User login
Update On Insulin Management in Type 2 Diabetes

JOURNAL SCANSummary of Key ArticlesIdentifying Challenges With Insulin Therapy and Assessing Treatment Strategies With Pramlintide
Summary of Key Articles
Identifying Challenges With Insulin Therapy and Assessing Treatment Strategies With Pramlintide
A supplement to Clinical Endocrinology News.
This supplement was sponsored by Amylin.

• Introduction
• Should Minimal Blood Glucose Variability Become the Gold Standard of Glycemic Control?
• Contributions of Fasting and Postprandial Plasma Glucose Increments to the Overall Diurnal Hyperglycemia of Type 2 Diabetic Patients
• Addition of Biphasic, Prandial, or Basal Insulin to Oral Therapy in Type 2 Diabetes
• Effects of Intensive Glucose Lowering in Type 2 Diabetes
• Pramlintide as an Adjunct to Insulin in Patients With Type 2 Diabetes in a Clinical Practice Setting Reduced A1C, Postprandial Glucose Excursions, and Weight
• Pramlintide as an Adjunct to Insulin Therapy Improves Long-Term Glycemic and Weight Control in Patients With Type 2 Diabetes: A 1-Year Randomized Controlled Trial
• Amylin Replacement with Primlintide as an Adjunct to Insulin Therapy Improves Long-Term Glycemic and Weight Control in Type 1 Diabetes Mellitus: A 1-Year, Randomized Controlled Trial
• Important Safety Information and SYMLIN Prescribing Information
Faculty/Faculty Disclosure
Steven V. Edelman, MD
Professor of Medicine, University of California, San Diego
Veterans Affairs Medical Center, San Diego, California
Founder and Director, Taking Control of Your Diabetes, 501(3)
Del Mar, California
Associate Clinical Professor of Medicine
Dr. Edelman is a consultant to and speaker for Amylin Pharmaceuticals, Inc., Eli Lilly and Company, Novo Nordisk A/S, and sanofi-aventis U.S., LLC.
Copyright © 2009 Elsevier Inc.
A supplement to Clinical Endocrinology News.
This supplement was sponsored by Amylin.
• Introduction
• Should Minimal Blood Glucose Variability Become the Gold Standard of Glycemic Control?
• Contributions of Fasting and Postprandial Plasma Glucose Increments to the Overall Diurnal Hyperglycemia of Type 2 Diabetic Patients
• Addition of Biphasic, Prandial, or Basal Insulin to Oral Therapy in Type 2 Diabetes
• Effects of Intensive Glucose Lowering in Type 2 Diabetes
• Pramlintide as an Adjunct to Insulin in Patients With Type 2 Diabetes in a Clinical Practice Setting Reduced A1C, Postprandial Glucose Excursions, and Weight
• Pramlintide as an Adjunct to Insulin Therapy Improves Long-Term Glycemic and Weight Control in Patients With Type 2 Diabetes: A 1-Year Randomized Controlled Trial
• Amylin Replacement with Primlintide as an Adjunct to Insulin Therapy Improves Long-Term Glycemic and Weight Control in Type 1 Diabetes Mellitus: A 1-Year, Randomized Controlled Trial
• Important Safety Information and SYMLIN Prescribing Information
Faculty/Faculty Disclosure
Steven V. Edelman, MD
Professor of Medicine, University of California, San Diego
Veterans Affairs Medical Center, San Diego, California
Founder and Director, Taking Control of Your Diabetes, 501(3)
Del Mar, California
Associate Clinical Professor of Medicine
Dr. Edelman is a consultant to and speaker for Amylin Pharmaceuticals, Inc., Eli Lilly and Company, Novo Nordisk A/S, and sanofi-aventis U.S., LLC.
Copyright © 2009 Elsevier Inc.
A supplement to Clinical Endocrinology News.
This supplement was sponsored by Amylin.
• Introduction
• Should Minimal Blood Glucose Variability Become the Gold Standard of Glycemic Control?
• Contributions of Fasting and Postprandial Plasma Glucose Increments to the Overall Diurnal Hyperglycemia of Type 2 Diabetic Patients
• Addition of Biphasic, Prandial, or Basal Insulin to Oral Therapy in Type 2 Diabetes
• Effects of Intensive Glucose Lowering in Type 2 Diabetes
• Pramlintide as an Adjunct to Insulin in Patients With Type 2 Diabetes in a Clinical Practice Setting Reduced A1C, Postprandial Glucose Excursions, and Weight
• Pramlintide as an Adjunct to Insulin Therapy Improves Long-Term Glycemic and Weight Control in Patients With Type 2 Diabetes: A 1-Year Randomized Controlled Trial
• Amylin Replacement with Primlintide as an Adjunct to Insulin Therapy Improves Long-Term Glycemic and Weight Control in Type 1 Diabetes Mellitus: A 1-Year, Randomized Controlled Trial
• Important Safety Information and SYMLIN Prescribing Information
Faculty/Faculty Disclosure
Steven V. Edelman, MD
Professor of Medicine, University of California, San Diego
Veterans Affairs Medical Center, San Diego, California
Founder and Director, Taking Control of Your Diabetes, 501(3)
Del Mar, California
Associate Clinical Professor of Medicine
Dr. Edelman is a consultant to and speaker for Amylin Pharmaceuticals, Inc., Eli Lilly and Company, Novo Nordisk A/S, and sanofi-aventis U.S., LLC.
Copyright © 2009 Elsevier Inc.
Summary of Key Articles
Identifying Challenges With Insulin Therapy and Assessing Treatment Strategies With Pramlintide
Summary of Key Articles
Identifying Challenges With Insulin Therapy and Assessing Treatment Strategies With Pramlintide

Case 1: Management Decisions in an Adult Comorbid Patient With Type 2 Diabetes Having Primary HyperlipidemiaCase 2: Colesevelam Hydrochloride for Management of a Patient With Type 2 Diabetes Mellitus and Hyperlipidemia
Case 2: Colesevelam Hydrochloride for Management of a Patient With Type 2 Diabetes Mellitus and Hyperlipidemia
A Case Studies Compendium supplement to Clinical Endocrinology News. This supplement was sponsored by Daiichi Sankyo, Inc.

• Background
• Current Visit
• Laboratory Results
• Clinical Discussion
• Endocrinologist Consultation
• New Treatment Regimen With Add-On Therapy
• Conclusions
Case 2 Topics
• Background
• Current Visit: Exam Findings
• Current Treatment Regimen
• Health History
• Laboratory Results
• Clinical Discussion
• Cardiologist Visit
• Three Months After Visiting the Cardiologist
• Add-On Therapy With Welchol for Patients With T2DM and CHD
• Treatment Goals for Alice
• Conclusions
Faculty/Faculty Disclosures
Yehuda Handelsman, MD, FACP, FACE
Medical Director
Metabolic Institute of America
Chair and Program Director
7th World Congress on InsulinResistance
Chair, International Committeefor Insulin Resistance
18372 Clark Street, Suite 212
Tarzana, CA 91356
E-mail:[email protected]
Web Site:www.TheMetabolicCenter.com
Dr Handelsman is a consultant for Bristol-Myers Squibb
Company, Daiichi Sankyo, Inc., GlaxoSmithKline, Medtronic, Merck, Tethys,
and Xoma; he has received clinical research grant funding from Daiichi Sankyo, Inc., GlaxoSmithKline, Novo Nordisk, and Takeda; and he ison the speakers bureau for AstraZeneca, Bristol-Myers Squibb, Daiichi Sankyo, Inc., GlaxoSmithKline, Merck, and Novartis. He also serves on the advisory board for CLINICAL ENDOCRINOLOGY NEWS.
Peter H. Jones, MD, FACP
Co-Director, Lipid Metabolism
and Atherosclerosis Clinic
Medical Director, Weight
Management Center
The Methodist Hospital
Associate Professor of Medicine
Section of Atherosclerosis andLipid Research
Baylor College of Medicine
Houston, TX 77030
E-mail: [email protected]
Dr Jones has disclosed that he has received support in the form of consulting agreements from Abbott Laboratories, AstraZeneca Pharmaceuticals LP, Daiichi Sankyo, Inc., and Merck.
Copyright © 2010 Elsevier Inc.
A Case Studies Compendium supplement to Clinical Endocrinology News. This supplement was sponsored by Daiichi Sankyo, Inc.
• Background
• Current Visit
• Laboratory Results
• Clinical Discussion
• Endocrinologist Consultation
• New Treatment Regimen With Add-On Therapy
• Conclusions
Case 2 Topics
• Background
• Current Visit: Exam Findings
• Current Treatment Regimen
• Health History
• Laboratory Results
• Clinical Discussion
• Cardiologist Visit
• Three Months After Visiting the Cardiologist
• Add-On Therapy With Welchol for Patients With T2DM and CHD
• Treatment Goals for Alice
• Conclusions
Faculty/Faculty Disclosures
Yehuda Handelsman, MD, FACP, FACE
Medical Director
Metabolic Institute of America
Chair and Program Director
7th World Congress on InsulinResistance
Chair, International Committeefor Insulin Resistance
18372 Clark Street, Suite 212
Tarzana, CA 91356
E-mail:[email protected]
Web Site:www.TheMetabolicCenter.com
Dr Handelsman is a consultant for Bristol-Myers Squibb
Company, Daiichi Sankyo, Inc., GlaxoSmithKline, Medtronic, Merck, Tethys,
and Xoma; he has received clinical research grant funding from Daiichi Sankyo, Inc., GlaxoSmithKline, Novo Nordisk, and Takeda; and he ison the speakers bureau for AstraZeneca, Bristol-Myers Squibb, Daiichi Sankyo, Inc., GlaxoSmithKline, Merck, and Novartis. He also serves on the advisory board for CLINICAL ENDOCRINOLOGY NEWS.
Peter H. Jones, MD, FACP
Co-Director, Lipid Metabolism
and Atherosclerosis Clinic
Medical Director, Weight
Management Center
The Methodist Hospital
Associate Professor of Medicine
Section of Atherosclerosis andLipid Research
Baylor College of Medicine
Houston, TX 77030
E-mail: [email protected]
Dr Jones has disclosed that he has received support in the form of consulting agreements from Abbott Laboratories, AstraZeneca Pharmaceuticals LP, Daiichi Sankyo, Inc., and Merck.
Copyright © 2010 Elsevier Inc.
A Case Studies Compendium supplement to Clinical Endocrinology News. This supplement was sponsored by Daiichi Sankyo, Inc.
• Background
• Current Visit
• Laboratory Results
• Clinical Discussion
• Endocrinologist Consultation
• New Treatment Regimen With Add-On Therapy
• Conclusions
Case 2 Topics
• Background
• Current Visit: Exam Findings
• Current Treatment Regimen
• Health History
• Laboratory Results
• Clinical Discussion
• Cardiologist Visit
• Three Months After Visiting the Cardiologist
• Add-On Therapy With Welchol for Patients With T2DM and CHD
• Treatment Goals for Alice
• Conclusions
Faculty/Faculty Disclosures
Yehuda Handelsman, MD, FACP, FACE
Medical Director
Metabolic Institute of America
Chair and Program Director
7th World Congress on InsulinResistance
Chair, International Committeefor Insulin Resistance
18372 Clark Street, Suite 212
Tarzana, CA 91356
E-mail:[email protected]
Web Site:www.TheMetabolicCenter.com
Dr Handelsman is a consultant for Bristol-Myers Squibb
Company, Daiichi Sankyo, Inc., GlaxoSmithKline, Medtronic, Merck, Tethys,
and Xoma; he has received clinical research grant funding from Daiichi Sankyo, Inc., GlaxoSmithKline, Novo Nordisk, and Takeda; and he ison the speakers bureau for AstraZeneca, Bristol-Myers Squibb, Daiichi Sankyo, Inc., GlaxoSmithKline, Merck, and Novartis. He also serves on the advisory board for CLINICAL ENDOCRINOLOGY NEWS.
Peter H. Jones, MD, FACP
Co-Director, Lipid Metabolism
and Atherosclerosis Clinic
Medical Director, Weight
Management Center
The Methodist Hospital
Associate Professor of Medicine
Section of Atherosclerosis andLipid Research
Baylor College of Medicine
Houston, TX 77030
E-mail: [email protected]
Dr Jones has disclosed that he has received support in the form of consulting agreements from Abbott Laboratories, AstraZeneca Pharmaceuticals LP, Daiichi Sankyo, Inc., and Merck.
Copyright © 2010 Elsevier Inc.
Case 2: Colesevelam Hydrochloride for Management of a Patient With Type 2 Diabetes Mellitus and Hyperlipidemia
Case 2: Colesevelam Hydrochloride for Management of a Patient With Type 2 Diabetes Mellitus and Hyperlipidemia
An Approach to the Management of Type 2 Diabetes Mellitus in Patients Receiving Add-On Therapy With Colesevelam HCl
A Journal Scan supplement to Clinical Endocrinology News. This supplement was sponsored by Daiichi Sankyo, Inc.

• Introduction
• Results of the Glucose-Lowering Effect of WelChol Study (GLOWS): A Randomized, Double-Blind, Placebo-Controlled Pilot Study Evaluating the Effect of Colesevelam Hydrochloride on Glycemic Control in Subjects with Type 2 Diabetes
• Efficacy and Safety of Colesevelam in Patients With Type 2 Diabetes Mellitus and Inadequate Glycemic Control Receiving Insulin-Based Therapy
• Colesevelam HCl Improves Glycemic Control and Reduces LDL Cholesterol in Patients With Inadequately Controlled Type 2 Diabetes on Sulfonylurea-Based Therapy
• Colesevelam Hydrochloride Therapy in Patients With Type 2 Diabetes Mellitus Treated With Metformin: Glucose and Lipid Effects
Faculty/Faculty Disclosures
Endocrinologist:
Harold E. Bays, MD, FACP, FACE
Medical Director/President
Louisville Metabolic and
Atherosclerosis Research Center
Louisville, Kentucky
Dr Bays has research grants, consultant fees, and speaker fees with Abbott Laboratories, Aegerion Pharmaceuticals, Akros Pharma Inc, Amarin, Amgen Inc., Amylin Pharmaceuticals, Inc., Arena Pharmaceuticals, Inc., Arete Therapeutics Inc., AstraZeneca, Bristol-Myers Squibb, Boehringer Ingelheim Corporation, Cargill, Inc., Daiichi Sankyo, Inc., Eli Lilly and Company, Essentialis, Inc., GlaxoSmithKline plc, Hoffmann-La Roche Inc., Home Access Health Corporation, InteKrin Therapeutics Inc., Isis Pharmaceuticals, Inc., Johnson & Johnson Services, Inc., Merck & Co., Inc.,Merck/Schering-Plough Pharmaceuticals, Metabolex, Inc., Neuromed Pharmaceuticals Ltd., NicOx, Novo Nordisk A/S, Orexigen Therapeutics, Inc., Pfizer Inc., Purdue Pharma L.P., sanofi-aventis US LLC, Sciele Pharma, Inc., Surface Logix, Inc., Takeda Pharmaceutical Company Limited, and VIVUS Inc.
Cardiologist:
Peter H. Jones, MD
Associate Professor of Medicine
Baylor College of Medicine
Houston, Texas
Dr Jones has consulting agreements with Abbott Laboratories, AstraZeneca, Daiichi Sankyo, Inc., and Merck/Schering-Plough Pharmaceuticals.
Copyright © 2010 Elsevier Inc.
A Journal Scan supplement to Clinical Endocrinology News. This supplement was sponsored by Daiichi Sankyo, Inc.
• Introduction
• Results of the Glucose-Lowering Effect of WelChol Study (GLOWS): A Randomized, Double-Blind, Placebo-Controlled Pilot Study Evaluating the Effect of Colesevelam Hydrochloride on Glycemic Control in Subjects with Type 2 Diabetes
• Efficacy and Safety of Colesevelam in Patients With Type 2 Diabetes Mellitus and Inadequate Glycemic Control Receiving Insulin-Based Therapy
• Colesevelam HCl Improves Glycemic Control and Reduces LDL Cholesterol in Patients With Inadequately Controlled Type 2 Diabetes on Sulfonylurea-Based Therapy
• Colesevelam Hydrochloride Therapy in Patients With Type 2 Diabetes Mellitus Treated With Metformin: Glucose and Lipid Effects
Faculty/Faculty Disclosures
Endocrinologist:
Harold E. Bays, MD, FACP, FACE
Medical Director/President
Louisville Metabolic and
Atherosclerosis Research Center
Louisville, Kentucky
Dr Bays has research grants, consultant fees, and speaker fees with Abbott Laboratories, Aegerion Pharmaceuticals, Akros Pharma Inc, Amarin, Amgen Inc., Amylin Pharmaceuticals, Inc., Arena Pharmaceuticals, Inc., Arete Therapeutics Inc., AstraZeneca, Bristol-Myers Squibb, Boehringer Ingelheim Corporation, Cargill, Inc., Daiichi Sankyo, Inc., Eli Lilly and Company, Essentialis, Inc., GlaxoSmithKline plc, Hoffmann-La Roche Inc., Home Access Health Corporation, InteKrin Therapeutics Inc., Isis Pharmaceuticals, Inc., Johnson & Johnson Services, Inc., Merck & Co., Inc.,Merck/Schering-Plough Pharmaceuticals, Metabolex, Inc., Neuromed Pharmaceuticals Ltd., NicOx, Novo Nordisk A/S, Orexigen Therapeutics, Inc., Pfizer Inc., Purdue Pharma L.P., sanofi-aventis US LLC, Sciele Pharma, Inc., Surface Logix, Inc., Takeda Pharmaceutical Company Limited, and VIVUS Inc.
Cardiologist:
Peter H. Jones, MD
Associate Professor of Medicine
Baylor College of Medicine
Houston, Texas
Dr Jones has consulting agreements with Abbott Laboratories, AstraZeneca, Daiichi Sankyo, Inc., and Merck/Schering-Plough Pharmaceuticals.
Copyright © 2010 Elsevier Inc.
A Journal Scan supplement to Clinical Endocrinology News. This supplement was sponsored by Daiichi Sankyo, Inc.
• Introduction
• Results of the Glucose-Lowering Effect of WelChol Study (GLOWS): A Randomized, Double-Blind, Placebo-Controlled Pilot Study Evaluating the Effect of Colesevelam Hydrochloride on Glycemic Control in Subjects with Type 2 Diabetes
• Efficacy and Safety of Colesevelam in Patients With Type 2 Diabetes Mellitus and Inadequate Glycemic Control Receiving Insulin-Based Therapy
• Colesevelam HCl Improves Glycemic Control and Reduces LDL Cholesterol in Patients With Inadequately Controlled Type 2 Diabetes on Sulfonylurea-Based Therapy
• Colesevelam Hydrochloride Therapy in Patients With Type 2 Diabetes Mellitus Treated With Metformin: Glucose and Lipid Effects
Faculty/Faculty Disclosures
Endocrinologist:
Harold E. Bays, MD, FACP, FACE
Medical Director/President
Louisville Metabolic and
Atherosclerosis Research Center
Louisville, Kentucky
Dr Bays has research grants, consultant fees, and speaker fees with Abbott Laboratories, Aegerion Pharmaceuticals, Akros Pharma Inc, Amarin, Amgen Inc., Amylin Pharmaceuticals, Inc., Arena Pharmaceuticals, Inc., Arete Therapeutics Inc., AstraZeneca, Bristol-Myers Squibb, Boehringer Ingelheim Corporation, Cargill, Inc., Daiichi Sankyo, Inc., Eli Lilly and Company, Essentialis, Inc., GlaxoSmithKline plc, Hoffmann-La Roche Inc., Home Access Health Corporation, InteKrin Therapeutics Inc., Isis Pharmaceuticals, Inc., Johnson & Johnson Services, Inc., Merck & Co., Inc.,Merck/Schering-Plough Pharmaceuticals, Metabolex, Inc., Neuromed Pharmaceuticals Ltd., NicOx, Novo Nordisk A/S, Orexigen Therapeutics, Inc., Pfizer Inc., Purdue Pharma L.P., sanofi-aventis US LLC, Sciele Pharma, Inc., Surface Logix, Inc., Takeda Pharmaceutical Company Limited, and VIVUS Inc.
Cardiologist:
Peter H. Jones, MD
Associate Professor of Medicine
Baylor College of Medicine
Houston, Texas
Dr Jones has consulting agreements with Abbott Laboratories, AstraZeneca, Daiichi Sankyo, Inc., and Merck/Schering-Plough Pharmaceuticals.
Copyright © 2010 Elsevier Inc.
CASE STUDY: Management Decisions in a Comorbid Patient With Type 2 Diabetes Having Primary Hyperlipidemia
A supplement to Clinical Endocrinology News. This supplement was sponsored by Daiichi Sankyo, Inc.

• Background
• Current Visit
• Laboratory Results
• Clinical Discussion
• Endocrinologist Consultation
• New Treatment Regimen With Add-On Therapy
• Conclusions
Faculty
Yehuda Handelsman, MD, FACP, FACE
Medical Director, Metabolic Institute of America
Chair and Program Director, 7th World Congress on Insulin Resistance Chair, International Committee for Insulin Resistance
18372 Clark Street, Suite 212
Tarzana, CA 91356
E-mail:[email protected]
Web site:www.TheMetabolicCenter.com
Dr Handelsman is a consultant for Bristol-Myers Squibb Company, Daiichi Sankyo, Inc., GlaxoSmithKline, Medtronic, Merck, Xoma, and Tethys;he has received clinical research grant funding from Takeda, Daiichi Sankyo Inc., GlaxoSmithKline, and Novo Nordisk; and he is on the speakers bureau for AstraZeneca, Bristol-Myers Squibb, Daiichi Sankyo Inc., GlaxoSmithKline, Merck, and Novartis. He also serves on the advisory board for CLINICAL ENDOCRINOLOGY NEWS.
Copyright © 2010 Elsevier Inc.
A supplement to Clinical Endocrinology News. This supplement was sponsored by Daiichi Sankyo, Inc.
• Background
• Current Visit
• Laboratory Results
• Clinical Discussion
• Endocrinologist Consultation
• New Treatment Regimen With Add-On Therapy
• Conclusions
Faculty
Yehuda Handelsman, MD, FACP, FACE
Medical Director, Metabolic Institute of America
Chair and Program Director, 7th World Congress on Insulin Resistance Chair, International Committee for Insulin Resistance
18372 Clark Street, Suite 212
Tarzana, CA 91356
E-mail:[email protected]
Web site:www.TheMetabolicCenter.com
Dr Handelsman is a consultant for Bristol-Myers Squibb Company, Daiichi Sankyo, Inc., GlaxoSmithKline, Medtronic, Merck, Xoma, and Tethys;he has received clinical research grant funding from Takeda, Daiichi Sankyo Inc., GlaxoSmithKline, and Novo Nordisk; and he is on the speakers bureau for AstraZeneca, Bristol-Myers Squibb, Daiichi Sankyo Inc., GlaxoSmithKline, Merck, and Novartis. He also serves on the advisory board for CLINICAL ENDOCRINOLOGY NEWS.
Copyright © 2010 Elsevier Inc.
A supplement to Clinical Endocrinology News. This supplement was sponsored by Daiichi Sankyo, Inc.
• Background
• Current Visit
• Laboratory Results
• Clinical Discussion
• Endocrinologist Consultation
• New Treatment Regimen With Add-On Therapy
• Conclusions
Faculty
Yehuda Handelsman, MD, FACP, FACE
Medical Director, Metabolic Institute of America
Chair and Program Director, 7th World Congress on Insulin Resistance Chair, International Committee for Insulin Resistance
18372 Clark Street, Suite 212
Tarzana, CA 91356
E-mail:[email protected]
Web site:www.TheMetabolicCenter.com
Dr Handelsman is a consultant for Bristol-Myers Squibb Company, Daiichi Sankyo, Inc., GlaxoSmithKline, Medtronic, Merck, Xoma, and Tethys;he has received clinical research grant funding from Takeda, Daiichi Sankyo Inc., GlaxoSmithKline, and Novo Nordisk; and he is on the speakers bureau for AstraZeneca, Bristol-Myers Squibb, Daiichi Sankyo Inc., GlaxoSmithKline, Merck, and Novartis. He also serves on the advisory board for CLINICAL ENDOCRINOLOGY NEWS.
Copyright © 2010 Elsevier Inc.

Central pain states: a shift in thinking about chronic pain
What do we mean when we talk about pain? Traditionally pain is defined as an unpleasant sensory and emotional experience associated with actual or potential tissue damage.1 Pain can result when intense or noxious stimuli activate peripheral nociceptors. It serves as a warning against impending tissue damage and acts reflectively to protect against or minimize that damage.
We have known since the time of Descartes about the existence of an ascending sensory pain pathway that sends “distress” signals from the source of tissue damage to the brain. We also know of the Gate Control theory described by Melzack and Wall in 1965, in which stimulation of the skin evokes responses that transmit signal injury to transmission cells (the “gate”) in the dorsal horn of the spinal cord that continues to the brain, triggering response signals that modulate the activity of inhibitory cells (which close the “gate”), thereby decreasing the intensity of pain.2 But how do we explain pain in the absence of tissue damage, pain that is not triggered in the periphery, that often appears long after the noxious stimulus has stopped exerting its unpleasant effect?
Types of chronic pain
An estimated 116 million American adults suffer from chronic pain, defined as pain that lasts more than 3 months after onset and well into the phase of healing.1,3 According to a 2006 report from the Centers for Disease Control and Prevention with a special focus on pain, almost 57% of adults age 65 or older and 37% of younger adults ages 20–44 reported pain that lasted one year or more [Figure 1].4 Chronic pain exacts a cost of between $560 billion and $635 billion annually in medical treatment and lost productivity.5 There is a tremendous need to understand the molecular and cellular mechanisms of chronic pain in an effort to develop new, more effective treatments for these patients. This understanding may come as a result of our recent advances in visualizing the peripheral and central processes involved in pain. The emerging data suggest that for some individuals central factors play a key role in the maintenance and establishment of certain chronic pain conditions. That is, for some, the problem is really not inthe periphery.
| FIGURE 1: Pain duration by age group, 1999-2002 |
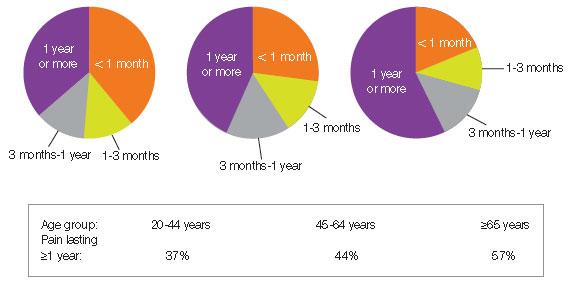
| Source: Centers for Disease Control and Prevention, National Center for Health Statistics, Health, United States, 2006. Data from theNational Health and Nutrition Examination Survey. |
Knee and hip pain. When peripheral tissue damage is unavoidable, the inflamed tissues and those nearby become hypersensitive, a protective response to guard the area during the period of healing. Conditions like chronic low-back pain and knee or hip osteoarthritis classically have been thought to be due to inflammation or damage to tissues in the back, knee, or hip. However, recent studies show that these conditions may have complex factors entailing both the peripheral and central nervous systems.
Analysis of data from the National Health and Nutrition Examination Survey (NHANES I) of patients with radiographic evidence of structural damage to the knee due to osteoarthritis found discordance between the amount of damage visible on x-ray and patients’ self-report of the degree of pain. In 319 patients with radiographic stage 2–4 knee osteoarthritis, only 47% reported knee pain, suggesting that something more than the degree of tissue injury was involved in the perception of pain.6,7 One explanation of these findings is that pain is a complex system incorporating structural changes, peripheral and central pain mechanisms, and subjective factors, including the patient’s history, psychological experience, genetics, and culture.
Diabetic neuropathy and postherpetic neuralgia. Chronic neuropathic pain results when there is actual damage to the nervous system—the peripheral nerve, dorsal root, or central nervous system. Peripheral neuropathic pain occurs after damage or alterations to sensory neurons. Some neuropathic pain disorders, such as diabetic neuropathy and postherpetic neuralgia, are well-defined disorders in which symptoms are unrelated to a stimulus and pain is related to peripheral as well as central processing.8
Stroke. Central poststroke pain, in which pain and hypersensitivity occurs in a body part due to injury to the corresponding part of the brain affected by the cerebrovascular lesion, is also considered a neuropathic pain syndrome. The onset of central poststroke pain typically occurs more than one month after the stroke, and exists with somatosensory abnormalities.9-11 For these types of neuropathies, altered function due to loss or damage of neuronal tissue is likely the cause of the pain condition.
Many of the people suffering from these central chronic pain conditions find it difficult to obtain relief, and probably will not benefit from surgeries or manipulations in the periphery. Instead, they may benefit from a targeted approach that addresses the central nervous system.
Recent studies on fibromyalgia and pain
Fibromyalgia (FM) may be considered the prototypical central pain disorder, in which the pain originates or is maintained in part in the central nervous system. Although new diagnostic criteria are being validated for this disorder, FM classically has been diagnosed by the detection of 11 of 18 tender points and the presence of chronic widespread pain for 3 months or longer.12
FM is a common disorder found to affect between 2% and 4% of the US population.13 It was one of the first disorders shown to have central factors predominant in the pathology, and as a result it has been the focus of numerous studies. Irritable bowel syndrome and chronic fatigue syndrome, often comorbid with FM, are also commonly studied. Until recently, these disorders have largely been considered “wastebasket” terms to categorize the complaints of patients with unexplained symptoms, because there were no objective signs to support their complaints. However with the advent of new imaging techniques to look into the brain and the central nervous system, researchers are finding very real physiological differences. For example, one study using sensory testing with thermal, mechanical, and electrical stimuli showed a correlation between FM patients’ subjective reports of pain and significantly altered cold and heat thresholds when compared with controls.14 Based on such studies it appears that patients with FM perceive stimuli as noxious at lower levels than healthy, pain-free controls.
Recent studies of FM have incorporated the use of functional magnetic resonance imaging (fMRI) to look at brain activations in response to painful stimuli. A study that included patients with FM and others with chronic low-back pain used fMRI to visualize the participants’ response to equal amounts of thumbnail pressure. In the FM and groups, 5 areas of neuronal activation within the cortex related to pain were detected, compared with only one activation in controls.15 Another study to evaluate the pattern of cerebral activation in FM patients found that in response to similar thumbnail pressures there were 13 regions of greater activation in the FM group compared with one region in the healthy control group.16 Additionally, mild pressure resulted in subjective pain reports and cerebral responses in the FM group that were similar to responses produced by twice the pressure applied in controls.
Another important area of research in pain processing looks at gray matter in the brain using voxel-based morphometry. A study of patients with FM found significantly less volume of gray matter and an age-associated decrease in gray matter that was 3.3 times greater than healthy controls.17
Using MRI to look at gray matter volume in patients with chronic musculoskeletal pain, significant differences in gray matter volume were found in osteoarthritis patients prior to hip arthroplasty compared with healthy controls. Specifically, areas of the thalamus, understood to play a role in central pain processing, showed decreased gray matter volume in the osteoarthritis group. Significantly, a comparison of gray matter volume 9 months after surgery showed that the levels of reduced thalamic gray matter volume in osteoarthritis patients “reversed” to levels similar to the those of the healthy control group.18
Although the mechanism that drives the loss or degradation of brain tissue in patients with chronic pain remains to be determined, one theory is that pain is associated with certain areas of the brain becoming hyperactive. Imaging studies using fMRI show that a constellation of regions typically are activated in pain processing, including the insula,
cingulate, primary somatosensory and secondary somatosensory cortices, amygdala, and thalamus [Figure 2].19 These regions have been shown to be more active in chronic pain states when patients respond to stimuli such as painful pressure or heat. Indeed, these regions have shown overamplification or augmentation of neural activity.
| FIGURE 2: Neuroanatomy of pain processing. Main brain regions that activate during a painful experience are highlighted as bilaterally active but with more dominant activation on the contralateral hemisphere (red). |
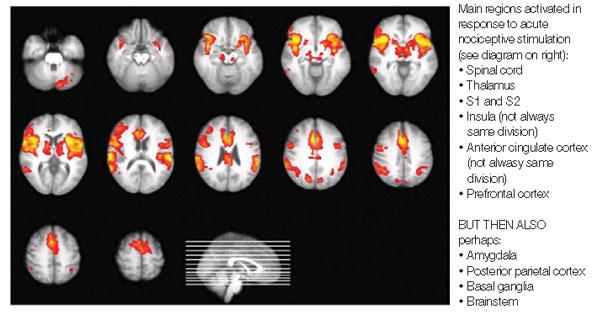
| Source: Tracey I. Br J Anaesth. 2008;101:32-39. |
Since overstimulation of nerve cells can trigger a toxic release of glutamate into surrounding tissues of the brain, this may cause nerve cells to die, ultimately reducing the amount of gray matter visualized in the brains of patients with chronic pain. In addition, some studies of FM have shown elevated levels of glutamate, an excitatory neurotransmitter that is known to cause excitotoxicity.20
Another significant consequence of long-term pain appears to be alterations in the normal connectivity of the brain, including the “default mode network” (DMN) which is noted to be important during the resting state. Recent studies of chronic pain suggest alterations in key DMN regions that may be related to the chronic pain state and existing comorbidities.21
The role of stress and depression in pain
The association among physical and psychosocial stressors, depression, and chronic pain syndromes has been the subject of numerous studies.
Posttraumatic stress disorder (PTSD) has been closely correlated with chronic pain. An example of one such stressor may be deployment to a military conflict. Soldiers and military personnel throughout history have reported a cluster of symptoms such as pain, fatigue, and cognitive impairment that are very similar to FM. From US military conflicts, these syndromes include Gulf War illness, the condition known as “shell shock” in World War I, and “soldier’s heart” during the Civil War.
A review of the literature addressing the association between chronic pain and PTSD by the Department of Veterans Affairs found such a high degree of correlation that the authors suggested clinicians who conduct diagnostic assessments for one disorder should also assess for the other.22 In a study that evaluated patients for FM, chronic fatigue, and psychiatric symptoms, patients with FM who had both tender points and diffuse pain were significantly more likely to have an increased prevalence of lifetime PTSD.23
The relationship between depression and chronic pain has been well documented. Kaiser Permanente surveyed patients seen in primary care and found that a significantly higher proportion of patients with major depressive disorder (MDD) reported chronic pain than did patients without MDD (66% vs 43%, respectively).24 These conditions share common physiologic features and a high degree of comorbidity.
A study of patients with FM and depressive symptoms or MDD looked at neural responses to painful pressure and found no association between the extent of depressive symptoms or MDD and neural activation in the primary and secondary cortices, areas associated with the sensation of pain. However, activation was seen in the amygdala and contralateral anterior insula, areas associated with affective pain processing.25
These findings were supported in a more recent study in which patients who met the criteria for FM were given a series of questionnaires to assess depressive symptoms, anxiety, and catastrophizing, and were tested for painful pressure responses using fMRI. The results established a correlation between this cluster of affective symptoms, but there was no correlation with clinical pain symptoms or responses to painful pressure.26 Rather than suggesting that there is no alignment between the mental and physical aspects of pain, results from both of these studies suggest that 2 independent pain networks exist to process the sensory and affective dimensions of pain, and that these pathways may operate simultaneously.
Pain in the clinical setting
The evidence is strong that many patients experience chronic pain that is not site-specific and arises not merely from the periphery but from intricate neural systems. With a new appreciation for the complexity of pain processing, the clinician is compelled to probe beyond, “Where does it hurt?” [Table].
| TABLE: Clinical diagnosis of central pain
|
When patients complain of widespread or chronic pain, the clinician is well advised to take the time to examine further by inquiring about depression, anxiety, fatigue, sleep disturbances, and cognitive difficulties in order to understand what is driving the patient’s symptoms.13 The results may be revealing. In a study of primary care patients, participants who complained of muscle pain, headache, and stomach pain were found to be 2.5 to 10 times more likely to screen positively for panic disorder, generalized anxiety, or MDD.27
An article in a following issue will discuss practical tools that can be used to assess comorbidities such as anxiety and depression, and interventions that might be helpful for central pain and neurorehabilitation. An approach that acknowledges the patient’s account of pain, recognizes the cluster of symptoms and conditions that can accompany pain, and utilizes a multidisciplinary approach for diagnosis and treatment will have the best chance of yielding positive outcomes.
Acknowledgement—The author wishes to thank Kristen Georgi for her assistance in the research and writing of this article.
REFERENCES
1. International Association for the Study of Pain. IASP taxonomy: pain terms. Pain. Available at: http://www.iasp-pain.org/AM/Template.cfm?Section=Pain_Defi...isplay.cfm&ContentID=1728#Pain.
2. Melzack R, Wall PD. Pain mechanisms. A new theory. Science. 1965;150:971-979.
3. Carr DB. How prevalent is chronic pain? Pain Clinical Updates. 2003;11:1-4. Available at: http://www.iasp-pain.org/AM/AMTemplate.cfm?Section=Home&CONTENTID=7594&TEMPLATE=/CM/ContentDisplay.cfm&SECTION=Home.
4. Washington, DC: US Department of Health and Human Services, Centers for Disease Control and Prevention; 2006. Bernstein AB, Makuc DM, Bilheimer LT. Health, United States, 2006. Available at: http: //www.cdc.gov/nchs/data/hus/hus06.pdf.
5. Institute of Medicine. Relieving pain in America: a blueprint for transforming prevention, care, education, and research. Washington, DC: National Academies Press; 2011.
6. Hannan MT, Felson DT, Pincus T. Analysis of the discordance between radiographic changes and knee pain in osteoarthritis of the knee. J Rheumatol. 2000;27:1513-1517.
7. Creamer P, Hochberg MC. Why does osteoarthritis of the knee hurt—sometimes? Br J Rheumatol. 1997;36:726-728.
8. Woolf CJ, Mannion RJ. Neuropathic pain: aetiology, symptoms, mechanisms, and management. Lancet. 1999;353:1959-1964.
9. Andersen G, Vestergaard K, Ingeman-Nielsen M, et al. Incidence of central post-stroke pain. Pain. 1995;61:187-193.
10. Bowsher D. Central pain: clinical and physiological characteristics. J Neurol Neurosurg Psychiatry. 1996;61:62-69.
11. Klit H, Finnerup NB, Jensen TS. Central post-stroke pain: clinical characteristics, pathophysiology, and management. Lancet. 2009;8:857-868.
12. Wolfe F, Smythe HA, Yunus MB, et al. The American College of Rheumatology 1990 criteria for the classification of fibromyalgia: report of the multicenter criteria committee. Arthritis Rheum. 1990;33:160-172.
13. Wolfe F, Ross K, Anderson J, et al. Aspects of fibromyalgia in the general population: sex, pain threshold, and fibromyalgia symptoms. J Rheumatol. 1995;22:151-156.
14. Desmeules JA, Cedraschi C, Rapiti E, et al. Neurolopshysiologic evidence for a central sensitization in patients with fibromyalgia. Arthritis Rheum. 2003;48:1420-1429.
15. Giesecke T, Gracely RH, Grant MAB, et al. Evidence of augmented central pain processing in idiopathic chronic low back pain. Arthritis Rheum. 2004;50:613-623.
16. Gracely RH, Petzke F, Wolf JM, et al. Functional magnetic resonance imaging evidence of augmented pain processing in fibromyalgia. Arthritis Rheum. 2002;46:1333-1343.
17. Kuchinad A, Schweinhardt P, Seminowicz DA, et al. Accelerated brain gray matter loss in fibromyalgia patients: premature aging of the brain? J Neurosci. 2007;27:4004-4007.
18. Gwilym SE, Fillipini N, Douaud G, et al. Thalamic atrophy associated with painful osteoarthritis of the hip is reversible after arthroplasty. Arthritis Rheum. 2010;62:2930-2940.
19. Tracey I. Imaging pain. Br J Anaesth. 2008;101:32-39.
20. Harris RE, Sundgren PC, Craig AD, et al. Elevated insular glutamate in fibromyalgia is associated with experimental pain. Arthritis Rheum. 2009;60:3146-3152.
21. Baliki MN, Geha PY, Apkarian AV, et al. Beyond feeling: chronic pain hurts the brain, disrupting the default-mode network dynamics. J Neurosci. 2008;28:
1398-1403.
22. Otis JD, Keane TM, Kerns RD. An examination of the relationship between chronic pain and posttraumatic stress disorder. J Rehabil Res Dev. 2003;40:397-406.
23. Roy-Byrne P, Smith WR, Goldberg N, et al. Posttraumatic stress disorder among patients with chronic pain and chronic fatigue. Psychol Med. 2004;34:
363-368.
24. Arnow BA, Hunkeler EM, Blasey CM, et al. Comorbid depression, chronic pain, and disability in primary care. Psychosom Med. 2006;68:262-268.
25. Giesecke T, Gracely RH, Williams DA, et al. The relationship between depression, clinical pain, and experimental pain in a chronic pain cohort. Arthritis Rheum. 2005;52:1577-1584.
26. Jensen KB, Petzke F, Carville S, et al. Anxiety and depressive symptoms in fibromyalgia are related to poor perception of health but not to pain sensitivity or cerebral processing of pain. Arthritis Rheum. 2010;62:3488-3495.
27. Means-Christensen AJ, Roy-Byrne PR, Sherbourne CD, et al. Relationships among pain, anxiety, and depression in primary care. Depress Anxiety. 2008;25:
593-600.
What do we mean when we talk about pain? Traditionally pain is defined as an unpleasant sensory and emotional experience associated with actual or potential tissue damage.1 Pain can result when intense or noxious stimuli activate peripheral nociceptors. It serves as a warning against impending tissue damage and acts reflectively to protect against or minimize that damage.
We have known since the time of Descartes about the existence of an ascending sensory pain pathway that sends “distress” signals from the source of tissue damage to the brain. We also know of the Gate Control theory described by Melzack and Wall in 1965, in which stimulation of the skin evokes responses that transmit signal injury to transmission cells (the “gate”) in the dorsal horn of the spinal cord that continues to the brain, triggering response signals that modulate the activity of inhibitory cells (which close the “gate”), thereby decreasing the intensity of pain.2 But how do we explain pain in the absence of tissue damage, pain that is not triggered in the periphery, that often appears long after the noxious stimulus has stopped exerting its unpleasant effect?
Types of chronic pain
An estimated 116 million American adults suffer from chronic pain, defined as pain that lasts more than 3 months after onset and well into the phase of healing.1,3 According to a 2006 report from the Centers for Disease Control and Prevention with a special focus on pain, almost 57% of adults age 65 or older and 37% of younger adults ages 20–44 reported pain that lasted one year or more [Figure 1].4 Chronic pain exacts a cost of between $560 billion and $635 billion annually in medical treatment and lost productivity.5 There is a tremendous need to understand the molecular and cellular mechanisms of chronic pain in an effort to develop new, more effective treatments for these patients. This understanding may come as a result of our recent advances in visualizing the peripheral and central processes involved in pain. The emerging data suggest that for some individuals central factors play a key role in the maintenance and establishment of certain chronic pain conditions. That is, for some, the problem is really not inthe periphery.
| FIGURE 1: Pain duration by age group, 1999-2002 |
| Source: Centers for Disease Control and Prevention, National Center for Health Statistics, Health, United States, 2006. Data from theNational Health and Nutrition Examination Survey. |
Knee and hip pain. When peripheral tissue damage is unavoidable, the inflamed tissues and those nearby become hypersensitive, a protective response to guard the area during the period of healing. Conditions like chronic low-back pain and knee or hip osteoarthritis classically have been thought to be due to inflammation or damage to tissues in the back, knee, or hip. However, recent studies show that these conditions may have complex factors entailing both the peripheral and central nervous systems.
Analysis of data from the National Health and Nutrition Examination Survey (NHANES I) of patients with radiographic evidence of structural damage to the knee due to osteoarthritis found discordance between the amount of damage visible on x-ray and patients’ self-report of the degree of pain. In 319 patients with radiographic stage 2–4 knee osteoarthritis, only 47% reported knee pain, suggesting that something more than the degree of tissue injury was involved in the perception of pain.6,7 One explanation of these findings is that pain is a complex system incorporating structural changes, peripheral and central pain mechanisms, and subjective factors, including the patient’s history, psychological experience, genetics, and culture.
Diabetic neuropathy and postherpetic neuralgia. Chronic neuropathic pain results when there is actual damage to the nervous system—the peripheral nerve, dorsal root, or central nervous system. Peripheral neuropathic pain occurs after damage or alterations to sensory neurons. Some neuropathic pain disorders, such as diabetic neuropathy and postherpetic neuralgia, are well-defined disorders in which symptoms are unrelated to a stimulus and pain is related to peripheral as well as central processing.8
Stroke. Central poststroke pain, in which pain and hypersensitivity occurs in a body part due to injury to the corresponding part of the brain affected by the cerebrovascular lesion, is also considered a neuropathic pain syndrome. The onset of central poststroke pain typically occurs more than one month after the stroke, and exists with somatosensory abnormalities.9-11 For these types of neuropathies, altered function due to loss or damage of neuronal tissue is likely the cause of the pain condition.
Many of the people suffering from these central chronic pain conditions find it difficult to obtain relief, and probably will not benefit from surgeries or manipulations in the periphery. Instead, they may benefit from a targeted approach that addresses the central nervous system.
Recent studies on fibromyalgia and pain
Fibromyalgia (FM) may be considered the prototypical central pain disorder, in which the pain originates or is maintained in part in the central nervous system. Although new diagnostic criteria are being validated for this disorder, FM classically has been diagnosed by the detection of 11 of 18 tender points and the presence of chronic widespread pain for 3 months or longer.12
FM is a common disorder found to affect between 2% and 4% of the US population.13 It was one of the first disorders shown to have central factors predominant in the pathology, and as a result it has been the focus of numerous studies. Irritable bowel syndrome and chronic fatigue syndrome, often comorbid with FM, are also commonly studied. Until recently, these disorders have largely been considered “wastebasket” terms to categorize the complaints of patients with unexplained symptoms, because there were no objective signs to support their complaints. However with the advent of new imaging techniques to look into the brain and the central nervous system, researchers are finding very real physiological differences. For example, one study using sensory testing with thermal, mechanical, and electrical stimuli showed a correlation between FM patients’ subjective reports of pain and significantly altered cold and heat thresholds when compared with controls.14 Based on such studies it appears that patients with FM perceive stimuli as noxious at lower levels than healthy, pain-free controls.
Recent studies of FM have incorporated the use of functional magnetic resonance imaging (fMRI) to look at brain activations in response to painful stimuli. A study that included patients with FM and others with chronic low-back pain used fMRI to visualize the participants’ response to equal amounts of thumbnail pressure. In the FM and groups, 5 areas of neuronal activation within the cortex related to pain were detected, compared with only one activation in controls.15 Another study to evaluate the pattern of cerebral activation in FM patients found that in response to similar thumbnail pressures there were 13 regions of greater activation in the FM group compared with one region in the healthy control group.16 Additionally, mild pressure resulted in subjective pain reports and cerebral responses in the FM group that were similar to responses produced by twice the pressure applied in controls.
Another important area of research in pain processing looks at gray matter in the brain using voxel-based morphometry. A study of patients with FM found significantly less volume of gray matter and an age-associated decrease in gray matter that was 3.3 times greater than healthy controls.17
Using MRI to look at gray matter volume in patients with chronic musculoskeletal pain, significant differences in gray matter volume were found in osteoarthritis patients prior to hip arthroplasty compared with healthy controls. Specifically, areas of the thalamus, understood to play a role in central pain processing, showed decreased gray matter volume in the osteoarthritis group. Significantly, a comparison of gray matter volume 9 months after surgery showed that the levels of reduced thalamic gray matter volume in osteoarthritis patients “reversed” to levels similar to the those of the healthy control group.18
Although the mechanism that drives the loss or degradation of brain tissue in patients with chronic pain remains to be determined, one theory is that pain is associated with certain areas of the brain becoming hyperactive. Imaging studies using fMRI show that a constellation of regions typically are activated in pain processing, including the insula,
cingulate, primary somatosensory and secondary somatosensory cortices, amygdala, and thalamus [Figure 2].19 These regions have been shown to be more active in chronic pain states when patients respond to stimuli such as painful pressure or heat. Indeed, these regions have shown overamplification or augmentation of neural activity.
| FIGURE 2: Neuroanatomy of pain processing. Main brain regions that activate during a painful experience are highlighted as bilaterally active but with more dominant activation on the contralateral hemisphere (red). |
| Source: Tracey I. Br J Anaesth. 2008;101:32-39. |
Since overstimulation of nerve cells can trigger a toxic release of glutamate into surrounding tissues of the brain, this may cause nerve cells to die, ultimately reducing the amount of gray matter visualized in the brains of patients with chronic pain. In addition, some studies of FM have shown elevated levels of glutamate, an excitatory neurotransmitter that is known to cause excitotoxicity.20
Another significant consequence of long-term pain appears to be alterations in the normal connectivity of the brain, including the “default mode network” (DMN) which is noted to be important during the resting state. Recent studies of chronic pain suggest alterations in key DMN regions that may be related to the chronic pain state and existing comorbidities.21
The role of stress and depression in pain
The association among physical and psychosocial stressors, depression, and chronic pain syndromes has been the subject of numerous studies.
Posttraumatic stress disorder (PTSD) has been closely correlated with chronic pain. An example of one such stressor may be deployment to a military conflict. Soldiers and military personnel throughout history have reported a cluster of symptoms such as pain, fatigue, and cognitive impairment that are very similar to FM. From US military conflicts, these syndromes include Gulf War illness, the condition known as “shell shock” in World War I, and “soldier’s heart” during the Civil War.
A review of the literature addressing the association between chronic pain and PTSD by the Department of Veterans Affairs found such a high degree of correlation that the authors suggested clinicians who conduct diagnostic assessments for one disorder should also assess for the other.22 In a study that evaluated patients for FM, chronic fatigue, and psychiatric symptoms, patients with FM who had both tender points and diffuse pain were significantly more likely to have an increased prevalence of lifetime PTSD.23
The relationship between depression and chronic pain has been well documented. Kaiser Permanente surveyed patients seen in primary care and found that a significantly higher proportion of patients with major depressive disorder (MDD) reported chronic pain than did patients without MDD (66% vs 43%, respectively).24 These conditions share common physiologic features and a high degree of comorbidity.
A study of patients with FM and depressive symptoms or MDD looked at neural responses to painful pressure and found no association between the extent of depressive symptoms or MDD and neural activation in the primary and secondary cortices, areas associated with the sensation of pain. However, activation was seen in the amygdala and contralateral anterior insula, areas associated with affective pain processing.25
These findings were supported in a more recent study in which patients who met the criteria for FM were given a series of questionnaires to assess depressive symptoms, anxiety, and catastrophizing, and were tested for painful pressure responses using fMRI. The results established a correlation between this cluster of affective symptoms, but there was no correlation with clinical pain symptoms or responses to painful pressure.26 Rather than suggesting that there is no alignment between the mental and physical aspects of pain, results from both of these studies suggest that 2 independent pain networks exist to process the sensory and affective dimensions of pain, and that these pathways may operate simultaneously.
Pain in the clinical setting
The evidence is strong that many patients experience chronic pain that is not site-specific and arises not merely from the periphery but from intricate neural systems. With a new appreciation for the complexity of pain processing, the clinician is compelled to probe beyond, “Where does it hurt?” [Table].
| TABLE: Clinical diagnosis of central pain
|
When patients complain of widespread or chronic pain, the clinician is well advised to take the time to examine further by inquiring about depression, anxiety, fatigue, sleep disturbances, and cognitive difficulties in order to understand what is driving the patient’s symptoms.13 The results may be revealing. In a study of primary care patients, participants who complained of muscle pain, headache, and stomach pain were found to be 2.5 to 10 times more likely to screen positively for panic disorder, generalized anxiety, or MDD.27
An article in a following issue will discuss practical tools that can be used to assess comorbidities such as anxiety and depression, and interventions that might be helpful for central pain and neurorehabilitation. An approach that acknowledges the patient’s account of pain, recognizes the cluster of symptoms and conditions that can accompany pain, and utilizes a multidisciplinary approach for diagnosis and treatment will have the best chance of yielding positive outcomes.
Acknowledgement—The author wishes to thank Kristen Georgi for her assistance in the research and writing of this article.
REFERENCES
1. International Association for the Study of Pain. IASP taxonomy: pain terms. Pain. Available at: http://www.iasp-pain.org/AM/Template.cfm?Section=Pain_Defi...isplay.cfm&ContentID=1728#Pain.
2. Melzack R, Wall PD. Pain mechanisms. A new theory. Science. 1965;150:971-979.
3. Carr DB. How prevalent is chronic pain? Pain Clinical Updates. 2003;11:1-4. Available at: http://www.iasp-pain.org/AM/AMTemplate.cfm?Section=Home&CONTENTID=7594&TEMPLATE=/CM/ContentDisplay.cfm&SECTION=Home.
4. Washington, DC: US Department of Health and Human Services, Centers for Disease Control and Prevention; 2006. Bernstein AB, Makuc DM, Bilheimer LT. Health, United States, 2006. Available at: http: //www.cdc.gov/nchs/data/hus/hus06.pdf.
5. Institute of Medicine. Relieving pain in America: a blueprint for transforming prevention, care, education, and research. Washington, DC: National Academies Press; 2011.
6. Hannan MT, Felson DT, Pincus T. Analysis of the discordance between radiographic changes and knee pain in osteoarthritis of the knee. J Rheumatol. 2000;27:1513-1517.
7. Creamer P, Hochberg MC. Why does osteoarthritis of the knee hurt—sometimes? Br J Rheumatol. 1997;36:726-728.
8. Woolf CJ, Mannion RJ. Neuropathic pain: aetiology, symptoms, mechanisms, and management. Lancet. 1999;353:1959-1964.
9. Andersen G, Vestergaard K, Ingeman-Nielsen M, et al. Incidence of central post-stroke pain. Pain. 1995;61:187-193.
10. Bowsher D. Central pain: clinical and physiological characteristics. J Neurol Neurosurg Psychiatry. 1996;61:62-69.
11. Klit H, Finnerup NB, Jensen TS. Central post-stroke pain: clinical characteristics, pathophysiology, and management. Lancet. 2009;8:857-868.
12. Wolfe F, Smythe HA, Yunus MB, et al. The American College of Rheumatology 1990 criteria for the classification of fibromyalgia: report of the multicenter criteria committee. Arthritis Rheum. 1990;33:160-172.
13. Wolfe F, Ross K, Anderson J, et al. Aspects of fibromyalgia in the general population: sex, pain threshold, and fibromyalgia symptoms. J Rheumatol. 1995;22:151-156.
14. Desmeules JA, Cedraschi C, Rapiti E, et al. Neurolopshysiologic evidence for a central sensitization in patients with fibromyalgia. Arthritis Rheum. 2003;48:1420-1429.
15. Giesecke T, Gracely RH, Grant MAB, et al. Evidence of augmented central pain processing in idiopathic chronic low back pain. Arthritis Rheum. 2004;50:613-623.
16. Gracely RH, Petzke F, Wolf JM, et al. Functional magnetic resonance imaging evidence of augmented pain processing in fibromyalgia. Arthritis Rheum. 2002;46:1333-1343.
17. Kuchinad A, Schweinhardt P, Seminowicz DA, et al. Accelerated brain gray matter loss in fibromyalgia patients: premature aging of the brain? J Neurosci. 2007;27:4004-4007.
18. Gwilym SE, Fillipini N, Douaud G, et al. Thalamic atrophy associated with painful osteoarthritis of the hip is reversible after arthroplasty. Arthritis Rheum. 2010;62:2930-2940.
19. Tracey I. Imaging pain. Br J Anaesth. 2008;101:32-39.
20. Harris RE, Sundgren PC, Craig AD, et al. Elevated insular glutamate in fibromyalgia is associated with experimental pain. Arthritis Rheum. 2009;60:3146-3152.
21. Baliki MN, Geha PY, Apkarian AV, et al. Beyond feeling: chronic pain hurts the brain, disrupting the default-mode network dynamics. J Neurosci. 2008;28:
1398-1403.
22. Otis JD, Keane TM, Kerns RD. An examination of the relationship between chronic pain and posttraumatic stress disorder. J Rehabil Res Dev. 2003;40:397-406.
23. Roy-Byrne P, Smith WR, Goldberg N, et al. Posttraumatic stress disorder among patients with chronic pain and chronic fatigue. Psychol Med. 2004;34:
363-368.
24. Arnow BA, Hunkeler EM, Blasey CM, et al. Comorbid depression, chronic pain, and disability in primary care. Psychosom Med. 2006;68:262-268.
25. Giesecke T, Gracely RH, Williams DA, et al. The relationship between depression, clinical pain, and experimental pain in a chronic pain cohort. Arthritis Rheum. 2005;52:1577-1584.
26. Jensen KB, Petzke F, Carville S, et al. Anxiety and depressive symptoms in fibromyalgia are related to poor perception of health but not to pain sensitivity or cerebral processing of pain. Arthritis Rheum. 2010;62:3488-3495.
27. Means-Christensen AJ, Roy-Byrne PR, Sherbourne CD, et al. Relationships among pain, anxiety, and depression in primary care. Depress Anxiety. 2008;25:
593-600.
What do we mean when we talk about pain? Traditionally pain is defined as an unpleasant sensory and emotional experience associated with actual or potential tissue damage.1 Pain can result when intense or noxious stimuli activate peripheral nociceptors. It serves as a warning against impending tissue damage and acts reflectively to protect against or minimize that damage.
We have known since the time of Descartes about the existence of an ascending sensory pain pathway that sends “distress” signals from the source of tissue damage to the brain. We also know of the Gate Control theory described by Melzack and Wall in 1965, in which stimulation of the skin evokes responses that transmit signal injury to transmission cells (the “gate”) in the dorsal horn of the spinal cord that continues to the brain, triggering response signals that modulate the activity of inhibitory cells (which close the “gate”), thereby decreasing the intensity of pain.2 But how do we explain pain in the absence of tissue damage, pain that is not triggered in the periphery, that often appears long after the noxious stimulus has stopped exerting its unpleasant effect?
Types of chronic pain
An estimated 116 million American adults suffer from chronic pain, defined as pain that lasts more than 3 months after onset and well into the phase of healing.1,3 According to a 2006 report from the Centers for Disease Control and Prevention with a special focus on pain, almost 57% of adults age 65 or older and 37% of younger adults ages 20–44 reported pain that lasted one year or more [Figure 1].4 Chronic pain exacts a cost of between $560 billion and $635 billion annually in medical treatment and lost productivity.5 There is a tremendous need to understand the molecular and cellular mechanisms of chronic pain in an effort to develop new, more effective treatments for these patients. This understanding may come as a result of our recent advances in visualizing the peripheral and central processes involved in pain. The emerging data suggest that for some individuals central factors play a key role in the maintenance and establishment of certain chronic pain conditions. That is, for some, the problem is really not inthe periphery.
| FIGURE 1: Pain duration by age group, 1999-2002 |
| Source: Centers for Disease Control and Prevention, National Center for Health Statistics, Health, United States, 2006. Data from theNational Health and Nutrition Examination Survey. |
Knee and hip pain. When peripheral tissue damage is unavoidable, the inflamed tissues and those nearby become hypersensitive, a protective response to guard the area during the period of healing. Conditions like chronic low-back pain and knee or hip osteoarthritis classically have been thought to be due to inflammation or damage to tissues in the back, knee, or hip. However, recent studies show that these conditions may have complex factors entailing both the peripheral and central nervous systems.
Analysis of data from the National Health and Nutrition Examination Survey (NHANES I) of patients with radiographic evidence of structural damage to the knee due to osteoarthritis found discordance between the amount of damage visible on x-ray and patients’ self-report of the degree of pain. In 319 patients with radiographic stage 2–4 knee osteoarthritis, only 47% reported knee pain, suggesting that something more than the degree of tissue injury was involved in the perception of pain.6,7 One explanation of these findings is that pain is a complex system incorporating structural changes, peripheral and central pain mechanisms, and subjective factors, including the patient’s history, psychological experience, genetics, and culture.
Diabetic neuropathy and postherpetic neuralgia. Chronic neuropathic pain results when there is actual damage to the nervous system—the peripheral nerve, dorsal root, or central nervous system. Peripheral neuropathic pain occurs after damage or alterations to sensory neurons. Some neuropathic pain disorders, such as diabetic neuropathy and postherpetic neuralgia, are well-defined disorders in which symptoms are unrelated to a stimulus and pain is related to peripheral as well as central processing.8
Stroke. Central poststroke pain, in which pain and hypersensitivity occurs in a body part due to injury to the corresponding part of the brain affected by the cerebrovascular lesion, is also considered a neuropathic pain syndrome. The onset of central poststroke pain typically occurs more than one month after the stroke, and exists with somatosensory abnormalities.9-11 For these types of neuropathies, altered function due to loss or damage of neuronal tissue is likely the cause of the pain condition.
Many of the people suffering from these central chronic pain conditions find it difficult to obtain relief, and probably will not benefit from surgeries or manipulations in the periphery. Instead, they may benefit from a targeted approach that addresses the central nervous system.
Recent studies on fibromyalgia and pain
Fibromyalgia (FM) may be considered the prototypical central pain disorder, in which the pain originates or is maintained in part in the central nervous system. Although new diagnostic criteria are being validated for this disorder, FM classically has been diagnosed by the detection of 11 of 18 tender points and the presence of chronic widespread pain for 3 months or longer.12
FM is a common disorder found to affect between 2% and 4% of the US population.13 It was one of the first disorders shown to have central factors predominant in the pathology, and as a result it has been the focus of numerous studies. Irritable bowel syndrome and chronic fatigue syndrome, often comorbid with FM, are also commonly studied. Until recently, these disorders have largely been considered “wastebasket” terms to categorize the complaints of patients with unexplained symptoms, because there were no objective signs to support their complaints. However with the advent of new imaging techniques to look into the brain and the central nervous system, researchers are finding very real physiological differences. For example, one study using sensory testing with thermal, mechanical, and electrical stimuli showed a correlation between FM patients’ subjective reports of pain and significantly altered cold and heat thresholds when compared with controls.14 Based on such studies it appears that patients with FM perceive stimuli as noxious at lower levels than healthy, pain-free controls.
Recent studies of FM have incorporated the use of functional magnetic resonance imaging (fMRI) to look at brain activations in response to painful stimuli. A study that included patients with FM and others with chronic low-back pain used fMRI to visualize the participants’ response to equal amounts of thumbnail pressure. In the FM and groups, 5 areas of neuronal activation within the cortex related to pain were detected, compared with only one activation in controls.15 Another study to evaluate the pattern of cerebral activation in FM patients found that in response to similar thumbnail pressures there were 13 regions of greater activation in the FM group compared with one region in the healthy control group.16 Additionally, mild pressure resulted in subjective pain reports and cerebral responses in the FM group that were similar to responses produced by twice the pressure applied in controls.
Another important area of research in pain processing looks at gray matter in the brain using voxel-based morphometry. A study of patients with FM found significantly less volume of gray matter and an age-associated decrease in gray matter that was 3.3 times greater than healthy controls.17
Using MRI to look at gray matter volume in patients with chronic musculoskeletal pain, significant differences in gray matter volume were found in osteoarthritis patients prior to hip arthroplasty compared with healthy controls. Specifically, areas of the thalamus, understood to play a role in central pain processing, showed decreased gray matter volume in the osteoarthritis group. Significantly, a comparison of gray matter volume 9 months after surgery showed that the levels of reduced thalamic gray matter volume in osteoarthritis patients “reversed” to levels similar to the those of the healthy control group.18
Although the mechanism that drives the loss or degradation of brain tissue in patients with chronic pain remains to be determined, one theory is that pain is associated with certain areas of the brain becoming hyperactive. Imaging studies using fMRI show that a constellation of regions typically are activated in pain processing, including the insula,
cingulate, primary somatosensory and secondary somatosensory cortices, amygdala, and thalamus [Figure 2].19 These regions have been shown to be more active in chronic pain states when patients respond to stimuli such as painful pressure or heat. Indeed, these regions have shown overamplification or augmentation of neural activity.
| FIGURE 2: Neuroanatomy of pain processing. Main brain regions that activate during a painful experience are highlighted as bilaterally active but with more dominant activation on the contralateral hemisphere (red). |
| Source: Tracey I. Br J Anaesth. 2008;101:32-39. |
Since overstimulation of nerve cells can trigger a toxic release of glutamate into surrounding tissues of the brain, this may cause nerve cells to die, ultimately reducing the amount of gray matter visualized in the brains of patients with chronic pain. In addition, some studies of FM have shown elevated levels of glutamate, an excitatory neurotransmitter that is known to cause excitotoxicity.20
Another significant consequence of long-term pain appears to be alterations in the normal connectivity of the brain, including the “default mode network” (DMN) which is noted to be important during the resting state. Recent studies of chronic pain suggest alterations in key DMN regions that may be related to the chronic pain state and existing comorbidities.21
The role of stress and depression in pain
The association among physical and psychosocial stressors, depression, and chronic pain syndromes has been the subject of numerous studies.
Posttraumatic stress disorder (PTSD) has been closely correlated with chronic pain. An example of one such stressor may be deployment to a military conflict. Soldiers and military personnel throughout history have reported a cluster of symptoms such as pain, fatigue, and cognitive impairment that are very similar to FM. From US military conflicts, these syndromes include Gulf War illness, the condition known as “shell shock” in World War I, and “soldier’s heart” during the Civil War.
A review of the literature addressing the association between chronic pain and PTSD by the Department of Veterans Affairs found such a high degree of correlation that the authors suggested clinicians who conduct diagnostic assessments for one disorder should also assess for the other.22 In a study that evaluated patients for FM, chronic fatigue, and psychiatric symptoms, patients with FM who had both tender points and diffuse pain were significantly more likely to have an increased prevalence of lifetime PTSD.23
The relationship between depression and chronic pain has been well documented. Kaiser Permanente surveyed patients seen in primary care and found that a significantly higher proportion of patients with major depressive disorder (MDD) reported chronic pain than did patients without MDD (66% vs 43%, respectively).24 These conditions share common physiologic features and a high degree of comorbidity.
A study of patients with FM and depressive symptoms or MDD looked at neural responses to painful pressure and found no association between the extent of depressive symptoms or MDD and neural activation in the primary and secondary cortices, areas associated with the sensation of pain. However, activation was seen in the amygdala and contralateral anterior insula, areas associated with affective pain processing.25
These findings were supported in a more recent study in which patients who met the criteria for FM were given a series of questionnaires to assess depressive symptoms, anxiety, and catastrophizing, and were tested for painful pressure responses using fMRI. The results established a correlation between this cluster of affective symptoms, but there was no correlation with clinical pain symptoms or responses to painful pressure.26 Rather than suggesting that there is no alignment between the mental and physical aspects of pain, results from both of these studies suggest that 2 independent pain networks exist to process the sensory and affective dimensions of pain, and that these pathways may operate simultaneously.
Pain in the clinical setting
The evidence is strong that many patients experience chronic pain that is not site-specific and arises not merely from the periphery but from intricate neural systems. With a new appreciation for the complexity of pain processing, the clinician is compelled to probe beyond, “Where does it hurt?” [Table].
| TABLE: Clinical diagnosis of central pain
|
When patients complain of widespread or chronic pain, the clinician is well advised to take the time to examine further by inquiring about depression, anxiety, fatigue, sleep disturbances, and cognitive difficulties in order to understand what is driving the patient’s symptoms.13 The results may be revealing. In a study of primary care patients, participants who complained of muscle pain, headache, and stomach pain were found to be 2.5 to 10 times more likely to screen positively for panic disorder, generalized anxiety, or MDD.27
An article in a following issue will discuss practical tools that can be used to assess comorbidities such as anxiety and depression, and interventions that might be helpful for central pain and neurorehabilitation. An approach that acknowledges the patient’s account of pain, recognizes the cluster of symptoms and conditions that can accompany pain, and utilizes a multidisciplinary approach for diagnosis and treatment will have the best chance of yielding positive outcomes.
Acknowledgement—The author wishes to thank Kristen Georgi for her assistance in the research and writing of this article.
REFERENCES
1. International Association for the Study of Pain. IASP taxonomy: pain terms. Pain. Available at: http://www.iasp-pain.org/AM/Template.cfm?Section=Pain_Defi...isplay.cfm&ContentID=1728#Pain.
2. Melzack R, Wall PD. Pain mechanisms. A new theory. Science. 1965;150:971-979.
3. Carr DB. How prevalent is chronic pain? Pain Clinical Updates. 2003;11:1-4. Available at: http://www.iasp-pain.org/AM/AMTemplate.cfm?Section=Home&CONTENTID=7594&TEMPLATE=/CM/ContentDisplay.cfm&SECTION=Home.
4. Washington, DC: US Department of Health and Human Services, Centers for Disease Control and Prevention; 2006. Bernstein AB, Makuc DM, Bilheimer LT. Health, United States, 2006. Available at: http: //www.cdc.gov/nchs/data/hus/hus06.pdf.
5. Institute of Medicine. Relieving pain in America: a blueprint for transforming prevention, care, education, and research. Washington, DC: National Academies Press; 2011.
6. Hannan MT, Felson DT, Pincus T. Analysis of the discordance between radiographic changes and knee pain in osteoarthritis of the knee. J Rheumatol. 2000;27:1513-1517.
7. Creamer P, Hochberg MC. Why does osteoarthritis of the knee hurt—sometimes? Br J Rheumatol. 1997;36:726-728.
8. Woolf CJ, Mannion RJ. Neuropathic pain: aetiology, symptoms, mechanisms, and management. Lancet. 1999;353:1959-1964.
9. Andersen G, Vestergaard K, Ingeman-Nielsen M, et al. Incidence of central post-stroke pain. Pain. 1995;61:187-193.
10. Bowsher D. Central pain: clinical and physiological characteristics. J Neurol Neurosurg Psychiatry. 1996;61:62-69.
11. Klit H, Finnerup NB, Jensen TS. Central post-stroke pain: clinical characteristics, pathophysiology, and management. Lancet. 2009;8:857-868.
12. Wolfe F, Smythe HA, Yunus MB, et al. The American College of Rheumatology 1990 criteria for the classification of fibromyalgia: report of the multicenter criteria committee. Arthritis Rheum. 1990;33:160-172.
13. Wolfe F, Ross K, Anderson J, et al. Aspects of fibromyalgia in the general population: sex, pain threshold, and fibromyalgia symptoms. J Rheumatol. 1995;22:151-156.
14. Desmeules JA, Cedraschi C, Rapiti E, et al. Neurolopshysiologic evidence for a central sensitization in patients with fibromyalgia. Arthritis Rheum. 2003;48:1420-1429.
15. Giesecke T, Gracely RH, Grant MAB, et al. Evidence of augmented central pain processing in idiopathic chronic low back pain. Arthritis Rheum. 2004;50:613-623.
16. Gracely RH, Petzke F, Wolf JM, et al. Functional magnetic resonance imaging evidence of augmented pain processing in fibromyalgia. Arthritis Rheum. 2002;46:1333-1343.
17. Kuchinad A, Schweinhardt P, Seminowicz DA, et al. Accelerated brain gray matter loss in fibromyalgia patients: premature aging of the brain? J Neurosci. 2007;27:4004-4007.
18. Gwilym SE, Fillipini N, Douaud G, et al. Thalamic atrophy associated with painful osteoarthritis of the hip is reversible after arthroplasty. Arthritis Rheum. 2010;62:2930-2940.
19. Tracey I. Imaging pain. Br J Anaesth. 2008;101:32-39.
20. Harris RE, Sundgren PC, Craig AD, et al. Elevated insular glutamate in fibromyalgia is associated with experimental pain. Arthritis Rheum. 2009;60:3146-3152.
21. Baliki MN, Geha PY, Apkarian AV, et al. Beyond feeling: chronic pain hurts the brain, disrupting the default-mode network dynamics. J Neurosci. 2008;28:
1398-1403.
22. Otis JD, Keane TM, Kerns RD. An examination of the relationship between chronic pain and posttraumatic stress disorder. J Rehabil Res Dev. 2003;40:397-406.
23. Roy-Byrne P, Smith WR, Goldberg N, et al. Posttraumatic stress disorder among patients with chronic pain and chronic fatigue. Psychol Med. 2004;34:
363-368.
24. Arnow BA, Hunkeler EM, Blasey CM, et al. Comorbid depression, chronic pain, and disability in primary care. Psychosom Med. 2006;68:262-268.
25. Giesecke T, Gracely RH, Williams DA, et al. The relationship between depression, clinical pain, and experimental pain in a chronic pain cohort. Arthritis Rheum. 2005;52:1577-1584.
26. Jensen KB, Petzke F, Carville S, et al. Anxiety and depressive symptoms in fibromyalgia are related to poor perception of health but not to pain sensitivity or cerebral processing of pain. Arthritis Rheum. 2010;62:3488-3495.
27. Means-Christensen AJ, Roy-Byrne PR, Sherbourne CD, et al. Relationships among pain, anxiety, and depression in primary care. Depress Anxiety. 2008;25:
593-600.
Exploring the Role of Modified-Release Doxycycline in Rosacea

Topics
- Introduction - Exploring the Role of Modified-Release
- Doxycycline in Rosacea
- Comparing Antimicrobial and Anti-Inflammatory Doses of Oral Doxycycline in the Treatment of Rosacea
- Impact of Antibiotic Resistance on Dermatologic Practice
- The Effects of Modified-Release Doxycycline on Quality of Life
- Combining Anti-Inflammatory–Dose Doxycycline With Topical Metronidazole
To view the supplement, click the image above.
Faculty/Faculty Disclosure
Brian Berman, MD, PhD
Voluntary Professor of Dermatology and Cutaneous Surgery
University of Miami, Miller School of Medicine
Co-Director
Center for Clinical and Cosmetic Research, Skin & Cancer Associates, LLP,
Aventura, FL
Dr Berman has received funding for clinical grants from, is an investigator for, and is a consultant to, Galderma Laboratories, L.P.
Copyright © 2012 by Elsevier Inc.
Topics
- Introduction - Exploring the Role of Modified-Release
- Doxycycline in Rosacea
- Comparing Antimicrobial and Anti-Inflammatory Doses of Oral Doxycycline in the Treatment of Rosacea
- Impact of Antibiotic Resistance on Dermatologic Practice
- The Effects of Modified-Release Doxycycline on Quality of Life
- Combining Anti-Inflammatory–Dose Doxycycline With Topical Metronidazole
To view the supplement, click the image above.
Faculty/Faculty Disclosure
Brian Berman, MD, PhD
Voluntary Professor of Dermatology and Cutaneous Surgery
University of Miami, Miller School of Medicine
Co-Director
Center for Clinical and Cosmetic Research, Skin & Cancer Associates, LLP,
Aventura, FL
Dr Berman has received funding for clinical grants from, is an investigator for, and is a consultant to, Galderma Laboratories, L.P.
Copyright © 2012 by Elsevier Inc.
Topics
- Introduction - Exploring the Role of Modified-Release
- Doxycycline in Rosacea
- Comparing Antimicrobial and Anti-Inflammatory Doses of Oral Doxycycline in the Treatment of Rosacea
- Impact of Antibiotic Resistance on Dermatologic Practice
- The Effects of Modified-Release Doxycycline on Quality of Life
- Combining Anti-Inflammatory–Dose Doxycycline With Topical Metronidazole
To view the supplement, click the image above.
Faculty/Faculty Disclosure
Brian Berman, MD, PhD
Voluntary Professor of Dermatology and Cutaneous Surgery
University of Miami, Miller School of Medicine
Co-Director
Center for Clinical and Cosmetic Research, Skin & Cancer Associates, LLP,
Aventura, FL
Dr Berman has received funding for clinical grants from, is an investigator for, and is a consultant to, Galderma Laboratories, L.P.
Copyright © 2012 by Elsevier Inc.
Exploring the Role of Modified-Release Doxycycline in Rosacea

- Introduction - Exploring the Role of Modified-Release
- Doxycycline in Rosacea
- Comparing Antimicrobial and Anti-Inflammatory Doses of Oral Doxycycline in the Treatment of Rosacea
- Impact of Antibiotic Resistance on Dermatologic Practice
- The Effects of Modified-Release Doxycycline on Quality of Life
- Combining Anti-Inflammatory–Dose Doxycycline With Topical Metronidazole
To view the supplement, click the image above.
Faculty/Faculty Disclosure
Brian Berman, MD, PhD
Voluntary Professor of Dermatology and Cutaneous Surgery
University of Miami, Miller School of Medicine Co-Director
Center for Clinical and Cosmetic Research, Skin & Cancer Associates, LLP, Aventura, FL
Copyright (c) 2012 by Elsevier Inc.
- Introduction - Exploring the Role of Modified-Release
- Doxycycline in Rosacea
- Comparing Antimicrobial and Anti-Inflammatory Doses of Oral Doxycycline in the Treatment of Rosacea
- Impact of Antibiotic Resistance on Dermatologic Practice
- The Effects of Modified-Release Doxycycline on Quality of Life
- Combining Anti-Inflammatory–Dose Doxycycline With Topical Metronidazole
To view the supplement, click the image above.
Faculty/Faculty Disclosure
Brian Berman, MD, PhD
Voluntary Professor of Dermatology and Cutaneous Surgery
University of Miami, Miller School of Medicine Co-Director
Center for Clinical and Cosmetic Research, Skin & Cancer Associates, LLP, Aventura, FL
Copyright (c) 2012 by Elsevier Inc.
- Introduction - Exploring the Role of Modified-Release
- Doxycycline in Rosacea
- Comparing Antimicrobial and Anti-Inflammatory Doses of Oral Doxycycline in the Treatment of Rosacea
- Impact of Antibiotic Resistance on Dermatologic Practice
- The Effects of Modified-Release Doxycycline on Quality of Life
- Combining Anti-Inflammatory–Dose Doxycycline With Topical Metronidazole
To view the supplement, click the image above.
Faculty/Faculty Disclosure
Brian Berman, MD, PhD
Voluntary Professor of Dermatology and Cutaneous Surgery
University of Miami, Miller School of Medicine Co-Director
Center for Clinical and Cosmetic Research, Skin & Cancer Associates, LLP, Aventura, FL
Copyright (c) 2012 by Elsevier Inc.

Men, women, and migraine: The role of sex, hormones, obesity, and PTSD
Migraine is a common neurologic disorder that occurs in approximately 3 times as many females as males in the United States. Among 30,000 respondents, the American Migraine Study II found that the prevalence of migraine was 18.2% among females and 6.5% among males, and was much higher in females from age 12 across the lifespan.1 In comparison, for tension-type headache the female to male ratio of occurrence is 5:4, occurring only slightly more in females.2 The reasons for this disparity in migraine prevalence are not well understood. The disproportionate number of women of reproductive age with migraine suggests that hormonal factors may play a role, but the complex pathophysiology of migraine indicates additional factors are involved.3
Recent research on menstrual-related migraine and two significant comorbidities of migraine—obesity and posttraumatic stress disorder (PTSD)—shed new light on the differences in how men and women present with and experience this often disabling disorder.
Epidemiologic differences
The incidence of migraine, defined here as age of first onset, is different in boys and girls. For migraine without aura, age of first onset is approximately 10 to 11 years in boys versus 14 to 17 years in girls. For migraine with aura, age of first onset is approximately 5 years in boys and 12 to 13 years in girls.4
The picture of migraine differs by sex before and after puberty. Before age 12, boys have a higher incidence and prevalence of migraine. After age 12, prevalence increases for both sexes, peaking between age 35 to 45, with an increase in the female-to-male ratio from 2:1 at age 20 to 3.3:1 at age 40.5,6
Disparities in migraine symptoms
Common symptoms associated with severe or unilateral migraine pain include photophobia, phonophobia, and nausea. In the American Migraine Study II, the most frequently reported symptoms were pulsatile pain (85%of migraineurs), light sensitivity (80%), sound sensitivity (76%), nausea (73%), unilateral pain (59%), blurred vision (44%), aura (36%), and vomiting (29%).1 Females were more likely than males to report light sensitivity, sound sensitivity, and nausea. More females experienced 1 to 2 days of migraine-associated activity restriction than males (30.5% vs 22.9%).1 Separate studies have shown neck pain to be second after menstruation in its predictive value for onset of migraine, and to be more prevalent than nausea at the time of treatment.7,8
Migraine comorbidities
Migraine is known to be comorbid with a variety of disorders including psychiatric conditions such as depression and anxiety,9,10 and medical comorbidities such as stroke, epilepsy, and hypothyroidism.11-13 In women, migraine is also comorbid with endometriosis.14
Hormonal factors: Menstrual-related migraine
With migraine disproportionately affecting women of reproductive age, as many as 70% of female migraineurs are aware of a menstrual association with their headaches.15 A menstrual migraine is defined as migraine without aura that occurs during the 5-day window that begins 2 days before the onset of bleeding and extends through the third day of active bleeding—and that occurs in at least two-thirds of menstrual cycles.16 Approximately 14% of women experience what is termed pure menstrual migraine, meaning the only time they experience migraine is during menstruation. For women who also have migraines triggered by other mechanisms, the menstrual migraine is typically their most severe migraine of the month.
For many women, menstrual migraines are more painful, longer lasting, and more resistant to acute therapy than migraines occurring at other times.17,18 It is specifically the reduction in estradiol in the late luteal phase that appears to be the greatest trigger for menstrual migraine.
About two-thirds of women with migraine improve in menopause, particularly those for whom migraine attacks were associated with menstruation.19,20 As disabling as menstrual related migraine can be, clinically it is often found to coexist with chronic migraine and medication overuse headache.21
In a study that looked at the impact of eliminating menstrual migraine, investigators treated women with hormonal preventives based on the hypothesis that, because these agents confer no known benefit for migraines that are not hormonally triggered, use of these agents might allow them to separate out menstrual-related migraine and its effect on the overall clinical picture.21 Among 229 consecutive women seen in follow-up, 81% of those patients who were taking the hormonal preventive as prescribed had a complete resolution of menstrual-related migraine. Among those in whom menstrual migraine was eliminated, 58.9% reverted back to episodic migraine, compared with only 11% of patients whose menstrual-migraine was not eliminated.21 Resolution of menstrual-related migraine also was associated with resolution of medication overuse. Patients in whom menstrual-related migraine resolved were >2 times as likely to stop medication overuse as those in whom the migraines were not eliminated. The results offer preliminary evidence that hormonal regimens may be of benefit in preventing menstrual-related migraine.
Migraine and obesity
Obesity, which results from excessive adipose tissue in relation to fat free mass, has been shown in clinical and population-based studies to be associated with migraine.22-25 Both migraine and the distribution of adipose tissue change substantially based on age and sex.25 Following puberty, girls have an increase in the subcutaneous to visceral adipose tissue ratio as compared with boys, a pattern that continues through the reproductive years for women. Postmenopausal women see an increase in visceral
adipose tissue volume and a decrease in the subcutaneous to visceral adipose tissue volume compared with premenopausal women. Similarly, migraine prevalence increases in women of reproductive age as compared with those of postreproductive age and it is greater in women of reproductive age as compared with men.25
To evaluate the prevalence of migraine and severe headaches in men and women with and without total body obesity (TBO), as measured by body mass index (BMI) and abdominal obesity (Abd-O), Peterlin and colleagues analyzed data from 21,783 participants in the National Health and Nutrition Examination Survey.26 The investigators found that the relationship between migraine and obesity varies by age, sex, and the distribution of adipose tissue. For men and women of reproductive age, migraine prevalence increased in those with either TBO or Abd-O compared with those without. For postreproductive aged men and women (>55 years), migraine prevalence was not increased in those with either Abd-O or TBO. [Figure 1]
FIGURE 1: Migraine prevalence in men and women in relation to TBO and Abd-O
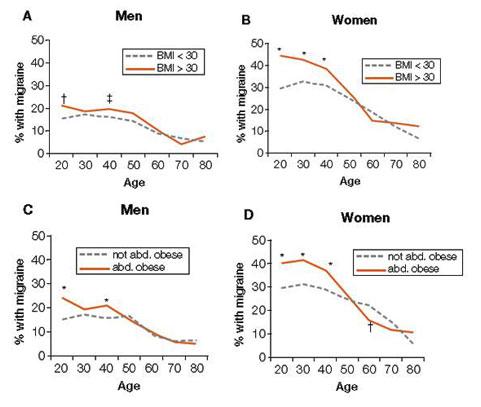
Total body obesity (TBO) was estimated based on BMI. Abdominal obesity (Abd-O) was estimated
based on waist circumference.
*P ≤ .001; † P ≤ .01; ‡ P ≤ .05
Source: Adapted with permission from Peterlin BL, et al. Migraine and obesity: Epidemiology,
mechanisms, and implications. Headache. 2010;50:631-636.
Vo et al observed similar findings for women of reproductive age in analyses of data from the Omega study. In a cohort of 3,733 women during early pregnancy, researchers found that obesity was associated with increased odds for migraine and that the risk of migraine increased with increasing obesity.27 Specifically, while the overall odds of migraine in women with obesity of any level was 48% greater than in women without obesity (OR 1.48; 95%CI: 1.12-1.96), those women with severe or class II obesity (BMI 35 to 39.9) had a >200% increased risk (OR 2.07; 95%CI: 1.27-3.39), and those with morbid or class III obesity (BMI ≥40) had a 275% increased risk of migraine, (OR 2.75; 95%CI: 1.60-4.70).27 Furthermore, Vo et al demonstrated that women with a history of pediatric migraine had 67% increased odds of gaining ≥22 pounds above their weight at the age of 18 (OR 1.67; 95% CI:1.13-2.47).27
An association between obesity and migraine was also found in two small studies that assessed the effects of bariatric surgery on headache frequency in morbidly obese, episodic migraineurs.28,29 In these studies, at 6 months after surgery the monthly headache frequency declined from approximately 4 headache days per month at baseline to just 1 to 2 headache days per month. Researchers also noted that following bariatric surgery, the migraine-associated symptoms were reduced and headache related disability improved significantly. Larger, controlled studies will be needed to substantiate these findings and determine the true effect size before bariatric surgery could be considered as a component of migraine therapy.30 However, these results highlight the observation that clinicians should give consideration to obesity as a potentially modifiable risk factor for episodic migraine.
Migraine and PTSD
Posttraumatic stress disorder (PTSD), the result of traumatic life stressors, has a lifetime prevalence of approximately 7%—3.6% among men and 9.7% among women—according to the National Comorbidity Survey Replication (NCS-R), a cross-sectional, general population survey of mental disorders.31 Interpersonal trauma (such as physical or sexual abuse) is the most common cause of PTSD, but it can also result from life-threatening situations such as natural and man-made disasters or military combat.32,33 In a secondary analysis of a the NCS-R, Peterlin and colleagues and found that 21.5% of episodic migraineurs and 19.2% of chronic daily headache sufferers fulfilled PTSD criteria.34
Although both migraine and PTSD are up to 3 times more common in women than men, recent data suggest that the association between migraine and PTSD is stronger in men.34,35 Using the NCS-R data, Peterlin and colleagues found a more than 3-4 fold increase in the odds ratio of PTSD in men with migraine versus women with migraine—a result that renders PTSD, to the knowledge of the investigators, the first mental disorder to be reported as having a greater prevalence in men with migraine than women with migraine.34[Figure 2]
FIGURE 2: Sex-specific odds ratio of PTSD in episodic migraine
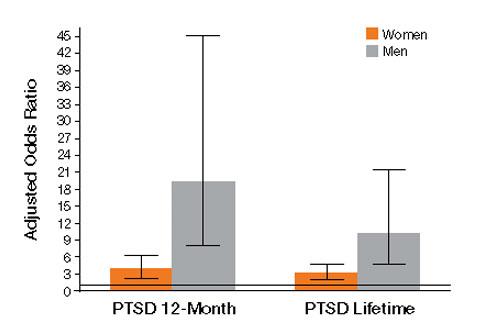
Source: Adapted with permission from Peterlin BL, et al. Post-traumatic distress disorder and migraine:
Epidemiology, sex differences, and potential mechanisms. Headache. 2011;51(6)860-868.
The neurobiological mechanism linking PTSD to migraine is not known. Although a variety of theories exist—including low serotonin levels, dysfunctions of the autonomic system and hypothalamic-pituitary-adrenal axis (HPA) in both migraine and PTSD, and elevated baseline cortisol levels in migraineurs—it remains unclear why the association is stronger in men than in women.34 Some studies suggest that sex-related differences of the HPA axis may play a role.36,37 Others consider fMRI findings of sex differences in cerebral blood flow to pain centers in response to psychological distress.37 Further research into the sex-related differences of migraineurs with PTSD will likely reveal insights into new therapeutic directions for men and women with these disorders.
Implications for clinicians
The preceding data add to the understanding that numerous comorbidities exist in individuals with migraine. If a patient is a migraineur, screen for PTSD as well as depression and anxiety. Treatment with cognitive behavioral therapy—alone or in combination with pharmacological therapy—should be considered, since treatment of PTSD alone has been shown to have a beneficial effect on both pain and disability in chronic pain patients.38
Given that obesity is a modifiable risk factor, educate all migraine patients about the association with obesity in general, the increasing risk of migraine associated with increasing obesity, and the potential effect of weight gain/loss on headache frequency.26,27 Also inform patients about the potential effects migraine medications may have on their weight, and encourage them to eat a healthy diet, exercise, and avoid gaining excessive weight. If other comorbidities are involved, tailor the therapeutic regimen based on that combination. If a migraine patient is obese and has high blood pressure, look for an antihypertensive agent that is relatively weight-neutral.
Eliminating menstrual migraine should be an important treatment goal for patients in whom it is the most disabling migraine of the month. Hormonal preventives may be the best approach for women whose menstrual attacks are resistant to acute treatment.21
Disclosures
B. Lee Peterlin, DO, has received grant/research support from GlaxoSmithKline, has served as a consultant to Nautilus, and has served on the speaker’s bureau of Zogenix. She holds a provisional patent for use of adiponectin-modulating drugs for migraine.
Anne H. Calhoun, MD, has no conflicts of interest to report.
Fred Balzac has no conflicts of interest to report.
1. Lipton RB, Stewart WF, Diamond S, et al. Prevalence and burden of migraine in the United States: data from the American Migraine Study II. Headache. 2001;41:646-657.
2. Rasmussen BK, Jensen R, Schroll M, et al. Epidemiology of headache in a general population—a prevalence study. J Clin Epidemiol. 1991;44(11)1147-1157.
3. Peterlin BL, Katsnelson MJ, Calhoun AH. The associations between migraine, unipolar psychiatric comorbidities, and stress-related disorders and the role of estrogen. Curr Pain Headache Rep. 2009;13:404-412.
4. Stewart WF, Linet MS, Celentano DD, et al. Age- and sex-specific incidence rates of migraine with and without visual aura. Am J Epidemiol. 1991;134(10):1111-1120.
5. Stewart WF, Lipton RB, Celentano DD, et al. Prevalence of migraine headache in the United States: relation to age, income, race, and other sociodemographic factors. JAMA. 1992;267:64- 69.
6. Lipton RB, Stewart WF. Migraine in the United States: a review of epidemiology and health care use. Neurology. 1993;43(suppl 3):S6-10.
7. Wober C, Brannath W, Schmidt K, et al. Prospective analysis of factors related to migraine attacks: The PAMINA study. Cephalalgia. 2007;27:304-314.
8. Calhoun AH, Ford S, Millen C, et al. The prevalence of neck pain in migraine. Headache. 2010;50:1273-1277.
9. Breslau N, Lipton RB, Stewart WF, et al. Comorbidity of migraine and depression: Investigating potential etiology and prognosis. Neurology. 2003;60:1308-1312.
10. Stewart W, Breslau N, Keck PE Jr. Comorbidity of migraine and panic disorder. Neurology. 1994;44:S23-S27.
11. Scher AI, Terwindt GM, Picavet HS, et al. Cardiovascular risk factors and migraine: The GEM population based study. Neurology. 2005;64:614-620.
12. Ottman R, Lipton RB. Comorbidity of migraine and epilepsy. Neurology. 1994;44:2105-2110.
13. Moreau T, Manceau E, Giroud-Baleydier F, et al. Headache in hypothyroidism. Prevalence and outcome under thyroid hormone therapy. Cephalalgia. 1998;18:687-689.
14. Ferrero S, Pretta S, Bertoldi S, et al. Increased frequency of migraine among women with endometriosis. Hum Reprod. 2004;19:2927-2932.
15. MacGregor EA. “Menstrual” migraine: Towards a definition. Cephalalgia. 1996;16:11-21.
16. Calhoun AH, Hutchinson S. Hormonal therapies for menstrual migraine. Curr Pain Headache Rep.2009;13:381-385.
17. Granella F, Sances G, Allais G, et al. Characteristics of menstrual and nonmenstrual attacks in women with menstrually related migraine referred to headache centres. Cephalalgia. 2004;24:707-716.
18. MacGregor EA, Hackshaw A. Prevalence of migraine on each day of the natural menstrual cycle. Neurology. 2004;63:351-353.
19. Neri I, Granella F, Nappi R, et al. Characteristics of headache at menopause: a clinico-epidemiologic study. Maturitas.1993;17:31-37.
20. Brandes JL. The influence of estrogen on migraine: a systematic review. JAMA. 2006;295(15):1824-1830.
21. Calhoun A, Ford S. Elimination of menstrual-related migraine beneficially impacts chronification and medication overuse. Headache. 2008;48:1186-1193.
22. Scher AI, Stewart WF, Ricci JA, et al. Factors associated with the onset and remission of chronic daily headache in a population-based study. Pain. 2003;106:81-89.
23. Horev A, Wirguin I, Lantsberg L, et al. A high incidence of migraine with aura among morbidly obese women. Headache. 2005;45:936-938.
24. Ford ES, Li C, Pearson WS, et al. Body mass index and headaches: Findings from a national sample of US adults. Cephalalgia. 2008;28(12):1270-1276.
25. Peterlin BL, Rapoport AM, Kurth T. Migraine and obesity: Epidemiology, mechanisms, and implications. Headache. 2012;50:631-648.
26. Peterlin BL, Rosso AL, Rapoport AM, et al. Obesity and migraine: the effect of age, gender and adipose tissue distribution. Headache. 2010;50:52-62.
27. Vo M, Ainalem A, Qiu C, et al. Body mass index and adult weight gain among reproductive age women with migraine. Headache. 2011;51:559-569.
28. Novack V, Fuchs L, Lantsberg L, et al. Changes in headache frequency in premenopausal obese women with migraine after bariatric surgery: A case series. Cephalalgia. 2011;31(13):1336-1342.
29. Bond DS, Vithiananthan S, Nash JM, et al. Improvement of migraine headaches in severely obese patients after bariatric surgery. Neurology. 2011;76(13)1135-1138.
30. Peterlin BL. Bariatric surgery in obese migraineurs: Mounting evidence but important questions remain. Cephalalgia. 2011;31(13):1333-1335.
31. Kessler RC, Berglund P, Delmer O, et al. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):593-602.
32. Butterfield MI, Becker M, Marx CE. Posttraumatic stress disorder in women: Current concepts and treatments. Curr Psychiatry Rep. 2002;4:474-486.
33. Breslau N. The epidemiology of trauma, PTSD, and other posttrauma disorders. Trauma Violence Abuse. 2009;10(3):198-210.
34. Peterlin BL, Rosso AL, Sheftell FD, et al. Post-traumatic stress disorder, drug abuse and migraine: new findings from the National Comorbidity Survey Replication (NCS-R). Cephalalgia. 2011;31:235-244.
35. Peterlin BL, Nijjar SS, Tietjen GE. Post-traumatic stress disorder and migraine: epidemiology, sex differences, and potential mechanisms. Headache. 2011;51:860-868.
36. Rainero I, Ferrero M, Rubino E, et al. Endocrine function is altered in chronic migraine patient with medication-overuse. Headache. 2006;46:597-603.
37. Wang J, Korczykowski, Rao H, et al. Gender difference in neural response to psychological stress. Soc Cog Affect Neurosci. 2007;2:227-239.
38. Peterlin BL, Tietjen GE, Brandes JL, et al. Posttraumatic stress disorder in migraine. Headache. 2009;49:541-551.
Migraine is a common neurologic disorder that occurs in approximately 3 times as many females as males in the United States. Among 30,000 respondents, the American Migraine Study II found that the prevalence of migraine was 18.2% among females and 6.5% among males, and was much higher in females from age 12 across the lifespan.1 In comparison, for tension-type headache the female to male ratio of occurrence is 5:4, occurring only slightly more in females.2 The reasons for this disparity in migraine prevalence are not well understood. The disproportionate number of women of reproductive age with migraine suggests that hormonal factors may play a role, but the complex pathophysiology of migraine indicates additional factors are involved.3
Recent research on menstrual-related migraine and two significant comorbidities of migraine—obesity and posttraumatic stress disorder (PTSD)—shed new light on the differences in how men and women present with and experience this often disabling disorder.
Epidemiologic differences
The incidence of migraine, defined here as age of first onset, is different in boys and girls. For migraine without aura, age of first onset is approximately 10 to 11 years in boys versus 14 to 17 years in girls. For migraine with aura, age of first onset is approximately 5 years in boys and 12 to 13 years in girls.4
The picture of migraine differs by sex before and after puberty. Before age 12, boys have a higher incidence and prevalence of migraine. After age 12, prevalence increases for both sexes, peaking between age 35 to 45, with an increase in the female-to-male ratio from 2:1 at age 20 to 3.3:1 at age 40.5,6
Disparities in migraine symptoms
Common symptoms associated with severe or unilateral migraine pain include photophobia, phonophobia, and nausea. In the American Migraine Study II, the most frequently reported symptoms were pulsatile pain (85%of migraineurs), light sensitivity (80%), sound sensitivity (76%), nausea (73%), unilateral pain (59%), blurred vision (44%), aura (36%), and vomiting (29%).1 Females were more likely than males to report light sensitivity, sound sensitivity, and nausea. More females experienced 1 to 2 days of migraine-associated activity restriction than males (30.5% vs 22.9%).1 Separate studies have shown neck pain to be second after menstruation in its predictive value for onset of migraine, and to be more prevalent than nausea at the time of treatment.7,8
Migraine comorbidities
Migraine is known to be comorbid with a variety of disorders including psychiatric conditions such as depression and anxiety,9,10 and medical comorbidities such as stroke, epilepsy, and hypothyroidism.11-13 In women, migraine is also comorbid with endometriosis.14
Hormonal factors: Menstrual-related migraine
With migraine disproportionately affecting women of reproductive age, as many as 70% of female migraineurs are aware of a menstrual association with their headaches.15 A menstrual migraine is defined as migraine without aura that occurs during the 5-day window that begins 2 days before the onset of bleeding and extends through the third day of active bleeding—and that occurs in at least two-thirds of menstrual cycles.16 Approximately 14% of women experience what is termed pure menstrual migraine, meaning the only time they experience migraine is during menstruation. For women who also have migraines triggered by other mechanisms, the menstrual migraine is typically their most severe migraine of the month.
For many women, menstrual migraines are more painful, longer lasting, and more resistant to acute therapy than migraines occurring at other times.17,18 It is specifically the reduction in estradiol in the late luteal phase that appears to be the greatest trigger for menstrual migraine.
About two-thirds of women with migraine improve in menopause, particularly those for whom migraine attacks were associated with menstruation.19,20 As disabling as menstrual related migraine can be, clinically it is often found to coexist with chronic migraine and medication overuse headache.21
In a study that looked at the impact of eliminating menstrual migraine, investigators treated women with hormonal preventives based on the hypothesis that, because these agents confer no known benefit for migraines that are not hormonally triggered, use of these agents might allow them to separate out menstrual-related migraine and its effect on the overall clinical picture.21 Among 229 consecutive women seen in follow-up, 81% of those patients who were taking the hormonal preventive as prescribed had a complete resolution of menstrual-related migraine. Among those in whom menstrual migraine was eliminated, 58.9% reverted back to episodic migraine, compared with only 11% of patients whose menstrual-migraine was not eliminated.21 Resolution of menstrual-related migraine also was associated with resolution of medication overuse. Patients in whom menstrual-related migraine resolved were >2 times as likely to stop medication overuse as those in whom the migraines were not eliminated. The results offer preliminary evidence that hormonal regimens may be of benefit in preventing menstrual-related migraine.
Migraine and obesity
Obesity, which results from excessive adipose tissue in relation to fat free mass, has been shown in clinical and population-based studies to be associated with migraine.22-25 Both migraine and the distribution of adipose tissue change substantially based on age and sex.25 Following puberty, girls have an increase in the subcutaneous to visceral adipose tissue ratio as compared with boys, a pattern that continues through the reproductive years for women. Postmenopausal women see an increase in visceral
adipose tissue volume and a decrease in the subcutaneous to visceral adipose tissue volume compared with premenopausal women. Similarly, migraine prevalence increases in women of reproductive age as compared with those of postreproductive age and it is greater in women of reproductive age as compared with men.25
To evaluate the prevalence of migraine and severe headaches in men and women with and without total body obesity (TBO), as measured by body mass index (BMI) and abdominal obesity (Abd-O), Peterlin and colleagues analyzed data from 21,783 participants in the National Health and Nutrition Examination Survey.26 The investigators found that the relationship between migraine and obesity varies by age, sex, and the distribution of adipose tissue. For men and women of reproductive age, migraine prevalence increased in those with either TBO or Abd-O compared with those without. For postreproductive aged men and women (>55 years), migraine prevalence was not increased in those with either Abd-O or TBO. [Figure 1]
FIGURE 1: Migraine prevalence in men and women in relation to TBO and Abd-O
Total body obesity (TBO) was estimated based on BMI. Abdominal obesity (Abd-O) was estimated
based on waist circumference.
*P ≤ .001; † P ≤ .01; ‡ P ≤ .05
Source: Adapted with permission from Peterlin BL, et al. Migraine and obesity: Epidemiology,
mechanisms, and implications. Headache. 2010;50:631-636.
Vo et al observed similar findings for women of reproductive age in analyses of data from the Omega study. In a cohort of 3,733 women during early pregnancy, researchers found that obesity was associated with increased odds for migraine and that the risk of migraine increased with increasing obesity.27 Specifically, while the overall odds of migraine in women with obesity of any level was 48% greater than in women without obesity (OR 1.48; 95%CI: 1.12-1.96), those women with severe or class II obesity (BMI 35 to 39.9) had a >200% increased risk (OR 2.07; 95%CI: 1.27-3.39), and those with morbid or class III obesity (BMI ≥40) had a 275% increased risk of migraine, (OR 2.75; 95%CI: 1.60-4.70).27 Furthermore, Vo et al demonstrated that women with a history of pediatric migraine had 67% increased odds of gaining ≥22 pounds above their weight at the age of 18 (OR 1.67; 95% CI:1.13-2.47).27
An association between obesity and migraine was also found in two small studies that assessed the effects of bariatric surgery on headache frequency in morbidly obese, episodic migraineurs.28,29 In these studies, at 6 months after surgery the monthly headache frequency declined from approximately 4 headache days per month at baseline to just 1 to 2 headache days per month. Researchers also noted that following bariatric surgery, the migraine-associated symptoms were reduced and headache related disability improved significantly. Larger, controlled studies will be needed to substantiate these findings and determine the true effect size before bariatric surgery could be considered as a component of migraine therapy.30 However, these results highlight the observation that clinicians should give consideration to obesity as a potentially modifiable risk factor for episodic migraine.
Migraine and PTSD
Posttraumatic stress disorder (PTSD), the result of traumatic life stressors, has a lifetime prevalence of approximately 7%—3.6% among men and 9.7% among women—according to the National Comorbidity Survey Replication (NCS-R), a cross-sectional, general population survey of mental disorders.31 Interpersonal trauma (such as physical or sexual abuse) is the most common cause of PTSD, but it can also result from life-threatening situations such as natural and man-made disasters or military combat.32,33 In a secondary analysis of a the NCS-R, Peterlin and colleagues and found that 21.5% of episodic migraineurs and 19.2% of chronic daily headache sufferers fulfilled PTSD criteria.34
Although both migraine and PTSD are up to 3 times more common in women than men, recent data suggest that the association between migraine and PTSD is stronger in men.34,35 Using the NCS-R data, Peterlin and colleagues found a more than 3-4 fold increase in the odds ratio of PTSD in men with migraine versus women with migraine—a result that renders PTSD, to the knowledge of the investigators, the first mental disorder to be reported as having a greater prevalence in men with migraine than women with migraine.34[Figure 2]
FIGURE 2: Sex-specific odds ratio of PTSD in episodic migraine
Source: Adapted with permission from Peterlin BL, et al. Post-traumatic distress disorder and migraine:
Epidemiology, sex differences, and potential mechanisms. Headache. 2011;51(6)860-868.
The neurobiological mechanism linking PTSD to migraine is not known. Although a variety of theories exist—including low serotonin levels, dysfunctions of the autonomic system and hypothalamic-pituitary-adrenal axis (HPA) in both migraine and PTSD, and elevated baseline cortisol levels in migraineurs—it remains unclear why the association is stronger in men than in women.34 Some studies suggest that sex-related differences of the HPA axis may play a role.36,37 Others consider fMRI findings of sex differences in cerebral blood flow to pain centers in response to psychological distress.37 Further research into the sex-related differences of migraineurs with PTSD will likely reveal insights into new therapeutic directions for men and women with these disorders.
Implications for clinicians
The preceding data add to the understanding that numerous comorbidities exist in individuals with migraine. If a patient is a migraineur, screen for PTSD as well as depression and anxiety. Treatment with cognitive behavioral therapy—alone or in combination with pharmacological therapy—should be considered, since treatment of PTSD alone has been shown to have a beneficial effect on both pain and disability in chronic pain patients.38
Given that obesity is a modifiable risk factor, educate all migraine patients about the association with obesity in general, the increasing risk of migraine associated with increasing obesity, and the potential effect of weight gain/loss on headache frequency.26,27 Also inform patients about the potential effects migraine medications may have on their weight, and encourage them to eat a healthy diet, exercise, and avoid gaining excessive weight. If other comorbidities are involved, tailor the therapeutic regimen based on that combination. If a migraine patient is obese and has high blood pressure, look for an antihypertensive agent that is relatively weight-neutral.
Eliminating menstrual migraine should be an important treatment goal for patients in whom it is the most disabling migraine of the month. Hormonal preventives may be the best approach for women whose menstrual attacks are resistant to acute treatment.21
Disclosures
B. Lee Peterlin, DO, has received grant/research support from GlaxoSmithKline, has served as a consultant to Nautilus, and has served on the speaker’s bureau of Zogenix. She holds a provisional patent for use of adiponectin-modulating drugs for migraine.
Anne H. Calhoun, MD, has no conflicts of interest to report.
Fred Balzac has no conflicts of interest to report.
Migraine is a common neurologic disorder that occurs in approximately 3 times as many females as males in the United States. Among 30,000 respondents, the American Migraine Study II found that the prevalence of migraine was 18.2% among females and 6.5% among males, and was much higher in females from age 12 across the lifespan.1 In comparison, for tension-type headache the female to male ratio of occurrence is 5:4, occurring only slightly more in females.2 The reasons for this disparity in migraine prevalence are not well understood. The disproportionate number of women of reproductive age with migraine suggests that hormonal factors may play a role, but the complex pathophysiology of migraine indicates additional factors are involved.3
Recent research on menstrual-related migraine and two significant comorbidities of migraine—obesity and posttraumatic stress disorder (PTSD)—shed new light on the differences in how men and women present with and experience this often disabling disorder.
Epidemiologic differences
The incidence of migraine, defined here as age of first onset, is different in boys and girls. For migraine without aura, age of first onset is approximately 10 to 11 years in boys versus 14 to 17 years in girls. For migraine with aura, age of first onset is approximately 5 years in boys and 12 to 13 years in girls.4
The picture of migraine differs by sex before and after puberty. Before age 12, boys have a higher incidence and prevalence of migraine. After age 12, prevalence increases for both sexes, peaking between age 35 to 45, with an increase in the female-to-male ratio from 2:1 at age 20 to 3.3:1 at age 40.5,6
Disparities in migraine symptoms
Common symptoms associated with severe or unilateral migraine pain include photophobia, phonophobia, and nausea. In the American Migraine Study II, the most frequently reported symptoms were pulsatile pain (85%of migraineurs), light sensitivity (80%), sound sensitivity (76%), nausea (73%), unilateral pain (59%), blurred vision (44%), aura (36%), and vomiting (29%).1 Females were more likely than males to report light sensitivity, sound sensitivity, and nausea. More females experienced 1 to 2 days of migraine-associated activity restriction than males (30.5% vs 22.9%).1 Separate studies have shown neck pain to be second after menstruation in its predictive value for onset of migraine, and to be more prevalent than nausea at the time of treatment.7,8
Migraine comorbidities
Migraine is known to be comorbid with a variety of disorders including psychiatric conditions such as depression and anxiety,9,10 and medical comorbidities such as stroke, epilepsy, and hypothyroidism.11-13 In women, migraine is also comorbid with endometriosis.14
Hormonal factors: Menstrual-related migraine
With migraine disproportionately affecting women of reproductive age, as many as 70% of female migraineurs are aware of a menstrual association with their headaches.15 A menstrual migraine is defined as migraine without aura that occurs during the 5-day window that begins 2 days before the onset of bleeding and extends through the third day of active bleeding—and that occurs in at least two-thirds of menstrual cycles.16 Approximately 14% of women experience what is termed pure menstrual migraine, meaning the only time they experience migraine is during menstruation. For women who also have migraines triggered by other mechanisms, the menstrual migraine is typically their most severe migraine of the month.
For many women, menstrual migraines are more painful, longer lasting, and more resistant to acute therapy than migraines occurring at other times.17,18 It is specifically the reduction in estradiol in the late luteal phase that appears to be the greatest trigger for menstrual migraine.
About two-thirds of women with migraine improve in menopause, particularly those for whom migraine attacks were associated with menstruation.19,20 As disabling as menstrual related migraine can be, clinically it is often found to coexist with chronic migraine and medication overuse headache.21
In a study that looked at the impact of eliminating menstrual migraine, investigators treated women with hormonal preventives based on the hypothesis that, because these agents confer no known benefit for migraines that are not hormonally triggered, use of these agents might allow them to separate out menstrual-related migraine and its effect on the overall clinical picture.21 Among 229 consecutive women seen in follow-up, 81% of those patients who were taking the hormonal preventive as prescribed had a complete resolution of menstrual-related migraine. Among those in whom menstrual migraine was eliminated, 58.9% reverted back to episodic migraine, compared with only 11% of patients whose menstrual-migraine was not eliminated.21 Resolution of menstrual-related migraine also was associated with resolution of medication overuse. Patients in whom menstrual-related migraine resolved were >2 times as likely to stop medication overuse as those in whom the migraines were not eliminated. The results offer preliminary evidence that hormonal regimens may be of benefit in preventing menstrual-related migraine.
Migraine and obesity
Obesity, which results from excessive adipose tissue in relation to fat free mass, has been shown in clinical and population-based studies to be associated with migraine.22-25 Both migraine and the distribution of adipose tissue change substantially based on age and sex.25 Following puberty, girls have an increase in the subcutaneous to visceral adipose tissue ratio as compared with boys, a pattern that continues through the reproductive years for women. Postmenopausal women see an increase in visceral
adipose tissue volume and a decrease in the subcutaneous to visceral adipose tissue volume compared with premenopausal women. Similarly, migraine prevalence increases in women of reproductive age as compared with those of postreproductive age and it is greater in women of reproductive age as compared with men.25
To evaluate the prevalence of migraine and severe headaches in men and women with and without total body obesity (TBO), as measured by body mass index (BMI) and abdominal obesity (Abd-O), Peterlin and colleagues analyzed data from 21,783 participants in the National Health and Nutrition Examination Survey.26 The investigators found that the relationship between migraine and obesity varies by age, sex, and the distribution of adipose tissue. For men and women of reproductive age, migraine prevalence increased in those with either TBO or Abd-O compared with those without. For postreproductive aged men and women (>55 years), migraine prevalence was not increased in those with either Abd-O or TBO. [Figure 1]
FIGURE 1: Migraine prevalence in men and women in relation to TBO and Abd-O
Total body obesity (TBO) was estimated based on BMI. Abdominal obesity (Abd-O) was estimated
based on waist circumference.
*P ≤ .001; † P ≤ .01; ‡ P ≤ .05
Source: Adapted with permission from Peterlin BL, et al. Migraine and obesity: Epidemiology,
mechanisms, and implications. Headache. 2010;50:631-636.
Vo et al observed similar findings for women of reproductive age in analyses of data from the Omega study. In a cohort of 3,733 women during early pregnancy, researchers found that obesity was associated with increased odds for migraine and that the risk of migraine increased with increasing obesity.27 Specifically, while the overall odds of migraine in women with obesity of any level was 48% greater than in women without obesity (OR 1.48; 95%CI: 1.12-1.96), those women with severe or class II obesity (BMI 35 to 39.9) had a >200% increased risk (OR 2.07; 95%CI: 1.27-3.39), and those with morbid or class III obesity (BMI ≥40) had a 275% increased risk of migraine, (OR 2.75; 95%CI: 1.60-4.70).27 Furthermore, Vo et al demonstrated that women with a history of pediatric migraine had 67% increased odds of gaining ≥22 pounds above their weight at the age of 18 (OR 1.67; 95% CI:1.13-2.47).27
An association between obesity and migraine was also found in two small studies that assessed the effects of bariatric surgery on headache frequency in morbidly obese, episodic migraineurs.28,29 In these studies, at 6 months after surgery the monthly headache frequency declined from approximately 4 headache days per month at baseline to just 1 to 2 headache days per month. Researchers also noted that following bariatric surgery, the migraine-associated symptoms were reduced and headache related disability improved significantly. Larger, controlled studies will be needed to substantiate these findings and determine the true effect size before bariatric surgery could be considered as a component of migraine therapy.30 However, these results highlight the observation that clinicians should give consideration to obesity as a potentially modifiable risk factor for episodic migraine.
Migraine and PTSD
Posttraumatic stress disorder (PTSD), the result of traumatic life stressors, has a lifetime prevalence of approximately 7%—3.6% among men and 9.7% among women—according to the National Comorbidity Survey Replication (NCS-R), a cross-sectional, general population survey of mental disorders.31 Interpersonal trauma (such as physical or sexual abuse) is the most common cause of PTSD, but it can also result from life-threatening situations such as natural and man-made disasters or military combat.32,33 In a secondary analysis of a the NCS-R, Peterlin and colleagues and found that 21.5% of episodic migraineurs and 19.2% of chronic daily headache sufferers fulfilled PTSD criteria.34
Although both migraine and PTSD are up to 3 times more common in women than men, recent data suggest that the association between migraine and PTSD is stronger in men.34,35 Using the NCS-R data, Peterlin and colleagues found a more than 3-4 fold increase in the odds ratio of PTSD in men with migraine versus women with migraine—a result that renders PTSD, to the knowledge of the investigators, the first mental disorder to be reported as having a greater prevalence in men with migraine than women with migraine.34[Figure 2]
FIGURE 2: Sex-specific odds ratio of PTSD in episodic migraine
Source: Adapted with permission from Peterlin BL, et al. Post-traumatic distress disorder and migraine:
Epidemiology, sex differences, and potential mechanisms. Headache. 2011;51(6)860-868.
The neurobiological mechanism linking PTSD to migraine is not known. Although a variety of theories exist—including low serotonin levels, dysfunctions of the autonomic system and hypothalamic-pituitary-adrenal axis (HPA) in both migraine and PTSD, and elevated baseline cortisol levels in migraineurs—it remains unclear why the association is stronger in men than in women.34 Some studies suggest that sex-related differences of the HPA axis may play a role.36,37 Others consider fMRI findings of sex differences in cerebral blood flow to pain centers in response to psychological distress.37 Further research into the sex-related differences of migraineurs with PTSD will likely reveal insights into new therapeutic directions for men and women with these disorders.
Implications for clinicians
The preceding data add to the understanding that numerous comorbidities exist in individuals with migraine. If a patient is a migraineur, screen for PTSD as well as depression and anxiety. Treatment with cognitive behavioral therapy—alone or in combination with pharmacological therapy—should be considered, since treatment of PTSD alone has been shown to have a beneficial effect on both pain and disability in chronic pain patients.38
Given that obesity is a modifiable risk factor, educate all migraine patients about the association with obesity in general, the increasing risk of migraine associated with increasing obesity, and the potential effect of weight gain/loss on headache frequency.26,27 Also inform patients about the potential effects migraine medications may have on their weight, and encourage them to eat a healthy diet, exercise, and avoid gaining excessive weight. If other comorbidities are involved, tailor the therapeutic regimen based on that combination. If a migraine patient is obese and has high blood pressure, look for an antihypertensive agent that is relatively weight-neutral.
Eliminating menstrual migraine should be an important treatment goal for patients in whom it is the most disabling migraine of the month. Hormonal preventives may be the best approach for women whose menstrual attacks are resistant to acute treatment.21
Disclosures
B. Lee Peterlin, DO, has received grant/research support from GlaxoSmithKline, has served as a consultant to Nautilus, and has served on the speaker’s bureau of Zogenix. She holds a provisional patent for use of adiponectin-modulating drugs for migraine.
Anne H. Calhoun, MD, has no conflicts of interest to report.
Fred Balzac has no conflicts of interest to report.
1. Lipton RB, Stewart WF, Diamond S, et al. Prevalence and burden of migraine in the United States: data from the American Migraine Study II. Headache. 2001;41:646-657.
2. Rasmussen BK, Jensen R, Schroll M, et al. Epidemiology of headache in a general population—a prevalence study. J Clin Epidemiol. 1991;44(11)1147-1157.
3. Peterlin BL, Katsnelson MJ, Calhoun AH. The associations between migraine, unipolar psychiatric comorbidities, and stress-related disorders and the role of estrogen. Curr Pain Headache Rep. 2009;13:404-412.
4. Stewart WF, Linet MS, Celentano DD, et al. Age- and sex-specific incidence rates of migraine with and without visual aura. Am J Epidemiol. 1991;134(10):1111-1120.
5. Stewart WF, Lipton RB, Celentano DD, et al. Prevalence of migraine headache in the United States: relation to age, income, race, and other sociodemographic factors. JAMA. 1992;267:64- 69.
6. Lipton RB, Stewart WF. Migraine in the United States: a review of epidemiology and health care use. Neurology. 1993;43(suppl 3):S6-10.
7. Wober C, Brannath W, Schmidt K, et al. Prospective analysis of factors related to migraine attacks: The PAMINA study. Cephalalgia. 2007;27:304-314.
8. Calhoun AH, Ford S, Millen C, et al. The prevalence of neck pain in migraine. Headache. 2010;50:1273-1277.
9. Breslau N, Lipton RB, Stewart WF, et al. Comorbidity of migraine and depression: Investigating potential etiology and prognosis. Neurology. 2003;60:1308-1312.
10. Stewart W, Breslau N, Keck PE Jr. Comorbidity of migraine and panic disorder. Neurology. 1994;44:S23-S27.
11. Scher AI, Terwindt GM, Picavet HS, et al. Cardiovascular risk factors and migraine: The GEM population based study. Neurology. 2005;64:614-620.
12. Ottman R, Lipton RB. Comorbidity of migraine and epilepsy. Neurology. 1994;44:2105-2110.
13. Moreau T, Manceau E, Giroud-Baleydier F, et al. Headache in hypothyroidism. Prevalence and outcome under thyroid hormone therapy. Cephalalgia. 1998;18:687-689.
14. Ferrero S, Pretta S, Bertoldi S, et al. Increased frequency of migraine among women with endometriosis. Hum Reprod. 2004;19:2927-2932.
15. MacGregor EA. “Menstrual” migraine: Towards a definition. Cephalalgia. 1996;16:11-21.
16. Calhoun AH, Hutchinson S. Hormonal therapies for menstrual migraine. Curr Pain Headache Rep.2009;13:381-385.
17. Granella F, Sances G, Allais G, et al. Characteristics of menstrual and nonmenstrual attacks in women with menstrually related migraine referred to headache centres. Cephalalgia. 2004;24:707-716.
18. MacGregor EA, Hackshaw A. Prevalence of migraine on each day of the natural menstrual cycle. Neurology. 2004;63:351-353.
19. Neri I, Granella F, Nappi R, et al. Characteristics of headache at menopause: a clinico-epidemiologic study. Maturitas.1993;17:31-37.
20. Brandes JL. The influence of estrogen on migraine: a systematic review. JAMA. 2006;295(15):1824-1830.
21. Calhoun A, Ford S. Elimination of menstrual-related migraine beneficially impacts chronification and medication overuse. Headache. 2008;48:1186-1193.
22. Scher AI, Stewart WF, Ricci JA, et al. Factors associated with the onset and remission of chronic daily headache in a population-based study. Pain. 2003;106:81-89.
23. Horev A, Wirguin I, Lantsberg L, et al. A high incidence of migraine with aura among morbidly obese women. Headache. 2005;45:936-938.
24. Ford ES, Li C, Pearson WS, et al. Body mass index and headaches: Findings from a national sample of US adults. Cephalalgia. 2008;28(12):1270-1276.
25. Peterlin BL, Rapoport AM, Kurth T. Migraine and obesity: Epidemiology, mechanisms, and implications. Headache. 2012;50:631-648.
26. Peterlin BL, Rosso AL, Rapoport AM, et al. Obesity and migraine: the effect of age, gender and adipose tissue distribution. Headache. 2010;50:52-62.
27. Vo M, Ainalem A, Qiu C, et al. Body mass index and adult weight gain among reproductive age women with migraine. Headache. 2011;51:559-569.
28. Novack V, Fuchs L, Lantsberg L, et al. Changes in headache frequency in premenopausal obese women with migraine after bariatric surgery: A case series. Cephalalgia. 2011;31(13):1336-1342.
29. Bond DS, Vithiananthan S, Nash JM, et al. Improvement of migraine headaches in severely obese patients after bariatric surgery. Neurology. 2011;76(13)1135-1138.
30. Peterlin BL. Bariatric surgery in obese migraineurs: Mounting evidence but important questions remain. Cephalalgia. 2011;31(13):1333-1335.
31. Kessler RC, Berglund P, Delmer O, et al. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):593-602.
32. Butterfield MI, Becker M, Marx CE. Posttraumatic stress disorder in women: Current concepts and treatments. Curr Psychiatry Rep. 2002;4:474-486.
33. Breslau N. The epidemiology of trauma, PTSD, and other posttrauma disorders. Trauma Violence Abuse. 2009;10(3):198-210.
34. Peterlin BL, Rosso AL, Sheftell FD, et al. Post-traumatic stress disorder, drug abuse and migraine: new findings from the National Comorbidity Survey Replication (NCS-R). Cephalalgia. 2011;31:235-244.
35. Peterlin BL, Nijjar SS, Tietjen GE. Post-traumatic stress disorder and migraine: epidemiology, sex differences, and potential mechanisms. Headache. 2011;51:860-868.
36. Rainero I, Ferrero M, Rubino E, et al. Endocrine function is altered in chronic migraine patient with medication-overuse. Headache. 2006;46:597-603.
37. Wang J, Korczykowski, Rao H, et al. Gender difference in neural response to psychological stress. Soc Cog Affect Neurosci. 2007;2:227-239.
38. Peterlin BL, Tietjen GE, Brandes JL, et al. Posttraumatic stress disorder in migraine. Headache. 2009;49:541-551.
1. Lipton RB, Stewart WF, Diamond S, et al. Prevalence and burden of migraine in the United States: data from the American Migraine Study II. Headache. 2001;41:646-657.
2. Rasmussen BK, Jensen R, Schroll M, et al. Epidemiology of headache in a general population—a prevalence study. J Clin Epidemiol. 1991;44(11)1147-1157.
3. Peterlin BL, Katsnelson MJ, Calhoun AH. The associations between migraine, unipolar psychiatric comorbidities, and stress-related disorders and the role of estrogen. Curr Pain Headache Rep. 2009;13:404-412.
4. Stewart WF, Linet MS, Celentano DD, et al. Age- and sex-specific incidence rates of migraine with and without visual aura. Am J Epidemiol. 1991;134(10):1111-1120.
5. Stewart WF, Lipton RB, Celentano DD, et al. Prevalence of migraine headache in the United States: relation to age, income, race, and other sociodemographic factors. JAMA. 1992;267:64- 69.
6. Lipton RB, Stewart WF. Migraine in the United States: a review of epidemiology and health care use. Neurology. 1993;43(suppl 3):S6-10.
7. Wober C, Brannath W, Schmidt K, et al. Prospective analysis of factors related to migraine attacks: The PAMINA study. Cephalalgia. 2007;27:304-314.
8. Calhoun AH, Ford S, Millen C, et al. The prevalence of neck pain in migraine. Headache. 2010;50:1273-1277.
9. Breslau N, Lipton RB, Stewart WF, et al. Comorbidity of migraine and depression: Investigating potential etiology and prognosis. Neurology. 2003;60:1308-1312.
10. Stewart W, Breslau N, Keck PE Jr. Comorbidity of migraine and panic disorder. Neurology. 1994;44:S23-S27.
11. Scher AI, Terwindt GM, Picavet HS, et al. Cardiovascular risk factors and migraine: The GEM population based study. Neurology. 2005;64:614-620.
12. Ottman R, Lipton RB. Comorbidity of migraine and epilepsy. Neurology. 1994;44:2105-2110.
13. Moreau T, Manceau E, Giroud-Baleydier F, et al. Headache in hypothyroidism. Prevalence and outcome under thyroid hormone therapy. Cephalalgia. 1998;18:687-689.
14. Ferrero S, Pretta S, Bertoldi S, et al. Increased frequency of migraine among women with endometriosis. Hum Reprod. 2004;19:2927-2932.
15. MacGregor EA. “Menstrual” migraine: Towards a definition. Cephalalgia. 1996;16:11-21.
16. Calhoun AH, Hutchinson S. Hormonal therapies for menstrual migraine. Curr Pain Headache Rep.2009;13:381-385.
17. Granella F, Sances G, Allais G, et al. Characteristics of menstrual and nonmenstrual attacks in women with menstrually related migraine referred to headache centres. Cephalalgia. 2004;24:707-716.
18. MacGregor EA, Hackshaw A. Prevalence of migraine on each day of the natural menstrual cycle. Neurology. 2004;63:351-353.
19. Neri I, Granella F, Nappi R, et al. Characteristics of headache at menopause: a clinico-epidemiologic study. Maturitas.1993;17:31-37.
20. Brandes JL. The influence of estrogen on migraine: a systematic review. JAMA. 2006;295(15):1824-1830.
21. Calhoun A, Ford S. Elimination of menstrual-related migraine beneficially impacts chronification and medication overuse. Headache. 2008;48:1186-1193.
22. Scher AI, Stewart WF, Ricci JA, et al. Factors associated with the onset and remission of chronic daily headache in a population-based study. Pain. 2003;106:81-89.
23. Horev A, Wirguin I, Lantsberg L, et al. A high incidence of migraine with aura among morbidly obese women. Headache. 2005;45:936-938.
24. Ford ES, Li C, Pearson WS, et al. Body mass index and headaches: Findings from a national sample of US adults. Cephalalgia. 2008;28(12):1270-1276.
25. Peterlin BL, Rapoport AM, Kurth T. Migraine and obesity: Epidemiology, mechanisms, and implications. Headache. 2012;50:631-648.
26. Peterlin BL, Rosso AL, Rapoport AM, et al. Obesity and migraine: the effect of age, gender and adipose tissue distribution. Headache. 2010;50:52-62.
27. Vo M, Ainalem A, Qiu C, et al. Body mass index and adult weight gain among reproductive age women with migraine. Headache. 2011;51:559-569.
28. Novack V, Fuchs L, Lantsberg L, et al. Changes in headache frequency in premenopausal obese women with migraine after bariatric surgery: A case series. Cephalalgia. 2011;31(13):1336-1342.
29. Bond DS, Vithiananthan S, Nash JM, et al. Improvement of migraine headaches in severely obese patients after bariatric surgery. Neurology. 2011;76(13)1135-1138.
30. Peterlin BL. Bariatric surgery in obese migraineurs: Mounting evidence but important questions remain. Cephalalgia. 2011;31(13):1333-1335.
31. Kessler RC, Berglund P, Delmer O, et al. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):593-602.
32. Butterfield MI, Becker M, Marx CE. Posttraumatic stress disorder in women: Current concepts and treatments. Curr Psychiatry Rep. 2002;4:474-486.
33. Breslau N. The epidemiology of trauma, PTSD, and other posttrauma disorders. Trauma Violence Abuse. 2009;10(3):198-210.
34. Peterlin BL, Rosso AL, Sheftell FD, et al. Post-traumatic stress disorder, drug abuse and migraine: new findings from the National Comorbidity Survey Replication (NCS-R). Cephalalgia. 2011;31:235-244.
35. Peterlin BL, Nijjar SS, Tietjen GE. Post-traumatic stress disorder and migraine: epidemiology, sex differences, and potential mechanisms. Headache. 2011;51:860-868.
36. Rainero I, Ferrero M, Rubino E, et al. Endocrine function is altered in chronic migraine patient with medication-overuse. Headache. 2006;46:597-603.
37. Wang J, Korczykowski, Rao H, et al. Gender difference in neural response to psychological stress. Soc Cog Affect Neurosci. 2007;2:227-239.
38. Peterlin BL, Tietjen GE, Brandes JL, et al. Posttraumatic stress disorder in migraine. Headache. 2009;49:541-551.
Chronic Pain Perspectives - September 2011
- Central pain states: a shift in thinking about chronic pain
- Use of complementary therapies to treat the pain of osteoarthritis
- The promise of telemedicine: providing curbside consults for chronic care, acute care, and pain
- REMS: red tape, or a remedy for opioid abuse?
- Central pain states: a shift in thinking about chronic pain
- Use of complementary therapies to treat the pain of osteoarthritis
- The promise of telemedicine: providing curbside consults for chronic care, acute care, and pain
- REMS: red tape, or a remedy for opioid abuse?
- Central pain states: a shift in thinking about chronic pain
- Use of complementary therapies to treat the pain of osteoarthritis
- The promise of telemedicine: providing curbside consults for chronic care, acute care, and pain
- REMS: red tape, or a remedy for opioid abuse?
