User login
Monitoring calcium with lithium treatment
I appreciate Dr. McInnis’s article and his recommendation to monitor the comprehensive metabolic profile, including the calcium level, before and during lithium treatment. There is an association among lithium treatment, hypercalcemia, and hyperparathyroidism.1,2 This can occur by lithium reducing parathyroid hormone suppression or stimulating parathyroid glands.3
Surprisingly, many guidelines do not include a recommendation to monitor the calcium level; however, the International Society for Bipolar Disorders and other experts do recommend obtaining a calcium level before initiating lithium therapy and at least annually thereafter.1,4 If hypercalcemia is present, assessing lithium and the parathyroid hormone level is recommended.3
Clinicians can continue lithium and monitor calcium if treatment is beneficial, hypercalcemia is mild, and the patient is asymptomatic.2 For a symptomatic patient or one who has significant hypercalcemia, clinicians should consider discontinuing lithium and monitoring for a normalizing calcium level.2 For patients with significant hypercalcemia who need lithium therapy, consultation with an endocrinologist is advised.3
Jonathan R. Scarff, MD
VA Outpatient Clinic
Spartanburg, South Carolina
Dr. McInnis responds
Generally, calcium is included in the comprehensive biochemistry panel (Table 1). Typically, magnesium or phosphorus is overlooked, and therefore was specifically included in the table of recommendations. There is a complex relationship between lithium and calcium; Dr. Scarff’s points highlight this. It is noteworthy that lithium normalizes the calcium amplitude during action potentials in neurons derived from induced pluripotent stem cells from persons with BD1; this suggests that there might be a direct mode of action in BD involving lithium and calcium. This finding further emphasizes the importance of monitoring calcium, and the wise clinician will verify that it is included in the comprehensive biochemistry panel.
1. McKnight RF, Adida M, Budge K, et al. Lithium toxicity profile: a systematic review and meta-analysis. Lancet. 2012;379(9817):721-728.
2. Lehmann SW, Lee J. Lithium-associated hyper-calcemia and hyperparathyroidism in the elderly: what do we know? J Affect Disord. 2013;146(2): 151-157.
3. Broome JT, Solorzano CC. Lithium use and primary hyperparathyroidism. Endocr Pract. 2011; 17(suppl 1):31-35.
4. Ng F, Mammen OK, Wilting I, et al. The International Society for Bipolar Disorders (ISBD) consensus guidelines for the safety monitoring of bipolar disorder treatments. Bipolar Disord. 2009; 11(6):559-595.
Reference
1. Chen HM, DeLong CJ, Bame M, et al. Transcripts involved in calcium signaling and telencephalic neuronal fate are altered in induced pluripotent stem cells from bipolar disorder patients. Transl Psychiatry. 2014;4:e375. doi:10.1038/tp.2014.12.
I appreciate Dr. McInnis’s article and his recommendation to monitor the comprehensive metabolic profile, including the calcium level, before and during lithium treatment. There is an association among lithium treatment, hypercalcemia, and hyperparathyroidism.1,2 This can occur by lithium reducing parathyroid hormone suppression or stimulating parathyroid glands.3
Surprisingly, many guidelines do not include a recommendation to monitor the calcium level; however, the International Society for Bipolar Disorders and other experts do recommend obtaining a calcium level before initiating lithium therapy and at least annually thereafter.1,4 If hypercalcemia is present, assessing lithium and the parathyroid hormone level is recommended.3
Clinicians can continue lithium and monitor calcium if treatment is beneficial, hypercalcemia is mild, and the patient is asymptomatic.2 For a symptomatic patient or one who has significant hypercalcemia, clinicians should consider discontinuing lithium and monitoring for a normalizing calcium level.2 For patients with significant hypercalcemia who need lithium therapy, consultation with an endocrinologist is advised.3
Jonathan R. Scarff, MD
VA Outpatient Clinic
Spartanburg, South Carolina
Dr. McInnis responds
Generally, calcium is included in the comprehensive biochemistry panel (Table 1). Typically, magnesium or phosphorus is overlooked, and therefore was specifically included in the table of recommendations. There is a complex relationship between lithium and calcium; Dr. Scarff’s points highlight this. It is noteworthy that lithium normalizes the calcium amplitude during action potentials in neurons derived from induced pluripotent stem cells from persons with BD1; this suggests that there might be a direct mode of action in BD involving lithium and calcium. This finding further emphasizes the importance of monitoring calcium, and the wise clinician will verify that it is included in the comprehensive biochemistry panel.
I appreciate Dr. McInnis’s article and his recommendation to monitor the comprehensive metabolic profile, including the calcium level, before and during lithium treatment. There is an association among lithium treatment, hypercalcemia, and hyperparathyroidism.1,2 This can occur by lithium reducing parathyroid hormone suppression or stimulating parathyroid glands.3
Surprisingly, many guidelines do not include a recommendation to monitor the calcium level; however, the International Society for Bipolar Disorders and other experts do recommend obtaining a calcium level before initiating lithium therapy and at least annually thereafter.1,4 If hypercalcemia is present, assessing lithium and the parathyroid hormone level is recommended.3
Clinicians can continue lithium and monitor calcium if treatment is beneficial, hypercalcemia is mild, and the patient is asymptomatic.2 For a symptomatic patient or one who has significant hypercalcemia, clinicians should consider discontinuing lithium and monitoring for a normalizing calcium level.2 For patients with significant hypercalcemia who need lithium therapy, consultation with an endocrinologist is advised.3
Jonathan R. Scarff, MD
VA Outpatient Clinic
Spartanburg, South Carolina
Dr. McInnis responds
Generally, calcium is included in the comprehensive biochemistry panel (Table 1). Typically, magnesium or phosphorus is overlooked, and therefore was specifically included in the table of recommendations. There is a complex relationship between lithium and calcium; Dr. Scarff’s points highlight this. It is noteworthy that lithium normalizes the calcium amplitude during action potentials in neurons derived from induced pluripotent stem cells from persons with BD1; this suggests that there might be a direct mode of action in BD involving lithium and calcium. This finding further emphasizes the importance of monitoring calcium, and the wise clinician will verify that it is included in the comprehensive biochemistry panel.
1. McKnight RF, Adida M, Budge K, et al. Lithium toxicity profile: a systematic review and meta-analysis. Lancet. 2012;379(9817):721-728.
2. Lehmann SW, Lee J. Lithium-associated hyper-calcemia and hyperparathyroidism in the elderly: what do we know? J Affect Disord. 2013;146(2): 151-157.
3. Broome JT, Solorzano CC. Lithium use and primary hyperparathyroidism. Endocr Pract. 2011; 17(suppl 1):31-35.
4. Ng F, Mammen OK, Wilting I, et al. The International Society for Bipolar Disorders (ISBD) consensus guidelines for the safety monitoring of bipolar disorder treatments. Bipolar Disord. 2009; 11(6):559-595.
Reference
1. Chen HM, DeLong CJ, Bame M, et al. Transcripts involved in calcium signaling and telencephalic neuronal fate are altered in induced pluripotent stem cells from bipolar disorder patients. Transl Psychiatry. 2014;4:e375. doi:10.1038/tp.2014.12.
1. McKnight RF, Adida M, Budge K, et al. Lithium toxicity profile: a systematic review and meta-analysis. Lancet. 2012;379(9817):721-728.
2. Lehmann SW, Lee J. Lithium-associated hyper-calcemia and hyperparathyroidism in the elderly: what do we know? J Affect Disord. 2013;146(2): 151-157.
3. Broome JT, Solorzano CC. Lithium use and primary hyperparathyroidism. Endocr Pract. 2011; 17(suppl 1):31-35.
4. Ng F, Mammen OK, Wilting I, et al. The International Society for Bipolar Disorders (ISBD) consensus guidelines for the safety monitoring of bipolar disorder treatments. Bipolar Disord. 2009; 11(6):559-595.
Reference
1. Chen HM, DeLong CJ, Bame M, et al. Transcripts involved in calcium signaling and telencephalic neuronal fate are altered in induced pluripotent stem cells from bipolar disorder patients. Transl Psychiatry. 2014;4:e375. doi:10.1038/tp.2014.12.
Cautions when prescribing lithium
I was astonished that Dr. Melvin G. McInnis’ article on using lithium to treat bipolar disorder (BD) (Current Psychiatry, June 2014, p. 38-44; [http://bit.ly/1sszAUr]) did not address all the potential hazards of the medication. He discussed side effects, but only how to manage them so that patients will adhere to treatment.
I have used lithium for patients with BD, and often it is efficacious, although hazardous in overdose. Lithium toxicity can cause cardiac arrhythmias, and must be monitored closely. In addition, the effects of hydration and exercise on the lithium level, especially during summer, often are ignored.
Two of my patients, an adolescent and an adult, were well-maintained on lithium, adhered to treatment, and had no concurrent medical problems, but developed significant toxicity for no reason that I could determine. The adult had a lithium level of 2.0 mEq/L in the emergency room; the adolescent had a lithium level of 1.8 mEq/L. Levels this high are considered potentially lethal, and because it happened without warning and without a cause that I could determine, I consider lithium to be one of the riskier mood stabilizers. I still prescribe it, but with great caution.
Dr. McInnis also did not mention the possibility of lithium-induced diabetes insipidus, a condition in which the kidneys are no longer able to concentrate urine and that is marked by excessive urination, concomitant water intake, and low urine specific gravity. It is uncommon, but I have seen it 3 times in 30 years, in a practice that specializes in psychotherapy and does not see a high percentage of patients with BD. I consider it a condition that must be kept in mind as we follow our patients in long-term treatment.
Mary Davis, MD
Lancaster, Pennsylvania
Dr. McInnis responds
Dr. Davis raises the issue of lithium toxicity and provides examples of 2 patients who developed levels of 2.0 mEq/L and 1.8 mEq/L. These levels clearly are well beyond the toxicity threshold of 1.3 mEq/L, and the patients wisely sought urgent care. These scenarios exemplify the need for regular monitoring of the lithium level—in particular, when there is any change in physical or mental health status. Development of significant toxicity generally has some lead-time with emerging short-term side effects (outlined in Table 2 of my article), which underscores the importance of discussing the nature of emerging side effects with your patient.
Dr. Davis is correct in noting that the practitioner must be aware of long-term side effects of lithium. I find it helpful to discuss these effects with the patient in the context of short-term (days or weeks), intermediate (weeks or months), and long-term (months or years) time frames (Table 2). Diabetes insipidus is listed as an intermediate side effect.
I am grateful to Dr. Davis for raising the issue of hydration and summer heat, a concern among parents and coaches when student athletes practice strenuously for extended hours.1 Miller et al2 found that the concentration of lithium was between 1.2- and 4.6-fold in forearm sweat compared with serum levels, with the implication that heat-induced sweating may lower lithium levels. Jefferson et al3 studied 4 athletes after a 20-km race and found that all had become dehydrated but had a decrease in the serum lithium level. This is contrary to the widely held belief that excessive sweating predisposes to lithium toxicity.
BD is among the more lethal psychiatric disorders, and lithium is among the few medications shown to mitigate suicidal behavior.4 As with any medication, lithium is not without risk, and there is a clear need for informed medical management. Any notable change in health status or physical activity in a patient taking lithium is worthy of review, with recommendations based on knowledge of the patient and medical science.
1. Reardon CL, Factor RM. Sport psychiatry: a systematic review of diagnosis and medical treatment of mental illness in athletes. Sports Med. 2010;40:961-980.
2. Miller EB, Pain RW, Skripal PJ. Sweat lithium in manic-depression. Br J Psychiatry. 1978;133:477-478.
3. Jefferson JW, Greist JH, Clagnaz PJ, et al. Effect of strenuous exercise on serum lithium level in man. Am J Psychiatry. 1982;139(12):1593-1595.
4. Goodwin FK, Fireman B, Simon GE, et al. Suicide risk in bipolar disorder during treatment with lithium and divalproex. JAMA. 2003;290(11):1467-1473.
I was astonished that Dr. Melvin G. McInnis’ article on using lithium to treat bipolar disorder (BD) (Current Psychiatry, June 2014, p. 38-44; [http://bit.ly/1sszAUr]) did not address all the potential hazards of the medication. He discussed side effects, but only how to manage them so that patients will adhere to treatment.
I have used lithium for patients with BD, and often it is efficacious, although hazardous in overdose. Lithium toxicity can cause cardiac arrhythmias, and must be monitored closely. In addition, the effects of hydration and exercise on the lithium level, especially during summer, often are ignored.
Two of my patients, an adolescent and an adult, were well-maintained on lithium, adhered to treatment, and had no concurrent medical problems, but developed significant toxicity for no reason that I could determine. The adult had a lithium level of 2.0 mEq/L in the emergency room; the adolescent had a lithium level of 1.8 mEq/L. Levels this high are considered potentially lethal, and because it happened without warning and without a cause that I could determine, I consider lithium to be one of the riskier mood stabilizers. I still prescribe it, but with great caution.
Dr. McInnis also did not mention the possibility of lithium-induced diabetes insipidus, a condition in which the kidneys are no longer able to concentrate urine and that is marked by excessive urination, concomitant water intake, and low urine specific gravity. It is uncommon, but I have seen it 3 times in 30 years, in a practice that specializes in psychotherapy and does not see a high percentage of patients with BD. I consider it a condition that must be kept in mind as we follow our patients in long-term treatment.
Mary Davis, MD
Lancaster, Pennsylvania
Dr. McInnis responds
Dr. Davis raises the issue of lithium toxicity and provides examples of 2 patients who developed levels of 2.0 mEq/L and 1.8 mEq/L. These levels clearly are well beyond the toxicity threshold of 1.3 mEq/L, and the patients wisely sought urgent care. These scenarios exemplify the need for regular monitoring of the lithium level—in particular, when there is any change in physical or mental health status. Development of significant toxicity generally has some lead-time with emerging short-term side effects (outlined in Table 2 of my article), which underscores the importance of discussing the nature of emerging side effects with your patient.
Dr. Davis is correct in noting that the practitioner must be aware of long-term side effects of lithium. I find it helpful to discuss these effects with the patient in the context of short-term (days or weeks), intermediate (weeks or months), and long-term (months or years) time frames (Table 2). Diabetes insipidus is listed as an intermediate side effect.
I am grateful to Dr. Davis for raising the issue of hydration and summer heat, a concern among parents and coaches when student athletes practice strenuously for extended hours.1 Miller et al2 found that the concentration of lithium was between 1.2- and 4.6-fold in forearm sweat compared with serum levels, with the implication that heat-induced sweating may lower lithium levels. Jefferson et al3 studied 4 athletes after a 20-km race and found that all had become dehydrated but had a decrease in the serum lithium level. This is contrary to the widely held belief that excessive sweating predisposes to lithium toxicity.
BD is among the more lethal psychiatric disorders, and lithium is among the few medications shown to mitigate suicidal behavior.4 As with any medication, lithium is not without risk, and there is a clear need for informed medical management. Any notable change in health status or physical activity in a patient taking lithium is worthy of review, with recommendations based on knowledge of the patient and medical science.
I was astonished that Dr. Melvin G. McInnis’ article on using lithium to treat bipolar disorder (BD) (Current Psychiatry, June 2014, p. 38-44; [http://bit.ly/1sszAUr]) did not address all the potential hazards of the medication. He discussed side effects, but only how to manage them so that patients will adhere to treatment.
I have used lithium for patients with BD, and often it is efficacious, although hazardous in overdose. Lithium toxicity can cause cardiac arrhythmias, and must be monitored closely. In addition, the effects of hydration and exercise on the lithium level, especially during summer, often are ignored.
Two of my patients, an adolescent and an adult, were well-maintained on lithium, adhered to treatment, and had no concurrent medical problems, but developed significant toxicity for no reason that I could determine. The adult had a lithium level of 2.0 mEq/L in the emergency room; the adolescent had a lithium level of 1.8 mEq/L. Levels this high are considered potentially lethal, and because it happened without warning and without a cause that I could determine, I consider lithium to be one of the riskier mood stabilizers. I still prescribe it, but with great caution.
Dr. McInnis also did not mention the possibility of lithium-induced diabetes insipidus, a condition in which the kidneys are no longer able to concentrate urine and that is marked by excessive urination, concomitant water intake, and low urine specific gravity. It is uncommon, but I have seen it 3 times in 30 years, in a practice that specializes in psychotherapy and does not see a high percentage of patients with BD. I consider it a condition that must be kept in mind as we follow our patients in long-term treatment.
Mary Davis, MD
Lancaster, Pennsylvania
Dr. McInnis responds
Dr. Davis raises the issue of lithium toxicity and provides examples of 2 patients who developed levels of 2.0 mEq/L and 1.8 mEq/L. These levels clearly are well beyond the toxicity threshold of 1.3 mEq/L, and the patients wisely sought urgent care. These scenarios exemplify the need for regular monitoring of the lithium level—in particular, when there is any change in physical or mental health status. Development of significant toxicity generally has some lead-time with emerging short-term side effects (outlined in Table 2 of my article), which underscores the importance of discussing the nature of emerging side effects with your patient.
Dr. Davis is correct in noting that the practitioner must be aware of long-term side effects of lithium. I find it helpful to discuss these effects with the patient in the context of short-term (days or weeks), intermediate (weeks or months), and long-term (months or years) time frames (Table 2). Diabetes insipidus is listed as an intermediate side effect.
I am grateful to Dr. Davis for raising the issue of hydration and summer heat, a concern among parents and coaches when student athletes practice strenuously for extended hours.1 Miller et al2 found that the concentration of lithium was between 1.2- and 4.6-fold in forearm sweat compared with serum levels, with the implication that heat-induced sweating may lower lithium levels. Jefferson et al3 studied 4 athletes after a 20-km race and found that all had become dehydrated but had a decrease in the serum lithium level. This is contrary to the widely held belief that excessive sweating predisposes to lithium toxicity.
BD is among the more lethal psychiatric disorders, and lithium is among the few medications shown to mitigate suicidal behavior.4 As with any medication, lithium is not without risk, and there is a clear need for informed medical management. Any notable change in health status or physical activity in a patient taking lithium is worthy of review, with recommendations based on knowledge of the patient and medical science.
1. Reardon CL, Factor RM. Sport psychiatry: a systematic review of diagnosis and medical treatment of mental illness in athletes. Sports Med. 2010;40:961-980.
2. Miller EB, Pain RW, Skripal PJ. Sweat lithium in manic-depression. Br J Psychiatry. 1978;133:477-478.
3. Jefferson JW, Greist JH, Clagnaz PJ, et al. Effect of strenuous exercise on serum lithium level in man. Am J Psychiatry. 1982;139(12):1593-1595.
4. Goodwin FK, Fireman B, Simon GE, et al. Suicide risk in bipolar disorder during treatment with lithium and divalproex. JAMA. 2003;290(11):1467-1473.
1. Reardon CL, Factor RM. Sport psychiatry: a systematic review of diagnosis and medical treatment of mental illness in athletes. Sports Med. 2010;40:961-980.
2. Miller EB, Pain RW, Skripal PJ. Sweat lithium in manic-depression. Br J Psychiatry. 1978;133:477-478.
3. Jefferson JW, Greist JH, Clagnaz PJ, et al. Effect of strenuous exercise on serum lithium level in man. Am J Psychiatry. 1982;139(12):1593-1595.
4. Goodwin FK, Fireman B, Simon GE, et al. Suicide risk in bipolar disorder during treatment with lithium and divalproex. JAMA. 2003;290(11):1467-1473.
Severity of side effects key to choosing between lithium and quetiapine in bipolar I and II
HOLLYWOOD, FLA. – Because there is no clinically significant difference in bipolar spectrum symptom relief offered by either lithium or quetiapine, which mood stabilizer clinicians choose to prescribe should largely depend on what side effects patients can tolerate.
That’s the conclusion of a panel of experts who presented data from the Bipolar CHOICE (Clinical Health Outcomes Initiative in Comparative Effectiveness for Bipolar Disorder) clinical trial at a meeting of the American Society of Clinical Psychopharmacology, formerly known as the New Clinical Drug Evaluation Unit meeting.

By randomly assigning the study’s 482 participating outpatient adults to either lithium or quetiapine, while allowing clinicians to prescribe adjunctive treatment as necessary; and by using a broader-than-usual set of inclusion criteria, the investigators hoped to provide clinicians with "real world" data on how the respective mood stabilizers perform.
"To my knowledge, this is the first randomized comparative effectiveness study of regular, expert care that looks at lithium versus quetiapine strategies of treatment, both with adjunctive personalized treatment when necessary," study coauthor Dr. Andrew A. Nierenberg told the audience in a well-attended session.
"We tortured the data to get a P value to pop out," said Dr. Nierenberg, who is the director of the Bipolar Clinic and Research Program at Massachusetts General Hospital in Boston. "The bottom line was that the treatment strategies, based on either lithium or quetiapine, were very similar. I think the clinical implication is that the choice of treatment really depends on someone’s tolerability. This may resurrect lithium as something [clinicians] should at least consider, because its use has gone down dramatically in the last 20 years or so."
Side effects such as metabolic or sleep disturbances were slightly less frequent in the lithium group, although the difference was not statistically significant; rates of suicidality and discontinuation of medication due to side effects were also similar across the two groups, according to Dr. David E. Kemp of the psychiatry department at Case Western Reserve University, Cleveland, and a study coauthor who also presented data during the session. Changes from baseline in mood stabilization were also virtually the same across the groups.
‘Rules of engagement’
The study enrolled adults aged 18-68 years who were at least mildly ill with either bipolar disorder I (68%) or II, with a Clinical Global Impression (CGI) score of at least 3, although the average CGI score was 4.5 (standard deviation of plus or minus 0.9). Of the 482 enrolled, 364 completed the study.
The so-called rules of engagement for clinicians from the 11 participating centers were that "they do everything they could to get their patients well," with the caveat that the lithium patient group not receive any antipsychotic, and the quetiapine patient group not receive lithium or any other antipsychotic.
"But they could get anything else that they needed," Dr. Nierenberg said.
At the time of enrollment, subjects were, in the estimation of their treating physician, experiencing symptoms that warranted a change in treatment, and that either lithium or quetiapine would be viable therapeutic options. Patients did not need to be lithium- or quetiapine-naive, but they could not have been treated with either drug in the previous 30 days. If they were already taking a second-generation antipsychotic, participants had to be willing to discontinue that medication and to be randomly assigned to either of the study drugs.
This strict adherence to one mood stabilizer, combined with adjunctive personalized treatments such as antidepressants or benzodiazepines, prescribed at the discretion of the treating clinician, ensured that the study tested the strategy of using either lithium or quetiapine as the base of treatment, Dr. Nierenberg said.
‘Similar’ results
Clinicians also were instructed to use the maximum tolerated dose of the respective mood stabilizer. For the 240 patients in the lithium group, the mean maximum tolerated dose was 1,007.5 mg, with the median dose being a "perfectly reasonable 900 mg," Dr. Nierenberg said. Blood lithium levels were taken at weeks 2, 16, and 24 and also were all found to be "reasonable," with most patients getting to at least 0.6 mEq/L by week 24.
For the 242 members of the quetiapine group, the maximum tolerated dose was 344.9 mg, with a median tolerated dose of 300 mg, which Dr. Nierenberg said was "what you would expect."
The overall result was that regardless of which mood stabilizer was prescribed along with adjunctive personalized treatment, the coprimary outcomes of the benefits and harms ratio from treatment effects over time (the CGI efficacy index), and the number of necessary clinical adjustments (changes in medication excluding titrations according to scale), were virtually parallel: For each primary outcome, the P value for the estimated change in baseline was less than .0001 for both lithium plus adjunctive treatment, and quetiapine plus adjunctive treatment.
Further, Dr. Nierenberg reported the "unexpected" result that at 6 months, about a quarter of each group was observed to be doing well without any adjunctive personalized treatments (23.8% of the lithium group; 27.3% of the quetiapine group; P = .14). "We thought that everybody would be on multiple things," Dr. Nierenberg said.
There was also no real difference in the time to discontinuation. "We were actually surprised that at 6 months, about three-quarters of the patients were still on the study drug, which was pretty good considering that this was a very ill population," Dr. Nierenberg said.
Using a CGI bipolar severity scale rating of up to 2, maintained for at least 8 weeks, the investigators found that overall, 20% were considered doing "really well"; it was also about 20% for the lithium plus adjunctive therapy group and the quetiapine and adjunctive therapy group (P = .14 for all three).
Because the Agency for Healthcare Research and Quality–funded study mandated that researchers end their investigation at precisely 36 months, Dr. Nierenberg said the study sites "randomized the 482 patients to 6 months of treatment within 36 months from start to finish," but he added that the investigators would have preferred to conduct a full 2-year study of participants.
"The good news was that most of the patients actually did improve substantially; the bad news is that while maybe a quarter did really well by the end of 6 months, we don’t know whether if we were to extend the study out further, we would see a difference between the two groups, whether they would continue to improve, or whether they would relapse," he said.
Adverse effects, predictors of response
Because study participants were followed for only 6 months, the long-term adverse effects of many years of exposure to either mood stabilizer, such as renal impairment with lithium or type II diabetes with quetiapine, were not considered, Dr. Kemp said. The adverse-effect profile for lithium generally includes a narrow therapeutic index; nausea, vomiting, and diarrhea; renal impairment; and hypothyroidism. Although Dr. Kemp said that the long-term adverse effects of quetiapine are understudied, known short-term side effects include the potential for sedation or somnolence, and weight gain.
Changes in baseline on the Frequency and Intensity of Side Effects Ratings for the quetiapine plus adjunctive personalized treatment arm were slightly more adverse than for the lithium and additional treatment arm. For the lithium plus adjunctive treatment group, the mean frequency of side effects was –1.41 (–1.78, –1.04 SD); the mean intensity of side effects was –1.48 (–1.80, –1.15 SD); and the mean level of impairment was –1.13 (–1.43, –0.82 SD). For the quetiapine and adjunctive treatment group, the mean frequency measure was –1.08 (–1.45, –0.72 SD); the intensity was –1.12 (–1.44, –0.79 SD); and the impairment was –0.77 (–1.07, –0.47 SD). For all scores in both groups, P was less than .001.
The changes from baseline on the Bipolar Index Severity Scale (BISS) overall for the quetiapine plus adjunctive treatment group was –28.56 (–10.91, –26.21 SD; P less than .0001). For the lithium plus adjunctive treatment group, it was –27.61 (–29.99, –25.24 SD; P less than .0001). The overall difference between the two groups was 0.94 (–2.10, 3.99 SD; P = .54).
Scores on the Longitudinal Interval Follow-up Evaluation Range of Impaired Functioning Tool also slightly favored lithium: –3.74 (–4.29, –3.19 SD) vs. –3.6 (–4.15, –3.07 SD) for quetiapine (P less than .0001 for all).
To the investigators’ surprise, among those with comorbid anxiety, the lithium plus adjunctive treatment group had fewer necessary clinical adjustments per month than did the quetiapine plus adjunctive treatment group, according to Dr. Nierenberg: –0.83 vs. 1.11 (P = .02).
"That seemed counterintuitive, and this difference was only with anxiety, not with any other comorbid psychiatric conditions," Dr. Nierenberg said. He hypothesized that it was possible benzodiazepines were used more frequently and easily with lithium than with quetiapine, but said future analyses would give a clearer answer. "We have a detailed database of every other medication used: when it was started, when it was stopped, and the reason why everything was done."
Not having current anxiety disorder was predictive of a better outcome (odds ratio, 1.81; P = .02), as was employment (OR, 1.67; P = .04). Those with bipolar II disorder responded better to treatment than those with bipolar disorder I, having an OR of response to treatment of nearly 1.8 P = .03). "That was a surprise to us, too," Dr. Nierenberg said.
Just over a quarter (27%) of the study population had metabolic syndrome, according to Dr. Kemp, who said this was not found to influence treatment outcomes.
Nearly half of the overall population was obese (48%), and slightly less than half (44%) had adipose. Prospective analysis indicated that patients with either obesity or adiposity tended to show less improvement in their CGI scores in a statistically significant way, regardless of which mood stabilizer they were on.
"Part of that might be due to overlapping pathophysiology between bipolar disorder and obesity," Dr. Kemp said. "Much of that is centered around inflammation in the central nervous system, as well as alterations in adipokines receptor levels and mitochondrial dysfunction."
"A key issue is to take care of obesity," said panel discussant Dr. Mauricio Tohen, chairman of psychiatry at the University of New Mexico in Albuquerque. "Regardless of the treatment, when there is obesity, the outcome will not be as good."
Efficacy vs. ‘generalizability’
Adjunctive personalized treatment was measured to help minimize the lack of assay sensitivity and internal validity typically inherent in comparative effectiveness trials, while also achieving more broadly applicable results.
"The right study depends on the right question," Dr. Tohen said. "If the question is whether a particular treatment has efficacy and is safe, then of course, we need an efficacy study. The problem with efficacy studies is that they limit the generalizability."
Instead, Dr. Tohen, who disclosed he spent more than a decade evaluating efficacy studies for both Eli Lily and AstraZeneca (makers of quetiapine), praised the metric of the adjunctive personalized treatments, and said a study should answer the question, "Of all the patients in my clinic, who will do better on which treatment? With efficacy studies you cannot answer that question because of the exclusion criteria that need to be taken into account."
In addition, Dr. Tohen said the metric likely would increase in importance under the Affordable Care Act, where efficacy is not the only consideration. "For example, if a patient relapses earlier, it might not be reimbursed, so asking what other outcomes we need to measure in [these kinds of] comparative effectiveness studies is very important."
In the CHOICE study, which had no placebo group, participating physicians were asked to track each patient’s dosage changes, missed doses, new medications added, discontinued medications, and the specific reasons for any of these changes. Changes that were made because of lack of effectiveness or intolerance were measured; however, planned dosage titrations according to normal scales were not considered necessary clinical adjustments but simply the regular course of treatment.
This heterogeneity of adjunctive treatment was seen by the investigators as a way to reflect "real world" practice, although they also noted it could be seen as a limitation to the study.
Another way the study was designed to reflect real-world practice was the inclusion of a broader-than-usual group of participants, and asking them for their feedback at the end of the study period.
"Before we put together these data, we held a stakeholder summit," Dr. Nierenberg said. "We invited patients and their advocates to help us interpret the study. They felt strongly that this was a reasonably positive study, because they thought that people really did get better. You could report these data toward the negative or the positive, but we reported toward the positive because that is what the stakeholders asked us to do." Dr. Tohen said that this kind of feedback in a comparative effectiveness study was another way these kinds of studies could help guide practice in the era of the Affordable Care Act.
As for who was actually admitted to the study, "exclusions were minimal," said Dr. Edward S. Friedman of the psychiatry department at the University of Pittsburgh. Those with a history of drug or alcohol dependence in the previous 30 days, a demonstrated intolerance to either study drug, or severe cardiovascular or renal disease were excluded, as were those with unstable thyroid disease, and pregnant or breastfeeding women.
Overall, the group was multiethnic, although nearly three-quarters were white and 20% were black. Roughly a third of the entire study population was employed, a third unemployed, and the rest were students, retirees, or those on disability.
The overall BISS score at enrollment averaged 56.1 (SD plus or minus 18.8). The average BISS depression score was 37.6 (SD plus or minus 14.0), and the average BISS mania score was 18.5 (SD plus or minus 12.1).
There were many comorbid psychiatric conditions, ranging from panic disorder to agoraphobia, although substance use was highest (61.4%). Current anxiety disorder also was prevalent at 58%.
"The CHOICE sample was similar in age and gender to previous efficacy studies," Dr. Friedman said. "It was more representative of the U.S. population than efficacy studies such as STEP-BD or LITMUS."
The 283 women (59% of the study) were more likely to report having spent a greater percentage of time depressed in the previous year, although the percentage of time spent in manic or hypomanic states was equal across both genders.
"This study was composed of sick individuals who had been sick for a considerable period of time," Dr. Friedman said.
For example, in the CHOICE study, 47% had been hospitalized for their bipolar disorder previously, vs. 43% in the LITMUS study. CHOICE participants had an attempted suicide rate of 36%, which fell between the 41% in the LITMUS trial and the 33.3% in an efficacy study conducted by Dr. Joseph R. Calabrese and his colleagues (J. Clin. Psychiatry 1999;60:79-88).
The average age for the first depressive episode for CHOICE participants was 16.4 years; the first manic episode tended to be at 20 years; and the first mood episode tended to be around 15.5 years. These data were similar to those in the LITMUS study, but differed from data in several efficacy studies such as the one by Dr. Calabrese, where the average age was 31.3 years.
"You might anticipate that in these specialty clinics we would have very few medication-naive patients, and yet we did," Dr. Friedman said during a postpanel audience participation session. "Looking for patients with a low threshold, we brought in patients who were very sick. They were also older, with lots of previous episodes. Maybe we missed younger patients who didn’t have as many previous episodes."
"These are the patients you would see in your practice," Dr. Nierenberg said before asking the audience what they think should be studied next in a comparative effectiveness trial. "We could look at the use of different antipsychotics, the combinations we use, with or without lamotrigine," he said.
"Most of the decisions that are made in medicine are made without evidence. Most of the things that are done are done without evidence. You have combinations that were never studied before or never even used before, and it’s across all medicine." Because medicine needs to be learning more, he said the audience needed to participate. "What are the questions that need to be asked?"
On Twitter @whitneymcknight
HOLLYWOOD, FLA. – Because there is no clinically significant difference in bipolar spectrum symptom relief offered by either lithium or quetiapine, which mood stabilizer clinicians choose to prescribe should largely depend on what side effects patients can tolerate.
That’s the conclusion of a panel of experts who presented data from the Bipolar CHOICE (Clinical Health Outcomes Initiative in Comparative Effectiveness for Bipolar Disorder) clinical trial at a meeting of the American Society of Clinical Psychopharmacology, formerly known as the New Clinical Drug Evaluation Unit meeting.
By randomly assigning the study’s 482 participating outpatient adults to either lithium or quetiapine, while allowing clinicians to prescribe adjunctive treatment as necessary; and by using a broader-than-usual set of inclusion criteria, the investigators hoped to provide clinicians with "real world" data on how the respective mood stabilizers perform.
"To my knowledge, this is the first randomized comparative effectiveness study of regular, expert care that looks at lithium versus quetiapine strategies of treatment, both with adjunctive personalized treatment when necessary," study coauthor Dr. Andrew A. Nierenberg told the audience in a well-attended session.
"We tortured the data to get a P value to pop out," said Dr. Nierenberg, who is the director of the Bipolar Clinic and Research Program at Massachusetts General Hospital in Boston. "The bottom line was that the treatment strategies, based on either lithium or quetiapine, were very similar. I think the clinical implication is that the choice of treatment really depends on someone’s tolerability. This may resurrect lithium as something [clinicians] should at least consider, because its use has gone down dramatically in the last 20 years or so."
Side effects such as metabolic or sleep disturbances were slightly less frequent in the lithium group, although the difference was not statistically significant; rates of suicidality and discontinuation of medication due to side effects were also similar across the two groups, according to Dr. David E. Kemp of the psychiatry department at Case Western Reserve University, Cleveland, and a study coauthor who also presented data during the session. Changes from baseline in mood stabilization were also virtually the same across the groups.
‘Rules of engagement’
The study enrolled adults aged 18-68 years who were at least mildly ill with either bipolar disorder I (68%) or II, with a Clinical Global Impression (CGI) score of at least 3, although the average CGI score was 4.5 (standard deviation of plus or minus 0.9). Of the 482 enrolled, 364 completed the study.
The so-called rules of engagement for clinicians from the 11 participating centers were that "they do everything they could to get their patients well," with the caveat that the lithium patient group not receive any antipsychotic, and the quetiapine patient group not receive lithium or any other antipsychotic.
"But they could get anything else that they needed," Dr. Nierenberg said.
At the time of enrollment, subjects were, in the estimation of their treating physician, experiencing symptoms that warranted a change in treatment, and that either lithium or quetiapine would be viable therapeutic options. Patients did not need to be lithium- or quetiapine-naive, but they could not have been treated with either drug in the previous 30 days. If they were already taking a second-generation antipsychotic, participants had to be willing to discontinue that medication and to be randomly assigned to either of the study drugs.
This strict adherence to one mood stabilizer, combined with adjunctive personalized treatments such as antidepressants or benzodiazepines, prescribed at the discretion of the treating clinician, ensured that the study tested the strategy of using either lithium or quetiapine as the base of treatment, Dr. Nierenberg said.
‘Similar’ results
Clinicians also were instructed to use the maximum tolerated dose of the respective mood stabilizer. For the 240 patients in the lithium group, the mean maximum tolerated dose was 1,007.5 mg, with the median dose being a "perfectly reasonable 900 mg," Dr. Nierenberg said. Blood lithium levels were taken at weeks 2, 16, and 24 and also were all found to be "reasonable," with most patients getting to at least 0.6 mEq/L by week 24.
For the 242 members of the quetiapine group, the maximum tolerated dose was 344.9 mg, with a median tolerated dose of 300 mg, which Dr. Nierenberg said was "what you would expect."
The overall result was that regardless of which mood stabilizer was prescribed along with adjunctive personalized treatment, the coprimary outcomes of the benefits and harms ratio from treatment effects over time (the CGI efficacy index), and the number of necessary clinical adjustments (changes in medication excluding titrations according to scale), were virtually parallel: For each primary outcome, the P value for the estimated change in baseline was less than .0001 for both lithium plus adjunctive treatment, and quetiapine plus adjunctive treatment.
Further, Dr. Nierenberg reported the "unexpected" result that at 6 months, about a quarter of each group was observed to be doing well without any adjunctive personalized treatments (23.8% of the lithium group; 27.3% of the quetiapine group; P = .14). "We thought that everybody would be on multiple things," Dr. Nierenberg said.
There was also no real difference in the time to discontinuation. "We were actually surprised that at 6 months, about three-quarters of the patients were still on the study drug, which was pretty good considering that this was a very ill population," Dr. Nierenberg said.
Using a CGI bipolar severity scale rating of up to 2, maintained for at least 8 weeks, the investigators found that overall, 20% were considered doing "really well"; it was also about 20% for the lithium plus adjunctive therapy group and the quetiapine and adjunctive therapy group (P = .14 for all three).
Because the Agency for Healthcare Research and Quality–funded study mandated that researchers end their investigation at precisely 36 months, Dr. Nierenberg said the study sites "randomized the 482 patients to 6 months of treatment within 36 months from start to finish," but he added that the investigators would have preferred to conduct a full 2-year study of participants.
"The good news was that most of the patients actually did improve substantially; the bad news is that while maybe a quarter did really well by the end of 6 months, we don’t know whether if we were to extend the study out further, we would see a difference between the two groups, whether they would continue to improve, or whether they would relapse," he said.
Adverse effects, predictors of response
Because study participants were followed for only 6 months, the long-term adverse effects of many years of exposure to either mood stabilizer, such as renal impairment with lithium or type II diabetes with quetiapine, were not considered, Dr. Kemp said. The adverse-effect profile for lithium generally includes a narrow therapeutic index; nausea, vomiting, and diarrhea; renal impairment; and hypothyroidism. Although Dr. Kemp said that the long-term adverse effects of quetiapine are understudied, known short-term side effects include the potential for sedation or somnolence, and weight gain.
Changes in baseline on the Frequency and Intensity of Side Effects Ratings for the quetiapine plus adjunctive personalized treatment arm were slightly more adverse than for the lithium and additional treatment arm. For the lithium plus adjunctive treatment group, the mean frequency of side effects was –1.41 (–1.78, –1.04 SD); the mean intensity of side effects was –1.48 (–1.80, –1.15 SD); and the mean level of impairment was –1.13 (–1.43, –0.82 SD). For the quetiapine and adjunctive treatment group, the mean frequency measure was –1.08 (–1.45, –0.72 SD); the intensity was –1.12 (–1.44, –0.79 SD); and the impairment was –0.77 (–1.07, –0.47 SD). For all scores in both groups, P was less than .001.
The changes from baseline on the Bipolar Index Severity Scale (BISS) overall for the quetiapine plus adjunctive treatment group was –28.56 (–10.91, –26.21 SD; P less than .0001). For the lithium plus adjunctive treatment group, it was –27.61 (–29.99, –25.24 SD; P less than .0001). The overall difference between the two groups was 0.94 (–2.10, 3.99 SD; P = .54).
Scores on the Longitudinal Interval Follow-up Evaluation Range of Impaired Functioning Tool also slightly favored lithium: –3.74 (–4.29, –3.19 SD) vs. –3.6 (–4.15, –3.07 SD) for quetiapine (P less than .0001 for all).
To the investigators’ surprise, among those with comorbid anxiety, the lithium plus adjunctive treatment group had fewer necessary clinical adjustments per month than did the quetiapine plus adjunctive treatment group, according to Dr. Nierenberg: –0.83 vs. 1.11 (P = .02).
"That seemed counterintuitive, and this difference was only with anxiety, not with any other comorbid psychiatric conditions," Dr. Nierenberg said. He hypothesized that it was possible benzodiazepines were used more frequently and easily with lithium than with quetiapine, but said future analyses would give a clearer answer. "We have a detailed database of every other medication used: when it was started, when it was stopped, and the reason why everything was done."
Not having current anxiety disorder was predictive of a better outcome (odds ratio, 1.81; P = .02), as was employment (OR, 1.67; P = .04). Those with bipolar II disorder responded better to treatment than those with bipolar disorder I, having an OR of response to treatment of nearly 1.8 P = .03). "That was a surprise to us, too," Dr. Nierenberg said.
Just over a quarter (27%) of the study population had metabolic syndrome, according to Dr. Kemp, who said this was not found to influence treatment outcomes.
Nearly half of the overall population was obese (48%), and slightly less than half (44%) had adipose. Prospective analysis indicated that patients with either obesity or adiposity tended to show less improvement in their CGI scores in a statistically significant way, regardless of which mood stabilizer they were on.
"Part of that might be due to overlapping pathophysiology between bipolar disorder and obesity," Dr. Kemp said. "Much of that is centered around inflammation in the central nervous system, as well as alterations in adipokines receptor levels and mitochondrial dysfunction."
"A key issue is to take care of obesity," said panel discussant Dr. Mauricio Tohen, chairman of psychiatry at the University of New Mexico in Albuquerque. "Regardless of the treatment, when there is obesity, the outcome will not be as good."
Efficacy vs. ‘generalizability’
Adjunctive personalized treatment was measured to help minimize the lack of assay sensitivity and internal validity typically inherent in comparative effectiveness trials, while also achieving more broadly applicable results.
"The right study depends on the right question," Dr. Tohen said. "If the question is whether a particular treatment has efficacy and is safe, then of course, we need an efficacy study. The problem with efficacy studies is that they limit the generalizability."
Instead, Dr. Tohen, who disclosed he spent more than a decade evaluating efficacy studies for both Eli Lily and AstraZeneca (makers of quetiapine), praised the metric of the adjunctive personalized treatments, and said a study should answer the question, "Of all the patients in my clinic, who will do better on which treatment? With efficacy studies you cannot answer that question because of the exclusion criteria that need to be taken into account."
In addition, Dr. Tohen said the metric likely would increase in importance under the Affordable Care Act, where efficacy is not the only consideration. "For example, if a patient relapses earlier, it might not be reimbursed, so asking what other outcomes we need to measure in [these kinds of] comparative effectiveness studies is very important."
In the CHOICE study, which had no placebo group, participating physicians were asked to track each patient’s dosage changes, missed doses, new medications added, discontinued medications, and the specific reasons for any of these changes. Changes that were made because of lack of effectiveness or intolerance were measured; however, planned dosage titrations according to normal scales were not considered necessary clinical adjustments but simply the regular course of treatment.
This heterogeneity of adjunctive treatment was seen by the investigators as a way to reflect "real world" practice, although they also noted it could be seen as a limitation to the study.
Another way the study was designed to reflect real-world practice was the inclusion of a broader-than-usual group of participants, and asking them for their feedback at the end of the study period.
"Before we put together these data, we held a stakeholder summit," Dr. Nierenberg said. "We invited patients and their advocates to help us interpret the study. They felt strongly that this was a reasonably positive study, because they thought that people really did get better. You could report these data toward the negative or the positive, but we reported toward the positive because that is what the stakeholders asked us to do." Dr. Tohen said that this kind of feedback in a comparative effectiveness study was another way these kinds of studies could help guide practice in the era of the Affordable Care Act.
As for who was actually admitted to the study, "exclusions were minimal," said Dr. Edward S. Friedman of the psychiatry department at the University of Pittsburgh. Those with a history of drug or alcohol dependence in the previous 30 days, a demonstrated intolerance to either study drug, or severe cardiovascular or renal disease were excluded, as were those with unstable thyroid disease, and pregnant or breastfeeding women.
Overall, the group was multiethnic, although nearly three-quarters were white and 20% were black. Roughly a third of the entire study population was employed, a third unemployed, and the rest were students, retirees, or those on disability.
The overall BISS score at enrollment averaged 56.1 (SD plus or minus 18.8). The average BISS depression score was 37.6 (SD plus or minus 14.0), and the average BISS mania score was 18.5 (SD plus or minus 12.1).
There were many comorbid psychiatric conditions, ranging from panic disorder to agoraphobia, although substance use was highest (61.4%). Current anxiety disorder also was prevalent at 58%.
"The CHOICE sample was similar in age and gender to previous efficacy studies," Dr. Friedman said. "It was more representative of the U.S. population than efficacy studies such as STEP-BD or LITMUS."
The 283 women (59% of the study) were more likely to report having spent a greater percentage of time depressed in the previous year, although the percentage of time spent in manic or hypomanic states was equal across both genders.
"This study was composed of sick individuals who had been sick for a considerable period of time," Dr. Friedman said.
For example, in the CHOICE study, 47% had been hospitalized for their bipolar disorder previously, vs. 43% in the LITMUS study. CHOICE participants had an attempted suicide rate of 36%, which fell between the 41% in the LITMUS trial and the 33.3% in an efficacy study conducted by Dr. Joseph R. Calabrese and his colleagues (J. Clin. Psychiatry 1999;60:79-88).
The average age for the first depressive episode for CHOICE participants was 16.4 years; the first manic episode tended to be at 20 years; and the first mood episode tended to be around 15.5 years. These data were similar to those in the LITMUS study, but differed from data in several efficacy studies such as the one by Dr. Calabrese, where the average age was 31.3 years.
"You might anticipate that in these specialty clinics we would have very few medication-naive patients, and yet we did," Dr. Friedman said during a postpanel audience participation session. "Looking for patients with a low threshold, we brought in patients who were very sick. They were also older, with lots of previous episodes. Maybe we missed younger patients who didn’t have as many previous episodes."
"These are the patients you would see in your practice," Dr. Nierenberg said before asking the audience what they think should be studied next in a comparative effectiveness trial. "We could look at the use of different antipsychotics, the combinations we use, with or without lamotrigine," he said.
"Most of the decisions that are made in medicine are made without evidence. Most of the things that are done are done without evidence. You have combinations that were never studied before or never even used before, and it’s across all medicine." Because medicine needs to be learning more, he said the audience needed to participate. "What are the questions that need to be asked?"
On Twitter @whitneymcknight
HOLLYWOOD, FLA. – Because there is no clinically significant difference in bipolar spectrum symptom relief offered by either lithium or quetiapine, which mood stabilizer clinicians choose to prescribe should largely depend on what side effects patients can tolerate.
That’s the conclusion of a panel of experts who presented data from the Bipolar CHOICE (Clinical Health Outcomes Initiative in Comparative Effectiveness for Bipolar Disorder) clinical trial at a meeting of the American Society of Clinical Psychopharmacology, formerly known as the New Clinical Drug Evaluation Unit meeting.
By randomly assigning the study’s 482 participating outpatient adults to either lithium or quetiapine, while allowing clinicians to prescribe adjunctive treatment as necessary; and by using a broader-than-usual set of inclusion criteria, the investigators hoped to provide clinicians with "real world" data on how the respective mood stabilizers perform.
"To my knowledge, this is the first randomized comparative effectiveness study of regular, expert care that looks at lithium versus quetiapine strategies of treatment, both with adjunctive personalized treatment when necessary," study coauthor Dr. Andrew A. Nierenberg told the audience in a well-attended session.
"We tortured the data to get a P value to pop out," said Dr. Nierenberg, who is the director of the Bipolar Clinic and Research Program at Massachusetts General Hospital in Boston. "The bottom line was that the treatment strategies, based on either lithium or quetiapine, were very similar. I think the clinical implication is that the choice of treatment really depends on someone’s tolerability. This may resurrect lithium as something [clinicians] should at least consider, because its use has gone down dramatically in the last 20 years or so."
Side effects such as metabolic or sleep disturbances were slightly less frequent in the lithium group, although the difference was not statistically significant; rates of suicidality and discontinuation of medication due to side effects were also similar across the two groups, according to Dr. David E. Kemp of the psychiatry department at Case Western Reserve University, Cleveland, and a study coauthor who also presented data during the session. Changes from baseline in mood stabilization were also virtually the same across the groups.
‘Rules of engagement’
The study enrolled adults aged 18-68 years who were at least mildly ill with either bipolar disorder I (68%) or II, with a Clinical Global Impression (CGI) score of at least 3, although the average CGI score was 4.5 (standard deviation of plus or minus 0.9). Of the 482 enrolled, 364 completed the study.
The so-called rules of engagement for clinicians from the 11 participating centers were that "they do everything they could to get their patients well," with the caveat that the lithium patient group not receive any antipsychotic, and the quetiapine patient group not receive lithium or any other antipsychotic.
"But they could get anything else that they needed," Dr. Nierenberg said.
At the time of enrollment, subjects were, in the estimation of their treating physician, experiencing symptoms that warranted a change in treatment, and that either lithium or quetiapine would be viable therapeutic options. Patients did not need to be lithium- or quetiapine-naive, but they could not have been treated with either drug in the previous 30 days. If they were already taking a second-generation antipsychotic, participants had to be willing to discontinue that medication and to be randomly assigned to either of the study drugs.
This strict adherence to one mood stabilizer, combined with adjunctive personalized treatments such as antidepressants or benzodiazepines, prescribed at the discretion of the treating clinician, ensured that the study tested the strategy of using either lithium or quetiapine as the base of treatment, Dr. Nierenberg said.
‘Similar’ results
Clinicians also were instructed to use the maximum tolerated dose of the respective mood stabilizer. For the 240 patients in the lithium group, the mean maximum tolerated dose was 1,007.5 mg, with the median dose being a "perfectly reasonable 900 mg," Dr. Nierenberg said. Blood lithium levels were taken at weeks 2, 16, and 24 and also were all found to be "reasonable," with most patients getting to at least 0.6 mEq/L by week 24.
For the 242 members of the quetiapine group, the maximum tolerated dose was 344.9 mg, with a median tolerated dose of 300 mg, which Dr. Nierenberg said was "what you would expect."
The overall result was that regardless of which mood stabilizer was prescribed along with adjunctive personalized treatment, the coprimary outcomes of the benefits and harms ratio from treatment effects over time (the CGI efficacy index), and the number of necessary clinical adjustments (changes in medication excluding titrations according to scale), were virtually parallel: For each primary outcome, the P value for the estimated change in baseline was less than .0001 for both lithium plus adjunctive treatment, and quetiapine plus adjunctive treatment.
Further, Dr. Nierenberg reported the "unexpected" result that at 6 months, about a quarter of each group was observed to be doing well without any adjunctive personalized treatments (23.8% of the lithium group; 27.3% of the quetiapine group; P = .14). "We thought that everybody would be on multiple things," Dr. Nierenberg said.
There was also no real difference in the time to discontinuation. "We were actually surprised that at 6 months, about three-quarters of the patients were still on the study drug, which was pretty good considering that this was a very ill population," Dr. Nierenberg said.
Using a CGI bipolar severity scale rating of up to 2, maintained for at least 8 weeks, the investigators found that overall, 20% were considered doing "really well"; it was also about 20% for the lithium plus adjunctive therapy group and the quetiapine and adjunctive therapy group (P = .14 for all three).
Because the Agency for Healthcare Research and Quality–funded study mandated that researchers end their investigation at precisely 36 months, Dr. Nierenberg said the study sites "randomized the 482 patients to 6 months of treatment within 36 months from start to finish," but he added that the investigators would have preferred to conduct a full 2-year study of participants.
"The good news was that most of the patients actually did improve substantially; the bad news is that while maybe a quarter did really well by the end of 6 months, we don’t know whether if we were to extend the study out further, we would see a difference between the two groups, whether they would continue to improve, or whether they would relapse," he said.
Adverse effects, predictors of response
Because study participants were followed for only 6 months, the long-term adverse effects of many years of exposure to either mood stabilizer, such as renal impairment with lithium or type II diabetes with quetiapine, were not considered, Dr. Kemp said. The adverse-effect profile for lithium generally includes a narrow therapeutic index; nausea, vomiting, and diarrhea; renal impairment; and hypothyroidism. Although Dr. Kemp said that the long-term adverse effects of quetiapine are understudied, known short-term side effects include the potential for sedation or somnolence, and weight gain.
Changes in baseline on the Frequency and Intensity of Side Effects Ratings for the quetiapine plus adjunctive personalized treatment arm were slightly more adverse than for the lithium and additional treatment arm. For the lithium plus adjunctive treatment group, the mean frequency of side effects was –1.41 (–1.78, –1.04 SD); the mean intensity of side effects was –1.48 (–1.80, –1.15 SD); and the mean level of impairment was –1.13 (–1.43, –0.82 SD). For the quetiapine and adjunctive treatment group, the mean frequency measure was –1.08 (–1.45, –0.72 SD); the intensity was –1.12 (–1.44, –0.79 SD); and the impairment was –0.77 (–1.07, –0.47 SD). For all scores in both groups, P was less than .001.
The changes from baseline on the Bipolar Index Severity Scale (BISS) overall for the quetiapine plus adjunctive treatment group was –28.56 (–10.91, –26.21 SD; P less than .0001). For the lithium plus adjunctive treatment group, it was –27.61 (–29.99, –25.24 SD; P less than .0001). The overall difference between the two groups was 0.94 (–2.10, 3.99 SD; P = .54).
Scores on the Longitudinal Interval Follow-up Evaluation Range of Impaired Functioning Tool also slightly favored lithium: –3.74 (–4.29, –3.19 SD) vs. –3.6 (–4.15, –3.07 SD) for quetiapine (P less than .0001 for all).
To the investigators’ surprise, among those with comorbid anxiety, the lithium plus adjunctive treatment group had fewer necessary clinical adjustments per month than did the quetiapine plus adjunctive treatment group, according to Dr. Nierenberg: –0.83 vs. 1.11 (P = .02).
"That seemed counterintuitive, and this difference was only with anxiety, not with any other comorbid psychiatric conditions," Dr. Nierenberg said. He hypothesized that it was possible benzodiazepines were used more frequently and easily with lithium than with quetiapine, but said future analyses would give a clearer answer. "We have a detailed database of every other medication used: when it was started, when it was stopped, and the reason why everything was done."
Not having current anxiety disorder was predictive of a better outcome (odds ratio, 1.81; P = .02), as was employment (OR, 1.67; P = .04). Those with bipolar II disorder responded better to treatment than those with bipolar disorder I, having an OR of response to treatment of nearly 1.8 P = .03). "That was a surprise to us, too," Dr. Nierenberg said.
Just over a quarter (27%) of the study population had metabolic syndrome, according to Dr. Kemp, who said this was not found to influence treatment outcomes.
Nearly half of the overall population was obese (48%), and slightly less than half (44%) had adipose. Prospective analysis indicated that patients with either obesity or adiposity tended to show less improvement in their CGI scores in a statistically significant way, regardless of which mood stabilizer they were on.
"Part of that might be due to overlapping pathophysiology between bipolar disorder and obesity," Dr. Kemp said. "Much of that is centered around inflammation in the central nervous system, as well as alterations in adipokines receptor levels and mitochondrial dysfunction."
"A key issue is to take care of obesity," said panel discussant Dr. Mauricio Tohen, chairman of psychiatry at the University of New Mexico in Albuquerque. "Regardless of the treatment, when there is obesity, the outcome will not be as good."
Efficacy vs. ‘generalizability’
Adjunctive personalized treatment was measured to help minimize the lack of assay sensitivity and internal validity typically inherent in comparative effectiveness trials, while also achieving more broadly applicable results.
"The right study depends on the right question," Dr. Tohen said. "If the question is whether a particular treatment has efficacy and is safe, then of course, we need an efficacy study. The problem with efficacy studies is that they limit the generalizability."
Instead, Dr. Tohen, who disclosed he spent more than a decade evaluating efficacy studies for both Eli Lily and AstraZeneca (makers of quetiapine), praised the metric of the adjunctive personalized treatments, and said a study should answer the question, "Of all the patients in my clinic, who will do better on which treatment? With efficacy studies you cannot answer that question because of the exclusion criteria that need to be taken into account."
In addition, Dr. Tohen said the metric likely would increase in importance under the Affordable Care Act, where efficacy is not the only consideration. "For example, if a patient relapses earlier, it might not be reimbursed, so asking what other outcomes we need to measure in [these kinds of] comparative effectiveness studies is very important."
In the CHOICE study, which had no placebo group, participating physicians were asked to track each patient’s dosage changes, missed doses, new medications added, discontinued medications, and the specific reasons for any of these changes. Changes that were made because of lack of effectiveness or intolerance were measured; however, planned dosage titrations according to normal scales were not considered necessary clinical adjustments but simply the regular course of treatment.
This heterogeneity of adjunctive treatment was seen by the investigators as a way to reflect "real world" practice, although they also noted it could be seen as a limitation to the study.
Another way the study was designed to reflect real-world practice was the inclusion of a broader-than-usual group of participants, and asking them for their feedback at the end of the study period.
"Before we put together these data, we held a stakeholder summit," Dr. Nierenberg said. "We invited patients and their advocates to help us interpret the study. They felt strongly that this was a reasonably positive study, because they thought that people really did get better. You could report these data toward the negative or the positive, but we reported toward the positive because that is what the stakeholders asked us to do." Dr. Tohen said that this kind of feedback in a comparative effectiveness study was another way these kinds of studies could help guide practice in the era of the Affordable Care Act.
As for who was actually admitted to the study, "exclusions were minimal," said Dr. Edward S. Friedman of the psychiatry department at the University of Pittsburgh. Those with a history of drug or alcohol dependence in the previous 30 days, a demonstrated intolerance to either study drug, or severe cardiovascular or renal disease were excluded, as were those with unstable thyroid disease, and pregnant or breastfeeding women.
Overall, the group was multiethnic, although nearly three-quarters were white and 20% were black. Roughly a third of the entire study population was employed, a third unemployed, and the rest were students, retirees, or those on disability.
The overall BISS score at enrollment averaged 56.1 (SD plus or minus 18.8). The average BISS depression score was 37.6 (SD plus or minus 14.0), and the average BISS mania score was 18.5 (SD plus or minus 12.1).
There were many comorbid psychiatric conditions, ranging from panic disorder to agoraphobia, although substance use was highest (61.4%). Current anxiety disorder also was prevalent at 58%.
"The CHOICE sample was similar in age and gender to previous efficacy studies," Dr. Friedman said. "It was more representative of the U.S. population than efficacy studies such as STEP-BD or LITMUS."
The 283 women (59% of the study) were more likely to report having spent a greater percentage of time depressed in the previous year, although the percentage of time spent in manic or hypomanic states was equal across both genders.
"This study was composed of sick individuals who had been sick for a considerable period of time," Dr. Friedman said.
For example, in the CHOICE study, 47% had been hospitalized for their bipolar disorder previously, vs. 43% in the LITMUS study. CHOICE participants had an attempted suicide rate of 36%, which fell between the 41% in the LITMUS trial and the 33.3% in an efficacy study conducted by Dr. Joseph R. Calabrese and his colleagues (J. Clin. Psychiatry 1999;60:79-88).
The average age for the first depressive episode for CHOICE participants was 16.4 years; the first manic episode tended to be at 20 years; and the first mood episode tended to be around 15.5 years. These data were similar to those in the LITMUS study, but differed from data in several efficacy studies such as the one by Dr. Calabrese, where the average age was 31.3 years.
"You might anticipate that in these specialty clinics we would have very few medication-naive patients, and yet we did," Dr. Friedman said during a postpanel audience participation session. "Looking for patients with a low threshold, we brought in patients who were very sick. They were also older, with lots of previous episodes. Maybe we missed younger patients who didn’t have as many previous episodes."
"These are the patients you would see in your practice," Dr. Nierenberg said before asking the audience what they think should be studied next in a comparative effectiveness trial. "We could look at the use of different antipsychotics, the combinations we use, with or without lamotrigine," he said.
"Most of the decisions that are made in medicine are made without evidence. Most of the things that are done are done without evidence. You have combinations that were never studied before or never even used before, and it’s across all medicine." Because medicine needs to be learning more, he said the audience needed to participate. "What are the questions that need to be asked?"
On Twitter @whitneymcknight
AT THE ASCP ANNUAL MEETING
Key clinical point: Determining whether to use lithium or quetiapine in bipolar I and II comes down to side effects.
Major finding: No clinically significant difference was found for bipolar I and bipolar II symptom improvements in patients given lithium or quetiapine (P less than .0001).
Data source: Multicenter, randomized comparative effectiveness study of 482 outpatients on the bipolar spectrum, followed for 6 months as they were given either lithium plus adjunctive therapy, quetiapine plus adjunctive therapy, or monotherapy of either mood stabilizer.
Disclosures: The Agency for Healthcare Research and Quality funded this study in its entirety.

Telepsychiatry is a tool that we must exploit
As psychiatrists, we are particularly attuned to the value of face-to-face contact with patients. After all, so much is communicated nonverbally.
Fortunately, telepsychiatry has the capacity to give us the information we need to provide effective interventions for patients with mental illness. Even patients with serious mental illness can benefit from these interventions.

Take, for example, a literature review of 390 studies using terms that included "schizophrenia" and/or "telepsychiatry," "telemedicine," or "telepsychology" (Clin. Schizophr. Relat. Psychoses 2014 [doi:10.3371/CSRP.KAFE.021513]). The review, conducted by Dr. John Kasckow of the Veterans Affairs Pittsburgh Health Care System, found that modalities involving the telephone, the Internet, and videoconferencing "appear to be feasible in patients with schizophrenia." Furthermore, they found that those modalities appear to improve patient outcomes, although they acknowledge that more research is needed.
A subset of patients that can benefit from telepsychiatry is those in correctional facilities. Another literature review that looked at the implementation of telepsychiatry in correctional facilities in seven states, including my own state of California, and found that the modality "may improve living conditions and safety inside correctional facilities" (Perm. J. 2013 Summer;17:80-6). This review, conducted by Stacie Anne Deslich of the Marshall University in South Charleston, W.Va., and her colleagues, also found that using telepsychiatry improved access and saved those facilities $12,000 to more than $1 million.
These researchers also called for more study, particularly a case-control examination of the cost of providing psychiatric care through telemedicine vs. face-to-face psychiatric treatment. Using telepsychiatry for this population of patients is particularly important in light of depth and breadth of untreated mental illness in correctional facilities, such as depression, anxiety, bipolar disorders, and schizophrenia. "In addition, costs for providers traveling to distant facilities have been a deterrent to providing adequate care to inmates," Ms. Deslich wrote.
Yet another population of patients that can benefit from telepsychiatry is those with mental illness who come to emergency departments. A program implemented in Elizabeth City, N.C., connected patients in the ED with psychiatric providers who were at remote locations using telemedicine carts that were equipped with wireless technology (ED Manag. 2013;25:121-4). The program’s administrators reported that almost 30% of the patients who had involuntary commitment orders were stabilized to the extent that those orders could be rescinded and they were discharged to outpatient care. Furthermore, the researchers reported, the average length of stay for ED patients who were discharged to inpatient treatment facilities dropped by more than half, from 48 hours to 22.5 hours.
Not so surprisingly, telepsychiatry also is establishing a solid track record among young patients. A study of the perspectives of psychiatrists who provide consultation services to schools found "students were more likely to disclose clinical information via video, compared with face-to-face contact" (Telemed. J.E. Health 2013; 19;794-9). However, the psychiatrists did express concerns about technological difficulties, logistics, and information sharing.
Telepsychiatry also is gaining a foothold in other areas, such as in geriatric and consultation psychiatry. In other settings, telepsychiatry is being introduced, and evidence is still accumulating.
The primary driver of telepsychiatry is the psychiatrist shortage. In 2009, a total of 77% of U.S. counties reported a shortage. Additionally, recent increases in coverage for mental health care create a demand for more psychiatrist time. These factors, coupled with an aging psychiatry workforce, led to a growing imbalance between supply and demand that telepsychiatry can help to alleviate. Telepsychiatry can increase the efficiency of psychiatric care by allowing one psychiatrist to serve patients in multiple settings without burdensome travel. Although telepsychiatry was first used more than 30 years ago, only recently have demographic, economic, and cultural trends led to its rapid expansion.
Opportunities for telepsychiatry implementation exist across the spectrum of psychiatric care. So far, research has shown little or no difference between the outcomes yielded by traditional care and telepsychiatry. Work remains to be done, but clearly telepsychiatry is here to stay.
Dr. Kornbluh is assistant medical director for program improvement and telepsychiatry at the California Department of State Hospitals.
As psychiatrists, we are particularly attuned to the value of face-to-face contact with patients. After all, so much is communicated nonverbally.
Fortunately, telepsychiatry has the capacity to give us the information we need to provide effective interventions for patients with mental illness. Even patients with serious mental illness can benefit from these interventions.
Take, for example, a literature review of 390 studies using terms that included "schizophrenia" and/or "telepsychiatry," "telemedicine," or "telepsychology" (Clin. Schizophr. Relat. Psychoses 2014 [doi:10.3371/CSRP.KAFE.021513]). The review, conducted by Dr. John Kasckow of the Veterans Affairs Pittsburgh Health Care System, found that modalities involving the telephone, the Internet, and videoconferencing "appear to be feasible in patients with schizophrenia." Furthermore, they found that those modalities appear to improve patient outcomes, although they acknowledge that more research is needed.
A subset of patients that can benefit from telepsychiatry is those in correctional facilities. Another literature review that looked at the implementation of telepsychiatry in correctional facilities in seven states, including my own state of California, and found that the modality "may improve living conditions and safety inside correctional facilities" (Perm. J. 2013 Summer;17:80-6). This review, conducted by Stacie Anne Deslich of the Marshall University in South Charleston, W.Va., and her colleagues, also found that using telepsychiatry improved access and saved those facilities $12,000 to more than $1 million.
These researchers also called for more study, particularly a case-control examination of the cost of providing psychiatric care through telemedicine vs. face-to-face psychiatric treatment. Using telepsychiatry for this population of patients is particularly important in light of depth and breadth of untreated mental illness in correctional facilities, such as depression, anxiety, bipolar disorders, and schizophrenia. "In addition, costs for providers traveling to distant facilities have been a deterrent to providing adequate care to inmates," Ms. Deslich wrote.
Yet another population of patients that can benefit from telepsychiatry is those with mental illness who come to emergency departments. A program implemented in Elizabeth City, N.C., connected patients in the ED with psychiatric providers who were at remote locations using telemedicine carts that were equipped with wireless technology (ED Manag. 2013;25:121-4). The program’s administrators reported that almost 30% of the patients who had involuntary commitment orders were stabilized to the extent that those orders could be rescinded and they were discharged to outpatient care. Furthermore, the researchers reported, the average length of stay for ED patients who were discharged to inpatient treatment facilities dropped by more than half, from 48 hours to 22.5 hours.
Not so surprisingly, telepsychiatry also is establishing a solid track record among young patients. A study of the perspectives of psychiatrists who provide consultation services to schools found "students were more likely to disclose clinical information via video, compared with face-to-face contact" (Telemed. J.E. Health 2013; 19;794-9). However, the psychiatrists did express concerns about technological difficulties, logistics, and information sharing.
Telepsychiatry also is gaining a foothold in other areas, such as in geriatric and consultation psychiatry. In other settings, telepsychiatry is being introduced, and evidence is still accumulating.
The primary driver of telepsychiatry is the psychiatrist shortage. In 2009, a total of 77% of U.S. counties reported a shortage. Additionally, recent increases in coverage for mental health care create a demand for more psychiatrist time. These factors, coupled with an aging psychiatry workforce, led to a growing imbalance between supply and demand that telepsychiatry can help to alleviate. Telepsychiatry can increase the efficiency of psychiatric care by allowing one psychiatrist to serve patients in multiple settings without burdensome travel. Although telepsychiatry was first used more than 30 years ago, only recently have demographic, economic, and cultural trends led to its rapid expansion.
Opportunities for telepsychiatry implementation exist across the spectrum of psychiatric care. So far, research has shown little or no difference between the outcomes yielded by traditional care and telepsychiatry. Work remains to be done, but clearly telepsychiatry is here to stay.
Dr. Kornbluh is assistant medical director for program improvement and telepsychiatry at the California Department of State Hospitals.
As psychiatrists, we are particularly attuned to the value of face-to-face contact with patients. After all, so much is communicated nonverbally.
Fortunately, telepsychiatry has the capacity to give us the information we need to provide effective interventions for patients with mental illness. Even patients with serious mental illness can benefit from these interventions.
Take, for example, a literature review of 390 studies using terms that included "schizophrenia" and/or "telepsychiatry," "telemedicine," or "telepsychology" (Clin. Schizophr. Relat. Psychoses 2014 [doi:10.3371/CSRP.KAFE.021513]). The review, conducted by Dr. John Kasckow of the Veterans Affairs Pittsburgh Health Care System, found that modalities involving the telephone, the Internet, and videoconferencing "appear to be feasible in patients with schizophrenia." Furthermore, they found that those modalities appear to improve patient outcomes, although they acknowledge that more research is needed.
A subset of patients that can benefit from telepsychiatry is those in correctional facilities. Another literature review that looked at the implementation of telepsychiatry in correctional facilities in seven states, including my own state of California, and found that the modality "may improve living conditions and safety inside correctional facilities" (Perm. J. 2013 Summer;17:80-6). This review, conducted by Stacie Anne Deslich of the Marshall University in South Charleston, W.Va., and her colleagues, also found that using telepsychiatry improved access and saved those facilities $12,000 to more than $1 million.
These researchers also called for more study, particularly a case-control examination of the cost of providing psychiatric care through telemedicine vs. face-to-face psychiatric treatment. Using telepsychiatry for this population of patients is particularly important in light of depth and breadth of untreated mental illness in correctional facilities, such as depression, anxiety, bipolar disorders, and schizophrenia. "In addition, costs for providers traveling to distant facilities have been a deterrent to providing adequate care to inmates," Ms. Deslich wrote.
Yet another population of patients that can benefit from telepsychiatry is those with mental illness who come to emergency departments. A program implemented in Elizabeth City, N.C., connected patients in the ED with psychiatric providers who were at remote locations using telemedicine carts that were equipped with wireless technology (ED Manag. 2013;25:121-4). The program’s administrators reported that almost 30% of the patients who had involuntary commitment orders were stabilized to the extent that those orders could be rescinded and they were discharged to outpatient care. Furthermore, the researchers reported, the average length of stay for ED patients who were discharged to inpatient treatment facilities dropped by more than half, from 48 hours to 22.5 hours.
Not so surprisingly, telepsychiatry also is establishing a solid track record among young patients. A study of the perspectives of psychiatrists who provide consultation services to schools found "students were more likely to disclose clinical information via video, compared with face-to-face contact" (Telemed. J.E. Health 2013; 19;794-9). However, the psychiatrists did express concerns about technological difficulties, logistics, and information sharing.
Telepsychiatry also is gaining a foothold in other areas, such as in geriatric and consultation psychiatry. In other settings, telepsychiatry is being introduced, and evidence is still accumulating.
The primary driver of telepsychiatry is the psychiatrist shortage. In 2009, a total of 77% of U.S. counties reported a shortage. Additionally, recent increases in coverage for mental health care create a demand for more psychiatrist time. These factors, coupled with an aging psychiatry workforce, led to a growing imbalance between supply and demand that telepsychiatry can help to alleviate. Telepsychiatry can increase the efficiency of psychiatric care by allowing one psychiatrist to serve patients in multiple settings without burdensome travel. Although telepsychiatry was first used more than 30 years ago, only recently have demographic, economic, and cultural trends led to its rapid expansion.
Opportunities for telepsychiatry implementation exist across the spectrum of psychiatric care. So far, research has shown little or no difference between the outcomes yielded by traditional care and telepsychiatry. Work remains to be done, but clearly telepsychiatry is here to stay.
Dr. Kornbluh is assistant medical director for program improvement and telepsychiatry at the California Department of State Hospitals.

Should lithium and ECT be used concurrently in geriatric patients?
Delirium has been described as a potential complication of concurrent lithium and electroconvulsive therapy (ECT) for depression, in association with a range of serum lithium levels. Although debate persists about the safety of continuing previously established lithium therapy during a course of ECT for mood symptoms, withholding lithium for 24 hours before administering ECT and measuring the serum lithium level before ECT were found to decrease the risk of post-ECT neurocognitive effects.1
We have found that the conventional practice of holding lithium for 24 hours before ECT might need to be re-evaluated in geriatric patients, as the following case demonstrates. Only 24 hours of holding lithium therapy might result in a lithium level sufficient to contribute to delirium after ECT.
CASE REPORT
An older woman with recurrent unipolar psychotic depression
Mrs. A, age 81, was admitted to the hospital with a 1-week history of depressed mood, anhedonia, insomnia, anergia, anorexia, and nihilistic somatic delusions that her organs were “rotting and shutting down.” Treatment included nortriptyline, 40 mg/d; lithium, 150 mg/d; and haloperidol, 0.5 mg/d. Her serum lithium level was 0.3 mEq/L (reference range, 0.6 to 1.2 mEq/L); the serum nortriptyline level was 68 ng/mL (reference range, 50 to 150 ng/mL). CT of the head and an electrocardiogram were unremarkable.
A twice-weekly course of ECT was initiated.
The day before Treatment 1 of ECT, the serum lithium level (drawn 12 hours after the last dose) was 0.4 mEq/L. Lithium was withheld 24 hours before ECT; nortriptyline and haloperidol were continued at prescribed dosages.
Right unilateral stimulation was used at 50%/mC energy (Thymatron DG, with methohexital anesthesia, and succinylcholine for muscle relaxation). Seizure duration, measured by EEG, was 57 seconds.
Mrs. A developed postictal delirium after the first 2 ECT sessions. The serum lithium level was unchanged. Subsequently, lithium treatment was discontinued and ECT was continued; once lithium was stopped, delirium resolved. ECT sessions 3 and 4 were uneventful, with no post-treatment delirium. Seizure duration for Treatment 4 was 58 seconds. She started breathing easily after all ECT sessions.
After Treatment 4, Mrs. A experienced full remission of depressive and psychotic symptoms. Repeat CT of head, after Treatment 4, was unchanged from baseline.
What is the role of lithium?
Mrs. A did not exhibit typical signs of lithium intoxication (diarrhea, vomiting, tremor). Notably, lithium has an intrinsic anticholinergic activity2; concurrent nortriptyline, a secondary amine tricyclic antidepressant with fewer anticholinergic side effects than other tricyclics,2 could precipitate delirium in a vulnerable patient secondary to excessive cumulative anticholinergic exposure.
No prolonged time-to-respiration or time-to-awakening occurred during treatments in which concurrent lithium and ECT were used; seizure duration with and without concurrent lithium was relatively similar.
There are potential complications of concurrent use of lithium and ECT:
• prolongation of the duration of muscle paralysis and apnea induced by commonly used neuromuscular-blocking agents (eg, succinylcholine)
• post-ECT cognitive disturbance.1,3,4
There is debate about the safety of continuing lithium during, or in close proximity to, ECT. In a case series of 12 patients who underwent combined lithium therapy and ECT, the authors concluded that this combination can be safe, regardless of age, as long as appropriate clinical monitoring is provided.4 In Mrs. A’s case, once post-ECT delirium was noted, lithium was discontinued for subsequent ECT sessions.
Because further ECT was uneventful without lithium, and no other clear acute cause of delirium could be identified, we concluded that lithium likely played a role in Mrs. A’s delirium. Notably, nortriptyline had been continued, suggesting that the degree of anticholinergic blockade provided by nortriptyline was insufficient to provoke delirium post-ECT in the absence of potentiation of this effect, as it had been when lithium also was used initially.
Guidelines for dosing and serum lithium concentrations in geriatric patients are not well-established; the current traditional range of 0.6 to 1.2 mEq/L, is too high for geriatric patients and can result in episodes of lithium toxicity, including delirium.5 Although our patient’s lithium level was below the reference range for all patients, a level of 0.3 mEq/L can be considered at the low end of the reference range for geriatric patients.5 Inasmuch as the lithium-assisted post-ECT delirium could represent a clinical sign of lithium toxicity, perhaps even a subtherapeutic level in a certain patient could be paradoxically “toxic.”
Although the serum lithium level in our patient remained below the toxic level for the general population (>1.5 mEq/L), delirium in a geriatric patient could result from:
• age-related changes in the pharmacokinetics of lithium, a water-soluble drug; these changes reduce renal clearance of the drug and extend plasma elimination half-life of a single dose to 36 hours, with the result that lithium remains in the body longer and necessitating a lower dosage (ie, a dosage that yields a serum level of approximately 0.5 mEq/L)
• the CNS tissue concentration of lithium, which can be high even though the serum level is not toxic
• an age-related increase in blood-brain barrier permeability, making the barrier more porous for drugs
• changes in blood-brain barrier permeability by post-ECT biochemical induction, with subsequent increased drug availability in the CNS.5,6
What we recommend
Possible interactions between lithium and ECT that lead to ECT-associated delirium need further elucidation, but discontinuing lithium during the course of ECT in a geriatric patient warrants your consideration. Following a safe interval after the last ECT session, lithium likely can be safely re-introduced 1) if there is clinical need and 2) as long as clinical surveillance for cognitive side effects is provided— especially if ECT will need to be reconsidered in the future.
Two additional considerations:
• Actively reassess lithium dosing in all geriatric psychiatric patients, especially those with renal insufficiency and other systemic metabolic considerations.
• Actively examine the use of all other anticholinergic agents in the course of evaluating a patient’s candidacy for ECT.
Disclosures
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
1. American Psychiatric Association. The practice of electroconvulsive therapy: recommendations for treatment, training, and privileging. A task force report of the American Psychiatric Association. 2nd ed. Washington, DC: American Psychiatric Publishing; 2001.
2. Chew ML, Mulsant BH, Pollock BG, et al. Anticholinergic activity of 107 medications commonly used by older adults. J Am Geriatr Soc. 2008;56(7):1333-1341.
3. Hill GE, Wong KC, Hodges MR. Potentiation of succinylcholine neuromuscular blockade by lithium carbonate. Anesthesiology. 1976;44(5):439-442.
4. Dolenc TJ, Rasmussen KG. The safety of electroconvulsive therapy and lithium in combination: a case series and review of the literature. J ECT. 2005;21(3):165-170.
5. Shulman KI. Lithium for older adults with bipolar disorder: should it still be considered a first line agent? Drugs Aging. 2010;27(8):607-615.
6. Grandjean EM, Aubry JM. Lithium: updated human knowledge using an evidence-based approach. Part II: clinical pharmacology and therapeutic monitoring. CNS Drugs. 2009;23(4):331-349.
Delirium has been described as a potential complication of concurrent lithium and electroconvulsive therapy (ECT) for depression, in association with a range of serum lithium levels. Although debate persists about the safety of continuing previously established lithium therapy during a course of ECT for mood symptoms, withholding lithium for 24 hours before administering ECT and measuring the serum lithium level before ECT were found to decrease the risk of post-ECT neurocognitive effects.1
We have found that the conventional practice of holding lithium for 24 hours before ECT might need to be re-evaluated in geriatric patients, as the following case demonstrates. Only 24 hours of holding lithium therapy might result in a lithium level sufficient to contribute to delirium after ECT.
CASE REPORT
An older woman with recurrent unipolar psychotic depression
Mrs. A, age 81, was admitted to the hospital with a 1-week history of depressed mood, anhedonia, insomnia, anergia, anorexia, and nihilistic somatic delusions that her organs were “rotting and shutting down.” Treatment included nortriptyline, 40 mg/d; lithium, 150 mg/d; and haloperidol, 0.5 mg/d. Her serum lithium level was 0.3 mEq/L (reference range, 0.6 to 1.2 mEq/L); the serum nortriptyline level was 68 ng/mL (reference range, 50 to 150 ng/mL). CT of the head and an electrocardiogram were unremarkable.
A twice-weekly course of ECT was initiated.
The day before Treatment 1 of ECT, the serum lithium level (drawn 12 hours after the last dose) was 0.4 mEq/L. Lithium was withheld 24 hours before ECT; nortriptyline and haloperidol were continued at prescribed dosages.
Right unilateral stimulation was used at 50%/mC energy (Thymatron DG, with methohexital anesthesia, and succinylcholine for muscle relaxation). Seizure duration, measured by EEG, was 57 seconds.
Mrs. A developed postictal delirium after the first 2 ECT sessions. The serum lithium level was unchanged. Subsequently, lithium treatment was discontinued and ECT was continued; once lithium was stopped, delirium resolved. ECT sessions 3 and 4 were uneventful, with no post-treatment delirium. Seizure duration for Treatment 4 was 58 seconds. She started breathing easily after all ECT sessions.
After Treatment 4, Mrs. A experienced full remission of depressive and psychotic symptoms. Repeat CT of head, after Treatment 4, was unchanged from baseline.
What is the role of lithium?
Mrs. A did not exhibit typical signs of lithium intoxication (diarrhea, vomiting, tremor). Notably, lithium has an intrinsic anticholinergic activity2; concurrent nortriptyline, a secondary amine tricyclic antidepressant with fewer anticholinergic side effects than other tricyclics,2 could precipitate delirium in a vulnerable patient secondary to excessive cumulative anticholinergic exposure.
No prolonged time-to-respiration or time-to-awakening occurred during treatments in which concurrent lithium and ECT were used; seizure duration with and without concurrent lithium was relatively similar.
There are potential complications of concurrent use of lithium and ECT:
• prolongation of the duration of muscle paralysis and apnea induced by commonly used neuromuscular-blocking agents (eg, succinylcholine)
• post-ECT cognitive disturbance.1,3,4
There is debate about the safety of continuing lithium during, or in close proximity to, ECT. In a case series of 12 patients who underwent combined lithium therapy and ECT, the authors concluded that this combination can be safe, regardless of age, as long as appropriate clinical monitoring is provided.4 In Mrs. A’s case, once post-ECT delirium was noted, lithium was discontinued for subsequent ECT sessions.
Because further ECT was uneventful without lithium, and no other clear acute cause of delirium could be identified, we concluded that lithium likely played a role in Mrs. A’s delirium. Notably, nortriptyline had been continued, suggesting that the degree of anticholinergic blockade provided by nortriptyline was insufficient to provoke delirium post-ECT in the absence of potentiation of this effect, as it had been when lithium also was used initially.
Guidelines for dosing and serum lithium concentrations in geriatric patients are not well-established; the current traditional range of 0.6 to 1.2 mEq/L, is too high for geriatric patients and can result in episodes of lithium toxicity, including delirium.5 Although our patient’s lithium level was below the reference range for all patients, a level of 0.3 mEq/L can be considered at the low end of the reference range for geriatric patients.5 Inasmuch as the lithium-assisted post-ECT delirium could represent a clinical sign of lithium toxicity, perhaps even a subtherapeutic level in a certain patient could be paradoxically “toxic.”
Although the serum lithium level in our patient remained below the toxic level for the general population (>1.5 mEq/L), delirium in a geriatric patient could result from:
• age-related changes in the pharmacokinetics of lithium, a water-soluble drug; these changes reduce renal clearance of the drug and extend plasma elimination half-life of a single dose to 36 hours, with the result that lithium remains in the body longer and necessitating a lower dosage (ie, a dosage that yields a serum level of approximately 0.5 mEq/L)
• the CNS tissue concentration of lithium, which can be high even though the serum level is not toxic
• an age-related increase in blood-brain barrier permeability, making the barrier more porous for drugs
• changes in blood-brain barrier permeability by post-ECT biochemical induction, with subsequent increased drug availability in the CNS.5,6
What we recommend
Possible interactions between lithium and ECT that lead to ECT-associated delirium need further elucidation, but discontinuing lithium during the course of ECT in a geriatric patient warrants your consideration. Following a safe interval after the last ECT session, lithium likely can be safely re-introduced 1) if there is clinical need and 2) as long as clinical surveillance for cognitive side effects is provided— especially if ECT will need to be reconsidered in the future.
Two additional considerations:
• Actively reassess lithium dosing in all geriatric psychiatric patients, especially those with renal insufficiency and other systemic metabolic considerations.
• Actively examine the use of all other anticholinergic agents in the course of evaluating a patient’s candidacy for ECT.
Disclosures
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
Delirium has been described as a potential complication of concurrent lithium and electroconvulsive therapy (ECT) for depression, in association with a range of serum lithium levels. Although debate persists about the safety of continuing previously established lithium therapy during a course of ECT for mood symptoms, withholding lithium for 24 hours before administering ECT and measuring the serum lithium level before ECT were found to decrease the risk of post-ECT neurocognitive effects.1
We have found that the conventional practice of holding lithium for 24 hours before ECT might need to be re-evaluated in geriatric patients, as the following case demonstrates. Only 24 hours of holding lithium therapy might result in a lithium level sufficient to contribute to delirium after ECT.
CASE REPORT
An older woman with recurrent unipolar psychotic depression
Mrs. A, age 81, was admitted to the hospital with a 1-week history of depressed mood, anhedonia, insomnia, anergia, anorexia, and nihilistic somatic delusions that her organs were “rotting and shutting down.” Treatment included nortriptyline, 40 mg/d; lithium, 150 mg/d; and haloperidol, 0.5 mg/d. Her serum lithium level was 0.3 mEq/L (reference range, 0.6 to 1.2 mEq/L); the serum nortriptyline level was 68 ng/mL (reference range, 50 to 150 ng/mL). CT of the head and an electrocardiogram were unremarkable.
A twice-weekly course of ECT was initiated.
The day before Treatment 1 of ECT, the serum lithium level (drawn 12 hours after the last dose) was 0.4 mEq/L. Lithium was withheld 24 hours before ECT; nortriptyline and haloperidol were continued at prescribed dosages.
Right unilateral stimulation was used at 50%/mC energy (Thymatron DG, with methohexital anesthesia, and succinylcholine for muscle relaxation). Seizure duration, measured by EEG, was 57 seconds.
Mrs. A developed postictal delirium after the first 2 ECT sessions. The serum lithium level was unchanged. Subsequently, lithium treatment was discontinued and ECT was continued; once lithium was stopped, delirium resolved. ECT sessions 3 and 4 were uneventful, with no post-treatment delirium. Seizure duration for Treatment 4 was 58 seconds. She started breathing easily after all ECT sessions.
After Treatment 4, Mrs. A experienced full remission of depressive and psychotic symptoms. Repeat CT of head, after Treatment 4, was unchanged from baseline.
What is the role of lithium?
Mrs. A did not exhibit typical signs of lithium intoxication (diarrhea, vomiting, tremor). Notably, lithium has an intrinsic anticholinergic activity2; concurrent nortriptyline, a secondary amine tricyclic antidepressant with fewer anticholinergic side effects than other tricyclics,2 could precipitate delirium in a vulnerable patient secondary to excessive cumulative anticholinergic exposure.
No prolonged time-to-respiration or time-to-awakening occurred during treatments in which concurrent lithium and ECT were used; seizure duration with and without concurrent lithium was relatively similar.
There are potential complications of concurrent use of lithium and ECT:
• prolongation of the duration of muscle paralysis and apnea induced by commonly used neuromuscular-blocking agents (eg, succinylcholine)
• post-ECT cognitive disturbance.1,3,4
There is debate about the safety of continuing lithium during, or in close proximity to, ECT. In a case series of 12 patients who underwent combined lithium therapy and ECT, the authors concluded that this combination can be safe, regardless of age, as long as appropriate clinical monitoring is provided.4 In Mrs. A’s case, once post-ECT delirium was noted, lithium was discontinued for subsequent ECT sessions.
Because further ECT was uneventful without lithium, and no other clear acute cause of delirium could be identified, we concluded that lithium likely played a role in Mrs. A’s delirium. Notably, nortriptyline had been continued, suggesting that the degree of anticholinergic blockade provided by nortriptyline was insufficient to provoke delirium post-ECT in the absence of potentiation of this effect, as it had been when lithium also was used initially.
Guidelines for dosing and serum lithium concentrations in geriatric patients are not well-established; the current traditional range of 0.6 to 1.2 mEq/L, is too high for geriatric patients and can result in episodes of lithium toxicity, including delirium.5 Although our patient’s lithium level was below the reference range for all patients, a level of 0.3 mEq/L can be considered at the low end of the reference range for geriatric patients.5 Inasmuch as the lithium-assisted post-ECT delirium could represent a clinical sign of lithium toxicity, perhaps even a subtherapeutic level in a certain patient could be paradoxically “toxic.”
Although the serum lithium level in our patient remained below the toxic level for the general population (>1.5 mEq/L), delirium in a geriatric patient could result from:
• age-related changes in the pharmacokinetics of lithium, a water-soluble drug; these changes reduce renal clearance of the drug and extend plasma elimination half-life of a single dose to 36 hours, with the result that lithium remains in the body longer and necessitating a lower dosage (ie, a dosage that yields a serum level of approximately 0.5 mEq/L)
• the CNS tissue concentration of lithium, which can be high even though the serum level is not toxic
• an age-related increase in blood-brain barrier permeability, making the barrier more porous for drugs
• changes in blood-brain barrier permeability by post-ECT biochemical induction, with subsequent increased drug availability in the CNS.5,6
What we recommend
Possible interactions between lithium and ECT that lead to ECT-associated delirium need further elucidation, but discontinuing lithium during the course of ECT in a geriatric patient warrants your consideration. Following a safe interval after the last ECT session, lithium likely can be safely re-introduced 1) if there is clinical need and 2) as long as clinical surveillance for cognitive side effects is provided— especially if ECT will need to be reconsidered in the future.
Two additional considerations:
• Actively reassess lithium dosing in all geriatric psychiatric patients, especially those with renal insufficiency and other systemic metabolic considerations.
• Actively examine the use of all other anticholinergic agents in the course of evaluating a patient’s candidacy for ECT.
Disclosures
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
1. American Psychiatric Association. The practice of electroconvulsive therapy: recommendations for treatment, training, and privileging. A task force report of the American Psychiatric Association. 2nd ed. Washington, DC: American Psychiatric Publishing; 2001.
2. Chew ML, Mulsant BH, Pollock BG, et al. Anticholinergic activity of 107 medications commonly used by older adults. J Am Geriatr Soc. 2008;56(7):1333-1341.
3. Hill GE, Wong KC, Hodges MR. Potentiation of succinylcholine neuromuscular blockade by lithium carbonate. Anesthesiology. 1976;44(5):439-442.
4. Dolenc TJ, Rasmussen KG. The safety of electroconvulsive therapy and lithium in combination: a case series and review of the literature. J ECT. 2005;21(3):165-170.
5. Shulman KI. Lithium for older adults with bipolar disorder: should it still be considered a first line agent? Drugs Aging. 2010;27(8):607-615.
6. Grandjean EM, Aubry JM. Lithium: updated human knowledge using an evidence-based approach. Part II: clinical pharmacology and therapeutic monitoring. CNS Drugs. 2009;23(4):331-349.
1. American Psychiatric Association. The practice of electroconvulsive therapy: recommendations for treatment, training, and privileging. A task force report of the American Psychiatric Association. 2nd ed. Washington, DC: American Psychiatric Publishing; 2001.
2. Chew ML, Mulsant BH, Pollock BG, et al. Anticholinergic activity of 107 medications commonly used by older adults. J Am Geriatr Soc. 2008;56(7):1333-1341.
3. Hill GE, Wong KC, Hodges MR. Potentiation of succinylcholine neuromuscular blockade by lithium carbonate. Anesthesiology. 1976;44(5):439-442.
4. Dolenc TJ, Rasmussen KG. The safety of electroconvulsive therapy and lithium in combination: a case series and review of the literature. J ECT. 2005;21(3):165-170.
5. Shulman KI. Lithium for older adults with bipolar disorder: should it still be considered a first line agent? Drugs Aging. 2010;27(8):607-615.
6. Grandjean EM, Aubry JM. Lithium: updated human knowledge using an evidence-based approach. Part II: clinical pharmacology and therapeutic monitoring. CNS Drugs. 2009;23(4):331-349.
For couples seeking to conceive, offer advice on reducing the risk of schizophrenia in their child
I explained to them that schizophrenia is a neurodevelopmental syndrome that comprises hundreds of different disorders of genetic or non-genetic etiology, all of which share a similar psychotic phenotype. Although the various genetic causes of schizophrenia are difficult to prevent—but may be prevented in the future with epigenetic techniques—the many non-genetic (environmental) pathways to schizophrenia can be avoided to significantly reduce the incidence of schizophrenia by 40% to 50%, according to some estimates.
I will share what I told this couple, because even couples without any family history of psychosis may have a child who develops schizophrenia because of a variety of environmental risk factors.
Genetic risk factors
One-half of the 20,000 genes in the 23 chromosomes of the human genome participate in constructing and sculpting the extremely intricate and complex human brain. There are many ways that genetic factors can increase the risk of schizophrenia,1 and only some are transmitted by parents:
Risk genes. More than 30 risk genes have been identified as heritable in schizophrenia. They are spread over many chromosomes and more are likely to be discovered. Most of those risk genes regulate glutamate— not dopamine—pathways, and each increases the risk by 2% to 4%.
Copy number variations (CNVs) are produced via meiosis mishaps, where 1 or 3 alleles of certain genes are formed instead of the usual 2. A high frequency of CNVs have been found in schizophrenia compared with the general population—but also are found in autism and bipolar disorders—and are believed to disrupt brain development in various ways.
De novo mutations. Recent studies on large samples of people with schizophrenia (50,000 to 100,000) uncovered a much higher rate of mutations (some code for proteins while others are nonsense mutations that code for nothing). Obviously, these mutations led to anomalous neurodevelopment.
There are hundreds, maybe thousands, of genetic subtypes within the schizophrenia syndrome. Advances in epigenetics, which allow silencing of culprit genes or overexpression of protective genes, one day may enable psychiatric geneticists to prevent schizophrenia in fetuses at risk.
Non-genetic risk factors
Just as with the genetic patho-genic heterogeneity, the schizophrenia syndrome can be caused by numerous environmental adverse events,2 many of which can be avoided, including:
Older paternal age (>45) at time of conception doubles or triples the risk of schizophrenia3 as well as autism and bipolar disorder. Aging sperm are associated with a higher rate of DNA fragmentation and genetic mutations.
Prenatal complications, especially during the second trimester when CNS development takes place. These adverse prenatal events skew fetal brain development to produce psychosis in adulthood and can be minimized with optimal prenatal care, which sadly is lacking among the poor. These include:
• Vaginal infections before pregnancy,4 such as herpes simplex virus, can cause fetal brain inflammation and increased risk of schizophrenia.
• Infections during pregnancy— whether bacterial, viral, or protozoan (Toxoplasma gondii)—have been shown to significantly increase the risk of schizophrenia in offspring.5 An increase in serum C-reactive protein during pregnancy also is a biomarker of increased risk.
• Poor diet, especially starvation, can double or triple the risk of schizophrenia.
• Vitamin deficiency, especially folate and vitamin D, are critical for normal brain development.6 Vitamin D is vital to mitigate neuroinflammation.
• Smoking before and during pregnancy.4
• Medical illness during pregnancy, especially gestational diabetes, increases the risk of schizophrenia in the fetus by 800%.7
• Severe stress during pregnancy, such as the death of the spouse, doubles the risk of schizophrenia.2
• Schizophrenia risk is 400% to 500% higher among those born and raised in an urban area, compared with a rural area.8
• Babies born in northern latitudes, such as in Sweden, Norway, or Canada, have a 10-fold risk of schizophrenia in adulthood compared with babies born near the equator.6 This has been attributed to lack of sunshine and the risk of severe vitamin D deficiency in northern latitudes.
• High maternal body mass index during the first trimester7 increases the child’s risk of schizophrenia.
• Low number of prenatal visits is associated with higher risk of schizophrenia.
• Obstetric complications that cause hypoxia and a low Apgar score after birth increase the risk of schizophrenia. This includes long labor, cord around the neck, meconium spillage into the amniotic fluid, and mechanical injury with forceps delivery.
• Infection in the newborn shortly after birth.
Severe physical or sexual abuse before age 5 is associated with increased risk of schizophrenia in adulthood.2 This may be because of stress-induced epigenetic mechanisms (silencing or overexpressing certain genes).
Migration has been shown to increase the risk of schizophrenia by 3 to 5 fold. The exact reason is unclear, but it could be a combination of social stress, exposure to new types of germs, less sunshine, and even a different diet.
My advice to the couple? Get a good obstetrician well before conception; get the mother immunized against infections; eat a lot of fish (omega-3 fatty acids); take adequate doses of folate and vitamin D, perhaps even choline9; avoid smoking before and during pregnancy; adopt a healthy, balanced diet; avoid excessive weight gain and/or gestational diabetes; avoid contact with people with infections; avoid exposure to cat feces (toxoplasmosis); schedule frequent prenatal visits; and hope for a smooth and uneventful delivery and a newborn with an Apgar score of 9 or 10. All this will greatly reduce the non-genetic risks of schizophrenia, but is unlikely to modify the genetic risks. However, it has been shown that a combination of both genetic and non-genetic risk factors is associated with a more severe form of schizophrenia.10
Optimal prenatal and postnatal care can be helpful for couples with a family history of schizophrenia (without moving to deliver their baby in a rural village near the equator). However, if their child starts using marijuana during adolescence, all bets are off. The risk of schizophrenia and serious cortical tissue loss increases dramatically when a carrier of risk genes use Cannabis. But that’s another editorial, to be read by clinicians in states where marijuana has been (foolishly, I believe) legalized.
1. Rodriguez-Murillo L, Gogos JA, Karayiorgou M. The genetic architecture of schizophrenia: new mutations and emerging paradigms. Annu Rev Med. 2012;63:63-80.
2. van Os J, Kenis G, Rutten BP. The environment and schizophrenia. Nature. 2010;468(7321):203-212.
3. Brown AS, Schefer CA, Wyatt RJ, et al. Paternal age and risk of schizophrenia in adult offspring. Am J Psychiatry. 2002;159(9):1528-1533.
4. Betts KS, Williams GM, Najman JM, et al. Maternal prenatal infection, early susceptibility to illness and adult psychotic experiences: a birth cohort study. Schizophr Res. 2014;156(2- 3):161-167.
5. Brown AS, Derkits EJ. Prental infection and schizophrenia: a review of epidemiologic and translational studies. Am J Psychiatry. 2010;167(3):261-280.
6. Kinney DK, Teixeira P, Hsu D, et al. Relation of schizophrenia prevalence to latitude, climate, fish consumption, infant mortality, and skin color: a role for prenatal vitamin d deficiency and infections? Schizophr Bull. 2009;35(3): 582-595.
7. Kawai M, Minabe Y, Takagai S, et al. Poor maternal care and high maternal body mass index in pregnancy as a risk factor for schizophrenia in offspring. Acta Psychiatry Scand. 2004;110(4):257-263.
8. Kelly BD, O’Callaghan E, Waddington JL, et al. Schizophrenia and the city: a review of literature and prospective study of psychosis and urbanicity in Ireland. Schizophr Res. 2010;116(1):75-89.
9. Ross RG, Hunter SK, McCarthy L, et al. Perinatal choline effects on neonatal pathophysiology related to later schizophrenia risk. Am J Psychiatry. 2013; 170(3):290-298.
10. Maynard TM, Sikich L, Lieberman JA, et al. Neural development, cell-cell signaling, and the “two-hit” hypothesis of schizophrenia. Schizophr Bull. 2001;27(3): 457-476.
I explained to them that schizophrenia is a neurodevelopmental syndrome that comprises hundreds of different disorders of genetic or non-genetic etiology, all of which share a similar psychotic phenotype. Although the various genetic causes of schizophrenia are difficult to prevent—but may be prevented in the future with epigenetic techniques—the many non-genetic (environmental) pathways to schizophrenia can be avoided to significantly reduce the incidence of schizophrenia by 40% to 50%, according to some estimates.
I will share what I told this couple, because even couples without any family history of psychosis may have a child who develops schizophrenia because of a variety of environmental risk factors.
Genetic risk factors
One-half of the 20,000 genes in the 23 chromosomes of the human genome participate in constructing and sculpting the extremely intricate and complex human brain. There are many ways that genetic factors can increase the risk of schizophrenia,1 and only some are transmitted by parents:
Risk genes. More than 30 risk genes have been identified as heritable in schizophrenia. They are spread over many chromosomes and more are likely to be discovered. Most of those risk genes regulate glutamate— not dopamine—pathways, and each increases the risk by 2% to 4%.
Copy number variations (CNVs) are produced via meiosis mishaps, where 1 or 3 alleles of certain genes are formed instead of the usual 2. A high frequency of CNVs have been found in schizophrenia compared with the general population—but also are found in autism and bipolar disorders—and are believed to disrupt brain development in various ways.
De novo mutations. Recent studies on large samples of people with schizophrenia (50,000 to 100,000) uncovered a much higher rate of mutations (some code for proteins while others are nonsense mutations that code for nothing). Obviously, these mutations led to anomalous neurodevelopment.
There are hundreds, maybe thousands, of genetic subtypes within the schizophrenia syndrome. Advances in epigenetics, which allow silencing of culprit genes or overexpression of protective genes, one day may enable psychiatric geneticists to prevent schizophrenia in fetuses at risk.
Non-genetic risk factors
Just as with the genetic patho-genic heterogeneity, the schizophrenia syndrome can be caused by numerous environmental adverse events,2 many of which can be avoided, including:
Older paternal age (>45) at time of conception doubles or triples the risk of schizophrenia3 as well as autism and bipolar disorder. Aging sperm are associated with a higher rate of DNA fragmentation and genetic mutations.
Prenatal complications, especially during the second trimester when CNS development takes place. These adverse prenatal events skew fetal brain development to produce psychosis in adulthood and can be minimized with optimal prenatal care, which sadly is lacking among the poor. These include:
• Vaginal infections before pregnancy,4 such as herpes simplex virus, can cause fetal brain inflammation and increased risk of schizophrenia.
• Infections during pregnancy— whether bacterial, viral, or protozoan (Toxoplasma gondii)—have been shown to significantly increase the risk of schizophrenia in offspring.5 An increase in serum C-reactive protein during pregnancy also is a biomarker of increased risk.
• Poor diet, especially starvation, can double or triple the risk of schizophrenia.
• Vitamin deficiency, especially folate and vitamin D, are critical for normal brain development.6 Vitamin D is vital to mitigate neuroinflammation.
• Smoking before and during pregnancy.4
• Medical illness during pregnancy, especially gestational diabetes, increases the risk of schizophrenia in the fetus by 800%.7
• Severe stress during pregnancy, such as the death of the spouse, doubles the risk of schizophrenia.2
• Schizophrenia risk is 400% to 500% higher among those born and raised in an urban area, compared with a rural area.8
• Babies born in northern latitudes, such as in Sweden, Norway, or Canada, have a 10-fold risk of schizophrenia in adulthood compared with babies born near the equator.6 This has been attributed to lack of sunshine and the risk of severe vitamin D deficiency in northern latitudes.
• High maternal body mass index during the first trimester7 increases the child’s risk of schizophrenia.
• Low number of prenatal visits is associated with higher risk of schizophrenia.
• Obstetric complications that cause hypoxia and a low Apgar score after birth increase the risk of schizophrenia. This includes long labor, cord around the neck, meconium spillage into the amniotic fluid, and mechanical injury with forceps delivery.
• Infection in the newborn shortly after birth.
Severe physical or sexual abuse before age 5 is associated with increased risk of schizophrenia in adulthood.2 This may be because of stress-induced epigenetic mechanisms (silencing or overexpressing certain genes).
Migration has been shown to increase the risk of schizophrenia by 3 to 5 fold. The exact reason is unclear, but it could be a combination of social stress, exposure to new types of germs, less sunshine, and even a different diet.
My advice to the couple? Get a good obstetrician well before conception; get the mother immunized against infections; eat a lot of fish (omega-3 fatty acids); take adequate doses of folate and vitamin D, perhaps even choline9; avoid smoking before and during pregnancy; adopt a healthy, balanced diet; avoid excessive weight gain and/or gestational diabetes; avoid contact with people with infections; avoid exposure to cat feces (toxoplasmosis); schedule frequent prenatal visits; and hope for a smooth and uneventful delivery and a newborn with an Apgar score of 9 or 10. All this will greatly reduce the non-genetic risks of schizophrenia, but is unlikely to modify the genetic risks. However, it has been shown that a combination of both genetic and non-genetic risk factors is associated with a more severe form of schizophrenia.10
Optimal prenatal and postnatal care can be helpful for couples with a family history of schizophrenia (without moving to deliver their baby in a rural village near the equator). However, if their child starts using marijuana during adolescence, all bets are off. The risk of schizophrenia and serious cortical tissue loss increases dramatically when a carrier of risk genes use Cannabis. But that’s another editorial, to be read by clinicians in states where marijuana has been (foolishly, I believe) legalized.
I explained to them that schizophrenia is a neurodevelopmental syndrome that comprises hundreds of different disorders of genetic or non-genetic etiology, all of which share a similar psychotic phenotype. Although the various genetic causes of schizophrenia are difficult to prevent—but may be prevented in the future with epigenetic techniques—the many non-genetic (environmental) pathways to schizophrenia can be avoided to significantly reduce the incidence of schizophrenia by 40% to 50%, according to some estimates.
I will share what I told this couple, because even couples without any family history of psychosis may have a child who develops schizophrenia because of a variety of environmental risk factors.
Genetic risk factors
One-half of the 20,000 genes in the 23 chromosomes of the human genome participate in constructing and sculpting the extremely intricate and complex human brain. There are many ways that genetic factors can increase the risk of schizophrenia,1 and only some are transmitted by parents:
Risk genes. More than 30 risk genes have been identified as heritable in schizophrenia. They are spread over many chromosomes and more are likely to be discovered. Most of those risk genes regulate glutamate— not dopamine—pathways, and each increases the risk by 2% to 4%.
Copy number variations (CNVs) are produced via meiosis mishaps, where 1 or 3 alleles of certain genes are formed instead of the usual 2. A high frequency of CNVs have been found in schizophrenia compared with the general population—but also are found in autism and bipolar disorders—and are believed to disrupt brain development in various ways.
De novo mutations. Recent studies on large samples of people with schizophrenia (50,000 to 100,000) uncovered a much higher rate of mutations (some code for proteins while others are nonsense mutations that code for nothing). Obviously, these mutations led to anomalous neurodevelopment.
There are hundreds, maybe thousands, of genetic subtypes within the schizophrenia syndrome. Advances in epigenetics, which allow silencing of culprit genes or overexpression of protective genes, one day may enable psychiatric geneticists to prevent schizophrenia in fetuses at risk.
Non-genetic risk factors
Just as with the genetic patho-genic heterogeneity, the schizophrenia syndrome can be caused by numerous environmental adverse events,2 many of which can be avoided, including:
Older paternal age (>45) at time of conception doubles or triples the risk of schizophrenia3 as well as autism and bipolar disorder. Aging sperm are associated with a higher rate of DNA fragmentation and genetic mutations.
Prenatal complications, especially during the second trimester when CNS development takes place. These adverse prenatal events skew fetal brain development to produce psychosis in adulthood and can be minimized with optimal prenatal care, which sadly is lacking among the poor. These include:
• Vaginal infections before pregnancy,4 such as herpes simplex virus, can cause fetal brain inflammation and increased risk of schizophrenia.
• Infections during pregnancy— whether bacterial, viral, or protozoan (Toxoplasma gondii)—have been shown to significantly increase the risk of schizophrenia in offspring.5 An increase in serum C-reactive protein during pregnancy also is a biomarker of increased risk.
• Poor diet, especially starvation, can double or triple the risk of schizophrenia.
• Vitamin deficiency, especially folate and vitamin D, are critical for normal brain development.6 Vitamin D is vital to mitigate neuroinflammation.
• Smoking before and during pregnancy.4
• Medical illness during pregnancy, especially gestational diabetes, increases the risk of schizophrenia in the fetus by 800%.7
• Severe stress during pregnancy, such as the death of the spouse, doubles the risk of schizophrenia.2
• Schizophrenia risk is 400% to 500% higher among those born and raised in an urban area, compared with a rural area.8
• Babies born in northern latitudes, such as in Sweden, Norway, or Canada, have a 10-fold risk of schizophrenia in adulthood compared with babies born near the equator.6 This has been attributed to lack of sunshine and the risk of severe vitamin D deficiency in northern latitudes.
• High maternal body mass index during the first trimester7 increases the child’s risk of schizophrenia.
• Low number of prenatal visits is associated with higher risk of schizophrenia.
• Obstetric complications that cause hypoxia and a low Apgar score after birth increase the risk of schizophrenia. This includes long labor, cord around the neck, meconium spillage into the amniotic fluid, and mechanical injury with forceps delivery.
• Infection in the newborn shortly after birth.
Severe physical or sexual abuse before age 5 is associated with increased risk of schizophrenia in adulthood.2 This may be because of stress-induced epigenetic mechanisms (silencing or overexpressing certain genes).
Migration has been shown to increase the risk of schizophrenia by 3 to 5 fold. The exact reason is unclear, but it could be a combination of social stress, exposure to new types of germs, less sunshine, and even a different diet.
My advice to the couple? Get a good obstetrician well before conception; get the mother immunized against infections; eat a lot of fish (omega-3 fatty acids); take adequate doses of folate and vitamin D, perhaps even choline9; avoid smoking before and during pregnancy; adopt a healthy, balanced diet; avoid excessive weight gain and/or gestational diabetes; avoid contact with people with infections; avoid exposure to cat feces (toxoplasmosis); schedule frequent prenatal visits; and hope for a smooth and uneventful delivery and a newborn with an Apgar score of 9 or 10. All this will greatly reduce the non-genetic risks of schizophrenia, but is unlikely to modify the genetic risks. However, it has been shown that a combination of both genetic and non-genetic risk factors is associated with a more severe form of schizophrenia.10
Optimal prenatal and postnatal care can be helpful for couples with a family history of schizophrenia (without moving to deliver their baby in a rural village near the equator). However, if their child starts using marijuana during adolescence, all bets are off. The risk of schizophrenia and serious cortical tissue loss increases dramatically when a carrier of risk genes use Cannabis. But that’s another editorial, to be read by clinicians in states where marijuana has been (foolishly, I believe) legalized.
1. Rodriguez-Murillo L, Gogos JA, Karayiorgou M. The genetic architecture of schizophrenia: new mutations and emerging paradigms. Annu Rev Med. 2012;63:63-80.
2. van Os J, Kenis G, Rutten BP. The environment and schizophrenia. Nature. 2010;468(7321):203-212.
3. Brown AS, Schefer CA, Wyatt RJ, et al. Paternal age and risk of schizophrenia in adult offspring. Am J Psychiatry. 2002;159(9):1528-1533.
4. Betts KS, Williams GM, Najman JM, et al. Maternal prenatal infection, early susceptibility to illness and adult psychotic experiences: a birth cohort study. Schizophr Res. 2014;156(2- 3):161-167.
5. Brown AS, Derkits EJ. Prental infection and schizophrenia: a review of epidemiologic and translational studies. Am J Psychiatry. 2010;167(3):261-280.
6. Kinney DK, Teixeira P, Hsu D, et al. Relation of schizophrenia prevalence to latitude, climate, fish consumption, infant mortality, and skin color: a role for prenatal vitamin d deficiency and infections? Schizophr Bull. 2009;35(3): 582-595.
7. Kawai M, Minabe Y, Takagai S, et al. Poor maternal care and high maternal body mass index in pregnancy as a risk factor for schizophrenia in offspring. Acta Psychiatry Scand. 2004;110(4):257-263.
8. Kelly BD, O’Callaghan E, Waddington JL, et al. Schizophrenia and the city: a review of literature and prospective study of psychosis and urbanicity in Ireland. Schizophr Res. 2010;116(1):75-89.
9. Ross RG, Hunter SK, McCarthy L, et al. Perinatal choline effects on neonatal pathophysiology related to later schizophrenia risk. Am J Psychiatry. 2013; 170(3):290-298.
10. Maynard TM, Sikich L, Lieberman JA, et al. Neural development, cell-cell signaling, and the “two-hit” hypothesis of schizophrenia. Schizophr Bull. 2001;27(3): 457-476.
1. Rodriguez-Murillo L, Gogos JA, Karayiorgou M. The genetic architecture of schizophrenia: new mutations and emerging paradigms. Annu Rev Med. 2012;63:63-80.
2. van Os J, Kenis G, Rutten BP. The environment and schizophrenia. Nature. 2010;468(7321):203-212.
3. Brown AS, Schefer CA, Wyatt RJ, et al. Paternal age and risk of schizophrenia in adult offspring. Am J Psychiatry. 2002;159(9):1528-1533.
4. Betts KS, Williams GM, Najman JM, et al. Maternal prenatal infection, early susceptibility to illness and adult psychotic experiences: a birth cohort study. Schizophr Res. 2014;156(2- 3):161-167.
5. Brown AS, Derkits EJ. Prental infection and schizophrenia: a review of epidemiologic and translational studies. Am J Psychiatry. 2010;167(3):261-280.
6. Kinney DK, Teixeira P, Hsu D, et al. Relation of schizophrenia prevalence to latitude, climate, fish consumption, infant mortality, and skin color: a role for prenatal vitamin d deficiency and infections? Schizophr Bull. 2009;35(3): 582-595.
7. Kawai M, Minabe Y, Takagai S, et al. Poor maternal care and high maternal body mass index in pregnancy as a risk factor for schizophrenia in offspring. Acta Psychiatry Scand. 2004;110(4):257-263.
8. Kelly BD, O’Callaghan E, Waddington JL, et al. Schizophrenia and the city: a review of literature and prospective study of psychosis and urbanicity in Ireland. Schizophr Res. 2010;116(1):75-89.
9. Ross RG, Hunter SK, McCarthy L, et al. Perinatal choline effects on neonatal pathophysiology related to later schizophrenia risk. Am J Psychiatry. 2013; 170(3):290-298.
10. Maynard TM, Sikich L, Lieberman JA, et al. Neural development, cell-cell signaling, and the “two-hit” hypothesis of schizophrenia. Schizophr Bull. 2001;27(3): 457-476.
Dissociation found to mediate ketamine’s antidepressive effects
HOLLYWOOD, FLA. – Dissociative side effects in patients given a ketamine infusion to treat either major depressive disorder or bipolar disorder predicted a more robust antidepressive response, according to a small secondary analysis.
"Patients who don’t have acute dissociation are more likely not to have antidepressant efficacy in the postinfusion period," Dr. Mark J. Niciu said during an interview discussing his poster presentation at a meeting of the American Society of Clinical Psychopharmacology, formerly known as the New Clinical Drug Evaluation Unit meeting.
"The patients with more disassociation might be the ones to have greater antidepressant efficacy, but they are also the patients we need to keep a closer clinical eye on because they’re having perceptual alterations during the postinfusion period," he said.
Dr. Niciu, a clinical research fellow at the National Institute of Mental Health in Bethesda, Md., reviewed data from 108 treatment-resistant inpatients who met criteria for major depressive disorder or bipolar I or II and were given a subanesthetic ketamine infusion. They examined whether dissociation and psychotic-like experiences, as measured by the Clinician Administered Dissociative States Scale (CADSS), the Brief Psychiatric Rating Scale (BPRS), and the Young Mania Rating Scale (YMRS), and vital sign changes correlated with improvements in the Hamilton Depression Rating Scale (HDRS) at 40 minutes and 230 minutes post infusion, and at 1 and 7 days post infusion.
Pearson correlations indicated that there was a significant association between increased CADSS scores at 40 minutes post infusion and improvement with ketamine in HDRS scores at 230 minutes (r = –0.35, P = .007). Changes in the YMRS or BPRS Positive Symptom score at 40 minutes did not significantly correlate with HDRS improvement at any time point with ketamine. Similarly, none of the vital signs analyzed (changes in systolic or diastolic blood pressure and pulse) significantly correlated to HDRS change.
The question of whether there was an "unblinding" effect was of concern to Dr. Niciu. "The subjects who received ketamine that had greater disassociation might also expect to have greater antidepressive efficacy post infusion," he said. To account for that possibility, he said some researchers are using more active placebos such as midazolam, but he did not think that it was a complete solution because the ideal active placebo would affect glutamate, dopamine, and noradrenaline without having an antidepressant effect.
The overall goal is to discover medications that have keen effects on glutamate receptors such as NMDA (N-methyl-D-aspartate) receptors, as ketamine does, but that do not also have dissociative side effects. "But maybe that’s not possible," Dr. Niciu said. "Maybe we need to have some degree of dissociation as a proxy for the strength of the NMDA receptor blockade because of its antidepressant effects downstream post infusion."
This study was funded by the Intramural Research Program at the National Institute of Mental Health, a NARSAD Independent Investigator Award, and a Brain and Behavior Mood Disorders Research Award. Both of the awards were given to Dr. Carlos A. Zarate.
On Twitter @whitneymcknight
HOLLYWOOD, FLA. – Dissociative side effects in patients given a ketamine infusion to treat either major depressive disorder or bipolar disorder predicted a more robust antidepressive response, according to a small secondary analysis.
"Patients who don’t have acute dissociation are more likely not to have antidepressant efficacy in the postinfusion period," Dr. Mark J. Niciu said during an interview discussing his poster presentation at a meeting of the American Society of Clinical Psychopharmacology, formerly known as the New Clinical Drug Evaluation Unit meeting.
"The patients with more disassociation might be the ones to have greater antidepressant efficacy, but they are also the patients we need to keep a closer clinical eye on because they’re having perceptual alterations during the postinfusion period," he said.
Dr. Niciu, a clinical research fellow at the National Institute of Mental Health in Bethesda, Md., reviewed data from 108 treatment-resistant inpatients who met criteria for major depressive disorder or bipolar I or II and were given a subanesthetic ketamine infusion. They examined whether dissociation and psychotic-like experiences, as measured by the Clinician Administered Dissociative States Scale (CADSS), the Brief Psychiatric Rating Scale (BPRS), and the Young Mania Rating Scale (YMRS), and vital sign changes correlated with improvements in the Hamilton Depression Rating Scale (HDRS) at 40 minutes and 230 minutes post infusion, and at 1 and 7 days post infusion.
Pearson correlations indicated that there was a significant association between increased CADSS scores at 40 minutes post infusion and improvement with ketamine in HDRS scores at 230 minutes (r = –0.35, P = .007). Changes in the YMRS or BPRS Positive Symptom score at 40 minutes did not significantly correlate with HDRS improvement at any time point with ketamine. Similarly, none of the vital signs analyzed (changes in systolic or diastolic blood pressure and pulse) significantly correlated to HDRS change.
The question of whether there was an "unblinding" effect was of concern to Dr. Niciu. "The subjects who received ketamine that had greater disassociation might also expect to have greater antidepressive efficacy post infusion," he said. To account for that possibility, he said some researchers are using more active placebos such as midazolam, but he did not think that it was a complete solution because the ideal active placebo would affect glutamate, dopamine, and noradrenaline without having an antidepressant effect.
The overall goal is to discover medications that have keen effects on glutamate receptors such as NMDA (N-methyl-D-aspartate) receptors, as ketamine does, but that do not also have dissociative side effects. "But maybe that’s not possible," Dr. Niciu said. "Maybe we need to have some degree of dissociation as a proxy for the strength of the NMDA receptor blockade because of its antidepressant effects downstream post infusion."
This study was funded by the Intramural Research Program at the National Institute of Mental Health, a NARSAD Independent Investigator Award, and a Brain and Behavior Mood Disorders Research Award. Both of the awards were given to Dr. Carlos A. Zarate.
On Twitter @whitneymcknight
HOLLYWOOD, FLA. – Dissociative side effects in patients given a ketamine infusion to treat either major depressive disorder or bipolar disorder predicted a more robust antidepressive response, according to a small secondary analysis.
"Patients who don’t have acute dissociation are more likely not to have antidepressant efficacy in the postinfusion period," Dr. Mark J. Niciu said during an interview discussing his poster presentation at a meeting of the American Society of Clinical Psychopharmacology, formerly known as the New Clinical Drug Evaluation Unit meeting.
"The patients with more disassociation might be the ones to have greater antidepressant efficacy, but they are also the patients we need to keep a closer clinical eye on because they’re having perceptual alterations during the postinfusion period," he said.
Dr. Niciu, a clinical research fellow at the National Institute of Mental Health in Bethesda, Md., reviewed data from 108 treatment-resistant inpatients who met criteria for major depressive disorder or bipolar I or II and were given a subanesthetic ketamine infusion. They examined whether dissociation and psychotic-like experiences, as measured by the Clinician Administered Dissociative States Scale (CADSS), the Brief Psychiatric Rating Scale (BPRS), and the Young Mania Rating Scale (YMRS), and vital sign changes correlated with improvements in the Hamilton Depression Rating Scale (HDRS) at 40 minutes and 230 minutes post infusion, and at 1 and 7 days post infusion.
Pearson correlations indicated that there was a significant association between increased CADSS scores at 40 minutes post infusion and improvement with ketamine in HDRS scores at 230 minutes (r = –0.35, P = .007). Changes in the YMRS or BPRS Positive Symptom score at 40 minutes did not significantly correlate with HDRS improvement at any time point with ketamine. Similarly, none of the vital signs analyzed (changes in systolic or diastolic blood pressure and pulse) significantly correlated to HDRS change.
The question of whether there was an "unblinding" effect was of concern to Dr. Niciu. "The subjects who received ketamine that had greater disassociation might also expect to have greater antidepressive efficacy post infusion," he said. To account for that possibility, he said some researchers are using more active placebos such as midazolam, but he did not think that it was a complete solution because the ideal active placebo would affect glutamate, dopamine, and noradrenaline without having an antidepressant effect.
The overall goal is to discover medications that have keen effects on glutamate receptors such as NMDA (N-methyl-D-aspartate) receptors, as ketamine does, but that do not also have dissociative side effects. "But maybe that’s not possible," Dr. Niciu said. "Maybe we need to have some degree of dissociation as a proxy for the strength of the NMDA receptor blockade because of its antidepressant effects downstream post infusion."
This study was funded by the Intramural Research Program at the National Institute of Mental Health, a NARSAD Independent Investigator Award, and a Brain and Behavior Mood Disorders Research Award. Both of the awards were given to Dr. Carlos A. Zarate.
On Twitter @whitneymcknight
AT THE ASCP ANNUAL MEETING
Key clinical point: Some degree of dissociation might be needed "as a proxy for the strength of the NMDA receptor blockade because of its antidepressant effects downstream post infusion."
Major finding: A significant association was found between increased CADSS scores at 40 minutes post infusion and improvement with ketamine in HDRS scores at 230 minutes (r = –0.35, P = .007).
Data source: Secondary analysis of 108 inpatients treated for MDD or BP I or II with ketamine infusion.
Disclosures: This study was funded by the Intramural Research Program at the National Institute of Mental Health, a NARSAD Independent Investigator Award, and a Brain and Behavior Mood Disorders Research Award. Both of the awards were given to Dr. Carlos A. Zarate.
Lurasidone monotherapy improves quality of life in bipolar I
HOLLYWOOD, FLA. – Lurasidone as monotherapy in the dosage range of either 20-60 mg/day* or 80-120 mg/day significantly improved functioning and quality-of-life in patients with bipolar depression, a post hoc analysis has shown.
In a previously published study of 318 patients randomized to either lurasidone dosage groups or placebo, the drug’s association at both dose ranges with reduced Montgomery-sberg Depression Scale total scores and Clinical Global Impressions scale for bipolar depression severity scores from baseline to week 6 was significant. The study also noted that both lurasidone groups had significant improvements in patient-reported measures of quality of life and functional impairment, compared with the placebo group (P less than .001 for each) (Am. J. Psychiatry 2014;171:160-8).
The findings led Dr. Terence A. Ketter, professor of psychiatry and chief of the bipolar disorders clinic at Stanford (Calif.) University, to wonder how the improvements in functionality and quality of life had happened in such relatively short order.
"It kind of makes sense that it’s related to the mood improvement," Dr. Ketter said in an interview during a poster session at a meeting of the American Society of Clinical Psychopharmacology, formerly known as the New Clinical Drug Evaluation Unit meeting.
To investigate further, Dr. Ketter and his colleagues performed a mediation regression analysis using data from phase III of the original trial. The results were that reduced depressive symptoms from baseline to week 6 mediated the effect of lurasidone on Sheehan Disability Scale functional recovery and Quality of Life Enjoyment and Satisfaction Questionnaire scores at week 6 (P less than .05 for each).
"This suggests that, at least in the first 6 weeks, most of the improvement [in functionality and quality of life] is related to the improvement in depressive symptoms," Dr. Ketter said. "Functional recovery is something that takes months, and it may be that beyond this by a month or two, you’re looking at a degree of mood improvement by duration interaction to get functional improvement." He added that there likely would be a "huge improvement" in cognition, simply because of the removal of depressive symptoms.
"Is it enough to be able to go out and get a job? Well, maybe not. Maybe you need things to integrate for months before you can go out and work." But, he added, over time, the less interference with one’s cognitive ability, the greater likelihood that person is employable.
In the original study in bipolar I patients, "the company wanted to know which was the right dose," Dr. Ketter said. "As it turned out, both worked. The higher one was a little bit harder to tolerate, but not horribly so."
As a result, Dr. Ketter said the drug has a "pretty flexible label." In his own practice, he said he starts patients on monotherapy with lurasidone 20 mg/day at dinner time, titrating upward in 20-mg increments each week until his patients reach the dosage that works best for them. "The average dose seems to be about 60 mg/day," he said.
Lurasidone, a second-generation antipsychotic, originally was approved by the Food and Drug Administration in 2010 to treat schizophrenia in adults; the indication was expanded in 2013 to include bipolar I, either as monotherapy or as an adjunct to lithium or valproate.
Because of its relatively low impact on metabolic function and its low sedative effect, compared with other second-generation antipsychotics, Dr. Ketter said he favors using lurasidone in his patients. "It’s like an easier to use quetiapine," he noted.
This study was supported by Sunovion Pharmaceuticals. Dr. Ketter disclosed that he has received funding from Sunovion, as well as from AstraZeneca Pharmaceuticals, Cephalon, Eli Lilly, and others.
On Twitter @whitneymcknight
*Correction, 7/2/2014: An earlier version of this story misstated the lurasidone dosage range.
HOLLYWOOD, FLA. – Lurasidone as monotherapy in the dosage range of either 20-60 mg/day* or 80-120 mg/day significantly improved functioning and quality-of-life in patients with bipolar depression, a post hoc analysis has shown.
In a previously published study of 318 patients randomized to either lurasidone dosage groups or placebo, the drug’s association at both dose ranges with reduced Montgomery-sberg Depression Scale total scores and Clinical Global Impressions scale for bipolar depression severity scores from baseline to week 6 was significant. The study also noted that both lurasidone groups had significant improvements in patient-reported measures of quality of life and functional impairment, compared with the placebo group (P less than .001 for each) (Am. J. Psychiatry 2014;171:160-8).
The findings led Dr. Terence A. Ketter, professor of psychiatry and chief of the bipolar disorders clinic at Stanford (Calif.) University, to wonder how the improvements in functionality and quality of life had happened in such relatively short order.
"It kind of makes sense that it’s related to the mood improvement," Dr. Ketter said in an interview during a poster session at a meeting of the American Society of Clinical Psychopharmacology, formerly known as the New Clinical Drug Evaluation Unit meeting.
To investigate further, Dr. Ketter and his colleagues performed a mediation regression analysis using data from phase III of the original trial. The results were that reduced depressive symptoms from baseline to week 6 mediated the effect of lurasidone on Sheehan Disability Scale functional recovery and Quality of Life Enjoyment and Satisfaction Questionnaire scores at week 6 (P less than .05 for each).
"This suggests that, at least in the first 6 weeks, most of the improvement [in functionality and quality of life] is related to the improvement in depressive symptoms," Dr. Ketter said. "Functional recovery is something that takes months, and it may be that beyond this by a month or two, you’re looking at a degree of mood improvement by duration interaction to get functional improvement." He added that there likely would be a "huge improvement" in cognition, simply because of the removal of depressive symptoms.
"Is it enough to be able to go out and get a job? Well, maybe not. Maybe you need things to integrate for months before you can go out and work." But, he added, over time, the less interference with one’s cognitive ability, the greater likelihood that person is employable.
In the original study in bipolar I patients, "the company wanted to know which was the right dose," Dr. Ketter said. "As it turned out, both worked. The higher one was a little bit harder to tolerate, but not horribly so."
As a result, Dr. Ketter said the drug has a "pretty flexible label." In his own practice, he said he starts patients on monotherapy with lurasidone 20 mg/day at dinner time, titrating upward in 20-mg increments each week until his patients reach the dosage that works best for them. "The average dose seems to be about 60 mg/day," he said.
Lurasidone, a second-generation antipsychotic, originally was approved by the Food and Drug Administration in 2010 to treat schizophrenia in adults; the indication was expanded in 2013 to include bipolar I, either as monotherapy or as an adjunct to lithium or valproate.
Because of its relatively low impact on metabolic function and its low sedative effect, compared with other second-generation antipsychotics, Dr. Ketter said he favors using lurasidone in his patients. "It’s like an easier to use quetiapine," he noted.
This study was supported by Sunovion Pharmaceuticals. Dr. Ketter disclosed that he has received funding from Sunovion, as well as from AstraZeneca Pharmaceuticals, Cephalon, Eli Lilly, and others.
On Twitter @whitneymcknight
*Correction, 7/2/2014: An earlier version of this story misstated the lurasidone dosage range.
HOLLYWOOD, FLA. – Lurasidone as monotherapy in the dosage range of either 20-60 mg/day* or 80-120 mg/day significantly improved functioning and quality-of-life in patients with bipolar depression, a post hoc analysis has shown.
In a previously published study of 318 patients randomized to either lurasidone dosage groups or placebo, the drug’s association at both dose ranges with reduced Montgomery-sberg Depression Scale total scores and Clinical Global Impressions scale for bipolar depression severity scores from baseline to week 6 was significant. The study also noted that both lurasidone groups had significant improvements in patient-reported measures of quality of life and functional impairment, compared with the placebo group (P less than .001 for each) (Am. J. Psychiatry 2014;171:160-8).
The findings led Dr. Terence A. Ketter, professor of psychiatry and chief of the bipolar disorders clinic at Stanford (Calif.) University, to wonder how the improvements in functionality and quality of life had happened in such relatively short order.
"It kind of makes sense that it’s related to the mood improvement," Dr. Ketter said in an interview during a poster session at a meeting of the American Society of Clinical Psychopharmacology, formerly known as the New Clinical Drug Evaluation Unit meeting.
To investigate further, Dr. Ketter and his colleagues performed a mediation regression analysis using data from phase III of the original trial. The results were that reduced depressive symptoms from baseline to week 6 mediated the effect of lurasidone on Sheehan Disability Scale functional recovery and Quality of Life Enjoyment and Satisfaction Questionnaire scores at week 6 (P less than .05 for each).
"This suggests that, at least in the first 6 weeks, most of the improvement [in functionality and quality of life] is related to the improvement in depressive symptoms," Dr. Ketter said. "Functional recovery is something that takes months, and it may be that beyond this by a month or two, you’re looking at a degree of mood improvement by duration interaction to get functional improvement." He added that there likely would be a "huge improvement" in cognition, simply because of the removal of depressive symptoms.
"Is it enough to be able to go out and get a job? Well, maybe not. Maybe you need things to integrate for months before you can go out and work." But, he added, over time, the less interference with one’s cognitive ability, the greater likelihood that person is employable.
In the original study in bipolar I patients, "the company wanted to know which was the right dose," Dr. Ketter said. "As it turned out, both worked. The higher one was a little bit harder to tolerate, but not horribly so."
As a result, Dr. Ketter said the drug has a "pretty flexible label." In his own practice, he said he starts patients on monotherapy with lurasidone 20 mg/day at dinner time, titrating upward in 20-mg increments each week until his patients reach the dosage that works best for them. "The average dose seems to be about 60 mg/day," he said.
Lurasidone, a second-generation antipsychotic, originally was approved by the Food and Drug Administration in 2010 to treat schizophrenia in adults; the indication was expanded in 2013 to include bipolar I, either as monotherapy or as an adjunct to lithium or valproate.
Because of its relatively low impact on metabolic function and its low sedative effect, compared with other second-generation antipsychotics, Dr. Ketter said he favors using lurasidone in his patients. "It’s like an easier to use quetiapine," he noted.
This study was supported by Sunovion Pharmaceuticals. Dr. Ketter disclosed that he has received funding from Sunovion, as well as from AstraZeneca Pharmaceuticals, Cephalon, Eli Lilly, and others.
On Twitter @whitneymcknight
*Correction, 7/2/2014: An earlier version of this story misstated the lurasidone dosage range.
AT THE ASCP ANNUAL MEETING
Key clinical point: Lurasidone appears to reduce depressive symptoms in patients with bipolar I depression without the metabolic complications characteristic of other second-generation antipsychotics.
Major finding: In 318 patients with bipolar I depression, reduced depressive symptoms from baseline to week 6 mediated the effect of lurasidone vs. placebo (P less than .05 in each) on functioning and quality of life.
Data source: A post hoc analysis of phase III data from a randomized, double-blind, placebo controlled trial in 318 intent-to-treat patients with bipolar I.
Disclosures: This study was supported by Sunovion Pharmaceuticals. Dr. Ketter disclosed he has received funding from Sunovion, as well as from AstraZeneca Pharmaceuticals, Cephalon, Eli Lilly, and others.
ADHD or bipolar disorder?

Confused and nearly naked after going on spending sprees
CASE Nearly naked
Mr. A, age 68, is found sitting in his car, wearing only a jacket, underpants, and boots. He speaks of spreading a message about Osama bin Laden and “taking a census.” Police officers bring him to a hospital emergency department for evaluation.
The examining clinician determines that Mr. A is a danger to himself and others because of mental illness, leading to admission to our state psychiatric hospital.
Mr. A’s wife describes recent spending sprees with large purchases. She had obtained a restraining order against her husband because of his threatening remarks and behaviors. Within days of the order issuance, he got a home equity loan and purchased a $300,000 house.
The medical history is notable for type 2 diabetes mellitus. Although he is not taking medications, his blood sugar is well controlled. Other than an initial resting heart rate of 116 beats per minute, vital signs are stable and within normal limits. Physical examination is unremarkable. Screening laboratory studies are notable for mildly elevated hepatic function, which approaches normal range several days after admission.
Mr. A reports a remote history of alcohol abuse but says he had not been drinking recently, and does not detail his pattern of use. Urine toxicology screen is negative for all substances of abuse.
Mental status examination reveals disheveled appearance, motor agitation, pressured speech, labile affect, loosening of associations, grandiose delusions, and auditory hallucinations. Mr. A’s thought processes are grossly disorganized, such that we could not gather a meaningful history. He believes God is speaking directly to him about plans to build a carousel at Disney World. He makes strange gestures with his hands throughout the interview, as if attempting to trace the shapes of letters and numbers. He frequently speaks of seeing an array of colors. Cognitive examination reveals a score of 5 of 30 on the Montreal Cognitive Assessment (Figure 1), indicating a severe impairment in neurocognitive functioning. He demonstrates limited insight and markedly impaired judgment, and denies having a mental illness.

What should be the next step in managing Mr. A?
a) obtain records from other facilities and collateral history
b) start an antipsychotic
c) order a brain MRI
d) start an alcohol withdrawal protocol
The authors’ observations
Mr. A showed elements of mania, psychosis, and delirium. We considered a broad differential diagnosis (Table). Mr. A initially could not provide reliable or accurate information. The least invasive next step was to obtain additional history from his wife and other medical records to refine the differential diagnosis. 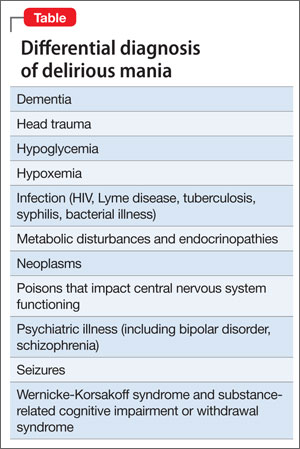
HISTORY Bizarre behavior
Mr. A allows staff to speak with his wife and obtain records from a psychiatric hospitalization 3 years earlier. Mrs. A reports significant and rapid changes in her husband’s behavior and personality over 3 months, but does not describe a recent alcohol relapse. Mr. A sleeps very little, remaining awake and active throughout the night. He frequently rearranges the furniture in their home for no clear reason. Once, he knocked on the door of a young female neighbor asking if she found him attractive.
Mr. A has a significant criminal history. Approximately 30 years ago, he was charged with attempted murder of his ex-wife and he had faced charges of attempted kidnapping and assaulting a police officer. However, he has no recent legal issues.
Mr. A has a history of episodes that are similar to this presentation. Seven years ago, he impulsively purchased a $650,000 house after his fourth wife died. He then had a $90,000 heart-shaped pool installed. He also drove a tractor through his stepdaughter’s car for no apparent reason. Also, 3 years ago, he displayed symptoms similar to his current presentation, including insomnia, irritability, and grandiosity. He engaged in strange behaviors, such as dressing up and imitating homeless people at his church.
During the hospitalization 3 years ago, clinicians gave Mr. A a diagnosis of bipolar disorder, current episode manic, and delirium of an unclear cause. A medical workup, including brain MRI, did not uncover a basis for his delirium. Antipsychotics (risperidone and perphenazine) and mood stabilizers (lithium and valproic acid), stabilized his condition; after 7 weeks, Mr. A was discharged, but he did not pursue outpatient psychiatric care.
What is the most likely DSM-5 diagnosis?
a) major neurocognitive disorder (dementia)
b) alcohol use disorder (eg, Wernicke- Korsakoff syndrome)
c) delirium secondary to mania
d) psychotic disorder
The authors’ observations
DSM-51 suggests a stepwise approach to diagnosis, with consideration of:
• signs and symptoms
• substance use
• general medical condition
• developmental conflict or stage
• whether a mental disorder is present.
Mr. A’s age and severe cognitive impairment raise the possibility of dementia. Rapid onset, history of similar episodes, and apparent inter-episode recovery make dementia unlikely. The history of alcohol abuse and mildly elevated hepatic function tests suggest a substance use disorder such as Wernicke-Korsakoff syndrome or a withdrawal syndrome. However, there is no evidence of excessive alcohol use over the past several months, toxicology studies were negative, and vital signs were stable. General medical causes for Mr. A’s presentation, such as hypoglycemia, head trauma, intracranial infection, and metabolic disturbance were considered, but physical examination and laboratory studies did not suggest any condition that would explain his condition.
Mr. A’s previous psychiatric hospitalization is critical in clarifying the more likely diagnosis. A similar presentation yielded the diagnosis of bipolar disorder, manic phase. Our working diagnosis, therefore, was bipolar disorder with features of delirious mania.
Delirious mania
Delirious mania was first described by Luther Bell in 1849 and is characterized by an acute and simultaneous onset of mania— severe insomnia, poor judgment, grandiosity, excitement, emotional lability, bizarre hallucinations, and delusions—and delirium—altered consciousness, disorientation, and confusion.2,3 Although there are no diagnostic criteria, some authors suggest that delirious mania is characterized by inappropriate toileting, denudation, profound lack of sleep, and episodic memory impairment that can last hours or days.4 Catatonia frequently is seen with delirious mania.5 Initial case descriptions described a high mortality rate, approaching 75% of patients.6 There is little published literature and no classification of delirious mania in DSM-5.1 Estimates are that delirium is concomitant in 20% to 33% of patients with mania.7,8
Several theories try to clarify the underlying etiology of delirious mania. Jacobowski et al9 summarized the etiology and proposed that it is:
• 1 of 3 types of mania, including: acute and delusional manias, as initially proposed by Kraeplin
• a severe form of catatonia
• a condition akin to, but distinct from, delirium with similar underlying medical causes
• a primary psychiatric disorder underlying the cause of delirium.
EVALUATION Brain changes
For several days, Mr. A continues to engage in strange behavior. He tries to take patients’ belongings, is denudative, crawls on floors, licks walls, is unable to feed himself, and exhibits odd motor movements with purposeless motor activity.
We consult our internal medicine team to identify treatable, medical causes. Results of serum B12, thyroid-stimulating hormone, and rapid plasma reagin studies are within normal limits. Urinalysis is negative. A brain MRI reveals numerous white-matter T2-weighted and FLAIR hyperintensities, indicating small-vessel ischemic changes that are consistent with the findings of an MRI 3 years ago. A sleep-deprived EEG with temporal leads obtained on Day 4 of hospitalization demonstrates a diffusely slow and marginally to poorly organized background, believed to indicate global cerebral dysfunction that is most consistent with nonfocal global encephalopathy. There is no seizure activity. We do not perform a lumbar puncture because of Mr. A’s absence of focal neurologic deficits, lack of fever, and normal white blood cell count.
What is the most appropriate treatment?
a) electroconvulsive therapy (ECT)
b) high-dose benzodiazepine
c) mood stabilizer
d) antipsychotic
The authors’ observations
We strongly suspect that Mr. A has delirious mania. Symptoms and signs of mania include labile mood, excessive spending, grandiosity, insomnia, and psychosis together with delirium (marked disorientation, confusion). We ascribed Mr. A’s odd motor behaviors to catatonia, a hallmark of delirious mania. The literature has little description of EEG findings in suspected cases of delirious mania; however, abnormal EEG tracings have been reported.10 We also speculated that Mr. A’s EEG reflected effects produced by his prescribed antipsychotic regimen.
Treatment
There is no clear consensus on treating delirious mania. Because catatonia is a key feature of delirious mania—whether etiologically or as a prominent sign of the condition—ECT and benzodiazepines are proposed as primary treatments. In a study of 16 patients with delirious mania, Karmacharya et al4 found ECT to be effective, with patients showing improvement after 1 to 4 treatments. Lee et al10 reported similar findings. Although a high-dose benzodiazepine is not as effective as ECT, a 1-time oral dose of 3 to 4 mg of lorazepam has been used to treat delirious mania.
The efficacy of antipsychotic and mood-stabilizing pharmacotherapy is not clear. Bond3 described 3 cases in which patients were treated effectively with a typical antipsychotic (haloperidol or chlorpromazine) and lithium. Jung and Lee11demonstrated the efficacy of atypical antipsychotics, with a marked improvement in symptoms within 1 week. However, other studies do not support these findings. Karmacharya et al4 found that typical antipsychotics 1) make the clinical picture worse by increasing extrapyramidal symptoms and 2) produce inconsistent effects. Mood stabilizers sometimes proved beneficial.
Karmacharya et al4 further argued that the delay in improvement seen with any antipsychotics and mood stabilizers suggest they should not be considered a first-line treatment. These discordant findings are the result of a small number of studies and a lack of understanding of the exact nature of delirious mania.
TREATMENT Quick Response
Mr. A’s symptoms rapidly resolve with a combination of quetiapine, 800 mg/d, haloperidol, 10 mg/d, and lithium, 1,200 mg/d. His mood returns to euthymia and his psychotic symptoms abate. He is able to attend to all activities of daily living. Mental status clears and he is fully oriented and able to hold a logical conversation. He scores 28 out of 30 on a subsequent Montreal Cognitive Assessment, administered 11 days after the initial assessment (Figure 2), indicating normal neurocognitive function. He returns to his baseline level of functioning and is discharged in psychiatrically stable condition. Mr. A has no recollection of the bizarre behaviors he displayed earlier in his hospitalization. 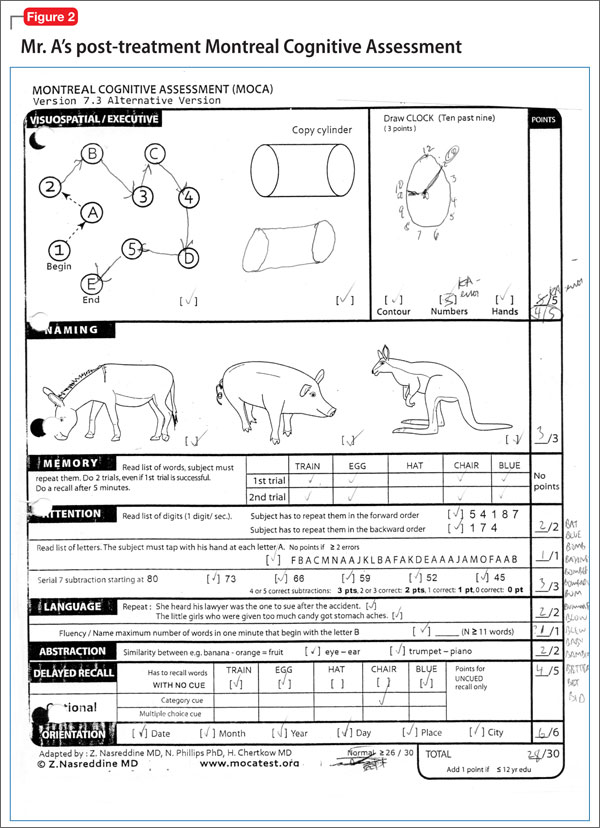
The authors’ observations
We started Mr. A on antipsychotics because of his initial level of agitation. In reviewing pharmacotherapy options for Mr. A’s mania and delirium, we contemplated several options. Quetiapine and lithium were chosen after a review of outside hospital records demonstrated a combination of a mood stabilizer and an antipsychotic was effective in treating a previous similar episode, which led to remission of Mr. A’s symptoms. We chose quetiapine because of it highly sedating properties, suspecting that it would help treat his insomnia. We thought that the risk that lithium would make delirium worse was mitigated by Mr. A’s previous therapeutic response to it. Haloperidol was added for treating delirium, given its more potent D2 antagonism. Mr. A responded quickly to these interventions.
We did not consider ECT at the beginning of Mr. A’s admission, and we avoided sedative-hypnotic agents because we were concerned that a benzodiazepine might make his delirium worse. In light of available data suggesting that ECT and benzodiazepines are preferred treatments for delirious mania, it is noteworthy that Mr. A responded so robustly and rapidly to an antipsychotic and a mood stabilizer.
Bottom Line
Consider delirious mania in any patient who has a history of bipolar disorder presenting with co-occuring symptoms of mania and delirium. Collateral information is vital to establishing a diagnosis. With suspected delirium, rule out concomitant reversible medical problems. Electroconvulsive therapy, high-dose benzodiazepines, antipsychotics, and mood stabilizers have shown efficacy.
Related Resources
• Nunes AL, Cheniaux E. Delirium and mania with catatonic features in a Brazilian patient: response to ECT. J Neuropsychiatry Clin Neurosci. 2014;26(1):E1-E3.
• Danivas V, Behere RV, Varambally S, et al. Electroconvulsive therapy in the treatment of delirious mania: a report of 2 patients. J ECT. 2010;26(4):278-279.
Drug Brand Names
Chlorpromazine • Thorazine Perphenazine • Trilafon
Haloperidol • Haldol Quetiapine • Seroquel
Lithium • Eskalith Risperidone • Risperdal
Lorazepam • Ativan Valproic acid • Depakene
Disclosure
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE Nearly naked
Mr. A, age 68, is found sitting in his car, wearing only a jacket, underpants, and boots. He speaks of spreading a message about Osama bin Laden and “taking a census.” Police officers bring him to a hospital emergency department for evaluation.
The examining clinician determines that Mr. A is a danger to himself and others because of mental illness, leading to admission to our state psychiatric hospital.
Mr. A’s wife describes recent spending sprees with large purchases. She had obtained a restraining order against her husband because of his threatening remarks and behaviors. Within days of the order issuance, he got a home equity loan and purchased a $300,000 house.
The medical history is notable for type 2 diabetes mellitus. Although he is not taking medications, his blood sugar is well controlled. Other than an initial resting heart rate of 116 beats per minute, vital signs are stable and within normal limits. Physical examination is unremarkable. Screening laboratory studies are notable for mildly elevated hepatic function, which approaches normal range several days after admission.
Mr. A reports a remote history of alcohol abuse but says he had not been drinking recently, and does not detail his pattern of use. Urine toxicology screen is negative for all substances of abuse.
Mental status examination reveals disheveled appearance, motor agitation, pressured speech, labile affect, loosening of associations, grandiose delusions, and auditory hallucinations. Mr. A’s thought processes are grossly disorganized, such that we could not gather a meaningful history. He believes God is speaking directly to him about plans to build a carousel at Disney World. He makes strange gestures with his hands throughout the interview, as if attempting to trace the shapes of letters and numbers. He frequently speaks of seeing an array of colors. Cognitive examination reveals a score of 5 of 30 on the Montreal Cognitive Assessment (Figure 1), indicating a severe impairment in neurocognitive functioning. He demonstrates limited insight and markedly impaired judgment, and denies having a mental illness.
What should be the next step in managing Mr. A?
a) obtain records from other facilities and collateral history
b) start an antipsychotic
c) order a brain MRI
d) start an alcohol withdrawal protocol
The authors’ observations
Mr. A showed elements of mania, psychosis, and delirium. We considered a broad differential diagnosis (Table). Mr. A initially could not provide reliable or accurate information. The least invasive next step was to obtain additional history from his wife and other medical records to refine the differential diagnosis.
HISTORY Bizarre behavior
Mr. A allows staff to speak with his wife and obtain records from a psychiatric hospitalization 3 years earlier. Mrs. A reports significant and rapid changes in her husband’s behavior and personality over 3 months, but does not describe a recent alcohol relapse. Mr. A sleeps very little, remaining awake and active throughout the night. He frequently rearranges the furniture in their home for no clear reason. Once, he knocked on the door of a young female neighbor asking if she found him attractive.
Mr. A has a significant criminal history. Approximately 30 years ago, he was charged with attempted murder of his ex-wife and he had faced charges of attempted kidnapping and assaulting a police officer. However, he has no recent legal issues.
Mr. A has a history of episodes that are similar to this presentation. Seven years ago, he impulsively purchased a $650,000 house after his fourth wife died. He then had a $90,000 heart-shaped pool installed. He also drove a tractor through his stepdaughter’s car for no apparent reason. Also, 3 years ago, he displayed symptoms similar to his current presentation, including insomnia, irritability, and grandiosity. He engaged in strange behaviors, such as dressing up and imitating homeless people at his church.
During the hospitalization 3 years ago, clinicians gave Mr. A a diagnosis of bipolar disorder, current episode manic, and delirium of an unclear cause. A medical workup, including brain MRI, did not uncover a basis for his delirium. Antipsychotics (risperidone and perphenazine) and mood stabilizers (lithium and valproic acid), stabilized his condition; after 7 weeks, Mr. A was discharged, but he did not pursue outpatient psychiatric care.
What is the most likely DSM-5 diagnosis?
a) major neurocognitive disorder (dementia)
b) alcohol use disorder (eg, Wernicke- Korsakoff syndrome)
c) delirium secondary to mania
d) psychotic disorder
The authors’ observations
DSM-51 suggests a stepwise approach to diagnosis, with consideration of:
• signs and symptoms
• substance use
• general medical condition
• developmental conflict or stage
• whether a mental disorder is present.
Mr. A’s age and severe cognitive impairment raise the possibility of dementia. Rapid onset, history of similar episodes, and apparent inter-episode recovery make dementia unlikely. The history of alcohol abuse and mildly elevated hepatic function tests suggest a substance use disorder such as Wernicke-Korsakoff syndrome or a withdrawal syndrome. However, there is no evidence of excessive alcohol use over the past several months, toxicology studies were negative, and vital signs were stable. General medical causes for Mr. A’s presentation, such as hypoglycemia, head trauma, intracranial infection, and metabolic disturbance were considered, but physical examination and laboratory studies did not suggest any condition that would explain his condition.
Mr. A’s previous psychiatric hospitalization is critical in clarifying the more likely diagnosis. A similar presentation yielded the diagnosis of bipolar disorder, manic phase. Our working diagnosis, therefore, was bipolar disorder with features of delirious mania.
Delirious mania
Delirious mania was first described by Luther Bell in 1849 and is characterized by an acute and simultaneous onset of mania— severe insomnia, poor judgment, grandiosity, excitement, emotional lability, bizarre hallucinations, and delusions—and delirium—altered consciousness, disorientation, and confusion.2,3 Although there are no diagnostic criteria, some authors suggest that delirious mania is characterized by inappropriate toileting, denudation, profound lack of sleep, and episodic memory impairment that can last hours or days.4 Catatonia frequently is seen with delirious mania.5 Initial case descriptions described a high mortality rate, approaching 75% of patients.6 There is little published literature and no classification of delirious mania in DSM-5.1 Estimates are that delirium is concomitant in 20% to 33% of patients with mania.7,8
Several theories try to clarify the underlying etiology of delirious mania. Jacobowski et al9 summarized the etiology and proposed that it is:
• 1 of 3 types of mania, including: acute and delusional manias, as initially proposed by Kraeplin
• a severe form of catatonia
• a condition akin to, but distinct from, delirium with similar underlying medical causes
• a primary psychiatric disorder underlying the cause of delirium.
EVALUATION Brain changes
For several days, Mr. A continues to engage in strange behavior. He tries to take patients’ belongings, is denudative, crawls on floors, licks walls, is unable to feed himself, and exhibits odd motor movements with purposeless motor activity.
We consult our internal medicine team to identify treatable, medical causes. Results of serum B12, thyroid-stimulating hormone, and rapid plasma reagin studies are within normal limits. Urinalysis is negative. A brain MRI reveals numerous white-matter T2-weighted and FLAIR hyperintensities, indicating small-vessel ischemic changes that are consistent with the findings of an MRI 3 years ago. A sleep-deprived EEG with temporal leads obtained on Day 4 of hospitalization demonstrates a diffusely slow and marginally to poorly organized background, believed to indicate global cerebral dysfunction that is most consistent with nonfocal global encephalopathy. There is no seizure activity. We do not perform a lumbar puncture because of Mr. A’s absence of focal neurologic deficits, lack of fever, and normal white blood cell count.
What is the most appropriate treatment?
a) electroconvulsive therapy (ECT)
b) high-dose benzodiazepine
c) mood stabilizer
d) antipsychotic
The authors’ observations
We strongly suspect that Mr. A has delirious mania. Symptoms and signs of mania include labile mood, excessive spending, grandiosity, insomnia, and psychosis together with delirium (marked disorientation, confusion). We ascribed Mr. A’s odd motor behaviors to catatonia, a hallmark of delirious mania. The literature has little description of EEG findings in suspected cases of delirious mania; however, abnormal EEG tracings have been reported.10 We also speculated that Mr. A’s EEG reflected effects produced by his prescribed antipsychotic regimen.
Treatment
There is no clear consensus on treating delirious mania. Because catatonia is a key feature of delirious mania—whether etiologically or as a prominent sign of the condition—ECT and benzodiazepines are proposed as primary treatments. In a study of 16 patients with delirious mania, Karmacharya et al4 found ECT to be effective, with patients showing improvement after 1 to 4 treatments. Lee et al10 reported similar findings. Although a high-dose benzodiazepine is not as effective as ECT, a 1-time oral dose of 3 to 4 mg of lorazepam has been used to treat delirious mania.
The efficacy of antipsychotic and mood-stabilizing pharmacotherapy is not clear. Bond3 described 3 cases in which patients were treated effectively with a typical antipsychotic (haloperidol or chlorpromazine) and lithium. Jung and Lee11demonstrated the efficacy of atypical antipsychotics, with a marked improvement in symptoms within 1 week. However, other studies do not support these findings. Karmacharya et al4 found that typical antipsychotics 1) make the clinical picture worse by increasing extrapyramidal symptoms and 2) produce inconsistent effects. Mood stabilizers sometimes proved beneficial.
Karmacharya et al4 further argued that the delay in improvement seen with any antipsychotics and mood stabilizers suggest they should not be considered a first-line treatment. These discordant findings are the result of a small number of studies and a lack of understanding of the exact nature of delirious mania.
TREATMENT Quick Response
Mr. A’s symptoms rapidly resolve with a combination of quetiapine, 800 mg/d, haloperidol, 10 mg/d, and lithium, 1,200 mg/d. His mood returns to euthymia and his psychotic symptoms abate. He is able to attend to all activities of daily living. Mental status clears and he is fully oriented and able to hold a logical conversation. He scores 28 out of 30 on a subsequent Montreal Cognitive Assessment, administered 11 days after the initial assessment (Figure 2), indicating normal neurocognitive function. He returns to his baseline level of functioning and is discharged in psychiatrically stable condition. Mr. A has no recollection of the bizarre behaviors he displayed earlier in his hospitalization.
The authors’ observations
We started Mr. A on antipsychotics because of his initial level of agitation. In reviewing pharmacotherapy options for Mr. A’s mania and delirium, we contemplated several options. Quetiapine and lithium were chosen after a review of outside hospital records demonstrated a combination of a mood stabilizer and an antipsychotic was effective in treating a previous similar episode, which led to remission of Mr. A’s symptoms. We chose quetiapine because of it highly sedating properties, suspecting that it would help treat his insomnia. We thought that the risk that lithium would make delirium worse was mitigated by Mr. A’s previous therapeutic response to it. Haloperidol was added for treating delirium, given its more potent D2 antagonism. Mr. A responded quickly to these interventions.
We did not consider ECT at the beginning of Mr. A’s admission, and we avoided sedative-hypnotic agents because we were concerned that a benzodiazepine might make his delirium worse. In light of available data suggesting that ECT and benzodiazepines are preferred treatments for delirious mania, it is noteworthy that Mr. A responded so robustly and rapidly to an antipsychotic and a mood stabilizer.
Bottom Line
Consider delirious mania in any patient who has a history of bipolar disorder presenting with co-occuring symptoms of mania and delirium. Collateral information is vital to establishing a diagnosis. With suspected delirium, rule out concomitant reversible medical problems. Electroconvulsive therapy, high-dose benzodiazepines, antipsychotics, and mood stabilizers have shown efficacy.
Related Resources
• Nunes AL, Cheniaux E. Delirium and mania with catatonic features in a Brazilian patient: response to ECT. J Neuropsychiatry Clin Neurosci. 2014;26(1):E1-E3.
• Danivas V, Behere RV, Varambally S, et al. Electroconvulsive therapy in the treatment of delirious mania: a report of 2 patients. J ECT. 2010;26(4):278-279.
Drug Brand Names
Chlorpromazine • Thorazine Perphenazine • Trilafon
Haloperidol • Haldol Quetiapine • Seroquel
Lithium • Eskalith Risperidone • Risperdal
Lorazepam • Ativan Valproic acid • Depakene
Disclosure
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE Nearly naked
Mr. A, age 68, is found sitting in his car, wearing only a jacket, underpants, and boots. He speaks of spreading a message about Osama bin Laden and “taking a census.” Police officers bring him to a hospital emergency department for evaluation.
The examining clinician determines that Mr. A is a danger to himself and others because of mental illness, leading to admission to our state psychiatric hospital.
Mr. A’s wife describes recent spending sprees with large purchases. She had obtained a restraining order against her husband because of his threatening remarks and behaviors. Within days of the order issuance, he got a home equity loan and purchased a $300,000 house.
The medical history is notable for type 2 diabetes mellitus. Although he is not taking medications, his blood sugar is well controlled. Other than an initial resting heart rate of 116 beats per minute, vital signs are stable and within normal limits. Physical examination is unremarkable. Screening laboratory studies are notable for mildly elevated hepatic function, which approaches normal range several days after admission.
Mr. A reports a remote history of alcohol abuse but says he had not been drinking recently, and does not detail his pattern of use. Urine toxicology screen is negative for all substances of abuse.
Mental status examination reveals disheveled appearance, motor agitation, pressured speech, labile affect, loosening of associations, grandiose delusions, and auditory hallucinations. Mr. A’s thought processes are grossly disorganized, such that we could not gather a meaningful history. He believes God is speaking directly to him about plans to build a carousel at Disney World. He makes strange gestures with his hands throughout the interview, as if attempting to trace the shapes of letters and numbers. He frequently speaks of seeing an array of colors. Cognitive examination reveals a score of 5 of 30 on the Montreal Cognitive Assessment (Figure 1), indicating a severe impairment in neurocognitive functioning. He demonstrates limited insight and markedly impaired judgment, and denies having a mental illness.
What should be the next step in managing Mr. A?
a) obtain records from other facilities and collateral history
b) start an antipsychotic
c) order a brain MRI
d) start an alcohol withdrawal protocol
The authors’ observations
Mr. A showed elements of mania, psychosis, and delirium. We considered a broad differential diagnosis (Table). Mr. A initially could not provide reliable or accurate information. The least invasive next step was to obtain additional history from his wife and other medical records to refine the differential diagnosis.
HISTORY Bizarre behavior
Mr. A allows staff to speak with his wife and obtain records from a psychiatric hospitalization 3 years earlier. Mrs. A reports significant and rapid changes in her husband’s behavior and personality over 3 months, but does not describe a recent alcohol relapse. Mr. A sleeps very little, remaining awake and active throughout the night. He frequently rearranges the furniture in their home for no clear reason. Once, he knocked on the door of a young female neighbor asking if she found him attractive.
Mr. A has a significant criminal history. Approximately 30 years ago, he was charged with attempted murder of his ex-wife and he had faced charges of attempted kidnapping and assaulting a police officer. However, he has no recent legal issues.
Mr. A has a history of episodes that are similar to this presentation. Seven years ago, he impulsively purchased a $650,000 house after his fourth wife died. He then had a $90,000 heart-shaped pool installed. He also drove a tractor through his stepdaughter’s car for no apparent reason. Also, 3 years ago, he displayed symptoms similar to his current presentation, including insomnia, irritability, and grandiosity. He engaged in strange behaviors, such as dressing up and imitating homeless people at his church.
During the hospitalization 3 years ago, clinicians gave Mr. A a diagnosis of bipolar disorder, current episode manic, and delirium of an unclear cause. A medical workup, including brain MRI, did not uncover a basis for his delirium. Antipsychotics (risperidone and perphenazine) and mood stabilizers (lithium and valproic acid), stabilized his condition; after 7 weeks, Mr. A was discharged, but he did not pursue outpatient psychiatric care.
What is the most likely DSM-5 diagnosis?
a) major neurocognitive disorder (dementia)
b) alcohol use disorder (eg, Wernicke- Korsakoff syndrome)
c) delirium secondary to mania
d) psychotic disorder
The authors’ observations
DSM-51 suggests a stepwise approach to diagnosis, with consideration of:
• signs and symptoms
• substance use
• general medical condition
• developmental conflict or stage
• whether a mental disorder is present.
Mr. A’s age and severe cognitive impairment raise the possibility of dementia. Rapid onset, history of similar episodes, and apparent inter-episode recovery make dementia unlikely. The history of alcohol abuse and mildly elevated hepatic function tests suggest a substance use disorder such as Wernicke-Korsakoff syndrome or a withdrawal syndrome. However, there is no evidence of excessive alcohol use over the past several months, toxicology studies were negative, and vital signs were stable. General medical causes for Mr. A’s presentation, such as hypoglycemia, head trauma, intracranial infection, and metabolic disturbance were considered, but physical examination and laboratory studies did not suggest any condition that would explain his condition.
Mr. A’s previous psychiatric hospitalization is critical in clarifying the more likely diagnosis. A similar presentation yielded the diagnosis of bipolar disorder, manic phase. Our working diagnosis, therefore, was bipolar disorder with features of delirious mania.
Delirious mania
Delirious mania was first described by Luther Bell in 1849 and is characterized by an acute and simultaneous onset of mania— severe insomnia, poor judgment, grandiosity, excitement, emotional lability, bizarre hallucinations, and delusions—and delirium—altered consciousness, disorientation, and confusion.2,3 Although there are no diagnostic criteria, some authors suggest that delirious mania is characterized by inappropriate toileting, denudation, profound lack of sleep, and episodic memory impairment that can last hours or days.4 Catatonia frequently is seen with delirious mania.5 Initial case descriptions described a high mortality rate, approaching 75% of patients.6 There is little published literature and no classification of delirious mania in DSM-5.1 Estimates are that delirium is concomitant in 20% to 33% of patients with mania.7,8
Several theories try to clarify the underlying etiology of delirious mania. Jacobowski et al9 summarized the etiology and proposed that it is:
• 1 of 3 types of mania, including: acute and delusional manias, as initially proposed by Kraeplin
• a severe form of catatonia
• a condition akin to, but distinct from, delirium with similar underlying medical causes
• a primary psychiatric disorder underlying the cause of delirium.
EVALUATION Brain changes
For several days, Mr. A continues to engage in strange behavior. He tries to take patients’ belongings, is denudative, crawls on floors, licks walls, is unable to feed himself, and exhibits odd motor movements with purposeless motor activity.
We consult our internal medicine team to identify treatable, medical causes. Results of serum B12, thyroid-stimulating hormone, and rapid plasma reagin studies are within normal limits. Urinalysis is negative. A brain MRI reveals numerous white-matter T2-weighted and FLAIR hyperintensities, indicating small-vessel ischemic changes that are consistent with the findings of an MRI 3 years ago. A sleep-deprived EEG with temporal leads obtained on Day 4 of hospitalization demonstrates a diffusely slow and marginally to poorly organized background, believed to indicate global cerebral dysfunction that is most consistent with nonfocal global encephalopathy. There is no seizure activity. We do not perform a lumbar puncture because of Mr. A’s absence of focal neurologic deficits, lack of fever, and normal white blood cell count.
What is the most appropriate treatment?
a) electroconvulsive therapy (ECT)
b) high-dose benzodiazepine
c) mood stabilizer
d) antipsychotic
The authors’ observations
We strongly suspect that Mr. A has delirious mania. Symptoms and signs of mania include labile mood, excessive spending, grandiosity, insomnia, and psychosis together with delirium (marked disorientation, confusion). We ascribed Mr. A’s odd motor behaviors to catatonia, a hallmark of delirious mania. The literature has little description of EEG findings in suspected cases of delirious mania; however, abnormal EEG tracings have been reported.10 We also speculated that Mr. A’s EEG reflected effects produced by his prescribed antipsychotic regimen.
Treatment
There is no clear consensus on treating delirious mania. Because catatonia is a key feature of delirious mania—whether etiologically or as a prominent sign of the condition—ECT and benzodiazepines are proposed as primary treatments. In a study of 16 patients with delirious mania, Karmacharya et al4 found ECT to be effective, with patients showing improvement after 1 to 4 treatments. Lee et al10 reported similar findings. Although a high-dose benzodiazepine is not as effective as ECT, a 1-time oral dose of 3 to 4 mg of lorazepam has been used to treat delirious mania.
The efficacy of antipsychotic and mood-stabilizing pharmacotherapy is not clear. Bond3 described 3 cases in which patients were treated effectively with a typical antipsychotic (haloperidol or chlorpromazine) and lithium. Jung and Lee11demonstrated the efficacy of atypical antipsychotics, with a marked improvement in symptoms within 1 week. However, other studies do not support these findings. Karmacharya et al4 found that typical antipsychotics 1) make the clinical picture worse by increasing extrapyramidal symptoms and 2) produce inconsistent effects. Mood stabilizers sometimes proved beneficial.
Karmacharya et al4 further argued that the delay in improvement seen with any antipsychotics and mood stabilizers suggest they should not be considered a first-line treatment. These discordant findings are the result of a small number of studies and a lack of understanding of the exact nature of delirious mania.
TREATMENT Quick Response
Mr. A’s symptoms rapidly resolve with a combination of quetiapine, 800 mg/d, haloperidol, 10 mg/d, and lithium, 1,200 mg/d. His mood returns to euthymia and his psychotic symptoms abate. He is able to attend to all activities of daily living. Mental status clears and he is fully oriented and able to hold a logical conversation. He scores 28 out of 30 on a subsequent Montreal Cognitive Assessment, administered 11 days after the initial assessment (Figure 2), indicating normal neurocognitive function. He returns to his baseline level of functioning and is discharged in psychiatrically stable condition. Mr. A has no recollection of the bizarre behaviors he displayed earlier in his hospitalization.
The authors’ observations
We started Mr. A on antipsychotics because of his initial level of agitation. In reviewing pharmacotherapy options for Mr. A’s mania and delirium, we contemplated several options. Quetiapine and lithium were chosen after a review of outside hospital records demonstrated a combination of a mood stabilizer and an antipsychotic was effective in treating a previous similar episode, which led to remission of Mr. A’s symptoms. We chose quetiapine because of it highly sedating properties, suspecting that it would help treat his insomnia. We thought that the risk that lithium would make delirium worse was mitigated by Mr. A’s previous therapeutic response to it. Haloperidol was added for treating delirium, given its more potent D2 antagonism. Mr. A responded quickly to these interventions.
We did not consider ECT at the beginning of Mr. A’s admission, and we avoided sedative-hypnotic agents because we were concerned that a benzodiazepine might make his delirium worse. In light of available data suggesting that ECT and benzodiazepines are preferred treatments for delirious mania, it is noteworthy that Mr. A responded so robustly and rapidly to an antipsychotic and a mood stabilizer.
Bottom Line
Consider delirious mania in any patient who has a history of bipolar disorder presenting with co-occuring symptoms of mania and delirium. Collateral information is vital to establishing a diagnosis. With suspected delirium, rule out concomitant reversible medical problems. Electroconvulsive therapy, high-dose benzodiazepines, antipsychotics, and mood stabilizers have shown efficacy.
Related Resources
• Nunes AL, Cheniaux E. Delirium and mania with catatonic features in a Brazilian patient: response to ECT. J Neuropsychiatry Clin Neurosci. 2014;26(1):E1-E3.
• Danivas V, Behere RV, Varambally S, et al. Electroconvulsive therapy in the treatment of delirious mania: a report of 2 patients. J ECT. 2010;26(4):278-279.
Drug Brand Names
Chlorpromazine • Thorazine Perphenazine • Trilafon
Haloperidol • Haldol Quetiapine • Seroquel
Lithium • Eskalith Risperidone • Risperdal
Lorazepam • Ativan Valproic acid • Depakene
Disclosure
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.