User login
Hospitalist as consultant
Hospitalists may provide expert medical opinion regarding the care of hospitalized patients or may serve as consultants for patients under the care of other medical and surgical services. The hospitalist consultant may provide opinions and recommendations or actively manage the patient's hospital care. Effective and frequent communication between the hospitalist and the requesting physician ensures safe and quality care. Hospitalists should promote communication between services to improve the care of the hospitalized patient, optimize resource utilization, and enhance patient safety.
KNOWLEDGE
Hospitalists should be able to:
Define the role of the hospitalist consultant.
Describe the components of an effective consultation.
Assess the urgency of the consultation and the questions posed by the requesting physician.
List factors that may affect implementation of consultant's recommendations.
SKILLS
Hospitalists should be able to:
Obtain a thorough and relevant history and review the medical record.
Perform a relevant physical examination.
Interpret indicated diagnostic studies.
Synthesize a treatment plan based on the data obtained from the history, physical examination and diagnostic studies.
Summarize the findings in the patient record.
List concise but specific recommendations for management.
Communicate recommendations to the consulting physician in an expedient and efficient manner.
Assess the level of care required, and communicate with the requesting physician if a transition of care is advised.
ATTITUDES
Hospitalists should be able to:
Determine the hospitalist consultant's role in collaboration with the requesting physician.
Respond promptly to the requesting physician's need for consultation.
Lead by example by performing consultations in a collegial, professional and non‐confrontational manner.
Inform and educate the requesting physician of potential complications and opportunities for prevention of complications.
Provide frequent follow‐up, including review of pertinent findings and laboratory data, and ensure that critical recommendations have been followed.
Provide timely and effective communication with the requesting physician/team.
Transmit written communication legibly and with clear contact information.
Recognize when the hospitalist's role in the patient's care is complete, document final recommendations in the medical record, and maintain availability.
Communicate with patient and family to convey recommendations and treatment plans.
Recognize the importance of arranging appropriate follow‐up.
Lead, coordinate or participate in multidisciplinary initiatives to promote patient safety and optimize resource utilization.
Hospitalists may provide expert medical opinion regarding the care of hospitalized patients or may serve as consultants for patients under the care of other medical and surgical services. The hospitalist consultant may provide opinions and recommendations or actively manage the patient's hospital care. Effective and frequent communication between the hospitalist and the requesting physician ensures safe and quality care. Hospitalists should promote communication between services to improve the care of the hospitalized patient, optimize resource utilization, and enhance patient safety.
KNOWLEDGE
Hospitalists should be able to:
Define the role of the hospitalist consultant.
Describe the components of an effective consultation.
Assess the urgency of the consultation and the questions posed by the requesting physician.
List factors that may affect implementation of consultant's recommendations.
SKILLS
Hospitalists should be able to:
Obtain a thorough and relevant history and review the medical record.
Perform a relevant physical examination.
Interpret indicated diagnostic studies.
Synthesize a treatment plan based on the data obtained from the history, physical examination and diagnostic studies.
Summarize the findings in the patient record.
List concise but specific recommendations for management.
Communicate recommendations to the consulting physician in an expedient and efficient manner.
Assess the level of care required, and communicate with the requesting physician if a transition of care is advised.
ATTITUDES
Hospitalists should be able to:
Determine the hospitalist consultant's role in collaboration with the requesting physician.
Respond promptly to the requesting physician's need for consultation.
Lead by example by performing consultations in a collegial, professional and non‐confrontational manner.
Inform and educate the requesting physician of potential complications and opportunities for prevention of complications.
Provide frequent follow‐up, including review of pertinent findings and laboratory data, and ensure that critical recommendations have been followed.
Provide timely and effective communication with the requesting physician/team.
Transmit written communication legibly and with clear contact information.
Recognize when the hospitalist's role in the patient's care is complete, document final recommendations in the medical record, and maintain availability.
Communicate with patient and family to convey recommendations and treatment plans.
Recognize the importance of arranging appropriate follow‐up.
Lead, coordinate or participate in multidisciplinary initiatives to promote patient safety and optimize resource utilization.
Hospitalists may provide expert medical opinion regarding the care of hospitalized patients or may serve as consultants for patients under the care of other medical and surgical services. The hospitalist consultant may provide opinions and recommendations or actively manage the patient's hospital care. Effective and frequent communication between the hospitalist and the requesting physician ensures safe and quality care. Hospitalists should promote communication between services to improve the care of the hospitalized patient, optimize resource utilization, and enhance patient safety.
KNOWLEDGE
Hospitalists should be able to:
Define the role of the hospitalist consultant.
Describe the components of an effective consultation.
Assess the urgency of the consultation and the questions posed by the requesting physician.
List factors that may affect implementation of consultant's recommendations.
SKILLS
Hospitalists should be able to:
Obtain a thorough and relevant history and review the medical record.
Perform a relevant physical examination.
Interpret indicated diagnostic studies.
Synthesize a treatment plan based on the data obtained from the history, physical examination and diagnostic studies.
Summarize the findings in the patient record.
List concise but specific recommendations for management.
Communicate recommendations to the consulting physician in an expedient and efficient manner.
Assess the level of care required, and communicate with the requesting physician if a transition of care is advised.
ATTITUDES
Hospitalists should be able to:
Determine the hospitalist consultant's role in collaboration with the requesting physician.
Respond promptly to the requesting physician's need for consultation.
Lead by example by performing consultations in a collegial, professional and non‐confrontational manner.
Inform and educate the requesting physician of potential complications and opportunities for prevention of complications.
Provide frequent follow‐up, including review of pertinent findings and laboratory data, and ensure that critical recommendations have been followed.
Provide timely and effective communication with the requesting physician/team.
Transmit written communication legibly and with clear contact information.
Recognize when the hospitalist's role in the patient's care is complete, document final recommendations in the medical record, and maintain availability.
Communicate with patient and family to convey recommendations and treatment plans.
Recognize the importance of arranging appropriate follow‐up.
Lead, coordinate or participate in multidisciplinary initiatives to promote patient safety and optimize resource utilization.
Copyright © 2006 Society of Hospital Medicine
Chest radiograph interpretation
Chest radiographs (CXRs) utilize low‐level radiation to form images of the chest anatomy. They are non‐invasive and readily available. CXRs are an integral part of the initial evaluation of cardiopulmonary pathology. Hospitalists interpret the results of CXRs, often before radiologists, to diagnose disease and develop treatment plans in hospitalized patients.
KNOWLEDGE
Hospitalists should be able to:
Explain the normal anatomy of the thorax with particular attention to spatial relationships.
Explain the images seen on a CXR, including bone and soft tissue structures, airway, lungs, cardiac structure and silhouette, aorta, and diaphragm.
List the indications for ordering a CXR.
Describe evidence based national guidelines for ordering CXRs.
Compare the diagnostic utility and limitations of portable radiographs to posteroanterior and lateral radiographs.
Explain the indications for a lateral decubitus CXR.
Describe the effects of film exposure, inspiratory effort, and patient position on the radiographic image.
Explain the effect of cardiovascular, systemic, and traumatic processes on the CXR.
Explain the limitations of various CXR findings.
SKILLS
Hospitalists should be able to:
Review a CXR utilizing a systemic approach.
Identify normal variants.
Identify abnormalities shown on a CSR and, when possible, correlate with clinical presentation and/or prior procedures.
Correlate physical examination findings with CXR abnormalities.
Synthesize CXR findings with other clinical and diagnostic information to diagnose disease and develop a clinical plan.
ATTITUDES
Hospitalists should be able to:
Communicate with patients and families to explain results of CXRs and how the findings influence the care plan.
Personally and promptly interpret CXRs and compare them to previously obtained CXRs, when available.
Review each CXR with a standard and consistent approach.
Consult and collaborate with radiologists in interpreting complex CXRs and in ordering further diagnostic studies or procedures based on CXR interpretation.
Utilize evidence based national guidelines to ensure cost efficiency and to minimize unnecessary patient imaging.
SYSTEM ORGANIZATION AND IMPROVEMENT
To improve quality and efficiency within their organizations, Hospitalists should:
Lead, coordinate or participate in efforts to develop protocols to minimize unnecessary CXRs.
Identify and convey the need for system improvements related to acquisition and interpretation of CXRs for hospitalized patients.
Chest radiographs (CXRs) utilize low‐level radiation to form images of the chest anatomy. They are non‐invasive and readily available. CXRs are an integral part of the initial evaluation of cardiopulmonary pathology. Hospitalists interpret the results of CXRs, often before radiologists, to diagnose disease and develop treatment plans in hospitalized patients.
KNOWLEDGE
Hospitalists should be able to:
Explain the normal anatomy of the thorax with particular attention to spatial relationships.
Explain the images seen on a CXR, including bone and soft tissue structures, airway, lungs, cardiac structure and silhouette, aorta, and diaphragm.
List the indications for ordering a CXR.
Describe evidence based national guidelines for ordering CXRs.
Compare the diagnostic utility and limitations of portable radiographs to posteroanterior and lateral radiographs.
Explain the indications for a lateral decubitus CXR.
Describe the effects of film exposure, inspiratory effort, and patient position on the radiographic image.
Explain the effect of cardiovascular, systemic, and traumatic processes on the CXR.
Explain the limitations of various CXR findings.
SKILLS
Hospitalists should be able to:
Review a CXR utilizing a systemic approach.
Identify normal variants.
Identify abnormalities shown on a CSR and, when possible, correlate with clinical presentation and/or prior procedures.
Correlate physical examination findings with CXR abnormalities.
Synthesize CXR findings with other clinical and diagnostic information to diagnose disease and develop a clinical plan.
ATTITUDES
Hospitalists should be able to:
Communicate with patients and families to explain results of CXRs and how the findings influence the care plan.
Personally and promptly interpret CXRs and compare them to previously obtained CXRs, when available.
Review each CXR with a standard and consistent approach.
Consult and collaborate with radiologists in interpreting complex CXRs and in ordering further diagnostic studies or procedures based on CXR interpretation.
Utilize evidence based national guidelines to ensure cost efficiency and to minimize unnecessary patient imaging.
SYSTEM ORGANIZATION AND IMPROVEMENT
To improve quality and efficiency within their organizations, Hospitalists should:
Lead, coordinate or participate in efforts to develop protocols to minimize unnecessary CXRs.
Identify and convey the need for system improvements related to acquisition and interpretation of CXRs for hospitalized patients.
Chest radiographs (CXRs) utilize low‐level radiation to form images of the chest anatomy. They are non‐invasive and readily available. CXRs are an integral part of the initial evaluation of cardiopulmonary pathology. Hospitalists interpret the results of CXRs, often before radiologists, to diagnose disease and develop treatment plans in hospitalized patients.
KNOWLEDGE
Hospitalists should be able to:
Explain the normal anatomy of the thorax with particular attention to spatial relationships.
Explain the images seen on a CXR, including bone and soft tissue structures, airway, lungs, cardiac structure and silhouette, aorta, and diaphragm.
List the indications for ordering a CXR.
Describe evidence based national guidelines for ordering CXRs.
Compare the diagnostic utility and limitations of portable radiographs to posteroanterior and lateral radiographs.
Explain the indications for a lateral decubitus CXR.
Describe the effects of film exposure, inspiratory effort, and patient position on the radiographic image.
Explain the effect of cardiovascular, systemic, and traumatic processes on the CXR.
Explain the limitations of various CXR findings.
SKILLS
Hospitalists should be able to:
Review a CXR utilizing a systemic approach.
Identify normal variants.
Identify abnormalities shown on a CSR and, when possible, correlate with clinical presentation and/or prior procedures.
Correlate physical examination findings with CXR abnormalities.
Synthesize CXR findings with other clinical and diagnostic information to diagnose disease and develop a clinical plan.
ATTITUDES
Hospitalists should be able to:
Communicate with patients and families to explain results of CXRs and how the findings influence the care plan.
Personally and promptly interpret CXRs and compare them to previously obtained CXRs, when available.
Review each CXR with a standard and consistent approach.
Consult and collaborate with radiologists in interpreting complex CXRs and in ordering further diagnostic studies or procedures based on CXR interpretation.
Utilize evidence based national guidelines to ensure cost efficiency and to minimize unnecessary patient imaging.
SYSTEM ORGANIZATION AND IMPROVEMENT
To improve quality and efficiency within their organizations, Hospitalists should:
Lead, coordinate or participate in efforts to develop protocols to minimize unnecessary CXRs.
Identify and convey the need for system improvements related to acquisition and interpretation of CXRs for hospitalized patients.
Copyright © 2006 Society of Hospital Medicine
Sepsis syndrome
Sepsis syndrome is defined as infection associated with the Systemic Inflammatory Response Syndrome (SIRS). Sepsis has various etiologies and clinical presentations. It accounts for substantial morbidity and mortality. The Healthcare Cost and Utilization Project (HCUP) estimated 300,000 discharges for sepsis syndrome in 2002, with an in‐hospital mortality of 18.6%. The mean length‐of‐stay was 7.3 days with approximately $26,000 in charges per patient. Sepsis requires expeditious diagnosis and standardized treatment plans to favorably impact patient morbidity and mortality. Hospitalists play a key role in the early identification of patients with sepsis, and practice aggressive evidence based evaluation and interventions. Hospitalists lead their institutions to implement early diagnostic strategies, initiate evidence based medical therapies, and incorporate multidisciplinary approaches to the care of patients with sepsis.
KNOWLEDGE
Hospitalists should be able to:
Define and differentiate bacteremia and the clinical spectrum of SIRS, sepsis, severe sepsis, and septic shock.
Describe the symptoms and signs of SIRS, sepsis, severe sepsis, and septic shock.
Describe the inflammatory cascade that leads to SIRS and sepsis.
Distinguish infectious causes of SIRS from other etiologies.
Distinguish septic shock from other causes of shock.
Describe the indicated tests required to evaluate sepsis.
Identify patient groups with increased risk for the development of sepsis, increased morbidity or mortality, or uncommon etiologic organisms.
Discuss the evidence based diagnostic choices available in the evaluation of sepsis.
Describe the indications, contraindications and side effects of therapeutic agents including fluids, vasopressors, antibiotics, steroids, activated protein C, and blood products in the treatment of sepsis.
Explain indications, contraindications and mechanisms of action of pharmacologic agents used to treat sepsis syndrome.
Describe the indications for and limitations of central venous access and its value for hemodynamic monitoring and administration of vasoactive agents.
Describe the role of established scoring systems to estimate the severity of sepsis.
Explain patient characteristics that on admission portend poor prognosis.
Explain goals for hospital discharge, including specific measures of clinical stability for safe care transition.
SKILLS
Hospitalists should be able to:
Utilize all available information, including medical records and history provided by patient and care givers, to identify factors that contribute to the development of sepsis.
Perform a rapid and targeted physical examination to identify potential sources of sepsis.
Recognize the value and limitations of the history and physical examination in determining the cause of sepsis.
Order indicated diagnostic testing to identify the source of sepsis and determine severity of organ dysfunction.
Rapidly identify patients with septic shock and aggressively treat in parallel with transfer to a critical care setting.
Assess cardiopulmonary stability and implement aggressive fluid resuscitation, airway maintenance and circulatory support.
Initiate empiric antimicrobial therapy based on the suspected etiologic source of infection.
Assess the need for central venous access and monitoring; when needed, coordinate or establish central venous access.
Determine or coordinate appropriate nutritional and metabolic interventions.
Support organ function and correct metabolic derangements when indicated.
Implement measures to ensure strict glycemic control.
Adopt measures to prevent complications, which may include aspiration precautions, stress ulcer and VTE prophylaxis, and decubitus ulcer prevention.
Measure and interpret indicated hemodynamic monitoring parameters.
ATTITUDES
Hospitalists should be able to:
Communicate with patients and families to explain the history and prognosis of sepsis and indicators of functional improvement or decline.
Communicate with patients and families to explain goals of care plan, including clinical stability criteria, discharge instructions and management after release from hospital.
Communicate with patients and families to explain tests and procedures and their indications, and to obtain informed consent.
Recognize the indications for specialty consultations, which may include critical care medicine.
Employ an early and multidisciplinary approach, which may include respiratory therapy, nursing, pharmacy, nutrition, rehabilitation and social services, that begins at admission and continues through all care transitions.
Establish and maintain an open dialogue with patients and families regarding care goals and limitations, including palliative care and end‐of‐life wishes.
Address resuscitation status early during hospital stay, and discuss and implement end of life decisions by patient or family when indicated or desired.
Ensure good communication with patients and receiving physicians during care transitions.
Utilize evidence based recommendations to guide diagnosis, monitoring and treatment of sepsis.
SYSTEM ORGANIZATION AND IMPROVEMENT
To improve efficiency and quality within their organizations, Hospitalists should:
Lead, coordinate or participate in the development and promotion of guidelines and/or pathways that facilitate efficient and timely evaluation and treatment of patients with sepsis.
Implement systems to ensure hospital‐wide adherence to national standards, and document those measures as specified by recognized organizations.
Lead, coordinate or participate in multidisciplinary initiatives to promote patient safety and optimize resource utilization.
Lead, coordinate or participate in intra‐ and inter‐institutional efforts to develop protocols for the rapid identification and transfer of patients with sepsis to appropriate facilities.
Lead, coordinate or participate in multidisciplinary teams, which may include nutrition, pharmacy, rehabilitation, social services and respiratory therapy, early in the hospital course to improve patient function and outcomes.
Integrate outcomes research, institution‐specific laboratory policies, and hospital formulary to create indicated and cost‐effective diagnostic and management strategies for patients with sepsis.
Sepsis syndrome is defined as infection associated with the Systemic Inflammatory Response Syndrome (SIRS). Sepsis has various etiologies and clinical presentations. It accounts for substantial morbidity and mortality. The Healthcare Cost and Utilization Project (HCUP) estimated 300,000 discharges for sepsis syndrome in 2002, with an in‐hospital mortality of 18.6%. The mean length‐of‐stay was 7.3 days with approximately $26,000 in charges per patient. Sepsis requires expeditious diagnosis and standardized treatment plans to favorably impact patient morbidity and mortality. Hospitalists play a key role in the early identification of patients with sepsis, and practice aggressive evidence based evaluation and interventions. Hospitalists lead their institutions to implement early diagnostic strategies, initiate evidence based medical therapies, and incorporate multidisciplinary approaches to the care of patients with sepsis.
KNOWLEDGE
Hospitalists should be able to:
Define and differentiate bacteremia and the clinical spectrum of SIRS, sepsis, severe sepsis, and septic shock.
Describe the symptoms and signs of SIRS, sepsis, severe sepsis, and septic shock.
Describe the inflammatory cascade that leads to SIRS and sepsis.
Distinguish infectious causes of SIRS from other etiologies.
Distinguish septic shock from other causes of shock.
Describe the indicated tests required to evaluate sepsis.
Identify patient groups with increased risk for the development of sepsis, increased morbidity or mortality, or uncommon etiologic organisms.
Discuss the evidence based diagnostic choices available in the evaluation of sepsis.
Describe the indications, contraindications and side effects of therapeutic agents including fluids, vasopressors, antibiotics, steroids, activated protein C, and blood products in the treatment of sepsis.
Explain indications, contraindications and mechanisms of action of pharmacologic agents used to treat sepsis syndrome.
Describe the indications for and limitations of central venous access and its value for hemodynamic monitoring and administration of vasoactive agents.
Describe the role of established scoring systems to estimate the severity of sepsis.
Explain patient characteristics that on admission portend poor prognosis.
Explain goals for hospital discharge, including specific measures of clinical stability for safe care transition.
SKILLS
Hospitalists should be able to:
Utilize all available information, including medical records and history provided by patient and care givers, to identify factors that contribute to the development of sepsis.
Perform a rapid and targeted physical examination to identify potential sources of sepsis.
Recognize the value and limitations of the history and physical examination in determining the cause of sepsis.
Order indicated diagnostic testing to identify the source of sepsis and determine severity of organ dysfunction.
Rapidly identify patients with septic shock and aggressively treat in parallel with transfer to a critical care setting.
Assess cardiopulmonary stability and implement aggressive fluid resuscitation, airway maintenance and circulatory support.
Initiate empiric antimicrobial therapy based on the suspected etiologic source of infection.
Assess the need for central venous access and monitoring; when needed, coordinate or establish central venous access.
Determine or coordinate appropriate nutritional and metabolic interventions.
Support organ function and correct metabolic derangements when indicated.
Implement measures to ensure strict glycemic control.
Adopt measures to prevent complications, which may include aspiration precautions, stress ulcer and VTE prophylaxis, and decubitus ulcer prevention.
Measure and interpret indicated hemodynamic monitoring parameters.
ATTITUDES
Hospitalists should be able to:
Communicate with patients and families to explain the history and prognosis of sepsis and indicators of functional improvement or decline.
Communicate with patients and families to explain goals of care plan, including clinical stability criteria, discharge instructions and management after release from hospital.
Communicate with patients and families to explain tests and procedures and their indications, and to obtain informed consent.
Recognize the indications for specialty consultations, which may include critical care medicine.
Employ an early and multidisciplinary approach, which may include respiratory therapy, nursing, pharmacy, nutrition, rehabilitation and social services, that begins at admission and continues through all care transitions.
Establish and maintain an open dialogue with patients and families regarding care goals and limitations, including palliative care and end‐of‐life wishes.
Address resuscitation status early during hospital stay, and discuss and implement end of life decisions by patient or family when indicated or desired.
Ensure good communication with patients and receiving physicians during care transitions.
Utilize evidence based recommendations to guide diagnosis, monitoring and treatment of sepsis.
SYSTEM ORGANIZATION AND IMPROVEMENT
To improve efficiency and quality within their organizations, Hospitalists should:
Lead, coordinate or participate in the development and promotion of guidelines and/or pathways that facilitate efficient and timely evaluation and treatment of patients with sepsis.
Implement systems to ensure hospital‐wide adherence to national standards, and document those measures as specified by recognized organizations.
Lead, coordinate or participate in multidisciplinary initiatives to promote patient safety and optimize resource utilization.
Lead, coordinate or participate in intra‐ and inter‐institutional efforts to develop protocols for the rapid identification and transfer of patients with sepsis to appropriate facilities.
Lead, coordinate or participate in multidisciplinary teams, which may include nutrition, pharmacy, rehabilitation, social services and respiratory therapy, early in the hospital course to improve patient function and outcomes.
Integrate outcomes research, institution‐specific laboratory policies, and hospital formulary to create indicated and cost‐effective diagnostic and management strategies for patients with sepsis.
Sepsis syndrome is defined as infection associated with the Systemic Inflammatory Response Syndrome (SIRS). Sepsis has various etiologies and clinical presentations. It accounts for substantial morbidity and mortality. The Healthcare Cost and Utilization Project (HCUP) estimated 300,000 discharges for sepsis syndrome in 2002, with an in‐hospital mortality of 18.6%. The mean length‐of‐stay was 7.3 days with approximately $26,000 in charges per patient. Sepsis requires expeditious diagnosis and standardized treatment plans to favorably impact patient morbidity and mortality. Hospitalists play a key role in the early identification of patients with sepsis, and practice aggressive evidence based evaluation and interventions. Hospitalists lead their institutions to implement early diagnostic strategies, initiate evidence based medical therapies, and incorporate multidisciplinary approaches to the care of patients with sepsis.
KNOWLEDGE
Hospitalists should be able to:
Define and differentiate bacteremia and the clinical spectrum of SIRS, sepsis, severe sepsis, and septic shock.
Describe the symptoms and signs of SIRS, sepsis, severe sepsis, and septic shock.
Describe the inflammatory cascade that leads to SIRS and sepsis.
Distinguish infectious causes of SIRS from other etiologies.
Distinguish septic shock from other causes of shock.
Describe the indicated tests required to evaluate sepsis.
Identify patient groups with increased risk for the development of sepsis, increased morbidity or mortality, or uncommon etiologic organisms.
Discuss the evidence based diagnostic choices available in the evaluation of sepsis.
Describe the indications, contraindications and side effects of therapeutic agents including fluids, vasopressors, antibiotics, steroids, activated protein C, and blood products in the treatment of sepsis.
Explain indications, contraindications and mechanisms of action of pharmacologic agents used to treat sepsis syndrome.
Describe the indications for and limitations of central venous access and its value for hemodynamic monitoring and administration of vasoactive agents.
Describe the role of established scoring systems to estimate the severity of sepsis.
Explain patient characteristics that on admission portend poor prognosis.
Explain goals for hospital discharge, including specific measures of clinical stability for safe care transition.
SKILLS
Hospitalists should be able to:
Utilize all available information, including medical records and history provided by patient and care givers, to identify factors that contribute to the development of sepsis.
Perform a rapid and targeted physical examination to identify potential sources of sepsis.
Recognize the value and limitations of the history and physical examination in determining the cause of sepsis.
Order indicated diagnostic testing to identify the source of sepsis and determine severity of organ dysfunction.
Rapidly identify patients with septic shock and aggressively treat in parallel with transfer to a critical care setting.
Assess cardiopulmonary stability and implement aggressive fluid resuscitation, airway maintenance and circulatory support.
Initiate empiric antimicrobial therapy based on the suspected etiologic source of infection.
Assess the need for central venous access and monitoring; when needed, coordinate or establish central venous access.
Determine or coordinate appropriate nutritional and metabolic interventions.
Support organ function and correct metabolic derangements when indicated.
Implement measures to ensure strict glycemic control.
Adopt measures to prevent complications, which may include aspiration precautions, stress ulcer and VTE prophylaxis, and decubitus ulcer prevention.
Measure and interpret indicated hemodynamic monitoring parameters.
ATTITUDES
Hospitalists should be able to:
Communicate with patients and families to explain the history and prognosis of sepsis and indicators of functional improvement or decline.
Communicate with patients and families to explain goals of care plan, including clinical stability criteria, discharge instructions and management after release from hospital.
Communicate with patients and families to explain tests and procedures and their indications, and to obtain informed consent.
Recognize the indications for specialty consultations, which may include critical care medicine.
Employ an early and multidisciplinary approach, which may include respiratory therapy, nursing, pharmacy, nutrition, rehabilitation and social services, that begins at admission and continues through all care transitions.
Establish and maintain an open dialogue with patients and families regarding care goals and limitations, including palliative care and end‐of‐life wishes.
Address resuscitation status early during hospital stay, and discuss and implement end of life decisions by patient or family when indicated or desired.
Ensure good communication with patients and receiving physicians during care transitions.
Utilize evidence based recommendations to guide diagnosis, monitoring and treatment of sepsis.
SYSTEM ORGANIZATION AND IMPROVEMENT
To improve efficiency and quality within their organizations, Hospitalists should:
Lead, coordinate or participate in the development and promotion of guidelines and/or pathways that facilitate efficient and timely evaluation and treatment of patients with sepsis.
Implement systems to ensure hospital‐wide adherence to national standards, and document those measures as specified by recognized organizations.
Lead, coordinate or participate in multidisciplinary initiatives to promote patient safety and optimize resource utilization.
Lead, coordinate or participate in intra‐ and inter‐institutional efforts to develop protocols for the rapid identification and transfer of patients with sepsis to appropriate facilities.
Lead, coordinate or participate in multidisciplinary teams, which may include nutrition, pharmacy, rehabilitation, social services and respiratory therapy, early in the hospital course to improve patient function and outcomes.
Integrate outcomes research, institution‐specific laboratory policies, and hospital formulary to create indicated and cost‐effective diagnostic and management strategies for patients with sepsis.
Copyright © 2006 Society of Hospital Medicine
Palliative care
Palliative care refers to a collaborative, comprehensive, interdisciplinary approach to improve the quality of life of patients living with debilitating, chronic or terminal illness. Palliative care is appropriate at any stage of illness and should be provided simultaneously with all other medical treatments. This approach includes the prevention and relief of suffering by means of early identification, assessment, and treatment of pain and other distressing symptoms such as dyspnea, nausea, fatigue, anxiety and depression; and attention to the physical, psychosocial and spiritual needs of patients and their families.
Hospitalists provide palliative care in multiple realms including 1) patients dying in the hospital; 2) patients discharged to home or another institution for end‐of‐life care; 3) patients with newly diagnosed life‐threatening illness; 4) patients requiring complex inpatient symptom management interventions; 5) patients for whom it is appropriate to shift the goal of care away from disease cure or stabilization and toward the maximization of comfort; and 6) patients with serious, chronic illness such as heart failure, COPD, liver disease, dementia, and cancer. Hospitalists lead, coordinate, and participate in initiatives to improve the identification and treatment of patients and families in need of palliative care.
KNOWLEDGE
Hospitalists should be able to:
Determine effective management strategies for patients requiring palliative care.
Describe potential adverse effects from medications and procedures directed at palliation.
Formulate strategies for prevention and treatment of complications of palliative care interventions.
Assess the impact of interventions including feeding tubes, parenteral nutrition, mechanical ventilation, and intravenous fluids on patient comfort and prognosis.
Describe the concept of double effect with respect to palliative care intervention.
Name the basic tenets of hospice care and the Medicare hospice benefit.
Identify indicators of clinical stability that allow for safe transitions of care and continuity after discharge.
Explain the role of palliative care throughout the course of illness and how it can be provided alongside all other appropriate medical treatments.
Describe signs and symptoms of the last 24 hours of life and how to discuss these observations with families.
Describe the responsibilities of the hospitalist after a patient dies, including pronouncing a person dead, completing the death certificate, requesting an autopsy, notifying family and PCP, and contacting the organ donor network.
SKILLS
Hospitalists should be able to:
Obtain a thorough and relevant history, review the medical record, and perform a comprehensive physical examination to identify symptoms, co‐morbidities, medications or social influences that impact the palliative care plan.
Direct individual patient's palliative care delivery from admission to discharge.
Formulate a communication plan for delivering prognostic information.
Conduct effective and compassionate family meetings.
Formulate specific patient centered palliative care plans that include pain management; integration of psychiatric, social, spiritual and other support services; and discharge planning.
Recognize and address the psychosocial effects of complex, acute life threatening illness in hospitalized patients.
Assess and respond to patient's symptoms, which may include pain, dyspnea, nausea, constipation, fatigue, anorexia, anxiety, depression and delirium.
Anticipate adverse effects and double effect from interventions and initiate measures to minimize such problems.
Communicate effectively with patients and families about patient's values and goals of care.
Communicate effectively with patients and families about hospice and know how to refer a patient to hospice.
Respond to patient requests for assisted suicide and identify and address other important ethical issues.
ATTITUDES
Hospitalists should be able to:
Convey diagnosis, prognosis, treatment and support options available for patients and families in a clear, concise, compassionate, culturally sensitive and timely manner.
Determine patient and family understanding of severity of illness, prognosis and their role in determining the goals of their care.
Promote the ethical imperative of frequent pain assessment and adequate control.
Appreciate that all pain is subjective and acknowledge patient's self reports of pain.
Discuss with patients and families goals for pain management strategies and functional status and set targets for pain control.
Appreciate that good palliative care for patients with certain conditions often involves the use of therapies typically thought of as curative.
Conduct meetings with patients and families to establish goals of care that reflect the patient's wishes.
Determine existence of advance directives and provide patients and families with resources to understand and execute such directives.
Advocate incorporation of patient wishes into care plans.
Recognize the need for frequent family meetings.
Address resuscitation status and patient preferences for care early during hospital stay.
Maintain rapport with patients and families and a consistent approach to management during transfers of care.
Recognize impact of cultural and spiritual factors to the provision of palliative care.
Appreciate the role of other members of the healthcare team including nursing and social services, pharmacy, psychology and pastoral care in providing comprehensive palliative care, and work closely with these team members in caring for patients with serious, chronic and terminal illnesses and their families.
Provide reassurance to patients and families that clinical providers will be available to provide ongoing care and relief of symptoms.
Formulate a comprehensive discharge plan that will empower the patient, family and subsequent providers to anticipate and manage changing symptoms, emergency situations, and increasing dependency.
Lead, coordinate or participate in efforts to establish or improve palliative care in the hospital, which may include establishing a palliative care consultation service.
Consider palliative care issues at hospital management and committee meetings.
Engage providers and administrators in the study of local palliative care delivery to include efficacy of pain assessment and intervention, patient and family satisfaction with care delivery, impact on hospital occupancy and costs, and fulfilled expectations of referring and collaborating providers and services.
Palliative care refers to a collaborative, comprehensive, interdisciplinary approach to improve the quality of life of patients living with debilitating, chronic or terminal illness. Palliative care is appropriate at any stage of illness and should be provided simultaneously with all other medical treatments. This approach includes the prevention and relief of suffering by means of early identification, assessment, and treatment of pain and other distressing symptoms such as dyspnea, nausea, fatigue, anxiety and depression; and attention to the physical, psychosocial and spiritual needs of patients and their families.
Hospitalists provide palliative care in multiple realms including 1) patients dying in the hospital; 2) patients discharged to home or another institution for end‐of‐life care; 3) patients with newly diagnosed life‐threatening illness; 4) patients requiring complex inpatient symptom management interventions; 5) patients for whom it is appropriate to shift the goal of care away from disease cure or stabilization and toward the maximization of comfort; and 6) patients with serious, chronic illness such as heart failure, COPD, liver disease, dementia, and cancer. Hospitalists lead, coordinate, and participate in initiatives to improve the identification and treatment of patients and families in need of palliative care.
KNOWLEDGE
Hospitalists should be able to:
Determine effective management strategies for patients requiring palliative care.
Describe potential adverse effects from medications and procedures directed at palliation.
Formulate strategies for prevention and treatment of complications of palliative care interventions.
Assess the impact of interventions including feeding tubes, parenteral nutrition, mechanical ventilation, and intravenous fluids on patient comfort and prognosis.
Describe the concept of double effect with respect to palliative care intervention.
Name the basic tenets of hospice care and the Medicare hospice benefit.
Identify indicators of clinical stability that allow for safe transitions of care and continuity after discharge.
Explain the role of palliative care throughout the course of illness and how it can be provided alongside all other appropriate medical treatments.
Describe signs and symptoms of the last 24 hours of life and how to discuss these observations with families.
Describe the responsibilities of the hospitalist after a patient dies, including pronouncing a person dead, completing the death certificate, requesting an autopsy, notifying family and PCP, and contacting the organ donor network.
SKILLS
Hospitalists should be able to:
Obtain a thorough and relevant history, review the medical record, and perform a comprehensive physical examination to identify symptoms, co‐morbidities, medications or social influences that impact the palliative care plan.
Direct individual patient's palliative care delivery from admission to discharge.
Formulate a communication plan for delivering prognostic information.
Conduct effective and compassionate family meetings.
Formulate specific patient centered palliative care plans that include pain management; integration of psychiatric, social, spiritual and other support services; and discharge planning.
Recognize and address the psychosocial effects of complex, acute life threatening illness in hospitalized patients.
Assess and respond to patient's symptoms, which may include pain, dyspnea, nausea, constipation, fatigue, anorexia, anxiety, depression and delirium.
Anticipate adverse effects and double effect from interventions and initiate measures to minimize such problems.
Communicate effectively with patients and families about patient's values and goals of care.
Communicate effectively with patients and families about hospice and know how to refer a patient to hospice.
Respond to patient requests for assisted suicide and identify and address other important ethical issues.
ATTITUDES
Hospitalists should be able to:
Convey diagnosis, prognosis, treatment and support options available for patients and families in a clear, concise, compassionate, culturally sensitive and timely manner.
Determine patient and family understanding of severity of illness, prognosis and their role in determining the goals of their care.
Promote the ethical imperative of frequent pain assessment and adequate control.
Appreciate that all pain is subjective and acknowledge patient's self reports of pain.
Discuss with patients and families goals for pain management strategies and functional status and set targets for pain control.
Appreciate that good palliative care for patients with certain conditions often involves the use of therapies typically thought of as curative.
Conduct meetings with patients and families to establish goals of care that reflect the patient's wishes.
Determine existence of advance directives and provide patients and families with resources to understand and execute such directives.
Advocate incorporation of patient wishes into care plans.
Recognize the need for frequent family meetings.
Address resuscitation status and patient preferences for care early during hospital stay.
Maintain rapport with patients and families and a consistent approach to management during transfers of care.
Recognize impact of cultural and spiritual factors to the provision of palliative care.
Appreciate the role of other members of the healthcare team including nursing and social services, pharmacy, psychology and pastoral care in providing comprehensive palliative care, and work closely with these team members in caring for patients with serious, chronic and terminal illnesses and their families.
Provide reassurance to patients and families that clinical providers will be available to provide ongoing care and relief of symptoms.
Formulate a comprehensive discharge plan that will empower the patient, family and subsequent providers to anticipate and manage changing symptoms, emergency situations, and increasing dependency.
Lead, coordinate or participate in efforts to establish or improve palliative care in the hospital, which may include establishing a palliative care consultation service.
Consider palliative care issues at hospital management and committee meetings.
Engage providers and administrators in the study of local palliative care delivery to include efficacy of pain assessment and intervention, patient and family satisfaction with care delivery, impact on hospital occupancy and costs, and fulfilled expectations of referring and collaborating providers and services.
Palliative care refers to a collaborative, comprehensive, interdisciplinary approach to improve the quality of life of patients living with debilitating, chronic or terminal illness. Palliative care is appropriate at any stage of illness and should be provided simultaneously with all other medical treatments. This approach includes the prevention and relief of suffering by means of early identification, assessment, and treatment of pain and other distressing symptoms such as dyspnea, nausea, fatigue, anxiety and depression; and attention to the physical, psychosocial and spiritual needs of patients and their families.
Hospitalists provide palliative care in multiple realms including 1) patients dying in the hospital; 2) patients discharged to home or another institution for end‐of‐life care; 3) patients with newly diagnosed life‐threatening illness; 4) patients requiring complex inpatient symptom management interventions; 5) patients for whom it is appropriate to shift the goal of care away from disease cure or stabilization and toward the maximization of comfort; and 6) patients with serious, chronic illness such as heart failure, COPD, liver disease, dementia, and cancer. Hospitalists lead, coordinate, and participate in initiatives to improve the identification and treatment of patients and families in need of palliative care.
KNOWLEDGE
Hospitalists should be able to:
Determine effective management strategies for patients requiring palliative care.
Describe potential adverse effects from medications and procedures directed at palliation.
Formulate strategies for prevention and treatment of complications of palliative care interventions.
Assess the impact of interventions including feeding tubes, parenteral nutrition, mechanical ventilation, and intravenous fluids on patient comfort and prognosis.
Describe the concept of double effect with respect to palliative care intervention.
Name the basic tenets of hospice care and the Medicare hospice benefit.
Identify indicators of clinical stability that allow for safe transitions of care and continuity after discharge.
Explain the role of palliative care throughout the course of illness and how it can be provided alongside all other appropriate medical treatments.
Describe signs and symptoms of the last 24 hours of life and how to discuss these observations with families.
Describe the responsibilities of the hospitalist after a patient dies, including pronouncing a person dead, completing the death certificate, requesting an autopsy, notifying family and PCP, and contacting the organ donor network.
SKILLS
Hospitalists should be able to:
Obtain a thorough and relevant history, review the medical record, and perform a comprehensive physical examination to identify symptoms, co‐morbidities, medications or social influences that impact the palliative care plan.
Direct individual patient's palliative care delivery from admission to discharge.
Formulate a communication plan for delivering prognostic information.
Conduct effective and compassionate family meetings.
Formulate specific patient centered palliative care plans that include pain management; integration of psychiatric, social, spiritual and other support services; and discharge planning.
Recognize and address the psychosocial effects of complex, acute life threatening illness in hospitalized patients.
Assess and respond to patient's symptoms, which may include pain, dyspnea, nausea, constipation, fatigue, anorexia, anxiety, depression and delirium.
Anticipate adverse effects and double effect from interventions and initiate measures to minimize such problems.
Communicate effectively with patients and families about patient's values and goals of care.
Communicate effectively with patients and families about hospice and know how to refer a patient to hospice.
Respond to patient requests for assisted suicide and identify and address other important ethical issues.
ATTITUDES
Hospitalists should be able to:
Convey diagnosis, prognosis, treatment and support options available for patients and families in a clear, concise, compassionate, culturally sensitive and timely manner.
Determine patient and family understanding of severity of illness, prognosis and their role in determining the goals of their care.
Promote the ethical imperative of frequent pain assessment and adequate control.
Appreciate that all pain is subjective and acknowledge patient's self reports of pain.
Discuss with patients and families goals for pain management strategies and functional status and set targets for pain control.
Appreciate that good palliative care for patients with certain conditions often involves the use of therapies typically thought of as curative.
Conduct meetings with patients and families to establish goals of care that reflect the patient's wishes.
Determine existence of advance directives and provide patients and families with resources to understand and execute such directives.
Advocate incorporation of patient wishes into care plans.
Recognize the need for frequent family meetings.
Address resuscitation status and patient preferences for care early during hospital stay.
Maintain rapport with patients and families and a consistent approach to management during transfers of care.
Recognize impact of cultural and spiritual factors to the provision of palliative care.
Appreciate the role of other members of the healthcare team including nursing and social services, pharmacy, psychology and pastoral care in providing comprehensive palliative care, and work closely with these team members in caring for patients with serious, chronic and terminal illnesses and their families.
Provide reassurance to patients and families that clinical providers will be available to provide ongoing care and relief of symptoms.
Formulate a comprehensive discharge plan that will empower the patient, family and subsequent providers to anticipate and manage changing symptoms, emergency situations, and increasing dependency.
Lead, coordinate or participate in efforts to establish or improve palliative care in the hospital, which may include establishing a palliative care consultation service.
Consider palliative care issues at hospital management and committee meetings.
Engage providers and administrators in the study of local palliative care delivery to include efficacy of pain assessment and intervention, patient and family satisfaction with care delivery, impact on hospital occupancy and costs, and fulfilled expectations of referring and collaborating providers and services.
Copyright © 2006 Society of Hospital Medicine
Community‐acquired pneumonia
Community‐acquired pneumonia (cap) is an infection of the lung parenchyma that begins in the community and is diagnosed within 48 hours of admission to the hospital. in the u.s. each year, cap is the most common infectious cause of death and the sixth leading cause of death overall in the united states. the healthcare cost and utilization project (hcup) attributed 831,000 discharges to the diagnosis related group (drg) for simple pneumonia in 2002. these patients were hospitalized for a mean of 5.4 days and had an in‐hospital mortality of 4.9%. the mean charges for these patients were $13,000 per patient and the mean length‐of‐stay was 4.7 days with in‐house mortality of 1.7%. quality indicators have been created around the key processes of care for patients with cap, and these indicators are used to evaluate performance of states, healthcare organizations, physician groups, and individual physicians. from admission to discharge, hospitalists apply evidence based practice guidelines to the management of cap and lead initiatives to improve quality of care and reduce practice variability.
KNOWLEDGE
Hospitalists should be able to:
Define cap, list the likely etiologies and signs and symptoms, and distinguish from hospital‐acquired pneumonia.
Differentiate cap from other processes that may mimic cap or other causes of infiltrates on chest x‐ray.
Describe the indicated tests required to evaluate and treat cap.
Explain indications for respiratory isolation.
Identify patients with co‐morbidities (such as the immunocompromised patient and those with diabetes mellitus) and extremes of age (the elderly and very young) who are at risk for a complicated course of cap.
Identify specific pathogens that predispose patients to a complicated course of cap.
Explain patient specific risk factors and presence of specific organisms that predispose patients to a complicated course of cap.
Describe indicated therapeutic modalities for cap including oxygen therapy, respiratory care modalities and antibiotic selection.
Predict patient risk for morbidity and mortality from cap using an evidence based tool such as the pneumonia patient outcomes research team (port) / pneumonia severity index (psi) validated risk score.
Explain goals for hospital discharge, including evidence based measures of clinical stability for safe care transition.
SKILLS
Hospitalists should be able to:
Elicit a focused history to identify symptoms consistent with cap and demographic factors that may predispose patients to cap.
Perform a targeted physical examination to elicit signs consistent with cap and differentiate it from other mimicking conditions.
Select and interpret indicated laboratory, microbiologic and radiological studies to confirm diagnosis of cap, and risk stratify patients.
Apply evidence based tools such as the pneumonia severity index, to triage decisions and identify factors that support the need for intensive care unit (icu) admission.
Initiate empiric antibiotic selection based on exposure to long term or group care, severity of illness, and evidence based national guidelines, taking into account local resistance patterns.
Formulate a subsequent treatment plan that includes narrowing antibiotic therapies based on available culture data and patient response to treatment.
Recognize and address complications of cap and/or inadequate response to therapy including respiratory failure and emerging parapneumonic effusions.
ATTITUDES
Hospitalists should be able to:
Communicate with patients and families to explain the history and prognosis of cap.
Communicate with patients and families to explain the goals of care plan, including clinical stability criteria, the importance of prevention measures such as smoking cessation, and required follow‐up care.
Communicate with patients and families to explain tests and procedures, and the use and potential side effects of pharmacologic agents.
Recognize indications for specialty consultation.
Promote prevention strategies, which may include smoking cessation and indicated vaccinations.
Collaborate with primary care physicians and emergency physicians in making the admission decision.
Document treatment plan and discharge instructions, and identify the outpatient clinician responsible for follow‐up of pending tests.
Recognize and address barriers to follow‐up care and anticipated post‐discharge requirements.
Utilize evidence based recommendations for the treatment of patients with cap
SYSTEM ORGANIZATION AND IMPROVEMENT
To improve efficiency and quality within their organizations, hospitalists should:
Lead, coordinate or participate in efforts to identify, address and monitor quality indicators for cap including assessment of oxygenation, obtaining blood cultures prior to administration of antibiotics, prompt administration of antibiotics, and providing indicated vaccinations and smoking cessation education.
Implement systems to ensure hospital wide adherence to national standards and document those measures as specified by recognized organizations (jcaho, idsa, ats)
Integrate port score / psi in conjunction with patient specific factors and clinical judgment into the admission decision.
Lead, coordinate or participate in multidisciplinary initiatives, which may include collaboration with infectious disease and pulmonary specialists, to promote patient safety and cost effective diagnostic and management strategies for patients with cap.
Lead efforts to educate staff on the importance of smoking cessation counseling and other prevention measures.
Community‐acquired pneumonia (cap) is an infection of the lung parenchyma that begins in the community and is diagnosed within 48 hours of admission to the hospital. in the u.s. each year, cap is the most common infectious cause of death and the sixth leading cause of death overall in the united states. the healthcare cost and utilization project (hcup) attributed 831,000 discharges to the diagnosis related group (drg) for simple pneumonia in 2002. these patients were hospitalized for a mean of 5.4 days and had an in‐hospital mortality of 4.9%. the mean charges for these patients were $13,000 per patient and the mean length‐of‐stay was 4.7 days with in‐house mortality of 1.7%. quality indicators have been created around the key processes of care for patients with cap, and these indicators are used to evaluate performance of states, healthcare organizations, physician groups, and individual physicians. from admission to discharge, hospitalists apply evidence based practice guidelines to the management of cap and lead initiatives to improve quality of care and reduce practice variability.
KNOWLEDGE
Hospitalists should be able to:
Define cap, list the likely etiologies and signs and symptoms, and distinguish from hospital‐acquired pneumonia.
Differentiate cap from other processes that may mimic cap or other causes of infiltrates on chest x‐ray.
Describe the indicated tests required to evaluate and treat cap.
Explain indications for respiratory isolation.
Identify patients with co‐morbidities (such as the immunocompromised patient and those with diabetes mellitus) and extremes of age (the elderly and very young) who are at risk for a complicated course of cap.
Identify specific pathogens that predispose patients to a complicated course of cap.
Explain patient specific risk factors and presence of specific organisms that predispose patients to a complicated course of cap.
Describe indicated therapeutic modalities for cap including oxygen therapy, respiratory care modalities and antibiotic selection.
Predict patient risk for morbidity and mortality from cap using an evidence based tool such as the pneumonia patient outcomes research team (port) / pneumonia severity index (psi) validated risk score.
Explain goals for hospital discharge, including evidence based measures of clinical stability for safe care transition.
SKILLS
Hospitalists should be able to:
Elicit a focused history to identify symptoms consistent with cap and demographic factors that may predispose patients to cap.
Perform a targeted physical examination to elicit signs consistent with cap and differentiate it from other mimicking conditions.
Select and interpret indicated laboratory, microbiologic and radiological studies to confirm diagnosis of cap, and risk stratify patients.
Apply evidence based tools such as the pneumonia severity index, to triage decisions and identify factors that support the need for intensive care unit (icu) admission.
Initiate empiric antibiotic selection based on exposure to long term or group care, severity of illness, and evidence based national guidelines, taking into account local resistance patterns.
Formulate a subsequent treatment plan that includes narrowing antibiotic therapies based on available culture data and patient response to treatment.
Recognize and address complications of cap and/or inadequate response to therapy including respiratory failure and emerging parapneumonic effusions.
ATTITUDES
Hospitalists should be able to:
Communicate with patients and families to explain the history and prognosis of cap.
Communicate with patients and families to explain the goals of care plan, including clinical stability criteria, the importance of prevention measures such as smoking cessation, and required follow‐up care.
Communicate with patients and families to explain tests and procedures, and the use and potential side effects of pharmacologic agents.
Recognize indications for specialty consultation.
Promote prevention strategies, which may include smoking cessation and indicated vaccinations.
Collaborate with primary care physicians and emergency physicians in making the admission decision.
Document treatment plan and discharge instructions, and identify the outpatient clinician responsible for follow‐up of pending tests.
Recognize and address barriers to follow‐up care and anticipated post‐discharge requirements.
Utilize evidence based recommendations for the treatment of patients with cap
SYSTEM ORGANIZATION AND IMPROVEMENT
To improve efficiency and quality within their organizations, hospitalists should:
Lead, coordinate or participate in efforts to identify, address and monitor quality indicators for cap including assessment of oxygenation, obtaining blood cultures prior to administration of antibiotics, prompt administration of antibiotics, and providing indicated vaccinations and smoking cessation education.
Implement systems to ensure hospital wide adherence to national standards and document those measures as specified by recognized organizations (jcaho, idsa, ats)
Integrate port score / psi in conjunction with patient specific factors and clinical judgment into the admission decision.
Lead, coordinate or participate in multidisciplinary initiatives, which may include collaboration with infectious disease and pulmonary specialists, to promote patient safety and cost effective diagnostic and management strategies for patients with cap.
Lead efforts to educate staff on the importance of smoking cessation counseling and other prevention measures.
Community‐acquired pneumonia (cap) is an infection of the lung parenchyma that begins in the community and is diagnosed within 48 hours of admission to the hospital. in the u.s. each year, cap is the most common infectious cause of death and the sixth leading cause of death overall in the united states. the healthcare cost and utilization project (hcup) attributed 831,000 discharges to the diagnosis related group (drg) for simple pneumonia in 2002. these patients were hospitalized for a mean of 5.4 days and had an in‐hospital mortality of 4.9%. the mean charges for these patients were $13,000 per patient and the mean length‐of‐stay was 4.7 days with in‐house mortality of 1.7%. quality indicators have been created around the key processes of care for patients with cap, and these indicators are used to evaluate performance of states, healthcare organizations, physician groups, and individual physicians. from admission to discharge, hospitalists apply evidence based practice guidelines to the management of cap and lead initiatives to improve quality of care and reduce practice variability.
KNOWLEDGE
Hospitalists should be able to:
Define cap, list the likely etiologies and signs and symptoms, and distinguish from hospital‐acquired pneumonia.
Differentiate cap from other processes that may mimic cap or other causes of infiltrates on chest x‐ray.
Describe the indicated tests required to evaluate and treat cap.
Explain indications for respiratory isolation.
Identify patients with co‐morbidities (such as the immunocompromised patient and those with diabetes mellitus) and extremes of age (the elderly and very young) who are at risk for a complicated course of cap.
Identify specific pathogens that predispose patients to a complicated course of cap.
Explain patient specific risk factors and presence of specific organisms that predispose patients to a complicated course of cap.
Describe indicated therapeutic modalities for cap including oxygen therapy, respiratory care modalities and antibiotic selection.
Predict patient risk for morbidity and mortality from cap using an evidence based tool such as the pneumonia patient outcomes research team (port) / pneumonia severity index (psi) validated risk score.
Explain goals for hospital discharge, including evidence based measures of clinical stability for safe care transition.
SKILLS
Hospitalists should be able to:
Elicit a focused history to identify symptoms consistent with cap and demographic factors that may predispose patients to cap.
Perform a targeted physical examination to elicit signs consistent with cap and differentiate it from other mimicking conditions.
Select and interpret indicated laboratory, microbiologic and radiological studies to confirm diagnosis of cap, and risk stratify patients.
Apply evidence based tools such as the pneumonia severity index, to triage decisions and identify factors that support the need for intensive care unit (icu) admission.
Initiate empiric antibiotic selection based on exposure to long term or group care, severity of illness, and evidence based national guidelines, taking into account local resistance patterns.
Formulate a subsequent treatment plan that includes narrowing antibiotic therapies based on available culture data and patient response to treatment.
Recognize and address complications of cap and/or inadequate response to therapy including respiratory failure and emerging parapneumonic effusions.
ATTITUDES
Hospitalists should be able to:
Communicate with patients and families to explain the history and prognosis of cap.
Communicate with patients and families to explain the goals of care plan, including clinical stability criteria, the importance of prevention measures such as smoking cessation, and required follow‐up care.
Communicate with patients and families to explain tests and procedures, and the use and potential side effects of pharmacologic agents.
Recognize indications for specialty consultation.
Promote prevention strategies, which may include smoking cessation and indicated vaccinations.
Collaborate with primary care physicians and emergency physicians in making the admission decision.
Document treatment plan and discharge instructions, and identify the outpatient clinician responsible for follow‐up of pending tests.
Recognize and address barriers to follow‐up care and anticipated post‐discharge requirements.
Utilize evidence based recommendations for the treatment of patients with cap
SYSTEM ORGANIZATION AND IMPROVEMENT
To improve efficiency and quality within their organizations, hospitalists should:
Lead, coordinate or participate in efforts to identify, address and monitor quality indicators for cap including assessment of oxygenation, obtaining blood cultures prior to administration of antibiotics, prompt administration of antibiotics, and providing indicated vaccinations and smoking cessation education.
Implement systems to ensure hospital wide adherence to national standards and document those measures as specified by recognized organizations (jcaho, idsa, ats)
Integrate port score / psi in conjunction with patient specific factors and clinical judgment into the admission decision.
Lead, coordinate or participate in multidisciplinary initiatives, which may include collaboration with infectious disease and pulmonary specialists, to promote patient safety and cost effective diagnostic and management strategies for patients with cap.
Lead efforts to educate staff on the importance of smoking cessation counseling and other prevention measures.
Copyright © 2006 Society of Hospital Medicine
The Evolution of Azelaic Acid

Nicotinamide and Zinc in the Treatment of Acne and Rosacea
Current Concepts in Pelvic Anatomy and Reconstructive Surgery
Supplement Editor:
G. Willy Davila, MD
Contents
Preface: Sizing up the evolution of reconstructive pelvic surgery
G. Willy Davila, MD
Contemporary views on female pelvic anatomy
Matthew D. Barber, MD, MHS
Vaginal vault prolapse: Identification and surgical options
Daniel H. Biller, MD, and G. Willy Davila, MD
Anterior vaginal wall prolapse: Innovative surgical approaches
Mark D. Waters, MD, and Marie Fidela R. Paraiso, MD
Optimizing pelvic surgery outcomes
G. Willy Davila, MD
Supplement Editor:
G. Willy Davila, MD
Contents
Preface: Sizing up the evolution of reconstructive pelvic surgery
G. Willy Davila, MD
Contemporary views on female pelvic anatomy
Matthew D. Barber, MD, MHS
Vaginal vault prolapse: Identification and surgical options
Daniel H. Biller, MD, and G. Willy Davila, MD
Anterior vaginal wall prolapse: Innovative surgical approaches
Mark D. Waters, MD, and Marie Fidela R. Paraiso, MD
Optimizing pelvic surgery outcomes
G. Willy Davila, MD
Supplement Editor:
G. Willy Davila, MD
Contents
Preface: Sizing up the evolution of reconstructive pelvic surgery
G. Willy Davila, MD
Contemporary views on female pelvic anatomy
Matthew D. Barber, MD, MHS
Vaginal vault prolapse: Identification and surgical options
Daniel H. Biller, MD, and G. Willy Davila, MD
Anterior vaginal wall prolapse: Innovative surgical approaches
Mark D. Waters, MD, and Marie Fidela R. Paraiso, MD
Optimizing pelvic surgery outcomes
G. Willy Davila, MD
DIAGNOSTIC CHALLENGES: Differentiating Nighttime GERD
- Reflux episodes with nighttime GERD occur less frequently but are more prolonged than those with daytime GERD. (SOR: B)
- Esophageal complications are generally more severe and nonesophageal complications more common in nighttime than in daytime GERD. (SOR: B)
- Nighttime GERD-induced alterations in sleep cause significant patient morbidity and reduced quality of life and productivity. (SOR: B)
- Several factors are associated with nighttime GERD, including increased body mass index, carbonated soft drink consumption, hypertension, benzodiazepine use, obstructive sleep apnea, and asthma. (SOR: B)
- The history and physical examination generally provide the most useful information in making the diagnosis. (SOR: C)
- Sleep-induced physiologic alterations are thought to be important factors responsible for the more common and severe symptoms and complications in nighttime vs daytime GERD. (SOR: C)
Prevalence estimates for gastroesophageal reflux disease (GERD) range from 8% to 40%, depending on the definition and diagnostic criteria.1-4 While heartburn and regurgitation are considered the hallmark symptoms, GERD actually represents a spectrum of disorders that generally result from transient relaxations of the lower esophageal sphincter (LES), so that gastric refluxate comes into contact with the esophageal epithelium. Additionally, differences in rates of acid secretion and clearance and the time since food ingestion affect symptoms, potentially leading to differing presentations of GERD associated with daytime and nocturnal episodes. To facilitate accurate diagnosis of GERD, it may be helpful for clinicians to distinguish between the symptoms that occur during the day or in an upright position and those that occur at night or when a person is supine.4 This paper reviews the differences in symptoms and explains the pathophysiologic mechanisms involved.
Issues of GERD and quality of life
Patients’ quality of life and ability to function is negatively impacted by factors associated specifically with nocturnal episodes of GERD. Patients who experience GERD primarily at night may complain of sleep disturbances. Symptoms associated with nighttime GERD generally are more severe,5 and the complications more diverse and frequent,4 due to the prolonged length of nighttime reflux.6 For these reasons, determining if the underlying cause of a group of symptoms is nighttime episodes of GERD is an important treatment step.
Complications of reflux: associations with nighttime occurrences
Esophageal complications of GERD include erosive esophagitis, esophageal hemorrhage, ulceration, and strictures and appear to be more severe in patients with nighttime episodes of GERD than in those complaining of daytime reflux. An early study showed that patients who experience reflux only in the supine position have a higher incidence of esophagitis compared with patients who only refluxed in an upright position.7 Prolonged acid contact time increases the risk that esophagitis will become erosive. This was demonstrated in a study that concluded particularly that the presence of nocturnal reflux events lasting more than 5 minutes was a powerful predictor of erosive damage.6
Overall, approximately 7% to 12% of patients with chronic GERD develop Barrett’s esophagus compared with fewer than 1% of those in the general population.8 Potentially, more severe nocturnal symptoms may be among the factors that increase the risk of Barrett’s esophagus.9,10 Esophageal adenocarcinoma also is more likely in patients with nocturnal episodes of GERD: In a national, population-based, case-controlled trial, an 11-fold increased risk for esophageal adenocarcinoma was reported in patients who experienced once-weekly episodes of nighttime heartburn, regurgitation, or both. Overall, an 8-fold increased risk of esophageal adenocarcinoma was observed in all patients with GERD.11
Impact of nighttime episodes on sleep
Not surprisingly, sleep is significantly affected by nighttime GERD episodes. A recent Internet-based survey of full-time working adults in the United States identified 1002 patients with symptomatic GERD.12 Using the validated GERD Symptom and Medication Questionnaire, symptomatic GERD was defined as a score of 10 or greater for at least one episode of heartburn or acid regurgitation within the past 7 days. Symptomatic nighttime GERD was defined as at least 2 nights with symptoms during the past 7 days. GERD-related sleep problems were twice as frequent in patients with nighttime compared with daytime GERD. Patients with nighttime episodes of GERD experienced GERD-related sleep impairment an average of 1.6 to 1.9 nights per week compared with 0.3 to 0.4 nights per week for the daytime GERD group.
In both groups, the most commonly reported sleep problem was awakening due to symptoms (75% vs 37%, respectively). Sixty-five percent of nighttime and 28% of daytime GERD patients indicated that GERD symptoms prevented them from feeling rested in the morning.12 In addition, respondents with nighttime GERD experienced an additional 2.7 hours per week of lost work productivity when compared to those with daytime GERD.13 A similar survey also found that in those with nighttime GERD, the number of nights with sleep interference was associated with reduced work productivity.14
These results are consistent with 2 previous telephone surveys. In one survey, 13% of 1000 adults who experienced heartburn at least weekly had only nighttime episodes; 20% reported only daytime heartburn.15 Altogether, 79% of the heartburn sufferers reported experiencing heartburn at night. Of these, 75% reported that heartburn had a negative impact on sleep; 63% indicated that heartburn adversely affected their ability to sleep well; and 40% reported impaired functioning the next day. The prevalence of sleep disturbances increased directly with the incidence of nighttime heartburn.
The second telephone survey of persons with nighttime GERD had lower scores using the Short-Form 36 Health Survey (a measure of quality of life) than did persons with daytime GERD or controls (TABLE 1).4 In another study, the greatest differences between groups occurred in terms of physical and emotional role functioning, vitality, and general health.16 A comparison with other major disorders affirmed the substantial impairment in health-related quality of life caused by nighttime GERD (TABLE 2).4
In summary, although heartburn and regurgitation are common in daytime and nighttime GERD, patients with nighttime GERD are more likely to experience impaired sleep, fatigue, reduced work productivity, and decreased quality of life.
TABLE 1
Adjusted medical outcomes study Short-Form 36 Health Survey scores
| Scale | Nocturnal GERD (n=945) | Non-nocturnal GERD (n=339) | Controls (n=268) |
|---|---|---|---|
| Physical functioning | 63† | 68† | 69 |
| Role limitations—physical | 53*† | 64† | 67* |
| Bodily pain | 54*† | 63† | 69* |
| General health | 48*† | 53†‡ | 59*‡ |
| Vitality | 41*† | 47†‡ | 54*‡ |
| Social functioning | 70*† | 76† | 78* |
| Role limitations—emotional | 69*† | 80† | 81* |
| Mental health | 66*† | 71† | 74* |
| Physical component summary | 39*† | 42† | 43* |
| Mental component summary | 47† | 50† | 51 |
| Analysis of covariance, adjusted for age, sex, and comorbidity. | |||
| *P<.001 nocturnal GERD vs controls; †P<.001 nocturnal vs non-nocturnal; ‡P<.001 non-nocturnal GERD vs controls. | |||
| Farup C, et al. Arch Intern Med. 2001;161:45-52.4 | |||
| Copyright © 2001 American Medical Association. Reproduced with permission. | |||
TABLE 2
Mean medical outcomes study Short-Form 36 Health Survey scores
| Scale | Nocturnal GERD (n=945) | Hypertension (n=2089) | Type 2 diabetes (n=541) | Congestive heart failure (n=216) | Clinical depression (n=502) | Angina (n=256) |
|---|---|---|---|---|---|---|
| Physical functioning | 77 | 73 | 68* | 48* | 72* | 63* |
| Role limitations—physical | 69 | 62* | 57* | 34* | 44* | 44* |
| Bodily pain | 62 | 72* | 69* | 63 | 59 | 62 |
| General health | 63 | 63 | 56* | 47* | 53* | 52* |
| Vitality | 49 | 58* | 56* | 44 | 40* | 49 |
| Social functioning | 79 | 87* | 82 | 71 | 57* | 80 |
| Role limitations—emotional | 75 | 77 | 76 | 64* | 39* | 70 |
| Mental health | 71 | 78* | 77* | 75 | 46* | 73 |
| Physical component summary | 45 | 44 | 42* | 35* | 45 | 39* |
| Mental component summary | 48 | 52* | 52* | 50 | 35* | 50 |
| *P<.001 vs nocturnal GERD Norms for non-GERD disorders were obtained from the Short-Form 36 Health Survey: Manual and Interpretation Guide. | ||||||
| Farup C, et al. Arch Intern Med. 2001;161:45-52.4 Copyright © 2001 American Medical Association. Reproduced with permission. | ||||||
Diagnosis: evaluation of symptoms
Physicians should inquire specifically about GERD symptoms to ensure diagnosis, as the signs of GERD are often subtle, nonspecific, or judged to be trivial by patients. Symptoms of GERD may include esophageal or nonesophageal complaints, or both. Importantly, heartburn or regurgitation may be absent in many patients: One group of investigators reported that neither heartburn nor regurgitation was experienced by approximately half of all patients who had nonclassical symptoms of GERD.3
Nonesophageal symptoms associated with GERD
Laryngitis, laryngospasm, chronic cough, hoarseness, excessive throat clearing, and globus pharyngeus are common nonesophageal symptoms in patients with GERD (TABLE 3).17,18 In a recent investigation, 86% and 77% of patients with nighttime and daytime episodes of GERD, respectively, reported one or more nonesophageal symptom. In patients experiencing GERD at night, the most common symptoms were sinusitis (52%), dry cough/throat clearing (49%), and snoring (47%). Symptom severity scores were significantly higher in the nighttime vs daytime GERD groups (2.42 vs 1.80, respectively).5
In a cross-sectional international population survey of 2202 randomly selected persons and 459 additional individuals with asthma, Gislason et al estimated the possible association between reported symptoms of nighttime GERD, sleep-disordered breathing, respiratory symptoms, and asthma. The investigators reported a 2- to 3-fold increased prevalence of asthma and other respiratory symptoms (such as wheezing, chest tightness, breathlessness, and nighttime cough) in patients with nighttime reflux.19
TABLE 3
Nonesophageal conditions associated with GERD
|
| Fass R, et al. Aliment Pharmacol Ther. 2004;20(suppl 9):26-38.17 |
| McGuigan JE, et al. Aliment Pharmacol Ther. 2004;20(suppl 9):57-72.18 |
Patient history
The patient’s history is the primary focus of the diagnostic workup and the physician should explore patient risk factors for GERD. For patients with atypical symptoms of GERD, the history is especially important to determine the diagnosis.
The presence of at least one esophageal or non-esophageal sign and symptom should prompt consideration of GERD as the cause, and discussion with the patient may help classify GERD further. The symptoms of nighttime GERD range from mild to severe. Though they can be similar to the symptoms of daytime GERD, nocturnal symptoms may be exacerbated by lying down or may differ in their manifestation. Asking questions about a patient’s quality of sleep, with input from the patient’s sleep partner, if possible, is useful in assessing nighttime GERD (TABLE 4).
TABLE 4
Key questions in the assessment of nighttime GERD
|
| Note: Input should also be sought from the patient’s sleep partner. |
| Farup C, et al. Arch Intern Med. 2001;161:45-52.4 |
Predictors of nighttime reflux
A high body mass index (BMI) may lead to a reduction in LES pressure and is a risk factor for GERD.20,21 Social habits such as smoking and alcohol use are often cited as risk factors for GERD; however, data to confirm this premise are lacking.11 Several other factors and the presence of some pulmonary disorders may be specific predictors and indications of nighttime GERD episodes.
A recent large prospective cohort study specifically evaluated predictors of heartburn during sleep. Symptoms of GERD were strongly associated with increased BMI, carbonated soft drink consumption (possibly due to low pH), snoring and daytime sleepiness, insomnia, hypertension, asthma, and usage of benzodiazepines (TABLE 5).20 It was noted that the association of hypertension with nighttime heartburn likely is a reflection of factors associated with hypertension rather than hypertension itself. Possible factors of hypertension include antihypertensive medications, comorbidities, diet, and body habitus.20
Several sleep-related and respiratory factors are associated with nighttime GERD. Among these, insomnia and sleepiness are probably consequences rather than causes of nighttime reflux. An association of GERD with obstructive sleep apnea has been established, although causality has not been determined. Similarly, asthma is clearly associated with GERD, but the extent of causality remains unclear. Nonetheless, nighttime GERD should be suspected in patients who present with one of these sleep disturbances, particularly obstructive sleep apnea, or adult-onset or difficult-to-treat asthma.20
TABLE 5
Factors associated with nighttime GERD
|
| Lagergren J, et al. N Engl J Med. 1999;340:825-831.11 |
| Fass R, et al. Chest. 2005;127:1658-1666.20 |
| Fisher BL, et al. Dig Dis Sci. 1999;44:2290-2294.21 |
Diagnostic tests for GERD
Various tests have been investigated for the diagnosis of all types of GERD, and there is no difference in the tests used when nighttime GERD is suspected. Endoscopy is an important diagnostic tool for either identifying or ruling out complications such as erosions or Barrett’s esophagus. Esophageal pH monitoring can be helpful in diagnosis.
Pathophysiology: potential differences between daytime and nighttime GERD
Several mechanisms have been established to contribute to the development of GERD. Included are transient LES relaxations and, less frequently, sustained LES pressure abnormalities. Other factors that contribute to the pathophysiology of GERD include hiatal hernia, which reduces LES pressure and impairs acid clearance, and poor esophageal clearance.22
Despite their similarities, important pathophysiologic differences between daytime and nighttime gastroesophageal reflux can be seen. Increased acid secretion and gastric volume are associated with food consumption, so daytime reflux and associated symptoms tend to occur after meals. Nighttime gastroesophageal reflux occurs less frequently, but the episodes are of longer duration than those of daytime reflux, as a result of delayed acid clearance from the esophagus at night.6,7,23
Sleep-related mechanisms combined with impairment of the LES and the supine position help explain the more common and severe symptoms and wider range of complications seen in nighttime compared with daytime GERD.
Protective processes impaired during sleep
Differences between daytime and nighttime GERD are thought to be due to the sleep state rather than just to differences in posture (TABLE 6).24,25 Processes that occur normally during the day to facilitate refluxed acid clearance from the esophagus, such as swallowing and acid neutralization (via bicarbonate-containing salivation), are suppressed during sleep.25
Saliva, composed of mucus, bicarbonate, and epidermal growth factor, neutralizes refluxed acid and protects esophageal tissue. Saliva production is diminished during sleep, with implications for GERD symptoms.26,27 Swallowing is reduced during sleep and may not occur during deeper stages of sleep.28 Absence of the voluntary swallow-initiated peristaltic wave of esophageal contractions during sleep also results in reduced volume clearance.29
Delayed gastric emptying during sleep may result in increased gastric distention and contribute to the occurrence of nighttime reflux.25,30
TABLE 6
Sleep-related mechanisms contributing to nighttime GERD
|
| Orr WC, et al. Am J Gastroenterol. 2000;95:37-42.24 |
| Orr WC, et al. Aliment Pharmacol Ther. 2004;20(suppl 9):39-46.25 |
Effect of reduced consciousness
Reflux during sleep may be accompanied by a brief period of arousal, which helps to hasten esophageal clearance of refluxate and protect the airway against aspiration and acid exposure.25 However, arousal does not occur in all reflux episodes, since the conscious perception of heartburn is absent during sleep. Consequently, the sleep-induced mechanisms are allowed to persist leading to prolonged periods of acid exposure.25
Summary
For the purposes of understanding symptoms and facilitating diagnosis, GERD can be divided into daytime and nighttime GERD. Compared with daytime GERD, nighttime reflux episodes occur less frequently but are more prolonged. In addition, nighttime symptoms are more common and more severe, and esophageal and nonesophageal complications are more likely. The presence of severe symptoms or at least one esophageal and/or nonesophageal symptom should prompt an investigation of nighttime GERD. In doing so, the history and physical examination findings are the most helpful; laboratory values and other test results are generally less so. Physiologic alterations during sleep are thought to be the primary factors that contribute to nighttime symptoms.
EDITOR’S NOTE:
This article is meant to alert the reader to different symptomatology in GERD at night; therefore, treatment will not be discussed.
1. Jones R, Galmiche JP. Review: what do we mean by GERD?—definition and diagnosis. Aliment Pharmacol Ther. 2005;22(suppl 1):2-10.
2. Frank L, Kleinman L, Ganoczy D, et al. Upper gastrointestinal symptoms in North America: prevalence and relationship to healthcare utilization and quality of life. Dig Dis Sci. 2000;45:809-818.
3. Locke GR, III, Talley NJ, Fett SL, Zinsmeister AR, Melton LJ, III. Prevalence and clinical spectrum of gastroesophageal reflux: a population-based study in Olmsted County, Minnesota. Gastroenterology. 1997;112:1448-1456.
4. Farup C, Kleinman L, Sloan S, et al. The impact of nocturnal symptoms associated with gastroesophageal reflux disease on health-related quality of life. Arch Intern Med. 2001;161:45-52.
5. Dubois RW, Fass R, Johnson LF, et al. Atypical nighttime symptoms of GERD among individuals with nighttime versus daytime GERD [abstract]. Gastroenterology. 2005;128(suppl 2):A288.-Abstract M999.
6. Orr WC, Allen ML, Robinson M. The pattern of nocturnal and diurnal esophageal acid exposure in the pathogenesis of erosive mucosal damage. Am J Gastroenterol. 1994;89:509-512.
7. Demeester TR, Johnson LF, Joseph GJ, Toscano MS, Hall AW, Skinner DB. Patterns of gastroesophageal reflux in health and disease. Ann Surg. 1976;184:459-470.
8. Cameron AJ, Lomboy CT. Barrett’s esophagus: age, prevalence, and extent of columnar epithelium. Gastroenterology. 1992;103:1241-1245.
9. Orr WC, Lackey C, Robinson MG, Johnson LF, Welsh JD. Esophageal acid clearance during sleep in patients with Barrett’s esophagus. Dig Dis Sci. 1988;33:654-659.
10. Eisen GM, Sandler RS, Murray S, Gottfried M. The relationship between gastroesophageal reflux disease and its complications with Barrett’s esophagus. Am J Gastroenterol. 1997;92:27-31.
11. Lagergren J, Bergstrom R, Lindgren A, Nyren O. Symptomatic gastroesophageal reflux as a risk factor for esophageal adenocarcinoma. N Engl J Med. 1999;340:825-831.
12. Dubois RW, Orr WC, Lange SM, et al. GERD-related sleep impairment among individuals with nighttime versus daytime GERD [abstract]. Gastroenterology. 2005;128(suppl 2):A288.-Abstract M998.
13. Dubois RW, Lange SM, Fass R, et al. Work productivity loss associated with nighttime GERD [abstract]. Gastroenterology. 2005;128(suppl 2):A286.-Abstract M988.
14. Dean BB, Crawley JA, Schmitt CM, Wong J, Ofman JJ. The burden of illness of gastro-oesophageal reflux disease: impact on work productivity. Aliment Pharmacol Ther. 2003;17:1309-1317.
15. Shaker R, Castell DO, Schoenfeld PS, Spechler SJ. Nighttime heartburn is an under-appreciated clinical problem that impacts sleep and daytime function the results of a Gallup survey conducted on behalf of the American Gastroenterological Association. Am J Gastroenterol. 2003;98:1487-1493.
16. Dubois RW, Fass R, Lange SM, et al. Impact of nighttime GERD on health-related quality of life [abstract]. Gastroenterology. 2005;128:(4 Suppl 2):A286.-Abstract M989.
17. Fass R, Achem SR, Harding S, Mittal RK, Quigley E. Review article: supra-oesophageal manifestations of gastro-oesophageal reflux disease and the role of night-time gastro-oesophageal reflux. Aliment Pharmacol Ther. 2004;20(suppl 9):26-38.
18. McGuigan JE, Belafsky PC, Fromer L, et al. Review article: diagnosis and management of night-time reflux. Aliment Pharmacol Ther. 2004;20(suppl 9):57-72.
19. Gislason T, Janson C, Vermeire P, et al. Respiratory symptoms and nocturnal gastroesophageal reflux: a population-based study of young adults in three European countries. Chest. 2002;121:158-163.
20. Fass R, Quan SF, O’Connor GT, Ervin A, Iber C. Predictors of heartburn during sleep in a large prospective cohort study. Chest. 2005;127:1658-1666.
21. Fisher BL, Pennathur A, Mutnick JL, Little AG. Obesity correlates with gastroesophageal reflux. Dig Dis Sci. 1999;44:2290-2294.
22. Castell DO, Murray JA, Tutuian R, Orlando RC, Arnold R. Review article: the pathophysiology of gastro-oesophageal reflux disease - oesophageal manifestations. Aliment Pharmacol Ther. 2004;20(suppl 9):14-25.
23. Orr WC, Johnson LF. Responses to different levels of esophageal acidification during waking and sleeping. Dig Dis Sci. 1998;43:241-245.
24. Orr WC, Elsenbruch S, Harnish MJ, Johnson LF. Proximal migration of esophageal acid perfusions during waking and sleep. Am J Gastroenterol. 2000;95:37-42.
25. Orr WC, Heading R, Johnson LF, Kryger M. Review article: sleep and its relationship to gastro-oesophageal reflux. Aliment Pharmacol Ther. 2004;20(suppl 9):39-46.
26. Schneyer LH, Pigman WW, Hanahan LL, Gilmore R. Rate of flow of human parotid sublingual, and submaxillary secretions during sleep. J Dent Res. 1956;35:109-114.
27. Dawes C. Circadian rhythms in human salivary flow rate and composition. J Physiol. 1972;220:529-545.
28. Lear CS, Flanagan JB, Jr, Moorrees CF. The frequency of deglutition in man. Arch Oral Biol. 1965;10:83-100.
29. Orr WC, Johnson LF, Robinson MG. Effect of sleep on swallowing, esophageal peristalsis, and acid clearance. Gastroenterology. 1984;86 (pt 1):814-819.
30. Elsenbruch S, Orr WC, Harnish MJ, Chen JD. Disruption of normal gastric myoelectric functioning by sleep. Sleep. 1999;22:453-458.
- Reflux episodes with nighttime GERD occur less frequently but are more prolonged than those with daytime GERD. (SOR: B)
- Esophageal complications are generally more severe and nonesophageal complications more common in nighttime than in daytime GERD. (SOR: B)
- Nighttime GERD-induced alterations in sleep cause significant patient morbidity and reduced quality of life and productivity. (SOR: B)
- Several factors are associated with nighttime GERD, including increased body mass index, carbonated soft drink consumption, hypertension, benzodiazepine use, obstructive sleep apnea, and asthma. (SOR: B)
- The history and physical examination generally provide the most useful information in making the diagnosis. (SOR: C)
- Sleep-induced physiologic alterations are thought to be important factors responsible for the more common and severe symptoms and complications in nighttime vs daytime GERD. (SOR: C)
Prevalence estimates for gastroesophageal reflux disease (GERD) range from 8% to 40%, depending on the definition and diagnostic criteria.1-4 While heartburn and regurgitation are considered the hallmark symptoms, GERD actually represents a spectrum of disorders that generally result from transient relaxations of the lower esophageal sphincter (LES), so that gastric refluxate comes into contact with the esophageal epithelium. Additionally, differences in rates of acid secretion and clearance and the time since food ingestion affect symptoms, potentially leading to differing presentations of GERD associated with daytime and nocturnal episodes. To facilitate accurate diagnosis of GERD, it may be helpful for clinicians to distinguish between the symptoms that occur during the day or in an upright position and those that occur at night or when a person is supine.4 This paper reviews the differences in symptoms and explains the pathophysiologic mechanisms involved.
Issues of GERD and quality of life
Patients’ quality of life and ability to function is negatively impacted by factors associated specifically with nocturnal episodes of GERD. Patients who experience GERD primarily at night may complain of sleep disturbances. Symptoms associated with nighttime GERD generally are more severe,5 and the complications more diverse and frequent,4 due to the prolonged length of nighttime reflux.6 For these reasons, determining if the underlying cause of a group of symptoms is nighttime episodes of GERD is an important treatment step.
Complications of reflux: associations with nighttime occurrences
Esophageal complications of GERD include erosive esophagitis, esophageal hemorrhage, ulceration, and strictures and appear to be more severe in patients with nighttime episodes of GERD than in those complaining of daytime reflux. An early study showed that patients who experience reflux only in the supine position have a higher incidence of esophagitis compared with patients who only refluxed in an upright position.7 Prolonged acid contact time increases the risk that esophagitis will become erosive. This was demonstrated in a study that concluded particularly that the presence of nocturnal reflux events lasting more than 5 minutes was a powerful predictor of erosive damage.6
Overall, approximately 7% to 12% of patients with chronic GERD develop Barrett’s esophagus compared with fewer than 1% of those in the general population.8 Potentially, more severe nocturnal symptoms may be among the factors that increase the risk of Barrett’s esophagus.9,10 Esophageal adenocarcinoma also is more likely in patients with nocturnal episodes of GERD: In a national, population-based, case-controlled trial, an 11-fold increased risk for esophageal adenocarcinoma was reported in patients who experienced once-weekly episodes of nighttime heartburn, regurgitation, or both. Overall, an 8-fold increased risk of esophageal adenocarcinoma was observed in all patients with GERD.11
Impact of nighttime episodes on sleep
Not surprisingly, sleep is significantly affected by nighttime GERD episodes. A recent Internet-based survey of full-time working adults in the United States identified 1002 patients with symptomatic GERD.12 Using the validated GERD Symptom and Medication Questionnaire, symptomatic GERD was defined as a score of 10 or greater for at least one episode of heartburn or acid regurgitation within the past 7 days. Symptomatic nighttime GERD was defined as at least 2 nights with symptoms during the past 7 days. GERD-related sleep problems were twice as frequent in patients with nighttime compared with daytime GERD. Patients with nighttime episodes of GERD experienced GERD-related sleep impairment an average of 1.6 to 1.9 nights per week compared with 0.3 to 0.4 nights per week for the daytime GERD group.
In both groups, the most commonly reported sleep problem was awakening due to symptoms (75% vs 37%, respectively). Sixty-five percent of nighttime and 28% of daytime GERD patients indicated that GERD symptoms prevented them from feeling rested in the morning.12 In addition, respondents with nighttime GERD experienced an additional 2.7 hours per week of lost work productivity when compared to those with daytime GERD.13 A similar survey also found that in those with nighttime GERD, the number of nights with sleep interference was associated with reduced work productivity.14
These results are consistent with 2 previous telephone surveys. In one survey, 13% of 1000 adults who experienced heartburn at least weekly had only nighttime episodes; 20% reported only daytime heartburn.15 Altogether, 79% of the heartburn sufferers reported experiencing heartburn at night. Of these, 75% reported that heartburn had a negative impact on sleep; 63% indicated that heartburn adversely affected their ability to sleep well; and 40% reported impaired functioning the next day. The prevalence of sleep disturbances increased directly with the incidence of nighttime heartburn.
The second telephone survey of persons with nighttime GERD had lower scores using the Short-Form 36 Health Survey (a measure of quality of life) than did persons with daytime GERD or controls (TABLE 1).4 In another study, the greatest differences between groups occurred in terms of physical and emotional role functioning, vitality, and general health.16 A comparison with other major disorders affirmed the substantial impairment in health-related quality of life caused by nighttime GERD (TABLE 2).4
In summary, although heartburn and regurgitation are common in daytime and nighttime GERD, patients with nighttime GERD are more likely to experience impaired sleep, fatigue, reduced work productivity, and decreased quality of life.
TABLE 1
Adjusted medical outcomes study Short-Form 36 Health Survey scores
| Scale | Nocturnal GERD (n=945) | Non-nocturnal GERD (n=339) | Controls (n=268) |
|---|---|---|---|
| Physical functioning | 63† | 68† | 69 |
| Role limitations—physical | 53*† | 64† | 67* |
| Bodily pain | 54*† | 63† | 69* |
| General health | 48*† | 53†‡ | 59*‡ |
| Vitality | 41*† | 47†‡ | 54*‡ |
| Social functioning | 70*† | 76† | 78* |
| Role limitations—emotional | 69*† | 80† | 81* |
| Mental health | 66*† | 71† | 74* |
| Physical component summary | 39*† | 42† | 43* |
| Mental component summary | 47† | 50† | 51 |
| Analysis of covariance, adjusted for age, sex, and comorbidity. | |||
| *P<.001 nocturnal GERD vs controls; †P<.001 nocturnal vs non-nocturnal; ‡P<.001 non-nocturnal GERD vs controls. | |||
| Farup C, et al. Arch Intern Med. 2001;161:45-52.4 | |||
| Copyright © 2001 American Medical Association. Reproduced with permission. | |||
TABLE 2
Mean medical outcomes study Short-Form 36 Health Survey scores
| Scale | Nocturnal GERD (n=945) | Hypertension (n=2089) | Type 2 diabetes (n=541) | Congestive heart failure (n=216) | Clinical depression (n=502) | Angina (n=256) |
|---|---|---|---|---|---|---|
| Physical functioning | 77 | 73 | 68* | 48* | 72* | 63* |
| Role limitations—physical | 69 | 62* | 57* | 34* | 44* | 44* |
| Bodily pain | 62 | 72* | 69* | 63 | 59 | 62 |
| General health | 63 | 63 | 56* | 47* | 53* | 52* |
| Vitality | 49 | 58* | 56* | 44 | 40* | 49 |
| Social functioning | 79 | 87* | 82 | 71 | 57* | 80 |
| Role limitations—emotional | 75 | 77 | 76 | 64* | 39* | 70 |
| Mental health | 71 | 78* | 77* | 75 | 46* | 73 |
| Physical component summary | 45 | 44 | 42* | 35* | 45 | 39* |
| Mental component summary | 48 | 52* | 52* | 50 | 35* | 50 |
| *P<.001 vs nocturnal GERD Norms for non-GERD disorders were obtained from the Short-Form 36 Health Survey: Manual and Interpretation Guide. | ||||||
| Farup C, et al. Arch Intern Med. 2001;161:45-52.4 Copyright © 2001 American Medical Association. Reproduced with permission. | ||||||
Diagnosis: evaluation of symptoms
Physicians should inquire specifically about GERD symptoms to ensure diagnosis, as the signs of GERD are often subtle, nonspecific, or judged to be trivial by patients. Symptoms of GERD may include esophageal or nonesophageal complaints, or both. Importantly, heartburn or regurgitation may be absent in many patients: One group of investigators reported that neither heartburn nor regurgitation was experienced by approximately half of all patients who had nonclassical symptoms of GERD.3
Nonesophageal symptoms associated with GERD
Laryngitis, laryngospasm, chronic cough, hoarseness, excessive throat clearing, and globus pharyngeus are common nonesophageal symptoms in patients with GERD (TABLE 3).17,18 In a recent investigation, 86% and 77% of patients with nighttime and daytime episodes of GERD, respectively, reported one or more nonesophageal symptom. In patients experiencing GERD at night, the most common symptoms were sinusitis (52%), dry cough/throat clearing (49%), and snoring (47%). Symptom severity scores were significantly higher in the nighttime vs daytime GERD groups (2.42 vs 1.80, respectively).5
In a cross-sectional international population survey of 2202 randomly selected persons and 459 additional individuals with asthma, Gislason et al estimated the possible association between reported symptoms of nighttime GERD, sleep-disordered breathing, respiratory symptoms, and asthma. The investigators reported a 2- to 3-fold increased prevalence of asthma and other respiratory symptoms (such as wheezing, chest tightness, breathlessness, and nighttime cough) in patients with nighttime reflux.19
TABLE 3
Nonesophageal conditions associated with GERD
|
| Fass R, et al. Aliment Pharmacol Ther. 2004;20(suppl 9):26-38.17 |
| McGuigan JE, et al. Aliment Pharmacol Ther. 2004;20(suppl 9):57-72.18 |
Patient history
The patient’s history is the primary focus of the diagnostic workup and the physician should explore patient risk factors for GERD. For patients with atypical symptoms of GERD, the history is especially important to determine the diagnosis.
The presence of at least one esophageal or non-esophageal sign and symptom should prompt consideration of GERD as the cause, and discussion with the patient may help classify GERD further. The symptoms of nighttime GERD range from mild to severe. Though they can be similar to the symptoms of daytime GERD, nocturnal symptoms may be exacerbated by lying down or may differ in their manifestation. Asking questions about a patient’s quality of sleep, with input from the patient’s sleep partner, if possible, is useful in assessing nighttime GERD (TABLE 4).
TABLE 4
Key questions in the assessment of nighttime GERD
|
| Note: Input should also be sought from the patient’s sleep partner. |
| Farup C, et al. Arch Intern Med. 2001;161:45-52.4 |
Predictors of nighttime reflux
A high body mass index (BMI) may lead to a reduction in LES pressure and is a risk factor for GERD.20,21 Social habits such as smoking and alcohol use are often cited as risk factors for GERD; however, data to confirm this premise are lacking.11 Several other factors and the presence of some pulmonary disorders may be specific predictors and indications of nighttime GERD episodes.
A recent large prospective cohort study specifically evaluated predictors of heartburn during sleep. Symptoms of GERD were strongly associated with increased BMI, carbonated soft drink consumption (possibly due to low pH), snoring and daytime sleepiness, insomnia, hypertension, asthma, and usage of benzodiazepines (TABLE 5).20 It was noted that the association of hypertension with nighttime heartburn likely is a reflection of factors associated with hypertension rather than hypertension itself. Possible factors of hypertension include antihypertensive medications, comorbidities, diet, and body habitus.20
Several sleep-related and respiratory factors are associated with nighttime GERD. Among these, insomnia and sleepiness are probably consequences rather than causes of nighttime reflux. An association of GERD with obstructive sleep apnea has been established, although causality has not been determined. Similarly, asthma is clearly associated with GERD, but the extent of causality remains unclear. Nonetheless, nighttime GERD should be suspected in patients who present with one of these sleep disturbances, particularly obstructive sleep apnea, or adult-onset or difficult-to-treat asthma.20
TABLE 5
Factors associated with nighttime GERD
|
| Lagergren J, et al. N Engl J Med. 1999;340:825-831.11 |
| Fass R, et al. Chest. 2005;127:1658-1666.20 |
| Fisher BL, et al. Dig Dis Sci. 1999;44:2290-2294.21 |
Diagnostic tests for GERD
Various tests have been investigated for the diagnosis of all types of GERD, and there is no difference in the tests used when nighttime GERD is suspected. Endoscopy is an important diagnostic tool for either identifying or ruling out complications such as erosions or Barrett’s esophagus. Esophageal pH monitoring can be helpful in diagnosis.
Pathophysiology: potential differences between daytime and nighttime GERD
Several mechanisms have been established to contribute to the development of GERD. Included are transient LES relaxations and, less frequently, sustained LES pressure abnormalities. Other factors that contribute to the pathophysiology of GERD include hiatal hernia, which reduces LES pressure and impairs acid clearance, and poor esophageal clearance.22
Despite their similarities, important pathophysiologic differences between daytime and nighttime gastroesophageal reflux can be seen. Increased acid secretion and gastric volume are associated with food consumption, so daytime reflux and associated symptoms tend to occur after meals. Nighttime gastroesophageal reflux occurs less frequently, but the episodes are of longer duration than those of daytime reflux, as a result of delayed acid clearance from the esophagus at night.6,7,23
Sleep-related mechanisms combined with impairment of the LES and the supine position help explain the more common and severe symptoms and wider range of complications seen in nighttime compared with daytime GERD.
Protective processes impaired during sleep
Differences between daytime and nighttime GERD are thought to be due to the sleep state rather than just to differences in posture (TABLE 6).24,25 Processes that occur normally during the day to facilitate refluxed acid clearance from the esophagus, such as swallowing and acid neutralization (via bicarbonate-containing salivation), are suppressed during sleep.25
Saliva, composed of mucus, bicarbonate, and epidermal growth factor, neutralizes refluxed acid and protects esophageal tissue. Saliva production is diminished during sleep, with implications for GERD symptoms.26,27 Swallowing is reduced during sleep and may not occur during deeper stages of sleep.28 Absence of the voluntary swallow-initiated peristaltic wave of esophageal contractions during sleep also results in reduced volume clearance.29
Delayed gastric emptying during sleep may result in increased gastric distention and contribute to the occurrence of nighttime reflux.25,30
TABLE 6
Sleep-related mechanisms contributing to nighttime GERD
|
| Orr WC, et al. Am J Gastroenterol. 2000;95:37-42.24 |
| Orr WC, et al. Aliment Pharmacol Ther. 2004;20(suppl 9):39-46.25 |
Effect of reduced consciousness
Reflux during sleep may be accompanied by a brief period of arousal, which helps to hasten esophageal clearance of refluxate and protect the airway against aspiration and acid exposure.25 However, arousal does not occur in all reflux episodes, since the conscious perception of heartburn is absent during sleep. Consequently, the sleep-induced mechanisms are allowed to persist leading to prolonged periods of acid exposure.25
Summary
For the purposes of understanding symptoms and facilitating diagnosis, GERD can be divided into daytime and nighttime GERD. Compared with daytime GERD, nighttime reflux episodes occur less frequently but are more prolonged. In addition, nighttime symptoms are more common and more severe, and esophageal and nonesophageal complications are more likely. The presence of severe symptoms or at least one esophageal and/or nonesophageal symptom should prompt an investigation of nighttime GERD. In doing so, the history and physical examination findings are the most helpful; laboratory values and other test results are generally less so. Physiologic alterations during sleep are thought to be the primary factors that contribute to nighttime symptoms.
EDITOR’S NOTE:
This article is meant to alert the reader to different symptomatology in GERD at night; therefore, treatment will not be discussed.
- Reflux episodes with nighttime GERD occur less frequently but are more prolonged than those with daytime GERD. (SOR: B)
- Esophageal complications are generally more severe and nonesophageal complications more common in nighttime than in daytime GERD. (SOR: B)
- Nighttime GERD-induced alterations in sleep cause significant patient morbidity and reduced quality of life and productivity. (SOR: B)
- Several factors are associated with nighttime GERD, including increased body mass index, carbonated soft drink consumption, hypertension, benzodiazepine use, obstructive sleep apnea, and asthma. (SOR: B)
- The history and physical examination generally provide the most useful information in making the diagnosis. (SOR: C)
- Sleep-induced physiologic alterations are thought to be important factors responsible for the more common and severe symptoms and complications in nighttime vs daytime GERD. (SOR: C)
Prevalence estimates for gastroesophageal reflux disease (GERD) range from 8% to 40%, depending on the definition and diagnostic criteria.1-4 While heartburn and regurgitation are considered the hallmark symptoms, GERD actually represents a spectrum of disorders that generally result from transient relaxations of the lower esophageal sphincter (LES), so that gastric refluxate comes into contact with the esophageal epithelium. Additionally, differences in rates of acid secretion and clearance and the time since food ingestion affect symptoms, potentially leading to differing presentations of GERD associated with daytime and nocturnal episodes. To facilitate accurate diagnosis of GERD, it may be helpful for clinicians to distinguish between the symptoms that occur during the day or in an upright position and those that occur at night or when a person is supine.4 This paper reviews the differences in symptoms and explains the pathophysiologic mechanisms involved.
Issues of GERD and quality of life
Patients’ quality of life and ability to function is negatively impacted by factors associated specifically with nocturnal episodes of GERD. Patients who experience GERD primarily at night may complain of sleep disturbances. Symptoms associated with nighttime GERD generally are more severe,5 and the complications more diverse and frequent,4 due to the prolonged length of nighttime reflux.6 For these reasons, determining if the underlying cause of a group of symptoms is nighttime episodes of GERD is an important treatment step.
Complications of reflux: associations with nighttime occurrences
Esophageal complications of GERD include erosive esophagitis, esophageal hemorrhage, ulceration, and strictures and appear to be more severe in patients with nighttime episodes of GERD than in those complaining of daytime reflux. An early study showed that patients who experience reflux only in the supine position have a higher incidence of esophagitis compared with patients who only refluxed in an upright position.7 Prolonged acid contact time increases the risk that esophagitis will become erosive. This was demonstrated in a study that concluded particularly that the presence of nocturnal reflux events lasting more than 5 minutes was a powerful predictor of erosive damage.6
Overall, approximately 7% to 12% of patients with chronic GERD develop Barrett’s esophagus compared with fewer than 1% of those in the general population.8 Potentially, more severe nocturnal symptoms may be among the factors that increase the risk of Barrett’s esophagus.9,10 Esophageal adenocarcinoma also is more likely in patients with nocturnal episodes of GERD: In a national, population-based, case-controlled trial, an 11-fold increased risk for esophageal adenocarcinoma was reported in patients who experienced once-weekly episodes of nighttime heartburn, regurgitation, or both. Overall, an 8-fold increased risk of esophageal adenocarcinoma was observed in all patients with GERD.11
Impact of nighttime episodes on sleep
Not surprisingly, sleep is significantly affected by nighttime GERD episodes. A recent Internet-based survey of full-time working adults in the United States identified 1002 patients with symptomatic GERD.12 Using the validated GERD Symptom and Medication Questionnaire, symptomatic GERD was defined as a score of 10 or greater for at least one episode of heartburn or acid regurgitation within the past 7 days. Symptomatic nighttime GERD was defined as at least 2 nights with symptoms during the past 7 days. GERD-related sleep problems were twice as frequent in patients with nighttime compared with daytime GERD. Patients with nighttime episodes of GERD experienced GERD-related sleep impairment an average of 1.6 to 1.9 nights per week compared with 0.3 to 0.4 nights per week for the daytime GERD group.
In both groups, the most commonly reported sleep problem was awakening due to symptoms (75% vs 37%, respectively). Sixty-five percent of nighttime and 28% of daytime GERD patients indicated that GERD symptoms prevented them from feeling rested in the morning.12 In addition, respondents with nighttime GERD experienced an additional 2.7 hours per week of lost work productivity when compared to those with daytime GERD.13 A similar survey also found that in those with nighttime GERD, the number of nights with sleep interference was associated with reduced work productivity.14
These results are consistent with 2 previous telephone surveys. In one survey, 13% of 1000 adults who experienced heartburn at least weekly had only nighttime episodes; 20% reported only daytime heartburn.15 Altogether, 79% of the heartburn sufferers reported experiencing heartburn at night. Of these, 75% reported that heartburn had a negative impact on sleep; 63% indicated that heartburn adversely affected their ability to sleep well; and 40% reported impaired functioning the next day. The prevalence of sleep disturbances increased directly with the incidence of nighttime heartburn.
The second telephone survey of persons with nighttime GERD had lower scores using the Short-Form 36 Health Survey (a measure of quality of life) than did persons with daytime GERD or controls (TABLE 1).4 In another study, the greatest differences between groups occurred in terms of physical and emotional role functioning, vitality, and general health.16 A comparison with other major disorders affirmed the substantial impairment in health-related quality of life caused by nighttime GERD (TABLE 2).4
In summary, although heartburn and regurgitation are common in daytime and nighttime GERD, patients with nighttime GERD are more likely to experience impaired sleep, fatigue, reduced work productivity, and decreased quality of life.
TABLE 1
Adjusted medical outcomes study Short-Form 36 Health Survey scores
| Scale | Nocturnal GERD (n=945) | Non-nocturnal GERD (n=339) | Controls (n=268) |
|---|---|---|---|
| Physical functioning | 63† | 68† | 69 |
| Role limitations—physical | 53*† | 64† | 67* |
| Bodily pain | 54*† | 63† | 69* |
| General health | 48*† | 53†‡ | 59*‡ |
| Vitality | 41*† | 47†‡ | 54*‡ |
| Social functioning | 70*† | 76† | 78* |
| Role limitations—emotional | 69*† | 80† | 81* |
| Mental health | 66*† | 71† | 74* |
| Physical component summary | 39*† | 42† | 43* |
| Mental component summary | 47† | 50† | 51 |
| Analysis of covariance, adjusted for age, sex, and comorbidity. | |||
| *P<.001 nocturnal GERD vs controls; †P<.001 nocturnal vs non-nocturnal; ‡P<.001 non-nocturnal GERD vs controls. | |||
| Farup C, et al. Arch Intern Med. 2001;161:45-52.4 | |||
| Copyright © 2001 American Medical Association. Reproduced with permission. | |||
TABLE 2
Mean medical outcomes study Short-Form 36 Health Survey scores
| Scale | Nocturnal GERD (n=945) | Hypertension (n=2089) | Type 2 diabetes (n=541) | Congestive heart failure (n=216) | Clinical depression (n=502) | Angina (n=256) |
|---|---|---|---|---|---|---|
| Physical functioning | 77 | 73 | 68* | 48* | 72* | 63* |
| Role limitations—physical | 69 | 62* | 57* | 34* | 44* | 44* |
| Bodily pain | 62 | 72* | 69* | 63 | 59 | 62 |
| General health | 63 | 63 | 56* | 47* | 53* | 52* |
| Vitality | 49 | 58* | 56* | 44 | 40* | 49 |
| Social functioning | 79 | 87* | 82 | 71 | 57* | 80 |
| Role limitations—emotional | 75 | 77 | 76 | 64* | 39* | 70 |
| Mental health | 71 | 78* | 77* | 75 | 46* | 73 |
| Physical component summary | 45 | 44 | 42* | 35* | 45 | 39* |
| Mental component summary | 48 | 52* | 52* | 50 | 35* | 50 |
| *P<.001 vs nocturnal GERD Norms for non-GERD disorders were obtained from the Short-Form 36 Health Survey: Manual and Interpretation Guide. | ||||||
| Farup C, et al. Arch Intern Med. 2001;161:45-52.4 Copyright © 2001 American Medical Association. Reproduced with permission. | ||||||
Diagnosis: evaluation of symptoms
Physicians should inquire specifically about GERD symptoms to ensure diagnosis, as the signs of GERD are often subtle, nonspecific, or judged to be trivial by patients. Symptoms of GERD may include esophageal or nonesophageal complaints, or both. Importantly, heartburn or regurgitation may be absent in many patients: One group of investigators reported that neither heartburn nor regurgitation was experienced by approximately half of all patients who had nonclassical symptoms of GERD.3
Nonesophageal symptoms associated with GERD
Laryngitis, laryngospasm, chronic cough, hoarseness, excessive throat clearing, and globus pharyngeus are common nonesophageal symptoms in patients with GERD (TABLE 3).17,18 In a recent investigation, 86% and 77% of patients with nighttime and daytime episodes of GERD, respectively, reported one or more nonesophageal symptom. In patients experiencing GERD at night, the most common symptoms were sinusitis (52%), dry cough/throat clearing (49%), and snoring (47%). Symptom severity scores were significantly higher in the nighttime vs daytime GERD groups (2.42 vs 1.80, respectively).5
In a cross-sectional international population survey of 2202 randomly selected persons and 459 additional individuals with asthma, Gislason et al estimated the possible association between reported symptoms of nighttime GERD, sleep-disordered breathing, respiratory symptoms, and asthma. The investigators reported a 2- to 3-fold increased prevalence of asthma and other respiratory symptoms (such as wheezing, chest tightness, breathlessness, and nighttime cough) in patients with nighttime reflux.19
TABLE 3
Nonesophageal conditions associated with GERD
|
| Fass R, et al. Aliment Pharmacol Ther. 2004;20(suppl 9):26-38.17 |
| McGuigan JE, et al. Aliment Pharmacol Ther. 2004;20(suppl 9):57-72.18 |
Patient history
The patient’s history is the primary focus of the diagnostic workup and the physician should explore patient risk factors for GERD. For patients with atypical symptoms of GERD, the history is especially important to determine the diagnosis.
The presence of at least one esophageal or non-esophageal sign and symptom should prompt consideration of GERD as the cause, and discussion with the patient may help classify GERD further. The symptoms of nighttime GERD range from mild to severe. Though they can be similar to the symptoms of daytime GERD, nocturnal symptoms may be exacerbated by lying down or may differ in their manifestation. Asking questions about a patient’s quality of sleep, with input from the patient’s sleep partner, if possible, is useful in assessing nighttime GERD (TABLE 4).
TABLE 4
Key questions in the assessment of nighttime GERD
|
| Note: Input should also be sought from the patient’s sleep partner. |
| Farup C, et al. Arch Intern Med. 2001;161:45-52.4 |
Predictors of nighttime reflux
A high body mass index (BMI) may lead to a reduction in LES pressure and is a risk factor for GERD.20,21 Social habits such as smoking and alcohol use are often cited as risk factors for GERD; however, data to confirm this premise are lacking.11 Several other factors and the presence of some pulmonary disorders may be specific predictors and indications of nighttime GERD episodes.
A recent large prospective cohort study specifically evaluated predictors of heartburn during sleep. Symptoms of GERD were strongly associated with increased BMI, carbonated soft drink consumption (possibly due to low pH), snoring and daytime sleepiness, insomnia, hypertension, asthma, and usage of benzodiazepines (TABLE 5).20 It was noted that the association of hypertension with nighttime heartburn likely is a reflection of factors associated with hypertension rather than hypertension itself. Possible factors of hypertension include antihypertensive medications, comorbidities, diet, and body habitus.20
Several sleep-related and respiratory factors are associated with nighttime GERD. Among these, insomnia and sleepiness are probably consequences rather than causes of nighttime reflux. An association of GERD with obstructive sleep apnea has been established, although causality has not been determined. Similarly, asthma is clearly associated with GERD, but the extent of causality remains unclear. Nonetheless, nighttime GERD should be suspected in patients who present with one of these sleep disturbances, particularly obstructive sleep apnea, or adult-onset or difficult-to-treat asthma.20
TABLE 5
Factors associated with nighttime GERD
|
| Lagergren J, et al. N Engl J Med. 1999;340:825-831.11 |
| Fass R, et al. Chest. 2005;127:1658-1666.20 |
| Fisher BL, et al. Dig Dis Sci. 1999;44:2290-2294.21 |
Diagnostic tests for GERD
Various tests have been investigated for the diagnosis of all types of GERD, and there is no difference in the tests used when nighttime GERD is suspected. Endoscopy is an important diagnostic tool for either identifying or ruling out complications such as erosions or Barrett’s esophagus. Esophageal pH monitoring can be helpful in diagnosis.
Pathophysiology: potential differences between daytime and nighttime GERD
Several mechanisms have been established to contribute to the development of GERD. Included are transient LES relaxations and, less frequently, sustained LES pressure abnormalities. Other factors that contribute to the pathophysiology of GERD include hiatal hernia, which reduces LES pressure and impairs acid clearance, and poor esophageal clearance.22
Despite their similarities, important pathophysiologic differences between daytime and nighttime gastroesophageal reflux can be seen. Increased acid secretion and gastric volume are associated with food consumption, so daytime reflux and associated symptoms tend to occur after meals. Nighttime gastroesophageal reflux occurs less frequently, but the episodes are of longer duration than those of daytime reflux, as a result of delayed acid clearance from the esophagus at night.6,7,23
Sleep-related mechanisms combined with impairment of the LES and the supine position help explain the more common and severe symptoms and wider range of complications seen in nighttime compared with daytime GERD.
Protective processes impaired during sleep
Differences between daytime and nighttime GERD are thought to be due to the sleep state rather than just to differences in posture (TABLE 6).24,25 Processes that occur normally during the day to facilitate refluxed acid clearance from the esophagus, such as swallowing and acid neutralization (via bicarbonate-containing salivation), are suppressed during sleep.25
Saliva, composed of mucus, bicarbonate, and epidermal growth factor, neutralizes refluxed acid and protects esophageal tissue. Saliva production is diminished during sleep, with implications for GERD symptoms.26,27 Swallowing is reduced during sleep and may not occur during deeper stages of sleep.28 Absence of the voluntary swallow-initiated peristaltic wave of esophageal contractions during sleep also results in reduced volume clearance.29
Delayed gastric emptying during sleep may result in increased gastric distention and contribute to the occurrence of nighttime reflux.25,30
TABLE 6
Sleep-related mechanisms contributing to nighttime GERD
|
| Orr WC, et al. Am J Gastroenterol. 2000;95:37-42.24 |
| Orr WC, et al. Aliment Pharmacol Ther. 2004;20(suppl 9):39-46.25 |
Effect of reduced consciousness
Reflux during sleep may be accompanied by a brief period of arousal, which helps to hasten esophageal clearance of refluxate and protect the airway against aspiration and acid exposure.25 However, arousal does not occur in all reflux episodes, since the conscious perception of heartburn is absent during sleep. Consequently, the sleep-induced mechanisms are allowed to persist leading to prolonged periods of acid exposure.25
Summary
For the purposes of understanding symptoms and facilitating diagnosis, GERD can be divided into daytime and nighttime GERD. Compared with daytime GERD, nighttime reflux episodes occur less frequently but are more prolonged. In addition, nighttime symptoms are more common and more severe, and esophageal and nonesophageal complications are more likely. The presence of severe symptoms or at least one esophageal and/or nonesophageal symptom should prompt an investigation of nighttime GERD. In doing so, the history and physical examination findings are the most helpful; laboratory values and other test results are generally less so. Physiologic alterations during sleep are thought to be the primary factors that contribute to nighttime symptoms.
EDITOR’S NOTE:
This article is meant to alert the reader to different symptomatology in GERD at night; therefore, treatment will not be discussed.
1. Jones R, Galmiche JP. Review: what do we mean by GERD?—definition and diagnosis. Aliment Pharmacol Ther. 2005;22(suppl 1):2-10.
2. Frank L, Kleinman L, Ganoczy D, et al. Upper gastrointestinal symptoms in North America: prevalence and relationship to healthcare utilization and quality of life. Dig Dis Sci. 2000;45:809-818.
3. Locke GR, III, Talley NJ, Fett SL, Zinsmeister AR, Melton LJ, III. Prevalence and clinical spectrum of gastroesophageal reflux: a population-based study in Olmsted County, Minnesota. Gastroenterology. 1997;112:1448-1456.
4. Farup C, Kleinman L, Sloan S, et al. The impact of nocturnal symptoms associated with gastroesophageal reflux disease on health-related quality of life. Arch Intern Med. 2001;161:45-52.
5. Dubois RW, Fass R, Johnson LF, et al. Atypical nighttime symptoms of GERD among individuals with nighttime versus daytime GERD [abstract]. Gastroenterology. 2005;128(suppl 2):A288.-Abstract M999.
6. Orr WC, Allen ML, Robinson M. The pattern of nocturnal and diurnal esophageal acid exposure in the pathogenesis of erosive mucosal damage. Am J Gastroenterol. 1994;89:509-512.
7. Demeester TR, Johnson LF, Joseph GJ, Toscano MS, Hall AW, Skinner DB. Patterns of gastroesophageal reflux in health and disease. Ann Surg. 1976;184:459-470.
8. Cameron AJ, Lomboy CT. Barrett’s esophagus: age, prevalence, and extent of columnar epithelium. Gastroenterology. 1992;103:1241-1245.
9. Orr WC, Lackey C, Robinson MG, Johnson LF, Welsh JD. Esophageal acid clearance during sleep in patients with Barrett’s esophagus. Dig Dis Sci. 1988;33:654-659.
10. Eisen GM, Sandler RS, Murray S, Gottfried M. The relationship between gastroesophageal reflux disease and its complications with Barrett’s esophagus. Am J Gastroenterol. 1997;92:27-31.
11. Lagergren J, Bergstrom R, Lindgren A, Nyren O. Symptomatic gastroesophageal reflux as a risk factor for esophageal adenocarcinoma. N Engl J Med. 1999;340:825-831.
12. Dubois RW, Orr WC, Lange SM, et al. GERD-related sleep impairment among individuals with nighttime versus daytime GERD [abstract]. Gastroenterology. 2005;128(suppl 2):A288.-Abstract M998.
13. Dubois RW, Lange SM, Fass R, et al. Work productivity loss associated with nighttime GERD [abstract]. Gastroenterology. 2005;128(suppl 2):A286.-Abstract M988.
14. Dean BB, Crawley JA, Schmitt CM, Wong J, Ofman JJ. The burden of illness of gastro-oesophageal reflux disease: impact on work productivity. Aliment Pharmacol Ther. 2003;17:1309-1317.
15. Shaker R, Castell DO, Schoenfeld PS, Spechler SJ. Nighttime heartburn is an under-appreciated clinical problem that impacts sleep and daytime function the results of a Gallup survey conducted on behalf of the American Gastroenterological Association. Am J Gastroenterol. 2003;98:1487-1493.
16. Dubois RW, Fass R, Lange SM, et al. Impact of nighttime GERD on health-related quality of life [abstract]. Gastroenterology. 2005;128:(4 Suppl 2):A286.-Abstract M989.
17. Fass R, Achem SR, Harding S, Mittal RK, Quigley E. Review article: supra-oesophageal manifestations of gastro-oesophageal reflux disease and the role of night-time gastro-oesophageal reflux. Aliment Pharmacol Ther. 2004;20(suppl 9):26-38.
18. McGuigan JE, Belafsky PC, Fromer L, et al. Review article: diagnosis and management of night-time reflux. Aliment Pharmacol Ther. 2004;20(suppl 9):57-72.
19. Gislason T, Janson C, Vermeire P, et al. Respiratory symptoms and nocturnal gastroesophageal reflux: a population-based study of young adults in three European countries. Chest. 2002;121:158-163.
20. Fass R, Quan SF, O’Connor GT, Ervin A, Iber C. Predictors of heartburn during sleep in a large prospective cohort study. Chest. 2005;127:1658-1666.
21. Fisher BL, Pennathur A, Mutnick JL, Little AG. Obesity correlates with gastroesophageal reflux. Dig Dis Sci. 1999;44:2290-2294.
22. Castell DO, Murray JA, Tutuian R, Orlando RC, Arnold R. Review article: the pathophysiology of gastro-oesophageal reflux disease - oesophageal manifestations. Aliment Pharmacol Ther. 2004;20(suppl 9):14-25.
23. Orr WC, Johnson LF. Responses to different levels of esophageal acidification during waking and sleeping. Dig Dis Sci. 1998;43:241-245.
24. Orr WC, Elsenbruch S, Harnish MJ, Johnson LF. Proximal migration of esophageal acid perfusions during waking and sleep. Am J Gastroenterol. 2000;95:37-42.
25. Orr WC, Heading R, Johnson LF, Kryger M. Review article: sleep and its relationship to gastro-oesophageal reflux. Aliment Pharmacol Ther. 2004;20(suppl 9):39-46.
26. Schneyer LH, Pigman WW, Hanahan LL, Gilmore R. Rate of flow of human parotid sublingual, and submaxillary secretions during sleep. J Dent Res. 1956;35:109-114.
27. Dawes C. Circadian rhythms in human salivary flow rate and composition. J Physiol. 1972;220:529-545.
28. Lear CS, Flanagan JB, Jr, Moorrees CF. The frequency of deglutition in man. Arch Oral Biol. 1965;10:83-100.
29. Orr WC, Johnson LF, Robinson MG. Effect of sleep on swallowing, esophageal peristalsis, and acid clearance. Gastroenterology. 1984;86 (pt 1):814-819.
30. Elsenbruch S, Orr WC, Harnish MJ, Chen JD. Disruption of normal gastric myoelectric functioning by sleep. Sleep. 1999;22:453-458.
1. Jones R, Galmiche JP. Review: what do we mean by GERD?—definition and diagnosis. Aliment Pharmacol Ther. 2005;22(suppl 1):2-10.
2. Frank L, Kleinman L, Ganoczy D, et al. Upper gastrointestinal symptoms in North America: prevalence and relationship to healthcare utilization and quality of life. Dig Dis Sci. 2000;45:809-818.
3. Locke GR, III, Talley NJ, Fett SL, Zinsmeister AR, Melton LJ, III. Prevalence and clinical spectrum of gastroesophageal reflux: a population-based study in Olmsted County, Minnesota. Gastroenterology. 1997;112:1448-1456.
4. Farup C, Kleinman L, Sloan S, et al. The impact of nocturnal symptoms associated with gastroesophageal reflux disease on health-related quality of life. Arch Intern Med. 2001;161:45-52.
5. Dubois RW, Fass R, Johnson LF, et al. Atypical nighttime symptoms of GERD among individuals with nighttime versus daytime GERD [abstract]. Gastroenterology. 2005;128(suppl 2):A288.-Abstract M999.
6. Orr WC, Allen ML, Robinson M. The pattern of nocturnal and diurnal esophageal acid exposure in the pathogenesis of erosive mucosal damage. Am J Gastroenterol. 1994;89:509-512.
7. Demeester TR, Johnson LF, Joseph GJ, Toscano MS, Hall AW, Skinner DB. Patterns of gastroesophageal reflux in health and disease. Ann Surg. 1976;184:459-470.
8. Cameron AJ, Lomboy CT. Barrett’s esophagus: age, prevalence, and extent of columnar epithelium. Gastroenterology. 1992;103:1241-1245.
9. Orr WC, Lackey C, Robinson MG, Johnson LF, Welsh JD. Esophageal acid clearance during sleep in patients with Barrett’s esophagus. Dig Dis Sci. 1988;33:654-659.
10. Eisen GM, Sandler RS, Murray S, Gottfried M. The relationship between gastroesophageal reflux disease and its complications with Barrett’s esophagus. Am J Gastroenterol. 1997;92:27-31.
11. Lagergren J, Bergstrom R, Lindgren A, Nyren O. Symptomatic gastroesophageal reflux as a risk factor for esophageal adenocarcinoma. N Engl J Med. 1999;340:825-831.
12. Dubois RW, Orr WC, Lange SM, et al. GERD-related sleep impairment among individuals with nighttime versus daytime GERD [abstract]. Gastroenterology. 2005;128(suppl 2):A288.-Abstract M998.
13. Dubois RW, Lange SM, Fass R, et al. Work productivity loss associated with nighttime GERD [abstract]. Gastroenterology. 2005;128(suppl 2):A286.-Abstract M988.
14. Dean BB, Crawley JA, Schmitt CM, Wong J, Ofman JJ. The burden of illness of gastro-oesophageal reflux disease: impact on work productivity. Aliment Pharmacol Ther. 2003;17:1309-1317.
15. Shaker R, Castell DO, Schoenfeld PS, Spechler SJ. Nighttime heartburn is an under-appreciated clinical problem that impacts sleep and daytime function the results of a Gallup survey conducted on behalf of the American Gastroenterological Association. Am J Gastroenterol. 2003;98:1487-1493.
16. Dubois RW, Fass R, Lange SM, et al. Impact of nighttime GERD on health-related quality of life [abstract]. Gastroenterology. 2005;128:(4 Suppl 2):A286.-Abstract M989.
17. Fass R, Achem SR, Harding S, Mittal RK, Quigley E. Review article: supra-oesophageal manifestations of gastro-oesophageal reflux disease and the role of night-time gastro-oesophageal reflux. Aliment Pharmacol Ther. 2004;20(suppl 9):26-38.
18. McGuigan JE, Belafsky PC, Fromer L, et al. Review article: diagnosis and management of night-time reflux. Aliment Pharmacol Ther. 2004;20(suppl 9):57-72.
19. Gislason T, Janson C, Vermeire P, et al. Respiratory symptoms and nocturnal gastroesophageal reflux: a population-based study of young adults in three European countries. Chest. 2002;121:158-163.
20. Fass R, Quan SF, O’Connor GT, Ervin A, Iber C. Predictors of heartburn during sleep in a large prospective cohort study. Chest. 2005;127:1658-1666.
21. Fisher BL, Pennathur A, Mutnick JL, Little AG. Obesity correlates with gastroesophageal reflux. Dig Dis Sci. 1999;44:2290-2294.
22. Castell DO, Murray JA, Tutuian R, Orlando RC, Arnold R. Review article: the pathophysiology of gastro-oesophageal reflux disease - oesophageal manifestations. Aliment Pharmacol Ther. 2004;20(suppl 9):14-25.
23. Orr WC, Johnson LF. Responses to different levels of esophageal acidification during waking and sleeping. Dig Dis Sci. 1998;43:241-245.
24. Orr WC, Elsenbruch S, Harnish MJ, Johnson LF. Proximal migration of esophageal acid perfusions during waking and sleep. Am J Gastroenterol. 2000;95:37-42.
25. Orr WC, Heading R, Johnson LF, Kryger M. Review article: sleep and its relationship to gastro-oesophageal reflux. Aliment Pharmacol Ther. 2004;20(suppl 9):39-46.
26. Schneyer LH, Pigman WW, Hanahan LL, Gilmore R. Rate of flow of human parotid sublingual, and submaxillary secretions during sleep. J Dent Res. 1956;35:109-114.
27. Dawes C. Circadian rhythms in human salivary flow rate and composition. J Physiol. 1972;220:529-545.
28. Lear CS, Flanagan JB, Jr, Moorrees CF. The frequency of deglutition in man. Arch Oral Biol. 1965;10:83-100.
29. Orr WC, Johnson LF, Robinson MG. Effect of sleep on swallowing, esophageal peristalsis, and acid clearance. Gastroenterology. 1984;86 (pt 1):814-819.
30. Elsenbruch S, Orr WC, Harnish MJ, Chen JD. Disruption of normal gastric myoelectric functioning by sleep. Sleep. 1999;22:453-458.
Acute Otitis Media: Influence of the PCV-7 vaccine on changes in the disease and its management
- Widespread use of the 7-valent pneumococcal conjugate vaccine has resulted in a shift in frequency of causative bacterial pathogens responsible for recurrent and persistent acute otitis media (AOM); disease management practice should encompass this change (SOR: B).
- High-dose amoxicillin is the first choice for antibiotic therapy in uncomplicated bacterial AOM, although β-lactamase–producing pathogens are increasingly common primary causative agents, and amoxicillin is susceptible to β-lactamase (SOR: B).
- Adding clavulanate to amoxicillin increases resistance to and improves effectiveness against β-lactamase–producing pathogens. Specific third-generation cephalosporins also should be included as antibiotic choices because of excellent activity against β-lactamase–producing pathogens and because of compliance advantages, such as better taste, less frequent dosing, and even shorter duration of therapy (SOR: B).
Since the approval of the 7-valent pneumococcal conjugate vaccine (PCV-7) for use in children younger than 24 months in February 2000, occurrences of acute otitis media (AOM) and the frequency of recurrent AOM have declined. Based on results from early clinical trials, PCV-7 may reduce total AOM by 6% to 8%, recurrent AOM by 10% to 26%, and tympanostomy tube placements by 24%.1,2
Acute otitis media occurs most frequently in children between the ages of 6 months and 18 months. By the end of their first year, approximately 86% of children will experience at least 1 episode of AOM.3
The condition remains a leading reason for visits to pediatricians and family physicians in the United States.4 It accounted for 16 million visits in 2000.4 This is a decrease from almost 25 million visits in 1995, prior to use of PCV-7. Additionally, AOM is associated with significant costs: In 1995, the direct and indirect costs of AOM were estimated to be about $3 billion.5
Changes in pathogen frequency for AOM in the ERA of PCV-7
The true impact of PCV-7 on management practice is not characterized by the modest reduction in incidence of uncomplicated AOM but in the PCV-7–associated shift in causative pathogens. Pre-PCV-7, 40% to 50% of cases of AOM in young children were caused by Streptococcus pneumoniae, 20% to 30% by Haemophilus influenzae, and 10% to 15% by Moraxella catarrhalis.6 In studies conducted prior to 2000, diagnostic tympanocentesis isolated S pneumoniae from 25% to 55% of all middle ear aspirates from children with AOM.6-8
Conversely, 1 study published in 2001 and 2 studies published in 2004 appear to document a reverse trend with the advent of the conjugate pneumococcal vaccine.9,10 Compared with children studied in an earlier era, those vaccinated with PCV-7 may be more likely to have H influenzae isolates. These studies will be described in detail below.
Bacterial AOM: initial antibiotic therapy and specific pathogens
Current guidelines recommend amoxicillin (45 mg/kg/day) or high-dose amoxicillin (80-90 mg/kg/day) as initial therapy in presumed or documented bacterial AOM.5 Although amoxicillin is effective against pneumococcus and β-lactamase–negative strains of H influenzae, it is ineffective against β-lactamase–positive strains of H influenzae.9 Significant initial failures may point to a changing pathogen per population frequency. A 2004 review assessed children with continued (persistence of infection detected within 30 days after treatment completion) or refractory (clinical failure while receiving antimicrobial therapy) AOM who have received high-dose amoxicillin as initial empiric therapy. The authors noted that the rate of infection due to H influenzae has increased from 43% among those treated prior to the licensure of PCV-7 to 57% among those who received 2 or more doses of PCV-7.10
Evidence from the medical literature
Three studies provide the major evidence concerning the pathogen shift associated with the adoption of the PCV-7 conjugate vaccine:
- The Finnish Otitis Media Vaccine Trial2
- A published collection of clinical trial results from a rural practice in Kentucky in which 94% of children were immunized with PCV-79
- A prospective study conducted in a suburban community-based private practice in Rochester, NY that evaluated children with persistent or nonresponsive AOM.10
The Finnish Otitis Media Vaccine Trial
In this trial, 1662 infants received either the PCV-7 vaccine or a control vaccine at ages 2, 4, 6, and 12 months and were monitored from ages 6.5 months to 24 months.2 An overall 6.9% reduction in episodes of clinical AOM were diagnosed (n=1251) in PCV-7–vaccinated children compared with the control group (n=1345). This suggested that fewer AOM cases were caused by the S pneumoniae vaccine serotypes than nonvaccine serotypes. The bacteriologic findings in the samples of middle ear fluid taken during 93% of the visits for AOM (TABLE 1) show a 34% reduction in culture-confirmed episodes in the PCV-7–vaccinated group, a decrease of more than 50% in pneumococcal AOM episodes caused by vaccine or vaccine cross-reactive serotypes, a 33% increase in infections caused by other pneumococcal serotypes, and an 11% increase in the proportion of AOM cases due to H influenzae.2
TABLE 1
Finnish Otitis Media Vaccine Trial: Causes of AOM Episodes and Impact of PCV-7 Immunization on Incidence
| CAUSE | PCV-7 EPISODES | CONTROL EPISODES | DIFFERENCE (%) |
|---|---|---|---|
| Culture-confirmed pneumococcus | 271 | 414 | 34 |
| Pneumococcal serotype in vaccine | 107 | 250 | 57 |
| Vaccine cross-reactive serotypes* | 41 | 84 | 51 |
| Other pneumococcal serotypes | 125 | 95 | 33 |
| Haemophilus influenzae | 315 | 287 | 11 |
| Moraxella catarrhalis | 379 | 381 | 1 |
| *6A, 9N, 18B, 19A, 23A. | |||
| AOM, acute otitis media; PCV-7, 7-valent pneumococcal conjugate vaccine. | |||
| Adapted with permission from Eskola J, et al. N Engl J Med. 2001;344:403-409. Copyright 2001 Massachusetts Medical Society. All rights reserved. | |||
Study Results From a Rural Kentucky Practice
In this practice, data on isolates from middle ear fluid were collected in children with severe or refractory AOM aged 7 to 24 months.9 Data were obtained from 1992 to 1998, before the introduction of PCV-7, and from 2000 to 2003, following immunization with 3 or 4 doses of PCV-7 during the first 18 months of life.
As shown in TABLE 2, the pre-PCV-7 group of children (N=336; 1992-1998) had a proportion of 48% culture-confirmed pneumococcus vs a proportion of 31% in the PCV-7-vaccinated group (N=83; 2000-2003), a 17% decrease. The decrease in proportion of AOM episodes resulting from vaccine serotypes was 34%.
In this investigation, 28% of the pre-PCV-7 group and 34% of the post-PCV-7 group had received antibiotic therapy within the previous 3 days. Additionally, 59% and 76%, respectively, had received antibiotic therapy within the preceding 30 days. There were increases of 30% in vaccine cross-reactive serotypes and 45% in nonvaccine serotypes. Vaccine cross-reactive serotypes 6A and 19A accounted for most of the penicillin-nonsusceptible S pneumoniae strains in the vaccinated population.
Most impressive, however, in the post-PCV-7 group, was that gram-negative bacteria, mainly H influenzae, accounted for two thirds of AOM isolates, an increase from 41% in the pre-PCV-7 group to 56% in the vaccinated group. A 56% increase was noted in β-lactamase–positive organisms from the pre-PCV-7 group to the post-PCV-7 group. The combined H influenzae and M catarrhalis β-lactamase–producing organisms accounted for nearly half of all isolates.9
TABLE 2
Results From a Rural Kentucky Practice: Change in AOM Microbiology From Pre-PCV-7 (1992–1998) to Post-PCV-7 (2000–2003)
| PATHOGEN | PRE-PCV-7 1992-1998 (N=336) | POST-PCV-7 2000-2003 (N=83) | CHANGE (%) | P VALUE | ||
|---|---|---|---|---|---|---|
| n | % | n | % | |||
| Culture-confirmed pneumococcus | 160 | 48 | 26 | 31 | 17 | .007 |
| Pneumococcal serotype in vaccine | 236 | 70 | 30 | 36 | 34 | .003 |
| Vaccine cross-reactive serotypes* | 27 | 8 | 27 | 32 | 24 | .003 |
| Other pneumococcal serotypes† | 74 | 22 | 27 | 32 | 10 | NS |
| Haemophilus influenzae | 137 | 41 | 46 | 32 | 15 | .01 |
| β-lactamase-positive | 108 | 23 | 39 | 36 | 15 | .007 |
| Moraxella catarrhalis, β-lactamase-positive | 31 | 9 | 9 | 11 | 2 | NS |
| AOM, acute otitis media; n, total isolates; NS, nonsignificant; PCV-7, 7-valent pneumococcal conjugate vaccine. | ||||||
| *Includes 6A and 19A. | ||||||
| †Nonvaccine serotypes in post-PCV-7 group: 1, 11A, 15A, 29, and 33F. | ||||||
| Adapted with permission from Block SL, et al. Pediatr Infect Dis J. 2004;23:829-833. | ||||||
The Prospective Rochester, New York Study
Changes in pre- and post-PVC-7 patterns also were seen in a prospective study of 551 children with persistent or nonresponsive AOM (defined as nonresponders after 1 or 2 empiric antibiotic courses or failures after 48 hours of treatment). These children underwent tympanocentesis to identify bacterial isolates during the 9-year period from 1995 to 2003.10
From 1995 to 1997, enrollees received a standard dose of amoxicillin (40-50 mg/kg, divided into 3 doses daily) as initial empiric treatment. From 1998 to 2000 and 2001 to 2003, all children received high-dose amoxicillin (80-100 mg/kg, divided into twice-daily doses).
During the latter period, the children also were vaccinated with PCV-7, with 63% receiving the primary series of 3 doses and 10% receiving the booster dose. In this investigation, shortages in vaccine supply, discussed below, caused vaccination schedules to be compromised.
Study results (TABLE 3) show that in the post-PCV-7 group, there was a 13% decrease in the proportion of S pneumoniae isolates and a 14% increase in the proportion of H influenzae isolates compared with the pre-PCV-7 group (1998-2000 enrollees). An increase of 22% for β-lactamase–positive bacteria was also observed, along with a trend toward an increased proportion of penicillin-susceptible S pneumoniae isolates (58% vs 72%; P=.017) post-PCV-7.10 A 24% reduction (P=.009) in the frequency of the diagnosis of persistent or AOM treatment failure occurred in the period after PCV-7 vaccination. These changes were considered to be the result of the use of the conjugate pneumococcal vaccine rather than of the change in amoxicillin dosing.10
TABLE 3
The Prospective Rochester, New York Study: Pathogens Isolated in Persistent AOM and AOM Treatment Failure Pre- and Post-PCV-7
| PATHOGEN | PRE-PCV-7 1998-2000 (N=204) | POST-PCV-7 2000-2003 (N=152) | CHANGE (%) | P VALUE | ||
|---|---|---|---|---|---|---|
| n | % | n | % | |||
| Streptococcus pneumoniae* | 50 | 44 | 28 | 31 | 13 | .017 |
| Penicillin nonsusceptible | 12 | 24 | 4 | 14 | 10 | NS |
| Haemophilus influenzae | 49 | 43 | 51 | 57 | 14 | .012 |
| β-lactamase-positive | 16 | 33 | 28 | 55 | 22 | .044 |
| Moraxella catarrhalis | 6 | 5 | 1 | 1 | 4 | NS |
| AOM, acute otitis media; N, total isolates; NS, nonsignificant; PCV-7, 7-valent pneumococcal conjugate vaccine. | ||||||
| *Pneumococcal serotyping was not done. | ||||||
| Adapted with permission from Casey JR, Pichichero ME. Pediatr Infect Dis J. 2004;23:824-828. | ||||||
Pneumococcal serotype shifts
In addition to the change in causative pathogens, use of the conjugate pneumococcal vaccine appears to have led to a significant shift in the pneumococcal strains causing AOM. Studies at urban medical centers and in the Kentucky practice documented an increase in the proportion of nonvaccine serotypes, accounting for 32% to 38% of pneumococcal AOM.10-12 A 33% increase was seen in the Finnish Trial.2 These nonvaccine pneumococcal serotypes do not carry the same level of resistance seen with those serotypes included in PCV-7.
PCV-7 conjugate vaccine
The PCV-7 conjugate vaccine was approved for use in February 2000. It is a 7-valent pneumococcal conjugate of the capsular antigens of the S pneumoniae serotypes 4, 6B, 9V, 14, 18C, 19F, and 23F, individually conjugated to diphtheria CRM197 protein.13 These serotypes have been responsible for approximately 80% of invasive pneumococcal disease in children younger than 6 years in the United States.13,14 They also accounted for 74% of penicillin-susceptible S pneumoniae and 100% of pneumococci with high-level penicillin resistance isolated from children younger than age 6 years with invasive disease during a 1993-1994 surveillance by the Centers for Disease Control and Prevention (CDC).13
Mechanism of Action and Recommended Immunization Schedule
The conjugate vaccine is converted to a T-cell–dependent antigen, antibody formation is enhanced, and memory B cells are primed.14
The recommended immunization schedule was established as 3 primary doses at ages 2, 4, and 6 months and a booster dose at 12 to 15 months.1 It is the first multivalent pneumococcal vaccine approved for use in children younger than 24 months.
An 89% reduction in invasive pneumococcal disease was observed in children receiving 1 or more doses, and the vaccine appears to reduce nasopharyngeal carriage of vaccine serotypes.15,16
The older 23-valent polysaccharide vaccine does not stimulate good response in children younger than 2 years of age14 and does not reduce mucosal carriage or limit the spread of resistant strains.15
PCV-7 Supply Since 2000
In August 2001, a serious shortage of the vaccine developed in 34 state immunization programs.17 The following month, the CDC advised physicians to administer it only to children younger than 12 months and to those aged 1 to 5 years at increased risk of pneumococcal disease.18 As demand continued despite the change in recommendations, the CDC further changed recommendations to conserve vaccine supply, first suspending the fourth dose temporarily in healthy children19 and then discontinuing both the third and fourth doses.11 In July 2004, production problems seemed to have resolved; the CDC recommended that every child receive 3 doses. In September, supplies were adequate for return to the 4-dose schedule.12 As of June 2004, 67.7% of children aged 24 months had received 3 or more doses of PCV-7.20 Thus, the effects of PCV-7 on the changing microbiology of AOM may only now, at the end of 2005, be fully realized.
Herd Immunity and Reduction in Carriage
Despite the shortages of vaccine during the first years of use, evidence of herd immunity and a decrease in antibiotic resistance in pneumococcal pathogens has been reported throughout the United States.21,22 A 29% decrease in the rate of pneumococcal disease in both young children and adults has also been observed, along with a 35% reduction in the rate of disease caused by nonpenicillin-susceptible pneumococcal strains.21 The reduction in carriage among vaccinated children may be the reason.21,22 Because of the impact of PCV-7, it will be important to record immunization history when collecting AOM data.
AOM treatment choices
The basis of recommendations for treating AOM depends on the presumed responsible pathogens, their susceptibility to antibiotics, and concerns for developing resistance, all influenced by clinical trial data. In practice, however, empiric choices are often made based on knowledge of local resistance patterns and of other patient characteristics; that is cost concerns, adverse event profiles, need to avoid initial treatment failure, adherence issues (eg, taste or palatability), convenience, and duration of dosing regimen.
All current guidelines recommend oral amoxicillin as first-line therapy in documented or presumed bacterial AOM. The 2004 American Academy of Pediatrics/American Academy of Family Physicians’ (AAP/AAFP) guidelines4 recommended increasing the dosage used for empiric treatment from 40 to 45 mg/kg/day to 80 to 90 mg/kg/day for all children. This was a result of concerns about the prevalence of penicillin-resistant S pneumoniae for which standard-dose amoxicillin is inadequate.23
The guidelines were written and published before the data from the Kentucky and New York studies were available; therefore, although the guidelines recommended that empiric treatment of bacterial AOM should target S pneumoniae, H influenzae, and M catarrhalis, the pathogen shift discussed previously might today produce a modified antibiotic selection paradigm. The pathogen mix in persistent or recurrent AOM has already led to a guideline recommendation for high-dose amoxicillin/clavulanate, 90/6.4 mg/kg/day, cefdinir, cefprozil, cefpodoxime, cefuroxime, or ceftriaxone in these patients.23
If an increase in the proportion of β-lactamase–producing pathogens due to PCV-7 occurs, amoxicillin may no longer be the best first choice.
Selecting Among Recommended Antibiotic Choices
As antibiotic preparations for treating bacterial AOM are oral suspensions, taste is a major factor for pediatric patients. TABLE 4 summarizes comparative taste ratings for antibiotic suspensions based on several studies and shows the range, from those that can enhance compliance to those that discourage compliance.23
Adverse events, especially diarrhea, nausea/vomiting, and gastritis, are also of concern. These are shortcomings of amoxicillin/clavulanate, which has a higher incidence of diarrhea and nausea than cephalosporins.24
Dosing frequency is also a factor among recommended agents. Amoxicillin, amoxicillin/clavulanate, cefprozil, and cefpodoxime require twice-daily dosing. Cefdinir can be effective at once-daily dosing.24
Duration of approved therapy is perhaps the most critical selection factor given the reality of patient behaviors. Cefpodoxime and cefdinir are the only 2 FDA-approved agents for 5-day treatment of bacterial AOM that are also guideline-recommended.
TABLE 4
Compliance-Enhancing Ranking of Antibiotic Suspensions
| STRONGLY COMPLIANCE-ENHANCING | |
|
|
| MODERATELY COMPLIANCE-ENHANCING | |
|
|
| EQUIVOCAL COMPLIANCE-ENHANCING | |
| |
| NOT COMPLIANCE-ENHANCING | |
| |
| DISCOURAGES COMPLIANCE | |
|
|
| TMP-SMX, trimethoprim sulfamethoxazole | |
| Sources: Adapted from Steele RW, et al. Pediatr Infect Dis J. 2001;20:1-5. | |
| Demers DM, et al. Pediatr Infect Dis J. 1994;13:87-89. | |
| Ruff ME, et al. Pediatr Infect Dis J. 1991;10:30-33. | |
Choices for Effective Initial Therapy
Considering the changing microbial population in bacterial AOM and the increasing concern of effectiveness of amoxicillin and other antibiotics against β-lactamase–producing H influenzae, the choice of therapy may need modification. Specifically, that may mean changing the choice of effective antibiotic, taking into consideration the compliance-enhancing advantages of available options.
Based on efficacy, the overall prevalence of antibiotic-resistant AOM pathogens for PCV-7-vaccinated children, the potential for adverse effects, and patient compliance issues, Block and Harrison developed an algorithm (FIGURE) for the management of AOM diagnosed by strict criteria in an otherwise healthy child between 4 months and 36 months old.24 As the environment of AOM evolves, the choices for treatment must be not only effective but also the best and most appropriate.
FIGURE Antibiotic Choices for Acute Otitis Media in the 2000s
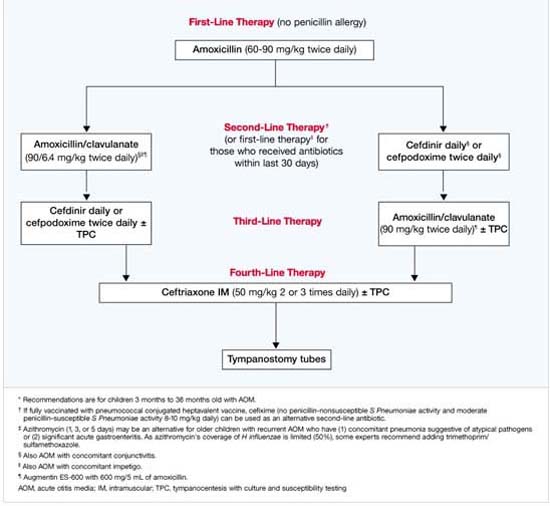
1. Fireman B, Black SB, Shinefield HR, et al. Impact of the pneumococcal conjugate vaccine on otitis media. Pediatr Infect Dis J. 2003;22:10-16.
2. Eskola J, Kilpi T, Palmu A, et al. Efficacy of a pneumococcal conjugate vaccine against acute otitis media. N Engl J Med. 2001;344:403-409.
3. Block SL, Harrison CH, Hedrick J, et al. Restricted use of antibiotic prophylaxis for recurrent acute otitis media in the era of penicillin non-susceptible Streptococcus pneumoniae. Int J Pediatr Otorhinolaryngol. 2001;61:47-60.
4. Advisory Committee on Immunization Practices. Preventing pneumococcal disease among infants and young children: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2000;49(RR-9):1-35.
5. American Academy of Family Physicians Subcommittee on Management of Acute Otitis Media. Diagnosis and management of acute otitis media. Pediatrics. 2004;113:1451-1465.
6. Dowell SF, Butler JC, Giebink GS, et al. Acute otitis media: management and surveillance in an era of pneumococcal resistance—a report from the Drug-resistant Streptococcus pneumoniae Therapeutic Working Group. Pediatr Infect Dis J. 1999;18:1-9.
7. Block SL. Causative pathogens, antibiotic resistance and therapeutic considerations in acute otitis media. Pediatr Infect Dis J. 1997;16:449-456.
8. Bluestone CD, Stephenson JS, Martin LM. Ten-year review of otitis media pathogens. Pediatr Infect Dis J. 1992;11(suppl 8):S7-S11.
9. Block SL, Hedrick J, Harrison CJ, et al. Community-wide vaccination with the heptavalent pneumococcal conjugate significantly alters the microbiology of acute otitis media. Pediatr Infect Dis J. 2004;23:829-833.
10. Casey JR, Pichichero ME. Changes in frequency and pathogens causing acute otitis media in 1995-2003. Pediatr Infect Dis J. 2004;23:824-828.
11. Centers for Disease Control and Prevention. Updated recommendations on the use of pneumococcal conjugate vaccine: suspension of recommendation for third and fourth dose. MMWR Morb Mortal Wkly Rep. 2004;53:177-178.
12. Centers for Disease Control and Prevention. Pneumococcal conjugate vaccine shortage resolved. MMWR Morb Mortal Wkly Rep. 2004;53:851-852.
13. Prevnar® (pneumococcal 7-valent vaccine) [prescribing information]. Philadelphia, Pa: Wyeth Pharmaceuticals. Rev. 01/04.
14. Watson W. Pneumococcal conjugate vaccines. Pediatr Infect Dis J. 2000;19:331-332.
15. Giebink GS. The prevention of pneumococcal disease in children. N Engl J Med. 2001;345:1177-1183.
16. Pelton SI, Loughlin AM, Marchand CD. Seven valent pneumococcal conjugate vaccine immunization in two Boston communities: changes in serotypes and antimicrobial susceptibility among Streptococcus pneumoniae isolates. Pediatr Infect Dis J. 2003;23:1015-1022.
17. Freed GL, Davis MM, Clark SJ. Variation in public and private supply of pneumococcal conjugate vaccine during a shortage. JAMA. 2003;289:575-578.
18. Centers for Disease Control and Prevention. Decreased availability of pneumococcal conjugate vaccine. MMWR Morb Mortal Wkly Rep. 2001;50:783-784.
19. Centers for Disease Control and Prevention. Limited supply of pneumococcal conjugate vaccine: suspension of recommendation for fourth dose. MMWR Morb Mortal Wkly Rep. 2004;53:108-109.
20. CDC National Immunization Survey. Estimated vaccination coverage with individual vaccines and selected vaccination series by 24 months of age by state and immunization action plan area US, Q3/2003-Q4/2004. Available at: http://www2a.cdc.gov/nip/coverage/nis/nis_iap.asp?fmt=v&rpt=tab09_24mo_iap_0304&qtr=Q3/2003-Q2/2004. Accessed September 20, 2005.
21. Whitney CG, Farley MM, Hadler J, et al. Decline in invasive pneumococcal disease after the introduction of protein-polysaccharide conjugate vaccine. N Engl J Med. 2003;348:1737-1746.
22. Black S, Shinefield H, Baxter R, et al. Postlicensure surveillance for pneumococcal invasive disease after use of heptavalent pneumococcal vaccine in Northern California Kaiser Permanente. Pediatr Infect Dis J. 2004;23:485-489.
23. Pichichero ME, Casey JR. Acute otitis media: Making sense of recent guidelines on antimicrobial treatment. J Fam Pract. 2005;54:313-332.
24. Block SL, Harrison CJ. Diagnosis and Management of Acute Otitis Media, 3rd ed. In press.
- Widespread use of the 7-valent pneumococcal conjugate vaccine has resulted in a shift in frequency of causative bacterial pathogens responsible for recurrent and persistent acute otitis media (AOM); disease management practice should encompass this change (SOR: B).
- High-dose amoxicillin is the first choice for antibiotic therapy in uncomplicated bacterial AOM, although β-lactamase–producing pathogens are increasingly common primary causative agents, and amoxicillin is susceptible to β-lactamase (SOR: B).
- Adding clavulanate to amoxicillin increases resistance to and improves effectiveness against β-lactamase–producing pathogens. Specific third-generation cephalosporins also should be included as antibiotic choices because of excellent activity against β-lactamase–producing pathogens and because of compliance advantages, such as better taste, less frequent dosing, and even shorter duration of therapy (SOR: B).
Since the approval of the 7-valent pneumococcal conjugate vaccine (PCV-7) for use in children younger than 24 months in February 2000, occurrences of acute otitis media (AOM) and the frequency of recurrent AOM have declined. Based on results from early clinical trials, PCV-7 may reduce total AOM by 6% to 8%, recurrent AOM by 10% to 26%, and tympanostomy tube placements by 24%.1,2
Acute otitis media occurs most frequently in children between the ages of 6 months and 18 months. By the end of their first year, approximately 86% of children will experience at least 1 episode of AOM.3
The condition remains a leading reason for visits to pediatricians and family physicians in the United States.4 It accounted for 16 million visits in 2000.4 This is a decrease from almost 25 million visits in 1995, prior to use of PCV-7. Additionally, AOM is associated with significant costs: In 1995, the direct and indirect costs of AOM were estimated to be about $3 billion.5
Changes in pathogen frequency for AOM in the ERA of PCV-7
The true impact of PCV-7 on management practice is not characterized by the modest reduction in incidence of uncomplicated AOM but in the PCV-7–associated shift in causative pathogens. Pre-PCV-7, 40% to 50% of cases of AOM in young children were caused by Streptococcus pneumoniae, 20% to 30% by Haemophilus influenzae, and 10% to 15% by Moraxella catarrhalis.6 In studies conducted prior to 2000, diagnostic tympanocentesis isolated S pneumoniae from 25% to 55% of all middle ear aspirates from children with AOM.6-8
Conversely, 1 study published in 2001 and 2 studies published in 2004 appear to document a reverse trend with the advent of the conjugate pneumococcal vaccine.9,10 Compared with children studied in an earlier era, those vaccinated with PCV-7 may be more likely to have H influenzae isolates. These studies will be described in detail below.
Bacterial AOM: initial antibiotic therapy and specific pathogens
Current guidelines recommend amoxicillin (45 mg/kg/day) or high-dose amoxicillin (80-90 mg/kg/day) as initial therapy in presumed or documented bacterial AOM.5 Although amoxicillin is effective against pneumococcus and β-lactamase–negative strains of H influenzae, it is ineffective against β-lactamase–positive strains of H influenzae.9 Significant initial failures may point to a changing pathogen per population frequency. A 2004 review assessed children with continued (persistence of infection detected within 30 days after treatment completion) or refractory (clinical failure while receiving antimicrobial therapy) AOM who have received high-dose amoxicillin as initial empiric therapy. The authors noted that the rate of infection due to H influenzae has increased from 43% among those treated prior to the licensure of PCV-7 to 57% among those who received 2 or more doses of PCV-7.10
Evidence from the medical literature
Three studies provide the major evidence concerning the pathogen shift associated with the adoption of the PCV-7 conjugate vaccine:
- The Finnish Otitis Media Vaccine Trial2
- A published collection of clinical trial results from a rural practice in Kentucky in which 94% of children were immunized with PCV-79
- A prospective study conducted in a suburban community-based private practice in Rochester, NY that evaluated children with persistent or nonresponsive AOM.10
The Finnish Otitis Media Vaccine Trial
In this trial, 1662 infants received either the PCV-7 vaccine or a control vaccine at ages 2, 4, 6, and 12 months and were monitored from ages 6.5 months to 24 months.2 An overall 6.9% reduction in episodes of clinical AOM were diagnosed (n=1251) in PCV-7–vaccinated children compared with the control group (n=1345). This suggested that fewer AOM cases were caused by the S pneumoniae vaccine serotypes than nonvaccine serotypes. The bacteriologic findings in the samples of middle ear fluid taken during 93% of the visits for AOM (TABLE 1) show a 34% reduction in culture-confirmed episodes in the PCV-7–vaccinated group, a decrease of more than 50% in pneumococcal AOM episodes caused by vaccine or vaccine cross-reactive serotypes, a 33% increase in infections caused by other pneumococcal serotypes, and an 11% increase in the proportion of AOM cases due to H influenzae.2
TABLE 1
Finnish Otitis Media Vaccine Trial: Causes of AOM Episodes and Impact of PCV-7 Immunization on Incidence
| CAUSE | PCV-7 EPISODES | CONTROL EPISODES | DIFFERENCE (%) |
|---|---|---|---|
| Culture-confirmed pneumococcus | 271 | 414 | 34 |
| Pneumococcal serotype in vaccine | 107 | 250 | 57 |
| Vaccine cross-reactive serotypes* | 41 | 84 | 51 |
| Other pneumococcal serotypes | 125 | 95 | 33 |
| Haemophilus influenzae | 315 | 287 | 11 |
| Moraxella catarrhalis | 379 | 381 | 1 |
| *6A, 9N, 18B, 19A, 23A. | |||
| AOM, acute otitis media; PCV-7, 7-valent pneumococcal conjugate vaccine. | |||
| Adapted with permission from Eskola J, et al. N Engl J Med. 2001;344:403-409. Copyright 2001 Massachusetts Medical Society. All rights reserved. | |||
Study Results From a Rural Kentucky Practice
In this practice, data on isolates from middle ear fluid were collected in children with severe or refractory AOM aged 7 to 24 months.9 Data were obtained from 1992 to 1998, before the introduction of PCV-7, and from 2000 to 2003, following immunization with 3 or 4 doses of PCV-7 during the first 18 months of life.
As shown in TABLE 2, the pre-PCV-7 group of children (N=336; 1992-1998) had a proportion of 48% culture-confirmed pneumococcus vs a proportion of 31% in the PCV-7-vaccinated group (N=83; 2000-2003), a 17% decrease. The decrease in proportion of AOM episodes resulting from vaccine serotypes was 34%.
In this investigation, 28% of the pre-PCV-7 group and 34% of the post-PCV-7 group had received antibiotic therapy within the previous 3 days. Additionally, 59% and 76%, respectively, had received antibiotic therapy within the preceding 30 days. There were increases of 30% in vaccine cross-reactive serotypes and 45% in nonvaccine serotypes. Vaccine cross-reactive serotypes 6A and 19A accounted for most of the penicillin-nonsusceptible S pneumoniae strains in the vaccinated population.
Most impressive, however, in the post-PCV-7 group, was that gram-negative bacteria, mainly H influenzae, accounted for two thirds of AOM isolates, an increase from 41% in the pre-PCV-7 group to 56% in the vaccinated group. A 56% increase was noted in β-lactamase–positive organisms from the pre-PCV-7 group to the post-PCV-7 group. The combined H influenzae and M catarrhalis β-lactamase–producing organisms accounted for nearly half of all isolates.9
TABLE 2
Results From a Rural Kentucky Practice: Change in AOM Microbiology From Pre-PCV-7 (1992–1998) to Post-PCV-7 (2000–2003)
| PATHOGEN | PRE-PCV-7 1992-1998 (N=336) | POST-PCV-7 2000-2003 (N=83) | CHANGE (%) | P VALUE | ||
|---|---|---|---|---|---|---|
| n | % | n | % | |||
| Culture-confirmed pneumococcus | 160 | 48 | 26 | 31 | 17 | .007 |
| Pneumococcal serotype in vaccine | 236 | 70 | 30 | 36 | 34 | .003 |
| Vaccine cross-reactive serotypes* | 27 | 8 | 27 | 32 | 24 | .003 |
| Other pneumococcal serotypes† | 74 | 22 | 27 | 32 | 10 | NS |
| Haemophilus influenzae | 137 | 41 | 46 | 32 | 15 | .01 |
| β-lactamase-positive | 108 | 23 | 39 | 36 | 15 | .007 |
| Moraxella catarrhalis, β-lactamase-positive | 31 | 9 | 9 | 11 | 2 | NS |
| AOM, acute otitis media; n, total isolates; NS, nonsignificant; PCV-7, 7-valent pneumococcal conjugate vaccine. | ||||||
| *Includes 6A and 19A. | ||||||
| †Nonvaccine serotypes in post-PCV-7 group: 1, 11A, 15A, 29, and 33F. | ||||||
| Adapted with permission from Block SL, et al. Pediatr Infect Dis J. 2004;23:829-833. | ||||||
The Prospective Rochester, New York Study
Changes in pre- and post-PVC-7 patterns also were seen in a prospective study of 551 children with persistent or nonresponsive AOM (defined as nonresponders after 1 or 2 empiric antibiotic courses or failures after 48 hours of treatment). These children underwent tympanocentesis to identify bacterial isolates during the 9-year period from 1995 to 2003.10
From 1995 to 1997, enrollees received a standard dose of amoxicillin (40-50 mg/kg, divided into 3 doses daily) as initial empiric treatment. From 1998 to 2000 and 2001 to 2003, all children received high-dose amoxicillin (80-100 mg/kg, divided into twice-daily doses).
During the latter period, the children also were vaccinated with PCV-7, with 63% receiving the primary series of 3 doses and 10% receiving the booster dose. In this investigation, shortages in vaccine supply, discussed below, caused vaccination schedules to be compromised.
Study results (TABLE 3) show that in the post-PCV-7 group, there was a 13% decrease in the proportion of S pneumoniae isolates and a 14% increase in the proportion of H influenzae isolates compared with the pre-PCV-7 group (1998-2000 enrollees). An increase of 22% for β-lactamase–positive bacteria was also observed, along with a trend toward an increased proportion of penicillin-susceptible S pneumoniae isolates (58% vs 72%; P=.017) post-PCV-7.10 A 24% reduction (P=.009) in the frequency of the diagnosis of persistent or AOM treatment failure occurred in the period after PCV-7 vaccination. These changes were considered to be the result of the use of the conjugate pneumococcal vaccine rather than of the change in amoxicillin dosing.10
TABLE 3
The Prospective Rochester, New York Study: Pathogens Isolated in Persistent AOM and AOM Treatment Failure Pre- and Post-PCV-7
| PATHOGEN | PRE-PCV-7 1998-2000 (N=204) | POST-PCV-7 2000-2003 (N=152) | CHANGE (%) | P VALUE | ||
|---|---|---|---|---|---|---|
| n | % | n | % | |||
| Streptococcus pneumoniae* | 50 | 44 | 28 | 31 | 13 | .017 |
| Penicillin nonsusceptible | 12 | 24 | 4 | 14 | 10 | NS |
| Haemophilus influenzae | 49 | 43 | 51 | 57 | 14 | .012 |
| β-lactamase-positive | 16 | 33 | 28 | 55 | 22 | .044 |
| Moraxella catarrhalis | 6 | 5 | 1 | 1 | 4 | NS |
| AOM, acute otitis media; N, total isolates; NS, nonsignificant; PCV-7, 7-valent pneumococcal conjugate vaccine. | ||||||
| *Pneumococcal serotyping was not done. | ||||||
| Adapted with permission from Casey JR, Pichichero ME. Pediatr Infect Dis J. 2004;23:824-828. | ||||||
Pneumococcal serotype shifts
In addition to the change in causative pathogens, use of the conjugate pneumococcal vaccine appears to have led to a significant shift in the pneumococcal strains causing AOM. Studies at urban medical centers and in the Kentucky practice documented an increase in the proportion of nonvaccine serotypes, accounting for 32% to 38% of pneumococcal AOM.10-12 A 33% increase was seen in the Finnish Trial.2 These nonvaccine pneumococcal serotypes do not carry the same level of resistance seen with those serotypes included in PCV-7.
PCV-7 conjugate vaccine
The PCV-7 conjugate vaccine was approved for use in February 2000. It is a 7-valent pneumococcal conjugate of the capsular antigens of the S pneumoniae serotypes 4, 6B, 9V, 14, 18C, 19F, and 23F, individually conjugated to diphtheria CRM197 protein.13 These serotypes have been responsible for approximately 80% of invasive pneumococcal disease in children younger than 6 years in the United States.13,14 They also accounted for 74% of penicillin-susceptible S pneumoniae and 100% of pneumococci with high-level penicillin resistance isolated from children younger than age 6 years with invasive disease during a 1993-1994 surveillance by the Centers for Disease Control and Prevention (CDC).13
Mechanism of Action and Recommended Immunization Schedule
The conjugate vaccine is converted to a T-cell–dependent antigen, antibody formation is enhanced, and memory B cells are primed.14
The recommended immunization schedule was established as 3 primary doses at ages 2, 4, and 6 months and a booster dose at 12 to 15 months.1 It is the first multivalent pneumococcal vaccine approved for use in children younger than 24 months.
An 89% reduction in invasive pneumococcal disease was observed in children receiving 1 or more doses, and the vaccine appears to reduce nasopharyngeal carriage of vaccine serotypes.15,16
The older 23-valent polysaccharide vaccine does not stimulate good response in children younger than 2 years of age14 and does not reduce mucosal carriage or limit the spread of resistant strains.15
PCV-7 Supply Since 2000
In August 2001, a serious shortage of the vaccine developed in 34 state immunization programs.17 The following month, the CDC advised physicians to administer it only to children younger than 12 months and to those aged 1 to 5 years at increased risk of pneumococcal disease.18 As demand continued despite the change in recommendations, the CDC further changed recommendations to conserve vaccine supply, first suspending the fourth dose temporarily in healthy children19 and then discontinuing both the third and fourth doses.11 In July 2004, production problems seemed to have resolved; the CDC recommended that every child receive 3 doses. In September, supplies were adequate for return to the 4-dose schedule.12 As of June 2004, 67.7% of children aged 24 months had received 3 or more doses of PCV-7.20 Thus, the effects of PCV-7 on the changing microbiology of AOM may only now, at the end of 2005, be fully realized.
Herd Immunity and Reduction in Carriage
Despite the shortages of vaccine during the first years of use, evidence of herd immunity and a decrease in antibiotic resistance in pneumococcal pathogens has been reported throughout the United States.21,22 A 29% decrease in the rate of pneumococcal disease in both young children and adults has also been observed, along with a 35% reduction in the rate of disease caused by nonpenicillin-susceptible pneumococcal strains.21 The reduction in carriage among vaccinated children may be the reason.21,22 Because of the impact of PCV-7, it will be important to record immunization history when collecting AOM data.
AOM treatment choices
The basis of recommendations for treating AOM depends on the presumed responsible pathogens, their susceptibility to antibiotics, and concerns for developing resistance, all influenced by clinical trial data. In practice, however, empiric choices are often made based on knowledge of local resistance patterns and of other patient characteristics; that is cost concerns, adverse event profiles, need to avoid initial treatment failure, adherence issues (eg, taste or palatability), convenience, and duration of dosing regimen.
All current guidelines recommend oral amoxicillin as first-line therapy in documented or presumed bacterial AOM. The 2004 American Academy of Pediatrics/American Academy of Family Physicians’ (AAP/AAFP) guidelines4 recommended increasing the dosage used for empiric treatment from 40 to 45 mg/kg/day to 80 to 90 mg/kg/day for all children. This was a result of concerns about the prevalence of penicillin-resistant S pneumoniae for which standard-dose amoxicillin is inadequate.23
The guidelines were written and published before the data from the Kentucky and New York studies were available; therefore, although the guidelines recommended that empiric treatment of bacterial AOM should target S pneumoniae, H influenzae, and M catarrhalis, the pathogen shift discussed previously might today produce a modified antibiotic selection paradigm. The pathogen mix in persistent or recurrent AOM has already led to a guideline recommendation for high-dose amoxicillin/clavulanate, 90/6.4 mg/kg/day, cefdinir, cefprozil, cefpodoxime, cefuroxime, or ceftriaxone in these patients.23
If an increase in the proportion of β-lactamase–producing pathogens due to PCV-7 occurs, amoxicillin may no longer be the best first choice.
Selecting Among Recommended Antibiotic Choices
As antibiotic preparations for treating bacterial AOM are oral suspensions, taste is a major factor for pediatric patients. TABLE 4 summarizes comparative taste ratings for antibiotic suspensions based on several studies and shows the range, from those that can enhance compliance to those that discourage compliance.23
Adverse events, especially diarrhea, nausea/vomiting, and gastritis, are also of concern. These are shortcomings of amoxicillin/clavulanate, which has a higher incidence of diarrhea and nausea than cephalosporins.24
Dosing frequency is also a factor among recommended agents. Amoxicillin, amoxicillin/clavulanate, cefprozil, and cefpodoxime require twice-daily dosing. Cefdinir can be effective at once-daily dosing.24
Duration of approved therapy is perhaps the most critical selection factor given the reality of patient behaviors. Cefpodoxime and cefdinir are the only 2 FDA-approved agents for 5-day treatment of bacterial AOM that are also guideline-recommended.
TABLE 4
Compliance-Enhancing Ranking of Antibiotic Suspensions
| STRONGLY COMPLIANCE-ENHANCING | |
|
|
| MODERATELY COMPLIANCE-ENHANCING | |
|
|
| EQUIVOCAL COMPLIANCE-ENHANCING | |
| |
| NOT COMPLIANCE-ENHANCING | |
| |
| DISCOURAGES COMPLIANCE | |
|
|
| TMP-SMX, trimethoprim sulfamethoxazole | |
| Sources: Adapted from Steele RW, et al. Pediatr Infect Dis J. 2001;20:1-5. | |
| Demers DM, et al. Pediatr Infect Dis J. 1994;13:87-89. | |
| Ruff ME, et al. Pediatr Infect Dis J. 1991;10:30-33. | |
Choices for Effective Initial Therapy
Considering the changing microbial population in bacterial AOM and the increasing concern of effectiveness of amoxicillin and other antibiotics against β-lactamase–producing H influenzae, the choice of therapy may need modification. Specifically, that may mean changing the choice of effective antibiotic, taking into consideration the compliance-enhancing advantages of available options.
Based on efficacy, the overall prevalence of antibiotic-resistant AOM pathogens for PCV-7-vaccinated children, the potential for adverse effects, and patient compliance issues, Block and Harrison developed an algorithm (FIGURE) for the management of AOM diagnosed by strict criteria in an otherwise healthy child between 4 months and 36 months old.24 As the environment of AOM evolves, the choices for treatment must be not only effective but also the best and most appropriate.
FIGURE Antibiotic Choices for Acute Otitis Media in the 2000s
- Widespread use of the 7-valent pneumococcal conjugate vaccine has resulted in a shift in frequency of causative bacterial pathogens responsible for recurrent and persistent acute otitis media (AOM); disease management practice should encompass this change (SOR: B).
- High-dose amoxicillin is the first choice for antibiotic therapy in uncomplicated bacterial AOM, although β-lactamase–producing pathogens are increasingly common primary causative agents, and amoxicillin is susceptible to β-lactamase (SOR: B).
- Adding clavulanate to amoxicillin increases resistance to and improves effectiveness against β-lactamase–producing pathogens. Specific third-generation cephalosporins also should be included as antibiotic choices because of excellent activity against β-lactamase–producing pathogens and because of compliance advantages, such as better taste, less frequent dosing, and even shorter duration of therapy (SOR: B).
Since the approval of the 7-valent pneumococcal conjugate vaccine (PCV-7) for use in children younger than 24 months in February 2000, occurrences of acute otitis media (AOM) and the frequency of recurrent AOM have declined. Based on results from early clinical trials, PCV-7 may reduce total AOM by 6% to 8%, recurrent AOM by 10% to 26%, and tympanostomy tube placements by 24%.1,2
Acute otitis media occurs most frequently in children between the ages of 6 months and 18 months. By the end of their first year, approximately 86% of children will experience at least 1 episode of AOM.3
The condition remains a leading reason for visits to pediatricians and family physicians in the United States.4 It accounted for 16 million visits in 2000.4 This is a decrease from almost 25 million visits in 1995, prior to use of PCV-7. Additionally, AOM is associated with significant costs: In 1995, the direct and indirect costs of AOM were estimated to be about $3 billion.5
Changes in pathogen frequency for AOM in the ERA of PCV-7
The true impact of PCV-7 on management practice is not characterized by the modest reduction in incidence of uncomplicated AOM but in the PCV-7–associated shift in causative pathogens. Pre-PCV-7, 40% to 50% of cases of AOM in young children were caused by Streptococcus pneumoniae, 20% to 30% by Haemophilus influenzae, and 10% to 15% by Moraxella catarrhalis.6 In studies conducted prior to 2000, diagnostic tympanocentesis isolated S pneumoniae from 25% to 55% of all middle ear aspirates from children with AOM.6-8
Conversely, 1 study published in 2001 and 2 studies published in 2004 appear to document a reverse trend with the advent of the conjugate pneumococcal vaccine.9,10 Compared with children studied in an earlier era, those vaccinated with PCV-7 may be more likely to have H influenzae isolates. These studies will be described in detail below.
Bacterial AOM: initial antibiotic therapy and specific pathogens
Current guidelines recommend amoxicillin (45 mg/kg/day) or high-dose amoxicillin (80-90 mg/kg/day) as initial therapy in presumed or documented bacterial AOM.5 Although amoxicillin is effective against pneumococcus and β-lactamase–negative strains of H influenzae, it is ineffective against β-lactamase–positive strains of H influenzae.9 Significant initial failures may point to a changing pathogen per population frequency. A 2004 review assessed children with continued (persistence of infection detected within 30 days after treatment completion) or refractory (clinical failure while receiving antimicrobial therapy) AOM who have received high-dose amoxicillin as initial empiric therapy. The authors noted that the rate of infection due to H influenzae has increased from 43% among those treated prior to the licensure of PCV-7 to 57% among those who received 2 or more doses of PCV-7.10
Evidence from the medical literature
Three studies provide the major evidence concerning the pathogen shift associated with the adoption of the PCV-7 conjugate vaccine:
- The Finnish Otitis Media Vaccine Trial2
- A published collection of clinical trial results from a rural practice in Kentucky in which 94% of children were immunized with PCV-79
- A prospective study conducted in a suburban community-based private practice in Rochester, NY that evaluated children with persistent or nonresponsive AOM.10
The Finnish Otitis Media Vaccine Trial
In this trial, 1662 infants received either the PCV-7 vaccine or a control vaccine at ages 2, 4, 6, and 12 months and were monitored from ages 6.5 months to 24 months.2 An overall 6.9% reduction in episodes of clinical AOM were diagnosed (n=1251) in PCV-7–vaccinated children compared with the control group (n=1345). This suggested that fewer AOM cases were caused by the S pneumoniae vaccine serotypes than nonvaccine serotypes. The bacteriologic findings in the samples of middle ear fluid taken during 93% of the visits for AOM (TABLE 1) show a 34% reduction in culture-confirmed episodes in the PCV-7–vaccinated group, a decrease of more than 50% in pneumococcal AOM episodes caused by vaccine or vaccine cross-reactive serotypes, a 33% increase in infections caused by other pneumococcal serotypes, and an 11% increase in the proportion of AOM cases due to H influenzae.2
TABLE 1
Finnish Otitis Media Vaccine Trial: Causes of AOM Episodes and Impact of PCV-7 Immunization on Incidence
| CAUSE | PCV-7 EPISODES | CONTROL EPISODES | DIFFERENCE (%) |
|---|---|---|---|
| Culture-confirmed pneumococcus | 271 | 414 | 34 |
| Pneumococcal serotype in vaccine | 107 | 250 | 57 |
| Vaccine cross-reactive serotypes* | 41 | 84 | 51 |
| Other pneumococcal serotypes | 125 | 95 | 33 |
| Haemophilus influenzae | 315 | 287 | 11 |
| Moraxella catarrhalis | 379 | 381 | 1 |
| *6A, 9N, 18B, 19A, 23A. | |||
| AOM, acute otitis media; PCV-7, 7-valent pneumococcal conjugate vaccine. | |||
| Adapted with permission from Eskola J, et al. N Engl J Med. 2001;344:403-409. Copyright 2001 Massachusetts Medical Society. All rights reserved. | |||
Study Results From a Rural Kentucky Practice
In this practice, data on isolates from middle ear fluid were collected in children with severe or refractory AOM aged 7 to 24 months.9 Data were obtained from 1992 to 1998, before the introduction of PCV-7, and from 2000 to 2003, following immunization with 3 or 4 doses of PCV-7 during the first 18 months of life.
As shown in TABLE 2, the pre-PCV-7 group of children (N=336; 1992-1998) had a proportion of 48% culture-confirmed pneumococcus vs a proportion of 31% in the PCV-7-vaccinated group (N=83; 2000-2003), a 17% decrease. The decrease in proportion of AOM episodes resulting from vaccine serotypes was 34%.
In this investigation, 28% of the pre-PCV-7 group and 34% of the post-PCV-7 group had received antibiotic therapy within the previous 3 days. Additionally, 59% and 76%, respectively, had received antibiotic therapy within the preceding 30 days. There were increases of 30% in vaccine cross-reactive serotypes and 45% in nonvaccine serotypes. Vaccine cross-reactive serotypes 6A and 19A accounted for most of the penicillin-nonsusceptible S pneumoniae strains in the vaccinated population.
Most impressive, however, in the post-PCV-7 group, was that gram-negative bacteria, mainly H influenzae, accounted for two thirds of AOM isolates, an increase from 41% in the pre-PCV-7 group to 56% in the vaccinated group. A 56% increase was noted in β-lactamase–positive organisms from the pre-PCV-7 group to the post-PCV-7 group. The combined H influenzae and M catarrhalis β-lactamase–producing organisms accounted for nearly half of all isolates.9
TABLE 2
Results From a Rural Kentucky Practice: Change in AOM Microbiology From Pre-PCV-7 (1992–1998) to Post-PCV-7 (2000–2003)
| PATHOGEN | PRE-PCV-7 1992-1998 (N=336) | POST-PCV-7 2000-2003 (N=83) | CHANGE (%) | P VALUE | ||
|---|---|---|---|---|---|---|
| n | % | n | % | |||
| Culture-confirmed pneumococcus | 160 | 48 | 26 | 31 | 17 | .007 |
| Pneumococcal serotype in vaccine | 236 | 70 | 30 | 36 | 34 | .003 |
| Vaccine cross-reactive serotypes* | 27 | 8 | 27 | 32 | 24 | .003 |
| Other pneumococcal serotypes† | 74 | 22 | 27 | 32 | 10 | NS |
| Haemophilus influenzae | 137 | 41 | 46 | 32 | 15 | .01 |
| β-lactamase-positive | 108 | 23 | 39 | 36 | 15 | .007 |
| Moraxella catarrhalis, β-lactamase-positive | 31 | 9 | 9 | 11 | 2 | NS |
| AOM, acute otitis media; n, total isolates; NS, nonsignificant; PCV-7, 7-valent pneumococcal conjugate vaccine. | ||||||
| *Includes 6A and 19A. | ||||||
| †Nonvaccine serotypes in post-PCV-7 group: 1, 11A, 15A, 29, and 33F. | ||||||
| Adapted with permission from Block SL, et al. Pediatr Infect Dis J. 2004;23:829-833. | ||||||
The Prospective Rochester, New York Study
Changes in pre- and post-PVC-7 patterns also were seen in a prospective study of 551 children with persistent or nonresponsive AOM (defined as nonresponders after 1 or 2 empiric antibiotic courses or failures after 48 hours of treatment). These children underwent tympanocentesis to identify bacterial isolates during the 9-year period from 1995 to 2003.10
From 1995 to 1997, enrollees received a standard dose of amoxicillin (40-50 mg/kg, divided into 3 doses daily) as initial empiric treatment. From 1998 to 2000 and 2001 to 2003, all children received high-dose amoxicillin (80-100 mg/kg, divided into twice-daily doses).
During the latter period, the children also were vaccinated with PCV-7, with 63% receiving the primary series of 3 doses and 10% receiving the booster dose. In this investigation, shortages in vaccine supply, discussed below, caused vaccination schedules to be compromised.
Study results (TABLE 3) show that in the post-PCV-7 group, there was a 13% decrease in the proportion of S pneumoniae isolates and a 14% increase in the proportion of H influenzae isolates compared with the pre-PCV-7 group (1998-2000 enrollees). An increase of 22% for β-lactamase–positive bacteria was also observed, along with a trend toward an increased proportion of penicillin-susceptible S pneumoniae isolates (58% vs 72%; P=.017) post-PCV-7.10 A 24% reduction (P=.009) in the frequency of the diagnosis of persistent or AOM treatment failure occurred in the period after PCV-7 vaccination. These changes were considered to be the result of the use of the conjugate pneumococcal vaccine rather than of the change in amoxicillin dosing.10
TABLE 3
The Prospective Rochester, New York Study: Pathogens Isolated in Persistent AOM and AOM Treatment Failure Pre- and Post-PCV-7
| PATHOGEN | PRE-PCV-7 1998-2000 (N=204) | POST-PCV-7 2000-2003 (N=152) | CHANGE (%) | P VALUE | ||
|---|---|---|---|---|---|---|
| n | % | n | % | |||
| Streptococcus pneumoniae* | 50 | 44 | 28 | 31 | 13 | .017 |
| Penicillin nonsusceptible | 12 | 24 | 4 | 14 | 10 | NS |
| Haemophilus influenzae | 49 | 43 | 51 | 57 | 14 | .012 |
| β-lactamase-positive | 16 | 33 | 28 | 55 | 22 | .044 |
| Moraxella catarrhalis | 6 | 5 | 1 | 1 | 4 | NS |
| AOM, acute otitis media; N, total isolates; NS, nonsignificant; PCV-7, 7-valent pneumococcal conjugate vaccine. | ||||||
| *Pneumococcal serotyping was not done. | ||||||
| Adapted with permission from Casey JR, Pichichero ME. Pediatr Infect Dis J. 2004;23:824-828. | ||||||
Pneumococcal serotype shifts
In addition to the change in causative pathogens, use of the conjugate pneumococcal vaccine appears to have led to a significant shift in the pneumococcal strains causing AOM. Studies at urban medical centers and in the Kentucky practice documented an increase in the proportion of nonvaccine serotypes, accounting for 32% to 38% of pneumococcal AOM.10-12 A 33% increase was seen in the Finnish Trial.2 These nonvaccine pneumococcal serotypes do not carry the same level of resistance seen with those serotypes included in PCV-7.
PCV-7 conjugate vaccine
The PCV-7 conjugate vaccine was approved for use in February 2000. It is a 7-valent pneumococcal conjugate of the capsular antigens of the S pneumoniae serotypes 4, 6B, 9V, 14, 18C, 19F, and 23F, individually conjugated to diphtheria CRM197 protein.13 These serotypes have been responsible for approximately 80% of invasive pneumococcal disease in children younger than 6 years in the United States.13,14 They also accounted for 74% of penicillin-susceptible S pneumoniae and 100% of pneumococci with high-level penicillin resistance isolated from children younger than age 6 years with invasive disease during a 1993-1994 surveillance by the Centers for Disease Control and Prevention (CDC).13
Mechanism of Action and Recommended Immunization Schedule
The conjugate vaccine is converted to a T-cell–dependent antigen, antibody formation is enhanced, and memory B cells are primed.14
The recommended immunization schedule was established as 3 primary doses at ages 2, 4, and 6 months and a booster dose at 12 to 15 months.1 It is the first multivalent pneumococcal vaccine approved for use in children younger than 24 months.
An 89% reduction in invasive pneumococcal disease was observed in children receiving 1 or more doses, and the vaccine appears to reduce nasopharyngeal carriage of vaccine serotypes.15,16
The older 23-valent polysaccharide vaccine does not stimulate good response in children younger than 2 years of age14 and does not reduce mucosal carriage or limit the spread of resistant strains.15
PCV-7 Supply Since 2000
In August 2001, a serious shortage of the vaccine developed in 34 state immunization programs.17 The following month, the CDC advised physicians to administer it only to children younger than 12 months and to those aged 1 to 5 years at increased risk of pneumococcal disease.18 As demand continued despite the change in recommendations, the CDC further changed recommendations to conserve vaccine supply, first suspending the fourth dose temporarily in healthy children19 and then discontinuing both the third and fourth doses.11 In July 2004, production problems seemed to have resolved; the CDC recommended that every child receive 3 doses. In September, supplies were adequate for return to the 4-dose schedule.12 As of June 2004, 67.7% of children aged 24 months had received 3 or more doses of PCV-7.20 Thus, the effects of PCV-7 on the changing microbiology of AOM may only now, at the end of 2005, be fully realized.
Herd Immunity and Reduction in Carriage
Despite the shortages of vaccine during the first years of use, evidence of herd immunity and a decrease in antibiotic resistance in pneumococcal pathogens has been reported throughout the United States.21,22 A 29% decrease in the rate of pneumococcal disease in both young children and adults has also been observed, along with a 35% reduction in the rate of disease caused by nonpenicillin-susceptible pneumococcal strains.21 The reduction in carriage among vaccinated children may be the reason.21,22 Because of the impact of PCV-7, it will be important to record immunization history when collecting AOM data.
AOM treatment choices
The basis of recommendations for treating AOM depends on the presumed responsible pathogens, their susceptibility to antibiotics, and concerns for developing resistance, all influenced by clinical trial data. In practice, however, empiric choices are often made based on knowledge of local resistance patterns and of other patient characteristics; that is cost concerns, adverse event profiles, need to avoid initial treatment failure, adherence issues (eg, taste or palatability), convenience, and duration of dosing regimen.
All current guidelines recommend oral amoxicillin as first-line therapy in documented or presumed bacterial AOM. The 2004 American Academy of Pediatrics/American Academy of Family Physicians’ (AAP/AAFP) guidelines4 recommended increasing the dosage used for empiric treatment from 40 to 45 mg/kg/day to 80 to 90 mg/kg/day for all children. This was a result of concerns about the prevalence of penicillin-resistant S pneumoniae for which standard-dose amoxicillin is inadequate.23
The guidelines were written and published before the data from the Kentucky and New York studies were available; therefore, although the guidelines recommended that empiric treatment of bacterial AOM should target S pneumoniae, H influenzae, and M catarrhalis, the pathogen shift discussed previously might today produce a modified antibiotic selection paradigm. The pathogen mix in persistent or recurrent AOM has already led to a guideline recommendation for high-dose amoxicillin/clavulanate, 90/6.4 mg/kg/day, cefdinir, cefprozil, cefpodoxime, cefuroxime, or ceftriaxone in these patients.23
If an increase in the proportion of β-lactamase–producing pathogens due to PCV-7 occurs, amoxicillin may no longer be the best first choice.
Selecting Among Recommended Antibiotic Choices
As antibiotic preparations for treating bacterial AOM are oral suspensions, taste is a major factor for pediatric patients. TABLE 4 summarizes comparative taste ratings for antibiotic suspensions based on several studies and shows the range, from those that can enhance compliance to those that discourage compliance.23
Adverse events, especially diarrhea, nausea/vomiting, and gastritis, are also of concern. These are shortcomings of amoxicillin/clavulanate, which has a higher incidence of diarrhea and nausea than cephalosporins.24
Dosing frequency is also a factor among recommended agents. Amoxicillin, amoxicillin/clavulanate, cefprozil, and cefpodoxime require twice-daily dosing. Cefdinir can be effective at once-daily dosing.24
Duration of approved therapy is perhaps the most critical selection factor given the reality of patient behaviors. Cefpodoxime and cefdinir are the only 2 FDA-approved agents for 5-day treatment of bacterial AOM that are also guideline-recommended.
TABLE 4
Compliance-Enhancing Ranking of Antibiotic Suspensions
| STRONGLY COMPLIANCE-ENHANCING | |
|
|
| MODERATELY COMPLIANCE-ENHANCING | |
|
|
| EQUIVOCAL COMPLIANCE-ENHANCING | |
| |
| NOT COMPLIANCE-ENHANCING | |
| |
| DISCOURAGES COMPLIANCE | |
|
|
| TMP-SMX, trimethoprim sulfamethoxazole | |
| Sources: Adapted from Steele RW, et al. Pediatr Infect Dis J. 2001;20:1-5. | |
| Demers DM, et al. Pediatr Infect Dis J. 1994;13:87-89. | |
| Ruff ME, et al. Pediatr Infect Dis J. 1991;10:30-33. | |
Choices for Effective Initial Therapy
Considering the changing microbial population in bacterial AOM and the increasing concern of effectiveness of amoxicillin and other antibiotics against β-lactamase–producing H influenzae, the choice of therapy may need modification. Specifically, that may mean changing the choice of effective antibiotic, taking into consideration the compliance-enhancing advantages of available options.
Based on efficacy, the overall prevalence of antibiotic-resistant AOM pathogens for PCV-7-vaccinated children, the potential for adverse effects, and patient compliance issues, Block and Harrison developed an algorithm (FIGURE) for the management of AOM diagnosed by strict criteria in an otherwise healthy child between 4 months and 36 months old.24 As the environment of AOM evolves, the choices for treatment must be not only effective but also the best and most appropriate.
FIGURE Antibiotic Choices for Acute Otitis Media in the 2000s
1. Fireman B, Black SB, Shinefield HR, et al. Impact of the pneumococcal conjugate vaccine on otitis media. Pediatr Infect Dis J. 2003;22:10-16.
2. Eskola J, Kilpi T, Palmu A, et al. Efficacy of a pneumococcal conjugate vaccine against acute otitis media. N Engl J Med. 2001;344:403-409.
3. Block SL, Harrison CH, Hedrick J, et al. Restricted use of antibiotic prophylaxis for recurrent acute otitis media in the era of penicillin non-susceptible Streptococcus pneumoniae. Int J Pediatr Otorhinolaryngol. 2001;61:47-60.
4. Advisory Committee on Immunization Practices. Preventing pneumococcal disease among infants and young children: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2000;49(RR-9):1-35.
5. American Academy of Family Physicians Subcommittee on Management of Acute Otitis Media. Diagnosis and management of acute otitis media. Pediatrics. 2004;113:1451-1465.
6. Dowell SF, Butler JC, Giebink GS, et al. Acute otitis media: management and surveillance in an era of pneumococcal resistance—a report from the Drug-resistant Streptococcus pneumoniae Therapeutic Working Group. Pediatr Infect Dis J. 1999;18:1-9.
7. Block SL. Causative pathogens, antibiotic resistance and therapeutic considerations in acute otitis media. Pediatr Infect Dis J. 1997;16:449-456.
8. Bluestone CD, Stephenson JS, Martin LM. Ten-year review of otitis media pathogens. Pediatr Infect Dis J. 1992;11(suppl 8):S7-S11.
9. Block SL, Hedrick J, Harrison CJ, et al. Community-wide vaccination with the heptavalent pneumococcal conjugate significantly alters the microbiology of acute otitis media. Pediatr Infect Dis J. 2004;23:829-833.
10. Casey JR, Pichichero ME. Changes in frequency and pathogens causing acute otitis media in 1995-2003. Pediatr Infect Dis J. 2004;23:824-828.
11. Centers for Disease Control and Prevention. Updated recommendations on the use of pneumococcal conjugate vaccine: suspension of recommendation for third and fourth dose. MMWR Morb Mortal Wkly Rep. 2004;53:177-178.
12. Centers for Disease Control and Prevention. Pneumococcal conjugate vaccine shortage resolved. MMWR Morb Mortal Wkly Rep. 2004;53:851-852.
13. Prevnar® (pneumococcal 7-valent vaccine) [prescribing information]. Philadelphia, Pa: Wyeth Pharmaceuticals. Rev. 01/04.
14. Watson W. Pneumococcal conjugate vaccines. Pediatr Infect Dis J. 2000;19:331-332.
15. Giebink GS. The prevention of pneumococcal disease in children. N Engl J Med. 2001;345:1177-1183.
16. Pelton SI, Loughlin AM, Marchand CD. Seven valent pneumococcal conjugate vaccine immunization in two Boston communities: changes in serotypes and antimicrobial susceptibility among Streptococcus pneumoniae isolates. Pediatr Infect Dis J. 2003;23:1015-1022.
17. Freed GL, Davis MM, Clark SJ. Variation in public and private supply of pneumococcal conjugate vaccine during a shortage. JAMA. 2003;289:575-578.
18. Centers for Disease Control and Prevention. Decreased availability of pneumococcal conjugate vaccine. MMWR Morb Mortal Wkly Rep. 2001;50:783-784.
19. Centers for Disease Control and Prevention. Limited supply of pneumococcal conjugate vaccine: suspension of recommendation for fourth dose. MMWR Morb Mortal Wkly Rep. 2004;53:108-109.
20. CDC National Immunization Survey. Estimated vaccination coverage with individual vaccines and selected vaccination series by 24 months of age by state and immunization action plan area US, Q3/2003-Q4/2004. Available at: http://www2a.cdc.gov/nip/coverage/nis/nis_iap.asp?fmt=v&rpt=tab09_24mo_iap_0304&qtr=Q3/2003-Q2/2004. Accessed September 20, 2005.
21. Whitney CG, Farley MM, Hadler J, et al. Decline in invasive pneumococcal disease after the introduction of protein-polysaccharide conjugate vaccine. N Engl J Med. 2003;348:1737-1746.
22. Black S, Shinefield H, Baxter R, et al. Postlicensure surveillance for pneumococcal invasive disease after use of heptavalent pneumococcal vaccine in Northern California Kaiser Permanente. Pediatr Infect Dis J. 2004;23:485-489.
23. Pichichero ME, Casey JR. Acute otitis media: Making sense of recent guidelines on antimicrobial treatment. J Fam Pract. 2005;54:313-332.
24. Block SL, Harrison CJ. Diagnosis and Management of Acute Otitis Media, 3rd ed. In press.
1. Fireman B, Black SB, Shinefield HR, et al. Impact of the pneumococcal conjugate vaccine on otitis media. Pediatr Infect Dis J. 2003;22:10-16.
2. Eskola J, Kilpi T, Palmu A, et al. Efficacy of a pneumococcal conjugate vaccine against acute otitis media. N Engl J Med. 2001;344:403-409.
3. Block SL, Harrison CH, Hedrick J, et al. Restricted use of antibiotic prophylaxis for recurrent acute otitis media in the era of penicillin non-susceptible Streptococcus pneumoniae. Int J Pediatr Otorhinolaryngol. 2001;61:47-60.
4. Advisory Committee on Immunization Practices. Preventing pneumococcal disease among infants and young children: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2000;49(RR-9):1-35.
5. American Academy of Family Physicians Subcommittee on Management of Acute Otitis Media. Diagnosis and management of acute otitis media. Pediatrics. 2004;113:1451-1465.
6. Dowell SF, Butler JC, Giebink GS, et al. Acute otitis media: management and surveillance in an era of pneumococcal resistance—a report from the Drug-resistant Streptococcus pneumoniae Therapeutic Working Group. Pediatr Infect Dis J. 1999;18:1-9.
7. Block SL. Causative pathogens, antibiotic resistance and therapeutic considerations in acute otitis media. Pediatr Infect Dis J. 1997;16:449-456.
8. Bluestone CD, Stephenson JS, Martin LM. Ten-year review of otitis media pathogens. Pediatr Infect Dis J. 1992;11(suppl 8):S7-S11.
9. Block SL, Hedrick J, Harrison CJ, et al. Community-wide vaccination with the heptavalent pneumococcal conjugate significantly alters the microbiology of acute otitis media. Pediatr Infect Dis J. 2004;23:829-833.
10. Casey JR, Pichichero ME. Changes in frequency and pathogens causing acute otitis media in 1995-2003. Pediatr Infect Dis J. 2004;23:824-828.
11. Centers for Disease Control and Prevention. Updated recommendations on the use of pneumococcal conjugate vaccine: suspension of recommendation for third and fourth dose. MMWR Morb Mortal Wkly Rep. 2004;53:177-178.
12. Centers for Disease Control and Prevention. Pneumococcal conjugate vaccine shortage resolved. MMWR Morb Mortal Wkly Rep. 2004;53:851-852.
13. Prevnar® (pneumococcal 7-valent vaccine) [prescribing information]. Philadelphia, Pa: Wyeth Pharmaceuticals. Rev. 01/04.
14. Watson W. Pneumococcal conjugate vaccines. Pediatr Infect Dis J. 2000;19:331-332.
15. Giebink GS. The prevention of pneumococcal disease in children. N Engl J Med. 2001;345:1177-1183.
16. Pelton SI, Loughlin AM, Marchand CD. Seven valent pneumococcal conjugate vaccine immunization in two Boston communities: changes in serotypes and antimicrobial susceptibility among Streptococcus pneumoniae isolates. Pediatr Infect Dis J. 2003;23:1015-1022.
17. Freed GL, Davis MM, Clark SJ. Variation in public and private supply of pneumococcal conjugate vaccine during a shortage. JAMA. 2003;289:575-578.
18. Centers for Disease Control and Prevention. Decreased availability of pneumococcal conjugate vaccine. MMWR Morb Mortal Wkly Rep. 2001;50:783-784.
19. Centers for Disease Control and Prevention. Limited supply of pneumococcal conjugate vaccine: suspension of recommendation for fourth dose. MMWR Morb Mortal Wkly Rep. 2004;53:108-109.
20. CDC National Immunization Survey. Estimated vaccination coverage with individual vaccines and selected vaccination series by 24 months of age by state and immunization action plan area US, Q3/2003-Q4/2004. Available at: http://www2a.cdc.gov/nip/coverage/nis/nis_iap.asp?fmt=v&rpt=tab09_24mo_iap_0304&qtr=Q3/2003-Q2/2004. Accessed September 20, 2005.
21. Whitney CG, Farley MM, Hadler J, et al. Decline in invasive pneumococcal disease after the introduction of protein-polysaccharide conjugate vaccine. N Engl J Med. 2003;348:1737-1746.
22. Black S, Shinefield H, Baxter R, et al. Postlicensure surveillance for pneumococcal invasive disease after use of heptavalent pneumococcal vaccine in Northern California Kaiser Permanente. Pediatr Infect Dis J. 2004;23:485-489.
23. Pichichero ME, Casey JR. Acute otitis media: Making sense of recent guidelines on antimicrobial treatment. J Fam Pract. 2005;54:313-332.
24. Block SL, Harrison CJ. Diagnosis and Management of Acute Otitis Media, 3rd ed. In press.