User login
Malaria vaccine disappoints in phase II trial
The efficacy of an investigational malaria vaccine waned from 36% to 2.5% over a period of 7 years in Kenya, at which time it was even associated with an excess of cases in areas of high malaria transmission.
The overall vaccine efficacy during the entire follow-up period was 4.4%, Ally Olotu, PhD, and colleagues wrote in the June 29 issue of the New England Journal of Medicine (2016;374:2519-29. doi: 10.1056/NEJMoa1515257). But after 7 years, in areas of high malaria risk, the vaccine was associated with 141 excess cases per 1,000 vaccinated children.

“We found that RTS,S/AS01 provided protective efficacy in the first year after vaccination but that the efficacy subsequently waned,” wrote Dr. Olotu of the Kenya Medical Research Institute in Africa and associates. “Efficacy was close to zero in the fourth year and may have been negative in the fifth year. This result eroded the benefits that were seen in early years.”
The rebound in cases probably occurred because the vaccine targets only a particular early-stage form of Plasmodium falciparum, they noted. “[It] protects against malaria sporozoites but does not induce clinical immunity against blood-stage parasites. We and others have previously found lower levels of antibodies against blood-stage parasites in children who have been immunized with the RTS,S/AS01 vaccine than in those given the control vaccine. The reduced exposure to blood-stage parasites among persons who have received the vaccine may lead to a slower acquisition of immunity to blood-stage parasites, leading to an increase in episodes of clinical malaria in later life.”
The phase II study comprised 447 children aged 5-17 months who were randomized to three doses of RTS,S/AS01 or a control rabies vaccine, administered at baseline and at 1 and 2 months. Children were followed for 7 years. The study had a large attrition rate, with 312 children completing all the follow-up visits.
In an intent-to-treat analysis, 150 incident cases of malaria developed among 223 children in the active group, and 157 cases among 224 in the control group. This equated to a vaccine efficacy of 27% against a first episode of malaria.
Overall, there were 1,002 episodes of malaria in the vaccine group and 992 in the control group. When the investigators grouped the children according to the endemic potential of their environment (high- vs. low-risk exposure), they observed that efficacy was consistently better in the low-risk group than the high-risk group (16.6% vs. –2.4%)
They then examined this finding year by year. Vaccine efficacy declined from 36% in year 1 to 3.6% in year 7. At year 5, there was significant negative efficacy in the high-risk exposure cohort (–56.8%, P = .008).
Overall, the vaccine averted 317 cases of clinical malaria per 1,000 children vaccinated, but the investigators noted that this finding was nonsignificant. In the low-exposure cohort, the vaccine did better, averting 718 cases per 1,000 vaccinated children. “However, in the high-exposure cohort … there were more cumulative cases among participants in the RTS,S/AS01 group than among those in the control group … which more than offset the cases that were averted in earlier years,” leading to an excess of 141 cases per 1,000 vaccinated children over baseline levels.
The rate of serious adverse events was similar between the vaccine and control groups (17.9% vs. 25.4%). No cases of meningitis occurred.
The investigators said a larger, phase III trial is being conducted in several areas with varying levels of transmission, and with different dosing schedules. “It will be essential to monitor efficacy in longer-term follow-up for year 5 and beyond to accurately measure the benefit and potential risk of vaccination with the RTS,S/AS01 vaccine,” they wrote.
The study was funded by grants from the PATH Malaria Vaccine Initiative, GlaxoSmithKline Biologicals, the Bill and Melinda Gates Foundation, and the Wellcome Trust. Two of the investigators, Amanda Leach and Marc Lievens, reported receiving personal fees and other support from GlaxoSmithKline Vaccines.
On Twitter @Alz_Gal
The findings of this extended follow-up of a 2008 phase II trial suggest that the RTS,S/AS01 malaria vaccine should be further investigated, but shouldn’t impede studies to prepare for large-scale vaccine deployment by the World Health Organization, according to John Clemens, MD, and Vasee Moorthy, PhD, in an editorial accompanying the study (N Engl J Med. 2016;374:2596-7. doi:10.1056/NEJMe1606007).
The three-dose regimen examined in the study is not the one that WHO agreed upon based on the vaccine’s most recent phase III trial, conducted in 15,500 children. That study looked at a three- and four-dose regimen in two different age groups. While efficacy waned in both groups over the 32-month study period, the four-dose regimen declined more slowly. WHO has thus given its support only to the four-dose regimen in the 5- to 17-month age group, and recommended pilot implementation studies in several sub-Saharan countries with moderate to high levels of malaria transmission.
The new data from the phase II trial cast even more negative light on the complex interplay of this vaccine and the malaria risk in areas in which it is to be deployed. But, the authors said, it should not be cause for abandoning the vaccine protocol.
“The interpretation of these findings requires caution, in view of the high attrition of the original cohort over time and the emergence of these findings in the context of many analyses, with the attendant risk of increased type I error,” the authors of the editorial wrote. “Fortunately, three other sites participating in the phase III trial are extending surveillance beyond the 4th year and include cohorts receiving either a three-dose or four-dose regimen; these sites will provide an important resource to test and better understand the findings of this trial. To maximize the usefulness and ensure the validity of these additional trials, it will be critical that the analyses be done conjointly, with the use of common a priori analytic plans and definitions. In the meantime, it would be unwise to postpone the planning of the WHO-recommended pilot implementation studies, which will be designed to yield data of importance to decisions regarding the deployment of this vaccine.”
Dr. Clemens is professor and vice chairman in the department of epidemiology, as well as the founding director of the center for global infectious diseases at the University of California, Los Angeles. He has received grant support from GlaxoSmithKline. Dr. Moorthy is an infectious disease specialist with the World Health Organization. He had no financial conflicts to disclose.
The findings of this extended follow-up of a 2008 phase II trial suggest that the RTS,S/AS01 malaria vaccine should be further investigated, but shouldn’t impede studies to prepare for large-scale vaccine deployment by the World Health Organization, according to John Clemens, MD, and Vasee Moorthy, PhD, in an editorial accompanying the study (N Engl J Med. 2016;374:2596-7. doi:10.1056/NEJMe1606007).
The three-dose regimen examined in the study is not the one that WHO agreed upon based on the vaccine’s most recent phase III trial, conducted in 15,500 children. That study looked at a three- and four-dose regimen in two different age groups. While efficacy waned in both groups over the 32-month study period, the four-dose regimen declined more slowly. WHO has thus given its support only to the four-dose regimen in the 5- to 17-month age group, and recommended pilot implementation studies in several sub-Saharan countries with moderate to high levels of malaria transmission.
The new data from the phase II trial cast even more negative light on the complex interplay of this vaccine and the malaria risk in areas in which it is to be deployed. But, the authors said, it should not be cause for abandoning the vaccine protocol.
“The interpretation of these findings requires caution, in view of the high attrition of the original cohort over time and the emergence of these findings in the context of many analyses, with the attendant risk of increased type I error,” the authors of the editorial wrote. “Fortunately, three other sites participating in the phase III trial are extending surveillance beyond the 4th year and include cohorts receiving either a three-dose or four-dose regimen; these sites will provide an important resource to test and better understand the findings of this trial. To maximize the usefulness and ensure the validity of these additional trials, it will be critical that the analyses be done conjointly, with the use of common a priori analytic plans and definitions. In the meantime, it would be unwise to postpone the planning of the WHO-recommended pilot implementation studies, which will be designed to yield data of importance to decisions regarding the deployment of this vaccine.”
Dr. Clemens is professor and vice chairman in the department of epidemiology, as well as the founding director of the center for global infectious diseases at the University of California, Los Angeles. He has received grant support from GlaxoSmithKline. Dr. Moorthy is an infectious disease specialist with the World Health Organization. He had no financial conflicts to disclose.
The findings of this extended follow-up of a 2008 phase II trial suggest that the RTS,S/AS01 malaria vaccine should be further investigated, but shouldn’t impede studies to prepare for large-scale vaccine deployment by the World Health Organization, according to John Clemens, MD, and Vasee Moorthy, PhD, in an editorial accompanying the study (N Engl J Med. 2016;374:2596-7. doi:10.1056/NEJMe1606007).
The three-dose regimen examined in the study is not the one that WHO agreed upon based on the vaccine’s most recent phase III trial, conducted in 15,500 children. That study looked at a three- and four-dose regimen in two different age groups. While efficacy waned in both groups over the 32-month study period, the four-dose regimen declined more slowly. WHO has thus given its support only to the four-dose regimen in the 5- to 17-month age group, and recommended pilot implementation studies in several sub-Saharan countries with moderate to high levels of malaria transmission.
The new data from the phase II trial cast even more negative light on the complex interplay of this vaccine and the malaria risk in areas in which it is to be deployed. But, the authors said, it should not be cause for abandoning the vaccine protocol.
“The interpretation of these findings requires caution, in view of the high attrition of the original cohort over time and the emergence of these findings in the context of many analyses, with the attendant risk of increased type I error,” the authors of the editorial wrote. “Fortunately, three other sites participating in the phase III trial are extending surveillance beyond the 4th year and include cohorts receiving either a three-dose or four-dose regimen; these sites will provide an important resource to test and better understand the findings of this trial. To maximize the usefulness and ensure the validity of these additional trials, it will be critical that the analyses be done conjointly, with the use of common a priori analytic plans and definitions. In the meantime, it would be unwise to postpone the planning of the WHO-recommended pilot implementation studies, which will be designed to yield data of importance to decisions regarding the deployment of this vaccine.”
Dr. Clemens is professor and vice chairman in the department of epidemiology, as well as the founding director of the center for global infectious diseases at the University of California, Los Angeles. He has received grant support from GlaxoSmithKline. Dr. Moorthy is an infectious disease specialist with the World Health Organization. He had no financial conflicts to disclose.
The efficacy of an investigational malaria vaccine waned from 36% to 2.5% over a period of 7 years in Kenya, at which time it was even associated with an excess of cases in areas of high malaria transmission.
The overall vaccine efficacy during the entire follow-up period was 4.4%, Ally Olotu, PhD, and colleagues wrote in the June 29 issue of the New England Journal of Medicine (2016;374:2519-29. doi: 10.1056/NEJMoa1515257). But after 7 years, in areas of high malaria risk, the vaccine was associated with 141 excess cases per 1,000 vaccinated children.
“We found that RTS,S/AS01 provided protective efficacy in the first year after vaccination but that the efficacy subsequently waned,” wrote Dr. Olotu of the Kenya Medical Research Institute in Africa and associates. “Efficacy was close to zero in the fourth year and may have been negative in the fifth year. This result eroded the benefits that were seen in early years.”
The rebound in cases probably occurred because the vaccine targets only a particular early-stage form of Plasmodium falciparum, they noted. “[It] protects against malaria sporozoites but does not induce clinical immunity against blood-stage parasites. We and others have previously found lower levels of antibodies against blood-stage parasites in children who have been immunized with the RTS,S/AS01 vaccine than in those given the control vaccine. The reduced exposure to blood-stage parasites among persons who have received the vaccine may lead to a slower acquisition of immunity to blood-stage parasites, leading to an increase in episodes of clinical malaria in later life.”
The phase II study comprised 447 children aged 5-17 months who were randomized to three doses of RTS,S/AS01 or a control rabies vaccine, administered at baseline and at 1 and 2 months. Children were followed for 7 years. The study had a large attrition rate, with 312 children completing all the follow-up visits.
In an intent-to-treat analysis, 150 incident cases of malaria developed among 223 children in the active group, and 157 cases among 224 in the control group. This equated to a vaccine efficacy of 27% against a first episode of malaria.
Overall, there were 1,002 episodes of malaria in the vaccine group and 992 in the control group. When the investigators grouped the children according to the endemic potential of their environment (high- vs. low-risk exposure), they observed that efficacy was consistently better in the low-risk group than the high-risk group (16.6% vs. –2.4%)
They then examined this finding year by year. Vaccine efficacy declined from 36% in year 1 to 3.6% in year 7. At year 5, there was significant negative efficacy in the high-risk exposure cohort (–56.8%, P = .008).
Overall, the vaccine averted 317 cases of clinical malaria per 1,000 children vaccinated, but the investigators noted that this finding was nonsignificant. In the low-exposure cohort, the vaccine did better, averting 718 cases per 1,000 vaccinated children. “However, in the high-exposure cohort … there were more cumulative cases among participants in the RTS,S/AS01 group than among those in the control group … which more than offset the cases that were averted in earlier years,” leading to an excess of 141 cases per 1,000 vaccinated children over baseline levels.
The rate of serious adverse events was similar between the vaccine and control groups (17.9% vs. 25.4%). No cases of meningitis occurred.
The investigators said a larger, phase III trial is being conducted in several areas with varying levels of transmission, and with different dosing schedules. “It will be essential to monitor efficacy in longer-term follow-up for year 5 and beyond to accurately measure the benefit and potential risk of vaccination with the RTS,S/AS01 vaccine,” they wrote.
The study was funded by grants from the PATH Malaria Vaccine Initiative, GlaxoSmithKline Biologicals, the Bill and Melinda Gates Foundation, and the Wellcome Trust. Two of the investigators, Amanda Leach and Marc Lievens, reported receiving personal fees and other support from GlaxoSmithKline Vaccines.
On Twitter @Alz_Gal
The efficacy of an investigational malaria vaccine waned from 36% to 2.5% over a period of 7 years in Kenya, at which time it was even associated with an excess of cases in areas of high malaria transmission.
The overall vaccine efficacy during the entire follow-up period was 4.4%, Ally Olotu, PhD, and colleagues wrote in the June 29 issue of the New England Journal of Medicine (2016;374:2519-29. doi: 10.1056/NEJMoa1515257). But after 7 years, in areas of high malaria risk, the vaccine was associated with 141 excess cases per 1,000 vaccinated children.
“We found that RTS,S/AS01 provided protective efficacy in the first year after vaccination but that the efficacy subsequently waned,” wrote Dr. Olotu of the Kenya Medical Research Institute in Africa and associates. “Efficacy was close to zero in the fourth year and may have been negative in the fifth year. This result eroded the benefits that were seen in early years.”
The rebound in cases probably occurred because the vaccine targets only a particular early-stage form of Plasmodium falciparum, they noted. “[It] protects against malaria sporozoites but does not induce clinical immunity against blood-stage parasites. We and others have previously found lower levels of antibodies against blood-stage parasites in children who have been immunized with the RTS,S/AS01 vaccine than in those given the control vaccine. The reduced exposure to blood-stage parasites among persons who have received the vaccine may lead to a slower acquisition of immunity to blood-stage parasites, leading to an increase in episodes of clinical malaria in later life.”
The phase II study comprised 447 children aged 5-17 months who were randomized to three doses of RTS,S/AS01 or a control rabies vaccine, administered at baseline and at 1 and 2 months. Children were followed for 7 years. The study had a large attrition rate, with 312 children completing all the follow-up visits.
In an intent-to-treat analysis, 150 incident cases of malaria developed among 223 children in the active group, and 157 cases among 224 in the control group. This equated to a vaccine efficacy of 27% against a first episode of malaria.
Overall, there were 1,002 episodes of malaria in the vaccine group and 992 in the control group. When the investigators grouped the children according to the endemic potential of their environment (high- vs. low-risk exposure), they observed that efficacy was consistently better in the low-risk group than the high-risk group (16.6% vs. –2.4%)
They then examined this finding year by year. Vaccine efficacy declined from 36% in year 1 to 3.6% in year 7. At year 5, there was significant negative efficacy in the high-risk exposure cohort (–56.8%, P = .008).
Overall, the vaccine averted 317 cases of clinical malaria per 1,000 children vaccinated, but the investigators noted that this finding was nonsignificant. In the low-exposure cohort, the vaccine did better, averting 718 cases per 1,000 vaccinated children. “However, in the high-exposure cohort … there were more cumulative cases among participants in the RTS,S/AS01 group than among those in the control group … which more than offset the cases that were averted in earlier years,” leading to an excess of 141 cases per 1,000 vaccinated children over baseline levels.
The rate of serious adverse events was similar between the vaccine and control groups (17.9% vs. 25.4%). No cases of meningitis occurred.
The investigators said a larger, phase III trial is being conducted in several areas with varying levels of transmission, and with different dosing schedules. “It will be essential to monitor efficacy in longer-term follow-up for year 5 and beyond to accurately measure the benefit and potential risk of vaccination with the RTS,S/AS01 vaccine,” they wrote.
The study was funded by grants from the PATH Malaria Vaccine Initiative, GlaxoSmithKline Biologicals, the Bill and Melinda Gates Foundation, and the Wellcome Trust. Two of the investigators, Amanda Leach and Marc Lievens, reported receiving personal fees and other support from GlaxoSmithKline Vaccines.
On Twitter @Alz_Gal
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: An investigational malaria vaccine lost efficacy over a 7-year period, and was associated with increased cases in late follow-up.
Major finding: Vaccine efficacy waned from 36% to 2.5% over 7 years, when 141 excess cases per 1,000 children were observed.
Data source: The phase II study randomized 447 children to three doses of the malaria vaccine or a control rabies vaccine.
Disclosures: The study was funded by grants from the PATH Malaria Vaccine Initiative, GlaxoSmithKline Biologicals, the Bill and Melinda Gates Foundation, and the Wellcome Trust. Two of the investigators, Amanda Leach and Marc Lievens, reported receiving personal fees and other support from GlaxoSmithKline Vaccines.

Abortion requests surged in Latin American countries after Zika warnings
Requests for medication abortions have risen significantly in nine Latin American countries since the Pan American Health Organization issued an epidemiologic warning about Zika virus in November 2015.
All of the countries have legal restrictions that make abortions impossible or very difficult to obtain. Nevertheless, women are seeking them in increasing numbers using Women on Web, a nonprofit, international group that supplies information on abortions and facilitates contact with physicians who provide abortifacient medications.
Dr. Abigail Aiken of the University of Texas, Austin, and her colleagues reported the findings June 22 in the New England Journal of Medicine (2016 Jun. doi: 10.1056/NEJMc1605389).
Most of the increased requests occurred in countries that issued a national advisory to pregnant women, the researchers noted. But increases also occurred in two countries with local Zika transmission but no national advisory.
“We cannot definitively attribute the rapid acceleration in requests … to concern about Zika virus exposure,” the researchers wrote in a letter to the editor. However, “In Latin American countries that issued warnings to pregnant women about complications associated with Zika virus infection, requests for abortion through [Women on Web] increased significantly. Our approach may underestimate the effect of the advisories on demand for abortion, since many women may have used an unsafe method, accessed misoprostol from local pharmacies or the black market, or visited local underground providers.”
The authors worked with Women on Web to assess requests for medical abortion consultations from women in 19 Latin American countries between Jan. 1, 2010, and March 2, 2016. They compared these numbers before and after the November 2015 Zika announcement from the Pan American Health Organization.
They divided the data into three groups: countries with local Zika transmission, legally restricted abortion, and a national advisory to pregnant women; countries with no Zika transmission and legally restricted abortion; and countries with local Zika transmission, legally restricted abortion, and no national advisory to pregnant women. The study also included three control countries with no Zika transmission anticipated (Chile, Poland, and Uruguay).
All of the eight countries with local Zika transmission, legally restricted abortion, and a national advisory to pregnant women showed significant increases in Women on Web requests, except Jamaica. The increases were highest in Brazil and Ecuador (108%) and lowest in El Salvador and Costa Rica (36%). The increases reported reflect the relative change between actual and expected requests for abortion medications.
Two of the four countries with no Zika transmission and legally restricted abortion also showed increases: Peru (20.5%) and Argentina (21.8%).
There were no significant increases in requests in any of the seven countries with local Zika transmission, legally restricted abortion, and no national advisory to pregnant women.
The findings suggest a difficult future for many women who desire pregnancy or who conceive in areas of Zika activity, the researchers wrote. “Models that were developed by the World Health Organization predict that 3 million to 4 million persons across the Americas will contract Zika virus infection through 2017, and the virus will inevitably spread to other countries where access to safe abortion is restricted. Official information and advice about potential exposure to the Zika virus should be accompanied by efforts to ensure that all reproductive choices are safe, legal, and accessible.”
Dr. Thomas Gellhaus, president of the American Congress of Obstetricians and Gynecologists (ACOG), said the study “presents alarming insight on how the Zika virus is affecting the lives of pregnant women.”
“ACOG has long recognized that access to reproductive services, including abortion care, is essential for all women,” he said. “All women, must have the legal right to abortion, unconstrained by harassment, unavailability of care, procedure bans, or other legislative or regulatory barriers. The Zika crisis makes it impossible to ignore that women around the world do not have access to this basic health care need.”
ACOG updated its Zika clinical guidelines on June 13.
Two of the researchers are affiliated with Women on Web.
Requests for medication abortions have risen significantly in nine Latin American countries since the Pan American Health Organization issued an epidemiologic warning about Zika virus in November 2015.
All of the countries have legal restrictions that make abortions impossible or very difficult to obtain. Nevertheless, women are seeking them in increasing numbers using Women on Web, a nonprofit, international group that supplies information on abortions and facilitates contact with physicians who provide abortifacient medications.
Dr. Abigail Aiken of the University of Texas, Austin, and her colleagues reported the findings June 22 in the New England Journal of Medicine (2016 Jun. doi: 10.1056/NEJMc1605389).
Most of the increased requests occurred in countries that issued a national advisory to pregnant women, the researchers noted. But increases also occurred in two countries with local Zika transmission but no national advisory.
“We cannot definitively attribute the rapid acceleration in requests … to concern about Zika virus exposure,” the researchers wrote in a letter to the editor. However, “In Latin American countries that issued warnings to pregnant women about complications associated with Zika virus infection, requests for abortion through [Women on Web] increased significantly. Our approach may underestimate the effect of the advisories on demand for abortion, since many women may have used an unsafe method, accessed misoprostol from local pharmacies or the black market, or visited local underground providers.”
The authors worked with Women on Web to assess requests for medical abortion consultations from women in 19 Latin American countries between Jan. 1, 2010, and March 2, 2016. They compared these numbers before and after the November 2015 Zika announcement from the Pan American Health Organization.
They divided the data into three groups: countries with local Zika transmission, legally restricted abortion, and a national advisory to pregnant women; countries with no Zika transmission and legally restricted abortion; and countries with local Zika transmission, legally restricted abortion, and no national advisory to pregnant women. The study also included three control countries with no Zika transmission anticipated (Chile, Poland, and Uruguay).
All of the eight countries with local Zika transmission, legally restricted abortion, and a national advisory to pregnant women showed significant increases in Women on Web requests, except Jamaica. The increases were highest in Brazil and Ecuador (108%) and lowest in El Salvador and Costa Rica (36%). The increases reported reflect the relative change between actual and expected requests for abortion medications.
Two of the four countries with no Zika transmission and legally restricted abortion also showed increases: Peru (20.5%) and Argentina (21.8%).
There were no significant increases in requests in any of the seven countries with local Zika transmission, legally restricted abortion, and no national advisory to pregnant women.
The findings suggest a difficult future for many women who desire pregnancy or who conceive in areas of Zika activity, the researchers wrote. “Models that were developed by the World Health Organization predict that 3 million to 4 million persons across the Americas will contract Zika virus infection through 2017, and the virus will inevitably spread to other countries where access to safe abortion is restricted. Official information and advice about potential exposure to the Zika virus should be accompanied by efforts to ensure that all reproductive choices are safe, legal, and accessible.”
Dr. Thomas Gellhaus, president of the American Congress of Obstetricians and Gynecologists (ACOG), said the study “presents alarming insight on how the Zika virus is affecting the lives of pregnant women.”
“ACOG has long recognized that access to reproductive services, including abortion care, is essential for all women,” he said. “All women, must have the legal right to abortion, unconstrained by harassment, unavailability of care, procedure bans, or other legislative or regulatory barriers. The Zika crisis makes it impossible to ignore that women around the world do not have access to this basic health care need.”
ACOG updated its Zika clinical guidelines on June 13.
Two of the researchers are affiliated with Women on Web.
Requests for medication abortions have risen significantly in nine Latin American countries since the Pan American Health Organization issued an epidemiologic warning about Zika virus in November 2015.
All of the countries have legal restrictions that make abortions impossible or very difficult to obtain. Nevertheless, women are seeking them in increasing numbers using Women on Web, a nonprofit, international group that supplies information on abortions and facilitates contact with physicians who provide abortifacient medications.
Dr. Abigail Aiken of the University of Texas, Austin, and her colleagues reported the findings June 22 in the New England Journal of Medicine (2016 Jun. doi: 10.1056/NEJMc1605389).
Most of the increased requests occurred in countries that issued a national advisory to pregnant women, the researchers noted. But increases also occurred in two countries with local Zika transmission but no national advisory.
“We cannot definitively attribute the rapid acceleration in requests … to concern about Zika virus exposure,” the researchers wrote in a letter to the editor. However, “In Latin American countries that issued warnings to pregnant women about complications associated with Zika virus infection, requests for abortion through [Women on Web] increased significantly. Our approach may underestimate the effect of the advisories on demand for abortion, since many women may have used an unsafe method, accessed misoprostol from local pharmacies or the black market, or visited local underground providers.”
The authors worked with Women on Web to assess requests for medical abortion consultations from women in 19 Latin American countries between Jan. 1, 2010, and March 2, 2016. They compared these numbers before and after the November 2015 Zika announcement from the Pan American Health Organization.
They divided the data into three groups: countries with local Zika transmission, legally restricted abortion, and a national advisory to pregnant women; countries with no Zika transmission and legally restricted abortion; and countries with local Zika transmission, legally restricted abortion, and no national advisory to pregnant women. The study also included three control countries with no Zika transmission anticipated (Chile, Poland, and Uruguay).
All of the eight countries with local Zika transmission, legally restricted abortion, and a national advisory to pregnant women showed significant increases in Women on Web requests, except Jamaica. The increases were highest in Brazil and Ecuador (108%) and lowest in El Salvador and Costa Rica (36%). The increases reported reflect the relative change between actual and expected requests for abortion medications.
Two of the four countries with no Zika transmission and legally restricted abortion also showed increases: Peru (20.5%) and Argentina (21.8%).
There were no significant increases in requests in any of the seven countries with local Zika transmission, legally restricted abortion, and no national advisory to pregnant women.
The findings suggest a difficult future for many women who desire pregnancy or who conceive in areas of Zika activity, the researchers wrote. “Models that were developed by the World Health Organization predict that 3 million to 4 million persons across the Americas will contract Zika virus infection through 2017, and the virus will inevitably spread to other countries where access to safe abortion is restricted. Official information and advice about potential exposure to the Zika virus should be accompanied by efforts to ensure that all reproductive choices are safe, legal, and accessible.”
Dr. Thomas Gellhaus, president of the American Congress of Obstetricians and Gynecologists (ACOG), said the study “presents alarming insight on how the Zika virus is affecting the lives of pregnant women.”
“ACOG has long recognized that access to reproductive services, including abortion care, is essential for all women,” he said. “All women, must have the legal right to abortion, unconstrained by harassment, unavailability of care, procedure bans, or other legislative or regulatory barriers. The Zika crisis makes it impossible to ignore that women around the world do not have access to this basic health care need.”
ACOG updated its Zika clinical guidelines on June 13.
Two of the researchers are affiliated with Women on Web.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Requests for medication abortions have risen in nine Latin American countries since the first Zika warning last November.
Major finding: Requests for abortifacient medications in Brazil and Ecuador rose by about 108%, compared with expected requests.
Data source: The study compared data between Jan. 1, 2010, and March 2, 2016.
Disclosures: Two of the researchers are affiliated with Women on Web, a nonprofit, international group that supplies information on abortions and facilitates contact with physicians who provide abortifacient medications.
Enhanced recovery protocol speeds discharge, decreases readmissions for ventral hernia repair
A postsurgical recovery program featuring early feeding and multimodal pain management hastened the return of bowel function and shortened hospital stay by 2 days for patients undergoing complex ventral hernia repair.
Despite leaving the hospital sooner, however, patients were 75% less likely to be readmitted within 90 days, Dr. Arnab Majumder and his colleagues wrote in the June issue of the Journal of the American College of Surgeons (2016 Jun;222:1106-15). Most of those who did return had wound complications, a stark contrast to readmissions among patients who didn’t experience the enhanced recovery program. Among that group, 75% of the readmissions were caused by bowel obstruction/ileus, deep venous thrombosis or pulmonary embolism, pneumonia, and urinary tract infections – all of them “problems [that] could be related to prolonged hospitalizations,” said Dr. Majumder of the University Hospitals Case Medical Center, Cleveland.

The investigators created an Enhanced Recovery After Surgery (ERAS) pathway specifically for patients undergoing complex ventral hernia repairs using transversus abdominis release and sublay synthetic mesh placement. The patients “present formidable challenges to the surgeon, not only in the operating room but also during perioperative management,” the authors noted.
The ERAS the team preemptively addressed patient issues in the preoperative, intra- and perioperative, and postoperative periods. They compared the outcomes of 100 patients treated with the protocol to those in a control group of 100 who underwent the same surgery before the protocol was implemented. The main outcomes measures were time to diet advancement, time to return of bowel function, time to oral narcotics, length of stay, and 90-day readmissions.
The ERAS begins with preoperative optimization. This consists of weight loss, smoking cessation, and managing diabetes and obstructive sleep apnea. No surgery occurs until the HbA1c is less than 8 and patients have been tobacco free for at least 1 month.
All patients receive an arginine and omega-3 supplement thrice daily for 5 days before surgery. The night before surgery, they have a nasal swab screen for methicillin-resistant Staphylococcus aureus (MRSA), and decolonization with mupirocin ointment and a chlorhexidine bath.
Preoperatively, they receive 5,000 units of unfractionated heparin, along with sequential compression devices for deep vein thrombosis protection. Use of both continue postoperatively, with heparin given every 8 hours until the patient is ambulatory.
Those without a history of narcotic use receive a preoperative dose of alvimopan. Everyone also receives oral gabapentin and preoperative antibiotics.
Intraoperatively, intravenous fluids are given judiciously to minimize bowel edema and decrease the risk of respiratory side effects. The surgeon also employs a transversus abdominis plane (TAP) block with liposomal bupivacaine.
There is a multimodal pain management program, which includes intravenous hydromorphone by patient-controlled anesthesia pump and oral gabapentin three times daily. Patients switch to oral analgesics on postoperative day 2. These consist of acetaminophen and NSAIDs on an alternating schedule. Intravenous diazepam can be added as an antispasmodic. Alvimopan is continued twice daily until first bowel movement or hospital discharge.
Clear liquids are limited to 250 mL/8 hours on postoperative day 1, along with a clear protein drink. By day 2, patients are advanced to unrestricted volumes of clear liquids, and on day 3, to a regular solid diet. At that point, the clear protein drink is switched for a regular protein drink (Boost Plus).
Patients who vomit or require a nasogastric tube for decompression, and those with severe persistent nausea are made NPO, but can resume diet when these symptoms improve. Those with mild-moderate nausea receive intravenous ondansetron and are allowed to self-limit oral intake.
Patients were a mean of 57 years old with a mean body mass index of about 33 kg/m2. The hernia was recurrent for about 60% of each group, with a mean area of about 300 cm2, and a mean width of 14 cm. The mean mesh size was about 1,000 cm2. The mean operative time was significantly shorter in the control group: 197 vs. 245 minutes.
Diet was advanced significantly more quickly in the ERAS group than the control group: 1 vs. 2 days on a liquid diet and 3 vs. 4.8 days to regular diet. Emesis after diet advancement was similar (4% for ERAS and 5% for control).
Compared with the control group, the ERAS group experienced significantly shorter average times to flatus (3.1 vs. 3.9 days), bowel movement (3.6 vs. 5.2 days), and reaching GI-3 status (3.4 vs. 4.8 days). Those in the ERAS group switched to oral narcotics sooner (2.2 vs. 3.6 days) also.
The average length of stay was significantly lower in ERAS group as well (4 vs. 6 days). About 18% of those in the ERAS group had a stay of less than 3 days, compared with 2% of the control group.
Readmissions within 90 days occurred in 16% of the control group and 4% of the ERAS group – a significant difference. There were four surgical site complications in the control group and three in the ERAS group. Bowel obstruction occurred in three control patients and one ERAS patient. All other complications requiring readmission occurred in the control group: two pulmonary embolisms, two deep vein thromboses, one pneumonia, one urinary tract infection and three other unspecified causes.
The authors noted that the shift to multimodal pain management and shorter-term use of IV opiates is a large contributor to the protocol’s good bowel outcomes. “Introduction of preoperative and postoperative gabapentin, intraoperative surgeon-delivered TAP block with long-acting liposomal bupivacaine, postoperative use of acetaminophen, and nonsteroidal agents have all appeared to contribute to better pain control and likely decrease in opioid consumption,” they said.
The use of diazepam as a pain medication is unusual, they said, but effective.
“We believe a large component of postoperative pain in hernia patients is due to muscle spasms after myofascial release, irritation from mesh placement, and transabdominal suture fixation. Therefore, in the context of our frequent use of myofascial releases for large incisional hernias, we believe the antispasmodic effects of diazepam potentially alleviate some of the postoperative discomfort caused by major abdominal wall reconstruction.”
None of the investigators reported financial conflicts.
A postsurgical recovery program featuring early feeding and multimodal pain management hastened the return of bowel function and shortened hospital stay by 2 days for patients undergoing complex ventral hernia repair.
Despite leaving the hospital sooner, however, patients were 75% less likely to be readmitted within 90 days, Dr. Arnab Majumder and his colleagues wrote in the June issue of the Journal of the American College of Surgeons (2016 Jun;222:1106-15). Most of those who did return had wound complications, a stark contrast to readmissions among patients who didn’t experience the enhanced recovery program. Among that group, 75% of the readmissions were caused by bowel obstruction/ileus, deep venous thrombosis or pulmonary embolism, pneumonia, and urinary tract infections – all of them “problems [that] could be related to prolonged hospitalizations,” said Dr. Majumder of the University Hospitals Case Medical Center, Cleveland.
The investigators created an Enhanced Recovery After Surgery (ERAS) pathway specifically for patients undergoing complex ventral hernia repairs using transversus abdominis release and sublay synthetic mesh placement. The patients “present formidable challenges to the surgeon, not only in the operating room but also during perioperative management,” the authors noted.
The ERAS the team preemptively addressed patient issues in the preoperative, intra- and perioperative, and postoperative periods. They compared the outcomes of 100 patients treated with the protocol to those in a control group of 100 who underwent the same surgery before the protocol was implemented. The main outcomes measures were time to diet advancement, time to return of bowel function, time to oral narcotics, length of stay, and 90-day readmissions.
The ERAS begins with preoperative optimization. This consists of weight loss, smoking cessation, and managing diabetes and obstructive sleep apnea. No surgery occurs until the HbA1c is less than 8 and patients have been tobacco free for at least 1 month.
All patients receive an arginine and omega-3 supplement thrice daily for 5 days before surgery. The night before surgery, they have a nasal swab screen for methicillin-resistant Staphylococcus aureus (MRSA), and decolonization with mupirocin ointment and a chlorhexidine bath.
Preoperatively, they receive 5,000 units of unfractionated heparin, along with sequential compression devices for deep vein thrombosis protection. Use of both continue postoperatively, with heparin given every 8 hours until the patient is ambulatory.
Those without a history of narcotic use receive a preoperative dose of alvimopan. Everyone also receives oral gabapentin and preoperative antibiotics.
Intraoperatively, intravenous fluids are given judiciously to minimize bowel edema and decrease the risk of respiratory side effects. The surgeon also employs a transversus abdominis plane (TAP) block with liposomal bupivacaine.
There is a multimodal pain management program, which includes intravenous hydromorphone by patient-controlled anesthesia pump and oral gabapentin three times daily. Patients switch to oral analgesics on postoperative day 2. These consist of acetaminophen and NSAIDs on an alternating schedule. Intravenous diazepam can be added as an antispasmodic. Alvimopan is continued twice daily until first bowel movement or hospital discharge.
Clear liquids are limited to 250 mL/8 hours on postoperative day 1, along with a clear protein drink. By day 2, patients are advanced to unrestricted volumes of clear liquids, and on day 3, to a regular solid diet. At that point, the clear protein drink is switched for a regular protein drink (Boost Plus).
Patients who vomit or require a nasogastric tube for decompression, and those with severe persistent nausea are made NPO, but can resume diet when these symptoms improve. Those with mild-moderate nausea receive intravenous ondansetron and are allowed to self-limit oral intake.
Patients were a mean of 57 years old with a mean body mass index of about 33 kg/m2. The hernia was recurrent for about 60% of each group, with a mean area of about 300 cm2, and a mean width of 14 cm. The mean mesh size was about 1,000 cm2. The mean operative time was significantly shorter in the control group: 197 vs. 245 minutes.
Diet was advanced significantly more quickly in the ERAS group than the control group: 1 vs. 2 days on a liquid diet and 3 vs. 4.8 days to regular diet. Emesis after diet advancement was similar (4% for ERAS and 5% for control).
Compared with the control group, the ERAS group experienced significantly shorter average times to flatus (3.1 vs. 3.9 days), bowel movement (3.6 vs. 5.2 days), and reaching GI-3 status (3.4 vs. 4.8 days). Those in the ERAS group switched to oral narcotics sooner (2.2 vs. 3.6 days) also.
The average length of stay was significantly lower in ERAS group as well (4 vs. 6 days). About 18% of those in the ERAS group had a stay of less than 3 days, compared with 2% of the control group.
Readmissions within 90 days occurred in 16% of the control group and 4% of the ERAS group – a significant difference. There were four surgical site complications in the control group and three in the ERAS group. Bowel obstruction occurred in three control patients and one ERAS patient. All other complications requiring readmission occurred in the control group: two pulmonary embolisms, two deep vein thromboses, one pneumonia, one urinary tract infection and three other unspecified causes.
The authors noted that the shift to multimodal pain management and shorter-term use of IV opiates is a large contributor to the protocol’s good bowel outcomes. “Introduction of preoperative and postoperative gabapentin, intraoperative surgeon-delivered TAP block with long-acting liposomal bupivacaine, postoperative use of acetaminophen, and nonsteroidal agents have all appeared to contribute to better pain control and likely decrease in opioid consumption,” they said.
The use of diazepam as a pain medication is unusual, they said, but effective.
“We believe a large component of postoperative pain in hernia patients is due to muscle spasms after myofascial release, irritation from mesh placement, and transabdominal suture fixation. Therefore, in the context of our frequent use of myofascial releases for large incisional hernias, we believe the antispasmodic effects of diazepam potentially alleviate some of the postoperative discomfort caused by major abdominal wall reconstruction.”
None of the investigators reported financial conflicts.
A postsurgical recovery program featuring early feeding and multimodal pain management hastened the return of bowel function and shortened hospital stay by 2 days for patients undergoing complex ventral hernia repair.
Despite leaving the hospital sooner, however, patients were 75% less likely to be readmitted within 90 days, Dr. Arnab Majumder and his colleagues wrote in the June issue of the Journal of the American College of Surgeons (2016 Jun;222:1106-15). Most of those who did return had wound complications, a stark contrast to readmissions among patients who didn’t experience the enhanced recovery program. Among that group, 75% of the readmissions were caused by bowel obstruction/ileus, deep venous thrombosis or pulmonary embolism, pneumonia, and urinary tract infections – all of them “problems [that] could be related to prolonged hospitalizations,” said Dr. Majumder of the University Hospitals Case Medical Center, Cleveland.
The investigators created an Enhanced Recovery After Surgery (ERAS) pathway specifically for patients undergoing complex ventral hernia repairs using transversus abdominis release and sublay synthetic mesh placement. The patients “present formidable challenges to the surgeon, not only in the operating room but also during perioperative management,” the authors noted.
The ERAS the team preemptively addressed patient issues in the preoperative, intra- and perioperative, and postoperative periods. They compared the outcomes of 100 patients treated with the protocol to those in a control group of 100 who underwent the same surgery before the protocol was implemented. The main outcomes measures were time to diet advancement, time to return of bowel function, time to oral narcotics, length of stay, and 90-day readmissions.
The ERAS begins with preoperative optimization. This consists of weight loss, smoking cessation, and managing diabetes and obstructive sleep apnea. No surgery occurs until the HbA1c is less than 8 and patients have been tobacco free for at least 1 month.
All patients receive an arginine and omega-3 supplement thrice daily for 5 days before surgery. The night before surgery, they have a nasal swab screen for methicillin-resistant Staphylococcus aureus (MRSA), and decolonization with mupirocin ointment and a chlorhexidine bath.
Preoperatively, they receive 5,000 units of unfractionated heparin, along with sequential compression devices for deep vein thrombosis protection. Use of both continue postoperatively, with heparin given every 8 hours until the patient is ambulatory.
Those without a history of narcotic use receive a preoperative dose of alvimopan. Everyone also receives oral gabapentin and preoperative antibiotics.
Intraoperatively, intravenous fluids are given judiciously to minimize bowel edema and decrease the risk of respiratory side effects. The surgeon also employs a transversus abdominis plane (TAP) block with liposomal bupivacaine.
There is a multimodal pain management program, which includes intravenous hydromorphone by patient-controlled anesthesia pump and oral gabapentin three times daily. Patients switch to oral analgesics on postoperative day 2. These consist of acetaminophen and NSAIDs on an alternating schedule. Intravenous diazepam can be added as an antispasmodic. Alvimopan is continued twice daily until first bowel movement or hospital discharge.
Clear liquids are limited to 250 mL/8 hours on postoperative day 1, along with a clear protein drink. By day 2, patients are advanced to unrestricted volumes of clear liquids, and on day 3, to a regular solid diet. At that point, the clear protein drink is switched for a regular protein drink (Boost Plus).
Patients who vomit or require a nasogastric tube for decompression, and those with severe persistent nausea are made NPO, but can resume diet when these symptoms improve. Those with mild-moderate nausea receive intravenous ondansetron and are allowed to self-limit oral intake.
Patients were a mean of 57 years old with a mean body mass index of about 33 kg/m2. The hernia was recurrent for about 60% of each group, with a mean area of about 300 cm2, and a mean width of 14 cm. The mean mesh size was about 1,000 cm2. The mean operative time was significantly shorter in the control group: 197 vs. 245 minutes.
Diet was advanced significantly more quickly in the ERAS group than the control group: 1 vs. 2 days on a liquid diet and 3 vs. 4.8 days to regular diet. Emesis after diet advancement was similar (4% for ERAS and 5% for control).
Compared with the control group, the ERAS group experienced significantly shorter average times to flatus (3.1 vs. 3.9 days), bowel movement (3.6 vs. 5.2 days), and reaching GI-3 status (3.4 vs. 4.8 days). Those in the ERAS group switched to oral narcotics sooner (2.2 vs. 3.6 days) also.
The average length of stay was significantly lower in ERAS group as well (4 vs. 6 days). About 18% of those in the ERAS group had a stay of less than 3 days, compared with 2% of the control group.
Readmissions within 90 days occurred in 16% of the control group and 4% of the ERAS group – a significant difference. There were four surgical site complications in the control group and three in the ERAS group. Bowel obstruction occurred in three control patients and one ERAS patient. All other complications requiring readmission occurred in the control group: two pulmonary embolisms, two deep vein thromboses, one pneumonia, one urinary tract infection and three other unspecified causes.
The authors noted that the shift to multimodal pain management and shorter-term use of IV opiates is a large contributor to the protocol’s good bowel outcomes. “Introduction of preoperative and postoperative gabapentin, intraoperative surgeon-delivered TAP block with long-acting liposomal bupivacaine, postoperative use of acetaminophen, and nonsteroidal agents have all appeared to contribute to better pain control and likely decrease in opioid consumption,” they said.
The use of diazepam as a pain medication is unusual, they said, but effective.
“We believe a large component of postoperative pain in hernia patients is due to muscle spasms after myofascial release, irritation from mesh placement, and transabdominal suture fixation. Therefore, in the context of our frequent use of myofascial releases for large incisional hernias, we believe the antispasmodic effects of diazepam potentially alleviate some of the postoperative discomfort caused by major abdominal wall reconstruction.”
None of the investigators reported financial conflicts.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF SURGEONS
Key clinical point: Early enteral feeding and multimodal pain management both contributed to early return of bowel function.
Major finding: Length of stay was 2 days shorter, and readmissions decreased by 75%, compared with a control group.
Data source: The prospective study comprised 200 patients.
Disclosures: Neither Dr. Majumder nor his colleagues had any financial disclosures.

2015-2016 flu season slower and milder than past 3 years
The 2015-2016 flu season was less severe than the last three seasons, with a lower hospitalization rate and fewer pediatric deaths.
Cases of influenza appeared later in the season than typically seen, and activity didn’t peak until March, Stacy L. Davlin, Ph.D., wrote in the June 10 issue of the Morbidity and Mortality Weekly Report (MMWR 2016;22:567-75)
“During the most recent 18 influenza seasons, only two other seasons have peaked in March (2011-2012 and 2005-2006),” wrote Dr. Davlin, an epidemiologist at the Centers for Disease Control and Prevention, Atlanta. This serves as a reminder that influenza can and does occur outside the traditionally expected season, and that clinicians shouldn’t discount the possibility of flu when a patient presents with typical symptoms.
“Although summer influenza activity in the United States typically is low, influenza cases and outbreaks have occurred during summer months, and clinicians should remain vigilant in considering influenza in the differential diagnosis of summer respiratory illnesses,” Dr. Davlin said.
The most common influenza virus of the last season was A(H1N1), which accounted for about half of cases in those aged 5-24 years, and about 70% of cases in those younger than 5 years and those 65 years and older.
Three novel viruses were seen as well: variants of A(H1N1), A(H1N2), and A(H3N2). The A(H1N1) variant occurred in a Minnesota resident who lived and worked in an area of swine farming, but who denied direct contact with pigs. The A(H3N2) variant occurred in a New Jersey resident who reported visiting a farm shortly before symptom onset. There was no evidence of human-to-human transmission. Both recovered fully without hospitalization. The A(H1N2) variant occurred in a Minnesota resident who was hospitalized but who recovered. This person was not interviewed so no possible source of infection was identified.
The CDC tested 2,408 viral specimens for susceptibility to antiviral medications. Among the 2,193 A(H1N1) specimens, less than 1% were resistant to oseltamivir and peramivir. All were susceptible to zanamivir. However, the testing found persistent high levels of resistance to amantadine and rimantadine in the A viruses. Amantadine is not effective on the B strains at all. Therefore, CDC does not recommend the use of amantadine as an anti-influenza medication.
Reports of influenza first exceeded the 2.1% baseline level in the week ending Dec. 26, 2015, according to the U.S. Outpatient Influenza-Like Illness Surveillance Network (ILINet). They remained elevated for the next 17 weeks, with a peak of 3.6% of all outpatient visits in the week ending March 12. From October 2015-April 2016, the overall hospitalization rate for influenza-like illness was 31 per 100,000. This was highest in those aged 65 years and older (85/100,000), and lowest in those aged 5-17 years (10/100,000). About 92% of adults hospitalized for flu-like illness had at least one underlying medical comorbidity, including obesity (42%), cardiovascular disease (40%), and metabolic disorders (38%). Almost half of children (48%) also had medical comorbidities, including asthma or other reactive airway disease (22%) and neurologic disorders (18%).
CDC’s National Center for Health Statistics Mortality Surveillance System found that the percentage of deaths attributed to pneumonia and influenza peaked at 8% during the week ending March 19. This is slightly lower than the death rate seen in the last 5 years, which ranged from 9% in 2011-2012 to 11% in 2012-2013.
Of this season’s deaths, 74 occurred in children. The mean and median ages of these patients were 7 years and 6 years, respectively; the range was 2 months-16 years. This total was lower than that recorded in any of the past three influenza seasons: 171 pediatric deaths in 2012-2013, 111 in 2013-2014, and 148 in 2014-2015.
Dr. Davlin also announced the Food and Drug Administration’s recommendations for composition of the 2016-2017 influenza vaccine.
Trivalent vaccines should contain an A/California/7/2009 (H1N1) pdm09-like virus, an A/Hong Kong/4801/2014 (H3N2)-like virus, and a B/Brisbane/60/2008-like virus (B/Victoria lineage). Quadrivalent vaccines, which have two influenza B viruses, should include the viruses recommended for the trivalent vaccines, as well as a B/Phuket/3073/2013-like virus (B/Yamagata lineage).
“The vaccine viruses recommended for inclusion in the 2016-2017 Northern Hemisphere influenza vaccines are the same vaccine viruses that were chosen for inclusion in 2016 Southern Hemisphere seasonal influenza vaccines,” Dr. Davlin noted. “These vaccine recommendations were based on a number of factors, including global influenza virologic and epidemiologic surveillance, genetic and antigenic characterization, antiviral susceptibility, and the availability of candidate vaccine viruses for production.”
As a CDC employee, Dr. Davlin had no financial disclosures.
On Twitter @Alz_Gal
The 2015-2016 flu season was less severe than the last three seasons, with a lower hospitalization rate and fewer pediatric deaths.
Cases of influenza appeared later in the season than typically seen, and activity didn’t peak until March, Stacy L. Davlin, Ph.D., wrote in the June 10 issue of the Morbidity and Mortality Weekly Report (MMWR 2016;22:567-75)
“During the most recent 18 influenza seasons, only two other seasons have peaked in March (2011-2012 and 2005-2006),” wrote Dr. Davlin, an epidemiologist at the Centers for Disease Control and Prevention, Atlanta. This serves as a reminder that influenza can and does occur outside the traditionally expected season, and that clinicians shouldn’t discount the possibility of flu when a patient presents with typical symptoms.
“Although summer influenza activity in the United States typically is low, influenza cases and outbreaks have occurred during summer months, and clinicians should remain vigilant in considering influenza in the differential diagnosis of summer respiratory illnesses,” Dr. Davlin said.
The most common influenza virus of the last season was A(H1N1), which accounted for about half of cases in those aged 5-24 years, and about 70% of cases in those younger than 5 years and those 65 years and older.
Three novel viruses were seen as well: variants of A(H1N1), A(H1N2), and A(H3N2). The A(H1N1) variant occurred in a Minnesota resident who lived and worked in an area of swine farming, but who denied direct contact with pigs. The A(H3N2) variant occurred in a New Jersey resident who reported visiting a farm shortly before symptom onset. There was no evidence of human-to-human transmission. Both recovered fully without hospitalization. The A(H1N2) variant occurred in a Minnesota resident who was hospitalized but who recovered. This person was not interviewed so no possible source of infection was identified.
The CDC tested 2,408 viral specimens for susceptibility to antiviral medications. Among the 2,193 A(H1N1) specimens, less than 1% were resistant to oseltamivir and peramivir. All were susceptible to zanamivir. However, the testing found persistent high levels of resistance to amantadine and rimantadine in the A viruses. Amantadine is not effective on the B strains at all. Therefore, CDC does not recommend the use of amantadine as an anti-influenza medication.
Reports of influenza first exceeded the 2.1% baseline level in the week ending Dec. 26, 2015, according to the U.S. Outpatient Influenza-Like Illness Surveillance Network (ILINet). They remained elevated for the next 17 weeks, with a peak of 3.6% of all outpatient visits in the week ending March 12. From October 2015-April 2016, the overall hospitalization rate for influenza-like illness was 31 per 100,000. This was highest in those aged 65 years and older (85/100,000), and lowest in those aged 5-17 years (10/100,000). About 92% of adults hospitalized for flu-like illness had at least one underlying medical comorbidity, including obesity (42%), cardiovascular disease (40%), and metabolic disorders (38%). Almost half of children (48%) also had medical comorbidities, including asthma or other reactive airway disease (22%) and neurologic disorders (18%).
CDC’s National Center for Health Statistics Mortality Surveillance System found that the percentage of deaths attributed to pneumonia and influenza peaked at 8% during the week ending March 19. This is slightly lower than the death rate seen in the last 5 years, which ranged from 9% in 2011-2012 to 11% in 2012-2013.
Of this season’s deaths, 74 occurred in children. The mean and median ages of these patients were 7 years and 6 years, respectively; the range was 2 months-16 years. This total was lower than that recorded in any of the past three influenza seasons: 171 pediatric deaths in 2012-2013, 111 in 2013-2014, and 148 in 2014-2015.
Dr. Davlin also announced the Food and Drug Administration’s recommendations for composition of the 2016-2017 influenza vaccine.
Trivalent vaccines should contain an A/California/7/2009 (H1N1) pdm09-like virus, an A/Hong Kong/4801/2014 (H3N2)-like virus, and a B/Brisbane/60/2008-like virus (B/Victoria lineage). Quadrivalent vaccines, which have two influenza B viruses, should include the viruses recommended for the trivalent vaccines, as well as a B/Phuket/3073/2013-like virus (B/Yamagata lineage).
“The vaccine viruses recommended for inclusion in the 2016-2017 Northern Hemisphere influenza vaccines are the same vaccine viruses that were chosen for inclusion in 2016 Southern Hemisphere seasonal influenza vaccines,” Dr. Davlin noted. “These vaccine recommendations were based on a number of factors, including global influenza virologic and epidemiologic surveillance, genetic and antigenic characterization, antiviral susceptibility, and the availability of candidate vaccine viruses for production.”
As a CDC employee, Dr. Davlin had no financial disclosures.
On Twitter @Alz_Gal
The 2015-2016 flu season was less severe than the last three seasons, with a lower hospitalization rate and fewer pediatric deaths.
Cases of influenza appeared later in the season than typically seen, and activity didn’t peak until March, Stacy L. Davlin, Ph.D., wrote in the June 10 issue of the Morbidity and Mortality Weekly Report (MMWR 2016;22:567-75)
“During the most recent 18 influenza seasons, only two other seasons have peaked in March (2011-2012 and 2005-2006),” wrote Dr. Davlin, an epidemiologist at the Centers for Disease Control and Prevention, Atlanta. This serves as a reminder that influenza can and does occur outside the traditionally expected season, and that clinicians shouldn’t discount the possibility of flu when a patient presents with typical symptoms.
“Although summer influenza activity in the United States typically is low, influenza cases and outbreaks have occurred during summer months, and clinicians should remain vigilant in considering influenza in the differential diagnosis of summer respiratory illnesses,” Dr. Davlin said.
The most common influenza virus of the last season was A(H1N1), which accounted for about half of cases in those aged 5-24 years, and about 70% of cases in those younger than 5 years and those 65 years and older.
Three novel viruses were seen as well: variants of A(H1N1), A(H1N2), and A(H3N2). The A(H1N1) variant occurred in a Minnesota resident who lived and worked in an area of swine farming, but who denied direct contact with pigs. The A(H3N2) variant occurred in a New Jersey resident who reported visiting a farm shortly before symptom onset. There was no evidence of human-to-human transmission. Both recovered fully without hospitalization. The A(H1N2) variant occurred in a Minnesota resident who was hospitalized but who recovered. This person was not interviewed so no possible source of infection was identified.
The CDC tested 2,408 viral specimens for susceptibility to antiviral medications. Among the 2,193 A(H1N1) specimens, less than 1% were resistant to oseltamivir and peramivir. All were susceptible to zanamivir. However, the testing found persistent high levels of resistance to amantadine and rimantadine in the A viruses. Amantadine is not effective on the B strains at all. Therefore, CDC does not recommend the use of amantadine as an anti-influenza medication.
Reports of influenza first exceeded the 2.1% baseline level in the week ending Dec. 26, 2015, according to the U.S. Outpatient Influenza-Like Illness Surveillance Network (ILINet). They remained elevated for the next 17 weeks, with a peak of 3.6% of all outpatient visits in the week ending March 12. From October 2015-April 2016, the overall hospitalization rate for influenza-like illness was 31 per 100,000. This was highest in those aged 65 years and older (85/100,000), and lowest in those aged 5-17 years (10/100,000). About 92% of adults hospitalized for flu-like illness had at least one underlying medical comorbidity, including obesity (42%), cardiovascular disease (40%), and metabolic disorders (38%). Almost half of children (48%) also had medical comorbidities, including asthma or other reactive airway disease (22%) and neurologic disorders (18%).
CDC’s National Center for Health Statistics Mortality Surveillance System found that the percentage of deaths attributed to pneumonia and influenza peaked at 8% during the week ending March 19. This is slightly lower than the death rate seen in the last 5 years, which ranged from 9% in 2011-2012 to 11% in 2012-2013.
Of this season’s deaths, 74 occurred in children. The mean and median ages of these patients were 7 years and 6 years, respectively; the range was 2 months-16 years. This total was lower than that recorded in any of the past three influenza seasons: 171 pediatric deaths in 2012-2013, 111 in 2013-2014, and 148 in 2014-2015.
Dr. Davlin also announced the Food and Drug Administration’s recommendations for composition of the 2016-2017 influenza vaccine.
Trivalent vaccines should contain an A/California/7/2009 (H1N1) pdm09-like virus, an A/Hong Kong/4801/2014 (H3N2)-like virus, and a B/Brisbane/60/2008-like virus (B/Victoria lineage). Quadrivalent vaccines, which have two influenza B viruses, should include the viruses recommended for the trivalent vaccines, as well as a B/Phuket/3073/2013-like virus (B/Yamagata lineage).
“The vaccine viruses recommended for inclusion in the 2016-2017 Northern Hemisphere influenza vaccines are the same vaccine viruses that were chosen for inclusion in 2016 Southern Hemisphere seasonal influenza vaccines,” Dr. Davlin noted. “These vaccine recommendations were based on a number of factors, including global influenza virologic and epidemiologic surveillance, genetic and antigenic characterization, antiviral susceptibility, and the availability of candidate vaccine viruses for production.”
As a CDC employee, Dr. Davlin had no financial disclosures.
On Twitter @Alz_Gal
FROM THE MMWR
2015-2016 flu season slower and milder than past 3 years
The 2015-2016 flu season was less severe than the last three seasons, with a lower hospitalization rate and fewer pediatric deaths.
Cases of influenza appeared later in the season that typically seen, and activity didn’t peak until March, Stacy L. Davlin, Ph.D., wrote in the June 10 issue of the Morbidity and Mortality report (MMWR 2016; 22:567-75)
“During the most recent 18 influenza seasons, only two other seasons have peaked in March (2011-2012 and 2005-2006),” wrote Dr. Davlin, an epidemiologist at the Centers for Disease Control and Prevention, Atlanta. This serves as a reminder that influenza can and does occur outside the traditionally expected season, and that clinicians shouldn’t discount the possibility of flu when a patient presents with typical symptoms.

“Although summer influenza activity in the United States typically is low, influenza cases and outbreaks have occurred during summer months, and clinicians should remain vigilant in considering influenza in the differential diagnosis of summer respiratory illnesses,” Dr. Davlin said.
The most common influenza virus of the last season was A(H1N1), which accounted for about half of cases in those aged 5-24 years, and about 70% of cases in those younger than 5 years and those 65 years and older.
Three novel viruses were seen as well: variants of A(H1N1), A(H1N2), and A(H3N2). The A(H1N1) variant occurred in a Minnesota resident who lived and worked in an area of swine farming, but who denied direct contact with pigs. The A(H3N2) variant occurred in a New Jersey resident who reported visiting a farm shortly before symptom onset. There was no evidence of human-to-human transmission. Both recovered fully without hospitalization. The A(H1N2) variant occurred in a Minnesota resident who was hospitalized but who recovered. This person was not interviewed so no possible source of infection was identified.
The CDC tested 2,408 viral specimens for susceptibility to antiviral medications. Among the 2,193 A(H1N1) specimens, less than 1% were resistant to oseltamivir and peramivir. All were susceptible to zanamivir. However, the testing found persistent high levels of resistant to amantadine and rimantadine in the A viruses. Amantadine is not effective on the B strains at all. Therefore, CDC does not recommend the use of amantadine as an anti-influenza medication.
Reports of influenza first exceeded the 2.1% baseline level in the week ending Dec. 26, 2015, according to the U.S. Outpatient Influenza-Like Illness Surveillance Network (ILINet). They remained elevated for the next 17 weeks, with a peak of 3.6% of all outpatient visits in the week ending March 12. From October 2015-April 2016, the overall hospitalization rate for influenza-like illness was 31 per 100,000. This was highest in those aged 65 years and older (85/100,000), and lowest in those aged 5-17 years (10/100,000). About 92% of adults hospitalized for flu-like illness had at least one underlying medical comorbidity, including obesity (42%), cardiovascular disease (40%), and metabolic disorders (38%). Almost half of children (48%) also had medical comorbidities, including asthma or other reactive airway disease (22%) and neurologic disorders (18%).
CDC’s National Center for Health Statistics Mortality Surveillance System found that the percentage of deaths attributed to pneumonia and influenza peaked at 8% during the week ending March 19. This is slightly lower than the death rate seen in the last 5 years, which ranged from 9% in 2011-2012 to 11% in 2012-2013.
Of this season’s deaths, 74 occurred in children. The mean and median ages of these patients were 7 years and 6 years, respectively; the range was 2 months-16 years. This total was lower than that recorded in any of the past three influenza seasons: 171 pediatric deaths in 2012-2013, 111 in 2013-2014, and 148 in 2014-2015.
Dr. Davlin also announced the Food and Drug Administration’s recommendations for composition of the 2016-2017 influenza vaccine.
Trivalent vaccines should contain an A/California/7/2009 (H1N1) pdm09-like virus, an A/Hong Kong/4801/2014 (H3N2)-like virus, and a B/Brisbane/60/2008-like virus (B/Victoria lineage). Quadrivalent vaccines, which have two influenza B viruses, should include the viruses recommended for the trivalent vaccines, as well as a B/Phuket/3073/2013-like virus (B/Yamagata lineage).
“The vaccine viruses recommended for inclusion in the 2016-2017 Northern Hemisphere influenza vaccines are the same vaccine viruses that were chosen for inclusion in 2016 Southern Hemisphere seasonal influenza vaccines,” Dr. Davlin noted. “These vaccine recommendations were based on a number of factors, including global influenza virologic and epidemiologic surveillance, genetic and antigenic characterization, antiviral susceptibility, and the availability of candidate vaccine viruses for production.”
As a CDC employee, Dr. Davlin had no financial disclosures.
On Twitter @Alz_Gal
The 2015-2016 flu season was less severe than the last three seasons, with a lower hospitalization rate and fewer pediatric deaths.
Cases of influenza appeared later in the season that typically seen, and activity didn’t peak until March, Stacy L. Davlin, Ph.D., wrote in the June 10 issue of the Morbidity and Mortality report (MMWR 2016; 22:567-75)
“During the most recent 18 influenza seasons, only two other seasons have peaked in March (2011-2012 and 2005-2006),” wrote Dr. Davlin, an epidemiologist at the Centers for Disease Control and Prevention, Atlanta. This serves as a reminder that influenza can and does occur outside the traditionally expected season, and that clinicians shouldn’t discount the possibility of flu when a patient presents with typical symptoms.
“Although summer influenza activity in the United States typically is low, influenza cases and outbreaks have occurred during summer months, and clinicians should remain vigilant in considering influenza in the differential diagnosis of summer respiratory illnesses,” Dr. Davlin said.
The most common influenza virus of the last season was A(H1N1), which accounted for about half of cases in those aged 5-24 years, and about 70% of cases in those younger than 5 years and those 65 years and older.
Three novel viruses were seen as well: variants of A(H1N1), A(H1N2), and A(H3N2). The A(H1N1) variant occurred in a Minnesota resident who lived and worked in an area of swine farming, but who denied direct contact with pigs. The A(H3N2) variant occurred in a New Jersey resident who reported visiting a farm shortly before symptom onset. There was no evidence of human-to-human transmission. Both recovered fully without hospitalization. The A(H1N2) variant occurred in a Minnesota resident who was hospitalized but who recovered. This person was not interviewed so no possible source of infection was identified.
The CDC tested 2,408 viral specimens for susceptibility to antiviral medications. Among the 2,193 A(H1N1) specimens, less than 1% were resistant to oseltamivir and peramivir. All were susceptible to zanamivir. However, the testing found persistent high levels of resistant to amantadine and rimantadine in the A viruses. Amantadine is not effective on the B strains at all. Therefore, CDC does not recommend the use of amantadine as an anti-influenza medication.
Reports of influenza first exceeded the 2.1% baseline level in the week ending Dec. 26, 2015, according to the U.S. Outpatient Influenza-Like Illness Surveillance Network (ILINet). They remained elevated for the next 17 weeks, with a peak of 3.6% of all outpatient visits in the week ending March 12. From October 2015-April 2016, the overall hospitalization rate for influenza-like illness was 31 per 100,000. This was highest in those aged 65 years and older (85/100,000), and lowest in those aged 5-17 years (10/100,000). About 92% of adults hospitalized for flu-like illness had at least one underlying medical comorbidity, including obesity (42%), cardiovascular disease (40%), and metabolic disorders (38%). Almost half of children (48%) also had medical comorbidities, including asthma or other reactive airway disease (22%) and neurologic disorders (18%).
CDC’s National Center for Health Statistics Mortality Surveillance System found that the percentage of deaths attributed to pneumonia and influenza peaked at 8% during the week ending March 19. This is slightly lower than the death rate seen in the last 5 years, which ranged from 9% in 2011-2012 to 11% in 2012-2013.
Of this season’s deaths, 74 occurred in children. The mean and median ages of these patients were 7 years and 6 years, respectively; the range was 2 months-16 years. This total was lower than that recorded in any of the past three influenza seasons: 171 pediatric deaths in 2012-2013, 111 in 2013-2014, and 148 in 2014-2015.
Dr. Davlin also announced the Food and Drug Administration’s recommendations for composition of the 2016-2017 influenza vaccine.
Trivalent vaccines should contain an A/California/7/2009 (H1N1) pdm09-like virus, an A/Hong Kong/4801/2014 (H3N2)-like virus, and a B/Brisbane/60/2008-like virus (B/Victoria lineage). Quadrivalent vaccines, which have two influenza B viruses, should include the viruses recommended for the trivalent vaccines, as well as a B/Phuket/3073/2013-like virus (B/Yamagata lineage).
“The vaccine viruses recommended for inclusion in the 2016-2017 Northern Hemisphere influenza vaccines are the same vaccine viruses that were chosen for inclusion in 2016 Southern Hemisphere seasonal influenza vaccines,” Dr. Davlin noted. “These vaccine recommendations were based on a number of factors, including global influenza virologic and epidemiologic surveillance, genetic and antigenic characterization, antiviral susceptibility, and the availability of candidate vaccine viruses for production.”
As a CDC employee, Dr. Davlin had no financial disclosures.
On Twitter @Alz_Gal
The 2015-2016 flu season was less severe than the last three seasons, with a lower hospitalization rate and fewer pediatric deaths.
Cases of influenza appeared later in the season that typically seen, and activity didn’t peak until March, Stacy L. Davlin, Ph.D., wrote in the June 10 issue of the Morbidity and Mortality report (MMWR 2016; 22:567-75)
“During the most recent 18 influenza seasons, only two other seasons have peaked in March (2011-2012 and 2005-2006),” wrote Dr. Davlin, an epidemiologist at the Centers for Disease Control and Prevention, Atlanta. This serves as a reminder that influenza can and does occur outside the traditionally expected season, and that clinicians shouldn’t discount the possibility of flu when a patient presents with typical symptoms.
“Although summer influenza activity in the United States typically is low, influenza cases and outbreaks have occurred during summer months, and clinicians should remain vigilant in considering influenza in the differential diagnosis of summer respiratory illnesses,” Dr. Davlin said.
The most common influenza virus of the last season was A(H1N1), which accounted for about half of cases in those aged 5-24 years, and about 70% of cases in those younger than 5 years and those 65 years and older.
Three novel viruses were seen as well: variants of A(H1N1), A(H1N2), and A(H3N2). The A(H1N1) variant occurred in a Minnesota resident who lived and worked in an area of swine farming, but who denied direct contact with pigs. The A(H3N2) variant occurred in a New Jersey resident who reported visiting a farm shortly before symptom onset. There was no evidence of human-to-human transmission. Both recovered fully without hospitalization. The A(H1N2) variant occurred in a Minnesota resident who was hospitalized but who recovered. This person was not interviewed so no possible source of infection was identified.
The CDC tested 2,408 viral specimens for susceptibility to antiviral medications. Among the 2,193 A(H1N1) specimens, less than 1% were resistant to oseltamivir and peramivir. All were susceptible to zanamivir. However, the testing found persistent high levels of resistant to amantadine and rimantadine in the A viruses. Amantadine is not effective on the B strains at all. Therefore, CDC does not recommend the use of amantadine as an anti-influenza medication.
Reports of influenza first exceeded the 2.1% baseline level in the week ending Dec. 26, 2015, according to the U.S. Outpatient Influenza-Like Illness Surveillance Network (ILINet). They remained elevated for the next 17 weeks, with a peak of 3.6% of all outpatient visits in the week ending March 12. From October 2015-April 2016, the overall hospitalization rate for influenza-like illness was 31 per 100,000. This was highest in those aged 65 years and older (85/100,000), and lowest in those aged 5-17 years (10/100,000). About 92% of adults hospitalized for flu-like illness had at least one underlying medical comorbidity, including obesity (42%), cardiovascular disease (40%), and metabolic disorders (38%). Almost half of children (48%) also had medical comorbidities, including asthma or other reactive airway disease (22%) and neurologic disorders (18%).
CDC’s National Center for Health Statistics Mortality Surveillance System found that the percentage of deaths attributed to pneumonia and influenza peaked at 8% during the week ending March 19. This is slightly lower than the death rate seen in the last 5 years, which ranged from 9% in 2011-2012 to 11% in 2012-2013.
Of this season’s deaths, 74 occurred in children. The mean and median ages of these patients were 7 years and 6 years, respectively; the range was 2 months-16 years. This total was lower than that recorded in any of the past three influenza seasons: 171 pediatric deaths in 2012-2013, 111 in 2013-2014, and 148 in 2014-2015.
Dr. Davlin also announced the Food and Drug Administration’s recommendations for composition of the 2016-2017 influenza vaccine.
Trivalent vaccines should contain an A/California/7/2009 (H1N1) pdm09-like virus, an A/Hong Kong/4801/2014 (H3N2)-like virus, and a B/Brisbane/60/2008-like virus (B/Victoria lineage). Quadrivalent vaccines, which have two influenza B viruses, should include the viruses recommended for the trivalent vaccines, as well as a B/Phuket/3073/2013-like virus (B/Yamagata lineage).
“The vaccine viruses recommended for inclusion in the 2016-2017 Northern Hemisphere influenza vaccines are the same vaccine viruses that were chosen for inclusion in 2016 Southern Hemisphere seasonal influenza vaccines,” Dr. Davlin noted. “These vaccine recommendations were based on a number of factors, including global influenza virologic and epidemiologic surveillance, genetic and antigenic characterization, antiviral susceptibility, and the availability of candidate vaccine viruses for production.”
As a CDC employee, Dr. Davlin had no financial disclosures.
On Twitter @Alz_Gal
FROM THE MMWR
Key clinical point: The last flu season peaked later, and killed fewer people than the last three seasons.
Major finding: The overall death rate was 31/100,000, with a peak of 8% occurring in March.
Data source: Numbers were drawn from CDC databases and other national influenza surveillance programs.
Disclosures: As a CDC employee, Dr. Davlin had no financial disclosures.
Anxiety before Mohs surgery can be easily managed
ORLANDO – Assessment, education, and a judicious dose of medication can make a big difference to patients who are feeling anxious about undergoing Mohs surgery.
No studies or guidelines lay out a step-by-step management plan for anxious patients. But a little bit of common sense and empathy go a long way in easing the feeling, according to presenters at the annual meeting of the American College of Mohs Surgery.

“We don’t have an algorithm for reducing anxiety,” said Dr. Joseph Sobanko of the University of Pennsylvania, Philadelphia. “But we do have a lot of studies showing that better psychosocial health is related to better surgical outcomes.”
The lack of definitive guidance means that anxious patients might be identified and assessed by gut instinct, he continued. “Those of you who see patients probably have a gestalt technique of identifying the anxious ones. I would suggest this might not be the best way.”
Instead of guessing, he recommends assessing all patients with a validated screening tool, and dealing with anxiety proactively.
Assessing anxiety
Although anxiety assessment may not be part of a typical Mohs surgery intake, it probably should be, Dr. Sobanko said. There are a number of excellent, well-validated tools, and none of them require expertise in psychology to administer.
The Beck Anxiety Inventory is a 21-question index that takes about 10 minutes to complete. It assesses subjective, somatic, and panic-related symptoms of anxiety, and has been validated in a variety of clinical settings. It focuses quite a bit on strong physical symptoms, however, which Dr. Sobanko feels “may not be as relevant for our patients.”
The State-Trait Anxiety Inventory consists of 40 questions and takes about 15 minutes to complete. “I like it because it not only assesses how they generally feel, but how they feel at the moment,” he said. “We think it’s good and we do use it, but it takes a while to complete.”
The Hospital Anxiety and Depression Scale is short, with only 14 questions, and takes only about 5 minutes to complete. “It’s validated for hospital patients, but we are often working with patients who are less sick than that,” Dr. Sobanko said.
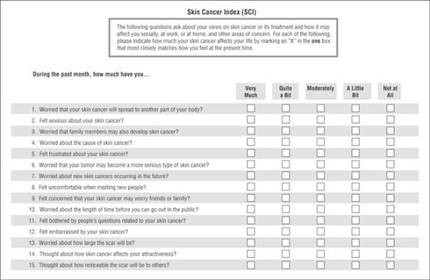
The Skin Cancer Index is his go-to anxiety screen for Mohs patients. It includes 15 questions that “really get to the heart of things that matter to our patients: emotional, social, and appearance issues,” he noted. Created in 2006, it was validated in a large cohort of Mohs surgery patients (Arch Facial Plast Surg. 2006;8[5]:314-318). The questions probe patients’ feelings about the seriousness of their skin cancer, its long-term health effect, and the impact the lesion – and its treatment – will have on appearance.
Tackling anxiety
Dr. Sobanko described his own, soon-to-be-published study of 104 Mohs surgery patients, who were randomized to receive a presurgical phone call to discuss anxiety, or the usual presurgical consultation. It was easy to implement the call, he said, noting that 70% were reached on the first try, and the interaction only took about 7 minutes.
Anxiety was common, with 43% reporting being anxious about the procedure. A frequent worry (25%) was whether their skin cancer would threaten their health over the long term. But both groups reported about the same reduction in anxiety after their discussion with the provider, whether it occurred over the phone or in person. After surgery, they expressed similar levels of satisfaction with the experience.
Clearly, the most effective method of dealing with patient anxiety has yet to be identified, Dr. Sobanko noted. Others are being explored, including music and educational videos.
In 2013, he and colleagues published a small study showing that music significantly reduced anxiety during Mohs surgery (Dermatol Surg. 2013 Feb;39[2]:298-305). It randomized 100 patients to surgery without music, or to listening to a playlist they had selected for themselves. Anxiety was measured using the State-Trait Anxiety Inventory and on a visual analog scale. Subjects in the music group experienced statistically significantly lower scores on both measures, Dr. Sobanko said.
A study presented at the meeting found that a preoperative education video helped as well. Dr. Sidney Smith of the Georgia Skin and Cancer Clinic, Savannah, examined the benefit of a 9-minute video created by the American College of Mohs Surgery. The video interviews patients about their experiences, describes the surgery and overall cure rates, and touches on reconstruction and follow-up.
The study comprised 200 patients; 100 saw the movie, and then completed a 24 question survey about their perception of the procedure. Almost all (94%) of those who viewed it said the video answered their questions; 85% said it relieved their fear about undergoing the surgery.
Treating anxiety
Anxiolytics can be easily employed to help ease day-of-surgery anxiety, Dr. Jerry Brewer said at the meeting. Generally speaking, the medications are safe, well-tolerated, and very effective.
“One thing we should remember, however, is that anxiolytics do not affect pain. They have no effect on pain receptors, although they may affect a patient’s memory of pain. For people who are anxious, though, this can be a really great help,” said Dr. Brewer of the Mayo Clinic, Rochester, Minn.
He favors the short-acting benzodiazepines, particularly midazolam. It has a peak concentration of 17-55 minutes, so it’s particularly well suited for shorter cases. It also has a very rapid metabolization profile, with an elimination half life of 3-7 hours.
Since midazolam has twice the affinity for the benzodiazepine receptors as does diazepam, it can be effective in relatively small doses – usually about 0.25 mg/kg. The dose should be reduced by half for elderly patients and for those with renal or hepatic failure. In those patients, the elimination half-life can be increased up to 13 hours.
The typical dose for both adults and children is 10-20 mg. “We should remember that patients who take narcotics and those who take a benzodiazepine as a sleep aide may be quite tolerant and need a higher dose,” Dr. Brewer said.
Diazepam has a peak concentration of about 2 hours, but a much longer elimination half-life – up to 48 hours in a healthy adult and up to 80 hours in an elderly person. “It’s important that patients know they’re going to have this drug in their system for a couple days. This should be part of the consenting process,” Dr. Brewer pointed out.
Lorazepam has a peak concentration of about 2 hours as well, but a shorter half-life of 12-18 hours. That can be prolonged by 75% in patients with renal problems.
With the right clinical supervision, these medications are very safe, he said. “We treat about 800 patients per year with these and have data on about 12,000. Of those, we have had very few problems. Two have fallen out of bed. One patient wrote and said he was discharged too early, as he was very tired. One person fell and hit his head in the bathroom. One was sedated enough to need a sternal rub to improve responsiveness. And one gentleman enjoyed the medication so much that when the nurse left the room for a moment he grabbed the rest of the dose and drank it.”
Safe discharge is crucial when using anxiolytics, he added. “They absolutely cannot drive themselves home and they cannot go back to work. We make sure there is a reliable person to stay with the patient for at least 4 hours after discharge.”
Dr. Brewer does not discharge any patient until that person displays a zero rating on the Richmond Agitation-Sedation Scale (RASS) sedation scale. “That means he is awake, alert, and calmly interacting with you.”
Neither Dr. Sobanko nor Dr. Brewer had any financial declarations.
ORLANDO – Assessment, education, and a judicious dose of medication can make a big difference to patients who are feeling anxious about undergoing Mohs surgery.
No studies or guidelines lay out a step-by-step management plan for anxious patients. But a little bit of common sense and empathy go a long way in easing the feeling, according to presenters at the annual meeting of the American College of Mohs Surgery.
“We don’t have an algorithm for reducing anxiety,” said Dr. Joseph Sobanko of the University of Pennsylvania, Philadelphia. “But we do have a lot of studies showing that better psychosocial health is related to better surgical outcomes.”
The lack of definitive guidance means that anxious patients might be identified and assessed by gut instinct, he continued. “Those of you who see patients probably have a gestalt technique of identifying the anxious ones. I would suggest this might not be the best way.”
Instead of guessing, he recommends assessing all patients with a validated screening tool, and dealing with anxiety proactively.
Assessing anxiety
Although anxiety assessment may not be part of a typical Mohs surgery intake, it probably should be, Dr. Sobanko said. There are a number of excellent, well-validated tools, and none of them require expertise in psychology to administer.
The Beck Anxiety Inventory is a 21-question index that takes about 10 minutes to complete. It assesses subjective, somatic, and panic-related symptoms of anxiety, and has been validated in a variety of clinical settings. It focuses quite a bit on strong physical symptoms, however, which Dr. Sobanko feels “may not be as relevant for our patients.”
The State-Trait Anxiety Inventory consists of 40 questions and takes about 15 minutes to complete. “I like it because it not only assesses how they generally feel, but how they feel at the moment,” he said. “We think it’s good and we do use it, but it takes a while to complete.”
The Hospital Anxiety and Depression Scale is short, with only 14 questions, and takes only about 5 minutes to complete. “It’s validated for hospital patients, but we are often working with patients who are less sick than that,” Dr. Sobanko said.
The Skin Cancer Index is his go-to anxiety screen for Mohs patients. It includes 15 questions that “really get to the heart of things that matter to our patients: emotional, social, and appearance issues,” he noted. Created in 2006, it was validated in a large cohort of Mohs surgery patients (Arch Facial Plast Surg. 2006;8[5]:314-318). The questions probe patients’ feelings about the seriousness of their skin cancer, its long-term health effect, and the impact the lesion – and its treatment – will have on appearance.
Tackling anxiety
Dr. Sobanko described his own, soon-to-be-published study of 104 Mohs surgery patients, who were randomized to receive a presurgical phone call to discuss anxiety, or the usual presurgical consultation. It was easy to implement the call, he said, noting that 70% were reached on the first try, and the interaction only took about 7 minutes.
Anxiety was common, with 43% reporting being anxious about the procedure. A frequent worry (25%) was whether their skin cancer would threaten their health over the long term. But both groups reported about the same reduction in anxiety after their discussion with the provider, whether it occurred over the phone or in person. After surgery, they expressed similar levels of satisfaction with the experience.
Clearly, the most effective method of dealing with patient anxiety has yet to be identified, Dr. Sobanko noted. Others are being explored, including music and educational videos.
In 2013, he and colleagues published a small study showing that music significantly reduced anxiety during Mohs surgery (Dermatol Surg. 2013 Feb;39[2]:298-305). It randomized 100 patients to surgery without music, or to listening to a playlist they had selected for themselves. Anxiety was measured using the State-Trait Anxiety Inventory and on a visual analog scale. Subjects in the music group experienced statistically significantly lower scores on both measures, Dr. Sobanko said.
A study presented at the meeting found that a preoperative education video helped as well. Dr. Sidney Smith of the Georgia Skin and Cancer Clinic, Savannah, examined the benefit of a 9-minute video created by the American College of Mohs Surgery. The video interviews patients about their experiences, describes the surgery and overall cure rates, and touches on reconstruction and follow-up.
The study comprised 200 patients; 100 saw the movie, and then completed a 24 question survey about their perception of the procedure. Almost all (94%) of those who viewed it said the video answered their questions; 85% said it relieved their fear about undergoing the surgery.
Treating anxiety
Anxiolytics can be easily employed to help ease day-of-surgery anxiety, Dr. Jerry Brewer said at the meeting. Generally speaking, the medications are safe, well-tolerated, and very effective.
“One thing we should remember, however, is that anxiolytics do not affect pain. They have no effect on pain receptors, although they may affect a patient’s memory of pain. For people who are anxious, though, this can be a really great help,” said Dr. Brewer of the Mayo Clinic, Rochester, Minn.
He favors the short-acting benzodiazepines, particularly midazolam. It has a peak concentration of 17-55 minutes, so it’s particularly well suited for shorter cases. It also has a very rapid metabolization profile, with an elimination half life of 3-7 hours.
Since midazolam has twice the affinity for the benzodiazepine receptors as does diazepam, it can be effective in relatively small doses – usually about 0.25 mg/kg. The dose should be reduced by half for elderly patients and for those with renal or hepatic failure. In those patients, the elimination half-life can be increased up to 13 hours.
The typical dose for both adults and children is 10-20 mg. “We should remember that patients who take narcotics and those who take a benzodiazepine as a sleep aide may be quite tolerant and need a higher dose,” Dr. Brewer said.
Diazepam has a peak concentration of about 2 hours, but a much longer elimination half-life – up to 48 hours in a healthy adult and up to 80 hours in an elderly person. “It’s important that patients know they’re going to have this drug in their system for a couple days. This should be part of the consenting process,” Dr. Brewer pointed out.
Lorazepam has a peak concentration of about 2 hours as well, but a shorter half-life of 12-18 hours. That can be prolonged by 75% in patients with renal problems.
With the right clinical supervision, these medications are very safe, he said. “We treat about 800 patients per year with these and have data on about 12,000. Of those, we have had very few problems. Two have fallen out of bed. One patient wrote and said he was discharged too early, as he was very tired. One person fell and hit his head in the bathroom. One was sedated enough to need a sternal rub to improve responsiveness. And one gentleman enjoyed the medication so much that when the nurse left the room for a moment he grabbed the rest of the dose and drank it.”
Safe discharge is crucial when using anxiolytics, he added. “They absolutely cannot drive themselves home and they cannot go back to work. We make sure there is a reliable person to stay with the patient for at least 4 hours after discharge.”
Dr. Brewer does not discharge any patient until that person displays a zero rating on the Richmond Agitation-Sedation Scale (RASS) sedation scale. “That means he is awake, alert, and calmly interacting with you.”
Neither Dr. Sobanko nor Dr. Brewer had any financial declarations.
ORLANDO – Assessment, education, and a judicious dose of medication can make a big difference to patients who are feeling anxious about undergoing Mohs surgery.
No studies or guidelines lay out a step-by-step management plan for anxious patients. But a little bit of common sense and empathy go a long way in easing the feeling, according to presenters at the annual meeting of the American College of Mohs Surgery.
“We don’t have an algorithm for reducing anxiety,” said Dr. Joseph Sobanko of the University of Pennsylvania, Philadelphia. “But we do have a lot of studies showing that better psychosocial health is related to better surgical outcomes.”
The lack of definitive guidance means that anxious patients might be identified and assessed by gut instinct, he continued. “Those of you who see patients probably have a gestalt technique of identifying the anxious ones. I would suggest this might not be the best way.”
Instead of guessing, he recommends assessing all patients with a validated screening tool, and dealing with anxiety proactively.
Assessing anxiety
Although anxiety assessment may not be part of a typical Mohs surgery intake, it probably should be, Dr. Sobanko said. There are a number of excellent, well-validated tools, and none of them require expertise in psychology to administer.
The Beck Anxiety Inventory is a 21-question index that takes about 10 minutes to complete. It assesses subjective, somatic, and panic-related symptoms of anxiety, and has been validated in a variety of clinical settings. It focuses quite a bit on strong physical symptoms, however, which Dr. Sobanko feels “may not be as relevant for our patients.”
The State-Trait Anxiety Inventory consists of 40 questions and takes about 15 minutes to complete. “I like it because it not only assesses how they generally feel, but how they feel at the moment,” he said. “We think it’s good and we do use it, but it takes a while to complete.”
The Hospital Anxiety and Depression Scale is short, with only 14 questions, and takes only about 5 minutes to complete. “It’s validated for hospital patients, but we are often working with patients who are less sick than that,” Dr. Sobanko said.
The Skin Cancer Index is his go-to anxiety screen for Mohs patients. It includes 15 questions that “really get to the heart of things that matter to our patients: emotional, social, and appearance issues,” he noted. Created in 2006, it was validated in a large cohort of Mohs surgery patients (Arch Facial Plast Surg. 2006;8[5]:314-318). The questions probe patients’ feelings about the seriousness of their skin cancer, its long-term health effect, and the impact the lesion – and its treatment – will have on appearance.
Tackling anxiety
Dr. Sobanko described his own, soon-to-be-published study of 104 Mohs surgery patients, who were randomized to receive a presurgical phone call to discuss anxiety, or the usual presurgical consultation. It was easy to implement the call, he said, noting that 70% were reached on the first try, and the interaction only took about 7 minutes.
Anxiety was common, with 43% reporting being anxious about the procedure. A frequent worry (25%) was whether their skin cancer would threaten their health over the long term. But both groups reported about the same reduction in anxiety after their discussion with the provider, whether it occurred over the phone or in person. After surgery, they expressed similar levels of satisfaction with the experience.
Clearly, the most effective method of dealing with patient anxiety has yet to be identified, Dr. Sobanko noted. Others are being explored, including music and educational videos.
In 2013, he and colleagues published a small study showing that music significantly reduced anxiety during Mohs surgery (Dermatol Surg. 2013 Feb;39[2]:298-305). It randomized 100 patients to surgery without music, or to listening to a playlist they had selected for themselves. Anxiety was measured using the State-Trait Anxiety Inventory and on a visual analog scale. Subjects in the music group experienced statistically significantly lower scores on both measures, Dr. Sobanko said.
A study presented at the meeting found that a preoperative education video helped as well. Dr. Sidney Smith of the Georgia Skin and Cancer Clinic, Savannah, examined the benefit of a 9-minute video created by the American College of Mohs Surgery. The video interviews patients about their experiences, describes the surgery and overall cure rates, and touches on reconstruction and follow-up.
The study comprised 200 patients; 100 saw the movie, and then completed a 24 question survey about their perception of the procedure. Almost all (94%) of those who viewed it said the video answered their questions; 85% said it relieved their fear about undergoing the surgery.
Treating anxiety
Anxiolytics can be easily employed to help ease day-of-surgery anxiety, Dr. Jerry Brewer said at the meeting. Generally speaking, the medications are safe, well-tolerated, and very effective.
“One thing we should remember, however, is that anxiolytics do not affect pain. They have no effect on pain receptors, although they may affect a patient’s memory of pain. For people who are anxious, though, this can be a really great help,” said Dr. Brewer of the Mayo Clinic, Rochester, Minn.
He favors the short-acting benzodiazepines, particularly midazolam. It has a peak concentration of 17-55 minutes, so it’s particularly well suited for shorter cases. It also has a very rapid metabolization profile, with an elimination half life of 3-7 hours.
Since midazolam has twice the affinity for the benzodiazepine receptors as does diazepam, it can be effective in relatively small doses – usually about 0.25 mg/kg. The dose should be reduced by half for elderly patients and for those with renal or hepatic failure. In those patients, the elimination half-life can be increased up to 13 hours.
The typical dose for both adults and children is 10-20 mg. “We should remember that patients who take narcotics and those who take a benzodiazepine as a sleep aide may be quite tolerant and need a higher dose,” Dr. Brewer said.
Diazepam has a peak concentration of about 2 hours, but a much longer elimination half-life – up to 48 hours in a healthy adult and up to 80 hours in an elderly person. “It’s important that patients know they’re going to have this drug in their system for a couple days. This should be part of the consenting process,” Dr. Brewer pointed out.
Lorazepam has a peak concentration of about 2 hours as well, but a shorter half-life of 12-18 hours. That can be prolonged by 75% in patients with renal problems.
With the right clinical supervision, these medications are very safe, he said. “We treat about 800 patients per year with these and have data on about 12,000. Of those, we have had very few problems. Two have fallen out of bed. One patient wrote and said he was discharged too early, as he was very tired. One person fell and hit his head in the bathroom. One was sedated enough to need a sternal rub to improve responsiveness. And one gentleman enjoyed the medication so much that when the nurse left the room for a moment he grabbed the rest of the dose and drank it.”
Safe discharge is crucial when using anxiolytics, he added. “They absolutely cannot drive themselves home and they cannot go back to work. We make sure there is a reliable person to stay with the patient for at least 4 hours after discharge.”
Dr. Brewer does not discharge any patient until that person displays a zero rating on the Richmond Agitation-Sedation Scale (RASS) sedation scale. “That means he is awake, alert, and calmly interacting with you.”
Neither Dr. Sobanko nor Dr. Brewer had any financial declarations.
EXPERT ANALYSIS FROM THE ACMS ANNUAL MEETING

Maternal flu shot offers far-reaching protection
WASHINGTON – The influenza vaccine is highly recommended for pregnant women, protecting the woman, the newborn, and even the fetus, according to Dr. Sonja Rasmussen.
Multiple prospective and retrospective studies have shown that the inactivated influenza shot is safe and effective for pregnant women. And not only does it confer a transient passive immunity upon the newborn, the vaccine also guards against the dangers the flu poses to fetuses, she said at the annual meeting of the American College of Obstetricians and Gynecologists.
Among the benefits seen with the flu shot are healthier birth weights, less preterm birth, and a much lower risk of birth defects that are associated with maternal fever in the first trimester, said Dr. Rasmussen, director of public health information dissemination at the Centers for Disease Control and Prevention.

“Fever in the first trimester doubles the risk of neural tube defects in the fetus,” said Dr. Rasmussen. She cited a 2014 meta-analysis that found increased risks of other fetal anomalies associated with first trimester flu: hydrocephaly (odds ratio, 5.74), congenital heart defects (OR, 1.56), cleft lip (OR, 3.12), limb abnormalities (OR, 2.03) and digestive system defects (OR, 1.72) (Hum Reprod. 2014 Apr;29[4]:809-23).
“We don’t know if these are more due to the hyperthermia of fever or to the flu virus crossing the placenta,” she said. “But we do know these are real risks.”
Newborns come with an immature immune system that takes a while to get ramped up. In the first 6 months of life, they’re especially vulnerable to communicable illnesses, and they can become severely ill and even die from flu, Dr. Rasmussen said. A new study of nearly 250,000 mother-child pairs confirmed that maternal vaccination reduces the risks of flu hospitalization by more than 80% in infants younger than 6 months (Pediatrics. 2016 May 2. doi: 10.1542/peds.2015-2360).
For most women, the understanding that a flu shot protects their baby before and after birth is good enough reason to get one, Dr. Rasmussen said, but the benefits for the woman are extremely important. “Pregnant women experience a lot of changes in immune function and heart and lung function that increase the risk for complications from influenza. In prior pandemics, we have seen pregnant women at an increased risk of severe illness, hospitalization, and death.”
She cited data from the 2009 H1N1 epidemic that showed that 5% of those who died from H1N1 flu were pregnant women, despite the fact that they represented only 1% of the U.S. population (JAMA. 2010;303[15]:1517-25).
Despite the well-documented benefits and reassuring safety data, flu vaccine coverage remains suboptimal for pregnant women, Dr. Rasmussen said. The most recent CDC data suggest that just half of pregnant women were immunized in 2014-2015, a rate that has remained steady since 2012.
The most effective way to boost this number, Dr. Rasmussen suggested, is to stress to women that the vaccine protects both the fetus and newborn from a potentially fatal illness. “We know that a large number of babies and children die of influenza every year,” she said. “The biggest motivator for moms is their desire to protect their baby – much more so than protecting themselves.”
Dr. Rasmussen reported having no relevant financial disclosures.
WASHINGTON – The influenza vaccine is highly recommended for pregnant women, protecting the woman, the newborn, and even the fetus, according to Dr. Sonja Rasmussen.
Multiple prospective and retrospective studies have shown that the inactivated influenza shot is safe and effective for pregnant women. And not only does it confer a transient passive immunity upon the newborn, the vaccine also guards against the dangers the flu poses to fetuses, she said at the annual meeting of the American College of Obstetricians and Gynecologists.
Among the benefits seen with the flu shot are healthier birth weights, less preterm birth, and a much lower risk of birth defects that are associated with maternal fever in the first trimester, said Dr. Rasmussen, director of public health information dissemination at the Centers for Disease Control and Prevention.
“Fever in the first trimester doubles the risk of neural tube defects in the fetus,” said Dr. Rasmussen. She cited a 2014 meta-analysis that found increased risks of other fetal anomalies associated with first trimester flu: hydrocephaly (odds ratio, 5.74), congenital heart defects (OR, 1.56), cleft lip (OR, 3.12), limb abnormalities (OR, 2.03) and digestive system defects (OR, 1.72) (Hum Reprod. 2014 Apr;29[4]:809-23).
“We don’t know if these are more due to the hyperthermia of fever or to the flu virus crossing the placenta,” she said. “But we do know these are real risks.”
Newborns come with an immature immune system that takes a while to get ramped up. In the first 6 months of life, they’re especially vulnerable to communicable illnesses, and they can become severely ill and even die from flu, Dr. Rasmussen said. A new study of nearly 250,000 mother-child pairs confirmed that maternal vaccination reduces the risks of flu hospitalization by more than 80% in infants younger than 6 months (Pediatrics. 2016 May 2. doi: 10.1542/peds.2015-2360).
For most women, the understanding that a flu shot protects their baby before and after birth is good enough reason to get one, Dr. Rasmussen said, but the benefits for the woman are extremely important. “Pregnant women experience a lot of changes in immune function and heart and lung function that increase the risk for complications from influenza. In prior pandemics, we have seen pregnant women at an increased risk of severe illness, hospitalization, and death.”
She cited data from the 2009 H1N1 epidemic that showed that 5% of those who died from H1N1 flu were pregnant women, despite the fact that they represented only 1% of the U.S. population (JAMA. 2010;303[15]:1517-25).
Despite the well-documented benefits and reassuring safety data, flu vaccine coverage remains suboptimal for pregnant women, Dr. Rasmussen said. The most recent CDC data suggest that just half of pregnant women were immunized in 2014-2015, a rate that has remained steady since 2012.
The most effective way to boost this number, Dr. Rasmussen suggested, is to stress to women that the vaccine protects both the fetus and newborn from a potentially fatal illness. “We know that a large number of babies and children die of influenza every year,” she said. “The biggest motivator for moms is their desire to protect their baby – much more so than protecting themselves.”
Dr. Rasmussen reported having no relevant financial disclosures.
WASHINGTON – The influenza vaccine is highly recommended for pregnant women, protecting the woman, the newborn, and even the fetus, according to Dr. Sonja Rasmussen.
Multiple prospective and retrospective studies have shown that the inactivated influenza shot is safe and effective for pregnant women. And not only does it confer a transient passive immunity upon the newborn, the vaccine also guards against the dangers the flu poses to fetuses, she said at the annual meeting of the American College of Obstetricians and Gynecologists.
Among the benefits seen with the flu shot are healthier birth weights, less preterm birth, and a much lower risk of birth defects that are associated with maternal fever in the first trimester, said Dr. Rasmussen, director of public health information dissemination at the Centers for Disease Control and Prevention.
“Fever in the first trimester doubles the risk of neural tube defects in the fetus,” said Dr. Rasmussen. She cited a 2014 meta-analysis that found increased risks of other fetal anomalies associated with first trimester flu: hydrocephaly (odds ratio, 5.74), congenital heart defects (OR, 1.56), cleft lip (OR, 3.12), limb abnormalities (OR, 2.03) and digestive system defects (OR, 1.72) (Hum Reprod. 2014 Apr;29[4]:809-23).
“We don’t know if these are more due to the hyperthermia of fever or to the flu virus crossing the placenta,” she said. “But we do know these are real risks.”
Newborns come with an immature immune system that takes a while to get ramped up. In the first 6 months of life, they’re especially vulnerable to communicable illnesses, and they can become severely ill and even die from flu, Dr. Rasmussen said. A new study of nearly 250,000 mother-child pairs confirmed that maternal vaccination reduces the risks of flu hospitalization by more than 80% in infants younger than 6 months (Pediatrics. 2016 May 2. doi: 10.1542/peds.2015-2360).
For most women, the understanding that a flu shot protects their baby before and after birth is good enough reason to get one, Dr. Rasmussen said, but the benefits for the woman are extremely important. “Pregnant women experience a lot of changes in immune function and heart and lung function that increase the risk for complications from influenza. In prior pandemics, we have seen pregnant women at an increased risk of severe illness, hospitalization, and death.”
She cited data from the 2009 H1N1 epidemic that showed that 5% of those who died from H1N1 flu were pregnant women, despite the fact that they represented only 1% of the U.S. population (JAMA. 2010;303[15]:1517-25).
Despite the well-documented benefits and reassuring safety data, flu vaccine coverage remains suboptimal for pregnant women, Dr. Rasmussen said. The most recent CDC data suggest that just half of pregnant women were immunized in 2014-2015, a rate that has remained steady since 2012.
The most effective way to boost this number, Dr. Rasmussen suggested, is to stress to women that the vaccine protects both the fetus and newborn from a potentially fatal illness. “We know that a large number of babies and children die of influenza every year,” she said. “The biggest motivator for moms is their desire to protect their baby – much more so than protecting themselves.”
Dr. Rasmussen reported having no relevant financial disclosures.
EXPERT ANALYSIS FROM ACOG 2016

HPV vaccine doesn’t provide herd immunity or cross-protection
WASHINGTON – The prevalence of human papillomavirus (HPV) types 16 and 18 has significantly decreased, but only among vaccinated women; national data show no evidence that the vaccine targeting them has conferred herd immunity or encouraged a shift toward lower-risk types.
From 2003, before the vaccine was introduced, to 2012, the prevalence of HPV 16 and 18 fell from 10% to about 4% in completely vaccinated women, Dr. Christopher Tarney said at the annual meeting of the American College of Obstetricians and Gynecologists. The prevalence among unvaccinated women, however, was virtually unchanged.

“Our study didn’t demonstrate cross-protection, type replacement, or herd immunity,” said Dr. Tarney of the Womack Army Medical Center, Ft. Bragg, N.C. “This is in contrast to some global data” that have recently shown such positive changes were linked to high HPV vaccine coverage in Scotland and Australia.
The lack of these findings in the United States probably has to do with the low rate of vaccine acceptance, Dr. Tarney said. Although 60% of eligible girls got at least one dose of the vaccine in 2014, only about 40% received the entire series.
Dr. Tarney compared data from the 2003 National Health and Nutrition Examination Survey (NHANES) for women 18-29 years old, with NHANES waves in 2007-2008, 2009-2010, and 2011-2012. He looked at the prevalence of high-risk HPV serotypes, and at the specific prevalence of HPV 16 and 18, which are specifically targeted in the vaccine. The study comprised 1,628 women who had submitted self-collected vaginal swabs for HPV analysis. The group was representative of more than 21 million U.S. women, Dr. Tarney said.
The prevalence of HPV 16 and 18 decreased significantly among vaccinated women, from 10% in 2003 to 4% in 2012. Even women who didn’t complete the series reaped some benefit from it. Among those who had at least one immunization, all high-risk HPV decreased from 67% in 2007-2008 to 41% in 2012.
Despite the vaccine’s effectiveness, it is not exerting cross-protection against other high-risk types, Dr. Tarney said, nor is there evidence of herd immunity. Among women who did not receive the vaccine, high-risk HPV prevalence was unchanged at about 49% in 2007-2008 and 51% in 2011-2012.
He expressed frustration that the vaccine has not been more widely adopted.
“During this postvaccine era, over 16 million eligible females didn’t get it. As women’s health care physicians, we must reduce missed clinical opportunities to administer this vaccine. We must strive to maximize access to it and increase support for it,” Dr. Tarney said. “We have a great opportunity to have a profound impact on the prevention of cervical cancer, but only when we can drastically increase the vaccination rates will we see these vaccines begin to contribute to the eradication of cervical cancer in the U.S.”
He reported having no relevant financial disclosures.
WASHINGTON – The prevalence of human papillomavirus (HPV) types 16 and 18 has significantly decreased, but only among vaccinated women; national data show no evidence that the vaccine targeting them has conferred herd immunity or encouraged a shift toward lower-risk types.
From 2003, before the vaccine was introduced, to 2012, the prevalence of HPV 16 and 18 fell from 10% to about 4% in completely vaccinated women, Dr. Christopher Tarney said at the annual meeting of the American College of Obstetricians and Gynecologists. The prevalence among unvaccinated women, however, was virtually unchanged.
“Our study didn’t demonstrate cross-protection, type replacement, or herd immunity,” said Dr. Tarney of the Womack Army Medical Center, Ft. Bragg, N.C. “This is in contrast to some global data” that have recently shown such positive changes were linked to high HPV vaccine coverage in Scotland and Australia.
The lack of these findings in the United States probably has to do with the low rate of vaccine acceptance, Dr. Tarney said. Although 60% of eligible girls got at least one dose of the vaccine in 2014, only about 40% received the entire series.
Dr. Tarney compared data from the 2003 National Health and Nutrition Examination Survey (NHANES) for women 18-29 years old, with NHANES waves in 2007-2008, 2009-2010, and 2011-2012. He looked at the prevalence of high-risk HPV serotypes, and at the specific prevalence of HPV 16 and 18, which are specifically targeted in the vaccine. The study comprised 1,628 women who had submitted self-collected vaginal swabs for HPV analysis. The group was representative of more than 21 million U.S. women, Dr. Tarney said.
The prevalence of HPV 16 and 18 decreased significantly among vaccinated women, from 10% in 2003 to 4% in 2012. Even women who didn’t complete the series reaped some benefit from it. Among those who had at least one immunization, all high-risk HPV decreased from 67% in 2007-2008 to 41% in 2012.
Despite the vaccine’s effectiveness, it is not exerting cross-protection against other high-risk types, Dr. Tarney said, nor is there evidence of herd immunity. Among women who did not receive the vaccine, high-risk HPV prevalence was unchanged at about 49% in 2007-2008 and 51% in 2011-2012.
He expressed frustration that the vaccine has not been more widely adopted.
“During this postvaccine era, over 16 million eligible females didn’t get it. As women’s health care physicians, we must reduce missed clinical opportunities to administer this vaccine. We must strive to maximize access to it and increase support for it,” Dr. Tarney said. “We have a great opportunity to have a profound impact on the prevention of cervical cancer, but only when we can drastically increase the vaccination rates will we see these vaccines begin to contribute to the eradication of cervical cancer in the U.S.”
He reported having no relevant financial disclosures.
WASHINGTON – The prevalence of human papillomavirus (HPV) types 16 and 18 has significantly decreased, but only among vaccinated women; national data show no evidence that the vaccine targeting them has conferred herd immunity or encouraged a shift toward lower-risk types.
From 2003, before the vaccine was introduced, to 2012, the prevalence of HPV 16 and 18 fell from 10% to about 4% in completely vaccinated women, Dr. Christopher Tarney said at the annual meeting of the American College of Obstetricians and Gynecologists. The prevalence among unvaccinated women, however, was virtually unchanged.
“Our study didn’t demonstrate cross-protection, type replacement, or herd immunity,” said Dr. Tarney of the Womack Army Medical Center, Ft. Bragg, N.C. “This is in contrast to some global data” that have recently shown such positive changes were linked to high HPV vaccine coverage in Scotland and Australia.
The lack of these findings in the United States probably has to do with the low rate of vaccine acceptance, Dr. Tarney said. Although 60% of eligible girls got at least one dose of the vaccine in 2014, only about 40% received the entire series.
Dr. Tarney compared data from the 2003 National Health and Nutrition Examination Survey (NHANES) for women 18-29 years old, with NHANES waves in 2007-2008, 2009-2010, and 2011-2012. He looked at the prevalence of high-risk HPV serotypes, and at the specific prevalence of HPV 16 and 18, which are specifically targeted in the vaccine. The study comprised 1,628 women who had submitted self-collected vaginal swabs for HPV analysis. The group was representative of more than 21 million U.S. women, Dr. Tarney said.
The prevalence of HPV 16 and 18 decreased significantly among vaccinated women, from 10% in 2003 to 4% in 2012. Even women who didn’t complete the series reaped some benefit from it. Among those who had at least one immunization, all high-risk HPV decreased from 67% in 2007-2008 to 41% in 2012.
Despite the vaccine’s effectiveness, it is not exerting cross-protection against other high-risk types, Dr. Tarney said, nor is there evidence of herd immunity. Among women who did not receive the vaccine, high-risk HPV prevalence was unchanged at about 49% in 2007-2008 and 51% in 2011-2012.
He expressed frustration that the vaccine has not been more widely adopted.
“During this postvaccine era, over 16 million eligible females didn’t get it. As women’s health care physicians, we must reduce missed clinical opportunities to administer this vaccine. We must strive to maximize access to it and increase support for it,” Dr. Tarney said. “We have a great opportunity to have a profound impact on the prevention of cervical cancer, but only when we can drastically increase the vaccination rates will we see these vaccines begin to contribute to the eradication of cervical cancer in the U.S.”
He reported having no relevant financial disclosures.
AT ACOG 2016

HPV vaccine doesn’t provide herd immunity or crossprotection
WASHINGTON – The prevalence of human papillomavirus (HPV) types 16 and 18 has significantly decreased, but only among vaccinated women; national data show no evidence that the vaccine targeting them has conferred herd immunity or encouraged a shift toward lower-risk types.
From 2003, before the vaccine was introduced, to 2012, the prevalence of HPV 16 and 18 fell from 10% to about 4% in completely vaccinated women, Dr. Christopher Tarney said at the annual meeting of the American College of Obstetricians and Gynecologists. The prevalence among unvaccinated women, however, was virtually unchanged.

“Our study didn’t demonstrate crossprotection, type replacement, or herd immunity,” said Dr. Tarney of the Womack Army Medical Center, Ft. Bragg, N.C. “This is in contrast to some global data” that have recently shown such positive changes were linked to high HPV vaccine coverage in Scotland and Australia.
The lack of these findings in the United States probably has to do with the low rate of vaccine acceptance, Dr. Tarney said. Although 60% of eligible girls got at least one dose of the vaccine in 2014, only about 40% received the entire series.
Dr. Tarney compared data from the 2003 National Health and Nutrition Examination Survey (NHANES) for women 18-29 years old, with NHANES waves in 2007-2008, 2009-2010, and 2011-2012. He looked at the prevalence of high-risk HPV serotypes, and at the specific prevalence of HPV 16 and 18, which are specifically targeted in the vaccine. The study comprised 1,628 women who had submitted self-collected vaginal swabs for HPV analysis. The group was representative of more than 21 million U.S. women, Dr. Tarney said.
The prevalence of HPV 16 and 18 decreased significantly among vaccinated women, from 10% in 2003 to 4% in 2012. Even women who didn’t complete the series reaped some benefit from it. Among those who had at least one immunization, all high-risk HPV decreased from 67% in 2007-2008 to 41% in 2012.
Despite the vaccine’s effectiveness, it is not exerting crossprotection against other high-risk types, Dr. Tarney said, nor is there evidence of herd immunity. Among women who did not receive the vaccine, high-risk HPV prevalence was unchanged at about 49% in 2007-2008 and 51% in 2011-2012.
He expressed frustration that the vaccine has not been more widely adopted.
“During this postvaccine era, over 16 million eligible females didn’t get it. As women’s health care physicians, we must reduce missed clinical opportunities to administer this vaccine. We must strive to maximize access to it and increase support for it,” Dr. Tarney said. “We have a great opportunity to have a profound impact on the prevention of cervical cancer, but only when we can drastically increase the vaccination rates will we see these vaccines begin to contribute to the eradication of cervical cancer in the U.S.”
He reported having no relevant financial disclosures.
WASHINGTON – The prevalence of human papillomavirus (HPV) types 16 and 18 has significantly decreased, but only among vaccinated women; national data show no evidence that the vaccine targeting them has conferred herd immunity or encouraged a shift toward lower-risk types.
From 2003, before the vaccine was introduced, to 2012, the prevalence of HPV 16 and 18 fell from 10% to about 4% in completely vaccinated women, Dr. Christopher Tarney said at the annual meeting of the American College of Obstetricians and Gynecologists. The prevalence among unvaccinated women, however, was virtually unchanged.
“Our study didn’t demonstrate crossprotection, type replacement, or herd immunity,” said Dr. Tarney of the Womack Army Medical Center, Ft. Bragg, N.C. “This is in contrast to some global data” that have recently shown such positive changes were linked to high HPV vaccine coverage in Scotland and Australia.
The lack of these findings in the United States probably has to do with the low rate of vaccine acceptance, Dr. Tarney said. Although 60% of eligible girls got at least one dose of the vaccine in 2014, only about 40% received the entire series.
Dr. Tarney compared data from the 2003 National Health and Nutrition Examination Survey (NHANES) for women 18-29 years old, with NHANES waves in 2007-2008, 2009-2010, and 2011-2012. He looked at the prevalence of high-risk HPV serotypes, and at the specific prevalence of HPV 16 and 18, which are specifically targeted in the vaccine. The study comprised 1,628 women who had submitted self-collected vaginal swabs for HPV analysis. The group was representative of more than 21 million U.S. women, Dr. Tarney said.
The prevalence of HPV 16 and 18 decreased significantly among vaccinated women, from 10% in 2003 to 4% in 2012. Even women who didn’t complete the series reaped some benefit from it. Among those who had at least one immunization, all high-risk HPV decreased from 67% in 2007-2008 to 41% in 2012.
Despite the vaccine’s effectiveness, it is not exerting crossprotection against other high-risk types, Dr. Tarney said, nor is there evidence of herd immunity. Among women who did not receive the vaccine, high-risk HPV prevalence was unchanged at about 49% in 2007-2008 and 51% in 2011-2012.
He expressed frustration that the vaccine has not been more widely adopted.
“During this postvaccine era, over 16 million eligible females didn’t get it. As women’s health care physicians, we must reduce missed clinical opportunities to administer this vaccine. We must strive to maximize access to it and increase support for it,” Dr. Tarney said. “We have a great opportunity to have a profound impact on the prevention of cervical cancer, but only when we can drastically increase the vaccination rates will we see these vaccines begin to contribute to the eradication of cervical cancer in the U.S.”
He reported having no relevant financial disclosures.
WASHINGTON – The prevalence of human papillomavirus (HPV) types 16 and 18 has significantly decreased, but only among vaccinated women; national data show no evidence that the vaccine targeting them has conferred herd immunity or encouraged a shift toward lower-risk types.
From 2003, before the vaccine was introduced, to 2012, the prevalence of HPV 16 and 18 fell from 10% to about 4% in completely vaccinated women, Dr. Christopher Tarney said at the annual meeting of the American College of Obstetricians and Gynecologists. The prevalence among unvaccinated women, however, was virtually unchanged.
“Our study didn’t demonstrate crossprotection, type replacement, or herd immunity,” said Dr. Tarney of the Womack Army Medical Center, Ft. Bragg, N.C. “This is in contrast to some global data” that have recently shown such positive changes were linked to high HPV vaccine coverage in Scotland and Australia.
The lack of these findings in the United States probably has to do with the low rate of vaccine acceptance, Dr. Tarney said. Although 60% of eligible girls got at least one dose of the vaccine in 2014, only about 40% received the entire series.
Dr. Tarney compared data from the 2003 National Health and Nutrition Examination Survey (NHANES) for women 18-29 years old, with NHANES waves in 2007-2008, 2009-2010, and 2011-2012. He looked at the prevalence of high-risk HPV serotypes, and at the specific prevalence of HPV 16 and 18, which are specifically targeted in the vaccine. The study comprised 1,628 women who had submitted self-collected vaginal swabs for HPV analysis. The group was representative of more than 21 million U.S. women, Dr. Tarney said.
The prevalence of HPV 16 and 18 decreased significantly among vaccinated women, from 10% in 2003 to 4% in 2012. Even women who didn’t complete the series reaped some benefit from it. Among those who had at least one immunization, all high-risk HPV decreased from 67% in 2007-2008 to 41% in 2012.
Despite the vaccine’s effectiveness, it is not exerting crossprotection against other high-risk types, Dr. Tarney said, nor is there evidence of herd immunity. Among women who did not receive the vaccine, high-risk HPV prevalence was unchanged at about 49% in 2007-2008 and 51% in 2011-2012.
He expressed frustration that the vaccine has not been more widely adopted.
“During this postvaccine era, over 16 million eligible females didn’t get it. As women’s health care physicians, we must reduce missed clinical opportunities to administer this vaccine. We must strive to maximize access to it and increase support for it,” Dr. Tarney said. “We have a great opportunity to have a profound impact on the prevention of cervical cancer, but only when we can drastically increase the vaccination rates will we see these vaccines begin to contribute to the eradication of cervical cancer in the U.S.”
He reported having no relevant financial disclosures.
AT ACOG 2016
Key clinical point: HPV types 16 and 18 have significantly decreased since the advent of the vaccine, but only among vaccinated women.
Major finding: HPV 16 and 18 prevalence dropped from 10% in 2003 to 4% in 2012 among vaccinated women.
Data source: A prospective study of 1,628 women.
Disclosures: Dr. Tarney reported having no relevant financial disclosures.

Gene expression test predicts melanoma metastasis
ORLANDO – A commercially available melanoma gene expression test had a negative predictive value of 98% for metastasis, but also correctly identified patients at very high risk of disease spread.
In a retrospective study, the DecisionDx-Melanoma test, which examines 28 risk genes, showed that patients stratified as high risk with the test were 22 times more likely to develop metastatic disease than were those stratified as low risk, Dr. Bradley Greenhaw said at the annual meeting of the American College of Mohs Surgery. The test classifies patients with stage I and stage II melanoma as having a low risk (class 1) or a high risk (class 2) of metastasis within 5 years.
“Our mean follow-up time is less than half of the 5-year risk this test is able to predict,” said Dr. Greenhaw, a Mohs surgeon in Tupelo, Miss. “So if the test is performing as it’s supposed to, there would be even more events – you would see this gap widen even more as time passes. Seeing this with our limited follow-up period is pretty significant.”
The test also added valuable prognostic information to the American Joint Committee on Cancer (AJCC) staging method, he said. “For example, based on AJCC staging alone, we would expect to see a 5-year metastatic rate of 5%-10% for stage I melanomas. We saw less than a 1% rate. That is a pretty significant negative predictive value.”

The genes in the panel were selected from those examined in eight different genetic risk studies of cutaneous melanomas. The panel divides tumors into the high- and low-risk groups. A validation study published last year concluded that the 5-year disease-free survival rates were 97% for class 1 tumors and 31% for class 2 tumors (Clin Cancer Res 2015;21[1];175-83).
In the retrospective study, Dr. Greenhaw and his associates examined the test’s accuracy in a cohort of 256 patients treated at his center. The mean follow-up time was 23 months, although some patients have completed 5 years of follow-up.
Of the tumor blocks analyzed, 214 were class 1 and 42 were class 2. He noted significant differences between the class 1 and class 2 tumors, including mean patient age (66 years vs. 74 years, respectively), mean Breslow’s depth (0.7 mm vs. 2.3 mm), mitotic rate (0.8 vs. 3.3), and ulceration (4% vs. 41%).
Over the mean 2-year follow-up time, three class 1 tumors and 10 class 2 tumors metastasized (1.4% vs. 23.8%). The test’s negative predictive value was 98%; class 2 tumors were 22 times more likely to metastasize. “About 77% of metastatic tumors were correctly identified as high risk by this test,” Dr. Greenhaw said in an interview. “For comparison, more than 80% were correctly identified in the validation study, so our study was in line with it.”
The test showed a link between metastatic risk and ulceration at presentation. Of the class 1 tumors, 4% were ulcerated, compared to 41% of class 2 tumors; class 2 tumors were 16 times more likely to be ulcerated. Among the ulcerated lesions, metastasis occurred in 11% of class 1 and 41% of class 2 tumors.
Dr. Greenhaw also compared the gene test’s characterization of tumors to the AJCC staging.
Of the 214 class 1 tumors, 94% were stage IA or IB. Among these, there was no metastasis. Of the class 2 tumors, 17% were stage IA and 26% were stage IB. Interestingly, Dr. Greenhaw said, despite the high-risk genetic signature, none of these tumors metastasized. “This could have been because although the gene expression showed them to be associated with a high risk of metastases, the tumors were completely excised prior to the metastatic event, or because our follow-up is still relatively short,” he noted.
In the class 1 group, 4% of the tumors were stage IIA and 2% were stage IIB. Of these 13 tumors, two metastasized. “This 15% metastatic rate is a lower rate than we would predict by the AJCC staging,” Dr. Greenhaw said.
In the class 2 groups, 24% were stage IIA, 26% were stage IIB, and 7% were stage IIC. Of these 24 tumors, 10 metastasized. “This is a higher rate than the AJCC staging would predict, and it occurred rather quickly, with our abbreviated follow-up period,” Dr. Greenhaw noted.
Based on these findings, Dr. Greenhaw suggested a clinical management algorithm:
• All patients with invasive melanoma should be offered the gene expression profiling.
• Those with class 1 tumors have a high chance of cure and a low risk of metastasis. They can be reasonably managed with clinical skin and nodal exams every 6 months for 2 years, and then annually.
• Those with class 2 tumors have a much higher risk of metastatic disease. They should receive clinical skin and nodal exams every 3 months for 2 years, then every 6-12 months for 5 years. After that, a yearly exam should suffice.
Tests like this are an important advance in managing melanoma, Dr. Greenhaw said. “I think this is where the future of melanoma prognosis is. The keys are found in the genes and DNA of these tumors. These tests are being used in other types of cancer and I think it’s where we need to go in our field as well.”
Dr. Greenhaw has no financial disclosures to report.
ORLANDO – A commercially available melanoma gene expression test had a negative predictive value of 98% for metastasis, but also correctly identified patients at very high risk of disease spread.
In a retrospective study, the DecisionDx-Melanoma test, which examines 28 risk genes, showed that patients stratified as high risk with the test were 22 times more likely to develop metastatic disease than were those stratified as low risk, Dr. Bradley Greenhaw said at the annual meeting of the American College of Mohs Surgery. The test classifies patients with stage I and stage II melanoma as having a low risk (class 1) or a high risk (class 2) of metastasis within 5 years.
“Our mean follow-up time is less than half of the 5-year risk this test is able to predict,” said Dr. Greenhaw, a Mohs surgeon in Tupelo, Miss. “So if the test is performing as it’s supposed to, there would be even more events – you would see this gap widen even more as time passes. Seeing this with our limited follow-up period is pretty significant.”
The test also added valuable prognostic information to the American Joint Committee on Cancer (AJCC) staging method, he said. “For example, based on AJCC staging alone, we would expect to see a 5-year metastatic rate of 5%-10% for stage I melanomas. We saw less than a 1% rate. That is a pretty significant negative predictive value.”
The genes in the panel were selected from those examined in eight different genetic risk studies of cutaneous melanomas. The panel divides tumors into the high- and low-risk groups. A validation study published last year concluded that the 5-year disease-free survival rates were 97% for class 1 tumors and 31% for class 2 tumors (Clin Cancer Res 2015;21[1];175-83).
In the retrospective study, Dr. Greenhaw and his associates examined the test’s accuracy in a cohort of 256 patients treated at his center. The mean follow-up time was 23 months, although some patients have completed 5 years of follow-up.
Of the tumor blocks analyzed, 214 were class 1 and 42 were class 2. He noted significant differences between the class 1 and class 2 tumors, including mean patient age (66 years vs. 74 years, respectively), mean Breslow’s depth (0.7 mm vs. 2.3 mm), mitotic rate (0.8 vs. 3.3), and ulceration (4% vs. 41%).
Over the mean 2-year follow-up time, three class 1 tumors and 10 class 2 tumors metastasized (1.4% vs. 23.8%). The test’s negative predictive value was 98%; class 2 tumors were 22 times more likely to metastasize. “About 77% of metastatic tumors were correctly identified as high risk by this test,” Dr. Greenhaw said in an interview. “For comparison, more than 80% were correctly identified in the validation study, so our study was in line with it.”
The test showed a link between metastatic risk and ulceration at presentation. Of the class 1 tumors, 4% were ulcerated, compared to 41% of class 2 tumors; class 2 tumors were 16 times more likely to be ulcerated. Among the ulcerated lesions, metastasis occurred in 11% of class 1 and 41% of class 2 tumors.
Dr. Greenhaw also compared the gene test’s characterization of tumors to the AJCC staging.
Of the 214 class 1 tumors, 94% were stage IA or IB. Among these, there was no metastasis. Of the class 2 tumors, 17% were stage IA and 26% were stage IB. Interestingly, Dr. Greenhaw said, despite the high-risk genetic signature, none of these tumors metastasized. “This could have been because although the gene expression showed them to be associated with a high risk of metastases, the tumors were completely excised prior to the metastatic event, or because our follow-up is still relatively short,” he noted.
In the class 1 group, 4% of the tumors were stage IIA and 2% were stage IIB. Of these 13 tumors, two metastasized. “This 15% metastatic rate is a lower rate than we would predict by the AJCC staging,” Dr. Greenhaw said.
In the class 2 groups, 24% were stage IIA, 26% were stage IIB, and 7% were stage IIC. Of these 24 tumors, 10 metastasized. “This is a higher rate than the AJCC staging would predict, and it occurred rather quickly, with our abbreviated follow-up period,” Dr. Greenhaw noted.
Based on these findings, Dr. Greenhaw suggested a clinical management algorithm:
• All patients with invasive melanoma should be offered the gene expression profiling.
• Those with class 1 tumors have a high chance of cure and a low risk of metastasis. They can be reasonably managed with clinical skin and nodal exams every 6 months for 2 years, and then annually.
• Those with class 2 tumors have a much higher risk of metastatic disease. They should receive clinical skin and nodal exams every 3 months for 2 years, then every 6-12 months for 5 years. After that, a yearly exam should suffice.
Tests like this are an important advance in managing melanoma, Dr. Greenhaw said. “I think this is where the future of melanoma prognosis is. The keys are found in the genes and DNA of these tumors. These tests are being used in other types of cancer and I think it’s where we need to go in our field as well.”
Dr. Greenhaw has no financial disclosures to report.
ORLANDO – A commercially available melanoma gene expression test had a negative predictive value of 98% for metastasis, but also correctly identified patients at very high risk of disease spread.
In a retrospective study, the DecisionDx-Melanoma test, which examines 28 risk genes, showed that patients stratified as high risk with the test were 22 times more likely to develop metastatic disease than were those stratified as low risk, Dr. Bradley Greenhaw said at the annual meeting of the American College of Mohs Surgery. The test classifies patients with stage I and stage II melanoma as having a low risk (class 1) or a high risk (class 2) of metastasis within 5 years.
“Our mean follow-up time is less than half of the 5-year risk this test is able to predict,” said Dr. Greenhaw, a Mohs surgeon in Tupelo, Miss. “So if the test is performing as it’s supposed to, there would be even more events – you would see this gap widen even more as time passes. Seeing this with our limited follow-up period is pretty significant.”
The test also added valuable prognostic information to the American Joint Committee on Cancer (AJCC) staging method, he said. “For example, based on AJCC staging alone, we would expect to see a 5-year metastatic rate of 5%-10% for stage I melanomas. We saw less than a 1% rate. That is a pretty significant negative predictive value.”
The genes in the panel were selected from those examined in eight different genetic risk studies of cutaneous melanomas. The panel divides tumors into the high- and low-risk groups. A validation study published last year concluded that the 5-year disease-free survival rates were 97% for class 1 tumors and 31% for class 2 tumors (Clin Cancer Res 2015;21[1];175-83).
In the retrospective study, Dr. Greenhaw and his associates examined the test’s accuracy in a cohort of 256 patients treated at his center. The mean follow-up time was 23 months, although some patients have completed 5 years of follow-up.
Of the tumor blocks analyzed, 214 were class 1 and 42 were class 2. He noted significant differences between the class 1 and class 2 tumors, including mean patient age (66 years vs. 74 years, respectively), mean Breslow’s depth (0.7 mm vs. 2.3 mm), mitotic rate (0.8 vs. 3.3), and ulceration (4% vs. 41%).
Over the mean 2-year follow-up time, three class 1 tumors and 10 class 2 tumors metastasized (1.4% vs. 23.8%). The test’s negative predictive value was 98%; class 2 tumors were 22 times more likely to metastasize. “About 77% of metastatic tumors were correctly identified as high risk by this test,” Dr. Greenhaw said in an interview. “For comparison, more than 80% were correctly identified in the validation study, so our study was in line with it.”
The test showed a link between metastatic risk and ulceration at presentation. Of the class 1 tumors, 4% were ulcerated, compared to 41% of class 2 tumors; class 2 tumors were 16 times more likely to be ulcerated. Among the ulcerated lesions, metastasis occurred in 11% of class 1 and 41% of class 2 tumors.
Dr. Greenhaw also compared the gene test’s characterization of tumors to the AJCC staging.
Of the 214 class 1 tumors, 94% were stage IA or IB. Among these, there was no metastasis. Of the class 2 tumors, 17% were stage IA and 26% were stage IB. Interestingly, Dr. Greenhaw said, despite the high-risk genetic signature, none of these tumors metastasized. “This could have been because although the gene expression showed them to be associated with a high risk of metastases, the tumors were completely excised prior to the metastatic event, or because our follow-up is still relatively short,” he noted.
In the class 1 group, 4% of the tumors were stage IIA and 2% were stage IIB. Of these 13 tumors, two metastasized. “This 15% metastatic rate is a lower rate than we would predict by the AJCC staging,” Dr. Greenhaw said.
In the class 2 groups, 24% were stage IIA, 26% were stage IIB, and 7% were stage IIC. Of these 24 tumors, 10 metastasized. “This is a higher rate than the AJCC staging would predict, and it occurred rather quickly, with our abbreviated follow-up period,” Dr. Greenhaw noted.
Based on these findings, Dr. Greenhaw suggested a clinical management algorithm:
• All patients with invasive melanoma should be offered the gene expression profiling.
• Those with class 1 tumors have a high chance of cure and a low risk of metastasis. They can be reasonably managed with clinical skin and nodal exams every 6 months for 2 years, and then annually.
• Those with class 2 tumors have a much higher risk of metastatic disease. They should receive clinical skin and nodal exams every 3 months for 2 years, then every 6-12 months for 5 years. After that, a yearly exam should suffice.
Tests like this are an important advance in managing melanoma, Dr. Greenhaw said. “I think this is where the future of melanoma prognosis is. The keys are found in the genes and DNA of these tumors. These tests are being used in other types of cancer and I think it’s where we need to go in our field as well.”
Dr. Greenhaw has no financial disclosures to report.
AT THE ACMS ANNUAL MEETING
Key clinical point: A commercially available gene expression test can help predict metastasis in early melanoma cases.
Major finding: The test had a 98% negative predictive value.
Data source: A retrospective study that evaluated the gene expression test in 256 patients with melanoma.
Disclosures: Dr. Greenhaw has no financial interest in the test.
