User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Three surprising studies on exercise restriction and an exercise sweet spot
LIVE HCM: Surprising result No. 1
Rachel Lampert, MD, from Yale University, New Haven, Conn., presented results of the LIVE-HCM observational study of vigorous exercise in more than 1,600 patients with hypertrophic cardiomyopathy (40% female). The investigators aimed to determine whether engagement in vigorous exercise, including competitive sports, is associated with increased risk for life-threatening ventricular arrhythmia and/or mortality in patients with HCM.
Because of the myocardial disease, HCM comes with a risk for ventricular arrhythmia. Prevailing wisdom held that vigorous exercise in these patients would be hazardous. It was all expert opinion; there were no data. Now there are.
Dr. Lampert and colleagues recruited patients from 42 international HCM centers. Patients self-enrolled and the researchers created three groups based on self-reported levels of exercise – vigorous, moderate, and sedentary. The main comparison was between vigorous versus nonvigorous exercisers (including moderate and sedentary). The two groups were mostly matched on baseline characteristics and typical of patients with HCM.
The primary endpoint was a composite of death, resuscitated cardiac arrest, syncope likely caused by an arrhythmia, or an appropriate shock from an ICD.
The event rates were low in all groups and almost identical in vigorous versus nonvigorous exercisers. Sub-group analyses found no increased risk in HCM patients who identified as competitive athletes.
Dr. Lampert said these data “do not support universal restriction of vigorous exercise in patients with HCM.”
Return to play: Surprising result No. 2
Undergraduate student Katherine Martinez from Loyola University, Chicago, presented an observational analysis of 76 elite athletes with genetic heart disease who gained a return-to-play approval from four expert centers in the United States.
The three-step, return-to-play protocol from these specialized centers deserves emphasis. First was the initial evaluation, including two ECGs, 24-hour ECG monitor, echocardiography, and treadmill exercise testing. Second was a discussion between clinicians and patients regarding the athlete’s situation. The third step was to inform coaches and staff of the team and instruct athletes to obtain a personal AED, stay replenished with electrolytes, avoid QT-prolonging drugs, and continue with annual follow-up.
Slightly more than half of these patients had HCM and almost a third had long QT syndrome. Nearly one-third had an ICD implant and 22 were women.
Of the 76 athletes, 73 chose to return to play; however, 4 of these remained disqualified because of their team’s decision. Of the remaining 69, only 3 had one or more breakthrough cardiac events during 200 patient-years of follow-up.
These comprised one male Division I basketball player with HCM who had an ICD shock while moving furniture; another male Division 1 hockey player with long QT syndrome who was taking beta-blockers experienced syncope while coming off the bench and while cooking; and a third male professional hockey player with HCM, on beta-blockers, had syncope without exertion.
The authors concluded that when there was careful evaluation by experts and shared decision-making, a specific plan to return to sport can be put into place for the highest-level athletes.
Masters@Heart: Surprising result No. 3
Ruben De Bosscher MD, PhD, from KU Leuven (Belgium), presented the Masters@Heart study on behalf of a Belgian team of researchers. The question they asked was whether lifelong endurance exercise is associated with more coronary atherosclerosis than standard “normal” exercise levels.
That question brings up the paradox of exercise, which is that numerous observational studies find that exercise strongly associates with lower rates of cardiovascular events, but imaging studies also report high rates of coronary artery calcium in endurance athletes, especially in those who have run multiple marathons.
Masters@Heart investigators sought to explore this paradox by performing detailed coronary imaging in three groups – lifelong athletes, late-onset athletes (after age 30 years), and super-healthy controls. Through advertisements they obtained about 1,100 middle-aged male volunteers (mean age, 55 years). Of these, 605 men were selected at random to participate to reduce the chance of enrolling people who responded to the ads because of health concerns.
Investigators assigned those selected based on self-report of exercise. The control group was notable for their good health: they were free of any risk factors, took (almost) no meds, exercised regularly but not excessively (about 3 hours per week) and had a VO2 max of 122% of predicted.
The groups were well matched on baseline characteristics. Cycling predominated as the exercise of choice (this is a Belgian study after all). All patients had an extensive evaluation including coronary CT imaging.
European Heart Journal published the provocative results.
- Lifelong exercisers had a significantly higher CAC burden than controls, which confirms previous work.
- Lifelong exercisers had a higher percentage of multiple coronary plaques, plaques of at least 50%, and proximal plaques.
- There were no significant differences in the mixture of plaque types in the three groups. About two thirds of the plaques in each group were calcified and the remainder were deemed noncalcified or mixed.
- When looking only at noncalcified plaques, lifelong exercisers tended to have a higher prevalence of multiple plaques, plaques of at least 50%, and proximal plaques.
- So named “vulnerable” plaques were extremely infrequent in all three groups.
The authors concluded that lifelong endurance sport relative to a generic healthy lifestyle was not associated with more favorable coronary plaque composition.
Comments
Each of these three studies provided data where there was none. That is always a good thing.
The major theme from the first two studies is that expert opinion was too cautious. Doctors have long held the idea that patients with genetic heart disease, especially hypertrophic cardiomyopathy, are vulnerable, fragile even, when it comes to vigorous sport.
This new evidence upends this belief, as long as return to sport occurs in the setting of robust patient education and expert evaluation and surveillance.
Paternalism in prohibiting participation in sport because of genetic heart disease has joined the long list of medical reversals.
Masters@Heart provides a slightly different message. It finds that lifelong high-level exercise does not prevent coronary atherosclerosis in men. And, more provocatively, if replicated, might even show that long-term exposure to the biochemical, inflammatory, or hormonal effects of endurance training may actually be atherogenic. Like all good science, these findings raise more questions to explore in the realm of atherogenesis.
Two of the main limitations of the Belgian study was that the control arm was quite healthy; had the comparison arm been typical of sedentary controls in say, the Southeastern United States, the coronary lesions found in longtime exercisers may have looked more favorable. The more significant limitation is the lack of outcomes. Images of coronary arteries remain a surrogate marker. It’s possible that, like statins, higher levels of exercise may stabilize plaque and actually lower the risk for events.
The Belgian authors suggest – as many have – a J-curve of exercise benefits, wherein too little exercise is clearly bad, but too much exercise may also increase risk. In other words, for maximizing health, there may be a Goldilocks amount of exercise.
The problem with this idea comes in its pragmatic translation. The number of lifelong high-level, middle-aged endurance athletes that cite heart health reasons for their affliction is ... almost zero. Nearly everyone I have met in the endurance sport fraternity harbors no notion that racing a bike or running multiple marathons per year is a healthy endeavor.
Paternalism, therefore, would also fall in the realm of limiting lifelong exercise in addicted middle-aged athletes.
Via email, sports cardiologist Michael Emery, MD, reiterated the main immediate message from Masters@Heart: “Exercise does not make you immune from heart disease (which is a message a lot of athletes need to hear honestly).”
I for one cannot give up on endurance exercise. I won’t likely race anymore but I am like the lab rat who needs to run on the wheel. Whether this affects my coronary plaque burden matters not to me.
Dr. Mandrola is a clinical electrophysiologist at Baptist Medical Associates, Louisville, Ky. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
LIVE HCM: Surprising result No. 1
Rachel Lampert, MD, from Yale University, New Haven, Conn., presented results of the LIVE-HCM observational study of vigorous exercise in more than 1,600 patients with hypertrophic cardiomyopathy (40% female). The investigators aimed to determine whether engagement in vigorous exercise, including competitive sports, is associated with increased risk for life-threatening ventricular arrhythmia and/or mortality in patients with HCM.
Because of the myocardial disease, HCM comes with a risk for ventricular arrhythmia. Prevailing wisdom held that vigorous exercise in these patients would be hazardous. It was all expert opinion; there were no data. Now there are.
Dr. Lampert and colleagues recruited patients from 42 international HCM centers. Patients self-enrolled and the researchers created three groups based on self-reported levels of exercise – vigorous, moderate, and sedentary. The main comparison was between vigorous versus nonvigorous exercisers (including moderate and sedentary). The two groups were mostly matched on baseline characteristics and typical of patients with HCM.
The primary endpoint was a composite of death, resuscitated cardiac arrest, syncope likely caused by an arrhythmia, or an appropriate shock from an ICD.
The event rates were low in all groups and almost identical in vigorous versus nonvigorous exercisers. Sub-group analyses found no increased risk in HCM patients who identified as competitive athletes.
Dr. Lampert said these data “do not support universal restriction of vigorous exercise in patients with HCM.”
Return to play: Surprising result No. 2
Undergraduate student Katherine Martinez from Loyola University, Chicago, presented an observational analysis of 76 elite athletes with genetic heart disease who gained a return-to-play approval from four expert centers in the United States.
The three-step, return-to-play protocol from these specialized centers deserves emphasis. First was the initial evaluation, including two ECGs, 24-hour ECG monitor, echocardiography, and treadmill exercise testing. Second was a discussion between clinicians and patients regarding the athlete’s situation. The third step was to inform coaches and staff of the team and instruct athletes to obtain a personal AED, stay replenished with electrolytes, avoid QT-prolonging drugs, and continue with annual follow-up.
Slightly more than half of these patients had HCM and almost a third had long QT syndrome. Nearly one-third had an ICD implant and 22 were women.
Of the 76 athletes, 73 chose to return to play; however, 4 of these remained disqualified because of their team’s decision. Of the remaining 69, only 3 had one or more breakthrough cardiac events during 200 patient-years of follow-up.
These comprised one male Division I basketball player with HCM who had an ICD shock while moving furniture; another male Division 1 hockey player with long QT syndrome who was taking beta-blockers experienced syncope while coming off the bench and while cooking; and a third male professional hockey player with HCM, on beta-blockers, had syncope without exertion.
The authors concluded that when there was careful evaluation by experts and shared decision-making, a specific plan to return to sport can be put into place for the highest-level athletes.
Masters@Heart: Surprising result No. 3
Ruben De Bosscher MD, PhD, from KU Leuven (Belgium), presented the Masters@Heart study on behalf of a Belgian team of researchers. The question they asked was whether lifelong endurance exercise is associated with more coronary atherosclerosis than standard “normal” exercise levels.
That question brings up the paradox of exercise, which is that numerous observational studies find that exercise strongly associates with lower rates of cardiovascular events, but imaging studies also report high rates of coronary artery calcium in endurance athletes, especially in those who have run multiple marathons.
Masters@Heart investigators sought to explore this paradox by performing detailed coronary imaging in three groups – lifelong athletes, late-onset athletes (after age 30 years), and super-healthy controls. Through advertisements they obtained about 1,100 middle-aged male volunteers (mean age, 55 years). Of these, 605 men were selected at random to participate to reduce the chance of enrolling people who responded to the ads because of health concerns.
Investigators assigned those selected based on self-report of exercise. The control group was notable for their good health: they were free of any risk factors, took (almost) no meds, exercised regularly but not excessively (about 3 hours per week) and had a VO2 max of 122% of predicted.
The groups were well matched on baseline characteristics. Cycling predominated as the exercise of choice (this is a Belgian study after all). All patients had an extensive evaluation including coronary CT imaging.
European Heart Journal published the provocative results.
- Lifelong exercisers had a significantly higher CAC burden than controls, which confirms previous work.
- Lifelong exercisers had a higher percentage of multiple coronary plaques, plaques of at least 50%, and proximal plaques.
- There were no significant differences in the mixture of plaque types in the three groups. About two thirds of the plaques in each group were calcified and the remainder were deemed noncalcified or mixed.
- When looking only at noncalcified plaques, lifelong exercisers tended to have a higher prevalence of multiple plaques, plaques of at least 50%, and proximal plaques.
- So named “vulnerable” plaques were extremely infrequent in all three groups.
The authors concluded that lifelong endurance sport relative to a generic healthy lifestyle was not associated with more favorable coronary plaque composition.
Comments
Each of these three studies provided data where there was none. That is always a good thing.
The major theme from the first two studies is that expert opinion was too cautious. Doctors have long held the idea that patients with genetic heart disease, especially hypertrophic cardiomyopathy, are vulnerable, fragile even, when it comes to vigorous sport.
This new evidence upends this belief, as long as return to sport occurs in the setting of robust patient education and expert evaluation and surveillance.
Paternalism in prohibiting participation in sport because of genetic heart disease has joined the long list of medical reversals.
Masters@Heart provides a slightly different message. It finds that lifelong high-level exercise does not prevent coronary atherosclerosis in men. And, more provocatively, if replicated, might even show that long-term exposure to the biochemical, inflammatory, or hormonal effects of endurance training may actually be atherogenic. Like all good science, these findings raise more questions to explore in the realm of atherogenesis.
Two of the main limitations of the Belgian study was that the control arm was quite healthy; had the comparison arm been typical of sedentary controls in say, the Southeastern United States, the coronary lesions found in longtime exercisers may have looked more favorable. The more significant limitation is the lack of outcomes. Images of coronary arteries remain a surrogate marker. It’s possible that, like statins, higher levels of exercise may stabilize plaque and actually lower the risk for events.
The Belgian authors suggest – as many have – a J-curve of exercise benefits, wherein too little exercise is clearly bad, but too much exercise may also increase risk. In other words, for maximizing health, there may be a Goldilocks amount of exercise.
The problem with this idea comes in its pragmatic translation. The number of lifelong high-level, middle-aged endurance athletes that cite heart health reasons for their affliction is ... almost zero. Nearly everyone I have met in the endurance sport fraternity harbors no notion that racing a bike or running multiple marathons per year is a healthy endeavor.
Paternalism, therefore, would also fall in the realm of limiting lifelong exercise in addicted middle-aged athletes.
Via email, sports cardiologist Michael Emery, MD, reiterated the main immediate message from Masters@Heart: “Exercise does not make you immune from heart disease (which is a message a lot of athletes need to hear honestly).”
I for one cannot give up on endurance exercise. I won’t likely race anymore but I am like the lab rat who needs to run on the wheel. Whether this affects my coronary plaque burden matters not to me.
Dr. Mandrola is a clinical electrophysiologist at Baptist Medical Associates, Louisville, Ky. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
LIVE HCM: Surprising result No. 1
Rachel Lampert, MD, from Yale University, New Haven, Conn., presented results of the LIVE-HCM observational study of vigorous exercise in more than 1,600 patients with hypertrophic cardiomyopathy (40% female). The investigators aimed to determine whether engagement in vigorous exercise, including competitive sports, is associated with increased risk for life-threatening ventricular arrhythmia and/or mortality in patients with HCM.
Because of the myocardial disease, HCM comes with a risk for ventricular arrhythmia. Prevailing wisdom held that vigorous exercise in these patients would be hazardous. It was all expert opinion; there were no data. Now there are.
Dr. Lampert and colleagues recruited patients from 42 international HCM centers. Patients self-enrolled and the researchers created three groups based on self-reported levels of exercise – vigorous, moderate, and sedentary. The main comparison was between vigorous versus nonvigorous exercisers (including moderate and sedentary). The two groups were mostly matched on baseline characteristics and typical of patients with HCM.
The primary endpoint was a composite of death, resuscitated cardiac arrest, syncope likely caused by an arrhythmia, or an appropriate shock from an ICD.
The event rates were low in all groups and almost identical in vigorous versus nonvigorous exercisers. Sub-group analyses found no increased risk in HCM patients who identified as competitive athletes.
Dr. Lampert said these data “do not support universal restriction of vigorous exercise in patients with HCM.”
Return to play: Surprising result No. 2
Undergraduate student Katherine Martinez from Loyola University, Chicago, presented an observational analysis of 76 elite athletes with genetic heart disease who gained a return-to-play approval from four expert centers in the United States.
The three-step, return-to-play protocol from these specialized centers deserves emphasis. First was the initial evaluation, including two ECGs, 24-hour ECG monitor, echocardiography, and treadmill exercise testing. Second was a discussion between clinicians and patients regarding the athlete’s situation. The third step was to inform coaches and staff of the team and instruct athletes to obtain a personal AED, stay replenished with electrolytes, avoid QT-prolonging drugs, and continue with annual follow-up.
Slightly more than half of these patients had HCM and almost a third had long QT syndrome. Nearly one-third had an ICD implant and 22 were women.
Of the 76 athletes, 73 chose to return to play; however, 4 of these remained disqualified because of their team’s decision. Of the remaining 69, only 3 had one or more breakthrough cardiac events during 200 patient-years of follow-up.
These comprised one male Division I basketball player with HCM who had an ICD shock while moving furniture; another male Division 1 hockey player with long QT syndrome who was taking beta-blockers experienced syncope while coming off the bench and while cooking; and a third male professional hockey player with HCM, on beta-blockers, had syncope without exertion.
The authors concluded that when there was careful evaluation by experts and shared decision-making, a specific plan to return to sport can be put into place for the highest-level athletes.
Masters@Heart: Surprising result No. 3
Ruben De Bosscher MD, PhD, from KU Leuven (Belgium), presented the Masters@Heart study on behalf of a Belgian team of researchers. The question they asked was whether lifelong endurance exercise is associated with more coronary atherosclerosis than standard “normal” exercise levels.
That question brings up the paradox of exercise, which is that numerous observational studies find that exercise strongly associates with lower rates of cardiovascular events, but imaging studies also report high rates of coronary artery calcium in endurance athletes, especially in those who have run multiple marathons.
Masters@Heart investigators sought to explore this paradox by performing detailed coronary imaging in three groups – lifelong athletes, late-onset athletes (after age 30 years), and super-healthy controls. Through advertisements they obtained about 1,100 middle-aged male volunteers (mean age, 55 years). Of these, 605 men were selected at random to participate to reduce the chance of enrolling people who responded to the ads because of health concerns.
Investigators assigned those selected based on self-report of exercise. The control group was notable for their good health: they were free of any risk factors, took (almost) no meds, exercised regularly but not excessively (about 3 hours per week) and had a VO2 max of 122% of predicted.
The groups were well matched on baseline characteristics. Cycling predominated as the exercise of choice (this is a Belgian study after all). All patients had an extensive evaluation including coronary CT imaging.
European Heart Journal published the provocative results.
- Lifelong exercisers had a significantly higher CAC burden than controls, which confirms previous work.
- Lifelong exercisers had a higher percentage of multiple coronary plaques, plaques of at least 50%, and proximal plaques.
- There were no significant differences in the mixture of plaque types in the three groups. About two thirds of the plaques in each group were calcified and the remainder were deemed noncalcified or mixed.
- When looking only at noncalcified plaques, lifelong exercisers tended to have a higher prevalence of multiple plaques, plaques of at least 50%, and proximal plaques.
- So named “vulnerable” plaques were extremely infrequent in all three groups.
The authors concluded that lifelong endurance sport relative to a generic healthy lifestyle was not associated with more favorable coronary plaque composition.
Comments
Each of these three studies provided data where there was none. That is always a good thing.
The major theme from the first two studies is that expert opinion was too cautious. Doctors have long held the idea that patients with genetic heart disease, especially hypertrophic cardiomyopathy, are vulnerable, fragile even, when it comes to vigorous sport.
This new evidence upends this belief, as long as return to sport occurs in the setting of robust patient education and expert evaluation and surveillance.
Paternalism in prohibiting participation in sport because of genetic heart disease has joined the long list of medical reversals.
Masters@Heart provides a slightly different message. It finds that lifelong high-level exercise does not prevent coronary atherosclerosis in men. And, more provocatively, if replicated, might even show that long-term exposure to the biochemical, inflammatory, or hormonal effects of endurance training may actually be atherogenic. Like all good science, these findings raise more questions to explore in the realm of atherogenesis.
Two of the main limitations of the Belgian study was that the control arm was quite healthy; had the comparison arm been typical of sedentary controls in say, the Southeastern United States, the coronary lesions found in longtime exercisers may have looked more favorable. The more significant limitation is the lack of outcomes. Images of coronary arteries remain a surrogate marker. It’s possible that, like statins, higher levels of exercise may stabilize plaque and actually lower the risk for events.
The Belgian authors suggest – as many have – a J-curve of exercise benefits, wherein too little exercise is clearly bad, but too much exercise may also increase risk. In other words, for maximizing health, there may be a Goldilocks amount of exercise.
The problem with this idea comes in its pragmatic translation. The number of lifelong high-level, middle-aged endurance athletes that cite heart health reasons for their affliction is ... almost zero. Nearly everyone I have met in the endurance sport fraternity harbors no notion that racing a bike or running multiple marathons per year is a healthy endeavor.
Paternalism, therefore, would also fall in the realm of limiting lifelong exercise in addicted middle-aged athletes.
Via email, sports cardiologist Michael Emery, MD, reiterated the main immediate message from Masters@Heart: “Exercise does not make you immune from heart disease (which is a message a lot of athletes need to hear honestly).”
I for one cannot give up on endurance exercise. I won’t likely race anymore but I am like the lab rat who needs to run on the wheel. Whether this affects my coronary plaque burden matters not to me.
Dr. Mandrola is a clinical electrophysiologist at Baptist Medical Associates, Louisville, Ky. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Fixed-dose combo pill for PAH promises accelerated benefit: A DUE
Already commonly used in combination for the treatment of pulmonary arterial hypertension (PAH), macitentan and tadalafil are safe and effective in a fixed-dose combination even as first-line therapy, according to a randomized multicenter comparative trial.
The fixed-dose combination “led to a highly significant and marked improvement in pulmonary vascular resistance when compared to macitentan and tadalafil as monotherapies,” Kelly Chin, MD, reported at the joint scientific sessions of the American College of Cardiology and the World Heart Federation.
Guidelines encourage rapid PVR reductions
In practice, it is common to start treatment with either the endothelial receptor antagonist (ERA) macitentan, the phosphodiesterase-5 (PDE-5) inhibitor tadalafil, or other frequently used medications for PAH, and to then add additional treatments, according to Dr. Chin. She pointed out, however, that guidelines, including those issued jointly by the European Society of Cardiology and the European Respiratory Society, encourage rapid escalation of therapy to quickly lower pulmonary vascular resistance (PVR).
In general, both macitentan and tadalafil are well tolerated, but the advantage and the safety of rapidly reducing PVR when these are initiated together in a single pill had not been evaluated previously in a major trial. In this double-blind phase III trial, called A DUE, 187 patients in functional class II or III PAH were randomized. The three-arm study included both treatment naive patients and patients who had been on stable doses (> 3 months) of an ERA or a PDE5 inhibitor, explained Dr. Chin, director of pulmonary hypertension at the UT Southwestern, Dallas.
Treatment naive patients, representing about 53% of the study population, were randomized to 10 mg macitentan monotherapy, 40 mg tadalafil monotherapy, or a fixed-dose, single-pill combination containing both. If on a stable dose of an ERA at trial entry, patients were randomized to 10 macitentan as a monotherapy or to the fixed dose combination. Patients entering the trial already on a stable dose of a PDE5 inhibitor were randomized to 40 mg tadalafil or the combination.
PVR reduced twofold on combination therapy
Relative to macitentan monotherapy, the percentage change from baseline in PVR by ratio of geometric mean, which was the primary outcome, was about twice as high on the combination (45% vs. 23%) at the end of the 16-week trial. This translates into a 29% PVR reduction (hazard ratio, 0.71; P < .0001).
For combination therapy relative to tadalafil monotherapy, the advantage for the fixed dose combination (44% vs. 22%) was about the same, also providing a nearly 30% relative reduction (HR, 0.72; P < .0001).
The increases in 6-minute walk distance (6MWD) at 16 weeks, a secondary endpoint, numerically favored the combination pill over both macitentan monotherapy (52.9 vs. 39.5 meters; P = .38) and tadalafil (43.4 vs. 15.9 meters; P = .059), but only the improvement relative to tadalafil monotherapy was considered a trend.
The proportion of patients who experienced at least one serious adverse event was higher in the combination arm (14.0%) relative to single agent macitentan (8.6%) or single agent tadalafil (9.1%). The adverse events and serious adverse events more common on the combination included hypotension, fluid retention, and anemia. This latter side effect occurred in 18.7%, 2.9%, and 2.3% in the combination, macitentan monotherapy, and tadalafil arms, respectively.
Several of those invited by the ACC to discuss the paper, including Lee R. Goldberg, MD, section chief of advanced heart failure and cardiac transplant, University of Pennsylvania, Philadelphia, raised concern about the increased rate of anemia among those in the combination pill. Two of the patients (2%) treated with the combination developed a hemoglobin < 8 g/dL.
Overall, nine (8.4%) of those on the fixed-dose combination, two (4.5%) of those randomized to tadalafil monotherapy, and none of the patients randomized to macitentan discontinued therapy due to side effects.
Anemia risk unexpected
Based on “the unexpected signal of an anemia risk,” Biykem Bozkurt, MD, PhD, chair of cardiology at Baylor College of Medicine, Houston, said that a larger scale trial with a longer follow-up is needed. While the concept of front-loading two drugs is attractive “for the very challenging PAH population,” she called for further evaluation of this safety signal before clinicians switch from the current practice of starting with one PAH therapy before adding others.

In addition, Dr. Bozkurt said a more definitive study would be helpful in determining whether starting with a fixed-pill combination is better than sequential treatment to improve quality of life. Dr. Bozkurt said it is likely that the lack of significant benefit on 6MWD in this study was due to the relatively small sample size, but an improvement in this measure would be another reason to consider a front-line fixed-dose combination.
Dr. Chin, in an interview, did not agree. She agreed that a larger sample size might have yielded a significant improvement in 6MWD, but she noted this outcome was moving in the right direction and was not the primary endpoint. In her opinion, this phase 3 trial does confirm that fixed-dose combination is well tolerated, has acceptable safety, and markedly improves PVR, fulfilling the guideline goal of controlling PAH more quickly.
Dr. Chin reports financial relationships with Altavant, Arena, Gossamer Bio, Janssen, Merck, ShouTi, and United Therapeutics. Dr. Goldberg reports financial relationships with Abbott, Respicardia/Zoll, and Viscardia. Dr. Bozkurt reports financial relationships with Abbott, Amgen, AstraZeneca, Boehringer Ingelheim, Cardurion, LivaNova, Relypsa, Renovacor, Sanofi-Aventis, and Vifor.
Already commonly used in combination for the treatment of pulmonary arterial hypertension (PAH), macitentan and tadalafil are safe and effective in a fixed-dose combination even as first-line therapy, according to a randomized multicenter comparative trial.
The fixed-dose combination “led to a highly significant and marked improvement in pulmonary vascular resistance when compared to macitentan and tadalafil as monotherapies,” Kelly Chin, MD, reported at the joint scientific sessions of the American College of Cardiology and the World Heart Federation.
Guidelines encourage rapid PVR reductions
In practice, it is common to start treatment with either the endothelial receptor antagonist (ERA) macitentan, the phosphodiesterase-5 (PDE-5) inhibitor tadalafil, or other frequently used medications for PAH, and to then add additional treatments, according to Dr. Chin. She pointed out, however, that guidelines, including those issued jointly by the European Society of Cardiology and the European Respiratory Society, encourage rapid escalation of therapy to quickly lower pulmonary vascular resistance (PVR).
In general, both macitentan and tadalafil are well tolerated, but the advantage and the safety of rapidly reducing PVR when these are initiated together in a single pill had not been evaluated previously in a major trial. In this double-blind phase III trial, called A DUE, 187 patients in functional class II or III PAH were randomized. The three-arm study included both treatment naive patients and patients who had been on stable doses (> 3 months) of an ERA or a PDE5 inhibitor, explained Dr. Chin, director of pulmonary hypertension at the UT Southwestern, Dallas.
Treatment naive patients, representing about 53% of the study population, were randomized to 10 mg macitentan monotherapy, 40 mg tadalafil monotherapy, or a fixed-dose, single-pill combination containing both. If on a stable dose of an ERA at trial entry, patients were randomized to 10 macitentan as a monotherapy or to the fixed dose combination. Patients entering the trial already on a stable dose of a PDE5 inhibitor were randomized to 40 mg tadalafil or the combination.
PVR reduced twofold on combination therapy
Relative to macitentan monotherapy, the percentage change from baseline in PVR by ratio of geometric mean, which was the primary outcome, was about twice as high on the combination (45% vs. 23%) at the end of the 16-week trial. This translates into a 29% PVR reduction (hazard ratio, 0.71; P < .0001).
For combination therapy relative to tadalafil monotherapy, the advantage for the fixed dose combination (44% vs. 22%) was about the same, also providing a nearly 30% relative reduction (HR, 0.72; P < .0001).
The increases in 6-minute walk distance (6MWD) at 16 weeks, a secondary endpoint, numerically favored the combination pill over both macitentan monotherapy (52.9 vs. 39.5 meters; P = .38) and tadalafil (43.4 vs. 15.9 meters; P = .059), but only the improvement relative to tadalafil monotherapy was considered a trend.
The proportion of patients who experienced at least one serious adverse event was higher in the combination arm (14.0%) relative to single agent macitentan (8.6%) or single agent tadalafil (9.1%). The adverse events and serious adverse events more common on the combination included hypotension, fluid retention, and anemia. This latter side effect occurred in 18.7%, 2.9%, and 2.3% in the combination, macitentan monotherapy, and tadalafil arms, respectively.
Several of those invited by the ACC to discuss the paper, including Lee R. Goldberg, MD, section chief of advanced heart failure and cardiac transplant, University of Pennsylvania, Philadelphia, raised concern about the increased rate of anemia among those in the combination pill. Two of the patients (2%) treated with the combination developed a hemoglobin < 8 g/dL.
Overall, nine (8.4%) of those on the fixed-dose combination, two (4.5%) of those randomized to tadalafil monotherapy, and none of the patients randomized to macitentan discontinued therapy due to side effects.
Anemia risk unexpected
Based on “the unexpected signal of an anemia risk,” Biykem Bozkurt, MD, PhD, chair of cardiology at Baylor College of Medicine, Houston, said that a larger scale trial with a longer follow-up is needed. While the concept of front-loading two drugs is attractive “for the very challenging PAH population,” she called for further evaluation of this safety signal before clinicians switch from the current practice of starting with one PAH therapy before adding others.
In addition, Dr. Bozkurt said a more definitive study would be helpful in determining whether starting with a fixed-pill combination is better than sequential treatment to improve quality of life. Dr. Bozkurt said it is likely that the lack of significant benefit on 6MWD in this study was due to the relatively small sample size, but an improvement in this measure would be another reason to consider a front-line fixed-dose combination.
Dr. Chin, in an interview, did not agree. She agreed that a larger sample size might have yielded a significant improvement in 6MWD, but she noted this outcome was moving in the right direction and was not the primary endpoint. In her opinion, this phase 3 trial does confirm that fixed-dose combination is well tolerated, has acceptable safety, and markedly improves PVR, fulfilling the guideline goal of controlling PAH more quickly.
Dr. Chin reports financial relationships with Altavant, Arena, Gossamer Bio, Janssen, Merck, ShouTi, and United Therapeutics. Dr. Goldberg reports financial relationships with Abbott, Respicardia/Zoll, and Viscardia. Dr. Bozkurt reports financial relationships with Abbott, Amgen, AstraZeneca, Boehringer Ingelheim, Cardurion, LivaNova, Relypsa, Renovacor, Sanofi-Aventis, and Vifor.
Already commonly used in combination for the treatment of pulmonary arterial hypertension (PAH), macitentan and tadalafil are safe and effective in a fixed-dose combination even as first-line therapy, according to a randomized multicenter comparative trial.
The fixed-dose combination “led to a highly significant and marked improvement in pulmonary vascular resistance when compared to macitentan and tadalafil as monotherapies,” Kelly Chin, MD, reported at the joint scientific sessions of the American College of Cardiology and the World Heart Federation.
Guidelines encourage rapid PVR reductions
In practice, it is common to start treatment with either the endothelial receptor antagonist (ERA) macitentan, the phosphodiesterase-5 (PDE-5) inhibitor tadalafil, or other frequently used medications for PAH, and to then add additional treatments, according to Dr. Chin. She pointed out, however, that guidelines, including those issued jointly by the European Society of Cardiology and the European Respiratory Society, encourage rapid escalation of therapy to quickly lower pulmonary vascular resistance (PVR).
In general, both macitentan and tadalafil are well tolerated, but the advantage and the safety of rapidly reducing PVR when these are initiated together in a single pill had not been evaluated previously in a major trial. In this double-blind phase III trial, called A DUE, 187 patients in functional class II or III PAH were randomized. The three-arm study included both treatment naive patients and patients who had been on stable doses (> 3 months) of an ERA or a PDE5 inhibitor, explained Dr. Chin, director of pulmonary hypertension at the UT Southwestern, Dallas.
Treatment naive patients, representing about 53% of the study population, were randomized to 10 mg macitentan monotherapy, 40 mg tadalafil monotherapy, or a fixed-dose, single-pill combination containing both. If on a stable dose of an ERA at trial entry, patients were randomized to 10 macitentan as a monotherapy or to the fixed dose combination. Patients entering the trial already on a stable dose of a PDE5 inhibitor were randomized to 40 mg tadalafil or the combination.
PVR reduced twofold on combination therapy
Relative to macitentan monotherapy, the percentage change from baseline in PVR by ratio of geometric mean, which was the primary outcome, was about twice as high on the combination (45% vs. 23%) at the end of the 16-week trial. This translates into a 29% PVR reduction (hazard ratio, 0.71; P < .0001).
For combination therapy relative to tadalafil monotherapy, the advantage for the fixed dose combination (44% vs. 22%) was about the same, also providing a nearly 30% relative reduction (HR, 0.72; P < .0001).
The increases in 6-minute walk distance (6MWD) at 16 weeks, a secondary endpoint, numerically favored the combination pill over both macitentan monotherapy (52.9 vs. 39.5 meters; P = .38) and tadalafil (43.4 vs. 15.9 meters; P = .059), but only the improvement relative to tadalafil monotherapy was considered a trend.
The proportion of patients who experienced at least one serious adverse event was higher in the combination arm (14.0%) relative to single agent macitentan (8.6%) or single agent tadalafil (9.1%). The adverse events and serious adverse events more common on the combination included hypotension, fluid retention, and anemia. This latter side effect occurred in 18.7%, 2.9%, and 2.3% in the combination, macitentan monotherapy, and tadalafil arms, respectively.
Several of those invited by the ACC to discuss the paper, including Lee R. Goldberg, MD, section chief of advanced heart failure and cardiac transplant, University of Pennsylvania, Philadelphia, raised concern about the increased rate of anemia among those in the combination pill. Two of the patients (2%) treated with the combination developed a hemoglobin < 8 g/dL.
Overall, nine (8.4%) of those on the fixed-dose combination, two (4.5%) of those randomized to tadalafil monotherapy, and none of the patients randomized to macitentan discontinued therapy due to side effects.
Anemia risk unexpected
Based on “the unexpected signal of an anemia risk,” Biykem Bozkurt, MD, PhD, chair of cardiology at Baylor College of Medicine, Houston, said that a larger scale trial with a longer follow-up is needed. While the concept of front-loading two drugs is attractive “for the very challenging PAH population,” she called for further evaluation of this safety signal before clinicians switch from the current practice of starting with one PAH therapy before adding others.
In addition, Dr. Bozkurt said a more definitive study would be helpful in determining whether starting with a fixed-pill combination is better than sequential treatment to improve quality of life. Dr. Bozkurt said it is likely that the lack of significant benefit on 6MWD in this study was due to the relatively small sample size, but an improvement in this measure would be another reason to consider a front-line fixed-dose combination.
Dr. Chin, in an interview, did not agree. She agreed that a larger sample size might have yielded a significant improvement in 6MWD, but she noted this outcome was moving in the right direction and was not the primary endpoint. In her opinion, this phase 3 trial does confirm that fixed-dose combination is well tolerated, has acceptable safety, and markedly improves PVR, fulfilling the guideline goal of controlling PAH more quickly.
Dr. Chin reports financial relationships with Altavant, Arena, Gossamer Bio, Janssen, Merck, ShouTi, and United Therapeutics. Dr. Goldberg reports financial relationships with Abbott, Respicardia/Zoll, and Viscardia. Dr. Bozkurt reports financial relationships with Abbott, Amgen, AstraZeneca, Boehringer Ingelheim, Cardurion, LivaNova, Relypsa, Renovacor, Sanofi-Aventis, and Vifor.
AT ACC 2023
Depressive symptoms tied to higher stroke risk, worse outcomes
new research suggests.
Data from the international INTERSTROKE study also showed that those with depressive symptoms before a stroke had worse outcomes, including a significantly higher mortality rate in the first month after a stroke.
These findings build on prior research on the link between depression and stroke, including one study that showed an increased risk for incident stroke among those with a high number of depressive symptoms and another that found that worsening depression can precede stroke in older adults.
“Depression is an important risk factor for acute stroke and is potentially a modifiable contributor to the global burden of stroke,” lead investigator Robert Murphy, MB, a consultant in stroke and geriatric medicine and a researcher with the clinical research facility at the University of Galway, Ireland, told this news organization. “Even mild depressive symptoms were found in this study to be associated with increased risk of stroke and this adds to the literature that across the full range of depressive symptoms there is an association with increased risk of stroke.”
The findings were published online March 8 in Neurology.
Significant stroke risk
For the analysis, investigators collected data on 26,877 cases and controls across 32 countries who participated in INTERSTROKE, an international case-control study of risk factors for a first acute stroke. Participants were recruited between 2007 and 2015 and completed a series of questionnaires about stroke risk factors, including measures of depressive symptoms experienced in the past 12 months.
After adjustment for occupation, education, wealth index, diet, physical activity, alcohol consumption, and smoking history, having prestroke depressive symptoms was associated with greater odds for acute stroke (adjusted odds ratio [aOR], 1.46; 95% confidence interval [CI], 1.34-1.58), including both intracerebral hemorrhage (aOR, 1.56; 95% CI, 1.28-1.91) and ischemic stroke (aOR, 1.44; 95% CI, 1.31-1.58).
Stroke risk increased with increasing severity of depression, but even those with mild depression had a 35% increased risk (aOR, 1.35; 95% CI, 1.19-1.53).
The increased risk held even after the researchers adjusted further for diabetes, hypertension, atrial fibrillation, and body mass index, and work, home, and financial stress.
The association was consistent across geographical regions and age groups, but was stronger in men and in those without hypertension.
“This study looks at different constructs of depression and identifies that across the spectrum of mild, moderate, and severe depressive symptoms that there is an association present with acute stroke and that a biological gradient emerges with increasing burden of depressive symptoms associated with increasing risk,” Dr. Murphy said.
An antidepressant mediating effect?
While prestroke depressive symptoms were not associated with a greater odds of worse stroke severity, they were associated with worse outcomes (P < .001) and higher mortality (10% vs. 8.1%; P = .003) 1 month after a stroke.
In a subgroup analysis, researchers found no association between depressive symptoms and stroke risk in patients who were taking antidepressants.
While no assumptions of causality can be drawn from these findings, “this subgroup analysis does suggest that an increased risk of stroke in those with depression may be attenuated if a patient is on appropriate treatment,” Dr. Murphy said. “This is an area that warrants further exploration.”
The mechanisms that link depression to stroke are unclear, but these findings offer strong evidence that this link exists, Dr. Murphy said.
“We adjusted for potential confounders in sequential models and after adjusting for traditional cardiovascular risk factors there was a consistent association between depressive symptoms and stroke identifying that there is likely an independent association between depression and stroke,” Dr. Murphy said.
Questions remain
Commenting on the study, Daniel T. Lackland DrPH, professor, division of translational neurosciences and population studies, department of neurology, Medical University of South Carolina, Charleston, said it adds to a growing body of work on the association of stroke and depression.
“In this case, depression may be a risk factor for having a stroke,” said Dr. Lackland, who was not part of the study. In addition, the study suggests that “treating depression can have additional benefits beyond mental health, in this case, reduced stroke risks.”
However, it’s important, as with any observational study, that there may be confounding factors that may offer an alternative explanation for the findings.
“Further, it is often difficult to accurately assess depression in all individuals, and specifically in individuals who have had a stroke,” Dr. Lackland said. “While this particular study adds depression as a risk factor and suggests treatment of depression in reducing risks, it is important to emphasize that the traditional stroke risk factors including hypertension should [be] continually recognized and treat[ed] with high rigor.”
The INTERSTROKE study was funded by the Canadian Institutes of Health Research, the Heart and Stroke Foundation of Canada, the Canadian Stroke Network, the Swedish Research Council, the Swedish Heart Lung Foundation, AFA Insurance, The Health & Medical Care Committee of the Regional Executive Board, Region Västra Götaland, and through unrestricted grants from several pharmaceutical companies with major contributions from AstraZeneca, Boehringer Ingelheim (Canada), Pfizer (Canada), Merck Sharp & Dohme, the Swedish Heart Lung Foundation, Chest Heart & Stroke Scotland, and the Stroke Association (United Kingdom). Dr. Murphy and Dr. Lackland have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new research suggests.
Data from the international INTERSTROKE study also showed that those with depressive symptoms before a stroke had worse outcomes, including a significantly higher mortality rate in the first month after a stroke.
These findings build on prior research on the link between depression and stroke, including one study that showed an increased risk for incident stroke among those with a high number of depressive symptoms and another that found that worsening depression can precede stroke in older adults.
“Depression is an important risk factor for acute stroke and is potentially a modifiable contributor to the global burden of stroke,” lead investigator Robert Murphy, MB, a consultant in stroke and geriatric medicine and a researcher with the clinical research facility at the University of Galway, Ireland, told this news organization. “Even mild depressive symptoms were found in this study to be associated with increased risk of stroke and this adds to the literature that across the full range of depressive symptoms there is an association with increased risk of stroke.”
The findings were published online March 8 in Neurology.
Significant stroke risk
For the analysis, investigators collected data on 26,877 cases and controls across 32 countries who participated in INTERSTROKE, an international case-control study of risk factors for a first acute stroke. Participants were recruited between 2007 and 2015 and completed a series of questionnaires about stroke risk factors, including measures of depressive symptoms experienced in the past 12 months.
After adjustment for occupation, education, wealth index, diet, physical activity, alcohol consumption, and smoking history, having prestroke depressive symptoms was associated with greater odds for acute stroke (adjusted odds ratio [aOR], 1.46; 95% confidence interval [CI], 1.34-1.58), including both intracerebral hemorrhage (aOR, 1.56; 95% CI, 1.28-1.91) and ischemic stroke (aOR, 1.44; 95% CI, 1.31-1.58).
Stroke risk increased with increasing severity of depression, but even those with mild depression had a 35% increased risk (aOR, 1.35; 95% CI, 1.19-1.53).
The increased risk held even after the researchers adjusted further for diabetes, hypertension, atrial fibrillation, and body mass index, and work, home, and financial stress.
The association was consistent across geographical regions and age groups, but was stronger in men and in those without hypertension.
“This study looks at different constructs of depression and identifies that across the spectrum of mild, moderate, and severe depressive symptoms that there is an association present with acute stroke and that a biological gradient emerges with increasing burden of depressive symptoms associated with increasing risk,” Dr. Murphy said.
An antidepressant mediating effect?
While prestroke depressive symptoms were not associated with a greater odds of worse stroke severity, they were associated with worse outcomes (P < .001) and higher mortality (10% vs. 8.1%; P = .003) 1 month after a stroke.
In a subgroup analysis, researchers found no association between depressive symptoms and stroke risk in patients who were taking antidepressants.
While no assumptions of causality can be drawn from these findings, “this subgroup analysis does suggest that an increased risk of stroke in those with depression may be attenuated if a patient is on appropriate treatment,” Dr. Murphy said. “This is an area that warrants further exploration.”
The mechanisms that link depression to stroke are unclear, but these findings offer strong evidence that this link exists, Dr. Murphy said.
“We adjusted for potential confounders in sequential models and after adjusting for traditional cardiovascular risk factors there was a consistent association between depressive symptoms and stroke identifying that there is likely an independent association between depression and stroke,” Dr. Murphy said.
Questions remain
Commenting on the study, Daniel T. Lackland DrPH, professor, division of translational neurosciences and population studies, department of neurology, Medical University of South Carolina, Charleston, said it adds to a growing body of work on the association of stroke and depression.
“In this case, depression may be a risk factor for having a stroke,” said Dr. Lackland, who was not part of the study. In addition, the study suggests that “treating depression can have additional benefits beyond mental health, in this case, reduced stroke risks.”
However, it’s important, as with any observational study, that there may be confounding factors that may offer an alternative explanation for the findings.
“Further, it is often difficult to accurately assess depression in all individuals, and specifically in individuals who have had a stroke,” Dr. Lackland said. “While this particular study adds depression as a risk factor and suggests treatment of depression in reducing risks, it is important to emphasize that the traditional stroke risk factors including hypertension should [be] continually recognized and treat[ed] with high rigor.”
The INTERSTROKE study was funded by the Canadian Institutes of Health Research, the Heart and Stroke Foundation of Canada, the Canadian Stroke Network, the Swedish Research Council, the Swedish Heart Lung Foundation, AFA Insurance, The Health & Medical Care Committee of the Regional Executive Board, Region Västra Götaland, and through unrestricted grants from several pharmaceutical companies with major contributions from AstraZeneca, Boehringer Ingelheim (Canada), Pfizer (Canada), Merck Sharp & Dohme, the Swedish Heart Lung Foundation, Chest Heart & Stroke Scotland, and the Stroke Association (United Kingdom). Dr. Murphy and Dr. Lackland have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new research suggests.
Data from the international INTERSTROKE study also showed that those with depressive symptoms before a stroke had worse outcomes, including a significantly higher mortality rate in the first month after a stroke.
These findings build on prior research on the link between depression and stroke, including one study that showed an increased risk for incident stroke among those with a high number of depressive symptoms and another that found that worsening depression can precede stroke in older adults.
“Depression is an important risk factor for acute stroke and is potentially a modifiable contributor to the global burden of stroke,” lead investigator Robert Murphy, MB, a consultant in stroke and geriatric medicine and a researcher with the clinical research facility at the University of Galway, Ireland, told this news organization. “Even mild depressive symptoms were found in this study to be associated with increased risk of stroke and this adds to the literature that across the full range of depressive symptoms there is an association with increased risk of stroke.”
The findings were published online March 8 in Neurology.
Significant stroke risk
For the analysis, investigators collected data on 26,877 cases and controls across 32 countries who participated in INTERSTROKE, an international case-control study of risk factors for a first acute stroke. Participants were recruited between 2007 and 2015 and completed a series of questionnaires about stroke risk factors, including measures of depressive symptoms experienced in the past 12 months.
After adjustment for occupation, education, wealth index, diet, physical activity, alcohol consumption, and smoking history, having prestroke depressive symptoms was associated with greater odds for acute stroke (adjusted odds ratio [aOR], 1.46; 95% confidence interval [CI], 1.34-1.58), including both intracerebral hemorrhage (aOR, 1.56; 95% CI, 1.28-1.91) and ischemic stroke (aOR, 1.44; 95% CI, 1.31-1.58).
Stroke risk increased with increasing severity of depression, but even those with mild depression had a 35% increased risk (aOR, 1.35; 95% CI, 1.19-1.53).
The increased risk held even after the researchers adjusted further for diabetes, hypertension, atrial fibrillation, and body mass index, and work, home, and financial stress.
The association was consistent across geographical regions and age groups, but was stronger in men and in those without hypertension.
“This study looks at different constructs of depression and identifies that across the spectrum of mild, moderate, and severe depressive symptoms that there is an association present with acute stroke and that a biological gradient emerges with increasing burden of depressive symptoms associated with increasing risk,” Dr. Murphy said.
An antidepressant mediating effect?
While prestroke depressive symptoms were not associated with a greater odds of worse stroke severity, they were associated with worse outcomes (P < .001) and higher mortality (10% vs. 8.1%; P = .003) 1 month after a stroke.
In a subgroup analysis, researchers found no association between depressive symptoms and stroke risk in patients who were taking antidepressants.
While no assumptions of causality can be drawn from these findings, “this subgroup analysis does suggest that an increased risk of stroke in those with depression may be attenuated if a patient is on appropriate treatment,” Dr. Murphy said. “This is an area that warrants further exploration.”
The mechanisms that link depression to stroke are unclear, but these findings offer strong evidence that this link exists, Dr. Murphy said.
“We adjusted for potential confounders in sequential models and after adjusting for traditional cardiovascular risk factors there was a consistent association between depressive symptoms and stroke identifying that there is likely an independent association between depression and stroke,” Dr. Murphy said.
Questions remain
Commenting on the study, Daniel T. Lackland DrPH, professor, division of translational neurosciences and population studies, department of neurology, Medical University of South Carolina, Charleston, said it adds to a growing body of work on the association of stroke and depression.
“In this case, depression may be a risk factor for having a stroke,” said Dr. Lackland, who was not part of the study. In addition, the study suggests that “treating depression can have additional benefits beyond mental health, in this case, reduced stroke risks.”
However, it’s important, as with any observational study, that there may be confounding factors that may offer an alternative explanation for the findings.
“Further, it is often difficult to accurately assess depression in all individuals, and specifically in individuals who have had a stroke,” Dr. Lackland said. “While this particular study adds depression as a risk factor and suggests treatment of depression in reducing risks, it is important to emphasize that the traditional stroke risk factors including hypertension should [be] continually recognized and treat[ed] with high rigor.”
The INTERSTROKE study was funded by the Canadian Institutes of Health Research, the Heart and Stroke Foundation of Canada, the Canadian Stroke Network, the Swedish Research Council, the Swedish Heart Lung Foundation, AFA Insurance, The Health & Medical Care Committee of the Regional Executive Board, Region Västra Götaland, and through unrestricted grants from several pharmaceutical companies with major contributions from AstraZeneca, Boehringer Ingelheim (Canada), Pfizer (Canada), Merck Sharp & Dohme, the Swedish Heart Lung Foundation, Chest Heart & Stroke Scotland, and the Stroke Association (United Kingdom). Dr. Murphy and Dr. Lackland have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM NEUROLOGY
Telehealth doctor indicted on health care fraud, opioid distribution charges
Sangita Patel, MD, 50, practiced at Advance Medical Home Physicians in Troy.
According to court documents, between July 2020 and June 2022 Patel was responsible for submitting Medicare claims for improper telehealth visits she didn’t conduct herself.
Dr. Patel, who accepted patients who paid in cash as well as those with Medicare and Medicaid coverage, billed approximately $3.4 million to Medicare between 2018 and 2022, according to court documents. An unusual number of these visits were billed using complex codes, an indication of health care fraud. The investigation also found that on many days, Dr. Patel billed for more than 24 hours of services. During this period, according to the document, 76% of Dr. Patel’s Medicare reimbursements were for telehealth.
Prosecutors say that Dr. Patel prescribed Schedule II controlled substances to more than 90% of the patients in these telehealth visits. She delegated her prescription authority to an unlicensed medical assistant. Through undercover visits and cell site search warrant data, the investigation found that Dr. Patel directed patients to contact, via cell phone, this assistant, who then entered electronic prescriptions into the electronic medical records system. Dr. Patel then signed the prescriptions and sent them to the pharmacies without ever interacting with the patients. Prosecutors also used text messages, obtained by search warrant, between Dr. Patel and her assistant and between the assistant and undercover informers to build their case.
Dr. Patel is also accused of referring patients to other providers, who in turn billed Medicare for claims associated with those patients. Advance Medical received $143,000 from these providers, potentially in violation of anti-kickback laws, according to bank records obtained by subpoena.
If convicted, Dr. Patel could be sentenced to up to 10 years in federal prison.
A version of this article first appeared on Medscape.com.
Sangita Patel, MD, 50, practiced at Advance Medical Home Physicians in Troy.
According to court documents, between July 2020 and June 2022 Patel was responsible for submitting Medicare claims for improper telehealth visits she didn’t conduct herself.
Dr. Patel, who accepted patients who paid in cash as well as those with Medicare and Medicaid coverage, billed approximately $3.4 million to Medicare between 2018 and 2022, according to court documents. An unusual number of these visits were billed using complex codes, an indication of health care fraud. The investigation also found that on many days, Dr. Patel billed for more than 24 hours of services. During this period, according to the document, 76% of Dr. Patel’s Medicare reimbursements were for telehealth.
Prosecutors say that Dr. Patel prescribed Schedule II controlled substances to more than 90% of the patients in these telehealth visits. She delegated her prescription authority to an unlicensed medical assistant. Through undercover visits and cell site search warrant data, the investigation found that Dr. Patel directed patients to contact, via cell phone, this assistant, who then entered electronic prescriptions into the electronic medical records system. Dr. Patel then signed the prescriptions and sent them to the pharmacies without ever interacting with the patients. Prosecutors also used text messages, obtained by search warrant, between Dr. Patel and her assistant and between the assistant and undercover informers to build their case.
Dr. Patel is also accused of referring patients to other providers, who in turn billed Medicare for claims associated with those patients. Advance Medical received $143,000 from these providers, potentially in violation of anti-kickback laws, according to bank records obtained by subpoena.
If convicted, Dr. Patel could be sentenced to up to 10 years in federal prison.
A version of this article first appeared on Medscape.com.
Sangita Patel, MD, 50, practiced at Advance Medical Home Physicians in Troy.
According to court documents, between July 2020 and June 2022 Patel was responsible for submitting Medicare claims for improper telehealth visits she didn’t conduct herself.
Dr. Patel, who accepted patients who paid in cash as well as those with Medicare and Medicaid coverage, billed approximately $3.4 million to Medicare between 2018 and 2022, according to court documents. An unusual number of these visits were billed using complex codes, an indication of health care fraud. The investigation also found that on many days, Dr. Patel billed for more than 24 hours of services. During this period, according to the document, 76% of Dr. Patel’s Medicare reimbursements were for telehealth.
Prosecutors say that Dr. Patel prescribed Schedule II controlled substances to more than 90% of the patients in these telehealth visits. She delegated her prescription authority to an unlicensed medical assistant. Through undercover visits and cell site search warrant data, the investigation found that Dr. Patel directed patients to contact, via cell phone, this assistant, who then entered electronic prescriptions into the electronic medical records system. Dr. Patel then signed the prescriptions and sent them to the pharmacies without ever interacting with the patients. Prosecutors also used text messages, obtained by search warrant, between Dr. Patel and her assistant and between the assistant and undercover informers to build their case.
Dr. Patel is also accused of referring patients to other providers, who in turn billed Medicare for claims associated with those patients. Advance Medical received $143,000 from these providers, potentially in violation of anti-kickback laws, according to bank records obtained by subpoena.
If convicted, Dr. Patel could be sentenced to up to 10 years in federal prison.
A version of this article first appeared on Medscape.com.
What’s it like to take Ozempic? A doctor’s own story
With the rising popularity of weight-loss drug injections, I’ve received many questions from patients about the pros, cons, and costs. While Ozempic (semaglutide) is perhaps the best known, it’s technically an agent approved only for type 2 diabetes that has been used off label for obesity. The same substance, semaglutide, is approved for use in obesity, but at a higher dose, under the brand name Wegovy. Alternatives are available, and results will vary depending on the specific agent used and the individual.
Ultimately, I decided to try these new injections for myself. I am not a paid representative for, nor an advocate of, any of these medications; I’m here only to share my personal experience.
In my discussions with patients about weight, I sometimes felt like an imposter. While I was overweight by medical standards, I fortunately had none of the underlying health problems. I wasn’t on medications for blood pressure nor did I have diabetes, but I was counseling people to lose weight and eat better while not always following my own advice.
Since having children and turning 40, my metabolism, like many other women’s, seems to have plummeted. I tried a number of older weight-loss medications, like phentermine and phendimetrazine, under the supervision of medical professionals.
Each time, the efforts worked for a short while, particularly when I followed good portion control and practiced moderate exercise. Once the side effects (that is, tachycardia, palpitations, mood changes, constipation) became intolerable, or I became tired or fearful of being on the medications too long, I’d stop and I would regain some of the weight.
When the newer subcutaneous injectable medications arrived on the scene and I started to talk to my patients about them, I was intrigued by their novel mode of action and seeming benefits.
These medications, glucagonlike peptide–1 (GLP-1) receptor agonists, were first approved for type 2 diabetes, and it soon became apparent that patients were losing significant amounts of weight taking them, so manufacturers conducted further trials in obesity patients without type 2 diabetes.
The first of these, liraglutide, is injected daily and was first approved as Victoza for type 2 diabetes; it later received an additional approval for obesity, in December 2014, as Saxenda.
Semaglutide, another of the new GLP-1 agonists, was first approved for type 2 diabetes as Ozempic but again was found to lead to substantial weight loss, so a subsequent approval of the drug for obesity, as Wegovy, came in June 2021. Semaglutide is injected once a week.
Semaglutide was branded a “game changer” when it was licensed for obesity because the mean weight loss seen in trials was around 15%, more than for any other drug and approaching what could be achieved with bariatric surgery, some doctors said.
These medications work in a different way from the older weight loss drugs, which had focused on the use of amphetamines. The newer medications became very popular because treating obesity helps lower blood glucose, blood pressure, cholesterol, kidney disease risk, and other comorbidities that occur with diabetes. Plus, for most people, there were fewer side effects.
I first tried Saxenda when it arrived on the market, via some samples that our pharmaceutical representative brought, both out of curiosity and to see if it would help me lose the stubborn baby weight. I ended up stopping the daily injections after my second or third week because of nausea and vomiting. I took a break, got a prescription for antinausea medicine, and tried again because it did indeed decrease my appetite. However, when I took my prescription to the pharmacy, my insurance wouldn’t cover it. It happens to doctors, too.
Fast-forward to 2017-2018. The baby weight was still holding on despite lifestyle changes, diet, and exercising. The newer drug classes hit the market, and again we had samples from our reps.
When Ozempic was on backorder, I switched to a low dose of Mounjaro (tirzepatide), a new dual GLP-1 and glucose-dependent insulinotropic polypeptide agonist, approved for type 2 diabetes in May 2022, again using it off label as a weekly injection, as it isn’t currently approved for weight loss. However, it does produce significant weight loss and is awaiting approval for obesity.
With these new medications, I noticed that both my patients and I didn’t complain as much about nausea and vomiting, but I did experience stomach upset, constipation, and acid reflux.
The appetite suppression is effective. It slows down the emptying of the gut so I feel full longer. I’ve lost 30 lb with these weekly injections and would like to lose another 20 lb. I follow a routine of reasonable, portion-controlled eating and moderate exercise (30 minutes of cardiovascular activity at least two to three times a week).
Discontinuing the medications may cause rebound weight gain, especially if I’m no longer following a routine of healthy eating and/or moderate exercise. I deal with minimal constipation by taking stool softeners, and I take antacids for acid reflux.
Here’s what I recommend applying when working with patients who have obesity: First, explain how these medications work. Then conduct a health history to make sure these injections are right for them. Patients with a family history of pancreatic cancer can’t take these medications. You also want to monitor use in patients with a history of hypoglycemia so their blood sugar doesn’t drop too low. It’s also important to make sure your patients are able to afford the medication. My husband takes Ozempic for diabetes, and recently we were told that a refill would cost about $1,500 a month, even with insurance. “Covered” doesn’t necessarily mean affordable.
Take a baseline hemoglobin A1c and repeat it after the patient has been on the medication for 2-3 weeks. Also remind them that they can’t rely solely on the medication but need to practice portion control and healthier eating and to exercise more.
For myself, I want to lose those remaining 20 lb or so by eating healthy and being physically active without having to rely on medication for the rest of my life. Research on these medications is still early so we don’t know the long-term effects yet.
As clinicians, I feel it’s okay to be honest with our patients about our own personal struggles to help them understand that they are not alone and that losing weight is a challenge for everyone.
Dr. Swiner is a family physician in Durham, N.C. She reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
With the rising popularity of weight-loss drug injections, I’ve received many questions from patients about the pros, cons, and costs. While Ozempic (semaglutide) is perhaps the best known, it’s technically an agent approved only for type 2 diabetes that has been used off label for obesity. The same substance, semaglutide, is approved for use in obesity, but at a higher dose, under the brand name Wegovy. Alternatives are available, and results will vary depending on the specific agent used and the individual.
Ultimately, I decided to try these new injections for myself. I am not a paid representative for, nor an advocate of, any of these medications; I’m here only to share my personal experience.
In my discussions with patients about weight, I sometimes felt like an imposter. While I was overweight by medical standards, I fortunately had none of the underlying health problems. I wasn’t on medications for blood pressure nor did I have diabetes, but I was counseling people to lose weight and eat better while not always following my own advice.
Since having children and turning 40, my metabolism, like many other women’s, seems to have plummeted. I tried a number of older weight-loss medications, like phentermine and phendimetrazine, under the supervision of medical professionals.
Each time, the efforts worked for a short while, particularly when I followed good portion control and practiced moderate exercise. Once the side effects (that is, tachycardia, palpitations, mood changes, constipation) became intolerable, or I became tired or fearful of being on the medications too long, I’d stop and I would regain some of the weight.
When the newer subcutaneous injectable medications arrived on the scene and I started to talk to my patients about them, I was intrigued by their novel mode of action and seeming benefits.
These medications, glucagonlike peptide–1 (GLP-1) receptor agonists, were first approved for type 2 diabetes, and it soon became apparent that patients were losing significant amounts of weight taking them, so manufacturers conducted further trials in obesity patients without type 2 diabetes.
The first of these, liraglutide, is injected daily and was first approved as Victoza for type 2 diabetes; it later received an additional approval for obesity, in December 2014, as Saxenda.
Semaglutide, another of the new GLP-1 agonists, was first approved for type 2 diabetes as Ozempic but again was found to lead to substantial weight loss, so a subsequent approval of the drug for obesity, as Wegovy, came in June 2021. Semaglutide is injected once a week.
Semaglutide was branded a “game changer” when it was licensed for obesity because the mean weight loss seen in trials was around 15%, more than for any other drug and approaching what could be achieved with bariatric surgery, some doctors said.
These medications work in a different way from the older weight loss drugs, which had focused on the use of amphetamines. The newer medications became very popular because treating obesity helps lower blood glucose, blood pressure, cholesterol, kidney disease risk, and other comorbidities that occur with diabetes. Plus, for most people, there were fewer side effects.
I first tried Saxenda when it arrived on the market, via some samples that our pharmaceutical representative brought, both out of curiosity and to see if it would help me lose the stubborn baby weight. I ended up stopping the daily injections after my second or third week because of nausea and vomiting. I took a break, got a prescription for antinausea medicine, and tried again because it did indeed decrease my appetite. However, when I took my prescription to the pharmacy, my insurance wouldn’t cover it. It happens to doctors, too.
Fast-forward to 2017-2018. The baby weight was still holding on despite lifestyle changes, diet, and exercising. The newer drug classes hit the market, and again we had samples from our reps.
When Ozempic was on backorder, I switched to a low dose of Mounjaro (tirzepatide), a new dual GLP-1 and glucose-dependent insulinotropic polypeptide agonist, approved for type 2 diabetes in May 2022, again using it off label as a weekly injection, as it isn’t currently approved for weight loss. However, it does produce significant weight loss and is awaiting approval for obesity.
With these new medications, I noticed that both my patients and I didn’t complain as much about nausea and vomiting, but I did experience stomach upset, constipation, and acid reflux.
The appetite suppression is effective. It slows down the emptying of the gut so I feel full longer. I’ve lost 30 lb with these weekly injections and would like to lose another 20 lb. I follow a routine of reasonable, portion-controlled eating and moderate exercise (30 minutes of cardiovascular activity at least two to three times a week).
Discontinuing the medications may cause rebound weight gain, especially if I’m no longer following a routine of healthy eating and/or moderate exercise. I deal with minimal constipation by taking stool softeners, and I take antacids for acid reflux.
Here’s what I recommend applying when working with patients who have obesity: First, explain how these medications work. Then conduct a health history to make sure these injections are right for them. Patients with a family history of pancreatic cancer can’t take these medications. You also want to monitor use in patients with a history of hypoglycemia so their blood sugar doesn’t drop too low. It’s also important to make sure your patients are able to afford the medication. My husband takes Ozempic for diabetes, and recently we were told that a refill would cost about $1,500 a month, even with insurance. “Covered” doesn’t necessarily mean affordable.
Take a baseline hemoglobin A1c and repeat it after the patient has been on the medication for 2-3 weeks. Also remind them that they can’t rely solely on the medication but need to practice portion control and healthier eating and to exercise more.
For myself, I want to lose those remaining 20 lb or so by eating healthy and being physically active without having to rely on medication for the rest of my life. Research on these medications is still early so we don’t know the long-term effects yet.
As clinicians, I feel it’s okay to be honest with our patients about our own personal struggles to help them understand that they are not alone and that losing weight is a challenge for everyone.
Dr. Swiner is a family physician in Durham, N.C. She reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
With the rising popularity of weight-loss drug injections, I’ve received many questions from patients about the pros, cons, and costs. While Ozempic (semaglutide) is perhaps the best known, it’s technically an agent approved only for type 2 diabetes that has been used off label for obesity. The same substance, semaglutide, is approved for use in obesity, but at a higher dose, under the brand name Wegovy. Alternatives are available, and results will vary depending on the specific agent used and the individual.
Ultimately, I decided to try these new injections for myself. I am not a paid representative for, nor an advocate of, any of these medications; I’m here only to share my personal experience.
In my discussions with patients about weight, I sometimes felt like an imposter. While I was overweight by medical standards, I fortunately had none of the underlying health problems. I wasn’t on medications for blood pressure nor did I have diabetes, but I was counseling people to lose weight and eat better while not always following my own advice.
Since having children and turning 40, my metabolism, like many other women’s, seems to have plummeted. I tried a number of older weight-loss medications, like phentermine and phendimetrazine, under the supervision of medical professionals.
Each time, the efforts worked for a short while, particularly when I followed good portion control and practiced moderate exercise. Once the side effects (that is, tachycardia, palpitations, mood changes, constipation) became intolerable, or I became tired or fearful of being on the medications too long, I’d stop and I would regain some of the weight.
When the newer subcutaneous injectable medications arrived on the scene and I started to talk to my patients about them, I was intrigued by their novel mode of action and seeming benefits.
These medications, glucagonlike peptide–1 (GLP-1) receptor agonists, were first approved for type 2 diabetes, and it soon became apparent that patients were losing significant amounts of weight taking them, so manufacturers conducted further trials in obesity patients without type 2 diabetes.
The first of these, liraglutide, is injected daily and was first approved as Victoza for type 2 diabetes; it later received an additional approval for obesity, in December 2014, as Saxenda.
Semaglutide, another of the new GLP-1 agonists, was first approved for type 2 diabetes as Ozempic but again was found to lead to substantial weight loss, so a subsequent approval of the drug for obesity, as Wegovy, came in June 2021. Semaglutide is injected once a week.
Semaglutide was branded a “game changer” when it was licensed for obesity because the mean weight loss seen in trials was around 15%, more than for any other drug and approaching what could be achieved with bariatric surgery, some doctors said.
These medications work in a different way from the older weight loss drugs, which had focused on the use of amphetamines. The newer medications became very popular because treating obesity helps lower blood glucose, blood pressure, cholesterol, kidney disease risk, and other comorbidities that occur with diabetes. Plus, for most people, there were fewer side effects.
I first tried Saxenda when it arrived on the market, via some samples that our pharmaceutical representative brought, both out of curiosity and to see if it would help me lose the stubborn baby weight. I ended up stopping the daily injections after my second or third week because of nausea and vomiting. I took a break, got a prescription for antinausea medicine, and tried again because it did indeed decrease my appetite. However, when I took my prescription to the pharmacy, my insurance wouldn’t cover it. It happens to doctors, too.
Fast-forward to 2017-2018. The baby weight was still holding on despite lifestyle changes, diet, and exercising. The newer drug classes hit the market, and again we had samples from our reps.
When Ozempic was on backorder, I switched to a low dose of Mounjaro (tirzepatide), a new dual GLP-1 and glucose-dependent insulinotropic polypeptide agonist, approved for type 2 diabetes in May 2022, again using it off label as a weekly injection, as it isn’t currently approved for weight loss. However, it does produce significant weight loss and is awaiting approval for obesity.
With these new medications, I noticed that both my patients and I didn’t complain as much about nausea and vomiting, but I did experience stomach upset, constipation, and acid reflux.
The appetite suppression is effective. It slows down the emptying of the gut so I feel full longer. I’ve lost 30 lb with these weekly injections and would like to lose another 20 lb. I follow a routine of reasonable, portion-controlled eating and moderate exercise (30 minutes of cardiovascular activity at least two to three times a week).
Discontinuing the medications may cause rebound weight gain, especially if I’m no longer following a routine of healthy eating and/or moderate exercise. I deal with minimal constipation by taking stool softeners, and I take antacids for acid reflux.
Here’s what I recommend applying when working with patients who have obesity: First, explain how these medications work. Then conduct a health history to make sure these injections are right for them. Patients with a family history of pancreatic cancer can’t take these medications. You also want to monitor use in patients with a history of hypoglycemia so their blood sugar doesn’t drop too low. It’s also important to make sure your patients are able to afford the medication. My husband takes Ozempic for diabetes, and recently we were told that a refill would cost about $1,500 a month, even with insurance. “Covered” doesn’t necessarily mean affordable.
Take a baseline hemoglobin A1c and repeat it after the patient has been on the medication for 2-3 weeks. Also remind them that they can’t rely solely on the medication but need to practice portion control and healthier eating and to exercise more.
For myself, I want to lose those remaining 20 lb or so by eating healthy and being physically active without having to rely on medication for the rest of my life. Research on these medications is still early so we don’t know the long-term effects yet.
As clinicians, I feel it’s okay to be honest with our patients about our own personal struggles to help them understand that they are not alone and that losing weight is a challenge for everyone.
Dr. Swiner is a family physician in Durham, N.C. She reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
New documentary highlights human toll of high insulin cost
A new documentary premiering at the 2023 South by Southwest (SXSW) Festival illustrates the human consequences of insulin’s high cost in the United States. Its creators hope that it will help spur action toward overall prescription pricing reform.
Pay or Die: A Documentary is scheduled to premiere March 11. It will be shown twice more during the festival, which runs from March 10 to 19 in Austin, Texas. The documentary was co-created and directed by filmmaker and cinematographer Scott Alexander Ruderman, who has type 1 diabetes, and his partner, producer and journalist Rachael Dyer. One of the executive producers is Sarah Silverman, a comic, actor, producer, and health care reform advocate.
The 90-minute film follows three human stories: A mother and young daughter who both have type 1 diabetes and become homeless after spending their rent money on insulin, a young adult diagnosed during the COVID-19 pandemic, and a mother whose 26-year-old son died from diabetic ketoacidosis (DKA) after his insulin was rationed.
“As an Australian now living in the U.S. and seeing how the health care system works here, especially for people with type 1 diabetes like Scott, and how access to insulin is a life-or-death situation, has been very eye-opening for me. I’m also half Canadian, and both are countries where access to health care is a human right, not a business,” Ms. Dyer said in an interview.
In response to the March 1 announcement from Eli Lilly about its insulin price cut, the film’s team told this news organization: “While we commend Eli Lilly in taking this first step and hope that Novo Nordisk and Sanofi [the two other major insulin manufacturers] follow suit, it is important to remember that the key issue is not about these companies voluntarily slashing prices; it’s about changing laws so the insulin manufacturers do not have the ability to raise the prices again.
“This is the life-or-death issue that we focus on in our documentary Pay or Die. It’s also important to note that insulin is just one of the many expensive prescription drugs in the U.S., which is why we need to call for reform. Affordable medication needs to be a basic human right within reach for all Americans.”
Physician perspective: Good news on insulin, but broader issues
The film features four physicians. One, Mayo Clinic oncologist/hematologist S. Vincent Rajkumar, MD, has spoken and published widely on insulin prices specifically and U.S. drug costs more broadly.
The other three are Joslin Clinic endocrinologist Elizabeth Halprin, MD, Massachusetts General Hospital internist Leigh Simmons, MD, and New York University physician and essayist Danielle Ofri, MD, PhD.
In an interview after the Lilly announcement, Dr. Rajkumar said, “I think this is very, very good news for patients. ... The fact that they’re doing it means they’re listening to us and listening to patients, which is good. And I do hope that other insulin manufacturers do the same shortly.”
However, he added, “for prescription drug prices and particularly cancer drug prices, there’s more reform that’s needed, and that’s at the policy level. ... The goal of the film was to use insulin to highlight the prescription drug price problem in the U.S.”
‘Then life changed’
The filmmaker, Mr. Ruderman, was diagnosed at age 19, during his freshman year in college. He spent several days hospitalized with DKA, and “then life changed,” he said in an interview. He went into photography first and later filmmaking, always with the uneasy knowledge that he could lose access to insulin at any time.
The impetus for the film came after he and Ms. Dyer walked into a pharmacy while visiting Canada in 2018 and discovered how much cheaper insulin was compared to the United States – roughly $20 per vial, compared to $300 in the U.S.
“When Rachael [Dyer] and I came back to the U.S., we were actually quite shocked about how many people are struggling to afford their medication ... the uninsured, those aging off their parents’ health insurance. So that was really the kickoff to us going into the field for the last 4 years making this documentary.”
As a freelancer, Mr. Ruderman has been personally paying for expensive “premium” health insurance that covers the pump and glucose monitors he uses. He buys insulin overseas as often as possible.
“Fortunately, I haven’t been in a situation where I’ve had to ration my insulin, but the fear is instilled in me. What if there’s a month when I can’t afford it? What am I going to do?” (Note: The writer of this article is in the same situation, which could be alleviated by Lilly’s action.)
Timing is everything
To be sure, even before Lilly’s announcement, some progress had been made since work on the film began.
The issue of insulin pricing has received wide media attention. More than 20 states have passed copay caps on insulin, and a new law capping the cost of insulin for Medicare beneficiaries at $35/month went into effect in January 2023. President Biden mentioned insulin during his State of the Union address, and Georgia Senator Raphael Warnock made the issue a centerpiece of his campaign.
But there have also been losses, including the failure thus far to pass a nationwide copay cap.
These recent developments make this a good time for the film’s debut, producer Yael Melamede said in an interview. “There’s a lot happening in the space, but also a lot of incredible disappointments along the way, so we are really interested in getting this film out now.”
Ms. Melamede, who owns a film production company, said, “I’ve done a lot of films that have some issue advocacy side to them. I love this film because it’s grounded in the stories of real people. ... We feel this is a perfect catalyst to keep the energy going and for people to say this is super-important and not get distracted.”
While the film doesn’t advocate for specific policies, there is a “call to action” at the end that points viewers to resources on the website for writing to their members of Congress along with additional ways to become personally involved.
Ms. Dyer told this news organization, “This film is not only focusing on type 1 diabetes. That is obviously the crux of the issue, but it is a broader health care message for everyone wanting to make a change for health care in this country, the richest country in the world.”
At SXSW, Pay or Die will be competing with seven other films in the documentary feature competition, and it is eligible to win other awards.
Several other activities at the festival will address the topics of diabetes and U.S. health care costs, including a panel discussion titled Crushing: The Burden of Diabetes on Patients, featuring musician and actor Nick Jonas, who has type 1 diabetes, and a representative from the continuous glucose monitor manufacturer Dexcom.
Another panel, Young and Uninsured: Pay or Die, will include Dr. Rajkumar, Mr. Ruderman, Texas Representative James Talarico, who is advancing an insulin cap bill in that state, and Nicole Smith-Holt, the Minnesota mother of the young man who died because he couldn’t afford his insulin.
Mr. Ruderman, Ms. Dyer, Ms. Melamede, and Dr. Rajkumar have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
A new documentary premiering at the 2023 South by Southwest (SXSW) Festival illustrates the human consequences of insulin’s high cost in the United States. Its creators hope that it will help spur action toward overall prescription pricing reform.
Pay or Die: A Documentary is scheduled to premiere March 11. It will be shown twice more during the festival, which runs from March 10 to 19 in Austin, Texas. The documentary was co-created and directed by filmmaker and cinematographer Scott Alexander Ruderman, who has type 1 diabetes, and his partner, producer and journalist Rachael Dyer. One of the executive producers is Sarah Silverman, a comic, actor, producer, and health care reform advocate.
The 90-minute film follows three human stories: A mother and young daughter who both have type 1 diabetes and become homeless after spending their rent money on insulin, a young adult diagnosed during the COVID-19 pandemic, and a mother whose 26-year-old son died from diabetic ketoacidosis (DKA) after his insulin was rationed.
“As an Australian now living in the U.S. and seeing how the health care system works here, especially for people with type 1 diabetes like Scott, and how access to insulin is a life-or-death situation, has been very eye-opening for me. I’m also half Canadian, and both are countries where access to health care is a human right, not a business,” Ms. Dyer said in an interview.
In response to the March 1 announcement from Eli Lilly about its insulin price cut, the film’s team told this news organization: “While we commend Eli Lilly in taking this first step and hope that Novo Nordisk and Sanofi [the two other major insulin manufacturers] follow suit, it is important to remember that the key issue is not about these companies voluntarily slashing prices; it’s about changing laws so the insulin manufacturers do not have the ability to raise the prices again.
“This is the life-or-death issue that we focus on in our documentary Pay or Die. It’s also important to note that insulin is just one of the many expensive prescription drugs in the U.S., which is why we need to call for reform. Affordable medication needs to be a basic human right within reach for all Americans.”
Physician perspective: Good news on insulin, but broader issues
The film features four physicians. One, Mayo Clinic oncologist/hematologist S. Vincent Rajkumar, MD, has spoken and published widely on insulin prices specifically and U.S. drug costs more broadly.
The other three are Joslin Clinic endocrinologist Elizabeth Halprin, MD, Massachusetts General Hospital internist Leigh Simmons, MD, and New York University physician and essayist Danielle Ofri, MD, PhD.
In an interview after the Lilly announcement, Dr. Rajkumar said, “I think this is very, very good news for patients. ... The fact that they’re doing it means they’re listening to us and listening to patients, which is good. And I do hope that other insulin manufacturers do the same shortly.”
However, he added, “for prescription drug prices and particularly cancer drug prices, there’s more reform that’s needed, and that’s at the policy level. ... The goal of the film was to use insulin to highlight the prescription drug price problem in the U.S.”
‘Then life changed’
The filmmaker, Mr. Ruderman, was diagnosed at age 19, during his freshman year in college. He spent several days hospitalized with DKA, and “then life changed,” he said in an interview. He went into photography first and later filmmaking, always with the uneasy knowledge that he could lose access to insulin at any time.
The impetus for the film came after he and Ms. Dyer walked into a pharmacy while visiting Canada in 2018 and discovered how much cheaper insulin was compared to the United States – roughly $20 per vial, compared to $300 in the U.S.
“When Rachael [Dyer] and I came back to the U.S., we were actually quite shocked about how many people are struggling to afford their medication ... the uninsured, those aging off their parents’ health insurance. So that was really the kickoff to us going into the field for the last 4 years making this documentary.”
As a freelancer, Mr. Ruderman has been personally paying for expensive “premium” health insurance that covers the pump and glucose monitors he uses. He buys insulin overseas as often as possible.
“Fortunately, I haven’t been in a situation where I’ve had to ration my insulin, but the fear is instilled in me. What if there’s a month when I can’t afford it? What am I going to do?” (Note: The writer of this article is in the same situation, which could be alleviated by Lilly’s action.)
Timing is everything
To be sure, even before Lilly’s announcement, some progress had been made since work on the film began.
The issue of insulin pricing has received wide media attention. More than 20 states have passed copay caps on insulin, and a new law capping the cost of insulin for Medicare beneficiaries at $35/month went into effect in January 2023. President Biden mentioned insulin during his State of the Union address, and Georgia Senator Raphael Warnock made the issue a centerpiece of his campaign.
But there have also been losses, including the failure thus far to pass a nationwide copay cap.
These recent developments make this a good time for the film’s debut, producer Yael Melamede said in an interview. “There’s a lot happening in the space, but also a lot of incredible disappointments along the way, so we are really interested in getting this film out now.”
Ms. Melamede, who owns a film production company, said, “I’ve done a lot of films that have some issue advocacy side to them. I love this film because it’s grounded in the stories of real people. ... We feel this is a perfect catalyst to keep the energy going and for people to say this is super-important and not get distracted.”
While the film doesn’t advocate for specific policies, there is a “call to action” at the end that points viewers to resources on the website for writing to their members of Congress along with additional ways to become personally involved.
Ms. Dyer told this news organization, “This film is not only focusing on type 1 diabetes. That is obviously the crux of the issue, but it is a broader health care message for everyone wanting to make a change for health care in this country, the richest country in the world.”
At SXSW, Pay or Die will be competing with seven other films in the documentary feature competition, and it is eligible to win other awards.
Several other activities at the festival will address the topics of diabetes and U.S. health care costs, including a panel discussion titled Crushing: The Burden of Diabetes on Patients, featuring musician and actor Nick Jonas, who has type 1 diabetes, and a representative from the continuous glucose monitor manufacturer Dexcom.
Another panel, Young and Uninsured: Pay or Die, will include Dr. Rajkumar, Mr. Ruderman, Texas Representative James Talarico, who is advancing an insulin cap bill in that state, and Nicole Smith-Holt, the Minnesota mother of the young man who died because he couldn’t afford his insulin.
Mr. Ruderman, Ms. Dyer, Ms. Melamede, and Dr. Rajkumar have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
A new documentary premiering at the 2023 South by Southwest (SXSW) Festival illustrates the human consequences of insulin’s high cost in the United States. Its creators hope that it will help spur action toward overall prescription pricing reform.
Pay or Die: A Documentary is scheduled to premiere March 11. It will be shown twice more during the festival, which runs from March 10 to 19 in Austin, Texas. The documentary was co-created and directed by filmmaker and cinematographer Scott Alexander Ruderman, who has type 1 diabetes, and his partner, producer and journalist Rachael Dyer. One of the executive producers is Sarah Silverman, a comic, actor, producer, and health care reform advocate.
The 90-minute film follows three human stories: A mother and young daughter who both have type 1 diabetes and become homeless after spending their rent money on insulin, a young adult diagnosed during the COVID-19 pandemic, and a mother whose 26-year-old son died from diabetic ketoacidosis (DKA) after his insulin was rationed.
“As an Australian now living in the U.S. and seeing how the health care system works here, especially for people with type 1 diabetes like Scott, and how access to insulin is a life-or-death situation, has been very eye-opening for me. I’m also half Canadian, and both are countries where access to health care is a human right, not a business,” Ms. Dyer said in an interview.
In response to the March 1 announcement from Eli Lilly about its insulin price cut, the film’s team told this news organization: “While we commend Eli Lilly in taking this first step and hope that Novo Nordisk and Sanofi [the two other major insulin manufacturers] follow suit, it is important to remember that the key issue is not about these companies voluntarily slashing prices; it’s about changing laws so the insulin manufacturers do not have the ability to raise the prices again.
“This is the life-or-death issue that we focus on in our documentary Pay or Die. It’s also important to note that insulin is just one of the many expensive prescription drugs in the U.S., which is why we need to call for reform. Affordable medication needs to be a basic human right within reach for all Americans.”
Physician perspective: Good news on insulin, but broader issues
The film features four physicians. One, Mayo Clinic oncologist/hematologist S. Vincent Rajkumar, MD, has spoken and published widely on insulin prices specifically and U.S. drug costs more broadly.
The other three are Joslin Clinic endocrinologist Elizabeth Halprin, MD, Massachusetts General Hospital internist Leigh Simmons, MD, and New York University physician and essayist Danielle Ofri, MD, PhD.
In an interview after the Lilly announcement, Dr. Rajkumar said, “I think this is very, very good news for patients. ... The fact that they’re doing it means they’re listening to us and listening to patients, which is good. And I do hope that other insulin manufacturers do the same shortly.”
However, he added, “for prescription drug prices and particularly cancer drug prices, there’s more reform that’s needed, and that’s at the policy level. ... The goal of the film was to use insulin to highlight the prescription drug price problem in the U.S.”
‘Then life changed’
The filmmaker, Mr. Ruderman, was diagnosed at age 19, during his freshman year in college. He spent several days hospitalized with DKA, and “then life changed,” he said in an interview. He went into photography first and later filmmaking, always with the uneasy knowledge that he could lose access to insulin at any time.
The impetus for the film came after he and Ms. Dyer walked into a pharmacy while visiting Canada in 2018 and discovered how much cheaper insulin was compared to the United States – roughly $20 per vial, compared to $300 in the U.S.
“When Rachael [Dyer] and I came back to the U.S., we were actually quite shocked about how many people are struggling to afford their medication ... the uninsured, those aging off their parents’ health insurance. So that was really the kickoff to us going into the field for the last 4 years making this documentary.”
As a freelancer, Mr. Ruderman has been personally paying for expensive “premium” health insurance that covers the pump and glucose monitors he uses. He buys insulin overseas as often as possible.
“Fortunately, I haven’t been in a situation where I’ve had to ration my insulin, but the fear is instilled in me. What if there’s a month when I can’t afford it? What am I going to do?” (Note: The writer of this article is in the same situation, which could be alleviated by Lilly’s action.)
Timing is everything
To be sure, even before Lilly’s announcement, some progress had been made since work on the film began.
The issue of insulin pricing has received wide media attention. More than 20 states have passed copay caps on insulin, and a new law capping the cost of insulin for Medicare beneficiaries at $35/month went into effect in January 2023. President Biden mentioned insulin during his State of the Union address, and Georgia Senator Raphael Warnock made the issue a centerpiece of his campaign.
But there have also been losses, including the failure thus far to pass a nationwide copay cap.
These recent developments make this a good time for the film’s debut, producer Yael Melamede said in an interview. “There’s a lot happening in the space, but also a lot of incredible disappointments along the way, so we are really interested in getting this film out now.”
Ms. Melamede, who owns a film production company, said, “I’ve done a lot of films that have some issue advocacy side to them. I love this film because it’s grounded in the stories of real people. ... We feel this is a perfect catalyst to keep the energy going and for people to say this is super-important and not get distracted.”
While the film doesn’t advocate for specific policies, there is a “call to action” at the end that points viewers to resources on the website for writing to their members of Congress along with additional ways to become personally involved.
Ms. Dyer told this news organization, “This film is not only focusing on type 1 diabetes. That is obviously the crux of the issue, but it is a broader health care message for everyone wanting to make a change for health care in this country, the richest country in the world.”
At SXSW, Pay or Die will be competing with seven other films in the documentary feature competition, and it is eligible to win other awards.
Several other activities at the festival will address the topics of diabetes and U.S. health care costs, including a panel discussion titled Crushing: The Burden of Diabetes on Patients, featuring musician and actor Nick Jonas, who has type 1 diabetes, and a representative from the continuous glucose monitor manufacturer Dexcom.
Another panel, Young and Uninsured: Pay or Die, will include Dr. Rajkumar, Mr. Ruderman, Texas Representative James Talarico, who is advancing an insulin cap bill in that state, and Nicole Smith-Holt, the Minnesota mother of the young man who died because he couldn’t afford his insulin.
Mr. Ruderman, Ms. Dyer, Ms. Melamede, and Dr. Rajkumar have disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Causal link found between childhood obesity and adult-onset diabetes
Childhood obesity is a risk factor for four of the five subtypes of adult-onset diabetes, emphasizing the importance of childhood weight control, according to a collaborative study from the Karolinska Institutet in Stockholm, the University of Bristol (England), and Sun Yat-Sen University in China.
“Our finding is that children who have a bigger body size than the average have increased risks of developing almost all subtypes of adult-onset diabetes, except for the mild age-related subtype,” lead author Yuxia Wei, a PhD student from the Karolinska Institutet, said in an interview. “This tells us that it is important to prevent overweight/obesity in children and important for pediatric patients to lose weight if they have already been overweight/obese,” she added, while acknowledging that the study did not examine whether childhood weight loss would prevent adult-onset diabetes.
The study, published online in Diabetologia, used Mendelian randomization (MR), with data from genome-wide association studies (GWAS) of childhood obesity and the five subtypes of adult-onset diabetes: latent autoimmune diabetes in adults (LADA, proxy for severe autoimmune diabetes), severe insulin-deficient diabetes (SIDD), severe insulin-resistant diabetes (SIRD), mild obesity-related diabetes (MOD), and mild age-related diabetes (MARD). MR is “a rather new but commonly used and established technique that uses genetic information to study the causal link between an environmental risk factor and a disease, while accounting for the influence of other risk factors,” Ms. Wei explained.
To identify genetic variations associated with obesity, the study used statistics from a GWAS of 453,169 Europeans who self-reported body size at age 10 years in the UK Biobank study. After adjustment for sex, age at baseline, type of genotyping array, and month of birth, they identified 295 independent single nucleotide polymorphisms (SNPs) for childhood body size.
The researchers also used data from two GWAS of European adults with newly diagnosed diabetes, or without diabetes, to identify SNPs in 8,581 individuals with LADA, 3,937 with SIDD, 3,874 with SIRD, 4,118 with MOD, and 5,605 with MARD.
They then used MR to assess the association of genetically predicted childhood body size with the different diabetes subtypes.
The analysis showed that, with the exception of MARD, all other adult-onset diabetes subtypes were causally associated with childhood obesity, with odds ratio of 1.62 for LADA, 2.11 for SIDD, 2.76 for SIRD, and 7.30 for MOD. However, a genetic correlation between childhood obesity and adult-onset diabetes was found only for MOD, and no other subtypes. “The weak genetic correlation between childhood obesity and adult diabetes indicates that the genes promoting childhood adiposity are largely distinct from those promoting diabetes during adulthood,” noted the authors.
The findings indicate that “childhood body size and MOD may share some genetic mutations,” added Ms. Wei. “That is to say, some genes may affect childhood body size and MOD simultaneously.” But the shared genes do demonstrate the causal effect of childhood obesity on MOD, she explained. The causal effect is demonstrated through the MR analysis.
Additionally, they noted that while “the link between childhood body size and SIRD is expected, given the adverse effects of adiposity on insulin sensitivity ... the smaller OR for SIRD than for MOD suggests that non–obesity-related and/or nongenetic effects may be the main factors underlying the development of SIRD.” Asked for her theory on how childhood body size could affect diabetes subtypes characterized by autoimmunity (LADA) or impaired insulin secretion (SIDD), Ms. Wei speculated that “excess fat around the pancreas can affect insulin secretion and that impaired insulin secretion is also an important problem for LADA.”
Another theory is that it might be “metabolic memory,” suggested Jordi Merino, PhD, of the University of Copenhagen and Harvard University, Boston, who was not involved in the research. “Being exposed to obesity during childhood will tell the body to produce more insulin/aberrant immunity responses later in life.”
Dr. Merino said that, overall, the study’s findings “highlight the long and lasting effect of early-life adiposity and metabolic alterations on different forms of adult-onset diabetes,” adding that this is the first evidence “that childhood adiposity is not only linked to the more traditional diabetes subtype consequence of increased insulin resistance but also subtypes driven by autoimmunity or impaired insulin secretion.” He explained that genetics is “only part of the story” driving increased diabetes risk and “we do not know much about other factors interacting with genetics, but the results from this Mendelian randomization analysis suggest that childhood obesity is a causal factor for all adult-onset diabetes subtypes. Identifying causal factors instead of associative factors is critical to implement more targeted preventive and therapeutic strategies.”
He acknowledged, “There is a long path for these results to be eventually implemented in clinical practice, but they can support early weight control strategies for preventing different diabetes subtypes.”
The study was supported by the Swedish Research Council, Research Council for Health, Working Life and Welfare, and Novo Nordisk Foundation. Ms. Wei received a scholarship from the China Scholarship Council. One coauthor is an employee of GlaxoSmithKline. Dr. Merino reported no conflicts of interest.
Childhood obesity is a risk factor for four of the five subtypes of adult-onset diabetes, emphasizing the importance of childhood weight control, according to a collaborative study from the Karolinska Institutet in Stockholm, the University of Bristol (England), and Sun Yat-Sen University in China.
“Our finding is that children who have a bigger body size than the average have increased risks of developing almost all subtypes of adult-onset diabetes, except for the mild age-related subtype,” lead author Yuxia Wei, a PhD student from the Karolinska Institutet, said in an interview. “This tells us that it is important to prevent overweight/obesity in children and important for pediatric patients to lose weight if they have already been overweight/obese,” she added, while acknowledging that the study did not examine whether childhood weight loss would prevent adult-onset diabetes.
The study, published online in Diabetologia, used Mendelian randomization (MR), with data from genome-wide association studies (GWAS) of childhood obesity and the five subtypes of adult-onset diabetes: latent autoimmune diabetes in adults (LADA, proxy for severe autoimmune diabetes), severe insulin-deficient diabetes (SIDD), severe insulin-resistant diabetes (SIRD), mild obesity-related diabetes (MOD), and mild age-related diabetes (MARD). MR is “a rather new but commonly used and established technique that uses genetic information to study the causal link between an environmental risk factor and a disease, while accounting for the influence of other risk factors,” Ms. Wei explained.
To identify genetic variations associated with obesity, the study used statistics from a GWAS of 453,169 Europeans who self-reported body size at age 10 years in the UK Biobank study. After adjustment for sex, age at baseline, type of genotyping array, and month of birth, they identified 295 independent single nucleotide polymorphisms (SNPs) for childhood body size.
The researchers also used data from two GWAS of European adults with newly diagnosed diabetes, or without diabetes, to identify SNPs in 8,581 individuals with LADA, 3,937 with SIDD, 3,874 with SIRD, 4,118 with MOD, and 5,605 with MARD.
They then used MR to assess the association of genetically predicted childhood body size with the different diabetes subtypes.
The analysis showed that, with the exception of MARD, all other adult-onset diabetes subtypes were causally associated with childhood obesity, with odds ratio of 1.62 for LADA, 2.11 for SIDD, 2.76 for SIRD, and 7.30 for MOD. However, a genetic correlation between childhood obesity and adult-onset diabetes was found only for MOD, and no other subtypes. “The weak genetic correlation between childhood obesity and adult diabetes indicates that the genes promoting childhood adiposity are largely distinct from those promoting diabetes during adulthood,” noted the authors.
The findings indicate that “childhood body size and MOD may share some genetic mutations,” added Ms. Wei. “That is to say, some genes may affect childhood body size and MOD simultaneously.” But the shared genes do demonstrate the causal effect of childhood obesity on MOD, she explained. The causal effect is demonstrated through the MR analysis.
Additionally, they noted that while “the link between childhood body size and SIRD is expected, given the adverse effects of adiposity on insulin sensitivity ... the smaller OR for SIRD than for MOD suggests that non–obesity-related and/or nongenetic effects may be the main factors underlying the development of SIRD.” Asked for her theory on how childhood body size could affect diabetes subtypes characterized by autoimmunity (LADA) or impaired insulin secretion (SIDD), Ms. Wei speculated that “excess fat around the pancreas can affect insulin secretion and that impaired insulin secretion is also an important problem for LADA.”
Another theory is that it might be “metabolic memory,” suggested Jordi Merino, PhD, of the University of Copenhagen and Harvard University, Boston, who was not involved in the research. “Being exposed to obesity during childhood will tell the body to produce more insulin/aberrant immunity responses later in life.”
Dr. Merino said that, overall, the study’s findings “highlight the long and lasting effect of early-life adiposity and metabolic alterations on different forms of adult-onset diabetes,” adding that this is the first evidence “that childhood adiposity is not only linked to the more traditional diabetes subtype consequence of increased insulin resistance but also subtypes driven by autoimmunity or impaired insulin secretion.” He explained that genetics is “only part of the story” driving increased diabetes risk and “we do not know much about other factors interacting with genetics, but the results from this Mendelian randomization analysis suggest that childhood obesity is a causal factor for all adult-onset diabetes subtypes. Identifying causal factors instead of associative factors is critical to implement more targeted preventive and therapeutic strategies.”
He acknowledged, “There is a long path for these results to be eventually implemented in clinical practice, but they can support early weight control strategies for preventing different diabetes subtypes.”
The study was supported by the Swedish Research Council, Research Council for Health, Working Life and Welfare, and Novo Nordisk Foundation. Ms. Wei received a scholarship from the China Scholarship Council. One coauthor is an employee of GlaxoSmithKline. Dr. Merino reported no conflicts of interest.
Childhood obesity is a risk factor for four of the five subtypes of adult-onset diabetes, emphasizing the importance of childhood weight control, according to a collaborative study from the Karolinska Institutet in Stockholm, the University of Bristol (England), and Sun Yat-Sen University in China.
“Our finding is that children who have a bigger body size than the average have increased risks of developing almost all subtypes of adult-onset diabetes, except for the mild age-related subtype,” lead author Yuxia Wei, a PhD student from the Karolinska Institutet, said in an interview. “This tells us that it is important to prevent overweight/obesity in children and important for pediatric patients to lose weight if they have already been overweight/obese,” she added, while acknowledging that the study did not examine whether childhood weight loss would prevent adult-onset diabetes.
The study, published online in Diabetologia, used Mendelian randomization (MR), with data from genome-wide association studies (GWAS) of childhood obesity and the five subtypes of adult-onset diabetes: latent autoimmune diabetes in adults (LADA, proxy for severe autoimmune diabetes), severe insulin-deficient diabetes (SIDD), severe insulin-resistant diabetes (SIRD), mild obesity-related diabetes (MOD), and mild age-related diabetes (MARD). MR is “a rather new but commonly used and established technique that uses genetic information to study the causal link between an environmental risk factor and a disease, while accounting for the influence of other risk factors,” Ms. Wei explained.
To identify genetic variations associated with obesity, the study used statistics from a GWAS of 453,169 Europeans who self-reported body size at age 10 years in the UK Biobank study. After adjustment for sex, age at baseline, type of genotyping array, and month of birth, they identified 295 independent single nucleotide polymorphisms (SNPs) for childhood body size.
The researchers also used data from two GWAS of European adults with newly diagnosed diabetes, or without diabetes, to identify SNPs in 8,581 individuals with LADA, 3,937 with SIDD, 3,874 with SIRD, 4,118 with MOD, and 5,605 with MARD.
They then used MR to assess the association of genetically predicted childhood body size with the different diabetes subtypes.
The analysis showed that, with the exception of MARD, all other adult-onset diabetes subtypes were causally associated with childhood obesity, with odds ratio of 1.62 for LADA, 2.11 for SIDD, 2.76 for SIRD, and 7.30 for MOD. However, a genetic correlation between childhood obesity and adult-onset diabetes was found only for MOD, and no other subtypes. “The weak genetic correlation between childhood obesity and adult diabetes indicates that the genes promoting childhood adiposity are largely distinct from those promoting diabetes during adulthood,” noted the authors.
The findings indicate that “childhood body size and MOD may share some genetic mutations,” added Ms. Wei. “That is to say, some genes may affect childhood body size and MOD simultaneously.” But the shared genes do demonstrate the causal effect of childhood obesity on MOD, she explained. The causal effect is demonstrated through the MR analysis.
Additionally, they noted that while “the link between childhood body size and SIRD is expected, given the adverse effects of adiposity on insulin sensitivity ... the smaller OR for SIRD than for MOD suggests that non–obesity-related and/or nongenetic effects may be the main factors underlying the development of SIRD.” Asked for her theory on how childhood body size could affect diabetes subtypes characterized by autoimmunity (LADA) or impaired insulin secretion (SIDD), Ms. Wei speculated that “excess fat around the pancreas can affect insulin secretion and that impaired insulin secretion is also an important problem for LADA.”
Another theory is that it might be “metabolic memory,” suggested Jordi Merino, PhD, of the University of Copenhagen and Harvard University, Boston, who was not involved in the research. “Being exposed to obesity during childhood will tell the body to produce more insulin/aberrant immunity responses later in life.”
Dr. Merino said that, overall, the study’s findings “highlight the long and lasting effect of early-life adiposity and metabolic alterations on different forms of adult-onset diabetes,” adding that this is the first evidence “that childhood adiposity is not only linked to the more traditional diabetes subtype consequence of increased insulin resistance but also subtypes driven by autoimmunity or impaired insulin secretion.” He explained that genetics is “only part of the story” driving increased diabetes risk and “we do not know much about other factors interacting with genetics, but the results from this Mendelian randomization analysis suggest that childhood obesity is a causal factor for all adult-onset diabetes subtypes. Identifying causal factors instead of associative factors is critical to implement more targeted preventive and therapeutic strategies.”
He acknowledged, “There is a long path for these results to be eventually implemented in clinical practice, but they can support early weight control strategies for preventing different diabetes subtypes.”
The study was supported by the Swedish Research Council, Research Council for Health, Working Life and Welfare, and Novo Nordisk Foundation. Ms. Wei received a scholarship from the China Scholarship Council. One coauthor is an employee of GlaxoSmithKline. Dr. Merino reported no conflicts of interest.
FROM DIABETOLOGIA
We have seen the future of healthy muffins, and its name is Roselle
Get ‘em while they’re hot … for your health
Today on the Eating Channel, it’s a very special episode of “Much Ado About Muffin.”
The muffin. For some of us, it’s a good way to pretend we’re not having dessert for breakfast. A bran muffin can be loaded with calcium and fiber, and our beloved blueberry is full of yummy antioxidants and vitamins. Definitely not dessert.
Well, the muffin denial can stop there because there’s a new flavor on the scene, and research suggests it may actually be healthy. (Disclaimer: Muffin may not be considered healthy in Norway.) This new muffin has a name, Roselle, that comes from the calyx extract used in it, which is found in the Hibiscus sabdariffa plant of the same name.
Now, when it comes to new foods, especially ones that are supposed to be healthy, the No. 1 criteria is the same: It has to taste good. Researchers at the Norwegian University of Science and Technology and Amity University in India agreed, but they also set out to make it nutritionally valuable and give it a long shelf life without the addition of preservatives.
Sounds like a tall order, but they figured it out.
Not only is it tasty, but the properties of it could rival your morning multivitamin. Hibiscus extract has huge amounts of antioxidants, like phenolics, which are believed to help prevent cell membrane damage. Foods like vegetables, flax seed, and whole grains also have these antioxidants, but why not just have a Roselle muffin instead? You also get a dose of ascorbic acid without the glass of OJ in the morning.
The ascorbic acid, however, is not there just to help you. It also helps to check the researcher’s third box, shelf life. These naturally rosy-colored pastries will stay mold-free for 6 days without refrigeration at room temperature and without added preservatives.
Our guess, though, is they won’t be on the kitchen counter long enough to find out.
A sobering proposition
If Hollywood is to be believed, there’s no amount of drunkenness that can’t be cured with a cup of coffee or a stern slap in the face. Unfortunately, here in the real world the only thing that can make you less drunk is time. Maybe next time you’ll stop after that seventh Manhattan.
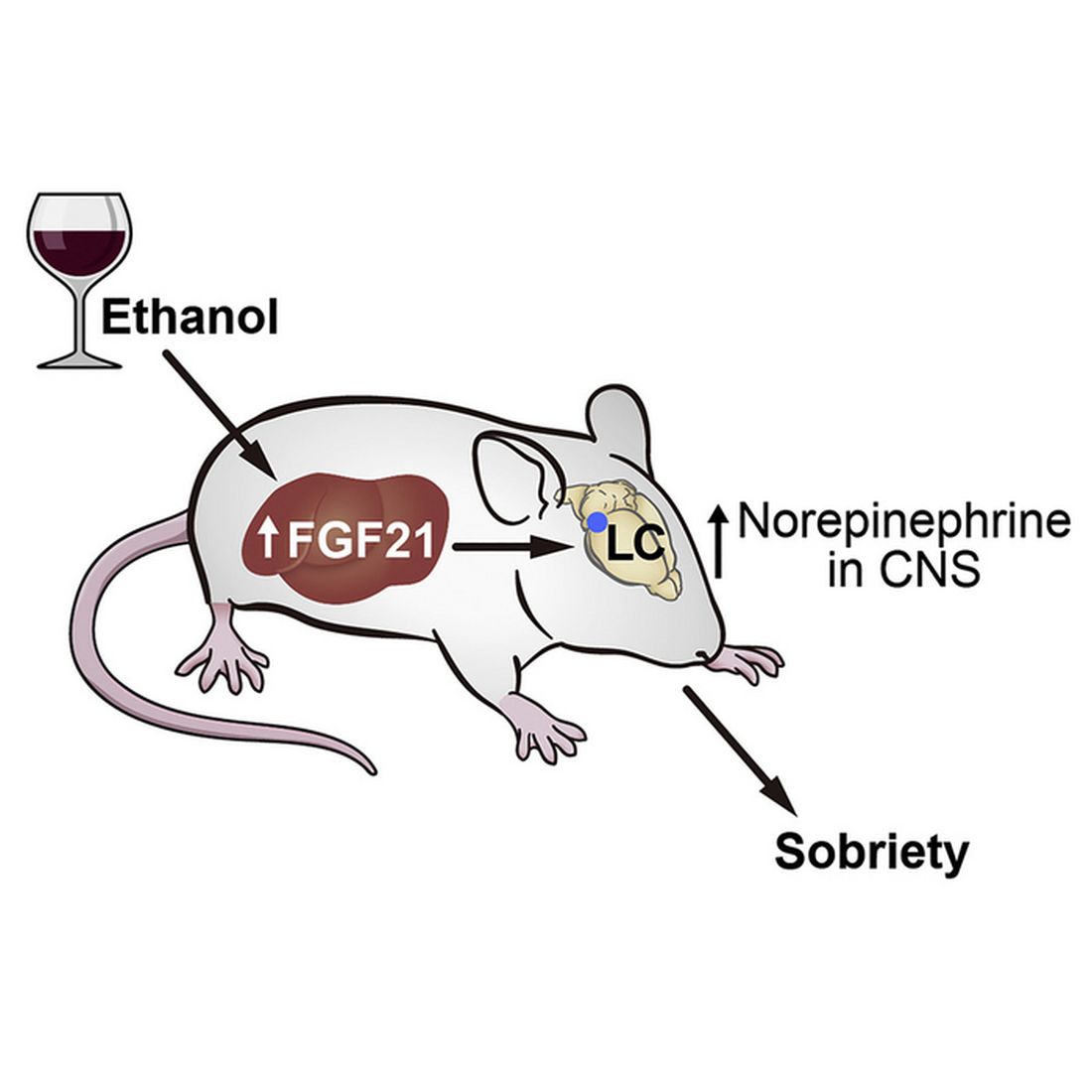
But what if we could beat time? What if there’s an actual sobriety drug out there?
Say hello to fibroblast growth factor 21. Although the liver already does good work filtering out what is essentially poison, it then goes the extra mile and produces fibroblast growth factor 21 (or, as her friends call her, FGF21), a hormone that suppresses the desire to drink, makes you desire water, and protects the liver all at the same time.
Now, FGF21 in its current role is great, but if you’ve ever seen or been a drunk person before, you’ve experienced the lack of interest in listening to reason, especially when it comes from within our own bodies. Who are you to tell us what to do, body? You’re not the boss of us! So a group of scientists decided to push the limits of FGF21. Could it do more than it already does?
First off, they genetically altered a group of mice so that they didn’t produce FGF21 on their own. Then they got them drunk. We’re going to assume they built a scale model of the bar from Cheers and had the mice filter in through the front door as they served their subjects beer out of tiny little glasses.
Once the mice were nice and liquored up, some were given a treatment of FGF21 while others were given a placebo. Lo and behold, the mice given FGF21 recovered about 50% faster than those that received the control treatment. Not exactly instant, but 50% is nothing to sniff at.
Before you bring your FGF21 supplement to the bar, though, this research only applies to mice. We don’t know if it works in people. And make sure you stick to booze. If your choice of intoxication is a bit more exotic, FGF21 isn’t going to do anything for you. Yes, the scientists tried. Yes, those mice are living a very interesting life. And yes, we are jealous of drugged-up lab mice.
Supersize your imagination, shrink your snacks
Have you ever heard of the meal-recall effect? Did you know that, in England, a biscuit is really a cookie? Did you also know that the magazine Bon Appétit is not the same as the peer-reviewed journal Appetite? We do … now.

The meal-recall effect is the subsequent reduction in snacking that comes from remembering a recent meal. It was used to great effect in a recent study conducted at the University of Cambridge, which is in England, where they feed their experimental humans cookies but, for some reason, call them biscuits.
For the first part of the study, the participants were invited to dine at Che Laboratory, where they “were given a microwave ready meal of rice and sauce and a cup of water,” according to a statement from the university. As our Uncle Ernie would say, “Gourmet all the way.”
The test subjects were instructed not to eat anything for 3 hours and “then invited back to the lab to perform imagination tasks.” Those who did come back were randomly divided into five different groups, each with a different task:
- Imagine moving their recent lunch at the lab around a plate.
- Recall eating their recent lunch in detail.
- Imagine that the lunch was twice as big and filling as it really was.
- Look at a photograph of spaghetti hoops in tomato sauce and write a description of it before imagining moving the food around a plate.
- Look at a photo of paper clips and rubber bands and imagine moving them around.
Now, at last, we get to the biscuits/cookies, which were the subject of a taste test that “was simply a rouse for covertly assessing snacking,” the investigators explained. As part of that test, participants were told they could eat as many biscuits as they wanted.
When the tables were cleared and the leftovers examined, the group that imagined spaghetti hoops had eaten the most biscuits (75.9 g), followed by the group that imagined paper clips (75.5 g), the moving-their-lunch-around-the-plate group (72.0 g), and the group that relived eating their lunch (70.0 g).
In a victory for the meal-recall effect, the people who imagined their meal being twice as big ate the fewest biscuits (51.1 g). “Your mind can be more powerful than your stomach in dictating how much you eat,” lead author Joanna Szypula, PhD, said in the university statement.
Oh! One more thing. The study appeared in Appetite, which is a peer-reviewed journal, not in Bon Appétit, which is not a peer-reviewed journal. Thanks to the fine folks at both publications for pointing that out to us.
Get ‘em while they’re hot … for your health
Today on the Eating Channel, it’s a very special episode of “Much Ado About Muffin.”
The muffin. For some of us, it’s a good way to pretend we’re not having dessert for breakfast. A bran muffin can be loaded with calcium and fiber, and our beloved blueberry is full of yummy antioxidants and vitamins. Definitely not dessert.
Well, the muffin denial can stop there because there’s a new flavor on the scene, and research suggests it may actually be healthy. (Disclaimer: Muffin may not be considered healthy in Norway.) This new muffin has a name, Roselle, that comes from the calyx extract used in it, which is found in the Hibiscus sabdariffa plant of the same name.
Now, when it comes to new foods, especially ones that are supposed to be healthy, the No. 1 criteria is the same: It has to taste good. Researchers at the Norwegian University of Science and Technology and Amity University in India agreed, but they also set out to make it nutritionally valuable and give it a long shelf life without the addition of preservatives.
Sounds like a tall order, but they figured it out.
Not only is it tasty, but the properties of it could rival your morning multivitamin. Hibiscus extract has huge amounts of antioxidants, like phenolics, which are believed to help prevent cell membrane damage. Foods like vegetables, flax seed, and whole grains also have these antioxidants, but why not just have a Roselle muffin instead? You also get a dose of ascorbic acid without the glass of OJ in the morning.
The ascorbic acid, however, is not there just to help you. It also helps to check the researcher’s third box, shelf life. These naturally rosy-colored pastries will stay mold-free for 6 days without refrigeration at room temperature and without added preservatives.
Our guess, though, is they won’t be on the kitchen counter long enough to find out.
A sobering proposition
If Hollywood is to be believed, there’s no amount of drunkenness that can’t be cured with a cup of coffee or a stern slap in the face. Unfortunately, here in the real world the only thing that can make you less drunk is time. Maybe next time you’ll stop after that seventh Manhattan.
But what if we could beat time? What if there’s an actual sobriety drug out there?
Say hello to fibroblast growth factor 21. Although the liver already does good work filtering out what is essentially poison, it then goes the extra mile and produces fibroblast growth factor 21 (or, as her friends call her, FGF21), a hormone that suppresses the desire to drink, makes you desire water, and protects the liver all at the same time.
Now, FGF21 in its current role is great, but if you’ve ever seen or been a drunk person before, you’ve experienced the lack of interest in listening to reason, especially when it comes from within our own bodies. Who are you to tell us what to do, body? You’re not the boss of us! So a group of scientists decided to push the limits of FGF21. Could it do more than it already does?
First off, they genetically altered a group of mice so that they didn’t produce FGF21 on their own. Then they got them drunk. We’re going to assume they built a scale model of the bar from Cheers and had the mice filter in through the front door as they served their subjects beer out of tiny little glasses.
Once the mice were nice and liquored up, some were given a treatment of FGF21 while others were given a placebo. Lo and behold, the mice given FGF21 recovered about 50% faster than those that received the control treatment. Not exactly instant, but 50% is nothing to sniff at.
Before you bring your FGF21 supplement to the bar, though, this research only applies to mice. We don’t know if it works in people. And make sure you stick to booze. If your choice of intoxication is a bit more exotic, FGF21 isn’t going to do anything for you. Yes, the scientists tried. Yes, those mice are living a very interesting life. And yes, we are jealous of drugged-up lab mice.
Supersize your imagination, shrink your snacks
Have you ever heard of the meal-recall effect? Did you know that, in England, a biscuit is really a cookie? Did you also know that the magazine Bon Appétit is not the same as the peer-reviewed journal Appetite? We do … now.
The meal-recall effect is the subsequent reduction in snacking that comes from remembering a recent meal. It was used to great effect in a recent study conducted at the University of Cambridge, which is in England, where they feed their experimental humans cookies but, for some reason, call them biscuits.
For the first part of the study, the participants were invited to dine at Che Laboratory, where they “were given a microwave ready meal of rice and sauce and a cup of water,” according to a statement from the university. As our Uncle Ernie would say, “Gourmet all the way.”
The test subjects were instructed not to eat anything for 3 hours and “then invited back to the lab to perform imagination tasks.” Those who did come back were randomly divided into five different groups, each with a different task:
- Imagine moving their recent lunch at the lab around a plate.
- Recall eating their recent lunch in detail.
- Imagine that the lunch was twice as big and filling as it really was.
- Look at a photograph of spaghetti hoops in tomato sauce and write a description of it before imagining moving the food around a plate.
- Look at a photo of paper clips and rubber bands and imagine moving them around.
Now, at last, we get to the biscuits/cookies, which were the subject of a taste test that “was simply a rouse for covertly assessing snacking,” the investigators explained. As part of that test, participants were told they could eat as many biscuits as they wanted.
When the tables were cleared and the leftovers examined, the group that imagined spaghetti hoops had eaten the most biscuits (75.9 g), followed by the group that imagined paper clips (75.5 g), the moving-their-lunch-around-the-plate group (72.0 g), and the group that relived eating their lunch (70.0 g).
In a victory for the meal-recall effect, the people who imagined their meal being twice as big ate the fewest biscuits (51.1 g). “Your mind can be more powerful than your stomach in dictating how much you eat,” lead author Joanna Szypula, PhD, said in the university statement.
Oh! One more thing. The study appeared in Appetite, which is a peer-reviewed journal, not in Bon Appétit, which is not a peer-reviewed journal. Thanks to the fine folks at both publications for pointing that out to us.
Get ‘em while they’re hot … for your health
Today on the Eating Channel, it’s a very special episode of “Much Ado About Muffin.”
The muffin. For some of us, it’s a good way to pretend we’re not having dessert for breakfast. A bran muffin can be loaded with calcium and fiber, and our beloved blueberry is full of yummy antioxidants and vitamins. Definitely not dessert.
Well, the muffin denial can stop there because there’s a new flavor on the scene, and research suggests it may actually be healthy. (Disclaimer: Muffin may not be considered healthy in Norway.) This new muffin has a name, Roselle, that comes from the calyx extract used in it, which is found in the Hibiscus sabdariffa plant of the same name.
Now, when it comes to new foods, especially ones that are supposed to be healthy, the No. 1 criteria is the same: It has to taste good. Researchers at the Norwegian University of Science and Technology and Amity University in India agreed, but they also set out to make it nutritionally valuable and give it a long shelf life without the addition of preservatives.
Sounds like a tall order, but they figured it out.
Not only is it tasty, but the properties of it could rival your morning multivitamin. Hibiscus extract has huge amounts of antioxidants, like phenolics, which are believed to help prevent cell membrane damage. Foods like vegetables, flax seed, and whole grains also have these antioxidants, but why not just have a Roselle muffin instead? You also get a dose of ascorbic acid without the glass of OJ in the morning.
The ascorbic acid, however, is not there just to help you. It also helps to check the researcher’s third box, shelf life. These naturally rosy-colored pastries will stay mold-free for 6 days without refrigeration at room temperature and without added preservatives.
Our guess, though, is they won’t be on the kitchen counter long enough to find out.
A sobering proposition
If Hollywood is to be believed, there’s no amount of drunkenness that can’t be cured with a cup of coffee or a stern slap in the face. Unfortunately, here in the real world the only thing that can make you less drunk is time. Maybe next time you’ll stop after that seventh Manhattan.
But what if we could beat time? What if there’s an actual sobriety drug out there?
Say hello to fibroblast growth factor 21. Although the liver already does good work filtering out what is essentially poison, it then goes the extra mile and produces fibroblast growth factor 21 (or, as her friends call her, FGF21), a hormone that suppresses the desire to drink, makes you desire water, and protects the liver all at the same time.
Now, FGF21 in its current role is great, but if you’ve ever seen or been a drunk person before, you’ve experienced the lack of interest in listening to reason, especially when it comes from within our own bodies. Who are you to tell us what to do, body? You’re not the boss of us! So a group of scientists decided to push the limits of FGF21. Could it do more than it already does?
First off, they genetically altered a group of mice so that they didn’t produce FGF21 on their own. Then they got them drunk. We’re going to assume they built a scale model of the bar from Cheers and had the mice filter in through the front door as they served their subjects beer out of tiny little glasses.
Once the mice were nice and liquored up, some were given a treatment of FGF21 while others were given a placebo. Lo and behold, the mice given FGF21 recovered about 50% faster than those that received the control treatment. Not exactly instant, but 50% is nothing to sniff at.
Before you bring your FGF21 supplement to the bar, though, this research only applies to mice. We don’t know if it works in people. And make sure you stick to booze. If your choice of intoxication is a bit more exotic, FGF21 isn’t going to do anything for you. Yes, the scientists tried. Yes, those mice are living a very interesting life. And yes, we are jealous of drugged-up lab mice.
Supersize your imagination, shrink your snacks
Have you ever heard of the meal-recall effect? Did you know that, in England, a biscuit is really a cookie? Did you also know that the magazine Bon Appétit is not the same as the peer-reviewed journal Appetite? We do … now.
The meal-recall effect is the subsequent reduction in snacking that comes from remembering a recent meal. It was used to great effect in a recent study conducted at the University of Cambridge, which is in England, where they feed their experimental humans cookies but, for some reason, call them biscuits.
For the first part of the study, the participants were invited to dine at Che Laboratory, where they “were given a microwave ready meal of rice and sauce and a cup of water,” according to a statement from the university. As our Uncle Ernie would say, “Gourmet all the way.”
The test subjects were instructed not to eat anything for 3 hours and “then invited back to the lab to perform imagination tasks.” Those who did come back were randomly divided into five different groups, each with a different task:
- Imagine moving their recent lunch at the lab around a plate.
- Recall eating their recent lunch in detail.
- Imagine that the lunch was twice as big and filling as it really was.
- Look at a photograph of spaghetti hoops in tomato sauce and write a description of it before imagining moving the food around a plate.
- Look at a photo of paper clips and rubber bands and imagine moving them around.
Now, at last, we get to the biscuits/cookies, which were the subject of a taste test that “was simply a rouse for covertly assessing snacking,” the investigators explained. As part of that test, participants were told they could eat as many biscuits as they wanted.
When the tables were cleared and the leftovers examined, the group that imagined spaghetti hoops had eaten the most biscuits (75.9 g), followed by the group that imagined paper clips (75.5 g), the moving-their-lunch-around-the-plate group (72.0 g), and the group that relived eating their lunch (70.0 g).
In a victory for the meal-recall effect, the people who imagined their meal being twice as big ate the fewest biscuits (51.1 g). “Your mind can be more powerful than your stomach in dictating how much you eat,” lead author Joanna Szypula, PhD, said in the university statement.
Oh! One more thing. The study appeared in Appetite, which is a peer-reviewed journal, not in Bon Appétit, which is not a peer-reviewed journal. Thanks to the fine folks at both publications for pointing that out to us.
Encouraging 3-year data for TAVR in low-risk patients: EVOLUT
Three-year results from the Evolut trial seem to provide more reassurance on the use of transcatheter aortic valve replacement (TAVR) in low-surgical-risk patients.
The 3-year results show that low-surgical-risk patients undergoing aortic valve replacement continue to show lower rates of all-cause mortality and disabling stroke with TAVR, compared with surgery.
The rates of all-cause mortality or disabling stroke (the primary endpoint) at 3 years were 7.4% with TAVR and 10.4% with surgery.
Rates of new pacemaker implantation continued to be higher after TAVR and the frequency of new onset atrial fibrillation was more common after surgery.
“At 3 years, the rate of all-cause mortality or disabling stroke after TAVR with the Evolut valve compared very favorably to surgery. The absolute difference between treatment arms remained consistent with a 30% relative reduction in the hazard of death or disabling stroke, with a P value that just missed statistical significance,” said Evolut investigator John Forrest, MD, Yale University School of Medicine, New Haven, Conn.
“The Kaplan-Meier curves show what we’ve come to expect – an early separation of the curves – but what’s unique here, and seen for the first time, is that the early separation is maintained at year 1 and year 2, and between years 2 and 3 the curve didn’t start to come together, but, if anything, separated a little,” Dr. Forrest commented.
“Both components of the primary endpoint – all cause mortality and disabling stroke – numerically favor TAVR. The separation of the curves for stroke are maintained, and if anything, we see a further slight separation of the curves as we go forward out to 3 years in terms of all-cause mortality,” he added.
Dr. Forrest presented the 3-year results from the Evolut trial at the joint scientific sessions of the American College of Cardiology and the World Heart Federation. They were simultaneously published online in the Journal of the American College of Cardiology.
Dr. Forrest also reported that TAVR patients continued to have better valve hemodynamics at 3 years and very low rates of valve thrombosis; moreover, rates of moderate or greater paravalvular regurgitation and paravalvular leak (factors that can affect valve durability) were also low, although mild paravalvular regurgitation was higher with TAVR.
“In these low-risk patients, the durability of the valve is going to be critically important,” Dr. Forrest commented. “The excellent valve performance and durable outcomes out to 3 years in low-risk patients affirms the role of TAVR in this population,” he concluded.
On how these results may affect clinical practice, Dr. Forrest said: “I think in the U.S. these results reaffirm what we are doing. It gives us confidence to continue treating low-risk patients and being comfortable with that.”
He added: “Outside the U.S., the guidelines are a little different. Maybe we should reconsider some of these guidelines based on these data.”
David Moliterno, MD, Gill Heart and Vascular Institute, Lexington, Ky., who is not involved in the TAVR studies, said: “The results provide a little more reassurance ... that will go a little way further.”
“Uncertainty remains regarding long-term durability of the transcatheter valve in low-risk patients who are generally younger and likely more active than higher-risk cohorts,” he added. “The current 3-year results provide more confidence as the outcome curves for death and disabling stroke are trending in the right direction for TAVR versus surgery.”
Dr. Moliterno pointed out that while rates of paravalvular regurgitation and permanent pacemaker placement are decreasing with newer generation Evolut devices and implantation techniques, he noted that according to the U.S. Social Security Administration, patients aged 74 years as enrolled in this low-risk cohort have an additional life expectancy of approximately 12 years. “So, we have more device durability (and coronary access feasibility) to prove.”
In his presentation, Dr. Forrest explained that TAVR is now approved in the United States for all patients with aortic stenosis regardless of surgical risk and has become the dominant form of aortic valve replacement. Current ACC/AHA guidelines recommend that heart teams utilize a shared decision-making process when discussing aortic valve replacement with patients aged 65-80 years. In younger, lower-risk patients, the faster recovery and short-term benefits after TAVR must be balanced with long-term durability; however, only limited intermediate and long-term data exist to guide such discussions in this patient population.
The Evolut Low Risk trial randomly assigned 1,414 patients in need of aortic valve replacement to TAVR with a self-expanding, supra-annular valve or surgery. Results at 1 and 2 years have shown a similar benefit in the primary endpoint of all-cause mortality/disabling stroke for the less invasive TAVR procedure.
The current 3-year results suggest the benefit appears to be maintained out for another year.
The main results show that the rate of death or disabling stroke was 7.4% in the TAVR group versus 10.4% in the surgery group, giving a hazard ratio of 0.70 (P = .051).
In the JACC paper, the authors report that the absolute difference between treatment arms for all-cause mortality or disabling stroke remained broadly consistent over time: –1.8% at year 1; –2.0% at year 2; and –2.9% at year 3.
Other key results on valve durability show that mild paravalvular regurgitation was increased in the TAVR group (20.3%) versus 2.5% with surgery. However, rates of moderate or greater paravalvular regurgitation for both groups were below 1% and not significantly different between groups.
Patients who underwent TAVR had significantly improved valve hemodynamics (mean gradient 9.1 mm Hg TAVR vs. 12.1 mm Hg surgery; P < .001) at 3 years.
However, pacemaker placement was much higher in the TAVR group (23.2%), compared with 9.1% in the surgery group.
On the other hand, the surgery group had a greater incidence of atrial fibrillation (40%) versus 13% with TAVR.
Quality-of-life results looked good in both groups.
“As we’ve come to expect, patients recover more quickly after TAVR, so at 30 days their quality of life is better than those who have undergone surgery,” Dr. Forrest commented. “But by 1 year, both groups are doing exceptionally well and, remarkably, here by 3 years both groups have greater than a 20-point increase in their KCCQ score, showing a very large improvement in quality of life.”
Discussant of these latest results at the ACC late-breaking trials session, James Hermiller, MD, St. Vincent Ascension Heart Center, Indianapolis, said: “This 3-year data continues to demonstrate that the gift of TAVR keeps giving.”
Noting that the divergence in the effect curves was primarily driven by mortality rather than stroke, he asked whether this was cardiac or noncardiac mortality that was reduced.
Dr. Forrest responded: “It was a fairly equal contribution – a little bit more cardiac death. We have to remember that although the average age in this study was 74, there were some patients over 80 who were still low-surgical-risk included so we are going to see noncardiac death as well.”
Dr. Hermiller drew attention to the high pacemaker rate in the TAVR group and asked how these patients fared in comparison to those who didn’t need a pacemaker.
Dr. Forrest replied: “I think it’s fair to say that putting in a pacemaker is not a benign procedure. Patients who got a pacemaker did slightly worse than those who didn’t get a pacemaker, so we need to try to drive that rate down.”
He added that the number of patients needing a pacemaker after TAVR has come down with new implantation techniques and new generation valves.
“We realize that using a cusp overlap technique can significantly reduce the need for a pacemaker, and we see from registry data that with the use of this new technique the need for a pacemaker has dropped down to 8%-9%, significantly less than seen in this study,” Dr. Forrest commented.
Dr. Hermiller also asked about how TAVR affects future access for catheterization or percutaneous coronary intervention.
Dr. Forrest noted that 24 patients in the TAVR group required PCI in first 3 years, and all the PCI procedures had been successful. He noted that operators reported the procedure to be easy or moderately easy in about 75%-80% of cases and difficult in about 20% of patients. “So, it is slightly more challenging to engage the coronaries and have to go through the frame, but it is very feasible.”
Dr. Forrest concluded that: “These results provide patients and heart teams important data to aid in the shared decision-making process.”
But he acknowledged that longer term data are still needed. “And the potential impact that hemodynamics, valve design, new pacemakers, and other secondary endpoints have on long-term outcomes will be important to follow in this group of low-risk patients.”
The Evolut Low Risk trial was funded by Medtronic. Dr. Forrest has received grant support/research contracts and consultant fees/honoraria/speakers bureau fees from Edwards Lifesciences and Medtronic.
A version of this article first appeared on Medscape.com.
Three-year results from the Evolut trial seem to provide more reassurance on the use of transcatheter aortic valve replacement (TAVR) in low-surgical-risk patients.
The 3-year results show that low-surgical-risk patients undergoing aortic valve replacement continue to show lower rates of all-cause mortality and disabling stroke with TAVR, compared with surgery.
The rates of all-cause mortality or disabling stroke (the primary endpoint) at 3 years were 7.4% with TAVR and 10.4% with surgery.
Rates of new pacemaker implantation continued to be higher after TAVR and the frequency of new onset atrial fibrillation was more common after surgery.
“At 3 years, the rate of all-cause mortality or disabling stroke after TAVR with the Evolut valve compared very favorably to surgery. The absolute difference between treatment arms remained consistent with a 30% relative reduction in the hazard of death or disabling stroke, with a P value that just missed statistical significance,” said Evolut investigator John Forrest, MD, Yale University School of Medicine, New Haven, Conn.
“The Kaplan-Meier curves show what we’ve come to expect – an early separation of the curves – but what’s unique here, and seen for the first time, is that the early separation is maintained at year 1 and year 2, and between years 2 and 3 the curve didn’t start to come together, but, if anything, separated a little,” Dr. Forrest commented.
“Both components of the primary endpoint – all cause mortality and disabling stroke – numerically favor TAVR. The separation of the curves for stroke are maintained, and if anything, we see a further slight separation of the curves as we go forward out to 3 years in terms of all-cause mortality,” he added.
Dr. Forrest presented the 3-year results from the Evolut trial at the joint scientific sessions of the American College of Cardiology and the World Heart Federation. They were simultaneously published online in the Journal of the American College of Cardiology.
Dr. Forrest also reported that TAVR patients continued to have better valve hemodynamics at 3 years and very low rates of valve thrombosis; moreover, rates of moderate or greater paravalvular regurgitation and paravalvular leak (factors that can affect valve durability) were also low, although mild paravalvular regurgitation was higher with TAVR.
“In these low-risk patients, the durability of the valve is going to be critically important,” Dr. Forrest commented. “The excellent valve performance and durable outcomes out to 3 years in low-risk patients affirms the role of TAVR in this population,” he concluded.
On how these results may affect clinical practice, Dr. Forrest said: “I think in the U.S. these results reaffirm what we are doing. It gives us confidence to continue treating low-risk patients and being comfortable with that.”
He added: “Outside the U.S., the guidelines are a little different. Maybe we should reconsider some of these guidelines based on these data.”
David Moliterno, MD, Gill Heart and Vascular Institute, Lexington, Ky., who is not involved in the TAVR studies, said: “The results provide a little more reassurance ... that will go a little way further.”
“Uncertainty remains regarding long-term durability of the transcatheter valve in low-risk patients who are generally younger and likely more active than higher-risk cohorts,” he added. “The current 3-year results provide more confidence as the outcome curves for death and disabling stroke are trending in the right direction for TAVR versus surgery.”
Dr. Moliterno pointed out that while rates of paravalvular regurgitation and permanent pacemaker placement are decreasing with newer generation Evolut devices and implantation techniques, he noted that according to the U.S. Social Security Administration, patients aged 74 years as enrolled in this low-risk cohort have an additional life expectancy of approximately 12 years. “So, we have more device durability (and coronary access feasibility) to prove.”
In his presentation, Dr. Forrest explained that TAVR is now approved in the United States for all patients with aortic stenosis regardless of surgical risk and has become the dominant form of aortic valve replacement. Current ACC/AHA guidelines recommend that heart teams utilize a shared decision-making process when discussing aortic valve replacement with patients aged 65-80 years. In younger, lower-risk patients, the faster recovery and short-term benefits after TAVR must be balanced with long-term durability; however, only limited intermediate and long-term data exist to guide such discussions in this patient population.
The Evolut Low Risk trial randomly assigned 1,414 patients in need of aortic valve replacement to TAVR with a self-expanding, supra-annular valve or surgery. Results at 1 and 2 years have shown a similar benefit in the primary endpoint of all-cause mortality/disabling stroke for the less invasive TAVR procedure.
The current 3-year results suggest the benefit appears to be maintained out for another year.
The main results show that the rate of death or disabling stroke was 7.4% in the TAVR group versus 10.4% in the surgery group, giving a hazard ratio of 0.70 (P = .051).
In the JACC paper, the authors report that the absolute difference between treatment arms for all-cause mortality or disabling stroke remained broadly consistent over time: –1.8% at year 1; –2.0% at year 2; and –2.9% at year 3.
Other key results on valve durability show that mild paravalvular regurgitation was increased in the TAVR group (20.3%) versus 2.5% with surgery. However, rates of moderate or greater paravalvular regurgitation for both groups were below 1% and not significantly different between groups.
Patients who underwent TAVR had significantly improved valve hemodynamics (mean gradient 9.1 mm Hg TAVR vs. 12.1 mm Hg surgery; P < .001) at 3 years.
However, pacemaker placement was much higher in the TAVR group (23.2%), compared with 9.1% in the surgery group.
On the other hand, the surgery group had a greater incidence of atrial fibrillation (40%) versus 13% with TAVR.
Quality-of-life results looked good in both groups.
“As we’ve come to expect, patients recover more quickly after TAVR, so at 30 days their quality of life is better than those who have undergone surgery,” Dr. Forrest commented. “But by 1 year, both groups are doing exceptionally well and, remarkably, here by 3 years both groups have greater than a 20-point increase in their KCCQ score, showing a very large improvement in quality of life.”
Discussant of these latest results at the ACC late-breaking trials session, James Hermiller, MD, St. Vincent Ascension Heart Center, Indianapolis, said: “This 3-year data continues to demonstrate that the gift of TAVR keeps giving.”
Noting that the divergence in the effect curves was primarily driven by mortality rather than stroke, he asked whether this was cardiac or noncardiac mortality that was reduced.
Dr. Forrest responded: “It was a fairly equal contribution – a little bit more cardiac death. We have to remember that although the average age in this study was 74, there were some patients over 80 who were still low-surgical-risk included so we are going to see noncardiac death as well.”
Dr. Hermiller drew attention to the high pacemaker rate in the TAVR group and asked how these patients fared in comparison to those who didn’t need a pacemaker.
Dr. Forrest replied: “I think it’s fair to say that putting in a pacemaker is not a benign procedure. Patients who got a pacemaker did slightly worse than those who didn’t get a pacemaker, so we need to try to drive that rate down.”
He added that the number of patients needing a pacemaker after TAVR has come down with new implantation techniques and new generation valves.
“We realize that using a cusp overlap technique can significantly reduce the need for a pacemaker, and we see from registry data that with the use of this new technique the need for a pacemaker has dropped down to 8%-9%, significantly less than seen in this study,” Dr. Forrest commented.
Dr. Hermiller also asked about how TAVR affects future access for catheterization or percutaneous coronary intervention.
Dr. Forrest noted that 24 patients in the TAVR group required PCI in first 3 years, and all the PCI procedures had been successful. He noted that operators reported the procedure to be easy or moderately easy in about 75%-80% of cases and difficult in about 20% of patients. “So, it is slightly more challenging to engage the coronaries and have to go through the frame, but it is very feasible.”
Dr. Forrest concluded that: “These results provide patients and heart teams important data to aid in the shared decision-making process.”
But he acknowledged that longer term data are still needed. “And the potential impact that hemodynamics, valve design, new pacemakers, and other secondary endpoints have on long-term outcomes will be important to follow in this group of low-risk patients.”
The Evolut Low Risk trial was funded by Medtronic. Dr. Forrest has received grant support/research contracts and consultant fees/honoraria/speakers bureau fees from Edwards Lifesciences and Medtronic.
A version of this article first appeared on Medscape.com.
Three-year results from the Evolut trial seem to provide more reassurance on the use of transcatheter aortic valve replacement (TAVR) in low-surgical-risk patients.
The 3-year results show that low-surgical-risk patients undergoing aortic valve replacement continue to show lower rates of all-cause mortality and disabling stroke with TAVR, compared with surgery.
The rates of all-cause mortality or disabling stroke (the primary endpoint) at 3 years were 7.4% with TAVR and 10.4% with surgery.
Rates of new pacemaker implantation continued to be higher after TAVR and the frequency of new onset atrial fibrillation was more common after surgery.
“At 3 years, the rate of all-cause mortality or disabling stroke after TAVR with the Evolut valve compared very favorably to surgery. The absolute difference between treatment arms remained consistent with a 30% relative reduction in the hazard of death or disabling stroke, with a P value that just missed statistical significance,” said Evolut investigator John Forrest, MD, Yale University School of Medicine, New Haven, Conn.
“The Kaplan-Meier curves show what we’ve come to expect – an early separation of the curves – but what’s unique here, and seen for the first time, is that the early separation is maintained at year 1 and year 2, and between years 2 and 3 the curve didn’t start to come together, but, if anything, separated a little,” Dr. Forrest commented.
“Both components of the primary endpoint – all cause mortality and disabling stroke – numerically favor TAVR. The separation of the curves for stroke are maintained, and if anything, we see a further slight separation of the curves as we go forward out to 3 years in terms of all-cause mortality,” he added.
Dr. Forrest presented the 3-year results from the Evolut trial at the joint scientific sessions of the American College of Cardiology and the World Heart Federation. They were simultaneously published online in the Journal of the American College of Cardiology.
Dr. Forrest also reported that TAVR patients continued to have better valve hemodynamics at 3 years and very low rates of valve thrombosis; moreover, rates of moderate or greater paravalvular regurgitation and paravalvular leak (factors that can affect valve durability) were also low, although mild paravalvular regurgitation was higher with TAVR.
“In these low-risk patients, the durability of the valve is going to be critically important,” Dr. Forrest commented. “The excellent valve performance and durable outcomes out to 3 years in low-risk patients affirms the role of TAVR in this population,” he concluded.
On how these results may affect clinical practice, Dr. Forrest said: “I think in the U.S. these results reaffirm what we are doing. It gives us confidence to continue treating low-risk patients and being comfortable with that.”
He added: “Outside the U.S., the guidelines are a little different. Maybe we should reconsider some of these guidelines based on these data.”
David Moliterno, MD, Gill Heart and Vascular Institute, Lexington, Ky., who is not involved in the TAVR studies, said: “The results provide a little more reassurance ... that will go a little way further.”
“Uncertainty remains regarding long-term durability of the transcatheter valve in low-risk patients who are generally younger and likely more active than higher-risk cohorts,” he added. “The current 3-year results provide more confidence as the outcome curves for death and disabling stroke are trending in the right direction for TAVR versus surgery.”
Dr. Moliterno pointed out that while rates of paravalvular regurgitation and permanent pacemaker placement are decreasing with newer generation Evolut devices and implantation techniques, he noted that according to the U.S. Social Security Administration, patients aged 74 years as enrolled in this low-risk cohort have an additional life expectancy of approximately 12 years. “So, we have more device durability (and coronary access feasibility) to prove.”
In his presentation, Dr. Forrest explained that TAVR is now approved in the United States for all patients with aortic stenosis regardless of surgical risk and has become the dominant form of aortic valve replacement. Current ACC/AHA guidelines recommend that heart teams utilize a shared decision-making process when discussing aortic valve replacement with patients aged 65-80 years. In younger, lower-risk patients, the faster recovery and short-term benefits after TAVR must be balanced with long-term durability; however, only limited intermediate and long-term data exist to guide such discussions in this patient population.
The Evolut Low Risk trial randomly assigned 1,414 patients in need of aortic valve replacement to TAVR with a self-expanding, supra-annular valve or surgery. Results at 1 and 2 years have shown a similar benefit in the primary endpoint of all-cause mortality/disabling stroke for the less invasive TAVR procedure.
The current 3-year results suggest the benefit appears to be maintained out for another year.
The main results show that the rate of death or disabling stroke was 7.4% in the TAVR group versus 10.4% in the surgery group, giving a hazard ratio of 0.70 (P = .051).
In the JACC paper, the authors report that the absolute difference between treatment arms for all-cause mortality or disabling stroke remained broadly consistent over time: –1.8% at year 1; –2.0% at year 2; and –2.9% at year 3.
Other key results on valve durability show that mild paravalvular regurgitation was increased in the TAVR group (20.3%) versus 2.5% with surgery. However, rates of moderate or greater paravalvular regurgitation for both groups were below 1% and not significantly different between groups.
Patients who underwent TAVR had significantly improved valve hemodynamics (mean gradient 9.1 mm Hg TAVR vs. 12.1 mm Hg surgery; P < .001) at 3 years.
However, pacemaker placement was much higher in the TAVR group (23.2%), compared with 9.1% in the surgery group.
On the other hand, the surgery group had a greater incidence of atrial fibrillation (40%) versus 13% with TAVR.
Quality-of-life results looked good in both groups.
“As we’ve come to expect, patients recover more quickly after TAVR, so at 30 days their quality of life is better than those who have undergone surgery,” Dr. Forrest commented. “But by 1 year, both groups are doing exceptionally well and, remarkably, here by 3 years both groups have greater than a 20-point increase in their KCCQ score, showing a very large improvement in quality of life.”
Discussant of these latest results at the ACC late-breaking trials session, James Hermiller, MD, St. Vincent Ascension Heart Center, Indianapolis, said: “This 3-year data continues to demonstrate that the gift of TAVR keeps giving.”
Noting that the divergence in the effect curves was primarily driven by mortality rather than stroke, he asked whether this was cardiac or noncardiac mortality that was reduced.
Dr. Forrest responded: “It was a fairly equal contribution – a little bit more cardiac death. We have to remember that although the average age in this study was 74, there were some patients over 80 who were still low-surgical-risk included so we are going to see noncardiac death as well.”
Dr. Hermiller drew attention to the high pacemaker rate in the TAVR group and asked how these patients fared in comparison to those who didn’t need a pacemaker.
Dr. Forrest replied: “I think it’s fair to say that putting in a pacemaker is not a benign procedure. Patients who got a pacemaker did slightly worse than those who didn’t get a pacemaker, so we need to try to drive that rate down.”
He added that the number of patients needing a pacemaker after TAVR has come down with new implantation techniques and new generation valves.
“We realize that using a cusp overlap technique can significantly reduce the need for a pacemaker, and we see from registry data that with the use of this new technique the need for a pacemaker has dropped down to 8%-9%, significantly less than seen in this study,” Dr. Forrest commented.
Dr. Hermiller also asked about how TAVR affects future access for catheterization or percutaneous coronary intervention.
Dr. Forrest noted that 24 patients in the TAVR group required PCI in first 3 years, and all the PCI procedures had been successful. He noted that operators reported the procedure to be easy or moderately easy in about 75%-80% of cases and difficult in about 20% of patients. “So, it is slightly more challenging to engage the coronaries and have to go through the frame, but it is very feasible.”
Dr. Forrest concluded that: “These results provide patients and heart teams important data to aid in the shared decision-making process.”
But he acknowledged that longer term data are still needed. “And the potential impact that hemodynamics, valve design, new pacemakers, and other secondary endpoints have on long-term outcomes will be important to follow in this group of low-risk patients.”
The Evolut Low Risk trial was funded by Medtronic. Dr. Forrest has received grant support/research contracts and consultant fees/honoraria/speakers bureau fees from Edwards Lifesciences and Medtronic.
A version of this article first appeared on Medscape.com.
FROM ACC 2023
Two FDA clearances add diabetes technology options
Two diabetes management devices that aid in the precision of insulin delivery have been recently cleared by the Food and Drug Administration.
On March 2, the FDA cleared the Android version of Bigfoot Biomedical’s Unity Mobile App for use with its system of smart pen caps that are compatible with different disposable insulin pens for administering both long-acting and rapid-acting insulin.
The system, which has been compatible with iOS devices since May 2021, is “the first and only FDA-cleared smart injection system that turns CGM [continuous glucose monitoring] data into dosing recommendations displayed right on the pen cap for people using multiple daily [insulin] injection therapy,” according to a company statement.
The Bigfoot app allows users to input and review provider treatment recommendations, displays current glucose ranges, and delivers real-time alerts.
Once it is commercially launched, the Android phone application will be available via the Google Play Store. “Given that 41% of U.S. smartphone users choose Android devices, this clearance enables expanded access to a large group of people with diabetes,” the company said.
On March 6, the FDA cleared the Abbott FreeStyle Libre 2 and FreeStyle Libre 3 devices as “integrated” CGM sensors. This means that they can now be used as components in automated insulin delivery systems, along with insulin pumps and connectivity software.
Abbott is working with insulin pump manufacturers Insulet and Tandem in the United States for integration with the FreeStyle Libre versions 2 and 3. Outside the United States, the Libre 3 is already authorized to work with mylife Loop from Ypsomed and CamDiab in Germany. Further launches are expected in the United Kingdom, Switzerland, and the Netherlands later this year.
The modified FreeStyle Libre 2 and FreeStyle Libre 3 sensors have been cleared for use by patients as young as age 2 years and for up to 15 days, in contrast to the previous versions, which were available for patients as young as 4 years for use up to 14 days. The FDA has cleared all Libre sensors – 2 and 3, current and future versions – for use by pregnant women with any type of diabetes.
The modified sensors will be available in the United States later this year and will eventually replace the Libre sensors in current use, the company said in a statement.
“The FreeStyle Libre portfolio is still the most affordable CGM on the market,” an Abbott representative said in an interview.
A version of this article first appeared on Medscape.com.
Two diabetes management devices that aid in the precision of insulin delivery have been recently cleared by the Food and Drug Administration.
On March 2, the FDA cleared the Android version of Bigfoot Biomedical’s Unity Mobile App for use with its system of smart pen caps that are compatible with different disposable insulin pens for administering both long-acting and rapid-acting insulin.
The system, which has been compatible with iOS devices since May 2021, is “the first and only FDA-cleared smart injection system that turns CGM [continuous glucose monitoring] data into dosing recommendations displayed right on the pen cap for people using multiple daily [insulin] injection therapy,” according to a company statement.
The Bigfoot app allows users to input and review provider treatment recommendations, displays current glucose ranges, and delivers real-time alerts.
Once it is commercially launched, the Android phone application will be available via the Google Play Store. “Given that 41% of U.S. smartphone users choose Android devices, this clearance enables expanded access to a large group of people with diabetes,” the company said.
On March 6, the FDA cleared the Abbott FreeStyle Libre 2 and FreeStyle Libre 3 devices as “integrated” CGM sensors. This means that they can now be used as components in automated insulin delivery systems, along with insulin pumps and connectivity software.
Abbott is working with insulin pump manufacturers Insulet and Tandem in the United States for integration with the FreeStyle Libre versions 2 and 3. Outside the United States, the Libre 3 is already authorized to work with mylife Loop from Ypsomed and CamDiab in Germany. Further launches are expected in the United Kingdom, Switzerland, and the Netherlands later this year.
The modified FreeStyle Libre 2 and FreeStyle Libre 3 sensors have been cleared for use by patients as young as age 2 years and for up to 15 days, in contrast to the previous versions, which were available for patients as young as 4 years for use up to 14 days. The FDA has cleared all Libre sensors – 2 and 3, current and future versions – for use by pregnant women with any type of diabetes.
The modified sensors will be available in the United States later this year and will eventually replace the Libre sensors in current use, the company said in a statement.
“The FreeStyle Libre portfolio is still the most affordable CGM on the market,” an Abbott representative said in an interview.
A version of this article first appeared on Medscape.com.
Two diabetes management devices that aid in the precision of insulin delivery have been recently cleared by the Food and Drug Administration.
On March 2, the FDA cleared the Android version of Bigfoot Biomedical’s Unity Mobile App for use with its system of smart pen caps that are compatible with different disposable insulin pens for administering both long-acting and rapid-acting insulin.
The system, which has been compatible with iOS devices since May 2021, is “the first and only FDA-cleared smart injection system that turns CGM [continuous glucose monitoring] data into dosing recommendations displayed right on the pen cap for people using multiple daily [insulin] injection therapy,” according to a company statement.
The Bigfoot app allows users to input and review provider treatment recommendations, displays current glucose ranges, and delivers real-time alerts.
Once it is commercially launched, the Android phone application will be available via the Google Play Store. “Given that 41% of U.S. smartphone users choose Android devices, this clearance enables expanded access to a large group of people with diabetes,” the company said.
On March 6, the FDA cleared the Abbott FreeStyle Libre 2 and FreeStyle Libre 3 devices as “integrated” CGM sensors. This means that they can now be used as components in automated insulin delivery systems, along with insulin pumps and connectivity software.
Abbott is working with insulin pump manufacturers Insulet and Tandem in the United States for integration with the FreeStyle Libre versions 2 and 3. Outside the United States, the Libre 3 is already authorized to work with mylife Loop from Ypsomed and CamDiab in Germany. Further launches are expected in the United Kingdom, Switzerland, and the Netherlands later this year.
The modified FreeStyle Libre 2 and FreeStyle Libre 3 sensors have been cleared for use by patients as young as age 2 years and for up to 15 days, in contrast to the previous versions, which were available for patients as young as 4 years for use up to 14 days. The FDA has cleared all Libre sensors – 2 and 3, current and future versions – for use by pregnant women with any type of diabetes.
The modified sensors will be available in the United States later this year and will eventually replace the Libre sensors in current use, the company said in a statement.
“The FreeStyle Libre portfolio is still the most affordable CGM on the market,” an Abbott representative said in an interview.
A version of this article first appeared on Medscape.com.