biomarkers known as BAX, BIM, and cleaved CASPASE-3 was up-regulated in GDMUB-exosomes and HG-exos groups, but the antiapoptotic protein BCL-2 was down-regulated; this further supported the negative impact of GDM exomes on fetal lung development, the researchers said.
The researchers then conducted miRNA sequencing, which showed that the miRNA in placenta-derived exosomes from GDM pregnancies were distinct from the miRNA in exosomes from healthy control pregnancies.
The study findings were limited by several factors including the impurity of the isolated placenta-derived exosomes from the umbilical cord blood plasma, which were not placenta specific, the researchers noted. Other limitations included the lack of data on different stages of lung development, and more research is needed to validate miRNAs and to explore the signally pathways involved in fetal lung development.
However, the study is the first known to demonstrate an adverse effect of GDM on fetal lung development via in vitro, ex vivo, and in vitro models, they said.
“These data highlight an emerging role of placenta-derived exosomes in the pathogenesis of fetal lung underdevelopment in GDM pregnancies, and provide a novel strategy for maternal-fetal communication,” they concluded.
The study received no outside funding. The researchers had no financial conflicts to disclose.
FROM THE INTERNATIONAL JOURNAL OF NANOMEDICINE
Are early childhood viral infections linked with asthma?
MARSEILLE, France – It is well known that viral infections, especially respiratory syncytial virus (RSV) and rhinovirus (RV), exacerbate symptoms of asthma. But could they also play a part in triggering the onset of asthma?
The link between RSV and RV infections in early childhood and the development of asthma symptoms is well established, said Camille Taillé, MD, PhD, of the department of respiratory medicine and the rare diseases center of excellence at Bichat Hospital, Paris. But getting asthma is probably not just a matter of having a viral infection at a young age or of having a severe form of it. Gene polymorphisms, immune system disorders, and preexisting atopy are also associated with the risk of asthma. This was the focus of the 27th French-language respiratory medicine conference, held in Marseille, France.
RV and RSV
Persons with asthma are vulnerable to certain viral respiratory infections, in particular the flu and RV, which can exacerbate asthma symptoms. Inhaled corticosteroids have an overall protective effect against viral-induced exacerbations. For worsening asthma symptoms during an epidemic or pandemic, there is no contraindication to inhaled or oral corticosteroids.
Young children from the time of birth to 4 years of age are particularly susceptible to viral respiratory infections. According to data from France’s clinical surveillance network, Sentinelles, from the period covering winter 2021-2022, the rate of incidence per 100,000 inhabitants was systematically greater for the 0 to 4-year age range than for older age ranges.
Of the most common viruses that infect young children, RV, the virus that causes the common cold, is a nonenveloped RNA virus from the enterovirus family. There are 160 types, which are classified into three strains (A, B, and C). Of those strains, A and C confer the most severe infections. The virus is highly variable, which makes developing a vaccine challenging. The virus circulates year round, usually peaking in the fall and at the end of spring. RSV is an RNA virus that is classed as a respiratory virus. It comprises two serotypes: type A and B. Almost all children will have been infected with RSV by the time they are 2 years old. Epidemics occur each year during winter or in early spring in temperate climates. Vaccines are currently being developed and will soon be marketed. A monoclonal antibody (palivizumab), which targets fusion proteins of the virus, is available as prophylactic treatment for at-risk children.
RSV infection
During an RSV infection, the severe inflammation of the bronchial and alveolar wall causes acute respiratory distress. “But not all infants will develop severe forms of bronchiolitis,” said Dr. Taillé. “The risk factors for the severe form of the illness are well known: being under 6 months of age, prematurity, comorbidities (neurovascular, cardiovascular, respiratory, etc.), history of a stay in a neonatal intensive care unit at birth, living in low socioeconomic status towns, and exposure to smoking.”
Asthma development
The issue of whether or not viral diseases cause asthma has been the subject of intense debate. The studies are starting to stack up, however. They seem to show that RSV or RV infections are associated with the risk of subsequent asthma development. “For example, in a study published in 2022,” said Dr. Taillé, “in children admitted with an RSV infection, 60% of those who had been admitted to neonatal intensive care presented with symptoms of asthma between 3 and 6 years of age, compared with 18% of those who had had a milder case of RSV (admitted to nonintensive care settings). A serious RSV infection is a risk factor for later development of asthma.”
However, the link between RSV and later onset of asthma is also seen in milder cases of the infection. The American COAST study was designed to examine the effect of childhood respiratory infections on the risk of developing asthma. Researchers followed 259 newborns prospectively for 1, 3, and 6 years. To qualify, at least one parent was required to have respiratory allergies (defined as one or more positive aeroallergen skin tests) or a history of physician-diagnosed asthma. Regular samples taken during infectious episodes identified a virus in 90% of cases.
“We now know that RSV is not the only pathogen responsible for bronchiolitis. RV is often found, now that it can routinely be detected by PCR tests,” said Dr. Taillé. In the COAST study, the onset of wheezing during an RSV or RV infection in children aged 0-3 years was associated with an increased risk of asthma at 6 years of age. Globally, 28% of children infected by either virus were deemed to have asthma at 6 years of age. “There is clearly a link between having had a respiratory virus like RV or RSV and getting asthma symptoms at 6 years of age,” said Dr. Taillé. “What’s more, the effect of RV is not changed in this study by allergic sensitization.”
Many articles have been published on this topic. The results of cohort studies, from Japan to Finland and the United States, Italy, and Australia, are consistent with each other. Persons who have contracted RV or RSV are more likely to suffer from recurrent wheezing or asthma, especially if the infection is contracted in infancy or if it is severe. “Some studies even suggest that viral-induced asthma is more severe,” said Dr. Taillé. “For example, a Scottish study ... showed that children with a previous history of RSV infection had more hospital admissions and required more medication than asthmatics with no history of an RSV infection, suggesting the link between a previous history of RSV infection and the development of a more severe form of asthma.”
Reaching adulthood
Few longitudinal cohorts explore this issue in adulthood. A relatively old study reported an increased rate of asthma among adults who had required hospital admission for bronchiolitis in early childhood, as well as the effect on respiratory function. A 2023 study of the effects of respiratory illnesses in childhood reported similar findings. The authors evaluated lung structure and function via CT scans of 39 patients aged 26 years and concluded that participants who had been infected with RSV in childhood presented with increased air trapping, which is suggestive of airway abnormalities, possibly linked to a direct effect of viruses on lung development.
Mechanisms of action
“The real question is understanding if it’s the virus itself that causes asthma, or if the virus is simply uncovering underlying asthma in predisposed children,” said Dr. Taillé. From 30% to 40% of children who have had RSV will go on to develop wheezing or asthma in childhood. This observation suggests that there are factors favoring the development of asthma after infection with RSV. It has been shown that there is a genetic predisposition for RV. The roles of cigarette smoke, air pollution, environmental exposures to allergens, rapid urbanization, low vitamin D levels, low maternal omega-3 long-chain polyunsaturated fatty acid levels, maternal stress, and depression have also been highlighted.
It would seem that RSV and RV are a bit different. RV is thought to be associated with the development of asthma and wheezing, especially in people with a preexisting atopy or a reduced interferon immune response, while RSV, which occurs at a younger age and among the most vulnerable populations, seems to act independently of a person’s predisposition to allergies. RV stands out from other viral factors, owing to its tendency to create a Th2-biased inflammatory environment and its association with specific risk genes in people predisposed to asthma development (CDHR3).
Dr. Taillé has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
MARSEILLE, France – It is well known that viral infections, especially respiratory syncytial virus (RSV) and rhinovirus (RV), exacerbate symptoms of asthma. But could they also play a part in triggering the onset of asthma?
The link between RSV and RV infections in early childhood and the development of asthma symptoms is well established, said Camille Taillé, MD, PhD, of the department of respiratory medicine and the rare diseases center of excellence at Bichat Hospital, Paris. But getting asthma is probably not just a matter of having a viral infection at a young age or of having a severe form of it. Gene polymorphisms, immune system disorders, and preexisting atopy are also associated with the risk of asthma. This was the focus of the 27th French-language respiratory medicine conference, held in Marseille, France.
RV and RSV
Persons with asthma are vulnerable to certain viral respiratory infections, in particular the flu and RV, which can exacerbate asthma symptoms. Inhaled corticosteroids have an overall protective effect against viral-induced exacerbations. For worsening asthma symptoms during an epidemic or pandemic, there is no contraindication to inhaled or oral corticosteroids.
Young children from the time of birth to 4 years of age are particularly susceptible to viral respiratory infections. According to data from France’s clinical surveillance network, Sentinelles, from the period covering winter 2021-2022, the rate of incidence per 100,000 inhabitants was systematically greater for the 0 to 4-year age range than for older age ranges.
Of the most common viruses that infect young children, RV, the virus that causes the common cold, is a nonenveloped RNA virus from the enterovirus family. There are 160 types, which are classified into three strains (A, B, and C). Of those strains, A and C confer the most severe infections. The virus is highly variable, which makes developing a vaccine challenging. The virus circulates year round, usually peaking in the fall and at the end of spring. RSV is an RNA virus that is classed as a respiratory virus. It comprises two serotypes: type A and B. Almost all children will have been infected with RSV by the time they are 2 years old. Epidemics occur each year during winter or in early spring in temperate climates. Vaccines are currently being developed and will soon be marketed. A monoclonal antibody (palivizumab), which targets fusion proteins of the virus, is available as prophylactic treatment for at-risk children.
RSV infection
During an RSV infection, the severe inflammation of the bronchial and alveolar wall causes acute respiratory distress. “But not all infants will develop severe forms of bronchiolitis,” said Dr. Taillé. “The risk factors for the severe form of the illness are well known: being under 6 months of age, prematurity, comorbidities (neurovascular, cardiovascular, respiratory, etc.), history of a stay in a neonatal intensive care unit at birth, living in low socioeconomic status towns, and exposure to smoking.”
Asthma development
The issue of whether or not viral diseases cause asthma has been the subject of intense debate. The studies are starting to stack up, however. They seem to show that RSV or RV infections are associated with the risk of subsequent asthma development. “For example, in a study published in 2022,” said Dr. Taillé, “in children admitted with an RSV infection, 60% of those who had been admitted to neonatal intensive care presented with symptoms of asthma between 3 and 6 years of age, compared with 18% of those who had had a milder case of RSV (admitted to nonintensive care settings). A serious RSV infection is a risk factor for later development of asthma.”
However, the link between RSV and later onset of asthma is also seen in milder cases of the infection. The American COAST study was designed to examine the effect of childhood respiratory infections on the risk of developing asthma. Researchers followed 259 newborns prospectively for 1, 3, and 6 years. To qualify, at least one parent was required to have respiratory allergies (defined as one or more positive aeroallergen skin tests) or a history of physician-diagnosed asthma. Regular samples taken during infectious episodes identified a virus in 90% of cases.
“We now know that RSV is not the only pathogen responsible for bronchiolitis. RV is often found, now that it can routinely be detected by PCR tests,” said Dr. Taillé. In the COAST study, the onset of wheezing during an RSV or RV infection in children aged 0-3 years was associated with an increased risk of asthma at 6 years of age. Globally, 28% of children infected by either virus were deemed to have asthma at 6 years of age. “There is clearly a link between having had a respiratory virus like RV or RSV and getting asthma symptoms at 6 years of age,” said Dr. Taillé. “What’s more, the effect of RV is not changed in this study by allergic sensitization.”
Many articles have been published on this topic. The results of cohort studies, from Japan to Finland and the United States, Italy, and Australia, are consistent with each other. Persons who have contracted RV or RSV are more likely to suffer from recurrent wheezing or asthma, especially if the infection is contracted in infancy or if it is severe. “Some studies even suggest that viral-induced asthma is more severe,” said Dr. Taillé. “For example, a Scottish study ... showed that children with a previous history of RSV infection had more hospital admissions and required more medication than asthmatics with no history of an RSV infection, suggesting the link between a previous history of RSV infection and the development of a more severe form of asthma.”
Reaching adulthood
Few longitudinal cohorts explore this issue in adulthood. A relatively old study reported an increased rate of asthma among adults who had required hospital admission for bronchiolitis in early childhood, as well as the effect on respiratory function. A 2023 study of the effects of respiratory illnesses in childhood reported similar findings. The authors evaluated lung structure and function via CT scans of 39 patients aged 26 years and concluded that participants who had been infected with RSV in childhood presented with increased air trapping, which is suggestive of airway abnormalities, possibly linked to a direct effect of viruses on lung development.
Mechanisms of action
“The real question is understanding if it’s the virus itself that causes asthma, or if the virus is simply uncovering underlying asthma in predisposed children,” said Dr. Taillé. From 30% to 40% of children who have had RSV will go on to develop wheezing or asthma in childhood. This observation suggests that there are factors favoring the development of asthma after infection with RSV. It has been shown that there is a genetic predisposition for RV. The roles of cigarette smoke, air pollution, environmental exposures to allergens, rapid urbanization, low vitamin D levels, low maternal omega-3 long-chain polyunsaturated fatty acid levels, maternal stress, and depression have also been highlighted.
It would seem that RSV and RV are a bit different. RV is thought to be associated with the development of asthma and wheezing, especially in people with a preexisting atopy or a reduced interferon immune response, while RSV, which occurs at a younger age and among the most vulnerable populations, seems to act independently of a person’s predisposition to allergies. RV stands out from other viral factors, owing to its tendency to create a Th2-biased inflammatory environment and its association with specific risk genes in people predisposed to asthma development (CDHR3).
Dr. Taillé has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
MARSEILLE, France – It is well known that viral infections, especially respiratory syncytial virus (RSV) and rhinovirus (RV), exacerbate symptoms of asthma. But could they also play a part in triggering the onset of asthma?
The link between RSV and RV infections in early childhood and the development of asthma symptoms is well established, said Camille Taillé, MD, PhD, of the department of respiratory medicine and the rare diseases center of excellence at Bichat Hospital, Paris. But getting asthma is probably not just a matter of having a viral infection at a young age or of having a severe form of it. Gene polymorphisms, immune system disorders, and preexisting atopy are also associated with the risk of asthma. This was the focus of the 27th French-language respiratory medicine conference, held in Marseille, France.
RV and RSV
Persons with asthma are vulnerable to certain viral respiratory infections, in particular the flu and RV, which can exacerbate asthma symptoms. Inhaled corticosteroids have an overall protective effect against viral-induced exacerbations. For worsening asthma symptoms during an epidemic or pandemic, there is no contraindication to inhaled or oral corticosteroids.
Young children from the time of birth to 4 years of age are particularly susceptible to viral respiratory infections. According to data from France’s clinical surveillance network, Sentinelles, from the period covering winter 2021-2022, the rate of incidence per 100,000 inhabitants was systematically greater for the 0 to 4-year age range than for older age ranges.
Of the most common viruses that infect young children, RV, the virus that causes the common cold, is a nonenveloped RNA virus from the enterovirus family. There are 160 types, which are classified into three strains (A, B, and C). Of those strains, A and C confer the most severe infections. The virus is highly variable, which makes developing a vaccine challenging. The virus circulates year round, usually peaking in the fall and at the end of spring. RSV is an RNA virus that is classed as a respiratory virus. It comprises two serotypes: type A and B. Almost all children will have been infected with RSV by the time they are 2 years old. Epidemics occur each year during winter or in early spring in temperate climates. Vaccines are currently being developed and will soon be marketed. A monoclonal antibody (palivizumab), which targets fusion proteins of the virus, is available as prophylactic treatment for at-risk children.
RSV infection
During an RSV infection, the severe inflammation of the bronchial and alveolar wall causes acute respiratory distress. “But not all infants will develop severe forms of bronchiolitis,” said Dr. Taillé. “The risk factors for the severe form of the illness are well known: being under 6 months of age, prematurity, comorbidities (neurovascular, cardiovascular, respiratory, etc.), history of a stay in a neonatal intensive care unit at birth, living in low socioeconomic status towns, and exposure to smoking.”
Asthma development
The issue of whether or not viral diseases cause asthma has been the subject of intense debate. The studies are starting to stack up, however. They seem to show that RSV or RV infections are associated with the risk of subsequent asthma development. “For example, in a study published in 2022,” said Dr. Taillé, “in children admitted with an RSV infection, 60% of those who had been admitted to neonatal intensive care presented with symptoms of asthma between 3 and 6 years of age, compared with 18% of those who had had a milder case of RSV (admitted to nonintensive care settings). A serious RSV infection is a risk factor for later development of asthma.”
However, the link between RSV and later onset of asthma is also seen in milder cases of the infection. The American COAST study was designed to examine the effect of childhood respiratory infections on the risk of developing asthma. Researchers followed 259 newborns prospectively for 1, 3, and 6 years. To qualify, at least one parent was required to have respiratory allergies (defined as one or more positive aeroallergen skin tests) or a history of physician-diagnosed asthma. Regular samples taken during infectious episodes identified a virus in 90% of cases.
“We now know that RSV is not the only pathogen responsible for bronchiolitis. RV is often found, now that it can routinely be detected by PCR tests,” said Dr. Taillé. In the COAST study, the onset of wheezing during an RSV or RV infection in children aged 0-3 years was associated with an increased risk of asthma at 6 years of age. Globally, 28% of children infected by either virus were deemed to have asthma at 6 years of age. “There is clearly a link between having had a respiratory virus like RV or RSV and getting asthma symptoms at 6 years of age,” said Dr. Taillé. “What’s more, the effect of RV is not changed in this study by allergic sensitization.”
Many articles have been published on this topic. The results of cohort studies, from Japan to Finland and the United States, Italy, and Australia, are consistent with each other. Persons who have contracted RV or RSV are more likely to suffer from recurrent wheezing or asthma, especially if the infection is contracted in infancy or if it is severe. “Some studies even suggest that viral-induced asthma is more severe,” said Dr. Taillé. “For example, a Scottish study ... showed that children with a previous history of RSV infection had more hospital admissions and required more medication than asthmatics with no history of an RSV infection, suggesting the link between a previous history of RSV infection and the development of a more severe form of asthma.”
Reaching adulthood
Few longitudinal cohorts explore this issue in adulthood. A relatively old study reported an increased rate of asthma among adults who had required hospital admission for bronchiolitis in early childhood, as well as the effect on respiratory function. A 2023 study of the effects of respiratory illnesses in childhood reported similar findings. The authors evaluated lung structure and function via CT scans of 39 patients aged 26 years and concluded that participants who had been infected with RSV in childhood presented with increased air trapping, which is suggestive of airway abnormalities, possibly linked to a direct effect of viruses on lung development.
Mechanisms of action
“The real question is understanding if it’s the virus itself that causes asthma, or if the virus is simply uncovering underlying asthma in predisposed children,” said Dr. Taillé. From 30% to 40% of children who have had RSV will go on to develop wheezing or asthma in childhood. This observation suggests that there are factors favoring the development of asthma after infection with RSV. It has been shown that there is a genetic predisposition for RV. The roles of cigarette smoke, air pollution, environmental exposures to allergens, rapid urbanization, low vitamin D levels, low maternal omega-3 long-chain polyunsaturated fatty acid levels, maternal stress, and depression have also been highlighted.
It would seem that RSV and RV are a bit different. RV is thought to be associated with the development of asthma and wheezing, especially in people with a preexisting atopy or a reduced interferon immune response, while RSV, which occurs at a younger age and among the most vulnerable populations, seems to act independently of a person’s predisposition to allergies. RV stands out from other viral factors, owing to its tendency to create a Th2-biased inflammatory environment and its association with specific risk genes in people predisposed to asthma development (CDHR3).
Dr. Taillé has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
‘Unheard of’ PAH improvement with novel drug: STELLAR
NEW ORLEANS – An investigational, first-in class agent that delivers a completely new type of intervention to patients with pulmonary arterial hypertension (PAH) scored a clear win in the STELLAR trial, the first to complete among three phase 3 trials that are testing this agent.
Sotatercept, administered subcutaneously every 3 weeks for 24 weeks, improved from baseline average 6-minute walk distance (6MWD) by a significant and clinically meaningful 40.8 meters, compared with placebo, for the trial’s primary efficacy endpoint (P < .001). The treatment also “delivered broad clinical benefit across multiple domains including hemodynamics, World Health Organization functional class, disease biomarkers, risk scores and patient-reported outcomes,” Marius M. Hoeper, MD, said at the joint scientific sessions of the American College of Cardiology and the World Heart Federation.

“These results establish the clinical utility of sotatercept, administered in combination with approved PAH therapies, as a new treatment for PAH,” added Dr. Hoeper, professor and deputy director of the department of respiratory medicine at Hannover (Germany) Medical School,
“The most important aspect was the hemodynamic improvement,” with sotatercept treatment, which led to an average 235 dyn/sec per cm−5 reduction in pulmonary vascular resistance from baseline and an average cut in pulmonary artery pressure of 13.9 mm Hg from baseline, compared with placebo, a result that’s “unheard of,” Dr. Hoeper said in a press conference during the meeting.
“With other tested agents we usually see very little improvement in pulmonary artery pressure. This is a signal that we achieved some reversing of the pathological changes in the pulmonary vessels that lead to” PAH, he added.
Simultaneously with his report the findings also appeared online in the New England Journal of Medicine.
‘A new hope’ for patients with PAH
Based on the reported findings, sotatercept is a “very exciting boutique molecule” that will “offer patients with PAH a very exciting new treatment,” commented Rhonda Cooper-DeHoff, PharmD, a designated discussant and a researcher at the University of Florida, Gainesville.

“This study is a new hope for patients with PAH. Until now, they’ve had really bad outcomes, but [in this study] we see significant differences in 6MWD, hemodynamics, and risk factors. Overall, I think the benefit is greater than the risk” it may pose to patients through potential adverse effects, commented Julia Grapsa, MD, PhD, a cardiologist at St. Thomas Hospital in London, and another discussant at the meeting.
“The results are impressive” and “encouraging,” and “suggest that sotatercept may represent a new and clinically consequential addition to current medications for PAH,” wrote three clinicians from Canyons Region Intermountain Medical Center in Murray, Utah, in an editorial that accompanied the published report.
But the authors of the editorial also raised several cautions and concerns. They questioned the generalizability of the findings, noting that the patients with PAH enrolled in the study were all adults who were clinically stable and an average of more than 8 years out from their initial PAH diagnosis, and more than 90% were on stable treatment for PAH with two or three agents specific for treating the disorder. The study cohort also had a disproportionately high enrollment of patients with idiopathic (59%) or heritable (18%) forms of PAH, and the 15% of patients in the trial with connective tissue disease represented a disproportionately low prevalence of this PAH subtype.
The editorialists also called for “ongoing vigilance” for adverse effects from sotatercept treatment, although they acknowledged that the adverse effects reported to date from sotatercept are “largely reassuring.”
Death or clinical worsening cut by 84%
STELLAR randomized 323 patients at 91 sites in 21 countries with WHO Group 1 PAH and with WHO functional class II or III disease to receive either sotatercept or placebo for 24 weeks, with an option for treatment to continue beyond that until the last patient in the study reached 24 weeks on treatment, resulting in an overall median treatment duration of nearly 33 weeks.
In addition to the significant result for the primary endpoint, the 163 patients who received sotatercept had significant improvements, compared with 160 placebo-treated patients, for eight of nine secondary endpoints. The only secondary endpoint with a neutral result was for a measure of cognitive and emotional wellbeing, a parameter that was already at a normal level at baseline in most enrolled patients, Dr. Hoeper explained.
The incidence of either death or an event indicative of clinical worsening during the overall median follow-up of almost 33 weeks was 26.3% among the control patients and 5.5% among those who received sotatercept. This translated into a significant reduction for this endpoint of 84% with sotatercept treatment, compared with placebo.
The rates of treatment-emergent adverse events leading to discontinuation were roughly the same in the control and sotatercept arms, and the incidence of severe or serious treatment-emergent adverse events was higher among the control patients.
The most common adverse event on sotatercept was bleeding events, which occurred in 32% of those on sotatercept and in 16% of the control patients, but the events in the sotatercept arm were “mostly mild,” said Dr. Hoeper. The next most frequent adverse event during sotatercept treatment was appearance of telangiectasias, which occurred in 14% of those on sotatercept and in 4% of control patients.
“It’s an uncommon adverse event profile, but not unexpected for a drug with its mechanism of action,” he said.
Drug binds activin, a pathologic driver of PAH
Sotatercept is an engineered molecule that combines a section of a human immunoglobulin G molecule with a portion of the receptor for activin. This structure allows sotatercept to bind free activin molecules in a patient’s blood, thereby removing a key driver of the pulmonary vascular wall remodeling that is at the pathologic root of PAH.
“Hyperproliferation of blood vessel–wall cells” caused by activin signaling “is perhaps the most important driver of PAH,” Dr. Hoeper said. “Sotatercept allows us for the first time to target the underlying mechanism behind PAH.”
Still ongoing are the HYPERION and ZENITH phase 3 trials of sotatercept. HYPERION is enrolling patients with newly diagnosed or high-risk PAH and is expected to complete in 2028. ZENITH is enrolling patients with more advanced PAH and a higher mortality risk, with results expected in 2026.
Sotatercept has received “Breakthrough Therapy” designation and “Orphan Drug” designation by the Food and Drug Administration, and “Priority Medicines” designation and “Orphan Drug” designation by the European Medicines Agency for the treatment of PAH. One recent review estimated a worldwide PAH prevalence of about 3-4 cases/100,000, which for the United States translates into a total prevalence of perhaps 10,000-15,000 affected people.
STELLAR was funded by Acceleron Pharma, a subsidiary of Merck. Dr. Hoeper is a consultant to Acceleron. Dr. Cooper-DeHoff, Dr. Grapsa, and the authors of the editorial on STELLAR have no relevant disclosures.
NEW ORLEANS – An investigational, first-in class agent that delivers a completely new type of intervention to patients with pulmonary arterial hypertension (PAH) scored a clear win in the STELLAR trial, the first to complete among three phase 3 trials that are testing this agent.
Sotatercept, administered subcutaneously every 3 weeks for 24 weeks, improved from baseline average 6-minute walk distance (6MWD) by a significant and clinically meaningful 40.8 meters, compared with placebo, for the trial’s primary efficacy endpoint (P < .001). The treatment also “delivered broad clinical benefit across multiple domains including hemodynamics, World Health Organization functional class, disease biomarkers, risk scores and patient-reported outcomes,” Marius M. Hoeper, MD, said at the joint scientific sessions of the American College of Cardiology and the World Heart Federation.
“These results establish the clinical utility of sotatercept, administered in combination with approved PAH therapies, as a new treatment for PAH,” added Dr. Hoeper, professor and deputy director of the department of respiratory medicine at Hannover (Germany) Medical School,
“The most important aspect was the hemodynamic improvement,” with sotatercept treatment, which led to an average 235 dyn/sec per cm−5 reduction in pulmonary vascular resistance from baseline and an average cut in pulmonary artery pressure of 13.9 mm Hg from baseline, compared with placebo, a result that’s “unheard of,” Dr. Hoeper said in a press conference during the meeting.
“With other tested agents we usually see very little improvement in pulmonary artery pressure. This is a signal that we achieved some reversing of the pathological changes in the pulmonary vessels that lead to” PAH, he added.
Simultaneously with his report the findings also appeared online in the New England Journal of Medicine.
‘A new hope’ for patients with PAH
Based on the reported findings, sotatercept is a “very exciting boutique molecule” that will “offer patients with PAH a very exciting new treatment,” commented Rhonda Cooper-DeHoff, PharmD, a designated discussant and a researcher at the University of Florida, Gainesville.
“This study is a new hope for patients with PAH. Until now, they’ve had really bad outcomes, but [in this study] we see significant differences in 6MWD, hemodynamics, and risk factors. Overall, I think the benefit is greater than the risk” it may pose to patients through potential adverse effects, commented Julia Grapsa, MD, PhD, a cardiologist at St. Thomas Hospital in London, and another discussant at the meeting.
“The results are impressive” and “encouraging,” and “suggest that sotatercept may represent a new and clinically consequential addition to current medications for PAH,” wrote three clinicians from Canyons Region Intermountain Medical Center in Murray, Utah, in an editorial that accompanied the published report.
But the authors of the editorial also raised several cautions and concerns. They questioned the generalizability of the findings, noting that the patients with PAH enrolled in the study were all adults who were clinically stable and an average of more than 8 years out from their initial PAH diagnosis, and more than 90% were on stable treatment for PAH with two or three agents specific for treating the disorder. The study cohort also had a disproportionately high enrollment of patients with idiopathic (59%) or heritable (18%) forms of PAH, and the 15% of patients in the trial with connective tissue disease represented a disproportionately low prevalence of this PAH subtype.
The editorialists also called for “ongoing vigilance” for adverse effects from sotatercept treatment, although they acknowledged that the adverse effects reported to date from sotatercept are “largely reassuring.”
Death or clinical worsening cut by 84%
STELLAR randomized 323 patients at 91 sites in 21 countries with WHO Group 1 PAH and with WHO functional class II or III disease to receive either sotatercept or placebo for 24 weeks, with an option for treatment to continue beyond that until the last patient in the study reached 24 weeks on treatment, resulting in an overall median treatment duration of nearly 33 weeks.
In addition to the significant result for the primary endpoint, the 163 patients who received sotatercept had significant improvements, compared with 160 placebo-treated patients, for eight of nine secondary endpoints. The only secondary endpoint with a neutral result was for a measure of cognitive and emotional wellbeing, a parameter that was already at a normal level at baseline in most enrolled patients, Dr. Hoeper explained.
The incidence of either death or an event indicative of clinical worsening during the overall median follow-up of almost 33 weeks was 26.3% among the control patients and 5.5% among those who received sotatercept. This translated into a significant reduction for this endpoint of 84% with sotatercept treatment, compared with placebo.
The rates of treatment-emergent adverse events leading to discontinuation were roughly the same in the control and sotatercept arms, and the incidence of severe or serious treatment-emergent adverse events was higher among the control patients.
The most common adverse event on sotatercept was bleeding events, which occurred in 32% of those on sotatercept and in 16% of the control patients, but the events in the sotatercept arm were “mostly mild,” said Dr. Hoeper. The next most frequent adverse event during sotatercept treatment was appearance of telangiectasias, which occurred in 14% of those on sotatercept and in 4% of control patients.
“It’s an uncommon adverse event profile, but not unexpected for a drug with its mechanism of action,” he said.
Drug binds activin, a pathologic driver of PAH
Sotatercept is an engineered molecule that combines a section of a human immunoglobulin G molecule with a portion of the receptor for activin. This structure allows sotatercept to bind free activin molecules in a patient’s blood, thereby removing a key driver of the pulmonary vascular wall remodeling that is at the pathologic root of PAH.
“Hyperproliferation of blood vessel–wall cells” caused by activin signaling “is perhaps the most important driver of PAH,” Dr. Hoeper said. “Sotatercept allows us for the first time to target the underlying mechanism behind PAH.”
Still ongoing are the HYPERION and ZENITH phase 3 trials of sotatercept. HYPERION is enrolling patients with newly diagnosed or high-risk PAH and is expected to complete in 2028. ZENITH is enrolling patients with more advanced PAH and a higher mortality risk, with results expected in 2026.
Sotatercept has received “Breakthrough Therapy” designation and “Orphan Drug” designation by the Food and Drug Administration, and “Priority Medicines” designation and “Orphan Drug” designation by the European Medicines Agency for the treatment of PAH. One recent review estimated a worldwide PAH prevalence of about 3-4 cases/100,000, which for the United States translates into a total prevalence of perhaps 10,000-15,000 affected people.
STELLAR was funded by Acceleron Pharma, a subsidiary of Merck. Dr. Hoeper is a consultant to Acceleron. Dr. Cooper-DeHoff, Dr. Grapsa, and the authors of the editorial on STELLAR have no relevant disclosures.
NEW ORLEANS – An investigational, first-in class agent that delivers a completely new type of intervention to patients with pulmonary arterial hypertension (PAH) scored a clear win in the STELLAR trial, the first to complete among three phase 3 trials that are testing this agent.
Sotatercept, administered subcutaneously every 3 weeks for 24 weeks, improved from baseline average 6-minute walk distance (6MWD) by a significant and clinically meaningful 40.8 meters, compared with placebo, for the trial’s primary efficacy endpoint (P < .001). The treatment also “delivered broad clinical benefit across multiple domains including hemodynamics, World Health Organization functional class, disease biomarkers, risk scores and patient-reported outcomes,” Marius M. Hoeper, MD, said at the joint scientific sessions of the American College of Cardiology and the World Heart Federation.
“These results establish the clinical utility of sotatercept, administered in combination with approved PAH therapies, as a new treatment for PAH,” added Dr. Hoeper, professor and deputy director of the department of respiratory medicine at Hannover (Germany) Medical School,
“The most important aspect was the hemodynamic improvement,” with sotatercept treatment, which led to an average 235 dyn/sec per cm−5 reduction in pulmonary vascular resistance from baseline and an average cut in pulmonary artery pressure of 13.9 mm Hg from baseline, compared with placebo, a result that’s “unheard of,” Dr. Hoeper said in a press conference during the meeting.
“With other tested agents we usually see very little improvement in pulmonary artery pressure. This is a signal that we achieved some reversing of the pathological changes in the pulmonary vessels that lead to” PAH, he added.
Simultaneously with his report the findings also appeared online in the New England Journal of Medicine.
‘A new hope’ for patients with PAH
Based on the reported findings, sotatercept is a “very exciting boutique molecule” that will “offer patients with PAH a very exciting new treatment,” commented Rhonda Cooper-DeHoff, PharmD, a designated discussant and a researcher at the University of Florida, Gainesville.
“This study is a new hope for patients with PAH. Until now, they’ve had really bad outcomes, but [in this study] we see significant differences in 6MWD, hemodynamics, and risk factors. Overall, I think the benefit is greater than the risk” it may pose to patients through potential adverse effects, commented Julia Grapsa, MD, PhD, a cardiologist at St. Thomas Hospital in London, and another discussant at the meeting.
“The results are impressive” and “encouraging,” and “suggest that sotatercept may represent a new and clinically consequential addition to current medications for PAH,” wrote three clinicians from Canyons Region Intermountain Medical Center in Murray, Utah, in an editorial that accompanied the published report.
But the authors of the editorial also raised several cautions and concerns. They questioned the generalizability of the findings, noting that the patients with PAH enrolled in the study were all adults who were clinically stable and an average of more than 8 years out from their initial PAH diagnosis, and more than 90% were on stable treatment for PAH with two or three agents specific for treating the disorder. The study cohort also had a disproportionately high enrollment of patients with idiopathic (59%) or heritable (18%) forms of PAH, and the 15% of patients in the trial with connective tissue disease represented a disproportionately low prevalence of this PAH subtype.
The editorialists also called for “ongoing vigilance” for adverse effects from sotatercept treatment, although they acknowledged that the adverse effects reported to date from sotatercept are “largely reassuring.”
Death or clinical worsening cut by 84%
STELLAR randomized 323 patients at 91 sites in 21 countries with WHO Group 1 PAH and with WHO functional class II or III disease to receive either sotatercept or placebo for 24 weeks, with an option for treatment to continue beyond that until the last patient in the study reached 24 weeks on treatment, resulting in an overall median treatment duration of nearly 33 weeks.
In addition to the significant result for the primary endpoint, the 163 patients who received sotatercept had significant improvements, compared with 160 placebo-treated patients, for eight of nine secondary endpoints. The only secondary endpoint with a neutral result was for a measure of cognitive and emotional wellbeing, a parameter that was already at a normal level at baseline in most enrolled patients, Dr. Hoeper explained.
The incidence of either death or an event indicative of clinical worsening during the overall median follow-up of almost 33 weeks was 26.3% among the control patients and 5.5% among those who received sotatercept. This translated into a significant reduction for this endpoint of 84% with sotatercept treatment, compared with placebo.
The rates of treatment-emergent adverse events leading to discontinuation were roughly the same in the control and sotatercept arms, and the incidence of severe or serious treatment-emergent adverse events was higher among the control patients.
The most common adverse event on sotatercept was bleeding events, which occurred in 32% of those on sotatercept and in 16% of the control patients, but the events in the sotatercept arm were “mostly mild,” said Dr. Hoeper. The next most frequent adverse event during sotatercept treatment was appearance of telangiectasias, which occurred in 14% of those on sotatercept and in 4% of control patients.
“It’s an uncommon adverse event profile, but not unexpected for a drug with its mechanism of action,” he said.
Drug binds activin, a pathologic driver of PAH
Sotatercept is an engineered molecule that combines a section of a human immunoglobulin G molecule with a portion of the receptor for activin. This structure allows sotatercept to bind free activin molecules in a patient’s blood, thereby removing a key driver of the pulmonary vascular wall remodeling that is at the pathologic root of PAH.
“Hyperproliferation of blood vessel–wall cells” caused by activin signaling “is perhaps the most important driver of PAH,” Dr. Hoeper said. “Sotatercept allows us for the first time to target the underlying mechanism behind PAH.”
Still ongoing are the HYPERION and ZENITH phase 3 trials of sotatercept. HYPERION is enrolling patients with newly diagnosed or high-risk PAH and is expected to complete in 2028. ZENITH is enrolling patients with more advanced PAH and a higher mortality risk, with results expected in 2026.
Sotatercept has received “Breakthrough Therapy” designation and “Orphan Drug” designation by the Food and Drug Administration, and “Priority Medicines” designation and “Orphan Drug” designation by the European Medicines Agency for the treatment of PAH. One recent review estimated a worldwide PAH prevalence of about 3-4 cases/100,000, which for the United States translates into a total prevalence of perhaps 10,000-15,000 affected people.
STELLAR was funded by Acceleron Pharma, a subsidiary of Merck. Dr. Hoeper is a consultant to Acceleron. Dr. Cooper-DeHoff, Dr. Grapsa, and the authors of the editorial on STELLAR have no relevant disclosures.
At ACC 2023
The 2023 ‘Meddy’ awards
Without further ado (or comedy skits or musical numbers or extended tributes or commercials), the Meddys go to ...
Best depiction of emergency medicine’s rollercoaster
M*A*S*H (1970)
The original film, not the TV show, jumps from Frank Burns being hauled away in a straitjacket to a soldier’s spurting neck wound. Hawkeye Pierce calmly steps in and we see the entire sequence of him applying pressure, then stepping back to gown-and-glove (“it’s going to spurt a bit”), then jumping back in with arterial sutures, quipping, “Baby, we’re gonna see some stitchin’ like you never saw before.” After that, cocktail hour. Yes, medicine in Hollywood can be overdramatized and even inaccurate, but Robert Altman’s take on the novel by former U.S. Army surgeon Richard Hooker still stands tall for just how crazy emergency medicine can be.
Best ‘is there a doctor in the house?’ moment
Field of Dreams (1989)
When Ray Kinsella’s daughter gets knocked off the back of the bleachers, everything stops. No one knows what to do … except Doc “Moonlight” Graham, who gives up his life’s (and afterlife’s) dream to step off the field and save the girl from choking to death. Burt Lancaster, in his final movie role, embodies everything people wish a doctor to be: Calm, kind, and able to offer a quick, effective solution to a crisis. “Hey rookie! You were good.” Yes, he sure was.
Most unethical doctor
Elvis (2022)
No doctor wants to be remembered as the guy who killed Elvis. But that legacy clings to Dr. George Nichopoulos, Elvis’s personal physician in the 1970s. In Elvis, Dr. Nichopoulos, played by Tony Nixon, hovers in the background, enabling the King’s worsening addictions. Taking late-night calls for narcotics and injecting the unconscious star with stimulants, “unethical” is an understatement for the fictional “Dr. Nick.” The real Dr. Nichopoulos was acquitted of wrongdoing in Elvis’ death, although there is little doubt that the thousands of medication doses he prescribed played a role. When his license was finally revoked for overprescribing in the 1990s, the obliging doc reportedly claimed, “I cared too much.”
Best self-use of a defibrillator
Casino Royale (2006)
We expect backlash in the post-award press conference since James Bond technically only attempted to self-defibrillate in the passenger seat of his car. He never attached the device to the leads. Vesper Lynd had to pick up his slack and save the day. Also, supporters of fellow self-defibrillating nominee Jason Statham in Crank will no doubt raise a stink on Twitter. But we stand by our choice because it was such an, ahem, heart-stopper of a scene.
Best worst patient lying about an injury
Tár (2022)
Love it or hate it, few recent movies have been as polarizing as Tár. Cate Blanchett’s portrayal of a musical genius might be toweringly brilliant or outrageously offensive (or both) depending on whom you ask. But clearly the character has a loose relationship with facts. More than a few doctors might have raised an eyebrow had Lydia Tár appeared with injuries to her face, claiming to have been attacked in a mugging. In reality, Lydia tripped and fell while pursuing an attractive young cellist into a hazardous basement. Did she lie to protect her image, preserve her marriage, or – like many patients – avoid a lecture on unhealthy behavior? We pick D, all of the above.
Best therapy for a speech disorder
The King’s Speech (2010)
Public speaking might cause anxiety for many of us, but how about doing it in front of a global radio audience while wrestling with a speech disorder? Based on a true story, The King’s Speech revealed that terrifying experience for England’s King George VI. Enter Lionel Logue, played by Geoffrey Rush. Irreverent, unconventional, and untrained, the Australian pioneer in speech and language therapy uses a range of strategies – some of which are still used today – to help the royal find his voice. But when singing, shouting swear words, and provoking rage don’t do the trick, Mr. Logue turns to psychotherapy to unearth the childhood traumas at the root of the king’s disability. Experience, as Mr. Logue tells his patient, matters just as much as “letters after your name.”
A version of this article first appeared on Medscape.com.
Without further ado (or comedy skits or musical numbers or extended tributes or commercials), the Meddys go to ...
Best depiction of emergency medicine’s rollercoaster
M*A*S*H (1970)
The original film, not the TV show, jumps from Frank Burns being hauled away in a straitjacket to a soldier’s spurting neck wound. Hawkeye Pierce calmly steps in and we see the entire sequence of him applying pressure, then stepping back to gown-and-glove (“it’s going to spurt a bit”), then jumping back in with arterial sutures, quipping, “Baby, we’re gonna see some stitchin’ like you never saw before.” After that, cocktail hour. Yes, medicine in Hollywood can be overdramatized and even inaccurate, but Robert Altman’s take on the novel by former U.S. Army surgeon Richard Hooker still stands tall for just how crazy emergency medicine can be.
Best ‘is there a doctor in the house?’ moment
Field of Dreams (1989)
When Ray Kinsella’s daughter gets knocked off the back of the bleachers, everything stops. No one knows what to do … except Doc “Moonlight” Graham, who gives up his life’s (and afterlife’s) dream to step off the field and save the girl from choking to death. Burt Lancaster, in his final movie role, embodies everything people wish a doctor to be: Calm, kind, and able to offer a quick, effective solution to a crisis. “Hey rookie! You were good.” Yes, he sure was.
Most unethical doctor
Elvis (2022)
No doctor wants to be remembered as the guy who killed Elvis. But that legacy clings to Dr. George Nichopoulos, Elvis’s personal physician in the 1970s. In Elvis, Dr. Nichopoulos, played by Tony Nixon, hovers in the background, enabling the King’s worsening addictions. Taking late-night calls for narcotics and injecting the unconscious star with stimulants, “unethical” is an understatement for the fictional “Dr. Nick.” The real Dr. Nichopoulos was acquitted of wrongdoing in Elvis’ death, although there is little doubt that the thousands of medication doses he prescribed played a role. When his license was finally revoked for overprescribing in the 1990s, the obliging doc reportedly claimed, “I cared too much.”
Best self-use of a defibrillator
Casino Royale (2006)
We expect backlash in the post-award press conference since James Bond technically only attempted to self-defibrillate in the passenger seat of his car. He never attached the device to the leads. Vesper Lynd had to pick up his slack and save the day. Also, supporters of fellow self-defibrillating nominee Jason Statham in Crank will no doubt raise a stink on Twitter. But we stand by our choice because it was such an, ahem, heart-stopper of a scene.
Best worst patient lying about an injury
Tár (2022)
Love it or hate it, few recent movies have been as polarizing as Tár. Cate Blanchett’s portrayal of a musical genius might be toweringly brilliant or outrageously offensive (or both) depending on whom you ask. But clearly the character has a loose relationship with facts. More than a few doctors might have raised an eyebrow had Lydia Tár appeared with injuries to her face, claiming to have been attacked in a mugging. In reality, Lydia tripped and fell while pursuing an attractive young cellist into a hazardous basement. Did she lie to protect her image, preserve her marriage, or – like many patients – avoid a lecture on unhealthy behavior? We pick D, all of the above.
Best therapy for a speech disorder
The King’s Speech (2010)
Public speaking might cause anxiety for many of us, but how about doing it in front of a global radio audience while wrestling with a speech disorder? Based on a true story, The King’s Speech revealed that terrifying experience for England’s King George VI. Enter Lionel Logue, played by Geoffrey Rush. Irreverent, unconventional, and untrained, the Australian pioneer in speech and language therapy uses a range of strategies – some of which are still used today – to help the royal find his voice. But when singing, shouting swear words, and provoking rage don’t do the trick, Mr. Logue turns to psychotherapy to unearth the childhood traumas at the root of the king’s disability. Experience, as Mr. Logue tells his patient, matters just as much as “letters after your name.”
A version of this article first appeared on Medscape.com.
Without further ado (or comedy skits or musical numbers or extended tributes or commercials), the Meddys go to ...
Best depiction of emergency medicine’s rollercoaster
M*A*S*H (1970)
The original film, not the TV show, jumps from Frank Burns being hauled away in a straitjacket to a soldier’s spurting neck wound. Hawkeye Pierce calmly steps in and we see the entire sequence of him applying pressure, then stepping back to gown-and-glove (“it’s going to spurt a bit”), then jumping back in with arterial sutures, quipping, “Baby, we’re gonna see some stitchin’ like you never saw before.” After that, cocktail hour. Yes, medicine in Hollywood can be overdramatized and even inaccurate, but Robert Altman’s take on the novel by former U.S. Army surgeon Richard Hooker still stands tall for just how crazy emergency medicine can be.
Best ‘is there a doctor in the house?’ moment
Field of Dreams (1989)
When Ray Kinsella’s daughter gets knocked off the back of the bleachers, everything stops. No one knows what to do … except Doc “Moonlight” Graham, who gives up his life’s (and afterlife’s) dream to step off the field and save the girl from choking to death. Burt Lancaster, in his final movie role, embodies everything people wish a doctor to be: Calm, kind, and able to offer a quick, effective solution to a crisis. “Hey rookie! You were good.” Yes, he sure was.
Most unethical doctor
Elvis (2022)
No doctor wants to be remembered as the guy who killed Elvis. But that legacy clings to Dr. George Nichopoulos, Elvis’s personal physician in the 1970s. In Elvis, Dr. Nichopoulos, played by Tony Nixon, hovers in the background, enabling the King’s worsening addictions. Taking late-night calls for narcotics and injecting the unconscious star with stimulants, “unethical” is an understatement for the fictional “Dr. Nick.” The real Dr. Nichopoulos was acquitted of wrongdoing in Elvis’ death, although there is little doubt that the thousands of medication doses he prescribed played a role. When his license was finally revoked for overprescribing in the 1990s, the obliging doc reportedly claimed, “I cared too much.”
Best self-use of a defibrillator
Casino Royale (2006)
We expect backlash in the post-award press conference since James Bond technically only attempted to self-defibrillate in the passenger seat of his car. He never attached the device to the leads. Vesper Lynd had to pick up his slack and save the day. Also, supporters of fellow self-defibrillating nominee Jason Statham in Crank will no doubt raise a stink on Twitter. But we stand by our choice because it was such an, ahem, heart-stopper of a scene.
Best worst patient lying about an injury
Tár (2022)
Love it or hate it, few recent movies have been as polarizing as Tár. Cate Blanchett’s portrayal of a musical genius might be toweringly brilliant or outrageously offensive (or both) depending on whom you ask. But clearly the character has a loose relationship with facts. More than a few doctors might have raised an eyebrow had Lydia Tár appeared with injuries to her face, claiming to have been attacked in a mugging. In reality, Lydia tripped and fell while pursuing an attractive young cellist into a hazardous basement. Did she lie to protect her image, preserve her marriage, or – like many patients – avoid a lecture on unhealthy behavior? We pick D, all of the above.
Best therapy for a speech disorder
The King’s Speech (2010)
Public speaking might cause anxiety for many of us, but how about doing it in front of a global radio audience while wrestling with a speech disorder? Based on a true story, The King’s Speech revealed that terrifying experience for England’s King George VI. Enter Lionel Logue, played by Geoffrey Rush. Irreverent, unconventional, and untrained, the Australian pioneer in speech and language therapy uses a range of strategies – some of which are still used today – to help the royal find his voice. But when singing, shouting swear words, and provoking rage don’t do the trick, Mr. Logue turns to psychotherapy to unearth the childhood traumas at the root of the king’s disability. Experience, as Mr. Logue tells his patient, matters just as much as “letters after your name.”
A version of this article first appeared on Medscape.com.
Novel therapies for neuromuscular disease: What are the respiratory and sleep implications?
Sleep Medicine Network
Home-Based Mechanical Ventilation & Neuromuscular Disease Section
Novel therapies for neuromuscular disease: What are the respiratory and sleep implications?
The natural history of respiratory impairment in children and adults with progressive neuromuscular disease (NMD) often follows a predictable progression. Muscle weakness leads to sleep-disordered breathing and sleep-related hypoventilation, followed by diurnal hypoventilation, and, ultimately leads to respiratory failure. A number of disease-specific and society guidelines provide protocols for anticipatory respiratory monitoring, such as the role of polysomnography, pulmonary function testing, and respiratory muscle strength testing. They also guide the treatment of respiratory symptoms, such as when to initiate cough augmentation and assisted ventilation.
including spinal muscular atrophy (SMA) and Duchenne muscular dystrophy. There are now cases of children with SMA type 1, who subsequent to treatment, are walking independently. Studies examining the impact of these therapies on motor function use standardized assessments, but there are limited studies assessing pulmonary and sleep outcomes (Gurbani N, et al. Pediatr Pulmonol. 2021;56[4]:700).
Researchers are also assessing the role of home testing to diagnose hypoventilation (Shi J, et al. Sleep Med. 2023;101:221-7) and using tools like positive airway pressure device data to guide treatment with noninvasive ventilation (Perrem L et al. Pediatr Pulmonol. 2020;55[1]:58-67). While these advances in therapy are exciting, we still do not know what the long-term respiratory function, prognosis, or disease progression may be. Questions remain regarding how to best monitor, and at what frequency to assess, the respiratory status in these patients.
Moshe Y. Prero, MD
Section Member-at-Large
Sleep Medicine Network
Home-Based Mechanical Ventilation & Neuromuscular Disease Section
Novel therapies for neuromuscular disease: What are the respiratory and sleep implications?
The natural history of respiratory impairment in children and adults with progressive neuromuscular disease (NMD) often follows a predictable progression. Muscle weakness leads to sleep-disordered breathing and sleep-related hypoventilation, followed by diurnal hypoventilation, and, ultimately leads to respiratory failure. A number of disease-specific and society guidelines provide protocols for anticipatory respiratory monitoring, such as the role of polysomnography, pulmonary function testing, and respiratory muscle strength testing. They also guide the treatment of respiratory symptoms, such as when to initiate cough augmentation and assisted ventilation.
including spinal muscular atrophy (SMA) and Duchenne muscular dystrophy. There are now cases of children with SMA type 1, who subsequent to treatment, are walking independently. Studies examining the impact of these therapies on motor function use standardized assessments, but there are limited studies assessing pulmonary and sleep outcomes (Gurbani N, et al. Pediatr Pulmonol. 2021;56[4]:700).
Researchers are also assessing the role of home testing to diagnose hypoventilation (Shi J, et al. Sleep Med. 2023;101:221-7) and using tools like positive airway pressure device data to guide treatment with noninvasive ventilation (Perrem L et al. Pediatr Pulmonol. 2020;55[1]:58-67). While these advances in therapy are exciting, we still do not know what the long-term respiratory function, prognosis, or disease progression may be. Questions remain regarding how to best monitor, and at what frequency to assess, the respiratory status in these patients.
Moshe Y. Prero, MD
Section Member-at-Large
Sleep Medicine Network
Home-Based Mechanical Ventilation & Neuromuscular Disease Section
Novel therapies for neuromuscular disease: What are the respiratory and sleep implications?
The natural history of respiratory impairment in children and adults with progressive neuromuscular disease (NMD) often follows a predictable progression. Muscle weakness leads to sleep-disordered breathing and sleep-related hypoventilation, followed by diurnal hypoventilation, and, ultimately leads to respiratory failure. A number of disease-specific and society guidelines provide protocols for anticipatory respiratory monitoring, such as the role of polysomnography, pulmonary function testing, and respiratory muscle strength testing. They also guide the treatment of respiratory symptoms, such as when to initiate cough augmentation and assisted ventilation.
including spinal muscular atrophy (SMA) and Duchenne muscular dystrophy. There are now cases of children with SMA type 1, who subsequent to treatment, are walking independently. Studies examining the impact of these therapies on motor function use standardized assessments, but there are limited studies assessing pulmonary and sleep outcomes (Gurbani N, et al. Pediatr Pulmonol. 2021;56[4]:700).
Researchers are also assessing the role of home testing to diagnose hypoventilation (Shi J, et al. Sleep Med. 2023;101:221-7) and using tools like positive airway pressure device data to guide treatment with noninvasive ventilation (Perrem L et al. Pediatr Pulmonol. 2020;55[1]:58-67). While these advances in therapy are exciting, we still do not know what the long-term respiratory function, prognosis, or disease progression may be. Questions remain regarding how to best monitor, and at what frequency to assess, the respiratory status in these patients.
Moshe Y. Prero, MD
Section Member-at-Large
Tobramycin inhaled solution and quality of life in patients with bronchiectasis
Airway Disorders Network
Bronchiectasis Section
Bronchiectasis is a condition of dilated, inflamed airways and mucous production caused by a myriad of diseases. Bronchiectasis entails chronic productive cough and an increased risk of infections leading to exacerbations. Chronic bacterial infections are often a hallmark of severe disease, especially with Pseudomonas aeruginosa (O’Donnell AE. N Engl J Med. 2022;387[6]:533). Prophylactic inhaled antibiotics have been used as off-label therapies with mixed evidence, particularly in non-cystic fibrosis bronchiectasis (Rubin BK, et al. Respiration. 2014;88[3]:177).
In a recent publication, Guan and colleagues evaluated the efficacy and safety of tobramycin inhaled solution (TIS) for bronchiectasis with chronic P. aeruginosa in a phase 3, 16-week, multicenter, double-blind randomized, controlled trial (Guan W-J, et al. Chest. 2023;163[1]:64). A regimen of twice-daily TIS, compared with nebulized normal saline, demonstrated a more significant reduction in P. aeruginosa sputum density after two cycles of 28 days on-treatment and 28 days off-treatment (adjusted mean difference, 1.74 log10 colony-forming units/g; 95% CI, 1.12-2.35; (P < .001), and more patients became culture-negative for P. aeruginosa in the TIS group than in the placebo group on day 29 (29.3% vs 10.6%). Adverse events were similar in both groups. Importantly, there was an improvement in quality-of-life bronchiectasis respiratory symptom score by 7.91 points at day 29 and 6.72 points at day 85; all three were statistically significant but just below the minimal clinically important difference of 8 points.
Dr. Conroy Wong and Dr. Miguel Angel Martinez-Garcia (Chest. 2023 Jan;163[1]:3) highlighted in their accompanying editorial that use of health-related quality of life score was a “distinguishing feature” of the trial as “most studies have used the change in microbial density as the primary outcome measure alone.”
Future studies evaluating cyclical vs continuous antibiotic administration, treatment duration, and impact on exacerbations continue to be needed.
Alicia Mirza, MD
Section Member-at-Large
Airway Disorders Network
Bronchiectasis Section
Bronchiectasis is a condition of dilated, inflamed airways and mucous production caused by a myriad of diseases. Bronchiectasis entails chronic productive cough and an increased risk of infections leading to exacerbations. Chronic bacterial infections are often a hallmark of severe disease, especially with Pseudomonas aeruginosa (O’Donnell AE. N Engl J Med. 2022;387[6]:533). Prophylactic inhaled antibiotics have been used as off-label therapies with mixed evidence, particularly in non-cystic fibrosis bronchiectasis (Rubin BK, et al. Respiration. 2014;88[3]:177).
In a recent publication, Guan and colleagues evaluated the efficacy and safety of tobramycin inhaled solution (TIS) for bronchiectasis with chronic P. aeruginosa in a phase 3, 16-week, multicenter, double-blind randomized, controlled trial (Guan W-J, et al. Chest. 2023;163[1]:64). A regimen of twice-daily TIS, compared with nebulized normal saline, demonstrated a more significant reduction in P. aeruginosa sputum density after two cycles of 28 days on-treatment and 28 days off-treatment (adjusted mean difference, 1.74 log10 colony-forming units/g; 95% CI, 1.12-2.35; (P < .001), and more patients became culture-negative for P. aeruginosa in the TIS group than in the placebo group on day 29 (29.3% vs 10.6%). Adverse events were similar in both groups. Importantly, there was an improvement in quality-of-life bronchiectasis respiratory symptom score by 7.91 points at day 29 and 6.72 points at day 85; all three were statistically significant but just below the minimal clinically important difference of 8 points.
Dr. Conroy Wong and Dr. Miguel Angel Martinez-Garcia (Chest. 2023 Jan;163[1]:3) highlighted in their accompanying editorial that use of health-related quality of life score was a “distinguishing feature” of the trial as “most studies have used the change in microbial density as the primary outcome measure alone.”
Future studies evaluating cyclical vs continuous antibiotic administration, treatment duration, and impact on exacerbations continue to be needed.
Alicia Mirza, MD
Section Member-at-Large
Airway Disorders Network
Bronchiectasis Section
Bronchiectasis is a condition of dilated, inflamed airways and mucous production caused by a myriad of diseases. Bronchiectasis entails chronic productive cough and an increased risk of infections leading to exacerbations. Chronic bacterial infections are often a hallmark of severe disease, especially with Pseudomonas aeruginosa (O’Donnell AE. N Engl J Med. 2022;387[6]:533). Prophylactic inhaled antibiotics have been used as off-label therapies with mixed evidence, particularly in non-cystic fibrosis bronchiectasis (Rubin BK, et al. Respiration. 2014;88[3]:177).
In a recent publication, Guan and colleagues evaluated the efficacy and safety of tobramycin inhaled solution (TIS) for bronchiectasis with chronic P. aeruginosa in a phase 3, 16-week, multicenter, double-blind randomized, controlled trial (Guan W-J, et al. Chest. 2023;163[1]:64). A regimen of twice-daily TIS, compared with nebulized normal saline, demonstrated a more significant reduction in P. aeruginosa sputum density after two cycles of 28 days on-treatment and 28 days off-treatment (adjusted mean difference, 1.74 log10 colony-forming units/g; 95% CI, 1.12-2.35; (P < .001), and more patients became culture-negative for P. aeruginosa in the TIS group than in the placebo group on day 29 (29.3% vs 10.6%). Adverse events were similar in both groups. Importantly, there was an improvement in quality-of-life bronchiectasis respiratory symptom score by 7.91 points at day 29 and 6.72 points at day 85; all three were statistically significant but just below the minimal clinically important difference of 8 points.
Dr. Conroy Wong and Dr. Miguel Angel Martinez-Garcia (Chest. 2023 Jan;163[1]:3) highlighted in their accompanying editorial that use of health-related quality of life score was a “distinguishing feature” of the trial as “most studies have used the change in microbial density as the primary outcome measure alone.”
Future studies evaluating cyclical vs continuous antibiotic administration, treatment duration, and impact on exacerbations continue to be needed.
Alicia Mirza, MD
Section Member-at-Large