User login
Team planning cuts pancreatectomy readmissions
MIAMI BEACH – A combination of teamwork and leadership led to a 50% reduction in readmission after pancreatectomy in a large academic facility.
The readmission rate at Indiana University Hospital fell from a high of 23% to just over 11% over 5 years – even though length of stay and mortality remained stable, Dr. Eugene Ceppa reported at the annual meeting of the Americas Hepato-Pancreato-Biliary Association.

The multifaceted project made some progress during the first few years of implementation, said Dr. Ceppa of Indiana University Hospital, Indianapolis. But the biggest changes really came in years 4 and 5, after the team adopted its own version of a national readmission prevention plan, and created a "discharge coach" – a staff member dedicated to ensuring that patients were ready to leave the hospital, with plenty of support at home.
Studies generally show that pancreatectomy has a very high readmission rate, hovering around 18%. The situation was tolerated over the years, according to Dr. Henry Pitt, who coauthored the paper. But in 2008, the Centers for Medicare & Medicaid Services introduced the idea that hospital readmissions were eating away at health care dollars.
In a landmark paper, Dr. Brian Jack and colleagues noted that only 13% of discharged patients needed repeat hospitalizations, but these patients used up to 60% of the $753 billion spent on discharge in 2003.
Project RED (ReEngineering Discharge), originating from Boston University Medical Center, suggested that reducing readmissions could save $5 billion each year. Originally focused on reducing readmissions for heart failure, Project RED has been successfully adapted to multiple models – including surgery.
Changes have not come about overnight, said Dr. Pitt, now chief quality officer for Temple University Health System in Philadelphia. "There was denial at first that readmission was a problem," he said in an interview. "Then there was a period of time when there was acceptance but no idea of how to fix it. Now we are beginning to do so."
As pay-for-performance became ever more important, pancreatic surgeons at Indiana University Hospital decided to attack the problem of readmission for their pancreatectomy patients. Over a 5-year period, from 2007 to 2012, they implemented a number of reforms, beginning with renewed efforts to decrease surgical morbidity – especially their 24% rate of surgical site infections after pancreatectomy. Dr. Pitt and his colleagues had already shown that these infections were a leading cause of surgical morbidity, and reducing them was a logical first step toward reducing readmission.
The next step was to create a discharge team that would work cooperatively to make sure patients were in optimal condition to leave the hospital. The Readmission Quality Improvement Team consisted of physicians, nurses, physical and occupational therapists, case managers, pharmacists, and dietitians. Because of their efforts, the number of pancreatectomy patients discharged with some kind of home health care support increased from 20% to 50%.
At the same time, the surgeons made a policy change: There would be no readmissions without the approval of the attending surgeon. Because patients often traveled far to the university hospital, they would frequently go to their local hospitals when problems arose after they went home.
"A lot of the calls to us from patients would go to residents," Dr. Pitt said. "The default was to send them to their local emergency department, because the patients were so far away. And then we would get calls for transfers. We said that house staff would no longer have the authority to make those admissions. If they thought readmission was necessary, they had to call the attending surgeon. Just improving that decision-making process made a big difference, with fewer people going to the ED in the first place. Often it was just a matter of reassuring the patient."
By 2010, readmissions had dropped from 24% to 16%. In 2011, the team employed its own adaptation of Project RED. Each discharge included an 11-point checklist of things that had to be completed before a patient could leave. Those tasks include the following:
• Reconcile medications.
• Reconcile discharge plan with national guidelines.
• Make follow-up appointments.
• Follow up on any outstanding tests.
• Arrange for postdischarge services.
• Explain to the patient what do if a problem arises.
• Conduct patient education.
• Communicate discharge information to primary care physician.
• Make a follow-up call within 3 days of discharge.
The final puzzle piece was the discharge coach, Dr. Pitt said. The coach is a highly experienced nurse whose job it is to make sure each patient receives consistent discharge care and follow-through.
Last year, the team reviewed the project’s results, which Dr. Ceppa presented during the meeting. From 2007 to 2012, 1,147 patients underwent pancreatectomy at the facility. The mean age was 58 years. Pancreatic adenocarcinoma was the most common indication for surgery.
During the study period, neither mortality (2.7%) nor mean length of stay (10 days) changed. But readmission steadily decreased from the 2007 high of 23%. From 2008 through 2011, the readmission ranged from 18% to 15%. But after the changes implemented in 2011, the rate dropped to 11% – a significant decrease from baseline. Dr. Ceppa and Dr. Pitt attributed this to a combination of factors: stepped up discharge planning, attending-only readmission, and the discharge coach.
"I think the major thing we learned is that improving something like this isn’t simple or quick," Dr Pitt said. "You have to be persistent and really work on all the puzzle pieces until they fit into place."
Neither Dr. Pitt nor Dr. Ceppa had any financial disclosures.
MIAMI BEACH – A combination of teamwork and leadership led to a 50% reduction in readmission after pancreatectomy in a large academic facility.
The readmission rate at Indiana University Hospital fell from a high of 23% to just over 11% over 5 years – even though length of stay and mortality remained stable, Dr. Eugene Ceppa reported at the annual meeting of the Americas Hepato-Pancreato-Biliary Association.
The multifaceted project made some progress during the first few years of implementation, said Dr. Ceppa of Indiana University Hospital, Indianapolis. But the biggest changes really came in years 4 and 5, after the team adopted its own version of a national readmission prevention plan, and created a "discharge coach" – a staff member dedicated to ensuring that patients were ready to leave the hospital, with plenty of support at home.
Studies generally show that pancreatectomy has a very high readmission rate, hovering around 18%. The situation was tolerated over the years, according to Dr. Henry Pitt, who coauthored the paper. But in 2008, the Centers for Medicare & Medicaid Services introduced the idea that hospital readmissions were eating away at health care dollars.
In a landmark paper, Dr. Brian Jack and colleagues noted that only 13% of discharged patients needed repeat hospitalizations, but these patients used up to 60% of the $753 billion spent on discharge in 2003.
Project RED (ReEngineering Discharge), originating from Boston University Medical Center, suggested that reducing readmissions could save $5 billion each year. Originally focused on reducing readmissions for heart failure, Project RED has been successfully adapted to multiple models – including surgery.
Changes have not come about overnight, said Dr. Pitt, now chief quality officer for Temple University Health System in Philadelphia. "There was denial at first that readmission was a problem," he said in an interview. "Then there was a period of time when there was acceptance but no idea of how to fix it. Now we are beginning to do so."
As pay-for-performance became ever more important, pancreatic surgeons at Indiana University Hospital decided to attack the problem of readmission for their pancreatectomy patients. Over a 5-year period, from 2007 to 2012, they implemented a number of reforms, beginning with renewed efforts to decrease surgical morbidity – especially their 24% rate of surgical site infections after pancreatectomy. Dr. Pitt and his colleagues had already shown that these infections were a leading cause of surgical morbidity, and reducing them was a logical first step toward reducing readmission.
The next step was to create a discharge team that would work cooperatively to make sure patients were in optimal condition to leave the hospital. The Readmission Quality Improvement Team consisted of physicians, nurses, physical and occupational therapists, case managers, pharmacists, and dietitians. Because of their efforts, the number of pancreatectomy patients discharged with some kind of home health care support increased from 20% to 50%.
At the same time, the surgeons made a policy change: There would be no readmissions without the approval of the attending surgeon. Because patients often traveled far to the university hospital, they would frequently go to their local hospitals when problems arose after they went home.
"A lot of the calls to us from patients would go to residents," Dr. Pitt said. "The default was to send them to their local emergency department, because the patients were so far away. And then we would get calls for transfers. We said that house staff would no longer have the authority to make those admissions. If they thought readmission was necessary, they had to call the attending surgeon. Just improving that decision-making process made a big difference, with fewer people going to the ED in the first place. Often it was just a matter of reassuring the patient."
By 2010, readmissions had dropped from 24% to 16%. In 2011, the team employed its own adaptation of Project RED. Each discharge included an 11-point checklist of things that had to be completed before a patient could leave. Those tasks include the following:
• Reconcile medications.
• Reconcile discharge plan with national guidelines.
• Make follow-up appointments.
• Follow up on any outstanding tests.
• Arrange for postdischarge services.
• Explain to the patient what do if a problem arises.
• Conduct patient education.
• Communicate discharge information to primary care physician.
• Make a follow-up call within 3 days of discharge.
The final puzzle piece was the discharge coach, Dr. Pitt said. The coach is a highly experienced nurse whose job it is to make sure each patient receives consistent discharge care and follow-through.
Last year, the team reviewed the project’s results, which Dr. Ceppa presented during the meeting. From 2007 to 2012, 1,147 patients underwent pancreatectomy at the facility. The mean age was 58 years. Pancreatic adenocarcinoma was the most common indication for surgery.
During the study period, neither mortality (2.7%) nor mean length of stay (10 days) changed. But readmission steadily decreased from the 2007 high of 23%. From 2008 through 2011, the readmission ranged from 18% to 15%. But after the changes implemented in 2011, the rate dropped to 11% – a significant decrease from baseline. Dr. Ceppa and Dr. Pitt attributed this to a combination of factors: stepped up discharge planning, attending-only readmission, and the discharge coach.
"I think the major thing we learned is that improving something like this isn’t simple or quick," Dr Pitt said. "You have to be persistent and really work on all the puzzle pieces until they fit into place."
Neither Dr. Pitt nor Dr. Ceppa had any financial disclosures.
MIAMI BEACH – A combination of teamwork and leadership led to a 50% reduction in readmission after pancreatectomy in a large academic facility.
The readmission rate at Indiana University Hospital fell from a high of 23% to just over 11% over 5 years – even though length of stay and mortality remained stable, Dr. Eugene Ceppa reported at the annual meeting of the Americas Hepato-Pancreato-Biliary Association.
The multifaceted project made some progress during the first few years of implementation, said Dr. Ceppa of Indiana University Hospital, Indianapolis. But the biggest changes really came in years 4 and 5, after the team adopted its own version of a national readmission prevention plan, and created a "discharge coach" – a staff member dedicated to ensuring that patients were ready to leave the hospital, with plenty of support at home.
Studies generally show that pancreatectomy has a very high readmission rate, hovering around 18%. The situation was tolerated over the years, according to Dr. Henry Pitt, who coauthored the paper. But in 2008, the Centers for Medicare & Medicaid Services introduced the idea that hospital readmissions were eating away at health care dollars.
In a landmark paper, Dr. Brian Jack and colleagues noted that only 13% of discharged patients needed repeat hospitalizations, but these patients used up to 60% of the $753 billion spent on discharge in 2003.
Project RED (ReEngineering Discharge), originating from Boston University Medical Center, suggested that reducing readmissions could save $5 billion each year. Originally focused on reducing readmissions for heart failure, Project RED has been successfully adapted to multiple models – including surgery.
Changes have not come about overnight, said Dr. Pitt, now chief quality officer for Temple University Health System in Philadelphia. "There was denial at first that readmission was a problem," he said in an interview. "Then there was a period of time when there was acceptance but no idea of how to fix it. Now we are beginning to do so."
As pay-for-performance became ever more important, pancreatic surgeons at Indiana University Hospital decided to attack the problem of readmission for their pancreatectomy patients. Over a 5-year period, from 2007 to 2012, they implemented a number of reforms, beginning with renewed efforts to decrease surgical morbidity – especially their 24% rate of surgical site infections after pancreatectomy. Dr. Pitt and his colleagues had already shown that these infections were a leading cause of surgical morbidity, and reducing them was a logical first step toward reducing readmission.
The next step was to create a discharge team that would work cooperatively to make sure patients were in optimal condition to leave the hospital. The Readmission Quality Improvement Team consisted of physicians, nurses, physical and occupational therapists, case managers, pharmacists, and dietitians. Because of their efforts, the number of pancreatectomy patients discharged with some kind of home health care support increased from 20% to 50%.
At the same time, the surgeons made a policy change: There would be no readmissions without the approval of the attending surgeon. Because patients often traveled far to the university hospital, they would frequently go to their local hospitals when problems arose after they went home.
"A lot of the calls to us from patients would go to residents," Dr. Pitt said. "The default was to send them to their local emergency department, because the patients were so far away. And then we would get calls for transfers. We said that house staff would no longer have the authority to make those admissions. If they thought readmission was necessary, they had to call the attending surgeon. Just improving that decision-making process made a big difference, with fewer people going to the ED in the first place. Often it was just a matter of reassuring the patient."
By 2010, readmissions had dropped from 24% to 16%. In 2011, the team employed its own adaptation of Project RED. Each discharge included an 11-point checklist of things that had to be completed before a patient could leave. Those tasks include the following:
• Reconcile medications.
• Reconcile discharge plan with national guidelines.
• Make follow-up appointments.
• Follow up on any outstanding tests.
• Arrange for postdischarge services.
• Explain to the patient what do if a problem arises.
• Conduct patient education.
• Communicate discharge information to primary care physician.
• Make a follow-up call within 3 days of discharge.
The final puzzle piece was the discharge coach, Dr. Pitt said. The coach is a highly experienced nurse whose job it is to make sure each patient receives consistent discharge care and follow-through.
Last year, the team reviewed the project’s results, which Dr. Ceppa presented during the meeting. From 2007 to 2012, 1,147 patients underwent pancreatectomy at the facility. The mean age was 58 years. Pancreatic adenocarcinoma was the most common indication for surgery.
During the study period, neither mortality (2.7%) nor mean length of stay (10 days) changed. But readmission steadily decreased from the 2007 high of 23%. From 2008 through 2011, the readmission ranged from 18% to 15%. But after the changes implemented in 2011, the rate dropped to 11% – a significant decrease from baseline. Dr. Ceppa and Dr. Pitt attributed this to a combination of factors: stepped up discharge planning, attending-only readmission, and the discharge coach.
"I think the major thing we learned is that improving something like this isn’t simple or quick," Dr Pitt said. "You have to be persistent and really work on all the puzzle pieces until they fit into place."
Neither Dr. Pitt nor Dr. Ceppa had any financial disclosures.
AT AHPBA 2014
Major finding: Readmission after pancreatectomy dropped from 24% to 11% after implementation of a multifaceted effort to reduce infections and improve discharge planning,
Data source: A retrospective study of 1,147 patients.
Disclosures: Neither Dr. Ceppa nor Dr. Pitt had any financial disclosures.

Intraoperative ultrasound can change approach to liver resection
MIAMI BEACH – Intraoperative ultrasound during resection of colorectal liver metastases changed operative management in 43% of cases, according to a retrospective study.
Ultrasound employed during surgery identified new lesions not seen on preoperative imaging, and gave additional details about known lesions, said Dr. Sarah Knowles, a surgical resident at the University of Western Ontario, London (Canada).
"Intraoperative ultrasound provided new information about the number, size, location, and appearance of the lesions," she said at the annual meeting of the Americas Hepato-Pancreato-Biliary Association. The procedure was associated with significantly more blood loss, however, and there were no differences in negative surgical margins between patients who had ultrasound during surgery and those who did not.

Dr. Knowles presented a retrospective study of 103 patients who, from 2009 to 2012, underwent liver resection of colorectal cancer metastases. Mean age of the patients was 62 years. Most (94%) had undergone preoperative computerized tomography; the rest had undergone magnetic resonance imaging. The mean time from preoperative imaging to surgery was 66 days. Most of the patients (72) had intraoperative ultrasound imaging.
There were 45 anatomic resections and 27 nonanatomic resections in the group that had intraoperative ultrasound. This was significantly different from the nonultrasound group, which had 25 anatomic and 6 nonanatomic resections.
Ultrasound changed surgical strategy in 43% (31) of those who had it. Surgical strategy changed in 10% of those who had no intraoperative imaging – a significant difference (P = less than .001). Blood loss was significantly greater in the ultrasound group (650 mL vs. 350 mL).
The bulk of the strategic changes in the ultrasound group (17) were due to additional information about the location of lesions – either deeper or more superficial than preoperative imaging suggested. Other reasons for a shift in strategy were the discovery of new lesions (13), a disappearing lesion (1), larger-than-expected lesions (5), smaller-than-expected lesions (2), or a difference in the lesions’ appearance (3).
Resection margins were similar in the two groups. In the ultrasound group, 85% had R0 margins and 15% had R1 margins. In the group without ultrasound, 87% had R0 margins and 13% had R1 margins. There was no significant difference in disease-free 5-year survival.
Dr. Knowles had no financial disclosures.
MIAMI BEACH – Intraoperative ultrasound during resection of colorectal liver metastases changed operative management in 43% of cases, according to a retrospective study.
Ultrasound employed during surgery identified new lesions not seen on preoperative imaging, and gave additional details about known lesions, said Dr. Sarah Knowles, a surgical resident at the University of Western Ontario, London (Canada).
"Intraoperative ultrasound provided new information about the number, size, location, and appearance of the lesions," she said at the annual meeting of the Americas Hepato-Pancreato-Biliary Association. The procedure was associated with significantly more blood loss, however, and there were no differences in negative surgical margins between patients who had ultrasound during surgery and those who did not.
Dr. Knowles presented a retrospective study of 103 patients who, from 2009 to 2012, underwent liver resection of colorectal cancer metastases. Mean age of the patients was 62 years. Most (94%) had undergone preoperative computerized tomography; the rest had undergone magnetic resonance imaging. The mean time from preoperative imaging to surgery was 66 days. Most of the patients (72) had intraoperative ultrasound imaging.
There were 45 anatomic resections and 27 nonanatomic resections in the group that had intraoperative ultrasound. This was significantly different from the nonultrasound group, which had 25 anatomic and 6 nonanatomic resections.
Ultrasound changed surgical strategy in 43% (31) of those who had it. Surgical strategy changed in 10% of those who had no intraoperative imaging – a significant difference (P = less than .001). Blood loss was significantly greater in the ultrasound group (650 mL vs. 350 mL).
The bulk of the strategic changes in the ultrasound group (17) were due to additional information about the location of lesions – either deeper or more superficial than preoperative imaging suggested. Other reasons for a shift in strategy were the discovery of new lesions (13), a disappearing lesion (1), larger-than-expected lesions (5), smaller-than-expected lesions (2), or a difference in the lesions’ appearance (3).
Resection margins were similar in the two groups. In the ultrasound group, 85% had R0 margins and 15% had R1 margins. In the group without ultrasound, 87% had R0 margins and 13% had R1 margins. There was no significant difference in disease-free 5-year survival.
Dr. Knowles had no financial disclosures.
MIAMI BEACH – Intraoperative ultrasound during resection of colorectal liver metastases changed operative management in 43% of cases, according to a retrospective study.
Ultrasound employed during surgery identified new lesions not seen on preoperative imaging, and gave additional details about known lesions, said Dr. Sarah Knowles, a surgical resident at the University of Western Ontario, London (Canada).
"Intraoperative ultrasound provided new information about the number, size, location, and appearance of the lesions," she said at the annual meeting of the Americas Hepato-Pancreato-Biliary Association. The procedure was associated with significantly more blood loss, however, and there were no differences in negative surgical margins between patients who had ultrasound during surgery and those who did not.
Dr. Knowles presented a retrospective study of 103 patients who, from 2009 to 2012, underwent liver resection of colorectal cancer metastases. Mean age of the patients was 62 years. Most (94%) had undergone preoperative computerized tomography; the rest had undergone magnetic resonance imaging. The mean time from preoperative imaging to surgery was 66 days. Most of the patients (72) had intraoperative ultrasound imaging.
There were 45 anatomic resections and 27 nonanatomic resections in the group that had intraoperative ultrasound. This was significantly different from the nonultrasound group, which had 25 anatomic and 6 nonanatomic resections.
Ultrasound changed surgical strategy in 43% (31) of those who had it. Surgical strategy changed in 10% of those who had no intraoperative imaging – a significant difference (P = less than .001). Blood loss was significantly greater in the ultrasound group (650 mL vs. 350 mL).
The bulk of the strategic changes in the ultrasound group (17) were due to additional information about the location of lesions – either deeper or more superficial than preoperative imaging suggested. Other reasons for a shift in strategy were the discovery of new lesions (13), a disappearing lesion (1), larger-than-expected lesions (5), smaller-than-expected lesions (2), or a difference in the lesions’ appearance (3).
Resection margins were similar in the two groups. In the ultrasound group, 85% had R0 margins and 15% had R1 margins. In the group without ultrasound, 87% had R0 margins and 13% had R1 margins. There was no significant difference in disease-free 5-year survival.
Dr. Knowles had no financial disclosures.
AT AHPBA 2014
Major finding: Intraoperative ultrasound changed surgical strategy in 43% of patients undergoing liver resections of colorectal cancer metastases.
Data source: A retrospective study of 103 patients.
Disclosures: Dr. Knowles had no financial disclosures.

Group issues recommendations for genetic susceptibility testing for carbamazepine skin reactions
Genetic testing for alleles that affect histocompatibility should be the rule for patients who initiate the drug carbamazepine, according to new recommendations issued by the Canadian Pharmacogenomics Network for Drug Safety.
Two variants are associated with the severe, sometimes deadly, skin reactions that carbamazepine can bring on, usually within the first 3 months of therapy. One (HLA-B*15-02) is a particularly high-risk allele that is not uncommon in patients of Chinese, Thai, Malaysian, and Indian descent. It’s strongly associated with Stevens-Johnson syndrome and toxic epidermal necrolysis in those taking carbamazepine.
HLA-A*31:01 has been found among white, Japanese, Korean, and Chinese patients; in fact, it is somewhat common in most ethnic groups and people of mixed descent. This allele is associated with Stevens-Johnson, toxic epidermal necrolysis, and acute generalized exanthematous pustulosis, as well as some of the less-severe skin reactions, said Dr. Ursula Amstutz of the University of British Columbia, Vancouver, and her colleagues in the Network’s clinical recommendation group (Epilepsia 2014 March 5 [doi:10.1111/epi.12564]).
Genetic testing for the variants should be carried out before initiating treatment or within the first 3 months of treatment. But patients who have not had a reaction after at least 3 months’ treatment don’t need to be screened, advised the group, which used a systematic review of the literature to develop an expert consensus on the recommendations.
The group’s other recommendations include:
• Testing for HLA-B*15-02 should be done in all patients of the susceptible ethnic groups before treatment begins. It’s optional in groups where it is uncommon, but all drug-naïve patients should probably undergo the test.
• All patients, regardless of ethnicity, should undergo testing for HLA-A*31:01.
• Genetic testing should be done in patients who have previously experienced a skin reaction while taking carbamazepine, regardless of how long they have taken it.
• Negative tests don’t entirely rule out the possibility of a reaction, so patients, families, and physicians should still be alert for any early signs that one could develop.
One author was been a paid consultant for Novartis in legal cases relevant to carbamazepine-induced hypersensitivity. The others reported no relevant financial conflicts.
On Twitter @alz_gal
Genetic testing for alleles that affect histocompatibility should be the rule for patients who initiate the drug carbamazepine, according to new recommendations issued by the Canadian Pharmacogenomics Network for Drug Safety.
Two variants are associated with the severe, sometimes deadly, skin reactions that carbamazepine can bring on, usually within the first 3 months of therapy. One (HLA-B*15-02) is a particularly high-risk allele that is not uncommon in patients of Chinese, Thai, Malaysian, and Indian descent. It’s strongly associated with Stevens-Johnson syndrome and toxic epidermal necrolysis in those taking carbamazepine.
HLA-A*31:01 has been found among white, Japanese, Korean, and Chinese patients; in fact, it is somewhat common in most ethnic groups and people of mixed descent. This allele is associated with Stevens-Johnson, toxic epidermal necrolysis, and acute generalized exanthematous pustulosis, as well as some of the less-severe skin reactions, said Dr. Ursula Amstutz of the University of British Columbia, Vancouver, and her colleagues in the Network’s clinical recommendation group (Epilepsia 2014 March 5 [doi:10.1111/epi.12564]).
Genetic testing for the variants should be carried out before initiating treatment or within the first 3 months of treatment. But patients who have not had a reaction after at least 3 months’ treatment don’t need to be screened, advised the group, which used a systematic review of the literature to develop an expert consensus on the recommendations.
The group’s other recommendations include:
• Testing for HLA-B*15-02 should be done in all patients of the susceptible ethnic groups before treatment begins. It’s optional in groups where it is uncommon, but all drug-naïve patients should probably undergo the test.
• All patients, regardless of ethnicity, should undergo testing for HLA-A*31:01.
• Genetic testing should be done in patients who have previously experienced a skin reaction while taking carbamazepine, regardless of how long they have taken it.
• Negative tests don’t entirely rule out the possibility of a reaction, so patients, families, and physicians should still be alert for any early signs that one could develop.
One author was been a paid consultant for Novartis in legal cases relevant to carbamazepine-induced hypersensitivity. The others reported no relevant financial conflicts.
On Twitter @alz_gal
Genetic testing for alleles that affect histocompatibility should be the rule for patients who initiate the drug carbamazepine, according to new recommendations issued by the Canadian Pharmacogenomics Network for Drug Safety.
Two variants are associated with the severe, sometimes deadly, skin reactions that carbamazepine can bring on, usually within the first 3 months of therapy. One (HLA-B*15-02) is a particularly high-risk allele that is not uncommon in patients of Chinese, Thai, Malaysian, and Indian descent. It’s strongly associated with Stevens-Johnson syndrome and toxic epidermal necrolysis in those taking carbamazepine.
HLA-A*31:01 has been found among white, Japanese, Korean, and Chinese patients; in fact, it is somewhat common in most ethnic groups and people of mixed descent. This allele is associated with Stevens-Johnson, toxic epidermal necrolysis, and acute generalized exanthematous pustulosis, as well as some of the less-severe skin reactions, said Dr. Ursula Amstutz of the University of British Columbia, Vancouver, and her colleagues in the Network’s clinical recommendation group (Epilepsia 2014 March 5 [doi:10.1111/epi.12564]).
Genetic testing for the variants should be carried out before initiating treatment or within the first 3 months of treatment. But patients who have not had a reaction after at least 3 months’ treatment don’t need to be screened, advised the group, which used a systematic review of the literature to develop an expert consensus on the recommendations.
The group’s other recommendations include:
• Testing for HLA-B*15-02 should be done in all patients of the susceptible ethnic groups before treatment begins. It’s optional in groups where it is uncommon, but all drug-naïve patients should probably undergo the test.
• All patients, regardless of ethnicity, should undergo testing for HLA-A*31:01.
• Genetic testing should be done in patients who have previously experienced a skin reaction while taking carbamazepine, regardless of how long they have taken it.
• Negative tests don’t entirely rule out the possibility of a reaction, so patients, families, and physicians should still be alert for any early signs that one could develop.
One author was been a paid consultant for Novartis in legal cases relevant to carbamazepine-induced hypersensitivity. The others reported no relevant financial conflicts.
On Twitter @alz_gal
FROM EPILEPSIA
Volume matters: Whipple success hinges on surgeon experience
MIAMI BEACH – Studies continue to confirm it: When it comes to complex surgical procedures, higher volume equals better outcomes. But like the chicken-or-egg conundrum, researchers are asking which factor comes first – surgeon or facility.
Data presented at the annual meeting of the Americas Hepato-Pancreato-Biliary Association suggest that personal experience makes the biggest difference, at least for the difficult Whipple procedure. Surgeons who performed the highest number of pancreaticoduodenectomies each year had the best outcomes; when they transferred to low-volume hospitals with historically poor results, these surgeons improved perioperative complications, mortality, and readmissions, and lowered costs.
"The salutary effects of being a high-volume hospital for pancreaticoduodenectomy are transferred when high-volume surgeons relocate," said Dr. Paul Toomey. "It seems that the benefits of a high-volume hospital are more due to who does the surgery rather than where it’s undertaken."
Dr. Toomey, a surgical fellow at the Florida Hospital, Tampa, had a unique opportunity to study what happens when two surgeons highly experienced in the Whipple procedure transferred from a busy hospital to low-volume facilities. The surgeons, who together performed more than 100 of the procedures each year, moved for personal reasons, Dr. Toomey said in an interview.
The study focused on perioperative outcomes, mortality, and readmissions in two groups of Whipple patients: the last 50 undertaken at the high-volume hospital (more than 12 pancreaticoduodenectomies per year), and the first 50 at the low-volume hospital where they worked afterward.
The patient groups were similar. Their mean age was 78 years, a little more than half were men, and the average American Society of Anesthesiologists class was 3. The rates of malignancy were similar in the high- and low-volume centers (88% vs. 82%, respectively).
Overall, the average operative time was 252 minutes, with an estimated blood loss of 300 mL. Patients were in intensive care for 2 days, with an average hospital stay of 9 days. The readmission rate was 19% and 30-day mortality, 5%.
But when Dr. Toomey compared the two time periods, he found significant differences in outcomes, which appeared to be associated with the transfer of the highly experienced surgeons. In fact, he said, outcomes were actually much better at the low- than the high-volume centers after the transfer.
The mean operative time at the low-volume centers was 205 minutes, compared with 305 minutes at the high-volume centers. Estimated blood loss was also less at the low-volume centers (350 vs. 255 mL). ICU stays were significantly shorter (1 vs. 3 days), as was total length of stay (7 vs. 12 days). Readmission rates over 30 days were similar (20% vs. 18%), as was 30-day mortality (4% vs. 6%).
"The salutary benefits of being a high-volume hospital for pancreaticoduodenectomy seem to be transferred when high-volume surgeons relocate," Dr. Toomey said. "The benefits of a high-volume hospital may be more due to who does the pancreaticoduodenectomy rather than where the pancreaticoduodenectomy is undertaken."
Dr. Thomas Wood, also of the Florida Hospital, found a similar trend in his study, which examined Whipple outcomes statewide over 20 years. He related the outcomes to concentration, rather decentralization, of care.
For his study, Dr. Wood examined data from the Florida Agency for Health Care Administration, collected over three 3-year epochs: 1992-1994, 2001-2003, and 2010-2012. The data were sorted by surgeon volume of pancreaticoduodenectomy during these periods and correlated to length of stay, in-hospital mortality, and hospital charges, which were adjusted to 2012 dollars.
Over the 9 years, 893 surgeons performed 3,531 pancreaticoduodenectomies. During each epoch, the number of surgeons went down as the number of operations increased.
In the first epoch, 363 surgeons performed 729 operations. In the second, 334 surgeons performed 1,233 surgeries, and in the third, 196 performed 1,569 operations.
"By 2010-2012, 46% fewer surgeons undertook 115% more surgeries compared to the first period," Dr. Wood said. "In 1992-1994, 62% of pancreaticoduodenectomies were undertaken by surgeons who performed one or fewer per year. This fell to 13% by 2010-2012."
At the same time, the number of surgeons who performed more than 36 procedures in each 3-year period (12 per year) grew significantly. In the first epoch, one surgeon alone performed 45 procedures. In the second, six surgeons performed a total of 361. And in the third epoch, 11 surgeons performed 806 Whipples.
"From [the first through third periods,] there was an 11-fold increase in the number of high-volume surgeons and a corresponding 18-fold increase in the number of pancreaticoduodenectomies by surgeons who were performing at least 12 each year. They were performing more than 50% of these operations."
A separate analysis of just the 2010-2012 data evaluated outcomes by surgeons’ operation volume.
In the first epoch, in-hospital mortality was about 12%. In the second, it fell to 8%, and by the third, to 4%. Patients whose surgeons performed one to nine procedures (up to three per year) were hospitalized an average of about 14 days. Those whose surgeons performed 19 to 36 procedures (up to 12 per year) stayed an average of 8 days – a significant difference.
Mortality followed the same pattern. About 9% of patients whose surgeons performed one to three procedures per year died after surgery, compared with 2% of those whose doctors performed 12 procedures per year.
These more experienced surgeons also discharged more patients to home rather than nursing facilities (88% vs. 82%, a significant difference).
Both hospital and surgeon volume also affected costs. Overall, hospital costs increased significantly, even after adjustment for inflation, jumping from $93,000 to $133,000. But surgeons who performed at least 12 Whipples per year did so at a half the cost of those who performed 1-3 per year ($100,000 vs. $200,000).
"Suffice it to say, the busiest surgeons got the best results," Dr. Wood said.

Despite advances in centralizing this kind of specialized care, though, many low-volume centers are still performing the operations, said Dr. Jeffrey Sutton of the University of Cincinnati. "Research continues to show that high-volume centers have better outcomes," he said. "And yet a significant number of cases are still being done at hospitals that do less than one per year."
If research data aren’t enough to persuade hospitals to send patients to regional centers, Dr. Sutton wondered, could money be a motivating factor? He examined the records of almost 10,000 Whipple operations performed at 419 centers that are part of the University Health Systems Consortium clinical database. Of these, 120 were academic centers and 299 were affiliated hospitals. The procedures were performed from 2009 to 2011. Clinical outcomes included length of stay, mortality, and readmissions. He also assessed the cost of both the index admission and readmissions.
Hospitals were divided into volume quintiles of lowest, low, middle, high, and highest. The lowest-volume centers performed up to 21 cases/year in 2009 to up to 23 in 2011. The highest-volume centers performed up to 180 cases/year in 2009 and up to 216 in 2011.
Intraoperative mortality hovered around 2% at the middle-, high-, and highest-volume centers. At the low-volume centers, it reached 2.5% – not significantly different. But at the lowest-volume centers, 30-day mortality was significantly higher – nearly 4%.
Length of stay was similarly associated with volume. In low-, middle-, and high-volume centers, it was about 9 days. But in the lowest-volume centers, the average length of stay was 11 days – significantly longer than any of the others.
Readmission rates over the first postoperative month were also lowest in the highest-volume centers (16.5%). In the low-volume centers, 30-day readmission was just under 19%. But in the middle-, low-, and lowest-volume centers, it was significantly greater, hovering at nearly 20%.
"It’s not only that lower-volume centers are holding on to patients longer, they also are readmitting those same patients significantly more often," Dr. Sutton noted.
The cost analysis looked at Medicare charge data. "When both index and readmission costs were considered, the median per-patient cost at the lowest-volume centers was $23,005 – 11% more than at the highest-volume center."
But there was no significant difference in the cost of readmissions. "That means that the difference of about $2,263 extra per case was based solely on the index admission," Dr. Sutton said. "Essentially what we saw was that the more cases that are performed, the cheaper each individual case becomes."
"To put it bluntly, some low-volume centers are currently reimbursed higher sums of money for delivering suboptimal care to patients," Dr. Sutton said in an interview. In our current health care climate, which emphasizes improved outcomes at lower costs, this is a travesty. As health service researchers, it is our obligation to our patients to analyze and disseminate these data in an effort to urge policymakers to limit the financial reimbursements for poorer-performing providers."
None of the researchers quoted in this article reported any financial disclosures.
MIAMI BEACH – Studies continue to confirm it: When it comes to complex surgical procedures, higher volume equals better outcomes. But like the chicken-or-egg conundrum, researchers are asking which factor comes first – surgeon or facility.
Data presented at the annual meeting of the Americas Hepato-Pancreato-Biliary Association suggest that personal experience makes the biggest difference, at least for the difficult Whipple procedure. Surgeons who performed the highest number of pancreaticoduodenectomies each year had the best outcomes; when they transferred to low-volume hospitals with historically poor results, these surgeons improved perioperative complications, mortality, and readmissions, and lowered costs.
"The salutary effects of being a high-volume hospital for pancreaticoduodenectomy are transferred when high-volume surgeons relocate," said Dr. Paul Toomey. "It seems that the benefits of a high-volume hospital are more due to who does the surgery rather than where it’s undertaken."
Dr. Toomey, a surgical fellow at the Florida Hospital, Tampa, had a unique opportunity to study what happens when two surgeons highly experienced in the Whipple procedure transferred from a busy hospital to low-volume facilities. The surgeons, who together performed more than 100 of the procedures each year, moved for personal reasons, Dr. Toomey said in an interview.
The study focused on perioperative outcomes, mortality, and readmissions in two groups of Whipple patients: the last 50 undertaken at the high-volume hospital (more than 12 pancreaticoduodenectomies per year), and the first 50 at the low-volume hospital where they worked afterward.
The patient groups were similar. Their mean age was 78 years, a little more than half were men, and the average American Society of Anesthesiologists class was 3. The rates of malignancy were similar in the high- and low-volume centers (88% vs. 82%, respectively).
Overall, the average operative time was 252 minutes, with an estimated blood loss of 300 mL. Patients were in intensive care for 2 days, with an average hospital stay of 9 days. The readmission rate was 19% and 30-day mortality, 5%.
But when Dr. Toomey compared the two time periods, he found significant differences in outcomes, which appeared to be associated with the transfer of the highly experienced surgeons. In fact, he said, outcomes were actually much better at the low- than the high-volume centers after the transfer.
The mean operative time at the low-volume centers was 205 minutes, compared with 305 minutes at the high-volume centers. Estimated blood loss was also less at the low-volume centers (350 vs. 255 mL). ICU stays were significantly shorter (1 vs. 3 days), as was total length of stay (7 vs. 12 days). Readmission rates over 30 days were similar (20% vs. 18%), as was 30-day mortality (4% vs. 6%).
"The salutary benefits of being a high-volume hospital for pancreaticoduodenectomy seem to be transferred when high-volume surgeons relocate," Dr. Toomey said. "The benefits of a high-volume hospital may be more due to who does the pancreaticoduodenectomy rather than where the pancreaticoduodenectomy is undertaken."
Dr. Thomas Wood, also of the Florida Hospital, found a similar trend in his study, which examined Whipple outcomes statewide over 20 years. He related the outcomes to concentration, rather decentralization, of care.
For his study, Dr. Wood examined data from the Florida Agency for Health Care Administration, collected over three 3-year epochs: 1992-1994, 2001-2003, and 2010-2012. The data were sorted by surgeon volume of pancreaticoduodenectomy during these periods and correlated to length of stay, in-hospital mortality, and hospital charges, which were adjusted to 2012 dollars.
Over the 9 years, 893 surgeons performed 3,531 pancreaticoduodenectomies. During each epoch, the number of surgeons went down as the number of operations increased.
In the first epoch, 363 surgeons performed 729 operations. In the second, 334 surgeons performed 1,233 surgeries, and in the third, 196 performed 1,569 operations.
"By 2010-2012, 46% fewer surgeons undertook 115% more surgeries compared to the first period," Dr. Wood said. "In 1992-1994, 62% of pancreaticoduodenectomies were undertaken by surgeons who performed one or fewer per year. This fell to 13% by 2010-2012."
At the same time, the number of surgeons who performed more than 36 procedures in each 3-year period (12 per year) grew significantly. In the first epoch, one surgeon alone performed 45 procedures. In the second, six surgeons performed a total of 361. And in the third epoch, 11 surgeons performed 806 Whipples.
"From [the first through third periods,] there was an 11-fold increase in the number of high-volume surgeons and a corresponding 18-fold increase in the number of pancreaticoduodenectomies by surgeons who were performing at least 12 each year. They were performing more than 50% of these operations."
A separate analysis of just the 2010-2012 data evaluated outcomes by surgeons’ operation volume.
In the first epoch, in-hospital mortality was about 12%. In the second, it fell to 8%, and by the third, to 4%. Patients whose surgeons performed one to nine procedures (up to three per year) were hospitalized an average of about 14 days. Those whose surgeons performed 19 to 36 procedures (up to 12 per year) stayed an average of 8 days – a significant difference.
Mortality followed the same pattern. About 9% of patients whose surgeons performed one to three procedures per year died after surgery, compared with 2% of those whose doctors performed 12 procedures per year.
These more experienced surgeons also discharged more patients to home rather than nursing facilities (88% vs. 82%, a significant difference).
Both hospital and surgeon volume also affected costs. Overall, hospital costs increased significantly, even after adjustment for inflation, jumping from $93,000 to $133,000. But surgeons who performed at least 12 Whipples per year did so at a half the cost of those who performed 1-3 per year ($100,000 vs. $200,000).
"Suffice it to say, the busiest surgeons got the best results," Dr. Wood said.
Despite advances in centralizing this kind of specialized care, though, many low-volume centers are still performing the operations, said Dr. Jeffrey Sutton of the University of Cincinnati. "Research continues to show that high-volume centers have better outcomes," he said. "And yet a significant number of cases are still being done at hospitals that do less than one per year."
If research data aren’t enough to persuade hospitals to send patients to regional centers, Dr. Sutton wondered, could money be a motivating factor? He examined the records of almost 10,000 Whipple operations performed at 419 centers that are part of the University Health Systems Consortium clinical database. Of these, 120 were academic centers and 299 were affiliated hospitals. The procedures were performed from 2009 to 2011. Clinical outcomes included length of stay, mortality, and readmissions. He also assessed the cost of both the index admission and readmissions.
Hospitals were divided into volume quintiles of lowest, low, middle, high, and highest. The lowest-volume centers performed up to 21 cases/year in 2009 to up to 23 in 2011. The highest-volume centers performed up to 180 cases/year in 2009 and up to 216 in 2011.
Intraoperative mortality hovered around 2% at the middle-, high-, and highest-volume centers. At the low-volume centers, it reached 2.5% – not significantly different. But at the lowest-volume centers, 30-day mortality was significantly higher – nearly 4%.
Length of stay was similarly associated with volume. In low-, middle-, and high-volume centers, it was about 9 days. But in the lowest-volume centers, the average length of stay was 11 days – significantly longer than any of the others.
Readmission rates over the first postoperative month were also lowest in the highest-volume centers (16.5%). In the low-volume centers, 30-day readmission was just under 19%. But in the middle-, low-, and lowest-volume centers, it was significantly greater, hovering at nearly 20%.
"It’s not only that lower-volume centers are holding on to patients longer, they also are readmitting those same patients significantly more often," Dr. Sutton noted.
The cost analysis looked at Medicare charge data. "When both index and readmission costs were considered, the median per-patient cost at the lowest-volume centers was $23,005 – 11% more than at the highest-volume center."
But there was no significant difference in the cost of readmissions. "That means that the difference of about $2,263 extra per case was based solely on the index admission," Dr. Sutton said. "Essentially what we saw was that the more cases that are performed, the cheaper each individual case becomes."
"To put it bluntly, some low-volume centers are currently reimbursed higher sums of money for delivering suboptimal care to patients," Dr. Sutton said in an interview. In our current health care climate, which emphasizes improved outcomes at lower costs, this is a travesty. As health service researchers, it is our obligation to our patients to analyze and disseminate these data in an effort to urge policymakers to limit the financial reimbursements for poorer-performing providers."
None of the researchers quoted in this article reported any financial disclosures.
MIAMI BEACH – Studies continue to confirm it: When it comes to complex surgical procedures, higher volume equals better outcomes. But like the chicken-or-egg conundrum, researchers are asking which factor comes first – surgeon or facility.
Data presented at the annual meeting of the Americas Hepato-Pancreato-Biliary Association suggest that personal experience makes the biggest difference, at least for the difficult Whipple procedure. Surgeons who performed the highest number of pancreaticoduodenectomies each year had the best outcomes; when they transferred to low-volume hospitals with historically poor results, these surgeons improved perioperative complications, mortality, and readmissions, and lowered costs.
"The salutary effects of being a high-volume hospital for pancreaticoduodenectomy are transferred when high-volume surgeons relocate," said Dr. Paul Toomey. "It seems that the benefits of a high-volume hospital are more due to who does the surgery rather than where it’s undertaken."
Dr. Toomey, a surgical fellow at the Florida Hospital, Tampa, had a unique opportunity to study what happens when two surgeons highly experienced in the Whipple procedure transferred from a busy hospital to low-volume facilities. The surgeons, who together performed more than 100 of the procedures each year, moved for personal reasons, Dr. Toomey said in an interview.
The study focused on perioperative outcomes, mortality, and readmissions in two groups of Whipple patients: the last 50 undertaken at the high-volume hospital (more than 12 pancreaticoduodenectomies per year), and the first 50 at the low-volume hospital where they worked afterward.
The patient groups were similar. Their mean age was 78 years, a little more than half were men, and the average American Society of Anesthesiologists class was 3. The rates of malignancy were similar in the high- and low-volume centers (88% vs. 82%, respectively).
Overall, the average operative time was 252 minutes, with an estimated blood loss of 300 mL. Patients were in intensive care for 2 days, with an average hospital stay of 9 days. The readmission rate was 19% and 30-day mortality, 5%.
But when Dr. Toomey compared the two time periods, he found significant differences in outcomes, which appeared to be associated with the transfer of the highly experienced surgeons. In fact, he said, outcomes were actually much better at the low- than the high-volume centers after the transfer.
The mean operative time at the low-volume centers was 205 minutes, compared with 305 minutes at the high-volume centers. Estimated blood loss was also less at the low-volume centers (350 vs. 255 mL). ICU stays were significantly shorter (1 vs. 3 days), as was total length of stay (7 vs. 12 days). Readmission rates over 30 days were similar (20% vs. 18%), as was 30-day mortality (4% vs. 6%).
"The salutary benefits of being a high-volume hospital for pancreaticoduodenectomy seem to be transferred when high-volume surgeons relocate," Dr. Toomey said. "The benefits of a high-volume hospital may be more due to who does the pancreaticoduodenectomy rather than where the pancreaticoduodenectomy is undertaken."
Dr. Thomas Wood, also of the Florida Hospital, found a similar trend in his study, which examined Whipple outcomes statewide over 20 years. He related the outcomes to concentration, rather decentralization, of care.
For his study, Dr. Wood examined data from the Florida Agency for Health Care Administration, collected over three 3-year epochs: 1992-1994, 2001-2003, and 2010-2012. The data were sorted by surgeon volume of pancreaticoduodenectomy during these periods and correlated to length of stay, in-hospital mortality, and hospital charges, which were adjusted to 2012 dollars.
Over the 9 years, 893 surgeons performed 3,531 pancreaticoduodenectomies. During each epoch, the number of surgeons went down as the number of operations increased.
In the first epoch, 363 surgeons performed 729 operations. In the second, 334 surgeons performed 1,233 surgeries, and in the third, 196 performed 1,569 operations.
"By 2010-2012, 46% fewer surgeons undertook 115% more surgeries compared to the first period," Dr. Wood said. "In 1992-1994, 62% of pancreaticoduodenectomies were undertaken by surgeons who performed one or fewer per year. This fell to 13% by 2010-2012."
At the same time, the number of surgeons who performed more than 36 procedures in each 3-year period (12 per year) grew significantly. In the first epoch, one surgeon alone performed 45 procedures. In the second, six surgeons performed a total of 361. And in the third epoch, 11 surgeons performed 806 Whipples.
"From [the first through third periods,] there was an 11-fold increase in the number of high-volume surgeons and a corresponding 18-fold increase in the number of pancreaticoduodenectomies by surgeons who were performing at least 12 each year. They were performing more than 50% of these operations."
A separate analysis of just the 2010-2012 data evaluated outcomes by surgeons’ operation volume.
In the first epoch, in-hospital mortality was about 12%. In the second, it fell to 8%, and by the third, to 4%. Patients whose surgeons performed one to nine procedures (up to three per year) were hospitalized an average of about 14 days. Those whose surgeons performed 19 to 36 procedures (up to 12 per year) stayed an average of 8 days – a significant difference.
Mortality followed the same pattern. About 9% of patients whose surgeons performed one to three procedures per year died after surgery, compared with 2% of those whose doctors performed 12 procedures per year.
These more experienced surgeons also discharged more patients to home rather than nursing facilities (88% vs. 82%, a significant difference).
Both hospital and surgeon volume also affected costs. Overall, hospital costs increased significantly, even after adjustment for inflation, jumping from $93,000 to $133,000. But surgeons who performed at least 12 Whipples per year did so at a half the cost of those who performed 1-3 per year ($100,000 vs. $200,000).
"Suffice it to say, the busiest surgeons got the best results," Dr. Wood said.
Despite advances in centralizing this kind of specialized care, though, many low-volume centers are still performing the operations, said Dr. Jeffrey Sutton of the University of Cincinnati. "Research continues to show that high-volume centers have better outcomes," he said. "And yet a significant number of cases are still being done at hospitals that do less than one per year."
If research data aren’t enough to persuade hospitals to send patients to regional centers, Dr. Sutton wondered, could money be a motivating factor? He examined the records of almost 10,000 Whipple operations performed at 419 centers that are part of the University Health Systems Consortium clinical database. Of these, 120 were academic centers and 299 were affiliated hospitals. The procedures were performed from 2009 to 2011. Clinical outcomes included length of stay, mortality, and readmissions. He also assessed the cost of both the index admission and readmissions.
Hospitals were divided into volume quintiles of lowest, low, middle, high, and highest. The lowest-volume centers performed up to 21 cases/year in 2009 to up to 23 in 2011. The highest-volume centers performed up to 180 cases/year in 2009 and up to 216 in 2011.
Intraoperative mortality hovered around 2% at the middle-, high-, and highest-volume centers. At the low-volume centers, it reached 2.5% – not significantly different. But at the lowest-volume centers, 30-day mortality was significantly higher – nearly 4%.
Length of stay was similarly associated with volume. In low-, middle-, and high-volume centers, it was about 9 days. But in the lowest-volume centers, the average length of stay was 11 days – significantly longer than any of the others.
Readmission rates over the first postoperative month were also lowest in the highest-volume centers (16.5%). In the low-volume centers, 30-day readmission was just under 19%. But in the middle-, low-, and lowest-volume centers, it was significantly greater, hovering at nearly 20%.
"It’s not only that lower-volume centers are holding on to patients longer, they also are readmitting those same patients significantly more often," Dr. Sutton noted.
The cost analysis looked at Medicare charge data. "When both index and readmission costs were considered, the median per-patient cost at the lowest-volume centers was $23,005 – 11% more than at the highest-volume center."
But there was no significant difference in the cost of readmissions. "That means that the difference of about $2,263 extra per case was based solely on the index admission," Dr. Sutton said. "Essentially what we saw was that the more cases that are performed, the cheaper each individual case becomes."
"To put it bluntly, some low-volume centers are currently reimbursed higher sums of money for delivering suboptimal care to patients," Dr. Sutton said in an interview. In our current health care climate, which emphasizes improved outcomes at lower costs, this is a travesty. As health service researchers, it is our obligation to our patients to analyze and disseminate these data in an effort to urge policymakers to limit the financial reimbursements for poorer-performing providers."
None of the researchers quoted in this article reported any financial disclosures.
AT AHPBA 2014
Major finding: When high-volume surgeons transferred to low-volume institutions, these surgeons improved perioperative complications, mortality, and readmissions, and lowered costs in the low-volume institutions. The mean operative time at the low-volume centers was 205 minutes, compared with 305 minutes at the high-volume centers. Estimated blood loss was also less at the low-volume centers (350 vs. 255 mL), as was total length of stay (7 vs. 12 days).
Data source: Data from more than 100 Whipple procedures performed by two experienced surgeons who transferred to low-volume institutions.
Disclosures: None of the researchers quoted in this article reported any financial disclosures.

Outcomes similar for two reconstruction techniques, except for risk of severe complications
MIAMI BEACH* – There appears to be no difference in the rate of anastomotic leak in pancreaticogastrostomy compared with pancreaticojejunostomy reconstruction after a Whipple procedure, but pancreaticogastrostomy does appear to increase the risk of some serious postoperative complications, a study found.
"We didn’t show any significant differences in terms of leaks, severity of leaks, or even overall complications," Dr. Jan Grendar said at the annual meeting of the Americas Hepato-Pancreato-Biliary Association. "But we did show a significant difference in complications of Clavien grades III-V severity. This anastomosis just did a little bit worse in terms of severe complications."
Grade III Clavien complications are those that require a second invasive procedure, like reoperation or drainage, with local or general anesthesia. Grade IV complications are more serious – they include organ failures such as renal failure requiring hemodialysis, heart failure, and liver failure, and intubation. The Grade V complication is patient death.
Dr. Grendar, a surgical resident at the University of Calgary (Alta.), and his colleagues randomized 98 patients with benign or malignant pancreatic disease to either of the two reconstruction techniques after a Whipple procedure. Pancreaticojejunostomy (PJ) is the procedure typically performed in North America. Pancreaticogastrostomy (PG) is typically performed in Europe. The hepatobiliary pancreatic surgeons and residents at the university, however, have become adept at this second procedure and employ it as an alternative reconstruction, depending on the characteristics of the pancreas discovered during surgery. They most often use it on patients who have a soft pancreas or small pancreatic duct.
All of the patients in the study had a pancreatic or periampullary neoplasm that appeared resectable on preoperative imaging. There were no differences in baseline patient characteristics. The mean age was 64 in the PG group and 68 in the PJ group. The median Charlson comorbidity index score was 2.
The intraoperative outcomes were mostly similar. Gland mobilization occurred significantly more often in the PG group (31 vs. 18 mm). Significantly fewer PG patients had a two-layer anastomosis (77% vs. 94%). The mean pancreatic duct size was smaller in the PG patients (3.8 vs. 4.3 mm), but this wasn’t statistically significant. Significantly fewer PG patients had a pancreatic duct stent placed (22% vs. 83%).
Postoperative outcomes included pancreatic fistula, any postoperative complications, severe complications, and length of stay.
There was no difference between the groups in Clavien grade complications separately, but significantly more PG patients had severe, Clavien grade III-V complications (31% vs. 12%). But these didn’t affect the mean length of stay, which was similar between the groups (17 vs. 14 days).
In a multivariate analysis, only having a soft pancreas significantly increased the risk of developing a pancreatic fistula (odds ratio, 5.87). Female gender significantly decreased the risk (OR, 0.31). This most likely represents a correlation between pancreatic texture and patient sex rather than a true protective property of being female. Having a soft pancreas also significantly increased the risk of any postoperative complications (OR, 3.08).
Several factors significantly increased the risk of a severe complication. These included a baseline American Society of Anesthesiologists grade of 2 or 3 (OR, 12.75 and 29.56, respectively). Being randomized to the PJ procedure significantly decreased the risk of a severe complication (OR, 0.11).
"Unlike the European centers that report different outcomes, these results are coming from a center that wasn’t very enthusiastic about this type of reconstruction prior to this study," Dr. Grendar said in an interview. "Despite the initial preference, high-risk patients in Calgary, those with soft pancreatic glands and small pancreatic ducts, are now likely to be offered a pancreaticogastrostomy"
Dr. Grendar said he had no relevant financial disclosures.
*Correction, 3/11/2014: An earlier version of the article misstated the name of the city where the AHPBA meeting took place.
MIAMI BEACH* – There appears to be no difference in the rate of anastomotic leak in pancreaticogastrostomy compared with pancreaticojejunostomy reconstruction after a Whipple procedure, but pancreaticogastrostomy does appear to increase the risk of some serious postoperative complications, a study found.
"We didn’t show any significant differences in terms of leaks, severity of leaks, or even overall complications," Dr. Jan Grendar said at the annual meeting of the Americas Hepato-Pancreato-Biliary Association. "But we did show a significant difference in complications of Clavien grades III-V severity. This anastomosis just did a little bit worse in terms of severe complications."
Grade III Clavien complications are those that require a second invasive procedure, like reoperation or drainage, with local or general anesthesia. Grade IV complications are more serious – they include organ failures such as renal failure requiring hemodialysis, heart failure, and liver failure, and intubation. The Grade V complication is patient death.
Dr. Grendar, a surgical resident at the University of Calgary (Alta.), and his colleagues randomized 98 patients with benign or malignant pancreatic disease to either of the two reconstruction techniques after a Whipple procedure. Pancreaticojejunostomy (PJ) is the procedure typically performed in North America. Pancreaticogastrostomy (PG) is typically performed in Europe. The hepatobiliary pancreatic surgeons and residents at the university, however, have become adept at this second procedure and employ it as an alternative reconstruction, depending on the characteristics of the pancreas discovered during surgery. They most often use it on patients who have a soft pancreas or small pancreatic duct.
All of the patients in the study had a pancreatic or periampullary neoplasm that appeared resectable on preoperative imaging. There were no differences in baseline patient characteristics. The mean age was 64 in the PG group and 68 in the PJ group. The median Charlson comorbidity index score was 2.
The intraoperative outcomes were mostly similar. Gland mobilization occurred significantly more often in the PG group (31 vs. 18 mm). Significantly fewer PG patients had a two-layer anastomosis (77% vs. 94%). The mean pancreatic duct size was smaller in the PG patients (3.8 vs. 4.3 mm), but this wasn’t statistically significant. Significantly fewer PG patients had a pancreatic duct stent placed (22% vs. 83%).
Postoperative outcomes included pancreatic fistula, any postoperative complications, severe complications, and length of stay.
There was no difference between the groups in Clavien grade complications separately, but significantly more PG patients had severe, Clavien grade III-V complications (31% vs. 12%). But these didn’t affect the mean length of stay, which was similar between the groups (17 vs. 14 days).
In a multivariate analysis, only having a soft pancreas significantly increased the risk of developing a pancreatic fistula (odds ratio, 5.87). Female gender significantly decreased the risk (OR, 0.31). This most likely represents a correlation between pancreatic texture and patient sex rather than a true protective property of being female. Having a soft pancreas also significantly increased the risk of any postoperative complications (OR, 3.08).
Several factors significantly increased the risk of a severe complication. These included a baseline American Society of Anesthesiologists grade of 2 or 3 (OR, 12.75 and 29.56, respectively). Being randomized to the PJ procedure significantly decreased the risk of a severe complication (OR, 0.11).
"Unlike the European centers that report different outcomes, these results are coming from a center that wasn’t very enthusiastic about this type of reconstruction prior to this study," Dr. Grendar said in an interview. "Despite the initial preference, high-risk patients in Calgary, those with soft pancreatic glands and small pancreatic ducts, are now likely to be offered a pancreaticogastrostomy"
Dr. Grendar said he had no relevant financial disclosures.
*Correction, 3/11/2014: An earlier version of the article misstated the name of the city where the AHPBA meeting took place.
MIAMI BEACH* – There appears to be no difference in the rate of anastomotic leak in pancreaticogastrostomy compared with pancreaticojejunostomy reconstruction after a Whipple procedure, but pancreaticogastrostomy does appear to increase the risk of some serious postoperative complications, a study found.
"We didn’t show any significant differences in terms of leaks, severity of leaks, or even overall complications," Dr. Jan Grendar said at the annual meeting of the Americas Hepato-Pancreato-Biliary Association. "But we did show a significant difference in complications of Clavien grades III-V severity. This anastomosis just did a little bit worse in terms of severe complications."
Grade III Clavien complications are those that require a second invasive procedure, like reoperation or drainage, with local or general anesthesia. Grade IV complications are more serious – they include organ failures such as renal failure requiring hemodialysis, heart failure, and liver failure, and intubation. The Grade V complication is patient death.
Dr. Grendar, a surgical resident at the University of Calgary (Alta.), and his colleagues randomized 98 patients with benign or malignant pancreatic disease to either of the two reconstruction techniques after a Whipple procedure. Pancreaticojejunostomy (PJ) is the procedure typically performed in North America. Pancreaticogastrostomy (PG) is typically performed in Europe. The hepatobiliary pancreatic surgeons and residents at the university, however, have become adept at this second procedure and employ it as an alternative reconstruction, depending on the characteristics of the pancreas discovered during surgery. They most often use it on patients who have a soft pancreas or small pancreatic duct.
All of the patients in the study had a pancreatic or periampullary neoplasm that appeared resectable on preoperative imaging. There were no differences in baseline patient characteristics. The mean age was 64 in the PG group and 68 in the PJ group. The median Charlson comorbidity index score was 2.
The intraoperative outcomes were mostly similar. Gland mobilization occurred significantly more often in the PG group (31 vs. 18 mm). Significantly fewer PG patients had a two-layer anastomosis (77% vs. 94%). The mean pancreatic duct size was smaller in the PG patients (3.8 vs. 4.3 mm), but this wasn’t statistically significant. Significantly fewer PG patients had a pancreatic duct stent placed (22% vs. 83%).
Postoperative outcomes included pancreatic fistula, any postoperative complications, severe complications, and length of stay.
There was no difference between the groups in Clavien grade complications separately, but significantly more PG patients had severe, Clavien grade III-V complications (31% vs. 12%). But these didn’t affect the mean length of stay, which was similar between the groups (17 vs. 14 days).
In a multivariate analysis, only having a soft pancreas significantly increased the risk of developing a pancreatic fistula (odds ratio, 5.87). Female gender significantly decreased the risk (OR, 0.31). This most likely represents a correlation between pancreatic texture and patient sex rather than a true protective property of being female. Having a soft pancreas also significantly increased the risk of any postoperative complications (OR, 3.08).
Several factors significantly increased the risk of a severe complication. These included a baseline American Society of Anesthesiologists grade of 2 or 3 (OR, 12.75 and 29.56, respectively). Being randomized to the PJ procedure significantly decreased the risk of a severe complication (OR, 0.11).
"Unlike the European centers that report different outcomes, these results are coming from a center that wasn’t very enthusiastic about this type of reconstruction prior to this study," Dr. Grendar said in an interview. "Despite the initial preference, high-risk patients in Calgary, those with soft pancreatic glands and small pancreatic ducts, are now likely to be offered a pancreaticogastrostomy"
Dr. Grendar said he had no relevant financial disclosures.
*Correction, 3/11/2014: An earlier version of the article misstated the name of the city where the AHPBA meeting took place.
AT AHPBA 2014
Major finding: Severe complications occurred in significantly more Whipple patients who had a pancreaticogastrostomy reconstruction than a pancreaticojejunostomy (31% vs. 12%).
Data source: A randomized study involving 98 patients.
Disclosures: Dr. Grendar said he had no relevant financial disclosures.
Obesity a driving factor in stillbirth
NEW ORLEANS – Almost 20% of the stillbirths that occurred over an 8-year period appeared to be associated with obesity.
A database review of nearly 3 million births found that the risk of stillbirth increased along with body mass index and gestational age. For women with the highest BMI – 50 kg/m2 – the incidence of a stillbirth jumped from 1.8/1,000 pregnancies at 39 weeks to 3/1,000 at 40 weeks and to more than 5/1,000 by 41 weeks, Dr. Ruofan Yao reported at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
"There is a dose-response relationship where the greater the BMI, the higher the risk of stillbirth. Obesity is a major contributing risk for stillbirth, where 20% of all stillbirths happen to women who are obese, and 1 in 4 stillbirths after 37 weeks is associated with obesity," said Dr. Yao of Drexel University, Philadelphia. "This is significantly higher than the population-attributable risk for chronic hypertension or pregestational diabetes."
Dr. Yao used birth and death records from Texas and Washington to determine the associations between weight and stillbirth. The Texas cohort included data on about 2 million births that occurred from 2006 to 2011. The Washington cohort included data on about 1 million from 2003 to 2011. Of the nearly 3 million births analyzed, about 9,000 were stillbirths. Fetuses with severe congenital anomalies were excluded from the analysis, as were pregnancies with a gestational age of less than 20 weeks.
Overall, 51% of the mothers in the analysis were of normal weight. About a quarter were overweight. Class I obesity was present in 13%, class II in 6%, and class III in 3.5%. The remaining 0.5% had a BMI of 50 or higher.
Although the risk of stillbirth rose with BMI and gestational age, overweight women were at no significantly increased risk of stillbirth compared with normal-weight women.
Women in class I were about twice as likely to have a stillbirth at both 37-39 weeks and 40-42 weeks. For women in class II, the risk was about 2.5 times higher at 37-39 weeks and twice as high at 40-42 weeks. In class III, the risk of stillbirth was three times higher at both time points.
The risk was sharply elevated for women with a BMI of 50 or more. At 37-39 weeks, they had a threefold increased risk. That jumped to a ninefold increased risk by 40-42 weeks, Dr. Yao said.
A separate analysis quantified population-attributable risk (PAR) for obesity and stillbirth. For all obesity (30 or higher), the risk was almost 20% overall. The PAR was 24% for early-term pregnancies and 28% for late-term pregnancies.
"Furthermore, over 5% of stillbirths from 37-39 weeks were associated with the much smaller subset of women who are morbidly obese, and this number jumps to 8% from 40-42 weeks," he said.
"Our data pointed to 39 weeks as a pivotal point in the pregnancy where the risk of stillbirth increases at a dramatic pace for women with BMI more than 50," Dr. Yao said in an interview. "I believe it is reasonable to have a discussion with patients in this BMI group regarding their maternal and fetal risks for expectant management verses delivery at 39 weeks. Whether to extend this recommendation to other obese women is unclear until more studies can delineate the risks and benefits more clearly."
The pathophysiology behind the association of obesity and preterm birth isn’t yet clear, he added.
"It is known in endocrine and medicine literature that obesity increases the baseline inflammatory response, and this may lead to abnormal placental growth and the development of uteroplacental insufficiency," Dr. Yao said.
"Obesity is also commonly associated with sleep apnea, which often worsens in pregnancy and can lead to transient hypoxic state, hindering normal fetal growth, and increase the risk of preeclampsia. Obesity also leads to glucose intolerance and increased serum lipid and triglyceride levels, leading to accelerated fetal growth velocity, and may contribute to the development of uteroplacental insufficiency. Additionally, the dietary habits of many obese women tend to exacerbate that problem."
Dr. Yao reported that he had no financial disclosures.
NEW ORLEANS – Almost 20% of the stillbirths that occurred over an 8-year period appeared to be associated with obesity.
A database review of nearly 3 million births found that the risk of stillbirth increased along with body mass index and gestational age. For women with the highest BMI – 50 kg/m2 – the incidence of a stillbirth jumped from 1.8/1,000 pregnancies at 39 weeks to 3/1,000 at 40 weeks and to more than 5/1,000 by 41 weeks, Dr. Ruofan Yao reported at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
"There is a dose-response relationship where the greater the BMI, the higher the risk of stillbirth. Obesity is a major contributing risk for stillbirth, where 20% of all stillbirths happen to women who are obese, and 1 in 4 stillbirths after 37 weeks is associated with obesity," said Dr. Yao of Drexel University, Philadelphia. "This is significantly higher than the population-attributable risk for chronic hypertension or pregestational diabetes."
Dr. Yao used birth and death records from Texas and Washington to determine the associations between weight and stillbirth. The Texas cohort included data on about 2 million births that occurred from 2006 to 2011. The Washington cohort included data on about 1 million from 2003 to 2011. Of the nearly 3 million births analyzed, about 9,000 were stillbirths. Fetuses with severe congenital anomalies were excluded from the analysis, as were pregnancies with a gestational age of less than 20 weeks.
Overall, 51% of the mothers in the analysis were of normal weight. About a quarter were overweight. Class I obesity was present in 13%, class II in 6%, and class III in 3.5%. The remaining 0.5% had a BMI of 50 or higher.
Although the risk of stillbirth rose with BMI and gestational age, overweight women were at no significantly increased risk of stillbirth compared with normal-weight women.
Women in class I were about twice as likely to have a stillbirth at both 37-39 weeks and 40-42 weeks. For women in class II, the risk was about 2.5 times higher at 37-39 weeks and twice as high at 40-42 weeks. In class III, the risk of stillbirth was three times higher at both time points.
The risk was sharply elevated for women with a BMI of 50 or more. At 37-39 weeks, they had a threefold increased risk. That jumped to a ninefold increased risk by 40-42 weeks, Dr. Yao said.
A separate analysis quantified population-attributable risk (PAR) for obesity and stillbirth. For all obesity (30 or higher), the risk was almost 20% overall. The PAR was 24% for early-term pregnancies and 28% for late-term pregnancies.
"Furthermore, over 5% of stillbirths from 37-39 weeks were associated with the much smaller subset of women who are morbidly obese, and this number jumps to 8% from 40-42 weeks," he said.
"Our data pointed to 39 weeks as a pivotal point in the pregnancy where the risk of stillbirth increases at a dramatic pace for women with BMI more than 50," Dr. Yao said in an interview. "I believe it is reasonable to have a discussion with patients in this BMI group regarding their maternal and fetal risks for expectant management verses delivery at 39 weeks. Whether to extend this recommendation to other obese women is unclear until more studies can delineate the risks and benefits more clearly."
The pathophysiology behind the association of obesity and preterm birth isn’t yet clear, he added.
"It is known in endocrine and medicine literature that obesity increases the baseline inflammatory response, and this may lead to abnormal placental growth and the development of uteroplacental insufficiency," Dr. Yao said.
"Obesity is also commonly associated with sleep apnea, which often worsens in pregnancy and can lead to transient hypoxic state, hindering normal fetal growth, and increase the risk of preeclampsia. Obesity also leads to glucose intolerance and increased serum lipid and triglyceride levels, leading to accelerated fetal growth velocity, and may contribute to the development of uteroplacental insufficiency. Additionally, the dietary habits of many obese women tend to exacerbate that problem."
Dr. Yao reported that he had no financial disclosures.
NEW ORLEANS – Almost 20% of the stillbirths that occurred over an 8-year period appeared to be associated with obesity.
A database review of nearly 3 million births found that the risk of stillbirth increased along with body mass index and gestational age. For women with the highest BMI – 50 kg/m2 – the incidence of a stillbirth jumped from 1.8/1,000 pregnancies at 39 weeks to 3/1,000 at 40 weeks and to more than 5/1,000 by 41 weeks, Dr. Ruofan Yao reported at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
"There is a dose-response relationship where the greater the BMI, the higher the risk of stillbirth. Obesity is a major contributing risk for stillbirth, where 20% of all stillbirths happen to women who are obese, and 1 in 4 stillbirths after 37 weeks is associated with obesity," said Dr. Yao of Drexel University, Philadelphia. "This is significantly higher than the population-attributable risk for chronic hypertension or pregestational diabetes."
Dr. Yao used birth and death records from Texas and Washington to determine the associations between weight and stillbirth. The Texas cohort included data on about 2 million births that occurred from 2006 to 2011. The Washington cohort included data on about 1 million from 2003 to 2011. Of the nearly 3 million births analyzed, about 9,000 were stillbirths. Fetuses with severe congenital anomalies were excluded from the analysis, as were pregnancies with a gestational age of less than 20 weeks.
Overall, 51% of the mothers in the analysis were of normal weight. About a quarter were overweight. Class I obesity was present in 13%, class II in 6%, and class III in 3.5%. The remaining 0.5% had a BMI of 50 or higher.
Although the risk of stillbirth rose with BMI and gestational age, overweight women were at no significantly increased risk of stillbirth compared with normal-weight women.
Women in class I were about twice as likely to have a stillbirth at both 37-39 weeks and 40-42 weeks. For women in class II, the risk was about 2.5 times higher at 37-39 weeks and twice as high at 40-42 weeks. In class III, the risk of stillbirth was three times higher at both time points.
The risk was sharply elevated for women with a BMI of 50 or more. At 37-39 weeks, they had a threefold increased risk. That jumped to a ninefold increased risk by 40-42 weeks, Dr. Yao said.
A separate analysis quantified population-attributable risk (PAR) for obesity and stillbirth. For all obesity (30 or higher), the risk was almost 20% overall. The PAR was 24% for early-term pregnancies and 28% for late-term pregnancies.
"Furthermore, over 5% of stillbirths from 37-39 weeks were associated with the much smaller subset of women who are morbidly obese, and this number jumps to 8% from 40-42 weeks," he said.
"Our data pointed to 39 weeks as a pivotal point in the pregnancy where the risk of stillbirth increases at a dramatic pace for women with BMI more than 50," Dr. Yao said in an interview. "I believe it is reasonable to have a discussion with patients in this BMI group regarding their maternal and fetal risks for expectant management verses delivery at 39 weeks. Whether to extend this recommendation to other obese women is unclear until more studies can delineate the risks and benefits more clearly."
The pathophysiology behind the association of obesity and preterm birth isn’t yet clear, he added.
"It is known in endocrine and medicine literature that obesity increases the baseline inflammatory response, and this may lead to abnormal placental growth and the development of uteroplacental insufficiency," Dr. Yao said.
"Obesity is also commonly associated with sleep apnea, which often worsens in pregnancy and can lead to transient hypoxic state, hindering normal fetal growth, and increase the risk of preeclampsia. Obesity also leads to glucose intolerance and increased serum lipid and triglyceride levels, leading to accelerated fetal growth velocity, and may contribute to the development of uteroplacental insufficiency. Additionally, the dietary habits of many obese women tend to exacerbate that problem."
Dr. Yao reported that he had no financial disclosures.
AT THE PREGNANCY MEETING
Major finding: Nearly 20% of stillbirths that occurred over an 8-year period were associated with obesity.
Data source: Population-based data with information on almost 3 million births.
Disclosures: Dr. Yao reported that he had no financial disclosures.
Delivery of identical twins near 33 weeks balances outcomes
NEW ORLEANS – The optimal time to deliver monoamniotic twins is right around 33 weeks, when the risks of intrauterine death and neonatal complications are both very low.
"Monoamniotic twin pregnancies are at extremely high risk of intrauterine death before 28 weeks’ gestation," Dr. Tim Van Mieghem said at the Pregnancy Meeting, sponsored by the Society for Maternal Fetal Medicine. "But with regular fetal monitoring and ultrasound, that risk is extremely low from 28 to 32 weeks."

At the same time, the risk of neonatal complications decreases as the pregnancy advances. The fulcrum that balances both optimal outcomes is 33 weeks, 4 days.
To determine this, Dr. Van Mieghem looked at a retrospective cohort of monoamniotic twin pregnancies followed during 2003-2013 in Canada and Europe. The group comprised 193 pregnancies (386 fetuses); the investigators excluded conjoined twins and cases of twin reversed arterial perfusion. The rate of twin-twin transfusion syndrome was low (3%).
The rate of fetal anomalies was quite high (53; 14%), said Dr. Van Mieghem of the University Hospital of Leuven, Belgium. Twelve of the pregnancies were terminated. There were 28 double intrauterine deaths and 14 single intrauterine deaths. Most of these were caused by cord events; seven were iatrogenic.
Most of the fetuses (76%) were born alive at an average of 32 weeks’ gestation. Most of the mothers received corticosteroids (91%), and most deliveries were by cesarean section (97%). The mean birth weight was 1,749 g. The neonatal death rate was 5.7%.
The most common neonatal complications were respiratory; 80% of the infants needed respiratory support and 40% had respiratory distress syndrome. The rate of nonrespiratory complications was about 15%. Sepsis occurred in about 10%. The remainder of the complications were necrotizing enterocolitis, intraventricular hemorrhage, and periventricular leukomalacia.
The risk of intrauterine death decreased as the pregnancy advanced. At 24 weeks, it was about 5%, but by 28 weeks had dropped to a low of 1.4%. Thereafter, the risk began to rise, reaching about 7% by week 35.
The risk of neonatal complications also decreased as the pregnancy advanced. It reached its nadir of about 2% at around 28 weeks and stayed low until about 33 weeks, when it began to rise. By 34 weeks it was near 7%, but dropped to close to 0 shortly after 35 weeks.
"The risk curves intersected at 32 weeks, 4 days," Dr. Van Mieghem said. "Based on these curves, it seems prudent to deliver these fetuses at 32 weeks, when the risk of both intrauterine demise and neonatal complications is about 3%."
He added that there were no significant differences in neonatal outcomes between pregnancies that were monitored on an inpatient and outpatient basis. The gestational age at delivery was about a week earlier in inpatients (32 vs. 33 weeks.) The rate of fetal distress was slightly higher among inpatients (21% vs. 23%). The outpatient pregnancies resulted in larger infants (mean 1,827 g vs. 1,776 g).
The rate of nonrespiratory neonatal complications was about 9% in each group. However, significantly more infants in the inpatient group needed ventilation (76% vs. 63%). They were also on ventilation about a day longer (5 days vs. 4 days).
There were one single and two double intrauterine deaths in the outpatient group, and one single intrauterine death in the inpatient group. But because all of the outpatient deaths occurred before 28 weeks, Dr. Van Mieghem said they probably could not have been averted by inpatient management.
"If you were looking at the rate of truly preventable deaths, it likely would have been 0 in both groups," he said.
Dr. Van Mieghem had no financial disclosures.
On Twitter @alz_gal
NEW ORLEANS – The optimal time to deliver monoamniotic twins is right around 33 weeks, when the risks of intrauterine death and neonatal complications are both very low.
"Monoamniotic twin pregnancies are at extremely high risk of intrauterine death before 28 weeks’ gestation," Dr. Tim Van Mieghem said at the Pregnancy Meeting, sponsored by the Society for Maternal Fetal Medicine. "But with regular fetal monitoring and ultrasound, that risk is extremely low from 28 to 32 weeks."
At the same time, the risk of neonatal complications decreases as the pregnancy advances. The fulcrum that balances both optimal outcomes is 33 weeks, 4 days.
To determine this, Dr. Van Mieghem looked at a retrospective cohort of monoamniotic twin pregnancies followed during 2003-2013 in Canada and Europe. The group comprised 193 pregnancies (386 fetuses); the investigators excluded conjoined twins and cases of twin reversed arterial perfusion. The rate of twin-twin transfusion syndrome was low (3%).
The rate of fetal anomalies was quite high (53; 14%), said Dr. Van Mieghem of the University Hospital of Leuven, Belgium. Twelve of the pregnancies were terminated. There were 28 double intrauterine deaths and 14 single intrauterine deaths. Most of these were caused by cord events; seven were iatrogenic.
Most of the fetuses (76%) were born alive at an average of 32 weeks’ gestation. Most of the mothers received corticosteroids (91%), and most deliveries were by cesarean section (97%). The mean birth weight was 1,749 g. The neonatal death rate was 5.7%.
The most common neonatal complications were respiratory; 80% of the infants needed respiratory support and 40% had respiratory distress syndrome. The rate of nonrespiratory complications was about 15%. Sepsis occurred in about 10%. The remainder of the complications were necrotizing enterocolitis, intraventricular hemorrhage, and periventricular leukomalacia.
The risk of intrauterine death decreased as the pregnancy advanced. At 24 weeks, it was about 5%, but by 28 weeks had dropped to a low of 1.4%. Thereafter, the risk began to rise, reaching about 7% by week 35.
The risk of neonatal complications also decreased as the pregnancy advanced. It reached its nadir of about 2% at around 28 weeks and stayed low until about 33 weeks, when it began to rise. By 34 weeks it was near 7%, but dropped to close to 0 shortly after 35 weeks.
"The risk curves intersected at 32 weeks, 4 days," Dr. Van Mieghem said. "Based on these curves, it seems prudent to deliver these fetuses at 32 weeks, when the risk of both intrauterine demise and neonatal complications is about 3%."
He added that there were no significant differences in neonatal outcomes between pregnancies that were monitored on an inpatient and outpatient basis. The gestational age at delivery was about a week earlier in inpatients (32 vs. 33 weeks.) The rate of fetal distress was slightly higher among inpatients (21% vs. 23%). The outpatient pregnancies resulted in larger infants (mean 1,827 g vs. 1,776 g).
The rate of nonrespiratory neonatal complications was about 9% in each group. However, significantly more infants in the inpatient group needed ventilation (76% vs. 63%). They were also on ventilation about a day longer (5 days vs. 4 days).
There were one single and two double intrauterine deaths in the outpatient group, and one single intrauterine death in the inpatient group. But because all of the outpatient deaths occurred before 28 weeks, Dr. Van Mieghem said they probably could not have been averted by inpatient management.
"If you were looking at the rate of truly preventable deaths, it likely would have been 0 in both groups," he said.
Dr. Van Mieghem had no financial disclosures.
On Twitter @alz_gal
NEW ORLEANS – The optimal time to deliver monoamniotic twins is right around 33 weeks, when the risks of intrauterine death and neonatal complications are both very low.
"Monoamniotic twin pregnancies are at extremely high risk of intrauterine death before 28 weeks’ gestation," Dr. Tim Van Mieghem said at the Pregnancy Meeting, sponsored by the Society for Maternal Fetal Medicine. "But with regular fetal monitoring and ultrasound, that risk is extremely low from 28 to 32 weeks."
At the same time, the risk of neonatal complications decreases as the pregnancy advances. The fulcrum that balances both optimal outcomes is 33 weeks, 4 days.
To determine this, Dr. Van Mieghem looked at a retrospective cohort of monoamniotic twin pregnancies followed during 2003-2013 in Canada and Europe. The group comprised 193 pregnancies (386 fetuses); the investigators excluded conjoined twins and cases of twin reversed arterial perfusion. The rate of twin-twin transfusion syndrome was low (3%).
The rate of fetal anomalies was quite high (53; 14%), said Dr. Van Mieghem of the University Hospital of Leuven, Belgium. Twelve of the pregnancies were terminated. There were 28 double intrauterine deaths and 14 single intrauterine deaths. Most of these were caused by cord events; seven were iatrogenic.
Most of the fetuses (76%) were born alive at an average of 32 weeks’ gestation. Most of the mothers received corticosteroids (91%), and most deliveries were by cesarean section (97%). The mean birth weight was 1,749 g. The neonatal death rate was 5.7%.
The most common neonatal complications were respiratory; 80% of the infants needed respiratory support and 40% had respiratory distress syndrome. The rate of nonrespiratory complications was about 15%. Sepsis occurred in about 10%. The remainder of the complications were necrotizing enterocolitis, intraventricular hemorrhage, and periventricular leukomalacia.
The risk of intrauterine death decreased as the pregnancy advanced. At 24 weeks, it was about 5%, but by 28 weeks had dropped to a low of 1.4%. Thereafter, the risk began to rise, reaching about 7% by week 35.
The risk of neonatal complications also decreased as the pregnancy advanced. It reached its nadir of about 2% at around 28 weeks and stayed low until about 33 weeks, when it began to rise. By 34 weeks it was near 7%, but dropped to close to 0 shortly after 35 weeks.
"The risk curves intersected at 32 weeks, 4 days," Dr. Van Mieghem said. "Based on these curves, it seems prudent to deliver these fetuses at 32 weeks, when the risk of both intrauterine demise and neonatal complications is about 3%."
He added that there were no significant differences in neonatal outcomes between pregnancies that were monitored on an inpatient and outpatient basis. The gestational age at delivery was about a week earlier in inpatients (32 vs. 33 weeks.) The rate of fetal distress was slightly higher among inpatients (21% vs. 23%). The outpatient pregnancies resulted in larger infants (mean 1,827 g vs. 1,776 g).
The rate of nonrespiratory neonatal complications was about 9% in each group. However, significantly more infants in the inpatient group needed ventilation (76% vs. 63%). They were also on ventilation about a day longer (5 days vs. 4 days).
There were one single and two double intrauterine deaths in the outpatient group, and one single intrauterine death in the inpatient group. But because all of the outpatient deaths occurred before 28 weeks, Dr. Van Mieghem said they probably could not have been averted by inpatient management.
"If you were looking at the rate of truly preventable deaths, it likely would have been 0 in both groups," he said.
Dr. Van Mieghem had no financial disclosures.
On Twitter @alz_gal
AT THE PREGNANCY MEETING
Major finding: For monoamniotic twins, the risks of intrauterine death and neonatal complications are both about 3% at 33 weeks’ gestation, making that the best time to deliver these babies.
Data source: The retrospective study comprised 193 monoamniotic twin pregnancies during 2003-2013.
Disclosures: Dr. Tim Van Mieghem had no financial disclosures.

Renal insufficiency tied to risk of post–liver surgery problems
MIAMI BEACH – Renal insufficiency significantly increased the risk of major complications after liver surgery.
However, it wasn’t associated with an increased risk of 90-day mortality, suggesting that patients with poor renal function shouldn’t be ruled out as surgical candidates, Dr. Malcolm Squires III said at the annual meeting of the Americas Hepato-Pancreato-Biliary Association.
"While they may be at a potential risk of major complications – renal failure and respiratory failure – we are ultimately able to get these patients through the postoperative period without any significant increase in mortality," said Dr. Squires of Emory University, Atlanta.
He presented a large retrospective study that examined postoperative outcomes in 1,170 patients (mean age, 57 years) who underwent major hepatectomy at three national academic hospitals from 2000 to 2012. The study determined the link between major complications and preoperative serum creatinine levels. These levels were dichotomized as normal (1.8 mg/dL or less) and elevated (greater than 1.8 mg/dL).
Most patients (1,148) had normal levels; only 22 had elevated serum creatinine, considered to be reflective of chronic renal insufficiency.
Pathology included cholangiocarcinoma, hepatocellular carcinoma, metastatic colorectal cancer, other cancers, and benign lesions. Cirrhosis was present in 4% and steatosis in 39%.
Most (83%) had open surgery; 17% had a laparoscopic procedure. The mean blood loss was 510 cc; 25% needed an intraoperative blood transfusion.
Postoperative complications arose in 56% of the group. A quarter (24%) had a major complication, including renal failure (3%) and respiratory failure (5%). Three-month mortality in the entire group was 5%.
In a multivariate model, preoperative renal insufficiency conferred a fourfold increased risk of developing a major postoperative complication. Other significant predictors were a high American Society of Anesthesiologists classification score (odds ratio, 1.6), having a bile duct resection (OR, 1.7), and a low preoperative albumin level (OR, 1.6).
Renal insufficiency also significantly predicted postoperative respiratory failure (OR, 4.4). Other predictors of respiratory failure were older age (OR, 1.06) and cirrhosis (OR, 6.6).
Renal insufficiency was also a significant risk factor for renal failure, increasing the odds by 4.6.
The biggest predictor of 90-day mortality was hepatitis C, which conferred a ninefold increased risk. Cardiac disease also significantly increased the risk (OR, 2), as did bile duct resection (OR, 2.3), intraoperative transfusion (OR, 2) and cirrhosis (OR, 4.7).
Preoperative renal insufficiency did not significantly increase the risk of death, Dr. Squires noted.
"These findings should be taken into consideration when evaluating patients with preoperative renal insufficiency for hepatic resection," he said. "Careful patient selection and appropriate preoperative counseling are critical."
Dr. Squires had no financial disclosures.
MIAMI BEACH – Renal insufficiency significantly increased the risk of major complications after liver surgery.
However, it wasn’t associated with an increased risk of 90-day mortality, suggesting that patients with poor renal function shouldn’t be ruled out as surgical candidates, Dr. Malcolm Squires III said at the annual meeting of the Americas Hepato-Pancreato-Biliary Association.
"While they may be at a potential risk of major complications – renal failure and respiratory failure – we are ultimately able to get these patients through the postoperative period without any significant increase in mortality," said Dr. Squires of Emory University, Atlanta.
He presented a large retrospective study that examined postoperative outcomes in 1,170 patients (mean age, 57 years) who underwent major hepatectomy at three national academic hospitals from 2000 to 2012. The study determined the link between major complications and preoperative serum creatinine levels. These levels were dichotomized as normal (1.8 mg/dL or less) and elevated (greater than 1.8 mg/dL).
Most patients (1,148) had normal levels; only 22 had elevated serum creatinine, considered to be reflective of chronic renal insufficiency.
Pathology included cholangiocarcinoma, hepatocellular carcinoma, metastatic colorectal cancer, other cancers, and benign lesions. Cirrhosis was present in 4% and steatosis in 39%.
Most (83%) had open surgery; 17% had a laparoscopic procedure. The mean blood loss was 510 cc; 25% needed an intraoperative blood transfusion.
Postoperative complications arose in 56% of the group. A quarter (24%) had a major complication, including renal failure (3%) and respiratory failure (5%). Three-month mortality in the entire group was 5%.
In a multivariate model, preoperative renal insufficiency conferred a fourfold increased risk of developing a major postoperative complication. Other significant predictors were a high American Society of Anesthesiologists classification score (odds ratio, 1.6), having a bile duct resection (OR, 1.7), and a low preoperative albumin level (OR, 1.6).
Renal insufficiency also significantly predicted postoperative respiratory failure (OR, 4.4). Other predictors of respiratory failure were older age (OR, 1.06) and cirrhosis (OR, 6.6).
Renal insufficiency was also a significant risk factor for renal failure, increasing the odds by 4.6.
The biggest predictor of 90-day mortality was hepatitis C, which conferred a ninefold increased risk. Cardiac disease also significantly increased the risk (OR, 2), as did bile duct resection (OR, 2.3), intraoperative transfusion (OR, 2) and cirrhosis (OR, 4.7).
Preoperative renal insufficiency did not significantly increase the risk of death, Dr. Squires noted.
"These findings should be taken into consideration when evaluating patients with preoperative renal insufficiency for hepatic resection," he said. "Careful patient selection and appropriate preoperative counseling are critical."
Dr. Squires had no financial disclosures.
MIAMI BEACH – Renal insufficiency significantly increased the risk of major complications after liver surgery.
However, it wasn’t associated with an increased risk of 90-day mortality, suggesting that patients with poor renal function shouldn’t be ruled out as surgical candidates, Dr. Malcolm Squires III said at the annual meeting of the Americas Hepato-Pancreato-Biliary Association.
"While they may be at a potential risk of major complications – renal failure and respiratory failure – we are ultimately able to get these patients through the postoperative period without any significant increase in mortality," said Dr. Squires of Emory University, Atlanta.
He presented a large retrospective study that examined postoperative outcomes in 1,170 patients (mean age, 57 years) who underwent major hepatectomy at three national academic hospitals from 2000 to 2012. The study determined the link between major complications and preoperative serum creatinine levels. These levels were dichotomized as normal (1.8 mg/dL or less) and elevated (greater than 1.8 mg/dL).
Most patients (1,148) had normal levels; only 22 had elevated serum creatinine, considered to be reflective of chronic renal insufficiency.
Pathology included cholangiocarcinoma, hepatocellular carcinoma, metastatic colorectal cancer, other cancers, and benign lesions. Cirrhosis was present in 4% and steatosis in 39%.
Most (83%) had open surgery; 17% had a laparoscopic procedure. The mean blood loss was 510 cc; 25% needed an intraoperative blood transfusion.
Postoperative complications arose in 56% of the group. A quarter (24%) had a major complication, including renal failure (3%) and respiratory failure (5%). Three-month mortality in the entire group was 5%.
In a multivariate model, preoperative renal insufficiency conferred a fourfold increased risk of developing a major postoperative complication. Other significant predictors were a high American Society of Anesthesiologists classification score (odds ratio, 1.6), having a bile duct resection (OR, 1.7), and a low preoperative albumin level (OR, 1.6).
Renal insufficiency also significantly predicted postoperative respiratory failure (OR, 4.4). Other predictors of respiratory failure were older age (OR, 1.06) and cirrhosis (OR, 6.6).
Renal insufficiency was also a significant risk factor for renal failure, increasing the odds by 4.6.
The biggest predictor of 90-day mortality was hepatitis C, which conferred a ninefold increased risk. Cardiac disease also significantly increased the risk (OR, 2), as did bile duct resection (OR, 2.3), intraoperative transfusion (OR, 2) and cirrhosis (OR, 4.7).
Preoperative renal insufficiency did not significantly increase the risk of death, Dr. Squires noted.
"These findings should be taken into consideration when evaluating patients with preoperative renal insufficiency for hepatic resection," he said. "Careful patient selection and appropriate preoperative counseling are critical."
Dr. Squires had no financial disclosures.
AT AHPBA 2014
Major finding: Chronic preoperative renal insufficiency confers a fourfold increase in the risk of major complications after hepatic resection, although it did not increase the risk of 90-day mortality.
Data source: The retrospective study looked at postoperative outcomes in 1,170 patients.
Disclosures: Dr. Squires had no financial disclosures.
Study finds increased infant mortality for home births
NEW ORLEANS – Midwife-attended home births appear to have a higher mortality rate than midwife-attended hospital births, a new national database study suggests.
But for both physicians and families, the findings lie at the center of a tangled knot of statistics, philosophy, fear, and determination.
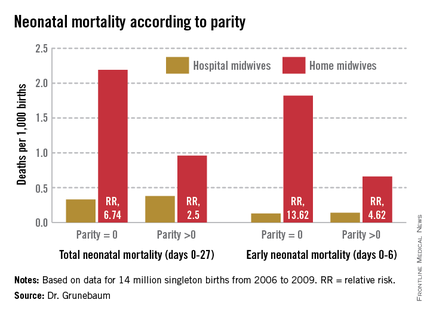
According to a new study of national birth and death statistics, total neonatal mortality in midwife-assisted hospital births was 0.32/1,000. For a midwife-attended home birth, that number was 1.26/1,000 – almost a fourfold increase in relative risk, Dr. Amos Grunebaum said at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
His study drew its data from linked birth and death records available through the Centers for Disease Control and Prevention’s (CDC’s) database. The study looked at 14 million births from 2006 to 2009. Only healthy singleton infants of normal birth weight and vertex presentation were included; gestation was 38-42 weeks.
The figures for nulliparous women giving birth at home were even more striking, said Dr. Grunebaum, director of obstetrics at Weill Cornell Medical College, New York. Total neonatal mortality (deaths from day 0 to 27) was 2.19/1,000 for home-birthed infants, compared with 0.38/1,000 for hospital-born infants (relative risk, 6.74). The rates of early neonatal mortality (deaths from day 0 to 6) were 1.82/1,000 vs. 0.13/1,000, respectively (RR, 13.6).
"When we calculate the excess total neonatal deaths associated with home birth, we arrive at 9/10,000," he said during an interview. "If the trend of increasing home birth holds over the next few years, in 2016 we could have 32 excess neonatal deaths per year – a whole school class of children."
"It’s possible these risks are even higher," he added, because any babies born in the hospital after an emergency transfer from home are counted as hospital births.
It’s tough to parse out the details in his analysis, however. Because lay midwives would never have had hospital privileges, the in-hospital midwife group was likely composed entirely of certified nurse-midwives (CNMs), whose specialized training makes them highly skilled birth attendants. But the midwives who attended home births were a heterogenous group. In addition to CNMs, the analysis included anyone else who would register as "midwife" on a birth certificate – a group that represents an extremely varied range of skill.
These attendants could be could have been CNMs, certified midwives, certified professional midwives, licensed midwives, or lay midwives. CNMs must have a bachelor’s degree as a registered nurse and then graduate from an accredited school of nurse-midwifery. A certified midwife is a graduate of the same school of midwifery program, but can hold a degree in a field other than nursing. The American College of Nurse-Midwives (ACNM) regulates these providers.
No college degree is required for a certified professional midwife. They can obtain licensure based on an apprenticeship portfolio or from other schools of midwifery. The Midwives Alliance of North America and the National Association of Certified Professional Midwives regulate this group. Lay midwives are allowed to practice in some states, but there is no regulatory board, and no licensure or educational requirements.
In all probability, very few CNMs attended the home births in Dr. Grunebaum’s study, according to Jesse Bushman, ACNM’s director of advocacy and government affairs. The college’s own data indicate that 90% of deliveries performed by members are in hospitals. Only 30% of home births recorded in the CDC data were performed by CNMs, he said.
"That is one issue we have with Dr. Grunebaum’s results," Mr. Bushman* said in an interview. "There are many people who could call themselves a midwife who may not have the training or competencies that CNMs do. To lump them together is quite problematic."
In an interview, Dr. Grunebaum said that he had parsed out the mortality results by specific provider group. However, he would not release those numbers, saying it could jeopardize his study’s peer-reviewed publication. "I will tell you that CNMs at home did much, much worse than CNMs in the hospital, and that other midwives at home were not far behind."
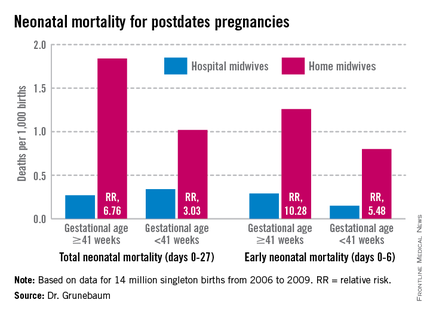
Birth outcomes data just released by the Midwives Alliance of North America (MANA) align with Dr. Grunebaum’s numbers (J. Midwifery Womens Health 2014 Jan. 30 [doi: 10.1111/jmwh.12172]). But the interpretation – if not the numbers – lies in the eye of the beholder. Dr. Grunebaum said the study illustrates the danger of home birth. MANA hailed it as proof of home birth’s safety.
"The results of this study ... confirm the safety and overwhelmingly positive health benefits for low-risk mothers and babies who choose to birth at home with a midwife," the group noted on its website. "At every step of the way, midwives are providing excellent care. This study enables families, providers, and policy makers to have a transparent look at the risks and benefits of planned home birth, as well as the health benefits of normal physiologic birth."
The study was a voluntary survey that examined data from almost 17,000 home births. The voluntary nature troubles Dr. Grunebaum, who pointed out that midwives with poor outcomes probably would not have submitted data.
There was an 11% hospital transfer rate in the cohort from the midwives study. There were 43 fetal deaths in the intrapartum, early, and late neonatal periods; 8 of these were from lethal congenital defects. The remaining deaths translated to a total neonatal mortality rate of 1.3/1,000.
Twenty-two died during labor, but before birth. For 13, the causes were known: placental abruption (2), intrauterine infection (2), cord accidents (3), complications of maternal gestational diabetes (2), meconium aspiration (1), shoulder dystocia (1), complications of preeclampsia (1), and liver rupture and hypoxia (1).
Seven babies died during the first 6 days of life. The causes were secondary to cord accidents (2, one with shoulder dystocia), and hypoxia or ischemia of unknown origin (5).
Six infants died in the late neonatal period. Two deaths were secondary to cord accidents, and four were from unknown causes.
Of 222 breech births, three infants died (13/1,000). Of 3,773 births to primiparous women, 11 infants died (2.9/1,000). Of 1,052 attempted vaginal births, 3 infants died (2.85/1,000)
"These numbers are horrible," Dr. Grunebaum said. "There is no longer room for the argument from home birth supporters that while the risk may be increased, it’s still very low in terms of absolute risk."
"This view has even been expressed by our own specialists," he added, referring to an American Academy of Pediatrics position paper on planned home birth (Pediatrics 2013;131:1016-20). While maintaining that birth is safest in a hospital or birthing center, the paper acknowledges that the two- or threefold overall increase in mortality associated with home birth is low – generally translating to about 1 in 1,000 newborns.
"That minimizes the extra risk involved in home birth," Dr. Grunebaum said. "We should have no acceptance for any increase in death or injury in exchange for parental convenience or for fewer interventions. We need to disclose these increased risks to mothers, and perform direct counseling against home birth."
His study fans a long-simmering debate about the best places to birth. Proponents of both philosophies want the same primary outcome: healthy mothers and infants. The debate? How to best get there.
Midwife-assisted home birth has grown exponentially over the past decade. According to CDC data, there were about 16,000 in 2007; by 2012, it was about 23,500. The rise is mostly seen in a very specific demographic – well-educated, financially secure white women with at least one other child who was, most frequently, born in a hospital.
Dr. Grunebaum attributed the rise to some women’s desire to avoid what they perceive as intrusive labor and birth management. With this thought, at least, others do agree.
Eugene DeClercq, Ph.D., a professor of obstetrics and gynecology and of public health at Boston University, has worked on three national surveys that poll new mothers about their experiences with pregnancy, labor and delivery, and postpartum life.
Childbirth Connection (childbirthconnection.org) conducted the Listening to Mothers surveys in 2002, 2006, and 2012. The survey reports are intended to serve as policy resources for improving the childbearing experience for women and their families.
"One of the real questions we need to look at is, what’s going on in hospitals that makes women consider giving birth outside the hospital," Dr. DeClercq said in an interview. "What has come through in our interviews is that many women are quite fine with the ways things go in a hospital. They are for any intervention that they think will make a safer birth. But many women are not. They report feeling pressured to have interventions, and worried that one will lead to another and another, in a cascade that can eventually end up in a cesarean section."
This is a legitimate concern in the United States, he said – a country in which the cesarean rate hovers around 30%, and ranges from 7% to 70% across hospitals. "If you lived ... where there was a 70% rate of cesarean – 70%! – might you be thinking about some way to avoid that?"
In the Listening to Mothers II survey, women were asked a series of questions about their experiences with labor and delivery. The results of the survey revealed that 47% of first-time mothers were induced. "Of those having an induction, 78% had an epidural, and of those mothers who had both an attempted induction and an epidural, the unplanned cesarean rate was 31%," the report noted. "Those who experienced either labor induction or an epidural, but not both, had cesarean rates of 19% to 20%. For those first-time mothers who experienced neither attempted induction nor an epidural, the unplanned cesarean rate was 5%."
Like it or not, he said, some women will go to almost any length to avoid interventions they fear may harm them and their babies.
The Listening to Mothers survey found that a quarter of women who had given birth in a hospital would consider a home birth. Most women in the survey (2/3) said a woman should be able to have a home birth if she wanted, and 11% said they would definitely want a home birth.
"If you look at the profile of home-birthers, it’s not like they are some crazy fringe group," Dr. DeClercq said. "These are very well-educated women, 75% of whom have already had a hospital birth. They are researching and weighing the pros and cons. They’re not just making some random decision."
His data also suggest that women who transfer to a hospital from a home birth fear judgment and even recrimination. "The consequences of that can be a delay in transfer when it’s necessary, and can lead to problems," even poor infant outcomes.
On this point at least, the two sides find common ground.
"Most of us will never attend a home birth," Dr. Grunebaum said. "But we will encounter patients asking us about home births and seeking hospital transfer for successful or complicated home births, and babies transferred after a home birth. And for these we need to provide compassionate, nonjudgmental care."
None of the sources interviewed for this story reported any financial disclosures.
*Correction, 3/4/2014: An earlier version of this story misstated Mr. Bushman's name.
NEW ORLEANS – Midwife-attended home births appear to have a higher mortality rate than midwife-attended hospital births, a new national database study suggests.
But for both physicians and families, the findings lie at the center of a tangled knot of statistics, philosophy, fear, and determination.
According to a new study of national birth and death statistics, total neonatal mortality in midwife-assisted hospital births was 0.32/1,000. For a midwife-attended home birth, that number was 1.26/1,000 – almost a fourfold increase in relative risk, Dr. Amos Grunebaum said at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
His study drew its data from linked birth and death records available through the Centers for Disease Control and Prevention’s (CDC’s) database. The study looked at 14 million births from 2006 to 2009. Only healthy singleton infants of normal birth weight and vertex presentation were included; gestation was 38-42 weeks.
The figures for nulliparous women giving birth at home were even more striking, said Dr. Grunebaum, director of obstetrics at Weill Cornell Medical College, New York. Total neonatal mortality (deaths from day 0 to 27) was 2.19/1,000 for home-birthed infants, compared with 0.38/1,000 for hospital-born infants (relative risk, 6.74). The rates of early neonatal mortality (deaths from day 0 to 6) were 1.82/1,000 vs. 0.13/1,000, respectively (RR, 13.6).
"When we calculate the excess total neonatal deaths associated with home birth, we arrive at 9/10,000," he said during an interview. "If the trend of increasing home birth holds over the next few years, in 2016 we could have 32 excess neonatal deaths per year – a whole school class of children."
"It’s possible these risks are even higher," he added, because any babies born in the hospital after an emergency transfer from home are counted as hospital births.
It’s tough to parse out the details in his analysis, however. Because lay midwives would never have had hospital privileges, the in-hospital midwife group was likely composed entirely of certified nurse-midwives (CNMs), whose specialized training makes them highly skilled birth attendants. But the midwives who attended home births were a heterogenous group. In addition to CNMs, the analysis included anyone else who would register as "midwife" on a birth certificate – a group that represents an extremely varied range of skill.
These attendants could be could have been CNMs, certified midwives, certified professional midwives, licensed midwives, or lay midwives. CNMs must have a bachelor’s degree as a registered nurse and then graduate from an accredited school of nurse-midwifery. A certified midwife is a graduate of the same school of midwifery program, but can hold a degree in a field other than nursing. The American College of Nurse-Midwives (ACNM) regulates these providers.
No college degree is required for a certified professional midwife. They can obtain licensure based on an apprenticeship portfolio or from other schools of midwifery. The Midwives Alliance of North America and the National Association of Certified Professional Midwives regulate this group. Lay midwives are allowed to practice in some states, but there is no regulatory board, and no licensure or educational requirements.
In all probability, very few CNMs attended the home births in Dr. Grunebaum’s study, according to Jesse Bushman, ACNM’s director of advocacy and government affairs. The college’s own data indicate that 90% of deliveries performed by members are in hospitals. Only 30% of home births recorded in the CDC data were performed by CNMs, he said.
"That is one issue we have with Dr. Grunebaum’s results," Mr. Bushman* said in an interview. "There are many people who could call themselves a midwife who may not have the training or competencies that CNMs do. To lump them together is quite problematic."
In an interview, Dr. Grunebaum said that he had parsed out the mortality results by specific provider group. However, he would not release those numbers, saying it could jeopardize his study’s peer-reviewed publication. "I will tell you that CNMs at home did much, much worse than CNMs in the hospital, and that other midwives at home were not far behind."
Birth outcomes data just released by the Midwives Alliance of North America (MANA) align with Dr. Grunebaum’s numbers (J. Midwifery Womens Health 2014 Jan. 30 [doi: 10.1111/jmwh.12172]). But the interpretation – if not the numbers – lies in the eye of the beholder. Dr. Grunebaum said the study illustrates the danger of home birth. MANA hailed it as proof of home birth’s safety.
"The results of this study ... confirm the safety and overwhelmingly positive health benefits for low-risk mothers and babies who choose to birth at home with a midwife," the group noted on its website. "At every step of the way, midwives are providing excellent care. This study enables families, providers, and policy makers to have a transparent look at the risks and benefits of planned home birth, as well as the health benefits of normal physiologic birth."
The study was a voluntary survey that examined data from almost 17,000 home births. The voluntary nature troubles Dr. Grunebaum, who pointed out that midwives with poor outcomes probably would not have submitted data.
There was an 11% hospital transfer rate in the cohort from the midwives study. There were 43 fetal deaths in the intrapartum, early, and late neonatal periods; 8 of these were from lethal congenital defects. The remaining deaths translated to a total neonatal mortality rate of 1.3/1,000.
Twenty-two died during labor, but before birth. For 13, the causes were known: placental abruption (2), intrauterine infection (2), cord accidents (3), complications of maternal gestational diabetes (2), meconium aspiration (1), shoulder dystocia (1), complications of preeclampsia (1), and liver rupture and hypoxia (1).
Seven babies died during the first 6 days of life. The causes were secondary to cord accidents (2, one with shoulder dystocia), and hypoxia or ischemia of unknown origin (5).
Six infants died in the late neonatal period. Two deaths were secondary to cord accidents, and four were from unknown causes.
Of 222 breech births, three infants died (13/1,000). Of 3,773 births to primiparous women, 11 infants died (2.9/1,000). Of 1,052 attempted vaginal births, 3 infants died (2.85/1,000)
"These numbers are horrible," Dr. Grunebaum said. "There is no longer room for the argument from home birth supporters that while the risk may be increased, it’s still very low in terms of absolute risk."
"This view has even been expressed by our own specialists," he added, referring to an American Academy of Pediatrics position paper on planned home birth (Pediatrics 2013;131:1016-20). While maintaining that birth is safest in a hospital or birthing center, the paper acknowledges that the two- or threefold overall increase in mortality associated with home birth is low – generally translating to about 1 in 1,000 newborns.
"That minimizes the extra risk involved in home birth," Dr. Grunebaum said. "We should have no acceptance for any increase in death or injury in exchange for parental convenience or for fewer interventions. We need to disclose these increased risks to mothers, and perform direct counseling against home birth."
His study fans a long-simmering debate about the best places to birth. Proponents of both philosophies want the same primary outcome: healthy mothers and infants. The debate? How to best get there.
Midwife-assisted home birth has grown exponentially over the past decade. According to CDC data, there were about 16,000 in 2007; by 2012, it was about 23,500. The rise is mostly seen in a very specific demographic – well-educated, financially secure white women with at least one other child who was, most frequently, born in a hospital.
Dr. Grunebaum attributed the rise to some women’s desire to avoid what they perceive as intrusive labor and birth management. With this thought, at least, others do agree.
Eugene DeClercq, Ph.D., a professor of obstetrics and gynecology and of public health at Boston University, has worked on three national surveys that poll new mothers about their experiences with pregnancy, labor and delivery, and postpartum life.
Childbirth Connection (childbirthconnection.org) conducted the Listening to Mothers surveys in 2002, 2006, and 2012. The survey reports are intended to serve as policy resources for improving the childbearing experience for women and their families.
"One of the real questions we need to look at is, what’s going on in hospitals that makes women consider giving birth outside the hospital," Dr. DeClercq said in an interview. "What has come through in our interviews is that many women are quite fine with the ways things go in a hospital. They are for any intervention that they think will make a safer birth. But many women are not. They report feeling pressured to have interventions, and worried that one will lead to another and another, in a cascade that can eventually end up in a cesarean section."
This is a legitimate concern in the United States, he said – a country in which the cesarean rate hovers around 30%, and ranges from 7% to 70% across hospitals. "If you lived ... where there was a 70% rate of cesarean – 70%! – might you be thinking about some way to avoid that?"
In the Listening to Mothers II survey, women were asked a series of questions about their experiences with labor and delivery. The results of the survey revealed that 47% of first-time mothers were induced. "Of those having an induction, 78% had an epidural, and of those mothers who had both an attempted induction and an epidural, the unplanned cesarean rate was 31%," the report noted. "Those who experienced either labor induction or an epidural, but not both, had cesarean rates of 19% to 20%. For those first-time mothers who experienced neither attempted induction nor an epidural, the unplanned cesarean rate was 5%."
Like it or not, he said, some women will go to almost any length to avoid interventions they fear may harm them and their babies.
The Listening to Mothers survey found that a quarter of women who had given birth in a hospital would consider a home birth. Most women in the survey (2/3) said a woman should be able to have a home birth if she wanted, and 11% said they would definitely want a home birth.
"If you look at the profile of home-birthers, it’s not like they are some crazy fringe group," Dr. DeClercq said. "These are very well-educated women, 75% of whom have already had a hospital birth. They are researching and weighing the pros and cons. They’re not just making some random decision."
His data also suggest that women who transfer to a hospital from a home birth fear judgment and even recrimination. "The consequences of that can be a delay in transfer when it’s necessary, and can lead to problems," even poor infant outcomes.
On this point at least, the two sides find common ground.
"Most of us will never attend a home birth," Dr. Grunebaum said. "But we will encounter patients asking us about home births and seeking hospital transfer for successful or complicated home births, and babies transferred after a home birth. And for these we need to provide compassionate, nonjudgmental care."
None of the sources interviewed for this story reported any financial disclosures.
*Correction, 3/4/2014: An earlier version of this story misstated Mr. Bushman's name.
NEW ORLEANS – Midwife-attended home births appear to have a higher mortality rate than midwife-attended hospital births, a new national database study suggests.
But for both physicians and families, the findings lie at the center of a tangled knot of statistics, philosophy, fear, and determination.
According to a new study of national birth and death statistics, total neonatal mortality in midwife-assisted hospital births was 0.32/1,000. For a midwife-attended home birth, that number was 1.26/1,000 – almost a fourfold increase in relative risk, Dr. Amos Grunebaum said at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
His study drew its data from linked birth and death records available through the Centers for Disease Control and Prevention’s (CDC’s) database. The study looked at 14 million births from 2006 to 2009. Only healthy singleton infants of normal birth weight and vertex presentation were included; gestation was 38-42 weeks.
The figures for nulliparous women giving birth at home were even more striking, said Dr. Grunebaum, director of obstetrics at Weill Cornell Medical College, New York. Total neonatal mortality (deaths from day 0 to 27) was 2.19/1,000 for home-birthed infants, compared with 0.38/1,000 for hospital-born infants (relative risk, 6.74). The rates of early neonatal mortality (deaths from day 0 to 6) were 1.82/1,000 vs. 0.13/1,000, respectively (RR, 13.6).
"When we calculate the excess total neonatal deaths associated with home birth, we arrive at 9/10,000," he said during an interview. "If the trend of increasing home birth holds over the next few years, in 2016 we could have 32 excess neonatal deaths per year – a whole school class of children."
"It’s possible these risks are even higher," he added, because any babies born in the hospital after an emergency transfer from home are counted as hospital births.
It’s tough to parse out the details in his analysis, however. Because lay midwives would never have had hospital privileges, the in-hospital midwife group was likely composed entirely of certified nurse-midwives (CNMs), whose specialized training makes them highly skilled birth attendants. But the midwives who attended home births were a heterogenous group. In addition to CNMs, the analysis included anyone else who would register as "midwife" on a birth certificate – a group that represents an extremely varied range of skill.
These attendants could be could have been CNMs, certified midwives, certified professional midwives, licensed midwives, or lay midwives. CNMs must have a bachelor’s degree as a registered nurse and then graduate from an accredited school of nurse-midwifery. A certified midwife is a graduate of the same school of midwifery program, but can hold a degree in a field other than nursing. The American College of Nurse-Midwives (ACNM) regulates these providers.
No college degree is required for a certified professional midwife. They can obtain licensure based on an apprenticeship portfolio or from other schools of midwifery. The Midwives Alliance of North America and the National Association of Certified Professional Midwives regulate this group. Lay midwives are allowed to practice in some states, but there is no regulatory board, and no licensure or educational requirements.
In all probability, very few CNMs attended the home births in Dr. Grunebaum’s study, according to Jesse Bushman, ACNM’s director of advocacy and government affairs. The college’s own data indicate that 90% of deliveries performed by members are in hospitals. Only 30% of home births recorded in the CDC data were performed by CNMs, he said.
"That is one issue we have with Dr. Grunebaum’s results," Mr. Bushman* said in an interview. "There are many people who could call themselves a midwife who may not have the training or competencies that CNMs do. To lump them together is quite problematic."
In an interview, Dr. Grunebaum said that he had parsed out the mortality results by specific provider group. However, he would not release those numbers, saying it could jeopardize his study’s peer-reviewed publication. "I will tell you that CNMs at home did much, much worse than CNMs in the hospital, and that other midwives at home were not far behind."
Birth outcomes data just released by the Midwives Alliance of North America (MANA) align with Dr. Grunebaum’s numbers (J. Midwifery Womens Health 2014 Jan. 30 [doi: 10.1111/jmwh.12172]). But the interpretation – if not the numbers – lies in the eye of the beholder. Dr. Grunebaum said the study illustrates the danger of home birth. MANA hailed it as proof of home birth’s safety.
"The results of this study ... confirm the safety and overwhelmingly positive health benefits for low-risk mothers and babies who choose to birth at home with a midwife," the group noted on its website. "At every step of the way, midwives are providing excellent care. This study enables families, providers, and policy makers to have a transparent look at the risks and benefits of planned home birth, as well as the health benefits of normal physiologic birth."
The study was a voluntary survey that examined data from almost 17,000 home births. The voluntary nature troubles Dr. Grunebaum, who pointed out that midwives with poor outcomes probably would not have submitted data.
There was an 11% hospital transfer rate in the cohort from the midwives study. There were 43 fetal deaths in the intrapartum, early, and late neonatal periods; 8 of these were from lethal congenital defects. The remaining deaths translated to a total neonatal mortality rate of 1.3/1,000.
Twenty-two died during labor, but before birth. For 13, the causes were known: placental abruption (2), intrauterine infection (2), cord accidents (3), complications of maternal gestational diabetes (2), meconium aspiration (1), shoulder dystocia (1), complications of preeclampsia (1), and liver rupture and hypoxia (1).
Seven babies died during the first 6 days of life. The causes were secondary to cord accidents (2, one with shoulder dystocia), and hypoxia or ischemia of unknown origin (5).
Six infants died in the late neonatal period. Two deaths were secondary to cord accidents, and four were from unknown causes.
Of 222 breech births, three infants died (13/1,000). Of 3,773 births to primiparous women, 11 infants died (2.9/1,000). Of 1,052 attempted vaginal births, 3 infants died (2.85/1,000)
"These numbers are horrible," Dr. Grunebaum said. "There is no longer room for the argument from home birth supporters that while the risk may be increased, it’s still very low in terms of absolute risk."
"This view has even been expressed by our own specialists," he added, referring to an American Academy of Pediatrics position paper on planned home birth (Pediatrics 2013;131:1016-20). While maintaining that birth is safest in a hospital or birthing center, the paper acknowledges that the two- or threefold overall increase in mortality associated with home birth is low – generally translating to about 1 in 1,000 newborns.
"That minimizes the extra risk involved in home birth," Dr. Grunebaum said. "We should have no acceptance for any increase in death or injury in exchange for parental convenience or for fewer interventions. We need to disclose these increased risks to mothers, and perform direct counseling against home birth."
His study fans a long-simmering debate about the best places to birth. Proponents of both philosophies want the same primary outcome: healthy mothers and infants. The debate? How to best get there.
Midwife-assisted home birth has grown exponentially over the past decade. According to CDC data, there were about 16,000 in 2007; by 2012, it was about 23,500. The rise is mostly seen in a very specific demographic – well-educated, financially secure white women with at least one other child who was, most frequently, born in a hospital.
Dr. Grunebaum attributed the rise to some women’s desire to avoid what they perceive as intrusive labor and birth management. With this thought, at least, others do agree.
Eugene DeClercq, Ph.D., a professor of obstetrics and gynecology and of public health at Boston University, has worked on three national surveys that poll new mothers about their experiences with pregnancy, labor and delivery, and postpartum life.
Childbirth Connection (childbirthconnection.org) conducted the Listening to Mothers surveys in 2002, 2006, and 2012. The survey reports are intended to serve as policy resources for improving the childbearing experience for women and their families.
"One of the real questions we need to look at is, what’s going on in hospitals that makes women consider giving birth outside the hospital," Dr. DeClercq said in an interview. "What has come through in our interviews is that many women are quite fine with the ways things go in a hospital. They are for any intervention that they think will make a safer birth. But many women are not. They report feeling pressured to have interventions, and worried that one will lead to another and another, in a cascade that can eventually end up in a cesarean section."
This is a legitimate concern in the United States, he said – a country in which the cesarean rate hovers around 30%, and ranges from 7% to 70% across hospitals. "If you lived ... where there was a 70% rate of cesarean – 70%! – might you be thinking about some way to avoid that?"
In the Listening to Mothers II survey, women were asked a series of questions about their experiences with labor and delivery. The results of the survey revealed that 47% of first-time mothers were induced. "Of those having an induction, 78% had an epidural, and of those mothers who had both an attempted induction and an epidural, the unplanned cesarean rate was 31%," the report noted. "Those who experienced either labor induction or an epidural, but not both, had cesarean rates of 19% to 20%. For those first-time mothers who experienced neither attempted induction nor an epidural, the unplanned cesarean rate was 5%."
Like it or not, he said, some women will go to almost any length to avoid interventions they fear may harm them and their babies.
The Listening to Mothers survey found that a quarter of women who had given birth in a hospital would consider a home birth. Most women in the survey (2/3) said a woman should be able to have a home birth if she wanted, and 11% said they would definitely want a home birth.
"If you look at the profile of home-birthers, it’s not like they are some crazy fringe group," Dr. DeClercq said. "These are very well-educated women, 75% of whom have already had a hospital birth. They are researching and weighing the pros and cons. They’re not just making some random decision."
His data also suggest that women who transfer to a hospital from a home birth fear judgment and even recrimination. "The consequences of that can be a delay in transfer when it’s necessary, and can lead to problems," even poor infant outcomes.
On this point at least, the two sides find common ground.
"Most of us will never attend a home birth," Dr. Grunebaum said. "But we will encounter patients asking us about home births and seeking hospital transfer for successful or complicated home births, and babies transferred after a home birth. And for these we need to provide compassionate, nonjudgmental care."
None of the sources interviewed for this story reported any financial disclosures.
*Correction, 3/4/2014: An earlier version of this story misstated Mr. Bushman's name.
AT THE PREGNANCY MEETING
Major finding: Total neonatal mortality in midwife-assisted hospital births was 0.32/1,000. For a midwife-attended home birth, that number was 1.26/1,000 – almost a fourfold increase in relative risk.
Data source: A Centers for Disease Control and Prevention database study that looked at 14 million births from 2006 to 2009.
Disclosures: None of the sources interviewed for this story reported any financial disclosures.
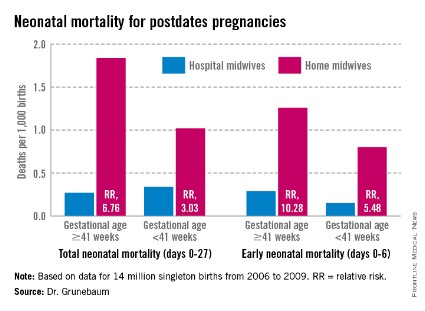
Suppressing interpregnancy HIV prevents infant transmission
NEW ORLEANS – There were no cases of HIV transmission to infants born of a second pregnancy to mothers who maintained viral suppression between their two pregnancies, a study showed.
In a retrospective cohort of 103 women, the mother-to-child transmission rate was 9% among women whose interpregnancy viral load was more than 1,000 copies/mL. But among those with a load of less than 1,000 copies/mL, the transmission rate was 0, Dr. Robert Stewart said at the annual Pregnancy Meeting, sponsored by the Society for Maternal-Fetal Medicine.

The data support the concept of treating HIV to help protect babies as well as mothers, said Dr. Stewart of the University of Texas Southwestern Medical Center, Dallas.
"Right now there are no recommendations for HIV treatment between pregnancies, or treatment for the benefit of the fetus," he said. The only treatment guidelines suggest that pregnant women be treated as nonpregnant women are, for their own health.
Dr. Stewart examined the issue in a cohort of 103 women who had a suppressed HIV load (less than 1,000 copies/mL) at their index pregnancy, and were seen at the same institution for their next pregnancy.
At baseline, the women were about 24 years old. Most (71%) were black. Gestational age at the first prenatal visit was 14 weeks; at the next pregnancy, the women came in earlier – a mean of 12 weeks. They also had more prenatal visits with their second pregnancy (mean of 10 compared with 9).
At presentation for the index pregnancy, the mean viral load for all women was 1,860 copies/mL, but the range was wide (0-21,700 copies/mL). The mean CD4 cell count was 456/mcL. Just over a third (35%) were already on antiretroviral therapy.
At presentation for the subsequent pregnancy, the overall mean viral load was 1,120 copies/mL (0-145,000 copies/mL). The mean CD4 count was 479 cells/mcL. These differences were not statistically significant. However, at the subsequent pregnancy, significantly more women were on antiretroviral therapy (56%).
The second pregnancy occurred a mean of 2.6 years later in both groups. At presentation for the second pregnancy, 57 had maintained that level of suppression and 46 had not. At that time, the mean viral load was 0 in those who had maintained suppression and 10,160 copies/mL among those who had not – a significant difference. CD4 cell count also was significantly different (596 vs. 342 cells/mcL). Significantly more of those who had maintained suppression were on antiretroviral therapy at the second pregnancy (75% vs. 59%).
By the time of delivery, however, HIV indices had improved in the group that had not maintained suppression. At that time, their mean viral load was also 0. Their CD4 count had increased to 427 cells/mcL, and 93% were on antiretroviral therapy.
There were no significant differences in the clinical parameters of the second pregnancy between those who had maintained suppression and those who had not. These included gestational age at delivery (38 weeks); birth weight (about 3,000 g); the use of intrapartum zidovudine (more than 90% of each group); cesarean delivery (32% vs. 52%; P = .18); length of labor; length of ruptured membranes; and incidence of clinical chorioamnionitis.
Vertical transmission was significantly higher among women who had not maintained an interpregnancy suppression (9% vs. 0 infants).
Dr. Stewart said he had no relevant financial disclosures.
On Twitter @alz_gal
NEW ORLEANS – There were no cases of HIV transmission to infants born of a second pregnancy to mothers who maintained viral suppression between their two pregnancies, a study showed.
In a retrospective cohort of 103 women, the mother-to-child transmission rate was 9% among women whose interpregnancy viral load was more than 1,000 copies/mL. But among those with a load of less than 1,000 copies/mL, the transmission rate was 0, Dr. Robert Stewart said at the annual Pregnancy Meeting, sponsored by the Society for Maternal-Fetal Medicine.
The data support the concept of treating HIV to help protect babies as well as mothers, said Dr. Stewart of the University of Texas Southwestern Medical Center, Dallas.
"Right now there are no recommendations for HIV treatment between pregnancies, or treatment for the benefit of the fetus," he said. The only treatment guidelines suggest that pregnant women be treated as nonpregnant women are, for their own health.
Dr. Stewart examined the issue in a cohort of 103 women who had a suppressed HIV load (less than 1,000 copies/mL) at their index pregnancy, and were seen at the same institution for their next pregnancy.
At baseline, the women were about 24 years old. Most (71%) were black. Gestational age at the first prenatal visit was 14 weeks; at the next pregnancy, the women came in earlier – a mean of 12 weeks. They also had more prenatal visits with their second pregnancy (mean of 10 compared with 9).
At presentation for the index pregnancy, the mean viral load for all women was 1,860 copies/mL, but the range was wide (0-21,700 copies/mL). The mean CD4 cell count was 456/mcL. Just over a third (35%) were already on antiretroviral therapy.
At presentation for the subsequent pregnancy, the overall mean viral load was 1,120 copies/mL (0-145,000 copies/mL). The mean CD4 count was 479 cells/mcL. These differences were not statistically significant. However, at the subsequent pregnancy, significantly more women were on antiretroviral therapy (56%).
The second pregnancy occurred a mean of 2.6 years later in both groups. At presentation for the second pregnancy, 57 had maintained that level of suppression and 46 had not. At that time, the mean viral load was 0 in those who had maintained suppression and 10,160 copies/mL among those who had not – a significant difference. CD4 cell count also was significantly different (596 vs. 342 cells/mcL). Significantly more of those who had maintained suppression were on antiretroviral therapy at the second pregnancy (75% vs. 59%).
By the time of delivery, however, HIV indices had improved in the group that had not maintained suppression. At that time, their mean viral load was also 0. Their CD4 count had increased to 427 cells/mcL, and 93% were on antiretroviral therapy.
There were no significant differences in the clinical parameters of the second pregnancy between those who had maintained suppression and those who had not. These included gestational age at delivery (38 weeks); birth weight (about 3,000 g); the use of intrapartum zidovudine (more than 90% of each group); cesarean delivery (32% vs. 52%; P = .18); length of labor; length of ruptured membranes; and incidence of clinical chorioamnionitis.
Vertical transmission was significantly higher among women who had not maintained an interpregnancy suppression (9% vs. 0 infants).
Dr. Stewart said he had no relevant financial disclosures.
On Twitter @alz_gal
NEW ORLEANS – There were no cases of HIV transmission to infants born of a second pregnancy to mothers who maintained viral suppression between their two pregnancies, a study showed.
In a retrospective cohort of 103 women, the mother-to-child transmission rate was 9% among women whose interpregnancy viral load was more than 1,000 copies/mL. But among those with a load of less than 1,000 copies/mL, the transmission rate was 0, Dr. Robert Stewart said at the annual Pregnancy Meeting, sponsored by the Society for Maternal-Fetal Medicine.
The data support the concept of treating HIV to help protect babies as well as mothers, said Dr. Stewart of the University of Texas Southwestern Medical Center, Dallas.
"Right now there are no recommendations for HIV treatment between pregnancies, or treatment for the benefit of the fetus," he said. The only treatment guidelines suggest that pregnant women be treated as nonpregnant women are, for their own health.
Dr. Stewart examined the issue in a cohort of 103 women who had a suppressed HIV load (less than 1,000 copies/mL) at their index pregnancy, and were seen at the same institution for their next pregnancy.
At baseline, the women were about 24 years old. Most (71%) were black. Gestational age at the first prenatal visit was 14 weeks; at the next pregnancy, the women came in earlier – a mean of 12 weeks. They also had more prenatal visits with their second pregnancy (mean of 10 compared with 9).
At presentation for the index pregnancy, the mean viral load for all women was 1,860 copies/mL, but the range was wide (0-21,700 copies/mL). The mean CD4 cell count was 456/mcL. Just over a third (35%) were already on antiretroviral therapy.
At presentation for the subsequent pregnancy, the overall mean viral load was 1,120 copies/mL (0-145,000 copies/mL). The mean CD4 count was 479 cells/mcL. These differences were not statistically significant. However, at the subsequent pregnancy, significantly more women were on antiretroviral therapy (56%).
The second pregnancy occurred a mean of 2.6 years later in both groups. At presentation for the second pregnancy, 57 had maintained that level of suppression and 46 had not. At that time, the mean viral load was 0 in those who had maintained suppression and 10,160 copies/mL among those who had not – a significant difference. CD4 cell count also was significantly different (596 vs. 342 cells/mcL). Significantly more of those who had maintained suppression were on antiretroviral therapy at the second pregnancy (75% vs. 59%).
By the time of delivery, however, HIV indices had improved in the group that had not maintained suppression. At that time, their mean viral load was also 0. Their CD4 count had increased to 427 cells/mcL, and 93% were on antiretroviral therapy.
There were no significant differences in the clinical parameters of the second pregnancy between those who had maintained suppression and those who had not. These included gestational age at delivery (38 weeks); birth weight (about 3,000 g); the use of intrapartum zidovudine (more than 90% of each group); cesarean delivery (32% vs. 52%; P = .18); length of labor; length of ruptured membranes; and incidence of clinical chorioamnionitis.
Vertical transmission was significantly higher among women who had not maintained an interpregnancy suppression (9% vs. 0 infants).
Dr. Stewart said he had no relevant financial disclosures.
On Twitter @alz_gal
AT THE PREGNANCY MEETING
Major finding: There were no cases of HIV transmission to infants among women who maintained a well-suppressed viral load between pregnancies, compared with 9% in those women whose interpregnancy viral load was more than 1,000 copies/mL.
Data source: A retrospective study that included 103 women who had an HIV viral load of less than 1,000 copies/mL at their index pregnancy.
Disclosures: Dr. Stewart said he had no financial disclosures.
