User login
For MD-IQ use only
PCPs play a small part in low-value care spending
according to a brief report published online Jan. 18 in Annals of Internal Medicine.
However, one expert said there are better ways to curb low-value care than focusing on which specialties are guilty of the practice.
Analyzing a 20% random sample of Medicare Part B claims, Aaron Baum, PhD, with the Icahn School of Medicine at Mount Sinai, New York, and colleagues found that the services primary care physicians performed or ordered made up on average 8.3% of the low-value care their patients received (interquartile range, 3.9%-15.1%; 95th percentile, 35.6%) and their referrals made up 15.4% (IQR, 6.3%-26.4%; 95th percentile, 44.6%).
By specialty, cardiology had the worst record with 27% of all spending on low-value services ($1.8 billion) attributed to that specialty. Yet, of the 25 highest-spending specialties in the report, 12 of them were associated with 1% or less than 1% each of all low-value spending, indicating the waste was widely distributed.
Dr. Baum said in an interview that though there are some PCPs guilty of high spending on low-value services, overall, most primary care physicians’ low-value services add up to only 0.3% of Part B spending. He noted that Part B spending is about one-third of all Medicare spending.
Primary care is often thought to be at the core of care management and spending and PCPs are often seen as the gatekeepers, but this analysis suggests that efforts to make big differences in curtailing low-value spending might be more effective elsewhere.
“There’s only so much spending you can reduce by changing primary care physicians’ services that they directly perform,” Dr. Baum said.
Low-value care is costly, can be harmful
Mark Fendrick, MD, director of the University of Michigan’s Center for Value-Based Insurance Design in Ann Arbor, said in an interview that the report adds confirmation to previous research that has consistently shown low-value care is “extremely common, very costly, and provided by primary care providers and specialists alike.” He noted that it can also be harmful.
“The math is simple,” he said. “If we want to improve coverage and lower patient costs for essential services like visits, diagnostic tests, and drugs, we have to reduce spending on those services that do not make Americans any healthier.”
The study ranked 31 clinical services judged to be low value by physician societies, Medicare and clinical guidelines, and their use among beneficiaries enrolled between 2007 and 2014. Here’s how the top six low-value services compare.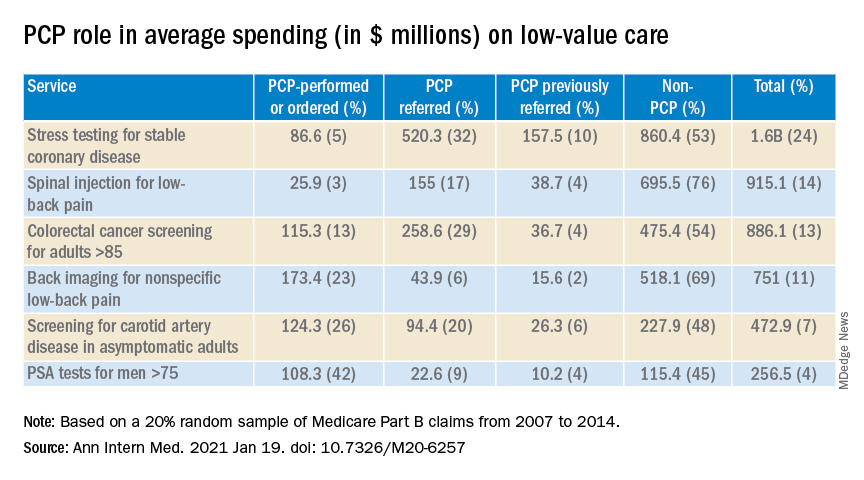
Dr. Fendrick said a weakness of the paper is the years of the data (2007-2014). Some of the criteria around low-value care have changed since then. The age that a prostate-specific antigen test becomes low-value is now 70 years, for instance, instead of 75. He added that some of the figures attributed to non-PCP providers appear out of date.
Dr. Fendrick said, “I understand that there are Medicare patients who end up at a gastroenterologist or surgeon’s office to get colorectal cancer screening, but it would be very hard for me to believe that half of stress tests and over half of colon cancer screening over [age] 85 [years] and half of PSA for people over 75 did not have some type of referring clinicians involved. I certainly don’t think that would be the case in 2020-2021.”
Dr. Baum said those years were the latest years available for the data points needed for this analysis, but he and his colleagues were working to update the data for future publication.
Dr. Fendrick said not much has changed in recent years in terms of waste on low-value care, even with campaigns such as Choosing Wisely dedicated to identifying low-value services or procedures in each specialty.
“I believe there’s not a particular group of clinicians one way or the other who are actually doing any better now than they were 7 years ago,” he said. He would rather focus less on which specialties are associated with the most low-value care and more on the underlying policies that encourage low-value care.
“If you’re going to get paid for doing a stress test and get paid nothing or significantly less if you don’t, the incentives are in the wrong direction,” he said.
Dr. Fendrick said the pandemic era provides an opportunity to eliminate low-value care because use of those services has dropped drastically as resources have been diverted to COVID-19 patients and many services have been delayed or canceled.
He said he has been pushing an approach that providers should be paid more after the pandemic “to do the things we want them to do.”
As an example, he said, instead of paying $886 million on colonoscopies for people over the age of 85, “why don’t we put a policy in place that would make it better for patients by lowering cost sharing and better for providers by paying them more to do the service on the people who need it as opposed to the people who don’t?”
The research was funded by the American Board of Family Medicine Foundation. Dr. Baum and a coauthor reported receiving personal fees from American Board of Family Medicine Foundation during the conduct of the study. Another coauthor reported receiving personal fees from Collective Health, HealthRight 360, PLOS Medicine, and the New England Journal of Medicine, outside the submitted work. Dr. Fendrick disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to a brief report published online Jan. 18 in Annals of Internal Medicine.
However, one expert said there are better ways to curb low-value care than focusing on which specialties are guilty of the practice.
Analyzing a 20% random sample of Medicare Part B claims, Aaron Baum, PhD, with the Icahn School of Medicine at Mount Sinai, New York, and colleagues found that the services primary care physicians performed or ordered made up on average 8.3% of the low-value care their patients received (interquartile range, 3.9%-15.1%; 95th percentile, 35.6%) and their referrals made up 15.4% (IQR, 6.3%-26.4%; 95th percentile, 44.6%).
By specialty, cardiology had the worst record with 27% of all spending on low-value services ($1.8 billion) attributed to that specialty. Yet, of the 25 highest-spending specialties in the report, 12 of them were associated with 1% or less than 1% each of all low-value spending, indicating the waste was widely distributed.
Dr. Baum said in an interview that though there are some PCPs guilty of high spending on low-value services, overall, most primary care physicians’ low-value services add up to only 0.3% of Part B spending. He noted that Part B spending is about one-third of all Medicare spending.
Primary care is often thought to be at the core of care management and spending and PCPs are often seen as the gatekeepers, but this analysis suggests that efforts to make big differences in curtailing low-value spending might be more effective elsewhere.
“There’s only so much spending you can reduce by changing primary care physicians’ services that they directly perform,” Dr. Baum said.
Low-value care is costly, can be harmful
Mark Fendrick, MD, director of the University of Michigan’s Center for Value-Based Insurance Design in Ann Arbor, said in an interview that the report adds confirmation to previous research that has consistently shown low-value care is “extremely common, very costly, and provided by primary care providers and specialists alike.” He noted that it can also be harmful.
“The math is simple,” he said. “If we want to improve coverage and lower patient costs for essential services like visits, diagnostic tests, and drugs, we have to reduce spending on those services that do not make Americans any healthier.”
The study ranked 31 clinical services judged to be low value by physician societies, Medicare and clinical guidelines, and their use among beneficiaries enrolled between 2007 and 2014. Here’s how the top six low-value services compare.
Dr. Fendrick said a weakness of the paper is the years of the data (2007-2014). Some of the criteria around low-value care have changed since then. The age that a prostate-specific antigen test becomes low-value is now 70 years, for instance, instead of 75. He added that some of the figures attributed to non-PCP providers appear out of date.
Dr. Fendrick said, “I understand that there are Medicare patients who end up at a gastroenterologist or surgeon’s office to get colorectal cancer screening, but it would be very hard for me to believe that half of stress tests and over half of colon cancer screening over [age] 85 [years] and half of PSA for people over 75 did not have some type of referring clinicians involved. I certainly don’t think that would be the case in 2020-2021.”
Dr. Baum said those years were the latest years available for the data points needed for this analysis, but he and his colleagues were working to update the data for future publication.
Dr. Fendrick said not much has changed in recent years in terms of waste on low-value care, even with campaigns such as Choosing Wisely dedicated to identifying low-value services or procedures in each specialty.
“I believe there’s not a particular group of clinicians one way or the other who are actually doing any better now than they were 7 years ago,” he said. He would rather focus less on which specialties are associated with the most low-value care and more on the underlying policies that encourage low-value care.
“If you’re going to get paid for doing a stress test and get paid nothing or significantly less if you don’t, the incentives are in the wrong direction,” he said.
Dr. Fendrick said the pandemic era provides an opportunity to eliminate low-value care because use of those services has dropped drastically as resources have been diverted to COVID-19 patients and many services have been delayed or canceled.
He said he has been pushing an approach that providers should be paid more after the pandemic “to do the things we want them to do.”
As an example, he said, instead of paying $886 million on colonoscopies for people over the age of 85, “why don’t we put a policy in place that would make it better for patients by lowering cost sharing and better for providers by paying them more to do the service on the people who need it as opposed to the people who don’t?”
The research was funded by the American Board of Family Medicine Foundation. Dr. Baum and a coauthor reported receiving personal fees from American Board of Family Medicine Foundation during the conduct of the study. Another coauthor reported receiving personal fees from Collective Health, HealthRight 360, PLOS Medicine, and the New England Journal of Medicine, outside the submitted work. Dr. Fendrick disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to a brief report published online Jan. 18 in Annals of Internal Medicine.
However, one expert said there are better ways to curb low-value care than focusing on which specialties are guilty of the practice.
Analyzing a 20% random sample of Medicare Part B claims, Aaron Baum, PhD, with the Icahn School of Medicine at Mount Sinai, New York, and colleagues found that the services primary care physicians performed or ordered made up on average 8.3% of the low-value care their patients received (interquartile range, 3.9%-15.1%; 95th percentile, 35.6%) and their referrals made up 15.4% (IQR, 6.3%-26.4%; 95th percentile, 44.6%).
By specialty, cardiology had the worst record with 27% of all spending on low-value services ($1.8 billion) attributed to that specialty. Yet, of the 25 highest-spending specialties in the report, 12 of them were associated with 1% or less than 1% each of all low-value spending, indicating the waste was widely distributed.
Dr. Baum said in an interview that though there are some PCPs guilty of high spending on low-value services, overall, most primary care physicians’ low-value services add up to only 0.3% of Part B spending. He noted that Part B spending is about one-third of all Medicare spending.
Primary care is often thought to be at the core of care management and spending and PCPs are often seen as the gatekeepers, but this analysis suggests that efforts to make big differences in curtailing low-value spending might be more effective elsewhere.
“There’s only so much spending you can reduce by changing primary care physicians’ services that they directly perform,” Dr. Baum said.
Low-value care is costly, can be harmful
Mark Fendrick, MD, director of the University of Michigan’s Center for Value-Based Insurance Design in Ann Arbor, said in an interview that the report adds confirmation to previous research that has consistently shown low-value care is “extremely common, very costly, and provided by primary care providers and specialists alike.” He noted that it can also be harmful.
“The math is simple,” he said. “If we want to improve coverage and lower patient costs for essential services like visits, diagnostic tests, and drugs, we have to reduce spending on those services that do not make Americans any healthier.”
The study ranked 31 clinical services judged to be low value by physician societies, Medicare and clinical guidelines, and their use among beneficiaries enrolled between 2007 and 2014. Here’s how the top six low-value services compare.
Dr. Fendrick said a weakness of the paper is the years of the data (2007-2014). Some of the criteria around low-value care have changed since then. The age that a prostate-specific antigen test becomes low-value is now 70 years, for instance, instead of 75. He added that some of the figures attributed to non-PCP providers appear out of date.
Dr. Fendrick said, “I understand that there are Medicare patients who end up at a gastroenterologist or surgeon’s office to get colorectal cancer screening, but it would be very hard for me to believe that half of stress tests and over half of colon cancer screening over [age] 85 [years] and half of PSA for people over 75 did not have some type of referring clinicians involved. I certainly don’t think that would be the case in 2020-2021.”
Dr. Baum said those years were the latest years available for the data points needed for this analysis, but he and his colleagues were working to update the data for future publication.
Dr. Fendrick said not much has changed in recent years in terms of waste on low-value care, even with campaigns such as Choosing Wisely dedicated to identifying low-value services or procedures in each specialty.
“I believe there’s not a particular group of clinicians one way or the other who are actually doing any better now than they were 7 years ago,” he said. He would rather focus less on which specialties are associated with the most low-value care and more on the underlying policies that encourage low-value care.
“If you’re going to get paid for doing a stress test and get paid nothing or significantly less if you don’t, the incentives are in the wrong direction,” he said.
Dr. Fendrick said the pandemic era provides an opportunity to eliminate low-value care because use of those services has dropped drastically as resources have been diverted to COVID-19 patients and many services have been delayed or canceled.
He said he has been pushing an approach that providers should be paid more after the pandemic “to do the things we want them to do.”
As an example, he said, instead of paying $886 million on colonoscopies for people over the age of 85, “why don’t we put a policy in place that would make it better for patients by lowering cost sharing and better for providers by paying them more to do the service on the people who need it as opposed to the people who don’t?”
The research was funded by the American Board of Family Medicine Foundation. Dr. Baum and a coauthor reported receiving personal fees from American Board of Family Medicine Foundation during the conduct of the study. Another coauthor reported receiving personal fees from Collective Health, HealthRight 360, PLOS Medicine, and the New England Journal of Medicine, outside the submitted work. Dr. Fendrick disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Finding meaning in ‘Lean’?
Using systems improvement strategies to support the Quadruple Aim
General background on well-being and burnout
With burnout increasingly recognized as a shared responsibility that requires addressing organizational drivers while supporting individuals to be well,1-4 practical strategies and examples of successful implementation of systems interventions to address burnout will be helpful for service directors to support their staff. The Charter on Physician Well-being, recently developed through collaborative input from multiple organizations, defines guiding principles and key commitments at the societal, organizational, interpersonal, and individual levels and may be a useful framework for organizations that are developing well-being initiatives.5

The charter advocates including physician well-being as a quality improvement metric for health systems, aligned with the concept of the Quadruple Aim of optimizing patient care by enhancing provider experience, promoting high-value care, and improving population health.6 Identifying areas of alignment between the charter’s recommendations and systems improvement strategies that seek to optimize efficiency and reduce waste, such as Lean Management, may help physician leaders to contextualize well-being initiatives more easily within ongoing systems improvement efforts. In this perspective, we provide one division’s experience using the Charter to assess successes and identify additional areas of improvement for well-being initiatives developed using Lean Management methodology.
Past and current state of affairs
In 2011, the division of hospital medicine at Zuckerberg San Francisco General Hospital was established and has seen continual expansion in terms of direct patient care, medical education, and hospital leadership.
In 2015, the division of hospital medicine experienced leadership transitions, faculty attrition, and insufficient recruitment resulting in staffing shortages, service line closure, schedule instability, and ultimately, low morale. A baseline survey conducted using the 2-Item Maslach Burnout Inventory. This survey, which uses one item in the domain of emotional exhaustion and one item in the domain of depersonalization, has shown good correlation with the full Maslach Burnout Inventory.7 At baseline, approximately one-third of the division’s physicians experienced burnout.
In response, a subsequent retreat focused on the three greatest areas of concern identified by the survey: scheduling, faculty development, and well-being.
Like many health systems, the hospital has adopted Lean as its preferred systems-improvement framework. The retreat was structured around the principles of Lean philosophy, and was designed to emulate that of a consolidated Kaizen workshop.
“Kaizen” in Japanese means “change for the better.” A typical Kaizen workshop revolves around rapid problem-solving over the course of 3-5 days, in which a team of people come together to identify and implement significant improvements for a selected process. To this end, the retreat was divided into subgroups for each area of concern. In turn, each subgroup mapped out existing workflows (“value stream”), identified areas of waste and non–value added time, and generated ideas of what an idealized process would be. Next, a root-cause analysis was performed and subsequent interventions (“countermeasures”) developed to address each problem. At the conclusion of the retreat, each subgroup shared a summary of their findings with the larger group.
Moving forward, this information served as a guiding framework for service and division leadership to run small tests of change. We enacted a series of countermeasures over the course of several years, and multiple cycles of improvement work addressed the three areas of concern. We developed an A3 report (a Lean project management tool that incorporates the plan-do-study-act cycle, organizes strategic efforts, and tracks progress on a single page) to summarize and present these initiatives to the Performance Improvement and Patient Safety Committee of the hospital executive leadership team. This structure illustrated alignment with the hospital’s core values (“true north”) of “developing people” and “care experience.”
In 2018, interval surveys demonstrated a gradual reduction of burnout to approximately one-fifth of division physicians as measured by the 2-item Maslach Burnout Inventory.
Initiatives in faculty well-being
The Charter of Physician Well-being outlines a framework to promote well-being among doctors by maximizing a sense of fulfillment and minimizing the harms of burnout. It shares this responsibility among societal, organizational, and interpersonal and individual commitments.5
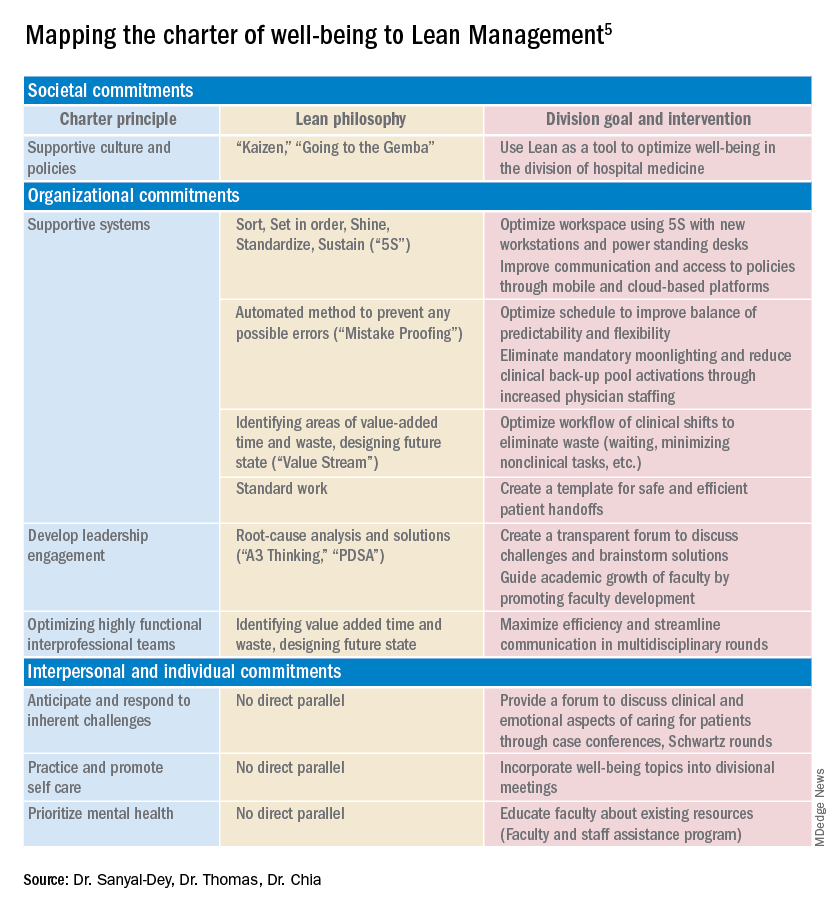
As illustrated above, we used principles of Lean Management to prospectively create initiatives to improve well-being in our division. Lean in health care is designed to optimize primarily the patient experience; its implementation has subsequently demonstrated mixed provider and staff experiences,8,9 and many providers are skeptical of Lean’s potential to improve their own well-being. If, however, Lean is aligned with best practice frameworks for well-being such as those outline in the charter, it may also help to meet the Quadruple Aim of optimizing both provider well-being and patient experience. To further test this hypothesis, we retrospectively categorized our Lean-based interventions into the commitments described by the charter to identify areas of alignment and gaps that were not initially addressed using Lean Management (Table).
Organizational commitments5Supportive systems
We optimized scheduling and enhanced physician staffing by budgeting for a physician staffing buffer each academic year in order to minimize mandatory moonlighting and jeopardy pool activations that result from operating on a thin staffing margin when expected personal leave and reductions in clinical effort occur. Furthermore, we revised scheduling principles to balance patient continuity and individual time off requests while setting limits on the maximum duration of clinical stretches and instituting mandatory minimum time off between them.
Leadership engagement
We initiated monthly operations meetings as a forum to discuss challenges, brainstorm solutions, and message new initiatives with group input. For example, as a result of these meetings, we designed and implemented an additional service line to address the high census, revised the distribution of new patient admissions to level-load clinical shifts, and established a maximum number of weekends worked per month and year. This approach aligns with recommendations to use participatory leadership strategies to enhance physician well-being.10 Engaging both executive level and service level management to focus on burnout and other related well-being metrics is necessary for sustaining such work.

Interprofessional teamwork
We revised multidisciplinary rounds with social work, utilization management, and physical therapy to maximize efficiency and streamline communication by developing standard approaches for each patient presentation.
Interpersonal and individual commitments5Address emotional challenges of physician work
Although these commitments did not have a direct corollary with Lean philosophy, some of these needs were identified by our physician group at our annual retreats. As a result, we initiated a monthly faculty-led noon conference series focused on the clinical challenges of caring for vulnerable populations, a particular source of distress in our practice setting, and revised the division schedule to encourage attendance at the hospital’s Schwartz rounds.
Mental health and self-care
We organized focus groups and faculty development sessions on provider well-being and burnout and dealing with challenging patients and invited the Faculty and Staff Assistance Program, our institution’s mental health service provider, to our weekly division meeting.
Future directions
After using Lean Management as an approach to prospectively improve physician well-being, we were able to use the Charter on Physician Well-being retrospectively as a “checklist” to identify additional gaps for targeted intervention to ensure all commitments are sufficiently addressed.
Overall, we found that, not surprisingly, Lean Management aligned best with the organizational commitments in the charter. Reviewing the organizational commitments, we found our biggest remaining challenges are in building supportive systems, namely ensuring sustainable workloads, offloading and delegating nonphysician tasks, and minimizing the burden of documentation and administration.

Reviewing the societal commitments helped us to identify opportunities for future directions that we may not have otherwise considered. As a safety-net institution, we benefit from a strong sense of mission and shared values within our hospital and division. However, we recognize the need to continue to be vigilant to ensure that our physicians perceive that their own values are aligned with the division’s stated mission. Devoting a Kaizen-style retreat to well-being likely helped, and allocating divisional resources to a well-being committee indirectly helped, to foster a culture of well-being; however, we could more deliberately identify local policies that may benefit from advocacy or revision. Although our faculty identified interventions to improve interpersonal and individual drivers of well-being, these charter commitments did not have direct parallels in Lean philosophy, and organizations may need to deliberately seek to address these commitments outside of a Lean approach. Specifically, by reviewing the charter, we identified opportunities to provide additional resources for peer support and protected time for mental health care and self-care.
Conclusion
Lean Management can be an effective strategy to address many of the organizational commitments outlined in the Charter on Physician Well-being. This approach may be particularly effective for solving local challenges with systems and workflows. Those who use Lean as a primary method to approach systems improvement in support of the Quadruple Aim may need to use additional strategies to address societal and interpersonal and individual commitments outlined in the charter.
Dr. Sanyal-Dey is visiting associate clinical professor of medicine at Zuckerberg San Francisco General Hospital and director of client services, LeanTaaS. Dr. Thomas is associate clinical professor of medicine at Zuckerberg San Francisco General Hospital. Dr. Chia is associate professor of clinical medicine at Zuckerberg San Francisco General Hospital.
References
1. West CP et al. Interventions to prevent and reduce physician burnout: A systematic review and meta-analysis. Lancet. 2016;388(10057):2272-81.
2. Shanafelt TD, Noseworthy JH. Executive leadership and physician: Nine organizational strategies to promote engagement and reduce burnout. Mayo Clin Proc. 2017;92(1):129-46.
3. Shanafelt T et al. The business case for investing in physician well-being. JAMA Intern Med. 2017;177(12):1826-32.
4. Shanafelt T et al. Building a program on well-being: Key design considerations to meet the unique needs of each organization. Acad Med. 2019 Feb;94(2):156-161.
5. Thomas LR et al. Charter on physician well-being. JAMA. 2018;319(15):1541-42.
6. Bodenheimer T, Sinsky C. From triple to quadruple aim: Care of the patient requires care of the provider. Ann Fam Med. 2014;12(6):573-6.
7. West CP et al. Concurrent Validity of Single-Item Measures of Emotional Exhaustion and Depersonalization in Burnout Assessment. J Gen Intern Med. 2012;27(11):1445-52.
8. Hung DY et al. Experiences of primary care physicians and staff following lean workflow redesign. BMC Health Serv Res. 2018 Apr 10;18(1):274.
9. Zibrowski E et al. Easier and faster is not always better: Grounded theory of the impact of large-scale system transformation on the clinical work of emergency medicine nurses and physicians. JMIR Hum Factors. 2018. doi: 10.2196/11013.
10. Shanafelt TD et al. Impact of organizational leadership on physician burnout and satisfaction. Mayo Clin Proc. 2015;90(4):432-40.
Using systems improvement strategies to support the Quadruple Aim
Using systems improvement strategies to support the Quadruple Aim
General background on well-being and burnout
With burnout increasingly recognized as a shared responsibility that requires addressing organizational drivers while supporting individuals to be well,1-4 practical strategies and examples of successful implementation of systems interventions to address burnout will be helpful for service directors to support their staff. The Charter on Physician Well-being, recently developed through collaborative input from multiple organizations, defines guiding principles and key commitments at the societal, organizational, interpersonal, and individual levels and may be a useful framework for organizations that are developing well-being initiatives.5
The charter advocates including physician well-being as a quality improvement metric for health systems, aligned with the concept of the Quadruple Aim of optimizing patient care by enhancing provider experience, promoting high-value care, and improving population health.6 Identifying areas of alignment between the charter’s recommendations and systems improvement strategies that seek to optimize efficiency and reduce waste, such as Lean Management, may help physician leaders to contextualize well-being initiatives more easily within ongoing systems improvement efforts. In this perspective, we provide one division’s experience using the Charter to assess successes and identify additional areas of improvement for well-being initiatives developed using Lean Management methodology.
Past and current state of affairs
In 2011, the division of hospital medicine at Zuckerberg San Francisco General Hospital was established and has seen continual expansion in terms of direct patient care, medical education, and hospital leadership.
In 2015, the division of hospital medicine experienced leadership transitions, faculty attrition, and insufficient recruitment resulting in staffing shortages, service line closure, schedule instability, and ultimately, low morale. A baseline survey conducted using the 2-Item Maslach Burnout Inventory. This survey, which uses one item in the domain of emotional exhaustion and one item in the domain of depersonalization, has shown good correlation with the full Maslach Burnout Inventory.7 At baseline, approximately one-third of the division’s physicians experienced burnout.
In response, a subsequent retreat focused on the three greatest areas of concern identified by the survey: scheduling, faculty development, and well-being.
Like many health systems, the hospital has adopted Lean as its preferred systems-improvement framework. The retreat was structured around the principles of Lean philosophy, and was designed to emulate that of a consolidated Kaizen workshop.
“Kaizen” in Japanese means “change for the better.” A typical Kaizen workshop revolves around rapid problem-solving over the course of 3-5 days, in which a team of people come together to identify and implement significant improvements for a selected process. To this end, the retreat was divided into subgroups for each area of concern. In turn, each subgroup mapped out existing workflows (“value stream”), identified areas of waste and non–value added time, and generated ideas of what an idealized process would be. Next, a root-cause analysis was performed and subsequent interventions (“countermeasures”) developed to address each problem. At the conclusion of the retreat, each subgroup shared a summary of their findings with the larger group.
Moving forward, this information served as a guiding framework for service and division leadership to run small tests of change. We enacted a series of countermeasures over the course of several years, and multiple cycles of improvement work addressed the three areas of concern. We developed an A3 report (a Lean project management tool that incorporates the plan-do-study-act cycle, organizes strategic efforts, and tracks progress on a single page) to summarize and present these initiatives to the Performance Improvement and Patient Safety Committee of the hospital executive leadership team. This structure illustrated alignment with the hospital’s core values (“true north”) of “developing people” and “care experience.”
In 2018, interval surveys demonstrated a gradual reduction of burnout to approximately one-fifth of division physicians as measured by the 2-item Maslach Burnout Inventory.
Initiatives in faculty well-being
The Charter of Physician Well-being outlines a framework to promote well-being among doctors by maximizing a sense of fulfillment and minimizing the harms of burnout. It shares this responsibility among societal, organizational, and interpersonal and individual commitments.5
As illustrated above, we used principles of Lean Management to prospectively create initiatives to improve well-being in our division. Lean in health care is designed to optimize primarily the patient experience; its implementation has subsequently demonstrated mixed provider and staff experiences,8,9 and many providers are skeptical of Lean’s potential to improve their own well-being. If, however, Lean is aligned with best practice frameworks for well-being such as those outline in the charter, it may also help to meet the Quadruple Aim of optimizing both provider well-being and patient experience. To further test this hypothesis, we retrospectively categorized our Lean-based interventions into the commitments described by the charter to identify areas of alignment and gaps that were not initially addressed using Lean Management (Table).
Organizational commitments5Supportive systems
We optimized scheduling and enhanced physician staffing by budgeting for a physician staffing buffer each academic year in order to minimize mandatory moonlighting and jeopardy pool activations that result from operating on a thin staffing margin when expected personal leave and reductions in clinical effort occur. Furthermore, we revised scheduling principles to balance patient continuity and individual time off requests while setting limits on the maximum duration of clinical stretches and instituting mandatory minimum time off between them.
Leadership engagement
We initiated monthly operations meetings as a forum to discuss challenges, brainstorm solutions, and message new initiatives with group input. For example, as a result of these meetings, we designed and implemented an additional service line to address the high census, revised the distribution of new patient admissions to level-load clinical shifts, and established a maximum number of weekends worked per month and year. This approach aligns with recommendations to use participatory leadership strategies to enhance physician well-being.10 Engaging both executive level and service level management to focus on burnout and other related well-being metrics is necessary for sustaining such work.
Interprofessional teamwork
We revised multidisciplinary rounds with social work, utilization management, and physical therapy to maximize efficiency and streamline communication by developing standard approaches for each patient presentation.
Interpersonal and individual commitments5Address emotional challenges of physician work
Although these commitments did not have a direct corollary with Lean philosophy, some of these needs were identified by our physician group at our annual retreats. As a result, we initiated a monthly faculty-led noon conference series focused on the clinical challenges of caring for vulnerable populations, a particular source of distress in our practice setting, and revised the division schedule to encourage attendance at the hospital’s Schwartz rounds.
Mental health and self-care
We organized focus groups and faculty development sessions on provider well-being and burnout and dealing with challenging patients and invited the Faculty and Staff Assistance Program, our institution’s mental health service provider, to our weekly division meeting.
Future directions
After using Lean Management as an approach to prospectively improve physician well-being, we were able to use the Charter on Physician Well-being retrospectively as a “checklist” to identify additional gaps for targeted intervention to ensure all commitments are sufficiently addressed.
Overall, we found that, not surprisingly, Lean Management aligned best with the organizational commitments in the charter. Reviewing the organizational commitments, we found our biggest remaining challenges are in building supportive systems, namely ensuring sustainable workloads, offloading and delegating nonphysician tasks, and minimizing the burden of documentation and administration.
Reviewing the societal commitments helped us to identify opportunities for future directions that we may not have otherwise considered. As a safety-net institution, we benefit from a strong sense of mission and shared values within our hospital and division. However, we recognize the need to continue to be vigilant to ensure that our physicians perceive that their own values are aligned with the division’s stated mission. Devoting a Kaizen-style retreat to well-being likely helped, and allocating divisional resources to a well-being committee indirectly helped, to foster a culture of well-being; however, we could more deliberately identify local policies that may benefit from advocacy or revision. Although our faculty identified interventions to improve interpersonal and individual drivers of well-being, these charter commitments did not have direct parallels in Lean philosophy, and organizations may need to deliberately seek to address these commitments outside of a Lean approach. Specifically, by reviewing the charter, we identified opportunities to provide additional resources for peer support and protected time for mental health care and self-care.
Conclusion
Lean Management can be an effective strategy to address many of the organizational commitments outlined in the Charter on Physician Well-being. This approach may be particularly effective for solving local challenges with systems and workflows. Those who use Lean as a primary method to approach systems improvement in support of the Quadruple Aim may need to use additional strategies to address societal and interpersonal and individual commitments outlined in the charter.
Dr. Sanyal-Dey is visiting associate clinical professor of medicine at Zuckerberg San Francisco General Hospital and director of client services, LeanTaaS. Dr. Thomas is associate clinical professor of medicine at Zuckerberg San Francisco General Hospital. Dr. Chia is associate professor of clinical medicine at Zuckerberg San Francisco General Hospital.
References
1. West CP et al. Interventions to prevent and reduce physician burnout: A systematic review and meta-analysis. Lancet. 2016;388(10057):2272-81.
2. Shanafelt TD, Noseworthy JH. Executive leadership and physician: Nine organizational strategies to promote engagement and reduce burnout. Mayo Clin Proc. 2017;92(1):129-46.
3. Shanafelt T et al. The business case for investing in physician well-being. JAMA Intern Med. 2017;177(12):1826-32.
4. Shanafelt T et al. Building a program on well-being: Key design considerations to meet the unique needs of each organization. Acad Med. 2019 Feb;94(2):156-161.
5. Thomas LR et al. Charter on physician well-being. JAMA. 2018;319(15):1541-42.
6. Bodenheimer T, Sinsky C. From triple to quadruple aim: Care of the patient requires care of the provider. Ann Fam Med. 2014;12(6):573-6.
7. West CP et al. Concurrent Validity of Single-Item Measures of Emotional Exhaustion and Depersonalization in Burnout Assessment. J Gen Intern Med. 2012;27(11):1445-52.
8. Hung DY et al. Experiences of primary care physicians and staff following lean workflow redesign. BMC Health Serv Res. 2018 Apr 10;18(1):274.
9. Zibrowski E et al. Easier and faster is not always better: Grounded theory of the impact of large-scale system transformation on the clinical work of emergency medicine nurses and physicians. JMIR Hum Factors. 2018. doi: 10.2196/11013.
10. Shanafelt TD et al. Impact of organizational leadership on physician burnout and satisfaction. Mayo Clin Proc. 2015;90(4):432-40.
General background on well-being and burnout
With burnout increasingly recognized as a shared responsibility that requires addressing organizational drivers while supporting individuals to be well,1-4 practical strategies and examples of successful implementation of systems interventions to address burnout will be helpful for service directors to support their staff. The Charter on Physician Well-being, recently developed through collaborative input from multiple organizations, defines guiding principles and key commitments at the societal, organizational, interpersonal, and individual levels and may be a useful framework for organizations that are developing well-being initiatives.5
The charter advocates including physician well-being as a quality improvement metric for health systems, aligned with the concept of the Quadruple Aim of optimizing patient care by enhancing provider experience, promoting high-value care, and improving population health.6 Identifying areas of alignment between the charter’s recommendations and systems improvement strategies that seek to optimize efficiency and reduce waste, such as Lean Management, may help physician leaders to contextualize well-being initiatives more easily within ongoing systems improvement efforts. In this perspective, we provide one division’s experience using the Charter to assess successes and identify additional areas of improvement for well-being initiatives developed using Lean Management methodology.
Past and current state of affairs
In 2011, the division of hospital medicine at Zuckerberg San Francisco General Hospital was established and has seen continual expansion in terms of direct patient care, medical education, and hospital leadership.
In 2015, the division of hospital medicine experienced leadership transitions, faculty attrition, and insufficient recruitment resulting in staffing shortages, service line closure, schedule instability, and ultimately, low morale. A baseline survey conducted using the 2-Item Maslach Burnout Inventory. This survey, which uses one item in the domain of emotional exhaustion and one item in the domain of depersonalization, has shown good correlation with the full Maslach Burnout Inventory.7 At baseline, approximately one-third of the division’s physicians experienced burnout.
In response, a subsequent retreat focused on the three greatest areas of concern identified by the survey: scheduling, faculty development, and well-being.
Like many health systems, the hospital has adopted Lean as its preferred systems-improvement framework. The retreat was structured around the principles of Lean philosophy, and was designed to emulate that of a consolidated Kaizen workshop.
“Kaizen” in Japanese means “change for the better.” A typical Kaizen workshop revolves around rapid problem-solving over the course of 3-5 days, in which a team of people come together to identify and implement significant improvements for a selected process. To this end, the retreat was divided into subgroups for each area of concern. In turn, each subgroup mapped out existing workflows (“value stream”), identified areas of waste and non–value added time, and generated ideas of what an idealized process would be. Next, a root-cause analysis was performed and subsequent interventions (“countermeasures”) developed to address each problem. At the conclusion of the retreat, each subgroup shared a summary of their findings with the larger group.
Moving forward, this information served as a guiding framework for service and division leadership to run small tests of change. We enacted a series of countermeasures over the course of several years, and multiple cycles of improvement work addressed the three areas of concern. We developed an A3 report (a Lean project management tool that incorporates the plan-do-study-act cycle, organizes strategic efforts, and tracks progress on a single page) to summarize and present these initiatives to the Performance Improvement and Patient Safety Committee of the hospital executive leadership team. This structure illustrated alignment with the hospital’s core values (“true north”) of “developing people” and “care experience.”
In 2018, interval surveys demonstrated a gradual reduction of burnout to approximately one-fifth of division physicians as measured by the 2-item Maslach Burnout Inventory.
Initiatives in faculty well-being
The Charter of Physician Well-being outlines a framework to promote well-being among doctors by maximizing a sense of fulfillment and minimizing the harms of burnout. It shares this responsibility among societal, organizational, and interpersonal and individual commitments.5
As illustrated above, we used principles of Lean Management to prospectively create initiatives to improve well-being in our division. Lean in health care is designed to optimize primarily the patient experience; its implementation has subsequently demonstrated mixed provider and staff experiences,8,9 and many providers are skeptical of Lean’s potential to improve their own well-being. If, however, Lean is aligned with best practice frameworks for well-being such as those outline in the charter, it may also help to meet the Quadruple Aim of optimizing both provider well-being and patient experience. To further test this hypothesis, we retrospectively categorized our Lean-based interventions into the commitments described by the charter to identify areas of alignment and gaps that were not initially addressed using Lean Management (Table).
Organizational commitments5Supportive systems
We optimized scheduling and enhanced physician staffing by budgeting for a physician staffing buffer each academic year in order to minimize mandatory moonlighting and jeopardy pool activations that result from operating on a thin staffing margin when expected personal leave and reductions in clinical effort occur. Furthermore, we revised scheduling principles to balance patient continuity and individual time off requests while setting limits on the maximum duration of clinical stretches and instituting mandatory minimum time off between them.
Leadership engagement
We initiated monthly operations meetings as a forum to discuss challenges, brainstorm solutions, and message new initiatives with group input. For example, as a result of these meetings, we designed and implemented an additional service line to address the high census, revised the distribution of new patient admissions to level-load clinical shifts, and established a maximum number of weekends worked per month and year. This approach aligns with recommendations to use participatory leadership strategies to enhance physician well-being.10 Engaging both executive level and service level management to focus on burnout and other related well-being metrics is necessary for sustaining such work.
Interprofessional teamwork
We revised multidisciplinary rounds with social work, utilization management, and physical therapy to maximize efficiency and streamline communication by developing standard approaches for each patient presentation.
Interpersonal and individual commitments5Address emotional challenges of physician work
Although these commitments did not have a direct corollary with Lean philosophy, some of these needs were identified by our physician group at our annual retreats. As a result, we initiated a monthly faculty-led noon conference series focused on the clinical challenges of caring for vulnerable populations, a particular source of distress in our practice setting, and revised the division schedule to encourage attendance at the hospital’s Schwartz rounds.
Mental health and self-care
We organized focus groups and faculty development sessions on provider well-being and burnout and dealing with challenging patients and invited the Faculty and Staff Assistance Program, our institution’s mental health service provider, to our weekly division meeting.
Future directions
After using Lean Management as an approach to prospectively improve physician well-being, we were able to use the Charter on Physician Well-being retrospectively as a “checklist” to identify additional gaps for targeted intervention to ensure all commitments are sufficiently addressed.
Overall, we found that, not surprisingly, Lean Management aligned best with the organizational commitments in the charter. Reviewing the organizational commitments, we found our biggest remaining challenges are in building supportive systems, namely ensuring sustainable workloads, offloading and delegating nonphysician tasks, and minimizing the burden of documentation and administration.
Reviewing the societal commitments helped us to identify opportunities for future directions that we may not have otherwise considered. As a safety-net institution, we benefit from a strong sense of mission and shared values within our hospital and division. However, we recognize the need to continue to be vigilant to ensure that our physicians perceive that their own values are aligned with the division’s stated mission. Devoting a Kaizen-style retreat to well-being likely helped, and allocating divisional resources to a well-being committee indirectly helped, to foster a culture of well-being; however, we could more deliberately identify local policies that may benefit from advocacy or revision. Although our faculty identified interventions to improve interpersonal and individual drivers of well-being, these charter commitments did not have direct parallels in Lean philosophy, and organizations may need to deliberately seek to address these commitments outside of a Lean approach. Specifically, by reviewing the charter, we identified opportunities to provide additional resources for peer support and protected time for mental health care and self-care.
Conclusion
Lean Management can be an effective strategy to address many of the organizational commitments outlined in the Charter on Physician Well-being. This approach may be particularly effective for solving local challenges with systems and workflows. Those who use Lean as a primary method to approach systems improvement in support of the Quadruple Aim may need to use additional strategies to address societal and interpersonal and individual commitments outlined in the charter.
Dr. Sanyal-Dey is visiting associate clinical professor of medicine at Zuckerberg San Francisco General Hospital and director of client services, LeanTaaS. Dr. Thomas is associate clinical professor of medicine at Zuckerberg San Francisco General Hospital. Dr. Chia is associate professor of clinical medicine at Zuckerberg San Francisco General Hospital.
References
1. West CP et al. Interventions to prevent and reduce physician burnout: A systematic review and meta-analysis. Lancet. 2016;388(10057):2272-81.
2. Shanafelt TD, Noseworthy JH. Executive leadership and physician: Nine organizational strategies to promote engagement and reduce burnout. Mayo Clin Proc. 2017;92(1):129-46.
3. Shanafelt T et al. The business case for investing in physician well-being. JAMA Intern Med. 2017;177(12):1826-32.
4. Shanafelt T et al. Building a program on well-being: Key design considerations to meet the unique needs of each organization. Acad Med. 2019 Feb;94(2):156-161.
5. Thomas LR et al. Charter on physician well-being. JAMA. 2018;319(15):1541-42.
6. Bodenheimer T, Sinsky C. From triple to quadruple aim: Care of the patient requires care of the provider. Ann Fam Med. 2014;12(6):573-6.
7. West CP et al. Concurrent Validity of Single-Item Measures of Emotional Exhaustion and Depersonalization in Burnout Assessment. J Gen Intern Med. 2012;27(11):1445-52.
8. Hung DY et al. Experiences of primary care physicians and staff following lean workflow redesign. BMC Health Serv Res. 2018 Apr 10;18(1):274.
9. Zibrowski E et al. Easier and faster is not always better: Grounded theory of the impact of large-scale system transformation on the clinical work of emergency medicine nurses and physicians. JMIR Hum Factors. 2018. doi: 10.2196/11013.
10. Shanafelt TD et al. Impact of organizational leadership on physician burnout and satisfaction. Mayo Clin Proc. 2015;90(4):432-40.
An introduction to Naikan
The list of things to be ungrateful for last year is long. You’re not supposed to make this list, though. The best practice is to list what you’re grateful for, even when living in trying times. That’s a long list too, but I find making it similarly unfruitful.
Of course, I’m grateful I don’t have COVID-19, thankful my practice hasn’t been significantly impacted, grateful I got the vaccine. But simply repeating these gratitudes daily seems ineffective. I’ve learned a different “gratefulness practice” that perhaps works better.

It’s a Japanese method called Naikan (pronounced “nye-kan”). The word means introspection and the practice is one of self-reflection. But . Yoshimoto Ishin developed Naikan in the 1940s. He was a Japanese businessman and devout Buddhist who wanted to make a difficult form of meditation more accessible. He removed the ascetic bits like sleep deprivation and refined the exercises such that they better see how others see us. The result is a way to reframe your life experiences and help you understand how much others do for us and how our actions and attitudes impact others. It can be done alone or with a partner. You can do it at the beginning or end of your day.
The method is simple. You ask three questions:
What have I received today from ___________?
What have I given today to ___________?
What difficulty or trouble have I caused to ___________?
The first question is similar to most gratitude practices. For example, you might ask, “What have I received from (my husband or nurse or friend, etc.)? Today, I received a beautifully tidied-up office from my wife who spent time last night sorting things. This made it easy for me to sit down and start writing this piece.

The second question is better. What have I given today to (my wife, or patient, or mom, etc.)? It can be simple as: Today, I slowed down to let everyone who was in the closed highway lane back into traffic (even though some were clearly undeserving of my generosity). Or last night, I worked to coordinate with anesthesia and scheduling to help a little girl who would benefit from conscious sedation for her procedure.
Combined, these two questions pull you 180 degrees from our default mode, which is complaining. We are wired to find, and talk about, all the inconveniences in our lives: Roadway construction caused a traffic backup that led to running late for clinic. First patient was peeved and had a list of complaints, the last of which was hair loss. Isn’t it much better to rave about how our dermatology nurse volunteered to work the hospital COVID-19 unit to give her colleagues a break? Or how my 10:15 patient came early to be sure she was on time? (It happens.)
The last question is the best. We all spend time thinking about what others think of us. We should spend time thinking about what impact we’ve had on them. Like a cold shower, it’s both briskly awakening and easy to do. Go back through your day and reflect on what you did that made things difficult for others. It can be as simple as I started whining about how a patient waylaid me with her silly complaints. That led to my colleague’s joining in about difficult patients. Or I was late turning in my article, which made my editor have to work harder to get it completed in time.
There’s plenty of things we should be grateful for. In doing these exercises you’ll learn just how much others have cared for you and, I hope, how you might do things to make them grateful for you.
If you’re interested in learning more about Naikan, I discovered this from Brett McKay’s The Art of Manliness podcast and the teaching of Gregg Krech, summarized in his book, “Naikan: Gratitude, Grace, and the Japanese Art of Self-Reflection.”
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected] .
The list of things to be ungrateful for last year is long. You’re not supposed to make this list, though. The best practice is to list what you’re grateful for, even when living in trying times. That’s a long list too, but I find making it similarly unfruitful.
Of course, I’m grateful I don’t have COVID-19, thankful my practice hasn’t been significantly impacted, grateful I got the vaccine. But simply repeating these gratitudes daily seems ineffective. I’ve learned a different “gratefulness practice” that perhaps works better.
It’s a Japanese method called Naikan (pronounced “nye-kan”). The word means introspection and the practice is one of self-reflection. But . Yoshimoto Ishin developed Naikan in the 1940s. He was a Japanese businessman and devout Buddhist who wanted to make a difficult form of meditation more accessible. He removed the ascetic bits like sleep deprivation and refined the exercises such that they better see how others see us. The result is a way to reframe your life experiences and help you understand how much others do for us and how our actions and attitudes impact others. It can be done alone or with a partner. You can do it at the beginning or end of your day.
The method is simple. You ask three questions:
What have I received today from ___________?
What have I given today to ___________?
What difficulty or trouble have I caused to ___________?
The first question is similar to most gratitude practices. For example, you might ask, “What have I received from (my husband or nurse or friend, etc.)? Today, I received a beautifully tidied-up office from my wife who spent time last night sorting things. This made it easy for me to sit down and start writing this piece.
The second question is better. What have I given today to (my wife, or patient, or mom, etc.)? It can be simple as: Today, I slowed down to let everyone who was in the closed highway lane back into traffic (even though some were clearly undeserving of my generosity). Or last night, I worked to coordinate with anesthesia and scheduling to help a little girl who would benefit from conscious sedation for her procedure.
Combined, these two questions pull you 180 degrees from our default mode, which is complaining. We are wired to find, and talk about, all the inconveniences in our lives: Roadway construction caused a traffic backup that led to running late for clinic. First patient was peeved and had a list of complaints, the last of which was hair loss. Isn’t it much better to rave about how our dermatology nurse volunteered to work the hospital COVID-19 unit to give her colleagues a break? Or how my 10:15 patient came early to be sure she was on time? (It happens.)
The last question is the best. We all spend time thinking about what others think of us. We should spend time thinking about what impact we’ve had on them. Like a cold shower, it’s both briskly awakening and easy to do. Go back through your day and reflect on what you did that made things difficult for others. It can be as simple as I started whining about how a patient waylaid me with her silly complaints. That led to my colleague’s joining in about difficult patients. Or I was late turning in my article, which made my editor have to work harder to get it completed in time.
There’s plenty of things we should be grateful for. In doing these exercises you’ll learn just how much others have cared for you and, I hope, how you might do things to make them grateful for you.
If you’re interested in learning more about Naikan, I discovered this from Brett McKay’s The Art of Manliness podcast and the teaching of Gregg Krech, summarized in his book, “Naikan: Gratitude, Grace, and the Japanese Art of Self-Reflection.”
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected] .
The list of things to be ungrateful for last year is long. You’re not supposed to make this list, though. The best practice is to list what you’re grateful for, even when living in trying times. That’s a long list too, but I find making it similarly unfruitful.
Of course, I’m grateful I don’t have COVID-19, thankful my practice hasn’t been significantly impacted, grateful I got the vaccine. But simply repeating these gratitudes daily seems ineffective. I’ve learned a different “gratefulness practice” that perhaps works better.
It’s a Japanese method called Naikan (pronounced “nye-kan”). The word means introspection and the practice is one of self-reflection. But . Yoshimoto Ishin developed Naikan in the 1940s. He was a Japanese businessman and devout Buddhist who wanted to make a difficult form of meditation more accessible. He removed the ascetic bits like sleep deprivation and refined the exercises such that they better see how others see us. The result is a way to reframe your life experiences and help you understand how much others do for us and how our actions and attitudes impact others. It can be done alone or with a partner. You can do it at the beginning or end of your day.
The method is simple. You ask three questions:
What have I received today from ___________?
What have I given today to ___________?
What difficulty or trouble have I caused to ___________?
The first question is similar to most gratitude practices. For example, you might ask, “What have I received from (my husband or nurse or friend, etc.)? Today, I received a beautifully tidied-up office from my wife who spent time last night sorting things. This made it easy for me to sit down and start writing this piece.
The second question is better. What have I given today to (my wife, or patient, or mom, etc.)? It can be simple as: Today, I slowed down to let everyone who was in the closed highway lane back into traffic (even though some were clearly undeserving of my generosity). Or last night, I worked to coordinate with anesthesia and scheduling to help a little girl who would benefit from conscious sedation for her procedure.
Combined, these two questions pull you 180 degrees from our default mode, which is complaining. We are wired to find, and talk about, all the inconveniences in our lives: Roadway construction caused a traffic backup that led to running late for clinic. First patient was peeved and had a list of complaints, the last of which was hair loss. Isn’t it much better to rave about how our dermatology nurse volunteered to work the hospital COVID-19 unit to give her colleagues a break? Or how my 10:15 patient came early to be sure she was on time? (It happens.)
The last question is the best. We all spend time thinking about what others think of us. We should spend time thinking about what impact we’ve had on them. Like a cold shower, it’s both briskly awakening and easy to do. Go back through your day and reflect on what you did that made things difficult for others. It can be as simple as I started whining about how a patient waylaid me with her silly complaints. That led to my colleague’s joining in about difficult patients. Or I was late turning in my article, which made my editor have to work harder to get it completed in time.
There’s plenty of things we should be grateful for. In doing these exercises you’ll learn just how much others have cared for you and, I hope, how you might do things to make them grateful for you.
If you’re interested in learning more about Naikan, I discovered this from Brett McKay’s The Art of Manliness podcast and the teaching of Gregg Krech, summarized in his book, “Naikan: Gratitude, Grace, and the Japanese Art of Self-Reflection.”
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected] .
Pityriasis rosea carries few risks for pregnant women
according to a review of 33 patients.
“Though generally considered benign, PR may be associated with an increased risk of birth complications if acquired during pregnancy,” and previous studies have shown increased rates of complications including miscarriage and neonatal hypotonia in these patients, wrote Julian Stashower of the University of Virginia, Charlottesville, and colleagues.
In a retrospective study published in the Journal of the American Academy of Dermatology, the researchers assessed pregnancy outcomes in women who developed PR during pregnancy. They were identified from medical records at three institutions between September 2010 and June 2020. Diagnosis of PR, a papulosquamous skin eruption associated with human herpesvirus (HHV)–6/7 reactivation, was based on history and physical examination.
Overall, 8 of the 33 women (24%) had birth complications; the rates of preterm delivery, spontaneous pregnancy loss in clinically detectable pregnancies, and oligohydramnios were 6%, 0%, and 3%, respectively. The average onset of PR during pregnancy was earlier among women with complications, compared with those without complications (10.75 weeks’ gestation vs. 15.21 weeks’ gestation), but the difference was not statistically significant.
The researchers noted that their findings differed from the most recent study of PR in pregnancy, which included 60 patients and found a notably higher incidence of overall birth complications (50%), as well as higher incidence of neonatal hypotonia (25%), and miscarriage (13%).
The previous study also showed an increased risk of birth complications when PR onset occurred prior to 15 weeks’ gestation, but the current study did not reflect that finding, they wrote.
The current study findings were limited by several factors including the small sample size, retrospective design, and lack of confirmation of PR with HHV-6/7 testing, as well as lack of exclusion of atypical PR cases, the researchers noted. However, the results suggest that birth complications associated with PR may be lower than previously reported. “Further research is needed to guide future care and fully elucidate this possible association, which has important implications for both pregnant women with PR and their providers.”
The study received no outside funding. The researchers had no financial conflict to disclose.
according to a review of 33 patients.
“Though generally considered benign, PR may be associated with an increased risk of birth complications if acquired during pregnancy,” and previous studies have shown increased rates of complications including miscarriage and neonatal hypotonia in these patients, wrote Julian Stashower of the University of Virginia, Charlottesville, and colleagues.
In a retrospective study published in the Journal of the American Academy of Dermatology, the researchers assessed pregnancy outcomes in women who developed PR during pregnancy. They were identified from medical records at three institutions between September 2010 and June 2020. Diagnosis of PR, a papulosquamous skin eruption associated with human herpesvirus (HHV)–6/7 reactivation, was based on history and physical examination.
Overall, 8 of the 33 women (24%) had birth complications; the rates of preterm delivery, spontaneous pregnancy loss in clinically detectable pregnancies, and oligohydramnios were 6%, 0%, and 3%, respectively. The average onset of PR during pregnancy was earlier among women with complications, compared with those without complications (10.75 weeks’ gestation vs. 15.21 weeks’ gestation), but the difference was not statistically significant.
The researchers noted that their findings differed from the most recent study of PR in pregnancy, which included 60 patients and found a notably higher incidence of overall birth complications (50%), as well as higher incidence of neonatal hypotonia (25%), and miscarriage (13%).
The previous study also showed an increased risk of birth complications when PR onset occurred prior to 15 weeks’ gestation, but the current study did not reflect that finding, they wrote.
The current study findings were limited by several factors including the small sample size, retrospective design, and lack of confirmation of PR with HHV-6/7 testing, as well as lack of exclusion of atypical PR cases, the researchers noted. However, the results suggest that birth complications associated with PR may be lower than previously reported. “Further research is needed to guide future care and fully elucidate this possible association, which has important implications for both pregnant women with PR and their providers.”
The study received no outside funding. The researchers had no financial conflict to disclose.
according to a review of 33 patients.
“Though generally considered benign, PR may be associated with an increased risk of birth complications if acquired during pregnancy,” and previous studies have shown increased rates of complications including miscarriage and neonatal hypotonia in these patients, wrote Julian Stashower of the University of Virginia, Charlottesville, and colleagues.
In a retrospective study published in the Journal of the American Academy of Dermatology, the researchers assessed pregnancy outcomes in women who developed PR during pregnancy. They were identified from medical records at three institutions between September 2010 and June 2020. Diagnosis of PR, a papulosquamous skin eruption associated with human herpesvirus (HHV)–6/7 reactivation, was based on history and physical examination.
Overall, 8 of the 33 women (24%) had birth complications; the rates of preterm delivery, spontaneous pregnancy loss in clinically detectable pregnancies, and oligohydramnios were 6%, 0%, and 3%, respectively. The average onset of PR during pregnancy was earlier among women with complications, compared with those without complications (10.75 weeks’ gestation vs. 15.21 weeks’ gestation), but the difference was not statistically significant.
The researchers noted that their findings differed from the most recent study of PR in pregnancy, which included 60 patients and found a notably higher incidence of overall birth complications (50%), as well as higher incidence of neonatal hypotonia (25%), and miscarriage (13%).
The previous study also showed an increased risk of birth complications when PR onset occurred prior to 15 weeks’ gestation, but the current study did not reflect that finding, they wrote.
The current study findings were limited by several factors including the small sample size, retrospective design, and lack of confirmation of PR with HHV-6/7 testing, as well as lack of exclusion of atypical PR cases, the researchers noted. However, the results suggest that birth complications associated with PR may be lower than previously reported. “Further research is needed to guide future care and fully elucidate this possible association, which has important implications for both pregnant women with PR and their providers.”
The study received no outside funding. The researchers had no financial conflict to disclose.
FROM THE JOURNAL OF THE AMERICAN ACADEMY OF DERMATOLOGY
Find and manage a kidney in crisis
“Kidney disease is the most common chronic disease in the United States and the world, and the incidence is on the rise,” said Kim Zuber, PA-C, executive director of the American Academy of Nephrology PAs and outreach chair for the National Kidney Foundation in St. Petersburg, Fla.

Kidney disease also is an expensive problem that accounts for approximately 20% of the Medicare budget in the United States, she said in a virtual presentation at the Metabolic & Endocrine Disease Summit by Global Academy for Medical Education.
“It’s important that we know how to identify it and how to slow the progression if possible, and what to do when we can no longer control the disease,” she said.
Notably, the rate of growth for kidney disease is highest among adults aged 20-45 years, said Ms. Zuber. “That is the group who will live for many years with kidney disease,” but should be in their peak years of working and earning. “That is the group we do not want to develop chronic diseases.”
“Look for kidney disease. It’s not always on the chart; it is often missed because people don’t think of it,” Ms. Zuber said. Anyone over 60 years has likely lost some kidney function. Other risk factors include minority/ethnicity, hypertension or cardiovascular disease, diabetes, and a family history of kidney disease.
Women are more likely to develop chronic kidney disease (CKD), but less likely to go on dialysis, said Ms. Zuber. “What I find fascinating is that a history of oophorectomy” increases risk. Other less obvious risk factors in a medical history that should prompt a kidney disease screening include mothers who drank during pregnancy, individuals with a history of acute kidney disease, lupus, sarcoid, amyloid, gout, or other autoimmune conditions, as well as a history of kidney stones of cancer. Kidney donors or transplant recipients are at increased risk, as are smokers, soda drinkers, and heavy salt users.
CKD is missed by many health care providers, Ms. Zuber said. For example, she cited data from more than 270,000 veterans treated at a Veterans Affairs hospital in Texas, which suggested that the likelihood of adding CKD to a patient’s diagnosis was 43.7% even if lab results confirmed CKD.
Find the patients
There are many formulas for defining kidney function, Ms. Zuber said. The estimation of creatinine clearance (eCrCl) and estimated glomerular filtration rate (eGFR) are among them. The most common definition is to calculate eGFR using the CKD-EPI formula. Cystatin C is more exact, but it is not standardized, so a lab in one state does not use the same formula as one in another state.
Overall, all these formulas are plus or minus 30%. “It is an estimate,” she said. Within the stages of CKD, “what we know is that, if you have a high GFR, that’s good, but patients who are losing albumin are at increased risk for CKD.” The albumin is more of a risk factor for CKD than GFR, so the GFR test used doesn’t make much difference, whereas, “if you have a lot of albumin in your urine, you are going downhill,” she said.
Normally, everyone loses kidney function with age, Ms. Zuber said. Starting at age 30, individuals lose about 1 mL/min per year in measures of GFR, however, this progression is more rapid among those with CKD, so “we need to find those people who are progressing more quickly than normal.”
The way to identify the high-risk patients is albumin, Ms. Zuber said. Health care providers need to test the urine and check albumin for high levels of albumin loss through urine, and many providers simply don’t routinely conduct urine tests for patients with other CKD risk factors such as diabetes or hypertension.
Albuminuria levels of 2,000 mg/g are the most concerning, and a urine-albumin-to-creatinine ratio (UACR) test is the most effective tool to monitor kidney function, Ms. Zuber said.
She recommends ordering a UACR test at least once a year to monitor kidney loss in all patients with hypertension, diabetes, lupus, and other risk factors including race and a history of acute kidney injury.
Keep them healthy
Managing patients with chronic kidney disease includes attention to several categories: hypertension, diabetes, obesity, and cardiovascular disease, and mental health, Ms. Zuber said.
“If hypertension doesn’t cause your CKD, your CKD will cause hypertension,” she said. The goal for patients with CKD is a target systolic blood pressure less than 120 mm Hg. “As kidney disease progresses, hypertension becomes harder to control,” she added. Lifestyle changes including exercise, low-fat diet, limited use of salt, weight loss if needed, and stress reduction strategies can help.
For patients with diabetes and CKD, work towards a target hemoglobin A1c of 7.0 for early CKD, and of 8% for stage 4/5 or for older patients with multiple comorbidities, Ms. Zuber said. All types of insulin are safe for CKD patients. “Kidney function declines at twice the normal rate for diabetes patients; however, SGLT2 inhibitors are very renoprotective. You may not see a drop in A1c, but you are protecting the kidney.”
For patients with obesity and CKD, data show that bariatric surgery (gastric bypass) lowers mortality in diabetes and also protects the heart and kidneys, said Ms. Zuber. Overall, central obesity increases CKD risk independent of any other risk factors, but losing weight, either by surgery or diet/lifestyle, helps save the kidneys.
Cardiovascular disease is the cause of death for more than 70% of kidney disease patients, Ms. Zuber said. CKD patients “are two to three times more likely to have atrial fibrillation, so take the time to listen with that stethoscope,” she added, also emphasizing the importance of statins for all CKD and diabetes patients, and decreasing smoking. In addition, “managing metabolic acidosis slows the loss of kidney function and protects the heart.”
Additional pearls for managing chronic kidney disease include paying attention to a patient’s mental health; depression occurs in roughly 25%-47% of CKD patients, and anxiety in approximately 27%, said Ms. Zuber. Depression “is believed to be the most common psychiatric disorder in patients with end stage renal disease,” and data suggest that managing depression can help improve survival in CKD patients.
Global Academy and this news organization are owned by the same parent company. Ms. Zuber had no financial conflicts to disclose.
“Kidney disease is the most common chronic disease in the United States and the world, and the incidence is on the rise,” said Kim Zuber, PA-C, executive director of the American Academy of Nephrology PAs and outreach chair for the National Kidney Foundation in St. Petersburg, Fla.
Kidney disease also is an expensive problem that accounts for approximately 20% of the Medicare budget in the United States, she said in a virtual presentation at the Metabolic & Endocrine Disease Summit by Global Academy for Medical Education.
“It’s important that we know how to identify it and how to slow the progression if possible, and what to do when we can no longer control the disease,” she said.
Notably, the rate of growth for kidney disease is highest among adults aged 20-45 years, said Ms. Zuber. “That is the group who will live for many years with kidney disease,” but should be in their peak years of working and earning. “That is the group we do not want to develop chronic diseases.”
“Look for kidney disease. It’s not always on the chart; it is often missed because people don’t think of it,” Ms. Zuber said. Anyone over 60 years has likely lost some kidney function. Other risk factors include minority/ethnicity, hypertension or cardiovascular disease, diabetes, and a family history of kidney disease.
Women are more likely to develop chronic kidney disease (CKD), but less likely to go on dialysis, said Ms. Zuber. “What I find fascinating is that a history of oophorectomy” increases risk. Other less obvious risk factors in a medical history that should prompt a kidney disease screening include mothers who drank during pregnancy, individuals with a history of acute kidney disease, lupus, sarcoid, amyloid, gout, or other autoimmune conditions, as well as a history of kidney stones of cancer. Kidney donors or transplant recipients are at increased risk, as are smokers, soda drinkers, and heavy salt users.
CKD is missed by many health care providers, Ms. Zuber said. For example, she cited data from more than 270,000 veterans treated at a Veterans Affairs hospital in Texas, which suggested that the likelihood of adding CKD to a patient’s diagnosis was 43.7% even if lab results confirmed CKD.
Find the patients
There are many formulas for defining kidney function, Ms. Zuber said. The estimation of creatinine clearance (eCrCl) and estimated glomerular filtration rate (eGFR) are among them. The most common definition is to calculate eGFR using the CKD-EPI formula. Cystatin C is more exact, but it is not standardized, so a lab in one state does not use the same formula as one in another state.
Overall, all these formulas are plus or minus 30%. “It is an estimate,” she said. Within the stages of CKD, “what we know is that, if you have a high GFR, that’s good, but patients who are losing albumin are at increased risk for CKD.” The albumin is more of a risk factor for CKD than GFR, so the GFR test used doesn’t make much difference, whereas, “if you have a lot of albumin in your urine, you are going downhill,” she said.
Normally, everyone loses kidney function with age, Ms. Zuber said. Starting at age 30, individuals lose about 1 mL/min per year in measures of GFR, however, this progression is more rapid among those with CKD, so “we need to find those people who are progressing more quickly than normal.”
The way to identify the high-risk patients is albumin, Ms. Zuber said. Health care providers need to test the urine and check albumin for high levels of albumin loss through urine, and many providers simply don’t routinely conduct urine tests for patients with other CKD risk factors such as diabetes or hypertension.
Albuminuria levels of 2,000 mg/g are the most concerning, and a urine-albumin-to-creatinine ratio (UACR) test is the most effective tool to monitor kidney function, Ms. Zuber said.
She recommends ordering a UACR test at least once a year to monitor kidney loss in all patients with hypertension, diabetes, lupus, and other risk factors including race and a history of acute kidney injury.
Keep them healthy
Managing patients with chronic kidney disease includes attention to several categories: hypertension, diabetes, obesity, and cardiovascular disease, and mental health, Ms. Zuber said.
“If hypertension doesn’t cause your CKD, your CKD will cause hypertension,” she said. The goal for patients with CKD is a target systolic blood pressure less than 120 mm Hg. “As kidney disease progresses, hypertension becomes harder to control,” she added. Lifestyle changes including exercise, low-fat diet, limited use of salt, weight loss if needed, and stress reduction strategies can help.
For patients with diabetes and CKD, work towards a target hemoglobin A1c of 7.0 for early CKD, and of 8% for stage 4/5 or for older patients with multiple comorbidities, Ms. Zuber said. All types of insulin are safe for CKD patients. “Kidney function declines at twice the normal rate for diabetes patients; however, SGLT2 inhibitors are very renoprotective. You may not see a drop in A1c, but you are protecting the kidney.”
For patients with obesity and CKD, data show that bariatric surgery (gastric bypass) lowers mortality in diabetes and also protects the heart and kidneys, said Ms. Zuber. Overall, central obesity increases CKD risk independent of any other risk factors, but losing weight, either by surgery or diet/lifestyle, helps save the kidneys.
Cardiovascular disease is the cause of death for more than 70% of kidney disease patients, Ms. Zuber said. CKD patients “are two to three times more likely to have atrial fibrillation, so take the time to listen with that stethoscope,” she added, also emphasizing the importance of statins for all CKD and diabetes patients, and decreasing smoking. In addition, “managing metabolic acidosis slows the loss of kidney function and protects the heart.”
Additional pearls for managing chronic kidney disease include paying attention to a patient’s mental health; depression occurs in roughly 25%-47% of CKD patients, and anxiety in approximately 27%, said Ms. Zuber. Depression “is believed to be the most common psychiatric disorder in patients with end stage renal disease,” and data suggest that managing depression can help improve survival in CKD patients.
Global Academy and this news organization are owned by the same parent company. Ms. Zuber had no financial conflicts to disclose.
“Kidney disease is the most common chronic disease in the United States and the world, and the incidence is on the rise,” said Kim Zuber, PA-C, executive director of the American Academy of Nephrology PAs and outreach chair for the National Kidney Foundation in St. Petersburg, Fla.
Kidney disease also is an expensive problem that accounts for approximately 20% of the Medicare budget in the United States, she said in a virtual presentation at the Metabolic & Endocrine Disease Summit by Global Academy for Medical Education.
“It’s important that we know how to identify it and how to slow the progression if possible, and what to do when we can no longer control the disease,” she said.
Notably, the rate of growth for kidney disease is highest among adults aged 20-45 years, said Ms. Zuber. “That is the group who will live for many years with kidney disease,” but should be in their peak years of working and earning. “That is the group we do not want to develop chronic diseases.”
“Look for kidney disease. It’s not always on the chart; it is often missed because people don’t think of it,” Ms. Zuber said. Anyone over 60 years has likely lost some kidney function. Other risk factors include minority/ethnicity, hypertension or cardiovascular disease, diabetes, and a family history of kidney disease.
Women are more likely to develop chronic kidney disease (CKD), but less likely to go on dialysis, said Ms. Zuber. “What I find fascinating is that a history of oophorectomy” increases risk. Other less obvious risk factors in a medical history that should prompt a kidney disease screening include mothers who drank during pregnancy, individuals with a history of acute kidney disease, lupus, sarcoid, amyloid, gout, or other autoimmune conditions, as well as a history of kidney stones of cancer. Kidney donors or transplant recipients are at increased risk, as are smokers, soda drinkers, and heavy salt users.
CKD is missed by many health care providers, Ms. Zuber said. For example, she cited data from more than 270,000 veterans treated at a Veterans Affairs hospital in Texas, which suggested that the likelihood of adding CKD to a patient’s diagnosis was 43.7% even if lab results confirmed CKD.
Find the patients
There are many formulas for defining kidney function, Ms. Zuber said. The estimation of creatinine clearance (eCrCl) and estimated glomerular filtration rate (eGFR) are among them. The most common definition is to calculate eGFR using the CKD-EPI formula. Cystatin C is more exact, but it is not standardized, so a lab in one state does not use the same formula as one in another state.
Overall, all these formulas are plus or minus 30%. “It is an estimate,” she said. Within the stages of CKD, “what we know is that, if you have a high GFR, that’s good, but patients who are losing albumin are at increased risk for CKD.” The albumin is more of a risk factor for CKD than GFR, so the GFR test used doesn’t make much difference, whereas, “if you have a lot of albumin in your urine, you are going downhill,” she said.
Normally, everyone loses kidney function with age, Ms. Zuber said. Starting at age 30, individuals lose about 1 mL/min per year in measures of GFR, however, this progression is more rapid among those with CKD, so “we need to find those people who are progressing more quickly than normal.”
The way to identify the high-risk patients is albumin, Ms. Zuber said. Health care providers need to test the urine and check albumin for high levels of albumin loss through urine, and many providers simply don’t routinely conduct urine tests for patients with other CKD risk factors such as diabetes or hypertension.
Albuminuria levels of 2,000 mg/g are the most concerning, and a urine-albumin-to-creatinine ratio (UACR) test is the most effective tool to monitor kidney function, Ms. Zuber said.
She recommends ordering a UACR test at least once a year to monitor kidney loss in all patients with hypertension, diabetes, lupus, and other risk factors including race and a history of acute kidney injury.
Keep them healthy
Managing patients with chronic kidney disease includes attention to several categories: hypertension, diabetes, obesity, and cardiovascular disease, and mental health, Ms. Zuber said.
“If hypertension doesn’t cause your CKD, your CKD will cause hypertension,” she said. The goal for patients with CKD is a target systolic blood pressure less than 120 mm Hg. “As kidney disease progresses, hypertension becomes harder to control,” she added. Lifestyle changes including exercise, low-fat diet, limited use of salt, weight loss if needed, and stress reduction strategies can help.
For patients with diabetes and CKD, work towards a target hemoglobin A1c of 7.0 for early CKD, and of 8% for stage 4/5 or for older patients with multiple comorbidities, Ms. Zuber said. All types of insulin are safe for CKD patients. “Kidney function declines at twice the normal rate for diabetes patients; however, SGLT2 inhibitors are very renoprotective. You may not see a drop in A1c, but you are protecting the kidney.”
For patients with obesity and CKD, data show that bariatric surgery (gastric bypass) lowers mortality in diabetes and also protects the heart and kidneys, said Ms. Zuber. Overall, central obesity increases CKD risk independent of any other risk factors, but losing weight, either by surgery or diet/lifestyle, helps save the kidneys.
Cardiovascular disease is the cause of death for more than 70% of kidney disease patients, Ms. Zuber said. CKD patients “are two to three times more likely to have atrial fibrillation, so take the time to listen with that stethoscope,” she added, also emphasizing the importance of statins for all CKD and diabetes patients, and decreasing smoking. In addition, “managing metabolic acidosis slows the loss of kidney function and protects the heart.”
Additional pearls for managing chronic kidney disease include paying attention to a patient’s mental health; depression occurs in roughly 25%-47% of CKD patients, and anxiety in approximately 27%, said Ms. Zuber. Depression “is believed to be the most common psychiatric disorder in patients with end stage renal disease,” and data suggest that managing depression can help improve survival in CKD patients.
Global Academy and this news organization are owned by the same parent company. Ms. Zuber had no financial conflicts to disclose.
FROM MEDS 2020
‘The Undoing’: A dramatization of ‘You Should Have Known’
Jean Hanff Korelitz’s ironic psychological thriller, “You Should Have Known,” (New York: Grand Central Publishing, 2014) was transformed into an HBO miniseries called “The Undoing,” written and produced by David E. Kelley and directed by Susanne Bier, which premiered on Oct. 25, 2020.

The television drama differed from the novel in fundamental ways, but both have themes related to the therapeutic process. In the novel, a New York City–based couples therapist, Grace Reinhart Sachs, had recently written a book called “You Should Have Known,” about women who married their spouses disregarding their gut instinct that their partner was not fundamentally right for them, or might potentially cheat on them, or whose stories contained contradictions. In the miniseries, Grace (played by Nicole Kidman), is a therapist but there is no mention of her having written a book. Grace in both the novel and the miniseries is married to a pediatric oncologist, Jonathan (his ethnicity and surname were changed in the miniseries from a Jewish New Yorker in the novel to a British Dr. Jonathan Fraser in the series, played by Hugh Grant).
[Spoiler alert]: Prepandemic New York City’s Upper East Side is scandalized when a murdered mother is found by her young son the day after a lavish fund-raising auction party for a private school. Grace and Jonathan’s son, Henry, attends this school as well, and Grace had served on the auction committee with the murdered mother. When two detectives question Grace in the course of their investigation, she assumes that they are questioning her as they would any parent in the school. However, when she tries to reach her husband about the news and the investigation, she cannot. She thought he was at a medical conference in Cleveland, but she realizes that she does not know exactly what conference and exactly where. After many failed attempts at calling and texting, she hears a familiar alert sound coming from his nightstand drawer where she retrieves the cell phone that had been deliberately placed.
In the novel, Jonathan never reappears from “Cleveland,” and although it takes Grace a while to understand that her husband is not who she thought he was, she eventually does. In the miniseries, Jonathan appears in their lake house and a trial ensues with Jonathan adamantly proclaiming his innocence despite all evidence to the contrary.
The Oxford Reference defines undoing as “an emotional conflict associated with an action is dealt with by negating the action or attempting ‘magically’ to cause it not to have occurred by substituting an approximately opposite action.” It is not that the consequences of the action are attempted to be negated (as in making amends or showing remorse), but the action itself. In this way, the miniseries is aptly named since both main characters, Grace and Jonathan, use this defense mechanism. Grace has difficulty acknowledging that her husband could be capable of any wrongdoing, even as she is faced with fact after fact that contradicts this premise – and counsels others about their relationship choices. Similarly, Jonathan’s choice of profession is likely an attempt to undo his 4-year-old sister’s death that occurred on his watch when he was 14. However, even treating children’s cancer cannot undo the many indiscretions he has apparently committed in his adult life.

In the portrayal of a doctor with narcissistic, and possibly psychopathic, traits, “The Undoing” joins multiple recent podcasts that document real-life bad doctors, including Wondery’s “The Shrink Next Door,” “Dr. Death” (seasons 1 and 2), and “Do No Harm.” While most physicians go into medicine to heal and improve peoples’ lives, others, such as the character of Dr. Jonathan Fraser, appear to become physicians for ulterior and sinister motivations. Jonathan’s difficulty with empathy was present when he was a child as a character trait – rather than being attributable to any childhood traumatic event, as Grace had let herself believe.
In a Dec. 11, 2020, New York Times op-ed, Richard A. Friedman, MD, a psychiatrist affiliated with New York Presbyterian-Cornell University, discussed three “dangerous doctors” during the pandemic who are potentially harming the nation. Scott Atlas, MD, a radiologist on leave from Stanford (Calif.) University, advised President Trump on the coronavirus despite having no training in public health or infectious disease. Before resigning, he questioned the use of face masks, contradicting scientific proof of their prevention of disease. Another doctor, a cardiologist in Washington, also publicly disputed scientific evidence of the efficacy of face masks and social distancing, and a third physician promoted hydroxychloroquine as a treatment for coronavirus despite scientific evidence that it has been ineffective and possibly even harmful to patients with the virus.
Both the novel “You Should Have Known” and the series “The Undoing” will be of interest to psychiatrists, especially therapists and forensic psychiatrists, because of the themes portrayed, such as defense mechanisms, therapeutic process, and a homicide investigation – as well as the common human experience of being an expert in something in one’s professional life, yet occasionally falling short of recognizing the same phenomena in one’s personal life.
Dr. Rosenbaum is a clinical and forensic psychiatrist in private practice in New York. She is an assistant clinical professor at New York University Langone Medical Center and is on the faculty at Weill-Cornell Medical Center. She has no conflicts of interest. Dr. Friedman serves as the Phillip Resnick Professor of Forensic Psychiatry at Case Western Reserve University, Cleveland. She is also editor of Family Murder: Pathologies of Love and Hate (Washington: American Psychiatric Publishing, 2019), which was written by the Group for the Advancement of Psychiatry’s Committee on Psychiatry & Law, and which was awarded the 2020 Manfred Gutmacher Award by the American Psychiatric Association. She has no conflicts of interest.
Jean Hanff Korelitz’s ironic psychological thriller, “You Should Have Known,” (New York: Grand Central Publishing, 2014) was transformed into an HBO miniseries called “The Undoing,” written and produced by David E. Kelley and directed by Susanne Bier, which premiered on Oct. 25, 2020.
The television drama differed from the novel in fundamental ways, but both have themes related to the therapeutic process. In the novel, a New York City–based couples therapist, Grace Reinhart Sachs, had recently written a book called “You Should Have Known,” about women who married their spouses disregarding their gut instinct that their partner was not fundamentally right for them, or might potentially cheat on them, or whose stories contained contradictions. In the miniseries, Grace (played by Nicole Kidman), is a therapist but there is no mention of her having written a book. Grace in both the novel and the miniseries is married to a pediatric oncologist, Jonathan (his ethnicity and surname were changed in the miniseries from a Jewish New Yorker in the novel to a British Dr. Jonathan Fraser in the series, played by Hugh Grant).
[Spoiler alert]: Prepandemic New York City’s Upper East Side is scandalized when a murdered mother is found by her young son the day after a lavish fund-raising auction party for a private school. Grace and Jonathan’s son, Henry, attends this school as well, and Grace had served on the auction committee with the murdered mother. When two detectives question Grace in the course of their investigation, she assumes that they are questioning her as they would any parent in the school. However, when she tries to reach her husband about the news and the investigation, she cannot. She thought he was at a medical conference in Cleveland, but she realizes that she does not know exactly what conference and exactly where. After many failed attempts at calling and texting, she hears a familiar alert sound coming from his nightstand drawer where she retrieves the cell phone that had been deliberately placed.
In the novel, Jonathan never reappears from “Cleveland,” and although it takes Grace a while to understand that her husband is not who she thought he was, she eventually does. In the miniseries, Jonathan appears in their lake house and a trial ensues with Jonathan adamantly proclaiming his innocence despite all evidence to the contrary.
The Oxford Reference defines undoing as “an emotional conflict associated with an action is dealt with by negating the action or attempting ‘magically’ to cause it not to have occurred by substituting an approximately opposite action.” It is not that the consequences of the action are attempted to be negated (as in making amends or showing remorse), but the action itself. In this way, the miniseries is aptly named since both main characters, Grace and Jonathan, use this defense mechanism. Grace has difficulty acknowledging that her husband could be capable of any wrongdoing, even as she is faced with fact after fact that contradicts this premise – and counsels others about their relationship choices. Similarly, Jonathan’s choice of profession is likely an attempt to undo his 4-year-old sister’s death that occurred on his watch when he was 14. However, even treating children’s cancer cannot undo the many indiscretions he has apparently committed in his adult life.
In the portrayal of a doctor with narcissistic, and possibly psychopathic, traits, “The Undoing” joins multiple recent podcasts that document real-life bad doctors, including Wondery’s “The Shrink Next Door,” “Dr. Death” (seasons 1 and 2), and “Do No Harm.” While most physicians go into medicine to heal and improve peoples’ lives, others, such as the character of Dr. Jonathan Fraser, appear to become physicians for ulterior and sinister motivations. Jonathan’s difficulty with empathy was present when he was a child as a character trait – rather than being attributable to any childhood traumatic event, as Grace had let herself believe.
In a Dec. 11, 2020, New York Times op-ed, Richard A. Friedman, MD, a psychiatrist affiliated with New York Presbyterian-Cornell University, discussed three “dangerous doctors” during the pandemic who are potentially harming the nation. Scott Atlas, MD, a radiologist on leave from Stanford (Calif.) University, advised President Trump on the coronavirus despite having no training in public health or infectious disease. Before resigning, he questioned the use of face masks, contradicting scientific proof of their prevention of disease. Another doctor, a cardiologist in Washington, also publicly disputed scientific evidence of the efficacy of face masks and social distancing, and a third physician promoted hydroxychloroquine as a treatment for coronavirus despite scientific evidence that it has been ineffective and possibly even harmful to patients with the virus.
Both the novel “You Should Have Known” and the series “The Undoing” will be of interest to psychiatrists, especially therapists and forensic psychiatrists, because of the themes portrayed, such as defense mechanisms, therapeutic process, and a homicide investigation – as well as the common human experience of being an expert in something in one’s professional life, yet occasionally falling short of recognizing the same phenomena in one’s personal life.
Dr. Rosenbaum is a clinical and forensic psychiatrist in private practice in New York. She is an assistant clinical professor at New York University Langone Medical Center and is on the faculty at Weill-Cornell Medical Center. She has no conflicts of interest. Dr. Friedman serves as the Phillip Resnick Professor of Forensic Psychiatry at Case Western Reserve University, Cleveland. She is also editor of Family Murder: Pathologies of Love and Hate (Washington: American Psychiatric Publishing, 2019), which was written by the Group for the Advancement of Psychiatry’s Committee on Psychiatry & Law, and which was awarded the 2020 Manfred Gutmacher Award by the American Psychiatric Association. She has no conflicts of interest.
Jean Hanff Korelitz’s ironic psychological thriller, “You Should Have Known,” (New York: Grand Central Publishing, 2014) was transformed into an HBO miniseries called “The Undoing,” written and produced by David E. Kelley and directed by Susanne Bier, which premiered on Oct. 25, 2020.
The television drama differed from the novel in fundamental ways, but both have themes related to the therapeutic process. In the novel, a New York City–based couples therapist, Grace Reinhart Sachs, had recently written a book called “You Should Have Known,” about women who married their spouses disregarding their gut instinct that their partner was not fundamentally right for them, or might potentially cheat on them, or whose stories contained contradictions. In the miniseries, Grace (played by Nicole Kidman), is a therapist but there is no mention of her having written a book. Grace in both the novel and the miniseries is married to a pediatric oncologist, Jonathan (his ethnicity and surname were changed in the miniseries from a Jewish New Yorker in the novel to a British Dr. Jonathan Fraser in the series, played by Hugh Grant).
[Spoiler alert]: Prepandemic New York City’s Upper East Side is scandalized when a murdered mother is found by her young son the day after a lavish fund-raising auction party for a private school. Grace and Jonathan’s son, Henry, attends this school as well, and Grace had served on the auction committee with the murdered mother. When two detectives question Grace in the course of their investigation, she assumes that they are questioning her as they would any parent in the school. However, when she tries to reach her husband about the news and the investigation, she cannot. She thought he was at a medical conference in Cleveland, but she realizes that she does not know exactly what conference and exactly where. After many failed attempts at calling and texting, she hears a familiar alert sound coming from his nightstand drawer where she retrieves the cell phone that had been deliberately placed.
In the novel, Jonathan never reappears from “Cleveland,” and although it takes Grace a while to understand that her husband is not who she thought he was, she eventually does. In the miniseries, Jonathan appears in their lake house and a trial ensues with Jonathan adamantly proclaiming his innocence despite all evidence to the contrary.
The Oxford Reference defines undoing as “an emotional conflict associated with an action is dealt with by negating the action or attempting ‘magically’ to cause it not to have occurred by substituting an approximately opposite action.” It is not that the consequences of the action are attempted to be negated (as in making amends or showing remorse), but the action itself. In this way, the miniseries is aptly named since both main characters, Grace and Jonathan, use this defense mechanism. Grace has difficulty acknowledging that her husband could be capable of any wrongdoing, even as she is faced with fact after fact that contradicts this premise – and counsels others about their relationship choices. Similarly, Jonathan’s choice of profession is likely an attempt to undo his 4-year-old sister’s death that occurred on his watch when he was 14. However, even treating children’s cancer cannot undo the many indiscretions he has apparently committed in his adult life.
In the portrayal of a doctor with narcissistic, and possibly psychopathic, traits, “The Undoing” joins multiple recent podcasts that document real-life bad doctors, including Wondery’s “The Shrink Next Door,” “Dr. Death” (seasons 1 and 2), and “Do No Harm.” While most physicians go into medicine to heal and improve peoples’ lives, others, such as the character of Dr. Jonathan Fraser, appear to become physicians for ulterior and sinister motivations. Jonathan’s difficulty with empathy was present when he was a child as a character trait – rather than being attributable to any childhood traumatic event, as Grace had let herself believe.
In a Dec. 11, 2020, New York Times op-ed, Richard A. Friedman, MD, a psychiatrist affiliated with New York Presbyterian-Cornell University, discussed three “dangerous doctors” during the pandemic who are potentially harming the nation. Scott Atlas, MD, a radiologist on leave from Stanford (Calif.) University, advised President Trump on the coronavirus despite having no training in public health or infectious disease. Before resigning, he questioned the use of face masks, contradicting scientific proof of their prevention of disease. Another doctor, a cardiologist in Washington, also publicly disputed scientific evidence of the efficacy of face masks and social distancing, and a third physician promoted hydroxychloroquine as a treatment for coronavirus despite scientific evidence that it has been ineffective and possibly even harmful to patients with the virus.
Both the novel “You Should Have Known” and the series “The Undoing” will be of interest to psychiatrists, especially therapists and forensic psychiatrists, because of the themes portrayed, such as defense mechanisms, therapeutic process, and a homicide investigation – as well as the common human experience of being an expert in something in one’s professional life, yet occasionally falling short of recognizing the same phenomena in one’s personal life.
Dr. Rosenbaum is a clinical and forensic psychiatrist in private practice in New York. She is an assistant clinical professor at New York University Langone Medical Center and is on the faculty at Weill-Cornell Medical Center. She has no conflicts of interest. Dr. Friedman serves as the Phillip Resnick Professor of Forensic Psychiatry at Case Western Reserve University, Cleveland. She is also editor of Family Murder: Pathologies of Love and Hate (Washington: American Psychiatric Publishing, 2019), which was written by the Group for the Advancement of Psychiatry’s Committee on Psychiatry & Law, and which was awarded the 2020 Manfred Gutmacher Award by the American Psychiatric Association. She has no conflicts of interest.
How can hospitalists change the status quo?
Lean framework for efficiency and empathy of care
“My census is too high.”
“I don’t have enough time to talk to patients.”
“These are outside our scope of practice.”

These are statements that I have heard from colleagues over the last fourteen years as a hospitalist. Back in 1996, when Dr. Bob Wachter coined the term ‘hospitalist,’ we were still in our infancy – the scope of what we could do had yet to be fully realized. Our focus was on providing care for hospitalized patients and improving quality of clinical care and patient safety. As health care organizations began to see the potential for our field, the demands on our services grew. We grew to comanage patients with our surgical colleagues, worked on patient satisfaction, facilitated transitions of care, and attempted to reduce readmissions – all of which improved patient care and the bottom line for our organizations.
Somewhere along the way, we were expected to staff high patient volumes to add more value, but this always seemed to come with compromise in another aspect of care or our own well-being. After all, there are only so many hours in the day and a limit on what one individual can accomplish in that time.
One of the reasons I love hospital medicine is the novelty of what we do – we are creative thinkers. We have the capacity to innovate solutions to hospital problems based on our expertise as frontline providers for our patients. Hospitalists of every discipline staff a large majority of inpatients, which makes our collective experience significant to the management of inpatient health care. We are often the ones tasked with executing improvement projects, but how often are we involved in their design? I know that we collectively have an enormous opportunity to improve our health care practice, both for ourselves, our patients, and the institutions we work for. But more than just being a voice of advocacy, we need to understand how to positively influence the health care structures that allow us to deliver quality patient care.
It is no surprise that the inefficiencies we deal with in our hospitals are many – daily workflow interruptions, delays in results, scheduling issues, communication difficulties. These are not unique to any one institution. The pandemic added more to that plate – PPE deficiencies, patient volume triage, and resource management are examples. Hospitals often contract consultants to help solve these problems, and many utilize a variety of frameworks to improve these system processes. The Lean framework is one of these, and it originated in the manufacturing industry to eliminate waste in systems in the pursuit of efficiency.
In my business training and prior hospital medicine leadership roles, I was educated in Lean thinking and methodologies for improving quality and applied its principles to projects for improving workflow. Last year I attended a virtual conference on ‘Lean Innovation during the pandemic’ for New York region hospitals, and it again highlighted how the Lean management methodology can help improve patient care but importantly, our workflow as clinicians. This got me thinking. Why is Lean well accepted in business and manufacturing circles, but less so in health care?
I think the answer is twofold – knowledge and people.
What is Lean and how can it help us?
The ‘Toyota Production System’-based philosophy has 14 core principles that help eliminate waste in systems in pursuit of efficiency. These principles are the “Toyota Way.” They center around two pillars: continuous improvement and respect for people. The cornerstone of this management methodology is based on efficient processes, developing employees to add value to the organization and continuous improvement through problem-solving and organizational learning.
Lean is often implemented with Six Sigma methodology. Six Sigma has its origins in Motorola. While Lean cuts waste in our systems to provide value, Six Sigma uses DMAIC (Define, Measure, Analyze, Improve, Control) to reduce variation in our processes. When done in its entirety, Lean Six Sigma methodology adds value by increasing efficiency, reducing cost, and improving our everyday work.
Statistical principles suggest that 80% of consequences comes from 20% of causes. Lean methodology and tools allow us to systematically identify root causes for the problems we face and help narrow it down to the ‘vital few.’ In other words, fixing these would give us the most bang for our buck. As hospitalists, we are able to do this better than most because we work in these hospital processes everyday – we truly know the strengths and weaknesses of our systems.
As a hospitalist, I would love for the process of seeing patients in hospitals to be more efficient, less variable, and be more cost-effective for my institution. By eliminating the time wasted performing unnecessary and redundant tasks in my everyday work, I can reallocate that time to patient care – the very reason I chose a career in medicine.
We, the people
There are two common rebuttals I hear for adopting Lean Six Sigma methodology in health care. A frequent misconception is that Lean is all about reducing staff or time with patients. The second is that manufacturing methodologies do not work for a service profession. For instance, an article published on Reuters Events (www.reutersevents.com/supplychain/supply-chain/end-just-time) talks about Lean JIT (Just In Time) inventory as a culprit for creating a supply chain deficit during COVID-19. It is not entirely without merit. However, if done the correct way, Lean is all about involving the frontline worker to create a workflow that would work best for them.
Reducing the waste in our processes and empowering our frontline doctors to be creative in finding solutions naturally leads to cost reduction. The cornerstone of Lean is creating a continuously learning organization and putting your employees at the forefront. I think it is important that Lean principles be utilized within health care – but we cannot push to fix every problem in our systems to perfection at a significant expense to the physician and other health care staff.
Why HM can benefit from Lean
There is no hard and fast rule about the way health care should adopt Lean thinking. It is a way of thinking that aims to balance purpose, people, and process – extremes of inventory management may not be necessary to be successful in health care. Lean tools alone would not create results. John Shook, chairman of Lean Global Network, has said that the social side of Lean needs to be in balance with the technical side. In other words, rigidity and efficiency is good, but so is encouraging creativity and flexibility in thinking within the workforce.
In the crisis created by the novel coronavirus, many hospitals in New York state, including my own, turned to Lean to respond quickly and effectively to the challenges. Lean principles helped them problem-solve and develop strategies to both recover from the pandemic surge and adapt to future problems that could occur. Geographic clustering of patients, PPE supply, OR shut down and ramp up, emergency management offices at the peak of the pandemic, telehealth streamlining, and post-COVID-19 care planning are some areas where the application of Lean resulted in successful responses to the challenges that 2020 brought to our work.
As Warren Bennis said, ‘The manager accepts the status quo; the leader challenges it.’ As hospitalists, we can lead the way our hospitals provide care. Lean is not just a way for hospitals to cut costs (although it helps quite a bit there). Its processes and philosophies could enable hospitalists to maximize potential, efficiency, quality of care, and allow for a balanced work environment. When applied in a manner that focuses on continuous improvement (and is cognizant of its limitations), it has the potential to increase the capability of our service lines and streamline our processes and workday for greater efficiency. As a specialty, we stand to benefit by taking the lead role in choosing how best to improve how we work. We should think outside the box. What better time to do this than now?
Dr. Kanikkannan is a practicing hospitalist and assistant professor of medicine at Albany (N.Y) Medical College. She is a former hospitalist medical director and has served on SHM’s national committees, and is a certified Lean Six Sigma black belt and MBA candidate.
Lean framework for efficiency and empathy of care
Lean framework for efficiency and empathy of care
“My census is too high.”
“I don’t have enough time to talk to patients.”
“These are outside our scope of practice.”
These are statements that I have heard from colleagues over the last fourteen years as a hospitalist. Back in 1996, when Dr. Bob Wachter coined the term ‘hospitalist,’ we were still in our infancy – the scope of what we could do had yet to be fully realized. Our focus was on providing care for hospitalized patients and improving quality of clinical care and patient safety. As health care organizations began to see the potential for our field, the demands on our services grew. We grew to comanage patients with our surgical colleagues, worked on patient satisfaction, facilitated transitions of care, and attempted to reduce readmissions – all of which improved patient care and the bottom line for our organizations.
Somewhere along the way, we were expected to staff high patient volumes to add more value, but this always seemed to come with compromise in another aspect of care or our own well-being. After all, there are only so many hours in the day and a limit on what one individual can accomplish in that time.
One of the reasons I love hospital medicine is the novelty of what we do – we are creative thinkers. We have the capacity to innovate solutions to hospital problems based on our expertise as frontline providers for our patients. Hospitalists of every discipline staff a large majority of inpatients, which makes our collective experience significant to the management of inpatient health care. We are often the ones tasked with executing improvement projects, but how often are we involved in their design? I know that we collectively have an enormous opportunity to improve our health care practice, both for ourselves, our patients, and the institutions we work for. But more than just being a voice of advocacy, we need to understand how to positively influence the health care structures that allow us to deliver quality patient care.
It is no surprise that the inefficiencies we deal with in our hospitals are many – daily workflow interruptions, delays in results, scheduling issues, communication difficulties. These are not unique to any one institution. The pandemic added more to that plate – PPE deficiencies, patient volume triage, and resource management are examples. Hospitals often contract consultants to help solve these problems, and many utilize a variety of frameworks to improve these system processes. The Lean framework is one of these, and it originated in the manufacturing industry to eliminate waste in systems in the pursuit of efficiency.
In my business training and prior hospital medicine leadership roles, I was educated in Lean thinking and methodologies for improving quality and applied its principles to projects for improving workflow. Last year I attended a virtual conference on ‘Lean Innovation during the pandemic’ for New York region hospitals, and it again highlighted how the Lean management methodology can help improve patient care but importantly, our workflow as clinicians. This got me thinking. Why is Lean well accepted in business and manufacturing circles, but less so in health care?
I think the answer is twofold – knowledge and people.
What is Lean and how can it help us?
The ‘Toyota Production System’-based philosophy has 14 core principles that help eliminate waste in systems in pursuit of efficiency. These principles are the “Toyota Way.” They center around two pillars: continuous improvement and respect for people. The cornerstone of this management methodology is based on efficient processes, developing employees to add value to the organization and continuous improvement through problem-solving and organizational learning.
Lean is often implemented with Six Sigma methodology. Six Sigma has its origins in Motorola. While Lean cuts waste in our systems to provide value, Six Sigma uses DMAIC (Define, Measure, Analyze, Improve, Control) to reduce variation in our processes. When done in its entirety, Lean Six Sigma methodology adds value by increasing efficiency, reducing cost, and improving our everyday work.
Statistical principles suggest that 80% of consequences comes from 20% of causes. Lean methodology and tools allow us to systematically identify root causes for the problems we face and help narrow it down to the ‘vital few.’ In other words, fixing these would give us the most bang for our buck. As hospitalists, we are able to do this better than most because we work in these hospital processes everyday – we truly know the strengths and weaknesses of our systems.
As a hospitalist, I would love for the process of seeing patients in hospitals to be more efficient, less variable, and be more cost-effective for my institution. By eliminating the time wasted performing unnecessary and redundant tasks in my everyday work, I can reallocate that time to patient care – the very reason I chose a career in medicine.
We, the people
There are two common rebuttals I hear for adopting Lean Six Sigma methodology in health care. A frequent misconception is that Lean is all about reducing staff or time with patients. The second is that manufacturing methodologies do not work for a service profession. For instance, an article published on Reuters Events (www.reutersevents.com/supplychain/supply-chain/end-just-time) talks about Lean JIT (Just In Time) inventory as a culprit for creating a supply chain deficit during COVID-19. It is not entirely without merit. However, if done the correct way, Lean is all about involving the frontline worker to create a workflow that would work best for them.
Reducing the waste in our processes and empowering our frontline doctors to be creative in finding solutions naturally leads to cost reduction. The cornerstone of Lean is creating a continuously learning organization and putting your employees at the forefront. I think it is important that Lean principles be utilized within health care – but we cannot push to fix every problem in our systems to perfection at a significant expense to the physician and other health care staff.
Why HM can benefit from Lean
There is no hard and fast rule about the way health care should adopt Lean thinking. It is a way of thinking that aims to balance purpose, people, and process – extremes of inventory management may not be necessary to be successful in health care. Lean tools alone would not create results. John Shook, chairman of Lean Global Network, has said that the social side of Lean needs to be in balance with the technical side. In other words, rigidity and efficiency is good, but so is encouraging creativity and flexibility in thinking within the workforce.
In the crisis created by the novel coronavirus, many hospitals in New York state, including my own, turned to Lean to respond quickly and effectively to the challenges. Lean principles helped them problem-solve and develop strategies to both recover from the pandemic surge and adapt to future problems that could occur. Geographic clustering of patients, PPE supply, OR shut down and ramp up, emergency management offices at the peak of the pandemic, telehealth streamlining, and post-COVID-19 care planning are some areas where the application of Lean resulted in successful responses to the challenges that 2020 brought to our work.
As Warren Bennis said, ‘The manager accepts the status quo; the leader challenges it.’ As hospitalists, we can lead the way our hospitals provide care. Lean is not just a way for hospitals to cut costs (although it helps quite a bit there). Its processes and philosophies could enable hospitalists to maximize potential, efficiency, quality of care, and allow for a balanced work environment. When applied in a manner that focuses on continuous improvement (and is cognizant of its limitations), it has the potential to increase the capability of our service lines and streamline our processes and workday for greater efficiency. As a specialty, we stand to benefit by taking the lead role in choosing how best to improve how we work. We should think outside the box. What better time to do this than now?
Dr. Kanikkannan is a practicing hospitalist and assistant professor of medicine at Albany (N.Y) Medical College. She is a former hospitalist medical director and has served on SHM’s national committees, and is a certified Lean Six Sigma black belt and MBA candidate.
“My census is too high.”
“I don’t have enough time to talk to patients.”
“These are outside our scope of practice.”
These are statements that I have heard from colleagues over the last fourteen years as a hospitalist. Back in 1996, when Dr. Bob Wachter coined the term ‘hospitalist,’ we were still in our infancy – the scope of what we could do had yet to be fully realized. Our focus was on providing care for hospitalized patients and improving quality of clinical care and patient safety. As health care organizations began to see the potential for our field, the demands on our services grew. We grew to comanage patients with our surgical colleagues, worked on patient satisfaction, facilitated transitions of care, and attempted to reduce readmissions – all of which improved patient care and the bottom line for our organizations.
Somewhere along the way, we were expected to staff high patient volumes to add more value, but this always seemed to come with compromise in another aspect of care or our own well-being. After all, there are only so many hours in the day and a limit on what one individual can accomplish in that time.
One of the reasons I love hospital medicine is the novelty of what we do – we are creative thinkers. We have the capacity to innovate solutions to hospital problems based on our expertise as frontline providers for our patients. Hospitalists of every discipline staff a large majority of inpatients, which makes our collective experience significant to the management of inpatient health care. We are often the ones tasked with executing improvement projects, but how often are we involved in their design? I know that we collectively have an enormous opportunity to improve our health care practice, both for ourselves, our patients, and the institutions we work for. But more than just being a voice of advocacy, we need to understand how to positively influence the health care structures that allow us to deliver quality patient care.
It is no surprise that the inefficiencies we deal with in our hospitals are many – daily workflow interruptions, delays in results, scheduling issues, communication difficulties. These are not unique to any one institution. The pandemic added more to that plate – PPE deficiencies, patient volume triage, and resource management are examples. Hospitals often contract consultants to help solve these problems, and many utilize a variety of frameworks to improve these system processes. The Lean framework is one of these, and it originated in the manufacturing industry to eliminate waste in systems in the pursuit of efficiency.
In my business training and prior hospital medicine leadership roles, I was educated in Lean thinking and methodologies for improving quality and applied its principles to projects for improving workflow. Last year I attended a virtual conference on ‘Lean Innovation during the pandemic’ for New York region hospitals, and it again highlighted how the Lean management methodology can help improve patient care but importantly, our workflow as clinicians. This got me thinking. Why is Lean well accepted in business and manufacturing circles, but less so in health care?
I think the answer is twofold – knowledge and people.
What is Lean and how can it help us?
The ‘Toyota Production System’-based philosophy has 14 core principles that help eliminate waste in systems in pursuit of efficiency. These principles are the “Toyota Way.” They center around two pillars: continuous improvement and respect for people. The cornerstone of this management methodology is based on efficient processes, developing employees to add value to the organization and continuous improvement through problem-solving and organizational learning.
Lean is often implemented with Six Sigma methodology. Six Sigma has its origins in Motorola. While Lean cuts waste in our systems to provide value, Six Sigma uses DMAIC (Define, Measure, Analyze, Improve, Control) to reduce variation in our processes. When done in its entirety, Lean Six Sigma methodology adds value by increasing efficiency, reducing cost, and improving our everyday work.
Statistical principles suggest that 80% of consequences comes from 20% of causes. Lean methodology and tools allow us to systematically identify root causes for the problems we face and help narrow it down to the ‘vital few.’ In other words, fixing these would give us the most bang for our buck. As hospitalists, we are able to do this better than most because we work in these hospital processes everyday – we truly know the strengths and weaknesses of our systems.
As a hospitalist, I would love for the process of seeing patients in hospitals to be more efficient, less variable, and be more cost-effective for my institution. By eliminating the time wasted performing unnecessary and redundant tasks in my everyday work, I can reallocate that time to patient care – the very reason I chose a career in medicine.
We, the people
There are two common rebuttals I hear for adopting Lean Six Sigma methodology in health care. A frequent misconception is that Lean is all about reducing staff or time with patients. The second is that manufacturing methodologies do not work for a service profession. For instance, an article published on Reuters Events (www.reutersevents.com/supplychain/supply-chain/end-just-time) talks about Lean JIT (Just In Time) inventory as a culprit for creating a supply chain deficit during COVID-19. It is not entirely without merit. However, if done the correct way, Lean is all about involving the frontline worker to create a workflow that would work best for them.
Reducing the waste in our processes and empowering our frontline doctors to be creative in finding solutions naturally leads to cost reduction. The cornerstone of Lean is creating a continuously learning organization and putting your employees at the forefront. I think it is important that Lean principles be utilized within health care – but we cannot push to fix every problem in our systems to perfection at a significant expense to the physician and other health care staff.
Why HM can benefit from Lean
There is no hard and fast rule about the way health care should adopt Lean thinking. It is a way of thinking that aims to balance purpose, people, and process – extremes of inventory management may not be necessary to be successful in health care. Lean tools alone would not create results. John Shook, chairman of Lean Global Network, has said that the social side of Lean needs to be in balance with the technical side. In other words, rigidity and efficiency is good, but so is encouraging creativity and flexibility in thinking within the workforce.
In the crisis created by the novel coronavirus, many hospitals in New York state, including my own, turned to Lean to respond quickly and effectively to the challenges. Lean principles helped them problem-solve and develop strategies to both recover from the pandemic surge and adapt to future problems that could occur. Geographic clustering of patients, PPE supply, OR shut down and ramp up, emergency management offices at the peak of the pandemic, telehealth streamlining, and post-COVID-19 care planning are some areas where the application of Lean resulted in successful responses to the challenges that 2020 brought to our work.
As Warren Bennis said, ‘The manager accepts the status quo; the leader challenges it.’ As hospitalists, we can lead the way our hospitals provide care. Lean is not just a way for hospitals to cut costs (although it helps quite a bit there). Its processes and philosophies could enable hospitalists to maximize potential, efficiency, quality of care, and allow for a balanced work environment. When applied in a manner that focuses on continuous improvement (and is cognizant of its limitations), it has the potential to increase the capability of our service lines and streamline our processes and workday for greater efficiency. As a specialty, we stand to benefit by taking the lead role in choosing how best to improve how we work. We should think outside the box. What better time to do this than now?
Dr. Kanikkannan is a practicing hospitalist and assistant professor of medicine at Albany (N.Y) Medical College. She is a former hospitalist medical director and has served on SHM’s national committees, and is a certified Lean Six Sigma black belt and MBA candidate.
Updated ACC decision pathway embraces new heart failure treatment strategies
A newly updated expert consensus from the American College of Cardiology for management of heart failure with reduced ejection fraction includes several new guideline-directed medical therapies among other substantial changes relative to its 2017 predecessor.

The advances in treatment of heart failure with reduced ejection fraction (HFrEF) have resulted in a substantial increase in complexity in reaching treatment goals, according to the authors of the new guidance. Structured similarly to the 2017 ACC Expert Consensus Decision Pathway, the update accommodates a series of practical tips to bring all patients on board with the newer as well as the established therapies with lifesaving potential.
The potential return from implementing these recommendations is not trivial. Relative to an ACE inhibitor and a beta-blocker alone, optimal implementation of the current guideline-directed medical therapies (GDMT) “can extend medical survival by more than 6 years,” according to Gregg C. Fonarow, MD, chief of cardiology at the University of California, Los Angeles.
A member of the writing committee for the 2021 update, Dr. Fonarow explained that the consensus pathway is more than a list of therapies and recommended doses. The detailed advice on how to overcome the barriers to GDMT is meant to close the substantial gap between current practice and unmet opportunities for inhibiting HFrEF progression.
“Optimal GDMT among HFrEF patients is distressingly low, due in part to the number and complexity of medications that now constitute GDMT,” said the chair of the writing committee, Thomas M. Maddox, MD, executive director, Healthcare Innovation Lab, BJC HealthCare/Washington University, St. Louis. Like Dr. Fonarow, Dr. Maddox emphasized that the importance of the update for the practical strategies it offers to place patients on optimal care.

In the 2017 guidance, 10 pivotal issues were tackled, ranging from advice of how to put HFrEF patients on the multiple drugs that now constitute optimal therapy to when to transition patients to hospice care. The 2021 update covers the same ground but incorporates new information that has changed the definition of optimal care.
Perhaps most importantly, sacubitril/valsartan, an angiotensin receptor neprilysin inhibitor (ARNi), and SGLT2 inhibitors represent major new additions in HFrEF GDMT. Dr. Maddox called the practical information about how these should be incorporated into HFrEF management represents one of the “major highlights” of the update.
Two algorithms outline the expert consensus recommendations of the order and the dose of the multiple drugs that now constitute the current GDMT. With the goal of explaining exactly how to place patients on all the HFrEF therapies associated with improved outcome, “I think these figures can really help us in guiding our patients to optimal medication regimens and dosages,” Dr. Maddox said. If successful, clinicians “can make a significant difference in these patients’ length and quality of life.”
Most cardiologists and others who treat HFrEF are likely aware of the major improvements in outcome documented in large trials when an ARNi and a SGLT2 inhibitor were added to previously established GDMT, but the update like the 2017 document is focused on the practical strategies of implementation, according to Larry A. Allen, MD, medical director of advanced heart failure at the University of Colorado at Denver, Aurora.
“The 2017 Expert Consensus Decision Pathway got a lot of attention because it takes a very practical approach to questions that clinicians and their patients have to tackle everyday but for which there was not always clean answers from the data,” said Dr. Allen, a member of the writing committee for both the 2017 expert consensus and the 2021 update. He noted that the earlier document was one of the most downloaded articles from the ACC’s journal in the year it appeared.
“There is excellent data on the benefits of beta-blockers, ARNi, mineralocorticoid antagonists, and SGLT2 inhibitors, but how does one decide what order to use them in?” Dr. Allen asked in outlining goals of the expert consensus.
While the new update “focuses on the newer drug classes, particularly SGLT2 inhibitors,” it traces care from first-line therapies to end-of-life management, according to Dr. Allen. This includes information on when to consider advanced therapies, such as left ventricular assist devices or transplant in order to get patients to these treatments before the opportunity for benefit is missed.
Both the 2017 version and the update offer a table to summarize triggers for referral. The complexity of individualizing care in a group of patients likely to have variable manifestations of disease and multiple comorbidities was a theme of the 2017 document that has been reprised in the 2021 update,
“Good communication and team-based care” is one of common management gaps that the update addresses, Dr. Allen said. He indicated that the checklists and algorithms in the update would help with complex decision-making and encourage the multidisciplinary care that ensures optimal management.
SOURCE: Maddox TM et al. J Am Coll Cardiol. 2021 Jan 11. doi: 10.1016/j.jacc.2020.11.022.
A newly updated expert consensus from the American College of Cardiology for management of heart failure with reduced ejection fraction includes several new guideline-directed medical therapies among other substantial changes relative to its 2017 predecessor.
The advances in treatment of heart failure with reduced ejection fraction (HFrEF) have resulted in a substantial increase in complexity in reaching treatment goals, according to the authors of the new guidance. Structured similarly to the 2017 ACC Expert Consensus Decision Pathway, the update accommodates a series of practical tips to bring all patients on board with the newer as well as the established therapies with lifesaving potential.
The potential return from implementing these recommendations is not trivial. Relative to an ACE inhibitor and a beta-blocker alone, optimal implementation of the current guideline-directed medical therapies (GDMT) “can extend medical survival by more than 6 years,” according to Gregg C. Fonarow, MD, chief of cardiology at the University of California, Los Angeles.
A member of the writing committee for the 2021 update, Dr. Fonarow explained that the consensus pathway is more than a list of therapies and recommended doses. The detailed advice on how to overcome the barriers to GDMT is meant to close the substantial gap between current practice and unmet opportunities for inhibiting HFrEF progression.
“Optimal GDMT among HFrEF patients is distressingly low, due in part to the number and complexity of medications that now constitute GDMT,” said the chair of the writing committee, Thomas M. Maddox, MD, executive director, Healthcare Innovation Lab, BJC HealthCare/Washington University, St. Louis. Like Dr. Fonarow, Dr. Maddox emphasized that the importance of the update for the practical strategies it offers to place patients on optimal care.
In the 2017 guidance, 10 pivotal issues were tackled, ranging from advice of how to put HFrEF patients on the multiple drugs that now constitute optimal therapy to when to transition patients to hospice care. The 2021 update covers the same ground but incorporates new information that has changed the definition of optimal care.
Perhaps most importantly, sacubitril/valsartan, an angiotensin receptor neprilysin inhibitor (ARNi), and SGLT2 inhibitors represent major new additions in HFrEF GDMT. Dr. Maddox called the practical information about how these should be incorporated into HFrEF management represents one of the “major highlights” of the update.
Two algorithms outline the expert consensus recommendations of the order and the dose of the multiple drugs that now constitute the current GDMT. With the goal of explaining exactly how to place patients on all the HFrEF therapies associated with improved outcome, “I think these figures can really help us in guiding our patients to optimal medication regimens and dosages,” Dr. Maddox said. If successful, clinicians “can make a significant difference in these patients’ length and quality of life.”
Most cardiologists and others who treat HFrEF are likely aware of the major improvements in outcome documented in large trials when an ARNi and a SGLT2 inhibitor were added to previously established GDMT, but the update like the 2017 document is focused on the practical strategies of implementation, according to Larry A. Allen, MD, medical director of advanced heart failure at the University of Colorado at Denver, Aurora.
“The 2017 Expert Consensus Decision Pathway got a lot of attention because it takes a very practical approach to questions that clinicians and their patients have to tackle everyday but for which there was not always clean answers from the data,” said Dr. Allen, a member of the writing committee for both the 2017 expert consensus and the 2021 update. He noted that the earlier document was one of the most downloaded articles from the ACC’s journal in the year it appeared.
“There is excellent data on the benefits of beta-blockers, ARNi, mineralocorticoid antagonists, and SGLT2 inhibitors, but how does one decide what order to use them in?” Dr. Allen asked in outlining goals of the expert consensus.
While the new update “focuses on the newer drug classes, particularly SGLT2 inhibitors,” it traces care from first-line therapies to end-of-life management, according to Dr. Allen. This includes information on when to consider advanced therapies, such as left ventricular assist devices or transplant in order to get patients to these treatments before the opportunity for benefit is missed.
Both the 2017 version and the update offer a table to summarize triggers for referral. The complexity of individualizing care in a group of patients likely to have variable manifestations of disease and multiple comorbidities was a theme of the 2017 document that has been reprised in the 2021 update,
“Good communication and team-based care” is one of common management gaps that the update addresses, Dr. Allen said. He indicated that the checklists and algorithms in the update would help with complex decision-making and encourage the multidisciplinary care that ensures optimal management.
SOURCE: Maddox TM et al. J Am Coll Cardiol. 2021 Jan 11. doi: 10.1016/j.jacc.2020.11.022.
A newly updated expert consensus from the American College of Cardiology for management of heart failure with reduced ejection fraction includes several new guideline-directed medical therapies among other substantial changes relative to its 2017 predecessor.
The advances in treatment of heart failure with reduced ejection fraction (HFrEF) have resulted in a substantial increase in complexity in reaching treatment goals, according to the authors of the new guidance. Structured similarly to the 2017 ACC Expert Consensus Decision Pathway, the update accommodates a series of practical tips to bring all patients on board with the newer as well as the established therapies with lifesaving potential.
The potential return from implementing these recommendations is not trivial. Relative to an ACE inhibitor and a beta-blocker alone, optimal implementation of the current guideline-directed medical therapies (GDMT) “can extend medical survival by more than 6 years,” according to Gregg C. Fonarow, MD, chief of cardiology at the University of California, Los Angeles.
A member of the writing committee for the 2021 update, Dr. Fonarow explained that the consensus pathway is more than a list of therapies and recommended doses. The detailed advice on how to overcome the barriers to GDMT is meant to close the substantial gap between current practice and unmet opportunities for inhibiting HFrEF progression.
“Optimal GDMT among HFrEF patients is distressingly low, due in part to the number and complexity of medications that now constitute GDMT,” said the chair of the writing committee, Thomas M. Maddox, MD, executive director, Healthcare Innovation Lab, BJC HealthCare/Washington University, St. Louis. Like Dr. Fonarow, Dr. Maddox emphasized that the importance of the update for the practical strategies it offers to place patients on optimal care.
In the 2017 guidance, 10 pivotal issues were tackled, ranging from advice of how to put HFrEF patients on the multiple drugs that now constitute optimal therapy to when to transition patients to hospice care. The 2021 update covers the same ground but incorporates new information that has changed the definition of optimal care.
Perhaps most importantly, sacubitril/valsartan, an angiotensin receptor neprilysin inhibitor (ARNi), and SGLT2 inhibitors represent major new additions in HFrEF GDMT. Dr. Maddox called the practical information about how these should be incorporated into HFrEF management represents one of the “major highlights” of the update.
Two algorithms outline the expert consensus recommendations of the order and the dose of the multiple drugs that now constitute the current GDMT. With the goal of explaining exactly how to place patients on all the HFrEF therapies associated with improved outcome, “I think these figures can really help us in guiding our patients to optimal medication regimens and dosages,” Dr. Maddox said. If successful, clinicians “can make a significant difference in these patients’ length and quality of life.”
Most cardiologists and others who treat HFrEF are likely aware of the major improvements in outcome documented in large trials when an ARNi and a SGLT2 inhibitor were added to previously established GDMT, but the update like the 2017 document is focused on the practical strategies of implementation, according to Larry A. Allen, MD, medical director of advanced heart failure at the University of Colorado at Denver, Aurora.
“The 2017 Expert Consensus Decision Pathway got a lot of attention because it takes a very practical approach to questions that clinicians and their patients have to tackle everyday but for which there was not always clean answers from the data,” said Dr. Allen, a member of the writing committee for both the 2017 expert consensus and the 2021 update. He noted that the earlier document was one of the most downloaded articles from the ACC’s journal in the year it appeared.
“There is excellent data on the benefits of beta-blockers, ARNi, mineralocorticoid antagonists, and SGLT2 inhibitors, but how does one decide what order to use them in?” Dr. Allen asked in outlining goals of the expert consensus.
While the new update “focuses on the newer drug classes, particularly SGLT2 inhibitors,” it traces care from first-line therapies to end-of-life management, according to Dr. Allen. This includes information on when to consider advanced therapies, such as left ventricular assist devices or transplant in order to get patients to these treatments before the opportunity for benefit is missed.
Both the 2017 version and the update offer a table to summarize triggers for referral. The complexity of individualizing care in a group of patients likely to have variable manifestations of disease and multiple comorbidities was a theme of the 2017 document that has been reprised in the 2021 update,
“Good communication and team-based care” is one of common management gaps that the update addresses, Dr. Allen said. He indicated that the checklists and algorithms in the update would help with complex decision-making and encourage the multidisciplinary care that ensures optimal management.
SOURCE: Maddox TM et al. J Am Coll Cardiol. 2021 Jan 11. doi: 10.1016/j.jacc.2020.11.022.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
AGA News
Career Development Workshops Series
The AGA Career Development Workshops equip trainees and early-career GIs with indispensable knowledge and skills to successfully navigate the career path ahead. Over the course of the workshops, you will gain vital insights and advice to advance in your career with education not formally part of the training program curriculum. Workshops take place virtually and include topics like “How to Evaluate a Job in 2021,” “How to Succeed in Academic or Private Practice During COVID-19,” “Life in Industry,” and more. Workshops continue to be added monthly. Register today.
Save the date for DDW Virtual™
In 2021, Digestive Disease Week® (DDW) moves online as a fully virtual meeting with slightly new dates: May 21-23, 2021.
For more than 50 years, members of the digestive disease community have connected over the best science, education, and networking at DDW, and we’re confident this year will be no exception. In fact, we’re excited by opportunities the new format provides to learn, share, and connect with each other.
Watch the DDW website for more information as it becomes available. In the meantime, check out our FAQs about DDW Virtual™. If you have a question we didn’t answer, please submit a ticket to our help desk.
DDW is jointly sponsored by AGA, the American Association for the Study of Liver Diseases, the American Society for Gastrointestinal Endoscopy, and the Society for Surgery of the Alimentary Tract.
Gastro.org/DDW2021.
We did it!
Thank you for helping us raise $231,357 on AGA Giving Day to fund health disparity research!
The past few months were unlike any we’ve ever experienced, and above all we knew we needed to take action to provide a better future for digestive health patients. That’s why AGA and the AGA Research Foundation launched AGA Giving Day to address health disparities that negatively affect our patients head on. We couldn’t have led the fight to eradicate disparities in GI without our loyal supporters.
AGA Giving Day provided an opportunity to do something about health care differences that lead to poorer outcomes due to race and socioeconomic status. Thanks to the support of all our donors and funders, we raised $231,357 to fund health disparities research.
All donations will go directly into research awards earmarked for GI health disparities research. Health disparities research is the key to understanding how we can improve disease management for every patient.
During these trying times, there is one thing that hasn’t and won’t change: our commitment to our mission of raising funds to support talented researchers in gastroenterology and hepatology. While there is still more work ahead, we know we can move forward with the help of friends like you.
Thank you for being part of our fight to eradicate disparities in GI. Learn more about our other efforts through the AGA Equity Project.
Gastro.org/GivingDay
Career Development Workshops Series
The AGA Career Development Workshops equip trainees and early-career GIs with indispensable knowledge and skills to successfully navigate the career path ahead. Over the course of the workshops, you will gain vital insights and advice to advance in your career with education not formally part of the training program curriculum. Workshops take place virtually and include topics like “How to Evaluate a Job in 2021,” “How to Succeed in Academic or Private Practice During COVID-19,” “Life in Industry,” and more. Workshops continue to be added monthly. Register today.
Save the date for DDW Virtual™
In 2021, Digestive Disease Week® (DDW) moves online as a fully virtual meeting with slightly new dates: May 21-23, 2021.
For more than 50 years, members of the digestive disease community have connected over the best science, education, and networking at DDW, and we’re confident this year will be no exception. In fact, we’re excited by opportunities the new format provides to learn, share, and connect with each other.
Watch the DDW website for more information as it becomes available. In the meantime, check out our FAQs about DDW Virtual™. If you have a question we didn’t answer, please submit a ticket to our help desk.
DDW is jointly sponsored by AGA, the American Association for the Study of Liver Diseases, the American Society for Gastrointestinal Endoscopy, and the Society for Surgery of the Alimentary Tract.
Gastro.org/DDW2021.
We did it!
Thank you for helping us raise $231,357 on AGA Giving Day to fund health disparity research!
The past few months were unlike any we’ve ever experienced, and above all we knew we needed to take action to provide a better future for digestive health patients. That’s why AGA and the AGA Research Foundation launched AGA Giving Day to address health disparities that negatively affect our patients head on. We couldn’t have led the fight to eradicate disparities in GI without our loyal supporters.
AGA Giving Day provided an opportunity to do something about health care differences that lead to poorer outcomes due to race and socioeconomic status. Thanks to the support of all our donors and funders, we raised $231,357 to fund health disparities research.
All donations will go directly into research awards earmarked for GI health disparities research. Health disparities research is the key to understanding how we can improve disease management for every patient.
During these trying times, there is one thing that hasn’t and won’t change: our commitment to our mission of raising funds to support talented researchers in gastroenterology and hepatology. While there is still more work ahead, we know we can move forward with the help of friends like you.
Thank you for being part of our fight to eradicate disparities in GI. Learn more about our other efforts through the AGA Equity Project.
Gastro.org/GivingDay
Career Development Workshops Series
The AGA Career Development Workshops equip trainees and early-career GIs with indispensable knowledge and skills to successfully navigate the career path ahead. Over the course of the workshops, you will gain vital insights and advice to advance in your career with education not formally part of the training program curriculum. Workshops take place virtually and include topics like “How to Evaluate a Job in 2021,” “How to Succeed in Academic or Private Practice During COVID-19,” “Life in Industry,” and more. Workshops continue to be added monthly. Register today.
Save the date for DDW Virtual™
In 2021, Digestive Disease Week® (DDW) moves online as a fully virtual meeting with slightly new dates: May 21-23, 2021.
For more than 50 years, members of the digestive disease community have connected over the best science, education, and networking at DDW, and we’re confident this year will be no exception. In fact, we’re excited by opportunities the new format provides to learn, share, and connect with each other.
Watch the DDW website for more information as it becomes available. In the meantime, check out our FAQs about DDW Virtual™. If you have a question we didn’t answer, please submit a ticket to our help desk.
DDW is jointly sponsored by AGA, the American Association for the Study of Liver Diseases, the American Society for Gastrointestinal Endoscopy, and the Society for Surgery of the Alimentary Tract.
Gastro.org/DDW2021.
We did it!
Thank you for helping us raise $231,357 on AGA Giving Day to fund health disparity research!
The past few months were unlike any we’ve ever experienced, and above all we knew we needed to take action to provide a better future for digestive health patients. That’s why AGA and the AGA Research Foundation launched AGA Giving Day to address health disparities that negatively affect our patients head on. We couldn’t have led the fight to eradicate disparities in GI without our loyal supporters.
AGA Giving Day provided an opportunity to do something about health care differences that lead to poorer outcomes due to race and socioeconomic status. Thanks to the support of all our donors and funders, we raised $231,357 to fund health disparities research.
All donations will go directly into research awards earmarked for GI health disparities research. Health disparities research is the key to understanding how we can improve disease management for every patient.
During these trying times, there is one thing that hasn’t and won’t change: our commitment to our mission of raising funds to support talented researchers in gastroenterology and hepatology. While there is still more work ahead, we know we can move forward with the help of friends like you.
Thank you for being part of our fight to eradicate disparities in GI. Learn more about our other efforts through the AGA Equity Project.
Gastro.org/GivingDay
Calendar
For more information about the American Gastroenterological Association’s upcoming events and award deadlines, please visit http://agau.gastro.org and http://www.gastro.org/research-funding.
Upcoming Events
May 1, 2021
2021 AGA Postgraduate Course (Virtual Event)
Discover emerging science, leverage new tools and technologies and build lasting collaborations that will transform GI research and patient care at the AGA Postgraduate Course. Receive updates here.

May 21-23, 2021
Digestive Disease Week® (Virtual Event)
Save the date for the world’s leading event in digestive disease. DDW® brings professionals in gastroenterology, hepatology, endoscopy, and GI surgery together. Experience growth when you share your research, converge with trailblazers, and improve the lives of patients suffering from GI and liver diseases.
Early bird registration: Jan. 20 to Mar. 31, 2021.
Award Deadlines
AGA Student Abstract Award
This award supports recipients who are graduate students, medical students, or medical residents (residents up to postgraduate year 3) giving abstract-based oral or poster presentations at Digestive Disease Week® (DDW). The top scoring abstract will be designated the Student Abstract of the Year.
Application Deadline: Feb. 24, 2021
AGA–Moti L. & Kamla Rustgi International Travel Awards
This award provides support to early career (i.e., 35 years of age or younger at the time of Digestive Disease Week® (DDW)) basic, translational or clinical investigators residing outside North America giving abstract-based oral or poster presentations at DDW.
Application Deadline: Feb. 24, 2021
AGA Fellow Abstract Award
This award supports recipients who are MD, PhD, or equivalent fellows giving abstract-based oral or poster presentations at Digestive Disease Week® (DDW). The top scoring abstract will be designated the Fellow Abstract of the Year.
Application Deadline: Feb. 24, 2021
AGA-Aman Armaan Ahmed Family Summer Undergraduate Research Fellowship (SURF)
These fellowships support undergraduate students from groups traditionally underrepresented in biomedical research to perform 10 weeks of research related to digestive diseases under the mentorship of top investigators in the fields of gastroenterology and hepatology. The award provides a stipend, funding to offset travel and meal expenses, and opportunities to learn about future training and career options.
Application Deadline: Feb. 24, 2021
For more information about the American Gastroenterological Association’s upcoming events and award deadlines, please visit http://agau.gastro.org and http://www.gastro.org/research-funding.
Upcoming Events
May 1, 2021
2021 AGA Postgraduate Course (Virtual Event)
Discover emerging science, leverage new tools and technologies and build lasting collaborations that will transform GI research and patient care at the AGA Postgraduate Course. Receive updates here.
May 21-23, 2021
Digestive Disease Week® (Virtual Event)
Save the date for the world’s leading event in digestive disease. DDW® brings professionals in gastroenterology, hepatology, endoscopy, and GI surgery together. Experience growth when you share your research, converge with trailblazers, and improve the lives of patients suffering from GI and liver diseases.
Early bird registration: Jan. 20 to Mar. 31, 2021.
Award Deadlines
AGA Student Abstract Award
This award supports recipients who are graduate students, medical students, or medical residents (residents up to postgraduate year 3) giving abstract-based oral or poster presentations at Digestive Disease Week® (DDW). The top scoring abstract will be designated the Student Abstract of the Year.
Application Deadline: Feb. 24, 2021
AGA–Moti L. & Kamla Rustgi International Travel Awards
This award provides support to early career (i.e., 35 years of age or younger at the time of Digestive Disease Week® (DDW)) basic, translational or clinical investigators residing outside North America giving abstract-based oral or poster presentations at DDW.
Application Deadline: Feb. 24, 2021
AGA Fellow Abstract Award
This award supports recipients who are MD, PhD, or equivalent fellows giving abstract-based oral or poster presentations at Digestive Disease Week® (DDW). The top scoring abstract will be designated the Fellow Abstract of the Year.
Application Deadline: Feb. 24, 2021
AGA-Aman Armaan Ahmed Family Summer Undergraduate Research Fellowship (SURF)
These fellowships support undergraduate students from groups traditionally underrepresented in biomedical research to perform 10 weeks of research related to digestive diseases under the mentorship of top investigators in the fields of gastroenterology and hepatology. The award provides a stipend, funding to offset travel and meal expenses, and opportunities to learn about future training and career options.
Application Deadline: Feb. 24, 2021
For more information about the American Gastroenterological Association’s upcoming events and award deadlines, please visit http://agau.gastro.org and http://www.gastro.org/research-funding.
Upcoming Events
May 1, 2021
2021 AGA Postgraduate Course (Virtual Event)
Discover emerging science, leverage new tools and technologies and build lasting collaborations that will transform GI research and patient care at the AGA Postgraduate Course. Receive updates here.
May 21-23, 2021
Digestive Disease Week® (Virtual Event)
Save the date for the world’s leading event in digestive disease. DDW® brings professionals in gastroenterology, hepatology, endoscopy, and GI surgery together. Experience growth when you share your research, converge with trailblazers, and improve the lives of patients suffering from GI and liver diseases.
Early bird registration: Jan. 20 to Mar. 31, 2021.
Award Deadlines
AGA Student Abstract Award
This award supports recipients who are graduate students, medical students, or medical residents (residents up to postgraduate year 3) giving abstract-based oral or poster presentations at Digestive Disease Week® (DDW). The top scoring abstract will be designated the Student Abstract of the Year.
Application Deadline: Feb. 24, 2021
AGA–Moti L. & Kamla Rustgi International Travel Awards
This award provides support to early career (i.e., 35 years of age or younger at the time of Digestive Disease Week® (DDW)) basic, translational or clinical investigators residing outside North America giving abstract-based oral or poster presentations at DDW.
Application Deadline: Feb. 24, 2021
AGA Fellow Abstract Award
This award supports recipients who are MD, PhD, or equivalent fellows giving abstract-based oral or poster presentations at Digestive Disease Week® (DDW). The top scoring abstract will be designated the Fellow Abstract of the Year.
Application Deadline: Feb. 24, 2021
AGA-Aman Armaan Ahmed Family Summer Undergraduate Research Fellowship (SURF)
These fellowships support undergraduate students from groups traditionally underrepresented in biomedical research to perform 10 weeks of research related to digestive diseases under the mentorship of top investigators in the fields of gastroenterology and hepatology. The award provides a stipend, funding to offset travel and meal expenses, and opportunities to learn about future training and career options.
Application Deadline: Feb. 24, 2021
