User login
For MD-IQ use only
Latest COVID-19 Shot May Cut Severe Outcomes in Veterans
TOPLINE:
Among US veterans, same-day receipt of both the 2024-2025 COVID19 vaccine and the influenza vaccine was associated with lower risks for emergency department visits, hospitalizations, and deaths compared with receipt of the influenza vaccine alone.
METHODOLOGY:
- Researchers conducted an observational study to assess the effectiveness of the 2024-2025 COVID-19 vaccine by comparing veterans who received both the COVID-19 and influenza vaccines on the same day with those who received only the influenza vaccine between September 3 and December 31, 2024.
- Data on participants (mean age, approximately 71.5 years; approximately 92% men) were sourced from electronic health records of the Department of Veterans Affairs and included 164,132 veterans who received both vaccines vs 131,839 who received only the seasonal influenza vaccine, with a follow-up duration of 180 days.
- The vaccines used were mainly the 2024-2025 mRNA COVID19 vaccines: Moderna mRNA1273, Pfizer BNT162b2, and the highdose trivalent 2024-2025 seasonal influenza vaccine.
- Primary outcomes were COVID-19-associated emergency department visits, hospitalizations, and deaths.
TAKEAWAY:
- Receipt of both the COVID-19 and influenza vaccines was associated with a lower risk for COVID-19-associated emergency department visits compared with receipt of the influenza vaccine alone, resulting in a vaccine effectiveness of 29.3% and a risk difference of 18.3 per 10,000 persons (95% CI, 10.8-27.6).
- Similarly, COVID-19 vaccine effectiveness was 39.2% (95% CI, 21.6-54.5) against COVID-19-associated hospitalizations, with a risk difference of 7.5 per 10,000 persons (95% CI, 3.4-13.0).
- For COVID-19-associated deaths, vaccine effectiveness was 64% (95% CI, 23.0-85.8), with a risk difference of 2.2 per 10,000 persons (95% CI, 0.5-6.9).
- Benefits were consistent across age groups (< 65, 65-75, and > 75 years) and among people with various comorbidities, including cardiovascular disease and immunocompromised status.
IN PRACTICE:
“The evidence may help inform ongoing discussions about the value of COVID-19 vaccines in the current epidemiologic landscape,” the authors wrote.
SOURCE:
The study was led by Miao Cai, PhD , Research and Development Service, Veterans Affairs St. Louis Health Care System, and the Veterans Research and Education Foundation of St. Louis, Missouri. It was published online in The New England Journal of Medicine .
LIMITATIONS:
The demographic composition of the cohort — predominantly older, White, male veterans — may limit the generalizability of the study. Although numerous covariates were adjusted for, residual confounding could not be fully ruled out. Safety and variantspecific effectiveness were not assessed.
DISCLOSURES:
The study was supported by a grant from the Department of Veterans Affairs. Two authors disclosed consulting for Pfizer.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Among US veterans, same-day receipt of both the 2024-2025 COVID19 vaccine and the influenza vaccine was associated with lower risks for emergency department visits, hospitalizations, and deaths compared with receipt of the influenza vaccine alone.
METHODOLOGY:
- Researchers conducted an observational study to assess the effectiveness of the 2024-2025 COVID-19 vaccine by comparing veterans who received both the COVID-19 and influenza vaccines on the same day with those who received only the influenza vaccine between September 3 and December 31, 2024.
- Data on participants (mean age, approximately 71.5 years; approximately 92% men) were sourced from electronic health records of the Department of Veterans Affairs and included 164,132 veterans who received both vaccines vs 131,839 who received only the seasonal influenza vaccine, with a follow-up duration of 180 days.
- The vaccines used were mainly the 2024-2025 mRNA COVID19 vaccines: Moderna mRNA1273, Pfizer BNT162b2, and the highdose trivalent 2024-2025 seasonal influenza vaccine.
- Primary outcomes were COVID-19-associated emergency department visits, hospitalizations, and deaths.
TAKEAWAY:
- Receipt of both the COVID-19 and influenza vaccines was associated with a lower risk for COVID-19-associated emergency department visits compared with receipt of the influenza vaccine alone, resulting in a vaccine effectiveness of 29.3% and a risk difference of 18.3 per 10,000 persons (95% CI, 10.8-27.6).
- Similarly, COVID-19 vaccine effectiveness was 39.2% (95% CI, 21.6-54.5) against COVID-19-associated hospitalizations, with a risk difference of 7.5 per 10,000 persons (95% CI, 3.4-13.0).
- For COVID-19-associated deaths, vaccine effectiveness was 64% (95% CI, 23.0-85.8), with a risk difference of 2.2 per 10,000 persons (95% CI, 0.5-6.9).
- Benefits were consistent across age groups (< 65, 65-75, and > 75 years) and among people with various comorbidities, including cardiovascular disease and immunocompromised status.
IN PRACTICE:
“The evidence may help inform ongoing discussions about the value of COVID-19 vaccines in the current epidemiologic landscape,” the authors wrote.
SOURCE:
The study was led by Miao Cai, PhD , Research and Development Service, Veterans Affairs St. Louis Health Care System, and the Veterans Research and Education Foundation of St. Louis, Missouri. It was published online in The New England Journal of Medicine .
LIMITATIONS:
The demographic composition of the cohort — predominantly older, White, male veterans — may limit the generalizability of the study. Although numerous covariates were adjusted for, residual confounding could not be fully ruled out. Safety and variantspecific effectiveness were not assessed.
DISCLOSURES:
The study was supported by a grant from the Department of Veterans Affairs. Two authors disclosed consulting for Pfizer.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Among US veterans, same-day receipt of both the 2024-2025 COVID19 vaccine and the influenza vaccine was associated with lower risks for emergency department visits, hospitalizations, and deaths compared with receipt of the influenza vaccine alone.
METHODOLOGY:
- Researchers conducted an observational study to assess the effectiveness of the 2024-2025 COVID-19 vaccine by comparing veterans who received both the COVID-19 and influenza vaccines on the same day with those who received only the influenza vaccine between September 3 and December 31, 2024.
- Data on participants (mean age, approximately 71.5 years; approximately 92% men) were sourced from electronic health records of the Department of Veterans Affairs and included 164,132 veterans who received both vaccines vs 131,839 who received only the seasonal influenza vaccine, with a follow-up duration of 180 days.
- The vaccines used were mainly the 2024-2025 mRNA COVID19 vaccines: Moderna mRNA1273, Pfizer BNT162b2, and the highdose trivalent 2024-2025 seasonal influenza vaccine.
- Primary outcomes were COVID-19-associated emergency department visits, hospitalizations, and deaths.
TAKEAWAY:
- Receipt of both the COVID-19 and influenza vaccines was associated with a lower risk for COVID-19-associated emergency department visits compared with receipt of the influenza vaccine alone, resulting in a vaccine effectiveness of 29.3% and a risk difference of 18.3 per 10,000 persons (95% CI, 10.8-27.6).
- Similarly, COVID-19 vaccine effectiveness was 39.2% (95% CI, 21.6-54.5) against COVID-19-associated hospitalizations, with a risk difference of 7.5 per 10,000 persons (95% CI, 3.4-13.0).
- For COVID-19-associated deaths, vaccine effectiveness was 64% (95% CI, 23.0-85.8), with a risk difference of 2.2 per 10,000 persons (95% CI, 0.5-6.9).
- Benefits were consistent across age groups (< 65, 65-75, and > 75 years) and among people with various comorbidities, including cardiovascular disease and immunocompromised status.
IN PRACTICE:
“The evidence may help inform ongoing discussions about the value of COVID-19 vaccines in the current epidemiologic landscape,” the authors wrote.
SOURCE:
The study was led by Miao Cai, PhD , Research and Development Service, Veterans Affairs St. Louis Health Care System, and the Veterans Research and Education Foundation of St. Louis, Missouri. It was published online in The New England Journal of Medicine .
LIMITATIONS:
The demographic composition of the cohort — predominantly older, White, male veterans — may limit the generalizability of the study. Although numerous covariates were adjusted for, residual confounding could not be fully ruled out. Safety and variantspecific effectiveness were not assessed.
DISCLOSURES:
The study was supported by a grant from the Department of Veterans Affairs. Two authors disclosed consulting for Pfizer.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.

Targeted Osteoporosis Program May Benefit At-Risk Older Men
Efforts to identify older men at risk for osteoporosis and treat those who are eligible received a boost from results reported from a Veterans Affairs (VA) study that showed a significant increase in screening, treatment, and medication adherence.
The cluster randomized trial used a centralized nurse-led intervention to assess men for traditional osteoporosis risk factors, offer bone density testing, and recommend treatment for eligible men. Over 2 years, the intervention group had a higher average femoral neck bone density than patients who underwent usual care.
“We designed this study to see if a risk factor-based approach, which is what most of the guidelines use, made sense and was feasible — that men would be accepting of screening and [the approach] would yield a similar proportion of people who need osteoporosis treatment as screening in women, which is widely recommended and implemented. And sure enough, we found that about 85% of the men in the VA primary care practices in our target age range of between 65 and 85 actually met criteria for screening, and over half of them had low bone mass. They were very accepting of screening, very accepting of treatment, and had excellent compliance rates. So, our study, we believe, supports the idea of identifying men with at least one risk factor for fracture and offering them osteoporosis screening starting at age 65, similar to what we do for women,” Cathleen S. Colón-Emeric, MD, MHS, said in an interview. She is the lead author of the study, a physician in the Durham VA Health Care System, and professor of medicine at Duke University School of Medicine, Durham, North Carolina.
“We were able to see a positive effect on bone density in the bone health group, compared with the usual care group, which suggests that if we followed these folks longer and had enough of them, we would be able to show a fracture reduction benefit,” Colón-Emeric said.
There have been few randomized trials of screening interventions in men, leading to inconsistencies in guidelines, according to the authors of the new study, published online in JAMA Internal Medicine . Both the US Preventive Services Task Force and the Veterans Health Administration National Center for Health Promotion and Disease Prevention consider there to be insufficient evidence to recommend for or against screening in men who have not experienced a fracture. Some professional societies recommend such screening, but there are inconsistencies in the recommended criteria, such as age range or risk factors.
Beyond the age of 50 years, one in five men will experience an osteoporosis-related fracture at some point in their life, according to a 2009 study. Treatment is inexpensive and effective in both men and women, and economic models suggest that screening using dual-energy x-ray absorptiometry (DXA) would be cost-effective. Still, screening is rare among men, with fewer than 10% of men getting screened before having an osteoporosis-related fracture.
“It’s important to screen men at risk for osteoporosis due to the dramatically increased mortality men suffer after a fragility fracture compared with women. Within 1 year of a hip fracture, mortality is as high as 36%. Studies have also shown that osteoporosis in men is undertreated, with only 10%-50% being prescribed antifracture treatment within 1 year of a hip fracture. Most individuals do not regain their prior level of function after a hip fracture,” said Joe C. Huang, MD, who was asked for comment. He is a clinical assistant professor of gerontology and geriatric medicine at Harborview Medical Center Senior Care Clinic and Healthy Bones Clinic in Seattle.
Details of the Intervention
The bone health service (BHS) intervention employed an electronic health record case-finding tool and a nurse care manager who undertook screening and treatment monitoring. They identified potential risk factors that included hyperthyroidism, hyperparathyroidism, rheumatoid arthritis, alcohol dependence, chronic lung disease, chronic liver disease, stroke, parkinsonism, prostate cancer, smoking, diabetes, pernicious anemia, gastrectomy, or high-risk medication use in at least 3 months of the prior 2 years. These medications included traditional antiepileptics, glucocorticoids, and androgen deprivation therapy.
The BHS nurse invited eligible men to be screened using an initial letter, followed by up to three phone calls. After DXA screening, the nurse scheduled an electronic consult with an osteoporosis expert, and patients with a T-score between -1 and -2.4 and an elevated 10-year fracture risk as measured by the Fracture Risk Assessment Tool were recommended for osteoporosis medication, vitamin D, and dietary or supplemental calcium. Following the prescription, the nurse provided patient education over the phone and mailed out written instructions. The nurse also made phone calls at 1 month, 6 months, and 12 months to encourage adherence and address common treatment barriers such as forgetting to take medication or dealing with gastrointestinal effects. The researchers recruited 38 primary care physicians from two VA health systems. The study included 3112 male veterans between the ages of 65 and 85 years (40.4% Black and 56% White). Nearly all participants (85.5%) had at least one indication for screening according to VA undersecretary guidelines, and almost a third (32.1%) had been prescribed androgen deprivation therapy, traditional antiepileptic drugs, or glucocorticoids.
Over a mean follow-up of 1.5 years, there was a much higher screening rate in the BHS group (49.2% vs 2.3%; P < .001), with a similar overall yield of DXA results recommending osteoporosis treatment (22.4% vs 27.2%). In the BHS group, 84.4% of patients who had treatment recommended followed through with treatment initiation. The mean persistence over follow-up was 657 days (SD, 366 days), and adherence was high with a mean proportion of days covered of 91.7%.
It was not possible to statistically compare adherence with the usual-care group because there were too few screened patients found to be eligible for treatment in that group, but the historic mean proportion of days covered at the two participating facilities was 52%.
After 2 years, the mean femoral neck T-score tested randomly in a subset of patients was better in the BHS arm, although it did not meet statistical significance according to the Bonferroni corrected criterion of P < .025 (-0.55 vs -0.70; P = .04). Fracture rates were similar between the two groups (1.8% vs 2.0%; P = .69).
Can the Findings Be Translated Across Clinics?
It remains to be seen how well the model could translate to other healthcare settings, according to Kenny Lin, MD, MPH, who was asked for comment on the study. “Outside of the VA health system and perhaps integrated HMOs [health maintenance organizations] such as Kaiser, Geisinger, etc., it seems unlikely that most primary care docs will have access to a centralized bone health service. Who’s going to pay for it? It leaves unanswered the question of whether it’s more efficient to address [osteoporosis] screening on a practice or population level. I suspect the latter is probably superior, but this study doesn’t provide any empiric evidence that this is so,” said Lin, associate director of the Penn Medicine Lancaster General Hospital’s Family Medicine Residency Program, Lancaster, Pennsylvania. The findings could help sway recommendations to screen men for osteoporosis, according to Susan Ott, MD, who was also asked for comment. Guideline committees “have been trying to be very scientific [about it]. I think they overdo it because they only look at one or two kinds of studies, and there are more kinds of science than just a randomized clinical trial. But they’re kind of stuck on that. The fact that this study was a randomized trial maybe they will finally change their recommendation, because there really shouldn’t be any difference in screening for men and for women. The men are actually discriminated against,” said Ott, emeritus professor of medicine at the University of Washington, Seattle.
In fact, she noted that the risks for men are similar to those for women, except that men tend to develop issues 5-10 years later in life. To screen and treat men, healthcare systems can “do the same thing they do with women. Just change the age range,” Ott said.
Lin sounded a different note, suggesting that the focus should remain on improvement of screening and treatment adherence in women. “We know that up to two thirds of women discontinue osteoporosis drugs within a year, and if we can’t figure out how to improve abysmal adherence in women, it’s unlikely we will persuade enough men to take these drugs to make a difference,” he said.
The study was funded by a grant from the VA Health Systems Research. Colón-Emeric, Lin, Ott, and Huang reported having no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
Efforts to identify older men at risk for osteoporosis and treat those who are eligible received a boost from results reported from a Veterans Affairs (VA) study that showed a significant increase in screening, treatment, and medication adherence.
The cluster randomized trial used a centralized nurse-led intervention to assess men for traditional osteoporosis risk factors, offer bone density testing, and recommend treatment for eligible men. Over 2 years, the intervention group had a higher average femoral neck bone density than patients who underwent usual care.
“We designed this study to see if a risk factor-based approach, which is what most of the guidelines use, made sense and was feasible — that men would be accepting of screening and [the approach] would yield a similar proportion of people who need osteoporosis treatment as screening in women, which is widely recommended and implemented. And sure enough, we found that about 85% of the men in the VA primary care practices in our target age range of between 65 and 85 actually met criteria for screening, and over half of them had low bone mass. They were very accepting of screening, very accepting of treatment, and had excellent compliance rates. So, our study, we believe, supports the idea of identifying men with at least one risk factor for fracture and offering them osteoporosis screening starting at age 65, similar to what we do for women,” Cathleen S. Colón-Emeric, MD, MHS, said in an interview. She is the lead author of the study, a physician in the Durham VA Health Care System, and professor of medicine at Duke University School of Medicine, Durham, North Carolina.
“We were able to see a positive effect on bone density in the bone health group, compared with the usual care group, which suggests that if we followed these folks longer and had enough of them, we would be able to show a fracture reduction benefit,” Colón-Emeric said.
There have been few randomized trials of screening interventions in men, leading to inconsistencies in guidelines, according to the authors of the new study, published online in JAMA Internal Medicine . Both the US Preventive Services Task Force and the Veterans Health Administration National Center for Health Promotion and Disease Prevention consider there to be insufficient evidence to recommend for or against screening in men who have not experienced a fracture. Some professional societies recommend such screening, but there are inconsistencies in the recommended criteria, such as age range or risk factors.
Beyond the age of 50 years, one in five men will experience an osteoporosis-related fracture at some point in their life, according to a 2009 study. Treatment is inexpensive and effective in both men and women, and economic models suggest that screening using dual-energy x-ray absorptiometry (DXA) would be cost-effective. Still, screening is rare among men, with fewer than 10% of men getting screened before having an osteoporosis-related fracture.
“It’s important to screen men at risk for osteoporosis due to the dramatically increased mortality men suffer after a fragility fracture compared with women. Within 1 year of a hip fracture, mortality is as high as 36%. Studies have also shown that osteoporosis in men is undertreated, with only 10%-50% being prescribed antifracture treatment within 1 year of a hip fracture. Most individuals do not regain their prior level of function after a hip fracture,” said Joe C. Huang, MD, who was asked for comment. He is a clinical assistant professor of gerontology and geriatric medicine at Harborview Medical Center Senior Care Clinic and Healthy Bones Clinic in Seattle.
Details of the Intervention
The bone health service (BHS) intervention employed an electronic health record case-finding tool and a nurse care manager who undertook screening and treatment monitoring. They identified potential risk factors that included hyperthyroidism, hyperparathyroidism, rheumatoid arthritis, alcohol dependence, chronic lung disease, chronic liver disease, stroke, parkinsonism, prostate cancer, smoking, diabetes, pernicious anemia, gastrectomy, or high-risk medication use in at least 3 months of the prior 2 years. These medications included traditional antiepileptics, glucocorticoids, and androgen deprivation therapy.
The BHS nurse invited eligible men to be screened using an initial letter, followed by up to three phone calls. After DXA screening, the nurse scheduled an electronic consult with an osteoporosis expert, and patients with a T-score between -1 and -2.4 and an elevated 10-year fracture risk as measured by the Fracture Risk Assessment Tool were recommended for osteoporosis medication, vitamin D, and dietary or supplemental calcium. Following the prescription, the nurse provided patient education over the phone and mailed out written instructions. The nurse also made phone calls at 1 month, 6 months, and 12 months to encourage adherence and address common treatment barriers such as forgetting to take medication or dealing with gastrointestinal effects. The researchers recruited 38 primary care physicians from two VA health systems. The study included 3112 male veterans between the ages of 65 and 85 years (40.4% Black and 56% White). Nearly all participants (85.5%) had at least one indication for screening according to VA undersecretary guidelines, and almost a third (32.1%) had been prescribed androgen deprivation therapy, traditional antiepileptic drugs, or glucocorticoids.
Over a mean follow-up of 1.5 years, there was a much higher screening rate in the BHS group (49.2% vs 2.3%; P < .001), with a similar overall yield of DXA results recommending osteoporosis treatment (22.4% vs 27.2%). In the BHS group, 84.4% of patients who had treatment recommended followed through with treatment initiation. The mean persistence over follow-up was 657 days (SD, 366 days), and adherence was high with a mean proportion of days covered of 91.7%.
It was not possible to statistically compare adherence with the usual-care group because there were too few screened patients found to be eligible for treatment in that group, but the historic mean proportion of days covered at the two participating facilities was 52%.
After 2 years, the mean femoral neck T-score tested randomly in a subset of patients was better in the BHS arm, although it did not meet statistical significance according to the Bonferroni corrected criterion of P < .025 (-0.55 vs -0.70; P = .04). Fracture rates were similar between the two groups (1.8% vs 2.0%; P = .69).
Can the Findings Be Translated Across Clinics?
It remains to be seen how well the model could translate to other healthcare settings, according to Kenny Lin, MD, MPH, who was asked for comment on the study. “Outside of the VA health system and perhaps integrated HMOs [health maintenance organizations] such as Kaiser, Geisinger, etc., it seems unlikely that most primary care docs will have access to a centralized bone health service. Who’s going to pay for it? It leaves unanswered the question of whether it’s more efficient to address [osteoporosis] screening on a practice or population level. I suspect the latter is probably superior, but this study doesn’t provide any empiric evidence that this is so,” said Lin, associate director of the Penn Medicine Lancaster General Hospital’s Family Medicine Residency Program, Lancaster, Pennsylvania. The findings could help sway recommendations to screen men for osteoporosis, according to Susan Ott, MD, who was also asked for comment. Guideline committees “have been trying to be very scientific [about it]. I think they overdo it because they only look at one or two kinds of studies, and there are more kinds of science than just a randomized clinical trial. But they’re kind of stuck on that. The fact that this study was a randomized trial maybe they will finally change their recommendation, because there really shouldn’t be any difference in screening for men and for women. The men are actually discriminated against,” said Ott, emeritus professor of medicine at the University of Washington, Seattle.
In fact, she noted that the risks for men are similar to those for women, except that men tend to develop issues 5-10 years later in life. To screen and treat men, healthcare systems can “do the same thing they do with women. Just change the age range,” Ott said.
Lin sounded a different note, suggesting that the focus should remain on improvement of screening and treatment adherence in women. “We know that up to two thirds of women discontinue osteoporosis drugs within a year, and if we can’t figure out how to improve abysmal adherence in women, it’s unlikely we will persuade enough men to take these drugs to make a difference,” he said.
The study was funded by a grant from the VA Health Systems Research. Colón-Emeric, Lin, Ott, and Huang reported having no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
Efforts to identify older men at risk for osteoporosis and treat those who are eligible received a boost from results reported from a Veterans Affairs (VA) study that showed a significant increase in screening, treatment, and medication adherence.
The cluster randomized trial used a centralized nurse-led intervention to assess men for traditional osteoporosis risk factors, offer bone density testing, and recommend treatment for eligible men. Over 2 years, the intervention group had a higher average femoral neck bone density than patients who underwent usual care.
“We designed this study to see if a risk factor-based approach, which is what most of the guidelines use, made sense and was feasible — that men would be accepting of screening and [the approach] would yield a similar proportion of people who need osteoporosis treatment as screening in women, which is widely recommended and implemented. And sure enough, we found that about 85% of the men in the VA primary care practices in our target age range of between 65 and 85 actually met criteria for screening, and over half of them had low bone mass. They were very accepting of screening, very accepting of treatment, and had excellent compliance rates. So, our study, we believe, supports the idea of identifying men with at least one risk factor for fracture and offering them osteoporosis screening starting at age 65, similar to what we do for women,” Cathleen S. Colón-Emeric, MD, MHS, said in an interview. She is the lead author of the study, a physician in the Durham VA Health Care System, and professor of medicine at Duke University School of Medicine, Durham, North Carolina.
“We were able to see a positive effect on bone density in the bone health group, compared with the usual care group, which suggests that if we followed these folks longer and had enough of them, we would be able to show a fracture reduction benefit,” Colón-Emeric said.
There have been few randomized trials of screening interventions in men, leading to inconsistencies in guidelines, according to the authors of the new study, published online in JAMA Internal Medicine . Both the US Preventive Services Task Force and the Veterans Health Administration National Center for Health Promotion and Disease Prevention consider there to be insufficient evidence to recommend for or against screening in men who have not experienced a fracture. Some professional societies recommend such screening, but there are inconsistencies in the recommended criteria, such as age range or risk factors.
Beyond the age of 50 years, one in five men will experience an osteoporosis-related fracture at some point in their life, according to a 2009 study. Treatment is inexpensive and effective in both men and women, and economic models suggest that screening using dual-energy x-ray absorptiometry (DXA) would be cost-effective. Still, screening is rare among men, with fewer than 10% of men getting screened before having an osteoporosis-related fracture.
“It’s important to screen men at risk for osteoporosis due to the dramatically increased mortality men suffer after a fragility fracture compared with women. Within 1 year of a hip fracture, mortality is as high as 36%. Studies have also shown that osteoporosis in men is undertreated, with only 10%-50% being prescribed antifracture treatment within 1 year of a hip fracture. Most individuals do not regain their prior level of function after a hip fracture,” said Joe C. Huang, MD, who was asked for comment. He is a clinical assistant professor of gerontology and geriatric medicine at Harborview Medical Center Senior Care Clinic and Healthy Bones Clinic in Seattle.
Details of the Intervention
The bone health service (BHS) intervention employed an electronic health record case-finding tool and a nurse care manager who undertook screening and treatment monitoring. They identified potential risk factors that included hyperthyroidism, hyperparathyroidism, rheumatoid arthritis, alcohol dependence, chronic lung disease, chronic liver disease, stroke, parkinsonism, prostate cancer, smoking, diabetes, pernicious anemia, gastrectomy, or high-risk medication use in at least 3 months of the prior 2 years. These medications included traditional antiepileptics, glucocorticoids, and androgen deprivation therapy.
The BHS nurse invited eligible men to be screened using an initial letter, followed by up to three phone calls. After DXA screening, the nurse scheduled an electronic consult with an osteoporosis expert, and patients with a T-score between -1 and -2.4 and an elevated 10-year fracture risk as measured by the Fracture Risk Assessment Tool were recommended for osteoporosis medication, vitamin D, and dietary or supplemental calcium. Following the prescription, the nurse provided patient education over the phone and mailed out written instructions. The nurse also made phone calls at 1 month, 6 months, and 12 months to encourage adherence and address common treatment barriers such as forgetting to take medication or dealing with gastrointestinal effects. The researchers recruited 38 primary care physicians from two VA health systems. The study included 3112 male veterans between the ages of 65 and 85 years (40.4% Black and 56% White). Nearly all participants (85.5%) had at least one indication for screening according to VA undersecretary guidelines, and almost a third (32.1%) had been prescribed androgen deprivation therapy, traditional antiepileptic drugs, or glucocorticoids.
Over a mean follow-up of 1.5 years, there was a much higher screening rate in the BHS group (49.2% vs 2.3%; P < .001), with a similar overall yield of DXA results recommending osteoporosis treatment (22.4% vs 27.2%). In the BHS group, 84.4% of patients who had treatment recommended followed through with treatment initiation. The mean persistence over follow-up was 657 days (SD, 366 days), and adherence was high with a mean proportion of days covered of 91.7%.
It was not possible to statistically compare adherence with the usual-care group because there were too few screened patients found to be eligible for treatment in that group, but the historic mean proportion of days covered at the two participating facilities was 52%.
After 2 years, the mean femoral neck T-score tested randomly in a subset of patients was better in the BHS arm, although it did not meet statistical significance according to the Bonferroni corrected criterion of P < .025 (-0.55 vs -0.70; P = .04). Fracture rates were similar between the two groups (1.8% vs 2.0%; P = .69).
Can the Findings Be Translated Across Clinics?
It remains to be seen how well the model could translate to other healthcare settings, according to Kenny Lin, MD, MPH, who was asked for comment on the study. “Outside of the VA health system and perhaps integrated HMOs [health maintenance organizations] such as Kaiser, Geisinger, etc., it seems unlikely that most primary care docs will have access to a centralized bone health service. Who’s going to pay for it? It leaves unanswered the question of whether it’s more efficient to address [osteoporosis] screening on a practice or population level. I suspect the latter is probably superior, but this study doesn’t provide any empiric evidence that this is so,” said Lin, associate director of the Penn Medicine Lancaster General Hospital’s Family Medicine Residency Program, Lancaster, Pennsylvania. The findings could help sway recommendations to screen men for osteoporosis, according to Susan Ott, MD, who was also asked for comment. Guideline committees “have been trying to be very scientific [about it]. I think they overdo it because they only look at one or two kinds of studies, and there are more kinds of science than just a randomized clinical trial. But they’re kind of stuck on that. The fact that this study was a randomized trial maybe they will finally change their recommendation, because there really shouldn’t be any difference in screening for men and for women. The men are actually discriminated against,” said Ott, emeritus professor of medicine at the University of Washington, Seattle.
In fact, she noted that the risks for men are similar to those for women, except that men tend to develop issues 5-10 years later in life. To screen and treat men, healthcare systems can “do the same thing they do with women. Just change the age range,” Ott said.
Lin sounded a different note, suggesting that the focus should remain on improvement of screening and treatment adherence in women. “We know that up to two thirds of women discontinue osteoporosis drugs within a year, and if we can’t figure out how to improve abysmal adherence in women, it’s unlikely we will persuade enough men to take these drugs to make a difference,” he said.
The study was funded by a grant from the VA Health Systems Research. Colón-Emeric, Lin, Ott, and Huang reported having no relevant financial disclosures.
A version of this article first appeared on Medscape.com.

U.S. Health Chief Kennedy Targets Vaccine Injury Compensation Program
WASHINGTON (Reuters) - U.S. Health Secretary Robert F. Kennedy Jr. said on July 28 that he will work to “fix” the program that compensates victims of vaccine injuries, the National Vaccine Injury Compensation Program.
Kennedy, a long-time vaccine skeptic and former vaccine injury plaintiff lawyer, accused the program and its so-called “Vaccine Court” of corruption and inefficiency in a post on X. He has long been an outspoken critic of the program.
“I will not allow the VICP to continue to ignore its mandate and fail its mission of quickly and fairly compensating vaccine-injured individuals,” he wrote, adding he was working with Attorney General Pam Bondi. “Together, we will steer the Vaccine Court back to its original congressional intent.”
He said the structure disadvantaged claimants because the Department of Health & Human Services – which he now leads – is the defendant, as opposed to vaccine makers.
Changing the VICP would be the latest in a series of far-reaching actions by Kennedy to reshape U.S. regulation of vaccines, food and medicine.
In June, he fired all 17 members of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices, a panel of vaccine experts, replacing them with 7 handpicked members, including known vaccine skeptics.
One of them earned thousands of dollars as an expert witness in litigation against Merck’s, Gardasil vaccine, court records show. Kennedy himself played an instrumental role in organizing mass litigation over the vaccine.
He also is planning to remove all the members of another advisory panel that determines what preventive health measures insurers must cover, the Wall Street Journal reported on July 25. An HHS spokesperson said Kennedy had not yet made a decision regarding the 16-member U.S. Preventive Services Task Force.
Kennedy has for years sown doubt about the safety and efficacy of vaccines. He has a history of clashing with the medical establishment and spreading misinformation about vaccines, including promoting a debunked link between vaccines and autism despite scientific evidence to the contrary.
He has also said the measles vaccine contains cells from aborted fetuses and that the mumps vaccination does not work, comments he made as the U.S. battles one of its worst outbreaks of measles in 25 years.
Kennedy made millions over the years from advocating against vaccines through case referrals, book sales, and consulting fees paid by a nonprofit he founded, according to ethics disclosures.
(Reporting by Ahmed Aboulenein; Additional reporting by Ryan Patrick Jones in Toronto; Editing by Doina Chiacu and Nia Williams)
A version of this article appeared on Medscape.com.
WASHINGTON (Reuters) - U.S. Health Secretary Robert F. Kennedy Jr. said on July 28 that he will work to “fix” the program that compensates victims of vaccine injuries, the National Vaccine Injury Compensation Program.
Kennedy, a long-time vaccine skeptic and former vaccine injury plaintiff lawyer, accused the program and its so-called “Vaccine Court” of corruption and inefficiency in a post on X. He has long been an outspoken critic of the program.
“I will not allow the VICP to continue to ignore its mandate and fail its mission of quickly and fairly compensating vaccine-injured individuals,” he wrote, adding he was working with Attorney General Pam Bondi. “Together, we will steer the Vaccine Court back to its original congressional intent.”
He said the structure disadvantaged claimants because the Department of Health & Human Services – which he now leads – is the defendant, as opposed to vaccine makers.
Changing the VICP would be the latest in a series of far-reaching actions by Kennedy to reshape U.S. regulation of vaccines, food and medicine.
In June, he fired all 17 members of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices, a panel of vaccine experts, replacing them with 7 handpicked members, including known vaccine skeptics.
One of them earned thousands of dollars as an expert witness in litigation against Merck’s, Gardasil vaccine, court records show. Kennedy himself played an instrumental role in organizing mass litigation over the vaccine.
He also is planning to remove all the members of another advisory panel that determines what preventive health measures insurers must cover, the Wall Street Journal reported on July 25. An HHS spokesperson said Kennedy had not yet made a decision regarding the 16-member U.S. Preventive Services Task Force.
Kennedy has for years sown doubt about the safety and efficacy of vaccines. He has a history of clashing with the medical establishment and spreading misinformation about vaccines, including promoting a debunked link between vaccines and autism despite scientific evidence to the contrary.
He has also said the measles vaccine contains cells from aborted fetuses and that the mumps vaccination does not work, comments he made as the U.S. battles one of its worst outbreaks of measles in 25 years.
Kennedy made millions over the years from advocating against vaccines through case referrals, book sales, and consulting fees paid by a nonprofit he founded, according to ethics disclosures.
(Reporting by Ahmed Aboulenein; Additional reporting by Ryan Patrick Jones in Toronto; Editing by Doina Chiacu and Nia Williams)
A version of this article appeared on Medscape.com.
WASHINGTON (Reuters) - U.S. Health Secretary Robert F. Kennedy Jr. said on July 28 that he will work to “fix” the program that compensates victims of vaccine injuries, the National Vaccine Injury Compensation Program.
Kennedy, a long-time vaccine skeptic and former vaccine injury plaintiff lawyer, accused the program and its so-called “Vaccine Court” of corruption and inefficiency in a post on X. He has long been an outspoken critic of the program.
“I will not allow the VICP to continue to ignore its mandate and fail its mission of quickly and fairly compensating vaccine-injured individuals,” he wrote, adding he was working with Attorney General Pam Bondi. “Together, we will steer the Vaccine Court back to its original congressional intent.”
He said the structure disadvantaged claimants because the Department of Health & Human Services – which he now leads – is the defendant, as opposed to vaccine makers.
Changing the VICP would be the latest in a series of far-reaching actions by Kennedy to reshape U.S. regulation of vaccines, food and medicine.
In June, he fired all 17 members of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices, a panel of vaccine experts, replacing them with 7 handpicked members, including known vaccine skeptics.
One of them earned thousands of dollars as an expert witness in litigation against Merck’s, Gardasil vaccine, court records show. Kennedy himself played an instrumental role in organizing mass litigation over the vaccine.
He also is planning to remove all the members of another advisory panel that determines what preventive health measures insurers must cover, the Wall Street Journal reported on July 25. An HHS spokesperson said Kennedy had not yet made a decision regarding the 16-member U.S. Preventive Services Task Force.
Kennedy has for years sown doubt about the safety and efficacy of vaccines. He has a history of clashing with the medical establishment and spreading misinformation about vaccines, including promoting a debunked link between vaccines and autism despite scientific evidence to the contrary.
He has also said the measles vaccine contains cells from aborted fetuses and that the mumps vaccination does not work, comments he made as the U.S. battles one of its worst outbreaks of measles in 25 years.
Kennedy made millions over the years from advocating against vaccines through case referrals, book sales, and consulting fees paid by a nonprofit he founded, according to ethics disclosures.
(Reporting by Ahmed Aboulenein; Additional reporting by Ryan Patrick Jones in Toronto; Editing by Doina Chiacu and Nia Williams)
A version of this article appeared on Medscape.com.

Rurality and Age May Shape Phone-Only Mental Health Care Access Among Veterans
TOPLINE:
Patients living in rural areas and those aged ≥ 65 y had increased odds of receiving mental health care exclusively by phone.
METHODOLOGY:
- Researchers explored factors linked to receiving phone-only mental health care among patients within the Department of Veterans Affairs.
- They included data for 1,156,146 veteran patients with at least one mental health-specific outpatient encounter between October 2021 and September 2022 and at least one between October 2022 and September 2023.
- Patients were categorized as those who received care through phone only (n = 49,125) and those who received care through other methods (n = 1,107,021. Care was received exclusively through video (6.39%), in-person (6.63%), or a combination of in-person, video, and/or phone (86.98%).
- Demographic and clinical predictors, including rurality, age, sex, race, ethnicity, and the number of mental health diagnoses (< 3 vs ≥ 3), were evaluated.
TAKEAWAY:
- The phone-only group had a mean of 6.27 phone visits, whereas those who received care through other methods had a mean of 4.79 phone visits.
- Highly rural patients had 1.50 times higher odds of receiving phone-only mental health care than their urban counterparts (adjusted odds ratio [aOR], 1.50; P < .0001).
- Patients aged 65 years or older were more than twice as likely to receive phone-only care than those younger than 30 years (aOR, ≥ 2.17; P < .0001).
- Having fewer than three mental health diagnoses and more than 50% of mental health visits conducted by medical providers was associated with higher odds of receiving mental health care exclusively by phone (aORs, 2.03 and 1.87, respectively; P < .0001).
IN PRACTICE:
“The results of this work help to characterize the phone-only patient population and can serve to inform future implementation efforts to ensure that patients are receiving care via the modality that best meets their needs,” the authors wrote.
SOURCE:
This study was led by Samantha L. Connolly, PhD, at the VA Boston Healthcare System in Boston. It was published online in The Journal of Rural Health.
LIMITATIONS:
This study focused on a veteran population which may limit the generalizability of the findings to other groups. Additionally, its cross-sectional design restricted the ability to determine cause-and-effect relationships between factors and phone-only care.
DISCLOSURES:
This study was supported by the US Department of Veterans Affairs. The authors declared having no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
Patients living in rural areas and those aged ≥ 65 y had increased odds of receiving mental health care exclusively by phone.
METHODOLOGY:
- Researchers explored factors linked to receiving phone-only mental health care among patients within the Department of Veterans Affairs.
- They included data for 1,156,146 veteran patients with at least one mental health-specific outpatient encounter between October 2021 and September 2022 and at least one between October 2022 and September 2023.
- Patients were categorized as those who received care through phone only (n = 49,125) and those who received care through other methods (n = 1,107,021. Care was received exclusively through video (6.39%), in-person (6.63%), or a combination of in-person, video, and/or phone (86.98%).
- Demographic and clinical predictors, including rurality, age, sex, race, ethnicity, and the number of mental health diagnoses (< 3 vs ≥ 3), were evaluated.
TAKEAWAY:
- The phone-only group had a mean of 6.27 phone visits, whereas those who received care through other methods had a mean of 4.79 phone visits.
- Highly rural patients had 1.50 times higher odds of receiving phone-only mental health care than their urban counterparts (adjusted odds ratio [aOR], 1.50; P < .0001).
- Patients aged 65 years or older were more than twice as likely to receive phone-only care than those younger than 30 years (aOR, ≥ 2.17; P < .0001).
- Having fewer than three mental health diagnoses and more than 50% of mental health visits conducted by medical providers was associated with higher odds of receiving mental health care exclusively by phone (aORs, 2.03 and 1.87, respectively; P < .0001).
IN PRACTICE:
“The results of this work help to characterize the phone-only patient population and can serve to inform future implementation efforts to ensure that patients are receiving care via the modality that best meets their needs,” the authors wrote.
SOURCE:
This study was led by Samantha L. Connolly, PhD, at the VA Boston Healthcare System in Boston. It was published online in The Journal of Rural Health.
LIMITATIONS:
This study focused on a veteran population which may limit the generalizability of the findings to other groups. Additionally, its cross-sectional design restricted the ability to determine cause-and-effect relationships between factors and phone-only care.
DISCLOSURES:
This study was supported by the US Department of Veterans Affairs. The authors declared having no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.
TOPLINE:
Patients living in rural areas and those aged ≥ 65 y had increased odds of receiving mental health care exclusively by phone.
METHODOLOGY:
- Researchers explored factors linked to receiving phone-only mental health care among patients within the Department of Veterans Affairs.
- They included data for 1,156,146 veteran patients with at least one mental health-specific outpatient encounter between October 2021 and September 2022 and at least one between October 2022 and September 2023.
- Patients were categorized as those who received care through phone only (n = 49,125) and those who received care through other methods (n = 1,107,021. Care was received exclusively through video (6.39%), in-person (6.63%), or a combination of in-person, video, and/or phone (86.98%).
- Demographic and clinical predictors, including rurality, age, sex, race, ethnicity, and the number of mental health diagnoses (< 3 vs ≥ 3), were evaluated.
TAKEAWAY:
- The phone-only group had a mean of 6.27 phone visits, whereas those who received care through other methods had a mean of 4.79 phone visits.
- Highly rural patients had 1.50 times higher odds of receiving phone-only mental health care than their urban counterparts (adjusted odds ratio [aOR], 1.50; P < .0001).
- Patients aged 65 years or older were more than twice as likely to receive phone-only care than those younger than 30 years (aOR, ≥ 2.17; P < .0001).
- Having fewer than three mental health diagnoses and more than 50% of mental health visits conducted by medical providers was associated with higher odds of receiving mental health care exclusively by phone (aORs, 2.03 and 1.87, respectively; P < .0001).
IN PRACTICE:
“The results of this work help to characterize the phone-only patient population and can serve to inform future implementation efforts to ensure that patients are receiving care via the modality that best meets their needs,” the authors wrote.
SOURCE:
This study was led by Samantha L. Connolly, PhD, at the VA Boston Healthcare System in Boston. It was published online in The Journal of Rural Health.
LIMITATIONS:
This study focused on a veteran population which may limit the generalizability of the findings to other groups. Additionally, its cross-sectional design restricted the ability to determine cause-and-effect relationships between factors and phone-only care.
DISCLOSURES:
This study was supported by the US Department of Veterans Affairs. The authors declared having no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.
A version of this article first appeared on Medscape.com.

Searching for the Optimal CRC Surveillance Test
About a third of the US population are eligible for colorectal cancer screening but aren’t up to date on screening.
Many patients are reluctant to test for colon cancer for a variety of reasons, said Jeffrey K. Lee, MD, MPH, a research scientist at the Kaiser Permanente Northern California Division of Research and an attending gastroenterologist at Kaiser Permanente San Francisco Medical Center.
“As a gastroenterologist, I strongly believe we should emphasize the importance of colorectal cancer screening. And there’s many tests available, not just a colonoscopy, to help reduce your chances of developing colorectal cancer and even dying from colorectal cancer,” said Dr. Lee.
Many patients prefer a test that’s more convenient, that doesn’t require them to take time out of their busy schedules. “We must educate our patients that there are some noninvasive screening options that are helpful, and to be able to share with them some of the benefits, but also some of the drawbacks compared to colonoscopy and allow them to have a choice,” he advised.

He is a recipient of the AGA Research Scholar Award, and has in turn supported other researchers by contributing to the AGA Research Foundation. In 2012, Dr. Lee received a grant from the Sylvia Allison Kaplan Clinical Research Fund to fund a study on long-term colorectal cancer risk in patients with normal colonoscopy results.
The findings, published in JAMA Internal Medicine, determined that 10 years after a negative colonoscopy, Kaiser Permanente members had a 46% lower risk of being diagnosed with CRC and were 88% less likely to die from disease compared with patients who didn’t undergo screening.
“Furthermore, the reduced risk of developing colorectal cancer, even dying from it, persisted for more than 12 years after the examination compared with an unscreened population,” said Dr. Lee. “I firmly believe our study really supports the ten-year screening interval after a normal colonoscopy, as currently recommended by our guidelines.”
In an interview, he discussed his research efforts to find the best detection regimens for CRC, and the mentors who guided his career path as a GI scientist.
Q: Why did you choose GI?
During medical school I was fortunate to work in the lab of Dr. John M. Carethers at UC San Diego. He introduced me to GI and inspired me to choose GI as a career. His mentorship was invaluable because he not only solidified my interest in GI, but also inspired me to become a physician scientist, focusing on colorectal cancer prevention and control. His amazing mentorship drew me to this field.
Q: One of your clinical focus areas is hereditary gastrointestinal cancer syndromes. How did you become interested in this area of GI medicine?
My interest in hereditary GI cancer syndromes stemmed from my work as a medical student in Dr. Carethers’ lab. One of my research projects was looking at certain gene mutations among patients with hereditary GI cancer syndromes, specifically, familial hamartomatous polyposis syndrome. It was through these research projects and seeing how these genetic mutations impacted their risk of developing colorectal cancer, inspired me to care for patients with hereditary GI cancer syndromes.
Q: Have you been doing any research on the reasons why more young people are getting colon cancer?
We recently published work looking at the potential factors that may be driving the rising rates of early onset colorectal cancer. One hypothesis that’s been floating around is antibiotic exposure in early adulthood or childhood because of its effect on the microbiome. Using our large database at Kaiser Permanente Northern California, we did not find an association between oral antibiotic use during early adulthood and the risk of early-onset colorectal cancer.
You have the usual suspects like obesity and diabetes, but it’s not explaining all that risk. While familial colorectal cancer syndromes contribute to a small proportion of early-onset colorectal, these syndromes are not increasing across generations. I really do feel it’s something in the diet or how foods are processed and environmental factors that’s driving some of the risk of early onset colorectal cancer and this should be explored further.
Q: In 2018, you issued a landmark study which found an association between a 10-year follow-up after negative colonoscopy and reduced risk of disease and mortality. Has there been any updates to these findings over the last 6 years?
We recently saw a study in JAMA Oncology of a Swedish cohort that showed a negative colonoscopy result was associated with a reduced risk of developing and even dying from colorectal cancer 15 years from that examination, compared to the general population of Sweden. I think there’s some things that we need to be cautious about regarding that study. We have to think about the comparison group that they used and the lack of information regarding the indication of the colonoscopy and the quality of the examination. So, it remains uncertain whether future guidelines are going to stretch out that 10-year interval to 15 years.
Q: What other CRC studies are you working on now?
We have several studies that we are working on right now. One is called the PREVENT CRC study, which is looking at whether a polygenic risk score can improve risk stratification following adenoma removal for colorectal cancer prevention and tailoring post-polypectomy surveillance. This is a large observational cohort study that we have teamed up with the Fred Hutchinson Cancer Center, Erasmus University, and Kaiser Permanente Northwest to answer this important question that may have implications for personalized medicine.
Then there’s the COOP study, funded by the Patient-Centered Outcomes Research Institute. This is looking at the best surveillance test to use among older adults 65 years and older with a history of polyps. The trial is randomizing them to either getting a colonoscopy for surveillance or annual fecal immunochemical test (FIT) for surveillance. This is to see which test is best for detecting colorectal cancer among older adults with a history of polyps.
Q: Do you think FIT tests could eventually replace colonoscopy, given that it’s less invasive?
Although FIT and other stool-based tests are less invasive and have been shown to have high accuracy for detecting colorectal cancer, I personally do not think they are going to replace colonoscopy as the most popular screening modality in the United States. Colonoscopy remains the gold standard for detecting and removing precancerous polyps and has the highest accuracy for detecting colorectal cancer.
Q: Besides Dr. Carethers, what teacher or mentor had the greatest impact on you?
Clinically it’s been Dr. Jonathan Terdiman from UCSF, who taught me everything I know about clinical GI, and the art of colonoscopy. In addition, Douglas A. Corley, MD, PhD, the Permanente Medical Group’s chief research officer, has made the greatest impact on my research career. He’s really taught me how to rigorously design a research study to answer important clinically relevant questions, and has given me the skill set to write NIH grants. I would not be here without these mentors who are truly giants in the field of GI.
Q: When you’re not being a GI, how do you spend your free weekend afternoons? Are you still a “Cal Bears” fan at your alma mater, UC Berkeley?
I spend a lot of time taking my kids to their activities on the weekends. I just took my son to a Cal Bears Game Day, which was hosted by ESPN at Berkeley.

It was an incredible experience hearing sports analyst Pat McAfee lead all the Cal chants, seeing Nick Saban from the University of Alabama take off his red tie and replace it with a Cal Bears tie, and watching a Cal student win a hundred thousand dollars by kicking a football through the goal posts wearing checkered vans.
Lightning Round
Texting or talking?
Text
Favorite breakfast?
Taiwanese breakfast
Place you most want to travel to?
Japan
Favorite junk food?
Trader Joe’s chili lime chips
Favorite season?
Springtime, baseball season
Favorite ice cream flavor?
Mint chocolate chip
How many cups of coffee do you drink per day?
2-3
Last movie you watched?
Oppenheimer
Best place you ever went on vacation?
Hawaii
If you weren’t a gastroenterologist, what would you be?
Barber
Best Halloween costume you ever wore?
SpongeBob SquarePants
Favorite sport?
Tennis
What song do you have to sing along with when you hear it?
Any classic 80s song
Introvert or extrovert?
Introvert
About a third of the US population are eligible for colorectal cancer screening but aren’t up to date on screening.
Many patients are reluctant to test for colon cancer for a variety of reasons, said Jeffrey K. Lee, MD, MPH, a research scientist at the Kaiser Permanente Northern California Division of Research and an attending gastroenterologist at Kaiser Permanente San Francisco Medical Center.
“As a gastroenterologist, I strongly believe we should emphasize the importance of colorectal cancer screening. And there’s many tests available, not just a colonoscopy, to help reduce your chances of developing colorectal cancer and even dying from colorectal cancer,” said Dr. Lee.
Many patients prefer a test that’s more convenient, that doesn’t require them to take time out of their busy schedules. “We must educate our patients that there are some noninvasive screening options that are helpful, and to be able to share with them some of the benefits, but also some of the drawbacks compared to colonoscopy and allow them to have a choice,” he advised.
He is a recipient of the AGA Research Scholar Award, and has in turn supported other researchers by contributing to the AGA Research Foundation. In 2012, Dr. Lee received a grant from the Sylvia Allison Kaplan Clinical Research Fund to fund a study on long-term colorectal cancer risk in patients with normal colonoscopy results.
The findings, published in JAMA Internal Medicine, determined that 10 years after a negative colonoscopy, Kaiser Permanente members had a 46% lower risk of being diagnosed with CRC and were 88% less likely to die from disease compared with patients who didn’t undergo screening.
“Furthermore, the reduced risk of developing colorectal cancer, even dying from it, persisted for more than 12 years after the examination compared with an unscreened population,” said Dr. Lee. “I firmly believe our study really supports the ten-year screening interval after a normal colonoscopy, as currently recommended by our guidelines.”
In an interview, he discussed his research efforts to find the best detection regimens for CRC, and the mentors who guided his career path as a GI scientist.
Q: Why did you choose GI?
During medical school I was fortunate to work in the lab of Dr. John M. Carethers at UC San Diego. He introduced me to GI and inspired me to choose GI as a career. His mentorship was invaluable because he not only solidified my interest in GI, but also inspired me to become a physician scientist, focusing on colorectal cancer prevention and control. His amazing mentorship drew me to this field.
Q: One of your clinical focus areas is hereditary gastrointestinal cancer syndromes. How did you become interested in this area of GI medicine?
My interest in hereditary GI cancer syndromes stemmed from my work as a medical student in Dr. Carethers’ lab. One of my research projects was looking at certain gene mutations among patients with hereditary GI cancer syndromes, specifically, familial hamartomatous polyposis syndrome. It was through these research projects and seeing how these genetic mutations impacted their risk of developing colorectal cancer, inspired me to care for patients with hereditary GI cancer syndromes.
Q: Have you been doing any research on the reasons why more young people are getting colon cancer?
We recently published work looking at the potential factors that may be driving the rising rates of early onset colorectal cancer. One hypothesis that’s been floating around is antibiotic exposure in early adulthood or childhood because of its effect on the microbiome. Using our large database at Kaiser Permanente Northern California, we did not find an association between oral antibiotic use during early adulthood and the risk of early-onset colorectal cancer.
You have the usual suspects like obesity and diabetes, but it’s not explaining all that risk. While familial colorectal cancer syndromes contribute to a small proportion of early-onset colorectal, these syndromes are not increasing across generations. I really do feel it’s something in the diet or how foods are processed and environmental factors that’s driving some of the risk of early onset colorectal cancer and this should be explored further.
Q: In 2018, you issued a landmark study which found an association between a 10-year follow-up after negative colonoscopy and reduced risk of disease and mortality. Has there been any updates to these findings over the last 6 years?
We recently saw a study in JAMA Oncology of a Swedish cohort that showed a negative colonoscopy result was associated with a reduced risk of developing and even dying from colorectal cancer 15 years from that examination, compared to the general population of Sweden. I think there’s some things that we need to be cautious about regarding that study. We have to think about the comparison group that they used and the lack of information regarding the indication of the colonoscopy and the quality of the examination. So, it remains uncertain whether future guidelines are going to stretch out that 10-year interval to 15 years.
Q: What other CRC studies are you working on now?
We have several studies that we are working on right now. One is called the PREVENT CRC study, which is looking at whether a polygenic risk score can improve risk stratification following adenoma removal for colorectal cancer prevention and tailoring post-polypectomy surveillance. This is a large observational cohort study that we have teamed up with the Fred Hutchinson Cancer Center, Erasmus University, and Kaiser Permanente Northwest to answer this important question that may have implications for personalized medicine.
Then there’s the COOP study, funded by the Patient-Centered Outcomes Research Institute. This is looking at the best surveillance test to use among older adults 65 years and older with a history of polyps. The trial is randomizing them to either getting a colonoscopy for surveillance or annual fecal immunochemical test (FIT) for surveillance. This is to see which test is best for detecting colorectal cancer among older adults with a history of polyps.
Q: Do you think FIT tests could eventually replace colonoscopy, given that it’s less invasive?
Although FIT and other stool-based tests are less invasive and have been shown to have high accuracy for detecting colorectal cancer, I personally do not think they are going to replace colonoscopy as the most popular screening modality in the United States. Colonoscopy remains the gold standard for detecting and removing precancerous polyps and has the highest accuracy for detecting colorectal cancer.
Q: Besides Dr. Carethers, what teacher or mentor had the greatest impact on you?
Clinically it’s been Dr. Jonathan Terdiman from UCSF, who taught me everything I know about clinical GI, and the art of colonoscopy. In addition, Douglas A. Corley, MD, PhD, the Permanente Medical Group’s chief research officer, has made the greatest impact on my research career. He’s really taught me how to rigorously design a research study to answer important clinically relevant questions, and has given me the skill set to write NIH grants. I would not be here without these mentors who are truly giants in the field of GI.
Q: When you’re not being a GI, how do you spend your free weekend afternoons? Are you still a “Cal Bears” fan at your alma mater, UC Berkeley?
I spend a lot of time taking my kids to their activities on the weekends. I just took my son to a Cal Bears Game Day, which was hosted by ESPN at Berkeley.
It was an incredible experience hearing sports analyst Pat McAfee lead all the Cal chants, seeing Nick Saban from the University of Alabama take off his red tie and replace it with a Cal Bears tie, and watching a Cal student win a hundred thousand dollars by kicking a football through the goal posts wearing checkered vans.
Lightning Round
Texting or talking?
Text
Favorite breakfast?
Taiwanese breakfast
Place you most want to travel to?
Japan
Favorite junk food?
Trader Joe’s chili lime chips
Favorite season?
Springtime, baseball season
Favorite ice cream flavor?
Mint chocolate chip
How many cups of coffee do you drink per day?
2-3
Last movie you watched?
Oppenheimer
Best place you ever went on vacation?
Hawaii
If you weren’t a gastroenterologist, what would you be?
Barber
Best Halloween costume you ever wore?
SpongeBob SquarePants
Favorite sport?
Tennis
What song do you have to sing along with when you hear it?
Any classic 80s song
Introvert or extrovert?
Introvert
About a third of the US population are eligible for colorectal cancer screening but aren’t up to date on screening.
Many patients are reluctant to test for colon cancer for a variety of reasons, said Jeffrey K. Lee, MD, MPH, a research scientist at the Kaiser Permanente Northern California Division of Research and an attending gastroenterologist at Kaiser Permanente San Francisco Medical Center.
“As a gastroenterologist, I strongly believe we should emphasize the importance of colorectal cancer screening. And there’s many tests available, not just a colonoscopy, to help reduce your chances of developing colorectal cancer and even dying from colorectal cancer,” said Dr. Lee.
Many patients prefer a test that’s more convenient, that doesn’t require them to take time out of their busy schedules. “We must educate our patients that there are some noninvasive screening options that are helpful, and to be able to share with them some of the benefits, but also some of the drawbacks compared to colonoscopy and allow them to have a choice,” he advised.
He is a recipient of the AGA Research Scholar Award, and has in turn supported other researchers by contributing to the AGA Research Foundation. In 2012, Dr. Lee received a grant from the Sylvia Allison Kaplan Clinical Research Fund to fund a study on long-term colorectal cancer risk in patients with normal colonoscopy results.
The findings, published in JAMA Internal Medicine, determined that 10 years after a negative colonoscopy, Kaiser Permanente members had a 46% lower risk of being diagnosed with CRC and were 88% less likely to die from disease compared with patients who didn’t undergo screening.
“Furthermore, the reduced risk of developing colorectal cancer, even dying from it, persisted for more than 12 years after the examination compared with an unscreened population,” said Dr. Lee. “I firmly believe our study really supports the ten-year screening interval after a normal colonoscopy, as currently recommended by our guidelines.”
In an interview, he discussed his research efforts to find the best detection regimens for CRC, and the mentors who guided his career path as a GI scientist.
Q: Why did you choose GI?
During medical school I was fortunate to work in the lab of Dr. John M. Carethers at UC San Diego. He introduced me to GI and inspired me to choose GI as a career. His mentorship was invaluable because he not only solidified my interest in GI, but also inspired me to become a physician scientist, focusing on colorectal cancer prevention and control. His amazing mentorship drew me to this field.
Q: One of your clinical focus areas is hereditary gastrointestinal cancer syndromes. How did you become interested in this area of GI medicine?
My interest in hereditary GI cancer syndromes stemmed from my work as a medical student in Dr. Carethers’ lab. One of my research projects was looking at certain gene mutations among patients with hereditary GI cancer syndromes, specifically, familial hamartomatous polyposis syndrome. It was through these research projects and seeing how these genetic mutations impacted their risk of developing colorectal cancer, inspired me to care for patients with hereditary GI cancer syndromes.
Q: Have you been doing any research on the reasons why more young people are getting colon cancer?
We recently published work looking at the potential factors that may be driving the rising rates of early onset colorectal cancer. One hypothesis that’s been floating around is antibiotic exposure in early adulthood or childhood because of its effect on the microbiome. Using our large database at Kaiser Permanente Northern California, we did not find an association between oral antibiotic use during early adulthood and the risk of early-onset colorectal cancer.
You have the usual suspects like obesity and diabetes, but it’s not explaining all that risk. While familial colorectal cancer syndromes contribute to a small proportion of early-onset colorectal, these syndromes are not increasing across generations. I really do feel it’s something in the diet or how foods are processed and environmental factors that’s driving some of the risk of early onset colorectal cancer and this should be explored further.
Q: In 2018, you issued a landmark study which found an association between a 10-year follow-up after negative colonoscopy and reduced risk of disease and mortality. Has there been any updates to these findings over the last 6 years?
We recently saw a study in JAMA Oncology of a Swedish cohort that showed a negative colonoscopy result was associated with a reduced risk of developing and even dying from colorectal cancer 15 years from that examination, compared to the general population of Sweden. I think there’s some things that we need to be cautious about regarding that study. We have to think about the comparison group that they used and the lack of information regarding the indication of the colonoscopy and the quality of the examination. So, it remains uncertain whether future guidelines are going to stretch out that 10-year interval to 15 years.
Q: What other CRC studies are you working on now?
We have several studies that we are working on right now. One is called the PREVENT CRC study, which is looking at whether a polygenic risk score can improve risk stratification following adenoma removal for colorectal cancer prevention and tailoring post-polypectomy surveillance. This is a large observational cohort study that we have teamed up with the Fred Hutchinson Cancer Center, Erasmus University, and Kaiser Permanente Northwest to answer this important question that may have implications for personalized medicine.
Then there’s the COOP study, funded by the Patient-Centered Outcomes Research Institute. This is looking at the best surveillance test to use among older adults 65 years and older with a history of polyps. The trial is randomizing them to either getting a colonoscopy for surveillance or annual fecal immunochemical test (FIT) for surveillance. This is to see which test is best for detecting colorectal cancer among older adults with a history of polyps.
Q: Do you think FIT tests could eventually replace colonoscopy, given that it’s less invasive?
Although FIT and other stool-based tests are less invasive and have been shown to have high accuracy for detecting colorectal cancer, I personally do not think they are going to replace colonoscopy as the most popular screening modality in the United States. Colonoscopy remains the gold standard for detecting and removing precancerous polyps and has the highest accuracy for detecting colorectal cancer.
Q: Besides Dr. Carethers, what teacher or mentor had the greatest impact on you?
Clinically it’s been Dr. Jonathan Terdiman from UCSF, who taught me everything I know about clinical GI, and the art of colonoscopy. In addition, Douglas A. Corley, MD, PhD, the Permanente Medical Group’s chief research officer, has made the greatest impact on my research career. He’s really taught me how to rigorously design a research study to answer important clinically relevant questions, and has given me the skill set to write NIH grants. I would not be here without these mentors who are truly giants in the field of GI.
Q: When you’re not being a GI, how do you spend your free weekend afternoons? Are you still a “Cal Bears” fan at your alma mater, UC Berkeley?
I spend a lot of time taking my kids to their activities on the weekends. I just took my son to a Cal Bears Game Day, which was hosted by ESPN at Berkeley.
It was an incredible experience hearing sports analyst Pat McAfee lead all the Cal chants, seeing Nick Saban from the University of Alabama take off his red tie and replace it with a Cal Bears tie, and watching a Cal student win a hundred thousand dollars by kicking a football through the goal posts wearing checkered vans.
Lightning Round
Texting or talking?
Text
Favorite breakfast?
Taiwanese breakfast
Place you most want to travel to?
Japan
Favorite junk food?
Trader Joe’s chili lime chips
Favorite season?
Springtime, baseball season
Favorite ice cream flavor?
Mint chocolate chip
How many cups of coffee do you drink per day?
2-3
Last movie you watched?
Oppenheimer
Best place you ever went on vacation?
Hawaii
If you weren’t a gastroenterologist, what would you be?
Barber
Best Halloween costume you ever wore?
SpongeBob SquarePants
Favorite sport?
Tennis
What song do you have to sing along with when you hear it?
Any classic 80s song
Introvert or extrovert?
Introvert

Clinical News Briefs
Clinical News Briefs
Randomized Trial Supports Sirolimus as Add-On Systemic Lupus Erythematosus Therapy
Adding sirolimus to standard treatment for active systemic lupus erythematosus improved disease control compared with placebo in a randomized phase 3 trial presented at the European Alliance of Associations for Rheumatology (EULAR) 2026 Annual Meeting. Patients receiving sirolimus were more likely to achieve a clinical response and showed greater improvement in disease activity and serologic markers. Treatment generally was well tolerated, although lipid abnormalities, leukopenia, and menstrual irregularities were more common. Sirolimus may become a useful oral option for refractory lupus, pending further confirmation and guidance.
Bimekizumab Trumps Risankizumab in Head-to-Head Psoriatic Arthritis Trial
Dual IL-17 blockade may offer greater joint benefit than IL-23 inhibition in psoriatic arthritis, potentially helping guide biologic selection for patients with skin and musculoskeletal disease. In the phase 3b BE BOLD trial, bimekizumab was more effective than risankizumab for joint disease, with more patients achieving a 50% improvement in American College of Rheumatology response criteria at 16 weeks. Bimekizumab also showed superior results across several secondary measures, including minimal disease activity and skin outcomes, while safety was broadly similar. The findings were presented at the EULAR 2026 Annual Meeting.
FDA Delays iPLEDGE Modifications Until November 2026
In a June 16 announcement, the US Food and Drug Administration said long-awaited modifications to the iPLEDGE Risk Evaluation and Mitigation Strategy program for isotretinoin—originally set to take effect on August 8, 2026—will be delayed until November 15, 2026. The agency said the extra time will allow testing of the system updates, reduce technical problems, and help avoid interruptions in patient access to isotretinoin. The planned changes are intended to reduce burdens on patients, prescribers, and pharmacies while maintaining safety, and they include allowing at-home pregnancy testing in some cases. Until the new date, the Food and Drug Administration will continue enforcement discretion for pregnancy testing requirements. The update also clarifies that monthly counseling documentation for patients who cannot become pregnant will no longer be required and that pharmacy staff training must be completed annually. iPledge work group chair John Barbieri, MD, MBA, told Medscape Medical News, “It’s important to make sure any changes to the program are implemented in a way that is effective…. I would rather it be done sooner than later, but it’s important it be done right.”
Smoking May Lower Sjögren Disease Risk and Mask Pathology
New data presented at EULAR 2026 suggest that smoking may be associated with a lower likelihood of Sjögren disease and milder salivary gland inflammation, although tobacco is harmful in many autoimmune diseases. In a cohort undergoing salivary gland biopsy for sicca symptoms, current smokers were less likely to have Sjögren disease; among those with disease, smokers had less inflammation and fewer advanced germinal centers. The key takeaway is not that smoking is beneficial, but that tobacco exposure may alter disease phenotype and biopsy interpretation, potentially masking severity and affecting diagnosis.
Skin Disorders in Transgender Patients: Treatment Recommendations
Hormonal therapy in transgender patients can substantially affect skin disease patterns, particularly acne, hair loss, melasma, and possibly hidradenitis suppurativa. In transmasculine patients receiving testosterone, acne is the most common dermatologic complaint and often develops early; isotretinoin is most effective, although pregnancy potential must be considered. Testosterone also contributes to androgenetic alopecia, managed with minoxidil and sometimes finasteride. In transfeminine patients, facial hair and melasma are common concerns. Dermatologists should anticipate these effects and provide gender-affirming care with counseling, examination practices, and preventive treatment.
Randomized Trial Supports Sirolimus as Add-On Systemic Lupus Erythematosus Therapy
Adding sirolimus to standard treatment for active systemic lupus erythematosus improved disease control compared with placebo in a randomized phase 3 trial presented at the European Alliance of Associations for Rheumatology (EULAR) 2026 Annual Meeting. Patients receiving sirolimus were more likely to achieve a clinical response and showed greater improvement in disease activity and serologic markers. Treatment generally was well tolerated, although lipid abnormalities, leukopenia, and menstrual irregularities were more common. Sirolimus may become a useful oral option for refractory lupus, pending further confirmation and guidance.
Bimekizumab Trumps Risankizumab in Head-to-Head Psoriatic Arthritis Trial
Dual IL-17 blockade may offer greater joint benefit than IL-23 inhibition in psoriatic arthritis, potentially helping guide biologic selection for patients with skin and musculoskeletal disease. In the phase 3b BE BOLD trial, bimekizumab was more effective than risankizumab for joint disease, with more patients achieving a 50% improvement in American College of Rheumatology response criteria at 16 weeks. Bimekizumab also showed superior results across several secondary measures, including minimal disease activity and skin outcomes, while safety was broadly similar. The findings were presented at the EULAR 2026 Annual Meeting.
FDA Delays iPLEDGE Modifications Until November 2026
In a June 16 announcement, the US Food and Drug Administration said long-awaited modifications to the iPLEDGE Risk Evaluation and Mitigation Strategy program for isotretinoin—originally set to take effect on August 8, 2026—will be delayed until November 15, 2026. The agency said the extra time will allow testing of the system updates, reduce technical problems, and help avoid interruptions in patient access to isotretinoin. The planned changes are intended to reduce burdens on patients, prescribers, and pharmacies while maintaining safety, and they include allowing at-home pregnancy testing in some cases. Until the new date, the Food and Drug Administration will continue enforcement discretion for pregnancy testing requirements. The update also clarifies that monthly counseling documentation for patients who cannot become pregnant will no longer be required and that pharmacy staff training must be completed annually. iPledge work group chair John Barbieri, MD, MBA, told Medscape Medical News, “It’s important to make sure any changes to the program are implemented in a way that is effective…. I would rather it be done sooner than later, but it’s important it be done right.”
Smoking May Lower Sjögren Disease Risk and Mask Pathology
New data presented at EULAR 2026 suggest that smoking may be associated with a lower likelihood of Sjögren disease and milder salivary gland inflammation, although tobacco is harmful in many autoimmune diseases. In a cohort undergoing salivary gland biopsy for sicca symptoms, current smokers were less likely to have Sjögren disease; among those with disease, smokers had less inflammation and fewer advanced germinal centers. The key takeaway is not that smoking is beneficial, but that tobacco exposure may alter disease phenotype and biopsy interpretation, potentially masking severity and affecting diagnosis.
Skin Disorders in Transgender Patients: Treatment Recommendations
Hormonal therapy in transgender patients can substantially affect skin disease patterns, particularly acne, hair loss, melasma, and possibly hidradenitis suppurativa. In transmasculine patients receiving testosterone, acne is the most common dermatologic complaint and often develops early; isotretinoin is most effective, although pregnancy potential must be considered. Testosterone also contributes to androgenetic alopecia, managed with minoxidil and sometimes finasteride. In transfeminine patients, facial hair and melasma are common concerns. Dermatologists should anticipate these effects and provide gender-affirming care with counseling, examination practices, and preventive treatment.
Randomized Trial Supports Sirolimus as Add-On Systemic Lupus Erythematosus Therapy
Adding sirolimus to standard treatment for active systemic lupus erythematosus improved disease control compared with placebo in a randomized phase 3 trial presented at the European Alliance of Associations for Rheumatology (EULAR) 2026 Annual Meeting. Patients receiving sirolimus were more likely to achieve a clinical response and showed greater improvement in disease activity and serologic markers. Treatment generally was well tolerated, although lipid abnormalities, leukopenia, and menstrual irregularities were more common. Sirolimus may become a useful oral option for refractory lupus, pending further confirmation and guidance.
Bimekizumab Trumps Risankizumab in Head-to-Head Psoriatic Arthritis Trial
Dual IL-17 blockade may offer greater joint benefit than IL-23 inhibition in psoriatic arthritis, potentially helping guide biologic selection for patients with skin and musculoskeletal disease. In the phase 3b BE BOLD trial, bimekizumab was more effective than risankizumab for joint disease, with more patients achieving a 50% improvement in American College of Rheumatology response criteria at 16 weeks. Bimekizumab also showed superior results across several secondary measures, including minimal disease activity and skin outcomes, while safety was broadly similar. The findings were presented at the EULAR 2026 Annual Meeting.
FDA Delays iPLEDGE Modifications Until November 2026
In a June 16 announcement, the US Food and Drug Administration said long-awaited modifications to the iPLEDGE Risk Evaluation and Mitigation Strategy program for isotretinoin—originally set to take effect on August 8, 2026—will be delayed until November 15, 2026. The agency said the extra time will allow testing of the system updates, reduce technical problems, and help avoid interruptions in patient access to isotretinoin. The planned changes are intended to reduce burdens on patients, prescribers, and pharmacies while maintaining safety, and they include allowing at-home pregnancy testing in some cases. Until the new date, the Food and Drug Administration will continue enforcement discretion for pregnancy testing requirements. The update also clarifies that monthly counseling documentation for patients who cannot become pregnant will no longer be required and that pharmacy staff training must be completed annually. iPledge work group chair John Barbieri, MD, MBA, told Medscape Medical News, “It’s important to make sure any changes to the program are implemented in a way that is effective…. I would rather it be done sooner than later, but it’s important it be done right.”
Smoking May Lower Sjögren Disease Risk and Mask Pathology
New data presented at EULAR 2026 suggest that smoking may be associated with a lower likelihood of Sjögren disease and milder salivary gland inflammation, although tobacco is harmful in many autoimmune diseases. In a cohort undergoing salivary gland biopsy for sicca symptoms, current smokers were less likely to have Sjögren disease; among those with disease, smokers had less inflammation and fewer advanced germinal centers. The key takeaway is not that smoking is beneficial, but that tobacco exposure may alter disease phenotype and biopsy interpretation, potentially masking severity and affecting diagnosis.
Skin Disorders in Transgender Patients: Treatment Recommendations
Hormonal therapy in transgender patients can substantially affect skin disease patterns, particularly acne, hair loss, melasma, and possibly hidradenitis suppurativa. In transmasculine patients receiving testosterone, acne is the most common dermatologic complaint and often develops early; isotretinoin is most effective, although pregnancy potential must be considered. Testosterone also contributes to androgenetic alopecia, managed with minoxidil and sometimes finasteride. In transfeminine patients, facial hair and melasma are common concerns. Dermatologists should anticipate these effects and provide gender-affirming care with counseling, examination practices, and preventive treatment.
Clinical News Briefs
Clinical News Briefs
Age- and Sex-Related Differences in Primary Cutaneous Lymphoma
Age- and Sex-Related Differences in Primary Cutaneous Lymphoma
Non-Hodgkin lymphomas (NHLs) are a heterogeneous group of lymphoproliferative malignancies originating from T, B, or natural killer (NK) lymphocytes.1 Compared to Hodgkin lymphomas, NHLs exhibit a broader clinical spectrum and have a poorer prognosis and frequent extranodal involvement, with the skin being the second most frequent extranodal site.2 Primary cutaneous lymphomas (PCLs) are NHLs that are first evident on the skin without evidence of extracutaneous disease at diagnosis. They include a heterogeneous group of cutaneous T-cell lymphomas (CTCLs) and cutaneous B-cell lymphomas. Among CTCLs, mycosis fungoides (MF) is the most prevalent subtype, generally following an indolent course. Cutaneous B-cell lymphomas primarily include follicle center lymphoma and diffuse large B-cell lymphoma.3,4
The clinical behavior and incidence of PCLs vary dramatically between children and adults, suggesting underlying biologic, immunologic, and genetic differences.5,6 However, there is a notable lack of comparative studies in the literature addressing these variations, limiting a comprehensive understanding of PCLs and hindering the development of tailored therapeutic strategies. The main objective of this study was to evaluate the different clinical characteristics, subtypes, treatment options, and prognosis in PCLs between pediatric and adult populations.7,8
Methods
This retrospective observational study included pediatric (aged ≤18 years at diagnosis) and adult (aged >18 years at diagnosis) patients with a clinical and histopathologic diagnosis of PCL who were diagnosed and treated at either of 2 tertiary institutions (Dr. Manuel Gea Gonzalez General Hospital or the National Institute of Pediatrics, both in Mexico City, Mexico) between January 1, 1999, and December 31, 2019. The data analysis included demographic and clinical characteristics, type of PCL (according to World Health Organization [WHO]/European Organisation for Research and Treatment of Cancer [EORTC]) classification,3,4 treatment administered, and outcome. Disease remission was defined as remittance of clinical PCL manifestations for 3 months or more. Disease control was defined as stable clinical manifestations with no change in PCL stage following treatment initiation. Disease progression was defined as worsening clinical manifestations with an increase in PCL stage and/or development of systemic lymphoma. Beyond similarities and differences across age groups, we also analyzed differences by sex. χ² and Mann-Whitney U tests were used to assess differences between groups. Statistical significance was set at P≤.05. Institutional approval was obtained from both tertiary centers.
Results
Our analysis included a total of 158 patients: 54 (34.2%) were children and 104 (65.8%) were adults. Eighty-eight (55.7%) patients were male (eTable 1). The mean (SD) age at diagnosis was 9.5 (1.9) years in children and 49.7 (18) years in adults. Regarding differences between age groups, adult patients had a similar sex distribution, while in children, the majority of patients were male (37/54 [68.5%]; P=.01).
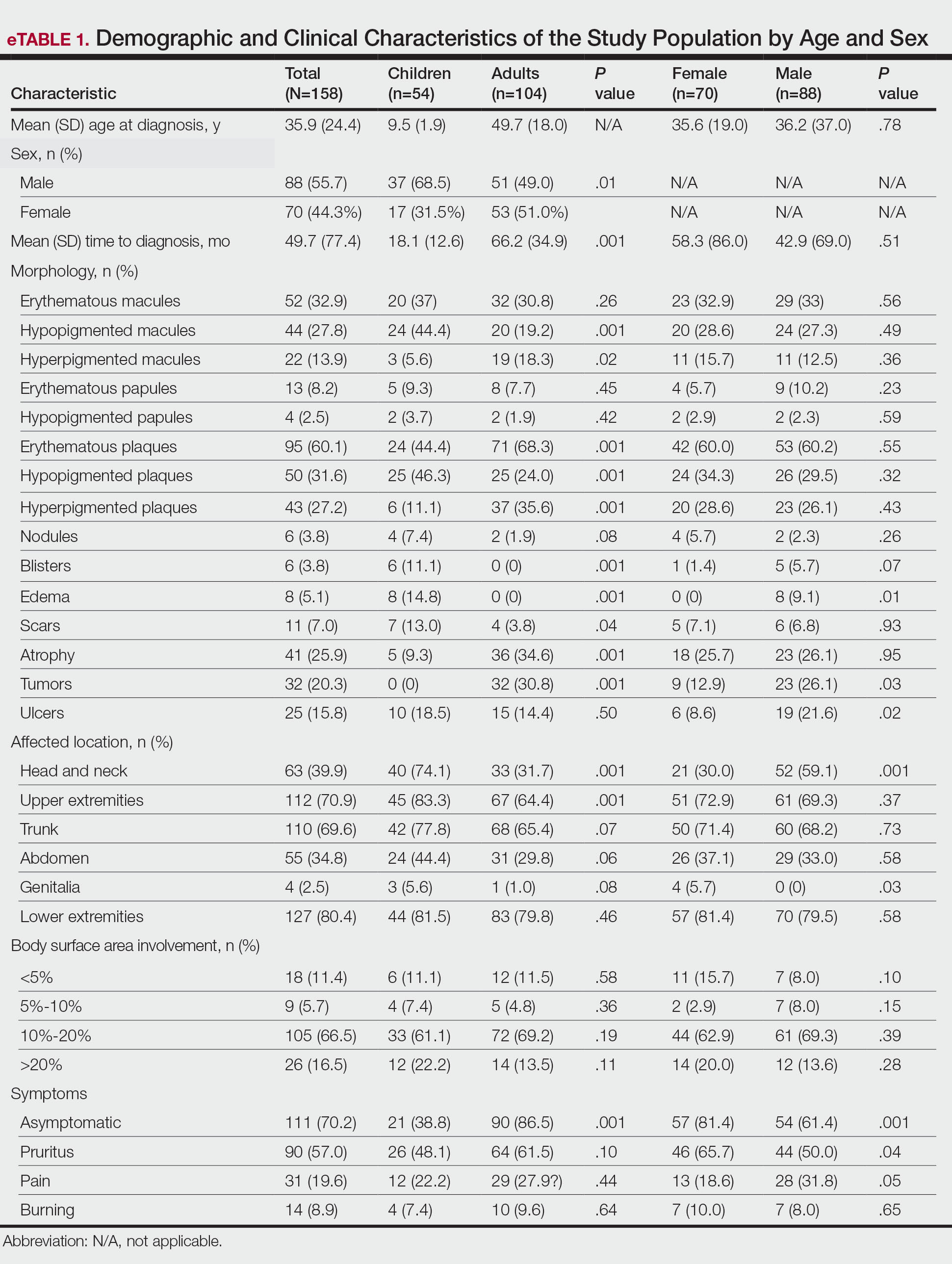
Overall, the most frequent diagnosis was MF, which occurred in 119 (75.3%) patients, and the most common lesions were erythematous plaques, noted in 95 (60.1%) patients. The lower extremities were the most affected body sites, impacting 127 (80.4%) patients, and the most common treatment was phototherapy, used to treat 110 (69.6%) patients. Reported outcomes included disease control in 45 (28.5%) patients and progression in 36 (22.8%) patients; 50 (31.6%) patients were lost to follow-up. Only 15 (9.5%) patients experienced disease remission, and 12 (7.6%) died.
The mean (SD) time between the onset of symptoms and diagnosis was shorter in children than in adults (18.1 [12.6] months vs 66.2 [34.9] months; P<.001). Regarding involved body sites, the head and neck more frequently affected children than adults (40 [74.1%] vs 33 [31.7%]; P<.001), while the upper extremities were more frequently involved in adults than in children (67 [64.4%] vs 45 [83.3%]; P<.001).
There were significant differences in the morphology of lesions and diagnoses. Children most frequently had hypopigmented plaques (25 [46.3%]) and macules (24 [44.4%])(P<.001) associated with MF, and scars (7 [13.0%]), blisters (6 [11.1%]), and edema (8 [14.8%])(P<.001) associated with positive Epstein-Barr virus (EBV) infection. Adults presented more frequently with hyperpigmented macules (19 [18.3%]) and plaques (37 [35.6%]), erythematous plaques (71 [68.3%]), atrophy (36 [34.6%]), and tumors (32 [30.8%])(P<.001). Adults were more often asymptomatic (86.5% vs 38.8%; P<.001).
Subtypes of PCL differed by age group (eTable 2), with MF being more frequent in adults (87 [83.6%] vs 32 [59.2%]; P<.001), while chronic active positive EBV infection (CAEBVI) manifesting as lymphoproliferative disease (LPD) was exclusive to male children (9 [16.6%])(P<.001). Accordingly, we found variations in systemic treatments used: monoclonal antibodies (mAb), thalidomide, intravenous immunoglobulin (IVIg), and hematopoietic stem cell transplantation (HSCT) were used exclusively for treating children (all P<.001). Outcomes were distributed similarly by age group.
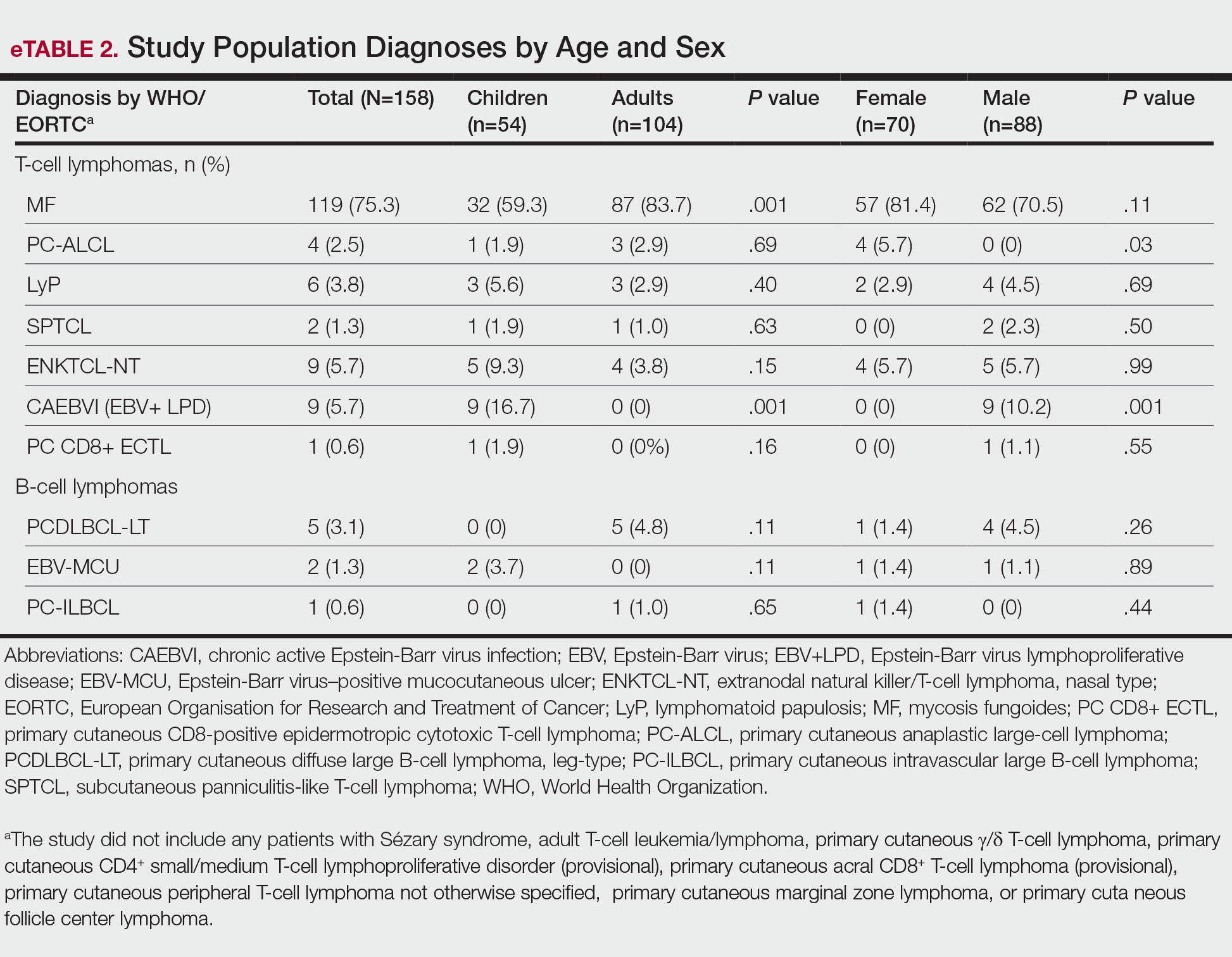
The type of PCL, clinical manifestations, and treatment also varied by sex (eTables 2 and 3). Only males had CAEBVI and presented with edema (8 [9.1%] vs 0%; P<.01). Males also had tumors (23 [26.1%] vs 9 [12.9%]; P=.03) and lesions affecting the head and neck (52 [59.1%] vs 21 [30.0%]; P<.001) more frequently than females. Males were more likely than females to report pain (28 [31.8%] vs 13 [18.6%]; P=.05) and receive systemic treatment with thalidomide (11 [12.5%] vs 1 [1.4%]; P<.001) and IVIg (6 [6.8%] vs 0%; P=.02). Only females were diagnosed with primary cutaneous anaplastic large cell lymphoma (PC-ALCL)(4 [5.7%] vs 0%; P=.03) and had genital involvement (4 [5.7%] vs 0%; P=.03). Females were more likely to be asymptomatic (57 [81.4%] vs 54 [61.4%]; P<.001) or report pruritus (46 [65.7%] vs 44 [50%]; P<.001) and receive local treatment with phototherapy (58 [82.9%] vs 52 [59.1%]; P<.001) compared to males. Although distribution of outcomes was similar by sex, we found males were more frequently lost to follow-up (38 [43.2%] vs 12 [17.1%]; P<.001).
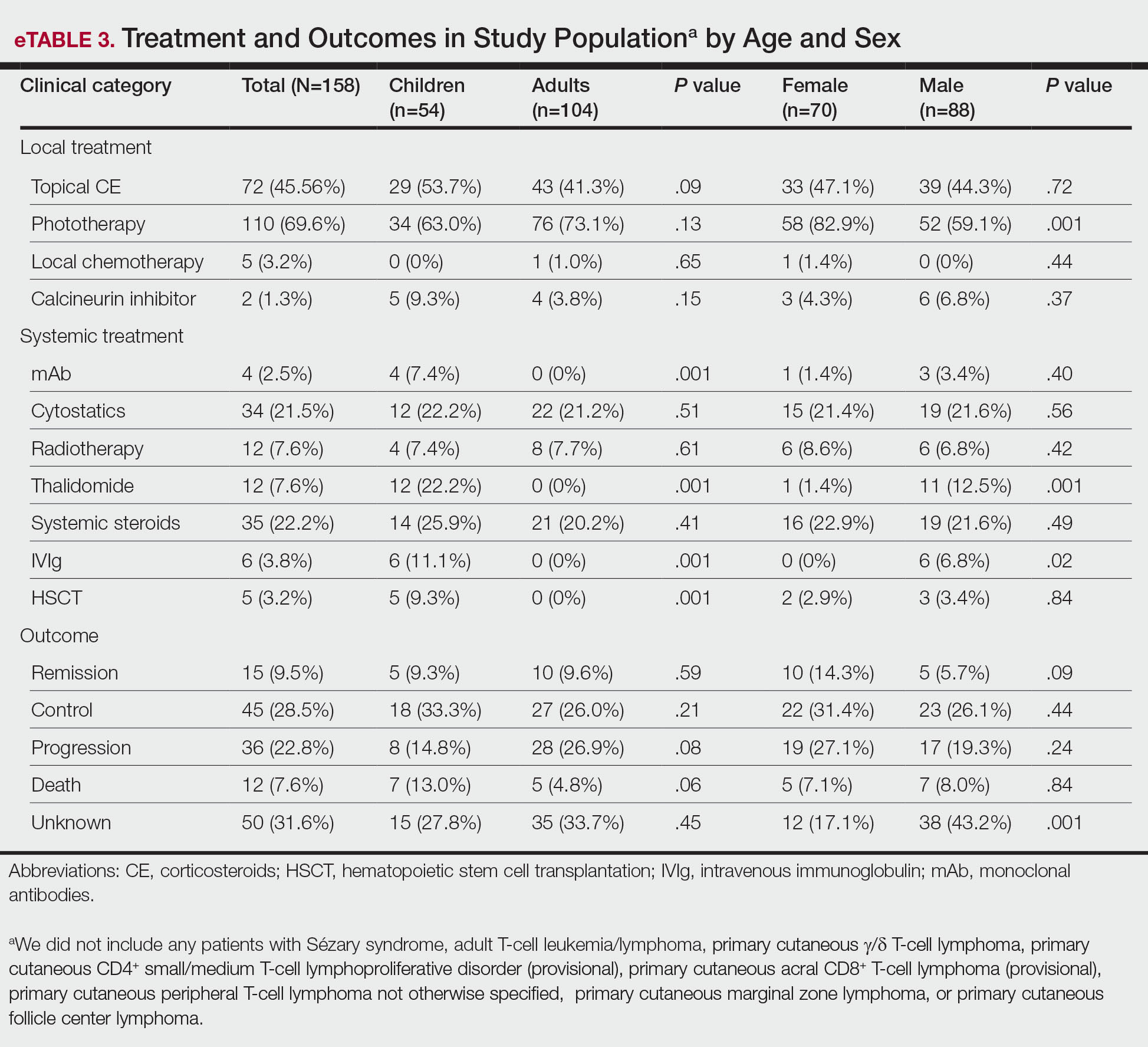
We further searched for differences in clinical manifestations according to the PCL subtype in each age group. The most frequent lesions in 32 children with MF were hypopigmented macules (21 [65.6%]; P<.001)(Figure 1). Three of 5 (60%) children with extranodal NK/T-cell lymphoma, nasal type (ENKTCL), had nodules (P=.002). Of 9 children with CAEBVI, 8 (88.9%) had edema (P<.001), ulcers (P<.001), erythematous plaques (P=.007), and hypopigmented plaques (P=.008); 5 (55.6%) children presented with scars (P<.001) and atrophy (P<.001); and 4 (44.4%) children had blisters (P=.005)(Figure 2). The 2 children with EBV-positive mucocutaneous ulcer (EBV-MCU) had crusts (P=.002) and blisters (P=.01).
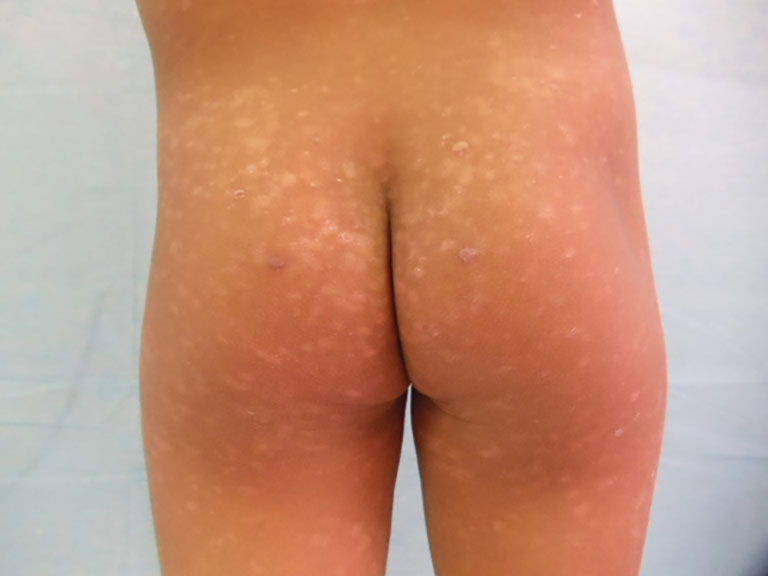

Of 87 adults with MF, 54 (62%) had scaly lesions (P=.006)(Figure 3). Of 3 adult patients with PC-ALCL, 2 (66.7%) had crusts (P=.04) and ulcers (P=.05). Two of 3 (66.7%) adults with lymphomatoid papulosis (LyP) had erythematous papules (P<.001). All 4 adult patients with ENKTCL (P=.008) and all 5 patients with primary cutaneous diffuse large B-cell lymphoma, leg-type, had tumors (P<.001).

Finally, we found no differences in outcomes according to types of PCL overall or by age group; however, when categorized by sex, we found males with EBV-MCU more frequently had disease progression than females with EBV-MCU (P=.04).
Comment
Primary cutaneous lymphomas were similarly distributed among males and females (55.6% vs 44.3%, respectively). This slight male predominance was similar to other reports in the literature: one US study reported a male-to-female incidence rate ratio of 1.72, indicating a significantly higher incidence in males (P<.001).6 Similar trends have been observed in other geographic regions, with reported male-to-female ratios of 1.56 in Greece and 1.35 in Argentina.9,10 These findings suggest that PCLs are slightly more prevalent in males across different populations; however, when we stratified by age, pediatric cases of PCL were significantly more frequent in males than in females (68.5% vs. 31.4%; P=.01).
Our analysis revealed that the time to diagnosis was significantly longer in adults than in children (66.2 months vs 18.1 months) for all PCLs (P<.001). The most common type of PCL in both age groups was MF, with a notably higher prevalence in adults than in children (87 [83.7%] vs 32 [59.2%]). The prolonged course of MF in adults, often taking years to progress from early to advanced stages (47.0-52.7 months) may contribute to delayed diagnosis.8,11,12 Additionally, classic lesions of MF (erythematous scaly plaques) may resemble other common dermatologic conditions, further complicating early recognition and treatment in adults more than in children.11,12 Conversely, more aggressive and rapidly progressing PCL subtypes, including CAEBVI and ENKTCL-NT, were more frequent in children and would likely be diagnosed more promptly because of the acute onset and fast evolution of signs and symptoms.13
Mycosis fungoides is the most common CTCL, followed by CD30+ T-cell disorders such as LyP and PC-ALCL.14 While MF was the predominant subtype in both age groups, similar to previous reports,6,7 pediatric patients in our study exhibited distinctive features, such as hypopigmented macules and plaques. Hypopigmented lesions may suggest an underlying immunologic mechanism unique to younger patients, specifically children, in contrast to the hyperpigmented or violaceous lesions predominating in adults.7 The hypopigmented variant of MF has been reported to be more prevalent in children, similar to our data, accounting for 54.5% of all pediatric MF cases. These hypopigmented lesions typically manifest at an early stage and follow an indolent course.15,16 Jung et al8 conducted a systematic review of children with MF and reported a mean age at diagnosis of 12.2 years, whereas in our cohort, the mean age was 9.5 years. These findings highlight the different clinical manifestations of MF in children, which may aid in early recognition and diagnosis.
In adults, MF most commonly manifested as hyperpigmented macules and plaques, erythematous plaques, atrophic lesions, and tumors. In this population, MF remained the most frequently diagnosed PCL subtype, followed by PC-ALCL.
There were notable differences in symptom presentation between age groups and sexes. Adults were more often asymptomatic, and males reported pain more frequently.
When analyzing PCL subtypes in our study, we found that CAEBVI was exclusive to children, specifically males. The updated WHO/EORTC classification contains a new section on EBV-positive LPD in childhood, including hydroa vacciniforme–like LPD and hypersensitivity reactions to mosquito bites.4 Both are cutaneous manifestations of CAEBVI with a risk for progression to systemic EBV-positive T-cell or NK-cell lymphoma. These disorders mainly affect children and adolescents from Asia or Indigenous populations from Mexico and Central and South America.3,4,17 Cases in both female and male patients have been reported, without a clear sex predominance; however, mutations in the Src homology 2 domain containing 1A (SH2D1A) gene recently have been shown to cause X-linked lymphoproliferative disease, which is associated with predilection for EBV infection and subsequent EBV-positive LPD, including CAEBVI.18,19 Thus, it is possible some of the children with CAEBVI in our study may have an underlying X-linked lymphoproliferative disease, accounting for the male predominance.
Similarly, ENKTCL-NT tended to occur more in children than in adults in our study. Both CAEBVI-LPD and ENKTCL-NT are aggressive lymphomas with a suboptimal prognosis. Although treatment with immunomodulatory agents may lead to temporary remission in most cases, disease progression has been reported in larger cohorts, emphasizing the need for long-term follow-up and more aggressive treatments in severe cases of CAEBVI.13,17 Treatment options for EBV-positive LPD include mAb such as rituximab, IVIg, HSCT, antiviral agents, interferons α and γ, and corticosteroids.20
Treatment approaches were notably different between children and adults (P<.0001). Monoclonal antibodies, immunomodulatory agents such as thalidomide, IVIg, and HSCT were exclusively used in pediatric patients, reflecting the presence of CAEBVI and ENKTCL-NT (P<.0001). Additionally, edema, blisters, and scars were observed more frequently in children, likely due to the clinical manifestations of these EBV-related disorders.
A recent review of systemic NHL highlighted various age-related differences in clinical presentation, biology, and outcomes.13 In general, children tend to present with more aggressive subtypes and achieve better outcomes compared to adults.13 These differences may be attributed to variations in tumor biology, immune responses, and/or the benefits of early and intensive interventions in pediatric populations. These findings resonate with our results, as pediatric PCL patients received more aggressive treatments—including mAb, thalidomide, IVIg, and HSCT—likely due to the higher frequency of CAEBVI/ENKTCL-NT; however, we were unable to properly assess treatment outcomes, as many patients, both adults and children, were lost to follow-up.
Overall, our findings and comparisons with existing studies highlight the need for age-specific research and management approaches for PCL. The distinct clinical and biological profiles across age groups highlight opportunities for personalized therapies and further investigation into the molecular drivers of these differences to optimize outcomes for pediatric and adult patients.
When analyzing differences by sex, we found that CAEBVI was diagnosed exclusively in male children, who correspondingly exhibited clinical features such as edema and tumors, with lesions predominantly located on the head and neck. This also influenced treatment approach, as these patients were more likely to receive thalidomide and IVIg. In contrast, PC-ALCL was observed only in female patients, a finding that deviates from previously reported epidemiology.14 Females with PC-ALCL were more likely to have genital involvement and be asymptomatic, which could suggest a sex-related bias in disease recognition and seeking health care.
Recognizing distinctive clinical manifestations across different diagnoses and age groups can aid health care providers in early identification and accurate diagnosis of PCL. Our findings revealed several notable differences: adults with MF more frequently had scaly lesions, those with PC-ALCL had crusts and ulcers, and those with LyP had erythematous papules. All adults with ENKTCL and primary cutaneous diffuse large B-cell lymphoma, leg-type, presented with tumors. While children with MF had an increased frequency of hypopigmented macules, those with ENKTCL more frequently developed nodules, and children with EBV-MCU often had crusts and ulcers. As has already been mentioned, children with CAEBVI displayed a broad range of lesions, including edema, ulcers, erythematous and hypopigmented plaques, atrophy, blisters, and scars.
Our study was limited by the retrospective design and missing data from one-third of patients, which prevented outcome comparison. We also lacked molecular profiling of patients, which could help refine therapeutic strategies for PCL.13 Finally, as both centers included are reference institutions, results may be biased and overestimated and could differ from the rest of the population.
Conclusion
This comparative study of PCL highlighted age-related differences in clinical presentation, diagnostic distribution, and treatment patterns, including a higher prevalence among male children than female children. Adult patients with PCL had a notably longer time to diagnosis than children. The most common type of PCL identified in both age groups and sex categories was MF, but hypopigmented lesions predominated in children with this condition. Epstein-Barr virus–associated PCL occurred almost exclusively in children and manifested with nodules, edema, blisters, and scars. In terms of treatment, children received more aggressive and advanced therapies, including mAb, thalidomide, IVIg, and HSCT. Further prospective research is needed to establish variations in clinical manifestations, diagnoses, treatments, and outcomes.
- Singh R, Shaik S, Negi BS, et al. Non-Hodgkin’s lymphoma: a review.J Family Med Prim Care. 2020;9:1834-1840.
- Armitage JO, Gascoyne RD, Lunning MA, et al. Non-Hodgkin lymphoma. Lancet. 2017;390:298-310.
- Swerdlow SH, Campo E, Pileri SA, et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood. 2016;127:2375-2390.
- Willemze R, Cerroni L, Kempf W, et al. The 2018 update of the WHO-EORTC classification for primary cutaneous lymphomas. Blood. 2019;133:1703-1714.
- Willemze R, Hodak E, Zinzani PL, et al; ESMO Guidelines Committee. Primary cutaneous lymphomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018;29:iv30-iv40.
- Bradford PT, Devesa SS, Anderson WF, et al. Cutaneous lymphoma incidence patterns in the United States: a population-based study of 3884 cases. Blood. 2009;113:5064-5073.
- Moon IJ, Won CH, Chang SE, et al. Prevalence, clinical features, and survival outcome trends of 627 patients with primary cutaneous lymphoma over 29 years: a retrospective review from a single tertiary center in Korea. Sci Rep. 2024;14:20118.
- Jung JM, Lim DJ, Won CH, et al. Mycosis fungoides in children and adolescents: a systematic review. JAMA Dermatol. 2021;157:431-438.
- Kaliampou S, Nikolaou V, Niforou A, et al. Epidemiological trends in cutaneous lymphomas in Greece. Eur J Dermatol. 2023;33:664-673.
- Abeldaño A, Enz P, Maskin M, et al. Primary cutaneous lymphoma in Argentina: a report of a nationwide study of 416 patients. Int J Dermatol. 2019;58:449-455.
- Cervini AB, Torres-Huamani AN, Sanchez-La-Rosa C, et al. Mycosis fungoides: experience in a pediatric hospital. Actas Dermosifiliogr. 2017;108:564-570.
- Welfringer-Morin A, Barroil M, Fraitag S, et al. Clinical features, histological characteristics, and disease outcomes of mycosis fungoides in children and adolescents: a nationwide multicentre cohort of 46 patients. Dermatology. 2023;239:132-139.
- Sandlund JT, Martin MG. Non-Hodgkin lymphoma across the pediatric and adolescent and young adult age spectrum. Hematology Am Soc Hematol Educ Program. 2016;2016:589-597.
- Ortiz-Hidalgo C, Pina-Oviedo S. Primary cutaneous anaplastic large cell lymphoma-a review of clinical, morphological, immunohistochemical, and molecular features. Cancers (Basel). 2023;15:4098.
- Nielsen PR, Eriksen JO, Wehkamp U, et al. Clinical and histological characteristics of mycosis fungoides and Sézary syndrome: a retrospective, single-centre study of 43 patients from eastern Denmark. Acta Derm Venereol. 2019;99:1231-1236.
- Suh KS, Jang MS, Jung JH, et al. Clinical characteristics and long-term outcome of 223 patients with mycosis fungoides at a single tertiary center in Korea: a 29-year review. J Am Acad Dermatol. 2022;86:1275-1284.
- Quintanilla-Martinez L, Ridaura C, Nagl F, et al. Hydroa vacciniforme-like lymphoma: a chronic EBV+ lymphoproliferative disorder with risk to develop a systemic lymphoma. Blood. 2013;122:3101-3110.
- Fujiwara S, Nakamura H. Chronic active Epstein-Barr virus infection: is it immunodeficiency, malignancy, or both? Cancers (Basel). 2020;12:3202.
- Sumazaki R, Kanegane H, Osaki M, et al. SH2D1A mutations in Japanese males with severe Epstein-Barr virus–associated illnesses. Blood. 2001;98:1268-1270.
- Kimura H. Pathogenesis of chronic active Epstein-Barr virus infection: is this an infectious disease, lymphoproliferative disorder, or immunodeficiency? Rev Med Virol. 2006;16:251-261.
Non-Hodgkin lymphomas (NHLs) are a heterogeneous group of lymphoproliferative malignancies originating from T, B, or natural killer (NK) lymphocytes.1 Compared to Hodgkin lymphomas, NHLs exhibit a broader clinical spectrum and have a poorer prognosis and frequent extranodal involvement, with the skin being the second most frequent extranodal site.2 Primary cutaneous lymphomas (PCLs) are NHLs that are first evident on the skin without evidence of extracutaneous disease at diagnosis. They include a heterogeneous group of cutaneous T-cell lymphomas (CTCLs) and cutaneous B-cell lymphomas. Among CTCLs, mycosis fungoides (MF) is the most prevalent subtype, generally following an indolent course. Cutaneous B-cell lymphomas primarily include follicle center lymphoma and diffuse large B-cell lymphoma.3,4
The clinical behavior and incidence of PCLs vary dramatically between children and adults, suggesting underlying biologic, immunologic, and genetic differences.5,6 However, there is a notable lack of comparative studies in the literature addressing these variations, limiting a comprehensive understanding of PCLs and hindering the development of tailored therapeutic strategies. The main objective of this study was to evaluate the different clinical characteristics, subtypes, treatment options, and prognosis in PCLs between pediatric and adult populations.7,8
Methods
This retrospective observational study included pediatric (aged ≤18 years at diagnosis) and adult (aged >18 years at diagnosis) patients with a clinical and histopathologic diagnosis of PCL who were diagnosed and treated at either of 2 tertiary institutions (Dr. Manuel Gea Gonzalez General Hospital or the National Institute of Pediatrics, both in Mexico City, Mexico) between January 1, 1999, and December 31, 2019. The data analysis included demographic and clinical characteristics, type of PCL (according to World Health Organization [WHO]/European Organisation for Research and Treatment of Cancer [EORTC]) classification,3,4 treatment administered, and outcome. Disease remission was defined as remittance of clinical PCL manifestations for 3 months or more. Disease control was defined as stable clinical manifestations with no change in PCL stage following treatment initiation. Disease progression was defined as worsening clinical manifestations with an increase in PCL stage and/or development of systemic lymphoma. Beyond similarities and differences across age groups, we also analyzed differences by sex. χ² and Mann-Whitney U tests were used to assess differences between groups. Statistical significance was set at P≤.05. Institutional approval was obtained from both tertiary centers.
Results
Our analysis included a total of 158 patients: 54 (34.2%) were children and 104 (65.8%) were adults. Eighty-eight (55.7%) patients were male (eTable 1). The mean (SD) age at diagnosis was 9.5 (1.9) years in children and 49.7 (18) years in adults. Regarding differences between age groups, adult patients had a similar sex distribution, while in children, the majority of patients were male (37/54 [68.5%]; P=.01).
Overall, the most frequent diagnosis was MF, which occurred in 119 (75.3%) patients, and the most common lesions were erythematous plaques, noted in 95 (60.1%) patients. The lower extremities were the most affected body sites, impacting 127 (80.4%) patients, and the most common treatment was phototherapy, used to treat 110 (69.6%) patients. Reported outcomes included disease control in 45 (28.5%) patients and progression in 36 (22.8%) patients; 50 (31.6%) patients were lost to follow-up. Only 15 (9.5%) patients experienced disease remission, and 12 (7.6%) died.
The mean (SD) time between the onset of symptoms and diagnosis was shorter in children than in adults (18.1 [12.6] months vs 66.2 [34.9] months; P<.001). Regarding involved body sites, the head and neck more frequently affected children than adults (40 [74.1%] vs 33 [31.7%]; P<.001), while the upper extremities were more frequently involved in adults than in children (67 [64.4%] vs 45 [83.3%]; P<.001).
There were significant differences in the morphology of lesions and diagnoses. Children most frequently had hypopigmented plaques (25 [46.3%]) and macules (24 [44.4%])(P<.001) associated with MF, and scars (7 [13.0%]), blisters (6 [11.1%]), and edema (8 [14.8%])(P<.001) associated with positive Epstein-Barr virus (EBV) infection. Adults presented more frequently with hyperpigmented macules (19 [18.3%]) and plaques (37 [35.6%]), erythematous plaques (71 [68.3%]), atrophy (36 [34.6%]), and tumors (32 [30.8%])(P<.001). Adults were more often asymptomatic (86.5% vs 38.8%; P<.001).
Subtypes of PCL differed by age group (eTable 2), with MF being more frequent in adults (87 [83.6%] vs 32 [59.2%]; P<.001), while chronic active positive EBV infection (CAEBVI) manifesting as lymphoproliferative disease (LPD) was exclusive to male children (9 [16.6%])(P<.001). Accordingly, we found variations in systemic treatments used: monoclonal antibodies (mAb), thalidomide, intravenous immunoglobulin (IVIg), and hematopoietic stem cell transplantation (HSCT) were used exclusively for treating children (all P<.001). Outcomes were distributed similarly by age group.
The type of PCL, clinical manifestations, and treatment also varied by sex (eTables 2 and 3). Only males had CAEBVI and presented with edema (8 [9.1%] vs 0%; P<.01). Males also had tumors (23 [26.1%] vs 9 [12.9%]; P=.03) and lesions affecting the head and neck (52 [59.1%] vs 21 [30.0%]; P<.001) more frequently than females. Males were more likely than females to report pain (28 [31.8%] vs 13 [18.6%]; P=.05) and receive systemic treatment with thalidomide (11 [12.5%] vs 1 [1.4%]; P<.001) and IVIg (6 [6.8%] vs 0%; P=.02). Only females were diagnosed with primary cutaneous anaplastic large cell lymphoma (PC-ALCL)(4 [5.7%] vs 0%; P=.03) and had genital involvement (4 [5.7%] vs 0%; P=.03). Females were more likely to be asymptomatic (57 [81.4%] vs 54 [61.4%]; P<.001) or report pruritus (46 [65.7%] vs 44 [50%]; P<.001) and receive local treatment with phototherapy (58 [82.9%] vs 52 [59.1%]; P<.001) compared to males. Although distribution of outcomes was similar by sex, we found males were more frequently lost to follow-up (38 [43.2%] vs 12 [17.1%]; P<.001).
We further searched for differences in clinical manifestations according to the PCL subtype in each age group. The most frequent lesions in 32 children with MF were hypopigmented macules (21 [65.6%]; P<.001)(Figure 1). Three of 5 (60%) children with extranodal NK/T-cell lymphoma, nasal type (ENKTCL), had nodules (P=.002). Of 9 children with CAEBVI, 8 (88.9%) had edema (P<.001), ulcers (P<.001), erythematous plaques (P=.007), and hypopigmented plaques (P=.008); 5 (55.6%) children presented with scars (P<.001) and atrophy (P<.001); and 4 (44.4%) children had blisters (P=.005)(Figure 2). The 2 children with EBV-positive mucocutaneous ulcer (EBV-MCU) had crusts (P=.002) and blisters (P=.01).
Of 87 adults with MF, 54 (62%) had scaly lesions (P=.006)(Figure 3). Of 3 adult patients with PC-ALCL, 2 (66.7%) had crusts (P=.04) and ulcers (P=.05). Two of 3 (66.7%) adults with lymphomatoid papulosis (LyP) had erythematous papules (P<.001). All 4 adult patients with ENKTCL (P=.008) and all 5 patients with primary cutaneous diffuse large B-cell lymphoma, leg-type, had tumors (P<.001).
Finally, we found no differences in outcomes according to types of PCL overall or by age group; however, when categorized by sex, we found males with EBV-MCU more frequently had disease progression than females with EBV-MCU (P=.04).
Comment
Primary cutaneous lymphomas were similarly distributed among males and females (55.6% vs 44.3%, respectively). This slight male predominance was similar to other reports in the literature: one US study reported a male-to-female incidence rate ratio of 1.72, indicating a significantly higher incidence in males (P<.001).6 Similar trends have been observed in other geographic regions, with reported male-to-female ratios of 1.56 in Greece and 1.35 in Argentina.9,10 These findings suggest that PCLs are slightly more prevalent in males across different populations; however, when we stratified by age, pediatric cases of PCL were significantly more frequent in males than in females (68.5% vs. 31.4%; P=.01).
Our analysis revealed that the time to diagnosis was significantly longer in adults than in children (66.2 months vs 18.1 months) for all PCLs (P<.001). The most common type of PCL in both age groups was MF, with a notably higher prevalence in adults than in children (87 [83.7%] vs 32 [59.2%]). The prolonged course of MF in adults, often taking years to progress from early to advanced stages (47.0-52.7 months) may contribute to delayed diagnosis.8,11,12 Additionally, classic lesions of MF (erythematous scaly plaques) may resemble other common dermatologic conditions, further complicating early recognition and treatment in adults more than in children.11,12 Conversely, more aggressive and rapidly progressing PCL subtypes, including CAEBVI and ENKTCL-NT, were more frequent in children and would likely be diagnosed more promptly because of the acute onset and fast evolution of signs and symptoms.13
Mycosis fungoides is the most common CTCL, followed by CD30+ T-cell disorders such as LyP and PC-ALCL.14 While MF was the predominant subtype in both age groups, similar to previous reports,6,7 pediatric patients in our study exhibited distinctive features, such as hypopigmented macules and plaques. Hypopigmented lesions may suggest an underlying immunologic mechanism unique to younger patients, specifically children, in contrast to the hyperpigmented or violaceous lesions predominating in adults.7 The hypopigmented variant of MF has been reported to be more prevalent in children, similar to our data, accounting for 54.5% of all pediatric MF cases. These hypopigmented lesions typically manifest at an early stage and follow an indolent course.15,16 Jung et al8 conducted a systematic review of children with MF and reported a mean age at diagnosis of 12.2 years, whereas in our cohort, the mean age was 9.5 years. These findings highlight the different clinical manifestations of MF in children, which may aid in early recognition and diagnosis.
In adults, MF most commonly manifested as hyperpigmented macules and plaques, erythematous plaques, atrophic lesions, and tumors. In this population, MF remained the most frequently diagnosed PCL subtype, followed by PC-ALCL.
There were notable differences in symptom presentation between age groups and sexes. Adults were more often asymptomatic, and males reported pain more frequently.
When analyzing PCL subtypes in our study, we found that CAEBVI was exclusive to children, specifically males. The updated WHO/EORTC classification contains a new section on EBV-positive LPD in childhood, including hydroa vacciniforme–like LPD and hypersensitivity reactions to mosquito bites.4 Both are cutaneous manifestations of CAEBVI with a risk for progression to systemic EBV-positive T-cell or NK-cell lymphoma. These disorders mainly affect children and adolescents from Asia or Indigenous populations from Mexico and Central and South America.3,4,17 Cases in both female and male patients have been reported, without a clear sex predominance; however, mutations in the Src homology 2 domain containing 1A (SH2D1A) gene recently have been shown to cause X-linked lymphoproliferative disease, which is associated with predilection for EBV infection and subsequent EBV-positive LPD, including CAEBVI.18,19 Thus, it is possible some of the children with CAEBVI in our study may have an underlying X-linked lymphoproliferative disease, accounting for the male predominance.
Similarly, ENKTCL-NT tended to occur more in children than in adults in our study. Both CAEBVI-LPD and ENKTCL-NT are aggressive lymphomas with a suboptimal prognosis. Although treatment with immunomodulatory agents may lead to temporary remission in most cases, disease progression has been reported in larger cohorts, emphasizing the need for long-term follow-up and more aggressive treatments in severe cases of CAEBVI.13,17 Treatment options for EBV-positive LPD include mAb such as rituximab, IVIg, HSCT, antiviral agents, interferons α and γ, and corticosteroids.20
Treatment approaches were notably different between children and adults (P<.0001). Monoclonal antibodies, immunomodulatory agents such as thalidomide, IVIg, and HSCT were exclusively used in pediatric patients, reflecting the presence of CAEBVI and ENKTCL-NT (P<.0001). Additionally, edema, blisters, and scars were observed more frequently in children, likely due to the clinical manifestations of these EBV-related disorders.
A recent review of systemic NHL highlighted various age-related differences in clinical presentation, biology, and outcomes.13 In general, children tend to present with more aggressive subtypes and achieve better outcomes compared to adults.13 These differences may be attributed to variations in tumor biology, immune responses, and/or the benefits of early and intensive interventions in pediatric populations. These findings resonate with our results, as pediatric PCL patients received more aggressive treatments—including mAb, thalidomide, IVIg, and HSCT—likely due to the higher frequency of CAEBVI/ENKTCL-NT; however, we were unable to properly assess treatment outcomes, as many patients, both adults and children, were lost to follow-up.
Overall, our findings and comparisons with existing studies highlight the need for age-specific research and management approaches for PCL. The distinct clinical and biological profiles across age groups highlight opportunities for personalized therapies and further investigation into the molecular drivers of these differences to optimize outcomes for pediatric and adult patients.
When analyzing differences by sex, we found that CAEBVI was diagnosed exclusively in male children, who correspondingly exhibited clinical features such as edema and tumors, with lesions predominantly located on the head and neck. This also influenced treatment approach, as these patients were more likely to receive thalidomide and IVIg. In contrast, PC-ALCL was observed only in female patients, a finding that deviates from previously reported epidemiology.14 Females with PC-ALCL were more likely to have genital involvement and be asymptomatic, which could suggest a sex-related bias in disease recognition and seeking health care.
Recognizing distinctive clinical manifestations across different diagnoses and age groups can aid health care providers in early identification and accurate diagnosis of PCL. Our findings revealed several notable differences: adults with MF more frequently had scaly lesions, those with PC-ALCL had crusts and ulcers, and those with LyP had erythematous papules. All adults with ENKTCL and primary cutaneous diffuse large B-cell lymphoma, leg-type, presented with tumors. While children with MF had an increased frequency of hypopigmented macules, those with ENKTCL more frequently developed nodules, and children with EBV-MCU often had crusts and ulcers. As has already been mentioned, children with CAEBVI displayed a broad range of lesions, including edema, ulcers, erythematous and hypopigmented plaques, atrophy, blisters, and scars.
Our study was limited by the retrospective design and missing data from one-third of patients, which prevented outcome comparison. We also lacked molecular profiling of patients, which could help refine therapeutic strategies for PCL.13 Finally, as both centers included are reference institutions, results may be biased and overestimated and could differ from the rest of the population.
Conclusion
This comparative study of PCL highlighted age-related differences in clinical presentation, diagnostic distribution, and treatment patterns, including a higher prevalence among male children than female children. Adult patients with PCL had a notably longer time to diagnosis than children. The most common type of PCL identified in both age groups and sex categories was MF, but hypopigmented lesions predominated in children with this condition. Epstein-Barr virus–associated PCL occurred almost exclusively in children and manifested with nodules, edema, blisters, and scars. In terms of treatment, children received more aggressive and advanced therapies, including mAb, thalidomide, IVIg, and HSCT. Further prospective research is needed to establish variations in clinical manifestations, diagnoses, treatments, and outcomes.
Non-Hodgkin lymphomas (NHLs) are a heterogeneous group of lymphoproliferative malignancies originating from T, B, or natural killer (NK) lymphocytes.1 Compared to Hodgkin lymphomas, NHLs exhibit a broader clinical spectrum and have a poorer prognosis and frequent extranodal involvement, with the skin being the second most frequent extranodal site.2 Primary cutaneous lymphomas (PCLs) are NHLs that are first evident on the skin without evidence of extracutaneous disease at diagnosis. They include a heterogeneous group of cutaneous T-cell lymphomas (CTCLs) and cutaneous B-cell lymphomas. Among CTCLs, mycosis fungoides (MF) is the most prevalent subtype, generally following an indolent course. Cutaneous B-cell lymphomas primarily include follicle center lymphoma and diffuse large B-cell lymphoma.3,4
The clinical behavior and incidence of PCLs vary dramatically between children and adults, suggesting underlying biologic, immunologic, and genetic differences.5,6 However, there is a notable lack of comparative studies in the literature addressing these variations, limiting a comprehensive understanding of PCLs and hindering the development of tailored therapeutic strategies. The main objective of this study was to evaluate the different clinical characteristics, subtypes, treatment options, and prognosis in PCLs between pediatric and adult populations.7,8
Methods
This retrospective observational study included pediatric (aged ≤18 years at diagnosis) and adult (aged >18 years at diagnosis) patients with a clinical and histopathologic diagnosis of PCL who were diagnosed and treated at either of 2 tertiary institutions (Dr. Manuel Gea Gonzalez General Hospital or the National Institute of Pediatrics, both in Mexico City, Mexico) between January 1, 1999, and December 31, 2019. The data analysis included demographic and clinical characteristics, type of PCL (according to World Health Organization [WHO]/European Organisation for Research and Treatment of Cancer [EORTC]) classification,3,4 treatment administered, and outcome. Disease remission was defined as remittance of clinical PCL manifestations for 3 months or more. Disease control was defined as stable clinical manifestations with no change in PCL stage following treatment initiation. Disease progression was defined as worsening clinical manifestations with an increase in PCL stage and/or development of systemic lymphoma. Beyond similarities and differences across age groups, we also analyzed differences by sex. χ² and Mann-Whitney U tests were used to assess differences between groups. Statistical significance was set at P≤.05. Institutional approval was obtained from both tertiary centers.
Results
Our analysis included a total of 158 patients: 54 (34.2%) were children and 104 (65.8%) were adults. Eighty-eight (55.7%) patients were male (eTable 1). The mean (SD) age at diagnosis was 9.5 (1.9) years in children and 49.7 (18) years in adults. Regarding differences between age groups, adult patients had a similar sex distribution, while in children, the majority of patients were male (37/54 [68.5%]; P=.01).
Overall, the most frequent diagnosis was MF, which occurred in 119 (75.3%) patients, and the most common lesions were erythematous plaques, noted in 95 (60.1%) patients. The lower extremities were the most affected body sites, impacting 127 (80.4%) patients, and the most common treatment was phototherapy, used to treat 110 (69.6%) patients. Reported outcomes included disease control in 45 (28.5%) patients and progression in 36 (22.8%) patients; 50 (31.6%) patients were lost to follow-up. Only 15 (9.5%) patients experienced disease remission, and 12 (7.6%) died.
The mean (SD) time between the onset of symptoms and diagnosis was shorter in children than in adults (18.1 [12.6] months vs 66.2 [34.9] months; P<.001). Regarding involved body sites, the head and neck more frequently affected children than adults (40 [74.1%] vs 33 [31.7%]; P<.001), while the upper extremities were more frequently involved in adults than in children (67 [64.4%] vs 45 [83.3%]; P<.001).
There were significant differences in the morphology of lesions and diagnoses. Children most frequently had hypopigmented plaques (25 [46.3%]) and macules (24 [44.4%])(P<.001) associated with MF, and scars (7 [13.0%]), blisters (6 [11.1%]), and edema (8 [14.8%])(P<.001) associated with positive Epstein-Barr virus (EBV) infection. Adults presented more frequently with hyperpigmented macules (19 [18.3%]) and plaques (37 [35.6%]), erythematous plaques (71 [68.3%]), atrophy (36 [34.6%]), and tumors (32 [30.8%])(P<.001). Adults were more often asymptomatic (86.5% vs 38.8%; P<.001).
Subtypes of PCL differed by age group (eTable 2), with MF being more frequent in adults (87 [83.6%] vs 32 [59.2%]; P<.001), while chronic active positive EBV infection (CAEBVI) manifesting as lymphoproliferative disease (LPD) was exclusive to male children (9 [16.6%])(P<.001). Accordingly, we found variations in systemic treatments used: monoclonal antibodies (mAb), thalidomide, intravenous immunoglobulin (IVIg), and hematopoietic stem cell transplantation (HSCT) were used exclusively for treating children (all P<.001). Outcomes were distributed similarly by age group.
The type of PCL, clinical manifestations, and treatment also varied by sex (eTables 2 and 3). Only males had CAEBVI and presented with edema (8 [9.1%] vs 0%; P<.01). Males also had tumors (23 [26.1%] vs 9 [12.9%]; P=.03) and lesions affecting the head and neck (52 [59.1%] vs 21 [30.0%]; P<.001) more frequently than females. Males were more likely than females to report pain (28 [31.8%] vs 13 [18.6%]; P=.05) and receive systemic treatment with thalidomide (11 [12.5%] vs 1 [1.4%]; P<.001) and IVIg (6 [6.8%] vs 0%; P=.02). Only females were diagnosed with primary cutaneous anaplastic large cell lymphoma (PC-ALCL)(4 [5.7%] vs 0%; P=.03) and had genital involvement (4 [5.7%] vs 0%; P=.03). Females were more likely to be asymptomatic (57 [81.4%] vs 54 [61.4%]; P<.001) or report pruritus (46 [65.7%] vs 44 [50%]; P<.001) and receive local treatment with phototherapy (58 [82.9%] vs 52 [59.1%]; P<.001) compared to males. Although distribution of outcomes was similar by sex, we found males were more frequently lost to follow-up (38 [43.2%] vs 12 [17.1%]; P<.001).
We further searched for differences in clinical manifestations according to the PCL subtype in each age group. The most frequent lesions in 32 children with MF were hypopigmented macules (21 [65.6%]; P<.001)(Figure 1). Three of 5 (60%) children with extranodal NK/T-cell lymphoma, nasal type (ENKTCL), had nodules (P=.002). Of 9 children with CAEBVI, 8 (88.9%) had edema (P<.001), ulcers (P<.001), erythematous plaques (P=.007), and hypopigmented plaques (P=.008); 5 (55.6%) children presented with scars (P<.001) and atrophy (P<.001); and 4 (44.4%) children had blisters (P=.005)(Figure 2). The 2 children with EBV-positive mucocutaneous ulcer (EBV-MCU) had crusts (P=.002) and blisters (P=.01).
Of 87 adults with MF, 54 (62%) had scaly lesions (P=.006)(Figure 3). Of 3 adult patients with PC-ALCL, 2 (66.7%) had crusts (P=.04) and ulcers (P=.05). Two of 3 (66.7%) adults with lymphomatoid papulosis (LyP) had erythematous papules (P<.001). All 4 adult patients with ENKTCL (P=.008) and all 5 patients with primary cutaneous diffuse large B-cell lymphoma, leg-type, had tumors (P<.001).
Finally, we found no differences in outcomes according to types of PCL overall or by age group; however, when categorized by sex, we found males with EBV-MCU more frequently had disease progression than females with EBV-MCU (P=.04).
Comment
Primary cutaneous lymphomas were similarly distributed among males and females (55.6% vs 44.3%, respectively). This slight male predominance was similar to other reports in the literature: one US study reported a male-to-female incidence rate ratio of 1.72, indicating a significantly higher incidence in males (P<.001).6 Similar trends have been observed in other geographic regions, with reported male-to-female ratios of 1.56 in Greece and 1.35 in Argentina.9,10 These findings suggest that PCLs are slightly more prevalent in males across different populations; however, when we stratified by age, pediatric cases of PCL were significantly more frequent in males than in females (68.5% vs. 31.4%; P=.01).
Our analysis revealed that the time to diagnosis was significantly longer in adults than in children (66.2 months vs 18.1 months) for all PCLs (P<.001). The most common type of PCL in both age groups was MF, with a notably higher prevalence in adults than in children (87 [83.7%] vs 32 [59.2%]). The prolonged course of MF in adults, often taking years to progress from early to advanced stages (47.0-52.7 months) may contribute to delayed diagnosis.8,11,12 Additionally, classic lesions of MF (erythematous scaly plaques) may resemble other common dermatologic conditions, further complicating early recognition and treatment in adults more than in children.11,12 Conversely, more aggressive and rapidly progressing PCL subtypes, including CAEBVI and ENKTCL-NT, were more frequent in children and would likely be diagnosed more promptly because of the acute onset and fast evolution of signs and symptoms.13
Mycosis fungoides is the most common CTCL, followed by CD30+ T-cell disorders such as LyP and PC-ALCL.14 While MF was the predominant subtype in both age groups, similar to previous reports,6,7 pediatric patients in our study exhibited distinctive features, such as hypopigmented macules and plaques. Hypopigmented lesions may suggest an underlying immunologic mechanism unique to younger patients, specifically children, in contrast to the hyperpigmented or violaceous lesions predominating in adults.7 The hypopigmented variant of MF has been reported to be more prevalent in children, similar to our data, accounting for 54.5% of all pediatric MF cases. These hypopigmented lesions typically manifest at an early stage and follow an indolent course.15,16 Jung et al8 conducted a systematic review of children with MF and reported a mean age at diagnosis of 12.2 years, whereas in our cohort, the mean age was 9.5 years. These findings highlight the different clinical manifestations of MF in children, which may aid in early recognition and diagnosis.
In adults, MF most commonly manifested as hyperpigmented macules and plaques, erythematous plaques, atrophic lesions, and tumors. In this population, MF remained the most frequently diagnosed PCL subtype, followed by PC-ALCL.
There were notable differences in symptom presentation between age groups and sexes. Adults were more often asymptomatic, and males reported pain more frequently.
When analyzing PCL subtypes in our study, we found that CAEBVI was exclusive to children, specifically males. The updated WHO/EORTC classification contains a new section on EBV-positive LPD in childhood, including hydroa vacciniforme–like LPD and hypersensitivity reactions to mosquito bites.4 Both are cutaneous manifestations of CAEBVI with a risk for progression to systemic EBV-positive T-cell or NK-cell lymphoma. These disorders mainly affect children and adolescents from Asia or Indigenous populations from Mexico and Central and South America.3,4,17 Cases in both female and male patients have been reported, without a clear sex predominance; however, mutations in the Src homology 2 domain containing 1A (SH2D1A) gene recently have been shown to cause X-linked lymphoproliferative disease, which is associated with predilection for EBV infection and subsequent EBV-positive LPD, including CAEBVI.18,19 Thus, it is possible some of the children with CAEBVI in our study may have an underlying X-linked lymphoproliferative disease, accounting for the male predominance.
Similarly, ENKTCL-NT tended to occur more in children than in adults in our study. Both CAEBVI-LPD and ENKTCL-NT are aggressive lymphomas with a suboptimal prognosis. Although treatment with immunomodulatory agents may lead to temporary remission in most cases, disease progression has been reported in larger cohorts, emphasizing the need for long-term follow-up and more aggressive treatments in severe cases of CAEBVI.13,17 Treatment options for EBV-positive LPD include mAb such as rituximab, IVIg, HSCT, antiviral agents, interferons α and γ, and corticosteroids.20
Treatment approaches were notably different between children and adults (P<.0001). Monoclonal antibodies, immunomodulatory agents such as thalidomide, IVIg, and HSCT were exclusively used in pediatric patients, reflecting the presence of CAEBVI and ENKTCL-NT (P<.0001). Additionally, edema, blisters, and scars were observed more frequently in children, likely due to the clinical manifestations of these EBV-related disorders.
A recent review of systemic NHL highlighted various age-related differences in clinical presentation, biology, and outcomes.13 In general, children tend to present with more aggressive subtypes and achieve better outcomes compared to adults.13 These differences may be attributed to variations in tumor biology, immune responses, and/or the benefits of early and intensive interventions in pediatric populations. These findings resonate with our results, as pediatric PCL patients received more aggressive treatments—including mAb, thalidomide, IVIg, and HSCT—likely due to the higher frequency of CAEBVI/ENKTCL-NT; however, we were unable to properly assess treatment outcomes, as many patients, both adults and children, were lost to follow-up.
Overall, our findings and comparisons with existing studies highlight the need for age-specific research and management approaches for PCL. The distinct clinical and biological profiles across age groups highlight opportunities for personalized therapies and further investigation into the molecular drivers of these differences to optimize outcomes for pediatric and adult patients.
When analyzing differences by sex, we found that CAEBVI was diagnosed exclusively in male children, who correspondingly exhibited clinical features such as edema and tumors, with lesions predominantly located on the head and neck. This also influenced treatment approach, as these patients were more likely to receive thalidomide and IVIg. In contrast, PC-ALCL was observed only in female patients, a finding that deviates from previously reported epidemiology.14 Females with PC-ALCL were more likely to have genital involvement and be asymptomatic, which could suggest a sex-related bias in disease recognition and seeking health care.
Recognizing distinctive clinical manifestations across different diagnoses and age groups can aid health care providers in early identification and accurate diagnosis of PCL. Our findings revealed several notable differences: adults with MF more frequently had scaly lesions, those with PC-ALCL had crusts and ulcers, and those with LyP had erythematous papules. All adults with ENKTCL and primary cutaneous diffuse large B-cell lymphoma, leg-type, presented with tumors. While children with MF had an increased frequency of hypopigmented macules, those with ENKTCL more frequently developed nodules, and children with EBV-MCU often had crusts and ulcers. As has already been mentioned, children with CAEBVI displayed a broad range of lesions, including edema, ulcers, erythematous and hypopigmented plaques, atrophy, blisters, and scars.
Our study was limited by the retrospective design and missing data from one-third of patients, which prevented outcome comparison. We also lacked molecular profiling of patients, which could help refine therapeutic strategies for PCL.13 Finally, as both centers included are reference institutions, results may be biased and overestimated and could differ from the rest of the population.
Conclusion
This comparative study of PCL highlighted age-related differences in clinical presentation, diagnostic distribution, and treatment patterns, including a higher prevalence among male children than female children. Adult patients with PCL had a notably longer time to diagnosis than children. The most common type of PCL identified in both age groups and sex categories was MF, but hypopigmented lesions predominated in children with this condition. Epstein-Barr virus–associated PCL occurred almost exclusively in children and manifested with nodules, edema, blisters, and scars. In terms of treatment, children received more aggressive and advanced therapies, including mAb, thalidomide, IVIg, and HSCT. Further prospective research is needed to establish variations in clinical manifestations, diagnoses, treatments, and outcomes.
- Singh R, Shaik S, Negi BS, et al. Non-Hodgkin’s lymphoma: a review.J Family Med Prim Care. 2020;9:1834-1840.
- Armitage JO, Gascoyne RD, Lunning MA, et al. Non-Hodgkin lymphoma. Lancet. 2017;390:298-310.
- Swerdlow SH, Campo E, Pileri SA, et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood. 2016;127:2375-2390.
- Willemze R, Cerroni L, Kempf W, et al. The 2018 update of the WHO-EORTC classification for primary cutaneous lymphomas. Blood. 2019;133:1703-1714.
- Willemze R, Hodak E, Zinzani PL, et al; ESMO Guidelines Committee. Primary cutaneous lymphomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018;29:iv30-iv40.
- Bradford PT, Devesa SS, Anderson WF, et al. Cutaneous lymphoma incidence patterns in the United States: a population-based study of 3884 cases. Blood. 2009;113:5064-5073.
- Moon IJ, Won CH, Chang SE, et al. Prevalence, clinical features, and survival outcome trends of 627 patients with primary cutaneous lymphoma over 29 years: a retrospective review from a single tertiary center in Korea. Sci Rep. 2024;14:20118.
- Jung JM, Lim DJ, Won CH, et al. Mycosis fungoides in children and adolescents: a systematic review. JAMA Dermatol. 2021;157:431-438.
- Kaliampou S, Nikolaou V, Niforou A, et al. Epidemiological trends in cutaneous lymphomas in Greece. Eur J Dermatol. 2023;33:664-673.
- Abeldaño A, Enz P, Maskin M, et al. Primary cutaneous lymphoma in Argentina: a report of a nationwide study of 416 patients. Int J Dermatol. 2019;58:449-455.
- Cervini AB, Torres-Huamani AN, Sanchez-La-Rosa C, et al. Mycosis fungoides: experience in a pediatric hospital. Actas Dermosifiliogr. 2017;108:564-570.
- Welfringer-Morin A, Barroil M, Fraitag S, et al. Clinical features, histological characteristics, and disease outcomes of mycosis fungoides in children and adolescents: a nationwide multicentre cohort of 46 patients. Dermatology. 2023;239:132-139.
- Sandlund JT, Martin MG. Non-Hodgkin lymphoma across the pediatric and adolescent and young adult age spectrum. Hematology Am Soc Hematol Educ Program. 2016;2016:589-597.
- Ortiz-Hidalgo C, Pina-Oviedo S. Primary cutaneous anaplastic large cell lymphoma-a review of clinical, morphological, immunohistochemical, and molecular features. Cancers (Basel). 2023;15:4098.
- Nielsen PR, Eriksen JO, Wehkamp U, et al. Clinical and histological characteristics of mycosis fungoides and Sézary syndrome: a retrospective, single-centre study of 43 patients from eastern Denmark. Acta Derm Venereol. 2019;99:1231-1236.
- Suh KS, Jang MS, Jung JH, et al. Clinical characteristics and long-term outcome of 223 patients with mycosis fungoides at a single tertiary center in Korea: a 29-year review. J Am Acad Dermatol. 2022;86:1275-1284.
- Quintanilla-Martinez L, Ridaura C, Nagl F, et al. Hydroa vacciniforme-like lymphoma: a chronic EBV+ lymphoproliferative disorder with risk to develop a systemic lymphoma. Blood. 2013;122:3101-3110.
- Fujiwara S, Nakamura H. Chronic active Epstein-Barr virus infection: is it immunodeficiency, malignancy, or both? Cancers (Basel). 2020;12:3202.
- Sumazaki R, Kanegane H, Osaki M, et al. SH2D1A mutations in Japanese males with severe Epstein-Barr virus–associated illnesses. Blood. 2001;98:1268-1270.
- Kimura H. Pathogenesis of chronic active Epstein-Barr virus infection: is this an infectious disease, lymphoproliferative disorder, or immunodeficiency? Rev Med Virol. 2006;16:251-261.
- Singh R, Shaik S, Negi BS, et al. Non-Hodgkin’s lymphoma: a review.J Family Med Prim Care. 2020;9:1834-1840.
- Armitage JO, Gascoyne RD, Lunning MA, et al. Non-Hodgkin lymphoma. Lancet. 2017;390:298-310.
- Swerdlow SH, Campo E, Pileri SA, et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood. 2016;127:2375-2390.
- Willemze R, Cerroni L, Kempf W, et al. The 2018 update of the WHO-EORTC classification for primary cutaneous lymphomas. Blood. 2019;133:1703-1714.
- Willemze R, Hodak E, Zinzani PL, et al; ESMO Guidelines Committee. Primary cutaneous lymphomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018;29:iv30-iv40.
- Bradford PT, Devesa SS, Anderson WF, et al. Cutaneous lymphoma incidence patterns in the United States: a population-based study of 3884 cases. Blood. 2009;113:5064-5073.
- Moon IJ, Won CH, Chang SE, et al. Prevalence, clinical features, and survival outcome trends of 627 patients with primary cutaneous lymphoma over 29 years: a retrospective review from a single tertiary center in Korea. Sci Rep. 2024;14:20118.
- Jung JM, Lim DJ, Won CH, et al. Mycosis fungoides in children and adolescents: a systematic review. JAMA Dermatol. 2021;157:431-438.
- Kaliampou S, Nikolaou V, Niforou A, et al. Epidemiological trends in cutaneous lymphomas in Greece. Eur J Dermatol. 2023;33:664-673.
- Abeldaño A, Enz P, Maskin M, et al. Primary cutaneous lymphoma in Argentina: a report of a nationwide study of 416 patients. Int J Dermatol. 2019;58:449-455.
- Cervini AB, Torres-Huamani AN, Sanchez-La-Rosa C, et al. Mycosis fungoides: experience in a pediatric hospital. Actas Dermosifiliogr. 2017;108:564-570.
- Welfringer-Morin A, Barroil M, Fraitag S, et al. Clinical features, histological characteristics, and disease outcomes of mycosis fungoides in children and adolescents: a nationwide multicentre cohort of 46 patients. Dermatology. 2023;239:132-139.
- Sandlund JT, Martin MG. Non-Hodgkin lymphoma across the pediatric and adolescent and young adult age spectrum. Hematology Am Soc Hematol Educ Program. 2016;2016:589-597.
- Ortiz-Hidalgo C, Pina-Oviedo S. Primary cutaneous anaplastic large cell lymphoma-a review of clinical, morphological, immunohistochemical, and molecular features. Cancers (Basel). 2023;15:4098.
- Nielsen PR, Eriksen JO, Wehkamp U, et al. Clinical and histological characteristics of mycosis fungoides and Sézary syndrome: a retrospective, single-centre study of 43 patients from eastern Denmark. Acta Derm Venereol. 2019;99:1231-1236.
- Suh KS, Jang MS, Jung JH, et al. Clinical characteristics and long-term outcome of 223 patients with mycosis fungoides at a single tertiary center in Korea: a 29-year review. J Am Acad Dermatol. 2022;86:1275-1284.
- Quintanilla-Martinez L, Ridaura C, Nagl F, et al. Hydroa vacciniforme-like lymphoma: a chronic EBV+ lymphoproliferative disorder with risk to develop a systemic lymphoma. Blood. 2013;122:3101-3110.
- Fujiwara S, Nakamura H. Chronic active Epstein-Barr virus infection: is it immunodeficiency, malignancy, or both? Cancers (Basel). 2020;12:3202.
- Sumazaki R, Kanegane H, Osaki M, et al. SH2D1A mutations in Japanese males with severe Epstein-Barr virus–associated illnesses. Blood. 2001;98:1268-1270.
- Kimura H. Pathogenesis of chronic active Epstein-Barr virus infection: is this an infectious disease, lymphoproliferative disorder, or immunodeficiency? Rev Med Virol. 2006;16:251-261.
Age- and Sex-Related Differences in Primary Cutaneous Lymphoma
Age- and Sex-Related Differences in Primary Cutaneous Lymphoma
Practice Points
- The clinical behavior and incidence of primary cutaneous lymphomas vary dramatically between children and adults, suggesting underlying biologic, immunologic, and genetic differences.
- Primary cutaneous lymphoma is more common among males, particularly in children.
- Adults experience longer diagnostic delays due to slower symptom progression and overlap with benign skin conditions, whereas children often present with rapidly progressive, severe variants requiring more aggressive therapies.

The Hair-Cut Sign for Scalp Biopsy Site Identification
The Hair-Cut Sign for Scalp Biopsy Site Identification
Practice Gap
Accurate biopsy site identification prior to Mohs micrographic surgery (MMS) can be challenging, particularly on the scalp, where excellent healing, field cancerization, prior procedures, large surface area, and hair density may complicate localization. Accurate site identification is further hindered when patients are unable to recall the biopsy location, when the biopsy and MMS are performed by different clinicians, or when photographic documentation is absent. Scalp lesions pose an additional challenge because even high-quality photographs may fail to capture subtle landmarks that are obscured by hair.
Wrong-site surgery was the most common serious error reported in a survey of 150 dermatologists, accounting for 19.0% of these errors.1 Research has shown that dermatologists may misidentify biopsy sites in up to 17.6% of cases, and patients (eg, if a patient goes to a dermatologic surgeon and is asked to identify the biopsy site for the surgeon) in up to 25.5% (N=278).2 Additionally, a survey of Mohs surgeons revealed that 14.0% of 42 malpractice cases were due to wrong-site surgery.3 A Delphi consensus study assessing possible preventive interventions found that the best way to document the site is with a photograph in association with landmarks and diagrams.4
The Technique
The hair-cut sign is a simple and effective technique for identifying biopsy sites on the scalp. Hair at the biopsy site typically is cut during biopsy; as the surrounding hair grows, the resulting short tuft serves as an anatomic marker that can persist for weeks to months to facilitate accurate site localization by the Mohs surgeon (Figure). This noninvasive, equipment-free method may be particularly useful when documentation or photography is limited. To maximize its effectiveness, clinical staff should avoid trimming the area before physician verification of the site. The technique is most effective in patients with longer hair and when the interval between biopsy and surgery is less than 3 months, as hair regrowth may reduce contrast with the surrounding scalp.
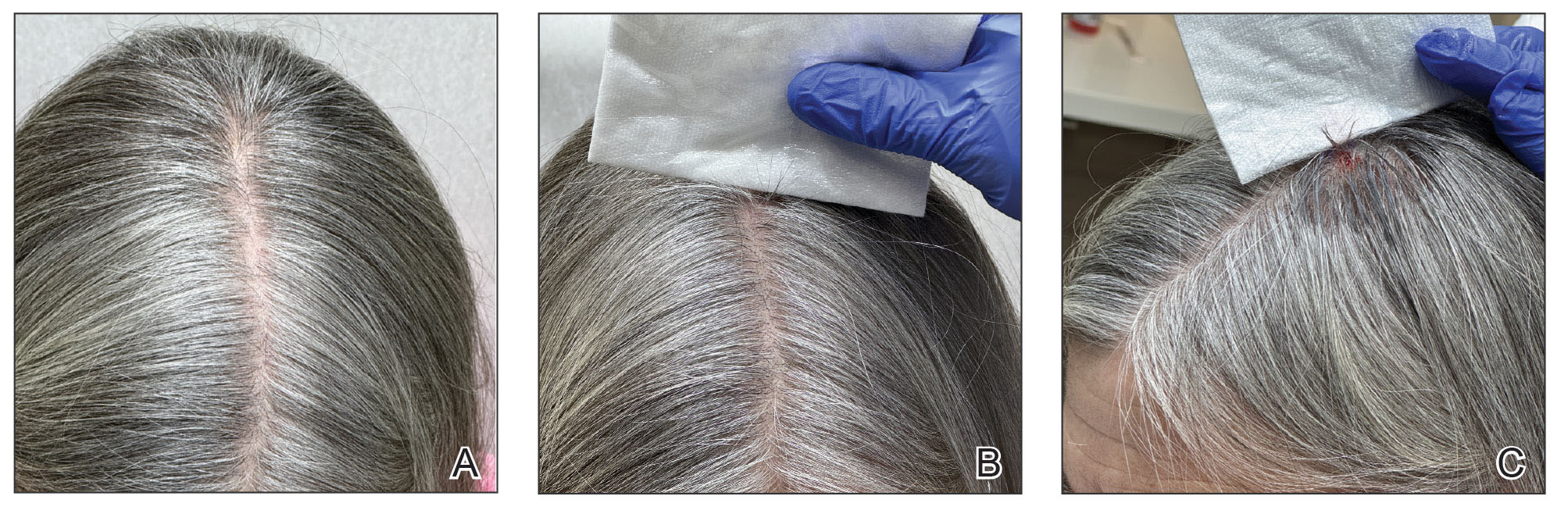
Practice Implications
Accurate biopsy site identification is a critical component of patient safety in dermatologic surgery, particularly on the scalp, where traditional localization strategies may be unreliable. The hair-cut sign is a simple, reliable, no-cost, and reproducible adjunct to photography, anatomic documentation, and patient verification that may improve site localization and help reduce the risk for wrong-site surgery in select patients to complement standard practices. Incorporating the hair-cut sign into routine scalp surgery workflow represents a low-burden intervention that may improve accuracy when other documentation is limited.
- Watson AJ, Redbord K, Taylor JS, et al. Medical error in dermatology practice: development of a classification system to drive priority setting in patient safety efforts. J Am Acad Dermatol. 2013;68:729-737. doi:10.1016/j.jaad.2012.10.058
- Nijhawan RI, Lee EH , Nehal KS. Biopsy site selfies—a quality improvement pilot study to assist with correct surgical site identification. Dermatol Surg. 2015;41:499-504. doi:10.1097/DSS.0000000000000305
- Perlis CS, Campbell RM, Perlis RH, et al. Incidence of and risk factors for medical malpractice lawsuits among Mohs surgeons. Dermatol Surg. 2006;32:79-83. doi:10.1111/1524-4725.2006.32009
- Alam M, Lee A, Ibrahimi OA, et al. A multistep approach to improving biopsy site identification in dermatology: physician, staff, and patient roles based on a Delphi consensus. JAMA Dermatol. 2014;150:550-558. doi:10.1001/jamadermatol.2013.9804
Practice Gap
Accurate biopsy site identification prior to Mohs micrographic surgery (MMS) can be challenging, particularly on the scalp, where excellent healing, field cancerization, prior procedures, large surface area, and hair density may complicate localization. Accurate site identification is further hindered when patients are unable to recall the biopsy location, when the biopsy and MMS are performed by different clinicians, or when photographic documentation is absent. Scalp lesions pose an additional challenge because even high-quality photographs may fail to capture subtle landmarks that are obscured by hair.
Wrong-site surgery was the most common serious error reported in a survey of 150 dermatologists, accounting for 19.0% of these errors.1 Research has shown that dermatologists may misidentify biopsy sites in up to 17.6% of cases, and patients (eg, if a patient goes to a dermatologic surgeon and is asked to identify the biopsy site for the surgeon) in up to 25.5% (N=278).2 Additionally, a survey of Mohs surgeons revealed that 14.0% of 42 malpractice cases were due to wrong-site surgery.3 A Delphi consensus study assessing possible preventive interventions found that the best way to document the site is with a photograph in association with landmarks and diagrams.4
The Technique
The hair-cut sign is a simple and effective technique for identifying biopsy sites on the scalp. Hair at the biopsy site typically is cut during biopsy; as the surrounding hair grows, the resulting short tuft serves as an anatomic marker that can persist for weeks to months to facilitate accurate site localization by the Mohs surgeon (Figure). This noninvasive, equipment-free method may be particularly useful when documentation or photography is limited. To maximize its effectiveness, clinical staff should avoid trimming the area before physician verification of the site. The technique is most effective in patients with longer hair and when the interval between biopsy and surgery is less than 3 months, as hair regrowth may reduce contrast with the surrounding scalp.
Practice Implications
Accurate biopsy site identification is a critical component of patient safety in dermatologic surgery, particularly on the scalp, where traditional localization strategies may be unreliable. The hair-cut sign is a simple, reliable, no-cost, and reproducible adjunct to photography, anatomic documentation, and patient verification that may improve site localization and help reduce the risk for wrong-site surgery in select patients to complement standard practices. Incorporating the hair-cut sign into routine scalp surgery workflow represents a low-burden intervention that may improve accuracy when other documentation is limited.
Practice Gap
Accurate biopsy site identification prior to Mohs micrographic surgery (MMS) can be challenging, particularly on the scalp, where excellent healing, field cancerization, prior procedures, large surface area, and hair density may complicate localization. Accurate site identification is further hindered when patients are unable to recall the biopsy location, when the biopsy and MMS are performed by different clinicians, or when photographic documentation is absent. Scalp lesions pose an additional challenge because even high-quality photographs may fail to capture subtle landmarks that are obscured by hair.
Wrong-site surgery was the most common serious error reported in a survey of 150 dermatologists, accounting for 19.0% of these errors.1 Research has shown that dermatologists may misidentify biopsy sites in up to 17.6% of cases, and patients (eg, if a patient goes to a dermatologic surgeon and is asked to identify the biopsy site for the surgeon) in up to 25.5% (N=278).2 Additionally, a survey of Mohs surgeons revealed that 14.0% of 42 malpractice cases were due to wrong-site surgery.3 A Delphi consensus study assessing possible preventive interventions found that the best way to document the site is with a photograph in association with landmarks and diagrams.4
The Technique
The hair-cut sign is a simple and effective technique for identifying biopsy sites on the scalp. Hair at the biopsy site typically is cut during biopsy; as the surrounding hair grows, the resulting short tuft serves as an anatomic marker that can persist for weeks to months to facilitate accurate site localization by the Mohs surgeon (Figure). This noninvasive, equipment-free method may be particularly useful when documentation or photography is limited. To maximize its effectiveness, clinical staff should avoid trimming the area before physician verification of the site. The technique is most effective in patients with longer hair and when the interval between biopsy and surgery is less than 3 months, as hair regrowth may reduce contrast with the surrounding scalp.
Practice Implications
Accurate biopsy site identification is a critical component of patient safety in dermatologic surgery, particularly on the scalp, where traditional localization strategies may be unreliable. The hair-cut sign is a simple, reliable, no-cost, and reproducible adjunct to photography, anatomic documentation, and patient verification that may improve site localization and help reduce the risk for wrong-site surgery in select patients to complement standard practices. Incorporating the hair-cut sign into routine scalp surgery workflow represents a low-burden intervention that may improve accuracy when other documentation is limited.
- Watson AJ, Redbord K, Taylor JS, et al. Medical error in dermatology practice: development of a classification system to drive priority setting in patient safety efforts. J Am Acad Dermatol. 2013;68:729-737. doi:10.1016/j.jaad.2012.10.058
- Nijhawan RI, Lee EH , Nehal KS. Biopsy site selfies—a quality improvement pilot study to assist with correct surgical site identification. Dermatol Surg. 2015;41:499-504. doi:10.1097/DSS.0000000000000305
- Perlis CS, Campbell RM, Perlis RH, et al. Incidence of and risk factors for medical malpractice lawsuits among Mohs surgeons. Dermatol Surg. 2006;32:79-83. doi:10.1111/1524-4725.2006.32009
- Alam M, Lee A, Ibrahimi OA, et al. A multistep approach to improving biopsy site identification in dermatology: physician, staff, and patient roles based on a Delphi consensus. JAMA Dermatol. 2014;150:550-558. doi:10.1001/jamadermatol.2013.9804
- Watson AJ, Redbord K, Taylor JS, et al. Medical error in dermatology practice: development of a classification system to drive priority setting in patient safety efforts. J Am Acad Dermatol. 2013;68:729-737. doi:10.1016/j.jaad.2012.10.058
- Nijhawan RI, Lee EH , Nehal KS. Biopsy site selfies—a quality improvement pilot study to assist with correct surgical site identification. Dermatol Surg. 2015;41:499-504. doi:10.1097/DSS.0000000000000305
- Perlis CS, Campbell RM, Perlis RH, et al. Incidence of and risk factors for medical malpractice lawsuits among Mohs surgeons. Dermatol Surg. 2006;32:79-83. doi:10.1111/1524-4725.2006.32009
- Alam M, Lee A, Ibrahimi OA, et al. A multistep approach to improving biopsy site identification in dermatology: physician, staff, and patient roles based on a Delphi consensus. JAMA Dermatol. 2014;150:550-558. doi:10.1001/jamadermatol.2013.9804
The Hair-Cut Sign for Scalp Biopsy Site Identification
The Hair-Cut Sign for Scalp Biopsy Site Identification

Black Malar Papules Following Use of Hydroquinone Cream 2% Purchased Online
Black Malar Papules Following Use of Hydroquinone Cream 2% Purchased Online
To the Editor:
Exogenous ochronosis (EO) is a rare dyschromia that affects individuals with darker skin tones and results from the application of skin-lightening topical agents, most commonly those containing hydroquinone. Hydroquinone-induced EO usually is reported outside the United States, mainly in African and South Asian patients,1 as well as after long-term use of high‑concentration hydroquinone. We report a case of stage II EO that developed in a patient in the United States following 6 months' use of hydroquinone cream 2% that was purchased online.
A 75-year-old Black man presented to the dermatology clinic with dark discoloration on the cheeks of 6 months’ duration. He reported that the hyperpigmentation had developed after 6 months of daily use of an over-the-counter (OTC) cream containing 2% hydroquinone, which he purchased online to treat melasma of the bilateral cheeks and temples that had been present for at least a decade. The patient was otherwise healthy and did not take any other daily medications. He was a landscaper by occupation and spent most days outdoors. He reported a history of recurrent blistering sunburns and reported that he applied sunscreen with a sun protection factor of 30 to the face on most days.
Physical examination revealed gray-black, coarsely textured papules and plaques on a background of brown pigmentation involving the malar cheeks. Reticulated, blue-black, caviarlike papules were present within the plaques (Figure 1). Dermoscopy revealed blue-black globules and globularlike structures on a brown background with the absence of follicular openings (Figure 2). A punch biopsy from the left malar cheek revealed banana-shaped, yellow-brown deposits with heavy elastosis in the superficial dermis (Figure 3). The patient was advised to permanently discontinue hydroquinone and was prescribed topical adapalene. He was evaluated for treatment with a fractional erbium-doped yttrium aluminum garnet laser but ultimately elected not to pursue treatment.

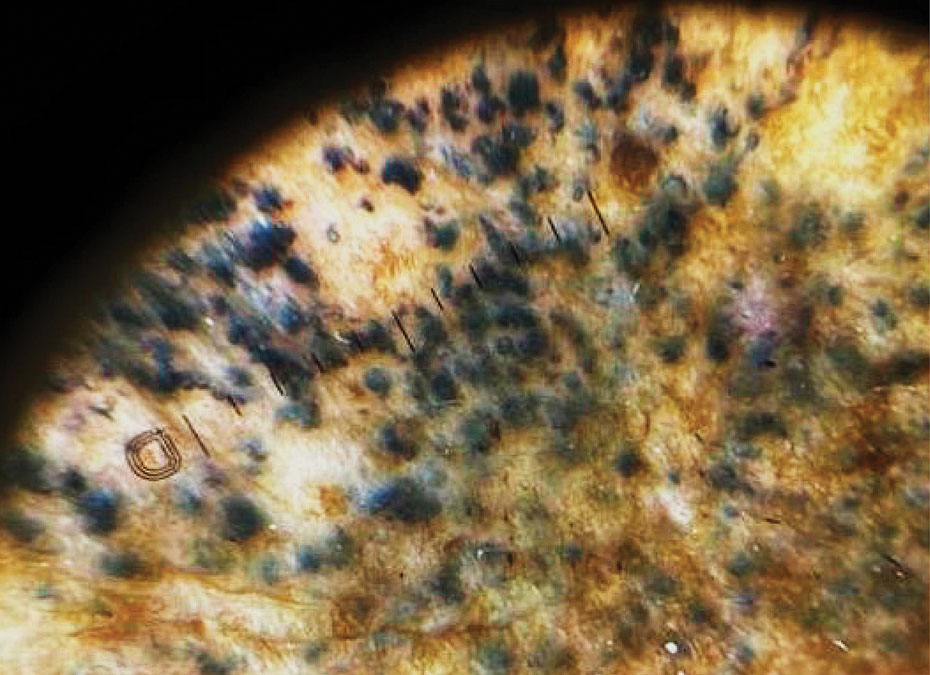
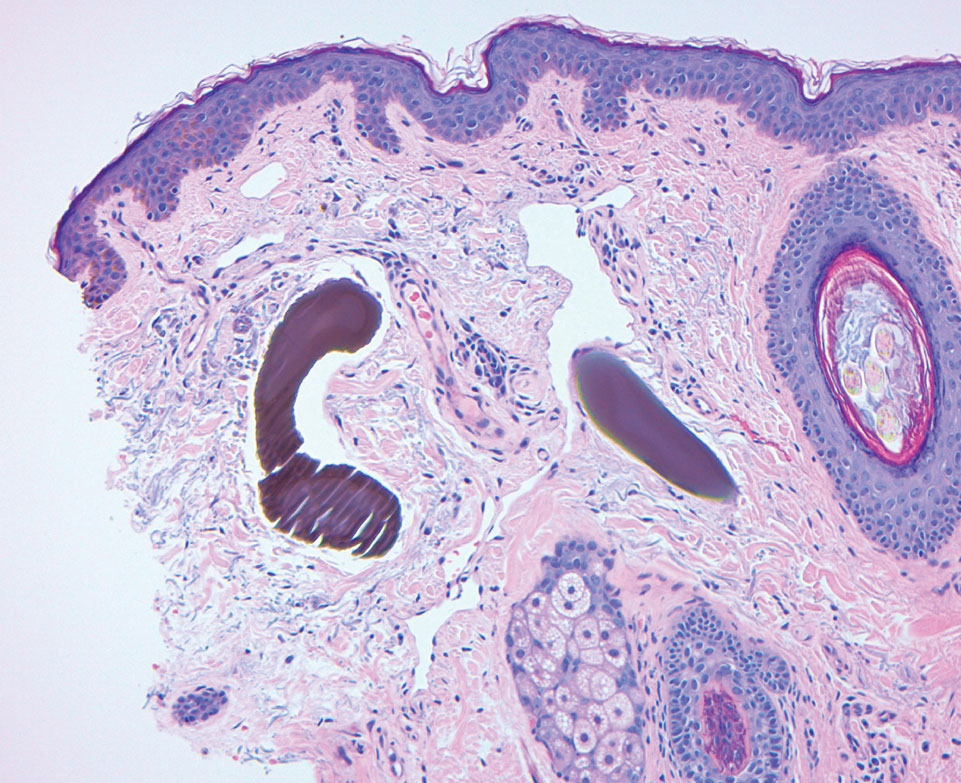
Hydroquinone has long been a first-line topical agent for the treatment of skin dyschromia. It generally is regarded as a safe and effective therapy when used under the supervision of a dermatologist. Prolonged use of topical hydroquinone is known to induce paradoxical EO. This acquired dyschromia is characterized by the development of blue-black or gray-blue pigmented patches as well as caviarlike black papules, papulonodules, and skin atrophy in more severe cases.2 Most cases are documented in African and South Asian countries, with fewer than 100 cases described in the United States.2 Despite the rarity of EO in the United States, concerns regarding the unsupervised use of hydroquinone contributed to regulatory changes. In response to the CARES Act and Over-the-Counter Drug Monograph Reform, the sale of OTC hydroquinone-based products became prohibited in September 2020 in the United States.³ Prior to the CARES Act, an estimated 10 million tubes of OTC hydroquinone were sold, and approximately 330,000 prescriptions were written in 2019.2,4 Subsequently, its availability was converted to prescription only in the United States.
Exogenous ochronosis occurs in 3 clinical stages: (I) erythema and hyperpigmentation, (II) black colloid milia (caviarlike papules) and atrophy, and (III) papulonodules.1 Our patient’s case was unusual, as EO is most commonly described after exposure to high concentrations and prolonged hydroquinone treatment. In a global retrospective review of 126 patients of varied racial and ethnic backgrounds with hydroquinone-induced ochronosis, EO was most frequently reported with concentrations exceeding 4%. The median duration of use was 5 years, and only 12 cases (9.5%) of EO were reported with 1 year of use or less, including 4 cases with 3 months or less of use.1
While large epidemiologic studies from South Africa have reported EO prevalence rates as high as 69% among users of skin-lightening products,6 a search of the PubMed, Scopus, and Web of Science databases using the terms exogenous ochronosis and hydroquinone identified only 39 cases in US-based literature between 1983 and 2020.2 In a retrospective review of 25 cases of EO in the United States, the average length of product use was 9.2 years, and the shortest duration was 1.5 years.7
The pathogenesis of EO is thought to occur due to the inhibitive effect of topical hydroquinone on homogentisic acid oxidase, resulting in the accumulation of homogentisic acid in tissues and ochronotic deposits.1,5 We suspect that our patient’s occupation as a landscaper and associated chronic sun exposure may have accelerated the development of EO, as UV exposure and inadequate photoprotection have been described as risk factors in the development and severity of EO.8 Although the patient reported daily application of sun protection factor 30 sunscreen, the extent of his outdoor occupational exposure may have exceeded the protection afforded.
Treatment of EO is notoriously challenging, and skin changes often are permanent. Of the 25 patients identified in a 10-year retrospective analysis of EO at a single US center, none responded to topical treatment alone.7 Among those who underwent procedural interventions, 3 patients treated with microneedling and 3 patients treated with Q-switched Alexandrite laser demonstrated favorable outcomes; however, this was a retrospective chart review, not a controlled trial with predefined treatment arms.7 Bellew et al9 reported 2 patients with EO who showed progressive lightening in response to Q-switched Alexandrite laser treatments. In this case series, the first patient received 6 treatments at 2-month intervals and the second received 4 treatments at 4-month intervals. Posttreatment biopsies demonstrated decreased dermal pigmentation, and neither patient experienced scarring or textural changes. Méndez Baca et al10 demonstrated successful lightening of pigmentation in a patient with medium-toned skin following 9 sessions with a fractional nonablative picosecond laser. Ceglio et al11 described a stepwise treatment approach in a patient with dark brown skin with EO, beginning with 12 sessions of a 1064-nm Q-switched Nd:YAG laser that yielded slight improvement, followed by 7 sessions of intense pulsed light therapy with partial response, and ultimately achieving marked improvement after 5 bimonthly sessions of fractional 10,600-nm carbon dioxide laser.
This case highlights the potential for EO to develop even with low-concentration (2%) hydroquinone obtained through unregulated online sources, underscoring the need for dermatologist supervision when hydroquinone is used. Despite the 2020 prohibition of OTC hydroquinone sales in the United States, patients continue to access these products online. Clinicians should maintain a high index of suspicion for EO in patients presenting with paradoxical facial hyperpigmentation and a history of unsupervised hydroquinone use.
- Ishack S, Lipner SR. Exogenous ochronosis associated with hydroquinone: a systematic review. Int J Dermatol. 2022;61:675-684. doi:10.1111/ijd.15878
- Qorbani A, Mubasher A, Sarantopoulos GP, et al. Exogenous ochronosis (EO): skin lightening cream causing rare caviar-like lesion with banana-like pigments; review of literature and histological comparison with endogenous counterpart. Autops Case Rep. 2020;10:E2020197. doi:10.4322/acr.2020.197
- Coronavirus Aid, Relief, and Economic Security (CARES) Act, Pub L No. 116-136, §3851, 134 Stat 281 (2020).
- Hydroquinone, found in skin lightening agents worldwide, linked with increased skin cancer risk. Medscape. August 26, 2022. Accessed June 5, 2026.
- Dogliotti M, Leibowitz M. Granulomatous ochronosis—a cosmetic-induced skin disorder in Blacks. S Afr Med J. 1979;56:757-760.
- Hardwick N, Van Gelder LW, Van der Merwe CA, Van der Merwe MP. Exogenous ochronosis: an epidemiological study. Br J Dermatol. 1989;120:229-238. doi:10.1111/j.1365-2133.1989.tb07787.x
- Lazar M, De La Garza H, Vashi NA. Exogenous ochronosis: characterizing a rare disorder in skin of color. J Clin Med. 2023;12:4341. doi:10.3390/jcm12134341
- Findlay GH, de Beer HA. Chronic hydroquinone poisoning of the skin from skin-lightening cosmetics. A South African epidemic of ochronosis of the face in dark-skinned individuals. S Afr Med J. 1980;57:187-190.
- Bellew SG, Alster TS. Treatment of exogenous ochronosis with a Q-switched alexandrite (755 nm) laser. Dermatol Surg. 2004;30:555-558. doi:10.1111/j.1524-4725.2004.30177.x
- Méndez Baca I, Al-Niaimi F, Colina C, et al. A case of ochronosis successfully treated with the picosecond laser. J Cosmet Dermatol. 2019;18:1322-1325. doi:10.1111/jocd.12834
- Ceglio WW, Careta MF, Patriota R, et al. Exogenous ochronosis successfully treated with the combination of intense pulsed light and fractional CO2 laser. An Bras Dermatol. 2023;98:138-140. doi:10.1016/j.abd.2021.08.013
To the Editor:
Exogenous ochronosis (EO) is a rare dyschromia that affects individuals with darker skin tones and results from the application of skin-lightening topical agents, most commonly those containing hydroquinone. Hydroquinone-induced EO usually is reported outside the United States, mainly in African and South Asian patients,1 as well as after long-term use of high‑concentration hydroquinone. We report a case of stage II EO that developed in a patient in the United States following 6 months' use of hydroquinone cream 2% that was purchased online.
A 75-year-old Black man presented to the dermatology clinic with dark discoloration on the cheeks of 6 months’ duration. He reported that the hyperpigmentation had developed after 6 months of daily use of an over-the-counter (OTC) cream containing 2% hydroquinone, which he purchased online to treat melasma of the bilateral cheeks and temples that had been present for at least a decade. The patient was otherwise healthy and did not take any other daily medications. He was a landscaper by occupation and spent most days outdoors. He reported a history of recurrent blistering sunburns and reported that he applied sunscreen with a sun protection factor of 30 to the face on most days.
Physical examination revealed gray-black, coarsely textured papules and plaques on a background of brown pigmentation involving the malar cheeks. Reticulated, blue-black, caviarlike papules were present within the plaques (Figure 1). Dermoscopy revealed blue-black globules and globularlike structures on a brown background with the absence of follicular openings (Figure 2). A punch biopsy from the left malar cheek revealed banana-shaped, yellow-brown deposits with heavy elastosis in the superficial dermis (Figure 3). The patient was advised to permanently discontinue hydroquinone and was prescribed topical adapalene. He was evaluated for treatment with a fractional erbium-doped yttrium aluminum garnet laser but ultimately elected not to pursue treatment.
Hydroquinone has long been a first-line topical agent for the treatment of skin dyschromia. It generally is regarded as a safe and effective therapy when used under the supervision of a dermatologist. Prolonged use of topical hydroquinone is known to induce paradoxical EO. This acquired dyschromia is characterized by the development of blue-black or gray-blue pigmented patches as well as caviarlike black papules, papulonodules, and skin atrophy in more severe cases.2 Most cases are documented in African and South Asian countries, with fewer than 100 cases described in the United States.2 Despite the rarity of EO in the United States, concerns regarding the unsupervised use of hydroquinone contributed to regulatory changes. In response to the CARES Act and Over-the-Counter Drug Monograph Reform, the sale of OTC hydroquinone-based products became prohibited in September 2020 in the United States.³ Prior to the CARES Act, an estimated 10 million tubes of OTC hydroquinone were sold, and approximately 330,000 prescriptions were written in 2019.2,4 Subsequently, its availability was converted to prescription only in the United States.
Exogenous ochronosis occurs in 3 clinical stages: (I) erythema and hyperpigmentation, (II) black colloid milia (caviarlike papules) and atrophy, and (III) papulonodules.1 Our patient’s case was unusual, as EO is most commonly described after exposure to high concentrations and prolonged hydroquinone treatment. In a global retrospective review of 126 patients of varied racial and ethnic backgrounds with hydroquinone-induced ochronosis, EO was most frequently reported with concentrations exceeding 4%. The median duration of use was 5 years, and only 12 cases (9.5%) of EO were reported with 1 year of use or less, including 4 cases with 3 months or less of use.1
While large epidemiologic studies from South Africa have reported EO prevalence rates as high as 69% among users of skin-lightening products,6 a search of the PubMed, Scopus, and Web of Science databases using the terms exogenous ochronosis and hydroquinone identified only 39 cases in US-based literature between 1983 and 2020.2 In a retrospective review of 25 cases of EO in the United States, the average length of product use was 9.2 years, and the shortest duration was 1.5 years.7
The pathogenesis of EO is thought to occur due to the inhibitive effect of topical hydroquinone on homogentisic acid oxidase, resulting in the accumulation of homogentisic acid in tissues and ochronotic deposits.1,5 We suspect that our patient’s occupation as a landscaper and associated chronic sun exposure may have accelerated the development of EO, as UV exposure and inadequate photoprotection have been described as risk factors in the development and severity of EO.8 Although the patient reported daily application of sun protection factor 30 sunscreen, the extent of his outdoor occupational exposure may have exceeded the protection afforded.
Treatment of EO is notoriously challenging, and skin changes often are permanent. Of the 25 patients identified in a 10-year retrospective analysis of EO at a single US center, none responded to topical treatment alone.7 Among those who underwent procedural interventions, 3 patients treated with microneedling and 3 patients treated with Q-switched Alexandrite laser demonstrated favorable outcomes; however, this was a retrospective chart review, not a controlled trial with predefined treatment arms.7 Bellew et al9 reported 2 patients with EO who showed progressive lightening in response to Q-switched Alexandrite laser treatments. In this case series, the first patient received 6 treatments at 2-month intervals and the second received 4 treatments at 4-month intervals. Posttreatment biopsies demonstrated decreased dermal pigmentation, and neither patient experienced scarring or textural changes. Méndez Baca et al10 demonstrated successful lightening of pigmentation in a patient with medium-toned skin following 9 sessions with a fractional nonablative picosecond laser. Ceglio et al11 described a stepwise treatment approach in a patient with dark brown skin with EO, beginning with 12 sessions of a 1064-nm Q-switched Nd:YAG laser that yielded slight improvement, followed by 7 sessions of intense pulsed light therapy with partial response, and ultimately achieving marked improvement after 5 bimonthly sessions of fractional 10,600-nm carbon dioxide laser.
This case highlights the potential for EO to develop even with low-concentration (2%) hydroquinone obtained through unregulated online sources, underscoring the need for dermatologist supervision when hydroquinone is used. Despite the 2020 prohibition of OTC hydroquinone sales in the United States, patients continue to access these products online. Clinicians should maintain a high index of suspicion for EO in patients presenting with paradoxical facial hyperpigmentation and a history of unsupervised hydroquinone use.
To the Editor:
Exogenous ochronosis (EO) is a rare dyschromia that affects individuals with darker skin tones and results from the application of skin-lightening topical agents, most commonly those containing hydroquinone. Hydroquinone-induced EO usually is reported outside the United States, mainly in African and South Asian patients,1 as well as after long-term use of high‑concentration hydroquinone. We report a case of stage II EO that developed in a patient in the United States following 6 months' use of hydroquinone cream 2% that was purchased online.
A 75-year-old Black man presented to the dermatology clinic with dark discoloration on the cheeks of 6 months’ duration. He reported that the hyperpigmentation had developed after 6 months of daily use of an over-the-counter (OTC) cream containing 2% hydroquinone, which he purchased online to treat melasma of the bilateral cheeks and temples that had been present for at least a decade. The patient was otherwise healthy and did not take any other daily medications. He was a landscaper by occupation and spent most days outdoors. He reported a history of recurrent blistering sunburns and reported that he applied sunscreen with a sun protection factor of 30 to the face on most days.
Physical examination revealed gray-black, coarsely textured papules and plaques on a background of brown pigmentation involving the malar cheeks. Reticulated, blue-black, caviarlike papules were present within the plaques (Figure 1). Dermoscopy revealed blue-black globules and globularlike structures on a brown background with the absence of follicular openings (Figure 2). A punch biopsy from the left malar cheek revealed banana-shaped, yellow-brown deposits with heavy elastosis in the superficial dermis (Figure 3). The patient was advised to permanently discontinue hydroquinone and was prescribed topical adapalene. He was evaluated for treatment with a fractional erbium-doped yttrium aluminum garnet laser but ultimately elected not to pursue treatment.
Hydroquinone has long been a first-line topical agent for the treatment of skin dyschromia. It generally is regarded as a safe and effective therapy when used under the supervision of a dermatologist. Prolonged use of topical hydroquinone is known to induce paradoxical EO. This acquired dyschromia is characterized by the development of blue-black or gray-blue pigmented patches as well as caviarlike black papules, papulonodules, and skin atrophy in more severe cases.2 Most cases are documented in African and South Asian countries, with fewer than 100 cases described in the United States.2 Despite the rarity of EO in the United States, concerns regarding the unsupervised use of hydroquinone contributed to regulatory changes. In response to the CARES Act and Over-the-Counter Drug Monograph Reform, the sale of OTC hydroquinone-based products became prohibited in September 2020 in the United States.³ Prior to the CARES Act, an estimated 10 million tubes of OTC hydroquinone were sold, and approximately 330,000 prescriptions were written in 2019.2,4 Subsequently, its availability was converted to prescription only in the United States.
Exogenous ochronosis occurs in 3 clinical stages: (I) erythema and hyperpigmentation, (II) black colloid milia (caviarlike papules) and atrophy, and (III) papulonodules.1 Our patient’s case was unusual, as EO is most commonly described after exposure to high concentrations and prolonged hydroquinone treatment. In a global retrospective review of 126 patients of varied racial and ethnic backgrounds with hydroquinone-induced ochronosis, EO was most frequently reported with concentrations exceeding 4%. The median duration of use was 5 years, and only 12 cases (9.5%) of EO were reported with 1 year of use or less, including 4 cases with 3 months or less of use.1
While large epidemiologic studies from South Africa have reported EO prevalence rates as high as 69% among users of skin-lightening products,6 a search of the PubMed, Scopus, and Web of Science databases using the terms exogenous ochronosis and hydroquinone identified only 39 cases in US-based literature between 1983 and 2020.2 In a retrospective review of 25 cases of EO in the United States, the average length of product use was 9.2 years, and the shortest duration was 1.5 years.7
The pathogenesis of EO is thought to occur due to the inhibitive effect of topical hydroquinone on homogentisic acid oxidase, resulting in the accumulation of homogentisic acid in tissues and ochronotic deposits.1,5 We suspect that our patient’s occupation as a landscaper and associated chronic sun exposure may have accelerated the development of EO, as UV exposure and inadequate photoprotection have been described as risk factors in the development and severity of EO.8 Although the patient reported daily application of sun protection factor 30 sunscreen, the extent of his outdoor occupational exposure may have exceeded the protection afforded.
Treatment of EO is notoriously challenging, and skin changes often are permanent. Of the 25 patients identified in a 10-year retrospective analysis of EO at a single US center, none responded to topical treatment alone.7 Among those who underwent procedural interventions, 3 patients treated with microneedling and 3 patients treated with Q-switched Alexandrite laser demonstrated favorable outcomes; however, this was a retrospective chart review, not a controlled trial with predefined treatment arms.7 Bellew et al9 reported 2 patients with EO who showed progressive lightening in response to Q-switched Alexandrite laser treatments. In this case series, the first patient received 6 treatments at 2-month intervals and the second received 4 treatments at 4-month intervals. Posttreatment biopsies demonstrated decreased dermal pigmentation, and neither patient experienced scarring or textural changes. Méndez Baca et al10 demonstrated successful lightening of pigmentation in a patient with medium-toned skin following 9 sessions with a fractional nonablative picosecond laser. Ceglio et al11 described a stepwise treatment approach in a patient with dark brown skin with EO, beginning with 12 sessions of a 1064-nm Q-switched Nd:YAG laser that yielded slight improvement, followed by 7 sessions of intense pulsed light therapy with partial response, and ultimately achieving marked improvement after 5 bimonthly sessions of fractional 10,600-nm carbon dioxide laser.
This case highlights the potential for EO to develop even with low-concentration (2%) hydroquinone obtained through unregulated online sources, underscoring the need for dermatologist supervision when hydroquinone is used. Despite the 2020 prohibition of OTC hydroquinone sales in the United States, patients continue to access these products online. Clinicians should maintain a high index of suspicion for EO in patients presenting with paradoxical facial hyperpigmentation and a history of unsupervised hydroquinone use.
- Ishack S, Lipner SR. Exogenous ochronosis associated with hydroquinone: a systematic review. Int J Dermatol. 2022;61:675-684. doi:10.1111/ijd.15878
- Qorbani A, Mubasher A, Sarantopoulos GP, et al. Exogenous ochronosis (EO): skin lightening cream causing rare caviar-like lesion with banana-like pigments; review of literature and histological comparison with endogenous counterpart. Autops Case Rep. 2020;10:E2020197. doi:10.4322/acr.2020.197
- Coronavirus Aid, Relief, and Economic Security (CARES) Act, Pub L No. 116-136, §3851, 134 Stat 281 (2020).
- Hydroquinone, found in skin lightening agents worldwide, linked with increased skin cancer risk. Medscape. August 26, 2022. Accessed June 5, 2026.
- Dogliotti M, Leibowitz M. Granulomatous ochronosis—a cosmetic-induced skin disorder in Blacks. S Afr Med J. 1979;56:757-760.
- Hardwick N, Van Gelder LW, Van der Merwe CA, Van der Merwe MP. Exogenous ochronosis: an epidemiological study. Br J Dermatol. 1989;120:229-238. doi:10.1111/j.1365-2133.1989.tb07787.x
- Lazar M, De La Garza H, Vashi NA. Exogenous ochronosis: characterizing a rare disorder in skin of color. J Clin Med. 2023;12:4341. doi:10.3390/jcm12134341
- Findlay GH, de Beer HA. Chronic hydroquinone poisoning of the skin from skin-lightening cosmetics. A South African epidemic of ochronosis of the face in dark-skinned individuals. S Afr Med J. 1980;57:187-190.
- Bellew SG, Alster TS. Treatment of exogenous ochronosis with a Q-switched alexandrite (755 nm) laser. Dermatol Surg. 2004;30:555-558. doi:10.1111/j.1524-4725.2004.30177.x
- Méndez Baca I, Al-Niaimi F, Colina C, et al. A case of ochronosis successfully treated with the picosecond laser. J Cosmet Dermatol. 2019;18:1322-1325. doi:10.1111/jocd.12834
- Ceglio WW, Careta MF, Patriota R, et al. Exogenous ochronosis successfully treated with the combination of intense pulsed light and fractional CO2 laser. An Bras Dermatol. 2023;98:138-140. doi:10.1016/j.abd.2021.08.013
- Ishack S, Lipner SR. Exogenous ochronosis associated with hydroquinone: a systematic review. Int J Dermatol. 2022;61:675-684. doi:10.1111/ijd.15878
- Qorbani A, Mubasher A, Sarantopoulos GP, et al. Exogenous ochronosis (EO): skin lightening cream causing rare caviar-like lesion with banana-like pigments; review of literature and histological comparison with endogenous counterpart. Autops Case Rep. 2020;10:E2020197. doi:10.4322/acr.2020.197
- Coronavirus Aid, Relief, and Economic Security (CARES) Act, Pub L No. 116-136, §3851, 134 Stat 281 (2020).
- Hydroquinone, found in skin lightening agents worldwide, linked with increased skin cancer risk. Medscape. August 26, 2022. Accessed June 5, 2026.
- Dogliotti M, Leibowitz M. Granulomatous ochronosis—a cosmetic-induced skin disorder in Blacks. S Afr Med J. 1979;56:757-760.
- Hardwick N, Van Gelder LW, Van der Merwe CA, Van der Merwe MP. Exogenous ochronosis: an epidemiological study. Br J Dermatol. 1989;120:229-238. doi:10.1111/j.1365-2133.1989.tb07787.x
- Lazar M, De La Garza H, Vashi NA. Exogenous ochronosis: characterizing a rare disorder in skin of color. J Clin Med. 2023;12:4341. doi:10.3390/jcm12134341
- Findlay GH, de Beer HA. Chronic hydroquinone poisoning of the skin from skin-lightening cosmetics. A South African epidemic of ochronosis of the face in dark-skinned individuals. S Afr Med J. 1980;57:187-190.
- Bellew SG, Alster TS. Treatment of exogenous ochronosis with a Q-switched alexandrite (755 nm) laser. Dermatol Surg. 2004;30:555-558. doi:10.1111/j.1524-4725.2004.30177.x
- Méndez Baca I, Al-Niaimi F, Colina C, et al. A case of ochronosis successfully treated with the picosecond laser. J Cosmet Dermatol. 2019;18:1322-1325. doi:10.1111/jocd.12834
- Ceglio WW, Careta MF, Patriota R, et al. Exogenous ochronosis successfully treated with the combination of intense pulsed light and fractional CO2 laser. An Bras Dermatol. 2023;98:138-140. doi:10.1016/j.abd.2021.08.013
Black Malar Papules Following Use of Hydroquinone Cream 2% Purchased Online
Black Malar Papules Following Use of Hydroquinone Cream 2% Purchased Online
Practice Points
- Exogenous ochronosis (EO) is a rare adverse effect of topical hydroquinone characterized by blue-black or gray-blue pigmentation, caviarlike papules, and distinctive banana-shaped dermal deposits on histopathology.
- Most reported cases of hydroquinone-induced EO occur after prolonged use of concentrations exceeding 4%; this case developed after only 6 months of exposure to hydroquinone cream 2% purchased online.
- Available evidence suggests that laser-based therapies may offer greater improvement than topical treatments in affected patients.

Asymptomatic Enlarging Lobulated Mass on the Lower Leg
Asymptomatic Enlarging Lobulated Mass on the Lower Leg
THE DIAGNOSIS: Dermatofibroma
Histopathologic examination of the shave biopsy revealed fascicles of plump fibroblasts and histiocytes interposed between thick collagen bundles within the dermis, consistent with a diagnosis of dermatofibroma (DF). Dermatofibroma is a common benign skin tumor that classically manifests as brownish or reddish-brown firm papules or nodules that dimple when compressed. While the exact etiology of DF remains uncertain, it is believed to arise from a combined neoplastic and reactive fibroblastic proliferation process in response to stimuli, such as minor trauma or insect bites (as in our patient).1
On histopathology, the most common findings associated with DF are dermal proliferation of spindle-shaped fibroblasts arranged in a storiform or whorled pattern.2 In this patient, fascicles of plump fibroblasts and histiocytes were observed interspersed among thick collagen bundles within the dermis (Figure). Other histologic variants of DF include cellular, histiocytic, lipidized, angiomatous, aneurysmal, clear cell, monster cell, myxoid, keloidal, palisading, osteoclastic, and epithelioid.
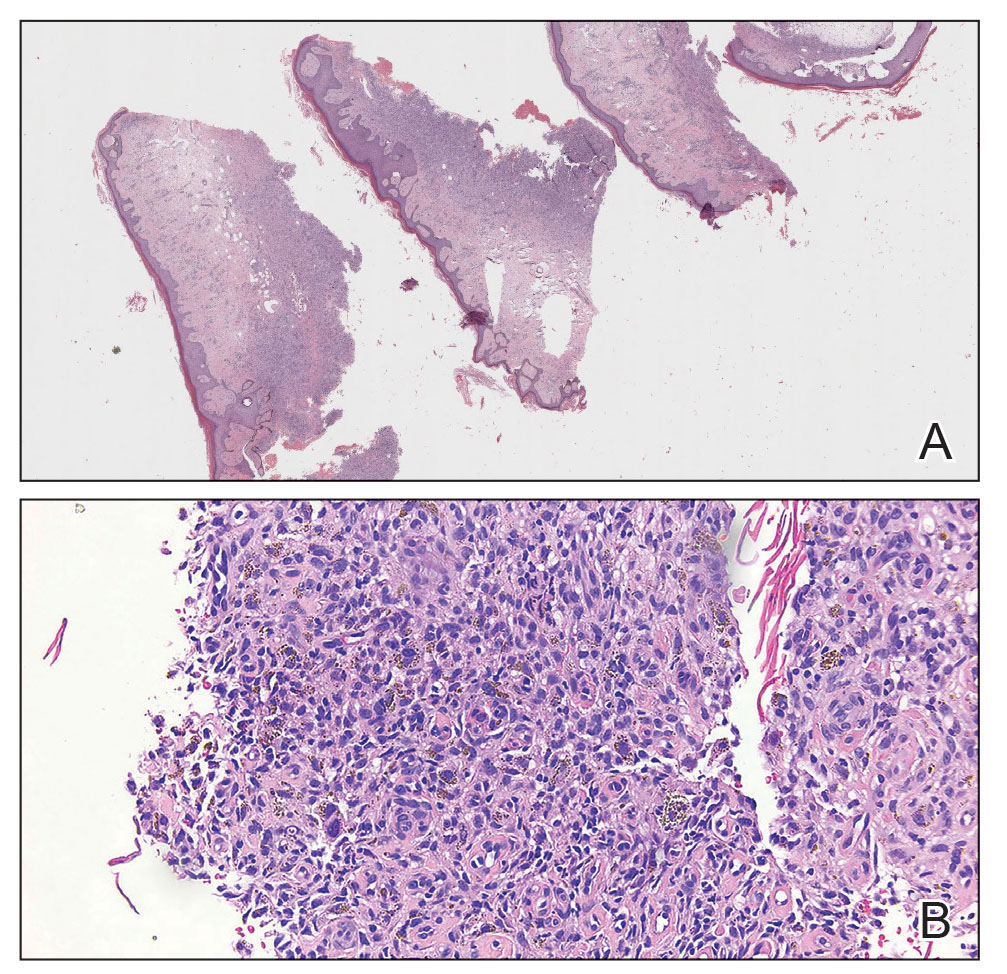
On dermatoscopic examination, a pigment network is the most common feature, followed by a white scarlike patch, brown dots and globules, and vascular structures.2 Atypical DF variants can manifest with diverse clinical morphologies; one example is giant DF, which exceeds 5 cm and may exhibit an ulcerated or pedunculated appearance, as seen in our case.3 In such cases, a thorough clinical examination coupled with histopathologic analysis becomes paramount for accurate diagnosis.
Most cases of DF do not require intervention unless there are cosmetic concerns or the lesions are symptomatic. Surgical excision is a common and effective treatment method but results in scarring. Intralesional steroid injection and cryotherapy are less aggressive treatment options but have limited efficacy. Lasers, including carbon dioxide and pulsed dye lasers, are infrequently used; however, recurrence is possible with any treatment modality.4 Local recurrence is common, occurring in 26% to 50% of cases, particularly in atypical dermatofibroma variants after treatment.5 Recurrence is more likely with primary lesions larger than 1 cm.5
Several conditions share clinical features with DF, necessitating a thorough differential diagnosis. Dermatofibrosarcoma protuberans (DFSP) is a rare, locally aggressive, malignant tumor with a propensity for recurrence. It manifests as a slow-growing, red-brown, indurated plaque with irregular nodularity. Immunohistochemical staining can be used to differentiate DF from DFSP, with DF typically expressing factor XIIIa and lacking CD34, whereas DFSP exhibits CD34 positivity and lacks factor XIIIa expression.6 Another diagnosis in the differential is fibrosarcoma, a malignant tumor of fibroblasts that manifests as a painless, enlarging, poorly defined mass on the lower extremities. Histopathologic features include atypical fibroblasts and collagen with proliferation of atypical spindle-shaped cells.
Other benign lesions to consider include neurofibroma, which may manifest as a firm nodule but is derived from nerve tissue. Clinically, neurofibromas can be differentiated by their association with neurofibromatosis and softer texture. Cutaneous squamous cell carcinoma also should be considered, as it is a malignant proliferation of cutaneous epithelium that clinically manifests as a hyperkeratotic papule or plaque.5
- Hui P, J. Glusac E, Sinard JH, et al. Clonal analysis of cutaneous fibrous histiocytoma (dermatofibroma). J Cutan Pathol. 2002;29:385-389.
- Şenel E, Yuyucu Karabulut Y, Doğruer Şenel S. Clinical, histopathological, dermatoscopic and digital microscopic features of dermatofibroma: a retrospective analysis of 200 lesions. J Eur Acad Derm Venereol. 2015;29:1958-1966.
- Requena L, Fariña MC, Fuente C, et al. Giant dermatofibroma: a little-known clinical variant of dermatofibroma. J Am Acad Dermatol. 1994;30:714-718.
- Alonso-Castro L, Boixeda P, Segura-Palacios JM, et al. Dermatofibromas treated with pulsed dye laser: clinical and dermoscopic outcomes. J Cosmet Laser Ther. 2012;14:98-101.
- Gaufin M, Michaelis T, Duffy K. Cellular dermatofibroma: clinicopathologic review of 218 cases of cellular dermatofibroma to determine the clinical recurrence rate. Dermatol Surg. 2019;45:1359-1364.
- West KL, Cardona DM, Su Z, et al. Immunohistochemical markers in fibrohistiocytic lesions: factor XIIIa, CD34, S-100 and p75. Am J Dermatopathol. 2014;36:414-419.
THE DIAGNOSIS: Dermatofibroma
Histopathologic examination of the shave biopsy revealed fascicles of plump fibroblasts and histiocytes interposed between thick collagen bundles within the dermis, consistent with a diagnosis of dermatofibroma (DF). Dermatofibroma is a common benign skin tumor that classically manifests as brownish or reddish-brown firm papules or nodules that dimple when compressed. While the exact etiology of DF remains uncertain, it is believed to arise from a combined neoplastic and reactive fibroblastic proliferation process in response to stimuli, such as minor trauma or insect bites (as in our patient).1
On histopathology, the most common findings associated with DF are dermal proliferation of spindle-shaped fibroblasts arranged in a storiform or whorled pattern.2 In this patient, fascicles of plump fibroblasts and histiocytes were observed interspersed among thick collagen bundles within the dermis (Figure). Other histologic variants of DF include cellular, histiocytic, lipidized, angiomatous, aneurysmal, clear cell, monster cell, myxoid, keloidal, palisading, osteoclastic, and epithelioid.
On dermatoscopic examination, a pigment network is the most common feature, followed by a white scarlike patch, brown dots and globules, and vascular structures.2 Atypical DF variants can manifest with diverse clinical morphologies; one example is giant DF, which exceeds 5 cm and may exhibit an ulcerated or pedunculated appearance, as seen in our case.3 In such cases, a thorough clinical examination coupled with histopathologic analysis becomes paramount for accurate diagnosis.
Most cases of DF do not require intervention unless there are cosmetic concerns or the lesions are symptomatic. Surgical excision is a common and effective treatment method but results in scarring. Intralesional steroid injection and cryotherapy are less aggressive treatment options but have limited efficacy. Lasers, including carbon dioxide and pulsed dye lasers, are infrequently used; however, recurrence is possible with any treatment modality.4 Local recurrence is common, occurring in 26% to 50% of cases, particularly in atypical dermatofibroma variants after treatment.5 Recurrence is more likely with primary lesions larger than 1 cm.5
Several conditions share clinical features with DF, necessitating a thorough differential diagnosis. Dermatofibrosarcoma protuberans (DFSP) is a rare, locally aggressive, malignant tumor with a propensity for recurrence. It manifests as a slow-growing, red-brown, indurated plaque with irregular nodularity. Immunohistochemical staining can be used to differentiate DF from DFSP, with DF typically expressing factor XIIIa and lacking CD34, whereas DFSP exhibits CD34 positivity and lacks factor XIIIa expression.6 Another diagnosis in the differential is fibrosarcoma, a malignant tumor of fibroblasts that manifests as a painless, enlarging, poorly defined mass on the lower extremities. Histopathologic features include atypical fibroblasts and collagen with proliferation of atypical spindle-shaped cells.
Other benign lesions to consider include neurofibroma, which may manifest as a firm nodule but is derived from nerve tissue. Clinically, neurofibromas can be differentiated by their association with neurofibromatosis and softer texture. Cutaneous squamous cell carcinoma also should be considered, as it is a malignant proliferation of cutaneous epithelium that clinically manifests as a hyperkeratotic papule or plaque.5
THE DIAGNOSIS: Dermatofibroma
Histopathologic examination of the shave biopsy revealed fascicles of plump fibroblasts and histiocytes interposed between thick collagen bundles within the dermis, consistent with a diagnosis of dermatofibroma (DF). Dermatofibroma is a common benign skin tumor that classically manifests as brownish or reddish-brown firm papules or nodules that dimple when compressed. While the exact etiology of DF remains uncertain, it is believed to arise from a combined neoplastic and reactive fibroblastic proliferation process in response to stimuli, such as minor trauma or insect bites (as in our patient).1
On histopathology, the most common findings associated with DF are dermal proliferation of spindle-shaped fibroblasts arranged in a storiform or whorled pattern.2 In this patient, fascicles of plump fibroblasts and histiocytes were observed interspersed among thick collagen bundles within the dermis (Figure). Other histologic variants of DF include cellular, histiocytic, lipidized, angiomatous, aneurysmal, clear cell, monster cell, myxoid, keloidal, palisading, osteoclastic, and epithelioid.
On dermatoscopic examination, a pigment network is the most common feature, followed by a white scarlike patch, brown dots and globules, and vascular structures.2 Atypical DF variants can manifest with diverse clinical morphologies; one example is giant DF, which exceeds 5 cm and may exhibit an ulcerated or pedunculated appearance, as seen in our case.3 In such cases, a thorough clinical examination coupled with histopathologic analysis becomes paramount for accurate diagnosis.
Most cases of DF do not require intervention unless there are cosmetic concerns or the lesions are symptomatic. Surgical excision is a common and effective treatment method but results in scarring. Intralesional steroid injection and cryotherapy are less aggressive treatment options but have limited efficacy. Lasers, including carbon dioxide and pulsed dye lasers, are infrequently used; however, recurrence is possible with any treatment modality.4 Local recurrence is common, occurring in 26% to 50% of cases, particularly in atypical dermatofibroma variants after treatment.5 Recurrence is more likely with primary lesions larger than 1 cm.5
Several conditions share clinical features with DF, necessitating a thorough differential diagnosis. Dermatofibrosarcoma protuberans (DFSP) is a rare, locally aggressive, malignant tumor with a propensity for recurrence. It manifests as a slow-growing, red-brown, indurated plaque with irregular nodularity. Immunohistochemical staining can be used to differentiate DF from DFSP, with DF typically expressing factor XIIIa and lacking CD34, whereas DFSP exhibits CD34 positivity and lacks factor XIIIa expression.6 Another diagnosis in the differential is fibrosarcoma, a malignant tumor of fibroblasts that manifests as a painless, enlarging, poorly defined mass on the lower extremities. Histopathologic features include atypical fibroblasts and collagen with proliferation of atypical spindle-shaped cells.
Other benign lesions to consider include neurofibroma, which may manifest as a firm nodule but is derived from nerve tissue. Clinically, neurofibromas can be differentiated by their association with neurofibromatosis and softer texture. Cutaneous squamous cell carcinoma also should be considered, as it is a malignant proliferation of cutaneous epithelium that clinically manifests as a hyperkeratotic papule or plaque.5
- Hui P, J. Glusac E, Sinard JH, et al. Clonal analysis of cutaneous fibrous histiocytoma (dermatofibroma). J Cutan Pathol. 2002;29:385-389.
- Şenel E, Yuyucu Karabulut Y, Doğruer Şenel S. Clinical, histopathological, dermatoscopic and digital microscopic features of dermatofibroma: a retrospective analysis of 200 lesions. J Eur Acad Derm Venereol. 2015;29:1958-1966.
- Requena L, Fariña MC, Fuente C, et al. Giant dermatofibroma: a little-known clinical variant of dermatofibroma. J Am Acad Dermatol. 1994;30:714-718.
- Alonso-Castro L, Boixeda P, Segura-Palacios JM, et al. Dermatofibromas treated with pulsed dye laser: clinical and dermoscopic outcomes. J Cosmet Laser Ther. 2012;14:98-101.
- Gaufin M, Michaelis T, Duffy K. Cellular dermatofibroma: clinicopathologic review of 218 cases of cellular dermatofibroma to determine the clinical recurrence rate. Dermatol Surg. 2019;45:1359-1364.
- West KL, Cardona DM, Su Z, et al. Immunohistochemical markers in fibrohistiocytic lesions: factor XIIIa, CD34, S-100 and p75. Am J Dermatopathol. 2014;36:414-419.
- Hui P, J. Glusac E, Sinard JH, et al. Clonal analysis of cutaneous fibrous histiocytoma (dermatofibroma). J Cutan Pathol. 2002;29:385-389.
- Şenel E, Yuyucu Karabulut Y, Doğruer Şenel S. Clinical, histopathological, dermatoscopic and digital microscopic features of dermatofibroma: a retrospective analysis of 200 lesions. J Eur Acad Derm Venereol. 2015;29:1958-1966.
- Requena L, Fariña MC, Fuente C, et al. Giant dermatofibroma: a little-known clinical variant of dermatofibroma. J Am Acad Dermatol. 1994;30:714-718.
- Alonso-Castro L, Boixeda P, Segura-Palacios JM, et al. Dermatofibromas treated with pulsed dye laser: clinical and dermoscopic outcomes. J Cosmet Laser Ther. 2012;14:98-101.
- Gaufin M, Michaelis T, Duffy K. Cellular dermatofibroma: clinicopathologic review of 218 cases of cellular dermatofibroma to determine the clinical recurrence rate. Dermatol Surg. 2019;45:1359-1364.
- West KL, Cardona DM, Su Z, et al. Immunohistochemical markers in fibrohistiocytic lesions: factor XIIIa, CD34, S-100 and p75. Am J Dermatopathol. 2014;36:414-419.
Asymptomatic Enlarging Lobulated Mass on the Lower Leg
Asymptomatic Enlarging Lobulated Mass on the Lower Leg
A 69-year-old woman presented to the dermatology clinic with enlarging nodules on the bilateral lower legs of several years’ duration. Cutaneous examination of the legs revealed a brown, pedunculated, lobulated nodule on the lateral right lower leg measuring 5.0×1.9 cm. The patient reported that the lesion first appeared after a mosquito bite and then slowly grew over several years. A shave biopsy of the lesion was performed.

