User login
MEK inhibitors can induce skin eruptions with distinctive duskiness
Case reports of unusual drug hypersensitivity to MEK inhibitors, involving skin eruptions with distinctive central duskiness, have been described online in JAMA Dermatology.
Three patients who were receiving different MEK inhibitors (selumetinib, cobimetinib, and trametinib) developed grade 2 or 3 eruptions, all associated with unique duskiness, reported Dr. Urvi Patel and associates at Washington University, St. Louis.
A 60-year-old man with pancreatic cancer who was receiving selumetinib as part of a clinical trial presented with a grade 2 generalized eruption and pruritus 12 days after initiating therapy. He had diffuse targetoid patches with central duskiness. Selumetinib and other study drugs were withheld, the patient was given topical corticosteroid treatment, and the eruption completely resolved after 4 weeks. The patient did not restart the study drugs because of an elevated alkaline phosphatase level and fatigue.
A woman in her 40s who was receiving cobimetinib and other medication for metastatic melanoma developed grade 2 coalescing urticarial patches with surrounding duskiness on day 28 of treatment. Histopathologic examination showed a superficial perivascular lymphocytic infiltrate with rare eosinophils. After treatment was halted for 7 days and a regimen of oral prednisone was started, cobimetinib therapy was reinstituted at a lower dose. There was no recurrence of the eruption 1 year after cobimetinib therapy was restarted, Dr. Patel and associates reported (JAMA Dermatol. 2015 Jan. 14 [doi:10.1001/jamadermatol.2014.3207]).
The third patient, a woman in her 50s with metastatic melanoma, developed a grade 3 eruption 7 weeks into trametinib treatment together with another drug. The worsening urticarial patches and plaques had surrounding diffuse duskiness. After trametinib treatment was withheld for a week, and a regimen of oral prednisone was begun, trametinib therapy was restarted and the eruption did not return.
“As shown in our patients, successful treatment of this MEK inhibitor–associated cutaneous eruption can include a drug holiday and oral corticosteroid therapy, with reinstitution of the drug at a lower dose without recurrence,” Dr. Patel and his associates wrote.
MEK inhibitors target the mitogen-activated protein kinase pathway. Trametinib has been approved for treating advanced melanoma, and more than a dozen other MEK inhibitors are in clinical trials (including selumetinib and cobimetinib) for treatment of melanoma and other solid-organ malignant neoplasms, including pancreatic, hepatocellular, colorectal, and non–small cell lung cancer, the authors noted.
On Twitter @nikolaideslaura
Case reports of unusual drug hypersensitivity to MEK inhibitors, involving skin eruptions with distinctive central duskiness, have been described online in JAMA Dermatology.
Three patients who were receiving different MEK inhibitors (selumetinib, cobimetinib, and trametinib) developed grade 2 or 3 eruptions, all associated with unique duskiness, reported Dr. Urvi Patel and associates at Washington University, St. Louis.
A 60-year-old man with pancreatic cancer who was receiving selumetinib as part of a clinical trial presented with a grade 2 generalized eruption and pruritus 12 days after initiating therapy. He had diffuse targetoid patches with central duskiness. Selumetinib and other study drugs were withheld, the patient was given topical corticosteroid treatment, and the eruption completely resolved after 4 weeks. The patient did not restart the study drugs because of an elevated alkaline phosphatase level and fatigue.
A woman in her 40s who was receiving cobimetinib and other medication for metastatic melanoma developed grade 2 coalescing urticarial patches with surrounding duskiness on day 28 of treatment. Histopathologic examination showed a superficial perivascular lymphocytic infiltrate with rare eosinophils. After treatment was halted for 7 days and a regimen of oral prednisone was started, cobimetinib therapy was reinstituted at a lower dose. There was no recurrence of the eruption 1 year after cobimetinib therapy was restarted, Dr. Patel and associates reported (JAMA Dermatol. 2015 Jan. 14 [doi:10.1001/jamadermatol.2014.3207]).
The third patient, a woman in her 50s with metastatic melanoma, developed a grade 3 eruption 7 weeks into trametinib treatment together with another drug. The worsening urticarial patches and plaques had surrounding diffuse duskiness. After trametinib treatment was withheld for a week, and a regimen of oral prednisone was begun, trametinib therapy was restarted and the eruption did not return.
“As shown in our patients, successful treatment of this MEK inhibitor–associated cutaneous eruption can include a drug holiday and oral corticosteroid therapy, with reinstitution of the drug at a lower dose without recurrence,” Dr. Patel and his associates wrote.
MEK inhibitors target the mitogen-activated protein kinase pathway. Trametinib has been approved for treating advanced melanoma, and more than a dozen other MEK inhibitors are in clinical trials (including selumetinib and cobimetinib) for treatment of melanoma and other solid-organ malignant neoplasms, including pancreatic, hepatocellular, colorectal, and non–small cell lung cancer, the authors noted.
On Twitter @nikolaideslaura
Case reports of unusual drug hypersensitivity to MEK inhibitors, involving skin eruptions with distinctive central duskiness, have been described online in JAMA Dermatology.
Three patients who were receiving different MEK inhibitors (selumetinib, cobimetinib, and trametinib) developed grade 2 or 3 eruptions, all associated with unique duskiness, reported Dr. Urvi Patel and associates at Washington University, St. Louis.
A 60-year-old man with pancreatic cancer who was receiving selumetinib as part of a clinical trial presented with a grade 2 generalized eruption and pruritus 12 days after initiating therapy. He had diffuse targetoid patches with central duskiness. Selumetinib and other study drugs were withheld, the patient was given topical corticosteroid treatment, and the eruption completely resolved after 4 weeks. The patient did not restart the study drugs because of an elevated alkaline phosphatase level and fatigue.
A woman in her 40s who was receiving cobimetinib and other medication for metastatic melanoma developed grade 2 coalescing urticarial patches with surrounding duskiness on day 28 of treatment. Histopathologic examination showed a superficial perivascular lymphocytic infiltrate with rare eosinophils. After treatment was halted for 7 days and a regimen of oral prednisone was started, cobimetinib therapy was reinstituted at a lower dose. There was no recurrence of the eruption 1 year after cobimetinib therapy was restarted, Dr. Patel and associates reported (JAMA Dermatol. 2015 Jan. 14 [doi:10.1001/jamadermatol.2014.3207]).
The third patient, a woman in her 50s with metastatic melanoma, developed a grade 3 eruption 7 weeks into trametinib treatment together with another drug. The worsening urticarial patches and plaques had surrounding diffuse duskiness. After trametinib treatment was withheld for a week, and a regimen of oral prednisone was begun, trametinib therapy was restarted and the eruption did not return.
“As shown in our patients, successful treatment of this MEK inhibitor–associated cutaneous eruption can include a drug holiday and oral corticosteroid therapy, with reinstitution of the drug at a lower dose without recurrence,” Dr. Patel and his associates wrote.
MEK inhibitors target the mitogen-activated protein kinase pathway. Trametinib has been approved for treating advanced melanoma, and more than a dozen other MEK inhibitors are in clinical trials (including selumetinib and cobimetinib) for treatment of melanoma and other solid-organ malignant neoplasms, including pancreatic, hepatocellular, colorectal, and non–small cell lung cancer, the authors noted.
On Twitter @nikolaideslaura
FROM JAMA DERMATOLOGY
Key clinical point: This MEK inhibitor–associated cutaneous eruption can be treated with a drug holiday and oral corticosteroid treatment, restarting the drug at a lower dose without recurrence.
Major finding: Three patients who were receiving different MEK inhibitors (selumetinib, cobimetinib, and trametinib) developed grade 2 or 3 eruptions, all associated with unique duskiness.
Data source: Three case studies of patients receiving different MEK inhibitors.
Disclosures: Dr. Lynn Cornelius has received a research grant from Genentech and is a clinical subinvestigator for GlaxoSmithKline. Dr. Milan J. Anadkat has received honoraria as a speaker and/or consultant from AstraZeneca, Bristol-Myers Squibb, Eisai, ImClone, and Therakos. No other disclosures were reported.
Maintenance tacrolimus for eczema boosts quality of life
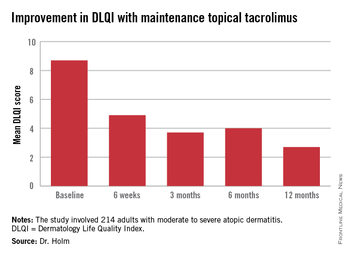
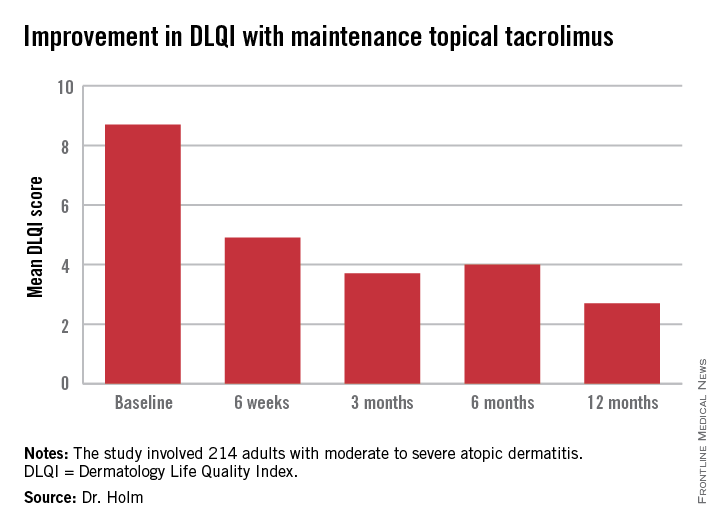
AMSTERDAM – Twice-weekly proactive maintenance therapy with 0.1% tacrolimus ointment in adults with moderate to severe atopic dermatitis resulted in dramatic improvement in self-reported quality of life in a 12-month observational study.
This prospective study was designed to assess patients’ own experiences in real-world clinical practice. For example, patients had to pay for their own medication, unlike in randomized clinical trials, where they get it for free. Study participants also didn’t check in for regularly scheduled office visits or receive pep talks to boost medication adherence. They simply reported their outcomes to investigators through mailed questionnaires instead, Dr. Elisabeth A. Holm explained at the annual congress of the European Academy of Dermatology and Venereology.
A previous clinical trial by other investigators showed that twice-weekly maintenance therapy with topical tacrolimus kept adult atopic dermatitis in remission for extended periods and reduced the incidence of eczema exacerbations (Allergy 2008;63:742-50). But Dr. Holm, a dermatologist at Copenhagen University, wondered what happens when maintenance topical tacrolimus is employed as a proactive treatment strategy in real daily life, particularly in light of a Danish study that found that dermatology patients never filled one in three prescriptions for new medications (J. Am. Acad. Dermatol. 2008;59:27-33).
The current observational study included 214 adults with moderate to severe atopic dermatitis previously treated with corticosteroids who presented to 41 sites in Denmark and Sweden. They were given a prescription for 0.1% tacrolimus ointment (Protopic) with instructions to apply it twice daily until their eczema was cleared or almost cleared, then switch to twice weekly maintenance therapy, shifting back to BID therapy as needed to combat flares.
The primary endpoint was change in health-related quality of life during 12 months of followup. This was assessed using the Dermatology Life Quality Index (DLQI), which was administered at baseline, 6 weeks, and 3, 6, and 12 months. Scores improved dramatically.
At baseline, 35% of patients had a DLQI of 6-10, indicative of a moderate adverse impact of their skin disease on daily life. Another 27% had a DLQI of 11-20, reflecting a very large adverse effect. At 12 months, however, DLQI scores had undergone a big shift in the favorable direction: 14% of subjects had a DLQI of 6-10, a mere 4% scored 11-20, and 52% of patients had a DLQI of 0 or 1, meaning they felt their atopic dermatitis had no effect upon their quality of life.
In other outcomes, patients reported that it took a mean of 35 and median of 27 days on twice-daily therapy to become free of atopic dermatitis.
“This is helpful information for us in telling new patients what to expect. They come in really hoping to be free of eczema after 2 days. If we inform them it will take several weeks they’ll probably be more adherent to therapy,” Dr. Holm said.
Once patients became clear or almost clear and switched to twice weekly maintenance therapy, they stayed that way for an average of 61 days.
Self-reported patient compliance with the maintenance regimen was excellent. Patients indicated they applied topical tacrolimus a median of two times per week. They also utilized emolliants an average of once per day or more, as physicians had encouraged. Patients didn’t report any adverse events on their questionnaires.
An interesting study finding was that even though 52% of patients had atopic dermatitis on the face -- the most visible and highly charged of all locations -- 75% of patients indicated the biggest difficulty posed by their skin disease was its itchiness, not its adverse impact on their appearance.
“This is what I find in my own daily practice, too. Patients come in and say, ‘Please give me a drug to remove my daily itch and I will be satisfied,’” according to Dr. Holm.
The study was sponsored by Astellas Pharma. Dr. Holm is a consultant to the company.
AMSTERDAM – Twice-weekly proactive maintenance therapy with 0.1% tacrolimus ointment in adults with moderate to severe atopic dermatitis resulted in dramatic improvement in self-reported quality of life in a 12-month observational study.
This prospective study was designed to assess patients’ own experiences in real-world clinical practice. For example, patients had to pay for their own medication, unlike in randomized clinical trials, where they get it for free. Study participants also didn’t check in for regularly scheduled office visits or receive pep talks to boost medication adherence. They simply reported their outcomes to investigators through mailed questionnaires instead, Dr. Elisabeth A. Holm explained at the annual congress of the European Academy of Dermatology and Venereology.
A previous clinical trial by other investigators showed that twice-weekly maintenance therapy with topical tacrolimus kept adult atopic dermatitis in remission for extended periods and reduced the incidence of eczema exacerbations (Allergy 2008;63:742-50). But Dr. Holm, a dermatologist at Copenhagen University, wondered what happens when maintenance topical tacrolimus is employed as a proactive treatment strategy in real daily life, particularly in light of a Danish study that found that dermatology patients never filled one in three prescriptions for new medications (J. Am. Acad. Dermatol. 2008;59:27-33).
The current observational study included 214 adults with moderate to severe atopic dermatitis previously treated with corticosteroids who presented to 41 sites in Denmark and Sweden. They were given a prescription for 0.1% tacrolimus ointment (Protopic) with instructions to apply it twice daily until their eczema was cleared or almost cleared, then switch to twice weekly maintenance therapy, shifting back to BID therapy as needed to combat flares.
The primary endpoint was change in health-related quality of life during 12 months of followup. This was assessed using the Dermatology Life Quality Index (DLQI), which was administered at baseline, 6 weeks, and 3, 6, and 12 months. Scores improved dramatically.
At baseline, 35% of patients had a DLQI of 6-10, indicative of a moderate adverse impact of their skin disease on daily life. Another 27% had a DLQI of 11-20, reflecting a very large adverse effect. At 12 months, however, DLQI scores had undergone a big shift in the favorable direction: 14% of subjects had a DLQI of 6-10, a mere 4% scored 11-20, and 52% of patients had a DLQI of 0 or 1, meaning they felt their atopic dermatitis had no effect upon their quality of life.
In other outcomes, patients reported that it took a mean of 35 and median of 27 days on twice-daily therapy to become free of atopic dermatitis.
“This is helpful information for us in telling new patients what to expect. They come in really hoping to be free of eczema after 2 days. If we inform them it will take several weeks they’ll probably be more adherent to therapy,” Dr. Holm said.
Once patients became clear or almost clear and switched to twice weekly maintenance therapy, they stayed that way for an average of 61 days.
Self-reported patient compliance with the maintenance regimen was excellent. Patients indicated they applied topical tacrolimus a median of two times per week. They also utilized emolliants an average of once per day or more, as physicians had encouraged. Patients didn’t report any adverse events on their questionnaires.
An interesting study finding was that even though 52% of patients had atopic dermatitis on the face -- the most visible and highly charged of all locations -- 75% of patients indicated the biggest difficulty posed by their skin disease was its itchiness, not its adverse impact on their appearance.
“This is what I find in my own daily practice, too. Patients come in and say, ‘Please give me a drug to remove my daily itch and I will be satisfied,’” according to Dr. Holm.
The study was sponsored by Astellas Pharma. Dr. Holm is a consultant to the company.
AMSTERDAM – Twice-weekly proactive maintenance therapy with 0.1% tacrolimus ointment in adults with moderate to severe atopic dermatitis resulted in dramatic improvement in self-reported quality of life in a 12-month observational study.
This prospective study was designed to assess patients’ own experiences in real-world clinical practice. For example, patients had to pay for their own medication, unlike in randomized clinical trials, where they get it for free. Study participants also didn’t check in for regularly scheduled office visits or receive pep talks to boost medication adherence. They simply reported their outcomes to investigators through mailed questionnaires instead, Dr. Elisabeth A. Holm explained at the annual congress of the European Academy of Dermatology and Venereology.
A previous clinical trial by other investigators showed that twice-weekly maintenance therapy with topical tacrolimus kept adult atopic dermatitis in remission for extended periods and reduced the incidence of eczema exacerbations (Allergy 2008;63:742-50). But Dr. Holm, a dermatologist at Copenhagen University, wondered what happens when maintenance topical tacrolimus is employed as a proactive treatment strategy in real daily life, particularly in light of a Danish study that found that dermatology patients never filled one in three prescriptions for new medications (J. Am. Acad. Dermatol. 2008;59:27-33).
The current observational study included 214 adults with moderate to severe atopic dermatitis previously treated with corticosteroids who presented to 41 sites in Denmark and Sweden. They were given a prescription for 0.1% tacrolimus ointment (Protopic) with instructions to apply it twice daily until their eczema was cleared or almost cleared, then switch to twice weekly maintenance therapy, shifting back to BID therapy as needed to combat flares.
The primary endpoint was change in health-related quality of life during 12 months of followup. This was assessed using the Dermatology Life Quality Index (DLQI), which was administered at baseline, 6 weeks, and 3, 6, and 12 months. Scores improved dramatically.
At baseline, 35% of patients had a DLQI of 6-10, indicative of a moderate adverse impact of their skin disease on daily life. Another 27% had a DLQI of 11-20, reflecting a very large adverse effect. At 12 months, however, DLQI scores had undergone a big shift in the favorable direction: 14% of subjects had a DLQI of 6-10, a mere 4% scored 11-20, and 52% of patients had a DLQI of 0 or 1, meaning they felt their atopic dermatitis had no effect upon their quality of life.
In other outcomes, patients reported that it took a mean of 35 and median of 27 days on twice-daily therapy to become free of atopic dermatitis.
“This is helpful information for us in telling new patients what to expect. They come in really hoping to be free of eczema after 2 days. If we inform them it will take several weeks they’ll probably be more adherent to therapy,” Dr. Holm said.
Once patients became clear or almost clear and switched to twice weekly maintenance therapy, they stayed that way for an average of 61 days.
Self-reported patient compliance with the maintenance regimen was excellent. Patients indicated they applied topical tacrolimus a median of two times per week. They also utilized emolliants an average of once per day or more, as physicians had encouraged. Patients didn’t report any adverse events on their questionnaires.
An interesting study finding was that even though 52% of patients had atopic dermatitis on the face -- the most visible and highly charged of all locations -- 75% of patients indicated the biggest difficulty posed by their skin disease was its itchiness, not its adverse impact on their appearance.
“This is what I find in my own daily practice, too. Patients come in and say, ‘Please give me a drug to remove my daily itch and I will be satisfied,’” according to Dr. Holm.
The study was sponsored by Astellas Pharma. Dr. Holm is a consultant to the company.
AT THE EADV CONGRESS
Key clinical point: Twice-weekly proactive application of topical tacrolimus in adults with moderate to severe atopic dermatitis not only reduces flares, it dramatically improves patients’ self-rated quality of life.
Major finding: Mean scores on the Dermatology Life Quality Index in patients on maintenance therapy improved from 8.7 at baseline to 2.7 at 12 months, indicative of minimal disease impact upon daily life.
Data source: This was a 41-site, two-nation study involving 214 adults with moderate to severe atopic dermatitis.
Disclosures: The study was sponsored by Astellas. The presenter is a consultant to the company.
Can patients be desensitized to nickel?
VANCOUVER, B.C. – Nickel has long ranked at the top of common contact allergens. In fact, it earned the No. 1 spot in the North American Contact Dermatitis Group patch test results in 2009-2010.
A team of Canadian researchers began to wonder: Is it feasible to induce tolerance to nickel, or to desensitize patients to this substance found in everything from jewelry and orthodontic devices to vitamins and herbal remedies? At the annual meeting of the Pacific Dermatologic Association, Dr. Gillian C. de Gannes, a dermatologist who directs the University of British Columbia Contact Dermatitis Clinic in Vancouver, discussed preliminary findings from a proof-of-principle study designed to answer that question.

“We have a nickel detection kit for our patients – the dimethylglyoxime test – but at this point, allergen avoidance counseling is how we treat nickel allergy,” she said. “The regulatory CD4-positive CD25-positive T cells (Tregs) modulate nickel sensitivity in humans, and topical application of calcipotriol induces Treg cells to prevent both the induction and elicitation of contact hypersensitivity in mice. It’s [also] been shown that topical vitamin D analogues prevented topical sensitization to DNCB [dinitrochlorobenzene] in humans: a very potent sensitizer,” she noted (Arch. Dermatol. 2006;142:1332-4).
In an effort to investigate whether topical immune modulators can stop preestablished contact hypersensitivity to nickel, Dr. de Gannes and her associates recruited 24 volunteers to participate in a double-blind, controlled trial, and randomized them to one of four groups: petrolatum ointment, betamethasone dipropionate ointment, calcipotriol ointment, and the combination of betamethasone dipropionate and calcipotriol ointments. “We first do a nickel patch test on the distal forearm to confirm that this person is sensitized to nickel,” she explained. “That’s our confirmation stage. On the opposite arm, we randomize them to one of the four groups of ointment, and we instruct them to apply a measured amount of ointment in a defined area twice daily for a week. They come back to us at the end of that week, and we repeat the nickel patch test where they applied their ointment to see whether they react or not.”
So far, preliminary results from 13 patients showed that application of some of the topical products induced tolerance and decreased reactivity to nickel, “but we’ve not yet been able to desensitize patients,” Dr. de Gannes noted. “This is just an interim analysis, and we have not unblinded the study yet. Hopefully we’ll have more meaningful results within the next year.”
The strategy is clinically relevant, she continued, because “we have hairstylists, for example, who come to us, allergic to the chemicals that they’re using. They really want to get back to their job. If this is a hand dermatitis caused by nickel or other contact allergens, and I can possibly give that hairstylist an ointment to apply to her hands in the morning and night and get back to her job, that’s a happy worker. That scenario would be a successful clinical outcome of this research, but we have a lot more work to do.”
Dr. de Gannes said that she had no relevant financial conflicts of interest to disclose.
On Twitter @dougbrunk
VANCOUVER, B.C. – Nickel has long ranked at the top of common contact allergens. In fact, it earned the No. 1 spot in the North American Contact Dermatitis Group patch test results in 2009-2010.
A team of Canadian researchers began to wonder: Is it feasible to induce tolerance to nickel, or to desensitize patients to this substance found in everything from jewelry and orthodontic devices to vitamins and herbal remedies? At the annual meeting of the Pacific Dermatologic Association, Dr. Gillian C. de Gannes, a dermatologist who directs the University of British Columbia Contact Dermatitis Clinic in Vancouver, discussed preliminary findings from a proof-of-principle study designed to answer that question.
“We have a nickel detection kit for our patients – the dimethylglyoxime test – but at this point, allergen avoidance counseling is how we treat nickel allergy,” she said. “The regulatory CD4-positive CD25-positive T cells (Tregs) modulate nickel sensitivity in humans, and topical application of calcipotriol induces Treg cells to prevent both the induction and elicitation of contact hypersensitivity in mice. It’s [also] been shown that topical vitamin D analogues prevented topical sensitization to DNCB [dinitrochlorobenzene] in humans: a very potent sensitizer,” she noted (Arch. Dermatol. 2006;142:1332-4).
In an effort to investigate whether topical immune modulators can stop preestablished contact hypersensitivity to nickel, Dr. de Gannes and her associates recruited 24 volunteers to participate in a double-blind, controlled trial, and randomized them to one of four groups: petrolatum ointment, betamethasone dipropionate ointment, calcipotriol ointment, and the combination of betamethasone dipropionate and calcipotriol ointments. “We first do a nickel patch test on the distal forearm to confirm that this person is sensitized to nickel,” she explained. “That’s our confirmation stage. On the opposite arm, we randomize them to one of the four groups of ointment, and we instruct them to apply a measured amount of ointment in a defined area twice daily for a week. They come back to us at the end of that week, and we repeat the nickel patch test where they applied their ointment to see whether they react or not.”
So far, preliminary results from 13 patients showed that application of some of the topical products induced tolerance and decreased reactivity to nickel, “but we’ve not yet been able to desensitize patients,” Dr. de Gannes noted. “This is just an interim analysis, and we have not unblinded the study yet. Hopefully we’ll have more meaningful results within the next year.”
The strategy is clinically relevant, she continued, because “we have hairstylists, for example, who come to us, allergic to the chemicals that they’re using. They really want to get back to their job. If this is a hand dermatitis caused by nickel or other contact allergens, and I can possibly give that hairstylist an ointment to apply to her hands in the morning and night and get back to her job, that’s a happy worker. That scenario would be a successful clinical outcome of this research, but we have a lot more work to do.”
Dr. de Gannes said that she had no relevant financial conflicts of interest to disclose.
On Twitter @dougbrunk
VANCOUVER, B.C. – Nickel has long ranked at the top of common contact allergens. In fact, it earned the No. 1 spot in the North American Contact Dermatitis Group patch test results in 2009-2010.
A team of Canadian researchers began to wonder: Is it feasible to induce tolerance to nickel, or to desensitize patients to this substance found in everything from jewelry and orthodontic devices to vitamins and herbal remedies? At the annual meeting of the Pacific Dermatologic Association, Dr. Gillian C. de Gannes, a dermatologist who directs the University of British Columbia Contact Dermatitis Clinic in Vancouver, discussed preliminary findings from a proof-of-principle study designed to answer that question.
“We have a nickel detection kit for our patients – the dimethylglyoxime test – but at this point, allergen avoidance counseling is how we treat nickel allergy,” she said. “The regulatory CD4-positive CD25-positive T cells (Tregs) modulate nickel sensitivity in humans, and topical application of calcipotriol induces Treg cells to prevent both the induction and elicitation of contact hypersensitivity in mice. It’s [also] been shown that topical vitamin D analogues prevented topical sensitization to DNCB [dinitrochlorobenzene] in humans: a very potent sensitizer,” she noted (Arch. Dermatol. 2006;142:1332-4).
In an effort to investigate whether topical immune modulators can stop preestablished contact hypersensitivity to nickel, Dr. de Gannes and her associates recruited 24 volunteers to participate in a double-blind, controlled trial, and randomized them to one of four groups: petrolatum ointment, betamethasone dipropionate ointment, calcipotriol ointment, and the combination of betamethasone dipropionate and calcipotriol ointments. “We first do a nickel patch test on the distal forearm to confirm that this person is sensitized to nickel,” she explained. “That’s our confirmation stage. On the opposite arm, we randomize them to one of the four groups of ointment, and we instruct them to apply a measured amount of ointment in a defined area twice daily for a week. They come back to us at the end of that week, and we repeat the nickel patch test where they applied their ointment to see whether they react or not.”
So far, preliminary results from 13 patients showed that application of some of the topical products induced tolerance and decreased reactivity to nickel, “but we’ve not yet been able to desensitize patients,” Dr. de Gannes noted. “This is just an interim analysis, and we have not unblinded the study yet. Hopefully we’ll have more meaningful results within the next year.”
The strategy is clinically relevant, she continued, because “we have hairstylists, for example, who come to us, allergic to the chemicals that they’re using. They really want to get back to their job. If this is a hand dermatitis caused by nickel or other contact allergens, and I can possibly give that hairstylist an ointment to apply to her hands in the morning and night and get back to her job, that’s a happy worker. That scenario would be a successful clinical outcome of this research, but we have a lot more work to do.”
Dr. de Gannes said that she had no relevant financial conflicts of interest to disclose.
On Twitter @dougbrunk
EXPERT ANALYSIS AT PDA 2014

Dupilumab advances for severe atopic dermatitis
AMSTERDAM – The novel biologic agent dupilumab showed strong dose-dependent efficacy in adults with moderate to severe atopic dermatitis not adequately controlled with topical medications in a 380-patient phase IIb dose-ranging study.
“Based on the results of this study, we’ll take the top two doses further to our phase III program. We’re also planning to conduct a maintenance study. At the end of 16 weeks of treatment, we’ll investigate lower-dose regimens that may be capable of maintaining clinical response,” Dr. Marius Ardeleanu said at the annual congress of the European Academy of Dermatology and Venereology.

Dupilumab is an investigational fully human monoclonal antibody that addresses a novel target: It is directed against the interleukin-4 receptor alpha subunit (IL-4Ra). Through this effect it blocks IL-4 and IL-13, the drivers of the type 2 helper T-cell–mediated inflammation responsible for the hallmark symptoms of atopic dermatitis (AD), explained Dr. Ardeleanu of Regeneron Pharmaceuticals in Tarrytown, N.Y.
Participants in this 16-week, double-blind, international phase IIb study were randomized to placebo or one of five dupilumab dosing regimens ranging from a low of 100 mg given subcutaneously every 4 weeks to a maximum of 300 mg once weekly or every 2 weeks.
These patients had a significant disease burden. They were typically in their mid- to late 30s and had a 27-year disease history, a mean baseline SCORAD of 67 on a 0-100 scale, a baseline Eczema Area and Severity Index (EASI) score of 32, an Investigator’s Global Assessment of disease severity score of 3.5 on a 0-4 scale, and 50% body surface area involvement. Their mean average weekly self-rated itching score was 6.8 on a 0-10 scale.
The primary study endpoint was change in the EASI score from baseline to 16 weeks. The score dropped by 20% in placebo-treated controls and by significantly greater margins in all five dupilumab arms. The largest reduction in EASI score – nearly 80% – occurred in the group on 300 mg/wk, with the 300 mg every 2 weeks group showing about a 70% reduction.
Roughly 80% of patients on 300 mg/wk or every 2 weeks showed an EASI 50 response at week 16, meaning a 50% reduction from baseline in their score, which is considered clinically meaningful improvement. One-third of patients on either of these top two–performing regimens achieved an Investigator’s Global Assessment score of 0 or 1, which is virtual remission; none of the controls did. Overall weekly average pruritus scores dropped by more than 60% with weekly treatment at 300 mg and by slightly less with biweekly therapy at 300 mg.
Safety data were similar to those from a recently published earlier phase IIa study (N. Engl. J. Med. 2014; 371:130-9). There were no dose-limiting toxicities. Headache and injection site reactions were the only adverse events more common with dupilumab than with placebo in the phase IIb trial, with the incidence of injection site reactions showing a possible dose-response relationship.
In addition to the large phase III studies now being planned, which will also evaluate step-down maintenance therapy, another study has been scheduled to investigate the use of dupilumab in combination with topical corticosteroid therapy. The earlier phase IIa study provided evidence to suggest this combination has even greater efficacy than dupilumab alone, and with modest use of the topical agent, according to Dr. Ardeleanu.
Dupilumab is also being developed as a treatment for tough-to-control moderate to severe asthma. It showed positive results in a phase II study, with reduced asthma exacerbations and improved lung function, compared with placebo (N. Engl. J. Med. 2013; 368:2455-66).
AMSTERDAM – The novel biologic agent dupilumab showed strong dose-dependent efficacy in adults with moderate to severe atopic dermatitis not adequately controlled with topical medications in a 380-patient phase IIb dose-ranging study.
“Based on the results of this study, we’ll take the top two doses further to our phase III program. We’re also planning to conduct a maintenance study. At the end of 16 weeks of treatment, we’ll investigate lower-dose regimens that may be capable of maintaining clinical response,” Dr. Marius Ardeleanu said at the annual congress of the European Academy of Dermatology and Venereology.
Dupilumab is an investigational fully human monoclonal antibody that addresses a novel target: It is directed against the interleukin-4 receptor alpha subunit (IL-4Ra). Through this effect it blocks IL-4 and IL-13, the drivers of the type 2 helper T-cell–mediated inflammation responsible for the hallmark symptoms of atopic dermatitis (AD), explained Dr. Ardeleanu of Regeneron Pharmaceuticals in Tarrytown, N.Y.
Participants in this 16-week, double-blind, international phase IIb study were randomized to placebo or one of five dupilumab dosing regimens ranging from a low of 100 mg given subcutaneously every 4 weeks to a maximum of 300 mg once weekly or every 2 weeks.
These patients had a significant disease burden. They were typically in their mid- to late 30s and had a 27-year disease history, a mean baseline SCORAD of 67 on a 0-100 scale, a baseline Eczema Area and Severity Index (EASI) score of 32, an Investigator’s Global Assessment of disease severity score of 3.5 on a 0-4 scale, and 50% body surface area involvement. Their mean average weekly self-rated itching score was 6.8 on a 0-10 scale.
The primary study endpoint was change in the EASI score from baseline to 16 weeks. The score dropped by 20% in placebo-treated controls and by significantly greater margins in all five dupilumab arms. The largest reduction in EASI score – nearly 80% – occurred in the group on 300 mg/wk, with the 300 mg every 2 weeks group showing about a 70% reduction.
Roughly 80% of patients on 300 mg/wk or every 2 weeks showed an EASI 50 response at week 16, meaning a 50% reduction from baseline in their score, which is considered clinically meaningful improvement. One-third of patients on either of these top two–performing regimens achieved an Investigator’s Global Assessment score of 0 or 1, which is virtual remission; none of the controls did. Overall weekly average pruritus scores dropped by more than 60% with weekly treatment at 300 mg and by slightly less with biweekly therapy at 300 mg.
Safety data were similar to those from a recently published earlier phase IIa study (N. Engl. J. Med. 2014; 371:130-9). There were no dose-limiting toxicities. Headache and injection site reactions were the only adverse events more common with dupilumab than with placebo in the phase IIb trial, with the incidence of injection site reactions showing a possible dose-response relationship.
In addition to the large phase III studies now being planned, which will also evaluate step-down maintenance therapy, another study has been scheduled to investigate the use of dupilumab in combination with topical corticosteroid therapy. The earlier phase IIa study provided evidence to suggest this combination has even greater efficacy than dupilumab alone, and with modest use of the topical agent, according to Dr. Ardeleanu.
Dupilumab is also being developed as a treatment for tough-to-control moderate to severe asthma. It showed positive results in a phase II study, with reduced asthma exacerbations and improved lung function, compared with placebo (N. Engl. J. Med. 2013; 368:2455-66).
AMSTERDAM – The novel biologic agent dupilumab showed strong dose-dependent efficacy in adults with moderate to severe atopic dermatitis not adequately controlled with topical medications in a 380-patient phase IIb dose-ranging study.
“Based on the results of this study, we’ll take the top two doses further to our phase III program. We’re also planning to conduct a maintenance study. At the end of 16 weeks of treatment, we’ll investigate lower-dose regimens that may be capable of maintaining clinical response,” Dr. Marius Ardeleanu said at the annual congress of the European Academy of Dermatology and Venereology.
Dupilumab is an investigational fully human monoclonal antibody that addresses a novel target: It is directed against the interleukin-4 receptor alpha subunit (IL-4Ra). Through this effect it blocks IL-4 and IL-13, the drivers of the type 2 helper T-cell–mediated inflammation responsible for the hallmark symptoms of atopic dermatitis (AD), explained Dr. Ardeleanu of Regeneron Pharmaceuticals in Tarrytown, N.Y.
Participants in this 16-week, double-blind, international phase IIb study were randomized to placebo or one of five dupilumab dosing regimens ranging from a low of 100 mg given subcutaneously every 4 weeks to a maximum of 300 mg once weekly or every 2 weeks.
These patients had a significant disease burden. They were typically in their mid- to late 30s and had a 27-year disease history, a mean baseline SCORAD of 67 on a 0-100 scale, a baseline Eczema Area and Severity Index (EASI) score of 32, an Investigator’s Global Assessment of disease severity score of 3.5 on a 0-4 scale, and 50% body surface area involvement. Their mean average weekly self-rated itching score was 6.8 on a 0-10 scale.
The primary study endpoint was change in the EASI score from baseline to 16 weeks. The score dropped by 20% in placebo-treated controls and by significantly greater margins in all five dupilumab arms. The largest reduction in EASI score – nearly 80% – occurred in the group on 300 mg/wk, with the 300 mg every 2 weeks group showing about a 70% reduction.
Roughly 80% of patients on 300 mg/wk or every 2 weeks showed an EASI 50 response at week 16, meaning a 50% reduction from baseline in their score, which is considered clinically meaningful improvement. One-third of patients on either of these top two–performing regimens achieved an Investigator’s Global Assessment score of 0 or 1, which is virtual remission; none of the controls did. Overall weekly average pruritus scores dropped by more than 60% with weekly treatment at 300 mg and by slightly less with biweekly therapy at 300 mg.
Safety data were similar to those from a recently published earlier phase IIa study (N. Engl. J. Med. 2014; 371:130-9). There were no dose-limiting toxicities. Headache and injection site reactions were the only adverse events more common with dupilumab than with placebo in the phase IIb trial, with the incidence of injection site reactions showing a possible dose-response relationship.
In addition to the large phase III studies now being planned, which will also evaluate step-down maintenance therapy, another study has been scheduled to investigate the use of dupilumab in combination with topical corticosteroid therapy. The earlier phase IIa study provided evidence to suggest this combination has even greater efficacy than dupilumab alone, and with modest use of the topical agent, according to Dr. Ardeleanu.
Dupilumab is also being developed as a treatment for tough-to-control moderate to severe asthma. It showed positive results in a phase II study, with reduced asthma exacerbations and improved lung function, compared with placebo (N. Engl. J. Med. 2013; 368:2455-66).
AT THE EADV CONGRESS
Key clinical point: A promising new therapy with a novel mechanism of action is progressing through the pipeline for adults with refractory atopic dermatitis.
Major finding: Patients on subcutaneous dupilumab at 300 mg once weekly showed nearly an 80% reduction from baseline in Eczema Area and Severity Index scores after 16 weeks of treatment.
Data source: A randomized, double-blind, placebo-controlled, international, 16-week phase IIb study of 380 adults with moderate to severe atopic dermatitis inadequately controlled by topical therapies.
Disclosures: The study was sponsored by Regeneron Pharmaceuticals and presented by the company’s senior director of clinical sciences.

Vulvar pruritus in young girls usually due to toilet hygiene
NEWPORT BEACH, CALIF. – All it takes to clear up vulvar pruritus in most young girls prior to puberty is a little reminder about proper toilet habits, according to Dr. Bethanee J. Schlosser.
“There are a whole slew of conditions that cause itching of the genitals in young girls, but the most common is poor hygiene,” explained Dr. Schlosser of the departments of dermatology and obstetrics and gynecology at Northwestern University in Chicago.

Afraid they might miss out on something, children often rush bathroom visits and don’t take the time to wipe properly. Itching and redness soon follow. Gentle guidance is mostly all that’s needed to clear the problem. Loose-fitting cotton underwear helps, too, along with quickly changing soiled underpants, avoiding wet wipes, and taking baths to make sure the genitalia are adequately rinsed, Dr. Schlosser said at the Skin Disease Education Foundation’s Women’s & Pediatric Dermatology Seminar.
Simple as those steps are, they can be overlooked in the clinic. One study found that young girls are sometimes misdiagnosed with candidiasis, and treated with topical antifungals for years, even though yeast infections – the most common cause of vulvovaginal pruritus in adult women – are estrogen dependent, and so far less likely before puberty (Australas. J. Dermatol. 2010;51:118-23). After hygiene issues, lichen sclerosus is perhaps the next most common cause of vulvar pruritus in young girls, and tends to present with more urinary problems and bleeding than in adults, and more GI complaints, especially constipation. It’s “the most common inflammatory vulvar dermatosis that we see, with the possible exception of contact dermatitis,” Dr. Schlosser wrote (Arch. Dermatol. 2004;140:702-6). As in adult women, the first-line treatment is once-daily clobetasol propionate ointment 0.05% for several weeks, followed by maintenance therapy. Dr. Schlosser said she used to switch patients to a less potent topical steroid, but “then I had a couple patients get confused about which tube they were supposed to use at home, so now I taper the frequency of their clobetasol ointment” to once or twice a week instead of switching them to a less potent topical steroid. It’s easier for them, but as with any topical steroid, “you need to continue ongoing monitoring for cutaneous atrophy,” she said.
In general, pelvic exams in pediatric patients “require special consideration. These are not 5-minute visits. You have to take the time to make yourself available. Educate patients and parents about what’s going to happen,” and use the child’s own terms for her genitals, asking parents beforehand what they are, so that the child understands what she’s hearing, Dr. Schlosser said.
“When I see young girls,” mom is in the room and “I only have gauze, gloves, and maybe a Q-tip [swab] here and there. I often” begin by asking the child if it’s okay to look at her scalp, face, and hands, then “gradually work my way down. I think that gives patients some sense of comfort and control,” she said.
Dr. Schlosser said she prefers the frog-leg position, with very young girls in their mothers’ laps. The literature sometimes advocates the prone knee-to-chest position, but “I find it makes people feel very vulnerable. They can’t see you, and they have no idea of what’s going on. I don’t advocate it,” she said.
Dr. Schlosser said she has no relevant financial disclosures.
SDEF and this news organization are owned by Frontline Medical Communications.
NEWPORT BEACH, CALIF. – All it takes to clear up vulvar pruritus in most young girls prior to puberty is a little reminder about proper toilet habits, according to Dr. Bethanee J. Schlosser.
“There are a whole slew of conditions that cause itching of the genitals in young girls, but the most common is poor hygiene,” explained Dr. Schlosser of the departments of dermatology and obstetrics and gynecology at Northwestern University in Chicago.
Afraid they might miss out on something, children often rush bathroom visits and don’t take the time to wipe properly. Itching and redness soon follow. Gentle guidance is mostly all that’s needed to clear the problem. Loose-fitting cotton underwear helps, too, along with quickly changing soiled underpants, avoiding wet wipes, and taking baths to make sure the genitalia are adequately rinsed, Dr. Schlosser said at the Skin Disease Education Foundation’s Women’s & Pediatric Dermatology Seminar.
Simple as those steps are, they can be overlooked in the clinic. One study found that young girls are sometimes misdiagnosed with candidiasis, and treated with topical antifungals for years, even though yeast infections – the most common cause of vulvovaginal pruritus in adult women – are estrogen dependent, and so far less likely before puberty (Australas. J. Dermatol. 2010;51:118-23). After hygiene issues, lichen sclerosus is perhaps the next most common cause of vulvar pruritus in young girls, and tends to present with more urinary problems and bleeding than in adults, and more GI complaints, especially constipation. It’s “the most common inflammatory vulvar dermatosis that we see, with the possible exception of contact dermatitis,” Dr. Schlosser wrote (Arch. Dermatol. 2004;140:702-6). As in adult women, the first-line treatment is once-daily clobetasol propionate ointment 0.05% for several weeks, followed by maintenance therapy. Dr. Schlosser said she used to switch patients to a less potent topical steroid, but “then I had a couple patients get confused about which tube they were supposed to use at home, so now I taper the frequency of their clobetasol ointment” to once or twice a week instead of switching them to a less potent topical steroid. It’s easier for them, but as with any topical steroid, “you need to continue ongoing monitoring for cutaneous atrophy,” she said.
In general, pelvic exams in pediatric patients “require special consideration. These are not 5-minute visits. You have to take the time to make yourself available. Educate patients and parents about what’s going to happen,” and use the child’s own terms for her genitals, asking parents beforehand what they are, so that the child understands what she’s hearing, Dr. Schlosser said.
“When I see young girls,” mom is in the room and “I only have gauze, gloves, and maybe a Q-tip [swab] here and there. I often” begin by asking the child if it’s okay to look at her scalp, face, and hands, then “gradually work my way down. I think that gives patients some sense of comfort and control,” she said.
Dr. Schlosser said she prefers the frog-leg position, with very young girls in their mothers’ laps. The literature sometimes advocates the prone knee-to-chest position, but “I find it makes people feel very vulnerable. They can’t see you, and they have no idea of what’s going on. I don’t advocate it,” she said.
Dr. Schlosser said she has no relevant financial disclosures.
SDEF and this news organization are owned by Frontline Medical Communications.
NEWPORT BEACH, CALIF. – All it takes to clear up vulvar pruritus in most young girls prior to puberty is a little reminder about proper toilet habits, according to Dr. Bethanee J. Schlosser.
“There are a whole slew of conditions that cause itching of the genitals in young girls, but the most common is poor hygiene,” explained Dr. Schlosser of the departments of dermatology and obstetrics and gynecology at Northwestern University in Chicago.
Afraid they might miss out on something, children often rush bathroom visits and don’t take the time to wipe properly. Itching and redness soon follow. Gentle guidance is mostly all that’s needed to clear the problem. Loose-fitting cotton underwear helps, too, along with quickly changing soiled underpants, avoiding wet wipes, and taking baths to make sure the genitalia are adequately rinsed, Dr. Schlosser said at the Skin Disease Education Foundation’s Women’s & Pediatric Dermatology Seminar.
Simple as those steps are, they can be overlooked in the clinic. One study found that young girls are sometimes misdiagnosed with candidiasis, and treated with topical antifungals for years, even though yeast infections – the most common cause of vulvovaginal pruritus in adult women – are estrogen dependent, and so far less likely before puberty (Australas. J. Dermatol. 2010;51:118-23). After hygiene issues, lichen sclerosus is perhaps the next most common cause of vulvar pruritus in young girls, and tends to present with more urinary problems and bleeding than in adults, and more GI complaints, especially constipation. It’s “the most common inflammatory vulvar dermatosis that we see, with the possible exception of contact dermatitis,” Dr. Schlosser wrote (Arch. Dermatol. 2004;140:702-6). As in adult women, the first-line treatment is once-daily clobetasol propionate ointment 0.05% for several weeks, followed by maintenance therapy. Dr. Schlosser said she used to switch patients to a less potent topical steroid, but “then I had a couple patients get confused about which tube they were supposed to use at home, so now I taper the frequency of their clobetasol ointment” to once or twice a week instead of switching them to a less potent topical steroid. It’s easier for them, but as with any topical steroid, “you need to continue ongoing monitoring for cutaneous atrophy,” she said.
In general, pelvic exams in pediatric patients “require special consideration. These are not 5-minute visits. You have to take the time to make yourself available. Educate patients and parents about what’s going to happen,” and use the child’s own terms for her genitals, asking parents beforehand what they are, so that the child understands what she’s hearing, Dr. Schlosser said.
“When I see young girls,” mom is in the room and “I only have gauze, gloves, and maybe a Q-tip [swab] here and there. I often” begin by asking the child if it’s okay to look at her scalp, face, and hands, then “gradually work my way down. I think that gives patients some sense of comfort and control,” she said.
Dr. Schlosser said she prefers the frog-leg position, with very young girls in their mothers’ laps. The literature sometimes advocates the prone knee-to-chest position, but “I find it makes people feel very vulnerable. They can’t see you, and they have no idea of what’s going on. I don’t advocate it,” she said.
Dr. Schlosser said she has no relevant financial disclosures.
SDEF and this news organization are owned by Frontline Medical Communications.
AT THE SDEF WOMEN’S & PEDIATRIC DERMATOLOGY SEMINAR

‘Shotgun’ skin prick testing for food allergy held flawed
VANCOUVER, B.C. – The “shotgun” style of skin prick testing in children and adolescents with suspected IgE-mediated food allergy shows sensitization, but not necessarily allergy, according to Dr. James Bergman.
A positive skin test measures the presence of a specific IgE antibody, which does not necessarily equate to an allergy. Consequently, children may have multiple positive skin prick tests yet clinically tolerate the tested food, he said. “Sensitization is just the presence of a specific IgE to a food. Allergy is sensitization plus signs or symptoms upon exposure to the food.”

Dr. Bergman, who also holds a faculty position in the department of dermatology and skin science at the University of British Columbia, said the practice of shotgun skin prick testing can lead to unnecessary avoidance of specific foods. One group of researchers conducted oral food challenge tests in 125 children aged 1-9 years with a diagnosis of food allergy based on IgE tests. Nearly all of them (93%) had no reactivity when challenged with the suspect food (J. Peds. 2011; 158[4]:578-83). “Ninety-three percent of the children would have been avoiding their ‘allergic foods’ perhaps indefinitely,” said Dr. Bergman, who was not involved with the study.
“The general rule is, if you’re not having clinical symptoms that suggest an IgE-mediated reaction, then don’t test,” Dr. Bergman, a dermatologist who practices in Vancouver, said at the annual meeting of the Pacific Dermatologic Association.
“I explain to parents that if they want to test for a food in the situation where there is no IgE-mediated reaction, then it can be done, but there is a significant risk of a false positive or ‘fake allergy,’ ” he said. “In this situation the only way of knowing for sure whether it is an allergy is to undertake a formal oral food challenge, which is the (highest) standard for diagnosing food allergy.”
Telltale symptoms of an IgE-mediated food allergy include hives, vomiting, diarrhea, breathing problems, and change in level of consciousness. “These symptoms typically occur within minutes of ingestion, sometimes within 30 minutes and rarely up to 2 hours,” Dr. Bergman said. “If it’s beyond 2 hours, it’s unlikely to be IgE mediated.”
“If someone has a true food allergy, advise them to avoid the culprit food, give them an epinephrine injector, and refer them to an allergist for testing, education, and follow-up,” he advised.
Food allergies affect 6%-8% of pediatric patients, yet 35%- 90% of families self-report food allergies depending on the population studied. Milk, egg, wheat, peanuts, nuts, soy, and seafood account for 90% of food allergens. Most children outgrow allergy to milk, egg, wheat, and soy, while few outgrow allergy to peanuts, nuts, fish, and shellfish.
Most patients and many physicians believe that eczema is caused by food allergies. In fact, only a small minority of patients have food allergies that directly cause eczema. “Eczema could occur secondary to scratching induced by an urticarial food reaction or by a primary irritant reaction, but food directly causing isolated eczema is rare,” Dr. Bergman said. “The belief that food allergies directly cause eczema is completely understandable given that eczema patients do have an increased rate of allergies, the cyclic pattern of eczema, and the parent’s desire to find a cause for the child’s rash. Eczema’s cyclic nature can easily lead to a specific food being implicated due to recall bias. The parent will remember the flares that occurred with exposure to the specific food, while not recalling the times when the food was tolerated or the flares that were not associated with the food.”
If a parent is worried about a food causing eczema and there are no IgE mediated symptoms, then instead of testing he will often recommend that the family keep a formal food symptom diary while they are intermittently ingesting the food of concern. “The vast majority of parents will see no consistent direct correlation with the food and they can feel comfortable with ongoing future ingestion,” he said.
Some clinicians are offering oral immune therapy to patients with IgE-mediated food allergy. Dr. Bergman characterized such practice as “risky” at this point in time. “It’s like the traditional allergy shots you’d get for your pollen allergy, except it’s done orally,” he explained. “Research is being done in this area by introducing small amounts [of the allergen], in an attempt to induce tolerance. The results are encouraging, but the problem is that patients can have bad reactions. We also don’t know how well or for how long it will work. At this point, while promising, the field is not yet ready for prime time.”
He also said there is no current evidence supporting IgG testing, Vega testing, or muscle strength testing in the investigation of suspected IgE-mediated food allergy. “What I tell patients is that if any of these tests identifies something, it probably identifies something that’s mild and very temporary, because in my experience patients with positive IgG tests are usually told to avoid the food for 1-4 months and then to reintroduce that food in a rotation basis. Avoidance of food allergens based on this type of testing is not necessary. However, for patients who still wish to practice short term avoidance of the food then this is fine provided the diet does not compromise nutrition.”
Dr. Bergman reported having no financial disclosures.
On Twitter @dougbrunk
VANCOUVER, B.C. – The “shotgun” style of skin prick testing in children and adolescents with suspected IgE-mediated food allergy shows sensitization, but not necessarily allergy, according to Dr. James Bergman.
A positive skin test measures the presence of a specific IgE antibody, which does not necessarily equate to an allergy. Consequently, children may have multiple positive skin prick tests yet clinically tolerate the tested food, he said. “Sensitization is just the presence of a specific IgE to a food. Allergy is sensitization plus signs or symptoms upon exposure to the food.”
Dr. Bergman, who also holds a faculty position in the department of dermatology and skin science at the University of British Columbia, said the practice of shotgun skin prick testing can lead to unnecessary avoidance of specific foods. One group of researchers conducted oral food challenge tests in 125 children aged 1-9 years with a diagnosis of food allergy based on IgE tests. Nearly all of them (93%) had no reactivity when challenged with the suspect food (J. Peds. 2011; 158[4]:578-83). “Ninety-three percent of the children would have been avoiding their ‘allergic foods’ perhaps indefinitely,” said Dr. Bergman, who was not involved with the study.
“The general rule is, if you’re not having clinical symptoms that suggest an IgE-mediated reaction, then don’t test,” Dr. Bergman, a dermatologist who practices in Vancouver, said at the annual meeting of the Pacific Dermatologic Association.
“I explain to parents that if they want to test for a food in the situation where there is no IgE-mediated reaction, then it can be done, but there is a significant risk of a false positive or ‘fake allergy,’ ” he said. “In this situation the only way of knowing for sure whether it is an allergy is to undertake a formal oral food challenge, which is the (highest) standard for diagnosing food allergy.”
Telltale symptoms of an IgE-mediated food allergy include hives, vomiting, diarrhea, breathing problems, and change in level of consciousness. “These symptoms typically occur within minutes of ingestion, sometimes within 30 minutes and rarely up to 2 hours,” Dr. Bergman said. “If it’s beyond 2 hours, it’s unlikely to be IgE mediated.”
“If someone has a true food allergy, advise them to avoid the culprit food, give them an epinephrine injector, and refer them to an allergist for testing, education, and follow-up,” he advised.
Food allergies affect 6%-8% of pediatric patients, yet 35%- 90% of families self-report food allergies depending on the population studied. Milk, egg, wheat, peanuts, nuts, soy, and seafood account for 90% of food allergens. Most children outgrow allergy to milk, egg, wheat, and soy, while few outgrow allergy to peanuts, nuts, fish, and shellfish.
Most patients and many physicians believe that eczema is caused by food allergies. In fact, only a small minority of patients have food allergies that directly cause eczema. “Eczema could occur secondary to scratching induced by an urticarial food reaction or by a primary irritant reaction, but food directly causing isolated eczema is rare,” Dr. Bergman said. “The belief that food allergies directly cause eczema is completely understandable given that eczema patients do have an increased rate of allergies, the cyclic pattern of eczema, and the parent’s desire to find a cause for the child’s rash. Eczema’s cyclic nature can easily lead to a specific food being implicated due to recall bias. The parent will remember the flares that occurred with exposure to the specific food, while not recalling the times when the food was tolerated or the flares that were not associated with the food.”
If a parent is worried about a food causing eczema and there are no IgE mediated symptoms, then instead of testing he will often recommend that the family keep a formal food symptom diary while they are intermittently ingesting the food of concern. “The vast majority of parents will see no consistent direct correlation with the food and they can feel comfortable with ongoing future ingestion,” he said.
Some clinicians are offering oral immune therapy to patients with IgE-mediated food allergy. Dr. Bergman characterized such practice as “risky” at this point in time. “It’s like the traditional allergy shots you’d get for your pollen allergy, except it’s done orally,” he explained. “Research is being done in this area by introducing small amounts [of the allergen], in an attempt to induce tolerance. The results are encouraging, but the problem is that patients can have bad reactions. We also don’t know how well or for how long it will work. At this point, while promising, the field is not yet ready for prime time.”
He also said there is no current evidence supporting IgG testing, Vega testing, or muscle strength testing in the investigation of suspected IgE-mediated food allergy. “What I tell patients is that if any of these tests identifies something, it probably identifies something that’s mild and very temporary, because in my experience patients with positive IgG tests are usually told to avoid the food for 1-4 months and then to reintroduce that food in a rotation basis. Avoidance of food allergens based on this type of testing is not necessary. However, for patients who still wish to practice short term avoidance of the food then this is fine provided the diet does not compromise nutrition.”
Dr. Bergman reported having no financial disclosures.
On Twitter @dougbrunk
VANCOUVER, B.C. – The “shotgun” style of skin prick testing in children and adolescents with suspected IgE-mediated food allergy shows sensitization, but not necessarily allergy, according to Dr. James Bergman.
A positive skin test measures the presence of a specific IgE antibody, which does not necessarily equate to an allergy. Consequently, children may have multiple positive skin prick tests yet clinically tolerate the tested food, he said. “Sensitization is just the presence of a specific IgE to a food. Allergy is sensitization plus signs or symptoms upon exposure to the food.”
Dr. Bergman, who also holds a faculty position in the department of dermatology and skin science at the University of British Columbia, said the practice of shotgun skin prick testing can lead to unnecessary avoidance of specific foods. One group of researchers conducted oral food challenge tests in 125 children aged 1-9 years with a diagnosis of food allergy based on IgE tests. Nearly all of them (93%) had no reactivity when challenged with the suspect food (J. Peds. 2011; 158[4]:578-83). “Ninety-three percent of the children would have been avoiding their ‘allergic foods’ perhaps indefinitely,” said Dr. Bergman, who was not involved with the study.
“The general rule is, if you’re not having clinical symptoms that suggest an IgE-mediated reaction, then don’t test,” Dr. Bergman, a dermatologist who practices in Vancouver, said at the annual meeting of the Pacific Dermatologic Association.
“I explain to parents that if they want to test for a food in the situation where there is no IgE-mediated reaction, then it can be done, but there is a significant risk of a false positive or ‘fake allergy,’ ” he said. “In this situation the only way of knowing for sure whether it is an allergy is to undertake a formal oral food challenge, which is the (highest) standard for diagnosing food allergy.”
Telltale symptoms of an IgE-mediated food allergy include hives, vomiting, diarrhea, breathing problems, and change in level of consciousness. “These symptoms typically occur within minutes of ingestion, sometimes within 30 minutes and rarely up to 2 hours,” Dr. Bergman said. “If it’s beyond 2 hours, it’s unlikely to be IgE mediated.”
“If someone has a true food allergy, advise them to avoid the culprit food, give them an epinephrine injector, and refer them to an allergist for testing, education, and follow-up,” he advised.
Food allergies affect 6%-8% of pediatric patients, yet 35%- 90% of families self-report food allergies depending on the population studied. Milk, egg, wheat, peanuts, nuts, soy, and seafood account for 90% of food allergens. Most children outgrow allergy to milk, egg, wheat, and soy, while few outgrow allergy to peanuts, nuts, fish, and shellfish.
Most patients and many physicians believe that eczema is caused by food allergies. In fact, only a small minority of patients have food allergies that directly cause eczema. “Eczema could occur secondary to scratching induced by an urticarial food reaction or by a primary irritant reaction, but food directly causing isolated eczema is rare,” Dr. Bergman said. “The belief that food allergies directly cause eczema is completely understandable given that eczema patients do have an increased rate of allergies, the cyclic pattern of eczema, and the parent’s desire to find a cause for the child’s rash. Eczema’s cyclic nature can easily lead to a specific food being implicated due to recall bias. The parent will remember the flares that occurred with exposure to the specific food, while not recalling the times when the food was tolerated or the flares that were not associated with the food.”
If a parent is worried about a food causing eczema and there are no IgE mediated symptoms, then instead of testing he will often recommend that the family keep a formal food symptom diary while they are intermittently ingesting the food of concern. “The vast majority of parents will see no consistent direct correlation with the food and they can feel comfortable with ongoing future ingestion,” he said.
Some clinicians are offering oral immune therapy to patients with IgE-mediated food allergy. Dr. Bergman characterized such practice as “risky” at this point in time. “It’s like the traditional allergy shots you’d get for your pollen allergy, except it’s done orally,” he explained. “Research is being done in this area by introducing small amounts [of the allergen], in an attempt to induce tolerance. The results are encouraging, but the problem is that patients can have bad reactions. We also don’t know how well or for how long it will work. At this point, while promising, the field is not yet ready for prime time.”
He also said there is no current evidence supporting IgG testing, Vega testing, or muscle strength testing in the investigation of suspected IgE-mediated food allergy. “What I tell patients is that if any of these tests identifies something, it probably identifies something that’s mild and very temporary, because in my experience patients with positive IgG tests are usually told to avoid the food for 1-4 months and then to reintroduce that food in a rotation basis. Avoidance of food allergens based on this type of testing is not necessary. However, for patients who still wish to practice short term avoidance of the food then this is fine provided the diet does not compromise nutrition.”
Dr. Bergman reported having no financial disclosures.
On Twitter @dougbrunk
EXPERT ANALYSIS FROM THE PDA ANNUAL MEETING

VIDEO: When atopic dermatitis and contact dermatitis collide
LAS VEGAS– Atopic dermatitis patients may be at increased risk for contact as well, Dr. Joseph Fowler said at Skin Disease Education Foundation’s annual Las Vegas dermatology seminar.
In an interview at the meeting, Dr. Fowler reviewed several emerging allergens, explained how contact dermatitis and atopic dermatitis interact, and shared some tips for identifying and managing both conditions when they occur simultaneously.
Dr. Fowler disclosed relationships with multiple pharmaceutical companies, none of which were relevant to the content of this video. SDEF and this news organization are owned by Frontline Medical Communications.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
LAS VEGAS– Atopic dermatitis patients may be at increased risk for contact as well, Dr. Joseph Fowler said at Skin Disease Education Foundation’s annual Las Vegas dermatology seminar.
In an interview at the meeting, Dr. Fowler reviewed several emerging allergens, explained how contact dermatitis and atopic dermatitis interact, and shared some tips for identifying and managing both conditions when they occur simultaneously.
Dr. Fowler disclosed relationships with multiple pharmaceutical companies, none of which were relevant to the content of this video. SDEF and this news organization are owned by Frontline Medical Communications.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
LAS VEGAS– Atopic dermatitis patients may be at increased risk for contact as well, Dr. Joseph Fowler said at Skin Disease Education Foundation’s annual Las Vegas dermatology seminar.
In an interview at the meeting, Dr. Fowler reviewed several emerging allergens, explained how contact dermatitis and atopic dermatitis interact, and shared some tips for identifying and managing both conditions when they occur simultaneously.
Dr. Fowler disclosed relationships with multiple pharmaceutical companies, none of which were relevant to the content of this video. SDEF and this news organization are owned by Frontline Medical Communications.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT SDEF LAS VEGAS DERMATOLOGY SEMINAR

Consider strep, not MRSA, when eczematous children suffer skin infections
NEWPORT BEACH, CALIF.– In children with atopic dermatitis, serious superinfections are more likely to be caused by group A beta-hemolytic Streptococcus than methicillin-resistant Staphylococcus aureus, according to Dr. Victoria Barrio of the University of California, San Diego.
Unless there are classic MRSA signs, “I wouldn’t start off with Bactrim [sulfamethoxazole and trimethoprim] assuming that they have MRSA; Bactrim doesn’t work for strep. You are going to be in trouble if they actually have strep,” she said at Skin Disease Education Foundation’s Women’s & Pediatric Dermatology Seminar.

Instead, Dr. Barrio is more likely to start empirically with cephalexin (Keflex) three times daily, which also covers staph in most communities. “It’s usually well tolerated, and it does pretty well,” she said, but adding that she adjusts treatment as needed depending on culture results.
This protocol is supported in part by findings from a study by colleagues of Dr. Barrio, which showed that children with atopic dermatitis carry more S. aureus on their skin than do children without eczema, so they are less likely to be infected with community-acquired MRSA, probably because non-MRSA strains outcompete it. In the study, the MRSA the investigators found responded to clindamycin (Pediatr. Dermatol. 2011;28:6-11).
Dr. Barrio cited another study suggesting that group A strep skin infections are a more serious problem than staph is in children with eczema; the children are more likely to be febrile, have systemic involvement, and need hospitalization than those with staph superinfections (Pediatr. Dermatol. 2011;28:230-4).
“These patients are often a lot sicker. You have to be aware that strep is out there, and it can be a problem for kids with eczema,” said Dr. Barrio.
In general, for bacterial superinfections, “bleach baths are a fantastic way to try to keep kids who are always getting infected under control,” she said. It really does keep that overload of bacteria down.”
Current data support her opinion. Following a course of antibiotics, another study showed that twice-weekly baths, followed by intranasal mupirocin ointment had “significantly greater mean reductions from baseline in Eczema Area and Severity Index scores,” compared with placebo (Pediatrics 2009;123:e808-14).
For older children who don’t want to take baths, a bleach soap (CLn Bodywash) is now available, Dr. Barrio noted.
Viral eczema coxsackium skin infections, recently characterized in the literature, remain a problem for children. Presentations can vary and include widespread blisters, erosions, purpura, and petechiae around the mouth or on the arms, legs, and torso. The infection can mimic bullous impetigo, eczema herpeticum, vasculitis, and primary immunobullous disease,and it is a common cause of onychomadesis as well, Dr. Barrio noted (Pediatrics 2013;132:e149-57).
“We saw a lot of it a few years ago. I am still seeing it around. You don’t really think about it as being hand, foot, and mouth” disease, she said.
Dr. Barrio added that eczema is hard on children emotionally as well as physically. They may lose sleep, have a tough time in school, and might blame the illness on themselves, and these and other problems can lead to depression, anxiety, and a big hit to self-esteem, she said.
Clinicians at the University of Nottingham (U.K.) have created a free web resource that might help, which features stories for children. The clinicians have posted several tales, like “The Princess and the Itch,” that make eczema the villain and the child the hero, which helps to externalize the disease. The child’s name can be entered into a template to personalize the story (Pediatr. Dermatol. 2013;30:765-7). Dr. Barrio had no relevant disclosures. SDEF and this news organization are owned by Frontline Medical Communications.
NEWPORT BEACH, CALIF.– In children with atopic dermatitis, serious superinfections are more likely to be caused by group A beta-hemolytic Streptococcus than methicillin-resistant Staphylococcus aureus, according to Dr. Victoria Barrio of the University of California, San Diego.
Unless there are classic MRSA signs, “I wouldn’t start off with Bactrim [sulfamethoxazole and trimethoprim] assuming that they have MRSA; Bactrim doesn’t work for strep. You are going to be in trouble if they actually have strep,” she said at Skin Disease Education Foundation’s Women’s & Pediatric Dermatology Seminar.
Instead, Dr. Barrio is more likely to start empirically with cephalexin (Keflex) three times daily, which also covers staph in most communities. “It’s usually well tolerated, and it does pretty well,” she said, but adding that she adjusts treatment as needed depending on culture results.
This protocol is supported in part by findings from a study by colleagues of Dr. Barrio, which showed that children with atopic dermatitis carry more S. aureus on their skin than do children without eczema, so they are less likely to be infected with community-acquired MRSA, probably because non-MRSA strains outcompete it. In the study, the MRSA the investigators found responded to clindamycin (Pediatr. Dermatol. 2011;28:6-11).
Dr. Barrio cited another study suggesting that group A strep skin infections are a more serious problem than staph is in children with eczema; the children are more likely to be febrile, have systemic involvement, and need hospitalization than those with staph superinfections (Pediatr. Dermatol. 2011;28:230-4).
“These patients are often a lot sicker. You have to be aware that strep is out there, and it can be a problem for kids with eczema,” said Dr. Barrio.
In general, for bacterial superinfections, “bleach baths are a fantastic way to try to keep kids who are always getting infected under control,” she said. It really does keep that overload of bacteria down.”
Current data support her opinion. Following a course of antibiotics, another study showed that twice-weekly baths, followed by intranasal mupirocin ointment had “significantly greater mean reductions from baseline in Eczema Area and Severity Index scores,” compared with placebo (Pediatrics 2009;123:e808-14).
For older children who don’t want to take baths, a bleach soap (CLn Bodywash) is now available, Dr. Barrio noted.
Viral eczema coxsackium skin infections, recently characterized in the literature, remain a problem for children. Presentations can vary and include widespread blisters, erosions, purpura, and petechiae around the mouth or on the arms, legs, and torso. The infection can mimic bullous impetigo, eczema herpeticum, vasculitis, and primary immunobullous disease,and it is a common cause of onychomadesis as well, Dr. Barrio noted (Pediatrics 2013;132:e149-57).
“We saw a lot of it a few years ago. I am still seeing it around. You don’t really think about it as being hand, foot, and mouth” disease, she said.
Dr. Barrio added that eczema is hard on children emotionally as well as physically. They may lose sleep, have a tough time in school, and might blame the illness on themselves, and these and other problems can lead to depression, anxiety, and a big hit to self-esteem, she said.
Clinicians at the University of Nottingham (U.K.) have created a free web resource that might help, which features stories for children. The clinicians have posted several tales, like “The Princess and the Itch,” that make eczema the villain and the child the hero, which helps to externalize the disease. The child’s name can be entered into a template to personalize the story (Pediatr. Dermatol. 2013;30:765-7). Dr. Barrio had no relevant disclosures. SDEF and this news organization are owned by Frontline Medical Communications.
NEWPORT BEACH, CALIF.– In children with atopic dermatitis, serious superinfections are more likely to be caused by group A beta-hemolytic Streptococcus than methicillin-resistant Staphylococcus aureus, according to Dr. Victoria Barrio of the University of California, San Diego.
Unless there are classic MRSA signs, “I wouldn’t start off with Bactrim [sulfamethoxazole and trimethoprim] assuming that they have MRSA; Bactrim doesn’t work for strep. You are going to be in trouble if they actually have strep,” she said at Skin Disease Education Foundation’s Women’s & Pediatric Dermatology Seminar.
Instead, Dr. Barrio is more likely to start empirically with cephalexin (Keflex) three times daily, which also covers staph in most communities. “It’s usually well tolerated, and it does pretty well,” she said, but adding that she adjusts treatment as needed depending on culture results.
This protocol is supported in part by findings from a study by colleagues of Dr. Barrio, which showed that children with atopic dermatitis carry more S. aureus on their skin than do children without eczema, so they are less likely to be infected with community-acquired MRSA, probably because non-MRSA strains outcompete it. In the study, the MRSA the investigators found responded to clindamycin (Pediatr. Dermatol. 2011;28:6-11).
Dr. Barrio cited another study suggesting that group A strep skin infections are a more serious problem than staph is in children with eczema; the children are more likely to be febrile, have systemic involvement, and need hospitalization than those with staph superinfections (Pediatr. Dermatol. 2011;28:230-4).
“These patients are often a lot sicker. You have to be aware that strep is out there, and it can be a problem for kids with eczema,” said Dr. Barrio.
In general, for bacterial superinfections, “bleach baths are a fantastic way to try to keep kids who are always getting infected under control,” she said. It really does keep that overload of bacteria down.”
Current data support her opinion. Following a course of antibiotics, another study showed that twice-weekly baths, followed by intranasal mupirocin ointment had “significantly greater mean reductions from baseline in Eczema Area and Severity Index scores,” compared with placebo (Pediatrics 2009;123:e808-14).
For older children who don’t want to take baths, a bleach soap (CLn Bodywash) is now available, Dr. Barrio noted.
Viral eczema coxsackium skin infections, recently characterized in the literature, remain a problem for children. Presentations can vary and include widespread blisters, erosions, purpura, and petechiae around the mouth or on the arms, legs, and torso. The infection can mimic bullous impetigo, eczema herpeticum, vasculitis, and primary immunobullous disease,and it is a common cause of onychomadesis as well, Dr. Barrio noted (Pediatrics 2013;132:e149-57).
“We saw a lot of it a few years ago. I am still seeing it around. You don’t really think about it as being hand, foot, and mouth” disease, she said.
Dr. Barrio added that eczema is hard on children emotionally as well as physically. They may lose sleep, have a tough time in school, and might blame the illness on themselves, and these and other problems can lead to depression, anxiety, and a big hit to self-esteem, she said.
Clinicians at the University of Nottingham (U.K.) have created a free web resource that might help, which features stories for children. The clinicians have posted several tales, like “The Princess and the Itch,” that make eczema the villain and the child the hero, which helps to externalize the disease. The child’s name can be entered into a template to personalize the story (Pediatr. Dermatol. 2013;30:765-7). Dr. Barrio had no relevant disclosures. SDEF and this news organization are owned by Frontline Medical Communications.
EXPERT ANALYSIS FROM SDEF WOMEN’S & PEDIATRIC DERMATOLOGY

Hard water linked to infant eczema
AMSTERDAM – Living in a locale with hard water – defined as a calcium carbonate concentration of 258 mg/L or more in the domestic water supply – was associated with significantly increased risk of eczema at 3 months of age in a large study conducted across England and Wales.
The study findings have potentially far-reaching implications for the prevention of childhood eczema, as well as halting what is often called the “atopic march” from eczema to food allergies to asthma. A national follow-up study is now being prepared in which families will be given an effective water softener machine when a child is born, with randomization to the machine being switched on or off.

“We want to see whether we might be able to prevent eczema by removing calcium carbonate from domestic water,” Dr. Carsten Flohr explained at a meeting of the European Task Force on Atopic Dermatitis held in conjunction with the annual congress of the European Academy of Dermatology and Venereology.
He reported on 1,303 infants who at 3 months of age underwent a structured skin examination with SCORAD (SCORing Atopic Dermatitis) measurement. Twenty-four percent were diagnosed as having eczema, which was typically mild.
Calcium carbonate concentrations in the local water supply vary enormously across England and Wales because rich limestone beds are found in some areas, notably the south and east, Dr. Flohr noted.
Babies living in areas with a calcium carbonate water concentration above the median level had a 45% increase in eczema risk. This risk was mediated by filaggrin loss-of-function (FLG) mutations. All study participants underwent testing for the six most common such mutations. In children without an FLG mutation, water hardness made little difference in eczema risk.
But FLG carriers living in the third quartile for water hardness – defined as a calcium carbonate concentration of 258-285 mg/L – had a 4.9-fold greater risk of eczema than did the general study population. Those in the highest quartile were at 2.67-fold increased risk, which just missed achieving statistical significance.
Looking at calcium carbonate concentration as a continuous variable, FLG carriers had an impressive 1% increase in the risk of eczema for each 1 mg/L rise in domestic water hardness, added Dr. Flohr, a pediatric dermatologist at St. Thomas’ Hospital, London.
The investigators also measured transepidermal water loss (TEWL) as an indicator of skin barrier function. FLG carriers without eczema living in hard-water areas had a high rate of excessive TEWL, defined as at least 15 g/m2 per hour. Those in the third quartile for calcium carbonate were at a 4.63-fold greater risk of abnormal TEWL, compared with FLG carriers living in areas in the two lowest quartiles of water hardness. The risk of excessive TEWL among FLG carriers without eczema rose by 1% for every 1 mg/L increase in calcium carbonate concentration.
“This suggests that the interaction between filaggrin mutation, water hardness, and eczema is related to a direct skin barrier effect,” Dr. Flohr said.

He and his coinvestigators have found supporting evidence in an adult population for their findings of a link between water hardness and infant eczema and TEWL. In a large national United Kingdom cohort of individuals born in 1958, who are part of an ongoing epidemiologic study, data show that those living in areas of high water hardness have increased rates of atopic disease.
As to the possible mechanism involved, Dr. Flohr said it’s known that as calcium carbonate concentration increases, it alters the skin surface pH. This could potentially have a detrimental effect on skin barrier function, although such an effect remains speculative. The attenuated risks of eczema and TEWL seen in FLG-carrying infants in the fourth water hardness quartile as compared to the third water hardness quartile warrants further study, but it might be the result of a calcium-scavenging effect, perhaps because of magnesium in the water, he added.
“I really think that the skin pH is involved in this,” Dr. Flohr emphasized.
Session cochair Dr. Ulf Darsow of Technical University, Munich, noted that Dr. Flohr’s countrymen at the University of Nottingham, England, have already performed an interventional study involving the use of water-softening devices. In the Softened Water Eczema Trial (SWET), the Nottingham group found no beneficial effect on pediatric eczema (PLoS Med. 2011; doi: 10.1371/journal.pmed.1000395).
“That is true, but it was a 12-week trial in children with established moderate to severe eczema,” Dr. Flohr replied. “What I’m suggesting is that potentially calcium carbonate concentration could be involved in the initiation of the skin inflammation, even if fitting a water softener once you’ve got established skin inflammation doesn’t seem to make much of a difference.”
“So this interesting story continues,” Dr. Darsow observed.
Dr. Flohr’s study was funded by the UK National Institute for Health Research. He reported having no financial conflicts.
AMSTERDAM – Living in a locale with hard water – defined as a calcium carbonate concentration of 258 mg/L or more in the domestic water supply – was associated with significantly increased risk of eczema at 3 months of age in a large study conducted across England and Wales.
The study findings have potentially far-reaching implications for the prevention of childhood eczema, as well as halting what is often called the “atopic march” from eczema to food allergies to asthma. A national follow-up study is now being prepared in which families will be given an effective water softener machine when a child is born, with randomization to the machine being switched on or off.
“We want to see whether we might be able to prevent eczema by removing calcium carbonate from domestic water,” Dr. Carsten Flohr explained at a meeting of the European Task Force on Atopic Dermatitis held in conjunction with the annual congress of the European Academy of Dermatology and Venereology.
He reported on 1,303 infants who at 3 months of age underwent a structured skin examination with SCORAD (SCORing Atopic Dermatitis) measurement. Twenty-four percent were diagnosed as having eczema, which was typically mild.
Calcium carbonate concentrations in the local water supply vary enormously across England and Wales because rich limestone beds are found in some areas, notably the south and east, Dr. Flohr noted.
Babies living in areas with a calcium carbonate water concentration above the median level had a 45% increase in eczema risk. This risk was mediated by filaggrin loss-of-function (FLG) mutations. All study participants underwent testing for the six most common such mutations. In children without an FLG mutation, water hardness made little difference in eczema risk.
But FLG carriers living in the third quartile for water hardness – defined as a calcium carbonate concentration of 258-285 mg/L – had a 4.9-fold greater risk of eczema than did the general study population. Those in the highest quartile were at 2.67-fold increased risk, which just missed achieving statistical significance.
Looking at calcium carbonate concentration as a continuous variable, FLG carriers had an impressive 1% increase in the risk of eczema for each 1 mg/L rise in domestic water hardness, added Dr. Flohr, a pediatric dermatologist at St. Thomas’ Hospital, London.
The investigators also measured transepidermal water loss (TEWL) as an indicator of skin barrier function. FLG carriers without eczema living in hard-water areas had a high rate of excessive TEWL, defined as at least 15 g/m2 per hour. Those in the third quartile for calcium carbonate were at a 4.63-fold greater risk of abnormal TEWL, compared with FLG carriers living in areas in the two lowest quartiles of water hardness. The risk of excessive TEWL among FLG carriers without eczema rose by 1% for every 1 mg/L increase in calcium carbonate concentration.
“This suggests that the interaction between filaggrin mutation, water hardness, and eczema is related to a direct skin barrier effect,” Dr. Flohr said.
He and his coinvestigators have found supporting evidence in an adult population for their findings of a link between water hardness and infant eczema and TEWL. In a large national United Kingdom cohort of individuals born in 1958, who are part of an ongoing epidemiologic study, data show that those living in areas of high water hardness have increased rates of atopic disease.
As to the possible mechanism involved, Dr. Flohr said it’s known that as calcium carbonate concentration increases, it alters the skin surface pH. This could potentially have a detrimental effect on skin barrier function, although such an effect remains speculative. The attenuated risks of eczema and TEWL seen in FLG-carrying infants in the fourth water hardness quartile as compared to the third water hardness quartile warrants further study, but it might be the result of a calcium-scavenging effect, perhaps because of magnesium in the water, he added.
“I really think that the skin pH is involved in this,” Dr. Flohr emphasized.
Session cochair Dr. Ulf Darsow of Technical University, Munich, noted that Dr. Flohr’s countrymen at the University of Nottingham, England, have already performed an interventional study involving the use of water-softening devices. In the Softened Water Eczema Trial (SWET), the Nottingham group found no beneficial effect on pediatric eczema (PLoS Med. 2011; doi: 10.1371/journal.pmed.1000395).
“That is true, but it was a 12-week trial in children with established moderate to severe eczema,” Dr. Flohr replied. “What I’m suggesting is that potentially calcium carbonate concentration could be involved in the initiation of the skin inflammation, even if fitting a water softener once you’ve got established skin inflammation doesn’t seem to make much of a difference.”
“So this interesting story continues,” Dr. Darsow observed.
Dr. Flohr’s study was funded by the UK National Institute for Health Research. He reported having no financial conflicts.
AMSTERDAM – Living in a locale with hard water – defined as a calcium carbonate concentration of 258 mg/L or more in the domestic water supply – was associated with significantly increased risk of eczema at 3 months of age in a large study conducted across England and Wales.
The study findings have potentially far-reaching implications for the prevention of childhood eczema, as well as halting what is often called the “atopic march” from eczema to food allergies to asthma. A national follow-up study is now being prepared in which families will be given an effective water softener machine when a child is born, with randomization to the machine being switched on or off.
“We want to see whether we might be able to prevent eczema by removing calcium carbonate from domestic water,” Dr. Carsten Flohr explained at a meeting of the European Task Force on Atopic Dermatitis held in conjunction with the annual congress of the European Academy of Dermatology and Venereology.
He reported on 1,303 infants who at 3 months of age underwent a structured skin examination with SCORAD (SCORing Atopic Dermatitis) measurement. Twenty-four percent were diagnosed as having eczema, which was typically mild.
Calcium carbonate concentrations in the local water supply vary enormously across England and Wales because rich limestone beds are found in some areas, notably the south and east, Dr. Flohr noted.
Babies living in areas with a calcium carbonate water concentration above the median level had a 45% increase in eczema risk. This risk was mediated by filaggrin loss-of-function (FLG) mutations. All study participants underwent testing for the six most common such mutations. In children without an FLG mutation, water hardness made little difference in eczema risk.
But FLG carriers living in the third quartile for water hardness – defined as a calcium carbonate concentration of 258-285 mg/L – had a 4.9-fold greater risk of eczema than did the general study population. Those in the highest quartile were at 2.67-fold increased risk, which just missed achieving statistical significance.
Looking at calcium carbonate concentration as a continuous variable, FLG carriers had an impressive 1% increase in the risk of eczema for each 1 mg/L rise in domestic water hardness, added Dr. Flohr, a pediatric dermatologist at St. Thomas’ Hospital, London.
The investigators also measured transepidermal water loss (TEWL) as an indicator of skin barrier function. FLG carriers without eczema living in hard-water areas had a high rate of excessive TEWL, defined as at least 15 g/m2 per hour. Those in the third quartile for calcium carbonate were at a 4.63-fold greater risk of abnormal TEWL, compared with FLG carriers living in areas in the two lowest quartiles of water hardness. The risk of excessive TEWL among FLG carriers without eczema rose by 1% for every 1 mg/L increase in calcium carbonate concentration.
“This suggests that the interaction between filaggrin mutation, water hardness, and eczema is related to a direct skin barrier effect,” Dr. Flohr said.
He and his coinvestigators have found supporting evidence in an adult population for their findings of a link between water hardness and infant eczema and TEWL. In a large national United Kingdom cohort of individuals born in 1958, who are part of an ongoing epidemiologic study, data show that those living in areas of high water hardness have increased rates of atopic disease.
As to the possible mechanism involved, Dr. Flohr said it’s known that as calcium carbonate concentration increases, it alters the skin surface pH. This could potentially have a detrimental effect on skin barrier function, although such an effect remains speculative. The attenuated risks of eczema and TEWL seen in FLG-carrying infants in the fourth water hardness quartile as compared to the third water hardness quartile warrants further study, but it might be the result of a calcium-scavenging effect, perhaps because of magnesium in the water, he added.
“I really think that the skin pH is involved in this,” Dr. Flohr emphasized.
Session cochair Dr. Ulf Darsow of Technical University, Munich, noted that Dr. Flohr’s countrymen at the University of Nottingham, England, have already performed an interventional study involving the use of water-softening devices. In the Softened Water Eczema Trial (SWET), the Nottingham group found no beneficial effect on pediatric eczema (PLoS Med. 2011; doi: 10.1371/journal.pmed.1000395).
“That is true, but it was a 12-week trial in children with established moderate to severe eczema,” Dr. Flohr replied. “What I’m suggesting is that potentially calcium carbonate concentration could be involved in the initiation of the skin inflammation, even if fitting a water softener once you’ve got established skin inflammation doesn’t seem to make much of a difference.”
“So this interesting story continues,” Dr. Darsow observed.
Dr. Flohr’s study was funded by the UK National Institute for Health Research. He reported having no financial conflicts.
AT THE EADV CONGRESS
Key clinical point: Infants living in areas with a high calcium carbonate concentration in the water supply are at increased risk for eczema, especially if they carry a filaggrin loss-of-function gene mutation.
Major finding: British 3-month-olds with a filaggrin mutation are at up to nearly fivefold increased likelihood of having eczema if they live in an area with above-average water hardness, compared with those in the lowest quartile in terms of water hardness.
Data source: A cross-sectional study of more than 1,300 infants across England and Wales who underwent a structured skin examination looking for eczema at age 3 months.
Disclosures: The study was funded by the UK National Institute for Health Research. The presenter reported having no financial conflicts.

VIDEO: Scabies epidemic plagues nursing homes
SONOMA, CALIF. – Dr. Miriam S. Bettencourt is seeing what she considers an epidemic of scabies among elderly patients in nursing homes.
The problem is a lack of detection, she said in an interview at the annual Coastal Dermatology Symposium.
Dermatologists who see elderly patients should look for scabies in unusual bodily locations and remember that scabies in the elderly can produce atypical lesions, said Dr. Bettencourt of the University of Nevada, Las Vegas.
Permethrin cream alone probably won’t be enough to treat these patients, she said at the symposium, jointly presented by the University of Louisville, Kentucky, and the Global Academy for Medical Education. This publication and the Global Academy for Medical Education are owned by the same parent company.
How would you treat scabies in an elderly patient? Dr. Bettencourt discussed several effective options.
Dr. Bettencourt reported having no financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @sherryboschert
SONOMA, CALIF. – Dr. Miriam S. Bettencourt is seeing what she considers an epidemic of scabies among elderly patients in nursing homes.
The problem is a lack of detection, she said in an interview at the annual Coastal Dermatology Symposium.
Dermatologists who see elderly patients should look for scabies in unusual bodily locations and remember that scabies in the elderly can produce atypical lesions, said Dr. Bettencourt of the University of Nevada, Las Vegas.
Permethrin cream alone probably won’t be enough to treat these patients, she said at the symposium, jointly presented by the University of Louisville, Kentucky, and the Global Academy for Medical Education. This publication and the Global Academy for Medical Education are owned by the same parent company.
How would you treat scabies in an elderly patient? Dr. Bettencourt discussed several effective options.
Dr. Bettencourt reported having no financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @sherryboschert
SONOMA, CALIF. – Dr. Miriam S. Bettencourt is seeing what she considers an epidemic of scabies among elderly patients in nursing homes.
The problem is a lack of detection, she said in an interview at the annual Coastal Dermatology Symposium.
Dermatologists who see elderly patients should look for scabies in unusual bodily locations and remember that scabies in the elderly can produce atypical lesions, said Dr. Bettencourt of the University of Nevada, Las Vegas.
Permethrin cream alone probably won’t be enough to treat these patients, she said at the symposium, jointly presented by the University of Louisville, Kentucky, and the Global Academy for Medical Education. This publication and the Global Academy for Medical Education are owned by the same parent company.
How would you treat scabies in an elderly patient? Dr. Bettencourt discussed several effective options.
Dr. Bettencourt reported having no financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @sherryboschert
AT THE COASTAL DERMATOLOGY SYMPOSIUM
