User login
For MD-IQ use only
ACIP issues adult vaccination schedule 2022
by the Advisory Committee on Immunization Practices (ACIP) of the Centers for Disease Control and Prevention (CDC).
The Clinical Guideline on the “Recommended Adult Immunization Schedule, United States, 2022” appears online Feb. 17 in Annals of Internal Medicine and in the CDC’s Morbidity and Mortality Weekly Report.
The document features changes to the zoster, pneumococcal, and hepatitis B vaccines. COVID-19 vaccinations are now included in the notes section of the schedule and can be co-administered with other vaccines, according to ACIP.
The 2022 schedule is particularly important because the pandemic has caused many adults to fall behind in routine vaccinations, according to lead author Neil Murthy, MD, MPH, MSJ, of the CDC’s immunization services division, National Center for Immunization and Respiratory Diseases, and colleagues.
“Providers should administer all due and overdue vaccines according to the routine immunization schedule during the same visit,” the group wrote. “In addition, providers should implement strategies to catch up all patients on any overdue vaccines.”
Among other changes appearing in the 2022 recommendations:
- A new step 4 in the form of an appendix lists all the contraindications and precautions for each vaccine.
- The zoster vaccine now is recommended for use in everyone aged 19 years and older who are or will be immunodeficient or immunosuppressed through disease or therapy. The new purple color bar reflects ACIP’s new two-dose series regimen for immunocompromised adults aged 19 to 49.
- The simplified pneumococcal recommendation includes guidance on using the new PCV15 and PCV20 vaccines.
- The hepatitis B recommendation has been made more inclusive, with vaccination recommended for all adults aged 19 to 59. The Special Situations section in the Notes outlines the risk-based recommendations for the hepatitis B vaccine in adults aged 60 and older. The schedule has been harmonized with the 2022 Child and Adolescent Immunization Schedule.
A welcome change
Sandra A. Fryhofer, MD, a member of the ACIP Combined Immunization Work Group, said the new pneumococcal recommendation is a particularly welcome change.
“The old recommendation was complicated and confusing. The new one is much more straightforward,” Dr. Fryhofer, an internist in Atlanta, said in an interview. Now there are only two options: a two-vaccine series of PCV15 (Vaxneuvance), in combination with the already familiar PPSV23 polysaccharide vaccine (Pneumovax 23), and a single dose of the new PCV20, Prevnar 20.
“Some work group members favored a universal age-based recommendation starting at 50 instead of 65,” Fryhofer said. “This would provide more opportunities to vaccinate adults but could lead to waning immunity later in life when risk of disease is higher.”
Although none of the updates is likely to stir controversy, discussion among ACIP members was particularly lively around hepatitis B vaccination, Dr. Fryhofer said. This vaccine has historically been recommended based on risk and has had poor uptake, while age-based vaccine recommendations generally have greater uptake.
“ACIP approved hepatitis B vaccine universally for those up to age 60, but for those 60 and older, the recommendation remains risk-based with a loophole: Anyone 60 and older who wants it can get it,” she told this news organization. “Some of the risk indications for hepatitis B vaccination may be uncomfortable or embarrassing to disclose, especially for older patients. The loophole takes care of that, but patients may have to ask for the vaccine.”
As usual, the graphics have been fine-tuned for greater accuracy and readability. “You can print a color copy to have in the exam room or at your workspace or give it a bookmark and check it online,” Dr. Fryhofer said. “It’s a great resource to have at your fingertips.”
Dr. Fryhofer has made a series of videos explaining ACIP’s approval process, the use of the schedule, and changes to vaccines including influenza. These can be accessed on the American College of Physicians website.
The authors of the recommendations stress that physicians should pay careful attention to the notes section for each vaccine, as these details clarify who needs what vaccine, when, and at what dose.
Co-author Henry Bernstein, DO, reported that he is the editor of Current Opinion in Pediatrics Office Pediatrics Series and received a presentation honorarium from the Florida chapter of the American Academy of Pediatrics. Co-author Kevin Ault, MD, reported having received a grant from the National Cancer Institute, consulting fees from PathoVax, and payments supporting attending meetings and/or travel from the American College of Obstetricians and Gynecologists.
A version of this article first appeared on Medscape.com.
by the Advisory Committee on Immunization Practices (ACIP) of the Centers for Disease Control and Prevention (CDC).
The Clinical Guideline on the “Recommended Adult Immunization Schedule, United States, 2022” appears online Feb. 17 in Annals of Internal Medicine and in the CDC’s Morbidity and Mortality Weekly Report.
The document features changes to the zoster, pneumococcal, and hepatitis B vaccines. COVID-19 vaccinations are now included in the notes section of the schedule and can be co-administered with other vaccines, according to ACIP.
The 2022 schedule is particularly important because the pandemic has caused many adults to fall behind in routine vaccinations, according to lead author Neil Murthy, MD, MPH, MSJ, of the CDC’s immunization services division, National Center for Immunization and Respiratory Diseases, and colleagues.
“Providers should administer all due and overdue vaccines according to the routine immunization schedule during the same visit,” the group wrote. “In addition, providers should implement strategies to catch up all patients on any overdue vaccines.”
Among other changes appearing in the 2022 recommendations:
- A new step 4 in the form of an appendix lists all the contraindications and precautions for each vaccine.
- The zoster vaccine now is recommended for use in everyone aged 19 years and older who are or will be immunodeficient or immunosuppressed through disease or therapy. The new purple color bar reflects ACIP’s new two-dose series regimen for immunocompromised adults aged 19 to 49.
- The simplified pneumococcal recommendation includes guidance on using the new PCV15 and PCV20 vaccines.
- The hepatitis B recommendation has been made more inclusive, with vaccination recommended for all adults aged 19 to 59. The Special Situations section in the Notes outlines the risk-based recommendations for the hepatitis B vaccine in adults aged 60 and older. The schedule has been harmonized with the 2022 Child and Adolescent Immunization Schedule.
A welcome change
Sandra A. Fryhofer, MD, a member of the ACIP Combined Immunization Work Group, said the new pneumococcal recommendation is a particularly welcome change.
“The old recommendation was complicated and confusing. The new one is much more straightforward,” Dr. Fryhofer, an internist in Atlanta, said in an interview. Now there are only two options: a two-vaccine series of PCV15 (Vaxneuvance), in combination with the already familiar PPSV23 polysaccharide vaccine (Pneumovax 23), and a single dose of the new PCV20, Prevnar 20.
“Some work group members favored a universal age-based recommendation starting at 50 instead of 65,” Fryhofer said. “This would provide more opportunities to vaccinate adults but could lead to waning immunity later in life when risk of disease is higher.”
Although none of the updates is likely to stir controversy, discussion among ACIP members was particularly lively around hepatitis B vaccination, Dr. Fryhofer said. This vaccine has historically been recommended based on risk and has had poor uptake, while age-based vaccine recommendations generally have greater uptake.
“ACIP approved hepatitis B vaccine universally for those up to age 60, but for those 60 and older, the recommendation remains risk-based with a loophole: Anyone 60 and older who wants it can get it,” she told this news organization. “Some of the risk indications for hepatitis B vaccination may be uncomfortable or embarrassing to disclose, especially for older patients. The loophole takes care of that, but patients may have to ask for the vaccine.”
As usual, the graphics have been fine-tuned for greater accuracy and readability. “You can print a color copy to have in the exam room or at your workspace or give it a bookmark and check it online,” Dr. Fryhofer said. “It’s a great resource to have at your fingertips.”
Dr. Fryhofer has made a series of videos explaining ACIP’s approval process, the use of the schedule, and changes to vaccines including influenza. These can be accessed on the American College of Physicians website.
The authors of the recommendations stress that physicians should pay careful attention to the notes section for each vaccine, as these details clarify who needs what vaccine, when, and at what dose.
Co-author Henry Bernstein, DO, reported that he is the editor of Current Opinion in Pediatrics Office Pediatrics Series and received a presentation honorarium from the Florida chapter of the American Academy of Pediatrics. Co-author Kevin Ault, MD, reported having received a grant from the National Cancer Institute, consulting fees from PathoVax, and payments supporting attending meetings and/or travel from the American College of Obstetricians and Gynecologists.
A version of this article first appeared on Medscape.com.
by the Advisory Committee on Immunization Practices (ACIP) of the Centers for Disease Control and Prevention (CDC).
The Clinical Guideline on the “Recommended Adult Immunization Schedule, United States, 2022” appears online Feb. 17 in Annals of Internal Medicine and in the CDC’s Morbidity and Mortality Weekly Report.
The document features changes to the zoster, pneumococcal, and hepatitis B vaccines. COVID-19 vaccinations are now included in the notes section of the schedule and can be co-administered with other vaccines, according to ACIP.
The 2022 schedule is particularly important because the pandemic has caused many adults to fall behind in routine vaccinations, according to lead author Neil Murthy, MD, MPH, MSJ, of the CDC’s immunization services division, National Center for Immunization and Respiratory Diseases, and colleagues.
“Providers should administer all due and overdue vaccines according to the routine immunization schedule during the same visit,” the group wrote. “In addition, providers should implement strategies to catch up all patients on any overdue vaccines.”
Among other changes appearing in the 2022 recommendations:
- A new step 4 in the form of an appendix lists all the contraindications and precautions for each vaccine.
- The zoster vaccine now is recommended for use in everyone aged 19 years and older who are or will be immunodeficient or immunosuppressed through disease or therapy. The new purple color bar reflects ACIP’s new two-dose series regimen for immunocompromised adults aged 19 to 49.
- The simplified pneumococcal recommendation includes guidance on using the new PCV15 and PCV20 vaccines.
- The hepatitis B recommendation has been made more inclusive, with vaccination recommended for all adults aged 19 to 59. The Special Situations section in the Notes outlines the risk-based recommendations for the hepatitis B vaccine in adults aged 60 and older. The schedule has been harmonized with the 2022 Child and Adolescent Immunization Schedule.
A welcome change
Sandra A. Fryhofer, MD, a member of the ACIP Combined Immunization Work Group, said the new pneumococcal recommendation is a particularly welcome change.
“The old recommendation was complicated and confusing. The new one is much more straightforward,” Dr. Fryhofer, an internist in Atlanta, said in an interview. Now there are only two options: a two-vaccine series of PCV15 (Vaxneuvance), in combination with the already familiar PPSV23 polysaccharide vaccine (Pneumovax 23), and a single dose of the new PCV20, Prevnar 20.
“Some work group members favored a universal age-based recommendation starting at 50 instead of 65,” Fryhofer said. “This would provide more opportunities to vaccinate adults but could lead to waning immunity later in life when risk of disease is higher.”
Although none of the updates is likely to stir controversy, discussion among ACIP members was particularly lively around hepatitis B vaccination, Dr. Fryhofer said. This vaccine has historically been recommended based on risk and has had poor uptake, while age-based vaccine recommendations generally have greater uptake.
“ACIP approved hepatitis B vaccine universally for those up to age 60, but for those 60 and older, the recommendation remains risk-based with a loophole: Anyone 60 and older who wants it can get it,” she told this news organization. “Some of the risk indications for hepatitis B vaccination may be uncomfortable or embarrassing to disclose, especially for older patients. The loophole takes care of that, but patients may have to ask for the vaccine.”
As usual, the graphics have been fine-tuned for greater accuracy and readability. “You can print a color copy to have in the exam room or at your workspace or give it a bookmark and check it online,” Dr. Fryhofer said. “It’s a great resource to have at your fingertips.”
Dr. Fryhofer has made a series of videos explaining ACIP’s approval process, the use of the schedule, and changes to vaccines including influenza. These can be accessed on the American College of Physicians website.
The authors of the recommendations stress that physicians should pay careful attention to the notes section for each vaccine, as these details clarify who needs what vaccine, when, and at what dose.
Co-author Henry Bernstein, DO, reported that he is the editor of Current Opinion in Pediatrics Office Pediatrics Series and received a presentation honorarium from the Florida chapter of the American Academy of Pediatrics. Co-author Kevin Ault, MD, reported having received a grant from the National Cancer Institute, consulting fees from PathoVax, and payments supporting attending meetings and/or travel from the American College of Obstetricians and Gynecologists.
A version of this article first appeared on Medscape.com.
Diversity among oncologists has not kept pace with the U.S. population
in these fields, according to a cross-sectional study of data from the Association of American Medical Colleges.
“Creating and maintaining a diverse health care workforce is a priority to help combat societal inequities and health disparities, particularly in light of the evolving demographic characteristics of the general U.S. population,” wrote authors who were led by Sophia C. Kamran, MD, a radiation oncologist with Massachusetts General Hospital, Boston.
The study, which was published Dec. 9 in JAMA Oncology, surveyed full-time U.S.-based faculty in radiation and medical oncology departments from 1970 through 2019.
Improved patient satisfaction, compliance, and outcomes have been documented when a health care workforce better reflects the demographic traits of those whom it serves, Dr. Kamran and associates wrote.
They point to recent increases in the number and urgency of calls for improved diversity in the health care workforce, citing also higher incidence and mortality of new cancer cases among Black, indigenous, and Hispanic populations, compared with their non-Hispanic White counterparts. Prior calls for health care work force diversity have led to some creation of opportunities and pathways for increased representation of women and racial and ethnic minority groups in medicine, and the overall diversity of medical school faculty has been increasing by race and ethnicity and sex.
The change, however, is of lesser magnitude than what has been seen among medical school applicants, students, and graduates, and the gains in medical school faculty diversity have not kept pace with increasing diversity of the U.S. population. It has remained unclear whether corresponding progress has occurred in the composition of radiation oncology and medical oncology departments during the last 5 decades.
Despite lack of diversity, total faculty numbers have increased
Dr. Kamran and associates’ analysis revealed that total faculty numbers increased over time in both radiation oncology and medical oncology, with faculty representation of underrepresented-in-medicine (URM) women proportionally increased by 0.1% per decade in both radiation oncology (95% confidence interval, 0.005%-0.110%; P < . 001 for trend) and medical oncology (95% CI, −0.03% to 0.16%; P = .06 for trend), compared with non–URM women faculty, which increased by 0.4% (95% CI, 0.25%-0.80%) per decade in radiation oncology and 0.7% (95% CI, 0.47%-0.87%) per decade in medical oncology (P < .001 for trend for both). Faculty representation of URM men did not significantly change for radiation oncology (0.03% per decade [95% CI, −0.008% to 0.065%]; P = .09 for trend) or for medical oncology (0.003% per decade [95% CI, −0.13% to 0.14%]; P = .94 for trend).
In both 2009 and 2019, representation of both women and URM individuals for both specialties was less than their representation in the U.S. population. Radiation oncology faculty had the lowest URM representation in 2019 at 5.1%. The number of total URM faculty represented among both medical oncology and radiation oncology remained low for every rank in 2019 (Medical oncology: instructor, 2 of 44 [5%]; assistant professor, 18 of 274 [7%]; associate professor, 13 of 177 [7%]; full professor, 13 of 276 [5%]. Radiation oncology: instructor, 9 of 147 [6%]; assistant professor, 57 of 927 [6%]; associate professor, 20 of 510 [4%]; full professor, 18 of 452 [4%]).
“Our results highlight significant diversity differences along the career ladder in both specialties, with women having lower academic rank than men throughout the study period, and underrepresented [racial and ethnic groups] at every rank,” the authors wrote.
And, although Black, Hispanic, and indigenous people make up about 31% of the U.S. population, their inclusion in the health care workforce trails at all stages in the pipeline, the investigators found.
Diversity among radiation and medical oncologists lags behind that of medical school diversity in general, which has grown through efforts by the Association of American Medical Colleges.
Despite some improvements, the authors suggest the need for more initiatives to retain racial and ethnic minorities in an effort to reflect the diversity of the U.S. cancer population.
“This is a multifactorial issue, with focus not only on increasing diversity of the upstream pipeline but maintaining diversity throughout the entire pipeline, requiring difficult but necessary conversations about racial and ethnic systemic bias, lack of exposure and opportunities, and financial toxicities and pressures, to name a few. Until these factors are further delineated and better addressed, focused and targeted mentorship is key,” the authors wrote.
Small steps can have a collective impact
In a commentary published with the study, Frederick Lansigan, MD, and Charles R. Thomas Jr, MD, both of the Norris Cotton Cancer Center at Dartmouth-Hitchcock Medical Center, Lebanon, N.H., called for a systemic change in hiring practices.
“Any small steps of change that contribute to supporting the issues highlighted by the Kamran et al. study can have a collective positive impact. A holistic evaluation of [underrepresented] applicants at all stages of education and training is paramount, and joining selection committees is necessary to ensure fair processes. Mentoring programs, leadership courses, and addressing microaggressions and mistreatment may improve retention of [underrepresented] medical school matriculants and trainees in oncology. Cancer centers can build and lead visible and tangible diversity, equity, inclusion, justice, and belonging efforts as we are doing at our institution,” the physicians wrote.
But above all, Dr. Lansigan and Dr. Thomas said that the oncology community needs to agree that intentionally increasing the number of underrepresented physicians in the U.S. workforce is necessary to better address health care inequities.
“We need all hands on deck to reduce structural barriers in early education. We need STEM programs that start in elementary school and offer support through college. Oncologists can mentor these early learners to highlight the positive aspects of a career in oncology, the importance of [underrepresented] physicians in oncology, and the resilience required in caring for those with serious illness, many of whom will come from underserved populations. “Physicians and public health experts themselves who are interested in tackling the discrepancy between [underrepresented] and [non-underrepresented] medical school [students] and oncology trainees need to seek and be elected into positions that can start to balance this equation. If more are willing to acknowledge the structural inequities that exist in the oncology workforce pipeline, we can start to solve the complex equation of structural inequities.”
Dr Lansigan reported being the Interim Associate Dean of Diversity, Equity, and Inclusion at the Geisel School of Medicine and the Principal of Diversity, Equity, and Inclusion for the department of medicine at Dartmouth-Hitchcock Medical Center. No other disclosures were reported.
in these fields, according to a cross-sectional study of data from the Association of American Medical Colleges.
“Creating and maintaining a diverse health care workforce is a priority to help combat societal inequities and health disparities, particularly in light of the evolving demographic characteristics of the general U.S. population,” wrote authors who were led by Sophia C. Kamran, MD, a radiation oncologist with Massachusetts General Hospital, Boston.
The study, which was published Dec. 9 in JAMA Oncology, surveyed full-time U.S.-based faculty in radiation and medical oncology departments from 1970 through 2019.
Improved patient satisfaction, compliance, and outcomes have been documented when a health care workforce better reflects the demographic traits of those whom it serves, Dr. Kamran and associates wrote.
They point to recent increases in the number and urgency of calls for improved diversity in the health care workforce, citing also higher incidence and mortality of new cancer cases among Black, indigenous, and Hispanic populations, compared with their non-Hispanic White counterparts. Prior calls for health care work force diversity have led to some creation of opportunities and pathways for increased representation of women and racial and ethnic minority groups in medicine, and the overall diversity of medical school faculty has been increasing by race and ethnicity and sex.
The change, however, is of lesser magnitude than what has been seen among medical school applicants, students, and graduates, and the gains in medical school faculty diversity have not kept pace with increasing diversity of the U.S. population. It has remained unclear whether corresponding progress has occurred in the composition of radiation oncology and medical oncology departments during the last 5 decades.
Despite lack of diversity, total faculty numbers have increased
Dr. Kamran and associates’ analysis revealed that total faculty numbers increased over time in both radiation oncology and medical oncology, with faculty representation of underrepresented-in-medicine (URM) women proportionally increased by 0.1% per decade in both radiation oncology (95% confidence interval, 0.005%-0.110%; P < . 001 for trend) and medical oncology (95% CI, −0.03% to 0.16%; P = .06 for trend), compared with non–URM women faculty, which increased by 0.4% (95% CI, 0.25%-0.80%) per decade in radiation oncology and 0.7% (95% CI, 0.47%-0.87%) per decade in medical oncology (P < .001 for trend for both). Faculty representation of URM men did not significantly change for radiation oncology (0.03% per decade [95% CI, −0.008% to 0.065%]; P = .09 for trend) or for medical oncology (0.003% per decade [95% CI, −0.13% to 0.14%]; P = .94 for trend).
In both 2009 and 2019, representation of both women and URM individuals for both specialties was less than their representation in the U.S. population. Radiation oncology faculty had the lowest URM representation in 2019 at 5.1%. The number of total URM faculty represented among both medical oncology and radiation oncology remained low for every rank in 2019 (Medical oncology: instructor, 2 of 44 [5%]; assistant professor, 18 of 274 [7%]; associate professor, 13 of 177 [7%]; full professor, 13 of 276 [5%]. Radiation oncology: instructor, 9 of 147 [6%]; assistant professor, 57 of 927 [6%]; associate professor, 20 of 510 [4%]; full professor, 18 of 452 [4%]).
“Our results highlight significant diversity differences along the career ladder in both specialties, with women having lower academic rank than men throughout the study period, and underrepresented [racial and ethnic groups] at every rank,” the authors wrote.
And, although Black, Hispanic, and indigenous people make up about 31% of the U.S. population, their inclusion in the health care workforce trails at all stages in the pipeline, the investigators found.
Diversity among radiation and medical oncologists lags behind that of medical school diversity in general, which has grown through efforts by the Association of American Medical Colleges.
Despite some improvements, the authors suggest the need for more initiatives to retain racial and ethnic minorities in an effort to reflect the diversity of the U.S. cancer population.
“This is a multifactorial issue, with focus not only on increasing diversity of the upstream pipeline but maintaining diversity throughout the entire pipeline, requiring difficult but necessary conversations about racial and ethnic systemic bias, lack of exposure and opportunities, and financial toxicities and pressures, to name a few. Until these factors are further delineated and better addressed, focused and targeted mentorship is key,” the authors wrote.
Small steps can have a collective impact
In a commentary published with the study, Frederick Lansigan, MD, and Charles R. Thomas Jr, MD, both of the Norris Cotton Cancer Center at Dartmouth-Hitchcock Medical Center, Lebanon, N.H., called for a systemic change in hiring practices.
“Any small steps of change that contribute to supporting the issues highlighted by the Kamran et al. study can have a collective positive impact. A holistic evaluation of [underrepresented] applicants at all stages of education and training is paramount, and joining selection committees is necessary to ensure fair processes. Mentoring programs, leadership courses, and addressing microaggressions and mistreatment may improve retention of [underrepresented] medical school matriculants and trainees in oncology. Cancer centers can build and lead visible and tangible diversity, equity, inclusion, justice, and belonging efforts as we are doing at our institution,” the physicians wrote.
But above all, Dr. Lansigan and Dr. Thomas said that the oncology community needs to agree that intentionally increasing the number of underrepresented physicians in the U.S. workforce is necessary to better address health care inequities.
“We need all hands on deck to reduce structural barriers in early education. We need STEM programs that start in elementary school and offer support through college. Oncologists can mentor these early learners to highlight the positive aspects of a career in oncology, the importance of [underrepresented] physicians in oncology, and the resilience required in caring for those with serious illness, many of whom will come from underserved populations. “Physicians and public health experts themselves who are interested in tackling the discrepancy between [underrepresented] and [non-underrepresented] medical school [students] and oncology trainees need to seek and be elected into positions that can start to balance this equation. If more are willing to acknowledge the structural inequities that exist in the oncology workforce pipeline, we can start to solve the complex equation of structural inequities.”
Dr Lansigan reported being the Interim Associate Dean of Diversity, Equity, and Inclusion at the Geisel School of Medicine and the Principal of Diversity, Equity, and Inclusion for the department of medicine at Dartmouth-Hitchcock Medical Center. No other disclosures were reported.
in these fields, according to a cross-sectional study of data from the Association of American Medical Colleges.
“Creating and maintaining a diverse health care workforce is a priority to help combat societal inequities and health disparities, particularly in light of the evolving demographic characteristics of the general U.S. population,” wrote authors who were led by Sophia C. Kamran, MD, a radiation oncologist with Massachusetts General Hospital, Boston.
The study, which was published Dec. 9 in JAMA Oncology, surveyed full-time U.S.-based faculty in radiation and medical oncology departments from 1970 through 2019.
Improved patient satisfaction, compliance, and outcomes have been documented when a health care workforce better reflects the demographic traits of those whom it serves, Dr. Kamran and associates wrote.
They point to recent increases in the number and urgency of calls for improved diversity in the health care workforce, citing also higher incidence and mortality of new cancer cases among Black, indigenous, and Hispanic populations, compared with their non-Hispanic White counterparts. Prior calls for health care work force diversity have led to some creation of opportunities and pathways for increased representation of women and racial and ethnic minority groups in medicine, and the overall diversity of medical school faculty has been increasing by race and ethnicity and sex.
The change, however, is of lesser magnitude than what has been seen among medical school applicants, students, and graduates, and the gains in medical school faculty diversity have not kept pace with increasing diversity of the U.S. population. It has remained unclear whether corresponding progress has occurred in the composition of radiation oncology and medical oncology departments during the last 5 decades.
Despite lack of diversity, total faculty numbers have increased
Dr. Kamran and associates’ analysis revealed that total faculty numbers increased over time in both radiation oncology and medical oncology, with faculty representation of underrepresented-in-medicine (URM) women proportionally increased by 0.1% per decade in both radiation oncology (95% confidence interval, 0.005%-0.110%; P < . 001 for trend) and medical oncology (95% CI, −0.03% to 0.16%; P = .06 for trend), compared with non–URM women faculty, which increased by 0.4% (95% CI, 0.25%-0.80%) per decade in radiation oncology and 0.7% (95% CI, 0.47%-0.87%) per decade in medical oncology (P < .001 for trend for both). Faculty representation of URM men did not significantly change for radiation oncology (0.03% per decade [95% CI, −0.008% to 0.065%]; P = .09 for trend) or for medical oncology (0.003% per decade [95% CI, −0.13% to 0.14%]; P = .94 for trend).
In both 2009 and 2019, representation of both women and URM individuals for both specialties was less than their representation in the U.S. population. Radiation oncology faculty had the lowest URM representation in 2019 at 5.1%. The number of total URM faculty represented among both medical oncology and radiation oncology remained low for every rank in 2019 (Medical oncology: instructor, 2 of 44 [5%]; assistant professor, 18 of 274 [7%]; associate professor, 13 of 177 [7%]; full professor, 13 of 276 [5%]. Radiation oncology: instructor, 9 of 147 [6%]; assistant professor, 57 of 927 [6%]; associate professor, 20 of 510 [4%]; full professor, 18 of 452 [4%]).
“Our results highlight significant diversity differences along the career ladder in both specialties, with women having lower academic rank than men throughout the study period, and underrepresented [racial and ethnic groups] at every rank,” the authors wrote.
And, although Black, Hispanic, and indigenous people make up about 31% of the U.S. population, their inclusion in the health care workforce trails at all stages in the pipeline, the investigators found.
Diversity among radiation and medical oncologists lags behind that of medical school diversity in general, which has grown through efforts by the Association of American Medical Colleges.
Despite some improvements, the authors suggest the need for more initiatives to retain racial and ethnic minorities in an effort to reflect the diversity of the U.S. cancer population.
“This is a multifactorial issue, with focus not only on increasing diversity of the upstream pipeline but maintaining diversity throughout the entire pipeline, requiring difficult but necessary conversations about racial and ethnic systemic bias, lack of exposure and opportunities, and financial toxicities and pressures, to name a few. Until these factors are further delineated and better addressed, focused and targeted mentorship is key,” the authors wrote.
Small steps can have a collective impact
In a commentary published with the study, Frederick Lansigan, MD, and Charles R. Thomas Jr, MD, both of the Norris Cotton Cancer Center at Dartmouth-Hitchcock Medical Center, Lebanon, N.H., called for a systemic change in hiring practices.
“Any small steps of change that contribute to supporting the issues highlighted by the Kamran et al. study can have a collective positive impact. A holistic evaluation of [underrepresented] applicants at all stages of education and training is paramount, and joining selection committees is necessary to ensure fair processes. Mentoring programs, leadership courses, and addressing microaggressions and mistreatment may improve retention of [underrepresented] medical school matriculants and trainees in oncology. Cancer centers can build and lead visible and tangible diversity, equity, inclusion, justice, and belonging efforts as we are doing at our institution,” the physicians wrote.
But above all, Dr. Lansigan and Dr. Thomas said that the oncology community needs to agree that intentionally increasing the number of underrepresented physicians in the U.S. workforce is necessary to better address health care inequities.
“We need all hands on deck to reduce structural barriers in early education. We need STEM programs that start in elementary school and offer support through college. Oncologists can mentor these early learners to highlight the positive aspects of a career in oncology, the importance of [underrepresented] physicians in oncology, and the resilience required in caring for those with serious illness, many of whom will come from underserved populations. “Physicians and public health experts themselves who are interested in tackling the discrepancy between [underrepresented] and [non-underrepresented] medical school [students] and oncology trainees need to seek and be elected into positions that can start to balance this equation. If more are willing to acknowledge the structural inequities that exist in the oncology workforce pipeline, we can start to solve the complex equation of structural inequities.”
Dr Lansigan reported being the Interim Associate Dean of Diversity, Equity, and Inclusion at the Geisel School of Medicine and the Principal of Diversity, Equity, and Inclusion for the department of medicine at Dartmouth-Hitchcock Medical Center. No other disclosures were reported.
FROM JAMA ONCOLOGY
Biden’s FDA chief nominee narrowly wins Senate confirmation
On Feb. 15, Robert Califf, MD, narrowly won Senate confirmation to once again serve as the commissioner of the Food and Drug Administration, overcoming protest votes from lawmakers about abortion and opioid issues.

The Senate voted 50-46 in favor of Dr. Califf’s nomination. A cardiologist long affiliated with Duke University and a noted expert on clinical trials, Dr. Califf also led the FDA from February 2016 through January 2017.
In 2016, the Senate confirmed him as FDA chief in an 89-4 vote. At that time, Sen. Joe Manchin, D-WV, and a few other senators said they were concerned that Dr. Califf’s links to the drug industry would hamper his ability to regulate drugmakers, particularly in terms of rules on prescription painkillers.
Sen. Manchin also objected to Dr. Califf’s second nomination as FDA commissioner, as did several fellow Democrats, including Sen. Edward Markey of Massachusetts. In a statement issued after the Feb. 15 vote, Sen. Markey said he has “consistently raised concerns about the FDA’s egregious mishandling of opioid approvals and its role in enabling the current opioid epidemic.”
“To date, the FDA still has not implemented many of the reforms necessary to ensure that it is fulfilling its role as our nation’s top pharmaceutical cop on the beat,” Sen. Markey said. “I have not received any real commitment from Dr. Califf to truly reform the FDA or to learn from the failures that fueled this public health crisis.”
This time, Dr. Califf lost support among Republican senators due to objections raised by groups seeking to end women’s access to abortion. Susan B. Anthony List and National Right to Life asked senators in a January letter to oppose Dr. Califf’s nomination, citing their objections to how the FDA handled reporting of adverse events from abortions by medication during Dr. Califf’s Tenure.
But some Republicans supported Califf in the Tuesday vote. Sens. Roy Blunt of Missouri, Richard Burr of North Carolina, Susan Collins of Maine, Lisa Murkowski of Alaska, Mitt Romney of Utah, and Pat Toomey of Pennsylvania all voted in his favor.
On Feb. 14, Sen. Patty Murray, D-WA, chairwoman of the Senate Health, Education, Labor, and Pensions Committee, urged her colleagues to vote for Dr. Califf to give the FDA strong leadership to tackle urgent health needs such as the opioid crisis, youth tobacco use, antimicrobial resistance, and inequities in health care.
“At this critical moment, we need a trusted hand to lead the FDA,” she said in a floor speech. Dr. Califf’s previous service at the FDA and his years spent as a research scientist “give him the experience to take on this challenge.”
Separately, three former FDA commissioners on Feb. 15 published an opinion article that appeared in The Hill. Republican presidents nominated two of these former FDA chiefs: Scott Gottlieb, MD, and Mark McClellan, MD. The third, Margaret Hamburg, MD, was nominated by President Barack Obama, as was Dr. Califf for his first time as FDA chief.
There’s an urgent need for a confirmed leader at the FDA as the United States seeks to move beyond the pandemic, the former FDA chiefs wrote. The work ahead includes continued efforts with vaccines as well as efforts to bolster medical supply chains, they said.
Dr. Califf “knows how to advance the safe development and use of medical products and to bring a sound, science-based foundation to the FDA’s regulatory actions. Because of this, he has earned the confidence of FDA’s professional career staff, as well as a broad base of patient groups, academic experts, medical professionals, and public health organizations,” Dr. Gottlieb, Dr. Hamburg, and Dr. McClellan wrote.
The article also was signed by former Centers for Medicare and Medicaid Services Administrator Andy Slavitt, who served in the Obama administration.
Support of medical community
The American Heart Association issued a statement on Feb.15, congratulating Dr. Califf on his second confirmation after the Senate vote.
“With a distinguished career in public service and a long-time volunteer leader at the American Heart Association, Dr. Califf has honed his ability to communicate and build trust with diverse constituencies,” CEO Nancy Brown said in the statement. “He will use his experience as a cardiologist to safeguard the health and well-being of people throughout the country, and his background in research to prioritize science and evidence-based policymaking.”
Dr. Califf was also backed by the Association of American Medical Colleges, the American Academy of Pediatrics, the American Academy of Family Physicians, and the American College of Physicians when he was nominated for the role last year by President Joe Biden.
A version of this article first appeared on Medscape.com.
On Feb. 15, Robert Califf, MD, narrowly won Senate confirmation to once again serve as the commissioner of the Food and Drug Administration, overcoming protest votes from lawmakers about abortion and opioid issues.
The Senate voted 50-46 in favor of Dr. Califf’s nomination. A cardiologist long affiliated with Duke University and a noted expert on clinical trials, Dr. Califf also led the FDA from February 2016 through January 2017.
In 2016, the Senate confirmed him as FDA chief in an 89-4 vote. At that time, Sen. Joe Manchin, D-WV, and a few other senators said they were concerned that Dr. Califf’s links to the drug industry would hamper his ability to regulate drugmakers, particularly in terms of rules on prescription painkillers.
Sen. Manchin also objected to Dr. Califf’s second nomination as FDA commissioner, as did several fellow Democrats, including Sen. Edward Markey of Massachusetts. In a statement issued after the Feb. 15 vote, Sen. Markey said he has “consistently raised concerns about the FDA’s egregious mishandling of opioid approvals and its role in enabling the current opioid epidemic.”
“To date, the FDA still has not implemented many of the reforms necessary to ensure that it is fulfilling its role as our nation’s top pharmaceutical cop on the beat,” Sen. Markey said. “I have not received any real commitment from Dr. Califf to truly reform the FDA or to learn from the failures that fueled this public health crisis.”
This time, Dr. Califf lost support among Republican senators due to objections raised by groups seeking to end women’s access to abortion. Susan B. Anthony List and National Right to Life asked senators in a January letter to oppose Dr. Califf’s nomination, citing their objections to how the FDA handled reporting of adverse events from abortions by medication during Dr. Califf’s Tenure.
But some Republicans supported Califf in the Tuesday vote. Sens. Roy Blunt of Missouri, Richard Burr of North Carolina, Susan Collins of Maine, Lisa Murkowski of Alaska, Mitt Romney of Utah, and Pat Toomey of Pennsylvania all voted in his favor.
On Feb. 14, Sen. Patty Murray, D-WA, chairwoman of the Senate Health, Education, Labor, and Pensions Committee, urged her colleagues to vote for Dr. Califf to give the FDA strong leadership to tackle urgent health needs such as the opioid crisis, youth tobacco use, antimicrobial resistance, and inequities in health care.
“At this critical moment, we need a trusted hand to lead the FDA,” she said in a floor speech. Dr. Califf’s previous service at the FDA and his years spent as a research scientist “give him the experience to take on this challenge.”
Separately, three former FDA commissioners on Feb. 15 published an opinion article that appeared in The Hill. Republican presidents nominated two of these former FDA chiefs: Scott Gottlieb, MD, and Mark McClellan, MD. The third, Margaret Hamburg, MD, was nominated by President Barack Obama, as was Dr. Califf for his first time as FDA chief.
There’s an urgent need for a confirmed leader at the FDA as the United States seeks to move beyond the pandemic, the former FDA chiefs wrote. The work ahead includes continued efforts with vaccines as well as efforts to bolster medical supply chains, they said.
Dr. Califf “knows how to advance the safe development and use of medical products and to bring a sound, science-based foundation to the FDA’s regulatory actions. Because of this, he has earned the confidence of FDA’s professional career staff, as well as a broad base of patient groups, academic experts, medical professionals, and public health organizations,” Dr. Gottlieb, Dr. Hamburg, and Dr. McClellan wrote.
The article also was signed by former Centers for Medicare and Medicaid Services Administrator Andy Slavitt, who served in the Obama administration.
Support of medical community
The American Heart Association issued a statement on Feb.15, congratulating Dr. Califf on his second confirmation after the Senate vote.
“With a distinguished career in public service and a long-time volunteer leader at the American Heart Association, Dr. Califf has honed his ability to communicate and build trust with diverse constituencies,” CEO Nancy Brown said in the statement. “He will use his experience as a cardiologist to safeguard the health and well-being of people throughout the country, and his background in research to prioritize science and evidence-based policymaking.”
Dr. Califf was also backed by the Association of American Medical Colleges, the American Academy of Pediatrics, the American Academy of Family Physicians, and the American College of Physicians when he was nominated for the role last year by President Joe Biden.
A version of this article first appeared on Medscape.com.
On Feb. 15, Robert Califf, MD, narrowly won Senate confirmation to once again serve as the commissioner of the Food and Drug Administration, overcoming protest votes from lawmakers about abortion and opioid issues.
The Senate voted 50-46 in favor of Dr. Califf’s nomination. A cardiologist long affiliated with Duke University and a noted expert on clinical trials, Dr. Califf also led the FDA from February 2016 through January 2017.
In 2016, the Senate confirmed him as FDA chief in an 89-4 vote. At that time, Sen. Joe Manchin, D-WV, and a few other senators said they were concerned that Dr. Califf’s links to the drug industry would hamper his ability to regulate drugmakers, particularly in terms of rules on prescription painkillers.
Sen. Manchin also objected to Dr. Califf’s second nomination as FDA commissioner, as did several fellow Democrats, including Sen. Edward Markey of Massachusetts. In a statement issued after the Feb. 15 vote, Sen. Markey said he has “consistently raised concerns about the FDA’s egregious mishandling of opioid approvals and its role in enabling the current opioid epidemic.”
“To date, the FDA still has not implemented many of the reforms necessary to ensure that it is fulfilling its role as our nation’s top pharmaceutical cop on the beat,” Sen. Markey said. “I have not received any real commitment from Dr. Califf to truly reform the FDA or to learn from the failures that fueled this public health crisis.”
This time, Dr. Califf lost support among Republican senators due to objections raised by groups seeking to end women’s access to abortion. Susan B. Anthony List and National Right to Life asked senators in a January letter to oppose Dr. Califf’s nomination, citing their objections to how the FDA handled reporting of adverse events from abortions by medication during Dr. Califf’s Tenure.
But some Republicans supported Califf in the Tuesday vote. Sens. Roy Blunt of Missouri, Richard Burr of North Carolina, Susan Collins of Maine, Lisa Murkowski of Alaska, Mitt Romney of Utah, and Pat Toomey of Pennsylvania all voted in his favor.
On Feb. 14, Sen. Patty Murray, D-WA, chairwoman of the Senate Health, Education, Labor, and Pensions Committee, urged her colleagues to vote for Dr. Califf to give the FDA strong leadership to tackle urgent health needs such as the opioid crisis, youth tobacco use, antimicrobial resistance, and inequities in health care.
“At this critical moment, we need a trusted hand to lead the FDA,” she said in a floor speech. Dr. Califf’s previous service at the FDA and his years spent as a research scientist “give him the experience to take on this challenge.”
Separately, three former FDA commissioners on Feb. 15 published an opinion article that appeared in The Hill. Republican presidents nominated two of these former FDA chiefs: Scott Gottlieb, MD, and Mark McClellan, MD. The third, Margaret Hamburg, MD, was nominated by President Barack Obama, as was Dr. Califf for his first time as FDA chief.
There’s an urgent need for a confirmed leader at the FDA as the United States seeks to move beyond the pandemic, the former FDA chiefs wrote. The work ahead includes continued efforts with vaccines as well as efforts to bolster medical supply chains, they said.
Dr. Califf “knows how to advance the safe development and use of medical products and to bring a sound, science-based foundation to the FDA’s regulatory actions. Because of this, he has earned the confidence of FDA’s professional career staff, as well as a broad base of patient groups, academic experts, medical professionals, and public health organizations,” Dr. Gottlieb, Dr. Hamburg, and Dr. McClellan wrote.
The article also was signed by former Centers for Medicare and Medicaid Services Administrator Andy Slavitt, who served in the Obama administration.
Support of medical community
The American Heart Association issued a statement on Feb.15, congratulating Dr. Califf on his second confirmation after the Senate vote.
“With a distinguished career in public service and a long-time volunteer leader at the American Heart Association, Dr. Califf has honed his ability to communicate and build trust with diverse constituencies,” CEO Nancy Brown said in the statement. “He will use his experience as a cardiologist to safeguard the health and well-being of people throughout the country, and his background in research to prioritize science and evidence-based policymaking.”
Dr. Califf was also backed by the Association of American Medical Colleges, the American Academy of Pediatrics, the American Academy of Family Physicians, and the American College of Physicians when he was nominated for the role last year by President Joe Biden.
A version of this article first appeared on Medscape.com.
Why is vitamin D hype so impervious to evidence?
The vitamin D story exudes teaching points: It offers a master class in critical appraisal, connecting the concepts of biologic plausibility, flawed surrogate markers, confounded observational studies, and slews of randomized controlled trials (RCTs) showing no benefits on health outcomes.

Yet despite the utter lack of benefit seen in trials, the hype continues. And the pandemic has only enhanced this hype as an onslaught of papers have reported the association of low vitamin D levels and COVID-19 disease.
My questions are simple: Why doesn’t the evidence persuade people? How many nonsignificant trials do we need before researchers stop studying vitamin D, doctors stop (routinely) measuring levels, and patients stop wasting money on the unhelpful supplement? What are the implications for this lack of persuasion?
Before exploring these questions, I want to set out that symptomatic vitamin deficiencies of any sort ought to be corrected.
Biologic plausibility and the pull of observational studies
It has long been known that vitamin D is crucial for bone health and that it can be produced in the skin with sun exposure. In the last decade, however, experts note that nearly every tissue and cell in our body has a vitamin D receptor. It then follows that if this many cells in the body can activate vitamin D, it must be vital for cardiovascular health, immune function, cancer prevention: basically, everything health related.
Oodles of observational studies have found that low serum levels of vitamin D correlate with higher mortality from all causes, cancer, cardiovascular disease, and now even COVID-19. Yet no matter the amount of statistical adjustment in these studies, we cannot know whether these associations are due to true causality.
The major issue is confounding: That is, people with low vitamin D levels have other conditions or diseases that lead to higher rates of ill health. Consider a patient with obesity, arthritis, and cognitive decline; this person is unlikely to do much exercise in the sun and may have low vitamin D levels. The low vitamin D level is simply a marker of overall poor health.
The randomized controlled trials tell a clear story
There are hundreds of vitamin D RCTs. The results simplify into one sentence: Vitamin D supplements do not improve health outcomes.
Here is a short summary of some recent studies.
VITAL, a massive (N > 25,000) RCT with 5 years of follow-up, compared vitamin D supplements to placebo and found no differences in the primary endpoints of cancer or cardiac events. Rates of death from any cause were nearly identical. Crucially, in subgroup analyses, the effects did not vary according to vitamin D levels at baseline.
The D-Health investigators randomly assigned more than 21,000 adults to vitamin D or placebo and after 5.7 years of follow-up reported no differences in the primary endpoint of overall mortality. There also were no differences in cardiovascular disease mortality.
Then you have the Mendelian randomized studies, which some have called nature’s RCT. These studies take advantage of the fact that some people are born with gene variations that predispose to low vitamin D levels. More than 60 Mendelian randomization studies have evaluated the consequences of lifelong genetically lowered vitamin D levels on various outcomes; most of these have found null effects.
Then there are the meta-analyses and systematic reviews. I loved the conclusion of this review of systematic reviews from the BMJ (emphasis mine):
“Despite a few hundred systematic reviews and meta-analyses, highly convincing evidence of a clear role of vitamin D does not exist for any outcome, but associations with a selection of outcomes are probable.”
The failure to persuade
My original plan was to emphasize the power of the RCT. Despite strong associations of low vitamin D levels with poor outcomes, the trials show no benefit to treatment. This strongly suggests (or nearly proves) that low vitamin D levels are akin to premature ventricular complexes after myocardial infarction: a marker for risk but not a target for therapy.
But I now see the more important issue as why scientists, funders, clinicians, and patients are not persuaded by clear evidence. Every day in clinic I see patients on vitamin D supplements; the journals keep publishing vitamin D studies. The proponents of vitamin D remain positive. And lately there is outsized attention and hope that vitamin D will mitigate SARS-CoV2 infection – based only on observational data.
You might argue against this point by saying vitamin D is natural and relatively innocuous, so who cares?
I offer three rebuttals to that point: Opportunity costs, distraction, and the insidious danger of poor critical appraisal skills. If you are burning money on vitamin D research, there is less available to study other important issues. If a patient is distracted by low vitamin D levels, she may pay less attention to her high body mass index or hypertension. And on the matter of critical appraisal, trust in medicine requires clinicians to be competent in critical appraisal. And these days, what could be more important than trust in medical professionals?
One major reason for the failure of persuasion of evidence is spin – or language that distracts from the primary endpoint. Here are two (of many) examples:
A meta-analysis of 50 vitamin D trials set out to study mortality. The authors found no significant difference in that primary endpoint. But the second sentence in their conclusion was that vitamin D supplements reduced the risk for cancer deaths by 15%. That’s a secondary endpoint in a study with nonsignificance in the primary endpoint. That is spin. This meta-analysis was completed before the Australian D-Health trial found that cancer deaths were 15% higher in the vitamin D arm, a difference that did not reach statistical significance.
The following example is worse: The authors of the VITAL trial, which found that vitamin D supplements had no effect on the primary endpoint of invasive cancer or cardiovascular disease, published a secondary analysis of the trial looking at a different endpoint: A composite incidence of metastatic and fatal invasive total cancer. They reported a 0.4% lower rate for the vitamin D group, a difference that barely made statistical significance at a P value of .04.
But everyone knows the dangers of reanalyzing data with a new endpoint after you have seen the data. What’s more, even if this were a reasonable post hoc analysis, the results are neither clinically meaningful nor statistically robust. Yet the fatally flawed paper has been viewed 60,000 times and picked up by 48 news outlets.
Another way to distract from nonsignificant primary outcomes is to nitpick the trials. The vitamin D dose wasn’t high enough, for instance. This might persuade me if there were one or two vitamin D trials, but there are hundreds of trials and meta-analyses, and their results are consistently null.
Conclusion: No, it is not hopeless
A nihilist would argue that fighting spin is futile. They would say you can’t fight incentives and business models. The incentive structure to publish is strong, and the journals and media know vitamin D studies garner attention – which is their currency.
I am not a nihilist and believe strongly that we must continue to teach critical appraisal and numerical literacy.
In fact, I would speculate that decades of poor critical appraisal by the medical profession have fostered outsized hope and created erroneous norms.
Imagine a counter-factual world in which clinicians have taught society that the human body is unlike an engine that can be repaired by fixing one part (i.e., the vitamin D level), that magic bullets (insulin) are rare, that most treatments fail, or that you can’t rely on association studies to prove efficacy.
In this world, people would be immune from spin and hype.
The norm would be that pills, supplements, and procedures are not what delivers good health. What delivers health is an amalgam of good luck, healthy habits, and lots of time spent outside playing in the sun.
Dr. Mandrola practices cardiac electrophysiology in Louisville, Ky., and is a writer and podcaster for Medscape. He espouses a conservative approach to medical practice. He participates in clinical research and writes often about the state of medical evidence. He has disclosed no relevant financial relationships. A version of this article first appeared on Medscape.com.
The vitamin D story exudes teaching points: It offers a master class in critical appraisal, connecting the concepts of biologic plausibility, flawed surrogate markers, confounded observational studies, and slews of randomized controlled trials (RCTs) showing no benefits on health outcomes.
Yet despite the utter lack of benefit seen in trials, the hype continues. And the pandemic has only enhanced this hype as an onslaught of papers have reported the association of low vitamin D levels and COVID-19 disease.
My questions are simple: Why doesn’t the evidence persuade people? How many nonsignificant trials do we need before researchers stop studying vitamin D, doctors stop (routinely) measuring levels, and patients stop wasting money on the unhelpful supplement? What are the implications for this lack of persuasion?
Before exploring these questions, I want to set out that symptomatic vitamin deficiencies of any sort ought to be corrected.
Biologic plausibility and the pull of observational studies
It has long been known that vitamin D is crucial for bone health and that it can be produced in the skin with sun exposure. In the last decade, however, experts note that nearly every tissue and cell in our body has a vitamin D receptor. It then follows that if this many cells in the body can activate vitamin D, it must be vital for cardiovascular health, immune function, cancer prevention: basically, everything health related.
Oodles of observational studies have found that low serum levels of vitamin D correlate with higher mortality from all causes, cancer, cardiovascular disease, and now even COVID-19. Yet no matter the amount of statistical adjustment in these studies, we cannot know whether these associations are due to true causality.
The major issue is confounding: That is, people with low vitamin D levels have other conditions or diseases that lead to higher rates of ill health. Consider a patient with obesity, arthritis, and cognitive decline; this person is unlikely to do much exercise in the sun and may have low vitamin D levels. The low vitamin D level is simply a marker of overall poor health.
The randomized controlled trials tell a clear story
There are hundreds of vitamin D RCTs. The results simplify into one sentence: Vitamin D supplements do not improve health outcomes.
Here is a short summary of some recent studies.
VITAL, a massive (N > 25,000) RCT with 5 years of follow-up, compared vitamin D supplements to placebo and found no differences in the primary endpoints of cancer or cardiac events. Rates of death from any cause were nearly identical. Crucially, in subgroup analyses, the effects did not vary according to vitamin D levels at baseline.
The D-Health investigators randomly assigned more than 21,000 adults to vitamin D or placebo and after 5.7 years of follow-up reported no differences in the primary endpoint of overall mortality. There also were no differences in cardiovascular disease mortality.
Then you have the Mendelian randomized studies, which some have called nature’s RCT. These studies take advantage of the fact that some people are born with gene variations that predispose to low vitamin D levels. More than 60 Mendelian randomization studies have evaluated the consequences of lifelong genetically lowered vitamin D levels on various outcomes; most of these have found null effects.
Then there are the meta-analyses and systematic reviews. I loved the conclusion of this review of systematic reviews from the BMJ (emphasis mine):
“Despite a few hundred systematic reviews and meta-analyses, highly convincing evidence of a clear role of vitamin D does not exist for any outcome, but associations with a selection of outcomes are probable.”
The failure to persuade
My original plan was to emphasize the power of the RCT. Despite strong associations of low vitamin D levels with poor outcomes, the trials show no benefit to treatment. This strongly suggests (or nearly proves) that low vitamin D levels are akin to premature ventricular complexes after myocardial infarction: a marker for risk but not a target for therapy.
But I now see the more important issue as why scientists, funders, clinicians, and patients are not persuaded by clear evidence. Every day in clinic I see patients on vitamin D supplements; the journals keep publishing vitamin D studies. The proponents of vitamin D remain positive. And lately there is outsized attention and hope that vitamin D will mitigate SARS-CoV2 infection – based only on observational data.
You might argue against this point by saying vitamin D is natural and relatively innocuous, so who cares?
I offer three rebuttals to that point: Opportunity costs, distraction, and the insidious danger of poor critical appraisal skills. If you are burning money on vitamin D research, there is less available to study other important issues. If a patient is distracted by low vitamin D levels, she may pay less attention to her high body mass index or hypertension. And on the matter of critical appraisal, trust in medicine requires clinicians to be competent in critical appraisal. And these days, what could be more important than trust in medical professionals?
One major reason for the failure of persuasion of evidence is spin – or language that distracts from the primary endpoint. Here are two (of many) examples:
A meta-analysis of 50 vitamin D trials set out to study mortality. The authors found no significant difference in that primary endpoint. But the second sentence in their conclusion was that vitamin D supplements reduced the risk for cancer deaths by 15%. That’s a secondary endpoint in a study with nonsignificance in the primary endpoint. That is spin. This meta-analysis was completed before the Australian D-Health trial found that cancer deaths were 15% higher in the vitamin D arm, a difference that did not reach statistical significance.
The following example is worse: The authors of the VITAL trial, which found that vitamin D supplements had no effect on the primary endpoint of invasive cancer or cardiovascular disease, published a secondary analysis of the trial looking at a different endpoint: A composite incidence of metastatic and fatal invasive total cancer. They reported a 0.4% lower rate for the vitamin D group, a difference that barely made statistical significance at a P value of .04.
But everyone knows the dangers of reanalyzing data with a new endpoint after you have seen the data. What’s more, even if this were a reasonable post hoc analysis, the results are neither clinically meaningful nor statistically robust. Yet the fatally flawed paper has been viewed 60,000 times and picked up by 48 news outlets.
Another way to distract from nonsignificant primary outcomes is to nitpick the trials. The vitamin D dose wasn’t high enough, for instance. This might persuade me if there were one or two vitamin D trials, but there are hundreds of trials and meta-analyses, and their results are consistently null.
Conclusion: No, it is not hopeless
A nihilist would argue that fighting spin is futile. They would say you can’t fight incentives and business models. The incentive structure to publish is strong, and the journals and media know vitamin D studies garner attention – which is their currency.
I am not a nihilist and believe strongly that we must continue to teach critical appraisal and numerical literacy.
In fact, I would speculate that decades of poor critical appraisal by the medical profession have fostered outsized hope and created erroneous norms.
Imagine a counter-factual world in which clinicians have taught society that the human body is unlike an engine that can be repaired by fixing one part (i.e., the vitamin D level), that magic bullets (insulin) are rare, that most treatments fail, or that you can’t rely on association studies to prove efficacy.
In this world, people would be immune from spin and hype.
The norm would be that pills, supplements, and procedures are not what delivers good health. What delivers health is an amalgam of good luck, healthy habits, and lots of time spent outside playing in the sun.
Dr. Mandrola practices cardiac electrophysiology in Louisville, Ky., and is a writer and podcaster for Medscape. He espouses a conservative approach to medical practice. He participates in clinical research and writes often about the state of medical evidence. He has disclosed no relevant financial relationships. A version of this article first appeared on Medscape.com.
The vitamin D story exudes teaching points: It offers a master class in critical appraisal, connecting the concepts of biologic plausibility, flawed surrogate markers, confounded observational studies, and slews of randomized controlled trials (RCTs) showing no benefits on health outcomes.
Yet despite the utter lack of benefit seen in trials, the hype continues. And the pandemic has only enhanced this hype as an onslaught of papers have reported the association of low vitamin D levels and COVID-19 disease.
My questions are simple: Why doesn’t the evidence persuade people? How many nonsignificant trials do we need before researchers stop studying vitamin D, doctors stop (routinely) measuring levels, and patients stop wasting money on the unhelpful supplement? What are the implications for this lack of persuasion?
Before exploring these questions, I want to set out that symptomatic vitamin deficiencies of any sort ought to be corrected.
Biologic plausibility and the pull of observational studies
It has long been known that vitamin D is crucial for bone health and that it can be produced in the skin with sun exposure. In the last decade, however, experts note that nearly every tissue and cell in our body has a vitamin D receptor. It then follows that if this many cells in the body can activate vitamin D, it must be vital for cardiovascular health, immune function, cancer prevention: basically, everything health related.
Oodles of observational studies have found that low serum levels of vitamin D correlate with higher mortality from all causes, cancer, cardiovascular disease, and now even COVID-19. Yet no matter the amount of statistical adjustment in these studies, we cannot know whether these associations are due to true causality.
The major issue is confounding: That is, people with low vitamin D levels have other conditions or diseases that lead to higher rates of ill health. Consider a patient with obesity, arthritis, and cognitive decline; this person is unlikely to do much exercise in the sun and may have low vitamin D levels. The low vitamin D level is simply a marker of overall poor health.
The randomized controlled trials tell a clear story
There are hundreds of vitamin D RCTs. The results simplify into one sentence: Vitamin D supplements do not improve health outcomes.
Here is a short summary of some recent studies.
VITAL, a massive (N > 25,000) RCT with 5 years of follow-up, compared vitamin D supplements to placebo and found no differences in the primary endpoints of cancer or cardiac events. Rates of death from any cause were nearly identical. Crucially, in subgroup analyses, the effects did not vary according to vitamin D levels at baseline.
The D-Health investigators randomly assigned more than 21,000 adults to vitamin D or placebo and after 5.7 years of follow-up reported no differences in the primary endpoint of overall mortality. There also were no differences in cardiovascular disease mortality.
Then you have the Mendelian randomized studies, which some have called nature’s RCT. These studies take advantage of the fact that some people are born with gene variations that predispose to low vitamin D levels. More than 60 Mendelian randomization studies have evaluated the consequences of lifelong genetically lowered vitamin D levels on various outcomes; most of these have found null effects.
Then there are the meta-analyses and systematic reviews. I loved the conclusion of this review of systematic reviews from the BMJ (emphasis mine):
“Despite a few hundred systematic reviews and meta-analyses, highly convincing evidence of a clear role of vitamin D does not exist for any outcome, but associations with a selection of outcomes are probable.”
The failure to persuade
My original plan was to emphasize the power of the RCT. Despite strong associations of low vitamin D levels with poor outcomes, the trials show no benefit to treatment. This strongly suggests (or nearly proves) that low vitamin D levels are akin to premature ventricular complexes after myocardial infarction: a marker for risk but not a target for therapy.
But I now see the more important issue as why scientists, funders, clinicians, and patients are not persuaded by clear evidence. Every day in clinic I see patients on vitamin D supplements; the journals keep publishing vitamin D studies. The proponents of vitamin D remain positive. And lately there is outsized attention and hope that vitamin D will mitigate SARS-CoV2 infection – based only on observational data.
You might argue against this point by saying vitamin D is natural and relatively innocuous, so who cares?
I offer three rebuttals to that point: Opportunity costs, distraction, and the insidious danger of poor critical appraisal skills. If you are burning money on vitamin D research, there is less available to study other important issues. If a patient is distracted by low vitamin D levels, she may pay less attention to her high body mass index or hypertension. And on the matter of critical appraisal, trust in medicine requires clinicians to be competent in critical appraisal. And these days, what could be more important than trust in medical professionals?
One major reason for the failure of persuasion of evidence is spin – or language that distracts from the primary endpoint. Here are two (of many) examples:
A meta-analysis of 50 vitamin D trials set out to study mortality. The authors found no significant difference in that primary endpoint. But the second sentence in their conclusion was that vitamin D supplements reduced the risk for cancer deaths by 15%. That’s a secondary endpoint in a study with nonsignificance in the primary endpoint. That is spin. This meta-analysis was completed before the Australian D-Health trial found that cancer deaths were 15% higher in the vitamin D arm, a difference that did not reach statistical significance.
The following example is worse: The authors of the VITAL trial, which found that vitamin D supplements had no effect on the primary endpoint of invasive cancer or cardiovascular disease, published a secondary analysis of the trial looking at a different endpoint: A composite incidence of metastatic and fatal invasive total cancer. They reported a 0.4% lower rate for the vitamin D group, a difference that barely made statistical significance at a P value of .04.
But everyone knows the dangers of reanalyzing data with a new endpoint after you have seen the data. What’s more, even if this were a reasonable post hoc analysis, the results are neither clinically meaningful nor statistically robust. Yet the fatally flawed paper has been viewed 60,000 times and picked up by 48 news outlets.
Another way to distract from nonsignificant primary outcomes is to nitpick the trials. The vitamin D dose wasn’t high enough, for instance. This might persuade me if there were one or two vitamin D trials, but there are hundreds of trials and meta-analyses, and their results are consistently null.
Conclusion: No, it is not hopeless
A nihilist would argue that fighting spin is futile. They would say you can’t fight incentives and business models. The incentive structure to publish is strong, and the journals and media know vitamin D studies garner attention – which is their currency.
I am not a nihilist and believe strongly that we must continue to teach critical appraisal and numerical literacy.
In fact, I would speculate that decades of poor critical appraisal by the medical profession have fostered outsized hope and created erroneous norms.
Imagine a counter-factual world in which clinicians have taught society that the human body is unlike an engine that can be repaired by fixing one part (i.e., the vitamin D level), that magic bullets (insulin) are rare, that most treatments fail, or that you can’t rely on association studies to prove efficacy.
In this world, people would be immune from spin and hype.
The norm would be that pills, supplements, and procedures are not what delivers good health. What delivers health is an amalgam of good luck, healthy habits, and lots of time spent outside playing in the sun.
Dr. Mandrola practices cardiac electrophysiology in Louisville, Ky., and is a writer and podcaster for Medscape. He espouses a conservative approach to medical practice. He participates in clinical research and writes often about the state of medical evidence. He has disclosed no relevant financial relationships. A version of this article first appeared on Medscape.com.

Tiny hitchhikers like to ride in the trunk
Junk (germs) in the trunk
It’s been a long drive, and you’ve got a long way to go. You pull into a rest stop to use the bathroom and get some food. Quick, which order do you do those things in?
If you’re not a crazy person, you’d use the bathroom and then get your food. Who would bring food into a dirty bathroom? That’s kind of gross. Most people would take care of business, grab food, then get back in the car, eating along the way. Unfortunately, if you’re searching for a sanitary eating environment, your car may not actually be much better than that bathroom, according to new research from Aston University in Birmingham, England.
Let’s start off with the good news. The steering wheels of the five used cars that were swabbed for bacteria were pretty clean. Definitely cleaner than either of the toilet seats analyzed, likely thanks to increased usage of sanitizer, courtesy of the current pandemic. It’s easy to wipe down the steering wheel. Things break down, though, once we look elsewhere. The interiors of the five cars all contained just as much, if not more, bacteria than the toilet seats, with fecal matter commonly appearing on the driver’s seat.
The car interiors were less than sanitary, but they paled in comparison with the real winner here: the trunk. In each of the five cars, bacteria levels there far exceeded those in the toilets, and included everyone’s favorites – Escherichia coli and Staphylococcus aureus.
So, snacking on a bag of chips as you drive along is probably okay, but the food that popped out of its bag and spent the last 5 minutes rolling around the back? Perhaps less okay. You may want to wash it. Or burn it. Or torch the entire car for good measure like we’re about to do. Next time we’ll buy a car without poop in it.
Shut the lid when you flush
Maybe you’ve never thought about this, but it’s actually extremely important to shut the toilet lid when you flush. Just think of all those germs flying around from the force of the flush. Is your toothbrush anywhere near the toilet? Ew. Those pesky little bacteria and viruses are everywhere, and we know we can’t really escape them, but we should really do our best once we’re made aware of where to find them.

It seems like a no-brainer these days since we’ve all been really focused on cleanliness during the pandemic, but according to a poll in the United Kingdom, 55% of the 2,000 participants said they don’t put the lid down while flushing.
The OnePoll survey commissioned by Harpic, a company that makes toilet-cleaning products, also advised that toilet water isn’t even completely clean after flushed several times and can still be contaminated with many germs. Company researchers took specialized pictures of flushing toilets and they looked like tiny little Fourth of July fireworks shows, minus the sparklers. The pictures proved that droplets can go all over the place, including on bathroom users.
“There has never been a more important time to take extra care around our homes, although the risks associated with germ spread in unhygienic bathrooms are high, the solution to keeping them clean is simple,” a Harpic researcher said. Since other studies have shown that coronavirus can be found in feces, it’s become increasingly important to keep ourselves and others safe. Fireworks are pretty, but not when they come out of your toilet.
The latest in MRI fashion
Do you see that photo just below? Looks like something you could buy at the Lego store, right? Well, it’s not. Nor is it the proverbial thinking cap come to life.
(Did someone just say “come to life”? That reminds us of our favorite scene from Frosty the Snowman.)
Anywaaay, about the photo. That funny-looking chapeau is what we in the science business call a metamaterial.
Nope, metamaterials have nothing to do with Facebook parent company Meta. We checked. According to a statement from Boston University, they are engineered structures “created from small unit cells that might be unspectacular alone, but when grouped together in a precise way, get new superpowers not found in nature.”
Superpowers, eh? Who doesn’t want superpowers? Even if they come with a funny hat.
The unit cells, known as resonators, are just plastic tubes wrapped in copper wiring, but when they are grouped in an array and precisely arranged into a helmet, they can channel the magnetic field of the MRI machine during a scan. In theory, that would create “crisper images that can be captured at twice the normal speed,” Xin Zhang, PhD, and her team at BU’s Photonics Center explained in the university statement.
In the future, the metamaterial device could “be used in conjunction with cheaper low-field MRI machines to make the technology more widely available, particularly in the developing world,” they suggested. Or, like so many other superpowers, it could fall into the wrong hands. Like those of Lex Luthor. Or Mark Zuckerberg. Or Frosty the Snowman.
The highway of the mind
How fast can you think on your feet? Well, according to a recently published study, it could be a legitimate measure of intelligence. Here’s the science.

Researchers from the University of Würzburg in Germany and Indiana University have suggested that a person’s intelligence score measures the ability, based on certain neuronal networks and their communication structures, to switch between resting state and different task states.
The investigators set up a study to observe almost 800 people while they completed seven tasks. By monitoring brain activity with functional magnetic resonance imaging, the teams found that subjects who had higher intelligence scores required “less adjustment when switching between different cognitive states,” they said in a separate statement.
It comes down to the network architecture of their brains.
Kirsten Hilger, PhD, head of the German group, described it in terms of highways. The resting state of the brain is normal traffic. It’s always moving. Holiday traffic is the task. The ability to handle the increased flow of commuters is a function of the highway infrastructure. The better the infrastructure, the higher the intelligence.
So the next time you’re stuck in traffic, think how efficient your brain would be with such a task. The quicker, the better.
Junk (germs) in the trunk
It’s been a long drive, and you’ve got a long way to go. You pull into a rest stop to use the bathroom and get some food. Quick, which order do you do those things in?
If you’re not a crazy person, you’d use the bathroom and then get your food. Who would bring food into a dirty bathroom? That’s kind of gross. Most people would take care of business, grab food, then get back in the car, eating along the way. Unfortunately, if you’re searching for a sanitary eating environment, your car may not actually be much better than that bathroom, according to new research from Aston University in Birmingham, England.
Let’s start off with the good news. The steering wheels of the five used cars that were swabbed for bacteria were pretty clean. Definitely cleaner than either of the toilet seats analyzed, likely thanks to increased usage of sanitizer, courtesy of the current pandemic. It’s easy to wipe down the steering wheel. Things break down, though, once we look elsewhere. The interiors of the five cars all contained just as much, if not more, bacteria than the toilet seats, with fecal matter commonly appearing on the driver’s seat.
The car interiors were less than sanitary, but they paled in comparison with the real winner here: the trunk. In each of the five cars, bacteria levels there far exceeded those in the toilets, and included everyone’s favorites – Escherichia coli and Staphylococcus aureus.
So, snacking on a bag of chips as you drive along is probably okay, but the food that popped out of its bag and spent the last 5 minutes rolling around the back? Perhaps less okay. You may want to wash it. Or burn it. Or torch the entire car for good measure like we’re about to do. Next time we’ll buy a car without poop in it.
Shut the lid when you flush
Maybe you’ve never thought about this, but it’s actually extremely important to shut the toilet lid when you flush. Just think of all those germs flying around from the force of the flush. Is your toothbrush anywhere near the toilet? Ew. Those pesky little bacteria and viruses are everywhere, and we know we can’t really escape them, but we should really do our best once we’re made aware of where to find them.
It seems like a no-brainer these days since we’ve all been really focused on cleanliness during the pandemic, but according to a poll in the United Kingdom, 55% of the 2,000 participants said they don’t put the lid down while flushing.
The OnePoll survey commissioned by Harpic, a company that makes toilet-cleaning products, also advised that toilet water isn’t even completely clean after flushed several times and can still be contaminated with many germs. Company researchers took specialized pictures of flushing toilets and they looked like tiny little Fourth of July fireworks shows, minus the sparklers. The pictures proved that droplets can go all over the place, including on bathroom users.
“There has never been a more important time to take extra care around our homes, although the risks associated with germ spread in unhygienic bathrooms are high, the solution to keeping them clean is simple,” a Harpic researcher said. Since other studies have shown that coronavirus can be found in feces, it’s become increasingly important to keep ourselves and others safe. Fireworks are pretty, but not when they come out of your toilet.
The latest in MRI fashion
Do you see that photo just below? Looks like something you could buy at the Lego store, right? Well, it’s not. Nor is it the proverbial thinking cap come to life.
(Did someone just say “come to life”? That reminds us of our favorite scene from Frosty the Snowman.)
Anywaaay, about the photo. That funny-looking chapeau is what we in the science business call a metamaterial.
Nope, metamaterials have nothing to do with Facebook parent company Meta. We checked. According to a statement from Boston University, they are engineered structures “created from small unit cells that might be unspectacular alone, but when grouped together in a precise way, get new superpowers not found in nature.”
Superpowers, eh? Who doesn’t want superpowers? Even if they come with a funny hat.
The unit cells, known as resonators, are just plastic tubes wrapped in copper wiring, but when they are grouped in an array and precisely arranged into a helmet, they can channel the magnetic field of the MRI machine during a scan. In theory, that would create “crisper images that can be captured at twice the normal speed,” Xin Zhang, PhD, and her team at BU’s Photonics Center explained in the university statement.
In the future, the metamaterial device could “be used in conjunction with cheaper low-field MRI machines to make the technology more widely available, particularly in the developing world,” they suggested. Or, like so many other superpowers, it could fall into the wrong hands. Like those of Lex Luthor. Or Mark Zuckerberg. Or Frosty the Snowman.
The highway of the mind
How fast can you think on your feet? Well, according to a recently published study, it could be a legitimate measure of intelligence. Here’s the science.
Researchers from the University of Würzburg in Germany and Indiana University have suggested that a person’s intelligence score measures the ability, based on certain neuronal networks and their communication structures, to switch between resting state and different task states.
The investigators set up a study to observe almost 800 people while they completed seven tasks. By monitoring brain activity with functional magnetic resonance imaging, the teams found that subjects who had higher intelligence scores required “less adjustment when switching between different cognitive states,” they said in a separate statement.
It comes down to the network architecture of their brains.
Kirsten Hilger, PhD, head of the German group, described it in terms of highways. The resting state of the brain is normal traffic. It’s always moving. Holiday traffic is the task. The ability to handle the increased flow of commuters is a function of the highway infrastructure. The better the infrastructure, the higher the intelligence.
So the next time you’re stuck in traffic, think how efficient your brain would be with such a task. The quicker, the better.
Junk (germs) in the trunk
It’s been a long drive, and you’ve got a long way to go. You pull into a rest stop to use the bathroom and get some food. Quick, which order do you do those things in?
If you’re not a crazy person, you’d use the bathroom and then get your food. Who would bring food into a dirty bathroom? That’s kind of gross. Most people would take care of business, grab food, then get back in the car, eating along the way. Unfortunately, if you’re searching for a sanitary eating environment, your car may not actually be much better than that bathroom, according to new research from Aston University in Birmingham, England.
Let’s start off with the good news. The steering wheels of the five used cars that were swabbed for bacteria were pretty clean. Definitely cleaner than either of the toilet seats analyzed, likely thanks to increased usage of sanitizer, courtesy of the current pandemic. It’s easy to wipe down the steering wheel. Things break down, though, once we look elsewhere. The interiors of the five cars all contained just as much, if not more, bacteria than the toilet seats, with fecal matter commonly appearing on the driver’s seat.
The car interiors were less than sanitary, but they paled in comparison with the real winner here: the trunk. In each of the five cars, bacteria levels there far exceeded those in the toilets, and included everyone’s favorites – Escherichia coli and Staphylococcus aureus.
So, snacking on a bag of chips as you drive along is probably okay, but the food that popped out of its bag and spent the last 5 minutes rolling around the back? Perhaps less okay. You may want to wash it. Or burn it. Or torch the entire car for good measure like we’re about to do. Next time we’ll buy a car without poop in it.
Shut the lid when you flush
Maybe you’ve never thought about this, but it’s actually extremely important to shut the toilet lid when you flush. Just think of all those germs flying around from the force of the flush. Is your toothbrush anywhere near the toilet? Ew. Those pesky little bacteria and viruses are everywhere, and we know we can’t really escape them, but we should really do our best once we’re made aware of where to find them.
It seems like a no-brainer these days since we’ve all been really focused on cleanliness during the pandemic, but according to a poll in the United Kingdom, 55% of the 2,000 participants said they don’t put the lid down while flushing.
The OnePoll survey commissioned by Harpic, a company that makes toilet-cleaning products, also advised that toilet water isn’t even completely clean after flushed several times and can still be contaminated with many germs. Company researchers took specialized pictures of flushing toilets and they looked like tiny little Fourth of July fireworks shows, minus the sparklers. The pictures proved that droplets can go all over the place, including on bathroom users.
“There has never been a more important time to take extra care around our homes, although the risks associated with germ spread in unhygienic bathrooms are high, the solution to keeping them clean is simple,” a Harpic researcher said. Since other studies have shown that coronavirus can be found in feces, it’s become increasingly important to keep ourselves and others safe. Fireworks are pretty, but not when they come out of your toilet.
The latest in MRI fashion
Do you see that photo just below? Looks like something you could buy at the Lego store, right? Well, it’s not. Nor is it the proverbial thinking cap come to life.
(Did someone just say “come to life”? That reminds us of our favorite scene from Frosty the Snowman.)
Anywaaay, about the photo. That funny-looking chapeau is what we in the science business call a metamaterial.
Nope, metamaterials have nothing to do with Facebook parent company Meta. We checked. According to a statement from Boston University, they are engineered structures “created from small unit cells that might be unspectacular alone, but when grouped together in a precise way, get new superpowers not found in nature.”
Superpowers, eh? Who doesn’t want superpowers? Even if they come with a funny hat.
The unit cells, known as resonators, are just plastic tubes wrapped in copper wiring, but when they are grouped in an array and precisely arranged into a helmet, they can channel the magnetic field of the MRI machine during a scan. In theory, that would create “crisper images that can be captured at twice the normal speed,” Xin Zhang, PhD, and her team at BU’s Photonics Center explained in the university statement.
In the future, the metamaterial device could “be used in conjunction with cheaper low-field MRI machines to make the technology more widely available, particularly in the developing world,” they suggested. Or, like so many other superpowers, it could fall into the wrong hands. Like those of Lex Luthor. Or Mark Zuckerberg. Or Frosty the Snowman.
The highway of the mind
How fast can you think on your feet? Well, according to a recently published study, it could be a legitimate measure of intelligence. Here’s the science.
Researchers from the University of Würzburg in Germany and Indiana University have suggested that a person’s intelligence score measures the ability, based on certain neuronal networks and their communication structures, to switch between resting state and different task states.
The investigators set up a study to observe almost 800 people while they completed seven tasks. By monitoring brain activity with functional magnetic resonance imaging, the teams found that subjects who had higher intelligence scores required “less adjustment when switching between different cognitive states,” they said in a separate statement.
It comes down to the network architecture of their brains.
Kirsten Hilger, PhD, head of the German group, described it in terms of highways. The resting state of the brain is normal traffic. It’s always moving. Holiday traffic is the task. The ability to handle the increased flow of commuters is a function of the highway infrastructure. The better the infrastructure, the higher the intelligence.
So the next time you’re stuck in traffic, think how efficient your brain would be with such a task. The quicker, the better.
Repeat Laparoscopic Cholecystectomy for Duplicated Gallbladder After 16-Year Interval
Gallbladder duplication is a congenital abnormality of the hepatobiliary system and often is not considered in the evaluation of a patient with right upper quadrant pain. Accuracy of the most commonly used imaging study to assess for biliary disease, abdominal ultrasound, is highly dependent on the skills of the ultrasonographer, and given its relative rarity, this condition is often not considered prior to planned cholecystectomy.1 Small case reviews found that < 50% of gallbladder duplications are diagnosed preoperatively despite use of ultrasound or computed tomography (CT) scan.2-4 Failure to recognize duplicate gallbladder anatomy in symptomatic patients may result in incomplete surgical management, an increase in perioperative complications, and years of morbidity due to unresolved symptoms. Once a patient has had a cholecystectomy, symptoms are presumed to be due to a nonbiliary etiology and an extensive, often repetitive, workup is pursued before “repeat cholecystectomy” is considered.5
Case Presentation
A 63-year-old man was referred to gastroenterology for recurrent episodic right upper quadrant pain. He reported intermittent both right and left upper abdominal pain that was variable in quality. At times it was associated with an empty stomach prior to meals; at other times, onset was 30 to 60 minutes after meals. The patient also reported significant flatulence and bloating and intermittent loose stools. Sixteen years before, he underwent a laparoscopic cholecystectomy. He reported that the pain he experienced before the cholecystectomy never resolved after surgery but occurred less frequently. For the next 16 years, the patient did not seek evaluation of his ongoing but infrequent symptoms until his pain became a daily occurrence. The patient’s surgical history included a remote open vagotomy and antrectomy for peptic ulcer disease, laparoscopic appendectomy, and a laparoscopic cholecystectomy for reported biliary colic.
The gastroenterology evaluation included a colonoscopy and esophagogastroduodenoscopy (EGD); both were benign and without findings specific to identify the etiology for the patient’s pain. The patient was given a course of rifaximin 1200 mg daily for 7 days for possible bacterial overgrowth and placed on a proton pump inhibitor twice daily. Neither of these interventions helped resolve the patient’s symptoms. Further workup was pursued by gastroenterology to include a right upper quadrant ultrasound that showed a structure most consistent with a small gallbladder containing a small polyp vs stone. Magnetic resonance cholangiopancreatography (MRCP) also was performed and showed the presence of a small gallbladder with a small 2-mm filling defect and an otherwise benign biliary tree. MRCP images and EGD documented a Billroth 1 reconstruction at the time of his remote antrectomy and vagotomy (Figure 1).

The patient was referred to general surgery for consideration of a repeat cholecystectomy. He confirmed the history of intermittent upper abdominal pain for the past 16 years, which was similar to the symptoms he had experienced before his original laparoscopic cholecystectomy. On examination, the patient had a body mass index of 38, had a large upper midline incision from his prior antrectomy and vagotomy procedure, and several scars presumed to be port incision scars to the right lateral abdominal wall. Hospital records were obtained from the patient’s prior workup for biliary colic and cholecystectomy 16 years before. The preoperative abdominal ultrasound examination showed a mildly distended gallbladder but was notably described as “quite limited due to patient’s body habitus and liver is not well seen.” No additional imaging was documented in his presurgical evaluation notes and imaging records.
The operative report described a gallbladder that was densely adherent to adjacent fat and omental tissue with significant adhesions secondary to the prior vagotomy and antrectomy procedure. The cystic duct and artery were dissected free at the level of their junction with the gallbladder infundibulum. The cystic artery was divided with a harmonic scalpel. Following this the gallbladder body was dissected free from the liver bed in top-down fashion. A 0 Vicryl Endoloop suture was placed over the gallbladder and secured just past the origin of the cystic duct on the gallbladder infundibulum and the cystic duct divided above this suture. No surgical clips were used, which corresponded with the lack of surgical clips seen in imaging in his recent gastroenterology workup. No documentation of an intraoperative cholangiogram existed or was considered in the operative report.
The pathology report from this first cholecystectomy procedure noted the removed specimen to be an unopened 6-cm gallbladder containing 2 small yellow stones that otherwise were benign. At the time of this patient’s re-presentation to general surgery, there was suspicion that the patient’s prior surgical procedure had not been a cholecystectomy but rather a subtotal cholecystectomy. However, after appropriate workup and review of prior records, the patient had, indeed, previously undergone cholecystectomy and represented a rare case of gallbladder duplication resulting in abdominal pain for 16 years after his index operation.
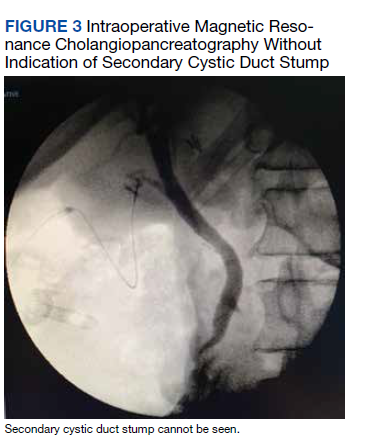
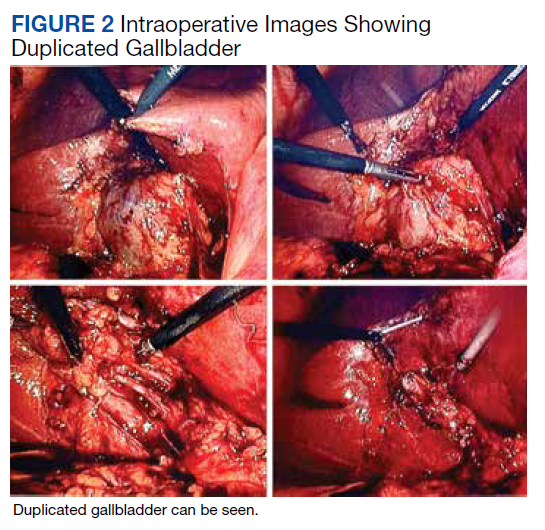
The patient was consented for repeat cholecystectomy and underwent a laparoscopic lysis of adhesions, cholecystectomy, and intraoperative cholangiogram. Significant scarring was found at the liver undersurface that would have been exposed during the original laparoscopic resection of the gallbladder from its liver bed. Deeper to this, a small saccular structure was identified as the duplicate gallbladder (Figure 2). Though the visualized gallbladder was small with a deep intrahepatic lie, the critical view of safety was achieved and was without additional variation. An intraoperative cholangiogram was performed to determine whether residual ductal stumps or other additional evidence of the previously removed gallbladder could be identified. The cholangiogram showed clear visualization of the cystic duct, common bile duct, right and left hepatic ducts, and contrast into the duodenum without abnormal variants. There was no visualized accessory or secondary cystic duct stump seen on the cholangiogram (Figure 3). Pathology of the repeat cholecystectomy specimen confirmed a 3-cm gallbladder with a distinct duct leading out of the gallbladder and the presence of several gallstones. The patient had an uneventful recovery after the repeat laparoscopic cholecystectomy with complete resolution of his upper abdominal pain.
Discussion
The first reported human case of gallbladder duplication was noted in a sacrificial victim of Emperor Augustus in 31 BCE. Sherren reported the first documented case of double accessory gallbladder in a living human in 1911.1,6 Though the exact incidence of gallbladder duplication is not fully known due to primary documentation from case reports, incidence is approximately 1 in 4000 to 5000 people. It was first formally classified by Boyden in 1926.7 Further anatomic classification based on morphology and embryogenesis was delineated by Harlaftis and colleagues in 1977, establishing type 1 and 2 structures of a duplicated gallbladder.8 Type 1 duplicated gallbladder anatomy shares a single cystic duct, whereas in type 2 each gallbladder has its own cystic duct. Later reports and studies identified triple gallbladders as well as trabecular variants with the most common classification used currently being the modified Harlaftis classification.9,10
The case presented here most likely represents either a Y-shaped type 1 primordial gallbladder or a type 2 accessory gallbladder based on historical data and intraoperative cholangiogram findings at the time of repeat cholecystectomy. Gallbladder duplication is clinically indistinguishable from regular gallbladder pathology preoperatively and can only be identified on imaging or intraoperatively.11 Prior case reports and studies have found that it is frequently missed on preoperative abdominal ultrasonography and CT in up to 50% of cases.12-14
The differential diagnosis of gallbladder duplication seen on preoperative imaging includes a gallbladder diverticulum, choledochal cyst, focal adenonomyomatosis, Phrygian cap, or folded gallbladder.1,2 Historically, the most definitive test for gallbladder duplication has been either intraoperative cholangiography, which can also clarify biliary anatomy, or endoscopic retrograde cholangiopancreatography with cholangiography.1,3 The debate over routine use of intraoperative cholangiography has been ongoing for the past several decades.15 Though intraoperative cholangiogram remains one of the most definitive tests for gallbladder duplication, given the overall low incidence of this variant, recommendation for routine intraoperative cholangiography solely to rule out gallbladder duplication cannot be definitively recommended based on our review of the literature. Currently, preoperative MRCP is the study of choice when there is concern from historical facts or from other imaging of gallbladder duplication as it is noninvasive and has a high degree of detail, particularly with 3D reconstructions.14,16 At the time of surgery, the most critical step to avoid inadvertent ductal injury is clear visualization of ductal anatomy and obtaining the critical view of safety.17 Though this will also assist in identifying some cases of gallbladder duplication, given the great variation of duplication, it will not prevent missing some variants. In our case, extensive local scarring from the patient’s prior antrectomy and vagotomy along with lack of the use of intraoperative cholangiography likely contributed to missing his duplication at the time of his index cholecystectomy.
Undiagnosed gallbladder duplication can lead to additional morbidity related to common entities associated with gallbladder pathology, such as biliary colic, cholecystitis, cholangitis, and pancreatitis. Additionally, case reports in the literature have documented more rare associations, such as empyema, carcinoma, cholecystoenteric fistula, and torsion, all associated with a duplicated gallbladder.18-21 Once identified pre- or intraoperatively, it is generally recommended that all gallbladders be removed in symptomatic patients and that intraoperative cholangiography be done to assure complete resection of the duplicated gallbladders and to avoid injury to the biliary trees.22-25
Conclusions
Gallbladder duplication and other congenital biliary anatomic variations should be considered before a biliary operation and included in the differential diagnosis when evaluating patients who have clinical symptoms consistent with biliary pathology. In addition, intraoperative cholangiogram should be performed during cholecystectomy if the inferior liver edge cannot be visualized well, as in the case of this patient where a prior foregut operation resulted in extensive adhesive disease. Intraoperative cholangiogram also should be considered in patients whose preoperative imaging does not visualize the right upper quadrant well due to patient habitus. Doing so may identify gallbladder duplication and allow for complete cholecystectomy as well as proper identification and management of cystic duct variants. Awareness and consideration of duplicated biliary variants can help prevent intraoperative complications related to biliary anomalies and avoid the morbidity related to recurrent biliary disease and the need for repeat operative procedures.
Acknowledgments
We extend our thanks to Veterans Affairs Puget Sound Healthcare System and the Departments of Surgery and Radiology for their support of this case report, and Lorrie Langdale, MD, and Roger Tatum, MD, for their mentorship of this project
1. Vezakis A, Pantiora E, Giannoulopoulos D, et al. A duplicated gallbladder in a patient presenting with acute cholangitis. A case study and a literature review. Ann Hepatol. 2019;18(1):240-245. doi:10.5604/01.3001.0012.7932
2. Barut Í, Tarhan ÖR, Dog^ru U, Bülbül M. Gallbladder duplication: diagnosed and treated by laparoscopy. Eur J Gen Med. 2006;3(3):142-145. doi:10.29333/ejgm/82396 3. Cozacov Y, Subhas G, Jacobs M, Parikh J. Total laparoscopic removal of accessory gallbladder: a case report and review of literature. World J Gastrointest Surg. 2015;7(12):398-402. doi:10.4240/wjgs.v7.i12.398
4. Musleh MG, Burnett H, Rajashanker B, Ammori BJ. Laparoscopic double cholecystectomy for duplicated gallbladder: a case report. Int J Surg Case Rep. 2017;41:502-504. Published 2017 Nov 27. doi:10.1016/j.ijscr.2017.11.046
5. Walbolt TD, Lalezarzadeh F. Laparoscopic management of a duplicated gallbladder: a case study and anatomic history. Surg Laparosc Endosc Percutan Tech. 2011;21(3):e156-e158. doi:10.1097/SLE.0b013e31821d47ce
6. Sherren J. A double gall-bladder removed by operation. Ann Surg. 1911;54(2):204-205. doi:10.1097/00000658-191108000-00009
7. Boyden EA. The accessory gall-bladder—an embryological and comparative study of aberrant biliary vesicles occurring in man and the domestic mammals. Am J Anat. 1926; 38(2):177-231. doi:10.1002/aja.1000380202
8. Harlaftis N, Gray SW, Skandalakis JE. Multiple gallbladders. Surg Gynecol Obstet. 1977;145(6):928-934.
9. Kim RD, Zendejas I, Velopulos C, et al. Duplicate gallbladder arising from the left hepatic duct: report of a case. Surg Today. 2009;39(6):536-539. doi:10.1007/s00595-008-3878-4
10. Causey MW, Miller S, Fernelius CA, Burgess JR, Brown TA, Newton C. Gallbladder duplication: evaluation, treatment, and classification. J Pediatr Surg. 2010;45(2):443-446. doi:10.1016/j.jpedsurg.2009.12.015
11. Apolo Romero EX, Gálvez Salazar PF, Estrada Chandi JA, et al. Gallbladder duplication and cholecystitis. J Surg Case Rep. 2018;2018(7):rjy158. Published 2018 Jul 3. doi:10.1093/jscr/rjy158
12. Gorecki PJ, Andrei VE, Musacchio T, Schein M. Double gallbladder originating from left hepatic duct: a case report and review of literature. JSLS. 1998;2(4):337-339.
13. Cueto García J, Weber A, Serrano Berry F, Tanur Tatz B. Double gallbladder treated successfully by laparoscopy. J Laparoendosc Surg. 1993;3(2):153-155. doi:10.1089/lps.1993.3.153
14. Fazio V, Damiano G, Palumbo VD, et al. An unexpected surprise at the end of a “quiet” cholecystectomy. A case report and review of the literature. Ann Ital Chir. 2012;83(3):265-267.
15. Flum DR, Dellinger EP, Cheadle A, Chan L, Koepsell T. Intraoperative cholangiography and risk of common bile duct injury during cholecystectomy. JAMA. 2003;289(13):1639-1644. doi:10.1001/jama.289.13.1639
16. Botsford A, McKay K, Hartery A, Hapgood C. MRCP imaging of duplicate gallbladder: a case report and review of the literature. Surg Radiol Anat. 2015;37(5):425-429. doi:10.1007/s00276-015-1456-1
17. Strasberg SM, Hertl M, Soper NJ. An analysis of the problem of biliary injury during laparoscopic cholecystectomy. J Am Coll Surg. 1995;180(1):101-125.
18. Raymond SW, Thrift CB. Carcinoma of a duplicated gall bladder. Ill Med J. 1956;110(5):239-240.
19. Cunningham JJ. Empyema of a duplicated gallbladder: echographic findings. J Clin Ultrasound. 1980;8(6):511-512. doi:10.1002/jcu.1870080612
20. Recht W. Torsion of a double gallbladder; a report of a case and a review of the literature. Br J Surg. 1952;39(156):342-344. doi:10.1002/bjs.18003915616
21. Ritchie AW, Crucioli V. Double gallbladder with cholecystocolic fistula: a case report. Br J Surg. 1980;67(2):145-146. doi:10.1002/bjs.1800670226
22. Shapiro T, Rennie W. Duplicate gallbladder cholecystitis after open cholecystectomy. Ann Emerg Med. 1999;33(5):584-587. doi:10.1016/s0196-0644(99)70348-3
23. Hobbs MS, Mai Q, Knuiman MW, Fletcher DR, Ridout SC. Surgeon experience and trends in intraoperative complications in laparoscopic cholecystectomy. Br J Surg. 2006;93(7):844-853. doi:10.1002/bjs.5333
24. Davidoff AM, Pappas TN, Murray EA, et al. Mechanisms of major biliary injury during laparoscopic cholecystectomy. Ann Surg. 1992;215(3):196-202. doi:10.1097/00000658-199203000-00002
25. Flowers JL, Zucker KA, Graham SM, Scovill WA, Imbembo AL, Bailey RW. Laparoscopic cholangiography. Results and indications. Ann Surg. 1992;215(3):209-216. doi:10.1097/00000658-199203000-00004
Gallbladder duplication is a congenital abnormality of the hepatobiliary system and often is not considered in the evaluation of a patient with right upper quadrant pain. Accuracy of the most commonly used imaging study to assess for biliary disease, abdominal ultrasound, is highly dependent on the skills of the ultrasonographer, and given its relative rarity, this condition is often not considered prior to planned cholecystectomy.1 Small case reviews found that < 50% of gallbladder duplications are diagnosed preoperatively despite use of ultrasound or computed tomography (CT) scan.2-4 Failure to recognize duplicate gallbladder anatomy in symptomatic patients may result in incomplete surgical management, an increase in perioperative complications, and years of morbidity due to unresolved symptoms. Once a patient has had a cholecystectomy, symptoms are presumed to be due to a nonbiliary etiology and an extensive, often repetitive, workup is pursued before “repeat cholecystectomy” is considered.5
Case Presentation
A 63-year-old man was referred to gastroenterology for recurrent episodic right upper quadrant pain. He reported intermittent both right and left upper abdominal pain that was variable in quality. At times it was associated with an empty stomach prior to meals; at other times, onset was 30 to 60 minutes after meals. The patient also reported significant flatulence and bloating and intermittent loose stools. Sixteen years before, he underwent a laparoscopic cholecystectomy. He reported that the pain he experienced before the cholecystectomy never resolved after surgery but occurred less frequently. For the next 16 years, the patient did not seek evaluation of his ongoing but infrequent symptoms until his pain became a daily occurrence. The patient’s surgical history included a remote open vagotomy and antrectomy for peptic ulcer disease, laparoscopic appendectomy, and a laparoscopic cholecystectomy for reported biliary colic.
The gastroenterology evaluation included a colonoscopy and esophagogastroduodenoscopy (EGD); both were benign and without findings specific to identify the etiology for the patient’s pain. The patient was given a course of rifaximin 1200 mg daily for 7 days for possible bacterial overgrowth and placed on a proton pump inhibitor twice daily. Neither of these interventions helped resolve the patient’s symptoms. Further workup was pursued by gastroenterology to include a right upper quadrant ultrasound that showed a structure most consistent with a small gallbladder containing a small polyp vs stone. Magnetic resonance cholangiopancreatography (MRCP) also was performed and showed the presence of a small gallbladder with a small 2-mm filling defect and an otherwise benign biliary tree. MRCP images and EGD documented a Billroth 1 reconstruction at the time of his remote antrectomy and vagotomy (Figure 1).
The patient was referred to general surgery for consideration of a repeat cholecystectomy. He confirmed the history of intermittent upper abdominal pain for the past 16 years, which was similar to the symptoms he had experienced before his original laparoscopic cholecystectomy. On examination, the patient had a body mass index of 38, had a large upper midline incision from his prior antrectomy and vagotomy procedure, and several scars presumed to be port incision scars to the right lateral abdominal wall. Hospital records were obtained from the patient’s prior workup for biliary colic and cholecystectomy 16 years before. The preoperative abdominal ultrasound examination showed a mildly distended gallbladder but was notably described as “quite limited due to patient’s body habitus and liver is not well seen.” No additional imaging was documented in his presurgical evaluation notes and imaging records.
The operative report described a gallbladder that was densely adherent to adjacent fat and omental tissue with significant adhesions secondary to the prior vagotomy and antrectomy procedure. The cystic duct and artery were dissected free at the level of their junction with the gallbladder infundibulum. The cystic artery was divided with a harmonic scalpel. Following this the gallbladder body was dissected free from the liver bed in top-down fashion. A 0 Vicryl Endoloop suture was placed over the gallbladder and secured just past the origin of the cystic duct on the gallbladder infundibulum and the cystic duct divided above this suture. No surgical clips were used, which corresponded with the lack of surgical clips seen in imaging in his recent gastroenterology workup. No documentation of an intraoperative cholangiogram existed or was considered in the operative report.
The pathology report from this first cholecystectomy procedure noted the removed specimen to be an unopened 6-cm gallbladder containing 2 small yellow stones that otherwise were benign. At the time of this patient’s re-presentation to general surgery, there was suspicion that the patient’s prior surgical procedure had not been a cholecystectomy but rather a subtotal cholecystectomy. However, after appropriate workup and review of prior records, the patient had, indeed, previously undergone cholecystectomy and represented a rare case of gallbladder duplication resulting in abdominal pain for 16 years after his index operation.
The patient was consented for repeat cholecystectomy and underwent a laparoscopic lysis of adhesions, cholecystectomy, and intraoperative cholangiogram. Significant scarring was found at the liver undersurface that would have been exposed during the original laparoscopic resection of the gallbladder from its liver bed. Deeper to this, a small saccular structure was identified as the duplicate gallbladder (Figure 2). Though the visualized gallbladder was small with a deep intrahepatic lie, the critical view of safety was achieved and was without additional variation. An intraoperative cholangiogram was performed to determine whether residual ductal stumps or other additional evidence of the previously removed gallbladder could be identified. The cholangiogram showed clear visualization of the cystic duct, common bile duct, right and left hepatic ducts, and contrast into the duodenum without abnormal variants. There was no visualized accessory or secondary cystic duct stump seen on the cholangiogram (Figure 3). Pathology of the repeat cholecystectomy specimen confirmed a 3-cm gallbladder with a distinct duct leading out of the gallbladder and the presence of several gallstones. The patient had an uneventful recovery after the repeat laparoscopic cholecystectomy with complete resolution of his upper abdominal pain.
Discussion
The first reported human case of gallbladder duplication was noted in a sacrificial victim of Emperor Augustus in 31 BCE. Sherren reported the first documented case of double accessory gallbladder in a living human in 1911.1,6 Though the exact incidence of gallbladder duplication is not fully known due to primary documentation from case reports, incidence is approximately 1 in 4000 to 5000 people. It was first formally classified by Boyden in 1926.7 Further anatomic classification based on morphology and embryogenesis was delineated by Harlaftis and colleagues in 1977, establishing type 1 and 2 structures of a duplicated gallbladder.8 Type 1 duplicated gallbladder anatomy shares a single cystic duct, whereas in type 2 each gallbladder has its own cystic duct. Later reports and studies identified triple gallbladders as well as trabecular variants with the most common classification used currently being the modified Harlaftis classification.9,10
The case presented here most likely represents either a Y-shaped type 1 primordial gallbladder or a type 2 accessory gallbladder based on historical data and intraoperative cholangiogram findings at the time of repeat cholecystectomy. Gallbladder duplication is clinically indistinguishable from regular gallbladder pathology preoperatively and can only be identified on imaging or intraoperatively.11 Prior case reports and studies have found that it is frequently missed on preoperative abdominal ultrasonography and CT in up to 50% of cases.12-14
The differential diagnosis of gallbladder duplication seen on preoperative imaging includes a gallbladder diverticulum, choledochal cyst, focal adenonomyomatosis, Phrygian cap, or folded gallbladder.1,2 Historically, the most definitive test for gallbladder duplication has been either intraoperative cholangiography, which can also clarify biliary anatomy, or endoscopic retrograde cholangiopancreatography with cholangiography.1,3 The debate over routine use of intraoperative cholangiography has been ongoing for the past several decades.15 Though intraoperative cholangiogram remains one of the most definitive tests for gallbladder duplication, given the overall low incidence of this variant, recommendation for routine intraoperative cholangiography solely to rule out gallbladder duplication cannot be definitively recommended based on our review of the literature. Currently, preoperative MRCP is the study of choice when there is concern from historical facts or from other imaging of gallbladder duplication as it is noninvasive and has a high degree of detail, particularly with 3D reconstructions.14,16 At the time of surgery, the most critical step to avoid inadvertent ductal injury is clear visualization of ductal anatomy and obtaining the critical view of safety.17 Though this will also assist in identifying some cases of gallbladder duplication, given the great variation of duplication, it will not prevent missing some variants. In our case, extensive local scarring from the patient’s prior antrectomy and vagotomy along with lack of the use of intraoperative cholangiography likely contributed to missing his duplication at the time of his index cholecystectomy.
Undiagnosed gallbladder duplication can lead to additional morbidity related to common entities associated with gallbladder pathology, such as biliary colic, cholecystitis, cholangitis, and pancreatitis. Additionally, case reports in the literature have documented more rare associations, such as empyema, carcinoma, cholecystoenteric fistula, and torsion, all associated with a duplicated gallbladder.18-21 Once identified pre- or intraoperatively, it is generally recommended that all gallbladders be removed in symptomatic patients and that intraoperative cholangiography be done to assure complete resection of the duplicated gallbladders and to avoid injury to the biliary trees.22-25
Conclusions
Gallbladder duplication and other congenital biliary anatomic variations should be considered before a biliary operation and included in the differential diagnosis when evaluating patients who have clinical symptoms consistent with biliary pathology. In addition, intraoperative cholangiogram should be performed during cholecystectomy if the inferior liver edge cannot be visualized well, as in the case of this patient where a prior foregut operation resulted in extensive adhesive disease. Intraoperative cholangiogram also should be considered in patients whose preoperative imaging does not visualize the right upper quadrant well due to patient habitus. Doing so may identify gallbladder duplication and allow for complete cholecystectomy as well as proper identification and management of cystic duct variants. Awareness and consideration of duplicated biliary variants can help prevent intraoperative complications related to biliary anomalies and avoid the morbidity related to recurrent biliary disease and the need for repeat operative procedures.
Acknowledgments
We extend our thanks to Veterans Affairs Puget Sound Healthcare System and the Departments of Surgery and Radiology for their support of this case report, and Lorrie Langdale, MD, and Roger Tatum, MD, for their mentorship of this project
Gallbladder duplication is a congenital abnormality of the hepatobiliary system and often is not considered in the evaluation of a patient with right upper quadrant pain. Accuracy of the most commonly used imaging study to assess for biliary disease, abdominal ultrasound, is highly dependent on the skills of the ultrasonographer, and given its relative rarity, this condition is often not considered prior to planned cholecystectomy.1 Small case reviews found that < 50% of gallbladder duplications are diagnosed preoperatively despite use of ultrasound or computed tomography (CT) scan.2-4 Failure to recognize duplicate gallbladder anatomy in symptomatic patients may result in incomplete surgical management, an increase in perioperative complications, and years of morbidity due to unresolved symptoms. Once a patient has had a cholecystectomy, symptoms are presumed to be due to a nonbiliary etiology and an extensive, often repetitive, workup is pursued before “repeat cholecystectomy” is considered.5
Case Presentation
A 63-year-old man was referred to gastroenterology for recurrent episodic right upper quadrant pain. He reported intermittent both right and left upper abdominal pain that was variable in quality. At times it was associated with an empty stomach prior to meals; at other times, onset was 30 to 60 minutes after meals. The patient also reported significant flatulence and bloating and intermittent loose stools. Sixteen years before, he underwent a laparoscopic cholecystectomy. He reported that the pain he experienced before the cholecystectomy never resolved after surgery but occurred less frequently. For the next 16 years, the patient did not seek evaluation of his ongoing but infrequent symptoms until his pain became a daily occurrence. The patient’s surgical history included a remote open vagotomy and antrectomy for peptic ulcer disease, laparoscopic appendectomy, and a laparoscopic cholecystectomy for reported biliary colic.
The gastroenterology evaluation included a colonoscopy and esophagogastroduodenoscopy (EGD); both were benign and without findings specific to identify the etiology for the patient’s pain. The patient was given a course of rifaximin 1200 mg daily for 7 days for possible bacterial overgrowth and placed on a proton pump inhibitor twice daily. Neither of these interventions helped resolve the patient’s symptoms. Further workup was pursued by gastroenterology to include a right upper quadrant ultrasound that showed a structure most consistent with a small gallbladder containing a small polyp vs stone. Magnetic resonance cholangiopancreatography (MRCP) also was performed and showed the presence of a small gallbladder with a small 2-mm filling defect and an otherwise benign biliary tree. MRCP images and EGD documented a Billroth 1 reconstruction at the time of his remote antrectomy and vagotomy (Figure 1).
The patient was referred to general surgery for consideration of a repeat cholecystectomy. He confirmed the history of intermittent upper abdominal pain for the past 16 years, which was similar to the symptoms he had experienced before his original laparoscopic cholecystectomy. On examination, the patient had a body mass index of 38, had a large upper midline incision from his prior antrectomy and vagotomy procedure, and several scars presumed to be port incision scars to the right lateral abdominal wall. Hospital records were obtained from the patient’s prior workup for biliary colic and cholecystectomy 16 years before. The preoperative abdominal ultrasound examination showed a mildly distended gallbladder but was notably described as “quite limited due to patient’s body habitus and liver is not well seen.” No additional imaging was documented in his presurgical evaluation notes and imaging records.
The operative report described a gallbladder that was densely adherent to adjacent fat and omental tissue with significant adhesions secondary to the prior vagotomy and antrectomy procedure. The cystic duct and artery were dissected free at the level of their junction with the gallbladder infundibulum. The cystic artery was divided with a harmonic scalpel. Following this the gallbladder body was dissected free from the liver bed in top-down fashion. A 0 Vicryl Endoloop suture was placed over the gallbladder and secured just past the origin of the cystic duct on the gallbladder infundibulum and the cystic duct divided above this suture. No surgical clips were used, which corresponded with the lack of surgical clips seen in imaging in his recent gastroenterology workup. No documentation of an intraoperative cholangiogram existed or was considered in the operative report.
The pathology report from this first cholecystectomy procedure noted the removed specimen to be an unopened 6-cm gallbladder containing 2 small yellow stones that otherwise were benign. At the time of this patient’s re-presentation to general surgery, there was suspicion that the patient’s prior surgical procedure had not been a cholecystectomy but rather a subtotal cholecystectomy. However, after appropriate workup and review of prior records, the patient had, indeed, previously undergone cholecystectomy and represented a rare case of gallbladder duplication resulting in abdominal pain for 16 years after his index operation.
The patient was consented for repeat cholecystectomy and underwent a laparoscopic lysis of adhesions, cholecystectomy, and intraoperative cholangiogram. Significant scarring was found at the liver undersurface that would have been exposed during the original laparoscopic resection of the gallbladder from its liver bed. Deeper to this, a small saccular structure was identified as the duplicate gallbladder (Figure 2). Though the visualized gallbladder was small with a deep intrahepatic lie, the critical view of safety was achieved and was without additional variation. An intraoperative cholangiogram was performed to determine whether residual ductal stumps or other additional evidence of the previously removed gallbladder could be identified. The cholangiogram showed clear visualization of the cystic duct, common bile duct, right and left hepatic ducts, and contrast into the duodenum without abnormal variants. There was no visualized accessory or secondary cystic duct stump seen on the cholangiogram (Figure 3). Pathology of the repeat cholecystectomy specimen confirmed a 3-cm gallbladder with a distinct duct leading out of the gallbladder and the presence of several gallstones. The patient had an uneventful recovery after the repeat laparoscopic cholecystectomy with complete resolution of his upper abdominal pain.
Discussion
The first reported human case of gallbladder duplication was noted in a sacrificial victim of Emperor Augustus in 31 BCE. Sherren reported the first documented case of double accessory gallbladder in a living human in 1911.1,6 Though the exact incidence of gallbladder duplication is not fully known due to primary documentation from case reports, incidence is approximately 1 in 4000 to 5000 people. It was first formally classified by Boyden in 1926.7 Further anatomic classification based on morphology and embryogenesis was delineated by Harlaftis and colleagues in 1977, establishing type 1 and 2 structures of a duplicated gallbladder.8 Type 1 duplicated gallbladder anatomy shares a single cystic duct, whereas in type 2 each gallbladder has its own cystic duct. Later reports and studies identified triple gallbladders as well as trabecular variants with the most common classification used currently being the modified Harlaftis classification.9,10
The case presented here most likely represents either a Y-shaped type 1 primordial gallbladder or a type 2 accessory gallbladder based on historical data and intraoperative cholangiogram findings at the time of repeat cholecystectomy. Gallbladder duplication is clinically indistinguishable from regular gallbladder pathology preoperatively and can only be identified on imaging or intraoperatively.11 Prior case reports and studies have found that it is frequently missed on preoperative abdominal ultrasonography and CT in up to 50% of cases.12-14
The differential diagnosis of gallbladder duplication seen on preoperative imaging includes a gallbladder diverticulum, choledochal cyst, focal adenonomyomatosis, Phrygian cap, or folded gallbladder.1,2 Historically, the most definitive test for gallbladder duplication has been either intraoperative cholangiography, which can also clarify biliary anatomy, or endoscopic retrograde cholangiopancreatography with cholangiography.1,3 The debate over routine use of intraoperative cholangiography has been ongoing for the past several decades.15 Though intraoperative cholangiogram remains one of the most definitive tests for gallbladder duplication, given the overall low incidence of this variant, recommendation for routine intraoperative cholangiography solely to rule out gallbladder duplication cannot be definitively recommended based on our review of the literature. Currently, preoperative MRCP is the study of choice when there is concern from historical facts or from other imaging of gallbladder duplication as it is noninvasive and has a high degree of detail, particularly with 3D reconstructions.14,16 At the time of surgery, the most critical step to avoid inadvertent ductal injury is clear visualization of ductal anatomy and obtaining the critical view of safety.17 Though this will also assist in identifying some cases of gallbladder duplication, given the great variation of duplication, it will not prevent missing some variants. In our case, extensive local scarring from the patient’s prior antrectomy and vagotomy along with lack of the use of intraoperative cholangiography likely contributed to missing his duplication at the time of his index cholecystectomy.
Undiagnosed gallbladder duplication can lead to additional morbidity related to common entities associated with gallbladder pathology, such as biliary colic, cholecystitis, cholangitis, and pancreatitis. Additionally, case reports in the literature have documented more rare associations, such as empyema, carcinoma, cholecystoenteric fistula, and torsion, all associated with a duplicated gallbladder.18-21 Once identified pre- or intraoperatively, it is generally recommended that all gallbladders be removed in symptomatic patients and that intraoperative cholangiography be done to assure complete resection of the duplicated gallbladders and to avoid injury to the biliary trees.22-25
Conclusions
Gallbladder duplication and other congenital biliary anatomic variations should be considered before a biliary operation and included in the differential diagnosis when evaluating patients who have clinical symptoms consistent with biliary pathology. In addition, intraoperative cholangiogram should be performed during cholecystectomy if the inferior liver edge cannot be visualized well, as in the case of this patient where a prior foregut operation resulted in extensive adhesive disease. Intraoperative cholangiogram also should be considered in patients whose preoperative imaging does not visualize the right upper quadrant well due to patient habitus. Doing so may identify gallbladder duplication and allow for complete cholecystectomy as well as proper identification and management of cystic duct variants. Awareness and consideration of duplicated biliary variants can help prevent intraoperative complications related to biliary anomalies and avoid the morbidity related to recurrent biliary disease and the need for repeat operative procedures.
Acknowledgments
We extend our thanks to Veterans Affairs Puget Sound Healthcare System and the Departments of Surgery and Radiology for their support of this case report, and Lorrie Langdale, MD, and Roger Tatum, MD, for their mentorship of this project
1. Vezakis A, Pantiora E, Giannoulopoulos D, et al. A duplicated gallbladder in a patient presenting with acute cholangitis. A case study and a literature review. Ann Hepatol. 2019;18(1):240-245. doi:10.5604/01.3001.0012.7932
2. Barut Í, Tarhan ÖR, Dog^ru U, Bülbül M. Gallbladder duplication: diagnosed and treated by laparoscopy. Eur J Gen Med. 2006;3(3):142-145. doi:10.29333/ejgm/82396 3. Cozacov Y, Subhas G, Jacobs M, Parikh J. Total laparoscopic removal of accessory gallbladder: a case report and review of literature. World J Gastrointest Surg. 2015;7(12):398-402. doi:10.4240/wjgs.v7.i12.398
4. Musleh MG, Burnett H, Rajashanker B, Ammori BJ. Laparoscopic double cholecystectomy for duplicated gallbladder: a case report. Int J Surg Case Rep. 2017;41:502-504. Published 2017 Nov 27. doi:10.1016/j.ijscr.2017.11.046
5. Walbolt TD, Lalezarzadeh F. Laparoscopic management of a duplicated gallbladder: a case study and anatomic history. Surg Laparosc Endosc Percutan Tech. 2011;21(3):e156-e158. doi:10.1097/SLE.0b013e31821d47ce
6. Sherren J. A double gall-bladder removed by operation. Ann Surg. 1911;54(2):204-205. doi:10.1097/00000658-191108000-00009
7. Boyden EA. The accessory gall-bladder—an embryological and comparative study of aberrant biliary vesicles occurring in man and the domestic mammals. Am J Anat. 1926; 38(2):177-231. doi:10.1002/aja.1000380202
8. Harlaftis N, Gray SW, Skandalakis JE. Multiple gallbladders. Surg Gynecol Obstet. 1977;145(6):928-934.
9. Kim RD, Zendejas I, Velopulos C, et al. Duplicate gallbladder arising from the left hepatic duct: report of a case. Surg Today. 2009;39(6):536-539. doi:10.1007/s00595-008-3878-4
10. Causey MW, Miller S, Fernelius CA, Burgess JR, Brown TA, Newton C. Gallbladder duplication: evaluation, treatment, and classification. J Pediatr Surg. 2010;45(2):443-446. doi:10.1016/j.jpedsurg.2009.12.015
11. Apolo Romero EX, Gálvez Salazar PF, Estrada Chandi JA, et al. Gallbladder duplication and cholecystitis. J Surg Case Rep. 2018;2018(7):rjy158. Published 2018 Jul 3. doi:10.1093/jscr/rjy158
12. Gorecki PJ, Andrei VE, Musacchio T, Schein M. Double gallbladder originating from left hepatic duct: a case report and review of literature. JSLS. 1998;2(4):337-339.
13. Cueto García J, Weber A, Serrano Berry F, Tanur Tatz B. Double gallbladder treated successfully by laparoscopy. J Laparoendosc Surg. 1993;3(2):153-155. doi:10.1089/lps.1993.3.153
14. Fazio V, Damiano G, Palumbo VD, et al. An unexpected surprise at the end of a “quiet” cholecystectomy. A case report and review of the literature. Ann Ital Chir. 2012;83(3):265-267.
15. Flum DR, Dellinger EP, Cheadle A, Chan L, Koepsell T. Intraoperative cholangiography and risk of common bile duct injury during cholecystectomy. JAMA. 2003;289(13):1639-1644. doi:10.1001/jama.289.13.1639
16. Botsford A, McKay K, Hartery A, Hapgood C. MRCP imaging of duplicate gallbladder: a case report and review of the literature. Surg Radiol Anat. 2015;37(5):425-429. doi:10.1007/s00276-015-1456-1
17. Strasberg SM, Hertl M, Soper NJ. An analysis of the problem of biliary injury during laparoscopic cholecystectomy. J Am Coll Surg. 1995;180(1):101-125.
18. Raymond SW, Thrift CB. Carcinoma of a duplicated gall bladder. Ill Med J. 1956;110(5):239-240.
19. Cunningham JJ. Empyema of a duplicated gallbladder: echographic findings. J Clin Ultrasound. 1980;8(6):511-512. doi:10.1002/jcu.1870080612
20. Recht W. Torsion of a double gallbladder; a report of a case and a review of the literature. Br J Surg. 1952;39(156):342-344. doi:10.1002/bjs.18003915616
21. Ritchie AW, Crucioli V. Double gallbladder with cholecystocolic fistula: a case report. Br J Surg. 1980;67(2):145-146. doi:10.1002/bjs.1800670226
22. Shapiro T, Rennie W. Duplicate gallbladder cholecystitis after open cholecystectomy. Ann Emerg Med. 1999;33(5):584-587. doi:10.1016/s0196-0644(99)70348-3
23. Hobbs MS, Mai Q, Knuiman MW, Fletcher DR, Ridout SC. Surgeon experience and trends in intraoperative complications in laparoscopic cholecystectomy. Br J Surg. 2006;93(7):844-853. doi:10.1002/bjs.5333
24. Davidoff AM, Pappas TN, Murray EA, et al. Mechanisms of major biliary injury during laparoscopic cholecystectomy. Ann Surg. 1992;215(3):196-202. doi:10.1097/00000658-199203000-00002
25. Flowers JL, Zucker KA, Graham SM, Scovill WA, Imbembo AL, Bailey RW. Laparoscopic cholangiography. Results and indications. Ann Surg. 1992;215(3):209-216. doi:10.1097/00000658-199203000-00004
1. Vezakis A, Pantiora E, Giannoulopoulos D, et al. A duplicated gallbladder in a patient presenting with acute cholangitis. A case study and a literature review. Ann Hepatol. 2019;18(1):240-245. doi:10.5604/01.3001.0012.7932
2. Barut Í, Tarhan ÖR, Dog^ru U, Bülbül M. Gallbladder duplication: diagnosed and treated by laparoscopy. Eur J Gen Med. 2006;3(3):142-145. doi:10.29333/ejgm/82396 3. Cozacov Y, Subhas G, Jacobs M, Parikh J. Total laparoscopic removal of accessory gallbladder: a case report and review of literature. World J Gastrointest Surg. 2015;7(12):398-402. doi:10.4240/wjgs.v7.i12.398
4. Musleh MG, Burnett H, Rajashanker B, Ammori BJ. Laparoscopic double cholecystectomy for duplicated gallbladder: a case report. Int J Surg Case Rep. 2017;41:502-504. Published 2017 Nov 27. doi:10.1016/j.ijscr.2017.11.046
5. Walbolt TD, Lalezarzadeh F. Laparoscopic management of a duplicated gallbladder: a case study and anatomic history. Surg Laparosc Endosc Percutan Tech. 2011;21(3):e156-e158. doi:10.1097/SLE.0b013e31821d47ce
6. Sherren J. A double gall-bladder removed by operation. Ann Surg. 1911;54(2):204-205. doi:10.1097/00000658-191108000-00009
7. Boyden EA. The accessory gall-bladder—an embryological and comparative study of aberrant biliary vesicles occurring in man and the domestic mammals. Am J Anat. 1926; 38(2):177-231. doi:10.1002/aja.1000380202
8. Harlaftis N, Gray SW, Skandalakis JE. Multiple gallbladders. Surg Gynecol Obstet. 1977;145(6):928-934.
9. Kim RD, Zendejas I, Velopulos C, et al. Duplicate gallbladder arising from the left hepatic duct: report of a case. Surg Today. 2009;39(6):536-539. doi:10.1007/s00595-008-3878-4
10. Causey MW, Miller S, Fernelius CA, Burgess JR, Brown TA, Newton C. Gallbladder duplication: evaluation, treatment, and classification. J Pediatr Surg. 2010;45(2):443-446. doi:10.1016/j.jpedsurg.2009.12.015
11. Apolo Romero EX, Gálvez Salazar PF, Estrada Chandi JA, et al. Gallbladder duplication and cholecystitis. J Surg Case Rep. 2018;2018(7):rjy158. Published 2018 Jul 3. doi:10.1093/jscr/rjy158
12. Gorecki PJ, Andrei VE, Musacchio T, Schein M. Double gallbladder originating from left hepatic duct: a case report and review of literature. JSLS. 1998;2(4):337-339.
13. Cueto García J, Weber A, Serrano Berry F, Tanur Tatz B. Double gallbladder treated successfully by laparoscopy. J Laparoendosc Surg. 1993;3(2):153-155. doi:10.1089/lps.1993.3.153
14. Fazio V, Damiano G, Palumbo VD, et al. An unexpected surprise at the end of a “quiet” cholecystectomy. A case report and review of the literature. Ann Ital Chir. 2012;83(3):265-267.
15. Flum DR, Dellinger EP, Cheadle A, Chan L, Koepsell T. Intraoperative cholangiography and risk of common bile duct injury during cholecystectomy. JAMA. 2003;289(13):1639-1644. doi:10.1001/jama.289.13.1639
16. Botsford A, McKay K, Hartery A, Hapgood C. MRCP imaging of duplicate gallbladder: a case report and review of the literature. Surg Radiol Anat. 2015;37(5):425-429. doi:10.1007/s00276-015-1456-1
17. Strasberg SM, Hertl M, Soper NJ. An analysis of the problem of biliary injury during laparoscopic cholecystectomy. J Am Coll Surg. 1995;180(1):101-125.
18. Raymond SW, Thrift CB. Carcinoma of a duplicated gall bladder. Ill Med J. 1956;110(5):239-240.
19. Cunningham JJ. Empyema of a duplicated gallbladder: echographic findings. J Clin Ultrasound. 1980;8(6):511-512. doi:10.1002/jcu.1870080612
20. Recht W. Torsion of a double gallbladder; a report of a case and a review of the literature. Br J Surg. 1952;39(156):342-344. doi:10.1002/bjs.18003915616
21. Ritchie AW, Crucioli V. Double gallbladder with cholecystocolic fistula: a case report. Br J Surg. 1980;67(2):145-146. doi:10.1002/bjs.1800670226
22. Shapiro T, Rennie W. Duplicate gallbladder cholecystitis after open cholecystectomy. Ann Emerg Med. 1999;33(5):584-587. doi:10.1016/s0196-0644(99)70348-3
23. Hobbs MS, Mai Q, Knuiman MW, Fletcher DR, Ridout SC. Surgeon experience and trends in intraoperative complications in laparoscopic cholecystectomy. Br J Surg. 2006;93(7):844-853. doi:10.1002/bjs.5333
24. Davidoff AM, Pappas TN, Murray EA, et al. Mechanisms of major biliary injury during laparoscopic cholecystectomy. Ann Surg. 1992;215(3):196-202. doi:10.1097/00000658-199203000-00002
25. Flowers JL, Zucker KA, Graham SM, Scovill WA, Imbembo AL, Bailey RW. Laparoscopic cholangiography. Results and indications. Ann Surg. 1992;215(3):209-216. doi:10.1097/00000658-199203000-00004
FDA hints at deadlines to meet accelerated approval requirements
The FDA launched its accelerated approval program in 1992 in response to the AIDS crisis, but the bulk of approvals since then have been for cancer drugs, wrote the authors who included Gautam U. Mehta, MD, a clinical reviewer with the FDA’s Center for Drug Evaluation and Research; R. Angelo de Claro, MD, associate director of the FDA’s Global Clinical Sciences division within the Oncology Center of Excellence; and Richard Pazdur, MD, director of the FDA’s Oncology Center of Excellence.
Accelerated approvals are typically granted in oncology based on overall response rate with a requirement that companies confirm that there’s actually a clinical benefit in postmarketing studies.
The system has inspired European nations and Australia to launch their own programs, but with a key difference: Conditional approvals expire within 1 year or 2.
To be reinstated and remain on the market, companies have to submit a timeline for when they’ll meet their outstanding obligations and demonstrate that the benefit of leaving their product on the market outweighs the risk.
The approach puts “the onus of timely completion of confirmatory trials and verification of benefit” on the drug maker. In the meantime, the system limits “public exposure to stale claims of effectiveness that cannot be expeditiously substantiated,” Dr. Mehta and colleagues wrote.
There aren’t any deadlines in the United States, however, so the FDA has “to initiate a resource-intensive withdrawal process” when proof of clinical benefit is not forthcoming, they said.
In the United States, only 14 of 167 oncology indications granted accelerated approval since 1992 were withdrawn voluntarily and one was withdrawn by FDA request, and one was forced by the agency. The median time from accelerated approval to withdrawal was 8.8 years.
The actual withdrawal process itself took 11 months when bevacizumab’s breast cancer indication was canceled in 2011.
The authors didn’t call for change outright, but they did say that “future discussions of the accelerated approval program in the U.S.” will seek “to coordinate regulatory processes” with other countries, with an eye towards building “harmony between” agencies.
Among other targets for possible harmonization, they noted that only new molecular entities are eligible for accelerated approval in Europe, whereas supplemental indications are also eligible in the United States
Europe also requires a risk-benefit assessment for conditional approvals, which “has led to relatively few approvals based on single-arm clinical trial data,” the authors said.
Dr. Mehta, Dr. de Claro, and Dr. Pazdur had no conflicts of interest.
The FDA launched its accelerated approval program in 1992 in response to the AIDS crisis, but the bulk of approvals since then have been for cancer drugs, wrote the authors who included Gautam U. Mehta, MD, a clinical reviewer with the FDA’s Center for Drug Evaluation and Research; R. Angelo de Claro, MD, associate director of the FDA’s Global Clinical Sciences division within the Oncology Center of Excellence; and Richard Pazdur, MD, director of the FDA’s Oncology Center of Excellence.
Accelerated approvals are typically granted in oncology based on overall response rate with a requirement that companies confirm that there’s actually a clinical benefit in postmarketing studies.
The system has inspired European nations and Australia to launch their own programs, but with a key difference: Conditional approvals expire within 1 year or 2.
To be reinstated and remain on the market, companies have to submit a timeline for when they’ll meet their outstanding obligations and demonstrate that the benefit of leaving their product on the market outweighs the risk.
The approach puts “the onus of timely completion of confirmatory trials and verification of benefit” on the drug maker. In the meantime, the system limits “public exposure to stale claims of effectiveness that cannot be expeditiously substantiated,” Dr. Mehta and colleagues wrote.
There aren’t any deadlines in the United States, however, so the FDA has “to initiate a resource-intensive withdrawal process” when proof of clinical benefit is not forthcoming, they said.
In the United States, only 14 of 167 oncology indications granted accelerated approval since 1992 were withdrawn voluntarily and one was withdrawn by FDA request, and one was forced by the agency. The median time from accelerated approval to withdrawal was 8.8 years.
The actual withdrawal process itself took 11 months when bevacizumab’s breast cancer indication was canceled in 2011.
The authors didn’t call for change outright, but they did say that “future discussions of the accelerated approval program in the U.S.” will seek “to coordinate regulatory processes” with other countries, with an eye towards building “harmony between” agencies.
Among other targets for possible harmonization, they noted that only new molecular entities are eligible for accelerated approval in Europe, whereas supplemental indications are also eligible in the United States
Europe also requires a risk-benefit assessment for conditional approvals, which “has led to relatively few approvals based on single-arm clinical trial data,” the authors said.
Dr. Mehta, Dr. de Claro, and Dr. Pazdur had no conflicts of interest.
The FDA launched its accelerated approval program in 1992 in response to the AIDS crisis, but the bulk of approvals since then have been for cancer drugs, wrote the authors who included Gautam U. Mehta, MD, a clinical reviewer with the FDA’s Center for Drug Evaluation and Research; R. Angelo de Claro, MD, associate director of the FDA’s Global Clinical Sciences division within the Oncology Center of Excellence; and Richard Pazdur, MD, director of the FDA’s Oncology Center of Excellence.
Accelerated approvals are typically granted in oncology based on overall response rate with a requirement that companies confirm that there’s actually a clinical benefit in postmarketing studies.
The system has inspired European nations and Australia to launch their own programs, but with a key difference: Conditional approvals expire within 1 year or 2.
To be reinstated and remain on the market, companies have to submit a timeline for when they’ll meet their outstanding obligations and demonstrate that the benefit of leaving their product on the market outweighs the risk.
The approach puts “the onus of timely completion of confirmatory trials and verification of benefit” on the drug maker. In the meantime, the system limits “public exposure to stale claims of effectiveness that cannot be expeditiously substantiated,” Dr. Mehta and colleagues wrote.
There aren’t any deadlines in the United States, however, so the FDA has “to initiate a resource-intensive withdrawal process” when proof of clinical benefit is not forthcoming, they said.
In the United States, only 14 of 167 oncology indications granted accelerated approval since 1992 were withdrawn voluntarily and one was withdrawn by FDA request, and one was forced by the agency. The median time from accelerated approval to withdrawal was 8.8 years.
The actual withdrawal process itself took 11 months when bevacizumab’s breast cancer indication was canceled in 2011.
The authors didn’t call for change outright, but they did say that “future discussions of the accelerated approval program in the U.S.” will seek “to coordinate regulatory processes” with other countries, with an eye towards building “harmony between” agencies.
Among other targets for possible harmonization, they noted that only new molecular entities are eligible for accelerated approval in Europe, whereas supplemental indications are also eligible in the United States
Europe also requires a risk-benefit assessment for conditional approvals, which “has led to relatively few approvals based on single-arm clinical trial data,” the authors said.
Dr. Mehta, Dr. de Claro, and Dr. Pazdur had no conflicts of interest.
FROM JAMA ONCOLOGY
Too much marijuana can make you unpleasantly, dangerously sick
At the center of the emerging science on the unintended consequences of daily long-term use of marijuana lies a paradox.
For years, medical marijuana has been used to ease nausea from cancer chemotherapy and GI conditions. Now, with greater legalization comes growing awareness that chronic use of marijuana – also known as cannabis – can trigger a condition where, ironically, a person has hard-to-control vomiting and nausea.
Some people with the disorder, known as “cannabinoid hyperemesis syndrome,” also report crippling belly pain.
Linda can relate. The 33-year-old Oregon resident, who asked to remain anonymous to protect her privacy, refers to a medieval spiky metal ball on a chain when describing the pain.
“Picture a mace inside your stomach, pushing up inside your chest and, at the same time, exploding out,” she said.
To seek relief, she gets down on her knees, adopts a child’s yoga pose, and runs hot water in the bathroom for hours on end, a trick many with the disorder says has provided relief. She also occasionally goes outside and tries walking it off.
“I would just wander around my neighborhood, a lot of times at like 4 or 5 in the morning,” she said. “The fresh air helps a little bit. I just keep walking down the street, take about 10 steps, stop, vomit – walk a little bit more, stop, vomit.”
Her first experience with the disorder began in the middle of one night in 2017 while she was at a conference in Las Vegas.
“We went out to eat the night before, and I woke up about 4 in the morning with just the most intense pain I’ve ever had,” she said. “I found myself in a really hot shower in between throwing up everything and trying to say get some water down. I was sharing an Airbnb with my colleagues, so it was less than ideal.”
Many people with cannabinoid hyperemesis syndrome find relief from hot baths or showers. Researchers believe that hot water helps because temperature sensors in the skin send signals to the brain that can help ease the symptoms, at least for a while.
The problem is that people with this syndrome “can’t live in the water,” said emergency doctor and medical cannabis expert Leigh Vinocur, MD.
Fast-forward 6 months to another event in Boulder, Colo. Again, Linda woke up and could not stop vomiting.
“I was not feeling any better. Showering wasn’t helping. I ended up in the hospital,” she said.
She received opioids for her pain. But neither she nor the ED staff were quite sure what was happening. Her discharge paperwork read “cannabis allergy.”
Cannabinoid hyperemesis syndrome “shatters that image of cannabis only being a good thing. It’s a bold statement, but, you know, once you start to think about it, it’s like a little too much of anything isn’t good,” Linda said.
Experts suggest greater awareness is needed to identify this syndrome earlier, by both cannabinoid users and doctors. The bouts of vomiting, in particular, can get so severe that people can end up hospitalized with dehydration, electrolyte disorders, and weight loss.
The severe electrolyte imbalances “can really be life-threatening,” said David Johnson, MD, a professor of medicine and chief of gastroenterology at Eastern Virginia Medical School, Norfolk.
“By the time they come into emergency care, they’re in bad shape,” Dr. Vinocur agreed. “Many try to ignore it, but they continue to vomit.”
Genetic risk factors?
One mystery is why some regular marijuana users get this syndrome while others do not.
“I can say that not everybody gets this, thank goodness,” said Ethan Russo, MD. “But there has to be a reason that certain people are susceptible and others are not.”
Interestingly, a new study from Dr. Russo and colleagues suggests that genes play a role. They identified five genetic changes that could make a chronic marijuana user more likely to have cannabinoid hyperemesis syndrome in a study published July 5, 2021, in the journal Cannabis and Cannabinoid Research.
They compared 28 people with the disorder with 12 other high-frequency marijuana users without these symptoms.
The results are not final but could help guide future research, Dr. Russo said.
“What we’ve discovered – and it was far more than we expected – is that there’s a lot more to this than a hypersensitivity to cannabis,” said Dr. Russo, a neurologist and founder/CEO of CReDO Science, a firm that promotes cannabis research and develops commercial products.
Also, he said, those affected by cannabinoid hyperemesis syndrome could be at higher risk for other conditions, such as addiction to alcohol or other substances, dementia, diabetes, and heart disease.
“Most people with [cannabinoid hyperemesis syndrome] are going to be younger,” he said. “What we’ve demonstrated is there is a risk for more serious problems for decades to come. So someone who has these symptoms really deserves a look at this genetic screening.”
Battling disbelief
Getting back to the paradox, many users don’t believe marijuana can trigger serious vomiting and nausea because of its reputation for doing the opposite.
“Folks that have this are just uniquely resistant to the concept that cannabis is actually the problem and not the solution,” Dr. Russo said.
“It’s kind of counterintuitive because people think: ‘Oh, cannabis helps with nausea,’ so they use more of it,” said Dr. Vinocur, who is also a spokesperson for the American College of Emergency Physicians and runs a medical cannabis practice.
Most kinds of marijuana act in this way – doing opposite things at different doses. Once a certain threshold is passed, people with cannabinoid hyperemesis syndrome are “just uniquely susceptible and really can’t tolerate any significant amount of THC,” Dr. Russo said, referring to tetrahydrocannabinol, the substance that gets marijuana users high.
Once diagnosed, quitting is the most effective strategy. But it can be tough to persuade someone to stop using marijuana.
“You do have to try and convince them ... to try abstinence and to watch and see what happens,” Dr. Vinocur said.
People should “realize the root cause of this is its cannabinoid ingestion, and the treatment is really best directed at absolute avoidance,” Dr. Johnson said.
Unfortunately, evidence also shows that once a person stops using marijuana and gets relief, going back to marijuana or other forms of cannabinoids can cause the syndrome to start all over again.
“We’ve had people that quit for a month, a year, 2 years and upon resumption, almost invariably, they’re back into bouts of the hyperemesis along with all the other [symptoms],” Dr. Russo said.
Marijuana and cannabinoids can cause digestive problems, Dr. Johnson said, which may cause more problems.
What recent research reveals
Cannabinoid hyperemesis syndrome is a relatively young disorder – first described in 2004 – and early reports and case studies are giving way now to studies looking into potential treatments.
So far, the strongest evidence suggests a role for an over-the-counter cream called capsaicin to help manage symptoms, but more studies are needed.
Similar to hot showers, this ingredient from chili peppers can warm the skin and trigger the temperature-sensitive skin sensors to lessen the symptoms, Dr. Johnson said.
An October 2021 study in Spain looked at 54 ED visits among 29 people with cannabinoid hyperemesis syndrome. For the 75% treated with capsaicin, vomiting stopped after an average of 18 minutes.
Lead author Guillermo Burillo-Putze, MD, PhD, said he is most surprised by the growing number of new cases of the disorder.
“This should be of concern given the increase in cannabis use due to its legalization and permissiveness,” said Dr. Burillo-Putze, an emergency doctor at Hospital Universitario de Canarias, Santa Cruz de Tenerife, Spain.
Cannabinoid hyperemesis syndrome appears not to discriminate across racial and ethic groups. Although most studies to date include White participants, a July 2021 study of 29 people, 90% of whom were Black, found repeat visits to the ED were common.
The study found that 16 people returned 42 times to the ED and accounted for 10 hospital admissions, for example.
Cannabis conspiracy theories
“Unfortunately, this condition has become the subject of great speculation hinging on conspiracy theories as its true cause,” Dr. Russo noted in a September 2021 letter to the editor in the American Journal of Emergency Medicine.
Some “myth busting” is in order, he said.
For example, cannabinoid hyperemesis syndrome does not happen because of exposure to products from a tree called neem or from pesticides applied to marijuana plants during cultivation, Dr. Russo said. It can also occur with high-dose synthetic cannabinoids.
The state of recreational and medical marijuana
Recreational marijuana is legal in 18 states, Washington, D.C., and Guam as of January 2022, according to a report in U.S. News. More states permit medical marijuana use – 37 in total, plus Washington, D.C., according to Britannica ProCon.
One of the states where only medicinal use is legal is Maryland, which is where Dr. Vinocur practices.
“We are seeing increasing numbers of cases” of cannabinoid hyperemesis syndrome, she said.
In addition to chronic use or higher doses, it’s likely that the higher potency levels of THC in the legal marijuana industry trigger the syndrome in some people as well.
Linda estimates she ended up in emergency rooms at least a half-dozen times in the last 5 years. In April 2021, she had a “pretty serious event.” She blames it on traveling a lot for work, not eating right, and not getting enough sleep. She broke her 2-year abstinence with alcohol.
“I basically didn’t listen to my body and paid a pretty significant price for it,” she said.
Linda did not stop altogether but said she “drastically changed the types and form of the cannabis I was using.”
“I can tell you on the record that I would be a hundred percent dead without this plant,” she said.
“The prospect of living without it was more detrimental to me than all of those things I just described to you, because addiction runs in my family and I had opiate problems myself that I overcame with cannabis.”
A version of this article first appeared on Medscape.com.
At the center of the emerging science on the unintended consequences of daily long-term use of marijuana lies a paradox.
For years, medical marijuana has been used to ease nausea from cancer chemotherapy and GI conditions. Now, with greater legalization comes growing awareness that chronic use of marijuana – also known as cannabis – can trigger a condition where, ironically, a person has hard-to-control vomiting and nausea.
Some people with the disorder, known as “cannabinoid hyperemesis syndrome,” also report crippling belly pain.
Linda can relate. The 33-year-old Oregon resident, who asked to remain anonymous to protect her privacy, refers to a medieval spiky metal ball on a chain when describing the pain.
“Picture a mace inside your stomach, pushing up inside your chest and, at the same time, exploding out,” she said.
To seek relief, she gets down on her knees, adopts a child’s yoga pose, and runs hot water in the bathroom for hours on end, a trick many with the disorder says has provided relief. She also occasionally goes outside and tries walking it off.
“I would just wander around my neighborhood, a lot of times at like 4 or 5 in the morning,” she said. “The fresh air helps a little bit. I just keep walking down the street, take about 10 steps, stop, vomit – walk a little bit more, stop, vomit.”
Her first experience with the disorder began in the middle of one night in 2017 while she was at a conference in Las Vegas.
“We went out to eat the night before, and I woke up about 4 in the morning with just the most intense pain I’ve ever had,” she said. “I found myself in a really hot shower in between throwing up everything and trying to say get some water down. I was sharing an Airbnb with my colleagues, so it was less than ideal.”
Many people with cannabinoid hyperemesis syndrome find relief from hot baths or showers. Researchers believe that hot water helps because temperature sensors in the skin send signals to the brain that can help ease the symptoms, at least for a while.
The problem is that people with this syndrome “can’t live in the water,” said emergency doctor and medical cannabis expert Leigh Vinocur, MD.
Fast-forward 6 months to another event in Boulder, Colo. Again, Linda woke up and could not stop vomiting.
“I was not feeling any better. Showering wasn’t helping. I ended up in the hospital,” she said.
She received opioids for her pain. But neither she nor the ED staff were quite sure what was happening. Her discharge paperwork read “cannabis allergy.”
Cannabinoid hyperemesis syndrome “shatters that image of cannabis only being a good thing. It’s a bold statement, but, you know, once you start to think about it, it’s like a little too much of anything isn’t good,” Linda said.
Experts suggest greater awareness is needed to identify this syndrome earlier, by both cannabinoid users and doctors. The bouts of vomiting, in particular, can get so severe that people can end up hospitalized with dehydration, electrolyte disorders, and weight loss.
The severe electrolyte imbalances “can really be life-threatening,” said David Johnson, MD, a professor of medicine and chief of gastroenterology at Eastern Virginia Medical School, Norfolk.
“By the time they come into emergency care, they’re in bad shape,” Dr. Vinocur agreed. “Many try to ignore it, but they continue to vomit.”
Genetic risk factors?
One mystery is why some regular marijuana users get this syndrome while others do not.
“I can say that not everybody gets this, thank goodness,” said Ethan Russo, MD. “But there has to be a reason that certain people are susceptible and others are not.”
Interestingly, a new study from Dr. Russo and colleagues suggests that genes play a role. They identified five genetic changes that could make a chronic marijuana user more likely to have cannabinoid hyperemesis syndrome in a study published July 5, 2021, in the journal Cannabis and Cannabinoid Research.
They compared 28 people with the disorder with 12 other high-frequency marijuana users without these symptoms.
The results are not final but could help guide future research, Dr. Russo said.
“What we’ve discovered – and it was far more than we expected – is that there’s a lot more to this than a hypersensitivity to cannabis,” said Dr. Russo, a neurologist and founder/CEO of CReDO Science, a firm that promotes cannabis research and develops commercial products.
Also, he said, those affected by cannabinoid hyperemesis syndrome could be at higher risk for other conditions, such as addiction to alcohol or other substances, dementia, diabetes, and heart disease.
“Most people with [cannabinoid hyperemesis syndrome] are going to be younger,” he said. “What we’ve demonstrated is there is a risk for more serious problems for decades to come. So someone who has these symptoms really deserves a look at this genetic screening.”
Battling disbelief
Getting back to the paradox, many users don’t believe marijuana can trigger serious vomiting and nausea because of its reputation for doing the opposite.
“Folks that have this are just uniquely resistant to the concept that cannabis is actually the problem and not the solution,” Dr. Russo said.
“It’s kind of counterintuitive because people think: ‘Oh, cannabis helps with nausea,’ so they use more of it,” said Dr. Vinocur, who is also a spokesperson for the American College of Emergency Physicians and runs a medical cannabis practice.
Most kinds of marijuana act in this way – doing opposite things at different doses. Once a certain threshold is passed, people with cannabinoid hyperemesis syndrome are “just uniquely susceptible and really can’t tolerate any significant amount of THC,” Dr. Russo said, referring to tetrahydrocannabinol, the substance that gets marijuana users high.
Once diagnosed, quitting is the most effective strategy. But it can be tough to persuade someone to stop using marijuana.
“You do have to try and convince them ... to try abstinence and to watch and see what happens,” Dr. Vinocur said.
People should “realize the root cause of this is its cannabinoid ingestion, and the treatment is really best directed at absolute avoidance,” Dr. Johnson said.
Unfortunately, evidence also shows that once a person stops using marijuana and gets relief, going back to marijuana or other forms of cannabinoids can cause the syndrome to start all over again.
“We’ve had people that quit for a month, a year, 2 years and upon resumption, almost invariably, they’re back into bouts of the hyperemesis along with all the other [symptoms],” Dr. Russo said.
Marijuana and cannabinoids can cause digestive problems, Dr. Johnson said, which may cause more problems.
What recent research reveals
Cannabinoid hyperemesis syndrome is a relatively young disorder – first described in 2004 – and early reports and case studies are giving way now to studies looking into potential treatments.
So far, the strongest evidence suggests a role for an over-the-counter cream called capsaicin to help manage symptoms, but more studies are needed.
Similar to hot showers, this ingredient from chili peppers can warm the skin and trigger the temperature-sensitive skin sensors to lessen the symptoms, Dr. Johnson said.
An October 2021 study in Spain looked at 54 ED visits among 29 people with cannabinoid hyperemesis syndrome. For the 75% treated with capsaicin, vomiting stopped after an average of 18 minutes.
Lead author Guillermo Burillo-Putze, MD, PhD, said he is most surprised by the growing number of new cases of the disorder.
“This should be of concern given the increase in cannabis use due to its legalization and permissiveness,” said Dr. Burillo-Putze, an emergency doctor at Hospital Universitario de Canarias, Santa Cruz de Tenerife, Spain.
Cannabinoid hyperemesis syndrome appears not to discriminate across racial and ethic groups. Although most studies to date include White participants, a July 2021 study of 29 people, 90% of whom were Black, found repeat visits to the ED were common.
The study found that 16 people returned 42 times to the ED and accounted for 10 hospital admissions, for example.
Cannabis conspiracy theories
“Unfortunately, this condition has become the subject of great speculation hinging on conspiracy theories as its true cause,” Dr. Russo noted in a September 2021 letter to the editor in the American Journal of Emergency Medicine.
Some “myth busting” is in order, he said.
For example, cannabinoid hyperemesis syndrome does not happen because of exposure to products from a tree called neem or from pesticides applied to marijuana plants during cultivation, Dr. Russo said. It can also occur with high-dose synthetic cannabinoids.
The state of recreational and medical marijuana
Recreational marijuana is legal in 18 states, Washington, D.C., and Guam as of January 2022, according to a report in U.S. News. More states permit medical marijuana use – 37 in total, plus Washington, D.C., according to Britannica ProCon.
One of the states where only medicinal use is legal is Maryland, which is where Dr. Vinocur practices.
“We are seeing increasing numbers of cases” of cannabinoid hyperemesis syndrome, she said.
In addition to chronic use or higher doses, it’s likely that the higher potency levels of THC in the legal marijuana industry trigger the syndrome in some people as well.
Linda estimates she ended up in emergency rooms at least a half-dozen times in the last 5 years. In April 2021, she had a “pretty serious event.” She blames it on traveling a lot for work, not eating right, and not getting enough sleep. She broke her 2-year abstinence with alcohol.
“I basically didn’t listen to my body and paid a pretty significant price for it,” she said.
Linda did not stop altogether but said she “drastically changed the types and form of the cannabis I was using.”
“I can tell you on the record that I would be a hundred percent dead without this plant,” she said.
“The prospect of living without it was more detrimental to me than all of those things I just described to you, because addiction runs in my family and I had opiate problems myself that I overcame with cannabis.”
A version of this article first appeared on Medscape.com.
At the center of the emerging science on the unintended consequences of daily long-term use of marijuana lies a paradox.
For years, medical marijuana has been used to ease nausea from cancer chemotherapy and GI conditions. Now, with greater legalization comes growing awareness that chronic use of marijuana – also known as cannabis – can trigger a condition where, ironically, a person has hard-to-control vomiting and nausea.
Some people with the disorder, known as “cannabinoid hyperemesis syndrome,” also report crippling belly pain.
Linda can relate. The 33-year-old Oregon resident, who asked to remain anonymous to protect her privacy, refers to a medieval spiky metal ball on a chain when describing the pain.
“Picture a mace inside your stomach, pushing up inside your chest and, at the same time, exploding out,” she said.
To seek relief, she gets down on her knees, adopts a child’s yoga pose, and runs hot water in the bathroom for hours on end, a trick many with the disorder says has provided relief. She also occasionally goes outside and tries walking it off.
“I would just wander around my neighborhood, a lot of times at like 4 or 5 in the morning,” she said. “The fresh air helps a little bit. I just keep walking down the street, take about 10 steps, stop, vomit – walk a little bit more, stop, vomit.”
Her first experience with the disorder began in the middle of one night in 2017 while she was at a conference in Las Vegas.
“We went out to eat the night before, and I woke up about 4 in the morning with just the most intense pain I’ve ever had,” she said. “I found myself in a really hot shower in between throwing up everything and trying to say get some water down. I was sharing an Airbnb with my colleagues, so it was less than ideal.”
Many people with cannabinoid hyperemesis syndrome find relief from hot baths or showers. Researchers believe that hot water helps because temperature sensors in the skin send signals to the brain that can help ease the symptoms, at least for a while.
The problem is that people with this syndrome “can’t live in the water,” said emergency doctor and medical cannabis expert Leigh Vinocur, MD.
Fast-forward 6 months to another event in Boulder, Colo. Again, Linda woke up and could not stop vomiting.
“I was not feeling any better. Showering wasn’t helping. I ended up in the hospital,” she said.
She received opioids for her pain. But neither she nor the ED staff were quite sure what was happening. Her discharge paperwork read “cannabis allergy.”
Cannabinoid hyperemesis syndrome “shatters that image of cannabis only being a good thing. It’s a bold statement, but, you know, once you start to think about it, it’s like a little too much of anything isn’t good,” Linda said.
Experts suggest greater awareness is needed to identify this syndrome earlier, by both cannabinoid users and doctors. The bouts of vomiting, in particular, can get so severe that people can end up hospitalized with dehydration, electrolyte disorders, and weight loss.
The severe electrolyte imbalances “can really be life-threatening,” said David Johnson, MD, a professor of medicine and chief of gastroenterology at Eastern Virginia Medical School, Norfolk.
“By the time they come into emergency care, they’re in bad shape,” Dr. Vinocur agreed. “Many try to ignore it, but they continue to vomit.”
Genetic risk factors?
One mystery is why some regular marijuana users get this syndrome while others do not.
“I can say that not everybody gets this, thank goodness,” said Ethan Russo, MD. “But there has to be a reason that certain people are susceptible and others are not.”
Interestingly, a new study from Dr. Russo and colleagues suggests that genes play a role. They identified five genetic changes that could make a chronic marijuana user more likely to have cannabinoid hyperemesis syndrome in a study published July 5, 2021, in the journal Cannabis and Cannabinoid Research.
They compared 28 people with the disorder with 12 other high-frequency marijuana users without these symptoms.
The results are not final but could help guide future research, Dr. Russo said.
“What we’ve discovered – and it was far more than we expected – is that there’s a lot more to this than a hypersensitivity to cannabis,” said Dr. Russo, a neurologist and founder/CEO of CReDO Science, a firm that promotes cannabis research and develops commercial products.
Also, he said, those affected by cannabinoid hyperemesis syndrome could be at higher risk for other conditions, such as addiction to alcohol or other substances, dementia, diabetes, and heart disease.
“Most people with [cannabinoid hyperemesis syndrome] are going to be younger,” he said. “What we’ve demonstrated is there is a risk for more serious problems for decades to come. So someone who has these symptoms really deserves a look at this genetic screening.”
Battling disbelief
Getting back to the paradox, many users don’t believe marijuana can trigger serious vomiting and nausea because of its reputation for doing the opposite.
“Folks that have this are just uniquely resistant to the concept that cannabis is actually the problem and not the solution,” Dr. Russo said.
“It’s kind of counterintuitive because people think: ‘Oh, cannabis helps with nausea,’ so they use more of it,” said Dr. Vinocur, who is also a spokesperson for the American College of Emergency Physicians and runs a medical cannabis practice.
Most kinds of marijuana act in this way – doing opposite things at different doses. Once a certain threshold is passed, people with cannabinoid hyperemesis syndrome are “just uniquely susceptible and really can’t tolerate any significant amount of THC,” Dr. Russo said, referring to tetrahydrocannabinol, the substance that gets marijuana users high.
Once diagnosed, quitting is the most effective strategy. But it can be tough to persuade someone to stop using marijuana.
“You do have to try and convince them ... to try abstinence and to watch and see what happens,” Dr. Vinocur said.
People should “realize the root cause of this is its cannabinoid ingestion, and the treatment is really best directed at absolute avoidance,” Dr. Johnson said.
Unfortunately, evidence also shows that once a person stops using marijuana and gets relief, going back to marijuana or other forms of cannabinoids can cause the syndrome to start all over again.
“We’ve had people that quit for a month, a year, 2 years and upon resumption, almost invariably, they’re back into bouts of the hyperemesis along with all the other [symptoms],” Dr. Russo said.
Marijuana and cannabinoids can cause digestive problems, Dr. Johnson said, which may cause more problems.
What recent research reveals
Cannabinoid hyperemesis syndrome is a relatively young disorder – first described in 2004 – and early reports and case studies are giving way now to studies looking into potential treatments.
So far, the strongest evidence suggests a role for an over-the-counter cream called capsaicin to help manage symptoms, but more studies are needed.
Similar to hot showers, this ingredient from chili peppers can warm the skin and trigger the temperature-sensitive skin sensors to lessen the symptoms, Dr. Johnson said.
An October 2021 study in Spain looked at 54 ED visits among 29 people with cannabinoid hyperemesis syndrome. For the 75% treated with capsaicin, vomiting stopped after an average of 18 minutes.
Lead author Guillermo Burillo-Putze, MD, PhD, said he is most surprised by the growing number of new cases of the disorder.
“This should be of concern given the increase in cannabis use due to its legalization and permissiveness,” said Dr. Burillo-Putze, an emergency doctor at Hospital Universitario de Canarias, Santa Cruz de Tenerife, Spain.
Cannabinoid hyperemesis syndrome appears not to discriminate across racial and ethic groups. Although most studies to date include White participants, a July 2021 study of 29 people, 90% of whom were Black, found repeat visits to the ED were common.
The study found that 16 people returned 42 times to the ED and accounted for 10 hospital admissions, for example.
Cannabis conspiracy theories
“Unfortunately, this condition has become the subject of great speculation hinging on conspiracy theories as its true cause,” Dr. Russo noted in a September 2021 letter to the editor in the American Journal of Emergency Medicine.
Some “myth busting” is in order, he said.
For example, cannabinoid hyperemesis syndrome does not happen because of exposure to products from a tree called neem or from pesticides applied to marijuana plants during cultivation, Dr. Russo said. It can also occur with high-dose synthetic cannabinoids.
The state of recreational and medical marijuana
Recreational marijuana is legal in 18 states, Washington, D.C., and Guam as of January 2022, according to a report in U.S. News. More states permit medical marijuana use – 37 in total, plus Washington, D.C., according to Britannica ProCon.
One of the states where only medicinal use is legal is Maryland, which is where Dr. Vinocur practices.
“We are seeing increasing numbers of cases” of cannabinoid hyperemesis syndrome, she said.
In addition to chronic use or higher doses, it’s likely that the higher potency levels of THC in the legal marijuana industry trigger the syndrome in some people as well.
Linda estimates she ended up in emergency rooms at least a half-dozen times in the last 5 years. In April 2021, she had a “pretty serious event.” She blames it on traveling a lot for work, not eating right, and not getting enough sleep. She broke her 2-year abstinence with alcohol.
“I basically didn’t listen to my body and paid a pretty significant price for it,” she said.
Linda did not stop altogether but said she “drastically changed the types and form of the cannabis I was using.”
“I can tell you on the record that I would be a hundred percent dead without this plant,” she said.
“The prospect of living without it was more detrimental to me than all of those things I just described to you, because addiction runs in my family and I had opiate problems myself that I overcame with cannabis.”
A version of this article first appeared on Medscape.com.
A third person living with HIV has been cured by transplant
In a first, If she remains off treatment without any hint of HIV, she would be only the third person in the world – after the Berlin Patient and the London Patient – to be cured through a transplant.
“Her own virus could not infect her cells,” said Yvonne Bryson, MD, chief of pediatric infectious diseases at the University of California, Los Angeles, who presented the study at the Conference on Retroviruses and Opportunistic Infections, which both presenters and the audience attended remotely.
The middle-aged New York woman of mixed race, who has asked that her specific race and age not be shared to protect her privacy, was diagnosed with HIV in 2013 when she was still in the very early stages of infection. She started treatment immediately and quickly achieved an undetectable viral load. An undetectable viral load not only prevents someone from transmitting HIV to others but also reduces or eliminates HIV replication, which means fewer variants and less time for the virus to infiltrate cells where it can hide.
But in 2017, she was diagnosed with leukemia. As a last resort to cure her of the cancer, she received a combination of adult stem cells from a relative’s blood that closely matched her own and umbilical cord blood obtained from a cord blood bank. That particular sample of cord blood was selected for its genetic mutation against the CCR5 receptor on immune cells, CD4 T cells. That mutation makes the immune system resistant to HIV.
The two previous HIV cures, of Berlin Patient Timothy Ray Brown and London Patient Adam Castillejo, also used stem cell transplantation with a CCR5 mutation, but theirs were bone marrow transplants. Bone marrow transplants are more arduous than cord blood transplants, which are commonly used in pediatric cancer treatment.
In this case, the physicians treating her used both.
“This allows the adult cells to accelerate and grow up until the cord blood takes over,” said Dr. Bryson. During her presentation, Dr. Bryson pointed to two types of data: First, she presented data showing the level of HIV in the patient’s blood. Soon after HIV diagnosis and treatment, her viral load dropped to undetectable levels. She had a spike of virus when she received the transplant, but then it went back to undetectable and has stayed that way ever since.
Meanwhile, following the transplant, her immune system started rebuilding itself using the new, HIV-resistant cells provided in the transplant. As her care team watched, no graft-versus-host (GVH) disease, a common side effect of stem cell transplants, emerged. In fact, the transplant went so well that she was discharged early from the hospital.
One hundred days after the transplant, the immune system contained within the cord blood had taken over. Her CD4 immune cells returned to normal levels a little more than a year after the transplant. By 27 months, she decided to stop all HIV treatment to see if the transplant had worked.
This was the real test. But as Dr. Bryson and colleagues continued to watch her HIV viral load and her CD4 counts and search for infectious virus, they didn’t find any. She tested negative for HIV by antibody test. Dr. Bryson grew 75 million of her cells in a lab to look for any HIV. None. Aside from one blip in detectable HIV DNA at 14 weeks, researchers never found HIV in the patient again.
“Her cells are resistant to HIV now – both her own strains and laboratory strains,” Dr. Bryson told this news organization. “It’s been 14 months since then. She has no rebound and no detectable virus.”
The presentation drew as raucous as praise gets in a virtual environment. The comments began pouring in.
“Impressive results,” wrote Jim Hoxie, MD, professor emeritus at the University of Pennsylvania, Philadelphia.
“Exciting case,” wrote Allison Agwu, MD, a professor of pediatrics at Johns Hopkins University, Baltimore.
And Dennis Copertino, a research specialist at Weill Cornell Medicine, New York, wrote: “Thank you so much for translating this important cure strategy to people of color.”
Most donors with CCR5 mutations are White, Dr. Bryson said, suggesting that this approach, in a mixed-race woman, could expand the pool of people living with HIV and cancer who are good candidates for the approach.
But other observers had questions, ones that may require more research to answer. Some asked why this woman’s virus, after transplantation, wasn’t just immune to viruses with CCR5 but also another variant, called CXCR4, that one wouldn’t expect. Luis Montaner, DVM, director of the Immunopathogenesis Laboratory at the Wistar Institute in Philadelphia, wondered whether it was more than the blood that had cleared HIV. Did it get into the tissue, too? That question has not yet been answered.
For Carl Dieffenbach, PhD, director of the division of AIDS at the National Institute of Allergy and Infectious Diseases, the lack of GVH disease was a powerful and hopeful finding.
“There’s been this ongoing hypothesis that maybe graft-versus-host disease was needed at some level to help clear out every last single CD4+ T cell that may or may not have been harboring replication-competent virus,” Dr. Dieffenbach said in an interview. “But there was no GVH disease. That’s incredible. It’s a wonderful thing.”
Now the challenge is to move from a single case to making cure available to other people living with HIV.
The case also got cure researchers thinking.
Dr. Montaner called the case “an encouraging roadmap supporting anti-CCR5 strategies by CRISPR Cas9,” studies that are now underway.
Steven Deeks, MD, called the case “perhaps a model for how we might do this using a person’s own cells. Because we were never really going to be transplanting cells from another person as a scalable cure.”
For people living with HIV, particularly women of color, the results raise hopes and questions. Nina Martinez knows something about being a “first.” In 2019, she was the first American woman of color living with HIV to donate a kidney to another person living with the virus. To her, the excitement over the first woman of color being cured of HIV just shines a light on how very White and male HIV cure studies have been until now.
“For me, I’m not looking for a cure in which the successful step forward is me getting cancer,” she said in an interview. “I’m looking at, what’s going to be sustainable? I want to know what’s going to work for a group of people.”
Gina Marie Brown, a social worker living with HIV in New Orleans, is also thinking of groups of people.
“Every time we get a breakthrough, it’s like the sun is taken from behind the clouds a little more,” said Ms. Brown. “I think about people in the South, who bear a huge burden of HIV. I think about trans women. I think about Black women, and gay, bisexual, and same-gender-loving men. This could really impact HIV – in the same way that PrEP [pre-exposure prophylaxis] has, the same way that one pill once a day has.”
When Ms. Brown was diagnosed with HIV 22 years ago, she started to plan her funeral.
“That’s how much I thought HIV was a death sentence,” she told this news organization. “Oh my goodness! Glad you stuck around, Gina.”
The study was funded by the National Institutes of Health. Dr. Bryson, Dr. Dieffenbach, Dr. Deeks, and Dr. Montaner disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a first, If she remains off treatment without any hint of HIV, she would be only the third person in the world – after the Berlin Patient and the London Patient – to be cured through a transplant.
“Her own virus could not infect her cells,” said Yvonne Bryson, MD, chief of pediatric infectious diseases at the University of California, Los Angeles, who presented the study at the Conference on Retroviruses and Opportunistic Infections, which both presenters and the audience attended remotely.
The middle-aged New York woman of mixed race, who has asked that her specific race and age not be shared to protect her privacy, was diagnosed with HIV in 2013 when she was still in the very early stages of infection. She started treatment immediately and quickly achieved an undetectable viral load. An undetectable viral load not only prevents someone from transmitting HIV to others but also reduces or eliminates HIV replication, which means fewer variants and less time for the virus to infiltrate cells where it can hide.
But in 2017, she was diagnosed with leukemia. As a last resort to cure her of the cancer, she received a combination of adult stem cells from a relative’s blood that closely matched her own and umbilical cord blood obtained from a cord blood bank. That particular sample of cord blood was selected for its genetic mutation against the CCR5 receptor on immune cells, CD4 T cells. That mutation makes the immune system resistant to HIV.
The two previous HIV cures, of Berlin Patient Timothy Ray Brown and London Patient Adam Castillejo, also used stem cell transplantation with a CCR5 mutation, but theirs were bone marrow transplants. Bone marrow transplants are more arduous than cord blood transplants, which are commonly used in pediatric cancer treatment.
In this case, the physicians treating her used both.
“This allows the adult cells to accelerate and grow up until the cord blood takes over,” said Dr. Bryson. During her presentation, Dr. Bryson pointed to two types of data: First, she presented data showing the level of HIV in the patient’s blood. Soon after HIV diagnosis and treatment, her viral load dropped to undetectable levels. She had a spike of virus when she received the transplant, but then it went back to undetectable and has stayed that way ever since.
Meanwhile, following the transplant, her immune system started rebuilding itself using the new, HIV-resistant cells provided in the transplant. As her care team watched, no graft-versus-host (GVH) disease, a common side effect of stem cell transplants, emerged. In fact, the transplant went so well that she was discharged early from the hospital.
One hundred days after the transplant, the immune system contained within the cord blood had taken over. Her CD4 immune cells returned to normal levels a little more than a year after the transplant. By 27 months, she decided to stop all HIV treatment to see if the transplant had worked.
This was the real test. But as Dr. Bryson and colleagues continued to watch her HIV viral load and her CD4 counts and search for infectious virus, they didn’t find any. She tested negative for HIV by antibody test. Dr. Bryson grew 75 million of her cells in a lab to look for any HIV. None. Aside from one blip in detectable HIV DNA at 14 weeks, researchers never found HIV in the patient again.
“Her cells are resistant to HIV now – both her own strains and laboratory strains,” Dr. Bryson told this news organization. “It’s been 14 months since then. She has no rebound and no detectable virus.”
The presentation drew as raucous as praise gets in a virtual environment. The comments began pouring in.
“Impressive results,” wrote Jim Hoxie, MD, professor emeritus at the University of Pennsylvania, Philadelphia.
“Exciting case,” wrote Allison Agwu, MD, a professor of pediatrics at Johns Hopkins University, Baltimore.
And Dennis Copertino, a research specialist at Weill Cornell Medicine, New York, wrote: “Thank you so much for translating this important cure strategy to people of color.”
Most donors with CCR5 mutations are White, Dr. Bryson said, suggesting that this approach, in a mixed-race woman, could expand the pool of people living with HIV and cancer who are good candidates for the approach.
But other observers had questions, ones that may require more research to answer. Some asked why this woman’s virus, after transplantation, wasn’t just immune to viruses with CCR5 but also another variant, called CXCR4, that one wouldn’t expect. Luis Montaner, DVM, director of the Immunopathogenesis Laboratory at the Wistar Institute in Philadelphia, wondered whether it was more than the blood that had cleared HIV. Did it get into the tissue, too? That question has not yet been answered.
For Carl Dieffenbach, PhD, director of the division of AIDS at the National Institute of Allergy and Infectious Diseases, the lack of GVH disease was a powerful and hopeful finding.
“There’s been this ongoing hypothesis that maybe graft-versus-host disease was needed at some level to help clear out every last single CD4+ T cell that may or may not have been harboring replication-competent virus,” Dr. Dieffenbach said in an interview. “But there was no GVH disease. That’s incredible. It’s a wonderful thing.”
Now the challenge is to move from a single case to making cure available to other people living with HIV.
The case also got cure researchers thinking.
Dr. Montaner called the case “an encouraging roadmap supporting anti-CCR5 strategies by CRISPR Cas9,” studies that are now underway.
Steven Deeks, MD, called the case “perhaps a model for how we might do this using a person’s own cells. Because we were never really going to be transplanting cells from another person as a scalable cure.”
For people living with HIV, particularly women of color, the results raise hopes and questions. Nina Martinez knows something about being a “first.” In 2019, she was the first American woman of color living with HIV to donate a kidney to another person living with the virus. To her, the excitement over the first woman of color being cured of HIV just shines a light on how very White and male HIV cure studies have been until now.
“For me, I’m not looking for a cure in which the successful step forward is me getting cancer,” she said in an interview. “I’m looking at, what’s going to be sustainable? I want to know what’s going to work for a group of people.”
Gina Marie Brown, a social worker living with HIV in New Orleans, is also thinking of groups of people.
“Every time we get a breakthrough, it’s like the sun is taken from behind the clouds a little more,” said Ms. Brown. “I think about people in the South, who bear a huge burden of HIV. I think about trans women. I think about Black women, and gay, bisexual, and same-gender-loving men. This could really impact HIV – in the same way that PrEP [pre-exposure prophylaxis] has, the same way that one pill once a day has.”
When Ms. Brown was diagnosed with HIV 22 years ago, she started to plan her funeral.
“That’s how much I thought HIV was a death sentence,” she told this news organization. “Oh my goodness! Glad you stuck around, Gina.”
The study was funded by the National Institutes of Health. Dr. Bryson, Dr. Dieffenbach, Dr. Deeks, and Dr. Montaner disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a first, If she remains off treatment without any hint of HIV, she would be only the third person in the world – after the Berlin Patient and the London Patient – to be cured through a transplant.
“Her own virus could not infect her cells,” said Yvonne Bryson, MD, chief of pediatric infectious diseases at the University of California, Los Angeles, who presented the study at the Conference on Retroviruses and Opportunistic Infections, which both presenters and the audience attended remotely.
The middle-aged New York woman of mixed race, who has asked that her specific race and age not be shared to protect her privacy, was diagnosed with HIV in 2013 when she was still in the very early stages of infection. She started treatment immediately and quickly achieved an undetectable viral load. An undetectable viral load not only prevents someone from transmitting HIV to others but also reduces or eliminates HIV replication, which means fewer variants and less time for the virus to infiltrate cells where it can hide.
But in 2017, she was diagnosed with leukemia. As a last resort to cure her of the cancer, she received a combination of adult stem cells from a relative’s blood that closely matched her own and umbilical cord blood obtained from a cord blood bank. That particular sample of cord blood was selected for its genetic mutation against the CCR5 receptor on immune cells, CD4 T cells. That mutation makes the immune system resistant to HIV.
The two previous HIV cures, of Berlin Patient Timothy Ray Brown and London Patient Adam Castillejo, also used stem cell transplantation with a CCR5 mutation, but theirs were bone marrow transplants. Bone marrow transplants are more arduous than cord blood transplants, which are commonly used in pediatric cancer treatment.
In this case, the physicians treating her used both.
“This allows the adult cells to accelerate and grow up until the cord blood takes over,” said Dr. Bryson. During her presentation, Dr. Bryson pointed to two types of data: First, she presented data showing the level of HIV in the patient’s blood. Soon after HIV diagnosis and treatment, her viral load dropped to undetectable levels. She had a spike of virus when she received the transplant, but then it went back to undetectable and has stayed that way ever since.
Meanwhile, following the transplant, her immune system started rebuilding itself using the new, HIV-resistant cells provided in the transplant. As her care team watched, no graft-versus-host (GVH) disease, a common side effect of stem cell transplants, emerged. In fact, the transplant went so well that she was discharged early from the hospital.
One hundred days after the transplant, the immune system contained within the cord blood had taken over. Her CD4 immune cells returned to normal levels a little more than a year after the transplant. By 27 months, she decided to stop all HIV treatment to see if the transplant had worked.
This was the real test. But as Dr. Bryson and colleagues continued to watch her HIV viral load and her CD4 counts and search for infectious virus, they didn’t find any. She tested negative for HIV by antibody test. Dr. Bryson grew 75 million of her cells in a lab to look for any HIV. None. Aside from one blip in detectable HIV DNA at 14 weeks, researchers never found HIV in the patient again.
“Her cells are resistant to HIV now – both her own strains and laboratory strains,” Dr. Bryson told this news organization. “It’s been 14 months since then. She has no rebound and no detectable virus.”
The presentation drew as raucous as praise gets in a virtual environment. The comments began pouring in.
“Impressive results,” wrote Jim Hoxie, MD, professor emeritus at the University of Pennsylvania, Philadelphia.
“Exciting case,” wrote Allison Agwu, MD, a professor of pediatrics at Johns Hopkins University, Baltimore.
And Dennis Copertino, a research specialist at Weill Cornell Medicine, New York, wrote: “Thank you so much for translating this important cure strategy to people of color.”
Most donors with CCR5 mutations are White, Dr. Bryson said, suggesting that this approach, in a mixed-race woman, could expand the pool of people living with HIV and cancer who are good candidates for the approach.
But other observers had questions, ones that may require more research to answer. Some asked why this woman’s virus, after transplantation, wasn’t just immune to viruses with CCR5 but also another variant, called CXCR4, that one wouldn’t expect. Luis Montaner, DVM, director of the Immunopathogenesis Laboratory at the Wistar Institute in Philadelphia, wondered whether it was more than the blood that had cleared HIV. Did it get into the tissue, too? That question has not yet been answered.
For Carl Dieffenbach, PhD, director of the division of AIDS at the National Institute of Allergy and Infectious Diseases, the lack of GVH disease was a powerful and hopeful finding.
“There’s been this ongoing hypothesis that maybe graft-versus-host disease was needed at some level to help clear out every last single CD4+ T cell that may or may not have been harboring replication-competent virus,” Dr. Dieffenbach said in an interview. “But there was no GVH disease. That’s incredible. It’s a wonderful thing.”
Now the challenge is to move from a single case to making cure available to other people living with HIV.
The case also got cure researchers thinking.
Dr. Montaner called the case “an encouraging roadmap supporting anti-CCR5 strategies by CRISPR Cas9,” studies that are now underway.
Steven Deeks, MD, called the case “perhaps a model for how we might do this using a person’s own cells. Because we were never really going to be transplanting cells from another person as a scalable cure.”
For people living with HIV, particularly women of color, the results raise hopes and questions. Nina Martinez knows something about being a “first.” In 2019, she was the first American woman of color living with HIV to donate a kidney to another person living with the virus. To her, the excitement over the first woman of color being cured of HIV just shines a light on how very White and male HIV cure studies have been until now.
“For me, I’m not looking for a cure in which the successful step forward is me getting cancer,” she said in an interview. “I’m looking at, what’s going to be sustainable? I want to know what’s going to work for a group of people.”
Gina Marie Brown, a social worker living with HIV in New Orleans, is also thinking of groups of people.
“Every time we get a breakthrough, it’s like the sun is taken from behind the clouds a little more,” said Ms. Brown. “I think about people in the South, who bear a huge burden of HIV. I think about trans women. I think about Black women, and gay, bisexual, and same-gender-loving men. This could really impact HIV – in the same way that PrEP [pre-exposure prophylaxis] has, the same way that one pill once a day has.”
When Ms. Brown was diagnosed with HIV 22 years ago, she started to plan her funeral.
“That’s how much I thought HIV was a death sentence,” she told this news organization. “Oh my goodness! Glad you stuck around, Gina.”
The study was funded by the National Institutes of Health. Dr. Bryson, Dr. Dieffenbach, Dr. Deeks, and Dr. Montaner disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM CROI 2022
Blind optimism only works in fantasy football. Time to get realistic
In the age of COVID, what exactly does it mean to be optimistic? I get this question quite a bit from virtually everyone I meet in one form or another through my work with the George Washington Resiliency and Well-Being Center in Washington, D.C. Giving a lecture on resilience and staying positive can be a significant challenge. Especially when we wake up to the news that 1 of every 100 older Americans has died secondary to COVID. The mind doesn’t really know how to process this type of loss. It is hard to maintain any form of a positive attitude when you’re still struggling just to accept the magnitude of what humanity has experienced over the past 2 years.

In “Resilience: The Science of Mastering Life’s Greatest Challenges,” (Cambridge, England: Cambridge University Press, 2018), Steven M. Southwick, MD, and Dennis S. Charney, MD, identify 10 critical factors associated with very resilient individuals. The authors based their work on science, personal experience, and interviews of people who have literally been through hell and back. One of the critical factors they identified is optimism.
“Optimism ignites resilience, providing energy to power the other resilience factors. It facilitates an active and creative approach to coping with challenging situations.”
Dr. Southwick and Dr. Charney are a lot smarter than me and far more patient to weave all this data together into a coherent story about optimism. Sounds like a damn good factor to focus a lecture on in my book! Slight problem: In my experience, many health professionals are already expert optimists. They literally eat, sleep, and sincerely breathe this stuff. So if we are going to talk about optimism, then we need to discuss realistic optimism.
How does realistic optimism differ from, say, blind optimism? Dr. Southwick and Dr. Charney’s review of the literature points to three features worthy of highlighting.
Realistic vs. blind optimism: Take-home points
- In realistic optimism, we notice the negative but don’t stay engaged with it. Realistic optimists moved on from problems that were not solvable.
- Blind optimism can lead to underestimating risk, overestimating abilities, and inadequate preparation.
Growing up in northeast Ohio, I can absolutely embrace the concept of realistic optimism. It’s overcast in Cleveland 8 months out of the year. To hope for 3 sunny days in a row in April is genuinely a fools’ errand. So you learn over time, the sun will shine; you just have to at times wait 3-4 months for it to occur.
From a skill perspective, realistic optimism could be conceptualized as a great mix of radical acceptance, emotion regulation, and focused problem solving. This is all fine, but to be realistically optimistic, we must first stop wishing for a better tomorrow. You may say, I don’t wish for or see rainbows and unicorns, et cetera, et cetera. Okay, so you don’t verbalize your wishes, but on a small level, you may engage in wishful thinking. Here are a few wishful thoughts that I would daydream about, which were not realistically optimistic at various points:
- “Once we get enough COVID-19 tests, things will improve.”
- “All we need to do is get vaccines, and then the new normal is right there.”
- “Once everyone gets the booster, then we got this thing beat.”
At this point, you could argue that I was engaged in blind optimism. I consider the above statements blind for a couple of reasons. They weren’t balanced (both positive and negative), didn’t have a clear definition of the outcome, and were more focused on external events I couldn’t control. These statements were the equivalent of wishes, and I don’t have a magic lamp with a genie, so I need to let go of my wishful thinking first. Let me rephrase that: I need to forcefully toss it into the sea of COVID variants and start figuring out how I’m going to tread water for another 6-12 months. So with this in mind, here are my initial thoughts on ways to navigate the next year of the pandemic:
- A multilayered form of protection gives me the best chance to survive the next 6 months of the pandemic.
- It will take time, but I’ll process the loss associated with a workplace that will never be the same.
- Until we have positivity test rates lower than 2% across the globe, COVID will remain a substantial disruption to humanity.
- I can’t bring back missed graduation or the first day of school, but I can share ways that I’ve countered and survived loneliness in my life with my children.
Okay, this is the starting point – hopefully not pessimistic, or blindly optimistic, just realistic. Now I can address other important topics, such as planning to rebuild my disappointing fantasy football team. I was No. 1 in our GW department of psychiatry fantasy football league until my star running back Derrick Henry went down. My residents will become attendings and still give me grief about this for many years to follow, and that is a very good thing.
Everyone be well and safe.
Dr. Norris is associate dean of student affairs; associate professor, department of psychiatry, George Washington University; chief wellness officer, GW Hospital, GW Medical Faculty Associates, and the GW School of Medicine and Health Sciences (GWU Medical Enterprise), Washington. He has disclosed having no relevant financial relationships. A version of this article first appeared on Medscape.com.
In the age of COVID, what exactly does it mean to be optimistic? I get this question quite a bit from virtually everyone I meet in one form or another through my work with the George Washington Resiliency and Well-Being Center in Washington, D.C. Giving a lecture on resilience and staying positive can be a significant challenge. Especially when we wake up to the news that 1 of every 100 older Americans has died secondary to COVID. The mind doesn’t really know how to process this type of loss. It is hard to maintain any form of a positive attitude when you’re still struggling just to accept the magnitude of what humanity has experienced over the past 2 years.
In “Resilience: The Science of Mastering Life’s Greatest Challenges,” (Cambridge, England: Cambridge University Press, 2018), Steven M. Southwick, MD, and Dennis S. Charney, MD, identify 10 critical factors associated with very resilient individuals. The authors based their work on science, personal experience, and interviews of people who have literally been through hell and back. One of the critical factors they identified is optimism.
“Optimism ignites resilience, providing energy to power the other resilience factors. It facilitates an active and creative approach to coping with challenging situations.”
Dr. Southwick and Dr. Charney are a lot smarter than me and far more patient to weave all this data together into a coherent story about optimism. Sounds like a damn good factor to focus a lecture on in my book! Slight problem: In my experience, many health professionals are already expert optimists. They literally eat, sleep, and sincerely breathe this stuff. So if we are going to talk about optimism, then we need to discuss realistic optimism.
How does realistic optimism differ from, say, blind optimism? Dr. Southwick and Dr. Charney’s review of the literature points to three features worthy of highlighting.
Realistic vs. blind optimism: Take-home points
- In realistic optimism, we notice the negative but don’t stay engaged with it. Realistic optimists moved on from problems that were not solvable.
- Blind optimism can lead to underestimating risk, overestimating abilities, and inadequate preparation.
Growing up in northeast Ohio, I can absolutely embrace the concept of realistic optimism. It’s overcast in Cleveland 8 months out of the year. To hope for 3 sunny days in a row in April is genuinely a fools’ errand. So you learn over time, the sun will shine; you just have to at times wait 3-4 months for it to occur.
From a skill perspective, realistic optimism could be conceptualized as a great mix of radical acceptance, emotion regulation, and focused problem solving. This is all fine, but to be realistically optimistic, we must first stop wishing for a better tomorrow. You may say, I don’t wish for or see rainbows and unicorns, et cetera, et cetera. Okay, so you don’t verbalize your wishes, but on a small level, you may engage in wishful thinking. Here are a few wishful thoughts that I would daydream about, which were not realistically optimistic at various points:
- “Once we get enough COVID-19 tests, things will improve.”
- “All we need to do is get vaccines, and then the new normal is right there.”
- “Once everyone gets the booster, then we got this thing beat.”
At this point, you could argue that I was engaged in blind optimism. I consider the above statements blind for a couple of reasons. They weren’t balanced (both positive and negative), didn’t have a clear definition of the outcome, and were more focused on external events I couldn’t control. These statements were the equivalent of wishes, and I don’t have a magic lamp with a genie, so I need to let go of my wishful thinking first. Let me rephrase that: I need to forcefully toss it into the sea of COVID variants and start figuring out how I’m going to tread water for another 6-12 months. So with this in mind, here are my initial thoughts on ways to navigate the next year of the pandemic:
- A multilayered form of protection gives me the best chance to survive the next 6 months of the pandemic.
- It will take time, but I’ll process the loss associated with a workplace that will never be the same.
- Until we have positivity test rates lower than 2% across the globe, COVID will remain a substantial disruption to humanity.
- I can’t bring back missed graduation or the first day of school, but I can share ways that I’ve countered and survived loneliness in my life with my children.
Okay, this is the starting point – hopefully not pessimistic, or blindly optimistic, just realistic. Now I can address other important topics, such as planning to rebuild my disappointing fantasy football team. I was No. 1 in our GW department of psychiatry fantasy football league until my star running back Derrick Henry went down. My residents will become attendings and still give me grief about this for many years to follow, and that is a very good thing.
Everyone be well and safe.
Dr. Norris is associate dean of student affairs; associate professor, department of psychiatry, George Washington University; chief wellness officer, GW Hospital, GW Medical Faculty Associates, and the GW School of Medicine and Health Sciences (GWU Medical Enterprise), Washington. He has disclosed having no relevant financial relationships. A version of this article first appeared on Medscape.com.
In the age of COVID, what exactly does it mean to be optimistic? I get this question quite a bit from virtually everyone I meet in one form or another through my work with the George Washington Resiliency and Well-Being Center in Washington, D.C. Giving a lecture on resilience and staying positive can be a significant challenge. Especially when we wake up to the news that 1 of every 100 older Americans has died secondary to COVID. The mind doesn’t really know how to process this type of loss. It is hard to maintain any form of a positive attitude when you’re still struggling just to accept the magnitude of what humanity has experienced over the past 2 years.
In “Resilience: The Science of Mastering Life’s Greatest Challenges,” (Cambridge, England: Cambridge University Press, 2018), Steven M. Southwick, MD, and Dennis S. Charney, MD, identify 10 critical factors associated with very resilient individuals. The authors based their work on science, personal experience, and interviews of people who have literally been through hell and back. One of the critical factors they identified is optimism.
“Optimism ignites resilience, providing energy to power the other resilience factors. It facilitates an active and creative approach to coping with challenging situations.”
Dr. Southwick and Dr. Charney are a lot smarter than me and far more patient to weave all this data together into a coherent story about optimism. Sounds like a damn good factor to focus a lecture on in my book! Slight problem: In my experience, many health professionals are already expert optimists. They literally eat, sleep, and sincerely breathe this stuff. So if we are going to talk about optimism, then we need to discuss realistic optimism.
How does realistic optimism differ from, say, blind optimism? Dr. Southwick and Dr. Charney’s review of the literature points to three features worthy of highlighting.
Realistic vs. blind optimism: Take-home points
- In realistic optimism, we notice the negative but don’t stay engaged with it. Realistic optimists moved on from problems that were not solvable.
- Blind optimism can lead to underestimating risk, overestimating abilities, and inadequate preparation.
Growing up in northeast Ohio, I can absolutely embrace the concept of realistic optimism. It’s overcast in Cleveland 8 months out of the year. To hope for 3 sunny days in a row in April is genuinely a fools’ errand. So you learn over time, the sun will shine; you just have to at times wait 3-4 months for it to occur.
From a skill perspective, realistic optimism could be conceptualized as a great mix of radical acceptance, emotion regulation, and focused problem solving. This is all fine, but to be realistically optimistic, we must first stop wishing for a better tomorrow. You may say, I don’t wish for or see rainbows and unicorns, et cetera, et cetera. Okay, so you don’t verbalize your wishes, but on a small level, you may engage in wishful thinking. Here are a few wishful thoughts that I would daydream about, which were not realistically optimistic at various points:
- “Once we get enough COVID-19 tests, things will improve.”
- “All we need to do is get vaccines, and then the new normal is right there.”
- “Once everyone gets the booster, then we got this thing beat.”
At this point, you could argue that I was engaged in blind optimism. I consider the above statements blind for a couple of reasons. They weren’t balanced (both positive and negative), didn’t have a clear definition of the outcome, and were more focused on external events I couldn’t control. These statements were the equivalent of wishes, and I don’t have a magic lamp with a genie, so I need to let go of my wishful thinking first. Let me rephrase that: I need to forcefully toss it into the sea of COVID variants and start figuring out how I’m going to tread water for another 6-12 months. So with this in mind, here are my initial thoughts on ways to navigate the next year of the pandemic:
- A multilayered form of protection gives me the best chance to survive the next 6 months of the pandemic.
- It will take time, but I’ll process the loss associated with a workplace that will never be the same.
- Until we have positivity test rates lower than 2% across the globe, COVID will remain a substantial disruption to humanity.
- I can’t bring back missed graduation or the first day of school, but I can share ways that I’ve countered and survived loneliness in my life with my children.
Okay, this is the starting point – hopefully not pessimistic, or blindly optimistic, just realistic. Now I can address other important topics, such as planning to rebuild my disappointing fantasy football team. I was No. 1 in our GW department of psychiatry fantasy football league until my star running back Derrick Henry went down. My residents will become attendings and still give me grief about this for many years to follow, and that is a very good thing.
Everyone be well and safe.
Dr. Norris is associate dean of student affairs; associate professor, department of psychiatry, George Washington University; chief wellness officer, GW Hospital, GW Medical Faculty Associates, and the GW School of Medicine and Health Sciences (GWU Medical Enterprise), Washington. He has disclosed having no relevant financial relationships. A version of this article first appeared on Medscape.com.