User login
Official Newspaper of the American College of Surgeons
CABG best for diabetes patients with CKD – or is it?
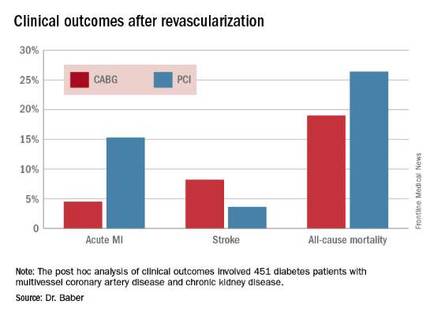
ROME – The use of coronary artery bypass graft surgery for revascularization in patients with multivessel CAD and comorbid diabetes plus chronic kidney disease was associated with a significantly lower risk of major cardiovascular and cerebrovascular events than was PCI with first-generation drug-eluting stents in a new secondary analysis from the landmark FREEDOM trial.
“The reason for this presentation is that even though chronic kidney disease is common in patients with diabetes, until now there has not been a large study of the efficacy and safety of coronary revascularization with drug-eluting stents versus CABG in this population in a randomized trial cohort,” explained Usman Baber, MD, who reported the results at the annual congress of the European Society of Cardiology.

FREEDOM (Future Revascularization Evaluation in Patients with Diabetes Mellitus: Optimal Management of Multivessel Disease) randomized 1,900 diabetic patients with multivessel CAD to PCI or CABG. As previously reported, CABG proved superior to PCI, with a significantly lower rate of the composite primary endpoint composed of all-cause mortality, MI, or stroke (N Engl J Med. 2012 Dec 20;367[25]:2375-84).
Dr. Baber presented a post hoc analysis of the 451 FREEDOM participants with baseline comorbid chronic kidney disease (CKD). Their mean SYNTAX score was 27, and their mean baseline estimated glomerular filtration rate was 44 mL/min per 1.73 m2, indicative of mild to moderate CKD.
“Only 28 patients in the FREEDOM trial had an estimated GFR below 30, therefore we can’t make any inferences about revascularization in that setting, which I think is a completely different population,” he noted.
The 5-year rate of major adverse cardiovascular and cerebrovascular events in patients with CKD was 26% in the CABG group, an absolute 9.4% less than the 35.6% rate in subjects randomized to PCI.
Roughly one-quarter of FREEDOM participants had CKD. They fared significantly worse than did those without CKD. The 5-year incidence of major adverse cardiovascular and cerebrovascular events was 30.8% in patients with CKD and 20.1% in patients without renal impairment. In a multivariate analysis adjusted for age, gender, hypertension, peripheral vascular disease, and other potential confounders, the risk of all-cause mortality was twofold higher in the CKD group. Their risk of cardiac death was increased 1.8-fold, and they were at 1.9-fold increased risk for stroke. Interestingly, however, the acute MI risk did not differ between patients with or without CKD, Dr. Baber observed.
Drilling deeper into the data, the cardiologist reported that CABG was associated with significantly lower rates of MI and a nonsignificant trend for fewer deaths, but with a significantly higher stroke rate than PCI.
One audience member rose to complain that this information won’t be helpful in counseling his diabetic patients with CKD and multivessel CAD because the choices look so grim: a higher risk of MI with percutaneous therapy, and a greater risk of stroke with surgery.
Dr. Baber replied by pointing out that the 10.8% absolute reduction in the risk of MI with CABG compared with PCI was more than twice as large as the absolute 4.6% increase in stroke risk with surgery.

“Most people would say that a heart attack is an inconvenience, and a stroke is a life-changing experience for them and their family,” said session cochair Kim A. Williams, MD, professor of medicine and chairman of cardiology at Rush University Medical Center in Chicago.
At that, Dr. Baber backtracked a bit, observing that since this was a post hoc analysis, the FREEDOM findings in patients with CKD must be viewed as hypothesis-generating rather than definitive. And, of course, contemporary second-generation drug-eluting stents have a better risk/benefit profile than do those used in FREEDOM.
“The number needed to treat/number needed to harm ratio for CABG and PCI probably ends up being roughly equal. The pertinence of an analysis like this is if you look at real-world registry-based data, you find a therapeutic nihilism that’s highly prevalent in CKD patients, where many patients who might benefit are not provided with revascularization therapy. It’s clear that we as clinicians – either because we don’t know there is a benefit or we are too concerned about potential harm – deprive patients of a treatment that might be beneficial. This analysis makes clinicians who might be concerned feel somewhat comforted that there is not unacceptable harm and that there is benefit,” Dr. Baber said.
Follow-up of FREEDOM participants continues and will be the subject of future reports, he added.
The FREEDOM trial was sponsored by the National Heart, Lung and Blood Institute. Dr. Baber reported having no financial conflicts of interest.
ROME – The use of coronary artery bypass graft surgery for revascularization in patients with multivessel CAD and comorbid diabetes plus chronic kidney disease was associated with a significantly lower risk of major cardiovascular and cerebrovascular events than was PCI with first-generation drug-eluting stents in a new secondary analysis from the landmark FREEDOM trial.
“The reason for this presentation is that even though chronic kidney disease is common in patients with diabetes, until now there has not been a large study of the efficacy and safety of coronary revascularization with drug-eluting stents versus CABG in this population in a randomized trial cohort,” explained Usman Baber, MD, who reported the results at the annual congress of the European Society of Cardiology.
FREEDOM (Future Revascularization Evaluation in Patients with Diabetes Mellitus: Optimal Management of Multivessel Disease) randomized 1,900 diabetic patients with multivessel CAD to PCI or CABG. As previously reported, CABG proved superior to PCI, with a significantly lower rate of the composite primary endpoint composed of all-cause mortality, MI, or stroke (N Engl J Med. 2012 Dec 20;367[25]:2375-84).
Dr. Baber presented a post hoc analysis of the 451 FREEDOM participants with baseline comorbid chronic kidney disease (CKD). Their mean SYNTAX score was 27, and their mean baseline estimated glomerular filtration rate was 44 mL/min per 1.73 m2, indicative of mild to moderate CKD.
“Only 28 patients in the FREEDOM trial had an estimated GFR below 30, therefore we can’t make any inferences about revascularization in that setting, which I think is a completely different population,” he noted.
The 5-year rate of major adverse cardiovascular and cerebrovascular events in patients with CKD was 26% in the CABG group, an absolute 9.4% less than the 35.6% rate in subjects randomized to PCI.
Roughly one-quarter of FREEDOM participants had CKD. They fared significantly worse than did those without CKD. The 5-year incidence of major adverse cardiovascular and cerebrovascular events was 30.8% in patients with CKD and 20.1% in patients without renal impairment. In a multivariate analysis adjusted for age, gender, hypertension, peripheral vascular disease, and other potential confounders, the risk of all-cause mortality was twofold higher in the CKD group. Their risk of cardiac death was increased 1.8-fold, and they were at 1.9-fold increased risk for stroke. Interestingly, however, the acute MI risk did not differ between patients with or without CKD, Dr. Baber observed.
Drilling deeper into the data, the cardiologist reported that CABG was associated with significantly lower rates of MI and a nonsignificant trend for fewer deaths, but with a significantly higher stroke rate than PCI.
One audience member rose to complain that this information won’t be helpful in counseling his diabetic patients with CKD and multivessel CAD because the choices look so grim: a higher risk of MI with percutaneous therapy, and a greater risk of stroke with surgery.
Dr. Baber replied by pointing out that the 10.8% absolute reduction in the risk of MI with CABG compared with PCI was more than twice as large as the absolute 4.6% increase in stroke risk with surgery.
“Most people would say that a heart attack is an inconvenience, and a stroke is a life-changing experience for them and their family,” said session cochair Kim A. Williams, MD, professor of medicine and chairman of cardiology at Rush University Medical Center in Chicago.
At that, Dr. Baber backtracked a bit, observing that since this was a post hoc analysis, the FREEDOM findings in patients with CKD must be viewed as hypothesis-generating rather than definitive. And, of course, contemporary second-generation drug-eluting stents have a better risk/benefit profile than do those used in FREEDOM.
“The number needed to treat/number needed to harm ratio for CABG and PCI probably ends up being roughly equal. The pertinence of an analysis like this is if you look at real-world registry-based data, you find a therapeutic nihilism that’s highly prevalent in CKD patients, where many patients who might benefit are not provided with revascularization therapy. It’s clear that we as clinicians – either because we don’t know there is a benefit or we are too concerned about potential harm – deprive patients of a treatment that might be beneficial. This analysis makes clinicians who might be concerned feel somewhat comforted that there is not unacceptable harm and that there is benefit,” Dr. Baber said.
Follow-up of FREEDOM participants continues and will be the subject of future reports, he added.
The FREEDOM trial was sponsored by the National Heart, Lung and Blood Institute. Dr. Baber reported having no financial conflicts of interest.
ROME – The use of coronary artery bypass graft surgery for revascularization in patients with multivessel CAD and comorbid diabetes plus chronic kidney disease was associated with a significantly lower risk of major cardiovascular and cerebrovascular events than was PCI with first-generation drug-eluting stents in a new secondary analysis from the landmark FREEDOM trial.
“The reason for this presentation is that even though chronic kidney disease is common in patients with diabetes, until now there has not been a large study of the efficacy and safety of coronary revascularization with drug-eluting stents versus CABG in this population in a randomized trial cohort,” explained Usman Baber, MD, who reported the results at the annual congress of the European Society of Cardiology.
FREEDOM (Future Revascularization Evaluation in Patients with Diabetes Mellitus: Optimal Management of Multivessel Disease) randomized 1,900 diabetic patients with multivessel CAD to PCI or CABG. As previously reported, CABG proved superior to PCI, with a significantly lower rate of the composite primary endpoint composed of all-cause mortality, MI, or stroke (N Engl J Med. 2012 Dec 20;367[25]:2375-84).
Dr. Baber presented a post hoc analysis of the 451 FREEDOM participants with baseline comorbid chronic kidney disease (CKD). Their mean SYNTAX score was 27, and their mean baseline estimated glomerular filtration rate was 44 mL/min per 1.73 m2, indicative of mild to moderate CKD.
“Only 28 patients in the FREEDOM trial had an estimated GFR below 30, therefore we can’t make any inferences about revascularization in that setting, which I think is a completely different population,” he noted.
The 5-year rate of major adverse cardiovascular and cerebrovascular events in patients with CKD was 26% in the CABG group, an absolute 9.4% less than the 35.6% rate in subjects randomized to PCI.
Roughly one-quarter of FREEDOM participants had CKD. They fared significantly worse than did those without CKD. The 5-year incidence of major adverse cardiovascular and cerebrovascular events was 30.8% in patients with CKD and 20.1% in patients without renal impairment. In a multivariate analysis adjusted for age, gender, hypertension, peripheral vascular disease, and other potential confounders, the risk of all-cause mortality was twofold higher in the CKD group. Their risk of cardiac death was increased 1.8-fold, and they were at 1.9-fold increased risk for stroke. Interestingly, however, the acute MI risk did not differ between patients with or without CKD, Dr. Baber observed.
Drilling deeper into the data, the cardiologist reported that CABG was associated with significantly lower rates of MI and a nonsignificant trend for fewer deaths, but with a significantly higher stroke rate than PCI.
One audience member rose to complain that this information won’t be helpful in counseling his diabetic patients with CKD and multivessel CAD because the choices look so grim: a higher risk of MI with percutaneous therapy, and a greater risk of stroke with surgery.
Dr. Baber replied by pointing out that the 10.8% absolute reduction in the risk of MI with CABG compared with PCI was more than twice as large as the absolute 4.6% increase in stroke risk with surgery.
“Most people would say that a heart attack is an inconvenience, and a stroke is a life-changing experience for them and their family,” said session cochair Kim A. Williams, MD, professor of medicine and chairman of cardiology at Rush University Medical Center in Chicago.
At that, Dr. Baber backtracked a bit, observing that since this was a post hoc analysis, the FREEDOM findings in patients with CKD must be viewed as hypothesis-generating rather than definitive. And, of course, contemporary second-generation drug-eluting stents have a better risk/benefit profile than do those used in FREEDOM.
“The number needed to treat/number needed to harm ratio for CABG and PCI probably ends up being roughly equal. The pertinence of an analysis like this is if you look at real-world registry-based data, you find a therapeutic nihilism that’s highly prevalent in CKD patients, where many patients who might benefit are not provided with revascularization therapy. It’s clear that we as clinicians – either because we don’t know there is a benefit or we are too concerned about potential harm – deprive patients of a treatment that might be beneficial. This analysis makes clinicians who might be concerned feel somewhat comforted that there is not unacceptable harm and that there is benefit,” Dr. Baber said.
Follow-up of FREEDOM participants continues and will be the subject of future reports, he added.
The FREEDOM trial was sponsored by the National Heart, Lung and Blood Institute. Dr. Baber reported having no financial conflicts of interest.
AT THE ESC CONGRESS 2016
Key clinical point: Coronary artery bypass graft surgery resulted in fewer myocardial infarctions but more strokes than did percutaneous coronary intervention at 5 years of follow-up in diabetic patients with multivessel coronary artery disease and chronic kidney disease.
Major finding: The cumulative MI rates in patients randomized to CABG versus PCI were 4.5% and 15.3%, respectively, while the stroke rates were 8.2% versus 3.6%.
Data source: A post hoc analysis of clinical outcomes in 451 diabetic patients with multivessel CAD and chronic kidney disease who were randomized to CABG or PCI in the prospective multicenter FREEDOM trial.
Disclosures: The FREEDOM trial was sponsored by the National Heart, Lung, and Blood Institute. The presenter reported having no financial conflicts of interest.

Nearly half of patients readmitted after liver transplant
Nearly half of patients were readmitted to the hospital within 90 days of liver transplantation, according to a single-center retrospective study.
“As readmission portends decreased survival, an emphasis should be placed on identifying and optimizing those at increased risk. If readmission does occur, however, it presents an opportunity to intervene, as virtually no patients died during initial readmission,” Madhukar S. Patel, MD, and his associates at Massachusetts General Hospital, Boston, wrote online in HPB.
Long wait times for liver transplantation in this part of the country lead to “high patient acuity,” the researchers noted. To better understand the correlates and consequences of posttransplant readmissions, they reviewed the records for 325 adults who underwent liver transplantation at their hospital between 2005 and 2015. Patients averaged 56 years old and had awaited transplant for a mean of 1 year (standard deviation, 506 days). Their average MELD (Model for End-Stage Liver Disease) scores were 30.3 at transplant (SD, 5.8), and 16.9 (SD, 9.4) on postoperative day 5. Their average hospital length of stay was 12 days, the investigators reported (HPB. 2016 Sep 15. doi: 10.1016/j.hpb.2016.08.003). A total of 149 patients (46%) were readmitted within 90 days of discharge, most often for infections (28% of readmissions), followed by medication issues (19%) and biliary complications (11%). The strongest predictor of posttransplant readmission was hepatitis C virus (HCV) infection, which more than doubled the odds of readmission, compared with alcoholic liver disease (odds ratio, 2.37; 95% confidence interval, 1.44-3.91; P = .001). Transplantees with HCV might benefit from closer outpatient follow-up to detect worsening liver function, diagnostic algorithms to help prevent unnecessary readmissions, and associated nosocomial infections, and pre- and posttransplant direct-acting antiviral therapy, “although the impact [of direct-acting antiviral] therapy on readmissions] is unknown at this time,” the investigators said.
The multivariable analysis also linked readmissions to longer hospital stays (OR, 1.03; P = .04), while age and male sex were protective factors, the investigators said. “Although speculative, it is possible that these factors may be protective due to differences in social support structures upon discharge,” they wrote, noting that women are more likely than men to outlive their partners and thus to live alone in later life.
Readmission within 90 days was associated with a significantly lower rate of survival at 5 years (75% vs. 88% for patients who were not readmitted; P = .008). But only one patient died during the initial readmission, “suggesting that when readmission does occur, it may be an opportunity to intervene,” the researchers said. Strategies include earlier extubation and removal of indwelling catheters, decreasing levels of immunosuppression, lowering treatment thresholds, and shifting patients with laboratory abnormalities to the outpatient setting, they noted. “At our center a process has been initiated in which the inpatient transplant attending surgeon directly passes off discharged patients to the outpatient team,” the investigators wrote. “Additionally, for patients discharged to an acute rehabilitation facility, a specific transplant physician point of contact is provided to the team at the rehab center in case any questions or issues arise [after] discharge. Although these strategies are a reasonable starting point, follow-up studies remain necessary in order to evaluate the impact of these interventions in this patient cohort.”
The researchers reported no funding sources and had no relevant financial disclosures.
Nearly half of patients were readmitted to the hospital within 90 days of liver transplantation, according to a single-center retrospective study.
“As readmission portends decreased survival, an emphasis should be placed on identifying and optimizing those at increased risk. If readmission does occur, however, it presents an opportunity to intervene, as virtually no patients died during initial readmission,” Madhukar S. Patel, MD, and his associates at Massachusetts General Hospital, Boston, wrote online in HPB.
Long wait times for liver transplantation in this part of the country lead to “high patient acuity,” the researchers noted. To better understand the correlates and consequences of posttransplant readmissions, they reviewed the records for 325 adults who underwent liver transplantation at their hospital between 2005 and 2015. Patients averaged 56 years old and had awaited transplant for a mean of 1 year (standard deviation, 506 days). Their average MELD (Model for End-Stage Liver Disease) scores were 30.3 at transplant (SD, 5.8), and 16.9 (SD, 9.4) on postoperative day 5. Their average hospital length of stay was 12 days, the investigators reported (HPB. 2016 Sep 15. doi: 10.1016/j.hpb.2016.08.003). A total of 149 patients (46%) were readmitted within 90 days of discharge, most often for infections (28% of readmissions), followed by medication issues (19%) and biliary complications (11%). The strongest predictor of posttransplant readmission was hepatitis C virus (HCV) infection, which more than doubled the odds of readmission, compared with alcoholic liver disease (odds ratio, 2.37; 95% confidence interval, 1.44-3.91; P = .001). Transplantees with HCV might benefit from closer outpatient follow-up to detect worsening liver function, diagnostic algorithms to help prevent unnecessary readmissions, and associated nosocomial infections, and pre- and posttransplant direct-acting antiviral therapy, “although the impact [of direct-acting antiviral] therapy on readmissions] is unknown at this time,” the investigators said.
The multivariable analysis also linked readmissions to longer hospital stays (OR, 1.03; P = .04), while age and male sex were protective factors, the investigators said. “Although speculative, it is possible that these factors may be protective due to differences in social support structures upon discharge,” they wrote, noting that women are more likely than men to outlive their partners and thus to live alone in later life.
Readmission within 90 days was associated with a significantly lower rate of survival at 5 years (75% vs. 88% for patients who were not readmitted; P = .008). But only one patient died during the initial readmission, “suggesting that when readmission does occur, it may be an opportunity to intervene,” the researchers said. Strategies include earlier extubation and removal of indwelling catheters, decreasing levels of immunosuppression, lowering treatment thresholds, and shifting patients with laboratory abnormalities to the outpatient setting, they noted. “At our center a process has been initiated in which the inpatient transplant attending surgeon directly passes off discharged patients to the outpatient team,” the investigators wrote. “Additionally, for patients discharged to an acute rehabilitation facility, a specific transplant physician point of contact is provided to the team at the rehab center in case any questions or issues arise [after] discharge. Although these strategies are a reasonable starting point, follow-up studies remain necessary in order to evaluate the impact of these interventions in this patient cohort.”
The researchers reported no funding sources and had no relevant financial disclosures.
Nearly half of patients were readmitted to the hospital within 90 days of liver transplantation, according to a single-center retrospective study.
“As readmission portends decreased survival, an emphasis should be placed on identifying and optimizing those at increased risk. If readmission does occur, however, it presents an opportunity to intervene, as virtually no patients died during initial readmission,” Madhukar S. Patel, MD, and his associates at Massachusetts General Hospital, Boston, wrote online in HPB.
Long wait times for liver transplantation in this part of the country lead to “high patient acuity,” the researchers noted. To better understand the correlates and consequences of posttransplant readmissions, they reviewed the records for 325 adults who underwent liver transplantation at their hospital between 2005 and 2015. Patients averaged 56 years old and had awaited transplant for a mean of 1 year (standard deviation, 506 days). Their average MELD (Model for End-Stage Liver Disease) scores were 30.3 at transplant (SD, 5.8), and 16.9 (SD, 9.4) on postoperative day 5. Their average hospital length of stay was 12 days, the investigators reported (HPB. 2016 Sep 15. doi: 10.1016/j.hpb.2016.08.003). A total of 149 patients (46%) were readmitted within 90 days of discharge, most often for infections (28% of readmissions), followed by medication issues (19%) and biliary complications (11%). The strongest predictor of posttransplant readmission was hepatitis C virus (HCV) infection, which more than doubled the odds of readmission, compared with alcoholic liver disease (odds ratio, 2.37; 95% confidence interval, 1.44-3.91; P = .001). Transplantees with HCV might benefit from closer outpatient follow-up to detect worsening liver function, diagnostic algorithms to help prevent unnecessary readmissions, and associated nosocomial infections, and pre- and posttransplant direct-acting antiviral therapy, “although the impact [of direct-acting antiviral] therapy on readmissions] is unknown at this time,” the investigators said.
The multivariable analysis also linked readmissions to longer hospital stays (OR, 1.03; P = .04), while age and male sex were protective factors, the investigators said. “Although speculative, it is possible that these factors may be protective due to differences in social support structures upon discharge,” they wrote, noting that women are more likely than men to outlive their partners and thus to live alone in later life.
Readmission within 90 days was associated with a significantly lower rate of survival at 5 years (75% vs. 88% for patients who were not readmitted; P = .008). But only one patient died during the initial readmission, “suggesting that when readmission does occur, it may be an opportunity to intervene,” the researchers said. Strategies include earlier extubation and removal of indwelling catheters, decreasing levels of immunosuppression, lowering treatment thresholds, and shifting patients with laboratory abnormalities to the outpatient setting, they noted. “At our center a process has been initiated in which the inpatient transplant attending surgeon directly passes off discharged patients to the outpatient team,” the investigators wrote. “Additionally, for patients discharged to an acute rehabilitation facility, a specific transplant physician point of contact is provided to the team at the rehab center in case any questions or issues arise [after] discharge. Although these strategies are a reasonable starting point, follow-up studies remain necessary in order to evaluate the impact of these interventions in this patient cohort.”
The researchers reported no funding sources and had no relevant financial disclosures.
FROM HPB
Key clinical point: Nearly half of liver recipients at Massachusetts General Hospital were readmitted within 90 days.
Major finding: A total of 46% of patients were readmitted, with hepatitis C virus infection being the strongest predictor of readmission (odds ratio, 2.37, compared with alcoholic liver disease).
Data source: A single-center retrospective study of 325 liver transplant patients between 2005 and 2015.
Disclosures: The researchers reported no funding sources and had no relevant financial disclosures.
Benefits of early endovascular thrombectomy outlined in five trials
For patients with large-vessel ischemic stroke, endovascular thrombectomy produces better functional outcomes at 90 days than does optimal medical therapy, as long as the procedure is started within 7.3 hours of symptom onset, according to a report published online Sept. 27 in JAMA.
The benefit of thrombectomy was greatest when the procedure was begun under 2 hours from symptom onset, and it became nonsignificant after 7 hours and 18 minutes elapsed. This emphasizes “the importance of programs to enhance patient awareness, out-of-hospital care, and in-hospital management to shorten symptom onset-to-treatment times,” wrote Jeffrey L. Saver, MD, of the University of California, Los Angeles, and his associates.

Five major randomized trials have demonstrated the benefit of second-generation endovascular recanalization therapies over medical therapy in this patient population, but uncertainties persist regarding the timing of the intervention. For example, practice guidelines in the United States recommend thrombectomy until 6 hours after symptom onset, but the Food and Drug Administration allows thrombectomy devices to be used up to 8 hours after symptom onset and Canadian guidelines recommend the procedure for selected patients up to 12 hours after symptom onset.
The investigators for the five trials formed the Highly Effective Reperfusion Evaluated in Multiple Endovascular Stroke Trials (HERMES) collaboration to pool their individual patient data and perform a meta-analysis to clarify the issue of timing. They assessed patients’ functional independence at 90 days using the modified Rankin Score (mRS). The study participants included 634 patients who had been randomly assigned to endovascular thrombectomy and 653 randomly assigned to medical therapy.
The intervention correlated with a substantially lower degree of patient disability at 90 days than did medical therapy: the mean mRS was 2.9 in the thrombectomy group and 3.6 in the medical therapy group. In addition, increasing delays in treatment were associated with higher levels of residual disability in the thrombectomy group but not in the medical therapy group, the investigators reported.
“Based on the current study, and assuming the findings are generalizable to the population of patients with acute ischemic stroke due to large-vessel occlusion, among every 1,000 patients achieving substantial endovascular reperfusion, for every 15-minute faster ED door-to-reperfusion time, an estimated 39 patients would have a less-disabled outcome at 3 months, including 25 more who would achieve functional independence (mRS 0-2),” Dr. Saver and his associates wrote (JAMA. 2016;316[12]:1279-88).
These findings reinforce current recommendations to attempt endovascular thrombectomy when the procedure can be initiated within 6 hours of symptom onset, and they also “provide evidence that potentially supports strengthening of the recommendation for treatment from 6 through 7.3 hours after symptom onset,” they added.
No specific sponsor of this study was cited. Dr. Saver reported ties to Medtronic, Stryker, Cognition Medical, Covidien, Neuravi, BrainsGate, Pfizer, Bristol-Myers Squibb, Boehringer Ingelheim, ZZ Biotech, St. Jude Medical, and Genentech. His associates reported ties to numerous industry sources.
Earlier thrombectomy has such a profound effect on stroke patients’ outcomes that substantial changes in the current medical system are warranted to shorten these times even further. In this study, median time from symptom onset to randomization was approximately 3 hours, median time to arterial puncture was approximately 4 hours, and median time to reperfusion was nearly 5 hours.
Reducing the number of patients who are transferred from community hospitals to facilities with stroke centers would shorten door-to-reperfusion time a great deal. It is estimated that direct transport to stroke centers would allow endovascular thrombectomy for an additional 13% of stroke patients. Telemedicine, mobile stroke units, and out-of-hospital administration of tissue plasminogen activator are other possibilities that should be investigated.
Steven Warach, MD, PhD, and S. Claiborne Johnston, MD, PhD, are with the University of Texas at Austin. They reported having no relevant financial disclosures. Dr. Warach and Dr. Johnston made these remarks in an editorial (JAMA. 2016;316[12]:1265-6) accompanying Dr. Saver’s report.
Earlier thrombectomy has such a profound effect on stroke patients’ outcomes that substantial changes in the current medical system are warranted to shorten these times even further. In this study, median time from symptom onset to randomization was approximately 3 hours, median time to arterial puncture was approximately 4 hours, and median time to reperfusion was nearly 5 hours.
Reducing the number of patients who are transferred from community hospitals to facilities with stroke centers would shorten door-to-reperfusion time a great deal. It is estimated that direct transport to stroke centers would allow endovascular thrombectomy for an additional 13% of stroke patients. Telemedicine, mobile stroke units, and out-of-hospital administration of tissue plasminogen activator are other possibilities that should be investigated.
Steven Warach, MD, PhD, and S. Claiborne Johnston, MD, PhD, are with the University of Texas at Austin. They reported having no relevant financial disclosures. Dr. Warach and Dr. Johnston made these remarks in an editorial (JAMA. 2016;316[12]:1265-6) accompanying Dr. Saver’s report.
Earlier thrombectomy has such a profound effect on stroke patients’ outcomes that substantial changes in the current medical system are warranted to shorten these times even further. In this study, median time from symptom onset to randomization was approximately 3 hours, median time to arterial puncture was approximately 4 hours, and median time to reperfusion was nearly 5 hours.
Reducing the number of patients who are transferred from community hospitals to facilities with stroke centers would shorten door-to-reperfusion time a great deal. It is estimated that direct transport to stroke centers would allow endovascular thrombectomy for an additional 13% of stroke patients. Telemedicine, mobile stroke units, and out-of-hospital administration of tissue plasminogen activator are other possibilities that should be investigated.
Steven Warach, MD, PhD, and S. Claiborne Johnston, MD, PhD, are with the University of Texas at Austin. They reported having no relevant financial disclosures. Dr. Warach and Dr. Johnston made these remarks in an editorial (JAMA. 2016;316[12]:1265-6) accompanying Dr. Saver’s report.
For patients with large-vessel ischemic stroke, endovascular thrombectomy produces better functional outcomes at 90 days than does optimal medical therapy, as long as the procedure is started within 7.3 hours of symptom onset, according to a report published online Sept. 27 in JAMA.
The benefit of thrombectomy was greatest when the procedure was begun under 2 hours from symptom onset, and it became nonsignificant after 7 hours and 18 minutes elapsed. This emphasizes “the importance of programs to enhance patient awareness, out-of-hospital care, and in-hospital management to shorten symptom onset-to-treatment times,” wrote Jeffrey L. Saver, MD, of the University of California, Los Angeles, and his associates.
Five major randomized trials have demonstrated the benefit of second-generation endovascular recanalization therapies over medical therapy in this patient population, but uncertainties persist regarding the timing of the intervention. For example, practice guidelines in the United States recommend thrombectomy until 6 hours after symptom onset, but the Food and Drug Administration allows thrombectomy devices to be used up to 8 hours after symptom onset and Canadian guidelines recommend the procedure for selected patients up to 12 hours after symptom onset.
The investigators for the five trials formed the Highly Effective Reperfusion Evaluated in Multiple Endovascular Stroke Trials (HERMES) collaboration to pool their individual patient data and perform a meta-analysis to clarify the issue of timing. They assessed patients’ functional independence at 90 days using the modified Rankin Score (mRS). The study participants included 634 patients who had been randomly assigned to endovascular thrombectomy and 653 randomly assigned to medical therapy.
The intervention correlated with a substantially lower degree of patient disability at 90 days than did medical therapy: the mean mRS was 2.9 in the thrombectomy group and 3.6 in the medical therapy group. In addition, increasing delays in treatment were associated with higher levels of residual disability in the thrombectomy group but not in the medical therapy group, the investigators reported.
“Based on the current study, and assuming the findings are generalizable to the population of patients with acute ischemic stroke due to large-vessel occlusion, among every 1,000 patients achieving substantial endovascular reperfusion, for every 15-minute faster ED door-to-reperfusion time, an estimated 39 patients would have a less-disabled outcome at 3 months, including 25 more who would achieve functional independence (mRS 0-2),” Dr. Saver and his associates wrote (JAMA. 2016;316[12]:1279-88).
These findings reinforce current recommendations to attempt endovascular thrombectomy when the procedure can be initiated within 6 hours of symptom onset, and they also “provide evidence that potentially supports strengthening of the recommendation for treatment from 6 through 7.3 hours after symptom onset,” they added.
No specific sponsor of this study was cited. Dr. Saver reported ties to Medtronic, Stryker, Cognition Medical, Covidien, Neuravi, BrainsGate, Pfizer, Bristol-Myers Squibb, Boehringer Ingelheim, ZZ Biotech, St. Jude Medical, and Genentech. His associates reported ties to numerous industry sources.
For patients with large-vessel ischemic stroke, endovascular thrombectomy produces better functional outcomes at 90 days than does optimal medical therapy, as long as the procedure is started within 7.3 hours of symptom onset, according to a report published online Sept. 27 in JAMA.
The benefit of thrombectomy was greatest when the procedure was begun under 2 hours from symptom onset, and it became nonsignificant after 7 hours and 18 minutes elapsed. This emphasizes “the importance of programs to enhance patient awareness, out-of-hospital care, and in-hospital management to shorten symptom onset-to-treatment times,” wrote Jeffrey L. Saver, MD, of the University of California, Los Angeles, and his associates.
Five major randomized trials have demonstrated the benefit of second-generation endovascular recanalization therapies over medical therapy in this patient population, but uncertainties persist regarding the timing of the intervention. For example, practice guidelines in the United States recommend thrombectomy until 6 hours after symptom onset, but the Food and Drug Administration allows thrombectomy devices to be used up to 8 hours after symptom onset and Canadian guidelines recommend the procedure for selected patients up to 12 hours after symptom onset.
The investigators for the five trials formed the Highly Effective Reperfusion Evaluated in Multiple Endovascular Stroke Trials (HERMES) collaboration to pool their individual patient data and perform a meta-analysis to clarify the issue of timing. They assessed patients’ functional independence at 90 days using the modified Rankin Score (mRS). The study participants included 634 patients who had been randomly assigned to endovascular thrombectomy and 653 randomly assigned to medical therapy.
The intervention correlated with a substantially lower degree of patient disability at 90 days than did medical therapy: the mean mRS was 2.9 in the thrombectomy group and 3.6 in the medical therapy group. In addition, increasing delays in treatment were associated with higher levels of residual disability in the thrombectomy group but not in the medical therapy group, the investigators reported.
“Based on the current study, and assuming the findings are generalizable to the population of patients with acute ischemic stroke due to large-vessel occlusion, among every 1,000 patients achieving substantial endovascular reperfusion, for every 15-minute faster ED door-to-reperfusion time, an estimated 39 patients would have a less-disabled outcome at 3 months, including 25 more who would achieve functional independence (mRS 0-2),” Dr. Saver and his associates wrote (JAMA. 2016;316[12]:1279-88).
These findings reinforce current recommendations to attempt endovascular thrombectomy when the procedure can be initiated within 6 hours of symptom onset, and they also “provide evidence that potentially supports strengthening of the recommendation for treatment from 6 through 7.3 hours after symptom onset,” they added.
No specific sponsor of this study was cited. Dr. Saver reported ties to Medtronic, Stryker, Cognition Medical, Covidien, Neuravi, BrainsGate, Pfizer, Bristol-Myers Squibb, Boehringer Ingelheim, ZZ Biotech, St. Jude Medical, and Genentech. His associates reported ties to numerous industry sources.
FROM JAMA
Key clinical point: Endovascular thrombectomy started within 7.3 hours of symptom onset for large-vessel ischemic stroke produces better outcomes than does optimal medical therapy.
Major finding: For every 15-minute shorter door-to-reperfusion time, an estimated 39 patients would have a less-disabled outcome at 3 months, including 25 more who would achieve functional independence.
Data source: A meta-analysis of pooled data from five randomized clinical trials involving 1,287 patients.
Disclosures: No specific sponsor of this study was cited. Dr. Saver reported ties to Medtronic, Stryker, Cognition Medical, Covidien, Neuravi, BrainsGate, Pfizer, Bristol Myers Squibb, Boehringer Ingelheim, ZZ Biotech, St. Jude Medical, and Genentech. His associates reported ties to numerous industry sources.

Survival shorter in extended-criteria lung recipients
The availability of lungs for transplant has been severely limited by usable donors, but organs from so-called extended criteria donors – those aged 65 years or older, had a 20 pack-years or more smoking history or history of diabetes mellitus, or were black – were found to be associated with shorter survival than lungs from standard donor lungs, and recipients with more severe lung disease had the lowest survival rates from extended-criteria organs, an analysis of the national donor database found.
“Matching donor quality to recipient severity is critical to achieve optimal outcomes in lung transplantation,” Matthew J. Mulligan, MD, and his colleagues from the University of Maryland, Baltimore, said in the September issue of the Journal of Thoracic and Cardiovascular Surgery (2016;152:891-8). Dr. Mulligan previously presented the study results in April 2015 at the annual meeting of the American Association for Thoracic Surgery in Seattle.
The researchers analyzed 10,995 patients who received donor lungs between May 2005 and December 2012, 3,792 of whom received extended-criteria donor (ECD) organs. The study population was taken from the Organ Procurement and Transplantation Network/United Network for Organ Sharing database. Dr. Mulligan and his coauthors said this is the largest study examining ECD in lung transplants to date.
The goal of the study was to identify donor factors associated with reduced 1-year survival after transplantation, Dr. Mulligan and his colleagues said. “In the current literature, there is a paucity of data to guide the decision of matching donor quality to recipient severity,” the study authors said.
Recipients of extended-criteria lungs had a 41% increased risk of death, compared with recipients standard donor lungs, but individuals with more severe lung disease were at even greater risk with extended-criterial lungs, Dr. Mulligan and his colleagues said. Those who had a lung allocation score (LAS) less than 70 had a 1-year survival of 87% with standard donor lungs vs. 82% with extended-criteria lungs, while those who had a LAS of 70 or greater had survival rates of 80% and 72%, respectively.
Other donor factors that were inconsequential in recipient survival, Dr. Mulligan and his coauthors reported, included an abnormal chest x-ray, purulent secretions on bronchoscopy, blood type, mechanism of death (stroke, blunt trauma, gunshot, asphyxiation, and so on), or diagnosis of coronary artery disease and hypertension.
The researchers also did a Cox regression analysis, and found that recipients of extended-criteria lungs with a LAS greater than 70 had an 81% greater risk of death, compared with 37% for those with a LAS of 70 or greater who received standard-donor lungs, and 42% with a LAS of 70 or less and an extended-criteria donor lung.
These findings support the idea of not using ECD lungs in high-risk individuals with LAS greater than 70. “More important, ECD lungs were associated with the worst survival when transplanted into high-risk recipients,” Dr. Mulligan and his colleagues said.
The authors did acknowledge the inherent limitations of a retrospective analysis, but the large patient population is a redeeming factor of the study, Dr. Mulligan and his colleagues said. “Notwithstanding these limitations, the current study provides a rigorous analysis of a large number of lung transplants in the modern era, and the results reported will be useful to the lung transplant community,” the study authors said.
Dr. Mulligan and his coauthors had no relationships to disclose.
This study provides “greater clarity to the definition and significance of using lungs from an extended-criteria donor,” Benjamin Wei, MD, of the University of Alabama at Birmingham said in his invited commentary (J Thorac Cardiovasc Surg. 2016;152:899-900). “Now, we have more data about what constitutes an ECD for lung transplantation.”
The study also brought clarity on components of donor factors that do not affect survival – namely radiologic, bronchoscope, or laboratory criteria – Dr. Wei said. At the same time, the study raises questions about how transplant surgeons should use the findings. “Do we shy away from using donors with these high risk factors in low-risk recipients, high-risk recipients, neither, or both?” Dr. Wei asks. The study did not compare ECD lungs vs. no transplant, and becoming more selective in donors could cause more patients to die on the waiting list, he said.
A host of other questions also remain unanswered, Dr. Wei said, such as how a single standard-donor lung transplant compares with bilateral ECD transplants, or a single ECD lung vs. bilateral ECD lungs, and if use of ECD lungs by the criteria Dr. Mulligan and his coauthors outlined influences allograft patient survival.
“Of note, this study also did not include recipients receiving donor after cardiac death lungs or extracorporeal membrane oxygenation, both increasingly common situations,” he said. Nonetheless, the findings provide more information that transplant surgeons can base their decision-making on.
Dr. Wei had no financial relationships to disclose.
This study provides “greater clarity to the definition and significance of using lungs from an extended-criteria donor,” Benjamin Wei, MD, of the University of Alabama at Birmingham said in his invited commentary (J Thorac Cardiovasc Surg. 2016;152:899-900). “Now, we have more data about what constitutes an ECD for lung transplantation.”
The study also brought clarity on components of donor factors that do not affect survival – namely radiologic, bronchoscope, or laboratory criteria – Dr. Wei said. At the same time, the study raises questions about how transplant surgeons should use the findings. “Do we shy away from using donors with these high risk factors in low-risk recipients, high-risk recipients, neither, or both?” Dr. Wei asks. The study did not compare ECD lungs vs. no transplant, and becoming more selective in donors could cause more patients to die on the waiting list, he said.
A host of other questions also remain unanswered, Dr. Wei said, such as how a single standard-donor lung transplant compares with bilateral ECD transplants, or a single ECD lung vs. bilateral ECD lungs, and if use of ECD lungs by the criteria Dr. Mulligan and his coauthors outlined influences allograft patient survival.
“Of note, this study also did not include recipients receiving donor after cardiac death lungs or extracorporeal membrane oxygenation, both increasingly common situations,” he said. Nonetheless, the findings provide more information that transplant surgeons can base their decision-making on.
Dr. Wei had no financial relationships to disclose.
This study provides “greater clarity to the definition and significance of using lungs from an extended-criteria donor,” Benjamin Wei, MD, of the University of Alabama at Birmingham said in his invited commentary (J Thorac Cardiovasc Surg. 2016;152:899-900). “Now, we have more data about what constitutes an ECD for lung transplantation.”
The study also brought clarity on components of donor factors that do not affect survival – namely radiologic, bronchoscope, or laboratory criteria – Dr. Wei said. At the same time, the study raises questions about how transplant surgeons should use the findings. “Do we shy away from using donors with these high risk factors in low-risk recipients, high-risk recipients, neither, or both?” Dr. Wei asks. The study did not compare ECD lungs vs. no transplant, and becoming more selective in donors could cause more patients to die on the waiting list, he said.
A host of other questions also remain unanswered, Dr. Wei said, such as how a single standard-donor lung transplant compares with bilateral ECD transplants, or a single ECD lung vs. bilateral ECD lungs, and if use of ECD lungs by the criteria Dr. Mulligan and his coauthors outlined influences allograft patient survival.
“Of note, this study also did not include recipients receiving donor after cardiac death lungs or extracorporeal membrane oxygenation, both increasingly common situations,” he said. Nonetheless, the findings provide more information that transplant surgeons can base their decision-making on.
Dr. Wei had no financial relationships to disclose.
The availability of lungs for transplant has been severely limited by usable donors, but organs from so-called extended criteria donors – those aged 65 years or older, had a 20 pack-years or more smoking history or history of diabetes mellitus, or were black – were found to be associated with shorter survival than lungs from standard donor lungs, and recipients with more severe lung disease had the lowest survival rates from extended-criteria organs, an analysis of the national donor database found.
“Matching donor quality to recipient severity is critical to achieve optimal outcomes in lung transplantation,” Matthew J. Mulligan, MD, and his colleagues from the University of Maryland, Baltimore, said in the September issue of the Journal of Thoracic and Cardiovascular Surgery (2016;152:891-8). Dr. Mulligan previously presented the study results in April 2015 at the annual meeting of the American Association for Thoracic Surgery in Seattle.
The researchers analyzed 10,995 patients who received donor lungs between May 2005 and December 2012, 3,792 of whom received extended-criteria donor (ECD) organs. The study population was taken from the Organ Procurement and Transplantation Network/United Network for Organ Sharing database. Dr. Mulligan and his coauthors said this is the largest study examining ECD in lung transplants to date.
The goal of the study was to identify donor factors associated with reduced 1-year survival after transplantation, Dr. Mulligan and his colleagues said. “In the current literature, there is a paucity of data to guide the decision of matching donor quality to recipient severity,” the study authors said.
Recipients of extended-criteria lungs had a 41% increased risk of death, compared with recipients standard donor lungs, but individuals with more severe lung disease were at even greater risk with extended-criterial lungs, Dr. Mulligan and his colleagues said. Those who had a lung allocation score (LAS) less than 70 had a 1-year survival of 87% with standard donor lungs vs. 82% with extended-criteria lungs, while those who had a LAS of 70 or greater had survival rates of 80% and 72%, respectively.
Other donor factors that were inconsequential in recipient survival, Dr. Mulligan and his coauthors reported, included an abnormal chest x-ray, purulent secretions on bronchoscopy, blood type, mechanism of death (stroke, blunt trauma, gunshot, asphyxiation, and so on), or diagnosis of coronary artery disease and hypertension.
The researchers also did a Cox regression analysis, and found that recipients of extended-criteria lungs with a LAS greater than 70 had an 81% greater risk of death, compared with 37% for those with a LAS of 70 or greater who received standard-donor lungs, and 42% with a LAS of 70 or less and an extended-criteria donor lung.
These findings support the idea of not using ECD lungs in high-risk individuals with LAS greater than 70. “More important, ECD lungs were associated with the worst survival when transplanted into high-risk recipients,” Dr. Mulligan and his colleagues said.
The authors did acknowledge the inherent limitations of a retrospective analysis, but the large patient population is a redeeming factor of the study, Dr. Mulligan and his colleagues said. “Notwithstanding these limitations, the current study provides a rigorous analysis of a large number of lung transplants in the modern era, and the results reported will be useful to the lung transplant community,” the study authors said.
Dr. Mulligan and his coauthors had no relationships to disclose.
The availability of lungs for transplant has been severely limited by usable donors, but organs from so-called extended criteria donors – those aged 65 years or older, had a 20 pack-years or more smoking history or history of diabetes mellitus, or were black – were found to be associated with shorter survival than lungs from standard donor lungs, and recipients with more severe lung disease had the lowest survival rates from extended-criteria organs, an analysis of the national donor database found.
“Matching donor quality to recipient severity is critical to achieve optimal outcomes in lung transplantation,” Matthew J. Mulligan, MD, and his colleagues from the University of Maryland, Baltimore, said in the September issue of the Journal of Thoracic and Cardiovascular Surgery (2016;152:891-8). Dr. Mulligan previously presented the study results in April 2015 at the annual meeting of the American Association for Thoracic Surgery in Seattle.
The researchers analyzed 10,995 patients who received donor lungs between May 2005 and December 2012, 3,792 of whom received extended-criteria donor (ECD) organs. The study population was taken from the Organ Procurement and Transplantation Network/United Network for Organ Sharing database. Dr. Mulligan and his coauthors said this is the largest study examining ECD in lung transplants to date.
The goal of the study was to identify donor factors associated with reduced 1-year survival after transplantation, Dr. Mulligan and his colleagues said. “In the current literature, there is a paucity of data to guide the decision of matching donor quality to recipient severity,” the study authors said.
Recipients of extended-criteria lungs had a 41% increased risk of death, compared with recipients standard donor lungs, but individuals with more severe lung disease were at even greater risk with extended-criterial lungs, Dr. Mulligan and his colleagues said. Those who had a lung allocation score (LAS) less than 70 had a 1-year survival of 87% with standard donor lungs vs. 82% with extended-criteria lungs, while those who had a LAS of 70 or greater had survival rates of 80% and 72%, respectively.
Other donor factors that were inconsequential in recipient survival, Dr. Mulligan and his coauthors reported, included an abnormal chest x-ray, purulent secretions on bronchoscopy, blood type, mechanism of death (stroke, blunt trauma, gunshot, asphyxiation, and so on), or diagnosis of coronary artery disease and hypertension.
The researchers also did a Cox regression analysis, and found that recipients of extended-criteria lungs with a LAS greater than 70 had an 81% greater risk of death, compared with 37% for those with a LAS of 70 or greater who received standard-donor lungs, and 42% with a LAS of 70 or less and an extended-criteria donor lung.
These findings support the idea of not using ECD lungs in high-risk individuals with LAS greater than 70. “More important, ECD lungs were associated with the worst survival when transplanted into high-risk recipients,” Dr. Mulligan and his colleagues said.
The authors did acknowledge the inherent limitations of a retrospective analysis, but the large patient population is a redeeming factor of the study, Dr. Mulligan and his colleagues said. “Notwithstanding these limitations, the current study provides a rigorous analysis of a large number of lung transplants in the modern era, and the results reported will be useful to the lung transplant community,” the study authors said.
Dr. Mulligan and his coauthors had no relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Lung transplant recipients who received extended-criteria donor (ECD) lungs have lower rates of 1-year survival than recipients of standard donor lungs.
Major finding: Recipients of ECD lungs had a 41% higher risk of death than recipients of standard lungs, and those who had more severe lung disease had lower rates of 1-year survival after receiving ECD lungs, compared with standard donor lungs.
Data source: Retrospective analysis of 10,995 lung recipients, from the Organ Procurement and Transplantation Network/United Network for Organ Sharing database, 3,792 of whom who received extended-criteria donor organs over 7.5 years.
Disclosures: Dr. Mulligan and his coauthors had no financial relationships to disclose.
Feds require more transparent reporting of clinical trial results
New federal regulations aim to strengthen the current requirements on reporting of clinical trial information.
The new rule offers a checklist to help determine which clinical trials are subject to regulations and who is responsible for information that appears on ClinicalTrials.gov. In addition, the rule does the following:

• Expands the scope of trials for which results must be submitted to include Food and Drug Administration–regulated products that have not yet been approved, licensed, or cleared.
• Requires additional information be submitted to ClinicalTrials.gov, including demographic information about trial participants.
• Expands adverse-event reporting.
• Adds potential penalties for noncompliance.
Simultaneously, the National Institutes of Health issued a complimentary policy for all trials it funds, regardless of whether the trials would be subject to the final rule.
Current federal requirements for reporting of clinical trial information were originally enacted as part of the FDA Amendments Act of 2007. However, a 2015 analysis of trials listed on ClinicalTrials.gov from 2007 to 2012 found a woeful lack of compliance: Study results were posted for 13% of trials covered by reporting requirements (N Engl J Med. 2015;372:1031-9).
“Organizations will need to ensure that their systems, procedures, and organizational values all promote complete and timely clinical trial reporting,” wrote Deborah Zarin, MD, of the National Library of Medicine, Bethesda, Md., and her colleagues in a special report on the final rule (N Engl J Med. 2016 Sep 16. doi: 10.1056/NEJMsr1611785). “In the end, the parties responsible for clinical trials will be held accountable by the public.”
The final rule applies to most interventional studies of drugs, biologics, and devices regulated by FDA, but it will not apply to phase I trials of pharmaceuticals or small feasibility studies of devices. It specifies how and when information collected in a clinical trial should be collected and submitted to ClinicalTrials.gov but does not dictate how clinical trials should be designed or conducted.
“Expanding the registration information in ClinicalTrials.gov improves people’s ability to find clinical trials in which they may be able to participate and access investigational therapies,” NIH officials said in a statement. “More information about the scientific results of trials, whether positive or negative, may help inform healthcare providers and patients regarding medical decisions. Additional information will help researchers avoid unnecessary duplication of studies, focus on areas in need of study and improve study design, ultimately advancing the development of clinical interventions.”
“Many U.S. academic medical centers, including those that conduct the most clinical trials, will find that the majority of their clinical trials fall under the [FDA Amendments Act], the NIH policy, or both,” Dr. Zarin and her colleagues wrote. “We hope that sponsors and other relevant entities will go considerably above and beyond the minimum requirements and expectations, making an effort to honor the contributions of all study participants and ensure that others in the scientific community have access to complete and high-quality information about every clinical trial under their stewardship.”
The final rule was published in the Federal Register on Sept. 21 and becomes effective on Jan. 18, 2017.
New federal regulations aim to strengthen the current requirements on reporting of clinical trial information.
The new rule offers a checklist to help determine which clinical trials are subject to regulations and who is responsible for information that appears on ClinicalTrials.gov. In addition, the rule does the following:
• Expands the scope of trials for which results must be submitted to include Food and Drug Administration–regulated products that have not yet been approved, licensed, or cleared.
• Requires additional information be submitted to ClinicalTrials.gov, including demographic information about trial participants.
• Expands adverse-event reporting.
• Adds potential penalties for noncompliance.
Simultaneously, the National Institutes of Health issued a complimentary policy for all trials it funds, regardless of whether the trials would be subject to the final rule.
Current federal requirements for reporting of clinical trial information were originally enacted as part of the FDA Amendments Act of 2007. However, a 2015 analysis of trials listed on ClinicalTrials.gov from 2007 to 2012 found a woeful lack of compliance: Study results were posted for 13% of trials covered by reporting requirements (N Engl J Med. 2015;372:1031-9).
“Organizations will need to ensure that their systems, procedures, and organizational values all promote complete and timely clinical trial reporting,” wrote Deborah Zarin, MD, of the National Library of Medicine, Bethesda, Md., and her colleagues in a special report on the final rule (N Engl J Med. 2016 Sep 16. doi: 10.1056/NEJMsr1611785). “In the end, the parties responsible for clinical trials will be held accountable by the public.”
The final rule applies to most interventional studies of drugs, biologics, and devices regulated by FDA, but it will not apply to phase I trials of pharmaceuticals or small feasibility studies of devices. It specifies how and when information collected in a clinical trial should be collected and submitted to ClinicalTrials.gov but does not dictate how clinical trials should be designed or conducted.
“Expanding the registration information in ClinicalTrials.gov improves people’s ability to find clinical trials in which they may be able to participate and access investigational therapies,” NIH officials said in a statement. “More information about the scientific results of trials, whether positive or negative, may help inform healthcare providers and patients regarding medical decisions. Additional information will help researchers avoid unnecessary duplication of studies, focus on areas in need of study and improve study design, ultimately advancing the development of clinical interventions.”
“Many U.S. academic medical centers, including those that conduct the most clinical trials, will find that the majority of their clinical trials fall under the [FDA Amendments Act], the NIH policy, or both,” Dr. Zarin and her colleagues wrote. “We hope that sponsors and other relevant entities will go considerably above and beyond the minimum requirements and expectations, making an effort to honor the contributions of all study participants and ensure that others in the scientific community have access to complete and high-quality information about every clinical trial under their stewardship.”
The final rule was published in the Federal Register on Sept. 21 and becomes effective on Jan. 18, 2017.
New federal regulations aim to strengthen the current requirements on reporting of clinical trial information.
The new rule offers a checklist to help determine which clinical trials are subject to regulations and who is responsible for information that appears on ClinicalTrials.gov. In addition, the rule does the following:
• Expands the scope of trials for which results must be submitted to include Food and Drug Administration–regulated products that have not yet been approved, licensed, or cleared.
• Requires additional information be submitted to ClinicalTrials.gov, including demographic information about trial participants.
• Expands adverse-event reporting.
• Adds potential penalties for noncompliance.
Simultaneously, the National Institutes of Health issued a complimentary policy for all trials it funds, regardless of whether the trials would be subject to the final rule.
Current federal requirements for reporting of clinical trial information were originally enacted as part of the FDA Amendments Act of 2007. However, a 2015 analysis of trials listed on ClinicalTrials.gov from 2007 to 2012 found a woeful lack of compliance: Study results were posted for 13% of trials covered by reporting requirements (N Engl J Med. 2015;372:1031-9).
“Organizations will need to ensure that their systems, procedures, and organizational values all promote complete and timely clinical trial reporting,” wrote Deborah Zarin, MD, of the National Library of Medicine, Bethesda, Md., and her colleagues in a special report on the final rule (N Engl J Med. 2016 Sep 16. doi: 10.1056/NEJMsr1611785). “In the end, the parties responsible for clinical trials will be held accountable by the public.”
The final rule applies to most interventional studies of drugs, biologics, and devices regulated by FDA, but it will not apply to phase I trials of pharmaceuticals or small feasibility studies of devices. It specifies how and when information collected in a clinical trial should be collected and submitted to ClinicalTrials.gov but does not dictate how clinical trials should be designed or conducted.
“Expanding the registration information in ClinicalTrials.gov improves people’s ability to find clinical trials in which they may be able to participate and access investigational therapies,” NIH officials said in a statement. “More information about the scientific results of trials, whether positive or negative, may help inform healthcare providers and patients regarding medical decisions. Additional information will help researchers avoid unnecessary duplication of studies, focus on areas in need of study and improve study design, ultimately advancing the development of clinical interventions.”
“Many U.S. academic medical centers, including those that conduct the most clinical trials, will find that the majority of their clinical trials fall under the [FDA Amendments Act], the NIH policy, or both,” Dr. Zarin and her colleagues wrote. “We hope that sponsors and other relevant entities will go considerably above and beyond the minimum requirements and expectations, making an effort to honor the contributions of all study participants and ensure that others in the scientific community have access to complete and high-quality information about every clinical trial under their stewardship.”
The final rule was published in the Federal Register on Sept. 21 and becomes effective on Jan. 18, 2017.
Transcatheter mitral valve therapy at ‘event horizon’
As investigational transcatheter mitral valve therapies continue to explode onto the scene, cardiac surgeons must act now to seize and assert their place in the multidisciplinary team with interventional, imaging, and heart failure colleagues to deliver these treatments to people with complex mitral valve regurgitation, an expert opinion report in the August issue of the Journal of Thoracic and Cardiovascular Surgery states (J Thorac Cardiovasc Surg. 2016;152:330-6).
“There is a growing population of patients with primary and secondary mitral regurgitation underserved by surgical therapy because of comorbid risk,” Vinay Badhwar, MD, of West Virginia University and his colleagues said. “This has led to a tremendous activity of device development.”
With more than 25 different transcatheter mitral valve devices in development (MitraClip, Abbott Vascular, is the only FDA-approved transcatheter for primary mitral regurgitation [MR]), cardiac surgeons will soon have the tools to offer transcatheter mitral valve repair (TMVr) and transcatheter mitral valve replacement (TMVR) to more complex patients who have MR along with other health problems. Today about half of those patients do not get surgery because they are too frail, Dr. Badhwar and his colleagues said.
The authors used the astrophysical phrase “event horizon” to define the current state of transcatheter mitral valve therapies – “a point of no return.” They expect surgery to remain the treatment of choice for MR for the next 10 years. “However, as our patient cohorts become increasingly more complex and transcatheter mitral therapies more facile, the day when this will become a daily clinical reality will soon be upon us,” Dr. Badhwar and his colleagues said.
The multidisciplinary team approach will be integral in achieving the full potential of transcatheter mitral valve replacement or repair, Dr. Badhwar and his coauthors said. While surgery is the most effective treatment for primary MR, cardiac surgeons are challenged to introduce transcatheter treatments in patients who have other health problems. “The best way to adjudicate innovative surgical and interventional mitral therapies is through a robust collaboration within a well-functioning heart team that includes not only a cardiac surgeon and interventional cardiologist but also an imaging specialist,” the authors said.
The time to reach out to those other specialties is now, before those investigational devices start emerging from the development pipeline, Dr. Badhwar and his colleagues said. “This will soon enable the team-based mitral specialist to be facile in safely transitioning patients from open mitral surgery to TMVr or TMVR as most appropriate for durable long-term outcomes.”
Dr. Badhwar disclosed he is an uncompensated member of the Abbott Vascular advisory board. Coauthor Vinod Thourani, MD, disclosed relationships with Edwards Lifesciences, Medtronic Cardiovascular, Abbott Vascular, St. Jude Medical, Mitralign, and AtriCure. Coauthor Michael Mack, MD, serves on the Edwards Lifesciences steering committee Partner Trial and is an uncompensated co-principal investigator of the Abbott Vascular Clinical Outcomes Assessment of the MitraClip Percutaneous Therapy Trial.
Channeling Bob Dylan’s “The Times They Are A-Changin’” in his invited commentary, W. Randolph Chitwood Jr., MD, of East Carolina University in Greenville, N.C., called Dr. Badhwar’s expert opinion “the clarion call for cardiac surgeons to become engaged in this rapidly evolving parade.”

|
Dr. W. Randolph Chitwood Jr. |
The evidence supporting the safety and efficacy of transcatheter aortic valve replacement (TAVR) is already strong, Dr. Chitwood noted. “It seems reasonable to suspect that the evolving pathway for the development of transcatheter mitral valve replacement (TMVR) could recapitulate the success of TAVR, with each generation having improved results,” he said (J Thorac Cardiovasc Surg. 2016;152:336-7).
Cardiac surgeons need to develop alternate access platforms and acquire the skills to use the new generation of transcatheter mitral devices, Dr. Chitwood said. The expert opinion “should encourage cardiac surgeons to become members of a heart team,” he said. “Guidewire skills are at the pinnacle of necessity to remain a player in this new world.”
Dr. Chitwood’s advice to colleagues: “Then you better start swimming or you’ll sink like a stone, For the times they are a-changin’.”
Dr. Chitwood disclosed he is a consultant to Direct Flow Medical and co-principal investigator for the Edwards Lifesciences Transform Trial.
Channeling Bob Dylan’s “The Times They Are A-Changin’” in his invited commentary, W. Randolph Chitwood Jr., MD, of East Carolina University in Greenville, N.C., called Dr. Badhwar’s expert opinion “the clarion call for cardiac surgeons to become engaged in this rapidly evolving parade.”
|
|
Dr. W. Randolph Chitwood Jr. |
The evidence supporting the safety and efficacy of transcatheter aortic valve replacement (TAVR) is already strong, Dr. Chitwood noted. “It seems reasonable to suspect that the evolving pathway for the development of transcatheter mitral valve replacement (TMVR) could recapitulate the success of TAVR, with each generation having improved results,” he said (J Thorac Cardiovasc Surg. 2016;152:336-7).
Cardiac surgeons need to develop alternate access platforms and acquire the skills to use the new generation of transcatheter mitral devices, Dr. Chitwood said. The expert opinion “should encourage cardiac surgeons to become members of a heart team,” he said. “Guidewire skills are at the pinnacle of necessity to remain a player in this new world.”
Dr. Chitwood’s advice to colleagues: “Then you better start swimming or you’ll sink like a stone, For the times they are a-changin’.”
Dr. Chitwood disclosed he is a consultant to Direct Flow Medical and co-principal investigator for the Edwards Lifesciences Transform Trial.
Channeling Bob Dylan’s “The Times They Are A-Changin’” in his invited commentary, W. Randolph Chitwood Jr., MD, of East Carolina University in Greenville, N.C., called Dr. Badhwar’s expert opinion “the clarion call for cardiac surgeons to become engaged in this rapidly evolving parade.”
|
|
Dr. W. Randolph Chitwood Jr. |
The evidence supporting the safety and efficacy of transcatheter aortic valve replacement (TAVR) is already strong, Dr. Chitwood noted. “It seems reasonable to suspect that the evolving pathway for the development of transcatheter mitral valve replacement (TMVR) could recapitulate the success of TAVR, with each generation having improved results,” he said (J Thorac Cardiovasc Surg. 2016;152:336-7).
Cardiac surgeons need to develop alternate access platforms and acquire the skills to use the new generation of transcatheter mitral devices, Dr. Chitwood said. The expert opinion “should encourage cardiac surgeons to become members of a heart team,” he said. “Guidewire skills are at the pinnacle of necessity to remain a player in this new world.”
Dr. Chitwood’s advice to colleagues: “Then you better start swimming or you’ll sink like a stone, For the times they are a-changin’.”
Dr. Chitwood disclosed he is a consultant to Direct Flow Medical and co-principal investigator for the Edwards Lifesciences Transform Trial.
As investigational transcatheter mitral valve therapies continue to explode onto the scene, cardiac surgeons must act now to seize and assert their place in the multidisciplinary team with interventional, imaging, and heart failure colleagues to deliver these treatments to people with complex mitral valve regurgitation, an expert opinion report in the August issue of the Journal of Thoracic and Cardiovascular Surgery states (J Thorac Cardiovasc Surg. 2016;152:330-6).
“There is a growing population of patients with primary and secondary mitral regurgitation underserved by surgical therapy because of comorbid risk,” Vinay Badhwar, MD, of West Virginia University and his colleagues said. “This has led to a tremendous activity of device development.”
With more than 25 different transcatheter mitral valve devices in development (MitraClip, Abbott Vascular, is the only FDA-approved transcatheter for primary mitral regurgitation [MR]), cardiac surgeons will soon have the tools to offer transcatheter mitral valve repair (TMVr) and transcatheter mitral valve replacement (TMVR) to more complex patients who have MR along with other health problems. Today about half of those patients do not get surgery because they are too frail, Dr. Badhwar and his colleagues said.
The authors used the astrophysical phrase “event horizon” to define the current state of transcatheter mitral valve therapies – “a point of no return.” They expect surgery to remain the treatment of choice for MR for the next 10 years. “However, as our patient cohorts become increasingly more complex and transcatheter mitral therapies more facile, the day when this will become a daily clinical reality will soon be upon us,” Dr. Badhwar and his colleagues said.
The multidisciplinary team approach will be integral in achieving the full potential of transcatheter mitral valve replacement or repair, Dr. Badhwar and his coauthors said. While surgery is the most effective treatment for primary MR, cardiac surgeons are challenged to introduce transcatheter treatments in patients who have other health problems. “The best way to adjudicate innovative surgical and interventional mitral therapies is through a robust collaboration within a well-functioning heart team that includes not only a cardiac surgeon and interventional cardiologist but also an imaging specialist,” the authors said.
The time to reach out to those other specialties is now, before those investigational devices start emerging from the development pipeline, Dr. Badhwar and his colleagues said. “This will soon enable the team-based mitral specialist to be facile in safely transitioning patients from open mitral surgery to TMVr or TMVR as most appropriate for durable long-term outcomes.”
Dr. Badhwar disclosed he is an uncompensated member of the Abbott Vascular advisory board. Coauthor Vinod Thourani, MD, disclosed relationships with Edwards Lifesciences, Medtronic Cardiovascular, Abbott Vascular, St. Jude Medical, Mitralign, and AtriCure. Coauthor Michael Mack, MD, serves on the Edwards Lifesciences steering committee Partner Trial and is an uncompensated co-principal investigator of the Abbott Vascular Clinical Outcomes Assessment of the MitraClip Percutaneous Therapy Trial.
As investigational transcatheter mitral valve therapies continue to explode onto the scene, cardiac surgeons must act now to seize and assert their place in the multidisciplinary team with interventional, imaging, and heart failure colleagues to deliver these treatments to people with complex mitral valve regurgitation, an expert opinion report in the August issue of the Journal of Thoracic and Cardiovascular Surgery states (J Thorac Cardiovasc Surg. 2016;152:330-6).
“There is a growing population of patients with primary and secondary mitral regurgitation underserved by surgical therapy because of comorbid risk,” Vinay Badhwar, MD, of West Virginia University and his colleagues said. “This has led to a tremendous activity of device development.”
With more than 25 different transcatheter mitral valve devices in development (MitraClip, Abbott Vascular, is the only FDA-approved transcatheter for primary mitral regurgitation [MR]), cardiac surgeons will soon have the tools to offer transcatheter mitral valve repair (TMVr) and transcatheter mitral valve replacement (TMVR) to more complex patients who have MR along with other health problems. Today about half of those patients do not get surgery because they are too frail, Dr. Badhwar and his colleagues said.
The authors used the astrophysical phrase “event horizon” to define the current state of transcatheter mitral valve therapies – “a point of no return.” They expect surgery to remain the treatment of choice for MR for the next 10 years. “However, as our patient cohorts become increasingly more complex and transcatheter mitral therapies more facile, the day when this will become a daily clinical reality will soon be upon us,” Dr. Badhwar and his colleagues said.
The multidisciplinary team approach will be integral in achieving the full potential of transcatheter mitral valve replacement or repair, Dr. Badhwar and his coauthors said. While surgery is the most effective treatment for primary MR, cardiac surgeons are challenged to introduce transcatheter treatments in patients who have other health problems. “The best way to adjudicate innovative surgical and interventional mitral therapies is through a robust collaboration within a well-functioning heart team that includes not only a cardiac surgeon and interventional cardiologist but also an imaging specialist,” the authors said.
The time to reach out to those other specialties is now, before those investigational devices start emerging from the development pipeline, Dr. Badhwar and his colleagues said. “This will soon enable the team-based mitral specialist to be facile in safely transitioning patients from open mitral surgery to TMVr or TMVR as most appropriate for durable long-term outcomes.”
Dr. Badhwar disclosed he is an uncompensated member of the Abbott Vascular advisory board. Coauthor Vinod Thourani, MD, disclosed relationships with Edwards Lifesciences, Medtronic Cardiovascular, Abbott Vascular, St. Jude Medical, Mitralign, and AtriCure. Coauthor Michael Mack, MD, serves on the Edwards Lifesciences steering committee Partner Trial and is an uncompensated co-principal investigator of the Abbott Vascular Clinical Outcomes Assessment of the MitraClip Percutaneous Therapy Trial.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Transcatheter mitral valve repair and replacement technology has reached a critical point that requires cardiac surgeons to assume their place in a multidisciplinary team.
Major finding: One transcatheter device is commercially available in the United States and more than 25 companies have devices in development.
Data source: Review of 22 published reports on transcatheter mitral valve technology.
Disclosures: Dr. Badhwar disclosed he is an uncompensated member of the Abbott Vascular advisory board. Coauthor Vinod Thourani, MD, disclosed relationships with Edwards Lifesciences, Medtronic Cardiovascular, Abbott Vascular, St. Jude Medical, Mitralign and AtriCure. Coauthor Michael Mack, MD, serves on the Edwards Lifesciences steering committee Partner Trial, and is an uncompensated co-principal investigator of the Abbott Vascular Clinical Outcomes Assessment of the MitraClip Percutaneous Therapy Trial.
VIDEO: When is it time to jump into MACRA with both feet?
LAS VEGAS – Change in federal reimbursement for physicians is coming. Though the change is inevitable, physicians still have to weigh choices about when they might want to jump in with both feet, since entry into the full incentive payment system will be optional – for a time.
The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) is “basically a reorganization of all of these disparate reward and penalty systems” that have existed within the federal health care reimbursement landscape, said Joseph S. Eastern, MD. “The idea was to collect them all within one system.”
The new system is called the Medicare Incentive Payment System, or MIPS. Physicians are already familiar with many MIPS components, including meaningful use of the electronic health record, “which everybody thought was going away, but it isn’t,” said Dr. Eastern, a dermatologist in private practice in Belleville, N.J., who’s affiliated with Seton Hall University, South Orange, N.J. Also included are the Physician Quality Reimbursement System (PQRS) and the value-based modifier system.
MIPS is designed so that “you’ll either get a reward or a penalty depending on how well you do, compared with other physicians,” said Dr. Eastern, speaking at the annual Perspectives in Rheumatic Diseases held by Global Academy for Medical Education.
The alternative, he said, is to opt for one of the Alternative Payment Models, or APMs. However, details about APMs are “really up in the air, because a lot of them have either not been doing very well, or have not been very well defined,” so that physicians often don’t currently have enough data to make an informed choice. He expects the APM landscape to sort out over the next year or two.
Opting not to comply and take the 1%-3% cut in Medicare reimbursement associated with noncompliance might make sense for just a few physicians, though it might seem tempting, Dr. Eastern said in a video interview. Since the penalties will escalate significantly over the next few years, he feels that only physicians who are considering retiring soon or selling their practices should consider opting out.
Global Academy for Medical Education and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @karioakes
LAS VEGAS – Change in federal reimbursement for physicians is coming. Though the change is inevitable, physicians still have to weigh choices about when they might want to jump in with both feet, since entry into the full incentive payment system will be optional – for a time.
The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) is “basically a reorganization of all of these disparate reward and penalty systems” that have existed within the federal health care reimbursement landscape, said Joseph S. Eastern, MD. “The idea was to collect them all within one system.”
The new system is called the Medicare Incentive Payment System, or MIPS. Physicians are already familiar with many MIPS components, including meaningful use of the electronic health record, “which everybody thought was going away, but it isn’t,” said Dr. Eastern, a dermatologist in private practice in Belleville, N.J., who’s affiliated with Seton Hall University, South Orange, N.J. Also included are the Physician Quality Reimbursement System (PQRS) and the value-based modifier system.
MIPS is designed so that “you’ll either get a reward or a penalty depending on how well you do, compared with other physicians,” said Dr. Eastern, speaking at the annual Perspectives in Rheumatic Diseases held by Global Academy for Medical Education.
The alternative, he said, is to opt for one of the Alternative Payment Models, or APMs. However, details about APMs are “really up in the air, because a lot of them have either not been doing very well, or have not been very well defined,” so that physicians often don’t currently have enough data to make an informed choice. He expects the APM landscape to sort out over the next year or two.
Opting not to comply and take the 1%-3% cut in Medicare reimbursement associated with noncompliance might make sense for just a few physicians, though it might seem tempting, Dr. Eastern said in a video interview. Since the penalties will escalate significantly over the next few years, he feels that only physicians who are considering retiring soon or selling their practices should consider opting out.
Global Academy for Medical Education and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @karioakes
LAS VEGAS – Change in federal reimbursement for physicians is coming. Though the change is inevitable, physicians still have to weigh choices about when they might want to jump in with both feet, since entry into the full incentive payment system will be optional – for a time.
The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) is “basically a reorganization of all of these disparate reward and penalty systems” that have existed within the federal health care reimbursement landscape, said Joseph S. Eastern, MD. “The idea was to collect them all within one system.”
The new system is called the Medicare Incentive Payment System, or MIPS. Physicians are already familiar with many MIPS components, including meaningful use of the electronic health record, “which everybody thought was going away, but it isn’t,” said Dr. Eastern, a dermatologist in private practice in Belleville, N.J., who’s affiliated with Seton Hall University, South Orange, N.J. Also included are the Physician Quality Reimbursement System (PQRS) and the value-based modifier system.
MIPS is designed so that “you’ll either get a reward or a penalty depending on how well you do, compared with other physicians,” said Dr. Eastern, speaking at the annual Perspectives in Rheumatic Diseases held by Global Academy for Medical Education.
The alternative, he said, is to opt for one of the Alternative Payment Models, or APMs. However, details about APMs are “really up in the air, because a lot of them have either not been doing very well, or have not been very well defined,” so that physicians often don’t currently have enough data to make an informed choice. He expects the APM landscape to sort out over the next year or two.
Opting not to comply and take the 1%-3% cut in Medicare reimbursement associated with noncompliance might make sense for just a few physicians, though it might seem tempting, Dr. Eastern said in a video interview. Since the penalties will escalate significantly over the next few years, he feels that only physicians who are considering retiring soon or selling their practices should consider opting out.
Global Academy for Medical Education and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @karioakes
EXPERT ANALYSIS FROM THE ANNUAL PERSPECTIVES IN RHEUMATIC DISEASES

Less pain, quicker discharge with post-TORS dexamethasone
SEATTLE – A longer course of dexamethasone was a bit better than the usual single intraoperative dose for controlling pain and dysphagia after transoral robotic surgery in a randomized trial from the Oregon Health and Science University, Portland.
Thirty-five subjects were randomized to the standard 10-mg intraoperative dexamethasone dose plus 8 mg every 8 hours for up to 4 days; 33 others were randomized to the intraoperative dose plus placebo. All the subjects had transoral robotic surgery (TORS) resection for T1 or T2 oropharyngeal squamous cell carcinoma, either partial pharyngectomy/radical tonsillectomy, base of tongue resection, or both.

The dexamethasone group had significantly less pain on postop day 3 (about 1.5 points less on the 10-point visual analogue scale) and were discharged, on average, a day earlier. They also advanced more quickly toward solid food at 1- and 3-weeks’ follow-up. “They were much more likely to be on a full-soft diet, while the placebo group was mostly still on purees, and just starting into soft foods,” said lead investigator Daniel Clayburgh, MD, a head and neck cancer specialist at the university.
Otherwise, however, the extra dexamethasone wasn’t much help; pain scores were the same in both groups for the first couple days after surgery and at follow-up, and both groups used the same amount of post-op opioids. Other than food tolerance, dysphagia metrics were pretty much the same.
“I was actually anticipating a little bit more of a benefit, but there are potentially some benefits to extended corticosteroid courses after TORS. It’s safe, and well tolerated so long as you screen out diabetes and other problems with hyperglycemia,” as was done in the study, he said. “It does decrease post-op length of stay and may provide a modest decrease in post-op pain, and may slightly accelerate advancement of dietary consistency,” Dr. Clayburgh said at the International Conference on Head and Neck Cancer, held by the American Head and Neck Society.
Although he and his colleagues are mulling over what to do with the findings in light of other initiatives to reduce post-TORS pain, they are now likely to extend dexamethasone courses when significant post-op pain seems likely, and doing so is not otherwise contraindicated, he said.
Intraoperative corticosteroids are now routine for TORS, based on the strength of benefit in the tonsillectomy literature. The team decided to try an extended course because “being rather simple minded surgeons, we thought that if one dose is good, more should be better,” Dr. Clayburgh said.
The dexamethasone group was slightly younger than the placebo group (56 vs. 61 years) but otherwise similar; most were men. In addition to patients with hyperglycemia issues, those with confounders for post-op speech and swallowing recovery were among those excluded from the trial. Subjects required nasogastric feeding tubes for a median of 6.5 days postoperatively, lost a mean of 10 pounds in the first 2 post-op weeks, and were hospitalized for a mean of about 5 days. Dexamethasone was delivered orally or by nasogastric tube.
There was no external funding for the study, and Dr. Clayburgh had no relevant financial disclosures.
SEATTLE – A longer course of dexamethasone was a bit better than the usual single intraoperative dose for controlling pain and dysphagia after transoral robotic surgery in a randomized trial from the Oregon Health and Science University, Portland.
Thirty-five subjects were randomized to the standard 10-mg intraoperative dexamethasone dose plus 8 mg every 8 hours for up to 4 days; 33 others were randomized to the intraoperative dose plus placebo. All the subjects had transoral robotic surgery (TORS) resection for T1 or T2 oropharyngeal squamous cell carcinoma, either partial pharyngectomy/radical tonsillectomy, base of tongue resection, or both.
The dexamethasone group had significantly less pain on postop day 3 (about 1.5 points less on the 10-point visual analogue scale) and were discharged, on average, a day earlier. They also advanced more quickly toward solid food at 1- and 3-weeks’ follow-up. “They were much more likely to be on a full-soft diet, while the placebo group was mostly still on purees, and just starting into soft foods,” said lead investigator Daniel Clayburgh, MD, a head and neck cancer specialist at the university.
Otherwise, however, the extra dexamethasone wasn’t much help; pain scores were the same in both groups for the first couple days after surgery and at follow-up, and both groups used the same amount of post-op opioids. Other than food tolerance, dysphagia metrics were pretty much the same.
“I was actually anticipating a little bit more of a benefit, but there are potentially some benefits to extended corticosteroid courses after TORS. It’s safe, and well tolerated so long as you screen out diabetes and other problems with hyperglycemia,” as was done in the study, he said. “It does decrease post-op length of stay and may provide a modest decrease in post-op pain, and may slightly accelerate advancement of dietary consistency,” Dr. Clayburgh said at the International Conference on Head and Neck Cancer, held by the American Head and Neck Society.
Although he and his colleagues are mulling over what to do with the findings in light of other initiatives to reduce post-TORS pain, they are now likely to extend dexamethasone courses when significant post-op pain seems likely, and doing so is not otherwise contraindicated, he said.
Intraoperative corticosteroids are now routine for TORS, based on the strength of benefit in the tonsillectomy literature. The team decided to try an extended course because “being rather simple minded surgeons, we thought that if one dose is good, more should be better,” Dr. Clayburgh said.
The dexamethasone group was slightly younger than the placebo group (56 vs. 61 years) but otherwise similar; most were men. In addition to patients with hyperglycemia issues, those with confounders for post-op speech and swallowing recovery were among those excluded from the trial. Subjects required nasogastric feeding tubes for a median of 6.5 days postoperatively, lost a mean of 10 pounds in the first 2 post-op weeks, and were hospitalized for a mean of about 5 days. Dexamethasone was delivered orally or by nasogastric tube.
There was no external funding for the study, and Dr. Clayburgh had no relevant financial disclosures.
SEATTLE – A longer course of dexamethasone was a bit better than the usual single intraoperative dose for controlling pain and dysphagia after transoral robotic surgery in a randomized trial from the Oregon Health and Science University, Portland.
Thirty-five subjects were randomized to the standard 10-mg intraoperative dexamethasone dose plus 8 mg every 8 hours for up to 4 days; 33 others were randomized to the intraoperative dose plus placebo. All the subjects had transoral robotic surgery (TORS) resection for T1 or T2 oropharyngeal squamous cell carcinoma, either partial pharyngectomy/radical tonsillectomy, base of tongue resection, or both.
The dexamethasone group had significantly less pain on postop day 3 (about 1.5 points less on the 10-point visual analogue scale) and were discharged, on average, a day earlier. They also advanced more quickly toward solid food at 1- and 3-weeks’ follow-up. “They were much more likely to be on a full-soft diet, while the placebo group was mostly still on purees, and just starting into soft foods,” said lead investigator Daniel Clayburgh, MD, a head and neck cancer specialist at the university.
Otherwise, however, the extra dexamethasone wasn’t much help; pain scores were the same in both groups for the first couple days after surgery and at follow-up, and both groups used the same amount of post-op opioids. Other than food tolerance, dysphagia metrics were pretty much the same.
“I was actually anticipating a little bit more of a benefit, but there are potentially some benefits to extended corticosteroid courses after TORS. It’s safe, and well tolerated so long as you screen out diabetes and other problems with hyperglycemia,” as was done in the study, he said. “It does decrease post-op length of stay and may provide a modest decrease in post-op pain, and may slightly accelerate advancement of dietary consistency,” Dr. Clayburgh said at the International Conference on Head and Neck Cancer, held by the American Head and Neck Society.
Although he and his colleagues are mulling over what to do with the findings in light of other initiatives to reduce post-TORS pain, they are now likely to extend dexamethasone courses when significant post-op pain seems likely, and doing so is not otherwise contraindicated, he said.
Intraoperative corticosteroids are now routine for TORS, based on the strength of benefit in the tonsillectomy literature. The team decided to try an extended course because “being rather simple minded surgeons, we thought that if one dose is good, more should be better,” Dr. Clayburgh said.
The dexamethasone group was slightly younger than the placebo group (56 vs. 61 years) but otherwise similar; most were men. In addition to patients with hyperglycemia issues, those with confounders for post-op speech and swallowing recovery were among those excluded from the trial. Subjects required nasogastric feeding tubes for a median of 6.5 days postoperatively, lost a mean of 10 pounds in the first 2 post-op weeks, and were hospitalized for a mean of about 5 days. Dexamethasone was delivered orally or by nasogastric tube.
There was no external funding for the study, and Dr. Clayburgh had no relevant financial disclosures.
AT AHNS 2016
Key clinical point: A longer course of dexamethasone is a bit better than the usual single intraoperative dose for controlling pain and dysphagia after transoral robotic surgery.
Major finding: The dexamethasone group had significantly less pain on post-op day 3 (about 1.5 points less on the 10-point visual analogue scale) and were discharged, on average, a day earlier. They also advanced more quickly toward solid food at 1- and 3-weeks’ follow-up.
Data source: A randomized trial of 68 TORS patients.
Disclosures: There was no external funding for the study, and the lead investigator had no relevant financial disclosures.

Blacks found to have higher amputation rates than whites
COLUMBUS, OHIO – The disparity in amputation rates between blacks and non-Hispanic whites in Chicago was higher than the national average and up to five times greater on the predominantly black South Side than on the predominantly white North Side of the city.
The reasons for this disparity are unclear, but a recent study of white and black Chicagoans has shown that the rates at which the races self-report claudication do not differ, suggesting that better utilization of public health resources in the black community could potentially reduce this disparity.

Reporting at the annual meeting of the Midwestern Vascular Surgery Society, lead investigator Samantha Minc, MD, of Rush University in Chicago, said the difference in amputation rates may be traced to later recognition of disease in nonwhites.
“Possible reasons for late recognition of disease include lack of access to care, communication issues with doctors, education issues, or the patient and/or caregiver and primary care provider having difficulty accessing specialists,” Dr. Minc said. “Another often-cited explanation for the late recognition is the possibility of differences in disease symptom manifestations in nonwhites, which is what we chose to study.”
Investigators from Rush University analyzed data from a combined cohort of Chicago residents age 65 years and older from two studies of aging: The Rush Memory and Aging Project and the Minority Aging Research Study.
Because of the segregated nature of Chicago – the North Side is mostly white, the South Side mostly black and the West Side mostly Hispanic – prior research has coupled census data with the Illinois Department of Public Health database to analyze care patterns. This data showed that the disparity in amputation rates among groups in Chicago was higher than the national average and up to five times greater on the South Side, compared with the North, Dr. Minc said.
The latest study matched blacks and whites from both studies 1:2 based on age, education, gender, and length of follow-up. In all, a cohort of 2,487 subjects was generated: 801 blacks and 1,686 non-Hispanic whites. Among blacks, 6.5% reported claudication at baseline, compared with 5.9% of whites, and at any point of the study 19.5% of blacks and 19.6% of non-Hispanic whites reported claudication, differences that were not statistically significant.
Blacks did have higher rates of diabetes, 27% vs. 12.6%, were more likely to have used tobacco, more likely to be female, and were slightly younger on average, but other demographic factors – such as income or rates of congestive heart failure and coronary artery disease – were not significantly different, Dr. Minc said.
The study findings will inform the Chicago Department of Public Health’s Healthy Chicago 2.0 initiative to reduce the disparity in amputation rates between whites and blacks by 10% by 2020.
Dr. Minc acknowledged limitations of the study, among them that participants were volunteers, aged 65 years and older, and 72% female, that Hispanics were excluded, and that the use of the Modified Rose/World Health Organization questionnaire to detect claudication is “specific, but not very sensitive.”
“Our findings suggest that the delay in recognition in disease in nonwhites is not due to a racial differences in disease manifestation or symptomatology and that addressing socioeconomic issues, such as access to care, communication, and education may reduce the racial disparity in amputation rates,” Dr. Minc said. “Public health resources should focus on early recognition of the disease in higher-risk groups to decrease this disparity.”
Dr. Minc and her coauthors had no relationships to disclose.
COLUMBUS, OHIO – The disparity in amputation rates between blacks and non-Hispanic whites in Chicago was higher than the national average and up to five times greater on the predominantly black South Side than on the predominantly white North Side of the city.
The reasons for this disparity are unclear, but a recent study of white and black Chicagoans has shown that the rates at which the races self-report claudication do not differ, suggesting that better utilization of public health resources in the black community could potentially reduce this disparity.
Reporting at the annual meeting of the Midwestern Vascular Surgery Society, lead investigator Samantha Minc, MD, of Rush University in Chicago, said the difference in amputation rates may be traced to later recognition of disease in nonwhites.
“Possible reasons for late recognition of disease include lack of access to care, communication issues with doctors, education issues, or the patient and/or caregiver and primary care provider having difficulty accessing specialists,” Dr. Minc said. “Another often-cited explanation for the late recognition is the possibility of differences in disease symptom manifestations in nonwhites, which is what we chose to study.”
Investigators from Rush University analyzed data from a combined cohort of Chicago residents age 65 years and older from two studies of aging: The Rush Memory and Aging Project and the Minority Aging Research Study.
Because of the segregated nature of Chicago – the North Side is mostly white, the South Side mostly black and the West Side mostly Hispanic – prior research has coupled census data with the Illinois Department of Public Health database to analyze care patterns. This data showed that the disparity in amputation rates among groups in Chicago was higher than the national average and up to five times greater on the South Side, compared with the North, Dr. Minc said.
The latest study matched blacks and whites from both studies 1:2 based on age, education, gender, and length of follow-up. In all, a cohort of 2,487 subjects was generated: 801 blacks and 1,686 non-Hispanic whites. Among blacks, 6.5% reported claudication at baseline, compared with 5.9% of whites, and at any point of the study 19.5% of blacks and 19.6% of non-Hispanic whites reported claudication, differences that were not statistically significant.
Blacks did have higher rates of diabetes, 27% vs. 12.6%, were more likely to have used tobacco, more likely to be female, and were slightly younger on average, but other demographic factors – such as income or rates of congestive heart failure and coronary artery disease – were not significantly different, Dr. Minc said.
The study findings will inform the Chicago Department of Public Health’s Healthy Chicago 2.0 initiative to reduce the disparity in amputation rates between whites and blacks by 10% by 2020.
Dr. Minc acknowledged limitations of the study, among them that participants were volunteers, aged 65 years and older, and 72% female, that Hispanics were excluded, and that the use of the Modified Rose/World Health Organization questionnaire to detect claudication is “specific, but not very sensitive.”
“Our findings suggest that the delay in recognition in disease in nonwhites is not due to a racial differences in disease manifestation or symptomatology and that addressing socioeconomic issues, such as access to care, communication, and education may reduce the racial disparity in amputation rates,” Dr. Minc said. “Public health resources should focus on early recognition of the disease in higher-risk groups to decrease this disparity.”
Dr. Minc and her coauthors had no relationships to disclose.
COLUMBUS, OHIO – The disparity in amputation rates between blacks and non-Hispanic whites in Chicago was higher than the national average and up to five times greater on the predominantly black South Side than on the predominantly white North Side of the city.
The reasons for this disparity are unclear, but a recent study of white and black Chicagoans has shown that the rates at which the races self-report claudication do not differ, suggesting that better utilization of public health resources in the black community could potentially reduce this disparity.
Reporting at the annual meeting of the Midwestern Vascular Surgery Society, lead investigator Samantha Minc, MD, of Rush University in Chicago, said the difference in amputation rates may be traced to later recognition of disease in nonwhites.
“Possible reasons for late recognition of disease include lack of access to care, communication issues with doctors, education issues, or the patient and/or caregiver and primary care provider having difficulty accessing specialists,” Dr. Minc said. “Another often-cited explanation for the late recognition is the possibility of differences in disease symptom manifestations in nonwhites, which is what we chose to study.”
Investigators from Rush University analyzed data from a combined cohort of Chicago residents age 65 years and older from two studies of aging: The Rush Memory and Aging Project and the Minority Aging Research Study.
Because of the segregated nature of Chicago – the North Side is mostly white, the South Side mostly black and the West Side mostly Hispanic – prior research has coupled census data with the Illinois Department of Public Health database to analyze care patterns. This data showed that the disparity in amputation rates among groups in Chicago was higher than the national average and up to five times greater on the South Side, compared with the North, Dr. Minc said.
The latest study matched blacks and whites from both studies 1:2 based on age, education, gender, and length of follow-up. In all, a cohort of 2,487 subjects was generated: 801 blacks and 1,686 non-Hispanic whites. Among blacks, 6.5% reported claudication at baseline, compared with 5.9% of whites, and at any point of the study 19.5% of blacks and 19.6% of non-Hispanic whites reported claudication, differences that were not statistically significant.
Blacks did have higher rates of diabetes, 27% vs. 12.6%, were more likely to have used tobacco, more likely to be female, and were slightly younger on average, but other demographic factors – such as income or rates of congestive heart failure and coronary artery disease – were not significantly different, Dr. Minc said.
The study findings will inform the Chicago Department of Public Health’s Healthy Chicago 2.0 initiative to reduce the disparity in amputation rates between whites and blacks by 10% by 2020.
Dr. Minc acknowledged limitations of the study, among them that participants were volunteers, aged 65 years and older, and 72% female, that Hispanics were excluded, and that the use of the Modified Rose/World Health Organization questionnaire to detect claudication is “specific, but not very sensitive.”
“Our findings suggest that the delay in recognition in disease in nonwhites is not due to a racial differences in disease manifestation or symptomatology and that addressing socioeconomic issues, such as access to care, communication, and education may reduce the racial disparity in amputation rates,” Dr. Minc said. “Public health resources should focus on early recognition of the disease in higher-risk groups to decrease this disparity.”
Dr. Minc and her coauthors had no relationships to disclose.
AT MIDWESTERN VASCULAR 2016
Key clinical point: Amputation rates in Chicago were up to five times greater on the predominantly black South Side of the city than on the predominantly white North Side of the city.
Major finding: Disparities in amputation rates suggest a need to address access to care and improve communication and education with regard to amputation risks in the nonwhite communities.
Data source: 2,487 subjects from the Rush Memory and Aging Project and the Minority Aging Research Study.
Disclosures: Dr. Minc and her coauthors had no relationships to disclose.

Patient-reported outcomes tied to long-term outcomes in bariatric surgery
Clinical outcomes of surgery and patient-reported outcomes of function, disability, and health status are two different measures of surgical success.
A large study of patients who had bariatric surgery showed that patient-reported outcomes were correlated with long-term weight loss but not with short-term complication rates. In addition, obesity-specific patient-reported quality of life scores were associated with a reduction in medications required for the treatment of obesity-related conditions.
“Clinical outcomes, such as perioperative morbidity and mortality, are commonly used to benchmark hospital performance,” reported Jennifer F. Waljee, MD, and her associates at the University of Michigan, Ann Arbor (Ann Surg. 2016. doi: 10.1097/SLA.0000000000001852).
“However, for many surgical procedures, such as bariatric surgery ... complications may be rare, and may not entirely reflect treatment effectiveness. Alternatively, patient-reported measures of function, disability, and health status may offer a unique and more reliable assessment of provider quality and performance,” she explained. Yet despite growing interest in using patient-reported measures, many important questions regarding their accuracy, applicability, and clinical utility remain. The purpose of this study was, therefore, to evaluate how patient-reported quality of life measures compared to short-term and long-term clinical outcomes in patients who underwent bariatric surgery.

The majority of the study’s 11,420 participants were female (79.8%), were white (84.1%), and underwent Roux-en-Y laparoscopic gastric bypass (56.8%). For each study participant, both short-term and long-term clinical outcome measures were obtained from medical board review. Short-term clinical outcomes were defined as the rate of perioperative complications within 30 days of bariatric surgery. Percent excess weight loss at 1 year post surgery was used as a long-term clinical outcome.
In addition, two patient-reported outcomes were collected: an overall health-related quality of life score called the Health and Activities Limitations Index (HALex) and an obesity-specific quality of life score, the Bariatric Quality of Life (BQL) index, which measures well-being, social and physical functioning, and obesity-related symptoms.
Multivariate and linear regression models demonstrated that short-term complication rates were not correlated to the overall patient-reported quality of life score (P = .32) or to the obesity-specific BQL score (P = .74).
However, the long-term measure of excess weight loss at 1 year post surgery was significantly associated with both overall and obesity-specific patient-reported measures of health-related quality of life (P less than .002 and P less than .001 respectively).
Moreover, scores indicating improved quality of life were associated with greater weight loss.
Finally, comorbidity resolution, estimated by the reduction in the use of medications taken to treat conditions related to obesity, was significantly associated with the obesity-specific measure, BQL, but not the overall quality of life measure, HALex.
“In conclusion, [patient-reported outcomes] are distinct from clinical outcomes,” investigators wrote. Patient-reported outcomes “provide an opportunity for improved population-based cost-effectiveness analyses using outcomes germane to procedures performed for symptomatology and improving QOL,” they added.
The Agency for Healthcare Research and Quality supported the research. The investigators reported having no disclosures.
On Twitter @jessnicolecraig
Clinical outcomes of surgery and patient-reported outcomes of function, disability, and health status are two different measures of surgical success.
A large study of patients who had bariatric surgery showed that patient-reported outcomes were correlated with long-term weight loss but not with short-term complication rates. In addition, obesity-specific patient-reported quality of life scores were associated with a reduction in medications required for the treatment of obesity-related conditions.
“Clinical outcomes, such as perioperative morbidity and mortality, are commonly used to benchmark hospital performance,” reported Jennifer F. Waljee, MD, and her associates at the University of Michigan, Ann Arbor (Ann Surg. 2016. doi: 10.1097/SLA.0000000000001852).
“However, for many surgical procedures, such as bariatric surgery ... complications may be rare, and may not entirely reflect treatment effectiveness. Alternatively, patient-reported measures of function, disability, and health status may offer a unique and more reliable assessment of provider quality and performance,” she explained. Yet despite growing interest in using patient-reported measures, many important questions regarding their accuracy, applicability, and clinical utility remain. The purpose of this study was, therefore, to evaluate how patient-reported quality of life measures compared to short-term and long-term clinical outcomes in patients who underwent bariatric surgery.
The majority of the study’s 11,420 participants were female (79.8%), were white (84.1%), and underwent Roux-en-Y laparoscopic gastric bypass (56.8%). For each study participant, both short-term and long-term clinical outcome measures were obtained from medical board review. Short-term clinical outcomes were defined as the rate of perioperative complications within 30 days of bariatric surgery. Percent excess weight loss at 1 year post surgery was used as a long-term clinical outcome.
In addition, two patient-reported outcomes were collected: an overall health-related quality of life score called the Health and Activities Limitations Index (HALex) and an obesity-specific quality of life score, the Bariatric Quality of Life (BQL) index, which measures well-being, social and physical functioning, and obesity-related symptoms.
Multivariate and linear regression models demonstrated that short-term complication rates were not correlated to the overall patient-reported quality of life score (P = .32) or to the obesity-specific BQL score (P = .74).
However, the long-term measure of excess weight loss at 1 year post surgery was significantly associated with both overall and obesity-specific patient-reported measures of health-related quality of life (P less than .002 and P less than .001 respectively).
Moreover, scores indicating improved quality of life were associated with greater weight loss.
Finally, comorbidity resolution, estimated by the reduction in the use of medications taken to treat conditions related to obesity, was significantly associated with the obesity-specific measure, BQL, but not the overall quality of life measure, HALex.
“In conclusion, [patient-reported outcomes] are distinct from clinical outcomes,” investigators wrote. Patient-reported outcomes “provide an opportunity for improved population-based cost-effectiveness analyses using outcomes germane to procedures performed for symptomatology and improving QOL,” they added.
The Agency for Healthcare Research and Quality supported the research. The investigators reported having no disclosures.
On Twitter @jessnicolecraig
Clinical outcomes of surgery and patient-reported outcomes of function, disability, and health status are two different measures of surgical success.
A large study of patients who had bariatric surgery showed that patient-reported outcomes were correlated with long-term weight loss but not with short-term complication rates. In addition, obesity-specific patient-reported quality of life scores were associated with a reduction in medications required for the treatment of obesity-related conditions.
“Clinical outcomes, such as perioperative morbidity and mortality, are commonly used to benchmark hospital performance,” reported Jennifer F. Waljee, MD, and her associates at the University of Michigan, Ann Arbor (Ann Surg. 2016. doi: 10.1097/SLA.0000000000001852).
“However, for many surgical procedures, such as bariatric surgery ... complications may be rare, and may not entirely reflect treatment effectiveness. Alternatively, patient-reported measures of function, disability, and health status may offer a unique and more reliable assessment of provider quality and performance,” she explained. Yet despite growing interest in using patient-reported measures, many important questions regarding their accuracy, applicability, and clinical utility remain. The purpose of this study was, therefore, to evaluate how patient-reported quality of life measures compared to short-term and long-term clinical outcomes in patients who underwent bariatric surgery.
The majority of the study’s 11,420 participants were female (79.8%), were white (84.1%), and underwent Roux-en-Y laparoscopic gastric bypass (56.8%). For each study participant, both short-term and long-term clinical outcome measures were obtained from medical board review. Short-term clinical outcomes were defined as the rate of perioperative complications within 30 days of bariatric surgery. Percent excess weight loss at 1 year post surgery was used as a long-term clinical outcome.
In addition, two patient-reported outcomes were collected: an overall health-related quality of life score called the Health and Activities Limitations Index (HALex) and an obesity-specific quality of life score, the Bariatric Quality of Life (BQL) index, which measures well-being, social and physical functioning, and obesity-related symptoms.
Multivariate and linear regression models demonstrated that short-term complication rates were not correlated to the overall patient-reported quality of life score (P = .32) or to the obesity-specific BQL score (P = .74).
However, the long-term measure of excess weight loss at 1 year post surgery was significantly associated with both overall and obesity-specific patient-reported measures of health-related quality of life (P less than .002 and P less than .001 respectively).
Moreover, scores indicating improved quality of life were associated with greater weight loss.
Finally, comorbidity resolution, estimated by the reduction in the use of medications taken to treat conditions related to obesity, was significantly associated with the obesity-specific measure, BQL, but not the overall quality of life measure, HALex.
“In conclusion, [patient-reported outcomes] are distinct from clinical outcomes,” investigators wrote. Patient-reported outcomes “provide an opportunity for improved population-based cost-effectiveness analyses using outcomes germane to procedures performed for symptomatology and improving QOL,” they added.
The Agency for Healthcare Research and Quality supported the research. The investigators reported having no disclosures.
On Twitter @jessnicolecraig
FROM ANNALS OF SURGERY
Key clinical point: Patient-reported quality of life measures were associated with long-term but not short-term clinical outcomes.
Major finding: Overall and obesity-specific patient-reported quality of life scores were associated with long-term excess weight loss (P less than .002 and P less than .001 respectively).
Data source: A retrospective study of 11,420 patients who underwent bariatric surgery.
Disclosures: The Agency for Healthcare Research and Quality supported the study. The investigators reported having no disclosures.
