User login
Suvorexant: An option for preventing delirium?
Delirium is characterized by a disturbance of consciousness or cognition that typically has a rapid onset and fluctuating course.1 Up to 42% of hospitalized geriatric patients experience delirium.1 Approximately 10% to 31% of these patients have the condition upon admission, and the remainder develop it during their hospitalization.1 Unfortunately, options for preventing or treating delirium are limited. Benzodiazepines and antipsychotic medications have been used to treat problematic behaviors associated with delirium, but they do not effectively reduce the occurrence, duration, or severity of this condition.2,3
Recent evidence suggests that suvorexant, which is FDA-approved for insomnia, may be useful for preventing delirium. Suvorexant—a dual orexin receptor (OX1R, OX2R) antagonist—promotes sleep onset and maintenance, and is associated with normal measures of sleep activity such as rapid eye movement (REM) sleep, non-REM sleep, and sleep stage–specific electroencephalographic profiles.4 Here we review 3 studies that evaluated suvorexant for preventing delirium.
Hatta et al.5 In this randomized, placebo-controlled, blinded, multicenter study, 72 patients (age 65 to 89) newly admitted to an ICU were randomized to suvorexant, 15 mg/d, (n = 36) or placebo (n = 36) for 3 days.5 None of the patients taking suvorexant developed delirium, whereas 17% (6 patients) in the placebo group did (P = .025).5
Azuma et al.6 In this 7-day, blinded, randomized study of 70 adult patients (age ≥20) admitted to an ICU, 34 participants received suvorexant (15 mg nightly for age <65, 20 mg nightly for age ≥65) and the rest received treatment as usual (TAU). Suvorexant was associated with a lower incidence of delirium symptoms (n = 6, 17.6%) compared with TAU (n = 17, 47.2%) (P = .011).6 The onset of delirium was earlier in the TAU group (P < .05).6
Hatta et al.7 In this large prospective, observational study of adults (age >65), 526 patients with significant risk factors for delirium were prescribed suvorexant and/or ramelteon. Approximately 16% of the patients who received either or both of these medications met DSM-5 criteria for delirium, compared with 24% who did not receive these medications (P = .005).7
Acknowledgment
The authors thank Jakob Evans, BS, for compiling much of the research for this article.
1. Siddiqi N, House AO, Holmes JD. Occurrence and outcome of delirium in medical in-patients: a systematic literature review. Age Ageing. 2006;35(4):350-364.
2. Lonergan E, Luxenberg J, Areosa Sastre A. Benzodiazepines for delirium. Cochrane Database Syst Rev. 2009;2009(4):CD006379.
3. Burry L, Mehta S, Perreault MM, et al. Antipsychotics for treatment of delirium in hospitalised non-ICU patients. Cochrane Database Syst Rev. 2018;6(6):CD005594.
4. Coleman PJ, Gotter AL, Herring WJ, et al. The discovery of suvorexant, the first orexin receptor drug for insomnia. Annu Rev Pharmacol Toxicol. 2017;57:509-533.
5. Hatta K, Kishi Y, Wada K, et al. Preventive effects of suvorexant on delirium: a randomized placebo-controlled trial. J Clin Psychiatry. 2017;78(8):e970-e979.
6. Azuma K, Takaesu Y, Soeda H, et al. Ability of suvorexant to prevent delirium in patients in the intensive care unit: a randomized controlled trial. Acute Med Surg. 2018;5(4):362-368.
7. Hatta K, Kishi Y, Wada K, et al. Real-world effectiveness of ramelteon and suvorexant for delirium prevention in 948 patients with delirium risk factors. J Clin Psychiatry. 2019;81(1):19m12865. doi: 10.4088/JCP.19m12865
Delirium is characterized by a disturbance of consciousness or cognition that typically has a rapid onset and fluctuating course.1 Up to 42% of hospitalized geriatric patients experience delirium.1 Approximately 10% to 31% of these patients have the condition upon admission, and the remainder develop it during their hospitalization.1 Unfortunately, options for preventing or treating delirium are limited. Benzodiazepines and antipsychotic medications have been used to treat problematic behaviors associated with delirium, but they do not effectively reduce the occurrence, duration, or severity of this condition.2,3
Recent evidence suggests that suvorexant, which is FDA-approved for insomnia, may be useful for preventing delirium. Suvorexant—a dual orexin receptor (OX1R, OX2R) antagonist—promotes sleep onset and maintenance, and is associated with normal measures of sleep activity such as rapid eye movement (REM) sleep, non-REM sleep, and sleep stage–specific electroencephalographic profiles.4 Here we review 3 studies that evaluated suvorexant for preventing delirium.
Hatta et al.5 In this randomized, placebo-controlled, blinded, multicenter study, 72 patients (age 65 to 89) newly admitted to an ICU were randomized to suvorexant, 15 mg/d, (n = 36) or placebo (n = 36) for 3 days.5 None of the patients taking suvorexant developed delirium, whereas 17% (6 patients) in the placebo group did (P = .025).5
Azuma et al.6 In this 7-day, blinded, randomized study of 70 adult patients (age ≥20) admitted to an ICU, 34 participants received suvorexant (15 mg nightly for age <65, 20 mg nightly for age ≥65) and the rest received treatment as usual (TAU). Suvorexant was associated with a lower incidence of delirium symptoms (n = 6, 17.6%) compared with TAU (n = 17, 47.2%) (P = .011).6 The onset of delirium was earlier in the TAU group (P < .05).6
Hatta et al.7 In this large prospective, observational study of adults (age >65), 526 patients with significant risk factors for delirium were prescribed suvorexant and/or ramelteon. Approximately 16% of the patients who received either or both of these medications met DSM-5 criteria for delirium, compared with 24% who did not receive these medications (P = .005).7
Acknowledgment
The authors thank Jakob Evans, BS, for compiling much of the research for this article.
Delirium is characterized by a disturbance of consciousness or cognition that typically has a rapid onset and fluctuating course.1 Up to 42% of hospitalized geriatric patients experience delirium.1 Approximately 10% to 31% of these patients have the condition upon admission, and the remainder develop it during their hospitalization.1 Unfortunately, options for preventing or treating delirium are limited. Benzodiazepines and antipsychotic medications have been used to treat problematic behaviors associated with delirium, but they do not effectively reduce the occurrence, duration, or severity of this condition.2,3
Recent evidence suggests that suvorexant, which is FDA-approved for insomnia, may be useful for preventing delirium. Suvorexant—a dual orexin receptor (OX1R, OX2R) antagonist—promotes sleep onset and maintenance, and is associated with normal measures of sleep activity such as rapid eye movement (REM) sleep, non-REM sleep, and sleep stage–specific electroencephalographic profiles.4 Here we review 3 studies that evaluated suvorexant for preventing delirium.
Hatta et al.5 In this randomized, placebo-controlled, blinded, multicenter study, 72 patients (age 65 to 89) newly admitted to an ICU were randomized to suvorexant, 15 mg/d, (n = 36) or placebo (n = 36) for 3 days.5 None of the patients taking suvorexant developed delirium, whereas 17% (6 patients) in the placebo group did (P = .025).5
Azuma et al.6 In this 7-day, blinded, randomized study of 70 adult patients (age ≥20) admitted to an ICU, 34 participants received suvorexant (15 mg nightly for age <65, 20 mg nightly for age ≥65) and the rest received treatment as usual (TAU). Suvorexant was associated with a lower incidence of delirium symptoms (n = 6, 17.6%) compared with TAU (n = 17, 47.2%) (P = .011).6 The onset of delirium was earlier in the TAU group (P < .05).6
Hatta et al.7 In this large prospective, observational study of adults (age >65), 526 patients with significant risk factors for delirium were prescribed suvorexant and/or ramelteon. Approximately 16% of the patients who received either or both of these medications met DSM-5 criteria for delirium, compared with 24% who did not receive these medications (P = .005).7
Acknowledgment
The authors thank Jakob Evans, BS, for compiling much of the research for this article.
1. Siddiqi N, House AO, Holmes JD. Occurrence and outcome of delirium in medical in-patients: a systematic literature review. Age Ageing. 2006;35(4):350-364.
2. Lonergan E, Luxenberg J, Areosa Sastre A. Benzodiazepines for delirium. Cochrane Database Syst Rev. 2009;2009(4):CD006379.
3. Burry L, Mehta S, Perreault MM, et al. Antipsychotics for treatment of delirium in hospitalised non-ICU patients. Cochrane Database Syst Rev. 2018;6(6):CD005594.
4. Coleman PJ, Gotter AL, Herring WJ, et al. The discovery of suvorexant, the first orexin receptor drug for insomnia. Annu Rev Pharmacol Toxicol. 2017;57:509-533.
5. Hatta K, Kishi Y, Wada K, et al. Preventive effects of suvorexant on delirium: a randomized placebo-controlled trial. J Clin Psychiatry. 2017;78(8):e970-e979.
6. Azuma K, Takaesu Y, Soeda H, et al. Ability of suvorexant to prevent delirium in patients in the intensive care unit: a randomized controlled trial. Acute Med Surg. 2018;5(4):362-368.
7. Hatta K, Kishi Y, Wada K, et al. Real-world effectiveness of ramelteon and suvorexant for delirium prevention in 948 patients with delirium risk factors. J Clin Psychiatry. 2019;81(1):19m12865. doi: 10.4088/JCP.19m12865
1. Siddiqi N, House AO, Holmes JD. Occurrence and outcome of delirium in medical in-patients: a systematic literature review. Age Ageing. 2006;35(4):350-364.
2. Lonergan E, Luxenberg J, Areosa Sastre A. Benzodiazepines for delirium. Cochrane Database Syst Rev. 2009;2009(4):CD006379.
3. Burry L, Mehta S, Perreault MM, et al. Antipsychotics for treatment of delirium in hospitalised non-ICU patients. Cochrane Database Syst Rev. 2018;6(6):CD005594.
4. Coleman PJ, Gotter AL, Herring WJ, et al. The discovery of suvorexant, the first orexin receptor drug for insomnia. Annu Rev Pharmacol Toxicol. 2017;57:509-533.
5. Hatta K, Kishi Y, Wada K, et al. Preventive effects of suvorexant on delirium: a randomized placebo-controlled trial. J Clin Psychiatry. 2017;78(8):e970-e979.
6. Azuma K, Takaesu Y, Soeda H, et al. Ability of suvorexant to prevent delirium in patients in the intensive care unit: a randomized controlled trial. Acute Med Surg. 2018;5(4):362-368.
7. Hatta K, Kishi Y, Wada K, et al. Real-world effectiveness of ramelteon and suvorexant for delirium prevention in 948 patients with delirium risk factors. J Clin Psychiatry. 2019;81(1):19m12865. doi: 10.4088/JCP.19m12865

Pandemic binge-watching: Is excessive screen time undermining mental health?
During the ongoing COVID-19 pandemic, many people are spending endless hours at home looking at computer, phone, and television screens. Our population has turned to Internet use and television watching as a coping mechanism to deal with their isolation, boredom, stress, and fear of the virus. Indeed, some people have become addicted to watching television and binge-watching entire series in a single sitting on subscription streaming services.

A U.K. study showed that, during the lockdown, adults averaged spending 40% of their waking hours in front of a screen. After a long binge-watch, folks often forget what happened in the episodes or even the name of the program they viewed. When someone finds himself in this situation and can’t remember very much about what he actually watched, he feels as though he has wasted his own time and might become dysphoric and depressed. This type of viewer feels disconnected and forgets what he watched because he is experiencing passive enjoyment, rather than actively relating to the world.
So should television binge-watching give people feelings of guilt?
Fortunately, there are some positive factors about spending excessive time engrossed in these screens during a pandemic; some people use television viewing as a coping mechanism to deal with the reality and the fear of the coronavirus. Some beneficial aspects of television watching include:
- Escaping from the reality and stress of the pandemic in an emotionally safe, isolated cocoon.
- Experiencing safety from contracting COVID-19 by sheltering in place, isolating, and physical distancing from other people in the outside world.
- Experiencing a subdued, private, and mentally relaxing environment.
- Being productive and multitasking while watching television, for example, knit, sew, fold clothes, pay bills, write a letter, etc.
Despite many beneficial aspects of excessive television watching during the pandemic, we have to ask: Can too much television prove detrimental to our mental or physical well-being?
Associated mental, and physical problems
Cause and effect between excessive screen time and sleep disturbances is scientifically unproven, but there is an association between those factors.
Excessive screen time is associated with a sleep deficit, and a proper amount of sleep is necessary for optimal brain function, a healthy immune system, good memory, and overall well-being. Sleep cleans out the short-term memory stage from the information learned that day to make room for new memories. This allows us to store memories every day. An inadequate amount of sleep causes memory problems and cognitive deficits because we are not storing as many memories from days when we are sleep deprived. A good night’s sleep will prevent stress from one day to be carried over to the next day.

Lack of sleep affects people differently, but in some cases, a shortage of sleep can cause feelings of depression and isolation. Television, computer, and phone screens convey excessive damaging LED and blue light, detrimentally affecting our melatonin production and circadian rhythm. Blue light has wavelengths between 380 nm and 500 nm, and although blue wavelengths are beneficial in the day and increase positive mental mood, attention, and reaction times, blue wavelengths are destructive at night. Blue-light exposure suppresses the secretion of melatonin, which, as we know, is a hormone that influences circadian rhythms. The negative disruption of circadian rhythm throws the body’s biological clock in disarray and makes it more difficult for the mind to shut down at night.
Unfortunately, electronics with LED screens increase the amount of exposure to these blue wavelengths. In addition, the U.S. National Toxicology Program has suggested that a link exists between blue-light exposure at night to diabetes, heart disease, cancer, and obesity (Sci Tot Environ. 2017 Dec 31;[607-8]:1073-84).
Advice for patients and clinicians
Time spent watching television and using the Internet should be done in moderation. Make sure that patients understand that they should not feel guilty about watching television during these periods of isolation.
Encourage patients to be selective in their television viewing and to research available programs on streaming services and TV – and limit their screen time only to programs that truly interest them. Discourage them from watching television endlessly, hour after hour. Also, discourage patients from watching too much news. Instead, tell them to limit news to 1 hour per day, because news they perceive as bad might increase their overall anxiety.
Tell patients to engage in physical exercise every day; walk or run outside if possible. When inside, advise them to get up and walk around at least once per hour. Other advice we would like to offer patients and clinicians alike are:
- Put yourself on a schedule and go to sleep the same time each night and try to get 8 hours of sleep in a 24-hour period.
- Put away your devices 1 hour before going to bed or at least use dark mode, and wear blue-block glasses, since they are easier on the eyes and brain. Do not use television to put yourself to sleep. Spending too much time reading news stories is not a good idea, either, because doing so is mentally stimulating and can cause more uncertainty – making it difficult to sleep.
- Protect your eye health by purchasing and installing light bulbs with more internal red coating than blue. These bulbs will produce a warmer tone than the blue, and warmer tones will be less likely to shift circadian rhythm and suppress melatonin, thus reducing blue-light exposure. Blink your eyes often, and use eye solution for dry eyes.
- Sleep in total darkness to reduce your exposure to blue light. Take supplements with lutein and zeaxanthin, which may reduce the oxidative effects of blue light.
Encouraging patients to follow these guidelines – and adhering to them ourselves – should help us emerge from the COVID-19 pandemic mentally and physically healthy.
Dr. Cohen is board certified in psychiatry and has had a private practice in Philadelphia for more than 35 years. His areas of specialty include sports psychiatry, agoraphobia, depression, and substance abuse. In addition, Dr. Cohen is a former professor of psychiatry, family medicine, and otolaryngology at Thomas Jefferson University, Philadelphia. He has no conflicts of interest.
Ms. Cohen holds an MBA from Temple University, Philadelphia, with a focus on health care administration. Previously, Ms. Cohen was an associate administrator at Hahnemann University Hospital and an executive at the Health Services Council, both in Philadelphia. She currently writes biographical summaries of notable 18th- and 19th-century women. Ms. Cohen has no conflicts of interest.
During the ongoing COVID-19 pandemic, many people are spending endless hours at home looking at computer, phone, and television screens. Our population has turned to Internet use and television watching as a coping mechanism to deal with their isolation, boredom, stress, and fear of the virus. Indeed, some people have become addicted to watching television and binge-watching entire series in a single sitting on subscription streaming services.
A U.K. study showed that, during the lockdown, adults averaged spending 40% of their waking hours in front of a screen. After a long binge-watch, folks often forget what happened in the episodes or even the name of the program they viewed. When someone finds himself in this situation and can’t remember very much about what he actually watched, he feels as though he has wasted his own time and might become dysphoric and depressed. This type of viewer feels disconnected and forgets what he watched because he is experiencing passive enjoyment, rather than actively relating to the world.
So should television binge-watching give people feelings of guilt?
Fortunately, there are some positive factors about spending excessive time engrossed in these screens during a pandemic; some people use television viewing as a coping mechanism to deal with the reality and the fear of the coronavirus. Some beneficial aspects of television watching include:
- Escaping from the reality and stress of the pandemic in an emotionally safe, isolated cocoon.
- Experiencing safety from contracting COVID-19 by sheltering in place, isolating, and physical distancing from other people in the outside world.
- Experiencing a subdued, private, and mentally relaxing environment.
- Being productive and multitasking while watching television, for example, knit, sew, fold clothes, pay bills, write a letter, etc.
Despite many beneficial aspects of excessive television watching during the pandemic, we have to ask: Can too much television prove detrimental to our mental or physical well-being?
Associated mental, and physical problems
Cause and effect between excessive screen time and sleep disturbances is scientifically unproven, but there is an association between those factors.
Excessive screen time is associated with a sleep deficit, and a proper amount of sleep is necessary for optimal brain function, a healthy immune system, good memory, and overall well-being. Sleep cleans out the short-term memory stage from the information learned that day to make room for new memories. This allows us to store memories every day. An inadequate amount of sleep causes memory problems and cognitive deficits because we are not storing as many memories from days when we are sleep deprived. A good night’s sleep will prevent stress from one day to be carried over to the next day.
Lack of sleep affects people differently, but in some cases, a shortage of sleep can cause feelings of depression and isolation. Television, computer, and phone screens convey excessive damaging LED and blue light, detrimentally affecting our melatonin production and circadian rhythm. Blue light has wavelengths between 380 nm and 500 nm, and although blue wavelengths are beneficial in the day and increase positive mental mood, attention, and reaction times, blue wavelengths are destructive at night. Blue-light exposure suppresses the secretion of melatonin, which, as we know, is a hormone that influences circadian rhythms. The negative disruption of circadian rhythm throws the body’s biological clock in disarray and makes it more difficult for the mind to shut down at night.
Unfortunately, electronics with LED screens increase the amount of exposure to these blue wavelengths. In addition, the U.S. National Toxicology Program has suggested that a link exists between blue-light exposure at night to diabetes, heart disease, cancer, and obesity (Sci Tot Environ. 2017 Dec 31;[607-8]:1073-84).
Advice for patients and clinicians
Time spent watching television and using the Internet should be done in moderation. Make sure that patients understand that they should not feel guilty about watching television during these periods of isolation.
Encourage patients to be selective in their television viewing and to research available programs on streaming services and TV – and limit their screen time only to programs that truly interest them. Discourage them from watching television endlessly, hour after hour. Also, discourage patients from watching too much news. Instead, tell them to limit news to 1 hour per day, because news they perceive as bad might increase their overall anxiety.
Tell patients to engage in physical exercise every day; walk or run outside if possible. When inside, advise them to get up and walk around at least once per hour. Other advice we would like to offer patients and clinicians alike are:
- Put yourself on a schedule and go to sleep the same time each night and try to get 8 hours of sleep in a 24-hour period.
- Put away your devices 1 hour before going to bed or at least use dark mode, and wear blue-block glasses, since they are easier on the eyes and brain. Do not use television to put yourself to sleep. Spending too much time reading news stories is not a good idea, either, because doing so is mentally stimulating and can cause more uncertainty – making it difficult to sleep.
- Protect your eye health by purchasing and installing light bulbs with more internal red coating than blue. These bulbs will produce a warmer tone than the blue, and warmer tones will be less likely to shift circadian rhythm and suppress melatonin, thus reducing blue-light exposure. Blink your eyes often, and use eye solution for dry eyes.
- Sleep in total darkness to reduce your exposure to blue light. Take supplements with lutein and zeaxanthin, which may reduce the oxidative effects of blue light.
Encouraging patients to follow these guidelines – and adhering to them ourselves – should help us emerge from the COVID-19 pandemic mentally and physically healthy.
Dr. Cohen is board certified in psychiatry and has had a private practice in Philadelphia for more than 35 years. His areas of specialty include sports psychiatry, agoraphobia, depression, and substance abuse. In addition, Dr. Cohen is a former professor of psychiatry, family medicine, and otolaryngology at Thomas Jefferson University, Philadelphia. He has no conflicts of interest.
Ms. Cohen holds an MBA from Temple University, Philadelphia, with a focus on health care administration. Previously, Ms. Cohen was an associate administrator at Hahnemann University Hospital and an executive at the Health Services Council, both in Philadelphia. She currently writes biographical summaries of notable 18th- and 19th-century women. Ms. Cohen has no conflicts of interest.
During the ongoing COVID-19 pandemic, many people are spending endless hours at home looking at computer, phone, and television screens. Our population has turned to Internet use and television watching as a coping mechanism to deal with their isolation, boredom, stress, and fear of the virus. Indeed, some people have become addicted to watching television and binge-watching entire series in a single sitting on subscription streaming services.
A U.K. study showed that, during the lockdown, adults averaged spending 40% of their waking hours in front of a screen. After a long binge-watch, folks often forget what happened in the episodes or even the name of the program they viewed. When someone finds himself in this situation and can’t remember very much about what he actually watched, he feels as though he has wasted his own time and might become dysphoric and depressed. This type of viewer feels disconnected and forgets what he watched because he is experiencing passive enjoyment, rather than actively relating to the world.
So should television binge-watching give people feelings of guilt?
Fortunately, there are some positive factors about spending excessive time engrossed in these screens during a pandemic; some people use television viewing as a coping mechanism to deal with the reality and the fear of the coronavirus. Some beneficial aspects of television watching include:
- Escaping from the reality and stress of the pandemic in an emotionally safe, isolated cocoon.
- Experiencing safety from contracting COVID-19 by sheltering in place, isolating, and physical distancing from other people in the outside world.
- Experiencing a subdued, private, and mentally relaxing environment.
- Being productive and multitasking while watching television, for example, knit, sew, fold clothes, pay bills, write a letter, etc.
Despite many beneficial aspects of excessive television watching during the pandemic, we have to ask: Can too much television prove detrimental to our mental or physical well-being?
Associated mental, and physical problems
Cause and effect between excessive screen time and sleep disturbances is scientifically unproven, but there is an association between those factors.
Excessive screen time is associated with a sleep deficit, and a proper amount of sleep is necessary for optimal brain function, a healthy immune system, good memory, and overall well-being. Sleep cleans out the short-term memory stage from the information learned that day to make room for new memories. This allows us to store memories every day. An inadequate amount of sleep causes memory problems and cognitive deficits because we are not storing as many memories from days when we are sleep deprived. A good night’s sleep will prevent stress from one day to be carried over to the next day.
Lack of sleep affects people differently, but in some cases, a shortage of sleep can cause feelings of depression and isolation. Television, computer, and phone screens convey excessive damaging LED and blue light, detrimentally affecting our melatonin production and circadian rhythm. Blue light has wavelengths between 380 nm and 500 nm, and although blue wavelengths are beneficial in the day and increase positive mental mood, attention, and reaction times, blue wavelengths are destructive at night. Blue-light exposure suppresses the secretion of melatonin, which, as we know, is a hormone that influences circadian rhythms. The negative disruption of circadian rhythm throws the body’s biological clock in disarray and makes it more difficult for the mind to shut down at night.
Unfortunately, electronics with LED screens increase the amount of exposure to these blue wavelengths. In addition, the U.S. National Toxicology Program has suggested that a link exists between blue-light exposure at night to diabetes, heart disease, cancer, and obesity (Sci Tot Environ. 2017 Dec 31;[607-8]:1073-84).
Advice for patients and clinicians
Time spent watching television and using the Internet should be done in moderation. Make sure that patients understand that they should not feel guilty about watching television during these periods of isolation.
Encourage patients to be selective in their television viewing and to research available programs on streaming services and TV – and limit their screen time only to programs that truly interest them. Discourage them from watching television endlessly, hour after hour. Also, discourage patients from watching too much news. Instead, tell them to limit news to 1 hour per day, because news they perceive as bad might increase their overall anxiety.
Tell patients to engage in physical exercise every day; walk or run outside if possible. When inside, advise them to get up and walk around at least once per hour. Other advice we would like to offer patients and clinicians alike are:
- Put yourself on a schedule and go to sleep the same time each night and try to get 8 hours of sleep in a 24-hour period.
- Put away your devices 1 hour before going to bed or at least use dark mode, and wear blue-block glasses, since they are easier on the eyes and brain. Do not use television to put yourself to sleep. Spending too much time reading news stories is not a good idea, either, because doing so is mentally stimulating and can cause more uncertainty – making it difficult to sleep.
- Protect your eye health by purchasing and installing light bulbs with more internal red coating than blue. These bulbs will produce a warmer tone than the blue, and warmer tones will be less likely to shift circadian rhythm and suppress melatonin, thus reducing blue-light exposure. Blink your eyes often, and use eye solution for dry eyes.
- Sleep in total darkness to reduce your exposure to blue light. Take supplements with lutein and zeaxanthin, which may reduce the oxidative effects of blue light.
Encouraging patients to follow these guidelines – and adhering to them ourselves – should help us emerge from the COVID-19 pandemic mentally and physically healthy.
Dr. Cohen is board certified in psychiatry and has had a private practice in Philadelphia for more than 35 years. His areas of specialty include sports psychiatry, agoraphobia, depression, and substance abuse. In addition, Dr. Cohen is a former professor of psychiatry, family medicine, and otolaryngology at Thomas Jefferson University, Philadelphia. He has no conflicts of interest.
Ms. Cohen holds an MBA from Temple University, Philadelphia, with a focus on health care administration. Previously, Ms. Cohen was an associate administrator at Hahnemann University Hospital and an executive at the Health Services Council, both in Philadelphia. She currently writes biographical summaries of notable 18th- and 19th-century women. Ms. Cohen has no conflicts of interest.
Coronasomnia: Pervasive sleeplessness, self-medicating raise concerns of sleep experts
Among the many losses suffered by millions worldwide during the COVID-19 pandemic, the loss of sleep may be the most widespread, with potentially long-lasting, negative consequences on physical, mental, and emotional health, sleep researchers have found.
Results from multiple studies and surveys conducted during the pandemic show that a majority of subjects report clinically meaningful changes in sleep quality, sleep patterns, and sleep disturbances.

For example, a cross-sectional international survey conducted from late March through late April 2020 found that among more than 3,000 responders from 49 countries, 58% reported dissatisfaction with their sleep, and 40% reported a decrease in sleep quality during the pandemic, compared with pre-COVID-19 sleep, according to Uri Mandelkorn of the Natural Sleep Clinic in Jerusalem, and colleagues.
“In particular, this research raises the need to screen for worsening sleep patterns and use of sleeping aids in the more susceptible populations identified in this study, namely, women and people with insecure livelihoods or those subjected to strict quarantine. Health care providers should pay special attention to physical and psychological problems that this surge in sleep disturbances may cause,” they wrote. The report is in the Journal of Clinical Sleep Medicine.
Sleeping, more or less
A coauthor of that study, David Gozal, MD, FCCP, a pediatric pulmonologist and sleep medicine specialist at the University of Missouri in Columbia, said that the pandemic has had paradoxical effects on sleeps patterns for many.
“At the beginning, with the initial phases of lockdown for COVID, for most of the people whose jobs were not affected and who did not lose their jobs, [for whom] there was not the anxiety of being jobless and financially strapped, but who now were staying at home, there was actually a benefit. People started reporting getting more sleep and, more importantly, more vivid dreams and things of that nature,” he said in an interview.
“But as the lockdown progressed, we saw progressively and increasingly more people having difficulty falling asleep and staying asleep, using more medicines such as hypnotics to induce sleep, and we saw a 20% increase in the overall consumption of sleeping pills,” he said.
Similar results were seen in a cross-sectional survey of 843 adults in the United Kingdom, which showed that nearly 70% of participants reported a change in sleep patterns, only 45% reported having refreshing sleep, and 46% reported being sleepier during lockdown than before. Two-thirds of the respondents reported that the pandemic affected their mental health, and one-fourth reported increased alcohol consumption during lockdown. Those with suspected COVID-19 infections reported having more nightmares and abnormal sleep rhythms.
It is possible that the effects of COVID-19 infection on sleep may linger long after the infection itself has resolved, results of a cohort study from China suggest. As reported in The Lancet, among 1,655 patients discharged from the Jin Yin-tan hospital in Wuhan, 26% reported sleep disturbances 6 months after acute COVID-19 infection.
Self-medicating
Among 5,525 Canadians surveyed from April 3 through June 24, 2020, a large proportion reported the use of pharmacologic sleeps aids, said Tetyana Kendzerska, MD, PhD, assistant professor of medicine in the division of respirology at the University of Ottawa.
“At the time of the survey completion, 27% of participants reported taking sleeping aids (prescribed or [over] the counter); across the entire sample, 8% of respondents reported an increase in the frequency of sleeping medication use during the outbreak compared to before the outbreak,” she said in an interview.
Many people resort to self-medicating with over-the-counter preparations such as melatonin and pain-relief nighttime formulations containing diphenhydramine (Benadryl), a first-generation antihistamine with sedative properties, noted Kannan Ramar, MBBS, MD, a critical care, pulmonary, and sleep medicine specialist at the Mayo Clinic in Rochester, Minn., and current president of the American Academy of Sleep Medicine.
“When people are self-medicating for what they think is difficulty sleeping, the concern is that even if a diagnosis of insomnia has been established, there could be another, ongoing sleep disorder that may be undiagnosed, which might be causing the problem with insomnia,” he said in an interview.
“For example, obstructive sleep apnea might be causing people to wake up in the night or even contribute to difficulty falling asleep in the first place. So medicating for something without a known diagnosis may leave an underlying sleep disorder untreated, which won’t help the patient in either the short or the long term,” Dr. Ramar said.
Causes for concern
“For those people who have COVID, we have seen quite a few sleep issues develop. Those were not reported in the actual study, but in the clinic and subsequent studies published from other places,” Dr. Gozal said.
“People who suffered from COVID, and even people who supposedly did very well and were virtually asymptomatic or maybe had only a headache or fever but did not need to go to the hospital, many of those people reported either excessive sleepiness for a long period of time, and would sleep 2 or 3 hours more per night. Or the opposite was reported: There were those that after recovering reported that they couldn’t sleep – they were sleeping 4 or 5 hours when they normally sleep 7 or 8,” he said.
It’s also unclear from current evidence whether the reported uptick in sleep problems is related to stress or, in patients who have had COVID-19 infections, to physiologic causes.
Dr. Gozal said that insomnia in the time of COVID-19 could be attributed to a number of factors such as less daily exposure to natural light from people sheltering indoors, stress related to financial or health worries, depression, or other psychological factors.
It’s also, possible, however, that COVID-19-related physiological changes could contribute to sleep disorders, he said, pointing to a recent study in the Journal of Experimental Medicine showing that SARS-CoV-2, the virus that causes COVID-19, can bind to neurons and cause metabolic changes in both infected and neighboring cells.
“My guess is that some of it is related more to behavioral impacts – people develop depression, changes in mood, anxiety, and so on, and all of these can translate into difficulties with sleep,” he said.
“It could be that in some instances – not very commonly – the virus will affect areas that control sleep in our brain, and that therefore we may see too much or too little sleep, and how to differentiate between all of these is the area that clearly needs to be explored, particularly in light of the finding that the virus can bind to brain cells and can induce substantial issues in the brain cells.”
Compromised immunity
It has been well documented that in addition to being, as Shakespeare called it, “the balm of hurt minds,” sleep has an important role in supporting the immune system.
“Sleep and immunity go together,” Dr. Ramar said. “When people have adequate sleep, their immune system is boosted. We know that there are good data from hepatitis A and hepatitis B vaccinations, and recently on flu vaccination, that if people get sufficient duration of sleep before and after they receive the shot, their likelihood of building an immune response to that particular vaccination tends to go up.”
It’s reasonable to assume that the same would hold true for COVID-19 vaccinations, but this has yet to be shown, he added.
“We do know from the previous studies that persistent sleep problems can make people more susceptible to infection or impair recovery; not yet, I believe, from the COVID-19 infection perspective,” Dr. Kendzerska said. “In our study, we did find that, among other factors, having a chronic illness was associated with new sleep difficulties during the pandemic. We did not look separately if sleep difficulties were associated with the COVID-19 infection or symptoms, but this is a great question to address with longitudinal data we have.”
What to do?
All three sleep experts contacted for this article agreed that for patients with insomnia, mitigating stress through relaxation techniques or cognitive behavioral therapy is more beneficial than medication.
“Medications, even over-the-counter medications, all have side effects, and if one is taking a medication that has stimulants in place, such as pseudoephedrine in antihistamine combinations, that can potentially contribute to or exacerbate any underlying sleep disorders,” Dr. Ramar said.
Dr. Kendzerska recommended reserving medications such as melatonin, a chronobiotic therapy, for patients with sleep disorders related to circadian rhythm problems, including a sleep phase delay. Supplemental, short-term treatment with hypnotic agents such as zolpidem (Ambien), eszopiclone (Lunesta), or zaleplon (Sonata) should be used only as a last resort, she said.
Sleep medicine specialists recommend good sleep hygiene as the best means of obtaining restful sleep, including regular bed and wake times, limited exposure to stressful news (including COVID-19 stories), reduced consumption of alcohol and stimulants such as coffee or caffeine drinks, avoiding use of electronic devices in bed or near bedtime, and healthy lifestyle, including diet and exercise.
They also frown on self-medication with over-the-counter aids, because these products may not be addressing the underlying issue, as noted before.
“It is also foreseeable that there may be an increase in individuals who may require professional guidance to taper off from sleeping medications started or increased during the pandemic. While some of these sleep problems may be transient, it should be a high priority to ensure they do not evolve into chronic sleep disorders,” Dr. Kendzerska and colleagues wrote.
Research avenues
If there’s anything that causes specialists to lose sleep, it’s the lack of data or evidence to guide clinical care and research. Dr. Gozal emphasized that little is still known about the potential central nervous system effects of COVID-19, and said that should be an important focus for research into the still novel coronavirus.
“What happens post COVID and how might that affect subsequent recovery is a great question, and I don’t think we have good data there,” Dr. Ramar said. “What we do know is that patients develop the symptoms of fatigue, disrupted sleep, even ongoing fever, and unfortunately, this may persist for a long period of time even among patients who have otherwise recovered from COVID-19. We know that leaving that untreated from a sleep disorder perspective can exacerbate their daytime symptoms, and that’s where I would strongly recommend that they seek help with a sleep provider or if there are symptoms other than insomnia at least with a primary care provider.”
Among the many losses suffered by millions worldwide during the COVID-19 pandemic, the loss of sleep may be the most widespread, with potentially long-lasting, negative consequences on physical, mental, and emotional health, sleep researchers have found.
Results from multiple studies and surveys conducted during the pandemic show that a majority of subjects report clinically meaningful changes in sleep quality, sleep patterns, and sleep disturbances.
For example, a cross-sectional international survey conducted from late March through late April 2020 found that among more than 3,000 responders from 49 countries, 58% reported dissatisfaction with their sleep, and 40% reported a decrease in sleep quality during the pandemic, compared with pre-COVID-19 sleep, according to Uri Mandelkorn of the Natural Sleep Clinic in Jerusalem, and colleagues.
“In particular, this research raises the need to screen for worsening sleep patterns and use of sleeping aids in the more susceptible populations identified in this study, namely, women and people with insecure livelihoods or those subjected to strict quarantine. Health care providers should pay special attention to physical and psychological problems that this surge in sleep disturbances may cause,” they wrote. The report is in the Journal of Clinical Sleep Medicine.
Sleeping, more or less
A coauthor of that study, David Gozal, MD, FCCP, a pediatric pulmonologist and sleep medicine specialist at the University of Missouri in Columbia, said that the pandemic has had paradoxical effects on sleeps patterns for many.
“At the beginning, with the initial phases of lockdown for COVID, for most of the people whose jobs were not affected and who did not lose their jobs, [for whom] there was not the anxiety of being jobless and financially strapped, but who now were staying at home, there was actually a benefit. People started reporting getting more sleep and, more importantly, more vivid dreams and things of that nature,” he said in an interview.
“But as the lockdown progressed, we saw progressively and increasingly more people having difficulty falling asleep and staying asleep, using more medicines such as hypnotics to induce sleep, and we saw a 20% increase in the overall consumption of sleeping pills,” he said.
Similar results were seen in a cross-sectional survey of 843 adults in the United Kingdom, which showed that nearly 70% of participants reported a change in sleep patterns, only 45% reported having refreshing sleep, and 46% reported being sleepier during lockdown than before. Two-thirds of the respondents reported that the pandemic affected their mental health, and one-fourth reported increased alcohol consumption during lockdown. Those with suspected COVID-19 infections reported having more nightmares and abnormal sleep rhythms.
It is possible that the effects of COVID-19 infection on sleep may linger long after the infection itself has resolved, results of a cohort study from China suggest. As reported in The Lancet, among 1,655 patients discharged from the Jin Yin-tan hospital in Wuhan, 26% reported sleep disturbances 6 months after acute COVID-19 infection.
Self-medicating
Among 5,525 Canadians surveyed from April 3 through June 24, 2020, a large proportion reported the use of pharmacologic sleeps aids, said Tetyana Kendzerska, MD, PhD, assistant professor of medicine in the division of respirology at the University of Ottawa.
“At the time of the survey completion, 27% of participants reported taking sleeping aids (prescribed or [over] the counter); across the entire sample, 8% of respondents reported an increase in the frequency of sleeping medication use during the outbreak compared to before the outbreak,” she said in an interview.
Many people resort to self-medicating with over-the-counter preparations such as melatonin and pain-relief nighttime formulations containing diphenhydramine (Benadryl), a first-generation antihistamine with sedative properties, noted Kannan Ramar, MBBS, MD, a critical care, pulmonary, and sleep medicine specialist at the Mayo Clinic in Rochester, Minn., and current president of the American Academy of Sleep Medicine.
“When people are self-medicating for what they think is difficulty sleeping, the concern is that even if a diagnosis of insomnia has been established, there could be another, ongoing sleep disorder that may be undiagnosed, which might be causing the problem with insomnia,” he said in an interview.
“For example, obstructive sleep apnea might be causing people to wake up in the night or even contribute to difficulty falling asleep in the first place. So medicating for something without a known diagnosis may leave an underlying sleep disorder untreated, which won’t help the patient in either the short or the long term,” Dr. Ramar said.
Causes for concern
“For those people who have COVID, we have seen quite a few sleep issues develop. Those were not reported in the actual study, but in the clinic and subsequent studies published from other places,” Dr. Gozal said.
“People who suffered from COVID, and even people who supposedly did very well and were virtually asymptomatic or maybe had only a headache or fever but did not need to go to the hospital, many of those people reported either excessive sleepiness for a long period of time, and would sleep 2 or 3 hours more per night. Or the opposite was reported: There were those that after recovering reported that they couldn’t sleep – they were sleeping 4 or 5 hours when they normally sleep 7 or 8,” he said.
It’s also unclear from current evidence whether the reported uptick in sleep problems is related to stress or, in patients who have had COVID-19 infections, to physiologic causes.
Dr. Gozal said that insomnia in the time of COVID-19 could be attributed to a number of factors such as less daily exposure to natural light from people sheltering indoors, stress related to financial or health worries, depression, or other psychological factors.
It’s also, possible, however, that COVID-19-related physiological changes could contribute to sleep disorders, he said, pointing to a recent study in the Journal of Experimental Medicine showing that SARS-CoV-2, the virus that causes COVID-19, can bind to neurons and cause metabolic changes in both infected and neighboring cells.
“My guess is that some of it is related more to behavioral impacts – people develop depression, changes in mood, anxiety, and so on, and all of these can translate into difficulties with sleep,” he said.
“It could be that in some instances – not very commonly – the virus will affect areas that control sleep in our brain, and that therefore we may see too much or too little sleep, and how to differentiate between all of these is the area that clearly needs to be explored, particularly in light of the finding that the virus can bind to brain cells and can induce substantial issues in the brain cells.”
Compromised immunity
It has been well documented that in addition to being, as Shakespeare called it, “the balm of hurt minds,” sleep has an important role in supporting the immune system.
“Sleep and immunity go together,” Dr. Ramar said. “When people have adequate sleep, their immune system is boosted. We know that there are good data from hepatitis A and hepatitis B vaccinations, and recently on flu vaccination, that if people get sufficient duration of sleep before and after they receive the shot, their likelihood of building an immune response to that particular vaccination tends to go up.”
It’s reasonable to assume that the same would hold true for COVID-19 vaccinations, but this has yet to be shown, he added.
“We do know from the previous studies that persistent sleep problems can make people more susceptible to infection or impair recovery; not yet, I believe, from the COVID-19 infection perspective,” Dr. Kendzerska said. “In our study, we did find that, among other factors, having a chronic illness was associated with new sleep difficulties during the pandemic. We did not look separately if sleep difficulties were associated with the COVID-19 infection or symptoms, but this is a great question to address with longitudinal data we have.”
What to do?
All three sleep experts contacted for this article agreed that for patients with insomnia, mitigating stress through relaxation techniques or cognitive behavioral therapy is more beneficial than medication.
“Medications, even over-the-counter medications, all have side effects, and if one is taking a medication that has stimulants in place, such as pseudoephedrine in antihistamine combinations, that can potentially contribute to or exacerbate any underlying sleep disorders,” Dr. Ramar said.
Dr. Kendzerska recommended reserving medications such as melatonin, a chronobiotic therapy, for patients with sleep disorders related to circadian rhythm problems, including a sleep phase delay. Supplemental, short-term treatment with hypnotic agents such as zolpidem (Ambien), eszopiclone (Lunesta), or zaleplon (Sonata) should be used only as a last resort, she said.
Sleep medicine specialists recommend good sleep hygiene as the best means of obtaining restful sleep, including regular bed and wake times, limited exposure to stressful news (including COVID-19 stories), reduced consumption of alcohol and stimulants such as coffee or caffeine drinks, avoiding use of electronic devices in bed or near bedtime, and healthy lifestyle, including diet and exercise.
They also frown on self-medication with over-the-counter aids, because these products may not be addressing the underlying issue, as noted before.
“It is also foreseeable that there may be an increase in individuals who may require professional guidance to taper off from sleeping medications started or increased during the pandemic. While some of these sleep problems may be transient, it should be a high priority to ensure they do not evolve into chronic sleep disorders,” Dr. Kendzerska and colleagues wrote.
Research avenues
If there’s anything that causes specialists to lose sleep, it’s the lack of data or evidence to guide clinical care and research. Dr. Gozal emphasized that little is still known about the potential central nervous system effects of COVID-19, and said that should be an important focus for research into the still novel coronavirus.
“What happens post COVID and how might that affect subsequent recovery is a great question, and I don’t think we have good data there,” Dr. Ramar said. “What we do know is that patients develop the symptoms of fatigue, disrupted sleep, even ongoing fever, and unfortunately, this may persist for a long period of time even among patients who have otherwise recovered from COVID-19. We know that leaving that untreated from a sleep disorder perspective can exacerbate their daytime symptoms, and that’s where I would strongly recommend that they seek help with a sleep provider or if there are symptoms other than insomnia at least with a primary care provider.”
Among the many losses suffered by millions worldwide during the COVID-19 pandemic, the loss of sleep may be the most widespread, with potentially long-lasting, negative consequences on physical, mental, and emotional health, sleep researchers have found.
Results from multiple studies and surveys conducted during the pandemic show that a majority of subjects report clinically meaningful changes in sleep quality, sleep patterns, and sleep disturbances.
For example, a cross-sectional international survey conducted from late March through late April 2020 found that among more than 3,000 responders from 49 countries, 58% reported dissatisfaction with their sleep, and 40% reported a decrease in sleep quality during the pandemic, compared with pre-COVID-19 sleep, according to Uri Mandelkorn of the Natural Sleep Clinic in Jerusalem, and colleagues.
“In particular, this research raises the need to screen for worsening sleep patterns and use of sleeping aids in the more susceptible populations identified in this study, namely, women and people with insecure livelihoods or those subjected to strict quarantine. Health care providers should pay special attention to physical and psychological problems that this surge in sleep disturbances may cause,” they wrote. The report is in the Journal of Clinical Sleep Medicine.
Sleeping, more or less
A coauthor of that study, David Gozal, MD, FCCP, a pediatric pulmonologist and sleep medicine specialist at the University of Missouri in Columbia, said that the pandemic has had paradoxical effects on sleeps patterns for many.
“At the beginning, with the initial phases of lockdown for COVID, for most of the people whose jobs were not affected and who did not lose their jobs, [for whom] there was not the anxiety of being jobless and financially strapped, but who now were staying at home, there was actually a benefit. People started reporting getting more sleep and, more importantly, more vivid dreams and things of that nature,” he said in an interview.
“But as the lockdown progressed, we saw progressively and increasingly more people having difficulty falling asleep and staying asleep, using more medicines such as hypnotics to induce sleep, and we saw a 20% increase in the overall consumption of sleeping pills,” he said.
Similar results were seen in a cross-sectional survey of 843 adults in the United Kingdom, which showed that nearly 70% of participants reported a change in sleep patterns, only 45% reported having refreshing sleep, and 46% reported being sleepier during lockdown than before. Two-thirds of the respondents reported that the pandemic affected their mental health, and one-fourth reported increased alcohol consumption during lockdown. Those with suspected COVID-19 infections reported having more nightmares and abnormal sleep rhythms.
It is possible that the effects of COVID-19 infection on sleep may linger long after the infection itself has resolved, results of a cohort study from China suggest. As reported in The Lancet, among 1,655 patients discharged from the Jin Yin-tan hospital in Wuhan, 26% reported sleep disturbances 6 months after acute COVID-19 infection.
Self-medicating
Among 5,525 Canadians surveyed from April 3 through June 24, 2020, a large proportion reported the use of pharmacologic sleeps aids, said Tetyana Kendzerska, MD, PhD, assistant professor of medicine in the division of respirology at the University of Ottawa.
“At the time of the survey completion, 27% of participants reported taking sleeping aids (prescribed or [over] the counter); across the entire sample, 8% of respondents reported an increase in the frequency of sleeping medication use during the outbreak compared to before the outbreak,” she said in an interview.
Many people resort to self-medicating with over-the-counter preparations such as melatonin and pain-relief nighttime formulations containing diphenhydramine (Benadryl), a first-generation antihistamine with sedative properties, noted Kannan Ramar, MBBS, MD, a critical care, pulmonary, and sleep medicine specialist at the Mayo Clinic in Rochester, Minn., and current president of the American Academy of Sleep Medicine.
“When people are self-medicating for what they think is difficulty sleeping, the concern is that even if a diagnosis of insomnia has been established, there could be another, ongoing sleep disorder that may be undiagnosed, which might be causing the problem with insomnia,” he said in an interview.
“For example, obstructive sleep apnea might be causing people to wake up in the night or even contribute to difficulty falling asleep in the first place. So medicating for something without a known diagnosis may leave an underlying sleep disorder untreated, which won’t help the patient in either the short or the long term,” Dr. Ramar said.
Causes for concern
“For those people who have COVID, we have seen quite a few sleep issues develop. Those were not reported in the actual study, but in the clinic and subsequent studies published from other places,” Dr. Gozal said.
“People who suffered from COVID, and even people who supposedly did very well and were virtually asymptomatic or maybe had only a headache or fever but did not need to go to the hospital, many of those people reported either excessive sleepiness for a long period of time, and would sleep 2 or 3 hours more per night. Or the opposite was reported: There were those that after recovering reported that they couldn’t sleep – they were sleeping 4 or 5 hours when they normally sleep 7 or 8,” he said.
It’s also unclear from current evidence whether the reported uptick in sleep problems is related to stress or, in patients who have had COVID-19 infections, to physiologic causes.
Dr. Gozal said that insomnia in the time of COVID-19 could be attributed to a number of factors such as less daily exposure to natural light from people sheltering indoors, stress related to financial or health worries, depression, or other psychological factors.
It’s also, possible, however, that COVID-19-related physiological changes could contribute to sleep disorders, he said, pointing to a recent study in the Journal of Experimental Medicine showing that SARS-CoV-2, the virus that causes COVID-19, can bind to neurons and cause metabolic changes in both infected and neighboring cells.
“My guess is that some of it is related more to behavioral impacts – people develop depression, changes in mood, anxiety, and so on, and all of these can translate into difficulties with sleep,” he said.
“It could be that in some instances – not very commonly – the virus will affect areas that control sleep in our brain, and that therefore we may see too much or too little sleep, and how to differentiate between all of these is the area that clearly needs to be explored, particularly in light of the finding that the virus can bind to brain cells and can induce substantial issues in the brain cells.”
Compromised immunity
It has been well documented that in addition to being, as Shakespeare called it, “the balm of hurt minds,” sleep has an important role in supporting the immune system.
“Sleep and immunity go together,” Dr. Ramar said. “When people have adequate sleep, their immune system is boosted. We know that there are good data from hepatitis A and hepatitis B vaccinations, and recently on flu vaccination, that if people get sufficient duration of sleep before and after they receive the shot, their likelihood of building an immune response to that particular vaccination tends to go up.”
It’s reasonable to assume that the same would hold true for COVID-19 vaccinations, but this has yet to be shown, he added.
“We do know from the previous studies that persistent sleep problems can make people more susceptible to infection or impair recovery; not yet, I believe, from the COVID-19 infection perspective,” Dr. Kendzerska said. “In our study, we did find that, among other factors, having a chronic illness was associated with new sleep difficulties during the pandemic. We did not look separately if sleep difficulties were associated with the COVID-19 infection or symptoms, but this is a great question to address with longitudinal data we have.”
What to do?
All three sleep experts contacted for this article agreed that for patients with insomnia, mitigating stress through relaxation techniques or cognitive behavioral therapy is more beneficial than medication.
“Medications, even over-the-counter medications, all have side effects, and if one is taking a medication that has stimulants in place, such as pseudoephedrine in antihistamine combinations, that can potentially contribute to or exacerbate any underlying sleep disorders,” Dr. Ramar said.
Dr. Kendzerska recommended reserving medications such as melatonin, a chronobiotic therapy, for patients with sleep disorders related to circadian rhythm problems, including a sleep phase delay. Supplemental, short-term treatment with hypnotic agents such as zolpidem (Ambien), eszopiclone (Lunesta), or zaleplon (Sonata) should be used only as a last resort, she said.
Sleep medicine specialists recommend good sleep hygiene as the best means of obtaining restful sleep, including regular bed and wake times, limited exposure to stressful news (including COVID-19 stories), reduced consumption of alcohol and stimulants such as coffee or caffeine drinks, avoiding use of electronic devices in bed or near bedtime, and healthy lifestyle, including diet and exercise.
They also frown on self-medication with over-the-counter aids, because these products may not be addressing the underlying issue, as noted before.
“It is also foreseeable that there may be an increase in individuals who may require professional guidance to taper off from sleeping medications started or increased during the pandemic. While some of these sleep problems may be transient, it should be a high priority to ensure they do not evolve into chronic sleep disorders,” Dr. Kendzerska and colleagues wrote.
Research avenues
If there’s anything that causes specialists to lose sleep, it’s the lack of data or evidence to guide clinical care and research. Dr. Gozal emphasized that little is still known about the potential central nervous system effects of COVID-19, and said that should be an important focus for research into the still novel coronavirus.
“What happens post COVID and how might that affect subsequent recovery is a great question, and I don’t think we have good data there,” Dr. Ramar said. “What we do know is that patients develop the symptoms of fatigue, disrupted sleep, even ongoing fever, and unfortunately, this may persist for a long period of time even among patients who have otherwise recovered from COVID-19. We know that leaving that untreated from a sleep disorder perspective can exacerbate their daytime symptoms, and that’s where I would strongly recommend that they seek help with a sleep provider or if there are symptoms other than insomnia at least with a primary care provider.”
American Academy of Sleep Medicine (AASM) advocates for year-round standard time
Although the United States has observed daylight saving time (DST) continuously, in some form, for the last 5 decades (Table), the twice a year switches have never been less popular. In 2019, an American Academy of Sleep Medicine (AASM) survey of more than 2,000 US adults found that 63% support the elimination of seasonal time changes in favor of a national, fixed, year-round time, and only 11% oppose it. Indeed, multiple states have pending legislations to adopt year-round daylight saving time or year-round standard time (Updated September 30, 2020, Congressional Research Service. https://crsreports.congress.gov. R45208 Daylight Saving Time. Accessed Dec 14, 2020). Adjacent states, to limit confusion to interstate travel and commerce, tend to lobby for similar changes together. Most importantly, because of the scientific evidence of detrimental health effects to the public and safety concerns, the American Academy of Sleep Medicine has issued a position statement for year-round standard time (Rishi MA, et al. Daylight saving time: an American Academy of Sleep Medicine position statement. J Clin Sleep Med. 2020;16(10):1781).

Railroad industry successfully lobbied the US government for consistent time in the United States to keep transportation schedules uniform in 1883; standard time was implemented. When war efforts were over, DST was dropped. Some regions, such as New York and Chicago, maintained DST, but no national standard was applied. Retailers and the recreational activity industry advocated for DST to increase business after work in the afternoon and evenings. In 1966, Congress passed the Uniform Time Act of 1966 to implement 6 months of DST and 6 months of standard time (Waxman OB. The real reason why daylight saving time is a thing. https://time.com/4549397/daylight-saving-time-history-politics/; November 1, 2017. Accessed Dec 14, 2020). Local jurisdictions can opt out of DST, but it requires an act of congress to enforce perennial DST.
When the OPEC embargo occurred, the Emergency Daylight Saving Time Energy Conservation Act was enacted in 1973, but it was quickly ended in October 1974 due to its unpopularity. The dairy industry was opposed to earlier rise time that disrupted the animals’ feeding schedules and their farm operations (Feldman R. Five myths about daylight saving time. https://www.washingtonpost.com/opinions/five-myths-about-daylight-saving-time/2015/03/06/970092d4-c2c1-11e4-9271-610273846239_story.html. Accessed Dec 14, 2020.). Public safety was raised as a concern as early as 1975. The Department of Transportation found increased fatalities of school-aged children in the mornings from January to April of 1974 as compared with 1973. However, the National Bureau of Standards, that performed a review subsequently, stated that other factors might also be at play. Further extension of DST from 6 months of the year to the subsequent 7, and then 8 months per year were enacted in 1986 and 2005, respectively (The reasoning behind changing daylight saving. https://www.npr.org/templates/story/story.php?storyId=7779869. NPR. Accessed Nov 1, 2020.)
An exemption of a state from DST is allowable under existing law, but to establish permanent DST will require an act of Congress. Since then, Arizona and Hawaii, as well as US territories, such as Puerto Rico, Guam, American Samoa and Northern Mariana Islands, and US Virgin Islands, have all opted out of DST by state exemption. Because of Hawaii’s proximity to the equator, the timing of sunrise and sunset were fairly constant throughout the year that made DST unnecessary. The Navajo Nation in Arizona, because of its extension into adjacent New Mexico and Utah, participates in DST. Most of the countries along the tropics, parts of Australia, China, Japan, South Korea, India, and majority of African countries do not observe DST. The European Union has voted to abolish twice yearly change in time in 2021; and individual member states will be able to decide whether they wish to remain on permanent standard time or DST. Since 2015, more than 45 states have proposed legislation to change their observance of DST.
The human biological rhythm is most consistent with standard time (Antle M. Circadian rhythm expert argues against permanent daylight saving time. https://www.ucalgary.ca/news/circadian-rhythm-expert-argues-against-permanent-daylight-saving-time. Accessed Dec 14, 2020.). Since the biological clock for most individuals is not exactly 24 hours long, zeitgebers such as sunlight, exercise, and feeding behaviors are important time cues to foster a regular rhythm. Acutely, the adjustment to 1 hour’s sleep loss at the spring switch from standard time to DST generally requires several days to adapt (Kalidindi A. Daylight saving time is bad for your health. https://massivesci.com/articles/daylight-saving-savings-time-dst-november-standard-time. Accessed Dec 14, 2020.). During this adjustment period, the internal bodily functions are disrupted. The sense of sleepiness and fatigue are increased with earlier morning awakenings, and the inability to fall asleep earlier leads to symptoms of insomnia and poor sleep quality.

The health and economic costs due to accidents, injuries, and medical errors are now well known. Individual biological rhythm disruptions at the spring switch from standard time to DST with the loss of sleep likely contributes to higher risks of myocardial infarctions (Janszky I, et al. Shifts to and from daylight saving time and incidence of myocardial infarction. N Engl J Med. 2008; 359(18):1966) that are not mostly seen during the fall switch from DST to standard time. An estimated 40 minutes of sleep loss occurs within the Sunday to Monday transition of DST in the spring. Medical errors, car crashes, suicide risks, and fatigue are all reportedly higher on the Monday after the spring switch. Some of these effects have been cited as remaining elevated through the first week and possibly chronically during the entire duration of DST. Some people have difficulty adapting to sleep loss from DST, creating social jetlag, and complaints of fatigue and increased prevalence of metabolic syndromes are more common in this population (Koopman ADM, et al. The association between social jetlag, the metabolic syndrome, and type 2 diabetes mellitus in the general population: The New Hoorn study. J Biol Rhythms. 2017 Aug:32(4):359; Roenneberg T, et al. Social jetlag and obesity. Curr Biol. 2012 May 22; 22(10):939). “Cyber-loafing,” describing those at work but who chose to peruse entertaining websites, reportedly occurred more during DST compared with the fall.
Delaying school start time has been associated with improved school attendance and performance. The American Academy of Pediatrics and AASM support delaying school start time; this measure has been adopted by California, and legislation is pending in other states (https://www.startschoollater.net/legislation.html). In spring, the loss of 1 hour’s sleep would negate any benefit of beginning the school day later. Students would suffer inattention, decrease ability to focus, and be less effective learners. Obesity and metabolic syndromes that have been found in adults, are also observed in children whose biological rhythms are delayed compared with their peers who have morning lark tendencies. Risks of mood disorder may be elevated at onset of DST due to earlier arise time or standard time when less sunlight is available in the evenings.
During the current pandemic with SARS-CoV-2, there are new reports of teens and college students able to obtain more sleep because of online education (How children’s sleep habits have changed in the pandemic. https://www.nytimes.com/2020/08/17/well/family/children-sleep-pandemic.html. Accessed Dec 14, 2020.) and they had more restful sleep and improved mood. This positive trend will be monitored closely with some schools returning to in-person instruction.
Societal costs of decreased productivity, on the job accidents and injuries, and increased risk of motor vehicle crashes (Robb D, et al. Accident rates and the impact of daylight saving transitions. Accid Anal Prev. 2018 Feb; 111:193), in addition to individual well-being, have also been reported. Energy savings that propelled arguments for DST did not translate into significant savings after all. Although less electricity was used with more abundance of sunlight in the afternoon, people drove more and used more gasoline to attend their after work activities.
Adaptation of a year-round time schedule will need to balance the impact and disruption to the health and well-being of its citizens, as well as the interests of its commercial sector. The argument for maintaining year-round standard time states that to prevent the loss of the 1 hour’s sleep that DST creates in the spring. Therefore, it preserves a more aligned biological rhythm, lowers the risks of preventable myocardial infarction, improves attention and focus, lessens daytime fatigue, and improves sense of well-being year round. Certainly, it will ensure that the teens who are likely to have later sleep schedules, will not lose more sleep and negate the benefit of starting school later.
Timeline for DST
1784 Benjamin Franklin advocated to rise earlier so as to burn fewer candles in the evenings.
1883 Railroads need standard time for operations.
1890 Merchants and retailers (clothing, cigars) advocated for longer shopping hours.
1916 Germany conserves energy.
1918 DST: fuel conservation during World War I.
1942 DST during World War II.
1963 “Chaos of clocks” needs uniform time for commerce.
1966 Uniform Time Act: DST 6 months per year.
1973 Emergency DST Energy Conservation Act: Arab oil embargo to extend DST to 8 months; ended prematurely in October 1974.
1986 Extended start date from last Sunday of April to first Sunday of November.
2005 Energy Act of 2005: 2nd week of March.
Dr. Yuen is Assistant Professor, UCSF Department of Internal Medicine-Pulmonary Department, and Adjunct Clinical Assistant Professor at Department of Psychiatry & Behavioral Sciences at Stanford (Calif.) University. Dr. Rishi is Consultant – Pulmonary, Critical Care and Sleep Medicine, Mayo Clinic Health System, Eau Claire, WI; and Assistant Professor of Medicine, Alix School of Medicine, Mayo Clinic, Rochester, MN.
Correction 3/16/21: A photo caption in an earlier version of this article misstated Dr. Kin Yuen's name.
Although the United States has observed daylight saving time (DST) continuously, in some form, for the last 5 decades (Table), the twice a year switches have never been less popular. In 2019, an American Academy of Sleep Medicine (AASM) survey of more than 2,000 US adults found that 63% support the elimination of seasonal time changes in favor of a national, fixed, year-round time, and only 11% oppose it. Indeed, multiple states have pending legislations to adopt year-round daylight saving time or year-round standard time (Updated September 30, 2020, Congressional Research Service. https://crsreports.congress.gov. R45208 Daylight Saving Time. Accessed Dec 14, 2020). Adjacent states, to limit confusion to interstate travel and commerce, tend to lobby for similar changes together. Most importantly, because of the scientific evidence of detrimental health effects to the public and safety concerns, the American Academy of Sleep Medicine has issued a position statement for year-round standard time (Rishi MA, et al. Daylight saving time: an American Academy of Sleep Medicine position statement. J Clin Sleep Med. 2020;16(10):1781).
Railroad industry successfully lobbied the US government for consistent time in the United States to keep transportation schedules uniform in 1883; standard time was implemented. When war efforts were over, DST was dropped. Some regions, such as New York and Chicago, maintained DST, but no national standard was applied. Retailers and the recreational activity industry advocated for DST to increase business after work in the afternoon and evenings. In 1966, Congress passed the Uniform Time Act of 1966 to implement 6 months of DST and 6 months of standard time (Waxman OB. The real reason why daylight saving time is a thing. https://time.com/4549397/daylight-saving-time-history-politics/; November 1, 2017. Accessed Dec 14, 2020). Local jurisdictions can opt out of DST, but it requires an act of congress to enforce perennial DST.
When the OPEC embargo occurred, the Emergency Daylight Saving Time Energy Conservation Act was enacted in 1973, but it was quickly ended in October 1974 due to its unpopularity. The dairy industry was opposed to earlier rise time that disrupted the animals’ feeding schedules and their farm operations (Feldman R. Five myths about daylight saving time. https://www.washingtonpost.com/opinions/five-myths-about-daylight-saving-time/2015/03/06/970092d4-c2c1-11e4-9271-610273846239_story.html. Accessed Dec 14, 2020.). Public safety was raised as a concern as early as 1975. The Department of Transportation found increased fatalities of school-aged children in the mornings from January to April of 1974 as compared with 1973. However, the National Bureau of Standards, that performed a review subsequently, stated that other factors might also be at play. Further extension of DST from 6 months of the year to the subsequent 7, and then 8 months per year were enacted in 1986 and 2005, respectively (The reasoning behind changing daylight saving. https://www.npr.org/templates/story/story.php?storyId=7779869. NPR. Accessed Nov 1, 2020.)
An exemption of a state from DST is allowable under existing law, but to establish permanent DST will require an act of Congress. Since then, Arizona and Hawaii, as well as US territories, such as Puerto Rico, Guam, American Samoa and Northern Mariana Islands, and US Virgin Islands, have all opted out of DST by state exemption. Because of Hawaii’s proximity to the equator, the timing of sunrise and sunset were fairly constant throughout the year that made DST unnecessary. The Navajo Nation in Arizona, because of its extension into adjacent New Mexico and Utah, participates in DST. Most of the countries along the tropics, parts of Australia, China, Japan, South Korea, India, and majority of African countries do not observe DST. The European Union has voted to abolish twice yearly change in time in 2021; and individual member states will be able to decide whether they wish to remain on permanent standard time or DST. Since 2015, more than 45 states have proposed legislation to change their observance of DST.
The human biological rhythm is most consistent with standard time (Antle M. Circadian rhythm expert argues against permanent daylight saving time. https://www.ucalgary.ca/news/circadian-rhythm-expert-argues-against-permanent-daylight-saving-time. Accessed Dec 14, 2020.). Since the biological clock for most individuals is not exactly 24 hours long, zeitgebers such as sunlight, exercise, and feeding behaviors are important time cues to foster a regular rhythm. Acutely, the adjustment to 1 hour’s sleep loss at the spring switch from standard time to DST generally requires several days to adapt (Kalidindi A. Daylight saving time is bad for your health. https://massivesci.com/articles/daylight-saving-savings-time-dst-november-standard-time. Accessed Dec 14, 2020.). During this adjustment period, the internal bodily functions are disrupted. The sense of sleepiness and fatigue are increased with earlier morning awakenings, and the inability to fall asleep earlier leads to symptoms of insomnia and poor sleep quality.
The health and economic costs due to accidents, injuries, and medical errors are now well known. Individual biological rhythm disruptions at the spring switch from standard time to DST with the loss of sleep likely contributes to higher risks of myocardial infarctions (Janszky I, et al. Shifts to and from daylight saving time and incidence of myocardial infarction. N Engl J Med. 2008; 359(18):1966) that are not mostly seen during the fall switch from DST to standard time. An estimated 40 minutes of sleep loss occurs within the Sunday to Monday transition of DST in the spring. Medical errors, car crashes, suicide risks, and fatigue are all reportedly higher on the Monday after the spring switch. Some of these effects have been cited as remaining elevated through the first week and possibly chronically during the entire duration of DST. Some people have difficulty adapting to sleep loss from DST, creating social jetlag, and complaints of fatigue and increased prevalence of metabolic syndromes are more common in this population (Koopman ADM, et al. The association between social jetlag, the metabolic syndrome, and type 2 diabetes mellitus in the general population: The New Hoorn study. J Biol Rhythms. 2017 Aug:32(4):359; Roenneberg T, et al. Social jetlag and obesity. Curr Biol. 2012 May 22; 22(10):939). “Cyber-loafing,” describing those at work but who chose to peruse entertaining websites, reportedly occurred more during DST compared with the fall.
Delaying school start time has been associated with improved school attendance and performance. The American Academy of Pediatrics and AASM support delaying school start time; this measure has been adopted by California, and legislation is pending in other states (https://www.startschoollater.net/legislation.html). In spring, the loss of 1 hour’s sleep would negate any benefit of beginning the school day later. Students would suffer inattention, decrease ability to focus, and be less effective learners. Obesity and metabolic syndromes that have been found in adults, are also observed in children whose biological rhythms are delayed compared with their peers who have morning lark tendencies. Risks of mood disorder may be elevated at onset of DST due to earlier arise time or standard time when less sunlight is available in the evenings.
During the current pandemic with SARS-CoV-2, there are new reports of teens and college students able to obtain more sleep because of online education (How children’s sleep habits have changed in the pandemic. https://www.nytimes.com/2020/08/17/well/family/children-sleep-pandemic.html. Accessed Dec 14, 2020.) and they had more restful sleep and improved mood. This positive trend will be monitored closely with some schools returning to in-person instruction.
Societal costs of decreased productivity, on the job accidents and injuries, and increased risk of motor vehicle crashes (Robb D, et al. Accident rates and the impact of daylight saving transitions. Accid Anal Prev. 2018 Feb; 111:193), in addition to individual well-being, have also been reported. Energy savings that propelled arguments for DST did not translate into significant savings after all. Although less electricity was used with more abundance of sunlight in the afternoon, people drove more and used more gasoline to attend their after work activities.
Adaptation of a year-round time schedule will need to balance the impact and disruption to the health and well-being of its citizens, as well as the interests of its commercial sector. The argument for maintaining year-round standard time states that to prevent the loss of the 1 hour’s sleep that DST creates in the spring. Therefore, it preserves a more aligned biological rhythm, lowers the risks of preventable myocardial infarction, improves attention and focus, lessens daytime fatigue, and improves sense of well-being year round. Certainly, it will ensure that the teens who are likely to have later sleep schedules, will not lose more sleep and negate the benefit of starting school later.
Timeline for DST
1784 Benjamin Franklin advocated to rise earlier so as to burn fewer candles in the evenings.
1883 Railroads need standard time for operations.
1890 Merchants and retailers (clothing, cigars) advocated for longer shopping hours.
1916 Germany conserves energy.
1918 DST: fuel conservation during World War I.
1942 DST during World War II.
1963 “Chaos of clocks” needs uniform time for commerce.
1966 Uniform Time Act: DST 6 months per year.
1973 Emergency DST Energy Conservation Act: Arab oil embargo to extend DST to 8 months; ended prematurely in October 1974.
1986 Extended start date from last Sunday of April to first Sunday of November.
2005 Energy Act of 2005: 2nd week of March.
Dr. Yuen is Assistant Professor, UCSF Department of Internal Medicine-Pulmonary Department, and Adjunct Clinical Assistant Professor at Department of Psychiatry & Behavioral Sciences at Stanford (Calif.) University. Dr. Rishi is Consultant – Pulmonary, Critical Care and Sleep Medicine, Mayo Clinic Health System, Eau Claire, WI; and Assistant Professor of Medicine, Alix School of Medicine, Mayo Clinic, Rochester, MN.
Correction 3/16/21: A photo caption in an earlier version of this article misstated Dr. Kin Yuen's name.
Although the United States has observed daylight saving time (DST) continuously, in some form, for the last 5 decades (Table), the twice a year switches have never been less popular. In 2019, an American Academy of Sleep Medicine (AASM) survey of more than 2,000 US adults found that 63% support the elimination of seasonal time changes in favor of a national, fixed, year-round time, and only 11% oppose it. Indeed, multiple states have pending legislations to adopt year-round daylight saving time or year-round standard time (Updated September 30, 2020, Congressional Research Service. https://crsreports.congress.gov. R45208 Daylight Saving Time. Accessed Dec 14, 2020). Adjacent states, to limit confusion to interstate travel and commerce, tend to lobby for similar changes together. Most importantly, because of the scientific evidence of detrimental health effects to the public and safety concerns, the American Academy of Sleep Medicine has issued a position statement for year-round standard time (Rishi MA, et al. Daylight saving time: an American Academy of Sleep Medicine position statement. J Clin Sleep Med. 2020;16(10):1781).
Railroad industry successfully lobbied the US government for consistent time in the United States to keep transportation schedules uniform in 1883; standard time was implemented. When war efforts were over, DST was dropped. Some regions, such as New York and Chicago, maintained DST, but no national standard was applied. Retailers and the recreational activity industry advocated for DST to increase business after work in the afternoon and evenings. In 1966, Congress passed the Uniform Time Act of 1966 to implement 6 months of DST and 6 months of standard time (Waxman OB. The real reason why daylight saving time is a thing. https://time.com/4549397/daylight-saving-time-history-politics/; November 1, 2017. Accessed Dec 14, 2020). Local jurisdictions can opt out of DST, but it requires an act of congress to enforce perennial DST.
When the OPEC embargo occurred, the Emergency Daylight Saving Time Energy Conservation Act was enacted in 1973, but it was quickly ended in October 1974 due to its unpopularity. The dairy industry was opposed to earlier rise time that disrupted the animals’ feeding schedules and their farm operations (Feldman R. Five myths about daylight saving time. https://www.washingtonpost.com/opinions/five-myths-about-daylight-saving-time/2015/03/06/970092d4-c2c1-11e4-9271-610273846239_story.html. Accessed Dec 14, 2020.). Public safety was raised as a concern as early as 1975. The Department of Transportation found increased fatalities of school-aged children in the mornings from January to April of 1974 as compared with 1973. However, the National Bureau of Standards, that performed a review subsequently, stated that other factors might also be at play. Further extension of DST from 6 months of the year to the subsequent 7, and then 8 months per year were enacted in 1986 and 2005, respectively (The reasoning behind changing daylight saving. https://www.npr.org/templates/story/story.php?storyId=7779869. NPR. Accessed Nov 1, 2020.)
An exemption of a state from DST is allowable under existing law, but to establish permanent DST will require an act of Congress. Since then, Arizona and Hawaii, as well as US territories, such as Puerto Rico, Guam, American Samoa and Northern Mariana Islands, and US Virgin Islands, have all opted out of DST by state exemption. Because of Hawaii’s proximity to the equator, the timing of sunrise and sunset were fairly constant throughout the year that made DST unnecessary. The Navajo Nation in Arizona, because of its extension into adjacent New Mexico and Utah, participates in DST. Most of the countries along the tropics, parts of Australia, China, Japan, South Korea, India, and majority of African countries do not observe DST. The European Union has voted to abolish twice yearly change in time in 2021; and individual member states will be able to decide whether they wish to remain on permanent standard time or DST. Since 2015, more than 45 states have proposed legislation to change their observance of DST.
The human biological rhythm is most consistent with standard time (Antle M. Circadian rhythm expert argues against permanent daylight saving time. https://www.ucalgary.ca/news/circadian-rhythm-expert-argues-against-permanent-daylight-saving-time. Accessed Dec 14, 2020.). Since the biological clock for most individuals is not exactly 24 hours long, zeitgebers such as sunlight, exercise, and feeding behaviors are important time cues to foster a regular rhythm. Acutely, the adjustment to 1 hour’s sleep loss at the spring switch from standard time to DST generally requires several days to adapt (Kalidindi A. Daylight saving time is bad for your health. https://massivesci.com/articles/daylight-saving-savings-time-dst-november-standard-time. Accessed Dec 14, 2020.). During this adjustment period, the internal bodily functions are disrupted. The sense of sleepiness and fatigue are increased with earlier morning awakenings, and the inability to fall asleep earlier leads to symptoms of insomnia and poor sleep quality.
The health and economic costs due to accidents, injuries, and medical errors are now well known. Individual biological rhythm disruptions at the spring switch from standard time to DST with the loss of sleep likely contributes to higher risks of myocardial infarctions (Janszky I, et al. Shifts to and from daylight saving time and incidence of myocardial infarction. N Engl J Med. 2008; 359(18):1966) that are not mostly seen during the fall switch from DST to standard time. An estimated 40 minutes of sleep loss occurs within the Sunday to Monday transition of DST in the spring. Medical errors, car crashes, suicide risks, and fatigue are all reportedly higher on the Monday after the spring switch. Some of these effects have been cited as remaining elevated through the first week and possibly chronically during the entire duration of DST. Some people have difficulty adapting to sleep loss from DST, creating social jetlag, and complaints of fatigue and increased prevalence of metabolic syndromes are more common in this population (Koopman ADM, et al. The association between social jetlag, the metabolic syndrome, and type 2 diabetes mellitus in the general population: The New Hoorn study. J Biol Rhythms. 2017 Aug:32(4):359; Roenneberg T, et al. Social jetlag and obesity. Curr Biol. 2012 May 22; 22(10):939). “Cyber-loafing,” describing those at work but who chose to peruse entertaining websites, reportedly occurred more during DST compared with the fall.
Delaying school start time has been associated with improved school attendance and performance. The American Academy of Pediatrics and AASM support delaying school start time; this measure has been adopted by California, and legislation is pending in other states (https://www.startschoollater.net/legislation.html). In spring, the loss of 1 hour’s sleep would negate any benefit of beginning the school day later. Students would suffer inattention, decrease ability to focus, and be less effective learners. Obesity and metabolic syndromes that have been found in adults, are also observed in children whose biological rhythms are delayed compared with their peers who have morning lark tendencies. Risks of mood disorder may be elevated at onset of DST due to earlier arise time or standard time when less sunlight is available in the evenings.
During the current pandemic with SARS-CoV-2, there are new reports of teens and college students able to obtain more sleep because of online education (How children’s sleep habits have changed in the pandemic. https://www.nytimes.com/2020/08/17/well/family/children-sleep-pandemic.html. Accessed Dec 14, 2020.) and they had more restful sleep and improved mood. This positive trend will be monitored closely with some schools returning to in-person instruction.
Societal costs of decreased productivity, on the job accidents and injuries, and increased risk of motor vehicle crashes (Robb D, et al. Accident rates and the impact of daylight saving transitions. Accid Anal Prev. 2018 Feb; 111:193), in addition to individual well-being, have also been reported. Energy savings that propelled arguments for DST did not translate into significant savings after all. Although less electricity was used with more abundance of sunlight in the afternoon, people drove more and used more gasoline to attend their after work activities.
Adaptation of a year-round time schedule will need to balance the impact and disruption to the health and well-being of its citizens, as well as the interests of its commercial sector. The argument for maintaining year-round standard time states that to prevent the loss of the 1 hour’s sleep that DST creates in the spring. Therefore, it preserves a more aligned biological rhythm, lowers the risks of preventable myocardial infarction, improves attention and focus, lessens daytime fatigue, and improves sense of well-being year round. Certainly, it will ensure that the teens who are likely to have later sleep schedules, will not lose more sleep and negate the benefit of starting school later.
Timeline for DST
1784 Benjamin Franklin advocated to rise earlier so as to burn fewer candles in the evenings.
1883 Railroads need standard time for operations.
1890 Merchants and retailers (clothing, cigars) advocated for longer shopping hours.
1916 Germany conserves energy.
1918 DST: fuel conservation during World War I.
1942 DST during World War II.
1963 “Chaos of clocks” needs uniform time for commerce.
1966 Uniform Time Act: DST 6 months per year.
1973 Emergency DST Energy Conservation Act: Arab oil embargo to extend DST to 8 months; ended prematurely in October 1974.
1986 Extended start date from last Sunday of April to first Sunday of November.
2005 Energy Act of 2005: 2nd week of March.
Dr. Yuen is Assistant Professor, UCSF Department of Internal Medicine-Pulmonary Department, and Adjunct Clinical Assistant Professor at Department of Psychiatry & Behavioral Sciences at Stanford (Calif.) University. Dr. Rishi is Consultant – Pulmonary, Critical Care and Sleep Medicine, Mayo Clinic Health System, Eau Claire, WI; and Assistant Professor of Medicine, Alix School of Medicine, Mayo Clinic, Rochester, MN.
Correction 3/16/21: A photo caption in an earlier version of this article misstated Dr. Kin Yuen's name.
COVID-19 symptoms persist months after acute infection
, according to a follow-up study involving 1,733 patients.
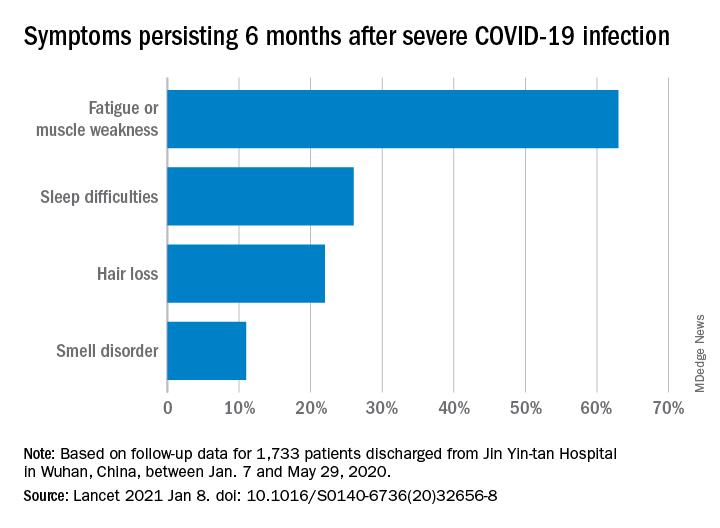
“Patients with COVID-19 had symptoms of fatigue or muscle weakness, sleep difficulties, and anxiety or depression,” and those with “more severe illness during their hospital stay had increasingly impaired pulmonary diffusion capacities and abnormal chest imaging manifestations,” Chaolin Huang, MD, of Jin Yin-tan Hospital in Wuhan, China, and associates wrote in the Lancet.
Fatigue or muscle weakness, reported by 63% of patients, was the most common symptom, followed by sleep difficulties, hair loss, and smell disorder. Altogether, 76% of those examined 6 months after discharge from Jin Yin-tan hospital – the first designated for patients with COVID-19 in Wuhan – reported at least one symptom, they said.
Symptoms were more common in women than men: 81% vs. 73% had at least one symptom, and 66% vs. 59% had fatigue or muscle weakness. Women were also more likely than men to report anxiety or depression at follow-up: 28% vs. 18% (23% overall), the investigators said.
Patients with the most severe COVID-19 were 2.4 times as likely to report any symptom later, compared with those who had the least severe levels of infection. Among the 349 participants who completed a lung function test at follow-up, lung diffusion impairment was seen in 56% of those with the most severe illness and 22% of those with the lowest level, Dr. Huang and associates reported.
In a different subset of 94 patients from whom plasma samples were collected, the “seropositivity and median titres of the neutralising antibodies were significantly lower than at the acute phase,” raising concern for reinfection, they said.
The results of the study, the investigators noted, “support that those with severe disease need post-discharge care. Longer follow-up studies in a larger population are necessary to understand the full spectrum of health consequences from COVID-19.”
, according to a follow-up study involving 1,733 patients.
“Patients with COVID-19 had symptoms of fatigue or muscle weakness, sleep difficulties, and anxiety or depression,” and those with “more severe illness during their hospital stay had increasingly impaired pulmonary diffusion capacities and abnormal chest imaging manifestations,” Chaolin Huang, MD, of Jin Yin-tan Hospital in Wuhan, China, and associates wrote in the Lancet.
Fatigue or muscle weakness, reported by 63% of patients, was the most common symptom, followed by sleep difficulties, hair loss, and smell disorder. Altogether, 76% of those examined 6 months after discharge from Jin Yin-tan hospital – the first designated for patients with COVID-19 in Wuhan – reported at least one symptom, they said.
Symptoms were more common in women than men: 81% vs. 73% had at least one symptom, and 66% vs. 59% had fatigue or muscle weakness. Women were also more likely than men to report anxiety or depression at follow-up: 28% vs. 18% (23% overall), the investigators said.
Patients with the most severe COVID-19 were 2.4 times as likely to report any symptom later, compared with those who had the least severe levels of infection. Among the 349 participants who completed a lung function test at follow-up, lung diffusion impairment was seen in 56% of those with the most severe illness and 22% of those with the lowest level, Dr. Huang and associates reported.
In a different subset of 94 patients from whom plasma samples were collected, the “seropositivity and median titres of the neutralising antibodies were significantly lower than at the acute phase,” raising concern for reinfection, they said.
The results of the study, the investigators noted, “support that those with severe disease need post-discharge care. Longer follow-up studies in a larger population are necessary to understand the full spectrum of health consequences from COVID-19.”
, according to a follow-up study involving 1,733 patients.
“Patients with COVID-19 had symptoms of fatigue or muscle weakness, sleep difficulties, and anxiety or depression,” and those with “more severe illness during their hospital stay had increasingly impaired pulmonary diffusion capacities and abnormal chest imaging manifestations,” Chaolin Huang, MD, of Jin Yin-tan Hospital in Wuhan, China, and associates wrote in the Lancet.
Fatigue or muscle weakness, reported by 63% of patients, was the most common symptom, followed by sleep difficulties, hair loss, and smell disorder. Altogether, 76% of those examined 6 months after discharge from Jin Yin-tan hospital – the first designated for patients with COVID-19 in Wuhan – reported at least one symptom, they said.
Symptoms were more common in women than men: 81% vs. 73% had at least one symptom, and 66% vs. 59% had fatigue or muscle weakness. Women were also more likely than men to report anxiety or depression at follow-up: 28% vs. 18% (23% overall), the investigators said.
Patients with the most severe COVID-19 were 2.4 times as likely to report any symptom later, compared with those who had the least severe levels of infection. Among the 349 participants who completed a lung function test at follow-up, lung diffusion impairment was seen in 56% of those with the most severe illness and 22% of those with the lowest level, Dr. Huang and associates reported.
In a different subset of 94 patients from whom plasma samples were collected, the “seropositivity and median titres of the neutralising antibodies were significantly lower than at the acute phase,” raising concern for reinfection, they said.
The results of the study, the investigators noted, “support that those with severe disease need post-discharge care. Longer follow-up studies in a larger population are necessary to understand the full spectrum of health consequences from COVID-19.”
FROM THE LANCET
New resilience center targets traumatized health care workers
A physician assistant participating in a virtual workshop began to cry, confessing that she felt overwhelmed with guilt because New Yorkers were hailing her as a frontline hero in the pandemic. That was when Joe Ciavarro knew he was in the right place.

“She was saying all the things I could not verbalize because I, too, didn’t feel like I deserved all this praise and thousands of people cheering for us every evening when people were losing jobs, didn’t have money for food, and their loved ones were dying without family at their side,” says Mr. Ciavarro, a PA at Mount Sinai Medical Center in New York.
Mr. Ciavarro, who also manages 170 other PAs on two of Mount Sinai’s campuses in Manhattan, has been on the front lines since COVID-19 first hit; he lost a colleague and friend to suicide in September.
The mental anguish from his job prompted him to sign up for the resilience workshop offered by Mount Sinai’s Center for Stress, Resilience, and Personal Growth. The center – the first of its kind in North America – was launched in June to help health care workers like him cope with the intense psychological pressures they were facing. The weekly workshops became a safe place where Mr. Ciavarro and other staff members could share their darkest fears and learn ways to help them deal with their situation.
“It’s been grueling but we learned how to take care of ourselves so we can take care of our patients,” said Mr. Ciavarro. “This has become like a guided group therapy session on ways to manage and develop resilience. And I feel like my emotions are validated, knowing that others feel the same way.”
Caring for their own
Medical professionals treating patients with COVID-19 are in similar predicaments, and the psychological fallout is enormous: They’re exhausted by the seemingly never-ending patient load and staffing shortages, and haunted by fears for their own safety and that of their families. Studies in China, Canada, and Italy have revealed that a significant number of doctors and nurses in the early days of the pandemic experienced high levels of distress, depression, anxiety, nightmares, and insomnia.
after witnessing the deaths of so many patients who were alone, without family.

But the resilience workshop that Mr. Ciavarro attended offers some hope and is part of a multifaceted program that aims to be a model for other institutions and communities. The Mount Sinai health system already had some programs in place, including centers for 9/11 responders, for spirituality and health, and a wellness program to aid burned-out doctors. But the leadership at Mount Sinai, which includes psychiatrist Dennis Charney, MD, dean of the medical school and a leading expert on PTSD, knew early in the pandemic that emotional and psychological distress would plague health care workers, according to Deborah Marin, MD, director of the new center.
“We decided to quickly put in place a program that we could do virtually, with workshops and apps, that would give access to several services above and beyond what was already going on,” says Dr. Marin, a professor of psychiatry at the Icahn School of Medicine at Mount Sinai, New York, who also directs their center for spirituality and health.
The key components include a comprehensive screening tool that helps doctors at the center identify which potential participants are most at risk. Participants build personal inventories that detail the intensity of work-related exposures, personal or family stressors that have arisen because of the pandemic, or any mental health conditions or substance abuse problems that may make staff members more vulnerable.
The weekly workshops led by trained staff are designed to give participants the tools to foster resilience and process their experiences. Online apps provide feedback on their progress and engage them with video and other resources around meditation, relaxation, and resilience techniques.
In addition, all 40,000 members of the Mount Sinai staff are eligible for up to 14 one-on-one sessions with psychologists and psychiatrists who specialize in treating trauma.
“That’s highly unusual – to offer this at no cost to everyone,” said Dr. Marin. “We also have a treatment service that is specifically focused on behavioral health care, so people can learn better coping strategies, and we also have social workers to provide coaching.”
While the center doesn’t have specific numbers on how many nurses, physicians, and other staff have participated in treatment, they have trained over 70 peer leaders for their five workshops that home in on the most important factors of resilience.

“We’ve gotten enthusiastic responses from PAs and nurses,” said Craig Katz, MD, an expert in disaster psychiatry at Mount Sinai and a workshop moderator. Physicians have been slower to get on board. “Doctors are a tough nut to crack – it’s largely a culture where they may burn out but don’t want to talk about it. And asking for help is a hard transition for physicians to make.”
How to protect in midst of trauma
In formulating the program’s platform, Mount Sinai experts drew upon their extensive experience aiding 9/11 responders at the World Trade Center (WTC), as well as their system-wide wellness program that aids demoralized and burned-out physicians. While the reach of the pandemic is much broader than 9/11, experts see some commonalities in conditions that emerge after traumatic events, and they also discovered what can help.

“We learned from our WTC experience about what are protective factors – what are the social supports that buffer against depression, anxiety, and PTSD,” said Jonathan DePierro, PhD, clinical director of CSRPG and a psychologist at the Mount Sinai WTC Mental Health Program. “We also learned that people who have more prolonged exposures are at greater risk of developing mental health difficulties.”
The program itself reflects these lessons – and that’s why it’s open to all employees, not just medical professionals. Housekeepers, security staffers, even construction workers are also dealing with their lives being in danger. “That wasn’t in their job description,” said Dr. DePierro. “These people tend to have fewer social and economic resources, make less money and have fewer structural supports, which makes them even more vulnerable.”
Dr. Charney’s strategies on building resilience became a bible of sorts for the workshops, according to Dr. Katz, who authored the training curriculum. Sessions deal with how to build up reservoirs of realistic optimism, keep gratitude journals, find spiritual meaning in their lives, maintain physical wellness and create networks of social support. The workshops are meant to help participants create action plans, to reach out for support in their social networks, and keep the focus on the positives.
The goal is to give demoralized health care workers a renewed sense of competence. “The resilience workshop is a launching point to get people to show up and talk,” said Dr. Katz. “And if we do that, we’ve accomplished a lot just getting people in the door.”
The center will also have a research component to identify what works and what doesn’t so their platform can provide a template for other institutions; Dr. Marin said they’ve gotten inquiries about the program from major hospital systems in Michigan and California. They’ll also conduct longitudinal research to determine what lingering problems persist among healthcare workers over time.
Since the center opened its virtual doors, the curriculum has also been altered in response to feedback from the support staff, many of whom live in the community that surrounds Mount Sinai in northern Manhattan, which is largely lower-income Latinx and Black individuals. Workshop materials have been translated into Spanish and now feature people who reflect a more diverse set of experiences.
“Many of our employees and the population we serve identify as non-White so we’ve been doing outreach with a lot of the local unions,” said Dr. Marin. “Our next step is to take what we’re doing and work with local community organizations.”
A version of this article first appeared on Medscape.com.
A physician assistant participating in a virtual workshop began to cry, confessing that she felt overwhelmed with guilt because New Yorkers were hailing her as a frontline hero in the pandemic. That was when Joe Ciavarro knew he was in the right place.
“She was saying all the things I could not verbalize because I, too, didn’t feel like I deserved all this praise and thousands of people cheering for us every evening when people were losing jobs, didn’t have money for food, and their loved ones were dying without family at their side,” says Mr. Ciavarro, a PA at Mount Sinai Medical Center in New York.
Mr. Ciavarro, who also manages 170 other PAs on two of Mount Sinai’s campuses in Manhattan, has been on the front lines since COVID-19 first hit; he lost a colleague and friend to suicide in September.
The mental anguish from his job prompted him to sign up for the resilience workshop offered by Mount Sinai’s Center for Stress, Resilience, and Personal Growth. The center – the first of its kind in North America – was launched in June to help health care workers like him cope with the intense psychological pressures they were facing. The weekly workshops became a safe place where Mr. Ciavarro and other staff members could share their darkest fears and learn ways to help them deal with their situation.
“It’s been grueling but we learned how to take care of ourselves so we can take care of our patients,” said Mr. Ciavarro. “This has become like a guided group therapy session on ways to manage and develop resilience. And I feel like my emotions are validated, knowing that others feel the same way.”
Caring for their own
Medical professionals treating patients with COVID-19 are in similar predicaments, and the psychological fallout is enormous: They’re exhausted by the seemingly never-ending patient load and staffing shortages, and haunted by fears for their own safety and that of their families. Studies in China, Canada, and Italy have revealed that a significant number of doctors and nurses in the early days of the pandemic experienced high levels of distress, depression, anxiety, nightmares, and insomnia.
after witnessing the deaths of so many patients who were alone, without family.
But the resilience workshop that Mr. Ciavarro attended offers some hope and is part of a multifaceted program that aims to be a model for other institutions and communities. The Mount Sinai health system already had some programs in place, including centers for 9/11 responders, for spirituality and health, and a wellness program to aid burned-out doctors. But the leadership at Mount Sinai, which includes psychiatrist Dennis Charney, MD, dean of the medical school and a leading expert on PTSD, knew early in the pandemic that emotional and psychological distress would plague health care workers, according to Deborah Marin, MD, director of the new center.
“We decided to quickly put in place a program that we could do virtually, with workshops and apps, that would give access to several services above and beyond what was already going on,” says Dr. Marin, a professor of psychiatry at the Icahn School of Medicine at Mount Sinai, New York, who also directs their center for spirituality and health.
The key components include a comprehensive screening tool that helps doctors at the center identify which potential participants are most at risk. Participants build personal inventories that detail the intensity of work-related exposures, personal or family stressors that have arisen because of the pandemic, or any mental health conditions or substance abuse problems that may make staff members more vulnerable.
The weekly workshops led by trained staff are designed to give participants the tools to foster resilience and process their experiences. Online apps provide feedback on their progress and engage them with video and other resources around meditation, relaxation, and resilience techniques.
In addition, all 40,000 members of the Mount Sinai staff are eligible for up to 14 one-on-one sessions with psychologists and psychiatrists who specialize in treating trauma.
“That’s highly unusual – to offer this at no cost to everyone,” said Dr. Marin. “We also have a treatment service that is specifically focused on behavioral health care, so people can learn better coping strategies, and we also have social workers to provide coaching.”
While the center doesn’t have specific numbers on how many nurses, physicians, and other staff have participated in treatment, they have trained over 70 peer leaders for their five workshops that home in on the most important factors of resilience.
“We’ve gotten enthusiastic responses from PAs and nurses,” said Craig Katz, MD, an expert in disaster psychiatry at Mount Sinai and a workshop moderator. Physicians have been slower to get on board. “Doctors are a tough nut to crack – it’s largely a culture where they may burn out but don’t want to talk about it. And asking for help is a hard transition for physicians to make.”
How to protect in midst of trauma
In formulating the program’s platform, Mount Sinai experts drew upon their extensive experience aiding 9/11 responders at the World Trade Center (WTC), as well as their system-wide wellness program that aids demoralized and burned-out physicians. While the reach of the pandemic is much broader than 9/11, experts see some commonalities in conditions that emerge after traumatic events, and they also discovered what can help.
“We learned from our WTC experience about what are protective factors – what are the social supports that buffer against depression, anxiety, and PTSD,” said Jonathan DePierro, PhD, clinical director of CSRPG and a psychologist at the Mount Sinai WTC Mental Health Program. “We also learned that people who have more prolonged exposures are at greater risk of developing mental health difficulties.”
The program itself reflects these lessons – and that’s why it’s open to all employees, not just medical professionals. Housekeepers, security staffers, even construction workers are also dealing with their lives being in danger. “That wasn’t in their job description,” said Dr. DePierro. “These people tend to have fewer social and economic resources, make less money and have fewer structural supports, which makes them even more vulnerable.”
Dr. Charney’s strategies on building resilience became a bible of sorts for the workshops, according to Dr. Katz, who authored the training curriculum. Sessions deal with how to build up reservoirs of realistic optimism, keep gratitude journals, find spiritual meaning in their lives, maintain physical wellness and create networks of social support. The workshops are meant to help participants create action plans, to reach out for support in their social networks, and keep the focus on the positives.
The goal is to give demoralized health care workers a renewed sense of competence. “The resilience workshop is a launching point to get people to show up and talk,” said Dr. Katz. “And if we do that, we’ve accomplished a lot just getting people in the door.”
The center will also have a research component to identify what works and what doesn’t so their platform can provide a template for other institutions; Dr. Marin said they’ve gotten inquiries about the program from major hospital systems in Michigan and California. They’ll also conduct longitudinal research to determine what lingering problems persist among healthcare workers over time.
Since the center opened its virtual doors, the curriculum has also been altered in response to feedback from the support staff, many of whom live in the community that surrounds Mount Sinai in northern Manhattan, which is largely lower-income Latinx and Black individuals. Workshop materials have been translated into Spanish and now feature people who reflect a more diverse set of experiences.
“Many of our employees and the population we serve identify as non-White so we’ve been doing outreach with a lot of the local unions,” said Dr. Marin. “Our next step is to take what we’re doing and work with local community organizations.”
A version of this article first appeared on Medscape.com.
A physician assistant participating in a virtual workshop began to cry, confessing that she felt overwhelmed with guilt because New Yorkers were hailing her as a frontline hero in the pandemic. That was when Joe Ciavarro knew he was in the right place.
“She was saying all the things I could not verbalize because I, too, didn’t feel like I deserved all this praise and thousands of people cheering for us every evening when people were losing jobs, didn’t have money for food, and their loved ones were dying without family at their side,” says Mr. Ciavarro, a PA at Mount Sinai Medical Center in New York.
Mr. Ciavarro, who also manages 170 other PAs on two of Mount Sinai’s campuses in Manhattan, has been on the front lines since COVID-19 first hit; he lost a colleague and friend to suicide in September.
The mental anguish from his job prompted him to sign up for the resilience workshop offered by Mount Sinai’s Center for Stress, Resilience, and Personal Growth. The center – the first of its kind in North America – was launched in June to help health care workers like him cope with the intense psychological pressures they were facing. The weekly workshops became a safe place where Mr. Ciavarro and other staff members could share their darkest fears and learn ways to help them deal with their situation.
“It’s been grueling but we learned how to take care of ourselves so we can take care of our patients,” said Mr. Ciavarro. “This has become like a guided group therapy session on ways to manage and develop resilience. And I feel like my emotions are validated, knowing that others feel the same way.”
Caring for their own
Medical professionals treating patients with COVID-19 are in similar predicaments, and the psychological fallout is enormous: They’re exhausted by the seemingly never-ending patient load and staffing shortages, and haunted by fears for their own safety and that of their families. Studies in China, Canada, and Italy have revealed that a significant number of doctors and nurses in the early days of the pandemic experienced high levels of distress, depression, anxiety, nightmares, and insomnia.
after witnessing the deaths of so many patients who were alone, without family.
But the resilience workshop that Mr. Ciavarro attended offers some hope and is part of a multifaceted program that aims to be a model for other institutions and communities. The Mount Sinai health system already had some programs in place, including centers for 9/11 responders, for spirituality and health, and a wellness program to aid burned-out doctors. But the leadership at Mount Sinai, which includes psychiatrist Dennis Charney, MD, dean of the medical school and a leading expert on PTSD, knew early in the pandemic that emotional and psychological distress would plague health care workers, according to Deborah Marin, MD, director of the new center.
“We decided to quickly put in place a program that we could do virtually, with workshops and apps, that would give access to several services above and beyond what was already going on,” says Dr. Marin, a professor of psychiatry at the Icahn School of Medicine at Mount Sinai, New York, who also directs their center for spirituality and health.
The key components include a comprehensive screening tool that helps doctors at the center identify which potential participants are most at risk. Participants build personal inventories that detail the intensity of work-related exposures, personal or family stressors that have arisen because of the pandemic, or any mental health conditions or substance abuse problems that may make staff members more vulnerable.
The weekly workshops led by trained staff are designed to give participants the tools to foster resilience and process their experiences. Online apps provide feedback on their progress and engage them with video and other resources around meditation, relaxation, and resilience techniques.
In addition, all 40,000 members of the Mount Sinai staff are eligible for up to 14 one-on-one sessions with psychologists and psychiatrists who specialize in treating trauma.
“That’s highly unusual – to offer this at no cost to everyone,” said Dr. Marin. “We also have a treatment service that is specifically focused on behavioral health care, so people can learn better coping strategies, and we also have social workers to provide coaching.”
While the center doesn’t have specific numbers on how many nurses, physicians, and other staff have participated in treatment, they have trained over 70 peer leaders for their five workshops that home in on the most important factors of resilience.
“We’ve gotten enthusiastic responses from PAs and nurses,” said Craig Katz, MD, an expert in disaster psychiatry at Mount Sinai and a workshop moderator. Physicians have been slower to get on board. “Doctors are a tough nut to crack – it’s largely a culture where they may burn out but don’t want to talk about it. And asking for help is a hard transition for physicians to make.”
How to protect in midst of trauma
In formulating the program’s platform, Mount Sinai experts drew upon their extensive experience aiding 9/11 responders at the World Trade Center (WTC), as well as their system-wide wellness program that aids demoralized and burned-out physicians. While the reach of the pandemic is much broader than 9/11, experts see some commonalities in conditions that emerge after traumatic events, and they also discovered what can help.
“We learned from our WTC experience about what are protective factors – what are the social supports that buffer against depression, anxiety, and PTSD,” said Jonathan DePierro, PhD, clinical director of CSRPG and a psychologist at the Mount Sinai WTC Mental Health Program. “We also learned that people who have more prolonged exposures are at greater risk of developing mental health difficulties.”
The program itself reflects these lessons – and that’s why it’s open to all employees, not just medical professionals. Housekeepers, security staffers, even construction workers are also dealing with their lives being in danger. “That wasn’t in their job description,” said Dr. DePierro. “These people tend to have fewer social and economic resources, make less money and have fewer structural supports, which makes them even more vulnerable.”
Dr. Charney’s strategies on building resilience became a bible of sorts for the workshops, according to Dr. Katz, who authored the training curriculum. Sessions deal with how to build up reservoirs of realistic optimism, keep gratitude journals, find spiritual meaning in their lives, maintain physical wellness and create networks of social support. The workshops are meant to help participants create action plans, to reach out for support in their social networks, and keep the focus on the positives.
The goal is to give demoralized health care workers a renewed sense of competence. “The resilience workshop is a launching point to get people to show up and talk,” said Dr. Katz. “And if we do that, we’ve accomplished a lot just getting people in the door.”
The center will also have a research component to identify what works and what doesn’t so their platform can provide a template for other institutions; Dr. Marin said they’ve gotten inquiries about the program from major hospital systems in Michigan and California. They’ll also conduct longitudinal research to determine what lingering problems persist among healthcare workers over time.
Since the center opened its virtual doors, the curriculum has also been altered in response to feedback from the support staff, many of whom live in the community that surrounds Mount Sinai in northern Manhattan, which is largely lower-income Latinx and Black individuals. Workshop materials have been translated into Spanish and now feature people who reflect a more diverse set of experiences.
“Many of our employees and the population we serve identify as non-White so we’ve been doing outreach with a lot of the local unions,” said Dr. Marin. “Our next step is to take what we’re doing and work with local community organizations.”
A version of this article first appeared on Medscape.com.
More severe AD correlates with worse sleep health and attention problems in children
, results from a national survey demonstrated.
“We think it’s important for dermatologists and pediatricians to be monitoring children with AD for sleep and attention dysregulation,” Nina Y. Zhou said during a late-breaking research session at the Revolutionizing Atopic Dermatitis virtual symposium. “It’s also important to highlight sleep hygiene habits to improve sleep health overall.”
In an effort to determine the impact of AD severity on these symptoms in young children with AD and characterize sleep health and attention regulation behaviors, Ms. Zhou, a medical student at Northwestern University, Chicago, and colleagues drew from a national survey distributed via panel company OP4G and the National Eczema Association that was conducted with parents of 60 children with AD aged 1-5 years. Questionnaires included the Patient Reported Outcomes Measurement Information System (PROMIS) Early Childhood Sleep Health Measures to assess sleep health, the Peak Pruritus NRS to measure itch severity, and the Multidimensional Assessment Profile of Attention Regulation (MAPS-AR) to measure attention dysregulation related to inattention and hyperactivity. The researchers performed linear regression to determine the predictors of sleep health and attention dysregulation.
The mean age of 60 children was 3 years, 55% were male, 32% were black, 42% had severe disease, 42% had moderate disease, and 16% had mild disease. Children with more extensive AD were significantly more likely to report worse sleep disturbance. The proportion of children who reported sleep disturbance on at least 5 nights per week was 67% among those with severe AD, 24% among those with moderate AD, and 0% among those with mild AD.
In addition, 72% of parents of children with severe AD reported trouble paying attention at least 3 times per week “no matter what was going on,” compared with 24% of those with moderate AD and none of those with mild AD.
Parents of children with more severe AD reported more itch-related burden and significantly decreased quality of life for their children. For example, 76% of parents with children who had severe AD reported “because of itch, their child was frustrated,” compared to 44% of those with moderate AD and 10% with mild AD.
In fully adjusted linear regression analysis, the strongest predictors of sleep disturbance were AD severity (unstandardized beta value = 0.79, P less than .01) and being Black (unstandardized beta value = 3.89, P = .03). AD severity (unstandardized beta value = 1.22, P less than .01) and being Black (unstandardized beta value = 7.79, P less than .01) also predicted more attention dysregulation.
Household income appeared to differ significantly based on AD severity groups. “If you have mild AD, you are more likely to come from a higher income household,” Ms. Zhou said.
She concluded her presentation by calling for future studies with larger samples sizes to establish causality and directional effects between AD severity, itch, sleep, race, and attention.
The study was funded by the Agency for Healthcare Research and Quality. Ms. Zhou reported having no financial disclosures.
, results from a national survey demonstrated.
“We think it’s important for dermatologists and pediatricians to be monitoring children with AD for sleep and attention dysregulation,” Nina Y. Zhou said during a late-breaking research session at the Revolutionizing Atopic Dermatitis virtual symposium. “It’s also important to highlight sleep hygiene habits to improve sleep health overall.”
In an effort to determine the impact of AD severity on these symptoms in young children with AD and characterize sleep health and attention regulation behaviors, Ms. Zhou, a medical student at Northwestern University, Chicago, and colleagues drew from a national survey distributed via panel company OP4G and the National Eczema Association that was conducted with parents of 60 children with AD aged 1-5 years. Questionnaires included the Patient Reported Outcomes Measurement Information System (PROMIS) Early Childhood Sleep Health Measures to assess sleep health, the Peak Pruritus NRS to measure itch severity, and the Multidimensional Assessment Profile of Attention Regulation (MAPS-AR) to measure attention dysregulation related to inattention and hyperactivity. The researchers performed linear regression to determine the predictors of sleep health and attention dysregulation.
The mean age of 60 children was 3 years, 55% were male, 32% were black, 42% had severe disease, 42% had moderate disease, and 16% had mild disease. Children with more extensive AD were significantly more likely to report worse sleep disturbance. The proportion of children who reported sleep disturbance on at least 5 nights per week was 67% among those with severe AD, 24% among those with moderate AD, and 0% among those with mild AD.
In addition, 72% of parents of children with severe AD reported trouble paying attention at least 3 times per week “no matter what was going on,” compared with 24% of those with moderate AD and none of those with mild AD.
Parents of children with more severe AD reported more itch-related burden and significantly decreased quality of life for their children. For example, 76% of parents with children who had severe AD reported “because of itch, their child was frustrated,” compared to 44% of those with moderate AD and 10% with mild AD.
In fully adjusted linear regression analysis, the strongest predictors of sleep disturbance were AD severity (unstandardized beta value = 0.79, P less than .01) and being Black (unstandardized beta value = 3.89, P = .03). AD severity (unstandardized beta value = 1.22, P less than .01) and being Black (unstandardized beta value = 7.79, P less than .01) also predicted more attention dysregulation.
Household income appeared to differ significantly based on AD severity groups. “If you have mild AD, you are more likely to come from a higher income household,” Ms. Zhou said.
She concluded her presentation by calling for future studies with larger samples sizes to establish causality and directional effects between AD severity, itch, sleep, race, and attention.
The study was funded by the Agency for Healthcare Research and Quality. Ms. Zhou reported having no financial disclosures.
, results from a national survey demonstrated.
“We think it’s important for dermatologists and pediatricians to be monitoring children with AD for sleep and attention dysregulation,” Nina Y. Zhou said during a late-breaking research session at the Revolutionizing Atopic Dermatitis virtual symposium. “It’s also important to highlight sleep hygiene habits to improve sleep health overall.”
In an effort to determine the impact of AD severity on these symptoms in young children with AD and characterize sleep health and attention regulation behaviors, Ms. Zhou, a medical student at Northwestern University, Chicago, and colleagues drew from a national survey distributed via panel company OP4G and the National Eczema Association that was conducted with parents of 60 children with AD aged 1-5 years. Questionnaires included the Patient Reported Outcomes Measurement Information System (PROMIS) Early Childhood Sleep Health Measures to assess sleep health, the Peak Pruritus NRS to measure itch severity, and the Multidimensional Assessment Profile of Attention Regulation (MAPS-AR) to measure attention dysregulation related to inattention and hyperactivity. The researchers performed linear regression to determine the predictors of sleep health and attention dysregulation.
The mean age of 60 children was 3 years, 55% were male, 32% were black, 42% had severe disease, 42% had moderate disease, and 16% had mild disease. Children with more extensive AD were significantly more likely to report worse sleep disturbance. The proportion of children who reported sleep disturbance on at least 5 nights per week was 67% among those with severe AD, 24% among those with moderate AD, and 0% among those with mild AD.
In addition, 72% of parents of children with severe AD reported trouble paying attention at least 3 times per week “no matter what was going on,” compared with 24% of those with moderate AD and none of those with mild AD.
Parents of children with more severe AD reported more itch-related burden and significantly decreased quality of life for their children. For example, 76% of parents with children who had severe AD reported “because of itch, their child was frustrated,” compared to 44% of those with moderate AD and 10% with mild AD.
In fully adjusted linear regression analysis, the strongest predictors of sleep disturbance were AD severity (unstandardized beta value = 0.79, P less than .01) and being Black (unstandardized beta value = 3.89, P = .03). AD severity (unstandardized beta value = 1.22, P less than .01) and being Black (unstandardized beta value = 7.79, P less than .01) also predicted more attention dysregulation.
Household income appeared to differ significantly based on AD severity groups. “If you have mild AD, you are more likely to come from a higher income household,” Ms. Zhou said.
She concluded her presentation by calling for future studies with larger samples sizes to establish causality and directional effects between AD severity, itch, sleep, race, and attention.
The study was funded by the Agency for Healthcare Research and Quality. Ms. Zhou reported having no financial disclosures.
FROM REVOLUTIONIZING AD 2020
Study links sleep meds and dementia risk in older adults
Sleep medications for older patients who report sleep problems may not be the best treatment given growing evidence of the link between these medications and the risk of incident dementia.

Adults aged 65 years and older who used sleep medications 5-7 days a week demonstrated a 30% increased risk of dementia, compared with those who did not use sleep medications, findings from a prospective study of 6,373 individuals show.
Adults aged 65 and older report a higher burden of sleep problems than other age groups, but major medical associations discourage the use of sleep medications by older adults because of growing evidence of a link between sleep medication use and cognitive decline, wrote Rebecca Robbins, MD, of Brigham and Women’s Hospital, Boston, and colleagues. However, data on this association among adults in the United States are limited, they said.
In a study published in Sleep Medicine, the researchers surveyed 6,373 adults aged 65 years and older who were enrolled in the nationally representative National Health and Aging Trends Study (NHATS). The majority of the participants were non-Hispanic White (71%), 59% were women, and 21% ranged in age from 70 to 74 years.
Participants responded to questions about routine sleep medication use. Routine was defined as “most nights” or “every night.” The data were collected for an 8-year period from 2011 to 2018. The study began in 2011, with a core interview administered annually.
Approximately 15% of the study population reported routine use of sleep medications. Overall, routine use of sleep medication was significantly associated with risk of incident dementia (hazard ratio, 1.30; P < .01) after controlling for multiple variables including age, sex, education level, and chronic conditions.
Dementia screening was conducted by participants rating their memory and then performing a memory-related activity (immediate and delayed 10-word recall) and other exercises to assess executive function and orientation. A separate eight-item informant screener was performed for patient proxies. The researcher noted, “Sensitivity of the NHATS probable dementia screening measure has been determined in previous research to be 66%, and specificity is 87%, with respect to a clinical dementia diagnosis.”
The study findings were limited by several factors including the use of self-reports, the lack of data on type or dose of sleep medication, and lack of data on the indication for the prescription, the researchers noted.
“Also, sleep medication use leads to worse performance on cognitive testing, such as the questionnaires used to screen for dementia in this study, and therefore could have resulted in a false diagnosis of dementia,” they added.
However, the results were strengthened by the large, nationally representative study population and support the need for quality geriatric care, the researchers said.
“Our findings provide further support and evidence that sleep medications are all too commonly administered, yet associated with greater risk for incident dementia, and that the U.S. health care system is in need of creative solutions for addressing poor sleep among older individuals,” they concluded.
Implications and alternatives
The study is important as the number of aging Americans increases, said Carolyn M. D’Ambrosio, MD, FCCP, of Brigham and Women’s Hospital and Harvard Medical School, Boston, in an interview. “In the elderly, inability to fall asleep or stay asleep are common issues that are brought to a health care provider,” she said. Dr. D’Ambrosio said she was not surprised by the study findings “as elderly patients often have sleep issues and sometimes a well-meaning health care provider gives them sleep medication to help. We have known that some of these sleep medications such as benzodiazepines affect cognitive performance,” she said.
Dr. D’Ambrosio said she avoids prescribing sleep medications for older adults if possible. “A deep dive into sleep habits, environment, and other things that disrupt sleep often gets to the problem rather than just masking it with a sleep medication,” she noted. Alternatives to improve sleep in older adults include exercise, exposure to bright light during the day, and good healthy sleep habits, all of which contribute to improved sleep in the elderly, said Dr. D’Ambrosio. She also recommends screening older adults for other issues that affect sleep, such as chronic pain.
The current study highlighted the association between sleep medication use and dementia, but it does not show causation, Dr. D’Ambrosio said. “So much more needs to be done to determine whether the sleep medications are causing worsening cognitive function long term, or if the dementia is starting but not yet diagnosed and the sleep medication is given but not the cause of the dementia, she noted.
Research gaps and treatment strategies
Older adults experiencing sleep difficulties may try various medications including pharmacologics (e.g., benzodiazepines), over-the-counter agents, such as diphenhydramine or doxylamine preparations, and/or herbal and nutritional supplements such as valerian or melatonin, said Mary Jo S. Farmer, MD, FCCP, of the University of Massachusetts Medical School–Baystate, Springfield, in an interview. “However, sleep medications, particularly benzodiazepines, are strongly discouraged by major medical associations including the American Geriatrics Society in part because of the growing evidence that use of sleep medications is associated with cognitive impairment and decline,” she said.

The current study results contribute to previous work demonstrating that both pharmacologic and nonpharmacologic sleep medication, although commonly administered, is associated with subsequent adverse outcomes in older adults, Dr. Farmer said. This association sets the stage for creative and different solutions for addressing poor sleep among older adults, such as behavioral treatments including cognitive-behavioral therapy, she noted.
Dr. Farmer said, “Areas for future research include exploring the causal link between prescription and/or over-the-counter sleep medication use and incident dementia in a randomized controlled trial,” she added.
“Another interesting opportunity for future research is to explore the indications for sleep medications among older adults since it has been shown in the general population that sleep difficulties represent only 12% of the indication for sleep medication prescriptions,” Dr. Farmer noted. “Future research could examine the strength of the underlying motivation to use sleep medication even in light of suggested long-term effects, and the effectiveness of other measures to avoid or minimize sleep difficulties,” she said.
“My experience is that the majority of ambulatory patients recently seen in sleep clinic want to avoid long-term use of sleep medications and will ask what other measures can be tried to consistently achieve a good night’s sleep without medication use,” Dr. Farmer said. “If medications are used, patients would rather try melatonin than a benzodiazepine. Many patients who come to sleep clinic with sleep medications already prescribed and are subsequently found to have sleep apnea and/or restless legs find that they no longer need sleep medication when these other medical conditions are appropriately diagnosed and managed,” she explained. “Finally, many patients tell me they feel less energetic upon awakening, almost feel hung over, and express being less sharp cognitively when taking pharmacologic sleep medication, whether for short or long periods of time, and therefore they want to avoid continuing with sleep medication use,” she said.
Dr. Farmer’s strategy for developing alternatives to sleep medications in older adults includes taking a careful history, including a complete list of medical problems, review of medications, and a thorough sleep history including usual time of sleep onset, awake time, and the frequency of daytime naps. “Tips for improving the quality of nighttime sleep may include adequately treating pain and other medical conditions such as heartburn, sleep apnea, and restless legs, creating a soothing environment to promote sleep by eliminating noise and bright lights, avoiding stimulant medications and substances such as caffeine and nicotine before bedtime, avoiding excessive amounts of alcohol, avoiding diuretics before bedtime, encouraging physical activity during the day, spending time in the sunlight as much as possible to help regulate the sleep cycle, limiting daytime naps, and establishing a regular sleep schedule,” she said.
The study was supported by National Institutes of Health awards K01HL150339, U54MD000538, K07AG052685, R01AG056531, R01AG056031. Lead author Dr. Robbins had no financial conflicts to disclose. Dr. D’Ambrosio disclosed serving as a section editor for sleep medicine for Dynamed and owning a patent on a circadian programming device. Dr. Farmer had no disclosures.
SOURCE: Robbins R et al. Sleep Med. 2020 Nov 11. doi: 10.1016/j.sleep.2020.11.004.
Sleep medications for older patients who report sleep problems may not be the best treatment given growing evidence of the link between these medications and the risk of incident dementia.
Adults aged 65 years and older who used sleep medications 5-7 days a week demonstrated a 30% increased risk of dementia, compared with those who did not use sleep medications, findings from a prospective study of 6,373 individuals show.
Adults aged 65 and older report a higher burden of sleep problems than other age groups, but major medical associations discourage the use of sleep medications by older adults because of growing evidence of a link between sleep medication use and cognitive decline, wrote Rebecca Robbins, MD, of Brigham and Women’s Hospital, Boston, and colleagues. However, data on this association among adults in the United States are limited, they said.
In a study published in Sleep Medicine, the researchers surveyed 6,373 adults aged 65 years and older who were enrolled in the nationally representative National Health and Aging Trends Study (NHATS). The majority of the participants were non-Hispanic White (71%), 59% were women, and 21% ranged in age from 70 to 74 years.
Participants responded to questions about routine sleep medication use. Routine was defined as “most nights” or “every night.” The data were collected for an 8-year period from 2011 to 2018. The study began in 2011, with a core interview administered annually.
Approximately 15% of the study population reported routine use of sleep medications. Overall, routine use of sleep medication was significantly associated with risk of incident dementia (hazard ratio, 1.30; P < .01) after controlling for multiple variables including age, sex, education level, and chronic conditions.
Dementia screening was conducted by participants rating their memory and then performing a memory-related activity (immediate and delayed 10-word recall) and other exercises to assess executive function and orientation. A separate eight-item informant screener was performed for patient proxies. The researcher noted, “Sensitivity of the NHATS probable dementia screening measure has been determined in previous research to be 66%, and specificity is 87%, with respect to a clinical dementia diagnosis.”
The study findings were limited by several factors including the use of self-reports, the lack of data on type or dose of sleep medication, and lack of data on the indication for the prescription, the researchers noted.
“Also, sleep medication use leads to worse performance on cognitive testing, such as the questionnaires used to screen for dementia in this study, and therefore could have resulted in a false diagnosis of dementia,” they added.
However, the results were strengthened by the large, nationally representative study population and support the need for quality geriatric care, the researchers said.
“Our findings provide further support and evidence that sleep medications are all too commonly administered, yet associated with greater risk for incident dementia, and that the U.S. health care system is in need of creative solutions for addressing poor sleep among older individuals,” they concluded.
Implications and alternatives
The study is important as the number of aging Americans increases, said Carolyn M. D’Ambrosio, MD, FCCP, of Brigham and Women’s Hospital and Harvard Medical School, Boston, in an interview. “In the elderly, inability to fall asleep or stay asleep are common issues that are brought to a health care provider,” she said. Dr. D’Ambrosio said she was not surprised by the study findings “as elderly patients often have sleep issues and sometimes a well-meaning health care provider gives them sleep medication to help. We have known that some of these sleep medications such as benzodiazepines affect cognitive performance,” she said.
Dr. D’Ambrosio said she avoids prescribing sleep medications for older adults if possible. “A deep dive into sleep habits, environment, and other things that disrupt sleep often gets to the problem rather than just masking it with a sleep medication,” she noted. Alternatives to improve sleep in older adults include exercise, exposure to bright light during the day, and good healthy sleep habits, all of which contribute to improved sleep in the elderly, said Dr. D’Ambrosio. She also recommends screening older adults for other issues that affect sleep, such as chronic pain.
The current study highlighted the association between sleep medication use and dementia, but it does not show causation, Dr. D’Ambrosio said. “So much more needs to be done to determine whether the sleep medications are causing worsening cognitive function long term, or if the dementia is starting but not yet diagnosed and the sleep medication is given but not the cause of the dementia, she noted.
Research gaps and treatment strategies
Older adults experiencing sleep difficulties may try various medications including pharmacologics (e.g., benzodiazepines), over-the-counter agents, such as diphenhydramine or doxylamine preparations, and/or herbal and nutritional supplements such as valerian or melatonin, said Mary Jo S. Farmer, MD, FCCP, of the University of Massachusetts Medical School–Baystate, Springfield, in an interview. “However, sleep medications, particularly benzodiazepines, are strongly discouraged by major medical associations including the American Geriatrics Society in part because of the growing evidence that use of sleep medications is associated with cognitive impairment and decline,” she said.
The current study results contribute to previous work demonstrating that both pharmacologic and nonpharmacologic sleep medication, although commonly administered, is associated with subsequent adverse outcomes in older adults, Dr. Farmer said. This association sets the stage for creative and different solutions for addressing poor sleep among older adults, such as behavioral treatments including cognitive-behavioral therapy, she noted.
Dr. Farmer said, “Areas for future research include exploring the causal link between prescription and/or over-the-counter sleep medication use and incident dementia in a randomized controlled trial,” she added.
“Another interesting opportunity for future research is to explore the indications for sleep medications among older adults since it has been shown in the general population that sleep difficulties represent only 12% of the indication for sleep medication prescriptions,” Dr. Farmer noted. “Future research could examine the strength of the underlying motivation to use sleep medication even in light of suggested long-term effects, and the effectiveness of other measures to avoid or minimize sleep difficulties,” she said.
“My experience is that the majority of ambulatory patients recently seen in sleep clinic want to avoid long-term use of sleep medications and will ask what other measures can be tried to consistently achieve a good night’s sleep without medication use,” Dr. Farmer said. “If medications are used, patients would rather try melatonin than a benzodiazepine. Many patients who come to sleep clinic with sleep medications already prescribed and are subsequently found to have sleep apnea and/or restless legs find that they no longer need sleep medication when these other medical conditions are appropriately diagnosed and managed,” she explained. “Finally, many patients tell me they feel less energetic upon awakening, almost feel hung over, and express being less sharp cognitively when taking pharmacologic sleep medication, whether for short or long periods of time, and therefore they want to avoid continuing with sleep medication use,” she said.
Dr. Farmer’s strategy for developing alternatives to sleep medications in older adults includes taking a careful history, including a complete list of medical problems, review of medications, and a thorough sleep history including usual time of sleep onset, awake time, and the frequency of daytime naps. “Tips for improving the quality of nighttime sleep may include adequately treating pain and other medical conditions such as heartburn, sleep apnea, and restless legs, creating a soothing environment to promote sleep by eliminating noise and bright lights, avoiding stimulant medications and substances such as caffeine and nicotine before bedtime, avoiding excessive amounts of alcohol, avoiding diuretics before bedtime, encouraging physical activity during the day, spending time in the sunlight as much as possible to help regulate the sleep cycle, limiting daytime naps, and establishing a regular sleep schedule,” she said.
The study was supported by National Institutes of Health awards K01HL150339, U54MD000538, K07AG052685, R01AG056531, R01AG056031. Lead author Dr. Robbins had no financial conflicts to disclose. Dr. D’Ambrosio disclosed serving as a section editor for sleep medicine for Dynamed and owning a patent on a circadian programming device. Dr. Farmer had no disclosures.
SOURCE: Robbins R et al. Sleep Med. 2020 Nov 11. doi: 10.1016/j.sleep.2020.11.004.
Sleep medications for older patients who report sleep problems may not be the best treatment given growing evidence of the link between these medications and the risk of incident dementia.
Adults aged 65 years and older who used sleep medications 5-7 days a week demonstrated a 30% increased risk of dementia, compared with those who did not use sleep medications, findings from a prospective study of 6,373 individuals show.
Adults aged 65 and older report a higher burden of sleep problems than other age groups, but major medical associations discourage the use of sleep medications by older adults because of growing evidence of a link between sleep medication use and cognitive decline, wrote Rebecca Robbins, MD, of Brigham and Women’s Hospital, Boston, and colleagues. However, data on this association among adults in the United States are limited, they said.
In a study published in Sleep Medicine, the researchers surveyed 6,373 adults aged 65 years and older who were enrolled in the nationally representative National Health and Aging Trends Study (NHATS). The majority of the participants were non-Hispanic White (71%), 59% were women, and 21% ranged in age from 70 to 74 years.
Participants responded to questions about routine sleep medication use. Routine was defined as “most nights” or “every night.” The data were collected for an 8-year period from 2011 to 2018. The study began in 2011, with a core interview administered annually.
Approximately 15% of the study population reported routine use of sleep medications. Overall, routine use of sleep medication was significantly associated with risk of incident dementia (hazard ratio, 1.30; P < .01) after controlling for multiple variables including age, sex, education level, and chronic conditions.
Dementia screening was conducted by participants rating their memory and then performing a memory-related activity (immediate and delayed 10-word recall) and other exercises to assess executive function and orientation. A separate eight-item informant screener was performed for patient proxies. The researcher noted, “Sensitivity of the NHATS probable dementia screening measure has been determined in previous research to be 66%, and specificity is 87%, with respect to a clinical dementia diagnosis.”
The study findings were limited by several factors including the use of self-reports, the lack of data on type or dose of sleep medication, and lack of data on the indication for the prescription, the researchers noted.
“Also, sleep medication use leads to worse performance on cognitive testing, such as the questionnaires used to screen for dementia in this study, and therefore could have resulted in a false diagnosis of dementia,” they added.
However, the results were strengthened by the large, nationally representative study population and support the need for quality geriatric care, the researchers said.
“Our findings provide further support and evidence that sleep medications are all too commonly administered, yet associated with greater risk for incident dementia, and that the U.S. health care system is in need of creative solutions for addressing poor sleep among older individuals,” they concluded.
Implications and alternatives
The study is important as the number of aging Americans increases, said Carolyn M. D’Ambrosio, MD, FCCP, of Brigham and Women’s Hospital and Harvard Medical School, Boston, in an interview. “In the elderly, inability to fall asleep or stay asleep are common issues that are brought to a health care provider,” she said. Dr. D’Ambrosio said she was not surprised by the study findings “as elderly patients often have sleep issues and sometimes a well-meaning health care provider gives them sleep medication to help. We have known that some of these sleep medications such as benzodiazepines affect cognitive performance,” she said.
Dr. D’Ambrosio said she avoids prescribing sleep medications for older adults if possible. “A deep dive into sleep habits, environment, and other things that disrupt sleep often gets to the problem rather than just masking it with a sleep medication,” she noted. Alternatives to improve sleep in older adults include exercise, exposure to bright light during the day, and good healthy sleep habits, all of which contribute to improved sleep in the elderly, said Dr. D’Ambrosio. She also recommends screening older adults for other issues that affect sleep, such as chronic pain.
The current study highlighted the association between sleep medication use and dementia, but it does not show causation, Dr. D’Ambrosio said. “So much more needs to be done to determine whether the sleep medications are causing worsening cognitive function long term, or if the dementia is starting but not yet diagnosed and the sleep medication is given but not the cause of the dementia, she noted.
Research gaps and treatment strategies
Older adults experiencing sleep difficulties may try various medications including pharmacologics (e.g., benzodiazepines), over-the-counter agents, such as diphenhydramine or doxylamine preparations, and/or herbal and nutritional supplements such as valerian or melatonin, said Mary Jo S. Farmer, MD, FCCP, of the University of Massachusetts Medical School–Baystate, Springfield, in an interview. “However, sleep medications, particularly benzodiazepines, are strongly discouraged by major medical associations including the American Geriatrics Society in part because of the growing evidence that use of sleep medications is associated with cognitive impairment and decline,” she said.
The current study results contribute to previous work demonstrating that both pharmacologic and nonpharmacologic sleep medication, although commonly administered, is associated with subsequent adverse outcomes in older adults, Dr. Farmer said. This association sets the stage for creative and different solutions for addressing poor sleep among older adults, such as behavioral treatments including cognitive-behavioral therapy, she noted.
Dr. Farmer said, “Areas for future research include exploring the causal link between prescription and/or over-the-counter sleep medication use and incident dementia in a randomized controlled trial,” she added.
“Another interesting opportunity for future research is to explore the indications for sleep medications among older adults since it has been shown in the general population that sleep difficulties represent only 12% of the indication for sleep medication prescriptions,” Dr. Farmer noted. “Future research could examine the strength of the underlying motivation to use sleep medication even in light of suggested long-term effects, and the effectiveness of other measures to avoid or minimize sleep difficulties,” she said.
“My experience is that the majority of ambulatory patients recently seen in sleep clinic want to avoid long-term use of sleep medications and will ask what other measures can be tried to consistently achieve a good night’s sleep without medication use,” Dr. Farmer said. “If medications are used, patients would rather try melatonin than a benzodiazepine. Many patients who come to sleep clinic with sleep medications already prescribed and are subsequently found to have sleep apnea and/or restless legs find that they no longer need sleep medication when these other medical conditions are appropriately diagnosed and managed,” she explained. “Finally, many patients tell me they feel less energetic upon awakening, almost feel hung over, and express being less sharp cognitively when taking pharmacologic sleep medication, whether for short or long periods of time, and therefore they want to avoid continuing with sleep medication use,” she said.
Dr. Farmer’s strategy for developing alternatives to sleep medications in older adults includes taking a careful history, including a complete list of medical problems, review of medications, and a thorough sleep history including usual time of sleep onset, awake time, and the frequency of daytime naps. “Tips for improving the quality of nighttime sleep may include adequately treating pain and other medical conditions such as heartburn, sleep apnea, and restless legs, creating a soothing environment to promote sleep by eliminating noise and bright lights, avoiding stimulant medications and substances such as caffeine and nicotine before bedtime, avoiding excessive amounts of alcohol, avoiding diuretics before bedtime, encouraging physical activity during the day, spending time in the sunlight as much as possible to help regulate the sleep cycle, limiting daytime naps, and establishing a regular sleep schedule,” she said.
The study was supported by National Institutes of Health awards K01HL150339, U54MD000538, K07AG052685, R01AG056531, R01AG056031. Lead author Dr. Robbins had no financial conflicts to disclose. Dr. D’Ambrosio disclosed serving as a section editor for sleep medicine for Dynamed and owning a patent on a circadian programming device. Dr. Farmer had no disclosures.
SOURCE: Robbins R et al. Sleep Med. 2020 Nov 11. doi: 10.1016/j.sleep.2020.11.004.
FROM SLEEP MEDICINE
Kennedy, NIMH demand urgent action on COVID-19 mental health toll
A public-private partnership, led by mental health advocate Patrick Kennedy and the head of the National Institute of Mental Health, Joshua Gordon, MD, PhD, want urgent action to address the wave of mental illness and suicide caused by COVID-19.
“Our country is in serious denial about the full impact of mental health in this country and certainly as part of this pandemic,” said former congressman Mr. Kennedy, cochair of the Action Alliance’s Mental Health & Suicide Prevention National Response to COVID-19, at a briefing unveiling the group’s new six-priority Action Plan.
“That’s reinforced when all we hear from is Dr. Fauci,” and only about the physical effects of the disease, said Mr. Kennedy, the founder of the Kennedy Forum, a nonprofit dedicated to changing the health system’s approach to mental health and substance use disorders.
“ he said. Mr. Kennedy noted the huge effort to speed therapeutics and vaccines to the American public. “We need to bring that same sense of urgency to these deaths of despair hiding in plain sight.”
Dr. Gordon, NIMH’s director and a cochair of the National Response group, was also at the briefing.
“We know many people report experiencing symptoms of distress, including anxiety, sleep problems, depression, substance use, and suicidal thoughts at rates two to three times higher than we might expect in times before the pandemic. Just as the country has come together to mitigate the physical impacts of pandemic, we also have to identify how to mitigate the mental health impacts,” said Dr. Gordon.
Plan of action
Mr. Kennedy emphasized that it is crucial that federal lawmakers and regulators find a way to increase parity between mental and physical health.
Paramount in that effort would be ensuring stronger enforcement of the Mental Health Parity and Addiction Equity Act, he said.
That 1996 law requires health plans to ensure that benefits for physical and mental health were equivalent, but it has frequently been ignored. In 2019, a U.S. federal court found that one of the nation’s largest behavioral health insurers, United Behavioral Health, had been violating the law. Mr. Kennedy said he expects this decision to continue to have a positive impact on achieving parity.
In November, United was ordered by a federal judge to reprocess 67,000 claims that it illegally denied.
The Alliance’s Action Plan has six priorities:
- Change the national conversation about mental health and suicide.
- Increase access to evidence-based treatments for substance use and mental health disorders in specialty and primary care, and include better reimbursement for services and make permanent reimbursement for telehealth services.
- Increase the use of nonpunitive and supportive crisis intervention services, including keeping people out of the criminal justice system.
- Establish near real-time data collection systems to promptly identify changes in rates of suicide, overdose, and other key events, and of clusters or spikes.
- Ensure the equitable delivery of comprehensive and effective suicide prevention and mental health services for Black Americans, Latin Americans, American Indian/Alaskan Natives, LGBTQ individuals, and others disproportionately impacted by the pandemic.
- Invest in prevention and early intervention approaches that treat the root causes of suicide and mental health problems.
Uptick in distress
Dr. Gordon noted that recent data indicate that, although ED visits for children are still down in 2020, compared with previous years, mental health ED visits are back to prepandemic levels.
A September survey showed an increase in suicidal thoughts and attempts, anxiety, and depression pandemic in youth because of the pandemic. Almost one-quarter of those surveyed said they knew a peer who developed suicidal thoughts since the start of the pandemic and 5% reported making a suicide attempt themselves.
In early December, research reported in JAMA Psychiatry showed the overall rate of overdose-related cardiac arrests in 2020 was about 50% higher than trends in 2018 and 2019, and that all overdose-related incidents were about 17% above baseline in 2020.
COVID-19 also appears to be striking individuals who are living in behavioral health facilities, and some of those facilities are reducing inpatient care and other programs because they don’t have enough personal protective equipment, testing supplies, or staff to cope with the disease.
The facilities are not required to report infections to the federal government. Sen. Elizabeth Warren (D-Mass.), Rep. Carolyn Maloney (D-N.Y.), and Rep. Katie Porter (D-Calif.) issued a report based on their own offices’ survey of 10 large behavioral health program operators.
Eight of those operators – covering 376 facilities and more than 100,000 patients in 40 states and Puerto Rico – provided substantive responses.
More than half had at least one COVID case and 14% had large outbreaks of 10 or more cases. The infection rate for patients was in line with that of the general public.
A version of this article originally appeared on Medscape.com.
A public-private partnership, led by mental health advocate Patrick Kennedy and the head of the National Institute of Mental Health, Joshua Gordon, MD, PhD, want urgent action to address the wave of mental illness and suicide caused by COVID-19.
“Our country is in serious denial about the full impact of mental health in this country and certainly as part of this pandemic,” said former congressman Mr. Kennedy, cochair of the Action Alliance’s Mental Health & Suicide Prevention National Response to COVID-19, at a briefing unveiling the group’s new six-priority Action Plan.
“That’s reinforced when all we hear from is Dr. Fauci,” and only about the physical effects of the disease, said Mr. Kennedy, the founder of the Kennedy Forum, a nonprofit dedicated to changing the health system’s approach to mental health and substance use disorders.
“ he said. Mr. Kennedy noted the huge effort to speed therapeutics and vaccines to the American public. “We need to bring that same sense of urgency to these deaths of despair hiding in plain sight.”
Dr. Gordon, NIMH’s director and a cochair of the National Response group, was also at the briefing.
“We know many people report experiencing symptoms of distress, including anxiety, sleep problems, depression, substance use, and suicidal thoughts at rates two to three times higher than we might expect in times before the pandemic. Just as the country has come together to mitigate the physical impacts of pandemic, we also have to identify how to mitigate the mental health impacts,” said Dr. Gordon.
Plan of action
Mr. Kennedy emphasized that it is crucial that federal lawmakers and regulators find a way to increase parity between mental and physical health.
Paramount in that effort would be ensuring stronger enforcement of the Mental Health Parity and Addiction Equity Act, he said.
That 1996 law requires health plans to ensure that benefits for physical and mental health were equivalent, but it has frequently been ignored. In 2019, a U.S. federal court found that one of the nation’s largest behavioral health insurers, United Behavioral Health, had been violating the law. Mr. Kennedy said he expects this decision to continue to have a positive impact on achieving parity.
In November, United was ordered by a federal judge to reprocess 67,000 claims that it illegally denied.
The Alliance’s Action Plan has six priorities:
- Change the national conversation about mental health and suicide.
- Increase access to evidence-based treatments for substance use and mental health disorders in specialty and primary care, and include better reimbursement for services and make permanent reimbursement for telehealth services.
- Increase the use of nonpunitive and supportive crisis intervention services, including keeping people out of the criminal justice system.
- Establish near real-time data collection systems to promptly identify changes in rates of suicide, overdose, and other key events, and of clusters or spikes.
- Ensure the equitable delivery of comprehensive and effective suicide prevention and mental health services for Black Americans, Latin Americans, American Indian/Alaskan Natives, LGBTQ individuals, and others disproportionately impacted by the pandemic.
- Invest in prevention and early intervention approaches that treat the root causes of suicide and mental health problems.
Uptick in distress
Dr. Gordon noted that recent data indicate that, although ED visits for children are still down in 2020, compared with previous years, mental health ED visits are back to prepandemic levels.
A September survey showed an increase in suicidal thoughts and attempts, anxiety, and depression pandemic in youth because of the pandemic. Almost one-quarter of those surveyed said they knew a peer who developed suicidal thoughts since the start of the pandemic and 5% reported making a suicide attempt themselves.
In early December, research reported in JAMA Psychiatry showed the overall rate of overdose-related cardiac arrests in 2020 was about 50% higher than trends in 2018 and 2019, and that all overdose-related incidents were about 17% above baseline in 2020.
COVID-19 also appears to be striking individuals who are living in behavioral health facilities, and some of those facilities are reducing inpatient care and other programs because they don’t have enough personal protective equipment, testing supplies, or staff to cope with the disease.
The facilities are not required to report infections to the federal government. Sen. Elizabeth Warren (D-Mass.), Rep. Carolyn Maloney (D-N.Y.), and Rep. Katie Porter (D-Calif.) issued a report based on their own offices’ survey of 10 large behavioral health program operators.
Eight of those operators – covering 376 facilities and more than 100,000 patients in 40 states and Puerto Rico – provided substantive responses.
More than half had at least one COVID case and 14% had large outbreaks of 10 or more cases. The infection rate for patients was in line with that of the general public.
A version of this article originally appeared on Medscape.com.
A public-private partnership, led by mental health advocate Patrick Kennedy and the head of the National Institute of Mental Health, Joshua Gordon, MD, PhD, want urgent action to address the wave of mental illness and suicide caused by COVID-19.
“Our country is in serious denial about the full impact of mental health in this country and certainly as part of this pandemic,” said former congressman Mr. Kennedy, cochair of the Action Alliance’s Mental Health & Suicide Prevention National Response to COVID-19, at a briefing unveiling the group’s new six-priority Action Plan.
“That’s reinforced when all we hear from is Dr. Fauci,” and only about the physical effects of the disease, said Mr. Kennedy, the founder of the Kennedy Forum, a nonprofit dedicated to changing the health system’s approach to mental health and substance use disorders.
“ he said. Mr. Kennedy noted the huge effort to speed therapeutics and vaccines to the American public. “We need to bring that same sense of urgency to these deaths of despair hiding in plain sight.”
Dr. Gordon, NIMH’s director and a cochair of the National Response group, was also at the briefing.
“We know many people report experiencing symptoms of distress, including anxiety, sleep problems, depression, substance use, and suicidal thoughts at rates two to three times higher than we might expect in times before the pandemic. Just as the country has come together to mitigate the physical impacts of pandemic, we also have to identify how to mitigate the mental health impacts,” said Dr. Gordon.
Plan of action
Mr. Kennedy emphasized that it is crucial that federal lawmakers and regulators find a way to increase parity between mental and physical health.
Paramount in that effort would be ensuring stronger enforcement of the Mental Health Parity and Addiction Equity Act, he said.
That 1996 law requires health plans to ensure that benefits for physical and mental health were equivalent, but it has frequently been ignored. In 2019, a U.S. federal court found that one of the nation’s largest behavioral health insurers, United Behavioral Health, had been violating the law. Mr. Kennedy said he expects this decision to continue to have a positive impact on achieving parity.
In November, United was ordered by a federal judge to reprocess 67,000 claims that it illegally denied.
The Alliance’s Action Plan has six priorities:
- Change the national conversation about mental health and suicide.
- Increase access to evidence-based treatments for substance use and mental health disorders in specialty and primary care, and include better reimbursement for services and make permanent reimbursement for telehealth services.
- Increase the use of nonpunitive and supportive crisis intervention services, including keeping people out of the criminal justice system.
- Establish near real-time data collection systems to promptly identify changes in rates of suicide, overdose, and other key events, and of clusters or spikes.
- Ensure the equitable delivery of comprehensive and effective suicide prevention and mental health services for Black Americans, Latin Americans, American Indian/Alaskan Natives, LGBTQ individuals, and others disproportionately impacted by the pandemic.
- Invest in prevention and early intervention approaches that treat the root causes of suicide and mental health problems.
Uptick in distress
Dr. Gordon noted that recent data indicate that, although ED visits for children are still down in 2020, compared with previous years, mental health ED visits are back to prepandemic levels.
A September survey showed an increase in suicidal thoughts and attempts, anxiety, and depression pandemic in youth because of the pandemic. Almost one-quarter of those surveyed said they knew a peer who developed suicidal thoughts since the start of the pandemic and 5% reported making a suicide attempt themselves.
In early December, research reported in JAMA Psychiatry showed the overall rate of overdose-related cardiac arrests in 2020 was about 50% higher than trends in 2018 and 2019, and that all overdose-related incidents were about 17% above baseline in 2020.
COVID-19 also appears to be striking individuals who are living in behavioral health facilities, and some of those facilities are reducing inpatient care and other programs because they don’t have enough personal protective equipment, testing supplies, or staff to cope with the disease.
The facilities are not required to report infections to the federal government. Sen. Elizabeth Warren (D-Mass.), Rep. Carolyn Maloney (D-N.Y.), and Rep. Katie Porter (D-Calif.) issued a report based on their own offices’ survey of 10 large behavioral health program operators.
Eight of those operators – covering 376 facilities and more than 100,000 patients in 40 states and Puerto Rico – provided substantive responses.
More than half had at least one COVID case and 14% had large outbreaks of 10 or more cases. The infection rate for patients was in line with that of the general public.
A version of this article originally appeared on Medscape.com.
Treating insomnia, anxiety in a pandemic
Since the start of the pandemic, we have been conducting an extra hour of Virtual Rounds at the Center for Women’s Mental Health. Virtual Rounds has been an opportunity to discuss cases around a spectrum of clinical management issues with respect to depression, bipolar disorder, and a spectrum of anxiety disorders like obsessive-compulsive disorder (OCD), posttraumatic stress disorder (PTSD), and generalized anxiety disorder. How to apply the calculus of risk-benefit decision-making around management of psychiatric disorder during pregnancy and the postpartum period has been the cornerstone of the work at our center for over 2 decades.

When we went virtual at our center in the early Spring, we decided to keep the format of our faculty rounds the way they have been for years and to sustain cohesiveness of our program during the pandemic. But we thought the needs of pregnant and postpartum women warranted being addressed in a context more specific to COVID-19, and also that reproductive psychiatrists and other clinicians could learn from each other about novel issues coming up for this group of patients during the pandemic. With that backdrop, Marlene Freeman, MD, and I founded “Virtual Rounds at the Center” to respond to queries from our colleagues across the country; we do this just after our own rounds on Wednesdays at 2:00 p.m.
As the pandemic has progressed, Virtual Rounds has blossomed into a virtual community on the Zoom platform, where social workers, psychologists, nurse prescribers, psychiatrists, and obstetricians discuss the needs of pregnant and postpartum women specific to COVID-19. Frequently, our discussions involve a review of the risks and benefits of treatment before, during, and after pregnancy.
Seemingly, week to week, more and more colleagues raise questions about the treatment of anxiety and insomnia during pregnancy and the postpartum period. I’ve spoken in previous columns about the enhanced use of telemedicine. Telemedicine not only facilitates efforts like Virtual Rounds and our ability to reach out to colleagues across the country and share cases, but also has allowed us to keep even closer tabs on the emotional well-being of our pregnant and postpartum women during COVID-19.
The question is not just about the effects of a medicine that a woman might take to treat anxiety or insomnia during pregnancy, but the experience of the pandemic per se, which we are measuring in multiple studies now using a variety of psychological instruments that patients complete. The pandemic is unequivocally taking a still unquantified toll on the mental health of Americans and potentially on the next generation to come.
Midcycle awakening during pregnancy
Complaints of insomnia and midcycle awakening during pregnancy are not new – it is the rule, rather than the exception for many pregnant women, particularly later in pregnancy. We have unequivocally seen a worsening of complaints of sleep disruption including insomnia and midcycle awakening during the pandemic that is greater than what we have seen previously. Both patients and colleagues have asked us the safest ways to manage it. One of the first things we consider when we hear about insomnia is whether it is part of an underlying mood disorder. While we see primary insomnia clinically, it really is important to remember that insomnia can be part and parcel of an underlying mood disorder.
With that in mind, what are the options? During the pandemic, we’ve seen an increased use of digital cognitive behavioral therapy for insomnia (CBT-I) for patients who cannot initiate sleep, which has a very strong evidence base for effectiveness as a first-line intervention for many.
If a patient has an incomplete response to CBT-I, what might be pursued next? In our center, we have a low threshold for using low doses of benzodiazepines, such as lorazepam or clonazepam, because the majority of data do not support an increased risk of major congenital malformations even when used in the first trimester. It is quite common to see medicines such as newer nonbenzodiazepine sedative hypnotics such as Ambien CR (zolpidem) or Lunesta (eszopiclone) used by our colleagues in ob.gyn. The reproductive safety data on those medicines are particularly sparse, and they may have greater risk of cognitive side effects the next day, so we tend to avoid them.
Another sometimes-forgotten option to consider is using low doses of tricyclic antidepressants (i.e., 10-25 mg of nortriptyline at bedtime), with tricyclics having a 40-year history and at least one pooled analysis showing the absence of increased risk for major congenital malformations when used. This may be a very easy way of managing insomnia, with low-dose tricyclics having an anxiolytic effect as well.
Anxiety during pregnancy
The most common rise in symptoms during COVID-19 for women who are pregnant or post partum has been an increase in anxiety. Women present with a spectrum of concerns leading to anxiety symptoms in the context of the pandemic. Earlier on in the pandemic, concerns focused mostly on how to stay healthy, and how to mitigate risk and not catch SARS-CoV-2 during pregnancy, as well as the very complex issues that were playing out in real time as hospital systems were figuring out how to manage pregnant women in labor and to keep both them and staff safe. Over time, anxiety has shifted to still staying safe during the pandemic and the potential impact of SARS-CoV-2 infection on pregnancy outcomes. The No. 1 concern is what the implications of COVID-19 disease are on mother and child. New mothers also are anxious about how they will practically navigate life with a newborn in the postpartum setting.
Early on in the pandemic, some hospital systems severely limited who was in the room with a woman during labor, potentially impeding the wishes of women during delivery who would have wanted their loved ones and/or a doula present, as an example. With enhanced testing available now, protocols have since relaxed in many hospitals to allow partners – but not a team – to remain in the hospital during the labor process. Still, the prospect of delivering during a pandemic is undoubtedly a source of anxiety for some women.
This sort of anxiety, particularly in patients with preexisting anxiety disorders, can be particularly challenging. Fortunately, there has been a rapid increase over the last several years of digital apps to mitigate anxiety. While many of them have not been systematically studied, the data on biobehavioral intervention for anxiety is enormous, and this should be used as first-line treatment for patients with mild to moderate symptoms; so many women would prefer to avoid pharmacological intervention during pregnancy, if possible, to avoid fetal drug exposure. For patients who meet criteria for frank anxiety disorder, other nonpharmacologic interventions such as CBT have been shown to be effective.
Frequently, we see women who are experiencing levels of anxiety where nonpharmacological interventions have an incomplete response, and colleagues have asked about the safest way to treat these patients. As has been discussed in multiple previous columns, selective serotonin reuptake inhibitors (SSRIs) should be thought of sooner rather than later, particularly with medicines with good reproductive safety data such as sertraline, citalopram, or fluoxetine.
We also reported over 15 years ago that at least 30%-40% of women presenting with histories of recurrent major depression at the beginning of pregnancy had comorbid anxiety disorders, and that the use of benzodiazepines in that population in addition to SSRIs was exceedingly common, with doses of approximately 0.5-1.5 mg of clonazepam or lorazepam being standard fare. Again, this is very appropriate treatment to mitigate anxiety symptoms because now have enough data as a field that support the existence of adverse outcomes associated with untreated anxiety during pregnancy in terms of both adverse obstetric and neonatal outcomes, higher rates of preterm birth, and other obstetric complications. Hence, managing anxiety during pregnancy should be considered like managing a toxic exposure – the same way that one would be concerned about anything else that a pregnant woman could be exposed to.
Lastly, although no atypical antipsychotic has been approved for the treatment of anxiety, its use off label is extremely common. More and more data support the absence of a signal of teratogenicity across the family of molecules including atypical antipsychotics. Beyond potential use of atypical antipsychotics, at Virtual Rounds last week, a colleague asked about the use of gabapentin in a patient who was diagnosed with substance use disorder and who had inadvertently conceived on gabapentin, which was being used to treat both anxiety and insomnia. We have typically avoided the use of gabapentin during pregnancy because prospective data have been limited to relatively small case series and one report, with a total of exposures in roughly the 300 range.
However, our colleagues at the Harvard School of Public Health have recently published an article that looked at the United States Medicaid Analytic eXtract (MAX) dataset, which has been used to publish other articles addressing atypical antipsychotics, SSRIs, lithium, and pharmacovigilance investigations among other important topics. In this study, the database was used to look specifically at 4,642 pregnancies with gabapentin exposure relative to 1,744,447 unexposed pregnancies, without a significant finding for increased risk for major congenital malformations.
The question of an increased risk of cardiac malformations and of increased risk for obstetric complications are difficult to untangle from anxiety and depression, as they also are associated with those same outcomes. With that said, the analysis is a welcome addition to our knowledge base for a medicine used more widely to treat symptoms such as anxiety and insomnia in the general population, with a question mark around where it may fit into the algorithm during pregnancy.
In our center, gabapentin still would not be used as a first-line treatment for the management of anxiety or insomnia during pregnancy. But these new data still are reassuring for patients who come in, frequently with unplanned pregnancies. It is an important reminder to those of us taking care of patients during the pandemic to review use of contraception, because although data are unavailable specific to the period of the pandemic, what is clear is that, even prior to COVID-19, 50% of pregnancies in America were unplanned. Addressing issues of reliable use of contraception, particularly during the pandemic, is that much more important.
In this particular case, our clinician colleague in Virtual Rounds decided to continue gabapentin across pregnancy in the context of these reassuring data, but others may choose to discontinue or pursue some of the other treatment options noted above.
Dr. Cohen is the director of the Ammon-Pinizzotto Center for Women’s Mental Health at Massachusetts General Hospital (MGH) in Boston, which provides information resources and conducts clinical care and research in reproductive mental health. He has been a consultant to manufacturers of psychiatric medications. Email Dr. Cohen at [email protected].
Since the start of the pandemic, we have been conducting an extra hour of Virtual Rounds at the Center for Women’s Mental Health. Virtual Rounds has been an opportunity to discuss cases around a spectrum of clinical management issues with respect to depression, bipolar disorder, and a spectrum of anxiety disorders like obsessive-compulsive disorder (OCD), posttraumatic stress disorder (PTSD), and generalized anxiety disorder. How to apply the calculus of risk-benefit decision-making around management of psychiatric disorder during pregnancy and the postpartum period has been the cornerstone of the work at our center for over 2 decades.
When we went virtual at our center in the early Spring, we decided to keep the format of our faculty rounds the way they have been for years and to sustain cohesiveness of our program during the pandemic. But we thought the needs of pregnant and postpartum women warranted being addressed in a context more specific to COVID-19, and also that reproductive psychiatrists and other clinicians could learn from each other about novel issues coming up for this group of patients during the pandemic. With that backdrop, Marlene Freeman, MD, and I founded “Virtual Rounds at the Center” to respond to queries from our colleagues across the country; we do this just after our own rounds on Wednesdays at 2:00 p.m.
As the pandemic has progressed, Virtual Rounds has blossomed into a virtual community on the Zoom platform, where social workers, psychologists, nurse prescribers, psychiatrists, and obstetricians discuss the needs of pregnant and postpartum women specific to COVID-19. Frequently, our discussions involve a review of the risks and benefits of treatment before, during, and after pregnancy.
Seemingly, week to week, more and more colleagues raise questions about the treatment of anxiety and insomnia during pregnancy and the postpartum period. I’ve spoken in previous columns about the enhanced use of telemedicine. Telemedicine not only facilitates efforts like Virtual Rounds and our ability to reach out to colleagues across the country and share cases, but also has allowed us to keep even closer tabs on the emotional well-being of our pregnant and postpartum women during COVID-19.
The question is not just about the effects of a medicine that a woman might take to treat anxiety or insomnia during pregnancy, but the experience of the pandemic per se, which we are measuring in multiple studies now using a variety of psychological instruments that patients complete. The pandemic is unequivocally taking a still unquantified toll on the mental health of Americans and potentially on the next generation to come.
Midcycle awakening during pregnancy
Complaints of insomnia and midcycle awakening during pregnancy are not new – it is the rule, rather than the exception for many pregnant women, particularly later in pregnancy. We have unequivocally seen a worsening of complaints of sleep disruption including insomnia and midcycle awakening during the pandemic that is greater than what we have seen previously. Both patients and colleagues have asked us the safest ways to manage it. One of the first things we consider when we hear about insomnia is whether it is part of an underlying mood disorder. While we see primary insomnia clinically, it really is important to remember that insomnia can be part and parcel of an underlying mood disorder.
With that in mind, what are the options? During the pandemic, we’ve seen an increased use of digital cognitive behavioral therapy for insomnia (CBT-I) for patients who cannot initiate sleep, which has a very strong evidence base for effectiveness as a first-line intervention for many.
If a patient has an incomplete response to CBT-I, what might be pursued next? In our center, we have a low threshold for using low doses of benzodiazepines, such as lorazepam or clonazepam, because the majority of data do not support an increased risk of major congenital malformations even when used in the first trimester. It is quite common to see medicines such as newer nonbenzodiazepine sedative hypnotics such as Ambien CR (zolpidem) or Lunesta (eszopiclone) used by our colleagues in ob.gyn. The reproductive safety data on those medicines are particularly sparse, and they may have greater risk of cognitive side effects the next day, so we tend to avoid them.
Another sometimes-forgotten option to consider is using low doses of tricyclic antidepressants (i.e., 10-25 mg of nortriptyline at bedtime), with tricyclics having a 40-year history and at least one pooled analysis showing the absence of increased risk for major congenital malformations when used. This may be a very easy way of managing insomnia, with low-dose tricyclics having an anxiolytic effect as well.
Anxiety during pregnancy
The most common rise in symptoms during COVID-19 for women who are pregnant or post partum has been an increase in anxiety. Women present with a spectrum of concerns leading to anxiety symptoms in the context of the pandemic. Earlier on in the pandemic, concerns focused mostly on how to stay healthy, and how to mitigate risk and not catch SARS-CoV-2 during pregnancy, as well as the very complex issues that were playing out in real time as hospital systems were figuring out how to manage pregnant women in labor and to keep both them and staff safe. Over time, anxiety has shifted to still staying safe during the pandemic and the potential impact of SARS-CoV-2 infection on pregnancy outcomes. The No. 1 concern is what the implications of COVID-19 disease are on mother and child. New mothers also are anxious about how they will practically navigate life with a newborn in the postpartum setting.
Early on in the pandemic, some hospital systems severely limited who was in the room with a woman during labor, potentially impeding the wishes of women during delivery who would have wanted their loved ones and/or a doula present, as an example. With enhanced testing available now, protocols have since relaxed in many hospitals to allow partners – but not a team – to remain in the hospital during the labor process. Still, the prospect of delivering during a pandemic is undoubtedly a source of anxiety for some women.
This sort of anxiety, particularly in patients with preexisting anxiety disorders, can be particularly challenging. Fortunately, there has been a rapid increase over the last several years of digital apps to mitigate anxiety. While many of them have not been systematically studied, the data on biobehavioral intervention for anxiety is enormous, and this should be used as first-line treatment for patients with mild to moderate symptoms; so many women would prefer to avoid pharmacological intervention during pregnancy, if possible, to avoid fetal drug exposure. For patients who meet criteria for frank anxiety disorder, other nonpharmacologic interventions such as CBT have been shown to be effective.
Frequently, we see women who are experiencing levels of anxiety where nonpharmacological interventions have an incomplete response, and colleagues have asked about the safest way to treat these patients. As has been discussed in multiple previous columns, selective serotonin reuptake inhibitors (SSRIs) should be thought of sooner rather than later, particularly with medicines with good reproductive safety data such as sertraline, citalopram, or fluoxetine.
We also reported over 15 years ago that at least 30%-40% of women presenting with histories of recurrent major depression at the beginning of pregnancy had comorbid anxiety disorders, and that the use of benzodiazepines in that population in addition to SSRIs was exceedingly common, with doses of approximately 0.5-1.5 mg of clonazepam or lorazepam being standard fare. Again, this is very appropriate treatment to mitigate anxiety symptoms because now have enough data as a field that support the existence of adverse outcomes associated with untreated anxiety during pregnancy in terms of both adverse obstetric and neonatal outcomes, higher rates of preterm birth, and other obstetric complications. Hence, managing anxiety during pregnancy should be considered like managing a toxic exposure – the same way that one would be concerned about anything else that a pregnant woman could be exposed to.
Lastly, although no atypical antipsychotic has been approved for the treatment of anxiety, its use off label is extremely common. More and more data support the absence of a signal of teratogenicity across the family of molecules including atypical antipsychotics. Beyond potential use of atypical antipsychotics, at Virtual Rounds last week, a colleague asked about the use of gabapentin in a patient who was diagnosed with substance use disorder and who had inadvertently conceived on gabapentin, which was being used to treat both anxiety and insomnia. We have typically avoided the use of gabapentin during pregnancy because prospective data have been limited to relatively small case series and one report, with a total of exposures in roughly the 300 range.
However, our colleagues at the Harvard School of Public Health have recently published an article that looked at the United States Medicaid Analytic eXtract (MAX) dataset, which has been used to publish other articles addressing atypical antipsychotics, SSRIs, lithium, and pharmacovigilance investigations among other important topics. In this study, the database was used to look specifically at 4,642 pregnancies with gabapentin exposure relative to 1,744,447 unexposed pregnancies, without a significant finding for increased risk for major congenital malformations.
The question of an increased risk of cardiac malformations and of increased risk for obstetric complications are difficult to untangle from anxiety and depression, as they also are associated with those same outcomes. With that said, the analysis is a welcome addition to our knowledge base for a medicine used more widely to treat symptoms such as anxiety and insomnia in the general population, with a question mark around where it may fit into the algorithm during pregnancy.
In our center, gabapentin still would not be used as a first-line treatment for the management of anxiety or insomnia during pregnancy. But these new data still are reassuring for patients who come in, frequently with unplanned pregnancies. It is an important reminder to those of us taking care of patients during the pandemic to review use of contraception, because although data are unavailable specific to the period of the pandemic, what is clear is that, even prior to COVID-19, 50% of pregnancies in America were unplanned. Addressing issues of reliable use of contraception, particularly during the pandemic, is that much more important.
In this particular case, our clinician colleague in Virtual Rounds decided to continue gabapentin across pregnancy in the context of these reassuring data, but others may choose to discontinue or pursue some of the other treatment options noted above.
Dr. Cohen is the director of the Ammon-Pinizzotto Center for Women’s Mental Health at Massachusetts General Hospital (MGH) in Boston, which provides information resources and conducts clinical care and research in reproductive mental health. He has been a consultant to manufacturers of psychiatric medications. Email Dr. Cohen at [email protected].
Since the start of the pandemic, we have been conducting an extra hour of Virtual Rounds at the Center for Women’s Mental Health. Virtual Rounds has been an opportunity to discuss cases around a spectrum of clinical management issues with respect to depression, bipolar disorder, and a spectrum of anxiety disorders like obsessive-compulsive disorder (OCD), posttraumatic stress disorder (PTSD), and generalized anxiety disorder. How to apply the calculus of risk-benefit decision-making around management of psychiatric disorder during pregnancy and the postpartum period has been the cornerstone of the work at our center for over 2 decades.
When we went virtual at our center in the early Spring, we decided to keep the format of our faculty rounds the way they have been for years and to sustain cohesiveness of our program during the pandemic. But we thought the needs of pregnant and postpartum women warranted being addressed in a context more specific to COVID-19, and also that reproductive psychiatrists and other clinicians could learn from each other about novel issues coming up for this group of patients during the pandemic. With that backdrop, Marlene Freeman, MD, and I founded “Virtual Rounds at the Center” to respond to queries from our colleagues across the country; we do this just after our own rounds on Wednesdays at 2:00 p.m.
As the pandemic has progressed, Virtual Rounds has blossomed into a virtual community on the Zoom platform, where social workers, psychologists, nurse prescribers, psychiatrists, and obstetricians discuss the needs of pregnant and postpartum women specific to COVID-19. Frequently, our discussions involve a review of the risks and benefits of treatment before, during, and after pregnancy.
Seemingly, week to week, more and more colleagues raise questions about the treatment of anxiety and insomnia during pregnancy and the postpartum period. I’ve spoken in previous columns about the enhanced use of telemedicine. Telemedicine not only facilitates efforts like Virtual Rounds and our ability to reach out to colleagues across the country and share cases, but also has allowed us to keep even closer tabs on the emotional well-being of our pregnant and postpartum women during COVID-19.
The question is not just about the effects of a medicine that a woman might take to treat anxiety or insomnia during pregnancy, but the experience of the pandemic per se, which we are measuring in multiple studies now using a variety of psychological instruments that patients complete. The pandemic is unequivocally taking a still unquantified toll on the mental health of Americans and potentially on the next generation to come.
Midcycle awakening during pregnancy
Complaints of insomnia and midcycle awakening during pregnancy are not new – it is the rule, rather than the exception for many pregnant women, particularly later in pregnancy. We have unequivocally seen a worsening of complaints of sleep disruption including insomnia and midcycle awakening during the pandemic that is greater than what we have seen previously. Both patients and colleagues have asked us the safest ways to manage it. One of the first things we consider when we hear about insomnia is whether it is part of an underlying mood disorder. While we see primary insomnia clinically, it really is important to remember that insomnia can be part and parcel of an underlying mood disorder.
With that in mind, what are the options? During the pandemic, we’ve seen an increased use of digital cognitive behavioral therapy for insomnia (CBT-I) for patients who cannot initiate sleep, which has a very strong evidence base for effectiveness as a first-line intervention for many.
If a patient has an incomplete response to CBT-I, what might be pursued next? In our center, we have a low threshold for using low doses of benzodiazepines, such as lorazepam or clonazepam, because the majority of data do not support an increased risk of major congenital malformations even when used in the first trimester. It is quite common to see medicines such as newer nonbenzodiazepine sedative hypnotics such as Ambien CR (zolpidem) or Lunesta (eszopiclone) used by our colleagues in ob.gyn. The reproductive safety data on those medicines are particularly sparse, and they may have greater risk of cognitive side effects the next day, so we tend to avoid them.
Another sometimes-forgotten option to consider is using low doses of tricyclic antidepressants (i.e., 10-25 mg of nortriptyline at bedtime), with tricyclics having a 40-year history and at least one pooled analysis showing the absence of increased risk for major congenital malformations when used. This may be a very easy way of managing insomnia, with low-dose tricyclics having an anxiolytic effect as well.
Anxiety during pregnancy
The most common rise in symptoms during COVID-19 for women who are pregnant or post partum has been an increase in anxiety. Women present with a spectrum of concerns leading to anxiety symptoms in the context of the pandemic. Earlier on in the pandemic, concerns focused mostly on how to stay healthy, and how to mitigate risk and not catch SARS-CoV-2 during pregnancy, as well as the very complex issues that were playing out in real time as hospital systems were figuring out how to manage pregnant women in labor and to keep both them and staff safe. Over time, anxiety has shifted to still staying safe during the pandemic and the potential impact of SARS-CoV-2 infection on pregnancy outcomes. The No. 1 concern is what the implications of COVID-19 disease are on mother and child. New mothers also are anxious about how they will practically navigate life with a newborn in the postpartum setting.
Early on in the pandemic, some hospital systems severely limited who was in the room with a woman during labor, potentially impeding the wishes of women during delivery who would have wanted their loved ones and/or a doula present, as an example. With enhanced testing available now, protocols have since relaxed in many hospitals to allow partners – but not a team – to remain in the hospital during the labor process. Still, the prospect of delivering during a pandemic is undoubtedly a source of anxiety for some women.
This sort of anxiety, particularly in patients with preexisting anxiety disorders, can be particularly challenging. Fortunately, there has been a rapid increase over the last several years of digital apps to mitigate anxiety. While many of them have not been systematically studied, the data on biobehavioral intervention for anxiety is enormous, and this should be used as first-line treatment for patients with mild to moderate symptoms; so many women would prefer to avoid pharmacological intervention during pregnancy, if possible, to avoid fetal drug exposure. For patients who meet criteria for frank anxiety disorder, other nonpharmacologic interventions such as CBT have been shown to be effective.
Frequently, we see women who are experiencing levels of anxiety where nonpharmacological interventions have an incomplete response, and colleagues have asked about the safest way to treat these patients. As has been discussed in multiple previous columns, selective serotonin reuptake inhibitors (SSRIs) should be thought of sooner rather than later, particularly with medicines with good reproductive safety data such as sertraline, citalopram, or fluoxetine.
We also reported over 15 years ago that at least 30%-40% of women presenting with histories of recurrent major depression at the beginning of pregnancy had comorbid anxiety disorders, and that the use of benzodiazepines in that population in addition to SSRIs was exceedingly common, with doses of approximately 0.5-1.5 mg of clonazepam or lorazepam being standard fare. Again, this is very appropriate treatment to mitigate anxiety symptoms because now have enough data as a field that support the existence of adverse outcomes associated with untreated anxiety during pregnancy in terms of both adverse obstetric and neonatal outcomes, higher rates of preterm birth, and other obstetric complications. Hence, managing anxiety during pregnancy should be considered like managing a toxic exposure – the same way that one would be concerned about anything else that a pregnant woman could be exposed to.
Lastly, although no atypical antipsychotic has been approved for the treatment of anxiety, its use off label is extremely common. More and more data support the absence of a signal of teratogenicity across the family of molecules including atypical antipsychotics. Beyond potential use of atypical antipsychotics, at Virtual Rounds last week, a colleague asked about the use of gabapentin in a patient who was diagnosed with substance use disorder and who had inadvertently conceived on gabapentin, which was being used to treat both anxiety and insomnia. We have typically avoided the use of gabapentin during pregnancy because prospective data have been limited to relatively small case series and one report, with a total of exposures in roughly the 300 range.
However, our colleagues at the Harvard School of Public Health have recently published an article that looked at the United States Medicaid Analytic eXtract (MAX) dataset, which has been used to publish other articles addressing atypical antipsychotics, SSRIs, lithium, and pharmacovigilance investigations among other important topics. In this study, the database was used to look specifically at 4,642 pregnancies with gabapentin exposure relative to 1,744,447 unexposed pregnancies, without a significant finding for increased risk for major congenital malformations.
The question of an increased risk of cardiac malformations and of increased risk for obstetric complications are difficult to untangle from anxiety and depression, as they also are associated with those same outcomes. With that said, the analysis is a welcome addition to our knowledge base for a medicine used more widely to treat symptoms such as anxiety and insomnia in the general population, with a question mark around where it may fit into the algorithm during pregnancy.
In our center, gabapentin still would not be used as a first-line treatment for the management of anxiety or insomnia during pregnancy. But these new data still are reassuring for patients who come in, frequently with unplanned pregnancies. It is an important reminder to those of us taking care of patients during the pandemic to review use of contraception, because although data are unavailable specific to the period of the pandemic, what is clear is that, even prior to COVID-19, 50% of pregnancies in America were unplanned. Addressing issues of reliable use of contraception, particularly during the pandemic, is that much more important.
In this particular case, our clinician colleague in Virtual Rounds decided to continue gabapentin across pregnancy in the context of these reassuring data, but others may choose to discontinue or pursue some of the other treatment options noted above.
Dr. Cohen is the director of the Ammon-Pinizzotto Center for Women’s Mental Health at Massachusetts General Hospital (MGH) in Boston, which provides information resources and conducts clinical care and research in reproductive mental health. He has been a consultant to manufacturers of psychiatric medications. Email Dr. Cohen at [email protected].