User login
Official Newspaper of the American College of Surgeons
Competitive surgical outcomes observed at critical access hospitals
Thirty-day mortality rates for several common operations were not significantly different for patients seen at “critical access” hospitals, compared with larger high-volume facilities, according to a study using a large, national Medicare database.
The findings suggest that such procedures can be performed safely in smaller, rural hospitals. The Medicare Provider Analysis and Review (MEDPAR) file was used by investigators to examine data from 2009 through 2013 on more than 1 million patients at both types of facilities. The findings were published in JAMA on May 17.

The study was important to conduct for two reasons, coauthors Dr. Andrew Ibrahim and Dr. Justin Dimick of the University of Michigan, Ann Arbor, said in an interview.
“First, this study helps inform important policy decision making regarding rural access to surgery. Critical access hospitals receive more than $9 billion dollars annually from Medicare under payment provisions established in the Medicare Rural Hospital Flexibility Program to help keep them financially viable,” they said. “Plans to modify and even eliminate this program have been proposed largely based on studies demonstrating lower quality of care for common medical conditions (such as heart failure, pneumonia, or heart attack.) This study provides important information about common surgical procedures done in these same hospitals,” they stated.
“Second, this study gives us a better understanding of how to ensure safe surgical care without limiting access for common procedures. We have years of research demonstrating that relatively rare, complex operations (such as open heart operations and cancer resections) should be centralized to high-volume centers where patients travel to obtain their care,” the researchers said. “On the other end of the spectrum, this paper describes common, less complex operations where it is safe for patients to stay at their local hospital without the burden of traveling. This is particularly important now as large health case systems are consolidating and developing strategies to regionalize procedures within their network,” they noted.

The researchers and their colleagues reviewed data from 28,512 patients treated at critical access hospitals and 1,603,392 seen at non–critical access hospitals (JAMA 2016;315:2095-2103. doi:10.1001/jama.2016.5618). The patients underwent one of four surgeries: appendectomy, cholecystectomy, colectomy, or hernia repair.
After the researchers controlled for confounding variables, 30-day mortality rates were not significantly different among patients at critical access and non–critical access hospitals (5.4% vs. 5.6%), although the rates of serious complications were significantly lower in critical access vs. non–critical access hospitals (6.5 vs. 14%). In addition, Medicare expenses were significantly lower at critical access vs. non–critical access hospitals after factoring in risk-adjustment and price standardization ($14,450 vs. $15,845).
Overall, patients treated at critical access hospitals were significantly less likely than were those seen at non–critical access hospitals to have chronic medical problems including heart failure (8% vs. 10%), diabetes (20% vs. 22%), obesity (7% vs. 11%), and two or more comorbidities (60% vs. 70%). The average age of the patients was 77 years, and approximately half were women.

The findings on 30-day mortality and Medicare expenses contradict previous studies of nonsurgical admissions in critical access and non–critical access settings, the researchers noted. However, patients were less likely to proceed to post–acute care facilities from critical access hospitals compared with non–critical access hospitals.
“Based on information about admissions for common medical problems to these hospitals having higher mortality rates and decreased compliance with process measures, we thought this might be the same for surgical admissions,” the researchers said in the interview. “Our findings, however, show that critical access hospitals perform well for common surgical admissions with no difference in their risk-adjusted 30-day mortality rates.”
The results were limited by the use of administrative data, the potential overestimation of complication rates, and the lack of data on younger patients. The data illustrate how new payment models might impact critical care facilities, but several areas of research should be explored, the investigators said.
“First, we need a better understanding of how these small rural hospitals appear to be providing safe care at lower costs. Our data suggest it may be related to patient-selection, but even when we accounted for that in our models they still perform well,” they explained.
“Second, as many of these hospitals may in fact close in the next year, studies will be needed to inform how this might impact cost and access to rural surgical care. Finally, there are many other operations that we do not yet understand if they should be centralized to a large urban hospital, of if they are safe to be done in small hospital settings. As large health care systems continue to consolidate, each one will need a ‘health care systems architect’ to help organize how surgical services should be centralized or decentralized across their network to optimize both quality and access,” they added.
Dr. Ibrahim has received funding from the Robert Wood Johnson Foundation and the U.S. Department of Veterans Affairs. Dr. Justin Dimick has a financial interest in ArborMetrix Inc. and has received funds from the Agency for Healthcare Research and Quality and the National Institutes of Health, as well as honoraria from Stanford University, Emory University, and the University of Texas.
Thirty-day mortality rates for several common operations were not significantly different for patients seen at “critical access” hospitals, compared with larger high-volume facilities, according to a study using a large, national Medicare database.
The findings suggest that such procedures can be performed safely in smaller, rural hospitals. The Medicare Provider Analysis and Review (MEDPAR) file was used by investigators to examine data from 2009 through 2013 on more than 1 million patients at both types of facilities. The findings were published in JAMA on May 17.
The study was important to conduct for two reasons, coauthors Dr. Andrew Ibrahim and Dr. Justin Dimick of the University of Michigan, Ann Arbor, said in an interview.
“First, this study helps inform important policy decision making regarding rural access to surgery. Critical access hospitals receive more than $9 billion dollars annually from Medicare under payment provisions established in the Medicare Rural Hospital Flexibility Program to help keep them financially viable,” they said. “Plans to modify and even eliminate this program have been proposed largely based on studies demonstrating lower quality of care for common medical conditions (such as heart failure, pneumonia, or heart attack.) This study provides important information about common surgical procedures done in these same hospitals,” they stated.
“Second, this study gives us a better understanding of how to ensure safe surgical care without limiting access for common procedures. We have years of research demonstrating that relatively rare, complex operations (such as open heart operations and cancer resections) should be centralized to high-volume centers where patients travel to obtain their care,” the researchers said. “On the other end of the spectrum, this paper describes common, less complex operations where it is safe for patients to stay at their local hospital without the burden of traveling. This is particularly important now as large health case systems are consolidating and developing strategies to regionalize procedures within their network,” they noted.
The researchers and their colleagues reviewed data from 28,512 patients treated at critical access hospitals and 1,603,392 seen at non–critical access hospitals (JAMA 2016;315:2095-2103. doi:10.1001/jama.2016.5618). The patients underwent one of four surgeries: appendectomy, cholecystectomy, colectomy, or hernia repair.
After the researchers controlled for confounding variables, 30-day mortality rates were not significantly different among patients at critical access and non–critical access hospitals (5.4% vs. 5.6%), although the rates of serious complications were significantly lower in critical access vs. non–critical access hospitals (6.5 vs. 14%). In addition, Medicare expenses were significantly lower at critical access vs. non–critical access hospitals after factoring in risk-adjustment and price standardization ($14,450 vs. $15,845).
Overall, patients treated at critical access hospitals were significantly less likely than were those seen at non–critical access hospitals to have chronic medical problems including heart failure (8% vs. 10%), diabetes (20% vs. 22%), obesity (7% vs. 11%), and two or more comorbidities (60% vs. 70%). The average age of the patients was 77 years, and approximately half were women.
The findings on 30-day mortality and Medicare expenses contradict previous studies of nonsurgical admissions in critical access and non–critical access settings, the researchers noted. However, patients were less likely to proceed to post–acute care facilities from critical access hospitals compared with non–critical access hospitals.
“Based on information about admissions for common medical problems to these hospitals having higher mortality rates and decreased compliance with process measures, we thought this might be the same for surgical admissions,” the researchers said in the interview. “Our findings, however, show that critical access hospitals perform well for common surgical admissions with no difference in their risk-adjusted 30-day mortality rates.”
The results were limited by the use of administrative data, the potential overestimation of complication rates, and the lack of data on younger patients. The data illustrate how new payment models might impact critical care facilities, but several areas of research should be explored, the investigators said.
“First, we need a better understanding of how these small rural hospitals appear to be providing safe care at lower costs. Our data suggest it may be related to patient-selection, but even when we accounted for that in our models they still perform well,” they explained.
“Second, as many of these hospitals may in fact close in the next year, studies will be needed to inform how this might impact cost and access to rural surgical care. Finally, there are many other operations that we do not yet understand if they should be centralized to a large urban hospital, of if they are safe to be done in small hospital settings. As large health care systems continue to consolidate, each one will need a ‘health care systems architect’ to help organize how surgical services should be centralized or decentralized across their network to optimize both quality and access,” they added.
Dr. Ibrahim has received funding from the Robert Wood Johnson Foundation and the U.S. Department of Veterans Affairs. Dr. Justin Dimick has a financial interest in ArborMetrix Inc. and has received funds from the Agency for Healthcare Research and Quality and the National Institutes of Health, as well as honoraria from Stanford University, Emory University, and the University of Texas.
Thirty-day mortality rates for several common operations were not significantly different for patients seen at “critical access” hospitals, compared with larger high-volume facilities, according to a study using a large, national Medicare database.
The findings suggest that such procedures can be performed safely in smaller, rural hospitals. The Medicare Provider Analysis and Review (MEDPAR) file was used by investigators to examine data from 2009 through 2013 on more than 1 million patients at both types of facilities. The findings were published in JAMA on May 17.
The study was important to conduct for two reasons, coauthors Dr. Andrew Ibrahim and Dr. Justin Dimick of the University of Michigan, Ann Arbor, said in an interview.
“First, this study helps inform important policy decision making regarding rural access to surgery. Critical access hospitals receive more than $9 billion dollars annually from Medicare under payment provisions established in the Medicare Rural Hospital Flexibility Program to help keep them financially viable,” they said. “Plans to modify and even eliminate this program have been proposed largely based on studies demonstrating lower quality of care for common medical conditions (such as heart failure, pneumonia, or heart attack.) This study provides important information about common surgical procedures done in these same hospitals,” they stated.
“Second, this study gives us a better understanding of how to ensure safe surgical care without limiting access for common procedures. We have years of research demonstrating that relatively rare, complex operations (such as open heart operations and cancer resections) should be centralized to high-volume centers where patients travel to obtain their care,” the researchers said. “On the other end of the spectrum, this paper describes common, less complex operations where it is safe for patients to stay at their local hospital without the burden of traveling. This is particularly important now as large health case systems are consolidating and developing strategies to regionalize procedures within their network,” they noted.
The researchers and their colleagues reviewed data from 28,512 patients treated at critical access hospitals and 1,603,392 seen at non–critical access hospitals (JAMA 2016;315:2095-2103. doi:10.1001/jama.2016.5618). The patients underwent one of four surgeries: appendectomy, cholecystectomy, colectomy, or hernia repair.
After the researchers controlled for confounding variables, 30-day mortality rates were not significantly different among patients at critical access and non–critical access hospitals (5.4% vs. 5.6%), although the rates of serious complications were significantly lower in critical access vs. non–critical access hospitals (6.5 vs. 14%). In addition, Medicare expenses were significantly lower at critical access vs. non–critical access hospitals after factoring in risk-adjustment and price standardization ($14,450 vs. $15,845).
Overall, patients treated at critical access hospitals were significantly less likely than were those seen at non–critical access hospitals to have chronic medical problems including heart failure (8% vs. 10%), diabetes (20% vs. 22%), obesity (7% vs. 11%), and two or more comorbidities (60% vs. 70%). The average age of the patients was 77 years, and approximately half were women.
The findings on 30-day mortality and Medicare expenses contradict previous studies of nonsurgical admissions in critical access and non–critical access settings, the researchers noted. However, patients were less likely to proceed to post–acute care facilities from critical access hospitals compared with non–critical access hospitals.
“Based on information about admissions for common medical problems to these hospitals having higher mortality rates and decreased compliance with process measures, we thought this might be the same for surgical admissions,” the researchers said in the interview. “Our findings, however, show that critical access hospitals perform well for common surgical admissions with no difference in their risk-adjusted 30-day mortality rates.”
The results were limited by the use of administrative data, the potential overestimation of complication rates, and the lack of data on younger patients. The data illustrate how new payment models might impact critical care facilities, but several areas of research should be explored, the investigators said.
“First, we need a better understanding of how these small rural hospitals appear to be providing safe care at lower costs. Our data suggest it may be related to patient-selection, but even when we accounted for that in our models they still perform well,” they explained.
“Second, as many of these hospitals may in fact close in the next year, studies will be needed to inform how this might impact cost and access to rural surgical care. Finally, there are many other operations that we do not yet understand if they should be centralized to a large urban hospital, of if they are safe to be done in small hospital settings. As large health care systems continue to consolidate, each one will need a ‘health care systems architect’ to help organize how surgical services should be centralized or decentralized across their network to optimize both quality and access,” they added.
Dr. Ibrahim has received funding from the Robert Wood Johnson Foundation and the U.S. Department of Veterans Affairs. Dr. Justin Dimick has a financial interest in ArborMetrix Inc. and has received funds from the Agency for Healthcare Research and Quality and the National Institutes of Health, as well as honoraria from Stanford University, Emory University, and the University of Texas.
FROM JAMA
Key clinical point: Common surgical procedures can be performed at smaller hospitals safety and cost-effectively for appropriate patients.
Major finding: Thirty-day mortality rates were similar among patients at critical access and non–critical access hospitals (5.4% vs. 5.6%).
Data source: A cross-sectional, retrospective review of 1,631,904 Medicare beneficiary admissions for appendectomy, cholecystectomy, colectomy, or hernia repair.
Disclosures: Dr. Ibrahim has received funding from the Robert Wood Johnson Foundation and the U.S. Department of Veterans Affairs; coauthor Dr. Dennis Dimick has a financial interest in ArborMetrix Inc. and has received funds from the Agency for Healthcare Research and Quality and the National Institutes of Health, as well as honoraria from Stanford University, Emory University, and the University of Texas.

ERAS protocol benefited colorectal surgery patients
LOS ANGELES – Implementation of a perioperative protocol designed to enhance recovery in patients undergoing elective laparoscopic colorectal surgery decreased hospital length of stay, the rate of complications, and overall direct costs, results from a single-center study showed.
“Until recently patients undergoing colorectal surgery were counseled to accept a 20%-25% risk of complications and a 7- to 10-day postoperative stay in the hospital,” lead study author Dr. Daniel S. Lavy said at the annual meeting of the American Society of Colon and Rectal Surgeons. “Studies from the 1990s have shown that length of stay rates improved when one single component of care was changed.”

Dr. Lavy of the department of surgery at Monmouth Medical Center, Long Branch, N.J., discussed results from a study of Enhanced Recovery After Surgery (ERAS), which he described as “a multimodal perioperative care pathway designed to achieve early recovery for patients undergoing major surgery. Many of its elements challenge existing surgical doctrine, including optimizing nutrition, standardized nonnarcotic and anesthetic regimens, early mobilization, and early initiation of enteral feeding.” The protocol also includes multimodal analgesia aimed at reducing the use of narcotics by intravenous Toradol (ketorolac), intravenous Tylenol (acetaminophen), and a transverse abdominis plane block; preoperative intravenous Solu-Medrol (methylprednisolone); prevention of fluid overload; preoperative and postoperative Entereg (alvimopan); preoperative enteral feedings and early postoperative diet initiation; and aggressive postoperative rehabilitation.
In an effort to evaluate the impact of the protocol in patients undergoing colorectal surgery, Dr. Lavy and his associates analyzed records from 283 elective laparoscopic colon procedures performed at Monmouth Medical Center from July 2013 to December 2015, a time period that included 11 months prior to implementation of ERAS and 18 months after implementation. The data were analyzed using control charts to assess for process changes, while open or emergent procedures were excluded from review. Key measures assessed included hospital length of stay, direct hospital costs, 30-day readmissions, and complications.
Dr. Lavy reported that following implementation of the ERAS protocol, the median length of stay decreased from 3.8 days to 2.8 days; the median direct hospital costs fell 8.5%, resulting in a savings of $876 per case; and the complication rate dropped from 20% to 16%. No changes were observed in the 30-day readmission rate, which held steady at 8%.
“This multifaceted approach has decreased hospital stay, decreased hospital cost and complication rate, did not change the 30-day readmission rate, and maintained patient safety while improving patient care,” Dr. Lavy said. “We suggest research be conducted to determine how this pathway can be altered to further improve quality of care given to patients while simultaneously reducing hospital costs. Also, these methods may be able to be applied to other surgical subspecialties, including ob.gyn., orthopedics, and urology.”
Dr. Lavy reported having no relevant financial disclosures.
LOS ANGELES – Implementation of a perioperative protocol designed to enhance recovery in patients undergoing elective laparoscopic colorectal surgery decreased hospital length of stay, the rate of complications, and overall direct costs, results from a single-center study showed.
“Until recently patients undergoing colorectal surgery were counseled to accept a 20%-25% risk of complications and a 7- to 10-day postoperative stay in the hospital,” lead study author Dr. Daniel S. Lavy said at the annual meeting of the American Society of Colon and Rectal Surgeons. “Studies from the 1990s have shown that length of stay rates improved when one single component of care was changed.”
Dr. Lavy of the department of surgery at Monmouth Medical Center, Long Branch, N.J., discussed results from a study of Enhanced Recovery After Surgery (ERAS), which he described as “a multimodal perioperative care pathway designed to achieve early recovery for patients undergoing major surgery. Many of its elements challenge existing surgical doctrine, including optimizing nutrition, standardized nonnarcotic and anesthetic regimens, early mobilization, and early initiation of enteral feeding.” The protocol also includes multimodal analgesia aimed at reducing the use of narcotics by intravenous Toradol (ketorolac), intravenous Tylenol (acetaminophen), and a transverse abdominis plane block; preoperative intravenous Solu-Medrol (methylprednisolone); prevention of fluid overload; preoperative and postoperative Entereg (alvimopan); preoperative enteral feedings and early postoperative diet initiation; and aggressive postoperative rehabilitation.
In an effort to evaluate the impact of the protocol in patients undergoing colorectal surgery, Dr. Lavy and his associates analyzed records from 283 elective laparoscopic colon procedures performed at Monmouth Medical Center from July 2013 to December 2015, a time period that included 11 months prior to implementation of ERAS and 18 months after implementation. The data were analyzed using control charts to assess for process changes, while open or emergent procedures were excluded from review. Key measures assessed included hospital length of stay, direct hospital costs, 30-day readmissions, and complications.
Dr. Lavy reported that following implementation of the ERAS protocol, the median length of stay decreased from 3.8 days to 2.8 days; the median direct hospital costs fell 8.5%, resulting in a savings of $876 per case; and the complication rate dropped from 20% to 16%. No changes were observed in the 30-day readmission rate, which held steady at 8%.
“This multifaceted approach has decreased hospital stay, decreased hospital cost and complication rate, did not change the 30-day readmission rate, and maintained patient safety while improving patient care,” Dr. Lavy said. “We suggest research be conducted to determine how this pathway can be altered to further improve quality of care given to patients while simultaneously reducing hospital costs. Also, these methods may be able to be applied to other surgical subspecialties, including ob.gyn., orthopedics, and urology.”
Dr. Lavy reported having no relevant financial disclosures.
LOS ANGELES – Implementation of a perioperative protocol designed to enhance recovery in patients undergoing elective laparoscopic colorectal surgery decreased hospital length of stay, the rate of complications, and overall direct costs, results from a single-center study showed.
“Until recently patients undergoing colorectal surgery were counseled to accept a 20%-25% risk of complications and a 7- to 10-day postoperative stay in the hospital,” lead study author Dr. Daniel S. Lavy said at the annual meeting of the American Society of Colon and Rectal Surgeons. “Studies from the 1990s have shown that length of stay rates improved when one single component of care was changed.”
Dr. Lavy of the department of surgery at Monmouth Medical Center, Long Branch, N.J., discussed results from a study of Enhanced Recovery After Surgery (ERAS), which he described as “a multimodal perioperative care pathway designed to achieve early recovery for patients undergoing major surgery. Many of its elements challenge existing surgical doctrine, including optimizing nutrition, standardized nonnarcotic and anesthetic regimens, early mobilization, and early initiation of enteral feeding.” The protocol also includes multimodal analgesia aimed at reducing the use of narcotics by intravenous Toradol (ketorolac), intravenous Tylenol (acetaminophen), and a transverse abdominis plane block; preoperative intravenous Solu-Medrol (methylprednisolone); prevention of fluid overload; preoperative and postoperative Entereg (alvimopan); preoperative enteral feedings and early postoperative diet initiation; and aggressive postoperative rehabilitation.
In an effort to evaluate the impact of the protocol in patients undergoing colorectal surgery, Dr. Lavy and his associates analyzed records from 283 elective laparoscopic colon procedures performed at Monmouth Medical Center from July 2013 to December 2015, a time period that included 11 months prior to implementation of ERAS and 18 months after implementation. The data were analyzed using control charts to assess for process changes, while open or emergent procedures were excluded from review. Key measures assessed included hospital length of stay, direct hospital costs, 30-day readmissions, and complications.
Dr. Lavy reported that following implementation of the ERAS protocol, the median length of stay decreased from 3.8 days to 2.8 days; the median direct hospital costs fell 8.5%, resulting in a savings of $876 per case; and the complication rate dropped from 20% to 16%. No changes were observed in the 30-day readmission rate, which held steady at 8%.
“This multifaceted approach has decreased hospital stay, decreased hospital cost and complication rate, did not change the 30-day readmission rate, and maintained patient safety while improving patient care,” Dr. Lavy said. “We suggest research be conducted to determine how this pathway can be altered to further improve quality of care given to patients while simultaneously reducing hospital costs. Also, these methods may be able to be applied to other surgical subspecialties, including ob.gyn., orthopedics, and urology.”
Dr. Lavy reported having no relevant financial disclosures.
AT THE ASCRS ANNUAL MEETING
Key clinical point: A multifaceted perioperative protocol benefited patients undergoing laparoscopic colorectal surgery.
Major finding: Following implementation of the protocol, the median length of stay decreased from 3.8 days to 2.8 days, the median direct hospital costs fell 8.5%, and the complication rate dropped from 20% to 16%.
Data source: A review of records from 283 elective laparoscopic colon procedures performed from July 2013 to December 2015.
Disclosures: Dr. Lavy reported having no relevant financial disclosures.

Watchman registry provides reassuring answers on device safety
PARIS – Results of the real-world EWOLUTION registry of recipients of the Watchman device for stroke prevention provide reassuring answers to several key questions which have slowed physician uptake of the left atrial appendage closure device, Dr. Martin W. Bergmann said at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“EWOLUTION, with more than 1,000 patients, is I think the study that we’ve needed to make this intervention happen in routine practice as a procedure for stroke prevention in atrial fibrillation,” declared Dr. Bergmann of Cardiologicum Hamburg, a large German group practice.

EWOLUTION is a prospective, single-arm, multicenter registry including 1,025 recipients of the first-generation version of the Watchman, a transcatheter device for left atrial appendage closure as a means of stroke prevention in patients with atrial fibrillation (AF). These were high-risk patients: 50% of them had a CHA2DS2-VASc score of 5 or higher, and 72% of participants were deemed unsuitable for warfarin. EWOLUTION was conducted at 47 sites in Europe, the Middle East, and Russia. Dr. Bergmann presented the 3-month outcomes, a key period for device-related complications because protective epithelialization of the device isn’t yet complete. Follow-up will continue at the 1- and 2-year marks.
Among the key findings in the domain of procedural success: The rate of successful device implantation was 98.5%. A complete seal or an echocardiographic color jet of 5 mm or less at the time of implantation was achieved in 99.7% of cases, and this remained the case in 98.9% at 3 months.
With regard to safety, the stroke rate was 0.4%, device embolization occurred in 0.4%, and the pericardial effusion/tamponade rate was 0.7%, all of which are lower rates than in earlier clinical trials.
Just over 4% of patients experienced device-related adverse events with full recovery at the 3-month follow-up. These were mostly bleeding events at the groin access site. More importantly, only 0.5% of patients had device-related serious adverse events that weren’t resolved at 3 months.
“This 0.5% is a major step forward,” Dr. Bergmann said. “This includes all pericardial effusions, all device embolizations, all periprocedural strokes – everything involving the procedure that puts a patient at risk. In fact, that 0.5% risk for left atrial appendage closure with the Watchman is pretty much the same risk as if you refer your patient with AF to an electrophysiologist for pulmonary vein isolation.”
One key question answered by EWOLUTION is, do you need to be an expert in the procedure in order to get excellent results? The answer, Dr. Bergmann said, is emphatically “no.” Interventionalists at the 47 participating sites varied widely in their experience with left atrial appendage occlusion, so investigators divided the sites into quartiles based upon experience and patient volumes contributed to the registry. While cardiologists in the most experienced centers had a significantly higher rate of successful device release on the first try, the most- and least-experienced centers did equally well on the endpoint that really counts: a complete or near-complete seal of the left atrial appendage at follow-up. Complication rates didn’t differ by site experience, either.
Another important practical question that’s been holding up wider adoption of the Watchman concerns how best to handle postimplantation antithrombotic therapy. Here the EWOLUTION registry provides a partial answer: 607 patients were on dual antiplatelet therapy, 113 were on a novel anticoagulant (NOAC), 159 were on warfarin, 67 were on nothing at all, and the rest were on a single antiplatelet agent. And there was no significant difference between any of these groups in the 3-month rates of thrombus on the device, bleeding events, stroke, or other adverse events.
“The main message is there is no difference in serious adverse events between any of the drug regimens. So if you’re in a situation where you can’t give any medication to reduce stroke risk because the bleeding risk is so high, you can go for left atrial appendage closure technology and give them nothing post implant,” according to Dr. Bergmann.
He added that he’d personally try to avoid that strategy: “You want to have some coverage.”

Also noteworthy is that 113 Watchman recipients did well with 3 months of NOAC monotherapy. The appeal of that approach is the short half-life of those agents in the event of a bleeding problem.
Discussant Dr. Farrel Hellig commented that EWOLUTION demonstrates that the Watchman procedure is predictable and safe, with an impressively low complication rate even in inexperienced centers. For that, he added, kudos goes to Boston Scientific, which markets the Watchman, for rolling out an effective physician training program.
“The most important topic to discuss is bleeding, because a bleeding rate of 4.1% at 3 months is certainly not insignificant,” he continued. “It appears, firstly, from EWOLUTION that it’s safe to omit warfarin. I think the most important thing we’d like to know now is could a postprocedure NOAC be the best option, and can aspirin be eliminated in the long term?”
“Is it too early to recommend a NOAC-only for a period of time post procedure? Perhaps. But I think this would be an important next clinical trial: a NOAC-only for a period post procedure with no aspirin to follow. This is the next piece of information we need to complete the puzzle and for left atrial appendage closure to reach its full potential,” according to Dr. Hellig of the University of Cape Town (South Africa).
The EWOLUTION registry is sponsored by Boston Scientific. Dr. Bergmann reported serving as a consultant to Boston Scientific and Biosense Webster and receiving honoraria from more than a half-dozen pharmaceutical and device companies.
PARIS – Results of the real-world EWOLUTION registry of recipients of the Watchman device for stroke prevention provide reassuring answers to several key questions which have slowed physician uptake of the left atrial appendage closure device, Dr. Martin W. Bergmann said at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“EWOLUTION, with more than 1,000 patients, is I think the study that we’ve needed to make this intervention happen in routine practice as a procedure for stroke prevention in atrial fibrillation,” declared Dr. Bergmann of Cardiologicum Hamburg, a large German group practice.
EWOLUTION is a prospective, single-arm, multicenter registry including 1,025 recipients of the first-generation version of the Watchman, a transcatheter device for left atrial appendage closure as a means of stroke prevention in patients with atrial fibrillation (AF). These were high-risk patients: 50% of them had a CHA2DS2-VASc score of 5 or higher, and 72% of participants were deemed unsuitable for warfarin. EWOLUTION was conducted at 47 sites in Europe, the Middle East, and Russia. Dr. Bergmann presented the 3-month outcomes, a key period for device-related complications because protective epithelialization of the device isn’t yet complete. Follow-up will continue at the 1- and 2-year marks.
Among the key findings in the domain of procedural success: The rate of successful device implantation was 98.5%. A complete seal or an echocardiographic color jet of 5 mm or less at the time of implantation was achieved in 99.7% of cases, and this remained the case in 98.9% at 3 months.
With regard to safety, the stroke rate was 0.4%, device embolization occurred in 0.4%, and the pericardial effusion/tamponade rate was 0.7%, all of which are lower rates than in earlier clinical trials.
Just over 4% of patients experienced device-related adverse events with full recovery at the 3-month follow-up. These were mostly bleeding events at the groin access site. More importantly, only 0.5% of patients had device-related serious adverse events that weren’t resolved at 3 months.
“This 0.5% is a major step forward,” Dr. Bergmann said. “This includes all pericardial effusions, all device embolizations, all periprocedural strokes – everything involving the procedure that puts a patient at risk. In fact, that 0.5% risk for left atrial appendage closure with the Watchman is pretty much the same risk as if you refer your patient with AF to an electrophysiologist for pulmonary vein isolation.”
One key question answered by EWOLUTION is, do you need to be an expert in the procedure in order to get excellent results? The answer, Dr. Bergmann said, is emphatically “no.” Interventionalists at the 47 participating sites varied widely in their experience with left atrial appendage occlusion, so investigators divided the sites into quartiles based upon experience and patient volumes contributed to the registry. While cardiologists in the most experienced centers had a significantly higher rate of successful device release on the first try, the most- and least-experienced centers did equally well on the endpoint that really counts: a complete or near-complete seal of the left atrial appendage at follow-up. Complication rates didn’t differ by site experience, either.
Another important practical question that’s been holding up wider adoption of the Watchman concerns how best to handle postimplantation antithrombotic therapy. Here the EWOLUTION registry provides a partial answer: 607 patients were on dual antiplatelet therapy, 113 were on a novel anticoagulant (NOAC), 159 were on warfarin, 67 were on nothing at all, and the rest were on a single antiplatelet agent. And there was no significant difference between any of these groups in the 3-month rates of thrombus on the device, bleeding events, stroke, or other adverse events.
“The main message is there is no difference in serious adverse events between any of the drug regimens. So if you’re in a situation where you can’t give any medication to reduce stroke risk because the bleeding risk is so high, you can go for left atrial appendage closure technology and give them nothing post implant,” according to Dr. Bergmann.
He added that he’d personally try to avoid that strategy: “You want to have some coverage.”
Also noteworthy is that 113 Watchman recipients did well with 3 months of NOAC monotherapy. The appeal of that approach is the short half-life of those agents in the event of a bleeding problem.
Discussant Dr. Farrel Hellig commented that EWOLUTION demonstrates that the Watchman procedure is predictable and safe, with an impressively low complication rate even in inexperienced centers. For that, he added, kudos goes to Boston Scientific, which markets the Watchman, for rolling out an effective physician training program.
“The most important topic to discuss is bleeding, because a bleeding rate of 4.1% at 3 months is certainly not insignificant,” he continued. “It appears, firstly, from EWOLUTION that it’s safe to omit warfarin. I think the most important thing we’d like to know now is could a postprocedure NOAC be the best option, and can aspirin be eliminated in the long term?”
“Is it too early to recommend a NOAC-only for a period of time post procedure? Perhaps. But I think this would be an important next clinical trial: a NOAC-only for a period post procedure with no aspirin to follow. This is the next piece of information we need to complete the puzzle and for left atrial appendage closure to reach its full potential,” according to Dr. Hellig of the University of Cape Town (South Africa).
The EWOLUTION registry is sponsored by Boston Scientific. Dr. Bergmann reported serving as a consultant to Boston Scientific and Biosense Webster and receiving honoraria from more than a half-dozen pharmaceutical and device companies.
PARIS – Results of the real-world EWOLUTION registry of recipients of the Watchman device for stroke prevention provide reassuring answers to several key questions which have slowed physician uptake of the left atrial appendage closure device, Dr. Martin W. Bergmann said at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
“EWOLUTION, with more than 1,000 patients, is I think the study that we’ve needed to make this intervention happen in routine practice as a procedure for stroke prevention in atrial fibrillation,” declared Dr. Bergmann of Cardiologicum Hamburg, a large German group practice.
EWOLUTION is a prospective, single-arm, multicenter registry including 1,025 recipients of the first-generation version of the Watchman, a transcatheter device for left atrial appendage closure as a means of stroke prevention in patients with atrial fibrillation (AF). These were high-risk patients: 50% of them had a CHA2DS2-VASc score of 5 or higher, and 72% of participants were deemed unsuitable for warfarin. EWOLUTION was conducted at 47 sites in Europe, the Middle East, and Russia. Dr. Bergmann presented the 3-month outcomes, a key period for device-related complications because protective epithelialization of the device isn’t yet complete. Follow-up will continue at the 1- and 2-year marks.
Among the key findings in the domain of procedural success: The rate of successful device implantation was 98.5%. A complete seal or an echocardiographic color jet of 5 mm or less at the time of implantation was achieved in 99.7% of cases, and this remained the case in 98.9% at 3 months.
With regard to safety, the stroke rate was 0.4%, device embolization occurred in 0.4%, and the pericardial effusion/tamponade rate was 0.7%, all of which are lower rates than in earlier clinical trials.
Just over 4% of patients experienced device-related adverse events with full recovery at the 3-month follow-up. These were mostly bleeding events at the groin access site. More importantly, only 0.5% of patients had device-related serious adverse events that weren’t resolved at 3 months.
“This 0.5% is a major step forward,” Dr. Bergmann said. “This includes all pericardial effusions, all device embolizations, all periprocedural strokes – everything involving the procedure that puts a patient at risk. In fact, that 0.5% risk for left atrial appendage closure with the Watchman is pretty much the same risk as if you refer your patient with AF to an electrophysiologist for pulmonary vein isolation.”
One key question answered by EWOLUTION is, do you need to be an expert in the procedure in order to get excellent results? The answer, Dr. Bergmann said, is emphatically “no.” Interventionalists at the 47 participating sites varied widely in their experience with left atrial appendage occlusion, so investigators divided the sites into quartiles based upon experience and patient volumes contributed to the registry. While cardiologists in the most experienced centers had a significantly higher rate of successful device release on the first try, the most- and least-experienced centers did equally well on the endpoint that really counts: a complete or near-complete seal of the left atrial appendage at follow-up. Complication rates didn’t differ by site experience, either.
Another important practical question that’s been holding up wider adoption of the Watchman concerns how best to handle postimplantation antithrombotic therapy. Here the EWOLUTION registry provides a partial answer: 607 patients were on dual antiplatelet therapy, 113 were on a novel anticoagulant (NOAC), 159 were on warfarin, 67 were on nothing at all, and the rest were on a single antiplatelet agent. And there was no significant difference between any of these groups in the 3-month rates of thrombus on the device, bleeding events, stroke, or other adverse events.
“The main message is there is no difference in serious adverse events between any of the drug regimens. So if you’re in a situation where you can’t give any medication to reduce stroke risk because the bleeding risk is so high, you can go for left atrial appendage closure technology and give them nothing post implant,” according to Dr. Bergmann.
He added that he’d personally try to avoid that strategy: “You want to have some coverage.”
Also noteworthy is that 113 Watchman recipients did well with 3 months of NOAC monotherapy. The appeal of that approach is the short half-life of those agents in the event of a bleeding problem.
Discussant Dr. Farrel Hellig commented that EWOLUTION demonstrates that the Watchman procedure is predictable and safe, with an impressively low complication rate even in inexperienced centers. For that, he added, kudos goes to Boston Scientific, which markets the Watchman, for rolling out an effective physician training program.
“The most important topic to discuss is bleeding, because a bleeding rate of 4.1% at 3 months is certainly not insignificant,” he continued. “It appears, firstly, from EWOLUTION that it’s safe to omit warfarin. I think the most important thing we’d like to know now is could a postprocedure NOAC be the best option, and can aspirin be eliminated in the long term?”
“Is it too early to recommend a NOAC-only for a period of time post procedure? Perhaps. But I think this would be an important next clinical trial: a NOAC-only for a period post procedure with no aspirin to follow. This is the next piece of information we need to complete the puzzle and for left atrial appendage closure to reach its full potential,” according to Dr. Hellig of the University of Cape Town (South Africa).
The EWOLUTION registry is sponsored by Boston Scientific. Dr. Bergmann reported serving as a consultant to Boston Scientific and Biosense Webster and receiving honoraria from more than a half-dozen pharmaceutical and device companies.
AT EUROPCR 2016
Key clinical point: You don’t have to be an expert at implanting the Watchman left atrial appendage closure device to achieve the same sort of sky-high procedural success and low complication rates the experts do.
Major finding: The Watchman device successfully sealed off the left atrial appendage in 98.9% of cases at 3 months follow-up, with rates closely similar at the least- and most-experienced centers.
Data source: EWOLUTION is a prospective, multicenter, real-world registry of 1,025 recipients of the Watchman left atrial appendage closure device at 47 sites in Europe, the Middle East, and Russia.
Disclosures: The EWOLUTION registry is sponsored by Boston Scientific. The presenter reported serving as a consultant to Boston Scientific and Biosense Webster and receiving honoraria from more than a half-dozen pharmaceutical and device companies.

VIDEO: EVLP may extend lung preservation, quality for transplants
BALTIMORE – The use of ex vivo lung perfusion (EVLP) may allow for the safe transplantation of lungs preserved for more than 12 hours, according to a study presented at the annual meeting of the American Association for Thoracic Surgery.
A research team at the University of Toronto evaluated the outcomes of transplant patients who received a lung with a preservation time of over 12 hours between January 2006 and April 2015 and compared them to the general lung transplant population. Median hospital and ICU length of stay were similar between the two groups, and Kaplan-Meier survival curves between the two groups did not show any difference. Preservation time, donor PO2, and use of EVLP were not significant variables affecting survival.
Dr. Bartley P. Griffith, chief of cardiac surgery at the University of Maryland, Baltimore, and a discussant on the paper at the meeting, said that the findings of the study open up the possibility of a more “planned” approach to transplantation.
“Anything that not only extends preservation time, but perhaps even improves quality of preservation, would be a godsend,” Dr. Griffith said in a video interview. He cautioned that the “devil is in the details,” and that the data had to be examined closely. Nevertheless, Dr. Griffith said transplant surgeons should be grateful for the important work done by the University of Toronto team.
Dr. Griffith reported no relevant financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @richpizzi
BALTIMORE – The use of ex vivo lung perfusion (EVLP) may allow for the safe transplantation of lungs preserved for more than 12 hours, according to a study presented at the annual meeting of the American Association for Thoracic Surgery.
A research team at the University of Toronto evaluated the outcomes of transplant patients who received a lung with a preservation time of over 12 hours between January 2006 and April 2015 and compared them to the general lung transplant population. Median hospital and ICU length of stay were similar between the two groups, and Kaplan-Meier survival curves between the two groups did not show any difference. Preservation time, donor PO2, and use of EVLP were not significant variables affecting survival.
Dr. Bartley P. Griffith, chief of cardiac surgery at the University of Maryland, Baltimore, and a discussant on the paper at the meeting, said that the findings of the study open up the possibility of a more “planned” approach to transplantation.
“Anything that not only extends preservation time, but perhaps even improves quality of preservation, would be a godsend,” Dr. Griffith said in a video interview. He cautioned that the “devil is in the details,” and that the data had to be examined closely. Nevertheless, Dr. Griffith said transplant surgeons should be grateful for the important work done by the University of Toronto team.
Dr. Griffith reported no relevant financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @richpizzi
BALTIMORE – The use of ex vivo lung perfusion (EVLP) may allow for the safe transplantation of lungs preserved for more than 12 hours, according to a study presented at the annual meeting of the American Association for Thoracic Surgery.
A research team at the University of Toronto evaluated the outcomes of transplant patients who received a lung with a preservation time of over 12 hours between January 2006 and April 2015 and compared them to the general lung transplant population. Median hospital and ICU length of stay were similar between the two groups, and Kaplan-Meier survival curves between the two groups did not show any difference. Preservation time, donor PO2, and use of EVLP were not significant variables affecting survival.
Dr. Bartley P. Griffith, chief of cardiac surgery at the University of Maryland, Baltimore, and a discussant on the paper at the meeting, said that the findings of the study open up the possibility of a more “planned” approach to transplantation.
“Anything that not only extends preservation time, but perhaps even improves quality of preservation, would be a godsend,” Dr. Griffith said in a video interview. He cautioned that the “devil is in the details,” and that the data had to be examined closely. Nevertheless, Dr. Griffith said transplant surgeons should be grateful for the important work done by the University of Toronto team.
Dr. Griffith reported no relevant financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @richpizzi
AT THE AATS ANNUAL MEETING
Repeat SICU admissions should trigger palliative care consult
ICU readmission was most predictive of the need for palliative care among patients in the surgical intensive care unit, based on a study of six potential trigger criteria associated with in-hospital death or discharge to hospice.
To facilitate proactive case findings of patients who would benefit from a palliative care consult, a team of surgical ICU and palliative care clinicians at the Icahn School of Medicine at Mount Sinai, N.Y., developed and tested a system of palliative care triggers. The study was published online in the Journal of Critical Care (http://dx.doi.org/10.1016/j.jcrc.2016.04.010).
Based on a literature review, the researchers created a six-item list of potential triggers for palliative care: length of stay over 10 days, ICU readmission, intensivist referral, status post cardiac arrest, metastatic cancer, and a match of two or more on a set of secondary criteria.

Data were collected for the period from Sept. 4, 2013, through May 30, 2014, at the surgical ICU of a 1,170-bed tertiary medical center. Patients who received a palliative care consultation were compared with those who did not, and the trigger list was tested for accuracy in predicting patient outcomes. The primary outcomes were hospital death, hospice discharge, and a combined endpoint of these two outcomes. Patients who died in the hospital or were released to hospice care were assumed to be those most in need of a palliative care consult.
Bivariate analysis was done to calculate the unadjusted odds ratios of individual triggers to each of these outcomes. Then, the team used logistic regression analysis to calculate the adjusted odds ratios of triggers to outcomes.
Of the 512 patients admitted to the SICU in the study period, those not discharged by the end of the study were excluded, leaving 492 patients in the study.
Bivariate analysis found that all of the triggers were significantly associated with in-hospital death. With the multivariate analysis and adjusted odds ratios, SICU readmission, status post cardiac arrest, metastatic cancer, and secondary triggers were significantly associated with hospital death.
For the combined outcome of hospital death or release to hospice care, the relationships were stronger. In particular, repeat SICU readmissions and metastatic cancer triggers were strongly associated with the combined outcome (odds ratio, 19.41, CI 5.81-54.86 and OR, 16.40, CI 4.69-57.36, respectively). The secondary triggers did not show the same strength of association, although they were associated significantly with the combined outcome (OR, 4.41, CI 2.05-9.53).
The most prominent finding is the strength of repeat SICU admissions with the hospital death or release to hospice. The strong relationship between repeat SICU admission and outcomes led the researchers to conclude “that one might consider adapting this clinical criterion as a standalone criterion. This would require all patients who are readmitted to the SICU to be seen by palliative care to assess their overall goals of care and understanding of their serious illness. This approach may be particularly useful for smaller palliative care teams that do not have the resources to screen daily with a series of triggers.”
The American Federation of Aging Research and the National Institute on Aging funded the study.
ICU readmission was most predictive of the need for palliative care among patients in the surgical intensive care unit, based on a study of six potential trigger criteria associated with in-hospital death or discharge to hospice.
To facilitate proactive case findings of patients who would benefit from a palliative care consult, a team of surgical ICU and palliative care clinicians at the Icahn School of Medicine at Mount Sinai, N.Y., developed and tested a system of palliative care triggers. The study was published online in the Journal of Critical Care (http://dx.doi.org/10.1016/j.jcrc.2016.04.010).
Based on a literature review, the researchers created a six-item list of potential triggers for palliative care: length of stay over 10 days, ICU readmission, intensivist referral, status post cardiac arrest, metastatic cancer, and a match of two or more on a set of secondary criteria.
Data were collected for the period from Sept. 4, 2013, through May 30, 2014, at the surgical ICU of a 1,170-bed tertiary medical center. Patients who received a palliative care consultation were compared with those who did not, and the trigger list was tested for accuracy in predicting patient outcomes. The primary outcomes were hospital death, hospice discharge, and a combined endpoint of these two outcomes. Patients who died in the hospital or were released to hospice care were assumed to be those most in need of a palliative care consult.
Bivariate analysis was done to calculate the unadjusted odds ratios of individual triggers to each of these outcomes. Then, the team used logistic regression analysis to calculate the adjusted odds ratios of triggers to outcomes.
Of the 512 patients admitted to the SICU in the study period, those not discharged by the end of the study were excluded, leaving 492 patients in the study.
Bivariate analysis found that all of the triggers were significantly associated with in-hospital death. With the multivariate analysis and adjusted odds ratios, SICU readmission, status post cardiac arrest, metastatic cancer, and secondary triggers were significantly associated with hospital death.
For the combined outcome of hospital death or release to hospice care, the relationships were stronger. In particular, repeat SICU readmissions and metastatic cancer triggers were strongly associated with the combined outcome (odds ratio, 19.41, CI 5.81-54.86 and OR, 16.40, CI 4.69-57.36, respectively). The secondary triggers did not show the same strength of association, although they were associated significantly with the combined outcome (OR, 4.41, CI 2.05-9.53).
The most prominent finding is the strength of repeat SICU admissions with the hospital death or release to hospice. The strong relationship between repeat SICU admission and outcomes led the researchers to conclude “that one might consider adapting this clinical criterion as a standalone criterion. This would require all patients who are readmitted to the SICU to be seen by palliative care to assess their overall goals of care and understanding of their serious illness. This approach may be particularly useful for smaller palliative care teams that do not have the resources to screen daily with a series of triggers.”
The American Federation of Aging Research and the National Institute on Aging funded the study.
ICU readmission was most predictive of the need for palliative care among patients in the surgical intensive care unit, based on a study of six potential trigger criteria associated with in-hospital death or discharge to hospice.
To facilitate proactive case findings of patients who would benefit from a palliative care consult, a team of surgical ICU and palliative care clinicians at the Icahn School of Medicine at Mount Sinai, N.Y., developed and tested a system of palliative care triggers. The study was published online in the Journal of Critical Care (http://dx.doi.org/10.1016/j.jcrc.2016.04.010).
Based on a literature review, the researchers created a six-item list of potential triggers for palliative care: length of stay over 10 days, ICU readmission, intensivist referral, status post cardiac arrest, metastatic cancer, and a match of two or more on a set of secondary criteria.
Data were collected for the period from Sept. 4, 2013, through May 30, 2014, at the surgical ICU of a 1,170-bed tertiary medical center. Patients who received a palliative care consultation were compared with those who did not, and the trigger list was tested for accuracy in predicting patient outcomes. The primary outcomes were hospital death, hospice discharge, and a combined endpoint of these two outcomes. Patients who died in the hospital or were released to hospice care were assumed to be those most in need of a palliative care consult.
Bivariate analysis was done to calculate the unadjusted odds ratios of individual triggers to each of these outcomes. Then, the team used logistic regression analysis to calculate the adjusted odds ratios of triggers to outcomes.
Of the 512 patients admitted to the SICU in the study period, those not discharged by the end of the study were excluded, leaving 492 patients in the study.
Bivariate analysis found that all of the triggers were significantly associated with in-hospital death. With the multivariate analysis and adjusted odds ratios, SICU readmission, status post cardiac arrest, metastatic cancer, and secondary triggers were significantly associated with hospital death.
For the combined outcome of hospital death or release to hospice care, the relationships were stronger. In particular, repeat SICU readmissions and metastatic cancer triggers were strongly associated with the combined outcome (odds ratio, 19.41, CI 5.81-54.86 and OR, 16.40, CI 4.69-57.36, respectively). The secondary triggers did not show the same strength of association, although they were associated significantly with the combined outcome (OR, 4.41, CI 2.05-9.53).
The most prominent finding is the strength of repeat SICU admissions with the hospital death or release to hospice. The strong relationship between repeat SICU admission and outcomes led the researchers to conclude “that one might consider adapting this clinical criterion as a standalone criterion. This would require all patients who are readmitted to the SICU to be seen by palliative care to assess their overall goals of care and understanding of their serious illness. This approach may be particularly useful for smaller palliative care teams that do not have the resources to screen daily with a series of triggers.”
The American Federation of Aging Research and the National Institute on Aging funded the study.
FROM THE JOURNAL OF CRITICAL CARE
Key clinical point: A list of tested triggers can predict the need of surgical ICU patients for a palliative care consultation.
Major finding: Readmission to the surgical ICU was strongly associated with the study endpoint of hospital death or release to hospice (odds ratio 19.41, CI 5.81-54.86).
Data source: A case review of all 492 patients admitted to the surgical intensive care facility at a 1,170-bed, tertiary care medical center.
Disclosures: The American Federation of Aging Research and the National Institute on Aging funded the study.

Resection of recurrence shows survival benefit for adrenocortical carcinoma
BALTIMORE – Patients who have recurrent adrenocortical carcinoma appear to have one option to increase their survival: surgery that includes complete tumor resection – but it may a viable path only if the recurrence occurred a year or more after the initial resection and diagnosis, according to an retrospective study of patients at five French university hospitals. “Adrenocortical carcinoma (ACC) is a rare, malignant tumor that has a poor prognosis, and recurrence of the tumor is considerable with 75% recurrence at 5 years,” Dr. Claire Blanchard of the Digestive and Endocrine Surgery Clinic at the Central University Hospital, Nantes, France, reported at the annual meeting of the American Association of Endocrine Surgeons. “Complete resection of recurrence is the only curative treatment.”
The researchers conducted a retrospective study of patients with at least one recurrence, diagnosed between 1980 and 2014, after initial resection of ACC, comparing outcomes in 29 patients who underwent surgery with 30 who had non-operative treatment, mainly chemotherapy and radiation.

Patients who had an operation for recurrence more often had local recurrence, 75% vs. 10% in the nonoperative group, and more frequently had a unique site of recurrence, 97% vs. 45%, than the nonoperative patients, Dr. Blanchard said.
These other demographic and tumor characteristics were similar between the operative and nonoperative groups, respectively: age, 49 years and 53 years; gender, 63% and 79% female; Weiss score, 6 and 7; Ki-67 protein index, 23% and 24%; tumor size, 99.2 mm and 115.5 mm; ENSAT stage, 65% and 45% stages I and II; and R0 resection status of the primary tumor at initial surgery, 83% and 71%.
The univariate analysis showed that appearance of the first recurrence more than 12 months after the initial diagnosis increased a patient’s chance of survival after treatment for recurrence, Dr. Blanchard said.
“Recurrences occurred at median delay of 12 months after the initial surgery,” Dr. Blanchard said. “In the 59 patients, 24 had local recurrences and 35 had distant metastases.”
Overall median survival after the first recurrence was 91 months for patients who had surgery vs. 15 months for those who did not. Overall median survival after initial resection of the primary tumor was 133 months, with a range of 14 to 252 months, in operated patients vs. 32 months, ranging from 21 to 43 months, in those who had no surgery, Dr. Blanchard said.
Of the 29 surgery patients in the surgery group, 22 had local-regional resections, 6 of whom had adjunctive radiation of the tumor bed.
“The type of resection in recurrent ACC depends on the location of the recurrence,” senior coauthor Dr. Eric Mirallié said. “In the case of local recurrence, we resected the adrenalectomy bed and all the adjacent invaded organs.”
In this series, 6 patients had resection of the tumor bed and 16 had adjacent organ resections; 8 patients (28%) had two or more operations for recurrences. These operations involved eight splenectomies, seven resections for abdominal nodules, six nephrectomies, three distal pancreatectomies, three segmental colectomies, and two minor hepatectomies. All operations were by laparotomy.
“In cases of distant recurrence, complete metastasectomy was performed,” Dr. Mirallié said. The series reported two right hepatectomies, one liver tumorectomy, one lung tumorectomy, and one brain tumorectomy.
“Nonoperative management is reserved for nonresectable patients with recurrent adrenocortical carcinoma,” Dr. Mirallié said. “Oral chemotherapy like mitotane was always given when possible. In cases of nonresectable local recurrence, radiotherapy can be used.”
During the discussion, Dr. Bradford K. Mitchell of Michigan State University, East Lansing, said that the benefit of improved survival in surgical patients in the study may have been a function of selection bias as patients who were not operated on may have had more advanced disease.
Dr. Blanchard and her coauthors had no financial relationships to disclose.
BALTIMORE – Patients who have recurrent adrenocortical carcinoma appear to have one option to increase their survival: surgery that includes complete tumor resection – but it may a viable path only if the recurrence occurred a year or more after the initial resection and diagnosis, according to an retrospective study of patients at five French university hospitals. “Adrenocortical carcinoma (ACC) is a rare, malignant tumor that has a poor prognosis, and recurrence of the tumor is considerable with 75% recurrence at 5 years,” Dr. Claire Blanchard of the Digestive and Endocrine Surgery Clinic at the Central University Hospital, Nantes, France, reported at the annual meeting of the American Association of Endocrine Surgeons. “Complete resection of recurrence is the only curative treatment.”
The researchers conducted a retrospective study of patients with at least one recurrence, diagnosed between 1980 and 2014, after initial resection of ACC, comparing outcomes in 29 patients who underwent surgery with 30 who had non-operative treatment, mainly chemotherapy and radiation.
Patients who had an operation for recurrence more often had local recurrence, 75% vs. 10% in the nonoperative group, and more frequently had a unique site of recurrence, 97% vs. 45%, than the nonoperative patients, Dr. Blanchard said.
These other demographic and tumor characteristics were similar between the operative and nonoperative groups, respectively: age, 49 years and 53 years; gender, 63% and 79% female; Weiss score, 6 and 7; Ki-67 protein index, 23% and 24%; tumor size, 99.2 mm and 115.5 mm; ENSAT stage, 65% and 45% stages I and II; and R0 resection status of the primary tumor at initial surgery, 83% and 71%.
The univariate analysis showed that appearance of the first recurrence more than 12 months after the initial diagnosis increased a patient’s chance of survival after treatment for recurrence, Dr. Blanchard said.
“Recurrences occurred at median delay of 12 months after the initial surgery,” Dr. Blanchard said. “In the 59 patients, 24 had local recurrences and 35 had distant metastases.”
Overall median survival after the first recurrence was 91 months for patients who had surgery vs. 15 months for those who did not. Overall median survival after initial resection of the primary tumor was 133 months, with a range of 14 to 252 months, in operated patients vs. 32 months, ranging from 21 to 43 months, in those who had no surgery, Dr. Blanchard said.
Of the 29 surgery patients in the surgery group, 22 had local-regional resections, 6 of whom had adjunctive radiation of the tumor bed.
“The type of resection in recurrent ACC depends on the location of the recurrence,” senior coauthor Dr. Eric Mirallié said. “In the case of local recurrence, we resected the adrenalectomy bed and all the adjacent invaded organs.”
In this series, 6 patients had resection of the tumor bed and 16 had adjacent organ resections; 8 patients (28%) had two or more operations for recurrences. These operations involved eight splenectomies, seven resections for abdominal nodules, six nephrectomies, three distal pancreatectomies, three segmental colectomies, and two minor hepatectomies. All operations were by laparotomy.
“In cases of distant recurrence, complete metastasectomy was performed,” Dr. Mirallié said. The series reported two right hepatectomies, one liver tumorectomy, one lung tumorectomy, and one brain tumorectomy.
“Nonoperative management is reserved for nonresectable patients with recurrent adrenocortical carcinoma,” Dr. Mirallié said. “Oral chemotherapy like mitotane was always given when possible. In cases of nonresectable local recurrence, radiotherapy can be used.”
During the discussion, Dr. Bradford K. Mitchell of Michigan State University, East Lansing, said that the benefit of improved survival in surgical patients in the study may have been a function of selection bias as patients who were not operated on may have had more advanced disease.
Dr. Blanchard and her coauthors had no financial relationships to disclose.
BALTIMORE – Patients who have recurrent adrenocortical carcinoma appear to have one option to increase their survival: surgery that includes complete tumor resection – but it may a viable path only if the recurrence occurred a year or more after the initial resection and diagnosis, according to an retrospective study of patients at five French university hospitals. “Adrenocortical carcinoma (ACC) is a rare, malignant tumor that has a poor prognosis, and recurrence of the tumor is considerable with 75% recurrence at 5 years,” Dr. Claire Blanchard of the Digestive and Endocrine Surgery Clinic at the Central University Hospital, Nantes, France, reported at the annual meeting of the American Association of Endocrine Surgeons. “Complete resection of recurrence is the only curative treatment.”
The researchers conducted a retrospective study of patients with at least one recurrence, diagnosed between 1980 and 2014, after initial resection of ACC, comparing outcomes in 29 patients who underwent surgery with 30 who had non-operative treatment, mainly chemotherapy and radiation.
Patients who had an operation for recurrence more often had local recurrence, 75% vs. 10% in the nonoperative group, and more frequently had a unique site of recurrence, 97% vs. 45%, than the nonoperative patients, Dr. Blanchard said.
These other demographic and tumor characteristics were similar between the operative and nonoperative groups, respectively: age, 49 years and 53 years; gender, 63% and 79% female; Weiss score, 6 and 7; Ki-67 protein index, 23% and 24%; tumor size, 99.2 mm and 115.5 mm; ENSAT stage, 65% and 45% stages I and II; and R0 resection status of the primary tumor at initial surgery, 83% and 71%.
The univariate analysis showed that appearance of the first recurrence more than 12 months after the initial diagnosis increased a patient’s chance of survival after treatment for recurrence, Dr. Blanchard said.
“Recurrences occurred at median delay of 12 months after the initial surgery,” Dr. Blanchard said. “In the 59 patients, 24 had local recurrences and 35 had distant metastases.”
Overall median survival after the first recurrence was 91 months for patients who had surgery vs. 15 months for those who did not. Overall median survival after initial resection of the primary tumor was 133 months, with a range of 14 to 252 months, in operated patients vs. 32 months, ranging from 21 to 43 months, in those who had no surgery, Dr. Blanchard said.
Of the 29 surgery patients in the surgery group, 22 had local-regional resections, 6 of whom had adjunctive radiation of the tumor bed.
“The type of resection in recurrent ACC depends on the location of the recurrence,” senior coauthor Dr. Eric Mirallié said. “In the case of local recurrence, we resected the adrenalectomy bed and all the adjacent invaded organs.”
In this series, 6 patients had resection of the tumor bed and 16 had adjacent organ resections; 8 patients (28%) had two or more operations for recurrences. These operations involved eight splenectomies, seven resections for abdominal nodules, six nephrectomies, three distal pancreatectomies, three segmental colectomies, and two minor hepatectomies. All operations were by laparotomy.
“In cases of distant recurrence, complete metastasectomy was performed,” Dr. Mirallié said. The series reported two right hepatectomies, one liver tumorectomy, one lung tumorectomy, and one brain tumorectomy.
“Nonoperative management is reserved for nonresectable patients with recurrent adrenocortical carcinoma,” Dr. Mirallié said. “Oral chemotherapy like mitotane was always given when possible. In cases of nonresectable local recurrence, radiotherapy can be used.”
During the discussion, Dr. Bradford K. Mitchell of Michigan State University, East Lansing, said that the benefit of improved survival in surgical patients in the study may have been a function of selection bias as patients who were not operated on may have had more advanced disease.
Dr. Blanchard and her coauthors had no financial relationships to disclose.
AT AAES 2016
Key clinical point: Surgery carries a significant survival benefit in patients with recurrent adrenocortical carcinoma (ACC).
Major finding: Overall median survival after the first recurrence was 91 months in patients who had surgery vs. 32 months in those who did not.
Data source: Retrospective case-control study of 59 patients at five French teaching hospitals who had treatment for recurrent ACC from 1980-2014.
Disclosures: Dr. Blanchard and her coauthors reported having no financial disclosures.

Histologic examination of anastomotic stapler doughnuts may not yield clinical benefit
LOS ANGELES – A multicenter of patients who had low anterior resection with stapled anastomosis for rectal cancer found no clinical or economic benefit in routinely sending anastomotic doughnuts for histopathological evaluation.
“Several small studies outside the United States have found no benefit in histologic examination of anastomotic stapler doughnuts,” lead study author Dr. Jeremy Sugrue said at the annual meeting of the American Society of Colon and Rectal Surgeons. “We wanted to see if this held true in our population.”

Dr. Sugrue, of the division of colon and rectal surgery in the department of surgery at the University of Illinois at Chicago, and his associates performed a retrospective review of 486 patients who underwent a low anterior resection with stapled anastomosis for rectal cancer between 2002 and 2015 at three medical institutions. The primary outcome was pathologic findings in the doughnuts and their impact on patient management. Secondary outcomes included tumor characteristics that may influence how often a surgeon may send a doughnut to pathology, along with approximate cost.
The mean age of the 486 patients was 60 years, 55% were male, and the mean gross distal margin of the primary tumor specimen was 2.9 cm. “The majority of tumors were located in the middle rectum, and the rest were evenly distributed between the lower rectum, upper rectum, and rectosigmoid regions,” said Dr. Sugrue, who is a general surgery resident. About half of the patients received neoadjuvant radiation or chemotherapy.
Benign findings were found in 33 patients. Among these, 16 had inflammatory changes, including 12 who had nonspecific changes, 3 who had changes from radiation, and 1 had inflammatory bowel disease changes. In addition, 13 patients with benign findings had polyps in their doughnuts (10 hyperplastic and 3 adenomatous), while 4 patients had miscellaneous changes including two cases of vessel micro calcification, one case of diverticuli, and one case of melanosis coli.
Among the 412 patients with malignant findings, 410 (99.5%) had no cancer in the doughnuts and no cancer at the distal resection margin in the primary tumor specimens. “In the two patients where we found cancer in the doughnuts, these patients also had a positive distal margin,” Dr. Sugrue said. “We did not find any patients with a positive distal margin and a negative doughnut. Likewise, we did not find any patients with a negative distal margin or an unexpectedly positive doughnut.”
The researchers also found that patients with low rectal tumors were significantly more likely to have their doughnut sent to pathology, compared with those with rectosigmoid tumors. “However, when we looked at distal margin comparing patients who had doughnuts reported on pathology with those who did not, there was no statistically significant difference,” Dr. Sugrue said. After averaging pathology professional fees and technical fees across all three institutions, he and his associates determined that doughnuts add $643 in cost when processed by pathology as a unique specimen.
Limitations of the study, he said, include its retrospective design, “which inherently introduces selection bias, and we did not perform a precise cost-benefit analysis.”
Dr. Sugrue reported having no financial disclosures.
LOS ANGELES – A multicenter of patients who had low anterior resection with stapled anastomosis for rectal cancer found no clinical or economic benefit in routinely sending anastomotic doughnuts for histopathological evaluation.
“Several small studies outside the United States have found no benefit in histologic examination of anastomotic stapler doughnuts,” lead study author Dr. Jeremy Sugrue said at the annual meeting of the American Society of Colon and Rectal Surgeons. “We wanted to see if this held true in our population.”
Dr. Sugrue, of the division of colon and rectal surgery in the department of surgery at the University of Illinois at Chicago, and his associates performed a retrospective review of 486 patients who underwent a low anterior resection with stapled anastomosis for rectal cancer between 2002 and 2015 at three medical institutions. The primary outcome was pathologic findings in the doughnuts and their impact on patient management. Secondary outcomes included tumor characteristics that may influence how often a surgeon may send a doughnut to pathology, along with approximate cost.
The mean age of the 486 patients was 60 years, 55% were male, and the mean gross distal margin of the primary tumor specimen was 2.9 cm. “The majority of tumors were located in the middle rectum, and the rest were evenly distributed between the lower rectum, upper rectum, and rectosigmoid regions,” said Dr. Sugrue, who is a general surgery resident. About half of the patients received neoadjuvant radiation or chemotherapy.
Benign findings were found in 33 patients. Among these, 16 had inflammatory changes, including 12 who had nonspecific changes, 3 who had changes from radiation, and 1 had inflammatory bowel disease changes. In addition, 13 patients with benign findings had polyps in their doughnuts (10 hyperplastic and 3 adenomatous), while 4 patients had miscellaneous changes including two cases of vessel micro calcification, one case of diverticuli, and one case of melanosis coli.
Among the 412 patients with malignant findings, 410 (99.5%) had no cancer in the doughnuts and no cancer at the distal resection margin in the primary tumor specimens. “In the two patients where we found cancer in the doughnuts, these patients also had a positive distal margin,” Dr. Sugrue said. “We did not find any patients with a positive distal margin and a negative doughnut. Likewise, we did not find any patients with a negative distal margin or an unexpectedly positive doughnut.”
The researchers also found that patients with low rectal tumors were significantly more likely to have their doughnut sent to pathology, compared with those with rectosigmoid tumors. “However, when we looked at distal margin comparing patients who had doughnuts reported on pathology with those who did not, there was no statistically significant difference,” Dr. Sugrue said. After averaging pathology professional fees and technical fees across all three institutions, he and his associates determined that doughnuts add $643 in cost when processed by pathology as a unique specimen.
Limitations of the study, he said, include its retrospective design, “which inherently introduces selection bias, and we did not perform a precise cost-benefit analysis.”
Dr. Sugrue reported having no financial disclosures.
LOS ANGELES – A multicenter of patients who had low anterior resection with stapled anastomosis for rectal cancer found no clinical or economic benefit in routinely sending anastomotic doughnuts for histopathological evaluation.
“Several small studies outside the United States have found no benefit in histologic examination of anastomotic stapler doughnuts,” lead study author Dr. Jeremy Sugrue said at the annual meeting of the American Society of Colon and Rectal Surgeons. “We wanted to see if this held true in our population.”
Dr. Sugrue, of the division of colon and rectal surgery in the department of surgery at the University of Illinois at Chicago, and his associates performed a retrospective review of 486 patients who underwent a low anterior resection with stapled anastomosis for rectal cancer between 2002 and 2015 at three medical institutions. The primary outcome was pathologic findings in the doughnuts and their impact on patient management. Secondary outcomes included tumor characteristics that may influence how often a surgeon may send a doughnut to pathology, along with approximate cost.
The mean age of the 486 patients was 60 years, 55% were male, and the mean gross distal margin of the primary tumor specimen was 2.9 cm. “The majority of tumors were located in the middle rectum, and the rest were evenly distributed between the lower rectum, upper rectum, and rectosigmoid regions,” said Dr. Sugrue, who is a general surgery resident. About half of the patients received neoadjuvant radiation or chemotherapy.
Benign findings were found in 33 patients. Among these, 16 had inflammatory changes, including 12 who had nonspecific changes, 3 who had changes from radiation, and 1 had inflammatory bowel disease changes. In addition, 13 patients with benign findings had polyps in their doughnuts (10 hyperplastic and 3 adenomatous), while 4 patients had miscellaneous changes including two cases of vessel micro calcification, one case of diverticuli, and one case of melanosis coli.
Among the 412 patients with malignant findings, 410 (99.5%) had no cancer in the doughnuts and no cancer at the distal resection margin in the primary tumor specimens. “In the two patients where we found cancer in the doughnuts, these patients also had a positive distal margin,” Dr. Sugrue said. “We did not find any patients with a positive distal margin and a negative doughnut. Likewise, we did not find any patients with a negative distal margin or an unexpectedly positive doughnut.”
The researchers also found that patients with low rectal tumors were significantly more likely to have their doughnut sent to pathology, compared with those with rectosigmoid tumors. “However, when we looked at distal margin comparing patients who had doughnuts reported on pathology with those who did not, there was no statistically significant difference,” Dr. Sugrue said. After averaging pathology professional fees and technical fees across all three institutions, he and his associates determined that doughnuts add $643 in cost when processed by pathology as a unique specimen.
Limitations of the study, he said, include its retrospective design, “which inherently introduces selection bias, and we did not perform a precise cost-benefit analysis.”
Dr. Sugrue reported having no financial disclosures.
AT THE ASCRS ANNUAL MEETING
Key clinical point: The routine histologic examination of anastomotic doughnuts at lower anterior resection for rectal cancer has no clinical benefit.
Major finding: Of the 412 patients with anastomotic doughnuts included in their pathology reports, only 2 had cancer cells in their doughnuts and both of these patients also had a positive distal margin in their primary tumor specimen.
Data source: A retrospective review of 486 patients who underwent a low anterior resection with stapled anastomosis for rectal cancer between 2002 and 2015 at three medical institutions.
Disclosures: Dr. Sugrue reported having no financial disclosures.

General surgeons each generate $2.17 million for hospitals
General surgeons are generating 16.6% more revenue for hospitals in 2015 than they did in 2012, according to a survey by physician recruitment firm Merritt Hawkins.
In 2015, general surgeons generated an average of $2.17 million in net revenue for their affiliated hospitals, compared with $1.86 million in 2012, when Merritt Hawkins last conducted its survey of hospital chief financial officers.
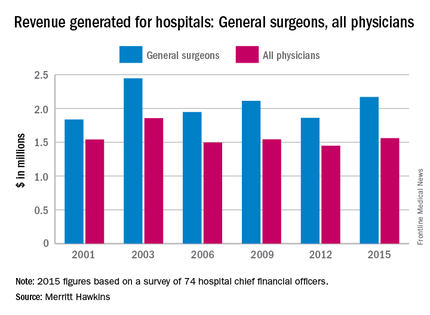
Of the 18 specialties included in the survey, only orthopedic surgeons ($2.75 million), invasive cardiologists ($2.448 million), and neurosurgeons ($2.446 million), produced more revenue than did general surgeons. Net revenue generated by physicians in all 18 specialties averaged $1.56 million in 2015, which was up 7.7% over the $1.45 million generated in 2012. Average revenue for specialists was up 12.8%, going from $1.42 million in 2012 to $1.61 million in 2015, the survey showed.
The survey (available for download here) was completed by 74 hospital chief financial officers. Despite the small number, Merritt Hawkins said that the “results are reliable and accurate, in large part because the overall number for average annual revenue generated by all physician specialties for their affiliated hospitals has remained virtually unchanged” over the course of six surveys spanning 14 years.
General surgeons are generating 16.6% more revenue for hospitals in 2015 than they did in 2012, according to a survey by physician recruitment firm Merritt Hawkins.
In 2015, general surgeons generated an average of $2.17 million in net revenue for their affiliated hospitals, compared with $1.86 million in 2012, when Merritt Hawkins last conducted its survey of hospital chief financial officers.
Of the 18 specialties included in the survey, only orthopedic surgeons ($2.75 million), invasive cardiologists ($2.448 million), and neurosurgeons ($2.446 million), produced more revenue than did general surgeons. Net revenue generated by physicians in all 18 specialties averaged $1.56 million in 2015, which was up 7.7% over the $1.45 million generated in 2012. Average revenue for specialists was up 12.8%, going from $1.42 million in 2012 to $1.61 million in 2015, the survey showed.
The survey (available for download here) was completed by 74 hospital chief financial officers. Despite the small number, Merritt Hawkins said that the “results are reliable and accurate, in large part because the overall number for average annual revenue generated by all physician specialties for their affiliated hospitals has remained virtually unchanged” over the course of six surveys spanning 14 years.
General surgeons are generating 16.6% more revenue for hospitals in 2015 than they did in 2012, according to a survey by physician recruitment firm Merritt Hawkins.
In 2015, general surgeons generated an average of $2.17 million in net revenue for their affiliated hospitals, compared with $1.86 million in 2012, when Merritt Hawkins last conducted its survey of hospital chief financial officers.
Of the 18 specialties included in the survey, only orthopedic surgeons ($2.75 million), invasive cardiologists ($2.448 million), and neurosurgeons ($2.446 million), produced more revenue than did general surgeons. Net revenue generated by physicians in all 18 specialties averaged $1.56 million in 2015, which was up 7.7% over the $1.45 million generated in 2012. Average revenue for specialists was up 12.8%, going from $1.42 million in 2012 to $1.61 million in 2015, the survey showed.
The survey (available for download here) was completed by 74 hospital chief financial officers. Despite the small number, Merritt Hawkins said that the “results are reliable and accurate, in large part because the overall number for average annual revenue generated by all physician specialties for their affiliated hospitals has remained virtually unchanged” over the course of six surveys spanning 14 years.
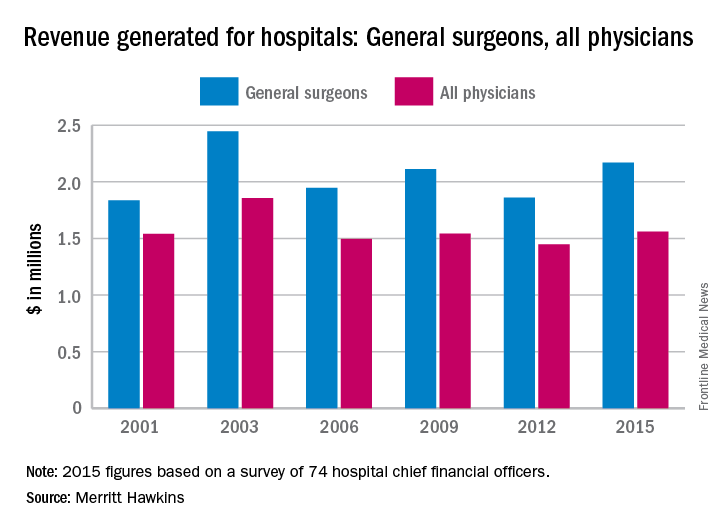
VIDEO: Identifying patients who will benefit from pulmonary metastasectomy
BALTIMORE – New research from Memorial Sloan Kettering Cancer Center in New York could help surgeons better determine which patients with soft tissue sarcoma may benefit most from pulmonary metastasectomy.
The results of the research, presented at the annual meeting of the American Association for Thoracic Surgery, suggest that preoperative factors such as primary tumor histology and size, number of metastases, time from initial resection of the primary, absence of extrapulmonary disease, and thoracoscopic resection are associated with improved survival in STS patients.
Dr. Garrett L. Walsh, professor of surgery at the University of Texas MD Anderson Cancer Center, Houston, and a discussant on the paper at the meeting, said the study was important because it showed the power of a prospective surgical database, retrospectively viewed in this particular case. He said that the Sloan Kettering research was likely “as good as it’s going to get,” given that a randomized controlled trial is unlikely ever to occur with STS patients.
“Trying to select the patients we think are going to do well with surgery has always been one of the challenging aspects of thoracic surgery,” Dr. Walsh said in a video interview. “This paper may help with better selection of patients from that large cohort who are referred to us for pulmonary metastasectomy.”
Dr. Walsh reported no relevant financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @richpizzi
BALTIMORE – New research from Memorial Sloan Kettering Cancer Center in New York could help surgeons better determine which patients with soft tissue sarcoma may benefit most from pulmonary metastasectomy.
The results of the research, presented at the annual meeting of the American Association for Thoracic Surgery, suggest that preoperative factors such as primary tumor histology and size, number of metastases, time from initial resection of the primary, absence of extrapulmonary disease, and thoracoscopic resection are associated with improved survival in STS patients.
Dr. Garrett L. Walsh, professor of surgery at the University of Texas MD Anderson Cancer Center, Houston, and a discussant on the paper at the meeting, said the study was important because it showed the power of a prospective surgical database, retrospectively viewed in this particular case. He said that the Sloan Kettering research was likely “as good as it’s going to get,” given that a randomized controlled trial is unlikely ever to occur with STS patients.
“Trying to select the patients we think are going to do well with surgery has always been one of the challenging aspects of thoracic surgery,” Dr. Walsh said in a video interview. “This paper may help with better selection of patients from that large cohort who are referred to us for pulmonary metastasectomy.”
Dr. Walsh reported no relevant financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @richpizzi
BALTIMORE – New research from Memorial Sloan Kettering Cancer Center in New York could help surgeons better determine which patients with soft tissue sarcoma may benefit most from pulmonary metastasectomy.
The results of the research, presented at the annual meeting of the American Association for Thoracic Surgery, suggest that preoperative factors such as primary tumor histology and size, number of metastases, time from initial resection of the primary, absence of extrapulmonary disease, and thoracoscopic resection are associated with improved survival in STS patients.
Dr. Garrett L. Walsh, professor of surgery at the University of Texas MD Anderson Cancer Center, Houston, and a discussant on the paper at the meeting, said the study was important because it showed the power of a prospective surgical database, retrospectively viewed in this particular case. He said that the Sloan Kettering research was likely “as good as it’s going to get,” given that a randomized controlled trial is unlikely ever to occur with STS patients.
“Trying to select the patients we think are going to do well with surgery has always been one of the challenging aspects of thoracic surgery,” Dr. Walsh said in a video interview. “This paper may help with better selection of patients from that large cohort who are referred to us for pulmonary metastasectomy.”
Dr. Walsh reported no relevant financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @richpizzi
AT THE AATS ANNUAL MEETING

Accuracy of gene test for thyroid nodules questioned
BALTIMORE – Biopsy results from a commercially available genetic test for ruling out malignancy of thyroid nodules may not provide reliable answers to clinicians and patients.
When fine-needle aspiration biopsy of thyroid nodules comes back inconclusive, clinicians have increasingly utilized the Afirma gene expression classifier (GEC) to rule out malignancy, but a retrospective analysis of almost 200 patients with indeterminate biopsy results along with a pooled analysis of 11 previous studies has raised questions about the negative predictive value of the test.

“The Afirma GEC test has substantial variability in performance,” said Dr. Zaid Al-Qurayshi of Tulane University, New Orleans, who reported the results at the annual meeting of the American Association of Endocrine Surgeons. “This variability cannot be explained based on differences in prevalence alone, but may also be the result of intrinsic test properties.”
The Afirma GEC measures the expression of 167 genes to more precisely determine the cancer risk of an indeterminate biopsied thyroid nodule and avoid unnecessary surgery. The test costs approximately $4,800 per nodule.
The researchers undertook the study in light of an American Thyroid Association (ATA) statement last year that concluded that test results are predicated on the clinician knowing the prevalence of malignancy within each indeterminate cytologic category at his/her own institution. Without this information, the performance of the diagnostic tests may vary substantially (Thyroid. 2015;25:760-8).
The single-center, retrospective cohort analysis included 192 patients with 210 indeterminate biopsy results, 145 of whom had surgery with 154 thyroid nodules. With a malignancy prevalence of 45%, the expected negative predictive value (NPV) of the test was estimated to be 85%, Dr. Al-Qurayshi said. However, the actual observed NPV was 69%. “If the prevalence was assumed to be 25%, the expected NPV was estimated to be 94%, while the observed NPV would have been 85%,” Dr. Al-Qurayshi said.
The researchers calculated the expected NPV by adopting the sensitivity and specificity rates of the test as reported in previous studies, while they calculated the observed NPV based on the actual negative rate among the Tulane cohort, Dr. Al-Qurayshi said.
Dr. Al-Qurayshi and colleagues then compared their results with pooled data from 11 other studies of the Afirma GEC. The pooled data analysis included 1,303 patients and yielded a malignancy prevalence of 31.1%, with a range of 29%-35%, and a pooled NPV of 92%, with a range of 87%-96%, Dr. Al-Qurayshi said.
“A lot of previously published studies took the sensitivity and specificity that were previously reported for granted, and now we are showing this sensitivity is all over the place,” Dr. Al-Qurayshi said. “Now, we don’t know which is the true one, and we need a larger clinical trial first to determine the true properties. Then we can ask how the prevalence in one’s institution is affecting the performance of the test.”
In an interview, Dr. Emad Kandil, senior study coauthor, also of Tulane, said the 69% NPV of the Tulane cohort puts the diagnostic scenario “back to ground zero, which is similar to what we had prior to the use of the new commercially available genetic tests.” He added, “A larger, randomized trial of the Afirma GEC test should answer those questions.”
The seminal study for the Afirma GEC, authored by Dr. Erik Alexander of Brigham and Women’s Hospital, Boston, in 2012, reported a 92% NPV with the test (N Engl J Med. 2012;367:705-15).
“The first thought was that they had different results because their population was different,” Dr. Al-Qurayshi said. “The ATA statement noted that it is the clinician’s responsibility to determine if this test is appropriate for their population or not, but the performance of the test doesn’t just depend on the population property, but it also depends on the intrinsic testing properties.”
Dr. Kandil disclosed that he has been a primary investigator in the ENHANCE multicenter study of the Afirma GEC. The other coauthors had no financial disclosures.
BALTIMORE – Biopsy results from a commercially available genetic test for ruling out malignancy of thyroid nodules may not provide reliable answers to clinicians and patients.
When fine-needle aspiration biopsy of thyroid nodules comes back inconclusive, clinicians have increasingly utilized the Afirma gene expression classifier (GEC) to rule out malignancy, but a retrospective analysis of almost 200 patients with indeterminate biopsy results along with a pooled analysis of 11 previous studies has raised questions about the negative predictive value of the test.
“The Afirma GEC test has substantial variability in performance,” said Dr. Zaid Al-Qurayshi of Tulane University, New Orleans, who reported the results at the annual meeting of the American Association of Endocrine Surgeons. “This variability cannot be explained based on differences in prevalence alone, but may also be the result of intrinsic test properties.”
The Afirma GEC measures the expression of 167 genes to more precisely determine the cancer risk of an indeterminate biopsied thyroid nodule and avoid unnecessary surgery. The test costs approximately $4,800 per nodule.
The researchers undertook the study in light of an American Thyroid Association (ATA) statement last year that concluded that test results are predicated on the clinician knowing the prevalence of malignancy within each indeterminate cytologic category at his/her own institution. Without this information, the performance of the diagnostic tests may vary substantially (Thyroid. 2015;25:760-8).
The single-center, retrospective cohort analysis included 192 patients with 210 indeterminate biopsy results, 145 of whom had surgery with 154 thyroid nodules. With a malignancy prevalence of 45%, the expected negative predictive value (NPV) of the test was estimated to be 85%, Dr. Al-Qurayshi said. However, the actual observed NPV was 69%. “If the prevalence was assumed to be 25%, the expected NPV was estimated to be 94%, while the observed NPV would have been 85%,” Dr. Al-Qurayshi said.
The researchers calculated the expected NPV by adopting the sensitivity and specificity rates of the test as reported in previous studies, while they calculated the observed NPV based on the actual negative rate among the Tulane cohort, Dr. Al-Qurayshi said.
Dr. Al-Qurayshi and colleagues then compared their results with pooled data from 11 other studies of the Afirma GEC. The pooled data analysis included 1,303 patients and yielded a malignancy prevalence of 31.1%, with a range of 29%-35%, and a pooled NPV of 92%, with a range of 87%-96%, Dr. Al-Qurayshi said.
“A lot of previously published studies took the sensitivity and specificity that were previously reported for granted, and now we are showing this sensitivity is all over the place,” Dr. Al-Qurayshi said. “Now, we don’t know which is the true one, and we need a larger clinical trial first to determine the true properties. Then we can ask how the prevalence in one’s institution is affecting the performance of the test.”
In an interview, Dr. Emad Kandil, senior study coauthor, also of Tulane, said the 69% NPV of the Tulane cohort puts the diagnostic scenario “back to ground zero, which is similar to what we had prior to the use of the new commercially available genetic tests.” He added, “A larger, randomized trial of the Afirma GEC test should answer those questions.”
The seminal study for the Afirma GEC, authored by Dr. Erik Alexander of Brigham and Women’s Hospital, Boston, in 2012, reported a 92% NPV with the test (N Engl J Med. 2012;367:705-15).
“The first thought was that they had different results because their population was different,” Dr. Al-Qurayshi said. “The ATA statement noted that it is the clinician’s responsibility to determine if this test is appropriate for their population or not, but the performance of the test doesn’t just depend on the population property, but it also depends on the intrinsic testing properties.”
Dr. Kandil disclosed that he has been a primary investigator in the ENHANCE multicenter study of the Afirma GEC. The other coauthors had no financial disclosures.
BALTIMORE – Biopsy results from a commercially available genetic test for ruling out malignancy of thyroid nodules may not provide reliable answers to clinicians and patients.
When fine-needle aspiration biopsy of thyroid nodules comes back inconclusive, clinicians have increasingly utilized the Afirma gene expression classifier (GEC) to rule out malignancy, but a retrospective analysis of almost 200 patients with indeterminate biopsy results along with a pooled analysis of 11 previous studies has raised questions about the negative predictive value of the test.
“The Afirma GEC test has substantial variability in performance,” said Dr. Zaid Al-Qurayshi of Tulane University, New Orleans, who reported the results at the annual meeting of the American Association of Endocrine Surgeons. “This variability cannot be explained based on differences in prevalence alone, but may also be the result of intrinsic test properties.”
The Afirma GEC measures the expression of 167 genes to more precisely determine the cancer risk of an indeterminate biopsied thyroid nodule and avoid unnecessary surgery. The test costs approximately $4,800 per nodule.
The researchers undertook the study in light of an American Thyroid Association (ATA) statement last year that concluded that test results are predicated on the clinician knowing the prevalence of malignancy within each indeterminate cytologic category at his/her own institution. Without this information, the performance of the diagnostic tests may vary substantially (Thyroid. 2015;25:760-8).
The single-center, retrospective cohort analysis included 192 patients with 210 indeterminate biopsy results, 145 of whom had surgery with 154 thyroid nodules. With a malignancy prevalence of 45%, the expected negative predictive value (NPV) of the test was estimated to be 85%, Dr. Al-Qurayshi said. However, the actual observed NPV was 69%. “If the prevalence was assumed to be 25%, the expected NPV was estimated to be 94%, while the observed NPV would have been 85%,” Dr. Al-Qurayshi said.
The researchers calculated the expected NPV by adopting the sensitivity and specificity rates of the test as reported in previous studies, while they calculated the observed NPV based on the actual negative rate among the Tulane cohort, Dr. Al-Qurayshi said.
Dr. Al-Qurayshi and colleagues then compared their results with pooled data from 11 other studies of the Afirma GEC. The pooled data analysis included 1,303 patients and yielded a malignancy prevalence of 31.1%, with a range of 29%-35%, and a pooled NPV of 92%, with a range of 87%-96%, Dr. Al-Qurayshi said.
“A lot of previously published studies took the sensitivity and specificity that were previously reported for granted, and now we are showing this sensitivity is all over the place,” Dr. Al-Qurayshi said. “Now, we don’t know which is the true one, and we need a larger clinical trial first to determine the true properties. Then we can ask how the prevalence in one’s institution is affecting the performance of the test.”
In an interview, Dr. Emad Kandil, senior study coauthor, also of Tulane, said the 69% NPV of the Tulane cohort puts the diagnostic scenario “back to ground zero, which is similar to what we had prior to the use of the new commercially available genetic tests.” He added, “A larger, randomized trial of the Afirma GEC test should answer those questions.”
The seminal study for the Afirma GEC, authored by Dr. Erik Alexander of Brigham and Women’s Hospital, Boston, in 2012, reported a 92% NPV with the test (N Engl J Med. 2012;367:705-15).
“The first thought was that they had different results because their population was different,” Dr. Al-Qurayshi said. “The ATA statement noted that it is the clinician’s responsibility to determine if this test is appropriate for their population or not, but the performance of the test doesn’t just depend on the population property, but it also depends on the intrinsic testing properties.”
Dr. Kandil disclosed that he has been a primary investigator in the ENHANCE multicenter study of the Afirma GEC. The other coauthors had no financial disclosures.
At AAES 2016
Key clinical point: Biopsy results from a commercially available genetic test for ruling out malignancy of thyroid nodules may not provide reliable answers to clinicians and patients.
Major finding: With a malignancy prevalence of 45%, the expected negative predictive value of the test was estimated to be 85%, but the actual observed NPV was 69%.
Data source: A single-center, retrospective cohort analysis involving 145 patients with 154 thyroid nodules.
Disclosures: Coauthor Dr. Emad Kandil disclosed that he has been a primary investigator in the ENHANCE multicenter study of the Afirma GEC. The other coauthors reported having no financial disclosures.
