User login
Cellular senescence, skin aging, and cosmeceuticals
I just completed the third edition of my Cosmetic Dermatology textbook (McGraw Hill), which will come out later this year. Although writing it is a huge effort, I really enjoy all the basic science. While I was working on the book, I was most surprised by the .

Right now, it is too early, and we don’t know enough yet, to have cosmeceuticals that affect cellular senescence and autophagy. But, it’s not too early to learn about this research, to avoid falling prey to any pseudoscience that invariably ends up affecting cosmeceuticals on the market. The following is a brief primer on cellular senescence, skin aging, and cosmeceuticals; it represents what we currently know.
Cell phases
Keratinocytes and fibroblasts go through five different phases: stem, proliferation, differentiation, senescence, and apoptosis. The difference between apoptotic cells and senescent cells is that apoptotic cells are not viable and are eliminated, while senescent cells, even though they have gone into cell cycle arrest, remain functional and are not eliminated from the skin.
What are senescent cells?
Senescent cells have lost the ability to proliferate but have not undergone apoptosis. Senescent human skin fibroblasts in cell culture lose the youthful spindlelike shape and become enlarged and flattened.1 Their lysosomes and mitochondria lose functionality.2 The presence of senescent cells is associated with increased aging and seems to speed aging.
Senescent cells and skin aging
Senescent cells are increased in the age-related phenotype3 because of an age-related decline of senescent cell removal systems, such as the immune system4 and the autophagy-lysosomal pathway.5 Senescent cells are deleterious because they develop into a senescence-associated secretory phenotype (SASP), which is believed to be one of the major causes of aging. SASP cells communicate with nearby cells using proinflammatory cytokines, which include catabolic modulators such as Matrix metalloproteinases. They are known to release growth factors, cytokines, chemokines, matrix-modeling enzymes, lipids, and extracellular vesicles. The last are lipid bilayer-lined vesicles that can transport functional RNA and microRNA and facilitate other modes of communication between cells.6
The SASP is likely a natural tumor suppressive mode employed by cells to prevent cells with cancerous mutations from undergoing replication;7 however, when it comes to aging, the deleterious effects of SASP outweigh the beneficial effects. For example, SASP contributes to a prolonged state of inflammation, known as “inflammaging,”8 which is detrimental to the skin’s appearance. Human fibroblasts that have assumed the SASP secrete proinflammatory cytokines and MMPs and release reactive oxygen species,9,10 resulting in degradation of the surrounding extracellular matrix (ECM). Loss of the ECM leads to fibroblast compaction and reduced DNA synthesis, all caused by SASPs.9
What causes cellular senescence?
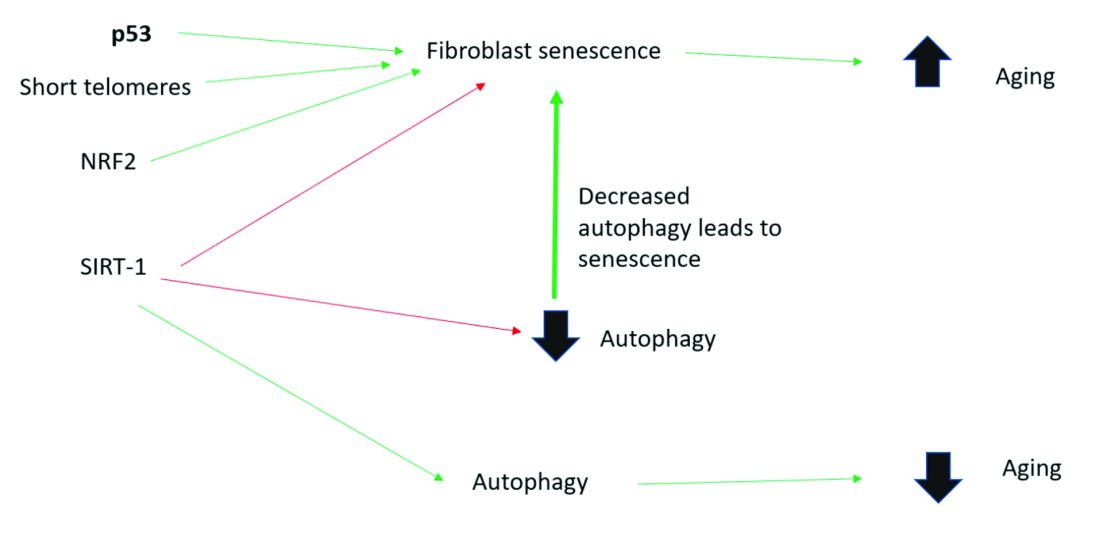
Activation of the nuclear factor-erythroid 2-related transcription factor 2 (NRF2) induces cellular senescence via direct targeting of certain ECM genes. NRF2 is a key regulator of the skin’s antioxidant defense system, which controls the transcription of genes encoding reactive oxygen species–detoxifying enzymes and various other antioxidant proteins.11 Loss of mitochondrial autophagy also induces senescence, as do activation of the TP53 gene, inactivity of SIRT-1, and short telomeres.
Cellular senescence and skin aging
Timely clearance of senescent cells before they create too much damage postpones the onset and severity of age-related diseases and extends the life span of mice.12,6 Antiaging treatments should focus on decreasing the number of senescent cells and reverting senescent cells to the more juvenile forms: proliferating or differentiating cells as an approach to prevent skin aging.13 Restoration of the lysosomal-mitochondrial axis has been shown to revert SASP back to a juvenile status. Normalization of the lysosomal-mitochondrial axis is a prerequisite to reverse senescence.14
Cellular senescence, autophagy, the lysosomal-mitochondrial axis, and cosmeceuticals
Autophagy is the important process of organelles, like mitochondria,15 self-digesting their cytoplasmic material into lysosomes for degradation. Mitochondrial autophagy is very important in slowing the aging process because damaged mitochondria generate free radicals. As you can imagine, much research is focused on this area, but it is too early for any research to translate to efficacious cosmeceuticals.
Conclusion
To summarize, activation of sirtuin-1 (SIRT-1) has been shown to extend the lifespan of mammals, as does caloric restriction.16 This extension occurs because SIRT-1 decreases senescence and activates autophagy.
Although we do not yet know whether topical skincare products could affect senescence or autophagy, there are data to show that oral resveratrol16 and melatonin17 activate SIRT-1 and increase autophagy. I am closely watching this research and will let you know if there are any similar data on topical cosmeceuticals targeting senescence or autophagy. Stay tuned!
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann has written two textbooks and a New York Times Best Sellers book for consumers. Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Galderma, Revance, Evolus, and Burt’s Bees. She is the CEO of Skin Type Solutions Inc., a company that independently tests skin care products and makes recommendations to physicians on which skin care technologies are best. Write to her at [email protected].
References
1. Papadopoulou A et al. Biogerontology. 2020 Dec;21(6):695-708.
2. López-Otin C et al. Cell. 2013 June 6;153, 1194–217.
3. Yoon J E et al. Theranostics. 2018 Sep 9;8(17):4620-32.
4. Rodier F, Campisi J. J Cell Biol. 2011 Feb 21;192(4):547-56.
5. Dutta D et al. Circ Res. 2012 Apr 13;110(8):1125-38.
6. Terlecki-Zaniewicz L et al. J Invest Dermatol. 2019 Dec;139(12):2425-36.e5.
7. Campisi J et al. Nat Rev Mol Cell Biol. 2007 Sep;8(9):729-40.
8. Franceschi C and Campisi J. J Gerontol A Biol Sci Med Sci. 2014 Jun;69 Suppl 1:S4-9.
9. Nelson G et al. Aging Cell. 2012 Apr;11(2):345-9.
10. Passos JF et al. PLoS Biol. 2007 May;5(5):e110.
11. Hiebert P et al. Dev Cell. 2018 Jul 16;46(2):145-61.e10.
12. Baker DJ et al. Nature. 2016 Feb 11:530(7589):184-9.
13. Mavrogonatou E et al. Matrix Biol. 2019 Jan;75-76:27-42.
14. Park JT et al. Ageing Res Rev. 2018 Nov;47:176-82.
15. Levine B and Kroemer G. Cell. 2019 Jan 10;176(1-2):11-42.
16. Morselli E et al. Cell Death Dis. 2010;1(1):e10.
17. Lee JH et al. Oncotarget. 2016 Mar 15;7(11):12075-88.
I just completed the third edition of my Cosmetic Dermatology textbook (McGraw Hill), which will come out later this year. Although writing it is a huge effort, I really enjoy all the basic science. While I was working on the book, I was most surprised by the .
Right now, it is too early, and we don’t know enough yet, to have cosmeceuticals that affect cellular senescence and autophagy. But, it’s not too early to learn about this research, to avoid falling prey to any pseudoscience that invariably ends up affecting cosmeceuticals on the market. The following is a brief primer on cellular senescence, skin aging, and cosmeceuticals; it represents what we currently know.
Cell phases
Keratinocytes and fibroblasts go through five different phases: stem, proliferation, differentiation, senescence, and apoptosis. The difference between apoptotic cells and senescent cells is that apoptotic cells are not viable and are eliminated, while senescent cells, even though they have gone into cell cycle arrest, remain functional and are not eliminated from the skin.
What are senescent cells?
Senescent cells have lost the ability to proliferate but have not undergone apoptosis. Senescent human skin fibroblasts in cell culture lose the youthful spindlelike shape and become enlarged and flattened.1 Their lysosomes and mitochondria lose functionality.2 The presence of senescent cells is associated with increased aging and seems to speed aging.
Senescent cells and skin aging
Senescent cells are increased in the age-related phenotype3 because of an age-related decline of senescent cell removal systems, such as the immune system4 and the autophagy-lysosomal pathway.5 Senescent cells are deleterious because they develop into a senescence-associated secretory phenotype (SASP), which is believed to be one of the major causes of aging. SASP cells communicate with nearby cells using proinflammatory cytokines, which include catabolic modulators such as Matrix metalloproteinases. They are known to release growth factors, cytokines, chemokines, matrix-modeling enzymes, lipids, and extracellular vesicles. The last are lipid bilayer-lined vesicles that can transport functional RNA and microRNA and facilitate other modes of communication between cells.6
The SASP is likely a natural tumor suppressive mode employed by cells to prevent cells with cancerous mutations from undergoing replication;7 however, when it comes to aging, the deleterious effects of SASP outweigh the beneficial effects. For example, SASP contributes to a prolonged state of inflammation, known as “inflammaging,”8 which is detrimental to the skin’s appearance. Human fibroblasts that have assumed the SASP secrete proinflammatory cytokines and MMPs and release reactive oxygen species,9,10 resulting in degradation of the surrounding extracellular matrix (ECM). Loss of the ECM leads to fibroblast compaction and reduced DNA synthesis, all caused by SASPs.9
What causes cellular senescence?
Activation of the nuclear factor-erythroid 2-related transcription factor 2 (NRF2) induces cellular senescence via direct targeting of certain ECM genes. NRF2 is a key regulator of the skin’s antioxidant defense system, which controls the transcription of genes encoding reactive oxygen species–detoxifying enzymes and various other antioxidant proteins.11 Loss of mitochondrial autophagy also induces senescence, as do activation of the TP53 gene, inactivity of SIRT-1, and short telomeres.
Cellular senescence and skin aging
Timely clearance of senescent cells before they create too much damage postpones the onset and severity of age-related diseases and extends the life span of mice.12,6 Antiaging treatments should focus on decreasing the number of senescent cells and reverting senescent cells to the more juvenile forms: proliferating or differentiating cells as an approach to prevent skin aging.13 Restoration of the lysosomal-mitochondrial axis has been shown to revert SASP back to a juvenile status. Normalization of the lysosomal-mitochondrial axis is a prerequisite to reverse senescence.14
Cellular senescence, autophagy, the lysosomal-mitochondrial axis, and cosmeceuticals
Autophagy is the important process of organelles, like mitochondria,15 self-digesting their cytoplasmic material into lysosomes for degradation. Mitochondrial autophagy is very important in slowing the aging process because damaged mitochondria generate free radicals. As you can imagine, much research is focused on this area, but it is too early for any research to translate to efficacious cosmeceuticals.
Conclusion
To summarize, activation of sirtuin-1 (SIRT-1) has been shown to extend the lifespan of mammals, as does caloric restriction.16 This extension occurs because SIRT-1 decreases senescence and activates autophagy.
Although we do not yet know whether topical skincare products could affect senescence or autophagy, there are data to show that oral resveratrol16 and melatonin17 activate SIRT-1 and increase autophagy. I am closely watching this research and will let you know if there are any similar data on topical cosmeceuticals targeting senescence or autophagy. Stay tuned!
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann has written two textbooks and a New York Times Best Sellers book for consumers. Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Galderma, Revance, Evolus, and Burt’s Bees. She is the CEO of Skin Type Solutions Inc., a company that independently tests skin care products and makes recommendations to physicians on which skin care technologies are best. Write to her at [email protected].
References
1. Papadopoulou A et al. Biogerontology. 2020 Dec;21(6):695-708.
2. López-Otin C et al. Cell. 2013 June 6;153, 1194–217.
3. Yoon J E et al. Theranostics. 2018 Sep 9;8(17):4620-32.
4. Rodier F, Campisi J. J Cell Biol. 2011 Feb 21;192(4):547-56.
5. Dutta D et al. Circ Res. 2012 Apr 13;110(8):1125-38.
6. Terlecki-Zaniewicz L et al. J Invest Dermatol. 2019 Dec;139(12):2425-36.e5.
7. Campisi J et al. Nat Rev Mol Cell Biol. 2007 Sep;8(9):729-40.
8. Franceschi C and Campisi J. J Gerontol A Biol Sci Med Sci. 2014 Jun;69 Suppl 1:S4-9.
9. Nelson G et al. Aging Cell. 2012 Apr;11(2):345-9.
10. Passos JF et al. PLoS Biol. 2007 May;5(5):e110.
11. Hiebert P et al. Dev Cell. 2018 Jul 16;46(2):145-61.e10.
12. Baker DJ et al. Nature. 2016 Feb 11:530(7589):184-9.
13. Mavrogonatou E et al. Matrix Biol. 2019 Jan;75-76:27-42.
14. Park JT et al. Ageing Res Rev. 2018 Nov;47:176-82.
15. Levine B and Kroemer G. Cell. 2019 Jan 10;176(1-2):11-42.
16. Morselli E et al. Cell Death Dis. 2010;1(1):e10.
17. Lee JH et al. Oncotarget. 2016 Mar 15;7(11):12075-88.
I just completed the third edition of my Cosmetic Dermatology textbook (McGraw Hill), which will come out later this year. Although writing it is a huge effort, I really enjoy all the basic science. While I was working on the book, I was most surprised by the .
Right now, it is too early, and we don’t know enough yet, to have cosmeceuticals that affect cellular senescence and autophagy. But, it’s not too early to learn about this research, to avoid falling prey to any pseudoscience that invariably ends up affecting cosmeceuticals on the market. The following is a brief primer on cellular senescence, skin aging, and cosmeceuticals; it represents what we currently know.
Cell phases
Keratinocytes and fibroblasts go through five different phases: stem, proliferation, differentiation, senescence, and apoptosis. The difference between apoptotic cells and senescent cells is that apoptotic cells are not viable and are eliminated, while senescent cells, even though they have gone into cell cycle arrest, remain functional and are not eliminated from the skin.
What are senescent cells?
Senescent cells have lost the ability to proliferate but have not undergone apoptosis. Senescent human skin fibroblasts in cell culture lose the youthful spindlelike shape and become enlarged and flattened.1 Their lysosomes and mitochondria lose functionality.2 The presence of senescent cells is associated with increased aging and seems to speed aging.
Senescent cells and skin aging
Senescent cells are increased in the age-related phenotype3 because of an age-related decline of senescent cell removal systems, such as the immune system4 and the autophagy-lysosomal pathway.5 Senescent cells are deleterious because they develop into a senescence-associated secretory phenotype (SASP), which is believed to be one of the major causes of aging. SASP cells communicate with nearby cells using proinflammatory cytokines, which include catabolic modulators such as Matrix metalloproteinases. They are known to release growth factors, cytokines, chemokines, matrix-modeling enzymes, lipids, and extracellular vesicles. The last are lipid bilayer-lined vesicles that can transport functional RNA and microRNA and facilitate other modes of communication between cells.6
The SASP is likely a natural tumor suppressive mode employed by cells to prevent cells with cancerous mutations from undergoing replication;7 however, when it comes to aging, the deleterious effects of SASP outweigh the beneficial effects. For example, SASP contributes to a prolonged state of inflammation, known as “inflammaging,”8 which is detrimental to the skin’s appearance. Human fibroblasts that have assumed the SASP secrete proinflammatory cytokines and MMPs and release reactive oxygen species,9,10 resulting in degradation of the surrounding extracellular matrix (ECM). Loss of the ECM leads to fibroblast compaction and reduced DNA synthesis, all caused by SASPs.9
What causes cellular senescence?
Activation of the nuclear factor-erythroid 2-related transcription factor 2 (NRF2) induces cellular senescence via direct targeting of certain ECM genes. NRF2 is a key regulator of the skin’s antioxidant defense system, which controls the transcription of genes encoding reactive oxygen species–detoxifying enzymes and various other antioxidant proteins.11 Loss of mitochondrial autophagy also induces senescence, as do activation of the TP53 gene, inactivity of SIRT-1, and short telomeres.
Cellular senescence and skin aging
Timely clearance of senescent cells before they create too much damage postpones the onset and severity of age-related diseases and extends the life span of mice.12,6 Antiaging treatments should focus on decreasing the number of senescent cells and reverting senescent cells to the more juvenile forms: proliferating or differentiating cells as an approach to prevent skin aging.13 Restoration of the lysosomal-mitochondrial axis has been shown to revert SASP back to a juvenile status. Normalization of the lysosomal-mitochondrial axis is a prerequisite to reverse senescence.14
Cellular senescence, autophagy, the lysosomal-mitochondrial axis, and cosmeceuticals
Autophagy is the important process of organelles, like mitochondria,15 self-digesting their cytoplasmic material into lysosomes for degradation. Mitochondrial autophagy is very important in slowing the aging process because damaged mitochondria generate free radicals. As you can imagine, much research is focused on this area, but it is too early for any research to translate to efficacious cosmeceuticals.
Conclusion
To summarize, activation of sirtuin-1 (SIRT-1) has been shown to extend the lifespan of mammals, as does caloric restriction.16 This extension occurs because SIRT-1 decreases senescence and activates autophagy.
Although we do not yet know whether topical skincare products could affect senescence or autophagy, there are data to show that oral resveratrol16 and melatonin17 activate SIRT-1 and increase autophagy. I am closely watching this research and will let you know if there are any similar data on topical cosmeceuticals targeting senescence or autophagy. Stay tuned!
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann has written two textbooks and a New York Times Best Sellers book for consumers. Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Galderma, Revance, Evolus, and Burt’s Bees. She is the CEO of Skin Type Solutions Inc., a company that independently tests skin care products and makes recommendations to physicians on which skin care technologies are best. Write to her at [email protected].
References
1. Papadopoulou A et al. Biogerontology. 2020 Dec;21(6):695-708.
2. López-Otin C et al. Cell. 2013 June 6;153, 1194–217.
3. Yoon J E et al. Theranostics. 2018 Sep 9;8(17):4620-32.
4. Rodier F, Campisi J. J Cell Biol. 2011 Feb 21;192(4):547-56.
5. Dutta D et al. Circ Res. 2012 Apr 13;110(8):1125-38.
6. Terlecki-Zaniewicz L et al. J Invest Dermatol. 2019 Dec;139(12):2425-36.e5.
7. Campisi J et al. Nat Rev Mol Cell Biol. 2007 Sep;8(9):729-40.
8. Franceschi C and Campisi J. J Gerontol A Biol Sci Med Sci. 2014 Jun;69 Suppl 1:S4-9.
9. Nelson G et al. Aging Cell. 2012 Apr;11(2):345-9.
10. Passos JF et al. PLoS Biol. 2007 May;5(5):e110.
11. Hiebert P et al. Dev Cell. 2018 Jul 16;46(2):145-61.e10.
12. Baker DJ et al. Nature. 2016 Feb 11:530(7589):184-9.
13. Mavrogonatou E et al. Matrix Biol. 2019 Jan;75-76:27-42.
14. Park JT et al. Ageing Res Rev. 2018 Nov;47:176-82.
15. Levine B and Kroemer G. Cell. 2019 Jan 10;176(1-2):11-42.
16. Morselli E et al. Cell Death Dis. 2010;1(1):e10.
17. Lee JH et al. Oncotarget. 2016 Mar 15;7(11):12075-88.
Screaming for screens: Digital well-being in the 2020s
Charlie is a 15-year-old male whose medical history includes overweight and autism spectrum disorder. While his autism symptoms are stable and he is doing fairly well in school, your sense is that he is underperforming and unhappy. His screening for anxiety and depression is not outstanding and you wonder whether to leave well enough alone.

Historically, pediatrician queries about media use happen in a minority of visits,1 overcrowded by the multitude of screening and acute care needs, let alone the pressures of electronic health record prompts, billing, and documentation. Yet the COVID-19 pandemic has emphasized what was already getting louder: screen life is becoming a ubiquitous, increasing, and normative function of child development. Digital well-being exhibits bidirectional interactions with most of the core indicators of child health: sleep, nutrition, safety, mood, relationships, and many other aspects of physical and mental health.1
The pandemic unveiled the blessings and curses of digital life by shifting many into remote work and school situations where screen time became both necessary and uncontrollable. Reeling with changes in employment, health, finances, and more, families struggled to forge a new screen-life balance that could bridge academic, professional, and recreational use.
Research has wavered in producing a verdict on the effects of screen time, in part because of limitations in methodology and follow-up time,2 and exacerbated by the quickly changing nature of screen use. Screen time may put youth at risk for obesity and behavior problems,3 but the latter may be mediated in part by loss of sleep because of late-night digital activity.4 While survey data at the population level show little link between screen time and well-being impairments,5 zooming in on individuals may tell a different story. Twenge and Campbell show light use of digital media (compared with nonuse) is associated with greater well-being while heavy use is associated with lower well-being and a higher risk for depression and suicidal behavior – especially in girls.6,7 Largely cross-sectional data show a small detriment to psychological well-being associated with digital technology, though this may be bidirectional and does not clearly differentiate types of technology.2
Recent neuroscience suggests that, compared with active play, sedentary screen time after school reduced impulse control and increased brain activity in regions associated with craving.8 This may explain some of the link between screen time and obesity. Brain imaging of preschoolers showed that greater screen time correlated with lower reading readiness as well as less integrity of white-matter tracts involved in language and executive function,9 whereas nurturing home reading practices were protective for language development and white matter integrity.10
Returning to the care of Charlie, providers may benefit from taking time to reflect on their own digital environment. What does the patient-side view of your office look like? Many offices use telephone reminders and patient portals, fill prescriptions electronically, and have waiting rooms with WiFi or devices for children’s use. Office visits share space with providers’ desktops, laptops, and smartphones, with EMRs guiding the visit. EMRs may come home for evening documentation. How does this affect provider digital well-being? How do you start the conversation with families about digital well-being?
The American Academy of Pediatrics recommends media screening be incorporated into routine pediatric care, with several tools available to support this. Adapting the HEADSSS model for psychosocial check-ins, Clark and colleagues propose an additional “S” to capture screen time.11 Their model queries which apps and social media are used, quantity of use, effects on self-confidence, and whether cyberbullying or sexting are occurring. Smartphones themselves provide an eye-opening and accessible dataset, with built-in features (for example, Screen Time for iOS) tracking not just daily duration of use, but also how frequently the phone is picked up and which apps get more use. Screening may be followed by motivational coaching, emphasizing nonjudgment, curiosity, empathy, and flexibility — for patient and provider.12
In Charlie’s case, screening reveals heavy use of social Internet games that connect him with like-minded peers. While he describes an inclusiveness and level of socialization that he has not found outside the home, the quantity of use is interfering with sleep, schoolwork, and physical activity.
Significant problematic Internet use may lead to intervention or referral – addictive behaviors and mental health symptoms may warrant connection with mental health providers. Cyberbullying or unsafe behaviors may additionally benefit from parental and school-based support. There is early and limited evidence that psychological and educational interventions may be of benefit for problematic Internet use.13
When digital life is not so dramatically affecting well-being, providers may begin by working with families on a media use plan. The AAP offers its own website to support this. Other well-researched and well-designed sites include Digital Wellness Lab For Parents, with developmentally staged information and plentiful research, and Common Sense Media, which reviews apps, movies, and more; plus they have a knowledge/advice section under “Parents Need to Know.” Keep in mind that digital media can also support youth in managing psychiatric problems, e.g., a digital intervention promoting positive psychology practices looked very helpful for young people with psychosis.14
For Charlie, a health coaching approach is adopted. Using Gabrielli’s TECH parenting rubric,15 Charlie’s parents are coached to make space to talk about and coview media and apps, as well as creating a Family Media Use Plan for everyone – parents included. Alongside setting limits on screen time; health promotion activities like exercise, reading, and schoolwork are also rewarded with extra screen time. When Charlie returns 3 months later, the family reports that, in recognition of their collective digital overload, they preserved dinnertime and after 10 p.m. as screen-free downtime. While they still have concerns about Charlie’s gaming and social life, his sleep is somewhat improved and family tension is lower.
Attention to digital well-being stands to benefit provider and patient alike, and over time may gain from the scaffolding of handouts, standardized assessments, and health coaching providers that may be in place to support other important domains like sleep hygiene, food security, and parenting.
Dr. Rosenfeld is assistant professor, University of Vermont, Vermont Center for Children, Youth, and Families, Burlington. He has no relevant disclosures.
References
1. Chassiakos YR et al. Pediatrics. 2016;138(5)e20162593.
2. Orben A. Soc Psychiatry Psych Epi. 2020;55(4):407.
3. Fang K et al. Child Care Health Dev. 2019;45(5):744-53.
4. Janssen X et al. Sleep Med Rev. 2020;49:101226.
5. George MJ et al. J Ped. 2020;219:180.
6. Twenge JM and Campbell WK. Psychiatry Q. 2019;90(2):311-31.
7. Twenge JM and Martin GN. J Adolesc. 2020;79:91.
8. Efraim M et al. Brain Imaging Behav. 2021;15(1):177-89.
9. Hutton JS et al. JAMA Pediatr. 2020;174(1):e193869.
10. Hutton JS et al. Acta Paediatr. 2020;109(7):1376-86.
11. Clark DL et al. Pediatrics. 2018;141(6).
12. Jericho M and Elliot A. Clin Child Psychol Psychiatry. 2020;25(3):662.
13. Malinauskas R and Malinauskine V. J Behav Addict. 2019;8(4):613.
14. Lim MH et al. Soc Psychiatry Psychiatr Epi. 2020;55(7):877-89.
15. Gabrielli J et al. Pediatrics. 2018;142(1)e20173718.
Charlie is a 15-year-old male whose medical history includes overweight and autism spectrum disorder. While his autism symptoms are stable and he is doing fairly well in school, your sense is that he is underperforming and unhappy. His screening for anxiety and depression is not outstanding and you wonder whether to leave well enough alone.
Historically, pediatrician queries about media use happen in a minority of visits,1 overcrowded by the multitude of screening and acute care needs, let alone the pressures of electronic health record prompts, billing, and documentation. Yet the COVID-19 pandemic has emphasized what was already getting louder: screen life is becoming a ubiquitous, increasing, and normative function of child development. Digital well-being exhibits bidirectional interactions with most of the core indicators of child health: sleep, nutrition, safety, mood, relationships, and many other aspects of physical and mental health.1
The pandemic unveiled the blessings and curses of digital life by shifting many into remote work and school situations where screen time became both necessary and uncontrollable. Reeling with changes in employment, health, finances, and more, families struggled to forge a new screen-life balance that could bridge academic, professional, and recreational use.
Research has wavered in producing a verdict on the effects of screen time, in part because of limitations in methodology and follow-up time,2 and exacerbated by the quickly changing nature of screen use. Screen time may put youth at risk for obesity and behavior problems,3 but the latter may be mediated in part by loss of sleep because of late-night digital activity.4 While survey data at the population level show little link between screen time and well-being impairments,5 zooming in on individuals may tell a different story. Twenge and Campbell show light use of digital media (compared with nonuse) is associated with greater well-being while heavy use is associated with lower well-being and a higher risk for depression and suicidal behavior – especially in girls.6,7 Largely cross-sectional data show a small detriment to psychological well-being associated with digital technology, though this may be bidirectional and does not clearly differentiate types of technology.2
Recent neuroscience suggests that, compared with active play, sedentary screen time after school reduced impulse control and increased brain activity in regions associated with craving.8 This may explain some of the link between screen time and obesity. Brain imaging of preschoolers showed that greater screen time correlated with lower reading readiness as well as less integrity of white-matter tracts involved in language and executive function,9 whereas nurturing home reading practices were protective for language development and white matter integrity.10
Returning to the care of Charlie, providers may benefit from taking time to reflect on their own digital environment. What does the patient-side view of your office look like? Many offices use telephone reminders and patient portals, fill prescriptions electronically, and have waiting rooms with WiFi or devices for children’s use. Office visits share space with providers’ desktops, laptops, and smartphones, with EMRs guiding the visit. EMRs may come home for evening documentation. How does this affect provider digital well-being? How do you start the conversation with families about digital well-being?
The American Academy of Pediatrics recommends media screening be incorporated into routine pediatric care, with several tools available to support this. Adapting the HEADSSS model for psychosocial check-ins, Clark and colleagues propose an additional “S” to capture screen time.11 Their model queries which apps and social media are used, quantity of use, effects on self-confidence, and whether cyberbullying or sexting are occurring. Smartphones themselves provide an eye-opening and accessible dataset, with built-in features (for example, Screen Time for iOS) tracking not just daily duration of use, but also how frequently the phone is picked up and which apps get more use. Screening may be followed by motivational coaching, emphasizing nonjudgment, curiosity, empathy, and flexibility — for patient and provider.12
In Charlie’s case, screening reveals heavy use of social Internet games that connect him with like-minded peers. While he describes an inclusiveness and level of socialization that he has not found outside the home, the quantity of use is interfering with sleep, schoolwork, and physical activity.
Significant problematic Internet use may lead to intervention or referral – addictive behaviors and mental health symptoms may warrant connection with mental health providers. Cyberbullying or unsafe behaviors may additionally benefit from parental and school-based support. There is early and limited evidence that psychological and educational interventions may be of benefit for problematic Internet use.13
When digital life is not so dramatically affecting well-being, providers may begin by working with families on a media use plan. The AAP offers its own website to support this. Other well-researched and well-designed sites include Digital Wellness Lab For Parents, with developmentally staged information and plentiful research, and Common Sense Media, which reviews apps, movies, and more; plus they have a knowledge/advice section under “Parents Need to Know.” Keep in mind that digital media can also support youth in managing psychiatric problems, e.g., a digital intervention promoting positive psychology practices looked very helpful for young people with psychosis.14
For Charlie, a health coaching approach is adopted. Using Gabrielli’s TECH parenting rubric,15 Charlie’s parents are coached to make space to talk about and coview media and apps, as well as creating a Family Media Use Plan for everyone – parents included. Alongside setting limits on screen time; health promotion activities like exercise, reading, and schoolwork are also rewarded with extra screen time. When Charlie returns 3 months later, the family reports that, in recognition of their collective digital overload, they preserved dinnertime and after 10 p.m. as screen-free downtime. While they still have concerns about Charlie’s gaming and social life, his sleep is somewhat improved and family tension is lower.
Attention to digital well-being stands to benefit provider and patient alike, and over time may gain from the scaffolding of handouts, standardized assessments, and health coaching providers that may be in place to support other important domains like sleep hygiene, food security, and parenting.
Dr. Rosenfeld is assistant professor, University of Vermont, Vermont Center for Children, Youth, and Families, Burlington. He has no relevant disclosures.
References
1. Chassiakos YR et al. Pediatrics. 2016;138(5)e20162593.
2. Orben A. Soc Psychiatry Psych Epi. 2020;55(4):407.
3. Fang K et al. Child Care Health Dev. 2019;45(5):744-53.
4. Janssen X et al. Sleep Med Rev. 2020;49:101226.
5. George MJ et al. J Ped. 2020;219:180.
6. Twenge JM and Campbell WK. Psychiatry Q. 2019;90(2):311-31.
7. Twenge JM and Martin GN. J Adolesc. 2020;79:91.
8. Efraim M et al. Brain Imaging Behav. 2021;15(1):177-89.
9. Hutton JS et al. JAMA Pediatr. 2020;174(1):e193869.
10. Hutton JS et al. Acta Paediatr. 2020;109(7):1376-86.
11. Clark DL et al. Pediatrics. 2018;141(6).
12. Jericho M and Elliot A. Clin Child Psychol Psychiatry. 2020;25(3):662.
13. Malinauskas R and Malinauskine V. J Behav Addict. 2019;8(4):613.
14. Lim MH et al. Soc Psychiatry Psychiatr Epi. 2020;55(7):877-89.
15. Gabrielli J et al. Pediatrics. 2018;142(1)e20173718.
Charlie is a 15-year-old male whose medical history includes overweight and autism spectrum disorder. While his autism symptoms are stable and he is doing fairly well in school, your sense is that he is underperforming and unhappy. His screening for anxiety and depression is not outstanding and you wonder whether to leave well enough alone.
Historically, pediatrician queries about media use happen in a minority of visits,1 overcrowded by the multitude of screening and acute care needs, let alone the pressures of electronic health record prompts, billing, and documentation. Yet the COVID-19 pandemic has emphasized what was already getting louder: screen life is becoming a ubiquitous, increasing, and normative function of child development. Digital well-being exhibits bidirectional interactions with most of the core indicators of child health: sleep, nutrition, safety, mood, relationships, and many other aspects of physical and mental health.1
The pandemic unveiled the blessings and curses of digital life by shifting many into remote work and school situations where screen time became both necessary and uncontrollable. Reeling with changes in employment, health, finances, and more, families struggled to forge a new screen-life balance that could bridge academic, professional, and recreational use.
Research has wavered in producing a verdict on the effects of screen time, in part because of limitations in methodology and follow-up time,2 and exacerbated by the quickly changing nature of screen use. Screen time may put youth at risk for obesity and behavior problems,3 but the latter may be mediated in part by loss of sleep because of late-night digital activity.4 While survey data at the population level show little link between screen time and well-being impairments,5 zooming in on individuals may tell a different story. Twenge and Campbell show light use of digital media (compared with nonuse) is associated with greater well-being while heavy use is associated with lower well-being and a higher risk for depression and suicidal behavior – especially in girls.6,7 Largely cross-sectional data show a small detriment to psychological well-being associated with digital technology, though this may be bidirectional and does not clearly differentiate types of technology.2
Recent neuroscience suggests that, compared with active play, sedentary screen time after school reduced impulse control and increased brain activity in regions associated with craving.8 This may explain some of the link between screen time and obesity. Brain imaging of preschoolers showed that greater screen time correlated with lower reading readiness as well as less integrity of white-matter tracts involved in language and executive function,9 whereas nurturing home reading practices were protective for language development and white matter integrity.10
Returning to the care of Charlie, providers may benefit from taking time to reflect on their own digital environment. What does the patient-side view of your office look like? Many offices use telephone reminders and patient portals, fill prescriptions electronically, and have waiting rooms with WiFi or devices for children’s use. Office visits share space with providers’ desktops, laptops, and smartphones, with EMRs guiding the visit. EMRs may come home for evening documentation. How does this affect provider digital well-being? How do you start the conversation with families about digital well-being?
The American Academy of Pediatrics recommends media screening be incorporated into routine pediatric care, with several tools available to support this. Adapting the HEADSSS model for psychosocial check-ins, Clark and colleagues propose an additional “S” to capture screen time.11 Their model queries which apps and social media are used, quantity of use, effects on self-confidence, and whether cyberbullying or sexting are occurring. Smartphones themselves provide an eye-opening and accessible dataset, with built-in features (for example, Screen Time for iOS) tracking not just daily duration of use, but also how frequently the phone is picked up and which apps get more use. Screening may be followed by motivational coaching, emphasizing nonjudgment, curiosity, empathy, and flexibility — for patient and provider.12
In Charlie’s case, screening reveals heavy use of social Internet games that connect him with like-minded peers. While he describes an inclusiveness and level of socialization that he has not found outside the home, the quantity of use is interfering with sleep, schoolwork, and physical activity.
Significant problematic Internet use may lead to intervention or referral – addictive behaviors and mental health symptoms may warrant connection with mental health providers. Cyberbullying or unsafe behaviors may additionally benefit from parental and school-based support. There is early and limited evidence that psychological and educational interventions may be of benefit for problematic Internet use.13
When digital life is not so dramatically affecting well-being, providers may begin by working with families on a media use plan. The AAP offers its own website to support this. Other well-researched and well-designed sites include Digital Wellness Lab For Parents, with developmentally staged information and plentiful research, and Common Sense Media, which reviews apps, movies, and more; plus they have a knowledge/advice section under “Parents Need to Know.” Keep in mind that digital media can also support youth in managing psychiatric problems, e.g., a digital intervention promoting positive psychology practices looked very helpful for young people with psychosis.14
For Charlie, a health coaching approach is adopted. Using Gabrielli’s TECH parenting rubric,15 Charlie’s parents are coached to make space to talk about and coview media and apps, as well as creating a Family Media Use Plan for everyone – parents included. Alongside setting limits on screen time; health promotion activities like exercise, reading, and schoolwork are also rewarded with extra screen time. When Charlie returns 3 months later, the family reports that, in recognition of their collective digital overload, they preserved dinnertime and after 10 p.m. as screen-free downtime. While they still have concerns about Charlie’s gaming and social life, his sleep is somewhat improved and family tension is lower.
Attention to digital well-being stands to benefit provider and patient alike, and over time may gain from the scaffolding of handouts, standardized assessments, and health coaching providers that may be in place to support other important domains like sleep hygiene, food security, and parenting.
Dr. Rosenfeld is assistant professor, University of Vermont, Vermont Center for Children, Youth, and Families, Burlington. He has no relevant disclosures.
References
1. Chassiakos YR et al. Pediatrics. 2016;138(5)e20162593.
2. Orben A. Soc Psychiatry Psych Epi. 2020;55(4):407.
3. Fang K et al. Child Care Health Dev. 2019;45(5):744-53.
4. Janssen X et al. Sleep Med Rev. 2020;49:101226.
5. George MJ et al. J Ped. 2020;219:180.
6. Twenge JM and Campbell WK. Psychiatry Q. 2019;90(2):311-31.
7. Twenge JM and Martin GN. J Adolesc. 2020;79:91.
8. Efraim M et al. Brain Imaging Behav. 2021;15(1):177-89.
9. Hutton JS et al. JAMA Pediatr. 2020;174(1):e193869.
10. Hutton JS et al. Acta Paediatr. 2020;109(7):1376-86.
11. Clark DL et al. Pediatrics. 2018;141(6).
12. Jericho M and Elliot A. Clin Child Psychol Psychiatry. 2020;25(3):662.
13. Malinauskas R and Malinauskine V. J Behav Addict. 2019;8(4):613.
14. Lim MH et al. Soc Psychiatry Psychiatr Epi. 2020;55(7):877-89.
15. Gabrielli J et al. Pediatrics. 2018;142(1)e20173718.
Is your patient having an existential crisis?
The news is portraying our modern time as an existential crisis as though our very existence is threatened. An existential crisis is a profound feeling of lack of meaning, choice, or freedom in one’s life that makes even existing seem worthless. It can emerge as early as 5 years old, especially in introspective, gifted children, when they realize that death is permanent and universal, after a real loss or a story of a loss or failure, or from a sense of guilt.

The past 18 months of COVID-19 have been a perfect storm for developing an existential crisis. One of the main sources of life meaning for children is friendships. COVID-19 has reduced or blocked access to old and new friends. Younger children, when asked what makes a friend, will say “we like to do the same things.” Virtual play dates help but don’t replace shared experiences.
School provides meaning for children not only from socializing but also from accomplishing academic tasks – fulfilling Erickson’s stages of “mastery” and “productivity.” Teachers were better able to carry out hands-on activities, group assignments, and field trips in person so that all children and learning styles were engaged and successful. Not having in-person school has also meant loss of extracurricular activities, sports, and clubs as sources of mastery.
Loss of the structure of daily life, common during COVID-19, for waking, dressing, meals, chores, homework time, bathing, or bedtime can be profoundly disorienting.
For adolescents, opportunities to contribute to society and become productive by volunteering or being employed have been stunted by quarantine and social distancing. Some teens have had to care for relatives at home so that parents can earn a living, which, while meaningful, blocks age-essential socializing.
Meaning can also be created at any age by community structures and agreed upon beliefs such as religion. While religious membership is low in the United States, members have been largely unable to attend services. Following sports teams, an alternate “religion” and source of identity, was on hold for many months.
Existential despair can also come from major life losses. COVID-19 has taken a terrible toll of lives, homes, and jobs for millions. As short-term thinkers, when children see so many of their plans and dreams for making the team, having a girlfriend, going to prom, attending summer camp, or graduating, it feels like the end of the world they had imagined. Even the most important source of meaning – connection to family – has been disrupted by lockdown, illness, or loss.
The loss of choice and freedom goes beyond being stuck indoors. Advanced classes and exams, as well as resume-building jobs or volunteering, which teens saw as essential to college, disappeared; sometimes also the money needed was exhausted by COVID-19 unemployment. Work-at-home parents supervising virtual school see their children’s malaise or panic and pressure them to work harder, which is impossible for despairing children. Observing a parent losing his or her job makes a teen’s own career aspirations uncertain. Teen depression and suicidal ideation/acts have shot up from hopelessness, with loss of meaning at the core.
A profound sense of powerlessness has taken over. COVID-19, an invisible threat, has taken down lives. Even with amazingly effective vaccines available, fear and helplessness have burned into our brains. Helplessness to stop structural racism and the arbitrary killings of our own Black citizens by police has finally registered. And climate change is now reported as an impending disaster that may not be stoppable.
So this must be the worst time in history, right? Actually, no. The past 60 years have been a period of historically remarkable stability of government, economy, and natural forces. Perhaps knowing no other world has made these problems appear unsolvable to the parents of our patients. Their own sense of meaning has been challenged in a way similar to that of their children. Perhaps from lack of privacy or peers, parents have been sharing their own sense of powerlessness with their children directly or indirectly, making it harder to reassure them.
With COVID-19 waning in the United States, many of the sources of meaning just discussed can be reinstated by way of in-person play dates, school, sports, socializing, practicing religion, volunteering, and getting jobs. Although there is “existential therapy,” what our children need most is adult leadership showing confidence in life’s meaning, even if we have to hide our own worries. Parents can point out that, even if it takes years, people have made it through difficult times in the past, and there are many positive alternatives for education and employment.
Children need to repeatedly hear about ways they are valued that are not dependent on accomplishments. Thanking them for and telling others about their effort, ideas, curiosity, integrity, love, and kindness point out meaning for their existence independent of world events. Parents need to establish routines and rules for children to demonstrate that life goes on as usual. Chores helpful to the family are a practical contribution. Family activities that are challenging and unpredictable set up for discussing, modeling, and building resilience; for example, visiting new places, camping, hiking, trying a new sport, or adopting a pet give opportunities to say: “Oh, well, we’ll find another way.”
Parents can share stories or books about people who made it through tougher times, such as Abraham Lincoln, or better, personal, or family experiences overcoming challenges. Recalling and nicknaming instances of the child’s own resilience is valuable. Books such as “The Little Engine That Could,” “Chicken Little,” and fairy tales of overcoming doubts when facing challenges can be helpful. “Stay calm and carry on,” a saying from the British when they were being bombed during World War II, has become a meme.
As clinicians we need to sort out significant complicated grief, anxiety, obsessive compulsive disorder, depression, or suicidal ideation, and provide assessment and treatment. But when children get stuck in existential futility, in addition to engaging them in meaningful activities, we can advise parents to coach them to distract themselves, “put the thoughts in a box in your head” to consider later, and/or write down or photograph things that make them grateful. Good lessons for us all to reinvent meaning in our lives.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. Email her at [email protected].
The news is portraying our modern time as an existential crisis as though our very existence is threatened. An existential crisis is a profound feeling of lack of meaning, choice, or freedom in one’s life that makes even existing seem worthless. It can emerge as early as 5 years old, especially in introspective, gifted children, when they realize that death is permanent and universal, after a real loss or a story of a loss or failure, or from a sense of guilt.
The past 18 months of COVID-19 have been a perfect storm for developing an existential crisis. One of the main sources of life meaning for children is friendships. COVID-19 has reduced or blocked access to old and new friends. Younger children, when asked what makes a friend, will say “we like to do the same things.” Virtual play dates help but don’t replace shared experiences.
School provides meaning for children not only from socializing but also from accomplishing academic tasks – fulfilling Erickson’s stages of “mastery” and “productivity.” Teachers were better able to carry out hands-on activities, group assignments, and field trips in person so that all children and learning styles were engaged and successful. Not having in-person school has also meant loss of extracurricular activities, sports, and clubs as sources of mastery.
Loss of the structure of daily life, common during COVID-19, for waking, dressing, meals, chores, homework time, bathing, or bedtime can be profoundly disorienting.
For adolescents, opportunities to contribute to society and become productive by volunteering or being employed have been stunted by quarantine and social distancing. Some teens have had to care for relatives at home so that parents can earn a living, which, while meaningful, blocks age-essential socializing.
Meaning can also be created at any age by community structures and agreed upon beliefs such as religion. While religious membership is low in the United States, members have been largely unable to attend services. Following sports teams, an alternate “religion” and source of identity, was on hold for many months.
Existential despair can also come from major life losses. COVID-19 has taken a terrible toll of lives, homes, and jobs for millions. As short-term thinkers, when children see so many of their plans and dreams for making the team, having a girlfriend, going to prom, attending summer camp, or graduating, it feels like the end of the world they had imagined. Even the most important source of meaning – connection to family – has been disrupted by lockdown, illness, or loss.
The loss of choice and freedom goes beyond being stuck indoors. Advanced classes and exams, as well as resume-building jobs or volunteering, which teens saw as essential to college, disappeared; sometimes also the money needed was exhausted by COVID-19 unemployment. Work-at-home parents supervising virtual school see their children’s malaise or panic and pressure them to work harder, which is impossible for despairing children. Observing a parent losing his or her job makes a teen’s own career aspirations uncertain. Teen depression and suicidal ideation/acts have shot up from hopelessness, with loss of meaning at the core.
A profound sense of powerlessness has taken over. COVID-19, an invisible threat, has taken down lives. Even with amazingly effective vaccines available, fear and helplessness have burned into our brains. Helplessness to stop structural racism and the arbitrary killings of our own Black citizens by police has finally registered. And climate change is now reported as an impending disaster that may not be stoppable.
So this must be the worst time in history, right? Actually, no. The past 60 years have been a period of historically remarkable stability of government, economy, and natural forces. Perhaps knowing no other world has made these problems appear unsolvable to the parents of our patients. Their own sense of meaning has been challenged in a way similar to that of their children. Perhaps from lack of privacy or peers, parents have been sharing their own sense of powerlessness with their children directly or indirectly, making it harder to reassure them.
With COVID-19 waning in the United States, many of the sources of meaning just discussed can be reinstated by way of in-person play dates, school, sports, socializing, practicing religion, volunteering, and getting jobs. Although there is “existential therapy,” what our children need most is adult leadership showing confidence in life’s meaning, even if we have to hide our own worries. Parents can point out that, even if it takes years, people have made it through difficult times in the past, and there are many positive alternatives for education and employment.
Children need to repeatedly hear about ways they are valued that are not dependent on accomplishments. Thanking them for and telling others about their effort, ideas, curiosity, integrity, love, and kindness point out meaning for their existence independent of world events. Parents need to establish routines and rules for children to demonstrate that life goes on as usual. Chores helpful to the family are a practical contribution. Family activities that are challenging and unpredictable set up for discussing, modeling, and building resilience; for example, visiting new places, camping, hiking, trying a new sport, or adopting a pet give opportunities to say: “Oh, well, we’ll find another way.”
Parents can share stories or books about people who made it through tougher times, such as Abraham Lincoln, or better, personal, or family experiences overcoming challenges. Recalling and nicknaming instances of the child’s own resilience is valuable. Books such as “The Little Engine That Could,” “Chicken Little,” and fairy tales of overcoming doubts when facing challenges can be helpful. “Stay calm and carry on,” a saying from the British when they were being bombed during World War II, has become a meme.
As clinicians we need to sort out significant complicated grief, anxiety, obsessive compulsive disorder, depression, or suicidal ideation, and provide assessment and treatment. But when children get stuck in existential futility, in addition to engaging them in meaningful activities, we can advise parents to coach them to distract themselves, “put the thoughts in a box in your head” to consider later, and/or write down or photograph things that make them grateful. Good lessons for us all to reinvent meaning in our lives.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. Email her at [email protected].
The news is portraying our modern time as an existential crisis as though our very existence is threatened. An existential crisis is a profound feeling of lack of meaning, choice, or freedom in one’s life that makes even existing seem worthless. It can emerge as early as 5 years old, especially in introspective, gifted children, when they realize that death is permanent and universal, after a real loss or a story of a loss or failure, or from a sense of guilt.
The past 18 months of COVID-19 have been a perfect storm for developing an existential crisis. One of the main sources of life meaning for children is friendships. COVID-19 has reduced or blocked access to old and new friends. Younger children, when asked what makes a friend, will say “we like to do the same things.” Virtual play dates help but don’t replace shared experiences.
School provides meaning for children not only from socializing but also from accomplishing academic tasks – fulfilling Erickson’s stages of “mastery” and “productivity.” Teachers were better able to carry out hands-on activities, group assignments, and field trips in person so that all children and learning styles were engaged and successful. Not having in-person school has also meant loss of extracurricular activities, sports, and clubs as sources of mastery.
Loss of the structure of daily life, common during COVID-19, for waking, dressing, meals, chores, homework time, bathing, or bedtime can be profoundly disorienting.
For adolescents, opportunities to contribute to society and become productive by volunteering or being employed have been stunted by quarantine and social distancing. Some teens have had to care for relatives at home so that parents can earn a living, which, while meaningful, blocks age-essential socializing.
Meaning can also be created at any age by community structures and agreed upon beliefs such as religion. While religious membership is low in the United States, members have been largely unable to attend services. Following sports teams, an alternate “religion” and source of identity, was on hold for many months.
Existential despair can also come from major life losses. COVID-19 has taken a terrible toll of lives, homes, and jobs for millions. As short-term thinkers, when children see so many of their plans and dreams for making the team, having a girlfriend, going to prom, attending summer camp, or graduating, it feels like the end of the world they had imagined. Even the most important source of meaning – connection to family – has been disrupted by lockdown, illness, or loss.
The loss of choice and freedom goes beyond being stuck indoors. Advanced classes and exams, as well as resume-building jobs or volunteering, which teens saw as essential to college, disappeared; sometimes also the money needed was exhausted by COVID-19 unemployment. Work-at-home parents supervising virtual school see their children’s malaise or panic and pressure them to work harder, which is impossible for despairing children. Observing a parent losing his or her job makes a teen’s own career aspirations uncertain. Teen depression and suicidal ideation/acts have shot up from hopelessness, with loss of meaning at the core.
A profound sense of powerlessness has taken over. COVID-19, an invisible threat, has taken down lives. Even with amazingly effective vaccines available, fear and helplessness have burned into our brains. Helplessness to stop structural racism and the arbitrary killings of our own Black citizens by police has finally registered. And climate change is now reported as an impending disaster that may not be stoppable.
So this must be the worst time in history, right? Actually, no. The past 60 years have been a period of historically remarkable stability of government, economy, and natural forces. Perhaps knowing no other world has made these problems appear unsolvable to the parents of our patients. Their own sense of meaning has been challenged in a way similar to that of their children. Perhaps from lack of privacy or peers, parents have been sharing their own sense of powerlessness with their children directly or indirectly, making it harder to reassure them.
With COVID-19 waning in the United States, many of the sources of meaning just discussed can be reinstated by way of in-person play dates, school, sports, socializing, practicing religion, volunteering, and getting jobs. Although there is “existential therapy,” what our children need most is adult leadership showing confidence in life’s meaning, even if we have to hide our own worries. Parents can point out that, even if it takes years, people have made it through difficult times in the past, and there are many positive alternatives for education and employment.
Children need to repeatedly hear about ways they are valued that are not dependent on accomplishments. Thanking them for and telling others about their effort, ideas, curiosity, integrity, love, and kindness point out meaning for their existence independent of world events. Parents need to establish routines and rules for children to demonstrate that life goes on as usual. Chores helpful to the family are a practical contribution. Family activities that are challenging and unpredictable set up for discussing, modeling, and building resilience; for example, visiting new places, camping, hiking, trying a new sport, or adopting a pet give opportunities to say: “Oh, well, we’ll find another way.”
Parents can share stories or books about people who made it through tougher times, such as Abraham Lincoln, or better, personal, or family experiences overcoming challenges. Recalling and nicknaming instances of the child’s own resilience is valuable. Books such as “The Little Engine That Could,” “Chicken Little,” and fairy tales of overcoming doubts when facing challenges can be helpful. “Stay calm and carry on,” a saying from the British when they were being bombed during World War II, has become a meme.
As clinicians we need to sort out significant complicated grief, anxiety, obsessive compulsive disorder, depression, or suicidal ideation, and provide assessment and treatment. But when children get stuck in existential futility, in addition to engaging them in meaningful activities, we can advise parents to coach them to distract themselves, “put the thoughts in a box in your head” to consider later, and/or write down or photograph things that make them grateful. Good lessons for us all to reinvent meaning in our lives.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. Email her at [email protected].
Updates in clinical practice guidelines for Lyme disease
According to the Centers for Disease Control and Prevention, Lyme disease is the fastest growing vector-borne disease, affecting approximately 300,000 Americans every year. It is caused by the spirochete, Borrelia burgdorferi which is transmitted to humans by the deer tick. Lyme disease is often an overlooked diagnosis for myriad reasons, including inaccurate test results.

Recent guidelines for the prevention, diagnosis, and treatment of Lyme disease have been developed by a panel from the Infectious Disease Society of America (IDSA), the American Academy of Neurology (AAN), and the American College of Rheumatology (ACR) using evidence-based recommendations.
Infection prevention
We all know that the best way to treat any disease is by preventing it. The following measures are recommended as tools to prevent infection: personal protective wear, repellents, and removal of the attached tick. Recommended repellents include DEET, picaridin, IR3535, oil of lemon, eucalyptus, para-Menthane-3,8-diol (PMD), 2-undecanone, and permethrin. If a tick is found, it should be removed promptly by mechanical measures, such as with tweezers. The tweezers should be inserted between the tick body and skin to ensure removal of the entire tick. Burning an attached tick or applying a noxious chemical to the tick is not recommended.
Diagnosis
Diagnosing Lyme disease is often difficult given that tests can be negative for some time after a tick bite, even when the infection is present. There is good evidence to show that submitting the removed tick for identification is good practice. However, there is no evidence supporting testing the removed tick for the presence of Borrelia burgdorferi as it does not reliably predict infection in humans. It also is recommended to avoid testing asymptomatic people following a tick bite.
Following a high-risk tick bite, adults and children can be given prophylactic antibiotics within 72 hours. It is not helpful for low-risk bites. If the risk level is uncertain, it is better to observe before giving antibiotics. For adults, a single 200-mg dose of doxycycline can be given. In children, 4.4 mg per kg of body weight, up to 200 mg max, can be used for those under 45 kg.
For patients with a tick exposure and erythema migrans, a clinical diagnosis of Lyme disease can be made without further testing. If the clinical presentation is not typical, it is recommended to do an antibody test on an acute phase serum sample followed by a convalescent serum sample in 2-3 weeks if the initial test is negative. Recommended antibiotics for treatment include doxycycline for 10 days or amoxicillin or cefuroxime for 14 days. If a patient is unable to take these, azithromycin may be used for 7 days.
The guidelines also make recommendations regarding testing for Lyme neuroborreliosis, for which neurologic presentations, for adults with psychiatric illnesses, and for children with developmental/behavioral/psychiatric disorders. They further make recommendations for treatment of Lyme disease involving the brain or spinal column, facial nerve palsy, carditis, cardiomyopathy, and arthritis, which are beyond the scope of this discussion.
As family doctors, we are often the first ones patients call upon after a tick bite. We are the ones who diagnosis and treat Lyme disease, so it is imperative that we stay up to date with current clinical guidelines and practice evidence-based medicine. These most recent guidelines from several specialty societies can provide the answers to many of our patients’ questions. They also serve as a great tool to help with our clinical decision-making regarding tick bites. Lyme disease can be a scary infection for patients but, if we offer them the recommended measures, it doesn’t have to be.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. You can contact her at [email protected].
According to the Centers for Disease Control and Prevention, Lyme disease is the fastest growing vector-borne disease, affecting approximately 300,000 Americans every year. It is caused by the spirochete, Borrelia burgdorferi which is transmitted to humans by the deer tick. Lyme disease is often an overlooked diagnosis for myriad reasons, including inaccurate test results.
Recent guidelines for the prevention, diagnosis, and treatment of Lyme disease have been developed by a panel from the Infectious Disease Society of America (IDSA), the American Academy of Neurology (AAN), and the American College of Rheumatology (ACR) using evidence-based recommendations.
Infection prevention
We all know that the best way to treat any disease is by preventing it. The following measures are recommended as tools to prevent infection: personal protective wear, repellents, and removal of the attached tick. Recommended repellents include DEET, picaridin, IR3535, oil of lemon, eucalyptus, para-Menthane-3,8-diol (PMD), 2-undecanone, and permethrin. If a tick is found, it should be removed promptly by mechanical measures, such as with tweezers. The tweezers should be inserted between the tick body and skin to ensure removal of the entire tick. Burning an attached tick or applying a noxious chemical to the tick is not recommended.
Diagnosis
Diagnosing Lyme disease is often difficult given that tests can be negative for some time after a tick bite, even when the infection is present. There is good evidence to show that submitting the removed tick for identification is good practice. However, there is no evidence supporting testing the removed tick for the presence of Borrelia burgdorferi as it does not reliably predict infection in humans. It also is recommended to avoid testing asymptomatic people following a tick bite.
Following a high-risk tick bite, adults and children can be given prophylactic antibiotics within 72 hours. It is not helpful for low-risk bites. If the risk level is uncertain, it is better to observe before giving antibiotics. For adults, a single 200-mg dose of doxycycline can be given. In children, 4.4 mg per kg of body weight, up to 200 mg max, can be used for those under 45 kg.
For patients with a tick exposure and erythema migrans, a clinical diagnosis of Lyme disease can be made without further testing. If the clinical presentation is not typical, it is recommended to do an antibody test on an acute phase serum sample followed by a convalescent serum sample in 2-3 weeks if the initial test is negative. Recommended antibiotics for treatment include doxycycline for 10 days or amoxicillin or cefuroxime for 14 days. If a patient is unable to take these, azithromycin may be used for 7 days.
The guidelines also make recommendations regarding testing for Lyme neuroborreliosis, for which neurologic presentations, for adults with psychiatric illnesses, and for children with developmental/behavioral/psychiatric disorders. They further make recommendations for treatment of Lyme disease involving the brain or spinal column, facial nerve palsy, carditis, cardiomyopathy, and arthritis, which are beyond the scope of this discussion.
As family doctors, we are often the first ones patients call upon after a tick bite. We are the ones who diagnosis and treat Lyme disease, so it is imperative that we stay up to date with current clinical guidelines and practice evidence-based medicine. These most recent guidelines from several specialty societies can provide the answers to many of our patients’ questions. They also serve as a great tool to help with our clinical decision-making regarding tick bites. Lyme disease can be a scary infection for patients but, if we offer them the recommended measures, it doesn’t have to be.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. You can contact her at [email protected].
According to the Centers for Disease Control and Prevention, Lyme disease is the fastest growing vector-borne disease, affecting approximately 300,000 Americans every year. It is caused by the spirochete, Borrelia burgdorferi which is transmitted to humans by the deer tick. Lyme disease is often an overlooked diagnosis for myriad reasons, including inaccurate test results.
Recent guidelines for the prevention, diagnosis, and treatment of Lyme disease have been developed by a panel from the Infectious Disease Society of America (IDSA), the American Academy of Neurology (AAN), and the American College of Rheumatology (ACR) using evidence-based recommendations.
Infection prevention
We all know that the best way to treat any disease is by preventing it. The following measures are recommended as tools to prevent infection: personal protective wear, repellents, and removal of the attached tick. Recommended repellents include DEET, picaridin, IR3535, oil of lemon, eucalyptus, para-Menthane-3,8-diol (PMD), 2-undecanone, and permethrin. If a tick is found, it should be removed promptly by mechanical measures, such as with tweezers. The tweezers should be inserted between the tick body and skin to ensure removal of the entire tick. Burning an attached tick or applying a noxious chemical to the tick is not recommended.
Diagnosis
Diagnosing Lyme disease is often difficult given that tests can be negative for some time after a tick bite, even when the infection is present. There is good evidence to show that submitting the removed tick for identification is good practice. However, there is no evidence supporting testing the removed tick for the presence of Borrelia burgdorferi as it does not reliably predict infection in humans. It also is recommended to avoid testing asymptomatic people following a tick bite.
Following a high-risk tick bite, adults and children can be given prophylactic antibiotics within 72 hours. It is not helpful for low-risk bites. If the risk level is uncertain, it is better to observe before giving antibiotics. For adults, a single 200-mg dose of doxycycline can be given. In children, 4.4 mg per kg of body weight, up to 200 mg max, can be used for those under 45 kg.
For patients with a tick exposure and erythema migrans, a clinical diagnosis of Lyme disease can be made without further testing. If the clinical presentation is not typical, it is recommended to do an antibody test on an acute phase serum sample followed by a convalescent serum sample in 2-3 weeks if the initial test is negative. Recommended antibiotics for treatment include doxycycline for 10 days or amoxicillin or cefuroxime for 14 days. If a patient is unable to take these, azithromycin may be used for 7 days.
The guidelines also make recommendations regarding testing for Lyme neuroborreliosis, for which neurologic presentations, for adults with psychiatric illnesses, and for children with developmental/behavioral/psychiatric disorders. They further make recommendations for treatment of Lyme disease involving the brain or spinal column, facial nerve palsy, carditis, cardiomyopathy, and arthritis, which are beyond the scope of this discussion.
As family doctors, we are often the first ones patients call upon after a tick bite. We are the ones who diagnosis and treat Lyme disease, so it is imperative that we stay up to date with current clinical guidelines and practice evidence-based medicine. These most recent guidelines from several specialty societies can provide the answers to many of our patients’ questions. They also serve as a great tool to help with our clinical decision-making regarding tick bites. Lyme disease can be a scary infection for patients but, if we offer them the recommended measures, it doesn’t have to be.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. You can contact her at [email protected].
Music and the human brain
Music has to be one of humanity’s most unique traits, and, at the same time, one of neurology’s greatest mysteries.

Where did it come from, and why?
When it started, we can only guess. The first known musical instrument is a flute carved from bear bone, made 67,000 years ago, but music is certainly older. The first instruments were probably clapped hands, then rocks and sticks.
Tens of thousands of cultures have developed over the course of human history. And, to date, not a single one is known that didn’t have music.
It takes energy to create music, too: to make and play instruments, think of songs, sing ... So at some point having music became an evolutionary advantage of some sort (one can imagine Bill and Ted saying “Dude, chicks dig it”) or it wouldn’t have lasted. Then, as people spread out, music forms got mixed and matched among cultures. Always changing, never leaving, and now somehow woven into the DNA of our brains.
The physics principles behind music are limited and simple: percussion, a vibrating string, air movement in a tube ... But from such simple things the human brain has adapted thousands of natural, and now synthetic, objects, to create an endless variety of unique sounds.
There are plenty of articles out there about how music can be relaxing or stimulating, capable of distracting you or helping you concentrate. Music can help you forget a bad day or remember a good one. They talk about PET scans and cortical activation and many other interesting things that show the effect of music on the remarkable human brain.
But at some level it doesn’t matter to me. I don’t try to understand music any more than I try to understand my dogs. I just know I couldn’t live without either. I’m not alone. Look around you: How many people on the train, or plane, or in the gym have earbuds on?
I have iTunes on my office computer, with roughly 5,000 songs covering the majority of genres from classical to rock. It’s the first program I switch on early each morning when I start the day. It gets me focused on the work at hand, and adds an enjoyable element to the day.
I’m not a musician. I took a few guitar lessons as a kid, but never really learned it. I used to joke that the only instrument I could play was the stereo (now I guess it’s iTunes). Coming from a maternal line of excellent musicians, it’s embarrassing to admit my lack of talent. But my inability to perform it myself doesn’t keep me from enjoying it.
There is no better example of the remarkable human memory than its ability to instantly recall the lyrics of songs you haven’t heard for 20, 30, 40, or more years. A few notes and it’s like you heard them yesterday. At this point, almost 30 years since my medical school graduation, I’ve likely forgotten a large portion of what I learned there. But 70s or 80s pop from my youth? Still there, and immediately recalled.
We process music everywhere – at stores, in elevators, in the car – without realizing it, like driving down the street and automatically reading signs as we pass them. But no matter where it is in our level of realization at the time, it’s a key part of our everyday lives.
Another marvel of the remarkable human brain.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Music has to be one of humanity’s most unique traits, and, at the same time, one of neurology’s greatest mysteries.
Where did it come from, and why?
When it started, we can only guess. The first known musical instrument is a flute carved from bear bone, made 67,000 years ago, but music is certainly older. The first instruments were probably clapped hands, then rocks and sticks.
Tens of thousands of cultures have developed over the course of human history. And, to date, not a single one is known that didn’t have music.
It takes energy to create music, too: to make and play instruments, think of songs, sing ... So at some point having music became an evolutionary advantage of some sort (one can imagine Bill and Ted saying “Dude, chicks dig it”) or it wouldn’t have lasted. Then, as people spread out, music forms got mixed and matched among cultures. Always changing, never leaving, and now somehow woven into the DNA of our brains.
The physics principles behind music are limited and simple: percussion, a vibrating string, air movement in a tube ... But from such simple things the human brain has adapted thousands of natural, and now synthetic, objects, to create an endless variety of unique sounds.
There are plenty of articles out there about how music can be relaxing or stimulating, capable of distracting you or helping you concentrate. Music can help you forget a bad day or remember a good one. They talk about PET scans and cortical activation and many other interesting things that show the effect of music on the remarkable human brain.
But at some level it doesn’t matter to me. I don’t try to understand music any more than I try to understand my dogs. I just know I couldn’t live without either. I’m not alone. Look around you: How many people on the train, or plane, or in the gym have earbuds on?
I have iTunes on my office computer, with roughly 5,000 songs covering the majority of genres from classical to rock. It’s the first program I switch on early each morning when I start the day. It gets me focused on the work at hand, and adds an enjoyable element to the day.
I’m not a musician. I took a few guitar lessons as a kid, but never really learned it. I used to joke that the only instrument I could play was the stereo (now I guess it’s iTunes). Coming from a maternal line of excellent musicians, it’s embarrassing to admit my lack of talent. But my inability to perform it myself doesn’t keep me from enjoying it.
There is no better example of the remarkable human memory than its ability to instantly recall the lyrics of songs you haven’t heard for 20, 30, 40, or more years. A few notes and it’s like you heard them yesterday. At this point, almost 30 years since my medical school graduation, I’ve likely forgotten a large portion of what I learned there. But 70s or 80s pop from my youth? Still there, and immediately recalled.
We process music everywhere – at stores, in elevators, in the car – without realizing it, like driving down the street and automatically reading signs as we pass them. But no matter where it is in our level of realization at the time, it’s a key part of our everyday lives.
Another marvel of the remarkable human brain.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Music has to be one of humanity’s most unique traits, and, at the same time, one of neurology’s greatest mysteries.
Where did it come from, and why?
When it started, we can only guess. The first known musical instrument is a flute carved from bear bone, made 67,000 years ago, but music is certainly older. The first instruments were probably clapped hands, then rocks and sticks.
Tens of thousands of cultures have developed over the course of human history. And, to date, not a single one is known that didn’t have music.
It takes energy to create music, too: to make and play instruments, think of songs, sing ... So at some point having music became an evolutionary advantage of some sort (one can imagine Bill and Ted saying “Dude, chicks dig it”) or it wouldn’t have lasted. Then, as people spread out, music forms got mixed and matched among cultures. Always changing, never leaving, and now somehow woven into the DNA of our brains.
The physics principles behind music are limited and simple: percussion, a vibrating string, air movement in a tube ... But from such simple things the human brain has adapted thousands of natural, and now synthetic, objects, to create an endless variety of unique sounds.
There are plenty of articles out there about how music can be relaxing or stimulating, capable of distracting you or helping you concentrate. Music can help you forget a bad day or remember a good one. They talk about PET scans and cortical activation and many other interesting things that show the effect of music on the remarkable human brain.
But at some level it doesn’t matter to me. I don’t try to understand music any more than I try to understand my dogs. I just know I couldn’t live without either. I’m not alone. Look around you: How many people on the train, or plane, or in the gym have earbuds on?
I have iTunes on my office computer, with roughly 5,000 songs covering the majority of genres from classical to rock. It’s the first program I switch on early each morning when I start the day. It gets me focused on the work at hand, and adds an enjoyable element to the day.
I’m not a musician. I took a few guitar lessons as a kid, but never really learned it. I used to joke that the only instrument I could play was the stereo (now I guess it’s iTunes). Coming from a maternal line of excellent musicians, it’s embarrassing to admit my lack of talent. But my inability to perform it myself doesn’t keep me from enjoying it.
There is no better example of the remarkable human memory than its ability to instantly recall the lyrics of songs you haven’t heard for 20, 30, 40, or more years. A few notes and it’s like you heard them yesterday. At this point, almost 30 years since my medical school graduation, I’ve likely forgotten a large portion of what I learned there. But 70s or 80s pop from my youth? Still there, and immediately recalled.
We process music everywhere – at stores, in elevators, in the car – without realizing it, like driving down the street and automatically reading signs as we pass them. But no matter where it is in our level of realization at the time, it’s a key part of our everyday lives.
Another marvel of the remarkable human brain.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
New world order: Reflecting on a year of COVID
I remember sitting at the pool in San Diego. I had been there before many years prior – one of my first medical conferences. I remember the clinking of metal sail stays in the morning breeze.

Flying out this time I packed a few surgical masks. I guiltily picked up an N95 from the hospital floors the day before leaving, but then left it at home thinking it overkill. I still have it in a ziplock bag a year later – it’s our emergency “what-if-we-have-to-care-for-one-another-with-COVID-in-this-tiny-house-full-of-kids” N95. Not that my husband has been fit tested. At the time, neither was I.
I returned after the conference to befuddlement over how we might fit test thousands of people, racing COVID to the front door. An overly complicated task, as we didn’t even know who was supposed to be responsible for orchestrating such an effort. We didn’t even know if we could spare the N95s.
Still in California, I sat by the pool wondering if anyone would acknowledge the impending new reality. At the conference we were told “don’t shake hands, don’t touch your face, wash your hands a lot.” I gave a workshop without a mask. I ate dinner in an actual restaurant worried only about gluten free soy sauce. I sat in a lecture hall with almost 5,000 people. I started to have a conversation with a friend from Seattle, but he needed to leave because they found a positive patient in his hospital. I listened to a prerecorded webinar by the pool from our chief safety officer saying there was a plan. I was not reassured.
When we flew home the world had already changed. There were patients in New York now. Masks had appeared in the airport news stand. Yet we breathed the air in the closed space of the red eye and forgot to be concerned. At work that Monday I asked my team – fist to 5, how worried are you about this? Brave faces and side eyes at each other and a lot of 1s or 2s held up in the air. My job this week, I told them, is to get you all to a 5.
I was working with a resident who 2 months prior I had told, as we worked together in the lounge, I don’t think you’re going to China on vacation. She hadn’t gone, of course. I wasn’t going on spring break either. On one of my last train rides a commuter friend (remember those?) told me we’ll all feel a lot better once we realize that none of us are going to get to do any of the things we want to do.
The med students were still there, helping the team and hanging onto their education. I told everyone not to see any patient with a respiratory complaint until we first discussed the case. On the third day of service I had to call infection control because a hypoxic febrile patient had come to the floor without isolation orders. “Are we testing?” No, I was informed, she hadn’t had exposures, hadn’t travelled. Speechless that we were screening for travel to Italy while living with one tiny state between us and the American epicenter, I can now recall thinking that our infection control officer did not sound well rested.
My N95 was still in a baggy at home. The PAPRS hadn’t appeared yet. Literally no one could agree what kind of mask the CDC or infection control or the ID consultant of the day recommended – today we are using surgical masks, I was told. Thursday will likely be different. “Anyway, she doesn’t sound like she has it.” I walked to the floors.
My med student started presenting our septic viral pneumonia patient including the very well done exam that I previously forbade him from obtaining. What happened to not seeing respiratory patients, I asked. Oh, they said, well night float said it didn’t sound like COVID. Insufficiently convinced by our second year resident’s unjustifiably overconfident, though ultimately correct, assessment – I held my head in my hands and give my first hallway COVID chalk talk of the new era. Complete with telling the team to question everything they thought they knew now including everything I said except “be careful.” That was about when Philadelphia ran out of toilet paper.
That weekend I sat in front of a bay of computers as our Medical Officer of the Day. Air traffic control for ED patients coming in for a landing on medical teams, I watched the new biohazard warnings line up indicating respiratory isolation patients waiting for a bed. I watched CRPs and D-dimers, and looked for leukopenia. I vowed I would follow up on tests to hone my COVID illness script. I soon realized that tests lie anyway.
By the end of that week we’d fallen through the looking glass. The old rules didn’t apply. We weren’t going to China, or Arizona; we didn’t know when the med students were coming back; the jobs we had were not the jobs we signed up for but were those that the world needed us to do; we couldn’t trust our intuition or our tests; we had no experts – and yet we started to grow the humble beginnings of expertise like spring garden sprouts.
In a chaotic world, seeds of order take shape and then scatter like a screensaver. The skills needed to manage chaos are different from those that leaders use in simple ordered times. Order cannot be pulled from chaos by force of will or cleverness, nor can it be delegated, cascaded, demanded, or launched. Order emerges when communities that are receptive to learning see patterns through noise, and slowly, lovingly, coax moments of stability into being.
Dr. Jaffe is division director for hospital medicine in the Department of Medicine at Thomas Jefferson University Hospital in Philadelphia.
I remember sitting at the pool in San Diego. I had been there before many years prior – one of my first medical conferences. I remember the clinking of metal sail stays in the morning breeze.
Flying out this time I packed a few surgical masks. I guiltily picked up an N95 from the hospital floors the day before leaving, but then left it at home thinking it overkill. I still have it in a ziplock bag a year later – it’s our emergency “what-if-we-have-to-care-for-one-another-with-COVID-in-this-tiny-house-full-of-kids” N95. Not that my husband has been fit tested. At the time, neither was I.
I returned after the conference to befuddlement over how we might fit test thousands of people, racing COVID to the front door. An overly complicated task, as we didn’t even know who was supposed to be responsible for orchestrating such an effort. We didn’t even know if we could spare the N95s.
Still in California, I sat by the pool wondering if anyone would acknowledge the impending new reality. At the conference we were told “don’t shake hands, don’t touch your face, wash your hands a lot.” I gave a workshop without a mask. I ate dinner in an actual restaurant worried only about gluten free soy sauce. I sat in a lecture hall with almost 5,000 people. I started to have a conversation with a friend from Seattle, but he needed to leave because they found a positive patient in his hospital. I listened to a prerecorded webinar by the pool from our chief safety officer saying there was a plan. I was not reassured.
When we flew home the world had already changed. There were patients in New York now. Masks had appeared in the airport news stand. Yet we breathed the air in the closed space of the red eye and forgot to be concerned. At work that Monday I asked my team – fist to 5, how worried are you about this? Brave faces and side eyes at each other and a lot of 1s or 2s held up in the air. My job this week, I told them, is to get you all to a 5.
I was working with a resident who 2 months prior I had told, as we worked together in the lounge, I don’t think you’re going to China on vacation. She hadn’t gone, of course. I wasn’t going on spring break either. On one of my last train rides a commuter friend (remember those?) told me we’ll all feel a lot better once we realize that none of us are going to get to do any of the things we want to do.
The med students were still there, helping the team and hanging onto their education. I told everyone not to see any patient with a respiratory complaint until we first discussed the case. On the third day of service I had to call infection control because a hypoxic febrile patient had come to the floor without isolation orders. “Are we testing?” No, I was informed, she hadn’t had exposures, hadn’t travelled. Speechless that we were screening for travel to Italy while living with one tiny state between us and the American epicenter, I can now recall thinking that our infection control officer did not sound well rested.
My N95 was still in a baggy at home. The PAPRS hadn’t appeared yet. Literally no one could agree what kind of mask the CDC or infection control or the ID consultant of the day recommended – today we are using surgical masks, I was told. Thursday will likely be different. “Anyway, she doesn’t sound like she has it.” I walked to the floors.
My med student started presenting our septic viral pneumonia patient including the very well done exam that I previously forbade him from obtaining. What happened to not seeing respiratory patients, I asked. Oh, they said, well night float said it didn’t sound like COVID. Insufficiently convinced by our second year resident’s unjustifiably overconfident, though ultimately correct, assessment – I held my head in my hands and give my first hallway COVID chalk talk of the new era. Complete with telling the team to question everything they thought they knew now including everything I said except “be careful.” That was about when Philadelphia ran out of toilet paper.
That weekend I sat in front of a bay of computers as our Medical Officer of the Day. Air traffic control for ED patients coming in for a landing on medical teams, I watched the new biohazard warnings line up indicating respiratory isolation patients waiting for a bed. I watched CRPs and D-dimers, and looked for leukopenia. I vowed I would follow up on tests to hone my COVID illness script. I soon realized that tests lie anyway.
By the end of that week we’d fallen through the looking glass. The old rules didn’t apply. We weren’t going to China, or Arizona; we didn’t know when the med students were coming back; the jobs we had were not the jobs we signed up for but were those that the world needed us to do; we couldn’t trust our intuition or our tests; we had no experts – and yet we started to grow the humble beginnings of expertise like spring garden sprouts.
In a chaotic world, seeds of order take shape and then scatter like a screensaver. The skills needed to manage chaos are different from those that leaders use in simple ordered times. Order cannot be pulled from chaos by force of will or cleverness, nor can it be delegated, cascaded, demanded, or launched. Order emerges when communities that are receptive to learning see patterns through noise, and slowly, lovingly, coax moments of stability into being.
Dr. Jaffe is division director for hospital medicine in the Department of Medicine at Thomas Jefferson University Hospital in Philadelphia.
I remember sitting at the pool in San Diego. I had been there before many years prior – one of my first medical conferences. I remember the clinking of metal sail stays in the morning breeze.
Flying out this time I packed a few surgical masks. I guiltily picked up an N95 from the hospital floors the day before leaving, but then left it at home thinking it overkill. I still have it in a ziplock bag a year later – it’s our emergency “what-if-we-have-to-care-for-one-another-with-COVID-in-this-tiny-house-full-of-kids” N95. Not that my husband has been fit tested. At the time, neither was I.
I returned after the conference to befuddlement over how we might fit test thousands of people, racing COVID to the front door. An overly complicated task, as we didn’t even know who was supposed to be responsible for orchestrating such an effort. We didn’t even know if we could spare the N95s.
Still in California, I sat by the pool wondering if anyone would acknowledge the impending new reality. At the conference we were told “don’t shake hands, don’t touch your face, wash your hands a lot.” I gave a workshop without a mask. I ate dinner in an actual restaurant worried only about gluten free soy sauce. I sat in a lecture hall with almost 5,000 people. I started to have a conversation with a friend from Seattle, but he needed to leave because they found a positive patient in his hospital. I listened to a prerecorded webinar by the pool from our chief safety officer saying there was a plan. I was not reassured.
When we flew home the world had already changed. There were patients in New York now. Masks had appeared in the airport news stand. Yet we breathed the air in the closed space of the red eye and forgot to be concerned. At work that Monday I asked my team – fist to 5, how worried are you about this? Brave faces and side eyes at each other and a lot of 1s or 2s held up in the air. My job this week, I told them, is to get you all to a 5.
I was working with a resident who 2 months prior I had told, as we worked together in the lounge, I don’t think you’re going to China on vacation. She hadn’t gone, of course. I wasn’t going on spring break either. On one of my last train rides a commuter friend (remember those?) told me we’ll all feel a lot better once we realize that none of us are going to get to do any of the things we want to do.
The med students were still there, helping the team and hanging onto their education. I told everyone not to see any patient with a respiratory complaint until we first discussed the case. On the third day of service I had to call infection control because a hypoxic febrile patient had come to the floor without isolation orders. “Are we testing?” No, I was informed, she hadn’t had exposures, hadn’t travelled. Speechless that we were screening for travel to Italy while living with one tiny state between us and the American epicenter, I can now recall thinking that our infection control officer did not sound well rested.
My N95 was still in a baggy at home. The PAPRS hadn’t appeared yet. Literally no one could agree what kind of mask the CDC or infection control or the ID consultant of the day recommended – today we are using surgical masks, I was told. Thursday will likely be different. “Anyway, she doesn’t sound like she has it.” I walked to the floors.
My med student started presenting our septic viral pneumonia patient including the very well done exam that I previously forbade him from obtaining. What happened to not seeing respiratory patients, I asked. Oh, they said, well night float said it didn’t sound like COVID. Insufficiently convinced by our second year resident’s unjustifiably overconfident, though ultimately correct, assessment – I held my head in my hands and give my first hallway COVID chalk talk of the new era. Complete with telling the team to question everything they thought they knew now including everything I said except “be careful.” That was about when Philadelphia ran out of toilet paper.
That weekend I sat in front of a bay of computers as our Medical Officer of the Day. Air traffic control for ED patients coming in for a landing on medical teams, I watched the new biohazard warnings line up indicating respiratory isolation patients waiting for a bed. I watched CRPs and D-dimers, and looked for leukopenia. I vowed I would follow up on tests to hone my COVID illness script. I soon realized that tests lie anyway.
By the end of that week we’d fallen through the looking glass. The old rules didn’t apply. We weren’t going to China, or Arizona; we didn’t know when the med students were coming back; the jobs we had were not the jobs we signed up for but were those that the world needed us to do; we couldn’t trust our intuition or our tests; we had no experts – and yet we started to grow the humble beginnings of expertise like spring garden sprouts.
In a chaotic world, seeds of order take shape and then scatter like a screensaver. The skills needed to manage chaos are different from those that leaders use in simple ordered times. Order cannot be pulled from chaos by force of will or cleverness, nor can it be delegated, cascaded, demanded, or launched. Order emerges when communities that are receptive to learning see patterns through noise, and slowly, lovingly, coax moments of stability into being.
Dr. Jaffe is division director for hospital medicine in the Department of Medicine at Thomas Jefferson University Hospital in Philadelphia.
Not your ordinary neuropathy
She has had a diagnosis of type 2 diabetes for the past 4 years. She initially presented with polyuria/polydipsia and a hemoglobin A1c level of 9.5. She has previously not tolerated metformin, and did not want to take any subsequent medications. She was seen 4 months ago and at that time had an A1c level of 12.5. She decided she wanted to really treat her diabetes as well as she could. She started consuming a low carbohydrate diet, restarted metformin and began using a continuous glucose monitor. She also started taking nighttime glargine insulin, and mealtime insulin apart. She reports she lost 20 pounds over the past 4 months, her blood sugars now run between 100-120 fasting, and up to 180 before meals. She has had a severe, sharp pain in both of her feet over the past month that is interfering with sleep and makes walking painful for her. An exam reveals hyperesthesia of both feet, and her A1c level is 7.5. What is the most likely cause of her neuropathic symptoms?

A. Vitamin B12 deficiency
B. Diabetic neuropathy
C. Insulin neuritis
D. Charcot-Marie-Tooth disease
The most likely cause
In this case, certainly considering vitamin B12 deficiency is reasonable. It is highly unlikely though, given the rapidity of onset of symptoms, and that the patient has been on metformin for a very short period of time. Chronic metformin use is associated with low B12 levels, and the American Diabetes Association has advised that regular monitoring of vitamin B12 levels should be done on patients who are on long-term metformin.1
Diabetic neuropathy is also unlikely, given the rapidity of symptoms in this patient. What is most likely in this patient is treatment-induced neuropathy (TIN), first described with the name “insulin neuritis”.
Research on TIN
Gibbons and colleagues evaluated 16 patients with diabetes with recent marked, rapid improvement in glycemic control who developed a sudden, painful neuropathy.2 All developed symptoms within 8 weeks of intensive glucose control, with 69% having autonomic dysfunction as well, and all developing worsening retinopathy.
Gibbons and Freeman did a retrospective study of patients referred to a diabetic neuropathy clinic over a 5-year period to try to understand how prevalent TIN is.3
A total of 954 patients were evaluated for diabetic neuropathy. Treatment induced neuropathy was defined as a painful neuropathy and/or autonomic dysfunction occurring within 8 weeks of intensified treatment and a drop of the A1c level greater than 2 over a 3-month period.
A total of 104 patients (10.9%) met the criteria for treatment induced neuropathy. Patients who had a decrease in A1c had a much greater chance of developing a painful or autonomic neuropathy than patients who had no change in A1c (P < .0001). The same patients had a much higher risk of developing retinopathy (P < .001). The greater the reduction in A1c, the greater the risk. Patients whose A1c decreased by 2%-3% over 3 months had an absolute risk of 20%, whereas those with a A1c decease of greater than 4% had an 80% absolute risk.
Siddique and colleagues reported on three cases with very different clinical presentations of TIN.4 One patient had an acute third nerve palsy, another patient had a lumbosacral radiculoplexus neuropathy, and the third patient presented with a diffuse painful sensory neuropathy and postural hypotension.
Most patients improve over time from their neuropathic symptoms, with better recovery in patients with type 1 diabetes.2
Pearl
Strongly consider treatment induced neuropathy in your patients with diabetes who present with acute painful neuropathy and/or autonomic dysfunction in the setting of rapid improvement of glucose control.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and serves as third-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact him at [email protected].
References
1. American Diabetes Association. Diabetes Care. 2019 Jan;42(Suppl 1):S90-102.
2. Gibbons CH and Freeman R. Ann Neurol 2010; 67:534–41.
3. Gibbons CH and Freeman R. Brain. 2015;138:43-52.
4. Siddique N et al. Endocrinol Diabetes Metab Case Rep. 2020 Feb 26;2020:19-0140.
She has had a diagnosis of type 2 diabetes for the past 4 years. She initially presented with polyuria/polydipsia and a hemoglobin A1c level of 9.5. She has previously not tolerated metformin, and did not want to take any subsequent medications. She was seen 4 months ago and at that time had an A1c level of 12.5. She decided she wanted to really treat her diabetes as well as she could. She started consuming a low carbohydrate diet, restarted metformin and began using a continuous glucose monitor. She also started taking nighttime glargine insulin, and mealtime insulin apart. She reports she lost 20 pounds over the past 4 months, her blood sugars now run between 100-120 fasting, and up to 180 before meals. She has had a severe, sharp pain in both of her feet over the past month that is interfering with sleep and makes walking painful for her. An exam reveals hyperesthesia of both feet, and her A1c level is 7.5. What is the most likely cause of her neuropathic symptoms?
A. Vitamin B12 deficiency
B. Diabetic neuropathy
C. Insulin neuritis
D. Charcot-Marie-Tooth disease
The most likely cause
In this case, certainly considering vitamin B12 deficiency is reasonable. It is highly unlikely though, given the rapidity of onset of symptoms, and that the patient has been on metformin for a very short period of time. Chronic metformin use is associated with low B12 levels, and the American Diabetes Association has advised that regular monitoring of vitamin B12 levels should be done on patients who are on long-term metformin.1
Diabetic neuropathy is also unlikely, given the rapidity of symptoms in this patient. What is most likely in this patient is treatment-induced neuropathy (TIN), first described with the name “insulin neuritis”.
Research on TIN
Gibbons and colleagues evaluated 16 patients with diabetes with recent marked, rapid improvement in glycemic control who developed a sudden, painful neuropathy.2 All developed symptoms within 8 weeks of intensive glucose control, with 69% having autonomic dysfunction as well, and all developing worsening retinopathy.
Gibbons and Freeman did a retrospective study of patients referred to a diabetic neuropathy clinic over a 5-year period to try to understand how prevalent TIN is.3
A total of 954 patients were evaluated for diabetic neuropathy. Treatment induced neuropathy was defined as a painful neuropathy and/or autonomic dysfunction occurring within 8 weeks of intensified treatment and a drop of the A1c level greater than 2 over a 3-month period.
A total of 104 patients (10.9%) met the criteria for treatment induced neuropathy. Patients who had a decrease in A1c had a much greater chance of developing a painful or autonomic neuropathy than patients who had no change in A1c (P < .0001). The same patients had a much higher risk of developing retinopathy (P < .001). The greater the reduction in A1c, the greater the risk. Patients whose A1c decreased by 2%-3% over 3 months had an absolute risk of 20%, whereas those with a A1c decease of greater than 4% had an 80% absolute risk.
Siddique and colleagues reported on three cases with very different clinical presentations of TIN.4 One patient had an acute third nerve palsy, another patient had a lumbosacral radiculoplexus neuropathy, and the third patient presented with a diffuse painful sensory neuropathy and postural hypotension.
Most patients improve over time from their neuropathic symptoms, with better recovery in patients with type 1 diabetes.2
Pearl
Strongly consider treatment induced neuropathy in your patients with diabetes who present with acute painful neuropathy and/or autonomic dysfunction in the setting of rapid improvement of glucose control.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and serves as third-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact him at [email protected].
References
1. American Diabetes Association. Diabetes Care. 2019 Jan;42(Suppl 1):S90-102.
2. Gibbons CH and Freeman R. Ann Neurol 2010; 67:534–41.
3. Gibbons CH and Freeman R. Brain. 2015;138:43-52.
4. Siddique N et al. Endocrinol Diabetes Metab Case Rep. 2020 Feb 26;2020:19-0140.
She has had a diagnosis of type 2 diabetes for the past 4 years. She initially presented with polyuria/polydipsia and a hemoglobin A1c level of 9.5. She has previously not tolerated metformin, and did not want to take any subsequent medications. She was seen 4 months ago and at that time had an A1c level of 12.5. She decided she wanted to really treat her diabetes as well as she could. She started consuming a low carbohydrate diet, restarted metformin and began using a continuous glucose monitor. She also started taking nighttime glargine insulin, and mealtime insulin apart. She reports she lost 20 pounds over the past 4 months, her blood sugars now run between 100-120 fasting, and up to 180 before meals. She has had a severe, sharp pain in both of her feet over the past month that is interfering with sleep and makes walking painful for her. An exam reveals hyperesthesia of both feet, and her A1c level is 7.5. What is the most likely cause of her neuropathic symptoms?
A. Vitamin B12 deficiency
B. Diabetic neuropathy
C. Insulin neuritis
D. Charcot-Marie-Tooth disease
The most likely cause
In this case, certainly considering vitamin B12 deficiency is reasonable. It is highly unlikely though, given the rapidity of onset of symptoms, and that the patient has been on metformin for a very short period of time. Chronic metformin use is associated with low B12 levels, and the American Diabetes Association has advised that regular monitoring of vitamin B12 levels should be done on patients who are on long-term metformin.1
Diabetic neuropathy is also unlikely, given the rapidity of symptoms in this patient. What is most likely in this patient is treatment-induced neuropathy (TIN), first described with the name “insulin neuritis”.
Research on TIN
Gibbons and colleagues evaluated 16 patients with diabetes with recent marked, rapid improvement in glycemic control who developed a sudden, painful neuropathy.2 All developed symptoms within 8 weeks of intensive glucose control, with 69% having autonomic dysfunction as well, and all developing worsening retinopathy.
Gibbons and Freeman did a retrospective study of patients referred to a diabetic neuropathy clinic over a 5-year period to try to understand how prevalent TIN is.3
A total of 954 patients were evaluated for diabetic neuropathy. Treatment induced neuropathy was defined as a painful neuropathy and/or autonomic dysfunction occurring within 8 weeks of intensified treatment and a drop of the A1c level greater than 2 over a 3-month period.
A total of 104 patients (10.9%) met the criteria for treatment induced neuropathy. Patients who had a decrease in A1c had a much greater chance of developing a painful or autonomic neuropathy than patients who had no change in A1c (P < .0001). The same patients had a much higher risk of developing retinopathy (P < .001). The greater the reduction in A1c, the greater the risk. Patients whose A1c decreased by 2%-3% over 3 months had an absolute risk of 20%, whereas those with a A1c decease of greater than 4% had an 80% absolute risk.
Siddique and colleagues reported on three cases with very different clinical presentations of TIN.4 One patient had an acute third nerve palsy, another patient had a lumbosacral radiculoplexus neuropathy, and the third patient presented with a diffuse painful sensory neuropathy and postural hypotension.
Most patients improve over time from their neuropathic symptoms, with better recovery in patients with type 1 diabetes.2
Pearl
Strongly consider treatment induced neuropathy in your patients with diabetes who present with acute painful neuropathy and/or autonomic dysfunction in the setting of rapid improvement of glucose control.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and serves as third-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact him at [email protected].
References
1. American Diabetes Association. Diabetes Care. 2019 Jan;42(Suppl 1):S90-102.
2. Gibbons CH and Freeman R. Ann Neurol 2010; 67:534–41.
3. Gibbons CH and Freeman R. Brain. 2015;138:43-52.
4. Siddique N et al. Endocrinol Diabetes Metab Case Rep. 2020 Feb 26;2020:19-0140.
Naomi Osaka withdraws from the French Open: When athletes struggle
In 2018, when Naomi Osaka won the U.S. Open by defeating Serena Williams, the trophy ceremony was painful to watch.

Ms. Williams had argued with an umpire over a controversial call, and the ceremony began with the crowd booing. Ms. Osaka, the victor, cried while Ms. Williams comforted her and quietly assured Ms. Osaka that the crowd was not booing at her. When asked how her dream of playing against Ms. Williams compared with the reality, the new champion, looking anything but victorious, responded: “Umm, I’m gonna sort of defer from your question, I’m sorry. I know that everyone was cheering for her, and I’m sorry it had to end like this.”
It was hardly the joyous moment it should have been in this young tennis player’s life.
Ms. Osaka, now 23, entered this year’s French Open as the Women’s Tennis Association’s second-ranked player and as the highest-paid female athlete of all time. She is known for her support of Black Lives Matter. Ms. Osaka announced that she would not be attending press conferences in an Instagram post days before the competition began. “If the organizations think they can keep saying, ‘do press or you’re going to get fined,’ and continue to ignore the mental health of the athletes that are the centerpiece of their cooperation then I just gotta laugh,” Ms. Osaka posted.
She was fined $15,000 on Sunday, May 30, when she did not appear at a press conference after winning her first match. Officials noted that she would be subjected to higher fines and expulsion from the tournament if she did not attend the mandatory media briefings. On June 1, Ms. Osaka withdrew from the French Open and explained her reasons on Instagram in a post where she announced that she has been struggling with depression and social anxiety and did not mean to become a distraction for the competition.
Psychiatrists weigh in
Sue Kim, MD, a psychiatrist who both plays and watches tennis, brought up Ms. Osaka’s resignation for discussion on the Maryland Psychiatric Society’s listserv. “[Ms.] Osaka put out on social media her depression and wanted to have rules reviewed and revised by the governing body of tennis, for future occasions. I feel it is so unfortunate and unfair and I am interested in hearing your opinions.”

Yusuke Sagawa, MD, a psychiatrist and tennis fan, wrote in: “During the COVID-19 pandemic, I rekindled my interest in tennis and I followed what transpired this past weekend. Naomi Osaka is an exceptionally shy and introverted person. I have noted that her speech is somewhat akin to (for lack of a better term) ‘Valley Girl’ talk, and from reading comments on tennis-related blogs, it appears she has garnered a significant amount of hatred as a result. Most of it is along the lines of people feeling her shyness and modesty is simply a masquerade.
“I have also seen YouTube videos of her signing autographs for fans. She is cooperative and pleasant, but clearly uncomfortable around large groups of people.
“Having seen many press conferences after a match,” Dr. Sagawa continued, “tennis journalists have a penchant for asking questions that are either personal or seemingly an attempt to stir up acrimony amongst players. Whatever the case, I truly do believe that this is not some sort of ruse on her part, and I hope that people come to her defense. It is disturbing to hear the comments already coming out from the ‘big names’ in the sport that have mostly been nonsupportive. Fortunately, there have also been a number of her contemporaries who have expressed this support for her.”
In the days following Ms. Osaka’s departure from the French Open, the situation has become more complex. as it is used in these types of communications.
Maryland psychiatrist Erik Roskes, MD, wrote: “I have followed this story from a distance and what strikes me is the intermixing of athleticism – which is presumably why we watch sports – and entertainment, the money-making part of it. The athletes are both athletes and entertainers, and [Ms.] Osaka seems to be unable to fully fulfill the latter part due to her unique traits. But like many, I wonder what if this had been Michael Phelps? Is there a gender issue at play?”
Stephanie Durruthy, MD, added: “[Ms.] Osaka brings complexity to the mental health conversations. There is no one answer to her current plight, but her being a person of color cannot be minimized. She magnified the race conversation in tennis to a higher level.
“When she was new to the Grand Slam scene, her Haitian, Japanese, and Black heritage became an issue with unending curiosity.
“[Ms.] Osaka used her platform during the 2020 U.S. Open to single-handedly highlight Black Lives Matter,” Dr. Durruthy continued. “Afterward, the tennis fans could not avoid seeing her face mask. In each match, she displayed another mask depicting the name of those killed. She described on social media her fears of being a Black person in America. The biases of gender and race are well described in the sports world.”
Lindsay Crouse wrote June 1 in the New York Times: “When Naomi Osaka dropped out of the French Open, after declining to attend media interviews that she said could trigger her anxiety, she wasn’t just protecting her mental health. She was sending a message to the establishment of one of the world’s most elite sports: I will not be controlled. This was a power move – and it packed more punch coming from a young woman of color. When the system hasn’t historically stood for you, why sacrifice yourself to uphold it? Especially when you have the power to change it instead.”

Professional sports are grueling on athletes, both physically and mentally. People will speculate about Ms. Osaka’s motives for refusing to participate in the media briefings that are mandated by her contract. Some will see it as manipulative, others as the desire of a young woman struggling with anxiety and depression to push back against a system that makes few allowances for those who suffer. As psychiatrists, we see how crippling these illnesses can be and admire those who achieve at these superhuman levels, often at the expense of their own well-being.
Dr. Kim, who started the MPS listserv discussion, ended it with: “I feel bad if Naomi Osaka needs to play a mental ‘illness’ card, as opposed to mental ‘wellness’ card.”
Let’s hope that Ms. Osaka’s withdrawal from the French Open sparks more conversation about how to accommodate athletes as they endeavor to meet both the demands of their contracts and when it might be more appropriate to be flexible for those with individual struggles.
Dr. Miller is coauthor of “ Committed: The Battle Over Involuntary Psychiatric Care ” (Baltimore: Johns Hopkins University Press, 2016). She has a private practice and is assistant professor of psychiatry and behavioral sciences at Johns Hopkins University, both in Baltimore.
In 2018, when Naomi Osaka won the U.S. Open by defeating Serena Williams, the trophy ceremony was painful to watch.
Ms. Williams had argued with an umpire over a controversial call, and the ceremony began with the crowd booing. Ms. Osaka, the victor, cried while Ms. Williams comforted her and quietly assured Ms. Osaka that the crowd was not booing at her. When asked how her dream of playing against Ms. Williams compared with the reality, the new champion, looking anything but victorious, responded: “Umm, I’m gonna sort of defer from your question, I’m sorry. I know that everyone was cheering for her, and I’m sorry it had to end like this.”
It was hardly the joyous moment it should have been in this young tennis player’s life.
Ms. Osaka, now 23, entered this year’s French Open as the Women’s Tennis Association’s second-ranked player and as the highest-paid female athlete of all time. She is known for her support of Black Lives Matter. Ms. Osaka announced that she would not be attending press conferences in an Instagram post days before the competition began. “If the organizations think they can keep saying, ‘do press or you’re going to get fined,’ and continue to ignore the mental health of the athletes that are the centerpiece of their cooperation then I just gotta laugh,” Ms. Osaka posted.
She was fined $15,000 on Sunday, May 30, when she did not appear at a press conference after winning her first match. Officials noted that she would be subjected to higher fines and expulsion from the tournament if she did not attend the mandatory media briefings. On June 1, Ms. Osaka withdrew from the French Open and explained her reasons on Instagram in a post where she announced that she has been struggling with depression and social anxiety and did not mean to become a distraction for the competition.
Psychiatrists weigh in
Sue Kim, MD, a psychiatrist who both plays and watches tennis, brought up Ms. Osaka’s resignation for discussion on the Maryland Psychiatric Society’s listserv. “[Ms.] Osaka put out on social media her depression and wanted to have rules reviewed and revised by the governing body of tennis, for future occasions. I feel it is so unfortunate and unfair and I am interested in hearing your opinions.”
Yusuke Sagawa, MD, a psychiatrist and tennis fan, wrote in: “During the COVID-19 pandemic, I rekindled my interest in tennis and I followed what transpired this past weekend. Naomi Osaka is an exceptionally shy and introverted person. I have noted that her speech is somewhat akin to (for lack of a better term) ‘Valley Girl’ talk, and from reading comments on tennis-related blogs, it appears she has garnered a significant amount of hatred as a result. Most of it is along the lines of people feeling her shyness and modesty is simply a masquerade.
“I have also seen YouTube videos of her signing autographs for fans. She is cooperative and pleasant, but clearly uncomfortable around large groups of people.
“Having seen many press conferences after a match,” Dr. Sagawa continued, “tennis journalists have a penchant for asking questions that are either personal or seemingly an attempt to stir up acrimony amongst players. Whatever the case, I truly do believe that this is not some sort of ruse on her part, and I hope that people come to her defense. It is disturbing to hear the comments already coming out from the ‘big names’ in the sport that have mostly been nonsupportive. Fortunately, there have also been a number of her contemporaries who have expressed this support for her.”
In the days following Ms. Osaka’s departure from the French Open, the situation has become more complex. as it is used in these types of communications.
Maryland psychiatrist Erik Roskes, MD, wrote: “I have followed this story from a distance and what strikes me is the intermixing of athleticism – which is presumably why we watch sports – and entertainment, the money-making part of it. The athletes are both athletes and entertainers, and [Ms.] Osaka seems to be unable to fully fulfill the latter part due to her unique traits. But like many, I wonder what if this had been Michael Phelps? Is there a gender issue at play?”
Stephanie Durruthy, MD, added: “[Ms.] Osaka brings complexity to the mental health conversations. There is no one answer to her current plight, but her being a person of color cannot be minimized. She magnified the race conversation in tennis to a higher level.
“When she was new to the Grand Slam scene, her Haitian, Japanese, and Black heritage became an issue with unending curiosity.
“[Ms.] Osaka used her platform during the 2020 U.S. Open to single-handedly highlight Black Lives Matter,” Dr. Durruthy continued. “Afterward, the tennis fans could not avoid seeing her face mask. In each match, she displayed another mask depicting the name of those killed. She described on social media her fears of being a Black person in America. The biases of gender and race are well described in the sports world.”
Lindsay Crouse wrote June 1 in the New York Times: “When Naomi Osaka dropped out of the French Open, after declining to attend media interviews that she said could trigger her anxiety, she wasn’t just protecting her mental health. She was sending a message to the establishment of one of the world’s most elite sports: I will not be controlled. This was a power move – and it packed more punch coming from a young woman of color. When the system hasn’t historically stood for you, why sacrifice yourself to uphold it? Especially when you have the power to change it instead.”
Professional sports are grueling on athletes, both physically and mentally. People will speculate about Ms. Osaka’s motives for refusing to participate in the media briefings that are mandated by her contract. Some will see it as manipulative, others as the desire of a young woman struggling with anxiety and depression to push back against a system that makes few allowances for those who suffer. As psychiatrists, we see how crippling these illnesses can be and admire those who achieve at these superhuman levels, often at the expense of their own well-being.
Dr. Kim, who started the MPS listserv discussion, ended it with: “I feel bad if Naomi Osaka needs to play a mental ‘illness’ card, as opposed to mental ‘wellness’ card.”
Let’s hope that Ms. Osaka’s withdrawal from the French Open sparks more conversation about how to accommodate athletes as they endeavor to meet both the demands of their contracts and when it might be more appropriate to be flexible for those with individual struggles.
Dr. Miller is coauthor of “ Committed: The Battle Over Involuntary Psychiatric Care ” (Baltimore: Johns Hopkins University Press, 2016). She has a private practice and is assistant professor of psychiatry and behavioral sciences at Johns Hopkins University, both in Baltimore.
In 2018, when Naomi Osaka won the U.S. Open by defeating Serena Williams, the trophy ceremony was painful to watch.
Ms. Williams had argued with an umpire over a controversial call, and the ceremony began with the crowd booing. Ms. Osaka, the victor, cried while Ms. Williams comforted her and quietly assured Ms. Osaka that the crowd was not booing at her. When asked how her dream of playing against Ms. Williams compared with the reality, the new champion, looking anything but victorious, responded: “Umm, I’m gonna sort of defer from your question, I’m sorry. I know that everyone was cheering for her, and I’m sorry it had to end like this.”
It was hardly the joyous moment it should have been in this young tennis player’s life.
Ms. Osaka, now 23, entered this year’s French Open as the Women’s Tennis Association’s second-ranked player and as the highest-paid female athlete of all time. She is known for her support of Black Lives Matter. Ms. Osaka announced that she would not be attending press conferences in an Instagram post days before the competition began. “If the organizations think they can keep saying, ‘do press or you’re going to get fined,’ and continue to ignore the mental health of the athletes that are the centerpiece of their cooperation then I just gotta laugh,” Ms. Osaka posted.
She was fined $15,000 on Sunday, May 30, when she did not appear at a press conference after winning her first match. Officials noted that she would be subjected to higher fines and expulsion from the tournament if she did not attend the mandatory media briefings. On June 1, Ms. Osaka withdrew from the French Open and explained her reasons on Instagram in a post where she announced that she has been struggling with depression and social anxiety and did not mean to become a distraction for the competition.
Psychiatrists weigh in
Sue Kim, MD, a psychiatrist who both plays and watches tennis, brought up Ms. Osaka’s resignation for discussion on the Maryland Psychiatric Society’s listserv. “[Ms.] Osaka put out on social media her depression and wanted to have rules reviewed and revised by the governing body of tennis, for future occasions. I feel it is so unfortunate and unfair and I am interested in hearing your opinions.”
Yusuke Sagawa, MD, a psychiatrist and tennis fan, wrote in: “During the COVID-19 pandemic, I rekindled my interest in tennis and I followed what transpired this past weekend. Naomi Osaka is an exceptionally shy and introverted person. I have noted that her speech is somewhat akin to (for lack of a better term) ‘Valley Girl’ talk, and from reading comments on tennis-related blogs, it appears she has garnered a significant amount of hatred as a result. Most of it is along the lines of people feeling her shyness and modesty is simply a masquerade.
“I have also seen YouTube videos of her signing autographs for fans. She is cooperative and pleasant, but clearly uncomfortable around large groups of people.
“Having seen many press conferences after a match,” Dr. Sagawa continued, “tennis journalists have a penchant for asking questions that are either personal or seemingly an attempt to stir up acrimony amongst players. Whatever the case, I truly do believe that this is not some sort of ruse on her part, and I hope that people come to her defense. It is disturbing to hear the comments already coming out from the ‘big names’ in the sport that have mostly been nonsupportive. Fortunately, there have also been a number of her contemporaries who have expressed this support for her.”
In the days following Ms. Osaka’s departure from the French Open, the situation has become more complex. as it is used in these types of communications.
Maryland psychiatrist Erik Roskes, MD, wrote: “I have followed this story from a distance and what strikes me is the intermixing of athleticism – which is presumably why we watch sports – and entertainment, the money-making part of it. The athletes are both athletes and entertainers, and [Ms.] Osaka seems to be unable to fully fulfill the latter part due to her unique traits. But like many, I wonder what if this had been Michael Phelps? Is there a gender issue at play?”
Stephanie Durruthy, MD, added: “[Ms.] Osaka brings complexity to the mental health conversations. There is no one answer to her current plight, but her being a person of color cannot be minimized. She magnified the race conversation in tennis to a higher level.
“When she was new to the Grand Slam scene, her Haitian, Japanese, and Black heritage became an issue with unending curiosity.
“[Ms.] Osaka used her platform during the 2020 U.S. Open to single-handedly highlight Black Lives Matter,” Dr. Durruthy continued. “Afterward, the tennis fans could not avoid seeing her face mask. In each match, she displayed another mask depicting the name of those killed. She described on social media her fears of being a Black person in America. The biases of gender and race are well described in the sports world.”
Lindsay Crouse wrote June 1 in the New York Times: “When Naomi Osaka dropped out of the French Open, after declining to attend media interviews that she said could trigger her anxiety, she wasn’t just protecting her mental health. She was sending a message to the establishment of one of the world’s most elite sports: I will not be controlled. This was a power move – and it packed more punch coming from a young woman of color. When the system hasn’t historically stood for you, why sacrifice yourself to uphold it? Especially when you have the power to change it instead.”
Professional sports are grueling on athletes, both physically and mentally. People will speculate about Ms. Osaka’s motives for refusing to participate in the media briefings that are mandated by her contract. Some will see it as manipulative, others as the desire of a young woman struggling with anxiety and depression to push back against a system that makes few allowances for those who suffer. As psychiatrists, we see how crippling these illnesses can be and admire those who achieve at these superhuman levels, often at the expense of their own well-being.
Dr. Kim, who started the MPS listserv discussion, ended it with: “I feel bad if Naomi Osaka needs to play a mental ‘illness’ card, as opposed to mental ‘wellness’ card.”
Let’s hope that Ms. Osaka’s withdrawal from the French Open sparks more conversation about how to accommodate athletes as they endeavor to meet both the demands of their contracts and when it might be more appropriate to be flexible for those with individual struggles.
Dr. Miller is coauthor of “ Committed: The Battle Over Involuntary Psychiatric Care ” (Baltimore: Johns Hopkins University Press, 2016). She has a private practice and is assistant professor of psychiatry and behavioral sciences at Johns Hopkins University, both in Baltimore.
Rethinking your journey to work every day
Burnout is seldom the result of a single factor. It is more often a tragic case of death by a thousand cuts: a balky user-unfriendly electronic medical record system, administrative pressure to see more patients and the resulting frustration of not being able to provide the care you feel they deserve, an overemphasis on documentation or you won’t get paid, the dark cloud of malpractice always overhead, and of course the difficult balance between family responsibilities and work. It often boils down to feeling that there aren’t enough hours in the day to get everything done and still have time to recharge your physical and psychological batteries.

A recent report in the Harvard Business School newsletter, Working Knowledge (“Commuting Hurts Productivity and Your Best Talent Suffers Most.” Lane Lambert. 2021 Mar 30) describes an interesting study by Andy Wu, assistant professor of business administration, in which he discovered that, for every 10 kilometers of commuting distance, there was a decrease in the productivity of high-tech inventors as measured by the number of patents registered by their companies. The quality of their inventions declined even more (7%) for each additional 10 kilometers of commute.
You might question the relevance of these findings with your work in an outpatient clinic, but a conscientious physician is also an inventor and a creator. Every patient, even those with what sounds like a routine complaint, presents a novel collection of management challenges. The best physicians treat their profession as an art and must be invent solutions on the fly.
There is abundant evidence that commuting also can have a negative effect on the physical and mental health of workers. (“The astonishing human potential wasted on commutes.” The Washington Post .Christopher Ingraham. 2016 Feb 25). Watching my father walk into the house after an hour-long train ride out of the city and listening to him grumble created an image that influenced every decision I made about where my wife and I would live and work.
Did I benefit from the luxury of growing up in a small suburban community? Of course I did and I shall be forever grateful for the sacrifice my father made to allow that to happen. But, I promised myself that, while I would make sacrifices for my family, a long or unpleasant commute was not going to be on that list. For a few years I tolerated a 10- to 12-minute car commute (three stoplights) but asked to dissolve the partnership because even that 9-mile ride was too much for me and instead spent the bulk of my 40-year career a 10-minute bike ride from my office and the two hospitals. It meant we didn’t have a view of the ocean or a gentleman’s farm but we had an extra hour together as a family and I arrived at work and at home happy.
The pandemic has been a wake-up call for many of the fortunate folks who have found that they can work from home, eliminating what may have been a time-gobbling commute that was creating more stress than they may have realized. Even if telemedicine continues to maintain some postpandemic presence, I suspect that most physicians will continue to be faced with the challenge of traveling to an office or hospital.
If work is losing some of its luster and/or you are arriving home grumpy from a long day in the office, it is easy to blame an insensitive office administrator or the clunky electronic medical record system ... they deserve it. But, it may be the journey and not just the destination that is the contributing to the problem. I realize that rethinking the decision about where one lives can be painful and the options may be limited. However, I hope that at least some of you can rethink the role your journey is playing in your life.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Burnout is seldom the result of a single factor. It is more often a tragic case of death by a thousand cuts: a balky user-unfriendly electronic medical record system, administrative pressure to see more patients and the resulting frustration of not being able to provide the care you feel they deserve, an overemphasis on documentation or you won’t get paid, the dark cloud of malpractice always overhead, and of course the difficult balance between family responsibilities and work. It often boils down to feeling that there aren’t enough hours in the day to get everything done and still have time to recharge your physical and psychological batteries.
A recent report in the Harvard Business School newsletter, Working Knowledge (“Commuting Hurts Productivity and Your Best Talent Suffers Most.” Lane Lambert. 2021 Mar 30) describes an interesting study by Andy Wu, assistant professor of business administration, in which he discovered that, for every 10 kilometers of commuting distance, there was a decrease in the productivity of high-tech inventors as measured by the number of patents registered by their companies. The quality of their inventions declined even more (7%) for each additional 10 kilometers of commute.
You might question the relevance of these findings with your work in an outpatient clinic, but a conscientious physician is also an inventor and a creator. Every patient, even those with what sounds like a routine complaint, presents a novel collection of management challenges. The best physicians treat their profession as an art and must be invent solutions on the fly.
There is abundant evidence that commuting also can have a negative effect on the physical and mental health of workers. (“The astonishing human potential wasted on commutes.” The Washington Post .Christopher Ingraham. 2016 Feb 25). Watching my father walk into the house after an hour-long train ride out of the city and listening to him grumble created an image that influenced every decision I made about where my wife and I would live and work.
Did I benefit from the luxury of growing up in a small suburban community? Of course I did and I shall be forever grateful for the sacrifice my father made to allow that to happen. But, I promised myself that, while I would make sacrifices for my family, a long or unpleasant commute was not going to be on that list. For a few years I tolerated a 10- to 12-minute car commute (three stoplights) but asked to dissolve the partnership because even that 9-mile ride was too much for me and instead spent the bulk of my 40-year career a 10-minute bike ride from my office and the two hospitals. It meant we didn’t have a view of the ocean or a gentleman’s farm but we had an extra hour together as a family and I arrived at work and at home happy.
The pandemic has been a wake-up call for many of the fortunate folks who have found that they can work from home, eliminating what may have been a time-gobbling commute that was creating more stress than they may have realized. Even if telemedicine continues to maintain some postpandemic presence, I suspect that most physicians will continue to be faced with the challenge of traveling to an office or hospital.
If work is losing some of its luster and/or you are arriving home grumpy from a long day in the office, it is easy to blame an insensitive office administrator or the clunky electronic medical record system ... they deserve it. But, it may be the journey and not just the destination that is the contributing to the problem. I realize that rethinking the decision about where one lives can be painful and the options may be limited. However, I hope that at least some of you can rethink the role your journey is playing in your life.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Burnout is seldom the result of a single factor. It is more often a tragic case of death by a thousand cuts: a balky user-unfriendly electronic medical record system, administrative pressure to see more patients and the resulting frustration of not being able to provide the care you feel they deserve, an overemphasis on documentation or you won’t get paid, the dark cloud of malpractice always overhead, and of course the difficult balance between family responsibilities and work. It often boils down to feeling that there aren’t enough hours in the day to get everything done and still have time to recharge your physical and psychological batteries.
A recent report in the Harvard Business School newsletter, Working Knowledge (“Commuting Hurts Productivity and Your Best Talent Suffers Most.” Lane Lambert. 2021 Mar 30) describes an interesting study by Andy Wu, assistant professor of business administration, in which he discovered that, for every 10 kilometers of commuting distance, there was a decrease in the productivity of high-tech inventors as measured by the number of patents registered by their companies. The quality of their inventions declined even more (7%) for each additional 10 kilometers of commute.
You might question the relevance of these findings with your work in an outpatient clinic, but a conscientious physician is also an inventor and a creator. Every patient, even those with what sounds like a routine complaint, presents a novel collection of management challenges. The best physicians treat their profession as an art and must be invent solutions on the fly.
There is abundant evidence that commuting also can have a negative effect on the physical and mental health of workers. (“The astonishing human potential wasted on commutes.” The Washington Post .Christopher Ingraham. 2016 Feb 25). Watching my father walk into the house after an hour-long train ride out of the city and listening to him grumble created an image that influenced every decision I made about where my wife and I would live and work.
Did I benefit from the luxury of growing up in a small suburban community? Of course I did and I shall be forever grateful for the sacrifice my father made to allow that to happen. But, I promised myself that, while I would make sacrifices for my family, a long or unpleasant commute was not going to be on that list. For a few years I tolerated a 10- to 12-minute car commute (three stoplights) but asked to dissolve the partnership because even that 9-mile ride was too much for me and instead spent the bulk of my 40-year career a 10-minute bike ride from my office and the two hospitals. It meant we didn’t have a view of the ocean or a gentleman’s farm but we had an extra hour together as a family and I arrived at work and at home happy.
The pandemic has been a wake-up call for many of the fortunate folks who have found that they can work from home, eliminating what may have been a time-gobbling commute that was creating more stress than they may have realized. Even if telemedicine continues to maintain some postpandemic presence, I suspect that most physicians will continue to be faced with the challenge of traveling to an office or hospital.
If work is losing some of its luster and/or you are arriving home grumpy from a long day in the office, it is easy to blame an insensitive office administrator or the clunky electronic medical record system ... they deserve it. But, it may be the journey and not just the destination that is the contributing to the problem. I realize that rethinking the decision about where one lives can be painful and the options may be limited. However, I hope that at least some of you can rethink the role your journey is playing in your life.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Sealing the envelope
Mike died last week.
He was a long-retired doc, in his mid-90s. One of my favorite patients to just chat with about nothing in particular. I learned more from him about restoring old grandfather clocks than I ever dreamed I’d know.
After receiving the sad news, I sat down, as I often do, to write a letter to his family. After 23 years I have a pretty standard idea of what I want to say, but it still always takes some thought.
Sealing the envelopes on these letters always seems to be more than just paperwork. There’s a symbolism to it, that I’m closing out my relationship, sometimes of 10-20 years, with the person involved.
Some patients become friends after a time. It’s a matter of chemistry. I don’t socialize with them outside my office, but still enjoy seeing them and talking about nonmedical stuff in the space around clinical questions and answers. They’re the ones it’s hardest to say goodbye to.
I’ll miss my 2-3 visits a year with Mike. We swapped medical war stories, family anecdotes, and the occasional tip about clock restoration that I’ll probably never use (but who knows, he didn’t start until after he retired).
Closing the envelope comes with the realization that I won’t be seeing him again. I don’t go to patient funerals, as I believe those are for families and close friends, and so writing the letter is the closest I’ll get to saying goodbye.
Medicine, and how we practice, is focused on what we do for the patient – which is what it should be.
But lost in the shuffle sometimes is realizing what the patient does for us. That’s also important, but harder to quantify. And sometimes we don’t realize it until we seal the envelope.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Mike died last week.
He was a long-retired doc, in his mid-90s. One of my favorite patients to just chat with about nothing in particular. I learned more from him about restoring old grandfather clocks than I ever dreamed I’d know.
After receiving the sad news, I sat down, as I often do, to write a letter to his family. After 23 years I have a pretty standard idea of what I want to say, but it still always takes some thought.
Sealing the envelopes on these letters always seems to be more than just paperwork. There’s a symbolism to it, that I’m closing out my relationship, sometimes of 10-20 years, with the person involved.
Some patients become friends after a time. It’s a matter of chemistry. I don’t socialize with them outside my office, but still enjoy seeing them and talking about nonmedical stuff in the space around clinical questions and answers. They’re the ones it’s hardest to say goodbye to.
I’ll miss my 2-3 visits a year with Mike. We swapped medical war stories, family anecdotes, and the occasional tip about clock restoration that I’ll probably never use (but who knows, he didn’t start until after he retired).
Closing the envelope comes with the realization that I won’t be seeing him again. I don’t go to patient funerals, as I believe those are for families and close friends, and so writing the letter is the closest I’ll get to saying goodbye.
Medicine, and how we practice, is focused on what we do for the patient – which is what it should be.
But lost in the shuffle sometimes is realizing what the patient does for us. That’s also important, but harder to quantify. And sometimes we don’t realize it until we seal the envelope.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Mike died last week.
He was a long-retired doc, in his mid-90s. One of my favorite patients to just chat with about nothing in particular. I learned more from him about restoring old grandfather clocks than I ever dreamed I’d know.
After receiving the sad news, I sat down, as I often do, to write a letter to his family. After 23 years I have a pretty standard idea of what I want to say, but it still always takes some thought.
Sealing the envelopes on these letters always seems to be more than just paperwork. There’s a symbolism to it, that I’m closing out my relationship, sometimes of 10-20 years, with the person involved.
Some patients become friends after a time. It’s a matter of chemistry. I don’t socialize with them outside my office, but still enjoy seeing them and talking about nonmedical stuff in the space around clinical questions and answers. They’re the ones it’s hardest to say goodbye to.
I’ll miss my 2-3 visits a year with Mike. We swapped medical war stories, family anecdotes, and the occasional tip about clock restoration that I’ll probably never use (but who knows, he didn’t start until after he retired).
Closing the envelope comes with the realization that I won’t be seeing him again. I don’t go to patient funerals, as I believe those are for families and close friends, and so writing the letter is the closest I’ll get to saying goodbye.
Medicine, and how we practice, is focused on what we do for the patient – which is what it should be.
But lost in the shuffle sometimes is realizing what the patient does for us. That’s also important, but harder to quantify. And sometimes we don’t realize it until we seal the envelope.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.