User login
FDA approves intramuscular administration for peginterferon beta-1a in MS
“The new IM administration offers people living with relapsing MS the well-characterized efficacy and safety of Plegridy with the potential for significantly reduced injection site reactions,” Biogen said in a news release announcing the FDA action.
Plegridy is a pegylated version of interferon beta-1a, which prolongs the circulation time of the molecule in the body by increasing its size. The process extends the drug’s half-life, allowing for a less-frequent dosing schedule.
Peginterferon beta-1a administered subcutaneously was first approved by the FDA in 2014 based on data showing it significantly reduces MS relapses, disability progression, and brain lesions.
The FDA approved IM administration for peginterferon beta-1a based on data evaluating bioequivalence and adverse reactions associated with IM administration compared with subcutaneous (SC) administration in healthy volunteers.
Bioequivalence of the IM and SC dosing regimens was confirmed and volunteers receiving the drug through IM administration experienced fewer injection site reactions relative to those receiving SC administration (14.4% vs. 32.1%), the company said.
The overall safety profiles of IM and SC administration were generally similar, with no new safety signals.
The European Commission allowed marketing authorization for IM administration of peginterferon beta-1a in December 2020.
A version of this article first appeared on Medscape.com.
“The new IM administration offers people living with relapsing MS the well-characterized efficacy and safety of Plegridy with the potential for significantly reduced injection site reactions,” Biogen said in a news release announcing the FDA action.
Plegridy is a pegylated version of interferon beta-1a, which prolongs the circulation time of the molecule in the body by increasing its size. The process extends the drug’s half-life, allowing for a less-frequent dosing schedule.
Peginterferon beta-1a administered subcutaneously was first approved by the FDA in 2014 based on data showing it significantly reduces MS relapses, disability progression, and brain lesions.
The FDA approved IM administration for peginterferon beta-1a based on data evaluating bioequivalence and adverse reactions associated with IM administration compared with subcutaneous (SC) administration in healthy volunteers.
Bioequivalence of the IM and SC dosing regimens was confirmed and volunteers receiving the drug through IM administration experienced fewer injection site reactions relative to those receiving SC administration (14.4% vs. 32.1%), the company said.
The overall safety profiles of IM and SC administration were generally similar, with no new safety signals.
The European Commission allowed marketing authorization for IM administration of peginterferon beta-1a in December 2020.
A version of this article first appeared on Medscape.com.
“The new IM administration offers people living with relapsing MS the well-characterized efficacy and safety of Plegridy with the potential for significantly reduced injection site reactions,” Biogen said in a news release announcing the FDA action.
Plegridy is a pegylated version of interferon beta-1a, which prolongs the circulation time of the molecule in the body by increasing its size. The process extends the drug’s half-life, allowing for a less-frequent dosing schedule.
Peginterferon beta-1a administered subcutaneously was first approved by the FDA in 2014 based on data showing it significantly reduces MS relapses, disability progression, and brain lesions.
The FDA approved IM administration for peginterferon beta-1a based on data evaluating bioequivalence and adverse reactions associated with IM administration compared with subcutaneous (SC) administration in healthy volunteers.
Bioequivalence of the IM and SC dosing regimens was confirmed and volunteers receiving the drug through IM administration experienced fewer injection site reactions relative to those receiving SC administration (14.4% vs. 32.1%), the company said.
The overall safety profiles of IM and SC administration were generally similar, with no new safety signals.
The European Commission allowed marketing authorization for IM administration of peginterferon beta-1a in December 2020.
A version of this article first appeared on Medscape.com.
New NIH database will track neurologic effects of COVID-19
“We know COVID-19 can disrupt multiple body systems, but the effects of the virus and the body’s response to COVID-19 infection on the brain, spinal cord, nerves, and muscle can be particularly devastating and contribute to persistence of disability even after the virus is cleared,” said Barbara Karp, MD, program director at the National Institute of Neurological Disorders and Stroke.
“There is an urgent need to understand COVID-19–related neurological problems, which not uncommonly include headaches, fatigue, cognitive difficulties, stroke, pain, and sleep disorders as well as some very rare complications of serious infections,” said Dr. Karp.
The COVID-19 NeuroDatabank/BioBank (NeuroCOVID) is funded by the NINDS. It was created and will be maintained by researchers at NYU Langone Health in New York.
The project is led by Andrea Troxel, ScD, professor of population health, and Eva Petkova, PhD, professor of population health and child and adolescent psychiatry, both at New York University.
“We’ve built a pretty comprehensive database that will accept deidentified patient information about new neurological issues that coincide with their COVID disease or worsening of preexisting neurological problems,” said Dr. Troxel. “In addition, we have a bio repository that will accept almost any kind of biological sample, such as blood, plasma, cerebrospinal fluid, and tissue,” she said.
“Neuroimages are very difficult to store because the files are so enormous, but we’ve had some questions about that, and we’re looking into whether we can accommodate neuroimages,” Dr. Troxel noted.
Dr. Troxel said a “blast of information and invitations” has gone out in an effort to acquire data and biospecimens. “We’ve been really pleased with the amount of interest already, interest not only from large academic medical centers, as you might expect, but also from some smaller stand-alone clinics and even some individuals who have either experienced some of these neurological problems of COVID or know those who have and are really eager to try to provide information,” she added.
Researchers interested in using data and biosamples from the database may submit requests to the NeuroCOVID Steering Committee. More information is available online on the NeuroCOVID website.
A version of this article first appeared on Medscape.com.
“We know COVID-19 can disrupt multiple body systems, but the effects of the virus and the body’s response to COVID-19 infection on the brain, spinal cord, nerves, and muscle can be particularly devastating and contribute to persistence of disability even after the virus is cleared,” said Barbara Karp, MD, program director at the National Institute of Neurological Disorders and Stroke.
“There is an urgent need to understand COVID-19–related neurological problems, which not uncommonly include headaches, fatigue, cognitive difficulties, stroke, pain, and sleep disorders as well as some very rare complications of serious infections,” said Dr. Karp.
The COVID-19 NeuroDatabank/BioBank (NeuroCOVID) is funded by the NINDS. It was created and will be maintained by researchers at NYU Langone Health in New York.
The project is led by Andrea Troxel, ScD, professor of population health, and Eva Petkova, PhD, professor of population health and child and adolescent psychiatry, both at New York University.
“We’ve built a pretty comprehensive database that will accept deidentified patient information about new neurological issues that coincide with their COVID disease or worsening of preexisting neurological problems,” said Dr. Troxel. “In addition, we have a bio repository that will accept almost any kind of biological sample, such as blood, plasma, cerebrospinal fluid, and tissue,” she said.
“Neuroimages are very difficult to store because the files are so enormous, but we’ve had some questions about that, and we’re looking into whether we can accommodate neuroimages,” Dr. Troxel noted.
Dr. Troxel said a “blast of information and invitations” has gone out in an effort to acquire data and biospecimens. “We’ve been really pleased with the amount of interest already, interest not only from large academic medical centers, as you might expect, but also from some smaller stand-alone clinics and even some individuals who have either experienced some of these neurological problems of COVID or know those who have and are really eager to try to provide information,” she added.
Researchers interested in using data and biosamples from the database may submit requests to the NeuroCOVID Steering Committee. More information is available online on the NeuroCOVID website.
A version of this article first appeared on Medscape.com.
“We know COVID-19 can disrupt multiple body systems, but the effects of the virus and the body’s response to COVID-19 infection on the brain, spinal cord, nerves, and muscle can be particularly devastating and contribute to persistence of disability even after the virus is cleared,” said Barbara Karp, MD, program director at the National Institute of Neurological Disorders and Stroke.
“There is an urgent need to understand COVID-19–related neurological problems, which not uncommonly include headaches, fatigue, cognitive difficulties, stroke, pain, and sleep disorders as well as some very rare complications of serious infections,” said Dr. Karp.
The COVID-19 NeuroDatabank/BioBank (NeuroCOVID) is funded by the NINDS. It was created and will be maintained by researchers at NYU Langone Health in New York.
The project is led by Andrea Troxel, ScD, professor of population health, and Eva Petkova, PhD, professor of population health and child and adolescent psychiatry, both at New York University.
“We’ve built a pretty comprehensive database that will accept deidentified patient information about new neurological issues that coincide with their COVID disease or worsening of preexisting neurological problems,” said Dr. Troxel. “In addition, we have a bio repository that will accept almost any kind of biological sample, such as blood, plasma, cerebrospinal fluid, and tissue,” she said.
“Neuroimages are very difficult to store because the files are so enormous, but we’ve had some questions about that, and we’re looking into whether we can accommodate neuroimages,” Dr. Troxel noted.
Dr. Troxel said a “blast of information and invitations” has gone out in an effort to acquire data and biospecimens. “We’ve been really pleased with the amount of interest already, interest not only from large academic medical centers, as you might expect, but also from some smaller stand-alone clinics and even some individuals who have either experienced some of these neurological problems of COVID or know those who have and are really eager to try to provide information,” she added.
Researchers interested in using data and biosamples from the database may submit requests to the NeuroCOVID Steering Committee. More information is available online on the NeuroCOVID website.
A version of this article first appeared on Medscape.com.
Plant-based or keto diet? Novel study yields surprising results
For appetite control, a low-fat, plant-based diet has advantages over a low-carbohydrate, animal-based ketogenic diet, although the keto diet wins when it comes to keeping post-meal glucose and insulin levels in check, new research suggests.
In a highly controlled crossover study conducted at the National Institutes of Health, people consumed fewer daily calories when on a low-fat, plant-based diet, but their insulin and blood glucose levels were higher than when they followed a low-carbohydrate, animal-based diet.
“There is this somewhat-outdated idea now that higher-fat diets, because they have more calories per gram, tend to make people overeat – something called the passive overconsumption model,” senior investigator Kevin Hall, PhD, National Institute of Diabetes and Digestive and Kidney Diseases, said in an interview.
The other more popular model these days, he explained, is the carbohydrate-insulin model, which holds that following a diet high in carbohydrates and sugar that causes insulin levels to spike will increase hunger and cause a person to overeat.
In this study, Dr. Hall and colleagues tested these two hypotheses head to head.
“The short answer is that we got exactly the opposite predictions from the carbohydrate-insulin model of obesity. In other words, instead of making people eat more and gaining weight and body fat, they actually ended up eating less on that diet and losing body fat compared to the higher-fat diet,” Dr. Hall said.
“Yet, the passive overconsumption model also failed, because despite them eating a very energy-dense diet and high fat, they didn’t gain weight and gain body fat. And so both of these models of why people overeat and gain weight seem to be inadequate in our study,” he said. “This suggests that things are a little bit more complicated.”
The study was published online Jan. 21, 2021 in Nature Medicine.
Pros and cons to both diets
For the study, the researchers housed 20 healthy adults who did not have diabetes for 4 continuous weeks at the NIH Clinical Center. The mean age of the participants was 29.9 years, and the mean body mass index was 27.8 kg/m2.
The participants were randomly allocated to consume ad libitum either a plant-based, low-fat diet (10.3% fat, 75.2% carbohydrate) with low-energy density (about 1 kcal/g−1), or an animal-based, ketogenic, low-carbohydrate diet (75.8% fat, 10.0% carbohydrate) with high energy density (about 2 kcal/g−1) for 2 weeks. They then crossed over to the alternate diet for 2 weeks.
Both diets contained about 14% protein and were matched for total calories, although the low-carb diet had twice as many calories per gram of food than the low-fat diet. Participants could eat what and however much they chose of the meals they were given.
One participant withdrew, owing to hypoglycemia during the low-carbohydrate diet phase. For the primary outcome, the researchers compared mean daily ad libitum energy intake between each 2-week diet period.
They found that energy intake from the low-fat diet was reduced by approximately 550-700 kcal/d−1, compared with the low-carbohydrate keto diet. Yet, despite the large differences in calorie intake, participants reported no differences in hunger, enjoyment of meals, or fullness between the two diets.
Participants lost weight on both diets (about 1-2 kg on average), but only the low-fat diet led to a significant loss of body fat.
“Interestingly, our findings suggest benefits to both diets, at least in the short term,” Dr. Hall said in a news release.
“While the low-fat, plant-based diet helps curb appetite, the animal-based, low-carb diet resulted in lower and more steady insulin and glucose levels. We don’t yet know if these differences would be sustained over the long term,” he said.
Dr. Hall added that it’s important to note that the study was not designed to make diet recommendations for weight loss, and the results might have been different had the participants been actively trying to lose weight.
“In fact, they didn’t even know what the study was about; we just said we want you to eat the two diets, and we’re going to see what happens in your body either as you eat as much or as little as you want,” he said.
“It’s a bit of a mixed bag in terms of which diet might be better for an individual. I think you can interpret this study as that there are positives and negatives for both diets,” Dr. Hall said.
Diet ‘tribes’
In a comment, Taylor Wallace, PhD, adjunct professor, department of nutrition and food studies, George Mason University, Fairfax, Va., said it’s important to note that “a ‘low-carb diet’ has yet to be defined, and many definitions exist.
“We really need a standard definition of what constitutes ‘low-carb’ so that studies can be designed and evaluated in a consistent manner. It’s problematic because, without a standard definition, the ‘diet tribe’ researchers (keto versus plant-based) always seem to find the answer that is in their own favor,” Dr. Wallace said. “This study does seem to use less than 20 grams of carbs per day, which in my mind is pretty low carb.”
Perhaps the most important caveat, he added, is that, in the real world, “most people don’t adhere to these very strict diets – not even for 2 weeks.”
The study was supported by the NIDDK Intramural Research Program, with additional NIH support from a National Institute of Nursing Research grant. One author has received reimbursement for speaking at conferences sponsored by companies selling nutritional products, serves on the scientific advisory council for Kerry Taste and Nutrition, and is part of an academic consortium that has received research funding from Abbott Nutrition, Nestec, and Danone. Dr. Hall and the other authors disclosed no relevant financial relationships. Dr. Wallace is principal and CEO of the Think Healthy Group, editor of the Journal of Dietary Supplements, and deputy editor of the Journal of the American College of Nutrition.
A version of this article first appeared on Medscape.com.
For appetite control, a low-fat, plant-based diet has advantages over a low-carbohydrate, animal-based ketogenic diet, although the keto diet wins when it comes to keeping post-meal glucose and insulin levels in check, new research suggests.
In a highly controlled crossover study conducted at the National Institutes of Health, people consumed fewer daily calories when on a low-fat, plant-based diet, but their insulin and blood glucose levels were higher than when they followed a low-carbohydrate, animal-based diet.
“There is this somewhat-outdated idea now that higher-fat diets, because they have more calories per gram, tend to make people overeat – something called the passive overconsumption model,” senior investigator Kevin Hall, PhD, National Institute of Diabetes and Digestive and Kidney Diseases, said in an interview.
The other more popular model these days, he explained, is the carbohydrate-insulin model, which holds that following a diet high in carbohydrates and sugar that causes insulin levels to spike will increase hunger and cause a person to overeat.
In this study, Dr. Hall and colleagues tested these two hypotheses head to head.
“The short answer is that we got exactly the opposite predictions from the carbohydrate-insulin model of obesity. In other words, instead of making people eat more and gaining weight and body fat, they actually ended up eating less on that diet and losing body fat compared to the higher-fat diet,” Dr. Hall said.
“Yet, the passive overconsumption model also failed, because despite them eating a very energy-dense diet and high fat, they didn’t gain weight and gain body fat. And so both of these models of why people overeat and gain weight seem to be inadequate in our study,” he said. “This suggests that things are a little bit more complicated.”
The study was published online Jan. 21, 2021 in Nature Medicine.
Pros and cons to both diets
For the study, the researchers housed 20 healthy adults who did not have diabetes for 4 continuous weeks at the NIH Clinical Center. The mean age of the participants was 29.9 years, and the mean body mass index was 27.8 kg/m2.
The participants were randomly allocated to consume ad libitum either a plant-based, low-fat diet (10.3% fat, 75.2% carbohydrate) with low-energy density (about 1 kcal/g−1), or an animal-based, ketogenic, low-carbohydrate diet (75.8% fat, 10.0% carbohydrate) with high energy density (about 2 kcal/g−1) for 2 weeks. They then crossed over to the alternate diet for 2 weeks.
Both diets contained about 14% protein and were matched for total calories, although the low-carb diet had twice as many calories per gram of food than the low-fat diet. Participants could eat what and however much they chose of the meals they were given.
One participant withdrew, owing to hypoglycemia during the low-carbohydrate diet phase. For the primary outcome, the researchers compared mean daily ad libitum energy intake between each 2-week diet period.
They found that energy intake from the low-fat diet was reduced by approximately 550-700 kcal/d−1, compared with the low-carbohydrate keto diet. Yet, despite the large differences in calorie intake, participants reported no differences in hunger, enjoyment of meals, or fullness between the two diets.
Participants lost weight on both diets (about 1-2 kg on average), but only the low-fat diet led to a significant loss of body fat.
“Interestingly, our findings suggest benefits to both diets, at least in the short term,” Dr. Hall said in a news release.
“While the low-fat, plant-based diet helps curb appetite, the animal-based, low-carb diet resulted in lower and more steady insulin and glucose levels. We don’t yet know if these differences would be sustained over the long term,” he said.
Dr. Hall added that it’s important to note that the study was not designed to make diet recommendations for weight loss, and the results might have been different had the participants been actively trying to lose weight.
“In fact, they didn’t even know what the study was about; we just said we want you to eat the two diets, and we’re going to see what happens in your body either as you eat as much or as little as you want,” he said.
“It’s a bit of a mixed bag in terms of which diet might be better for an individual. I think you can interpret this study as that there are positives and negatives for both diets,” Dr. Hall said.
Diet ‘tribes’
In a comment, Taylor Wallace, PhD, adjunct professor, department of nutrition and food studies, George Mason University, Fairfax, Va., said it’s important to note that “a ‘low-carb diet’ has yet to be defined, and many definitions exist.
“We really need a standard definition of what constitutes ‘low-carb’ so that studies can be designed and evaluated in a consistent manner. It’s problematic because, without a standard definition, the ‘diet tribe’ researchers (keto versus plant-based) always seem to find the answer that is in their own favor,” Dr. Wallace said. “This study does seem to use less than 20 grams of carbs per day, which in my mind is pretty low carb.”
Perhaps the most important caveat, he added, is that, in the real world, “most people don’t adhere to these very strict diets – not even for 2 weeks.”
The study was supported by the NIDDK Intramural Research Program, with additional NIH support from a National Institute of Nursing Research grant. One author has received reimbursement for speaking at conferences sponsored by companies selling nutritional products, serves on the scientific advisory council for Kerry Taste and Nutrition, and is part of an academic consortium that has received research funding from Abbott Nutrition, Nestec, and Danone. Dr. Hall and the other authors disclosed no relevant financial relationships. Dr. Wallace is principal and CEO of the Think Healthy Group, editor of the Journal of Dietary Supplements, and deputy editor of the Journal of the American College of Nutrition.
A version of this article first appeared on Medscape.com.
For appetite control, a low-fat, plant-based diet has advantages over a low-carbohydrate, animal-based ketogenic diet, although the keto diet wins when it comes to keeping post-meal glucose and insulin levels in check, new research suggests.
In a highly controlled crossover study conducted at the National Institutes of Health, people consumed fewer daily calories when on a low-fat, plant-based diet, but their insulin and blood glucose levels were higher than when they followed a low-carbohydrate, animal-based diet.
“There is this somewhat-outdated idea now that higher-fat diets, because they have more calories per gram, tend to make people overeat – something called the passive overconsumption model,” senior investigator Kevin Hall, PhD, National Institute of Diabetes and Digestive and Kidney Diseases, said in an interview.
The other more popular model these days, he explained, is the carbohydrate-insulin model, which holds that following a diet high in carbohydrates and sugar that causes insulin levels to spike will increase hunger and cause a person to overeat.
In this study, Dr. Hall and colleagues tested these two hypotheses head to head.
“The short answer is that we got exactly the opposite predictions from the carbohydrate-insulin model of obesity. In other words, instead of making people eat more and gaining weight and body fat, they actually ended up eating less on that diet and losing body fat compared to the higher-fat diet,” Dr. Hall said.
“Yet, the passive overconsumption model also failed, because despite them eating a very energy-dense diet and high fat, they didn’t gain weight and gain body fat. And so both of these models of why people overeat and gain weight seem to be inadequate in our study,” he said. “This suggests that things are a little bit more complicated.”
The study was published online Jan. 21, 2021 in Nature Medicine.
Pros and cons to both diets
For the study, the researchers housed 20 healthy adults who did not have diabetes for 4 continuous weeks at the NIH Clinical Center. The mean age of the participants was 29.9 years, and the mean body mass index was 27.8 kg/m2.
The participants were randomly allocated to consume ad libitum either a plant-based, low-fat diet (10.3% fat, 75.2% carbohydrate) with low-energy density (about 1 kcal/g−1), or an animal-based, ketogenic, low-carbohydrate diet (75.8% fat, 10.0% carbohydrate) with high energy density (about 2 kcal/g−1) for 2 weeks. They then crossed over to the alternate diet for 2 weeks.
Both diets contained about 14% protein and were matched for total calories, although the low-carb diet had twice as many calories per gram of food than the low-fat diet. Participants could eat what and however much they chose of the meals they were given.
One participant withdrew, owing to hypoglycemia during the low-carbohydrate diet phase. For the primary outcome, the researchers compared mean daily ad libitum energy intake between each 2-week diet period.
They found that energy intake from the low-fat diet was reduced by approximately 550-700 kcal/d−1, compared with the low-carbohydrate keto diet. Yet, despite the large differences in calorie intake, participants reported no differences in hunger, enjoyment of meals, or fullness between the two diets.
Participants lost weight on both diets (about 1-2 kg on average), but only the low-fat diet led to a significant loss of body fat.
“Interestingly, our findings suggest benefits to both diets, at least in the short term,” Dr. Hall said in a news release.
“While the low-fat, plant-based diet helps curb appetite, the animal-based, low-carb diet resulted in lower and more steady insulin and glucose levels. We don’t yet know if these differences would be sustained over the long term,” he said.
Dr. Hall added that it’s important to note that the study was not designed to make diet recommendations for weight loss, and the results might have been different had the participants been actively trying to lose weight.
“In fact, they didn’t even know what the study was about; we just said we want you to eat the two diets, and we’re going to see what happens in your body either as you eat as much or as little as you want,” he said.
“It’s a bit of a mixed bag in terms of which diet might be better for an individual. I think you can interpret this study as that there are positives and negatives for both diets,” Dr. Hall said.
Diet ‘tribes’
In a comment, Taylor Wallace, PhD, adjunct professor, department of nutrition and food studies, George Mason University, Fairfax, Va., said it’s important to note that “a ‘low-carb diet’ has yet to be defined, and many definitions exist.
“We really need a standard definition of what constitutes ‘low-carb’ so that studies can be designed and evaluated in a consistent manner. It’s problematic because, without a standard definition, the ‘diet tribe’ researchers (keto versus plant-based) always seem to find the answer that is in their own favor,” Dr. Wallace said. “This study does seem to use less than 20 grams of carbs per day, which in my mind is pretty low carb.”
Perhaps the most important caveat, he added, is that, in the real world, “most people don’t adhere to these very strict diets – not even for 2 weeks.”
The study was supported by the NIDDK Intramural Research Program, with additional NIH support from a National Institute of Nursing Research grant. One author has received reimbursement for speaking at conferences sponsored by companies selling nutritional products, serves on the scientific advisory council for Kerry Taste and Nutrition, and is part of an academic consortium that has received research funding from Abbott Nutrition, Nestec, and Danone. Dr. Hall and the other authors disclosed no relevant financial relationships. Dr. Wallace is principal and CEO of the Think Healthy Group, editor of the Journal of Dietary Supplements, and deputy editor of the Journal of the American College of Nutrition.
A version of this article first appeared on Medscape.com.
‘Alarming finding’ in schizophrenia patients with COVID-19
Schizophrenia spectrum disorder is associated with a significantly increased risk of dying from COVID-19, new research shows.
After adjusting for demographic and medical risk factors, the investigators found that patients who had been diagnosed with schizophrenia were two to three times more likely to die of COVID-19 if they contracted the disease.
“ and efforts should be taken to reduce risk of infection [social distancing, masks, etc.], particularly in people with schizophrenia who live in congregate living situations [hospitals and group residences],” Donald Goff, MD, department of psychiatry, New York University Langone Medical Center, said in an interview.
The study was published online Jan. 27 in JAMA Psychiatry.

The study included 7,348 adults with laboratory-confirmed SARS-CoV-2 infection from the NYU Langone Health System; 75 (1.0%) had a history of schizophrenia spectrum disorder, 564 (7.7%) had a history of a mood disorder, and 360 (4.9%) had a history of an anxiety disorder.
Overall, 864 patients (11.8%) died or were discharged to hospice within 45 days of a positive SARS-CoV-2 test.
In the fully adjusted model, a premorbid diagnosis of schizophrenia spectrum disorder, but not mood or anxiety disorder, was significantly associated with an increased risk of dying from COVID-19 within 45 days.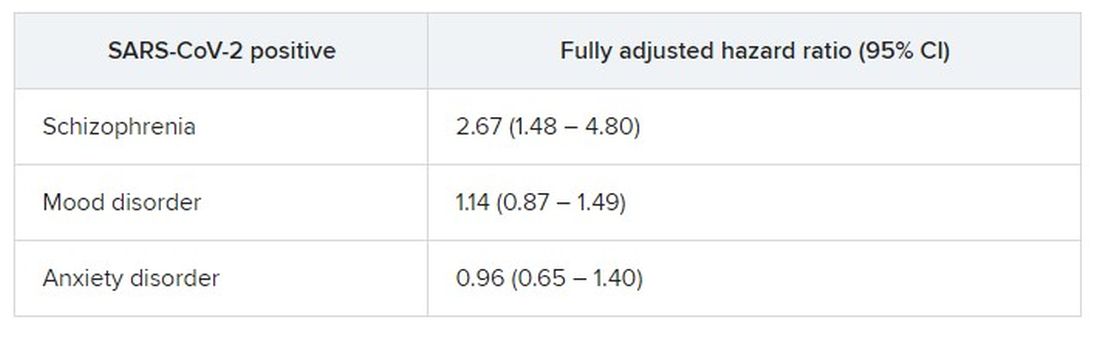
”A higher risk with schizophrenia spectrum diagnoses was expected based on previous studies of all-cause mortality, but the magnitude of the increase after adjusting for comorbid medical risk factors was unexpected,” the researchers wrote in the study, first authored by Katlyn Nemani, MD, research assistant professor of psychiatry at NYU Langone.
‘Alarming finding’
In an interview, Luming Li, MD, Yale New Haven (Conn.) Psychiatric Hospital, noted that, although the number patients with schizophrenia spectrum disorders in the sample is “fairly low,” she was not surprised by the increased risk for death from COVID-19.

“Schizophrenia falls into the serious mental illness category, and these patients are more often predisposed to homelessness, comorbid medical and substance use, living in congregate settings, lower socioeconomic status, etc,” Dr. Li noted.
Dr. Li’s advice for clinicians who treat patients who have schizophrenia during the COVID-19 pandemic is to minimize their risk in various care settings through the use of personal protective equipment and other infection prevention techniques.
“If a patient does contract COVID-19, make sure patient’s care is escalated appropriately, given the higher risk for mortality in patients with schizophrenia spectrum disorders,” she said.
Tom Pollak, PhD, MRCPsych, King’s College London, said that it has been known for some time that patients with serious mental illness have poorer physical health outcomes. More recently, it has been shown that those who have been diagnosed with psychiatric disorders appear to be at greater risk for poor COVID-19 outcomes.
“This study is the first to specifically highlight schizophrenia spectrum disorders as being particularly at risk. This is an alarming finding. These patients are already amongst the most vulnerable members of society and are probably underserved by most health care systems worldwide,” Dr. Pollak said in a statement.
“Although these findings need urgent replication in larger samples, there are clear reasons for policymakers to take notice now, including giving immediate consideration for prioritization of patients with serious mental illness in nationwide COVID-19 vaccination programs,” he added.
Matthew Hotopf, PhD, FRCPsych, FMedSci, also with King’s College London, said that the New York group has identified people with severe mental disorders as “a high-risk group, and this has immediate public health implications regarding vaccination – that’s the important message of the paper.
“Schizophrenia and other severe psychiatric disorders are risk factors for mortality in the general population before COVID. This is a group with a 10- to 20-year reduction in life expectancy – more than for many diseases we associated with early death,” said Dr. Hotopf.
“The reasons for this are multifactorial, including social deprivation, lifestyle factors (people with schizophrenia smoke more and have high rates of obesity), harms associated with some medications used to treat psychosis, and differential access to health care,” he noted.
“In COVID, we know that deprivation is associated with a much higher mortality, so we would therefore expect that people with severe mental illness will be particularly disadvantaged,” he said.
The study had no specific funding. Dr. Goff has received research support and travel reimbursement from Avanir Pharmaceuticals and Takeda. Dr. Nemani, Dr. Li, Dr. Pollak, and Dr. Hotopf disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Schizophrenia spectrum disorder is associated with a significantly increased risk of dying from COVID-19, new research shows.
After adjusting for demographic and medical risk factors, the investigators found that patients who had been diagnosed with schizophrenia were two to three times more likely to die of COVID-19 if they contracted the disease.
“ and efforts should be taken to reduce risk of infection [social distancing, masks, etc.], particularly in people with schizophrenia who live in congregate living situations [hospitals and group residences],” Donald Goff, MD, department of psychiatry, New York University Langone Medical Center, said in an interview.
The study was published online Jan. 27 in JAMA Psychiatry.
The study included 7,348 adults with laboratory-confirmed SARS-CoV-2 infection from the NYU Langone Health System; 75 (1.0%) had a history of schizophrenia spectrum disorder, 564 (7.7%) had a history of a mood disorder, and 360 (4.9%) had a history of an anxiety disorder.
Overall, 864 patients (11.8%) died or were discharged to hospice within 45 days of a positive SARS-CoV-2 test.
In the fully adjusted model, a premorbid diagnosis of schizophrenia spectrum disorder, but not mood or anxiety disorder, was significantly associated with an increased risk of dying from COVID-19 within 45 days.
”A higher risk with schizophrenia spectrum diagnoses was expected based on previous studies of all-cause mortality, but the magnitude of the increase after adjusting for comorbid medical risk factors was unexpected,” the researchers wrote in the study, first authored by Katlyn Nemani, MD, research assistant professor of psychiatry at NYU Langone.
‘Alarming finding’
In an interview, Luming Li, MD, Yale New Haven (Conn.) Psychiatric Hospital, noted that, although the number patients with schizophrenia spectrum disorders in the sample is “fairly low,” she was not surprised by the increased risk for death from COVID-19.
“Schizophrenia falls into the serious mental illness category, and these patients are more often predisposed to homelessness, comorbid medical and substance use, living in congregate settings, lower socioeconomic status, etc,” Dr. Li noted.
Dr. Li’s advice for clinicians who treat patients who have schizophrenia during the COVID-19 pandemic is to minimize their risk in various care settings through the use of personal protective equipment and other infection prevention techniques.
“If a patient does contract COVID-19, make sure patient’s care is escalated appropriately, given the higher risk for mortality in patients with schizophrenia spectrum disorders,” she said.
Tom Pollak, PhD, MRCPsych, King’s College London, said that it has been known for some time that patients with serious mental illness have poorer physical health outcomes. More recently, it has been shown that those who have been diagnosed with psychiatric disorders appear to be at greater risk for poor COVID-19 outcomes.
“This study is the first to specifically highlight schizophrenia spectrum disorders as being particularly at risk. This is an alarming finding. These patients are already amongst the most vulnerable members of society and are probably underserved by most health care systems worldwide,” Dr. Pollak said in a statement.
“Although these findings need urgent replication in larger samples, there are clear reasons for policymakers to take notice now, including giving immediate consideration for prioritization of patients with serious mental illness in nationwide COVID-19 vaccination programs,” he added.
Matthew Hotopf, PhD, FRCPsych, FMedSci, also with King’s College London, said that the New York group has identified people with severe mental disorders as “a high-risk group, and this has immediate public health implications regarding vaccination – that’s the important message of the paper.
“Schizophrenia and other severe psychiatric disorders are risk factors for mortality in the general population before COVID. This is a group with a 10- to 20-year reduction in life expectancy – more than for many diseases we associated with early death,” said Dr. Hotopf.
“The reasons for this are multifactorial, including social deprivation, lifestyle factors (people with schizophrenia smoke more and have high rates of obesity), harms associated with some medications used to treat psychosis, and differential access to health care,” he noted.
“In COVID, we know that deprivation is associated with a much higher mortality, so we would therefore expect that people with severe mental illness will be particularly disadvantaged,” he said.
The study had no specific funding. Dr. Goff has received research support and travel reimbursement from Avanir Pharmaceuticals and Takeda. Dr. Nemani, Dr. Li, Dr. Pollak, and Dr. Hotopf disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Schizophrenia spectrum disorder is associated with a significantly increased risk of dying from COVID-19, new research shows.
After adjusting for demographic and medical risk factors, the investigators found that patients who had been diagnosed with schizophrenia were two to three times more likely to die of COVID-19 if they contracted the disease.
“ and efforts should be taken to reduce risk of infection [social distancing, masks, etc.], particularly in people with schizophrenia who live in congregate living situations [hospitals and group residences],” Donald Goff, MD, department of psychiatry, New York University Langone Medical Center, said in an interview.
The study was published online Jan. 27 in JAMA Psychiatry.
The study included 7,348 adults with laboratory-confirmed SARS-CoV-2 infection from the NYU Langone Health System; 75 (1.0%) had a history of schizophrenia spectrum disorder, 564 (7.7%) had a history of a mood disorder, and 360 (4.9%) had a history of an anxiety disorder.
Overall, 864 patients (11.8%) died or were discharged to hospice within 45 days of a positive SARS-CoV-2 test.
In the fully adjusted model, a premorbid diagnosis of schizophrenia spectrum disorder, but not mood or anxiety disorder, was significantly associated with an increased risk of dying from COVID-19 within 45 days.
”A higher risk with schizophrenia spectrum diagnoses was expected based on previous studies of all-cause mortality, but the magnitude of the increase after adjusting for comorbid medical risk factors was unexpected,” the researchers wrote in the study, first authored by Katlyn Nemani, MD, research assistant professor of psychiatry at NYU Langone.
‘Alarming finding’
In an interview, Luming Li, MD, Yale New Haven (Conn.) Psychiatric Hospital, noted that, although the number patients with schizophrenia spectrum disorders in the sample is “fairly low,” she was not surprised by the increased risk for death from COVID-19.
“Schizophrenia falls into the serious mental illness category, and these patients are more often predisposed to homelessness, comorbid medical and substance use, living in congregate settings, lower socioeconomic status, etc,” Dr. Li noted.
Dr. Li’s advice for clinicians who treat patients who have schizophrenia during the COVID-19 pandemic is to minimize their risk in various care settings through the use of personal protective equipment and other infection prevention techniques.
“If a patient does contract COVID-19, make sure patient’s care is escalated appropriately, given the higher risk for mortality in patients with schizophrenia spectrum disorders,” she said.
Tom Pollak, PhD, MRCPsych, King’s College London, said that it has been known for some time that patients with serious mental illness have poorer physical health outcomes. More recently, it has been shown that those who have been diagnosed with psychiatric disorders appear to be at greater risk for poor COVID-19 outcomes.
“This study is the first to specifically highlight schizophrenia spectrum disorders as being particularly at risk. This is an alarming finding. These patients are already amongst the most vulnerable members of society and are probably underserved by most health care systems worldwide,” Dr. Pollak said in a statement.
“Although these findings need urgent replication in larger samples, there are clear reasons for policymakers to take notice now, including giving immediate consideration for prioritization of patients with serious mental illness in nationwide COVID-19 vaccination programs,” he added.
Matthew Hotopf, PhD, FRCPsych, FMedSci, also with King’s College London, said that the New York group has identified people with severe mental disorders as “a high-risk group, and this has immediate public health implications regarding vaccination – that’s the important message of the paper.
“Schizophrenia and other severe psychiatric disorders are risk factors for mortality in the general population before COVID. This is a group with a 10- to 20-year reduction in life expectancy – more than for many diseases we associated with early death,” said Dr. Hotopf.
“The reasons for this are multifactorial, including social deprivation, lifestyle factors (people with schizophrenia smoke more and have high rates of obesity), harms associated with some medications used to treat psychosis, and differential access to health care,” he noted.
“In COVID, we know that deprivation is associated with a much higher mortality, so we would therefore expect that people with severe mental illness will be particularly disadvantaged,” he said.
The study had no specific funding. Dr. Goff has received research support and travel reimbursement from Avanir Pharmaceuticals and Takeda. Dr. Nemani, Dr. Li, Dr. Pollak, and Dr. Hotopf disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.

APA apologizes for past support of racism in psychiatry
The American Psychiatric Association has issued a formal apology for its past support of structural racism in psychiatry.
The apology, issued Jan. 18, coincided with the federal holiday honoring the life and work of civil rights activist Dr. Martin Luther King Jr.
“We apologize for our role in perpetrating structural racism in this country, and we hope to begin to make amends for APA’s and psychiatry’s history of actions, intentional and not, that hurt Black, indigenous, and people of color,” APA President Jeffrey Geller, MD, MPH, said in a statement.
The apology was written and issued by the APA Board of Trustees. It acknowledges practices and events in psychiatry that contributed to racial inequality, and expresses the organization’s commitment to developing antiracist policies that promote equity in mental health for all.
“This apology is one important step we needed to take to move forward to a more equitable future. The board is issuing this document on Martin Luther King Jr. Day, because we hope that it honors his life’s work of reconciliation and equality. We do not take that legacy or his call to action lightly and will continue our important work,” said Dr. Geller.
One involved the Eastern State Hospital in Williamsburg, Va., the nation’s first psychiatric care facility, founded in 1773.
Eastern State, which for a time in the 1800s was called the Eastern Lunatic Asylum, was not segregated when founded. However, 70 years later, when the 13 founders of what is now the APA met to discuss improvements in mental health care delivery, the treatment system they created and the organization they founded aligned with that era’s racist social and political policies. In this system, Black patients received psychiatric care separately from White patients, the APA said.
The APA also acknowledged failing to act in Black Americans’ best interest at critical points in the United States’ sociopolitical evolution throughout the 19th and 20th centuries.
“This inactivity was notably evident while white supremacists lynched Black people during the Reconstruction Era as well as when Jim Crow segregation was in effect, which led to ‘separate but equal’ standards of care starting in 1896,” the APA said.
Later, the APA failed to declare support for Brown v. Board of Education of Topeka in 1954, along with further major civil rights legislation designed to improve social and psychological conditions for Black people, the organization admitted.
Throughout the decades that followed, psychiatric misdiagnosis among Black, indigenous, and people of color populations were also common, the APA acknowledged.
For example, late 20th century psychiatrists commonly attributed their minority patients’ frustrations to schizophrenia, while categorizing similar behaviors as “neuroticism” in White patients.
The APA pointed to one study which found that APA members diagnosed more Black than White patients with schizophrenia, even when both had otherwise identical clinical presentations.
“This reveals the basis for embedded discrimination within psychiatry that has contributed to reduced quality of care” for Black, indigenous, and people of color, and “perpetuation of dangerous stereotypes,” the APA said.
Saul Levin, MD, the APA’s medical director and CEO, said the Board of Trustees has taken “an important step in issuing this apology. The APA administration is committed to working toward inclusion, health equity, and fairness that everyone deserves.”
The APA Board of Trustees began drafting the apology late last year after it concluded that events and persistent inequities in health care and psychiatry had highlighted an organizational need for action.
The APA’s Presidential Task Force on Structural Racism is continuing with efforts to educate and engage members on the issue and implement changes within the organization.
A version of this article first appeared on Medscape.com.
The American Psychiatric Association has issued a formal apology for its past support of structural racism in psychiatry.
The apology, issued Jan. 18, coincided with the federal holiday honoring the life and work of civil rights activist Dr. Martin Luther King Jr.
“We apologize for our role in perpetrating structural racism in this country, and we hope to begin to make amends for APA’s and psychiatry’s history of actions, intentional and not, that hurt Black, indigenous, and people of color,” APA President Jeffrey Geller, MD, MPH, said in a statement.
The apology was written and issued by the APA Board of Trustees. It acknowledges practices and events in psychiatry that contributed to racial inequality, and expresses the organization’s commitment to developing antiracist policies that promote equity in mental health for all.
“This apology is one important step we needed to take to move forward to a more equitable future. The board is issuing this document on Martin Luther King Jr. Day, because we hope that it honors his life’s work of reconciliation and equality. We do not take that legacy or his call to action lightly and will continue our important work,” said Dr. Geller.
One involved the Eastern State Hospital in Williamsburg, Va., the nation’s first psychiatric care facility, founded in 1773.
Eastern State, which for a time in the 1800s was called the Eastern Lunatic Asylum, was not segregated when founded. However, 70 years later, when the 13 founders of what is now the APA met to discuss improvements in mental health care delivery, the treatment system they created and the organization they founded aligned with that era’s racist social and political policies. In this system, Black patients received psychiatric care separately from White patients, the APA said.
The APA also acknowledged failing to act in Black Americans’ best interest at critical points in the United States’ sociopolitical evolution throughout the 19th and 20th centuries.
“This inactivity was notably evident while white supremacists lynched Black people during the Reconstruction Era as well as when Jim Crow segregation was in effect, which led to ‘separate but equal’ standards of care starting in 1896,” the APA said.
Later, the APA failed to declare support for Brown v. Board of Education of Topeka in 1954, along with further major civil rights legislation designed to improve social and psychological conditions for Black people, the organization admitted.
Throughout the decades that followed, psychiatric misdiagnosis among Black, indigenous, and people of color populations were also common, the APA acknowledged.
For example, late 20th century psychiatrists commonly attributed their minority patients’ frustrations to schizophrenia, while categorizing similar behaviors as “neuroticism” in White patients.
The APA pointed to one study which found that APA members diagnosed more Black than White patients with schizophrenia, even when both had otherwise identical clinical presentations.
“This reveals the basis for embedded discrimination within psychiatry that has contributed to reduced quality of care” for Black, indigenous, and people of color, and “perpetuation of dangerous stereotypes,” the APA said.
Saul Levin, MD, the APA’s medical director and CEO, said the Board of Trustees has taken “an important step in issuing this apology. The APA administration is committed to working toward inclusion, health equity, and fairness that everyone deserves.”
The APA Board of Trustees began drafting the apology late last year after it concluded that events and persistent inequities in health care and psychiatry had highlighted an organizational need for action.
The APA’s Presidential Task Force on Structural Racism is continuing with efforts to educate and engage members on the issue and implement changes within the organization.
A version of this article first appeared on Medscape.com.
The American Psychiatric Association has issued a formal apology for its past support of structural racism in psychiatry.
The apology, issued Jan. 18, coincided with the federal holiday honoring the life and work of civil rights activist Dr. Martin Luther King Jr.
“We apologize for our role in perpetrating structural racism in this country, and we hope to begin to make amends for APA’s and psychiatry’s history of actions, intentional and not, that hurt Black, indigenous, and people of color,” APA President Jeffrey Geller, MD, MPH, said in a statement.
The apology was written and issued by the APA Board of Trustees. It acknowledges practices and events in psychiatry that contributed to racial inequality, and expresses the organization’s commitment to developing antiracist policies that promote equity in mental health for all.
“This apology is one important step we needed to take to move forward to a more equitable future. The board is issuing this document on Martin Luther King Jr. Day, because we hope that it honors his life’s work of reconciliation and equality. We do not take that legacy or his call to action lightly and will continue our important work,” said Dr. Geller.
One involved the Eastern State Hospital in Williamsburg, Va., the nation’s first psychiatric care facility, founded in 1773.
Eastern State, which for a time in the 1800s was called the Eastern Lunatic Asylum, was not segregated when founded. However, 70 years later, when the 13 founders of what is now the APA met to discuss improvements in mental health care delivery, the treatment system they created and the organization they founded aligned with that era’s racist social and political policies. In this system, Black patients received psychiatric care separately from White patients, the APA said.
The APA also acknowledged failing to act in Black Americans’ best interest at critical points in the United States’ sociopolitical evolution throughout the 19th and 20th centuries.
“This inactivity was notably evident while white supremacists lynched Black people during the Reconstruction Era as well as when Jim Crow segregation was in effect, which led to ‘separate but equal’ standards of care starting in 1896,” the APA said.
Later, the APA failed to declare support for Brown v. Board of Education of Topeka in 1954, along with further major civil rights legislation designed to improve social and psychological conditions for Black people, the organization admitted.
Throughout the decades that followed, psychiatric misdiagnosis among Black, indigenous, and people of color populations were also common, the APA acknowledged.
For example, late 20th century psychiatrists commonly attributed their minority patients’ frustrations to schizophrenia, while categorizing similar behaviors as “neuroticism” in White patients.
The APA pointed to one study which found that APA members diagnosed more Black than White patients with schizophrenia, even when both had otherwise identical clinical presentations.
“This reveals the basis for embedded discrimination within psychiatry that has contributed to reduced quality of care” for Black, indigenous, and people of color, and “perpetuation of dangerous stereotypes,” the APA said.
Saul Levin, MD, the APA’s medical director and CEO, said the Board of Trustees has taken “an important step in issuing this apology. The APA administration is committed to working toward inclusion, health equity, and fairness that everyone deserves.”
The APA Board of Trustees began drafting the apology late last year after it concluded that events and persistent inequities in health care and psychiatry had highlighted an organizational need for action.
The APA’s Presidential Task Force on Structural Racism is continuing with efforts to educate and engage members on the issue and implement changes within the organization.
A version of this article first appeared on Medscape.com.
FDA clears device to remove dead pancreatic tissue
The Food and Drug Administration has approved the EndoRotor System (Interscope, Inc.) for removal of necrotic tissue in patients with walled-off pancreatic necrosis (WOPN).
“This device has shown its potential to provide a minimally invasive way to remove harmful necrotic pancreatic tissue in patients with walled-off pancreatic necrosis,” Charles Viviano, MD, PhD, acting director, Reproductive, Gastro-Renal, Urological, General Hospital Device and Human Factors Office, FDA Center for Devices and Radiological Health, said in a statement.
“Currently, in order to remove dead tissue from a patient’s necrotic pancreatic cavity, health care providers need to perform an invasive surgery or use other endoscopic tools not specifically indicated to treat this condition. With [this] marketing authorization, patients with walled-off pancreatic necrosis now have a new treatment option,” said Dr. Viviano.
WOPN is a potentially deadly condition that occurs in about 15% of patients with severe pancreatitis. Often, the dead tissue must be removed.
The EndoRotor System is made up of a power console, foot control, specimen trap, and single-use catheter.
The device is used to perform endoscopic necrosectomy. In this procedure, a stent is used to create a portal between the stomach and the necrotic cavity in the pancreas to accommodate a standard endoscope through which the EndoRotor cuts and removes necrotized tissue.
The FDA approved the EndoRotor System on the basis of a clinical trial involving 30 patients with WOPN who underwent a total of 63 direct endoscopic necrosectomies with the EndoRotor System (average, 2.1 procedures per patient).
The effectiveness of the EndoRotor System was determined by how well it cleared pancreatic necrotic tissue measured during CT with contrast before and after the procedure, endoscopy, or MRI 14 to 28 days after the last procedure.
Results showed an average 85% reduction in the amount of necrotic tissue, with half of the patients having 98.5% clearance of necrotic tissue, the FDA said.
Three patients suffered procedure-related serious adverse events (10% complication rate). Two patients experienced gastrointestinal bleeding. One patient had a pneumoperitoneum and later died after suffering from sepsis and multiorgan system failure caused by massive collections of infected pancreatic necrotic tissue.
Other serious adverse events, which were thought to be due to the patient’s underlying condition and not related to the device or procedure, included hematemesis, deep vein thrombosis, and pancreatitis.
The EndoRotor System should not be used for patients with known or suspected pancreatic cancer, and the device will carry a boxed warning stating this.
The FDA said it knows of one patient who died from pancreatic cancer 3 months after having necrotic pancreatic tissue removed with the EndoRotor System.
“This patient did not have a diagnosis of pancreatic cancer prior to treatment, although the patient’s outcome is believed to be unrelated to the device or procedure,” the FDA said.
The EndoRotor System should be used only after patients have undergone other procedures to drain the WOPN.
It is also not appropriate for patients with walled-off necrosis who have a documented pseudoaneurysm greater than 1 cm within the cavity or with intervening gastric varices or unavoidable blood vessels within the access tract.
The EndoRotor System was approved under the de novo premarket review pathway for new low- to moderate-risk devices.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration has approved the EndoRotor System (Interscope, Inc.) for removal of necrotic tissue in patients with walled-off pancreatic necrosis (WOPN).
“This device has shown its potential to provide a minimally invasive way to remove harmful necrotic pancreatic tissue in patients with walled-off pancreatic necrosis,” Charles Viviano, MD, PhD, acting director, Reproductive, Gastro-Renal, Urological, General Hospital Device and Human Factors Office, FDA Center for Devices and Radiological Health, said in a statement.
“Currently, in order to remove dead tissue from a patient’s necrotic pancreatic cavity, health care providers need to perform an invasive surgery or use other endoscopic tools not specifically indicated to treat this condition. With [this] marketing authorization, patients with walled-off pancreatic necrosis now have a new treatment option,” said Dr. Viviano.
WOPN is a potentially deadly condition that occurs in about 15% of patients with severe pancreatitis. Often, the dead tissue must be removed.
The EndoRotor System is made up of a power console, foot control, specimen trap, and single-use catheter.
The device is used to perform endoscopic necrosectomy. In this procedure, a stent is used to create a portal between the stomach and the necrotic cavity in the pancreas to accommodate a standard endoscope through which the EndoRotor cuts and removes necrotized tissue.
The FDA approved the EndoRotor System on the basis of a clinical trial involving 30 patients with WOPN who underwent a total of 63 direct endoscopic necrosectomies with the EndoRotor System (average, 2.1 procedures per patient).
The effectiveness of the EndoRotor System was determined by how well it cleared pancreatic necrotic tissue measured during CT with contrast before and after the procedure, endoscopy, or MRI 14 to 28 days after the last procedure.
Results showed an average 85% reduction in the amount of necrotic tissue, with half of the patients having 98.5% clearance of necrotic tissue, the FDA said.
Three patients suffered procedure-related serious adverse events (10% complication rate). Two patients experienced gastrointestinal bleeding. One patient had a pneumoperitoneum and later died after suffering from sepsis and multiorgan system failure caused by massive collections of infected pancreatic necrotic tissue.
Other serious adverse events, which were thought to be due to the patient’s underlying condition and not related to the device or procedure, included hematemesis, deep vein thrombosis, and pancreatitis.
The EndoRotor System should not be used for patients with known or suspected pancreatic cancer, and the device will carry a boxed warning stating this.
The FDA said it knows of one patient who died from pancreatic cancer 3 months after having necrotic pancreatic tissue removed with the EndoRotor System.
“This patient did not have a diagnosis of pancreatic cancer prior to treatment, although the patient’s outcome is believed to be unrelated to the device or procedure,” the FDA said.
The EndoRotor System should be used only after patients have undergone other procedures to drain the WOPN.
It is also not appropriate for patients with walled-off necrosis who have a documented pseudoaneurysm greater than 1 cm within the cavity or with intervening gastric varices or unavoidable blood vessels within the access tract.
The EndoRotor System was approved under the de novo premarket review pathway for new low- to moderate-risk devices.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration has approved the EndoRotor System (Interscope, Inc.) for removal of necrotic tissue in patients with walled-off pancreatic necrosis (WOPN).
“This device has shown its potential to provide a minimally invasive way to remove harmful necrotic pancreatic tissue in patients with walled-off pancreatic necrosis,” Charles Viviano, MD, PhD, acting director, Reproductive, Gastro-Renal, Urological, General Hospital Device and Human Factors Office, FDA Center for Devices and Radiological Health, said in a statement.
“Currently, in order to remove dead tissue from a patient’s necrotic pancreatic cavity, health care providers need to perform an invasive surgery or use other endoscopic tools not specifically indicated to treat this condition. With [this] marketing authorization, patients with walled-off pancreatic necrosis now have a new treatment option,” said Dr. Viviano.
WOPN is a potentially deadly condition that occurs in about 15% of patients with severe pancreatitis. Often, the dead tissue must be removed.
The EndoRotor System is made up of a power console, foot control, specimen trap, and single-use catheter.
The device is used to perform endoscopic necrosectomy. In this procedure, a stent is used to create a portal between the stomach and the necrotic cavity in the pancreas to accommodate a standard endoscope through which the EndoRotor cuts and removes necrotized tissue.
The FDA approved the EndoRotor System on the basis of a clinical trial involving 30 patients with WOPN who underwent a total of 63 direct endoscopic necrosectomies with the EndoRotor System (average, 2.1 procedures per patient).
The effectiveness of the EndoRotor System was determined by how well it cleared pancreatic necrotic tissue measured during CT with contrast before and after the procedure, endoscopy, or MRI 14 to 28 days after the last procedure.
Results showed an average 85% reduction in the amount of necrotic tissue, with half of the patients having 98.5% clearance of necrotic tissue, the FDA said.
Three patients suffered procedure-related serious adverse events (10% complication rate). Two patients experienced gastrointestinal bleeding. One patient had a pneumoperitoneum and later died after suffering from sepsis and multiorgan system failure caused by massive collections of infected pancreatic necrotic tissue.
Other serious adverse events, which were thought to be due to the patient’s underlying condition and not related to the device or procedure, included hematemesis, deep vein thrombosis, and pancreatitis.
The EndoRotor System should not be used for patients with known or suspected pancreatic cancer, and the device will carry a boxed warning stating this.
The FDA said it knows of one patient who died from pancreatic cancer 3 months after having necrotic pancreatic tissue removed with the EndoRotor System.
“This patient did not have a diagnosis of pancreatic cancer prior to treatment, although the patient’s outcome is believed to be unrelated to the device or procedure,” the FDA said.
The EndoRotor System should be used only after patients have undergone other procedures to drain the WOPN.
It is also not appropriate for patients with walled-off necrosis who have a documented pseudoaneurysm greater than 1 cm within the cavity or with intervening gastric varices or unavoidable blood vessels within the access tract.
The EndoRotor System was approved under the de novo premarket review pathway for new low- to moderate-risk devices.
A version of this article first appeared on Medscape.com.
Cancer treatment delays are deadly: 5- and 10-year data
The COVID-19 pandemic has meant delays in cancer screening, diagnosis, and treatment — and a new study shows just how deadly delaying cancer treatment can be.
The study found evidence that longer time to starting treatment after diagnosis was generally associated with higher mortality across several common cancers, most notably for colon and early-stage lung cancer.
“There is a limit to how long we can safely defer treatment for cancer therapies, pandemic or not, which may be shorter than we think,” lead author Eugene Cone, MD, Combined Harvard Program in Urologic Oncology, Massachusetts General Hospital and Brigham & Women’s Hospital, Boston, told Medscape Medical News.
“When you consider that cancer screening may have been delayed during the pandemic, which would further increase the period between developing a disease and getting therapy, timely treatment for cancer has never been more important,” Cone added.
The study was published online December 14 in JAMA Network Open.
The sooner the better
Using the National Cancer Database, Cone and colleagues identified roughly 2.24 million patients diagnosed with nonmetastatic breast (52%), prostate (38%), colon (4%) and non-small cell lung cancer (NSCLC, 6%) between 2004 and 2015. Treatment and outcome data were analyzed from January to March 2020.
The time-to-treatment initiation (TTI) – the interval between cancer diagnosis and receipt of curative-intent therapy – was categorized as 8 to 60 days (reference), 61 to 120 days, 121 to 180 days, and 181 to 365 days. Median TTI was 32 days for breast, 79 days for prostate, 41 days for NSCLC, and 26 days for colon cancer.
All four cancers benefitted to some degree from a short interval between diagnosis and therapy, the researchers found.
Across all four cancers, increasing TTI was generally associated with higher predicted mortality at 5 and 10 years, although the degree varied by cancer type and stage. The most pronounced association between increasing TTI and mortality was observed for colon and lung cancer.
For example, for stage III colon cancer, 5- and 10-year predicted mortality was 38.9% and 54%, respectively, with TTI of 61 to 120 days, and increased to 47.8% and 63.8%, respectively, with TTI of 181 to 365 days.
Each additional 60-day delay was associated with a 3.2% to 6% increase in 5-year mortality for stage III colon cancer and a 0.9% to 4.6% increase for stage I colon cancer, with a longer 10-year time horizon showing larger effect sizes with increasing TTI.
For stage I NSCLC, 5- and 10-year predicted mortality was 47.4% and 72.6%, respectively, with TTI of 61 to 120 days compared with 47.6% and 72.8%, respectively, with TTI of 181 to 365 days.
For stage I NSCLC, there was a 4% to 6.2% absolute increase in 5-year mortality for increased TTI groups compared with the 8- to 60-day reference group, with larger effect sizes on 10-year mortality. The data precluded conclusions about stage II NSCLC.
“For prostate cancer, deferral of treatment by even a few months was associated with a significant impact on mortality,” Cone told Medscape Medical News.
For high-risk prostate cancer, 5- and 10-year predicted mortality was 12.8% and 31.2%, respectively, with TTI of 61-120 days increasing to 14.1% and 33.8%, respectively with TTI at 181-365 days.
For intermediate-risk prostate cancer, 5- and 10-year predicted mortality was 7.4% and 20.4% with TTI of 61-120 days vs 8.3% and 22.6% with TTI at 181-365 days.
The data show all-cause mortality differences of 2.2% at 5 years and 4.6% at 10 years between high-risk prostate cancer patients who were treated expeditiously vs those waiting 4 to 6 months and differences of 0.9% at 5 years and 2.4% at 10 years for similar intermediate-risk patients.
No surprises
Turning to breast cancer, increased TTI was associated with the most negative survival effects for stage II and III breast cancer.
For stage II breast cancer, for example, 5- and 10-year predicted mortality was 17.7% and 30.5%, respectively, with TTI of 61-120 days vs 21.7% and 36.5% with TTI at 181-365 days.
Even for stage I breast cancer patients, there were significant differences in all-cause mortality with delayed definitive therapy, although the effect size is clinically small, the researchers report.
Patients with stage IA or IB breast cancer who were not treated until 61 to 120 days after diagnosis had 1.3% and 2.3% increased mortality at 5 years and 10 years, respectively, and those waiting longer suffered even greater increases in mortality. “As such, our analysis underscores the importance of timely definitive treatment, even for stage I breast cancer,” the authors write.
Charles Shapiro, MD, director of translational breast cancer research for the Mount Sinai Health System, New York City, was not surprised by the data.
The observation that delays in initiating cancer treatment are associated with worse survival is “not new, as delays in primary surgical treatments and chemotherapy for early-stage disease is an adverse prognostic factor for clinical outcomes,” Shapiro told Medscape Medical News.
“The bottom line is primary surgery and the start of chemotherapy should probably occur as soon as clinically feasible,” said Shapiro, who was not involved in the study.
The authors of an accompanying editorial agree.
This study supports avoiding unnecessary treatment delays and prioritizing timely cancer care, even during the COVID-19 pandemic, write Laura Van Metre Baum, MD, Division of Hematology and Oncology, Vanderbilt University, Nashville, Tennessee, and colleagues.
They note, however, that primary care, “the most important conduit for cancer screening and initial evaluation of new symptoms, has been the hardest hit economically and the most subject to profound disruption and restructuring during the current COVID-19 pandemic.
“In many centers, cancer care delivery has been disrupted and nonstandard therapies offered in an effort to minimize exposure of this high-risk group to the virus. The implications in appropriately balancing the urgency of cancer care and the threat of COVID-19 exposure in the pandemic are more complex,” the editorialists conclude.
Cone, Shapiro, and Van Metre Baum have disclosed no relevant financial relationships. This work won first prize in the Commission on Cancer 2020 Cancer Research Paper Competition and was virtually presented at the Commission on Cancer Plenary Session on October 30, 2020.
A version of this article first appeared on Medscape.com.
The COVID-19 pandemic has meant delays in cancer screening, diagnosis, and treatment — and a new study shows just how deadly delaying cancer treatment can be.
The study found evidence that longer time to starting treatment after diagnosis was generally associated with higher mortality across several common cancers, most notably for colon and early-stage lung cancer.
“There is a limit to how long we can safely defer treatment for cancer therapies, pandemic or not, which may be shorter than we think,” lead author Eugene Cone, MD, Combined Harvard Program in Urologic Oncology, Massachusetts General Hospital and Brigham & Women’s Hospital, Boston, told Medscape Medical News.
“When you consider that cancer screening may have been delayed during the pandemic, which would further increase the period between developing a disease and getting therapy, timely treatment for cancer has never been more important,” Cone added.
The study was published online December 14 in JAMA Network Open.
The sooner the better
Using the National Cancer Database, Cone and colleagues identified roughly 2.24 million patients diagnosed with nonmetastatic breast (52%), prostate (38%), colon (4%) and non-small cell lung cancer (NSCLC, 6%) between 2004 and 2015. Treatment and outcome data were analyzed from January to March 2020.
The time-to-treatment initiation (TTI) – the interval between cancer diagnosis and receipt of curative-intent therapy – was categorized as 8 to 60 days (reference), 61 to 120 days, 121 to 180 days, and 181 to 365 days. Median TTI was 32 days for breast, 79 days for prostate, 41 days for NSCLC, and 26 days for colon cancer.
All four cancers benefitted to some degree from a short interval between diagnosis and therapy, the researchers found.
Across all four cancers, increasing TTI was generally associated with higher predicted mortality at 5 and 10 years, although the degree varied by cancer type and stage. The most pronounced association between increasing TTI and mortality was observed for colon and lung cancer.
For example, for stage III colon cancer, 5- and 10-year predicted mortality was 38.9% and 54%, respectively, with TTI of 61 to 120 days, and increased to 47.8% and 63.8%, respectively, with TTI of 181 to 365 days.
Each additional 60-day delay was associated with a 3.2% to 6% increase in 5-year mortality for stage III colon cancer and a 0.9% to 4.6% increase for stage I colon cancer, with a longer 10-year time horizon showing larger effect sizes with increasing TTI.
For stage I NSCLC, 5- and 10-year predicted mortality was 47.4% and 72.6%, respectively, with TTI of 61 to 120 days compared with 47.6% and 72.8%, respectively, with TTI of 181 to 365 days.
For stage I NSCLC, there was a 4% to 6.2% absolute increase in 5-year mortality for increased TTI groups compared with the 8- to 60-day reference group, with larger effect sizes on 10-year mortality. The data precluded conclusions about stage II NSCLC.
“For prostate cancer, deferral of treatment by even a few months was associated with a significant impact on mortality,” Cone told Medscape Medical News.
For high-risk prostate cancer, 5- and 10-year predicted mortality was 12.8% and 31.2%, respectively, with TTI of 61-120 days increasing to 14.1% and 33.8%, respectively with TTI at 181-365 days.
For intermediate-risk prostate cancer, 5- and 10-year predicted mortality was 7.4% and 20.4% with TTI of 61-120 days vs 8.3% and 22.6% with TTI at 181-365 days.
The data show all-cause mortality differences of 2.2% at 5 years and 4.6% at 10 years between high-risk prostate cancer patients who were treated expeditiously vs those waiting 4 to 6 months and differences of 0.9% at 5 years and 2.4% at 10 years for similar intermediate-risk patients.
No surprises
Turning to breast cancer, increased TTI was associated with the most negative survival effects for stage II and III breast cancer.
For stage II breast cancer, for example, 5- and 10-year predicted mortality was 17.7% and 30.5%, respectively, with TTI of 61-120 days vs 21.7% and 36.5% with TTI at 181-365 days.
Even for stage I breast cancer patients, there were significant differences in all-cause mortality with delayed definitive therapy, although the effect size is clinically small, the researchers report.
Patients with stage IA or IB breast cancer who were not treated until 61 to 120 days after diagnosis had 1.3% and 2.3% increased mortality at 5 years and 10 years, respectively, and those waiting longer suffered even greater increases in mortality. “As such, our analysis underscores the importance of timely definitive treatment, even for stage I breast cancer,” the authors write.
Charles Shapiro, MD, director of translational breast cancer research for the Mount Sinai Health System, New York City, was not surprised by the data.
The observation that delays in initiating cancer treatment are associated with worse survival is “not new, as delays in primary surgical treatments and chemotherapy for early-stage disease is an adverse prognostic factor for clinical outcomes,” Shapiro told Medscape Medical News.
“The bottom line is primary surgery and the start of chemotherapy should probably occur as soon as clinically feasible,” said Shapiro, who was not involved in the study.
The authors of an accompanying editorial agree.
This study supports avoiding unnecessary treatment delays and prioritizing timely cancer care, even during the COVID-19 pandemic, write Laura Van Metre Baum, MD, Division of Hematology and Oncology, Vanderbilt University, Nashville, Tennessee, and colleagues.
They note, however, that primary care, “the most important conduit for cancer screening and initial evaluation of new symptoms, has been the hardest hit economically and the most subject to profound disruption and restructuring during the current COVID-19 pandemic.
“In many centers, cancer care delivery has been disrupted and nonstandard therapies offered in an effort to minimize exposure of this high-risk group to the virus. The implications in appropriately balancing the urgency of cancer care and the threat of COVID-19 exposure in the pandemic are more complex,” the editorialists conclude.
Cone, Shapiro, and Van Metre Baum have disclosed no relevant financial relationships. This work won first prize in the Commission on Cancer 2020 Cancer Research Paper Competition and was virtually presented at the Commission on Cancer Plenary Session on October 30, 2020.
A version of this article first appeared on Medscape.com.
The COVID-19 pandemic has meant delays in cancer screening, diagnosis, and treatment — and a new study shows just how deadly delaying cancer treatment can be.
The study found evidence that longer time to starting treatment after diagnosis was generally associated with higher mortality across several common cancers, most notably for colon and early-stage lung cancer.
“There is a limit to how long we can safely defer treatment for cancer therapies, pandemic or not, which may be shorter than we think,” lead author Eugene Cone, MD, Combined Harvard Program in Urologic Oncology, Massachusetts General Hospital and Brigham & Women’s Hospital, Boston, told Medscape Medical News.
“When you consider that cancer screening may have been delayed during the pandemic, which would further increase the period between developing a disease and getting therapy, timely treatment for cancer has never been more important,” Cone added.
The study was published online December 14 in JAMA Network Open.
The sooner the better
Using the National Cancer Database, Cone and colleagues identified roughly 2.24 million patients diagnosed with nonmetastatic breast (52%), prostate (38%), colon (4%) and non-small cell lung cancer (NSCLC, 6%) between 2004 and 2015. Treatment and outcome data were analyzed from January to March 2020.
The time-to-treatment initiation (TTI) – the interval between cancer diagnosis and receipt of curative-intent therapy – was categorized as 8 to 60 days (reference), 61 to 120 days, 121 to 180 days, and 181 to 365 days. Median TTI was 32 days for breast, 79 days for prostate, 41 days for NSCLC, and 26 days for colon cancer.
All four cancers benefitted to some degree from a short interval between diagnosis and therapy, the researchers found.
Across all four cancers, increasing TTI was generally associated with higher predicted mortality at 5 and 10 years, although the degree varied by cancer type and stage. The most pronounced association between increasing TTI and mortality was observed for colon and lung cancer.
For example, for stage III colon cancer, 5- and 10-year predicted mortality was 38.9% and 54%, respectively, with TTI of 61 to 120 days, and increased to 47.8% and 63.8%, respectively, with TTI of 181 to 365 days.
Each additional 60-day delay was associated with a 3.2% to 6% increase in 5-year mortality for stage III colon cancer and a 0.9% to 4.6% increase for stage I colon cancer, with a longer 10-year time horizon showing larger effect sizes with increasing TTI.
For stage I NSCLC, 5- and 10-year predicted mortality was 47.4% and 72.6%, respectively, with TTI of 61 to 120 days compared with 47.6% and 72.8%, respectively, with TTI of 181 to 365 days.
For stage I NSCLC, there was a 4% to 6.2% absolute increase in 5-year mortality for increased TTI groups compared with the 8- to 60-day reference group, with larger effect sizes on 10-year mortality. The data precluded conclusions about stage II NSCLC.
“For prostate cancer, deferral of treatment by even a few months was associated with a significant impact on mortality,” Cone told Medscape Medical News.
For high-risk prostate cancer, 5- and 10-year predicted mortality was 12.8% and 31.2%, respectively, with TTI of 61-120 days increasing to 14.1% and 33.8%, respectively with TTI at 181-365 days.
For intermediate-risk prostate cancer, 5- and 10-year predicted mortality was 7.4% and 20.4% with TTI of 61-120 days vs 8.3% and 22.6% with TTI at 181-365 days.
The data show all-cause mortality differences of 2.2% at 5 years and 4.6% at 10 years between high-risk prostate cancer patients who were treated expeditiously vs those waiting 4 to 6 months and differences of 0.9% at 5 years and 2.4% at 10 years for similar intermediate-risk patients.
No surprises
Turning to breast cancer, increased TTI was associated with the most negative survival effects for stage II and III breast cancer.
For stage II breast cancer, for example, 5- and 10-year predicted mortality was 17.7% and 30.5%, respectively, with TTI of 61-120 days vs 21.7% and 36.5% with TTI at 181-365 days.
Even for stage I breast cancer patients, there were significant differences in all-cause mortality with delayed definitive therapy, although the effect size is clinically small, the researchers report.
Patients with stage IA or IB breast cancer who were not treated until 61 to 120 days after diagnosis had 1.3% and 2.3% increased mortality at 5 years and 10 years, respectively, and those waiting longer suffered even greater increases in mortality. “As such, our analysis underscores the importance of timely definitive treatment, even for stage I breast cancer,” the authors write.
Charles Shapiro, MD, director of translational breast cancer research for the Mount Sinai Health System, New York City, was not surprised by the data.
The observation that delays in initiating cancer treatment are associated with worse survival is “not new, as delays in primary surgical treatments and chemotherapy for early-stage disease is an adverse prognostic factor for clinical outcomes,” Shapiro told Medscape Medical News.
“The bottom line is primary surgery and the start of chemotherapy should probably occur as soon as clinically feasible,” said Shapiro, who was not involved in the study.
The authors of an accompanying editorial agree.
This study supports avoiding unnecessary treatment delays and prioritizing timely cancer care, even during the COVID-19 pandemic, write Laura Van Metre Baum, MD, Division of Hematology and Oncology, Vanderbilt University, Nashville, Tennessee, and colleagues.
They note, however, that primary care, “the most important conduit for cancer screening and initial evaluation of new symptoms, has been the hardest hit economically and the most subject to profound disruption and restructuring during the current COVID-19 pandemic.
“In many centers, cancer care delivery has been disrupted and nonstandard therapies offered in an effort to minimize exposure of this high-risk group to the virus. The implications in appropriately balancing the urgency of cancer care and the threat of COVID-19 exposure in the pandemic are more complex,” the editorialists conclude.
Cone, Shapiro, and Van Metre Baum have disclosed no relevant financial relationships. This work won first prize in the Commission on Cancer 2020 Cancer Research Paper Competition and was virtually presented at the Commission on Cancer Plenary Session on October 30, 2020.
A version of this article first appeared on Medscape.com.
FDA OKs osimertinib as first adjuvant drug for NSCLC
Osimertinib was first approved in the US in 2018 for the first-line treatment of patients with metastatic EGFR-mutated NSCLC.
With this new indication, “patients may be treated with this targeted therapy in an earlier and potentially more curative stage of non-small cell lung cancer,” Richard Pazdur, MD, director of the FDA’s Oncology Center of Excellence and acting director of the Office of Oncologic Diseases in the FDA’s Center for Drug Evaluation and Research, said in a news release.
The expanded indication is based on results of the ADAURA clinical trial, which compared osimertinib with placebo following complete resection of localized or locally advanced NSCLC with negative margins.
In the trial, adjuvant osimertinib reduced the relative risk of disease recurrence or death by 83% in patients with stage II and IIIA disease (hazard ratio [HR], 0.17; 95% CI, 0.12 - 0.23; P < .0001).
Disease-free survival (DFS) in the overall trial population of patients with stage IB-IIIA disease showed osimertinib reduced the risk of disease recurrence or death by 80% (HR, 0.20; 95% CI, 0.15 - 0.27; P < .0001).
At 2 years, 89% of patients treated with the targeted agent remained alive and disease free vs 52% on placebo after surgery. The safety and tolerability of osimertinib in the adjuvant setting was consistent with previous trials in the metastatic setting.
The trial of 682 patients was unblinded early and halted on the recommendation of the independent data-monitoring committee, because of the efficacy of osimertinib.
“If I were on the committee, I would have done the same thing. These are extraordinary results,” study investigator Roy S. Herbst, MD, PhD, chief of medical oncology at the Yale Cancer Center, New Haven, Connecticut, said at a press briefing prior to the study presentation at the American Society of Clinical Oncology’s (ASCO) virtual scientific program last spring.
In a Medscape commentary, Mark Kris, MD, of Memorial Sloan Kettering Cancer Center in New York City, said the data with osimertinib in the adjuvant setting are “important and practice-changing.”
“The potential for this drug to improve outcomes has been there for a long time. This phase 3 randomized trial presented at the plenary session of ASCO showed a more than doubling of disease-free survival at 2 years. It shows that we can use therapies in the earlier stages of disease,” Kris noted.
“This approval dispels the notion that treatment is over after surgery and chemotherapy, as the ADAURA results show that Tagrisso can dramatically change the course of this disease,” Dave Fredrickson, executive vice president, AstraZeneca oncology business unit, said in a news release.
Osimertinib had orphan drug status and breakthrough therapy designation for treatment of EGFR mutation-positive NSCLC.
A version of this article first appeared on Medscape.com.
Osimertinib was first approved in the US in 2018 for the first-line treatment of patients with metastatic EGFR-mutated NSCLC.
With this new indication, “patients may be treated with this targeted therapy in an earlier and potentially more curative stage of non-small cell lung cancer,” Richard Pazdur, MD, director of the FDA’s Oncology Center of Excellence and acting director of the Office of Oncologic Diseases in the FDA’s Center for Drug Evaluation and Research, said in a news release.
The expanded indication is based on results of the ADAURA clinical trial, which compared osimertinib with placebo following complete resection of localized or locally advanced NSCLC with negative margins.
In the trial, adjuvant osimertinib reduced the relative risk of disease recurrence or death by 83% in patients with stage II and IIIA disease (hazard ratio [HR], 0.17; 95% CI, 0.12 - 0.23; P < .0001).
Disease-free survival (DFS) in the overall trial population of patients with stage IB-IIIA disease showed osimertinib reduced the risk of disease recurrence or death by 80% (HR, 0.20; 95% CI, 0.15 - 0.27; P < .0001).
At 2 years, 89% of patients treated with the targeted agent remained alive and disease free vs 52% on placebo after surgery. The safety and tolerability of osimertinib in the adjuvant setting was consistent with previous trials in the metastatic setting.
The trial of 682 patients was unblinded early and halted on the recommendation of the independent data-monitoring committee, because of the efficacy of osimertinib.
“If I were on the committee, I would have done the same thing. These are extraordinary results,” study investigator Roy S. Herbst, MD, PhD, chief of medical oncology at the Yale Cancer Center, New Haven, Connecticut, said at a press briefing prior to the study presentation at the American Society of Clinical Oncology’s (ASCO) virtual scientific program last spring.
In a Medscape commentary, Mark Kris, MD, of Memorial Sloan Kettering Cancer Center in New York City, said the data with osimertinib in the adjuvant setting are “important and practice-changing.”
“The potential for this drug to improve outcomes has been there for a long time. This phase 3 randomized trial presented at the plenary session of ASCO showed a more than doubling of disease-free survival at 2 years. It shows that we can use therapies in the earlier stages of disease,” Kris noted.
“This approval dispels the notion that treatment is over after surgery and chemotherapy, as the ADAURA results show that Tagrisso can dramatically change the course of this disease,” Dave Fredrickson, executive vice president, AstraZeneca oncology business unit, said in a news release.
Osimertinib had orphan drug status and breakthrough therapy designation for treatment of EGFR mutation-positive NSCLC.
A version of this article first appeared on Medscape.com.
Osimertinib was first approved in the US in 2018 for the first-line treatment of patients with metastatic EGFR-mutated NSCLC.
With this new indication, “patients may be treated with this targeted therapy in an earlier and potentially more curative stage of non-small cell lung cancer,” Richard Pazdur, MD, director of the FDA’s Oncology Center of Excellence and acting director of the Office of Oncologic Diseases in the FDA’s Center for Drug Evaluation and Research, said in a news release.
The expanded indication is based on results of the ADAURA clinical trial, which compared osimertinib with placebo following complete resection of localized or locally advanced NSCLC with negative margins.
In the trial, adjuvant osimertinib reduced the relative risk of disease recurrence or death by 83% in patients with stage II and IIIA disease (hazard ratio [HR], 0.17; 95% CI, 0.12 - 0.23; P < .0001).
Disease-free survival (DFS) in the overall trial population of patients with stage IB-IIIA disease showed osimertinib reduced the risk of disease recurrence or death by 80% (HR, 0.20; 95% CI, 0.15 - 0.27; P < .0001).
At 2 years, 89% of patients treated with the targeted agent remained alive and disease free vs 52% on placebo after surgery. The safety and tolerability of osimertinib in the adjuvant setting was consistent with previous trials in the metastatic setting.
The trial of 682 patients was unblinded early and halted on the recommendation of the independent data-monitoring committee, because of the efficacy of osimertinib.
“If I were on the committee, I would have done the same thing. These are extraordinary results,” study investigator Roy S. Herbst, MD, PhD, chief of medical oncology at the Yale Cancer Center, New Haven, Connecticut, said at a press briefing prior to the study presentation at the American Society of Clinical Oncology’s (ASCO) virtual scientific program last spring.
In a Medscape commentary, Mark Kris, MD, of Memorial Sloan Kettering Cancer Center in New York City, said the data with osimertinib in the adjuvant setting are “important and practice-changing.”
“The potential for this drug to improve outcomes has been there for a long time. This phase 3 randomized trial presented at the plenary session of ASCO showed a more than doubling of disease-free survival at 2 years. It shows that we can use therapies in the earlier stages of disease,” Kris noted.
“This approval dispels the notion that treatment is over after surgery and chemotherapy, as the ADAURA results show that Tagrisso can dramatically change the course of this disease,” Dave Fredrickson, executive vice president, AstraZeneca oncology business unit, said in a news release.
Osimertinib had orphan drug status and breakthrough therapy designation for treatment of EGFR mutation-positive NSCLC.
A version of this article first appeared on Medscape.com.
Give psych patients the COVID vaccination now, experts say
With COVID-19 vaccinations now underway, mental health experts around the world continue to push for patients with serious mental illness (SMI) to be considered a high-priority group for the vaccine.
Research shows that patients with SMI are at increased risk of being infected with SARS-CoV-2 and have higher rates of hospitalization and poor outcomes, Nicola Warren, MBBS, University of Queensland, Brisbane, Australia, and coauthors write in a viewpoint published online Dec. 15 in JAMA Psychiatry

Factors behind the worse outcomes in individuals with SMI include concomitant medications, poorer premorbid general health, physical comorbidity, reduced access to medical care, and environmental and lifestyle factors such as lower socioeconomic status, overcrowding, smoking, and obesity.
“In light of these vulnerabilities, it is important that people with SMI are a priority group to receive a vaccination,” Dr. Warren and colleagues say.
Yet there are challenges at the individual and public health level in getting people with SMI vaccinated against COVID-19, they point out.
Challenges at the individual level include getting people with SMI to recognize the importance of the vaccine and combating negative beliefs about safety and misconceptions that the vaccine itself can make them sick with COVID-19.
Mental health professionals are “uniquely skilled” to deliver vaccine education, “being able to adapt for those with communication difficulties and balance factors influencing decision-making,” Dr. Warren and colleagues write.
, like getting to a vaccination clinic.
Research has shown that running vaccination clinics parallel to mental health services can boost vaccination rates by 25%, the authors note. Therefore, one solution may be to embed vaccination clinics within mental health services, Dr. Warren and colleagues suggest.
Join the chorus
Plans and policies to ensure rapid delivery of the COVID-19 vaccine are “vital,” they conclude. “Mental health clinicians have a key role in advocating for priority access to a COVID-19 vaccination for those with SMI, as well as facilitating its uptake,” they add.
Dr. Warren and her colleagues join a chorus of other mental health care providers who have sounded the alarm on the risks of COVID-19 for patients with SMI and the need to get them vaccinated early.
In a perspective article published last month in World Psychiatry, Marc De Hert, MD, PhD, professor of psychiatry at KU Leuven (Belgium), and coauthors called for individuals with SMI to have priority status for any COVID-19 vaccine, as reported by this news organization.
Dr. De Hert and colleagues noted that there is an ethical duty to prioritize vaccination for people with SMI given their increased risk of worse outcomes following COVID-19 infection and the structural barriers faced by people with SMI in accessing a vaccine.
Joining the chorus, Benjamin Druss, MD, MPH, from Emory University, Atlanta, Georgia, warned in a JAMA Psychiatry viewpoint in April that the COVID-19 pandemic represents a looming crisis for patients with SMI and the health care systems that serve them.
“Careful planning and execution at multiple levels will be essential for minimizing the adverse outcomes of this pandemic for this vulnerable population,” Dr. Druss wrote.
The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
With COVID-19 vaccinations now underway, mental health experts around the world continue to push for patients with serious mental illness (SMI) to be considered a high-priority group for the vaccine.
Research shows that patients with SMI are at increased risk of being infected with SARS-CoV-2 and have higher rates of hospitalization and poor outcomes, Nicola Warren, MBBS, University of Queensland, Brisbane, Australia, and coauthors write in a viewpoint published online Dec. 15 in JAMA Psychiatry
Factors behind the worse outcomes in individuals with SMI include concomitant medications, poorer premorbid general health, physical comorbidity, reduced access to medical care, and environmental and lifestyle factors such as lower socioeconomic status, overcrowding, smoking, and obesity.
“In light of these vulnerabilities, it is important that people with SMI are a priority group to receive a vaccination,” Dr. Warren and colleagues say.
Yet there are challenges at the individual and public health level in getting people with SMI vaccinated against COVID-19, they point out.
Challenges at the individual level include getting people with SMI to recognize the importance of the vaccine and combating negative beliefs about safety and misconceptions that the vaccine itself can make them sick with COVID-19.
Mental health professionals are “uniquely skilled” to deliver vaccine education, “being able to adapt for those with communication difficulties and balance factors influencing decision-making,” Dr. Warren and colleagues write.
, like getting to a vaccination clinic.
Research has shown that running vaccination clinics parallel to mental health services can boost vaccination rates by 25%, the authors note. Therefore, one solution may be to embed vaccination clinics within mental health services, Dr. Warren and colleagues suggest.
Join the chorus
Plans and policies to ensure rapid delivery of the COVID-19 vaccine are “vital,” they conclude. “Mental health clinicians have a key role in advocating for priority access to a COVID-19 vaccination for those with SMI, as well as facilitating its uptake,” they add.
Dr. Warren and her colleagues join a chorus of other mental health care providers who have sounded the alarm on the risks of COVID-19 for patients with SMI and the need to get them vaccinated early.
In a perspective article published last month in World Psychiatry, Marc De Hert, MD, PhD, professor of psychiatry at KU Leuven (Belgium), and coauthors called for individuals with SMI to have priority status for any COVID-19 vaccine, as reported by this news organization.
Dr. De Hert and colleagues noted that there is an ethical duty to prioritize vaccination for people with SMI given their increased risk of worse outcomes following COVID-19 infection and the structural barriers faced by people with SMI in accessing a vaccine.
Joining the chorus, Benjamin Druss, MD, MPH, from Emory University, Atlanta, Georgia, warned in a JAMA Psychiatry viewpoint in April that the COVID-19 pandemic represents a looming crisis for patients with SMI and the health care systems that serve them.
“Careful planning and execution at multiple levels will be essential for minimizing the adverse outcomes of this pandemic for this vulnerable population,” Dr. Druss wrote.
The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
With COVID-19 vaccinations now underway, mental health experts around the world continue to push for patients with serious mental illness (SMI) to be considered a high-priority group for the vaccine.
Research shows that patients with SMI are at increased risk of being infected with SARS-CoV-2 and have higher rates of hospitalization and poor outcomes, Nicola Warren, MBBS, University of Queensland, Brisbane, Australia, and coauthors write in a viewpoint published online Dec. 15 in JAMA Psychiatry
Factors behind the worse outcomes in individuals with SMI include concomitant medications, poorer premorbid general health, physical comorbidity, reduced access to medical care, and environmental and lifestyle factors such as lower socioeconomic status, overcrowding, smoking, and obesity.
“In light of these vulnerabilities, it is important that people with SMI are a priority group to receive a vaccination,” Dr. Warren and colleagues say.
Yet there are challenges at the individual and public health level in getting people with SMI vaccinated against COVID-19, they point out.
Challenges at the individual level include getting people with SMI to recognize the importance of the vaccine and combating negative beliefs about safety and misconceptions that the vaccine itself can make them sick with COVID-19.
Mental health professionals are “uniquely skilled” to deliver vaccine education, “being able to adapt for those with communication difficulties and balance factors influencing decision-making,” Dr. Warren and colleagues write.
, like getting to a vaccination clinic.
Research has shown that running vaccination clinics parallel to mental health services can boost vaccination rates by 25%, the authors note. Therefore, one solution may be to embed vaccination clinics within mental health services, Dr. Warren and colleagues suggest.
Join the chorus
Plans and policies to ensure rapid delivery of the COVID-19 vaccine are “vital,” they conclude. “Mental health clinicians have a key role in advocating for priority access to a COVID-19 vaccination for those with SMI, as well as facilitating its uptake,” they add.
Dr. Warren and her colleagues join a chorus of other mental health care providers who have sounded the alarm on the risks of COVID-19 for patients with SMI and the need to get them vaccinated early.
In a perspective article published last month in World Psychiatry, Marc De Hert, MD, PhD, professor of psychiatry at KU Leuven (Belgium), and coauthors called for individuals with SMI to have priority status for any COVID-19 vaccine, as reported by this news organization.
Dr. De Hert and colleagues noted that there is an ethical duty to prioritize vaccination for people with SMI given their increased risk of worse outcomes following COVID-19 infection and the structural barriers faced by people with SMI in accessing a vaccine.
Joining the chorus, Benjamin Druss, MD, MPH, from Emory University, Atlanta, Georgia, warned in a JAMA Psychiatry viewpoint in April that the COVID-19 pandemic represents a looming crisis for patients with SMI and the health care systems that serve them.
“Careful planning and execution at multiple levels will be essential for minimizing the adverse outcomes of this pandemic for this vulnerable population,” Dr. Druss wrote.
The authors have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FDA expands belimumab indication to adults with lupus nephritis
The U.S. Food and Drug Administration has expanded the indication for belimumab (Benlysta) to adults with active lupus nephritis who are receiving standard therapy.

Roughly 40% of patients with systemic lupus erythematosus (SLE) develop lupus nephritis (LN), which causes inflammation in the kidneys and can lead to end-stage kidney disease.
“Benlysta is the first medicine approved to treat systemic lupus and adults with active lupus nephritis, an important treatment advance for patients with this incurable autoimmune disease,” Hal Barron, MD, GlaxoSmithKline’s chief scientific officer and president of research and development, said in a company news release.
Belimumab IV infusion was first approved in the United States in March 2011 for adults with SLE. The FDA approved belimumab IV infusion for use in children as young as age 5 years with SLE in 2019.
Both the IV and subcutaneous formulations are now indicated in the United States for adults with SLE and LN.
Belimumab is a B-lymphocyte stimulator protein inhibitor that is thought to decrease the amount of abnormal B cells; the latter are thought to play a role in lupus.
The expanded indication for belimumab for patients with LN is based on findings from the BLISS-LN phase 3 trial, published in The New England Journal of Medicine in September.
“Neutralizing B-cell activating factor and down-regulating autoreactive B-cell function in kidneys” represents a “compelling therapeutic approach to lupus nephritis,” the lead investigator of BLISS-LN, Richard Furie, MD, told the online annual Perspectives in Rheumatic Diseases meeting recently.
“In the 4 decades I have been caring for people with lupus, we have not been able to achieve remission in more than just one-third of patients with lupus nephritis, and despite all of our efforts, 10%-30% of patients with lupus kidney disease still progress to end-stage kidney disease,” Dr. Furie, who is chief of the division of rheumatology at Northwell Health, notes in the GSK statement.
“The data from the BLISS-LN study show that Benlysta added to standard therapy not only increased response rates over 2 years, but it also prevented worsening of kidney disease in patients with active lupus nephritis, compared to standard therapy alone,” he added.
BLISS-LN study: Belimumab effect seen mostly in those on MMF
BLISS-LN enrolled 448 adults with biopsy-confirmed active LN. Half were randomly allocated to receive IV belimumab (10 mg/kg) plus standard therapy (mycophenolate mofetil for induction and maintenance or cyclophosphamide for induction followed by azathioprine for maintenance, with steroids) and half to receive placebo plus standard therapy.
At 2 years, significantly more patients in the belimumab group than in the placebo group had a primary efficacy renal response (43% vs. 32%; odds ratio, 1.6; 95% confidence interval, 1.0- 2.3; P = .03).
This primary endpoint was defined as a ratio of urinary protein to creatinine of ≤0.7, an estimated glomerular filtration rate that was no worse than 20% below the value before the renal flare or ≥60 mL per minute per 1.73 m2 of body surface area, without use of rescue therapy.
The risk for a renal-related event or death was also significantly lower among patients who received belimumab than among those who received placebo (hazard ratio, 0.51; P = .001). The safety profile of belimumab was consistent with that observed in prior studies.
But in a commentary that accompanied the publication of BLISS-LN, editorialists noted that “most of the treatment effect was seen in patients who had received mycophenolate mofetil. No benefit was present in the subgroup of patients who received cyclophosphamide-azathioprine.”
In addition, induction treatment was not randomly assigned, editorialists Michael Ward, MD, MPH, and Maria Tektonidou, MD, PhD, noted.
“If patients with more severe nephritis were preferentially treated with cyclophosphamide, a likely inclination among most physicians, the trial may be telling us that belimumab enhances responses only among less severely affected patients,” observed Dr. Ward, who is with the National Institutes of Health, and Dr. Tektonidou, of the National and Kopodistrian University, in Athens.
A version of this article first appeared on Medscape.com.
The U.S. Food and Drug Administration has expanded the indication for belimumab (Benlysta) to adults with active lupus nephritis who are receiving standard therapy.
Roughly 40% of patients with systemic lupus erythematosus (SLE) develop lupus nephritis (LN), which causes inflammation in the kidneys and can lead to end-stage kidney disease.
“Benlysta is the first medicine approved to treat systemic lupus and adults with active lupus nephritis, an important treatment advance for patients with this incurable autoimmune disease,” Hal Barron, MD, GlaxoSmithKline’s chief scientific officer and president of research and development, said in a company news release.
Belimumab IV infusion was first approved in the United States in March 2011 for adults with SLE. The FDA approved belimumab IV infusion for use in children as young as age 5 years with SLE in 2019.
Both the IV and subcutaneous formulations are now indicated in the United States for adults with SLE and LN.
Belimumab is a B-lymphocyte stimulator protein inhibitor that is thought to decrease the amount of abnormal B cells; the latter are thought to play a role in lupus.
The expanded indication for belimumab for patients with LN is based on findings from the BLISS-LN phase 3 trial, published in The New England Journal of Medicine in September.
“Neutralizing B-cell activating factor and down-regulating autoreactive B-cell function in kidneys” represents a “compelling therapeutic approach to lupus nephritis,” the lead investigator of BLISS-LN, Richard Furie, MD, told the online annual Perspectives in Rheumatic Diseases meeting recently.
“In the 4 decades I have been caring for people with lupus, we have not been able to achieve remission in more than just one-third of patients with lupus nephritis, and despite all of our efforts, 10%-30% of patients with lupus kidney disease still progress to end-stage kidney disease,” Dr. Furie, who is chief of the division of rheumatology at Northwell Health, notes in the GSK statement.
“The data from the BLISS-LN study show that Benlysta added to standard therapy not only increased response rates over 2 years, but it also prevented worsening of kidney disease in patients with active lupus nephritis, compared to standard therapy alone,” he added.
BLISS-LN study: Belimumab effect seen mostly in those on MMF
BLISS-LN enrolled 448 adults with biopsy-confirmed active LN. Half were randomly allocated to receive IV belimumab (10 mg/kg) plus standard therapy (mycophenolate mofetil for induction and maintenance or cyclophosphamide for induction followed by azathioprine for maintenance, with steroids) and half to receive placebo plus standard therapy.
At 2 years, significantly more patients in the belimumab group than in the placebo group had a primary efficacy renal response (43% vs. 32%; odds ratio, 1.6; 95% confidence interval, 1.0- 2.3; P = .03).
This primary endpoint was defined as a ratio of urinary protein to creatinine of ≤0.7, an estimated glomerular filtration rate that was no worse than 20% below the value before the renal flare or ≥60 mL per minute per 1.73 m2 of body surface area, without use of rescue therapy.
The risk for a renal-related event or death was also significantly lower among patients who received belimumab than among those who received placebo (hazard ratio, 0.51; P = .001). The safety profile of belimumab was consistent with that observed in prior studies.
But in a commentary that accompanied the publication of BLISS-LN, editorialists noted that “most of the treatment effect was seen in patients who had received mycophenolate mofetil. No benefit was present in the subgroup of patients who received cyclophosphamide-azathioprine.”
In addition, induction treatment was not randomly assigned, editorialists Michael Ward, MD, MPH, and Maria Tektonidou, MD, PhD, noted.
“If patients with more severe nephritis were preferentially treated with cyclophosphamide, a likely inclination among most physicians, the trial may be telling us that belimumab enhances responses only among less severely affected patients,” observed Dr. Ward, who is with the National Institutes of Health, and Dr. Tektonidou, of the National and Kopodistrian University, in Athens.
A version of this article first appeared on Medscape.com.
The U.S. Food and Drug Administration has expanded the indication for belimumab (Benlysta) to adults with active lupus nephritis who are receiving standard therapy.
Roughly 40% of patients with systemic lupus erythematosus (SLE) develop lupus nephritis (LN), which causes inflammation in the kidneys and can lead to end-stage kidney disease.
“Benlysta is the first medicine approved to treat systemic lupus and adults with active lupus nephritis, an important treatment advance for patients with this incurable autoimmune disease,” Hal Barron, MD, GlaxoSmithKline’s chief scientific officer and president of research and development, said in a company news release.
Belimumab IV infusion was first approved in the United States in March 2011 for adults with SLE. The FDA approved belimumab IV infusion for use in children as young as age 5 years with SLE in 2019.
Both the IV and subcutaneous formulations are now indicated in the United States for adults with SLE and LN.
Belimumab is a B-lymphocyte stimulator protein inhibitor that is thought to decrease the amount of abnormal B cells; the latter are thought to play a role in lupus.
The expanded indication for belimumab for patients with LN is based on findings from the BLISS-LN phase 3 trial, published in The New England Journal of Medicine in September.
“Neutralizing B-cell activating factor and down-regulating autoreactive B-cell function in kidneys” represents a “compelling therapeutic approach to lupus nephritis,” the lead investigator of BLISS-LN, Richard Furie, MD, told the online annual Perspectives in Rheumatic Diseases meeting recently.
“In the 4 decades I have been caring for people with lupus, we have not been able to achieve remission in more than just one-third of patients with lupus nephritis, and despite all of our efforts, 10%-30% of patients with lupus kidney disease still progress to end-stage kidney disease,” Dr. Furie, who is chief of the division of rheumatology at Northwell Health, notes in the GSK statement.
“The data from the BLISS-LN study show that Benlysta added to standard therapy not only increased response rates over 2 years, but it also prevented worsening of kidney disease in patients with active lupus nephritis, compared to standard therapy alone,” he added.
BLISS-LN study: Belimumab effect seen mostly in those on MMF
BLISS-LN enrolled 448 adults with biopsy-confirmed active LN. Half were randomly allocated to receive IV belimumab (10 mg/kg) plus standard therapy (mycophenolate mofetil for induction and maintenance or cyclophosphamide for induction followed by azathioprine for maintenance, with steroids) and half to receive placebo plus standard therapy.
At 2 years, significantly more patients in the belimumab group than in the placebo group had a primary efficacy renal response (43% vs. 32%; odds ratio, 1.6; 95% confidence interval, 1.0- 2.3; P = .03).
This primary endpoint was defined as a ratio of urinary protein to creatinine of ≤0.7, an estimated glomerular filtration rate that was no worse than 20% below the value before the renal flare or ≥60 mL per minute per 1.73 m2 of body surface area, without use of rescue therapy.
The risk for a renal-related event or death was also significantly lower among patients who received belimumab than among those who received placebo (hazard ratio, 0.51; P = .001). The safety profile of belimumab was consistent with that observed in prior studies.
But in a commentary that accompanied the publication of BLISS-LN, editorialists noted that “most of the treatment effect was seen in patients who had received mycophenolate mofetil. No benefit was present in the subgroup of patients who received cyclophosphamide-azathioprine.”
In addition, induction treatment was not randomly assigned, editorialists Michael Ward, MD, MPH, and Maria Tektonidou, MD, PhD, noted.
“If patients with more severe nephritis were preferentially treated with cyclophosphamide, a likely inclination among most physicians, the trial may be telling us that belimumab enhances responses only among less severely affected patients,” observed Dr. Ward, who is with the National Institutes of Health, and Dr. Tektonidou, of the National and Kopodistrian University, in Athens.
A version of this article first appeared on Medscape.com.