User login
Malpractice climate: ‘Stable, but still dysfunctional’
Fewer malpractice suits are resulting in paid claims against physicians while malpractice insurance premiums have remained stable or declined over the last 12 years, according to an analysis published Oct. 30 in JAMA.
Since 2002, the rate of paid malpractice claims against doctors of medicine has decreased by an estimated 6% annually; for doctors of osteopathy, the rate has declined about 5% annually, Michelle M. Mello of Stanford (Calif.) University and her colleagues reported (JAMA 2014 Oct. 30 [doi:10.1001/jama.2014.10705]).
Dr. Mello and her colleagues analyzed paid legal claims against MDs and DOs between 1994 and 2013 from the National Practitioner Data Bank and the American Medical Association’s Physician Masterfile. They also evaluated premium data from the Medical Liability Monitor’s Annual Rate Survey.

The rate of paid malpractice claims against MDs fell from 18.6 to 9.9 paid claims per 1,000 physicians between 2002 and 2013, they found. For DOs, rates dropped from about 19 in 2002 to about 12.2 paid claims per 1,000 physicians in 2013.
The median compensation paid to plaintiffs rose by 63% between 1994 and 2007, from $133,799 to $218,400, in adjusted 2013 dollars. However, since 2007, that number has declined, reaching $195,000 in 2013. Only 3.4% of payments made during the 20-year period resulted from jury verdicts; the others stemmed from settlements.
For the premiums review, Dr. Mello and colleagues analyzed insurance data from 2004 to 2013 from five geographical areas: Los Angeles, Orange, Kern, and Ventura counties in California; Nassau and Suffolk counties in New York; Cook, Madison, St. Clair, and Will counties in Illinois; and the states of Tennessee and Colorado. The locations were selected based on geographic diversity and because each had an insurer with a dominant market share.
In California, Illinois, and Tennessee, internists and ob.gyns. saw a 36% decrease in premiums charged by each state’s largest medical malpractice insurer from 2004 to 2013. Premiums charged to general surgeons fell by 30% in these states. In Colorado, internists saw a 20% decrease in premiums over the same time period, but general surgeons saw an increase of 13% and ob.gyns. experienced an 11% rise. In New York, rates charged by the largest insurer rose by 12% for ob.gyns, 16% for internists, and 35% for general surgeons.
It remains unclear why the rate of paid claims has decreased and why premiums have remained fairly stable, Dr. Mello and colleagues said. While medical organizations like to point to tort reform, traditional reforms such as award caps do not address problems within the malpractice system’s core functions – compensating negligently injured patients and deterring substandard care, they added.
“The weight of evidence suggests that the system’s effectiveness as both a compensation and a deterrence mechanism is mediocre at best, and there is little to suggest it has improved over the past decade,” they wrote. “Thus, ‘stable but still dysfunctional’ might describe today’s liability environment.”
The authors offered alternatives to traditional tort reform, such as communication and resolution programs, mandatory presuit notification laws, and judge-directed negotiation.
In communication and resolution programs, clinicians and institutions openly discuss adverse outcomes with patients and proactively seek resolution, including offering an apology, and, if the standard of care was not met, compensation. Mandatory presuit notification refers to requiring plaintiffs to give defendants advance notice that they intend to sue. Judge-directed negotiation centers on court policies in which malpractice litigants meet early and often with judges to discuss settlement. In such negotiations, the court employs an attorney with clinical training to help judges understand clinical issues.
The authors conclude that action to improve the medical liability system is necessary while the legal climate is stable, and not after a crisis.
“During malpractice crises, interest in liability reform intensifies, but one lesson of the last 40 years is that an atmosphere of crisis is not conducive to thoughtful and enduring solutions,” study authors said. “Action now to reduce the amplitude of the next medical liability cycle is both prudent and feasible. Further testing of nontraditional reforms, followed by wider implementation of those that work, holds the most promise.”
On Twitter @legal_med
Fewer malpractice suits are resulting in paid claims against physicians while malpractice insurance premiums have remained stable or declined over the last 12 years, according to an analysis published Oct. 30 in JAMA.
Since 2002, the rate of paid malpractice claims against doctors of medicine has decreased by an estimated 6% annually; for doctors of osteopathy, the rate has declined about 5% annually, Michelle M. Mello of Stanford (Calif.) University and her colleagues reported (JAMA 2014 Oct. 30 [doi:10.1001/jama.2014.10705]).
Dr. Mello and her colleagues analyzed paid legal claims against MDs and DOs between 1994 and 2013 from the National Practitioner Data Bank and the American Medical Association’s Physician Masterfile. They also evaluated premium data from the Medical Liability Monitor’s Annual Rate Survey.
The rate of paid malpractice claims against MDs fell from 18.6 to 9.9 paid claims per 1,000 physicians between 2002 and 2013, they found. For DOs, rates dropped from about 19 in 2002 to about 12.2 paid claims per 1,000 physicians in 2013.
The median compensation paid to plaintiffs rose by 63% between 1994 and 2007, from $133,799 to $218,400, in adjusted 2013 dollars. However, since 2007, that number has declined, reaching $195,000 in 2013. Only 3.4% of payments made during the 20-year period resulted from jury verdicts; the others stemmed from settlements.
For the premiums review, Dr. Mello and colleagues analyzed insurance data from 2004 to 2013 from five geographical areas: Los Angeles, Orange, Kern, and Ventura counties in California; Nassau and Suffolk counties in New York; Cook, Madison, St. Clair, and Will counties in Illinois; and the states of Tennessee and Colorado. The locations were selected based on geographic diversity and because each had an insurer with a dominant market share.
In California, Illinois, and Tennessee, internists and ob.gyns. saw a 36% decrease in premiums charged by each state’s largest medical malpractice insurer from 2004 to 2013. Premiums charged to general surgeons fell by 30% in these states. In Colorado, internists saw a 20% decrease in premiums over the same time period, but general surgeons saw an increase of 13% and ob.gyns. experienced an 11% rise. In New York, rates charged by the largest insurer rose by 12% for ob.gyns, 16% for internists, and 35% for general surgeons.
It remains unclear why the rate of paid claims has decreased and why premiums have remained fairly stable, Dr. Mello and colleagues said. While medical organizations like to point to tort reform, traditional reforms such as award caps do not address problems within the malpractice system’s core functions – compensating negligently injured patients and deterring substandard care, they added.
“The weight of evidence suggests that the system’s effectiveness as both a compensation and a deterrence mechanism is mediocre at best, and there is little to suggest it has improved over the past decade,” they wrote. “Thus, ‘stable but still dysfunctional’ might describe today’s liability environment.”
The authors offered alternatives to traditional tort reform, such as communication and resolution programs, mandatory presuit notification laws, and judge-directed negotiation.
In communication and resolution programs, clinicians and institutions openly discuss adverse outcomes with patients and proactively seek resolution, including offering an apology, and, if the standard of care was not met, compensation. Mandatory presuit notification refers to requiring plaintiffs to give defendants advance notice that they intend to sue. Judge-directed negotiation centers on court policies in which malpractice litigants meet early and often with judges to discuss settlement. In such negotiations, the court employs an attorney with clinical training to help judges understand clinical issues.
The authors conclude that action to improve the medical liability system is necessary while the legal climate is stable, and not after a crisis.
“During malpractice crises, interest in liability reform intensifies, but one lesson of the last 40 years is that an atmosphere of crisis is not conducive to thoughtful and enduring solutions,” study authors said. “Action now to reduce the amplitude of the next medical liability cycle is both prudent and feasible. Further testing of nontraditional reforms, followed by wider implementation of those that work, holds the most promise.”
On Twitter @legal_med
Fewer malpractice suits are resulting in paid claims against physicians while malpractice insurance premiums have remained stable or declined over the last 12 years, according to an analysis published Oct. 30 in JAMA.
Since 2002, the rate of paid malpractice claims against doctors of medicine has decreased by an estimated 6% annually; for doctors of osteopathy, the rate has declined about 5% annually, Michelle M. Mello of Stanford (Calif.) University and her colleagues reported (JAMA 2014 Oct. 30 [doi:10.1001/jama.2014.10705]).
Dr. Mello and her colleagues analyzed paid legal claims against MDs and DOs between 1994 and 2013 from the National Practitioner Data Bank and the American Medical Association’s Physician Masterfile. They also evaluated premium data from the Medical Liability Monitor’s Annual Rate Survey.
The rate of paid malpractice claims against MDs fell from 18.6 to 9.9 paid claims per 1,000 physicians between 2002 and 2013, they found. For DOs, rates dropped from about 19 in 2002 to about 12.2 paid claims per 1,000 physicians in 2013.
The median compensation paid to plaintiffs rose by 63% between 1994 and 2007, from $133,799 to $218,400, in adjusted 2013 dollars. However, since 2007, that number has declined, reaching $195,000 in 2013. Only 3.4% of payments made during the 20-year period resulted from jury verdicts; the others stemmed from settlements.
For the premiums review, Dr. Mello and colleagues analyzed insurance data from 2004 to 2013 from five geographical areas: Los Angeles, Orange, Kern, and Ventura counties in California; Nassau and Suffolk counties in New York; Cook, Madison, St. Clair, and Will counties in Illinois; and the states of Tennessee and Colorado. The locations were selected based on geographic diversity and because each had an insurer with a dominant market share.
In California, Illinois, and Tennessee, internists and ob.gyns. saw a 36% decrease in premiums charged by each state’s largest medical malpractice insurer from 2004 to 2013. Premiums charged to general surgeons fell by 30% in these states. In Colorado, internists saw a 20% decrease in premiums over the same time period, but general surgeons saw an increase of 13% and ob.gyns. experienced an 11% rise. In New York, rates charged by the largest insurer rose by 12% for ob.gyns, 16% for internists, and 35% for general surgeons.
It remains unclear why the rate of paid claims has decreased and why premiums have remained fairly stable, Dr. Mello and colleagues said. While medical organizations like to point to tort reform, traditional reforms such as award caps do not address problems within the malpractice system’s core functions – compensating negligently injured patients and deterring substandard care, they added.
“The weight of evidence suggests that the system’s effectiveness as both a compensation and a deterrence mechanism is mediocre at best, and there is little to suggest it has improved over the past decade,” they wrote. “Thus, ‘stable but still dysfunctional’ might describe today’s liability environment.”
The authors offered alternatives to traditional tort reform, such as communication and resolution programs, mandatory presuit notification laws, and judge-directed negotiation.
In communication and resolution programs, clinicians and institutions openly discuss adverse outcomes with patients and proactively seek resolution, including offering an apology, and, if the standard of care was not met, compensation. Mandatory presuit notification refers to requiring plaintiffs to give defendants advance notice that they intend to sue. Judge-directed negotiation centers on court policies in which malpractice litigants meet early and often with judges to discuss settlement. In such negotiations, the court employs an attorney with clinical training to help judges understand clinical issues.
The authors conclude that action to improve the medical liability system is necessary while the legal climate is stable, and not after a crisis.
“During malpractice crises, interest in liability reform intensifies, but one lesson of the last 40 years is that an atmosphere of crisis is not conducive to thoughtful and enduring solutions,” study authors said. “Action now to reduce the amplitude of the next medical liability cycle is both prudent and feasible. Further testing of nontraditional reforms, followed by wider implementation of those that work, holds the most promise.”
On Twitter @legal_med
Key clinical point: Doctors have experienced a steady decrease in paid malpractice claims since 2002.
Major finding: The rate of paid malpractice claims against MDs fell from 18.6 to 9.9 paid claims per 1,000 physicians between 2002 and 2013.
Data source: Data analysis of paid claims and insurance premiums
Disclosures: Michelle M. Mello, Ph.D., and Dr. Allen Kachalia report that they served as investigators on several of the demonstration projects described in the JAMA article. Dr Mello also reports that she is an investigator on the Agency for Healthcare Research and Quality’s toolkit project. Dr. Mello and Dr. Kachalia report that they have served as consultants to the state of Oregon on liability issues.
Child molesters’ motivations may include repressed sexuality
CHICAGO – Many factors motivate the actions of child molesters, including feelings of inadequacy, repressed sexuality, and childhood experiences, a small study showed.
In the study, the motivations of 18 child molesters receiving treatment were assessed. All subjects were adult men who had admitted to and been convicted of a hands-on sexual offense against a child. The offenders ranged in age from 24 to 73, with a mean age of 50. All molesters knew their victims, Natasha Knack reported at the American Academy of Psychiatry and the Law annual meeting.
The goal of the qualitative research was to better identify the motivations behind offenders who sexually abuse children in order to more effectively treat them, said Ms. Knack, forensic research assistant at the Royal Ottawa Mental Health Centre.*

“One of the things that makes treating sex offenders more complicated is that they are a very diverse group,” she said. “Even child molesters specifically are very heterogeneous, and they have different motivations for offending. It seems the general public assumes there’s basically one motivation for committing these offenses, and that’s sexual gratification. While that’s something that came out in the research, that is definitely not the only motivation that we found.”
Ms. Knack conducted in-depth interviews with each offender and asked questions pertaining to what factors led to their crimes. Factors that contributed to the abuse fell into categories of explicit or implicit motivations. Explicit motivations included sexual gratification with such underlying themes as opportunity and feelings of inadequacy among adults. Seeking intimacy and self-identifying as a teacher were some explicit, nonsexual gratification motivations that were found.
Implicit motivations included childhood experiences such as personal abuse, repressed sexuality, and a lack of sexual information. Other implicit motivations found were life experiences such as poor romantic relationships with adults and problems with substance abuse.
Ms. Knack noted that the absence of sexual information among victims and offenders when they were children played a part in the abuse. For example, some offenders admitted choosing victims who were naive about sex, had parents who did not openly discuss sex, and would be unlikely to tell their parents of the abuse. At the same time, some offenders noted they had developed misconceived ideas about sex as children, had parents who did not discuss the subject, or had learned about sexual topics from friends.
“Parents really need to talk about sex with their children more,” Ms. Knack said at the meeting. “It needs to come from parents. Children need to know they can talk to their parents if they need to. That makes them more likely to disclose abuse that happens and more likely to know what’s appropriate behavior with an adult and what’s not.”
Investigators hope the research into the motivations of child molesters will assist in more targeted and effective approaches to treatment and prevention.
The University of Ottawa Medical Research Fund funded the study.
On Twitter @legal_med
*Correction, 10/30/2014: An earlier version of this story misstated the title of Natasha Knack.
CHICAGO – Many factors motivate the actions of child molesters, including feelings of inadequacy, repressed sexuality, and childhood experiences, a small study showed.
In the study, the motivations of 18 child molesters receiving treatment were assessed. All subjects were adult men who had admitted to and been convicted of a hands-on sexual offense against a child. The offenders ranged in age from 24 to 73, with a mean age of 50. All molesters knew their victims, Natasha Knack reported at the American Academy of Psychiatry and the Law annual meeting.
The goal of the qualitative research was to better identify the motivations behind offenders who sexually abuse children in order to more effectively treat them, said Ms. Knack, forensic research assistant at the Royal Ottawa Mental Health Centre.*
“One of the things that makes treating sex offenders more complicated is that they are a very diverse group,” she said. “Even child molesters specifically are very heterogeneous, and they have different motivations for offending. It seems the general public assumes there’s basically one motivation for committing these offenses, and that’s sexual gratification. While that’s something that came out in the research, that is definitely not the only motivation that we found.”
Ms. Knack conducted in-depth interviews with each offender and asked questions pertaining to what factors led to their crimes. Factors that contributed to the abuse fell into categories of explicit or implicit motivations. Explicit motivations included sexual gratification with such underlying themes as opportunity and feelings of inadequacy among adults. Seeking intimacy and self-identifying as a teacher were some explicit, nonsexual gratification motivations that were found.
Implicit motivations included childhood experiences such as personal abuse, repressed sexuality, and a lack of sexual information. Other implicit motivations found were life experiences such as poor romantic relationships with adults and problems with substance abuse.
Ms. Knack noted that the absence of sexual information among victims and offenders when they were children played a part in the abuse. For example, some offenders admitted choosing victims who were naive about sex, had parents who did not openly discuss sex, and would be unlikely to tell their parents of the abuse. At the same time, some offenders noted they had developed misconceived ideas about sex as children, had parents who did not discuss the subject, or had learned about sexual topics from friends.
“Parents really need to talk about sex with their children more,” Ms. Knack said at the meeting. “It needs to come from parents. Children need to know they can talk to their parents if they need to. That makes them more likely to disclose abuse that happens and more likely to know what’s appropriate behavior with an adult and what’s not.”
Investigators hope the research into the motivations of child molesters will assist in more targeted and effective approaches to treatment and prevention.
The University of Ottawa Medical Research Fund funded the study.
On Twitter @legal_med
*Correction, 10/30/2014: An earlier version of this story misstated the title of Natasha Knack.
CHICAGO – Many factors motivate the actions of child molesters, including feelings of inadequacy, repressed sexuality, and childhood experiences, a small study showed.
In the study, the motivations of 18 child molesters receiving treatment were assessed. All subjects were adult men who had admitted to and been convicted of a hands-on sexual offense against a child. The offenders ranged in age from 24 to 73, with a mean age of 50. All molesters knew their victims, Natasha Knack reported at the American Academy of Psychiatry and the Law annual meeting.
The goal of the qualitative research was to better identify the motivations behind offenders who sexually abuse children in order to more effectively treat them, said Ms. Knack, forensic research assistant at the Royal Ottawa Mental Health Centre.*
“One of the things that makes treating sex offenders more complicated is that they are a very diverse group,” she said. “Even child molesters specifically are very heterogeneous, and they have different motivations for offending. It seems the general public assumes there’s basically one motivation for committing these offenses, and that’s sexual gratification. While that’s something that came out in the research, that is definitely not the only motivation that we found.”
Ms. Knack conducted in-depth interviews with each offender and asked questions pertaining to what factors led to their crimes. Factors that contributed to the abuse fell into categories of explicit or implicit motivations. Explicit motivations included sexual gratification with such underlying themes as opportunity and feelings of inadequacy among adults. Seeking intimacy and self-identifying as a teacher were some explicit, nonsexual gratification motivations that were found.
Implicit motivations included childhood experiences such as personal abuse, repressed sexuality, and a lack of sexual information. Other implicit motivations found were life experiences such as poor romantic relationships with adults and problems with substance abuse.
Ms. Knack noted that the absence of sexual information among victims and offenders when they were children played a part in the abuse. For example, some offenders admitted choosing victims who were naive about sex, had parents who did not openly discuss sex, and would be unlikely to tell their parents of the abuse. At the same time, some offenders noted they had developed misconceived ideas about sex as children, had parents who did not discuss the subject, or had learned about sexual topics from friends.
“Parents really need to talk about sex with their children more,” Ms. Knack said at the meeting. “It needs to come from parents. Children need to know they can talk to their parents if they need to. That makes them more likely to disclose abuse that happens and more likely to know what’s appropriate behavior with an adult and what’s not.”
Investigators hope the research into the motivations of child molesters will assist in more targeted and effective approaches to treatment and prevention.
The University of Ottawa Medical Research Fund funded the study.
On Twitter @legal_med
*Correction, 10/30/2014: An earlier version of this story misstated the title of Natasha Knack.
AT THE AAPL ANNUAL MEETING
Key clinical point: Parents should be encouraged to talk with their children about sex and sexuality.
Major finding: Key contributors to sex abuse against children by adults are childhood experiences, repressed sexuality, lack of sexual information as a child, and feelings of inadequacy among adults and peer groups.
Data source: A qualitative research study of 18 men aged 24-73 who were getting treatment, and had admitted to and been convicted of a hands-on sexual offense against a child.
Disclosures: The University of Ottawa Medical Research Fund funded the study.

Board provides more flexibility on MOC
CHICAGO – New flexibility should help make maintenance of certification efforts a bit more palatable for psychiatrists, according to Dr. Larry Faulkner, president and CEO fo the American Board of Psychiatry and Neurology.
Key changes include a more-relaxed approach to how psychiatrists and neurologists can complete the feedback module and the waiving of some continuing medical education credit hours upon completion of certain peer review activities, Dr. Faulkner said at the annual meeting of the American Academy of Psychiatry and the Law. The modifications come in response to new maintenance of certification (MOC) standards by the American Board of Medical Specialties (ABMS) that go into effect in 2015.

“We are trying to make sure our program is credible, but at the same time, we don’t want the program to be so exhausting that it brings people to their knees in order to accomplish our program,” Dr. Faulkner said. “We’re trying to strike this balance.”
The ABPN’s MOC program consists of four components: professional standing; self-assessment and continuing medication education (CME); cognitive expertise; and performance in practice (PIP). PIP units require two modules – clinical and feedback. The feedback module now can be fulfilled by completing a patient survey, a peer survey, an institutional peer review of general competencies, supervisor evaluations of general competencies, resident evaluations of general competencies, or a 360-degree evaluation of general competencies.
Additionally, some required CME credits to be waived for completing a non-CME self-assessment activity, Dr. Faulkner said. Diplomates are required to complete an average of 30 specialty and/or subspecialty CME credits averaged over 3 years. At least eight credits per year, averaged over 3 years, must involve self-assessment. In summer 2014, ABPN decided it would waive eight CME credits for such activities as passing an ABPN cognitive certification or recertification examination; receiving documented feedback on an approved scientific grant application. or by receiveing documented feedback on an academic/scientific journal article accepted for publication. The ABPN will waive a maximum of 16 self-assessment CME credits for two different non-CME self-assessment activities in a 3-year MOC block. Other options for receiving waived credits are listed on the ABPN’s website.
Dr. Faulkner acknowledged that many physicians have expressed dissatisfaction over MOC and its validity. In June, physicians at the American Medical Association House of Delegates meeting spoke out about MOC being too expensive, too lengthy, and having too little value. The AMA delegates defeated a resolution that asked the organization to put a moratorium on MOC until it was proven to improve the quality of care and patient outcomes. However, delegates agreed to directing the AMA to explore the feasibility of a study to evaluate the effect MOC requirements and maintenance of licensure principles have on workforce, practice costs, patient outcomes, patient safety, and patient access.
Despite some negative sentiments, Dr. Faulkner stressed that MOC is not going away, and that physicians should view the process as a way to demonstrate efforts of their ongoing professional learning.
“I’ve never heard somebody deny that life-long learning is important,” he said. “Maintenance of certification is a little more than a formal way for you to document your life-long learning efforts, and I would encourage you to think of maintenance of certification in that vein.”
On Twitter @legal_med
CHICAGO – New flexibility should help make maintenance of certification efforts a bit more palatable for psychiatrists, according to Dr. Larry Faulkner, president and CEO fo the American Board of Psychiatry and Neurology.
Key changes include a more-relaxed approach to how psychiatrists and neurologists can complete the feedback module and the waiving of some continuing medical education credit hours upon completion of certain peer review activities, Dr. Faulkner said at the annual meeting of the American Academy of Psychiatry and the Law. The modifications come in response to new maintenance of certification (MOC) standards by the American Board of Medical Specialties (ABMS) that go into effect in 2015.
“We are trying to make sure our program is credible, but at the same time, we don’t want the program to be so exhausting that it brings people to their knees in order to accomplish our program,” Dr. Faulkner said. “We’re trying to strike this balance.”
The ABPN’s MOC program consists of four components: professional standing; self-assessment and continuing medication education (CME); cognitive expertise; and performance in practice (PIP). PIP units require two modules – clinical and feedback. The feedback module now can be fulfilled by completing a patient survey, a peer survey, an institutional peer review of general competencies, supervisor evaluations of general competencies, resident evaluations of general competencies, or a 360-degree evaluation of general competencies.
Additionally, some required CME credits to be waived for completing a non-CME self-assessment activity, Dr. Faulkner said. Diplomates are required to complete an average of 30 specialty and/or subspecialty CME credits averaged over 3 years. At least eight credits per year, averaged over 3 years, must involve self-assessment. In summer 2014, ABPN decided it would waive eight CME credits for such activities as passing an ABPN cognitive certification or recertification examination; receiving documented feedback on an approved scientific grant application. or by receiveing documented feedback on an academic/scientific journal article accepted for publication. The ABPN will waive a maximum of 16 self-assessment CME credits for two different non-CME self-assessment activities in a 3-year MOC block. Other options for receiving waived credits are listed on the ABPN’s website.
Dr. Faulkner acknowledged that many physicians have expressed dissatisfaction over MOC and its validity. In June, physicians at the American Medical Association House of Delegates meeting spoke out about MOC being too expensive, too lengthy, and having too little value. The AMA delegates defeated a resolution that asked the organization to put a moratorium on MOC until it was proven to improve the quality of care and patient outcomes. However, delegates agreed to directing the AMA to explore the feasibility of a study to evaluate the effect MOC requirements and maintenance of licensure principles have on workforce, practice costs, patient outcomes, patient safety, and patient access.
Despite some negative sentiments, Dr. Faulkner stressed that MOC is not going away, and that physicians should view the process as a way to demonstrate efforts of their ongoing professional learning.
“I’ve never heard somebody deny that life-long learning is important,” he said. “Maintenance of certification is a little more than a formal way for you to document your life-long learning efforts, and I would encourage you to think of maintenance of certification in that vein.”
On Twitter @legal_med
CHICAGO – New flexibility should help make maintenance of certification efforts a bit more palatable for psychiatrists, according to Dr. Larry Faulkner, president and CEO fo the American Board of Psychiatry and Neurology.
Key changes include a more-relaxed approach to how psychiatrists and neurologists can complete the feedback module and the waiving of some continuing medical education credit hours upon completion of certain peer review activities, Dr. Faulkner said at the annual meeting of the American Academy of Psychiatry and the Law. The modifications come in response to new maintenance of certification (MOC) standards by the American Board of Medical Specialties (ABMS) that go into effect in 2015.
“We are trying to make sure our program is credible, but at the same time, we don’t want the program to be so exhausting that it brings people to their knees in order to accomplish our program,” Dr. Faulkner said. “We’re trying to strike this balance.”
The ABPN’s MOC program consists of four components: professional standing; self-assessment and continuing medication education (CME); cognitive expertise; and performance in practice (PIP). PIP units require two modules – clinical and feedback. The feedback module now can be fulfilled by completing a patient survey, a peer survey, an institutional peer review of general competencies, supervisor evaluations of general competencies, resident evaluations of general competencies, or a 360-degree evaluation of general competencies.
Additionally, some required CME credits to be waived for completing a non-CME self-assessment activity, Dr. Faulkner said. Diplomates are required to complete an average of 30 specialty and/or subspecialty CME credits averaged over 3 years. At least eight credits per year, averaged over 3 years, must involve self-assessment. In summer 2014, ABPN decided it would waive eight CME credits for such activities as passing an ABPN cognitive certification or recertification examination; receiving documented feedback on an approved scientific grant application. or by receiveing documented feedback on an academic/scientific journal article accepted for publication. The ABPN will waive a maximum of 16 self-assessment CME credits for two different non-CME self-assessment activities in a 3-year MOC block. Other options for receiving waived credits are listed on the ABPN’s website.
Dr. Faulkner acknowledged that many physicians have expressed dissatisfaction over MOC and its validity. In June, physicians at the American Medical Association House of Delegates meeting spoke out about MOC being too expensive, too lengthy, and having too little value. The AMA delegates defeated a resolution that asked the organization to put a moratorium on MOC until it was proven to improve the quality of care and patient outcomes. However, delegates agreed to directing the AMA to explore the feasibility of a study to evaluate the effect MOC requirements and maintenance of licensure principles have on workforce, practice costs, patient outcomes, patient safety, and patient access.
Despite some negative sentiments, Dr. Faulkner stressed that MOC is not going away, and that physicians should view the process as a way to demonstrate efforts of their ongoing professional learning.
“I’ve never heard somebody deny that life-long learning is important,” he said. “Maintenance of certification is a little more than a formal way for you to document your life-long learning efforts, and I would encourage you to think of maintenance of certification in that vein.”
On Twitter @legal_med
AT THE AAPL ANNUAL MEETING

Stalker risk assessment tool effectively predicts future offenses
CHICAGO– The Stalking Risk Profile, a tool designed to access recidivism risk, is effective in predicting the potential for future stalking in offenders. In an analysis of 230 stalkers, more than 1 in 3 with a high SRP score went on to stalk the same victim again, while fewer than 1 in 10 with a low SRP score stalked again, research presented at the American Academy of Psychiatry and the Law annual meeting showed.
“For us, this is really positive because it shows that the tool does work,” said Troy McEwan, D.Psych., a Melbourne-based forensic psychologist and lecturer for the Centre for Forensic Behavioural Science at Swinburne University of Technology. “It doesn’t mean if you are high risk that you are going to reoffend,” Dr. McEwan added at the AAPL meeting, “it means you reoffend at a higher base rate.”

The SRP is a structured, professional judgment tool developed by Dr. McEwan and several colleagues that accesses and manages risk in stalking cases. The tool measures whether a stalker will continue stalking, start stalking again once having stopped, and/or become violent in the context of stalking. SRP scores range from low to moderate to high.
The tool is structured differently from most risk assessment tools, said Dr. McEwan, who also practices at the Problem Behaviour Program at the Victorian Institute of Forensic Mental Health, Fairfield, Australia, known as Forensicare. Rather than approaching all offenders similarly and applying the same risk factors to all stalkers, the test identifies risk factors relevant to different stalker types. For instance, when accessing a rejected ex-partner for future violence, key risk factors include prior violence and threats. Additionally, having shared children is a unique risk factor for stalking recidivism among rejected ex-partners. However, for intimacy-seeking stalkers who pursue strangers, prior violence and paranoid ideation are specific risk factors to future violence, while erotomania is a factor in this group’s recidivism risk.
For the study, investigators administered the SRP to patients referred to Forensicare’s Problem Behaviour Program for stalking between 2010 and 2013 and also applied the tool retrospectively to clients assessed for stalking during 2004-2007. Of the 230 subjects, 51% had stalked an ex-partner, 33% had stalked an acquaintance, and 16% had stalked a stranger. Researchers followed up with police for subsequent charging data in July 2014. Of the subjects, 26.5% stalked again. About 14% stalked the same victim, 13.5% stalked a different victim, and 3% stalked the same and a different victim, according to research data.
Of a 16% base rate prevalence of reoffending against the same victim, fewer than 1 in 10 subjects with a low SRP went on to reoffend against the same victim, results found; more than 1 in 3 of those with a high SRP score went on to reoffend against the same victim. Of a 14% base rate prevalence of reoffending against a different victim, fewer than 1 in 10 of subjects went on to reoffend against a new victim, while about 1 in 3 of high SRP scorers pursued a new victim.
In addition, the reliability that individual evaluators would reach the same or similar SRP scores was high, the study found. The study found also a 72% probability that stalkers who reoffend against the same victim will score higher on the SRP than do stalkers who do not reoffend against the same victim. A 69% probability exists that a stalker who reoffends against a different victim will get a higher SRP score than would a subject who does not reoffend against a different victim.
The findings show the SRP is a strong and depending tool for measuring future stalking, Dr. McEwan said. The measurement enables clinicians to better target stalking interventions compared with general tools such as the The Historical Clinical Risk Management–20 (HCR-20), she noted.
“Essentially, it means we can use (the SRP) reliably, which is really positive,” she said at the meeting. “It means it does discriminate against offenders and non-offenders, and it does predict who is going to reoffend fairly well.”
Dr. McEwan reported no financial conflicts of interest.
On Twitter @legal_med
CHICAGO– The Stalking Risk Profile, a tool designed to access recidivism risk, is effective in predicting the potential for future stalking in offenders. In an analysis of 230 stalkers, more than 1 in 3 with a high SRP score went on to stalk the same victim again, while fewer than 1 in 10 with a low SRP score stalked again, research presented at the American Academy of Psychiatry and the Law annual meeting showed.
“For us, this is really positive because it shows that the tool does work,” said Troy McEwan, D.Psych., a Melbourne-based forensic psychologist and lecturer for the Centre for Forensic Behavioural Science at Swinburne University of Technology. “It doesn’t mean if you are high risk that you are going to reoffend,” Dr. McEwan added at the AAPL meeting, “it means you reoffend at a higher base rate.”
The SRP is a structured, professional judgment tool developed by Dr. McEwan and several colleagues that accesses and manages risk in stalking cases. The tool measures whether a stalker will continue stalking, start stalking again once having stopped, and/or become violent in the context of stalking. SRP scores range from low to moderate to high.
The tool is structured differently from most risk assessment tools, said Dr. McEwan, who also practices at the Problem Behaviour Program at the Victorian Institute of Forensic Mental Health, Fairfield, Australia, known as Forensicare. Rather than approaching all offenders similarly and applying the same risk factors to all stalkers, the test identifies risk factors relevant to different stalker types. For instance, when accessing a rejected ex-partner for future violence, key risk factors include prior violence and threats. Additionally, having shared children is a unique risk factor for stalking recidivism among rejected ex-partners. However, for intimacy-seeking stalkers who pursue strangers, prior violence and paranoid ideation are specific risk factors to future violence, while erotomania is a factor in this group’s recidivism risk.
For the study, investigators administered the SRP to patients referred to Forensicare’s Problem Behaviour Program for stalking between 2010 and 2013 and also applied the tool retrospectively to clients assessed for stalking during 2004-2007. Of the 230 subjects, 51% had stalked an ex-partner, 33% had stalked an acquaintance, and 16% had stalked a stranger. Researchers followed up with police for subsequent charging data in July 2014. Of the subjects, 26.5% stalked again. About 14% stalked the same victim, 13.5% stalked a different victim, and 3% stalked the same and a different victim, according to research data.
Of a 16% base rate prevalence of reoffending against the same victim, fewer than 1 in 10 subjects with a low SRP went on to reoffend against the same victim, results found; more than 1 in 3 of those with a high SRP score went on to reoffend against the same victim. Of a 14% base rate prevalence of reoffending against a different victim, fewer than 1 in 10 of subjects went on to reoffend against a new victim, while about 1 in 3 of high SRP scorers pursued a new victim.
In addition, the reliability that individual evaluators would reach the same or similar SRP scores was high, the study found. The study found also a 72% probability that stalkers who reoffend against the same victim will score higher on the SRP than do stalkers who do not reoffend against the same victim. A 69% probability exists that a stalker who reoffends against a different victim will get a higher SRP score than would a subject who does not reoffend against a different victim.
The findings show the SRP is a strong and depending tool for measuring future stalking, Dr. McEwan said. The measurement enables clinicians to better target stalking interventions compared with general tools such as the The Historical Clinical Risk Management–20 (HCR-20), she noted.
“Essentially, it means we can use (the SRP) reliably, which is really positive,” she said at the meeting. “It means it does discriminate against offenders and non-offenders, and it does predict who is going to reoffend fairly well.”
Dr. McEwan reported no financial conflicts of interest.
On Twitter @legal_med
CHICAGO– The Stalking Risk Profile, a tool designed to access recidivism risk, is effective in predicting the potential for future stalking in offenders. In an analysis of 230 stalkers, more than 1 in 3 with a high SRP score went on to stalk the same victim again, while fewer than 1 in 10 with a low SRP score stalked again, research presented at the American Academy of Psychiatry and the Law annual meeting showed.
“For us, this is really positive because it shows that the tool does work,” said Troy McEwan, D.Psych., a Melbourne-based forensic psychologist and lecturer for the Centre for Forensic Behavioural Science at Swinburne University of Technology. “It doesn’t mean if you are high risk that you are going to reoffend,” Dr. McEwan added at the AAPL meeting, “it means you reoffend at a higher base rate.”
The SRP is a structured, professional judgment tool developed by Dr. McEwan and several colleagues that accesses and manages risk in stalking cases. The tool measures whether a stalker will continue stalking, start stalking again once having stopped, and/or become violent in the context of stalking. SRP scores range from low to moderate to high.
The tool is structured differently from most risk assessment tools, said Dr. McEwan, who also practices at the Problem Behaviour Program at the Victorian Institute of Forensic Mental Health, Fairfield, Australia, known as Forensicare. Rather than approaching all offenders similarly and applying the same risk factors to all stalkers, the test identifies risk factors relevant to different stalker types. For instance, when accessing a rejected ex-partner for future violence, key risk factors include prior violence and threats. Additionally, having shared children is a unique risk factor for stalking recidivism among rejected ex-partners. However, for intimacy-seeking stalkers who pursue strangers, prior violence and paranoid ideation are specific risk factors to future violence, while erotomania is a factor in this group’s recidivism risk.
For the study, investigators administered the SRP to patients referred to Forensicare’s Problem Behaviour Program for stalking between 2010 and 2013 and also applied the tool retrospectively to clients assessed for stalking during 2004-2007. Of the 230 subjects, 51% had stalked an ex-partner, 33% had stalked an acquaintance, and 16% had stalked a stranger. Researchers followed up with police for subsequent charging data in July 2014. Of the subjects, 26.5% stalked again. About 14% stalked the same victim, 13.5% stalked a different victim, and 3% stalked the same and a different victim, according to research data.
Of a 16% base rate prevalence of reoffending against the same victim, fewer than 1 in 10 subjects with a low SRP went on to reoffend against the same victim, results found; more than 1 in 3 of those with a high SRP score went on to reoffend against the same victim. Of a 14% base rate prevalence of reoffending against a different victim, fewer than 1 in 10 of subjects went on to reoffend against a new victim, while about 1 in 3 of high SRP scorers pursued a new victim.
In addition, the reliability that individual evaluators would reach the same or similar SRP scores was high, the study found. The study found also a 72% probability that stalkers who reoffend against the same victim will score higher on the SRP than do stalkers who do not reoffend against the same victim. A 69% probability exists that a stalker who reoffends against a different victim will get a higher SRP score than would a subject who does not reoffend against a different victim.
The findings show the SRP is a strong and depending tool for measuring future stalking, Dr. McEwan said. The measurement enables clinicians to better target stalking interventions compared with general tools such as the The Historical Clinical Risk Management–20 (HCR-20), she noted.
“Essentially, it means we can use (the SRP) reliably, which is really positive,” she said at the meeting. “It means it does discriminate against offenders and non-offenders, and it does predict who is going to reoffend fairly well.”
Dr. McEwan reported no financial conflicts of interest.
On Twitter @legal_med
AT THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF PSYCHIATRY AND THE LAW
Key clinical point: The Stalker Risk Profile successfully predicts future stalking against same and new victims.
Major finding: In an analysis of 230 stalkers, more than 1 in 3 with a high SRP score went on to stalk the same victim again, while fewer than 1 in 10 with a low SRP score. This was based on a 16% base rate prevalence of reoffending against the same victim, and a 14% base rate prevalence of reoffending against a different victim.
Data source: Case study of prior offenders.
Disclosures: Dr. McEwan reported no financial conflicts of interest.

Diagnostic centers to pay $2.6 million for physician kickbacks
Two Houston-based diagnostic groups have agreed to pay the government $2.6 million to settle allegations that they had improper financial relationships with physicians and violated the False Claims Act.
Three whistle-blowers and Kenneth Magidson, U.S. Attorney for the Southern District of Texas, filed suit Oct. 4, 2012, against One Step Diagnostic centers and a group of six other Texas diagnostic centers as well as several physicians and podiatrists. Investigators alleged One Step Diagnostic and the doctors entered into sham consulting and medical director agreements that resulted in the unlawful referring of patients to One Step Diagnostic centers. The second group of diagnostic centers had inappropriate financial relationships with referring physicians and improperly billed Medicare using an unauthorized provider number the Justice Department said.

Employee whistle-blowers claimed staff were instructed to deliver checks to physicians and podiatrists involved in medical consultant and medical director agreements with the centers. The money was to be accompanied by a set of medical records that doctors would review as part of the agreement, according to court documents. However, employees claimed, on many occasions they delivered the checks without medical records. Investigators said the contracts were an attempt to disguise illegal kickbacks to doctors in exchange for referrals.
As part of the settlement, One Step Diagnostic will pay $1.2 million to the government, while the other group of centers agreed to pay about $1.5 million, according to an Oct. 17 statement from the U.S. Department of Justice. The U.S. Attorney for the Southern District of Texas does not plan to continue the False Claims Act lawsuit against the named physicians and podiatrists. However, the Office of Counsel to the Inspector General retains the right to seek civil monetary penalties against the health providers.
The diagnostic centers acknowledged no wrongdoing in the case, said Anna Grizzle, a Nashville-based attorney who represented the second group of diagnostic centers.
“Our clients did deny liability in the matter,” Ms. Grizzle said in an interview. “However, they fully cooperated with the government and took appropriate steps to resolve the matter.”
The Justice Department noted the settlements were finalized without an admission of liability by both groups of diagnostic centers.
On Twitter @legal_med
Two Houston-based diagnostic groups have agreed to pay the government $2.6 million to settle allegations that they had improper financial relationships with physicians and violated the False Claims Act.
Three whistle-blowers and Kenneth Magidson, U.S. Attorney for the Southern District of Texas, filed suit Oct. 4, 2012, against One Step Diagnostic centers and a group of six other Texas diagnostic centers as well as several physicians and podiatrists. Investigators alleged One Step Diagnostic and the doctors entered into sham consulting and medical director agreements that resulted in the unlawful referring of patients to One Step Diagnostic centers. The second group of diagnostic centers had inappropriate financial relationships with referring physicians and improperly billed Medicare using an unauthorized provider number the Justice Department said.
Employee whistle-blowers claimed staff were instructed to deliver checks to physicians and podiatrists involved in medical consultant and medical director agreements with the centers. The money was to be accompanied by a set of medical records that doctors would review as part of the agreement, according to court documents. However, employees claimed, on many occasions they delivered the checks without medical records. Investigators said the contracts were an attempt to disguise illegal kickbacks to doctors in exchange for referrals.
As part of the settlement, One Step Diagnostic will pay $1.2 million to the government, while the other group of centers agreed to pay about $1.5 million, according to an Oct. 17 statement from the U.S. Department of Justice. The U.S. Attorney for the Southern District of Texas does not plan to continue the False Claims Act lawsuit against the named physicians and podiatrists. However, the Office of Counsel to the Inspector General retains the right to seek civil monetary penalties against the health providers.
The diagnostic centers acknowledged no wrongdoing in the case, said Anna Grizzle, a Nashville-based attorney who represented the second group of diagnostic centers.
“Our clients did deny liability in the matter,” Ms. Grizzle said in an interview. “However, they fully cooperated with the government and took appropriate steps to resolve the matter.”
The Justice Department noted the settlements were finalized without an admission of liability by both groups of diagnostic centers.
On Twitter @legal_med
Two Houston-based diagnostic groups have agreed to pay the government $2.6 million to settle allegations that they had improper financial relationships with physicians and violated the False Claims Act.
Three whistle-blowers and Kenneth Magidson, U.S. Attorney for the Southern District of Texas, filed suit Oct. 4, 2012, against One Step Diagnostic centers and a group of six other Texas diagnostic centers as well as several physicians and podiatrists. Investigators alleged One Step Diagnostic and the doctors entered into sham consulting and medical director agreements that resulted in the unlawful referring of patients to One Step Diagnostic centers. The second group of diagnostic centers had inappropriate financial relationships with referring physicians and improperly billed Medicare using an unauthorized provider number the Justice Department said.
Employee whistle-blowers claimed staff were instructed to deliver checks to physicians and podiatrists involved in medical consultant and medical director agreements with the centers. The money was to be accompanied by a set of medical records that doctors would review as part of the agreement, according to court documents. However, employees claimed, on many occasions they delivered the checks without medical records. Investigators said the contracts were an attempt to disguise illegal kickbacks to doctors in exchange for referrals.
As part of the settlement, One Step Diagnostic will pay $1.2 million to the government, while the other group of centers agreed to pay about $1.5 million, according to an Oct. 17 statement from the U.S. Department of Justice. The U.S. Attorney for the Southern District of Texas does not plan to continue the False Claims Act lawsuit against the named physicians and podiatrists. However, the Office of Counsel to the Inspector General retains the right to seek civil monetary penalties against the health providers.
The diagnostic centers acknowledged no wrongdoing in the case, said Anna Grizzle, a Nashville-based attorney who represented the second group of diagnostic centers.
“Our clients did deny liability in the matter,” Ms. Grizzle said in an interview. “However, they fully cooperated with the government and took appropriate steps to resolve the matter.”
The Justice Department noted the settlements were finalized without an admission of liability by both groups of diagnostic centers.
On Twitter @legal_med
Court: Fla. malpractice reform doesn’t violate HIPAA
A federal appeals court has upheld a Florida tort reform law that enables physician defendants to have equal access to plaintiffs’ health information, ruling that the state law does not violate federal patient privacy protections.
The 11th U.S. Circuit Court of Appeals decision means Florida doctors can be better prepared for malpractice lawsuits and better able to defend themselves, said Jeff Scott, director of legal and governmental affairs for the Florida Medical Association. Before the reform, plaintiffs’ attorneys could obtain information from a patient’s treating physicians, but defense attorneys could not access the same doctors until the deposition period – and only with the patient’s attorney present.
“The impact (of the ruling) is: It’s going to level the playing field in medical malpractice cases by giving defendant physicians the same access to crucial expert witnesses that the plaintiff has,” Mr. Scott said in an interview.

As part of the 2013 law, prospective plaintiffs must execute a written form that authorizes defendants to obtain documents and conduct ex parte interviews of the plaintiff’s medical providers. The form is a precondition to filing a medical negligence claim.
A patient who planned to sue a Florida family physician asked a federal district court to vacate the rule, arguing that the law violated his privacy. The U.S. District Court for the Northern District of Florida concluded the law would result in disclosure of the patient’s HIPAA-protected health information without his consent. That court ruled HIPAA preempted the state law.
The appeals court overturned. In its opinion, the three-judge panel said the Florida law is fully compliant with HIPAA and should stand.
“Had the drafters of the HIPAA regulations wished to preclude a state legislature from conditioning a public benefit – such as filing a lawsuit – on signing a HIPAA authorization, they could have easily done so, just as they generally prohibited doctors from conditioning medical treatment on signing a HIPAA authorization,” the appellate judges said in their decision.
“Further, an individual’s decision to sign an authorization prior to bringing a medical negligence claim in state court is not an involuntary one,” the appeals court noted. “If an individual does not wish to execute such an authorization, he does not have to. He is, however, precluded from using the Florida courts to obtain relief through a medical negligence lawsuit against a health care provider.”
Florida is not the first state to adopt the ex parte communications lawsuit rule. Both Texas and Tennessee have enacted similar statutes. In 2009, the Texas Supreme Court upheld the state’s rule, and in 2013, the Tennessee Supreme Court followed suit.
On Twitter @legal_med
A federal appeals court has upheld a Florida tort reform law that enables physician defendants to have equal access to plaintiffs’ health information, ruling that the state law does not violate federal patient privacy protections.
The 11th U.S. Circuit Court of Appeals decision means Florida doctors can be better prepared for malpractice lawsuits and better able to defend themselves, said Jeff Scott, director of legal and governmental affairs for the Florida Medical Association. Before the reform, plaintiffs’ attorneys could obtain information from a patient’s treating physicians, but defense attorneys could not access the same doctors until the deposition period – and only with the patient’s attorney present.
“The impact (of the ruling) is: It’s going to level the playing field in medical malpractice cases by giving defendant physicians the same access to crucial expert witnesses that the plaintiff has,” Mr. Scott said in an interview.
As part of the 2013 law, prospective plaintiffs must execute a written form that authorizes defendants to obtain documents and conduct ex parte interviews of the plaintiff’s medical providers. The form is a precondition to filing a medical negligence claim.
A patient who planned to sue a Florida family physician asked a federal district court to vacate the rule, arguing that the law violated his privacy. The U.S. District Court for the Northern District of Florida concluded the law would result in disclosure of the patient’s HIPAA-protected health information without his consent. That court ruled HIPAA preempted the state law.
The appeals court overturned. In its opinion, the three-judge panel said the Florida law is fully compliant with HIPAA and should stand.
“Had the drafters of the HIPAA regulations wished to preclude a state legislature from conditioning a public benefit – such as filing a lawsuit – on signing a HIPAA authorization, they could have easily done so, just as they generally prohibited doctors from conditioning medical treatment on signing a HIPAA authorization,” the appellate judges said in their decision.
“Further, an individual’s decision to sign an authorization prior to bringing a medical negligence claim in state court is not an involuntary one,” the appeals court noted. “If an individual does not wish to execute such an authorization, he does not have to. He is, however, precluded from using the Florida courts to obtain relief through a medical negligence lawsuit against a health care provider.”
Florida is not the first state to adopt the ex parte communications lawsuit rule. Both Texas and Tennessee have enacted similar statutes. In 2009, the Texas Supreme Court upheld the state’s rule, and in 2013, the Tennessee Supreme Court followed suit.
On Twitter @legal_med
A federal appeals court has upheld a Florida tort reform law that enables physician defendants to have equal access to plaintiffs’ health information, ruling that the state law does not violate federal patient privacy protections.
The 11th U.S. Circuit Court of Appeals decision means Florida doctors can be better prepared for malpractice lawsuits and better able to defend themselves, said Jeff Scott, director of legal and governmental affairs for the Florida Medical Association. Before the reform, plaintiffs’ attorneys could obtain information from a patient’s treating physicians, but defense attorneys could not access the same doctors until the deposition period – and only with the patient’s attorney present.
“The impact (of the ruling) is: It’s going to level the playing field in medical malpractice cases by giving defendant physicians the same access to crucial expert witnesses that the plaintiff has,” Mr. Scott said in an interview.
As part of the 2013 law, prospective plaintiffs must execute a written form that authorizes defendants to obtain documents and conduct ex parte interviews of the plaintiff’s medical providers. The form is a precondition to filing a medical negligence claim.
A patient who planned to sue a Florida family physician asked a federal district court to vacate the rule, arguing that the law violated his privacy. The U.S. District Court for the Northern District of Florida concluded the law would result in disclosure of the patient’s HIPAA-protected health information without his consent. That court ruled HIPAA preempted the state law.
The appeals court overturned. In its opinion, the three-judge panel said the Florida law is fully compliant with HIPAA and should stand.
“Had the drafters of the HIPAA regulations wished to preclude a state legislature from conditioning a public benefit – such as filing a lawsuit – on signing a HIPAA authorization, they could have easily done so, just as they generally prohibited doctors from conditioning medical treatment on signing a HIPAA authorization,” the appellate judges said in their decision.
“Further, an individual’s decision to sign an authorization prior to bringing a medical negligence claim in state court is not an involuntary one,” the appeals court noted. “If an individual does not wish to execute such an authorization, he does not have to. He is, however, precluded from using the Florida courts to obtain relief through a medical negligence lawsuit against a health care provider.”
Florida is not the first state to adopt the ex parte communications lawsuit rule. Both Texas and Tennessee have enacted similar statutes. In 2009, the Texas Supreme Court upheld the state’s rule, and in 2013, the Tennessee Supreme Court followed suit.
On Twitter @legal_med

Malpractice premiums remained flat in 2014
Malpractice premiums for physicians stayed mostly the same in 2014, with 65% of liability insurance rates remaining steady nationwide, according to the Medical Liability Monitor’s annual survey and analysis of premiums nationwide.
Ongoing trends of slow lawsuit frequency and low plaintiff payouts are contributing to the steady market, said Chad C. Karls, editor of the 2014 Annual Rate Survey and a principal and consulting actuary for Milliman in Brookfield, Wis.
“We certainly do see those very large verdicts in the industry, but when we take it across all claims, the vast majority don’t have a verdict attached to them,” Mr. Karls said in an interview. “The vast majority get settled. That average claim has remained relatively stable.”
Unchanging insurance rates, however, can mean payment misery or relief depending on where physicians practice. Internists in southern Florida will pay a high of $47,707 for malpractice insurance this year, while their counterparts in South Dakota will pay just $3,697. For ob.gyns., malpractice insurance is priciest in the New York counties of Nassau and Suffolk, where they will pay $214,999 in malpractice premiums this year. But in Central California, ob.gyns. will pay just $16,240. General surgeons in southern Florida will dish out $190,829 in premiums in 2014, while Wisconsin surgeons will pay $10,868.
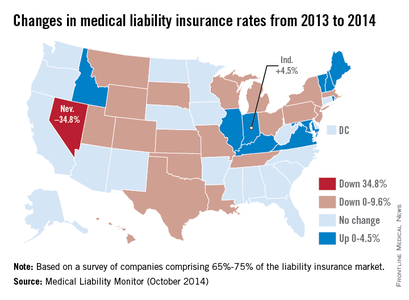
Premiums did increase in some areas in 2014. Indiana physicians saw the highest increase at 4.5%. Nevada doctors experienced a 34.8% decrease in premiums, by far the largest drop among states. (See map.) Nevada’s average percent change was driven by two companies that reported high rate decreases, the survey noted. (Acquisitions by some Nevada insurers may have affected the numbers.)
In general, Nevada’s large rate decline is not surprising, said Dr. Warren Volker, trustee-at-large for the Clark County (Nev.) Medical Society and chair of Premiere Physician Insurance Company in Nevada. Doctors in the state have experienced a stable medical liability climate for the last decade, he said.
“Our premiums have gone down dramatically, across the board,” Dr. Volker said in an interview. “Physicians have enjoyed cost savings as long as they have a good history.”
He attributed the declines to tort reform passed in 2002, including a $350,000 noneconomic damages cap in medical malpractice cases. Since then, the number of lawsuit filings has gone down and competition among liability insurers has increased, he said.
Legal reforms such as Nevada’s have probably contributed to the overall decrease in lawsuit frequency and payout severity across the country, Mr. Karls said. Patient safety initiatives and better risk management within medical practices also may be having an impact.

It remains to be seen how the Affordable Care Act will affect medical liability premiums. So far, industry analysts have not seen a definitive impact on medical malpractice insurance rates from the law, Mr. Karls said. The law could ultimately help lower liability claims if the ACA results in more proactive, preventive approaches to medical errors and less acute care, but in the short term, more patients covered under the ACA could mean a rise in lawsuits and, thus, premiums.
There are “more people getting care from the same number of health providers,” he said. “That puts additional pressure on an already strained system. Short term, the impact of the ACA could lead to additional [malpractice] claims.”
As for states with extremely high insurance rates, Dr. Volker does not see premium relief any time soon. He expects the trend of practice mergers and acquisitions to continue as more physicians seek to escape high premium costs and regulatory burdens.
“I think what you’re going to see in the hotbeds is more migration,” said Dr. Volker, who is licensed to practice in Nevada, California, Florida, and Arizona. “More doctors [will be] giving up their individual practices and joining larger groups.”
The MLM survey, published in October, gathered July 1 premium data from the major medical malpractice insurers and examines rates for mature, claims-made policies with $1 million/$3 million limits for internists, general surgeons, and ob.gyns.
On Twitter @legal_med
Malpractice premiums for physicians stayed mostly the same in 2014, with 65% of liability insurance rates remaining steady nationwide, according to the Medical Liability Monitor’s annual survey and analysis of premiums nationwide.
Ongoing trends of slow lawsuit frequency and low plaintiff payouts are contributing to the steady market, said Chad C. Karls, editor of the 2014 Annual Rate Survey and a principal and consulting actuary for Milliman in Brookfield, Wis.
“We certainly do see those very large verdicts in the industry, but when we take it across all claims, the vast majority don’t have a verdict attached to them,” Mr. Karls said in an interview. “The vast majority get settled. That average claim has remained relatively stable.”
Unchanging insurance rates, however, can mean payment misery or relief depending on where physicians practice. Internists in southern Florida will pay a high of $47,707 for malpractice insurance this year, while their counterparts in South Dakota will pay just $3,697. For ob.gyns., malpractice insurance is priciest in the New York counties of Nassau and Suffolk, where they will pay $214,999 in malpractice premiums this year. But in Central California, ob.gyns. will pay just $16,240. General surgeons in southern Florida will dish out $190,829 in premiums in 2014, while Wisconsin surgeons will pay $10,868.
Premiums did increase in some areas in 2014. Indiana physicians saw the highest increase at 4.5%. Nevada doctors experienced a 34.8% decrease in premiums, by far the largest drop among states. (See map.) Nevada’s average percent change was driven by two companies that reported high rate decreases, the survey noted. (Acquisitions by some Nevada insurers may have affected the numbers.)
In general, Nevada’s large rate decline is not surprising, said Dr. Warren Volker, trustee-at-large for the Clark County (Nev.) Medical Society and chair of Premiere Physician Insurance Company in Nevada. Doctors in the state have experienced a stable medical liability climate for the last decade, he said.
“Our premiums have gone down dramatically, across the board,” Dr. Volker said in an interview. “Physicians have enjoyed cost savings as long as they have a good history.”
He attributed the declines to tort reform passed in 2002, including a $350,000 noneconomic damages cap in medical malpractice cases. Since then, the number of lawsuit filings has gone down and competition among liability insurers has increased, he said.
Legal reforms such as Nevada’s have probably contributed to the overall decrease in lawsuit frequency and payout severity across the country, Mr. Karls said. Patient safety initiatives and better risk management within medical practices also may be having an impact.
It remains to be seen how the Affordable Care Act will affect medical liability premiums. So far, industry analysts have not seen a definitive impact on medical malpractice insurance rates from the law, Mr. Karls said. The law could ultimately help lower liability claims if the ACA results in more proactive, preventive approaches to medical errors and less acute care, but in the short term, more patients covered under the ACA could mean a rise in lawsuits and, thus, premiums.
There are “more people getting care from the same number of health providers,” he said. “That puts additional pressure on an already strained system. Short term, the impact of the ACA could lead to additional [malpractice] claims.”
As for states with extremely high insurance rates, Dr. Volker does not see premium relief any time soon. He expects the trend of practice mergers and acquisitions to continue as more physicians seek to escape high premium costs and regulatory burdens.
“I think what you’re going to see in the hotbeds is more migration,” said Dr. Volker, who is licensed to practice in Nevada, California, Florida, and Arizona. “More doctors [will be] giving up their individual practices and joining larger groups.”
The MLM survey, published in October, gathered July 1 premium data from the major medical malpractice insurers and examines rates for mature, claims-made policies with $1 million/$3 million limits for internists, general surgeons, and ob.gyns.
On Twitter @legal_med
Malpractice premiums for physicians stayed mostly the same in 2014, with 65% of liability insurance rates remaining steady nationwide, according to the Medical Liability Monitor’s annual survey and analysis of premiums nationwide.
Ongoing trends of slow lawsuit frequency and low plaintiff payouts are contributing to the steady market, said Chad C. Karls, editor of the 2014 Annual Rate Survey and a principal and consulting actuary for Milliman in Brookfield, Wis.
“We certainly do see those very large verdicts in the industry, but when we take it across all claims, the vast majority don’t have a verdict attached to them,” Mr. Karls said in an interview. “The vast majority get settled. That average claim has remained relatively stable.”
Unchanging insurance rates, however, can mean payment misery or relief depending on where physicians practice. Internists in southern Florida will pay a high of $47,707 for malpractice insurance this year, while their counterparts in South Dakota will pay just $3,697. For ob.gyns., malpractice insurance is priciest in the New York counties of Nassau and Suffolk, where they will pay $214,999 in malpractice premiums this year. But in Central California, ob.gyns. will pay just $16,240. General surgeons in southern Florida will dish out $190,829 in premiums in 2014, while Wisconsin surgeons will pay $10,868.
Premiums did increase in some areas in 2014. Indiana physicians saw the highest increase at 4.5%. Nevada doctors experienced a 34.8% decrease in premiums, by far the largest drop among states. (See map.) Nevada’s average percent change was driven by two companies that reported high rate decreases, the survey noted. (Acquisitions by some Nevada insurers may have affected the numbers.)
In general, Nevada’s large rate decline is not surprising, said Dr. Warren Volker, trustee-at-large for the Clark County (Nev.) Medical Society and chair of Premiere Physician Insurance Company in Nevada. Doctors in the state have experienced a stable medical liability climate for the last decade, he said.
“Our premiums have gone down dramatically, across the board,” Dr. Volker said in an interview. “Physicians have enjoyed cost savings as long as they have a good history.”
He attributed the declines to tort reform passed in 2002, including a $350,000 noneconomic damages cap in medical malpractice cases. Since then, the number of lawsuit filings has gone down and competition among liability insurers has increased, he said.
Legal reforms such as Nevada’s have probably contributed to the overall decrease in lawsuit frequency and payout severity across the country, Mr. Karls said. Patient safety initiatives and better risk management within medical practices also may be having an impact.
It remains to be seen how the Affordable Care Act will affect medical liability premiums. So far, industry analysts have not seen a definitive impact on medical malpractice insurance rates from the law, Mr. Karls said. The law could ultimately help lower liability claims if the ACA results in more proactive, preventive approaches to medical errors and less acute care, but in the short term, more patients covered under the ACA could mean a rise in lawsuits and, thus, premiums.
There are “more people getting care from the same number of health providers,” he said. “That puts additional pressure on an already strained system. Short term, the impact of the ACA could lead to additional [malpractice] claims.”
As for states with extremely high insurance rates, Dr. Volker does not see premium relief any time soon. He expects the trend of practice mergers and acquisitions to continue as more physicians seek to escape high premium costs and regulatory burdens.
“I think what you’re going to see in the hotbeds is more migration,” said Dr. Volker, who is licensed to practice in Nevada, California, Florida, and Arizona. “More doctors [will be] giving up their individual practices and joining larger groups.”
The MLM survey, published in October, gathered July 1 premium data from the major medical malpractice insurers and examines rates for mature, claims-made policies with $1 million/$3 million limits for internists, general surgeons, and ob.gyns.
On Twitter @legal_med

Audits are more likely under Medicare Advantage
If you see a lot of Medicare Advantage patients in your practice, you could be in line for an audit. That’s the message from Kim Harvey Looney, a Nashville-based health care regulatory and compliance attorney.
“It’s important for providers to know that if they have a significant portion of patients on Medicare Advantage, they’re more likely to be audited,” Ms. Looney said during a webinar held by the American Health Lawyers Association.

Continued growth of the Medicare Advantage (MA) program is one thing causing auditors – both federal and those who work for health insurers – to take a closer look, audit experts say. About 30% of all Medicare patients are enrolled in MA, according to a May report by the Kaiser Family Foundation. Since enactment of the Affordable Care Act, enrollment in the program has increased by 4.6 million, or by 41%. MA also accounts for a quarter of all Medicare spending, according to Kaiser Family Foundation data.
But the complex model under which MA operates can cause physicians to submit incorrect codes, Stephen M. Sullivan, a Los-Angeles health care attorney said.
The Centers for Medicare & Medicaid Services pays contracting health insurers per patient based on the patient’s risk adjustment scores. The scores are derived by the health status of the patient, so insurers get a higher stipend for sicker patients.
Risk adjustment scores themselves are based on diagnosis codes for previous visits to physicians; the plans then process and filter the information and send risk adjustment data to CMS.
“Risk adjustment in general, is complex, is very technical, and it is very data driven,” Mr. Sullivan said. “Because it is so data driven, there has been an acknowledgment within the industry, including from CMS, that there is a very high imprecision rate in the actual codes that are submitted.”
A July study published in the Medicare & Medicaid Research Review, a CMS publication, found that risk adjustment scores in the Medicare Advantage program were largely exaggerated by health plans and did not match enrollees’ morbidity. A June report by the Center for Public Integrity revealed similar findings.
Amid such criticism, the Office of Inspector General, in its 2014 Work Plan vowed to review the extent to which CMS is verifying the accuracy of MA encounter data and risk adjustment reporting.
For doctors, the spotlight on inaccurate risk scores means a sharper eye to coding and medical records from health plans and CMS auditors. Health plans, in particular, are searching both to ensure they were not underpaid by CMS because of undercoding, and that they aren’t audited due to overcoding.

“There is more focus now (by CMS), both looking at the plan and looking at the provider as to whether or not there is accurate information being submitted,” said George B. Breen, a Washington-based health care attorney and chair of his firm’s National Health Care and Life Sciences Practice Steering Committee. “From the plan’s perspective, they have the obligation to make sure the money being spent is, in fact, consistent with the diagnosis being reported, and that they have looked to see whether or not the record by the physician supports the condition.”
Some of the coding confusion comes from the critical differences in information required by MA as compared with fee-for-service Medicare, said Julie Nielsen, director of a Tampa, Fla.–based health care research and dispute resolution company. Rather than noting only services rendered for a primary condition, physicians coding an MA claim must include all conditions that affected the patient encounter.
“It’s been a very big transition for physicians and providers having to become more attuned to capturing all of the members’ diagnosis codes that impacted the visit when the member was there, not just that the member was there for a lab draw and an office visit,” Ms. Nielsen said.
Alleged coding errors found by health plans or CMS can result in a health provider being kicked out of the program or affect their payments from health plans. Inaccurate information that results in an overpayment by CMS can also lead to a False Claims Act (FCA) violation, said Mr. Breen, who defends health providers in billing, fraud, and FCA investigations.
“Even though the claim may not have been directly submitted to Medicare, but to the Medicare Advantage plan, the government can argue the provider either submitted a false claim or caused a false claim to be submitted,” he said.
To prevent and defend MA audits, develop a strong compliance program that includes ongoing internal risk assessments, Ms. Looney said. In some cases, it may be helpful to hire a third-party company to review coding submissions and offer conclusions.
“Try to figure out what you [should] be watching for and make sure you correct anything you’re doing wrong,” she said. “Find your weak links.”
Complete documentation and regular staff training is also essential, Mr. Breen added. Employees charged with coding or documentation duties should understand MA rules and regulations what information is required. If hit with a fraud or coding error accusation, doctors should be able to say that they made efforts to identify mistakes, he said.
“It’s not enough to say, ‘I made a mistake,’” he said. “You have to be able to say, ‘I looked for mistakes and tried to make sure we weren’t doing anything inappropriate.’ At the end of the day if you made a mistake, you have to demonstrate that you did something to prevent [such errors] in the first instance.”
On Twitter @legal_med
If you see a lot of Medicare Advantage patients in your practice, you could be in line for an audit. That’s the message from Kim Harvey Looney, a Nashville-based health care regulatory and compliance attorney.
“It’s important for providers to know that if they have a significant portion of patients on Medicare Advantage, they’re more likely to be audited,” Ms. Looney said during a webinar held by the American Health Lawyers Association.
Continued growth of the Medicare Advantage (MA) program is one thing causing auditors – both federal and those who work for health insurers – to take a closer look, audit experts say. About 30% of all Medicare patients are enrolled in MA, according to a May report by the Kaiser Family Foundation. Since enactment of the Affordable Care Act, enrollment in the program has increased by 4.6 million, or by 41%. MA also accounts for a quarter of all Medicare spending, according to Kaiser Family Foundation data.
But the complex model under which MA operates can cause physicians to submit incorrect codes, Stephen M. Sullivan, a Los-Angeles health care attorney said.
The Centers for Medicare & Medicaid Services pays contracting health insurers per patient based on the patient’s risk adjustment scores. The scores are derived by the health status of the patient, so insurers get a higher stipend for sicker patients.
Risk adjustment scores themselves are based on diagnosis codes for previous visits to physicians; the plans then process and filter the information and send risk adjustment data to CMS.
“Risk adjustment in general, is complex, is very technical, and it is very data driven,” Mr. Sullivan said. “Because it is so data driven, there has been an acknowledgment within the industry, including from CMS, that there is a very high imprecision rate in the actual codes that are submitted.”
A July study published in the Medicare & Medicaid Research Review, a CMS publication, found that risk adjustment scores in the Medicare Advantage program were largely exaggerated by health plans and did not match enrollees’ morbidity. A June report by the Center for Public Integrity revealed similar findings.
Amid such criticism, the Office of Inspector General, in its 2014 Work Plan vowed to review the extent to which CMS is verifying the accuracy of MA encounter data and risk adjustment reporting.
For doctors, the spotlight on inaccurate risk scores means a sharper eye to coding and medical records from health plans and CMS auditors. Health plans, in particular, are searching both to ensure they were not underpaid by CMS because of undercoding, and that they aren’t audited due to overcoding.
“There is more focus now (by CMS), both looking at the plan and looking at the provider as to whether or not there is accurate information being submitted,” said George B. Breen, a Washington-based health care attorney and chair of his firm’s National Health Care and Life Sciences Practice Steering Committee. “From the plan’s perspective, they have the obligation to make sure the money being spent is, in fact, consistent with the diagnosis being reported, and that they have looked to see whether or not the record by the physician supports the condition.”
Some of the coding confusion comes from the critical differences in information required by MA as compared with fee-for-service Medicare, said Julie Nielsen, director of a Tampa, Fla.–based health care research and dispute resolution company. Rather than noting only services rendered for a primary condition, physicians coding an MA claim must include all conditions that affected the patient encounter.
“It’s been a very big transition for physicians and providers having to become more attuned to capturing all of the members’ diagnosis codes that impacted the visit when the member was there, not just that the member was there for a lab draw and an office visit,” Ms. Nielsen said.
Alleged coding errors found by health plans or CMS can result in a health provider being kicked out of the program or affect their payments from health plans. Inaccurate information that results in an overpayment by CMS can also lead to a False Claims Act (FCA) violation, said Mr. Breen, who defends health providers in billing, fraud, and FCA investigations.
“Even though the claim may not have been directly submitted to Medicare, but to the Medicare Advantage plan, the government can argue the provider either submitted a false claim or caused a false claim to be submitted,” he said.
To prevent and defend MA audits, develop a strong compliance program that includes ongoing internal risk assessments, Ms. Looney said. In some cases, it may be helpful to hire a third-party company to review coding submissions and offer conclusions.
“Try to figure out what you [should] be watching for and make sure you correct anything you’re doing wrong,” she said. “Find your weak links.”
Complete documentation and regular staff training is also essential, Mr. Breen added. Employees charged with coding or documentation duties should understand MA rules and regulations what information is required. If hit with a fraud or coding error accusation, doctors should be able to say that they made efforts to identify mistakes, he said.
“It’s not enough to say, ‘I made a mistake,’” he said. “You have to be able to say, ‘I looked for mistakes and tried to make sure we weren’t doing anything inappropriate.’ At the end of the day if you made a mistake, you have to demonstrate that you did something to prevent [such errors] in the first instance.”
On Twitter @legal_med
If you see a lot of Medicare Advantage patients in your practice, you could be in line for an audit. That’s the message from Kim Harvey Looney, a Nashville-based health care regulatory and compliance attorney.
“It’s important for providers to know that if they have a significant portion of patients on Medicare Advantage, they’re more likely to be audited,” Ms. Looney said during a webinar held by the American Health Lawyers Association.
Continued growth of the Medicare Advantage (MA) program is one thing causing auditors – both federal and those who work for health insurers – to take a closer look, audit experts say. About 30% of all Medicare patients are enrolled in MA, according to a May report by the Kaiser Family Foundation. Since enactment of the Affordable Care Act, enrollment in the program has increased by 4.6 million, or by 41%. MA also accounts for a quarter of all Medicare spending, according to Kaiser Family Foundation data.
But the complex model under which MA operates can cause physicians to submit incorrect codes, Stephen M. Sullivan, a Los-Angeles health care attorney said.
The Centers for Medicare & Medicaid Services pays contracting health insurers per patient based on the patient’s risk adjustment scores. The scores are derived by the health status of the patient, so insurers get a higher stipend for sicker patients.
Risk adjustment scores themselves are based on diagnosis codes for previous visits to physicians; the plans then process and filter the information and send risk adjustment data to CMS.
“Risk adjustment in general, is complex, is very technical, and it is very data driven,” Mr. Sullivan said. “Because it is so data driven, there has been an acknowledgment within the industry, including from CMS, that there is a very high imprecision rate in the actual codes that are submitted.”
A July study published in the Medicare & Medicaid Research Review, a CMS publication, found that risk adjustment scores in the Medicare Advantage program were largely exaggerated by health plans and did not match enrollees’ morbidity. A June report by the Center for Public Integrity revealed similar findings.
Amid such criticism, the Office of Inspector General, in its 2014 Work Plan vowed to review the extent to which CMS is verifying the accuracy of MA encounter data and risk adjustment reporting.
For doctors, the spotlight on inaccurate risk scores means a sharper eye to coding and medical records from health plans and CMS auditors. Health plans, in particular, are searching both to ensure they were not underpaid by CMS because of undercoding, and that they aren’t audited due to overcoding.
“There is more focus now (by CMS), both looking at the plan and looking at the provider as to whether or not there is accurate information being submitted,” said George B. Breen, a Washington-based health care attorney and chair of his firm’s National Health Care and Life Sciences Practice Steering Committee. “From the plan’s perspective, they have the obligation to make sure the money being spent is, in fact, consistent with the diagnosis being reported, and that they have looked to see whether or not the record by the physician supports the condition.”
Some of the coding confusion comes from the critical differences in information required by MA as compared with fee-for-service Medicare, said Julie Nielsen, director of a Tampa, Fla.–based health care research and dispute resolution company. Rather than noting only services rendered for a primary condition, physicians coding an MA claim must include all conditions that affected the patient encounter.
“It’s been a very big transition for physicians and providers having to become more attuned to capturing all of the members’ diagnosis codes that impacted the visit when the member was there, not just that the member was there for a lab draw and an office visit,” Ms. Nielsen said.
Alleged coding errors found by health plans or CMS can result in a health provider being kicked out of the program or affect their payments from health plans. Inaccurate information that results in an overpayment by CMS can also lead to a False Claims Act (FCA) violation, said Mr. Breen, who defends health providers in billing, fraud, and FCA investigations.
“Even though the claim may not have been directly submitted to Medicare, but to the Medicare Advantage plan, the government can argue the provider either submitted a false claim or caused a false claim to be submitted,” he said.
To prevent and defend MA audits, develop a strong compliance program that includes ongoing internal risk assessments, Ms. Looney said. In some cases, it may be helpful to hire a third-party company to review coding submissions and offer conclusions.
“Try to figure out what you [should] be watching for and make sure you correct anything you’re doing wrong,” she said. “Find your weak links.”
Complete documentation and regular staff training is also essential, Mr. Breen added. Employees charged with coding or documentation duties should understand MA rules and regulations what information is required. If hit with a fraud or coding error accusation, doctors should be able to say that they made efforts to identify mistakes, he said.
“It’s not enough to say, ‘I made a mistake,’” he said. “You have to be able to say, ‘I looked for mistakes and tried to make sure we weren’t doing anything inappropriate.’ At the end of the day if you made a mistake, you have to demonstrate that you did something to prevent [such errors] in the first instance.”
On Twitter @legal_med
EXPERT ANALYSIS FROM AN AHLA WEBINAR

Auditors collected $57 million from physicians in 2013
Auditors with the Centers for Medicare & Medicaid Services collected more than $3 billion in overpayments from health providers in 2013, including nearly $57 million from doctors, according to a CMS Sept. 29 annual report to Congress.
Recovery audit contractors (RACs) corrected a total of $3.75 billion in improper payments in fiscal 2013, of which $3.65 billion were in overpayments, the report found. Underpayments made up $102 million of the incorrect fees. Physicians were responsible for $56.8 million of overpayments identified. Underpayments to doctors totaled $1.2 million in 2013. Overpayment recoveries from all health providers were up $1.3 billion from those collected in 2012, according to last year’s report.

After contingency and administrative costs, the RAC program returned $3 billion to the Medicare trust funds. Meanwhile, RACs received from 9% to 12.5% of the inaccurate payments they identified. In fiscal 2013, auditors were paid $301.7 million in contingency fees, according to the report.
The outcome of audit appeals varied widely depending on the type of provider. Appeals decisions were made in 720,416 Medicare Part A claims and 116,433 Part B durable medical equipment (DME) claims in fiscal 2013. Those numbers include first-, second-, third-, and fourth-level appeal decisions, and may count the same claim multiple times. Of total claims appealed, 31% were associated with overpayment findings. Sixty percent of Medicare Part B DME decisions were overturned in providers’ favor, while only 11% of Part A claims were overturned on appeal.
On Twitter @legal_med
Auditors with the Centers for Medicare & Medicaid Services collected more than $3 billion in overpayments from health providers in 2013, including nearly $57 million from doctors, according to a CMS Sept. 29 annual report to Congress.
Recovery audit contractors (RACs) corrected a total of $3.75 billion in improper payments in fiscal 2013, of which $3.65 billion were in overpayments, the report found. Underpayments made up $102 million of the incorrect fees. Physicians were responsible for $56.8 million of overpayments identified. Underpayments to doctors totaled $1.2 million in 2013. Overpayment recoveries from all health providers were up $1.3 billion from those collected in 2012, according to last year’s report.
After contingency and administrative costs, the RAC program returned $3 billion to the Medicare trust funds. Meanwhile, RACs received from 9% to 12.5% of the inaccurate payments they identified. In fiscal 2013, auditors were paid $301.7 million in contingency fees, according to the report.
The outcome of audit appeals varied widely depending on the type of provider. Appeals decisions were made in 720,416 Medicare Part A claims and 116,433 Part B durable medical equipment (DME) claims in fiscal 2013. Those numbers include first-, second-, third-, and fourth-level appeal decisions, and may count the same claim multiple times. Of total claims appealed, 31% were associated with overpayment findings. Sixty percent of Medicare Part B DME decisions were overturned in providers’ favor, while only 11% of Part A claims were overturned on appeal.
On Twitter @legal_med
Auditors with the Centers for Medicare & Medicaid Services collected more than $3 billion in overpayments from health providers in 2013, including nearly $57 million from doctors, according to a CMS Sept. 29 annual report to Congress.
Recovery audit contractors (RACs) corrected a total of $3.75 billion in improper payments in fiscal 2013, of which $3.65 billion were in overpayments, the report found. Underpayments made up $102 million of the incorrect fees. Physicians were responsible for $56.8 million of overpayments identified. Underpayments to doctors totaled $1.2 million in 2013. Overpayment recoveries from all health providers were up $1.3 billion from those collected in 2012, according to last year’s report.
After contingency and administrative costs, the RAC program returned $3 billion to the Medicare trust funds. Meanwhile, RACs received from 9% to 12.5% of the inaccurate payments they identified. In fiscal 2013, auditors were paid $301.7 million in contingency fees, according to the report.
The outcome of audit appeals varied widely depending on the type of provider. Appeals decisions were made in 720,416 Medicare Part A claims and 116,433 Part B durable medical equipment (DME) claims in fiscal 2013. Those numbers include first-, second-, third-, and fourth-level appeal decisions, and may count the same claim multiple times. Of total claims appealed, 31% were associated with overpayment findings. Sixty percent of Medicare Part B DME decisions were overturned in providers’ favor, while only 11% of Part A claims were overturned on appeal.
On Twitter @legal_med
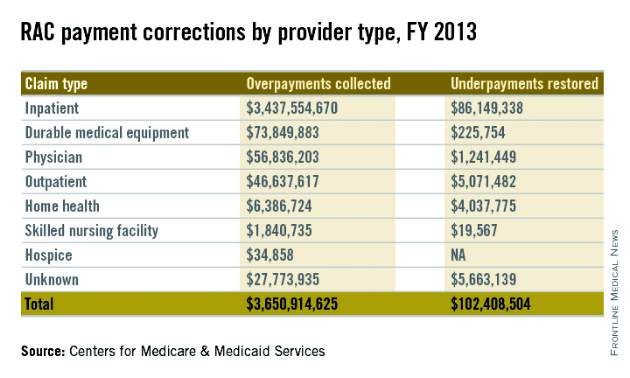
Study: Hospitals could be exploiting drug discount program
Hospital-affiliated clinics are using a federal program intended to provide low-income patients with discounted drugs to serve wealthier patients and likely generate profits, according to a study in the October Health Affairs (2014 [doi:10.1377/hlthaff.2014.0540]).
Rena M. Conti, Ph.D., and Dr. Peter B. Bach found that clinics that registered for the federal 340B program in 2004 or later serve more affluent communities than those that registered before 2004.
The findings support recent criticism that the 340B program is being used to enrich hospitals and affiliated clinics, rather than to serve vulnerable patient populations, the authors noted.

Named for section 340B of the Veterans Health Care Act of 1992, the medication program is aimed at providing aid to low-income and uninsured patients. The 340B program gives registered 340B entities, such as hospitals and other medical care providers, access to outpatient drug discounts similar to those offered through the Medicaid Drug Rebate Program.
To evaluate the patient populations of registered 340B health centers, Dr. Conti of the University of Chicago and Dr. Bach of Memorial Sloan-Kettering Cancer Center, New York, matched 340B program hospital data with Census Bureau community data. Specifically, the researchers compared data for 960 hospitals and 3,964 affiliated clinics registered with the 340B program in 2012 with the socioeconomic characteristics of their communities from the Census Bureau’s American Community Survey. They focused on 340B hospitals that also participated in Medicare’s disproportionate-share hospital (DSH) program.
Results showed that generally, DSH hospitals that registered for the 340B program in 2004 or later served communities with fewer low-income people (P < .05), compared to DSH hospitals that registered before 2004. Clinics affiliated with 340B entities that registered in 2004 or later served wealthier communities with higher levels of insurance (P < .01), compared with clinics that registered before 2004. In general, hospitals that registered in 2003 or before, had clinics that served significantly poorer communities than their parent institutions compared to facilities that registered after 2004 (P < .01), the study found.
Dr. Conti and Dr. Bach noted that 340B hospitals can generate profits by prescribing drugs to patients who have private insurance or Medicare. Hospitals can then potentially pocket the difference between the discounted price and the higher reimbursement paid by insurers and patients.
The study’s findings are consistent with recent claims by legislators that the 340B program is being misused by hospitals to gain profits. The researchers added that further national assessments of the 340B program are a necessary policy goal.
On Twitter @legal_med
Hospital-affiliated clinics are using a federal program intended to provide low-income patients with discounted drugs to serve wealthier patients and likely generate profits, according to a study in the October Health Affairs (2014 [doi:10.1377/hlthaff.2014.0540]).
Rena M. Conti, Ph.D., and Dr. Peter B. Bach found that clinics that registered for the federal 340B program in 2004 or later serve more affluent communities than those that registered before 2004.
The findings support recent criticism that the 340B program is being used to enrich hospitals and affiliated clinics, rather than to serve vulnerable patient populations, the authors noted.
Named for section 340B of the Veterans Health Care Act of 1992, the medication program is aimed at providing aid to low-income and uninsured patients. The 340B program gives registered 340B entities, such as hospitals and other medical care providers, access to outpatient drug discounts similar to those offered through the Medicaid Drug Rebate Program.
To evaluate the patient populations of registered 340B health centers, Dr. Conti of the University of Chicago and Dr. Bach of Memorial Sloan-Kettering Cancer Center, New York, matched 340B program hospital data with Census Bureau community data. Specifically, the researchers compared data for 960 hospitals and 3,964 affiliated clinics registered with the 340B program in 2012 with the socioeconomic characteristics of their communities from the Census Bureau’s American Community Survey. They focused on 340B hospitals that also participated in Medicare’s disproportionate-share hospital (DSH) program.
Results showed that generally, DSH hospitals that registered for the 340B program in 2004 or later served communities with fewer low-income people (P < .05), compared to DSH hospitals that registered before 2004. Clinics affiliated with 340B entities that registered in 2004 or later served wealthier communities with higher levels of insurance (P < .01), compared with clinics that registered before 2004. In general, hospitals that registered in 2003 or before, had clinics that served significantly poorer communities than their parent institutions compared to facilities that registered after 2004 (P < .01), the study found.
Dr. Conti and Dr. Bach noted that 340B hospitals can generate profits by prescribing drugs to patients who have private insurance or Medicare. Hospitals can then potentially pocket the difference between the discounted price and the higher reimbursement paid by insurers and patients.
The study’s findings are consistent with recent claims by legislators that the 340B program is being misused by hospitals to gain profits. The researchers added that further national assessments of the 340B program are a necessary policy goal.
On Twitter @legal_med
Hospital-affiliated clinics are using a federal program intended to provide low-income patients with discounted drugs to serve wealthier patients and likely generate profits, according to a study in the October Health Affairs (2014 [doi:10.1377/hlthaff.2014.0540]).
Rena M. Conti, Ph.D., and Dr. Peter B. Bach found that clinics that registered for the federal 340B program in 2004 or later serve more affluent communities than those that registered before 2004.
The findings support recent criticism that the 340B program is being used to enrich hospitals and affiliated clinics, rather than to serve vulnerable patient populations, the authors noted.
Named for section 340B of the Veterans Health Care Act of 1992, the medication program is aimed at providing aid to low-income and uninsured patients. The 340B program gives registered 340B entities, such as hospitals and other medical care providers, access to outpatient drug discounts similar to those offered through the Medicaid Drug Rebate Program.
To evaluate the patient populations of registered 340B health centers, Dr. Conti of the University of Chicago and Dr. Bach of Memorial Sloan-Kettering Cancer Center, New York, matched 340B program hospital data with Census Bureau community data. Specifically, the researchers compared data for 960 hospitals and 3,964 affiliated clinics registered with the 340B program in 2012 with the socioeconomic characteristics of their communities from the Census Bureau’s American Community Survey. They focused on 340B hospitals that also participated in Medicare’s disproportionate-share hospital (DSH) program.
Results showed that generally, DSH hospitals that registered for the 340B program in 2004 or later served communities with fewer low-income people (P < .05), compared to DSH hospitals that registered before 2004. Clinics affiliated with 340B entities that registered in 2004 or later served wealthier communities with higher levels of insurance (P < .01), compared with clinics that registered before 2004. In general, hospitals that registered in 2003 or before, had clinics that served significantly poorer communities than their parent institutions compared to facilities that registered after 2004 (P < .01), the study found.
Dr. Conti and Dr. Bach noted that 340B hospitals can generate profits by prescribing drugs to patients who have private insurance or Medicare. Hospitals can then potentially pocket the difference between the discounted price and the higher reimbursement paid by insurers and patients.
The study’s findings are consistent with recent claims by legislators that the 340B program is being misused by hospitals to gain profits. The researchers added that further national assessments of the 340B program are a necessary policy goal.
On Twitter @legal_med
FROM HEALTH AFFAIRS
