User login
ACO Insider: Not ready for an ACO? Think CPC+
The Centers for Medicare & Medicaid Services in April announced its newest initiative, Comprehensive Primary Care Plus, to target primary care practices of varying capabilities to participate in an innovative payment model designed to support the delivery of comprehensive primary care that rewards value and quality.
“Strengthening primary care is critical to an effective health care system,” said Patrick Conway, MD, CMS deputy administrator and chief medical officer. “By supporting primary care doctors and clinicians to spend time with patients, serve patients’ needs outside of the office visit, and better coordinate care with specialists, we can continue to build a health care system that results in healthier people and smarter spending of our health care dollars.”

As readers of this column know, these are also the engines of accountable care organization success. So, if you and your patient-centered medical home are not in a Medicare ACO, this gets you going on high-value activities – and pays you monthly to do it.
The rub is that once you are in the Medicare Shared Savings Program, you can’t continue with this initiative. But, it’s a great “on ramp” to prep you for ACO success. You get monthly payments instead of waiting 18 months for shared savings that you may or may not get under the Medicare Shared Savings Program.
CPC+ is an advanced primary medical home model, created from lessons learned in the Comprehensive Primary Care Initiative and the Multi-Payer Advanced Primary Care Practice Demonstration. Similar to these programs, multi-payer engagement is an essential component of the model.
In the CPC+ model, the CMS intends to nationally solicit a variety of payers committed to strengthening primary care in up to 20 regions and accept up to 5,000 practices to participate in those regions. The CPC+ program is further evidence that primary care should not only be a fundamental component to moving our health care system to one that awards clinicians based on the quality, not quantity, of care they give patients, but that payment redesign must provide flexibility to accommodate the diverse needs of primary care practices.
What to know about payment
To provide this flexibility and to attract practices of varying capabilities and levels of experience, the CPC+ program offers two tracks with different payment options, which include a monthly care management fee, comprehensive primary care payments, and performance-based incentive payments.
In track 1, the CMS will pay practices a risk-adjusted prospective monthly care management fee ($15 per beneficiary per month [PBPM] average across four risk tiers), in addition to the fee-for-service payments under the Medicare Physician Fee Schedule for activities.
In track 2, the Medicare monthly care management fees will average $28 PBPM across five risk tiers, which includes a $100 care management fee to support care for patients with the most complex needs. Instead of full Medicare fee-for-service payments for evaluation and management services, track 2 practices will receive a hybrid of reduced Medicare fee-for-service payments and up-front comprehensive primary care payments for those services.
In addition, the CMS is providing incentive payments at $2.50 PBPM for track 1 and $4 PBPM for track 2, based on practice performance on utilization metrics and quality, measured at the practice level. While these payments are prepaid at the beginning of a performance year, they are subject to recoupment if the practice does not meet thresholds for quality and utilization performance.
What to know about participation
To participate, your practice must be located within 1 of the 20 regional geographic areas selected by the CMS and must serve not only Medicare beneficiaries, but patients covered by one or more additional participating payers.
You may apply for either track 1 or track 2, but participation for the entire 5-year period will be within a single track.
All practices will be expected to deliver a set of five comprehensive primary care functions and have certified electronic health record technology capabilities. Track 2 practices will be expected to focus on a core set of advance capabilities for health information technology and must submit a letter of support from their health IT vendors. The CMS may require a track 2 applicant to participate in track 1.
Participating in the CPC+ program limits your ability to fully participate in or utilize other CMS initiatives, models, or demonstrations, however – including the Medicare Shared Savings Program and Next Generation ACO, or bill for the chronic care management fee. This is a big trade-off for practices well down the value transformation path, but an opportunity for those getting started.
Although the shift to payment for improved population health can herald the golden age of primary care, you cannot default on this opportunity through inaction. It is urgent that you choose a path to value-care delivery. CPC+ provides the ability for greater cash flow and flexibility for primary care practices to deliver high-quality, whole-person patient-centered care.
Mr. Bobbitt is head of the health law group at the Smith Anderson law firm in Raleigh, N.C. He is president of Value Health Partners, LLC, a health care strategic consulting company. He has years of experience assisting physicians to form integrated delivery systems and prepare for the value-based compensation era. Mr. Parker is a member of the health law group at Smith Anderson and works with Mr. Bobbitt to guide physicians regarding preparing for value-based care. This article is meant to be educational and does not constitute legal advice. For additional information, readers may contact the author at [email protected] or 919-821-6612.
The Centers for Medicare & Medicaid Services in April announced its newest initiative, Comprehensive Primary Care Plus, to target primary care practices of varying capabilities to participate in an innovative payment model designed to support the delivery of comprehensive primary care that rewards value and quality.
“Strengthening primary care is critical to an effective health care system,” said Patrick Conway, MD, CMS deputy administrator and chief medical officer. “By supporting primary care doctors and clinicians to spend time with patients, serve patients’ needs outside of the office visit, and better coordinate care with specialists, we can continue to build a health care system that results in healthier people and smarter spending of our health care dollars.”
As readers of this column know, these are also the engines of accountable care organization success. So, if you and your patient-centered medical home are not in a Medicare ACO, this gets you going on high-value activities – and pays you monthly to do it.
The rub is that once you are in the Medicare Shared Savings Program, you can’t continue with this initiative. But, it’s a great “on ramp” to prep you for ACO success. You get monthly payments instead of waiting 18 months for shared savings that you may or may not get under the Medicare Shared Savings Program.
CPC+ is an advanced primary medical home model, created from lessons learned in the Comprehensive Primary Care Initiative and the Multi-Payer Advanced Primary Care Practice Demonstration. Similar to these programs, multi-payer engagement is an essential component of the model.
In the CPC+ model, the CMS intends to nationally solicit a variety of payers committed to strengthening primary care in up to 20 regions and accept up to 5,000 practices to participate in those regions. The CPC+ program is further evidence that primary care should not only be a fundamental component to moving our health care system to one that awards clinicians based on the quality, not quantity, of care they give patients, but that payment redesign must provide flexibility to accommodate the diverse needs of primary care practices.
What to know about payment
To provide this flexibility and to attract practices of varying capabilities and levels of experience, the CPC+ program offers two tracks with different payment options, which include a monthly care management fee, comprehensive primary care payments, and performance-based incentive payments.
In track 1, the CMS will pay practices a risk-adjusted prospective monthly care management fee ($15 per beneficiary per month [PBPM] average across four risk tiers), in addition to the fee-for-service payments under the Medicare Physician Fee Schedule for activities.
In track 2, the Medicare monthly care management fees will average $28 PBPM across five risk tiers, which includes a $100 care management fee to support care for patients with the most complex needs. Instead of full Medicare fee-for-service payments for evaluation and management services, track 2 practices will receive a hybrid of reduced Medicare fee-for-service payments and up-front comprehensive primary care payments for those services.
In addition, the CMS is providing incentive payments at $2.50 PBPM for track 1 and $4 PBPM for track 2, based on practice performance on utilization metrics and quality, measured at the practice level. While these payments are prepaid at the beginning of a performance year, they are subject to recoupment if the practice does not meet thresholds for quality and utilization performance.
What to know about participation
To participate, your practice must be located within 1 of the 20 regional geographic areas selected by the CMS and must serve not only Medicare beneficiaries, but patients covered by one or more additional participating payers.
You may apply for either track 1 or track 2, but participation for the entire 5-year period will be within a single track.
All practices will be expected to deliver a set of five comprehensive primary care functions and have certified electronic health record technology capabilities. Track 2 practices will be expected to focus on a core set of advance capabilities for health information technology and must submit a letter of support from their health IT vendors. The CMS may require a track 2 applicant to participate in track 1.
Participating in the CPC+ program limits your ability to fully participate in or utilize other CMS initiatives, models, or demonstrations, however – including the Medicare Shared Savings Program and Next Generation ACO, or bill for the chronic care management fee. This is a big trade-off for practices well down the value transformation path, but an opportunity for those getting started.
Although the shift to payment for improved population health can herald the golden age of primary care, you cannot default on this opportunity through inaction. It is urgent that you choose a path to value-care delivery. CPC+ provides the ability for greater cash flow and flexibility for primary care practices to deliver high-quality, whole-person patient-centered care.
Mr. Bobbitt is head of the health law group at the Smith Anderson law firm in Raleigh, N.C. He is president of Value Health Partners, LLC, a health care strategic consulting company. He has years of experience assisting physicians to form integrated delivery systems and prepare for the value-based compensation era. Mr. Parker is a member of the health law group at Smith Anderson and works with Mr. Bobbitt to guide physicians regarding preparing for value-based care. This article is meant to be educational and does not constitute legal advice. For additional information, readers may contact the author at [email protected] or 919-821-6612.
The Centers for Medicare & Medicaid Services in April announced its newest initiative, Comprehensive Primary Care Plus, to target primary care practices of varying capabilities to participate in an innovative payment model designed to support the delivery of comprehensive primary care that rewards value and quality.
“Strengthening primary care is critical to an effective health care system,” said Patrick Conway, MD, CMS deputy administrator and chief medical officer. “By supporting primary care doctors and clinicians to spend time with patients, serve patients’ needs outside of the office visit, and better coordinate care with specialists, we can continue to build a health care system that results in healthier people and smarter spending of our health care dollars.”
As readers of this column know, these are also the engines of accountable care organization success. So, if you and your patient-centered medical home are not in a Medicare ACO, this gets you going on high-value activities – and pays you monthly to do it.
The rub is that once you are in the Medicare Shared Savings Program, you can’t continue with this initiative. But, it’s a great “on ramp” to prep you for ACO success. You get monthly payments instead of waiting 18 months for shared savings that you may or may not get under the Medicare Shared Savings Program.
CPC+ is an advanced primary medical home model, created from lessons learned in the Comprehensive Primary Care Initiative and the Multi-Payer Advanced Primary Care Practice Demonstration. Similar to these programs, multi-payer engagement is an essential component of the model.
In the CPC+ model, the CMS intends to nationally solicit a variety of payers committed to strengthening primary care in up to 20 regions and accept up to 5,000 practices to participate in those regions. The CPC+ program is further evidence that primary care should not only be a fundamental component to moving our health care system to one that awards clinicians based on the quality, not quantity, of care they give patients, but that payment redesign must provide flexibility to accommodate the diverse needs of primary care practices.
What to know about payment
To provide this flexibility and to attract practices of varying capabilities and levels of experience, the CPC+ program offers two tracks with different payment options, which include a monthly care management fee, comprehensive primary care payments, and performance-based incentive payments.
In track 1, the CMS will pay practices a risk-adjusted prospective monthly care management fee ($15 per beneficiary per month [PBPM] average across four risk tiers), in addition to the fee-for-service payments under the Medicare Physician Fee Schedule for activities.
In track 2, the Medicare monthly care management fees will average $28 PBPM across five risk tiers, which includes a $100 care management fee to support care for patients with the most complex needs. Instead of full Medicare fee-for-service payments for evaluation and management services, track 2 practices will receive a hybrid of reduced Medicare fee-for-service payments and up-front comprehensive primary care payments for those services.
In addition, the CMS is providing incentive payments at $2.50 PBPM for track 1 and $4 PBPM for track 2, based on practice performance on utilization metrics and quality, measured at the practice level. While these payments are prepaid at the beginning of a performance year, they are subject to recoupment if the practice does not meet thresholds for quality and utilization performance.
What to know about participation
To participate, your practice must be located within 1 of the 20 regional geographic areas selected by the CMS and must serve not only Medicare beneficiaries, but patients covered by one or more additional participating payers.
You may apply for either track 1 or track 2, but participation for the entire 5-year period will be within a single track.
All practices will be expected to deliver a set of five comprehensive primary care functions and have certified electronic health record technology capabilities. Track 2 practices will be expected to focus on a core set of advance capabilities for health information technology and must submit a letter of support from their health IT vendors. The CMS may require a track 2 applicant to participate in track 1.
Participating in the CPC+ program limits your ability to fully participate in or utilize other CMS initiatives, models, or demonstrations, however – including the Medicare Shared Savings Program and Next Generation ACO, or bill for the chronic care management fee. This is a big trade-off for practices well down the value transformation path, but an opportunity for those getting started.
Although the shift to payment for improved population health can herald the golden age of primary care, you cannot default on this opportunity through inaction. It is urgent that you choose a path to value-care delivery. CPC+ provides the ability for greater cash flow and flexibility for primary care practices to deliver high-quality, whole-person patient-centered care.
Mr. Bobbitt is head of the health law group at the Smith Anderson law firm in Raleigh, N.C. He is president of Value Health Partners, LLC, a health care strategic consulting company. He has years of experience assisting physicians to form integrated delivery systems and prepare for the value-based compensation era. Mr. Parker is a member of the health law group at Smith Anderson and works with Mr. Bobbitt to guide physicians regarding preparing for value-based care. This article is meant to be educational and does not constitute legal advice. For additional information, readers may contact the author at [email protected] or 919-821-6612.

Unresolved questions about the specialty lurk in the cortex of psychiatrists
But many of our own questions await an answer. The fact is that psychiatrists have serious, nagging questions—in every cortical fold of their collective brain—about patients’ welfare, psychiatric practice, and professional matters. Their questions about frustrations of daily practice deserve an honest and convincing response, yet go begging—expressed so well in songwriter Bob Dylan’s lyric, “The answer is blowin’ in the wind.”
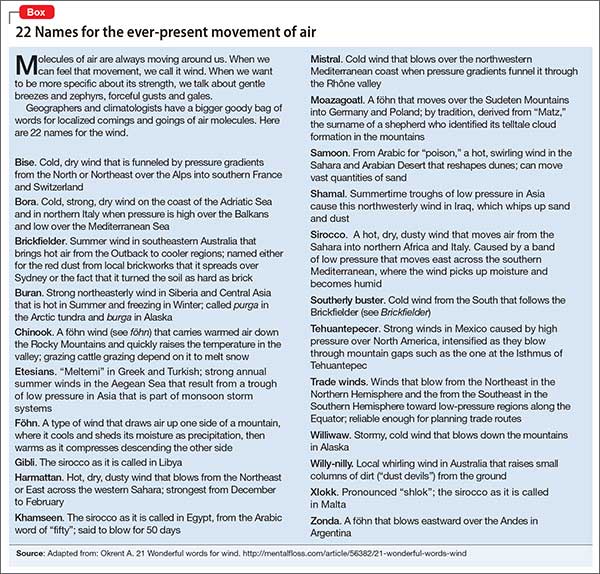
What follows are long-standing “Why?” questions whose answers are still blowin’ in the wind. (Dylan didn’t specify which wind is blowin’, so I’ve provided the names of 22 atmospheric movements of air molecules in the Box. Take your pick!)
Why is a jail OK for the mentally ill but an asylum is not? Why is it necessary to put armed guards in charge of psychiatric patients instead of a multidisciplinary team of psychiatrists, primary care providers, nurses, social workers, psychologists, and pharmacists? Why has a brain disease, such as psychosis or bipolar disorder, become a punishable felony instead of a treatable illness?
Why did the system of mental health care degenerate to the point that a severely depressed or suicidal, or acutely psychotic, patient can be hospitalized for only 4 or 5 days, then must be discharged before her (his) illness has been fully controlled? Why do health care insurers exhibit that atrocious combination of maximum greed and minimal compassion?
Why does a completely unjustified and hurtful stigma continue to plague mental brain disorders, patients who suffer from them, mental health professionals, and the very discipline of psychiatry?
Why do otherwise intelligent people show compassion toward people with a brain disorder such as stroke, Parkinson’s disease, multiple sclerosis, myasthenia gravis, or migraine, but express aversion and even disdain for psychiatric brain disorders such as schizophrenia, depression, obsessive-compulsive disorder, and panic disorder?
And why does this prejudice persist despite advances in psychiatric neuroscience that have used neurogenetics, neuroimaging, and molecular studies to establish, without a doubt, the neurobiological basis of all psychiatric disorders.
Why are there still no objective diagnostic criteria for psychiatric disorders? Why do we persist in using defining symptoms that have been volunteered by patients—symptoms that can be subject to distortion or malingering? Why aren’t the hundreds of established biomarkers being incorporated into the diagnostic formulation, to lessen subjectivity and improve reliability and validity?
Why is off-label prescribing, the judicious clinical repurposing of psychotropic medications, criticized and panned, even though there are no approved drugs for 88.5% psychiatric diagnoses?1 Why allow insurers to refuse to pay for a medication that can help a patient, just because the patient has not been given the “official” diagnosis for which the FDA approved that drug?
And why doesn’t the FDA solve this problem by revising its requirements that registration trials for new medications test their efficacy for a single symptom, rather than a diagnosis comprising multiple symptoms?
Why do people not accept the fact that all drugs have benefits and risks, and that it is impossible to have pure efficacy without side effects? Why empower lawyers to make clinical care adversarial? Why do lawyers refrain from suing oncologists or manufacturers of life-saving chemotherapy drugs because of terrible adverse effects, but pounce on other medications that might cause a serious side effect in a tiny percentage of patients that is clearly spelled out in the package insert?
Why do people demonize the pharmaceutical industry far more than other industries? No other entity discovers and develops life-saving medications.
Why don’t people realize that, without medications, massive numbers of patients would be hospitalized and the death rate would rise? Why can’t people weigh risks and benefits of having a pharmaceutical industry, just as they assess the risk-benefit ratio of everything in life?
Should the government impose a massive ($1 or $2 trillion) tax hike to establish infrastructure for drug research and development, for the benefit of psychiatry and all other medical specialties?
Why is there a severe shortage of psychiatrists but a glut of lawyers? Why doesn’t society rationally deploy its resources to meet urgent social needs and priorities? And why do lawyers bill us for every minute we talk to them, while we field telephone calls and e-mail messages from patients without compensation?
Why did the FDA allow the pharmaceutical industry to develop direct-to-consumer advertising? Why do they not realize how that decision has complicated the doctor–patient relationship, and how it preempts physicians’ evidence-based decision-making by encouraging consumers to demand a drug that they saw on television—a contorted version of prescribing by proxy?
Why (speaking of prescribing without a license), do politicians pass laws allowing people who do not have required medical training to take a short-cut to becoming a prescriber? Why not mandate that politicians, and their families, receive medical care exclusively from unqualified practitioners on whom they bestow prescribing privileges without requisite comprehensive medical training?Why do some psychiatrists resist changing their practice patterns despite continuous advances that update the care they provide? Why do reports of exciting therapeutic breakthroughs, published in top-tier journals, go unread by so many practitioners? Why do they say they are too busy to read journals or peruse PubMed?
Why don’t people realize that today’s research is tomorrow’s treatment? That research is not a luxury but an ongoing necessity? Why don’t more freshly minted, young psychiatrists pursue a career in research to accelerate the pace of progress about the biological causes and treatments of serious psychiatric disorders? Why aren’t there more incentives to grow the next generation of psychiatric discoverers and Nobel laureates? Why don’t clinicians support research by referring patients to clinical trials of medications or to National Institutes of Health-funded investigations of the neurobiology of psychiatric disorders?
Are these just rhetorical questions?
Some might sound that way. But they are not. These questions are brewing inside the hearts and minds of many psychiatrists, although only a few seem determined to relentlessly seek answers on which medical science and society can act.
We should collectively pose these “why” questions and not accept long-winded, hollow answers. We need to foster the winds of change—not resign ourselves to winds in which answers blow about but, ultimately, disappear.
1. Devulapalli KK, Nasrallah HA. An analysis of the high psychotropic off-label use in psychiatric disorders. Asian J Psychiatr. 2009;2(1):29-36.
But many of our own questions await an answer. The fact is that psychiatrists have serious, nagging questions—in every cortical fold of their collective brain—about patients’ welfare, psychiatric practice, and professional matters. Their questions about frustrations of daily practice deserve an honest and convincing response, yet go begging—expressed so well in songwriter Bob Dylan’s lyric, “The answer is blowin’ in the wind.”
What follows are long-standing “Why?” questions whose answers are still blowin’ in the wind. (Dylan didn’t specify which wind is blowin’, so I’ve provided the names of 22 atmospheric movements of air molecules in the Box. Take your pick!)
Why is a jail OK for the mentally ill but an asylum is not? Why is it necessary to put armed guards in charge of psychiatric patients instead of a multidisciplinary team of psychiatrists, primary care providers, nurses, social workers, psychologists, and pharmacists? Why has a brain disease, such as psychosis or bipolar disorder, become a punishable felony instead of a treatable illness?
Why did the system of mental health care degenerate to the point that a severely depressed or suicidal, or acutely psychotic, patient can be hospitalized for only 4 or 5 days, then must be discharged before her (his) illness has been fully controlled? Why do health care insurers exhibit that atrocious combination of maximum greed and minimal compassion?
Why does a completely unjustified and hurtful stigma continue to plague mental brain disorders, patients who suffer from them, mental health professionals, and the very discipline of psychiatry?
Why do otherwise intelligent people show compassion toward people with a brain disorder such as stroke, Parkinson’s disease, multiple sclerosis, myasthenia gravis, or migraine, but express aversion and even disdain for psychiatric brain disorders such as schizophrenia, depression, obsessive-compulsive disorder, and panic disorder?
And why does this prejudice persist despite advances in psychiatric neuroscience that have used neurogenetics, neuroimaging, and molecular studies to establish, without a doubt, the neurobiological basis of all psychiatric disorders.
Why are there still no objective diagnostic criteria for psychiatric disorders? Why do we persist in using defining symptoms that have been volunteered by patients—symptoms that can be subject to distortion or malingering? Why aren’t the hundreds of established biomarkers being incorporated into the diagnostic formulation, to lessen subjectivity and improve reliability and validity?
Why is off-label prescribing, the judicious clinical repurposing of psychotropic medications, criticized and panned, even though there are no approved drugs for 88.5% psychiatric diagnoses?1 Why allow insurers to refuse to pay for a medication that can help a patient, just because the patient has not been given the “official” diagnosis for which the FDA approved that drug?
And why doesn’t the FDA solve this problem by revising its requirements that registration trials for new medications test their efficacy for a single symptom, rather than a diagnosis comprising multiple symptoms?
Why do people not accept the fact that all drugs have benefits and risks, and that it is impossible to have pure efficacy without side effects? Why empower lawyers to make clinical care adversarial? Why do lawyers refrain from suing oncologists or manufacturers of life-saving chemotherapy drugs because of terrible adverse effects, but pounce on other medications that might cause a serious side effect in a tiny percentage of patients that is clearly spelled out in the package insert?
Why do people demonize the pharmaceutical industry far more than other industries? No other entity discovers and develops life-saving medications.
Why don’t people realize that, without medications, massive numbers of patients would be hospitalized and the death rate would rise? Why can’t people weigh risks and benefits of having a pharmaceutical industry, just as they assess the risk-benefit ratio of everything in life?
Should the government impose a massive ($1 or $2 trillion) tax hike to establish infrastructure for drug research and development, for the benefit of psychiatry and all other medical specialties?
Why is there a severe shortage of psychiatrists but a glut of lawyers? Why doesn’t society rationally deploy its resources to meet urgent social needs and priorities? And why do lawyers bill us for every minute we talk to them, while we field telephone calls and e-mail messages from patients without compensation?
Why did the FDA allow the pharmaceutical industry to develop direct-to-consumer advertising? Why do they not realize how that decision has complicated the doctor–patient relationship, and how it preempts physicians’ evidence-based decision-making by encouraging consumers to demand a drug that they saw on television—a contorted version of prescribing by proxy?
Why (speaking of prescribing without a license), do politicians pass laws allowing people who do not have required medical training to take a short-cut to becoming a prescriber? Why not mandate that politicians, and their families, receive medical care exclusively from unqualified practitioners on whom they bestow prescribing privileges without requisite comprehensive medical training?Why do some psychiatrists resist changing their practice patterns despite continuous advances that update the care they provide? Why do reports of exciting therapeutic breakthroughs, published in top-tier journals, go unread by so many practitioners? Why do they say they are too busy to read journals or peruse PubMed?
Why don’t people realize that today’s research is tomorrow’s treatment? That research is not a luxury but an ongoing necessity? Why don’t more freshly minted, young psychiatrists pursue a career in research to accelerate the pace of progress about the biological causes and treatments of serious psychiatric disorders? Why aren’t there more incentives to grow the next generation of psychiatric discoverers and Nobel laureates? Why don’t clinicians support research by referring patients to clinical trials of medications or to National Institutes of Health-funded investigations of the neurobiology of psychiatric disorders?
Are these just rhetorical questions?
Some might sound that way. But they are not. These questions are brewing inside the hearts and minds of many psychiatrists, although only a few seem determined to relentlessly seek answers on which medical science and society can act.
We should collectively pose these “why” questions and not accept long-winded, hollow answers. We need to foster the winds of change—not resign ourselves to winds in which answers blow about but, ultimately, disappear.
But many of our own questions await an answer. The fact is that psychiatrists have serious, nagging questions—in every cortical fold of their collective brain—about patients’ welfare, psychiatric practice, and professional matters. Their questions about frustrations of daily practice deserve an honest and convincing response, yet go begging—expressed so well in songwriter Bob Dylan’s lyric, “The answer is blowin’ in the wind.”
What follows are long-standing “Why?” questions whose answers are still blowin’ in the wind. (Dylan didn’t specify which wind is blowin’, so I’ve provided the names of 22 atmospheric movements of air molecules in the Box. Take your pick!)
Why is a jail OK for the mentally ill but an asylum is not? Why is it necessary to put armed guards in charge of psychiatric patients instead of a multidisciplinary team of psychiatrists, primary care providers, nurses, social workers, psychologists, and pharmacists? Why has a brain disease, such as psychosis or bipolar disorder, become a punishable felony instead of a treatable illness?
Why did the system of mental health care degenerate to the point that a severely depressed or suicidal, or acutely psychotic, patient can be hospitalized for only 4 or 5 days, then must be discharged before her (his) illness has been fully controlled? Why do health care insurers exhibit that atrocious combination of maximum greed and minimal compassion?
Why does a completely unjustified and hurtful stigma continue to plague mental brain disorders, patients who suffer from them, mental health professionals, and the very discipline of psychiatry?
Why do otherwise intelligent people show compassion toward people with a brain disorder such as stroke, Parkinson’s disease, multiple sclerosis, myasthenia gravis, or migraine, but express aversion and even disdain for psychiatric brain disorders such as schizophrenia, depression, obsessive-compulsive disorder, and panic disorder?
And why does this prejudice persist despite advances in psychiatric neuroscience that have used neurogenetics, neuroimaging, and molecular studies to establish, without a doubt, the neurobiological basis of all psychiatric disorders.
Why are there still no objective diagnostic criteria for psychiatric disorders? Why do we persist in using defining symptoms that have been volunteered by patients—symptoms that can be subject to distortion or malingering? Why aren’t the hundreds of established biomarkers being incorporated into the diagnostic formulation, to lessen subjectivity and improve reliability and validity?
Why is off-label prescribing, the judicious clinical repurposing of psychotropic medications, criticized and panned, even though there are no approved drugs for 88.5% psychiatric diagnoses?1 Why allow insurers to refuse to pay for a medication that can help a patient, just because the patient has not been given the “official” diagnosis for which the FDA approved that drug?
And why doesn’t the FDA solve this problem by revising its requirements that registration trials for new medications test their efficacy for a single symptom, rather than a diagnosis comprising multiple symptoms?
Why do people not accept the fact that all drugs have benefits and risks, and that it is impossible to have pure efficacy without side effects? Why empower lawyers to make clinical care adversarial? Why do lawyers refrain from suing oncologists or manufacturers of life-saving chemotherapy drugs because of terrible adverse effects, but pounce on other medications that might cause a serious side effect in a tiny percentage of patients that is clearly spelled out in the package insert?
Why do people demonize the pharmaceutical industry far more than other industries? No other entity discovers and develops life-saving medications.
Why don’t people realize that, without medications, massive numbers of patients would be hospitalized and the death rate would rise? Why can’t people weigh risks and benefits of having a pharmaceutical industry, just as they assess the risk-benefit ratio of everything in life?
Should the government impose a massive ($1 or $2 trillion) tax hike to establish infrastructure for drug research and development, for the benefit of psychiatry and all other medical specialties?
Why is there a severe shortage of psychiatrists but a glut of lawyers? Why doesn’t society rationally deploy its resources to meet urgent social needs and priorities? And why do lawyers bill us for every minute we talk to them, while we field telephone calls and e-mail messages from patients without compensation?
Why did the FDA allow the pharmaceutical industry to develop direct-to-consumer advertising? Why do they not realize how that decision has complicated the doctor–patient relationship, and how it preempts physicians’ evidence-based decision-making by encouraging consumers to demand a drug that they saw on television—a contorted version of prescribing by proxy?
Why (speaking of prescribing without a license), do politicians pass laws allowing people who do not have required medical training to take a short-cut to becoming a prescriber? Why not mandate that politicians, and their families, receive medical care exclusively from unqualified practitioners on whom they bestow prescribing privileges without requisite comprehensive medical training?Why do some psychiatrists resist changing their practice patterns despite continuous advances that update the care they provide? Why do reports of exciting therapeutic breakthroughs, published in top-tier journals, go unread by so many practitioners? Why do they say they are too busy to read journals or peruse PubMed?
Why don’t people realize that today’s research is tomorrow’s treatment? That research is not a luxury but an ongoing necessity? Why don’t more freshly minted, young psychiatrists pursue a career in research to accelerate the pace of progress about the biological causes and treatments of serious psychiatric disorders? Why aren’t there more incentives to grow the next generation of psychiatric discoverers and Nobel laureates? Why don’t clinicians support research by referring patients to clinical trials of medications or to National Institutes of Health-funded investigations of the neurobiology of psychiatric disorders?
Are these just rhetorical questions?
Some might sound that way. But they are not. These questions are brewing inside the hearts and minds of many psychiatrists, although only a few seem determined to relentlessly seek answers on which medical science and society can act.
We should collectively pose these “why” questions and not accept long-winded, hollow answers. We need to foster the winds of change—not resign ourselves to winds in which answers blow about but, ultimately, disappear.
1. Devulapalli KK, Nasrallah HA. An analysis of the high psychotropic off-label use in psychiatric disorders. Asian J Psychiatr. 2009;2(1):29-36.
1. Devulapalli KK, Nasrallah HA. An analysis of the high psychotropic off-label use in psychiatric disorders. Asian J Psychiatr. 2009;2(1):29-36.

Reversing Facial Fillers: How Much Hyaluronidase Is Needed to Dissolve Unwanted Filler?
Hyaluronic acid (HA) fillers are among the most commonly injected soft-tissue fillers worldwide. However, even with proper technique, there may be instances in which the filler becomes visible (Tyndall effect) or edematous, prompting the need to dissolve it. Not all HA fillers are identical; many differ in their degree of cross-linking or classification as monophasic or biphasic, which may affect the success in dissolving them with hyaluronidase. Rao et al (J Drugs Dermatol. 2014;13:1053-1056) published a study that looked at 2 commonly used hyaluronidase agents and how well they dissolved 4 commonly used HA fillers in the United States.
Rao et al performed an in vitro study using Vitrase (ovine testicular hyaluronidase)(Bausch & Lomb Incorporated) and Hylenex (recombinant human hyaluronidase)(Halozyme Therapeutics). The HA fillers tested were Restylane (Galderma Laboratories, LP), Juvéderm and Juvéderm Voluma (Allergan), and Belotero (Merz Aesthetics).
Phase 1 of the study looked at the volume of hyaluronidase on 3 of 4 fillers. The researchers utilized 0.1 mL of Vitrase or Hylenex to treat 0.2 mL of Restylane, Belotero, and Juvéderm. A control slide was kept for each filler. For Vitrase, 0.1 mL is 20 U of hyaluronidase. For Hylenex, 0.1 mL is 15 U of hyaluronidase. The filler and hyaluronidase were mixed together for 10 seconds using a 27-gauge needle. Photograph assessment of the slides was taken at 1 and 5 minutes.
Phase 2 of the study looked at the number of units of hyaluronidase on all 4 fillers. For this phase, 15 U and 30 U of Hylenex were mixed with 0.2 mL aliquots of each filler. Photographs and qualitative observations were taken at 1 and 5 minutes. The aliquots were observed for a total of 15 minutes.
For phase 1, the 2 hyaluronidase agents worked similarly on all 3 HA fillers. The greatest effect on dissolving or changing the shape of a filler was on Restylane, followed by Juvéderm and Belotero (a monophasic filler). The greatest effect was in the first minute and continued through the fifth minute. Even at 5 minutes, Belotero maintained most of its shape.
Phase 2 showed similar results with Restylane reacting the most to the hyaluronidase, followed by Juvéderm Voluma, Juvéderm, and Belotero. The higher dose (30 U) of hyaluronidase had a more dramatic effect on all fillers compared to the lower dose (15 U). Results were time dependent with the greatest changes seen at 5 minutes as opposed to 1 minute. The results of the 15-minute observation did not show any further changes. Belotero also maintained most of its shape during this phase.
What’s the issue?
With the increased number of HA fillers coming onto the market, it will become more important to understand the interaction between HA fillers and hyaluronidase. Hyaluronic acid fillers will vary in their degree of cross-linking, water absorption, and classification as monophasic (cohesive) or biphasic. Oftentimes, it is not until we use fillers in off-label manners that we realize some unintended consequences. We realized all too quickly that fillers, such as Restylane, placed superficially under eyelid skin gave an unsightly Tyndall effect. We then relied on hyaluronidase injections to resolve this issue. Furthermore, we learned that Juvéderm Ultra Plus XC could hold approximately 300% of its weight in water, causing unsightly eyelid edema in some patients. Luckily, the use of hyaluronidase can be a saving grace for physicians. However, the success of hyaluronidase injections varies. From the results of this study, it may be true that certain fillers need higher volumes or a higher number of units than other fillers to dissolve them. I would like to see this study expanded as newer HA fillers are brought onto the market.
Have you found that you have had to use varying amounts of hyaluronidase to address different filler complications?
Hyaluronic acid (HA) fillers are among the most commonly injected soft-tissue fillers worldwide. However, even with proper technique, there may be instances in which the filler becomes visible (Tyndall effect) or edematous, prompting the need to dissolve it. Not all HA fillers are identical; many differ in their degree of cross-linking or classification as monophasic or biphasic, which may affect the success in dissolving them with hyaluronidase. Rao et al (J Drugs Dermatol. 2014;13:1053-1056) published a study that looked at 2 commonly used hyaluronidase agents and how well they dissolved 4 commonly used HA fillers in the United States.
Rao et al performed an in vitro study using Vitrase (ovine testicular hyaluronidase)(Bausch & Lomb Incorporated) and Hylenex (recombinant human hyaluronidase)(Halozyme Therapeutics). The HA fillers tested were Restylane (Galderma Laboratories, LP), Juvéderm and Juvéderm Voluma (Allergan), and Belotero (Merz Aesthetics).
Phase 1 of the study looked at the volume of hyaluronidase on 3 of 4 fillers. The researchers utilized 0.1 mL of Vitrase or Hylenex to treat 0.2 mL of Restylane, Belotero, and Juvéderm. A control slide was kept for each filler. For Vitrase, 0.1 mL is 20 U of hyaluronidase. For Hylenex, 0.1 mL is 15 U of hyaluronidase. The filler and hyaluronidase were mixed together for 10 seconds using a 27-gauge needle. Photograph assessment of the slides was taken at 1 and 5 minutes.
Phase 2 of the study looked at the number of units of hyaluronidase on all 4 fillers. For this phase, 15 U and 30 U of Hylenex were mixed with 0.2 mL aliquots of each filler. Photographs and qualitative observations were taken at 1 and 5 minutes. The aliquots were observed for a total of 15 minutes.
For phase 1, the 2 hyaluronidase agents worked similarly on all 3 HA fillers. The greatest effect on dissolving or changing the shape of a filler was on Restylane, followed by Juvéderm and Belotero (a monophasic filler). The greatest effect was in the first minute and continued through the fifth minute. Even at 5 minutes, Belotero maintained most of its shape.
Phase 2 showed similar results with Restylane reacting the most to the hyaluronidase, followed by Juvéderm Voluma, Juvéderm, and Belotero. The higher dose (30 U) of hyaluronidase had a more dramatic effect on all fillers compared to the lower dose (15 U). Results were time dependent with the greatest changes seen at 5 minutes as opposed to 1 minute. The results of the 15-minute observation did not show any further changes. Belotero also maintained most of its shape during this phase.
What’s the issue?
With the increased number of HA fillers coming onto the market, it will become more important to understand the interaction between HA fillers and hyaluronidase. Hyaluronic acid fillers will vary in their degree of cross-linking, water absorption, and classification as monophasic (cohesive) or biphasic. Oftentimes, it is not until we use fillers in off-label manners that we realize some unintended consequences. We realized all too quickly that fillers, such as Restylane, placed superficially under eyelid skin gave an unsightly Tyndall effect. We then relied on hyaluronidase injections to resolve this issue. Furthermore, we learned that Juvéderm Ultra Plus XC could hold approximately 300% of its weight in water, causing unsightly eyelid edema in some patients. Luckily, the use of hyaluronidase can be a saving grace for physicians. However, the success of hyaluronidase injections varies. From the results of this study, it may be true that certain fillers need higher volumes or a higher number of units than other fillers to dissolve them. I would like to see this study expanded as newer HA fillers are brought onto the market.
Have you found that you have had to use varying amounts of hyaluronidase to address different filler complications?
Hyaluronic acid (HA) fillers are among the most commonly injected soft-tissue fillers worldwide. However, even with proper technique, there may be instances in which the filler becomes visible (Tyndall effect) or edematous, prompting the need to dissolve it. Not all HA fillers are identical; many differ in their degree of cross-linking or classification as monophasic or biphasic, which may affect the success in dissolving them with hyaluronidase. Rao et al (J Drugs Dermatol. 2014;13:1053-1056) published a study that looked at 2 commonly used hyaluronidase agents and how well they dissolved 4 commonly used HA fillers in the United States.
Rao et al performed an in vitro study using Vitrase (ovine testicular hyaluronidase)(Bausch & Lomb Incorporated) and Hylenex (recombinant human hyaluronidase)(Halozyme Therapeutics). The HA fillers tested were Restylane (Galderma Laboratories, LP), Juvéderm and Juvéderm Voluma (Allergan), and Belotero (Merz Aesthetics).
Phase 1 of the study looked at the volume of hyaluronidase on 3 of 4 fillers. The researchers utilized 0.1 mL of Vitrase or Hylenex to treat 0.2 mL of Restylane, Belotero, and Juvéderm. A control slide was kept for each filler. For Vitrase, 0.1 mL is 20 U of hyaluronidase. For Hylenex, 0.1 mL is 15 U of hyaluronidase. The filler and hyaluronidase were mixed together for 10 seconds using a 27-gauge needle. Photograph assessment of the slides was taken at 1 and 5 minutes.
Phase 2 of the study looked at the number of units of hyaluronidase on all 4 fillers. For this phase, 15 U and 30 U of Hylenex were mixed with 0.2 mL aliquots of each filler. Photographs and qualitative observations were taken at 1 and 5 minutes. The aliquots were observed for a total of 15 minutes.
For phase 1, the 2 hyaluronidase agents worked similarly on all 3 HA fillers. The greatest effect on dissolving or changing the shape of a filler was on Restylane, followed by Juvéderm and Belotero (a monophasic filler). The greatest effect was in the first minute and continued through the fifth minute. Even at 5 minutes, Belotero maintained most of its shape.
Phase 2 showed similar results with Restylane reacting the most to the hyaluronidase, followed by Juvéderm Voluma, Juvéderm, and Belotero. The higher dose (30 U) of hyaluronidase had a more dramatic effect on all fillers compared to the lower dose (15 U). Results were time dependent with the greatest changes seen at 5 minutes as opposed to 1 minute. The results of the 15-minute observation did not show any further changes. Belotero also maintained most of its shape during this phase.
What’s the issue?
With the increased number of HA fillers coming onto the market, it will become more important to understand the interaction between HA fillers and hyaluronidase. Hyaluronic acid fillers will vary in their degree of cross-linking, water absorption, and classification as monophasic (cohesive) or biphasic. Oftentimes, it is not until we use fillers in off-label manners that we realize some unintended consequences. We realized all too quickly that fillers, such as Restylane, placed superficially under eyelid skin gave an unsightly Tyndall effect. We then relied on hyaluronidase injections to resolve this issue. Furthermore, we learned that Juvéderm Ultra Plus XC could hold approximately 300% of its weight in water, causing unsightly eyelid edema in some patients. Luckily, the use of hyaluronidase can be a saving grace for physicians. However, the success of hyaluronidase injections varies. From the results of this study, it may be true that certain fillers need higher volumes or a higher number of units than other fillers to dissolve them. I would like to see this study expanded as newer HA fillers are brought onto the market.
Have you found that you have had to use varying amounts of hyaluronidase to address different filler complications?

Dermatologists Should Get the Point: Acupuncture for the Treatment of Skin Disorders

Complementary and alternative medicine has a definite adjunctive and even at times primary role in the medical management of patients. Its prevalence in the United States is estimated to be 38% and it is used to treat dermatologic conditions in 6% of patients (Harris et al; Smith et al). Acupuncture, a component of traditional Chinese medicine, has a prevalence of 0.6% to 1.4% and is used to treat 0.6% of dermatologic conditions (Smith et al; Cooper et al).
Acupuncture involves stimulation of specific points usually located along meridians. The source of stimulation on the skin can be elicited using needle points, pressure, or heat. Diseases disturb the body’s vital energy (qi), and stimulation along the appropriate meridian channel achieves balance and cures disease by restoring the normal circulation of the body’s qi.
Ma and Sivamani (J Altern Complement Med. 2015;21:520-529) performed a systematic review of articles indexed for MEDLINE, EMBASE, and the Cochrane Central Register using acupuncture therapy or acupuncture and skin diseases or dermatology as search terms to synthesize the evidence on the use of acupuncture as a primary treatment modality for dermatologic conditions. Twenty-four studies met inclusion criteria; of them, 17 showed statistically significant improvements (P<.05) in outcome measures. Specifically, acupuncture improved the outcome measures in the treatment of several dermatologic conditions including chloasma, dermatitis, facial elasticity, hyperhidrosis, pruritus, and urticaria.
What’s the issue?
Patients often have insight into potential available therapies for their medical problems. Hence, it is not unexpected that individuals with dermatologic conditions may not only be aware of complementary and alternative medicine approaches, such as acupuncture, but also seek dermatologists who can provide them with these possible therapeutic options. Although the frequency and duration of acupuncture treatments may not allow it to be a practical modality for all individuals, this treatment appears to be effective for reducing the severity of itch in patients with atopic dermatitis.
Should dermatologists incorporate acupuncture into their therapeutic armamentarium? Should national dermatology meetings provide courses on acupuncture technique? Should dermatology residency programs add competency in acupuncture management to their curriculum?
Suggested Readings
Cooper KL, Harris PE, Relton C, et al. Prevalence of visits to five types of complementary and alternative medicine practitioners by the general population: a systematic review. Complement Ther Clin Pract. 2013;19:214-220.
Harris PE, Cooper KL, Relton C, et al. Prevalence of complementary and alternative medicine (CAM) used by the general population: a systematic review and update. Int J Clin Pract. 2012;66:924-939.
Smith N, Shin DB, Brauer JA, et al. Use of complementary and alternative medicine among adults with skin disease: results from a national survey. J Am Acad Dermatol. 2009;60:419-425.
Complementary and alternative medicine has a definite adjunctive and even at times primary role in the medical management of patients. Its prevalence in the United States is estimated to be 38% and it is used to treat dermatologic conditions in 6% of patients (Harris et al; Smith et al). Acupuncture, a component of traditional Chinese medicine, has a prevalence of 0.6% to 1.4% and is used to treat 0.6% of dermatologic conditions (Smith et al; Cooper et al).
Acupuncture involves stimulation of specific points usually located along meridians. The source of stimulation on the skin can be elicited using needle points, pressure, or heat. Diseases disturb the body’s vital energy (qi), and stimulation along the appropriate meridian channel achieves balance and cures disease by restoring the normal circulation of the body’s qi.
Ma and Sivamani (J Altern Complement Med. 2015;21:520-529) performed a systematic review of articles indexed for MEDLINE, EMBASE, and the Cochrane Central Register using acupuncture therapy or acupuncture and skin diseases or dermatology as search terms to synthesize the evidence on the use of acupuncture as a primary treatment modality for dermatologic conditions. Twenty-four studies met inclusion criteria; of them, 17 showed statistically significant improvements (P<.05) in outcome measures. Specifically, acupuncture improved the outcome measures in the treatment of several dermatologic conditions including chloasma, dermatitis, facial elasticity, hyperhidrosis, pruritus, and urticaria.
What’s the issue?
Patients often have insight into potential available therapies for their medical problems. Hence, it is not unexpected that individuals with dermatologic conditions may not only be aware of complementary and alternative medicine approaches, such as acupuncture, but also seek dermatologists who can provide them with these possible therapeutic options. Although the frequency and duration of acupuncture treatments may not allow it to be a practical modality for all individuals, this treatment appears to be effective for reducing the severity of itch in patients with atopic dermatitis.
Should dermatologists incorporate acupuncture into their therapeutic armamentarium? Should national dermatology meetings provide courses on acupuncture technique? Should dermatology residency programs add competency in acupuncture management to their curriculum?
Complementary and alternative medicine has a definite adjunctive and even at times primary role in the medical management of patients. Its prevalence in the United States is estimated to be 38% and it is used to treat dermatologic conditions in 6% of patients (Harris et al; Smith et al). Acupuncture, a component of traditional Chinese medicine, has a prevalence of 0.6% to 1.4% and is used to treat 0.6% of dermatologic conditions (Smith et al; Cooper et al).
Acupuncture involves stimulation of specific points usually located along meridians. The source of stimulation on the skin can be elicited using needle points, pressure, or heat. Diseases disturb the body’s vital energy (qi), and stimulation along the appropriate meridian channel achieves balance and cures disease by restoring the normal circulation of the body’s qi.
Ma and Sivamani (J Altern Complement Med. 2015;21:520-529) performed a systematic review of articles indexed for MEDLINE, EMBASE, and the Cochrane Central Register using acupuncture therapy or acupuncture and skin diseases or dermatology as search terms to synthesize the evidence on the use of acupuncture as a primary treatment modality for dermatologic conditions. Twenty-four studies met inclusion criteria; of them, 17 showed statistically significant improvements (P<.05) in outcome measures. Specifically, acupuncture improved the outcome measures in the treatment of several dermatologic conditions including chloasma, dermatitis, facial elasticity, hyperhidrosis, pruritus, and urticaria.
What’s the issue?
Patients often have insight into potential available therapies for their medical problems. Hence, it is not unexpected that individuals with dermatologic conditions may not only be aware of complementary and alternative medicine approaches, such as acupuncture, but also seek dermatologists who can provide them with these possible therapeutic options. Although the frequency and duration of acupuncture treatments may not allow it to be a practical modality for all individuals, this treatment appears to be effective for reducing the severity of itch in patients with atopic dermatitis.
Should dermatologists incorporate acupuncture into their therapeutic armamentarium? Should national dermatology meetings provide courses on acupuncture technique? Should dermatology residency programs add competency in acupuncture management to their curriculum?
Suggested Readings
Cooper KL, Harris PE, Relton C, et al. Prevalence of visits to five types of complementary and alternative medicine practitioners by the general population: a systematic review. Complement Ther Clin Pract. 2013;19:214-220.
Harris PE, Cooper KL, Relton C, et al. Prevalence of complementary and alternative medicine (CAM) used by the general population: a systematic review and update. Int J Clin Pract. 2012;66:924-939.
Smith N, Shin DB, Brauer JA, et al. Use of complementary and alternative medicine among adults with skin disease: results from a national survey. J Am Acad Dermatol. 2009;60:419-425.
Suggested Readings
Cooper KL, Harris PE, Relton C, et al. Prevalence of visits to five types of complementary and alternative medicine practitioners by the general population: a systematic review. Complement Ther Clin Pract. 2013;19:214-220.
Harris PE, Cooper KL, Relton C, et al. Prevalence of complementary and alternative medicine (CAM) used by the general population: a systematic review and update. Int J Clin Pract. 2012;66:924-939.
Smith N, Shin DB, Brauer JA, et al. Use of complementary and alternative medicine among adults with skin disease: results from a national survey. J Am Acad Dermatol. 2009;60:419-425.

VIDEO: A case study in managing opioid addiction after a back injury
Has your patient’s opioid use escalated to opioid addiction? How can you tell, and what interventions can you take to help this patient in the context of a 15-minute appointment?
In this edition of Mental Health Consult, our panel discusses their recommendations for workup and next steps for managing a 45-year-old man who has no history of psychiatric disorders and appears to now be dependent on the opioid painkillers that he initially received after a back injury.
Join our panel of experts from George Washington University, Washington, including Daniel Lieberman, MD, professor of psychiatry and behavioral sciences clinical director; April Barbour, MD, MPH, director of the division of general internal medicine; and Lorenzo Norris, MD, medical director of psychiatric and behavioral services, as they discuss how to treat pain medication–related addiction, including when to refer to pain specialists and how various practice models drive treatment decisions and reimbursement.
On Twitter @whitneymcknight
Has your patient’s opioid use escalated to opioid addiction? How can you tell, and what interventions can you take to help this patient in the context of a 15-minute appointment?
In this edition of Mental Health Consult, our panel discusses their recommendations for workup and next steps for managing a 45-year-old man who has no history of psychiatric disorders and appears to now be dependent on the opioid painkillers that he initially received after a back injury.
Join our panel of experts from George Washington University, Washington, including Daniel Lieberman, MD, professor of psychiatry and behavioral sciences clinical director; April Barbour, MD, MPH, director of the division of general internal medicine; and Lorenzo Norris, MD, medical director of psychiatric and behavioral services, as they discuss how to treat pain medication–related addiction, including when to refer to pain specialists and how various practice models drive treatment decisions and reimbursement.
On Twitter @whitneymcknight
Has your patient’s opioid use escalated to opioid addiction? How can you tell, and what interventions can you take to help this patient in the context of a 15-minute appointment?
In this edition of Mental Health Consult, our panel discusses their recommendations for workup and next steps for managing a 45-year-old man who has no history of psychiatric disorders and appears to now be dependent on the opioid painkillers that he initially received after a back injury.
Join our panel of experts from George Washington University, Washington, including Daniel Lieberman, MD, professor of psychiatry and behavioral sciences clinical director; April Barbour, MD, MPH, director of the division of general internal medicine; and Lorenzo Norris, MD, medical director of psychiatric and behavioral services, as they discuss how to treat pain medication–related addiction, including when to refer to pain specialists and how various practice models drive treatment decisions and reimbursement.
On Twitter @whitneymcknight

Subclinical Joint Disease
We are aware of the clinical importance of diagnosing psoriatic arthritis (PsA) as early as possible to initiate appropriate therapy. Because psoriasis precedes PsA in the majority of cases, it is incumbent on clinicians to seek any evidence of joint involvement at each clinical encounter.
In a study published online on February 25 in Annals of the Rheumatic Diseases. Faustini et al reported that patients with psoriasis but without PsA experience structural joint changes at the entheses. Therefore, evidence for structural joint alterations may already exist at the time of apparently exclusive skin involvement in psoriatic disease.
In the analysis, 85 participants without arthritis, including 55 with psoriasis and 30 healthy controls, received high-field magnetic resonance imaging (MRI) of the hand. These scans were scored for synovitis, osteitis, tenosynovitis, and periarticular inflammation. Participants with psoriasis also received complete clinical investigation as well as high-resolution peripheral quantitative computed tomography for detecting erosions and enthesiophytes. All participants were followed for at least 1 year to evaluate for the development of PsA.
Magnetic resonance imaging evaluation showed that 47% (26/55) of participants with psoriasis possessed at least 1 inflammatory lesion. Synovitis was the most prevalent inflammatory lesion (38% [21/55]), while osteitis (11% [6/55]), tenosynovitis (4% [2/55]), and periarticular inflammation (4% [2/55]) were less frequent.
The incidence of enthesiophytes and bone erosions did not differ between patients with psoriasis, with or without inflammatory changes on MRI. The risk for developing PsA was as high as 60% in those with subclinical synovitis and symptoms related to arthralgia. However, the risk was only 13% if the patients had normal MRIs and did not report arthralgia. Faustini et al concluded that the prevalence of subclinical inflammatory lesions is high in patients with cutaneous psoriasis. Specifically, arthralgia in conjunction with MRI synovitis constitutes a high-risk constellation for the development of PsA.
What’s the issue?
These findings are critical, as they indicate the nature of the potential genesis of PsA in many patients. If the data are confirmed in future investigations, it may change the way we evaluate or treat early PsA. How will these findings affect your workup for early PsA?
We are aware of the clinical importance of diagnosing psoriatic arthritis (PsA) as early as possible to initiate appropriate therapy. Because psoriasis precedes PsA in the majority of cases, it is incumbent on clinicians to seek any evidence of joint involvement at each clinical encounter.
In a study published online on February 25 in Annals of the Rheumatic Diseases. Faustini et al reported that patients with psoriasis but without PsA experience structural joint changes at the entheses. Therefore, evidence for structural joint alterations may already exist at the time of apparently exclusive skin involvement in psoriatic disease.
In the analysis, 85 participants without arthritis, including 55 with psoriasis and 30 healthy controls, received high-field magnetic resonance imaging (MRI) of the hand. These scans were scored for synovitis, osteitis, tenosynovitis, and periarticular inflammation. Participants with psoriasis also received complete clinical investigation as well as high-resolution peripheral quantitative computed tomography for detecting erosions and enthesiophytes. All participants were followed for at least 1 year to evaluate for the development of PsA.
Magnetic resonance imaging evaluation showed that 47% (26/55) of participants with psoriasis possessed at least 1 inflammatory lesion. Synovitis was the most prevalent inflammatory lesion (38% [21/55]), while osteitis (11% [6/55]), tenosynovitis (4% [2/55]), and periarticular inflammation (4% [2/55]) were less frequent.
The incidence of enthesiophytes and bone erosions did not differ between patients with psoriasis, with or without inflammatory changes on MRI. The risk for developing PsA was as high as 60% in those with subclinical synovitis and symptoms related to arthralgia. However, the risk was only 13% if the patients had normal MRIs and did not report arthralgia. Faustini et al concluded that the prevalence of subclinical inflammatory lesions is high in patients with cutaneous psoriasis. Specifically, arthralgia in conjunction with MRI synovitis constitutes a high-risk constellation for the development of PsA.
What’s the issue?
These findings are critical, as they indicate the nature of the potential genesis of PsA in many patients. If the data are confirmed in future investigations, it may change the way we evaluate or treat early PsA. How will these findings affect your workup for early PsA?
We are aware of the clinical importance of diagnosing psoriatic arthritis (PsA) as early as possible to initiate appropriate therapy. Because psoriasis precedes PsA in the majority of cases, it is incumbent on clinicians to seek any evidence of joint involvement at each clinical encounter.
In a study published online on February 25 in Annals of the Rheumatic Diseases. Faustini et al reported that patients with psoriasis but without PsA experience structural joint changes at the entheses. Therefore, evidence for structural joint alterations may already exist at the time of apparently exclusive skin involvement in psoriatic disease.
In the analysis, 85 participants without arthritis, including 55 with psoriasis and 30 healthy controls, received high-field magnetic resonance imaging (MRI) of the hand. These scans were scored for synovitis, osteitis, tenosynovitis, and periarticular inflammation. Participants with psoriasis also received complete clinical investigation as well as high-resolution peripheral quantitative computed tomography for detecting erosions and enthesiophytes. All participants were followed for at least 1 year to evaluate for the development of PsA.
Magnetic resonance imaging evaluation showed that 47% (26/55) of participants with psoriasis possessed at least 1 inflammatory lesion. Synovitis was the most prevalent inflammatory lesion (38% [21/55]), while osteitis (11% [6/55]), tenosynovitis (4% [2/55]), and periarticular inflammation (4% [2/55]) were less frequent.
The incidence of enthesiophytes and bone erosions did not differ between patients with psoriasis, with or without inflammatory changes on MRI. The risk for developing PsA was as high as 60% in those with subclinical synovitis and symptoms related to arthralgia. However, the risk was only 13% if the patients had normal MRIs and did not report arthralgia. Faustini et al concluded that the prevalence of subclinical inflammatory lesions is high in patients with cutaneous psoriasis. Specifically, arthralgia in conjunction with MRI synovitis constitutes a high-risk constellation for the development of PsA.
What’s the issue?
These findings are critical, as they indicate the nature of the potential genesis of PsA in many patients. If the data are confirmed in future investigations, it may change the way we evaluate or treat early PsA. How will these findings affect your workup for early PsA?

VIDEO: Expert roundtable explores 50 years of contraception
WASHINGTON – What has the increased access to contraception over the last 50 years meant for American women?
We asked Ob.Gyn. News editorial advisory board member Dr. Eve Espey, professor and chair of the department of obstetrics and gynecology at the University of New Mexico, Albuquerque, along with three experts in family planning, to explore how expanded contraception options have affected public health, what barriers still remain, and what new products are in the pipeline.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Perhaps the biggest impact for women has been the ability to participate in the workforce, and that includes women entering medical school.
“Over the last 50 years, we’ve seen a big increase in the number of women who are professionals, who are physicians,” Dr. Espey said during the roundtable. “And during that same period of time, we’ve seen the growth of more focus on family planning.”
“I think that really would not be possible without the ability to control our fertility,” said Dr. Sarah W. Prager, associate professor of obstetrics and gynecology and director of the Ryan Family Planning Program at the University of Washington, Seattle.
And the widespread availability of contraception has translated into a decrease in maternal mortality as a result of fewer unintended pregnancies. “The implications for public health – for women and children in this country – is huge,” Dr. Prager said.
LARCs
One of the big shifts in contraceptive trends has been the slow but increasing uptake of long-acting reversible contraceptives (LARCs), such as IUDs and implants. After a drop-off in the 1970s following safety problems with the Dalkon Shield, there has been a resurgence in interest.
In the last decade, the rate of LARC use has grown from about 2% to 10%, corresponding to a slight drop in rates of unintended pregnancy, said Dr. Nikki B. Zite, professor and residency program director in the department of obstetrics and gynecology at the University of Tennessee, Knoxville.
The Contraceptive CHOICE Project, which enrolled more than 9,000 women who were provided with the no-cost reversible contraceptive method of their choice, found that about three-quarters of the women chose an IUD or an implant, which was associated with significant reductions in unintended and teen pregnancies.
“What we saw was that when we removed barriers to contraception in general, that uptake of IUDs and implants really went up,” said Dr. Tessa Madden, director of the division of family planning and associate professor in the department of obstetrics and gynecology at Washington University, St. Louis.
There is no “best” contraceptive method, Dr. Madden said. “Contraception really needs to be tailored to the individual woman [ensuring] that her values and preferences about contraception are taken into consideration during counseling, to help her choose the method that’s going to be the best fit for her.”
Resources
There are resources available to aid in tailoring contraception methods to the needs of patients.
U.S. Medical Eligibility Criteria for Contraceptive Use, guidance that is available through the Centers for Disease Control and Prevention, allows physicians to tailor the method to a patient’s comorbid medical conditions, Dr. Zite said. Physicians can search by contraceptive method or patient characteristic to determine the risk for a given patient, rated on a scale of 1-4 (where 1 or 2 means generally safe, 3 means that the risks may outweigh the benefits, and 4 means that the risks clearly outweigh the benefits).
“It’s a really easy starting-off point to use with patients and physicians when trying to decide what contraceptive method is safe for their patient,” Dr. Zite said.
Common medical comorbidities, including obesity, diabetes, thyroid disease, and hypertension, are all addressed in the medical eligibility criteria.
Another resource is the U.S. Selected Practice Recommendations for Contraceptive Use, which can help in deciding when it is appropriate to start a contraceptive method, what exams and tests are needed before initiation, what follow-up is needed, and how to handle problems such as missed pills or potential side effects.
Barriers
Over the years, many of the barriers to contraceptive access have been reduced. Some forms of emergency contraception are now available over the counter to women of all ages; more states are considering laws allowing women to access up to a year’s supply of hormonal contraceptives at one time; and a few states have passed laws allowing pharmacists to prescribe hormonal birth control directly. In addition, the Affordable Care Act’s mandate for insurers to cover approved methods of contraception without cost sharing has eliminated some cost barriers.
But other systems barriers still remain, such as making women return for multiple visits for the insertion of an IUD or implant, or limiting LARC use only to women who have already had a child. “There’s not a reason to avoid use of IUDs in women that have not had babies but there are still providers out there who will not insert an IUD, so we need to still do a better job to increase access even more,” Dr. Zite said.
Future trends
What new contraceptive options are in the pipeline? Dr. Prager predicted more development in the area of longer-acting injectables and implants, potentially even biodegradable implants. Also likely is the development of nonsurgical sterilization methods for women that eliminate some of the risk and cost barriers. And male contraceptive methods are in the works, both hormonal and nonhormonal, Dr. Prager said.
There’s an increasing interested in nonhormonal longer-acting methods, beyond just the copper IUD, Dr. Madden said, and there are new products on the horizon in that area. Researchers are exploring new methods to protect against HIV and other sexually transmitted infections, while offering contraception, Dr. Zite said.
Dr. Espey reported having no relevant financial disclosures. Dr. Prager is an unpaid trainer for Nexplanon (Merck). Dr. Zite is an unpaid trainer for Nexplanon and serves on an international IUD advisory board for Bayer. Dr. Madden serves on a scientific advisory board for Bayer and on a data safety monitoring board for phase IV safety studies of Bayer contraceptive products.
Throughout 2016, Ob.Gyn. News is celebrating its 50th anniversary with exclusive articles looking at the evolution of the specialty, including the history of infertility treatment, changes in gynecologic surgery, and the transformation of the well-woman visit. Look for these articles and more special features in the pages of Ob.Gyn. News and online at obgynnews.com.
On Twitter @maryellenny
WASHINGTON – What has the increased access to contraception over the last 50 years meant for American women?
We asked Ob.Gyn. News editorial advisory board member Dr. Eve Espey, professor and chair of the department of obstetrics and gynecology at the University of New Mexico, Albuquerque, along with three experts in family planning, to explore how expanded contraception options have affected public health, what barriers still remain, and what new products are in the pipeline.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Perhaps the biggest impact for women has been the ability to participate in the workforce, and that includes women entering medical school.
“Over the last 50 years, we’ve seen a big increase in the number of women who are professionals, who are physicians,” Dr. Espey said during the roundtable. “And during that same period of time, we’ve seen the growth of more focus on family planning.”
“I think that really would not be possible without the ability to control our fertility,” said Dr. Sarah W. Prager, associate professor of obstetrics and gynecology and director of the Ryan Family Planning Program at the University of Washington, Seattle.
And the widespread availability of contraception has translated into a decrease in maternal mortality as a result of fewer unintended pregnancies. “The implications for public health – for women and children in this country – is huge,” Dr. Prager said.
LARCs
One of the big shifts in contraceptive trends has been the slow but increasing uptake of long-acting reversible contraceptives (LARCs), such as IUDs and implants. After a drop-off in the 1970s following safety problems with the Dalkon Shield, there has been a resurgence in interest.
In the last decade, the rate of LARC use has grown from about 2% to 10%, corresponding to a slight drop in rates of unintended pregnancy, said Dr. Nikki B. Zite, professor and residency program director in the department of obstetrics and gynecology at the University of Tennessee, Knoxville.
The Contraceptive CHOICE Project, which enrolled more than 9,000 women who were provided with the no-cost reversible contraceptive method of their choice, found that about three-quarters of the women chose an IUD or an implant, which was associated with significant reductions in unintended and teen pregnancies.
“What we saw was that when we removed barriers to contraception in general, that uptake of IUDs and implants really went up,” said Dr. Tessa Madden, director of the division of family planning and associate professor in the department of obstetrics and gynecology at Washington University, St. Louis.
There is no “best” contraceptive method, Dr. Madden said. “Contraception really needs to be tailored to the individual woman [ensuring] that her values and preferences about contraception are taken into consideration during counseling, to help her choose the method that’s going to be the best fit for her.”
Resources
There are resources available to aid in tailoring contraception methods to the needs of patients.
U.S. Medical Eligibility Criteria for Contraceptive Use, guidance that is available through the Centers for Disease Control and Prevention, allows physicians to tailor the method to a patient’s comorbid medical conditions, Dr. Zite said. Physicians can search by contraceptive method or patient characteristic to determine the risk for a given patient, rated on a scale of 1-4 (where 1 or 2 means generally safe, 3 means that the risks may outweigh the benefits, and 4 means that the risks clearly outweigh the benefits).
“It’s a really easy starting-off point to use with patients and physicians when trying to decide what contraceptive method is safe for their patient,” Dr. Zite said.
Common medical comorbidities, including obesity, diabetes, thyroid disease, and hypertension, are all addressed in the medical eligibility criteria.
Another resource is the U.S. Selected Practice Recommendations for Contraceptive Use, which can help in deciding when it is appropriate to start a contraceptive method, what exams and tests are needed before initiation, what follow-up is needed, and how to handle problems such as missed pills or potential side effects.
Barriers
Over the years, many of the barriers to contraceptive access have been reduced. Some forms of emergency contraception are now available over the counter to women of all ages; more states are considering laws allowing women to access up to a year’s supply of hormonal contraceptives at one time; and a few states have passed laws allowing pharmacists to prescribe hormonal birth control directly. In addition, the Affordable Care Act’s mandate for insurers to cover approved methods of contraception without cost sharing has eliminated some cost barriers.
But other systems barriers still remain, such as making women return for multiple visits for the insertion of an IUD or implant, or limiting LARC use only to women who have already had a child. “There’s not a reason to avoid use of IUDs in women that have not had babies but there are still providers out there who will not insert an IUD, so we need to still do a better job to increase access even more,” Dr. Zite said.
Future trends
What new contraceptive options are in the pipeline? Dr. Prager predicted more development in the area of longer-acting injectables and implants, potentially even biodegradable implants. Also likely is the development of nonsurgical sterilization methods for women that eliminate some of the risk and cost barriers. And male contraceptive methods are in the works, both hormonal and nonhormonal, Dr. Prager said.
There’s an increasing interested in nonhormonal longer-acting methods, beyond just the copper IUD, Dr. Madden said, and there are new products on the horizon in that area. Researchers are exploring new methods to protect against HIV and other sexually transmitted infections, while offering contraception, Dr. Zite said.
Dr. Espey reported having no relevant financial disclosures. Dr. Prager is an unpaid trainer for Nexplanon (Merck). Dr. Zite is an unpaid trainer for Nexplanon and serves on an international IUD advisory board for Bayer. Dr. Madden serves on a scientific advisory board for Bayer and on a data safety monitoring board for phase IV safety studies of Bayer contraceptive products.
Throughout 2016, Ob.Gyn. News is celebrating its 50th anniversary with exclusive articles looking at the evolution of the specialty, including the history of infertility treatment, changes in gynecologic surgery, and the transformation of the well-woman visit. Look for these articles and more special features in the pages of Ob.Gyn. News and online at obgynnews.com.
On Twitter @maryellenny
WASHINGTON – What has the increased access to contraception over the last 50 years meant for American women?
We asked Ob.Gyn. News editorial advisory board member Dr. Eve Espey, professor and chair of the department of obstetrics and gynecology at the University of New Mexico, Albuquerque, along with three experts in family planning, to explore how expanded contraception options have affected public health, what barriers still remain, and what new products are in the pipeline.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Perhaps the biggest impact for women has been the ability to participate in the workforce, and that includes women entering medical school.
“Over the last 50 years, we’ve seen a big increase in the number of women who are professionals, who are physicians,” Dr. Espey said during the roundtable. “And during that same period of time, we’ve seen the growth of more focus on family planning.”
“I think that really would not be possible without the ability to control our fertility,” said Dr. Sarah W. Prager, associate professor of obstetrics and gynecology and director of the Ryan Family Planning Program at the University of Washington, Seattle.
And the widespread availability of contraception has translated into a decrease in maternal mortality as a result of fewer unintended pregnancies. “The implications for public health – for women and children in this country – is huge,” Dr. Prager said.
LARCs
One of the big shifts in contraceptive trends has been the slow but increasing uptake of long-acting reversible contraceptives (LARCs), such as IUDs and implants. After a drop-off in the 1970s following safety problems with the Dalkon Shield, there has been a resurgence in interest.
In the last decade, the rate of LARC use has grown from about 2% to 10%, corresponding to a slight drop in rates of unintended pregnancy, said Dr. Nikki B. Zite, professor and residency program director in the department of obstetrics and gynecology at the University of Tennessee, Knoxville.
The Contraceptive CHOICE Project, which enrolled more than 9,000 women who were provided with the no-cost reversible contraceptive method of their choice, found that about three-quarters of the women chose an IUD or an implant, which was associated with significant reductions in unintended and teen pregnancies.
“What we saw was that when we removed barriers to contraception in general, that uptake of IUDs and implants really went up,” said Dr. Tessa Madden, director of the division of family planning and associate professor in the department of obstetrics and gynecology at Washington University, St. Louis.
There is no “best” contraceptive method, Dr. Madden said. “Contraception really needs to be tailored to the individual woman [ensuring] that her values and preferences about contraception are taken into consideration during counseling, to help her choose the method that’s going to be the best fit for her.”
Resources
There are resources available to aid in tailoring contraception methods to the needs of patients.
U.S. Medical Eligibility Criteria for Contraceptive Use, guidance that is available through the Centers for Disease Control and Prevention, allows physicians to tailor the method to a patient’s comorbid medical conditions, Dr. Zite said. Physicians can search by contraceptive method or patient characteristic to determine the risk for a given patient, rated on a scale of 1-4 (where 1 or 2 means generally safe, 3 means that the risks may outweigh the benefits, and 4 means that the risks clearly outweigh the benefits).
“It’s a really easy starting-off point to use with patients and physicians when trying to decide what contraceptive method is safe for their patient,” Dr. Zite said.
Common medical comorbidities, including obesity, diabetes, thyroid disease, and hypertension, are all addressed in the medical eligibility criteria.
Another resource is the U.S. Selected Practice Recommendations for Contraceptive Use, which can help in deciding when it is appropriate to start a contraceptive method, what exams and tests are needed before initiation, what follow-up is needed, and how to handle problems such as missed pills or potential side effects.
Barriers
Over the years, many of the barriers to contraceptive access have been reduced. Some forms of emergency contraception are now available over the counter to women of all ages; more states are considering laws allowing women to access up to a year’s supply of hormonal contraceptives at one time; and a few states have passed laws allowing pharmacists to prescribe hormonal birth control directly. In addition, the Affordable Care Act’s mandate for insurers to cover approved methods of contraception without cost sharing has eliminated some cost barriers.
But other systems barriers still remain, such as making women return for multiple visits for the insertion of an IUD or implant, or limiting LARC use only to women who have already had a child. “There’s not a reason to avoid use of IUDs in women that have not had babies but there are still providers out there who will not insert an IUD, so we need to still do a better job to increase access even more,” Dr. Zite said.
Future trends
What new contraceptive options are in the pipeline? Dr. Prager predicted more development in the area of longer-acting injectables and implants, potentially even biodegradable implants. Also likely is the development of nonsurgical sterilization methods for women that eliminate some of the risk and cost barriers. And male contraceptive methods are in the works, both hormonal and nonhormonal, Dr. Prager said.
There’s an increasing interested in nonhormonal longer-acting methods, beyond just the copper IUD, Dr. Madden said, and there are new products on the horizon in that area. Researchers are exploring new methods to protect against HIV and other sexually transmitted infections, while offering contraception, Dr. Zite said.
Dr. Espey reported having no relevant financial disclosures. Dr. Prager is an unpaid trainer for Nexplanon (Merck). Dr. Zite is an unpaid trainer for Nexplanon and serves on an international IUD advisory board for Bayer. Dr. Madden serves on a scientific advisory board for Bayer and on a data safety monitoring board for phase IV safety studies of Bayer contraceptive products.
Throughout 2016, Ob.Gyn. News is celebrating its 50th anniversary with exclusive articles looking at the evolution of the specialty, including the history of infertility treatment, changes in gynecologic surgery, and the transformation of the well-woman visit. Look for these articles and more special features in the pages of Ob.Gyn. News and online at obgynnews.com.
On Twitter @maryellenny

Diet and Acne: Where Are We?
Over the past few years there have been studies published that support a relationship between acne and nutritional factors. Most suggest that high-glycemic-load diets and milk/dairy consumption might promote the development or exacerbation of acne vulgaris. So, what’s the mechanism? Some investigators believe that a high-glycemic-index diet induces hyperinsulinemia, which in turn elicits endocrine responses such as increasing androgen synthesis, ultimately inducing acne through mediators such as androgens, insulinlike growth factor (IGF) 1, and IGF binding protein 3. Insulinlike growth factor 1 itself can induce keratinocyte proliferation, sebocyte proliferation, and sebum production. We know that acne can be related to some endocrine diseases, such as polycystic ovary syndrome, which is characterized by peripheral insulin resistance and hyperinsulinemia, as well as acne, hirsutism, and androgenic alopecia.
In a study published by Çerman et al (J Am Acad Dermatol. 2016;75:155-162), investigators aimed to support the relationship between acne and diet and proposed that adiponectin levels, an adipocyte-derived hormone with established anti-inflammatory, antioxidant, and antidiabetic effects, are inversely associated with glycemic intake. Adiponectin inhibits proinflammatory cytokines, downregulates adhesion molecule expression, suppresses toll-like receptors and their ligands, and increases insulin sensitivity. In this small study of 50 patients with acne matched to 36 healthy controls, mean (SD) serum adiponectin concentrations were significantly lower in the patients with acne vulgaris than in the healthy controls (9.93 [2.29] ng/mL_1 vs 11.28 [2.74] ng/mL_1; P=.015), though milk and dairy product consumption, serum glucose, insulin, IGF-1, IGF binding protein 3, and homeostasis model assessment of insulin resistance values of the acne vulgaris and control groups did not differ significantly. The authors argued that this finding supports low-glycemic-load diets given the inverse correlation with adiponectin concentrations.
For every promising study comes one that may refute it. A study published online in February 2016 in Human & Experimental Toxicology aimed to evaluate several adipokines (adipocyte-derived cytokines) such as leptin, adiponectin, ghrelin and adiponectin levels, and adiponectin and leptin rates that indicate insulin resistance in nonobese patients with severe acne vulgaris. Although this study was smaller (30 acne patients and 15 controls), investigators found no difference between the 2 groups for any of these adipokines. It is important to note that patients studied were nonobese, nondiabetic, and glycemic load was not taken into account, so it is possible that this correlation is more significant for patients with factors such as insulin resistance and obesity.
What’s the issue?
Regardless of these findings, we have enough evidence to support that eating poorly can worsen acne and have other effects on the body. Are we all in agreement with this conclusion? Eating poorly is bad for more than just acne. High glycemic load leads to a proinflammatory state. Think psoriasis here. Chronic inflammation is detrimental for every organ system. Therefore, in addition to focusing on the pathways and elucidating the biology, let’s also design curricula to train current and future dermatologists how to counsel patients on diet or at the very least create resources to enable us to guide our patients. I published a survey study (J Am Acad Dermatol. 2014;71:1028-1029) showing that dermatologists are not comfortable counseling patients, specifically psoriasis patients, on diet, smoking, and drinking alcohol. It is time to create these tools. Do you want these types of resources?
Over the past few years there have been studies published that support a relationship between acne and nutritional factors. Most suggest that high-glycemic-load diets and milk/dairy consumption might promote the development or exacerbation of acne vulgaris. So, what’s the mechanism? Some investigators believe that a high-glycemic-index diet induces hyperinsulinemia, which in turn elicits endocrine responses such as increasing androgen synthesis, ultimately inducing acne through mediators such as androgens, insulinlike growth factor (IGF) 1, and IGF binding protein 3. Insulinlike growth factor 1 itself can induce keratinocyte proliferation, sebocyte proliferation, and sebum production. We know that acne can be related to some endocrine diseases, such as polycystic ovary syndrome, which is characterized by peripheral insulin resistance and hyperinsulinemia, as well as acne, hirsutism, and androgenic alopecia.
In a study published by Çerman et al (J Am Acad Dermatol. 2016;75:155-162), investigators aimed to support the relationship between acne and diet and proposed that adiponectin levels, an adipocyte-derived hormone with established anti-inflammatory, antioxidant, and antidiabetic effects, are inversely associated with glycemic intake. Adiponectin inhibits proinflammatory cytokines, downregulates adhesion molecule expression, suppresses toll-like receptors and their ligands, and increases insulin sensitivity. In this small study of 50 patients with acne matched to 36 healthy controls, mean (SD) serum adiponectin concentrations were significantly lower in the patients with acne vulgaris than in the healthy controls (9.93 [2.29] ng/mL_1 vs 11.28 [2.74] ng/mL_1; P=.015), though milk and dairy product consumption, serum glucose, insulin, IGF-1, IGF binding protein 3, and homeostasis model assessment of insulin resistance values of the acne vulgaris and control groups did not differ significantly. The authors argued that this finding supports low-glycemic-load diets given the inverse correlation with adiponectin concentrations.
For every promising study comes one that may refute it. A study published online in February 2016 in Human & Experimental Toxicology aimed to evaluate several adipokines (adipocyte-derived cytokines) such as leptin, adiponectin, ghrelin and adiponectin levels, and adiponectin and leptin rates that indicate insulin resistance in nonobese patients with severe acne vulgaris. Although this study was smaller (30 acne patients and 15 controls), investigators found no difference between the 2 groups for any of these adipokines. It is important to note that patients studied were nonobese, nondiabetic, and glycemic load was not taken into account, so it is possible that this correlation is more significant for patients with factors such as insulin resistance and obesity.
What’s the issue?
Regardless of these findings, we have enough evidence to support that eating poorly can worsen acne and have other effects on the body. Are we all in agreement with this conclusion? Eating poorly is bad for more than just acne. High glycemic load leads to a proinflammatory state. Think psoriasis here. Chronic inflammation is detrimental for every organ system. Therefore, in addition to focusing on the pathways and elucidating the biology, let’s also design curricula to train current and future dermatologists how to counsel patients on diet or at the very least create resources to enable us to guide our patients. I published a survey study (J Am Acad Dermatol. 2014;71:1028-1029) showing that dermatologists are not comfortable counseling patients, specifically psoriasis patients, on diet, smoking, and drinking alcohol. It is time to create these tools. Do you want these types of resources?
Over the past few years there have been studies published that support a relationship between acne and nutritional factors. Most suggest that high-glycemic-load diets and milk/dairy consumption might promote the development or exacerbation of acne vulgaris. So, what’s the mechanism? Some investigators believe that a high-glycemic-index diet induces hyperinsulinemia, which in turn elicits endocrine responses such as increasing androgen synthesis, ultimately inducing acne through mediators such as androgens, insulinlike growth factor (IGF) 1, and IGF binding protein 3. Insulinlike growth factor 1 itself can induce keratinocyte proliferation, sebocyte proliferation, and sebum production. We know that acne can be related to some endocrine diseases, such as polycystic ovary syndrome, which is characterized by peripheral insulin resistance and hyperinsulinemia, as well as acne, hirsutism, and androgenic alopecia.
In a study published by Çerman et al (J Am Acad Dermatol. 2016;75:155-162), investigators aimed to support the relationship between acne and diet and proposed that adiponectin levels, an adipocyte-derived hormone with established anti-inflammatory, antioxidant, and antidiabetic effects, are inversely associated with glycemic intake. Adiponectin inhibits proinflammatory cytokines, downregulates adhesion molecule expression, suppresses toll-like receptors and their ligands, and increases insulin sensitivity. In this small study of 50 patients with acne matched to 36 healthy controls, mean (SD) serum adiponectin concentrations were significantly lower in the patients with acne vulgaris than in the healthy controls (9.93 [2.29] ng/mL_1 vs 11.28 [2.74] ng/mL_1; P=.015), though milk and dairy product consumption, serum glucose, insulin, IGF-1, IGF binding protein 3, and homeostasis model assessment of insulin resistance values of the acne vulgaris and control groups did not differ significantly. The authors argued that this finding supports low-glycemic-load diets given the inverse correlation with adiponectin concentrations.
For every promising study comes one that may refute it. A study published online in February 2016 in Human & Experimental Toxicology aimed to evaluate several adipokines (adipocyte-derived cytokines) such as leptin, adiponectin, ghrelin and adiponectin levels, and adiponectin and leptin rates that indicate insulin resistance in nonobese patients with severe acne vulgaris. Although this study was smaller (30 acne patients and 15 controls), investigators found no difference between the 2 groups for any of these adipokines. It is important to note that patients studied were nonobese, nondiabetic, and glycemic load was not taken into account, so it is possible that this correlation is more significant for patients with factors such as insulin resistance and obesity.
What’s the issue?
Regardless of these findings, we have enough evidence to support that eating poorly can worsen acne and have other effects on the body. Are we all in agreement with this conclusion? Eating poorly is bad for more than just acne. High glycemic load leads to a proinflammatory state. Think psoriasis here. Chronic inflammation is detrimental for every organ system. Therefore, in addition to focusing on the pathways and elucidating the biology, let’s also design curricula to train current and future dermatologists how to counsel patients on diet or at the very least create resources to enable us to guide our patients. I published a survey study (J Am Acad Dermatol. 2014;71:1028-1029) showing that dermatologists are not comfortable counseling patients, specifically psoriasis patients, on diet, smoking, and drinking alcohol. It is time to create these tools. Do you want these types of resources?

Zika Understanding Unfolds
Inundating our popular and academic media circles is information regarding the Zika virus. A recent article by Farahnik et al in the Journal of the American Academy of Dermatology (2016;74:1286-1287) briefly outlines what is known about Zika infection thus far and its dermatologic manifestations. Pairing this article with Centers for Disease Control and Prevention guidelines on the topic, we are presented with an evolving introduction to this new entity. Here’s what we know:
- It is a single-stranded RNA arbovirus in the Flavivirus family transmitted by the bite of Aedes mosquitoes, with cases reported so far in Africa, Asia, and the Americas (particularly southern coastal and island destinations).
- It also is transmitted via transfusion of blood, sexual contact, and mother to fetus.
- There is theoretical risk for fetal microcephaly, intracranial calcifications, and other brain and eye abnormalities.
- Only 1 in 5 affected patients show any systemic manifestations of infection, including self-limited flulike symptoms and nonspecific exanthema, typically sparing acral sites and occurring within 1 to 2 weeks of virus exposure.
- Testing is recommended for pregnant women with possible Zika exposure (ie, travel to an area with active transmission of Zika virus, unprotected sex with a male with this travel history).
- Diagnosis can be made through state health departments, employing real-time reverse transcriptase–polymerase chain reaction (rRT-PCR) or enzyme-linked immunosorbent assay the week after symptom onset using serum, or rRT-PCR 2 weeks after symptom onset using urine. Further antibody testing can be done if a false-negative is suspected, but false-positives also are possible if a patient was exposed to or vaccinated against other flaviviruses (eg, dengue virus, West Nile virus, yellow fever virus)
- Testing is inaccurate if ordered within 7 days or more than 12 weeks following presumed exposure.
- If positive or inconclusive testing arises, serial fetal ultrasonography should be considered; if testing is negative, then a single fetal ultrasound is recommended to detect Zika abnormalities.
- Test results are automatically reported to respective state health departments.
- There is no treatment of this infection aside from supportive care.
What’s the issue?
As with any new outbreak, the applicability to the general population and true risks remain to be seen. Each of our clinics recalls the stark changes in patient intake and screening questions with infections as ubiquitous as methicillin-resistant Staphylococcus aureus to much rarer exposures such as Ebola virus, each with progressive understanding of risk groups, disease manifestations, and eradication and prevention measures.
By mid-June 2016, 30 hits on PubMed addressing Zika had already been cited just within the month, outlining various aspects of the infection, and many specialties, particularly neurology, obstetrics, primary care, infectious disease, and dermatology, are weighing in. Unfortunately, the majority of cases of primary Zika infection do not manifest with skin or systemic symptoms, and even cases that do are nonspecific, exanthematous, and flulike.
Vague as it may be so far, it is nonetheless imperative that clinicians be familiar with what is concretely known about Zika virus and acquaint ourselves with the travel distribution and restrictions, disease risk factors, known sequelae, testing availability and limitations, and reporting guidelines. From personal experience, as I traveled to Belize earlier this year during my first trimester of pregnancy before the travel restrictions were outlined, even obstetricians are not wholly familiar with the manner in which to order testing and the appropriate window to do so. I have been asymptomatic, my blood was drawn in a period of time that exceeded the interval for accurate results (as outlined above) and was therefore inappropriately recommended/ordered, and now serial fetal ultrasonography is being implemented every few weeks.
With lack of ubiquitous knowledge about the infection, clinicians are not universally certain of the appropriate next steps when a patient presents with Zika risk factors, and therefore anxiety remains high for pregnant patients and their contacts. The Centers for Disease Control and Prevention website is the official home base, and we should review it and await their further evolving specific recommendations as more cases unfortunately accumulate.
Have you encountered any patients this year with exposure to or symptoms of Zika infection, and what, if anything, have you outlined for them?
Inundating our popular and academic media circles is information regarding the Zika virus. A recent article by Farahnik et al in the Journal of the American Academy of Dermatology (2016;74:1286-1287) briefly outlines what is known about Zika infection thus far and its dermatologic manifestations. Pairing this article with Centers for Disease Control and Prevention guidelines on the topic, we are presented with an evolving introduction to this new entity. Here’s what we know:
- It is a single-stranded RNA arbovirus in the Flavivirus family transmitted by the bite of Aedes mosquitoes, with cases reported so far in Africa, Asia, and the Americas (particularly southern coastal and island destinations).
- It also is transmitted via transfusion of blood, sexual contact, and mother to fetus.
- There is theoretical risk for fetal microcephaly, intracranial calcifications, and other brain and eye abnormalities.
- Only 1 in 5 affected patients show any systemic manifestations of infection, including self-limited flulike symptoms and nonspecific exanthema, typically sparing acral sites and occurring within 1 to 2 weeks of virus exposure.
- Testing is recommended for pregnant women with possible Zika exposure (ie, travel to an area with active transmission of Zika virus, unprotected sex with a male with this travel history).
- Diagnosis can be made through state health departments, employing real-time reverse transcriptase–polymerase chain reaction (rRT-PCR) or enzyme-linked immunosorbent assay the week after symptom onset using serum, or rRT-PCR 2 weeks after symptom onset using urine. Further antibody testing can be done if a false-negative is suspected, but false-positives also are possible if a patient was exposed to or vaccinated against other flaviviruses (eg, dengue virus, West Nile virus, yellow fever virus)
- Testing is inaccurate if ordered within 7 days or more than 12 weeks following presumed exposure.
- If positive or inconclusive testing arises, serial fetal ultrasonography should be considered; if testing is negative, then a single fetal ultrasound is recommended to detect Zika abnormalities.
- Test results are automatically reported to respective state health departments.
- There is no treatment of this infection aside from supportive care.
What’s the issue?
As with any new outbreak, the applicability to the general population and true risks remain to be seen. Each of our clinics recalls the stark changes in patient intake and screening questions with infections as ubiquitous as methicillin-resistant Staphylococcus aureus to much rarer exposures such as Ebola virus, each with progressive understanding of risk groups, disease manifestations, and eradication and prevention measures.
By mid-June 2016, 30 hits on PubMed addressing Zika had already been cited just within the month, outlining various aspects of the infection, and many specialties, particularly neurology, obstetrics, primary care, infectious disease, and dermatology, are weighing in. Unfortunately, the majority of cases of primary Zika infection do not manifest with skin or systemic symptoms, and even cases that do are nonspecific, exanthematous, and flulike.
Vague as it may be so far, it is nonetheless imperative that clinicians be familiar with what is concretely known about Zika virus and acquaint ourselves with the travel distribution and restrictions, disease risk factors, known sequelae, testing availability and limitations, and reporting guidelines. From personal experience, as I traveled to Belize earlier this year during my first trimester of pregnancy before the travel restrictions were outlined, even obstetricians are not wholly familiar with the manner in which to order testing and the appropriate window to do so. I have been asymptomatic, my blood was drawn in a period of time that exceeded the interval for accurate results (as outlined above) and was therefore inappropriately recommended/ordered, and now serial fetal ultrasonography is being implemented every few weeks.
With lack of ubiquitous knowledge about the infection, clinicians are not universally certain of the appropriate next steps when a patient presents with Zika risk factors, and therefore anxiety remains high for pregnant patients and their contacts. The Centers for Disease Control and Prevention website is the official home base, and we should review it and await their further evolving specific recommendations as more cases unfortunately accumulate.
Have you encountered any patients this year with exposure to or symptoms of Zika infection, and what, if anything, have you outlined for them?
Inundating our popular and academic media circles is information regarding the Zika virus. A recent article by Farahnik et al in the Journal of the American Academy of Dermatology (2016;74:1286-1287) briefly outlines what is known about Zika infection thus far and its dermatologic manifestations. Pairing this article with Centers for Disease Control and Prevention guidelines on the topic, we are presented with an evolving introduction to this new entity. Here’s what we know:
- It is a single-stranded RNA arbovirus in the Flavivirus family transmitted by the bite of Aedes mosquitoes, with cases reported so far in Africa, Asia, and the Americas (particularly southern coastal and island destinations).
- It also is transmitted via transfusion of blood, sexual contact, and mother to fetus.
- There is theoretical risk for fetal microcephaly, intracranial calcifications, and other brain and eye abnormalities.
- Only 1 in 5 affected patients show any systemic manifestations of infection, including self-limited flulike symptoms and nonspecific exanthema, typically sparing acral sites and occurring within 1 to 2 weeks of virus exposure.
- Testing is recommended for pregnant women with possible Zika exposure (ie, travel to an area with active transmission of Zika virus, unprotected sex with a male with this travel history).
- Diagnosis can be made through state health departments, employing real-time reverse transcriptase–polymerase chain reaction (rRT-PCR) or enzyme-linked immunosorbent assay the week after symptom onset using serum, or rRT-PCR 2 weeks after symptom onset using urine. Further antibody testing can be done if a false-negative is suspected, but false-positives also are possible if a patient was exposed to or vaccinated against other flaviviruses (eg, dengue virus, West Nile virus, yellow fever virus)
- Testing is inaccurate if ordered within 7 days or more than 12 weeks following presumed exposure.
- If positive or inconclusive testing arises, serial fetal ultrasonography should be considered; if testing is negative, then a single fetal ultrasound is recommended to detect Zika abnormalities.
- Test results are automatically reported to respective state health departments.
- There is no treatment of this infection aside from supportive care.
What’s the issue?
As with any new outbreak, the applicability to the general population and true risks remain to be seen. Each of our clinics recalls the stark changes in patient intake and screening questions with infections as ubiquitous as methicillin-resistant Staphylococcus aureus to much rarer exposures such as Ebola virus, each with progressive understanding of risk groups, disease manifestations, and eradication and prevention measures.
By mid-June 2016, 30 hits on PubMed addressing Zika had already been cited just within the month, outlining various aspects of the infection, and many specialties, particularly neurology, obstetrics, primary care, infectious disease, and dermatology, are weighing in. Unfortunately, the majority of cases of primary Zika infection do not manifest with skin or systemic symptoms, and even cases that do are nonspecific, exanthematous, and flulike.
Vague as it may be so far, it is nonetheless imperative that clinicians be familiar with what is concretely known about Zika virus and acquaint ourselves with the travel distribution and restrictions, disease risk factors, known sequelae, testing availability and limitations, and reporting guidelines. From personal experience, as I traveled to Belize earlier this year during my first trimester of pregnancy before the travel restrictions were outlined, even obstetricians are not wholly familiar with the manner in which to order testing and the appropriate window to do so. I have been asymptomatic, my blood was drawn in a period of time that exceeded the interval for accurate results (as outlined above) and was therefore inappropriately recommended/ordered, and now serial fetal ultrasonography is being implemented every few weeks.
With lack of ubiquitous knowledge about the infection, clinicians are not universally certain of the appropriate next steps when a patient presents with Zika risk factors, and therefore anxiety remains high for pregnant patients and their contacts. The Centers for Disease Control and Prevention website is the official home base, and we should review it and await their further evolving specific recommendations as more cases unfortunately accumulate.
Have you encountered any patients this year with exposure to or symptoms of Zika infection, and what, if anything, have you outlined for them?

Fear and loathing abound in the ‘off-label’ presidential election of 2016
A day in the psychiatry clinic? No—just scenes from that high-stakes festival of intense human competitiveness gone awry: the current presidential election. Alas, we have no FDA-approved treatments for any of these unusual political behaviors.
More stunning is how blind some loyal voters are to the flaws of their candidate of choice. They seem to be joyfully intoxicated by sharing the unusual beliefs of the candidate, in a cultish folie en masse of epidemic proportion.
Other (rational) voters are stunned and jarred by what they see and hear; they appear to be in need of Rx: an intellectual antiemetic.
The rise of uber-narcissism
A certain amount of narcissism is, understandably, necessary to run for the nation’s highest office and to believe, against all odds, that winning is certain despite microscopic favorability in the polls. In this election cycle, the cup of narcissism has run over; yet, to adoring fans, narcissism only adds a wondrous halo to their candidate.
The history of the United States is rife with similar behavior by elected officials, including our revered Founding Fathers.1 But today’s psychiatrists, witnessing this national charade, are perplexed and question the rationality of the national psyche. Established rules for seeking the Presidency have been demolished and the show goes on as if heightened narcissism is the new normal in human behavior.
Giving voice to my colleagues’ consternation
Here are a few thoughts that might cross the mind of psychiatrists as they watch, with a frown and pursed lips, this unconventional election cycle:
From a psychoanalytic perspective, the id has left the ego in its dust, and the super-ego went home to hide.
When boorishness trumps civility, hillaryous consequences ensue.
The gullibility of voters deserves serious scientific study. Jeste and Harris2 reviewed the evidence for a neurobiology of wisdom; The National Institutes of Health should fund research into how some voters believe the candidate of their choice will provide them with everything they wish. The chicken in every pot expands to 100 in every pot, and money grows on trees (at least on 1% of the forest!).
From an evolutionary standpoint, survival of the fittest has become survival of the most bombastic.
The zeitgeist reflects an electorate that oscillates agonizingly from surprise to anger to cynicism to disgust.
The traditional internal conflict (studied by political scientists) of choosing between 2 reasonably meritorious candidates has been transformed into a conflict over whether to vote at all.
This is the least nuanced presidential campaign—ever.
All decision-making in politics is unconscious, political scientist Jon A. Krosnick proposed. In this election, however, candidates’ enunciations are so overt that it’s hard to believe there’s anything left in the unconscious. Freud spoke of the “primary process” arising from the unconscious; he definitely was not referring to the primary process we experienced during this election cycle.
From a neuropsychiatric perspective, the limbic system has kicked the cortex in the metaphorical derrière in this election campaign.
Unabashed display of character flaws, personal shortcomings, and biases prove that anyone can run for president in a democracy, and that some voters will display a flight of reason and vote for a flawed candidate.
Even an inept demagogue can be misperceived as a savior by followers. Some voters could use a few sessions of insight-oriented therapy or cognitive-behavioral therapy for their unrealistic expectations.
It is dizzying, mentally, to watch candidates’ verbal acrobatics as they try to pass several litmus tests to satisfy disparate demands of sundry constituencies and mendaciously flip-flop on many issues—ignoring the fact that everything they have said was recorded or videotaped. Intellectual transvestism is a political sin, and sinners abound.
Oh, for a Jenner, Pasteur, or Sabin to discover vaccines for the intellect
Writing this editorial has been therapeutic. It feels good to ventilate about this bizarre election process that has the nation in its grip. I would feel much better if neuroscientists would develop and license vaccines that would broadly inoculate candidates against demagoguery, dishonesty, and pandering and voters against mind-boggling gullibility.
That would make elections so boring. But also so on-label….
1. Gartner JD. The hypomanic edge: the link between (a little) craziness and (a lot of) success in America. New York, NY: Simon & Schuster; 2005.
2. Jeste DV, Harris JC. Wisdom—a neuroscience perspective. JAMA. 2013;304(14):1602-1603.
A day in the psychiatry clinic? No—just scenes from that high-stakes festival of intense human competitiveness gone awry: the current presidential election. Alas, we have no FDA-approved treatments for any of these unusual political behaviors.
More stunning is how blind some loyal voters are to the flaws of their candidate of choice. They seem to be joyfully intoxicated by sharing the unusual beliefs of the candidate, in a cultish folie en masse of epidemic proportion.
Other (rational) voters are stunned and jarred by what they see and hear; they appear to be in need of Rx: an intellectual antiemetic.
The rise of uber-narcissism
A certain amount of narcissism is, understandably, necessary to run for the nation’s highest office and to believe, against all odds, that winning is certain despite microscopic favorability in the polls. In this election cycle, the cup of narcissism has run over; yet, to adoring fans, narcissism only adds a wondrous halo to their candidate.
The history of the United States is rife with similar behavior by elected officials, including our revered Founding Fathers.1 But today’s psychiatrists, witnessing this national charade, are perplexed and question the rationality of the national psyche. Established rules for seeking the Presidency have been demolished and the show goes on as if heightened narcissism is the new normal in human behavior.
Giving voice to my colleagues’ consternation
Here are a few thoughts that might cross the mind of psychiatrists as they watch, with a frown and pursed lips, this unconventional election cycle:
From a psychoanalytic perspective, the id has left the ego in its dust, and the super-ego went home to hide.
When boorishness trumps civility, hillaryous consequences ensue.
The gullibility of voters deserves serious scientific study. Jeste and Harris2 reviewed the evidence for a neurobiology of wisdom; The National Institutes of Health should fund research into how some voters believe the candidate of their choice will provide them with everything they wish. The chicken in every pot expands to 100 in every pot, and money grows on trees (at least on 1% of the forest!).
From an evolutionary standpoint, survival of the fittest has become survival of the most bombastic.
The zeitgeist reflects an electorate that oscillates agonizingly from surprise to anger to cynicism to disgust.
The traditional internal conflict (studied by political scientists) of choosing between 2 reasonably meritorious candidates has been transformed into a conflict over whether to vote at all.
This is the least nuanced presidential campaign—ever.
All decision-making in politics is unconscious, political scientist Jon A. Krosnick proposed. In this election, however, candidates’ enunciations are so overt that it’s hard to believe there’s anything left in the unconscious. Freud spoke of the “primary process” arising from the unconscious; he definitely was not referring to the primary process we experienced during this election cycle.
From a neuropsychiatric perspective, the limbic system has kicked the cortex in the metaphorical derrière in this election campaign.
Unabashed display of character flaws, personal shortcomings, and biases prove that anyone can run for president in a democracy, and that some voters will display a flight of reason and vote for a flawed candidate.
Even an inept demagogue can be misperceived as a savior by followers. Some voters could use a few sessions of insight-oriented therapy or cognitive-behavioral therapy for their unrealistic expectations.
It is dizzying, mentally, to watch candidates’ verbal acrobatics as they try to pass several litmus tests to satisfy disparate demands of sundry constituencies and mendaciously flip-flop on many issues—ignoring the fact that everything they have said was recorded or videotaped. Intellectual transvestism is a political sin, and sinners abound.
Oh, for a Jenner, Pasteur, or Sabin to discover vaccines for the intellect
Writing this editorial has been therapeutic. It feels good to ventilate about this bizarre election process that has the nation in its grip. I would feel much better if neuroscientists would develop and license vaccines that would broadly inoculate candidates against demagoguery, dishonesty, and pandering and voters against mind-boggling gullibility.
That would make elections so boring. But also so on-label….
A day in the psychiatry clinic? No—just scenes from that high-stakes festival of intense human competitiveness gone awry: the current presidential election. Alas, we have no FDA-approved treatments for any of these unusual political behaviors.
More stunning is how blind some loyal voters are to the flaws of their candidate of choice. They seem to be joyfully intoxicated by sharing the unusual beliefs of the candidate, in a cultish folie en masse of epidemic proportion.
Other (rational) voters are stunned and jarred by what they see and hear; they appear to be in need of Rx: an intellectual antiemetic.
The rise of uber-narcissism
A certain amount of narcissism is, understandably, necessary to run for the nation’s highest office and to believe, against all odds, that winning is certain despite microscopic favorability in the polls. In this election cycle, the cup of narcissism has run over; yet, to adoring fans, narcissism only adds a wondrous halo to their candidate.
The history of the United States is rife with similar behavior by elected officials, including our revered Founding Fathers.1 But today’s psychiatrists, witnessing this national charade, are perplexed and question the rationality of the national psyche. Established rules for seeking the Presidency have been demolished and the show goes on as if heightened narcissism is the new normal in human behavior.
Giving voice to my colleagues’ consternation
Here are a few thoughts that might cross the mind of psychiatrists as they watch, with a frown and pursed lips, this unconventional election cycle:
From a psychoanalytic perspective, the id has left the ego in its dust, and the super-ego went home to hide.
When boorishness trumps civility, hillaryous consequences ensue.
The gullibility of voters deserves serious scientific study. Jeste and Harris2 reviewed the evidence for a neurobiology of wisdom; The National Institutes of Health should fund research into how some voters believe the candidate of their choice will provide them with everything they wish. The chicken in every pot expands to 100 in every pot, and money grows on trees (at least on 1% of the forest!).
From an evolutionary standpoint, survival of the fittest has become survival of the most bombastic.
The zeitgeist reflects an electorate that oscillates agonizingly from surprise to anger to cynicism to disgust.
The traditional internal conflict (studied by political scientists) of choosing between 2 reasonably meritorious candidates has been transformed into a conflict over whether to vote at all.
This is the least nuanced presidential campaign—ever.
All decision-making in politics is unconscious, political scientist Jon A. Krosnick proposed. In this election, however, candidates’ enunciations are so overt that it’s hard to believe there’s anything left in the unconscious. Freud spoke of the “primary process” arising from the unconscious; he definitely was not referring to the primary process we experienced during this election cycle.
From a neuropsychiatric perspective, the limbic system has kicked the cortex in the metaphorical derrière in this election campaign.
Unabashed display of character flaws, personal shortcomings, and biases prove that anyone can run for president in a democracy, and that some voters will display a flight of reason and vote for a flawed candidate.
Even an inept demagogue can be misperceived as a savior by followers. Some voters could use a few sessions of insight-oriented therapy or cognitive-behavioral therapy for their unrealistic expectations.
It is dizzying, mentally, to watch candidates’ verbal acrobatics as they try to pass several litmus tests to satisfy disparate demands of sundry constituencies and mendaciously flip-flop on many issues—ignoring the fact that everything they have said was recorded or videotaped. Intellectual transvestism is a political sin, and sinners abound.
Oh, for a Jenner, Pasteur, or Sabin to discover vaccines for the intellect
Writing this editorial has been therapeutic. It feels good to ventilate about this bizarre election process that has the nation in its grip. I would feel much better if neuroscientists would develop and license vaccines that would broadly inoculate candidates against demagoguery, dishonesty, and pandering and voters against mind-boggling gullibility.
That would make elections so boring. But also so on-label….
1. Gartner JD. The hypomanic edge: the link between (a little) craziness and (a lot of) success in America. New York, NY: Simon & Schuster; 2005.
2. Jeste DV, Harris JC. Wisdom—a neuroscience perspective. JAMA. 2013;304(14):1602-1603.
1. Gartner JD. The hypomanic edge: the link between (a little) craziness and (a lot of) success in America. New York, NY: Simon & Schuster; 2005.
2. Jeste DV, Harris JC. Wisdom—a neuroscience perspective. JAMA. 2013;304(14):1602-1603.
