User login
For MD-IQ use only
Burnout
Having taken the SVS “burnout” survey, I felt that it really never got into the “whys” of what was making individuals burn out. It dealt more with the consequences of the whys rather than the whys themselves, and it is these whys that must be addressed to assist in the prevention of burnout. I would like to comment on my experience of some, certainly not all, of the possible whys related to both inherent stressors and “administrator induced stressors” encountered in my 42-year vascular surgery practice that can easily cause burnout.

I believe there are several major areas that need to be evaluated to understand the causes of burnout because the complexities of today’s practice environment demand a different approach to the practice of vascular surgery for the well-being of the vascular surgeon. These complexities include the emotional baggage inherent in a practice, practice structure, unpredictable time management issues of running a practice, and hospital administration’s decisions creating unintended consequences for the vascular surgeon.
By its very nature, vascular surgery is a difficult field with many inherent stressors, endovascular innovations not withstanding. The initial emotional stressors may well be those of dealing with elderly patients with multiple severe comorbidities, poor outcomes, and the ensuing consequences. With the aging of the population, these stressors will only increase, yet compensation to treat these feeble patients has yet to rise to a level commensurate with the risk factors and complications the surgeon must deal with. Over time this will take its toll on some.
Which practice pattern one chooses to utilize – solo, group, or employed – also plays an important part. The presence or absence of appropriate help and backup for difficult cases, call coverage, and partnership financial packages can be either very stress producing or stress relieving. Are practice responsibilities and finances equally split so as to achieve a reasonable lifestyle, or is there a hierarchy of work and financial gain by which some must shoulder more of the burden for less pay than others? This is the beginning of the income versus lifestyle conflict and becomes a seriously stressful trap when one is short sighted and does not go for the long term. In our practice, we rotate the work and split the gain equally in return for the most valuable commodity of all: free time.
Time management is of paramount importance in completing a schedule, yet the paradox of the vascular world is its inherent unpredictability. There are difficult, time-consuming cases; unexpected, recurrent vascular problems in the same patient; urgent consults needing treatment within a few days; and the inevitable emergency room call for immediate treatment, day or night, for an embolism, vascular trauma, or ruptured aneurysm – not to mention the hospital committees or other responsibilities in the everyday life of a vascular surgeon.
One’s schedule requires dedicated time and attention yet the urgent/emergent issues interrupting one’s daily schedule ensures that the only predictability is unpredictability. This is a source of burnout. My experience over the years has been that about 25% of our practice load comes on an urgent to emergent basis, often causing considerable scheduling problems both in the operating room and at the office – again, issues that can cause tremendous stress for many. Without a large group, these constant stressors become difficult to shoulder.
Then there are the hospital-induced stressors caused by poorly conceived administrative decrees. One example is when emergency rooms need vascular services but no contracts are offered to secure these services, in which physicians are merely expected to provide 24/7 services. Once a physician has been called in for a case in the middle of the night, the stress of carrying on the next day becomes greater for that physician unless a system is in place for designated calls, which some larger groups have worked out.
Another example is the tendency to grant interventional privileges to those incapable of treating their operative complications without any consideration for who would reimburse those who come in after and how. Why is it assumed that vascular surgeons would/should take time out of their practice to answer the call without any additional compensation? If the compensation from these service lines is so lucrative, then compensation in the form of contracts needs to be offered to those who can provide the necessary services to treat the inevitable complications. This will in some way help compensate for time lost in the vascular surgeons’ practices.
The contracts should reflect the value to an institution vascular surgeons bring for their presence, including ED coverage for most if not all of the service lines, such as cardiology, radiology, orthopedics, gynecology, and general surgery. This also includes issues arising from the house staff inserting lines and from subsequent renal failure, as well as for angio-access patients who need immediate vascular backup to treat the vascular complications encountered.
In addition, these contracts should acknowledge the revenue generated by the presence of a vascular service line. With the burnout rate and unpredictable lifestyle, one would be concerned that vascular surgeons could be on the endangered species list; and given the current shortage of vascular surgeons, don’t our numbers reflect this concern?
There are no easy solutions because the field is a difficult one and is undercompensated for the risks assumed and services provided, which makes it an unattractive specialty, especially in today’s lifestyle-conscious generation. The vascular specialty is embattled, and the human toll extracted in the field speaks for itself. The rewards must improve to make things more appealing, and this will lead to an increase in the number of vascular surgeons, and more will join in groups to mitigate the effects of the stressors of the field. Until then, vascular surgeons need to demand that they receive fair compensation for their availability and the coverage they provide, which allows many other departments and specialties to function. This reality must be acknowledged and compensated.
Carlo A. Dall’Olmo, MD
Michigan Vascular Center
Flint, Michigan
Having taken the SVS “burnout” survey, I felt that it really never got into the “whys” of what was making individuals burn out. It dealt more with the consequences of the whys rather than the whys themselves, and it is these whys that must be addressed to assist in the prevention of burnout. I would like to comment on my experience of some, certainly not all, of the possible whys related to both inherent stressors and “administrator induced stressors” encountered in my 42-year vascular surgery practice that can easily cause burnout.
I believe there are several major areas that need to be evaluated to understand the causes of burnout because the complexities of today’s practice environment demand a different approach to the practice of vascular surgery for the well-being of the vascular surgeon. These complexities include the emotional baggage inherent in a practice, practice structure, unpredictable time management issues of running a practice, and hospital administration’s decisions creating unintended consequences for the vascular surgeon.
By its very nature, vascular surgery is a difficult field with many inherent stressors, endovascular innovations not withstanding. The initial emotional stressors may well be those of dealing with elderly patients with multiple severe comorbidities, poor outcomes, and the ensuing consequences. With the aging of the population, these stressors will only increase, yet compensation to treat these feeble patients has yet to rise to a level commensurate with the risk factors and complications the surgeon must deal with. Over time this will take its toll on some.
Which practice pattern one chooses to utilize – solo, group, or employed – also plays an important part. The presence or absence of appropriate help and backup for difficult cases, call coverage, and partnership financial packages can be either very stress producing or stress relieving. Are practice responsibilities and finances equally split so as to achieve a reasonable lifestyle, or is there a hierarchy of work and financial gain by which some must shoulder more of the burden for less pay than others? This is the beginning of the income versus lifestyle conflict and becomes a seriously stressful trap when one is short sighted and does not go for the long term. In our practice, we rotate the work and split the gain equally in return for the most valuable commodity of all: free time.
Time management is of paramount importance in completing a schedule, yet the paradox of the vascular world is its inherent unpredictability. There are difficult, time-consuming cases; unexpected, recurrent vascular problems in the same patient; urgent consults needing treatment within a few days; and the inevitable emergency room call for immediate treatment, day or night, for an embolism, vascular trauma, or ruptured aneurysm – not to mention the hospital committees or other responsibilities in the everyday life of a vascular surgeon.
One’s schedule requires dedicated time and attention yet the urgent/emergent issues interrupting one’s daily schedule ensures that the only predictability is unpredictability. This is a source of burnout. My experience over the years has been that about 25% of our practice load comes on an urgent to emergent basis, often causing considerable scheduling problems both in the operating room and at the office – again, issues that can cause tremendous stress for many. Without a large group, these constant stressors become difficult to shoulder.
Then there are the hospital-induced stressors caused by poorly conceived administrative decrees. One example is when emergency rooms need vascular services but no contracts are offered to secure these services, in which physicians are merely expected to provide 24/7 services. Once a physician has been called in for a case in the middle of the night, the stress of carrying on the next day becomes greater for that physician unless a system is in place for designated calls, which some larger groups have worked out.
Another example is the tendency to grant interventional privileges to those incapable of treating their operative complications without any consideration for who would reimburse those who come in after and how. Why is it assumed that vascular surgeons would/should take time out of their practice to answer the call without any additional compensation? If the compensation from these service lines is so lucrative, then compensation in the form of contracts needs to be offered to those who can provide the necessary services to treat the inevitable complications. This will in some way help compensate for time lost in the vascular surgeons’ practices.
The contracts should reflect the value to an institution vascular surgeons bring for their presence, including ED coverage for most if not all of the service lines, such as cardiology, radiology, orthopedics, gynecology, and general surgery. This also includes issues arising from the house staff inserting lines and from subsequent renal failure, as well as for angio-access patients who need immediate vascular backup to treat the vascular complications encountered.
In addition, these contracts should acknowledge the revenue generated by the presence of a vascular service line. With the burnout rate and unpredictable lifestyle, one would be concerned that vascular surgeons could be on the endangered species list; and given the current shortage of vascular surgeons, don’t our numbers reflect this concern?
There are no easy solutions because the field is a difficult one and is undercompensated for the risks assumed and services provided, which makes it an unattractive specialty, especially in today’s lifestyle-conscious generation. The vascular specialty is embattled, and the human toll extracted in the field speaks for itself. The rewards must improve to make things more appealing, and this will lead to an increase in the number of vascular surgeons, and more will join in groups to mitigate the effects of the stressors of the field. Until then, vascular surgeons need to demand that they receive fair compensation for their availability and the coverage they provide, which allows many other departments and specialties to function. This reality must be acknowledged and compensated.
Carlo A. Dall’Olmo, MD
Michigan Vascular Center
Flint, Michigan
Having taken the SVS “burnout” survey, I felt that it really never got into the “whys” of what was making individuals burn out. It dealt more with the consequences of the whys rather than the whys themselves, and it is these whys that must be addressed to assist in the prevention of burnout. I would like to comment on my experience of some, certainly not all, of the possible whys related to both inherent stressors and “administrator induced stressors” encountered in my 42-year vascular surgery practice that can easily cause burnout.
I believe there are several major areas that need to be evaluated to understand the causes of burnout because the complexities of today’s practice environment demand a different approach to the practice of vascular surgery for the well-being of the vascular surgeon. These complexities include the emotional baggage inherent in a practice, practice structure, unpredictable time management issues of running a practice, and hospital administration’s decisions creating unintended consequences for the vascular surgeon.
By its very nature, vascular surgery is a difficult field with many inherent stressors, endovascular innovations not withstanding. The initial emotional stressors may well be those of dealing with elderly patients with multiple severe comorbidities, poor outcomes, and the ensuing consequences. With the aging of the population, these stressors will only increase, yet compensation to treat these feeble patients has yet to rise to a level commensurate with the risk factors and complications the surgeon must deal with. Over time this will take its toll on some.
Which practice pattern one chooses to utilize – solo, group, or employed – also plays an important part. The presence or absence of appropriate help and backup for difficult cases, call coverage, and partnership financial packages can be either very stress producing or stress relieving. Are practice responsibilities and finances equally split so as to achieve a reasonable lifestyle, or is there a hierarchy of work and financial gain by which some must shoulder more of the burden for less pay than others? This is the beginning of the income versus lifestyle conflict and becomes a seriously stressful trap when one is short sighted and does not go for the long term. In our practice, we rotate the work and split the gain equally in return for the most valuable commodity of all: free time.
Time management is of paramount importance in completing a schedule, yet the paradox of the vascular world is its inherent unpredictability. There are difficult, time-consuming cases; unexpected, recurrent vascular problems in the same patient; urgent consults needing treatment within a few days; and the inevitable emergency room call for immediate treatment, day or night, for an embolism, vascular trauma, or ruptured aneurysm – not to mention the hospital committees or other responsibilities in the everyday life of a vascular surgeon.
One’s schedule requires dedicated time and attention yet the urgent/emergent issues interrupting one’s daily schedule ensures that the only predictability is unpredictability. This is a source of burnout. My experience over the years has been that about 25% of our practice load comes on an urgent to emergent basis, often causing considerable scheduling problems both in the operating room and at the office – again, issues that can cause tremendous stress for many. Without a large group, these constant stressors become difficult to shoulder.
Then there are the hospital-induced stressors caused by poorly conceived administrative decrees. One example is when emergency rooms need vascular services but no contracts are offered to secure these services, in which physicians are merely expected to provide 24/7 services. Once a physician has been called in for a case in the middle of the night, the stress of carrying on the next day becomes greater for that physician unless a system is in place for designated calls, which some larger groups have worked out.
Another example is the tendency to grant interventional privileges to those incapable of treating their operative complications without any consideration for who would reimburse those who come in after and how. Why is it assumed that vascular surgeons would/should take time out of their practice to answer the call without any additional compensation? If the compensation from these service lines is so lucrative, then compensation in the form of contracts needs to be offered to those who can provide the necessary services to treat the inevitable complications. This will in some way help compensate for time lost in the vascular surgeons’ practices.
The contracts should reflect the value to an institution vascular surgeons bring for their presence, including ED coverage for most if not all of the service lines, such as cardiology, radiology, orthopedics, gynecology, and general surgery. This also includes issues arising from the house staff inserting lines and from subsequent renal failure, as well as for angio-access patients who need immediate vascular backup to treat the vascular complications encountered.
In addition, these contracts should acknowledge the revenue generated by the presence of a vascular service line. With the burnout rate and unpredictable lifestyle, one would be concerned that vascular surgeons could be on the endangered species list; and given the current shortage of vascular surgeons, don’t our numbers reflect this concern?
There are no easy solutions because the field is a difficult one and is undercompensated for the risks assumed and services provided, which makes it an unattractive specialty, especially in today’s lifestyle-conscious generation. The vascular specialty is embattled, and the human toll extracted in the field speaks for itself. The rewards must improve to make things more appealing, and this will lead to an increase in the number of vascular surgeons, and more will join in groups to mitigate the effects of the stressors of the field. Until then, vascular surgeons need to demand that they receive fair compensation for their availability and the coverage they provide, which allows many other departments and specialties to function. This reality must be acknowledged and compensated.
Carlo A. Dall’Olmo, MD
Michigan Vascular Center
Flint, Michigan
What is your diagnosis? - January 2019
Primary intestinal lymphangiectasia
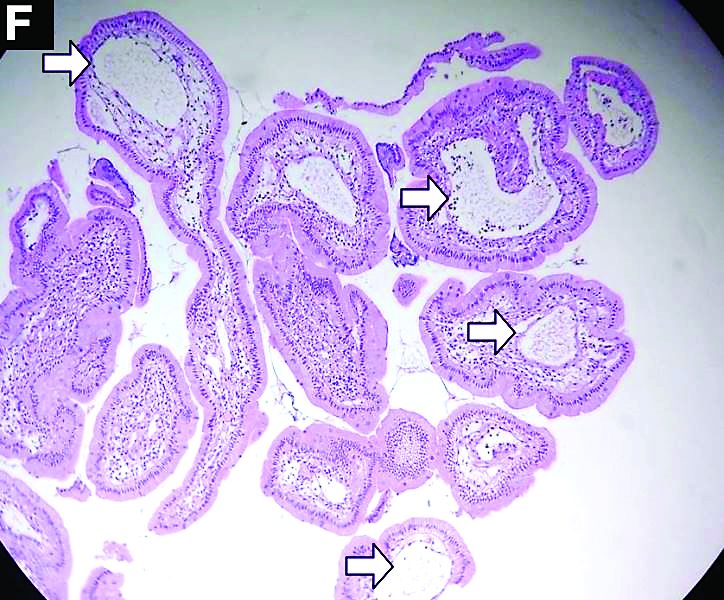
Histologic examination shows chronic inflammation of the ileum characterized by increased lymphoplasma cell infiltration of lamina propria without malignancy. Moreover, marked dilatation of lymphatic ducts that involved the mucosa was identified (Figure F, arrows; stain: hematoxylin and eosin; original magnification, ×100). On the basis of pathologic examinations, a diagnosis of primary intestinal lymphangiectasia (PIL) was made.
PIL is an extremely rare cause of protein-losing enteropathy characterized by the presence of dilated lymphatic channels in the mucosa, submucosa, or subserosa leading to protein-losing enteropathy.1 The true incidence and prevalence of this disease remains unclear. The disease affects males and females equally, and usually occurs in children and young adults. To date, less than 200 cases of PIL have been reported in the literature. The clinical manifestations of PIL may be asymptomatic or symptomatic such as abdominal pain, edema, diarrhea, and dyspnea. The diagnosis is based on the typical endoscopic findings of diffuse scattered mucosal white blebs with characteristic histologic findings of abnormal lymphatic dilatation. Double-balloon enteroscopy and capsule endoscopy are powerful modalities to evaluate the entire affected area of PIL.2 Although diet modification is a major treatment of PIL, several medicines have been reported to be useful such as corticosteroids, octreotide, and antiplasmin.3 Moreover, in patients with segmental lesions, surgery with local bowel resection is a useful treatment.3 In addition, PIL had a 5% risk of malignant transformation into lymphoma.3
References
1. Waldmann TA, Steinfeld JL, Dutcher TF, et al. The role of the gastrointestinal system in “idiopathic hypoproteinemia.” Gastroenterology. 1961;41:197-207.
2. Oh TG, Chung JW, Kim HM, et al. Primary intestinal lymphangiectasia diagnosed by capsule endoscopy and double balloon enteroscopy. World J Gastrointest Endosc. 2011;3:235-40.
3. Wen J, Tang Q, Wu, J. Primary intestinal lymphangiectasia: four case reports and a review of the literature. Dig Dis Sci. 2010;55:3466-72.
Primary intestinal lymphangiectasia
Histologic examination shows chronic inflammation of the ileum characterized by increased lymphoplasma cell infiltration of lamina propria without malignancy. Moreover, marked dilatation of lymphatic ducts that involved the mucosa was identified (Figure F, arrows; stain: hematoxylin and eosin; original magnification, ×100). On the basis of pathologic examinations, a diagnosis of primary intestinal lymphangiectasia (PIL) was made.
PIL is an extremely rare cause of protein-losing enteropathy characterized by the presence of dilated lymphatic channels in the mucosa, submucosa, or subserosa leading to protein-losing enteropathy.1 The true incidence and prevalence of this disease remains unclear. The disease affects males and females equally, and usually occurs in children and young adults. To date, less than 200 cases of PIL have been reported in the literature. The clinical manifestations of PIL may be asymptomatic or symptomatic such as abdominal pain, edema, diarrhea, and dyspnea. The diagnosis is based on the typical endoscopic findings of diffuse scattered mucosal white blebs with characteristic histologic findings of abnormal lymphatic dilatation. Double-balloon enteroscopy and capsule endoscopy are powerful modalities to evaluate the entire affected area of PIL.2 Although diet modification is a major treatment of PIL, several medicines have been reported to be useful such as corticosteroids, octreotide, and antiplasmin.3 Moreover, in patients with segmental lesions, surgery with local bowel resection is a useful treatment.3 In addition, PIL had a 5% risk of malignant transformation into lymphoma.3
References
1. Waldmann TA, Steinfeld JL, Dutcher TF, et al. The role of the gastrointestinal system in “idiopathic hypoproteinemia.” Gastroenterology. 1961;41:197-207.
2. Oh TG, Chung JW, Kim HM, et al. Primary intestinal lymphangiectasia diagnosed by capsule endoscopy and double balloon enteroscopy. World J Gastrointest Endosc. 2011;3:235-40.
3. Wen J, Tang Q, Wu, J. Primary intestinal lymphangiectasia: four case reports and a review of the literature. Dig Dis Sci. 2010;55:3466-72.
Primary intestinal lymphangiectasia
Histologic examination shows chronic inflammation of the ileum characterized by increased lymphoplasma cell infiltration of lamina propria without malignancy. Moreover, marked dilatation of lymphatic ducts that involved the mucosa was identified (Figure F, arrows; stain: hematoxylin and eosin; original magnification, ×100). On the basis of pathologic examinations, a diagnosis of primary intestinal lymphangiectasia (PIL) was made.
PIL is an extremely rare cause of protein-losing enteropathy characterized by the presence of dilated lymphatic channels in the mucosa, submucosa, or subserosa leading to protein-losing enteropathy.1 The true incidence and prevalence of this disease remains unclear. The disease affects males and females equally, and usually occurs in children and young adults. To date, less than 200 cases of PIL have been reported in the literature. The clinical manifestations of PIL may be asymptomatic or symptomatic such as abdominal pain, edema, diarrhea, and dyspnea. The diagnosis is based on the typical endoscopic findings of diffuse scattered mucosal white blebs with characteristic histologic findings of abnormal lymphatic dilatation. Double-balloon enteroscopy and capsule endoscopy are powerful modalities to evaluate the entire affected area of PIL.2 Although diet modification is a major treatment of PIL, several medicines have been reported to be useful such as corticosteroids, octreotide, and antiplasmin.3 Moreover, in patients with segmental lesions, surgery with local bowel resection is a useful treatment.3 In addition, PIL had a 5% risk of malignant transformation into lymphoma.3
References
1. Waldmann TA, Steinfeld JL, Dutcher TF, et al. The role of the gastrointestinal system in “idiopathic hypoproteinemia.” Gastroenterology. 1961;41:197-207.
2. Oh TG, Chung JW, Kim HM, et al. Primary intestinal lymphangiectasia diagnosed by capsule endoscopy and double balloon enteroscopy. World J Gastrointest Endosc. 2011;3:235-40.
3. Wen J, Tang Q, Wu, J. Primary intestinal lymphangiectasia: four case reports and a review of the literature. Dig Dis Sci. 2010;55:3466-72.
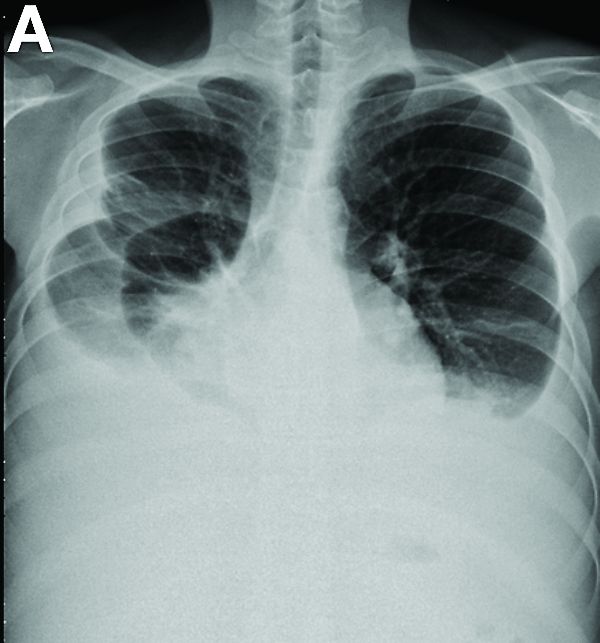
A 19-year-old boy presented to our hospital because of a 6-month history of progressive dyspnea and generalized edema. He developed cough, abdominal fullness, diarrhea, and leg edema 5 years ago.
Liver cirrhosis was suspected at that time. However, he seemed to have a poor response to medical treatment. Physical examination showed decreased breathing sounds and rales of the bilateral lower chest area, a distended abdomen with multiple purple striae, and edema of bilateral lower legs.
Laboratory tests showed a low serum total protein of 3.8 g/dL (normal range, 5.5–8), albumin of 2.0 g/dL (normal range, 3.8–5.4), total calcium of 7 mg/dL (normal range, 8.4–10.8), C-reactive protein of 11.02 mg/dL (normal, below 0.8). His hemogram showed a white blood cell count of 13,310 × 109/L (normal range, 3.5–11 × 109/L) with lymphocytopenia (9.8%).
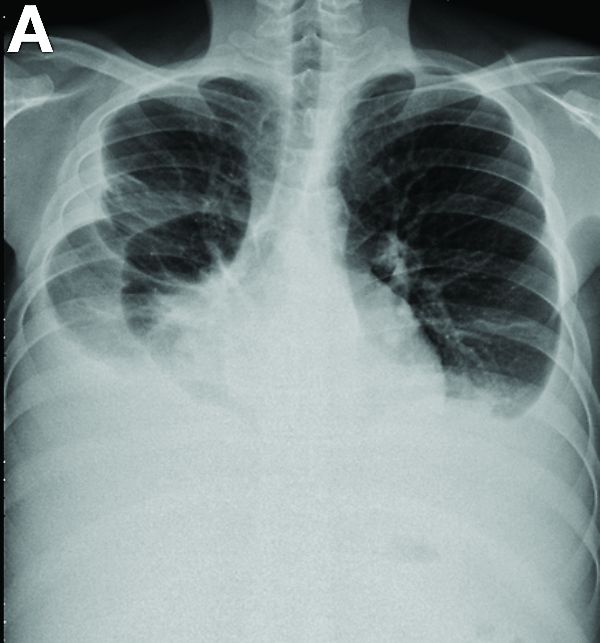
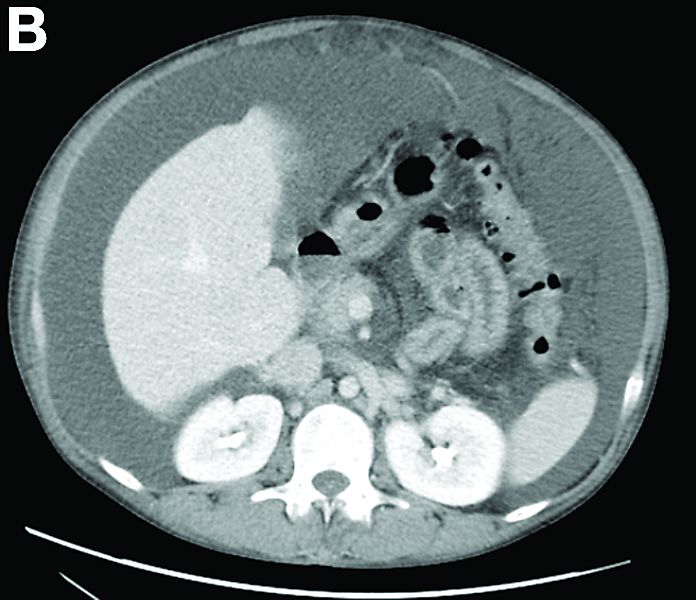
Other blood tests were within normal limits. The urinalysis and stool analysis were normal. Chest radiography showed bilateral pleural effusions (Figure A). Abdominal computed tomography demonstrated large ascites (Figure B). Paracentesis showed his serum ascites albumin gradient was 1.9 g/dL.

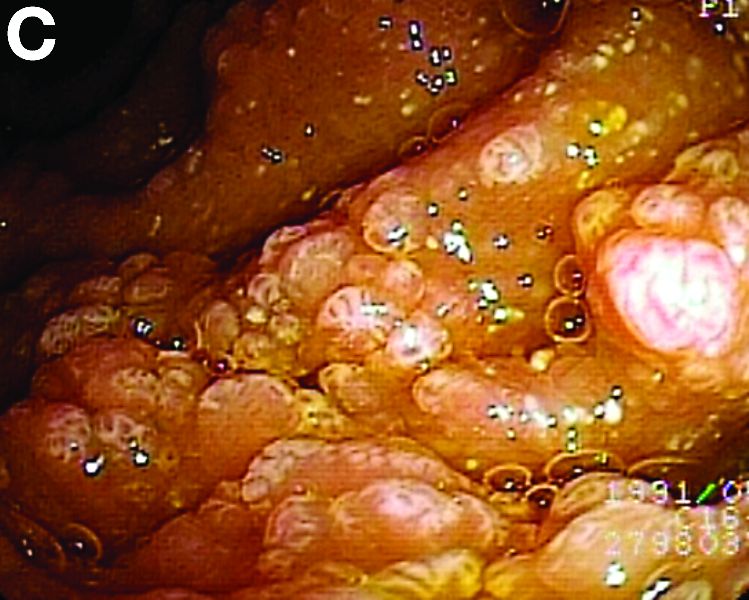
Subsequently, antegrade double-balloon enteroscopy (Fujinon EN-450T5; Fujinon, Saitama, Japan) demonstrated nodular mucosal lesions with a milk-like surface in the duodenum (Figure C).

Moreover, a snowflake appearance of mucosa was found in the jejunum and proximal ileum (Figure D). However, normal appearance of mucosa was identified in the middle ileum (Figure E). Biopsy specimens from these abnormal mucosal lesions were taken for pathology.
What is the diagnosis?
Deadly Marburg virus found in West Africa
Marburg virus has been found in fruit bats in Sierra Leone, marking the first appearance of the deadly, Ebola-like virus in West Africa, the Centers for Disease Control and Prevention (CDC) is reporting.

Five Egyptian rousette fruit bats found in three different districts tested positive for infection with Marburg virus, a cousin to Ebola that can cause a hemorrhagic fever with case fatality rates up to 90%, according to CDC.
While no confirmed cases of Marburg infection have been reported in Sierra Leone, the presence of virus in these bats indicates that people nearby may be at risk, according to scientists.
“We have known for a long time that rousette bats, which carry Marburg virus in other parts of Africa, also live in West Africa, so it’s not surprising that we’d find the virus in bats there,” CDC ecologist Jonathan S. Towner, PhD, said in a news release.
The Egyptian rousette bat (Rousettus aegyptiacus) is the natural reservoir for Marburg, shedding the virus in saliva, urine, and feces while feeding on fruit. People and are exposed to the virus when they eat contaminated fruit or capture bats for food, according to the CDC.
The most recent Marburg virus outbreak, which occurred in Uganda in 2017, was the 12th reported outbreak linked to Africa, according to the agency. The largest and deadliest outbreak occurred in 2005 in Angola, infecting 252 people, of whom 90% died.
Testing of the Marburg-positive bats revealed genetically diverse strains, suggesting the virus has been present in Sierra Leone bat colonies for many years, the agency said. Two of the four Marburg virus strains identified in the Sierra Leone bats were genetically similar to the strain implicated in the Angola outbreak.
Egyptian fruit bats are in fact common throughout Africa, living in caves or underground mines. Marburg-positive bats have been found in sub-Saharan Africa, according to researchers, mainly in Uganda and the Democratic Republic of Congo.
Colonies of Egyptian fruit bats can number more than 100,000 animals in eastern and central Africa, while in Sierra Leone, colonies are much smaller, which may explain the lack of Marburg virus disease outbreaks in that country, CDC said.
Discovery of Marburg virus in Sierra Leone was the result of two projects, one led by the CDC and Njala University in Freetown, Sierra Leone, and the other by the University of California, Davis, and the University of Makeni, Sierra Leone, which was funded by the United States Agency for International Development (USAID).
“This discovery is an excellent example of how our work can identify a threat and help us warn people of the risk before they get sick.” Dr. Towner said in the news release.
The two projects began in 2016 after the large Ebola outbreak in West Africa with the aim of identifying the reservoir of Ebola, according to CDC.
SOURCES: U.S. Department of Health and Human Services CDC Newsroom and Centers for Disease Control and Prevention (Marburg Virus).
Marburg virus has been found in fruit bats in Sierra Leone, marking the first appearance of the deadly, Ebola-like virus in West Africa, the Centers for Disease Control and Prevention (CDC) is reporting.
Five Egyptian rousette fruit bats found in three different districts tested positive for infection with Marburg virus, a cousin to Ebola that can cause a hemorrhagic fever with case fatality rates up to 90%, according to CDC.
While no confirmed cases of Marburg infection have been reported in Sierra Leone, the presence of virus in these bats indicates that people nearby may be at risk, according to scientists.
“We have known for a long time that rousette bats, which carry Marburg virus in other parts of Africa, also live in West Africa, so it’s not surprising that we’d find the virus in bats there,” CDC ecologist Jonathan S. Towner, PhD, said in a news release.
The Egyptian rousette bat (Rousettus aegyptiacus) is the natural reservoir for Marburg, shedding the virus in saliva, urine, and feces while feeding on fruit. People and are exposed to the virus when they eat contaminated fruit or capture bats for food, according to the CDC.
The most recent Marburg virus outbreak, which occurred in Uganda in 2017, was the 12th reported outbreak linked to Africa, according to the agency. The largest and deadliest outbreak occurred in 2005 in Angola, infecting 252 people, of whom 90% died.
Testing of the Marburg-positive bats revealed genetically diverse strains, suggesting the virus has been present in Sierra Leone bat colonies for many years, the agency said. Two of the four Marburg virus strains identified in the Sierra Leone bats were genetically similar to the strain implicated in the Angola outbreak.
Egyptian fruit bats are in fact common throughout Africa, living in caves or underground mines. Marburg-positive bats have been found in sub-Saharan Africa, according to researchers, mainly in Uganda and the Democratic Republic of Congo.
Colonies of Egyptian fruit bats can number more than 100,000 animals in eastern and central Africa, while in Sierra Leone, colonies are much smaller, which may explain the lack of Marburg virus disease outbreaks in that country, CDC said.
Discovery of Marburg virus in Sierra Leone was the result of two projects, one led by the CDC and Njala University in Freetown, Sierra Leone, and the other by the University of California, Davis, and the University of Makeni, Sierra Leone, which was funded by the United States Agency for International Development (USAID).
“This discovery is an excellent example of how our work can identify a threat and help us warn people of the risk before they get sick.” Dr. Towner said in the news release.
The two projects began in 2016 after the large Ebola outbreak in West Africa with the aim of identifying the reservoir of Ebola, according to CDC.
SOURCES: U.S. Department of Health and Human Services CDC Newsroom and Centers for Disease Control and Prevention (Marburg Virus).
Marburg virus has been found in fruit bats in Sierra Leone, marking the first appearance of the deadly, Ebola-like virus in West Africa, the Centers for Disease Control and Prevention (CDC) is reporting.
Five Egyptian rousette fruit bats found in three different districts tested positive for infection with Marburg virus, a cousin to Ebola that can cause a hemorrhagic fever with case fatality rates up to 90%, according to CDC.
While no confirmed cases of Marburg infection have been reported in Sierra Leone, the presence of virus in these bats indicates that people nearby may be at risk, according to scientists.
“We have known for a long time that rousette bats, which carry Marburg virus in other parts of Africa, also live in West Africa, so it’s not surprising that we’d find the virus in bats there,” CDC ecologist Jonathan S. Towner, PhD, said in a news release.
The Egyptian rousette bat (Rousettus aegyptiacus) is the natural reservoir for Marburg, shedding the virus in saliva, urine, and feces while feeding on fruit. People and are exposed to the virus when they eat contaminated fruit or capture bats for food, according to the CDC.
The most recent Marburg virus outbreak, which occurred in Uganda in 2017, was the 12th reported outbreak linked to Africa, according to the agency. The largest and deadliest outbreak occurred in 2005 in Angola, infecting 252 people, of whom 90% died.
Testing of the Marburg-positive bats revealed genetically diverse strains, suggesting the virus has been present in Sierra Leone bat colonies for many years, the agency said. Two of the four Marburg virus strains identified in the Sierra Leone bats were genetically similar to the strain implicated in the Angola outbreak.
Egyptian fruit bats are in fact common throughout Africa, living in caves or underground mines. Marburg-positive bats have been found in sub-Saharan Africa, according to researchers, mainly in Uganda and the Democratic Republic of Congo.
Colonies of Egyptian fruit bats can number more than 100,000 animals in eastern and central Africa, while in Sierra Leone, colonies are much smaller, which may explain the lack of Marburg virus disease outbreaks in that country, CDC said.
Discovery of Marburg virus in Sierra Leone was the result of two projects, one led by the CDC and Njala University in Freetown, Sierra Leone, and the other by the University of California, Davis, and the University of Makeni, Sierra Leone, which was funded by the United States Agency for International Development (USAID).
“This discovery is an excellent example of how our work can identify a threat and help us warn people of the risk before they get sick.” Dr. Towner said in the news release.
The two projects began in 2016 after the large Ebola outbreak in West Africa with the aim of identifying the reservoir of Ebola, according to CDC.
SOURCES: U.S. Department of Health and Human Services CDC Newsroom and Centers for Disease Control and Prevention (Marburg Virus).
FROM THE CENTERS FOR DISEASE CONTROL AND PREVENTION
ACA in peril after Texas ruling
Also today, baracitinib findings have immediate clinical relevance for patients with RA, a look at how often epileptic patients have treatment delayed, and the FDA issues an alert after e-cigarette liquids were found containing erectile dysfunction medication.
Also today, baracitinib findings have immediate clinical relevance for patients with RA, a look at how often epileptic patients have treatment delayed, and the FDA issues an alert after e-cigarette liquids were found containing erectile dysfunction medication.
Also today, baracitinib findings have immediate clinical relevance for patients with RA, a look at how often epileptic patients have treatment delayed, and the FDA issues an alert after e-cigarette liquids were found containing erectile dysfunction medication.
Be judicious with empiric antibiotics for febrile neutropenia
SAN FRANCISCO – Empiric antibiotic therapy for febrile neutropenia, a common and life-threatening complication of chemotherapy, hasn’t really changed much in 20 years, according to Alison Freifeld, MD, director of the section of oncology infectious diseases at the University of Nebraska, Omaha.

Antibiotic resistance has become a major problem over that time. Multidrug-resistant, gram-negative blood stream infections are not uncommon, particularly with extended-spectrum, beta-lactamase–producing Escherichia coli and Klebsiella pneumoniae. Carbapenemase-producing Enterobacteriaceae are also on the rise, among others.
“Our standard empiric antibiotics” – ceftazidime, cefepime, piperacillin/tazobactam, and carbapenems – “are generally not active against these organisms, putting us in a major dilemma about what to do” with patients who have them, Dr. Freifeld said.
“Our goal at the moment is to unpack this ship, take some of these loads of antibiotics off, and figure out how we can more effectively bridge the gap between risk factors and outcomes, with fewer and more stringently applied targeted antibiotics,” she said at ID Week, an annual scientific meeting on infectious diseases.
Dr. Freifeld shared her advice at the meeting on what to do as that plays out. The main driver is to protect the remaining potency of current antibiotics without sacrificing patient care while also keeping new options in reserve for the sickest patients, so “we do not overuse these precious commodities.”
For one thing, it’s okay to shorten treatment – traditionally around 2 weeks, until the absolute neutrophil count (ANC) tops 500 cells/mcg – once the fever abates and cultures turn negative, even if the ANC remains low.
A recent trial put the approach to the test. A total of 78 patients had their antibiotics stopped after they had been free of fever for 72 hours, with normal vital signs and no other signs of infection; 79 in the control group had usual care, continuing treatment until their ANC recovered.
Early withdrawal shortened treatment by about 3 days and there were no statistically significant differences in mortality, with one death in the short-arm group and three in the long-arm group. Over half of the patients in the short-arm group were neutropenic when antibiotics were discontinued.
Serious adverse events, meanwhile, were far less common in the short-arm group (18 vs. 38). The take-home lesson is that “interventions to shorten duration of empiric antibiotics are safe and effective and important to implement now,” Dr. Freifeld said (Lancet Haematol. 2017 Dec;4(12):e573-83).
Also, “use escalation and deescalation approaches,” she said. The basic idea is to begin with monotherapy – cefepime or piperacillin/tazobactam – in uncomplicated cases, bumped up as necessary, and, in complicated cases, to start with broad, multidrug regimens, deescalated as culture reports and other information comes in (Haematologica. 2013 Dec;98(12):1826-35).
Finally, fluoroquinolone prophylaxis, “once considered the wonder of the world,” Dr. Freifeld said, needs to be limited to the highest-risk patients, particularly those with neutropenia expected to last a week or more. It does seem to lower the rates of fever and bloodstream infections, but recent investigations have shown no mortality benefit, and fluoroquinolone prophylaxis makes patients more likely to be colonized by multidrug-resistant bacteria. Many centers have opted against it, even in higher-risk patients (J Infect. 2018 Jan;76(1):20-37).
Dr. Freifeld serves on a data adjudication committee for Merck, and reported research support from the company.
SAN FRANCISCO – Empiric antibiotic therapy for febrile neutropenia, a common and life-threatening complication of chemotherapy, hasn’t really changed much in 20 years, according to Alison Freifeld, MD, director of the section of oncology infectious diseases at the University of Nebraska, Omaha.
Antibiotic resistance has become a major problem over that time. Multidrug-resistant, gram-negative blood stream infections are not uncommon, particularly with extended-spectrum, beta-lactamase–producing Escherichia coli and Klebsiella pneumoniae. Carbapenemase-producing Enterobacteriaceae are also on the rise, among others.
“Our standard empiric antibiotics” – ceftazidime, cefepime, piperacillin/tazobactam, and carbapenems – “are generally not active against these organisms, putting us in a major dilemma about what to do” with patients who have them, Dr. Freifeld said.
“Our goal at the moment is to unpack this ship, take some of these loads of antibiotics off, and figure out how we can more effectively bridge the gap between risk factors and outcomes, with fewer and more stringently applied targeted antibiotics,” she said at ID Week, an annual scientific meeting on infectious diseases.
Dr. Freifeld shared her advice at the meeting on what to do as that plays out. The main driver is to protect the remaining potency of current antibiotics without sacrificing patient care while also keeping new options in reserve for the sickest patients, so “we do not overuse these precious commodities.”
For one thing, it’s okay to shorten treatment – traditionally around 2 weeks, until the absolute neutrophil count (ANC) tops 500 cells/mcg – once the fever abates and cultures turn negative, even if the ANC remains low.
A recent trial put the approach to the test. A total of 78 patients had their antibiotics stopped after they had been free of fever for 72 hours, with normal vital signs and no other signs of infection; 79 in the control group had usual care, continuing treatment until their ANC recovered.
Early withdrawal shortened treatment by about 3 days and there were no statistically significant differences in mortality, with one death in the short-arm group and three in the long-arm group. Over half of the patients in the short-arm group were neutropenic when antibiotics were discontinued.
Serious adverse events, meanwhile, were far less common in the short-arm group (18 vs. 38). The take-home lesson is that “interventions to shorten duration of empiric antibiotics are safe and effective and important to implement now,” Dr. Freifeld said (Lancet Haematol. 2017 Dec;4(12):e573-83).
Also, “use escalation and deescalation approaches,” she said. The basic idea is to begin with monotherapy – cefepime or piperacillin/tazobactam – in uncomplicated cases, bumped up as necessary, and, in complicated cases, to start with broad, multidrug regimens, deescalated as culture reports and other information comes in (Haematologica. 2013 Dec;98(12):1826-35).
Finally, fluoroquinolone prophylaxis, “once considered the wonder of the world,” Dr. Freifeld said, needs to be limited to the highest-risk patients, particularly those with neutropenia expected to last a week or more. It does seem to lower the rates of fever and bloodstream infections, but recent investigations have shown no mortality benefit, and fluoroquinolone prophylaxis makes patients more likely to be colonized by multidrug-resistant bacteria. Many centers have opted against it, even in higher-risk patients (J Infect. 2018 Jan;76(1):20-37).
Dr. Freifeld serves on a data adjudication committee for Merck, and reported research support from the company.
SAN FRANCISCO – Empiric antibiotic therapy for febrile neutropenia, a common and life-threatening complication of chemotherapy, hasn’t really changed much in 20 years, according to Alison Freifeld, MD, director of the section of oncology infectious diseases at the University of Nebraska, Omaha.
Antibiotic resistance has become a major problem over that time. Multidrug-resistant, gram-negative blood stream infections are not uncommon, particularly with extended-spectrum, beta-lactamase–producing Escherichia coli and Klebsiella pneumoniae. Carbapenemase-producing Enterobacteriaceae are also on the rise, among others.
“Our standard empiric antibiotics” – ceftazidime, cefepime, piperacillin/tazobactam, and carbapenems – “are generally not active against these organisms, putting us in a major dilemma about what to do” with patients who have them, Dr. Freifeld said.
“Our goal at the moment is to unpack this ship, take some of these loads of antibiotics off, and figure out how we can more effectively bridge the gap between risk factors and outcomes, with fewer and more stringently applied targeted antibiotics,” she said at ID Week, an annual scientific meeting on infectious diseases.
Dr. Freifeld shared her advice at the meeting on what to do as that plays out. The main driver is to protect the remaining potency of current antibiotics without sacrificing patient care while also keeping new options in reserve for the sickest patients, so “we do not overuse these precious commodities.”
For one thing, it’s okay to shorten treatment – traditionally around 2 weeks, until the absolute neutrophil count (ANC) tops 500 cells/mcg – once the fever abates and cultures turn negative, even if the ANC remains low.
A recent trial put the approach to the test. A total of 78 patients had their antibiotics stopped after they had been free of fever for 72 hours, with normal vital signs and no other signs of infection; 79 in the control group had usual care, continuing treatment until their ANC recovered.
Early withdrawal shortened treatment by about 3 days and there were no statistically significant differences in mortality, with one death in the short-arm group and three in the long-arm group. Over half of the patients in the short-arm group were neutropenic when antibiotics were discontinued.
Serious adverse events, meanwhile, were far less common in the short-arm group (18 vs. 38). The take-home lesson is that “interventions to shorten duration of empiric antibiotics are safe and effective and important to implement now,” Dr. Freifeld said (Lancet Haematol. 2017 Dec;4(12):e573-83).
Also, “use escalation and deescalation approaches,” she said. The basic idea is to begin with monotherapy – cefepime or piperacillin/tazobactam – in uncomplicated cases, bumped up as necessary, and, in complicated cases, to start with broad, multidrug regimens, deescalated as culture reports and other information comes in (Haematologica. 2013 Dec;98(12):1826-35).
Finally, fluoroquinolone prophylaxis, “once considered the wonder of the world,” Dr. Freifeld said, needs to be limited to the highest-risk patients, particularly those with neutropenia expected to last a week or more. It does seem to lower the rates of fever and bloodstream infections, but recent investigations have shown no mortality benefit, and fluoroquinolone prophylaxis makes patients more likely to be colonized by multidrug-resistant bacteria. Many centers have opted against it, even in higher-risk patients (J Infect. 2018 Jan;76(1):20-37).
Dr. Freifeld serves on a data adjudication committee for Merck, and reported research support from the company.
EXPERT ANALYSIS FROM IDWEEK 2018
Roberto Lewis-Fernandez: Cultural Assessments
More from Dr. Lewis-Fernandez, Curbside Consult: Chinese American man with high risk of psychosis.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
More from Dr. Lewis-Fernandez, Curbside Consult: Chinese American man with high risk of psychosis.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
More from Dr. Lewis-Fernandez, Curbside Consult: Chinese American man with high risk of psychosis.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
AHA reports statins are safe
Also today, acute stroke thrombolysis worked safely despite GI bleed or malignancy, legal advice on what to do if a patient sues you, and the link between childhood asthma and obesity.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
Also today, acute stroke thrombolysis worked safely despite GI bleed or malignancy, legal advice on what to do if a patient sues you, and the link between childhood asthma and obesity.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
Also today, acute stroke thrombolysis worked safely despite GI bleed or malignancy, legal advice on what to do if a patient sues you, and the link between childhood asthma and obesity.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify

Decreased insulin clearance and insulin resistance
Also today, tender joint count may confound assessment of RA inflammation, common AEDs confer moderately increased risk of major congenital malformations, and the ACR and the NPF unveil new treatment guidelines for psoriatic arthritis.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
Also today, tender joint count may confound assessment of RA inflammation, common AEDs confer moderately increased risk of major congenital malformations, and the ACR and the NPF unveil new treatment guidelines for psoriatic arthritis.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
Also today, tender joint count may confound assessment of RA inflammation, common AEDs confer moderately increased risk of major congenital malformations, and the ACR and the NPF unveil new treatment guidelines for psoriatic arthritis.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify

AHA: Statins associated with high degree of safety
The benefits of statins highly offset the associated risks in appropriate patients, according to a scientific statement issued by the American Heart Association.
“The review covers the general patient population, as well as demographic subgroups, including the elderly, children, pregnant women, East Asians, and patients with specific conditions.” wrote Connie B. Newman, MD, of New York University, together with her colleagues. The report is in Arteriosclerosis, Thrombosis, and Vascular Biology.
After an extensive review of the literature pertaining to statin safety and tolerability, Dr. Newman and her colleagues reported the compiled findings from several randomized controlled trials, in addition to observational data, where required. They found that the risk of serious muscle complications, such as rhabdomyolysis, attributable to statin use was less than 0.1%. Furthermore, they noted that the risk of serious hepatotoxicity was even less likely, occurring in about 1 in 10,000 patients treated with therapy.
“There is no convincing evidence for a causal relationship between statins and cancer, cataracts, cognitive dysfunction, peripheral neuropathy, erectile dysfunction, or tendinitis,” the experts wrote. “In U.S. clinical practices, roughly 10% of patients stop taking a statin because of subjective complaints, most commonly muscle symptoms without raised creatine kinase,” they further reported.
Contrastingly, data from randomized trials have shown that the change in the incidence of muscle-related symptoms in patients treated with statins versus placebo is less than 1%. Moreover, the incidence is even lower, with an estimated rate of 0.1%, in those who stopped statin therapy because of these symptoms. Given these results, Dr. Newman and her colleagues said that muscle-related symptoms among statin-treated patients are not due to the pharmacological activity of the statin.
“Restarting statin therapy in these patients can be challenging, but it is important, especially in patients at high risk of cardiovascular events, for whom prevention of these events is a priority,” they added.
A large proportion of the population takes statin therapy to lower the risk of major cardiovascular events, including ischemic stroke, myocardial infarction, and other adverse effects of cardiovascular disease. At maximal doses, statins may decrease LDL-cholesterol levels by roughly 55%-60%. In addition, given the multitude of available generics, statins are an economical treatment option for most patients.
However, Dr. Newman and her colleagues suggested that, when considering statin therapy in special populations, particularly in patients with end-stage renal failure or severe hepatic disease, commencing treatment is not recommended.
“The lack of proof of cardiovascular benefit in patients with end-stage renal disease suggests that initiating statin treatment in these patients is generally not warranted,” the experts wrote. “Data on safety in people with more serious liver disease are insufficient, and statin treatment is generally discouraged,” they added.
With respect to statin-induced adverse effects, they are usually reversible upon discontinuation of therapy, with the exception of hemorrhagic stroke. However, damage from an ischemic stroke or myocardial infarction may result in death. As a result, in patients who would benefit from statin therapy, based on most recent guidelines, cardiovascular benefits greatly exceed potential safety concerns.
Dr. Newman and her coauthors disclosed financial affiliations with Amgen, Kowa, Regeneron, Sanofi, and others.
SOURCE: Newman CB et al. Arterioscler Thromb Vasc Biol. 2018 Dec 10. doi: 10.1161/ATV.0000000000000073
The benefits of statins highly offset the associated risks in appropriate patients, according to a scientific statement issued by the American Heart Association.
“The review covers the general patient population, as well as demographic subgroups, including the elderly, children, pregnant women, East Asians, and patients with specific conditions.” wrote Connie B. Newman, MD, of New York University, together with her colleagues. The report is in Arteriosclerosis, Thrombosis, and Vascular Biology.
After an extensive review of the literature pertaining to statin safety and tolerability, Dr. Newman and her colleagues reported the compiled findings from several randomized controlled trials, in addition to observational data, where required. They found that the risk of serious muscle complications, such as rhabdomyolysis, attributable to statin use was less than 0.1%. Furthermore, they noted that the risk of serious hepatotoxicity was even less likely, occurring in about 1 in 10,000 patients treated with therapy.
“There is no convincing evidence for a causal relationship between statins and cancer, cataracts, cognitive dysfunction, peripheral neuropathy, erectile dysfunction, or tendinitis,” the experts wrote. “In U.S. clinical practices, roughly 10% of patients stop taking a statin because of subjective complaints, most commonly muscle symptoms without raised creatine kinase,” they further reported.
Contrastingly, data from randomized trials have shown that the change in the incidence of muscle-related symptoms in patients treated with statins versus placebo is less than 1%. Moreover, the incidence is even lower, with an estimated rate of 0.1%, in those who stopped statin therapy because of these symptoms. Given these results, Dr. Newman and her colleagues said that muscle-related symptoms among statin-treated patients are not due to the pharmacological activity of the statin.
“Restarting statin therapy in these patients can be challenging, but it is important, especially in patients at high risk of cardiovascular events, for whom prevention of these events is a priority,” they added.
A large proportion of the population takes statin therapy to lower the risk of major cardiovascular events, including ischemic stroke, myocardial infarction, and other adverse effects of cardiovascular disease. At maximal doses, statins may decrease LDL-cholesterol levels by roughly 55%-60%. In addition, given the multitude of available generics, statins are an economical treatment option for most patients.
However, Dr. Newman and her colleagues suggested that, when considering statin therapy in special populations, particularly in patients with end-stage renal failure or severe hepatic disease, commencing treatment is not recommended.
“The lack of proof of cardiovascular benefit in patients with end-stage renal disease suggests that initiating statin treatment in these patients is generally not warranted,” the experts wrote. “Data on safety in people with more serious liver disease are insufficient, and statin treatment is generally discouraged,” they added.
With respect to statin-induced adverse effects, they are usually reversible upon discontinuation of therapy, with the exception of hemorrhagic stroke. However, damage from an ischemic stroke or myocardial infarction may result in death. As a result, in patients who would benefit from statin therapy, based on most recent guidelines, cardiovascular benefits greatly exceed potential safety concerns.
Dr. Newman and her coauthors disclosed financial affiliations with Amgen, Kowa, Regeneron, Sanofi, and others.
SOURCE: Newman CB et al. Arterioscler Thromb Vasc Biol. 2018 Dec 10. doi: 10.1161/ATV.0000000000000073
The benefits of statins highly offset the associated risks in appropriate patients, according to a scientific statement issued by the American Heart Association.
“The review covers the general patient population, as well as demographic subgroups, including the elderly, children, pregnant women, East Asians, and patients with specific conditions.” wrote Connie B. Newman, MD, of New York University, together with her colleagues. The report is in Arteriosclerosis, Thrombosis, and Vascular Biology.
After an extensive review of the literature pertaining to statin safety and tolerability, Dr. Newman and her colleagues reported the compiled findings from several randomized controlled trials, in addition to observational data, where required. They found that the risk of serious muscle complications, such as rhabdomyolysis, attributable to statin use was less than 0.1%. Furthermore, they noted that the risk of serious hepatotoxicity was even less likely, occurring in about 1 in 10,000 patients treated with therapy.
“There is no convincing evidence for a causal relationship between statins and cancer, cataracts, cognitive dysfunction, peripheral neuropathy, erectile dysfunction, or tendinitis,” the experts wrote. “In U.S. clinical practices, roughly 10% of patients stop taking a statin because of subjective complaints, most commonly muscle symptoms without raised creatine kinase,” they further reported.
Contrastingly, data from randomized trials have shown that the change in the incidence of muscle-related symptoms in patients treated with statins versus placebo is less than 1%. Moreover, the incidence is even lower, with an estimated rate of 0.1%, in those who stopped statin therapy because of these symptoms. Given these results, Dr. Newman and her colleagues said that muscle-related symptoms among statin-treated patients are not due to the pharmacological activity of the statin.
“Restarting statin therapy in these patients can be challenging, but it is important, especially in patients at high risk of cardiovascular events, for whom prevention of these events is a priority,” they added.
A large proportion of the population takes statin therapy to lower the risk of major cardiovascular events, including ischemic stroke, myocardial infarction, and other adverse effects of cardiovascular disease. At maximal doses, statins may decrease LDL-cholesterol levels by roughly 55%-60%. In addition, given the multitude of available generics, statins are an economical treatment option for most patients.
However, Dr. Newman and her colleagues suggested that, when considering statin therapy in special populations, particularly in patients with end-stage renal failure or severe hepatic disease, commencing treatment is not recommended.
“The lack of proof of cardiovascular benefit in patients with end-stage renal disease suggests that initiating statin treatment in these patients is generally not warranted,” the experts wrote. “Data on safety in people with more serious liver disease are insufficient, and statin treatment is generally discouraged,” they added.
With respect to statin-induced adverse effects, they are usually reversible upon discontinuation of therapy, with the exception of hemorrhagic stroke. However, damage from an ischemic stroke or myocardial infarction may result in death. As a result, in patients who would benefit from statin therapy, based on most recent guidelines, cardiovascular benefits greatly exceed potential safety concerns.
Dr. Newman and her coauthors disclosed financial affiliations with Amgen, Kowa, Regeneron, Sanofi, and others.
SOURCE: Newman CB et al. Arterioscler Thromb Vasc Biol. 2018 Dec 10. doi: 10.1161/ATV.0000000000000073
FROM ARTERIOSCLEROSIS, THROMBOSIS, AND VASCULAR BIOLOGY
Key clinical point: After rigorous review, the benefits of statin therapy were found to markedly exceed associated risks.
Major finding: .
Study details: A scientific statement on statin safety and associated adverse events from the American Heart Association.
Disclosures: Several writing group members disclosed financial affiliations with Amgen, Kowa, Regeneron, Sanofi, and others.
Source: Newman CB et al. Arterioscler Thromb Vasc Biol. 2018 Dec 10. doi: 10.1161/ATV.0000000000000073.
Statin-diabetes link
Also today, should metabolic syndrome be renamed circadian syndrome? A smart phone application diagnoses STEMI nearly as well as ECG, and fewer people having insurance may have helped slow health spending growth in 2017.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
Also today, should metabolic syndrome be renamed circadian syndrome? A smart phone application diagnoses STEMI nearly as well as ECG, and fewer people having insurance may have helped slow health spending growth in 2017.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
Also today, should metabolic syndrome be renamed circadian syndrome? A smart phone application diagnoses STEMI nearly as well as ECG, and fewer people having insurance may have helped slow health spending growth in 2017.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
