User login
Oncology treatment errors: Emerging data shed light on risk factors, prevention
ORLANDO – Accumulating evidence is helping researchers better understand why errors occur during the delivery of cancer treatment and how to prevent them. Findings from a trio of studies were reported at a symposium on quality care sponsored by the American Society of Clinical Oncology.
Identifying causes of incidents in radiation therapy
In the first study, Greg D. Judy, MD, a radiation oncology resident at the University of North Carolina at Chapel Hill, and his colleagues retrospectively reviewed records in their institution’s reporting system, called Good Catch, to identify near-miss incidents (ones that didn’t reach the patient) and safety incidents (ones that did) among patients undergoing radiation therapy from October 2014 through April 2016.

Multivariate analysis showed that patients had a significantly higher risk of near-miss or safety incidents if they had stage T2 disease (odds ratio, 3.3), were being treated for cancer involving the head and neck (5.2), or were receiving image-guided intensity-modulated radiation therapy (3.0) or daily imaging as part of their treatment (7.0), Dr. Judy reported.
“Head and neck site and image-guided IMRT [intensity-modulated radiation therapy] are complex entities: They have multiple steps in both the planning and delivery phase,” he said. “Daily imaging as well. It’s a much more complex process to do daily imaging for setup verification than it is to do once-a-week or even once-every-2-weeks setup verification.”
On the other hand, it was unclear why T2 stage was a risk factor. “We kind of hypothesized that it might be more of the disease site that really drives this, as you can have HPV-positive oropharyngeal cancer which usually has lower T stages and more advanced nodal stages, but even then, that’s a head and neck site and we usually use image-guided IMRT, which are both very complex entities,” he said. The most common root causes for the incidents were issues related to documentation and scheduling (29% each), followed by issues related to communication (22%), technical treatment planning (14%), and technical treatment delivery (6%).
Incidents having a communication root cause were more likely than were others to affect patients (P less than .001), and those having a technical treatment delivery root cause were more likely to have higher severity (P = .005).
“Like some other studies, we found really the key factor was the complexity of the treatment plan and complexity of the overall process that is the real driving factor. This is important to understand because it promotes the idea of developing a more dedicated and robust QA system for complex cases,” said Dr. Judy. “It also highlights the importance of a strong reporting system to support a safety culture, as well as promote the continuous learning improvements within a department.”
The national Radiation Oncology Incident Learning System (RO-ILS) has been developed by the American Society for Radiation Oncology (ASTRO). “This is gaining membership very rapidly, and it’s good because it facilitates cooperative research and also safety standards for our field,” he maintained.

“I’ll argue that they did that for a variety of reasons,” he elaborated. “Strong and effective leadership by Dr. Larry Marks, who’s really created a departmental culture of safety in which people can feel free to speak up. They have this wonderful Good Catch program in place. And they have these simulation review huddles ... where people feel free to talk about what happened yesterday or today that may be relevant moving forward.”
As for the national RO-ILS initiative, “I would look out to the audience and say, why is it that we don’t have such a program in medical oncology?” Dr. Jacobson said. “It’s probably time for us to do this,” he maintained.
Reducing chemotherapy errors in pediatric oncology
In the second study, Brian D. Weiss, MD, associate director of safety and compliance at Cincinnati Children’s Hospital Medical Center, and his colleagues studied the impact of a safety initiative to prevent chemotherapy errors at their large urban pediatric academic center (J Clin Oncol 35, 2017 [suppl 8S; abstract 37]).
“Pediatric chemotherapy protocols are different from adult protocols. We dose based on age or weight or body surface area, and that can change within a protocol. You have to do adjustments every time they gain weight or grow some, which is different than for adult protocols,” he explained. “We have parents administering chemo at home. And the protocols most patients are on are very complicated, but there is no standardized format, so it makes crucial information for dose adjustments difficult to find.”

The team successively implemented about half a dozen interventions, such as dedicated chemotherapy safety zones where staff were not to be disturbed while checking orders and ear protectors as a visual deterrent to interruptions; a new chemotherapy registered nurse role with a detailed list of responsibilities; an event-reporting system to supplement the center’s error-reporting system and capture events not reaching the patient (near-miss events); and a daily chemotherapy huddle to discuss errors in a nonpunitive setting and review upcoming chemotherapy for readiness.
In the 6 years after the start of the initiative, 105,187 chemotherapy doses were administered at the center and 998 errors occurred, including 250 errors that reached the patient, according to results reported at the symposium and recently published (J Oncol Pract. 2017 April;13:e329-e336).
At the 22-month mark, the rate of chemotherapy errors reaching the patient had fallen from 3.8 in 1,000 doses at baseline to 1.9 in 1,000 doses. The reduction has since persisted for more than 4 years and translates to an estimated 155 fewer predicted errors reaching the patient because of the initiative.
“The errors that reached the patient were more often administration and dispensing errors,” Dr. Weiss said. “About two-thirds of those errors that didn’t reach the patient – because they got caught by the pharmacists and the nurses – were prescription errors.
“Our chemotherapy huddle has certainly increased our reporting of errors. We also now use it for patients on clinical trials ... any patient getting PK [pharmacokinetics] or PD [pharmacodynamics] sampled within the next 24 hours is reviewed at that meeting. And our missed samples have gone down significantly,” he noted. “It’s allowed us to manage our bed space better because now everybody knows who’s definitely coming in the next day and who’s maybe coming in the next day.”
“We are a large urban academic pediatric medical center. Some of these things may seem difficult to translate [to smaller facilities], but I’m not sure they are,” concluded Dr. Weiss.
Dr. Jacobson, the discussant, noted that the initiative was in keeping with this health system’s longstanding “obsessive” focus on patient safety and commended its rigorousness in, for example, setting clear goals, focusing on key drivers [processes] needed for change, and selecting a good outcome metric.
“This is very successful project,” he said. The success can be attributed to “strong and effective organization and leadership, building a culture of safety at Cincinnati Children’s Hospital, and an important predefined measurement program and methodology.”
Building chemotherapy regimens more accurately
In the third study, a team led by Andrea Crespo, BSc, BScPhm, BCOP, an oncology pharmacist and member of the Systemic Treatment Team at Cancer Care Ontario, Toronto, studied errors introduced when chemotherapy regimens were moved from publications into orders used by centers in the province (J Clin Oncol. 35, 2017 [suppl 8S; abstract 51]).
Nearly all outpatient intravenous systemic treatment visits in Ontario are supported by a Systemic Treatment Computerized Prescriber Order Entry (ST-CPOE) system, she noted. Such systems can reduce error rates but are not foolproof.

She and her colleagues asked all Ontario treatment centers to review their active chemotherapy regimens. Data were analyzed to determine whether the regimens were built as intended with respect to their component drugs and doses, leading to identification of any unintentional discrepancies with the original regimen.
A total of 33 centers performed the review, and the median number of regimens reviewed was 375 per center, Ms. Crespo reported.
Unintentional discrepancies in regimens were found at 27% of centers. The total number reported was 369 discrepancies, with a range from 2 to 198 per center.
All of the nine centers where discrepancies were found participated in the provincial ST-CPOE system, and most had for at least 20 years. Furthermore, eight of them used a team of at least two pharmacists and one oncologist to build their regimens. “So you can see that discrepancies occurred despite a fairly rigorous regimen-build process and many years of experience with the system,” she said.
Of the 369 total discrepancies, 41% were related to alignment with the Systemic Treatment Quality-Based Program regimen, and 32% were regimens flagged to be inactivated because of outdated information, new standards, or lack of use.
A detailed analysis of the remaining 27%, or 101 unintentional discrepancies, showed that the majority were due to missing information (35.6%) or missing drugs (13.9%), incorrect doses (10.9%), and incorrect or missing schedules (10.9%). Potential to cause harm was mild for 55%, moderate for 28%, and none for 17%.
“Corrective action has been taken to address the discrepancies identified,” said Ms. Crespo.
Only 6% of the 33 centers reported having an established regimen review and maintenance process in place before the study, but all now have such a process. In addition, some centers that did not find any regimen discrepancies nonetheless reported adding quality improvement activities, such as changes in the ways regimens were built and documented, and revising regimen names to facilitate accurate selection.
In discussing the study, Dr. Jacobson noted the low proportion of centers having an established process at baseline to ensure appropriate regimen maintenance and updates. “You might want to think to yourselves, the medical oncologists in the group, whether your center has such a process in place,” he proposed.
It is not yet known whether the project has met its goal of improving the quality and accuracy of oncology regimens in Ontario, he maintained. “We are going to have to invite [Ms. Crespo] back in a year or two to see whether that turns out to be true.” On the other hand, “clearly what they have achieved was the ability to measure the variance between what was intended and what was actually built.”
Chief among the reasons for success, again, “was a strong and effective leadership and organizational structure, not at the department level or hospital level, but across the entire province through Cancer Care Ontario,” Dr. Jacobson said. “It’s clear that they have a focus on quality and patient safety, and this measurement program that they have put in place turned out to be useful.”
Dr. Judy, Dr. Weiss, and Ms. Crespo disclosed that they had no relevant conflicts of interest.
ORLANDO – Accumulating evidence is helping researchers better understand why errors occur during the delivery of cancer treatment and how to prevent them. Findings from a trio of studies were reported at a symposium on quality care sponsored by the American Society of Clinical Oncology.
Identifying causes of incidents in radiation therapy
In the first study, Greg D. Judy, MD, a radiation oncology resident at the University of North Carolina at Chapel Hill, and his colleagues retrospectively reviewed records in their institution’s reporting system, called Good Catch, to identify near-miss incidents (ones that didn’t reach the patient) and safety incidents (ones that did) among patients undergoing radiation therapy from October 2014 through April 2016.
Multivariate analysis showed that patients had a significantly higher risk of near-miss or safety incidents if they had stage T2 disease (odds ratio, 3.3), were being treated for cancer involving the head and neck (5.2), or were receiving image-guided intensity-modulated radiation therapy (3.0) or daily imaging as part of their treatment (7.0), Dr. Judy reported.
“Head and neck site and image-guided IMRT [intensity-modulated radiation therapy] are complex entities: They have multiple steps in both the planning and delivery phase,” he said. “Daily imaging as well. It’s a much more complex process to do daily imaging for setup verification than it is to do once-a-week or even once-every-2-weeks setup verification.”
On the other hand, it was unclear why T2 stage was a risk factor. “We kind of hypothesized that it might be more of the disease site that really drives this, as you can have HPV-positive oropharyngeal cancer which usually has lower T stages and more advanced nodal stages, but even then, that’s a head and neck site and we usually use image-guided IMRT, which are both very complex entities,” he said. The most common root causes for the incidents were issues related to documentation and scheduling (29% each), followed by issues related to communication (22%), technical treatment planning (14%), and technical treatment delivery (6%).
Incidents having a communication root cause were more likely than were others to affect patients (P less than .001), and those having a technical treatment delivery root cause were more likely to have higher severity (P = .005).
“Like some other studies, we found really the key factor was the complexity of the treatment plan and complexity of the overall process that is the real driving factor. This is important to understand because it promotes the idea of developing a more dedicated and robust QA system for complex cases,” said Dr. Judy. “It also highlights the importance of a strong reporting system to support a safety culture, as well as promote the continuous learning improvements within a department.”
The national Radiation Oncology Incident Learning System (RO-ILS) has been developed by the American Society for Radiation Oncology (ASTRO). “This is gaining membership very rapidly, and it’s good because it facilitates cooperative research and also safety standards for our field,” he maintained.
“I’ll argue that they did that for a variety of reasons,” he elaborated. “Strong and effective leadership by Dr. Larry Marks, who’s really created a departmental culture of safety in which people can feel free to speak up. They have this wonderful Good Catch program in place. And they have these simulation review huddles ... where people feel free to talk about what happened yesterday or today that may be relevant moving forward.”
As for the national RO-ILS initiative, “I would look out to the audience and say, why is it that we don’t have such a program in medical oncology?” Dr. Jacobson said. “It’s probably time for us to do this,” he maintained.
Reducing chemotherapy errors in pediatric oncology
In the second study, Brian D. Weiss, MD, associate director of safety and compliance at Cincinnati Children’s Hospital Medical Center, and his colleagues studied the impact of a safety initiative to prevent chemotherapy errors at their large urban pediatric academic center (J Clin Oncol 35, 2017 [suppl 8S; abstract 37]).
“Pediatric chemotherapy protocols are different from adult protocols. We dose based on age or weight or body surface area, and that can change within a protocol. You have to do adjustments every time they gain weight or grow some, which is different than for adult protocols,” he explained. “We have parents administering chemo at home. And the protocols most patients are on are very complicated, but there is no standardized format, so it makes crucial information for dose adjustments difficult to find.”
The team successively implemented about half a dozen interventions, such as dedicated chemotherapy safety zones where staff were not to be disturbed while checking orders and ear protectors as a visual deterrent to interruptions; a new chemotherapy registered nurse role with a detailed list of responsibilities; an event-reporting system to supplement the center’s error-reporting system and capture events not reaching the patient (near-miss events); and a daily chemotherapy huddle to discuss errors in a nonpunitive setting and review upcoming chemotherapy for readiness.
In the 6 years after the start of the initiative, 105,187 chemotherapy doses were administered at the center and 998 errors occurred, including 250 errors that reached the patient, according to results reported at the symposium and recently published (J Oncol Pract. 2017 April;13:e329-e336).
At the 22-month mark, the rate of chemotherapy errors reaching the patient had fallen from 3.8 in 1,000 doses at baseline to 1.9 in 1,000 doses. The reduction has since persisted for more than 4 years and translates to an estimated 155 fewer predicted errors reaching the patient because of the initiative.
“The errors that reached the patient were more often administration and dispensing errors,” Dr. Weiss said. “About two-thirds of those errors that didn’t reach the patient – because they got caught by the pharmacists and the nurses – were prescription errors.
“Our chemotherapy huddle has certainly increased our reporting of errors. We also now use it for patients on clinical trials ... any patient getting PK [pharmacokinetics] or PD [pharmacodynamics] sampled within the next 24 hours is reviewed at that meeting. And our missed samples have gone down significantly,” he noted. “It’s allowed us to manage our bed space better because now everybody knows who’s definitely coming in the next day and who’s maybe coming in the next day.”
“We are a large urban academic pediatric medical center. Some of these things may seem difficult to translate [to smaller facilities], but I’m not sure they are,” concluded Dr. Weiss.
Dr. Jacobson, the discussant, noted that the initiative was in keeping with this health system’s longstanding “obsessive” focus on patient safety and commended its rigorousness in, for example, setting clear goals, focusing on key drivers [processes] needed for change, and selecting a good outcome metric.
“This is very successful project,” he said. The success can be attributed to “strong and effective organization and leadership, building a culture of safety at Cincinnati Children’s Hospital, and an important predefined measurement program and methodology.”
Building chemotherapy regimens more accurately
In the third study, a team led by Andrea Crespo, BSc, BScPhm, BCOP, an oncology pharmacist and member of the Systemic Treatment Team at Cancer Care Ontario, Toronto, studied errors introduced when chemotherapy regimens were moved from publications into orders used by centers in the province (J Clin Oncol. 35, 2017 [suppl 8S; abstract 51]).
Nearly all outpatient intravenous systemic treatment visits in Ontario are supported by a Systemic Treatment Computerized Prescriber Order Entry (ST-CPOE) system, she noted. Such systems can reduce error rates but are not foolproof.
She and her colleagues asked all Ontario treatment centers to review their active chemotherapy regimens. Data were analyzed to determine whether the regimens were built as intended with respect to their component drugs and doses, leading to identification of any unintentional discrepancies with the original regimen.
A total of 33 centers performed the review, and the median number of regimens reviewed was 375 per center, Ms. Crespo reported.
Unintentional discrepancies in regimens were found at 27% of centers. The total number reported was 369 discrepancies, with a range from 2 to 198 per center.
All of the nine centers where discrepancies were found participated in the provincial ST-CPOE system, and most had for at least 20 years. Furthermore, eight of them used a team of at least two pharmacists and one oncologist to build their regimens. “So you can see that discrepancies occurred despite a fairly rigorous regimen-build process and many years of experience with the system,” she said.
Of the 369 total discrepancies, 41% were related to alignment with the Systemic Treatment Quality-Based Program regimen, and 32% were regimens flagged to be inactivated because of outdated information, new standards, or lack of use.
A detailed analysis of the remaining 27%, or 101 unintentional discrepancies, showed that the majority were due to missing information (35.6%) or missing drugs (13.9%), incorrect doses (10.9%), and incorrect or missing schedules (10.9%). Potential to cause harm was mild for 55%, moderate for 28%, and none for 17%.
“Corrective action has been taken to address the discrepancies identified,” said Ms. Crespo.
Only 6% of the 33 centers reported having an established regimen review and maintenance process in place before the study, but all now have such a process. In addition, some centers that did not find any regimen discrepancies nonetheless reported adding quality improvement activities, such as changes in the ways regimens were built and documented, and revising regimen names to facilitate accurate selection.
In discussing the study, Dr. Jacobson noted the low proportion of centers having an established process at baseline to ensure appropriate regimen maintenance and updates. “You might want to think to yourselves, the medical oncologists in the group, whether your center has such a process in place,” he proposed.
It is not yet known whether the project has met its goal of improving the quality and accuracy of oncology regimens in Ontario, he maintained. “We are going to have to invite [Ms. Crespo] back in a year or two to see whether that turns out to be true.” On the other hand, “clearly what they have achieved was the ability to measure the variance between what was intended and what was actually built.”
Chief among the reasons for success, again, “was a strong and effective leadership and organizational structure, not at the department level or hospital level, but across the entire province through Cancer Care Ontario,” Dr. Jacobson said. “It’s clear that they have a focus on quality and patient safety, and this measurement program that they have put in place turned out to be useful.”
Dr. Judy, Dr. Weiss, and Ms. Crespo disclosed that they had no relevant conflicts of interest.
ORLANDO – Accumulating evidence is helping researchers better understand why errors occur during the delivery of cancer treatment and how to prevent them. Findings from a trio of studies were reported at a symposium on quality care sponsored by the American Society of Clinical Oncology.
Identifying causes of incidents in radiation therapy
In the first study, Greg D. Judy, MD, a radiation oncology resident at the University of North Carolina at Chapel Hill, and his colleagues retrospectively reviewed records in their institution’s reporting system, called Good Catch, to identify near-miss incidents (ones that didn’t reach the patient) and safety incidents (ones that did) among patients undergoing radiation therapy from October 2014 through April 2016.
Multivariate analysis showed that patients had a significantly higher risk of near-miss or safety incidents if they had stage T2 disease (odds ratio, 3.3), were being treated for cancer involving the head and neck (5.2), or were receiving image-guided intensity-modulated radiation therapy (3.0) or daily imaging as part of their treatment (7.0), Dr. Judy reported.
“Head and neck site and image-guided IMRT [intensity-modulated radiation therapy] are complex entities: They have multiple steps in both the planning and delivery phase,” he said. “Daily imaging as well. It’s a much more complex process to do daily imaging for setup verification than it is to do once-a-week or even once-every-2-weeks setup verification.”
On the other hand, it was unclear why T2 stage was a risk factor. “We kind of hypothesized that it might be more of the disease site that really drives this, as you can have HPV-positive oropharyngeal cancer which usually has lower T stages and more advanced nodal stages, but even then, that’s a head and neck site and we usually use image-guided IMRT, which are both very complex entities,” he said. The most common root causes for the incidents were issues related to documentation and scheduling (29% each), followed by issues related to communication (22%), technical treatment planning (14%), and technical treatment delivery (6%).
Incidents having a communication root cause were more likely than were others to affect patients (P less than .001), and those having a technical treatment delivery root cause were more likely to have higher severity (P = .005).
“Like some other studies, we found really the key factor was the complexity of the treatment plan and complexity of the overall process that is the real driving factor. This is important to understand because it promotes the idea of developing a more dedicated and robust QA system for complex cases,” said Dr. Judy. “It also highlights the importance of a strong reporting system to support a safety culture, as well as promote the continuous learning improvements within a department.”
The national Radiation Oncology Incident Learning System (RO-ILS) has been developed by the American Society for Radiation Oncology (ASTRO). “This is gaining membership very rapidly, and it’s good because it facilitates cooperative research and also safety standards for our field,” he maintained.
“I’ll argue that they did that for a variety of reasons,” he elaborated. “Strong and effective leadership by Dr. Larry Marks, who’s really created a departmental culture of safety in which people can feel free to speak up. They have this wonderful Good Catch program in place. And they have these simulation review huddles ... where people feel free to talk about what happened yesterday or today that may be relevant moving forward.”
As for the national RO-ILS initiative, “I would look out to the audience and say, why is it that we don’t have such a program in medical oncology?” Dr. Jacobson said. “It’s probably time for us to do this,” he maintained.
Reducing chemotherapy errors in pediatric oncology
In the second study, Brian D. Weiss, MD, associate director of safety and compliance at Cincinnati Children’s Hospital Medical Center, and his colleagues studied the impact of a safety initiative to prevent chemotherapy errors at their large urban pediatric academic center (J Clin Oncol 35, 2017 [suppl 8S; abstract 37]).
“Pediatric chemotherapy protocols are different from adult protocols. We dose based on age or weight or body surface area, and that can change within a protocol. You have to do adjustments every time they gain weight or grow some, which is different than for adult protocols,” he explained. “We have parents administering chemo at home. And the protocols most patients are on are very complicated, but there is no standardized format, so it makes crucial information for dose adjustments difficult to find.”
The team successively implemented about half a dozen interventions, such as dedicated chemotherapy safety zones where staff were not to be disturbed while checking orders and ear protectors as a visual deterrent to interruptions; a new chemotherapy registered nurse role with a detailed list of responsibilities; an event-reporting system to supplement the center’s error-reporting system and capture events not reaching the patient (near-miss events); and a daily chemotherapy huddle to discuss errors in a nonpunitive setting and review upcoming chemotherapy for readiness.
In the 6 years after the start of the initiative, 105,187 chemotherapy doses were administered at the center and 998 errors occurred, including 250 errors that reached the patient, according to results reported at the symposium and recently published (J Oncol Pract. 2017 April;13:e329-e336).
At the 22-month mark, the rate of chemotherapy errors reaching the patient had fallen from 3.8 in 1,000 doses at baseline to 1.9 in 1,000 doses. The reduction has since persisted for more than 4 years and translates to an estimated 155 fewer predicted errors reaching the patient because of the initiative.
“The errors that reached the patient were more often administration and dispensing errors,” Dr. Weiss said. “About two-thirds of those errors that didn’t reach the patient – because they got caught by the pharmacists and the nurses – were prescription errors.
“Our chemotherapy huddle has certainly increased our reporting of errors. We also now use it for patients on clinical trials ... any patient getting PK [pharmacokinetics] or PD [pharmacodynamics] sampled within the next 24 hours is reviewed at that meeting. And our missed samples have gone down significantly,” he noted. “It’s allowed us to manage our bed space better because now everybody knows who’s definitely coming in the next day and who’s maybe coming in the next day.”
“We are a large urban academic pediatric medical center. Some of these things may seem difficult to translate [to smaller facilities], but I’m not sure they are,” concluded Dr. Weiss.
Dr. Jacobson, the discussant, noted that the initiative was in keeping with this health system’s longstanding “obsessive” focus on patient safety and commended its rigorousness in, for example, setting clear goals, focusing on key drivers [processes] needed for change, and selecting a good outcome metric.
“This is very successful project,” he said. The success can be attributed to “strong and effective organization and leadership, building a culture of safety at Cincinnati Children’s Hospital, and an important predefined measurement program and methodology.”
Building chemotherapy regimens more accurately
In the third study, a team led by Andrea Crespo, BSc, BScPhm, BCOP, an oncology pharmacist and member of the Systemic Treatment Team at Cancer Care Ontario, Toronto, studied errors introduced when chemotherapy regimens were moved from publications into orders used by centers in the province (J Clin Oncol. 35, 2017 [suppl 8S; abstract 51]).
Nearly all outpatient intravenous systemic treatment visits in Ontario are supported by a Systemic Treatment Computerized Prescriber Order Entry (ST-CPOE) system, she noted. Such systems can reduce error rates but are not foolproof.
She and her colleagues asked all Ontario treatment centers to review their active chemotherapy regimens. Data were analyzed to determine whether the regimens were built as intended with respect to their component drugs and doses, leading to identification of any unintentional discrepancies with the original regimen.
A total of 33 centers performed the review, and the median number of regimens reviewed was 375 per center, Ms. Crespo reported.
Unintentional discrepancies in regimens were found at 27% of centers. The total number reported was 369 discrepancies, with a range from 2 to 198 per center.
All of the nine centers where discrepancies were found participated in the provincial ST-CPOE system, and most had for at least 20 years. Furthermore, eight of them used a team of at least two pharmacists and one oncologist to build their regimens. “So you can see that discrepancies occurred despite a fairly rigorous regimen-build process and many years of experience with the system,” she said.
Of the 369 total discrepancies, 41% were related to alignment with the Systemic Treatment Quality-Based Program regimen, and 32% were regimens flagged to be inactivated because of outdated information, new standards, or lack of use.
A detailed analysis of the remaining 27%, or 101 unintentional discrepancies, showed that the majority were due to missing information (35.6%) or missing drugs (13.9%), incorrect doses (10.9%), and incorrect or missing schedules (10.9%). Potential to cause harm was mild for 55%, moderate for 28%, and none for 17%.
“Corrective action has been taken to address the discrepancies identified,” said Ms. Crespo.
Only 6% of the 33 centers reported having an established regimen review and maintenance process in place before the study, but all now have such a process. In addition, some centers that did not find any regimen discrepancies nonetheless reported adding quality improvement activities, such as changes in the ways regimens were built and documented, and revising regimen names to facilitate accurate selection.
In discussing the study, Dr. Jacobson noted the low proportion of centers having an established process at baseline to ensure appropriate regimen maintenance and updates. “You might want to think to yourselves, the medical oncologists in the group, whether your center has such a process in place,” he proposed.
It is not yet known whether the project has met its goal of improving the quality and accuracy of oncology regimens in Ontario, he maintained. “We are going to have to invite [Ms. Crespo] back in a year or two to see whether that turns out to be true.” On the other hand, “clearly what they have achieved was the ability to measure the variance between what was intended and what was actually built.”
Chief among the reasons for success, again, “was a strong and effective leadership and organizational structure, not at the department level or hospital level, but across the entire province through Cancer Care Ontario,” Dr. Jacobson said. “It’s clear that they have a focus on quality and patient safety, and this measurement program that they have put in place turned out to be useful.”
Dr. Judy, Dr. Weiss, and Ms. Crespo disclosed that they had no relevant conflicts of interest.
AT THE QUALITY CARE SYMPOSIUM
Key clinical point:
Major finding: Risk factors for radiation therapy near-miss and safety incidents were T2 stage, H&N site, and more complex techniques (odds ratios, 3.0-7.0). A quality improvement initiative halved the rate of chemotherapy errors reaching the patient from 3.8 to 1.9 per 1,000 doses. Twenty-seven percent of centers found unintentional discrepancies in their chemotherapy regimens, 83% with potential to cause harm.
Data source: A retrospective case-control study of 400 patients receiving radiation therapy, a longitudinal cohort study of a quality improvement initiative at an urban pediatric academic medical center involving administration of 105,187 chemotherapy doses, and a cohort study of 33 Ontario treatment centers that reviewed a median of 375 chemotherapy regimens.
Disclosures: Dr. Judy, Dr. Weiss, and Ms. Crespo disclosed that they had no relevant conflicts of interest.
Chemo sequencing in elderly adults with NSCLC linked with survival
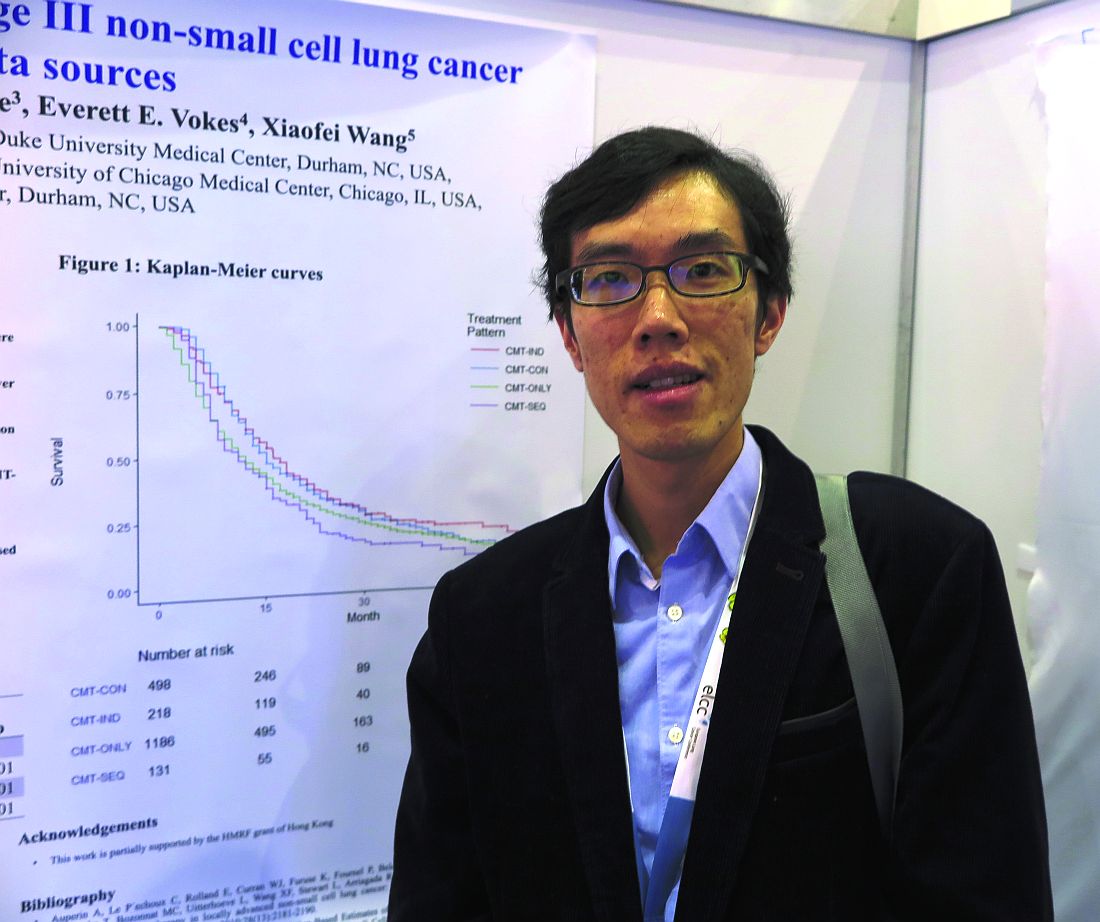
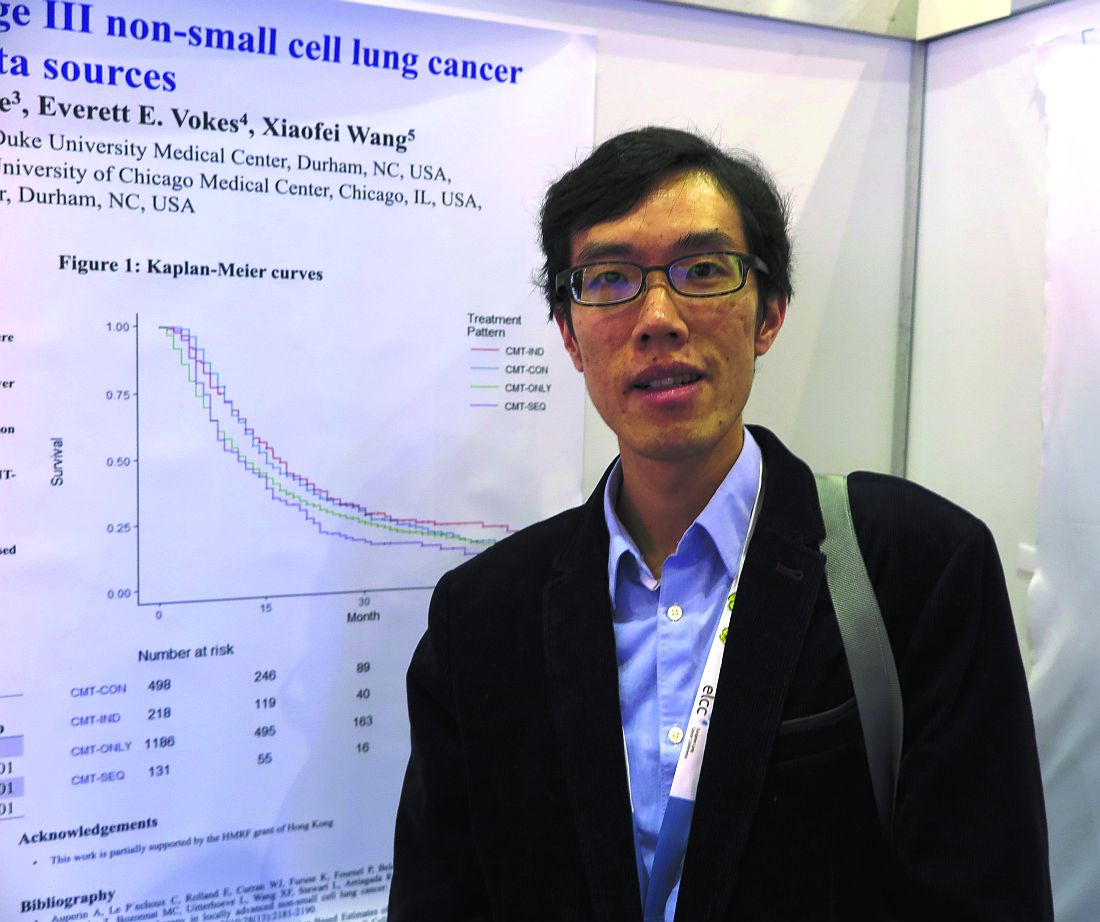
GENEVA – Among older adults with stage III non–small cell lung cancer (NSCLC), the sequencing of chemotherapy and radiation has a significant effect on overall survival, a team of investigators from Hong Kong and the United States reported.
Among 2,033 adults who were 65 years or older with locally advanced NSCLC and treated with one of four combined-modality therapy (CMT) schedules, both chemotherapy induction followed by concurrent therapy (CMT-IND) and concurrent therapy followed by consolidation chemoradiation (CMT-CON) were associated with an approximately 30% improvement in survival, compared with either sequential chemotherapy followed by radiation (CMT-SEQ) or concurrent therapy only (CMT-ONLY), reported Hei Man Herbert Pang, MD, of the University of Hong Kong and his colleagues.
The investigators used retrospective data from U.S. and Chinese sources to compare the relative survival benefits with various combined modality therapies. These included a Surveillance, Epidemiology, and End Results–Medicare cohort of patients 65 years and older with stage IIIA or IIIB NSCLC treated with CMT from 2006 through 2010 and a cohort of patients with the same age and NSCLC treated at Queen Mary Hospital in Hong Kong from 2007 through 2016.
They assessed neutropenia using inpatient claims data for episodes occurring within 130 days of the first chemotherapy cycle.
In an unadjusted analysis, they found that median overall survival, in descending order, was 16.1 months for CMT-SEQ,15.0 months for CMT-ONLY, 12.0 months for CMT-IND, and 11.0 months for CMT-CON.
When they controlled for variables, however, a different picture began to emerge.
For example, patients who were treated with CMT-SEQ had lower Charlson Comorbidity Index scores and, thus, were comparatively healthier than patients treated with other combined modalities.
Hospitalizations for neutropenia were most common with CMT-CON, occurring in 13.3% of patients, compared with 9.8% of patients treated with CMT-ONLY, 9.2% with CMT-IND, and 2.3% with CMT-SEQ.
In multivariable models controlling for sex, race, ethnicity, histology, and Charlson score, CMT-CON and CMT-IND were associated with significantly better overall, compared with CMT-SEQ, with respective hazard ratios for death of 0.68 (P less than .001) and 0.67 (P = .001). In this model, CMT-ONLY was not associated with significantly better survival.
In a propensity score model adjusted for the same factors, the respective HRs for CMT-CON, CMT-IND, and CMT-ONLY vs. CMT-SEQ were 0.69, 0.70, and 0.86 (P less than .001 for all three comparisons).
“The findings on efficacy and toxicity are quite consistent with previously reported studies based on clinical trials or observational databases,” the investigators said.
The study was supported by grants from the U.S. National Institutes of Health and the Hong Kong Health and Medical Research Fund. All authors have declared no conflicts of interest.
GENEVA – Among older adults with stage III non–small cell lung cancer (NSCLC), the sequencing of chemotherapy and radiation has a significant effect on overall survival, a team of investigators from Hong Kong and the United States reported.
Among 2,033 adults who were 65 years or older with locally advanced NSCLC and treated with one of four combined-modality therapy (CMT) schedules, both chemotherapy induction followed by concurrent therapy (CMT-IND) and concurrent therapy followed by consolidation chemoradiation (CMT-CON) were associated with an approximately 30% improvement in survival, compared with either sequential chemotherapy followed by radiation (CMT-SEQ) or concurrent therapy only (CMT-ONLY), reported Hei Man Herbert Pang, MD, of the University of Hong Kong and his colleagues.
The investigators used retrospective data from U.S. and Chinese sources to compare the relative survival benefits with various combined modality therapies. These included a Surveillance, Epidemiology, and End Results–Medicare cohort of patients 65 years and older with stage IIIA or IIIB NSCLC treated with CMT from 2006 through 2010 and a cohort of patients with the same age and NSCLC treated at Queen Mary Hospital in Hong Kong from 2007 through 2016.
They assessed neutropenia using inpatient claims data for episodes occurring within 130 days of the first chemotherapy cycle.
In an unadjusted analysis, they found that median overall survival, in descending order, was 16.1 months for CMT-SEQ,15.0 months for CMT-ONLY, 12.0 months for CMT-IND, and 11.0 months for CMT-CON.
When they controlled for variables, however, a different picture began to emerge.
For example, patients who were treated with CMT-SEQ had lower Charlson Comorbidity Index scores and, thus, were comparatively healthier than patients treated with other combined modalities.
Hospitalizations for neutropenia were most common with CMT-CON, occurring in 13.3% of patients, compared with 9.8% of patients treated with CMT-ONLY, 9.2% with CMT-IND, and 2.3% with CMT-SEQ.
In multivariable models controlling for sex, race, ethnicity, histology, and Charlson score, CMT-CON and CMT-IND were associated with significantly better overall, compared with CMT-SEQ, with respective hazard ratios for death of 0.68 (P less than .001) and 0.67 (P = .001). In this model, CMT-ONLY was not associated with significantly better survival.
In a propensity score model adjusted for the same factors, the respective HRs for CMT-CON, CMT-IND, and CMT-ONLY vs. CMT-SEQ were 0.69, 0.70, and 0.86 (P less than .001 for all three comparisons).
“The findings on efficacy and toxicity are quite consistent with previously reported studies based on clinical trials or observational databases,” the investigators said.
The study was supported by grants from the U.S. National Institutes of Health and the Hong Kong Health and Medical Research Fund. All authors have declared no conflicts of interest.
GENEVA – Among older adults with stage III non–small cell lung cancer (NSCLC), the sequencing of chemotherapy and radiation has a significant effect on overall survival, a team of investigators from Hong Kong and the United States reported.
Among 2,033 adults who were 65 years or older with locally advanced NSCLC and treated with one of four combined-modality therapy (CMT) schedules, both chemotherapy induction followed by concurrent therapy (CMT-IND) and concurrent therapy followed by consolidation chemoradiation (CMT-CON) were associated with an approximately 30% improvement in survival, compared with either sequential chemotherapy followed by radiation (CMT-SEQ) or concurrent therapy only (CMT-ONLY), reported Hei Man Herbert Pang, MD, of the University of Hong Kong and his colleagues.
The investigators used retrospective data from U.S. and Chinese sources to compare the relative survival benefits with various combined modality therapies. These included a Surveillance, Epidemiology, and End Results–Medicare cohort of patients 65 years and older with stage IIIA or IIIB NSCLC treated with CMT from 2006 through 2010 and a cohort of patients with the same age and NSCLC treated at Queen Mary Hospital in Hong Kong from 2007 through 2016.
They assessed neutropenia using inpatient claims data for episodes occurring within 130 days of the first chemotherapy cycle.
In an unadjusted analysis, they found that median overall survival, in descending order, was 16.1 months for CMT-SEQ,15.0 months for CMT-ONLY, 12.0 months for CMT-IND, and 11.0 months for CMT-CON.
When they controlled for variables, however, a different picture began to emerge.
For example, patients who were treated with CMT-SEQ had lower Charlson Comorbidity Index scores and, thus, were comparatively healthier than patients treated with other combined modalities.
Hospitalizations for neutropenia were most common with CMT-CON, occurring in 13.3% of patients, compared with 9.8% of patients treated with CMT-ONLY, 9.2% with CMT-IND, and 2.3% with CMT-SEQ.
In multivariable models controlling for sex, race, ethnicity, histology, and Charlson score, CMT-CON and CMT-IND were associated with significantly better overall, compared with CMT-SEQ, with respective hazard ratios for death of 0.68 (P less than .001) and 0.67 (P = .001). In this model, CMT-ONLY was not associated with significantly better survival.
In a propensity score model adjusted for the same factors, the respective HRs for CMT-CON, CMT-IND, and CMT-ONLY vs. CMT-SEQ were 0.69, 0.70, and 0.86 (P less than .001 for all three comparisons).
“The findings on efficacy and toxicity are quite consistent with previously reported studies based on clinical trials or observational databases,” the investigators said.
The study was supported by grants from the U.S. National Institutes of Health and the Hong Kong Health and Medical Research Fund. All authors have declared no conflicts of interest.
FROM ELCC
Key clinical point: Some combined modality therapy options for older adults with NSCLC are associated with better overall survival.
Major finding: CMT-IND and CMT-CON were associated with a 30% improvement in overall survival, compared with CMT-SEQ.
Data source: Retrospective review of data on 2,033 adults 65 years and older with NSCLC in the United States and Hong Kong.
Disclosures: The study was supported by grants from the U.S. National Institutes of Health and the Hong Kong Health and Medical Research Fund. All authors have declared no conflicts of interest.
Routine surveillance adds cost but little benefit following a pediatric tumor
MONTREAL – It can be a tough sell to worried patients or their caregivers, but surveillance imaging in children with a history of some treated solid tumors may not add anything to care except costs, a team of investigators suggested.
A study of the relationship between surveillance imaging and outcomes in patients who were followed after therapy for solid tumors found that “off therapy surveillance imaging did not affect outcomes in our relapsed solid tumor patients,” wrote Jacob Zimmerli and his coinvestigators at the University of Utah Huntsman Cancer Institute, Salt Lake City.
“In the case of rhabdomyosarcoma, we had a 31% relapse rate of our 39 unique cancer diagnoses that we looked at over a 10-year period. We had 12 relapses, and, of those relapses, 10 were found through nonroutine imaging,” Mr. Zimmerli said in an interview.
Survival rates for patients with rhabdomyosarcoma were identical whether their relapsed disease was detected via surveillance imaging or imaging performed when relapse was directly suspected because of clinical or physical findings, he said.
Surveillance imaging also came at a significant financial cost. Of the $345,000 total expenditure for imaging of rhabdomyosarcoma, $223,000 was spent on imaging for patients who never experienced a relapse. Additionally, $95,000 was spent on imaging for patients who had a relapse but whose relapses were not detected by routine surveillance imaging. Therefore, the investigators calculated, 92% of costs associated with surveillance did not lead to a relapse diagnosis.
“This finding in itself will lead us to look at a few more specific cancer subgroups and maybe do more cost analysis to see if there is a better way to treat these patients,” Mr. Zimmerli said.
To see whether surveillance imaging was associated with outcomes, the investigators performed a retrospective review of data on 292 patients treated at Primary Children’s Hospital in Salt Lake City for osteosarcoma, Wilms’ tumor, neuroblastoma, hepatoblastoma, Ewing sarcoma , or rhabdomyosarcoma.
All patients had either completed a minimum of 2 years of posttherapy follow-up or had a disease relapse within 2 years of completing therapy.
The investigators found that 8 of 10 osteosarcoma relapses, five of seven Wilms’ tumor relapses, and 9 of 15 neuroblastoma relapses were detected on routine imaging.
In contrast, only two of four hepatoblastoma relapses, three of nine Ewings sarcoma relapses, and 2 of 12 rhabdomyosarcoma relapses were found on routine imaging.
The overall survival rate for patients with relapses diagnosed on routine imaging was 51.72%, compared with 50% for patients whose relapses were diagnosed on imaging following the appearance of symptoms. The difference represented only one patient and was not statistically significant.
Mr. Zimmerli acknowledged that many routine posttherapy imaging studies are performed to assuage patient concerns and that it may be difficult to convince parents of children with a history of cancer that routine imaging of some tumors may not offer the assurances of relapse-free survival that they seek.
The study was supported by Intermountain Healthcare. The investigators reported no conflicts of interest.
MONTREAL – It can be a tough sell to worried patients or their caregivers, but surveillance imaging in children with a history of some treated solid tumors may not add anything to care except costs, a team of investigators suggested.
A study of the relationship between surveillance imaging and outcomes in patients who were followed after therapy for solid tumors found that “off therapy surveillance imaging did not affect outcomes in our relapsed solid tumor patients,” wrote Jacob Zimmerli and his coinvestigators at the University of Utah Huntsman Cancer Institute, Salt Lake City.
“In the case of rhabdomyosarcoma, we had a 31% relapse rate of our 39 unique cancer diagnoses that we looked at over a 10-year period. We had 12 relapses, and, of those relapses, 10 were found through nonroutine imaging,” Mr. Zimmerli said in an interview.
Survival rates for patients with rhabdomyosarcoma were identical whether their relapsed disease was detected via surveillance imaging or imaging performed when relapse was directly suspected because of clinical or physical findings, he said.
Surveillance imaging also came at a significant financial cost. Of the $345,000 total expenditure for imaging of rhabdomyosarcoma, $223,000 was spent on imaging for patients who never experienced a relapse. Additionally, $95,000 was spent on imaging for patients who had a relapse but whose relapses were not detected by routine surveillance imaging. Therefore, the investigators calculated, 92% of costs associated with surveillance did not lead to a relapse diagnosis.
“This finding in itself will lead us to look at a few more specific cancer subgroups and maybe do more cost analysis to see if there is a better way to treat these patients,” Mr. Zimmerli said.
To see whether surveillance imaging was associated with outcomes, the investigators performed a retrospective review of data on 292 patients treated at Primary Children’s Hospital in Salt Lake City for osteosarcoma, Wilms’ tumor, neuroblastoma, hepatoblastoma, Ewing sarcoma , or rhabdomyosarcoma.
All patients had either completed a minimum of 2 years of posttherapy follow-up or had a disease relapse within 2 years of completing therapy.
The investigators found that 8 of 10 osteosarcoma relapses, five of seven Wilms’ tumor relapses, and 9 of 15 neuroblastoma relapses were detected on routine imaging.
In contrast, only two of four hepatoblastoma relapses, three of nine Ewings sarcoma relapses, and 2 of 12 rhabdomyosarcoma relapses were found on routine imaging.
The overall survival rate for patients with relapses diagnosed on routine imaging was 51.72%, compared with 50% for patients whose relapses were diagnosed on imaging following the appearance of symptoms. The difference represented only one patient and was not statistically significant.
Mr. Zimmerli acknowledged that many routine posttherapy imaging studies are performed to assuage patient concerns and that it may be difficult to convince parents of children with a history of cancer that routine imaging of some tumors may not offer the assurances of relapse-free survival that they seek.
The study was supported by Intermountain Healthcare. The investigators reported no conflicts of interest.
MONTREAL – It can be a tough sell to worried patients or their caregivers, but surveillance imaging in children with a history of some treated solid tumors may not add anything to care except costs, a team of investigators suggested.
A study of the relationship between surveillance imaging and outcomes in patients who were followed after therapy for solid tumors found that “off therapy surveillance imaging did not affect outcomes in our relapsed solid tumor patients,” wrote Jacob Zimmerli and his coinvestigators at the University of Utah Huntsman Cancer Institute, Salt Lake City.
“In the case of rhabdomyosarcoma, we had a 31% relapse rate of our 39 unique cancer diagnoses that we looked at over a 10-year period. We had 12 relapses, and, of those relapses, 10 were found through nonroutine imaging,” Mr. Zimmerli said in an interview.
Survival rates for patients with rhabdomyosarcoma were identical whether their relapsed disease was detected via surveillance imaging or imaging performed when relapse was directly suspected because of clinical or physical findings, he said.
Surveillance imaging also came at a significant financial cost. Of the $345,000 total expenditure for imaging of rhabdomyosarcoma, $223,000 was spent on imaging for patients who never experienced a relapse. Additionally, $95,000 was spent on imaging for patients who had a relapse but whose relapses were not detected by routine surveillance imaging. Therefore, the investigators calculated, 92% of costs associated with surveillance did not lead to a relapse diagnosis.
“This finding in itself will lead us to look at a few more specific cancer subgroups and maybe do more cost analysis to see if there is a better way to treat these patients,” Mr. Zimmerli said.
To see whether surveillance imaging was associated with outcomes, the investigators performed a retrospective review of data on 292 patients treated at Primary Children’s Hospital in Salt Lake City for osteosarcoma, Wilms’ tumor, neuroblastoma, hepatoblastoma, Ewing sarcoma , or rhabdomyosarcoma.
All patients had either completed a minimum of 2 years of posttherapy follow-up or had a disease relapse within 2 years of completing therapy.
The investigators found that 8 of 10 osteosarcoma relapses, five of seven Wilms’ tumor relapses, and 9 of 15 neuroblastoma relapses were detected on routine imaging.
In contrast, only two of four hepatoblastoma relapses, three of nine Ewings sarcoma relapses, and 2 of 12 rhabdomyosarcoma relapses were found on routine imaging.
The overall survival rate for patients with relapses diagnosed on routine imaging was 51.72%, compared with 50% for patients whose relapses were diagnosed on imaging following the appearance of symptoms. The difference represented only one patient and was not statistically significant.
Mr. Zimmerli acknowledged that many routine posttherapy imaging studies are performed to assuage patient concerns and that it may be difficult to convince parents of children with a history of cancer that routine imaging of some tumors may not offer the assurances of relapse-free survival that they seek.
The study was supported by Intermountain Healthcare. The investigators reported no conflicts of interest.
FROM ASPHO
Key clinical point: Routine surveillance was less effective at detecting relapse of some pediatric solid tumors than imaging performed to confirm a clinical finding.
Major finding: Using imaging performed after symptoms appeared, 10 of 12 rhabdomyosarcoma relapses were detected.
Data source: A retrospective review of outcomes following routine and nonroutine imaging among children followed after treatment for one of six solid tumor types.
Disclosures: The study was supported by Intermountain Healthcare. The investigators reported no conflicts of interest.
Hospital infections top WHO’s list of priority pathogens
The World Health Organization is urging governments to focus antibiotic research efforts on a list of urgent bacterial threats, topped by several increasingly powerful superbugs that cause hospital-based infections and other potentially deadly conditions.
The WHO listed the top 20 bacteria that it believes are most harmful to human health, other than mycobacteria such as Mycobacterium tuberculosis, which causes tuberculosis. The germ was not included in the list because it’s generally accepted to be the most urgent priority for new antibiotic research and development, Marie-Paule Kieny, PhD, a WHO assistant director, said at a press conference.
The priority list is needed because the antibiotic pipeline is “practically dry,” thanks to scientific research challenges and a lack of financial incentives, according to Dr. Kieny. “Antibiotics are generally used for the short term, unlike therapies for chronic diseases, which bring in much higher returns on investment,” she said. The list “is intended to signal to the scientific community and the pharmaceutical industry the areas they should focus on to address urgent public health threats.”
The WHO list begins with Priority 1/“Critical” pathogens that it believes most urgently need to be targeted through antibiotic research and development: Acinetobacter baumannii, carbapenem-resistant; Pseudomonas aeruginosa, carbapenem-resistant; and Enterobacteriaceae (including Klebsiella pneumonia, Escherichia coli, Enterobacter spp., Serratia spp., Proteus spp., Providencia spp., and Morganella spp.), carbapenem-resistant, extended-spectrum beta-lactamase–producing.
“These bacteria are responsible for severe infections and high mortality rates, mostly in hospitalized patients, transplant recipients, those receiving chemotherapy, or patients in intensive care units,” Dr. Kieny said. “While these bacteria are not widespread and do not generally affect healthy individuals, the burden for patients and society is now alarming – and new, effective therapies are imperative.”
Priority 2/”High” pathogens are Enterococcus faecium, vancomycin-resistant; Staphylococcus aureus, methicillin-resistant, vancomycin intermediate and resistant; Helicobacter pylori, clarithromycin-resistant; Campylobacter, fluoroquinolone-resistant; Salmonella spp., fluoroquinolone-resistant; Neisseria gonorrhoeae, third-generation cephalosporin-resistant and fluoroquinolone-resistant.
Pathogens in this category can infect healthy individuals, Dr. Kieny noted. “These infections, although not associated with significant mortality, have a dramatic health and economic impact on communities and, in particular, in low-income countries.”
Priority 3/”Medium” pathogens are Streptococcus pneumoniae, penicillin–non-susceptible; Haemophilus influenzae, ampicillin-resistant; and Shigella spp., fluoroquinolone-resistant.
These pathogens “represent a threat because of increasing resistance but still have some effective antibiotic options available,” Dr. Kieny said.
According to a statement provided by the WHO, the priority list doesn’t include streptococcus A and B or chlamydia, because resistance hasn’t reached the level of a public health threat.
One goal of the list is to focus attention on the development of small-market, gram-negative drugs that combat hospital-based infections, explained Nicola Magrini, MD, a WHO scientist who also spoke at the press conference.
Over the last decade, he said, the pipeline has instead focused more on gram-positive agents – mostly linked to beta-lactamase – that have wider market potential and generate less resistance.
“From a clinical point of view, these multidrug-resistant gram-negative clinical trials are very difficult and expensive to do, more than for gram-positive,” noted Evelina Tacconelli, MD, PhD, a contributor to the WHO report. “Because when we talk about gram-negative, we need to cover multiple pathogens and not just one or two, as in the case of gram-positive.”
Dr. Magrini said he couldn’t provide estimates about how many people worldwide are affected by the listed pathogens. However, he said a full report with numbers will be released by June.
It does appear that patients with severe infection from antibiotic-resistant germs face a mortality rate of up to 60%, while extended-spectrum beta-lactamase–positive E. coli accounts for up to 70% of urinary tract infections in many countries, explained Dr. Tacconelli, head of the division of infectious diseases at the University of Tübingen, Germany.
“Even if we don’t know exactly how many,” she said, “we are talking about millions of people affected.”
The World Health Organization is urging governments to focus antibiotic research efforts on a list of urgent bacterial threats, topped by several increasingly powerful superbugs that cause hospital-based infections and other potentially deadly conditions.
The WHO listed the top 20 bacteria that it believes are most harmful to human health, other than mycobacteria such as Mycobacterium tuberculosis, which causes tuberculosis. The germ was not included in the list because it’s generally accepted to be the most urgent priority for new antibiotic research and development, Marie-Paule Kieny, PhD, a WHO assistant director, said at a press conference.
The priority list is needed because the antibiotic pipeline is “practically dry,” thanks to scientific research challenges and a lack of financial incentives, according to Dr. Kieny. “Antibiotics are generally used for the short term, unlike therapies for chronic diseases, which bring in much higher returns on investment,” she said. The list “is intended to signal to the scientific community and the pharmaceutical industry the areas they should focus on to address urgent public health threats.”
The WHO list begins with Priority 1/“Critical” pathogens that it believes most urgently need to be targeted through antibiotic research and development: Acinetobacter baumannii, carbapenem-resistant; Pseudomonas aeruginosa, carbapenem-resistant; and Enterobacteriaceae (including Klebsiella pneumonia, Escherichia coli, Enterobacter spp., Serratia spp., Proteus spp., Providencia spp., and Morganella spp.), carbapenem-resistant, extended-spectrum beta-lactamase–producing.
“These bacteria are responsible for severe infections and high mortality rates, mostly in hospitalized patients, transplant recipients, those receiving chemotherapy, or patients in intensive care units,” Dr. Kieny said. “While these bacteria are not widespread and do not generally affect healthy individuals, the burden for patients and society is now alarming – and new, effective therapies are imperative.”
Priority 2/”High” pathogens are Enterococcus faecium, vancomycin-resistant; Staphylococcus aureus, methicillin-resistant, vancomycin intermediate and resistant; Helicobacter pylori, clarithromycin-resistant; Campylobacter, fluoroquinolone-resistant; Salmonella spp., fluoroquinolone-resistant; Neisseria gonorrhoeae, third-generation cephalosporin-resistant and fluoroquinolone-resistant.
Pathogens in this category can infect healthy individuals, Dr. Kieny noted. “These infections, although not associated with significant mortality, have a dramatic health and economic impact on communities and, in particular, in low-income countries.”
Priority 3/”Medium” pathogens are Streptococcus pneumoniae, penicillin–non-susceptible; Haemophilus influenzae, ampicillin-resistant; and Shigella spp., fluoroquinolone-resistant.
These pathogens “represent a threat because of increasing resistance but still have some effective antibiotic options available,” Dr. Kieny said.
According to a statement provided by the WHO, the priority list doesn’t include streptococcus A and B or chlamydia, because resistance hasn’t reached the level of a public health threat.
One goal of the list is to focus attention on the development of small-market, gram-negative drugs that combat hospital-based infections, explained Nicola Magrini, MD, a WHO scientist who also spoke at the press conference.
Over the last decade, he said, the pipeline has instead focused more on gram-positive agents – mostly linked to beta-lactamase – that have wider market potential and generate less resistance.
“From a clinical point of view, these multidrug-resistant gram-negative clinical trials are very difficult and expensive to do, more than for gram-positive,” noted Evelina Tacconelli, MD, PhD, a contributor to the WHO report. “Because when we talk about gram-negative, we need to cover multiple pathogens and not just one or two, as in the case of gram-positive.”
Dr. Magrini said he couldn’t provide estimates about how many people worldwide are affected by the listed pathogens. However, he said a full report with numbers will be released by June.
It does appear that patients with severe infection from antibiotic-resistant germs face a mortality rate of up to 60%, while extended-spectrum beta-lactamase–positive E. coli accounts for up to 70% of urinary tract infections in many countries, explained Dr. Tacconelli, head of the division of infectious diseases at the University of Tübingen, Germany.
“Even if we don’t know exactly how many,” she said, “we are talking about millions of people affected.”
The World Health Organization is urging governments to focus antibiotic research efforts on a list of urgent bacterial threats, topped by several increasingly powerful superbugs that cause hospital-based infections and other potentially deadly conditions.
The WHO listed the top 20 bacteria that it believes are most harmful to human health, other than mycobacteria such as Mycobacterium tuberculosis, which causes tuberculosis. The germ was not included in the list because it’s generally accepted to be the most urgent priority for new antibiotic research and development, Marie-Paule Kieny, PhD, a WHO assistant director, said at a press conference.
The priority list is needed because the antibiotic pipeline is “practically dry,” thanks to scientific research challenges and a lack of financial incentives, according to Dr. Kieny. “Antibiotics are generally used for the short term, unlike therapies for chronic diseases, which bring in much higher returns on investment,” she said. The list “is intended to signal to the scientific community and the pharmaceutical industry the areas they should focus on to address urgent public health threats.”
The WHO list begins with Priority 1/“Critical” pathogens that it believes most urgently need to be targeted through antibiotic research and development: Acinetobacter baumannii, carbapenem-resistant; Pseudomonas aeruginosa, carbapenem-resistant; and Enterobacteriaceae (including Klebsiella pneumonia, Escherichia coli, Enterobacter spp., Serratia spp., Proteus spp., Providencia spp., and Morganella spp.), carbapenem-resistant, extended-spectrum beta-lactamase–producing.
“These bacteria are responsible for severe infections and high mortality rates, mostly in hospitalized patients, transplant recipients, those receiving chemotherapy, or patients in intensive care units,” Dr. Kieny said. “While these bacteria are not widespread and do not generally affect healthy individuals, the burden for patients and society is now alarming – and new, effective therapies are imperative.”
Priority 2/”High” pathogens are Enterococcus faecium, vancomycin-resistant; Staphylococcus aureus, methicillin-resistant, vancomycin intermediate and resistant; Helicobacter pylori, clarithromycin-resistant; Campylobacter, fluoroquinolone-resistant; Salmonella spp., fluoroquinolone-resistant; Neisseria gonorrhoeae, third-generation cephalosporin-resistant and fluoroquinolone-resistant.
Pathogens in this category can infect healthy individuals, Dr. Kieny noted. “These infections, although not associated with significant mortality, have a dramatic health and economic impact on communities and, in particular, in low-income countries.”
Priority 3/”Medium” pathogens are Streptococcus pneumoniae, penicillin–non-susceptible; Haemophilus influenzae, ampicillin-resistant; and Shigella spp., fluoroquinolone-resistant.
These pathogens “represent a threat because of increasing resistance but still have some effective antibiotic options available,” Dr. Kieny said.
According to a statement provided by the WHO, the priority list doesn’t include streptococcus A and B or chlamydia, because resistance hasn’t reached the level of a public health threat.
One goal of the list is to focus attention on the development of small-market, gram-negative drugs that combat hospital-based infections, explained Nicola Magrini, MD, a WHO scientist who also spoke at the press conference.
Over the last decade, he said, the pipeline has instead focused more on gram-positive agents – mostly linked to beta-lactamase – that have wider market potential and generate less resistance.
“From a clinical point of view, these multidrug-resistant gram-negative clinical trials are very difficult and expensive to do, more than for gram-positive,” noted Evelina Tacconelli, MD, PhD, a contributor to the WHO report. “Because when we talk about gram-negative, we need to cover multiple pathogens and not just one or two, as in the case of gram-positive.”
Dr. Magrini said he couldn’t provide estimates about how many people worldwide are affected by the listed pathogens. However, he said a full report with numbers will be released by June.
It does appear that patients with severe infection from antibiotic-resistant germs face a mortality rate of up to 60%, while extended-spectrum beta-lactamase–positive E. coli accounts for up to 70% of urinary tract infections in many countries, explained Dr. Tacconelli, head of the division of infectious diseases at the University of Tübingen, Germany.
“Even if we don’t know exactly how many,” she said, “we are talking about millions of people affected.”
Extended maraviroc helps prevent graft-versus-host disease
ORLANDO – The use of the CCR5 antagonist maraviroc for 90 days is safe and effective for graft-versus-host disease (GVHD) prophylaxis in patients undergoing allogeneic stem cell transplantation, according to findings from a phase II study.
An earlier study showed that CCR5 blockade using maraviroc for 33 days was associated with a low incidence of acute GVHD, as well as with absence of early liver and gut GVHD – although delayed severe cases of visceral GVHD still occurred.
The current study was performed because the prior findings raised concerns that brief blockade was insufficient for preventing GVHD over a longer period of time. The new findings show that an extended course may indeed provide additional benefits, Ran Reshef, MD, reported at the combined annual meetings of the Center for International Blood & Marrow Transplant Research and the American Society for Blood and Marrow Transplantation.
In 37 high-risk patients who received allogeneic stem cell transplantation from unrelated donors using fludarabine/busulfan (Flu/Bu2) conditioning followed by peripheral blood stem cells, maraviroc was given at a dose of 300 mg twice daily, in addition to standard tacrolimus and methotrexate.
The 180-day rates of grade 2-4 and grade 3-4 acute GVHD (the primary endpoint of the study) in these patients were 27% and 5%, respectively. These rates were very similar to the 24% and 6% rates seen in the first study at 6 months after 30 days of maraviroc treatment, said Dr. Reshef of Columbia University Medical Center, New York.
The earlier results were “driven not so much by a reduction in the rates of skin GVHD, but by low rates of visceral GVHD of the gut and the liver – with a striking absence of gut and liver GVHD in the first 100 days,” he said.
Dr. Reshef also noted that the current study had a less favorable donor mix, as no matched related donors were included because of the earlier study’s very low rates of GVHD – with or without maraviroc – in those with related donors, who composed a third of donors.
Long-term follow-up of results from the earlier study, with comparison of a large contemporary control cohort, showed that “there is in fact an impact ... on grade 2-4 and grade 3-4 [GVHD], although the number of events is small, and the study was not powered enough to reach statistical significance,” Dr. Reshef said. The rates of chronic GVHD did not differ between the study subjects and contemporary controls, he noted.
At 100 days in the current study, there were no cases of liver GVHD, two cases of mild upper-GI GVHD, and one case of severe gut GVHD. At 1 year, the disease relapse rate was “fairly reasonable” at 30%, nonrelapse mortality was 12% with only one case of death from GVHD, and the incidence of chronic GVHD was 8%, which was significantly lower than in the prior study, he said.
The low rate of chronic GVHD led to a GVHD/relapse-free survival (GRFS) rate of 49%.
“To put this in context, the [Center for International Blood & Marrow Transplant Research] data for reduced-intensity transplants ... have shown 25% for acute myeloid leukemia and 12% for myelodysplastic syndrome,” he said. “So, we feel that these are by far improved numbers, compared with this benchmark.”
To determine which patients develop GVHD despite chemotaxis blockade and why, Dr. Reshef and his colleagues developed a pharmacodynamic assay to assess the activity of maraviroc in fresh blood samples. They found that those with insufficient CCR5 blockade on day 0 were those with higher incidence of severe acute GVHD, nonrelapse mortality, GRFS, and overall survival.
The investigators performed pharmacokinetic analysis using combined data from both trials to improve understanding of why some patients have insufficient CCR5 blockade. This showed significant variability in day 0 trough of maraviroc among patients (median of 65 ng/mL, range 12-316 ng/mL); levels above the median were associated with a significantly lower incidence of acute grade 2-4 GVHD and a trend toward improved GRFS.
These studies of maraviroc, which was originally developed for the treatment of HIV infection, were done to test the belief that blocking lymphocyte migration might prevent GVHD without interfering with graft-versus-tumor activity. Based on the earlier findings, Dr. Reshef and his colleagues hypothesized that treatment up to day 90 would decrease the rate to less than 30%, from a historical rate of 52%.
Patients in the study were high risk by virtue of age (median, 64 years), HLA matching (matched unrelated, 84%; mismatched unrelated, 16%), and comorbidities (comorbidity index greater than 2 in 49%). Underlying diseases were acute leukemia (78%), myelodysplastic syndrome (16%), and myeloproliferative neoplasm and cutaneous T-cell lymphomas (3% each).
At a median follow-up of 21 months, the 3-month course of maraviroc was well tolerated. Eight patients did not complete treatment because of disease relapse (five patients), skin reaction (one patient), early infection-related death (one patient), or poor tolerance of oral drugs (one patient). Neutrophil, platelet, and T-cell engraftment were similar to historical controls, and rates of infections were also similar, Dr Reshef noted.
“To conclude, an extended course of maraviroc up to day 90 is feasible and safe in the majority of patients,” he said. “This study confirms the effect of CCR5 blockade on visceral GVHD. I’m still awaiting a randomized study to confirm that further.
“A long course of maraviroc does not necessarily affect the rates of acute GVHD, but may help reduce chronic GVHD and improve GRFS,” Dr. Reshef said. “We should look further into the pharmacodynamic and pharmacokinetic variables.”
Dr. Reshef reported receiving research funding from Pfizer.
ORLANDO – The use of the CCR5 antagonist maraviroc for 90 days is safe and effective for graft-versus-host disease (GVHD) prophylaxis in patients undergoing allogeneic stem cell transplantation, according to findings from a phase II study.
An earlier study showed that CCR5 blockade using maraviroc for 33 days was associated with a low incidence of acute GVHD, as well as with absence of early liver and gut GVHD – although delayed severe cases of visceral GVHD still occurred.
The current study was performed because the prior findings raised concerns that brief blockade was insufficient for preventing GVHD over a longer period of time. The new findings show that an extended course may indeed provide additional benefits, Ran Reshef, MD, reported at the combined annual meetings of the Center for International Blood & Marrow Transplant Research and the American Society for Blood and Marrow Transplantation.
In 37 high-risk patients who received allogeneic stem cell transplantation from unrelated donors using fludarabine/busulfan (Flu/Bu2) conditioning followed by peripheral blood stem cells, maraviroc was given at a dose of 300 mg twice daily, in addition to standard tacrolimus and methotrexate.
The 180-day rates of grade 2-4 and grade 3-4 acute GVHD (the primary endpoint of the study) in these patients were 27% and 5%, respectively. These rates were very similar to the 24% and 6% rates seen in the first study at 6 months after 30 days of maraviroc treatment, said Dr. Reshef of Columbia University Medical Center, New York.
The earlier results were “driven not so much by a reduction in the rates of skin GVHD, but by low rates of visceral GVHD of the gut and the liver – with a striking absence of gut and liver GVHD in the first 100 days,” he said.
Dr. Reshef also noted that the current study had a less favorable donor mix, as no matched related donors were included because of the earlier study’s very low rates of GVHD – with or without maraviroc – in those with related donors, who composed a third of donors.
Long-term follow-up of results from the earlier study, with comparison of a large contemporary control cohort, showed that “there is in fact an impact ... on grade 2-4 and grade 3-4 [GVHD], although the number of events is small, and the study was not powered enough to reach statistical significance,” Dr. Reshef said. The rates of chronic GVHD did not differ between the study subjects and contemporary controls, he noted.
At 100 days in the current study, there were no cases of liver GVHD, two cases of mild upper-GI GVHD, and one case of severe gut GVHD. At 1 year, the disease relapse rate was “fairly reasonable” at 30%, nonrelapse mortality was 12% with only one case of death from GVHD, and the incidence of chronic GVHD was 8%, which was significantly lower than in the prior study, he said.
The low rate of chronic GVHD led to a GVHD/relapse-free survival (GRFS) rate of 49%.
“To put this in context, the [Center for International Blood & Marrow Transplant Research] data for reduced-intensity transplants ... have shown 25% for acute myeloid leukemia and 12% for myelodysplastic syndrome,” he said. “So, we feel that these are by far improved numbers, compared with this benchmark.”
To determine which patients develop GVHD despite chemotaxis blockade and why, Dr. Reshef and his colleagues developed a pharmacodynamic assay to assess the activity of maraviroc in fresh blood samples. They found that those with insufficient CCR5 blockade on day 0 were those with higher incidence of severe acute GVHD, nonrelapse mortality, GRFS, and overall survival.
The investigators performed pharmacokinetic analysis using combined data from both trials to improve understanding of why some patients have insufficient CCR5 blockade. This showed significant variability in day 0 trough of maraviroc among patients (median of 65 ng/mL, range 12-316 ng/mL); levels above the median were associated with a significantly lower incidence of acute grade 2-4 GVHD and a trend toward improved GRFS.
These studies of maraviroc, which was originally developed for the treatment of HIV infection, were done to test the belief that blocking lymphocyte migration might prevent GVHD without interfering with graft-versus-tumor activity. Based on the earlier findings, Dr. Reshef and his colleagues hypothesized that treatment up to day 90 would decrease the rate to less than 30%, from a historical rate of 52%.
Patients in the study were high risk by virtue of age (median, 64 years), HLA matching (matched unrelated, 84%; mismatched unrelated, 16%), and comorbidities (comorbidity index greater than 2 in 49%). Underlying diseases were acute leukemia (78%), myelodysplastic syndrome (16%), and myeloproliferative neoplasm and cutaneous T-cell lymphomas (3% each).
At a median follow-up of 21 months, the 3-month course of maraviroc was well tolerated. Eight patients did not complete treatment because of disease relapse (five patients), skin reaction (one patient), early infection-related death (one patient), or poor tolerance of oral drugs (one patient). Neutrophil, platelet, and T-cell engraftment were similar to historical controls, and rates of infections were also similar, Dr Reshef noted.
“To conclude, an extended course of maraviroc up to day 90 is feasible and safe in the majority of patients,” he said. “This study confirms the effect of CCR5 blockade on visceral GVHD. I’m still awaiting a randomized study to confirm that further.
“A long course of maraviroc does not necessarily affect the rates of acute GVHD, but may help reduce chronic GVHD and improve GRFS,” Dr. Reshef said. “We should look further into the pharmacodynamic and pharmacokinetic variables.”
Dr. Reshef reported receiving research funding from Pfizer.
ORLANDO – The use of the CCR5 antagonist maraviroc for 90 days is safe and effective for graft-versus-host disease (GVHD) prophylaxis in patients undergoing allogeneic stem cell transplantation, according to findings from a phase II study.
An earlier study showed that CCR5 blockade using maraviroc for 33 days was associated with a low incidence of acute GVHD, as well as with absence of early liver and gut GVHD – although delayed severe cases of visceral GVHD still occurred.
The current study was performed because the prior findings raised concerns that brief blockade was insufficient for preventing GVHD over a longer period of time. The new findings show that an extended course may indeed provide additional benefits, Ran Reshef, MD, reported at the combined annual meetings of the Center for International Blood & Marrow Transplant Research and the American Society for Blood and Marrow Transplantation.
In 37 high-risk patients who received allogeneic stem cell transplantation from unrelated donors using fludarabine/busulfan (Flu/Bu2) conditioning followed by peripheral blood stem cells, maraviroc was given at a dose of 300 mg twice daily, in addition to standard tacrolimus and methotrexate.
The 180-day rates of grade 2-4 and grade 3-4 acute GVHD (the primary endpoint of the study) in these patients were 27% and 5%, respectively. These rates were very similar to the 24% and 6% rates seen in the first study at 6 months after 30 days of maraviroc treatment, said Dr. Reshef of Columbia University Medical Center, New York.
The earlier results were “driven not so much by a reduction in the rates of skin GVHD, but by low rates of visceral GVHD of the gut and the liver – with a striking absence of gut and liver GVHD in the first 100 days,” he said.
Dr. Reshef also noted that the current study had a less favorable donor mix, as no matched related donors were included because of the earlier study’s very low rates of GVHD – with or without maraviroc – in those with related donors, who composed a third of donors.
Long-term follow-up of results from the earlier study, with comparison of a large contemporary control cohort, showed that “there is in fact an impact ... on grade 2-4 and grade 3-4 [GVHD], although the number of events is small, and the study was not powered enough to reach statistical significance,” Dr. Reshef said. The rates of chronic GVHD did not differ between the study subjects and contemporary controls, he noted.
At 100 days in the current study, there were no cases of liver GVHD, two cases of mild upper-GI GVHD, and one case of severe gut GVHD. At 1 year, the disease relapse rate was “fairly reasonable” at 30%, nonrelapse mortality was 12% with only one case of death from GVHD, and the incidence of chronic GVHD was 8%, which was significantly lower than in the prior study, he said.
The low rate of chronic GVHD led to a GVHD/relapse-free survival (GRFS) rate of 49%.
“To put this in context, the [Center for International Blood & Marrow Transplant Research] data for reduced-intensity transplants ... have shown 25% for acute myeloid leukemia and 12% for myelodysplastic syndrome,” he said. “So, we feel that these are by far improved numbers, compared with this benchmark.”
To determine which patients develop GVHD despite chemotaxis blockade and why, Dr. Reshef and his colleagues developed a pharmacodynamic assay to assess the activity of maraviroc in fresh blood samples. They found that those with insufficient CCR5 blockade on day 0 were those with higher incidence of severe acute GVHD, nonrelapse mortality, GRFS, and overall survival.
The investigators performed pharmacokinetic analysis using combined data from both trials to improve understanding of why some patients have insufficient CCR5 blockade. This showed significant variability in day 0 trough of maraviroc among patients (median of 65 ng/mL, range 12-316 ng/mL); levels above the median were associated with a significantly lower incidence of acute grade 2-4 GVHD and a trend toward improved GRFS.
These studies of maraviroc, which was originally developed for the treatment of HIV infection, were done to test the belief that blocking lymphocyte migration might prevent GVHD without interfering with graft-versus-tumor activity. Based on the earlier findings, Dr. Reshef and his colleagues hypothesized that treatment up to day 90 would decrease the rate to less than 30%, from a historical rate of 52%.
Patients in the study were high risk by virtue of age (median, 64 years), HLA matching (matched unrelated, 84%; mismatched unrelated, 16%), and comorbidities (comorbidity index greater than 2 in 49%). Underlying diseases were acute leukemia (78%), myelodysplastic syndrome (16%), and myeloproliferative neoplasm and cutaneous T-cell lymphomas (3% each).
At a median follow-up of 21 months, the 3-month course of maraviroc was well tolerated. Eight patients did not complete treatment because of disease relapse (five patients), skin reaction (one patient), early infection-related death (one patient), or poor tolerance of oral drugs (one patient). Neutrophil, platelet, and T-cell engraftment were similar to historical controls, and rates of infections were also similar, Dr Reshef noted.
“To conclude, an extended course of maraviroc up to day 90 is feasible and safe in the majority of patients,” he said. “This study confirms the effect of CCR5 blockade on visceral GVHD. I’m still awaiting a randomized study to confirm that further.
“A long course of maraviroc does not necessarily affect the rates of acute GVHD, but may help reduce chronic GVHD and improve GRFS,” Dr. Reshef said. “We should look further into the pharmacodynamic and pharmacokinetic variables.”
Dr. Reshef reported receiving research funding from Pfizer.
AT THE 2017 BMT TANDEM MEETINGS
Key clinical point:
Major finding: The 180-day rates of grade 2-4 and grade 3-4 acute GVHD were 27% and 5%, respectively.
Data source: A phase II study of 37 patients.
Disclosures: Dr. Reshef reported receiving research funding from Pfizer.
Biomarker algorithm sharpens GVHD treatment outcomes prediction
ORLANDO – A biomarker algorithm was better than was clinical response at predicting outcomes after 1 week of systemic steroid treatment for graft-versus-host disease, according to findings from a multicenter study.
The findings have implications for early decision making regarding treatment course, Hannah Major-Monfried reported at the combined annual meetings of the Center for International Blood & Marrow Transplant Research and the American Society for Blood and Marrow Transplantation.
“The same GVHD algorithm that stratifies patients at day 7 after transplant, at [GVHD] diagnosis, also stratifies them after 1 week of steroid treatment into two groups with distinct risks for treatment failure, 6-month nonrelapse mortality, and overall survival,” she said.
The biomarker algorithm, which includes measures of ST2 and REG3-alpha, was previously shown to predict day-28 treatment response and 6-month non-relapse mortality (NRM) when applied at day 7 post transplant before the onset of GVHD and at the time of diagnosis, said Ms. Major-Monfried, a third-year medical student at Icahn School of Medicine at Mount Sinai, New York.
For the current analysis, levels of the biomarkers were measured after 1 week of treatment in 378 patients with acute GVHD from 11 centers in the Mount Sinai Acute GVHD International Consortium.
In a test cohort that included 236 of the patients, the measurements were used to generate a new predicted probability, or treatment score, for 6-month NRM, which had a value between 0 and 1.
Of the 236 patients, 93 (39%) were considered to have high posttreatment probability of NRM, and the remaining patients (61%) had low posttreatment probability of NRM, based on their treatment scores.
“High-risk patients were significantly less likely to respond to treatment than low-risk patients,” she said, noting that very similar results were found in a validation cohort of the remaining 142 patients, which had a similar proportion of high- and low-risk patients as did the test cohort.
The overall 6-month NRM for patients treated for GVHD was 27% in the test cohort. When the biomarker algorithm was used to separate the cohort into high- and low-risk groups, the NRM rate was found to be approximately 4 times higher among the high-risk patients than among the low-risk patients.
Overall survival was also significantly worse among high- vs. low-risk patients in both the test and validation cohorts.
“We can conclude that the increased NRM seen in the high-risk groups can explain these large differences in overall survival,” Ms. Major-Monfried said.
Because treatment decisions are often made after 1 week based on early clinical response, she and her colleagues also explored whether treatment response after 1 week could similarly predict NRM.
In the test cohort, early response – which includes complete or partial response in GVHD symptoms after 1 week of steroids – was observed in 48% of patients, while 52% were early nonresponders. NRM occurred in 17% of the early responders, compared with 36% of the nonresponders in the test cohort, and similar results were found in the validation cohort.
“These differences are independent of biomarkers,” she noted. “These are solely based on observed clinical response.”
When the biomarker algorithm was applied, prediction of NRM was more precise.
“We started with the early responders,” she explained. “When we used the biomarker algorithm to stratify these patients into high- and low-risk groups, we found that 28% of early responders were actually high risk, and that they experienced 38% NRM – significantly higher than the 8% observed in low-risk patients. Similar results were found again in the validation cohort.”
When the biomarker algorithm was used to stratify patients who were nonresponders at 7 days into high- and low-risk groups, 50% were found to be low risk, and those patients experienced 17% NRM, significantly lower than the 57% seen in the high-risk patients. Similar results were again seen in the validation cohort.
“Early responders with high posttreatment probability have high NRM, and perhaps should not be tapered despite the improvement of their clinical symptoms, while early nonresponders with low posttreatment probability have lower NRM and may not need treatment escalation,” Ms. Major-Monfried said.
“In data not shown, many of these patients are actually what we could call ‘slow responders’ who ultimately fare well,” she noted.
Ms. Major-Monfried reported having no disclosures.
ORLANDO – A biomarker algorithm was better than was clinical response at predicting outcomes after 1 week of systemic steroid treatment for graft-versus-host disease, according to findings from a multicenter study.
The findings have implications for early decision making regarding treatment course, Hannah Major-Monfried reported at the combined annual meetings of the Center for International Blood & Marrow Transplant Research and the American Society for Blood and Marrow Transplantation.
“The same GVHD algorithm that stratifies patients at day 7 after transplant, at [GVHD] diagnosis, also stratifies them after 1 week of steroid treatment into two groups with distinct risks for treatment failure, 6-month nonrelapse mortality, and overall survival,” she said.
The biomarker algorithm, which includes measures of ST2 and REG3-alpha, was previously shown to predict day-28 treatment response and 6-month non-relapse mortality (NRM) when applied at day 7 post transplant before the onset of GVHD and at the time of diagnosis, said Ms. Major-Monfried, a third-year medical student at Icahn School of Medicine at Mount Sinai, New York.
For the current analysis, levels of the biomarkers were measured after 1 week of treatment in 378 patients with acute GVHD from 11 centers in the Mount Sinai Acute GVHD International Consortium.
In a test cohort that included 236 of the patients, the measurements were used to generate a new predicted probability, or treatment score, for 6-month NRM, which had a value between 0 and 1.
Of the 236 patients, 93 (39%) were considered to have high posttreatment probability of NRM, and the remaining patients (61%) had low posttreatment probability of NRM, based on their treatment scores.
“High-risk patients were significantly less likely to respond to treatment than low-risk patients,” she said, noting that very similar results were found in a validation cohort of the remaining 142 patients, which had a similar proportion of high- and low-risk patients as did the test cohort.
The overall 6-month NRM for patients treated for GVHD was 27% in the test cohort. When the biomarker algorithm was used to separate the cohort into high- and low-risk groups, the NRM rate was found to be approximately 4 times higher among the high-risk patients than among the low-risk patients.
Overall survival was also significantly worse among high- vs. low-risk patients in both the test and validation cohorts.
“We can conclude that the increased NRM seen in the high-risk groups can explain these large differences in overall survival,” Ms. Major-Monfried said.
Because treatment decisions are often made after 1 week based on early clinical response, she and her colleagues also explored whether treatment response after 1 week could similarly predict NRM.
In the test cohort, early response – which includes complete or partial response in GVHD symptoms after 1 week of steroids – was observed in 48% of patients, while 52% were early nonresponders. NRM occurred in 17% of the early responders, compared with 36% of the nonresponders in the test cohort, and similar results were found in the validation cohort.
“These differences are independent of biomarkers,” she noted. “These are solely based on observed clinical response.”
When the biomarker algorithm was applied, prediction of NRM was more precise.
“We started with the early responders,” she explained. “When we used the biomarker algorithm to stratify these patients into high- and low-risk groups, we found that 28% of early responders were actually high risk, and that they experienced 38% NRM – significantly higher than the 8% observed in low-risk patients. Similar results were found again in the validation cohort.”
When the biomarker algorithm was used to stratify patients who were nonresponders at 7 days into high- and low-risk groups, 50% were found to be low risk, and those patients experienced 17% NRM, significantly lower than the 57% seen in the high-risk patients. Similar results were again seen in the validation cohort.
“Early responders with high posttreatment probability have high NRM, and perhaps should not be tapered despite the improvement of their clinical symptoms, while early nonresponders with low posttreatment probability have lower NRM and may not need treatment escalation,” Ms. Major-Monfried said.
“In data not shown, many of these patients are actually what we could call ‘slow responders’ who ultimately fare well,” she noted.
Ms. Major-Monfried reported having no disclosures.
ORLANDO – A biomarker algorithm was better than was clinical response at predicting outcomes after 1 week of systemic steroid treatment for graft-versus-host disease, according to findings from a multicenter study.
The findings have implications for early decision making regarding treatment course, Hannah Major-Monfried reported at the combined annual meetings of the Center for International Blood & Marrow Transplant Research and the American Society for Blood and Marrow Transplantation.
“The same GVHD algorithm that stratifies patients at day 7 after transplant, at [GVHD] diagnosis, also stratifies them after 1 week of steroid treatment into two groups with distinct risks for treatment failure, 6-month nonrelapse mortality, and overall survival,” she said.
The biomarker algorithm, which includes measures of ST2 and REG3-alpha, was previously shown to predict day-28 treatment response and 6-month non-relapse mortality (NRM) when applied at day 7 post transplant before the onset of GVHD and at the time of diagnosis, said Ms. Major-Monfried, a third-year medical student at Icahn School of Medicine at Mount Sinai, New York.
For the current analysis, levels of the biomarkers were measured after 1 week of treatment in 378 patients with acute GVHD from 11 centers in the Mount Sinai Acute GVHD International Consortium.
In a test cohort that included 236 of the patients, the measurements were used to generate a new predicted probability, or treatment score, for 6-month NRM, which had a value between 0 and 1.
Of the 236 patients, 93 (39%) were considered to have high posttreatment probability of NRM, and the remaining patients (61%) had low posttreatment probability of NRM, based on their treatment scores.
“High-risk patients were significantly less likely to respond to treatment than low-risk patients,” she said, noting that very similar results were found in a validation cohort of the remaining 142 patients, which had a similar proportion of high- and low-risk patients as did the test cohort.
The overall 6-month NRM for patients treated for GVHD was 27% in the test cohort. When the biomarker algorithm was used to separate the cohort into high- and low-risk groups, the NRM rate was found to be approximately 4 times higher among the high-risk patients than among the low-risk patients.
Overall survival was also significantly worse among high- vs. low-risk patients in both the test and validation cohorts.
“We can conclude that the increased NRM seen in the high-risk groups can explain these large differences in overall survival,” Ms. Major-Monfried said.
Because treatment decisions are often made after 1 week based on early clinical response, she and her colleagues also explored whether treatment response after 1 week could similarly predict NRM.
In the test cohort, early response – which includes complete or partial response in GVHD symptoms after 1 week of steroids – was observed in 48% of patients, while 52% were early nonresponders. NRM occurred in 17% of the early responders, compared with 36% of the nonresponders in the test cohort, and similar results were found in the validation cohort.
“These differences are independent of biomarkers,” she noted. “These are solely based on observed clinical response.”
When the biomarker algorithm was applied, prediction of NRM was more precise.
“We started with the early responders,” she explained. “When we used the biomarker algorithm to stratify these patients into high- and low-risk groups, we found that 28% of early responders were actually high risk, and that they experienced 38% NRM – significantly higher than the 8% observed in low-risk patients. Similar results were found again in the validation cohort.”
When the biomarker algorithm was used to stratify patients who were nonresponders at 7 days into high- and low-risk groups, 50% were found to be low risk, and those patients experienced 17% NRM, significantly lower than the 57% seen in the high-risk patients. Similar results were again seen in the validation cohort.
“Early responders with high posttreatment probability have high NRM, and perhaps should not be tapered despite the improvement of their clinical symptoms, while early nonresponders with low posttreatment probability have lower NRM and may not need treatment escalation,” Ms. Major-Monfried said.
“In data not shown, many of these patients are actually what we could call ‘slow responders’ who ultimately fare well,” she noted.
Ms. Major-Monfried reported having no disclosures.
Key clinical point:
Major finding: High- vs. low-risk patients, based on the biomarker algorithm, had a fourfold higher rate of nonrelapse mortality.
Data source: A multicenter study of 378 patients.
Disclosures: Ms. Major-Monfried reported having no disclosures.
FDA: REMS no longer necessary for epoetin, darbepoetin
The Food and Drug Administration no longer requires certification of doctors and hospitals to prescribe epoetin alfa (Procrit, Epogen) or darbepoetin alfa (Aranesp) for chemotherapy anemia.
A Risk Evaluation and Mitigation Strategy (REMS) program was put in place in 2011 to make sure that the benefits of erythropoiesis-stimulating agents (ESAs) outweighed the risks when prescribed. Under the program, providers were required to become certified in the ESA REMS and to demonstrate that each patient had received counseling on the benefits and risks of the therapies prior to use.
Amgen’s prescriber surveys demonstrated “acceptable knowledge” of the need to counsel patients about the risks. Utilization data indicated “appropriate prescribing” as an alternative to transfusion.
In addition, in an evaluation of the impact of multiple regulatory actions, the FDA determined that full implementation of the ESA REMS in 2011 had minimal impact on trends in ESA utilization metrics, the FDA wrote.
The FDA concluded that regulatory actions and label changes – and the cut in payments for nonrenal indications from the Center for Medicare & Medicaid Services – were enough to reduce overuse in chemotherapy.
However, while the REMS is no longer necessary, the FDA says serious risks of shortened overall survival and/or increased risk of tumor progression or recurrence associated with these drugs remain and health care providers should continue to discuss the risks and benefits of using ESAs with each patient before initiating use.
The Food and Drug Administration no longer requires certification of doctors and hospitals to prescribe epoetin alfa (Procrit, Epogen) or darbepoetin alfa (Aranesp) for chemotherapy anemia.
A Risk Evaluation and Mitigation Strategy (REMS) program was put in place in 2011 to make sure that the benefits of erythropoiesis-stimulating agents (ESAs) outweighed the risks when prescribed. Under the program, providers were required to become certified in the ESA REMS and to demonstrate that each patient had received counseling on the benefits and risks of the therapies prior to use.
Amgen’s prescriber surveys demonstrated “acceptable knowledge” of the need to counsel patients about the risks. Utilization data indicated “appropriate prescribing” as an alternative to transfusion.
In addition, in an evaluation of the impact of multiple regulatory actions, the FDA determined that full implementation of the ESA REMS in 2011 had minimal impact on trends in ESA utilization metrics, the FDA wrote.
The FDA concluded that regulatory actions and label changes – and the cut in payments for nonrenal indications from the Center for Medicare & Medicaid Services – were enough to reduce overuse in chemotherapy.
However, while the REMS is no longer necessary, the FDA says serious risks of shortened overall survival and/or increased risk of tumor progression or recurrence associated with these drugs remain and health care providers should continue to discuss the risks and benefits of using ESAs with each patient before initiating use.
The Food and Drug Administration no longer requires certification of doctors and hospitals to prescribe epoetin alfa (Procrit, Epogen) or darbepoetin alfa (Aranesp) for chemotherapy anemia.
A Risk Evaluation and Mitigation Strategy (REMS) program was put in place in 2011 to make sure that the benefits of erythropoiesis-stimulating agents (ESAs) outweighed the risks when prescribed. Under the program, providers were required to become certified in the ESA REMS and to demonstrate that each patient had received counseling on the benefits and risks of the therapies prior to use.
Amgen’s prescriber surveys demonstrated “acceptable knowledge” of the need to counsel patients about the risks. Utilization data indicated “appropriate prescribing” as an alternative to transfusion.
In addition, in an evaluation of the impact of multiple regulatory actions, the FDA determined that full implementation of the ESA REMS in 2011 had minimal impact on trends in ESA utilization metrics, the FDA wrote.
The FDA concluded that regulatory actions and label changes – and the cut in payments for nonrenal indications from the Center for Medicare & Medicaid Services – were enough to reduce overuse in chemotherapy.
However, while the REMS is no longer necessary, the FDA says serious risks of shortened overall survival and/or increased risk of tumor progression or recurrence associated with these drugs remain and health care providers should continue to discuss the risks and benefits of using ESAs with each patient before initiating use.
Single-, low-dose cyclophosphamide-associated severe hyponatremia with seizures in a patient with breast cancer
Cyclophosphamide, an agent used to treat various malignant and autoimmune disorders, can cause severe hyponatremia with seizures in rare cases. The exact mechanism of cyclophosphamide-induced hyponatremia is poorly understood, but is thought to occur from a drug- associated antidiuretic hormone (ADH) release leading to free water retention.1 This unusual phenomenon of cyclophosphamide-associated syndrome of inappropriate antidiuretic hormone secretion (SIADH) has been described only in case reports, most of which reported the development of severe hyponatremia within a week after administration of cyclophosphamide.2-5 We report a unique case of a patient who developed severe, symptomatic hyponatremia with seizures, with her serum sodium decreasing from 137 mEq to 112 mEq within 30 hours after her first dose of low-dose cyclophosphamide (600 mg/m2).
Case presentation and summary
A 68-year-old white woman with a history of bilateral invasive ductal carcinoma of the breast (status-post bilateral mastectomy) presented to the emergency department (ED) at our facility with new onset seizure. The patient had been diagnosed 8 months earlier with stage I (T1c, N0, M0) poorly differentiated infiltrating ductal carcinoma (triple negative) of the left breast for which she underwent left segmental mastectomy about 1 month after diagnosis. She was subsequently found to have progressive disease with stage IIIC (T2, N3, and M0) infiltrating ductal carcinoma with lobular features (ER/PR+, Her2) of the right breast. She underwent a right modified radical mastectomy 5 months after her stage IIIC breast cancer diagnosis. She received her first cycle of adjuvant chemotherapy with intravenous doxorubicin (60 mg/m2) and cyclophosphamide (600 mg/m2), which included pre-hydration, a day before presenting to our facility.
According to the patient’s family who provided the initial history, the patient reported tightness in her left arm while sitting at the dinner table. She was confused and subsequently had jerking movement of her right upper extremity with left facial twitching which lasted about 40 seconds. There was no loss of consciousness, or bowel or bladder control. She became unresponsive after the episode. Review of systems was negative except for a report of nausea a few hours before the onset of seizures, which resolved with ondansetron. Her past medical history was significant for breast cancer as already mentioned, seasonal allergic rhinitis, and hypertension. Home medications included hydrochlorothiazide 12.5 mg oral daily, aspirin 81 mg oral daily, and fexofenadine and loratadine oral daily as needed for allergies. There were no other significant surgical history other than already stated. The patient lived at home with her family and was independent with her instrumental activities of daily living. She is a former smoker of tobacco and quit smoking 30 years ago.
On arrival at our facility, the patient had normal vital signs. Significant findings on physical examination were an elderly female who seemed somnolent; not able to follow commands with a documented Glasgow Coma Scale of 10 with eyes opening spontaneously, incomprehensible sounds, and flexion withdrawal from pain as her best responses. She had an increased tone in her left upper extremity and had a brisk, deep tendon reflexes without clonus or 3+ (range, 0-5+, with 2+ being normal). The remainder of her physical exam was unremarkable. Laboratory testing revealed a glucose level of 120 mg/dL (normal, 65-110 mg/dL), sodium of 112 mEq/L (normal, 135-145 mmol/L), and chloride of 78 mEq/L (normal, 95-105 mmol/L). Serum osmolality and urine osmolality were 242 mOsm/kg (normal, 282-295 mOsm/kg) and 449 mOsm/kg (normal, 500-800 mOsm/kg) respectively, indicative of suboptimally dilute urine despite relatively low serum osmolality or SIADH. Urine electrolytes were not obtained.
Imaging studies including computed-tomography scans of the head and chest x-ray performed in the ED were unremarkable. After a phenytoin load, an electroencephalogram was obtained which showed diffuse encephalopathy without active seizure foci. A non-contrast magnetic-resonance imaging (MRI) of the brain was performed but it failed to show acute infarct, mass, mass effect, or brain herniation. There was nonspecific white matter abnormality with compromise of the bilateral cerebral hemispheres, calloseptal junction, left posterior pillar, and bilateral anterior pillars of the fornix, possibly representative of chronic white matter microvascular ischemic changes or less likely vasculitis or demyelination. Correction of her hyponatremia with normal saline was started in the ED with a change in serum sodium from 112 mEq/L to 115 mEq/L within 2 hours. She was admitted to the intensive care unit (ICU) where her sodium correction with normal saline and free water restriction was continued with a goal correction rate of 8-12 mEq/L in 24 hours. The patient’s serum sodium as well as level of consciousness improved gradually over the course of her ICU stay. After 64 hours in the hospital, her sodium had corrected to 137 mEq/L (normal, 135-145 mmol/L; Figure). She was then alert and oriented to person, place, and time. All motor findings noted on presentation had resolved. Her saline infusion was discontinued and serum sodium remained within normal range. She was discharged to a rehabilitation facility. Her hydrochlorothiazide was also discontinued.

Discussion
Hyponatremia is a common finding in cancer patients caused usually by paraneoplastic syndrome, chemotherapy, immunotherapy, or other associated treatment.6 SIADH is a frequent cause of hyponatremia in cancer patients and should be suspected in patients with hyponatremia, hypo-osmolality, and a urine osmolality above 100 mOsmol/kg.7
Our patient’s presentation and laboratory findings suggested SIADH as the likely cause of hyponatremia with a low sodium, a serum osmolality 242 mOsm/kg and urine osmolality of 449 mOsm/kg.8-10 She had no known underlying contributory comorbid condition relating to her serum lipids, thyroid, adrenal, kidney, or heart to date. Her use of a thiazide diuretic was the only confounding factor. The most plausible cause of hyponatremia/SIADH in our patient was likely cyclophosphamide based on her history, timeline of symptoms, and the absence of other possible causes. Though the mechanism for many of the previously mentioned etiologies are known, the mechanism of cyclophosphamide-induced SIADH is difficult to elucidate since the imminent complication of hemorrhagic cystitis means patients receiving this drug are often aggressively hydrated to prevent this complication.11,12 The result is that there is marked retention of water leading to potentially fatal hyponatremia in selected cases.11 This phenomenon has been fairly well described in patients receiving doses of 6 g/m2 as given in the STAMP protocol for stem cell mobilization or at doses of 30-50 mg/kg used to treat malignancy.12 Our patient clearly falls in this category given that she received a dose of 600 mg/m2. We found no evidence in her history to suggest post-operative, genetic or other cause for her hyponatremia. Our case mirrors a report by Koo and colleagues who described severe hyponatremia occurring within 24 hours following a single dose of intravenous cyclophosphamide 700 mg followed by saline infusion.13 In the case reported by Jayachandra and colleagues in which suspected cyclophosphamide-induced hyponatremia led to seizures, the patient received 500 mg IV of cyclophosphamide and had serum sodium as low as 106 mEq/L within a 24-hour period,2 similar to our patient.
There is a paucity of data on cyclophosphamide-induced SIADH. The mechanism by which cyclophosphamide causes SIADH is currently unknown. In addition, there are currently no set criteria that help identify at-risk patients who may develop such an event, including the dosage of cyclophosphamide that may trigger the SIADH, because lower doses of the drug have been associated with this complication.14
In a retrospective analysis by Lee and colleagues, cyclophosphamide-induced hyponatremia was found to be associated with male sex on a univariate analysis, but no risk factors were found in a multivariate analysis.15 It is likely that the concomitant use of diuretics, hydration, and high-dose cyclophosphamide contributed to hyponatremia/SIADH in our patient, though it is not clear through what mechanism. Harlow and colleagues proposed a mechanism for this phenomenon in 1979 based on the autopsy of a patient who had received high-dose cyclophosphamide involving degranulation of hypothalamic neurosecretory organelles and loss of Herring’s bodies. They inferred that metabolites of cyclophosphamide indirectly triggered inappropriate secretion of antidiuretic hormone as seen with a use of the structurally related analogue ifosfamide,16 but to our knowledge, this has yet to be replicated. Cyclophosphamide metabolite may have a direct tubular effect on the collecting duct epithelium leading to water retention15 as established by Campbell and colleagues. In one case, an established diabetes insipidus patient developed cyclophosphamide-induced antidiuresis without vasopressin secretion.17 It is imperative that the scientific community conduct research into the risk factors, underlying mechanisms, and methods of prevention to reduce and/or eliminate SIADH associated with use of cyclophosphamide.
1. Gilbar PJ, Richmond J, Wood J, Sullivan A. Syndrome of inappropriate antidiuretic hormone secretion induced by a single dose of oral cyclophosphamide. Ann Pharmacother. 2012.46(9):e23.
2. Jayachandran NV, Chandrasekhara PK, Thomas J, Agrawal S, Narsimulu G. Cyclophosphamide-associated complications: we need to be aware of SIADH and central pontine myelinolysis. Rheumatology (Oxford). 2009;48(1):89-90.
3. Baker M, Markman M, Niu J. Cyclophosphamide-induced severe acute hyponatremic encephalopathy in patients with breast cancer: report of two cases. Case Rep Oncol. 2014;7(2):550-554.
4. Lazarevic V, Hägg E, Wahlin A. Hiccups and severe hyponatremia associated with high-dose cyclophosphamide in conditioning regimen for allogeneic stem cell transplantation. Am J Hematol. 2007;82(1):88.
5. Geng C, Tang P, Zhang Y, Gao W. Hyponatremia induced by low-dose cyclophosphamide in two patients with breast cancer. Breast J. 2014; 20(4):442-443.
6. Kamoi K, Ebe T, Hasegawa A, et al. Hyponatremia in small cell lung cancer. Mechanisms not involving inappropriate ADH secretion. Cancer. 1987;60(5):1089-1093.
7. Matwiejczuk S, Püsküllüoğlu M, Zygulska AL. Oncological emergencies: syndrome of inappropriate antidiuretic hormone secretion (SIADH). Przegl Lek. 2014;71(10):541-543.
8. Robertson GL. Regulation of arginine vasopressin in the syndrome of inappropriate antidiuresis. Am J Med. 2006;119(7 Suppl 1):S36-42.
9. Robertson GL, Shelton RL, Athar S. The osmoregulation of vasopressin. Kidney Int. 1976;10(1):25-37.
10. Decaux G, Musch W. Clinical laboratory evaluation of the syndrome of inappropriate secretion of antidiuretic hormone. Clin J Am Soc Nephrol. 2008;3(4):1175-1184.
11. Bressler RB, Huston DP. Water intoxication following moderate-dose intravenous cyclophosphamide. Arch Intern Med. 1985;145(3):548-549.
12. Salido M, Macarron P, Hernández-García C, D’Cruz DP, Khamashta MA, Hughes GR. Water intoxication induced by low-dose cyclophosphamide in two patients with systemic lupus erythematosus. Lupus. 2003;12(8):636-639.
13. Koo TY, Bae SC, Park JS, et al. Water intoxication following low-dose intravenous cyclophosphamide. Electrolyte Blood Press. 2007;5(1):50-54.
14. [No authors listed]. Nausea and vasopressin. Lancet. 1991;337(8750):1133-1134.
15 Lee YC1, Park JS, Lee CH, et al. Hyponatraemia induced by low-dose intravenous pulse cyclophosphamide. Nephrol Dial Transplant. 2010;25(5):1520-1524.
16. Harlow PJ, DeClerck YA, Shore NA, Ortega JA, Carranza A, Heuser E. A fatal case of inappropriate ADH secretion induced by cyclophosphamide therapy. Cancer. 1979;44(3):896-898.
17. Campbell DM, Atkinson A, Gillis D, Sochett EB. Cyclophosphamide and water retention: mechanism revisited. J Pediatr Endocrinol Metab. 2000;13(6):673-675.
Cyclophosphamide, an agent used to treat various malignant and autoimmune disorders, can cause severe hyponatremia with seizures in rare cases. The exact mechanism of cyclophosphamide-induced hyponatremia is poorly understood, but is thought to occur from a drug- associated antidiuretic hormone (ADH) release leading to free water retention.1 This unusual phenomenon of cyclophosphamide-associated syndrome of inappropriate antidiuretic hormone secretion (SIADH) has been described only in case reports, most of which reported the development of severe hyponatremia within a week after administration of cyclophosphamide.2-5 We report a unique case of a patient who developed severe, symptomatic hyponatremia with seizures, with her serum sodium decreasing from 137 mEq to 112 mEq within 30 hours after her first dose of low-dose cyclophosphamide (600 mg/m2).
Case presentation and summary
A 68-year-old white woman with a history of bilateral invasive ductal carcinoma of the breast (status-post bilateral mastectomy) presented to the emergency department (ED) at our facility with new onset seizure. The patient had been diagnosed 8 months earlier with stage I (T1c, N0, M0) poorly differentiated infiltrating ductal carcinoma (triple negative) of the left breast for which she underwent left segmental mastectomy about 1 month after diagnosis. She was subsequently found to have progressive disease with stage IIIC (T2, N3, and M0) infiltrating ductal carcinoma with lobular features (ER/PR+, Her2) of the right breast. She underwent a right modified radical mastectomy 5 months after her stage IIIC breast cancer diagnosis. She received her first cycle of adjuvant chemotherapy with intravenous doxorubicin (60 mg/m2) and cyclophosphamide (600 mg/m2), which included pre-hydration, a day before presenting to our facility.
According to the patient’s family who provided the initial history, the patient reported tightness in her left arm while sitting at the dinner table. She was confused and subsequently had jerking movement of her right upper extremity with left facial twitching which lasted about 40 seconds. There was no loss of consciousness, or bowel or bladder control. She became unresponsive after the episode. Review of systems was negative except for a report of nausea a few hours before the onset of seizures, which resolved with ondansetron. Her past medical history was significant for breast cancer as already mentioned, seasonal allergic rhinitis, and hypertension. Home medications included hydrochlorothiazide 12.5 mg oral daily, aspirin 81 mg oral daily, and fexofenadine and loratadine oral daily as needed for allergies. There were no other significant surgical history other than already stated. The patient lived at home with her family and was independent with her instrumental activities of daily living. She is a former smoker of tobacco and quit smoking 30 years ago.
On arrival at our facility, the patient had normal vital signs. Significant findings on physical examination were an elderly female who seemed somnolent; not able to follow commands with a documented Glasgow Coma Scale of 10 with eyes opening spontaneously, incomprehensible sounds, and flexion withdrawal from pain as her best responses. She had an increased tone in her left upper extremity and had a brisk, deep tendon reflexes without clonus or 3+ (range, 0-5+, with 2+ being normal). The remainder of her physical exam was unremarkable. Laboratory testing revealed a glucose level of 120 mg/dL (normal, 65-110 mg/dL), sodium of 112 mEq/L (normal, 135-145 mmol/L), and chloride of 78 mEq/L (normal, 95-105 mmol/L). Serum osmolality and urine osmolality were 242 mOsm/kg (normal, 282-295 mOsm/kg) and 449 mOsm/kg (normal, 500-800 mOsm/kg) respectively, indicative of suboptimally dilute urine despite relatively low serum osmolality or SIADH. Urine electrolytes were not obtained.
Imaging studies including computed-tomography scans of the head and chest x-ray performed in the ED were unremarkable. After a phenytoin load, an electroencephalogram was obtained which showed diffuse encephalopathy without active seizure foci. A non-contrast magnetic-resonance imaging (MRI) of the brain was performed but it failed to show acute infarct, mass, mass effect, or brain herniation. There was nonspecific white matter abnormality with compromise of the bilateral cerebral hemispheres, calloseptal junction, left posterior pillar, and bilateral anterior pillars of the fornix, possibly representative of chronic white matter microvascular ischemic changes or less likely vasculitis or demyelination. Correction of her hyponatremia with normal saline was started in the ED with a change in serum sodium from 112 mEq/L to 115 mEq/L within 2 hours. She was admitted to the intensive care unit (ICU) where her sodium correction with normal saline and free water restriction was continued with a goal correction rate of 8-12 mEq/L in 24 hours. The patient’s serum sodium as well as level of consciousness improved gradually over the course of her ICU stay. After 64 hours in the hospital, her sodium had corrected to 137 mEq/L (normal, 135-145 mmol/L; Figure). She was then alert and oriented to person, place, and time. All motor findings noted on presentation had resolved. Her saline infusion was discontinued and serum sodium remained within normal range. She was discharged to a rehabilitation facility. Her hydrochlorothiazide was also discontinued.
Discussion
Hyponatremia is a common finding in cancer patients caused usually by paraneoplastic syndrome, chemotherapy, immunotherapy, or other associated treatment.6 SIADH is a frequent cause of hyponatremia in cancer patients and should be suspected in patients with hyponatremia, hypo-osmolality, and a urine osmolality above 100 mOsmol/kg.7
Our patient’s presentation and laboratory findings suggested SIADH as the likely cause of hyponatremia with a low sodium, a serum osmolality 242 mOsm/kg and urine osmolality of 449 mOsm/kg.8-10 She had no known underlying contributory comorbid condition relating to her serum lipids, thyroid, adrenal, kidney, or heart to date. Her use of a thiazide diuretic was the only confounding factor. The most plausible cause of hyponatremia/SIADH in our patient was likely cyclophosphamide based on her history, timeline of symptoms, and the absence of other possible causes. Though the mechanism for many of the previously mentioned etiologies are known, the mechanism of cyclophosphamide-induced SIADH is difficult to elucidate since the imminent complication of hemorrhagic cystitis means patients receiving this drug are often aggressively hydrated to prevent this complication.11,12 The result is that there is marked retention of water leading to potentially fatal hyponatremia in selected cases.11 This phenomenon has been fairly well described in patients receiving doses of 6 g/m2 as given in the STAMP protocol for stem cell mobilization or at doses of 30-50 mg/kg used to treat malignancy.12 Our patient clearly falls in this category given that she received a dose of 600 mg/m2. We found no evidence in her history to suggest post-operative, genetic or other cause for her hyponatremia. Our case mirrors a report by Koo and colleagues who described severe hyponatremia occurring within 24 hours following a single dose of intravenous cyclophosphamide 700 mg followed by saline infusion.13 In the case reported by Jayachandra and colleagues in which suspected cyclophosphamide-induced hyponatremia led to seizures, the patient received 500 mg IV of cyclophosphamide and had serum sodium as low as 106 mEq/L within a 24-hour period,2 similar to our patient.
There is a paucity of data on cyclophosphamide-induced SIADH. The mechanism by which cyclophosphamide causes SIADH is currently unknown. In addition, there are currently no set criteria that help identify at-risk patients who may develop such an event, including the dosage of cyclophosphamide that may trigger the SIADH, because lower doses of the drug have been associated with this complication.14
In a retrospective analysis by Lee and colleagues, cyclophosphamide-induced hyponatremia was found to be associated with male sex on a univariate analysis, but no risk factors were found in a multivariate analysis.15 It is likely that the concomitant use of diuretics, hydration, and high-dose cyclophosphamide contributed to hyponatremia/SIADH in our patient, though it is not clear through what mechanism. Harlow and colleagues proposed a mechanism for this phenomenon in 1979 based on the autopsy of a patient who had received high-dose cyclophosphamide involving degranulation of hypothalamic neurosecretory organelles and loss of Herring’s bodies. They inferred that metabolites of cyclophosphamide indirectly triggered inappropriate secretion of antidiuretic hormone as seen with a use of the structurally related analogue ifosfamide,16 but to our knowledge, this has yet to be replicated. Cyclophosphamide metabolite may have a direct tubular effect on the collecting duct epithelium leading to water retention15 as established by Campbell and colleagues. In one case, an established diabetes insipidus patient developed cyclophosphamide-induced antidiuresis without vasopressin secretion.17 It is imperative that the scientific community conduct research into the risk factors, underlying mechanisms, and methods of prevention to reduce and/or eliminate SIADH associated with use of cyclophosphamide.
Cyclophosphamide, an agent used to treat various malignant and autoimmune disorders, can cause severe hyponatremia with seizures in rare cases. The exact mechanism of cyclophosphamide-induced hyponatremia is poorly understood, but is thought to occur from a drug- associated antidiuretic hormone (ADH) release leading to free water retention.1 This unusual phenomenon of cyclophosphamide-associated syndrome of inappropriate antidiuretic hormone secretion (SIADH) has been described only in case reports, most of which reported the development of severe hyponatremia within a week after administration of cyclophosphamide.2-5 We report a unique case of a patient who developed severe, symptomatic hyponatremia with seizures, with her serum sodium decreasing from 137 mEq to 112 mEq within 30 hours after her first dose of low-dose cyclophosphamide (600 mg/m2).
Case presentation and summary
A 68-year-old white woman with a history of bilateral invasive ductal carcinoma of the breast (status-post bilateral mastectomy) presented to the emergency department (ED) at our facility with new onset seizure. The patient had been diagnosed 8 months earlier with stage I (T1c, N0, M0) poorly differentiated infiltrating ductal carcinoma (triple negative) of the left breast for which she underwent left segmental mastectomy about 1 month after diagnosis. She was subsequently found to have progressive disease with stage IIIC (T2, N3, and M0) infiltrating ductal carcinoma with lobular features (ER/PR+, Her2) of the right breast. She underwent a right modified radical mastectomy 5 months after her stage IIIC breast cancer diagnosis. She received her first cycle of adjuvant chemotherapy with intravenous doxorubicin (60 mg/m2) and cyclophosphamide (600 mg/m2), which included pre-hydration, a day before presenting to our facility.
According to the patient’s family who provided the initial history, the patient reported tightness in her left arm while sitting at the dinner table. She was confused and subsequently had jerking movement of her right upper extremity with left facial twitching which lasted about 40 seconds. There was no loss of consciousness, or bowel or bladder control. She became unresponsive after the episode. Review of systems was negative except for a report of nausea a few hours before the onset of seizures, which resolved with ondansetron. Her past medical history was significant for breast cancer as already mentioned, seasonal allergic rhinitis, and hypertension. Home medications included hydrochlorothiazide 12.5 mg oral daily, aspirin 81 mg oral daily, and fexofenadine and loratadine oral daily as needed for allergies. There were no other significant surgical history other than already stated. The patient lived at home with her family and was independent with her instrumental activities of daily living. She is a former smoker of tobacco and quit smoking 30 years ago.
On arrival at our facility, the patient had normal vital signs. Significant findings on physical examination were an elderly female who seemed somnolent; not able to follow commands with a documented Glasgow Coma Scale of 10 with eyes opening spontaneously, incomprehensible sounds, and flexion withdrawal from pain as her best responses. She had an increased tone in her left upper extremity and had a brisk, deep tendon reflexes without clonus or 3+ (range, 0-5+, with 2+ being normal). The remainder of her physical exam was unremarkable. Laboratory testing revealed a glucose level of 120 mg/dL (normal, 65-110 mg/dL), sodium of 112 mEq/L (normal, 135-145 mmol/L), and chloride of 78 mEq/L (normal, 95-105 mmol/L). Serum osmolality and urine osmolality were 242 mOsm/kg (normal, 282-295 mOsm/kg) and 449 mOsm/kg (normal, 500-800 mOsm/kg) respectively, indicative of suboptimally dilute urine despite relatively low serum osmolality or SIADH. Urine electrolytes were not obtained.
Imaging studies including computed-tomography scans of the head and chest x-ray performed in the ED were unremarkable. After a phenytoin load, an electroencephalogram was obtained which showed diffuse encephalopathy without active seizure foci. A non-contrast magnetic-resonance imaging (MRI) of the brain was performed but it failed to show acute infarct, mass, mass effect, or brain herniation. There was nonspecific white matter abnormality with compromise of the bilateral cerebral hemispheres, calloseptal junction, left posterior pillar, and bilateral anterior pillars of the fornix, possibly representative of chronic white matter microvascular ischemic changes or less likely vasculitis or demyelination. Correction of her hyponatremia with normal saline was started in the ED with a change in serum sodium from 112 mEq/L to 115 mEq/L within 2 hours. She was admitted to the intensive care unit (ICU) where her sodium correction with normal saline and free water restriction was continued with a goal correction rate of 8-12 mEq/L in 24 hours. The patient’s serum sodium as well as level of consciousness improved gradually over the course of her ICU stay. After 64 hours in the hospital, her sodium had corrected to 137 mEq/L (normal, 135-145 mmol/L; Figure). She was then alert and oriented to person, place, and time. All motor findings noted on presentation had resolved. Her saline infusion was discontinued and serum sodium remained within normal range. She was discharged to a rehabilitation facility. Her hydrochlorothiazide was also discontinued.
Discussion
Hyponatremia is a common finding in cancer patients caused usually by paraneoplastic syndrome, chemotherapy, immunotherapy, or other associated treatment.6 SIADH is a frequent cause of hyponatremia in cancer patients and should be suspected in patients with hyponatremia, hypo-osmolality, and a urine osmolality above 100 mOsmol/kg.7
Our patient’s presentation and laboratory findings suggested SIADH as the likely cause of hyponatremia with a low sodium, a serum osmolality 242 mOsm/kg and urine osmolality of 449 mOsm/kg.8-10 She had no known underlying contributory comorbid condition relating to her serum lipids, thyroid, adrenal, kidney, or heart to date. Her use of a thiazide diuretic was the only confounding factor. The most plausible cause of hyponatremia/SIADH in our patient was likely cyclophosphamide based on her history, timeline of symptoms, and the absence of other possible causes. Though the mechanism for many of the previously mentioned etiologies are known, the mechanism of cyclophosphamide-induced SIADH is difficult to elucidate since the imminent complication of hemorrhagic cystitis means patients receiving this drug are often aggressively hydrated to prevent this complication.11,12 The result is that there is marked retention of water leading to potentially fatal hyponatremia in selected cases.11 This phenomenon has been fairly well described in patients receiving doses of 6 g/m2 as given in the STAMP protocol for stem cell mobilization or at doses of 30-50 mg/kg used to treat malignancy.12 Our patient clearly falls in this category given that she received a dose of 600 mg/m2. We found no evidence in her history to suggest post-operative, genetic or other cause for her hyponatremia. Our case mirrors a report by Koo and colleagues who described severe hyponatremia occurring within 24 hours following a single dose of intravenous cyclophosphamide 700 mg followed by saline infusion.13 In the case reported by Jayachandra and colleagues in which suspected cyclophosphamide-induced hyponatremia led to seizures, the patient received 500 mg IV of cyclophosphamide and had serum sodium as low as 106 mEq/L within a 24-hour period,2 similar to our patient.
There is a paucity of data on cyclophosphamide-induced SIADH. The mechanism by which cyclophosphamide causes SIADH is currently unknown. In addition, there are currently no set criteria that help identify at-risk patients who may develop such an event, including the dosage of cyclophosphamide that may trigger the SIADH, because lower doses of the drug have been associated with this complication.14
In a retrospective analysis by Lee and colleagues, cyclophosphamide-induced hyponatremia was found to be associated with male sex on a univariate analysis, but no risk factors were found in a multivariate analysis.15 It is likely that the concomitant use of diuretics, hydration, and high-dose cyclophosphamide contributed to hyponatremia/SIADH in our patient, though it is not clear through what mechanism. Harlow and colleagues proposed a mechanism for this phenomenon in 1979 based on the autopsy of a patient who had received high-dose cyclophosphamide involving degranulation of hypothalamic neurosecretory organelles and loss of Herring’s bodies. They inferred that metabolites of cyclophosphamide indirectly triggered inappropriate secretion of antidiuretic hormone as seen with a use of the structurally related analogue ifosfamide,16 but to our knowledge, this has yet to be replicated. Cyclophosphamide metabolite may have a direct tubular effect on the collecting duct epithelium leading to water retention15 as established by Campbell and colleagues. In one case, an established diabetes insipidus patient developed cyclophosphamide-induced antidiuresis without vasopressin secretion.17 It is imperative that the scientific community conduct research into the risk factors, underlying mechanisms, and methods of prevention to reduce and/or eliminate SIADH associated with use of cyclophosphamide.
1. Gilbar PJ, Richmond J, Wood J, Sullivan A. Syndrome of inappropriate antidiuretic hormone secretion induced by a single dose of oral cyclophosphamide. Ann Pharmacother. 2012.46(9):e23.
2. Jayachandran NV, Chandrasekhara PK, Thomas J, Agrawal S, Narsimulu G. Cyclophosphamide-associated complications: we need to be aware of SIADH and central pontine myelinolysis. Rheumatology (Oxford). 2009;48(1):89-90.
3. Baker M, Markman M, Niu J. Cyclophosphamide-induced severe acute hyponatremic encephalopathy in patients with breast cancer: report of two cases. Case Rep Oncol. 2014;7(2):550-554.
4. Lazarevic V, Hägg E, Wahlin A. Hiccups and severe hyponatremia associated with high-dose cyclophosphamide in conditioning regimen for allogeneic stem cell transplantation. Am J Hematol. 2007;82(1):88.
5. Geng C, Tang P, Zhang Y, Gao W. Hyponatremia induced by low-dose cyclophosphamide in two patients with breast cancer. Breast J. 2014; 20(4):442-443.
6. Kamoi K, Ebe T, Hasegawa A, et al. Hyponatremia in small cell lung cancer. Mechanisms not involving inappropriate ADH secretion. Cancer. 1987;60(5):1089-1093.
7. Matwiejczuk S, Püsküllüoğlu M, Zygulska AL. Oncological emergencies: syndrome of inappropriate antidiuretic hormone secretion (SIADH). Przegl Lek. 2014;71(10):541-543.
8. Robertson GL. Regulation of arginine vasopressin in the syndrome of inappropriate antidiuresis. Am J Med. 2006;119(7 Suppl 1):S36-42.
9. Robertson GL, Shelton RL, Athar S. The osmoregulation of vasopressin. Kidney Int. 1976;10(1):25-37.
10. Decaux G, Musch W. Clinical laboratory evaluation of the syndrome of inappropriate secretion of antidiuretic hormone. Clin J Am Soc Nephrol. 2008;3(4):1175-1184.
11. Bressler RB, Huston DP. Water intoxication following moderate-dose intravenous cyclophosphamide. Arch Intern Med. 1985;145(3):548-549.
12. Salido M, Macarron P, Hernández-García C, D’Cruz DP, Khamashta MA, Hughes GR. Water intoxication induced by low-dose cyclophosphamide in two patients with systemic lupus erythematosus. Lupus. 2003;12(8):636-639.
13. Koo TY, Bae SC, Park JS, et al. Water intoxication following low-dose intravenous cyclophosphamide. Electrolyte Blood Press. 2007;5(1):50-54.
14. [No authors listed]. Nausea and vasopressin. Lancet. 1991;337(8750):1133-1134.
15 Lee YC1, Park JS, Lee CH, et al. Hyponatraemia induced by low-dose intravenous pulse cyclophosphamide. Nephrol Dial Transplant. 2010;25(5):1520-1524.
16. Harlow PJ, DeClerck YA, Shore NA, Ortega JA, Carranza A, Heuser E. A fatal case of inappropriate ADH secretion induced by cyclophosphamide therapy. Cancer. 1979;44(3):896-898.
17. Campbell DM, Atkinson A, Gillis D, Sochett EB. Cyclophosphamide and water retention: mechanism revisited. J Pediatr Endocrinol Metab. 2000;13(6):673-675.
1. Gilbar PJ, Richmond J, Wood J, Sullivan A. Syndrome of inappropriate antidiuretic hormone secretion induced by a single dose of oral cyclophosphamide. Ann Pharmacother. 2012.46(9):e23.
2. Jayachandran NV, Chandrasekhara PK, Thomas J, Agrawal S, Narsimulu G. Cyclophosphamide-associated complications: we need to be aware of SIADH and central pontine myelinolysis. Rheumatology (Oxford). 2009;48(1):89-90.
3. Baker M, Markman M, Niu J. Cyclophosphamide-induced severe acute hyponatremic encephalopathy in patients with breast cancer: report of two cases. Case Rep Oncol. 2014;7(2):550-554.
4. Lazarevic V, Hägg E, Wahlin A. Hiccups and severe hyponatremia associated with high-dose cyclophosphamide in conditioning regimen for allogeneic stem cell transplantation. Am J Hematol. 2007;82(1):88.
5. Geng C, Tang P, Zhang Y, Gao W. Hyponatremia induced by low-dose cyclophosphamide in two patients with breast cancer. Breast J. 2014; 20(4):442-443.
6. Kamoi K, Ebe T, Hasegawa A, et al. Hyponatremia in small cell lung cancer. Mechanisms not involving inappropriate ADH secretion. Cancer. 1987;60(5):1089-1093.
7. Matwiejczuk S, Püsküllüoğlu M, Zygulska AL. Oncological emergencies: syndrome of inappropriate antidiuretic hormone secretion (SIADH). Przegl Lek. 2014;71(10):541-543.
8. Robertson GL. Regulation of arginine vasopressin in the syndrome of inappropriate antidiuresis. Am J Med. 2006;119(7 Suppl 1):S36-42.
9. Robertson GL, Shelton RL, Athar S. The osmoregulation of vasopressin. Kidney Int. 1976;10(1):25-37.
10. Decaux G, Musch W. Clinical laboratory evaluation of the syndrome of inappropriate secretion of antidiuretic hormone. Clin J Am Soc Nephrol. 2008;3(4):1175-1184.
11. Bressler RB, Huston DP. Water intoxication following moderate-dose intravenous cyclophosphamide. Arch Intern Med. 1985;145(3):548-549.
12. Salido M, Macarron P, Hernández-García C, D’Cruz DP, Khamashta MA, Hughes GR. Water intoxication induced by low-dose cyclophosphamide in two patients with systemic lupus erythematosus. Lupus. 2003;12(8):636-639.
13. Koo TY, Bae SC, Park JS, et al. Water intoxication following low-dose intravenous cyclophosphamide. Electrolyte Blood Press. 2007;5(1):50-54.
14. [No authors listed]. Nausea and vasopressin. Lancet. 1991;337(8750):1133-1134.
15 Lee YC1, Park JS, Lee CH, et al. Hyponatraemia induced by low-dose intravenous pulse cyclophosphamide. Nephrol Dial Transplant. 2010;25(5):1520-1524.
16. Harlow PJ, DeClerck YA, Shore NA, Ortega JA, Carranza A, Heuser E. A fatal case of inappropriate ADH secretion induced by cyclophosphamide therapy. Cancer. 1979;44(3):896-898.
17. Campbell DM, Atkinson A, Gillis D, Sochett EB. Cyclophosphamide and water retention: mechanism revisited. J Pediatr Endocrinol Metab. 2000;13(6):673-675.
Paraneoplastic leukemoid reaction – poor prognostic marker in urothelial bladder carcinoma
Certain cancers have been observed to cause symptoms called paraneoplastic syndromes that are not directly attributed to tumor invasion or compression. This phenomenon is believed to be secondary to a tumor’s secretion of functional hormones, peptides, cytokines, or its immune cross-reactivity. One such variant is a paraneoplastic leukemoid reaction (PLR), defined as a leukocytosis level of >50 x 103 cells/mm³, where the white blood cell (WBC) count differential exhibits a neutrophilia or left-shift, in which a predominance of early neutrophil precursors is observed. A PLR is believed to be incited by the tumor cell’s production of its own growth factors such as granulocyte-colony stimulating factor (G-CSF) and a number of different cytokines. These reactions may at first be mistaken for infectious processes, and it is only after an infection has been ruled out or when a leukocytosis is disproportionately high in the setting of a treated infection, that a paraneoplastic leukemoid reaction (PLR) is considered and an oncologic work-up pursued.
PLR has been previously described in a variety of malignancies including lung, esophageal, nasopharyngeal and laryngeal, gastric, cholangiocarcinoma, melanoma, multiple myeloma, renal, prostate, and hepatocellular carcinoma, but has rarely been described in urothelial carcinoma.1 Leukemoid reactions and autocrine growth induced by paraneoplastic production of G-CSF have rarely been associated with urothelial carcinoma of the bladder,2 as in the case we present here of a 67-year-old white man with invasive high-grade urothelial carcinoma of the bladder. The case highlights PLR as a negative prognostic marker, secondary to urothelial bladder cancer cells’ presumed production of G-CSF, rarely reported as in the literature previously.
Case presentation and summary
A 67-year-old white man was diagnosed with clinical stage III (T3N0M0), invasive high-grade urothelial carcinoma of the bladder (Figure 1). He received neoadjuvant chemotherapy with the standard gemcitabine-cisplatin combination (1,000 mg/m2 of gemcitabine on days 1, 8, and 15 with 70 mg/m2 of cisplatin on day 1 of a 28-day cycle for 3 cycles), and had less than partial response at the end of a 3-month course. A computed tomography scan of his pelvis obtained at treatment completion revealed persistent disease with noted enhancement of the right distal ureter and a right posterior bladder mass at the ureterovesical junction measuring 1.7 x 2.6 x 2.6 cm (0.6 x 1 x 1 in), for which, a cystoprostatectomy was recommended to remove remaining disease. The patient was seen in routine follow-up 3 weeks after his last chemotherapy treatment, when his WBC count was noted to be within normal limits at a value of 8.4 x 103 cells/mm³ (normal range, 4.5-11 x 103 cells/mm³).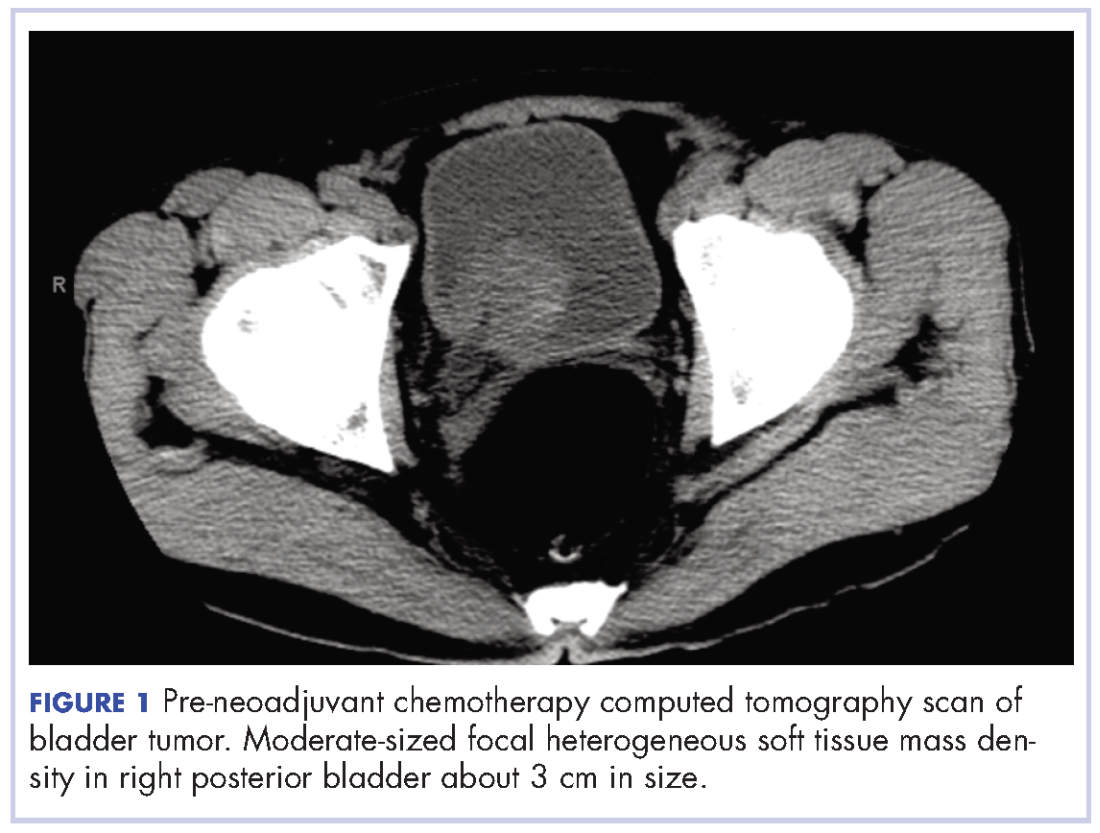
One week later (a month after treatment completion), the patient presented to the emergency department with complaints of dysuria, urinary frequency, and suprapubic pain. He was found to have leukocytosis, with a WBC count of 47 x 103 cells/mm³, (normal range, 4.5-11 x 103 cells/mm³), with an elevated neutrophil count of 82.7% (normal range 40%-60%), without clinical signs of systemic infection (fevers, chills, or rigors). A urinalysis revealed pyuria with 25-50 WBC/high power field, negative nitrite, positive leukocyte esterase, and moderate bacteria, consistent with what was presumed to be a urinary tract infection. The patient was discharged home with a 1-week course of the antibiotic levofloxacin and the alpha-blocker tamsulosin to make urination easier. Of note, the final results of the urine culture, which returned 48 hours after discharge, showed no growth.
One week prior to surgery, the patient underwent a cystoscopy for ureteral stent exchange, which revealed a necrotic tumor at the right bladder base surrounding the ureteral orifice and stent. Renal pelvis urine, sampled during stent exchange, revealed >100,000 CFU/ml (colony forming units; normal value, <10³) Candida albicans, for which the patient was started on intravenous fluconazole for fungal infection. We consulted with our colleagues in the infectious disease department and continued to follow the patient throughout his hospital course, which included several antibiotic regimens, a comprehensive hematological work-up and eventual urologic surgery. Work-ups for myeloproliferative disorders, leukemia, JAK-2, and BCR-ABL were all negative. A peripheral blood smear analysis showed mostly neutrophils, no immature cells, and occasional hypersegmented neutrophils, but was overall inconsistent with myeloproliferative disease. Despite the patient’s persistent leukocytosis, he remained completely asymptomatic and his neutrophilia was attributed to his malignancy.
The patient subsequently underwent a cystoprostatectomy with ileal conduit. The surgical pathologic analysis showed a high-grade, invasive urothelial (transitional cell) carcinoma measuring 5.2 x 5.0 x 4.5 cm (2 x 1.9 x 1.8 in) with squamous differentiation, extensive tumor necrosis, lymphovascular invasion, invasion into the adjacent seminal vesicle and prostatic stroma, and negative margins (pT4a pN0 pMX; Figure 2). On the day of surgical resection, the patient’s leukocytosis was 70 x 103 cells/mm³.
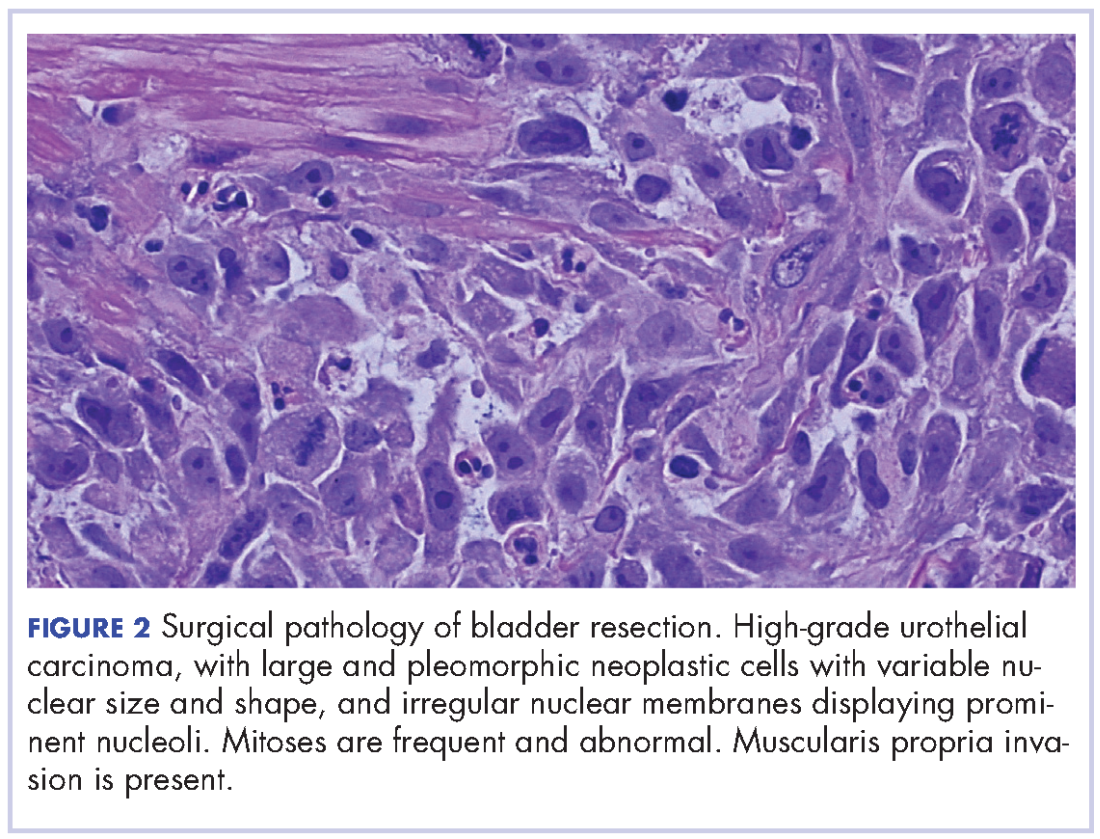
Despite a transient improvement in his leukocytosis to 37.7 x 103 cells/mm³ on postoperative day 1, the patient remained in the medical intensive care unit for uncontrolled pain and management of his leukocytosis. It is worth noting that the patient remained afebrile throughout his entire 45-day hospitalization, with negative culture data, and despite receiving an extensive broad spectrum antibiotic regimen (levofloxacin, piperacillin-tazobactam, cefazolin, metronidazole, ceftriaxone and fluconazole), his leukocytosis continued to progress, peaking at 161.5 x 103 cells/mm³ less than a month after his surgery (Figure 3).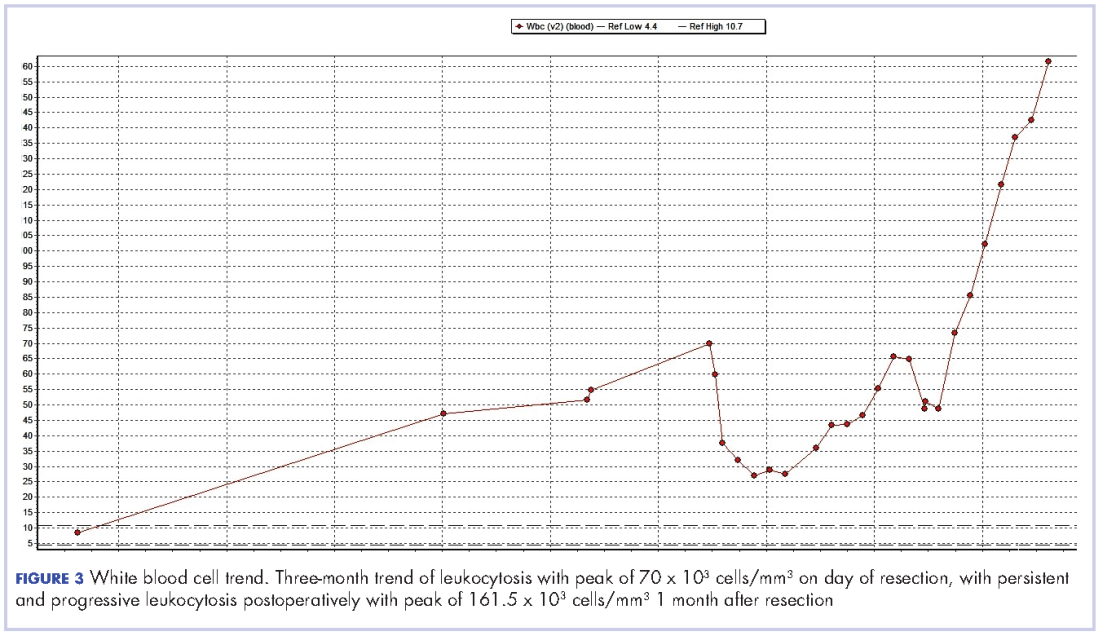
The patient continued to deteriorate rapidly, with a progressive leukocytosis, and developing metastases to the lung, perineum, and penis. He died a month after surgery (2 months after completion of neoadjuvant chemotherapy). The leukocytosis exhibited in this patient and the aggressive tumor cell growth are believed to have been secondary to a paraneoplastic leukemoid reaction incited by the urothelial bladder cancer cells’ presumed production of G-CSF, which has been rarely reported in the literature previously.
Discussion
We report here on the rare occurrence of PLR in a urothelial bladder cancer. Several mechanisms have been proposed to explain the pathophysiology of PLR. The levels of IL-1[alpha and beta], IL-3, G-CSF, GM-CSF, IL-6, and TNF-[alpha] have all been reported to be elevated in various solid tumors and suggested to contribute to an elevated leukocyte count.3 With previous reports that receptors for G-CSF have been found on cell surfaces of several nonhematopoietic cell types, Tachibana and Murai have proposed the mechanism of a cancer cell’s simultaneous acquisition of the ligand promotion and its receptor expression conferring an autocrine growth advantage.4 They have also reported on the capability of bladder cancer cells to induce a leukemoid reaction in their host through the stimulation of leukocyte production, which has been associated with aggressive tumor cell growth and a poor clinical outcome. In addition, He and colleagues have also described the correlation between PLR and high degree of malignancy, high probability of metastasis, recurrence, and poor prognosis.5
We observed the leukocytosis of 70 x 103 cells/mm³ on the day of resection with a slight drop postoperatively, peaking at 161.5 x 103 cells/mm³ less than a month after resection of the tumor. There is no clear understanding of the cause of the persistent and rapid progression of leukocytosis seen in this patient postoperatively. There is also a dearth of literature describing similar occurrences, with even fewer attempting to explain the pathophysiology of this occurrence.
When faced with similar occurrences in patients, clinicians usually treat for occult infection. Once infections and myeloproliferative diseases have been ruled out, clinicians may consider obtaining a patient’s serum G-CSF level or performing an immunohistochemistry analysis of urothelial cells for overexpression of G-CSF, when available.5 However, despite any efforts to diagnose earlier, there is little clinicians currently have to offer these patients as treatment.
As presented in this report, PLR portends a worse prognosis for patients because of its ability to not only masquerade as an infection leading to a delay in the proper treatment, but also because of its association with a more aggressive tumor cell behavior and growth, making it critically important for clinicians to be able to identify these patients early on. With further investigation into immune regulation and G-CSF receptor signaling, there may be future discoveries of novel methods to diagnose this condition and also advancements in the treatment options made available to these patients.
1. Chakraborty S, Keenportz B, Woodward S, Anderson J, Colan D. Paraneoplastic leukemoid reaction in solid tumors. Am J Clin Oncol. 2015;38(3):326-330.
2. Kumar AK, Satyan MT, Holzbeierlein J, Mirza M, Van Veldhuizen P. Leukemoid reaction and autocrine growth of bladder cancer induced by paraneoplastic production of granulocyte colony-stimulating factor-a potential neoplastic marker: a case report and review of the literature. J Med Case Rep. 2014;8(1):147.
3. Azuma T, Sakai I, Matsumoto T, et al. Leukemoid reaction in association with bone marrow necrosis due to metastatic prostate cancer. Intern Med. 2005;44(10):1093-1096.
4. Tachibana M, Murai M. G-CSF production in human bladder cancer and its ability to promote autocrine growth: a review. Cytokines Cell Mol Ther. 1998;4(2):113-120.
5. He H, Zhang Z, Ge J, Zhou W. Leukemoid reaction associated with transitional cell carcinoma: a case report and literature review. Niger J Clin Pract. 2014;17(3):391-394.
Certain cancers have been observed to cause symptoms called paraneoplastic syndromes that are not directly attributed to tumor invasion or compression. This phenomenon is believed to be secondary to a tumor’s secretion of functional hormones, peptides, cytokines, or its immune cross-reactivity. One such variant is a paraneoplastic leukemoid reaction (PLR), defined as a leukocytosis level of >50 x 103 cells/mm³, where the white blood cell (WBC) count differential exhibits a neutrophilia or left-shift, in which a predominance of early neutrophil precursors is observed. A PLR is believed to be incited by the tumor cell’s production of its own growth factors such as granulocyte-colony stimulating factor (G-CSF) and a number of different cytokines. These reactions may at first be mistaken for infectious processes, and it is only after an infection has been ruled out or when a leukocytosis is disproportionately high in the setting of a treated infection, that a paraneoplastic leukemoid reaction (PLR) is considered and an oncologic work-up pursued.
PLR has been previously described in a variety of malignancies including lung, esophageal, nasopharyngeal and laryngeal, gastric, cholangiocarcinoma, melanoma, multiple myeloma, renal, prostate, and hepatocellular carcinoma, but has rarely been described in urothelial carcinoma.1 Leukemoid reactions and autocrine growth induced by paraneoplastic production of G-CSF have rarely been associated with urothelial carcinoma of the bladder,2 as in the case we present here of a 67-year-old white man with invasive high-grade urothelial carcinoma of the bladder. The case highlights PLR as a negative prognostic marker, secondary to urothelial bladder cancer cells’ presumed production of G-CSF, rarely reported as in the literature previously.
Case presentation and summary
A 67-year-old white man was diagnosed with clinical stage III (T3N0M0), invasive high-grade urothelial carcinoma of the bladder (Figure 1). He received neoadjuvant chemotherapy with the standard gemcitabine-cisplatin combination (1,000 mg/m2 of gemcitabine on days 1, 8, and 15 with 70 mg/m2 of cisplatin on day 1 of a 28-day cycle for 3 cycles), and had less than partial response at the end of a 3-month course. A computed tomography scan of his pelvis obtained at treatment completion revealed persistent disease with noted enhancement of the right distal ureter and a right posterior bladder mass at the ureterovesical junction measuring 1.7 x 2.6 x 2.6 cm (0.6 x 1 x 1 in), for which, a cystoprostatectomy was recommended to remove remaining disease. The patient was seen in routine follow-up 3 weeks after his last chemotherapy treatment, when his WBC count was noted to be within normal limits at a value of 8.4 x 103 cells/mm³ (normal range, 4.5-11 x 103 cells/mm³).
One week later (a month after treatment completion), the patient presented to the emergency department with complaints of dysuria, urinary frequency, and suprapubic pain. He was found to have leukocytosis, with a WBC count of 47 x 103 cells/mm³, (normal range, 4.5-11 x 103 cells/mm³), with an elevated neutrophil count of 82.7% (normal range 40%-60%), without clinical signs of systemic infection (fevers, chills, or rigors). A urinalysis revealed pyuria with 25-50 WBC/high power field, negative nitrite, positive leukocyte esterase, and moderate bacteria, consistent with what was presumed to be a urinary tract infection. The patient was discharged home with a 1-week course of the antibiotic levofloxacin and the alpha-blocker tamsulosin to make urination easier. Of note, the final results of the urine culture, which returned 48 hours after discharge, showed no growth.
One week prior to surgery, the patient underwent a cystoscopy for ureteral stent exchange, which revealed a necrotic tumor at the right bladder base surrounding the ureteral orifice and stent. Renal pelvis urine, sampled during stent exchange, revealed >100,000 CFU/ml (colony forming units; normal value, <10³) Candida albicans, for which the patient was started on intravenous fluconazole for fungal infection. We consulted with our colleagues in the infectious disease department and continued to follow the patient throughout his hospital course, which included several antibiotic regimens, a comprehensive hematological work-up and eventual urologic surgery. Work-ups for myeloproliferative disorders, leukemia, JAK-2, and BCR-ABL were all negative. A peripheral blood smear analysis showed mostly neutrophils, no immature cells, and occasional hypersegmented neutrophils, but was overall inconsistent with myeloproliferative disease. Despite the patient’s persistent leukocytosis, he remained completely asymptomatic and his neutrophilia was attributed to his malignancy.
The patient subsequently underwent a cystoprostatectomy with ileal conduit. The surgical pathologic analysis showed a high-grade, invasive urothelial (transitional cell) carcinoma measuring 5.2 x 5.0 x 4.5 cm (2 x 1.9 x 1.8 in) with squamous differentiation, extensive tumor necrosis, lymphovascular invasion, invasion into the adjacent seminal vesicle and prostatic stroma, and negative margins (pT4a pN0 pMX; Figure 2). On the day of surgical resection, the patient’s leukocytosis was 70 x 103 cells/mm³.
Despite a transient improvement in his leukocytosis to 37.7 x 103 cells/mm³ on postoperative day 1, the patient remained in the medical intensive care unit for uncontrolled pain and management of his leukocytosis. It is worth noting that the patient remained afebrile throughout his entire 45-day hospitalization, with negative culture data, and despite receiving an extensive broad spectrum antibiotic regimen (levofloxacin, piperacillin-tazobactam, cefazolin, metronidazole, ceftriaxone and fluconazole), his leukocytosis continued to progress, peaking at 161.5 x 103 cells/mm³ less than a month after his surgery (Figure 3).
The patient continued to deteriorate rapidly, with a progressive leukocytosis, and developing metastases to the lung, perineum, and penis. He died a month after surgery (2 months after completion of neoadjuvant chemotherapy). The leukocytosis exhibited in this patient and the aggressive tumor cell growth are believed to have been secondary to a paraneoplastic leukemoid reaction incited by the urothelial bladder cancer cells’ presumed production of G-CSF, which has been rarely reported in the literature previously.
Discussion
We report here on the rare occurrence of PLR in a urothelial bladder cancer. Several mechanisms have been proposed to explain the pathophysiology of PLR. The levels of IL-1[alpha and beta], IL-3, G-CSF, GM-CSF, IL-6, and TNF-[alpha] have all been reported to be elevated in various solid tumors and suggested to contribute to an elevated leukocyte count.3 With previous reports that receptors for G-CSF have been found on cell surfaces of several nonhematopoietic cell types, Tachibana and Murai have proposed the mechanism of a cancer cell’s simultaneous acquisition of the ligand promotion and its receptor expression conferring an autocrine growth advantage.4 They have also reported on the capability of bladder cancer cells to induce a leukemoid reaction in their host through the stimulation of leukocyte production, which has been associated with aggressive tumor cell growth and a poor clinical outcome. In addition, He and colleagues have also described the correlation between PLR and high degree of malignancy, high probability of metastasis, recurrence, and poor prognosis.5
We observed the leukocytosis of 70 x 103 cells/mm³ on the day of resection with a slight drop postoperatively, peaking at 161.5 x 103 cells/mm³ less than a month after resection of the tumor. There is no clear understanding of the cause of the persistent and rapid progression of leukocytosis seen in this patient postoperatively. There is also a dearth of literature describing similar occurrences, with even fewer attempting to explain the pathophysiology of this occurrence.
When faced with similar occurrences in patients, clinicians usually treat for occult infection. Once infections and myeloproliferative diseases have been ruled out, clinicians may consider obtaining a patient’s serum G-CSF level or performing an immunohistochemistry analysis of urothelial cells for overexpression of G-CSF, when available.5 However, despite any efforts to diagnose earlier, there is little clinicians currently have to offer these patients as treatment.
As presented in this report, PLR portends a worse prognosis for patients because of its ability to not only masquerade as an infection leading to a delay in the proper treatment, but also because of its association with a more aggressive tumor cell behavior and growth, making it critically important for clinicians to be able to identify these patients early on. With further investigation into immune regulation and G-CSF receptor signaling, there may be future discoveries of novel methods to diagnose this condition and also advancements in the treatment options made available to these patients.
Certain cancers have been observed to cause symptoms called paraneoplastic syndromes that are not directly attributed to tumor invasion or compression. This phenomenon is believed to be secondary to a tumor’s secretion of functional hormones, peptides, cytokines, or its immune cross-reactivity. One such variant is a paraneoplastic leukemoid reaction (PLR), defined as a leukocytosis level of >50 x 103 cells/mm³, where the white blood cell (WBC) count differential exhibits a neutrophilia or left-shift, in which a predominance of early neutrophil precursors is observed. A PLR is believed to be incited by the tumor cell’s production of its own growth factors such as granulocyte-colony stimulating factor (G-CSF) and a number of different cytokines. These reactions may at first be mistaken for infectious processes, and it is only after an infection has been ruled out or when a leukocytosis is disproportionately high in the setting of a treated infection, that a paraneoplastic leukemoid reaction (PLR) is considered and an oncologic work-up pursued.
PLR has been previously described in a variety of malignancies including lung, esophageal, nasopharyngeal and laryngeal, gastric, cholangiocarcinoma, melanoma, multiple myeloma, renal, prostate, and hepatocellular carcinoma, but has rarely been described in urothelial carcinoma.1 Leukemoid reactions and autocrine growth induced by paraneoplastic production of G-CSF have rarely been associated with urothelial carcinoma of the bladder,2 as in the case we present here of a 67-year-old white man with invasive high-grade urothelial carcinoma of the bladder. The case highlights PLR as a negative prognostic marker, secondary to urothelial bladder cancer cells’ presumed production of G-CSF, rarely reported as in the literature previously.
Case presentation and summary
A 67-year-old white man was diagnosed with clinical stage III (T3N0M0), invasive high-grade urothelial carcinoma of the bladder (Figure 1). He received neoadjuvant chemotherapy with the standard gemcitabine-cisplatin combination (1,000 mg/m2 of gemcitabine on days 1, 8, and 15 with 70 mg/m2 of cisplatin on day 1 of a 28-day cycle for 3 cycles), and had less than partial response at the end of a 3-month course. A computed tomography scan of his pelvis obtained at treatment completion revealed persistent disease with noted enhancement of the right distal ureter and a right posterior bladder mass at the ureterovesical junction measuring 1.7 x 2.6 x 2.6 cm (0.6 x 1 x 1 in), for which, a cystoprostatectomy was recommended to remove remaining disease. The patient was seen in routine follow-up 3 weeks after his last chemotherapy treatment, when his WBC count was noted to be within normal limits at a value of 8.4 x 103 cells/mm³ (normal range, 4.5-11 x 103 cells/mm³).
One week later (a month after treatment completion), the patient presented to the emergency department with complaints of dysuria, urinary frequency, and suprapubic pain. He was found to have leukocytosis, with a WBC count of 47 x 103 cells/mm³, (normal range, 4.5-11 x 103 cells/mm³), with an elevated neutrophil count of 82.7% (normal range 40%-60%), without clinical signs of systemic infection (fevers, chills, or rigors). A urinalysis revealed pyuria with 25-50 WBC/high power field, negative nitrite, positive leukocyte esterase, and moderate bacteria, consistent with what was presumed to be a urinary tract infection. The patient was discharged home with a 1-week course of the antibiotic levofloxacin and the alpha-blocker tamsulosin to make urination easier. Of note, the final results of the urine culture, which returned 48 hours after discharge, showed no growth.
One week prior to surgery, the patient underwent a cystoscopy for ureteral stent exchange, which revealed a necrotic tumor at the right bladder base surrounding the ureteral orifice and stent. Renal pelvis urine, sampled during stent exchange, revealed >100,000 CFU/ml (colony forming units; normal value, <10³) Candida albicans, for which the patient was started on intravenous fluconazole for fungal infection. We consulted with our colleagues in the infectious disease department and continued to follow the patient throughout his hospital course, which included several antibiotic regimens, a comprehensive hematological work-up and eventual urologic surgery. Work-ups for myeloproliferative disorders, leukemia, JAK-2, and BCR-ABL were all negative. A peripheral blood smear analysis showed mostly neutrophils, no immature cells, and occasional hypersegmented neutrophils, but was overall inconsistent with myeloproliferative disease. Despite the patient’s persistent leukocytosis, he remained completely asymptomatic and his neutrophilia was attributed to his malignancy.
The patient subsequently underwent a cystoprostatectomy with ileal conduit. The surgical pathologic analysis showed a high-grade, invasive urothelial (transitional cell) carcinoma measuring 5.2 x 5.0 x 4.5 cm (2 x 1.9 x 1.8 in) with squamous differentiation, extensive tumor necrosis, lymphovascular invasion, invasion into the adjacent seminal vesicle and prostatic stroma, and negative margins (pT4a pN0 pMX; Figure 2). On the day of surgical resection, the patient’s leukocytosis was 70 x 103 cells/mm³.
Despite a transient improvement in his leukocytosis to 37.7 x 103 cells/mm³ on postoperative day 1, the patient remained in the medical intensive care unit for uncontrolled pain and management of his leukocytosis. It is worth noting that the patient remained afebrile throughout his entire 45-day hospitalization, with negative culture data, and despite receiving an extensive broad spectrum antibiotic regimen (levofloxacin, piperacillin-tazobactam, cefazolin, metronidazole, ceftriaxone and fluconazole), his leukocytosis continued to progress, peaking at 161.5 x 103 cells/mm³ less than a month after his surgery (Figure 3).
The patient continued to deteriorate rapidly, with a progressive leukocytosis, and developing metastases to the lung, perineum, and penis. He died a month after surgery (2 months after completion of neoadjuvant chemotherapy). The leukocytosis exhibited in this patient and the aggressive tumor cell growth are believed to have been secondary to a paraneoplastic leukemoid reaction incited by the urothelial bladder cancer cells’ presumed production of G-CSF, which has been rarely reported in the literature previously.
Discussion
We report here on the rare occurrence of PLR in a urothelial bladder cancer. Several mechanisms have been proposed to explain the pathophysiology of PLR. The levels of IL-1[alpha and beta], IL-3, G-CSF, GM-CSF, IL-6, and TNF-[alpha] have all been reported to be elevated in various solid tumors and suggested to contribute to an elevated leukocyte count.3 With previous reports that receptors for G-CSF have been found on cell surfaces of several nonhematopoietic cell types, Tachibana and Murai have proposed the mechanism of a cancer cell’s simultaneous acquisition of the ligand promotion and its receptor expression conferring an autocrine growth advantage.4 They have also reported on the capability of bladder cancer cells to induce a leukemoid reaction in their host through the stimulation of leukocyte production, which has been associated with aggressive tumor cell growth and a poor clinical outcome. In addition, He and colleagues have also described the correlation between PLR and high degree of malignancy, high probability of metastasis, recurrence, and poor prognosis.5
We observed the leukocytosis of 70 x 103 cells/mm³ on the day of resection with a slight drop postoperatively, peaking at 161.5 x 103 cells/mm³ less than a month after resection of the tumor. There is no clear understanding of the cause of the persistent and rapid progression of leukocytosis seen in this patient postoperatively. There is also a dearth of literature describing similar occurrences, with even fewer attempting to explain the pathophysiology of this occurrence.
When faced with similar occurrences in patients, clinicians usually treat for occult infection. Once infections and myeloproliferative diseases have been ruled out, clinicians may consider obtaining a patient’s serum G-CSF level or performing an immunohistochemistry analysis of urothelial cells for overexpression of G-CSF, when available.5 However, despite any efforts to diagnose earlier, there is little clinicians currently have to offer these patients as treatment.
As presented in this report, PLR portends a worse prognosis for patients because of its ability to not only masquerade as an infection leading to a delay in the proper treatment, but also because of its association with a more aggressive tumor cell behavior and growth, making it critically important for clinicians to be able to identify these patients early on. With further investigation into immune regulation and G-CSF receptor signaling, there may be future discoveries of novel methods to diagnose this condition and also advancements in the treatment options made available to these patients.
1. Chakraborty S, Keenportz B, Woodward S, Anderson J, Colan D. Paraneoplastic leukemoid reaction in solid tumors. Am J Clin Oncol. 2015;38(3):326-330.
2. Kumar AK, Satyan MT, Holzbeierlein J, Mirza M, Van Veldhuizen P. Leukemoid reaction and autocrine growth of bladder cancer induced by paraneoplastic production of granulocyte colony-stimulating factor-a potential neoplastic marker: a case report and review of the literature. J Med Case Rep. 2014;8(1):147.
3. Azuma T, Sakai I, Matsumoto T, et al. Leukemoid reaction in association with bone marrow necrosis due to metastatic prostate cancer. Intern Med. 2005;44(10):1093-1096.
4. Tachibana M, Murai M. G-CSF production in human bladder cancer and its ability to promote autocrine growth: a review. Cytokines Cell Mol Ther. 1998;4(2):113-120.
5. He H, Zhang Z, Ge J, Zhou W. Leukemoid reaction associated with transitional cell carcinoma: a case report and literature review. Niger J Clin Pract. 2014;17(3):391-394.
1. Chakraborty S, Keenportz B, Woodward S, Anderson J, Colan D. Paraneoplastic leukemoid reaction in solid tumors. Am J Clin Oncol. 2015;38(3):326-330.
2. Kumar AK, Satyan MT, Holzbeierlein J, Mirza M, Van Veldhuizen P. Leukemoid reaction and autocrine growth of bladder cancer induced by paraneoplastic production of granulocyte colony-stimulating factor-a potential neoplastic marker: a case report and review of the literature. J Med Case Rep. 2014;8(1):147.
3. Azuma T, Sakai I, Matsumoto T, et al. Leukemoid reaction in association with bone marrow necrosis due to metastatic prostate cancer. Intern Med. 2005;44(10):1093-1096.
4. Tachibana M, Murai M. G-CSF production in human bladder cancer and its ability to promote autocrine growth: a review. Cytokines Cell Mol Ther. 1998;4(2):113-120.
5. He H, Zhang Z, Ge J, Zhou W. Leukemoid reaction associated with transitional cell carcinoma: a case report and literature review. Niger J Clin Pract. 2014;17(3):391-394.
Three factors linked to rhinovirus pneumonia in HCT patients
ORLANDO – For patients who have received hematopoietic cell transplants, a rhinovirus infection can become much more than a cold.
“It holds true that rhinovirus is just as likely to be associated with mortality as are other respiratory viruses” among HCT recipients, Alpana Waghmare, MD, said at the combined annual meetings of the Center for International Blood & Marrow Transplant Research and the American Society for Blood and Marrow Transplantation.
In a new retrospective study, Dr. Waghmare and her coinvestigators found that the median time for a rhinovirus infection to progress from an upper to a lower respiratory tract infection was about 2 weeks among post-HCT patients.
Clinical and demographic risk factors for progression to lower respiratory tract infection included higher levels of steroid use (2 mg/kg per day or more) before developing the upper respiratory infection, a low white blood cell count, and a low monocyte count, said Dr. Waghmare, an infectious disease specialist and professor of pediatrics at the University of Washington, Seattle.
Of 3,445 HCT patients treated at the university center during the 6-year study, 732 patients (21%) were positive for human rhinovirus. Patients were classified as having upper respiratory infections if they had a PCR-positive nasal swab.
Patients were classed in one of three categories for potential lower respiratory infections: Proven lower respiratory infections were those detected by bronchoalveolar lavage or biopsy in patients who had a new radiographic abnormality. Probable lower respiratory infections were those with positive findings on bronchoalveolar lavage or biopsy but without radiographic changes. In possible lower respiratory infections, patients had upper tract virus detected on nasal swabs but did have a new radiographic abnormality.
Among the patients positive for human rhinovirus, 85% (665 patients) presented with upper respiratory infections and 15% (117 patients) with lower respiratory tract infections. By day 90, 16% of patients progressed from upper to lower respiratory tract infections. The median time to progression was 13.5 days. Progression to proven lower respiratory tract infection affected 5% of the HCT recipients.
In multivariable analytic models, a minimum white blood cell count of 1,000 or less was associated with a hazard ratio (HR) of 2.21 for progression to lower respiratory tract infection. A minimum monocyte count of 1,000 or less was associated with a HR of 3.66 for progression to lower respiratory tract infection.
The model also found a HR of 3.37 for lower respiratory tract infection with steroid use of 2 mg/kg per day or more. The patient’s conditioning regimen and donor type were not significantly associated with risk of progression to lower respiratory infection.
Viral copathogens, prior respiratory virus episodes, and the duration of time since HCT were not associated with risk of progress to lower respiratory infections. Neither were patient age, baseline lung function, and the year the transplant occurred.
“These data provide an initial framework for patient risk stratification and the development of rational prevention and treatment strategies in HCT recipients,” she said.
Dr. Waghmare reported receiving research funding from Aviragen, the maker of vapendavir, an investigational drug for human rhinovirus infection, and Gilead Sciences.
[email protected]
On Twitter @karioakes
ORLANDO – For patients who have received hematopoietic cell transplants, a rhinovirus infection can become much more than a cold.
“It holds true that rhinovirus is just as likely to be associated with mortality as are other respiratory viruses” among HCT recipients, Alpana Waghmare, MD, said at the combined annual meetings of the Center for International Blood & Marrow Transplant Research and the American Society for Blood and Marrow Transplantation.
In a new retrospective study, Dr. Waghmare and her coinvestigators found that the median time for a rhinovirus infection to progress from an upper to a lower respiratory tract infection was about 2 weeks among post-HCT patients.
Clinical and demographic risk factors for progression to lower respiratory tract infection included higher levels of steroid use (2 mg/kg per day or more) before developing the upper respiratory infection, a low white blood cell count, and a low monocyte count, said Dr. Waghmare, an infectious disease specialist and professor of pediatrics at the University of Washington, Seattle.
Of 3,445 HCT patients treated at the university center during the 6-year study, 732 patients (21%) were positive for human rhinovirus. Patients were classified as having upper respiratory infections if they had a PCR-positive nasal swab.
Patients were classed in one of three categories for potential lower respiratory infections: Proven lower respiratory infections were those detected by bronchoalveolar lavage or biopsy in patients who had a new radiographic abnormality. Probable lower respiratory infections were those with positive findings on bronchoalveolar lavage or biopsy but without radiographic changes. In possible lower respiratory infections, patients had upper tract virus detected on nasal swabs but did have a new radiographic abnormality.
Among the patients positive for human rhinovirus, 85% (665 patients) presented with upper respiratory infections and 15% (117 patients) with lower respiratory tract infections. By day 90, 16% of patients progressed from upper to lower respiratory tract infections. The median time to progression was 13.5 days. Progression to proven lower respiratory tract infection affected 5% of the HCT recipients.
In multivariable analytic models, a minimum white blood cell count of 1,000 or less was associated with a hazard ratio (HR) of 2.21 for progression to lower respiratory tract infection. A minimum monocyte count of 1,000 or less was associated with a HR of 3.66 for progression to lower respiratory tract infection.
The model also found a HR of 3.37 for lower respiratory tract infection with steroid use of 2 mg/kg per day or more. The patient’s conditioning regimen and donor type were not significantly associated with risk of progression to lower respiratory infection.
Viral copathogens, prior respiratory virus episodes, and the duration of time since HCT were not associated with risk of progress to lower respiratory infections. Neither were patient age, baseline lung function, and the year the transplant occurred.
“These data provide an initial framework for patient risk stratification and the development of rational prevention and treatment strategies in HCT recipients,” she said.
Dr. Waghmare reported receiving research funding from Aviragen, the maker of vapendavir, an investigational drug for human rhinovirus infection, and Gilead Sciences.
[email protected]
On Twitter @karioakes
ORLANDO – For patients who have received hematopoietic cell transplants, a rhinovirus infection can become much more than a cold.
“It holds true that rhinovirus is just as likely to be associated with mortality as are other respiratory viruses” among HCT recipients, Alpana Waghmare, MD, said at the combined annual meetings of the Center for International Blood & Marrow Transplant Research and the American Society for Blood and Marrow Transplantation.
In a new retrospective study, Dr. Waghmare and her coinvestigators found that the median time for a rhinovirus infection to progress from an upper to a lower respiratory tract infection was about 2 weeks among post-HCT patients.
Clinical and demographic risk factors for progression to lower respiratory tract infection included higher levels of steroid use (2 mg/kg per day or more) before developing the upper respiratory infection, a low white blood cell count, and a low monocyte count, said Dr. Waghmare, an infectious disease specialist and professor of pediatrics at the University of Washington, Seattle.
Of 3,445 HCT patients treated at the university center during the 6-year study, 732 patients (21%) were positive for human rhinovirus. Patients were classified as having upper respiratory infections if they had a PCR-positive nasal swab.
Patients were classed in one of three categories for potential lower respiratory infections: Proven lower respiratory infections were those detected by bronchoalveolar lavage or biopsy in patients who had a new radiographic abnormality. Probable lower respiratory infections were those with positive findings on bronchoalveolar lavage or biopsy but without radiographic changes. In possible lower respiratory infections, patients had upper tract virus detected on nasal swabs but did have a new radiographic abnormality.
Among the patients positive for human rhinovirus, 85% (665 patients) presented with upper respiratory infections and 15% (117 patients) with lower respiratory tract infections. By day 90, 16% of patients progressed from upper to lower respiratory tract infections. The median time to progression was 13.5 days. Progression to proven lower respiratory tract infection affected 5% of the HCT recipients.
In multivariable analytic models, a minimum white blood cell count of 1,000 or less was associated with a hazard ratio (HR) of 2.21 for progression to lower respiratory tract infection. A minimum monocyte count of 1,000 or less was associated with a HR of 3.66 for progression to lower respiratory tract infection.
The model also found a HR of 3.37 for lower respiratory tract infection with steroid use of 2 mg/kg per day or more. The patient’s conditioning regimen and donor type were not significantly associated with risk of progression to lower respiratory infection.
Viral copathogens, prior respiratory virus episodes, and the duration of time since HCT were not associated with risk of progress to lower respiratory infections. Neither were patient age, baseline lung function, and the year the transplant occurred.
“These data provide an initial framework for patient risk stratification and the development of rational prevention and treatment strategies in HCT recipients,” she said.
Dr. Waghmare reported receiving research funding from Aviragen, the maker of vapendavir, an investigational drug for human rhinovirus infection, and Gilead Sciences.
[email protected]
On Twitter @karioakes
AT THE BMT TANDEM MEETINGS
Key clinical point:
Major finding: Of 3,445 HCT patients, 732 patients (21%) were positive for human rhinovirus.
Data source: Single-center, 6-year retrospective study of 732 HCT patients with human rhinovirus infection.
Disclosures: Dr. Waghmare reported receiving research funding from Aviragen, the maker of vapendavir, an investigational drug for human rhinovirus infection, and Gilead Sciences.