User login
Codes, Contracts, and Commitments: Who Defines What is a Profession?
Codes, Contracts, and Commitments: Who Defines What is a Profession?
A professional is someone who can do his best work when he doesn’t feel like it.
Alistair Cooke
When I was a young person with no idea about growing up to be something, my father used to tell me there were 4 learned professions: medicine to heal the body, law to protect the body politic, teaching to nurture the mind, and the clergy to care for the soul.1 That adage, or some version of it, is attributed to a variety of sources, likely because it captures something essential and timeless about the learned professions. I write this as a much older person, and it has been my privilege to have worked in some capacity in all 4 of these venerable vocations.
There are many more recognized professions now than in my father’s time with new ones still emerging as the world becomes more complicated and specialized. In November 2025, however, the growth of the professions was dealt a serious blow when the US Department of Education (DOE) redefined what constitutes a profession for the purpose of federal funding of graduate degrees.2 The internet is understandably abuzz with opinions across the political spectrum. What is missing from many of these discussions is an understanding of the criteria for a profession and, even more importantly, who has the authority to decide when an individual or a group has met that standard.
But first, what and why did the DOE make this change? The One Big Beautiful Bill Act charged the DOE with reducing what it claims is massive overspending on graduate education by limiting the programs that meet the definition of a “professional degree” eligible for higher funding. Of my father’s 4, medicine (including dentistry) and law made the cut with students in those professions able to borrow up to $200,000 in direct unsubsidized student loans while those in other programs would be limited to $100,000.2
As one of the oldest and most respected professions in America, nursing has received the most media attention, yet there are also other important and valued professions that are missing from the DOE list.3 The excluded professions also include: physician assistants, physical therapists, audiologists, architects, accountants, educators, and social workers. The proposed regulatory changes are not yet finalized and Congressional representatives, health care experts, and a myriad of professional associations have rightly objected the reclassification will only worsen the critical shortage of nurses, teachers, and other helping professions the country is already facing.4
There are thousands of federal health care professionals who worked long and hard to achieve their goals whom this Act undervalues. Moreover, the regulatory change leaves many students enrolled in education and training programs under federal practice auspices confused and overwhelmed. Perhaps they can take some hope and inspiration from the recognition that historically and philosophically, no agency or administration can unilaterally define what is a profession.
The literature on professionalism is voluminous, in large part because it has been surprisingly difficult to reach a consensus definition. A proposed definition from scholars captures most of the key aspects of a profession. While it is drawn from the medical literature, it applies to most of the caring professions the DOE disqualified. For pedagogic purposes, the definition is parsed into discrete criteria in the Table.5
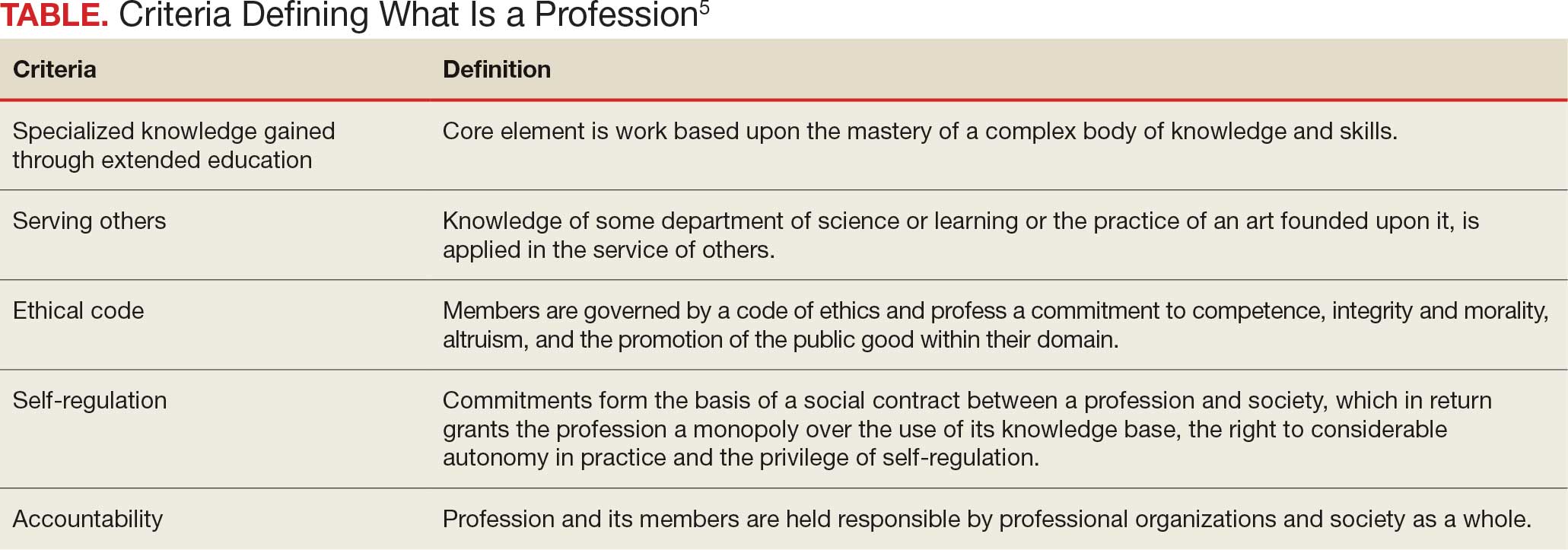
Even this simple summary makes it obvious that a government agency alone could not possibly have the competence to determine who meets these complex technical and moral criteria. The members of the profession must assume a primary role in that determination. The complicated history of the professions shows that the locus of these decisions has resided in various combinations of educational institutions, such as nursing schools,6 professional societies (eg, National Association of Social Workers),7 and certifying boards (eg, National Commission on Certification of Physician Assistants).8 States, not the federal government, have long played a key part in defining professions in the US, through their authority to grant licenses to practice.9
In response to criticism, the DOE has stated that “the definition of a ‘professional degree’ is an internal definition used by the Department of Education to distinguish among programs that qualify for higher loan limits, not a value judgment about the importance of programs. It has no bearing on whether a program is professional in nature or not.”2 Given the ancient compact between society and the professions in which the government subsidizes the training of professionals dedicated to public service, it is hard to see how these changes can be dismissed as merely semantic and not a promissory breach.10
I recognize that this abstract editorial is little comfort to beleaguered and demoralized professionals and students. Still, it offers a voice of support for each federal practitioner or trainee who fulfills the epigraph’s description of a professional day after day. The nurse who works the extra shift without complaint or resentment so that veterans receive the care they deserve, the social worker who responds on a weekend night to an active duty family without food so they do not spend another night hungry, and the physician assistant who makes it into the isolated public health clinic despite the terrible weather so there is someone ready to take care for patients in need. The proposed policy shift cannot in any meaningful sense rob them of their identity as individuals committed to a code of caring. However, without an intact social compact, it may well remove their practical ability to remain and enter the helping professions to the detriment of us all.
- Wade JW. Public responsibilities of the learned professions. Louisiana Law Rev. 1960;21:130-148
- US Department of Education. Myth vs. fact: the definition of professional degrees. Press Release. November 24, 2025. Accessed December 22, 2025. https://www.ed.gov/about/news/press-release/myth-vs-fact-definition-of-professional-degrees
- Laws J. Full list of degrees not classed as “professional” by Trump admin. Newsweek. Updated November 26, 2025. Accessed December 22, 2025. https://www.newsweek.com/full-list-degrees-professional-trump-administration-11085695
- New York Academy of Medicine. Response to stripping “professional status” as proposed by the Department of Education. New York Academy of Medicine. November 24, 2025. Accessed December 22, 2025. https://nyam.org/article/response-to-stripping-professional-status-as-proposed-by-the-department-of-education
- Cruess SR, Johnston S, Cruess RL. “Profession”: a working definition for medical educators. Teach Learn Med. 2004;16:74-76. doi:10.1207/s15328015tlm1601_15
- American Association of Colleges of Nursing. Nursing is a professional degree. American Association of Colleges of Nursing. Accessed December 20, 2025. https://www.aacnnursing.org/policy-advocacy/take-action/nursing-is-a-professional-degree
- National Association of Social Workers. Social work is a profession. Social Workers. Accessed December 20, 2025. https://www.socialworkers.org
- National Commission on Certification of Physician Assistants. Accessed December 20, 2025. https://www.nccpa.net/about-nccpa/#who-we-are
- The Federation of State Boards of Physical Therapy. Accessed December 20, 2025. https://www.fsbpt.org/About-Us/Staff-Home
- Cruess SR, Cruess RL. Professionalism and medicine’s contract with social contract with society. Virtual Mentor. 2004;6:185-188. doi:10.1001/virtualmentor.2004.6.4.msoc1-040
A professional is someone who can do his best work when he doesn’t feel like it.
Alistair Cooke
When I was a young person with no idea about growing up to be something, my father used to tell me there were 4 learned professions: medicine to heal the body, law to protect the body politic, teaching to nurture the mind, and the clergy to care for the soul.1 That adage, or some version of it, is attributed to a variety of sources, likely because it captures something essential and timeless about the learned professions. I write this as a much older person, and it has been my privilege to have worked in some capacity in all 4 of these venerable vocations.
There are many more recognized professions now than in my father’s time with new ones still emerging as the world becomes more complicated and specialized. In November 2025, however, the growth of the professions was dealt a serious blow when the US Department of Education (DOE) redefined what constitutes a profession for the purpose of federal funding of graduate degrees.2 The internet is understandably abuzz with opinions across the political spectrum. What is missing from many of these discussions is an understanding of the criteria for a profession and, even more importantly, who has the authority to decide when an individual or a group has met that standard.
But first, what and why did the DOE make this change? The One Big Beautiful Bill Act charged the DOE with reducing what it claims is massive overspending on graduate education by limiting the programs that meet the definition of a “professional degree” eligible for higher funding. Of my father’s 4, medicine (including dentistry) and law made the cut with students in those professions able to borrow up to $200,000 in direct unsubsidized student loans while those in other programs would be limited to $100,000.2
As one of the oldest and most respected professions in America, nursing has received the most media attention, yet there are also other important and valued professions that are missing from the DOE list.3 The excluded professions also include: physician assistants, physical therapists, audiologists, architects, accountants, educators, and social workers. The proposed regulatory changes are not yet finalized and Congressional representatives, health care experts, and a myriad of professional associations have rightly objected the reclassification will only worsen the critical shortage of nurses, teachers, and other helping professions the country is already facing.4
There are thousands of federal health care professionals who worked long and hard to achieve their goals whom this Act undervalues. Moreover, the regulatory change leaves many students enrolled in education and training programs under federal practice auspices confused and overwhelmed. Perhaps they can take some hope and inspiration from the recognition that historically and philosophically, no agency or administration can unilaterally define what is a profession.
The literature on professionalism is voluminous, in large part because it has been surprisingly difficult to reach a consensus definition. A proposed definition from scholars captures most of the key aspects of a profession. While it is drawn from the medical literature, it applies to most of the caring professions the DOE disqualified. For pedagogic purposes, the definition is parsed into discrete criteria in the Table.5
Even this simple summary makes it obvious that a government agency alone could not possibly have the competence to determine who meets these complex technical and moral criteria. The members of the profession must assume a primary role in that determination. The complicated history of the professions shows that the locus of these decisions has resided in various combinations of educational institutions, such as nursing schools,6 professional societies (eg, National Association of Social Workers),7 and certifying boards (eg, National Commission on Certification of Physician Assistants).8 States, not the federal government, have long played a key part in defining professions in the US, through their authority to grant licenses to practice.9
In response to criticism, the DOE has stated that “the definition of a ‘professional degree’ is an internal definition used by the Department of Education to distinguish among programs that qualify for higher loan limits, not a value judgment about the importance of programs. It has no bearing on whether a program is professional in nature or not.”2 Given the ancient compact between society and the professions in which the government subsidizes the training of professionals dedicated to public service, it is hard to see how these changes can be dismissed as merely semantic and not a promissory breach.10
I recognize that this abstract editorial is little comfort to beleaguered and demoralized professionals and students. Still, it offers a voice of support for each federal practitioner or trainee who fulfills the epigraph’s description of a professional day after day. The nurse who works the extra shift without complaint or resentment so that veterans receive the care they deserve, the social worker who responds on a weekend night to an active duty family without food so they do not spend another night hungry, and the physician assistant who makes it into the isolated public health clinic despite the terrible weather so there is someone ready to take care for patients in need. The proposed policy shift cannot in any meaningful sense rob them of their identity as individuals committed to a code of caring. However, without an intact social compact, it may well remove their practical ability to remain and enter the helping professions to the detriment of us all.
A professional is someone who can do his best work when he doesn’t feel like it.
Alistair Cooke
When I was a young person with no idea about growing up to be something, my father used to tell me there were 4 learned professions: medicine to heal the body, law to protect the body politic, teaching to nurture the mind, and the clergy to care for the soul.1 That adage, or some version of it, is attributed to a variety of sources, likely because it captures something essential and timeless about the learned professions. I write this as a much older person, and it has been my privilege to have worked in some capacity in all 4 of these venerable vocations.
There are many more recognized professions now than in my father’s time with new ones still emerging as the world becomes more complicated and specialized. In November 2025, however, the growth of the professions was dealt a serious blow when the US Department of Education (DOE) redefined what constitutes a profession for the purpose of federal funding of graduate degrees.2 The internet is understandably abuzz with opinions across the political spectrum. What is missing from many of these discussions is an understanding of the criteria for a profession and, even more importantly, who has the authority to decide when an individual or a group has met that standard.
But first, what and why did the DOE make this change? The One Big Beautiful Bill Act charged the DOE with reducing what it claims is massive overspending on graduate education by limiting the programs that meet the definition of a “professional degree” eligible for higher funding. Of my father’s 4, medicine (including dentistry) and law made the cut with students in those professions able to borrow up to $200,000 in direct unsubsidized student loans while those in other programs would be limited to $100,000.2
As one of the oldest and most respected professions in America, nursing has received the most media attention, yet there are also other important and valued professions that are missing from the DOE list.3 The excluded professions also include: physician assistants, physical therapists, audiologists, architects, accountants, educators, and social workers. The proposed regulatory changes are not yet finalized and Congressional representatives, health care experts, and a myriad of professional associations have rightly objected the reclassification will only worsen the critical shortage of nurses, teachers, and other helping professions the country is already facing.4
There are thousands of federal health care professionals who worked long and hard to achieve their goals whom this Act undervalues. Moreover, the regulatory change leaves many students enrolled in education and training programs under federal practice auspices confused and overwhelmed. Perhaps they can take some hope and inspiration from the recognition that historically and philosophically, no agency or administration can unilaterally define what is a profession.
The literature on professionalism is voluminous, in large part because it has been surprisingly difficult to reach a consensus definition. A proposed definition from scholars captures most of the key aspects of a profession. While it is drawn from the medical literature, it applies to most of the caring professions the DOE disqualified. For pedagogic purposes, the definition is parsed into discrete criteria in the Table.5
Even this simple summary makes it obvious that a government agency alone could not possibly have the competence to determine who meets these complex technical and moral criteria. The members of the profession must assume a primary role in that determination. The complicated history of the professions shows that the locus of these decisions has resided in various combinations of educational institutions, such as nursing schools,6 professional societies (eg, National Association of Social Workers),7 and certifying boards (eg, National Commission on Certification of Physician Assistants).8 States, not the federal government, have long played a key part in defining professions in the US, through their authority to grant licenses to practice.9
In response to criticism, the DOE has stated that “the definition of a ‘professional degree’ is an internal definition used by the Department of Education to distinguish among programs that qualify for higher loan limits, not a value judgment about the importance of programs. It has no bearing on whether a program is professional in nature or not.”2 Given the ancient compact between society and the professions in which the government subsidizes the training of professionals dedicated to public service, it is hard to see how these changes can be dismissed as merely semantic and not a promissory breach.10
I recognize that this abstract editorial is little comfort to beleaguered and demoralized professionals and students. Still, it offers a voice of support for each federal practitioner or trainee who fulfills the epigraph’s description of a professional day after day. The nurse who works the extra shift without complaint or resentment so that veterans receive the care they deserve, the social worker who responds on a weekend night to an active duty family without food so they do not spend another night hungry, and the physician assistant who makes it into the isolated public health clinic despite the terrible weather so there is someone ready to take care for patients in need. The proposed policy shift cannot in any meaningful sense rob them of their identity as individuals committed to a code of caring. However, without an intact social compact, it may well remove their practical ability to remain and enter the helping professions to the detriment of us all.
- Wade JW. Public responsibilities of the learned professions. Louisiana Law Rev. 1960;21:130-148
- US Department of Education. Myth vs. fact: the definition of professional degrees. Press Release. November 24, 2025. Accessed December 22, 2025. https://www.ed.gov/about/news/press-release/myth-vs-fact-definition-of-professional-degrees
- Laws J. Full list of degrees not classed as “professional” by Trump admin. Newsweek. Updated November 26, 2025. Accessed December 22, 2025. https://www.newsweek.com/full-list-degrees-professional-trump-administration-11085695
- New York Academy of Medicine. Response to stripping “professional status” as proposed by the Department of Education. New York Academy of Medicine. November 24, 2025. Accessed December 22, 2025. https://nyam.org/article/response-to-stripping-professional-status-as-proposed-by-the-department-of-education
- Cruess SR, Johnston S, Cruess RL. “Profession”: a working definition for medical educators. Teach Learn Med. 2004;16:74-76. doi:10.1207/s15328015tlm1601_15
- American Association of Colleges of Nursing. Nursing is a professional degree. American Association of Colleges of Nursing. Accessed December 20, 2025. https://www.aacnnursing.org/policy-advocacy/take-action/nursing-is-a-professional-degree
- National Association of Social Workers. Social work is a profession. Social Workers. Accessed December 20, 2025. https://www.socialworkers.org
- National Commission on Certification of Physician Assistants. Accessed December 20, 2025. https://www.nccpa.net/about-nccpa/#who-we-are
- The Federation of State Boards of Physical Therapy. Accessed December 20, 2025. https://www.fsbpt.org/About-Us/Staff-Home
- Cruess SR, Cruess RL. Professionalism and medicine’s contract with social contract with society. Virtual Mentor. 2004;6:185-188. doi:10.1001/virtualmentor.2004.6.4.msoc1-040
- Wade JW. Public responsibilities of the learned professions. Louisiana Law Rev. 1960;21:130-148
- US Department of Education. Myth vs. fact: the definition of professional degrees. Press Release. November 24, 2025. Accessed December 22, 2025. https://www.ed.gov/about/news/press-release/myth-vs-fact-definition-of-professional-degrees
- Laws J. Full list of degrees not classed as “professional” by Trump admin. Newsweek. Updated November 26, 2025. Accessed December 22, 2025. https://www.newsweek.com/full-list-degrees-professional-trump-administration-11085695
- New York Academy of Medicine. Response to stripping “professional status” as proposed by the Department of Education. New York Academy of Medicine. November 24, 2025. Accessed December 22, 2025. https://nyam.org/article/response-to-stripping-professional-status-as-proposed-by-the-department-of-education
- Cruess SR, Johnston S, Cruess RL. “Profession”: a working definition for medical educators. Teach Learn Med. 2004;16:74-76. doi:10.1207/s15328015tlm1601_15
- American Association of Colleges of Nursing. Nursing is a professional degree. American Association of Colleges of Nursing. Accessed December 20, 2025. https://www.aacnnursing.org/policy-advocacy/take-action/nursing-is-a-professional-degree
- National Association of Social Workers. Social work is a profession. Social Workers. Accessed December 20, 2025. https://www.socialworkers.org
- National Commission on Certification of Physician Assistants. Accessed December 20, 2025. https://www.nccpa.net/about-nccpa/#who-we-are
- The Federation of State Boards of Physical Therapy. Accessed December 20, 2025. https://www.fsbpt.org/About-Us/Staff-Home
- Cruess SR, Cruess RL. Professionalism and medicine’s contract with social contract with society. Virtual Mentor. 2004;6:185-188. doi:10.1001/virtualmentor.2004.6.4.msoc1-040
Codes, Contracts, and Commitments: Who Defines What is a Profession?
Codes, Contracts, and Commitments: Who Defines What is a Profession?

Can Telehealth Improve Access to Amyloid-Targeting Therapies for Veterans Living With Alzheimer Disease?
Can Telehealth Improve Access to Amyloid-Targeting Therapies for Veterans Living With Alzheimer Disease?
The Veterans Health Administration (VHA) is the largest US integrated health care system, providing health care to > 9 million veterans annually. Dementia affects > 7.2 million Americans, and an estimated 450,000 veterans live with Alzheimer disease (AD).1,2 Compared with the general population, veterans have a higher burden of chronic medical conditions and are disproportionately affected by AD due to exposure to military-related risk factors (eg, traumatic brain injury and posttraumatic stress disorder) and the high prevalence of nonmilitary risk factors, such as cardiovascular disease. The VHA is a pioneer in dementia care, having established a Dementia System of Care to provide primary and specialty care to veterans with dementia. The VHA also is leading the way in implementing the Institute for Healthcare Improvement Age-Friendly Health Systems (AFHS) framework for providing goal-concordant care in > 100 VHA medical centers. The VHA aims to be the largest AFHS in the country.
AD profoundly affects individuals and their families. The progressive nature of the most common form of dementia diminishes the quality of life for patients as well as their care partners in an ongoing fashion, often leading to emotional, physical, and financial strain. Costs for health and long-term care for people living with AD and other dementias were projected at $360 billion in 2024, largely due to the need for nursing home care.1 Although several oral medications are available, their capacity to effectively mitigate the negative effects of AD is limited. Cholinesterase inhibitors and memantine may offer temporary symptomatic relief, but they do not alter disease progression.3 The use of these agents is relatively low, with about one-third of patients diagnosed with AD receiving these medications.4
Amyloid-Targeting Therapies
Recent advancements in biologics, particularly amyloid-targeting therapies, such as lecanemab and donanemab, offer new hope for managing AD. Older adults treated with these medications show less decline on measures of cognition and function than those receiving a placebo at 18 months.5,6 However, accessing and using these medications is challenging.
Use of amyloid-targeting therapies poses challenges. The medications are expensive, potentially placing a financial burden on patients, families, and health care systems.7 Determining initial eligibility for treatment requires a battery of cognitive assessments, laboratory tests, advanced radiologic studies (eg, magnetic resonance imaging [MRI] of the brain and amyloid positron emission tomography [PET] scans), and possible cerebrospinal fluid (CSF) testing. Frequent ongoing assessments are necessary to monitor safety and efficacy. These treatments carry substantial risks, particularly amyloid-related imaging abnormalities (ARIA) such as cerebral edema, microhemorrhages, and superficial siderosis. Therefore, follow-up assessments typically occur around months 2, 3, 4, and 7, depending on which medication is selected. Finally, at present, both agents must be intravenous (IV)-administered in a monitored clinical setting, which requires additional coordination, transportation, and cost.
Ongoing evaluations and in-person administration particularly affect patients and care partners with limitations regarding transportation, time off work, and navigating complex health care systems.8 VHA clinicians at sites that have implemented or are interested in implementing amyloid-targeting therapy programs endorse similar challenges when implementing these therapies in their US Department of Veterans Affairs (VA) medical centers (VAMCs).9
The VHA was one of the first health care systems to use amyloid-targeting therapies, covering the cost of lecanemab and donanemab, in addition to costs associated with concomitant evaluation and testing. However, given the safety concerns with this novel class of medications, the VHA National Formulary Committee developed criteria for use and recommended the VA Center for Medication Safety (VAMedSAFE) conduct a mandatory real-time medication use evaluation (MUE). VAMedSAFE developed the MUE to monitor the safe and appropriate use of amyloid-targeting therapy for AD. Two authors (AJO, SMH) partnered with VAMedSAFE through the VA Pittsburgh Healthcare System Technology Enhancing Cognition and Health–Geriatric Research, Education, and Clinical Center (TECH-GRECC) to provide clinical expertise, substantive feedback for the development of the MUE, and guidance for VHA sites starting amyloid targeting-therapy programs. We started a VHA Amyloid-Targeting Therapy for AD SharePoint collaborative platform and VHA AD Therapeutics Community of Practice (CoP) for shared learning (Figure). The private SharePoint platform houses an array of implementation materials for VAMCs starting programs: key documents and links; educational materials; sample guidelines; note templates; and electronic health record screenshots. The CoP allows VHAs to share best practices and discuss challenges.
Even with these advantages, we found that ensuring the safe and appropriate use of amyloid-targeting therapies did not overcome the barriers associated with their complexity. This was especially true for veterans living in rural areas. Only 4 VAMCs had administered amyloid-targeting therapies in the first year they were available. Preliminary data demonstrated that 27 (84%) of 32 veterans who initiated lecanemab in the VHA between October 2023 and September 2024 resided in urban areas.10 To address the underutilization of amyloid-targeting therapy, we propose leveraging the strengths of VHA telehealth to facilitate expansion of access to these medications for veterans with early AD. Telehealth may substantially increase access to evaluation for veterans with early dementia and, when medically appropriate, to receive amyloid-targeting therapies by reducing transportation needs and mitigating costs while ensuring appropriate monitoring through ongoing clinical assessments.
Using Telehealth
The VHA is a pioneer in telehealth, with programs dating back to 2003.11 Between October 1, 2018, and September 30, 2019, the VHA served > 900,000 veterans through the provision of > 2.6 million episodes of care via telehealth.12 The COVID-19 pandemic further cemented the role of telemedicine as an essential component of health care. Telehealth has demonstrated success in the assessment and management of individuals living with dementia. At the VHA, the GRECC-Connect Project is a partnership between 9 urban GRECC sites that seek to provide consultative geriatric and dementia care to rural veterans through telehealth.13 Additional evidence supports the potential to leverage telehealth to effectively communicate results of amyloid PET scans.14
This approach is not without limitations such as the digital divide, or the gap that separates technology-enabled individuals and those unprepared to adopt technology due to limited digital literacy levels or access to needed hardware, software, and connectivity. The VHA has taken steps to address these digital divide barriers by broadly providing tools—such as tablets and broadband connectivity—to veterans. Specifically, the VHA has instituted digital divide consults to determine whether telehealth could be a potential solution for appropriate veterans and to provide an iPad (if eligible) to connect with VA clinicians. Complementary to the digital divide consult, a VHA-specific telehealth preparedness assessment tool is under development and being tested by 2 authors (JF, SMH). This telehealth preparedness assessment tool is designed to aid in the seamless integration of telehealth services with the support of tailored education materials specific to gaps in digital literacy that a veteran might experience.
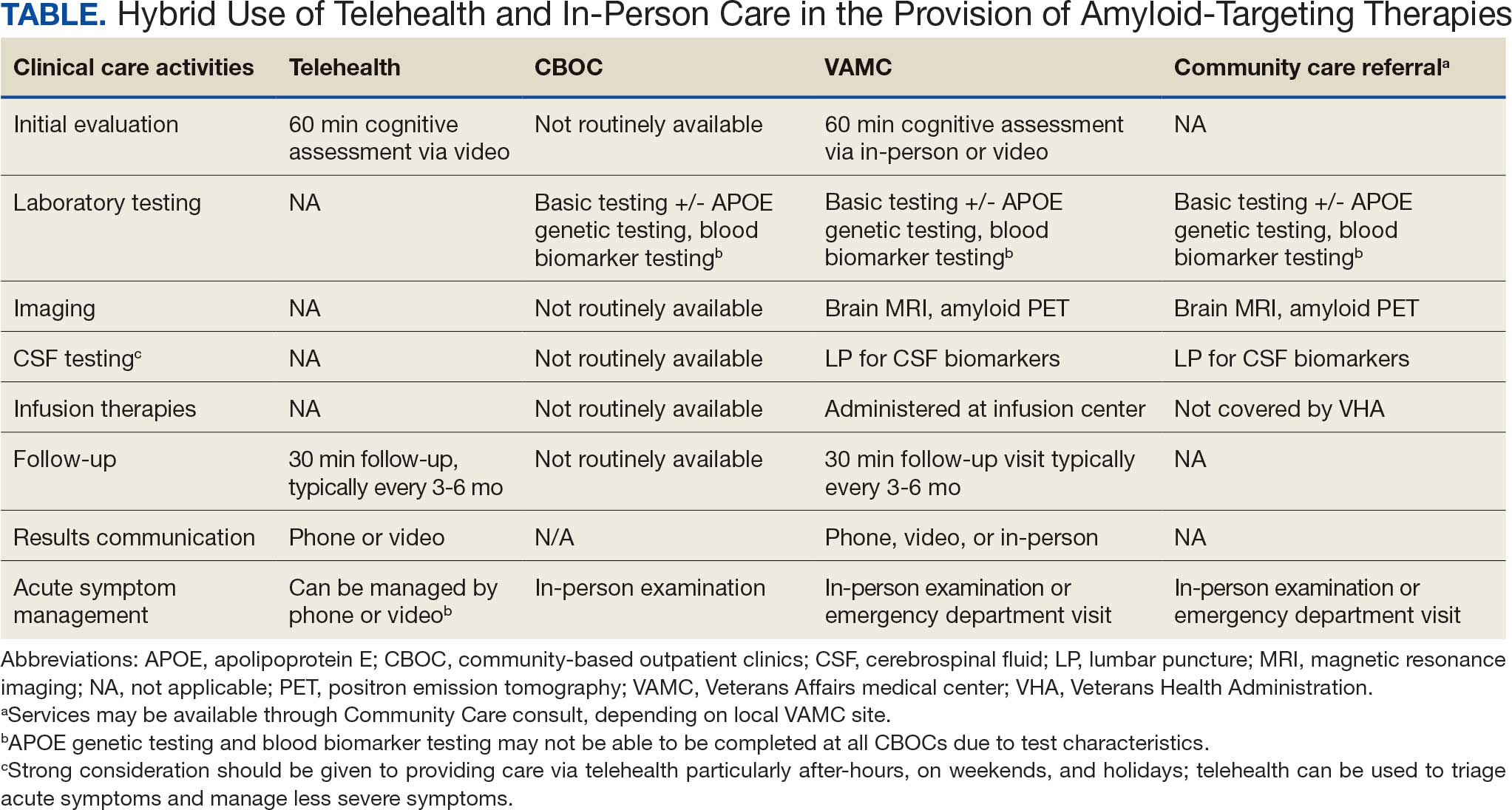
Building on these initiatives, there is an opportunity to expand access to amyloid-targeting therapies, regardless of distance to large VAMCs, by leveraging telehealth as an alternative method of connecting patients with specialty care. Specifically, a hybrid approach could be used to accomplish the myriad initial and follow-up tasks involved in the provision of amyloid-targeting therapies (Table). Not all VHA facilities possess the specialty expertise to prescribe these medications, and local clinicians may not have sufficient knowledge and clinical support to prescribe and monitor these therapies.
The first step is identifying local and regional subject matter experts, followed by the development and expansion of these networks. The National TeleNeurology Program is a good example of a national telehealth program that leverages technology to bring specialty services to rural areas with limited access to care. Although amyloid-targeting therapies often require more complex logistics, such as laboratory tests and imaging, these initial hurdles can be overcome through localized services and collaboration between VAMCs.
While treatment and imaging will most likely need to occur at a VAMC, most basic laboratory studies can be performed at community-based outpatient clinics (CBOCs). Some CBOCs may not be able to process more specialized laboratory tests such as apolipoprotein E genetic testing. Samples for these tests can be collected and processed at VAMCs, which usually have contracts with outside laboratories capable of performing these studies. Most, although not all, VAMCs offer advanced imaging, including MRI of the brain and amyloid PETs. VAMCs without those modalities may need to coordinate with other regional VAMCs. Additionally, a pilot program is already underway whereby VAMCs without the ability to quantify the amount of amyloid on PETs are able to leverage technology and collaborations with other VAMCs to obtain these data.
Once the initial phases of evaluation and care are completed, telemedicine can be leveraged for follow-up and ongoing management. Interdisciplinary teams can help facilitate care related to amyloid-targeting therapies, including the close monitoring of veterans for development of ARIA.15 To achieve this monitoring, specialty clinic teams prescribing amyloid-targeting therapies, which may be geographically distant, need to coordinate with local primary care clinical teams and emergency clinicians. All of these health care team members, along with neurologists and neurosurgeons, should be involved in the development and implementation of protocols in the event that patients present to their local primary or specialty care clinics or emergency department with ARIA symptoms.
If amyloid-targeting therapies are to be provided along with other emerging treatments for rural veterans, telehealth must be part of the solution. There is a pressing need to explore innovative evaluation and delivery models for these therapies, particularly as we expect additional diagnostics and therapeutics to be available in the future. With the advent of commercially available blood tests (ie, blood biomarkers) for AD, there is hope for a transition away from PETs and CSF testing given their cost, limited access, and invasiveness for diagnosis and monitoring of AD. These advances will increase the utility of telehealth to help rural veterans access amyloid-targeting therapies.
Additionally, administering the drug at home or at local clinics, supported by a dedicated health care team or home health agency, could further improve accessibility. Telehealth can be leveraged in this scenario, allowing specialty clinics and specialists to connect with patients and clinicians based out of local clinics or even home health agencies. In this scenario, specialists can provide hands-on care guidance and oversight even though they may be geographically distant from care recipients. Transitioning from IV administration to subcutaneous formulations would further enhance convenience and reduce barriers; these formulations may be available soon.16 Addressing logistical challenges to care and access through technology-based solutions will require coordinated efforts and continued VHA investment.
Conclusions
The VHA has a large population of veterans with dementia, and the costs to care for these veterans will only increase. While the current benefits of amyloid-targeting therapies are modest, now is the time to establish care processes that will support future innovations in amyloid-targeting therapies and other treatments and diagnostics. We are developing better ways to detect AD using clinical decision support tools, improving care pathways and the management of AD, and leveraging telehealth to improve access. The VA is conducting research to investigate whether a cognitive screening and laboratory evaluation that includes a telehealth preparedness assessment will be feasible and effective for improving the detection of AD and access to treatment, and we plan to publish the results.
The lessons learned can be extended to non-VHA care settings to help achieve potential benefits for other patients with early AD. Emerging therapies have the potential to improve the quality of life for both patients and care partners, adding life to years and not just years to life. Policymakers and payors must prioritize research funding to evaluate the safety and efficacy of these approaches to the delivery of health services, ensuring that emerging therapies are accessible for all individuals affected by AD.
- Alzheimer’s Association. 2025 Alzheimer’s disease facts and figures. Alzheimers Dement. 2025;21(4):e70235. doi:10.1002/alz.70235
- US Department of Veterans Affairs. Statistical Projections of Alzheimer’s Dementia for VA Patients, VA Enrollees, and US Veterans. December 18, 2020. Accessed November 2, 2025. https://www.va.gov/GERIATRICS/docs/VHA_ALZHEIMERS_DEMENTIA_Statistical_Projections_FY21_and_FY33_sgc121820.pdf
- Casey DA, Antimisiaris D, O’Brien J. Drugs for Alzheimer’s disease: are they effective? P T. 2010;35(4):208-211.
- Barthold D, Joyce G, Ferido P, et al. Pharmaceutical treatment for Alzheimer’s disease and related dementias: utilization and disparities. J Alzheimers Dis. 2020;76(2):579-589. doi:10.3233/JAD-200133
- Sims JR, Zimmer JA, Evans CD, et al. Donanemab in early symptomatic Alzheimer disease: the TRAILBLAZER-ALZ 2 randomized clinical trial. JAMA. 2023;330(6):512-527. doi:10.1001/jama.2023.13239
- van Dyck CH, Swanson CJ, Aisen P, et al. Lecanemab in early Alzheimer’s disease. N Engl J Med. 2023;388(1):9-21. doi:10.1056/NEJMoa2212948
- Tanne JH. Lecanemab: US Veterans Health Administration will cover cost of new Alzheimer’s drug. BMJ. 2023;380:p628. doi:10.1136/bmj.p628
- Nadeau SE. Lecanemab questions. Neurology. 2024;102(7):e209320. doi:10.1212/WNL.0000000000209320 9. O’Donnell AJ, Fortunato AT, Spitznogle BL, et al. Implementation of lecanemab for Alzheimer’s disease: facilitators and barriers. Presented at: American Geriatrics Society 2025 Annual Scientific Meeting, Chicago. May 2025.
- O’Donnell AJ, Zhao X, Parr A, et al. Use of lecanemab for Alzheimer’s disease within the Veteran’s Health Foundation: early findings. Abstract presented at: Alzheimer’s Association International Conference 2025; July 27, 2025; Toronto, Canada.
- O’Donnell AJ, Zhao X, Parr A, et al. Use of lecanemab for Alzheimer’s disease within the Veteran’s Health Foundation: early findings. Abstract presented at: Alzheimer’s Association International Conference 2025; July 27, 2025; Toronto, Canada.
- Hopp F, Whitten P, Subramanian U, et al. Perspectives from the Veterans Health Administration about opportunities and barriers in telemedicine. J Telemed Telecare. 2006;12(8):404-409. doi:10.1258/135763306779378717
- VA reports significant increase in veteran use of telehealth services. News release. US Department of Veterans Affairs. November 22, 2019. Accessed November 19, 2025. https://news.va.gov/press-room/va-reports-significant-increase-in-veteran-use-of-telehealth-services/
- Powers BB, Homer MC, Morone N, et al. Creation of an interprofessional teledementia clinic for rural veterans: preliminary data. J Am Geriatr Soc. 2017;65(5):1092-1099. doi:10.1111/jgs.14839
- Erickson CM, Chin NA, Rosario HL, et al. Feasibility of virtual Alzheimer’s biomarker disclosure: findings from an observational cohort. Alzheimers Dement (N Y). 2023;9(3):e12413. doi:10.1002/trc2.12413
- Turk KW, Knobel MD, Nothern A, et al. An interprofessional team for disease-modifying therapy in Alzheimer disease implementation. Neurol Clin Pract. 2024;14(6):e200346. doi:10.1212/CPJ.0000000000200346
- FDA accepts LEQEMBI® (lecanemab-irmb) biologics license application for subcutaneous maintenance dosing for the treatment of early Alzheimer’s disease. News release. Elsai US. January 13, 2025. Accessed November 2, 2025. https://media-us.eisai.com/2025-01-13-FDA-Accepts-LEQEMBI-R-lecanemab-irmb-Biologics-License-Application-for-Subcutaneous-Maintenance-Dosing-for-the-Treatment-of-Early-Alzheimers-Disease
The Veterans Health Administration (VHA) is the largest US integrated health care system, providing health care to > 9 million veterans annually. Dementia affects > 7.2 million Americans, and an estimated 450,000 veterans live with Alzheimer disease (AD).1,2 Compared with the general population, veterans have a higher burden of chronic medical conditions and are disproportionately affected by AD due to exposure to military-related risk factors (eg, traumatic brain injury and posttraumatic stress disorder) and the high prevalence of nonmilitary risk factors, such as cardiovascular disease. The VHA is a pioneer in dementia care, having established a Dementia System of Care to provide primary and specialty care to veterans with dementia. The VHA also is leading the way in implementing the Institute for Healthcare Improvement Age-Friendly Health Systems (AFHS) framework for providing goal-concordant care in > 100 VHA medical centers. The VHA aims to be the largest AFHS in the country.
AD profoundly affects individuals and their families. The progressive nature of the most common form of dementia diminishes the quality of life for patients as well as their care partners in an ongoing fashion, often leading to emotional, physical, and financial strain. Costs for health and long-term care for people living with AD and other dementias were projected at $360 billion in 2024, largely due to the need for nursing home care.1 Although several oral medications are available, their capacity to effectively mitigate the negative effects of AD is limited. Cholinesterase inhibitors and memantine may offer temporary symptomatic relief, but they do not alter disease progression.3 The use of these agents is relatively low, with about one-third of patients diagnosed with AD receiving these medications.4
Amyloid-Targeting Therapies
Recent advancements in biologics, particularly amyloid-targeting therapies, such as lecanemab and donanemab, offer new hope for managing AD. Older adults treated with these medications show less decline on measures of cognition and function than those receiving a placebo at 18 months.5,6 However, accessing and using these medications is challenging.
Use of amyloid-targeting therapies poses challenges. The medications are expensive, potentially placing a financial burden on patients, families, and health care systems.7 Determining initial eligibility for treatment requires a battery of cognitive assessments, laboratory tests, advanced radiologic studies (eg, magnetic resonance imaging [MRI] of the brain and amyloid positron emission tomography [PET] scans), and possible cerebrospinal fluid (CSF) testing. Frequent ongoing assessments are necessary to monitor safety and efficacy. These treatments carry substantial risks, particularly amyloid-related imaging abnormalities (ARIA) such as cerebral edema, microhemorrhages, and superficial siderosis. Therefore, follow-up assessments typically occur around months 2, 3, 4, and 7, depending on which medication is selected. Finally, at present, both agents must be intravenous (IV)-administered in a monitored clinical setting, which requires additional coordination, transportation, and cost.
Ongoing evaluations and in-person administration particularly affect patients and care partners with limitations regarding transportation, time off work, and navigating complex health care systems.8 VHA clinicians at sites that have implemented or are interested in implementing amyloid-targeting therapy programs endorse similar challenges when implementing these therapies in their US Department of Veterans Affairs (VA) medical centers (VAMCs).9
The VHA was one of the first health care systems to use amyloid-targeting therapies, covering the cost of lecanemab and donanemab, in addition to costs associated with concomitant evaluation and testing. However, given the safety concerns with this novel class of medications, the VHA National Formulary Committee developed criteria for use and recommended the VA Center for Medication Safety (VAMedSAFE) conduct a mandatory real-time medication use evaluation (MUE). VAMedSAFE developed the MUE to monitor the safe and appropriate use of amyloid-targeting therapy for AD. Two authors (AJO, SMH) partnered with VAMedSAFE through the VA Pittsburgh Healthcare System Technology Enhancing Cognition and Health–Geriatric Research, Education, and Clinical Center (TECH-GRECC) to provide clinical expertise, substantive feedback for the development of the MUE, and guidance for VHA sites starting amyloid targeting-therapy programs. We started a VHA Amyloid-Targeting Therapy for AD SharePoint collaborative platform and VHA AD Therapeutics Community of Practice (CoP) for shared learning (Figure). The private SharePoint platform houses an array of implementation materials for VAMCs starting programs: key documents and links; educational materials; sample guidelines; note templates; and electronic health record screenshots. The CoP allows VHAs to share best practices and discuss challenges.
Even with these advantages, we found that ensuring the safe and appropriate use of amyloid-targeting therapies did not overcome the barriers associated with their complexity. This was especially true for veterans living in rural areas. Only 4 VAMCs had administered amyloid-targeting therapies in the first year they were available. Preliminary data demonstrated that 27 (84%) of 32 veterans who initiated lecanemab in the VHA between October 2023 and September 2024 resided in urban areas.10 To address the underutilization of amyloid-targeting therapy, we propose leveraging the strengths of VHA telehealth to facilitate expansion of access to these medications for veterans with early AD. Telehealth may substantially increase access to evaluation for veterans with early dementia and, when medically appropriate, to receive amyloid-targeting therapies by reducing transportation needs and mitigating costs while ensuring appropriate monitoring through ongoing clinical assessments.
Using Telehealth
The VHA is a pioneer in telehealth, with programs dating back to 2003.11 Between October 1, 2018, and September 30, 2019, the VHA served > 900,000 veterans through the provision of > 2.6 million episodes of care via telehealth.12 The COVID-19 pandemic further cemented the role of telemedicine as an essential component of health care. Telehealth has demonstrated success in the assessment and management of individuals living with dementia. At the VHA, the GRECC-Connect Project is a partnership between 9 urban GRECC sites that seek to provide consultative geriatric and dementia care to rural veterans through telehealth.13 Additional evidence supports the potential to leverage telehealth to effectively communicate results of amyloid PET scans.14
This approach is not without limitations such as the digital divide, or the gap that separates technology-enabled individuals and those unprepared to adopt technology due to limited digital literacy levels or access to needed hardware, software, and connectivity. The VHA has taken steps to address these digital divide barriers by broadly providing tools—such as tablets and broadband connectivity—to veterans. Specifically, the VHA has instituted digital divide consults to determine whether telehealth could be a potential solution for appropriate veterans and to provide an iPad (if eligible) to connect with VA clinicians. Complementary to the digital divide consult, a VHA-specific telehealth preparedness assessment tool is under development and being tested by 2 authors (JF, SMH). This telehealth preparedness assessment tool is designed to aid in the seamless integration of telehealth services with the support of tailored education materials specific to gaps in digital literacy that a veteran might experience.
Building on these initiatives, there is an opportunity to expand access to amyloid-targeting therapies, regardless of distance to large VAMCs, by leveraging telehealth as an alternative method of connecting patients with specialty care. Specifically, a hybrid approach could be used to accomplish the myriad initial and follow-up tasks involved in the provision of amyloid-targeting therapies (Table). Not all VHA facilities possess the specialty expertise to prescribe these medications, and local clinicians may not have sufficient knowledge and clinical support to prescribe and monitor these therapies.
The first step is identifying local and regional subject matter experts, followed by the development and expansion of these networks. The National TeleNeurology Program is a good example of a national telehealth program that leverages technology to bring specialty services to rural areas with limited access to care. Although amyloid-targeting therapies often require more complex logistics, such as laboratory tests and imaging, these initial hurdles can be overcome through localized services and collaboration between VAMCs.
While treatment and imaging will most likely need to occur at a VAMC, most basic laboratory studies can be performed at community-based outpatient clinics (CBOCs). Some CBOCs may not be able to process more specialized laboratory tests such as apolipoprotein E genetic testing. Samples for these tests can be collected and processed at VAMCs, which usually have contracts with outside laboratories capable of performing these studies. Most, although not all, VAMCs offer advanced imaging, including MRI of the brain and amyloid PETs. VAMCs without those modalities may need to coordinate with other regional VAMCs. Additionally, a pilot program is already underway whereby VAMCs without the ability to quantify the amount of amyloid on PETs are able to leverage technology and collaborations with other VAMCs to obtain these data.
Once the initial phases of evaluation and care are completed, telemedicine can be leveraged for follow-up and ongoing management. Interdisciplinary teams can help facilitate care related to amyloid-targeting therapies, including the close monitoring of veterans for development of ARIA.15 To achieve this monitoring, specialty clinic teams prescribing amyloid-targeting therapies, which may be geographically distant, need to coordinate with local primary care clinical teams and emergency clinicians. All of these health care team members, along with neurologists and neurosurgeons, should be involved in the development and implementation of protocols in the event that patients present to their local primary or specialty care clinics or emergency department with ARIA symptoms.
If amyloid-targeting therapies are to be provided along with other emerging treatments for rural veterans, telehealth must be part of the solution. There is a pressing need to explore innovative evaluation and delivery models for these therapies, particularly as we expect additional diagnostics and therapeutics to be available in the future. With the advent of commercially available blood tests (ie, blood biomarkers) for AD, there is hope for a transition away from PETs and CSF testing given their cost, limited access, and invasiveness for diagnosis and monitoring of AD. These advances will increase the utility of telehealth to help rural veterans access amyloid-targeting therapies.
Additionally, administering the drug at home or at local clinics, supported by a dedicated health care team or home health agency, could further improve accessibility. Telehealth can be leveraged in this scenario, allowing specialty clinics and specialists to connect with patients and clinicians based out of local clinics or even home health agencies. In this scenario, specialists can provide hands-on care guidance and oversight even though they may be geographically distant from care recipients. Transitioning from IV administration to subcutaneous formulations would further enhance convenience and reduce barriers; these formulations may be available soon.16 Addressing logistical challenges to care and access through technology-based solutions will require coordinated efforts and continued VHA investment.
Conclusions
The VHA has a large population of veterans with dementia, and the costs to care for these veterans will only increase. While the current benefits of amyloid-targeting therapies are modest, now is the time to establish care processes that will support future innovations in amyloid-targeting therapies and other treatments and diagnostics. We are developing better ways to detect AD using clinical decision support tools, improving care pathways and the management of AD, and leveraging telehealth to improve access. The VA is conducting research to investigate whether a cognitive screening and laboratory evaluation that includes a telehealth preparedness assessment will be feasible and effective for improving the detection of AD and access to treatment, and we plan to publish the results.
The lessons learned can be extended to non-VHA care settings to help achieve potential benefits for other patients with early AD. Emerging therapies have the potential to improve the quality of life for both patients and care partners, adding life to years and not just years to life. Policymakers and payors must prioritize research funding to evaluate the safety and efficacy of these approaches to the delivery of health services, ensuring that emerging therapies are accessible for all individuals affected by AD.
The Veterans Health Administration (VHA) is the largest US integrated health care system, providing health care to > 9 million veterans annually. Dementia affects > 7.2 million Americans, and an estimated 450,000 veterans live with Alzheimer disease (AD).1,2 Compared with the general population, veterans have a higher burden of chronic medical conditions and are disproportionately affected by AD due to exposure to military-related risk factors (eg, traumatic brain injury and posttraumatic stress disorder) and the high prevalence of nonmilitary risk factors, such as cardiovascular disease. The VHA is a pioneer in dementia care, having established a Dementia System of Care to provide primary and specialty care to veterans with dementia. The VHA also is leading the way in implementing the Institute for Healthcare Improvement Age-Friendly Health Systems (AFHS) framework for providing goal-concordant care in > 100 VHA medical centers. The VHA aims to be the largest AFHS in the country.
AD profoundly affects individuals and their families. The progressive nature of the most common form of dementia diminishes the quality of life for patients as well as their care partners in an ongoing fashion, often leading to emotional, physical, and financial strain. Costs for health and long-term care for people living with AD and other dementias were projected at $360 billion in 2024, largely due to the need for nursing home care.1 Although several oral medications are available, their capacity to effectively mitigate the negative effects of AD is limited. Cholinesterase inhibitors and memantine may offer temporary symptomatic relief, but they do not alter disease progression.3 The use of these agents is relatively low, with about one-third of patients diagnosed with AD receiving these medications.4
Amyloid-Targeting Therapies
Recent advancements in biologics, particularly amyloid-targeting therapies, such as lecanemab and donanemab, offer new hope for managing AD. Older adults treated with these medications show less decline on measures of cognition and function than those receiving a placebo at 18 months.5,6 However, accessing and using these medications is challenging.
Use of amyloid-targeting therapies poses challenges. The medications are expensive, potentially placing a financial burden on patients, families, and health care systems.7 Determining initial eligibility for treatment requires a battery of cognitive assessments, laboratory tests, advanced radiologic studies (eg, magnetic resonance imaging [MRI] of the brain and amyloid positron emission tomography [PET] scans), and possible cerebrospinal fluid (CSF) testing. Frequent ongoing assessments are necessary to monitor safety and efficacy. These treatments carry substantial risks, particularly amyloid-related imaging abnormalities (ARIA) such as cerebral edema, microhemorrhages, and superficial siderosis. Therefore, follow-up assessments typically occur around months 2, 3, 4, and 7, depending on which medication is selected. Finally, at present, both agents must be intravenous (IV)-administered in a monitored clinical setting, which requires additional coordination, transportation, and cost.
Ongoing evaluations and in-person administration particularly affect patients and care partners with limitations regarding transportation, time off work, and navigating complex health care systems.8 VHA clinicians at sites that have implemented or are interested in implementing amyloid-targeting therapy programs endorse similar challenges when implementing these therapies in their US Department of Veterans Affairs (VA) medical centers (VAMCs).9
The VHA was one of the first health care systems to use amyloid-targeting therapies, covering the cost of lecanemab and donanemab, in addition to costs associated with concomitant evaluation and testing. However, given the safety concerns with this novel class of medications, the VHA National Formulary Committee developed criteria for use and recommended the VA Center for Medication Safety (VAMedSAFE) conduct a mandatory real-time medication use evaluation (MUE). VAMedSAFE developed the MUE to monitor the safe and appropriate use of amyloid-targeting therapy for AD. Two authors (AJO, SMH) partnered with VAMedSAFE through the VA Pittsburgh Healthcare System Technology Enhancing Cognition and Health–Geriatric Research, Education, and Clinical Center (TECH-GRECC) to provide clinical expertise, substantive feedback for the development of the MUE, and guidance for VHA sites starting amyloid targeting-therapy programs. We started a VHA Amyloid-Targeting Therapy for AD SharePoint collaborative platform and VHA AD Therapeutics Community of Practice (CoP) for shared learning (Figure). The private SharePoint platform houses an array of implementation materials for VAMCs starting programs: key documents and links; educational materials; sample guidelines; note templates; and electronic health record screenshots. The CoP allows VHAs to share best practices and discuss challenges.
Even with these advantages, we found that ensuring the safe and appropriate use of amyloid-targeting therapies did not overcome the barriers associated with their complexity. This was especially true for veterans living in rural areas. Only 4 VAMCs had administered amyloid-targeting therapies in the first year they were available. Preliminary data demonstrated that 27 (84%) of 32 veterans who initiated lecanemab in the VHA between October 2023 and September 2024 resided in urban areas.10 To address the underutilization of amyloid-targeting therapy, we propose leveraging the strengths of VHA telehealth to facilitate expansion of access to these medications for veterans with early AD. Telehealth may substantially increase access to evaluation for veterans with early dementia and, when medically appropriate, to receive amyloid-targeting therapies by reducing transportation needs and mitigating costs while ensuring appropriate monitoring through ongoing clinical assessments.
Using Telehealth
The VHA is a pioneer in telehealth, with programs dating back to 2003.11 Between October 1, 2018, and September 30, 2019, the VHA served > 900,000 veterans through the provision of > 2.6 million episodes of care via telehealth.12 The COVID-19 pandemic further cemented the role of telemedicine as an essential component of health care. Telehealth has demonstrated success in the assessment and management of individuals living with dementia. At the VHA, the GRECC-Connect Project is a partnership between 9 urban GRECC sites that seek to provide consultative geriatric and dementia care to rural veterans through telehealth.13 Additional evidence supports the potential to leverage telehealth to effectively communicate results of amyloid PET scans.14
This approach is not without limitations such as the digital divide, or the gap that separates technology-enabled individuals and those unprepared to adopt technology due to limited digital literacy levels or access to needed hardware, software, and connectivity. The VHA has taken steps to address these digital divide barriers by broadly providing tools—such as tablets and broadband connectivity—to veterans. Specifically, the VHA has instituted digital divide consults to determine whether telehealth could be a potential solution for appropriate veterans and to provide an iPad (if eligible) to connect with VA clinicians. Complementary to the digital divide consult, a VHA-specific telehealth preparedness assessment tool is under development and being tested by 2 authors (JF, SMH). This telehealth preparedness assessment tool is designed to aid in the seamless integration of telehealth services with the support of tailored education materials specific to gaps in digital literacy that a veteran might experience.
Building on these initiatives, there is an opportunity to expand access to amyloid-targeting therapies, regardless of distance to large VAMCs, by leveraging telehealth as an alternative method of connecting patients with specialty care. Specifically, a hybrid approach could be used to accomplish the myriad initial and follow-up tasks involved in the provision of amyloid-targeting therapies (Table). Not all VHA facilities possess the specialty expertise to prescribe these medications, and local clinicians may not have sufficient knowledge and clinical support to prescribe and monitor these therapies.
The first step is identifying local and regional subject matter experts, followed by the development and expansion of these networks. The National TeleNeurology Program is a good example of a national telehealth program that leverages technology to bring specialty services to rural areas with limited access to care. Although amyloid-targeting therapies often require more complex logistics, such as laboratory tests and imaging, these initial hurdles can be overcome through localized services and collaboration between VAMCs.
While treatment and imaging will most likely need to occur at a VAMC, most basic laboratory studies can be performed at community-based outpatient clinics (CBOCs). Some CBOCs may not be able to process more specialized laboratory tests such as apolipoprotein E genetic testing. Samples for these tests can be collected and processed at VAMCs, which usually have contracts with outside laboratories capable of performing these studies. Most, although not all, VAMCs offer advanced imaging, including MRI of the brain and amyloid PETs. VAMCs without those modalities may need to coordinate with other regional VAMCs. Additionally, a pilot program is already underway whereby VAMCs without the ability to quantify the amount of amyloid on PETs are able to leverage technology and collaborations with other VAMCs to obtain these data.
Once the initial phases of evaluation and care are completed, telemedicine can be leveraged for follow-up and ongoing management. Interdisciplinary teams can help facilitate care related to amyloid-targeting therapies, including the close monitoring of veterans for development of ARIA.15 To achieve this monitoring, specialty clinic teams prescribing amyloid-targeting therapies, which may be geographically distant, need to coordinate with local primary care clinical teams and emergency clinicians. All of these health care team members, along with neurologists and neurosurgeons, should be involved in the development and implementation of protocols in the event that patients present to their local primary or specialty care clinics or emergency department with ARIA symptoms.
If amyloid-targeting therapies are to be provided along with other emerging treatments for rural veterans, telehealth must be part of the solution. There is a pressing need to explore innovative evaluation and delivery models for these therapies, particularly as we expect additional diagnostics and therapeutics to be available in the future. With the advent of commercially available blood tests (ie, blood biomarkers) for AD, there is hope for a transition away from PETs and CSF testing given their cost, limited access, and invasiveness for diagnosis and monitoring of AD. These advances will increase the utility of telehealth to help rural veterans access amyloid-targeting therapies.
Additionally, administering the drug at home or at local clinics, supported by a dedicated health care team or home health agency, could further improve accessibility. Telehealth can be leveraged in this scenario, allowing specialty clinics and specialists to connect with patients and clinicians based out of local clinics or even home health agencies. In this scenario, specialists can provide hands-on care guidance and oversight even though they may be geographically distant from care recipients. Transitioning from IV administration to subcutaneous formulations would further enhance convenience and reduce barriers; these formulations may be available soon.16 Addressing logistical challenges to care and access through technology-based solutions will require coordinated efforts and continued VHA investment.
Conclusions
The VHA has a large population of veterans with dementia, and the costs to care for these veterans will only increase. While the current benefits of amyloid-targeting therapies are modest, now is the time to establish care processes that will support future innovations in amyloid-targeting therapies and other treatments and diagnostics. We are developing better ways to detect AD using clinical decision support tools, improving care pathways and the management of AD, and leveraging telehealth to improve access. The VA is conducting research to investigate whether a cognitive screening and laboratory evaluation that includes a telehealth preparedness assessment will be feasible and effective for improving the detection of AD and access to treatment, and we plan to publish the results.
The lessons learned can be extended to non-VHA care settings to help achieve potential benefits for other patients with early AD. Emerging therapies have the potential to improve the quality of life for both patients and care partners, adding life to years and not just years to life. Policymakers and payors must prioritize research funding to evaluate the safety and efficacy of these approaches to the delivery of health services, ensuring that emerging therapies are accessible for all individuals affected by AD.
- Alzheimer’s Association. 2025 Alzheimer’s disease facts and figures. Alzheimers Dement. 2025;21(4):e70235. doi:10.1002/alz.70235
- US Department of Veterans Affairs. Statistical Projections of Alzheimer’s Dementia for VA Patients, VA Enrollees, and US Veterans. December 18, 2020. Accessed November 2, 2025. https://www.va.gov/GERIATRICS/docs/VHA_ALZHEIMERS_DEMENTIA_Statistical_Projections_FY21_and_FY33_sgc121820.pdf
- Casey DA, Antimisiaris D, O’Brien J. Drugs for Alzheimer’s disease: are they effective? P T. 2010;35(4):208-211.
- Barthold D, Joyce G, Ferido P, et al. Pharmaceutical treatment for Alzheimer’s disease and related dementias: utilization and disparities. J Alzheimers Dis. 2020;76(2):579-589. doi:10.3233/JAD-200133
- Sims JR, Zimmer JA, Evans CD, et al. Donanemab in early symptomatic Alzheimer disease: the TRAILBLAZER-ALZ 2 randomized clinical trial. JAMA. 2023;330(6):512-527. doi:10.1001/jama.2023.13239
- van Dyck CH, Swanson CJ, Aisen P, et al. Lecanemab in early Alzheimer’s disease. N Engl J Med. 2023;388(1):9-21. doi:10.1056/NEJMoa2212948
- Tanne JH. Lecanemab: US Veterans Health Administration will cover cost of new Alzheimer’s drug. BMJ. 2023;380:p628. doi:10.1136/bmj.p628
- Nadeau SE. Lecanemab questions. Neurology. 2024;102(7):e209320. doi:10.1212/WNL.0000000000209320 9. O’Donnell AJ, Fortunato AT, Spitznogle BL, et al. Implementation of lecanemab for Alzheimer’s disease: facilitators and barriers. Presented at: American Geriatrics Society 2025 Annual Scientific Meeting, Chicago. May 2025.
- O’Donnell AJ, Zhao X, Parr A, et al. Use of lecanemab for Alzheimer’s disease within the Veteran’s Health Foundation: early findings. Abstract presented at: Alzheimer’s Association International Conference 2025; July 27, 2025; Toronto, Canada.
- O’Donnell AJ, Zhao X, Parr A, et al. Use of lecanemab for Alzheimer’s disease within the Veteran’s Health Foundation: early findings. Abstract presented at: Alzheimer’s Association International Conference 2025; July 27, 2025; Toronto, Canada.
- Hopp F, Whitten P, Subramanian U, et al. Perspectives from the Veterans Health Administration about opportunities and barriers in telemedicine. J Telemed Telecare. 2006;12(8):404-409. doi:10.1258/135763306779378717
- VA reports significant increase in veteran use of telehealth services. News release. US Department of Veterans Affairs. November 22, 2019. Accessed November 19, 2025. https://news.va.gov/press-room/va-reports-significant-increase-in-veteran-use-of-telehealth-services/
- Powers BB, Homer MC, Morone N, et al. Creation of an interprofessional teledementia clinic for rural veterans: preliminary data. J Am Geriatr Soc. 2017;65(5):1092-1099. doi:10.1111/jgs.14839
- Erickson CM, Chin NA, Rosario HL, et al. Feasibility of virtual Alzheimer’s biomarker disclosure: findings from an observational cohort. Alzheimers Dement (N Y). 2023;9(3):e12413. doi:10.1002/trc2.12413
- Turk KW, Knobel MD, Nothern A, et al. An interprofessional team for disease-modifying therapy in Alzheimer disease implementation. Neurol Clin Pract. 2024;14(6):e200346. doi:10.1212/CPJ.0000000000200346
- FDA accepts LEQEMBI® (lecanemab-irmb) biologics license application for subcutaneous maintenance dosing for the treatment of early Alzheimer’s disease. News release. Elsai US. January 13, 2025. Accessed November 2, 2025. https://media-us.eisai.com/2025-01-13-FDA-Accepts-LEQEMBI-R-lecanemab-irmb-Biologics-License-Application-for-Subcutaneous-Maintenance-Dosing-for-the-Treatment-of-Early-Alzheimers-Disease
- Alzheimer’s Association. 2025 Alzheimer’s disease facts and figures. Alzheimers Dement. 2025;21(4):e70235. doi:10.1002/alz.70235
- US Department of Veterans Affairs. Statistical Projections of Alzheimer’s Dementia for VA Patients, VA Enrollees, and US Veterans. December 18, 2020. Accessed November 2, 2025. https://www.va.gov/GERIATRICS/docs/VHA_ALZHEIMERS_DEMENTIA_Statistical_Projections_FY21_and_FY33_sgc121820.pdf
- Casey DA, Antimisiaris D, O’Brien J. Drugs for Alzheimer’s disease: are they effective? P T. 2010;35(4):208-211.
- Barthold D, Joyce G, Ferido P, et al. Pharmaceutical treatment for Alzheimer’s disease and related dementias: utilization and disparities. J Alzheimers Dis. 2020;76(2):579-589. doi:10.3233/JAD-200133
- Sims JR, Zimmer JA, Evans CD, et al. Donanemab in early symptomatic Alzheimer disease: the TRAILBLAZER-ALZ 2 randomized clinical trial. JAMA. 2023;330(6):512-527. doi:10.1001/jama.2023.13239
- van Dyck CH, Swanson CJ, Aisen P, et al. Lecanemab in early Alzheimer’s disease. N Engl J Med. 2023;388(1):9-21. doi:10.1056/NEJMoa2212948
- Tanne JH. Lecanemab: US Veterans Health Administration will cover cost of new Alzheimer’s drug. BMJ. 2023;380:p628. doi:10.1136/bmj.p628
- Nadeau SE. Lecanemab questions. Neurology. 2024;102(7):e209320. doi:10.1212/WNL.0000000000209320 9. O’Donnell AJ, Fortunato AT, Spitznogle BL, et al. Implementation of lecanemab for Alzheimer’s disease: facilitators and barriers. Presented at: American Geriatrics Society 2025 Annual Scientific Meeting, Chicago. May 2025.
- O’Donnell AJ, Zhao X, Parr A, et al. Use of lecanemab for Alzheimer’s disease within the Veteran’s Health Foundation: early findings. Abstract presented at: Alzheimer’s Association International Conference 2025; July 27, 2025; Toronto, Canada.
- O’Donnell AJ, Zhao X, Parr A, et al. Use of lecanemab for Alzheimer’s disease within the Veteran’s Health Foundation: early findings. Abstract presented at: Alzheimer’s Association International Conference 2025; July 27, 2025; Toronto, Canada.
- Hopp F, Whitten P, Subramanian U, et al. Perspectives from the Veterans Health Administration about opportunities and barriers in telemedicine. J Telemed Telecare. 2006;12(8):404-409. doi:10.1258/135763306779378717
- VA reports significant increase in veteran use of telehealth services. News release. US Department of Veterans Affairs. November 22, 2019. Accessed November 19, 2025. https://news.va.gov/press-room/va-reports-significant-increase-in-veteran-use-of-telehealth-services/
- Powers BB, Homer MC, Morone N, et al. Creation of an interprofessional teledementia clinic for rural veterans: preliminary data. J Am Geriatr Soc. 2017;65(5):1092-1099. doi:10.1111/jgs.14839
- Erickson CM, Chin NA, Rosario HL, et al. Feasibility of virtual Alzheimer’s biomarker disclosure: findings from an observational cohort. Alzheimers Dement (N Y). 2023;9(3):e12413. doi:10.1002/trc2.12413
- Turk KW, Knobel MD, Nothern A, et al. An interprofessional team for disease-modifying therapy in Alzheimer disease implementation. Neurol Clin Pract. 2024;14(6):e200346. doi:10.1212/CPJ.0000000000200346
- FDA accepts LEQEMBI® (lecanemab-irmb) biologics license application for subcutaneous maintenance dosing for the treatment of early Alzheimer’s disease. News release. Elsai US. January 13, 2025. Accessed November 2, 2025. https://media-us.eisai.com/2025-01-13-FDA-Accepts-LEQEMBI-R-lecanemab-irmb-Biologics-License-Application-for-Subcutaneous-Maintenance-Dosing-for-the-Treatment-of-Early-Alzheimers-Disease
Can Telehealth Improve Access to Amyloid-Targeting Therapies for Veterans Living With Alzheimer Disease?
Can Telehealth Improve Access to Amyloid-Targeting Therapies for Veterans Living With Alzheimer Disease?
The Once and Future Veterans Health Administration
The Once and Future Veterans Health Administration
He who thus considers things in their first growth and origin ... will obtain the clearest view of them. Politics, Book I, Part II by Aristotle
Many seasoned observers of federal practice have signaled that the future of US Department of Veterans Affairs (VA) health care is threatened as never before. Political forces and economic interests are siphoning Veterans Health Administration (VHA) capital and human resources into the community with an ineluctable push toward privatization.1
This Veterans Day, the vitality, if not the very viability of veteran health care, is in serious jeopardy, so it seems fitting to review the rationale for having institutions dedicated to the specialized medical treatment of veterans. Aristotle advises us on how to undertake this intellectual exercise in the epigraph. This column will revisit the historical origins of VA medicine to better appreciate the justification of an agency committed to this unique purpose and what may be sacrificed if it is decimated.
The provision of medical care focused on the injuries and illnesses of warriors is as old as war. The ancient Romans had among the first veterans’ hospital, named a valetudinarium. Sick and injured members of the Roman legions received state-of-the-art medical and surgical care from military doctors inside these facilities.2
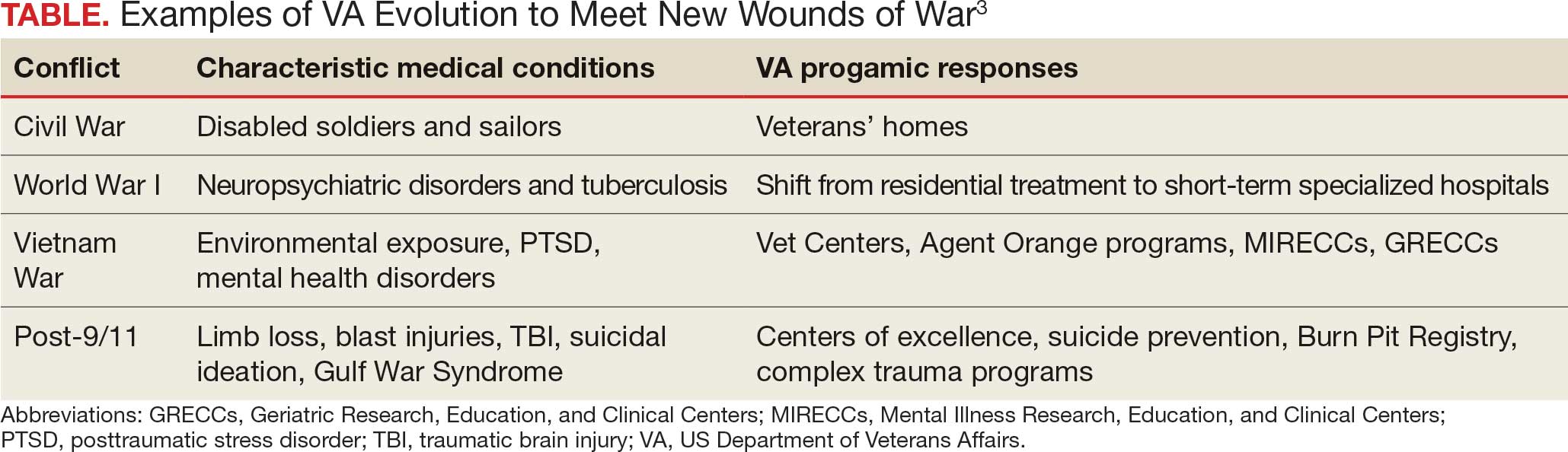
In the United States, federal practice emerged almost simultaneously with the birth of a nation. Wounded troops and families of slain soldiers required rehabilitation and support from the fledgling federal government. This began a pattern of development in which each war generated novel injuries and disorders that required the VA to evolve (Table).3
Many arguments can be marshalled to demonstrate the importance of not just ensuring VA health care survives but also has the resources needed to thrive. I will highlight what I argue are the most important justifications for its existence.
The ethical argument: President Abraham Lincoln and a long line of government officials for more than 2 centuries have called the provision of high-quality health care focused on veterans a sacred trust. Failing to fulfill that promise is a violation of the deepest principles of veracity and fidelity that those who govern owe to the citizens who selflessly sacrificed time, health, and even in some cases life, for the safety and well-being of their country.4
The quality argument: Dozens of studies have found that compared to the community, many areas of veteran medical care are just plain better. Two surveys particularly salient in the aging veteran population illustrate this growing body of positive research. The most recent and largest survey of Medicare patients found that VHA hospitals surpassed community-based hospitals on all 10 metrics.5 A retrospective cohort study of mortality compared veterans transported by ambulance to VHA or community-based hospitals. The researchers found that those taken to VHA facilities had a 30-day all cause adjustment mortality 20 times lower than those taken to civilian hospitals, especially among minoritized populations who generally have higher mortality.6
The cultural argument: Glance at almost any form of communication from veterans or about their health care and you will apprehend common cultural themes. Even when frustrated that the system has not lived up to their expectations, and perhaps because of their sense of belonging, they voice ownership of VHA as their medical home. Surveys of veteran experiences have shown many feel more comfortable receiving care in the company of comrades in arms and from health care professionals with expertise and experience with veterans’ distinctive medical problems and the military values that inform their preferences for care.7
The complexity argument: Anyone who has worked even a short time in a VHA hospital or clinic knows the patients are in general more complicated than similar patients in the community. Multiple medical, geriatric, neuropsychiatric, substance use, and social comorbidities are the expectation, not the exception, as in some civilian systems. Many of the conditions common in the VHA such as traumatic brain injury, service-connected cancers, suicidal ideation, environmental exposures, and posttraumatic stress disorder would be encountered in community health care settings. The differences between VHA and community care led the RAND Corporation to caution that “Community care providers might not be equipped to handle the needs of veterans.”8
Let me bring this 1000-foot view of the crisis facing federal practice down to the literal level of my own home. For many years I have had a wonderful mechanic who has a mobile bike service. I was talking to him as he fixed my trike. I never knew he was a Vietnam era veteran, and he didn’t realize that I was a career VA health care professional at the very VHA hospital where he received care. He spontaneously told me that, “when I first got out, the VA was awful, but now it is wonderful and they are so good to me. I would not go anywhere else.” For the many veterans of that era who would echo his sentiments, we must not allow the VA to lose all it has gained since that painful time
Another philosopher, Søren Kierkegaard, wrote that “life must be understood backwards but lived forwards.”9 Our own brief back to the future journey in this editorial has, I hope, shown that VHA medical institutions and health professionals cannot be replaced with or replicated by civilian systems and clinicians. Continued attempts to do so betray the trust and risks the health and well-being of veterans. It also would deprive the country of research, innovation, and education that make unparalleled contributions to public health. Ultimately, these efforts to diminish VHA compromise the solidarity of service members with each other and with their federal practitioners. If this trend to dismantle an organization that originated with the sole purpose of caring for veterans continues, then the public expressions of respect and gratitude will sound shallower and more tentative with each passing Veterans Day.
- Quil L. Hundreds of VA clinicians warn that cuts threaten vet’s health care. National Public Radio. October 1, 2025. Accessed October 27, 2025. https://www.npr.org/2025/10/01/nx-s1-5554394/hundreds-of-va-clinicians-warn-that-cuts-threaten-vets-health-care
- Nutton V. Ancient Medicine. 2nd ed. Routledge; 2012.
- US Department of Veterans Affairs. VA History Summary. Updated June 13, 2025. Accessed October 27, 2025. https://department.va.gov/history/history-overview/
- Geppert CMA. Learning from history: the ethical foundation of VA health care. Fed Pract. 2016;33:6-7.
- US Department of Veterans Affairs. Nationwide patient survey shows VA hospitals outperform non-VA hospitals. News release. June 14, 2023. Accessed October 27, 2025. https://news.va.gov/press-room/nationwide-patient-survey-shows-va-hospitals-outperform-non-va-hospitals
- Chan DC, Danesh K, Costantini S, Card D, Taylor L, Studdert DM. Mortality among US veterans after emergency visits to Veterans Affairs and other hospitals: retrospective cohort study. BMJ. 2022;376:e068099. doi:10.1136/bmj-2021-068099
- Vigilante K, Batten SV, Shang Q, et al. Camaraderie among US veterans and their preferences for health care systems and practitioners. JAMA Netw Open. 2025;8(4):e255253. doi:10.1001/jamanetworkopen.2025.5253
- Rasmussen P, Farmer CM. The promise and challenges of VA community care: veterans’ issues in focus. Rand Health Q. 2023;10:9.
- Kierkegaard S. Journalen JJ:167 (1843) in: Søren Kierkegaards Skrifter. Vol 18. Copenhagen; 1997:306.
He who thus considers things in their first growth and origin ... will obtain the clearest view of them. Politics, Book I, Part II by Aristotle
Many seasoned observers of federal practice have signaled that the future of US Department of Veterans Affairs (VA) health care is threatened as never before. Political forces and economic interests are siphoning Veterans Health Administration (VHA) capital and human resources into the community with an ineluctable push toward privatization.1
This Veterans Day, the vitality, if not the very viability of veteran health care, is in serious jeopardy, so it seems fitting to review the rationale for having institutions dedicated to the specialized medical treatment of veterans. Aristotle advises us on how to undertake this intellectual exercise in the epigraph. This column will revisit the historical origins of VA medicine to better appreciate the justification of an agency committed to this unique purpose and what may be sacrificed if it is decimated.
The provision of medical care focused on the injuries and illnesses of warriors is as old as war. The ancient Romans had among the first veterans’ hospital, named a valetudinarium. Sick and injured members of the Roman legions received state-of-the-art medical and surgical care from military doctors inside these facilities.2
In the United States, federal practice emerged almost simultaneously with the birth of a nation. Wounded troops and families of slain soldiers required rehabilitation and support from the fledgling federal government. This began a pattern of development in which each war generated novel injuries and disorders that required the VA to evolve (Table).3
Many arguments can be marshalled to demonstrate the importance of not just ensuring VA health care survives but also has the resources needed to thrive. I will highlight what I argue are the most important justifications for its existence.
The ethical argument: President Abraham Lincoln and a long line of government officials for more than 2 centuries have called the provision of high-quality health care focused on veterans a sacred trust. Failing to fulfill that promise is a violation of the deepest principles of veracity and fidelity that those who govern owe to the citizens who selflessly sacrificed time, health, and even in some cases life, for the safety and well-being of their country.4
The quality argument: Dozens of studies have found that compared to the community, many areas of veteran medical care are just plain better. Two surveys particularly salient in the aging veteran population illustrate this growing body of positive research. The most recent and largest survey of Medicare patients found that VHA hospitals surpassed community-based hospitals on all 10 metrics.5 A retrospective cohort study of mortality compared veterans transported by ambulance to VHA or community-based hospitals. The researchers found that those taken to VHA facilities had a 30-day all cause adjustment mortality 20 times lower than those taken to civilian hospitals, especially among minoritized populations who generally have higher mortality.6
The cultural argument: Glance at almost any form of communication from veterans or about their health care and you will apprehend common cultural themes. Even when frustrated that the system has not lived up to their expectations, and perhaps because of their sense of belonging, they voice ownership of VHA as their medical home. Surveys of veteran experiences have shown many feel more comfortable receiving care in the company of comrades in arms and from health care professionals with expertise and experience with veterans’ distinctive medical problems and the military values that inform their preferences for care.7
The complexity argument: Anyone who has worked even a short time in a VHA hospital or clinic knows the patients are in general more complicated than similar patients in the community. Multiple medical, geriatric, neuropsychiatric, substance use, and social comorbidities are the expectation, not the exception, as in some civilian systems. Many of the conditions common in the VHA such as traumatic brain injury, service-connected cancers, suicidal ideation, environmental exposures, and posttraumatic stress disorder would be encountered in community health care settings. The differences between VHA and community care led the RAND Corporation to caution that “Community care providers might not be equipped to handle the needs of veterans.”8
Let me bring this 1000-foot view of the crisis facing federal practice down to the literal level of my own home. For many years I have had a wonderful mechanic who has a mobile bike service. I was talking to him as he fixed my trike. I never knew he was a Vietnam era veteran, and he didn’t realize that I was a career VA health care professional at the very VHA hospital where he received care. He spontaneously told me that, “when I first got out, the VA was awful, but now it is wonderful and they are so good to me. I would not go anywhere else.” For the many veterans of that era who would echo his sentiments, we must not allow the VA to lose all it has gained since that painful time
Another philosopher, Søren Kierkegaard, wrote that “life must be understood backwards but lived forwards.”9 Our own brief back to the future journey in this editorial has, I hope, shown that VHA medical institutions and health professionals cannot be replaced with or replicated by civilian systems and clinicians. Continued attempts to do so betray the trust and risks the health and well-being of veterans. It also would deprive the country of research, innovation, and education that make unparalleled contributions to public health. Ultimately, these efforts to diminish VHA compromise the solidarity of service members with each other and with their federal practitioners. If this trend to dismantle an organization that originated with the sole purpose of caring for veterans continues, then the public expressions of respect and gratitude will sound shallower and more tentative with each passing Veterans Day.
He who thus considers things in their first growth and origin ... will obtain the clearest view of them. Politics, Book I, Part II by Aristotle
Many seasoned observers of federal practice have signaled that the future of US Department of Veterans Affairs (VA) health care is threatened as never before. Political forces and economic interests are siphoning Veterans Health Administration (VHA) capital and human resources into the community with an ineluctable push toward privatization.1
This Veterans Day, the vitality, if not the very viability of veteran health care, is in serious jeopardy, so it seems fitting to review the rationale for having institutions dedicated to the specialized medical treatment of veterans. Aristotle advises us on how to undertake this intellectual exercise in the epigraph. This column will revisit the historical origins of VA medicine to better appreciate the justification of an agency committed to this unique purpose and what may be sacrificed if it is decimated.
The provision of medical care focused on the injuries and illnesses of warriors is as old as war. The ancient Romans had among the first veterans’ hospital, named a valetudinarium. Sick and injured members of the Roman legions received state-of-the-art medical and surgical care from military doctors inside these facilities.2
In the United States, federal practice emerged almost simultaneously with the birth of a nation. Wounded troops and families of slain soldiers required rehabilitation and support from the fledgling federal government. This began a pattern of development in which each war generated novel injuries and disorders that required the VA to evolve (Table).3
Many arguments can be marshalled to demonstrate the importance of not just ensuring VA health care survives but also has the resources needed to thrive. I will highlight what I argue are the most important justifications for its existence.
The ethical argument: President Abraham Lincoln and a long line of government officials for more than 2 centuries have called the provision of high-quality health care focused on veterans a sacred trust. Failing to fulfill that promise is a violation of the deepest principles of veracity and fidelity that those who govern owe to the citizens who selflessly sacrificed time, health, and even in some cases life, for the safety and well-being of their country.4
The quality argument: Dozens of studies have found that compared to the community, many areas of veteran medical care are just plain better. Two surveys particularly salient in the aging veteran population illustrate this growing body of positive research. The most recent and largest survey of Medicare patients found that VHA hospitals surpassed community-based hospitals on all 10 metrics.5 A retrospective cohort study of mortality compared veterans transported by ambulance to VHA or community-based hospitals. The researchers found that those taken to VHA facilities had a 30-day all cause adjustment mortality 20 times lower than those taken to civilian hospitals, especially among minoritized populations who generally have higher mortality.6
The cultural argument: Glance at almost any form of communication from veterans or about their health care and you will apprehend common cultural themes. Even when frustrated that the system has not lived up to their expectations, and perhaps because of their sense of belonging, they voice ownership of VHA as their medical home. Surveys of veteran experiences have shown many feel more comfortable receiving care in the company of comrades in arms and from health care professionals with expertise and experience with veterans’ distinctive medical problems and the military values that inform their preferences for care.7
The complexity argument: Anyone who has worked even a short time in a VHA hospital or clinic knows the patients are in general more complicated than similar patients in the community. Multiple medical, geriatric, neuropsychiatric, substance use, and social comorbidities are the expectation, not the exception, as in some civilian systems. Many of the conditions common in the VHA such as traumatic brain injury, service-connected cancers, suicidal ideation, environmental exposures, and posttraumatic stress disorder would be encountered in community health care settings. The differences between VHA and community care led the RAND Corporation to caution that “Community care providers might not be equipped to handle the needs of veterans.”8
Let me bring this 1000-foot view of the crisis facing federal practice down to the literal level of my own home. For many years I have had a wonderful mechanic who has a mobile bike service. I was talking to him as he fixed my trike. I never knew he was a Vietnam era veteran, and he didn’t realize that I was a career VA health care professional at the very VHA hospital where he received care. He spontaneously told me that, “when I first got out, the VA was awful, but now it is wonderful and they are so good to me. I would not go anywhere else.” For the many veterans of that era who would echo his sentiments, we must not allow the VA to lose all it has gained since that painful time
Another philosopher, Søren Kierkegaard, wrote that “life must be understood backwards but lived forwards.”9 Our own brief back to the future journey in this editorial has, I hope, shown that VHA medical institutions and health professionals cannot be replaced with or replicated by civilian systems and clinicians. Continued attempts to do so betray the trust and risks the health and well-being of veterans. It also would deprive the country of research, innovation, and education that make unparalleled contributions to public health. Ultimately, these efforts to diminish VHA compromise the solidarity of service members with each other and with their federal practitioners. If this trend to dismantle an organization that originated with the sole purpose of caring for veterans continues, then the public expressions of respect and gratitude will sound shallower and more tentative with each passing Veterans Day.
- Quil L. Hundreds of VA clinicians warn that cuts threaten vet’s health care. National Public Radio. October 1, 2025. Accessed October 27, 2025. https://www.npr.org/2025/10/01/nx-s1-5554394/hundreds-of-va-clinicians-warn-that-cuts-threaten-vets-health-care
- Nutton V. Ancient Medicine. 2nd ed. Routledge; 2012.
- US Department of Veterans Affairs. VA History Summary. Updated June 13, 2025. Accessed October 27, 2025. https://department.va.gov/history/history-overview/
- Geppert CMA. Learning from history: the ethical foundation of VA health care. Fed Pract. 2016;33:6-7.
- US Department of Veterans Affairs. Nationwide patient survey shows VA hospitals outperform non-VA hospitals. News release. June 14, 2023. Accessed October 27, 2025. https://news.va.gov/press-room/nationwide-patient-survey-shows-va-hospitals-outperform-non-va-hospitals
- Chan DC, Danesh K, Costantini S, Card D, Taylor L, Studdert DM. Mortality among US veterans after emergency visits to Veterans Affairs and other hospitals: retrospective cohort study. BMJ. 2022;376:e068099. doi:10.1136/bmj-2021-068099
- Vigilante K, Batten SV, Shang Q, et al. Camaraderie among US veterans and their preferences for health care systems and practitioners. JAMA Netw Open. 2025;8(4):e255253. doi:10.1001/jamanetworkopen.2025.5253
- Rasmussen P, Farmer CM. The promise and challenges of VA community care: veterans’ issues in focus. Rand Health Q. 2023;10:9.
- Kierkegaard S. Journalen JJ:167 (1843) in: Søren Kierkegaards Skrifter. Vol 18. Copenhagen; 1997:306.
- Quil L. Hundreds of VA clinicians warn that cuts threaten vet’s health care. National Public Radio. October 1, 2025. Accessed October 27, 2025. https://www.npr.org/2025/10/01/nx-s1-5554394/hundreds-of-va-clinicians-warn-that-cuts-threaten-vets-health-care
- Nutton V. Ancient Medicine. 2nd ed. Routledge; 2012.
- US Department of Veterans Affairs. VA History Summary. Updated June 13, 2025. Accessed October 27, 2025. https://department.va.gov/history/history-overview/
- Geppert CMA. Learning from history: the ethical foundation of VA health care. Fed Pract. 2016;33:6-7.
- US Department of Veterans Affairs. Nationwide patient survey shows VA hospitals outperform non-VA hospitals. News release. June 14, 2023. Accessed October 27, 2025. https://news.va.gov/press-room/nationwide-patient-survey-shows-va-hospitals-outperform-non-va-hospitals
- Chan DC, Danesh K, Costantini S, Card D, Taylor L, Studdert DM. Mortality among US veterans after emergency visits to Veterans Affairs and other hospitals: retrospective cohort study. BMJ. 2022;376:e068099. doi:10.1136/bmj-2021-068099
- Vigilante K, Batten SV, Shang Q, et al. Camaraderie among US veterans and their preferences for health care systems and practitioners. JAMA Netw Open. 2025;8(4):e255253. doi:10.1001/jamanetworkopen.2025.5253
- Rasmussen P, Farmer CM. The promise and challenges of VA community care: veterans’ issues in focus. Rand Health Q. 2023;10:9.
- Kierkegaard S. Journalen JJ:167 (1843) in: Søren Kierkegaards Skrifter. Vol 18. Copenhagen; 1997:306.
The Once and Future Veterans Health Administration
The Once and Future Veterans Health Administration

Special Report II: Tackling Burnout
Last month, we introduced the epidemic of burnout and the adverse consequences for both our vascular surgery patients and ourselves. Today we will outline a framework for addressing these issues. The foundation of this framework is informed by the social and neurosciences.
From the perspective of the social scientist: Christina Maslach, the originator of the widely used Maslach Burnout Inventory, theorized that burnout arises from a chronic mismatch between people and their work setting in some or all of the following domains: Workload (too much, wrong kind); control (lack of autonomy, or insufficient control over resources); reward (insufficient financial or social rewards commensurate with achievements); community (loss of positive connection with others); fairness (lack of perceived fairness, inequity of work, pay, or promotion); and values (conflict of personal and organizational values). The reality of practicing medicine in today’s business milieu – of achieving service efficiencies by meeting performance targets – brings many of these mismatches into sharp focus.
From the perspective of the neuroscientist: Recent advances, including functional MRI, have demonstrated that the human brain is hard wired for compassion. Compassion is the deep feeling that arises when confronted with another’s suffering, coupled with a strong desire to alleviate that suffering. There are at least two neural pathways: one activated during empathy, having us experience another’s pain; and the other activated during compassion, resulting in our sense of reward. Thus, burnout is thought to occur when you know what your patient needs but you are unable to deliver it. Compassionate medical care is purposeful work, which promotes a sense of reward and mitigates burnout.
Because burnout affects all caregivers (anyone who touches the patient), a successful program addressing workforce well-being must be comprehensive and organization wide, similar to successful patient safety, CPI [continuous process improvement] and LEAN [Six Sigma] initiatives.
There are no shortcuts. Creating a culture of compassionate, collaborative care requires an understanding of the interrelationships between the individual provider, the unit or team, and organizational leadership.
1) The individual provider: There is evidence to support the use of programs that build personal resilience. A recently published meta-analysis by West and colleagues concluded that while no specific physician burnout intervention has been shown to be better than other types of interventions, mindfulness, stress management, and small-group discussions can be effective approaches to reducing burnout scores. Strategies to build individual resilience, such as mindfulness and meditation, are easy to teach but place the burden for success on the individual. No amount of resilience can withstand an unsupportive or toxic workplace environment, so both individual and organizational strategies in combination are necessary.
2) The unit or team: Scheduling time for open and honest discussion of social and emotional issues that arise in caring for patients helps nourish caregiver to caregiver compassion. The Schwartz Center for Compassionate Healthcare is a national nonprofit leading the movement to bring compassion to every patient-caregiver interaction. More than 425 health care organization are Schwartz Center members and conduct Schwartz Rounds™ to bring doctors, nurses, and other caregivers together to discuss the human side of health care. (www.theschwartzcenter.org). Team member to team member support is essential for navigating the stressors of practice. With having lunch in front of your computer being the norm, and the disappearance of traditional spaces for colleagues to connect (for example, nurses’ lounge, physician dining rooms), the opportunity for caregivers to have a safe place to escape, a place to have their own humanity reaffirmed, a place to offer support to their peers, has been eliminated.
3) Organizational Leadership: Making compassion a core value, articulating it, and establishing metrics whereby it can be measured, is a good start. The barriers to a culture of compassion are related to our systems of care. There are burgeoning administrative and documentation tasks to be performed, and productivity expectations that turn our clinics and hospitals into assembly lines. No, we cannot expect the EMR [electronic medical records] to be eliminated, but workforce well-being cannot be sustainable in the context of inadequate resources. A culture of compassionate collaborative care requires programs and policies that are implemented by the organization itself. Examples of organization-wide initiatives that support workforce well-being and provider engagement include: screening for caregiver burnout, establishing policies for managing adverse events with an eye toward the second victim, and most importantly, supporting systems that preserve work control autonomy of physicians and nurses in clinical settings. The business sector has long recognized that workplace stress is a function of how demanding a person’s job is and how much control that person has over his or her responsibilities. The business community has also recognized that the experience of the worker (provider) drives the experience of the customer (patient). In a study of hospital compassionate practices and HCAHPS [the Hospital Consumer Assessment of Healthcare Providers and Systems], McClelland and Vogus reported that how well a hospital compassionately supports it employees and rewards compassionate acts is significantly and positively is associated with that hospital’s ratings and likelihood of patients recommending it.
How does the Society of Vascular Surgery, or any professional medical/nursing society for that matter, fit into this model?
We propose that the SVS find ways to empower their members to be agents for culture change within their own health care organizations. How might this be done:
- Teach organizational leadership skills, starting with the SVS Board of Directors, the presidential line, and the chairs of committees. Offer leadership courses at the Annual Meeting.
- Develop a community of caregivers committed to creating a compassionate collaborative culture. The SVS is a founding member of the Schwartz Center Healthcare Society Leadership Council, and you, as members of the SVS benefit from reduced registration at the Annual Compassion in Action Healthcare Conference, June 24-27, 2017 in Boston. (http://compassioninactionconference.org) This conference is designed to be highly experiential, using a hands-on “how to do it” model.
- The SVS should make improving the overall wellness of its members a specific goal and find specific metrics to monitor our progress towards this goal. Members can be provided with the tools to identify, monitor, and measure burnout and compassion. Each committee and council of the SVS can reexamine their objectives through the lens of reducing burnout and improving the wellness of vascular surgeons.
- Provide members with evidence-based programs that build personal resilience. This will not be a successful initiative unless our surgeons recognize and acknowledge the symptoms of burnout, and are willing to admit vulnerability. Without doing so, it is difficult to reach out for help.
- Redesign postgraduate resident and fellowship education. Standardizing clinical care may reduce variation and promote efficiency. However, when processes such as time-limited appointment scheduling, EMR templates, and protocols that drive physician-patient interactions are embedded in Resident and Fellowship education, the result may well be inflexibility in practice, reduced face time with patients, and interactions that lack compassion; all leading to burnout. Graduate Medical Education leaders must develop programs that support the learner’s ability to connect with patients and families, cultivate and role-model skills and behaviors that strengthen compassionate interactions, and strive to develop clinical practice models that increase Resident and Fellow work control autonomy.
The SVS should work proactively to optimize workload, fairness, and reward on a larger scale for its members as it relates to the EMR, reimbursement, and systems coverage. While we may be relatively small in size, as leaders, we are perfectly poised to address these larger, global issues. Perhaps working within the current system (i.e., PAC and APM task force) and considering innovative solutions at a national leadership scale, the SVS can direct real change!
Changing culture is not easy, nor quick, nor does it have an easy-to-follow blueprint. The first step is recognizing the need. The second is taking a leadership role. The third is thinking deeply about implementation.
*The authors extend their thanks and appreciation for the guidance, resources and support of Michael Goldberg, MD, scholar in residence, Schwartz Center for Compassionate Care, Boston and clinical professor of orthopedics at Seattle Children’s Hospital.
REFERENCES
1. J Managerial Psychol. (2007) 22:309-28
2. Annu Rev Neurosci. (2012) 35:1-23
3. Medicine. (2016) 44:583-5
4. J Health Organization Manag. (2015) 29:973-87
5. De Zulueta P Developing compassionate leadership in health care: an integrative review. J Healthcare Leadership. (2016) 8:1-10
6. Dolan ED, Morh D, Lempa M et al. Using a single item to measure burnout in primary care staff: A psychometry evaluation. J Gen Intern Med. (2015) 30:582-7
7. Karasek RA Job demands, job decision latitude, and mental strain: implications for job design. Administrative Sciences Quarterly (1979) 24: 285-308
8. Lee VS, Miller T, Daniels C, et al. Creating the exceptional patient experience in one academic health system. Acad Med. (2016) 91:338-44
9. Linzer M, Levine R, Meltzer D, et al. 10 bold steps to prevent burnout in general internal medicine. J Gen Intern Med. (2013) 29:18-20
10. Lown BA, Manning CF The Schwartz Center Rounds: Evaluation of an interdisciplinary approach to enhancing patient-centered communication, teamwork, and provider support. Acad Med. (2010) 85:1073-81
11. Lown BA, Muncer SJ, Chadwick R Can compassionate healthcare be measured? The Schwartz Center Compassionate Care Scale. Patient Education and Counseling (2015) 98:1005-10
12. Lown BA, McIntosh S, Gaines ME, et. al. Integrating compassionate collaborative care (“the Triple C”) into health professional education to advance the triple aim of health care. Acad Med (2016) 91:1-7
13. Lown BA A social neuroscience-informed model for teaching and practicing compassion in health care. Medical Education (2016) 50: 332-342
14. Maslach C, Schaufeli WG, Leiter MP Job burnout. Annu Rev Psychol (2001) 52:397-422
15. McClelland LE, Vogus TJ Compassion practices and HCAHPS: Does rewarding and supporting workplace compassion influence patient perceptions? HSR: Health Serv Res. (2014) 49:1670-83
16. Shanafelt TD, Noseworthy JH Executive leadership and physician well-being: Nine organizational strategies to promote engagement and reduce burnout. Mayo Clin Proc. (2016) 6:1-18
17. Shanafelt TD, Dyrbye LN, West CP Addressing physician burnout: the way forward. JAMA (2017) 317:901-2
18. Singer T, Klimecki OM Empathy and compassion Curr Biol. (2014) 24: R875-8
19. West CP, Dyrbye LN, Satele DV et. al. Concurrent validity of single-item measures of emotional exhaustion and depersonalization in burnout assessment. J Gen Intern Med. (2012) 27:1445-52
20. West CP, Dyrbye LN, Erwin PJ, et al. Interventions to address and reduce physician burnout: a systematic review and meta-analysis. Lancet. (2016) 388:2272-81
21. Wuest TK, Goldberg MJ, Kelly JD Clinical faceoff: Physician burnout-Fact, fantasy, or the fourth component of the triple aim? Clin Orthop Relat Res. (2016) doi: 10.1007/5-11999-016-5193-5
Last month, we introduced the epidemic of burnout and the adverse consequences for both our vascular surgery patients and ourselves. Today we will outline a framework for addressing these issues. The foundation of this framework is informed by the social and neurosciences.
From the perspective of the social scientist: Christina Maslach, the originator of the widely used Maslach Burnout Inventory, theorized that burnout arises from a chronic mismatch between people and their work setting in some or all of the following domains: Workload (too much, wrong kind); control (lack of autonomy, or insufficient control over resources); reward (insufficient financial or social rewards commensurate with achievements); community (loss of positive connection with others); fairness (lack of perceived fairness, inequity of work, pay, or promotion); and values (conflict of personal and organizational values). The reality of practicing medicine in today’s business milieu – of achieving service efficiencies by meeting performance targets – brings many of these mismatches into sharp focus.
From the perspective of the neuroscientist: Recent advances, including functional MRI, have demonstrated that the human brain is hard wired for compassion. Compassion is the deep feeling that arises when confronted with another’s suffering, coupled with a strong desire to alleviate that suffering. There are at least two neural pathways: one activated during empathy, having us experience another’s pain; and the other activated during compassion, resulting in our sense of reward. Thus, burnout is thought to occur when you know what your patient needs but you are unable to deliver it. Compassionate medical care is purposeful work, which promotes a sense of reward and mitigates burnout.
Because burnout affects all caregivers (anyone who touches the patient), a successful program addressing workforce well-being must be comprehensive and organization wide, similar to successful patient safety, CPI [continuous process improvement] and LEAN [Six Sigma] initiatives.
There are no shortcuts. Creating a culture of compassionate, collaborative care requires an understanding of the interrelationships between the individual provider, the unit or team, and organizational leadership.
1) The individual provider: There is evidence to support the use of programs that build personal resilience. A recently published meta-analysis by West and colleagues concluded that while no specific physician burnout intervention has been shown to be better than other types of interventions, mindfulness, stress management, and small-group discussions can be effective approaches to reducing burnout scores. Strategies to build individual resilience, such as mindfulness and meditation, are easy to teach but place the burden for success on the individual. No amount of resilience can withstand an unsupportive or toxic workplace environment, so both individual and organizational strategies in combination are necessary.
2) The unit or team: Scheduling time for open and honest discussion of social and emotional issues that arise in caring for patients helps nourish caregiver to caregiver compassion. The Schwartz Center for Compassionate Healthcare is a national nonprofit leading the movement to bring compassion to every patient-caregiver interaction. More than 425 health care organization are Schwartz Center members and conduct Schwartz Rounds™ to bring doctors, nurses, and other caregivers together to discuss the human side of health care. (www.theschwartzcenter.org). Team member to team member support is essential for navigating the stressors of practice. With having lunch in front of your computer being the norm, and the disappearance of traditional spaces for colleagues to connect (for example, nurses’ lounge, physician dining rooms), the opportunity for caregivers to have a safe place to escape, a place to have their own humanity reaffirmed, a place to offer support to their peers, has been eliminated.
3) Organizational Leadership: Making compassion a core value, articulating it, and establishing metrics whereby it can be measured, is a good start. The barriers to a culture of compassion are related to our systems of care. There are burgeoning administrative and documentation tasks to be performed, and productivity expectations that turn our clinics and hospitals into assembly lines. No, we cannot expect the EMR [electronic medical records] to be eliminated, but workforce well-being cannot be sustainable in the context of inadequate resources. A culture of compassionate collaborative care requires programs and policies that are implemented by the organization itself. Examples of organization-wide initiatives that support workforce well-being and provider engagement include: screening for caregiver burnout, establishing policies for managing adverse events with an eye toward the second victim, and most importantly, supporting systems that preserve work control autonomy of physicians and nurses in clinical settings. The business sector has long recognized that workplace stress is a function of how demanding a person’s job is and how much control that person has over his or her responsibilities. The business community has also recognized that the experience of the worker (provider) drives the experience of the customer (patient). In a study of hospital compassionate practices and HCAHPS [the Hospital Consumer Assessment of Healthcare Providers and Systems], McClelland and Vogus reported that how well a hospital compassionately supports it employees and rewards compassionate acts is significantly and positively is associated with that hospital’s ratings and likelihood of patients recommending it.
How does the Society of Vascular Surgery, or any professional medical/nursing society for that matter, fit into this model?
We propose that the SVS find ways to empower their members to be agents for culture change within their own health care organizations. How might this be done:
- Teach organizational leadership skills, starting with the SVS Board of Directors, the presidential line, and the chairs of committees. Offer leadership courses at the Annual Meeting.
- Develop a community of caregivers committed to creating a compassionate collaborative culture. The SVS is a founding member of the Schwartz Center Healthcare Society Leadership Council, and you, as members of the SVS benefit from reduced registration at the Annual Compassion in Action Healthcare Conference, June 24-27, 2017 in Boston. (http://compassioninactionconference.org) This conference is designed to be highly experiential, using a hands-on “how to do it” model.
- The SVS should make improving the overall wellness of its members a specific goal and find specific metrics to monitor our progress towards this goal. Members can be provided with the tools to identify, monitor, and measure burnout and compassion. Each committee and council of the SVS can reexamine their objectives through the lens of reducing burnout and improving the wellness of vascular surgeons.
- Provide members with evidence-based programs that build personal resilience. This will not be a successful initiative unless our surgeons recognize and acknowledge the symptoms of burnout, and are willing to admit vulnerability. Without doing so, it is difficult to reach out for help.
- Redesign postgraduate resident and fellowship education. Standardizing clinical care may reduce variation and promote efficiency. However, when processes such as time-limited appointment scheduling, EMR templates, and protocols that drive physician-patient interactions are embedded in Resident and Fellowship education, the result may well be inflexibility in practice, reduced face time with patients, and interactions that lack compassion; all leading to burnout. Graduate Medical Education leaders must develop programs that support the learner’s ability to connect with patients and families, cultivate and role-model skills and behaviors that strengthen compassionate interactions, and strive to develop clinical practice models that increase Resident and Fellow work control autonomy.
The SVS should work proactively to optimize workload, fairness, and reward on a larger scale for its members as it relates to the EMR, reimbursement, and systems coverage. While we may be relatively small in size, as leaders, we are perfectly poised to address these larger, global issues. Perhaps working within the current system (i.e., PAC and APM task force) and considering innovative solutions at a national leadership scale, the SVS can direct real change!
Changing culture is not easy, nor quick, nor does it have an easy-to-follow blueprint. The first step is recognizing the need. The second is taking a leadership role. The third is thinking deeply about implementation.
*The authors extend their thanks and appreciation for the guidance, resources and support of Michael Goldberg, MD, scholar in residence, Schwartz Center for Compassionate Care, Boston and clinical professor of orthopedics at Seattle Children’s Hospital.
REFERENCES
1. J Managerial Psychol. (2007) 22:309-28
2. Annu Rev Neurosci. (2012) 35:1-23
3. Medicine. (2016) 44:583-5
4. J Health Organization Manag. (2015) 29:973-87
5. De Zulueta P Developing compassionate leadership in health care: an integrative review. J Healthcare Leadership. (2016) 8:1-10
6. Dolan ED, Morh D, Lempa M et al. Using a single item to measure burnout in primary care staff: A psychometry evaluation. J Gen Intern Med. (2015) 30:582-7
7. Karasek RA Job demands, job decision latitude, and mental strain: implications for job design. Administrative Sciences Quarterly (1979) 24: 285-308
8. Lee VS, Miller T, Daniels C, et al. Creating the exceptional patient experience in one academic health system. Acad Med. (2016) 91:338-44
9. Linzer M, Levine R, Meltzer D, et al. 10 bold steps to prevent burnout in general internal medicine. J Gen Intern Med. (2013) 29:18-20
10. Lown BA, Manning CF The Schwartz Center Rounds: Evaluation of an interdisciplinary approach to enhancing patient-centered communication, teamwork, and provider support. Acad Med. (2010) 85:1073-81
11. Lown BA, Muncer SJ, Chadwick R Can compassionate healthcare be measured? The Schwartz Center Compassionate Care Scale. Patient Education and Counseling (2015) 98:1005-10
12. Lown BA, McIntosh S, Gaines ME, et. al. Integrating compassionate collaborative care (“the Triple C”) into health professional education to advance the triple aim of health care. Acad Med (2016) 91:1-7
13. Lown BA A social neuroscience-informed model for teaching and practicing compassion in health care. Medical Education (2016) 50: 332-342
14. Maslach C, Schaufeli WG, Leiter MP Job burnout. Annu Rev Psychol (2001) 52:397-422
15. McClelland LE, Vogus TJ Compassion practices and HCAHPS: Does rewarding and supporting workplace compassion influence patient perceptions? HSR: Health Serv Res. (2014) 49:1670-83
16. Shanafelt TD, Noseworthy JH Executive leadership and physician well-being: Nine organizational strategies to promote engagement and reduce burnout. Mayo Clin Proc. (2016) 6:1-18
17. Shanafelt TD, Dyrbye LN, West CP Addressing physician burnout: the way forward. JAMA (2017) 317:901-2
18. Singer T, Klimecki OM Empathy and compassion Curr Biol. (2014) 24: R875-8
19. West CP, Dyrbye LN, Satele DV et. al. Concurrent validity of single-item measures of emotional exhaustion and depersonalization in burnout assessment. J Gen Intern Med. (2012) 27:1445-52
20. West CP, Dyrbye LN, Erwin PJ, et al. Interventions to address and reduce physician burnout: a systematic review and meta-analysis. Lancet. (2016) 388:2272-81
21. Wuest TK, Goldberg MJ, Kelly JD Clinical faceoff: Physician burnout-Fact, fantasy, or the fourth component of the triple aim? Clin Orthop Relat Res. (2016) doi: 10.1007/5-11999-016-5193-5
Last month, we introduced the epidemic of burnout and the adverse consequences for both our vascular surgery patients and ourselves. Today we will outline a framework for addressing these issues. The foundation of this framework is informed by the social and neurosciences.
From the perspective of the social scientist: Christina Maslach, the originator of the widely used Maslach Burnout Inventory, theorized that burnout arises from a chronic mismatch between people and their work setting in some or all of the following domains: Workload (too much, wrong kind); control (lack of autonomy, or insufficient control over resources); reward (insufficient financial or social rewards commensurate with achievements); community (loss of positive connection with others); fairness (lack of perceived fairness, inequity of work, pay, or promotion); and values (conflict of personal and organizational values). The reality of practicing medicine in today’s business milieu – of achieving service efficiencies by meeting performance targets – brings many of these mismatches into sharp focus.
From the perspective of the neuroscientist: Recent advances, including functional MRI, have demonstrated that the human brain is hard wired for compassion. Compassion is the deep feeling that arises when confronted with another’s suffering, coupled with a strong desire to alleviate that suffering. There are at least two neural pathways: one activated during empathy, having us experience another’s pain; and the other activated during compassion, resulting in our sense of reward. Thus, burnout is thought to occur when you know what your patient needs but you are unable to deliver it. Compassionate medical care is purposeful work, which promotes a sense of reward and mitigates burnout.
Because burnout affects all caregivers (anyone who touches the patient), a successful program addressing workforce well-being must be comprehensive and organization wide, similar to successful patient safety, CPI [continuous process improvement] and LEAN [Six Sigma] initiatives.
There are no shortcuts. Creating a culture of compassionate, collaborative care requires an understanding of the interrelationships between the individual provider, the unit or team, and organizational leadership.
1) The individual provider: There is evidence to support the use of programs that build personal resilience. A recently published meta-analysis by West and colleagues concluded that while no specific physician burnout intervention has been shown to be better than other types of interventions, mindfulness, stress management, and small-group discussions can be effective approaches to reducing burnout scores. Strategies to build individual resilience, such as mindfulness and meditation, are easy to teach but place the burden for success on the individual. No amount of resilience can withstand an unsupportive or toxic workplace environment, so both individual and organizational strategies in combination are necessary.
2) The unit or team: Scheduling time for open and honest discussion of social and emotional issues that arise in caring for patients helps nourish caregiver to caregiver compassion. The Schwartz Center for Compassionate Healthcare is a national nonprofit leading the movement to bring compassion to every patient-caregiver interaction. More than 425 health care organization are Schwartz Center members and conduct Schwartz Rounds™ to bring doctors, nurses, and other caregivers together to discuss the human side of health care. (www.theschwartzcenter.org). Team member to team member support is essential for navigating the stressors of practice. With having lunch in front of your computer being the norm, and the disappearance of traditional spaces for colleagues to connect (for example, nurses’ lounge, physician dining rooms), the opportunity for caregivers to have a safe place to escape, a place to have their own humanity reaffirmed, a place to offer support to their peers, has been eliminated.
3) Organizational Leadership: Making compassion a core value, articulating it, and establishing metrics whereby it can be measured, is a good start. The barriers to a culture of compassion are related to our systems of care. There are burgeoning administrative and documentation tasks to be performed, and productivity expectations that turn our clinics and hospitals into assembly lines. No, we cannot expect the EMR [electronic medical records] to be eliminated, but workforce well-being cannot be sustainable in the context of inadequate resources. A culture of compassionate collaborative care requires programs and policies that are implemented by the organization itself. Examples of organization-wide initiatives that support workforce well-being and provider engagement include: screening for caregiver burnout, establishing policies for managing adverse events with an eye toward the second victim, and most importantly, supporting systems that preserve work control autonomy of physicians and nurses in clinical settings. The business sector has long recognized that workplace stress is a function of how demanding a person’s job is and how much control that person has over his or her responsibilities. The business community has also recognized that the experience of the worker (provider) drives the experience of the customer (patient). In a study of hospital compassionate practices and HCAHPS [the Hospital Consumer Assessment of Healthcare Providers and Systems], McClelland and Vogus reported that how well a hospital compassionately supports it employees and rewards compassionate acts is significantly and positively is associated with that hospital’s ratings and likelihood of patients recommending it.
How does the Society of Vascular Surgery, or any professional medical/nursing society for that matter, fit into this model?
We propose that the SVS find ways to empower their members to be agents for culture change within their own health care organizations. How might this be done:
- Teach organizational leadership skills, starting with the SVS Board of Directors, the presidential line, and the chairs of committees. Offer leadership courses at the Annual Meeting.
- Develop a community of caregivers committed to creating a compassionate collaborative culture. The SVS is a founding member of the Schwartz Center Healthcare Society Leadership Council, and you, as members of the SVS benefit from reduced registration at the Annual Compassion in Action Healthcare Conference, June 24-27, 2017 in Boston. (http://compassioninactionconference.org) This conference is designed to be highly experiential, using a hands-on “how to do it” model.
- The SVS should make improving the overall wellness of its members a specific goal and find specific metrics to monitor our progress towards this goal. Members can be provided with the tools to identify, monitor, and measure burnout and compassion. Each committee and council of the SVS can reexamine their objectives through the lens of reducing burnout and improving the wellness of vascular surgeons.
- Provide members with evidence-based programs that build personal resilience. This will not be a successful initiative unless our surgeons recognize and acknowledge the symptoms of burnout, and are willing to admit vulnerability. Without doing so, it is difficult to reach out for help.
- Redesign postgraduate resident and fellowship education. Standardizing clinical care may reduce variation and promote efficiency. However, when processes such as time-limited appointment scheduling, EMR templates, and protocols that drive physician-patient interactions are embedded in Resident and Fellowship education, the result may well be inflexibility in practice, reduced face time with patients, and interactions that lack compassion; all leading to burnout. Graduate Medical Education leaders must develop programs that support the learner’s ability to connect with patients and families, cultivate and role-model skills and behaviors that strengthen compassionate interactions, and strive to develop clinical practice models that increase Resident and Fellow work control autonomy.
The SVS should work proactively to optimize workload, fairness, and reward on a larger scale for its members as it relates to the EMR, reimbursement, and systems coverage. While we may be relatively small in size, as leaders, we are perfectly poised to address these larger, global issues. Perhaps working within the current system (i.e., PAC and APM task force) and considering innovative solutions at a national leadership scale, the SVS can direct real change!
Changing culture is not easy, nor quick, nor does it have an easy-to-follow blueprint. The first step is recognizing the need. The second is taking a leadership role. The third is thinking deeply about implementation.
*The authors extend their thanks and appreciation for the guidance, resources and support of Michael Goldberg, MD, scholar in residence, Schwartz Center for Compassionate Care, Boston and clinical professor of orthopedics at Seattle Children’s Hospital.
REFERENCES
1. J Managerial Psychol. (2007) 22:309-28
2. Annu Rev Neurosci. (2012) 35:1-23
3. Medicine. (2016) 44:583-5
4. J Health Organization Manag. (2015) 29:973-87
5. De Zulueta P Developing compassionate leadership in health care: an integrative review. J Healthcare Leadership. (2016) 8:1-10
6. Dolan ED, Morh D, Lempa M et al. Using a single item to measure burnout in primary care staff: A psychometry evaluation. J Gen Intern Med. (2015) 30:582-7
7. Karasek RA Job demands, job decision latitude, and mental strain: implications for job design. Administrative Sciences Quarterly (1979) 24: 285-308
8. Lee VS, Miller T, Daniels C, et al. Creating the exceptional patient experience in one academic health system. Acad Med. (2016) 91:338-44
9. Linzer M, Levine R, Meltzer D, et al. 10 bold steps to prevent burnout in general internal medicine. J Gen Intern Med. (2013) 29:18-20
10. Lown BA, Manning CF The Schwartz Center Rounds: Evaluation of an interdisciplinary approach to enhancing patient-centered communication, teamwork, and provider support. Acad Med. (2010) 85:1073-81
11. Lown BA, Muncer SJ, Chadwick R Can compassionate healthcare be measured? The Schwartz Center Compassionate Care Scale. Patient Education and Counseling (2015) 98:1005-10
12. Lown BA, McIntosh S, Gaines ME, et. al. Integrating compassionate collaborative care (“the Triple C”) into health professional education to advance the triple aim of health care. Acad Med (2016) 91:1-7
13. Lown BA A social neuroscience-informed model for teaching and practicing compassion in health care. Medical Education (2016) 50: 332-342
14. Maslach C, Schaufeli WG, Leiter MP Job burnout. Annu Rev Psychol (2001) 52:397-422
15. McClelland LE, Vogus TJ Compassion practices and HCAHPS: Does rewarding and supporting workplace compassion influence patient perceptions? HSR: Health Serv Res. (2014) 49:1670-83
16. Shanafelt TD, Noseworthy JH Executive leadership and physician well-being: Nine organizational strategies to promote engagement and reduce burnout. Mayo Clin Proc. (2016) 6:1-18
17. Shanafelt TD, Dyrbye LN, West CP Addressing physician burnout: the way forward. JAMA (2017) 317:901-2
18. Singer T, Klimecki OM Empathy and compassion Curr Biol. (2014) 24: R875-8
19. West CP, Dyrbye LN, Satele DV et. al. Concurrent validity of single-item measures of emotional exhaustion and depersonalization in burnout assessment. J Gen Intern Med. (2012) 27:1445-52
20. West CP, Dyrbye LN, Erwin PJ, et al. Interventions to address and reduce physician burnout: a systematic review and meta-analysis. Lancet. (2016) 388:2272-81
21. Wuest TK, Goldberg MJ, Kelly JD Clinical faceoff: Physician burnout-Fact, fantasy, or the fourth component of the triple aim? Clin Orthop Relat Res. (2016) doi: 10.1007/5-11999-016-5193-5
Transplantation palliative care: The time is ripe
Over 10 years ago, a challenge was made in a surgical publication for increased collaboration between the fields of transplantation and palliative care.1
Since that time not much progress has been made bringing these fields together in a consistent way that would mutually benefit patients and the specialties. However, other progress has been made, particularly in the field of palliative care, which could brighten the prospects and broaden the opportunities to accomplish collaboration between palliative care and transplantation.
Growth of palliative services
During the past decade there has been a robust proliferation of hospital-based palliative care programs in the United States. In all, 67% of U.S. hospitals with 50 or more beds report palliative care teams, up from 63% in 2011 and 53% in 2008.
Only a decade ago, critical care and palliative care were generally considered mutually exclusive. Evidence is trickling in to suggest that this is no longer the case. Although palliative care was not an integral part of critical care at that time, patients, families, and even practitioners began to demand these services. Cook and Rocker have eloquently advocated the rightful place of palliative care in the ICU.2
Studies in recent years have shown that the integration of palliative care into critical care decreases in length of ICU and hospital stay, decreases costs, enhances patient/family satisfaction, and promotes a more rapid consensus about goals of care, without increasing mortality. The ICU experience to date could be considered a reassuring precedent for transplantation palliative care.
Integration of palliative care with transplantation
Early palliative care intervention has been shown to improve symptom burden and depression scores in end-stage liver disease patients awaiting transplant. In addition, early palliative care consultation in conjunction with cancer treatment has been associated with increased survival in non–small-cell lung cancer patients. It has been demonstrated that early integration of palliative care in the surgical ICU alongside disease-directed curative care can be accomplished without change in mortality, while improving end-of-life practice in liver transplant patients.3

What palliative care can do for transplant patients
What does palliative care mean for the person (and family) awaiting transplantation? For the cirrhotic patient with cachexia, ascites, and encephalopathy, it means access to the services of a team trained in the management of these symptoms. Palliative care teams can also provide psychosocial and spiritual support for patients and families who are intimidated by the complex navigation of the health care system and the existential threat that end-stage organ failure presents to them. Skilled palliative care and services can be the difference between failing and extended life with a higher quality of life for these very sick patients
Resuscitation of a patient, whether through restoration of organ function or interdicting the progression of disease, begins with resuscitation of hope. Nothing achieves this more quickly than amelioration of burdensome symptoms for the patient and family.
The barriers for transplant surgeons and teams referring and incorporating palliative care services in their practices are multiple and profound. The unique dilemma facing the transplant team is to balance the treatment of the failing organ, the treatment of the patient (and family and friends), and the best use of the graft, a precious gift of society.
Palliative surgery has been defined as any invasive procedure in which the main intention is to mitigate physical symptoms in patients with noncurable disease without causing premature death. The very success of transplantation over the past 3 decades has obscured our memory of transplantation as a type of palliative surgery. It is a well-known axiom of reconstructive surgery that the reconstructed site should be compared to what was there, not to “normal.” Even in the current era of improved immunosuppression and posttransplant support services, one could hardly describe even a successful transplant patient’s experience as “normal.” These patients’ lives may be extended and/or enhanced but they need palliative care before, during, and after transplantation. The growing availability of trained palliative care clinicians and teams, the increased familiarity of palliative and end-of-life care to surgical residents and fellows, and quality metrics measuring palliative care outcomes will provide reassurance and guidance to address reservations about the convergence of the two seemingly opposite realities.
A modest proposal
We propose that palliative care be presented to the entire spectrum of transplantation care: on the ward, in the ICU, and after transplantation. More specific “triggers” for palliative care for referral of transplant patients should be identified. Wentlandt et al.4 have described a promising model for an ambulatory clinic, which provides early, integrated palliative care to patients awaiting and receiving organ transplantation. In addition, we propose an application for grant funding for a conference and eventual formation of a work group of transplant surgeons and team members, palliative care clinicians, and patient/families who have experienced one of the aspects of the transplant spectrum. We await the subspecialty certification in hospice and palliative medicine of a transplant surgeon. Outside of transplantation, every other surgical specialty in the United States has diplomates certified in hospice and palliative medicine. We await the benefits that will accrue from research about the merging of these fields.
1. Molmenti EP, Dunn GP: Transplantation and palliative care: The convergence of two seemingly opposite realities. Surg Clin North Am. 2005;85:373-82.
2. Cook D, Rocker G. Dying with dignity in the intensive care unit. N Engl J Med. 2014;370:2506-14.
3. Lamba S, Murphy P, McVicker S, Smith JH, and Mosenthal AC. Changing end-of-life care practice for liver transplant patients: structured palliative care intervention in the surgical intensive care unit. J Pain Symptom Manage. 2012; 44(4):508-19.
4. Wentlandt, K., Dall’Osto, A., Freeman, N., Le, L. W., Kaya, E., Ross, H., Singer, L. G., Abbey, S., Clarke, H. and Zimmermann, C. (2016), The Transplant Palliative Care Clinic: An early palliative care model for patients in a transplant program. Clin Transplant. 2016 Nov 4; doi: 10.1111/ctr.12838.
Dr. Azoulay is a transplantation specialist of Assistance Publique – Hôpitaux de Paris, and the University of Paris. Dr. Dunn is medical director of the Palliative Care Consultation Service at the University of Pittsburgh Medical Center Hamot, and vice-chair of the ACS Committee on Surgical Palliative Care.
Over 10 years ago, a challenge was made in a surgical publication for increased collaboration between the fields of transplantation and palliative care.1
Since that time not much progress has been made bringing these fields together in a consistent way that would mutually benefit patients and the specialties. However, other progress has been made, particularly in the field of palliative care, which could brighten the prospects and broaden the opportunities to accomplish collaboration between palliative care and transplantation.
Growth of palliative services
During the past decade there has been a robust proliferation of hospital-based palliative care programs in the United States. In all, 67% of U.S. hospitals with 50 or more beds report palliative care teams, up from 63% in 2011 and 53% in 2008.
Only a decade ago, critical care and palliative care were generally considered mutually exclusive. Evidence is trickling in to suggest that this is no longer the case. Although palliative care was not an integral part of critical care at that time, patients, families, and even practitioners began to demand these services. Cook and Rocker have eloquently advocated the rightful place of palliative care in the ICU.2
Studies in recent years have shown that the integration of palliative care into critical care decreases in length of ICU and hospital stay, decreases costs, enhances patient/family satisfaction, and promotes a more rapid consensus about goals of care, without increasing mortality. The ICU experience to date could be considered a reassuring precedent for transplantation palliative care.
Integration of palliative care with transplantation
Early palliative care intervention has been shown to improve symptom burden and depression scores in end-stage liver disease patients awaiting transplant. In addition, early palliative care consultation in conjunction with cancer treatment has been associated with increased survival in non–small-cell lung cancer patients. It has been demonstrated that early integration of palliative care in the surgical ICU alongside disease-directed curative care can be accomplished without change in mortality, while improving end-of-life practice in liver transplant patients.3
What palliative care can do for transplant patients
What does palliative care mean for the person (and family) awaiting transplantation? For the cirrhotic patient with cachexia, ascites, and encephalopathy, it means access to the services of a team trained in the management of these symptoms. Palliative care teams can also provide psychosocial and spiritual support for patients and families who are intimidated by the complex navigation of the health care system and the existential threat that end-stage organ failure presents to them. Skilled palliative care and services can be the difference between failing and extended life with a higher quality of life for these very sick patients
Resuscitation of a patient, whether through restoration of organ function or interdicting the progression of disease, begins with resuscitation of hope. Nothing achieves this more quickly than amelioration of burdensome symptoms for the patient and family.
The barriers for transplant surgeons and teams referring and incorporating palliative care services in their practices are multiple and profound. The unique dilemma facing the transplant team is to balance the treatment of the failing organ, the treatment of the patient (and family and friends), and the best use of the graft, a precious gift of society.
Palliative surgery has been defined as any invasive procedure in which the main intention is to mitigate physical symptoms in patients with noncurable disease without causing premature death. The very success of transplantation over the past 3 decades has obscured our memory of transplantation as a type of palliative surgery. It is a well-known axiom of reconstructive surgery that the reconstructed site should be compared to what was there, not to “normal.” Even in the current era of improved immunosuppression and posttransplant support services, one could hardly describe even a successful transplant patient’s experience as “normal.” These patients’ lives may be extended and/or enhanced but they need palliative care before, during, and after transplantation. The growing availability of trained palliative care clinicians and teams, the increased familiarity of palliative and end-of-life care to surgical residents and fellows, and quality metrics measuring palliative care outcomes will provide reassurance and guidance to address reservations about the convergence of the two seemingly opposite realities.
A modest proposal
We propose that palliative care be presented to the entire spectrum of transplantation care: on the ward, in the ICU, and after transplantation. More specific “triggers” for palliative care for referral of transplant patients should be identified. Wentlandt et al.4 have described a promising model for an ambulatory clinic, which provides early, integrated palliative care to patients awaiting and receiving organ transplantation. In addition, we propose an application for grant funding for a conference and eventual formation of a work group of transplant surgeons and team members, palliative care clinicians, and patient/families who have experienced one of the aspects of the transplant spectrum. We await the subspecialty certification in hospice and palliative medicine of a transplant surgeon. Outside of transplantation, every other surgical specialty in the United States has diplomates certified in hospice and palliative medicine. We await the benefits that will accrue from research about the merging of these fields.
1. Molmenti EP, Dunn GP: Transplantation and palliative care: The convergence of two seemingly opposite realities. Surg Clin North Am. 2005;85:373-82.
2. Cook D, Rocker G. Dying with dignity in the intensive care unit. N Engl J Med. 2014;370:2506-14.
3. Lamba S, Murphy P, McVicker S, Smith JH, and Mosenthal AC. Changing end-of-life care practice for liver transplant patients: structured palliative care intervention in the surgical intensive care unit. J Pain Symptom Manage. 2012; 44(4):508-19.
4. Wentlandt, K., Dall’Osto, A., Freeman, N., Le, L. W., Kaya, E., Ross, H., Singer, L. G., Abbey, S., Clarke, H. and Zimmermann, C. (2016), The Transplant Palliative Care Clinic: An early palliative care model for patients in a transplant program. Clin Transplant. 2016 Nov 4; doi: 10.1111/ctr.12838.
Dr. Azoulay is a transplantation specialist of Assistance Publique – Hôpitaux de Paris, and the University of Paris. Dr. Dunn is medical director of the Palliative Care Consultation Service at the University of Pittsburgh Medical Center Hamot, and vice-chair of the ACS Committee on Surgical Palliative Care.
Over 10 years ago, a challenge was made in a surgical publication for increased collaboration between the fields of transplantation and palliative care.1
Since that time not much progress has been made bringing these fields together in a consistent way that would mutually benefit patients and the specialties. However, other progress has been made, particularly in the field of palliative care, which could brighten the prospects and broaden the opportunities to accomplish collaboration between palliative care and transplantation.
Growth of palliative services
During the past decade there has been a robust proliferation of hospital-based palliative care programs in the United States. In all, 67% of U.S. hospitals with 50 or more beds report palliative care teams, up from 63% in 2011 and 53% in 2008.
Only a decade ago, critical care and palliative care were generally considered mutually exclusive. Evidence is trickling in to suggest that this is no longer the case. Although palliative care was not an integral part of critical care at that time, patients, families, and even practitioners began to demand these services. Cook and Rocker have eloquently advocated the rightful place of palliative care in the ICU.2
Studies in recent years have shown that the integration of palliative care into critical care decreases in length of ICU and hospital stay, decreases costs, enhances patient/family satisfaction, and promotes a more rapid consensus about goals of care, without increasing mortality. The ICU experience to date could be considered a reassuring precedent for transplantation palliative care.
Integration of palliative care with transplantation
Early palliative care intervention has been shown to improve symptom burden and depression scores in end-stage liver disease patients awaiting transplant. In addition, early palliative care consultation in conjunction with cancer treatment has been associated with increased survival in non–small-cell lung cancer patients. It has been demonstrated that early integration of palliative care in the surgical ICU alongside disease-directed curative care can be accomplished without change in mortality, while improving end-of-life practice in liver transplant patients.3
What palliative care can do for transplant patients
What does palliative care mean for the person (and family) awaiting transplantation? For the cirrhotic patient with cachexia, ascites, and encephalopathy, it means access to the services of a team trained in the management of these symptoms. Palliative care teams can also provide psychosocial and spiritual support for patients and families who are intimidated by the complex navigation of the health care system and the existential threat that end-stage organ failure presents to them. Skilled palliative care and services can be the difference between failing and extended life with a higher quality of life for these very sick patients
Resuscitation of a patient, whether through restoration of organ function or interdicting the progression of disease, begins with resuscitation of hope. Nothing achieves this more quickly than amelioration of burdensome symptoms for the patient and family.
The barriers for transplant surgeons and teams referring and incorporating palliative care services in their practices are multiple and profound. The unique dilemma facing the transplant team is to balance the treatment of the failing organ, the treatment of the patient (and family and friends), and the best use of the graft, a precious gift of society.
Palliative surgery has been defined as any invasive procedure in which the main intention is to mitigate physical symptoms in patients with noncurable disease without causing premature death. The very success of transplantation over the past 3 decades has obscured our memory of transplantation as a type of palliative surgery. It is a well-known axiom of reconstructive surgery that the reconstructed site should be compared to what was there, not to “normal.” Even in the current era of improved immunosuppression and posttransplant support services, one could hardly describe even a successful transplant patient’s experience as “normal.” These patients’ lives may be extended and/or enhanced but they need palliative care before, during, and after transplantation. The growing availability of trained palliative care clinicians and teams, the increased familiarity of palliative and end-of-life care to surgical residents and fellows, and quality metrics measuring palliative care outcomes will provide reassurance and guidance to address reservations about the convergence of the two seemingly opposite realities.
A modest proposal
We propose that palliative care be presented to the entire spectrum of transplantation care: on the ward, in the ICU, and after transplantation. More specific “triggers” for palliative care for referral of transplant patients should be identified. Wentlandt et al.4 have described a promising model for an ambulatory clinic, which provides early, integrated palliative care to patients awaiting and receiving organ transplantation. In addition, we propose an application for grant funding for a conference and eventual formation of a work group of transplant surgeons and team members, palliative care clinicians, and patient/families who have experienced one of the aspects of the transplant spectrum. We await the subspecialty certification in hospice and palliative medicine of a transplant surgeon. Outside of transplantation, every other surgical specialty in the United States has diplomates certified in hospice and palliative medicine. We await the benefits that will accrue from research about the merging of these fields.
1. Molmenti EP, Dunn GP: Transplantation and palliative care: The convergence of two seemingly opposite realities. Surg Clin North Am. 2005;85:373-82.
2. Cook D, Rocker G. Dying with dignity in the intensive care unit. N Engl J Med. 2014;370:2506-14.
3. Lamba S, Murphy P, McVicker S, Smith JH, and Mosenthal AC. Changing end-of-life care practice for liver transplant patients: structured palliative care intervention in the surgical intensive care unit. J Pain Symptom Manage. 2012; 44(4):508-19.
4. Wentlandt, K., Dall’Osto, A., Freeman, N., Le, L. W., Kaya, E., Ross, H., Singer, L. G., Abbey, S., Clarke, H. and Zimmermann, C. (2016), The Transplant Palliative Care Clinic: An early palliative care model for patients in a transplant program. Clin Transplant. 2016 Nov 4; doi: 10.1111/ctr.12838.
Dr. Azoulay is a transplantation specialist of Assistance Publique – Hôpitaux de Paris, and the University of Paris. Dr. Dunn is medical director of the Palliative Care Consultation Service at the University of Pittsburgh Medical Center Hamot, and vice-chair of the ACS Committee on Surgical Palliative Care.
A Cost-Effectiveness and Psychological Evaluation of Early Skin Biopsies vs Later-Onset Surgeries in Melanoma Management
Compared to later-onset procedures, early diagnosis of melanoma using affordable skin biopsies can result in better patient outcomes, lower health care expenditures, and enhanced psychological well-being.1 Numerous research and economic evaluations that highlight the possible advantages of early intervention in melanoma care lend support to this strategy. In health care systems, the cost of early identification and screening for skin cancer is a critical factor.1 There has been debate in the literature regarding performing more frequent biopsies earlier for skin cancers, which may greatly improve patient outcomes at the expense of increased financial cost, compared with performing fewer biopsies, which reduces costs at the potential expense of managing later-onset melanoma.1,2 We sought to summarize the current literature and address some considerations that may help bring more clarity to this topic.
According to a study of a large health care system, the average cost of a skin cancer screening visit was $150, of which $105 (70%) went toward the costs of the office visit and $45 (30%) went toward the costs of the biopsy.1 In the changing health care landscape, it is crucial to take into account the possible compounded savings from early diagnosis and treatment. While biopsies do involve some expenses, consideration of immunotherapy costs for advanced melanoma also should be considered, as they provide an alternative viewpoint on the financial effects of melanoma treatment.2 The use of new systemic treatments such as immunotherapy has led to a notable rise in Medicare users’ first-year melanoma treatment expenses. The average expense of treating stage IV melanoma rose from $47,739 in 2007 through 2012 to $117,450 in 2018 through 2019. This sharp rise highlights how much more expensive treating advanced melanoma is than performing biopsies for early detection and treatment. Hundreds of biopsies might be carried out for the cost of a single advanced melanoma therapy, possibly identifying several cases at an earlier, more manageable stage.2
Patient quality of life and survival rates also can be considerably improved by early melanoma detection through screening.3 Compared to patients with later-stage diagnoses, those with early-stage melanoma reported a higher overall quality of life. Better physical functioning and reduced levels of anxiety and sadness were linked to early identification using skin biopsies. Patients with more advanced melanoma who had later-onset procedures, on the other hand, experience worsening psychological symptoms and physical health.3
A cost-effectiveness analysis using a Markov cohort model compared the long-term economic impact of early detection and primary prevention of melanoma. It found that daily use of sunscreen could prevent a substantial number of new skin tumors and melanoma deaths and reduce health care costs when compared to early detection strategies such as performing extra biopsies.4 There already are programs across the United States that aim to educate the public on the importance of wearing sunscreen; this has, in turn, reduced the prevalence of skin cancer in certain communities. Primary prevention resulted in just 1364 new melanomas and more than $430 million in expenditures per 100,000 individuals, whereas early diagnosis produced 2446 new melanomas and more than $660 million in economic expenses per 100,000 individuals.4 It is imperative to acknowledge that skin biopsies remain a vital tool for the early identification of melanoma, particularly in high-risk groups.
By using technologies such as teledermoscopy, the cost-effectiveness of skin cancer referral and consultation can be further enhanced; for example, teledermoscopy for skin cancer referral and triage would result in faster clinical resolution at an average cost of $54.64 per case. This method may reduce the need for redundant in-person consultations and increase the effectiveness of melanoma identification.5
Large-scale public health initiatives in skin cancer prevention and early detection have the potential to be very effective, as evidenced by the War on Melanoma project at Oregon Health & Science University (Portland, Oregon). This all-encompassing strategy, which uses cutting-edge technologies, public education, and health care professional training, has improved melanoma outcomes and decreased health care expenditures with encouraging results.6
A few tactics can be used to best balance the costs of later-onset procedures and early skin biopsies. These include using advanced technologies such as teledermoscopy and dermoscopy, provider training to increase diagnostic accuracy, public health campaigns to raise awareness and promote prevention, and a comprehensive strategy combining targeted early detection strategies with primary prevention.5,6 Health care systems can optimize the financial efficiency and clinical results of melanoma treatment by putting these principles into practice.
Compared to later-onset melanoma procedures, early skin biopsies typically are more cost-effective, produce better patient outcomes, and offer psychological advantages, even if they may have a higher initial cost. Health care systems can optimize the trade-off between early detection and cost effectiveness in melanoma management by putting sophisticated technology to use, enhancing provider training, and implementing focused screening programs.5,6 To support evidence-based policies and guidelines, future research should assess the long-term economic impact of different melanoma prevention and detection measures.
- Matsumoto M, Secrest A, Anderson A, et al. Estimating the cost of skin cancer detection by dermatology providers in a large health care system. J Am Acad Dermatol. 2018;78:701-709.e1. doi:10.1016/j.jaad.2017.11.033
- Gogebakan KC, Mukherjee K, Berry EG, et al. Impact of novel systemic therapies on the first-year costs of care for melanoma among Medicare beneficiaries. Cancer. 2021;127:2926-2933. doi:10.1002/cncr.33515
- Young JN, Griffith-Bauer K, Hill E, et al. The benefit of early-stage diagnosis: a registry-based survey evaluating the quality of life in patients with melanoma. Skin Health Dis. 2023;3:E237. doi:10.1002/ski2.237
- Gordon L, Olsen C, Whiteman DC, et al. Prevention versus early detection for long-term control of melanoma and keratinocyte carcinomas: a cost-effectiveness modelling study. BMJ Open. 2020;10:E034388. doi:10.1136/bmjopen-2019-034388
- Buja A, Rivera M, Girardi G, et al. Cost-effectiveness of a melanoma screening programme using whole disease modelling. J Med Screen. 2020;27:157-167. doi:10.1177/0969141319885998
- Gogebakan KC, Berry EG, Geller AC, et al. Strategizing screening for melanoma in an era of novel treatments: a model-based approach. Cancer Epidemiol Biomarkers Prev. 2020;29:2599-2607. doi:10.1158/1055-9965.EPI-20-0881
Compared to later-onset procedures, early diagnosis of melanoma using affordable skin biopsies can result in better patient outcomes, lower health care expenditures, and enhanced psychological well-being.1 Numerous research and economic evaluations that highlight the possible advantages of early intervention in melanoma care lend support to this strategy. In health care systems, the cost of early identification and screening for skin cancer is a critical factor.1 There has been debate in the literature regarding performing more frequent biopsies earlier for skin cancers, which may greatly improve patient outcomes at the expense of increased financial cost, compared with performing fewer biopsies, which reduces costs at the potential expense of managing later-onset melanoma.1,2 We sought to summarize the current literature and address some considerations that may help bring more clarity to this topic.
According to a study of a large health care system, the average cost of a skin cancer screening visit was $150, of which $105 (70%) went toward the costs of the office visit and $45 (30%) went toward the costs of the biopsy.1 In the changing health care landscape, it is crucial to take into account the possible compounded savings from early diagnosis and treatment. While biopsies do involve some expenses, consideration of immunotherapy costs for advanced melanoma also should be considered, as they provide an alternative viewpoint on the financial effects of melanoma treatment.2 The use of new systemic treatments such as immunotherapy has led to a notable rise in Medicare users’ first-year melanoma treatment expenses. The average expense of treating stage IV melanoma rose from $47,739 in 2007 through 2012 to $117,450 in 2018 through 2019. This sharp rise highlights how much more expensive treating advanced melanoma is than performing biopsies for early detection and treatment. Hundreds of biopsies might be carried out for the cost of a single advanced melanoma therapy, possibly identifying several cases at an earlier, more manageable stage.2
Patient quality of life and survival rates also can be considerably improved by early melanoma detection through screening.3 Compared to patients with later-stage diagnoses, those with early-stage melanoma reported a higher overall quality of life. Better physical functioning and reduced levels of anxiety and sadness were linked to early identification using skin biopsies. Patients with more advanced melanoma who had later-onset procedures, on the other hand, experience worsening psychological symptoms and physical health.3
A cost-effectiveness analysis using a Markov cohort model compared the long-term economic impact of early detection and primary prevention of melanoma. It found that daily use of sunscreen could prevent a substantial number of new skin tumors and melanoma deaths and reduce health care costs when compared to early detection strategies such as performing extra biopsies.4 There already are programs across the United States that aim to educate the public on the importance of wearing sunscreen; this has, in turn, reduced the prevalence of skin cancer in certain communities. Primary prevention resulted in just 1364 new melanomas and more than $430 million in expenditures per 100,000 individuals, whereas early diagnosis produced 2446 new melanomas and more than $660 million in economic expenses per 100,000 individuals.4 It is imperative to acknowledge that skin biopsies remain a vital tool for the early identification of melanoma, particularly in high-risk groups.
By using technologies such as teledermoscopy, the cost-effectiveness of skin cancer referral and consultation can be further enhanced; for example, teledermoscopy for skin cancer referral and triage would result in faster clinical resolution at an average cost of $54.64 per case. This method may reduce the need for redundant in-person consultations and increase the effectiveness of melanoma identification.5
Large-scale public health initiatives in skin cancer prevention and early detection have the potential to be very effective, as evidenced by the War on Melanoma project at Oregon Health & Science University (Portland, Oregon). This all-encompassing strategy, which uses cutting-edge technologies, public education, and health care professional training, has improved melanoma outcomes and decreased health care expenditures with encouraging results.6
A few tactics can be used to best balance the costs of later-onset procedures and early skin biopsies. These include using advanced technologies such as teledermoscopy and dermoscopy, provider training to increase diagnostic accuracy, public health campaigns to raise awareness and promote prevention, and a comprehensive strategy combining targeted early detection strategies with primary prevention.5,6 Health care systems can optimize the financial efficiency and clinical results of melanoma treatment by putting these principles into practice.
Compared to later-onset melanoma procedures, early skin biopsies typically are more cost-effective, produce better patient outcomes, and offer psychological advantages, even if they may have a higher initial cost. Health care systems can optimize the trade-off between early detection and cost effectiveness in melanoma management by putting sophisticated technology to use, enhancing provider training, and implementing focused screening programs.5,6 To support evidence-based policies and guidelines, future research should assess the long-term economic impact of different melanoma prevention and detection measures.
Compared to later-onset procedures, early diagnosis of melanoma using affordable skin biopsies can result in better patient outcomes, lower health care expenditures, and enhanced psychological well-being.1 Numerous research and economic evaluations that highlight the possible advantages of early intervention in melanoma care lend support to this strategy. In health care systems, the cost of early identification and screening for skin cancer is a critical factor.1 There has been debate in the literature regarding performing more frequent biopsies earlier for skin cancers, which may greatly improve patient outcomes at the expense of increased financial cost, compared with performing fewer biopsies, which reduces costs at the potential expense of managing later-onset melanoma.1,2 We sought to summarize the current literature and address some considerations that may help bring more clarity to this topic.
According to a study of a large health care system, the average cost of a skin cancer screening visit was $150, of which $105 (70%) went toward the costs of the office visit and $45 (30%) went toward the costs of the biopsy.1 In the changing health care landscape, it is crucial to take into account the possible compounded savings from early diagnosis and treatment. While biopsies do involve some expenses, consideration of immunotherapy costs for advanced melanoma also should be considered, as they provide an alternative viewpoint on the financial effects of melanoma treatment.2 The use of new systemic treatments such as immunotherapy has led to a notable rise in Medicare users’ first-year melanoma treatment expenses. The average expense of treating stage IV melanoma rose from $47,739 in 2007 through 2012 to $117,450 in 2018 through 2019. This sharp rise highlights how much more expensive treating advanced melanoma is than performing biopsies for early detection and treatment. Hundreds of biopsies might be carried out for the cost of a single advanced melanoma therapy, possibly identifying several cases at an earlier, more manageable stage.2
Patient quality of life and survival rates also can be considerably improved by early melanoma detection through screening.3 Compared to patients with later-stage diagnoses, those with early-stage melanoma reported a higher overall quality of life. Better physical functioning and reduced levels of anxiety and sadness were linked to early identification using skin biopsies. Patients with more advanced melanoma who had later-onset procedures, on the other hand, experience worsening psychological symptoms and physical health.3
A cost-effectiveness analysis using a Markov cohort model compared the long-term economic impact of early detection and primary prevention of melanoma. It found that daily use of sunscreen could prevent a substantial number of new skin tumors and melanoma deaths and reduce health care costs when compared to early detection strategies such as performing extra biopsies.4 There already are programs across the United States that aim to educate the public on the importance of wearing sunscreen; this has, in turn, reduced the prevalence of skin cancer in certain communities. Primary prevention resulted in just 1364 new melanomas and more than $430 million in expenditures per 100,000 individuals, whereas early diagnosis produced 2446 new melanomas and more than $660 million in economic expenses per 100,000 individuals.4 It is imperative to acknowledge that skin biopsies remain a vital tool for the early identification of melanoma, particularly in high-risk groups.
By using technologies such as teledermoscopy, the cost-effectiveness of skin cancer referral and consultation can be further enhanced; for example, teledermoscopy for skin cancer referral and triage would result in faster clinical resolution at an average cost of $54.64 per case. This method may reduce the need for redundant in-person consultations and increase the effectiveness of melanoma identification.5
Large-scale public health initiatives in skin cancer prevention and early detection have the potential to be very effective, as evidenced by the War on Melanoma project at Oregon Health & Science University (Portland, Oregon). This all-encompassing strategy, which uses cutting-edge technologies, public education, and health care professional training, has improved melanoma outcomes and decreased health care expenditures with encouraging results.6
A few tactics can be used to best balance the costs of later-onset procedures and early skin biopsies. These include using advanced technologies such as teledermoscopy and dermoscopy, provider training to increase diagnostic accuracy, public health campaigns to raise awareness and promote prevention, and a comprehensive strategy combining targeted early detection strategies with primary prevention.5,6 Health care systems can optimize the financial efficiency and clinical results of melanoma treatment by putting these principles into practice.
Compared to later-onset melanoma procedures, early skin biopsies typically are more cost-effective, produce better patient outcomes, and offer psychological advantages, even if they may have a higher initial cost. Health care systems can optimize the trade-off between early detection and cost effectiveness in melanoma management by putting sophisticated technology to use, enhancing provider training, and implementing focused screening programs.5,6 To support evidence-based policies and guidelines, future research should assess the long-term economic impact of different melanoma prevention and detection measures.
- Matsumoto M, Secrest A, Anderson A, et al. Estimating the cost of skin cancer detection by dermatology providers in a large health care system. J Am Acad Dermatol. 2018;78:701-709.e1. doi:10.1016/j.jaad.2017.11.033
- Gogebakan KC, Mukherjee K, Berry EG, et al. Impact of novel systemic therapies on the first-year costs of care for melanoma among Medicare beneficiaries. Cancer. 2021;127:2926-2933. doi:10.1002/cncr.33515
- Young JN, Griffith-Bauer K, Hill E, et al. The benefit of early-stage diagnosis: a registry-based survey evaluating the quality of life in patients with melanoma. Skin Health Dis. 2023;3:E237. doi:10.1002/ski2.237
- Gordon L, Olsen C, Whiteman DC, et al. Prevention versus early detection for long-term control of melanoma and keratinocyte carcinomas: a cost-effectiveness modelling study. BMJ Open. 2020;10:E034388. doi:10.1136/bmjopen-2019-034388
- Buja A, Rivera M, Girardi G, et al. Cost-effectiveness of a melanoma screening programme using whole disease modelling. J Med Screen. 2020;27:157-167. doi:10.1177/0969141319885998
- Gogebakan KC, Berry EG, Geller AC, et al. Strategizing screening for melanoma in an era of novel treatments: a model-based approach. Cancer Epidemiol Biomarkers Prev. 2020;29:2599-2607. doi:10.1158/1055-9965.EPI-20-0881
- Matsumoto M, Secrest A, Anderson A, et al. Estimating the cost of skin cancer detection by dermatology providers in a large health care system. J Am Acad Dermatol. 2018;78:701-709.e1. doi:10.1016/j.jaad.2017.11.033
- Gogebakan KC, Mukherjee K, Berry EG, et al. Impact of novel systemic therapies on the first-year costs of care for melanoma among Medicare beneficiaries. Cancer. 2021;127:2926-2933. doi:10.1002/cncr.33515
- Young JN, Griffith-Bauer K, Hill E, et al. The benefit of early-stage diagnosis: a registry-based survey evaluating the quality of life in patients with melanoma. Skin Health Dis. 2023;3:E237. doi:10.1002/ski2.237
- Gordon L, Olsen C, Whiteman DC, et al. Prevention versus early detection for long-term control of melanoma and keratinocyte carcinomas: a cost-effectiveness modelling study. BMJ Open. 2020;10:E034388. doi:10.1136/bmjopen-2019-034388
- Buja A, Rivera M, Girardi G, et al. Cost-effectiveness of a melanoma screening programme using whole disease modelling. J Med Screen. 2020;27:157-167. doi:10.1177/0969141319885998
- Gogebakan KC, Berry EG, Geller AC, et al. Strategizing screening for melanoma in an era of novel treatments: a model-based approach. Cancer Epidemiol Biomarkers Prev. 2020;29:2599-2607. doi:10.1158/1055-9965.EPI-20-0881
Practice Points
- Early melanoma detection via skin biopsy is generally more cost-effective than managing advanced-stage disease, largely due to the high costs associated with systemic therapies (eg, immunotherapy) used in later-stage melanoma.
- Earlier diagnosis is associated with improved patient outcomes, including better quality of life and reduced psychological distress, compared with later-stage melanoma diagnoses requiring more extensive intervention.
- Integrated prevention and early detection strategies—such as dermoscopy, teledermoscopy, and public health initiatives—may optimize melanoma outcomes while reducing overall health care expenditures.
VA Advanced Training for Clinician Researchers and Data Scientists in Mental Health
VA Advanced Training for Clinician Researchers and Data Scientists in Mental Health
The US Department of Veterans Affairs (VA) mission realizes President Abraham Lincoln’s promise to “to care for him who shall have borne the battle, and for his widow, and his orphan.”1 Evidence-based care fulfills this promise and is the backbone of Veterans Health Administration (VHA) mental health care.2,3 To ensure veterans receive state-of-the-art clinical care, a skilled workforce and investment in data-driven approaches are necessary to identify best treatments and strategies to implement them in practice.
Through scientific and clinical training tailored to VA, the 23 VA Advanced Fellowships have secured a steady flow of highly trained PhD professionals (ie, psychologists and other allied health professionals), and medical doctors (ie, psychiatrists and neurologists) into the VA workforce.4 The VA Advanced Fellows are funded by the Office of Academic Affiliations (OAA) and offer 2-year training opportunities for postresidency MDs and postdoctoral PhDs. This article describes a VA Advanced Fellowship in mental health as an example of how these programs can have a broad and positive impact on the VA health care system.
Advanced Fellows Program
The VA Advanced Fellowship in Mental Illness Research and Treatment (AF MIRT), formerly known as the VA Special Fellowship Program in Advanced Psychiatry and Psychology, educates and trains clinician and nonclinician researchers to meet VA priority mental health care needs.5 Clinical AF MIRT fellows dedicate 75% of their time to training and research activities and 25% to direct clinical services. Data science fellows complete projects that inform veteran clinical care through qualitative data collection, program evaluation, and analysis of large datasets. The full translational pathway to evidence-based clinical care is represented by fellow research spanning basic animal models, genetics, and neuroimaging to implementation science and applied clinical care for veterans.
In 2025, AF MIRT marked its 25th year of training postdoctoral-level mental health scientific practitioners and scholars. This investment in clinical research training has had profound benefits for innovation and retention of clinicians and scientists within the VA system. As of April 1, 2026, AF MIRT trained 700 fellows, including 152 MD or MD/PhD fellows, 544 PhD or PsyD fellows, 3 PharmDs fellows, and 1 doctor of nursing practice fellow.
Fellowship Structure
The AF MIRT coordinating center provides key administrative support to fellowship site directors and topical didactic training to Advanced Fellows, ensuring consistent standard of quality training across locations in 15 states and 4 times zones. The training provided by the AF MIRT coordinating center deepens the nationally-mandated focus of local translational clinical centers (eg, Mental Illness Research Education and Clinical Centers, Centers of Excellence) on posttraumatic stress disorder (PTSD), serious mental illness, dementia, and other areas.
The AF MIRT coordinating center also promotes VA workforce sustainability. Advanced Fellows in programs with a coordinating center are much more likely to be retained in VA for postfellowship employment compared with fellows in programs without such a coordinating center (60% vs 38%) according to unpublished Office of Academic Affiliations data (Joel Schmidt, oral communication, May 15, 2025). The AF MIRT coordinating center provides central standardization and uses evidence-based approaches to ensure fellows receive consistent support, resources, and training. More specifically, the coordinating center develops and delivers a standardized, core curriculum to the program’s 28 sites. The program pioneered video delivery of integrated didactics that enlist national experts, many of them VA researchers and clinicians themselves. Didactics include high priority veteran mental health topics, such as suicide prevention, new and emerging evidence-based treatments (eg, neurostimulation for treatment resistant PTSD, psychotherapeutic approaches for traumatic brain injury), and VA health system considerations for mental health treatment delivery.
This curated didactic series also covers professional and technical issues, such as statistical and methodological considerations for clinical trials, scientific writing, and grant-writing skill development. These offerings support the career pathways of advanced fellows to pursue careers as researchers, scientifically-informed clinicians, or data scientists at VA or academic medical centers. The coordinating center prepares fellows to apply for mentored career award funding or independent investigator awards through the VA, National Institutes of Health (NIH), US Department of Defense, and other organizations by offering an annual mock grant review session and monthly reviews and discussions of fellows’ grant applications.
AF MIRT continuously fine tunes the didactic series curriculum based on feedback from fellows on how the program meets their training needs. For example, learning about the strategies Advanced Fellows used to remain productive during COVID-19 pandemic lockdowns revealed a strong trend toward use of secondary data (eg, publicly available data or VA electronic health record data). This fueled curriculum adjustments to include more topics relevant to fellow interests and needs for accessing secondary data resources for high priority veteran mental health topics.6
VA Advanced Fellowships Successes
From July 2020 to June 2025, MIRT advanced fellows published 906 peer-reviewed articles in psychiatry, psychology, and other disciplines. Each year, about 20 to 25 articles are published in high-impact journals. In this 5-year period, fellows have received 153 grants (114 VA grants) as principal investigators– many examining new innovations to improve the quality of care of veterans. Of the 165 fellows who graduated since 2020, 63% continued working in veteran health care: 38% transitioned to full-time VA employment and 25% moved to VA employment with an academic-affiliated role. Nineteen percent transitioned to academic positions, 12% transitioned to the private sector, and 5% transitioned to other government, industry, or nonprofit employment where these professionals contribute to scientific and clinical innovation benefiting the US public; 1% did not provide postfellowship employment information. The Figure displays geographic locations of graduated fellows’ postfellowship employment from July 2020 to June 2025.
employment across all settings, July 2020 to June 2025.
The accomplishments of fellows are wide-ranging and aligned with VA’s mission. Each year, roughly 15 fellows receive new investigator awards, travel awards, and poster or presentation awards from prominent professional societies. Fellows have obtained VA Career Development Awards in diverse topics, including suicide prevention through clinician resources and training programs, firearm safety discussions, digital phenotyping and neuroimaging to enhance social integration in veterans with schizophrenia, rapid transcranial magnetic stimulation to treat nicotine use and PTSD, and evidence-based psychotherapy techniques for female veterans experiencing issues in menopause.
Several recent MIRT fellows have also received highly competitive NIH K Career Development Awards. One notable example is a fellow who studied pharmacologic approaches for treatment-resistant depression informed by novel brain circuit findings, first testing these approaches in community samples through a NIH K grant and translating findings to veterans. Fellows have gone on to become directors of important national research centers and studies, chairs of academic departments, and presidents of national medical organizations. Importantly, many MIRT fellows have become local directors and mentors to a new generation of VA fellows and researchers.
Conclusions
The AF MIRT coordinating center supports the VA’s mission of fulfilling President Lincoln’s promise to care for veterans. There are multiple benefits to evidence-based work that helps veterans and fosters a highly skilled VA workforce. Veterans are at the center of the MIRT data-driven approach, which is critical given their complex needs. Approaches to building the AF MIRT’s evidence base include randomized controlled trials open to veteran participants; program evaluation of current local, regional, or national VHA clinical services through measurement-based care and evaluation of national clinician training programs; and even smaller quality improvement projects in local VA clinics. These efforts support effective, efficient, and accessible provision of treatments that benefit veterans.
- US Department of Veterans Affairs. Our VA mission and core values. Updated April 17, 2025. Accessed March 2, 2026. https://department.va.gov/icare/
- Holliday R, Holder N. VA is a leader in mental health and social service research and operations. Fed Pract. 2025;42:S5. doi:10.12788/fp.0578
- Zeiss AM, Karlin BE. Integrating mental health and primary care services in the Department of Veterans Affairs health care system. J Clin Psychol Med Settings. 2008;15:73-78. doi:10.1007/s10880-008-9100-4
- O’Hara R, Cassidy-Eagle EL, Beaudreau SA, et al. Increasing the ranks of academic researchers in mental health: a multisite approach to postdoctoral fellowship training. Acad Med. 2010;85:41-47. doi:10.1097/ACM.0b013e3181c47c51
- US Department of Veterans Affairs. Office of Academic Affiliations. Updated March 13, 2025. Accessed March 2, 2026. https://www.va.gov/oaa/advancedfellowships /advanced-fellowships.asp
- Hantke NC, Samarina V, Hallmayer J, et al. Preparing the next generation of academic researchers during the pandemic: lessons from a national mental health research postdoctoral fellowship. Acad Psychiatry. 2022;46:466- 469. doi:10.1007/s40596-022-01613-4
The US Department of Veterans Affairs (VA) mission realizes President Abraham Lincoln’s promise to “to care for him who shall have borne the battle, and for his widow, and his orphan.”1 Evidence-based care fulfills this promise and is the backbone of Veterans Health Administration (VHA) mental health care.2,3 To ensure veterans receive state-of-the-art clinical care, a skilled workforce and investment in data-driven approaches are necessary to identify best treatments and strategies to implement them in practice.
Through scientific and clinical training tailored to VA, the 23 VA Advanced Fellowships have secured a steady flow of highly trained PhD professionals (ie, psychologists and other allied health professionals), and medical doctors (ie, psychiatrists and neurologists) into the VA workforce.4 The VA Advanced Fellows are funded by the Office of Academic Affiliations (OAA) and offer 2-year training opportunities for postresidency MDs and postdoctoral PhDs. This article describes a VA Advanced Fellowship in mental health as an example of how these programs can have a broad and positive impact on the VA health care system.
Advanced Fellows Program
The VA Advanced Fellowship in Mental Illness Research and Treatment (AF MIRT), formerly known as the VA Special Fellowship Program in Advanced Psychiatry and Psychology, educates and trains clinician and nonclinician researchers to meet VA priority mental health care needs.5 Clinical AF MIRT fellows dedicate 75% of their time to training and research activities and 25% to direct clinical services. Data science fellows complete projects that inform veteran clinical care through qualitative data collection, program evaluation, and analysis of large datasets. The full translational pathway to evidence-based clinical care is represented by fellow research spanning basic animal models, genetics, and neuroimaging to implementation science and applied clinical care for veterans.
In 2025, AF MIRT marked its 25th year of training postdoctoral-level mental health scientific practitioners and scholars. This investment in clinical research training has had profound benefits for innovation and retention of clinicians and scientists within the VA system. As of April 1, 2026, AF MIRT trained 700 fellows, including 152 MD or MD/PhD fellows, 544 PhD or PsyD fellows, 3 PharmDs fellows, and 1 doctor of nursing practice fellow.
Fellowship Structure
The AF MIRT coordinating center provides key administrative support to fellowship site directors and topical didactic training to Advanced Fellows, ensuring consistent standard of quality training across locations in 15 states and 4 times zones. The training provided by the AF MIRT coordinating center deepens the nationally-mandated focus of local translational clinical centers (eg, Mental Illness Research Education and Clinical Centers, Centers of Excellence) on posttraumatic stress disorder (PTSD), serious mental illness, dementia, and other areas.
The AF MIRT coordinating center also promotes VA workforce sustainability. Advanced Fellows in programs with a coordinating center are much more likely to be retained in VA for postfellowship employment compared with fellows in programs without such a coordinating center (60% vs 38%) according to unpublished Office of Academic Affiliations data (Joel Schmidt, oral communication, May 15, 2025). The AF MIRT coordinating center provides central standardization and uses evidence-based approaches to ensure fellows receive consistent support, resources, and training. More specifically, the coordinating center develops and delivers a standardized, core curriculum to the program’s 28 sites. The program pioneered video delivery of integrated didactics that enlist national experts, many of them VA researchers and clinicians themselves. Didactics include high priority veteran mental health topics, such as suicide prevention, new and emerging evidence-based treatments (eg, neurostimulation for treatment resistant PTSD, psychotherapeutic approaches for traumatic brain injury), and VA health system considerations for mental health treatment delivery.
This curated didactic series also covers professional and technical issues, such as statistical and methodological considerations for clinical trials, scientific writing, and grant-writing skill development. These offerings support the career pathways of advanced fellows to pursue careers as researchers, scientifically-informed clinicians, or data scientists at VA or academic medical centers. The coordinating center prepares fellows to apply for mentored career award funding or independent investigator awards through the VA, National Institutes of Health (NIH), US Department of Defense, and other organizations by offering an annual mock grant review session and monthly reviews and discussions of fellows’ grant applications.
AF MIRT continuously fine tunes the didactic series curriculum based on feedback from fellows on how the program meets their training needs. For example, learning about the strategies Advanced Fellows used to remain productive during COVID-19 pandemic lockdowns revealed a strong trend toward use of secondary data (eg, publicly available data or VA electronic health record data). This fueled curriculum adjustments to include more topics relevant to fellow interests and needs for accessing secondary data resources for high priority veteran mental health topics.6
VA Advanced Fellowships Successes
From July 2020 to June 2025, MIRT advanced fellows published 906 peer-reviewed articles in psychiatry, psychology, and other disciplines. Each year, about 20 to 25 articles are published in high-impact journals. In this 5-year period, fellows have received 153 grants (114 VA grants) as principal investigators– many examining new innovations to improve the quality of care of veterans. Of the 165 fellows who graduated since 2020, 63% continued working in veteran health care: 38% transitioned to full-time VA employment and 25% moved to VA employment with an academic-affiliated role. Nineteen percent transitioned to academic positions, 12% transitioned to the private sector, and 5% transitioned to other government, industry, or nonprofit employment where these professionals contribute to scientific and clinical innovation benefiting the US public; 1% did not provide postfellowship employment information. The Figure displays geographic locations of graduated fellows’ postfellowship employment from July 2020 to June 2025.
employment across all settings, July 2020 to June 2025.
The accomplishments of fellows are wide-ranging and aligned with VA’s mission. Each year, roughly 15 fellows receive new investigator awards, travel awards, and poster or presentation awards from prominent professional societies. Fellows have obtained VA Career Development Awards in diverse topics, including suicide prevention through clinician resources and training programs, firearm safety discussions, digital phenotyping and neuroimaging to enhance social integration in veterans with schizophrenia, rapid transcranial magnetic stimulation to treat nicotine use and PTSD, and evidence-based psychotherapy techniques for female veterans experiencing issues in menopause.
Several recent MIRT fellows have also received highly competitive NIH K Career Development Awards. One notable example is a fellow who studied pharmacologic approaches for treatment-resistant depression informed by novel brain circuit findings, first testing these approaches in community samples through a NIH K grant and translating findings to veterans. Fellows have gone on to become directors of important national research centers and studies, chairs of academic departments, and presidents of national medical organizations. Importantly, many MIRT fellows have become local directors and mentors to a new generation of VA fellows and researchers.
Conclusions
The AF MIRT coordinating center supports the VA’s mission of fulfilling President Lincoln’s promise to care for veterans. There are multiple benefits to evidence-based work that helps veterans and fosters a highly skilled VA workforce. Veterans are at the center of the MIRT data-driven approach, which is critical given their complex needs. Approaches to building the AF MIRT’s evidence base include randomized controlled trials open to veteran participants; program evaluation of current local, regional, or national VHA clinical services through measurement-based care and evaluation of national clinician training programs; and even smaller quality improvement projects in local VA clinics. These efforts support effective, efficient, and accessible provision of treatments that benefit veterans.
The US Department of Veterans Affairs (VA) mission realizes President Abraham Lincoln’s promise to “to care for him who shall have borne the battle, and for his widow, and his orphan.”1 Evidence-based care fulfills this promise and is the backbone of Veterans Health Administration (VHA) mental health care.2,3 To ensure veterans receive state-of-the-art clinical care, a skilled workforce and investment in data-driven approaches are necessary to identify best treatments and strategies to implement them in practice.
Through scientific and clinical training tailored to VA, the 23 VA Advanced Fellowships have secured a steady flow of highly trained PhD professionals (ie, psychologists and other allied health professionals), and medical doctors (ie, psychiatrists and neurologists) into the VA workforce.4 The VA Advanced Fellows are funded by the Office of Academic Affiliations (OAA) and offer 2-year training opportunities for postresidency MDs and postdoctoral PhDs. This article describes a VA Advanced Fellowship in mental health as an example of how these programs can have a broad and positive impact on the VA health care system.
Advanced Fellows Program
The VA Advanced Fellowship in Mental Illness Research and Treatment (AF MIRT), formerly known as the VA Special Fellowship Program in Advanced Psychiatry and Psychology, educates and trains clinician and nonclinician researchers to meet VA priority mental health care needs.5 Clinical AF MIRT fellows dedicate 75% of their time to training and research activities and 25% to direct clinical services. Data science fellows complete projects that inform veteran clinical care through qualitative data collection, program evaluation, and analysis of large datasets. The full translational pathway to evidence-based clinical care is represented by fellow research spanning basic animal models, genetics, and neuroimaging to implementation science and applied clinical care for veterans.
In 2025, AF MIRT marked its 25th year of training postdoctoral-level mental health scientific practitioners and scholars. This investment in clinical research training has had profound benefits for innovation and retention of clinicians and scientists within the VA system. As of April 1, 2026, AF MIRT trained 700 fellows, including 152 MD or MD/PhD fellows, 544 PhD or PsyD fellows, 3 PharmDs fellows, and 1 doctor of nursing practice fellow.
Fellowship Structure
The AF MIRT coordinating center provides key administrative support to fellowship site directors and topical didactic training to Advanced Fellows, ensuring consistent standard of quality training across locations in 15 states and 4 times zones. The training provided by the AF MIRT coordinating center deepens the nationally-mandated focus of local translational clinical centers (eg, Mental Illness Research Education and Clinical Centers, Centers of Excellence) on posttraumatic stress disorder (PTSD), serious mental illness, dementia, and other areas.
The AF MIRT coordinating center also promotes VA workforce sustainability. Advanced Fellows in programs with a coordinating center are much more likely to be retained in VA for postfellowship employment compared with fellows in programs without such a coordinating center (60% vs 38%) according to unpublished Office of Academic Affiliations data (Joel Schmidt, oral communication, May 15, 2025). The AF MIRT coordinating center provides central standardization and uses evidence-based approaches to ensure fellows receive consistent support, resources, and training. More specifically, the coordinating center develops and delivers a standardized, core curriculum to the program’s 28 sites. The program pioneered video delivery of integrated didactics that enlist national experts, many of them VA researchers and clinicians themselves. Didactics include high priority veteran mental health topics, such as suicide prevention, new and emerging evidence-based treatments (eg, neurostimulation for treatment resistant PTSD, psychotherapeutic approaches for traumatic brain injury), and VA health system considerations for mental health treatment delivery.
This curated didactic series also covers professional and technical issues, such as statistical and methodological considerations for clinical trials, scientific writing, and grant-writing skill development. These offerings support the career pathways of advanced fellows to pursue careers as researchers, scientifically-informed clinicians, or data scientists at VA or academic medical centers. The coordinating center prepares fellows to apply for mentored career award funding or independent investigator awards through the VA, National Institutes of Health (NIH), US Department of Defense, and other organizations by offering an annual mock grant review session and monthly reviews and discussions of fellows’ grant applications.
AF MIRT continuously fine tunes the didactic series curriculum based on feedback from fellows on how the program meets their training needs. For example, learning about the strategies Advanced Fellows used to remain productive during COVID-19 pandemic lockdowns revealed a strong trend toward use of secondary data (eg, publicly available data or VA electronic health record data). This fueled curriculum adjustments to include more topics relevant to fellow interests and needs for accessing secondary data resources for high priority veteran mental health topics.6
VA Advanced Fellowships Successes
From July 2020 to June 2025, MIRT advanced fellows published 906 peer-reviewed articles in psychiatry, psychology, and other disciplines. Each year, about 20 to 25 articles are published in high-impact journals. In this 5-year period, fellows have received 153 grants (114 VA grants) as principal investigators– many examining new innovations to improve the quality of care of veterans. Of the 165 fellows who graduated since 2020, 63% continued working in veteran health care: 38% transitioned to full-time VA employment and 25% moved to VA employment with an academic-affiliated role. Nineteen percent transitioned to academic positions, 12% transitioned to the private sector, and 5% transitioned to other government, industry, or nonprofit employment where these professionals contribute to scientific and clinical innovation benefiting the US public; 1% did not provide postfellowship employment information. The Figure displays geographic locations of graduated fellows’ postfellowship employment from July 2020 to June 2025.
employment across all settings, July 2020 to June 2025.
The accomplishments of fellows are wide-ranging and aligned with VA’s mission. Each year, roughly 15 fellows receive new investigator awards, travel awards, and poster or presentation awards from prominent professional societies. Fellows have obtained VA Career Development Awards in diverse topics, including suicide prevention through clinician resources and training programs, firearm safety discussions, digital phenotyping and neuroimaging to enhance social integration in veterans with schizophrenia, rapid transcranial magnetic stimulation to treat nicotine use and PTSD, and evidence-based psychotherapy techniques for female veterans experiencing issues in menopause.
Several recent MIRT fellows have also received highly competitive NIH K Career Development Awards. One notable example is a fellow who studied pharmacologic approaches for treatment-resistant depression informed by novel brain circuit findings, first testing these approaches in community samples through a NIH K grant and translating findings to veterans. Fellows have gone on to become directors of important national research centers and studies, chairs of academic departments, and presidents of national medical organizations. Importantly, many MIRT fellows have become local directors and mentors to a new generation of VA fellows and researchers.
Conclusions
The AF MIRT coordinating center supports the VA’s mission of fulfilling President Lincoln’s promise to care for veterans. There are multiple benefits to evidence-based work that helps veterans and fosters a highly skilled VA workforce. Veterans are at the center of the MIRT data-driven approach, which is critical given their complex needs. Approaches to building the AF MIRT’s evidence base include randomized controlled trials open to veteran participants; program evaluation of current local, regional, or national VHA clinical services through measurement-based care and evaluation of national clinician training programs; and even smaller quality improvement projects in local VA clinics. These efforts support effective, efficient, and accessible provision of treatments that benefit veterans.
- US Department of Veterans Affairs. Our VA mission and core values. Updated April 17, 2025. Accessed March 2, 2026. https://department.va.gov/icare/
- Holliday R, Holder N. VA is a leader in mental health and social service research and operations. Fed Pract. 2025;42:S5. doi:10.12788/fp.0578
- Zeiss AM, Karlin BE. Integrating mental health and primary care services in the Department of Veterans Affairs health care system. J Clin Psychol Med Settings. 2008;15:73-78. doi:10.1007/s10880-008-9100-4
- O’Hara R, Cassidy-Eagle EL, Beaudreau SA, et al. Increasing the ranks of academic researchers in mental health: a multisite approach to postdoctoral fellowship training. Acad Med. 2010;85:41-47. doi:10.1097/ACM.0b013e3181c47c51
- US Department of Veterans Affairs. Office of Academic Affiliations. Updated March 13, 2025. Accessed March 2, 2026. https://www.va.gov/oaa/advancedfellowships /advanced-fellowships.asp
- Hantke NC, Samarina V, Hallmayer J, et al. Preparing the next generation of academic researchers during the pandemic: lessons from a national mental health research postdoctoral fellowship. Acad Psychiatry. 2022;46:466- 469. doi:10.1007/s40596-022-01613-4
- US Department of Veterans Affairs. Our VA mission and core values. Updated April 17, 2025. Accessed March 2, 2026. https://department.va.gov/icare/
- Holliday R, Holder N. VA is a leader in mental health and social service research and operations. Fed Pract. 2025;42:S5. doi:10.12788/fp.0578
- Zeiss AM, Karlin BE. Integrating mental health and primary care services in the Department of Veterans Affairs health care system. J Clin Psychol Med Settings. 2008;15:73-78. doi:10.1007/s10880-008-9100-4
- O’Hara R, Cassidy-Eagle EL, Beaudreau SA, et al. Increasing the ranks of academic researchers in mental health: a multisite approach to postdoctoral fellowship training. Acad Med. 2010;85:41-47. doi:10.1097/ACM.0b013e3181c47c51
- US Department of Veterans Affairs. Office of Academic Affiliations. Updated March 13, 2025. Accessed March 2, 2026. https://www.va.gov/oaa/advancedfellowships /advanced-fellowships.asp
- Hantke NC, Samarina V, Hallmayer J, et al. Preparing the next generation of academic researchers during the pandemic: lessons from a national mental health research postdoctoral fellowship. Acad Psychiatry. 2022;46:466- 469. doi:10.1007/s40596-022-01613-4
VA Advanced Training for Clinician Researchers and Data Scientists in Mental Health
VA Advanced Training for Clinician Researchers and Data Scientists in Mental Health

Consumer Trends Driving Contact Dermatitis: Insights from JiaDe Yu, MD, MS
Consumer Trends Driving Contact Dermatitis: Insights from JiaDe Yu, MD, MS
How do social media trends and influencer driven product fads affect the patterns of contact dermatitis you are seeing?
DR. YU: Social media and influencers are huge marketing opportunities for cosmetic and personal care companies and drive consumer demand. One example from a few years ago is slime as a toy for kids. For a period of time, every kid was making slime at home, resulting in high numbers of hand allergic contact dermatitis. Making slime requires a combination of borax (irritant), glue (irritant and allergen), laundry detergent or dish soap (irritant and allergen), and fragrances (irritant and allergen). This fad has been slowing since I cowrote an article on it (doi:10.1111 /pde.13792). More recently, the rise of “Sephora kids” (preteens and adolescents influenced by social media trends promoting multistep skin care and anti-aging products) has raised concerns about contact dermatitis, as many of these products contain ingredients that can disrupt the skin barrier or trigger sensitization in younger patients.
How can products labeled free of fragrances or preservatives still trigger allergic contact dermatitis?
DR. YU: Fragrances are frequently in the top 10 ingredients that cause allergic contact dermatitis in adults and children. For people with sensitive skin, we almost unequivocally recommend fragrance-free products. Now, not all fragrance-free products are truly free of fragrance allergens. Some fragrance chemicals may be used for another purpose (benzyl alcohol as a preservative, for example), so the product can still be fragrance free even though benzyl alcohol has a fragrance. Most products cannot truly be preservative free if they are expected to have a shelf life. One-time-use products do exist and can be preservative free, but they are very rare and very expensive to manufacture and maintain.
Have you seen spikes in reactions from trendy products like CBD-infused creams, botanical serums, or exfoliating acids?
DR. YU: Not yet, but I would not be surprised that this is rising in prevalence. The issue might not be CBD itself; it’s really the other additives in these CBD products that will cause problems. Looking at some CBD products for sale from major retailers, many contain fragrances such as lemongrass oil and botanical extracts such as calendula that have been noted to cause allergic contact dermatitis.
Do certain patient behaviors (eg, layering multiple natural products, frequent product switching, prolonged leave-on use) increase the risk for ACD?
DR. YU: Absolutely possible. The more products you use, the more likely you will develop allergic contact dermatitis due to increased exposure to potential allergens. We know that leave-on products are higher risk than rinse-offs in general. Furthermore, more products used also increase the risk for irritant dermatitis that might break the skin barrier, increasing the odds that someone will develop allergic contact dermatitis. We see this often with facial skin care products where some people might layer on glycolic acid with retinoid acid with vitamin C oil with kojic acid, etc, all leading to irritation on the face.
How do emerging consumer product trends influence your patch-testing approach?
DR. YU: We try to customize our patch-tested allergens to the patient’s rash and symptoms. If it’s a patient with facial dermatitis, for example, we would patch test the patient to a core allergen series (eg, American Contact Dermatitis Society 90, North American Comprehensive 80, North American Contact Dermatitis Group 80) and add on other supplemental panels including cosmetic series if applicable. It is also preferable to patch test for products that are used and/or suspected of causing the rash. For example, if a blush is a suspected cause of dermatitis, we would certainly patch test to that as well. We generally try to encourage the patient to bring in all their products so we can evaluate them for appropriateness for patch testing.
Which consumer-driven ingredients do you now consider high-yield targets for testing?
DR. YU: Fragrances, preservatives, and botanical extracts are all likely causes of allergic contact dermatitis. We are uncovering new allergens all the time, so testing directly to patient products is also important. Just because something has not been reported to be a contact allergen doesn’t mean it can’t become one.
Have you observed any demographic or cultural trends in patients with allergic contact dermatitis related to consumer products?
DR. YU: There are various papers that outline different allergens in adults vs children vs older adults. However, in general, the prevalence of contact dermatitis is very similar across all age groups and distributions. I do think there are definitely gender and cultural variations. Women are more likely to be allergic to nickel, for example, which is more often found in jewelry. However, there really aren’t studies that demonstrate one population is more likely to develop allergic contact dermatitis than others. It really comes down to exposure. For example, neomycin, which is contained in triple antibiotics in the United States and is sold over the counter, is a common allergen here. However, it’s not readily available in other countries, and therefore, neomycin is a rare allergen in those countries.
Looking forward, which emerging consumer trends do you anticipate will create the next wave of contact dermatitis cases?
DR. YU: We have seen an increase in allergic contact dermatitis in the wearables industry, especially in continuous glucose monitors. They are now being sold over the counter so people without diabetes and without a prescription will be able to purchase them from retailers like Amazon or CVS. The adhesives in these glucose monitors have been shown to cause allergic contact dermatitis in a sizeable number of kids and adults. I suspect this problem will continue to increase with increased exposure to the allergens in these adhesives.
How do social media trends and influencer driven product fads affect the patterns of contact dermatitis you are seeing?
DR. YU: Social media and influencers are huge marketing opportunities for cosmetic and personal care companies and drive consumer demand. One example from a few years ago is slime as a toy for kids. For a period of time, every kid was making slime at home, resulting in high numbers of hand allergic contact dermatitis. Making slime requires a combination of borax (irritant), glue (irritant and allergen), laundry detergent or dish soap (irritant and allergen), and fragrances (irritant and allergen). This fad has been slowing since I cowrote an article on it (doi:10.1111 /pde.13792). More recently, the rise of “Sephora kids” (preteens and adolescents influenced by social media trends promoting multistep skin care and anti-aging products) has raised concerns about contact dermatitis, as many of these products contain ingredients that can disrupt the skin barrier or trigger sensitization in younger patients.
How can products labeled free of fragrances or preservatives still trigger allergic contact dermatitis?
DR. YU: Fragrances are frequently in the top 10 ingredients that cause allergic contact dermatitis in adults and children. For people with sensitive skin, we almost unequivocally recommend fragrance-free products. Now, not all fragrance-free products are truly free of fragrance allergens. Some fragrance chemicals may be used for another purpose (benzyl alcohol as a preservative, for example), so the product can still be fragrance free even though benzyl alcohol has a fragrance. Most products cannot truly be preservative free if they are expected to have a shelf life. One-time-use products do exist and can be preservative free, but they are very rare and very expensive to manufacture and maintain.
Have you seen spikes in reactions from trendy products like CBD-infused creams, botanical serums, or exfoliating acids?
DR. YU: Not yet, but I would not be surprised that this is rising in prevalence. The issue might not be CBD itself; it’s really the other additives in these CBD products that will cause problems. Looking at some CBD products for sale from major retailers, many contain fragrances such as lemongrass oil and botanical extracts such as calendula that have been noted to cause allergic contact dermatitis.
Do certain patient behaviors (eg, layering multiple natural products, frequent product switching, prolonged leave-on use) increase the risk for ACD?
DR. YU: Absolutely possible. The more products you use, the more likely you will develop allergic contact dermatitis due to increased exposure to potential allergens. We know that leave-on products are higher risk than rinse-offs in general. Furthermore, more products used also increase the risk for irritant dermatitis that might break the skin barrier, increasing the odds that someone will develop allergic contact dermatitis. We see this often with facial skin care products where some people might layer on glycolic acid with retinoid acid with vitamin C oil with kojic acid, etc, all leading to irritation on the face.
How do emerging consumer product trends influence your patch-testing approach?
DR. YU: We try to customize our patch-tested allergens to the patient’s rash and symptoms. If it’s a patient with facial dermatitis, for example, we would patch test the patient to a core allergen series (eg, American Contact Dermatitis Society 90, North American Comprehensive 80, North American Contact Dermatitis Group 80) and add on other supplemental panels including cosmetic series if applicable. It is also preferable to patch test for products that are used and/or suspected of causing the rash. For example, if a blush is a suspected cause of dermatitis, we would certainly patch test to that as well. We generally try to encourage the patient to bring in all their products so we can evaluate them for appropriateness for patch testing.
Which consumer-driven ingredients do you now consider high-yield targets for testing?
DR. YU: Fragrances, preservatives, and botanical extracts are all likely causes of allergic contact dermatitis. We are uncovering new allergens all the time, so testing directly to patient products is also important. Just because something has not been reported to be a contact allergen doesn’t mean it can’t become one.
Have you observed any demographic or cultural trends in patients with allergic contact dermatitis related to consumer products?
DR. YU: There are various papers that outline different allergens in adults vs children vs older adults. However, in general, the prevalence of contact dermatitis is very similar across all age groups and distributions. I do think there are definitely gender and cultural variations. Women are more likely to be allergic to nickel, for example, which is more often found in jewelry. However, there really aren’t studies that demonstrate one population is more likely to develop allergic contact dermatitis than others. It really comes down to exposure. For example, neomycin, which is contained in triple antibiotics in the United States and is sold over the counter, is a common allergen here. However, it’s not readily available in other countries, and therefore, neomycin is a rare allergen in those countries.
Looking forward, which emerging consumer trends do you anticipate will create the next wave of contact dermatitis cases?
DR. YU: We have seen an increase in allergic contact dermatitis in the wearables industry, especially in continuous glucose monitors. They are now being sold over the counter so people without diabetes and without a prescription will be able to purchase them from retailers like Amazon or CVS. The adhesives in these glucose monitors have been shown to cause allergic contact dermatitis in a sizeable number of kids and adults. I suspect this problem will continue to increase with increased exposure to the allergens in these adhesives.
How do social media trends and influencer driven product fads affect the patterns of contact dermatitis you are seeing?
DR. YU: Social media and influencers are huge marketing opportunities for cosmetic and personal care companies and drive consumer demand. One example from a few years ago is slime as a toy for kids. For a period of time, every kid was making slime at home, resulting in high numbers of hand allergic contact dermatitis. Making slime requires a combination of borax (irritant), glue (irritant and allergen), laundry detergent or dish soap (irritant and allergen), and fragrances (irritant and allergen). This fad has been slowing since I cowrote an article on it (doi:10.1111 /pde.13792). More recently, the rise of “Sephora kids” (preteens and adolescents influenced by social media trends promoting multistep skin care and anti-aging products) has raised concerns about contact dermatitis, as many of these products contain ingredients that can disrupt the skin barrier or trigger sensitization in younger patients.
How can products labeled free of fragrances or preservatives still trigger allergic contact dermatitis?
DR. YU: Fragrances are frequently in the top 10 ingredients that cause allergic contact dermatitis in adults and children. For people with sensitive skin, we almost unequivocally recommend fragrance-free products. Now, not all fragrance-free products are truly free of fragrance allergens. Some fragrance chemicals may be used for another purpose (benzyl alcohol as a preservative, for example), so the product can still be fragrance free even though benzyl alcohol has a fragrance. Most products cannot truly be preservative free if they are expected to have a shelf life. One-time-use products do exist and can be preservative free, but they are very rare and very expensive to manufacture and maintain.
Have you seen spikes in reactions from trendy products like CBD-infused creams, botanical serums, or exfoliating acids?
DR. YU: Not yet, but I would not be surprised that this is rising in prevalence. The issue might not be CBD itself; it’s really the other additives in these CBD products that will cause problems. Looking at some CBD products for sale from major retailers, many contain fragrances such as lemongrass oil and botanical extracts such as calendula that have been noted to cause allergic contact dermatitis.
Do certain patient behaviors (eg, layering multiple natural products, frequent product switching, prolonged leave-on use) increase the risk for ACD?
DR. YU: Absolutely possible. The more products you use, the more likely you will develop allergic contact dermatitis due to increased exposure to potential allergens. We know that leave-on products are higher risk than rinse-offs in general. Furthermore, more products used also increase the risk for irritant dermatitis that might break the skin barrier, increasing the odds that someone will develop allergic contact dermatitis. We see this often with facial skin care products where some people might layer on glycolic acid with retinoid acid with vitamin C oil with kojic acid, etc, all leading to irritation on the face.
How do emerging consumer product trends influence your patch-testing approach?
DR. YU: We try to customize our patch-tested allergens to the patient’s rash and symptoms. If it’s a patient with facial dermatitis, for example, we would patch test the patient to a core allergen series (eg, American Contact Dermatitis Society 90, North American Comprehensive 80, North American Contact Dermatitis Group 80) and add on other supplemental panels including cosmetic series if applicable. It is also preferable to patch test for products that are used and/or suspected of causing the rash. For example, if a blush is a suspected cause of dermatitis, we would certainly patch test to that as well. We generally try to encourage the patient to bring in all their products so we can evaluate them for appropriateness for patch testing.
Which consumer-driven ingredients do you now consider high-yield targets for testing?
DR. YU: Fragrances, preservatives, and botanical extracts are all likely causes of allergic contact dermatitis. We are uncovering new allergens all the time, so testing directly to patient products is also important. Just because something has not been reported to be a contact allergen doesn’t mean it can’t become one.
Have you observed any demographic or cultural trends in patients with allergic contact dermatitis related to consumer products?
DR. YU: There are various papers that outline different allergens in adults vs children vs older adults. However, in general, the prevalence of contact dermatitis is very similar across all age groups and distributions. I do think there are definitely gender and cultural variations. Women are more likely to be allergic to nickel, for example, which is more often found in jewelry. However, there really aren’t studies that demonstrate one population is more likely to develop allergic contact dermatitis than others. It really comes down to exposure. For example, neomycin, which is contained in triple antibiotics in the United States and is sold over the counter, is a common allergen here. However, it’s not readily available in other countries, and therefore, neomycin is a rare allergen in those countries.
Looking forward, which emerging consumer trends do you anticipate will create the next wave of contact dermatitis cases?
DR. YU: We have seen an increase in allergic contact dermatitis in the wearables industry, especially in continuous glucose monitors. They are now being sold over the counter so people without diabetes and without a prescription will be able to purchase them from retailers like Amazon or CVS. The adhesives in these glucose monitors have been shown to cause allergic contact dermatitis in a sizeable number of kids and adults. I suspect this problem will continue to increase with increased exposure to the allergens in these adhesives.
Consumer Trends Driving Contact Dermatitis: Insights from JiaDe Yu, MD, MS
Consumer Trends Driving Contact Dermatitis: Insights from JiaDe Yu, MD, MS

Limitations of Fitzpatrick Skin Type as a Proxy for Skin Color and Race
Limitations of Fitzpatrick Skin Type as a Proxy for Skin Color and Race
Recognizing inflammation in darker skin tones has important implications for diagnosis and management of skin disease, particularly in patients with skin of color.1 In this context, classification systems commonly are used—both in research and clinical practice—to standardize descriptions of skin tone across diverse populations. Fitzpatrick skin type (FST) originally was developed to classify cutaneous response to UV radiation exposure and remains one of the most widely used frameworks in dermatology.2 However, FST often is used beyond its intended purpose as a proxy for differentiating skin color and race.3,4 This mismatch risks obscuring clinically meaningful differences and limiting the accuracy of dermatologic research. Herein, we review the intended use of FST, its limitations in representing skin color and race, and considerations for more accurate characterization of skin pigmentation in clinical practice and research.
Origins and Intended Use of the FST Scale
Fitzpatrick skin type was developed by Thomas B. Fitzpatrick in the 1970s to guide UVA dosing for psoralen plus UVA therapy in patients with psoriasis.5,6 The scale was intended to estimate an individual’s erythematous and pigmentary response to UV exposure.6,7 Early iterations of FST largely were based on lighter skin types, reflecting its initial use in predominantly White populations, which limited representation of the full spectrum of skin tone diversity.5
Clinical, Educational, and Research Limitations of FST
Fitzpatrick skin type now is widely, albeit inaccurately, used in both research and clinical practice as a proxy for skin color and race,7,8 which reflects its ease of use and the lack of standardized alternatives; however, FST does not adequately capture variability in baseline skin pigmentation, undertone, or inflammatory response. These limitations are especially pronounced in phototypes IV to VI, which encompass highly heterogeneous populations. As a result, grouping patients by FST alone to describe skin color and race may obscure important differences and limit meaningful interpretation of clinical and research findings.
Clinically, recognition of dermatologic conditions such as erythema may be more challenging in darker skin tones, in which classic visual cues are less apparent.1,7 Relying on FST to stratify skin color may further compound diagnostic uncertainty by oversimplifying the cutaneous presentation. In addition, treatment decisions, including laser settings and assessment of pigmentary risk, often are guided by FST despite within-group variability.7 Further, educational frameworks that rely heavily on FST may inadequately prepare clinicians to recognize disease across diverse skin tones, contributing to delayed diagnosis and disparities in care in populations with skin of color.
The implications also extend to dermatologic research. Fitzpatrick skin type frequently is used to assess study populations; however, its limited ability to reflect true variation in pigmentation and ethnicity introduces misclassification bias.3,7 The broad FST scale may group heterogeneous populations, obscuring differences in treatment response. As a result, studies relying on FST to represent skin color or race may have reduced generalizability across diverse populations. Importantly, these limitations are not merely conceptual but may contribute to measurable disparities in dermatologic diagnosis and outcomes.
Rethinking Skin Classification Frameworks
Despite these shortcomings, FST remains deeply embedded in dermatology. Its decades-long use has led to widespread familiarity and integration into clinical guidelines, education, and research. At the same time, the absence of a universally accepted alternative has reinforced the continued use of FST as a proxy for skin color and race.
Alternative strategies for characterizing skin pigmentation include objective measures such as spectrophotometry and melanin index assessment.9
Although these approaches may provide more precise quantification of pigmentation, their use may be limited by the need for specialized equipment and reduced feasibility in routine clinical settings. Other proposed approaches incorporate multidimensional factors such as pigmentation, photoreactivity, and genetic ancestry.4 While these techniques represent important advances, none has achieved widespread adoption yet, and each presents challenges related to feasibility and standardization.
In the absence of a single ideal system, a more nuanced approach is needed. Fitzpatrick skin type should be used in the context for which it was designed: estimating UV response. Incorporating additional descriptors, including self-identified race and ethnicity, alongside more detailed assessments of pigmentation may improve the accuracy and relevance of both clinical evaluation and research. Combining FST with more precise and inclusive frameworks represents a pragmatic step toward better reflecting patient diversity.
- Taylor SC. Recognizing erythema in skin of color. J Am Acad Dermatol.
- Fitzpatrick TB. The validity and practicality of sun-reactive skin types I through VI. Arch Dermatol. 1988;124:869-871. doi:10.1001 /archderm.124.6.869
- Eilers S, Bach DQ, Gaber R, et al. Accuracy of self-reported Fitzpatrick skin phototype classification in US Hispanic and Latino populations. JAMA Dermatol. 2013;149:797-803. doi:10.1001 /jamadermatol.2013.4091
- Del Bino S, Bernerd F. Variations in skin colour and the biological consequences of ultraviolet radiation exposure. Br J Dermatol. 2013;169(S3):33-40. doi:10.1111/bjd.12529
- Goon P, Banfield C, Bello O, et al. Skin cancers in skin types IV–VI: does the Fitzpatrick scale give a false sense of security? Clin Exp Dermatol. 2022;47:1112-1117. doi:10.1002/ski2.40
- Fitzpatrick TB. Soleil et peau. J Med Asthet. 1975;2:33-34.
- Ware OR, Dawson JE, Shinohara MM, et al. Racial limitations of Fitzpatrick skin type. Cutis. 2020;105:77-80.
- Lester JC, Taylor SC, Chren MM. Under-representation of skin of colour in dermatology images: not just an educational issue. Br J Dermatol. 2019;180:1521-1522. doi:10.1111/bjd.17608
- Fullerton A, Fischer T, Lahti A, et al. Guidelines for measurement of skin colour and erythema. a report from the Standardization Group of the European Society of Contact Dermatitis. Contact Dermatitis. 1996;35:1-10. doi:10.1111/j.1600-0536.1996.tb02242.x
Recognizing inflammation in darker skin tones has important implications for diagnosis and management of skin disease, particularly in patients with skin of color.1 In this context, classification systems commonly are used—both in research and clinical practice—to standardize descriptions of skin tone across diverse populations. Fitzpatrick skin type (FST) originally was developed to classify cutaneous response to UV radiation exposure and remains one of the most widely used frameworks in dermatology.2 However, FST often is used beyond its intended purpose as a proxy for differentiating skin color and race.3,4 This mismatch risks obscuring clinically meaningful differences and limiting the accuracy of dermatologic research. Herein, we review the intended use of FST, its limitations in representing skin color and race, and considerations for more accurate characterization of skin pigmentation in clinical practice and research.
Origins and Intended Use of the FST Scale
Fitzpatrick skin type was developed by Thomas B. Fitzpatrick in the 1970s to guide UVA dosing for psoralen plus UVA therapy in patients with psoriasis.5,6 The scale was intended to estimate an individual’s erythematous and pigmentary response to UV exposure.6,7 Early iterations of FST largely were based on lighter skin types, reflecting its initial use in predominantly White populations, which limited representation of the full spectrum of skin tone diversity.5
Clinical, Educational, and Research Limitations of FST
Fitzpatrick skin type now is widely, albeit inaccurately, used in both research and clinical practice as a proxy for skin color and race,7,8 which reflects its ease of use and the lack of standardized alternatives; however, FST does not adequately capture variability in baseline skin pigmentation, undertone, or inflammatory response. These limitations are especially pronounced in phototypes IV to VI, which encompass highly heterogeneous populations. As a result, grouping patients by FST alone to describe skin color and race may obscure important differences and limit meaningful interpretation of clinical and research findings.
Clinically, recognition of dermatologic conditions such as erythema may be more challenging in darker skin tones, in which classic visual cues are less apparent.1,7 Relying on FST to stratify skin color may further compound diagnostic uncertainty by oversimplifying the cutaneous presentation. In addition, treatment decisions, including laser settings and assessment of pigmentary risk, often are guided by FST despite within-group variability.7 Further, educational frameworks that rely heavily on FST may inadequately prepare clinicians to recognize disease across diverse skin tones, contributing to delayed diagnosis and disparities in care in populations with skin of color.
The implications also extend to dermatologic research. Fitzpatrick skin type frequently is used to assess study populations; however, its limited ability to reflect true variation in pigmentation and ethnicity introduces misclassification bias.3,7 The broad FST scale may group heterogeneous populations, obscuring differences in treatment response. As a result, studies relying on FST to represent skin color or race may have reduced generalizability across diverse populations. Importantly, these limitations are not merely conceptual but may contribute to measurable disparities in dermatologic diagnosis and outcomes.
Rethinking Skin Classification Frameworks
Despite these shortcomings, FST remains deeply embedded in dermatology. Its decades-long use has led to widespread familiarity and integration into clinical guidelines, education, and research. At the same time, the absence of a universally accepted alternative has reinforced the continued use of FST as a proxy for skin color and race.
Alternative strategies for characterizing skin pigmentation include objective measures such as spectrophotometry and melanin index assessment.9
Although these approaches may provide more precise quantification of pigmentation, their use may be limited by the need for specialized equipment and reduced feasibility in routine clinical settings. Other proposed approaches incorporate multidimensional factors such as pigmentation, photoreactivity, and genetic ancestry.4 While these techniques represent important advances, none has achieved widespread adoption yet, and each presents challenges related to feasibility and standardization.
In the absence of a single ideal system, a more nuanced approach is needed. Fitzpatrick skin type should be used in the context for which it was designed: estimating UV response. Incorporating additional descriptors, including self-identified race and ethnicity, alongside more detailed assessments of pigmentation may improve the accuracy and relevance of both clinical evaluation and research. Combining FST with more precise and inclusive frameworks represents a pragmatic step toward better reflecting patient diversity.
Recognizing inflammation in darker skin tones has important implications for diagnosis and management of skin disease, particularly in patients with skin of color.1 In this context, classification systems commonly are used—both in research and clinical practice—to standardize descriptions of skin tone across diverse populations. Fitzpatrick skin type (FST) originally was developed to classify cutaneous response to UV radiation exposure and remains one of the most widely used frameworks in dermatology.2 However, FST often is used beyond its intended purpose as a proxy for differentiating skin color and race.3,4 This mismatch risks obscuring clinically meaningful differences and limiting the accuracy of dermatologic research. Herein, we review the intended use of FST, its limitations in representing skin color and race, and considerations for more accurate characterization of skin pigmentation in clinical practice and research.
Origins and Intended Use of the FST Scale
Fitzpatrick skin type was developed by Thomas B. Fitzpatrick in the 1970s to guide UVA dosing for psoralen plus UVA therapy in patients with psoriasis.5,6 The scale was intended to estimate an individual’s erythematous and pigmentary response to UV exposure.6,7 Early iterations of FST largely were based on lighter skin types, reflecting its initial use in predominantly White populations, which limited representation of the full spectrum of skin tone diversity.5
Clinical, Educational, and Research Limitations of FST
Fitzpatrick skin type now is widely, albeit inaccurately, used in both research and clinical practice as a proxy for skin color and race,7,8 which reflects its ease of use and the lack of standardized alternatives; however, FST does not adequately capture variability in baseline skin pigmentation, undertone, or inflammatory response. These limitations are especially pronounced in phototypes IV to VI, which encompass highly heterogeneous populations. As a result, grouping patients by FST alone to describe skin color and race may obscure important differences and limit meaningful interpretation of clinical and research findings.
Clinically, recognition of dermatologic conditions such as erythema may be more challenging in darker skin tones, in which classic visual cues are less apparent.1,7 Relying on FST to stratify skin color may further compound diagnostic uncertainty by oversimplifying the cutaneous presentation. In addition, treatment decisions, including laser settings and assessment of pigmentary risk, often are guided by FST despite within-group variability.7 Further, educational frameworks that rely heavily on FST may inadequately prepare clinicians to recognize disease across diverse skin tones, contributing to delayed diagnosis and disparities in care in populations with skin of color.
The implications also extend to dermatologic research. Fitzpatrick skin type frequently is used to assess study populations; however, its limited ability to reflect true variation in pigmentation and ethnicity introduces misclassification bias.3,7 The broad FST scale may group heterogeneous populations, obscuring differences in treatment response. As a result, studies relying on FST to represent skin color or race may have reduced generalizability across diverse populations. Importantly, these limitations are not merely conceptual but may contribute to measurable disparities in dermatologic diagnosis and outcomes.
Rethinking Skin Classification Frameworks
Despite these shortcomings, FST remains deeply embedded in dermatology. Its decades-long use has led to widespread familiarity and integration into clinical guidelines, education, and research. At the same time, the absence of a universally accepted alternative has reinforced the continued use of FST as a proxy for skin color and race.
Alternative strategies for characterizing skin pigmentation include objective measures such as spectrophotometry and melanin index assessment.9
Although these approaches may provide more precise quantification of pigmentation, their use may be limited by the need for specialized equipment and reduced feasibility in routine clinical settings. Other proposed approaches incorporate multidimensional factors such as pigmentation, photoreactivity, and genetic ancestry.4 While these techniques represent important advances, none has achieved widespread adoption yet, and each presents challenges related to feasibility and standardization.
In the absence of a single ideal system, a more nuanced approach is needed. Fitzpatrick skin type should be used in the context for which it was designed: estimating UV response. Incorporating additional descriptors, including self-identified race and ethnicity, alongside more detailed assessments of pigmentation may improve the accuracy and relevance of both clinical evaluation and research. Combining FST with more precise and inclusive frameworks represents a pragmatic step toward better reflecting patient diversity.
- Taylor SC. Recognizing erythema in skin of color. J Am Acad Dermatol.
- Fitzpatrick TB. The validity and practicality of sun-reactive skin types I through VI. Arch Dermatol. 1988;124:869-871. doi:10.1001 /archderm.124.6.869
- Eilers S, Bach DQ, Gaber R, et al. Accuracy of self-reported Fitzpatrick skin phototype classification in US Hispanic and Latino populations. JAMA Dermatol. 2013;149:797-803. doi:10.1001 /jamadermatol.2013.4091
- Del Bino S, Bernerd F. Variations in skin colour and the biological consequences of ultraviolet radiation exposure. Br J Dermatol. 2013;169(S3):33-40. doi:10.1111/bjd.12529
- Goon P, Banfield C, Bello O, et al. Skin cancers in skin types IV–VI: does the Fitzpatrick scale give a false sense of security? Clin Exp Dermatol. 2022;47:1112-1117. doi:10.1002/ski2.40
- Fitzpatrick TB. Soleil et peau. J Med Asthet. 1975;2:33-34.
- Ware OR, Dawson JE, Shinohara MM, et al. Racial limitations of Fitzpatrick skin type. Cutis. 2020;105:77-80.
- Lester JC, Taylor SC, Chren MM. Under-representation of skin of colour in dermatology images: not just an educational issue. Br J Dermatol. 2019;180:1521-1522. doi:10.1111/bjd.17608
- Fullerton A, Fischer T, Lahti A, et al. Guidelines for measurement of skin colour and erythema. a report from the Standardization Group of the European Society of Contact Dermatitis. Contact Dermatitis. 1996;35:1-10. doi:10.1111/j.1600-0536.1996.tb02242.x
- Taylor SC. Recognizing erythema in skin of color. J Am Acad Dermatol.
- Fitzpatrick TB. The validity and practicality of sun-reactive skin types I through VI. Arch Dermatol. 1988;124:869-871. doi:10.1001 /archderm.124.6.869
- Eilers S, Bach DQ, Gaber R, et al. Accuracy of self-reported Fitzpatrick skin phototype classification in US Hispanic and Latino populations. JAMA Dermatol. 2013;149:797-803. doi:10.1001 /jamadermatol.2013.4091
- Del Bino S, Bernerd F. Variations in skin colour and the biological consequences of ultraviolet radiation exposure. Br J Dermatol. 2013;169(S3):33-40. doi:10.1111/bjd.12529
- Goon P, Banfield C, Bello O, et al. Skin cancers in skin types IV–VI: does the Fitzpatrick scale give a false sense of security? Clin Exp Dermatol. 2022;47:1112-1117. doi:10.1002/ski2.40
- Fitzpatrick TB. Soleil et peau. J Med Asthet. 1975;2:33-34.
- Ware OR, Dawson JE, Shinohara MM, et al. Racial limitations of Fitzpatrick skin type. Cutis. 2020;105:77-80.
- Lester JC, Taylor SC, Chren MM. Under-representation of skin of colour in dermatology images: not just an educational issue. Br J Dermatol. 2019;180:1521-1522. doi:10.1111/bjd.17608
- Fullerton A, Fischer T, Lahti A, et al. Guidelines for measurement of skin colour and erythema. a report from the Standardization Group of the European Society of Contact Dermatitis. Contact Dermatitis. 1996;35:1-10. doi:10.1111/j.1600-0536.1996.tb02242.x
Limitations of Fitzpatrick Skin Type as a Proxy for Skin Color and Race
Limitations of Fitzpatrick Skin Type as a Proxy for Skin Color and Race

Hypochlorous Acid: A Multipurpose New Addition to the Military Med Bag?
Hypochlorous Acid: A Multipurpose New Addition to the Military Med Bag?
Exogenously, hypochlorous acid (HOCl) is a powerful oxidizing agent formed from chlorine dissolved in water. Within the body, it is part of the immune response, created by activated leukocytes, which form HOCl from hydrogen peroxide and chloride. HOCl has been used as a disinfectant in wound care due to its antimicrobial properties via inhibition of DNA synthesis, protein synthesis, and decreased adenosine triphosphate production. It specifically targets bacteria by blocking bacterial cell wall synthesis and decreasing DNA replication.1
During the COVID-19 pandemic, HOCl was recommended by the US Environmental Protection Agency as a disinfectant.2 HOCl can be purchased from a supplier, though its major limitation is its shelf life. The main environmental factors affecting its stability are sunlight exposure, temperatures > 25 °C, and air exposure. HOCl is stable and most potent when the pH falls between 3.5 and 5.5.3 It is best stored in a cool, dark environment to maintain efficacy for 2 weeks. Rossi-Fedele et al found that when exposed to sunlight, chlorine reduction starts on day 4, whereas solutions kept in dark storage remained more stable, with this process starting after day 14.4
HOCl can also be made on-site via a machine, which ranges in price from a portable version costing < $200 to a large commercial option that can cost $7000 to $25,000. HOCl is produced by mixing noniodinated salt and water, and using electrolysis, which generally takes less than 10 minutes before it is ready for use.2 Given the cost and nonreusable nature of disinfecting wipes, HOCl may be more worthwhile for economic and disposal purposes in the long term.
Different concentrations of HOCl are readily available commercially. Because topical application of 1% HOCl may cause skin irritation, solutions with lower concentrations have been developed including Vashe (0.03% HOCl; SteadMed), PhaseOne (0.025% HOCl solution; IHT), OCuSOFT (0.02% HOCl; OCuSOFT), Bruder (0.02% HOCl; Bruder Healthcare), Acuicyn (0.01% HOCl solution in dilute saline; Sonoma Pharmaceuticals), and Avenova (0.01% HOCl solution; NovaBay Pharmaceuticals).5
Aside from its surface utility, HOCl has been researched for its beneficial effects on skin. HOCl has been shown to be helpful intraoperatively and postoperatively in improving adverse effects (AEs) after hair restoration, including erythema and pruritus, and in optimizing healing by reducing inflammation, likely due to its antimicrobial properties and ability to promote oxygenation.6 Bucko et al demonstrated that Microcyn scar gel (with HOCl) was a superior nonirritating, nontoxic method of not only improving scar appearance (vascularity, scar height, and pliability) but also reducing scar symptoms of pain and pruritus in comparison to 100% silicone scar gel (traditional application used to improve scarring).7 Zhang et al demonstrated that HOCl consistently improved symptom relief of blepharitis, including meibomian gland, eyelash, and eyelid redness, irritation, and appearance in comparison as well as were better tolerated in comparison to traditional recommendations of eyelid compresses and wash (tea tree oil, diluted baby shampoo, and topical antibiotics).8 In children with moderate to severe atopic dermatitis, Majewski et al compared a traditional bleach bath with a body wash containing hypochlorite (NaOCl; hypochlorous acid in alkaline aqueous solution). The body wash proved to be more convenient (showering vs 10-minute bath) and significantly improved symptoms while reducing the need for topical corticosteroids (common treatment modality for atopic dermatitis).9
The skin is the body’s primary defense against both dermatologic and respiratory infections. The face is especially vulnerable to microbes via airborne or environmental transmission, mechanical irritation, and touch. In the military environment, personal protective equipment (PPE) or uniform items may increase the risk of dermatologic conditions such as allergic or irritant dermatitis, infection, and friction blisters.
In a literature review of 312 dermatologic articles published between 2002 and 2022, Singal and Lipner found that among deployed soldiers serving in hot and dry climates, dermatitis and eczematous conditions were the most common, whereas bacterial and fungal conditions were most common in hot and humid settings. In the nondeployed setting, dermatitis and eczematous, acne, and fungal infections were the most common skin conditions. This is reflected by the unique circumstances that service members face at home and while deployed, when they may be more vulnerable to developing new or worsening chronic skin conditions depending on the environment (access to shelter, humid vs dry environments), and decreased access or time for hygiene (shared quarters at home in barracks or on deployment). Occupation-related conditions also play a large role in military dermatologic conditions.10
Dever et al noted the unique risks and exposures in the environment itself (plants, arthropods) as well as uniform items (protective gear) that carry an increased risk of friction irritation and dermatitis. Occupational exposures commonly associated with irritant contact dermatitis include alcohols, oils, fuel, disinfectants, and solvents. Chemicals in military uniforms themselves (eg, formaldehyde resins, disperse dyes, and chromate-containing dyes) also have the potential to cause allergic contact dermatitis, which can be challenging to address given the emphasis on uniformity and standards.11 PPE also may exacerbate rosacea and acne.
Some pathologies are associated specifically with bacteria, such as Cutibacterium acnes, as seen in acne vulgaris. Colonization of bacteria on the face may create biofilms that are difficult to detect, may be resistant to antibiotic therapy, and are implicated in other dermatologic conditions, such as persistent wounds, atopic dermatitis, and candidiasis.12
Biofilm and antibiotic resistance already pose a risk to patient care, but the unique environmental conditions and exposures of military settings can amplify this risk in the military population.13 Using HOCl in austere environments or the field for wound care may help reduce microbial load and the subsequent need for systemic antibiotics which carry the risk of gastrointestinal AEs and resistance.1
An optimized healing rate would support operational objectives by enabling service members to remain on full duty and avoid medications, which may prevent them from special duty, such as aviation. Sakarya et al found that HOCl solution enhanced wound healing in contrast with povidone-iodine (PI), while a study by Dharap et al discussed how HOCl provided major improvement in ulcer wound size (and infection), as well as significant reduction of inflammation.13
Anagnostopoulos et al studied the efficacy of 0.01% HOCl vs other disinfectants (5% PI, 4% chlorhexidine gluconate [CHG] and 70% isopropyl alcohol [IPA]) against common skin organisms, including methicillin-susceptible Staphylococcus aureus and methicillin-susceptible Staphylococcus epidermidis. The study found that HOCl had at least equal if not greater efficacy to PI, CHG, and IPA depending on the bacterial strain, demonstrating immediate bactericidal effects.14
Furthermore, HOCl has been shown to be useful in suturing and wound closure by reducing microbial load when soaked gauze is placed in wound beds prior to closure, while not harming surrounding tissue.15 This would be especially advantageous for military health care when specialist follow-up would be delayed or to prevent infection risk while en route to higher care. Aside from its disinfectant strength, it’s also well tolerated. HOCl studies on human tissue demonstrate its efficacy to prevent irritation and AEs while also preventing infection and promoting wound healing.
Gozukucuk and Cakiroglu studied the use of HOCl as a skin disinfectant before neonatal circumcision and demonstrated fewer adverse effects compared with the more commonly used PI. Neonates treated with PI prior to circumcision resulted in greater postoperative edema and increased duration of wound healing compared with infants treated with HOCl.16 Furthermore, studies have shown that PI can lead to irritant dermatitis or chemical burns if not properly dried or if it becomes pooled because of occlusion dressings.17
Aside from its indicated use for infection or wound care, anti-inflammatory properties of HOCl also may be beneficial for off-label use in preventing flareups of chronic conditions as well as for treating symptoms while awaiting specialist evaluation. This might be the case during US-based training exercises, in remote locations without nearby dermatologists, or during virtual care because of internet constraints. For chronic conditions such as rosacea or atopic dermatitis, which research has shown are related to mast cell activation and degranulation and cytokine release, HOCl has been shown to reduce histamine, neutrophil-generated leukotrienes, in addition to interleukin-6 and interleukin-2 to improve symptoms by reducing inflammation.18
Limitations of HOCl to explore would be extending its shelf life, exploring its various forms (eg, spray, topical) and storage limitations, and training of the machine and materials needed to be made in-house if not purchased. There are also no official guidelines for clinicians to recommend HOCl to patients, and research should be expanded on its use in humans, though it generally is well tolerated without AEs. HOCl has the potential to be a potent, nontoxic, inexpensive tool in med bags or at austere clinics to help maintain a sterile space for procedures, prevent infection while rendering care, and help with exacerbations or prevent flare-ups of chronic conditions such as psoriasis, acne, and atopic dermatitis while specialist care is pending.
- Natarelli N, et al. Hypochlorous acid: applications in dermatology. J Integr Dermatol. December 22, 2022. Accessed March 2, 2026. https://www.jintegrativederm.org/article/56663-hypochlorous-acid-applications-in-dermatology
- Block MS, Rowan BG. Hypochlorous acid: a review. J Oral Maxillofac Surg. 2020;78:1461-1466. doi:10.1016/j.joms.2020.06.029
- Menta N, Vidal SI, Friedman A. Hypochlorous acid: a blast from the past. J Drugs Dermatol. 2024;23:909-910.
- Rossi-Fedele G, Dogramaci E, Steier L, et al. Some factors influencing the stability of Sterilox®, a super-oxidised water. Br Dent J. 2011;210:E23. doi:10.1038/sj.bdj.2011.143
- Tran AQ, Topilow N, Rong A, et al. Comparison of skin antiseptic agents and the role of 0.01% hypochlorous acid. Aesthet Surg J. 2021;41:1170-1175. doi:10.1093/asj/sjaa322
- Stough D. Topical stabilized super-oxidized hypochlorous acid for wound healing in hair restoration surgery: a real-time usage-controlled trial evaluating safety, efficacy, and tolerability. J Drugs Dermatol. 2023;22:1191-1196. doi:10.36849/JDD.7172
- Bucko AD, Draelos Z, Dubois JC, Jones TM. A doubleblind, randomized study to compare Microcyn scar management hydrogel, K103163, and Kelo-cote scar gel for hypertrophic or keloid scars. Dermatologist. 2015;23:113-122.
- Zhang H, Wu Y, Wan X, et al. Effect of hypochlorous acid on blepharitis through ultrasonic atomization: a randomized clinical trial. J Clin Med. 2023;12(3):1164. doi:10.3390/jcm12031164
- Majewski S, Bhattacharya T, Asztalos M, et al. Sodium hypochlorite body wash in the management of Staphylococcus aureus-colonized moderate-to-severe atopic dermatitis in infants, children, and adolescents. Pediatr Dermatol. 2019;36:442-447. doi:10.1111/pde.13842
- Singal A, Lipner SR. A review of skin disease in military soldiers: challenges and potential solutions. Ann Med. 2023;55:2267425. doi:10.1080/07853890.2023.2267425
- Dever TT, Walters M, Jacob S. Contact dermatitis in military personnel. Dermatitis. 2011;22:313-319. doi:10.2310/6620.2011.11024
- Nowbuth AA, Armstrong J, Cloete T, et al. A potential benefit of hypochlorous acid-facial sanitisation: a review. Preprints. 2021. doi:10.20944/preprints202107.0129.v2
- Gold MH, Andriessen A, Bhatia AC, et al. Topical stabilized hypochlorous acid: the future gold standard for wound care and scar management in dermatologic and plastic surgery procedures. J Cosmet Dermatol. 2020;19:270-277. doi:10.1111/jocd.13280
- Anagnostopoulos AG, Rong A, Miller D, et al. 0.01% hypochlorous acid as an alternative skin antiseptic: an in vitro comparison. Dermatol Surg. 2018;44:1489-1493. doi:10.1097/DSS.0000000000001594
- Odom EB, Mundschenk MB, Hard KA, et al. The utility of hypochlorous acid wound therapy in wound bed preparation and skin graft salvage. Plast Reconstr Surg. 2019;143:677e-678e. doi:10.1097/PRS.0000000000005359
- Gozukucuk A, Cakiroglu B. Comparison of hypochlorous acid and povidone-iodine as a disinfectant in neonatal circumcision. J Pediatr Urol. 2022;18:341.e1-341.e5. doi:10.1016/j.jpurol.2022.03.011
- Borrego L, Hernández N, Hernández Z, et al. Povidoneiodine-induced postsurgical irritant contact dermatitis localized outside of the surgical incision area: report of 27 cases and a literature review. Int J Dermatol. 2016;55:540- 545. doi:10.1111/ijd.12957
- Del Rosso JQ, Bhatia N. Status report on topical hypochlorous acid: clinical relevance of specific formulations, potential modes of action, and study outcomes. J Clin Aesthet Dermatol. 2018;11:36-39.
Exogenously, hypochlorous acid (HOCl) is a powerful oxidizing agent formed from chlorine dissolved in water. Within the body, it is part of the immune response, created by activated leukocytes, which form HOCl from hydrogen peroxide and chloride. HOCl has been used as a disinfectant in wound care due to its antimicrobial properties via inhibition of DNA synthesis, protein synthesis, and decreased adenosine triphosphate production. It specifically targets bacteria by blocking bacterial cell wall synthesis and decreasing DNA replication.1
During the COVID-19 pandemic, HOCl was recommended by the US Environmental Protection Agency as a disinfectant.2 HOCl can be purchased from a supplier, though its major limitation is its shelf life. The main environmental factors affecting its stability are sunlight exposure, temperatures > 25 °C, and air exposure. HOCl is stable and most potent when the pH falls between 3.5 and 5.5.3 It is best stored in a cool, dark environment to maintain efficacy for 2 weeks. Rossi-Fedele et al found that when exposed to sunlight, chlorine reduction starts on day 4, whereas solutions kept in dark storage remained more stable, with this process starting after day 14.4
HOCl can also be made on-site via a machine, which ranges in price from a portable version costing < $200 to a large commercial option that can cost $7000 to $25,000. HOCl is produced by mixing noniodinated salt and water, and using electrolysis, which generally takes less than 10 minutes before it is ready for use.2 Given the cost and nonreusable nature of disinfecting wipes, HOCl may be more worthwhile for economic and disposal purposes in the long term.
Different concentrations of HOCl are readily available commercially. Because topical application of 1% HOCl may cause skin irritation, solutions with lower concentrations have been developed including Vashe (0.03% HOCl; SteadMed), PhaseOne (0.025% HOCl solution; IHT), OCuSOFT (0.02% HOCl; OCuSOFT), Bruder (0.02% HOCl; Bruder Healthcare), Acuicyn (0.01% HOCl solution in dilute saline; Sonoma Pharmaceuticals), and Avenova (0.01% HOCl solution; NovaBay Pharmaceuticals).5
Aside from its surface utility, HOCl has been researched for its beneficial effects on skin. HOCl has been shown to be helpful intraoperatively and postoperatively in improving adverse effects (AEs) after hair restoration, including erythema and pruritus, and in optimizing healing by reducing inflammation, likely due to its antimicrobial properties and ability to promote oxygenation.6 Bucko et al demonstrated that Microcyn scar gel (with HOCl) was a superior nonirritating, nontoxic method of not only improving scar appearance (vascularity, scar height, and pliability) but also reducing scar symptoms of pain and pruritus in comparison to 100% silicone scar gel (traditional application used to improve scarring).7 Zhang et al demonstrated that HOCl consistently improved symptom relief of blepharitis, including meibomian gland, eyelash, and eyelid redness, irritation, and appearance in comparison as well as were better tolerated in comparison to traditional recommendations of eyelid compresses and wash (tea tree oil, diluted baby shampoo, and topical antibiotics).8 In children with moderate to severe atopic dermatitis, Majewski et al compared a traditional bleach bath with a body wash containing hypochlorite (NaOCl; hypochlorous acid in alkaline aqueous solution). The body wash proved to be more convenient (showering vs 10-minute bath) and significantly improved symptoms while reducing the need for topical corticosteroids (common treatment modality for atopic dermatitis).9
The skin is the body’s primary defense against both dermatologic and respiratory infections. The face is especially vulnerable to microbes via airborne or environmental transmission, mechanical irritation, and touch. In the military environment, personal protective equipment (PPE) or uniform items may increase the risk of dermatologic conditions such as allergic or irritant dermatitis, infection, and friction blisters.
In a literature review of 312 dermatologic articles published between 2002 and 2022, Singal and Lipner found that among deployed soldiers serving in hot and dry climates, dermatitis and eczematous conditions were the most common, whereas bacterial and fungal conditions were most common in hot and humid settings. In the nondeployed setting, dermatitis and eczematous, acne, and fungal infections were the most common skin conditions. This is reflected by the unique circumstances that service members face at home and while deployed, when they may be more vulnerable to developing new or worsening chronic skin conditions depending on the environment (access to shelter, humid vs dry environments), and decreased access or time for hygiene (shared quarters at home in barracks or on deployment). Occupation-related conditions also play a large role in military dermatologic conditions.10
Dever et al noted the unique risks and exposures in the environment itself (plants, arthropods) as well as uniform items (protective gear) that carry an increased risk of friction irritation and dermatitis. Occupational exposures commonly associated with irritant contact dermatitis include alcohols, oils, fuel, disinfectants, and solvents. Chemicals in military uniforms themselves (eg, formaldehyde resins, disperse dyes, and chromate-containing dyes) also have the potential to cause allergic contact dermatitis, which can be challenging to address given the emphasis on uniformity and standards.11 PPE also may exacerbate rosacea and acne.
Some pathologies are associated specifically with bacteria, such as Cutibacterium acnes, as seen in acne vulgaris. Colonization of bacteria on the face may create biofilms that are difficult to detect, may be resistant to antibiotic therapy, and are implicated in other dermatologic conditions, such as persistent wounds, atopic dermatitis, and candidiasis.12
Biofilm and antibiotic resistance already pose a risk to patient care, but the unique environmental conditions and exposures of military settings can amplify this risk in the military population.13 Using HOCl in austere environments or the field for wound care may help reduce microbial load and the subsequent need for systemic antibiotics which carry the risk of gastrointestinal AEs and resistance.1
An optimized healing rate would support operational objectives by enabling service members to remain on full duty and avoid medications, which may prevent them from special duty, such as aviation. Sakarya et al found that HOCl solution enhanced wound healing in contrast with povidone-iodine (PI), while a study by Dharap et al discussed how HOCl provided major improvement in ulcer wound size (and infection), as well as significant reduction of inflammation.13
Anagnostopoulos et al studied the efficacy of 0.01% HOCl vs other disinfectants (5% PI, 4% chlorhexidine gluconate [CHG] and 70% isopropyl alcohol [IPA]) against common skin organisms, including methicillin-susceptible Staphylococcus aureus and methicillin-susceptible Staphylococcus epidermidis. The study found that HOCl had at least equal if not greater efficacy to PI, CHG, and IPA depending on the bacterial strain, demonstrating immediate bactericidal effects.14
Furthermore, HOCl has been shown to be useful in suturing and wound closure by reducing microbial load when soaked gauze is placed in wound beds prior to closure, while not harming surrounding tissue.15 This would be especially advantageous for military health care when specialist follow-up would be delayed or to prevent infection risk while en route to higher care. Aside from its disinfectant strength, it’s also well tolerated. HOCl studies on human tissue demonstrate its efficacy to prevent irritation and AEs while also preventing infection and promoting wound healing.
Gozukucuk and Cakiroglu studied the use of HOCl as a skin disinfectant before neonatal circumcision and demonstrated fewer adverse effects compared with the more commonly used PI. Neonates treated with PI prior to circumcision resulted in greater postoperative edema and increased duration of wound healing compared with infants treated with HOCl.16 Furthermore, studies have shown that PI can lead to irritant dermatitis or chemical burns if not properly dried or if it becomes pooled because of occlusion dressings.17
Aside from its indicated use for infection or wound care, anti-inflammatory properties of HOCl also may be beneficial for off-label use in preventing flareups of chronic conditions as well as for treating symptoms while awaiting specialist evaluation. This might be the case during US-based training exercises, in remote locations without nearby dermatologists, or during virtual care because of internet constraints. For chronic conditions such as rosacea or atopic dermatitis, which research has shown are related to mast cell activation and degranulation and cytokine release, HOCl has been shown to reduce histamine, neutrophil-generated leukotrienes, in addition to interleukin-6 and interleukin-2 to improve symptoms by reducing inflammation.18
Limitations of HOCl to explore would be extending its shelf life, exploring its various forms (eg, spray, topical) and storage limitations, and training of the machine and materials needed to be made in-house if not purchased. There are also no official guidelines for clinicians to recommend HOCl to patients, and research should be expanded on its use in humans, though it generally is well tolerated without AEs. HOCl has the potential to be a potent, nontoxic, inexpensive tool in med bags or at austere clinics to help maintain a sterile space for procedures, prevent infection while rendering care, and help with exacerbations or prevent flare-ups of chronic conditions such as psoriasis, acne, and atopic dermatitis while specialist care is pending.
Exogenously, hypochlorous acid (HOCl) is a powerful oxidizing agent formed from chlorine dissolved in water. Within the body, it is part of the immune response, created by activated leukocytes, which form HOCl from hydrogen peroxide and chloride. HOCl has been used as a disinfectant in wound care due to its antimicrobial properties via inhibition of DNA synthesis, protein synthesis, and decreased adenosine triphosphate production. It specifically targets bacteria by blocking bacterial cell wall synthesis and decreasing DNA replication.1
During the COVID-19 pandemic, HOCl was recommended by the US Environmental Protection Agency as a disinfectant.2 HOCl can be purchased from a supplier, though its major limitation is its shelf life. The main environmental factors affecting its stability are sunlight exposure, temperatures > 25 °C, and air exposure. HOCl is stable and most potent when the pH falls between 3.5 and 5.5.3 It is best stored in a cool, dark environment to maintain efficacy for 2 weeks. Rossi-Fedele et al found that when exposed to sunlight, chlorine reduction starts on day 4, whereas solutions kept in dark storage remained more stable, with this process starting after day 14.4
HOCl can also be made on-site via a machine, which ranges in price from a portable version costing < $200 to a large commercial option that can cost $7000 to $25,000. HOCl is produced by mixing noniodinated salt and water, and using electrolysis, which generally takes less than 10 minutes before it is ready for use.2 Given the cost and nonreusable nature of disinfecting wipes, HOCl may be more worthwhile for economic and disposal purposes in the long term.
Different concentrations of HOCl are readily available commercially. Because topical application of 1% HOCl may cause skin irritation, solutions with lower concentrations have been developed including Vashe (0.03% HOCl; SteadMed), PhaseOne (0.025% HOCl solution; IHT), OCuSOFT (0.02% HOCl; OCuSOFT), Bruder (0.02% HOCl; Bruder Healthcare), Acuicyn (0.01% HOCl solution in dilute saline; Sonoma Pharmaceuticals), and Avenova (0.01% HOCl solution; NovaBay Pharmaceuticals).5
Aside from its surface utility, HOCl has been researched for its beneficial effects on skin. HOCl has been shown to be helpful intraoperatively and postoperatively in improving adverse effects (AEs) after hair restoration, including erythema and pruritus, and in optimizing healing by reducing inflammation, likely due to its antimicrobial properties and ability to promote oxygenation.6 Bucko et al demonstrated that Microcyn scar gel (with HOCl) was a superior nonirritating, nontoxic method of not only improving scar appearance (vascularity, scar height, and pliability) but also reducing scar symptoms of pain and pruritus in comparison to 100% silicone scar gel (traditional application used to improve scarring).7 Zhang et al demonstrated that HOCl consistently improved symptom relief of blepharitis, including meibomian gland, eyelash, and eyelid redness, irritation, and appearance in comparison as well as were better tolerated in comparison to traditional recommendations of eyelid compresses and wash (tea tree oil, diluted baby shampoo, and topical antibiotics).8 In children with moderate to severe atopic dermatitis, Majewski et al compared a traditional bleach bath with a body wash containing hypochlorite (NaOCl; hypochlorous acid in alkaline aqueous solution). The body wash proved to be more convenient (showering vs 10-minute bath) and significantly improved symptoms while reducing the need for topical corticosteroids (common treatment modality for atopic dermatitis).9
The skin is the body’s primary defense against both dermatologic and respiratory infections. The face is especially vulnerable to microbes via airborne or environmental transmission, mechanical irritation, and touch. In the military environment, personal protective equipment (PPE) or uniform items may increase the risk of dermatologic conditions such as allergic or irritant dermatitis, infection, and friction blisters.
In a literature review of 312 dermatologic articles published between 2002 and 2022, Singal and Lipner found that among deployed soldiers serving in hot and dry climates, dermatitis and eczematous conditions were the most common, whereas bacterial and fungal conditions were most common in hot and humid settings. In the nondeployed setting, dermatitis and eczematous, acne, and fungal infections were the most common skin conditions. This is reflected by the unique circumstances that service members face at home and while deployed, when they may be more vulnerable to developing new or worsening chronic skin conditions depending on the environment (access to shelter, humid vs dry environments), and decreased access or time for hygiene (shared quarters at home in barracks or on deployment). Occupation-related conditions also play a large role in military dermatologic conditions.10
Dever et al noted the unique risks and exposures in the environment itself (plants, arthropods) as well as uniform items (protective gear) that carry an increased risk of friction irritation and dermatitis. Occupational exposures commonly associated with irritant contact dermatitis include alcohols, oils, fuel, disinfectants, and solvents. Chemicals in military uniforms themselves (eg, formaldehyde resins, disperse dyes, and chromate-containing dyes) also have the potential to cause allergic contact dermatitis, which can be challenging to address given the emphasis on uniformity and standards.11 PPE also may exacerbate rosacea and acne.
Some pathologies are associated specifically with bacteria, such as Cutibacterium acnes, as seen in acne vulgaris. Colonization of bacteria on the face may create biofilms that are difficult to detect, may be resistant to antibiotic therapy, and are implicated in other dermatologic conditions, such as persistent wounds, atopic dermatitis, and candidiasis.12
Biofilm and antibiotic resistance already pose a risk to patient care, but the unique environmental conditions and exposures of military settings can amplify this risk in the military population.13 Using HOCl in austere environments or the field for wound care may help reduce microbial load and the subsequent need for systemic antibiotics which carry the risk of gastrointestinal AEs and resistance.1
An optimized healing rate would support operational objectives by enabling service members to remain on full duty and avoid medications, which may prevent them from special duty, such as aviation. Sakarya et al found that HOCl solution enhanced wound healing in contrast with povidone-iodine (PI), while a study by Dharap et al discussed how HOCl provided major improvement in ulcer wound size (and infection), as well as significant reduction of inflammation.13
Anagnostopoulos et al studied the efficacy of 0.01% HOCl vs other disinfectants (5% PI, 4% chlorhexidine gluconate [CHG] and 70% isopropyl alcohol [IPA]) against common skin organisms, including methicillin-susceptible Staphylococcus aureus and methicillin-susceptible Staphylococcus epidermidis. The study found that HOCl had at least equal if not greater efficacy to PI, CHG, and IPA depending on the bacterial strain, demonstrating immediate bactericidal effects.14
Furthermore, HOCl has been shown to be useful in suturing and wound closure by reducing microbial load when soaked gauze is placed in wound beds prior to closure, while not harming surrounding tissue.15 This would be especially advantageous for military health care when specialist follow-up would be delayed or to prevent infection risk while en route to higher care. Aside from its disinfectant strength, it’s also well tolerated. HOCl studies on human tissue demonstrate its efficacy to prevent irritation and AEs while also preventing infection and promoting wound healing.
Gozukucuk and Cakiroglu studied the use of HOCl as a skin disinfectant before neonatal circumcision and demonstrated fewer adverse effects compared with the more commonly used PI. Neonates treated with PI prior to circumcision resulted in greater postoperative edema and increased duration of wound healing compared with infants treated with HOCl.16 Furthermore, studies have shown that PI can lead to irritant dermatitis or chemical burns if not properly dried or if it becomes pooled because of occlusion dressings.17
Aside from its indicated use for infection or wound care, anti-inflammatory properties of HOCl also may be beneficial for off-label use in preventing flareups of chronic conditions as well as for treating symptoms while awaiting specialist evaluation. This might be the case during US-based training exercises, in remote locations without nearby dermatologists, or during virtual care because of internet constraints. For chronic conditions such as rosacea or atopic dermatitis, which research has shown are related to mast cell activation and degranulation and cytokine release, HOCl has been shown to reduce histamine, neutrophil-generated leukotrienes, in addition to interleukin-6 and interleukin-2 to improve symptoms by reducing inflammation.18
Limitations of HOCl to explore would be extending its shelf life, exploring its various forms (eg, spray, topical) and storage limitations, and training of the machine and materials needed to be made in-house if not purchased. There are also no official guidelines for clinicians to recommend HOCl to patients, and research should be expanded on its use in humans, though it generally is well tolerated without AEs. HOCl has the potential to be a potent, nontoxic, inexpensive tool in med bags or at austere clinics to help maintain a sterile space for procedures, prevent infection while rendering care, and help with exacerbations or prevent flare-ups of chronic conditions such as psoriasis, acne, and atopic dermatitis while specialist care is pending.
- Natarelli N, et al. Hypochlorous acid: applications in dermatology. J Integr Dermatol. December 22, 2022. Accessed March 2, 2026. https://www.jintegrativederm.org/article/56663-hypochlorous-acid-applications-in-dermatology
- Block MS, Rowan BG. Hypochlorous acid: a review. J Oral Maxillofac Surg. 2020;78:1461-1466. doi:10.1016/j.joms.2020.06.029
- Menta N, Vidal SI, Friedman A. Hypochlorous acid: a blast from the past. J Drugs Dermatol. 2024;23:909-910.
- Rossi-Fedele G, Dogramaci E, Steier L, et al. Some factors influencing the stability of Sterilox®, a super-oxidised water. Br Dent J. 2011;210:E23. doi:10.1038/sj.bdj.2011.143
- Tran AQ, Topilow N, Rong A, et al. Comparison of skin antiseptic agents and the role of 0.01% hypochlorous acid. Aesthet Surg J. 2021;41:1170-1175. doi:10.1093/asj/sjaa322
- Stough D. Topical stabilized super-oxidized hypochlorous acid for wound healing in hair restoration surgery: a real-time usage-controlled trial evaluating safety, efficacy, and tolerability. J Drugs Dermatol. 2023;22:1191-1196. doi:10.36849/JDD.7172
- Bucko AD, Draelos Z, Dubois JC, Jones TM. A doubleblind, randomized study to compare Microcyn scar management hydrogel, K103163, and Kelo-cote scar gel for hypertrophic or keloid scars. Dermatologist. 2015;23:113-122.
- Zhang H, Wu Y, Wan X, et al. Effect of hypochlorous acid on blepharitis through ultrasonic atomization: a randomized clinical trial. J Clin Med. 2023;12(3):1164. doi:10.3390/jcm12031164
- Majewski S, Bhattacharya T, Asztalos M, et al. Sodium hypochlorite body wash in the management of Staphylococcus aureus-colonized moderate-to-severe atopic dermatitis in infants, children, and adolescents. Pediatr Dermatol. 2019;36:442-447. doi:10.1111/pde.13842
- Singal A, Lipner SR. A review of skin disease in military soldiers: challenges and potential solutions. Ann Med. 2023;55:2267425. doi:10.1080/07853890.2023.2267425
- Dever TT, Walters M, Jacob S. Contact dermatitis in military personnel. Dermatitis. 2011;22:313-319. doi:10.2310/6620.2011.11024
- Nowbuth AA, Armstrong J, Cloete T, et al. A potential benefit of hypochlorous acid-facial sanitisation: a review. Preprints. 2021. doi:10.20944/preprints202107.0129.v2
- Gold MH, Andriessen A, Bhatia AC, et al. Topical stabilized hypochlorous acid: the future gold standard for wound care and scar management in dermatologic and plastic surgery procedures. J Cosmet Dermatol. 2020;19:270-277. doi:10.1111/jocd.13280
- Anagnostopoulos AG, Rong A, Miller D, et al. 0.01% hypochlorous acid as an alternative skin antiseptic: an in vitro comparison. Dermatol Surg. 2018;44:1489-1493. doi:10.1097/DSS.0000000000001594
- Odom EB, Mundschenk MB, Hard KA, et al. The utility of hypochlorous acid wound therapy in wound bed preparation and skin graft salvage. Plast Reconstr Surg. 2019;143:677e-678e. doi:10.1097/PRS.0000000000005359
- Gozukucuk A, Cakiroglu B. Comparison of hypochlorous acid and povidone-iodine as a disinfectant in neonatal circumcision. J Pediatr Urol. 2022;18:341.e1-341.e5. doi:10.1016/j.jpurol.2022.03.011
- Borrego L, Hernández N, Hernández Z, et al. Povidoneiodine-induced postsurgical irritant contact dermatitis localized outside of the surgical incision area: report of 27 cases and a literature review. Int J Dermatol. 2016;55:540- 545. doi:10.1111/ijd.12957
- Del Rosso JQ, Bhatia N. Status report on topical hypochlorous acid: clinical relevance of specific formulations, potential modes of action, and study outcomes. J Clin Aesthet Dermatol. 2018;11:36-39.
- Natarelli N, et al. Hypochlorous acid: applications in dermatology. J Integr Dermatol. December 22, 2022. Accessed March 2, 2026. https://www.jintegrativederm.org/article/56663-hypochlorous-acid-applications-in-dermatology
- Block MS, Rowan BG. Hypochlorous acid: a review. J Oral Maxillofac Surg. 2020;78:1461-1466. doi:10.1016/j.joms.2020.06.029
- Menta N, Vidal SI, Friedman A. Hypochlorous acid: a blast from the past. J Drugs Dermatol. 2024;23:909-910.
- Rossi-Fedele G, Dogramaci E, Steier L, et al. Some factors influencing the stability of Sterilox®, a super-oxidised water. Br Dent J. 2011;210:E23. doi:10.1038/sj.bdj.2011.143
- Tran AQ, Topilow N, Rong A, et al. Comparison of skin antiseptic agents and the role of 0.01% hypochlorous acid. Aesthet Surg J. 2021;41:1170-1175. doi:10.1093/asj/sjaa322
- Stough D. Topical stabilized super-oxidized hypochlorous acid for wound healing in hair restoration surgery: a real-time usage-controlled trial evaluating safety, efficacy, and tolerability. J Drugs Dermatol. 2023;22:1191-1196. doi:10.36849/JDD.7172
- Bucko AD, Draelos Z, Dubois JC, Jones TM. A doubleblind, randomized study to compare Microcyn scar management hydrogel, K103163, and Kelo-cote scar gel for hypertrophic or keloid scars. Dermatologist. 2015;23:113-122.
- Zhang H, Wu Y, Wan X, et al. Effect of hypochlorous acid on blepharitis through ultrasonic atomization: a randomized clinical trial. J Clin Med. 2023;12(3):1164. doi:10.3390/jcm12031164
- Majewski S, Bhattacharya T, Asztalos M, et al. Sodium hypochlorite body wash in the management of Staphylococcus aureus-colonized moderate-to-severe atopic dermatitis in infants, children, and adolescents. Pediatr Dermatol. 2019;36:442-447. doi:10.1111/pde.13842
- Singal A, Lipner SR. A review of skin disease in military soldiers: challenges and potential solutions. Ann Med. 2023;55:2267425. doi:10.1080/07853890.2023.2267425
- Dever TT, Walters M, Jacob S. Contact dermatitis in military personnel. Dermatitis. 2011;22:313-319. doi:10.2310/6620.2011.11024
- Nowbuth AA, Armstrong J, Cloete T, et al. A potential benefit of hypochlorous acid-facial sanitisation: a review. Preprints. 2021. doi:10.20944/preprints202107.0129.v2
- Gold MH, Andriessen A, Bhatia AC, et al. Topical stabilized hypochlorous acid: the future gold standard for wound care and scar management in dermatologic and plastic surgery procedures. J Cosmet Dermatol. 2020;19:270-277. doi:10.1111/jocd.13280
- Anagnostopoulos AG, Rong A, Miller D, et al. 0.01% hypochlorous acid as an alternative skin antiseptic: an in vitro comparison. Dermatol Surg. 2018;44:1489-1493. doi:10.1097/DSS.0000000000001594
- Odom EB, Mundschenk MB, Hard KA, et al. The utility of hypochlorous acid wound therapy in wound bed preparation and skin graft salvage. Plast Reconstr Surg. 2019;143:677e-678e. doi:10.1097/PRS.0000000000005359
- Gozukucuk A, Cakiroglu B. Comparison of hypochlorous acid and povidone-iodine as a disinfectant in neonatal circumcision. J Pediatr Urol. 2022;18:341.e1-341.e5. doi:10.1016/j.jpurol.2022.03.011
- Borrego L, Hernández N, Hernández Z, et al. Povidoneiodine-induced postsurgical irritant contact dermatitis localized outside of the surgical incision area: report of 27 cases and a literature review. Int J Dermatol. 2016;55:540- 545. doi:10.1111/ijd.12957
- Del Rosso JQ, Bhatia N. Status report on topical hypochlorous acid: clinical relevance of specific formulations, potential modes of action, and study outcomes. J Clin Aesthet Dermatol. 2018;11:36-39.
Hypochlorous Acid: A Multipurpose New Addition to the Military Med Bag?
Hypochlorous Acid: A Multipurpose New Addition to the Military Med Bag?
