User login
Lifetime Estrogen Exposure Linked to Depression Risk in Perimenopause
PHOENIX – Estrogen exposure across the lifespan appears to be associated with risk of depression during the menopausal transition, according to findings from the Study of Women's Health Across the Nation, or SWAN.
Specifically, a longer total duration of estradiol exposure was found to be protective against depression during the menopausal transition, Dr. Claudio N. Soares reported at the annual meeting of the New Clinical Drug Evaluation Unit, sponsored by the National Institute of Mental Health.

"What the data show is that for each year of increased premenopausal exposure to estrogen, you reduce by 15% the risk for developing depression after entering the menopausal transition. So the longer the exposure, the lower the risk," said Dr. Soares of McMaster University, Hamilton, Ont.
The menopausal transition has been shown in numerous studies to be a time of increased depression risk, and endocrinologic factors have been hypothesized as contributing to vulnerability to depression. It has remained unclear, however, why some women are at increased risk compared with others.
Studies have shown that estrogen exposure can improve depression, but the question of whether estrogen exposure prior to the menopausal transition would affect depression risk during the transition had not been addressed, Dr. Soares noted.
To assess factors – including lifetime exposure to estrogen (based on the time from age at menarche to the age at menopause) – that might contribute to depression risk during this reproductive phase, Dr. Soares and his colleagues analyzed data from more than 1,200 women who participated in SWAN, a seven-site, longitudinal, epidemiologic study designed to examine the physical, biological, and psychological changes that women undergo during their middle and menopausal years.
The average duration of estradiol exposure in the women (who were aged 42-52 years at study entry and who have been followed for nearly 10 years) was about 36 years. A longer duration of exposure prior to the menopausal transition was associated with a lower risk of having a score of less than 16 on the CES-D (Center for Epidemiologic Studies-Depression) scale during the transition (hazard ratio, 0.847 after adjustment for numerous factors, including age, ethnicity, education, study site, premenopausal depression, current and ever antidepressant use, baseline smoking, and time in study), Dr. Soares said.
"The next question is, what is happening during that time of exposure that could be exacerbating risk?" he said, noting, for example, that some interesting data show that oral contraceptive use may affect depression exacerbations. When investigators looked at oral contraceptive use as a continuous variable in this study, it was shown to be associated with an even greater protective effect.
However, other factors also could modulate exposure to estrogen exposure, such as the number of pregnancies and duration of breastfeeding. The next step of the analysis will look at such interactions, he said.
Thus far, the findings indicate that the relationship between depression and the menopausal transition is complex and is associated with both current and historic reproductive endocrinology, Dr. Soares said.
This study was supported by the North American Menopause Society. SWAN was supported by grants from the National Institutes of Health. Dr. Soares disclosed financial relationships with AstraZeneca, Bristol-Myers Squibb, CIHR, Eli Lilly, Lundbeck, Moven Pharmaceuticals, NARSAD, and Pfizer, but reported having no conflicts with respect to this study.
PHOENIX – Estrogen exposure across the lifespan appears to be associated with risk of depression during the menopausal transition, according to findings from the Study of Women's Health Across the Nation, or SWAN.
Specifically, a longer total duration of estradiol exposure was found to be protective against depression during the menopausal transition, Dr. Claudio N. Soares reported at the annual meeting of the New Clinical Drug Evaluation Unit, sponsored by the National Institute of Mental Health.
"What the data show is that for each year of increased premenopausal exposure to estrogen, you reduce by 15% the risk for developing depression after entering the menopausal transition. So the longer the exposure, the lower the risk," said Dr. Soares of McMaster University, Hamilton, Ont.
The menopausal transition has been shown in numerous studies to be a time of increased depression risk, and endocrinologic factors have been hypothesized as contributing to vulnerability to depression. It has remained unclear, however, why some women are at increased risk compared with others.
Studies have shown that estrogen exposure can improve depression, but the question of whether estrogen exposure prior to the menopausal transition would affect depression risk during the transition had not been addressed, Dr. Soares noted.
To assess factors – including lifetime exposure to estrogen (based on the time from age at menarche to the age at menopause) – that might contribute to depression risk during this reproductive phase, Dr. Soares and his colleagues analyzed data from more than 1,200 women who participated in SWAN, a seven-site, longitudinal, epidemiologic study designed to examine the physical, biological, and psychological changes that women undergo during their middle and menopausal years.
The average duration of estradiol exposure in the women (who were aged 42-52 years at study entry and who have been followed for nearly 10 years) was about 36 years. A longer duration of exposure prior to the menopausal transition was associated with a lower risk of having a score of less than 16 on the CES-D (Center for Epidemiologic Studies-Depression) scale during the transition (hazard ratio, 0.847 after adjustment for numerous factors, including age, ethnicity, education, study site, premenopausal depression, current and ever antidepressant use, baseline smoking, and time in study), Dr. Soares said.
"The next question is, what is happening during that time of exposure that could be exacerbating risk?" he said, noting, for example, that some interesting data show that oral contraceptive use may affect depression exacerbations. When investigators looked at oral contraceptive use as a continuous variable in this study, it was shown to be associated with an even greater protective effect.
However, other factors also could modulate exposure to estrogen exposure, such as the number of pregnancies and duration of breastfeeding. The next step of the analysis will look at such interactions, he said.
Thus far, the findings indicate that the relationship between depression and the menopausal transition is complex and is associated with both current and historic reproductive endocrinology, Dr. Soares said.
This study was supported by the North American Menopause Society. SWAN was supported by grants from the National Institutes of Health. Dr. Soares disclosed financial relationships with AstraZeneca, Bristol-Myers Squibb, CIHR, Eli Lilly, Lundbeck, Moven Pharmaceuticals, NARSAD, and Pfizer, but reported having no conflicts with respect to this study.
PHOENIX – Estrogen exposure across the lifespan appears to be associated with risk of depression during the menopausal transition, according to findings from the Study of Women's Health Across the Nation, or SWAN.
Specifically, a longer total duration of estradiol exposure was found to be protective against depression during the menopausal transition, Dr. Claudio N. Soares reported at the annual meeting of the New Clinical Drug Evaluation Unit, sponsored by the National Institute of Mental Health.
"What the data show is that for each year of increased premenopausal exposure to estrogen, you reduce by 15% the risk for developing depression after entering the menopausal transition. So the longer the exposure, the lower the risk," said Dr. Soares of McMaster University, Hamilton, Ont.
The menopausal transition has been shown in numerous studies to be a time of increased depression risk, and endocrinologic factors have been hypothesized as contributing to vulnerability to depression. It has remained unclear, however, why some women are at increased risk compared with others.
Studies have shown that estrogen exposure can improve depression, but the question of whether estrogen exposure prior to the menopausal transition would affect depression risk during the transition had not been addressed, Dr. Soares noted.
To assess factors – including lifetime exposure to estrogen (based on the time from age at menarche to the age at menopause) – that might contribute to depression risk during this reproductive phase, Dr. Soares and his colleagues analyzed data from more than 1,200 women who participated in SWAN, a seven-site, longitudinal, epidemiologic study designed to examine the physical, biological, and psychological changes that women undergo during their middle and menopausal years.
The average duration of estradiol exposure in the women (who were aged 42-52 years at study entry and who have been followed for nearly 10 years) was about 36 years. A longer duration of exposure prior to the menopausal transition was associated with a lower risk of having a score of less than 16 on the CES-D (Center for Epidemiologic Studies-Depression) scale during the transition (hazard ratio, 0.847 after adjustment for numerous factors, including age, ethnicity, education, study site, premenopausal depression, current and ever antidepressant use, baseline smoking, and time in study), Dr. Soares said.
"The next question is, what is happening during that time of exposure that could be exacerbating risk?" he said, noting, for example, that some interesting data show that oral contraceptive use may affect depression exacerbations. When investigators looked at oral contraceptive use as a continuous variable in this study, it was shown to be associated with an even greater protective effect.
However, other factors also could modulate exposure to estrogen exposure, such as the number of pregnancies and duration of breastfeeding. The next step of the analysis will look at such interactions, he said.
Thus far, the findings indicate that the relationship between depression and the menopausal transition is complex and is associated with both current and historic reproductive endocrinology, Dr. Soares said.
This study was supported by the North American Menopause Society. SWAN was supported by grants from the National Institutes of Health. Dr. Soares disclosed financial relationships with AstraZeneca, Bristol-Myers Squibb, CIHR, Eli Lilly, Lundbeck, Moven Pharmaceuticals, NARSAD, and Pfizer, but reported having no conflicts with respect to this study.
AT A MEETING OF THE NEW CLINICAL DRUG EVALUATION UNIT SPONSORED BY THE NATIONAL INSTITUTE OF MENTAL HEALTH
Major Finding: A longer duration of estrogen exposure before the menopausal transition was associated with a lower risk of having a score of less than 16 on the CES-D during the transition (HR, 0.847).
Data Source: Data are from more than 1,200 women participating in SWAN (Study of Women’s Health Across the Nation).
Disclosures: This study was supported by the North American Menopause Society. SWAN was supported by grants from the National Institutes of Health. Dr. Soares disclosed financial relationships with AstraZeneca, Bristol Myers Squibb, CIHR, Eli Lilly, Lundbeck, Moven Pharmaceuticals, NARSAD, and Pfizer, but reported having no conflicts with respect to this study.

The Women's Health Initiative -- Looking Back
The Women's Health Initiative was a groundbreaking study, but it became the center of news and controversy on July 9, 2002, when one of its arms was stopped after results showed that combination hormone therapy (estrogen plus progestin) caused serious health problems such as stroke and cancer in otherwise healthy women. We caught up with Dr. Vivian Pinn, former director of the Office of Research on Women's Health, to hear about her reflections on the past decade and about the data that the large randomized trial is still providing.
The Women's Health Initiative was a groundbreaking study, but it became the center of news and controversy on July 9, 2002, when one of its arms was stopped after results showed that combination hormone therapy (estrogen plus progestin) caused serious health problems such as stroke and cancer in otherwise healthy women. We caught up with Dr. Vivian Pinn, former director of the Office of Research on Women's Health, to hear about her reflections on the past decade and about the data that the large randomized trial is still providing.
The Women's Health Initiative was a groundbreaking study, but it became the center of news and controversy on July 9, 2002, when one of its arms was stopped after results showed that combination hormone therapy (estrogen plus progestin) caused serious health problems such as stroke and cancer in otherwise healthy women. We caught up with Dr. Vivian Pinn, former director of the Office of Research on Women's Health, to hear about her reflections on the past decade and about the data that the large randomized trial is still providing.

Only High Vitamin D Intake Cuts Fracture Risk
Only high intake of vitamin D supplementation with 800 IU or more per day appears to reduce the risk of fracture significantly in the elderly, according to the latest meta-analysis on the subject reported online July 4 in the New England Journal of Medicine.
Such high levels of supplementation appear to reduce the risk of hip fracture by 30% and the risk of nonvertebral fracture by 14% in people aged 65 years and older, said Dr. Heike A. Bischoff-Ferrari, of the Center on Aging and Mobility at the University of Zurich, and her associates.
Many previous meta-analyses of the protective effect of vitamin D supplements, like the numerous clinical trials they reviewed, have produced markedly conflicting results. Some have found reductions in fracture risk of up to 20%, others have found no beneficial effect, and a few have even found negative effects on fracture risk.
Dr. Bischoff-Ferrari and her colleagues reasoned that many of these clinical trials, as well as the meta-analyses that pooled their findings, were flawed by relying on the doses of vitamin D that were prescribed for subjects rather than the actual amount that subjects took. Many also were flawed in that they did not take into account subjects’ baseline levels of 25-hydroxyvitamin D, an indicator of the degree of their vitamin D deficiency.
So for their meta-analysis, the investigators included only double-blind, randomized, controlled trials that either recorded subjects’ actual intake of oral vitamin D supplements or controlled for their adherence to prescribed supplementation. Thus, the investigators were able to include only 11 studies, with a pooled population of 31,022 subjects, in their meta-analysis.
The intention-to-treat analysis, which examined the prescribed supplementation, showed a nonsignificant 10% reduction in the risk of hip fracture. However, a comparison of subjects’ actual intake of vitamin D supplements showed a significant 30% reduction in risk of hip fracture at the highest levels of intake (800-2,000 IU daily).
"Notably, there was no reduction in risk of hip fracture at any actual intake level lower than 792 IU per day," Dr. Bischoff-Ferrari and her associates said (N. Engl. J. Med. 2012 July 4 [doi: 10.1056/NEJMoa1109617]).
Similarly, the intention-to-treat analysis showed a nonsignificant 7% reduction in the risk of nonvertebral fracture, while a comparison of actual intake levels showed a significant 14% decline in risk at the highest levels of intake.
Internal validation analyses supported these results, and indicated that there was a dose-response relationship between vitamin D dose actually ingested and fracture risk. Several sensitivity analyses also bolstered the findings, and showed that the benefit of vitamin D supplements extended across several subgroups of patients, including all ages and both sexes.
"Previous meta-analyses have suggested that the benefits of vitamin D may be limited to older persons who live in institutions. Our subgroup analyses suggest that at the highest actual intake level, the risk of hip fracture is reduced among all persons 65 years of age or older, whether they live in the community or in an institution.
"Our data further suggest that persons who are most vulnerable to vitamin D deficiency – those 85 years of age or older and those with very low baseline levels of 25-hydroxyvitamin D – benefit from vitamin D supplementation at least as much as others do," they added.
Overall, the study results support the Institute of Medicine’s recommendation that people aged 65 years and older receive 800 IU of vitamin D each day, the investigators noted.
In addition, "our findings suggest that some previous high-quality trials of vitamin D supplementation either showed no benefit owing to lower-than-intended doses of vitamin D or showed an unexpected benefit owing to higher-than-intended doses," they said.
This study was supported by the Swiss National Foundation, the European Commission Framework 7 Program, and DSM Nutritional Products. Dr. Bischoff-Ferrari reported ties to DSM Nutritional Products, Amgen, MSD, Novartis, Roche, and Nestle, and her associates reported ties to numerous industry sources.
Vitamin D is like most nutrients in that people who have different levels at baseline and then receive identical supplementation may or may not show a measurable response to the supplementation, said Dr. Robert P. Heaney.
"Unfortunately, most of the randomized, controlled trials of vitamin D that have been published to date have paid little attention to baseline status. Among 31,022 patients whose results were analyzed by [Dr. Bischoff-Ferrari and colleagues], data on baseline concentrations of 25-hydroxyvitamin D were available for only 4,383 patients (barely 14%)," he noted.
"The question of how much vitamin D is enough is likely to remain muddled as long as meta-analyses focus on trial methodology rather than on biology," Dr. Heaney added.
Nonetheless, "given the congruence of the findings of this latest meta-analysis with the guidelines from the Endocrine Society [1,500-2,000 IU/ day], it would appear to be prudent, and probably helpful as well, to ensure an intake at the upper end of the range at which Bischoff-Ferrari et al. found a reduction in fracture risk," he concluded.
Dr. Heaney is with the osteoporosis research center at Creighton University in Omaha, Neb. He reported ties to Coca-Cola, the International Dairy Foods Commission, the Federal Trade Commission, the National Dairy Council, and the Council for Responsible Nutrition. These remarks were taken from his editorial accompanying Dr. Bischoff-Ferrari’s report (N. Engl. J. Med. 2012 July 4 [doi:10.1056/NEJMe1206858]).
Vitamin D is like most nutrients in that people who have different levels at baseline and then receive identical supplementation may or may not show a measurable response to the supplementation, said Dr. Robert P. Heaney.
"Unfortunately, most of the randomized, controlled trials of vitamin D that have been published to date have paid little attention to baseline status. Among 31,022 patients whose results were analyzed by [Dr. Bischoff-Ferrari and colleagues], data on baseline concentrations of 25-hydroxyvitamin D were available for only 4,383 patients (barely 14%)," he noted.
"The question of how much vitamin D is enough is likely to remain muddled as long as meta-analyses focus on trial methodology rather than on biology," Dr. Heaney added.
Nonetheless, "given the congruence of the findings of this latest meta-analysis with the guidelines from the Endocrine Society [1,500-2,000 IU/ day], it would appear to be prudent, and probably helpful as well, to ensure an intake at the upper end of the range at which Bischoff-Ferrari et al. found a reduction in fracture risk," he concluded.
Dr. Heaney is with the osteoporosis research center at Creighton University in Omaha, Neb. He reported ties to Coca-Cola, the International Dairy Foods Commission, the Federal Trade Commission, the National Dairy Council, and the Council for Responsible Nutrition. These remarks were taken from his editorial accompanying Dr. Bischoff-Ferrari’s report (N. Engl. J. Med. 2012 July 4 [doi:10.1056/NEJMe1206858]).
Vitamin D is like most nutrients in that people who have different levels at baseline and then receive identical supplementation may or may not show a measurable response to the supplementation, said Dr. Robert P. Heaney.
"Unfortunately, most of the randomized, controlled trials of vitamin D that have been published to date have paid little attention to baseline status. Among 31,022 patients whose results were analyzed by [Dr. Bischoff-Ferrari and colleagues], data on baseline concentrations of 25-hydroxyvitamin D were available for only 4,383 patients (barely 14%)," he noted.
"The question of how much vitamin D is enough is likely to remain muddled as long as meta-analyses focus on trial methodology rather than on biology," Dr. Heaney added.
Nonetheless, "given the congruence of the findings of this latest meta-analysis with the guidelines from the Endocrine Society [1,500-2,000 IU/ day], it would appear to be prudent, and probably helpful as well, to ensure an intake at the upper end of the range at which Bischoff-Ferrari et al. found a reduction in fracture risk," he concluded.
Dr. Heaney is with the osteoporosis research center at Creighton University in Omaha, Neb. He reported ties to Coca-Cola, the International Dairy Foods Commission, the Federal Trade Commission, the National Dairy Council, and the Council for Responsible Nutrition. These remarks were taken from his editorial accompanying Dr. Bischoff-Ferrari’s report (N. Engl. J. Med. 2012 July 4 [doi:10.1056/NEJMe1206858]).
Only high intake of vitamin D supplementation with 800 IU or more per day appears to reduce the risk of fracture significantly in the elderly, according to the latest meta-analysis on the subject reported online July 4 in the New England Journal of Medicine.
Such high levels of supplementation appear to reduce the risk of hip fracture by 30% and the risk of nonvertebral fracture by 14% in people aged 65 years and older, said Dr. Heike A. Bischoff-Ferrari, of the Center on Aging and Mobility at the University of Zurich, and her associates.
Many previous meta-analyses of the protective effect of vitamin D supplements, like the numerous clinical trials they reviewed, have produced markedly conflicting results. Some have found reductions in fracture risk of up to 20%, others have found no beneficial effect, and a few have even found negative effects on fracture risk.
Dr. Bischoff-Ferrari and her colleagues reasoned that many of these clinical trials, as well as the meta-analyses that pooled their findings, were flawed by relying on the doses of vitamin D that were prescribed for subjects rather than the actual amount that subjects took. Many also were flawed in that they did not take into account subjects’ baseline levels of 25-hydroxyvitamin D, an indicator of the degree of their vitamin D deficiency.
So for their meta-analysis, the investigators included only double-blind, randomized, controlled trials that either recorded subjects’ actual intake of oral vitamin D supplements or controlled for their adherence to prescribed supplementation. Thus, the investigators were able to include only 11 studies, with a pooled population of 31,022 subjects, in their meta-analysis.
The intention-to-treat analysis, which examined the prescribed supplementation, showed a nonsignificant 10% reduction in the risk of hip fracture. However, a comparison of subjects’ actual intake of vitamin D supplements showed a significant 30% reduction in risk of hip fracture at the highest levels of intake (800-2,000 IU daily).
"Notably, there was no reduction in risk of hip fracture at any actual intake level lower than 792 IU per day," Dr. Bischoff-Ferrari and her associates said (N. Engl. J. Med. 2012 July 4 [doi: 10.1056/NEJMoa1109617]).
Similarly, the intention-to-treat analysis showed a nonsignificant 7% reduction in the risk of nonvertebral fracture, while a comparison of actual intake levels showed a significant 14% decline in risk at the highest levels of intake.
Internal validation analyses supported these results, and indicated that there was a dose-response relationship between vitamin D dose actually ingested and fracture risk. Several sensitivity analyses also bolstered the findings, and showed that the benefit of vitamin D supplements extended across several subgroups of patients, including all ages and both sexes.
"Previous meta-analyses have suggested that the benefits of vitamin D may be limited to older persons who live in institutions. Our subgroup analyses suggest that at the highest actual intake level, the risk of hip fracture is reduced among all persons 65 years of age or older, whether they live in the community or in an institution.
"Our data further suggest that persons who are most vulnerable to vitamin D deficiency – those 85 years of age or older and those with very low baseline levels of 25-hydroxyvitamin D – benefit from vitamin D supplementation at least as much as others do," they added.
Overall, the study results support the Institute of Medicine’s recommendation that people aged 65 years and older receive 800 IU of vitamin D each day, the investigators noted.
In addition, "our findings suggest that some previous high-quality trials of vitamin D supplementation either showed no benefit owing to lower-than-intended doses of vitamin D or showed an unexpected benefit owing to higher-than-intended doses," they said.
This study was supported by the Swiss National Foundation, the European Commission Framework 7 Program, and DSM Nutritional Products. Dr. Bischoff-Ferrari reported ties to DSM Nutritional Products, Amgen, MSD, Novartis, Roche, and Nestle, and her associates reported ties to numerous industry sources.
Only high intake of vitamin D supplementation with 800 IU or more per day appears to reduce the risk of fracture significantly in the elderly, according to the latest meta-analysis on the subject reported online July 4 in the New England Journal of Medicine.
Such high levels of supplementation appear to reduce the risk of hip fracture by 30% and the risk of nonvertebral fracture by 14% in people aged 65 years and older, said Dr. Heike A. Bischoff-Ferrari, of the Center on Aging and Mobility at the University of Zurich, and her associates.
Many previous meta-analyses of the protective effect of vitamin D supplements, like the numerous clinical trials they reviewed, have produced markedly conflicting results. Some have found reductions in fracture risk of up to 20%, others have found no beneficial effect, and a few have even found negative effects on fracture risk.
Dr. Bischoff-Ferrari and her colleagues reasoned that many of these clinical trials, as well as the meta-analyses that pooled their findings, were flawed by relying on the doses of vitamin D that were prescribed for subjects rather than the actual amount that subjects took. Many also were flawed in that they did not take into account subjects’ baseline levels of 25-hydroxyvitamin D, an indicator of the degree of their vitamin D deficiency.
So for their meta-analysis, the investigators included only double-blind, randomized, controlled trials that either recorded subjects’ actual intake of oral vitamin D supplements or controlled for their adherence to prescribed supplementation. Thus, the investigators were able to include only 11 studies, with a pooled population of 31,022 subjects, in their meta-analysis.
The intention-to-treat analysis, which examined the prescribed supplementation, showed a nonsignificant 10% reduction in the risk of hip fracture. However, a comparison of subjects’ actual intake of vitamin D supplements showed a significant 30% reduction in risk of hip fracture at the highest levels of intake (800-2,000 IU daily).
"Notably, there was no reduction in risk of hip fracture at any actual intake level lower than 792 IU per day," Dr. Bischoff-Ferrari and her associates said (N. Engl. J. Med. 2012 July 4 [doi: 10.1056/NEJMoa1109617]).
Similarly, the intention-to-treat analysis showed a nonsignificant 7% reduction in the risk of nonvertebral fracture, while a comparison of actual intake levels showed a significant 14% decline in risk at the highest levels of intake.
Internal validation analyses supported these results, and indicated that there was a dose-response relationship between vitamin D dose actually ingested and fracture risk. Several sensitivity analyses also bolstered the findings, and showed that the benefit of vitamin D supplements extended across several subgroups of patients, including all ages and both sexes.
"Previous meta-analyses have suggested that the benefits of vitamin D may be limited to older persons who live in institutions. Our subgroup analyses suggest that at the highest actual intake level, the risk of hip fracture is reduced among all persons 65 years of age or older, whether they live in the community or in an institution.
"Our data further suggest that persons who are most vulnerable to vitamin D deficiency – those 85 years of age or older and those with very low baseline levels of 25-hydroxyvitamin D – benefit from vitamin D supplementation at least as much as others do," they added.
Overall, the study results support the Institute of Medicine’s recommendation that people aged 65 years and older receive 800 IU of vitamin D each day, the investigators noted.
In addition, "our findings suggest that some previous high-quality trials of vitamin D supplementation either showed no benefit owing to lower-than-intended doses of vitamin D or showed an unexpected benefit owing to higher-than-intended doses," they said.
This study was supported by the Swiss National Foundation, the European Commission Framework 7 Program, and DSM Nutritional Products. Dr. Bischoff-Ferrari reported ties to DSM Nutritional Products, Amgen, MSD, Novartis, Roche, and Nestle, and her associates reported ties to numerous industry sources.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
PRODUCT UPDATE
DISPOSABLE EXTRA-SMALL SPECULUM
Welch Allyn introduced the industry’s first extra-small KleenSpec® Disposable Vaginal Speculum for virginal and pediatric patients as well as postmenopausal and posthysterectomy women. Available in August, this speculum joins the company’s suite of vaginal specula designed to work with the Welch Allyn Cordless Illumination System. The KleenSpec line is constructed of smooth, molded acrylic with wide handles for improved ergonomics and manipulation, says Welch Allyn.
FOR MORE INFORMATION, VISIT www.welchallyn.com
SCARAWAY® SILICONE SCAR SHEETS
ScarAway® Silicone Scar Sheets are an effective, affordable, over-the-counter treatment to reduce and prevent hypertrophic and keloid scars that may result from surgery, injuries, or burns, reports Mitchell-Vance Laboratories. Unlike scar-minimizing creams and ointments, ScarAway delivers a slight pressure directly to the scar, and mimics the natural barrier function of healthy skin, diminishing the scar’s appearance and restoring skin to its natural texture and color. The sheeting is nongreasy, ultra-thin, flexible, breathable, and durable with a soft fabric backing.
FOR MORE INFORMATION, VISIT www.MyScarAway.com
PREMAMA LIQUID PRENATAL VITAMINS
Premama, a flavorless prenatal vitamin drink mix, can be added to juices, milk, iced tea, and more. Premama includes the necessary vitamins and minerals, including folic acid, iron, DHA, CoQ10, and calcium, to support prepregnant, pregnant, and breast-feeding mothers. The unique mix of ingredients has been shown to help relieve common prenatal vitamin side-effects, such as nausea and constipation. Premama is 100% natural, lactate-free, gluten-free, and certified kosher.
FOR MORE INFORMATION, VISIT www.drinkpremama.com
HARMONY™ PRENATAL TEST DETECTS COMMON FETAL TRISOMIES
The Harmony Prenatal Test from Ariosa Diagnostics and available through LabCorp, is designed as a safe and highly accurate option to test pregnant woman for fetal anomalies using a directed approach to analyze cell-free DNA (cfDNA) in maternal blood. The Harmony Prenatal Test detects common fetal trisomies such as Trisomy 21 (associated with Down Syndrome) in pregnant women of at least 10 weeks’ gestation with a single fetus conceived without the use of an egg donor.
FOR MORE INFORMATION, VISIT www.ariosadx.com
GE HEALTHCARE’S NEW VSCAN: MORE SCAN TIME, BETTER RESOLUTION, EXPORT OPTION
GE Healthcare has upgraded Vscan, its pocket-sized, hand-held ultrasound (US) tool. New features include 50% more scan time (extended battery life), a more user-friendly interface, enhanced resolution, and an “export to PDF” option that allows physicians to more efficiently document findings. Vscan provides black and white anatomic and color-coded blood flow images. While Vscan is not intended to replace a full fetal US survey, it can provide physicians a quick look to assess fetal viability, says the manufacturer.
FOR MORE INFORMATION, VISIT https://vscan.gehealthcare.com
SODEXO HEALTH CARE SERVICES
Sodexo Health Care Services provides food and facilities services to hospitals across the country. Using the latest technologies, Sodexo employees implement environmental services and cleaning programs that have reduced hospital-acquired infections, improved patient and staff satisfaction, and contributed to cost savings for more than 1,700 client hospitals.
FOR MORE INFORMATION, VISIT www.sodexousa.com
DISPOSABLE EXTRA-SMALL SPECULUM
Welch Allyn introduced the industry’s first extra-small KleenSpec® Disposable Vaginal Speculum for virginal and pediatric patients as well as postmenopausal and posthysterectomy women. Available in August, this speculum joins the company’s suite of vaginal specula designed to work with the Welch Allyn Cordless Illumination System. The KleenSpec line is constructed of smooth, molded acrylic with wide handles for improved ergonomics and manipulation, says Welch Allyn.
FOR MORE INFORMATION, VISIT www.welchallyn.com
SCARAWAY® SILICONE SCAR SHEETS
ScarAway® Silicone Scar Sheets are an effective, affordable, over-the-counter treatment to reduce and prevent hypertrophic and keloid scars that may result from surgery, injuries, or burns, reports Mitchell-Vance Laboratories. Unlike scar-minimizing creams and ointments, ScarAway delivers a slight pressure directly to the scar, and mimics the natural barrier function of healthy skin, diminishing the scar’s appearance and restoring skin to its natural texture and color. The sheeting is nongreasy, ultra-thin, flexible, breathable, and durable with a soft fabric backing.
FOR MORE INFORMATION, VISIT www.MyScarAway.com
PREMAMA LIQUID PRENATAL VITAMINS
Premama, a flavorless prenatal vitamin drink mix, can be added to juices, milk, iced tea, and more. Premama includes the necessary vitamins and minerals, including folic acid, iron, DHA, CoQ10, and calcium, to support prepregnant, pregnant, and breast-feeding mothers. The unique mix of ingredients has been shown to help relieve common prenatal vitamin side-effects, such as nausea and constipation. Premama is 100% natural, lactate-free, gluten-free, and certified kosher.
FOR MORE INFORMATION, VISIT www.drinkpremama.com
HARMONY™ PRENATAL TEST DETECTS COMMON FETAL TRISOMIES
The Harmony Prenatal Test from Ariosa Diagnostics and available through LabCorp, is designed as a safe and highly accurate option to test pregnant woman for fetal anomalies using a directed approach to analyze cell-free DNA (cfDNA) in maternal blood. The Harmony Prenatal Test detects common fetal trisomies such as Trisomy 21 (associated with Down Syndrome) in pregnant women of at least 10 weeks’ gestation with a single fetus conceived without the use of an egg donor.
FOR MORE INFORMATION, VISIT www.ariosadx.com
GE HEALTHCARE’S NEW VSCAN: MORE SCAN TIME, BETTER RESOLUTION, EXPORT OPTION
GE Healthcare has upgraded Vscan, its pocket-sized, hand-held ultrasound (US) tool. New features include 50% more scan time (extended battery life), a more user-friendly interface, enhanced resolution, and an “export to PDF” option that allows physicians to more efficiently document findings. Vscan provides black and white anatomic and color-coded blood flow images. While Vscan is not intended to replace a full fetal US survey, it can provide physicians a quick look to assess fetal viability, says the manufacturer.
FOR MORE INFORMATION, VISIT https://vscan.gehealthcare.com
SODEXO HEALTH CARE SERVICES
Sodexo Health Care Services provides food and facilities services to hospitals across the country. Using the latest technologies, Sodexo employees implement environmental services and cleaning programs that have reduced hospital-acquired infections, improved patient and staff satisfaction, and contributed to cost savings for more than 1,700 client hospitals.
FOR MORE INFORMATION, VISIT www.sodexousa.com
DISPOSABLE EXTRA-SMALL SPECULUM
Welch Allyn introduced the industry’s first extra-small KleenSpec® Disposable Vaginal Speculum for virginal and pediatric patients as well as postmenopausal and posthysterectomy women. Available in August, this speculum joins the company’s suite of vaginal specula designed to work with the Welch Allyn Cordless Illumination System. The KleenSpec line is constructed of smooth, molded acrylic with wide handles for improved ergonomics and manipulation, says Welch Allyn.
FOR MORE INFORMATION, VISIT www.welchallyn.com
SCARAWAY® SILICONE SCAR SHEETS
ScarAway® Silicone Scar Sheets are an effective, affordable, over-the-counter treatment to reduce and prevent hypertrophic and keloid scars that may result from surgery, injuries, or burns, reports Mitchell-Vance Laboratories. Unlike scar-minimizing creams and ointments, ScarAway delivers a slight pressure directly to the scar, and mimics the natural barrier function of healthy skin, diminishing the scar’s appearance and restoring skin to its natural texture and color. The sheeting is nongreasy, ultra-thin, flexible, breathable, and durable with a soft fabric backing.
FOR MORE INFORMATION, VISIT www.MyScarAway.com
PREMAMA LIQUID PRENATAL VITAMINS
Premama, a flavorless prenatal vitamin drink mix, can be added to juices, milk, iced tea, and more. Premama includes the necessary vitamins and minerals, including folic acid, iron, DHA, CoQ10, and calcium, to support prepregnant, pregnant, and breast-feeding mothers. The unique mix of ingredients has been shown to help relieve common prenatal vitamin side-effects, such as nausea and constipation. Premama is 100% natural, lactate-free, gluten-free, and certified kosher.
FOR MORE INFORMATION, VISIT www.drinkpremama.com
HARMONY™ PRENATAL TEST DETECTS COMMON FETAL TRISOMIES
The Harmony Prenatal Test from Ariosa Diagnostics and available through LabCorp, is designed as a safe and highly accurate option to test pregnant woman for fetal anomalies using a directed approach to analyze cell-free DNA (cfDNA) in maternal blood. The Harmony Prenatal Test detects common fetal trisomies such as Trisomy 21 (associated with Down Syndrome) in pregnant women of at least 10 weeks’ gestation with a single fetus conceived without the use of an egg donor.
FOR MORE INFORMATION, VISIT www.ariosadx.com
GE HEALTHCARE’S NEW VSCAN: MORE SCAN TIME, BETTER RESOLUTION, EXPORT OPTION
GE Healthcare has upgraded Vscan, its pocket-sized, hand-held ultrasound (US) tool. New features include 50% more scan time (extended battery life), a more user-friendly interface, enhanced resolution, and an “export to PDF” option that allows physicians to more efficiently document findings. Vscan provides black and white anatomic and color-coded blood flow images. While Vscan is not intended to replace a full fetal US survey, it can provide physicians a quick look to assess fetal viability, says the manufacturer.
FOR MORE INFORMATION, VISIT https://vscan.gehealthcare.com
SODEXO HEALTH CARE SERVICES
Sodexo Health Care Services provides food and facilities services to hospitals across the country. Using the latest technologies, Sodexo employees implement environmental services and cleaning programs that have reduced hospital-acquired infections, improved patient and staff satisfaction, and contributed to cost savings for more than 1,700 client hospitals.
FOR MORE INFORMATION, VISIT www.sodexousa.com
Complexities of counseling women about HT
Related article Update on Menopause Andrew Kaunitz, MD (May 2012)
Related article Update on Menopause Andrew Kaunitz, MD (May 2012)
Related article Update on Menopause Andrew Kaunitz, MD (May 2012)
UPDATE: MENOPAUSE
Important developments in the care of menopausal women in the past 12 months include:
- new evidence about the duration, and nonhormonal management, of hot flushes
- new data on the risk of venous thromboembolism when oral and transdermal hormone therapy (HT) are compared
- trends in thinking regarding ovarian conservation at the time of hysterectomy, as well as a new report on the impact of hysterectomy on subsequent ovarian function
- a new Position Statement on HT from the North American Menopause Society.
Hot flushes can last 10 years or longer
Freeman EW, Sammel MD, Lin H, Liu Z, Gracia CR. Duration of menopausal hot flushes and associated risk factors. Obstet Gynecol. 2011;117(5):1095–1104.
Levis S, Strickman-Stein N, Ganjei-Azar P, Xu P, Doerge DR, Krischer J. Soy isoflavones in the prevention of menopausal bone loss and menopausal symptoms: A randomized, double-blind trial. Arch Intern Med. 2011;171(15):1363–1369.
Hot flushes are more persistent than has been recognized
Previous reports have suggested that hot flushes, the most prevalent menopausal symptom, persist from 6 months to longer than 5 years. Freeman and colleagues carried out a prospective, population-based study in the Northeastern United States that enrolled more than 250 women (age range at enrollment, 35 to 47 years) who did not use HT. Subjects in this cohort were followed for 13 years as they progressed through menopause.
Surprisingly, the researchers found that the median duration of moderate-to-severe hot flushes was 10.2 years. Hot flushes persisted longer in black women than in white women (P = .02) and longer in non-obese women than in obese women (P = .003). Duration of symptoms was similar in smokers and nonsmokers.
Once again, soy fails to relieve menopausal symptoms
A number of clinical trials performed since the 2002 publication of the initial findings of the Women’s Health Initiative (WHI) have failed to demonstrate that soy is efficacious for treating menopausal symptoms. Nevertheless, many women remain intrigued by the potential for obtaining symptom relief with over-the-counter supplements.
Investigators in Florida randomized women who had been menopausal for at least 5 years to receive daily soy isoflavones (equivalent to about twice the amount ingested in a typical Asian diet) or placebo for 2 years. Outcomes assessed at baseline and again at 12 and at 24 months included spine and hip bone-mineral density (BMD), menopausal symptoms, and vaginal epithelial maturation. Almost 250 women (mean age, 52 years) were randomized.
At 2 years, researchers found that:
- BMD had declined at all sites by about 2% in both groups
- approximately one half of subjects in the soy group and approximately one third who were randomized to the placebo group reported experiencing hot flushes (P = .02)
- vaginal epithelial maturation did not change appreciably from baseline in either group
- constipation was reported by 31% of women in the soy group and 21% in the placebo group—a difference that only marginally achieved statistical significance.
Hormone therapy remains far and away the most effective treatment for vasomotor symptoms. The long-term prospective study of Freeman and colleagues clarifies that bothersome symptoms may persist for many years—an important (though not upbeat) counseling point for symptomatic women.
Highly effective nonhormonal treatment of vasomotor symptoms would represent a major advance for our menopausal patients. Regrettably, neither soy nor black cohosh1 offers relief greater than placebo.
Gabapentin and some serotonin reuptake inhibitor and serotonin–norepinephrine reuptake inhibitor antidepressants do offer a modestly more effective off-label treatment of hot flushes than does placebo,2 but their efficacy does not approach that of HT. In my practice, I find that many patients who suffer bothersome hot flushes are reluctant to try off-label use of antidepressants.
Hormone therapy and risk of venous thromboembolism
Laliberté F, Dea K, Duh MS, Kahler KH, Rolli M, Lefebvre P. Does the route of administration for estrogen hormone therapy impact the risk of venous thromboembolism? Estradiol transdermal system versus oral estrogen-only hormone therapy. Menopause. 2011;18(10):1052–1059.
Olié V, Plu-Bureau G, Conard J, Horellou MH, Canonico M, Scarabin PY. Hormone therapy and recurrence of venous thromboembolism among postmenopausal women. Menopause. 2011;18(5):488–493.
Transdermal HT appears to be safer than oral therapy
Yet another observational study adds evidence that venous thromboembolism (VTE) is less of a risk in women using transdermal estrogen therapy than it is in women taking oral therapy.
To compare oral and transdermal estrogen formulations in regard to the risk of VTE that they pose, Laliberte and colleagues conducted a retrospective cohort study of US and Canadian women, using health insurance claims data from women who were starting transdermal or oral estrogen. In all, 27,018 users of transdermal estrogen were matched with an equal number of oral users.
VTE was diagnosed in 115 women using transdermal estradiol and 164 women using oral estrogen. Compared with the rate in women initiating oral estrogen, women using transdermal estradiol had a significantly lower incidence of VTE than oral estrogen users (adjusted incidence rate ratio, 0.67).
Is HT safe for women who have a history of VTE?
The US Food and Drug Administration has designated a personal history of VTE as a contraindication to all estrogen and estrogen-progestin HT formulations in the package labeling for these products. Because accumulating evidence is reassuring in regard to the risk of VTE with transdermal HT, however, it seems reasonable to consider using HT in selected women who have a history of VTE.
In a retrospective cohort study, French investigators assessed the impact of oral and transdermal estrogen on the risk of recurrent VTE in 1,023 postmenopausal women who had an earlier diagnosis of VTE. During follow-up, most of the subjects did not use HT, although 103 used transdermal estrogen and 10 used oral estrogen.
Seventy-seven women experienced recurrent VTE during a mean of 79 months after discontinuing anticoagulation. Compared with non-use of estrogen therapy, use of transdermal estrogen was not significantly associated with recurrent VTE (hazard ratio [HR], 1.0); oral estrogen, however, was associated with a substantial and significantly increased risk of recurrent VTE (HR, 6.4).
In the 2011 OBG Management Update on Menopause, I examined two large observational studies3,4—one from France, the other from Great Britain—that provided convincing evidence that transdermal HT does not, in contrast with oral HT, raise the risk of VTE. These new reports, from North America and France, provide further support for the hypothesis that transdermal HT is safer from the perspective of VTE risk. Although a randomized trial that compares the risk of VTE in women using oral estrogen with the risk in women using transdermal estrogen might put this matter to rest, I don’t anticipate that a trial to address this outcome, with adequate statistical power, will be performed any time soon.
In my practice, most of the estrogen that I prescribe for menopausal women is transdermal. Using transdermal estrogen may be particularly important in patients who are at increased risk of VTE at baseline, including obese women.
The small numbers of thrombotic events in the cohort of women who had a history of VTE limits confidence in the findings of this French report. Nevertheless, this study provides a small measure of reassurance regarding use of transdermal estrogen after VTE.
Only rarely have I prescribed HT to women who have a history of VTE. These exceptional patients have been highly symptomatic and extensively counseled about the risk of recurrent thrombosis as well as the off-label status of hormone use, given their medical history. Certainly, if you consider prescribing HT to such women, the transdermal route (preferably at a dosage of 0.05 mg, or lower) would be more prudent that oral HT.
Hysterectomy may accelerate the onset of menopause
Moorman PG, Myers ER, Schildkraut JM, Iversen ES, Wang F, Warren N. Effect of hysterectomy with ovarian preservation on ovarian function. Obstet Gynecol. 2011;118(6):1271–1279.
Novetsky AP, Boyd LR, Curtin JP. Trends in bilateral oophorectomy at the time of hysterectomy for benign disease. Obstet Gynecol. 2011;118(6):1280–1286.
Does hysterectomy hasten ovarian failure?
In a prospective cohort study from North Carolina, Moorman and colleagues followed 1) 406 women who did not have malignancy who underwent hysterectomy, with conservation of at least one ovary and 2) 465 women who had an intact uterus (overall age range, 30 to 47 years). Within 5 years of follow-up, ovarian failure had occurred in 60 women who had undergone a hysterectomy and in 46 women who had an intact uterus (adjusted HR, 1.9).
Ovarian failure occurred almost 2 years earlier in women who had undergone a hysterectomy than it did in those whose uterus was intact. The likelihood of ovarian failure was higher in the setting of unilateral oophorectomy than when both ovaries had been conserved.
Hysterectomy for benign disease: Are we performing fewer oophorectomies?
Investigators in New York State followed trends in concomitant bilateral oophorectomy among women undergoing hysterectomy for benign disease, from 2000 to 2006. Overall, the rate of concomitant oophorectomy declined by 8% during this period; among women younger than 55 years, the rate of oophorectomy declined by more than 10%. The rate of concomitant bilateral oophorectomy was higher among women who had a family history of breast or ovarian cancer and among those who had a personal history of breast cancer, ovarian cysts, or endometriosis.
Early menopause puts our patients at elevated risk of osteoporosis, cardiovascular disease, neurodegenerative disease (possibly), and sexual dysfunction. We have long suspected that hysterectomy may accelerate the onset of menopause, and the North Carolina cohort study provides strong support for this hypothesis.
The New York State report reveals that ObGyns are more often practicing ovarian conservation in women (particularly younger women) undergoing hysterectomy for benign indications.
In 2008, ACOG revised its guidance on this matter—stating that “strong consideration should be given to retaining normal ovaries in premenopausal women who are not at increased genetic risk of ovarian cancer.”5 Evidence that we are increasingly following this prudent guideline is welcome news.
Breaking news: NAMS updates guidance on hormone therapy
Position Statement emphasizes differences in the benefit-risk profile of estrogen–only HT and estrogen-progestin HT
Periodically, NAMS assembles a multidisciplinary panel of clinicians and researchers to evaluate new evidence about HT and reach consensus on guidance about using hormones, and then publishes a Position Statement on the subject. In March, NAMS published its updated (2012) position on HT.
Two recent, and important, analyses of data from the Women’s Health Initiative (WHI)6,7 made an impact on the current revision to an earlier (2010) Position Statement; I had summarized those studies in the 2011 OBG Management Update on Menopause. One focused on breast cancer characteristics and mortality associated with use of combination estrogen-progestin HT; the other, outcomes after use of estrogen-only HT. Recap. Initial findings in the estrogen– progestin arm of the WHI, published in 2002,8 found that, after participants had used study medications (HT or placebo) for a mean of 5.2 years, their risk of invasive breast cancer was increased (HR, 1.26). This modestly elevated risk was only marginally significant (95% confidence limit, 1.00–1.59).
In 2010, investigators reported on breast cancer characteristics and mortality in WHI participants at a mean follow-up of 11 years. They found that combination HT users had breast cancer histology similar to that of subjects assigned to placebo, but that the tumors were more likely to be node-positive in combination HT users (23.7%, compared with 16.2% among placebo users). In addition, breast cancer mortality was slightly higher among users of HT (2.6 deaths, compared with 1.3 deaths, for every 10,000 woman-years of use) (HR, 1.96; 95% confidence interval [CI], 1.00–4.04); again, this elevated risk reached only marginal statistical significance.
Then, in 2011, WHI investigators reported their findings from the estrogen-alone arm of the study, in which post-menopausal, hysterectomized women were randomized to oral estrogen or placebo and took study medications for a mean of 6.8 years. (Recall that initial findings from the estrogen-only arm of WHI, published in 2004, found that the risk of invasive cancer was lower in women randomized to estrogen [HR, 0.77]—a reduction in risk that approached, but did not achieve, statistical significance [95% CI, 0.59–1.01].9) In the 2011 report, the lower risk of breast cancer in the estrogen group persisted; with almost 11 years mean follow-up, this prevention was found to be robust and statistically significant (HR, 0.77; 95% CI, 0.62–0.95).
The sobering increased risk of advanced-stage tumors and the marginally higher likelihood of fatal breast cancer associated with use of estrogen–progestin HT stands in stark contrast with the significant reduction in breast cancer associated with estrogen- only HT.
Estrogen. Most of my patients who are taking systemic menopausal hormone therapy (HT) use transdermal estrogen, with 0.05 mg the most common starting dose. Given the elevated baseline risk of thrombosis among obese women, I particularly encourage them to use transdermal estrogen when starting systemic HT.
When I prescribe oral estrogen, the formulation I use most often is generic micronized estradiol; the most common starting dosage is a 1 mg tablet.
Progestin. To protect the endometrium in menopausal women whose uterus is intact and who are opting for systemic HT, I often use micronized progesterone, 100 mg nightly (provided no peanut allergy is present). My rationale? Progesterone is less likely than other progestational agents to cause unpleasant mood changes, and may offer a safety advantage vis a vis breast cancer.
When cost is a concern, generic medroxyprogesterone acetate tablets are well studied and inexpensive (2.5 mg tablets are appropriate when using the dosages of transdermal or oral estradiol given above).
When treating vasomotor symptoms/irregular bleeding in perimenopausal women, symptomatic relief may be more likely if HT formulations with sufficient progestin to consistently suppress ovulation are employed. Therefore, in such patients, I often use approaches such as femHRT 1/5 (also available as a generic) and Activella (also available as a generic).
Last, my experience is favorable using a combination of transdermal estrogen and the progestin-releasing IUD in symptomatic perimenopausal women.
Note: Using any sex steroids to manage perimenopausal symptoms constitutes an off-label use.
Accordingly, NAMS has modified its guidance. To step back for a moment, in the abstract of its 2010 Position Statement, NAMS had concluded that:
- Recent data support the initiation of HT around the time of menopause to treat menopause-related symptoms; to treat or reduce the risk of certain disorders, such as osteoporosis or fractures in select postmenopausal women; or both. The benefit-risk ratio for menopausal HT is favorable for women who initiate HT close to menopause but decreases in older women and with time since menopause in previously untreated women.
Contrast that with the conclusion in the abstract of the Society’s 2012 Position Statement:
- Recent data support the initiation of HT around the time of menopause to treat menopause-related symptoms and to prevent osteoporosis in women at high risk of fracture. The more favorable benefit-risk ratio for ET allows more flexibility in extending duration of use compared to EPT where the earlier appearance of increased breast cancer risk precludes a recommendation for use beyond 3 to 5 years.
When counseling menopausal women who are considering starting or continuing HT, I point out that HT represents the most effective treatment for bothersome menopausal symptoms and is highly effective for preventing osteoporotic fractures and genital atrophy.
Almost all of my patients who are considering starting systemic HT are in their late 40s or in their 50s—within a decade of the onset of menopause. If these women have had a hysterectomy, I counsel them that estrogen-only HT is likely to reduce their risk of coronary artery disease (CAD). On the other hand, if these women have an intact uterus, I counsel them that combination estrogen–progestin HT does not increase their risk of CAD—and might prevent it.
I also point out that starting HT and continuing it over the long term may reduce their risk of dementia later in life.
I do prescribe oral and transdermal estrogen, but I more often prescribe transdermal formulations because of their apparent safety in regard to the risk of venous thromboembolism. This preference for transdermal estrogen applies, in particular, to overweight women because their baseline risk of VTE is elevated.
Regarding breast cancer, I point out to estrogen-only HT candidates that HT prevents breast cancer. I counsel women whose uterus is intact that women who use combination HT for longer than 3 to 5 years experience a modest increase in their risk of having a diagnosis of breast cancer—similar to the elevation associated with moderate alcohol consumption. I also point out that the risk of dying from breast cancer might be increased with long-term combination HT use.
In women for whom the only indication for HT is prevention of genital atrophy, I prefer to prescribe vaginal formulations of estrogen.
Some of my patients—particularly those who do not have a uterus—who are extensively counseled, choose to continue HT indefinitely. Such very-long-term users often focus on either 1) their greater sense of well-being with HT or 2) the benefit of the prevention of osteoporosis in the face of their desire to avoid long-term bisphosphonate therapy.
Last, over the course of patients’ years of taking HT, I encourage them to try lower dosages, until they either discontinue HT or remain on a very low dosage.
We want to hear from you! Tell us what you think.
1. Geller SE, Shulman LP, van Breemen RB, et al. Safety and efficacy of black cohosh and red clover for the management of vasomotor symptoms: A randomized controlled trial. Menopause. 2009;16(6):1156-1166.
2. Pachman DR, Jones JM, Loprinzi CL. Management of menopause-associated vasomotor symptoms: Current treatment options challenges and future directions. Int J Womens Health. 2010;2:123-135.
3. Canonico M, Fournier A, Carcaillon L, et al. Postmenopausal hormone therapy and risk of idiopathic venous thromboembolism: results from the E3N cohort study. Arterioscler Thromb Vasc Biol. 2010;30(2):340-345.
4. Renoux C, Dell’aniello S, Garbe E, Suissa S. Transdermal and oral hormone replacement therapy and the risk of stroke: a nested case-control study. BMJ. 2010;340:c2519. doi: 10.1136/bmj.c2519.
5. ACOG Practice Bulletin No 89. Elective and risk-reducing salpingo-oophorectomy. American College of Obstetricians and Gynecologists. Obstet Gynecol. 2008;111(1):231-241.
6. Chlebowski RT, Anderson GL, Gass M, et al. Estrogen plus progestin and breast cancer incidence and mortality in postmenopausal women. JAMA. 2010;304(15):1684-1692.
7. LaCroix AZ, Chlebowski RT, Manson JE, et al; WHI Investigators. Health outcomes after stopping conjugated equine estrogens among postmenopausal women with prior hysterectomy: A randomized controlled trial. JAMA. 2011;305(13):1305-1314.
8. Rossouw JE, Anderson GL, Prentice RL, et al; Writing Group for the Women’s Health Initiative Investigators. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: Principal results from the Women’s Health Initiative Randomized Controlled Trial. JAMA. 2002;288(3):321-333.
9. Anderson GL, Limacher M, Assaf AR, et al. Effects of conjugated equine estrogen in postmenopausal women with hysterectomy: the Women’s Health Initiative randomized controlled trial. JAMA. 2004;291(14):1701-1712.
| Dr. Kaunitz describes how he counsels patients about hormone therapy |

Andrew M. Kaunitz, MD
Dr. Kaunitz is Professor and Associate Chairman, Department of Obstetrics and Gynecology, University of Florida College of Medicine–Jacksonville. He serves on the OBG MANAGEMENT Board of Editors.
Dr. Kaunitz receives grant or research support from Bayer, Agile, Noven, Teva, Endoceutics, and Medical Diagnostic Laboratories; is a consultant to Bayer and Merck; and owns stock in Becton Dickinson.
| Dr. Kaunitz describes how he counsels patients about hormone therapy |
Andrew M. Kaunitz, MD
Dr. Kaunitz is Professor and Associate Chairman, Department of Obstetrics and Gynecology, University of Florida College of Medicine–Jacksonville. He serves on the OBG MANAGEMENT Board of Editors.
Dr. Kaunitz receives grant or research support from Bayer, Agile, Noven, Teva, Endoceutics, and Medical Diagnostic Laboratories; is a consultant to Bayer and Merck; and owns stock in Becton Dickinson.
| Dr. Kaunitz describes how he counsels patients about hormone therapy |
Andrew M. Kaunitz, MD
Dr. Kaunitz is Professor and Associate Chairman, Department of Obstetrics and Gynecology, University of Florida College of Medicine–Jacksonville. He serves on the OBG MANAGEMENT Board of Editors.
Dr. Kaunitz receives grant or research support from Bayer, Agile, Noven, Teva, Endoceutics, and Medical Diagnostic Laboratories; is a consultant to Bayer and Merck; and owns stock in Becton Dickinson.
Important developments in the care of menopausal women in the past 12 months include:
- new evidence about the duration, and nonhormonal management, of hot flushes
- new data on the risk of venous thromboembolism when oral and transdermal hormone therapy (HT) are compared
- trends in thinking regarding ovarian conservation at the time of hysterectomy, as well as a new report on the impact of hysterectomy on subsequent ovarian function
- a new Position Statement on HT from the North American Menopause Society.
Hot flushes can last 10 years or longer
Freeman EW, Sammel MD, Lin H, Liu Z, Gracia CR. Duration of menopausal hot flushes and associated risk factors. Obstet Gynecol. 2011;117(5):1095–1104.
Levis S, Strickman-Stein N, Ganjei-Azar P, Xu P, Doerge DR, Krischer J. Soy isoflavones in the prevention of menopausal bone loss and menopausal symptoms: A randomized, double-blind trial. Arch Intern Med. 2011;171(15):1363–1369.
Hot flushes are more persistent than has been recognized
Previous reports have suggested that hot flushes, the most prevalent menopausal symptom, persist from 6 months to longer than 5 years. Freeman and colleagues carried out a prospective, population-based study in the Northeastern United States that enrolled more than 250 women (age range at enrollment, 35 to 47 years) who did not use HT. Subjects in this cohort were followed for 13 years as they progressed through menopause.
Surprisingly, the researchers found that the median duration of moderate-to-severe hot flushes was 10.2 years. Hot flushes persisted longer in black women than in white women (P = .02) and longer in non-obese women than in obese women (P = .003). Duration of symptoms was similar in smokers and nonsmokers.
Once again, soy fails to relieve menopausal symptoms
A number of clinical trials performed since the 2002 publication of the initial findings of the Women’s Health Initiative (WHI) have failed to demonstrate that soy is efficacious for treating menopausal symptoms. Nevertheless, many women remain intrigued by the potential for obtaining symptom relief with over-the-counter supplements.
Investigators in Florida randomized women who had been menopausal for at least 5 years to receive daily soy isoflavones (equivalent to about twice the amount ingested in a typical Asian diet) or placebo for 2 years. Outcomes assessed at baseline and again at 12 and at 24 months included spine and hip bone-mineral density (BMD), menopausal symptoms, and vaginal epithelial maturation. Almost 250 women (mean age, 52 years) were randomized.
At 2 years, researchers found that:
- BMD had declined at all sites by about 2% in both groups
- approximately one half of subjects in the soy group and approximately one third who were randomized to the placebo group reported experiencing hot flushes (P = .02)
- vaginal epithelial maturation did not change appreciably from baseline in either group
- constipation was reported by 31% of women in the soy group and 21% in the placebo group—a difference that only marginally achieved statistical significance.
Hormone therapy remains far and away the most effective treatment for vasomotor symptoms. The long-term prospective study of Freeman and colleagues clarifies that bothersome symptoms may persist for many years—an important (though not upbeat) counseling point for symptomatic women.
Highly effective nonhormonal treatment of vasomotor symptoms would represent a major advance for our menopausal patients. Regrettably, neither soy nor black cohosh1 offers relief greater than placebo.
Gabapentin and some serotonin reuptake inhibitor and serotonin–norepinephrine reuptake inhibitor antidepressants do offer a modestly more effective off-label treatment of hot flushes than does placebo,2 but their efficacy does not approach that of HT. In my practice, I find that many patients who suffer bothersome hot flushes are reluctant to try off-label use of antidepressants.
Hormone therapy and risk of venous thromboembolism
Laliberté F, Dea K, Duh MS, Kahler KH, Rolli M, Lefebvre P. Does the route of administration for estrogen hormone therapy impact the risk of venous thromboembolism? Estradiol transdermal system versus oral estrogen-only hormone therapy. Menopause. 2011;18(10):1052–1059.
Olié V, Plu-Bureau G, Conard J, Horellou MH, Canonico M, Scarabin PY. Hormone therapy and recurrence of venous thromboembolism among postmenopausal women. Menopause. 2011;18(5):488–493.
Transdermal HT appears to be safer than oral therapy
Yet another observational study adds evidence that venous thromboembolism (VTE) is less of a risk in women using transdermal estrogen therapy than it is in women taking oral therapy.
To compare oral and transdermal estrogen formulations in regard to the risk of VTE that they pose, Laliberte and colleagues conducted a retrospective cohort study of US and Canadian women, using health insurance claims data from women who were starting transdermal or oral estrogen. In all, 27,018 users of transdermal estrogen were matched with an equal number of oral users.
VTE was diagnosed in 115 women using transdermal estradiol and 164 women using oral estrogen. Compared with the rate in women initiating oral estrogen, women using transdermal estradiol had a significantly lower incidence of VTE than oral estrogen users (adjusted incidence rate ratio, 0.67).
Is HT safe for women who have a history of VTE?
The US Food and Drug Administration has designated a personal history of VTE as a contraindication to all estrogen and estrogen-progestin HT formulations in the package labeling for these products. Because accumulating evidence is reassuring in regard to the risk of VTE with transdermal HT, however, it seems reasonable to consider using HT in selected women who have a history of VTE.
In a retrospective cohort study, French investigators assessed the impact of oral and transdermal estrogen on the risk of recurrent VTE in 1,023 postmenopausal women who had an earlier diagnosis of VTE. During follow-up, most of the subjects did not use HT, although 103 used transdermal estrogen and 10 used oral estrogen.
Seventy-seven women experienced recurrent VTE during a mean of 79 months after discontinuing anticoagulation. Compared with non-use of estrogen therapy, use of transdermal estrogen was not significantly associated with recurrent VTE (hazard ratio [HR], 1.0); oral estrogen, however, was associated with a substantial and significantly increased risk of recurrent VTE (HR, 6.4).
In the 2011 OBG Management Update on Menopause, I examined two large observational studies3,4—one from France, the other from Great Britain—that provided convincing evidence that transdermal HT does not, in contrast with oral HT, raise the risk of VTE. These new reports, from North America and France, provide further support for the hypothesis that transdermal HT is safer from the perspective of VTE risk. Although a randomized trial that compares the risk of VTE in women using oral estrogen with the risk in women using transdermal estrogen might put this matter to rest, I don’t anticipate that a trial to address this outcome, with adequate statistical power, will be performed any time soon.
In my practice, most of the estrogen that I prescribe for menopausal women is transdermal. Using transdermal estrogen may be particularly important in patients who are at increased risk of VTE at baseline, including obese women.
The small numbers of thrombotic events in the cohort of women who had a history of VTE limits confidence in the findings of this French report. Nevertheless, this study provides a small measure of reassurance regarding use of transdermal estrogen after VTE.
Only rarely have I prescribed HT to women who have a history of VTE. These exceptional patients have been highly symptomatic and extensively counseled about the risk of recurrent thrombosis as well as the off-label status of hormone use, given their medical history. Certainly, if you consider prescribing HT to such women, the transdermal route (preferably at a dosage of 0.05 mg, or lower) would be more prudent that oral HT.
Hysterectomy may accelerate the onset of menopause
Moorman PG, Myers ER, Schildkraut JM, Iversen ES, Wang F, Warren N. Effect of hysterectomy with ovarian preservation on ovarian function. Obstet Gynecol. 2011;118(6):1271–1279.
Novetsky AP, Boyd LR, Curtin JP. Trends in bilateral oophorectomy at the time of hysterectomy for benign disease. Obstet Gynecol. 2011;118(6):1280–1286.
Does hysterectomy hasten ovarian failure?
In a prospective cohort study from North Carolina, Moorman and colleagues followed 1) 406 women who did not have malignancy who underwent hysterectomy, with conservation of at least one ovary and 2) 465 women who had an intact uterus (overall age range, 30 to 47 years). Within 5 years of follow-up, ovarian failure had occurred in 60 women who had undergone a hysterectomy and in 46 women who had an intact uterus (adjusted HR, 1.9).
Ovarian failure occurred almost 2 years earlier in women who had undergone a hysterectomy than it did in those whose uterus was intact. The likelihood of ovarian failure was higher in the setting of unilateral oophorectomy than when both ovaries had been conserved.
Hysterectomy for benign disease: Are we performing fewer oophorectomies?
Investigators in New York State followed trends in concomitant bilateral oophorectomy among women undergoing hysterectomy for benign disease, from 2000 to 2006. Overall, the rate of concomitant oophorectomy declined by 8% during this period; among women younger than 55 years, the rate of oophorectomy declined by more than 10%. The rate of concomitant bilateral oophorectomy was higher among women who had a family history of breast or ovarian cancer and among those who had a personal history of breast cancer, ovarian cysts, or endometriosis.
Early menopause puts our patients at elevated risk of osteoporosis, cardiovascular disease, neurodegenerative disease (possibly), and sexual dysfunction. We have long suspected that hysterectomy may accelerate the onset of menopause, and the North Carolina cohort study provides strong support for this hypothesis.
The New York State report reveals that ObGyns are more often practicing ovarian conservation in women (particularly younger women) undergoing hysterectomy for benign indications.
In 2008, ACOG revised its guidance on this matter—stating that “strong consideration should be given to retaining normal ovaries in premenopausal women who are not at increased genetic risk of ovarian cancer.”5 Evidence that we are increasingly following this prudent guideline is welcome news.
Breaking news: NAMS updates guidance on hormone therapy
Position Statement emphasizes differences in the benefit-risk profile of estrogen–only HT and estrogen-progestin HT
Periodically, NAMS assembles a multidisciplinary panel of clinicians and researchers to evaluate new evidence about HT and reach consensus on guidance about using hormones, and then publishes a Position Statement on the subject. In March, NAMS published its updated (2012) position on HT.
Two recent, and important, analyses of data from the Women’s Health Initiative (WHI)6,7 made an impact on the current revision to an earlier (2010) Position Statement; I had summarized those studies in the 2011 OBG Management Update on Menopause. One focused on breast cancer characteristics and mortality associated with use of combination estrogen-progestin HT; the other, outcomes after use of estrogen-only HT. Recap. Initial findings in the estrogen– progestin arm of the WHI, published in 2002,8 found that, after participants had used study medications (HT or placebo) for a mean of 5.2 years, their risk of invasive breast cancer was increased (HR, 1.26). This modestly elevated risk was only marginally significant (95% confidence limit, 1.00–1.59).
In 2010, investigators reported on breast cancer characteristics and mortality in WHI participants at a mean follow-up of 11 years. They found that combination HT users had breast cancer histology similar to that of subjects assigned to placebo, but that the tumors were more likely to be node-positive in combination HT users (23.7%, compared with 16.2% among placebo users). In addition, breast cancer mortality was slightly higher among users of HT (2.6 deaths, compared with 1.3 deaths, for every 10,000 woman-years of use) (HR, 1.96; 95% confidence interval [CI], 1.00–4.04); again, this elevated risk reached only marginal statistical significance.
Then, in 2011, WHI investigators reported their findings from the estrogen-alone arm of the study, in which post-menopausal, hysterectomized women were randomized to oral estrogen or placebo and took study medications for a mean of 6.8 years. (Recall that initial findings from the estrogen-only arm of WHI, published in 2004, found that the risk of invasive cancer was lower in women randomized to estrogen [HR, 0.77]—a reduction in risk that approached, but did not achieve, statistical significance [95% CI, 0.59–1.01].9) In the 2011 report, the lower risk of breast cancer in the estrogen group persisted; with almost 11 years mean follow-up, this prevention was found to be robust and statistically significant (HR, 0.77; 95% CI, 0.62–0.95).
The sobering increased risk of advanced-stage tumors and the marginally higher likelihood of fatal breast cancer associated with use of estrogen–progestin HT stands in stark contrast with the significant reduction in breast cancer associated with estrogen- only HT.
Estrogen. Most of my patients who are taking systemic menopausal hormone therapy (HT) use transdermal estrogen, with 0.05 mg the most common starting dose. Given the elevated baseline risk of thrombosis among obese women, I particularly encourage them to use transdermal estrogen when starting systemic HT.
When I prescribe oral estrogen, the formulation I use most often is generic micronized estradiol; the most common starting dosage is a 1 mg tablet.
Progestin. To protect the endometrium in menopausal women whose uterus is intact and who are opting for systemic HT, I often use micronized progesterone, 100 mg nightly (provided no peanut allergy is present). My rationale? Progesterone is less likely than other progestational agents to cause unpleasant mood changes, and may offer a safety advantage vis a vis breast cancer.
When cost is a concern, generic medroxyprogesterone acetate tablets are well studied and inexpensive (2.5 mg tablets are appropriate when using the dosages of transdermal or oral estradiol given above).
When treating vasomotor symptoms/irregular bleeding in perimenopausal women, symptomatic relief may be more likely if HT formulations with sufficient progestin to consistently suppress ovulation are employed. Therefore, in such patients, I often use approaches such as femHRT 1/5 (also available as a generic) and Activella (also available as a generic).
Last, my experience is favorable using a combination of transdermal estrogen and the progestin-releasing IUD in symptomatic perimenopausal women.
Note: Using any sex steroids to manage perimenopausal symptoms constitutes an off-label use.
Accordingly, NAMS has modified its guidance. To step back for a moment, in the abstract of its 2010 Position Statement, NAMS had concluded that:
- Recent data support the initiation of HT around the time of menopause to treat menopause-related symptoms; to treat or reduce the risk of certain disorders, such as osteoporosis or fractures in select postmenopausal women; or both. The benefit-risk ratio for menopausal HT is favorable for women who initiate HT close to menopause but decreases in older women and with time since menopause in previously untreated women.
Contrast that with the conclusion in the abstract of the Society’s 2012 Position Statement:
- Recent data support the initiation of HT around the time of menopause to treat menopause-related symptoms and to prevent osteoporosis in women at high risk of fracture. The more favorable benefit-risk ratio for ET allows more flexibility in extending duration of use compared to EPT where the earlier appearance of increased breast cancer risk precludes a recommendation for use beyond 3 to 5 years.
When counseling menopausal women who are considering starting or continuing HT, I point out that HT represents the most effective treatment for bothersome menopausal symptoms and is highly effective for preventing osteoporotic fractures and genital atrophy.
Almost all of my patients who are considering starting systemic HT are in their late 40s or in their 50s—within a decade of the onset of menopause. If these women have had a hysterectomy, I counsel them that estrogen-only HT is likely to reduce their risk of coronary artery disease (CAD). On the other hand, if these women have an intact uterus, I counsel them that combination estrogen–progestin HT does not increase their risk of CAD—and might prevent it.
I also point out that starting HT and continuing it over the long term may reduce their risk of dementia later in life.
I do prescribe oral and transdermal estrogen, but I more often prescribe transdermal formulations because of their apparent safety in regard to the risk of venous thromboembolism. This preference for transdermal estrogen applies, in particular, to overweight women because their baseline risk of VTE is elevated.
Regarding breast cancer, I point out to estrogen-only HT candidates that HT prevents breast cancer. I counsel women whose uterus is intact that women who use combination HT for longer than 3 to 5 years experience a modest increase in their risk of having a diagnosis of breast cancer—similar to the elevation associated with moderate alcohol consumption. I also point out that the risk of dying from breast cancer might be increased with long-term combination HT use.
In women for whom the only indication for HT is prevention of genital atrophy, I prefer to prescribe vaginal formulations of estrogen.
Some of my patients—particularly those who do not have a uterus—who are extensively counseled, choose to continue HT indefinitely. Such very-long-term users often focus on either 1) their greater sense of well-being with HT or 2) the benefit of the prevention of osteoporosis in the face of their desire to avoid long-term bisphosphonate therapy.
Last, over the course of patients’ years of taking HT, I encourage them to try lower dosages, until they either discontinue HT or remain on a very low dosage.
We want to hear from you! Tell us what you think.
Important developments in the care of menopausal women in the past 12 months include:
- new evidence about the duration, and nonhormonal management, of hot flushes
- new data on the risk of venous thromboembolism when oral and transdermal hormone therapy (HT) are compared
- trends in thinking regarding ovarian conservation at the time of hysterectomy, as well as a new report on the impact of hysterectomy on subsequent ovarian function
- a new Position Statement on HT from the North American Menopause Society.
Hot flushes can last 10 years or longer
Freeman EW, Sammel MD, Lin H, Liu Z, Gracia CR. Duration of menopausal hot flushes and associated risk factors. Obstet Gynecol. 2011;117(5):1095–1104.
Levis S, Strickman-Stein N, Ganjei-Azar P, Xu P, Doerge DR, Krischer J. Soy isoflavones in the prevention of menopausal bone loss and menopausal symptoms: A randomized, double-blind trial. Arch Intern Med. 2011;171(15):1363–1369.
Hot flushes are more persistent than has been recognized
Previous reports have suggested that hot flushes, the most prevalent menopausal symptom, persist from 6 months to longer than 5 years. Freeman and colleagues carried out a prospective, population-based study in the Northeastern United States that enrolled more than 250 women (age range at enrollment, 35 to 47 years) who did not use HT. Subjects in this cohort were followed for 13 years as they progressed through menopause.
Surprisingly, the researchers found that the median duration of moderate-to-severe hot flushes was 10.2 years. Hot flushes persisted longer in black women than in white women (P = .02) and longer in non-obese women than in obese women (P = .003). Duration of symptoms was similar in smokers and nonsmokers.
Once again, soy fails to relieve menopausal symptoms
A number of clinical trials performed since the 2002 publication of the initial findings of the Women’s Health Initiative (WHI) have failed to demonstrate that soy is efficacious for treating menopausal symptoms. Nevertheless, many women remain intrigued by the potential for obtaining symptom relief with over-the-counter supplements.
Investigators in Florida randomized women who had been menopausal for at least 5 years to receive daily soy isoflavones (equivalent to about twice the amount ingested in a typical Asian diet) or placebo for 2 years. Outcomes assessed at baseline and again at 12 and at 24 months included spine and hip bone-mineral density (BMD), menopausal symptoms, and vaginal epithelial maturation. Almost 250 women (mean age, 52 years) were randomized.
At 2 years, researchers found that:
- BMD had declined at all sites by about 2% in both groups
- approximately one half of subjects in the soy group and approximately one third who were randomized to the placebo group reported experiencing hot flushes (P = .02)
- vaginal epithelial maturation did not change appreciably from baseline in either group
- constipation was reported by 31% of women in the soy group and 21% in the placebo group—a difference that only marginally achieved statistical significance.
Hormone therapy remains far and away the most effective treatment for vasomotor symptoms. The long-term prospective study of Freeman and colleagues clarifies that bothersome symptoms may persist for many years—an important (though not upbeat) counseling point for symptomatic women.
Highly effective nonhormonal treatment of vasomotor symptoms would represent a major advance for our menopausal patients. Regrettably, neither soy nor black cohosh1 offers relief greater than placebo.
Gabapentin and some serotonin reuptake inhibitor and serotonin–norepinephrine reuptake inhibitor antidepressants do offer a modestly more effective off-label treatment of hot flushes than does placebo,2 but their efficacy does not approach that of HT. In my practice, I find that many patients who suffer bothersome hot flushes are reluctant to try off-label use of antidepressants.
Hormone therapy and risk of venous thromboembolism
Laliberté F, Dea K, Duh MS, Kahler KH, Rolli M, Lefebvre P. Does the route of administration for estrogen hormone therapy impact the risk of venous thromboembolism? Estradiol transdermal system versus oral estrogen-only hormone therapy. Menopause. 2011;18(10):1052–1059.
Olié V, Plu-Bureau G, Conard J, Horellou MH, Canonico M, Scarabin PY. Hormone therapy and recurrence of venous thromboembolism among postmenopausal women. Menopause. 2011;18(5):488–493.
Transdermal HT appears to be safer than oral therapy
Yet another observational study adds evidence that venous thromboembolism (VTE) is less of a risk in women using transdermal estrogen therapy than it is in women taking oral therapy.
To compare oral and transdermal estrogen formulations in regard to the risk of VTE that they pose, Laliberte and colleagues conducted a retrospective cohort study of US and Canadian women, using health insurance claims data from women who were starting transdermal or oral estrogen. In all, 27,018 users of transdermal estrogen were matched with an equal number of oral users.
VTE was diagnosed in 115 women using transdermal estradiol and 164 women using oral estrogen. Compared with the rate in women initiating oral estrogen, women using transdermal estradiol had a significantly lower incidence of VTE than oral estrogen users (adjusted incidence rate ratio, 0.67).
Is HT safe for women who have a history of VTE?
The US Food and Drug Administration has designated a personal history of VTE as a contraindication to all estrogen and estrogen-progestin HT formulations in the package labeling for these products. Because accumulating evidence is reassuring in regard to the risk of VTE with transdermal HT, however, it seems reasonable to consider using HT in selected women who have a history of VTE.
In a retrospective cohort study, French investigators assessed the impact of oral and transdermal estrogen on the risk of recurrent VTE in 1,023 postmenopausal women who had an earlier diagnosis of VTE. During follow-up, most of the subjects did not use HT, although 103 used transdermal estrogen and 10 used oral estrogen.
Seventy-seven women experienced recurrent VTE during a mean of 79 months after discontinuing anticoagulation. Compared with non-use of estrogen therapy, use of transdermal estrogen was not significantly associated with recurrent VTE (hazard ratio [HR], 1.0); oral estrogen, however, was associated with a substantial and significantly increased risk of recurrent VTE (HR, 6.4).
In the 2011 OBG Management Update on Menopause, I examined two large observational studies3,4—one from France, the other from Great Britain—that provided convincing evidence that transdermal HT does not, in contrast with oral HT, raise the risk of VTE. These new reports, from North America and France, provide further support for the hypothesis that transdermal HT is safer from the perspective of VTE risk. Although a randomized trial that compares the risk of VTE in women using oral estrogen with the risk in women using transdermal estrogen might put this matter to rest, I don’t anticipate that a trial to address this outcome, with adequate statistical power, will be performed any time soon.
In my practice, most of the estrogen that I prescribe for menopausal women is transdermal. Using transdermal estrogen may be particularly important in patients who are at increased risk of VTE at baseline, including obese women.
The small numbers of thrombotic events in the cohort of women who had a history of VTE limits confidence in the findings of this French report. Nevertheless, this study provides a small measure of reassurance regarding use of transdermal estrogen after VTE.
Only rarely have I prescribed HT to women who have a history of VTE. These exceptional patients have been highly symptomatic and extensively counseled about the risk of recurrent thrombosis as well as the off-label status of hormone use, given their medical history. Certainly, if you consider prescribing HT to such women, the transdermal route (preferably at a dosage of 0.05 mg, or lower) would be more prudent that oral HT.
Hysterectomy may accelerate the onset of menopause
Moorman PG, Myers ER, Schildkraut JM, Iversen ES, Wang F, Warren N. Effect of hysterectomy with ovarian preservation on ovarian function. Obstet Gynecol. 2011;118(6):1271–1279.
Novetsky AP, Boyd LR, Curtin JP. Trends in bilateral oophorectomy at the time of hysterectomy for benign disease. Obstet Gynecol. 2011;118(6):1280–1286.
Does hysterectomy hasten ovarian failure?
In a prospective cohort study from North Carolina, Moorman and colleagues followed 1) 406 women who did not have malignancy who underwent hysterectomy, with conservation of at least one ovary and 2) 465 women who had an intact uterus (overall age range, 30 to 47 years). Within 5 years of follow-up, ovarian failure had occurred in 60 women who had undergone a hysterectomy and in 46 women who had an intact uterus (adjusted HR, 1.9).
Ovarian failure occurred almost 2 years earlier in women who had undergone a hysterectomy than it did in those whose uterus was intact. The likelihood of ovarian failure was higher in the setting of unilateral oophorectomy than when both ovaries had been conserved.
Hysterectomy for benign disease: Are we performing fewer oophorectomies?
Investigators in New York State followed trends in concomitant bilateral oophorectomy among women undergoing hysterectomy for benign disease, from 2000 to 2006. Overall, the rate of concomitant oophorectomy declined by 8% during this period; among women younger than 55 years, the rate of oophorectomy declined by more than 10%. The rate of concomitant bilateral oophorectomy was higher among women who had a family history of breast or ovarian cancer and among those who had a personal history of breast cancer, ovarian cysts, or endometriosis.
Early menopause puts our patients at elevated risk of osteoporosis, cardiovascular disease, neurodegenerative disease (possibly), and sexual dysfunction. We have long suspected that hysterectomy may accelerate the onset of menopause, and the North Carolina cohort study provides strong support for this hypothesis.
The New York State report reveals that ObGyns are more often practicing ovarian conservation in women (particularly younger women) undergoing hysterectomy for benign indications.
In 2008, ACOG revised its guidance on this matter—stating that “strong consideration should be given to retaining normal ovaries in premenopausal women who are not at increased genetic risk of ovarian cancer.”5 Evidence that we are increasingly following this prudent guideline is welcome news.
Breaking news: NAMS updates guidance on hormone therapy
Position Statement emphasizes differences in the benefit-risk profile of estrogen–only HT and estrogen-progestin HT
Periodically, NAMS assembles a multidisciplinary panel of clinicians and researchers to evaluate new evidence about HT and reach consensus on guidance about using hormones, and then publishes a Position Statement on the subject. In March, NAMS published its updated (2012) position on HT.
Two recent, and important, analyses of data from the Women’s Health Initiative (WHI)6,7 made an impact on the current revision to an earlier (2010) Position Statement; I had summarized those studies in the 2011 OBG Management Update on Menopause. One focused on breast cancer characteristics and mortality associated with use of combination estrogen-progestin HT; the other, outcomes after use of estrogen-only HT. Recap. Initial findings in the estrogen– progestin arm of the WHI, published in 2002,8 found that, after participants had used study medications (HT or placebo) for a mean of 5.2 years, their risk of invasive breast cancer was increased (HR, 1.26). This modestly elevated risk was only marginally significant (95% confidence limit, 1.00–1.59).
In 2010, investigators reported on breast cancer characteristics and mortality in WHI participants at a mean follow-up of 11 years. They found that combination HT users had breast cancer histology similar to that of subjects assigned to placebo, but that the tumors were more likely to be node-positive in combination HT users (23.7%, compared with 16.2% among placebo users). In addition, breast cancer mortality was slightly higher among users of HT (2.6 deaths, compared with 1.3 deaths, for every 10,000 woman-years of use) (HR, 1.96; 95% confidence interval [CI], 1.00–4.04); again, this elevated risk reached only marginal statistical significance.
Then, in 2011, WHI investigators reported their findings from the estrogen-alone arm of the study, in which post-menopausal, hysterectomized women were randomized to oral estrogen or placebo and took study medications for a mean of 6.8 years. (Recall that initial findings from the estrogen-only arm of WHI, published in 2004, found that the risk of invasive cancer was lower in women randomized to estrogen [HR, 0.77]—a reduction in risk that approached, but did not achieve, statistical significance [95% CI, 0.59–1.01].9) In the 2011 report, the lower risk of breast cancer in the estrogen group persisted; with almost 11 years mean follow-up, this prevention was found to be robust and statistically significant (HR, 0.77; 95% CI, 0.62–0.95).
The sobering increased risk of advanced-stage tumors and the marginally higher likelihood of fatal breast cancer associated with use of estrogen–progestin HT stands in stark contrast with the significant reduction in breast cancer associated with estrogen- only HT.
Estrogen. Most of my patients who are taking systemic menopausal hormone therapy (HT) use transdermal estrogen, with 0.05 mg the most common starting dose. Given the elevated baseline risk of thrombosis among obese women, I particularly encourage them to use transdermal estrogen when starting systemic HT.
When I prescribe oral estrogen, the formulation I use most often is generic micronized estradiol; the most common starting dosage is a 1 mg tablet.
Progestin. To protect the endometrium in menopausal women whose uterus is intact and who are opting for systemic HT, I often use micronized progesterone, 100 mg nightly (provided no peanut allergy is present). My rationale? Progesterone is less likely than other progestational agents to cause unpleasant mood changes, and may offer a safety advantage vis a vis breast cancer.
When cost is a concern, generic medroxyprogesterone acetate tablets are well studied and inexpensive (2.5 mg tablets are appropriate when using the dosages of transdermal or oral estradiol given above).
When treating vasomotor symptoms/irregular bleeding in perimenopausal women, symptomatic relief may be more likely if HT formulations with sufficient progestin to consistently suppress ovulation are employed. Therefore, in such patients, I often use approaches such as femHRT 1/5 (also available as a generic) and Activella (also available as a generic).
Last, my experience is favorable using a combination of transdermal estrogen and the progestin-releasing IUD in symptomatic perimenopausal women.
Note: Using any sex steroids to manage perimenopausal symptoms constitutes an off-label use.
Accordingly, NAMS has modified its guidance. To step back for a moment, in the abstract of its 2010 Position Statement, NAMS had concluded that:
- Recent data support the initiation of HT around the time of menopause to treat menopause-related symptoms; to treat or reduce the risk of certain disorders, such as osteoporosis or fractures in select postmenopausal women; or both. The benefit-risk ratio for menopausal HT is favorable for women who initiate HT close to menopause but decreases in older women and with time since menopause in previously untreated women.
Contrast that with the conclusion in the abstract of the Society’s 2012 Position Statement:
- Recent data support the initiation of HT around the time of menopause to treat menopause-related symptoms and to prevent osteoporosis in women at high risk of fracture. The more favorable benefit-risk ratio for ET allows more flexibility in extending duration of use compared to EPT where the earlier appearance of increased breast cancer risk precludes a recommendation for use beyond 3 to 5 years.
When counseling menopausal women who are considering starting or continuing HT, I point out that HT represents the most effective treatment for bothersome menopausal symptoms and is highly effective for preventing osteoporotic fractures and genital atrophy.
Almost all of my patients who are considering starting systemic HT are in their late 40s or in their 50s—within a decade of the onset of menopause. If these women have had a hysterectomy, I counsel them that estrogen-only HT is likely to reduce their risk of coronary artery disease (CAD). On the other hand, if these women have an intact uterus, I counsel them that combination estrogen–progestin HT does not increase their risk of CAD—and might prevent it.
I also point out that starting HT and continuing it over the long term may reduce their risk of dementia later in life.
I do prescribe oral and transdermal estrogen, but I more often prescribe transdermal formulations because of their apparent safety in regard to the risk of venous thromboembolism. This preference for transdermal estrogen applies, in particular, to overweight women because their baseline risk of VTE is elevated.
Regarding breast cancer, I point out to estrogen-only HT candidates that HT prevents breast cancer. I counsel women whose uterus is intact that women who use combination HT for longer than 3 to 5 years experience a modest increase in their risk of having a diagnosis of breast cancer—similar to the elevation associated with moderate alcohol consumption. I also point out that the risk of dying from breast cancer might be increased with long-term combination HT use.
In women for whom the only indication for HT is prevention of genital atrophy, I prefer to prescribe vaginal formulations of estrogen.
Some of my patients—particularly those who do not have a uterus—who are extensively counseled, choose to continue HT indefinitely. Such very-long-term users often focus on either 1) their greater sense of well-being with HT or 2) the benefit of the prevention of osteoporosis in the face of their desire to avoid long-term bisphosphonate therapy.
Last, over the course of patients’ years of taking HT, I encourage them to try lower dosages, until they either discontinue HT or remain on a very low dosage.
We want to hear from you! Tell us what you think.
1. Geller SE, Shulman LP, van Breemen RB, et al. Safety and efficacy of black cohosh and red clover for the management of vasomotor symptoms: A randomized controlled trial. Menopause. 2009;16(6):1156-1166.
2. Pachman DR, Jones JM, Loprinzi CL. Management of menopause-associated vasomotor symptoms: Current treatment options challenges and future directions. Int J Womens Health. 2010;2:123-135.
3. Canonico M, Fournier A, Carcaillon L, et al. Postmenopausal hormone therapy and risk of idiopathic venous thromboembolism: results from the E3N cohort study. Arterioscler Thromb Vasc Biol. 2010;30(2):340-345.
4. Renoux C, Dell’aniello S, Garbe E, Suissa S. Transdermal and oral hormone replacement therapy and the risk of stroke: a nested case-control study. BMJ. 2010;340:c2519. doi: 10.1136/bmj.c2519.
5. ACOG Practice Bulletin No 89. Elective and risk-reducing salpingo-oophorectomy. American College of Obstetricians and Gynecologists. Obstet Gynecol. 2008;111(1):231-241.
6. Chlebowski RT, Anderson GL, Gass M, et al. Estrogen plus progestin and breast cancer incidence and mortality in postmenopausal women. JAMA. 2010;304(15):1684-1692.
7. LaCroix AZ, Chlebowski RT, Manson JE, et al; WHI Investigators. Health outcomes after stopping conjugated equine estrogens among postmenopausal women with prior hysterectomy: A randomized controlled trial. JAMA. 2011;305(13):1305-1314.
8. Rossouw JE, Anderson GL, Prentice RL, et al; Writing Group for the Women’s Health Initiative Investigators. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: Principal results from the Women’s Health Initiative Randomized Controlled Trial. JAMA. 2002;288(3):321-333.
9. Anderson GL, Limacher M, Assaf AR, et al. Effects of conjugated equine estrogen in postmenopausal women with hysterectomy: the Women’s Health Initiative randomized controlled trial. JAMA. 2004;291(14):1701-1712.
1. Geller SE, Shulman LP, van Breemen RB, et al. Safety and efficacy of black cohosh and red clover for the management of vasomotor symptoms: A randomized controlled trial. Menopause. 2009;16(6):1156-1166.
2. Pachman DR, Jones JM, Loprinzi CL. Management of menopause-associated vasomotor symptoms: Current treatment options challenges and future directions. Int J Womens Health. 2010;2:123-135.
3. Canonico M, Fournier A, Carcaillon L, et al. Postmenopausal hormone therapy and risk of idiopathic venous thromboembolism: results from the E3N cohort study. Arterioscler Thromb Vasc Biol. 2010;30(2):340-345.
4. Renoux C, Dell’aniello S, Garbe E, Suissa S. Transdermal and oral hormone replacement therapy and the risk of stroke: a nested case-control study. BMJ. 2010;340:c2519. doi: 10.1136/bmj.c2519.
5. ACOG Practice Bulletin No 89. Elective and risk-reducing salpingo-oophorectomy. American College of Obstetricians and Gynecologists. Obstet Gynecol. 2008;111(1):231-241.
6. Chlebowski RT, Anderson GL, Gass M, et al. Estrogen plus progestin and breast cancer incidence and mortality in postmenopausal women. JAMA. 2010;304(15):1684-1692.
7. LaCroix AZ, Chlebowski RT, Manson JE, et al; WHI Investigators. Health outcomes after stopping conjugated equine estrogens among postmenopausal women with prior hysterectomy: A randomized controlled trial. JAMA. 2011;305(13):1305-1314.
8. Rossouw JE, Anderson GL, Prentice RL, et al; Writing Group for the Women’s Health Initiative Investigators. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: Principal results from the Women’s Health Initiative Randomized Controlled Trial. JAMA. 2002;288(3):321-333.
9. Anderson GL, Limacher M, Assaf AR, et al. Effects of conjugated equine estrogen in postmenopausal women with hysterectomy: the Women’s Health Initiative randomized controlled trial. JAMA. 2004;291(14):1701-1712.
Vulvar pain syndromes: Making the correct diagnosis
Although the incidence of vulvar pain has increased over the past decade—thanks to both greater awareness and increasing numbers of affected women—the phenomenon is not a recent development. As early as 1874, T. Galliard Thomas wrote, “[T]his disorder, although fortunately not very frequent, is by no means very rare.”1 He went on to express “surprise” that it had not been “more generally and fully described.”
Despite the focus Thomas directed to the issue, vulvar pain did not get much attention until the 21st century, when a number of studies began to gauge its prevalence. For example, in a study in Boston of about 5,000 women, the lifetime prevalence of chronic vulvar pain was 16%.2 And in a study in Texas, the prevalence of vulvar pain in an urban, largely minority population was estimated to be 11%.3 The Boston study also reported that “nearly 40% of women chose not to seek treatment, and, of those who did, 60% saw three or more doctors, many of whom could not provide a diagnosis.”2
Clearly, there is a need for comprehensive information on vulvar pain and its causes, symptoms, diagnosis, and treatment. To address the lack of guidance, OBG Management Contributing Editor Neal M. Lonky, MD, assembled a panel of experts on vulvar pain syndromes and invited them to share their considerable knowledge. The ensuing discussion, presented in three parts, offers a gold mine of information. In this opening article, the panel focuses on causes, symptomatology, and diagnosis of this common complaint.
|
The lower vagina and vulva are richly supplied with peripheral nerves and are, therefore, sensitive to pain, particularly the region of the hymeneal ring. Although the pudendal nerve (arrow) courses through the area, it is an uncommon source of vulvar pain. |
![]()
Dr. Lonky: What are the most common diagnoses when vulvar pain is the complaint?
Dr. Gunter: The most common cause of chronic vulvar pain is vulvodynia, although lichen simplex chronicus, chronic yeast infections, and non-neoplastic epithelial disorders, such as lichen sclerosus and lichen planus, can also produce irritation and pain. In postmenopausal women, atrophic vaginitis can also cause a burning pain, although symptoms are typically more vaginal than vulvar. Yeast and lichen simplex chronicus typically produce itching, although sometimes they can present with irritation and pain, so they must be considered in the differential diagnosis. It is important to remember that many women with vulvodynia have used multiple topical agents and may have developed complex hygiene rituals in an attempt to treat their symptoms, which can result in a secondary lichen simplex chronicus.
That said, there is a high frequency of misdiagnosis with yeast. For example, in a study by Nyirjesy and colleagues, two thirds of women who were referred to a tertiary clinic for chronic vulvovaginal candidiasis were found to have a noninfectious entity instead—most commonly lichen simplex chronicus and vulvodynia.4
Dr. Edwards: The most common “diagnosis” for vulvar pain is vulvodynia. However, the definition of vulvodynia is pain—i.e., burning, rawness, irritation, soreness, aching, or stabbing or stinging sensations—in the absence of skin disease, infection, or specific neurologic disease. Therefore, even though the usual cause of vulvar pain is vulvodynia, it is a diagnosis of exclusion, and skin disease, infection, and neurologic disease must be ruled out.
In regard to infection, Candida albicans and bacterial vaginosis (BV) are usually the first conditions that are considered when a patient complains of vulvar pain, but they are not common causes of vulvar pain and are never causes of chronic vulvar pain. Very rarely they may cause recurrent pain that clears, at least briefly, with treatment.
Candida albicans is usually primarily pruritic, and BV produces discharge and odor, sometimes with minor symptoms. Non-albicans Candida (e.g., Candida glabrata) is nearly always asymptomatic, but it occasionally causes irritation and burning.
Group B streptococcus is another infectious entity that very, very occasionally causes irritation and dyspareunia but is usually only a colonizer.
Herpes simplex virus is a cause of recurrent but not chronic pain.
Chronic pain is more likely to be caused by skin disease than by infection. Lichen simplex chronicus causes itching; any pain is due to erosions from scratching.
Dr. Haefner: Several other infectious conditions or their treatments can cause vulvar pain. For example, herpes (particularly primary herpes infection) is classically associated with vulvar pain. The pain is so great that, at times, the patient requires admission for pain control. Surprisingly, despite the known pain of herpes, approximately 80% of patients who have it are unaware of their diagnosis.
Although condyloma is generally a painless condition, many patients complain of pain following treatment for it, whether treatment involves topical medications or laser surgery.
Chancroid is a painful vulvar ulcer. Trichomonas can sometimes be associated with vulvar pain.
Dr. Lonky: What terminology do we use when we discuss vulvar pain?
Dr. Haefner: The current terminology used to describe vulvar pain was published in 2004, after years of debate over nomenclature within the International Society for the Study of Vulvovaginal Disease.5 The terminology lists two major categories of vulvar pain:
-
pain related to a specific disorder. This category encompasses numerous conditions that feature an abnormal appearance of the vulva (Table 1).
TABLE 1
Terminology and classification of vulvar pain from the International Society for the Study of Vulvovaginal Disease
| SOURCE: Moyal-Barracco and Lynch.5 Reproduced with permission from the Journal of Reproductive Medicine. |
|
-
vulvodynia, in which the vulva appears normal, other than occasional erythema, which is most prominent at the duct openings (vestibular ducts—Bartholin’s and Skene’s).
As for vulvar pain, there are two major forms:
-
hyperalgesia (a low threshold for pain)
-
allodynia (pain in response to light touch).
Some diseases that are associated with vulvar pain do not qualify for the diagnosis of vulvodynia (Table 2) because they are associated with an abnormal appearance of the vulva.
TABLE 2
Conditions other than vulvodynia that are associated with vulvar pain
| Acute irritant contact dermatitis (e.g., erosion due to podofilox, imiquimod, cantharidin, fluorouracil, or podophyllin toxin) |
| Aphthous ulcer |
| Atrophy |
| Bartholin’s abscess |
| Candidiasis |
| Carcinoma |
| Chronic irritant contact dermatitis |
| Endometriosis |
| Herpes (simplex and zoster) |
| Immunobullous diseases (including cicatricial pemphigoid, pemphigus vulgaris, linear immunoglobulin A disease, etc.) |
| Lichen planus |
| Lichen sclerosus |
| Podophyllin overdose (see above) |
| Prolapsed urethra |
| Sjögren’s syndrome |
| Trauma |
| Trichomoniasis |
| Vulvar intraepithelial neoplasia |
![]()
Dr. Lonky: What skin diseases need to be ruled out before vulvodynia can be diagnosed?
Dr. Edwards: Skin diseases that affect the vulva are usually pruritic—pain is a later sign. Lichen simplex chronicus (also known as eczema) is pruritus caused by any irritant; any pain that arises is produced by visible excoriations from scratching.
Lichen sclerosus manifests as white epithelium that has a crinkling, shiny, or waxy texture. It can produce pain, especially dyspareunia. The pain is caused by erosions that arise from fragility and introital narrowing and inelasticity.
Vulvovaginal lichen planus is usually erosive and preferentially affects mucous membranes, especially the vestibule; it sometimes affects the vagina and mouth, as well.
Desquamative inflammatory vaginitis is most likely a skin disease that affects only the vagina. It involves introital redness and a clinically and microscopically purulent vaginal discharge that also reveals parabasal cells and absent lactobacilli.
Dr. Lonky: You mentioned that neurologic diseases can sometimes cause vulvar pain. Which ones?
Dr. Edwards: Pudendal neuralgia, diabetic neuropathy, and post-herpetic neuralgia are the most common specific neurologic causes of vulvar pain. Multiple sclerosis can also produce pain syndromes. Post-herpetic neuralgia follows herpes zoster—not herpes simplex—virus infection.
Dr. Lonky: Any other conditions that can cause vulvar pain?
Dr. Haefner: Aphthous ulcers are common and are often flared by stress.
Non-neoplastic epithelial disorders are also seen frequently in health-care providers’ offices; many patients who experience them report pain on the vulva.
It is always important to consider cancer when a patient has an abnormal vulvar appearance and pain that has persisted despite treatment.
![]()
Dr. Lonky: If you were to rank vulvar pain syndromes according to their prevalence, what would the most common syndromes be?
Dr. Gunter: Given the misdiagnosis of many women, who are told they have chronic yeast infection, as I mentioned, it’s hard to know which vulvar pain syndromes are most prevalent. I suspect that lichen simplex chronicus is most common, followed by vulvodynia, with chronic yeast infection a distant third.
My experience reflects what Nyirjesy and colleagues4 found: 65% to 75% of women referred to my clinic with chronic yeast actually have lichen simplex chronicus or vulvodynia. In postmenopausal women, atrophic vaginitis is also a consideration; it’s becoming more common now that the use of systemic hormone replacement therapy is decreasing.
Dr. Lonky: What about subsets of vulvodynia? Which ones are most common?
Dr. Edwards: There is good evidence of marked overlap among subsets of vulvodynia. The vast majority of women who have vulvodynia experience primarily provoked vestibular pain, regardless of age. However, I find that almost all patients also report pain that extends beyond the vestibule at times, as well as occasional unprovoked pain.
The diagnosis requires the exclusion of other causes of vulvar pain, and the subset is identified by the location of pain (that is, is it strictly localized or generalized or even migratory?) and its provoked or unprovoked nature.
Localized clitoral pain and vulvar pain localized to one side of the vulva are extremely uncommon, but they do occur. And although I rarely encounter teenagers and prepubertal children who have vulvodynia, I do have patients in both age groups who have vulvodynia.
Dr. Lonky: Are there racial differences in the prevalence of vulvodynia?
Dr. Edwards: Although several good studies show that women of African descent and white patients are equally likely to experience vulvodynia, the vast majority (99%) of my patients who have vulvodynia are white. My patients of African descent consult me primarily for itching or discharge.
My local demographics prevent me from judging the likelihood of Asians having vulvodynia, and our Hispanic population has limited access to health care.
In general, I don’t think that demographics are useful in making the diagnosis of vulvodynia.
![]()
Dr. Lonky: Do your patients who have vulvodynia or another vulvar pain syndrome tend to have comorbidities? If so, is this information helpful in establishing the diagnosis and planning therapy?
Dr. Haefner: Women who have vulvodynia often have other medical problems as well. In my practice, when new patients who have vulvodynia complete their intake survey, they often report a history of headache, irritable bowel syndrome, interstitial cystitis, fibromyalgia,6 chronic fatigue syndrome, back pain, and temporomandibular joint (TMJ) disorder. These comorbidities are not particularly helpful in establishing the diagnosis of vulvodynia, but they are an important consideration when choosing therapy for the patient. Often, the medications chosen to treat one condition will also benefit another condition. However, it’s important to check for potential interactions between drugs before prescribing a new treatment.
Dr. Gunter: A significant number of women who have vulvodynia also have other chronic pain syndromes. For example, the incidence of bladder pain syndrome–interstitial cystitis is 68% to 82% among women who have vulvodynia, compared with a baseline rate among all women of 6% to 11%.7-10 The rate of irritable bowel syndrome is more than doubled among women who have vulvodynia, compared with the general population (27% versus 12%).8 Another common comorbidity, hypertonic somatic dysfunction of the pelvic floor, is identified in 10% to 90% of women who have chronic vulvar pain.8,11,12 These women also have a higher incidence of nongenital pain syndromes, such as fibromyalgia, migraine, and TMJ dysfunction, than the general population, as Dr. Haefner noted.8,12,13
Many studies have evaluated psychological and emotional contributions to chronic vulvar pain. Pain and depression are intimately related—the incidence of depression among all people who experience chronic pain ranges from 27% to 54%, compared with 5% to 17% among the general population.14-16 The relationship is complex because chronic illness in general is associated with depression. Nevertheless, several studies have noted an increase in anxiety, stress, and depression among women who have vulvodynia.17-19
I screen every patient for depression using a Patient Health Questionnaire (PHQ-9); I also screen for anxiety. I find that a significant percentage of patients in my clinic are depressed or have an anxiety disorder. Failure to address these comorbidities makes treatment very difficult. I typically prescribe citalopram (Celexa), although there is some question whether it can safely be combined with a tricyclic antidepressant. We also offer stress-reduction classes, teach every patient the value of diaphragmatic breathing, offer mind-body classes for anxiety and stress, and provide intensive programs where the patient can learn important self-care skills, such as pacing (spacing activities throughout the day in a manner that avoids aggravating the pain), and address her anxiety and stress in a more guided manner. We also have a psychologist who specializes in pain for any patient who may need one-on-one counseling.
Dr. Edwards: The presence of comorbidities is somewhat useful in making the diagnosis of vulvodynia. I question my diagnosis, in fact, when a patient who has vulvodynia does not have headaches, low energy, depression, anxiety, irritable bowel syndrome, constipation, fibromyalgia, chronic fatigue, sensitivity to medications, TMJ dysfunction, or urinary symptoms.
![]()
Dr. Lonky: How prevalent is a finding of pudendal neuralgia?
Dr. Edwards: The prevalence and incidence of pudendal neuralgia are not known. Those who specialize in this condition think it is relatively common. I do not identify or suspect it very often. Its definitive diagnosis and management are outside the purview of the general gynecologist, but the general gynecologist should recognize the symptoms of pudendal neuralgia and refer the patient for evaluation and therapy.
Dr. Lonky: What are those symptoms?
Dr. Haefner: Pudendal neuralgia often occurs following trauma to the pudendal nerve. The pudendal nerve arises from sacral nerves, generally sacral nerves 2 to 4. Several tests can be utilized to diagnose this condition, including quantitative sensor tests, pudendal nerve motor latency tests, electromyography (EMG), and pudendal nerve blocks.20
Nantes Criteria allow for making a diagnosis of pudendal neuralgia (Table 3).21
TABLE 3
Nantes Criteria for pudendal neuralgia by pudendal nerve entrapment
| SOURCE: Labat et al.21 Reproduced with permission from Neurology and Urodynamics. |
Essential criteria
|
Complementary diagnostic criteria
|
Exclusion criteria
|
Associated signs not excluding the diagnosis
|
Initial treatments for pudendal neuralgia should be conservative. Treatments consist of lifestyle changes to prevent flare of disease. Physical therapy, medical management, nerve blocks, and alternative treatments may be beneficial.
Pudendal nerve entrapment is often exacerbated by sitting (not on a toilet seat, however) and is reduced in a standing position. It tends to increase in intensity throughout the day.22 The final treatment for pudendal nerve entrapment is surgery if the nerve is compressed. By this time, the generalist is not generally the provider who performs the surgery.
Dr. Gunter: I believe pudendal neuralgia is sometimes overdiagnosed. EMG studies of the pudendal nerve, often touted as a diagnostic tool, are unreliable (they can be abnormal after vaginal delivery or vaginal hysterectomy, for example). In my experience, bilateral pain is less likely to be pudendal neuralgia; spontaneous bilateral compression neuropathy at exactly the same level is not a common phenomenon in chronic pain.
I reserve the diagnosis of pudendal neuralgia for women who have allodynia in the distribution of the pudendal nerve with severe pain on sitting, and who have exquisite tenderness when pressure is applied over the pudendal nerve (at the level of the ischial spine on vaginal examination). Typically, the vaginal sidewall on the affected side is very sensitive to light touch. I do see pudendal nerve pain after vaginal surgery when there has been some compromise of the pudendal nerve or the sacral plexus. This is typically unilateral pain.
Dr. Lonky: Thank you all. We’ll continue our discussion, with a focus on treatment.
|
MORE TO COME
|
References
1. Thomas TG. Practical Treatise on the Diseases of Women. Philadelphia Pa: Henry C. Lea; 1874.
2. Harlow BL, Stewart EG. A population-based assessment of chronic unexplained vulvar pain: have we underestimated the prevalence of vulvodynia? J Am Med Womens Assoc. 2003;58(2):82–88.
3. Lavy RJ, Hynan LS, Haley RW. Prevalence of vulvar pain in an urban minority population. J Reprod Med. 2007;52(1):59–62.
4. Nyirjesy P, Peyton C, Weitz MV, Mathew L, Culhane JF. Causes of chronic vaginitis: analysis of a prospective database of affected women. Obstet Gynecol. 2006;108(5):1185–1191.
5. Moyal-Barracco M, Lynch PJ. 2003 ISSVD terminology and classification of vulvodynia: a historical perspective. J Reprod Med. 2004;49(10):772–777.
6. Yunas MB. Fibromyalgia and overlapping disorders: the unifying concept of central sensitivity syndromes. Semin Arthritis Rheum. 2007;36(6):339–356.
7. Kahn BS, Tatro C, Parsons CL, Willems JJ. Prevalence of interstitial cystitis in vulvodynia patients detected by bladder potassium sensitivity. J Sex Med. 2010;7(2 Pt 2):996–1002.
8. Arnold JD, Bachman GS, Rosen R, Kelly S, Rhoads GG. Vulvodynia: characteristics and associations with comorbidities and quality of life. Obstet Gynecol. 2006;107(3):617–624.
9. Parsons CL, Dell J, Stanford EJ, et al. The prevalence of interstitial cystitis in gynecologic patients with pelvic pain, as detected by intravesical potassium sensitivity. Am J Obstet Gynecol. 2002;187(5):1395–1400.
10. Clemens JQ, Meenan RT, O’Keefe Rosetti MC, et al. Prevalence of interstitial cystitis symptoms in a managed care population. J Urol. 2005;174(2):576–580.
11. Engman M, Lindehammar H, Wijma B. Surface electromyography diagnostics in women with partial vaginismus with or without vulvar vestibulitis and in asymptomatic women. J Psychosom Obstet Gynecol. 2004;25(3-4):281–294.
12. Gunter J. Vulvodynia: new thoughts on a devastating condition. Obstet Gynecol Surv. 2007;62(12):812–819.
13. Gordon AS, Panahlan-Jand M, McComb F, Melegari C, Sharp S. Characteristics of women with vulvar pain disorders: a Web-based survey. J Sex Marital Ther. 2003;29(suppl 1):45.
14. Whitten CE, Cristobal K. Chronic pain is a chronic condition not just a symptom. Permanente J. 2005;9(3):43.
15. Manchikanti L, Fellows B, Pampati V, et al. Comparison of psychological status of chronic pain patients and the general population. Pain Physician. 2002;5(1):40–48.
16. Banks SM, Kerns RD. Explaining the high rates of depression in chronic pain: a diathesis-stress framework. Psychological Bulletin. 1996;119(1):95–110.
17. Sadownik LA. Clinical correlates of vulvodynia patients. A prospective study of 300 patients. J Reprod Med. 2000;5:40–48. Editor found in PubMed: Sadownik LA. Clinical profile of vulvodynia patients. A prospective study of 300 patients. J Reprod Med. 2000;45(8):679–684. Could not find the citation listed. Please confirm.
18. Reed BD, Haefner HK, Punch MR, Roth RS, Gorenflo DW, Gillespie BW. Psychosocial and sexual functioning in women with vulvodynia and chronic pelvic pain. A comparative evaluation. J Reprod Med. 2000;45(8):624–632.
19. Landry T, Bergeron S. Biopsychosocial factors associated with dyspareunia in a community sample of adolescent girls. Arch Sex Behav. 2011; June 22.
20. Goldstein A, Pukall C, Goldstein I. When Sex Hurts: A Woman’s Guide to Banishing Sexual Pain. Cambridge Mass: Da Capo Lifelong Books; 2011;117–126.
21. Labat JJ, Riant T, Robert R, Amarenco G, Lefaucheur JP, Rigaud J. Diagnostic criteria for pudendal neuralgia by pudendal nerve entrapment (Nantes criteria). Neurol Urodyn. 2008;27(4):306–310.
22. Popeney C, Answell V, Renney K. Pudendal entrapment as an etiology of chronic perineal pain: Diagnosis and treatment. Neurol Urodyn. 2007;26(6):820–827.
Although the incidence of vulvar pain has increased over the past decade—thanks to both greater awareness and increasing numbers of affected women—the phenomenon is not a recent development. As early as 1874, T. Galliard Thomas wrote, “[T]his disorder, although fortunately not very frequent, is by no means very rare.”1 He went on to express “surprise” that it had not been “more generally and fully described.”
Despite the focus Thomas directed to the issue, vulvar pain did not get much attention until the 21st century, when a number of studies began to gauge its prevalence. For example, in a study in Boston of about 5,000 women, the lifetime prevalence of chronic vulvar pain was 16%.2 And in a study in Texas, the prevalence of vulvar pain in an urban, largely minority population was estimated to be 11%.3 The Boston study also reported that “nearly 40% of women chose not to seek treatment, and, of those who did, 60% saw three or more doctors, many of whom could not provide a diagnosis.”2
Clearly, there is a need for comprehensive information on vulvar pain and its causes, symptoms, diagnosis, and treatment. To address the lack of guidance, OBG Management Contributing Editor Neal M. Lonky, MD, assembled a panel of experts on vulvar pain syndromes and invited them to share their considerable knowledge. The ensuing discussion, presented in three parts, offers a gold mine of information. In this opening article, the panel focuses on causes, symptomatology, and diagnosis of this common complaint.
|
The lower vagina and vulva are richly supplied with peripheral nerves and are, therefore, sensitive to pain, particularly the region of the hymeneal ring. Although the pudendal nerve (arrow) courses through the area, it is an uncommon source of vulvar pain. |
![]()
Dr. Lonky: What are the most common diagnoses when vulvar pain is the complaint?
Dr. Gunter: The most common cause of chronic vulvar pain is vulvodynia, although lichen simplex chronicus, chronic yeast infections, and non-neoplastic epithelial disorders, such as lichen sclerosus and lichen planus, can also produce irritation and pain. In postmenopausal women, atrophic vaginitis can also cause a burning pain, although symptoms are typically more vaginal than vulvar. Yeast and lichen simplex chronicus typically produce itching, although sometimes they can present with irritation and pain, so they must be considered in the differential diagnosis. It is important to remember that many women with vulvodynia have used multiple topical agents and may have developed complex hygiene rituals in an attempt to treat their symptoms, which can result in a secondary lichen simplex chronicus.
That said, there is a high frequency of misdiagnosis with yeast. For example, in a study by Nyirjesy and colleagues, two thirds of women who were referred to a tertiary clinic for chronic vulvovaginal candidiasis were found to have a noninfectious entity instead—most commonly lichen simplex chronicus and vulvodynia.4
Dr. Edwards: The most common “diagnosis” for vulvar pain is vulvodynia. However, the definition of vulvodynia is pain—i.e., burning, rawness, irritation, soreness, aching, or stabbing or stinging sensations—in the absence of skin disease, infection, or specific neurologic disease. Therefore, even though the usual cause of vulvar pain is vulvodynia, it is a diagnosis of exclusion, and skin disease, infection, and neurologic disease must be ruled out.
In regard to infection, Candida albicans and bacterial vaginosis (BV) are usually the first conditions that are considered when a patient complains of vulvar pain, but they are not common causes of vulvar pain and are never causes of chronic vulvar pain. Very rarely they may cause recurrent pain that clears, at least briefly, with treatment.
Candida albicans is usually primarily pruritic, and BV produces discharge and odor, sometimes with minor symptoms. Non-albicans Candida (e.g., Candida glabrata) is nearly always asymptomatic, but it occasionally causes irritation and burning.
Group B streptococcus is another infectious entity that very, very occasionally causes irritation and dyspareunia but is usually only a colonizer.
Herpes simplex virus is a cause of recurrent but not chronic pain.
Chronic pain is more likely to be caused by skin disease than by infection. Lichen simplex chronicus causes itching; any pain is due to erosions from scratching.
Dr. Haefner: Several other infectious conditions or their treatments can cause vulvar pain. For example, herpes (particularly primary herpes infection) is classically associated with vulvar pain. The pain is so great that, at times, the patient requires admission for pain control. Surprisingly, despite the known pain of herpes, approximately 80% of patients who have it are unaware of their diagnosis.
Although condyloma is generally a painless condition, many patients complain of pain following treatment for it, whether treatment involves topical medications or laser surgery.
Chancroid is a painful vulvar ulcer. Trichomonas can sometimes be associated with vulvar pain.
Dr. Lonky: What terminology do we use when we discuss vulvar pain?
Dr. Haefner: The current terminology used to describe vulvar pain was published in 2004, after years of debate over nomenclature within the International Society for the Study of Vulvovaginal Disease.5 The terminology lists two major categories of vulvar pain:
-
pain related to a specific disorder. This category encompasses numerous conditions that feature an abnormal appearance of the vulva (Table 1).
TABLE 1
Terminology and classification of vulvar pain from the International Society for the Study of Vulvovaginal Disease
| SOURCE: Moyal-Barracco and Lynch.5 Reproduced with permission from the Journal of Reproductive Medicine. |
|
-
vulvodynia, in which the vulva appears normal, other than occasional erythema, which is most prominent at the duct openings (vestibular ducts—Bartholin’s and Skene’s).
As for vulvar pain, there are two major forms:
-
hyperalgesia (a low threshold for pain)
-
allodynia (pain in response to light touch).
Some diseases that are associated with vulvar pain do not qualify for the diagnosis of vulvodynia (Table 2) because they are associated with an abnormal appearance of the vulva.
TABLE 2
Conditions other than vulvodynia that are associated with vulvar pain
| Acute irritant contact dermatitis (e.g., erosion due to podofilox, imiquimod, cantharidin, fluorouracil, or podophyllin toxin) |
| Aphthous ulcer |
| Atrophy |
| Bartholin’s abscess |
| Candidiasis |
| Carcinoma |
| Chronic irritant contact dermatitis |
| Endometriosis |
| Herpes (simplex and zoster) |
| Immunobullous diseases (including cicatricial pemphigoid, pemphigus vulgaris, linear immunoglobulin A disease, etc.) |
| Lichen planus |
| Lichen sclerosus |
| Podophyllin overdose (see above) |
| Prolapsed urethra |
| Sjögren’s syndrome |
| Trauma |
| Trichomoniasis |
| Vulvar intraepithelial neoplasia |
![]()
Dr. Lonky: What skin diseases need to be ruled out before vulvodynia can be diagnosed?
Dr. Edwards: Skin diseases that affect the vulva are usually pruritic—pain is a later sign. Lichen simplex chronicus (also known as eczema) is pruritus caused by any irritant; any pain that arises is produced by visible excoriations from scratching.
Lichen sclerosus manifests as white epithelium that has a crinkling, shiny, or waxy texture. It can produce pain, especially dyspareunia. The pain is caused by erosions that arise from fragility and introital narrowing and inelasticity.
Vulvovaginal lichen planus is usually erosive and preferentially affects mucous membranes, especially the vestibule; it sometimes affects the vagina and mouth, as well.
Desquamative inflammatory vaginitis is most likely a skin disease that affects only the vagina. It involves introital redness and a clinically and microscopically purulent vaginal discharge that also reveals parabasal cells and absent lactobacilli.
Dr. Lonky: You mentioned that neurologic diseases can sometimes cause vulvar pain. Which ones?
Dr. Edwards: Pudendal neuralgia, diabetic neuropathy, and post-herpetic neuralgia are the most common specific neurologic causes of vulvar pain. Multiple sclerosis can also produce pain syndromes. Post-herpetic neuralgia follows herpes zoster—not herpes simplex—virus infection.
Dr. Lonky: Any other conditions that can cause vulvar pain?
Dr. Haefner: Aphthous ulcers are common and are often flared by stress.
Non-neoplastic epithelial disorders are also seen frequently in health-care providers’ offices; many patients who experience them report pain on the vulva.
It is always important to consider cancer when a patient has an abnormal vulvar appearance and pain that has persisted despite treatment.
![]()
Dr. Lonky: If you were to rank vulvar pain syndromes according to their prevalence, what would the most common syndromes be?
Dr. Gunter: Given the misdiagnosis of many women, who are told they have chronic yeast infection, as I mentioned, it’s hard to know which vulvar pain syndromes are most prevalent. I suspect that lichen simplex chronicus is most common, followed by vulvodynia, with chronic yeast infection a distant third.
My experience reflects what Nyirjesy and colleagues4 found: 65% to 75% of women referred to my clinic with chronic yeast actually have lichen simplex chronicus or vulvodynia. In postmenopausal women, atrophic vaginitis is also a consideration; it’s becoming more common now that the use of systemic hormone replacement therapy is decreasing.
Dr. Lonky: What about subsets of vulvodynia? Which ones are most common?
Dr. Edwards: There is good evidence of marked overlap among subsets of vulvodynia. The vast majority of women who have vulvodynia experience primarily provoked vestibular pain, regardless of age. However, I find that almost all patients also report pain that extends beyond the vestibule at times, as well as occasional unprovoked pain.
The diagnosis requires the exclusion of other causes of vulvar pain, and the subset is identified by the location of pain (that is, is it strictly localized or generalized or even migratory?) and its provoked or unprovoked nature.
Localized clitoral pain and vulvar pain localized to one side of the vulva are extremely uncommon, but they do occur. And although I rarely encounter teenagers and prepubertal children who have vulvodynia, I do have patients in both age groups who have vulvodynia.
Dr. Lonky: Are there racial differences in the prevalence of vulvodynia?
Dr. Edwards: Although several good studies show that women of African descent and white patients are equally likely to experience vulvodynia, the vast majority (99%) of my patients who have vulvodynia are white. My patients of African descent consult me primarily for itching or discharge.
My local demographics prevent me from judging the likelihood of Asians having vulvodynia, and our Hispanic population has limited access to health care.
In general, I don’t think that demographics are useful in making the diagnosis of vulvodynia.
![]()
Dr. Lonky: Do your patients who have vulvodynia or another vulvar pain syndrome tend to have comorbidities? If so, is this information helpful in establishing the diagnosis and planning therapy?
Dr. Haefner: Women who have vulvodynia often have other medical problems as well. In my practice, when new patients who have vulvodynia complete their intake survey, they often report a history of headache, irritable bowel syndrome, interstitial cystitis, fibromyalgia,6 chronic fatigue syndrome, back pain, and temporomandibular joint (TMJ) disorder. These comorbidities are not particularly helpful in establishing the diagnosis of vulvodynia, but they are an important consideration when choosing therapy for the patient. Often, the medications chosen to treat one condition will also benefit another condition. However, it’s important to check for potential interactions between drugs before prescribing a new treatment.
Dr. Gunter: A significant number of women who have vulvodynia also have other chronic pain syndromes. For example, the incidence of bladder pain syndrome–interstitial cystitis is 68% to 82% among women who have vulvodynia, compared with a baseline rate among all women of 6% to 11%.7-10 The rate of irritable bowel syndrome is more than doubled among women who have vulvodynia, compared with the general population (27% versus 12%).8 Another common comorbidity, hypertonic somatic dysfunction of the pelvic floor, is identified in 10% to 90% of women who have chronic vulvar pain.8,11,12 These women also have a higher incidence of nongenital pain syndromes, such as fibromyalgia, migraine, and TMJ dysfunction, than the general population, as Dr. Haefner noted.8,12,13
Many studies have evaluated psychological and emotional contributions to chronic vulvar pain. Pain and depression are intimately related—the incidence of depression among all people who experience chronic pain ranges from 27% to 54%, compared with 5% to 17% among the general population.14-16 The relationship is complex because chronic illness in general is associated with depression. Nevertheless, several studies have noted an increase in anxiety, stress, and depression among women who have vulvodynia.17-19
I screen every patient for depression using a Patient Health Questionnaire (PHQ-9); I also screen for anxiety. I find that a significant percentage of patients in my clinic are depressed or have an anxiety disorder. Failure to address these comorbidities makes treatment very difficult. I typically prescribe citalopram (Celexa), although there is some question whether it can safely be combined with a tricyclic antidepressant. We also offer stress-reduction classes, teach every patient the value of diaphragmatic breathing, offer mind-body classes for anxiety and stress, and provide intensive programs where the patient can learn important self-care skills, such as pacing (spacing activities throughout the day in a manner that avoids aggravating the pain), and address her anxiety and stress in a more guided manner. We also have a psychologist who specializes in pain for any patient who may need one-on-one counseling.
Dr. Edwards: The presence of comorbidities is somewhat useful in making the diagnosis of vulvodynia. I question my diagnosis, in fact, when a patient who has vulvodynia does not have headaches, low energy, depression, anxiety, irritable bowel syndrome, constipation, fibromyalgia, chronic fatigue, sensitivity to medications, TMJ dysfunction, or urinary symptoms.
![]()
Dr. Lonky: How prevalent is a finding of pudendal neuralgia?
Dr. Edwards: The prevalence and incidence of pudendal neuralgia are not known. Those who specialize in this condition think it is relatively common. I do not identify or suspect it very often. Its definitive diagnosis and management are outside the purview of the general gynecologist, but the general gynecologist should recognize the symptoms of pudendal neuralgia and refer the patient for evaluation and therapy.
Dr. Lonky: What are those symptoms?
Dr. Haefner: Pudendal neuralgia often occurs following trauma to the pudendal nerve. The pudendal nerve arises from sacral nerves, generally sacral nerves 2 to 4. Several tests can be utilized to diagnose this condition, including quantitative sensor tests, pudendal nerve motor latency tests, electromyography (EMG), and pudendal nerve blocks.20
Nantes Criteria allow for making a diagnosis of pudendal neuralgia (Table 3).21
TABLE 3
Nantes Criteria for pudendal neuralgia by pudendal nerve entrapment
| SOURCE: Labat et al.21 Reproduced with permission from Neurology and Urodynamics. |
Essential criteria
|
Complementary diagnostic criteria
|
Exclusion criteria
|
Associated signs not excluding the diagnosis
|
Initial treatments for pudendal neuralgia should be conservative. Treatments consist of lifestyle changes to prevent flare of disease. Physical therapy, medical management, nerve blocks, and alternative treatments may be beneficial.
Pudendal nerve entrapment is often exacerbated by sitting (not on a toilet seat, however) and is reduced in a standing position. It tends to increase in intensity throughout the day.22 The final treatment for pudendal nerve entrapment is surgery if the nerve is compressed. By this time, the generalist is not generally the provider who performs the surgery.
Dr. Gunter: I believe pudendal neuralgia is sometimes overdiagnosed. EMG studies of the pudendal nerve, often touted as a diagnostic tool, are unreliable (they can be abnormal after vaginal delivery or vaginal hysterectomy, for example). In my experience, bilateral pain is less likely to be pudendal neuralgia; spontaneous bilateral compression neuropathy at exactly the same level is not a common phenomenon in chronic pain.
I reserve the diagnosis of pudendal neuralgia for women who have allodynia in the distribution of the pudendal nerve with severe pain on sitting, and who have exquisite tenderness when pressure is applied over the pudendal nerve (at the level of the ischial spine on vaginal examination). Typically, the vaginal sidewall on the affected side is very sensitive to light touch. I do see pudendal nerve pain after vaginal surgery when there has been some compromise of the pudendal nerve or the sacral plexus. This is typically unilateral pain.
Dr. Lonky: Thank you all. We’ll continue our discussion, with a focus on treatment.
|
MORE TO COME
|
References
1. Thomas TG. Practical Treatise on the Diseases of Women. Philadelphia Pa: Henry C. Lea; 1874.
2. Harlow BL, Stewart EG. A population-based assessment of chronic unexplained vulvar pain: have we underestimated the prevalence of vulvodynia? J Am Med Womens Assoc. 2003;58(2):82–88.
3. Lavy RJ, Hynan LS, Haley RW. Prevalence of vulvar pain in an urban minority population. J Reprod Med. 2007;52(1):59–62.
4. Nyirjesy P, Peyton C, Weitz MV, Mathew L, Culhane JF. Causes of chronic vaginitis: analysis of a prospective database of affected women. Obstet Gynecol. 2006;108(5):1185–1191.
5. Moyal-Barracco M, Lynch PJ. 2003 ISSVD terminology and classification of vulvodynia: a historical perspective. J Reprod Med. 2004;49(10):772–777.
6. Yunas MB. Fibromyalgia and overlapping disorders: the unifying concept of central sensitivity syndromes. Semin Arthritis Rheum. 2007;36(6):339–356.
7. Kahn BS, Tatro C, Parsons CL, Willems JJ. Prevalence of interstitial cystitis in vulvodynia patients detected by bladder potassium sensitivity. J Sex Med. 2010;7(2 Pt 2):996–1002.
8. Arnold JD, Bachman GS, Rosen R, Kelly S, Rhoads GG. Vulvodynia: characteristics and associations with comorbidities and quality of life. Obstet Gynecol. 2006;107(3):617–624.
9. Parsons CL, Dell J, Stanford EJ, et al. The prevalence of interstitial cystitis in gynecologic patients with pelvic pain, as detected by intravesical potassium sensitivity. Am J Obstet Gynecol. 2002;187(5):1395–1400.
10. Clemens JQ, Meenan RT, O’Keefe Rosetti MC, et al. Prevalence of interstitial cystitis symptoms in a managed care population. J Urol. 2005;174(2):576–580.
11. Engman M, Lindehammar H, Wijma B. Surface electromyography diagnostics in women with partial vaginismus with or without vulvar vestibulitis and in asymptomatic women. J Psychosom Obstet Gynecol. 2004;25(3-4):281–294.
12. Gunter J. Vulvodynia: new thoughts on a devastating condition. Obstet Gynecol Surv. 2007;62(12):812–819.
13. Gordon AS, Panahlan-Jand M, McComb F, Melegari C, Sharp S. Characteristics of women with vulvar pain disorders: a Web-based survey. J Sex Marital Ther. 2003;29(suppl 1):45.
14. Whitten CE, Cristobal K. Chronic pain is a chronic condition not just a symptom. Permanente J. 2005;9(3):43.
15. Manchikanti L, Fellows B, Pampati V, et al. Comparison of psychological status of chronic pain patients and the general population. Pain Physician. 2002;5(1):40–48.
16. Banks SM, Kerns RD. Explaining the high rates of depression in chronic pain: a diathesis-stress framework. Psychological Bulletin. 1996;119(1):95–110.
17. Sadownik LA. Clinical correlates of vulvodynia patients. A prospective study of 300 patients. J Reprod Med. 2000;5:40–48. Editor found in PubMed: Sadownik LA. Clinical profile of vulvodynia patients. A prospective study of 300 patients. J Reprod Med. 2000;45(8):679–684. Could not find the citation listed. Please confirm.
18. Reed BD, Haefner HK, Punch MR, Roth RS, Gorenflo DW, Gillespie BW. Psychosocial and sexual functioning in women with vulvodynia and chronic pelvic pain. A comparative evaluation. J Reprod Med. 2000;45(8):624–632.
19. Landry T, Bergeron S. Biopsychosocial factors associated with dyspareunia in a community sample of adolescent girls. Arch Sex Behav. 2011; June 22.
20. Goldstein A, Pukall C, Goldstein I. When Sex Hurts: A Woman’s Guide to Banishing Sexual Pain. Cambridge Mass: Da Capo Lifelong Books; 2011;117–126.
21. Labat JJ, Riant T, Robert R, Amarenco G, Lefaucheur JP, Rigaud J. Diagnostic criteria for pudendal neuralgia by pudendal nerve entrapment (Nantes criteria). Neurol Urodyn. 2008;27(4):306–310.
22. Popeney C, Answell V, Renney K. Pudendal entrapment as an etiology of chronic perineal pain: Diagnosis and treatment. Neurol Urodyn. 2007;26(6):820–827.
Although the incidence of vulvar pain has increased over the past decade—thanks to both greater awareness and increasing numbers of affected women—the phenomenon is not a recent development. As early as 1874, T. Galliard Thomas wrote, “[T]his disorder, although fortunately not very frequent, is by no means very rare.”1 He went on to express “surprise” that it had not been “more generally and fully described.”
Despite the focus Thomas directed to the issue, vulvar pain did not get much attention until the 21st century, when a number of studies began to gauge its prevalence. For example, in a study in Boston of about 5,000 women, the lifetime prevalence of chronic vulvar pain was 16%.2 And in a study in Texas, the prevalence of vulvar pain in an urban, largely minority population was estimated to be 11%.3 The Boston study also reported that “nearly 40% of women chose not to seek treatment, and, of those who did, 60% saw three or more doctors, many of whom could not provide a diagnosis.”2
Clearly, there is a need for comprehensive information on vulvar pain and its causes, symptoms, diagnosis, and treatment. To address the lack of guidance, OBG Management Contributing Editor Neal M. Lonky, MD, assembled a panel of experts on vulvar pain syndromes and invited them to share their considerable knowledge. The ensuing discussion, presented in three parts, offers a gold mine of information. In this opening article, the panel focuses on causes, symptomatology, and diagnosis of this common complaint.
|
The lower vagina and vulva are richly supplied with peripheral nerves and are, therefore, sensitive to pain, particularly the region of the hymeneal ring. Although the pudendal nerve (arrow) courses through the area, it is an uncommon source of vulvar pain. |
![]()
Dr. Lonky: What are the most common diagnoses when vulvar pain is the complaint?
Dr. Gunter: The most common cause of chronic vulvar pain is vulvodynia, although lichen simplex chronicus, chronic yeast infections, and non-neoplastic epithelial disorders, such as lichen sclerosus and lichen planus, can also produce irritation and pain. In postmenopausal women, atrophic vaginitis can also cause a burning pain, although symptoms are typically more vaginal than vulvar. Yeast and lichen simplex chronicus typically produce itching, although sometimes they can present with irritation and pain, so they must be considered in the differential diagnosis. It is important to remember that many women with vulvodynia have used multiple topical agents and may have developed complex hygiene rituals in an attempt to treat their symptoms, which can result in a secondary lichen simplex chronicus.
That said, there is a high frequency of misdiagnosis with yeast. For example, in a study by Nyirjesy and colleagues, two thirds of women who were referred to a tertiary clinic for chronic vulvovaginal candidiasis were found to have a noninfectious entity instead—most commonly lichen simplex chronicus and vulvodynia.4
Dr. Edwards: The most common “diagnosis” for vulvar pain is vulvodynia. However, the definition of vulvodynia is pain—i.e., burning, rawness, irritation, soreness, aching, or stabbing or stinging sensations—in the absence of skin disease, infection, or specific neurologic disease. Therefore, even though the usual cause of vulvar pain is vulvodynia, it is a diagnosis of exclusion, and skin disease, infection, and neurologic disease must be ruled out.
In regard to infection, Candida albicans and bacterial vaginosis (BV) are usually the first conditions that are considered when a patient complains of vulvar pain, but they are not common causes of vulvar pain and are never causes of chronic vulvar pain. Very rarely they may cause recurrent pain that clears, at least briefly, with treatment.
Candida albicans is usually primarily pruritic, and BV produces discharge and odor, sometimes with minor symptoms. Non-albicans Candida (e.g., Candida glabrata) is nearly always asymptomatic, but it occasionally causes irritation and burning.
Group B streptococcus is another infectious entity that very, very occasionally causes irritation and dyspareunia but is usually only a colonizer.
Herpes simplex virus is a cause of recurrent but not chronic pain.
Chronic pain is more likely to be caused by skin disease than by infection. Lichen simplex chronicus causes itching; any pain is due to erosions from scratching.
Dr. Haefner: Several other infectious conditions or their treatments can cause vulvar pain. For example, herpes (particularly primary herpes infection) is classically associated with vulvar pain. The pain is so great that, at times, the patient requires admission for pain control. Surprisingly, despite the known pain of herpes, approximately 80% of patients who have it are unaware of their diagnosis.
Although condyloma is generally a painless condition, many patients complain of pain following treatment for it, whether treatment involves topical medications or laser surgery.
Chancroid is a painful vulvar ulcer. Trichomonas can sometimes be associated with vulvar pain.
Dr. Lonky: What terminology do we use when we discuss vulvar pain?
Dr. Haefner: The current terminology used to describe vulvar pain was published in 2004, after years of debate over nomenclature within the International Society for the Study of Vulvovaginal Disease.5 The terminology lists two major categories of vulvar pain:
-
pain related to a specific disorder. This category encompasses numerous conditions that feature an abnormal appearance of the vulva (Table 1).
TABLE 1
Terminology and classification of vulvar pain from the International Society for the Study of Vulvovaginal Disease
| SOURCE: Moyal-Barracco and Lynch.5 Reproduced with permission from the Journal of Reproductive Medicine. |
|
-
vulvodynia, in which the vulva appears normal, other than occasional erythema, which is most prominent at the duct openings (vestibular ducts—Bartholin’s and Skene’s).
As for vulvar pain, there are two major forms:
-
hyperalgesia (a low threshold for pain)
-
allodynia (pain in response to light touch).
Some diseases that are associated with vulvar pain do not qualify for the diagnosis of vulvodynia (Table 2) because they are associated with an abnormal appearance of the vulva.
TABLE 2
Conditions other than vulvodynia that are associated with vulvar pain
| Acute irritant contact dermatitis (e.g., erosion due to podofilox, imiquimod, cantharidin, fluorouracil, or podophyllin toxin) |
| Aphthous ulcer |
| Atrophy |
| Bartholin’s abscess |
| Candidiasis |
| Carcinoma |
| Chronic irritant contact dermatitis |
| Endometriosis |
| Herpes (simplex and zoster) |
| Immunobullous diseases (including cicatricial pemphigoid, pemphigus vulgaris, linear immunoglobulin A disease, etc.) |
| Lichen planus |
| Lichen sclerosus |
| Podophyllin overdose (see above) |
| Prolapsed urethra |
| Sjögren’s syndrome |
| Trauma |
| Trichomoniasis |
| Vulvar intraepithelial neoplasia |
![]()
Dr. Lonky: What skin diseases need to be ruled out before vulvodynia can be diagnosed?
Dr. Edwards: Skin diseases that affect the vulva are usually pruritic—pain is a later sign. Lichen simplex chronicus (also known as eczema) is pruritus caused by any irritant; any pain that arises is produced by visible excoriations from scratching.
Lichen sclerosus manifests as white epithelium that has a crinkling, shiny, or waxy texture. It can produce pain, especially dyspareunia. The pain is caused by erosions that arise from fragility and introital narrowing and inelasticity.
Vulvovaginal lichen planus is usually erosive and preferentially affects mucous membranes, especially the vestibule; it sometimes affects the vagina and mouth, as well.
Desquamative inflammatory vaginitis is most likely a skin disease that affects only the vagina. It involves introital redness and a clinically and microscopically purulent vaginal discharge that also reveals parabasal cells and absent lactobacilli.
Dr. Lonky: You mentioned that neurologic diseases can sometimes cause vulvar pain. Which ones?
Dr. Edwards: Pudendal neuralgia, diabetic neuropathy, and post-herpetic neuralgia are the most common specific neurologic causes of vulvar pain. Multiple sclerosis can also produce pain syndromes. Post-herpetic neuralgia follows herpes zoster—not herpes simplex—virus infection.
Dr. Lonky: Any other conditions that can cause vulvar pain?
Dr. Haefner: Aphthous ulcers are common and are often flared by stress.
Non-neoplastic epithelial disorders are also seen frequently in health-care providers’ offices; many patients who experience them report pain on the vulva.
It is always important to consider cancer when a patient has an abnormal vulvar appearance and pain that has persisted despite treatment.
![]()
Dr. Lonky: If you were to rank vulvar pain syndromes according to their prevalence, what would the most common syndromes be?
Dr. Gunter: Given the misdiagnosis of many women, who are told they have chronic yeast infection, as I mentioned, it’s hard to know which vulvar pain syndromes are most prevalent. I suspect that lichen simplex chronicus is most common, followed by vulvodynia, with chronic yeast infection a distant third.
My experience reflects what Nyirjesy and colleagues4 found: 65% to 75% of women referred to my clinic with chronic yeast actually have lichen simplex chronicus or vulvodynia. In postmenopausal women, atrophic vaginitis is also a consideration; it’s becoming more common now that the use of systemic hormone replacement therapy is decreasing.
Dr. Lonky: What about subsets of vulvodynia? Which ones are most common?
Dr. Edwards: There is good evidence of marked overlap among subsets of vulvodynia. The vast majority of women who have vulvodynia experience primarily provoked vestibular pain, regardless of age. However, I find that almost all patients also report pain that extends beyond the vestibule at times, as well as occasional unprovoked pain.
The diagnosis requires the exclusion of other causes of vulvar pain, and the subset is identified by the location of pain (that is, is it strictly localized or generalized or even migratory?) and its provoked or unprovoked nature.
Localized clitoral pain and vulvar pain localized to one side of the vulva are extremely uncommon, but they do occur. And although I rarely encounter teenagers and prepubertal children who have vulvodynia, I do have patients in both age groups who have vulvodynia.
Dr. Lonky: Are there racial differences in the prevalence of vulvodynia?
Dr. Edwards: Although several good studies show that women of African descent and white patients are equally likely to experience vulvodynia, the vast majority (99%) of my patients who have vulvodynia are white. My patients of African descent consult me primarily for itching or discharge.
My local demographics prevent me from judging the likelihood of Asians having vulvodynia, and our Hispanic population has limited access to health care.
In general, I don’t think that demographics are useful in making the diagnosis of vulvodynia.
![]()
Dr. Lonky: Do your patients who have vulvodynia or another vulvar pain syndrome tend to have comorbidities? If so, is this information helpful in establishing the diagnosis and planning therapy?
Dr. Haefner: Women who have vulvodynia often have other medical problems as well. In my practice, when new patients who have vulvodynia complete their intake survey, they often report a history of headache, irritable bowel syndrome, interstitial cystitis, fibromyalgia,6 chronic fatigue syndrome, back pain, and temporomandibular joint (TMJ) disorder. These comorbidities are not particularly helpful in establishing the diagnosis of vulvodynia, but they are an important consideration when choosing therapy for the patient. Often, the medications chosen to treat one condition will also benefit another condition. However, it’s important to check for potential interactions between drugs before prescribing a new treatment.
Dr. Gunter: A significant number of women who have vulvodynia also have other chronic pain syndromes. For example, the incidence of bladder pain syndrome–interstitial cystitis is 68% to 82% among women who have vulvodynia, compared with a baseline rate among all women of 6% to 11%.7-10 The rate of irritable bowel syndrome is more than doubled among women who have vulvodynia, compared with the general population (27% versus 12%).8 Another common comorbidity, hypertonic somatic dysfunction of the pelvic floor, is identified in 10% to 90% of women who have chronic vulvar pain.8,11,12 These women also have a higher incidence of nongenital pain syndromes, such as fibromyalgia, migraine, and TMJ dysfunction, than the general population, as Dr. Haefner noted.8,12,13
Many studies have evaluated psychological and emotional contributions to chronic vulvar pain. Pain and depression are intimately related—the incidence of depression among all people who experience chronic pain ranges from 27% to 54%, compared with 5% to 17% among the general population.14-16 The relationship is complex because chronic illness in general is associated with depression. Nevertheless, several studies have noted an increase in anxiety, stress, and depression among women who have vulvodynia.17-19
I screen every patient for depression using a Patient Health Questionnaire (PHQ-9); I also screen for anxiety. I find that a significant percentage of patients in my clinic are depressed or have an anxiety disorder. Failure to address these comorbidities makes treatment very difficult. I typically prescribe citalopram (Celexa), although there is some question whether it can safely be combined with a tricyclic antidepressant. We also offer stress-reduction classes, teach every patient the value of diaphragmatic breathing, offer mind-body classes for anxiety and stress, and provide intensive programs where the patient can learn important self-care skills, such as pacing (spacing activities throughout the day in a manner that avoids aggravating the pain), and address her anxiety and stress in a more guided manner. We also have a psychologist who specializes in pain for any patient who may need one-on-one counseling.
Dr. Edwards: The presence of comorbidities is somewhat useful in making the diagnosis of vulvodynia. I question my diagnosis, in fact, when a patient who has vulvodynia does not have headaches, low energy, depression, anxiety, irritable bowel syndrome, constipation, fibromyalgia, chronic fatigue, sensitivity to medications, TMJ dysfunction, or urinary symptoms.
![]()
Dr. Lonky: How prevalent is a finding of pudendal neuralgia?
Dr. Edwards: The prevalence and incidence of pudendal neuralgia are not known. Those who specialize in this condition think it is relatively common. I do not identify or suspect it very often. Its definitive diagnosis and management are outside the purview of the general gynecologist, but the general gynecologist should recognize the symptoms of pudendal neuralgia and refer the patient for evaluation and therapy.
Dr. Lonky: What are those symptoms?
Dr. Haefner: Pudendal neuralgia often occurs following trauma to the pudendal nerve. The pudendal nerve arises from sacral nerves, generally sacral nerves 2 to 4. Several tests can be utilized to diagnose this condition, including quantitative sensor tests, pudendal nerve motor latency tests, electromyography (EMG), and pudendal nerve blocks.20
Nantes Criteria allow for making a diagnosis of pudendal neuralgia (Table 3).21
TABLE 3
Nantes Criteria for pudendal neuralgia by pudendal nerve entrapment
| SOURCE: Labat et al.21 Reproduced with permission from Neurology and Urodynamics. |
Essential criteria
|
Complementary diagnostic criteria
|
Exclusion criteria
|
Associated signs not excluding the diagnosis
|
Initial treatments for pudendal neuralgia should be conservative. Treatments consist of lifestyle changes to prevent flare of disease. Physical therapy, medical management, nerve blocks, and alternative treatments may be beneficial.
Pudendal nerve entrapment is often exacerbated by sitting (not on a toilet seat, however) and is reduced in a standing position. It tends to increase in intensity throughout the day.22 The final treatment for pudendal nerve entrapment is surgery if the nerve is compressed. By this time, the generalist is not generally the provider who performs the surgery.
Dr. Gunter: I believe pudendal neuralgia is sometimes overdiagnosed. EMG studies of the pudendal nerve, often touted as a diagnostic tool, are unreliable (they can be abnormal after vaginal delivery or vaginal hysterectomy, for example). In my experience, bilateral pain is less likely to be pudendal neuralgia; spontaneous bilateral compression neuropathy at exactly the same level is not a common phenomenon in chronic pain.
I reserve the diagnosis of pudendal neuralgia for women who have allodynia in the distribution of the pudendal nerve with severe pain on sitting, and who have exquisite tenderness when pressure is applied over the pudendal nerve (at the level of the ischial spine on vaginal examination). Typically, the vaginal sidewall on the affected side is very sensitive to light touch. I do see pudendal nerve pain after vaginal surgery when there has been some compromise of the pudendal nerve or the sacral plexus. This is typically unilateral pain.
Dr. Lonky: Thank you all. We’ll continue our discussion, with a focus on treatment.
|
MORE TO COME
|
References
1. Thomas TG. Practical Treatise on the Diseases of Women. Philadelphia Pa: Henry C. Lea; 1874.
2. Harlow BL, Stewart EG. A population-based assessment of chronic unexplained vulvar pain: have we underestimated the prevalence of vulvodynia? J Am Med Womens Assoc. 2003;58(2):82–88.
3. Lavy RJ, Hynan LS, Haley RW. Prevalence of vulvar pain in an urban minority population. J Reprod Med. 2007;52(1):59–62.
4. Nyirjesy P, Peyton C, Weitz MV, Mathew L, Culhane JF. Causes of chronic vaginitis: analysis of a prospective database of affected women. Obstet Gynecol. 2006;108(5):1185–1191.
5. Moyal-Barracco M, Lynch PJ. 2003 ISSVD terminology and classification of vulvodynia: a historical perspective. J Reprod Med. 2004;49(10):772–777.
6. Yunas MB. Fibromyalgia and overlapping disorders: the unifying concept of central sensitivity syndromes. Semin Arthritis Rheum. 2007;36(6):339–356.
7. Kahn BS, Tatro C, Parsons CL, Willems JJ. Prevalence of interstitial cystitis in vulvodynia patients detected by bladder potassium sensitivity. J Sex Med. 2010;7(2 Pt 2):996–1002.
8. Arnold JD, Bachman GS, Rosen R, Kelly S, Rhoads GG. Vulvodynia: characteristics and associations with comorbidities and quality of life. Obstet Gynecol. 2006;107(3):617–624.
9. Parsons CL, Dell J, Stanford EJ, et al. The prevalence of interstitial cystitis in gynecologic patients with pelvic pain, as detected by intravesical potassium sensitivity. Am J Obstet Gynecol. 2002;187(5):1395–1400.
10. Clemens JQ, Meenan RT, O’Keefe Rosetti MC, et al. Prevalence of interstitial cystitis symptoms in a managed care population. J Urol. 2005;174(2):576–580.
11. Engman M, Lindehammar H, Wijma B. Surface electromyography diagnostics in women with partial vaginismus with or without vulvar vestibulitis and in asymptomatic women. J Psychosom Obstet Gynecol. 2004;25(3-4):281–294.
12. Gunter J. Vulvodynia: new thoughts on a devastating condition. Obstet Gynecol Surv. 2007;62(12):812–819.
13. Gordon AS, Panahlan-Jand M, McComb F, Melegari C, Sharp S. Characteristics of women with vulvar pain disorders: a Web-based survey. J Sex Marital Ther. 2003;29(suppl 1):45.
14. Whitten CE, Cristobal K. Chronic pain is a chronic condition not just a symptom. Permanente J. 2005;9(3):43.
15. Manchikanti L, Fellows B, Pampati V, et al. Comparison of psychological status of chronic pain patients and the general population. Pain Physician. 2002;5(1):40–48.
16. Banks SM, Kerns RD. Explaining the high rates of depression in chronic pain: a diathesis-stress framework. Psychological Bulletin. 1996;119(1):95–110.
17. Sadownik LA. Clinical correlates of vulvodynia patients. A prospective study of 300 patients. J Reprod Med. 2000;5:40–48. Editor found in PubMed: Sadownik LA. Clinical profile of vulvodynia patients. A prospective study of 300 patients. J Reprod Med. 2000;45(8):679–684. Could not find the citation listed. Please confirm.
18. Reed BD, Haefner HK, Punch MR, Roth RS, Gorenflo DW, Gillespie BW. Psychosocial and sexual functioning in women with vulvodynia and chronic pelvic pain. A comparative evaluation. J Reprod Med. 2000;45(8):624–632.
19. Landry T, Bergeron S. Biopsychosocial factors associated with dyspareunia in a community sample of adolescent girls. Arch Sex Behav. 2011; June 22.
20. Goldstein A, Pukall C, Goldstein I. When Sex Hurts: A Woman’s Guide to Banishing Sexual Pain. Cambridge Mass: Da Capo Lifelong Books; 2011;117–126.
21. Labat JJ, Riant T, Robert R, Amarenco G, Lefaucheur JP, Rigaud J. Diagnostic criteria for pudendal neuralgia by pudendal nerve entrapment (Nantes criteria). Neurol Urodyn. 2008;27(4):306–310.
22. Popeney C, Answell V, Renney K. Pudendal entrapment as an etiology of chronic perineal pain: Diagnosis and treatment. Neurol Urodyn. 2007;26(6):820–827.
Hypnosis Chills Out Severe Postmenopausal Hot Flashes
NEW ORLEANS – A five-session hypnosis program reduced the frequency and severity of postmenopausal hot flashes by 80%, according to the results of a randomized controlled trial presented at the annual meeting of the Society of Behavioral Medicine.
"It appears that hypnosis, when properly applied, can be a safe and effective treatment for hot flashes. And side benefits appear likely. We had a lot of women comment that they were generally feeling better; improvement in sleep was a big deal," Gary Elkins, Ph.D., said in presenting the results at the meeting. This trial was honored by the society as the outstanding study in the field of complementary and alternative medicine during the past year.
Dr. Elkins and his colleagues randomized 184 postmenopausal women with moderate to severe hot flashes to either five weekly hypnosis sessions or a structured attention control condition of equal duration.
Hot flash frequency and severity scores as recorded in patients’ daily hot flash diaries fell by about 70% at 5 weeks and even further to 80% at 12 weeks of follow-up, 7 weeks after the intervention ended, reported Dr. Elkins, professor of psychology and neuroscience at Baylor University in Waco, Tex.
Another key study end point was change in physiologically measured hot flashes obtained via a 24-hour skin conductance monitor sensitive to sweating; this tool was particularly helpful in getting objective data on nighttime hot flashes. Hot flashes as documented by the monitor, the Biologic HF Recorder with computer linkage, declined by about 50% at 5 weeks and 60% at 12 weeks. In contrast, the control group showed a 10% decrease in hot flashes at 5 weeks and a 15% reduction at 12 weeks.
Secondary end points assessing sleep, depression, and hot flash–related interference with daily life also showed marked improvement in the hypnosis group.
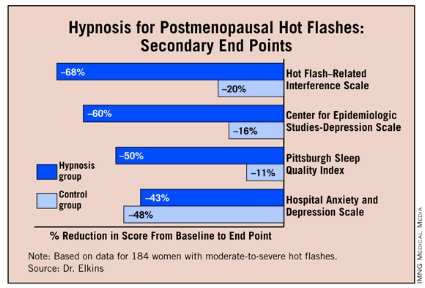
The intervention entailed hypnotic induction with relaxation and direct and indirect suggestions, dissociation, and mental imagery evoking coolness, such as walking down a mountain path on a cool day. The imagery was individualized to incorporate places a patient had been and things she’d experienced. The emphasis was on teaching patients self-hypnosis with the goal of patient empowerment, the psychologist explained.
Results with the hypnosis intervention compare favorably with studies of other proposed treatments for hot flashes. For instance, the nonpharmacologic therapies black cohosh, soy, and vitamin E have been shown "virtually indistinguishable" from placebo, according to Dr. Elkins.
Venlafaxine and SSRIs have achieved roughly a 50% reduction in hot flashes in clinical trials. While that’s a clinically meaningful improvement, it’s a weaker effect than seen in the hypnosis trial. Moreover, Dr. Elkins noted, some women don’t want to take drugs or they experience limiting side effects. Hormone replacement therapy, formerly the standard treatment for hot flashes, has fallen into disfavor since the 16,000-subject Women’s Health Initiative was halted early due to a 26% increase in breast cancer, a 29% increase in coronary heart disease, and a 41% greater risk of stroke than in the placebo arm (JAMA 2004; 29:1701-12).
The critical next step in this hypnosis research project is to disseminate the required therapeutic skills as widely as possible. After all, it’s estimated that more than 25 million American women experience hot flashes, and 4 million of them are severely affected.
"I think we’ve shown this is a very effective therapy, but we need to find a way to make it widely available," the researcher observed.

He and his coinvestigators are pursuing a twofold dissemination strategy. They are developing a treatment manual for interested health care professionals, although "that’s still not going to create an army of practitioners," Dr. Elkins noted. So in addition, the investigators plan to put a guided hypnotic intervention on a CD for self-treatment.
"That could be very widely distributed. Even if it’s not quite as effective, I think that’s going to be the long-term way to go," according to the psychologist.
In an earlier, smaller randomized trial, Dr. Elkins showed that hypnosis also was highly effective in reducing hot flashes in breast cancer survivors on hormone-suppressing therapy (J. Clin. Oncol. 2008;26:5022-6). Unlike the new study in women with postmenopausal hot flashes, however, the study in breast cancer patients relied solely on patient self-reported symptoms without physiologic monitoring.
The trial was funded by the National Institutes of Health’s National Center for Complementary and Alternative Medicine. Dr. Elkins and his colleagues reported having no financial conflict.
Venlafaxine, SSRIs,
NEW ORLEANS – A five-session hypnosis program reduced the frequency and severity of postmenopausal hot flashes by 80%, according to the results of a randomized controlled trial presented at the annual meeting of the Society of Behavioral Medicine.
"It appears that hypnosis, when properly applied, can be a safe and effective treatment for hot flashes. And side benefits appear likely. We had a lot of women comment that they were generally feeling better; improvement in sleep was a big deal," Gary Elkins, Ph.D., said in presenting the results at the meeting. This trial was honored by the society as the outstanding study in the field of complementary and alternative medicine during the past year.
Dr. Elkins and his colleagues randomized 184 postmenopausal women with moderate to severe hot flashes to either five weekly hypnosis sessions or a structured attention control condition of equal duration.
Hot flash frequency and severity scores as recorded in patients’ daily hot flash diaries fell by about 70% at 5 weeks and even further to 80% at 12 weeks of follow-up, 7 weeks after the intervention ended, reported Dr. Elkins, professor of psychology and neuroscience at Baylor University in Waco, Tex.
Another key study end point was change in physiologically measured hot flashes obtained via a 24-hour skin conductance monitor sensitive to sweating; this tool was particularly helpful in getting objective data on nighttime hot flashes. Hot flashes as documented by the monitor, the Biologic HF Recorder with computer linkage, declined by about 50% at 5 weeks and 60% at 12 weeks. In contrast, the control group showed a 10% decrease in hot flashes at 5 weeks and a 15% reduction at 12 weeks.
Secondary end points assessing sleep, depression, and hot flash–related interference with daily life also showed marked improvement in the hypnosis group.
The intervention entailed hypnotic induction with relaxation and direct and indirect suggestions, dissociation, and mental imagery evoking coolness, such as walking down a mountain path on a cool day. The imagery was individualized to incorporate places a patient had been and things she’d experienced. The emphasis was on teaching patients self-hypnosis with the goal of patient empowerment, the psychologist explained.
Results with the hypnosis intervention compare favorably with studies of other proposed treatments for hot flashes. For instance, the nonpharmacologic therapies black cohosh, soy, and vitamin E have been shown "virtually indistinguishable" from placebo, according to Dr. Elkins.
Venlafaxine and SSRIs have achieved roughly a 50% reduction in hot flashes in clinical trials. While that’s a clinically meaningful improvement, it’s a weaker effect than seen in the hypnosis trial. Moreover, Dr. Elkins noted, some women don’t want to take drugs or they experience limiting side effects. Hormone replacement therapy, formerly the standard treatment for hot flashes, has fallen into disfavor since the 16,000-subject Women’s Health Initiative was halted early due to a 26% increase in breast cancer, a 29% increase in coronary heart disease, and a 41% greater risk of stroke than in the placebo arm (JAMA 2004; 29:1701-12).
The critical next step in this hypnosis research project is to disseminate the required therapeutic skills as widely as possible. After all, it’s estimated that more than 25 million American women experience hot flashes, and 4 million of them are severely affected.
"I think we’ve shown this is a very effective therapy, but we need to find a way to make it widely available," the researcher observed.
He and his coinvestigators are pursuing a twofold dissemination strategy. They are developing a treatment manual for interested health care professionals, although "that’s still not going to create an army of practitioners," Dr. Elkins noted. So in addition, the investigators plan to put a guided hypnotic intervention on a CD for self-treatment.
"That could be very widely distributed. Even if it’s not quite as effective, I think that’s going to be the long-term way to go," according to the psychologist.
In an earlier, smaller randomized trial, Dr. Elkins showed that hypnosis also was highly effective in reducing hot flashes in breast cancer survivors on hormone-suppressing therapy (J. Clin. Oncol. 2008;26:5022-6). Unlike the new study in women with postmenopausal hot flashes, however, the study in breast cancer patients relied solely on patient self-reported symptoms without physiologic monitoring.
The trial was funded by the National Institutes of Health’s National Center for Complementary and Alternative Medicine. Dr. Elkins and his colleagues reported having no financial conflict.
NEW ORLEANS – A five-session hypnosis program reduced the frequency and severity of postmenopausal hot flashes by 80%, according to the results of a randomized controlled trial presented at the annual meeting of the Society of Behavioral Medicine.
"It appears that hypnosis, when properly applied, can be a safe and effective treatment for hot flashes. And side benefits appear likely. We had a lot of women comment that they were generally feeling better; improvement in sleep was a big deal," Gary Elkins, Ph.D., said in presenting the results at the meeting. This trial was honored by the society as the outstanding study in the field of complementary and alternative medicine during the past year.
Dr. Elkins and his colleagues randomized 184 postmenopausal women with moderate to severe hot flashes to either five weekly hypnosis sessions or a structured attention control condition of equal duration.
Hot flash frequency and severity scores as recorded in patients’ daily hot flash diaries fell by about 70% at 5 weeks and even further to 80% at 12 weeks of follow-up, 7 weeks after the intervention ended, reported Dr. Elkins, professor of psychology and neuroscience at Baylor University in Waco, Tex.
Another key study end point was change in physiologically measured hot flashes obtained via a 24-hour skin conductance monitor sensitive to sweating; this tool was particularly helpful in getting objective data on nighttime hot flashes. Hot flashes as documented by the monitor, the Biologic HF Recorder with computer linkage, declined by about 50% at 5 weeks and 60% at 12 weeks. In contrast, the control group showed a 10% decrease in hot flashes at 5 weeks and a 15% reduction at 12 weeks.
Secondary end points assessing sleep, depression, and hot flash–related interference with daily life also showed marked improvement in the hypnosis group.
The intervention entailed hypnotic induction with relaxation and direct and indirect suggestions, dissociation, and mental imagery evoking coolness, such as walking down a mountain path on a cool day. The imagery was individualized to incorporate places a patient had been and things she’d experienced. The emphasis was on teaching patients self-hypnosis with the goal of patient empowerment, the psychologist explained.
Results with the hypnosis intervention compare favorably with studies of other proposed treatments for hot flashes. For instance, the nonpharmacologic therapies black cohosh, soy, and vitamin E have been shown "virtually indistinguishable" from placebo, according to Dr. Elkins.
Venlafaxine and SSRIs have achieved roughly a 50% reduction in hot flashes in clinical trials. While that’s a clinically meaningful improvement, it’s a weaker effect than seen in the hypnosis trial. Moreover, Dr. Elkins noted, some women don’t want to take drugs or they experience limiting side effects. Hormone replacement therapy, formerly the standard treatment for hot flashes, has fallen into disfavor since the 16,000-subject Women’s Health Initiative was halted early due to a 26% increase in breast cancer, a 29% increase in coronary heart disease, and a 41% greater risk of stroke than in the placebo arm (JAMA 2004; 29:1701-12).
The critical next step in this hypnosis research project is to disseminate the required therapeutic skills as widely as possible. After all, it’s estimated that more than 25 million American women experience hot flashes, and 4 million of them are severely affected.
"I think we’ve shown this is a very effective therapy, but we need to find a way to make it widely available," the researcher observed.
He and his coinvestigators are pursuing a twofold dissemination strategy. They are developing a treatment manual for interested health care professionals, although "that’s still not going to create an army of practitioners," Dr. Elkins noted. So in addition, the investigators plan to put a guided hypnotic intervention on a CD for self-treatment.
"That could be very widely distributed. Even if it’s not quite as effective, I think that’s going to be the long-term way to go," according to the psychologist.
In an earlier, smaller randomized trial, Dr. Elkins showed that hypnosis also was highly effective in reducing hot flashes in breast cancer survivors on hormone-suppressing therapy (J. Clin. Oncol. 2008;26:5022-6). Unlike the new study in women with postmenopausal hot flashes, however, the study in breast cancer patients relied solely on patient self-reported symptoms without physiologic monitoring.
The trial was funded by the National Institutes of Health’s National Center for Complementary and Alternative Medicine. Dr. Elkins and his colleagues reported having no financial conflict.
Venlafaxine, SSRIs,
Venlafaxine, SSRIs,
FROM THE ANNUAL MEETING OF THE SOCIETY OF BEHAVIORAL MEDICINE
Estrogen-Only HT Also Increases Breast Cancer Risk
CHICAGO – Long-term use of estrogen-only therapy increases the risk of postmenopausal women developing breast cancer, according to new data from the Nurses’ Health Study.
The finding, reported April 1 by Dr. Wendy Chen at the annual meeting of the American Association for Cancer Research, suggests that opting for progesterone-free hormone therapy for the treatment of menopause symptoms should not be considered the risk-free alternative to combination progesterone plus estrogen formulations.
Still, the absolute risks were small. During the study’s 1.57 million person-years of follow-up from 1980 through 2008, 5,631 incident invasive breast cancers were diagnosed and 884 of the women died of breast cancer.
To evaluate the breast cancer risk associated with long-term use of both combined and estrogen-only hormone therapy, Dr. Chen of Brigham and Women’s Hospital in Boston and her colleagues evaluated data collected over 28 years through the Nurses’ Health Study. Of the 121,700 study participants who were aged 30-55 years in 1976, women who used estrogen-only therapy for 10.0-14.9 years and for 15.0-19.9 years had, respectively, a 22% and 43% increased risk of developing breast cancer relative to those women not on hormone therapy (HT).
"Our data also confirmed the previously reported increased risk associated with combined hormone therapy," Dr. Chen stated, noting that women in the study who used progesterone plus estrogen for 10-14.9 years had an 88% increased risk of developing breast cancer relative to those not on HT and the risk increased to more than twofold in women using it for up to 20 years. Further, the risk of developing breast cancer does not appear to plateau over time, but rather continues to increase. "The longer women use [HT]. The higher their risk," she said.
In a separate analysis, the investigators restricted the study population to healthy, active postmenopausal women 50-79 years with an intact uterus – the same population observed in the Women’s Health Initiative. "What we saw was a decline in breast cancer risk among women using estrogen-only therapy for less than 10 years, but an increased risk among those women using estrogen for 15-20 years," Dr. Chen said.
Importantly, although breast cancer incidence was increased in the HT groups, "there was no increase in the risk of fatal breast cancer, either with combined or estrogen-only therapy," Dr. Chen stressed. "This is something we are continuing to investigate."
The findings have the potential to increase the confusion regarding HT and to perhaps reignite the hormone therapy debate, Dr. Chen acknowledged in an interview. However, they should be considered in their proper context. "While the relative risk of developing breast cancer in increased, the absolute risk associated with [HT] are low," she said.
The observed effects associated with HT were stronger for estrogen receptor–positive tumors and among thinner women, Dr. Chen noted, adding that the results were similar when limited to women who underwent regular breast cancer screening.
The study was funded by the National Cancer Institute. Dr. Chen disclosed no financial conflicts of interest.
CHICAGO – Long-term use of estrogen-only therapy increases the risk of postmenopausal women developing breast cancer, according to new data from the Nurses’ Health Study.
The finding, reported April 1 by Dr. Wendy Chen at the annual meeting of the American Association for Cancer Research, suggests that opting for progesterone-free hormone therapy for the treatment of menopause symptoms should not be considered the risk-free alternative to combination progesterone plus estrogen formulations.
Still, the absolute risks were small. During the study’s 1.57 million person-years of follow-up from 1980 through 2008, 5,631 incident invasive breast cancers were diagnosed and 884 of the women died of breast cancer.
To evaluate the breast cancer risk associated with long-term use of both combined and estrogen-only hormone therapy, Dr. Chen of Brigham and Women’s Hospital in Boston and her colleagues evaluated data collected over 28 years through the Nurses’ Health Study. Of the 121,700 study participants who were aged 30-55 years in 1976, women who used estrogen-only therapy for 10.0-14.9 years and for 15.0-19.9 years had, respectively, a 22% and 43% increased risk of developing breast cancer relative to those women not on hormone therapy (HT).
"Our data also confirmed the previously reported increased risk associated with combined hormone therapy," Dr. Chen stated, noting that women in the study who used progesterone plus estrogen for 10-14.9 years had an 88% increased risk of developing breast cancer relative to those not on HT and the risk increased to more than twofold in women using it for up to 20 years. Further, the risk of developing breast cancer does not appear to plateau over time, but rather continues to increase. "The longer women use [HT]. The higher their risk," she said.
In a separate analysis, the investigators restricted the study population to healthy, active postmenopausal women 50-79 years with an intact uterus – the same population observed in the Women’s Health Initiative. "What we saw was a decline in breast cancer risk among women using estrogen-only therapy for less than 10 years, but an increased risk among those women using estrogen for 15-20 years," Dr. Chen said.
Importantly, although breast cancer incidence was increased in the HT groups, "there was no increase in the risk of fatal breast cancer, either with combined or estrogen-only therapy," Dr. Chen stressed. "This is something we are continuing to investigate."
The findings have the potential to increase the confusion regarding HT and to perhaps reignite the hormone therapy debate, Dr. Chen acknowledged in an interview. However, they should be considered in their proper context. "While the relative risk of developing breast cancer in increased, the absolute risk associated with [HT] are low," she said.
The observed effects associated with HT were stronger for estrogen receptor–positive tumors and among thinner women, Dr. Chen noted, adding that the results were similar when limited to women who underwent regular breast cancer screening.
The study was funded by the National Cancer Institute. Dr. Chen disclosed no financial conflicts of interest.
CHICAGO – Long-term use of estrogen-only therapy increases the risk of postmenopausal women developing breast cancer, according to new data from the Nurses’ Health Study.
The finding, reported April 1 by Dr. Wendy Chen at the annual meeting of the American Association for Cancer Research, suggests that opting for progesterone-free hormone therapy for the treatment of menopause symptoms should not be considered the risk-free alternative to combination progesterone plus estrogen formulations.
Still, the absolute risks were small. During the study’s 1.57 million person-years of follow-up from 1980 through 2008, 5,631 incident invasive breast cancers were diagnosed and 884 of the women died of breast cancer.
To evaluate the breast cancer risk associated with long-term use of both combined and estrogen-only hormone therapy, Dr. Chen of Brigham and Women’s Hospital in Boston and her colleagues evaluated data collected over 28 years through the Nurses’ Health Study. Of the 121,700 study participants who were aged 30-55 years in 1976, women who used estrogen-only therapy for 10.0-14.9 years and for 15.0-19.9 years had, respectively, a 22% and 43% increased risk of developing breast cancer relative to those women not on hormone therapy (HT).
"Our data also confirmed the previously reported increased risk associated with combined hormone therapy," Dr. Chen stated, noting that women in the study who used progesterone plus estrogen for 10-14.9 years had an 88% increased risk of developing breast cancer relative to those not on HT and the risk increased to more than twofold in women using it for up to 20 years. Further, the risk of developing breast cancer does not appear to plateau over time, but rather continues to increase. "The longer women use [HT]. The higher their risk," she said.
In a separate analysis, the investigators restricted the study population to healthy, active postmenopausal women 50-79 years with an intact uterus – the same population observed in the Women’s Health Initiative. "What we saw was a decline in breast cancer risk among women using estrogen-only therapy for less than 10 years, but an increased risk among those women using estrogen for 15-20 years," Dr. Chen said.
Importantly, although breast cancer incidence was increased in the HT groups, "there was no increase in the risk of fatal breast cancer, either with combined or estrogen-only therapy," Dr. Chen stressed. "This is something we are continuing to investigate."
The findings have the potential to increase the confusion regarding HT and to perhaps reignite the hormone therapy debate, Dr. Chen acknowledged in an interview. However, they should be considered in their proper context. "While the relative risk of developing breast cancer in increased, the absolute risk associated with [HT] are low," she said.
The observed effects associated with HT were stronger for estrogen receptor–positive tumors and among thinner women, Dr. Chen noted, adding that the results were similar when limited to women who underwent regular breast cancer screening.
The study was funded by the National Cancer Institute. Dr. Chen disclosed no financial conflicts of interest.
FROM THE ANNUAL MEETING OF THE AMERICAN ASSOCIATION OF CANCER RESEARCH
Major Finding: Of the 121,700 study participants in the Nurses’ Health Study who were aged 30-55 years in 1976, women who used estrogen-only therapy for 10.0-14.9 years and for 15.0-19.9 years had, respectively, a 22% and 43% increased risk of developing breast cancer relative to those not on hormone therapy.
Data Source: The Nurses’ Health Study of data collected during 1980-2008 from 121,700 postmenopausal women aged 30-55 years in 1976.
Disclosures: Dr. Chen disclosed no financial conflicts of interest.
Estrogen Protects Against Breast Cancer Long After Treatment
In a study of postmenopausal women who had undergone hysterectomy, the use of unopposed estrogen significantly reduced the incidence of invasive breast cancer for up to 5 years after they stopped taking the hormone, according to a report published online March 7 in the Lancet Oncology.
For study subjects who did develop breast cancer, estrogen use reduced breast-cancer mortality and all-cause mortality, Garnet L. Anderson, Ph.D., and her associates reported in an extended follow-up study of 7,645 participants in the Women’s Health Initiative (WHI).
"Our findings ... provide reassurance about breast cancer safety for postmenopausal women with [a] previous hysterectomy who receive unopposed estrogen to reduce climacteric symptoms," they noted.
The WHI, a multicenter, randomized clinical trial involving more than 10,000 women, compared outcomes between those who took conjugated equine estrogen and those who took a matching placebo.
The intervention phase of the WHI was terminated early in February 2004, after a mean follow-up of 7 years. Approximately 78% of the study subjects – 3,778 who had been randomly assigned to receive estrogen and 3,867 to receive placebo – agreed to extended follow-up until August 2009, for a total median follow-up of 11.8 years.
At this final assessment, women who had taken estrogen for a median of 6 years during the intervention phase had an overall incidence of invasive breast cancer of 0.27% per year (151 cases), which was significantly lower than the 0.35% per year rate (199 cases) among women who had taken placebo, said Dr. Anderson of the Fred Hutchinson Cancer Research Center, Seattle, and her colleagues.
"The continued, postintervention effect of estrogen on breast cancer incidence is akin to that reported for other hormone-targeted drugs shown to reduce breast cancer incidence," the investigators said (Lancet Oncol. 2012 March 7 [doi:10.1016/S1470-2045(12)70075-x]).
Estrogen was associated with a reduced risk of developing infiltrating ductal carcinoma but not infiltrating lobular cancers. It also decreased the risk of human epidermal growth factor receptor 2 (HER-2)–negative tumors but not HER-2–positive tumors, and appeared to reduce the risk of small and node-negative cancers but not large (2 cm or larger) or node-positive cancers. However, these differences among tumor subtypes did not reach statistical significance.
Among the study subjects who did develop breast cancer, those in the estrogen group were significantly less likely to die of any cause (30 deaths, for a mortality of 0.046% per year) than were those in the placebo group (50 deaths, for a mortality of 0.076% per year).
Breast-cancer-specific mortality also was significantly lower in the estrogen recipients (6 deaths, for a mortality of 0.009% per year) than in the placebo recipients (16 deaths, for a mortality of 0.024% per year).
However, the number of deaths was small, limiting the strength of these associations, Dr. Anderson and her associates noted.
These protective effects appeared to be restricted to women who had a lower risk for breast cancer. They did not apply to women with a history of benign breast disease or those with a first-degree family history of breast cancer.
In subgroup analyses, estrogen’s protective effects showed no interactions with patient age, body mass index, oophorectomy status, years since the onset of menopause, previous estrogen use, or the presence of vasomotor symptoms.
The WHI was limited in that it assessed "only one dose and schedule of oral conjugated equine estrogens; whether these findings apply to lower doses, other estrogen preparations, or longer durations of use is not known," the researchers noted.
They reported no relevant financial disclosures. The WHI was supported by the National Heart, Lung, and Blood Institute; the National Institutes of Health; the Department of Health and Human Services; and Wyeth. One of Dr. Anderson’s associates reported ties to AstraZeneca, Novartis, Amgen, and Pfizer. Dr. Anderson and the other investigators said they had no relevant financial disclosures.
These WHI results are significant though "modest," said Dr. Anthony Howell and Dr. Jack Cuzick.
The findings should be viewed "in the context of the update of the study in 2011 reporting the effects of estrogen on overall health. No overall difference was noted in participants’ global index of health (including cardiovascular disease, thrombosis and embolism, breast and colorectal cancer, hip fracture, and death from all causes)," they noted.
However, "this null result masked an unexpected but significant interaction with age," in which younger women (aged 50-59 years) showed health improvements while older women showed health decrements, Dr. Howell and Dr. Cuzick said.
Dr. Howell is with the University Hospital of South Manchester (England). Dr. Cuzick is at the center for cancer prevention at Queen Mary University of London. They reported no relevant financial disclosures. These remarks were taken from their editorial comment accompanying Dr. Anderson’s report (Lancet Oncol. 2012 March 7 [doi:10.1016/S1470-2045(12)70110-9]).
These WHI results are significant though "modest," said Dr. Anthony Howell and Dr. Jack Cuzick.
The findings should be viewed "in the context of the update of the study in 2011 reporting the effects of estrogen on overall health. No overall difference was noted in participants’ global index of health (including cardiovascular disease, thrombosis and embolism, breast and colorectal cancer, hip fracture, and death from all causes)," they noted.
However, "this null result masked an unexpected but significant interaction with age," in which younger women (aged 50-59 years) showed health improvements while older women showed health decrements, Dr. Howell and Dr. Cuzick said.
Dr. Howell is with the University Hospital of South Manchester (England). Dr. Cuzick is at the center for cancer prevention at Queen Mary University of London. They reported no relevant financial disclosures. These remarks were taken from their editorial comment accompanying Dr. Anderson’s report (Lancet Oncol. 2012 March 7 [doi:10.1016/S1470-2045(12)70110-9]).
These WHI results are significant though "modest," said Dr. Anthony Howell and Dr. Jack Cuzick.
The findings should be viewed "in the context of the update of the study in 2011 reporting the effects of estrogen on overall health. No overall difference was noted in participants’ global index of health (including cardiovascular disease, thrombosis and embolism, breast and colorectal cancer, hip fracture, and death from all causes)," they noted.
However, "this null result masked an unexpected but significant interaction with age," in which younger women (aged 50-59 years) showed health improvements while older women showed health decrements, Dr. Howell and Dr. Cuzick said.
Dr. Howell is with the University Hospital of South Manchester (England). Dr. Cuzick is at the center for cancer prevention at Queen Mary University of London. They reported no relevant financial disclosures. These remarks were taken from their editorial comment accompanying Dr. Anderson’s report (Lancet Oncol. 2012 March 7 [doi:10.1016/S1470-2045(12)70110-9]).
In a study of postmenopausal women who had undergone hysterectomy, the use of unopposed estrogen significantly reduced the incidence of invasive breast cancer for up to 5 years after they stopped taking the hormone, according to a report published online March 7 in the Lancet Oncology.
For study subjects who did develop breast cancer, estrogen use reduced breast-cancer mortality and all-cause mortality, Garnet L. Anderson, Ph.D., and her associates reported in an extended follow-up study of 7,645 participants in the Women’s Health Initiative (WHI).
"Our findings ... provide reassurance about breast cancer safety for postmenopausal women with [a] previous hysterectomy who receive unopposed estrogen to reduce climacteric symptoms," they noted.
The WHI, a multicenter, randomized clinical trial involving more than 10,000 women, compared outcomes between those who took conjugated equine estrogen and those who took a matching placebo.
The intervention phase of the WHI was terminated early in February 2004, after a mean follow-up of 7 years. Approximately 78% of the study subjects – 3,778 who had been randomly assigned to receive estrogen and 3,867 to receive placebo – agreed to extended follow-up until August 2009, for a total median follow-up of 11.8 years.
At this final assessment, women who had taken estrogen for a median of 6 years during the intervention phase had an overall incidence of invasive breast cancer of 0.27% per year (151 cases), which was significantly lower than the 0.35% per year rate (199 cases) among women who had taken placebo, said Dr. Anderson of the Fred Hutchinson Cancer Research Center, Seattle, and her colleagues.
"The continued, postintervention effect of estrogen on breast cancer incidence is akin to that reported for other hormone-targeted drugs shown to reduce breast cancer incidence," the investigators said (Lancet Oncol. 2012 March 7 [doi:10.1016/S1470-2045(12)70075-x]).
Estrogen was associated with a reduced risk of developing infiltrating ductal carcinoma but not infiltrating lobular cancers. It also decreased the risk of human epidermal growth factor receptor 2 (HER-2)–negative tumors but not HER-2–positive tumors, and appeared to reduce the risk of small and node-negative cancers but not large (2 cm or larger) or node-positive cancers. However, these differences among tumor subtypes did not reach statistical significance.
Among the study subjects who did develop breast cancer, those in the estrogen group were significantly less likely to die of any cause (30 deaths, for a mortality of 0.046% per year) than were those in the placebo group (50 deaths, for a mortality of 0.076% per year).
Breast-cancer-specific mortality also was significantly lower in the estrogen recipients (6 deaths, for a mortality of 0.009% per year) than in the placebo recipients (16 deaths, for a mortality of 0.024% per year).
However, the number of deaths was small, limiting the strength of these associations, Dr. Anderson and her associates noted.
These protective effects appeared to be restricted to women who had a lower risk for breast cancer. They did not apply to women with a history of benign breast disease or those with a first-degree family history of breast cancer.
In subgroup analyses, estrogen’s protective effects showed no interactions with patient age, body mass index, oophorectomy status, years since the onset of menopause, previous estrogen use, or the presence of vasomotor symptoms.
The WHI was limited in that it assessed "only one dose and schedule of oral conjugated equine estrogens; whether these findings apply to lower doses, other estrogen preparations, or longer durations of use is not known," the researchers noted.
They reported no relevant financial disclosures. The WHI was supported by the National Heart, Lung, and Blood Institute; the National Institutes of Health; the Department of Health and Human Services; and Wyeth. One of Dr. Anderson’s associates reported ties to AstraZeneca, Novartis, Amgen, and Pfizer. Dr. Anderson and the other investigators said they had no relevant financial disclosures.
In a study of postmenopausal women who had undergone hysterectomy, the use of unopposed estrogen significantly reduced the incidence of invasive breast cancer for up to 5 years after they stopped taking the hormone, according to a report published online March 7 in the Lancet Oncology.
For study subjects who did develop breast cancer, estrogen use reduced breast-cancer mortality and all-cause mortality, Garnet L. Anderson, Ph.D., and her associates reported in an extended follow-up study of 7,645 participants in the Women’s Health Initiative (WHI).
"Our findings ... provide reassurance about breast cancer safety for postmenopausal women with [a] previous hysterectomy who receive unopposed estrogen to reduce climacteric symptoms," they noted.
The WHI, a multicenter, randomized clinical trial involving more than 10,000 women, compared outcomes between those who took conjugated equine estrogen and those who took a matching placebo.
The intervention phase of the WHI was terminated early in February 2004, after a mean follow-up of 7 years. Approximately 78% of the study subjects – 3,778 who had been randomly assigned to receive estrogen and 3,867 to receive placebo – agreed to extended follow-up until August 2009, for a total median follow-up of 11.8 years.
At this final assessment, women who had taken estrogen for a median of 6 years during the intervention phase had an overall incidence of invasive breast cancer of 0.27% per year (151 cases), which was significantly lower than the 0.35% per year rate (199 cases) among women who had taken placebo, said Dr. Anderson of the Fred Hutchinson Cancer Research Center, Seattle, and her colleagues.
"The continued, postintervention effect of estrogen on breast cancer incidence is akin to that reported for other hormone-targeted drugs shown to reduce breast cancer incidence," the investigators said (Lancet Oncol. 2012 March 7 [doi:10.1016/S1470-2045(12)70075-x]).
Estrogen was associated with a reduced risk of developing infiltrating ductal carcinoma but not infiltrating lobular cancers. It also decreased the risk of human epidermal growth factor receptor 2 (HER-2)–negative tumors but not HER-2–positive tumors, and appeared to reduce the risk of small and node-negative cancers but not large (2 cm or larger) or node-positive cancers. However, these differences among tumor subtypes did not reach statistical significance.
Among the study subjects who did develop breast cancer, those in the estrogen group were significantly less likely to die of any cause (30 deaths, for a mortality of 0.046% per year) than were those in the placebo group (50 deaths, for a mortality of 0.076% per year).
Breast-cancer-specific mortality also was significantly lower in the estrogen recipients (6 deaths, for a mortality of 0.009% per year) than in the placebo recipients (16 deaths, for a mortality of 0.024% per year).
However, the number of deaths was small, limiting the strength of these associations, Dr. Anderson and her associates noted.
These protective effects appeared to be restricted to women who had a lower risk for breast cancer. They did not apply to women with a history of benign breast disease or those with a first-degree family history of breast cancer.
In subgroup analyses, estrogen’s protective effects showed no interactions with patient age, body mass index, oophorectomy status, years since the onset of menopause, previous estrogen use, or the presence of vasomotor symptoms.
The WHI was limited in that it assessed "only one dose and schedule of oral conjugated equine estrogens; whether these findings apply to lower doses, other estrogen preparations, or longer durations of use is not known," the researchers noted.
They reported no relevant financial disclosures. The WHI was supported by the National Heart, Lung, and Blood Institute; the National Institutes of Health; the Department of Health and Human Services; and Wyeth. One of Dr. Anderson’s associates reported ties to AstraZeneca, Novartis, Amgen, and Pfizer. Dr. Anderson and the other investigators said they had no relevant financial disclosures.
FROM THE LANCET ONCOLOGY
Major Finding: After 12 years of follow-up, women in the WHI who had taken estrogen had a significantly lower rate of invasive breast cancer (0.27% per year) than did those who had taken placebo (0.35% per year).
Data Source: Extended follow-up of 7,645 women who had participated in the multicenter, randomized double-blind WHI, involving 3,778 who received estrogen and 3,867 who received placebo for a median of 6 years.
Disclosures: The WHI was supported by the National Heart, Lung, and Blood Institute; the National Institutes of Health; the Department of Health and Human Services; and Wyeth. One of Dr. Anderson’s associates reported ties to AstraZeneca, Novartis, Amgen, and Pfizer. Dr. Anderson and the other investigators said they had no relevant financial disclosures.