User login
ESC heart failure guideline to integrate bounty of new meds
Today there are so many evidence-based drug therapies for heart failure with reduced ejection fraction (HFrEF) that physicians treating HF patients almost don’t know what to do them.
It’s an exciting new age that way, but to many vexingly unclear how best to merge the shiny new options with mainstay regimens based on time-honored renin-angiotensin system (RAS) inhibitors and beta-blockers.
To impart some clarity, the authors of a new HF guideline document recently took center stage at the Heart Failure Association of the European Society of Cardiology (ESC-HFA) annual meeting to preview their updated recommendations, with novel twists based on recent major trials, for the new age of HF pharmacotherapeutics.
The guideline committee considered the evidence base that existed “up until the end of March of this year,” Theresa A. McDonagh, MD, King’s College London, said during the presentation. The document “is now finalized, it’s with the publishers, and it will be presented in full with simultaneous publication at the ESC meeting” that starts August 27.
It describes a game plan, already followed by some clinicians in practice without official guidance, for initiating drugs from each of four classes in virtually all patients with HFrEF.
New indicated drugs, new perspective for HFrEF
Three of the drug categories are old acquaintances. Among them are the RAS inhibitors, which include angiotensin-receptor/neprilysin inhibitors, beta-blockers, and the mineralocorticoid receptor antagonists. The latter drugs are gaining new respect after having been underplayed in HF prescribing despite longstanding evidence of efficacy.
Completing the quartet of first-line HFrEF drug classes is a recent arrival to the HF arena, the sodium-glucose cotransporter 2 inhibitors.

“We now have new data and a simplified treatment algorithm for heart failure with reduced ejection fraction based on the early administration of the four major classes of drugs,” said Marco Metra, MD, University of Brescia (Italy), previewing the medical-therapy portions of the new guideline at the ESC-HFA sessions, which launched virtually and live in Florence, Italy, on July 29.
The new game plan offers a simple answer to a once-common but complex question: How and in what order are the different drug classes initiated in patients with HFrEF? In the new document, the stated goal is to get them all on board expeditiously and safely, by any means possible.
The guideline writers did not specify a sequence, preferring to leave that decision to physicians, said Dr. Metra, who stated only two guiding principles. The first is to consider the patient’s unique circumstances. The order in which the drugs are introduced might vary, depending on, for example, whether the patient has low or high blood pressure or renal dysfunction.
Second, “it is very important that we try to give all four classes of drugs to the patient in the shortest time possible, because this saves lives,” he said.

That there is no recommendation on sequencing the drugs has led some to the wrong interpretation that all should be started at once, observed coauthor Javed Butler, MD, MPH, University of Mississippi, Jackson, as a panelist during the presentation. Far from it, he said. “The doctor with the patient in front of you can make the best decision. The idea here is to get all the therapies on as soon as possible, as safely as possible.”
“The order in which they are introduced is not really important,” agreed Vijay Chopra, MD, Max Super Specialty Hospital Saket, New Delhi, another coauthor on the panel. “The important thing is that at least some dose of all the four drugs needs to be introduced in the first 4-6 weeks, and then up-titrated.”
Other medical therapy can be more tailored, Dr. Metra noted, such as loop diuretics for patients with congestion, iron for those with iron deficiency, and other drugs depending on whether there is, for example, atrial fibrillation or coronary disease.
Adoption of emerging definitions
The document adopts the emerging characterization of HFrEF by a left ventricular ejection fraction (LVEF) up to 40%.
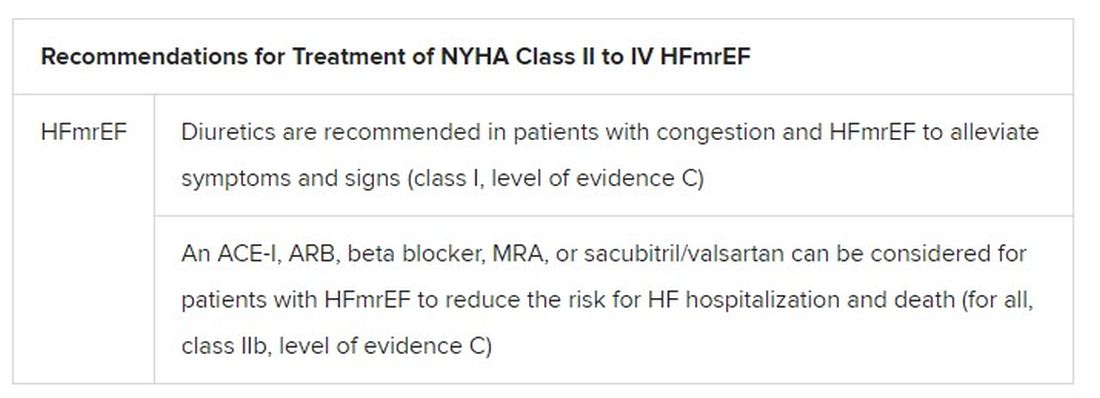
And it will leverage an expanding evidence base for medication in a segment of patients once said to have HF with preserved ejection fraction (HFpEF), who had therefore lacked specific, guideline-directed medical therapies. Now, patients with an LVEF of 41%-49% will be said to have HF with mildly reduced ejection fraction (HFmrEF), a tweak to the recently introduced HF with “mid-range” LVEF that is designed to assert its nature as something to treat. The new document’s HFmrEF recommendations come with various class and level-of-evidence ratings.
That leaves HFpEF to be characterized by an LVEF of 50% in combination with structural or functional abnormalities associated with LV diastolic dysfunction or raised LV filling pressures, including raised natriuretic peptide levels.
The definitions are consistent with those proposed internationally by the ESC-HFA, the Heart Failure Society of America, and other groups in a statement published in March.
Expanded HFrEF med landscape
Since the 2016 ESC guideline on HF therapy, Dr. McDonagh said, “there’s been no substantial change in the evidence for many of the classical drugs that we use in heart failure. However, we had a lot of new and exciting evidence to consider,” especially in support of the SGLT2 inhibitors as one of the core medications in HFrEF.
The new data came from two controlled trials in particular. In DAPA-HF, patients with HFrEF who were initially without diabetes and who went on dapagliflozin (Farxiga, AstraZeneca) showed a 27% drop in cardiovascular (CV) death or worsening-HF events over a median of 18 months.
“That was followed up with very concordant results with empagliflozin [Jardiance, Boehringer Ingelheim/Eli Lilly] in HFrEF in the EMPEROR-Reduced trial,” Dr. McDonagh said. In that trial, comparable patients who took empagliflozin showed a 25% drop in a primary endpoint similar to that in DAPA-HF over the median 16-month follow-up.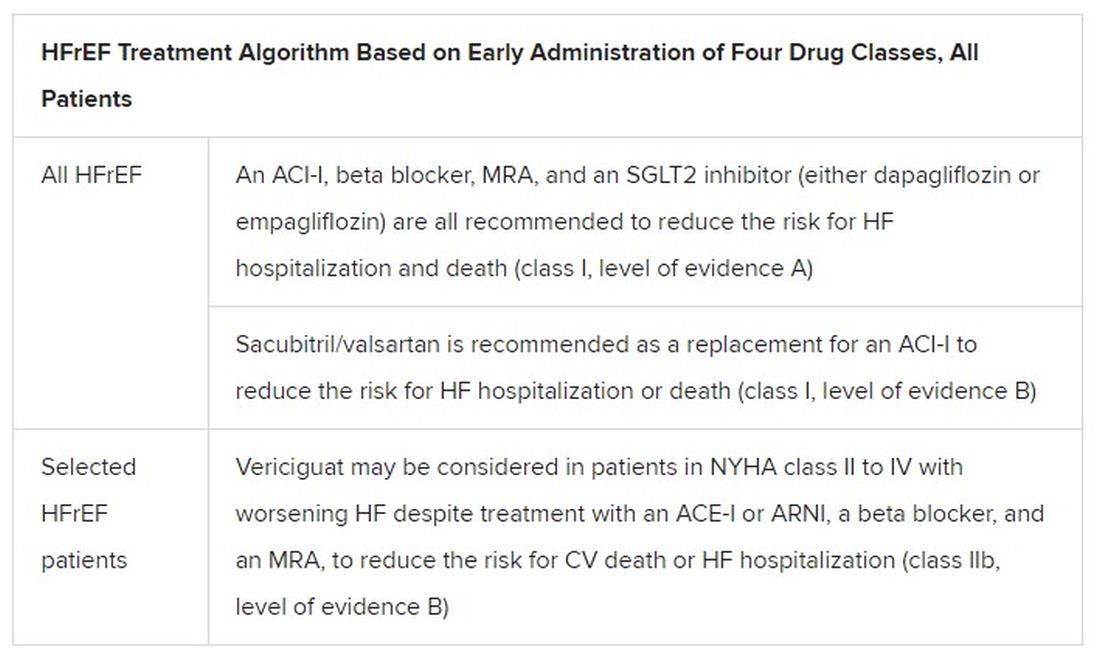
Other HFrEF recommendations are for selected patients. They include ivabradine, already in the guidelines, for patients in sinus rhythm with an elevated resting heart rate who can’t take beta-blockers for whatever reason. But, Dr. McDonagh noted, “we had some new classes of drugs to consider as well.”
In particular, the oral soluble guanylate-cyclase receptor stimulator vericiguat (Verquvo) emerged about a year ago from the VICTORIA trial as a modest success for patients with HFrEF and a previous HF hospitalization. In the trial with more than 5,000 patients, treatment with vericiguat atop standard drug and device therapy was followed by a significant 10% drop in risk for CV death or HF hospitalization.
Available now or likely to be available in the United States, the European Union, Japan, and other countries, vericiguat is recommended in the new guideline for VICTORIA-like patients who don’t adequately respond to other indicated medications.
Little for HFpEF as newly defined
“Almost nothing is new” in the guidelines for HFpEF, Dr. Metra said. The document recommends screening for and treatment of any underlying disorder and comorbidities, plus diuretics for any congestion. “That’s what we have to date.”
But that evidence base might soon change. The new HFpEF recommendations could possibly be up-staged at the ESC sessions by the August 27 scheduled presentation of EMPEROR-Preserved, a randomized test of empagliflozin in HFpEF and – it could be said – HFmrEF. The trial entered patients with chronic HF and an LVEF greater than 40%.
Eli Lilly and Boehringer Ingelheim offered the world a peek at the results, which suggest the SGLT2 inhibitor had a positive impact on the primary endpoint of CV death or HF hospitalization. They announced the cursory top-line outcomes in early July as part of its regulatory obligations, noting that the trial had “met” its primary endpoint.
But many unknowns remain, including the degree of benefit and whether it varied among subgroups, and especially whether outcomes were different for HFmrEF than for HFpEF.
Upgrades for familiar agents
Still, HFmrEF gets noteworthy attention in the document. “For the first time, we have recommendations for these patients,” Dr. Metra said. “We already knew that diuretics are indicated for the treatment of congestion. But now, ACE inhibitors, ARBs, beta-blockers, mineralocorticoid antagonists, as well as sacubitril/valsartan, may be considered to improve outcomes in these patients.” Their upgrades in the new guidelines were based on review of trials in the CHARM program and of TOPCAT and PARAGON-HF, among others, he said.
The new document also includes “treatment algorithms based on phenotypes”; that is, comorbidities and less common HF precipitants. For example, “assessment of iron status is now mandated in all patients with heart failure,” Dr. Metra said.
AFFIRM-HF is the key trial in this arena, with its more than 1,100 iron-deficient patients with LVEF less than 50% who had been recently hospitalized for HF. A year of treatment with ferric carboxymaltose (Ferinject/Injectafer, Vifor) led to a 26% drop in risk for HF hospitalization, but without affecting mortality.
For those who are iron deficient, Dr. Metra said, “ferric carboxymaltose intravenously should be considered not only in patients with low ejection fraction and outpatients, but also in patients recently hospitalized for acute heart failure.”
The SGLT2 inhibitors are recommended in HFrEF patients with type 2 diabetes. And treatment with tafamidis (Vyndaqel, Pfizer) in patients with genetic or wild-type transthyretin cardiac amyloidosis gets a class I recommendation based on survival gains seen in the ATTR-ACT trial.
Also recommended is a full CV assessment for patients with cancer who are on cardiotoxic agents or otherwise might be at risk for chemotherapy cardiotoxicity. “Beta-blockers and ACE inhibitors should be considered in those who develop left ventricular systolic dysfunction after anticancer therapy,” Dr. Metra said.
The ongoing pandemic made its mark on the document’s genesis, as it has with most everything else. “For better or worse, we were a ‘COVID guideline,’ ” Dr. McDonagh said. The writing committee consisted of “a large task force of 31 individuals, including two patients,” and there were “only two face-to-face meetings prior to the first wave of COVID hitting Europe.”
The committee voted on each of the recommendations, “and we had to have agreement of more than 75% of the task force to assign a class of recommendation or level of evidence,” she said. “I think we did the best we could in the circumstances. We had the benefit of many discussions over Zoom, and I think at the end of the day we have achieved a consensus.”
With such a large body of participants and the 75% threshold for agreement, “you end up with perhaps a conservative guideline. But that’s not a bad thing for clinical practice, for guidelines to be conservative,” Dr. McDonagh said. “They’re mainly concerned with looking at evidence and safety.”
A version of this article first appeared on Medscape.com.
Today there are so many evidence-based drug therapies for heart failure with reduced ejection fraction (HFrEF) that physicians treating HF patients almost don’t know what to do them.
It’s an exciting new age that way, but to many vexingly unclear how best to merge the shiny new options with mainstay regimens based on time-honored renin-angiotensin system (RAS) inhibitors and beta-blockers.
To impart some clarity, the authors of a new HF guideline document recently took center stage at the Heart Failure Association of the European Society of Cardiology (ESC-HFA) annual meeting to preview their updated recommendations, with novel twists based on recent major trials, for the new age of HF pharmacotherapeutics.
The guideline committee considered the evidence base that existed “up until the end of March of this year,” Theresa A. McDonagh, MD, King’s College London, said during the presentation. The document “is now finalized, it’s with the publishers, and it will be presented in full with simultaneous publication at the ESC meeting” that starts August 27.
It describes a game plan, already followed by some clinicians in practice without official guidance, for initiating drugs from each of four classes in virtually all patients with HFrEF.
New indicated drugs, new perspective for HFrEF
Three of the drug categories are old acquaintances. Among them are the RAS inhibitors, which include angiotensin-receptor/neprilysin inhibitors, beta-blockers, and the mineralocorticoid receptor antagonists. The latter drugs are gaining new respect after having been underplayed in HF prescribing despite longstanding evidence of efficacy.
Completing the quartet of first-line HFrEF drug classes is a recent arrival to the HF arena, the sodium-glucose cotransporter 2 inhibitors.
“We now have new data and a simplified treatment algorithm for heart failure with reduced ejection fraction based on the early administration of the four major classes of drugs,” said Marco Metra, MD, University of Brescia (Italy), previewing the medical-therapy portions of the new guideline at the ESC-HFA sessions, which launched virtually and live in Florence, Italy, on July 29.
The new game plan offers a simple answer to a once-common but complex question: How and in what order are the different drug classes initiated in patients with HFrEF? In the new document, the stated goal is to get them all on board expeditiously and safely, by any means possible.
The guideline writers did not specify a sequence, preferring to leave that decision to physicians, said Dr. Metra, who stated only two guiding principles. The first is to consider the patient’s unique circumstances. The order in which the drugs are introduced might vary, depending on, for example, whether the patient has low or high blood pressure or renal dysfunction.
Second, “it is very important that we try to give all four classes of drugs to the patient in the shortest time possible, because this saves lives,” he said.
That there is no recommendation on sequencing the drugs has led some to the wrong interpretation that all should be started at once, observed coauthor Javed Butler, MD, MPH, University of Mississippi, Jackson, as a panelist during the presentation. Far from it, he said. “The doctor with the patient in front of you can make the best decision. The idea here is to get all the therapies on as soon as possible, as safely as possible.”
“The order in which they are introduced is not really important,” agreed Vijay Chopra, MD, Max Super Specialty Hospital Saket, New Delhi, another coauthor on the panel. “The important thing is that at least some dose of all the four drugs needs to be introduced in the first 4-6 weeks, and then up-titrated.”
Other medical therapy can be more tailored, Dr. Metra noted, such as loop diuretics for patients with congestion, iron for those with iron deficiency, and other drugs depending on whether there is, for example, atrial fibrillation or coronary disease.
Adoption of emerging definitions
The document adopts the emerging characterization of HFrEF by a left ventricular ejection fraction (LVEF) up to 40%.
And it will leverage an expanding evidence base for medication in a segment of patients once said to have HF with preserved ejection fraction (HFpEF), who had therefore lacked specific, guideline-directed medical therapies. Now, patients with an LVEF of 41%-49% will be said to have HF with mildly reduced ejection fraction (HFmrEF), a tweak to the recently introduced HF with “mid-range” LVEF that is designed to assert its nature as something to treat. The new document’s HFmrEF recommendations come with various class and level-of-evidence ratings.
That leaves HFpEF to be characterized by an LVEF of 50% in combination with structural or functional abnormalities associated with LV diastolic dysfunction or raised LV filling pressures, including raised natriuretic peptide levels.
The definitions are consistent with those proposed internationally by the ESC-HFA, the Heart Failure Society of America, and other groups in a statement published in March.
Expanded HFrEF med landscape
Since the 2016 ESC guideline on HF therapy, Dr. McDonagh said, “there’s been no substantial change in the evidence for many of the classical drugs that we use in heart failure. However, we had a lot of new and exciting evidence to consider,” especially in support of the SGLT2 inhibitors as one of the core medications in HFrEF.
The new data came from two controlled trials in particular. In DAPA-HF, patients with HFrEF who were initially without diabetes and who went on dapagliflozin (Farxiga, AstraZeneca) showed a 27% drop in cardiovascular (CV) death or worsening-HF events over a median of 18 months.
“That was followed up with very concordant results with empagliflozin [Jardiance, Boehringer Ingelheim/Eli Lilly] in HFrEF in the EMPEROR-Reduced trial,” Dr. McDonagh said. In that trial, comparable patients who took empagliflozin showed a 25% drop in a primary endpoint similar to that in DAPA-HF over the median 16-month follow-up.
Other HFrEF recommendations are for selected patients. They include ivabradine, already in the guidelines, for patients in sinus rhythm with an elevated resting heart rate who can’t take beta-blockers for whatever reason. But, Dr. McDonagh noted, “we had some new classes of drugs to consider as well.”
In particular, the oral soluble guanylate-cyclase receptor stimulator vericiguat (Verquvo) emerged about a year ago from the VICTORIA trial as a modest success for patients with HFrEF and a previous HF hospitalization. In the trial with more than 5,000 patients, treatment with vericiguat atop standard drug and device therapy was followed by a significant 10% drop in risk for CV death or HF hospitalization.
Available now or likely to be available in the United States, the European Union, Japan, and other countries, vericiguat is recommended in the new guideline for VICTORIA-like patients who don’t adequately respond to other indicated medications.
Little for HFpEF as newly defined
“Almost nothing is new” in the guidelines for HFpEF, Dr. Metra said. The document recommends screening for and treatment of any underlying disorder and comorbidities, plus diuretics for any congestion. “That’s what we have to date.”
But that evidence base might soon change. The new HFpEF recommendations could possibly be up-staged at the ESC sessions by the August 27 scheduled presentation of EMPEROR-Preserved, a randomized test of empagliflozin in HFpEF and – it could be said – HFmrEF. The trial entered patients with chronic HF and an LVEF greater than 40%.
Eli Lilly and Boehringer Ingelheim offered the world a peek at the results, which suggest the SGLT2 inhibitor had a positive impact on the primary endpoint of CV death or HF hospitalization. They announced the cursory top-line outcomes in early July as part of its regulatory obligations, noting that the trial had “met” its primary endpoint.
But many unknowns remain, including the degree of benefit and whether it varied among subgroups, and especially whether outcomes were different for HFmrEF than for HFpEF.
Upgrades for familiar agents
Still, HFmrEF gets noteworthy attention in the document. “For the first time, we have recommendations for these patients,” Dr. Metra said. “We already knew that diuretics are indicated for the treatment of congestion. But now, ACE inhibitors, ARBs, beta-blockers, mineralocorticoid antagonists, as well as sacubitril/valsartan, may be considered to improve outcomes in these patients.” Their upgrades in the new guidelines were based on review of trials in the CHARM program and of TOPCAT and PARAGON-HF, among others, he said.
The new document also includes “treatment algorithms based on phenotypes”; that is, comorbidities and less common HF precipitants. For example, “assessment of iron status is now mandated in all patients with heart failure,” Dr. Metra said.
AFFIRM-HF is the key trial in this arena, with its more than 1,100 iron-deficient patients with LVEF less than 50% who had been recently hospitalized for HF. A year of treatment with ferric carboxymaltose (Ferinject/Injectafer, Vifor) led to a 26% drop in risk for HF hospitalization, but without affecting mortality.
For those who are iron deficient, Dr. Metra said, “ferric carboxymaltose intravenously should be considered not only in patients with low ejection fraction and outpatients, but also in patients recently hospitalized for acute heart failure.”
The SGLT2 inhibitors are recommended in HFrEF patients with type 2 diabetes. And treatment with tafamidis (Vyndaqel, Pfizer) in patients with genetic or wild-type transthyretin cardiac amyloidosis gets a class I recommendation based on survival gains seen in the ATTR-ACT trial.
Also recommended is a full CV assessment for patients with cancer who are on cardiotoxic agents or otherwise might be at risk for chemotherapy cardiotoxicity. “Beta-blockers and ACE inhibitors should be considered in those who develop left ventricular systolic dysfunction after anticancer therapy,” Dr. Metra said.
The ongoing pandemic made its mark on the document’s genesis, as it has with most everything else. “For better or worse, we were a ‘COVID guideline,’ ” Dr. McDonagh said. The writing committee consisted of “a large task force of 31 individuals, including two patients,” and there were “only two face-to-face meetings prior to the first wave of COVID hitting Europe.”
The committee voted on each of the recommendations, “and we had to have agreement of more than 75% of the task force to assign a class of recommendation or level of evidence,” she said. “I think we did the best we could in the circumstances. We had the benefit of many discussions over Zoom, and I think at the end of the day we have achieved a consensus.”
With such a large body of participants and the 75% threshold for agreement, “you end up with perhaps a conservative guideline. But that’s not a bad thing for clinical practice, for guidelines to be conservative,” Dr. McDonagh said. “They’re mainly concerned with looking at evidence and safety.”
A version of this article first appeared on Medscape.com.
Today there are so many evidence-based drug therapies for heart failure with reduced ejection fraction (HFrEF) that physicians treating HF patients almost don’t know what to do them.
It’s an exciting new age that way, but to many vexingly unclear how best to merge the shiny new options with mainstay regimens based on time-honored renin-angiotensin system (RAS) inhibitors and beta-blockers.
To impart some clarity, the authors of a new HF guideline document recently took center stage at the Heart Failure Association of the European Society of Cardiology (ESC-HFA) annual meeting to preview their updated recommendations, with novel twists based on recent major trials, for the new age of HF pharmacotherapeutics.
The guideline committee considered the evidence base that existed “up until the end of March of this year,” Theresa A. McDonagh, MD, King’s College London, said during the presentation. The document “is now finalized, it’s with the publishers, and it will be presented in full with simultaneous publication at the ESC meeting” that starts August 27.
It describes a game plan, already followed by some clinicians in practice without official guidance, for initiating drugs from each of four classes in virtually all patients with HFrEF.
New indicated drugs, new perspective for HFrEF
Three of the drug categories are old acquaintances. Among them are the RAS inhibitors, which include angiotensin-receptor/neprilysin inhibitors, beta-blockers, and the mineralocorticoid receptor antagonists. The latter drugs are gaining new respect after having been underplayed in HF prescribing despite longstanding evidence of efficacy.
Completing the quartet of first-line HFrEF drug classes is a recent arrival to the HF arena, the sodium-glucose cotransporter 2 inhibitors.
“We now have new data and a simplified treatment algorithm for heart failure with reduced ejection fraction based on the early administration of the four major classes of drugs,” said Marco Metra, MD, University of Brescia (Italy), previewing the medical-therapy portions of the new guideline at the ESC-HFA sessions, which launched virtually and live in Florence, Italy, on July 29.
The new game plan offers a simple answer to a once-common but complex question: How and in what order are the different drug classes initiated in patients with HFrEF? In the new document, the stated goal is to get them all on board expeditiously and safely, by any means possible.
The guideline writers did not specify a sequence, preferring to leave that decision to physicians, said Dr. Metra, who stated only two guiding principles. The first is to consider the patient’s unique circumstances. The order in which the drugs are introduced might vary, depending on, for example, whether the patient has low or high blood pressure or renal dysfunction.
Second, “it is very important that we try to give all four classes of drugs to the patient in the shortest time possible, because this saves lives,” he said.
That there is no recommendation on sequencing the drugs has led some to the wrong interpretation that all should be started at once, observed coauthor Javed Butler, MD, MPH, University of Mississippi, Jackson, as a panelist during the presentation. Far from it, he said. “The doctor with the patient in front of you can make the best decision. The idea here is to get all the therapies on as soon as possible, as safely as possible.”
“The order in which they are introduced is not really important,” agreed Vijay Chopra, MD, Max Super Specialty Hospital Saket, New Delhi, another coauthor on the panel. “The important thing is that at least some dose of all the four drugs needs to be introduced in the first 4-6 weeks, and then up-titrated.”
Other medical therapy can be more tailored, Dr. Metra noted, such as loop diuretics for patients with congestion, iron for those with iron deficiency, and other drugs depending on whether there is, for example, atrial fibrillation or coronary disease.
Adoption of emerging definitions
The document adopts the emerging characterization of HFrEF by a left ventricular ejection fraction (LVEF) up to 40%.
And it will leverage an expanding evidence base for medication in a segment of patients once said to have HF with preserved ejection fraction (HFpEF), who had therefore lacked specific, guideline-directed medical therapies. Now, patients with an LVEF of 41%-49% will be said to have HF with mildly reduced ejection fraction (HFmrEF), a tweak to the recently introduced HF with “mid-range” LVEF that is designed to assert its nature as something to treat. The new document’s HFmrEF recommendations come with various class and level-of-evidence ratings.
That leaves HFpEF to be characterized by an LVEF of 50% in combination with structural or functional abnormalities associated with LV diastolic dysfunction or raised LV filling pressures, including raised natriuretic peptide levels.
The definitions are consistent with those proposed internationally by the ESC-HFA, the Heart Failure Society of America, and other groups in a statement published in March.
Expanded HFrEF med landscape
Since the 2016 ESC guideline on HF therapy, Dr. McDonagh said, “there’s been no substantial change in the evidence for many of the classical drugs that we use in heart failure. However, we had a lot of new and exciting evidence to consider,” especially in support of the SGLT2 inhibitors as one of the core medications in HFrEF.
The new data came from two controlled trials in particular. In DAPA-HF, patients with HFrEF who were initially without diabetes and who went on dapagliflozin (Farxiga, AstraZeneca) showed a 27% drop in cardiovascular (CV) death or worsening-HF events over a median of 18 months.
“That was followed up with very concordant results with empagliflozin [Jardiance, Boehringer Ingelheim/Eli Lilly] in HFrEF in the EMPEROR-Reduced trial,” Dr. McDonagh said. In that trial, comparable patients who took empagliflozin showed a 25% drop in a primary endpoint similar to that in DAPA-HF over the median 16-month follow-up.
Other HFrEF recommendations are for selected patients. They include ivabradine, already in the guidelines, for patients in sinus rhythm with an elevated resting heart rate who can’t take beta-blockers for whatever reason. But, Dr. McDonagh noted, “we had some new classes of drugs to consider as well.”
In particular, the oral soluble guanylate-cyclase receptor stimulator vericiguat (Verquvo) emerged about a year ago from the VICTORIA trial as a modest success for patients with HFrEF and a previous HF hospitalization. In the trial with more than 5,000 patients, treatment with vericiguat atop standard drug and device therapy was followed by a significant 10% drop in risk for CV death or HF hospitalization.
Available now or likely to be available in the United States, the European Union, Japan, and other countries, vericiguat is recommended in the new guideline for VICTORIA-like patients who don’t adequately respond to other indicated medications.
Little for HFpEF as newly defined
“Almost nothing is new” in the guidelines for HFpEF, Dr. Metra said. The document recommends screening for and treatment of any underlying disorder and comorbidities, plus diuretics for any congestion. “That’s what we have to date.”
But that evidence base might soon change. The new HFpEF recommendations could possibly be up-staged at the ESC sessions by the August 27 scheduled presentation of EMPEROR-Preserved, a randomized test of empagliflozin in HFpEF and – it could be said – HFmrEF. The trial entered patients with chronic HF and an LVEF greater than 40%.
Eli Lilly and Boehringer Ingelheim offered the world a peek at the results, which suggest the SGLT2 inhibitor had a positive impact on the primary endpoint of CV death or HF hospitalization. They announced the cursory top-line outcomes in early July as part of its regulatory obligations, noting that the trial had “met” its primary endpoint.
But many unknowns remain, including the degree of benefit and whether it varied among subgroups, and especially whether outcomes were different for HFmrEF than for HFpEF.
Upgrades for familiar agents
Still, HFmrEF gets noteworthy attention in the document. “For the first time, we have recommendations for these patients,” Dr. Metra said. “We already knew that diuretics are indicated for the treatment of congestion. But now, ACE inhibitors, ARBs, beta-blockers, mineralocorticoid antagonists, as well as sacubitril/valsartan, may be considered to improve outcomes in these patients.” Their upgrades in the new guidelines were based on review of trials in the CHARM program and of TOPCAT and PARAGON-HF, among others, he said.
The new document also includes “treatment algorithms based on phenotypes”; that is, comorbidities and less common HF precipitants. For example, “assessment of iron status is now mandated in all patients with heart failure,” Dr. Metra said.
AFFIRM-HF is the key trial in this arena, with its more than 1,100 iron-deficient patients with LVEF less than 50% who had been recently hospitalized for HF. A year of treatment with ferric carboxymaltose (Ferinject/Injectafer, Vifor) led to a 26% drop in risk for HF hospitalization, but without affecting mortality.
For those who are iron deficient, Dr. Metra said, “ferric carboxymaltose intravenously should be considered not only in patients with low ejection fraction and outpatients, but also in patients recently hospitalized for acute heart failure.”
The SGLT2 inhibitors are recommended in HFrEF patients with type 2 diabetes. And treatment with tafamidis (Vyndaqel, Pfizer) in patients with genetic or wild-type transthyretin cardiac amyloidosis gets a class I recommendation based on survival gains seen in the ATTR-ACT trial.
Also recommended is a full CV assessment for patients with cancer who are on cardiotoxic agents or otherwise might be at risk for chemotherapy cardiotoxicity. “Beta-blockers and ACE inhibitors should be considered in those who develop left ventricular systolic dysfunction after anticancer therapy,” Dr. Metra said.
The ongoing pandemic made its mark on the document’s genesis, as it has with most everything else. “For better or worse, we were a ‘COVID guideline,’ ” Dr. McDonagh said. The writing committee consisted of “a large task force of 31 individuals, including two patients,” and there were “only two face-to-face meetings prior to the first wave of COVID hitting Europe.”
The committee voted on each of the recommendations, “and we had to have agreement of more than 75% of the task force to assign a class of recommendation or level of evidence,” she said. “I think we did the best we could in the circumstances. We had the benefit of many discussions over Zoom, and I think at the end of the day we have achieved a consensus.”
With such a large body of participants and the 75% threshold for agreement, “you end up with perhaps a conservative guideline. But that’s not a bad thing for clinical practice, for guidelines to be conservative,” Dr. McDonagh said. “They’re mainly concerned with looking at evidence and safety.”
A version of this article first appeared on Medscape.com.
In sickness and in health: Spouses can share risk for cardiac events
A study from Japan suggests that a history of cardiovascular events in a spouse may elevate risk for future CV events in the other partner, with one caveat: Men in the cohort study were at increased risk if their wives had such a history, but the association was only one way. The risk of events didn’t go up for women with husbands who had previously experienced a CV event.

The results highlight the need for clinicians to screen and possibly intervene with a primary CV prevention strategy “not only first-degree relatives but also spouses with a history of cardiovascular disease,” which is not currently part of the primary prevention guidelines, Hiroyuki Ohbe, MD, University of Tokyo, told this news organization.
In their study published online July 9 in Circulation: Cardiovascular Quality and Outcomes, Dr. Ohbe and Hideo Yasunaga, MD, PhD, of the same institution, assessed the risk of subsequent CV events in adults with a spouse who had experienced a stroke of any kind or had clinical ischemic heart disease such as angina or myocardial infarction.
Johanna Contreras, MD, director of heart failure at Mount Sinai Health System in New York, is not surprised by the finding that a wife’s CV history is linked to the CV risk in the husband.
“I see this often in my practice. When you live with someone, you also behave in a similar way as the other person,” Dr. Contreras told this news organization. “For example, couples who live together are likely to both exercise and have a healthy diet and not smoke.”
And most notably, she said, “the women are usually the ones who drive the healthy behaviors in the family; they watch what the family eats, where they eat, when they eat, and the men tend to allow the women to guide this behavior.”
Dr. Ohbe and Dr. Yasunaga agree, proposing that different results for men and women in the analysis may be because of the dependence of working-aged men on their wives for major aspects of lifestyle, such as diet and exercise. Moreover, they write, increased psychological and physical stress from taking care of a spouse with CV disease may also play a role, as caregivers often neglect their own health.
The team identified 13,759 adults in a large administrative database with no history of CV disease whose spouse had such a history at their first health checkup; they were the exposure group. The team matched each of them with up to four individuals (n = 55,027) who had no CV disease history and spouses without CV disease at their first health checkup; they were the nonexposure group.
The mean observation period was 7.9 years from the first health checkup, at which the subjects’ mean age was 56 years. During the follow-up, more people in the exposure group than the nonexposure group had a history of CV events, 0.6% versus 0.4%.
In the overall cohort, the hazard ratio for future severe CV events – heart failure hospitalization or MI – in those with spouses with a history of CV disease was 1.48 (95% confidence interval, 1.15-1.90).
When stratified by sex, men whose wives had CV disease showed a significantly increased risk of a future severe CV event (HR, 1.68; 95% CI, 1.22-2.32). But women with husbands with CV disease did not (HR, 1.22; 95% CI, 0.82-1.83).
The results of all four sensitivity analyses were similar to those of the primary analysis, both in the overall cohort and in the cohorts stratified by sex. The investigators performed multivariate survival analyses: one that excluded people whose partners had died, one that included death by any cause as an outcome, and one with propensity score matching.
Further studies are needed to confirm their observations and test whether a primary prevention strategy targeted at married couples could reduce CV events, note Dr. Ohbe and Dr. Yasunaga.
The findings have implications for everyday clinical practice, Dr. Contreras said. “When I see a patient who is married and has had a heart attack, I will insist on seeing the partner as well, and I will counsel them on working together to change their lifestyle,” she said in an interview.
“Often when you have that discussion with the couple after one has a heart attack, they quit smoking together, they go the gym together, and they get healthier together,” she said. “That’s now a very important conversation we have before they leave the hospital.”
The study was supported by grants from the Japan Ministry of Health, Ministry of Labour and Welfare, and the Ministry of Education, Culture, Sports, Science and Technology. Dr. Ohbe, Dr. Yasunaga, and Dr. Contreras have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A study from Japan suggests that a history of cardiovascular events in a spouse may elevate risk for future CV events in the other partner, with one caveat: Men in the cohort study were at increased risk if their wives had such a history, but the association was only one way. The risk of events didn’t go up for women with husbands who had previously experienced a CV event.
The results highlight the need for clinicians to screen and possibly intervene with a primary CV prevention strategy “not only first-degree relatives but also spouses with a history of cardiovascular disease,” which is not currently part of the primary prevention guidelines, Hiroyuki Ohbe, MD, University of Tokyo, told this news organization.
In their study published online July 9 in Circulation: Cardiovascular Quality and Outcomes, Dr. Ohbe and Hideo Yasunaga, MD, PhD, of the same institution, assessed the risk of subsequent CV events in adults with a spouse who had experienced a stroke of any kind or had clinical ischemic heart disease such as angina or myocardial infarction.
Johanna Contreras, MD, director of heart failure at Mount Sinai Health System in New York, is not surprised by the finding that a wife’s CV history is linked to the CV risk in the husband.
“I see this often in my practice. When you live with someone, you also behave in a similar way as the other person,” Dr. Contreras told this news organization. “For example, couples who live together are likely to both exercise and have a healthy diet and not smoke.”
And most notably, she said, “the women are usually the ones who drive the healthy behaviors in the family; they watch what the family eats, where they eat, when they eat, and the men tend to allow the women to guide this behavior.”
Dr. Ohbe and Dr. Yasunaga agree, proposing that different results for men and women in the analysis may be because of the dependence of working-aged men on their wives for major aspects of lifestyle, such as diet and exercise. Moreover, they write, increased psychological and physical stress from taking care of a spouse with CV disease may also play a role, as caregivers often neglect their own health.
The team identified 13,759 adults in a large administrative database with no history of CV disease whose spouse had such a history at their first health checkup; they were the exposure group. The team matched each of them with up to four individuals (n = 55,027) who had no CV disease history and spouses without CV disease at their first health checkup; they were the nonexposure group.
The mean observation period was 7.9 years from the first health checkup, at which the subjects’ mean age was 56 years. During the follow-up, more people in the exposure group than the nonexposure group had a history of CV events, 0.6% versus 0.4%.
In the overall cohort, the hazard ratio for future severe CV events – heart failure hospitalization or MI – in those with spouses with a history of CV disease was 1.48 (95% confidence interval, 1.15-1.90).
When stratified by sex, men whose wives had CV disease showed a significantly increased risk of a future severe CV event (HR, 1.68; 95% CI, 1.22-2.32). But women with husbands with CV disease did not (HR, 1.22; 95% CI, 0.82-1.83).
The results of all four sensitivity analyses were similar to those of the primary analysis, both in the overall cohort and in the cohorts stratified by sex. The investigators performed multivariate survival analyses: one that excluded people whose partners had died, one that included death by any cause as an outcome, and one with propensity score matching.
Further studies are needed to confirm their observations and test whether a primary prevention strategy targeted at married couples could reduce CV events, note Dr. Ohbe and Dr. Yasunaga.
The findings have implications for everyday clinical practice, Dr. Contreras said. “When I see a patient who is married and has had a heart attack, I will insist on seeing the partner as well, and I will counsel them on working together to change their lifestyle,” she said in an interview.
“Often when you have that discussion with the couple after one has a heart attack, they quit smoking together, they go the gym together, and they get healthier together,” she said. “That’s now a very important conversation we have before they leave the hospital.”
The study was supported by grants from the Japan Ministry of Health, Ministry of Labour and Welfare, and the Ministry of Education, Culture, Sports, Science and Technology. Dr. Ohbe, Dr. Yasunaga, and Dr. Contreras have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A study from Japan suggests that a history of cardiovascular events in a spouse may elevate risk for future CV events in the other partner, with one caveat: Men in the cohort study were at increased risk if their wives had such a history, but the association was only one way. The risk of events didn’t go up for women with husbands who had previously experienced a CV event.
The results highlight the need for clinicians to screen and possibly intervene with a primary CV prevention strategy “not only first-degree relatives but also spouses with a history of cardiovascular disease,” which is not currently part of the primary prevention guidelines, Hiroyuki Ohbe, MD, University of Tokyo, told this news organization.
In their study published online July 9 in Circulation: Cardiovascular Quality and Outcomes, Dr. Ohbe and Hideo Yasunaga, MD, PhD, of the same institution, assessed the risk of subsequent CV events in adults with a spouse who had experienced a stroke of any kind or had clinical ischemic heart disease such as angina or myocardial infarction.
Johanna Contreras, MD, director of heart failure at Mount Sinai Health System in New York, is not surprised by the finding that a wife’s CV history is linked to the CV risk in the husband.
“I see this often in my practice. When you live with someone, you also behave in a similar way as the other person,” Dr. Contreras told this news organization. “For example, couples who live together are likely to both exercise and have a healthy diet and not smoke.”
And most notably, she said, “the women are usually the ones who drive the healthy behaviors in the family; they watch what the family eats, where they eat, when they eat, and the men tend to allow the women to guide this behavior.”
Dr. Ohbe and Dr. Yasunaga agree, proposing that different results for men and women in the analysis may be because of the dependence of working-aged men on their wives for major aspects of lifestyle, such as diet and exercise. Moreover, they write, increased psychological and physical stress from taking care of a spouse with CV disease may also play a role, as caregivers often neglect their own health.
The team identified 13,759 adults in a large administrative database with no history of CV disease whose spouse had such a history at their first health checkup; they were the exposure group. The team matched each of them with up to four individuals (n = 55,027) who had no CV disease history and spouses without CV disease at their first health checkup; they were the nonexposure group.
The mean observation period was 7.9 years from the first health checkup, at which the subjects’ mean age was 56 years. During the follow-up, more people in the exposure group than the nonexposure group had a history of CV events, 0.6% versus 0.4%.
In the overall cohort, the hazard ratio for future severe CV events – heart failure hospitalization or MI – in those with spouses with a history of CV disease was 1.48 (95% confidence interval, 1.15-1.90).
When stratified by sex, men whose wives had CV disease showed a significantly increased risk of a future severe CV event (HR, 1.68; 95% CI, 1.22-2.32). But women with husbands with CV disease did not (HR, 1.22; 95% CI, 0.82-1.83).
The results of all four sensitivity analyses were similar to those of the primary analysis, both in the overall cohort and in the cohorts stratified by sex. The investigators performed multivariate survival analyses: one that excluded people whose partners had died, one that included death by any cause as an outcome, and one with propensity score matching.
Further studies are needed to confirm their observations and test whether a primary prevention strategy targeted at married couples could reduce CV events, note Dr. Ohbe and Dr. Yasunaga.
The findings have implications for everyday clinical practice, Dr. Contreras said. “When I see a patient who is married and has had a heart attack, I will insist on seeing the partner as well, and I will counsel them on working together to change their lifestyle,” she said in an interview.
“Often when you have that discussion with the couple after one has a heart attack, they quit smoking together, they go the gym together, and they get healthier together,” she said. “That’s now a very important conversation we have before they leave the hospital.”
The study was supported by grants from the Japan Ministry of Health, Ministry of Labour and Welfare, and the Ministry of Education, Culture, Sports, Science and Technology. Dr. Ohbe, Dr. Yasunaga, and Dr. Contreras have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Diabetes duration linked to increasing heart failure risk

In a multivariable analysis the rate of incident heart failure increased steadily and significantly as diabetes duration increased. Among the 168 study subjects (2% of the total study group) who had diabetes for at least 15 years, the subsequent incidence of heart failure was nearly threefold higher than among the 4,802 subjects (49%) who never had diabetes or prediabetes, reported Justin B. Echouffo-Tcheugui, MD, PhD, and coauthors in an article published in JACC Heart Failure.
People with prediabetes (32% of the study population) had a significant but modest increased rate of incident heart failure that was 16% higher than in control subjects who never developed diabetes. People with diabetes for durations of 0-4.9 years, 5.0-9.9 years, or 10-14.9 years, had steadily increasing relative incident heart failure rates of 29%, 97%, and 210%, respectively, compared with controls, reported Dr. Echouffo-Tcheugui, an endocrinologist at Johns Hopkins Medicine in Baltimore.
Similar rates of HFrEF and HFpEF
Among all 1,841 people in the dataset with diabetes for any length of time each additional 5 years of the disorder linked with a significant, relative 17% increase in the rate of incident heart failure. Incidence of heart failure rose even more sharply with added duration among those with a hemoglobin A1c of 7% or greater, compared with those with better glycemic control. And the rate of incident heart failure with reduced ejection fraction (HFrEF) roughly matched the rate of incident heart failure with preserved ejection fraction (HFpEF).
The study dataset included 9,734 adults enrolled into the Atherosclerosis Risk in Communities (ARIC) study, and during a median follow-up of 22.5 years they had nearly 2,000 episodes of either hospitalization or death secondary to incident heart failure. This included 617 (31%) events involving HFpEF, 495 events (25%) involving HFrEF, and 876 unclassified heart failure events.
The cohort averaged 63 years of age; 58% were women, 23% were Black, and 77% were White (the study design excluded people with other racial and ethnic backgrounds). The study design also excluded people with a history of heart failure or coronary artery disease, as well as those diagnosed with diabetes prior to age 18 resulting in a study group that presumably mostly had type 2 diabetes when diabetes was present. The report provided no data on the specific numbers of patients with type 1 or type 2 diabetes.
“It’s not surprising that a longer duration of diabetes is associated with heart failure, but the etiology remains problematic,” commented Robert H. Eckel, MD, an endocrinologist at the University of Colorado at Denver, Aurora. “The impact of diabetes on incident heart failure is not well know, particularly duration of diabetes,” although disorders often found in patients with diabetes, such as hypertension and diabetic cardiomyopathy, likely have roles in causing heart failure, he said.
Diabetes duration may signal need for an SGLT2 inhibitor
“With emerging novel treatments like the SGLT2 [sodium-glucose cotransporter 2] inhibitors for preventing heart failure hospitalizations and deaths in patients with type 2 diabetes, this is a timely analysis,” Dr. Eckel said in an interview.
“There is no question that with increased duration of type 2 diabetes” the need for an agent from the SGLT2-inhibitor class increases. Although, because of the proven protection these drugs give against heart failure events and progression of chronic kidney disease, treatment with this drug class should start early in patients with type 2 diabetes, he added.
Dr. Echouffo-Tcheugui and his coauthors agreed, citing two important clinical take-aways from their findings:
First, interventions that delay the onset of diabetes may potentially reduce incident heart failure; second, patients with diabetes might benefit from cardioprotective treatments such as SGLT2 inhibitors, the report said.
“Our observations suggest the potential prognostic relevance of diabetes duration in assessing heart failure,” the authors wrote. Integrating diabetes duration into heart failure risk estimation in people with diabetes “could help refine the selection of high-risk individuals who may derive the greatest absolute benefit from aggressive cardioprotective therapies such as SGLT2 inhibitors.”
The analysis also identified several other demographic and clinical factors that influenced the relative effect of diabetes duration. Longer duration was linked with higher rates of incident heart failure in women compared with men, in Blacks compared with Whites, in people younger than 65 compared with older people, in people with an A1c of 7% or higher, and in those with a body mass index of 30 kg/m2 or greater.
The ARIC study and the analyses run by Dr. Echouffo-Tcheugui and his coauthors received no commercial funding. Dr. Echouffo-Tcheugui and Dr. Eckel had no relevant disclosures.
In a multivariable analysis the rate of incident heart failure increased steadily and significantly as diabetes duration increased. Among the 168 study subjects (2% of the total study group) who had diabetes for at least 15 years, the subsequent incidence of heart failure was nearly threefold higher than among the 4,802 subjects (49%) who never had diabetes or prediabetes, reported Justin B. Echouffo-Tcheugui, MD, PhD, and coauthors in an article published in JACC Heart Failure.
People with prediabetes (32% of the study population) had a significant but modest increased rate of incident heart failure that was 16% higher than in control subjects who never developed diabetes. People with diabetes for durations of 0-4.9 years, 5.0-9.9 years, or 10-14.9 years, had steadily increasing relative incident heart failure rates of 29%, 97%, and 210%, respectively, compared with controls, reported Dr. Echouffo-Tcheugui, an endocrinologist at Johns Hopkins Medicine in Baltimore.
Similar rates of HFrEF and HFpEF
Among all 1,841 people in the dataset with diabetes for any length of time each additional 5 years of the disorder linked with a significant, relative 17% increase in the rate of incident heart failure. Incidence of heart failure rose even more sharply with added duration among those with a hemoglobin A1c of 7% or greater, compared with those with better glycemic control. And the rate of incident heart failure with reduced ejection fraction (HFrEF) roughly matched the rate of incident heart failure with preserved ejection fraction (HFpEF).
The study dataset included 9,734 adults enrolled into the Atherosclerosis Risk in Communities (ARIC) study, and during a median follow-up of 22.5 years they had nearly 2,000 episodes of either hospitalization or death secondary to incident heart failure. This included 617 (31%) events involving HFpEF, 495 events (25%) involving HFrEF, and 876 unclassified heart failure events.
The cohort averaged 63 years of age; 58% were women, 23% were Black, and 77% were White (the study design excluded people with other racial and ethnic backgrounds). The study design also excluded people with a history of heart failure or coronary artery disease, as well as those diagnosed with diabetes prior to age 18 resulting in a study group that presumably mostly had type 2 diabetes when diabetes was present. The report provided no data on the specific numbers of patients with type 1 or type 2 diabetes.
“It’s not surprising that a longer duration of diabetes is associated with heart failure, but the etiology remains problematic,” commented Robert H. Eckel, MD, an endocrinologist at the University of Colorado at Denver, Aurora. “The impact of diabetes on incident heart failure is not well know, particularly duration of diabetes,” although disorders often found in patients with diabetes, such as hypertension and diabetic cardiomyopathy, likely have roles in causing heart failure, he said.
Diabetes duration may signal need for an SGLT2 inhibitor
“With emerging novel treatments like the SGLT2 [sodium-glucose cotransporter 2] inhibitors for preventing heart failure hospitalizations and deaths in patients with type 2 diabetes, this is a timely analysis,” Dr. Eckel said in an interview.
“There is no question that with increased duration of type 2 diabetes” the need for an agent from the SGLT2-inhibitor class increases. Although, because of the proven protection these drugs give against heart failure events and progression of chronic kidney disease, treatment with this drug class should start early in patients with type 2 diabetes, he added.
Dr. Echouffo-Tcheugui and his coauthors agreed, citing two important clinical take-aways from their findings:
First, interventions that delay the onset of diabetes may potentially reduce incident heart failure; second, patients with diabetes might benefit from cardioprotective treatments such as SGLT2 inhibitors, the report said.
“Our observations suggest the potential prognostic relevance of diabetes duration in assessing heart failure,” the authors wrote. Integrating diabetes duration into heart failure risk estimation in people with diabetes “could help refine the selection of high-risk individuals who may derive the greatest absolute benefit from aggressive cardioprotective therapies such as SGLT2 inhibitors.”
The analysis also identified several other demographic and clinical factors that influenced the relative effect of diabetes duration. Longer duration was linked with higher rates of incident heart failure in women compared with men, in Blacks compared with Whites, in people younger than 65 compared with older people, in people with an A1c of 7% or higher, and in those with a body mass index of 30 kg/m2 or greater.
The ARIC study and the analyses run by Dr. Echouffo-Tcheugui and his coauthors received no commercial funding. Dr. Echouffo-Tcheugui and Dr. Eckel had no relevant disclosures.
In a multivariable analysis the rate of incident heart failure increased steadily and significantly as diabetes duration increased. Among the 168 study subjects (2% of the total study group) who had diabetes for at least 15 years, the subsequent incidence of heart failure was nearly threefold higher than among the 4,802 subjects (49%) who never had diabetes or prediabetes, reported Justin B. Echouffo-Tcheugui, MD, PhD, and coauthors in an article published in JACC Heart Failure.
People with prediabetes (32% of the study population) had a significant but modest increased rate of incident heart failure that was 16% higher than in control subjects who never developed diabetes. People with diabetes for durations of 0-4.9 years, 5.0-9.9 years, or 10-14.9 years, had steadily increasing relative incident heart failure rates of 29%, 97%, and 210%, respectively, compared with controls, reported Dr. Echouffo-Tcheugui, an endocrinologist at Johns Hopkins Medicine in Baltimore.
Similar rates of HFrEF and HFpEF
Among all 1,841 people in the dataset with diabetes for any length of time each additional 5 years of the disorder linked with a significant, relative 17% increase in the rate of incident heart failure. Incidence of heart failure rose even more sharply with added duration among those with a hemoglobin A1c of 7% or greater, compared with those with better glycemic control. And the rate of incident heart failure with reduced ejection fraction (HFrEF) roughly matched the rate of incident heart failure with preserved ejection fraction (HFpEF).
The study dataset included 9,734 adults enrolled into the Atherosclerosis Risk in Communities (ARIC) study, and during a median follow-up of 22.5 years they had nearly 2,000 episodes of either hospitalization or death secondary to incident heart failure. This included 617 (31%) events involving HFpEF, 495 events (25%) involving HFrEF, and 876 unclassified heart failure events.
The cohort averaged 63 years of age; 58% were women, 23% were Black, and 77% were White (the study design excluded people with other racial and ethnic backgrounds). The study design also excluded people with a history of heart failure or coronary artery disease, as well as those diagnosed with diabetes prior to age 18 resulting in a study group that presumably mostly had type 2 diabetes when diabetes was present. The report provided no data on the specific numbers of patients with type 1 or type 2 diabetes.
“It’s not surprising that a longer duration of diabetes is associated with heart failure, but the etiology remains problematic,” commented Robert H. Eckel, MD, an endocrinologist at the University of Colorado at Denver, Aurora. “The impact of diabetes on incident heart failure is not well know, particularly duration of diabetes,” although disorders often found in patients with diabetes, such as hypertension and diabetic cardiomyopathy, likely have roles in causing heart failure, he said.
Diabetes duration may signal need for an SGLT2 inhibitor
“With emerging novel treatments like the SGLT2 [sodium-glucose cotransporter 2] inhibitors for preventing heart failure hospitalizations and deaths in patients with type 2 diabetes, this is a timely analysis,” Dr. Eckel said in an interview.
“There is no question that with increased duration of type 2 diabetes” the need for an agent from the SGLT2-inhibitor class increases. Although, because of the proven protection these drugs give against heart failure events and progression of chronic kidney disease, treatment with this drug class should start early in patients with type 2 diabetes, he added.
Dr. Echouffo-Tcheugui and his coauthors agreed, citing two important clinical take-aways from their findings:
First, interventions that delay the onset of diabetes may potentially reduce incident heart failure; second, patients with diabetes might benefit from cardioprotective treatments such as SGLT2 inhibitors, the report said.
“Our observations suggest the potential prognostic relevance of diabetes duration in assessing heart failure,” the authors wrote. Integrating diabetes duration into heart failure risk estimation in people with diabetes “could help refine the selection of high-risk individuals who may derive the greatest absolute benefit from aggressive cardioprotective therapies such as SGLT2 inhibitors.”
The analysis also identified several other demographic and clinical factors that influenced the relative effect of diabetes duration. Longer duration was linked with higher rates of incident heart failure in women compared with men, in Blacks compared with Whites, in people younger than 65 compared with older people, in people with an A1c of 7% or higher, and in those with a body mass index of 30 kg/m2 or greater.
The ARIC study and the analyses run by Dr. Echouffo-Tcheugui and his coauthors received no commercial funding. Dr. Echouffo-Tcheugui and Dr. Eckel had no relevant disclosures.
FROM JACC HEART FAILURE
Rising meth-related heart failure admissions a ‘crisis,’ costly for society
Rates of heart failure (HF) caused by methamphetamine abuse are climbing quickly in the western United States, at great financial and societal cost, suggests an analysis that documents the trends in California over a recent decade.
In the new study, methamphetamine-associated HF (meth-HF) admissions in the state rose by 585% between 2008 and 2018, and charges related those hospitalizations jumped 840%. Cases of HF unrelated to meth fell by 6% during the same period.
The recent explosion in meth-HF hospitalizations has also been costly for society in general, because most cases are younger adults in their most productive, prime earning years, Susan X. Zhao, MD, Santa Clara Valley Medical Center, San Jose, Calif., said in an interview.
“Over the past 11 years, especially since 2018, it has really started to take off, with a pretty dramatic rise. And it happened without much attention, because when we think about drugs, we think about acute overdose and not so much about the chronic, smoldering, long-term effects,” said Dr. Zhao, who is lead author on the study published July 13, 2021, in Circulation: Cardiovascular Quality and Outcomes.
“It’s really affecting a section of the population that is not supposed to be having heart failure problems. I think it is going to continue for the next decade until we put a stop to the parent problem, which is methamphetamine,” Dr. Zhao said. “We’re at the beginning, even though the rise has been pretty dramatic. The worst is yet to come.”
Under the radar
Methamphetamine-associated HF has been a growing problem for many years but has largely been “flying under the radar” because HF hospitalization data focus on Medicare-age patients, not the overwhelmingly younger meth-HF population, the report notes.
“We have to get this message out. Many of my patients with meth heart failure had no idea this would happen to them. They didn’t know,” Dr. Zhao said. “Once I tell them that this is what methamphetamines will do to you after years and years of use, they say they wish someone had told them.”
Dr. Zhao and colleagues looked at HF admission data collected by California’s Health and Human Services Agency to assess meth-HF trends and disease burden. They identified 1,033,076 HF hospitalizations during the decade, of which 42,565 (4.12%) were for meth-HF.
Patients hospitalized with meth-HF had a mean age of 49.6 years, compared with 72.2 for the other patients admitted with HF (P < .001). Virtually all of the patients hospitalized for meth-HF were younger than 65 years: 94.5%, compared with 30% for the other HF patients (P < .001).
Hospitalized patients with meth-HF were mostly men, their prevalence of 80% contrasting with 52.4% for patients with non–meth-related HF (P < .001).
Rates of hospitalization for meth-HF steadily increased during the study period. The age-adjusted rate of meth-HF hospitalization per 100,000 rose from 4.1 in 2008 to 28.1 in 2018. The rate of hospitalization for HF unrelated to meth actually declined, going from 342.3 in 2008 to 321.6 in 2018.
Charges for hospitalizations related to meth-HF shot up more than eight times, from $41.5 million in 2008 to $390.2 million in 2018. In contrast, charges for other HF hospitalizations rose by only 82%, from $3.5 billion to $6.3 billion.
Multiple layers of prevention
Dr. Zhao proposed ways that clinicians can communicate with their patients who are using or considering to use meth. “There are multiple layers of prevention. For people who are thinking of using meth, they need to get the message that something really bad can happen to them years down the road. They’re not going to die from it overnight, but it will damage the heart slowly,” she said.
The next layer of prevention can potentially help meth users who have not yet developed heart problems, Dr. Zhao said. “This would be the time to say, ‘you’re so lucky, your heart is still good. It’s time to stop because people like you, a few years from now are going to die prematurely from a very horrible, very suffering kind of death’.”
Importantly, in meth users who have already developed HF, even then it may not be too late to reverse the cardiomyopathy and symptoms. For up to a third of people with established meth-HF, “if they stop using meth, if they take good cardiac medications, and if the heart failure is in an early enough course, their heart can entirely revert to normal,” Dr. Zhao said, citing an earlier work from her and her colleagues.
Currently, methamphetamine abuse has taken especially strong root in rural areas in California and the Midwest. But Dr. Zhao predicts it will soon become prevalent throughout the United States.
Spotlight on an ‘epidemic’
The rapid growth of the methamphetamine “epidemic” has been well-documented in the United States and around the world, observed an accompanying editorial from Pavan Reddy, MD, Icahn School of Medicine at Mount Sinai Morningside, New York, and Uri Elkayam, MD, University of Southern California, Los Angeles.
They contend that more attention has been given to opioid overdose deaths; meth abuse does not seem to command the same attention, likely because meth is not as strongly associated with acute overdose.
But meth, wrote Dr. Reddy and Dr. Elkayam, “is a different drug with its own M.O., equally dangerous and costly to society but more insidious in nature, its effects potentially causing decades of mental and physical debilitation before ending in premature death.”
The current study “has turned a spotlight on a public health crisis that has grown unfettered for over 2 decades,” and is a call for the “medical community to recognize and manage cases of meth-HF with a comprehensive approach that addresses both mental and physical illness,” they concluded. “Only then can we hope to properly help these patients and with that, reduce the socioeconomic burden of meth-HF.”
A quietly building crisis
The sharp rise in meth-HF hospitalizations is an expected reflection of the methamphetamine crisis, which has been quietly building over the last few years, addiction psychiatrist Corneliu N. Stanciu, MD, Dartmouth-Hitchcock Medical Center, Lebanon, N.H., said in an interview.
“This new version of methamphetamines looks like ice and is more potent and toxic than former versions traditionally made in home-built labs,” he said. Lately the vast majority of methamphetamines in the United States have come from Mexico, are less expensive with higher purity, “and can be manufactured in greater quantities.”
Some patients with opioid use disorder (OUD) also inject methamphetamines, which can make OUD treatment clinics good places to screen for meth abuse and educate about its cardiovascular implications, Dr. Stanciu said.
“Just as addiction treatment centers present an opportunity to implement cardiac screening and referrals,” he said, “cardiology visits and hospitalizations such as those for meth-HF also present a golden opportunity for involvement of substance use disorder interventions and referrals to get patients into treatment and prevent further damage through ongoing use.”
Dr. Zhao, Dr. Reddy, Dr. Eklayam, and Dr. Stanciu report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Rates of heart failure (HF) caused by methamphetamine abuse are climbing quickly in the western United States, at great financial and societal cost, suggests an analysis that documents the trends in California over a recent decade.
In the new study, methamphetamine-associated HF (meth-HF) admissions in the state rose by 585% between 2008 and 2018, and charges related those hospitalizations jumped 840%. Cases of HF unrelated to meth fell by 6% during the same period.
The recent explosion in meth-HF hospitalizations has also been costly for society in general, because most cases are younger adults in their most productive, prime earning years, Susan X. Zhao, MD, Santa Clara Valley Medical Center, San Jose, Calif., said in an interview.
“Over the past 11 years, especially since 2018, it has really started to take off, with a pretty dramatic rise. And it happened without much attention, because when we think about drugs, we think about acute overdose and not so much about the chronic, smoldering, long-term effects,” said Dr. Zhao, who is lead author on the study published July 13, 2021, in Circulation: Cardiovascular Quality and Outcomes.
“It’s really affecting a section of the population that is not supposed to be having heart failure problems. I think it is going to continue for the next decade until we put a stop to the parent problem, which is methamphetamine,” Dr. Zhao said. “We’re at the beginning, even though the rise has been pretty dramatic. The worst is yet to come.”
Under the radar
Methamphetamine-associated HF has been a growing problem for many years but has largely been “flying under the radar” because HF hospitalization data focus on Medicare-age patients, not the overwhelmingly younger meth-HF population, the report notes.
“We have to get this message out. Many of my patients with meth heart failure had no idea this would happen to them. They didn’t know,” Dr. Zhao said. “Once I tell them that this is what methamphetamines will do to you after years and years of use, they say they wish someone had told them.”
Dr. Zhao and colleagues looked at HF admission data collected by California’s Health and Human Services Agency to assess meth-HF trends and disease burden. They identified 1,033,076 HF hospitalizations during the decade, of which 42,565 (4.12%) were for meth-HF.
Patients hospitalized with meth-HF had a mean age of 49.6 years, compared with 72.2 for the other patients admitted with HF (P < .001). Virtually all of the patients hospitalized for meth-HF were younger than 65 years: 94.5%, compared with 30% for the other HF patients (P < .001).
Hospitalized patients with meth-HF were mostly men, their prevalence of 80% contrasting with 52.4% for patients with non–meth-related HF (P < .001).
Rates of hospitalization for meth-HF steadily increased during the study period. The age-adjusted rate of meth-HF hospitalization per 100,000 rose from 4.1 in 2008 to 28.1 in 2018. The rate of hospitalization for HF unrelated to meth actually declined, going from 342.3 in 2008 to 321.6 in 2018.
Charges for hospitalizations related to meth-HF shot up more than eight times, from $41.5 million in 2008 to $390.2 million in 2018. In contrast, charges for other HF hospitalizations rose by only 82%, from $3.5 billion to $6.3 billion.
Multiple layers of prevention
Dr. Zhao proposed ways that clinicians can communicate with their patients who are using or considering to use meth. “There are multiple layers of prevention. For people who are thinking of using meth, they need to get the message that something really bad can happen to them years down the road. They’re not going to die from it overnight, but it will damage the heart slowly,” she said.
The next layer of prevention can potentially help meth users who have not yet developed heart problems, Dr. Zhao said. “This would be the time to say, ‘you’re so lucky, your heart is still good. It’s time to stop because people like you, a few years from now are going to die prematurely from a very horrible, very suffering kind of death’.”
Importantly, in meth users who have already developed HF, even then it may not be too late to reverse the cardiomyopathy and symptoms. For up to a third of people with established meth-HF, “if they stop using meth, if they take good cardiac medications, and if the heart failure is in an early enough course, their heart can entirely revert to normal,” Dr. Zhao said, citing an earlier work from her and her colleagues.
Currently, methamphetamine abuse has taken especially strong root in rural areas in California and the Midwest. But Dr. Zhao predicts it will soon become prevalent throughout the United States.
Spotlight on an ‘epidemic’
The rapid growth of the methamphetamine “epidemic” has been well-documented in the United States and around the world, observed an accompanying editorial from Pavan Reddy, MD, Icahn School of Medicine at Mount Sinai Morningside, New York, and Uri Elkayam, MD, University of Southern California, Los Angeles.
They contend that more attention has been given to opioid overdose deaths; meth abuse does not seem to command the same attention, likely because meth is not as strongly associated with acute overdose.
But meth, wrote Dr. Reddy and Dr. Elkayam, “is a different drug with its own M.O., equally dangerous and costly to society but more insidious in nature, its effects potentially causing decades of mental and physical debilitation before ending in premature death.”
The current study “has turned a spotlight on a public health crisis that has grown unfettered for over 2 decades,” and is a call for the “medical community to recognize and manage cases of meth-HF with a comprehensive approach that addresses both mental and physical illness,” they concluded. “Only then can we hope to properly help these patients and with that, reduce the socioeconomic burden of meth-HF.”
A quietly building crisis
The sharp rise in meth-HF hospitalizations is an expected reflection of the methamphetamine crisis, which has been quietly building over the last few years, addiction psychiatrist Corneliu N. Stanciu, MD, Dartmouth-Hitchcock Medical Center, Lebanon, N.H., said in an interview.
“This new version of methamphetamines looks like ice and is more potent and toxic than former versions traditionally made in home-built labs,” he said. Lately the vast majority of methamphetamines in the United States have come from Mexico, are less expensive with higher purity, “and can be manufactured in greater quantities.”
Some patients with opioid use disorder (OUD) also inject methamphetamines, which can make OUD treatment clinics good places to screen for meth abuse and educate about its cardiovascular implications, Dr. Stanciu said.
“Just as addiction treatment centers present an opportunity to implement cardiac screening and referrals,” he said, “cardiology visits and hospitalizations such as those for meth-HF also present a golden opportunity for involvement of substance use disorder interventions and referrals to get patients into treatment and prevent further damage through ongoing use.”
Dr. Zhao, Dr. Reddy, Dr. Eklayam, and Dr. Stanciu report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Rates of heart failure (HF) caused by methamphetamine abuse are climbing quickly in the western United States, at great financial and societal cost, suggests an analysis that documents the trends in California over a recent decade.
In the new study, methamphetamine-associated HF (meth-HF) admissions in the state rose by 585% between 2008 and 2018, and charges related those hospitalizations jumped 840%. Cases of HF unrelated to meth fell by 6% during the same period.
The recent explosion in meth-HF hospitalizations has also been costly for society in general, because most cases are younger adults in their most productive, prime earning years, Susan X. Zhao, MD, Santa Clara Valley Medical Center, San Jose, Calif., said in an interview.
“Over the past 11 years, especially since 2018, it has really started to take off, with a pretty dramatic rise. And it happened without much attention, because when we think about drugs, we think about acute overdose and not so much about the chronic, smoldering, long-term effects,” said Dr. Zhao, who is lead author on the study published July 13, 2021, in Circulation: Cardiovascular Quality and Outcomes.
“It’s really affecting a section of the population that is not supposed to be having heart failure problems. I think it is going to continue for the next decade until we put a stop to the parent problem, which is methamphetamine,” Dr. Zhao said. “We’re at the beginning, even though the rise has been pretty dramatic. The worst is yet to come.”
Under the radar
Methamphetamine-associated HF has been a growing problem for many years but has largely been “flying under the radar” because HF hospitalization data focus on Medicare-age patients, not the overwhelmingly younger meth-HF population, the report notes.
“We have to get this message out. Many of my patients with meth heart failure had no idea this would happen to them. They didn’t know,” Dr. Zhao said. “Once I tell them that this is what methamphetamines will do to you after years and years of use, they say they wish someone had told them.”
Dr. Zhao and colleagues looked at HF admission data collected by California’s Health and Human Services Agency to assess meth-HF trends and disease burden. They identified 1,033,076 HF hospitalizations during the decade, of which 42,565 (4.12%) were for meth-HF.
Patients hospitalized with meth-HF had a mean age of 49.6 years, compared with 72.2 for the other patients admitted with HF (P < .001). Virtually all of the patients hospitalized for meth-HF were younger than 65 years: 94.5%, compared with 30% for the other HF patients (P < .001).
Hospitalized patients with meth-HF were mostly men, their prevalence of 80% contrasting with 52.4% for patients with non–meth-related HF (P < .001).
Rates of hospitalization for meth-HF steadily increased during the study period. The age-adjusted rate of meth-HF hospitalization per 100,000 rose from 4.1 in 2008 to 28.1 in 2018. The rate of hospitalization for HF unrelated to meth actually declined, going from 342.3 in 2008 to 321.6 in 2018.
Charges for hospitalizations related to meth-HF shot up more than eight times, from $41.5 million in 2008 to $390.2 million in 2018. In contrast, charges for other HF hospitalizations rose by only 82%, from $3.5 billion to $6.3 billion.
Multiple layers of prevention
Dr. Zhao proposed ways that clinicians can communicate with their patients who are using or considering to use meth. “There are multiple layers of prevention. For people who are thinking of using meth, they need to get the message that something really bad can happen to them years down the road. They’re not going to die from it overnight, but it will damage the heart slowly,” she said.
The next layer of prevention can potentially help meth users who have not yet developed heart problems, Dr. Zhao said. “This would be the time to say, ‘you’re so lucky, your heart is still good. It’s time to stop because people like you, a few years from now are going to die prematurely from a very horrible, very suffering kind of death’.”
Importantly, in meth users who have already developed HF, even then it may not be too late to reverse the cardiomyopathy and symptoms. For up to a third of people with established meth-HF, “if they stop using meth, if they take good cardiac medications, and if the heart failure is in an early enough course, their heart can entirely revert to normal,” Dr. Zhao said, citing an earlier work from her and her colleagues.
Currently, methamphetamine abuse has taken especially strong root in rural areas in California and the Midwest. But Dr. Zhao predicts it will soon become prevalent throughout the United States.
Spotlight on an ‘epidemic’
The rapid growth of the methamphetamine “epidemic” has been well-documented in the United States and around the world, observed an accompanying editorial from Pavan Reddy, MD, Icahn School of Medicine at Mount Sinai Morningside, New York, and Uri Elkayam, MD, University of Southern California, Los Angeles.
They contend that more attention has been given to opioid overdose deaths; meth abuse does not seem to command the same attention, likely because meth is not as strongly associated with acute overdose.
But meth, wrote Dr. Reddy and Dr. Elkayam, “is a different drug with its own M.O., equally dangerous and costly to society but more insidious in nature, its effects potentially causing decades of mental and physical debilitation before ending in premature death.”
The current study “has turned a spotlight on a public health crisis that has grown unfettered for over 2 decades,” and is a call for the “medical community to recognize and manage cases of meth-HF with a comprehensive approach that addresses both mental and physical illness,” they concluded. “Only then can we hope to properly help these patients and with that, reduce the socioeconomic burden of meth-HF.”
A quietly building crisis
The sharp rise in meth-HF hospitalizations is an expected reflection of the methamphetamine crisis, which has been quietly building over the last few years, addiction psychiatrist Corneliu N. Stanciu, MD, Dartmouth-Hitchcock Medical Center, Lebanon, N.H., said in an interview.
“This new version of methamphetamines looks like ice and is more potent and toxic than former versions traditionally made in home-built labs,” he said. Lately the vast majority of methamphetamines in the United States have come from Mexico, are less expensive with higher purity, “and can be manufactured in greater quantities.”
Some patients with opioid use disorder (OUD) also inject methamphetamines, which can make OUD treatment clinics good places to screen for meth abuse and educate about its cardiovascular implications, Dr. Stanciu said.
“Just as addiction treatment centers present an opportunity to implement cardiac screening and referrals,” he said, “cardiology visits and hospitalizations such as those for meth-HF also present a golden opportunity for involvement of substance use disorder interventions and referrals to get patients into treatment and prevent further damage through ongoing use.”
Dr. Zhao, Dr. Reddy, Dr. Eklayam, and Dr. Stanciu report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Dapagliflozin safe, protective in advanced kidney disease
Patients with stage 4 chronic kidney disease (CKD) who were in the DAPA-CKD trial had cardiorenal benefits from dapagliflozin that were similar to those of patients in the overall trial, with no added safety signal.

DAPA-CKD (Dapagliflozin and Prevention of Adverse Outcomes in Chronic Kidney Disease) was a landmark study of more than 4,000 patients with CKD, with an estimated glomerular filtration rate (eGFR) of 25-75 mL/min per 1.73 m2 and albuminuria with/without type 2 diabetes.
The primary results showed that patients who received the sodium-glucose cotransporter 2 (SGLT2) inhibitor dapagliflozin for a median of 2.4 years were significantly less likely to have worsening kidney disease or die from all causes than were patients who received placebo.
“This prespecified subanalysis of people with an eGFR < 30 mL/min/1.73 m2 [stage 4 CKD] in the DAPA-CKD study shows first, that in this very vulnerable population, use of the SGLT2 inhibitor is safe,” said Chantal Mathieu, MD, PhD.
Furthermore, there was no signal whatsoever of more adverse events and even a trend to fewer events, she said in an email to this news organization.
The analysis also showed that “although now in small numbers (around 300 each in the treated group vs. placebo group), there is no suggestion that the protective effect of dapagliflozin on the renal and cardiovascular front would not happen in this group” with advanced CKD. The efficacy findings just missed statistical significance, noted Dr. Mathieu, of Catholic University, Leuven, Belgium, who was not involved in the study.
Although dapagliflozin is now approved for treating patients with CKD who are at risk of kidney disease progression (on the basis of the DAPA-CKD results), guidelines have not yet been updated to reflect this, lead investigator Glenn M. Chertow, MD, MPH, of Stanford (Calif.) University, told this news organization in an email.

“For clinicians,” Dr. Mathieu said, “this is now the absolute reassurance that we do not have to stop an SGLT2 inhibitor in people with eGFR < 30 mL/min for safety reasons and that we should maintain them at these values for renal and cardiovascular protection!
“I absolutely hope labels will change soon to reflect these observations (and indeed movement on that front is happening),” she continued.
“The American Diabetes Association/European Association for the Study of Diabetes consensus on glucose-lowering therapies in type 2 diabetes already advocated keeping these agents until eGFR 30 mL/min (on the basis of evidence in 2019),” Dr. Mathieu added, “but this study will probably push the statements even further.”
“Of note,” she pointed out, “at these low eGFRs, the glucose-lowering potential of the SGLT2 inhibitor is negligible.”
Dapagliflozin risks and benefits in advanced CKD
Based on the DAPA-CKD study, published in the New England Journal of Medicine Oct. 8, 2020, the Food and Drug Administration expanded the indication for dapagliflozin (Farxiga, AstraZeneca) in April of 2021.
However, relatively little is known about the safety and efficacy of SGLT2 inhibitors in patients with advanced CKD, who are particularly vulnerable to cardiovascular events and progressive kidney failure, Dr. Chertow and colleagues wrote.
The DAPA-CKD trial randomized 4,304 patients with CKD 1:1 to dapagliflozin 10 mg/day or placebo, including 624 patients (14%) who had eGFR < 30 mL/min per 1.73 m2 and albuminuria at baseline.
Patients in the subgroup with advanced CKD had a mean age of 62 years, and 37% were female. About two-thirds had type 2 diabetes and about one-third had cardiovascular disease.
A total of 293 patients received dapagliflozin and 331 patients received placebo.
During a median follow-up of 2.4 years, patients who received dapagliflozin as opposed to placebo had a lower risk of the primary efficacy outcome – a composite of a 50% or greater sustained decline in eGFR, end-stage kidney disease, or death from cardiovascular or renal causes (hazard ratio, 0.73; 95% confidence interval, 0.53-1.02).
In secondary efficacy outcomes, patients who received dapagliflozin as opposed to placebo also had a lower risk of the following:
- A renal composite outcome – a ≥ 50% sustained decline in eGFR, end-stage kidney disease, or death from renal causes (HR, 0.71; 95% CI, 0.49-1.02).
- A cardiovascular composite outcome comprising cardiovascular death or hospitalization for heart failure (HR, 0.83; 95% CI, 0.45-1.53).
- All-cause mortality (HR, 0.68; 95% CI, 0.39 to 1.21).
The eGFR slope declined by 2.15 mL/min per 1.73 m2 per year and by 3.38 mL/min per 1.73 m2 per year in the dapagliflozin and placebo groups, respectively (P = .005).
“The trial was not powered to detect a statistically significant difference in the primary and key secondary endpoints in modest-sized subgroups,” the researchers noted.
The researchers limited their safety analysis to serious adverse events or symptoms of volume depletion, kidney-related events, major hypoglycemia, bone fractures, amputations, and potential diabetic ketoacidosis.
There was no evidence of increased risk of these adverse events in patients who received dapagliflozin.
The subanalysis of the DAPA-CKD trial was published July 16 in the Journal of the American Society of Nephrology.
The study was funded by AstraZeneca. Dr. Chertow has received fees from AstraZeneca for the DAPA-CKD trial steering committee. The disclosures of the other authors are listed in the article. Dr. Mathieu has served on the advisory panel/speakers bureau for AstraZeneca. Dr. Chertow and Dr. Mathieu also have financial relationships with many other pharmaceutical companies.
Patients with stage 4 chronic kidney disease (CKD) who were in the DAPA-CKD trial had cardiorenal benefits from dapagliflozin that were similar to those of patients in the overall trial, with no added safety signal.
DAPA-CKD (Dapagliflozin and Prevention of Adverse Outcomes in Chronic Kidney Disease) was a landmark study of more than 4,000 patients with CKD, with an estimated glomerular filtration rate (eGFR) of 25-75 mL/min per 1.73 m2 and albuminuria with/without type 2 diabetes.
The primary results showed that patients who received the sodium-glucose cotransporter 2 (SGLT2) inhibitor dapagliflozin for a median of 2.4 years were significantly less likely to have worsening kidney disease or die from all causes than were patients who received placebo.
“This prespecified subanalysis of people with an eGFR < 30 mL/min/1.73 m2 [stage 4 CKD] in the DAPA-CKD study shows first, that in this very vulnerable population, use of the SGLT2 inhibitor is safe,” said Chantal Mathieu, MD, PhD.
Furthermore, there was no signal whatsoever of more adverse events and even a trend to fewer events, she said in an email to this news organization.
The analysis also showed that “although now in small numbers (around 300 each in the treated group vs. placebo group), there is no suggestion that the protective effect of dapagliflozin on the renal and cardiovascular front would not happen in this group” with advanced CKD. The efficacy findings just missed statistical significance, noted Dr. Mathieu, of Catholic University, Leuven, Belgium, who was not involved in the study.
Although dapagliflozin is now approved for treating patients with CKD who are at risk of kidney disease progression (on the basis of the DAPA-CKD results), guidelines have not yet been updated to reflect this, lead investigator Glenn M. Chertow, MD, MPH, of Stanford (Calif.) University, told this news organization in an email.
“For clinicians,” Dr. Mathieu said, “this is now the absolute reassurance that we do not have to stop an SGLT2 inhibitor in people with eGFR < 30 mL/min for safety reasons and that we should maintain them at these values for renal and cardiovascular protection!
“I absolutely hope labels will change soon to reflect these observations (and indeed movement on that front is happening),” she continued.
“The American Diabetes Association/European Association for the Study of Diabetes consensus on glucose-lowering therapies in type 2 diabetes already advocated keeping these agents until eGFR 30 mL/min (on the basis of evidence in 2019),” Dr. Mathieu added, “but this study will probably push the statements even further.”
“Of note,” she pointed out, “at these low eGFRs, the glucose-lowering potential of the SGLT2 inhibitor is negligible.”
Dapagliflozin risks and benefits in advanced CKD
Based on the DAPA-CKD study, published in the New England Journal of Medicine Oct. 8, 2020, the Food and Drug Administration expanded the indication for dapagliflozin (Farxiga, AstraZeneca) in April of 2021.
However, relatively little is known about the safety and efficacy of SGLT2 inhibitors in patients with advanced CKD, who are particularly vulnerable to cardiovascular events and progressive kidney failure, Dr. Chertow and colleagues wrote.
The DAPA-CKD trial randomized 4,304 patients with CKD 1:1 to dapagliflozin 10 mg/day or placebo, including 624 patients (14%) who had eGFR < 30 mL/min per 1.73 m2 and albuminuria at baseline.
Patients in the subgroup with advanced CKD had a mean age of 62 years, and 37% were female. About two-thirds had type 2 diabetes and about one-third had cardiovascular disease.
A total of 293 patients received dapagliflozin and 331 patients received placebo.
During a median follow-up of 2.4 years, patients who received dapagliflozin as opposed to placebo had a lower risk of the primary efficacy outcome – a composite of a 50% or greater sustained decline in eGFR, end-stage kidney disease, or death from cardiovascular or renal causes (hazard ratio, 0.73; 95% confidence interval, 0.53-1.02).
In secondary efficacy outcomes, patients who received dapagliflozin as opposed to placebo also had a lower risk of the following:
- A renal composite outcome – a ≥ 50% sustained decline in eGFR, end-stage kidney disease, or death from renal causes (HR, 0.71; 95% CI, 0.49-1.02).
- A cardiovascular composite outcome comprising cardiovascular death or hospitalization for heart failure (HR, 0.83; 95% CI, 0.45-1.53).
- All-cause mortality (HR, 0.68; 95% CI, 0.39 to 1.21).
The eGFR slope declined by 2.15 mL/min per 1.73 m2 per year and by 3.38 mL/min per 1.73 m2 per year in the dapagliflozin and placebo groups, respectively (P = .005).
“The trial was not powered to detect a statistically significant difference in the primary and key secondary endpoints in modest-sized subgroups,” the researchers noted.
The researchers limited their safety analysis to serious adverse events or symptoms of volume depletion, kidney-related events, major hypoglycemia, bone fractures, amputations, and potential diabetic ketoacidosis.
There was no evidence of increased risk of these adverse events in patients who received dapagliflozin.
The subanalysis of the DAPA-CKD trial was published July 16 in the Journal of the American Society of Nephrology.
The study was funded by AstraZeneca. Dr. Chertow has received fees from AstraZeneca for the DAPA-CKD trial steering committee. The disclosures of the other authors are listed in the article. Dr. Mathieu has served on the advisory panel/speakers bureau for AstraZeneca. Dr. Chertow and Dr. Mathieu also have financial relationships with many other pharmaceutical companies.
Patients with stage 4 chronic kidney disease (CKD) who were in the DAPA-CKD trial had cardiorenal benefits from dapagliflozin that were similar to those of patients in the overall trial, with no added safety signal.
DAPA-CKD (Dapagliflozin and Prevention of Adverse Outcomes in Chronic Kidney Disease) was a landmark study of more than 4,000 patients with CKD, with an estimated glomerular filtration rate (eGFR) of 25-75 mL/min per 1.73 m2 and albuminuria with/without type 2 diabetes.
The primary results showed that patients who received the sodium-glucose cotransporter 2 (SGLT2) inhibitor dapagliflozin for a median of 2.4 years were significantly less likely to have worsening kidney disease or die from all causes than were patients who received placebo.
“This prespecified subanalysis of people with an eGFR < 30 mL/min/1.73 m2 [stage 4 CKD] in the DAPA-CKD study shows first, that in this very vulnerable population, use of the SGLT2 inhibitor is safe,” said Chantal Mathieu, MD, PhD.
Furthermore, there was no signal whatsoever of more adverse events and even a trend to fewer events, she said in an email to this news organization.
The analysis also showed that “although now in small numbers (around 300 each in the treated group vs. placebo group), there is no suggestion that the protective effect of dapagliflozin on the renal and cardiovascular front would not happen in this group” with advanced CKD. The efficacy findings just missed statistical significance, noted Dr. Mathieu, of Catholic University, Leuven, Belgium, who was not involved in the study.
Although dapagliflozin is now approved for treating patients with CKD who are at risk of kidney disease progression (on the basis of the DAPA-CKD results), guidelines have not yet been updated to reflect this, lead investigator Glenn M. Chertow, MD, MPH, of Stanford (Calif.) University, told this news organization in an email.
“For clinicians,” Dr. Mathieu said, “this is now the absolute reassurance that we do not have to stop an SGLT2 inhibitor in people with eGFR < 30 mL/min for safety reasons and that we should maintain them at these values for renal and cardiovascular protection!
“I absolutely hope labels will change soon to reflect these observations (and indeed movement on that front is happening),” she continued.
“The American Diabetes Association/European Association for the Study of Diabetes consensus on glucose-lowering therapies in type 2 diabetes already advocated keeping these agents until eGFR 30 mL/min (on the basis of evidence in 2019),” Dr. Mathieu added, “but this study will probably push the statements even further.”
“Of note,” she pointed out, “at these low eGFRs, the glucose-lowering potential of the SGLT2 inhibitor is negligible.”
Dapagliflozin risks and benefits in advanced CKD
Based on the DAPA-CKD study, published in the New England Journal of Medicine Oct. 8, 2020, the Food and Drug Administration expanded the indication for dapagliflozin (Farxiga, AstraZeneca) in April of 2021.
However, relatively little is known about the safety and efficacy of SGLT2 inhibitors in patients with advanced CKD, who are particularly vulnerable to cardiovascular events and progressive kidney failure, Dr. Chertow and colleagues wrote.
The DAPA-CKD trial randomized 4,304 patients with CKD 1:1 to dapagliflozin 10 mg/day or placebo, including 624 patients (14%) who had eGFR < 30 mL/min per 1.73 m2 and albuminuria at baseline.
Patients in the subgroup with advanced CKD had a mean age of 62 years, and 37% were female. About two-thirds had type 2 diabetes and about one-third had cardiovascular disease.
A total of 293 patients received dapagliflozin and 331 patients received placebo.
During a median follow-up of 2.4 years, patients who received dapagliflozin as opposed to placebo had a lower risk of the primary efficacy outcome – a composite of a 50% or greater sustained decline in eGFR, end-stage kidney disease, or death from cardiovascular or renal causes (hazard ratio, 0.73; 95% confidence interval, 0.53-1.02).
In secondary efficacy outcomes, patients who received dapagliflozin as opposed to placebo also had a lower risk of the following:
- A renal composite outcome – a ≥ 50% sustained decline in eGFR, end-stage kidney disease, or death from renal causes (HR, 0.71; 95% CI, 0.49-1.02).
- A cardiovascular composite outcome comprising cardiovascular death or hospitalization for heart failure (HR, 0.83; 95% CI, 0.45-1.53).
- All-cause mortality (HR, 0.68; 95% CI, 0.39 to 1.21).
The eGFR slope declined by 2.15 mL/min per 1.73 m2 per year and by 3.38 mL/min per 1.73 m2 per year in the dapagliflozin and placebo groups, respectively (P = .005).
“The trial was not powered to detect a statistically significant difference in the primary and key secondary endpoints in modest-sized subgroups,” the researchers noted.
The researchers limited their safety analysis to serious adverse events or symptoms of volume depletion, kidney-related events, major hypoglycemia, bone fractures, amputations, and potential diabetic ketoacidosis.
There was no evidence of increased risk of these adverse events in patients who received dapagliflozin.
The subanalysis of the DAPA-CKD trial was published July 16 in the Journal of the American Society of Nephrology.
The study was funded by AstraZeneca. Dr. Chertow has received fees from AstraZeneca for the DAPA-CKD trial steering committee. The disclosures of the other authors are listed in the article. Dr. Mathieu has served on the advisory panel/speakers bureau for AstraZeneca. Dr. Chertow and Dr. Mathieu also have financial relationships with many other pharmaceutical companies.
FROM THE JOURNAL OF THE AMERICAN SOCIETY OF NEPHROLOGY
Cycling linked to longer life in people with type 2 diabetes
Bicycle riding may help people with diabetes live longer, new research suggests.

Among more than 7,000 adults with diabetes in 10 Western European countries followed for about 15 years, those who cycled regularly were significantly less likely to die of any cause or of cardiovascular causes, even after accounting for differences in factors such as sex, age, educational level, diet, comorbidities, and other physical activities.
“The association between cycling and all-cause and CVD [cardiovascular disease] mortality in this study of person[s] with diabetes was of the same magnitude and direction as observed in the healthy population,” wrote Mathias Ried-Larsen, PhD, of the Centre for Physical Activity Research, Rigshospitalet, Copenhagen, and colleagues. The findings were published online July 19, 2021, in JAMA Internal Medicine.
In an accompanying Editor’s Note, JAMA Internal Medicine editor Rita F. Redberg, MD, and two deputy editors said that the new data add to previous studies showing benefits of cycling, compared with other physical activities. “The analysis from Ried-Larsen and colleagues strengthens the epidemiologic data on cycling and strongly suggests that it may contribute directly to longer and healthier lives,” they wrote.
Dr. Redberg, of the University of California, San Francisco, told this news organization: “I think the number of cyclists grew greatly during pandemic, when there was little auto traffic, and people did not want to take public transportation. Cities that add bike lanes, especially protected bike lanes, see an increase in cyclists. I think Americans can cycle more, would enjoy cycling more, and would live longer [by] cycling, to work and for pleasure.”
Dr. Redberg disclosed that she is “an avid cyclist and am currently on a bike ride in Glacier National Park. ... This group [Climate Ride] raises money for more bike lanes, promotes climate change awareness, has paid for solar panels at Glacier, and more.”
However, Dr. Redberg and colleagues also “recognize that cycling requires fitness, a good sense of balance, and the means to purchase a bicycle. We also understand that regular cycling requires living in an area where it is reasonably safe, and we celebrate the installation of more bike lanes, particularly protected lanes, in many cities around the world.”
But, despite the limitations of an observational study and possible selection bias of people who are able to cycle, “it is important to share this evidence for the potentially large health benefits of cycling, which almost surely generalize to persons without diabetes.”
Cycling tied to lower all-cause and CVD mortality
The prospective cohort study included 7,459 adults with diabetes from the European Prospective Investigation into Cancer and Nutrition. All were assessed during 1992-1998 and again in 1996-2011, with a mean follow-up of roughly 15 years. During that time, there were 1,673 deaths from all causes, with 811 attributed to CVD.
Compared with no cycling, those who reported any cycling had a 24% lower risk of death from any cause over a 5-year period, after adjustment for confounders and for other physical activity. The greatest risk reduction was seen in those who reported cycling between 150-299 minutes per week, particularly in CVD mortality.
In a subanalysis of 5,423 individuals with 10.7 years of follow-up, there were 975 all-cause deaths and 429 from CVD. Individuals who began or continued cycling during follow-up experienced reductions of about 35% for both all-cause and CVD mortality, compared with those who never cycled.
Dr. Redberg and colleagues added that “there are environmental benefits to increasing the use of cycling for commuting and other transport because cycling helps to decrease the adverse environmental and health effects of automobile exhaust.”
They concluded: “As avid and/or aspiring cyclists ourselves, we are sold on the mental and physical benefits of getting to work and seeing the world on two wheels, self-propelled, and think it is well worth a try.”
The study work was supported by the Health Research Fund of Instituto de Salud Carlos III; the Spanish regional governments of Andalucía, Asturias, Basque Country, Murcia, and Navarra; and the Catalan Institute of Oncology. The Centre for Physical Activity Research is supported by a grant from TrygFonden. Dr. Ried-Larsen reported personal fees from Novo Nordisk. Dr. Redberg reported receiving grants from Arnold Ventures; the Greenwall Foundation; and the National Heart, Lung, and Blood Institute.
Bicycle riding may help people with diabetes live longer, new research suggests.
Among more than 7,000 adults with diabetes in 10 Western European countries followed for about 15 years, those who cycled regularly were significantly less likely to die of any cause or of cardiovascular causes, even after accounting for differences in factors such as sex, age, educational level, diet, comorbidities, and other physical activities.
“The association between cycling and all-cause and CVD [cardiovascular disease] mortality in this study of person[s] with diabetes was of the same magnitude and direction as observed in the healthy population,” wrote Mathias Ried-Larsen, PhD, of the Centre for Physical Activity Research, Rigshospitalet, Copenhagen, and colleagues. The findings were published online July 19, 2021, in JAMA Internal Medicine.
In an accompanying Editor’s Note, JAMA Internal Medicine editor Rita F. Redberg, MD, and two deputy editors said that the new data add to previous studies showing benefits of cycling, compared with other physical activities. “The analysis from Ried-Larsen and colleagues strengthens the epidemiologic data on cycling and strongly suggests that it may contribute directly to longer and healthier lives,” they wrote.
Dr. Redberg, of the University of California, San Francisco, told this news organization: “I think the number of cyclists grew greatly during pandemic, when there was little auto traffic, and people did not want to take public transportation. Cities that add bike lanes, especially protected bike lanes, see an increase in cyclists. I think Americans can cycle more, would enjoy cycling more, and would live longer [by] cycling, to work and for pleasure.”
Dr. Redberg disclosed that she is “an avid cyclist and am currently on a bike ride in Glacier National Park. ... This group [Climate Ride] raises money for more bike lanes, promotes climate change awareness, has paid for solar panels at Glacier, and more.”
However, Dr. Redberg and colleagues also “recognize that cycling requires fitness, a good sense of balance, and the means to purchase a bicycle. We also understand that regular cycling requires living in an area where it is reasonably safe, and we celebrate the installation of more bike lanes, particularly protected lanes, in many cities around the world.”
But, despite the limitations of an observational study and possible selection bias of people who are able to cycle, “it is important to share this evidence for the potentially large health benefits of cycling, which almost surely generalize to persons without diabetes.”
Cycling tied to lower all-cause and CVD mortality
The prospective cohort study included 7,459 adults with diabetes from the European Prospective Investigation into Cancer and Nutrition. All were assessed during 1992-1998 and again in 1996-2011, with a mean follow-up of roughly 15 years. During that time, there were 1,673 deaths from all causes, with 811 attributed to CVD.
Compared with no cycling, those who reported any cycling had a 24% lower risk of death from any cause over a 5-year period, after adjustment for confounders and for other physical activity. The greatest risk reduction was seen in those who reported cycling between 150-299 minutes per week, particularly in CVD mortality.
In a subanalysis of 5,423 individuals with 10.7 years of follow-up, there were 975 all-cause deaths and 429 from CVD. Individuals who began or continued cycling during follow-up experienced reductions of about 35% for both all-cause and CVD mortality, compared with those who never cycled.
Dr. Redberg and colleagues added that “there are environmental benefits to increasing the use of cycling for commuting and other transport because cycling helps to decrease the adverse environmental and health effects of automobile exhaust.”
They concluded: “As avid and/or aspiring cyclists ourselves, we are sold on the mental and physical benefits of getting to work and seeing the world on two wheels, self-propelled, and think it is well worth a try.”
The study work was supported by the Health Research Fund of Instituto de Salud Carlos III; the Spanish regional governments of Andalucía, Asturias, Basque Country, Murcia, and Navarra; and the Catalan Institute of Oncology. The Centre for Physical Activity Research is supported by a grant from TrygFonden. Dr. Ried-Larsen reported personal fees from Novo Nordisk. Dr. Redberg reported receiving grants from Arnold Ventures; the Greenwall Foundation; and the National Heart, Lung, and Blood Institute.
Bicycle riding may help people with diabetes live longer, new research suggests.
Among more than 7,000 adults with diabetes in 10 Western European countries followed for about 15 years, those who cycled regularly were significantly less likely to die of any cause or of cardiovascular causes, even after accounting for differences in factors such as sex, age, educational level, diet, comorbidities, and other physical activities.
“The association between cycling and all-cause and CVD [cardiovascular disease] mortality in this study of person[s] with diabetes was of the same magnitude and direction as observed in the healthy population,” wrote Mathias Ried-Larsen, PhD, of the Centre for Physical Activity Research, Rigshospitalet, Copenhagen, and colleagues. The findings were published online July 19, 2021, in JAMA Internal Medicine.
In an accompanying Editor’s Note, JAMA Internal Medicine editor Rita F. Redberg, MD, and two deputy editors said that the new data add to previous studies showing benefits of cycling, compared with other physical activities. “The analysis from Ried-Larsen and colleagues strengthens the epidemiologic data on cycling and strongly suggests that it may contribute directly to longer and healthier lives,” they wrote.
Dr. Redberg, of the University of California, San Francisco, told this news organization: “I think the number of cyclists grew greatly during pandemic, when there was little auto traffic, and people did not want to take public transportation. Cities that add bike lanes, especially protected bike lanes, see an increase in cyclists. I think Americans can cycle more, would enjoy cycling more, and would live longer [by] cycling, to work and for pleasure.”
Dr. Redberg disclosed that she is “an avid cyclist and am currently on a bike ride in Glacier National Park. ... This group [Climate Ride] raises money for more bike lanes, promotes climate change awareness, has paid for solar panels at Glacier, and more.”
However, Dr. Redberg and colleagues also “recognize that cycling requires fitness, a good sense of balance, and the means to purchase a bicycle. We also understand that regular cycling requires living in an area where it is reasonably safe, and we celebrate the installation of more bike lanes, particularly protected lanes, in many cities around the world.”
But, despite the limitations of an observational study and possible selection bias of people who are able to cycle, “it is important to share this evidence for the potentially large health benefits of cycling, which almost surely generalize to persons without diabetes.”
Cycling tied to lower all-cause and CVD mortality
The prospective cohort study included 7,459 adults with diabetes from the European Prospective Investigation into Cancer and Nutrition. All were assessed during 1992-1998 and again in 1996-2011, with a mean follow-up of roughly 15 years. During that time, there were 1,673 deaths from all causes, with 811 attributed to CVD.
Compared with no cycling, those who reported any cycling had a 24% lower risk of death from any cause over a 5-year period, after adjustment for confounders and for other physical activity. The greatest risk reduction was seen in those who reported cycling between 150-299 minutes per week, particularly in CVD mortality.
In a subanalysis of 5,423 individuals with 10.7 years of follow-up, there were 975 all-cause deaths and 429 from CVD. Individuals who began or continued cycling during follow-up experienced reductions of about 35% for both all-cause and CVD mortality, compared with those who never cycled.
Dr. Redberg and colleagues added that “there are environmental benefits to increasing the use of cycling for commuting and other transport because cycling helps to decrease the adverse environmental and health effects of automobile exhaust.”
They concluded: “As avid and/or aspiring cyclists ourselves, we are sold on the mental and physical benefits of getting to work and seeing the world on two wheels, self-propelled, and think it is well worth a try.”
The study work was supported by the Health Research Fund of Instituto de Salud Carlos III; the Spanish regional governments of Andalucía, Asturias, Basque Country, Murcia, and Navarra; and the Catalan Institute of Oncology. The Centre for Physical Activity Research is supported by a grant from TrygFonden. Dr. Ried-Larsen reported personal fees from Novo Nordisk. Dr. Redberg reported receiving grants from Arnold Ventures; the Greenwall Foundation; and the National Heart, Lung, and Blood Institute.
FROM JAMA INTERNAL MEDICINE
St. Jude to pay $27 million to end DOJ suit over faulty ICDs
St. Jude Medical, now part of Abbott Laboratories, will pay the American government $27 million to settle allegations that it knowingly sold defective implantable cardiac defibrillators to health care facilities, which were implanted into patients, causing injuries and two deaths, the U.S. Department of Justice (DOJ) has announced.
“Medical device manufacturers have an obligation to be truthful with the Food and Drug Administration, and the U.S. government will not pay for devices that are unsafe and risk injury or death,” Jonathan F. Lenzner, Acting U.S. Attorney for the District of Maryland, said in a July 8 statement.
“The government contends that St. Jude knowingly caused the submission of false claims and failed to inform the FDA with critical information about prior injuries and a death which, had the FDA been made aware, would have led to a recall,” Mr. Lenzner added.
Those claims were submitted to the Medicare, TRICARE, and Federal Employees Health Benefits programs, according to the settlement agreement.
“The U.S. Attorney’s Office is committed to protecting Medicare and other federal health care programs from fraud, and in doing so, strengthen[ing] patient safety,” Mr. Lenzner said.
Premature battery depletion
The government alleges that St. Jude failed to disclose “serious adverse health events” related to premature battery depletion of certain models of its Fortify, Fortify Assura, Quadra, and Unify implantable defibrillators.
The government further alleges that, by 2013, St. Jude knew that lithium clusters could form on the batteries, causing them to short and run out of power. But it took until late 2014 for St. Jude to ask the FDA to approve a change to prevent lithium clusters from draining the battery.
And at this point, St. Jude told the FDA that “no serious injury, permanent harm, or deaths have been reported associated with this” issue, the government alleges.
However, according to the government’s allegations, St. Jude was aware at that time of two reported serious injuries and one death associated with the faulty batteries and continued to distribute devices that had been manufactured without the new design.
Not until August 2016 did St. Jude inform the FDA that the number of premature battery depletion events had increased to 729, including two deaths and 29 events associated with loss of pacing, the government alleges.
In October 2016, St. Jude issued a medical advisory regarding the battery problem, which the FDA classified as a Class I recall, the most serious type.
After the recall, St. Jude no longer sold the older devices, but thousands of them had been implanted into patients between November 2014 and October 2016.
In September 2017, as reported by this news organization, a nationwide class-action lawsuit was filed against St. Jude Medical and parent company Abbott Laboratories alleging that, despite knowing about a battery-depletion defect in some of its cardiac defibrillators as early as 2011, St. Jude failed to adequately report the risk and waited nearly 5 years before issuing a recall.
“To ensure the health and safety of patients, manufacturers of implantable cardiac devices must be transparent when communicating with the government about safety issues and incidents,” Acting Assistant Attorney General Brian Boynton, from the DOJ’s Civil Division, said in the DOJ statement announcing the settlement.
“We will hold accountable those companies whose conduct violates the law and puts patients’ health at risk,” Mr. Boynton said.
The civil settlement includes the resolution of claims brought under the qui tam, or whistleblower, provisions of the False Claims Act by Debbie Burke, a patient who received one of the devices that was subject to recall.
The claims resolved by the settlement are allegations only; there has been no determination of liability, the DOJ noted. St. Jude denies the allegations raised in the lawsuit.
A version of this article first appeared on Medscape.com.
St. Jude Medical, now part of Abbott Laboratories, will pay the American government $27 million to settle allegations that it knowingly sold defective implantable cardiac defibrillators to health care facilities, which were implanted into patients, causing injuries and two deaths, the U.S. Department of Justice (DOJ) has announced.
“Medical device manufacturers have an obligation to be truthful with the Food and Drug Administration, and the U.S. government will not pay for devices that are unsafe and risk injury or death,” Jonathan F. Lenzner, Acting U.S. Attorney for the District of Maryland, said in a July 8 statement.
“The government contends that St. Jude knowingly caused the submission of false claims and failed to inform the FDA with critical information about prior injuries and a death which, had the FDA been made aware, would have led to a recall,” Mr. Lenzner added.
Those claims were submitted to the Medicare, TRICARE, and Federal Employees Health Benefits programs, according to the settlement agreement.
“The U.S. Attorney’s Office is committed to protecting Medicare and other federal health care programs from fraud, and in doing so, strengthen[ing] patient safety,” Mr. Lenzner said.
Premature battery depletion
The government alleges that St. Jude failed to disclose “serious adverse health events” related to premature battery depletion of certain models of its Fortify, Fortify Assura, Quadra, and Unify implantable defibrillators.
The government further alleges that, by 2013, St. Jude knew that lithium clusters could form on the batteries, causing them to short and run out of power. But it took until late 2014 for St. Jude to ask the FDA to approve a change to prevent lithium clusters from draining the battery.
And at this point, St. Jude told the FDA that “no serious injury, permanent harm, or deaths have been reported associated with this” issue, the government alleges.
However, according to the government’s allegations, St. Jude was aware at that time of two reported serious injuries and one death associated with the faulty batteries and continued to distribute devices that had been manufactured without the new design.
Not until August 2016 did St. Jude inform the FDA that the number of premature battery depletion events had increased to 729, including two deaths and 29 events associated with loss of pacing, the government alleges.
In October 2016, St. Jude issued a medical advisory regarding the battery problem, which the FDA classified as a Class I recall, the most serious type.
After the recall, St. Jude no longer sold the older devices, but thousands of them had been implanted into patients between November 2014 and October 2016.
In September 2017, as reported by this news organization, a nationwide class-action lawsuit was filed against St. Jude Medical and parent company Abbott Laboratories alleging that, despite knowing about a battery-depletion defect in some of its cardiac defibrillators as early as 2011, St. Jude failed to adequately report the risk and waited nearly 5 years before issuing a recall.
“To ensure the health and safety of patients, manufacturers of implantable cardiac devices must be transparent when communicating with the government about safety issues and incidents,” Acting Assistant Attorney General Brian Boynton, from the DOJ’s Civil Division, said in the DOJ statement announcing the settlement.
“We will hold accountable those companies whose conduct violates the law and puts patients’ health at risk,” Mr. Boynton said.
The civil settlement includes the resolution of claims brought under the qui tam, or whistleblower, provisions of the False Claims Act by Debbie Burke, a patient who received one of the devices that was subject to recall.
The claims resolved by the settlement are allegations only; there has been no determination of liability, the DOJ noted. St. Jude denies the allegations raised in the lawsuit.
A version of this article first appeared on Medscape.com.
St. Jude Medical, now part of Abbott Laboratories, will pay the American government $27 million to settle allegations that it knowingly sold defective implantable cardiac defibrillators to health care facilities, which were implanted into patients, causing injuries and two deaths, the U.S. Department of Justice (DOJ) has announced.
“Medical device manufacturers have an obligation to be truthful with the Food and Drug Administration, and the U.S. government will not pay for devices that are unsafe and risk injury or death,” Jonathan F. Lenzner, Acting U.S. Attorney for the District of Maryland, said in a July 8 statement.
“The government contends that St. Jude knowingly caused the submission of false claims and failed to inform the FDA with critical information about prior injuries and a death which, had the FDA been made aware, would have led to a recall,” Mr. Lenzner added.
Those claims were submitted to the Medicare, TRICARE, and Federal Employees Health Benefits programs, according to the settlement agreement.
“The U.S. Attorney’s Office is committed to protecting Medicare and other federal health care programs from fraud, and in doing so, strengthen[ing] patient safety,” Mr. Lenzner said.
Premature battery depletion
The government alleges that St. Jude failed to disclose “serious adverse health events” related to premature battery depletion of certain models of its Fortify, Fortify Assura, Quadra, and Unify implantable defibrillators.
The government further alleges that, by 2013, St. Jude knew that lithium clusters could form on the batteries, causing them to short and run out of power. But it took until late 2014 for St. Jude to ask the FDA to approve a change to prevent lithium clusters from draining the battery.
And at this point, St. Jude told the FDA that “no serious injury, permanent harm, or deaths have been reported associated with this” issue, the government alleges.
However, according to the government’s allegations, St. Jude was aware at that time of two reported serious injuries and one death associated with the faulty batteries and continued to distribute devices that had been manufactured without the new design.
Not until August 2016 did St. Jude inform the FDA that the number of premature battery depletion events had increased to 729, including two deaths and 29 events associated with loss of pacing, the government alleges.
In October 2016, St. Jude issued a medical advisory regarding the battery problem, which the FDA classified as a Class I recall, the most serious type.
After the recall, St. Jude no longer sold the older devices, but thousands of them had been implanted into patients between November 2014 and October 2016.
In September 2017, as reported by this news organization, a nationwide class-action lawsuit was filed against St. Jude Medical and parent company Abbott Laboratories alleging that, despite knowing about a battery-depletion defect in some of its cardiac defibrillators as early as 2011, St. Jude failed to adequately report the risk and waited nearly 5 years before issuing a recall.
“To ensure the health and safety of patients, manufacturers of implantable cardiac devices must be transparent when communicating with the government about safety issues and incidents,” Acting Assistant Attorney General Brian Boynton, from the DOJ’s Civil Division, said in the DOJ statement announcing the settlement.
“We will hold accountable those companies whose conduct violates the law and puts patients’ health at risk,” Mr. Boynton said.
The civil settlement includes the resolution of claims brought under the qui tam, or whistleblower, provisions of the False Claims Act by Debbie Burke, a patient who received one of the devices that was subject to recall.
The claims resolved by the settlement are allegations only; there has been no determination of liability, the DOJ noted. St. Jude denies the allegations raised in the lawsuit.
A version of this article first appeared on Medscape.com.
Meta-analysis supports cardiovascular benefits of EPA
Support for a cardiovascular benefit of omega-3 fatty acids, particularly eicosapentaenoic acid (EPA), has come from a new systematic review and meta-analysis of randomized trials.

The meta-analysis of 38 randomized controlled trials found that omega-3 fatty acids improved cardiovascular outcomes, with a greater reduction in cardiovascular risk in studies of EPA alone rather than of combined eicosapentaenoic plus docosahexaenoic acid (DHA) supplements.
The paper was published online in EClinicalMedicine.
Senior author Deepak Bhatt, MD, Brigham and Women’s Hospital, Boston, was also lead investigator of the REDUCE-IT trial, which is included in the analysis and showed a 25% relative risk reduction in major cardiovascular events with a high-dose EPA product.
But the REDUCE-IT trial has been mired in controversy, with suggestions that the benefit seen might have been exaggerated because of the use of a harmful placebo. In addition, a second large trial of high-dose omega-3 fatty acids, STRENGTH (which tested a combination EPA/DHA product) showed no benefit on cardiovascular outcomes.
Dr. Bhatt said the new meta-analysis provides “a totality of evidence” that “supports a robust and consistent benefit of EPA.”
In the review, the authors concluded: “In this systematic review and meta-analysis, we noted moderate certainty of evidence favoring omega-3 fatty acids for reducing cardiovascular mortality and outcomes. ... The magnitude of relative reductions was robust in EPA trials versus those of EPA+DHA, suggesting differential effects of EPA and DHA in cardiovascular risk reduction.”
Controversy continues
But commenting on the publication for an interview, Steven Nissen, MD, Cleveland Clinic, who led the STRENGTH trial, pointed out that 85% of the EPA data in the new meta-analysis came from REDUCE-IT, so the results were a “foregone conclusion.”

“The purpose of a meta-analysis is to answer scientific questions when existing studies are too small to yield statistically robust results. That is not the case here,” Dr. Nissen stated.
He added: “There are only two major trials of EPA and both have important flaws. REDUCE-IT used a questionable placebo (mineral oil) and JELIS was an open-label trial that studied patients with baseline LDL [cholesterol] of 180 mg/dL that was not appropriately treated. A meta-analysis is only as good as the studies that it includes. The other EPA plus DHA studies were essentially neutral.”
Dr. Bhatt responded that, “to date, every randomized trial of EPA only has been positive. Some have been placebo controlled, some have been open label. This meta-analysis corroborates the results of each of those trials in a statistically robust way.”
He added: “Of course, REDUCE-IT is the most rigorous, contemporary trial of EPA. However, in our meta-analysis, even when excluding REDUCE-IT (or for that matter, JELIS), the EPA trials still significantly reduced cardiovascular events.”
Dr. Bhatt also pointed out that two randomized imaging studies, CHERRY and EVAPORATE, have shown benefits of EPA.
“Beyond the clinical trial data, there is a growing amount of evidence supporting the unique biological actions of different omega-3 fatty acids. EPA, in particular, appears to have the strongest basic science evidence supporting cardiovascular benefits. Overall, it is a remarkably consistent scientific story in support of EPA’s beneficial effects on cardiovascular health,” he stated.
38 trials included
For the current paper, Dr. Bhatt and coauthors performed a comprehensive literature search for randomized trials comparing omega-3 fatty acids with control (placebo, no supplementation, or lower dose of omega-3 fatty acids) in adults, with a follow-up of at least 12 months, and mortality and cardiovascular outcomes as endpoints.
Ultimately, 38 trials encompassing 149,051 patients were included. Of these, four trials compared EPA with control, 34 trials compared EPA+DHA with control, and 22 trials were in primary prevention. The dose of omega-3 fatty acids ranged from 0.4 g/day to 5.5 g/day.
A total of 25 trials with 143,514 individuals reported 5,550 events of cardiovascular mortality, and 24 trials with 140,983 individuals reported 10,795 events of all-cause mortality.
Omega-3 fatty acids were associated with reduced cardiovascular mortality (rate ratio, 0.93; P = .01), but not all-cause mortality (RR, 0.97; P = .27). The meta-analysis showed reduction in cardiovascular mortality with EPA monotherapy (RR, 0.82; P = .04) and EPA+DHA combination (RR, 0.94; P = .02).
A total of 20 trials with 125,611 individuals reported 2,989 nonfatal myocardial infarction events, and 29 trials with 144,384 individuals reported 9,153 coronary heart disease (CHD) events.
Omega-3 fatty acids were associated with reducing nonfatal MI (RR, 0.87; P = .0001) and CHD (RR, 0.91; P = .0002). The meta-analysis showed higher risk reductions in nonfatal MI with EPA monotherapy (RR, 0.72; P = .00002) than with EPA+DHA combination (RR, 0.92; P = .05), and also for CHD events with EPA monotherapy (RR, 0.73; P = .00004) than with EPA+DHA combination (RR, 0.94; P = .01).
A total of 17 trials (n = 135,019) reported 13,234 events of MACE, and 13 trials (n = 117,890) reported 7,416 events of revascularization.
Omega-3 fatty acids were associated with reducing MACE (RR, 0.95; P = .002) and revascularization (RR, 0.91; P = .0001). The meta-analysis showed higher risk reductions in MACE with EPA monotherapy (RR, 0.78; P = .00000001), whereas EPA+DHA combination did not reduce MACE (RR, 0.99; P = .48). This effect was consistent for revascularization.
A total of eight trials with 65,404 individuals reported 935 nonfatal strokes, and eight trials with 51,336 individuals reported 1,572 events of atrial fibrillation (AFib).
Omega-3 fatty acids did not significantly reduce nonfatal stroke (RR, 1.04; P = .55), but EPA monotherapy was associated with a reduction of nonfatal stroke, compared with control (RR: 0.71; P = .01).
Conversely, omega-3 fatty acids were associated with increased risk for AFib (RR, 1.26; P = .004), with a higher risk with EPA monotherapy than with control (RR, 1.35; P = .004).
Overall, omega-3 fatty acids did not prevent sudden cardiac death or increase gastrointestinal-related adverse events, total bleeding, or major or minor bleeding; however, the meta-analysis showed a higher risk of total bleeding with EPA monotherapy than with control (RR, 1.49; P = .006).
An influence analysis with stepwise exclusion of one trial at a time, including REDUCE-IT, did not alter the overall summary estimates. “Despite the exclusion of REDUCE-IT, EPA monotherapy reduced MACE by 23%, compared with the control,” the authors reported.
They said these new findings also have important implications for clinical practice and treatment guidelines.
“After REDUCE-IT, several national and international guidelines endorsed EPA in their therapeutic recommendations. However, the publication of two recent negative trials of EPA + DHA has created some confusion in the scientific community about the value of omega-3 FAs in preventing atherosclerotic cardiovascular disease [ASCVD],” they stated.
“This meta-analysis provides reassurance about the role of omega-3 fatty acids, specifically EPA, in the current treatment framework of ASCVD residual cardiovascular risk reduction and encourages investigators to explore further the cardiovascular effects of EPA across different clinical settings,” they added.
REDUCE-IT was sponsored by Amarin. Brigham and Women’s Hospital receives research funding from Amarin for the work Dr. Bhatt did as the trial chair and as the international principal investigator. The present analysis was unfunded.
A version of this article first appeared on Medscape.com.
Support for a cardiovascular benefit of omega-3 fatty acids, particularly eicosapentaenoic acid (EPA), has come from a new systematic review and meta-analysis of randomized trials.
The meta-analysis of 38 randomized controlled trials found that omega-3 fatty acids improved cardiovascular outcomes, with a greater reduction in cardiovascular risk in studies of EPA alone rather than of combined eicosapentaenoic plus docosahexaenoic acid (DHA) supplements.
The paper was published online in EClinicalMedicine.
Senior author Deepak Bhatt, MD, Brigham and Women’s Hospital, Boston, was also lead investigator of the REDUCE-IT trial, which is included in the analysis and showed a 25% relative risk reduction in major cardiovascular events with a high-dose EPA product.
But the REDUCE-IT trial has been mired in controversy, with suggestions that the benefit seen might have been exaggerated because of the use of a harmful placebo. In addition, a second large trial of high-dose omega-3 fatty acids, STRENGTH (which tested a combination EPA/DHA product) showed no benefit on cardiovascular outcomes.
Dr. Bhatt said the new meta-analysis provides “a totality of evidence” that “supports a robust and consistent benefit of EPA.”
In the review, the authors concluded: “In this systematic review and meta-analysis, we noted moderate certainty of evidence favoring omega-3 fatty acids for reducing cardiovascular mortality and outcomes. ... The magnitude of relative reductions was robust in EPA trials versus those of EPA+DHA, suggesting differential effects of EPA and DHA in cardiovascular risk reduction.”
Controversy continues
But commenting on the publication for an interview, Steven Nissen, MD, Cleveland Clinic, who led the STRENGTH trial, pointed out that 85% of the EPA data in the new meta-analysis came from REDUCE-IT, so the results were a “foregone conclusion.”
“The purpose of a meta-analysis is to answer scientific questions when existing studies are too small to yield statistically robust results. That is not the case here,” Dr. Nissen stated.
He added: “There are only two major trials of EPA and both have important flaws. REDUCE-IT used a questionable placebo (mineral oil) and JELIS was an open-label trial that studied patients with baseline LDL [cholesterol] of 180 mg/dL that was not appropriately treated. A meta-analysis is only as good as the studies that it includes. The other EPA plus DHA studies were essentially neutral.”
Dr. Bhatt responded that, “to date, every randomized trial of EPA only has been positive. Some have been placebo controlled, some have been open label. This meta-analysis corroborates the results of each of those trials in a statistically robust way.”
He added: “Of course, REDUCE-IT is the most rigorous, contemporary trial of EPA. However, in our meta-analysis, even when excluding REDUCE-IT (or for that matter, JELIS), the EPA trials still significantly reduced cardiovascular events.”
Dr. Bhatt also pointed out that two randomized imaging studies, CHERRY and EVAPORATE, have shown benefits of EPA.
“Beyond the clinical trial data, there is a growing amount of evidence supporting the unique biological actions of different omega-3 fatty acids. EPA, in particular, appears to have the strongest basic science evidence supporting cardiovascular benefits. Overall, it is a remarkably consistent scientific story in support of EPA’s beneficial effects on cardiovascular health,” he stated.
38 trials included
For the current paper, Dr. Bhatt and coauthors performed a comprehensive literature search for randomized trials comparing omega-3 fatty acids with control (placebo, no supplementation, or lower dose of omega-3 fatty acids) in adults, with a follow-up of at least 12 months, and mortality and cardiovascular outcomes as endpoints.
Ultimately, 38 trials encompassing 149,051 patients were included. Of these, four trials compared EPA with control, 34 trials compared EPA+DHA with control, and 22 trials were in primary prevention. The dose of omega-3 fatty acids ranged from 0.4 g/day to 5.5 g/day.
A total of 25 trials with 143,514 individuals reported 5,550 events of cardiovascular mortality, and 24 trials with 140,983 individuals reported 10,795 events of all-cause mortality.
Omega-3 fatty acids were associated with reduced cardiovascular mortality (rate ratio, 0.93; P = .01), but not all-cause mortality (RR, 0.97; P = .27). The meta-analysis showed reduction in cardiovascular mortality with EPA monotherapy (RR, 0.82; P = .04) and EPA+DHA combination (RR, 0.94; P = .02).
A total of 20 trials with 125,611 individuals reported 2,989 nonfatal myocardial infarction events, and 29 trials with 144,384 individuals reported 9,153 coronary heart disease (CHD) events.
Omega-3 fatty acids were associated with reducing nonfatal MI (RR, 0.87; P = .0001) and CHD (RR, 0.91; P = .0002). The meta-analysis showed higher risk reductions in nonfatal MI with EPA monotherapy (RR, 0.72; P = .00002) than with EPA+DHA combination (RR, 0.92; P = .05), and also for CHD events with EPA monotherapy (RR, 0.73; P = .00004) than with EPA+DHA combination (RR, 0.94; P = .01).
A total of 17 trials (n = 135,019) reported 13,234 events of MACE, and 13 trials (n = 117,890) reported 7,416 events of revascularization.
Omega-3 fatty acids were associated with reducing MACE (RR, 0.95; P = .002) and revascularization (RR, 0.91; P = .0001). The meta-analysis showed higher risk reductions in MACE with EPA monotherapy (RR, 0.78; P = .00000001), whereas EPA+DHA combination did not reduce MACE (RR, 0.99; P = .48). This effect was consistent for revascularization.
A total of eight trials with 65,404 individuals reported 935 nonfatal strokes, and eight trials with 51,336 individuals reported 1,572 events of atrial fibrillation (AFib).
Omega-3 fatty acids did not significantly reduce nonfatal stroke (RR, 1.04; P = .55), but EPA monotherapy was associated with a reduction of nonfatal stroke, compared with control (RR: 0.71; P = .01).
Conversely, omega-3 fatty acids were associated with increased risk for AFib (RR, 1.26; P = .004), with a higher risk with EPA monotherapy than with control (RR, 1.35; P = .004).
Overall, omega-3 fatty acids did not prevent sudden cardiac death or increase gastrointestinal-related adverse events, total bleeding, or major or minor bleeding; however, the meta-analysis showed a higher risk of total bleeding with EPA monotherapy than with control (RR, 1.49; P = .006).
An influence analysis with stepwise exclusion of one trial at a time, including REDUCE-IT, did not alter the overall summary estimates. “Despite the exclusion of REDUCE-IT, EPA monotherapy reduced MACE by 23%, compared with the control,” the authors reported.
They said these new findings also have important implications for clinical practice and treatment guidelines.
“After REDUCE-IT, several national and international guidelines endorsed EPA in their therapeutic recommendations. However, the publication of two recent negative trials of EPA + DHA has created some confusion in the scientific community about the value of omega-3 FAs in preventing atherosclerotic cardiovascular disease [ASCVD],” they stated.
“This meta-analysis provides reassurance about the role of omega-3 fatty acids, specifically EPA, in the current treatment framework of ASCVD residual cardiovascular risk reduction and encourages investigators to explore further the cardiovascular effects of EPA across different clinical settings,” they added.
REDUCE-IT was sponsored by Amarin. Brigham and Women’s Hospital receives research funding from Amarin for the work Dr. Bhatt did as the trial chair and as the international principal investigator. The present analysis was unfunded.
A version of this article first appeared on Medscape.com.
Support for a cardiovascular benefit of omega-3 fatty acids, particularly eicosapentaenoic acid (EPA), has come from a new systematic review and meta-analysis of randomized trials.
The meta-analysis of 38 randomized controlled trials found that omega-3 fatty acids improved cardiovascular outcomes, with a greater reduction in cardiovascular risk in studies of EPA alone rather than of combined eicosapentaenoic plus docosahexaenoic acid (DHA) supplements.
The paper was published online in EClinicalMedicine.
Senior author Deepak Bhatt, MD, Brigham and Women’s Hospital, Boston, was also lead investigator of the REDUCE-IT trial, which is included in the analysis and showed a 25% relative risk reduction in major cardiovascular events with a high-dose EPA product.
But the REDUCE-IT trial has been mired in controversy, with suggestions that the benefit seen might have been exaggerated because of the use of a harmful placebo. In addition, a second large trial of high-dose omega-3 fatty acids, STRENGTH (which tested a combination EPA/DHA product) showed no benefit on cardiovascular outcomes.
Dr. Bhatt said the new meta-analysis provides “a totality of evidence” that “supports a robust and consistent benefit of EPA.”
In the review, the authors concluded: “In this systematic review and meta-analysis, we noted moderate certainty of evidence favoring omega-3 fatty acids for reducing cardiovascular mortality and outcomes. ... The magnitude of relative reductions was robust in EPA trials versus those of EPA+DHA, suggesting differential effects of EPA and DHA in cardiovascular risk reduction.”
Controversy continues
But commenting on the publication for an interview, Steven Nissen, MD, Cleveland Clinic, who led the STRENGTH trial, pointed out that 85% of the EPA data in the new meta-analysis came from REDUCE-IT, so the results were a “foregone conclusion.”
“The purpose of a meta-analysis is to answer scientific questions when existing studies are too small to yield statistically robust results. That is not the case here,” Dr. Nissen stated.
He added: “There are only two major trials of EPA and both have important flaws. REDUCE-IT used a questionable placebo (mineral oil) and JELIS was an open-label trial that studied patients with baseline LDL [cholesterol] of 180 mg/dL that was not appropriately treated. A meta-analysis is only as good as the studies that it includes. The other EPA plus DHA studies were essentially neutral.”
Dr. Bhatt responded that, “to date, every randomized trial of EPA only has been positive. Some have been placebo controlled, some have been open label. This meta-analysis corroborates the results of each of those trials in a statistically robust way.”
He added: “Of course, REDUCE-IT is the most rigorous, contemporary trial of EPA. However, in our meta-analysis, even when excluding REDUCE-IT (or for that matter, JELIS), the EPA trials still significantly reduced cardiovascular events.”
Dr. Bhatt also pointed out that two randomized imaging studies, CHERRY and EVAPORATE, have shown benefits of EPA.
“Beyond the clinical trial data, there is a growing amount of evidence supporting the unique biological actions of different omega-3 fatty acids. EPA, in particular, appears to have the strongest basic science evidence supporting cardiovascular benefits. Overall, it is a remarkably consistent scientific story in support of EPA’s beneficial effects on cardiovascular health,” he stated.
38 trials included
For the current paper, Dr. Bhatt and coauthors performed a comprehensive literature search for randomized trials comparing omega-3 fatty acids with control (placebo, no supplementation, or lower dose of omega-3 fatty acids) in adults, with a follow-up of at least 12 months, and mortality and cardiovascular outcomes as endpoints.
Ultimately, 38 trials encompassing 149,051 patients were included. Of these, four trials compared EPA with control, 34 trials compared EPA+DHA with control, and 22 trials were in primary prevention. The dose of omega-3 fatty acids ranged from 0.4 g/day to 5.5 g/day.
A total of 25 trials with 143,514 individuals reported 5,550 events of cardiovascular mortality, and 24 trials with 140,983 individuals reported 10,795 events of all-cause mortality.
Omega-3 fatty acids were associated with reduced cardiovascular mortality (rate ratio, 0.93; P = .01), but not all-cause mortality (RR, 0.97; P = .27). The meta-analysis showed reduction in cardiovascular mortality with EPA monotherapy (RR, 0.82; P = .04) and EPA+DHA combination (RR, 0.94; P = .02).
A total of 20 trials with 125,611 individuals reported 2,989 nonfatal myocardial infarction events, and 29 trials with 144,384 individuals reported 9,153 coronary heart disease (CHD) events.
Omega-3 fatty acids were associated with reducing nonfatal MI (RR, 0.87; P = .0001) and CHD (RR, 0.91; P = .0002). The meta-analysis showed higher risk reductions in nonfatal MI with EPA monotherapy (RR, 0.72; P = .00002) than with EPA+DHA combination (RR, 0.92; P = .05), and also for CHD events with EPA monotherapy (RR, 0.73; P = .00004) than with EPA+DHA combination (RR, 0.94; P = .01).
A total of 17 trials (n = 135,019) reported 13,234 events of MACE, and 13 trials (n = 117,890) reported 7,416 events of revascularization.
Omega-3 fatty acids were associated with reducing MACE (RR, 0.95; P = .002) and revascularization (RR, 0.91; P = .0001). The meta-analysis showed higher risk reductions in MACE with EPA monotherapy (RR, 0.78; P = .00000001), whereas EPA+DHA combination did not reduce MACE (RR, 0.99; P = .48). This effect was consistent for revascularization.
A total of eight trials with 65,404 individuals reported 935 nonfatal strokes, and eight trials with 51,336 individuals reported 1,572 events of atrial fibrillation (AFib).
Omega-3 fatty acids did not significantly reduce nonfatal stroke (RR, 1.04; P = .55), but EPA monotherapy was associated with a reduction of nonfatal stroke, compared with control (RR: 0.71; P = .01).
Conversely, omega-3 fatty acids were associated with increased risk for AFib (RR, 1.26; P = .004), with a higher risk with EPA monotherapy than with control (RR, 1.35; P = .004).
Overall, omega-3 fatty acids did not prevent sudden cardiac death or increase gastrointestinal-related adverse events, total bleeding, or major or minor bleeding; however, the meta-analysis showed a higher risk of total bleeding with EPA monotherapy than with control (RR, 1.49; P = .006).
An influence analysis with stepwise exclusion of one trial at a time, including REDUCE-IT, did not alter the overall summary estimates. “Despite the exclusion of REDUCE-IT, EPA monotherapy reduced MACE by 23%, compared with the control,” the authors reported.
They said these new findings also have important implications for clinical practice and treatment guidelines.
“After REDUCE-IT, several national and international guidelines endorsed EPA in their therapeutic recommendations. However, the publication of two recent negative trials of EPA + DHA has created some confusion in the scientific community about the value of omega-3 FAs in preventing atherosclerotic cardiovascular disease [ASCVD],” they stated.
“This meta-analysis provides reassurance about the role of omega-3 fatty acids, specifically EPA, in the current treatment framework of ASCVD residual cardiovascular risk reduction and encourages investigators to explore further the cardiovascular effects of EPA across different clinical settings,” they added.
REDUCE-IT was sponsored by Amarin. Brigham and Women’s Hospital receives research funding from Amarin for the work Dr. Bhatt did as the trial chair and as the international principal investigator. The present analysis was unfunded.
A version of this article first appeared on Medscape.com.

Heart failure med undertreatment because of older age common, flouts evidence
, suggests a large cohort study.
About 80% of patients aged 80 years or older were prescribed renin-angiotensin-system inhibitors (RASi) in a multivariate-adjusted analysis of more than 27,000 patients in the Swedish Heart Failure Registry (SwedeHF). In contrast, such drugs – which included angiotensin receptor-neprilysin inhibitors (ARNi), angiotensin receptor blockers, and ACE inhibitors – were prescribed to 95% of patients younger than 70 years.
Similarly, fewer of the oldest patients were offered meds from the two other drug classes core to HF management at the time: Beta blockers and mineralocorticoid receptor antagonists (MRA).
And among those in the 80-and-older age group who were prescribed RASi or beta blockers, their uptitration more often fell short of even half the target dosage, compared with the youngest patients in the analysis.
Physicians may hold back on full guideline-directed medical therapy in their very elderly patients with HFrEF for many reasons, including a perceived likelihood of drug intolerance due to frailty or multiple comorbidities, including renal dysfunction, Davide Stolfo, MD, Karolinska Institutet, Stockholm, and University of Trieste, Italy, told this news organization.
But the current analysis was adjusted for about 80 variables “that in our interpretation may be main reasons for not introducing drugs and using them in the older patients,” he said. They included care setting (that is, inpatient or outpatient), HF severity by several measures, a range of comorbidities, renal dysfunction, and history of serious illness such as cancer.
Even then, age emerged as a significant, independent predictor of medical therapy underuse in the oldest patients. Some physicians apparently see advanced age, by itself, as an “intrinsic reason” not to abide by HFrEF medical therapy recommendations, said Dr. Stolfo, who presented the analysis at HFA 2021, the annual meeting of the Heart Failure Association of the European Society of Cardiology (ESC-HFA), conducted both virtually and live in Florence, Italy.
Most major HF-drug trials have excluded or admitted few patients aged 80 years or older, but “the guidelines recommend treatment regardless of age, and in the trials there has been no influence from age on the effectiveness of drugs,” Dr. Stolfo observed.
Moreover, in a prior SwedeHF analysis with propensity matching, patients with HFrEF aged 80 or older showed steeper reductions in risk for death or HF hospitalization from treatment with RASi than those in younger age groups.
One of the few randomized trials to focus on the very elderly, called SENIORS, enrolled patients aged 70 years and older – the average age was 76 – and saw a significantly reduced risk of death or cardiovascular hospitalization for those assigned to the beta blocker nebivolol. The benefits in the trial, which was conducted 15 years ago, were independent of left ventricular function.
So in the oldest patients, “we could question the need to achieve full dose of an evidence-based drug, but we shouldn’t question the use of these drugs.”
The findings are consistent with a need to individualize medical therapy in senior patients with HFrEF, especially those of more advanced age, some of whom may be robust enough to be managed similarly to younger patients while others who may be less suitable for full guideline-directed medical therapy, Dr. Stolfo said.
Even for those who are more frail or have major comorbidities, drug therapy of HFrEF continues to be important for symptom control even if competing causes of death make it harder to prolong survival, Dr. Stolfo said.
“We should provide to all patients the best strategy they can tolerate,” he said. “If we cannot greatly impact on the long-term survival for these patients, treatment can be aimed to improve the quality of life and keep the patient out of the hospital.”
The analysis was supported by Boehringer Ingelheim. Dr. Stolfo disclosed personal fees from Novartis, Merck, GlaxoSmithKline, and Acceleron.
A version of this article first appeared on Medscape.com.
, suggests a large cohort study.
About 80% of patients aged 80 years or older were prescribed renin-angiotensin-system inhibitors (RASi) in a multivariate-adjusted analysis of more than 27,000 patients in the Swedish Heart Failure Registry (SwedeHF). In contrast, such drugs – which included angiotensin receptor-neprilysin inhibitors (ARNi), angiotensin receptor blockers, and ACE inhibitors – were prescribed to 95% of patients younger than 70 years.
Similarly, fewer of the oldest patients were offered meds from the two other drug classes core to HF management at the time: Beta blockers and mineralocorticoid receptor antagonists (MRA).
And among those in the 80-and-older age group who were prescribed RASi or beta blockers, their uptitration more often fell short of even half the target dosage, compared with the youngest patients in the analysis.
Physicians may hold back on full guideline-directed medical therapy in their very elderly patients with HFrEF for many reasons, including a perceived likelihood of drug intolerance due to frailty or multiple comorbidities, including renal dysfunction, Davide Stolfo, MD, Karolinska Institutet, Stockholm, and University of Trieste, Italy, told this news organization.
But the current analysis was adjusted for about 80 variables “that in our interpretation may be main reasons for not introducing drugs and using them in the older patients,” he said. They included care setting (that is, inpatient or outpatient), HF severity by several measures, a range of comorbidities, renal dysfunction, and history of serious illness such as cancer.
Even then, age emerged as a significant, independent predictor of medical therapy underuse in the oldest patients. Some physicians apparently see advanced age, by itself, as an “intrinsic reason” not to abide by HFrEF medical therapy recommendations, said Dr. Stolfo, who presented the analysis at HFA 2021, the annual meeting of the Heart Failure Association of the European Society of Cardiology (ESC-HFA), conducted both virtually and live in Florence, Italy.
Most major HF-drug trials have excluded or admitted few patients aged 80 years or older, but “the guidelines recommend treatment regardless of age, and in the trials there has been no influence from age on the effectiveness of drugs,” Dr. Stolfo observed.
Moreover, in a prior SwedeHF analysis with propensity matching, patients with HFrEF aged 80 or older showed steeper reductions in risk for death or HF hospitalization from treatment with RASi than those in younger age groups.
One of the few randomized trials to focus on the very elderly, called SENIORS, enrolled patients aged 70 years and older – the average age was 76 – and saw a significantly reduced risk of death or cardiovascular hospitalization for those assigned to the beta blocker nebivolol. The benefits in the trial, which was conducted 15 years ago, were independent of left ventricular function.
So in the oldest patients, “we could question the need to achieve full dose of an evidence-based drug, but we shouldn’t question the use of these drugs.”
The findings are consistent with a need to individualize medical therapy in senior patients with HFrEF, especially those of more advanced age, some of whom may be robust enough to be managed similarly to younger patients while others who may be less suitable for full guideline-directed medical therapy, Dr. Stolfo said.
Even for those who are more frail or have major comorbidities, drug therapy of HFrEF continues to be important for symptom control even if competing causes of death make it harder to prolong survival, Dr. Stolfo said.
“We should provide to all patients the best strategy they can tolerate,” he said. “If we cannot greatly impact on the long-term survival for these patients, treatment can be aimed to improve the quality of life and keep the patient out of the hospital.”
The analysis was supported by Boehringer Ingelheim. Dr. Stolfo disclosed personal fees from Novartis, Merck, GlaxoSmithKline, and Acceleron.
A version of this article first appeared on Medscape.com.
, suggests a large cohort study.
About 80% of patients aged 80 years or older were prescribed renin-angiotensin-system inhibitors (RASi) in a multivariate-adjusted analysis of more than 27,000 patients in the Swedish Heart Failure Registry (SwedeHF). In contrast, such drugs – which included angiotensin receptor-neprilysin inhibitors (ARNi), angiotensin receptor blockers, and ACE inhibitors – were prescribed to 95% of patients younger than 70 years.
Similarly, fewer of the oldest patients were offered meds from the two other drug classes core to HF management at the time: Beta blockers and mineralocorticoid receptor antagonists (MRA).
And among those in the 80-and-older age group who were prescribed RASi or beta blockers, their uptitration more often fell short of even half the target dosage, compared with the youngest patients in the analysis.
Physicians may hold back on full guideline-directed medical therapy in their very elderly patients with HFrEF for many reasons, including a perceived likelihood of drug intolerance due to frailty or multiple comorbidities, including renal dysfunction, Davide Stolfo, MD, Karolinska Institutet, Stockholm, and University of Trieste, Italy, told this news organization.
But the current analysis was adjusted for about 80 variables “that in our interpretation may be main reasons for not introducing drugs and using them in the older patients,” he said. They included care setting (that is, inpatient or outpatient), HF severity by several measures, a range of comorbidities, renal dysfunction, and history of serious illness such as cancer.
Even then, age emerged as a significant, independent predictor of medical therapy underuse in the oldest patients. Some physicians apparently see advanced age, by itself, as an “intrinsic reason” not to abide by HFrEF medical therapy recommendations, said Dr. Stolfo, who presented the analysis at HFA 2021, the annual meeting of the Heart Failure Association of the European Society of Cardiology (ESC-HFA), conducted both virtually and live in Florence, Italy.
Most major HF-drug trials have excluded or admitted few patients aged 80 years or older, but “the guidelines recommend treatment regardless of age, and in the trials there has been no influence from age on the effectiveness of drugs,” Dr. Stolfo observed.
Moreover, in a prior SwedeHF analysis with propensity matching, patients with HFrEF aged 80 or older showed steeper reductions in risk for death or HF hospitalization from treatment with RASi than those in younger age groups.
One of the few randomized trials to focus on the very elderly, called SENIORS, enrolled patients aged 70 years and older – the average age was 76 – and saw a significantly reduced risk of death or cardiovascular hospitalization for those assigned to the beta blocker nebivolol. The benefits in the trial, which was conducted 15 years ago, were independent of left ventricular function.
So in the oldest patients, “we could question the need to achieve full dose of an evidence-based drug, but we shouldn’t question the use of these drugs.”
The findings are consistent with a need to individualize medical therapy in senior patients with HFrEF, especially those of more advanced age, some of whom may be robust enough to be managed similarly to younger patients while others who may be less suitable for full guideline-directed medical therapy, Dr. Stolfo said.
Even for those who are more frail or have major comorbidities, drug therapy of HFrEF continues to be important for symptom control even if competing causes of death make it harder to prolong survival, Dr. Stolfo said.
“We should provide to all patients the best strategy they can tolerate,” he said. “If we cannot greatly impact on the long-term survival for these patients, treatment can be aimed to improve the quality of life and keep the patient out of the hospital.”
The analysis was supported by Boehringer Ingelheim. Dr. Stolfo disclosed personal fees from Novartis, Merck, GlaxoSmithKline, and Acceleron.
A version of this article first appeared on Medscape.com.
New details of myocarditis linked to COVID vaccines
Further details from multiple cases of myocarditis linked to the Pfizer and Moderna mRNA COVID vaccines have been described in recent papers in the medical literature.
The cases appear to occur almost exclusively in males and most often in younger age groups. While symptoms and signs of myocarditis mostly resolved with a few days of supportive care, long-term effects are unknown at present.
The authors of all the reports and of two accompanying editorials in JAMA Cardiology are unanimous in their opinion that the benefits of vaccination still outweigh the risks.
The Centers for Disease Control and Prevention’s but committee members delivered a strong endorsement for continuing to vaccinate young people with the mRNA vaccines.
The current case reports are published in two papers in JAMA Cardiology and in three in Circulation.
U.S. military reports 23 cases
In one report in JAMA Cardiology, authors led by Jay Montgomery, MD, from Walter Reed National Military Medical Center in Bethesda, Md., described 23 cases from the U.S. Military Health System of individuals with acute myocarditis who presented within 4 days after mRNA-based COVID-19 vaccination (7 Pfizer and 16 Moderna).
All patients were male, 22 of 23 were on active duty, and the median age was 25 years (range, 20-51); 20 of the 23 cases occurred after receipt of a second dose of an mRNA COVID-19 vaccine.
The patients all presented with acute onset of marked chest pain. All patients had significantly elevated cardiac troponin levels. Among eight patients who underwent cardiac MRI (cMRI), all had findings consistent with the clinical diagnosis of myocarditis.
Additional testing did not identify other possible causes of myocarditis. All patients received brief supportive care and were recovered or recovering.
The authors reported that the military administered more than 2.8 million doses of mRNA COVID-19 vaccine in this period, and while the observed number of myocarditis cases was small, the number was “substantially higher” than expected among male military members after a second vaccine dose.
They noted that, based on historical data, among the 544,000 second doses to military members there may have been 0-10 expected myocarditis cases, but they observed 19 cases.
“All patients in this series reflect substantial similarities in demographic characteristics, proximate vaccine dose, onset interval, and character of vaccine-associated myocarditis. The consistent pattern of clinical presentation, rapid recovery, and absence of evidence of other causes support the diagnosis of hypersensitivity myocarditis,” they stated.
They added that presentation after a second vaccine dose or, in three patients, when vaccination followed SARS-CoV-2 infection, suggests that prior exposure was relevant in the hypersensitivity response.
“The spectrum of clinical presentation and reliance on patients seeking health care and on health care professionals recognizing a rare vaccine-associated adverse event limits determination of the true incidence of this condition,” the authors wrote.
They stressed that recognition of vaccine-associated myocarditis is clinically important because diagnosis impacts management, recommendations for exercise, and monitoring for cardiomyopathy.
But the authors also acknowledged that it is important to frame concerns about potential vaccine-associated myocarditis within the context of the current pandemic.
“Infection with SARS-CoV-2 is a clear cause of serious cardiac injury in many patients. ... Prevalence of cardiac injury may be as high as 60% in seriously ill patients. Notably, nearly 1% of highly fit athletes with mild COVID-19 infection have evidence of myocarditis on cMRI,” they wrote.
“Given that COVID-19 vaccines are remarkably effective at preventing infection, any risk of rare adverse events following immunization must be carefully weighed against the very substantial benefit of vaccination,” they concluded.
Four cases at Duke
In the second paper in JAMA Cardiology, a group led by Han W. Kim, MD, reported four patients with acute myocarditis occurring within days of mRNA COVID-19 vaccination (two Pfizer and two Moderna) in patients treated at Duke University Medical Center, Durham, N.C. The hospital courses of the four patients with myocarditis following COVID-19 vaccination were uneventful, and they were discharged within 2-4 days.
The authors said that, although a causal relationship cannot be established, none of the patients had a viral prodrome or had coincident testing that revealed an alternative explanation.
They stated that these four patients represent the majority of patients with acute myocarditis identified in the past 3 months at their institution, and this led to the highest total number of patients with acute myocarditis, compared with the same 3-month period for the past 5 years.
“Additionally, we identified only those patients with severe unremitting chest pain who sought medical attention. Those with mild or moderate chest pain might not seek medical attention, and it is possible that subclinical myocarditis may occur and could be detected by active surveillance, as has been described with smallpox vaccination,” they wrote.
Further case reports
In one of the papers in Circulation, a group led by Kathryn F. Larson, MD, from the Mayo Clinic in Rochester, Minn., described eight patients hospitalized with chest pain who were diagnosed with myocarditis within 2-4 days of receiving either the Pfizer or Moderna vaccine.
Two of the patients had previously been infected by SARS-CoV-2 without need for hospitalization. All individuals were otherwise healthy males between the ages of 21 and 56 years. All but one patient developed symptoms after their second dose, and the one patient who developed myocarditis after the first vaccine dose had previously been infected with SARS-CoV-2.
Systemic symptoms began within 24 hours after vaccine administration in five of eight patients, with chest pain presenting between 48 and 96 hours later. Troponin values were elevated in all individuals and appeared to peak the day after admission, whereas none had eosinophilia.
Cardiac MRI revealed findings consistent with myocarditis in all patients. All patients had resolution of their chest pain and were discharged from the hospital in stable condition.
“The patients presented here demonstrated typical signs, symptoms, and diagnostic features of acute myocarditis. The temporal association between receiving an mRNA-based COVID-19 vaccine and the development of myocarditis is notable,” the authors said.
They added that they would consider the use of corticosteroids in these patients but cautioned that this could reduce the specific immune response against SARS-COV-2 triggered by the vaccine. “Thus, the duration of corticosteroid administration should be limited to the resolution of the symptoms or ventricular arrhythmias or the recovery of the left ventricular ejection fraction.”
Pending publication of long-term outcome data after SARS-CoV-2 vaccine–related myocarditis, they suggest adherence to the current consensus recommendation to abstain from competitive sports for a period of 3-6 months with reevaluation prior to sports participation.
In another of the Circulation papers, a group led by Carolyn M. Rosner, MSN, presented a case series of seven patients hospitalized for acute myocarditis-like illness following COVID-19 vaccination, from two U.S. medical centers, in Falls Church, Va., and Dallas. All patients were males below the age of 40 years and of White or Hispanic race/ethnicity. Only one patient reported prior history of COVID-19 infection. Six patients received mRNA (Moderna or Pfizer) and one received the adenovirus (Johnson & Johnson) vaccine. All patients presented 3-7 days post vaccination with acute onset chest pain and biochemical evidence of myocardial injury.
Hospital length of stay was 3 days, and all patients’ symptoms resolved by hospital discharge.
And finally, the third paper in Circulation reported a detailed description of one patient – a 52-year-old, previously healthy male who presented with acute myocarditis 3 days after the administration of the second dose of Moderna’s COVID-19 vaccine. The symptoms resolved, and there was a gradual improvement in cMRI findings. Ischemic injury and other potential causes of acute myocardial injury were excluded, as were other potential infectious causes of myocarditis, and there was no evidence of systemic autoimmune disease.
“Clinicians should be aware that myocarditis may be present in patients exhibiting cardiac signs and symptoms 2-4 days after COVID-19 vaccination,” the authors said.
They added that additional surveillance of such adverse events post–COVID-19 vaccination will help identify subgroups at higher risk for this vaccine-related effect, and whether additional precautions are necessary.
‘Benefits outweigh risk’
In an accompanying editorial in JAMA Cardiology, three doctors from the CDC cite several other reports of myocarditis after mRNA COVID vaccination. These include a case report published in Pediatrics of seven male adolescents aged 14-19 years who presented with myocarditis or myopericarditis within 4 days after receipt of a second dose of the Pfizer vaccine.
But the editorialists noted that the most comprehensive data about the risk for myocarditis following immunization with mRNA vaccines comes from Israel.
The Israeli Ministry of Health recently posted data describing 121 myocarditis cases occurring within 30 days of a second dose of mRNA vaccine among 5,049,424 persons, suggesting a crude incidence rate of approximately 24 cases per million.
On the current case reports, the CDC doctors wrote: “The striking clinical similarities in the presentations of these patients, their recent vaccination with an mRNA-based COVID-19 vaccine, and the lack of any alternative etiologies for acute myocarditis suggest an association with immunization.”
They said that acute onset of chest pain 3-5 days after vaccine administration, usually after a second dose, is a typical feature of reported cases and suggests an immune-mediated mechanism.
But SARS-CoV-2 infection also causes cardiac injury which may result in severe outcomes, and based on currently available data, myocarditis following immunization with current mRNA-based vaccines is rare.
“At present, the benefits of immunization in preventing severe morbidity favors continued COVID-19 vaccination, particularly considering the increasing COVID-19 hospitalization rates among adolescents reported during spring 2021,” the editorialists stated.
But they added that many questions remain. These include whether modifications are needed to the vaccine schedule among persons with a history of possible or confirmed myocarditis after COVID vaccine, how should postvaccine myocarditis be managed, how often should follow-up assessments be performed, how might follow-up assessments affect recommendations to avoid vigorous physical activity following the diagnosis of myocarditis, and do all likely cases of acute myocarditis that appear to be uncomplicated require cardiac MRI for more definitive diagnosis?
“While the data needed to answer such questions are being collected, there is an opportunity for researchers with expertise in myocarditis to develop a comprehensive, national assessment of the natural history, pathogenesis, and treatment of acute myocarditis associated with receipt of mRNA-based COVID-19 vaccines,” they concluded.
In a second editorial in JAMA Cardiology, a group of editors from the journal acknowledged that publication of the current case reports may contribute to additional public concern regarding immunization. But they added that clinicians discussing immunization with patients should recognize that these case series suggest that the symptomatic events consistent with myocarditis are still very rare and appear to be self-limiting.
“Given the risks of COVID-19, including the risk of myocarditis from COVID-19 infection, the editors do not believe these case reports are sufficient to interrupt the march toward maximal vaccination against SARS-CoV-2 as expeditiously as possible,” they said.
A version of this article first appeared on Medscape.com.
Further details from multiple cases of myocarditis linked to the Pfizer and Moderna mRNA COVID vaccines have been described in recent papers in the medical literature.
The cases appear to occur almost exclusively in males and most often in younger age groups. While symptoms and signs of myocarditis mostly resolved with a few days of supportive care, long-term effects are unknown at present.
The authors of all the reports and of two accompanying editorials in JAMA Cardiology are unanimous in their opinion that the benefits of vaccination still outweigh the risks.
The Centers for Disease Control and Prevention’s but committee members delivered a strong endorsement for continuing to vaccinate young people with the mRNA vaccines.
The current case reports are published in two papers in JAMA Cardiology and in three in Circulation.
U.S. military reports 23 cases
In one report in JAMA Cardiology, authors led by Jay Montgomery, MD, from Walter Reed National Military Medical Center in Bethesda, Md., described 23 cases from the U.S. Military Health System of individuals with acute myocarditis who presented within 4 days after mRNA-based COVID-19 vaccination (7 Pfizer and 16 Moderna).
All patients were male, 22 of 23 were on active duty, and the median age was 25 years (range, 20-51); 20 of the 23 cases occurred after receipt of a second dose of an mRNA COVID-19 vaccine.
The patients all presented with acute onset of marked chest pain. All patients had significantly elevated cardiac troponin levels. Among eight patients who underwent cardiac MRI (cMRI), all had findings consistent with the clinical diagnosis of myocarditis.
Additional testing did not identify other possible causes of myocarditis. All patients received brief supportive care and were recovered or recovering.
The authors reported that the military administered more than 2.8 million doses of mRNA COVID-19 vaccine in this period, and while the observed number of myocarditis cases was small, the number was “substantially higher” than expected among male military members after a second vaccine dose.
They noted that, based on historical data, among the 544,000 second doses to military members there may have been 0-10 expected myocarditis cases, but they observed 19 cases.
“All patients in this series reflect substantial similarities in demographic characteristics, proximate vaccine dose, onset interval, and character of vaccine-associated myocarditis. The consistent pattern of clinical presentation, rapid recovery, and absence of evidence of other causes support the diagnosis of hypersensitivity myocarditis,” they stated.
They added that presentation after a second vaccine dose or, in three patients, when vaccination followed SARS-CoV-2 infection, suggests that prior exposure was relevant in the hypersensitivity response.
“The spectrum of clinical presentation and reliance on patients seeking health care and on health care professionals recognizing a rare vaccine-associated adverse event limits determination of the true incidence of this condition,” the authors wrote.
They stressed that recognition of vaccine-associated myocarditis is clinically important because diagnosis impacts management, recommendations for exercise, and monitoring for cardiomyopathy.
But the authors also acknowledged that it is important to frame concerns about potential vaccine-associated myocarditis within the context of the current pandemic.
“Infection with SARS-CoV-2 is a clear cause of serious cardiac injury in many patients. ... Prevalence of cardiac injury may be as high as 60% in seriously ill patients. Notably, nearly 1% of highly fit athletes with mild COVID-19 infection have evidence of myocarditis on cMRI,” they wrote.
“Given that COVID-19 vaccines are remarkably effective at preventing infection, any risk of rare adverse events following immunization must be carefully weighed against the very substantial benefit of vaccination,” they concluded.
Four cases at Duke
In the second paper in JAMA Cardiology, a group led by Han W. Kim, MD, reported four patients with acute myocarditis occurring within days of mRNA COVID-19 vaccination (two Pfizer and two Moderna) in patients treated at Duke University Medical Center, Durham, N.C. The hospital courses of the four patients with myocarditis following COVID-19 vaccination were uneventful, and they were discharged within 2-4 days.
The authors said that, although a causal relationship cannot be established, none of the patients had a viral prodrome or had coincident testing that revealed an alternative explanation.
They stated that these four patients represent the majority of patients with acute myocarditis identified in the past 3 months at their institution, and this led to the highest total number of patients with acute myocarditis, compared with the same 3-month period for the past 5 years.
“Additionally, we identified only those patients with severe unremitting chest pain who sought medical attention. Those with mild or moderate chest pain might not seek medical attention, and it is possible that subclinical myocarditis may occur and could be detected by active surveillance, as has been described with smallpox vaccination,” they wrote.
Further case reports
In one of the papers in Circulation, a group led by Kathryn F. Larson, MD, from the Mayo Clinic in Rochester, Minn., described eight patients hospitalized with chest pain who were diagnosed with myocarditis within 2-4 days of receiving either the Pfizer or Moderna vaccine.
Two of the patients had previously been infected by SARS-CoV-2 without need for hospitalization. All individuals were otherwise healthy males between the ages of 21 and 56 years. All but one patient developed symptoms after their second dose, and the one patient who developed myocarditis after the first vaccine dose had previously been infected with SARS-CoV-2.
Systemic symptoms began within 24 hours after vaccine administration in five of eight patients, with chest pain presenting between 48 and 96 hours later. Troponin values were elevated in all individuals and appeared to peak the day after admission, whereas none had eosinophilia.
Cardiac MRI revealed findings consistent with myocarditis in all patients. All patients had resolution of their chest pain and were discharged from the hospital in stable condition.
“The patients presented here demonstrated typical signs, symptoms, and diagnostic features of acute myocarditis. The temporal association between receiving an mRNA-based COVID-19 vaccine and the development of myocarditis is notable,” the authors said.
They added that they would consider the use of corticosteroids in these patients but cautioned that this could reduce the specific immune response against SARS-COV-2 triggered by the vaccine. “Thus, the duration of corticosteroid administration should be limited to the resolution of the symptoms or ventricular arrhythmias or the recovery of the left ventricular ejection fraction.”
Pending publication of long-term outcome data after SARS-CoV-2 vaccine–related myocarditis, they suggest adherence to the current consensus recommendation to abstain from competitive sports for a period of 3-6 months with reevaluation prior to sports participation.
In another of the Circulation papers, a group led by Carolyn M. Rosner, MSN, presented a case series of seven patients hospitalized for acute myocarditis-like illness following COVID-19 vaccination, from two U.S. medical centers, in Falls Church, Va., and Dallas. All patients were males below the age of 40 years and of White or Hispanic race/ethnicity. Only one patient reported prior history of COVID-19 infection. Six patients received mRNA (Moderna or Pfizer) and one received the adenovirus (Johnson & Johnson) vaccine. All patients presented 3-7 days post vaccination with acute onset chest pain and biochemical evidence of myocardial injury.
Hospital length of stay was 3 days, and all patients’ symptoms resolved by hospital discharge.
And finally, the third paper in Circulation reported a detailed description of one patient – a 52-year-old, previously healthy male who presented with acute myocarditis 3 days after the administration of the second dose of Moderna’s COVID-19 vaccine. The symptoms resolved, and there was a gradual improvement in cMRI findings. Ischemic injury and other potential causes of acute myocardial injury were excluded, as were other potential infectious causes of myocarditis, and there was no evidence of systemic autoimmune disease.
“Clinicians should be aware that myocarditis may be present in patients exhibiting cardiac signs and symptoms 2-4 days after COVID-19 vaccination,” the authors said.
They added that additional surveillance of such adverse events post–COVID-19 vaccination will help identify subgroups at higher risk for this vaccine-related effect, and whether additional precautions are necessary.
‘Benefits outweigh risk’
In an accompanying editorial in JAMA Cardiology, three doctors from the CDC cite several other reports of myocarditis after mRNA COVID vaccination. These include a case report published in Pediatrics of seven male adolescents aged 14-19 years who presented with myocarditis or myopericarditis within 4 days after receipt of a second dose of the Pfizer vaccine.
But the editorialists noted that the most comprehensive data about the risk for myocarditis following immunization with mRNA vaccines comes from Israel.
The Israeli Ministry of Health recently posted data describing 121 myocarditis cases occurring within 30 days of a second dose of mRNA vaccine among 5,049,424 persons, suggesting a crude incidence rate of approximately 24 cases per million.
On the current case reports, the CDC doctors wrote: “The striking clinical similarities in the presentations of these patients, their recent vaccination with an mRNA-based COVID-19 vaccine, and the lack of any alternative etiologies for acute myocarditis suggest an association with immunization.”
They said that acute onset of chest pain 3-5 days after vaccine administration, usually after a second dose, is a typical feature of reported cases and suggests an immune-mediated mechanism.
But SARS-CoV-2 infection also causes cardiac injury which may result in severe outcomes, and based on currently available data, myocarditis following immunization with current mRNA-based vaccines is rare.
“At present, the benefits of immunization in preventing severe morbidity favors continued COVID-19 vaccination, particularly considering the increasing COVID-19 hospitalization rates among adolescents reported during spring 2021,” the editorialists stated.
But they added that many questions remain. These include whether modifications are needed to the vaccine schedule among persons with a history of possible or confirmed myocarditis after COVID vaccine, how should postvaccine myocarditis be managed, how often should follow-up assessments be performed, how might follow-up assessments affect recommendations to avoid vigorous physical activity following the diagnosis of myocarditis, and do all likely cases of acute myocarditis that appear to be uncomplicated require cardiac MRI for more definitive diagnosis?
“While the data needed to answer such questions are being collected, there is an opportunity for researchers with expertise in myocarditis to develop a comprehensive, national assessment of the natural history, pathogenesis, and treatment of acute myocarditis associated with receipt of mRNA-based COVID-19 vaccines,” they concluded.
In a second editorial in JAMA Cardiology, a group of editors from the journal acknowledged that publication of the current case reports may contribute to additional public concern regarding immunization. But they added that clinicians discussing immunization with patients should recognize that these case series suggest that the symptomatic events consistent with myocarditis are still very rare and appear to be self-limiting.
“Given the risks of COVID-19, including the risk of myocarditis from COVID-19 infection, the editors do not believe these case reports are sufficient to interrupt the march toward maximal vaccination against SARS-CoV-2 as expeditiously as possible,” they said.
A version of this article first appeared on Medscape.com.
Further details from multiple cases of myocarditis linked to the Pfizer and Moderna mRNA COVID vaccines have been described in recent papers in the medical literature.
The cases appear to occur almost exclusively in males and most often in younger age groups. While symptoms and signs of myocarditis mostly resolved with a few days of supportive care, long-term effects are unknown at present.
The authors of all the reports and of two accompanying editorials in JAMA Cardiology are unanimous in their opinion that the benefits of vaccination still outweigh the risks.
The Centers for Disease Control and Prevention’s but committee members delivered a strong endorsement for continuing to vaccinate young people with the mRNA vaccines.
The current case reports are published in two papers in JAMA Cardiology and in three in Circulation.
U.S. military reports 23 cases
In one report in JAMA Cardiology, authors led by Jay Montgomery, MD, from Walter Reed National Military Medical Center in Bethesda, Md., described 23 cases from the U.S. Military Health System of individuals with acute myocarditis who presented within 4 days after mRNA-based COVID-19 vaccination (7 Pfizer and 16 Moderna).
All patients were male, 22 of 23 were on active duty, and the median age was 25 years (range, 20-51); 20 of the 23 cases occurred after receipt of a second dose of an mRNA COVID-19 vaccine.
The patients all presented with acute onset of marked chest pain. All patients had significantly elevated cardiac troponin levels. Among eight patients who underwent cardiac MRI (cMRI), all had findings consistent with the clinical diagnosis of myocarditis.
Additional testing did not identify other possible causes of myocarditis. All patients received brief supportive care and were recovered or recovering.
The authors reported that the military administered more than 2.8 million doses of mRNA COVID-19 vaccine in this period, and while the observed number of myocarditis cases was small, the number was “substantially higher” than expected among male military members after a second vaccine dose.
They noted that, based on historical data, among the 544,000 second doses to military members there may have been 0-10 expected myocarditis cases, but they observed 19 cases.
“All patients in this series reflect substantial similarities in demographic characteristics, proximate vaccine dose, onset interval, and character of vaccine-associated myocarditis. The consistent pattern of clinical presentation, rapid recovery, and absence of evidence of other causes support the diagnosis of hypersensitivity myocarditis,” they stated.
They added that presentation after a second vaccine dose or, in three patients, when vaccination followed SARS-CoV-2 infection, suggests that prior exposure was relevant in the hypersensitivity response.
“The spectrum of clinical presentation and reliance on patients seeking health care and on health care professionals recognizing a rare vaccine-associated adverse event limits determination of the true incidence of this condition,” the authors wrote.
They stressed that recognition of vaccine-associated myocarditis is clinically important because diagnosis impacts management, recommendations for exercise, and monitoring for cardiomyopathy.
But the authors also acknowledged that it is important to frame concerns about potential vaccine-associated myocarditis within the context of the current pandemic.
“Infection with SARS-CoV-2 is a clear cause of serious cardiac injury in many patients. ... Prevalence of cardiac injury may be as high as 60% in seriously ill patients. Notably, nearly 1% of highly fit athletes with mild COVID-19 infection have evidence of myocarditis on cMRI,” they wrote.
“Given that COVID-19 vaccines are remarkably effective at preventing infection, any risk of rare adverse events following immunization must be carefully weighed against the very substantial benefit of vaccination,” they concluded.
Four cases at Duke
In the second paper in JAMA Cardiology, a group led by Han W. Kim, MD, reported four patients with acute myocarditis occurring within days of mRNA COVID-19 vaccination (two Pfizer and two Moderna) in patients treated at Duke University Medical Center, Durham, N.C. The hospital courses of the four patients with myocarditis following COVID-19 vaccination were uneventful, and they were discharged within 2-4 days.
The authors said that, although a causal relationship cannot be established, none of the patients had a viral prodrome or had coincident testing that revealed an alternative explanation.
They stated that these four patients represent the majority of patients with acute myocarditis identified in the past 3 months at their institution, and this led to the highest total number of patients with acute myocarditis, compared with the same 3-month period for the past 5 years.
“Additionally, we identified only those patients with severe unremitting chest pain who sought medical attention. Those with mild or moderate chest pain might not seek medical attention, and it is possible that subclinical myocarditis may occur and could be detected by active surveillance, as has been described with smallpox vaccination,” they wrote.
Further case reports
In one of the papers in Circulation, a group led by Kathryn F. Larson, MD, from the Mayo Clinic in Rochester, Minn., described eight patients hospitalized with chest pain who were diagnosed with myocarditis within 2-4 days of receiving either the Pfizer or Moderna vaccine.
Two of the patients had previously been infected by SARS-CoV-2 without need for hospitalization. All individuals were otherwise healthy males between the ages of 21 and 56 years. All but one patient developed symptoms after their second dose, and the one patient who developed myocarditis after the first vaccine dose had previously been infected with SARS-CoV-2.
Systemic symptoms began within 24 hours after vaccine administration in five of eight patients, with chest pain presenting between 48 and 96 hours later. Troponin values were elevated in all individuals and appeared to peak the day after admission, whereas none had eosinophilia.
Cardiac MRI revealed findings consistent with myocarditis in all patients. All patients had resolution of their chest pain and were discharged from the hospital in stable condition.
“The patients presented here demonstrated typical signs, symptoms, and diagnostic features of acute myocarditis. The temporal association between receiving an mRNA-based COVID-19 vaccine and the development of myocarditis is notable,” the authors said.
They added that they would consider the use of corticosteroids in these patients but cautioned that this could reduce the specific immune response against SARS-COV-2 triggered by the vaccine. “Thus, the duration of corticosteroid administration should be limited to the resolution of the symptoms or ventricular arrhythmias or the recovery of the left ventricular ejection fraction.”
Pending publication of long-term outcome data after SARS-CoV-2 vaccine–related myocarditis, they suggest adherence to the current consensus recommendation to abstain from competitive sports for a period of 3-6 months with reevaluation prior to sports participation.
In another of the Circulation papers, a group led by Carolyn M. Rosner, MSN, presented a case series of seven patients hospitalized for acute myocarditis-like illness following COVID-19 vaccination, from two U.S. medical centers, in Falls Church, Va., and Dallas. All patients were males below the age of 40 years and of White or Hispanic race/ethnicity. Only one patient reported prior history of COVID-19 infection. Six patients received mRNA (Moderna or Pfizer) and one received the adenovirus (Johnson & Johnson) vaccine. All patients presented 3-7 days post vaccination with acute onset chest pain and biochemical evidence of myocardial injury.
Hospital length of stay was 3 days, and all patients’ symptoms resolved by hospital discharge.
And finally, the third paper in Circulation reported a detailed description of one patient – a 52-year-old, previously healthy male who presented with acute myocarditis 3 days after the administration of the second dose of Moderna’s COVID-19 vaccine. The symptoms resolved, and there was a gradual improvement in cMRI findings. Ischemic injury and other potential causes of acute myocardial injury were excluded, as were other potential infectious causes of myocarditis, and there was no evidence of systemic autoimmune disease.
“Clinicians should be aware that myocarditis may be present in patients exhibiting cardiac signs and symptoms 2-4 days after COVID-19 vaccination,” the authors said.
They added that additional surveillance of such adverse events post–COVID-19 vaccination will help identify subgroups at higher risk for this vaccine-related effect, and whether additional precautions are necessary.
‘Benefits outweigh risk’
In an accompanying editorial in JAMA Cardiology, three doctors from the CDC cite several other reports of myocarditis after mRNA COVID vaccination. These include a case report published in Pediatrics of seven male adolescents aged 14-19 years who presented with myocarditis or myopericarditis within 4 days after receipt of a second dose of the Pfizer vaccine.
But the editorialists noted that the most comprehensive data about the risk for myocarditis following immunization with mRNA vaccines comes from Israel.
The Israeli Ministry of Health recently posted data describing 121 myocarditis cases occurring within 30 days of a second dose of mRNA vaccine among 5,049,424 persons, suggesting a crude incidence rate of approximately 24 cases per million.
On the current case reports, the CDC doctors wrote: “The striking clinical similarities in the presentations of these patients, their recent vaccination with an mRNA-based COVID-19 vaccine, and the lack of any alternative etiologies for acute myocarditis suggest an association with immunization.”
They said that acute onset of chest pain 3-5 days after vaccine administration, usually after a second dose, is a typical feature of reported cases and suggests an immune-mediated mechanism.
But SARS-CoV-2 infection also causes cardiac injury which may result in severe outcomes, and based on currently available data, myocarditis following immunization with current mRNA-based vaccines is rare.
“At present, the benefits of immunization in preventing severe morbidity favors continued COVID-19 vaccination, particularly considering the increasing COVID-19 hospitalization rates among adolescents reported during spring 2021,” the editorialists stated.
But they added that many questions remain. These include whether modifications are needed to the vaccine schedule among persons with a history of possible or confirmed myocarditis after COVID vaccine, how should postvaccine myocarditis be managed, how often should follow-up assessments be performed, how might follow-up assessments affect recommendations to avoid vigorous physical activity following the diagnosis of myocarditis, and do all likely cases of acute myocarditis that appear to be uncomplicated require cardiac MRI for more definitive diagnosis?
“While the data needed to answer such questions are being collected, there is an opportunity for researchers with expertise in myocarditis to develop a comprehensive, national assessment of the natural history, pathogenesis, and treatment of acute myocarditis associated with receipt of mRNA-based COVID-19 vaccines,” they concluded.
In a second editorial in JAMA Cardiology, a group of editors from the journal acknowledged that publication of the current case reports may contribute to additional public concern regarding immunization. But they added that clinicians discussing immunization with patients should recognize that these case series suggest that the symptomatic events consistent with myocarditis are still very rare and appear to be self-limiting.
“Given the risks of COVID-19, including the risk of myocarditis from COVID-19 infection, the editors do not believe these case reports are sufficient to interrupt the march toward maximal vaccination against SARS-CoV-2 as expeditiously as possible,” they said.
A version of this article first appeared on Medscape.com.