User login
Official Newspaper of the American College of Surgeons
Gas-filled gastric balloons achieve weight loss
A gas-filled gastric balloon may promote weight loss more effectively than does its water-filled cousin, according to data from a randomized study that was presented during a teleconference in advance of the annual Digestive Disease Week. A water-filled version of the device is on the market already.
The study enrolled 387 people aged 22 to 64 years old with a body mass index (BMI) from 30 to 40 kg/m2 at 15 different sites. People were randomized to the Obalon Balloon System or to a sham control group. People in the treatment group were asked to swallow three capsules: one every 3 weeks until week 12.
The balloon is contained within the capsule, and after swallowing each balloon was filled with 250 cubic centimeters (slightly more than 1 cup) of a nitrogen-based gas via a small catheter. The control group also swallowed sugar-filled capsules (sham treatment).
A total of 366 patients swallowed at least two capsules and were included in the per protocol analysis: 185 in the treatment group and 181 in the control group. All patients saw a registered dietitian every 3 weeks and also followed diet, exercise, and behavior modification lifestyle changes. Obalon balloons were removed endoscopically at week 24, when participants’ weight was assessed.
The balloon-treated group had a mean weight loss of 6.8%, compared with 3.59% in the control group. At least 5% of body weight loss was achieved by 64.3% of the balloon-treated group, compared with 32% of the control group. The balloon treatment group, but not controls, showed improvements in levels of systolic blood pressure, LDL cholesterol, and triglycerides.
The finding that obese participants who swallowed the Obalon 6-Month Balloon System lost nearly 7% of their body weight and experienced improvements in other health indicators “is important because weight loss is quite difficult to achieve and a significant number of people are not successful in achieving their weight loss goals with diet changes and exercise,” said lead author Dr. Shelby Sullivan, who presented the findings.
Adverse events were mostly mild and included diarrhea, cramping, and nausea in nine patients. No hospitalizations were required for these events. One patient with a pre-existing bleeding ulcer experienced a serious adverse event, which the investigators classified as being possibly related to treatment.
“This patient had an orthopedic procedure and was taking high doses of NSAIDs. That should have been excluded in the trial,” said Dr. Sullivan of Washington University, St. Louis.
“Treatment over time, and even with the initial swallowing of the balloon capsule is quite well tolerated, with only mild symptoms compared with other balloon systems,” she said. “Anecdotally, my impression is that patients liked the therapy because it allowed them to follow lifestyle therapy as well.”
The Obalon balloon is given in stages, giving patients’ stomachs time to adjust to the balloon. Unlike liquid-filled balloons, the gas floats up in the stomach and may cause fewer symptoms than liquid-filled balloons, she suggested.
Dr. Sullivan believes that when the Obalon system is used in the real world, it may lead to even greater weight loss. “This has been seen in other sham-controlled trials,” she noted.
Patients enrolled in the trial are being followed longitudinally and those in the sham control group are allowed to cross over to the Obalon balloons on an open-label basis.
“More than 640 million people globally have obesity, and at this time, there are more overweight than underweight people in the world. Some treatments that are alternatives to diet and exercise may be risky. Obalon swallowable balloon is a new treatment option that can help patients lose almost twice as much weight compared with lifestyle changes alone,” she said.
Dr. Sullivan received funding for this study from Obalon Therapeutics.
A gas-filled gastric balloon may promote weight loss more effectively than does its water-filled cousin, according to data from a randomized study that was presented during a teleconference in advance of the annual Digestive Disease Week. A water-filled version of the device is on the market already.
The study enrolled 387 people aged 22 to 64 years old with a body mass index (BMI) from 30 to 40 kg/m2 at 15 different sites. People were randomized to the Obalon Balloon System or to a sham control group. People in the treatment group were asked to swallow three capsules: one every 3 weeks until week 12.
The balloon is contained within the capsule, and after swallowing each balloon was filled with 250 cubic centimeters (slightly more than 1 cup) of a nitrogen-based gas via a small catheter. The control group also swallowed sugar-filled capsules (sham treatment).
A total of 366 patients swallowed at least two capsules and were included in the per protocol analysis: 185 in the treatment group and 181 in the control group. All patients saw a registered dietitian every 3 weeks and also followed diet, exercise, and behavior modification lifestyle changes. Obalon balloons were removed endoscopically at week 24, when participants’ weight was assessed.
The balloon-treated group had a mean weight loss of 6.8%, compared with 3.59% in the control group. At least 5% of body weight loss was achieved by 64.3% of the balloon-treated group, compared with 32% of the control group. The balloon treatment group, but not controls, showed improvements in levels of systolic blood pressure, LDL cholesterol, and triglycerides.
The finding that obese participants who swallowed the Obalon 6-Month Balloon System lost nearly 7% of their body weight and experienced improvements in other health indicators “is important because weight loss is quite difficult to achieve and a significant number of people are not successful in achieving their weight loss goals with diet changes and exercise,” said lead author Dr. Shelby Sullivan, who presented the findings.
Adverse events were mostly mild and included diarrhea, cramping, and nausea in nine patients. No hospitalizations were required for these events. One patient with a pre-existing bleeding ulcer experienced a serious adverse event, which the investigators classified as being possibly related to treatment.
“This patient had an orthopedic procedure and was taking high doses of NSAIDs. That should have been excluded in the trial,” said Dr. Sullivan of Washington University, St. Louis.
“Treatment over time, and even with the initial swallowing of the balloon capsule is quite well tolerated, with only mild symptoms compared with other balloon systems,” she said. “Anecdotally, my impression is that patients liked the therapy because it allowed them to follow lifestyle therapy as well.”
The Obalon balloon is given in stages, giving patients’ stomachs time to adjust to the balloon. Unlike liquid-filled balloons, the gas floats up in the stomach and may cause fewer symptoms than liquid-filled balloons, she suggested.
Dr. Sullivan believes that when the Obalon system is used in the real world, it may lead to even greater weight loss. “This has been seen in other sham-controlled trials,” she noted.
Patients enrolled in the trial are being followed longitudinally and those in the sham control group are allowed to cross over to the Obalon balloons on an open-label basis.
“More than 640 million people globally have obesity, and at this time, there are more overweight than underweight people in the world. Some treatments that are alternatives to diet and exercise may be risky. Obalon swallowable balloon is a new treatment option that can help patients lose almost twice as much weight compared with lifestyle changes alone,” she said.
Dr. Sullivan received funding for this study from Obalon Therapeutics.
A gas-filled gastric balloon may promote weight loss more effectively than does its water-filled cousin, according to data from a randomized study that was presented during a teleconference in advance of the annual Digestive Disease Week. A water-filled version of the device is on the market already.
The study enrolled 387 people aged 22 to 64 years old with a body mass index (BMI) from 30 to 40 kg/m2 at 15 different sites. People were randomized to the Obalon Balloon System or to a sham control group. People in the treatment group were asked to swallow three capsules: one every 3 weeks until week 12.
The balloon is contained within the capsule, and after swallowing each balloon was filled with 250 cubic centimeters (slightly more than 1 cup) of a nitrogen-based gas via a small catheter. The control group also swallowed sugar-filled capsules (sham treatment).
A total of 366 patients swallowed at least two capsules and were included in the per protocol analysis: 185 in the treatment group and 181 in the control group. All patients saw a registered dietitian every 3 weeks and also followed diet, exercise, and behavior modification lifestyle changes. Obalon balloons were removed endoscopically at week 24, when participants’ weight was assessed.
The balloon-treated group had a mean weight loss of 6.8%, compared with 3.59% in the control group. At least 5% of body weight loss was achieved by 64.3% of the balloon-treated group, compared with 32% of the control group. The balloon treatment group, but not controls, showed improvements in levels of systolic blood pressure, LDL cholesterol, and triglycerides.
The finding that obese participants who swallowed the Obalon 6-Month Balloon System lost nearly 7% of their body weight and experienced improvements in other health indicators “is important because weight loss is quite difficult to achieve and a significant number of people are not successful in achieving their weight loss goals with diet changes and exercise,” said lead author Dr. Shelby Sullivan, who presented the findings.
Adverse events were mostly mild and included diarrhea, cramping, and nausea in nine patients. No hospitalizations were required for these events. One patient with a pre-existing bleeding ulcer experienced a serious adverse event, which the investigators classified as being possibly related to treatment.
“This patient had an orthopedic procedure and was taking high doses of NSAIDs. That should have been excluded in the trial,” said Dr. Sullivan of Washington University, St. Louis.
“Treatment over time, and even with the initial swallowing of the balloon capsule is quite well tolerated, with only mild symptoms compared with other balloon systems,” she said. “Anecdotally, my impression is that patients liked the therapy because it allowed them to follow lifestyle therapy as well.”
The Obalon balloon is given in stages, giving patients’ stomachs time to adjust to the balloon. Unlike liquid-filled balloons, the gas floats up in the stomach and may cause fewer symptoms than liquid-filled balloons, she suggested.
Dr. Sullivan believes that when the Obalon system is used in the real world, it may lead to even greater weight loss. “This has been seen in other sham-controlled trials,” she noted.
Patients enrolled in the trial are being followed longitudinally and those in the sham control group are allowed to cross over to the Obalon balloons on an open-label basis.
“More than 640 million people globally have obesity, and at this time, there are more overweight than underweight people in the world. Some treatments that are alternatives to diet and exercise may be risky. Obalon swallowable balloon is a new treatment option that can help patients lose almost twice as much weight compared with lifestyle changes alone,” she said.
Dr. Sullivan received funding for this study from Obalon Therapeutics.
FROM DDW® 2016
Key clinical point: Gas-filled gastric balloons achieve more weight loss than lifestyle changes and are quite tolerable.
Major finding: Gas-filled balloons achieved nearly 7% loss of weight in obese people, compared with 3.59% in obese controls.
Data source: Randomized multicenter study that enrolled 387 obese people.
Disclosures: Dr. Sullivan received funding for this study from Obalon Therapeutics.
Oxandrolone, propranolol combo increases growth in severely burned children
CHICAGO – Combination therapy with oxandrolone and propranolol can attenuate burn-induced growth arrest and increase growth rate in severely burned children, according to findings from a prospective, randomized clinical trial.
Of 612 children with burns over at least 30% of their total body surface area (average of more than 50%), 103 were randomized to receive treatment with both oxandrolone and propranolol, 67 received oxandrolone alone, 194 received propranolol alone, and 248 served as controls. After a minimum of 1 year of treatment, the average growth rate was 5.9 cm in the control group and 7.6 cm in the group receiving combination therapy, Dr. David N. Herndon of the University of Texas Medical Branch at Galveston reported at the annual meeting of the American Surgical Association.
“The rate of growth with combination therapy was significantly greater than with either of the individual drugs alone,” Dr. Herndon said.
Further, the period of growth arrest was significantly shorter – by 84 days – among those in the combination-treatment group, compared with those in the control group.
Study subjects were children treated at Shriners Hospitals for Children – Galveston from 1997 to 2015. Boys aged 6 months to 14 years and girls aged 6 months to 12 years were included to eliminate the variable onset of postpubescent growth delay. About two-thirds in each group were boys, and the ages in the patient groups were similar. Mortality was low and was similar across the groups, as was hospital length of stay.
Dr. Herndon and his colleagues controlled for heterogeneous burn distribution between the groups in the course of their analyses, as well as age.
In children with severe, extensive burn injury, the hypercatabolic response is mediated by increased production of catecholamines and corticosteroids, coupled with decreased production of testosterone. This contributes to growth arrest and to decreased strength for up to 2 years after burn injury, he explained. Children with burns over 50% of their total body surface routinely survive acute hospitalization but, at 3 months post injury, are thin, have difficulty walking, and require occupational and physical therapy to help them perform even the simplest activities of daily living.
At 1 year, a raised inflammatory mass covers their wounds, they experience itching, and they have, in large part, stunted growth; there is severe loss of lean body mass and strength, and fracture risk is increased, Dr. Herndon said.
In previous work, he and his colleagues showed that administration of propranolol at an average dose of 4 mg/kg per day for 1 year decreased cardiac work and resting energy expenditure while increasing peripheral lean mass. Further, they found that the testosterone analog oxandrolone, given at 0.1 mg/kg twice per day for 1 year, improved lean body mass accretion and bone mineral content.
The current study was conducted to test the effects of administering both agents in combination.
“The combined use of oxandrolone and propranolol in severely burned children confers an additional benefit on growth over either treatment alone,” Dr. Herndon said, adding that the additive effects of combination therapy may be due to the effects of oxandrolone on bone growth and the anti-inflammatory effects of propranolol.
“The additional benefits point out mechanistic changes that may be eventful in the treatment of hypermetabolism generally and in inflammatory states,” he concluded.
Dr. Herndon reported having no disclosures.
CHICAGO – Combination therapy with oxandrolone and propranolol can attenuate burn-induced growth arrest and increase growth rate in severely burned children, according to findings from a prospective, randomized clinical trial.
Of 612 children with burns over at least 30% of their total body surface area (average of more than 50%), 103 were randomized to receive treatment with both oxandrolone and propranolol, 67 received oxandrolone alone, 194 received propranolol alone, and 248 served as controls. After a minimum of 1 year of treatment, the average growth rate was 5.9 cm in the control group and 7.6 cm in the group receiving combination therapy, Dr. David N. Herndon of the University of Texas Medical Branch at Galveston reported at the annual meeting of the American Surgical Association.
“The rate of growth with combination therapy was significantly greater than with either of the individual drugs alone,” Dr. Herndon said.
Further, the period of growth arrest was significantly shorter – by 84 days – among those in the combination-treatment group, compared with those in the control group.
Study subjects were children treated at Shriners Hospitals for Children – Galveston from 1997 to 2015. Boys aged 6 months to 14 years and girls aged 6 months to 12 years were included to eliminate the variable onset of postpubescent growth delay. About two-thirds in each group were boys, and the ages in the patient groups were similar. Mortality was low and was similar across the groups, as was hospital length of stay.
Dr. Herndon and his colleagues controlled for heterogeneous burn distribution between the groups in the course of their analyses, as well as age.
In children with severe, extensive burn injury, the hypercatabolic response is mediated by increased production of catecholamines and corticosteroids, coupled with decreased production of testosterone. This contributes to growth arrest and to decreased strength for up to 2 years after burn injury, he explained. Children with burns over 50% of their total body surface routinely survive acute hospitalization but, at 3 months post injury, are thin, have difficulty walking, and require occupational and physical therapy to help them perform even the simplest activities of daily living.
At 1 year, a raised inflammatory mass covers their wounds, they experience itching, and they have, in large part, stunted growth; there is severe loss of lean body mass and strength, and fracture risk is increased, Dr. Herndon said.
In previous work, he and his colleagues showed that administration of propranolol at an average dose of 4 mg/kg per day for 1 year decreased cardiac work and resting energy expenditure while increasing peripheral lean mass. Further, they found that the testosterone analog oxandrolone, given at 0.1 mg/kg twice per day for 1 year, improved lean body mass accretion and bone mineral content.
The current study was conducted to test the effects of administering both agents in combination.
“The combined use of oxandrolone and propranolol in severely burned children confers an additional benefit on growth over either treatment alone,” Dr. Herndon said, adding that the additive effects of combination therapy may be due to the effects of oxandrolone on bone growth and the anti-inflammatory effects of propranolol.
“The additional benefits point out mechanistic changes that may be eventful in the treatment of hypermetabolism generally and in inflammatory states,” he concluded.
Dr. Herndon reported having no disclosures.
CHICAGO – Combination therapy with oxandrolone and propranolol can attenuate burn-induced growth arrest and increase growth rate in severely burned children, according to findings from a prospective, randomized clinical trial.
Of 612 children with burns over at least 30% of their total body surface area (average of more than 50%), 103 were randomized to receive treatment with both oxandrolone and propranolol, 67 received oxandrolone alone, 194 received propranolol alone, and 248 served as controls. After a minimum of 1 year of treatment, the average growth rate was 5.9 cm in the control group and 7.6 cm in the group receiving combination therapy, Dr. David N. Herndon of the University of Texas Medical Branch at Galveston reported at the annual meeting of the American Surgical Association.
“The rate of growth with combination therapy was significantly greater than with either of the individual drugs alone,” Dr. Herndon said.
Further, the period of growth arrest was significantly shorter – by 84 days – among those in the combination-treatment group, compared with those in the control group.
Study subjects were children treated at Shriners Hospitals for Children – Galveston from 1997 to 2015. Boys aged 6 months to 14 years and girls aged 6 months to 12 years were included to eliminate the variable onset of postpubescent growth delay. About two-thirds in each group were boys, and the ages in the patient groups were similar. Mortality was low and was similar across the groups, as was hospital length of stay.
Dr. Herndon and his colleagues controlled for heterogeneous burn distribution between the groups in the course of their analyses, as well as age.
In children with severe, extensive burn injury, the hypercatabolic response is mediated by increased production of catecholamines and corticosteroids, coupled with decreased production of testosterone. This contributes to growth arrest and to decreased strength for up to 2 years after burn injury, he explained. Children with burns over 50% of their total body surface routinely survive acute hospitalization but, at 3 months post injury, are thin, have difficulty walking, and require occupational and physical therapy to help them perform even the simplest activities of daily living.
At 1 year, a raised inflammatory mass covers their wounds, they experience itching, and they have, in large part, stunted growth; there is severe loss of lean body mass and strength, and fracture risk is increased, Dr. Herndon said.
In previous work, he and his colleagues showed that administration of propranolol at an average dose of 4 mg/kg per day for 1 year decreased cardiac work and resting energy expenditure while increasing peripheral lean mass. Further, they found that the testosterone analog oxandrolone, given at 0.1 mg/kg twice per day for 1 year, improved lean body mass accretion and bone mineral content.
The current study was conducted to test the effects of administering both agents in combination.
“The combined use of oxandrolone and propranolol in severely burned children confers an additional benefit on growth over either treatment alone,” Dr. Herndon said, adding that the additive effects of combination therapy may be due to the effects of oxandrolone on bone growth and the anti-inflammatory effects of propranolol.
“The additional benefits point out mechanistic changes that may be eventful in the treatment of hypermetabolism generally and in inflammatory states,” he concluded.
Dr. Herndon reported having no disclosures.
AT THE ASA ANNUAL MEETING
Key clinical point: Combination therapy with oxandrolone and propranolol can attenuate burn-induced growth arrest and increase growth rate in severely burned children, according to findings from a prospective, randomized clinical trial.
Major finding: After a minimum of 1 year of treatment, the average growth rate was 5.9 cm in the control group and 7.6 cm in the group receiving combination therapy.
Data source: A prospective, randomized clinical trial involving 612 children.
Disclosures: Dr. Herndon reported having no disclosures.
Judge says feds overstepped on ACA cost-sharing subsidies
The Obama administration suffered another legal judgment against the Affordable Care Act when a district court judge ruled that the government has wrongly spent billions of dollars to repay insurers for health insurance provided to certain low-income patients
Congress never appropriated the money for those payments and “no public money can be spent without [an appropriation],” Judge Rosemary M. Collyer of the U.S. District Court for the District of Columbia wrote in her May 12 opinion.

If the ruling stands, the reimbursements could end, making health insurance too expensive for the millions of low-income patients who benefit from the ACA’s cost-sharing subsides, according to Jay Mark Waxman, a Boston-based health law attorney.
“If premiums become too expensive, you have people pulling out, then you have the so-called death spiral,” Mr. Waxman said in an interview. “The law could remain intact, but you could end up with not having very many people taking advantage of the marketplace, particularly the Silver Plan.”
The case in question, U.S. House of Representatives v. Burwell, revolves around two sections of the ACA. Section 1401 provides tax credits to certain patients in order to make insurance premiums more affordable, while Section 1402 requires insurers to reduce copayments, deductibles, and other out-of-pocket costs for certain low-income patients. The health law requires the federal government to reimburse insurers for the cost of these two sections.
While the first section received funding through the congressional appropriations process, the second section did not. In January 2014, HHS started repaying repay cost-sharing subsidies to insurers using federal funds. The House sued, claiming that HHS is illegally spending monies that Congress never appropriated. HHS has argued that other statutory provisions of the ACA authorize expenditures for cost-sharing reimbursements.
Judge Collyer ruled in the House’s favor, writing that paying out reimbursements without an appropriation violates the Constitution.
House members praised the court decision, calling it a victory for “the rule of law and the American taxpayer.”

“We received vindication of what we have known for quite some time – that the administration does not have the authority to spend over $150 billion for payments to insurance companies without an appropriation from Congress,” House Energy and Commerce Committee Chairman Fred Upton (R-Mich.) said in a statement. “The court’s message was clear: Complying with Article I of the Constitution is not optional for President Obama.”
White House Press Secretary Josh Earnest countered that the administration has seen its share of lawsuits over the ACA and that such legal challenges generally end in a government victory.
“This is not the first time that we’ve seen opponents of the Affordable Care Act go through the motions to try to win this political fight in the court system,” Mr. Earnest said during a press conference. “And it’s unfortunate that Republicans have resorted to a taxpayer-funded lawsuit to refight a political fight that they keep losing. They’ve been losing this fight for 6 years. And they’ll lose it again.”

It’s too early to predict how the legal case might be resolved, said Katherine Hempstead, who directs health insurance coverage for the Robert Wood Johnson Foundation.
“There’s a lot of potential endings that don’t lead to people losing their cost-sharing reductions,” Ms. Hempstead said in an interview. “There are a lot of twists and turns ahead, and the probability of people losing their reductions is remote.”
The House could lose the case on appeal, she said. Such a ruling could be made on the merits of the case or on procedural grounds. Whether the House has standing to sue HHS has been questioned as well, she noted. HHS continues to argue that the House has not established a concrete or imminent injury and therefore, the suit should be thrown out. In addition, some have suggested that the federal ruling could be interpreted as requiring Congress to appropriate money to pay for the cost-sharing reductions, she said.
The ultimate resolution could come from the U.S. Supreme Court, Mr. Waxman added. Another possibility is that the next administration will decline to pursue the case.
“Depending on the timing, it could just stop in the court of appeals,” he said. “The next administration could say, ‘We’re happy with where it is and not take it up. You don’t know what’s going to happen.”
Mr. Earnest said the U.S. Department of Justice is reviewing the ruling and will make an announcement about the next step after the analysis.
On Twitter @legal_med
The Obama administration suffered another legal judgment against the Affordable Care Act when a district court judge ruled that the government has wrongly spent billions of dollars to repay insurers for health insurance provided to certain low-income patients
Congress never appropriated the money for those payments and “no public money can be spent without [an appropriation],” Judge Rosemary M. Collyer of the U.S. District Court for the District of Columbia wrote in her May 12 opinion.
If the ruling stands, the reimbursements could end, making health insurance too expensive for the millions of low-income patients who benefit from the ACA’s cost-sharing subsides, according to Jay Mark Waxman, a Boston-based health law attorney.
“If premiums become too expensive, you have people pulling out, then you have the so-called death spiral,” Mr. Waxman said in an interview. “The law could remain intact, but you could end up with not having very many people taking advantage of the marketplace, particularly the Silver Plan.”
The case in question, U.S. House of Representatives v. Burwell, revolves around two sections of the ACA. Section 1401 provides tax credits to certain patients in order to make insurance premiums more affordable, while Section 1402 requires insurers to reduce copayments, deductibles, and other out-of-pocket costs for certain low-income patients. The health law requires the federal government to reimburse insurers for the cost of these two sections.
While the first section received funding through the congressional appropriations process, the second section did not. In January 2014, HHS started repaying repay cost-sharing subsidies to insurers using federal funds. The House sued, claiming that HHS is illegally spending monies that Congress never appropriated. HHS has argued that other statutory provisions of the ACA authorize expenditures for cost-sharing reimbursements.
Judge Collyer ruled in the House’s favor, writing that paying out reimbursements without an appropriation violates the Constitution.
House members praised the court decision, calling it a victory for “the rule of law and the American taxpayer.”
“We received vindication of what we have known for quite some time – that the administration does not have the authority to spend over $150 billion for payments to insurance companies without an appropriation from Congress,” House Energy and Commerce Committee Chairman Fred Upton (R-Mich.) said in a statement. “The court’s message was clear: Complying with Article I of the Constitution is not optional for President Obama.”
White House Press Secretary Josh Earnest countered that the administration has seen its share of lawsuits over the ACA and that such legal challenges generally end in a government victory.
“This is not the first time that we’ve seen opponents of the Affordable Care Act go through the motions to try to win this political fight in the court system,” Mr. Earnest said during a press conference. “And it’s unfortunate that Republicans have resorted to a taxpayer-funded lawsuit to refight a political fight that they keep losing. They’ve been losing this fight for 6 years. And they’ll lose it again.”
It’s too early to predict how the legal case might be resolved, said Katherine Hempstead, who directs health insurance coverage for the Robert Wood Johnson Foundation.
“There’s a lot of potential endings that don’t lead to people losing their cost-sharing reductions,” Ms. Hempstead said in an interview. “There are a lot of twists and turns ahead, and the probability of people losing their reductions is remote.”
The House could lose the case on appeal, she said. Such a ruling could be made on the merits of the case or on procedural grounds. Whether the House has standing to sue HHS has been questioned as well, she noted. HHS continues to argue that the House has not established a concrete or imminent injury and therefore, the suit should be thrown out. In addition, some have suggested that the federal ruling could be interpreted as requiring Congress to appropriate money to pay for the cost-sharing reductions, she said.
The ultimate resolution could come from the U.S. Supreme Court, Mr. Waxman added. Another possibility is that the next administration will decline to pursue the case.
“Depending on the timing, it could just stop in the court of appeals,” he said. “The next administration could say, ‘We’re happy with where it is and not take it up. You don’t know what’s going to happen.”
Mr. Earnest said the U.S. Department of Justice is reviewing the ruling and will make an announcement about the next step after the analysis.
On Twitter @legal_med
The Obama administration suffered another legal judgment against the Affordable Care Act when a district court judge ruled that the government has wrongly spent billions of dollars to repay insurers for health insurance provided to certain low-income patients
Congress never appropriated the money for those payments and “no public money can be spent without [an appropriation],” Judge Rosemary M. Collyer of the U.S. District Court for the District of Columbia wrote in her May 12 opinion.
If the ruling stands, the reimbursements could end, making health insurance too expensive for the millions of low-income patients who benefit from the ACA’s cost-sharing subsides, according to Jay Mark Waxman, a Boston-based health law attorney.
“If premiums become too expensive, you have people pulling out, then you have the so-called death spiral,” Mr. Waxman said in an interview. “The law could remain intact, but you could end up with not having very many people taking advantage of the marketplace, particularly the Silver Plan.”
The case in question, U.S. House of Representatives v. Burwell, revolves around two sections of the ACA. Section 1401 provides tax credits to certain patients in order to make insurance premiums more affordable, while Section 1402 requires insurers to reduce copayments, deductibles, and other out-of-pocket costs for certain low-income patients. The health law requires the federal government to reimburse insurers for the cost of these two sections.
While the first section received funding through the congressional appropriations process, the second section did not. In January 2014, HHS started repaying repay cost-sharing subsidies to insurers using federal funds. The House sued, claiming that HHS is illegally spending monies that Congress never appropriated. HHS has argued that other statutory provisions of the ACA authorize expenditures for cost-sharing reimbursements.
Judge Collyer ruled in the House’s favor, writing that paying out reimbursements without an appropriation violates the Constitution.
House members praised the court decision, calling it a victory for “the rule of law and the American taxpayer.”
“We received vindication of what we have known for quite some time – that the administration does not have the authority to spend over $150 billion for payments to insurance companies without an appropriation from Congress,” House Energy and Commerce Committee Chairman Fred Upton (R-Mich.) said in a statement. “The court’s message was clear: Complying with Article I of the Constitution is not optional for President Obama.”
White House Press Secretary Josh Earnest countered that the administration has seen its share of lawsuits over the ACA and that such legal challenges generally end in a government victory.
“This is not the first time that we’ve seen opponents of the Affordable Care Act go through the motions to try to win this political fight in the court system,” Mr. Earnest said during a press conference. “And it’s unfortunate that Republicans have resorted to a taxpayer-funded lawsuit to refight a political fight that they keep losing. They’ve been losing this fight for 6 years. And they’ll lose it again.”
It’s too early to predict how the legal case might be resolved, said Katherine Hempstead, who directs health insurance coverage for the Robert Wood Johnson Foundation.
“There’s a lot of potential endings that don’t lead to people losing their cost-sharing reductions,” Ms. Hempstead said in an interview. “There are a lot of twists and turns ahead, and the probability of people losing their reductions is remote.”
The House could lose the case on appeal, she said. Such a ruling could be made on the merits of the case or on procedural grounds. Whether the House has standing to sue HHS has been questioned as well, she noted. HHS continues to argue that the House has not established a concrete or imminent injury and therefore, the suit should be thrown out. In addition, some have suggested that the federal ruling could be interpreted as requiring Congress to appropriate money to pay for the cost-sharing reductions, she said.
The ultimate resolution could come from the U.S. Supreme Court, Mr. Waxman added. Another possibility is that the next administration will decline to pursue the case.
“Depending on the timing, it could just stop in the court of appeals,” he said. “The next administration could say, ‘We’re happy with where it is and not take it up. You don’t know what’s going to happen.”
Mr. Earnest said the U.S. Department of Justice is reviewing the ruling and will make an announcement about the next step after the analysis.
On Twitter @legal_med

Persistent SIRS, leukocytosis linked to unrecognized necrotizing pancreatitis
SAN DIEGO – Patients who have persistent leukocytosis (greater than 12 x 109 white blood cells per liter) or persistent systemic inflammatory response syndrome (SIRS) on the day of scheduled cholecystectomy may have unrecognized pancreatic necrosis, which increases the risk of postsurgical organ failure and infected necrosis, Dr. Wilson Kwong reported.
For these patients, “we recommend performing a contrast-enhanced CT scan on day 4 or 5 to reassess for necrosis,” Dr. Kwong of the gastroenterology department at the University California, San Diego, said in an interview. “Patients who have necrosis should undergo interval cholecystectomy instead, while those without necrosis are likely safe to proceed with laparoscopic cholecystectomy,” he added.
Guidelines recommend same-admission cholecystectomy for mild acute gallstone pancreatitis, although this approach will send some patients with unrecognized necrotizing pancreatitis to surgery, “with unknown consequences,” Dr. Kwong said at the annual Digestive Diseases Week.
To better understand presurgical predictors of necrotizing pancreatitis, Dr. Kwong and his coauthor, Dr. Santhi Swaroop Vege of the Mayo Clinic, Rochester, Minn., studied 46 Mayo Clinic patients with apparent mild acute gallstone pancreatitis who in fact had necrotizing pancreatitis diagnosed during same-admission laparoscopic cholecystectomies (SALCs).
The most frequent characteristics of patients with unrecognized necrotizing pancreatitis included persistent SIRS (area under the curve, 0.96) and persistent leukocytosis (AUC, 0.92) on the day of cholecystectomy (both P less than .0001). However, 82% of patients with unrecognized necrotizing pancreatitis met criteria for SIRS by their second day in the hospital, with SIRS continuing until the day of planned cholecystectomy.
Next, the investigators compared the SALC patients with 48 patients who had necrotizing pancreatitis, but did not undergo SALC. In all, 24% of SALC patients developed new organ failure, compared with none of the comparison group (P = .0003). The SALC patients also had nearly double the rate of culture-confirmed infected necrosis (52% vs. 27%, P = .02), and stayed about 1.5 days longer in the hospital (26 vs. 24.5 days, P = .049). The chances of undergoing an intervention for necrotizing pancreatitis, conversion to open cholecystectomy, or death were slightly higher for SALC patients, compared with controls, but none of these differences reached statistical significance. Two SALC patients (4%) died, compared with 2% of patients who did not undergo SALC, the investigators reported.
The researchers also compared the SALC patients with a second control group of 48 patients who were later confirmed during SALC to have true mild acute gallstone pancreatitis. Fully 91% of patients with necrotizing pancreatitis met criteria for SIRS on the day of surgery, compared with none of the patients with acute gallstone pancreatitis (P less than .0001). Furthermore, all 11 patients with necrotizing pancreatitis and available test results had persistent leukocytosis on the day of surgery, compared with only 21% of the gallstone pancreatitis group (P less than .0001).
Finally, the researchers looked at the magnitude of the problem of unrecognized necrotizing pancreatitis. “From January 2014 to August 2015, 102 consecutive patients were directly admitted to Mayo Clinic, Rochester, with acute gallstone pancreatitis and underwent SALC,” they reported. “After laparoscopic cholecystectomy, seven of these patients were discovered to have previously unrecognized necrotizing pancreatitis, thus giving a 7% occurrence rate for this complication during this recent time period.” Accurately identifying patients with emerging necrotizing pancreatitis is crucial to help prevent potentially severe complications after SALC, they emphasized.
Dr. Kwong had no relevant financial disclosures. Dr. Vege disclosed consulting fees and other compensation from Takeda and several other companies.
SAN DIEGO – Patients who have persistent leukocytosis (greater than 12 x 109 white blood cells per liter) or persistent systemic inflammatory response syndrome (SIRS) on the day of scheduled cholecystectomy may have unrecognized pancreatic necrosis, which increases the risk of postsurgical organ failure and infected necrosis, Dr. Wilson Kwong reported.
For these patients, “we recommend performing a contrast-enhanced CT scan on day 4 or 5 to reassess for necrosis,” Dr. Kwong of the gastroenterology department at the University California, San Diego, said in an interview. “Patients who have necrosis should undergo interval cholecystectomy instead, while those without necrosis are likely safe to proceed with laparoscopic cholecystectomy,” he added.
Guidelines recommend same-admission cholecystectomy for mild acute gallstone pancreatitis, although this approach will send some patients with unrecognized necrotizing pancreatitis to surgery, “with unknown consequences,” Dr. Kwong said at the annual Digestive Diseases Week.
To better understand presurgical predictors of necrotizing pancreatitis, Dr. Kwong and his coauthor, Dr. Santhi Swaroop Vege of the Mayo Clinic, Rochester, Minn., studied 46 Mayo Clinic patients with apparent mild acute gallstone pancreatitis who in fact had necrotizing pancreatitis diagnosed during same-admission laparoscopic cholecystectomies (SALCs).
The most frequent characteristics of patients with unrecognized necrotizing pancreatitis included persistent SIRS (area under the curve, 0.96) and persistent leukocytosis (AUC, 0.92) on the day of cholecystectomy (both P less than .0001). However, 82% of patients with unrecognized necrotizing pancreatitis met criteria for SIRS by their second day in the hospital, with SIRS continuing until the day of planned cholecystectomy.
Next, the investigators compared the SALC patients with 48 patients who had necrotizing pancreatitis, but did not undergo SALC. In all, 24% of SALC patients developed new organ failure, compared with none of the comparison group (P = .0003). The SALC patients also had nearly double the rate of culture-confirmed infected necrosis (52% vs. 27%, P = .02), and stayed about 1.5 days longer in the hospital (26 vs. 24.5 days, P = .049). The chances of undergoing an intervention for necrotizing pancreatitis, conversion to open cholecystectomy, or death were slightly higher for SALC patients, compared with controls, but none of these differences reached statistical significance. Two SALC patients (4%) died, compared with 2% of patients who did not undergo SALC, the investigators reported.
The researchers also compared the SALC patients with a second control group of 48 patients who were later confirmed during SALC to have true mild acute gallstone pancreatitis. Fully 91% of patients with necrotizing pancreatitis met criteria for SIRS on the day of surgery, compared with none of the patients with acute gallstone pancreatitis (P less than .0001). Furthermore, all 11 patients with necrotizing pancreatitis and available test results had persistent leukocytosis on the day of surgery, compared with only 21% of the gallstone pancreatitis group (P less than .0001).
Finally, the researchers looked at the magnitude of the problem of unrecognized necrotizing pancreatitis. “From January 2014 to August 2015, 102 consecutive patients were directly admitted to Mayo Clinic, Rochester, with acute gallstone pancreatitis and underwent SALC,” they reported. “After laparoscopic cholecystectomy, seven of these patients were discovered to have previously unrecognized necrotizing pancreatitis, thus giving a 7% occurrence rate for this complication during this recent time period.” Accurately identifying patients with emerging necrotizing pancreatitis is crucial to help prevent potentially severe complications after SALC, they emphasized.
Dr. Kwong had no relevant financial disclosures. Dr. Vege disclosed consulting fees and other compensation from Takeda and several other companies.
SAN DIEGO – Patients who have persistent leukocytosis (greater than 12 x 109 white blood cells per liter) or persistent systemic inflammatory response syndrome (SIRS) on the day of scheduled cholecystectomy may have unrecognized pancreatic necrosis, which increases the risk of postsurgical organ failure and infected necrosis, Dr. Wilson Kwong reported.
For these patients, “we recommend performing a contrast-enhanced CT scan on day 4 or 5 to reassess for necrosis,” Dr. Kwong of the gastroenterology department at the University California, San Diego, said in an interview. “Patients who have necrosis should undergo interval cholecystectomy instead, while those without necrosis are likely safe to proceed with laparoscopic cholecystectomy,” he added.
Guidelines recommend same-admission cholecystectomy for mild acute gallstone pancreatitis, although this approach will send some patients with unrecognized necrotizing pancreatitis to surgery, “with unknown consequences,” Dr. Kwong said at the annual Digestive Diseases Week.
To better understand presurgical predictors of necrotizing pancreatitis, Dr. Kwong and his coauthor, Dr. Santhi Swaroop Vege of the Mayo Clinic, Rochester, Minn., studied 46 Mayo Clinic patients with apparent mild acute gallstone pancreatitis who in fact had necrotizing pancreatitis diagnosed during same-admission laparoscopic cholecystectomies (SALCs).
The most frequent characteristics of patients with unrecognized necrotizing pancreatitis included persistent SIRS (area under the curve, 0.96) and persistent leukocytosis (AUC, 0.92) on the day of cholecystectomy (both P less than .0001). However, 82% of patients with unrecognized necrotizing pancreatitis met criteria for SIRS by their second day in the hospital, with SIRS continuing until the day of planned cholecystectomy.
Next, the investigators compared the SALC patients with 48 patients who had necrotizing pancreatitis, but did not undergo SALC. In all, 24% of SALC patients developed new organ failure, compared with none of the comparison group (P = .0003). The SALC patients also had nearly double the rate of culture-confirmed infected necrosis (52% vs. 27%, P = .02), and stayed about 1.5 days longer in the hospital (26 vs. 24.5 days, P = .049). The chances of undergoing an intervention for necrotizing pancreatitis, conversion to open cholecystectomy, or death were slightly higher for SALC patients, compared with controls, but none of these differences reached statistical significance. Two SALC patients (4%) died, compared with 2% of patients who did not undergo SALC, the investigators reported.
The researchers also compared the SALC patients with a second control group of 48 patients who were later confirmed during SALC to have true mild acute gallstone pancreatitis. Fully 91% of patients with necrotizing pancreatitis met criteria for SIRS on the day of surgery, compared with none of the patients with acute gallstone pancreatitis (P less than .0001). Furthermore, all 11 patients with necrotizing pancreatitis and available test results had persistent leukocytosis on the day of surgery, compared with only 21% of the gallstone pancreatitis group (P less than .0001).
Finally, the researchers looked at the magnitude of the problem of unrecognized necrotizing pancreatitis. “From January 2014 to August 2015, 102 consecutive patients were directly admitted to Mayo Clinic, Rochester, with acute gallstone pancreatitis and underwent SALC,” they reported. “After laparoscopic cholecystectomy, seven of these patients were discovered to have previously unrecognized necrotizing pancreatitis, thus giving a 7% occurrence rate for this complication during this recent time period.” Accurately identifying patients with emerging necrotizing pancreatitis is crucial to help prevent potentially severe complications after SALC, they emphasized.
Dr. Kwong had no relevant financial disclosures. Dr. Vege disclosed consulting fees and other compensation from Takeda and several other companies.
AT DDW® 2016
Key clinical point: Persistent leukocytosis (greater than 12 x 109 white blood cells per liter) and SIRS on the day of scheduled laparoscopic cholecystectomy may indicate unrecognized necrotizing pancreatitis.
Major finding: The highest areas under the curve were for SIRS (0.96), followed by a WBC at or above 12 x 109/L (0.92; both P less than .0001).
Data source: A single-center retrospective study of 46 patients with unrecognized pancreatitis who underwent same-admission laparoscopic cholecystectomy, 48 patients with necrotizing pancreatitis who did not undergo SALC, and 48 patients with true mild acute gallstone pancreatitis.
Disclosures: Dr. Kwong had no relevant financial disclosures. Dr. Vege disclosed consulting fees and other compensation from Takeda and several other companies.
Tacrolimus worsens IBD post liver transplant for primary sclerosing cholangitis
SAN DIEGO – A retrospective study provides insight as to why some patients have a milder versus a more severe course of inflammatory bowel disease (IBD) after liver transplant for primary sclerosing cholangitis (PSC).
Recurrent PSC, prolonged use of steroids, and cancer development after liver transplant were associated with a milder course of IBD, but tacrolimus use was associated with increased IBD flare post transplant.

“The course of IBD is highly variable after liver transplant for PSC. PSC is associated with IBD in 60% to 90% of patients, and IBD worsens in about 30% of PSC-IBD patients after transplant. We wanted to explore the risk factors for worsening IBD in this setting,” Dr. Mohamad Mouchli of the Mayo Clinic in Rochester, Minn., explained at the annual Digestive Disease Week.
For purposes of this study, progression of IBD was defined as the need for escalation of medical therapy, compared with before liver transplant, or need for colectomy for medically refractory IBD.
The study population included patients with PSC-IBD who underwent liver transplant for noncholangiocarcinoma indications at the Mayo Clinic from 1998 to 2012. Patients were followed through February 2015.
The investigators screened 373 patients: After exclusions for cancer, no IBD at transplant, and pretransplant colectomy, 151 patients with an intact colon were left and formed the basis of further analysis.
Median age at transplant was 46 years and two-thirds of the patients were male. Transplant-related variables included the following: 23% experienced allograft failure, 36% had recurrent PSC, 25.2% had CMV infection, 19.2% were retransplanted, 22.5% developed cancer after liver transplant, and 52.3% had acute cellular rejection.
Before transplant, 69 patients had quiescent IBD with no therapy and 62 were maintained on 5-aminosalicylates. Post transplant, despite transplant-related immunosuppression, 56 patients (37.1%) required escalation of therapy, 87 patients (57.6%) had a stable course, and 8 patients (5.3%) improved.
Risk of IBD progression at 1, 5, and 10 years was 4%, 18.5%, and 25.5%, respectively. Thirty-five patients underwent colectomy after transplant: the 1-, 5-, and 10-year risks of colectomy were 2%, 9.3%, and 17.2%, respectively. Fourteen percent of patients required anti–tumor necrosis factor therapy after transplant.
On multivariate analysis, tacrolimus exposure emerged as a risk factor for progression of IBD. Tacrolimus immunosuppression was twice as likely as cyclosporine-based immunosuppression to lead to IBD progression. By contrast, recurrent PSC, use of steroids for longer than 6 months, and cancer development after liver transplant were protective of IBD progression.
No association was found between progression of IBD and transplant-related infection or mismatch, immunosuppression with mycophenolate or azathioprine, or IBD-related factors such as pretransplant IBD status or empirical initiation of 5-aminosalicylates within 4 months of liver transplant. During the question-and-answer session following his presentation, Dr. Mouchli was asked whether these results justify prophylactic colectomy. He said that could be considered in patients with active IBD before transplant, but on a case-by-case basis.
SAN DIEGO – A retrospective study provides insight as to why some patients have a milder versus a more severe course of inflammatory bowel disease (IBD) after liver transplant for primary sclerosing cholangitis (PSC).
Recurrent PSC, prolonged use of steroids, and cancer development after liver transplant were associated with a milder course of IBD, but tacrolimus use was associated with increased IBD flare post transplant.
“The course of IBD is highly variable after liver transplant for PSC. PSC is associated with IBD in 60% to 90% of patients, and IBD worsens in about 30% of PSC-IBD patients after transplant. We wanted to explore the risk factors for worsening IBD in this setting,” Dr. Mohamad Mouchli of the Mayo Clinic in Rochester, Minn., explained at the annual Digestive Disease Week.
For purposes of this study, progression of IBD was defined as the need for escalation of medical therapy, compared with before liver transplant, or need for colectomy for medically refractory IBD.
The study population included patients with PSC-IBD who underwent liver transplant for noncholangiocarcinoma indications at the Mayo Clinic from 1998 to 2012. Patients were followed through February 2015.
The investigators screened 373 patients: After exclusions for cancer, no IBD at transplant, and pretransplant colectomy, 151 patients with an intact colon were left and formed the basis of further analysis.
Median age at transplant was 46 years and two-thirds of the patients were male. Transplant-related variables included the following: 23% experienced allograft failure, 36% had recurrent PSC, 25.2% had CMV infection, 19.2% were retransplanted, 22.5% developed cancer after liver transplant, and 52.3% had acute cellular rejection.
Before transplant, 69 patients had quiescent IBD with no therapy and 62 were maintained on 5-aminosalicylates. Post transplant, despite transplant-related immunosuppression, 56 patients (37.1%) required escalation of therapy, 87 patients (57.6%) had a stable course, and 8 patients (5.3%) improved.
Risk of IBD progression at 1, 5, and 10 years was 4%, 18.5%, and 25.5%, respectively. Thirty-five patients underwent colectomy after transplant: the 1-, 5-, and 10-year risks of colectomy were 2%, 9.3%, and 17.2%, respectively. Fourteen percent of patients required anti–tumor necrosis factor therapy after transplant.
On multivariate analysis, tacrolimus exposure emerged as a risk factor for progression of IBD. Tacrolimus immunosuppression was twice as likely as cyclosporine-based immunosuppression to lead to IBD progression. By contrast, recurrent PSC, use of steroids for longer than 6 months, and cancer development after liver transplant were protective of IBD progression.
No association was found between progression of IBD and transplant-related infection or mismatch, immunosuppression with mycophenolate or azathioprine, or IBD-related factors such as pretransplant IBD status or empirical initiation of 5-aminosalicylates within 4 months of liver transplant. During the question-and-answer session following his presentation, Dr. Mouchli was asked whether these results justify prophylactic colectomy. He said that could be considered in patients with active IBD before transplant, but on a case-by-case basis.
SAN DIEGO – A retrospective study provides insight as to why some patients have a milder versus a more severe course of inflammatory bowel disease (IBD) after liver transplant for primary sclerosing cholangitis (PSC).
Recurrent PSC, prolonged use of steroids, and cancer development after liver transplant were associated with a milder course of IBD, but tacrolimus use was associated with increased IBD flare post transplant.
“The course of IBD is highly variable after liver transplant for PSC. PSC is associated with IBD in 60% to 90% of patients, and IBD worsens in about 30% of PSC-IBD patients after transplant. We wanted to explore the risk factors for worsening IBD in this setting,” Dr. Mohamad Mouchli of the Mayo Clinic in Rochester, Minn., explained at the annual Digestive Disease Week.
For purposes of this study, progression of IBD was defined as the need for escalation of medical therapy, compared with before liver transplant, or need for colectomy for medically refractory IBD.
The study population included patients with PSC-IBD who underwent liver transplant for noncholangiocarcinoma indications at the Mayo Clinic from 1998 to 2012. Patients were followed through February 2015.
The investigators screened 373 patients: After exclusions for cancer, no IBD at transplant, and pretransplant colectomy, 151 patients with an intact colon were left and formed the basis of further analysis.
Median age at transplant was 46 years and two-thirds of the patients were male. Transplant-related variables included the following: 23% experienced allograft failure, 36% had recurrent PSC, 25.2% had CMV infection, 19.2% were retransplanted, 22.5% developed cancer after liver transplant, and 52.3% had acute cellular rejection.
Before transplant, 69 patients had quiescent IBD with no therapy and 62 were maintained on 5-aminosalicylates. Post transplant, despite transplant-related immunosuppression, 56 patients (37.1%) required escalation of therapy, 87 patients (57.6%) had a stable course, and 8 patients (5.3%) improved.
Risk of IBD progression at 1, 5, and 10 years was 4%, 18.5%, and 25.5%, respectively. Thirty-five patients underwent colectomy after transplant: the 1-, 5-, and 10-year risks of colectomy were 2%, 9.3%, and 17.2%, respectively. Fourteen percent of patients required anti–tumor necrosis factor therapy after transplant.
On multivariate analysis, tacrolimus exposure emerged as a risk factor for progression of IBD. Tacrolimus immunosuppression was twice as likely as cyclosporine-based immunosuppression to lead to IBD progression. By contrast, recurrent PSC, use of steroids for longer than 6 months, and cancer development after liver transplant were protective of IBD progression.
No association was found between progression of IBD and transplant-related infection or mismatch, immunosuppression with mycophenolate or azathioprine, or IBD-related factors such as pretransplant IBD status or empirical initiation of 5-aminosalicylates within 4 months of liver transplant. During the question-and-answer session following his presentation, Dr. Mouchli was asked whether these results justify prophylactic colectomy. He said that could be considered in patients with active IBD before transplant, but on a case-by-case basis.
AT DDW® 2016
Key clinical point: Tacrolimus exposure was an independent risk factor for IBD progression after liver transplant in patients with PSC-IBD.
Major finding: Tacrolimus immunosuppression was twice as likely as cyclosporine-based immunosuppression to lead to worsening IBC post liver transplant.
Data source: Retrospective study of the natural history of IBD following liver transplant in 151 patients with PSC-IBD.
Disclosures: Dr. Mouchli had no financial disclosures to report.

Operating with pain: Surgeon workplace injury underrecognized
BOSTON – For many surgeons, hours in the OR can translate into serious or chronic neck, back, and hand pain.
Studies of occupational injury related to performing surgery took off in the 1990s when laparoscopic surgery became widespread and put new physical demands on surgeons (Surg Endosc 1999:13:466-468; Arch Surg 1999;134:1011-1016). Findings from a study presented at the Society for Surgical Oncology suggest that the problem remains widespread.
Dr. Rachael K. Voss, a research resident at the University of Texas MD Anderson Cancer Center, Houston, and her colleagues conducted a survey among oncologic surgeons at the Center to explore the extent, sources and risk factors of workplace injuries.
“[Workplace injury] is a serious issue for surgeons, but it is something we don’t talk about and there is very little training and information as we are going through training. But these occupational hazards are something we need to acknowledge. We need to do more work in the future with ergonomics experts and occupational hygiene experts that can help us improve our posture and positions in the OR so we can prevent these injuries,” Dr. Voss said.
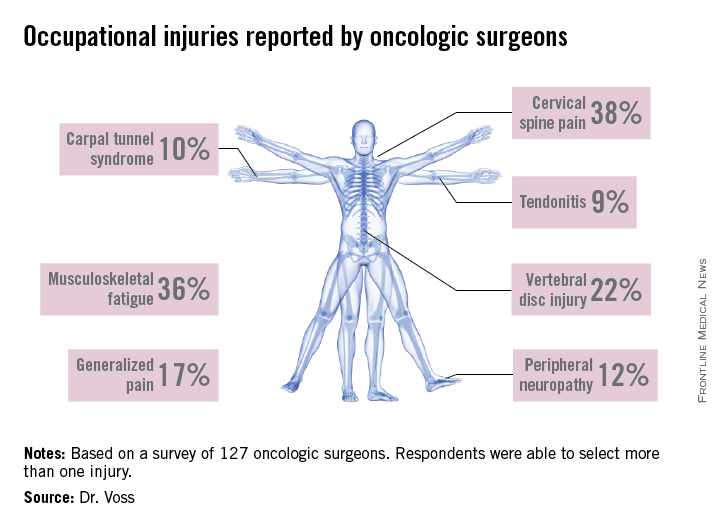
A high response rate of 58% yielded a total of 127 completed surveys. Most of the respondents were aged 35-64 and three-quarters spent 10 hours or more per week working in the OR. Among those responding, 92.3% experienced at least one occupation-related symptom over the past 6 weeks, and 27.6% reported sustaining an injury or chronic condition which they attributed to operating. The majority of injuries reported were cervical spine injury, musculoskeletal fatigue and vertebral disc injury. Other conditions mentioned were brachial plexus damage, carpal tunnel syndrome, peripheral neuropathy, and tendonitis.
A multivariate analysis identified some independent risk factors for injury: male gender, average case duration of 4 hours or longer, neck pain, and frequent use of a step for height adjustment. Age and years in practice were not associated with injury risk.
The good news is that, in this sample, 72% of the respondents reported seeking treatment for their injury. Physical therapy and medication were the most commonly utilized treatments, with about 20% resorting to surgery.
Plenty of evidence
The MD Anderson findings confirmed what other studies in this area have reported. William T. Davis and his colleagues surveyed Fellows of the Tennessee chapter of the American College of Surgeons on the issue of occupational musculoskeletal injury (J Surg Res 2014;184:207-212). Of the 793 surveys sent, 33% were completed. General surgeons accounted for 64% of respondents and 80% were male. Forty percent of respondents had sustained at least one injury related to operating. Most reported spine, hand, and neck injuries, but hip, knee, and shoulder pain was also mentioned. The majority of respondents reported the cause of their injury as chronic and 51% sought medical treatment. As with the MD Anderson study, no association was found between age or years in practice and workplace injury.
Mr. Davis and his colleagues conducted a similar study of orthopaedic surgeons and found similar rates of occupational injury (44%) among their 140 survey respondents (J Bone Joint Surg Am. 2013;95:e107). This study found that responding orthopaedic surgeons had more hand and lower back injuries, and correlation was found between years in practice and prevalence of injury.

A limitation of all of these studies is that the injury data are self-reported, and there is a potential selection bias. It is likely that the true extent of workplace injury among surgeons, and the costs and impact on surgeons’ life quality and productivity, are still largely unknown.
“There have been a few studies on this, but I think we’re just scratching the surface,” explained Dr. Adrian Park, chair of surgery at the Anne Arundel Medical Center in Annapolis, Md. Dr. Park was the lead author of a 2010 study that identified chronic pain among surgeons as a serious and underreported issue within medicine (J Am Coll Surg 2010;210;306-313).
The study, which evaluated 317 surgeons using a 23-question survey, found that 86.9% of surgeons experience “physical symptoms or discomfort,” with the most significant indicator of such symptoms being a high case load. Subsequent studies from Europe and eastern Asia also found rates of 80% or higher among surgeons in those regions.
Injuries downplayed
With so pervasive a problem, however, the relative paucity of data and conversation among medical professionals is something Dr. Park finds alarming. “As a surgeon leader, I can tell you surgeons complain about a lot of stuff, but one of the things they tend not to complain about is themselves and their own health and well-being,” said Dr. Park.
Dr. Mario Cerame is well aware of what a seemingly innocuous, relatively small chronic pain can do to a surgeon. A general surgeon practicing in North Carolina, Dr. Cerame began to experience symptoms of repetitive motion injury about 2 years ago, symptoms which he says “crept up on me.”

It began as numbness at the tips of his fingers, affecting the way he held laparoscopic tools during surgery and other, more menial, daily tasks. Initially suspecting it was carpal tunnel syndrome, Dr. Cerame brushed it off, until the numbness spread to three whole fingers and, eventually, his entire hand. His physician explained what was happening, instructing him that if he didn’t undergo orthopaedic surgery immediately, he ran the risk of paralysis.
“I got the diagnosis on Thursday, and had the operation on Tuesday,” said Dr. Cerame, explaining that the diagnosis was spinal stenosis. Two areas of his spinal column were pinching inward, causing the slow but steady paralysis he was experiencing. With physical therapy, Dr. Cerame could have returning function within 2 years of the operation.
“I’ve published an awful lot of papers, but the thing that struck me about [the 2010] paper is the response I got,” said Dr. Park. “Surgeons, literally from around the country, would call me saying ‘I used to be able to do this operation, I no longer can do that,’ or ‘this used to be what my case list looked like, I can no longer do this, you can use me as an example.’ People came forward.”
Risks of ignoring, self-medicating
Then there is the dark side of coping with chronic pain: risk of substance abuse. A study published in the Journal of Addiction Medicine (2013;7;349-353) on misuse of prescription medication among physicians found that surgeons were among the specialists at highest risk for substance abuse. According to this study, the beginning of addiction for many doctors is a prescription or self-medication for chronic pain. For surgeons, chronic pain from occupational injuries could lead to dependence on pain medication.
“When livelihoods are at stake, I think folks will take opportunities to stay in the game,” admitted Dr. Park.
The bottom line, according to both Dr. Park and Dr. Cerame, is for surgeons not to keep quiet about these issues if they ever do experience them. Asking for help and getting things checked right away is better, not only for a surgeon, but for family and patients, too. While Dr. Cerame has gone back to work, he is unable to handle the caseload he once had and isn’t sure if he’ll ever be able to.
“Surgeons and physicians in general have a tendency to get so consumed with other people’s health that they don’t focus on their own health issues,” said Dr. Cerame. “It took me almost 8 months from the time I had symptoms to actually get it checked out [because] I thought it would go away, [so] if you find something that you feel isn’t normal, take care of it.”
Dr. Voss, Dr. Park, and Dr. Cerame had no relevant financial disclosures.
Neil Osterweil contributed to this article.
BOSTON – For many surgeons, hours in the OR can translate into serious or chronic neck, back, and hand pain.
Studies of occupational injury related to performing surgery took off in the 1990s when laparoscopic surgery became widespread and put new physical demands on surgeons (Surg Endosc 1999:13:466-468; Arch Surg 1999;134:1011-1016). Findings from a study presented at the Society for Surgical Oncology suggest that the problem remains widespread.
Dr. Rachael K. Voss, a research resident at the University of Texas MD Anderson Cancer Center, Houston, and her colleagues conducted a survey among oncologic surgeons at the Center to explore the extent, sources and risk factors of workplace injuries.
“[Workplace injury] is a serious issue for surgeons, but it is something we don’t talk about and there is very little training and information as we are going through training. But these occupational hazards are something we need to acknowledge. We need to do more work in the future with ergonomics experts and occupational hygiene experts that can help us improve our posture and positions in the OR so we can prevent these injuries,” Dr. Voss said.
A high response rate of 58% yielded a total of 127 completed surveys. Most of the respondents were aged 35-64 and three-quarters spent 10 hours or more per week working in the OR. Among those responding, 92.3% experienced at least one occupation-related symptom over the past 6 weeks, and 27.6% reported sustaining an injury or chronic condition which they attributed to operating. The majority of injuries reported were cervical spine injury, musculoskeletal fatigue and vertebral disc injury. Other conditions mentioned were brachial plexus damage, carpal tunnel syndrome, peripheral neuropathy, and tendonitis.
A multivariate analysis identified some independent risk factors for injury: male gender, average case duration of 4 hours or longer, neck pain, and frequent use of a step for height adjustment. Age and years in practice were not associated with injury risk.
The good news is that, in this sample, 72% of the respondents reported seeking treatment for their injury. Physical therapy and medication were the most commonly utilized treatments, with about 20% resorting to surgery.
Plenty of evidence
The MD Anderson findings confirmed what other studies in this area have reported. William T. Davis and his colleagues surveyed Fellows of the Tennessee chapter of the American College of Surgeons on the issue of occupational musculoskeletal injury (J Surg Res 2014;184:207-212). Of the 793 surveys sent, 33% were completed. General surgeons accounted for 64% of respondents and 80% were male. Forty percent of respondents had sustained at least one injury related to operating. Most reported spine, hand, and neck injuries, but hip, knee, and shoulder pain was also mentioned. The majority of respondents reported the cause of their injury as chronic and 51% sought medical treatment. As with the MD Anderson study, no association was found between age or years in practice and workplace injury.
Mr. Davis and his colleagues conducted a similar study of orthopaedic surgeons and found similar rates of occupational injury (44%) among their 140 survey respondents (J Bone Joint Surg Am. 2013;95:e107). This study found that responding orthopaedic surgeons had more hand and lower back injuries, and correlation was found between years in practice and prevalence of injury.
A limitation of all of these studies is that the injury data are self-reported, and there is a potential selection bias. It is likely that the true extent of workplace injury among surgeons, and the costs and impact on surgeons’ life quality and productivity, are still largely unknown.
“There have been a few studies on this, but I think we’re just scratching the surface,” explained Dr. Adrian Park, chair of surgery at the Anne Arundel Medical Center in Annapolis, Md. Dr. Park was the lead author of a 2010 study that identified chronic pain among surgeons as a serious and underreported issue within medicine (J Am Coll Surg 2010;210;306-313).
The study, which evaluated 317 surgeons using a 23-question survey, found that 86.9% of surgeons experience “physical symptoms or discomfort,” with the most significant indicator of such symptoms being a high case load. Subsequent studies from Europe and eastern Asia also found rates of 80% or higher among surgeons in those regions.
Injuries downplayed
With so pervasive a problem, however, the relative paucity of data and conversation among medical professionals is something Dr. Park finds alarming. “As a surgeon leader, I can tell you surgeons complain about a lot of stuff, but one of the things they tend not to complain about is themselves and their own health and well-being,” said Dr. Park.
Dr. Mario Cerame is well aware of what a seemingly innocuous, relatively small chronic pain can do to a surgeon. A general surgeon practicing in North Carolina, Dr. Cerame began to experience symptoms of repetitive motion injury about 2 years ago, symptoms which he says “crept up on me.”
It began as numbness at the tips of his fingers, affecting the way he held laparoscopic tools during surgery and other, more menial, daily tasks. Initially suspecting it was carpal tunnel syndrome, Dr. Cerame brushed it off, until the numbness spread to three whole fingers and, eventually, his entire hand. His physician explained what was happening, instructing him that if he didn’t undergo orthopaedic surgery immediately, he ran the risk of paralysis.
“I got the diagnosis on Thursday, and had the operation on Tuesday,” said Dr. Cerame, explaining that the diagnosis was spinal stenosis. Two areas of his spinal column were pinching inward, causing the slow but steady paralysis he was experiencing. With physical therapy, Dr. Cerame could have returning function within 2 years of the operation.
“I’ve published an awful lot of papers, but the thing that struck me about [the 2010] paper is the response I got,” said Dr. Park. “Surgeons, literally from around the country, would call me saying ‘I used to be able to do this operation, I no longer can do that,’ or ‘this used to be what my case list looked like, I can no longer do this, you can use me as an example.’ People came forward.”
Risks of ignoring, self-medicating
Then there is the dark side of coping with chronic pain: risk of substance abuse. A study published in the Journal of Addiction Medicine (2013;7;349-353) on misuse of prescription medication among physicians found that surgeons were among the specialists at highest risk for substance abuse. According to this study, the beginning of addiction for many doctors is a prescription or self-medication for chronic pain. For surgeons, chronic pain from occupational injuries could lead to dependence on pain medication.
“When livelihoods are at stake, I think folks will take opportunities to stay in the game,” admitted Dr. Park.
The bottom line, according to both Dr. Park and Dr. Cerame, is for surgeons not to keep quiet about these issues if they ever do experience them. Asking for help and getting things checked right away is better, not only for a surgeon, but for family and patients, too. While Dr. Cerame has gone back to work, he is unable to handle the caseload he once had and isn’t sure if he’ll ever be able to.
“Surgeons and physicians in general have a tendency to get so consumed with other people’s health that they don’t focus on their own health issues,” said Dr. Cerame. “It took me almost 8 months from the time I had symptoms to actually get it checked out [because] I thought it would go away, [so] if you find something that you feel isn’t normal, take care of it.”
Dr. Voss, Dr. Park, and Dr. Cerame had no relevant financial disclosures.
Neil Osterweil contributed to this article.
BOSTON – For many surgeons, hours in the OR can translate into serious or chronic neck, back, and hand pain.
Studies of occupational injury related to performing surgery took off in the 1990s when laparoscopic surgery became widespread and put new physical demands on surgeons (Surg Endosc 1999:13:466-468; Arch Surg 1999;134:1011-1016). Findings from a study presented at the Society for Surgical Oncology suggest that the problem remains widespread.
Dr. Rachael K. Voss, a research resident at the University of Texas MD Anderson Cancer Center, Houston, and her colleagues conducted a survey among oncologic surgeons at the Center to explore the extent, sources and risk factors of workplace injuries.
“[Workplace injury] is a serious issue for surgeons, but it is something we don’t talk about and there is very little training and information as we are going through training. But these occupational hazards are something we need to acknowledge. We need to do more work in the future with ergonomics experts and occupational hygiene experts that can help us improve our posture and positions in the OR so we can prevent these injuries,” Dr. Voss said.
A high response rate of 58% yielded a total of 127 completed surveys. Most of the respondents were aged 35-64 and three-quarters spent 10 hours or more per week working in the OR. Among those responding, 92.3% experienced at least one occupation-related symptom over the past 6 weeks, and 27.6% reported sustaining an injury or chronic condition which they attributed to operating. The majority of injuries reported were cervical spine injury, musculoskeletal fatigue and vertebral disc injury. Other conditions mentioned were brachial plexus damage, carpal tunnel syndrome, peripheral neuropathy, and tendonitis.
A multivariate analysis identified some independent risk factors for injury: male gender, average case duration of 4 hours or longer, neck pain, and frequent use of a step for height adjustment. Age and years in practice were not associated with injury risk.
The good news is that, in this sample, 72% of the respondents reported seeking treatment for their injury. Physical therapy and medication were the most commonly utilized treatments, with about 20% resorting to surgery.
Plenty of evidence
The MD Anderson findings confirmed what other studies in this area have reported. William T. Davis and his colleagues surveyed Fellows of the Tennessee chapter of the American College of Surgeons on the issue of occupational musculoskeletal injury (J Surg Res 2014;184:207-212). Of the 793 surveys sent, 33% were completed. General surgeons accounted for 64% of respondents and 80% were male. Forty percent of respondents had sustained at least one injury related to operating. Most reported spine, hand, and neck injuries, but hip, knee, and shoulder pain was also mentioned. The majority of respondents reported the cause of their injury as chronic and 51% sought medical treatment. As with the MD Anderson study, no association was found between age or years in practice and workplace injury.
Mr. Davis and his colleagues conducted a similar study of orthopaedic surgeons and found similar rates of occupational injury (44%) among their 140 survey respondents (J Bone Joint Surg Am. 2013;95:e107). This study found that responding orthopaedic surgeons had more hand and lower back injuries, and correlation was found between years in practice and prevalence of injury.
A limitation of all of these studies is that the injury data are self-reported, and there is a potential selection bias. It is likely that the true extent of workplace injury among surgeons, and the costs and impact on surgeons’ life quality and productivity, are still largely unknown.
“There have been a few studies on this, but I think we’re just scratching the surface,” explained Dr. Adrian Park, chair of surgery at the Anne Arundel Medical Center in Annapolis, Md. Dr. Park was the lead author of a 2010 study that identified chronic pain among surgeons as a serious and underreported issue within medicine (J Am Coll Surg 2010;210;306-313).
The study, which evaluated 317 surgeons using a 23-question survey, found that 86.9% of surgeons experience “physical symptoms or discomfort,” with the most significant indicator of such symptoms being a high case load. Subsequent studies from Europe and eastern Asia also found rates of 80% or higher among surgeons in those regions.
Injuries downplayed
With so pervasive a problem, however, the relative paucity of data and conversation among medical professionals is something Dr. Park finds alarming. “As a surgeon leader, I can tell you surgeons complain about a lot of stuff, but one of the things they tend not to complain about is themselves and their own health and well-being,” said Dr. Park.
Dr. Mario Cerame is well aware of what a seemingly innocuous, relatively small chronic pain can do to a surgeon. A general surgeon practicing in North Carolina, Dr. Cerame began to experience symptoms of repetitive motion injury about 2 years ago, symptoms which he says “crept up on me.”
It began as numbness at the tips of his fingers, affecting the way he held laparoscopic tools during surgery and other, more menial, daily tasks. Initially suspecting it was carpal tunnel syndrome, Dr. Cerame brushed it off, until the numbness spread to three whole fingers and, eventually, his entire hand. His physician explained what was happening, instructing him that if he didn’t undergo orthopaedic surgery immediately, he ran the risk of paralysis.
“I got the diagnosis on Thursday, and had the operation on Tuesday,” said Dr. Cerame, explaining that the diagnosis was spinal stenosis. Two areas of his spinal column were pinching inward, causing the slow but steady paralysis he was experiencing. With physical therapy, Dr. Cerame could have returning function within 2 years of the operation.
“I’ve published an awful lot of papers, but the thing that struck me about [the 2010] paper is the response I got,” said Dr. Park. “Surgeons, literally from around the country, would call me saying ‘I used to be able to do this operation, I no longer can do that,’ or ‘this used to be what my case list looked like, I can no longer do this, you can use me as an example.’ People came forward.”
Risks of ignoring, self-medicating
Then there is the dark side of coping with chronic pain: risk of substance abuse. A study published in the Journal of Addiction Medicine (2013;7;349-353) on misuse of prescription medication among physicians found that surgeons were among the specialists at highest risk for substance abuse. According to this study, the beginning of addiction for many doctors is a prescription or self-medication for chronic pain. For surgeons, chronic pain from occupational injuries could lead to dependence on pain medication.
“When livelihoods are at stake, I think folks will take opportunities to stay in the game,” admitted Dr. Park.
The bottom line, according to both Dr. Park and Dr. Cerame, is for surgeons not to keep quiet about these issues if they ever do experience them. Asking for help and getting things checked right away is better, not only for a surgeon, but for family and patients, too. While Dr. Cerame has gone back to work, he is unable to handle the caseload he once had and isn’t sure if he’ll ever be able to.
“Surgeons and physicians in general have a tendency to get so consumed with other people’s health that they don’t focus on their own health issues,” said Dr. Cerame. “It took me almost 8 months from the time I had symptoms to actually get it checked out [because] I thought it would go away, [so] if you find something that you feel isn’t normal, take care of it.”
Dr. Voss, Dr. Park, and Dr. Cerame had no relevant financial disclosures.
Neil Osterweil contributed to this article.

Rotor ablation for atrial fibrillation strikes out in first randomized trial
SAN FRANCISCO – Focal impulse and rotor modulation-guided ablation for persistent atrial fibrillation – either alone or in conjunction with other procedures – increased procedural times without improving outcomes, according to the first randomized trial to assess its utility.
In fact, enrollment in the rotor ablation-only (RA) arm was halted early for futility. “There was 100% recurrence” of atrial fibrillation (AF), said senior investigator Dr. Andrea Natale, executive medical director of the Texas Cardiac Arrhythmia Institute, Austin.
“I’m surprised it took this long for a randomized study, because this system has been around for 5 or 6 years,” noted Dr. Natale. “Our community should demand these sorts of studies earlier, because it’s not fair for patients to go on with a procedure for years that has not been proven to be effective.

“For us, unless there is a new version of rotor mapping that I feel is significantly different, this will be the end of rotor ablation in my lab with this system [the Topera Physiologic Rotor Mapping Solution],” Dr. Natale said at the annual scientific sessions of the Heart Rhythm Society.
In the study, his team randomized 29 patients to RA only, 42 to RA plus pulmonary vein antral isolation (PVAI), and 42 to PVAI plus posterior wall and nonpulmonary vein trigger ablation.
At about 1 year, four RA-only patients (14%), 22 RA plus PVAI patients (52%), and 32 patients in the PVAI plus trigger group (76%) were free of AF and atrial tachycardias without antiarrhythmic drugs (P < .0001).
Meanwhile, RA alone and RA plus PVAI cases took about 230 minutes, while the more effective PVAI plus trigger approach took about 130 minutes (P < .001).
There was “a very poor outcome with rotor-only ablation,” Dr. Natale said. “There isn’t a benefit either alone or as an add-on strategy, at least with this mapping software.”
Perhaps “people who think rotors don’t exist are right,” he added. On the other hand, maybe the basket mapping catheter doesn’t touch enough of the left atrium, or the software that makes sense of what the catheter detects needs to be improved, Dr. Natale noted.
All the patients were undergoing their first ablation. They were in their early 60s, on average, and most were men. The mean left atrium diameter was about 47 mm, and mean left ventricle ejection fraction about 55%. There were no statistically significant differences between the study arms, and no significant differences in outcomes between the 70% of patients with persistent AF and the 30% with long-standing persistent AF.
There was no industry funding for the work. Dr. Natale disclosed relationships with Biosense Webster, Boston Scientific, Janssen, Medtronic, and St. Jude Medical.
My gut sense is that there’s something to rotor mapping, but we are not there yet. There are a lot of investment dollars and a lot of bright people working on this. It really is the Holy Grail to find the source of AF.
Dr. John Day is the director of Intermountain Heart Rhythm Specialists in Murray, Utah, and the current president of the Hearth Rhythm Society. He had no disclosures.
My gut sense is that there’s something to rotor mapping, but we are not there yet. There are a lot of investment dollars and a lot of bright people working on this. It really is the Holy Grail to find the source of AF.
Dr. John Day is the director of Intermountain Heart Rhythm Specialists in Murray, Utah, and the current president of the Hearth Rhythm Society. He had no disclosures.
My gut sense is that there’s something to rotor mapping, but we are not there yet. There are a lot of investment dollars and a lot of bright people working on this. It really is the Holy Grail to find the source of AF.
Dr. John Day is the director of Intermountain Heart Rhythm Specialists in Murray, Utah, and the current president of the Hearth Rhythm Society. He had no disclosures.
SAN FRANCISCO – Focal impulse and rotor modulation-guided ablation for persistent atrial fibrillation – either alone or in conjunction with other procedures – increased procedural times without improving outcomes, according to the first randomized trial to assess its utility.
In fact, enrollment in the rotor ablation-only (RA) arm was halted early for futility. “There was 100% recurrence” of atrial fibrillation (AF), said senior investigator Dr. Andrea Natale, executive medical director of the Texas Cardiac Arrhythmia Institute, Austin.
“I’m surprised it took this long for a randomized study, because this system has been around for 5 or 6 years,” noted Dr. Natale. “Our community should demand these sorts of studies earlier, because it’s not fair for patients to go on with a procedure for years that has not been proven to be effective.
“For us, unless there is a new version of rotor mapping that I feel is significantly different, this will be the end of rotor ablation in my lab with this system [the Topera Physiologic Rotor Mapping Solution],” Dr. Natale said at the annual scientific sessions of the Heart Rhythm Society.
In the study, his team randomized 29 patients to RA only, 42 to RA plus pulmonary vein antral isolation (PVAI), and 42 to PVAI plus posterior wall and nonpulmonary vein trigger ablation.
At about 1 year, four RA-only patients (14%), 22 RA plus PVAI patients (52%), and 32 patients in the PVAI plus trigger group (76%) were free of AF and atrial tachycardias without antiarrhythmic drugs (P < .0001).
Meanwhile, RA alone and RA plus PVAI cases took about 230 minutes, while the more effective PVAI plus trigger approach took about 130 minutes (P < .001).
There was “a very poor outcome with rotor-only ablation,” Dr. Natale said. “There isn’t a benefit either alone or as an add-on strategy, at least with this mapping software.”
Perhaps “people who think rotors don’t exist are right,” he added. On the other hand, maybe the basket mapping catheter doesn’t touch enough of the left atrium, or the software that makes sense of what the catheter detects needs to be improved, Dr. Natale noted.
All the patients were undergoing their first ablation. They were in their early 60s, on average, and most were men. The mean left atrium diameter was about 47 mm, and mean left ventricle ejection fraction about 55%. There were no statistically significant differences between the study arms, and no significant differences in outcomes between the 70% of patients with persistent AF and the 30% with long-standing persistent AF.
There was no industry funding for the work. Dr. Natale disclosed relationships with Biosense Webster, Boston Scientific, Janssen, Medtronic, and St. Jude Medical.
SAN FRANCISCO – Focal impulse and rotor modulation-guided ablation for persistent atrial fibrillation – either alone or in conjunction with other procedures – increased procedural times without improving outcomes, according to the first randomized trial to assess its utility.
In fact, enrollment in the rotor ablation-only (RA) arm was halted early for futility. “There was 100% recurrence” of atrial fibrillation (AF), said senior investigator Dr. Andrea Natale, executive medical director of the Texas Cardiac Arrhythmia Institute, Austin.
“I’m surprised it took this long for a randomized study, because this system has been around for 5 or 6 years,” noted Dr. Natale. “Our community should demand these sorts of studies earlier, because it’s not fair for patients to go on with a procedure for years that has not been proven to be effective.
“For us, unless there is a new version of rotor mapping that I feel is significantly different, this will be the end of rotor ablation in my lab with this system [the Topera Physiologic Rotor Mapping Solution],” Dr. Natale said at the annual scientific sessions of the Heart Rhythm Society.
In the study, his team randomized 29 patients to RA only, 42 to RA plus pulmonary vein antral isolation (PVAI), and 42 to PVAI plus posterior wall and nonpulmonary vein trigger ablation.
At about 1 year, four RA-only patients (14%), 22 RA plus PVAI patients (52%), and 32 patients in the PVAI plus trigger group (76%) were free of AF and atrial tachycardias without antiarrhythmic drugs (P < .0001).
Meanwhile, RA alone and RA plus PVAI cases took about 230 minutes, while the more effective PVAI plus trigger approach took about 130 minutes (P < .001).
There was “a very poor outcome with rotor-only ablation,” Dr. Natale said. “There isn’t a benefit either alone or as an add-on strategy, at least with this mapping software.”
Perhaps “people who think rotors don’t exist are right,” he added. On the other hand, maybe the basket mapping catheter doesn’t touch enough of the left atrium, or the software that makes sense of what the catheter detects needs to be improved, Dr. Natale noted.
All the patients were undergoing their first ablation. They were in their early 60s, on average, and most were men. The mean left atrium diameter was about 47 mm, and mean left ventricle ejection fraction about 55%. There were no statistically significant differences between the study arms, and no significant differences in outcomes between the 70% of patients with persistent AF and the 30% with long-standing persistent AF.
There was no industry funding for the work. Dr. Natale disclosed relationships with Biosense Webster, Boston Scientific, Janssen, Medtronic, and St. Jude Medical.
AT HEART RHYTHM 2016
Key clinical point: Focal impulse and rotor modulation-guided ablation for persistent atrial fibrillation – either alone or in conjunction with other procedures – increased procedural times without improving outcomes.
Major finding: At about 1 year, four rotor ablation-only patients (14%), 22 RA plus pulmonary vein antral isolation patients (52.4%), and 32 patients in the PVAI plus trigger group (76%) were free of atrial fibrillation and atrial tachycardias without antiarrhythmic drugs (P < .0001).
Data source: A randomized trial in 113 persistent AF patients.
Disclosures: There was no industry funding for the work. The senior investigator disclosed relationships with Biosense Webster, Boston Scientific, Janssen, Medtronic, and St. Jude Medical.

Commentary: Bones
I’ve always thought that “Bones” of the “Star Trek” series is the sort of surgeon I want to be. He is a treasure trove of wisdom that anyone worth their Federation credits who aspires to be a surgeon should study. Here are some of his truths we should follow in these primitive times, long before surgery becomes the ideal profession it is in the 23rd century (obviously it takes us a little time to solve universal health access).
“Permission to speak freely?” he asks the captain. “Are you out of your mind?” Even in the future, the ship’s surgeon is the one who sees clearly the hazards ahead with oblivious leadership at the helm. It is our job to point out the obvious and the dangerous and see the picture as clearly as possible – because if we don’t, bad things will happen. It seems that the good surgeon is the person who points out that ejecting the warp core of medicine might be the wrong move.

“I’d give a lot to see a hospital. I suppose they still cut and sew people like garments.” Since I cut and sew people like garments every day, one would think I would take offense at Dr. McCoy’s observation of 20th century medicine. But what would a surgeon do without the instruments of our originating profession, the barbers? No scissors and thread? It is now the 21st century, but we still use these basic tools and will probably do so for the foreseeable future.
Most good surgeons I know feel that we operate when it is the best option for our patients, and when that is not the case, we are pleased when a disease is best addressed by other means. Does anyone miss surgically putting sterile ping-pong balls into chests for TB? How about managing a leaking duodenum after an operation for a bleeding duodenal ulcer? That was a lot of fun, wasn’t it? I miss the excitement of operating on a perforated ulcer, an operation in which I could quickly take someone from agony and near death back to health. But I am glad that proton pump inhibitors and H. pylori were discovered. When I was a resident, esophageal cancer and rectal cancer were a death sentence. They are still ugly diseases; however, we now see people with no evidence of disease after chemoradiation. Will the world be a lesser place if esophagectomy and abdominal-perineal resection virtually disappear?
“Dammit Jim, I’m a surgeon not a …” This has to be the motto of every surgeon. We are a highly trained, highly strung set of individuals. In general, we were born to become surgeons, and I have no doubt that by the time Dr. McCoy is galloping about the cosmos, it will be common knowledge that the Cutter gene is found in people who become surgeons. Because this is true, society and surgeons make the mistake of thinking that being really good at surgery in some way equates to being an expert on business, health policy, home repair, or politics. The first thing a surgeon should do when asked to step outside the OR and begin messing with something he or she knows about only tangentially is to repeat Dr. McCoy’s mantra: I’m a surgeon, not an engineer. I’m a surgeon, not a CEO. I’m a surgeon, not a president. The surgeon, of course, can be all these things, but not until he or she has actually learned something in these areas. It would also be nice if nonsurgeons would refrain from posing as experts on surgery.
“He’s dead, Jim.” Dr. McCoy was great at being a realist and so should we surgeons. McCoy rarely made wildly ineffective attempts to save a life that was already gone. Surgeons have to be able to tell families and colleagues the truth about patients who are far beyond saving with today’s technology. It is often our role to do so, but sometimes we forget.
“I had to join Star Fleet – my wife took everything in the universe in the divorce. All I’ve got left is my bones.” This is the origin of Dr. McCoy’s nickname. I am grateful that this is one McCoy trait I’ve not emulated. Being married to one of the great creatures in the universe has made me a much better surgeon.
Sometimes when I look at how much has changed since I became a surgeon, I feel a little like Dr. McCoy. Even a country boy like me gets to work a miracle every now and then. I guess we may live long and prosper after all.
Dr. Hughes is an ACS Fellow with the department of general surgery, McPherson Hospital, McPherson, Kan., and is the Editor in Chief of ACS Communities. He is also Associate Editor for ACS Surgery News.
I’ve always thought that “Bones” of the “Star Trek” series is the sort of surgeon I want to be. He is a treasure trove of wisdom that anyone worth their Federation credits who aspires to be a surgeon should study. Here are some of his truths we should follow in these primitive times, long before surgery becomes the ideal profession it is in the 23rd century (obviously it takes us a little time to solve universal health access).
“Permission to speak freely?” he asks the captain. “Are you out of your mind?” Even in the future, the ship’s surgeon is the one who sees clearly the hazards ahead with oblivious leadership at the helm. It is our job to point out the obvious and the dangerous and see the picture as clearly as possible – because if we don’t, bad things will happen. It seems that the good surgeon is the person who points out that ejecting the warp core of medicine might be the wrong move.
“I’d give a lot to see a hospital. I suppose they still cut and sew people like garments.” Since I cut and sew people like garments every day, one would think I would take offense at Dr. McCoy’s observation of 20th century medicine. But what would a surgeon do without the instruments of our originating profession, the barbers? No scissors and thread? It is now the 21st century, but we still use these basic tools and will probably do so for the foreseeable future.
Most good surgeons I know feel that we operate when it is the best option for our patients, and when that is not the case, we are pleased when a disease is best addressed by other means. Does anyone miss surgically putting sterile ping-pong balls into chests for TB? How about managing a leaking duodenum after an operation for a bleeding duodenal ulcer? That was a lot of fun, wasn’t it? I miss the excitement of operating on a perforated ulcer, an operation in which I could quickly take someone from agony and near death back to health. But I am glad that proton pump inhibitors and H. pylori were discovered. When I was a resident, esophageal cancer and rectal cancer were a death sentence. They are still ugly diseases; however, we now see people with no evidence of disease after chemoradiation. Will the world be a lesser place if esophagectomy and abdominal-perineal resection virtually disappear?
“Dammit Jim, I’m a surgeon not a …” This has to be the motto of every surgeon. We are a highly trained, highly strung set of individuals. In general, we were born to become surgeons, and I have no doubt that by the time Dr. McCoy is galloping about the cosmos, it will be common knowledge that the Cutter gene is found in people who become surgeons. Because this is true, society and surgeons make the mistake of thinking that being really good at surgery in some way equates to being an expert on business, health policy, home repair, or politics. The first thing a surgeon should do when asked to step outside the OR and begin messing with something he or she knows about only tangentially is to repeat Dr. McCoy’s mantra: I’m a surgeon, not an engineer. I’m a surgeon, not a CEO. I’m a surgeon, not a president. The surgeon, of course, can be all these things, but not until he or she has actually learned something in these areas. It would also be nice if nonsurgeons would refrain from posing as experts on surgery.
“He’s dead, Jim.” Dr. McCoy was great at being a realist and so should we surgeons. McCoy rarely made wildly ineffective attempts to save a life that was already gone. Surgeons have to be able to tell families and colleagues the truth about patients who are far beyond saving with today’s technology. It is often our role to do so, but sometimes we forget.
“I had to join Star Fleet – my wife took everything in the universe in the divorce. All I’ve got left is my bones.” This is the origin of Dr. McCoy’s nickname. I am grateful that this is one McCoy trait I’ve not emulated. Being married to one of the great creatures in the universe has made me a much better surgeon.
Sometimes when I look at how much has changed since I became a surgeon, I feel a little like Dr. McCoy. Even a country boy like me gets to work a miracle every now and then. I guess we may live long and prosper after all.
Dr. Hughes is an ACS Fellow with the department of general surgery, McPherson Hospital, McPherson, Kan., and is the Editor in Chief of ACS Communities. He is also Associate Editor for ACS Surgery News.
I’ve always thought that “Bones” of the “Star Trek” series is the sort of surgeon I want to be. He is a treasure trove of wisdom that anyone worth their Federation credits who aspires to be a surgeon should study. Here are some of his truths we should follow in these primitive times, long before surgery becomes the ideal profession it is in the 23rd century (obviously it takes us a little time to solve universal health access).
“Permission to speak freely?” he asks the captain. “Are you out of your mind?” Even in the future, the ship’s surgeon is the one who sees clearly the hazards ahead with oblivious leadership at the helm. It is our job to point out the obvious and the dangerous and see the picture as clearly as possible – because if we don’t, bad things will happen. It seems that the good surgeon is the person who points out that ejecting the warp core of medicine might be the wrong move.
“I’d give a lot to see a hospital. I suppose they still cut and sew people like garments.” Since I cut and sew people like garments every day, one would think I would take offense at Dr. McCoy’s observation of 20th century medicine. But what would a surgeon do without the instruments of our originating profession, the barbers? No scissors and thread? It is now the 21st century, but we still use these basic tools and will probably do so for the foreseeable future.
Most good surgeons I know feel that we operate when it is the best option for our patients, and when that is not the case, we are pleased when a disease is best addressed by other means. Does anyone miss surgically putting sterile ping-pong balls into chests for TB? How about managing a leaking duodenum after an operation for a bleeding duodenal ulcer? That was a lot of fun, wasn’t it? I miss the excitement of operating on a perforated ulcer, an operation in which I could quickly take someone from agony and near death back to health. But I am glad that proton pump inhibitors and H. pylori were discovered. When I was a resident, esophageal cancer and rectal cancer were a death sentence. They are still ugly diseases; however, we now see people with no evidence of disease after chemoradiation. Will the world be a lesser place if esophagectomy and abdominal-perineal resection virtually disappear?
“Dammit Jim, I’m a surgeon not a …” This has to be the motto of every surgeon. We are a highly trained, highly strung set of individuals. In general, we were born to become surgeons, and I have no doubt that by the time Dr. McCoy is galloping about the cosmos, it will be common knowledge that the Cutter gene is found in people who become surgeons. Because this is true, society and surgeons make the mistake of thinking that being really good at surgery in some way equates to being an expert on business, health policy, home repair, or politics. The first thing a surgeon should do when asked to step outside the OR and begin messing with something he or she knows about only tangentially is to repeat Dr. McCoy’s mantra: I’m a surgeon, not an engineer. I’m a surgeon, not a CEO. I’m a surgeon, not a president. The surgeon, of course, can be all these things, but not until he or she has actually learned something in these areas. It would also be nice if nonsurgeons would refrain from posing as experts on surgery.
“He’s dead, Jim.” Dr. McCoy was great at being a realist and so should we surgeons. McCoy rarely made wildly ineffective attempts to save a life that was already gone. Surgeons have to be able to tell families and colleagues the truth about patients who are far beyond saving with today’s technology. It is often our role to do so, but sometimes we forget.
“I had to join Star Fleet – my wife took everything in the universe in the divorce. All I’ve got left is my bones.” This is the origin of Dr. McCoy’s nickname. I am grateful that this is one McCoy trait I’ve not emulated. Being married to one of the great creatures in the universe has made me a much better surgeon.
Sometimes when I look at how much has changed since I became a surgeon, I feel a little like Dr. McCoy. Even a country boy like me gets to work a miracle every now and then. I guess we may live long and prosper after all.
Dr. Hughes is an ACS Fellow with the department of general surgery, McPherson Hospital, McPherson, Kan., and is the Editor in Chief of ACS Communities. He is also Associate Editor for ACS Surgery News.

Drug-coated stent sets new standard in ACS patients at high bleeding risk
PARIS – In patients at high bleeding risk undergoing percutaneous coronary intervention for acute coronary syndrome, a unique drug-coated, polymer-free stent backed by just a single month of dual-antiplatelet therapy (DAPT) trounced a bare metal stent in both efficacy and safety at 1 year in a large randomized trial, Dr. Christoph K. Naber reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
The BioFreedom stent, coated with a proprietary sirolimus analogue called Biolimus-A9, rapidly transfers the drug to the vessel wall, leaving in place a metallic stent. This drug-coated stent (DCS) provides the antirestenotic benefits of a drug-eluting stent with the advantages of a shorter DAPT requirement and no potential polymer-related adverse events. The device’s performance in this prespecified subgroup analysis of the Leaders Free trial will be practice altering, predicted Dr. Naber of Elisabeth University Hospital in Essen, Germany.

“We believe that current guidelines and clinical practice need to change. Bare-metal stents can no longer be recommended for high–bleeding risk patients presenting with ACS. The Biolimus-A9–coated stent currently has the best supporting evidence for this indication,” he said.
“This was the last chance for bare metal stents to show a good indication. They were thought to be good only in high–bleeding risk patients. Now we see that a drug-coated stent provides better efficacy and is even safer,” the cardiologist continued.
Leaders Free was a randomized double-blind clinical trial in which 2,499 patients at high risk of bleeding who underwent PCI received either the DCS or the Gazelle bare-metal stent (BMS) and 1 month of dual-antiplatelet therapy. The main results, in which the DCS showed superior safety and efficacy at 12 months of follow-up, have been published (N Engl J Med. 2015 Nov 19;373[21]:2038-47).
Dr. Naber presented a prespecified subgroup analysis that included the 659 Leaders Free participants who presented with ACS.
The primary efficacy endpoint – the 12-month rate of clinically driven target lesion revascularization – was 3.9% in the DCS group, compared with 9% in patients randomized to the BMS, for an adjusted 59% relative risk reduction.
The composite safety endpoint was composed of the 1-year rate of cardiac death, acute MI, and definite or probable stent thrombosis. This occurred in 9.3% of the DCS- and 18.5% of the BMS-treated patients, for a relative risk reduction of 52%.
The BioFreedom stent has a selectively microstructured surface coated with Biolimus-A9, a drug that’s far more lipophilic than sirolimus, everolimus, or zotarolimus. As a result, 98% of the drug is transferred to the plaque-laden vessel within 30 days, which is why it’s safe to shorten DAPT to 1 month, Dr. Naber explained.
It’s estimated that up to 20% of patients undergoing PCI are at high bleeding risk for various reasons.
The DCS is marketed in Europe and in clinical trials in the United States aimed at getting Food and Drug Administration approval.
Discussant Dr. Thomas Cuisset of Timone Hospital in Marseille, France, agreed that “in 2016, bare-metal stents are no longer the gold standard in patients at high bleeding risk.”
He added that the Leaders Free ACS substudy leaves unanswered two major remaining questions: What’s the optimal duration of DAPT for DCS in non-ACS patients at high bleeding risk – is 1 month of DAPT as safe as 6 months? And how do contemporary drug-eluting, polymer-based stents compare to the BioFreedom stent for PCI in the setting of high bleeding risk?
In an interview, Dr. Naber said that before a head-to-head comparative clinical trial can even be considered, there will need to be evidence that drug-eluting stents are safe with shortened DAPT. That has yet to be shown.
The study was funded by Biosensors. Dr. Naber reported receiving consultant’s fees from that medical device company and several others. Dr. Cuisset serves as a consultant to or paid lecturer for more than a dozen medical companies.
Simultaneous with Dr. Naber’s presentation at EuroPCR in Paris, the Leaders Free ACS substudy results were published online (Eur Heart J. doi:10.1093/eurheartj/ehw203).
PARIS – In patients at high bleeding risk undergoing percutaneous coronary intervention for acute coronary syndrome, a unique drug-coated, polymer-free stent backed by just a single month of dual-antiplatelet therapy (DAPT) trounced a bare metal stent in both efficacy and safety at 1 year in a large randomized trial, Dr. Christoph K. Naber reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
The BioFreedom stent, coated with a proprietary sirolimus analogue called Biolimus-A9, rapidly transfers the drug to the vessel wall, leaving in place a metallic stent. This drug-coated stent (DCS) provides the antirestenotic benefits of a drug-eluting stent with the advantages of a shorter DAPT requirement and no potential polymer-related adverse events. The device’s performance in this prespecified subgroup analysis of the Leaders Free trial will be practice altering, predicted Dr. Naber of Elisabeth University Hospital in Essen, Germany.
“We believe that current guidelines and clinical practice need to change. Bare-metal stents can no longer be recommended for high–bleeding risk patients presenting with ACS. The Biolimus-A9–coated stent currently has the best supporting evidence for this indication,” he said.
“This was the last chance for bare metal stents to show a good indication. They were thought to be good only in high–bleeding risk patients. Now we see that a drug-coated stent provides better efficacy and is even safer,” the cardiologist continued.
Leaders Free was a randomized double-blind clinical trial in which 2,499 patients at high risk of bleeding who underwent PCI received either the DCS or the Gazelle bare-metal stent (BMS) and 1 month of dual-antiplatelet therapy. The main results, in which the DCS showed superior safety and efficacy at 12 months of follow-up, have been published (N Engl J Med. 2015 Nov 19;373[21]:2038-47).
Dr. Naber presented a prespecified subgroup analysis that included the 659 Leaders Free participants who presented with ACS.
The primary efficacy endpoint – the 12-month rate of clinically driven target lesion revascularization – was 3.9% in the DCS group, compared with 9% in patients randomized to the BMS, for an adjusted 59% relative risk reduction.
The composite safety endpoint was composed of the 1-year rate of cardiac death, acute MI, and definite or probable stent thrombosis. This occurred in 9.3% of the DCS- and 18.5% of the BMS-treated patients, for a relative risk reduction of 52%.
The BioFreedom stent has a selectively microstructured surface coated with Biolimus-A9, a drug that’s far more lipophilic than sirolimus, everolimus, or zotarolimus. As a result, 98% of the drug is transferred to the plaque-laden vessel within 30 days, which is why it’s safe to shorten DAPT to 1 month, Dr. Naber explained.
It’s estimated that up to 20% of patients undergoing PCI are at high bleeding risk for various reasons.
The DCS is marketed in Europe and in clinical trials in the United States aimed at getting Food and Drug Administration approval.
Discussant Dr. Thomas Cuisset of Timone Hospital in Marseille, France, agreed that “in 2016, bare-metal stents are no longer the gold standard in patients at high bleeding risk.”
He added that the Leaders Free ACS substudy leaves unanswered two major remaining questions: What’s the optimal duration of DAPT for DCS in non-ACS patients at high bleeding risk – is 1 month of DAPT as safe as 6 months? And how do contemporary drug-eluting, polymer-based stents compare to the BioFreedom stent for PCI in the setting of high bleeding risk?
In an interview, Dr. Naber said that before a head-to-head comparative clinical trial can even be considered, there will need to be evidence that drug-eluting stents are safe with shortened DAPT. That has yet to be shown.
The study was funded by Biosensors. Dr. Naber reported receiving consultant’s fees from that medical device company and several others. Dr. Cuisset serves as a consultant to or paid lecturer for more than a dozen medical companies.
Simultaneous with Dr. Naber’s presentation at EuroPCR in Paris, the Leaders Free ACS substudy results were published online (Eur Heart J. doi:10.1093/eurheartj/ehw203).
PARIS – In patients at high bleeding risk undergoing percutaneous coronary intervention for acute coronary syndrome, a unique drug-coated, polymer-free stent backed by just a single month of dual-antiplatelet therapy (DAPT) trounced a bare metal stent in both efficacy and safety at 1 year in a large randomized trial, Dr. Christoph K. Naber reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
The BioFreedom stent, coated with a proprietary sirolimus analogue called Biolimus-A9, rapidly transfers the drug to the vessel wall, leaving in place a metallic stent. This drug-coated stent (DCS) provides the antirestenotic benefits of a drug-eluting stent with the advantages of a shorter DAPT requirement and no potential polymer-related adverse events. The device’s performance in this prespecified subgroup analysis of the Leaders Free trial will be practice altering, predicted Dr. Naber of Elisabeth University Hospital in Essen, Germany.
“We believe that current guidelines and clinical practice need to change. Bare-metal stents can no longer be recommended for high–bleeding risk patients presenting with ACS. The Biolimus-A9–coated stent currently has the best supporting evidence for this indication,” he said.
“This was the last chance for bare metal stents to show a good indication. They were thought to be good only in high–bleeding risk patients. Now we see that a drug-coated stent provides better efficacy and is even safer,” the cardiologist continued.
Leaders Free was a randomized double-blind clinical trial in which 2,499 patients at high risk of bleeding who underwent PCI received either the DCS or the Gazelle bare-metal stent (BMS) and 1 month of dual-antiplatelet therapy. The main results, in which the DCS showed superior safety and efficacy at 12 months of follow-up, have been published (N Engl J Med. 2015 Nov 19;373[21]:2038-47).
Dr. Naber presented a prespecified subgroup analysis that included the 659 Leaders Free participants who presented with ACS.
The primary efficacy endpoint – the 12-month rate of clinically driven target lesion revascularization – was 3.9% in the DCS group, compared with 9% in patients randomized to the BMS, for an adjusted 59% relative risk reduction.
The composite safety endpoint was composed of the 1-year rate of cardiac death, acute MI, and definite or probable stent thrombosis. This occurred in 9.3% of the DCS- and 18.5% of the BMS-treated patients, for a relative risk reduction of 52%.
The BioFreedom stent has a selectively microstructured surface coated with Biolimus-A9, a drug that’s far more lipophilic than sirolimus, everolimus, or zotarolimus. As a result, 98% of the drug is transferred to the plaque-laden vessel within 30 days, which is why it’s safe to shorten DAPT to 1 month, Dr. Naber explained.
It’s estimated that up to 20% of patients undergoing PCI are at high bleeding risk for various reasons.
The DCS is marketed in Europe and in clinical trials in the United States aimed at getting Food and Drug Administration approval.
Discussant Dr. Thomas Cuisset of Timone Hospital in Marseille, France, agreed that “in 2016, bare-metal stents are no longer the gold standard in patients at high bleeding risk.”
He added that the Leaders Free ACS substudy leaves unanswered two major remaining questions: What’s the optimal duration of DAPT for DCS in non-ACS patients at high bleeding risk – is 1 month of DAPT as safe as 6 months? And how do contemporary drug-eluting, polymer-based stents compare to the BioFreedom stent for PCI in the setting of high bleeding risk?
In an interview, Dr. Naber said that before a head-to-head comparative clinical trial can even be considered, there will need to be evidence that drug-eluting stents are safe with shortened DAPT. That has yet to be shown.
The study was funded by Biosensors. Dr. Naber reported receiving consultant’s fees from that medical device company and several others. Dr. Cuisset serves as a consultant to or paid lecturer for more than a dozen medical companies.
Simultaneous with Dr. Naber’s presentation at EuroPCR in Paris, the Leaders Free ACS substudy results were published online (Eur Heart J. doi:10.1093/eurheartj/ehw203).
AT EUROPCR 2016
Key clinical point: There are no longer any good indications for implanting a bare-metal stent.
Major finding: The cumulative 1-year rate of cardiac death, MI, or definite or probable stent thrombosis in high–bleeding risk patients who underwent PCI for acute coronary syndrome was 9.3% in those randomized to a novel drug-coated stent, compared with 18.5% in those who got a bare-metal stent.
Data source: This was a prespecified subgroup analysis of the Leaders Free trial in which 659 acute coronary syndrome patients with high bleeding risk undergoing PCI for acute coronary syndrome were randomized to a unique drug-coated, polymer-free stent or a bare-metal stent, with 1 month of dual-antiplatelet therapy for all.
Disclosures: The study was funded by Biosensors. The presenter reported receiving consultant fees from that medical device company and several others.

Care bundle reduces cesarean surgical site infections
WASHINGTON – The rate of cesarean delivery surgical site infections fell significantly at Yale New Haven (Conn.) Hospital after implementation of a multidisciplinary care bundle with protocols covering preoperative, intraoperative, and postoperative care.
An analysis of two 3-month sampling periods – one before implementation of the bundle of care and one after – showed a drop in the surgical site infection (SSI) rate among total cesarean sections from 3.4% to 2.2%.
At the annual meeting of the American College of Obstetricians and Gynecologists, Dr. Ashley Pritchard of the hospital described the care bundle and urged obstetricians to consider the impact of even small reductions in SSIs after a cesarean.

“Infection is the most common complication following cesarean delivery … 2.5%-16% of all cesarean deliveries will result in a surgical site infection, and there is significant underestimation as between 15% to 80% of infections are diagnosed after patients leave the hospital,” she said.
A cesarean delivery SSI task force created by the hospital’s obstetric patient safety program developed the care bundle after reviewing best practices, guidelines, and evidence-based reviews.
Preoperative protocols for planned cesareans focused on patient education and included a preoperative appointment and instructions for showering the night before surgery, not shaving for more than 24 hours prior to scheduled surgery, using 2% chlorhexidine wipes both the night prior to surgery and the day of surgery, and other hygiene processes.
“We know from numerous studies that chlorhexidine is superior to iodine, but we also have found that with these wipes you get a level of antibiosis on the skin surface that decreases surgical site infections at the time of incisions,” Dr. Pritchard said.
For the operative care part of the bundle, staff were reeducated about the scrubbing protocol, proper attire and limits on operating room traffic, and the correct and timely use of antibiotics (for example, a cephalosporin administered within 30 minutes of incision). Staff also watched a video and were quizzed on the proper technique and timing for preoperative skin preparation.
Increased attention was paid to normothermia and included preoperative use of warming blankets and proper temperature in the operating room and post–anesthesia care unit.
“We’ve learned from colorectal and trauma surgery that normothermia and patient warming lead to reduced SSI,” Dr. Pritchard said. “This hasn’t been proven with cesarean delivery, but we know there’s improved maternal and fetal well-being with preoperative warming.”
Postoperatively, the use of supplemental oxygen was discontinued unless clinically indicated “since it’s been shown to have no positive effect on SSI,” she said. Incision dressing application and removal were also standardized, with sterile dressings maintained for at least 24 hours – with a tag labeling the date and time of application – and no more than 48 hours. At discharge, patients were given clear discharge instructions and a postpartum appointment for an incision check.
During the 3-month sampling period prior to implementation of the care bundle, there were 382 cesarean deliveries, and 147 patients presented for a postpartum appointment (either the prescribed visit or a later “issue visit”) within 30 days (38%). Of these patients, 8.6% were diagnosed with an SSI.
In the postimplementation sampling period, which began 6 months after rollout, there were 361 cesarean deliveries at the hospital, and 297 patients (77%) presented for postpartum care. Of these patients, 2.9% were diagnosed with an SSI.
An analysis based on the total number of cesarean deliveries performed at the hospital (planned and unplanned) during the two 3-month periods showed a decline in the cesarean delivery SSI rate from 3.4% to 2.2%. “This is statistically significant. It shows a dramatic decline in the SSI rate in our patient population … a clear impact of the bundle of care,” Dr. Pritchard said.
The Yale team attributes the significant increase in postoperative visit attendance to the preoperative protocol for planned cesareans. “We think it had something to do with our creating better relationships by having [patients] present preoperatively and starting their care prior to incision,” she said.
The preoperative visit also provided an opportunity to identify and treat any active skin infections, upper respiratory infections, or chronic colonizations (without evidence of completion of treatment) before delivery. “If necessary and if possible, [we could] push back their cesarean section date to ensure adequate treatment had been achieved,” Dr. Pritchard said.
All aspects of the care bundle were rolled out simultaneously. Next steps for the New Haven team include further analysis of provider and patient views, a look at the sustainability of the bundle of care and its impact, and a cost analysis. “We reduced our SSIs, but we’ve also added a number of elements to our care spectrum, pre- and postoperatively,” Dr. Pritchard said.
For now, one thing seems clear: “We learned from cardiac and colorectal surgery that there really is strength in the bundle, that the sum of the parts is greater than the individual aspects,” she said.
Dr. Pritchard reported that she and her coinvestigators have no relevant financial disclosures.
WASHINGTON – The rate of cesarean delivery surgical site infections fell significantly at Yale New Haven (Conn.) Hospital after implementation of a multidisciplinary care bundle with protocols covering preoperative, intraoperative, and postoperative care.
An analysis of two 3-month sampling periods – one before implementation of the bundle of care and one after – showed a drop in the surgical site infection (SSI) rate among total cesarean sections from 3.4% to 2.2%.
At the annual meeting of the American College of Obstetricians and Gynecologists, Dr. Ashley Pritchard of the hospital described the care bundle and urged obstetricians to consider the impact of even small reductions in SSIs after a cesarean.
“Infection is the most common complication following cesarean delivery … 2.5%-16% of all cesarean deliveries will result in a surgical site infection, and there is significant underestimation as between 15% to 80% of infections are diagnosed after patients leave the hospital,” she said.
A cesarean delivery SSI task force created by the hospital’s obstetric patient safety program developed the care bundle after reviewing best practices, guidelines, and evidence-based reviews.
Preoperative protocols for planned cesareans focused on patient education and included a preoperative appointment and instructions for showering the night before surgery, not shaving for more than 24 hours prior to scheduled surgery, using 2% chlorhexidine wipes both the night prior to surgery and the day of surgery, and other hygiene processes.
“We know from numerous studies that chlorhexidine is superior to iodine, but we also have found that with these wipes you get a level of antibiosis on the skin surface that decreases surgical site infections at the time of incisions,” Dr. Pritchard said.
For the operative care part of the bundle, staff were reeducated about the scrubbing protocol, proper attire and limits on operating room traffic, and the correct and timely use of antibiotics (for example, a cephalosporin administered within 30 minutes of incision). Staff also watched a video and were quizzed on the proper technique and timing for preoperative skin preparation.
Increased attention was paid to normothermia and included preoperative use of warming blankets and proper temperature in the operating room and post–anesthesia care unit.
“We’ve learned from colorectal and trauma surgery that normothermia and patient warming lead to reduced SSI,” Dr. Pritchard said. “This hasn’t been proven with cesarean delivery, but we know there’s improved maternal and fetal well-being with preoperative warming.”
Postoperatively, the use of supplemental oxygen was discontinued unless clinically indicated “since it’s been shown to have no positive effect on SSI,” she said. Incision dressing application and removal were also standardized, with sterile dressings maintained for at least 24 hours – with a tag labeling the date and time of application – and no more than 48 hours. At discharge, patients were given clear discharge instructions and a postpartum appointment for an incision check.
During the 3-month sampling period prior to implementation of the care bundle, there were 382 cesarean deliveries, and 147 patients presented for a postpartum appointment (either the prescribed visit or a later “issue visit”) within 30 days (38%). Of these patients, 8.6% were diagnosed with an SSI.
In the postimplementation sampling period, which began 6 months after rollout, there were 361 cesarean deliveries at the hospital, and 297 patients (77%) presented for postpartum care. Of these patients, 2.9% were diagnosed with an SSI.
An analysis based on the total number of cesarean deliveries performed at the hospital (planned and unplanned) during the two 3-month periods showed a decline in the cesarean delivery SSI rate from 3.4% to 2.2%. “This is statistically significant. It shows a dramatic decline in the SSI rate in our patient population … a clear impact of the bundle of care,” Dr. Pritchard said.
The Yale team attributes the significant increase in postoperative visit attendance to the preoperative protocol for planned cesareans. “We think it had something to do with our creating better relationships by having [patients] present preoperatively and starting their care prior to incision,” she said.
The preoperative visit also provided an opportunity to identify and treat any active skin infections, upper respiratory infections, or chronic colonizations (without evidence of completion of treatment) before delivery. “If necessary and if possible, [we could] push back their cesarean section date to ensure adequate treatment had been achieved,” Dr. Pritchard said.
All aspects of the care bundle were rolled out simultaneously. Next steps for the New Haven team include further analysis of provider and patient views, a look at the sustainability of the bundle of care and its impact, and a cost analysis. “We reduced our SSIs, but we’ve also added a number of elements to our care spectrum, pre- and postoperatively,” Dr. Pritchard said.
For now, one thing seems clear: “We learned from cardiac and colorectal surgery that there really is strength in the bundle, that the sum of the parts is greater than the individual aspects,” she said.
Dr. Pritchard reported that she and her coinvestigators have no relevant financial disclosures.
WASHINGTON – The rate of cesarean delivery surgical site infections fell significantly at Yale New Haven (Conn.) Hospital after implementation of a multidisciplinary care bundle with protocols covering preoperative, intraoperative, and postoperative care.
An analysis of two 3-month sampling periods – one before implementation of the bundle of care and one after – showed a drop in the surgical site infection (SSI) rate among total cesarean sections from 3.4% to 2.2%.
At the annual meeting of the American College of Obstetricians and Gynecologists, Dr. Ashley Pritchard of the hospital described the care bundle and urged obstetricians to consider the impact of even small reductions in SSIs after a cesarean.
“Infection is the most common complication following cesarean delivery … 2.5%-16% of all cesarean deliveries will result in a surgical site infection, and there is significant underestimation as between 15% to 80% of infections are diagnosed after patients leave the hospital,” she said.
A cesarean delivery SSI task force created by the hospital’s obstetric patient safety program developed the care bundle after reviewing best practices, guidelines, and evidence-based reviews.
Preoperative protocols for planned cesareans focused on patient education and included a preoperative appointment and instructions for showering the night before surgery, not shaving for more than 24 hours prior to scheduled surgery, using 2% chlorhexidine wipes both the night prior to surgery and the day of surgery, and other hygiene processes.
“We know from numerous studies that chlorhexidine is superior to iodine, but we also have found that with these wipes you get a level of antibiosis on the skin surface that decreases surgical site infections at the time of incisions,” Dr. Pritchard said.
For the operative care part of the bundle, staff were reeducated about the scrubbing protocol, proper attire and limits on operating room traffic, and the correct and timely use of antibiotics (for example, a cephalosporin administered within 30 minutes of incision). Staff also watched a video and were quizzed on the proper technique and timing for preoperative skin preparation.
Increased attention was paid to normothermia and included preoperative use of warming blankets and proper temperature in the operating room and post–anesthesia care unit.
“We’ve learned from colorectal and trauma surgery that normothermia and patient warming lead to reduced SSI,” Dr. Pritchard said. “This hasn’t been proven with cesarean delivery, but we know there’s improved maternal and fetal well-being with preoperative warming.”
Postoperatively, the use of supplemental oxygen was discontinued unless clinically indicated “since it’s been shown to have no positive effect on SSI,” she said. Incision dressing application and removal were also standardized, with sterile dressings maintained for at least 24 hours – with a tag labeling the date and time of application – and no more than 48 hours. At discharge, patients were given clear discharge instructions and a postpartum appointment for an incision check.
During the 3-month sampling period prior to implementation of the care bundle, there were 382 cesarean deliveries, and 147 patients presented for a postpartum appointment (either the prescribed visit or a later “issue visit”) within 30 days (38%). Of these patients, 8.6% were diagnosed with an SSI.
In the postimplementation sampling period, which began 6 months after rollout, there were 361 cesarean deliveries at the hospital, and 297 patients (77%) presented for postpartum care. Of these patients, 2.9% were diagnosed with an SSI.
An analysis based on the total number of cesarean deliveries performed at the hospital (planned and unplanned) during the two 3-month periods showed a decline in the cesarean delivery SSI rate from 3.4% to 2.2%. “This is statistically significant. It shows a dramatic decline in the SSI rate in our patient population … a clear impact of the bundle of care,” Dr. Pritchard said.
The Yale team attributes the significant increase in postoperative visit attendance to the preoperative protocol for planned cesareans. “We think it had something to do with our creating better relationships by having [patients] present preoperatively and starting their care prior to incision,” she said.
The preoperative visit also provided an opportunity to identify and treat any active skin infections, upper respiratory infections, or chronic colonizations (without evidence of completion of treatment) before delivery. “If necessary and if possible, [we could] push back their cesarean section date to ensure adequate treatment had been achieved,” Dr. Pritchard said.
All aspects of the care bundle were rolled out simultaneously. Next steps for the New Haven team include further analysis of provider and patient views, a look at the sustainability of the bundle of care and its impact, and a cost analysis. “We reduced our SSIs, but we’ve also added a number of elements to our care spectrum, pre- and postoperatively,” Dr. Pritchard said.
For now, one thing seems clear: “We learned from cardiac and colorectal surgery that there really is strength in the bundle, that the sum of the parts is greater than the individual aspects,” she said.
Dr. Pritchard reported that she and her coinvestigators have no relevant financial disclosures.
AT ACOG 2016
Key clinical point: A multidisciplinary bundle of care was effective in reducing the rate of surgical site infections with cesarean delivery.
Major finding: The rate of cesarean delivery SSIs decreased from 3.4% to 2.2% after implementation of a care bundle.
Data source: An analysis of a quality improvement project at Yale New Haven Hospital.
Disclosures: Dr. Pritchard reported that she and her coinvestigators have no relevant financial disclosures.
