User login
Flu Still a Killer for Neurologically Impaired Young People
A new report illustrates just how deadly influenza can be among children and young adults with neurological and neurodevelopmental disorders.
In a single Ohio residential facility last year, flu killed half of the patients in this population who developed a serious case. The case study points up the need for aggressive disease detection and treatment among this population, Dr. Mary DiOrio and colleagues reported in the Jan. 6 issue of the Morbidity and Mortality Weekly Report (MMWR 2012;60:1729-33).
"Prompt testing, early and aggressive antiviral treatment, and antiviral chemoprophylaxis are important for these patients," wrote Dr. DiOrio and her coauthors. "When influenza is suspected, antiviral treatment should be given as soon as possible after symptom onset, ideally within 48 hours. Treatment should not wait for laboratory confirmation of influenza."
All eligible residents and all staff members should be vaccinated each year, but during a flu outbreak all residential patients should also receive chemoprophylaxis with an antiviral medication, regardless of their vaccination status, the authors noted.
Dr. DiOrio, an epidemiologist for the Ohio Department of Health, and her coauthors reported on a 2011 flu outbreak in an Ohio facility that cares for children and young adults with neurologic and neurodevelopmental conditions. The outbreak ran for 6 weeks, from the beginning of February to the second week in March.
"When influenza is suspected, antiviral treatment should be given as soon as possible after symptom onset, ideally within 48 hours."
During the outbreak, 76 of the 130 (58%) patients experienced an acute onset of respiratory illness. Thirteen were severely ill; seven had influenza confirmed by laboratory testing and six had a suspected case. All of these had severe to profound neurologic and neurodevelopmental disabilities; nine had "do not resuscitate" orders.
All of the patients also had been vaccinated for the seasonal flu the previous fall. However, Dr. DiOrio’s investigation also revealed that the vaccine storage temperature might have affected its potency. The temperature of the storage refrigerator ranged from 10°-42° F during the investigation, with a mean of 27° F, which is below the vaccine’s recommended limit temperature.
The mean duration of illness was 18 days. Fever was the most common presenting sign, occurring in 12 patients. All seven deaths were due to respiratory failure secondary to influenza. Other diagnoses at the time of death or hospital discharge were pneumonia (5), septic shock (2), acute respiratory distress syndrome (2), and multiple organ failure (1).
Most of the cases (72) occurred before Feb. 28. Seven of the severe cases occurred from Feb 23-28. However, Dr. DiOrio noted, none of the facility residents received any oseltamivir prophylaxis until Feb 28. Eight of the cases received oseltamivir, but only four got the drug within 48 hours of symptom onset, as recommended for maximum benefit.
Although oseltamivir works best if administered within the first 48 hours of symptom onset, it can still mitigate the course of illness if given later. "Recent observational data indicate that, even when started more than 48 hours after illness onset, treatment can help prevent influenza-related complications and death in persons at higher risk or with more severe illness," the Centers for Disease Control and Prevention wrote in an editorial note.
While preventing flu with vaccination is the most effective way to combat the disease, vaccination may not completely protect patients who may have comorbid immunosuppression due to their medical status. "Because [these] persons ... are at high risk for complications and the vaccine might not protect them fully, vaccination should be one part of a larger program of influenza prevention in these settings," according to the CDC.
Such a program should include vaccination for all residents, as well as for all health care personnel in the facility, and any others who might expose the patient. "The program also should include use of infection control precautions and early use of influenza antiviral medications for treatment of persons with suspected or confirmed influenza and for prevention in other residents and staff members as soon as an outbreak is identified."
Proper vaccine storage is critically important. "Low temperatures for vaccine storage can lead to less than optimal vaccine potency. Influenza vaccine should be stored at 35 °–46° F. .... Many vaccines can be inactivated by exposure to temperatures colder than 33° F," according to the CDC.
It can be difficult diagnosing influenza in patients with severe neurologic or neurodevelopmental conditions because they "might have only subtle deviations from their baseline medical status and be unable to communicate symptoms effectively." These patients also might have "impaired pulmonary function resulting from muscle abnormalities or conditions such as severe scoliosis." Thus, they might "be less able to clear pulmonary secretions and be at increased risk for subsequent lower respiratory tract infection," the CDC said.
"Clinicians caring for patients with neurologic and neurodevelopmental conditions should be vigilant for signs and symptoms that might indicate early respiratory illness and should initiate influenza antiviral treatment as soon as warranted, especially during influenza season," according to the CDC.
A new report illustrates just how deadly influenza can be among children and young adults with neurological and neurodevelopmental disorders.
In a single Ohio residential facility last year, flu killed half of the patients in this population who developed a serious case. The case study points up the need for aggressive disease detection and treatment among this population, Dr. Mary DiOrio and colleagues reported in the Jan. 6 issue of the Morbidity and Mortality Weekly Report (MMWR 2012;60:1729-33).
"Prompt testing, early and aggressive antiviral treatment, and antiviral chemoprophylaxis are important for these patients," wrote Dr. DiOrio and her coauthors. "When influenza is suspected, antiviral treatment should be given as soon as possible after symptom onset, ideally within 48 hours. Treatment should not wait for laboratory confirmation of influenza."
All eligible residents and all staff members should be vaccinated each year, but during a flu outbreak all residential patients should also receive chemoprophylaxis with an antiviral medication, regardless of their vaccination status, the authors noted.
Dr. DiOrio, an epidemiologist for the Ohio Department of Health, and her coauthors reported on a 2011 flu outbreak in an Ohio facility that cares for children and young adults with neurologic and neurodevelopmental conditions. The outbreak ran for 6 weeks, from the beginning of February to the second week in March.
"When influenza is suspected, antiviral treatment should be given as soon as possible after symptom onset, ideally within 48 hours."
During the outbreak, 76 of the 130 (58%) patients experienced an acute onset of respiratory illness. Thirteen were severely ill; seven had influenza confirmed by laboratory testing and six had a suspected case. All of these had severe to profound neurologic and neurodevelopmental disabilities; nine had "do not resuscitate" orders.
All of the patients also had been vaccinated for the seasonal flu the previous fall. However, Dr. DiOrio’s investigation also revealed that the vaccine storage temperature might have affected its potency. The temperature of the storage refrigerator ranged from 10°-42° F during the investigation, with a mean of 27° F, which is below the vaccine’s recommended limit temperature.
The mean duration of illness was 18 days. Fever was the most common presenting sign, occurring in 12 patients. All seven deaths were due to respiratory failure secondary to influenza. Other diagnoses at the time of death or hospital discharge were pneumonia (5), septic shock (2), acute respiratory distress syndrome (2), and multiple organ failure (1).
Most of the cases (72) occurred before Feb. 28. Seven of the severe cases occurred from Feb 23-28. However, Dr. DiOrio noted, none of the facility residents received any oseltamivir prophylaxis until Feb 28. Eight of the cases received oseltamivir, but only four got the drug within 48 hours of symptom onset, as recommended for maximum benefit.
Although oseltamivir works best if administered within the first 48 hours of symptom onset, it can still mitigate the course of illness if given later. "Recent observational data indicate that, even when started more than 48 hours after illness onset, treatment can help prevent influenza-related complications and death in persons at higher risk or with more severe illness," the Centers for Disease Control and Prevention wrote in an editorial note.
While preventing flu with vaccination is the most effective way to combat the disease, vaccination may not completely protect patients who may have comorbid immunosuppression due to their medical status. "Because [these] persons ... are at high risk for complications and the vaccine might not protect them fully, vaccination should be one part of a larger program of influenza prevention in these settings," according to the CDC.
Such a program should include vaccination for all residents, as well as for all health care personnel in the facility, and any others who might expose the patient. "The program also should include use of infection control precautions and early use of influenza antiviral medications for treatment of persons with suspected or confirmed influenza and for prevention in other residents and staff members as soon as an outbreak is identified."
Proper vaccine storage is critically important. "Low temperatures for vaccine storage can lead to less than optimal vaccine potency. Influenza vaccine should be stored at 35 °–46° F. .... Many vaccines can be inactivated by exposure to temperatures colder than 33° F," according to the CDC.
It can be difficult diagnosing influenza in patients with severe neurologic or neurodevelopmental conditions because they "might have only subtle deviations from their baseline medical status and be unable to communicate symptoms effectively." These patients also might have "impaired pulmonary function resulting from muscle abnormalities or conditions such as severe scoliosis." Thus, they might "be less able to clear pulmonary secretions and be at increased risk for subsequent lower respiratory tract infection," the CDC said.
"Clinicians caring for patients with neurologic and neurodevelopmental conditions should be vigilant for signs and symptoms that might indicate early respiratory illness and should initiate influenza antiviral treatment as soon as warranted, especially during influenza season," according to the CDC.
A new report illustrates just how deadly influenza can be among children and young adults with neurological and neurodevelopmental disorders.
In a single Ohio residential facility last year, flu killed half of the patients in this population who developed a serious case. The case study points up the need for aggressive disease detection and treatment among this population, Dr. Mary DiOrio and colleagues reported in the Jan. 6 issue of the Morbidity and Mortality Weekly Report (MMWR 2012;60:1729-33).
"Prompt testing, early and aggressive antiviral treatment, and antiviral chemoprophylaxis are important for these patients," wrote Dr. DiOrio and her coauthors. "When influenza is suspected, antiviral treatment should be given as soon as possible after symptom onset, ideally within 48 hours. Treatment should not wait for laboratory confirmation of influenza."
All eligible residents and all staff members should be vaccinated each year, but during a flu outbreak all residential patients should also receive chemoprophylaxis with an antiviral medication, regardless of their vaccination status, the authors noted.
Dr. DiOrio, an epidemiologist for the Ohio Department of Health, and her coauthors reported on a 2011 flu outbreak in an Ohio facility that cares for children and young adults with neurologic and neurodevelopmental conditions. The outbreak ran for 6 weeks, from the beginning of February to the second week in March.
"When influenza is suspected, antiviral treatment should be given as soon as possible after symptom onset, ideally within 48 hours."
During the outbreak, 76 of the 130 (58%) patients experienced an acute onset of respiratory illness. Thirteen were severely ill; seven had influenza confirmed by laboratory testing and six had a suspected case. All of these had severe to profound neurologic and neurodevelopmental disabilities; nine had "do not resuscitate" orders.
All of the patients also had been vaccinated for the seasonal flu the previous fall. However, Dr. DiOrio’s investigation also revealed that the vaccine storage temperature might have affected its potency. The temperature of the storage refrigerator ranged from 10°-42° F during the investigation, with a mean of 27° F, which is below the vaccine’s recommended limit temperature.
The mean duration of illness was 18 days. Fever was the most common presenting sign, occurring in 12 patients. All seven deaths were due to respiratory failure secondary to influenza. Other diagnoses at the time of death or hospital discharge were pneumonia (5), septic shock (2), acute respiratory distress syndrome (2), and multiple organ failure (1).
Most of the cases (72) occurred before Feb. 28. Seven of the severe cases occurred from Feb 23-28. However, Dr. DiOrio noted, none of the facility residents received any oseltamivir prophylaxis until Feb 28. Eight of the cases received oseltamivir, but only four got the drug within 48 hours of symptom onset, as recommended for maximum benefit.
Although oseltamivir works best if administered within the first 48 hours of symptom onset, it can still mitigate the course of illness if given later. "Recent observational data indicate that, even when started more than 48 hours after illness onset, treatment can help prevent influenza-related complications and death in persons at higher risk or with more severe illness," the Centers for Disease Control and Prevention wrote in an editorial note.
While preventing flu with vaccination is the most effective way to combat the disease, vaccination may not completely protect patients who may have comorbid immunosuppression due to their medical status. "Because [these] persons ... are at high risk for complications and the vaccine might not protect them fully, vaccination should be one part of a larger program of influenza prevention in these settings," according to the CDC.
Such a program should include vaccination for all residents, as well as for all health care personnel in the facility, and any others who might expose the patient. "The program also should include use of infection control precautions and early use of influenza antiviral medications for treatment of persons with suspected or confirmed influenza and for prevention in other residents and staff members as soon as an outbreak is identified."
Proper vaccine storage is critically important. "Low temperatures for vaccine storage can lead to less than optimal vaccine potency. Influenza vaccine should be stored at 35 °–46° F. .... Many vaccines can be inactivated by exposure to temperatures colder than 33° F," according to the CDC.
It can be difficult diagnosing influenza in patients with severe neurologic or neurodevelopmental conditions because they "might have only subtle deviations from their baseline medical status and be unable to communicate symptoms effectively." These patients also might have "impaired pulmonary function resulting from muscle abnormalities or conditions such as severe scoliosis." Thus, they might "be less able to clear pulmonary secretions and be at increased risk for subsequent lower respiratory tract infection," the CDC said.
"Clinicians caring for patients with neurologic and neurodevelopmental conditions should be vigilant for signs and symptoms that might indicate early respiratory illness and should initiate influenza antiviral treatment as soon as warranted, especially during influenza season," according to the CDC.
FROM THE MORBIDITY AND MORTALITY REPORT
Major Finding: Among a group of patients with neurologic and neurodevelopmental disorders, influenza killed 7 of 13 (54%) who developed a severe case.
Data Source: A review of 76 influenza cases occurring in a single Ohio long-term care facility during February-March 2011.
Disclosures: As a government employee, Dr. DiOrio has no conflicts of interest.
Atorvastatin Failed to Slow Atherosclerosis in Pediatric Lupus
Atorvastatin did not confer any significantly lower progression of atherosclerosis in children and teens with systemic lupus erythematosus.
Although a 3-year course of the drug significantly improved lipid profiles, compared with placebo, it did not affect the mean progression of carotid intima media thickness, reported Dr. Laura E. Schanberg and colleagues in the January issue of Arthritis and Rheumatology (Arthritis Rheum 2012;64:285-96).

"Collectively, these results suggest that the potential benefits of statin therapy for slowing carotid intima medial progression are not large enough to warrant routine use in children with systemic lupus erythematosus," wrote Dr. Schanberg, professor of pediatrics and co-chief of the division of pediatric rheumatology at Duke University, Durham, N.C.
The APPLE (Atherosclerosis Prevention in Pediatric Lupus) trial randomized 180 young patients with systemic lupus erythematosus (SLE) to 3 years of either atorvastatin or placebo. The primary outcome was a clinically meaningful reduction in mean-mean carotid intima medial thickness (CIMT). Secondary outcomes included changes in lipid profile, changes in mean-maximum CIMT, safety and tolerability, and the drug’s relationship to development of new white matter hyperintensities in the brain as seen on MRI.
The patients were a mean of 16 years old at the start of the study; their mean duration of disease was 31 months. The average Severity of Disease Index was 81.
In all, 113 patients were treated with atorvastatin at a dose of either 10 mg or 20 mg/day based on their weight. All patients received diet and exercise counseling.
At the end of 3 years, the mean-mean progression of CIMT was not significantly different between the active and placebo groups (0.0010 mm/year vs. 0.0024 mm/year). The relationship remained nonsignificant even after adjustment for multiple possibly confounding factors.
The placebo group did show significantly greater progression from baseline in every secondary CIMT end point. But only mean-maximum internal CIMT progression was significantly worse than the treated group. "This was the only CIMT outcome where the estimated treatment effect met or exceeded the prespecified definition of clinical significance (0.0045 mm/year)," the authors wrote.
Compared with the placebo group, the active treatment group also showed significant lessening of levels of total cholesterol, LDL cholesterol, and high-sensitivity C-reactive protein.
There were no concerning safety issues, the authors wrote. A subset of the entire group (24 treated and 20 placebo patients) underwent brain MRI. Three in the active group and two in the placebo group had developed new hyperintense lesions.
There were 17 pregnancies over the 3-year study period, with no significant between-group differences in outcome. Seven were live births, including one atorvastatin-exposed infant who died 2 hours after birth from birth defects consistent with methotrexate exposure.
The rest of the pregnancies ended in spontaneous abortion (5) and elective abortion (4). One pregnancy was lost to follow-up.
Although findings from APPLE do not point to a compelling reason to routinely prescribe atorvastatin to young SLE patients, they did suggest higher-than-expected CIMT progression rates in placebo-treated patients (from 0.0023 mm/year to 0.0144 mm/year). "These results underscore that subclinical atherosclerosis does indeed begin early in pediatric SLE, with CIMT progression rates comparable with those in children with familial hypercholesterolemia, a disease that is clearly associated with premature atherosclerosis and cardiovascular morbidity and mortality."
The study was sponsored by the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Dr. Schanberg reported receiving consulting fees from Pfizer, which also supplied the study drug. The coauthors reported multiple financial relationships, including relationships with Pfizer. Dr. Ravelli did not disclose any financial conflicts of interest.
Although APPLE did not find atorvastatin to have any significant treatment benefit overall, it may identify subgroups who are more likely to benefit from statin therapy, Dr. Angelo Ravelli wrote in an accompanying editorial (Arthritis Rheum. 2012;64:33-6).
"Intriguingly, although statistical significance was not reached, the results suggest a trend in the direction of a positive effect of treatment," wrote Dr. Ravelli. "This observation, taken together with the average [low to moderate] level of disease activity in patients enrolled in the trial, indicates that statin therapy may not be necessary for every SLE patient, particularly those with less aggressive disease."
The key is to identify those patients who could reap the biggest benefit from treatment – a question that current post hoc analyses of APPLE may answer, he said.
Future studies "should assess the risk of early atherosclerosis and its progression by stratifying patients on the basis of the presence or absence of specific risk factors, such as family history of premature coronary heart disease, level of disease activity or severity, specific disease manifestations (namely, renal disease), burden of corticosteroid or immunosuppressive therapies, or sustained dyslipidemic state. These analyses may help select the patient subgroups that should be included in future clinical trials."
|

Until an appropriate subgroup may be identified, rheumatologists can still protect their young patients by helping them change those things that can be changed.
APPLE "underscores the importance of the routine identification and management of modifiable cardiovascular risk factors (dyslipidemia, hypertension, obesity, smoking, and low levels of physical exercise), an issue that is often neglected in pediatric rheumatology practice."
Dr. Ravelli is a pediatric rheumatologist at the University of Genoa (Italy). He did not disclose any financial conflicts of interest.
Although APPLE did not find atorvastatin to have any significant treatment benefit overall, it may identify subgroups who are more likely to benefit from statin therapy, Dr. Angelo Ravelli wrote in an accompanying editorial (Arthritis Rheum. 2012;64:33-6).
"Intriguingly, although statistical significance was not reached, the results suggest a trend in the direction of a positive effect of treatment," wrote Dr. Ravelli. "This observation, taken together with the average [low to moderate] level of disease activity in patients enrolled in the trial, indicates that statin therapy may not be necessary for every SLE patient, particularly those with less aggressive disease."
The key is to identify those patients who could reap the biggest benefit from treatment – a question that current post hoc analyses of APPLE may answer, he said.
Future studies "should assess the risk of early atherosclerosis and its progression by stratifying patients on the basis of the presence or absence of specific risk factors, such as family history of premature coronary heart disease, level of disease activity or severity, specific disease manifestations (namely, renal disease), burden of corticosteroid or immunosuppressive therapies, or sustained dyslipidemic state. These analyses may help select the patient subgroups that should be included in future clinical trials."
|
Until an appropriate subgroup may be identified, rheumatologists can still protect their young patients by helping them change those things that can be changed.
APPLE "underscores the importance of the routine identification and management of modifiable cardiovascular risk factors (dyslipidemia, hypertension, obesity, smoking, and low levels of physical exercise), an issue that is often neglected in pediatric rheumatology practice."
Dr. Ravelli is a pediatric rheumatologist at the University of Genoa (Italy). He did not disclose any financial conflicts of interest.
Although APPLE did not find atorvastatin to have any significant treatment benefit overall, it may identify subgroups who are more likely to benefit from statin therapy, Dr. Angelo Ravelli wrote in an accompanying editorial (Arthritis Rheum. 2012;64:33-6).
"Intriguingly, although statistical significance was not reached, the results suggest a trend in the direction of a positive effect of treatment," wrote Dr. Ravelli. "This observation, taken together with the average [low to moderate] level of disease activity in patients enrolled in the trial, indicates that statin therapy may not be necessary for every SLE patient, particularly those with less aggressive disease."
The key is to identify those patients who could reap the biggest benefit from treatment – a question that current post hoc analyses of APPLE may answer, he said.
Future studies "should assess the risk of early atherosclerosis and its progression by stratifying patients on the basis of the presence or absence of specific risk factors, such as family history of premature coronary heart disease, level of disease activity or severity, specific disease manifestations (namely, renal disease), burden of corticosteroid or immunosuppressive therapies, or sustained dyslipidemic state. These analyses may help select the patient subgroups that should be included in future clinical trials."
|
Until an appropriate subgroup may be identified, rheumatologists can still protect their young patients by helping them change those things that can be changed.
APPLE "underscores the importance of the routine identification and management of modifiable cardiovascular risk factors (dyslipidemia, hypertension, obesity, smoking, and low levels of physical exercise), an issue that is often neglected in pediatric rheumatology practice."
Dr. Ravelli is a pediatric rheumatologist at the University of Genoa (Italy). He did not disclose any financial conflicts of interest.
Atorvastatin did not confer any significantly lower progression of atherosclerosis in children and teens with systemic lupus erythematosus.
Although a 3-year course of the drug significantly improved lipid profiles, compared with placebo, it did not affect the mean progression of carotid intima media thickness, reported Dr. Laura E. Schanberg and colleagues in the January issue of Arthritis and Rheumatology (Arthritis Rheum 2012;64:285-96).
"Collectively, these results suggest that the potential benefits of statin therapy for slowing carotid intima medial progression are not large enough to warrant routine use in children with systemic lupus erythematosus," wrote Dr. Schanberg, professor of pediatrics and co-chief of the division of pediatric rheumatology at Duke University, Durham, N.C.
The APPLE (Atherosclerosis Prevention in Pediatric Lupus) trial randomized 180 young patients with systemic lupus erythematosus (SLE) to 3 years of either atorvastatin or placebo. The primary outcome was a clinically meaningful reduction in mean-mean carotid intima medial thickness (CIMT). Secondary outcomes included changes in lipid profile, changes in mean-maximum CIMT, safety and tolerability, and the drug’s relationship to development of new white matter hyperintensities in the brain as seen on MRI.
The patients were a mean of 16 years old at the start of the study; their mean duration of disease was 31 months. The average Severity of Disease Index was 81.
In all, 113 patients were treated with atorvastatin at a dose of either 10 mg or 20 mg/day based on their weight. All patients received diet and exercise counseling.
At the end of 3 years, the mean-mean progression of CIMT was not significantly different between the active and placebo groups (0.0010 mm/year vs. 0.0024 mm/year). The relationship remained nonsignificant even after adjustment for multiple possibly confounding factors.
The placebo group did show significantly greater progression from baseline in every secondary CIMT end point. But only mean-maximum internal CIMT progression was significantly worse than the treated group. "This was the only CIMT outcome where the estimated treatment effect met or exceeded the prespecified definition of clinical significance (0.0045 mm/year)," the authors wrote.
Compared with the placebo group, the active treatment group also showed significant lessening of levels of total cholesterol, LDL cholesterol, and high-sensitivity C-reactive protein.
There were no concerning safety issues, the authors wrote. A subset of the entire group (24 treated and 20 placebo patients) underwent brain MRI. Three in the active group and two in the placebo group had developed new hyperintense lesions.
There were 17 pregnancies over the 3-year study period, with no significant between-group differences in outcome. Seven were live births, including one atorvastatin-exposed infant who died 2 hours after birth from birth defects consistent with methotrexate exposure.
The rest of the pregnancies ended in spontaneous abortion (5) and elective abortion (4). One pregnancy was lost to follow-up.
Although findings from APPLE do not point to a compelling reason to routinely prescribe atorvastatin to young SLE patients, they did suggest higher-than-expected CIMT progression rates in placebo-treated patients (from 0.0023 mm/year to 0.0144 mm/year). "These results underscore that subclinical atherosclerosis does indeed begin early in pediatric SLE, with CIMT progression rates comparable with those in children with familial hypercholesterolemia, a disease that is clearly associated with premature atherosclerosis and cardiovascular morbidity and mortality."
The study was sponsored by the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Dr. Schanberg reported receiving consulting fees from Pfizer, which also supplied the study drug. The coauthors reported multiple financial relationships, including relationships with Pfizer. Dr. Ravelli did not disclose any financial conflicts of interest.
Atorvastatin did not confer any significantly lower progression of atherosclerosis in children and teens with systemic lupus erythematosus.
Although a 3-year course of the drug significantly improved lipid profiles, compared with placebo, it did not affect the mean progression of carotid intima media thickness, reported Dr. Laura E. Schanberg and colleagues in the January issue of Arthritis and Rheumatology (Arthritis Rheum 2012;64:285-96).
"Collectively, these results suggest that the potential benefits of statin therapy for slowing carotid intima medial progression are not large enough to warrant routine use in children with systemic lupus erythematosus," wrote Dr. Schanberg, professor of pediatrics and co-chief of the division of pediatric rheumatology at Duke University, Durham, N.C.
The APPLE (Atherosclerosis Prevention in Pediatric Lupus) trial randomized 180 young patients with systemic lupus erythematosus (SLE) to 3 years of either atorvastatin or placebo. The primary outcome was a clinically meaningful reduction in mean-mean carotid intima medial thickness (CIMT). Secondary outcomes included changes in lipid profile, changes in mean-maximum CIMT, safety and tolerability, and the drug’s relationship to development of new white matter hyperintensities in the brain as seen on MRI.
The patients were a mean of 16 years old at the start of the study; their mean duration of disease was 31 months. The average Severity of Disease Index was 81.
In all, 113 patients were treated with atorvastatin at a dose of either 10 mg or 20 mg/day based on their weight. All patients received diet and exercise counseling.
At the end of 3 years, the mean-mean progression of CIMT was not significantly different between the active and placebo groups (0.0010 mm/year vs. 0.0024 mm/year). The relationship remained nonsignificant even after adjustment for multiple possibly confounding factors.
The placebo group did show significantly greater progression from baseline in every secondary CIMT end point. But only mean-maximum internal CIMT progression was significantly worse than the treated group. "This was the only CIMT outcome where the estimated treatment effect met or exceeded the prespecified definition of clinical significance (0.0045 mm/year)," the authors wrote.
Compared with the placebo group, the active treatment group also showed significant lessening of levels of total cholesterol, LDL cholesterol, and high-sensitivity C-reactive protein.
There were no concerning safety issues, the authors wrote. A subset of the entire group (24 treated and 20 placebo patients) underwent brain MRI. Three in the active group and two in the placebo group had developed new hyperintense lesions.
There were 17 pregnancies over the 3-year study period, with no significant between-group differences in outcome. Seven were live births, including one atorvastatin-exposed infant who died 2 hours after birth from birth defects consistent with methotrexate exposure.
The rest of the pregnancies ended in spontaneous abortion (5) and elective abortion (4). One pregnancy was lost to follow-up.
Although findings from APPLE do not point to a compelling reason to routinely prescribe atorvastatin to young SLE patients, they did suggest higher-than-expected CIMT progression rates in placebo-treated patients (from 0.0023 mm/year to 0.0144 mm/year). "These results underscore that subclinical atherosclerosis does indeed begin early in pediatric SLE, with CIMT progression rates comparable with those in children with familial hypercholesterolemia, a disease that is clearly associated with premature atherosclerosis and cardiovascular morbidity and mortality."
The study was sponsored by the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Dr. Schanberg reported receiving consulting fees from Pfizer, which also supplied the study drug. The coauthors reported multiple financial relationships, including relationships with Pfizer. Dr. Ravelli did not disclose any financial conflicts of interest.
FROM ARTHRITIS AND RHEUMATOLOGY
Major Finding: After 3 years, young patients with SLE who took atorvastatin or placebo had similar rates of carotid intima media thickening (0.0010 mm/year vs. 0.0024 mm/year).
Data Source: A double-blinded, placebo-controlled trial of 180 children and teens.
Disclosures: The study was sponsored by the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Dr. Schanberg reported receiving consulting fees from Pfizer, which also supplied the study drug. The coauthors reported multiple financial relationships, including relationships with Pfizer.
Technique Maps Neural Connectivity to Detect Seizure Foci
BALTIMORE – A new study hints that mapping the functional connectivity of the brain may allow surgeons to pinpoint previously unidentified epileptogenic networks more precisely, leading to more effective epilepsy surgery.
Functional connectivity mapping could not only identify epileptogenic networks, but also could predict successful and failed epilepsy surgeries, Dr. Hyang Woon Lee reported in a study of the resting state functional MRI (fMRI) scans of 29 patients who underwent surgery for intractable partial epilepsy.
"I was quite thrilled to find that intrinsic functional connectivity changes stand out in the epileptogenic zones," Dr. Lee said in an interview at the annual meeting of the American Epilepsy Society. She is in the departments of neurology at Yale University, New Haven, Conn., and at Ewha Womans University in Seoul, South Korea.
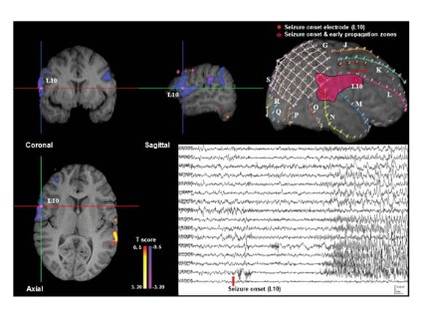
The research is based on a relatively new method of identifying brain regions that are structurally separate but functionally connected by previously unidentifiable neural networks. Dr. Lee’s colleague at Yale, R. Todd Constable, Ph.D., developed the technique of using a mathematical algorithm called intrinsic connectivity contrast (ICC) to identify interrelationships between the blood oxygenation level dependent signal of voxels measured with fMRI. A high degree of ICC for a particular voxel means that it has a strong connection to other brain areas. The resulting image shows the degree of these connections, and "provides a measure as to how well-connected any given tissue element is," Dr. Lee wrote in her poster.
The analysis can be done ipsilaterally, where connections to each voxel are compared with all others in the same hemisphere, and contralaterally, where connections to voxels in the other hemisphere are measured. The resulting maps identify functionally connected networks, Dr. Lee said. In the case of patients with focal epilepsy, they sometimes show that epileptogenic areas identified by intracranial EEG have additional connections, or are even part of a nodal network of abnormally functioning tissue.
Each of the 29 patients underwent presurgical fMRI and intracranial EEG to localize the seizure foci. Dr. Lee, Dr. Constable, and their coauthors analyzed the fMRI images with the ICC algorithm, both ipsilaterally and contralaterally. Dr. Lee then compared the ICC results to the intracranial EEG data that guided the epilepsy surgery. The ICC maps were a good match for the seizure onset and propagation zones detected by intracranial EEG, she said.
"Intracranial EEG seizure onset zones might have decreased ICCs, since the epileptogenic foci are likely to be abnormal brain tissue, often due to neuronal damage," she said.
Overall, 15 patients had good surgical outcomes, defined as an Engels class I, meaning they were free of disabling seizures. The other 14 patients had poor surgical outcomes: Engels classes II (rare disabling seizures), III (worthwhile improvement), and IV (no worthwhile improvement).
The determination of the seizure onset zones with ICC was concordant with presurgical intracranial EEG testing in 13 of the 15 patients with good surgical outcomes and in 7 of the 14 patients with poor outcomes.
The concordance between ICC and intracranial EEG also varied by the type of epilepsy. The techniques were 100% concordant among patients with extratemporal lobe epilepsy who had good outcomes. These patients often have ictal onset zones that are diffuse and sometimes difficult to determine.
The measurement of functional connectivity with fMRI has the potential to become a noninvasive presurgical diagnostic tool in epilepsy surgery based on its strong ability to identify the nodes of an epileptogenic network, Dr. Lee said.
"It might also help in the diagnosis of other neuropsychiatric disorders, such as Alzheimer’s disease, stroke, and schizophrenia by elucidating altered functional connectivity in the neural network. Although it’s still in the early stages of development, I believe this approach can be widely used for both clinical and scientific purposes with further validation."
Dr. Lee said that she had no financial disclosures.
BALTIMORE – A new study hints that mapping the functional connectivity of the brain may allow surgeons to pinpoint previously unidentified epileptogenic networks more precisely, leading to more effective epilepsy surgery.
Functional connectivity mapping could not only identify epileptogenic networks, but also could predict successful and failed epilepsy surgeries, Dr. Hyang Woon Lee reported in a study of the resting state functional MRI (fMRI) scans of 29 patients who underwent surgery for intractable partial epilepsy.
"I was quite thrilled to find that intrinsic functional connectivity changes stand out in the epileptogenic zones," Dr. Lee said in an interview at the annual meeting of the American Epilepsy Society. She is in the departments of neurology at Yale University, New Haven, Conn., and at Ewha Womans University in Seoul, South Korea.
The research is based on a relatively new method of identifying brain regions that are structurally separate but functionally connected by previously unidentifiable neural networks. Dr. Lee’s colleague at Yale, R. Todd Constable, Ph.D., developed the technique of using a mathematical algorithm called intrinsic connectivity contrast (ICC) to identify interrelationships between the blood oxygenation level dependent signal of voxels measured with fMRI. A high degree of ICC for a particular voxel means that it has a strong connection to other brain areas. The resulting image shows the degree of these connections, and "provides a measure as to how well-connected any given tissue element is," Dr. Lee wrote in her poster.
The analysis can be done ipsilaterally, where connections to each voxel are compared with all others in the same hemisphere, and contralaterally, where connections to voxels in the other hemisphere are measured. The resulting maps identify functionally connected networks, Dr. Lee said. In the case of patients with focal epilepsy, they sometimes show that epileptogenic areas identified by intracranial EEG have additional connections, or are even part of a nodal network of abnormally functioning tissue.
Each of the 29 patients underwent presurgical fMRI and intracranial EEG to localize the seizure foci. Dr. Lee, Dr. Constable, and their coauthors analyzed the fMRI images with the ICC algorithm, both ipsilaterally and contralaterally. Dr. Lee then compared the ICC results to the intracranial EEG data that guided the epilepsy surgery. The ICC maps were a good match for the seizure onset and propagation zones detected by intracranial EEG, she said.
"Intracranial EEG seizure onset zones might have decreased ICCs, since the epileptogenic foci are likely to be abnormal brain tissue, often due to neuronal damage," she said.
Overall, 15 patients had good surgical outcomes, defined as an Engels class I, meaning they were free of disabling seizures. The other 14 patients had poor surgical outcomes: Engels classes II (rare disabling seizures), III (worthwhile improvement), and IV (no worthwhile improvement).
The determination of the seizure onset zones with ICC was concordant with presurgical intracranial EEG testing in 13 of the 15 patients with good surgical outcomes and in 7 of the 14 patients with poor outcomes.
The concordance between ICC and intracranial EEG also varied by the type of epilepsy. The techniques were 100% concordant among patients with extratemporal lobe epilepsy who had good outcomes. These patients often have ictal onset zones that are diffuse and sometimes difficult to determine.
The measurement of functional connectivity with fMRI has the potential to become a noninvasive presurgical diagnostic tool in epilepsy surgery based on its strong ability to identify the nodes of an epileptogenic network, Dr. Lee said.
"It might also help in the diagnosis of other neuropsychiatric disorders, such as Alzheimer’s disease, stroke, and schizophrenia by elucidating altered functional connectivity in the neural network. Although it’s still in the early stages of development, I believe this approach can be widely used for both clinical and scientific purposes with further validation."
Dr. Lee said that she had no financial disclosures.
BALTIMORE – A new study hints that mapping the functional connectivity of the brain may allow surgeons to pinpoint previously unidentified epileptogenic networks more precisely, leading to more effective epilepsy surgery.
Functional connectivity mapping could not only identify epileptogenic networks, but also could predict successful and failed epilepsy surgeries, Dr. Hyang Woon Lee reported in a study of the resting state functional MRI (fMRI) scans of 29 patients who underwent surgery for intractable partial epilepsy.
"I was quite thrilled to find that intrinsic functional connectivity changes stand out in the epileptogenic zones," Dr. Lee said in an interview at the annual meeting of the American Epilepsy Society. She is in the departments of neurology at Yale University, New Haven, Conn., and at Ewha Womans University in Seoul, South Korea.
The research is based on a relatively new method of identifying brain regions that are structurally separate but functionally connected by previously unidentifiable neural networks. Dr. Lee’s colleague at Yale, R. Todd Constable, Ph.D., developed the technique of using a mathematical algorithm called intrinsic connectivity contrast (ICC) to identify interrelationships between the blood oxygenation level dependent signal of voxels measured with fMRI. A high degree of ICC for a particular voxel means that it has a strong connection to other brain areas. The resulting image shows the degree of these connections, and "provides a measure as to how well-connected any given tissue element is," Dr. Lee wrote in her poster.
The analysis can be done ipsilaterally, where connections to each voxel are compared with all others in the same hemisphere, and contralaterally, where connections to voxels in the other hemisphere are measured. The resulting maps identify functionally connected networks, Dr. Lee said. In the case of patients with focal epilepsy, they sometimes show that epileptogenic areas identified by intracranial EEG have additional connections, or are even part of a nodal network of abnormally functioning tissue.
Each of the 29 patients underwent presurgical fMRI and intracranial EEG to localize the seizure foci. Dr. Lee, Dr. Constable, and their coauthors analyzed the fMRI images with the ICC algorithm, both ipsilaterally and contralaterally. Dr. Lee then compared the ICC results to the intracranial EEG data that guided the epilepsy surgery. The ICC maps were a good match for the seizure onset and propagation zones detected by intracranial EEG, she said.
"Intracranial EEG seizure onset zones might have decreased ICCs, since the epileptogenic foci are likely to be abnormal brain tissue, often due to neuronal damage," she said.
Overall, 15 patients had good surgical outcomes, defined as an Engels class I, meaning they were free of disabling seizures. The other 14 patients had poor surgical outcomes: Engels classes II (rare disabling seizures), III (worthwhile improvement), and IV (no worthwhile improvement).
The determination of the seizure onset zones with ICC was concordant with presurgical intracranial EEG testing in 13 of the 15 patients with good surgical outcomes and in 7 of the 14 patients with poor outcomes.
The concordance between ICC and intracranial EEG also varied by the type of epilepsy. The techniques were 100% concordant among patients with extratemporal lobe epilepsy who had good outcomes. These patients often have ictal onset zones that are diffuse and sometimes difficult to determine.
The measurement of functional connectivity with fMRI has the potential to become a noninvasive presurgical diagnostic tool in epilepsy surgery based on its strong ability to identify the nodes of an epileptogenic network, Dr. Lee said.
"It might also help in the diagnosis of other neuropsychiatric disorders, such as Alzheimer’s disease, stroke, and schizophrenia by elucidating altered functional connectivity in the neural network. Although it’s still in the early stages of development, I believe this approach can be widely used for both clinical and scientific purposes with further validation."
Dr. Lee said that she had no financial disclosures.
FROM THE ANNUAL MEETING OF THE AMERICAN EPILEPSY SOCIETY
Major Finding: The determination of seizure onset zones with ICC was concordant with presurgical intracranial EEG testing in 13 of 15 patients with good surgical outcomes and in 7 of 14 patients with poor outcomes.
Data Source: A retrospective case study of 29 patients with intractable epilepsy who underwent presurgical fMRI and intracranial EEG to localize their seizure foci.
Disclosures: Dr. Lee said that she had no financial disclosures.
Hospital Infections Sharply Increase Death in Status Epilepticus
BALTIMORE – Patients who acquired a nosocomial infection during their hospital stay for status epilepticus had five times greater odds of dying than did noninfected patients in a single-center, observational cohort study.
The infections, most of which involved the respiratory tract, also were associated with having treatment-refractory status epilepticus, a longer ICU stay, and a worse overall outcome, Dr. Raoul Sutter said at the annual meeting of the American Epilepsy Society.

"Our findings underscore the importance of close observation of these patents and rigorous adherence to the prevention guidelines for hospital-acquired infections, as well as the urgent need for early diagnosis and treatment of status epilepticus and infection-related complications, especially in the first 3 days," said Dr. Sutter, who conducted the research while he was a member of the departments of neurology and intensive care medicine at University Hospital Basel (Switzerland). He is now a research fellow in the neurosciences critical care unit at Johns Hopkins University, Baltimore.
Dr. Sutter and his coinvestigators could not identify a reliable one-time marker for indicating the presence of infection at the onset of status.
He and his colleagues studied a cohort of 160 patients hospitalized for status epilepticus at University Hospital Basel (Switzerland) during a 5-year period. Their median age was 65 years (range 17-91 years) and more than half (55%) required mechanical ventilation.
About 22% of the cohort developed an infection during the first 3 days of hospital stay. Patients with an infection had a significantly longer ICU stay (mean of 11 days vs. 6 days) and five times greater odds of dying than did patients without infections, according to the study’s findings, which Dr. Sutter presented in two posters at the meeting.
Most of the infections involved the respiratory tract, with half being ventilator-associated pneumonias. Compared with patients without infections, patients with respiratory tract infections had a significantly longer duration of status (mean 7 vs. 2 days) and a longer ICU stay (mean 11 vs. 7 days). These infections also were associated with a significant increase in the odds of developing refractory status (odds ratio, 5.4) and dying (OR, 4). A majority (59%) with refractory status and an infection died (59%).
"Time of onset of infectious complications during status epilepticus was a critical element in outcome," Dr. Sutter said in an interview. "Patients who had a confirmed infection before admission had no significant increase in the risk of refractory status or death."
Early detection and treatment of infectious complications may mitigate their deleterious effects on these critically ill patients. Because early detection in this setting can be challenging, biomarkers could be useful for their diagnosis, he said.
In a search for a biomarker to indicate the presence of infection at the onset of status, the investigators found that serum procalcitonin, C-reactive protein (CRP), or white blood cell count did not accurately predict an oncoming hospital-acquired infection. However, a serial increase in CRP and white blood cell count over 3 days after status onset was significantly associated with infection.
Low levels tended to rule out infections. The negative predictive value of a low CRP over 3 days was 97%, but specificity remained low and did not improve despite using several cut-off values.
"Right now, we have identified the problem and deleterious impact of infections in status epilepticus, but we don’t really have an ideal solution to it," Dr. Sutter said.
The Society for Healthcare Epidemiology of America and the Infectious Diseases Society of America have issued practice recommendations to reduce the risk of ventilator-associated pneumonia. In addition to minimizing mechanical ventilation, the recommendations suggest measures to reduce colonization of the aerodigestive tract and prevent aspiration.
Selective digestive tract decontamination and selective oropharyngeal decontamination have recently been reported to reduce the mortality rate of critical ill patients by an estimated 3.5% and 2.9%, respectively, Dr. Sutter said.
"Despite the potential benefits described, selective decontamination of the digestive tract has not been largely adopted, most likely because of major concerns about promoting the growth of resistant bacteria," he said. "However, in light of the association of respiratory tract infections and worse outcomes that we observed, the benefit may outweigh this risk by far."
Dr. Sutter reported having no financial disclosures.
BALTIMORE – Patients who acquired a nosocomial infection during their hospital stay for status epilepticus had five times greater odds of dying than did noninfected patients in a single-center, observational cohort study.
The infections, most of which involved the respiratory tract, also were associated with having treatment-refractory status epilepticus, a longer ICU stay, and a worse overall outcome, Dr. Raoul Sutter said at the annual meeting of the American Epilepsy Society.
"Our findings underscore the importance of close observation of these patents and rigorous adherence to the prevention guidelines for hospital-acquired infections, as well as the urgent need for early diagnosis and treatment of status epilepticus and infection-related complications, especially in the first 3 days," said Dr. Sutter, who conducted the research while he was a member of the departments of neurology and intensive care medicine at University Hospital Basel (Switzerland). He is now a research fellow in the neurosciences critical care unit at Johns Hopkins University, Baltimore.
Dr. Sutter and his coinvestigators could not identify a reliable one-time marker for indicating the presence of infection at the onset of status.
He and his colleagues studied a cohort of 160 patients hospitalized for status epilepticus at University Hospital Basel (Switzerland) during a 5-year period. Their median age was 65 years (range 17-91 years) and more than half (55%) required mechanical ventilation.
About 22% of the cohort developed an infection during the first 3 days of hospital stay. Patients with an infection had a significantly longer ICU stay (mean of 11 days vs. 6 days) and five times greater odds of dying than did patients without infections, according to the study’s findings, which Dr. Sutter presented in two posters at the meeting.
Most of the infections involved the respiratory tract, with half being ventilator-associated pneumonias. Compared with patients without infections, patients with respiratory tract infections had a significantly longer duration of status (mean 7 vs. 2 days) and a longer ICU stay (mean 11 vs. 7 days). These infections also were associated with a significant increase in the odds of developing refractory status (odds ratio, 5.4) and dying (OR, 4). A majority (59%) with refractory status and an infection died (59%).
"Time of onset of infectious complications during status epilepticus was a critical element in outcome," Dr. Sutter said in an interview. "Patients who had a confirmed infection before admission had no significant increase in the risk of refractory status or death."
Early detection and treatment of infectious complications may mitigate their deleterious effects on these critically ill patients. Because early detection in this setting can be challenging, biomarkers could be useful for their diagnosis, he said.
In a search for a biomarker to indicate the presence of infection at the onset of status, the investigators found that serum procalcitonin, C-reactive protein (CRP), or white blood cell count did not accurately predict an oncoming hospital-acquired infection. However, a serial increase in CRP and white blood cell count over 3 days after status onset was significantly associated with infection.
Low levels tended to rule out infections. The negative predictive value of a low CRP over 3 days was 97%, but specificity remained low and did not improve despite using several cut-off values.
"Right now, we have identified the problem and deleterious impact of infections in status epilepticus, but we don’t really have an ideal solution to it," Dr. Sutter said.
The Society for Healthcare Epidemiology of America and the Infectious Diseases Society of America have issued practice recommendations to reduce the risk of ventilator-associated pneumonia. In addition to minimizing mechanical ventilation, the recommendations suggest measures to reduce colonization of the aerodigestive tract and prevent aspiration.
Selective digestive tract decontamination and selective oropharyngeal decontamination have recently been reported to reduce the mortality rate of critical ill patients by an estimated 3.5% and 2.9%, respectively, Dr. Sutter said.
"Despite the potential benefits described, selective decontamination of the digestive tract has not been largely adopted, most likely because of major concerns about promoting the growth of resistant bacteria," he said. "However, in light of the association of respiratory tract infections and worse outcomes that we observed, the benefit may outweigh this risk by far."
Dr. Sutter reported having no financial disclosures.
BALTIMORE – Patients who acquired a nosocomial infection during their hospital stay for status epilepticus had five times greater odds of dying than did noninfected patients in a single-center, observational cohort study.
The infections, most of which involved the respiratory tract, also were associated with having treatment-refractory status epilepticus, a longer ICU stay, and a worse overall outcome, Dr. Raoul Sutter said at the annual meeting of the American Epilepsy Society.
"Our findings underscore the importance of close observation of these patents and rigorous adherence to the prevention guidelines for hospital-acquired infections, as well as the urgent need for early diagnosis and treatment of status epilepticus and infection-related complications, especially in the first 3 days," said Dr. Sutter, who conducted the research while he was a member of the departments of neurology and intensive care medicine at University Hospital Basel (Switzerland). He is now a research fellow in the neurosciences critical care unit at Johns Hopkins University, Baltimore.
Dr. Sutter and his coinvestigators could not identify a reliable one-time marker for indicating the presence of infection at the onset of status.
He and his colleagues studied a cohort of 160 patients hospitalized for status epilepticus at University Hospital Basel (Switzerland) during a 5-year period. Their median age was 65 years (range 17-91 years) and more than half (55%) required mechanical ventilation.
About 22% of the cohort developed an infection during the first 3 days of hospital stay. Patients with an infection had a significantly longer ICU stay (mean of 11 days vs. 6 days) and five times greater odds of dying than did patients without infections, according to the study’s findings, which Dr. Sutter presented in two posters at the meeting.
Most of the infections involved the respiratory tract, with half being ventilator-associated pneumonias. Compared with patients without infections, patients with respiratory tract infections had a significantly longer duration of status (mean 7 vs. 2 days) and a longer ICU stay (mean 11 vs. 7 days). These infections also were associated with a significant increase in the odds of developing refractory status (odds ratio, 5.4) and dying (OR, 4). A majority (59%) with refractory status and an infection died (59%).
"Time of onset of infectious complications during status epilepticus was a critical element in outcome," Dr. Sutter said in an interview. "Patients who had a confirmed infection before admission had no significant increase in the risk of refractory status or death."
Early detection and treatment of infectious complications may mitigate their deleterious effects on these critically ill patients. Because early detection in this setting can be challenging, biomarkers could be useful for their diagnosis, he said.
In a search for a biomarker to indicate the presence of infection at the onset of status, the investigators found that serum procalcitonin, C-reactive protein (CRP), or white blood cell count did not accurately predict an oncoming hospital-acquired infection. However, a serial increase in CRP and white blood cell count over 3 days after status onset was significantly associated with infection.
Low levels tended to rule out infections. The negative predictive value of a low CRP over 3 days was 97%, but specificity remained low and did not improve despite using several cut-off values.
"Right now, we have identified the problem and deleterious impact of infections in status epilepticus, but we don’t really have an ideal solution to it," Dr. Sutter said.
The Society for Healthcare Epidemiology of America and the Infectious Diseases Society of America have issued practice recommendations to reduce the risk of ventilator-associated pneumonia. In addition to minimizing mechanical ventilation, the recommendations suggest measures to reduce colonization of the aerodigestive tract and prevent aspiration.
Selective digestive tract decontamination and selective oropharyngeal decontamination have recently been reported to reduce the mortality rate of critical ill patients by an estimated 3.5% and 2.9%, respectively, Dr. Sutter said.
"Despite the potential benefits described, selective decontamination of the digestive tract has not been largely adopted, most likely because of major concerns about promoting the growth of resistant bacteria," he said. "However, in light of the association of respiratory tract infections and worse outcomes that we observed, the benefit may outweigh this risk by far."
Dr. Sutter reported having no financial disclosures.
FROM THE ANNUAL MEETING OF THE AMERICAN EPILEPSY SOCIETY
Major Finding: A majority of patients (59%) with refractory status epilepticus and a hospital-acquired infection died.
Data Source: An observational cohort study of 160 patients hospitalized with status epilepticus.
Disclosures: Dr. Sutter reported having no financial disclosures.
FDA: Appropriate SSRI Use OK in Pregnancy
Pregnant women taking selective serotonin reuptake inhibitors for depression may continue to do so, despite a 2006 warning that the drugs may predispose infants to persistent pulmonary hypertension, the Food and Drug Administration has announced.
That earlier warning was based on a single study indicating that infants exposed to the drug in utero after the 20th week of pregnancy were six times more likely to develop persistent pulmonary hypertension (PPHN) than nonexposed infants (N. Engl. J. Med. 2006;354:579-87).
“Since then, there have been conflicting findings from new studies evaluating this potential risk, making it unclear whether use of SSRIs during pregnancy can cause persistent pulmonary hypertension,” the FDA said in a press statement.
The agency will update the drugs' warning labels to reflect data from new studies, which have produced conflicting results about the risk SSRIs may pose to an unborn child. Those studies include a large retrospective database study in 2009 that found no association between SSRI use and PPHN (Pharmacoepidemiol. Drug Saf. 2009;18:246-52), and a 2011 case-control study of 11,923 births that showed PPHN was associated with cesarean delivery but not with SSRI use in the second half of pregnancy (Am. J. Perinatol. 2011;28:19-24).
FDA officials concluded that the evidence is not sufficient to withhold SSRI treatment from pregnant women or take them off the antidepressants. “At present, FDA … recommends that health care providers treat depression during pregnancy as clinically appropriate,” according to the agency's statement.
Dr. Gideon Koren, professor of pediatrics, pharmacology, pharmacy, medicine, and medical genetics at the University of Toronto, commented in an interview, “I support FDA's hesitation in confirming causation of SSRIs in causing PPHN. The available studies are split in their ability to show an association between SSRIs taken in late pregnancy.
“Critically, several studies have shown that depression itself is also associated with increased risk of PPHN. Hence it is quite possible that depression and not its treatment cause this rare risk ('confounding by indication').” Dr. Koren also heads the Research Leadership for Better Pharmacotherapy During Pregnancy and Lactation at the Hospital for Sick Children, Toronto, where he is director of the Motherisk Program.
Physicians and their patients should carefully weigh the risks and benefits of any antidepressant use in pregnancy, the FDA added, given that there are “substantial risks associated with undertreatment or no treatment of depression during pregnancy.” Risks of untreated maternal depression can include low birth weight, preterm delivery, lower Apgar scores, poor prenatal care, failure to recognize or report impending labor, and increased risks of fetal abuse, neonaticide or maternal suicide, the FDA warned.
Both the American Psychiatric Association and the American College of Obstetricians and Gynecologists recommend monitoring pregnant women for depression and treating them appropriately.
Physicians should continue to report any possible adverse effects to the FDA's MedWatch program, www.fda.gov/MedWatch/report.htm
Reporting forms can also be requested by calling 800-332-1088.
Dr. Koren said he had no relevant financial disclosures.
View on the News
Cautious Treatment Makes Sense
Even at the time of the first publication regarding the link between SSRIs and PPHN in 2006, the conclusion of the authors was that if the link is causal, the absolute risk for PPHN following late pregnancy exposure to SSRIs is very low. Thus, the recommendation that clinicians treat pregnant women appropriately for their symptoms was consistent with the initial findings, and continues to be so.
Since the initial publication, three others have appeared in full manuscript form and one in abstract form (now in press). The two published U.S. studies were either underpowered, or had limitations in classifying the outcomes, whereas the two Scandinavian studies confirmed the initial findings in large cohort or linked database studies. Importantly, the European studies that confirmed the association also came to the conclusion that SSRIs pose a small increased risk for a very rare outcome of pregnancy. Thus, the recommendation to treat only if needed, but not to avoid necessary treatment because of concern for PPHN continues to make sense.
CHRISTINA CHAMBERS, Ph.D., M.P.H., is associate professor of pediatrics and family and preventive medicine at the University of California, San Diego. She is director of the California Teratogen Information Service and Clinical Research Program. Dr. Chambers is a past president of the Organization of Teratology Information Specialists and past president of the Teratology Society. She said she currently receives grant funding for two studies unrelated to SSRIs from GlaxoSmithKline and GlaxoSmithKline Bio.
{kind=link}
Pregnant women taking selective serotonin reuptake inhibitors for depression may continue to do so, despite a 2006 warning that the drugs may predispose infants to persistent pulmonary hypertension, the Food and Drug Administration has announced.
That earlier warning was based on a single study indicating that infants exposed to the drug in utero after the 20th week of pregnancy were six times more likely to develop persistent pulmonary hypertension (PPHN) than nonexposed infants (N. Engl. J. Med. 2006;354:579-87).
“Since then, there have been conflicting findings from new studies evaluating this potential risk, making it unclear whether use of SSRIs during pregnancy can cause persistent pulmonary hypertension,” the FDA said in a press statement.
The agency will update the drugs' warning labels to reflect data from new studies, which have produced conflicting results about the risk SSRIs may pose to an unborn child. Those studies include a large retrospective database study in 2009 that found no association between SSRI use and PPHN (Pharmacoepidemiol. Drug Saf. 2009;18:246-52), and a 2011 case-control study of 11,923 births that showed PPHN was associated with cesarean delivery but not with SSRI use in the second half of pregnancy (Am. J. Perinatol. 2011;28:19-24).
FDA officials concluded that the evidence is not sufficient to withhold SSRI treatment from pregnant women or take them off the antidepressants. “At present, FDA … recommends that health care providers treat depression during pregnancy as clinically appropriate,” according to the agency's statement.
Dr. Gideon Koren, professor of pediatrics, pharmacology, pharmacy, medicine, and medical genetics at the University of Toronto, commented in an interview, “I support FDA's hesitation in confirming causation of SSRIs in causing PPHN. The available studies are split in their ability to show an association between SSRIs taken in late pregnancy.
“Critically, several studies have shown that depression itself is also associated with increased risk of PPHN. Hence it is quite possible that depression and not its treatment cause this rare risk ('confounding by indication').” Dr. Koren also heads the Research Leadership for Better Pharmacotherapy During Pregnancy and Lactation at the Hospital for Sick Children, Toronto, where he is director of the Motherisk Program.
Physicians and their patients should carefully weigh the risks and benefits of any antidepressant use in pregnancy, the FDA added, given that there are “substantial risks associated with undertreatment or no treatment of depression during pregnancy.” Risks of untreated maternal depression can include low birth weight, preterm delivery, lower Apgar scores, poor prenatal care, failure to recognize or report impending labor, and increased risks of fetal abuse, neonaticide or maternal suicide, the FDA warned.
Both the American Psychiatric Association and the American College of Obstetricians and Gynecologists recommend monitoring pregnant women for depression and treating them appropriately.
Physicians should continue to report any possible adverse effects to the FDA's MedWatch program, www.fda.gov/MedWatch/report.htm
Reporting forms can also be requested by calling 800-332-1088.
Dr. Koren said he had no relevant financial disclosures.
View on the News
Cautious Treatment Makes Sense
Even at the time of the first publication regarding the link between SSRIs and PPHN in 2006, the conclusion of the authors was that if the link is causal, the absolute risk for PPHN following late pregnancy exposure to SSRIs is very low. Thus, the recommendation that clinicians treat pregnant women appropriately for their symptoms was consistent with the initial findings, and continues to be so.
Since the initial publication, three others have appeared in full manuscript form and one in abstract form (now in press). The two published U.S. studies were either underpowered, or had limitations in classifying the outcomes, whereas the two Scandinavian studies confirmed the initial findings in large cohort or linked database studies. Importantly, the European studies that confirmed the association also came to the conclusion that SSRIs pose a small increased risk for a very rare outcome of pregnancy. Thus, the recommendation to treat only if needed, but not to avoid necessary treatment because of concern for PPHN continues to make sense.
CHRISTINA CHAMBERS, Ph.D., M.P.H., is associate professor of pediatrics and family and preventive medicine at the University of California, San Diego. She is director of the California Teratogen Information Service and Clinical Research Program. Dr. Chambers is a past president of the Organization of Teratology Information Specialists and past president of the Teratology Society. She said she currently receives grant funding for two studies unrelated to SSRIs from GlaxoSmithKline and GlaxoSmithKline Bio.
Pregnant women taking selective serotonin reuptake inhibitors for depression may continue to do so, despite a 2006 warning that the drugs may predispose infants to persistent pulmonary hypertension, the Food and Drug Administration has announced.
That earlier warning was based on a single study indicating that infants exposed to the drug in utero after the 20th week of pregnancy were six times more likely to develop persistent pulmonary hypertension (PPHN) than nonexposed infants (N. Engl. J. Med. 2006;354:579-87).
“Since then, there have been conflicting findings from new studies evaluating this potential risk, making it unclear whether use of SSRIs during pregnancy can cause persistent pulmonary hypertension,” the FDA said in a press statement.
The agency will update the drugs' warning labels to reflect data from new studies, which have produced conflicting results about the risk SSRIs may pose to an unborn child. Those studies include a large retrospective database study in 2009 that found no association between SSRI use and PPHN (Pharmacoepidemiol. Drug Saf. 2009;18:246-52), and a 2011 case-control study of 11,923 births that showed PPHN was associated with cesarean delivery but not with SSRI use in the second half of pregnancy (Am. J. Perinatol. 2011;28:19-24).
FDA officials concluded that the evidence is not sufficient to withhold SSRI treatment from pregnant women or take them off the antidepressants. “At present, FDA … recommends that health care providers treat depression during pregnancy as clinically appropriate,” according to the agency's statement.
Dr. Gideon Koren, professor of pediatrics, pharmacology, pharmacy, medicine, and medical genetics at the University of Toronto, commented in an interview, “I support FDA's hesitation in confirming causation of SSRIs in causing PPHN. The available studies are split in their ability to show an association between SSRIs taken in late pregnancy.
“Critically, several studies have shown that depression itself is also associated with increased risk of PPHN. Hence it is quite possible that depression and not its treatment cause this rare risk ('confounding by indication').” Dr. Koren also heads the Research Leadership for Better Pharmacotherapy During Pregnancy and Lactation at the Hospital for Sick Children, Toronto, where he is director of the Motherisk Program.
Physicians and their patients should carefully weigh the risks and benefits of any antidepressant use in pregnancy, the FDA added, given that there are “substantial risks associated with undertreatment or no treatment of depression during pregnancy.” Risks of untreated maternal depression can include low birth weight, preterm delivery, lower Apgar scores, poor prenatal care, failure to recognize or report impending labor, and increased risks of fetal abuse, neonaticide or maternal suicide, the FDA warned.
Both the American Psychiatric Association and the American College of Obstetricians and Gynecologists recommend monitoring pregnant women for depression and treating them appropriately.
Physicians should continue to report any possible adverse effects to the FDA's MedWatch program, www.fda.gov/MedWatch/report.htm
Reporting forms can also be requested by calling 800-332-1088.
Dr. Koren said he had no relevant financial disclosures.
View on the News
Cautious Treatment Makes Sense
Even at the time of the first publication regarding the link between SSRIs and PPHN in 2006, the conclusion of the authors was that if the link is causal, the absolute risk for PPHN following late pregnancy exposure to SSRIs is very low. Thus, the recommendation that clinicians treat pregnant women appropriately for their symptoms was consistent with the initial findings, and continues to be so.
Since the initial publication, three others have appeared in full manuscript form and one in abstract form (now in press). The two published U.S. studies were either underpowered, or had limitations in classifying the outcomes, whereas the two Scandinavian studies confirmed the initial findings in large cohort or linked database studies. Importantly, the European studies that confirmed the association also came to the conclusion that SSRIs pose a small increased risk for a very rare outcome of pregnancy. Thus, the recommendation to treat only if needed, but not to avoid necessary treatment because of concern for PPHN continues to make sense.
CHRISTINA CHAMBERS, Ph.D., M.P.H., is associate professor of pediatrics and family and preventive medicine at the University of California, San Diego. She is director of the California Teratogen Information Service and Clinical Research Program. Dr. Chambers is a past president of the Organization of Teratology Information Specialists and past president of the Teratology Society. She said she currently receives grant funding for two studies unrelated to SSRIs from GlaxoSmithKline and GlaxoSmithKline Bio.
Joint Efforts Will Help Maternity Outcomes
If it takes an entire village to raise a child, it's going to take an entire country to raise maternal/fetal outcomes.
Everyone involved in maternity care – from payers and hospital administrators to laboring women and their nurses–needs to team up to improve the health of moms and newborns, even if that means admitting that mistakes can be made.
“Even the best people in obstetrical units can't do anything without leadership being willing to put moms' and babies' safety as the highest priority,” Maureen P. Corry said during a teleconference on patient safety. “Everyone needs to be respected, encouraged to speak up, and listened to. Right now, there is a hierarchy [in health care facilities] that makes people fear retaliation if they speak up – and this is an incredible barrier to improving care.”
Ms. Corry, executive director of Childbirth Connections, was one of several experts who spoke at the Partnership for Patients webinar, sponsored by the Department of Health and Human Services. Tasked with improving patient safety across the country, the initiative brings together all manner of health care stakeholders in webcast brainstorming sessions, with the aim of providing “take-home” strategies for systems improvement.
Wednesday's session focused on decreasing obstetrical adverse events. Although much of the data needed to succeed in this effort have long been available, many hospitals have yet to incorporate them into a cohesive obstetrical safety policy, the speakers said.
As cesarean section rates continue to rise (more than one-third of births in 2009), outcomes have continued to deteriorate, said Dr. Peter Cherouny, chair of the perinatal collaborative at the Institute for Healthcare Improvement. “No matter how much money we continue to throw at this, it's not a problem that has gone away. Maternal mortality in the United States has continued to increase at a rate of 2% per year for the last 20 years.”
Most mothers are healthy and leave the hospital with healthy babies, he said. But mistakes that put mothers and babies at risk continue to occur. The best way to view this is that all mistakes can be prevented.
“Communication errors are the sentinel event in the vast majority of perinatal adverse events,” he said. “That means up to 90% of birth trauma should be considered preventable.”
But people on the front line often ignore this possibility, partly because they resist the idea of being fallible and partly because they fear retaliation from someone higher in the administrative hierarchy.
This means that mothers can be intimidated by health care professionals, nurses can feel intimidated by physicians, physicians can fear administrators, and administrators fear those that make the hospital world go around – namely payers.
Instead of continuing this culture, Dr. Cherouny said, real change can only occur when everyone in the chain drops their shield against retaliation and adopts instead a stance of individual empowerment.
Mothers can be at the root of this cultural shift, Ms. Corry said, when they learn the risks and benefits of possible interventions and insist on having input into their own care.
Childbirth Connection recently published the results of its Listening to Mothers II survey. “We found that 97% of mothers wanted to know every or most of the possible complications of induction and cesarean, but that most of them couldn't correctly identify the adverse effects of either one,” Ms. Corry said.
The survey also showed that 45% of mothers with a prior cesarean section were interested in the option of a vaginal birth after cesarean, but were denied that option due to caregiver or facility unwillingness to perform it.
“Seventeen percent of the mothers reported that they also felt pressure from a health care professional to have an induction [before the onset of natural labor], and 25% felt pressure to have a cesarean section.”
Since risk increases with every unnecessary intervention, everyone would benefit by a more restrained approach to labor and delivery. Early induction of labor and elective cesareans are two good places to begin a shift toward safer childbirth.
Administrators sometimes fear that it may simply be too expensive to make institutional changes, the presenters agreed. But this is a short-sighted view, said Dr. Alan Fleischman, medical director of the March of Dimes.
“There are many published studies that reinforce the idea that this cultural change actually improves financial outcomes. Lawsuits decrease. Length of stay decreases. Overall costs decrease. And positive outcomes increase all the way around. These are good arguments that we can use to get these changes in motion.”
The Partnership for Patients webinar was sponsored by the Department of Health and Human Services.
If it takes an entire village to raise a child, it's going to take an entire country to raise maternal/fetal outcomes.
Everyone involved in maternity care – from payers and hospital administrators to laboring women and their nurses–needs to team up to improve the health of moms and newborns, even if that means admitting that mistakes can be made.
“Even the best people in obstetrical units can't do anything without leadership being willing to put moms' and babies' safety as the highest priority,” Maureen P. Corry said during a teleconference on patient safety. “Everyone needs to be respected, encouraged to speak up, and listened to. Right now, there is a hierarchy [in health care facilities] that makes people fear retaliation if they speak up – and this is an incredible barrier to improving care.”
Ms. Corry, executive director of Childbirth Connections, was one of several experts who spoke at the Partnership for Patients webinar, sponsored by the Department of Health and Human Services. Tasked with improving patient safety across the country, the initiative brings together all manner of health care stakeholders in webcast brainstorming sessions, with the aim of providing “take-home” strategies for systems improvement.
Wednesday's session focused on decreasing obstetrical adverse events. Although much of the data needed to succeed in this effort have long been available, many hospitals have yet to incorporate them into a cohesive obstetrical safety policy, the speakers said.
As cesarean section rates continue to rise (more than one-third of births in 2009), outcomes have continued to deteriorate, said Dr. Peter Cherouny, chair of the perinatal collaborative at the Institute for Healthcare Improvement. “No matter how much money we continue to throw at this, it's not a problem that has gone away. Maternal mortality in the United States has continued to increase at a rate of 2% per year for the last 20 years.”
Most mothers are healthy and leave the hospital with healthy babies, he said. But mistakes that put mothers and babies at risk continue to occur. The best way to view this is that all mistakes can be prevented.
“Communication errors are the sentinel event in the vast majority of perinatal adverse events,” he said. “That means up to 90% of birth trauma should be considered preventable.”
But people on the front line often ignore this possibility, partly because they resist the idea of being fallible and partly because they fear retaliation from someone higher in the administrative hierarchy.
This means that mothers can be intimidated by health care professionals, nurses can feel intimidated by physicians, physicians can fear administrators, and administrators fear those that make the hospital world go around – namely payers.
Instead of continuing this culture, Dr. Cherouny said, real change can only occur when everyone in the chain drops their shield against retaliation and adopts instead a stance of individual empowerment.
Mothers can be at the root of this cultural shift, Ms. Corry said, when they learn the risks and benefits of possible interventions and insist on having input into their own care.
Childbirth Connection recently published the results of its Listening to Mothers II survey. “We found that 97% of mothers wanted to know every or most of the possible complications of induction and cesarean, but that most of them couldn't correctly identify the adverse effects of either one,” Ms. Corry said.
The survey also showed that 45% of mothers with a prior cesarean section were interested in the option of a vaginal birth after cesarean, but were denied that option due to caregiver or facility unwillingness to perform it.
“Seventeen percent of the mothers reported that they also felt pressure from a health care professional to have an induction [before the onset of natural labor], and 25% felt pressure to have a cesarean section.”
Since risk increases with every unnecessary intervention, everyone would benefit by a more restrained approach to labor and delivery. Early induction of labor and elective cesareans are two good places to begin a shift toward safer childbirth.
Administrators sometimes fear that it may simply be too expensive to make institutional changes, the presenters agreed. But this is a short-sighted view, said Dr. Alan Fleischman, medical director of the March of Dimes.
“There are many published studies that reinforce the idea that this cultural change actually improves financial outcomes. Lawsuits decrease. Length of stay decreases. Overall costs decrease. And positive outcomes increase all the way around. These are good arguments that we can use to get these changes in motion.”
The Partnership for Patients webinar was sponsored by the Department of Health and Human Services.
If it takes an entire village to raise a child, it's going to take an entire country to raise maternal/fetal outcomes.
Everyone involved in maternity care – from payers and hospital administrators to laboring women and their nurses–needs to team up to improve the health of moms and newborns, even if that means admitting that mistakes can be made.
“Even the best people in obstetrical units can't do anything without leadership being willing to put moms' and babies' safety as the highest priority,” Maureen P. Corry said during a teleconference on patient safety. “Everyone needs to be respected, encouraged to speak up, and listened to. Right now, there is a hierarchy [in health care facilities] that makes people fear retaliation if they speak up – and this is an incredible barrier to improving care.”
Ms. Corry, executive director of Childbirth Connections, was one of several experts who spoke at the Partnership for Patients webinar, sponsored by the Department of Health and Human Services. Tasked with improving patient safety across the country, the initiative brings together all manner of health care stakeholders in webcast brainstorming sessions, with the aim of providing “take-home” strategies for systems improvement.
Wednesday's session focused on decreasing obstetrical adverse events. Although much of the data needed to succeed in this effort have long been available, many hospitals have yet to incorporate them into a cohesive obstetrical safety policy, the speakers said.
As cesarean section rates continue to rise (more than one-third of births in 2009), outcomes have continued to deteriorate, said Dr. Peter Cherouny, chair of the perinatal collaborative at the Institute for Healthcare Improvement. “No matter how much money we continue to throw at this, it's not a problem that has gone away. Maternal mortality in the United States has continued to increase at a rate of 2% per year for the last 20 years.”
Most mothers are healthy and leave the hospital with healthy babies, he said. But mistakes that put mothers and babies at risk continue to occur. The best way to view this is that all mistakes can be prevented.
“Communication errors are the sentinel event in the vast majority of perinatal adverse events,” he said. “That means up to 90% of birth trauma should be considered preventable.”
But people on the front line often ignore this possibility, partly because they resist the idea of being fallible and partly because they fear retaliation from someone higher in the administrative hierarchy.
This means that mothers can be intimidated by health care professionals, nurses can feel intimidated by physicians, physicians can fear administrators, and administrators fear those that make the hospital world go around – namely payers.
Instead of continuing this culture, Dr. Cherouny said, real change can only occur when everyone in the chain drops their shield against retaliation and adopts instead a stance of individual empowerment.
Mothers can be at the root of this cultural shift, Ms. Corry said, when they learn the risks and benefits of possible interventions and insist on having input into their own care.
Childbirth Connection recently published the results of its Listening to Mothers II survey. “We found that 97% of mothers wanted to know every or most of the possible complications of induction and cesarean, but that most of them couldn't correctly identify the adverse effects of either one,” Ms. Corry said.
The survey also showed that 45% of mothers with a prior cesarean section were interested in the option of a vaginal birth after cesarean, but were denied that option due to caregiver or facility unwillingness to perform it.
“Seventeen percent of the mothers reported that they also felt pressure from a health care professional to have an induction [before the onset of natural labor], and 25% felt pressure to have a cesarean section.”
Since risk increases with every unnecessary intervention, everyone would benefit by a more restrained approach to labor and delivery. Early induction of labor and elective cesareans are two good places to begin a shift toward safer childbirth.
Administrators sometimes fear that it may simply be too expensive to make institutional changes, the presenters agreed. But this is a short-sighted view, said Dr. Alan Fleischman, medical director of the March of Dimes.
“There are many published studies that reinforce the idea that this cultural change actually improves financial outcomes. Lawsuits decrease. Length of stay decreases. Overall costs decrease. And positive outcomes increase all the way around. These are good arguments that we can use to get these changes in motion.”
The Partnership for Patients webinar was sponsored by the Department of Health and Human Services.
From a Teleconference on Patient Safety
More Than 40% of Police Officers Have Sleep Disorders
Nearly half of North American police officers might be suffering from a sleep disorder that could interfere with the safe execution of their duties.
A survey of nearly 5,000 officers found that 40.4% of them screened positive for a sleep disorder, most of these undiagnosed. Those officers with a sleep disorder were significantly more likely to commit administrative errors, lose their temper with citizens, and even fall asleep while driving, Shantha M.W. Rajaratnam, Ph.D., and colleagues reported in the Dec. 21 issue of JAMA.

"Almost half [reported] having fallen asleep while driving" and about one-quarter said that this occurs one to two times per month, said Dr. Rajaratnam of Brigham and Women’s Hospital, Boston. "This is despite police officers apparently recognizing the dangers associated with drowsy driving." In a different survey of North American police officers, almost 90% regarded drowsy driving to be as dangerous as drunk driving, the investigators noted (JAMA 2011;306:2567-78).
The team conducted an online and in-person survey of 4,957 police officers, 97% of whom were based in the United States and 3% in Canada. The subjects responded to a variety of questionnaires that screen for sleep disorders, including obstructive sleep apnea, insomnia, restless legs syndrome, narcolepsy, and cataplexy. The survey also screened for shift-work disorder. Subjects provided basic health information, as well as information about alcohol intake and feelings of emotional burnout. They then completed monthly surveys for the next 2 years, with an accumulation of 15, 735 surveys.
The mean age of the cohort was 38.5 years; 82.3% were male. More than half (58%) reported their health as very good or excellent. However, 79.3% of the respondents were overweight or obese, and 33.5% were obese.
Most were patrol officers (66.5%), followed by managers (15%), criminal investigators (8.2%), and other job positions. Only 38% reported never having night-shift work; the rest worked overnight from once per month to nearly every shift.
Of the entire cohort, 2,003 (40.4%) screened positive for at least one sleep disorder. Obstructive sleep apnea was the most commonly identified problem, affecting 1,666 (33.6%) of the subjects. The next most commonly identified problem was moderate to severe insomnia, found in 281 (6.5%).
Other findings were shift-work disorder (269), restless legs syndrome (70), and narcolepsy with cataplexy (16).
The group with shift-work disorder represented 14% of those who worked overnight hours, the investigators noted. However, they said, if they applied the International Classification of Sleep Disorders–2 criteria for shift work disorder (excessive wake-time sleepiness or insomnia), then 1,004 (53.9%) of the police officers who worked night shifts screened positive.
The investigators found some significant associations between sleep disorders and health/safety outcomes. Those with a positive screen were almost three times as likely to report depression (odds ratio, 2.75) and emotional job burnout (OR, 2.87), and almost five times as likely to report having fallen asleep while driving after work (OR, 4.64). Of the entire cohort, 2,276 (46%) reported having fallen asleep while driving (56.9% at least once a month, and 13.5% once or twice a week).
At the 2-year follow-up, data were collected on 6,587 person-months for those with positive screens and 9,148 person-months for those with negative screens. Again, the authors found significant correlations between a sleep disorder and a behavioral or safety issue. Compared with those having a negative screen, those with a positive screen were 43% more likely to make an administrative error, 51% more likely to fall asleep while driving, and 63% more likely to make a fatigue-related safety error.
Sleep disorders also significantly correlated with public interaction. Those with positive screens were 25% more likely to experience uncontrolled anger at a citizen or suspect, and 35% more likely to incur a citizen complaint.
Over the follow-up period, those in the cohort experienced 287 motor vehicle accidents, which were 49% more common among those who had reported falling asleep while driving and 68% more common among those who reported falling asleep while stopped in traffic.
Dr. Rajaratnam reported numerous financial relationships with pharmaceutical and medical device companies. The study was sponsored by National Institute of Justice and the Centers for Disease Control and Prevention.
The study by Dr. Rajaratnam and colleagues points up the importance of a healthy and well-rested public safety force, Michael A. Grandner, Ph.D., and Dr. Allan I. Pack wrote in an accompanying editorial (JAMA 2011;306:2616-7).
The paper showed that inadequate sleep was related to a wide variety of both personal health problems and public safety. "Not only are police officers at high risk of having an undiagnosed sleep disorder, but the sleep disorder may have a detrimental effect on the officer’s health, productivity, and job performance," they noted.
Most officers in the study were aware of their personal and performance problems, but they had no idea that a sleep disorder was a key factor. Fortunately, the authors wrote, sleep problems can be corrected with adequate therapy – if they are diagnosed.
Some agencies already have recognized this problem and have taken steps to address it. "In the occupational arena, some employers are developing proactive educational programs, and a few are initiating programs for mandatory screening for common sleep disorders such as sleep apnea," wrote Dr. Grandner and Dr. Pack. "This is likely to be the most effective approach, but employees may have concerns that if they are found to have a sleep disorder, their employment will be adversely affected."
Indeed, some groups seem reluctant to introduce any type of screening and treatment program, despite having identified sleep issues as a major contributor to employee – and thus public – health.
"For example, in 2008 a medical expert panel created by the Federal Motor Carrier Safety Administration (responsible for the safety of commercial vehicles) gave recommendations on screening for sleep apnea, although to date the agency has not implemented any of the recommendations, which included provisions for sleep disorder screening and restrictions placed on those with untreated sleep apnea."
The situation is widespread and needs immediate attention for the health and safety of all, they said.
"As a matter of public safety, this study illustrates that the public at large may also be at risk when police officers are impaired in performing their duties because of sleep deprivation or an untreated sleep disorder.
"Now, the question is what police departments will do with this new information."
Dr. Grandner is a postdoctoral fellow at the center for sleep and respiratory neurobiology and Dr. Pack is the director of the center for sleep and circadian neurobiology, both at the University of Pennsylvania, Philadelphia. Both declared that they had no financial conflicts with regard to the study.
The study by Dr. Rajaratnam and colleagues points up the importance of a healthy and well-rested public safety force, Michael A. Grandner, Ph.D., and Dr. Allan I. Pack wrote in an accompanying editorial (JAMA 2011;306:2616-7).
The paper showed that inadequate sleep was related to a wide variety of both personal health problems and public safety. "Not only are police officers at high risk of having an undiagnosed sleep disorder, but the sleep disorder may have a detrimental effect on the officer’s health, productivity, and job performance," they noted.
Most officers in the study were aware of their personal and performance problems, but they had no idea that a sleep disorder was a key factor. Fortunately, the authors wrote, sleep problems can be corrected with adequate therapy – if they are diagnosed.
Some agencies already have recognized this problem and have taken steps to address it. "In the occupational arena, some employers are developing proactive educational programs, and a few are initiating programs for mandatory screening for common sleep disorders such as sleep apnea," wrote Dr. Grandner and Dr. Pack. "This is likely to be the most effective approach, but employees may have concerns that if they are found to have a sleep disorder, their employment will be adversely affected."
Indeed, some groups seem reluctant to introduce any type of screening and treatment program, despite having identified sleep issues as a major contributor to employee – and thus public – health.
"For example, in 2008 a medical expert panel created by the Federal Motor Carrier Safety Administration (responsible for the safety of commercial vehicles) gave recommendations on screening for sleep apnea, although to date the agency has not implemented any of the recommendations, which included provisions for sleep disorder screening and restrictions placed on those with untreated sleep apnea."
The situation is widespread and needs immediate attention for the health and safety of all, they said.
"As a matter of public safety, this study illustrates that the public at large may also be at risk when police officers are impaired in performing their duties because of sleep deprivation or an untreated sleep disorder.
"Now, the question is what police departments will do with this new information."
Dr. Grandner is a postdoctoral fellow at the center for sleep and respiratory neurobiology and Dr. Pack is the director of the center for sleep and circadian neurobiology, both at the University of Pennsylvania, Philadelphia. Both declared that they had no financial conflicts with regard to the study.
The study by Dr. Rajaratnam and colleagues points up the importance of a healthy and well-rested public safety force, Michael A. Grandner, Ph.D., and Dr. Allan I. Pack wrote in an accompanying editorial (JAMA 2011;306:2616-7).
The paper showed that inadequate sleep was related to a wide variety of both personal health problems and public safety. "Not only are police officers at high risk of having an undiagnosed sleep disorder, but the sleep disorder may have a detrimental effect on the officer’s health, productivity, and job performance," they noted.
Most officers in the study were aware of their personal and performance problems, but they had no idea that a sleep disorder was a key factor. Fortunately, the authors wrote, sleep problems can be corrected with adequate therapy – if they are diagnosed.
Some agencies already have recognized this problem and have taken steps to address it. "In the occupational arena, some employers are developing proactive educational programs, and a few are initiating programs for mandatory screening for common sleep disorders such as sleep apnea," wrote Dr. Grandner and Dr. Pack. "This is likely to be the most effective approach, but employees may have concerns that if they are found to have a sleep disorder, their employment will be adversely affected."
Indeed, some groups seem reluctant to introduce any type of screening and treatment program, despite having identified sleep issues as a major contributor to employee – and thus public – health.
"For example, in 2008 a medical expert panel created by the Federal Motor Carrier Safety Administration (responsible for the safety of commercial vehicles) gave recommendations on screening for sleep apnea, although to date the agency has not implemented any of the recommendations, which included provisions for sleep disorder screening and restrictions placed on those with untreated sleep apnea."
The situation is widespread and needs immediate attention for the health and safety of all, they said.
"As a matter of public safety, this study illustrates that the public at large may also be at risk when police officers are impaired in performing their duties because of sleep deprivation or an untreated sleep disorder.
"Now, the question is what police departments will do with this new information."
Dr. Grandner is a postdoctoral fellow at the center for sleep and respiratory neurobiology and Dr. Pack is the director of the center for sleep and circadian neurobiology, both at the University of Pennsylvania, Philadelphia. Both declared that they had no financial conflicts with regard to the study.
Nearly half of North American police officers might be suffering from a sleep disorder that could interfere with the safe execution of their duties.
A survey of nearly 5,000 officers found that 40.4% of them screened positive for a sleep disorder, most of these undiagnosed. Those officers with a sleep disorder were significantly more likely to commit administrative errors, lose their temper with citizens, and even fall asleep while driving, Shantha M.W. Rajaratnam, Ph.D., and colleagues reported in the Dec. 21 issue of JAMA.
"Almost half [reported] having fallen asleep while driving" and about one-quarter said that this occurs one to two times per month, said Dr. Rajaratnam of Brigham and Women’s Hospital, Boston. "This is despite police officers apparently recognizing the dangers associated with drowsy driving." In a different survey of North American police officers, almost 90% regarded drowsy driving to be as dangerous as drunk driving, the investigators noted (JAMA 2011;306:2567-78).
The team conducted an online and in-person survey of 4,957 police officers, 97% of whom were based in the United States and 3% in Canada. The subjects responded to a variety of questionnaires that screen for sleep disorders, including obstructive sleep apnea, insomnia, restless legs syndrome, narcolepsy, and cataplexy. The survey also screened for shift-work disorder. Subjects provided basic health information, as well as information about alcohol intake and feelings of emotional burnout. They then completed monthly surveys for the next 2 years, with an accumulation of 15, 735 surveys.
The mean age of the cohort was 38.5 years; 82.3% were male. More than half (58%) reported their health as very good or excellent. However, 79.3% of the respondents were overweight or obese, and 33.5% were obese.
Most were patrol officers (66.5%), followed by managers (15%), criminal investigators (8.2%), and other job positions. Only 38% reported never having night-shift work; the rest worked overnight from once per month to nearly every shift.
Of the entire cohort, 2,003 (40.4%) screened positive for at least one sleep disorder. Obstructive sleep apnea was the most commonly identified problem, affecting 1,666 (33.6%) of the subjects. The next most commonly identified problem was moderate to severe insomnia, found in 281 (6.5%).
Other findings were shift-work disorder (269), restless legs syndrome (70), and narcolepsy with cataplexy (16).
The group with shift-work disorder represented 14% of those who worked overnight hours, the investigators noted. However, they said, if they applied the International Classification of Sleep Disorders–2 criteria for shift work disorder (excessive wake-time sleepiness or insomnia), then 1,004 (53.9%) of the police officers who worked night shifts screened positive.
The investigators found some significant associations between sleep disorders and health/safety outcomes. Those with a positive screen were almost three times as likely to report depression (odds ratio, 2.75) and emotional job burnout (OR, 2.87), and almost five times as likely to report having fallen asleep while driving after work (OR, 4.64). Of the entire cohort, 2,276 (46%) reported having fallen asleep while driving (56.9% at least once a month, and 13.5% once or twice a week).
At the 2-year follow-up, data were collected on 6,587 person-months for those with positive screens and 9,148 person-months for those with negative screens. Again, the authors found significant correlations between a sleep disorder and a behavioral or safety issue. Compared with those having a negative screen, those with a positive screen were 43% more likely to make an administrative error, 51% more likely to fall asleep while driving, and 63% more likely to make a fatigue-related safety error.
Sleep disorders also significantly correlated with public interaction. Those with positive screens were 25% more likely to experience uncontrolled anger at a citizen or suspect, and 35% more likely to incur a citizen complaint.
Over the follow-up period, those in the cohort experienced 287 motor vehicle accidents, which were 49% more common among those who had reported falling asleep while driving and 68% more common among those who reported falling asleep while stopped in traffic.
Dr. Rajaratnam reported numerous financial relationships with pharmaceutical and medical device companies. The study was sponsored by National Institute of Justice and the Centers for Disease Control and Prevention.
Nearly half of North American police officers might be suffering from a sleep disorder that could interfere with the safe execution of their duties.
A survey of nearly 5,000 officers found that 40.4% of them screened positive for a sleep disorder, most of these undiagnosed. Those officers with a sleep disorder were significantly more likely to commit administrative errors, lose their temper with citizens, and even fall asleep while driving, Shantha M.W. Rajaratnam, Ph.D., and colleagues reported in the Dec. 21 issue of JAMA.
"Almost half [reported] having fallen asleep while driving" and about one-quarter said that this occurs one to two times per month, said Dr. Rajaratnam of Brigham and Women’s Hospital, Boston. "This is despite police officers apparently recognizing the dangers associated with drowsy driving." In a different survey of North American police officers, almost 90% regarded drowsy driving to be as dangerous as drunk driving, the investigators noted (JAMA 2011;306:2567-78).
The team conducted an online and in-person survey of 4,957 police officers, 97% of whom were based in the United States and 3% in Canada. The subjects responded to a variety of questionnaires that screen for sleep disorders, including obstructive sleep apnea, insomnia, restless legs syndrome, narcolepsy, and cataplexy. The survey also screened for shift-work disorder. Subjects provided basic health information, as well as information about alcohol intake and feelings of emotional burnout. They then completed monthly surveys for the next 2 years, with an accumulation of 15, 735 surveys.
The mean age of the cohort was 38.5 years; 82.3% were male. More than half (58%) reported their health as very good or excellent. However, 79.3% of the respondents were overweight or obese, and 33.5% were obese.
Most were patrol officers (66.5%), followed by managers (15%), criminal investigators (8.2%), and other job positions. Only 38% reported never having night-shift work; the rest worked overnight from once per month to nearly every shift.
Of the entire cohort, 2,003 (40.4%) screened positive for at least one sleep disorder. Obstructive sleep apnea was the most commonly identified problem, affecting 1,666 (33.6%) of the subjects. The next most commonly identified problem was moderate to severe insomnia, found in 281 (6.5%).
Other findings were shift-work disorder (269), restless legs syndrome (70), and narcolepsy with cataplexy (16).
The group with shift-work disorder represented 14% of those who worked overnight hours, the investigators noted. However, they said, if they applied the International Classification of Sleep Disorders–2 criteria for shift work disorder (excessive wake-time sleepiness or insomnia), then 1,004 (53.9%) of the police officers who worked night shifts screened positive.
The investigators found some significant associations between sleep disorders and health/safety outcomes. Those with a positive screen were almost three times as likely to report depression (odds ratio, 2.75) and emotional job burnout (OR, 2.87), and almost five times as likely to report having fallen asleep while driving after work (OR, 4.64). Of the entire cohort, 2,276 (46%) reported having fallen asleep while driving (56.9% at least once a month, and 13.5% once or twice a week).
At the 2-year follow-up, data were collected on 6,587 person-months for those with positive screens and 9,148 person-months for those with negative screens. Again, the authors found significant correlations between a sleep disorder and a behavioral or safety issue. Compared with those having a negative screen, those with a positive screen were 43% more likely to make an administrative error, 51% more likely to fall asleep while driving, and 63% more likely to make a fatigue-related safety error.
Sleep disorders also significantly correlated with public interaction. Those with positive screens were 25% more likely to experience uncontrolled anger at a citizen or suspect, and 35% more likely to incur a citizen complaint.
Over the follow-up period, those in the cohort experienced 287 motor vehicle accidents, which were 49% more common among those who had reported falling asleep while driving and 68% more common among those who reported falling asleep while stopped in traffic.
Dr. Rajaratnam reported numerous financial relationships with pharmaceutical and medical device companies. The study was sponsored by National Institute of Justice and the Centers for Disease Control and Prevention.
FROM JAMA
Major Finding: Sleep disorders among police officers increase the risk of their falling asleep while driving by five times, and are associated with a 49% increase in safety errors, a 25% increase in uncontrolled anger, and a 35% increase in citizen complaints.
Data Source: A prospective observational study of nearly 5,000 North American police officers.
Disclosures: Dr. Rajaratnam reported numerous financial relationships with pharmaceutical and medical device companies. The study was sponsored by National Institute of Justice and the Centers for Disease Control and Prevention.
FDA: New Acetaminophen Formula May Confuse Parents
A new, less-concentrated formula of infant acetaminophen has just hit the shelves, prompting the Food and Drug Administration to reinforce safety recommendations about the drug.
Until now, liquid acetaminophen for infants has been available in 80 mg/0.8 mL concentrations. The new product is a 160 mg/5 mL formula. Physicians should clearly specify which product to use, because confusion over the two formulas could lead to fatal overdoses, according to Carol Holtquist, director of FDA Division of Medical Error Prevention and Analysis.
"If a pediatrician prescribes a 5 mL dose of the less-concentrated liquid acetaminophen, but the parents administer a 5 mL dose of the more-concentrated liquid acetaminophen, the child can receive a potentially fatal overdose during the course of therapy," Ms. Holtquist said in a safety alert. "Conversely, if a physician prescribes a dose based on the more-concentrated liquid acetaminophen and the less-concentrated medication is used, the child might not receive enough medication to fight a fever."
The new formula may also be packaged with an oral syringe, instead of the dropper parents are accustomed to. It’s critical that adults giving the medication pay careful attention to the packaging directions, and use the correct device.
"Do not mix and match dosing devices," the FDA warned.
The new formulation is a response to the agency’s 2009 recommendation that manufacturers change their infants’ acetaminophen concentration to the lower 160 mg, to help prevent unintentional dosing errors that occurred with the 80-mg formula. The new product began appearing in stores earlier this year. "However, since this change is voluntary, products with the old concentration of acetaminophen marketed for infants are still available in stores and in medicine cabinets," the safety update noted.
Physicians should counsel parents carefully about giving acetaminophen to infants, the FDA said. Writing the desired dose and dosing directions on a prescription can help caregivers choose the recommended product and administer it correctly.
"[Physicians] should counsel caregivers on product differences," including how to read the label and instructions. "Caregivers should carefully read the Drug Facts label on the package to identify the concentration of the liquid acetaminophen (in mg/mL), dosage, and directions for use."
A new, less-concentrated formula of infant acetaminophen has just hit the shelves, prompting the Food and Drug Administration to reinforce safety recommendations about the drug.
Until now, liquid acetaminophen for infants has been available in 80 mg/0.8 mL concentrations. The new product is a 160 mg/5 mL formula. Physicians should clearly specify which product to use, because confusion over the two formulas could lead to fatal overdoses, according to Carol Holtquist, director of FDA Division of Medical Error Prevention and Analysis.
"If a pediatrician prescribes a 5 mL dose of the less-concentrated liquid acetaminophen, but the parents administer a 5 mL dose of the more-concentrated liquid acetaminophen, the child can receive a potentially fatal overdose during the course of therapy," Ms. Holtquist said in a safety alert. "Conversely, if a physician prescribes a dose based on the more-concentrated liquid acetaminophen and the less-concentrated medication is used, the child might not receive enough medication to fight a fever."
The new formula may also be packaged with an oral syringe, instead of the dropper parents are accustomed to. It’s critical that adults giving the medication pay careful attention to the packaging directions, and use the correct device.
"Do not mix and match dosing devices," the FDA warned.
The new formulation is a response to the agency’s 2009 recommendation that manufacturers change their infants’ acetaminophen concentration to the lower 160 mg, to help prevent unintentional dosing errors that occurred with the 80-mg formula. The new product began appearing in stores earlier this year. "However, since this change is voluntary, products with the old concentration of acetaminophen marketed for infants are still available in stores and in medicine cabinets," the safety update noted.
Physicians should counsel parents carefully about giving acetaminophen to infants, the FDA said. Writing the desired dose and dosing directions on a prescription can help caregivers choose the recommended product and administer it correctly.
"[Physicians] should counsel caregivers on product differences," including how to read the label and instructions. "Caregivers should carefully read the Drug Facts label on the package to identify the concentration of the liquid acetaminophen (in mg/mL), dosage, and directions for use."
A new, less-concentrated formula of infant acetaminophen has just hit the shelves, prompting the Food and Drug Administration to reinforce safety recommendations about the drug.
Until now, liquid acetaminophen for infants has been available in 80 mg/0.8 mL concentrations. The new product is a 160 mg/5 mL formula. Physicians should clearly specify which product to use, because confusion over the two formulas could lead to fatal overdoses, according to Carol Holtquist, director of FDA Division of Medical Error Prevention and Analysis.
"If a pediatrician prescribes a 5 mL dose of the less-concentrated liquid acetaminophen, but the parents administer a 5 mL dose of the more-concentrated liquid acetaminophen, the child can receive a potentially fatal overdose during the course of therapy," Ms. Holtquist said in a safety alert. "Conversely, if a physician prescribes a dose based on the more-concentrated liquid acetaminophen and the less-concentrated medication is used, the child might not receive enough medication to fight a fever."
The new formula may also be packaged with an oral syringe, instead of the dropper parents are accustomed to. It’s critical that adults giving the medication pay careful attention to the packaging directions, and use the correct device.
"Do not mix and match dosing devices," the FDA warned.
The new formulation is a response to the agency’s 2009 recommendation that manufacturers change their infants’ acetaminophen concentration to the lower 160 mg, to help prevent unintentional dosing errors that occurred with the 80-mg formula. The new product began appearing in stores earlier this year. "However, since this change is voluntary, products with the old concentration of acetaminophen marketed for infants are still available in stores and in medicine cabinets," the safety update noted.
Physicians should counsel parents carefully about giving acetaminophen to infants, the FDA said. Writing the desired dose and dosing directions on a prescription can help caregivers choose the recommended product and administer it correctly.
"[Physicians] should counsel caregivers on product differences," including how to read the label and instructions. "Caregivers should carefully read the Drug Facts label on the package to identify the concentration of the liquid acetaminophen (in mg/mL), dosage, and directions for use."
Depression, Physical Impairment Linger in ALI Survivors
Survivors of acute lung injury are likely to experience depression and physical impairment for up to 2 years after leaving the intensive care unit.
In a prospective study, 40% of patients had new-onset depression and 66% had new physical impairment after discharge. The findings seem inextricably linked on both psychological and physiological levels, Dr. Oscar J. Bienvenu and his colleagues wrote in the American Journal of Respiratory and Critical Care Medicine.

"Depressive symptoms may decrease motivation for and reward from the physical activities necessary for recovery of maintenance of functioning ... [they] can also amplify symptoms of general medical illnesses, and an increased physical symptom load could negatively affect functioning."
In addition, there may be less-understood links between depression and physical functioning, wrote Dr. Bienvenu of Johns Hopkins University, Baltimore, and his coauthors.
"Depressive symptoms could affect functioning through direct neurobiologic pathways, including neuroendocrine and inflammatory mechanisms."
The study comprised 2-year follow-up data on 186 patients. All of the patients were mechanically ventilated for acute lung injury (ALI). Baseline depression was present in 21% and baseline physical impairment in 40% (Am. J. Respir. Crit. Care Med. 2011 Dec. 8 [doi:10.1164/rccm.201103-0503OC]).
The patients’ mean age was 49 years; 56% were male. The mean length of stay in the intensive care unit (ICU) was 19 days. Patients were assessed for depression and physical function at 3, 6, 12, and 14 months after discharge.
During the entire follow-up period, 40% of the patients experienced new-onset depression and 66% had new-onset physical impairment. Remission occurred in 39% of those with depression and 54% of those with physical impairment, but there was recurrence in 20% and 14%, respectively. Most of those who developed depression or physical impairment had symptoms at 24 months (69% and 58%).
Patients who did remit, however, tended to do well. In those with remitted depression, the mean score on the Hospital and Anxiety Depression Scale remained about 5, indicating normal mood. In those whose symptoms did not remit, the score remained 10 or higher, indicating moderate to severe depression.
Similarly, those with remission of physical impairment had a mean of 1 impaired activity of daily living, compared with a mean of 4 or more in those with unremitted impairments.
When the authors looked at potential risk factors for new-onset depression and physical impairment, only two remained statistically significant in multivariate analyses. Education of 12 or fewer years increased the risk of new-onset depression by more than three times. Only depression at last follow-up significantly correlated with new-onset physical impairment (odds ratio, 2.7)
"Our analyses indicate that depressive symptoms are not only relatively persistent in ALI survivors, they are also an independent risk factor for subsequent impairment in physical function," the authors wrote. "Hence, early identification and treatment of depressive states should be evaluated as a potential intervention to minimize the suffering and impairment that affect too many of these patients."
The National Institutes of Health supported the study. None of the authors reported any financial conflicts.
Survivors of acute lung injury are likely to experience depression and physical impairment for up to 2 years after leaving the intensive care unit.
In a prospective study, 40% of patients had new-onset depression and 66% had new physical impairment after discharge. The findings seem inextricably linked on both psychological and physiological levels, Dr. Oscar J. Bienvenu and his colleagues wrote in the American Journal of Respiratory and Critical Care Medicine.
"Depressive symptoms may decrease motivation for and reward from the physical activities necessary for recovery of maintenance of functioning ... [they] can also amplify symptoms of general medical illnesses, and an increased physical symptom load could negatively affect functioning."
In addition, there may be less-understood links between depression and physical functioning, wrote Dr. Bienvenu of Johns Hopkins University, Baltimore, and his coauthors.
"Depressive symptoms could affect functioning through direct neurobiologic pathways, including neuroendocrine and inflammatory mechanisms."
The study comprised 2-year follow-up data on 186 patients. All of the patients were mechanically ventilated for acute lung injury (ALI). Baseline depression was present in 21% and baseline physical impairment in 40% (Am. J. Respir. Crit. Care Med. 2011 Dec. 8 [doi:10.1164/rccm.201103-0503OC]).
The patients’ mean age was 49 years; 56% were male. The mean length of stay in the intensive care unit (ICU) was 19 days. Patients were assessed for depression and physical function at 3, 6, 12, and 14 months after discharge.
During the entire follow-up period, 40% of the patients experienced new-onset depression and 66% had new-onset physical impairment. Remission occurred in 39% of those with depression and 54% of those with physical impairment, but there was recurrence in 20% and 14%, respectively. Most of those who developed depression or physical impairment had symptoms at 24 months (69% and 58%).
Patients who did remit, however, tended to do well. In those with remitted depression, the mean score on the Hospital and Anxiety Depression Scale remained about 5, indicating normal mood. In those whose symptoms did not remit, the score remained 10 or higher, indicating moderate to severe depression.
Similarly, those with remission of physical impairment had a mean of 1 impaired activity of daily living, compared with a mean of 4 or more in those with unremitted impairments.
When the authors looked at potential risk factors for new-onset depression and physical impairment, only two remained statistically significant in multivariate analyses. Education of 12 or fewer years increased the risk of new-onset depression by more than three times. Only depression at last follow-up significantly correlated with new-onset physical impairment (odds ratio, 2.7)
"Our analyses indicate that depressive symptoms are not only relatively persistent in ALI survivors, they are also an independent risk factor for subsequent impairment in physical function," the authors wrote. "Hence, early identification and treatment of depressive states should be evaluated as a potential intervention to minimize the suffering and impairment that affect too many of these patients."
The National Institutes of Health supported the study. None of the authors reported any financial conflicts.
Survivors of acute lung injury are likely to experience depression and physical impairment for up to 2 years after leaving the intensive care unit.
In a prospective study, 40% of patients had new-onset depression and 66% had new physical impairment after discharge. The findings seem inextricably linked on both psychological and physiological levels, Dr. Oscar J. Bienvenu and his colleagues wrote in the American Journal of Respiratory and Critical Care Medicine.
"Depressive symptoms may decrease motivation for and reward from the physical activities necessary for recovery of maintenance of functioning ... [they] can also amplify symptoms of general medical illnesses, and an increased physical symptom load could negatively affect functioning."
In addition, there may be less-understood links between depression and physical functioning, wrote Dr. Bienvenu of Johns Hopkins University, Baltimore, and his coauthors.
"Depressive symptoms could affect functioning through direct neurobiologic pathways, including neuroendocrine and inflammatory mechanisms."
The study comprised 2-year follow-up data on 186 patients. All of the patients were mechanically ventilated for acute lung injury (ALI). Baseline depression was present in 21% and baseline physical impairment in 40% (Am. J. Respir. Crit. Care Med. 2011 Dec. 8 [doi:10.1164/rccm.201103-0503OC]).
The patients’ mean age was 49 years; 56% were male. The mean length of stay in the intensive care unit (ICU) was 19 days. Patients were assessed for depression and physical function at 3, 6, 12, and 14 months after discharge.
During the entire follow-up period, 40% of the patients experienced new-onset depression and 66% had new-onset physical impairment. Remission occurred in 39% of those with depression and 54% of those with physical impairment, but there was recurrence in 20% and 14%, respectively. Most of those who developed depression or physical impairment had symptoms at 24 months (69% and 58%).
Patients who did remit, however, tended to do well. In those with remitted depression, the mean score on the Hospital and Anxiety Depression Scale remained about 5, indicating normal mood. In those whose symptoms did not remit, the score remained 10 or higher, indicating moderate to severe depression.
Similarly, those with remission of physical impairment had a mean of 1 impaired activity of daily living, compared with a mean of 4 or more in those with unremitted impairments.
When the authors looked at potential risk factors for new-onset depression and physical impairment, only two remained statistically significant in multivariate analyses. Education of 12 or fewer years increased the risk of new-onset depression by more than three times. Only depression at last follow-up significantly correlated with new-onset physical impairment (odds ratio, 2.7)
"Our analyses indicate that depressive symptoms are not only relatively persistent in ALI survivors, they are also an independent risk factor for subsequent impairment in physical function," the authors wrote. "Hence, early identification and treatment of depressive states should be evaluated as a potential intervention to minimize the suffering and impairment that affect too many of these patients."
The National Institutes of Health supported the study. None of the authors reported any financial conflicts.
FROM THE AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
Major Finding: New-onset depression occurred in 40% of ALI survivors, and new-onset physical impairment occurred in 66%. In most, those problems persisted at 2 years after hospital discharge.
Data Source: A 2-year prospective follow-up study of 186 patients.
Disclosures: The study was sponsored by the National Institutes of Health. The authors disclosed no financial conflicts.
Pediatric VNS Surgery: Pay Now or Pay More Later
BALTIMORE – "Pay now, save later" could be the motto in the case of vagus nerve stimulation surgery for young Medicaid patients who have intractable epilepsy.
In a study of 30-month outcomes in 445 children, vagus nerve stimulation (VNS) surgery had nearly paid for itself within a year, and began to save taxpayers money soon afterward, Dr. Sandra Helmers reported at the annual meeting of the American Epilepsy Society.

"When we looked at the annual costs of emergency department and hospitalization before and after VNS surgery, we found that the overall cost savings began in the fifth or sixth quarter after surgery," and continued to increase in succeeding quarters, said Dr. Helmers, a neurologist at Emory University Hospital and Clinic, Atlanta. "This is the way we need to look at these treatments, in terms of real-world outcomes in both health and finances."
She and her colleagues divided the group of children by age: patients aged 1-11 years (238) and patients aged 12-17 years (207). All were Medicaid recipients.
Among the younger group, the mean age at the time of surgery was 7 years. All had still been having seizures despite medical therapy. They had tried a mean of four antiepileptic drugs before surgery, and 63% were on polytherapy.
The mean age at the time of surgery in the older group was 15 years. They had tried a mean of four antiepileptic drugs before surgery, and 64% were on polytherapy.
The cost of the surgery ranged from about $20,000 to $30,000, which is "fairly high relative to the preimplant costs," Dr. Helmers said.
But it didn’t take long before the savings began to show, in terms of decreased hospital and ED visits, she said. In the first 6 months after the surgery, the younger patients were 27% less likely to have an ED visit and 26% less likely to have a hospital admission than they were in the prior 6 months. The surgery resulted in savings, but the overall costs were not quite statistically significant ($17,831 vs. $18,220 quarterly [P = .052]) in the 6 months before and after surgery.
During their 6-month postsurgery period, older patients were 57% less likely to go to the ED and 56% less likely to have a hospital admission. Average total health care costs were significantly lower in the 6 months after surgery than the 6 months before ($14,068 vs. $19,047 quarterly [P = .002]).
Although VNS surgery did positively affect hospitalizations, it did not significantly change the number of antiepileptic drugs the children took, Dr. Helmers noted. "We can’t really say anything about adding new medications, because these were refractory patients and for them, another trial of medicine typically does not give much benefit."
The findings are encouraging, because they show that the short-term expense of stabilizing children’s intractable epilepsy brings long-term savings.
"It is difficult for these children to get this intervention. Health insurance is the major barrier to good care for epilepsy. And if you don’t have insurance, you are unlikely to get this."
Policy makers need to know this kind of information, she said. "This pays off [in the United States] just as it has been shown to in other parts of the world. In our country we don’t use data like these to dictate policy – but that is coming. How that will play out in the future is something we still don’t know."
Dr. Helmers had no financial disclosures.
BALTIMORE – "Pay now, save later" could be the motto in the case of vagus nerve stimulation surgery for young Medicaid patients who have intractable epilepsy.
In a study of 30-month outcomes in 445 children, vagus nerve stimulation (VNS) surgery had nearly paid for itself within a year, and began to save taxpayers money soon afterward, Dr. Sandra Helmers reported at the annual meeting of the American Epilepsy Society.
"When we looked at the annual costs of emergency department and hospitalization before and after VNS surgery, we found that the overall cost savings began in the fifth or sixth quarter after surgery," and continued to increase in succeeding quarters, said Dr. Helmers, a neurologist at Emory University Hospital and Clinic, Atlanta. "This is the way we need to look at these treatments, in terms of real-world outcomes in both health and finances."
She and her colleagues divided the group of children by age: patients aged 1-11 years (238) and patients aged 12-17 years (207). All were Medicaid recipients.
Among the younger group, the mean age at the time of surgery was 7 years. All had still been having seizures despite medical therapy. They had tried a mean of four antiepileptic drugs before surgery, and 63% were on polytherapy.
The mean age at the time of surgery in the older group was 15 years. They had tried a mean of four antiepileptic drugs before surgery, and 64% were on polytherapy.
The cost of the surgery ranged from about $20,000 to $30,000, which is "fairly high relative to the preimplant costs," Dr. Helmers said.
But it didn’t take long before the savings began to show, in terms of decreased hospital and ED visits, she said. In the first 6 months after the surgery, the younger patients were 27% less likely to have an ED visit and 26% less likely to have a hospital admission than they were in the prior 6 months. The surgery resulted in savings, but the overall costs were not quite statistically significant ($17,831 vs. $18,220 quarterly [P = .052]) in the 6 months before and after surgery.
During their 6-month postsurgery period, older patients were 57% less likely to go to the ED and 56% less likely to have a hospital admission. Average total health care costs were significantly lower in the 6 months after surgery than the 6 months before ($14,068 vs. $19,047 quarterly [P = .002]).
Although VNS surgery did positively affect hospitalizations, it did not significantly change the number of antiepileptic drugs the children took, Dr. Helmers noted. "We can’t really say anything about adding new medications, because these were refractory patients and for them, another trial of medicine typically does not give much benefit."
The findings are encouraging, because they show that the short-term expense of stabilizing children’s intractable epilepsy brings long-term savings.
"It is difficult for these children to get this intervention. Health insurance is the major barrier to good care for epilepsy. And if you don’t have insurance, you are unlikely to get this."
Policy makers need to know this kind of information, she said. "This pays off [in the United States] just as it has been shown to in other parts of the world. In our country we don’t use data like these to dictate policy – but that is coming. How that will play out in the future is something we still don’t know."
Dr. Helmers had no financial disclosures.
BALTIMORE – "Pay now, save later" could be the motto in the case of vagus nerve stimulation surgery for young Medicaid patients who have intractable epilepsy.
In a study of 30-month outcomes in 445 children, vagus nerve stimulation (VNS) surgery had nearly paid for itself within a year, and began to save taxpayers money soon afterward, Dr. Sandra Helmers reported at the annual meeting of the American Epilepsy Society.
"When we looked at the annual costs of emergency department and hospitalization before and after VNS surgery, we found that the overall cost savings began in the fifth or sixth quarter after surgery," and continued to increase in succeeding quarters, said Dr. Helmers, a neurologist at Emory University Hospital and Clinic, Atlanta. "This is the way we need to look at these treatments, in terms of real-world outcomes in both health and finances."
She and her colleagues divided the group of children by age: patients aged 1-11 years (238) and patients aged 12-17 years (207). All were Medicaid recipients.
Among the younger group, the mean age at the time of surgery was 7 years. All had still been having seizures despite medical therapy. They had tried a mean of four antiepileptic drugs before surgery, and 63% were on polytherapy.
The mean age at the time of surgery in the older group was 15 years. They had tried a mean of four antiepileptic drugs before surgery, and 64% were on polytherapy.
The cost of the surgery ranged from about $20,000 to $30,000, which is "fairly high relative to the preimplant costs," Dr. Helmers said.
But it didn’t take long before the savings began to show, in terms of decreased hospital and ED visits, she said. In the first 6 months after the surgery, the younger patients were 27% less likely to have an ED visit and 26% less likely to have a hospital admission than they were in the prior 6 months. The surgery resulted in savings, but the overall costs were not quite statistically significant ($17,831 vs. $18,220 quarterly [P = .052]) in the 6 months before and after surgery.
During their 6-month postsurgery period, older patients were 57% less likely to go to the ED and 56% less likely to have a hospital admission. Average total health care costs were significantly lower in the 6 months after surgery than the 6 months before ($14,068 vs. $19,047 quarterly [P = .002]).
Although VNS surgery did positively affect hospitalizations, it did not significantly change the number of antiepileptic drugs the children took, Dr. Helmers noted. "We can’t really say anything about adding new medications, because these were refractory patients and for them, another trial of medicine typically does not give much benefit."
The findings are encouraging, because they show that the short-term expense of stabilizing children’s intractable epilepsy brings long-term savings.
"It is difficult for these children to get this intervention. Health insurance is the major barrier to good care for epilepsy. And if you don’t have insurance, you are unlikely to get this."
Policy makers need to know this kind of information, she said. "This pays off [in the United States] just as it has been shown to in other parts of the world. In our country we don’t use data like these to dictate policy – but that is coming. How that will play out in the future is something we still don’t know."
Dr. Helmers had no financial disclosures.
FROM THE ANNUAL MEETING OF THE AMERICAN EPILEPSY SOCIETY
Major Finding: VNS surgery reduced hospital admissions by up to 57% and saved up to $5,000 quarterly for pediatric patients on Medicaid.
Data Source: A Medicaid review of 445 pediatric patients with intractable epilepsy on Medicaid.
Disclosures: Dr. Helmers had no financial declarations.