User login
Adenoma detection rates affect CRC rates, mortality
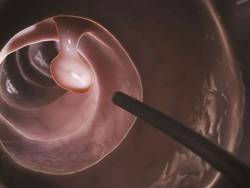
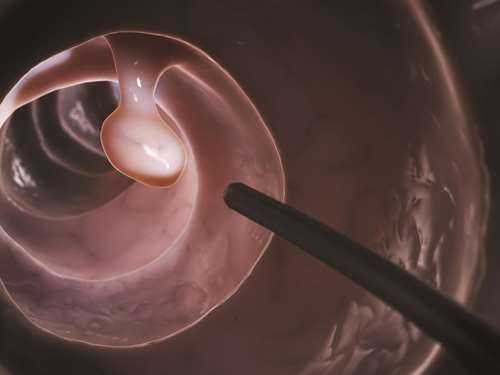
In an average-risk population, screening colonoscopies yield different incidences of colorectal cancer and different cancer-related mortality, depending on the operators’ adenoma detection rates, according to a report published online in JAMA.
Adenoma detection rates vary dramatically among gastroenterologists, and patients of physicians who have lower ADRs are known to have higher rates of both colorectal cancer and fatal colorectal cancer. But little is known about the effect different ADRs have on the lifetime benefits and risks of colonoscopy screening programs on average-risk populations. It is possible that the harms of high ADRs outweigh the benefits. For example, higher ADRs may signal increased detection of small low-risk polyps, leading to more surveillance colonoscopies as well as more complications – all from lesions that may well have been benign, said Reinier G.S. Meester of the department of public health, Erasmus University Medical Center, Rotterdam (the Netherlands), and his associat
They examined various possible outcomes for a colonoscopy screening program at different levels of adenoma detection using microsimulation modeling that incorporated data from a large U.S. HMO concerning 57,588 screening colonoscopies performed by 136 physicians between 1998 and 2010. Adenoma detection rates – the percentage of a physician’s screening colonoscopies that detected at least one histologically confirmed adenoma – ranged from 7.35% to 52.51%. The investigators categorized the data into five equal subsets according to the physicians’ ADRs; the first quintile had a mean ADR of 15.32%; the second quintile, 21.27%; the third quintile, 25.61%; the fourth quintile, 30.89%; and the fifth quintile, 38.66%.
The simulation cohort comprised 10 million men and women, and the investigators performed 1,000 simulation runs, varying 13 relevant parameters with each run. They found that patients of physicians in the first quintile had a lifetime risk of colorectal cancer of 26.6 per 1,000; this decreased in a linear fashion with each quintile, so that patients of physicians in the fifth quintile had a lifetime risk of colorectal cancer of 12.5 per 1,000. Lifetime risks of colorectal cancer death followed the same pattern, decreasing from 5.7 per 1,000 in the first quintile to 2.3 per 1,000 in the fifth quintile.
The simulated lifetime risk of colorectal cancer dropped an average of 11% with every 5% increase in ADR, and the simulated lifetime risk of colorectal cancer death dropped an average of 13% with every 5% increase in ADR. This translates to a 50%-60% lower incidence of colorectal cancer and 50%-60% lower cancer-related mortality for patients of physicians with the highest ADRs, compared with physicians with the lowest ADRs, wrote Mr. Meester and his associates (JAMA 2015 June 16 [doi:10.1001/jama.2015.6251]).
This article was updated July 15, 2015.
In an average-risk population, screening colonoscopies yield different incidences of colorectal cancer and different cancer-related mortality, depending on the operators’ adenoma detection rates, according to a report published online in JAMA.
Adenoma detection rates vary dramatically among gastroenterologists, and patients of physicians who have lower ADRs are known to have higher rates of both colorectal cancer and fatal colorectal cancer. But little is known about the effect different ADRs have on the lifetime benefits and risks of colonoscopy screening programs on average-risk populations. It is possible that the harms of high ADRs outweigh the benefits. For example, higher ADRs may signal increased detection of small low-risk polyps, leading to more surveillance colonoscopies as well as more complications – all from lesions that may well have been benign, said Reinier G.S. Meester of the department of public health, Erasmus University Medical Center, Rotterdam (the Netherlands), and his associat
They examined various possible outcomes for a colonoscopy screening program at different levels of adenoma detection using microsimulation modeling that incorporated data from a large U.S. HMO concerning 57,588 screening colonoscopies performed by 136 physicians between 1998 and 2010. Adenoma detection rates – the percentage of a physician’s screening colonoscopies that detected at least one histologically confirmed adenoma – ranged from 7.35% to 52.51%. The investigators categorized the data into five equal subsets according to the physicians’ ADRs; the first quintile had a mean ADR of 15.32%; the second quintile, 21.27%; the third quintile, 25.61%; the fourth quintile, 30.89%; and the fifth quintile, 38.66%.
The simulation cohort comprised 10 million men and women, and the investigators performed 1,000 simulation runs, varying 13 relevant parameters with each run. They found that patients of physicians in the first quintile had a lifetime risk of colorectal cancer of 26.6 per 1,000; this decreased in a linear fashion with each quintile, so that patients of physicians in the fifth quintile had a lifetime risk of colorectal cancer of 12.5 per 1,000. Lifetime risks of colorectal cancer death followed the same pattern, decreasing from 5.7 per 1,000 in the first quintile to 2.3 per 1,000 in the fifth quintile.
The simulated lifetime risk of colorectal cancer dropped an average of 11% with every 5% increase in ADR, and the simulated lifetime risk of colorectal cancer death dropped an average of 13% with every 5% increase in ADR. This translates to a 50%-60% lower incidence of colorectal cancer and 50%-60% lower cancer-related mortality for patients of physicians with the highest ADRs, compared with physicians with the lowest ADRs, wrote Mr. Meester and his associates (JAMA 2015 June 16 [doi:10.1001/jama.2015.6251]).
This article was updated July 15, 2015.
In an average-risk population, screening colonoscopies yield different incidences of colorectal cancer and different cancer-related mortality, depending on the operators’ adenoma detection rates, according to a report published online in JAMA.
Adenoma detection rates vary dramatically among gastroenterologists, and patients of physicians who have lower ADRs are known to have higher rates of both colorectal cancer and fatal colorectal cancer. But little is known about the effect different ADRs have on the lifetime benefits and risks of colonoscopy screening programs on average-risk populations. It is possible that the harms of high ADRs outweigh the benefits. For example, higher ADRs may signal increased detection of small low-risk polyps, leading to more surveillance colonoscopies as well as more complications – all from lesions that may well have been benign, said Reinier G.S. Meester of the department of public health, Erasmus University Medical Center, Rotterdam (the Netherlands), and his associat
They examined various possible outcomes for a colonoscopy screening program at different levels of adenoma detection using microsimulation modeling that incorporated data from a large U.S. HMO concerning 57,588 screening colonoscopies performed by 136 physicians between 1998 and 2010. Adenoma detection rates – the percentage of a physician’s screening colonoscopies that detected at least one histologically confirmed adenoma – ranged from 7.35% to 52.51%. The investigators categorized the data into five equal subsets according to the physicians’ ADRs; the first quintile had a mean ADR of 15.32%; the second quintile, 21.27%; the third quintile, 25.61%; the fourth quintile, 30.89%; and the fifth quintile, 38.66%.
The simulation cohort comprised 10 million men and women, and the investigators performed 1,000 simulation runs, varying 13 relevant parameters with each run. They found that patients of physicians in the first quintile had a lifetime risk of colorectal cancer of 26.6 per 1,000; this decreased in a linear fashion with each quintile, so that patients of physicians in the fifth quintile had a lifetime risk of colorectal cancer of 12.5 per 1,000. Lifetime risks of colorectal cancer death followed the same pattern, decreasing from 5.7 per 1,000 in the first quintile to 2.3 per 1,000 in the fifth quintile.
The simulated lifetime risk of colorectal cancer dropped an average of 11% with every 5% increase in ADR, and the simulated lifetime risk of colorectal cancer death dropped an average of 13% with every 5% increase in ADR. This translates to a 50%-60% lower incidence of colorectal cancer and 50%-60% lower cancer-related mortality for patients of physicians with the highest ADRs, compared with physicians with the lowest ADRs, wrote Mr. Meester and his associates (JAMA 2015 June 16 [doi:10.1001/jama.2015.6251]).
This article was updated July 15, 2015.
FROM JAMA
Key clinical point: Screening colonoscopies with higher adenoma detection rates are associated with lower rates of colorectal cancer and lower CRC mortality.
Major finding: The simulated lifetime risk of colorectal cancer dropped an average of 11% with every 5% increase in ADR, and the simulated lifetime risk of colorectal cancer death dropped an average of 13% with every 5% increase in ADR.
Data source: A microsimulation model using data from a large HMO to examine the possible benefits of a screening colonoscopy program at different levels of adenoma detection.
Disclosures: This study was supported by grants from the National Cancer Institute and the National Institutes of Health. Mr. Meester and his associates reported having no financial disclosures.
Antibiotic therapy an option for acute appendicitis
Antibiotic therapy failed to be shown as noninferior to surgery in a study of adults with uncomplicated acute appendicitis, but it did resolve the problem and avert surgery with no adverse effects in 73% of patients, according to a report published online June 15 in JAMA.
Moreover, patients who did require surgery after initial antibiotic treatment did not develop significant complications and arguably were no worse off than were those who were operated on immediately. In fact, the overall complication rate was 2.8% among patients assigned to antibiotics and 7% among those assigned to antibiotics who eventually underwent appendectomy, compared with a 20.5% complication rate among patients assigned to surgery, said Dr. Paulina Salminen of the division of digestive surgery and urology, Turku (Finland) University Hospital, and her associates.

Their findings indicate that acute uncomplicated appendicitis need no longer be considered a surgical emergency, and that delaying the operation while trying a course of antibiotics “has few consequences,” they noted.
The few previous studies that have compared the two approaches had many limitations, including small study populations.
For their study, the Appendicitis Acuta (AAPAC) trial, Dr. Salminen and her associates included 530 patients aged 18-60 years who presented to six Finnish hospitals with suspected appendicitis during a 2-year period and were followed for 1 year. Appendicitis was confirmed via computed tomography (CT). Patients who had an appendicolith, perforation, abscess, or tumor were excluded from the study.
A total of 273 patients were randomly assigned to undergo immediate open appendectomy (with preoperative prophylactic antibiotics) and the remaining 257 were assigned to a 3-day course of IV ertapenem followed by 7 days of oral levofloxacin and metronidazole. If progressive infection, perforation, or peritonitis was suspected, appendectomy was performed.
Previous studies of uncomplicated appendicitis treated with antibiotics found a 70%-80% success rate, so the researchers prespecified criteria for noninferiority to surgery at 75% for the study group.
The primary endpoint for the antibiotic group – resolution of acute appendicitis with no recurrences for a full year – occurred in 73%. The remaining 27% of patients in this group underwent appendectomy during follow-up, at a median of 102 days after initial presentation. None of these patients developed abscesses or serious infections, “suggesting that the decision to delay appendectomy ... can be made with a low likelihood of major complications,” the investigators said (JAMA 2015 June 15 [doi:10.1001/jama.2015.6154]). Nevertheless, antibiotic treatment did not qualify as noninferior to immediate surgery according to the study’s preset definitions, they said.
This study was supported by a government research grant from the EVO Foundation to Turku University Hospital. Dr. Salminen reported receiving lecture fees from Merck and Roche; there were no other financial disclosures.
This trial technically had a negative result because antibiotic therapy failed to meet the boundary for noninferiority, but in practical terms the findings fully justify a new approach to uncomplicated acute appendicitis.
The study findings dispel the notion that appendectomy is always an emergency and suggest instead that, given our current precise diagnostic capabilities and effective wide-spectrum antibiotics, a trial of antibiotic therapy is reasonable. However, it’s important to note that children, adolescents, pregnant women, and patients with complications were excluded from this trial so the findings do not apply to those patient groups.
Edward Livingston, M.D., is deputy editor of JAMA. Corrine Vons, M.D., Ph.D., is in the digestive surgery department at Jean-Verdier Hospital, Bondy, France. They reported having no financial conflicts of interest. Dr. Livingston and Dr. Vons made these remarks in an editorial accompanying Dr. Salminen’s report (JAMA 2015;313:2327-8).
This trial technically had a negative result because antibiotic therapy failed to meet the boundary for noninferiority, but in practical terms the findings fully justify a new approach to uncomplicated acute appendicitis.
The study findings dispel the notion that appendectomy is always an emergency and suggest instead that, given our current precise diagnostic capabilities and effective wide-spectrum antibiotics, a trial of antibiotic therapy is reasonable. However, it’s important to note that children, adolescents, pregnant women, and patients with complications were excluded from this trial so the findings do not apply to those patient groups.
Edward Livingston, M.D., is deputy editor of JAMA. Corrine Vons, M.D., Ph.D., is in the digestive surgery department at Jean-Verdier Hospital, Bondy, France. They reported having no financial conflicts of interest. Dr. Livingston and Dr. Vons made these remarks in an editorial accompanying Dr. Salminen’s report (JAMA 2015;313:2327-8).
This trial technically had a negative result because antibiotic therapy failed to meet the boundary for noninferiority, but in practical terms the findings fully justify a new approach to uncomplicated acute appendicitis.
The study findings dispel the notion that appendectomy is always an emergency and suggest instead that, given our current precise diagnostic capabilities and effective wide-spectrum antibiotics, a trial of antibiotic therapy is reasonable. However, it’s important to note that children, adolescents, pregnant women, and patients with complications were excluded from this trial so the findings do not apply to those patient groups.
Edward Livingston, M.D., is deputy editor of JAMA. Corrine Vons, M.D., Ph.D., is in the digestive surgery department at Jean-Verdier Hospital, Bondy, France. They reported having no financial conflicts of interest. Dr. Livingston and Dr. Vons made these remarks in an editorial accompanying Dr. Salminen’s report (JAMA 2015;313:2327-8).
Antibiotic therapy failed to be shown as noninferior to surgery in a study of adults with uncomplicated acute appendicitis, but it did resolve the problem and avert surgery with no adverse effects in 73% of patients, according to a report published online June 15 in JAMA.
Moreover, patients who did require surgery after initial antibiotic treatment did not develop significant complications and arguably were no worse off than were those who were operated on immediately. In fact, the overall complication rate was 2.8% among patients assigned to antibiotics and 7% among those assigned to antibiotics who eventually underwent appendectomy, compared with a 20.5% complication rate among patients assigned to surgery, said Dr. Paulina Salminen of the division of digestive surgery and urology, Turku (Finland) University Hospital, and her associates.
Their findings indicate that acute uncomplicated appendicitis need no longer be considered a surgical emergency, and that delaying the operation while trying a course of antibiotics “has few consequences,” they noted.
The few previous studies that have compared the two approaches had many limitations, including small study populations.
For their study, the Appendicitis Acuta (AAPAC) trial, Dr. Salminen and her associates included 530 patients aged 18-60 years who presented to six Finnish hospitals with suspected appendicitis during a 2-year period and were followed for 1 year. Appendicitis was confirmed via computed tomography (CT). Patients who had an appendicolith, perforation, abscess, or tumor were excluded from the study.
A total of 273 patients were randomly assigned to undergo immediate open appendectomy (with preoperative prophylactic antibiotics) and the remaining 257 were assigned to a 3-day course of IV ertapenem followed by 7 days of oral levofloxacin and metronidazole. If progressive infection, perforation, or peritonitis was suspected, appendectomy was performed.
Previous studies of uncomplicated appendicitis treated with antibiotics found a 70%-80% success rate, so the researchers prespecified criteria for noninferiority to surgery at 75% for the study group.
The primary endpoint for the antibiotic group – resolution of acute appendicitis with no recurrences for a full year – occurred in 73%. The remaining 27% of patients in this group underwent appendectomy during follow-up, at a median of 102 days after initial presentation. None of these patients developed abscesses or serious infections, “suggesting that the decision to delay appendectomy ... can be made with a low likelihood of major complications,” the investigators said (JAMA 2015 June 15 [doi:10.1001/jama.2015.6154]). Nevertheless, antibiotic treatment did not qualify as noninferior to immediate surgery according to the study’s preset definitions, they said.
This study was supported by a government research grant from the EVO Foundation to Turku University Hospital. Dr. Salminen reported receiving lecture fees from Merck and Roche; there were no other financial disclosures.
Antibiotic therapy failed to be shown as noninferior to surgery in a study of adults with uncomplicated acute appendicitis, but it did resolve the problem and avert surgery with no adverse effects in 73% of patients, according to a report published online June 15 in JAMA.
Moreover, patients who did require surgery after initial antibiotic treatment did not develop significant complications and arguably were no worse off than were those who were operated on immediately. In fact, the overall complication rate was 2.8% among patients assigned to antibiotics and 7% among those assigned to antibiotics who eventually underwent appendectomy, compared with a 20.5% complication rate among patients assigned to surgery, said Dr. Paulina Salminen of the division of digestive surgery and urology, Turku (Finland) University Hospital, and her associates.
Their findings indicate that acute uncomplicated appendicitis need no longer be considered a surgical emergency, and that delaying the operation while trying a course of antibiotics “has few consequences,” they noted.
The few previous studies that have compared the two approaches had many limitations, including small study populations.
For their study, the Appendicitis Acuta (AAPAC) trial, Dr. Salminen and her associates included 530 patients aged 18-60 years who presented to six Finnish hospitals with suspected appendicitis during a 2-year period and were followed for 1 year. Appendicitis was confirmed via computed tomography (CT). Patients who had an appendicolith, perforation, abscess, or tumor were excluded from the study.
A total of 273 patients were randomly assigned to undergo immediate open appendectomy (with preoperative prophylactic antibiotics) and the remaining 257 were assigned to a 3-day course of IV ertapenem followed by 7 days of oral levofloxacin and metronidazole. If progressive infection, perforation, or peritonitis was suspected, appendectomy was performed.
Previous studies of uncomplicated appendicitis treated with antibiotics found a 70%-80% success rate, so the researchers prespecified criteria for noninferiority to surgery at 75% for the study group.
The primary endpoint for the antibiotic group – resolution of acute appendicitis with no recurrences for a full year – occurred in 73%. The remaining 27% of patients in this group underwent appendectomy during follow-up, at a median of 102 days after initial presentation. None of these patients developed abscesses or serious infections, “suggesting that the decision to delay appendectomy ... can be made with a low likelihood of major complications,” the investigators said (JAMA 2015 June 15 [doi:10.1001/jama.2015.6154]). Nevertheless, antibiotic treatment did not qualify as noninferior to immediate surgery according to the study’s preset definitions, they said.
This study was supported by a government research grant from the EVO Foundation to Turku University Hospital. Dr. Salminen reported receiving lecture fees from Merck and Roche; there were no other financial disclosures.
FROM JAMA
Key clinical point: Antibiotic therapy was not noninferior to surgery for uncomplicated acute appendicitis, but it averted surgery in a clear majority without any adverse effects.
Major finding: The primary endpoint for the antibiotic group – resolution of acute appendicitis with no recurrences for a full year – occurred in 73% of patients.
Data source: An open-label randomized noninferiority trial involving 530 adults treated at six Finnish hospitals during a 2-year period.
Disclosures: This study was supported by a government research grant from the EVO Foundation to Turku University Hospital. Dr. Salminen reported receiving lecture fees from Merck and Roche; there were no other financial disclosures.

Giving patients choice of diet does not enhance weight loss
Allowing obese patients to choose between a low-carbohydrate or a low-fat diet according to their food preferences did not enhance their weight loss, dietary adherence, or weight-related quality of life, compared with randomly assigning them to one of the diets, according to a report published online June 15 in Annals of Internal Medicine.
Several studies have suggested that offering patients a choice among evidence-based dietary strategies for losing weight would facilitate their adherence and thus improve their results.
Researchers studied a 1-year weight-loss intervention among 207 overweight/obese adults (mean body mass index 36 kg/m2) who completed the Geiselman Food Preference Questionnaire to determine whether their preferences for 72 common foods aligned better with a low-carbohydrate or a low-fat diet.
Among the study participants, 105 were allowed to choose a low-carbohydrate or a low-fat diet, and 102 were randomly assigned to those diets. Mean age of the participants was 55 years; 73% were men; and 51% were African American.
All the participants received verbal and printed information about the efficacy and safety of the diets; sample menus; and a pocket guide to counting calories, fats, and carbohydrates. All were offered up to 19 group counseling sessions and individual telephone counseling from the study dietitian, and all were encouraged to aim for 30 minutes of moderate-intensity aerobic physical activity 5 days per week, said Dr. William S. Yancy Jr. of the Durham (N.C.) Veterans Affairs Medical Center and the VA’s Center for Health Services Research in Primary Care, and his associates.
Dietary adherence was similar between the two study groups. At final follow-up, the estimated mean weight loss for patients who chose their diet was 5.7 kg, or 5.6%, of their baseline body weight, compared with 6.7 kg, or 6.2%, of their baseline body weight, for patients who were assigned to a diet.
Final waist circumference and BMI were not significantly different between the two study groups, nor were scores on two measures of quality of life. “Contrary to expectations, the opportunity to choose a diet did not improve weight loss,” the investigators said (Ann. Intern. Med. 2015 June 15 [doi:10.7326/M14-2358]).
The findings indicate that providing a choice of diets may actually hinder weight loss, the researchers noted.
“One reason may be that persons are more likely to overeat when following a diet that emphasizes foods they find palatable,” Dr. Yancy and his associates explained. “Another reason may be a ‘personal trainer’ effect, in which persons may be more adherent to a fitness program if directed on what exercises to do rather than choosing their own.”
The U.S. Department of Veterans Affairs funded the study. Dr. Yancy reported receiving personal fees from Nutrisystem and the University of Pennsylvania.
Allowing obese patients to choose between a low-carbohydrate or a low-fat diet according to their food preferences did not enhance their weight loss, dietary adherence, or weight-related quality of life, compared with randomly assigning them to one of the diets, according to a report published online June 15 in Annals of Internal Medicine.
Several studies have suggested that offering patients a choice among evidence-based dietary strategies for losing weight would facilitate their adherence and thus improve their results.
Researchers studied a 1-year weight-loss intervention among 207 overweight/obese adults (mean body mass index 36 kg/m2) who completed the Geiselman Food Preference Questionnaire to determine whether their preferences for 72 common foods aligned better with a low-carbohydrate or a low-fat diet.
Among the study participants, 105 were allowed to choose a low-carbohydrate or a low-fat diet, and 102 were randomly assigned to those diets. Mean age of the participants was 55 years; 73% were men; and 51% were African American.
All the participants received verbal and printed information about the efficacy and safety of the diets; sample menus; and a pocket guide to counting calories, fats, and carbohydrates. All were offered up to 19 group counseling sessions and individual telephone counseling from the study dietitian, and all were encouraged to aim for 30 minutes of moderate-intensity aerobic physical activity 5 days per week, said Dr. William S. Yancy Jr. of the Durham (N.C.) Veterans Affairs Medical Center and the VA’s Center for Health Services Research in Primary Care, and his associates.
Dietary adherence was similar between the two study groups. At final follow-up, the estimated mean weight loss for patients who chose their diet was 5.7 kg, or 5.6%, of their baseline body weight, compared with 6.7 kg, or 6.2%, of their baseline body weight, for patients who were assigned to a diet.
Final waist circumference and BMI were not significantly different between the two study groups, nor were scores on two measures of quality of life. “Contrary to expectations, the opportunity to choose a diet did not improve weight loss,” the investigators said (Ann. Intern. Med. 2015 June 15 [doi:10.7326/M14-2358]).
The findings indicate that providing a choice of diets may actually hinder weight loss, the researchers noted.
“One reason may be that persons are more likely to overeat when following a diet that emphasizes foods they find palatable,” Dr. Yancy and his associates explained. “Another reason may be a ‘personal trainer’ effect, in which persons may be more adherent to a fitness program if directed on what exercises to do rather than choosing their own.”
The U.S. Department of Veterans Affairs funded the study. Dr. Yancy reported receiving personal fees from Nutrisystem and the University of Pennsylvania.
Allowing obese patients to choose between a low-carbohydrate or a low-fat diet according to their food preferences did not enhance their weight loss, dietary adherence, or weight-related quality of life, compared with randomly assigning them to one of the diets, according to a report published online June 15 in Annals of Internal Medicine.
Several studies have suggested that offering patients a choice among evidence-based dietary strategies for losing weight would facilitate their adherence and thus improve their results.
Researchers studied a 1-year weight-loss intervention among 207 overweight/obese adults (mean body mass index 36 kg/m2) who completed the Geiselman Food Preference Questionnaire to determine whether their preferences for 72 common foods aligned better with a low-carbohydrate or a low-fat diet.
Among the study participants, 105 were allowed to choose a low-carbohydrate or a low-fat diet, and 102 were randomly assigned to those diets. Mean age of the participants was 55 years; 73% were men; and 51% were African American.
All the participants received verbal and printed information about the efficacy and safety of the diets; sample menus; and a pocket guide to counting calories, fats, and carbohydrates. All were offered up to 19 group counseling sessions and individual telephone counseling from the study dietitian, and all were encouraged to aim for 30 minutes of moderate-intensity aerobic physical activity 5 days per week, said Dr. William S. Yancy Jr. of the Durham (N.C.) Veterans Affairs Medical Center and the VA’s Center for Health Services Research in Primary Care, and his associates.
Dietary adherence was similar between the two study groups. At final follow-up, the estimated mean weight loss for patients who chose their diet was 5.7 kg, or 5.6%, of their baseline body weight, compared with 6.7 kg, or 6.2%, of their baseline body weight, for patients who were assigned to a diet.
Final waist circumference and BMI were not significantly different between the two study groups, nor were scores on two measures of quality of life. “Contrary to expectations, the opportunity to choose a diet did not improve weight loss,” the investigators said (Ann. Intern. Med. 2015 June 15 [doi:10.7326/M14-2358]).
The findings indicate that providing a choice of diets may actually hinder weight loss, the researchers noted.
“One reason may be that persons are more likely to overeat when following a diet that emphasizes foods they find palatable,” Dr. Yancy and his associates explained. “Another reason may be a ‘personal trainer’ effect, in which persons may be more adherent to a fitness program if directed on what exercises to do rather than choosing their own.”
The U.S. Department of Veterans Affairs funded the study. Dr. Yancy reported receiving personal fees from Nutrisystem and the University of Pennsylvania.
FROM ANNALS OF INTERNAL MEDICINE
Key clinical point: Allowing patients to choose either a low-carbohydrate or a low-fat diet according to their food preferences failed to improve weight loss, dietary adherence, or weight-related quality of life.
Major finding: The estimated mean weight loss for patients who chose their diet was 5.7 kg, or 5.6% of their baseline body weight, compared with 6.7 kg, or 6.2% of their baseline body weight, for patients who were assigned to a diet.
Data source: A 1-year prospective, randomized trial comparing weight-loss outcomes between 105 obese patients allowed to choose their diet and 102 obese patients assigned to a specific diet.
Disclosures: The U.S. Department of Veterans Affairs funded the study. Dr. Yancy reported receiving personal fees from Nutrisystem and the University of Pennsylvania.
Stent-retriever thrombectomy reduces poststroke disability
For patients with proximal large-vessel anterior stroke, neurovascular thrombectomy with a stent retriever plus medical therapy in the REVASCAT trial reduced the severity of poststroke disability and raised the rate of functional independence, compared with medical therapy alone, according to a report in the New England Journal of Medicine.
To assess the efficacy and safety of thrombectomy with a stent retriever, investigators performed a prospective, open-label, phase III clinical trial involving 206 adults up to 85 years of age treated at four designated comprehensive stroke centers in Catalonia, Spain.
All the participants in the Randomized Trial of Revascularization With Solitaire FR Device Versus Best Medical Therapy in the Treatment of Acute Stroke Due to Anterior Circulation Large Vessel Occlusion Presenting Within Eight Hours of Symptom Onset (REVASCAT) had either not responded to intravenous alteplase administered within 4.5 hours of symptom onset or had contraindications to alteplase therapy. They were randomly assigned in equal numbers to undergo endovascular treatment with a stent retriever or medical therapy alone, said Dr. Tudor G. Jovin, director of the Stroke Institute, University of Pittsburgh Medical Center, and his associates.
The trial was halted early when the first interim analysis showed “lack of equipoise” between the two study groups, and because emerging results from three other studies demonstrated the superior efficacy of thrombectomy. The primary efficacy outcome measure – severity of disability at 90 days, as measured by expert assessors blinded to treatment assignment – significantly favored thrombectomy over medical therapy. The proportion of patients who achieved functional independence by day 90 on the modified Rankin scale also demonstrated the clear superiority of thrombectomy (43.7%) over medical therapy (28.2%).
Only 6.5 patients would need to be treated with thrombectomy to prevent 1 case of functional dependency or death. In addition, “thrombectomy was associated with a shift toward better outcomes across the entire spectrum of disability,” Dr. Jovin and his associates said (N. Engl. J. Med. 2015 [doi:10.1056/NEJMoa1503780]).
Regarding safety, the rate of death at 90 days did not differ significantly between patients who underwent thrombectomy (18.4%) and control subjects (15.5%). Rates of intracranial hemorrhage were the same, 1.9%, in both groups, and rates of other serious adverse events also were similar.
These findings are consistent with those of several other recently reported clinical trials and show that “in patients with acute stroke caused by a proximal large-vessel occlusion and an absence of a large infarct on baseline imaging, mechanical thrombectomy with [a] stent retriever was safe and led to improved clinical outcomes, as compared with medical therapy alone,” the investigators said.
REVASCAT was funded by an unrestricted grant from Covidien, maker of the stent retriever, and by grants from several Spanish research institutes. Dr. Jovin reported ties to Covidien, Silk Road Medical, Air Liquide, Medtronic, and Stryker Neurovascular.
For patients with proximal large-vessel anterior stroke, neurovascular thrombectomy with a stent retriever plus medical therapy in the REVASCAT trial reduced the severity of poststroke disability and raised the rate of functional independence, compared with medical therapy alone, according to a report in the New England Journal of Medicine.
To assess the efficacy and safety of thrombectomy with a stent retriever, investigators performed a prospective, open-label, phase III clinical trial involving 206 adults up to 85 years of age treated at four designated comprehensive stroke centers in Catalonia, Spain.
All the participants in the Randomized Trial of Revascularization With Solitaire FR Device Versus Best Medical Therapy in the Treatment of Acute Stroke Due to Anterior Circulation Large Vessel Occlusion Presenting Within Eight Hours of Symptom Onset (REVASCAT) had either not responded to intravenous alteplase administered within 4.5 hours of symptom onset or had contraindications to alteplase therapy. They were randomly assigned in equal numbers to undergo endovascular treatment with a stent retriever or medical therapy alone, said Dr. Tudor G. Jovin, director of the Stroke Institute, University of Pittsburgh Medical Center, and his associates.
The trial was halted early when the first interim analysis showed “lack of equipoise” between the two study groups, and because emerging results from three other studies demonstrated the superior efficacy of thrombectomy. The primary efficacy outcome measure – severity of disability at 90 days, as measured by expert assessors blinded to treatment assignment – significantly favored thrombectomy over medical therapy. The proportion of patients who achieved functional independence by day 90 on the modified Rankin scale also demonstrated the clear superiority of thrombectomy (43.7%) over medical therapy (28.2%).
Only 6.5 patients would need to be treated with thrombectomy to prevent 1 case of functional dependency or death. In addition, “thrombectomy was associated with a shift toward better outcomes across the entire spectrum of disability,” Dr. Jovin and his associates said (N. Engl. J. Med. 2015 [doi:10.1056/NEJMoa1503780]).
Regarding safety, the rate of death at 90 days did not differ significantly between patients who underwent thrombectomy (18.4%) and control subjects (15.5%). Rates of intracranial hemorrhage were the same, 1.9%, in both groups, and rates of other serious adverse events also were similar.
These findings are consistent with those of several other recently reported clinical trials and show that “in patients with acute stroke caused by a proximal large-vessel occlusion and an absence of a large infarct on baseline imaging, mechanical thrombectomy with [a] stent retriever was safe and led to improved clinical outcomes, as compared with medical therapy alone,” the investigators said.
REVASCAT was funded by an unrestricted grant from Covidien, maker of the stent retriever, and by grants from several Spanish research institutes. Dr. Jovin reported ties to Covidien, Silk Road Medical, Air Liquide, Medtronic, and Stryker Neurovascular.
For patients with proximal large-vessel anterior stroke, neurovascular thrombectomy with a stent retriever plus medical therapy in the REVASCAT trial reduced the severity of poststroke disability and raised the rate of functional independence, compared with medical therapy alone, according to a report in the New England Journal of Medicine.
To assess the efficacy and safety of thrombectomy with a stent retriever, investigators performed a prospective, open-label, phase III clinical trial involving 206 adults up to 85 years of age treated at four designated comprehensive stroke centers in Catalonia, Spain.
All the participants in the Randomized Trial of Revascularization With Solitaire FR Device Versus Best Medical Therapy in the Treatment of Acute Stroke Due to Anterior Circulation Large Vessel Occlusion Presenting Within Eight Hours of Symptom Onset (REVASCAT) had either not responded to intravenous alteplase administered within 4.5 hours of symptom onset or had contraindications to alteplase therapy. They were randomly assigned in equal numbers to undergo endovascular treatment with a stent retriever or medical therapy alone, said Dr. Tudor G. Jovin, director of the Stroke Institute, University of Pittsburgh Medical Center, and his associates.
The trial was halted early when the first interim analysis showed “lack of equipoise” between the two study groups, and because emerging results from three other studies demonstrated the superior efficacy of thrombectomy. The primary efficacy outcome measure – severity of disability at 90 days, as measured by expert assessors blinded to treatment assignment – significantly favored thrombectomy over medical therapy. The proportion of patients who achieved functional independence by day 90 on the modified Rankin scale also demonstrated the clear superiority of thrombectomy (43.7%) over medical therapy (28.2%).
Only 6.5 patients would need to be treated with thrombectomy to prevent 1 case of functional dependency or death. In addition, “thrombectomy was associated with a shift toward better outcomes across the entire spectrum of disability,” Dr. Jovin and his associates said (N. Engl. J. Med. 2015 [doi:10.1056/NEJMoa1503780]).
Regarding safety, the rate of death at 90 days did not differ significantly between patients who underwent thrombectomy (18.4%) and control subjects (15.5%). Rates of intracranial hemorrhage were the same, 1.9%, in both groups, and rates of other serious adverse events also were similar.
These findings are consistent with those of several other recently reported clinical trials and show that “in patients with acute stroke caused by a proximal large-vessel occlusion and an absence of a large infarct on baseline imaging, mechanical thrombectomy with [a] stent retriever was safe and led to improved clinical outcomes, as compared with medical therapy alone,” the investigators said.
REVASCAT was funded by an unrestricted grant from Covidien, maker of the stent retriever, and by grants from several Spanish research institutes. Dr. Jovin reported ties to Covidien, Silk Road Medical, Air Liquide, Medtronic, and Stryker Neurovascular.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Thrombectomy with a stent retriever reduced poststroke disability in patients with occlusion of the proximal anterior circulation.
Major finding: The proportion of patients who achieved functional independence by day 90 showed the clear superiority of thrombectomy (43.7%) over medical therapy (28.2%); only 6.5 patients would need to be treated with thrombectomy to prevent 1 case of functional dependency or death.
Data source: REVASCAT, a prospective, open-label, randomized phase III trial involving 206 adults treated during a 4-year period at four stroke centers in Spain.
Disclosures: REVASCAT was funded by an unrestricted grant from Covidien, maker of the stent retriever, and by grants from several Spanish research institutes. Dr. Jovin reported ties to Covidien, Silk Road Medical, Air Liquide, Medtronic, and Stryker Neurovascular.
‘Modest’ uptake of novel anticoagulants in real-world practice
The novel oral anticoagulants dabigatran and rivaroxaban have had only “modest” uptake into real-world clinical practice as thromboembolism prevention in high-risk patients with atrial fibrillation, according to a report published online June 9 in Circulation: Cardiovascular Outcomes and Quality.
These drugs have proved to be at least as effective as warfarin at prophylaxis in this patient population, appear to be safer than warfarin regarding the risk of intracranial hemorrhage, and are more practical because they don’t require routine monitoring and have more predictable treatment effects. Yet little is known about their adoption into real-world practice, said Dr. Priyesh A. Patel of Duke Clinical Research Institute in Durham, N.C., and his associates.
The investigators examined the issue by analyzing hospital records in the database of the Get With The Guidelines–Stroke initiative, a project aimed at improving overall stroke care. They focused on 61,655 patients with AF who were hospitalized for ischemic stroke or transient ischemic attack (TIA) and discharged on dabigatran, rivaroxaban, or warfarin during a 2-year period after FDA approval of the new agents. Dabigatran was prescribed to 9.6% of these patients, rivaroxaban to 1.5%, and warfarin to 88.9%.
“Our study shows modest early adoption rates for novel oral anticoagulant therapy” of 16%-17%. Yet this rate falls in the upper range of estimated uptakes in studies that describe early utilization patterns of drugs – including the initially modest adoption of warfarin for this indication, Dr. Patel and his associates said (Circ. Cardiovasc. Qual. Outcomes 2015 June 9 [doi:10.1161/circoutcomes.114.000907]).
The relative expense of the newer agents likely played a role in hindering diffusion into clinical practice because patients who lacked health insurance or were covered by Medicare/Medicaid were more likely to receive warfarin. In addition, clinicians may hesitate to prescribe dabigatran or rivaroxaban because real-world patients differ markedly from those included in clinical trials of these drugs. In this study, for example, participants were older, more likely to be female, less likely to be ambulatory, and had higher scores on measures of risk such as CHADS2 and CHA2DS2-VASc scores, compared with clinical study subjects, they said.
This study also uncovered one particularly worrying fact: 1.4% of patients discharged on dabigatran or rivaroxaban had prosthetic heart valves and 31% had known coronary artery disease, which can be contraindications to using these agents. “Further education on the risks and benefits of novel oral anticoagulation therapy may be needed to increase familiarity with these drugs and prevent risk-treatment mismatches or adverse events,” Dr. Patel and his associates added.
This study was funded by grants from the American Heart Association and the National Institutes of Health. Dr. Patel reported having no financial disclosures; his associates reported ties to numerous industry sources.
The novel oral anticoagulants dabigatran and rivaroxaban have had only “modest” uptake into real-world clinical practice as thromboembolism prevention in high-risk patients with atrial fibrillation, according to a report published online June 9 in Circulation: Cardiovascular Outcomes and Quality.
These drugs have proved to be at least as effective as warfarin at prophylaxis in this patient population, appear to be safer than warfarin regarding the risk of intracranial hemorrhage, and are more practical because they don’t require routine monitoring and have more predictable treatment effects. Yet little is known about their adoption into real-world practice, said Dr. Priyesh A. Patel of Duke Clinical Research Institute in Durham, N.C., and his associates.
The investigators examined the issue by analyzing hospital records in the database of the Get With The Guidelines–Stroke initiative, a project aimed at improving overall stroke care. They focused on 61,655 patients with AF who were hospitalized for ischemic stroke or transient ischemic attack (TIA) and discharged on dabigatran, rivaroxaban, or warfarin during a 2-year period after FDA approval of the new agents. Dabigatran was prescribed to 9.6% of these patients, rivaroxaban to 1.5%, and warfarin to 88.9%.
“Our study shows modest early adoption rates for novel oral anticoagulant therapy” of 16%-17%. Yet this rate falls in the upper range of estimated uptakes in studies that describe early utilization patterns of drugs – including the initially modest adoption of warfarin for this indication, Dr. Patel and his associates said (Circ. Cardiovasc. Qual. Outcomes 2015 June 9 [doi:10.1161/circoutcomes.114.000907]).
The relative expense of the newer agents likely played a role in hindering diffusion into clinical practice because patients who lacked health insurance or were covered by Medicare/Medicaid were more likely to receive warfarin. In addition, clinicians may hesitate to prescribe dabigatran or rivaroxaban because real-world patients differ markedly from those included in clinical trials of these drugs. In this study, for example, participants were older, more likely to be female, less likely to be ambulatory, and had higher scores on measures of risk such as CHADS2 and CHA2DS2-VASc scores, compared with clinical study subjects, they said.
This study also uncovered one particularly worrying fact: 1.4% of patients discharged on dabigatran or rivaroxaban had prosthetic heart valves and 31% had known coronary artery disease, which can be contraindications to using these agents. “Further education on the risks and benefits of novel oral anticoagulation therapy may be needed to increase familiarity with these drugs and prevent risk-treatment mismatches or adverse events,” Dr. Patel and his associates added.
This study was funded by grants from the American Heart Association and the National Institutes of Health. Dr. Patel reported having no financial disclosures; his associates reported ties to numerous industry sources.
The novel oral anticoagulants dabigatran and rivaroxaban have had only “modest” uptake into real-world clinical practice as thromboembolism prevention in high-risk patients with atrial fibrillation, according to a report published online June 9 in Circulation: Cardiovascular Outcomes and Quality.
These drugs have proved to be at least as effective as warfarin at prophylaxis in this patient population, appear to be safer than warfarin regarding the risk of intracranial hemorrhage, and are more practical because they don’t require routine monitoring and have more predictable treatment effects. Yet little is known about their adoption into real-world practice, said Dr. Priyesh A. Patel of Duke Clinical Research Institute in Durham, N.C., and his associates.
The investigators examined the issue by analyzing hospital records in the database of the Get With The Guidelines–Stroke initiative, a project aimed at improving overall stroke care. They focused on 61,655 patients with AF who were hospitalized for ischemic stroke or transient ischemic attack (TIA) and discharged on dabigatran, rivaroxaban, or warfarin during a 2-year period after FDA approval of the new agents. Dabigatran was prescribed to 9.6% of these patients, rivaroxaban to 1.5%, and warfarin to 88.9%.
“Our study shows modest early adoption rates for novel oral anticoagulant therapy” of 16%-17%. Yet this rate falls in the upper range of estimated uptakes in studies that describe early utilization patterns of drugs – including the initially modest adoption of warfarin for this indication, Dr. Patel and his associates said (Circ. Cardiovasc. Qual. Outcomes 2015 June 9 [doi:10.1161/circoutcomes.114.000907]).
The relative expense of the newer agents likely played a role in hindering diffusion into clinical practice because patients who lacked health insurance or were covered by Medicare/Medicaid were more likely to receive warfarin. In addition, clinicians may hesitate to prescribe dabigatran or rivaroxaban because real-world patients differ markedly from those included in clinical trials of these drugs. In this study, for example, participants were older, more likely to be female, less likely to be ambulatory, and had higher scores on measures of risk such as CHADS2 and CHA2DS2-VASc scores, compared with clinical study subjects, they said.
This study also uncovered one particularly worrying fact: 1.4% of patients discharged on dabigatran or rivaroxaban had prosthetic heart valves and 31% had known coronary artery disease, which can be contraindications to using these agents. “Further education on the risks and benefits of novel oral anticoagulation therapy may be needed to increase familiarity with these drugs and prevent risk-treatment mismatches or adverse events,” Dr. Patel and his associates added.
This study was funded by grants from the American Heart Association and the National Institutes of Health. Dr. Patel reported having no financial disclosures; his associates reported ties to numerous industry sources.
FROM CIRCULATION: CARDIOVASCULAR QUALITY AND OUTCOMES
Key clinical point: Clinicians have only modestly adopted novel oral anticoagulants into real-world clinical practice.
Major finding: Early adoption rates for novel oral anticoagulant therapy were deemed “modest” at 16%-17% of cases.
Data source: Analysis of 61,655 hospital records in the Get With The Guidelines–Stroke database concerning AF patients hospitalized for ischemic stroke or TIA in 2010-2012 who were discharged on warfarin, dabigatran, or rivaroxaban.
Disclosures: This study was funded by grants from the American Heart Association and the National Institutes of Health. Dr. Patel reported having no financial disclosures; his associates reported ties to numerous industry sources.
Rotavirus vaccine slashed hospitalizations for acute gastroenteritis
Hospitalizations for acute gastroenteritis in children aged 5 years and younger plummeted after routine rotavirus vaccination was implemented in 2006, with rotavirus-specific hospitalizations plunging 94% and all-cause gastroenteritis hospitalizations dropping 55% in the most recent year for which data are available, according to a report published online June 9 in JAMA.
Researchers assessed the vaccine’s effect by analyzing information in a Healthcare Cost and Utilization Project database covering community and academic hospitals. They focused on 1,201,458 hospitalizations coded for all-cause acute gastroenteritis, including 199,812 (17%) that were coded specifically for rotavirus, which occurred in 26 states during 2000 through 2012 among children under age 5 years.
The mean annual hospitalization rate for all-cause acute gastroenteritis was 76 per 10,000 before the vaccine was introduced, which declined by 31% in 2008, 33% in 2009, 48% in 2010, 47% in 2011, and 55% in 2012. The marked decrease occurred in both boys and girls, across all race/ethnicity categories, and at all ages. The reduction was greatest among children aged 6-23 months, Dr. Eyal Leshem of the Division of Viral Diseases, Centers for Disease Control and Prevention, Atlanta, and his associates said in a research letter.
The mean annual hospitalization rate for rotavirus-specific gastroenteritis dropped even more dramatically, from 16 per 10,000 before the vaccine was introduced by 70% in 2008, 63% in 2009, 90% in 2010, 79% in 2011, and 94% in 2012, the investigators said (JAMA 2015;313:2282-4).
The nonlinear pattern of both declines “might be explained by accumulation of susceptible, nonimmune population during seasons of markedly decreased transmission,” Dr. Leshem and his associates noted.
“Our findings support continued efforts to increase rotavirus vaccine coverage,” they added.
This study was supported by the Centers for Disease Control and Prevention and the Agency for Healthcare Research and Quality. Dr. Leshem and his associates reported having no relevant financial conflicts of interest.
Hospitalizations for acute gastroenteritis in children aged 5 years and younger plummeted after routine rotavirus vaccination was implemented in 2006, with rotavirus-specific hospitalizations plunging 94% and all-cause gastroenteritis hospitalizations dropping 55% in the most recent year for which data are available, according to a report published online June 9 in JAMA.
Researchers assessed the vaccine’s effect by analyzing information in a Healthcare Cost and Utilization Project database covering community and academic hospitals. They focused on 1,201,458 hospitalizations coded for all-cause acute gastroenteritis, including 199,812 (17%) that were coded specifically for rotavirus, which occurred in 26 states during 2000 through 2012 among children under age 5 years.
The mean annual hospitalization rate for all-cause acute gastroenteritis was 76 per 10,000 before the vaccine was introduced, which declined by 31% in 2008, 33% in 2009, 48% in 2010, 47% in 2011, and 55% in 2012. The marked decrease occurred in both boys and girls, across all race/ethnicity categories, and at all ages. The reduction was greatest among children aged 6-23 months, Dr. Eyal Leshem of the Division of Viral Diseases, Centers for Disease Control and Prevention, Atlanta, and his associates said in a research letter.
The mean annual hospitalization rate for rotavirus-specific gastroenteritis dropped even more dramatically, from 16 per 10,000 before the vaccine was introduced by 70% in 2008, 63% in 2009, 90% in 2010, 79% in 2011, and 94% in 2012, the investigators said (JAMA 2015;313:2282-4).
The nonlinear pattern of both declines “might be explained by accumulation of susceptible, nonimmune population during seasons of markedly decreased transmission,” Dr. Leshem and his associates noted.
“Our findings support continued efforts to increase rotavirus vaccine coverage,” they added.
This study was supported by the Centers for Disease Control and Prevention and the Agency for Healthcare Research and Quality. Dr. Leshem and his associates reported having no relevant financial conflicts of interest.
Hospitalizations for acute gastroenteritis in children aged 5 years and younger plummeted after routine rotavirus vaccination was implemented in 2006, with rotavirus-specific hospitalizations plunging 94% and all-cause gastroenteritis hospitalizations dropping 55% in the most recent year for which data are available, according to a report published online June 9 in JAMA.
Researchers assessed the vaccine’s effect by analyzing information in a Healthcare Cost and Utilization Project database covering community and academic hospitals. They focused on 1,201,458 hospitalizations coded for all-cause acute gastroenteritis, including 199,812 (17%) that were coded specifically for rotavirus, which occurred in 26 states during 2000 through 2012 among children under age 5 years.
The mean annual hospitalization rate for all-cause acute gastroenteritis was 76 per 10,000 before the vaccine was introduced, which declined by 31% in 2008, 33% in 2009, 48% in 2010, 47% in 2011, and 55% in 2012. The marked decrease occurred in both boys and girls, across all race/ethnicity categories, and at all ages. The reduction was greatest among children aged 6-23 months, Dr. Eyal Leshem of the Division of Viral Diseases, Centers for Disease Control and Prevention, Atlanta, and his associates said in a research letter.
The mean annual hospitalization rate for rotavirus-specific gastroenteritis dropped even more dramatically, from 16 per 10,000 before the vaccine was introduced by 70% in 2008, 63% in 2009, 90% in 2010, 79% in 2011, and 94% in 2012, the investigators said (JAMA 2015;313:2282-4).
The nonlinear pattern of both declines “might be explained by accumulation of susceptible, nonimmune population during seasons of markedly decreased transmission,” Dr. Leshem and his associates noted.
“Our findings support continued efforts to increase rotavirus vaccine coverage,” they added.
This study was supported by the Centers for Disease Control and Prevention and the Agency for Healthcare Research and Quality. Dr. Leshem and his associates reported having no relevant financial conflicts of interest.
FROM JAMA
Key clinical point: All hospitalizations for acute gastroenteritis in children aged 5 years and younger plummeted after routine rotavirus vaccination was implemented in 2006.
Major finding: The mean annual hospitalization rate for all-cause acute gastroenteritis was 76 per 10,000 before the vaccine was introduced, which declined by 31% in 2008, 33% in 2009, 48% in 2010, 47% in 2011, and 55% in 2012.
Data source: An analysis of information in a Healthcare Cost and Utilization Project database concerning 1,201,458 hospitalizations for acute gastroenteritis in 26 states from 2000 through 2012.
Disclosures: This study was supported by the Centers for Disease Control and Prevention and the Agency for Healthcare Research and Quality. Dr. Leshem and his associates reported having no relevant financial conflicts of interest.
Triple therapy added toxicity without survival benefit in multiple myeloma
Triple-agent bortezomib-based regimens yielded no survival or other advantages over a double-agent regimen in a phase-III clinical trial involving transplant-ineligible patients with multiple myeloma. The study was published online June 8 in the Journal of Clinical Oncology.
As the optimal therapy for transplant-ineligible patients has not yet been determined, researchers performed what they described as the first randomized trial comparing several bortezomib-based regimens. For this study, the researchers wanted to assess the regimens in more typical patients: elderly men and women of diverse ethnic and economic backgrounds who have common comorbidities and are treated in community oncology practices.
The 502 participants (mean age, 73 years) in this industry-sponsored study were treated at 159 oncology practices across the country during a 3-year period and followed up for a median of 43 months. Half had serious comorbidities such as diabetes, renal disease, and chronic pulmonary disease. They were randomly assigned to receive eight 21-day cycles of bortezomib-dexamethasone, bortezomib-thalidomide-dexamethasone, or bortezomib-melphalan-prednisone combination induction therapy, followed by five 35-day cycles of maintenance bortezomib, said Dr. Ruben Niesvizky of the myeloma center at New York Presbyterian Hospital and his associates.
The primary efficacy outcome – progression-free survival – was not significantly different among the three study groups at 14.7 months, 15.4 months, and 17.3 months, respectively. Overall response rates were 73%, 80%, and 70%, respectively; complete response rates were 3%, 4%, and 4%, respectively. Also not significantly different between the three groups were duration of response (18.3 months, 22.4 months, and 19.8 months) and median overall survival (49.8 months, 51.5 months, and 53.1 months), the researchers said (J. Clin. Oncol. 2015 June 8 [doi:10.1200/JCO.2014.58.7618]).
Peripheral neuropathy was the most common adverse effect in all three regimens and the most common reason for discontinuing therapy. Both the rates of adverse events and discontinuations due to adverse events were higher for bortezomib-thalidomide-dexamethasone treatment than for the other two regimens. Because of toxicity, only 30% of the total study population completed the full 13 cycles of treatment and only 40% received bortezomib maintenance therapy.
“Our results indicate that the type and number of agents(s) included in combination therapy for elderly persons are important, and offer caution to the current trend of incorporating 3 or even 4 agents into anti-multiple myeloma regimens to boost efficacy without confirmatory randomized studies,” Dr. Niesvizky and his associates noted.
Triple-agent bortezomib-based regimens yielded no survival or other advantages over a double-agent regimen in a phase-III clinical trial involving transplant-ineligible patients with multiple myeloma. The study was published online June 8 in the Journal of Clinical Oncology.
As the optimal therapy for transplant-ineligible patients has not yet been determined, researchers performed what they described as the first randomized trial comparing several bortezomib-based regimens. For this study, the researchers wanted to assess the regimens in more typical patients: elderly men and women of diverse ethnic and economic backgrounds who have common comorbidities and are treated in community oncology practices.
The 502 participants (mean age, 73 years) in this industry-sponsored study were treated at 159 oncology practices across the country during a 3-year period and followed up for a median of 43 months. Half had serious comorbidities such as diabetes, renal disease, and chronic pulmonary disease. They were randomly assigned to receive eight 21-day cycles of bortezomib-dexamethasone, bortezomib-thalidomide-dexamethasone, or bortezomib-melphalan-prednisone combination induction therapy, followed by five 35-day cycles of maintenance bortezomib, said Dr. Ruben Niesvizky of the myeloma center at New York Presbyterian Hospital and his associates.
The primary efficacy outcome – progression-free survival – was not significantly different among the three study groups at 14.7 months, 15.4 months, and 17.3 months, respectively. Overall response rates were 73%, 80%, and 70%, respectively; complete response rates were 3%, 4%, and 4%, respectively. Also not significantly different between the three groups were duration of response (18.3 months, 22.4 months, and 19.8 months) and median overall survival (49.8 months, 51.5 months, and 53.1 months), the researchers said (J. Clin. Oncol. 2015 June 8 [doi:10.1200/JCO.2014.58.7618]).
Peripheral neuropathy was the most common adverse effect in all three regimens and the most common reason for discontinuing therapy. Both the rates of adverse events and discontinuations due to adverse events were higher for bortezomib-thalidomide-dexamethasone treatment than for the other two regimens. Because of toxicity, only 30% of the total study population completed the full 13 cycles of treatment and only 40% received bortezomib maintenance therapy.
“Our results indicate that the type and number of agents(s) included in combination therapy for elderly persons are important, and offer caution to the current trend of incorporating 3 or even 4 agents into anti-multiple myeloma regimens to boost efficacy without confirmatory randomized studies,” Dr. Niesvizky and his associates noted.
Triple-agent bortezomib-based regimens yielded no survival or other advantages over a double-agent regimen in a phase-III clinical trial involving transplant-ineligible patients with multiple myeloma. The study was published online June 8 in the Journal of Clinical Oncology.
As the optimal therapy for transplant-ineligible patients has not yet been determined, researchers performed what they described as the first randomized trial comparing several bortezomib-based regimens. For this study, the researchers wanted to assess the regimens in more typical patients: elderly men and women of diverse ethnic and economic backgrounds who have common comorbidities and are treated in community oncology practices.
The 502 participants (mean age, 73 years) in this industry-sponsored study were treated at 159 oncology practices across the country during a 3-year period and followed up for a median of 43 months. Half had serious comorbidities such as diabetes, renal disease, and chronic pulmonary disease. They were randomly assigned to receive eight 21-day cycles of bortezomib-dexamethasone, bortezomib-thalidomide-dexamethasone, or bortezomib-melphalan-prednisone combination induction therapy, followed by five 35-day cycles of maintenance bortezomib, said Dr. Ruben Niesvizky of the myeloma center at New York Presbyterian Hospital and his associates.
The primary efficacy outcome – progression-free survival – was not significantly different among the three study groups at 14.7 months, 15.4 months, and 17.3 months, respectively. Overall response rates were 73%, 80%, and 70%, respectively; complete response rates were 3%, 4%, and 4%, respectively. Also not significantly different between the three groups were duration of response (18.3 months, 22.4 months, and 19.8 months) and median overall survival (49.8 months, 51.5 months, and 53.1 months), the researchers said (J. Clin. Oncol. 2015 June 8 [doi:10.1200/JCO.2014.58.7618]).
Peripheral neuropathy was the most common adverse effect in all three regimens and the most common reason for discontinuing therapy. Both the rates of adverse events and discontinuations due to adverse events were higher for bortezomib-thalidomide-dexamethasone treatment than for the other two regimens. Because of toxicity, only 30% of the total study population completed the full 13 cycles of treatment and only 40% received bortezomib maintenance therapy.
“Our results indicate that the type and number of agents(s) included in combination therapy for elderly persons are important, and offer caution to the current trend of incorporating 3 or even 4 agents into anti-multiple myeloma regimens to boost efficacy without confirmatory randomized studies,” Dr. Niesvizky and his associates noted.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Triple-agent bortezomib-based therapy offered no survival advantage over a double-agent regimen in elderly patients with multiple myeloma.
Major finding: The primary efficacy outcome – progression-free survival – was not significantly different among the three study groups at 14.7 months, 15.4 months, and 17.3 months, respectively.
Data source: An industry-sponsored randomized open-label phase-III clinical trial involving 502 patients followed for a median of 43 months at 159 U.S. medical centers.
Disclosures: This trial was supported by Millennium Pharmaceuticals, maker of bortezomib (Velcade). Dr. Niesvizky reported receiving research funding from Millennium, Celgene, and Onyx.
Advanced breast cancer: paclitaxel bests nab-paclitaxel, ixabepilone
Two newly developed agents, nab-paclitaxel and ixabepilone, both proved inferior to standard once-weekly paclitaxel and caused more toxicities in a phase III trial involving 783 patients with advanced chemotherapy-naive breast cancer, which was reported online June 8 in Journal of Clinical Oncology.
“On the basis of our data, once-per-week paclitaxel should remain the preferred microtubule inhibitor for patients with metastatic breast cancer in the first-line setting,” said Dr. Hope S. Rugo of the University of California, San Francisco, Helen Diller Family Comprehensive Cancer Center and her associates.

Nab-paclitaxel is a novel, solvent-free formulation of paclitaxel in albumin-bound nanoparticles, which precludes the need for premedication to prevent hypersensitivity reactions. Ixabepilone is a semisynthetic analog of epothilone B that binds to the same beta-tubulin site as does paclitaxel.
In phase II studies, both agents appeared to be more potent than paclitaxel and to have similar or superior toxicity profiles. In this trial, patients with metastatic or recurrent breast cancer not amenable to local therapy were randomly assigned to receive nab-paclitaxel (267 participants), ixabepilone (241 participants), or standard paclitaxel (275 participants) as well as bevacizumab; they were followed for a median of 25 months (maximum, 50 months).
The trial was halted early when interim analyses showed that both of the new agents crossed the futility boundary for superiority. The primary endpoint, progression-free survival, was 11 months with paclitaxel. Ixabepilone was clearly inferior, with a median progression-free survival of 7.4 months (HR, 1.59), and nab-paclitaxel trended toward inferiority, with a median progression-free survival of 9.3 months (HR, 1.20). Overall survival rates followed the same pattern. In addition, treatment response rates were lower with both new agents than with paclitaxel, as was palliation of disease-related symptoms.
Both hematologic and nonhematologic toxicities were more severe with the novel drugs than with paclitaxel. These included neutropenia, anemia, sensory neuropathy, fatigue, hypertension, motor neuropathy, pain, and nausea, the investigators said (J. Clin. Oncol. 2015 June 8 [doi:10.1200/JCO.2014.59.5298]).
Unfortunately, before these negative findings were published, the promising results of the phase II studies “led to widespread use of more costly and higher-dose nab-paclitaxel in many clinical practices,” Dr. Rugo and her associates noted.
“Our trial illustrates the importance of adequately powered prospective trials to confirm phase II reports. In addition, these results remind clinicians to be cautious when incorporating new agents, particularly those that are more expensive and potentially more toxic,” they added.
This study was supported by grants from the National Cancer Institute, the Alliance for Clinical Trials in Oncology’s Statistics and Data Center, and the Breast Cancer Research Foundation. Dr. Rugo reported ties to Genomic Health, Plexxikon, MacroGenics, OBI Pharma, Eisai, Pfizer, Novartis, Eli Lilly, GlaxoSmithKline, Genentech, Celsion, Nektar, Merck, Roche, OBI Ontology, and Mylan; her associates reported ties to some of those companies and to Myriad Genetics, Amgen, Celgene, and Verastem.
Two newly developed agents, nab-paclitaxel and ixabepilone, both proved inferior to standard once-weekly paclitaxel and caused more toxicities in a phase III trial involving 783 patients with advanced chemotherapy-naive breast cancer, which was reported online June 8 in Journal of Clinical Oncology.
“On the basis of our data, once-per-week paclitaxel should remain the preferred microtubule inhibitor for patients with metastatic breast cancer in the first-line setting,” said Dr. Hope S. Rugo of the University of California, San Francisco, Helen Diller Family Comprehensive Cancer Center and her associates.
Nab-paclitaxel is a novel, solvent-free formulation of paclitaxel in albumin-bound nanoparticles, which precludes the need for premedication to prevent hypersensitivity reactions. Ixabepilone is a semisynthetic analog of epothilone B that binds to the same beta-tubulin site as does paclitaxel.
In phase II studies, both agents appeared to be more potent than paclitaxel and to have similar or superior toxicity profiles. In this trial, patients with metastatic or recurrent breast cancer not amenable to local therapy were randomly assigned to receive nab-paclitaxel (267 participants), ixabepilone (241 participants), or standard paclitaxel (275 participants) as well as bevacizumab; they were followed for a median of 25 months (maximum, 50 months).
The trial was halted early when interim analyses showed that both of the new agents crossed the futility boundary for superiority. The primary endpoint, progression-free survival, was 11 months with paclitaxel. Ixabepilone was clearly inferior, with a median progression-free survival of 7.4 months (HR, 1.59), and nab-paclitaxel trended toward inferiority, with a median progression-free survival of 9.3 months (HR, 1.20). Overall survival rates followed the same pattern. In addition, treatment response rates were lower with both new agents than with paclitaxel, as was palliation of disease-related symptoms.
Both hematologic and nonhematologic toxicities were more severe with the novel drugs than with paclitaxel. These included neutropenia, anemia, sensory neuropathy, fatigue, hypertension, motor neuropathy, pain, and nausea, the investigators said (J. Clin. Oncol. 2015 June 8 [doi:10.1200/JCO.2014.59.5298]).
Unfortunately, before these negative findings were published, the promising results of the phase II studies “led to widespread use of more costly and higher-dose nab-paclitaxel in many clinical practices,” Dr. Rugo and her associates noted.
“Our trial illustrates the importance of adequately powered prospective trials to confirm phase II reports. In addition, these results remind clinicians to be cautious when incorporating new agents, particularly those that are more expensive and potentially more toxic,” they added.
This study was supported by grants from the National Cancer Institute, the Alliance for Clinical Trials in Oncology’s Statistics and Data Center, and the Breast Cancer Research Foundation. Dr. Rugo reported ties to Genomic Health, Plexxikon, MacroGenics, OBI Pharma, Eisai, Pfizer, Novartis, Eli Lilly, GlaxoSmithKline, Genentech, Celsion, Nektar, Merck, Roche, OBI Ontology, and Mylan; her associates reported ties to some of those companies and to Myriad Genetics, Amgen, Celgene, and Verastem.
Two newly developed agents, nab-paclitaxel and ixabepilone, both proved inferior to standard once-weekly paclitaxel and caused more toxicities in a phase III trial involving 783 patients with advanced chemotherapy-naive breast cancer, which was reported online June 8 in Journal of Clinical Oncology.
“On the basis of our data, once-per-week paclitaxel should remain the preferred microtubule inhibitor for patients with metastatic breast cancer in the first-line setting,” said Dr. Hope S. Rugo of the University of California, San Francisco, Helen Diller Family Comprehensive Cancer Center and her associates.
Nab-paclitaxel is a novel, solvent-free formulation of paclitaxel in albumin-bound nanoparticles, which precludes the need for premedication to prevent hypersensitivity reactions. Ixabepilone is a semisynthetic analog of epothilone B that binds to the same beta-tubulin site as does paclitaxel.
In phase II studies, both agents appeared to be more potent than paclitaxel and to have similar or superior toxicity profiles. In this trial, patients with metastatic or recurrent breast cancer not amenable to local therapy were randomly assigned to receive nab-paclitaxel (267 participants), ixabepilone (241 participants), or standard paclitaxel (275 participants) as well as bevacizumab; they were followed for a median of 25 months (maximum, 50 months).
The trial was halted early when interim analyses showed that both of the new agents crossed the futility boundary for superiority. The primary endpoint, progression-free survival, was 11 months with paclitaxel. Ixabepilone was clearly inferior, with a median progression-free survival of 7.4 months (HR, 1.59), and nab-paclitaxel trended toward inferiority, with a median progression-free survival of 9.3 months (HR, 1.20). Overall survival rates followed the same pattern. In addition, treatment response rates were lower with both new agents than with paclitaxel, as was palliation of disease-related symptoms.
Both hematologic and nonhematologic toxicities were more severe with the novel drugs than with paclitaxel. These included neutropenia, anemia, sensory neuropathy, fatigue, hypertension, motor neuropathy, pain, and nausea, the investigators said (J. Clin. Oncol. 2015 June 8 [doi:10.1200/JCO.2014.59.5298]).
Unfortunately, before these negative findings were published, the promising results of the phase II studies “led to widespread use of more costly and higher-dose nab-paclitaxel in many clinical practices,” Dr. Rugo and her associates noted.
“Our trial illustrates the importance of adequately powered prospective trials to confirm phase II reports. In addition, these results remind clinicians to be cautious when incorporating new agents, particularly those that are more expensive and potentially more toxic,” they added.
This study was supported by grants from the National Cancer Institute, the Alliance for Clinical Trials in Oncology’s Statistics and Data Center, and the Breast Cancer Research Foundation. Dr. Rugo reported ties to Genomic Health, Plexxikon, MacroGenics, OBI Pharma, Eisai, Pfizer, Novartis, Eli Lilly, GlaxoSmithKline, Genentech, Celsion, Nektar, Merck, Roche, OBI Ontology, and Mylan; her associates reported ties to some of those companies and to Myriad Genetics, Amgen, Celgene, and Verastem.
FROM JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Newly developed agents nab-paclitaxel and ixabepilone both failed to outperform paclitaxel against advanced breast cancer.
Major finding: Median progression-free survival was 11 months with paclitaxel, 7.4 months with ixabepilone (HR, 1.59), and 9.3 months with nab-paclitaxel (HR, 1.20).
Data source: A prospective, randomized phase III clinical trial comparing standard paclitaxel against nab-paclitaxel and ixabepilone as first-line chemotherapy in 783 patients with advanced breast cancer followed for a median of 25 months.
Disclosures: This study was supported by grants from the National Cancer Institute, the Alliance for Clinical Trials in Oncology’s Statistics and Data Center, and the Breast Cancer Research Foundation. Dr. Rugo reported ties to Genomic Health, Plexxikon, MacroGenics, OBI Pharma, Eisai, Pfizer, Novartis, Eli Lilly, GlaxoSmithKline, Genentech, Celsion, Nektar, Merck, Roche, OBI Ontology, and Mylan; her associates reported ties to some of those companies and to Myriad Genetics, Amgen, Celgene, and Verastem.

Patients in nursing homes show poor vascular outcomes
A substantial number of nursing home residents undergo lower-extremity revascularization each year, but very few of them gain any function and approximately half die within the year, according to an online report in JAMA Internal Medicine.
In a population-based analysis of Medicare claims and a database that tracks virtually all U.S. nursing homes, 82% of residents who underwent lower-extremity revascularization during a 3-year period had either died or were unable to walk a year afterward.
Most showed a clinically significant decline in function within 3 months of having the procedure, said Dr. Lawrence Oresanya of the department of surgery, University of California, San Francisco, and his associates. “Our findings can inform conversations between physicians, patients, and families about the risks and expected outcomes of surgery and whether the surgery is likely to be worthwhile. Our findings also highlight the importance of carefully considering a prognosis independent of vascular disease and assessing the goals of care. Ambulatory function … may be impossible to attain,” they wrote.
Lower-extremity revascularization is usually performed to maintain elderly patients’ functional independence by preserving their limbs. But a closer examination of these procedures is warranted in the nursing home population “because nursing home residents, in general, have high levels of functional dependence unrelated to peripheral arterial disease, and higher rates of mortality after most invasive procedures,” according to the investigators.
Dr. Oresanya and his colleagues identified 10,784 nursing home residents across the country who underwent lower-extremity revascularization.
The procedure was elective in 67% of cases and emergent or urgent in 33%. An endovascular approach was used in 56%, and an open approach in the remainder, with the endovacular approach being more associated with clinical success than open surgery.
The mean patient age was 82 years, and serious comorbidities were very common: 60% had cognitive impairment, 57% had heart failure, and 29% had renal failure. Three-fourths of the patients were nonambulatory at the time of surgery.
The investigators assumed that most patients in this setting had critical limb ischemia rather than claudication. They did not have information about the severity of the lower-extremity ischemia, or about the prevalence or duration of nonhealing wounds or gangrene.
One year after lower-extremity revascularization, mortality was 51% among ambulatory patients and 53% among nonambulatory patients.
Only 13% of the entire cohort were able to walk, and only 18% had maintained or improved their presurgical functional status.
“Revascularization rarely allowed a nonambulatory resident to become ambulatory,” Dr. Oresanya and his associates wrote (JAMA Intern. Med. 2015 April 6 [doi:10.1001/jamainternmed.2015.0486]).
The researchers were unable to determine whether these poor outcomes resulted from the surgery itself or were due to these patients’ “insufficient physiologic reserve.”
They also cautioned that they confined their study strictly to functional outcomes of lower-extremity revascularization, namely ambulation and mortality. Some patients may have derived other benefits from the procedure, such as relief of pain, healing of wounds, and avoidance of major amputation.
The authors reported having no relevant financial disclosures.
The recent study by Oresanya et al. is very controversial, especially in light of the recent NY Times article suggesting too many inappropriate procedures are occurring for PAD. However, the study must be looked at in context. This is a database study, which, as such, has inherent limitations. The authors admit they had no data on pain, wound healing, or avoidance of major amputations. Fully one-third of the cases in this study were urgent/emergent, again suggesting the critical nature of impaired perfusion in these patients. The only outcomes assessed were mortality and functional status. Seventy-five percent of the patients were already nonambulatory, again suggesting that the indications for intervention were likely critical limb ischemia. If this is correct, as the authors have also assumed, then the issue is not one of mortality or improving functional status, but rather one of limb salvage, and pain control – issues of quality of life. Further, the finding of endovascular cases being more successful suggests that the endovascular first approach is clearly appropriate in this debilitated population.
It is, unfortunately, not possible from this type of database study to ascertain whether the patients treated with open bypass were candidates for endovascular interventions, or had already failed an endovascular approach. It is also not possible to determine whether “success” was achieved, with pain relief, avoidance of major limb amputation with the inherent increased mortality risk, and wound healing.
However, what we can glean from this study is information to better counsel patients and families regarding functional status and life expectancy, as some families and patients have unrealistic expectations and push surgeons to intervene, despite initial attempts at counseling. Having additional data may allow surgeons to correctly convince some patients, whose pain is controlled and tissue loss is not immediately life or limb threatening, that because of limited life expectancy, medical management alone may be appropriate. This study, like most database studies, should lead to further evaluation in a situation in which clinical outcomes may be better assessed, such as a study of the Vascular Quality Initiative database, which does collect this type of information.
Dr. Linda Harris is professor of surgery and chief, division vascular surgery, University at Buffalo, State University of New York, and an associate medical editor for Vascular Specialist.
The recent study by Oresanya et al. is very controversial, especially in light of the recent NY Times article suggesting too many inappropriate procedures are occurring for PAD. However, the study must be looked at in context. This is a database study, which, as such, has inherent limitations. The authors admit they had no data on pain, wound healing, or avoidance of major amputations. Fully one-third of the cases in this study were urgent/emergent, again suggesting the critical nature of impaired perfusion in these patients. The only outcomes assessed were mortality and functional status. Seventy-five percent of the patients were already nonambulatory, again suggesting that the indications for intervention were likely critical limb ischemia. If this is correct, as the authors have also assumed, then the issue is not one of mortality or improving functional status, but rather one of limb salvage, and pain control – issues of quality of life. Further, the finding of endovascular cases being more successful suggests that the endovascular first approach is clearly appropriate in this debilitated population.
It is, unfortunately, not possible from this type of database study to ascertain whether the patients treated with open bypass were candidates for endovascular interventions, or had already failed an endovascular approach. It is also not possible to determine whether “success” was achieved, with pain relief, avoidance of major limb amputation with the inherent increased mortality risk, and wound healing.
However, what we can glean from this study is information to better counsel patients and families regarding functional status and life expectancy, as some families and patients have unrealistic expectations and push surgeons to intervene, despite initial attempts at counseling. Having additional data may allow surgeons to correctly convince some patients, whose pain is controlled and tissue loss is not immediately life or limb threatening, that because of limited life expectancy, medical management alone may be appropriate. This study, like most database studies, should lead to further evaluation in a situation in which clinical outcomes may be better assessed, such as a study of the Vascular Quality Initiative database, which does collect this type of information.
Dr. Linda Harris is professor of surgery and chief, division vascular surgery, University at Buffalo, State University of New York, and an associate medical editor for Vascular Specialist.
The recent study by Oresanya et al. is very controversial, especially in light of the recent NY Times article suggesting too many inappropriate procedures are occurring for PAD. However, the study must be looked at in context. This is a database study, which, as such, has inherent limitations. The authors admit they had no data on pain, wound healing, or avoidance of major amputations. Fully one-third of the cases in this study were urgent/emergent, again suggesting the critical nature of impaired perfusion in these patients. The only outcomes assessed were mortality and functional status. Seventy-five percent of the patients were already nonambulatory, again suggesting that the indications for intervention were likely critical limb ischemia. If this is correct, as the authors have also assumed, then the issue is not one of mortality or improving functional status, but rather one of limb salvage, and pain control – issues of quality of life. Further, the finding of endovascular cases being more successful suggests that the endovascular first approach is clearly appropriate in this debilitated population.
It is, unfortunately, not possible from this type of database study to ascertain whether the patients treated with open bypass were candidates for endovascular interventions, or had already failed an endovascular approach. It is also not possible to determine whether “success” was achieved, with pain relief, avoidance of major limb amputation with the inherent increased mortality risk, and wound healing.
However, what we can glean from this study is information to better counsel patients and families regarding functional status and life expectancy, as some families and patients have unrealistic expectations and push surgeons to intervene, despite initial attempts at counseling. Having additional data may allow surgeons to correctly convince some patients, whose pain is controlled and tissue loss is not immediately life or limb threatening, that because of limited life expectancy, medical management alone may be appropriate. This study, like most database studies, should lead to further evaluation in a situation in which clinical outcomes may be better assessed, such as a study of the Vascular Quality Initiative database, which does collect this type of information.
Dr. Linda Harris is professor of surgery and chief, division vascular surgery, University at Buffalo, State University of New York, and an associate medical editor for Vascular Specialist.
A substantial number of nursing home residents undergo lower-extremity revascularization each year, but very few of them gain any function and approximately half die within the year, according to an online report in JAMA Internal Medicine.
In a population-based analysis of Medicare claims and a database that tracks virtually all U.S. nursing homes, 82% of residents who underwent lower-extremity revascularization during a 3-year period had either died or were unable to walk a year afterward.
Most showed a clinically significant decline in function within 3 months of having the procedure, said Dr. Lawrence Oresanya of the department of surgery, University of California, San Francisco, and his associates. “Our findings can inform conversations between physicians, patients, and families about the risks and expected outcomes of surgery and whether the surgery is likely to be worthwhile. Our findings also highlight the importance of carefully considering a prognosis independent of vascular disease and assessing the goals of care. Ambulatory function … may be impossible to attain,” they wrote.
Lower-extremity revascularization is usually performed to maintain elderly patients’ functional independence by preserving their limbs. But a closer examination of these procedures is warranted in the nursing home population “because nursing home residents, in general, have high levels of functional dependence unrelated to peripheral arterial disease, and higher rates of mortality after most invasive procedures,” according to the investigators.
Dr. Oresanya and his colleagues identified 10,784 nursing home residents across the country who underwent lower-extremity revascularization.
The procedure was elective in 67% of cases and emergent or urgent in 33%. An endovascular approach was used in 56%, and an open approach in the remainder, with the endovacular approach being more associated with clinical success than open surgery.
The mean patient age was 82 years, and serious comorbidities were very common: 60% had cognitive impairment, 57% had heart failure, and 29% had renal failure. Three-fourths of the patients were nonambulatory at the time of surgery.
The investigators assumed that most patients in this setting had critical limb ischemia rather than claudication. They did not have information about the severity of the lower-extremity ischemia, or about the prevalence or duration of nonhealing wounds or gangrene.
One year after lower-extremity revascularization, mortality was 51% among ambulatory patients and 53% among nonambulatory patients.
Only 13% of the entire cohort were able to walk, and only 18% had maintained or improved their presurgical functional status.
“Revascularization rarely allowed a nonambulatory resident to become ambulatory,” Dr. Oresanya and his associates wrote (JAMA Intern. Med. 2015 April 6 [doi:10.1001/jamainternmed.2015.0486]).
The researchers were unable to determine whether these poor outcomes resulted from the surgery itself or were due to these patients’ “insufficient physiologic reserve.”
They also cautioned that they confined their study strictly to functional outcomes of lower-extremity revascularization, namely ambulation and mortality. Some patients may have derived other benefits from the procedure, such as relief of pain, healing of wounds, and avoidance of major amputation.
The authors reported having no relevant financial disclosures.
A substantial number of nursing home residents undergo lower-extremity revascularization each year, but very few of them gain any function and approximately half die within the year, according to an online report in JAMA Internal Medicine.
In a population-based analysis of Medicare claims and a database that tracks virtually all U.S. nursing homes, 82% of residents who underwent lower-extremity revascularization during a 3-year period had either died or were unable to walk a year afterward.
Most showed a clinically significant decline in function within 3 months of having the procedure, said Dr. Lawrence Oresanya of the department of surgery, University of California, San Francisco, and his associates. “Our findings can inform conversations between physicians, patients, and families about the risks and expected outcomes of surgery and whether the surgery is likely to be worthwhile. Our findings also highlight the importance of carefully considering a prognosis independent of vascular disease and assessing the goals of care. Ambulatory function … may be impossible to attain,” they wrote.
Lower-extremity revascularization is usually performed to maintain elderly patients’ functional independence by preserving their limbs. But a closer examination of these procedures is warranted in the nursing home population “because nursing home residents, in general, have high levels of functional dependence unrelated to peripheral arterial disease, and higher rates of mortality after most invasive procedures,” according to the investigators.
Dr. Oresanya and his colleagues identified 10,784 nursing home residents across the country who underwent lower-extremity revascularization.
The procedure was elective in 67% of cases and emergent or urgent in 33%. An endovascular approach was used in 56%, and an open approach in the remainder, with the endovacular approach being more associated with clinical success than open surgery.
The mean patient age was 82 years, and serious comorbidities were very common: 60% had cognitive impairment, 57% had heart failure, and 29% had renal failure. Three-fourths of the patients were nonambulatory at the time of surgery.
The investigators assumed that most patients in this setting had critical limb ischemia rather than claudication. They did not have information about the severity of the lower-extremity ischemia, or about the prevalence or duration of nonhealing wounds or gangrene.
One year after lower-extremity revascularization, mortality was 51% among ambulatory patients and 53% among nonambulatory patients.
Only 13% of the entire cohort were able to walk, and only 18% had maintained or improved their presurgical functional status.
“Revascularization rarely allowed a nonambulatory resident to become ambulatory,” Dr. Oresanya and his associates wrote (JAMA Intern. Med. 2015 April 6 [doi:10.1001/jamainternmed.2015.0486]).
The researchers were unable to determine whether these poor outcomes resulted from the surgery itself or were due to these patients’ “insufficient physiologic reserve.”
They also cautioned that they confined their study strictly to functional outcomes of lower-extremity revascularization, namely ambulation and mortality. Some patients may have derived other benefits from the procedure, such as relief of pain, healing of wounds, and avoidance of major amputation.
The authors reported having no relevant financial disclosures.
Annual US Incidence of BCC Pegged at 2 Million
Approximately 2 million basal cell carcinomas occur in the United States each year, a number that has increased only modestly during the past 15 years, according to a report published online June 3 in JAMA Dermatology.
The epidemiology of BCCs has been difficult to pin down because these tumors are excluded from cancer registries and national cancer surveillance programs, and because when they are tracked they are usually lumped together with squamous cell carcinomas. The most recent National Cancer Institute–funded survey of BCC was done more than 30 years ago.

So the current incidence of BCC “is not well characterized.” Nevertheless. some researchers have posited that the incidence has risen 80%-200% during the past 10-20 years, said Dr. Maryam M. Asgari of Kaiser Permanente Northern California, Oakland, and the department of dermatology at the University of California, San Francisco.
To estimate incidence more accurately, Dr. Asgari and her associates analyzed data from every electronic pathology report in a registry covering the 3.2 million participants in the HMO from 1998 through 2012. They identified 221,624 cases of BCC in patients aged 2-105 years. The annual incidence increased from 513 to 600 cases per 100,000 population during the study period – a 17% rise that was deemed “not remarkable.”
“In extrapolating our data to the United States, we estimate that approximately 2 million individuals develop at least one BCC in the U.S. in a given year,” Dr. Asgari and her associates wrote (JAMA Dermatol. 2015 June 3 [doi:10.1001/jamadermatol.2015.1188]).
This total is higher than that cited on the National Institutes of Health website, which estimates the annual incidence of all nonmelanoma skin cancers, not just BCC, at 2 million per year.
Males were at higher risk than were females for developing BCC (incidence rate ratio, 1.65), and risk increased with increasing patient age. As expected, whites were at 8- to 70-fold greater risk than were Hispanics, Asians, or blacks. Contrary to one previous report, the incidence of BCC did not increase among Hispanics during the study period.
The National Cancer Institute and the National Institutes of Health supported the study. Dr. Asgari reported receiving research grants from Kaiser Permanente, Pfizer, and Valeant Pharmaceuticals, but not for this project.
Approximately 2 million basal cell carcinomas occur in the United States each year, a number that has increased only modestly during the past 15 years, according to a report published online June 3 in JAMA Dermatology.
The epidemiology of BCCs has been difficult to pin down because these tumors are excluded from cancer registries and national cancer surveillance programs, and because when they are tracked they are usually lumped together with squamous cell carcinomas. The most recent National Cancer Institute–funded survey of BCC was done more than 30 years ago.
So the current incidence of BCC “is not well characterized.” Nevertheless. some researchers have posited that the incidence has risen 80%-200% during the past 10-20 years, said Dr. Maryam M. Asgari of Kaiser Permanente Northern California, Oakland, and the department of dermatology at the University of California, San Francisco.
To estimate incidence more accurately, Dr. Asgari and her associates analyzed data from every electronic pathology report in a registry covering the 3.2 million participants in the HMO from 1998 through 2012. They identified 221,624 cases of BCC in patients aged 2-105 years. The annual incidence increased from 513 to 600 cases per 100,000 population during the study period – a 17% rise that was deemed “not remarkable.”
“In extrapolating our data to the United States, we estimate that approximately 2 million individuals develop at least one BCC in the U.S. in a given year,” Dr. Asgari and her associates wrote (JAMA Dermatol. 2015 June 3 [doi:10.1001/jamadermatol.2015.1188]).
This total is higher than that cited on the National Institutes of Health website, which estimates the annual incidence of all nonmelanoma skin cancers, not just BCC, at 2 million per year.
Males were at higher risk than were females for developing BCC (incidence rate ratio, 1.65), and risk increased with increasing patient age. As expected, whites were at 8- to 70-fold greater risk than were Hispanics, Asians, or blacks. Contrary to one previous report, the incidence of BCC did not increase among Hispanics during the study period.
The National Cancer Institute and the National Institutes of Health supported the study. Dr. Asgari reported receiving research grants from Kaiser Permanente, Pfizer, and Valeant Pharmaceuticals, but not for this project.
Approximately 2 million basal cell carcinomas occur in the United States each year, a number that has increased only modestly during the past 15 years, according to a report published online June 3 in JAMA Dermatology.
The epidemiology of BCCs has been difficult to pin down because these tumors are excluded from cancer registries and national cancer surveillance programs, and because when they are tracked they are usually lumped together with squamous cell carcinomas. The most recent National Cancer Institute–funded survey of BCC was done more than 30 years ago.
So the current incidence of BCC “is not well characterized.” Nevertheless. some researchers have posited that the incidence has risen 80%-200% during the past 10-20 years, said Dr. Maryam M. Asgari of Kaiser Permanente Northern California, Oakland, and the department of dermatology at the University of California, San Francisco.
To estimate incidence more accurately, Dr. Asgari and her associates analyzed data from every electronic pathology report in a registry covering the 3.2 million participants in the HMO from 1998 through 2012. They identified 221,624 cases of BCC in patients aged 2-105 years. The annual incidence increased from 513 to 600 cases per 100,000 population during the study period – a 17% rise that was deemed “not remarkable.”
“In extrapolating our data to the United States, we estimate that approximately 2 million individuals develop at least one BCC in the U.S. in a given year,” Dr. Asgari and her associates wrote (JAMA Dermatol. 2015 June 3 [doi:10.1001/jamadermatol.2015.1188]).
This total is higher than that cited on the National Institutes of Health website, which estimates the annual incidence of all nonmelanoma skin cancers, not just BCC, at 2 million per year.
Males were at higher risk than were females for developing BCC (incidence rate ratio, 1.65), and risk increased with increasing patient age. As expected, whites were at 8- to 70-fold greater risk than were Hispanics, Asians, or blacks. Contrary to one previous report, the incidence of BCC did not increase among Hispanics during the study period.
The National Cancer Institute and the National Institutes of Health supported the study. Dr. Asgari reported receiving research grants from Kaiser Permanente, Pfizer, and Valeant Pharmaceuticals, but not for this project.
