User login
Improving transitions for elderly patients
Transitions are always a time of concern for hospitalists, and the transition from hospital to skilled nursing facilities (SNF) is no exception.
“During the transition and in the 30 days after discharge from the hospital to a SNF, patients are at high risk for death, rehospitalization, and high-cost health care,” said Amber Moore, MD, MPH, a hospitalist at Beth Israel Deaconess Medical Center, and instructor of medicine, Harvard Medical School. “Elderly adults are especially vulnerable because of impairments that may prevent them from participating in the discharge process and an increase in the risk that information is lost or incomplete during the care transition.”

To address this, she and several other physicians studied a novel video-conference program called Extension for Community Health Outcomes–Care Transitions (ECHO-CT) that connects an interdisciplinary hospital-based team with clinicians at SNFs to help reduce patient mortality, hospital readmission, skilled nursing facility length of stay, and 30-day health care costs.
The results of their study suggest that this intervention significantly decreased SNF length of stay, readmission rate, and costs of care, she says; the model they used is reproducible and has the potential to significantly improve care of these patients. “Our model was hospitalist run and is a mechanism to help hospitalists improve care to their patients during the transition time and beyond,” Dr. Moore said. “Furthermore, in participating in this model, hospitalists have the opportunity to better understand the challenges that face their patients after discharge and learn from postacute care providers.”
Ideally, she would like to see the model spread to other hospitals; she says hospitalists are well positioned to set up this program at their institution. “I also hope that our study highlights the incredible opportunity for improvement in the care of patients during transition from hospital to SNF and encourages hospitalists to look for innovative ways to improve care at this transition,” she said.
Reference
Moore AB, Krupp JE, Dufour AB, et al. Improving transitions to post-acute care for elderly patients using a novel video-conferencing program: ECHO-Care transitions. Am J Med. 2017 Oct;130(10):1199-204. Accessed June 6, 2017.
Transitions are always a time of concern for hospitalists, and the transition from hospital to skilled nursing facilities (SNF) is no exception.
“During the transition and in the 30 days after discharge from the hospital to a SNF, patients are at high risk for death, rehospitalization, and high-cost health care,” said Amber Moore, MD, MPH, a hospitalist at Beth Israel Deaconess Medical Center, and instructor of medicine, Harvard Medical School. “Elderly adults are especially vulnerable because of impairments that may prevent them from participating in the discharge process and an increase in the risk that information is lost or incomplete during the care transition.”
To address this, she and several other physicians studied a novel video-conference program called Extension for Community Health Outcomes–Care Transitions (ECHO-CT) that connects an interdisciplinary hospital-based team with clinicians at SNFs to help reduce patient mortality, hospital readmission, skilled nursing facility length of stay, and 30-day health care costs.
The results of their study suggest that this intervention significantly decreased SNF length of stay, readmission rate, and costs of care, she says; the model they used is reproducible and has the potential to significantly improve care of these patients. “Our model was hospitalist run and is a mechanism to help hospitalists improve care to their patients during the transition time and beyond,” Dr. Moore said. “Furthermore, in participating in this model, hospitalists have the opportunity to better understand the challenges that face their patients after discharge and learn from postacute care providers.”
Ideally, she would like to see the model spread to other hospitals; she says hospitalists are well positioned to set up this program at their institution. “I also hope that our study highlights the incredible opportunity for improvement in the care of patients during transition from hospital to SNF and encourages hospitalists to look for innovative ways to improve care at this transition,” she said.
Reference
Moore AB, Krupp JE, Dufour AB, et al. Improving transitions to post-acute care for elderly patients using a novel video-conferencing program: ECHO-Care transitions. Am J Med. 2017 Oct;130(10):1199-204. Accessed June 6, 2017.
Transitions are always a time of concern for hospitalists, and the transition from hospital to skilled nursing facilities (SNF) is no exception.
“During the transition and in the 30 days after discharge from the hospital to a SNF, patients are at high risk for death, rehospitalization, and high-cost health care,” said Amber Moore, MD, MPH, a hospitalist at Beth Israel Deaconess Medical Center, and instructor of medicine, Harvard Medical School. “Elderly adults are especially vulnerable because of impairments that may prevent them from participating in the discharge process and an increase in the risk that information is lost or incomplete during the care transition.”
To address this, she and several other physicians studied a novel video-conference program called Extension for Community Health Outcomes–Care Transitions (ECHO-CT) that connects an interdisciplinary hospital-based team with clinicians at SNFs to help reduce patient mortality, hospital readmission, skilled nursing facility length of stay, and 30-day health care costs.
The results of their study suggest that this intervention significantly decreased SNF length of stay, readmission rate, and costs of care, she says; the model they used is reproducible and has the potential to significantly improve care of these patients. “Our model was hospitalist run and is a mechanism to help hospitalists improve care to their patients during the transition time and beyond,” Dr. Moore said. “Furthermore, in participating in this model, hospitalists have the opportunity to better understand the challenges that face their patients after discharge and learn from postacute care providers.”
Ideally, she would like to see the model spread to other hospitals; she says hospitalists are well positioned to set up this program at their institution. “I also hope that our study highlights the incredible opportunity for improvement in the care of patients during transition from hospital to SNF and encourages hospitalists to look for innovative ways to improve care at this transition,” she said.
Reference
Moore AB, Krupp JE, Dufour AB, et al. Improving transitions to post-acute care for elderly patients using a novel video-conferencing program: ECHO-Care transitions. Am J Med. 2017 Oct;130(10):1199-204. Accessed June 6, 2017.
Some measures to control HAI sound better than they perform
SAN DIEGO – Some almost universally accepted measures against hospital-acquired infections are more costly, annoying, and time consuming than they’re worth, presenters agreed during a panel discussion at the annual clinical congress of the American College of Surgeons.
Intra-abdominal antibiotic irrigation, chlorhexidine bathing, and even postsurgical antibiotic infusions have not consistently been shown to reduce infections. These measures do, however, ratchet up costs and can contribute to antibiotic resistance.
Some of these and other measures to prevent nosocomial infections may indeed reduce the risk, but the gain is small, said Charles H. Cook, MD.
“Chlorhexidine bathing, for example, is touted by many as a panacea for all the infections we’re talking about,” said Dr. Cook, a critical care surgeon at Beth Israel Deaconess Medical Center, New York. “A recent meta-analysis in critical care units did find a reduced relative risk of 0.44 for central line bloodstream infections. But you needed to bathe 360 patients to prevent one infection. It’s what I call a long run for a short slide.”
Therese Duane, MD, FACS, agreed. A surgeon at the John Peter Smith Hospital, Ft. Worth, Tex., Dr. Duane reviewed three different guidelines for the prevention of surgical site infections: the ACS and Surgical Infection Society, the World Health Organization, and the Centers for Disease Control and Prevention. In looking for similarities between the documents, she said she found several well-accepted practices that just aren’t supported by good data.
Presurgical antimicrobial infusions got a strong thumbs-up from all the groups, but only under a very specific circumstance: The medication has to be administered well in advance of surgery for it to be effective.
“Your goal is to get the appropriate concentration into the tissues by the time of incision,” Dr. Duane said. “It takes time to get there – if you give it after the incision, you have bleeding and cellular death, and the antimicrobials cannot get to that incision and do their job. If I’m starting a case and they haven’t been given, I don’t ever start them after the incision, because then you have all of the risks and none of the benefits. In my opinion, we need to move to no further antimicrobials once the incision or case is over because it serves no purpose and is inconsistent with good antibiotic stewardship.”
Adhesive drapes got a resounding “eh” from the guidelines, Dr. Duane said. “You really do not need them. They’re expensive and they’re not improving outcomes, so don’t waste your time or money. We need to think about minimizing what isn’t helpful and maximizing the things that are worthwhile. That’s the way to practice good socially responsible surgery without breaking the bank,” she said.
Antimicrobial sutures got weak recommendations, Dr. Duane said. The evidence supporting their use was not very strong, although she said she feels triclosan-coated sutures are helpful in all kinds of surgery. Preoperative showering with an antiseptic received strong support, with alcohol-containing preps superior to chlorhexidine, which is better than povidone-iodine–containing solutions.
Deep-space irrigation with aqueous iodophor also received a weak recommendation, but Dr. Duane said the evidence does not support the use of antibiotic-containing irrigation in either the abdomen or the incision. “And the guidelines came out strongly against using antimicrobial agents on the incision,” she said. None of the guidelines issued a recommendation for or against antimicrobial dressings.
Protocolized infection-control bundles are a very great help in reducing the incidence of surgical site infections, Dr. Duane added. “They increase attention to detail and decrease the rates of infection.”
Dr. Cook agreed. “Central line bundles are one of the things that work” for line-associated bloodstream infections, he said. Since their large-scale adoption, mortality from these infections has dropped significantly; it was hovering around 28,000 per year in the mid-2000s, he said. “That’s about how many men die from prostate cancer every year.”
Central line infections are very costly too, he added – around $46,000 per event. “That comes to around $2 billion in direct and indirect costs every year.”
A 2006 study demonstrated the efficacy of central line bundles in the fight against these potentially devastating infections.
The bundled intervention comprised hand washing, using full-barrier precautions during the insertion of central venous catheters, cleaning the skin with chlorhexidine, avoiding the femoral site if possible, and removing unnecessary catheters. The median rate of catheter-related bloodstream infections per 1,000 catheter-days decreased from 2.7 at baseline to 0 at 3 months after implementation of the study intervention.
Antibiotic-coated or impregnated catheters do not work as well. A 2016 Cochrane review of 57 studies determined that the devices didn’t improve sepsis, all-cause mortality, or catheter-related local infections.
The jury may still be out on coated dressings or securing devices, however. Another Cochrane review, of 22 studies, found a 40% decrease in central line–associated bloodstream infections with these items. “There was moderate evidence that tip colonization was reduced, but the authors said more research is needed.”
The evidence looks stronger for alcohol-impregnated port protectors, Dr. Cook said. Two studies in particular support their use. In an oncology unit, the rate of these infections dropped from 2.3 to 0.3 per 1,000 catheter days after the port protectors were instituted.
In the second study, infection rates declined from 1.43 to 0.69 per 1,000 line-days after the protectors came on board.
“The advantage was seen mostly in ICUs, so the recommendations are to use them there,” Dr. Cook said.
Neither Dr. Cook nor Dr. Duane had any relevant financial disclosures.
[email protected]
On Twitter @Alz Gal
SAN DIEGO – Some almost universally accepted measures against hospital-acquired infections are more costly, annoying, and time consuming than they’re worth, presenters agreed during a panel discussion at the annual clinical congress of the American College of Surgeons.
Intra-abdominal antibiotic irrigation, chlorhexidine bathing, and even postsurgical antibiotic infusions have not consistently been shown to reduce infections. These measures do, however, ratchet up costs and can contribute to antibiotic resistance.
Some of these and other measures to prevent nosocomial infections may indeed reduce the risk, but the gain is small, said Charles H. Cook, MD.
“Chlorhexidine bathing, for example, is touted by many as a panacea for all the infections we’re talking about,” said Dr. Cook, a critical care surgeon at Beth Israel Deaconess Medical Center, New York. “A recent meta-analysis in critical care units did find a reduced relative risk of 0.44 for central line bloodstream infections. But you needed to bathe 360 patients to prevent one infection. It’s what I call a long run for a short slide.”
Therese Duane, MD, FACS, agreed. A surgeon at the John Peter Smith Hospital, Ft. Worth, Tex., Dr. Duane reviewed three different guidelines for the prevention of surgical site infections: the ACS and Surgical Infection Society, the World Health Organization, and the Centers for Disease Control and Prevention. In looking for similarities between the documents, she said she found several well-accepted practices that just aren’t supported by good data.
Presurgical antimicrobial infusions got a strong thumbs-up from all the groups, but only under a very specific circumstance: The medication has to be administered well in advance of surgery for it to be effective.
“Your goal is to get the appropriate concentration into the tissues by the time of incision,” Dr. Duane said. “It takes time to get there – if you give it after the incision, you have bleeding and cellular death, and the antimicrobials cannot get to that incision and do their job. If I’m starting a case and they haven’t been given, I don’t ever start them after the incision, because then you have all of the risks and none of the benefits. In my opinion, we need to move to no further antimicrobials once the incision or case is over because it serves no purpose and is inconsistent with good antibiotic stewardship.”
Adhesive drapes got a resounding “eh” from the guidelines, Dr. Duane said. “You really do not need them. They’re expensive and they’re not improving outcomes, so don’t waste your time or money. We need to think about minimizing what isn’t helpful and maximizing the things that are worthwhile. That’s the way to practice good socially responsible surgery without breaking the bank,” she said.
Antimicrobial sutures got weak recommendations, Dr. Duane said. The evidence supporting their use was not very strong, although she said she feels triclosan-coated sutures are helpful in all kinds of surgery. Preoperative showering with an antiseptic received strong support, with alcohol-containing preps superior to chlorhexidine, which is better than povidone-iodine–containing solutions.
Deep-space irrigation with aqueous iodophor also received a weak recommendation, but Dr. Duane said the evidence does not support the use of antibiotic-containing irrigation in either the abdomen or the incision. “And the guidelines came out strongly against using antimicrobial agents on the incision,” she said. None of the guidelines issued a recommendation for or against antimicrobial dressings.
Protocolized infection-control bundles are a very great help in reducing the incidence of surgical site infections, Dr. Duane added. “They increase attention to detail and decrease the rates of infection.”
Dr. Cook agreed. “Central line bundles are one of the things that work” for line-associated bloodstream infections, he said. Since their large-scale adoption, mortality from these infections has dropped significantly; it was hovering around 28,000 per year in the mid-2000s, he said. “That’s about how many men die from prostate cancer every year.”
Central line infections are very costly too, he added – around $46,000 per event. “That comes to around $2 billion in direct and indirect costs every year.”
A 2006 study demonstrated the efficacy of central line bundles in the fight against these potentially devastating infections.
The bundled intervention comprised hand washing, using full-barrier precautions during the insertion of central venous catheters, cleaning the skin with chlorhexidine, avoiding the femoral site if possible, and removing unnecessary catheters. The median rate of catheter-related bloodstream infections per 1,000 catheter-days decreased from 2.7 at baseline to 0 at 3 months after implementation of the study intervention.
Antibiotic-coated or impregnated catheters do not work as well. A 2016 Cochrane review of 57 studies determined that the devices didn’t improve sepsis, all-cause mortality, or catheter-related local infections.
The jury may still be out on coated dressings or securing devices, however. Another Cochrane review, of 22 studies, found a 40% decrease in central line–associated bloodstream infections with these items. “There was moderate evidence that tip colonization was reduced, but the authors said more research is needed.”
The evidence looks stronger for alcohol-impregnated port protectors, Dr. Cook said. Two studies in particular support their use. In an oncology unit, the rate of these infections dropped from 2.3 to 0.3 per 1,000 catheter days after the port protectors were instituted.
In the second study, infection rates declined from 1.43 to 0.69 per 1,000 line-days after the protectors came on board.
“The advantage was seen mostly in ICUs, so the recommendations are to use them there,” Dr. Cook said.
Neither Dr. Cook nor Dr. Duane had any relevant financial disclosures.
[email protected]
On Twitter @Alz Gal
SAN DIEGO – Some almost universally accepted measures against hospital-acquired infections are more costly, annoying, and time consuming than they’re worth, presenters agreed during a panel discussion at the annual clinical congress of the American College of Surgeons.
Intra-abdominal antibiotic irrigation, chlorhexidine bathing, and even postsurgical antibiotic infusions have not consistently been shown to reduce infections. These measures do, however, ratchet up costs and can contribute to antibiotic resistance.
Some of these and other measures to prevent nosocomial infections may indeed reduce the risk, but the gain is small, said Charles H. Cook, MD.
“Chlorhexidine bathing, for example, is touted by many as a panacea for all the infections we’re talking about,” said Dr. Cook, a critical care surgeon at Beth Israel Deaconess Medical Center, New York. “A recent meta-analysis in critical care units did find a reduced relative risk of 0.44 for central line bloodstream infections. But you needed to bathe 360 patients to prevent one infection. It’s what I call a long run for a short slide.”
Therese Duane, MD, FACS, agreed. A surgeon at the John Peter Smith Hospital, Ft. Worth, Tex., Dr. Duane reviewed three different guidelines for the prevention of surgical site infections: the ACS and Surgical Infection Society, the World Health Organization, and the Centers for Disease Control and Prevention. In looking for similarities between the documents, she said she found several well-accepted practices that just aren’t supported by good data.
Presurgical antimicrobial infusions got a strong thumbs-up from all the groups, but only under a very specific circumstance: The medication has to be administered well in advance of surgery for it to be effective.
“Your goal is to get the appropriate concentration into the tissues by the time of incision,” Dr. Duane said. “It takes time to get there – if you give it after the incision, you have bleeding and cellular death, and the antimicrobials cannot get to that incision and do their job. If I’m starting a case and they haven’t been given, I don’t ever start them after the incision, because then you have all of the risks and none of the benefits. In my opinion, we need to move to no further antimicrobials once the incision or case is over because it serves no purpose and is inconsistent with good antibiotic stewardship.”
Adhesive drapes got a resounding “eh” from the guidelines, Dr. Duane said. “You really do not need them. They’re expensive and they’re not improving outcomes, so don’t waste your time or money. We need to think about minimizing what isn’t helpful and maximizing the things that are worthwhile. That’s the way to practice good socially responsible surgery without breaking the bank,” she said.
Antimicrobial sutures got weak recommendations, Dr. Duane said. The evidence supporting their use was not very strong, although she said she feels triclosan-coated sutures are helpful in all kinds of surgery. Preoperative showering with an antiseptic received strong support, with alcohol-containing preps superior to chlorhexidine, which is better than povidone-iodine–containing solutions.
Deep-space irrigation with aqueous iodophor also received a weak recommendation, but Dr. Duane said the evidence does not support the use of antibiotic-containing irrigation in either the abdomen or the incision. “And the guidelines came out strongly against using antimicrobial agents on the incision,” she said. None of the guidelines issued a recommendation for or against antimicrobial dressings.
Protocolized infection-control bundles are a very great help in reducing the incidence of surgical site infections, Dr. Duane added. “They increase attention to detail and decrease the rates of infection.”
Dr. Cook agreed. “Central line bundles are one of the things that work” for line-associated bloodstream infections, he said. Since their large-scale adoption, mortality from these infections has dropped significantly; it was hovering around 28,000 per year in the mid-2000s, he said. “That’s about how many men die from prostate cancer every year.”
Central line infections are very costly too, he added – around $46,000 per event. “That comes to around $2 billion in direct and indirect costs every year.”
A 2006 study demonstrated the efficacy of central line bundles in the fight against these potentially devastating infections.
The bundled intervention comprised hand washing, using full-barrier precautions during the insertion of central venous catheters, cleaning the skin with chlorhexidine, avoiding the femoral site if possible, and removing unnecessary catheters. The median rate of catheter-related bloodstream infections per 1,000 catheter-days decreased from 2.7 at baseline to 0 at 3 months after implementation of the study intervention.
Antibiotic-coated or impregnated catheters do not work as well. A 2016 Cochrane review of 57 studies determined that the devices didn’t improve sepsis, all-cause mortality, or catheter-related local infections.
The jury may still be out on coated dressings or securing devices, however. Another Cochrane review, of 22 studies, found a 40% decrease in central line–associated bloodstream infections with these items. “There was moderate evidence that tip colonization was reduced, but the authors said more research is needed.”
The evidence looks stronger for alcohol-impregnated port protectors, Dr. Cook said. Two studies in particular support their use. In an oncology unit, the rate of these infections dropped from 2.3 to 0.3 per 1,000 catheter days after the port protectors were instituted.
In the second study, infection rates declined from 1.43 to 0.69 per 1,000 line-days after the protectors came on board.
“The advantage was seen mostly in ICUs, so the recommendations are to use them there,” Dr. Cook said.
Neither Dr. Cook nor Dr. Duane had any relevant financial disclosures.
[email protected]
On Twitter @Alz Gal
FROM THE ACS CLINICAL CONGRESS
Atrial fibrillation boosts VTE risk
BARCELONA – Atrial fibrillation is at least as strong a risk factor for venous thromboembolism as for ischemic stroke, Bjorn Hornestam, MD, asserted at the annual congress of the European Society of Cardiology.
This novel finding from a Swedish national registry study suggests it’s time for thoughtful consideration of a revision of risk scores in patients with atrial fibrillation (AF), according to Dr. Hornestam, director of cardiology at Sahlgrenska University Hospital in Gothenburg, Sweden.
“VTE risk is not included as an outcome in the CHA2DS2-VASc score, so we underestimate the total thromboembolic risk in AF patients,” he said.
Dr. Hornestam presented a Swedish registry study of 1.36 million patients, including 470,738 patients with new-onset AF and no previous diagnosis of VTE or ischemic stroke and twice as many controls without AF who were matched to the AF patients by age, gender, and county.

The VTE risk was highest during the first 30 days after diagnosis of AF. Women with new-onset AF had an 8.3-fold increased risk of VTE compared with controls during this early period, by a margin of 55.8 versus 6.4 cases per 1,000 person-years. Men with newly diagnosed AF had a 7.2-fold increased risk of VTE in the first 30 days, reflecting a rate of 40.1 per 1,000 person-years compared to 5.6 per 1,000 in controls.
The VTE risk dropped off precipitously in men after the first month. The rate was cut in half by 2 months after AF diagnosis and was no different from that of controls by 9 months.
In women, too, the early elevated VTE risk was halved by 2 months out, but thereafter the rate of decline in VTE risk slowed. Even 10 years after AF diagnosis, women had a 21% greater VTE risk than did matched controls.
Of note, the risk of VTE during the first 12 months after diagnosis of AF was nearly twice as great in both men and women under age 65 than in those older than 75.
These data raise the question of whether standard therapy in AF patients needs to be modified, especially during what now appears to be the critical time frame of the first 3-6 months after diagnosis of the arrhythmia, Dr. Hornestam said.
He reported having no financial conflicts of interest regarding this study.
BARCELONA – Atrial fibrillation is at least as strong a risk factor for venous thromboembolism as for ischemic stroke, Bjorn Hornestam, MD, asserted at the annual congress of the European Society of Cardiology.
This novel finding from a Swedish national registry study suggests it’s time for thoughtful consideration of a revision of risk scores in patients with atrial fibrillation (AF), according to Dr. Hornestam, director of cardiology at Sahlgrenska University Hospital in Gothenburg, Sweden.
“VTE risk is not included as an outcome in the CHA2DS2-VASc score, so we underestimate the total thromboembolic risk in AF patients,” he said.
Dr. Hornestam presented a Swedish registry study of 1.36 million patients, including 470,738 patients with new-onset AF and no previous diagnosis of VTE or ischemic stroke and twice as many controls without AF who were matched to the AF patients by age, gender, and county.
The VTE risk was highest during the first 30 days after diagnosis of AF. Women with new-onset AF had an 8.3-fold increased risk of VTE compared with controls during this early period, by a margin of 55.8 versus 6.4 cases per 1,000 person-years. Men with newly diagnosed AF had a 7.2-fold increased risk of VTE in the first 30 days, reflecting a rate of 40.1 per 1,000 person-years compared to 5.6 per 1,000 in controls.
The VTE risk dropped off precipitously in men after the first month. The rate was cut in half by 2 months after AF diagnosis and was no different from that of controls by 9 months.
In women, too, the early elevated VTE risk was halved by 2 months out, but thereafter the rate of decline in VTE risk slowed. Even 10 years after AF diagnosis, women had a 21% greater VTE risk than did matched controls.
Of note, the risk of VTE during the first 12 months after diagnosis of AF was nearly twice as great in both men and women under age 65 than in those older than 75.
These data raise the question of whether standard therapy in AF patients needs to be modified, especially during what now appears to be the critical time frame of the first 3-6 months after diagnosis of the arrhythmia, Dr. Hornestam said.
He reported having no financial conflicts of interest regarding this study.
BARCELONA – Atrial fibrillation is at least as strong a risk factor for venous thromboembolism as for ischemic stroke, Bjorn Hornestam, MD, asserted at the annual congress of the European Society of Cardiology.
This novel finding from a Swedish national registry study suggests it’s time for thoughtful consideration of a revision of risk scores in patients with atrial fibrillation (AF), according to Dr. Hornestam, director of cardiology at Sahlgrenska University Hospital in Gothenburg, Sweden.
“VTE risk is not included as an outcome in the CHA2DS2-VASc score, so we underestimate the total thromboembolic risk in AF patients,” he said.
Dr. Hornestam presented a Swedish registry study of 1.36 million patients, including 470,738 patients with new-onset AF and no previous diagnosis of VTE or ischemic stroke and twice as many controls without AF who were matched to the AF patients by age, gender, and county.
The VTE risk was highest during the first 30 days after diagnosis of AF. Women with new-onset AF had an 8.3-fold increased risk of VTE compared with controls during this early period, by a margin of 55.8 versus 6.4 cases per 1,000 person-years. Men with newly diagnosed AF had a 7.2-fold increased risk of VTE in the first 30 days, reflecting a rate of 40.1 per 1,000 person-years compared to 5.6 per 1,000 in controls.
The VTE risk dropped off precipitously in men after the first month. The rate was cut in half by 2 months after AF diagnosis and was no different from that of controls by 9 months.
In women, too, the early elevated VTE risk was halved by 2 months out, but thereafter the rate of decline in VTE risk slowed. Even 10 years after AF diagnosis, women had a 21% greater VTE risk than did matched controls.
Of note, the risk of VTE during the first 12 months after diagnosis of AF was nearly twice as great in both men and women under age 65 than in those older than 75.
These data raise the question of whether standard therapy in AF patients needs to be modified, especially during what now appears to be the critical time frame of the first 3-6 months after diagnosis of the arrhythmia, Dr. Hornestam said.
He reported having no financial conflicts of interest regarding this study.
AT THE ESC CONGRESS 2017
Key clinical point:
Major finding: The risk of a first venous thromboembolism is increased 7.2- to 8.3-fold during the first 30 days following diagnosis of AF and remains moderately elevated in women even 10 years later.
Data source: An observational Swedish national registry study of more than 1.3 million patients, including 470,738 with newly diagnosed atrial fibrillation and their matched controls.
Disclosures: The presenter reported having no financial conflicts of interest regarding this study, which was conducted free of commercial support.
Caprini score is not a good predictor of PE in patients with DVT
The Caprini score, commonly used to risk stratify patients for the development of venous thromboembolism and to determine the optimal dose of prophylaxis, failed to predict the development of pulmonary embolism and hemodynamically significant PE in patients presenting with deep vein thrombosis (DVT), according to the results of a large, retrospective single-center study.
Recent surgery was not associated with the development of hemodynamically significant PE, but the presence of proximal DVT was, according to a report published online in the Journal of Vascular Surgery: Venous and Lymphatic Disorders (2017. doi: 10.1016/j.jvsv.2017.08.015).

Their results showed that patients who had undergone recent surgery were less likely to develop hemodynamically significant PE (13.3% vs. 27.2%; P = .01). In contrast, patients with proximal DVT were at higher risk for development of hemodynamically significant PE (80.7% vs. 64.2%; P = .007). They found no association between Caprini score and PE severity (P = .17) or the Caprini score and proximal DVT (P = .89).
“This study shows that the Caprini score does not correlate with the occurrence of PE or the severity of PE. On the other hand, a proximal location of DVT seems to have a high association with hemodynamically significant PE. Such patients may benefit from more aggressive anticoagulant therapy and work-up for PE,” the researchers concluded.
The authors reported that they had no conflicts of interest.
The Caprini score, commonly used to risk stratify patients for the development of venous thromboembolism and to determine the optimal dose of prophylaxis, failed to predict the development of pulmonary embolism and hemodynamically significant PE in patients presenting with deep vein thrombosis (DVT), according to the results of a large, retrospective single-center study.
Recent surgery was not associated with the development of hemodynamically significant PE, but the presence of proximal DVT was, according to a report published online in the Journal of Vascular Surgery: Venous and Lymphatic Disorders (2017. doi: 10.1016/j.jvsv.2017.08.015).
Their results showed that patients who had undergone recent surgery were less likely to develop hemodynamically significant PE (13.3% vs. 27.2%; P = .01). In contrast, patients with proximal DVT were at higher risk for development of hemodynamically significant PE (80.7% vs. 64.2%; P = .007). They found no association between Caprini score and PE severity (P = .17) or the Caprini score and proximal DVT (P = .89).
“This study shows that the Caprini score does not correlate with the occurrence of PE or the severity of PE. On the other hand, a proximal location of DVT seems to have a high association with hemodynamically significant PE. Such patients may benefit from more aggressive anticoagulant therapy and work-up for PE,” the researchers concluded.
The authors reported that they had no conflicts of interest.
The Caprini score, commonly used to risk stratify patients for the development of venous thromboembolism and to determine the optimal dose of prophylaxis, failed to predict the development of pulmonary embolism and hemodynamically significant PE in patients presenting with deep vein thrombosis (DVT), according to the results of a large, retrospective single-center study.
Recent surgery was not associated with the development of hemodynamically significant PE, but the presence of proximal DVT was, according to a report published online in the Journal of Vascular Surgery: Venous and Lymphatic Disorders (2017. doi: 10.1016/j.jvsv.2017.08.015).
Their results showed that patients who had undergone recent surgery were less likely to develop hemodynamically significant PE (13.3% vs. 27.2%; P = .01). In contrast, patients with proximal DVT were at higher risk for development of hemodynamically significant PE (80.7% vs. 64.2%; P = .007). They found no association between Caprini score and PE severity (P = .17) or the Caprini score and proximal DVT (P = .89).
“This study shows that the Caprini score does not correlate with the occurrence of PE or the severity of PE. On the other hand, a proximal location of DVT seems to have a high association with hemodynamically significant PE. Such patients may benefit from more aggressive anticoagulant therapy and work-up for PE,” the researchers concluded.
The authors reported that they had no conflicts of interest.
FROM THE JOURNAL OF VASCULAR SURGERY: VENOUS AND LYMPHATIC DISORDERS
Key clinical point:
Major finding: Among 838 patients presenting with DVT, nearly 26% had concomitant PE, more than half of which was hemodynamically significant.
Data source: A single-center, retrospective review of 838 patients diagnosed with DVT.
Disclosures: The authors reported that they had no conflicts of interest.
VIDEO: How to manage surgical pain in opioid addiction treatment
NEW ORLEANS – How do you manage surgical pain when someone is in treatment for opioid addiction? And how do you manage chronic pain?
It is possible to give patients opioids for post-op pain without increasing the risk of relapse, according to Margaret Chaplin, MD, a staff psychiatrist at Community Mental Health Affiliates in New Britain, Conn.
Dr. Chaplin generally uses buprenorphine and naloxone (Suboxone) for opioid use disorder, and she likes to keep her patients on it for surgery. That often means, however, talking with skeptical surgeons and anesthesiologists beforehand, and reminding them that buprenorphine itself has analgesic effects. Meanwhile, when her patients have chronic pain, sometimes they need help understanding that aspirin and acetaminophen help, even if they don’t give patients a warm, fuzzy feeling.
Dr. Chaplin shared those tips and more about pain management in opioid addiction in an interview at the American Psychiatric Association’s Institute on Psychiatric Services.
NEW ORLEANS – How do you manage surgical pain when someone is in treatment for opioid addiction? And how do you manage chronic pain?
It is possible to give patients opioids for post-op pain without increasing the risk of relapse, according to Margaret Chaplin, MD, a staff psychiatrist at Community Mental Health Affiliates in New Britain, Conn.
Dr. Chaplin generally uses buprenorphine and naloxone (Suboxone) for opioid use disorder, and she likes to keep her patients on it for surgery. That often means, however, talking with skeptical surgeons and anesthesiologists beforehand, and reminding them that buprenorphine itself has analgesic effects. Meanwhile, when her patients have chronic pain, sometimes they need help understanding that aspirin and acetaminophen help, even if they don’t give patients a warm, fuzzy feeling.
Dr. Chaplin shared those tips and more about pain management in opioid addiction in an interview at the American Psychiatric Association’s Institute on Psychiatric Services.
NEW ORLEANS – How do you manage surgical pain when someone is in treatment for opioid addiction? And how do you manage chronic pain?
It is possible to give patients opioids for post-op pain without increasing the risk of relapse, according to Margaret Chaplin, MD, a staff psychiatrist at Community Mental Health Affiliates in New Britain, Conn.
Dr. Chaplin generally uses buprenorphine and naloxone (Suboxone) for opioid use disorder, and she likes to keep her patients on it for surgery. That often means, however, talking with skeptical surgeons and anesthesiologists beforehand, and reminding them that buprenorphine itself has analgesic effects. Meanwhile, when her patients have chronic pain, sometimes they need help understanding that aspirin and acetaminophen help, even if they don’t give patients a warm, fuzzy feeling.
Dr. Chaplin shared those tips and more about pain management in opioid addiction in an interview at the American Psychiatric Association’s Institute on Psychiatric Services.
AT IPS 2017

Naloxone: Difficult conversations about a potential lifesaver
New tools to help minimize the risk of opioid-related adverse events are becoming more widely available, although providers are still struggling over how best to implement them.
A recent study by Shane Mueller, MSW, and Ingrid Binswanger, MD, at Kaiser Permanente Colorado Institute for Health Research, Denver, for instance, found that doctors are frequently uncomfortable prescribing the opioid antagonist naloxone to counteract a potential overdose.1

Although much of the research was conducted in outpatient settings, the researchers say several lessons may be translated to the hospital readily. “Patients were really willing to embrace the idea of naloxone when it was framed to be used in a worst-case scenario,” Mr. Mueller said; some providers, for example, compared it to having a fire extinguisher in the house. “I think one patient said, ‘You know, I don’t plan on starting a fire in my kitchen, but it’s good to have there just in case something goes wrong.’ ”
Another important lesson, Mr. Mueller said, is to consider multiple factors that might heighten the overdose risk, such as a change in the prescription or a medical condition like renal failure. Including those considerations in a conversation might help destigmatize the topic and help patients who are concerned that they might be perceived as misusing the medication.

Ideally, opioid-safety interventions should be more patient centered, emphasizing safer home storage to prevent secondary exposures and educating patients fully about the medication’s downsides, she said. “They may have been on them a long time but never been fully informed of the risks,” she said. Among her group’s future research goals, Dr. Binswanger hopes to investigate how best to communicate such risks to patients.
References
1. Mueller SR, Koester S, Glanz JM, et al. Attitudes toward naloxone prescribing in clinical settings: A qualitative study of patients prescribed high dose opioids for chronic non-cancer pain. J Gen Intern Med. 2017 March;32(3):277-83.
New tools to help minimize the risk of opioid-related adverse events are becoming more widely available, although providers are still struggling over how best to implement them.
A recent study by Shane Mueller, MSW, and Ingrid Binswanger, MD, at Kaiser Permanente Colorado Institute for Health Research, Denver, for instance, found that doctors are frequently uncomfortable prescribing the opioid antagonist naloxone to counteract a potential overdose.1
Although much of the research was conducted in outpatient settings, the researchers say several lessons may be translated to the hospital readily. “Patients were really willing to embrace the idea of naloxone when it was framed to be used in a worst-case scenario,” Mr. Mueller said; some providers, for example, compared it to having a fire extinguisher in the house. “I think one patient said, ‘You know, I don’t plan on starting a fire in my kitchen, but it’s good to have there just in case something goes wrong.’ ”
Another important lesson, Mr. Mueller said, is to consider multiple factors that might heighten the overdose risk, such as a change in the prescription or a medical condition like renal failure. Including those considerations in a conversation might help destigmatize the topic and help patients who are concerned that they might be perceived as misusing the medication.
Ideally, opioid-safety interventions should be more patient centered, emphasizing safer home storage to prevent secondary exposures and educating patients fully about the medication’s downsides, she said. “They may have been on them a long time but never been fully informed of the risks,” she said. Among her group’s future research goals, Dr. Binswanger hopes to investigate how best to communicate such risks to patients.
References
1. Mueller SR, Koester S, Glanz JM, et al. Attitudes toward naloxone prescribing in clinical settings: A qualitative study of patients prescribed high dose opioids for chronic non-cancer pain. J Gen Intern Med. 2017 March;32(3):277-83.
New tools to help minimize the risk of opioid-related adverse events are becoming more widely available, although providers are still struggling over how best to implement them.
A recent study by Shane Mueller, MSW, and Ingrid Binswanger, MD, at Kaiser Permanente Colorado Institute for Health Research, Denver, for instance, found that doctors are frequently uncomfortable prescribing the opioid antagonist naloxone to counteract a potential overdose.1
Although much of the research was conducted in outpatient settings, the researchers say several lessons may be translated to the hospital readily. “Patients were really willing to embrace the idea of naloxone when it was framed to be used in a worst-case scenario,” Mr. Mueller said; some providers, for example, compared it to having a fire extinguisher in the house. “I think one patient said, ‘You know, I don’t plan on starting a fire in my kitchen, but it’s good to have there just in case something goes wrong.’ ”
Another important lesson, Mr. Mueller said, is to consider multiple factors that might heighten the overdose risk, such as a change in the prescription or a medical condition like renal failure. Including those considerations in a conversation might help destigmatize the topic and help patients who are concerned that they might be perceived as misusing the medication.
Ideally, opioid-safety interventions should be more patient centered, emphasizing safer home storage to prevent secondary exposures and educating patients fully about the medication’s downsides, she said. “They may have been on them a long time but never been fully informed of the risks,” she said. Among her group’s future research goals, Dr. Binswanger hopes to investigate how best to communicate such risks to patients.
References
1. Mueller SR, Koester S, Glanz JM, et al. Attitudes toward naloxone prescribing in clinical settings: A qualitative study of patients prescribed high dose opioids for chronic non-cancer pain. J Gen Intern Med. 2017 March;32(3):277-83.
Carvedilol fails to reduce variceal bleeds in acute-on-chronic liver failure
WASHINGTON – Treatment with carvedilol reduced the incidence of sepsis and acute kidney injury and improved survival at 28 days but did not significantly reduce the progression of esophageal varices in patients with acute-on-chronic liver failure.
A total of 136 patients with acute-on-chronic liver failure with small or no esophageal varices and a hepatic venous pressure gradient (HVPG) of 12 mm Hg or greater were enrolled in a single center, prospective, open-label, randomized controlled trial: 66 were randomized to carvedilol and 70 to placebo, according to Sumeet Kainth, MD, of the Institute of Liver and Biliary Sciences in New Delhi.

More than 90% of patients were men with a mean age of 44 years, and composition of the treatment and placebo groups was similar. About 70% in each group had alcoholic hepatitis (the reason for acute liver failure in most). Mean Model for End-Stage Liver Disease (MELD) scores were about 25. Hemodynamic parameters also were comparable, with a mean HVPG of about 19, Dr. Kainth said at the annual meeting of the American Association for the Study of Liver Diseases.
Patients in the treatment group received a median maximum tolerated dose of carvedilol of 12.5 mg, with a range of 3.13 mg to 25 mg.
Morbidity and mortality were high, as is expected with acute-on-chronic liver failure, he noted. A total of 36 patients died before the end of the 90-day study period. Another 23 experienced adverse events and 2 progressed to liver transplant.
HVPG at 90 days decreased significantly in both groups. In the carvedilol group, 90-day HVPG was 16 mm Hg, compared with 19.7 mm Hg at baseline (P less than .01). For placebo patients, 90-day HVPG spontaneously improved to 14.8 mm Hg, compared with a baseline of 17.2 mm Hg (P less than .01).
Carvedilol did not significantly slow the development or growth of varices, however, Dr. Kainth said. At 90 days, varices had progressed in 9 of 40 patients (22.5%) of patients on carvedilol and 8 of 31 (25.8%) of placebo patients.
Significantly fewer patients in the carvedilol group developed acute kidney injury at 28 days (14% vs. 38% on placebo) and sepsis (5% vs. 20%). Mortality also was reduced significantly at 28 days (11% vs. 24%), he reported.
Treatment with carvedilol did not achieve significant reductions in variceal bleeding, “possibly due to the low number of bleeds seen in the study [because of] the exclusion of patients with large varices,” Dr. Kainth said.
The study was sponsored by Institute of Liver and Biliary Sciences. Dr. Kainth reported no relevant conflicts of interest.
[email protected]
On Twitter @denisefulton
WASHINGTON – Treatment with carvedilol reduced the incidence of sepsis and acute kidney injury and improved survival at 28 days but did not significantly reduce the progression of esophageal varices in patients with acute-on-chronic liver failure.
A total of 136 patients with acute-on-chronic liver failure with small or no esophageal varices and a hepatic venous pressure gradient (HVPG) of 12 mm Hg or greater were enrolled in a single center, prospective, open-label, randomized controlled trial: 66 were randomized to carvedilol and 70 to placebo, according to Sumeet Kainth, MD, of the Institute of Liver and Biliary Sciences in New Delhi.
More than 90% of patients were men with a mean age of 44 years, and composition of the treatment and placebo groups was similar. About 70% in each group had alcoholic hepatitis (the reason for acute liver failure in most). Mean Model for End-Stage Liver Disease (MELD) scores were about 25. Hemodynamic parameters also were comparable, with a mean HVPG of about 19, Dr. Kainth said at the annual meeting of the American Association for the Study of Liver Diseases.
Patients in the treatment group received a median maximum tolerated dose of carvedilol of 12.5 mg, with a range of 3.13 mg to 25 mg.
Morbidity and mortality were high, as is expected with acute-on-chronic liver failure, he noted. A total of 36 patients died before the end of the 90-day study period. Another 23 experienced adverse events and 2 progressed to liver transplant.
HVPG at 90 days decreased significantly in both groups. In the carvedilol group, 90-day HVPG was 16 mm Hg, compared with 19.7 mm Hg at baseline (P less than .01). For placebo patients, 90-day HVPG spontaneously improved to 14.8 mm Hg, compared with a baseline of 17.2 mm Hg (P less than .01).
Carvedilol did not significantly slow the development or growth of varices, however, Dr. Kainth said. At 90 days, varices had progressed in 9 of 40 patients (22.5%) of patients on carvedilol and 8 of 31 (25.8%) of placebo patients.
Significantly fewer patients in the carvedilol group developed acute kidney injury at 28 days (14% vs. 38% on placebo) and sepsis (5% vs. 20%). Mortality also was reduced significantly at 28 days (11% vs. 24%), he reported.
Treatment with carvedilol did not achieve significant reductions in variceal bleeding, “possibly due to the low number of bleeds seen in the study [because of] the exclusion of patients with large varices,” Dr. Kainth said.
The study was sponsored by Institute of Liver and Biliary Sciences. Dr. Kainth reported no relevant conflicts of interest.
[email protected]
On Twitter @denisefulton
WASHINGTON – Treatment with carvedilol reduced the incidence of sepsis and acute kidney injury and improved survival at 28 days but did not significantly reduce the progression of esophageal varices in patients with acute-on-chronic liver failure.
A total of 136 patients with acute-on-chronic liver failure with small or no esophageal varices and a hepatic venous pressure gradient (HVPG) of 12 mm Hg or greater were enrolled in a single center, prospective, open-label, randomized controlled trial: 66 were randomized to carvedilol and 70 to placebo, according to Sumeet Kainth, MD, of the Institute of Liver and Biliary Sciences in New Delhi.
More than 90% of patients were men with a mean age of 44 years, and composition of the treatment and placebo groups was similar. About 70% in each group had alcoholic hepatitis (the reason for acute liver failure in most). Mean Model for End-Stage Liver Disease (MELD) scores were about 25. Hemodynamic parameters also were comparable, with a mean HVPG of about 19, Dr. Kainth said at the annual meeting of the American Association for the Study of Liver Diseases.
Patients in the treatment group received a median maximum tolerated dose of carvedilol of 12.5 mg, with a range of 3.13 mg to 25 mg.
Morbidity and mortality were high, as is expected with acute-on-chronic liver failure, he noted. A total of 36 patients died before the end of the 90-day study period. Another 23 experienced adverse events and 2 progressed to liver transplant.
HVPG at 90 days decreased significantly in both groups. In the carvedilol group, 90-day HVPG was 16 mm Hg, compared with 19.7 mm Hg at baseline (P less than .01). For placebo patients, 90-day HVPG spontaneously improved to 14.8 mm Hg, compared with a baseline of 17.2 mm Hg (P less than .01).
Carvedilol did not significantly slow the development or growth of varices, however, Dr. Kainth said. At 90 days, varices had progressed in 9 of 40 patients (22.5%) of patients on carvedilol and 8 of 31 (25.8%) of placebo patients.
Significantly fewer patients in the carvedilol group developed acute kidney injury at 28 days (14% vs. 38% on placebo) and sepsis (5% vs. 20%). Mortality also was reduced significantly at 28 days (11% vs. 24%), he reported.
Treatment with carvedilol did not achieve significant reductions in variceal bleeding, “possibly due to the low number of bleeds seen in the study [because of] the exclusion of patients with large varices,” Dr. Kainth said.
The study was sponsored by Institute of Liver and Biliary Sciences. Dr. Kainth reported no relevant conflicts of interest.
[email protected]
On Twitter @denisefulton
AT THE LIVER MEETING 2017
Key clinical point:
Major finding: At 90 days, varices had progressed in 9 of 40 (22.5%) patients on carvedilol vs. 8 of 31 (25.8%) of placebo patients.
Data source: A single-center, prospective, open-label, randomized controlled trial of 136 patients with acute-on-chronic liver failure.
Disclosures: The study was sponsored by the Institute of Liver and Biliary Sciences. Dr. Kainth reported no relevant conflicts of interest.
The opioid epidemic and its impact on the health care system
The United States is in the midst of a public health crisis. Every day, 91 Americans die from opioid overdoses.1 Opioid addiction has a tremendous negative effect on parents and children by destroying lives and breaking up families. When used appropriately, these drugs, such as morphine, hydrocodone, oxycodone, and fentanyl, provide much needed pain relief to patients, especially after a surgical procedure or during treatment for cancer. Unfortunately, opioids also have qualities that make them addictive and prone to overuse and abuse.
Heroin and other opioid drugs are affecting social, health, and economic welfare in communities throughout the United States. Opioid addiction does not discriminate among occupations, socioeconomic statuses, or ethnicities. Once addicted, users find it difficult to fight and overcome the habit. In this context, hospitalists who develop and use opioid policies and tactics are better equipped to deal with the increasing prevalence of opioid addiction and overdoses seen in the medical center environment.

Overview of opioid addiction
Opioids are more prevalent and easily available today in part because of the intense marketing campaigns by pharmaceutical companies. In fact, according to the 2014 National Survey on Drug Use and Health, almost 2 million Americans were dependent on or abused prescription opioids.2 Opioids create artificial endorphins in the brain, amplifying positive feelings and euphoria. Once they become dependent, patients feel sick and become depressed when they aren’t using narcotics. They experience uncontrollable cravings, relieved only by increasing opioid use. Personal relationships and finances are severely affected because patients will do whatever they can to acquire more opioids. Some resort to doctor shopping to obtain more opioids, while others will engage in drug trafficking to purchase and sell narcotics. Most new heroin users report that they started with nonmedical use of opioid pain relievers.3
Unfortunately, in 2015, there were more than 20,000 prescription opioid overdose deaths and almost 13,000 overdose deaths related to heroin.4 In addition to addiction and death, overuse of narcotics can cause many medical issues, including dizziness, constipation, depression, and immune dysfunction.
As with any addiction, there are many problems related to opiate withdrawal. Some of these include anxiety, rhinorrhea, lacrimation, piloerection, mydriasis, nausea, vomiting, abdominal pain, diarrhea, tachycardia, and hypertension. Methadone, buprenorphine, and extended-release naltrexone typically are used to help alleviate cravings and the symptoms of withdrawal. With more than 1,000 patients treated daily by emergency departments for misuse of prescription opioids, it’s imperative for the medical community to address this health care crisis.5
Impact on first responders and hospitalists
The impact of this epidemic on the medical community is dramatic. Emergency system resources, already on overload, are further taxed and drained by the increased 911 calls for overdose incidents. This means that instead of responding to heart attacks, strokes, or other emergencies, first responders are spending time stabilizing overdose patients and taking them to hospitals. This resource drain spreads to emergency rooms and hospitals as they treat these patients. Eventually, the epidemic results in higher insurance costs to cover the impact on medical resources.
Strategies for hospitalists
A multifaceted approach is required to combat this crisis, and hospitalists are one component of that solution. Here are strategies hospitalists can employ to combat the growing use and abuse of narcotics:
- Screen for high-risk conditions. Before prescribing opioids, screen patients for conditions that may be exacerbated by opioid use, including sleep apnea, obesity COPD, and heart failure, as well as whether they are using medications that cause sedation and respiratory depression.
- Develop and follow pain management clinical pathway protocols. For example, start with nonopioid analgesics, such as acetaminophen, ibuprofen, and naproxen, for patients with mild pain. If the patient is in moderate pain, or if the mild pain was unrelieved by the first type of medicine, continue with opioid analgesics including codeine, oxycodone, hydrocodone, or morphine. Finally, if the patient is experiencing severe pain, or if the mild to moderate pain was unrelieved by previous medications, prescribe higher doses of morphine, fentanyl, or hydromorphone or use a patient-controlled analgesia delivery of an intravenous opioid.
- Discuss other treatment options. Instead of prescribing narcotics, assess whether other treatment options are viable. These include physical and occupational therapy, steroid shots, massage, local nerve blocks, and muscle relaxers.
- Evaluate the reason(s) for current use of prescribed narcotics. It’s crucial to determine why patients are using opioids. The medical condition for which they were prescribed these medications may have resolved. If patients are using opioids without a medically indicated reason, offer alternative medications, such as methadone or naltrexone, and provide education to help them slowly taper off the drugs. Do not cease opioid use altogether unless the use is contraindicated because of other medical conditions or unstable vital signs (for example, low blood pressure).
- Train nurses on opioid use and addiction. Educate nurses about opioid addiction risk factors and symptoms of addiction. Instruct them on managing the Ramsay Sedation Scale and using an opioid sedation scale with patients receiving IV narcotics.
- Educate families on opioid use and addiction. Counsel patients and their families on the long-term effects of opioid use and about the warning signs of addiction. Teach them about alternatives to narcotics.
- Offer referrals to specialized clinics. Work with social workers, case managers, and local mental health professionals to refer patients to behavioral counseling, patient and family support groups, and monitored detoxification clinics qualified to treat opioid addiction.
Socioeconomic impact
The effects of the opioid epidemic are felt in all areas of the United States, especially in the health care industry. Emergency department visits are mounting while billions of dollars are spent on medical care for those addicted to opioids. Additionally, the socioeconomic effects of this crisis contribute to increasing depression, anxiety, missed days of work or school, unemployment, drop-out rates, and loss of productivity among those addicted to opioids. Also, the epidemic is adversely affecting families, leading to increased divorce rates, single parent families, and child abuse and neglect. By creating strategies and protocols for medical staff, patients, and families affected by opioid use, addiction, or overdose, hospitalists can have a positive influence on patients’ lives and ultimately the opioid epidemic.
Dr. Kasarla is a hospitalist with Apogee Physicians at Parkway Surgical & Cardiovascular Hospital in Fort Worth, Tex. He also works for Texas Health Physicians Group at Texas Health Harris Methodist Hospital and Texas Health Harris Methodist Hospital Southwest in Fort Worth, as well as at Texas Health Harris Methodist Hospital in Azle, Tex.
You can contact him at [email protected] or [email protected].
References
1. Understanding the Epidemic: Drug overdose deaths in the United States continue to increase in 2015. Accessed Sept. 11, 2017.
2. Behavioral health trends in the United States: Results from the 2014 national survey on drug use and health. Accessed Sept. 11, 2017.
3. Jones CM. Heroin use and heroin use risk behaviors among nonmedical users of prescription opioid pain relievers – United States, 2002-2004 and 2008-2010. Drug Alcohol Depend. 2013;132(1-2):95-100.
4. Rudd RA et al. Increases in drug and opioid-involved overdose deaths – United States, 2010-2015. MMWR Morb Mortal Wkly Rep. 2016;65(50-51):1445-52.
5. Highlights of the 2011 Drug Abuse Warning Network (DAWN) findings on drug-related emergency department visits. Accessed Sept. 11, 2017.
The United States is in the midst of a public health crisis. Every day, 91 Americans die from opioid overdoses.1 Opioid addiction has a tremendous negative effect on parents and children by destroying lives and breaking up families. When used appropriately, these drugs, such as morphine, hydrocodone, oxycodone, and fentanyl, provide much needed pain relief to patients, especially after a surgical procedure or during treatment for cancer. Unfortunately, opioids also have qualities that make them addictive and prone to overuse and abuse.
Heroin and other opioid drugs are affecting social, health, and economic welfare in communities throughout the United States. Opioid addiction does not discriminate among occupations, socioeconomic statuses, or ethnicities. Once addicted, users find it difficult to fight and overcome the habit. In this context, hospitalists who develop and use opioid policies and tactics are better equipped to deal with the increasing prevalence of opioid addiction and overdoses seen in the medical center environment.
Overview of opioid addiction
Opioids are more prevalent and easily available today in part because of the intense marketing campaigns by pharmaceutical companies. In fact, according to the 2014 National Survey on Drug Use and Health, almost 2 million Americans were dependent on or abused prescription opioids.2 Opioids create artificial endorphins in the brain, amplifying positive feelings and euphoria. Once they become dependent, patients feel sick and become depressed when they aren’t using narcotics. They experience uncontrollable cravings, relieved only by increasing opioid use. Personal relationships and finances are severely affected because patients will do whatever they can to acquire more opioids. Some resort to doctor shopping to obtain more opioids, while others will engage in drug trafficking to purchase and sell narcotics. Most new heroin users report that they started with nonmedical use of opioid pain relievers.3
Unfortunately, in 2015, there were more than 20,000 prescription opioid overdose deaths and almost 13,000 overdose deaths related to heroin.4 In addition to addiction and death, overuse of narcotics can cause many medical issues, including dizziness, constipation, depression, and immune dysfunction.
As with any addiction, there are many problems related to opiate withdrawal. Some of these include anxiety, rhinorrhea, lacrimation, piloerection, mydriasis, nausea, vomiting, abdominal pain, diarrhea, tachycardia, and hypertension. Methadone, buprenorphine, and extended-release naltrexone typically are used to help alleviate cravings and the symptoms of withdrawal. With more than 1,000 patients treated daily by emergency departments for misuse of prescription opioids, it’s imperative for the medical community to address this health care crisis.5
Impact on first responders and hospitalists
The impact of this epidemic on the medical community is dramatic. Emergency system resources, already on overload, are further taxed and drained by the increased 911 calls for overdose incidents. This means that instead of responding to heart attacks, strokes, or other emergencies, first responders are spending time stabilizing overdose patients and taking them to hospitals. This resource drain spreads to emergency rooms and hospitals as they treat these patients. Eventually, the epidemic results in higher insurance costs to cover the impact on medical resources.
Strategies for hospitalists
A multifaceted approach is required to combat this crisis, and hospitalists are one component of that solution. Here are strategies hospitalists can employ to combat the growing use and abuse of narcotics:
- Screen for high-risk conditions. Before prescribing opioids, screen patients for conditions that may be exacerbated by opioid use, including sleep apnea, obesity COPD, and heart failure, as well as whether they are using medications that cause sedation and respiratory depression.
- Develop and follow pain management clinical pathway protocols. For example, start with nonopioid analgesics, such as acetaminophen, ibuprofen, and naproxen, for patients with mild pain. If the patient is in moderate pain, or if the mild pain was unrelieved by the first type of medicine, continue with opioid analgesics including codeine, oxycodone, hydrocodone, or morphine. Finally, if the patient is experiencing severe pain, or if the mild to moderate pain was unrelieved by previous medications, prescribe higher doses of morphine, fentanyl, or hydromorphone or use a patient-controlled analgesia delivery of an intravenous opioid.
- Discuss other treatment options. Instead of prescribing narcotics, assess whether other treatment options are viable. These include physical and occupational therapy, steroid shots, massage, local nerve blocks, and muscle relaxers.
- Evaluate the reason(s) for current use of prescribed narcotics. It’s crucial to determine why patients are using opioids. The medical condition for which they were prescribed these medications may have resolved. If patients are using opioids without a medically indicated reason, offer alternative medications, such as methadone or naltrexone, and provide education to help them slowly taper off the drugs. Do not cease opioid use altogether unless the use is contraindicated because of other medical conditions or unstable vital signs (for example, low blood pressure).
- Train nurses on opioid use and addiction. Educate nurses about opioid addiction risk factors and symptoms of addiction. Instruct them on managing the Ramsay Sedation Scale and using an opioid sedation scale with patients receiving IV narcotics.
- Educate families on opioid use and addiction. Counsel patients and their families on the long-term effects of opioid use and about the warning signs of addiction. Teach them about alternatives to narcotics.
- Offer referrals to specialized clinics. Work with social workers, case managers, and local mental health professionals to refer patients to behavioral counseling, patient and family support groups, and monitored detoxification clinics qualified to treat opioid addiction.
Socioeconomic impact
The effects of the opioid epidemic are felt in all areas of the United States, especially in the health care industry. Emergency department visits are mounting while billions of dollars are spent on medical care for those addicted to opioids. Additionally, the socioeconomic effects of this crisis contribute to increasing depression, anxiety, missed days of work or school, unemployment, drop-out rates, and loss of productivity among those addicted to opioids. Also, the epidemic is adversely affecting families, leading to increased divorce rates, single parent families, and child abuse and neglect. By creating strategies and protocols for medical staff, patients, and families affected by opioid use, addiction, or overdose, hospitalists can have a positive influence on patients’ lives and ultimately the opioid epidemic.
Dr. Kasarla is a hospitalist with Apogee Physicians at Parkway Surgical & Cardiovascular Hospital in Fort Worth, Tex. He also works for Texas Health Physicians Group at Texas Health Harris Methodist Hospital and Texas Health Harris Methodist Hospital Southwest in Fort Worth, as well as at Texas Health Harris Methodist Hospital in Azle, Tex.
You can contact him at [email protected] or [email protected].
References
1. Understanding the Epidemic: Drug overdose deaths in the United States continue to increase in 2015. Accessed Sept. 11, 2017.
2. Behavioral health trends in the United States: Results from the 2014 national survey on drug use and health. Accessed Sept. 11, 2017.
3. Jones CM. Heroin use and heroin use risk behaviors among nonmedical users of prescription opioid pain relievers – United States, 2002-2004 and 2008-2010. Drug Alcohol Depend. 2013;132(1-2):95-100.
4. Rudd RA et al. Increases in drug and opioid-involved overdose deaths – United States, 2010-2015. MMWR Morb Mortal Wkly Rep. 2016;65(50-51):1445-52.
5. Highlights of the 2011 Drug Abuse Warning Network (DAWN) findings on drug-related emergency department visits. Accessed Sept. 11, 2017.
The United States is in the midst of a public health crisis. Every day, 91 Americans die from opioid overdoses.1 Opioid addiction has a tremendous negative effect on parents and children by destroying lives and breaking up families. When used appropriately, these drugs, such as morphine, hydrocodone, oxycodone, and fentanyl, provide much needed pain relief to patients, especially after a surgical procedure or during treatment for cancer. Unfortunately, opioids also have qualities that make them addictive and prone to overuse and abuse.
Heroin and other opioid drugs are affecting social, health, and economic welfare in communities throughout the United States. Opioid addiction does not discriminate among occupations, socioeconomic statuses, or ethnicities. Once addicted, users find it difficult to fight and overcome the habit. In this context, hospitalists who develop and use opioid policies and tactics are better equipped to deal with the increasing prevalence of opioid addiction and overdoses seen in the medical center environment.
Overview of opioid addiction
Opioids are more prevalent and easily available today in part because of the intense marketing campaigns by pharmaceutical companies. In fact, according to the 2014 National Survey on Drug Use and Health, almost 2 million Americans were dependent on or abused prescription opioids.2 Opioids create artificial endorphins in the brain, amplifying positive feelings and euphoria. Once they become dependent, patients feel sick and become depressed when they aren’t using narcotics. They experience uncontrollable cravings, relieved only by increasing opioid use. Personal relationships and finances are severely affected because patients will do whatever they can to acquire more opioids. Some resort to doctor shopping to obtain more opioids, while others will engage in drug trafficking to purchase and sell narcotics. Most new heroin users report that they started with nonmedical use of opioid pain relievers.3
Unfortunately, in 2015, there were more than 20,000 prescription opioid overdose deaths and almost 13,000 overdose deaths related to heroin.4 In addition to addiction and death, overuse of narcotics can cause many medical issues, including dizziness, constipation, depression, and immune dysfunction.
As with any addiction, there are many problems related to opiate withdrawal. Some of these include anxiety, rhinorrhea, lacrimation, piloerection, mydriasis, nausea, vomiting, abdominal pain, diarrhea, tachycardia, and hypertension. Methadone, buprenorphine, and extended-release naltrexone typically are used to help alleviate cravings and the symptoms of withdrawal. With more than 1,000 patients treated daily by emergency departments for misuse of prescription opioids, it’s imperative for the medical community to address this health care crisis.5
Impact on first responders and hospitalists
The impact of this epidemic on the medical community is dramatic. Emergency system resources, already on overload, are further taxed and drained by the increased 911 calls for overdose incidents. This means that instead of responding to heart attacks, strokes, or other emergencies, first responders are spending time stabilizing overdose patients and taking them to hospitals. This resource drain spreads to emergency rooms and hospitals as they treat these patients. Eventually, the epidemic results in higher insurance costs to cover the impact on medical resources.
Strategies for hospitalists
A multifaceted approach is required to combat this crisis, and hospitalists are one component of that solution. Here are strategies hospitalists can employ to combat the growing use and abuse of narcotics:
- Screen for high-risk conditions. Before prescribing opioids, screen patients for conditions that may be exacerbated by opioid use, including sleep apnea, obesity COPD, and heart failure, as well as whether they are using medications that cause sedation and respiratory depression.
- Develop and follow pain management clinical pathway protocols. For example, start with nonopioid analgesics, such as acetaminophen, ibuprofen, and naproxen, for patients with mild pain. If the patient is in moderate pain, or if the mild pain was unrelieved by the first type of medicine, continue with opioid analgesics including codeine, oxycodone, hydrocodone, or morphine. Finally, if the patient is experiencing severe pain, or if the mild to moderate pain was unrelieved by previous medications, prescribe higher doses of morphine, fentanyl, or hydromorphone or use a patient-controlled analgesia delivery of an intravenous opioid.
- Discuss other treatment options. Instead of prescribing narcotics, assess whether other treatment options are viable. These include physical and occupational therapy, steroid shots, massage, local nerve blocks, and muscle relaxers.
- Evaluate the reason(s) for current use of prescribed narcotics. It’s crucial to determine why patients are using opioids. The medical condition for which they were prescribed these medications may have resolved. If patients are using opioids without a medically indicated reason, offer alternative medications, such as methadone or naltrexone, and provide education to help them slowly taper off the drugs. Do not cease opioid use altogether unless the use is contraindicated because of other medical conditions or unstable vital signs (for example, low blood pressure).
- Train nurses on opioid use and addiction. Educate nurses about opioid addiction risk factors and symptoms of addiction. Instruct them on managing the Ramsay Sedation Scale and using an opioid sedation scale with patients receiving IV narcotics.
- Educate families on opioid use and addiction. Counsel patients and their families on the long-term effects of opioid use and about the warning signs of addiction. Teach them about alternatives to narcotics.
- Offer referrals to specialized clinics. Work with social workers, case managers, and local mental health professionals to refer patients to behavioral counseling, patient and family support groups, and monitored detoxification clinics qualified to treat opioid addiction.
Socioeconomic impact
The effects of the opioid epidemic are felt in all areas of the United States, especially in the health care industry. Emergency department visits are mounting while billions of dollars are spent on medical care for those addicted to opioids. Additionally, the socioeconomic effects of this crisis contribute to increasing depression, anxiety, missed days of work or school, unemployment, drop-out rates, and loss of productivity among those addicted to opioids. Also, the epidemic is adversely affecting families, leading to increased divorce rates, single parent families, and child abuse and neglect. By creating strategies and protocols for medical staff, patients, and families affected by opioid use, addiction, or overdose, hospitalists can have a positive influence on patients’ lives and ultimately the opioid epidemic.
Dr. Kasarla is a hospitalist with Apogee Physicians at Parkway Surgical & Cardiovascular Hospital in Fort Worth, Tex. He also works for Texas Health Physicians Group at Texas Health Harris Methodist Hospital and Texas Health Harris Methodist Hospital Southwest in Fort Worth, as well as at Texas Health Harris Methodist Hospital in Azle, Tex.
You can contact him at [email protected] or [email protected].
References
1. Understanding the Epidemic: Drug overdose deaths in the United States continue to increase in 2015. Accessed Sept. 11, 2017.
2. Behavioral health trends in the United States: Results from the 2014 national survey on drug use and health. Accessed Sept. 11, 2017.
3. Jones CM. Heroin use and heroin use risk behaviors among nonmedical users of prescription opioid pain relievers – United States, 2002-2004 and 2008-2010. Drug Alcohol Depend. 2013;132(1-2):95-100.
4. Rudd RA et al. Increases in drug and opioid-involved overdose deaths – United States, 2010-2015. MMWR Morb Mortal Wkly Rep. 2016;65(50-51):1445-52.
5. Highlights of the 2011 Drug Abuse Warning Network (DAWN) findings on drug-related emergency department visits. Accessed Sept. 11, 2017.
When do patients with SSTIs require hospital admission and IV antibiotics?
Case
A 54-year old gentleman with a history of type 2 diabetes mellitus presents with several days of progressive left lower extremity redness, pain, swelling, and subjective fevers.
On physical examination the patient is afebrile and hemodynamically stable. The left lower extremity is swollen, warm, and tender to light palpation with an irregular area of erythema extending anteriorly from the ankle to just below the knee. There are no areas of purulence or fluctuance. Labs are notable for a mild leukocytosis of 11,500 cells/mcL. An ultrasound shows no evidence of deep vein thrombosis and the patient is started on vancomycin and ceftazidime and admitted for intravenous antibiotics.
Does the patient require hospital admission and continuation of intravenous antibiotics?
Introduction

The clinical presentation of SSTIs can vary greatly. Consequently, the management of SSTIs can be as simple as a short course of outpatient oral antibiotics or escalate to as complicated as surgical intervention and/or prolonged courses of IV antibiotics. Given the frequency with which these infections result in hospital admission, it is essential for the practicing hospitalist to be able to appropriately triage and treat SSTIs in order to assure adequate therapy, while simultaneously reducing unnecessary hospital days and avoiding indiscriminate exposure to broad spectrum antibiotics.
Pathophysiology and clinical presentation
SSTIs represent a diverse range of presentations and severities from superficial impetigo to life-threatening necrotizing infections, with abscesses and cellulitis being most commonly diagnosed.1
All SSTIs emerge from microbial invasion of the layers of the skin and underlying soft tissues. The accepted minimal criteria for diagnosis of an SSTI are erythema, edema, and warmth and tenderness of the affected area. Comorbid conditions that impair skin integrity, such as lymphedema, chronic inflammation (for example, eczema), intertrigo, or venous insufficiency therefore increase the risk of infection. However, the strongest risk factor for development of an SSTI is disruption of the skin barrier via trauma (foreign body, bite wound), ulceration, laceration, fissures, or surgical wound.2,3
The hallmark features of SSTI are present in other noninfectious skin disorders, thus often yielding misdiagnosis. In a study of 259 patients hospitalized for lower extremity cellulitis, 79 patients (30.5%) were misdiagnosed.4 The most common mimic of SSTI is stasis dermatitis due to chronic venous insufficiency. Other conditions that are often misdiagnosed as SSTI include lymphedema, lipodermatosclerosis, contact dermatitis, papular urticaria and deep venous thrombosis. Differentiating between true SSTI and these “pseudo-cellulitic” conditions is essential to reducing unnecessary hospitalization and exposure to antibiotics, which contribute to nosocomial infection, iatrogenic injury (that is, Clostridium difficile infection, anaphylaxis) and avoidable health care costs.
Microbiology

In the majority of cases, the causative pathogen is not identified; superficial culture data is often confounded and positive results do not guarantee pathogenicity of the identified organism. However, the mechanism of bacterial entry, location of infection, and presence of underlying medical conditions also influence the infectious organism(s). For example, infections of the lower extremities may involve enteric organisms such as E. coli and Enterococcus due to fecal runoff. SSTIs due to cat and dog bites commonly involve Pasteurella multocida, while hot tub exposure and intravenous drug use increase the risk of infection with Pseudomonas aeruginosa. Patients with neutropenia are at increased risk for fungal and yeast infections. Consequently, an assessment for potential risk factors is essential in determining appropriate management. Common pathogens associated with various clinical presentations and risk factors are outlined in Table 2.
In addition to host risk factors, the type of SSTI may hint at the most likely organisms. Among purulent (“culturable”) SSTIs, up to 76% of infections are due to S. aureus, whereas in diffuse (“nonculturable”) cellulitis, the majority of cases are attributable to B-hemolytic streptococcus.7 The role of S. aureus in SSTIs is further complicated by the rise of methicillin-resistant S. aureus (MRSA), both nosocomial and community-acquired. It is estimated that between 25%-50% of all S. aureus isolates in the United States show methicillin resistance.6,8 Despite the rising prevalence of MRSA, reflexive treatment for MRSA should be avoided in the absence of high-risk presentations (for example, purulent SSTI) or patient risk factors for MRSA (Table 3).
Severity of infection
Given the variety of clinical presentations of SSTIs, an evaluation of the severity of disease is essential to determining appropriate initial management, including the need for hospitalization and intravenous antibiotics. Several grading systems have been proposed to assist in determining severity. High-risk features that are common to these systems include:
• Evidence of systemic infection (fever, tachycardia, altered mental status, tachypnea, hypotension);
• Location of infection with increased risk of local complication (face, brain, hand, perineum);
• Indication of deep tissue infection (for example, crepitus, bullae, or hemorrhage);
• Comorbid conditions predisposing to more severe infection (liver or renal disease, immunocompromised state including neutropenia or active chemotherapy, vascular insufficiency).
In assessing for necrotic infection, the Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score can help to distinguish severe cellulitis from necrotizing infections that require immediate surgical evaluation. The LRINEC score uses readily available laboratory markers to stratify patients into tertiles of risk for necrotizing fasciitis. While this objective score can identify patients who may require immediate surgical intervention, any patient with a clinical history or exam concerning for necrotizing infection should be urgently evaluated for possible surgical debridement.11,12
Management
Nonpurulent disease
Nonpurulent SSTIs include cellulitis and necrotizing infections such as necrotizing fasciitis. In the absence of risk factors for particular infectious agents (see above), mild infections can be managed with a trial of oral antibiotics with coverage for streptococcal species such as cephalexin, clindamycin, or amoxicillin-clavulanate.
Empiric coverage for MRSA is not recommended and has been shown to have little benefit. In a trial of 146 patients with mild nonpurulent cellulitis, there was no significant difference in cure rate at 2 weeks between cephalexin monotherapy and dual therapy with cephalexin and trimethoprim-sulfamethoxazole.13
Moderate infections warrant admission for intravenous antibiotics, also with coverage for streptococcal species and MSSA such as penicillin or cefazolin. In most cases, coverage for MRSA is not required but may be considered in patients with risk factors for MRSA. Generally, blood or cutaneous cultures are not recommended given an expected yield of positive culture to be less than 5%,14 but may be considered in patients with immunosuppression or neutropenia or evidence of systemic inflammatory response.
Severe infections should be evaluated for the need for surgical debridement. Empiric antibiotic coverage for Streptococcus pyogenes, MRSA, and gram-negative and anaerobic species is warranted. If necrotizing infection is suspected or diagnosed, immediate surgical debridement is indicated. Culture data from surgical debridement should be obtained and can be useful for tailoring therapy. While blood cultures remain unlikely to yield useful data, it is reasonable to obtain them in severe disease. Empiric antibiotic coverage should be broad and narrowed based on surgical specimens. The general recommendation regarding duration of antibiotics is 5 days; however, longer courses of up to 10-14 days may be required if there is minimal improvement after initial therapy.9
Purulent disease
Purulent SSTIs by definition involve collections of pus and include abscesses, furuncles, and carbuncles. In all purulent SSTIs, incision and drainage is indicated.
For mild disease, incision and drainage is considered definitive management and deep wound cultures and antibiotics are not required. In moderate purulent SSTI, culture of the drained fluid should be obtained, and antibiotics administered with empiric therapy to include coverage for MRSA. Patients at risk for community-acquired MRSA can be given oral agents such as trimethoprim-sulfamethoxazole, clindamycin, or doxycycline (depending upon local antibiogram data) with antibiotics narrowed based on culture data.
In order to minimize treatment failure with oral agents, dosing should be weight based with a minimum of 5 mg/kg per day of bactrim or 10 mg/kg per day of clindamycin.15 Those with risk factors for nosocomial MRSA may warrant intravenous antibiotics, even in moderate disease. Patients with severe purulent disease require intravenous antibiotics with coverage for MRSA with vancomycin, daptomycin or linezolid and subsequently narrowed based on culture data.9
Back to the case
Our patient presented with a case of mild, nonpurulent cellulitis. While he does have a mildly elevated white blood cell count, he has no other signs of systemic infection or underlying conditions predisposing to more severe disease. Hospital admission is not required and de-escalation of antibiotics to an oral agent is appropriate.
If the patient exhibited other signs of systemic infection (that is, fever or tachycardia) hospital admission or admission to observation status for IV antibiotics would be appropriate; however, de-escalation would still be recommended as MRSA coverage is not warranted. We suggest discharge from the emergency department with oral cephalexin, provided no prohibitive allergy is known, with outpatient follow-up to ensure resolution of infection.
Bottom line
SSTIs encompass a wide variety of clinical presentations and severity, and can be mimicked by a number of noninfectious medical conditions. If an infectious process is considered most likely, the need for hospitalization and broad-spectrum antibiotics should be individually determined based on specific criteria, and not empirically initiated for all presentations.
Dr. Perry is an instructor in the Yale Academic Hospitalist Program at Yale University, New Haven, Conn. Dr. Fogerty is associate professor of medicine in the Yale Academic Hospitalist Program. Dr. Sankey is assistant professor of medicine and interim inpatient medicine clerkship director in the Yale Academic Hospitalist Program.
Key Points
• SSTIs encompass a wide variety of clinical presentations and severity, and can be mimicked by a number of noninfectious medical conditions
• The majority of SSTIs are caused by gram-positive organisms, most notably Staphylococcus aureus and B-hemolytic streptococci
• Evaluation of the severity of disease, using a grading system, is essential to determining appropriate initial management
• Hospitalization and broad-spectrum antibiotics should be individually determined based on specific criteria, not empirically initiated for all presentations
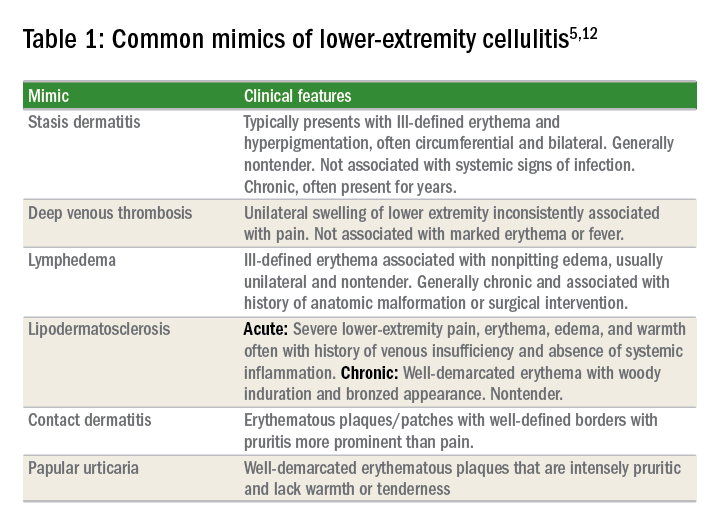
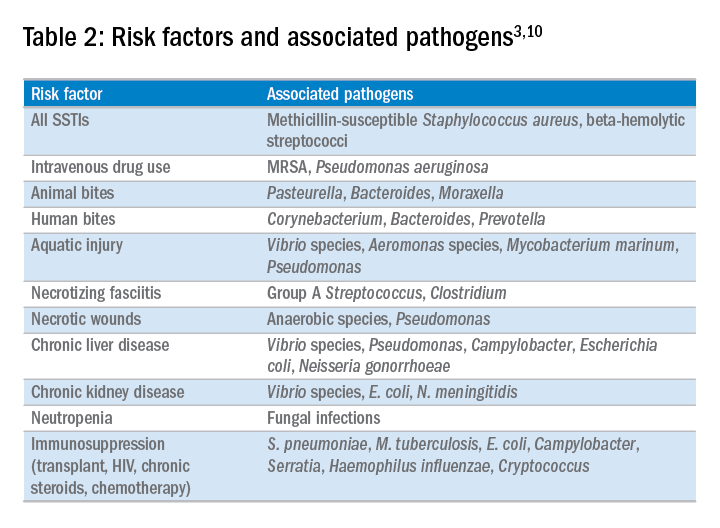
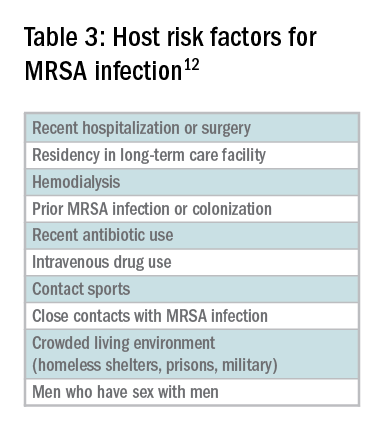
References
1. Miller L, Eisenberg D, Liu H, et al. Incidence of skin and soft tissue infections in ambulatory and inpatient settings, 2005-2010. BMC Infect Dis. 2015 Aug 21;15:362.
2. Dupuy A, Benchikhi H, Roujeau JC, et al. Risk factors for erysipelas of the leg (cellulitis): case control study. BMJ. 1999;318(7198):1591-4.
3. Ki V, Rotstein C. Bacterial skin and soft tissue infections in adults: A review of their epidemiology, pathogenesis, diagnosis, treatment and site of care. Can J Infect Dis Med Microbiol. 2008 Mar;19(2):173-84.
4. Weng QY, Raff AB, Cohen JM, et al. Costs and Consequences Associated with Misdiagnosed Lower Extremity Cellulitis. JAMA Dermatol. 2016 Nov 2.
5. Keller E, Tomecki K, Alraies M. Distinguishing cellulitis from its mimics. Cleve Clin J Med. 2012 Aug;79(8)547-52.
6. Bassetti, M, Carmelutti A, Righi E. The role of methicillin-resistant Staphylococcus aureus in skin and soft tissue infections. Curr Opin Infect Dis. 2017 Apr.
7. Jeng A, Beheshti M, Li J, Ramesh N. The Role of B-hemolytic Streptococci in Causing Diffuse, Nonculturable Cellulitis. Medicine (Baltimore). 2010 Jul;89(4):217-26.
8. Moran G, Krishnadasan A, Gorwitz R. Methicillin-Resistant S. aureus Infections among Patients in the Emergency Department. N Engl J Med. 2006; 355:666-74.
9. Stevens D, Bisno A, Chambers H, et al. Practice Guidelines for the Diagnosis and Management of Skin and Soft tissue Infections: 2014 Update by the Infectious Disease Society of America. Clin Infect Dis. 2014 Jul 15;59(2):e10-52.
10. Raff, AB and Kroshinsky D. Cellulitis: A Review. JAMA. 2016 Jul;316(3):325-37.
11. Wong, CH, Khin LW, Heng KS, Tan KC, Low CO. The LRINEC (Laboratory Risk Indicator for Necrotizing Fasciitis) score: a tool for distinguishing necrotizing fasciitis from other soft tissue infections. Crit Care Med. 2004 Jul;32(7):1535-41.
12. Gunderson CG. Cellulitis: Definition, etiology and clinical features. Am J Med 2011 Dec;124(12):1113-22.
13. Pallin D, et al. Comparative Effectiveness of Cephalexin Plus Trimethoprim-Sulfamethoxazole versus Cephalexin Alone for Treatment of Uncomplicated Cellulitis: A Randomized Controlled Trial. Clin Infect Dis. 2013 Jun;56(12):1754-62.
14. Gunderson CG, Martinello RA. A systematic review of bacteremias in cellulitis and erysipelas. J Infect. 2012;64(2):148-55.
15. Halilovic J, Heintz BH, Brown J.. Risk factors for clinical failure in patients hospitalized with cellulitis and cutaneous abscess. J Infect. 2012;65(2):128-34.
Case
A 54-year old gentleman with a history of type 2 diabetes mellitus presents with several days of progressive left lower extremity redness, pain, swelling, and subjective fevers.
On physical examination the patient is afebrile and hemodynamically stable. The left lower extremity is swollen, warm, and tender to light palpation with an irregular area of erythema extending anteriorly from the ankle to just below the knee. There are no areas of purulence or fluctuance. Labs are notable for a mild leukocytosis of 11,500 cells/mcL. An ultrasound shows no evidence of deep vein thrombosis and the patient is started on vancomycin and ceftazidime and admitted for intravenous antibiotics.
Does the patient require hospital admission and continuation of intravenous antibiotics?
Introduction
The clinical presentation of SSTIs can vary greatly. Consequently, the management of SSTIs can be as simple as a short course of outpatient oral antibiotics or escalate to as complicated as surgical intervention and/or prolonged courses of IV antibiotics. Given the frequency with which these infections result in hospital admission, it is essential for the practicing hospitalist to be able to appropriately triage and treat SSTIs in order to assure adequate therapy, while simultaneously reducing unnecessary hospital days and avoiding indiscriminate exposure to broad spectrum antibiotics.
Pathophysiology and clinical presentation
SSTIs represent a diverse range of presentations and severities from superficial impetigo to life-threatening necrotizing infections, with abscesses and cellulitis being most commonly diagnosed.1
All SSTIs emerge from microbial invasion of the layers of the skin and underlying soft tissues. The accepted minimal criteria for diagnosis of an SSTI are erythema, edema, and warmth and tenderness of the affected area. Comorbid conditions that impair skin integrity, such as lymphedema, chronic inflammation (for example, eczema), intertrigo, or venous insufficiency therefore increase the risk of infection. However, the strongest risk factor for development of an SSTI is disruption of the skin barrier via trauma (foreign body, bite wound), ulceration, laceration, fissures, or surgical wound.2,3
The hallmark features of SSTI are present in other noninfectious skin disorders, thus often yielding misdiagnosis. In a study of 259 patients hospitalized for lower extremity cellulitis, 79 patients (30.5%) were misdiagnosed.4 The most common mimic of SSTI is stasis dermatitis due to chronic venous insufficiency. Other conditions that are often misdiagnosed as SSTI include lymphedema, lipodermatosclerosis, contact dermatitis, papular urticaria and deep venous thrombosis. Differentiating between true SSTI and these “pseudo-cellulitic” conditions is essential to reducing unnecessary hospitalization and exposure to antibiotics, which contribute to nosocomial infection, iatrogenic injury (that is, Clostridium difficile infection, anaphylaxis) and avoidable health care costs.
Microbiology
In the majority of cases, the causative pathogen is not identified; superficial culture data is often confounded and positive results do not guarantee pathogenicity of the identified organism. However, the mechanism of bacterial entry, location of infection, and presence of underlying medical conditions also influence the infectious organism(s). For example, infections of the lower extremities may involve enteric organisms such as E. coli and Enterococcus due to fecal runoff. SSTIs due to cat and dog bites commonly involve Pasteurella multocida, while hot tub exposure and intravenous drug use increase the risk of infection with Pseudomonas aeruginosa. Patients with neutropenia are at increased risk for fungal and yeast infections. Consequently, an assessment for potential risk factors is essential in determining appropriate management. Common pathogens associated with various clinical presentations and risk factors are outlined in Table 2.
In addition to host risk factors, the type of SSTI may hint at the most likely organisms. Among purulent (“culturable”) SSTIs, up to 76% of infections are due to S. aureus, whereas in diffuse (“nonculturable”) cellulitis, the majority of cases are attributable to B-hemolytic streptococcus.7 The role of S. aureus in SSTIs is further complicated by the rise of methicillin-resistant S. aureus (MRSA), both nosocomial and community-acquired. It is estimated that between 25%-50% of all S. aureus isolates in the United States show methicillin resistance.6,8 Despite the rising prevalence of MRSA, reflexive treatment for MRSA should be avoided in the absence of high-risk presentations (for example, purulent SSTI) or patient risk factors for MRSA (Table 3).
Severity of infection
Given the variety of clinical presentations of SSTIs, an evaluation of the severity of disease is essential to determining appropriate initial management, including the need for hospitalization and intravenous antibiotics. Several grading systems have been proposed to assist in determining severity. High-risk features that are common to these systems include:
• Evidence of systemic infection (fever, tachycardia, altered mental status, tachypnea, hypotension);
• Location of infection with increased risk of local complication (face, brain, hand, perineum);
• Indication of deep tissue infection (for example, crepitus, bullae, or hemorrhage);
• Comorbid conditions predisposing to more severe infection (liver or renal disease, immunocompromised state including neutropenia or active chemotherapy, vascular insufficiency).
In assessing for necrotic infection, the Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score can help to distinguish severe cellulitis from necrotizing infections that require immediate surgical evaluation. The LRINEC score uses readily available laboratory markers to stratify patients into tertiles of risk for necrotizing fasciitis. While this objective score can identify patients who may require immediate surgical intervention, any patient with a clinical history or exam concerning for necrotizing infection should be urgently evaluated for possible surgical debridement.11,12
Management
Nonpurulent disease
Nonpurulent SSTIs include cellulitis and necrotizing infections such as necrotizing fasciitis. In the absence of risk factors for particular infectious agents (see above), mild infections can be managed with a trial of oral antibiotics with coverage for streptococcal species such as cephalexin, clindamycin, or amoxicillin-clavulanate.
Empiric coverage for MRSA is not recommended and has been shown to have little benefit. In a trial of 146 patients with mild nonpurulent cellulitis, there was no significant difference in cure rate at 2 weeks between cephalexin monotherapy and dual therapy with cephalexin and trimethoprim-sulfamethoxazole.13
Moderate infections warrant admission for intravenous antibiotics, also with coverage for streptococcal species and MSSA such as penicillin or cefazolin. In most cases, coverage for MRSA is not required but may be considered in patients with risk factors for MRSA. Generally, blood or cutaneous cultures are not recommended given an expected yield of positive culture to be less than 5%,14 but may be considered in patients with immunosuppression or neutropenia or evidence of systemic inflammatory response.
Severe infections should be evaluated for the need for surgical debridement. Empiric antibiotic coverage for Streptococcus pyogenes, MRSA, and gram-negative and anaerobic species is warranted. If necrotizing infection is suspected or diagnosed, immediate surgical debridement is indicated. Culture data from surgical debridement should be obtained and can be useful for tailoring therapy. While blood cultures remain unlikely to yield useful data, it is reasonable to obtain them in severe disease. Empiric antibiotic coverage should be broad and narrowed based on surgical specimens. The general recommendation regarding duration of antibiotics is 5 days; however, longer courses of up to 10-14 days may be required if there is minimal improvement after initial therapy.9
Purulent disease
Purulent SSTIs by definition involve collections of pus and include abscesses, furuncles, and carbuncles. In all purulent SSTIs, incision and drainage is indicated.
For mild disease, incision and drainage is considered definitive management and deep wound cultures and antibiotics are not required. In moderate purulent SSTI, culture of the drained fluid should be obtained, and antibiotics administered with empiric therapy to include coverage for MRSA. Patients at risk for community-acquired MRSA can be given oral agents such as trimethoprim-sulfamethoxazole, clindamycin, or doxycycline (depending upon local antibiogram data) with antibiotics narrowed based on culture data.
In order to minimize treatment failure with oral agents, dosing should be weight based with a minimum of 5 mg/kg per day of bactrim or 10 mg/kg per day of clindamycin.15 Those with risk factors for nosocomial MRSA may warrant intravenous antibiotics, even in moderate disease. Patients with severe purulent disease require intravenous antibiotics with coverage for MRSA with vancomycin, daptomycin or linezolid and subsequently narrowed based on culture data.9
Back to the case
Our patient presented with a case of mild, nonpurulent cellulitis. While he does have a mildly elevated white blood cell count, he has no other signs of systemic infection or underlying conditions predisposing to more severe disease. Hospital admission is not required and de-escalation of antibiotics to an oral agent is appropriate.
If the patient exhibited other signs of systemic infection (that is, fever or tachycardia) hospital admission or admission to observation status for IV antibiotics would be appropriate; however, de-escalation would still be recommended as MRSA coverage is not warranted. We suggest discharge from the emergency department with oral cephalexin, provided no prohibitive allergy is known, with outpatient follow-up to ensure resolution of infection.
Bottom line
SSTIs encompass a wide variety of clinical presentations and severity, and can be mimicked by a number of noninfectious medical conditions. If an infectious process is considered most likely, the need for hospitalization and broad-spectrum antibiotics should be individually determined based on specific criteria, and not empirically initiated for all presentations.
Dr. Perry is an instructor in the Yale Academic Hospitalist Program at Yale University, New Haven, Conn. Dr. Fogerty is associate professor of medicine in the Yale Academic Hospitalist Program. Dr. Sankey is assistant professor of medicine and interim inpatient medicine clerkship director in the Yale Academic Hospitalist Program.
Key Points
• SSTIs encompass a wide variety of clinical presentations and severity, and can be mimicked by a number of noninfectious medical conditions
• The majority of SSTIs are caused by gram-positive organisms, most notably Staphylococcus aureus and B-hemolytic streptococci
• Evaluation of the severity of disease, using a grading system, is essential to determining appropriate initial management
• Hospitalization and broad-spectrum antibiotics should be individually determined based on specific criteria, not empirically initiated for all presentations
References
1. Miller L, Eisenberg D, Liu H, et al. Incidence of skin and soft tissue infections in ambulatory and inpatient settings, 2005-2010. BMC Infect Dis. 2015 Aug 21;15:362.
2. Dupuy A, Benchikhi H, Roujeau JC, et al. Risk factors for erysipelas of the leg (cellulitis): case control study. BMJ. 1999;318(7198):1591-4.
3. Ki V, Rotstein C. Bacterial skin and soft tissue infections in adults: A review of their epidemiology, pathogenesis, diagnosis, treatment and site of care. Can J Infect Dis Med Microbiol. 2008 Mar;19(2):173-84.
4. Weng QY, Raff AB, Cohen JM, et al. Costs and Consequences Associated with Misdiagnosed Lower Extremity Cellulitis. JAMA Dermatol. 2016 Nov 2.
5. Keller E, Tomecki K, Alraies M. Distinguishing cellulitis from its mimics. Cleve Clin J Med. 2012 Aug;79(8)547-52.
6. Bassetti, M, Carmelutti A, Righi E. The role of methicillin-resistant Staphylococcus aureus in skin and soft tissue infections. Curr Opin Infect Dis. 2017 Apr.
7. Jeng A, Beheshti M, Li J, Ramesh N. The Role of B-hemolytic Streptococci in Causing Diffuse, Nonculturable Cellulitis. Medicine (Baltimore). 2010 Jul;89(4):217-26.
8. Moran G, Krishnadasan A, Gorwitz R. Methicillin-Resistant S. aureus Infections among Patients in the Emergency Department. N Engl J Med. 2006; 355:666-74.
9. Stevens D, Bisno A, Chambers H, et al. Practice Guidelines for the Diagnosis and Management of Skin and Soft tissue Infections: 2014 Update by the Infectious Disease Society of America. Clin Infect Dis. 2014 Jul 15;59(2):e10-52.
10. Raff, AB and Kroshinsky D. Cellulitis: A Review. JAMA. 2016 Jul;316(3):325-37.
11. Wong, CH, Khin LW, Heng KS, Tan KC, Low CO. The LRINEC (Laboratory Risk Indicator for Necrotizing Fasciitis) score: a tool for distinguishing necrotizing fasciitis from other soft tissue infections. Crit Care Med. 2004 Jul;32(7):1535-41.
12. Gunderson CG. Cellulitis: Definition, etiology and clinical features. Am J Med 2011 Dec;124(12):1113-22.
13. Pallin D, et al. Comparative Effectiveness of Cephalexin Plus Trimethoprim-Sulfamethoxazole versus Cephalexin Alone for Treatment of Uncomplicated Cellulitis: A Randomized Controlled Trial. Clin Infect Dis. 2013 Jun;56(12):1754-62.
14. Gunderson CG, Martinello RA. A systematic review of bacteremias in cellulitis and erysipelas. J Infect. 2012;64(2):148-55.
15. Halilovic J, Heintz BH, Brown J.. Risk factors for clinical failure in patients hospitalized with cellulitis and cutaneous abscess. J Infect. 2012;65(2):128-34.
Case
A 54-year old gentleman with a history of type 2 diabetes mellitus presents with several days of progressive left lower extremity redness, pain, swelling, and subjective fevers.
On physical examination the patient is afebrile and hemodynamically stable. The left lower extremity is swollen, warm, and tender to light palpation with an irregular area of erythema extending anteriorly from the ankle to just below the knee. There are no areas of purulence or fluctuance. Labs are notable for a mild leukocytosis of 11,500 cells/mcL. An ultrasound shows no evidence of deep vein thrombosis and the patient is started on vancomycin and ceftazidime and admitted for intravenous antibiotics.
Does the patient require hospital admission and continuation of intravenous antibiotics?
Introduction
The clinical presentation of SSTIs can vary greatly. Consequently, the management of SSTIs can be as simple as a short course of outpatient oral antibiotics or escalate to as complicated as surgical intervention and/or prolonged courses of IV antibiotics. Given the frequency with which these infections result in hospital admission, it is essential for the practicing hospitalist to be able to appropriately triage and treat SSTIs in order to assure adequate therapy, while simultaneously reducing unnecessary hospital days and avoiding indiscriminate exposure to broad spectrum antibiotics.
Pathophysiology and clinical presentation
SSTIs represent a diverse range of presentations and severities from superficial impetigo to life-threatening necrotizing infections, with abscesses and cellulitis being most commonly diagnosed.1
All SSTIs emerge from microbial invasion of the layers of the skin and underlying soft tissues. The accepted minimal criteria for diagnosis of an SSTI are erythema, edema, and warmth and tenderness of the affected area. Comorbid conditions that impair skin integrity, such as lymphedema, chronic inflammation (for example, eczema), intertrigo, or venous insufficiency therefore increase the risk of infection. However, the strongest risk factor for development of an SSTI is disruption of the skin barrier via trauma (foreign body, bite wound), ulceration, laceration, fissures, or surgical wound.2,3
The hallmark features of SSTI are present in other noninfectious skin disorders, thus often yielding misdiagnosis. In a study of 259 patients hospitalized for lower extremity cellulitis, 79 patients (30.5%) were misdiagnosed.4 The most common mimic of SSTI is stasis dermatitis due to chronic venous insufficiency. Other conditions that are often misdiagnosed as SSTI include lymphedema, lipodermatosclerosis, contact dermatitis, papular urticaria and deep venous thrombosis. Differentiating between true SSTI and these “pseudo-cellulitic” conditions is essential to reducing unnecessary hospitalization and exposure to antibiotics, which contribute to nosocomial infection, iatrogenic injury (that is, Clostridium difficile infection, anaphylaxis) and avoidable health care costs.
Microbiology
In the majority of cases, the causative pathogen is not identified; superficial culture data is often confounded and positive results do not guarantee pathogenicity of the identified organism. However, the mechanism of bacterial entry, location of infection, and presence of underlying medical conditions also influence the infectious organism(s). For example, infections of the lower extremities may involve enteric organisms such as E. coli and Enterococcus due to fecal runoff. SSTIs due to cat and dog bites commonly involve Pasteurella multocida, while hot tub exposure and intravenous drug use increase the risk of infection with Pseudomonas aeruginosa. Patients with neutropenia are at increased risk for fungal and yeast infections. Consequently, an assessment for potential risk factors is essential in determining appropriate management. Common pathogens associated with various clinical presentations and risk factors are outlined in Table 2.
In addition to host risk factors, the type of SSTI may hint at the most likely organisms. Among purulent (“culturable”) SSTIs, up to 76% of infections are due to S. aureus, whereas in diffuse (“nonculturable”) cellulitis, the majority of cases are attributable to B-hemolytic streptococcus.7 The role of S. aureus in SSTIs is further complicated by the rise of methicillin-resistant S. aureus (MRSA), both nosocomial and community-acquired. It is estimated that between 25%-50% of all S. aureus isolates in the United States show methicillin resistance.6,8 Despite the rising prevalence of MRSA, reflexive treatment for MRSA should be avoided in the absence of high-risk presentations (for example, purulent SSTI) or patient risk factors for MRSA (Table 3).
Severity of infection
Given the variety of clinical presentations of SSTIs, an evaluation of the severity of disease is essential to determining appropriate initial management, including the need for hospitalization and intravenous antibiotics. Several grading systems have been proposed to assist in determining severity. High-risk features that are common to these systems include:
• Evidence of systemic infection (fever, tachycardia, altered mental status, tachypnea, hypotension);
• Location of infection with increased risk of local complication (face, brain, hand, perineum);
• Indication of deep tissue infection (for example, crepitus, bullae, or hemorrhage);
• Comorbid conditions predisposing to more severe infection (liver or renal disease, immunocompromised state including neutropenia or active chemotherapy, vascular insufficiency).
In assessing for necrotic infection, the Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score can help to distinguish severe cellulitis from necrotizing infections that require immediate surgical evaluation. The LRINEC score uses readily available laboratory markers to stratify patients into tertiles of risk for necrotizing fasciitis. While this objective score can identify patients who may require immediate surgical intervention, any patient with a clinical history or exam concerning for necrotizing infection should be urgently evaluated for possible surgical debridement.11,12
Management
Nonpurulent disease
Nonpurulent SSTIs include cellulitis and necrotizing infections such as necrotizing fasciitis. In the absence of risk factors for particular infectious agents (see above), mild infections can be managed with a trial of oral antibiotics with coverage for streptococcal species such as cephalexin, clindamycin, or amoxicillin-clavulanate.
Empiric coverage for MRSA is not recommended and has been shown to have little benefit. In a trial of 146 patients with mild nonpurulent cellulitis, there was no significant difference in cure rate at 2 weeks between cephalexin monotherapy and dual therapy with cephalexin and trimethoprim-sulfamethoxazole.13
Moderate infections warrant admission for intravenous antibiotics, also with coverage for streptococcal species and MSSA such as penicillin or cefazolin. In most cases, coverage for MRSA is not required but may be considered in patients with risk factors for MRSA. Generally, blood or cutaneous cultures are not recommended given an expected yield of positive culture to be less than 5%,14 but may be considered in patients with immunosuppression or neutropenia or evidence of systemic inflammatory response.
Severe infections should be evaluated for the need for surgical debridement. Empiric antibiotic coverage for Streptococcus pyogenes, MRSA, and gram-negative and anaerobic species is warranted. If necrotizing infection is suspected or diagnosed, immediate surgical debridement is indicated. Culture data from surgical debridement should be obtained and can be useful for tailoring therapy. While blood cultures remain unlikely to yield useful data, it is reasonable to obtain them in severe disease. Empiric antibiotic coverage should be broad and narrowed based on surgical specimens. The general recommendation regarding duration of antibiotics is 5 days; however, longer courses of up to 10-14 days may be required if there is minimal improvement after initial therapy.9
Purulent disease
Purulent SSTIs by definition involve collections of pus and include abscesses, furuncles, and carbuncles. In all purulent SSTIs, incision and drainage is indicated.
For mild disease, incision and drainage is considered definitive management and deep wound cultures and antibiotics are not required. In moderate purulent SSTI, culture of the drained fluid should be obtained, and antibiotics administered with empiric therapy to include coverage for MRSA. Patients at risk for community-acquired MRSA can be given oral agents such as trimethoprim-sulfamethoxazole, clindamycin, or doxycycline (depending upon local antibiogram data) with antibiotics narrowed based on culture data.
In order to minimize treatment failure with oral agents, dosing should be weight based with a minimum of 5 mg/kg per day of bactrim or 10 mg/kg per day of clindamycin.15 Those with risk factors for nosocomial MRSA may warrant intravenous antibiotics, even in moderate disease. Patients with severe purulent disease require intravenous antibiotics with coverage for MRSA with vancomycin, daptomycin or linezolid and subsequently narrowed based on culture data.9
Back to the case
Our patient presented with a case of mild, nonpurulent cellulitis. While he does have a mildly elevated white blood cell count, he has no other signs of systemic infection or underlying conditions predisposing to more severe disease. Hospital admission is not required and de-escalation of antibiotics to an oral agent is appropriate.
If the patient exhibited other signs of systemic infection (that is, fever or tachycardia) hospital admission or admission to observation status for IV antibiotics would be appropriate; however, de-escalation would still be recommended as MRSA coverage is not warranted. We suggest discharge from the emergency department with oral cephalexin, provided no prohibitive allergy is known, with outpatient follow-up to ensure resolution of infection.
Bottom line
SSTIs encompass a wide variety of clinical presentations and severity, and can be mimicked by a number of noninfectious medical conditions. If an infectious process is considered most likely, the need for hospitalization and broad-spectrum antibiotics should be individually determined based on specific criteria, and not empirically initiated for all presentations.
Dr. Perry is an instructor in the Yale Academic Hospitalist Program at Yale University, New Haven, Conn. Dr. Fogerty is associate professor of medicine in the Yale Academic Hospitalist Program. Dr. Sankey is assistant professor of medicine and interim inpatient medicine clerkship director in the Yale Academic Hospitalist Program.
Key Points
• SSTIs encompass a wide variety of clinical presentations and severity, and can be mimicked by a number of noninfectious medical conditions
• The majority of SSTIs are caused by gram-positive organisms, most notably Staphylococcus aureus and B-hemolytic streptococci
• Evaluation of the severity of disease, using a grading system, is essential to determining appropriate initial management
• Hospitalization and broad-spectrum antibiotics should be individually determined based on specific criteria, not empirically initiated for all presentations
References
1. Miller L, Eisenberg D, Liu H, et al. Incidence of skin and soft tissue infections in ambulatory and inpatient settings, 2005-2010. BMC Infect Dis. 2015 Aug 21;15:362.
2. Dupuy A, Benchikhi H, Roujeau JC, et al. Risk factors for erysipelas of the leg (cellulitis): case control study. BMJ. 1999;318(7198):1591-4.
3. Ki V, Rotstein C. Bacterial skin and soft tissue infections in adults: A review of their epidemiology, pathogenesis, diagnosis, treatment and site of care. Can J Infect Dis Med Microbiol. 2008 Mar;19(2):173-84.
4. Weng QY, Raff AB, Cohen JM, et al. Costs and Consequences Associated with Misdiagnosed Lower Extremity Cellulitis. JAMA Dermatol. 2016 Nov 2.
5. Keller E, Tomecki K, Alraies M. Distinguishing cellulitis from its mimics. Cleve Clin J Med. 2012 Aug;79(8)547-52.
6. Bassetti, M, Carmelutti A, Righi E. The role of methicillin-resistant Staphylococcus aureus in skin and soft tissue infections. Curr Opin Infect Dis. 2017 Apr.
7. Jeng A, Beheshti M, Li J, Ramesh N. The Role of B-hemolytic Streptococci in Causing Diffuse, Nonculturable Cellulitis. Medicine (Baltimore). 2010 Jul;89(4):217-26.
8. Moran G, Krishnadasan A, Gorwitz R. Methicillin-Resistant S. aureus Infections among Patients in the Emergency Department. N Engl J Med. 2006; 355:666-74.
9. Stevens D, Bisno A, Chambers H, et al. Practice Guidelines for the Diagnosis and Management of Skin and Soft tissue Infections: 2014 Update by the Infectious Disease Society of America. Clin Infect Dis. 2014 Jul 15;59(2):e10-52.
10. Raff, AB and Kroshinsky D. Cellulitis: A Review. JAMA. 2016 Jul;316(3):325-37.
11. Wong, CH, Khin LW, Heng KS, Tan KC, Low CO. The LRINEC (Laboratory Risk Indicator for Necrotizing Fasciitis) score: a tool for distinguishing necrotizing fasciitis from other soft tissue infections. Crit Care Med. 2004 Jul;32(7):1535-41.
12. Gunderson CG. Cellulitis: Definition, etiology and clinical features. Am J Med 2011 Dec;124(12):1113-22.
13. Pallin D, et al. Comparative Effectiveness of Cephalexin Plus Trimethoprim-Sulfamethoxazole versus Cephalexin Alone for Treatment of Uncomplicated Cellulitis: A Randomized Controlled Trial. Clin Infect Dis. 2013 Jun;56(12):1754-62.
14. Gunderson CG, Martinello RA. A systematic review of bacteremias in cellulitis and erysipelas. J Infect. 2012;64(2):148-55.
15. Halilovic J, Heintz BH, Brown J.. Risk factors for clinical failure in patients hospitalized with cellulitis and cutaneous abscess. J Infect. 2012;65(2):128-34.
Sepsis response team does not improve mortality/organ dysfunction
A sepsis response team did not have a positive effect on mortality or organ dysfunction in septic patients, compared with standard treatment by a primary care team, according to a study abstract scheduled to be presented at CHEST 2017.

Compared with the primary care team, the sepsis team was more likely to intervene on patients with a quick Sepsis-Related Organ Failure Assessment score greater than 1 (33.8% vs. 22.8%), change or initiate antibiotics within 3 hours (64.6% vs. 37.2%), and obtain blood cultures on time (66.4% vs 45.2%). An additional difference between the two groups was that the sepsis team had better compliance with the 3-hour bundle (15.2% vs 8.4%).
Despite the sepsis team’s higher level of compliance with certain protocols, the combined outcome measure of mortality and organ dysfunction within 28 days was not significantly higher for patients treated by the sepsis team (11.3% vs. 9.8%; P = .6). In fact, there was at least one downside to being treated by the sepsis team, which was having a 14% longer hospital stay.
Chhaya Patel, MD, is scheduled to present the abstract on Sun., Oct. 29th, at 2:30-2:45 p.m. in Convention Center – 602B. This research is part of the Sepsis & Septic Shock session at the CHEST annual meeting, which will run from 1:30 to 3:00 p.m.
A sepsis response team did not have a positive effect on mortality or organ dysfunction in septic patients, compared with standard treatment by a primary care team, according to a study abstract scheduled to be presented at CHEST 2017.
Compared with the primary care team, the sepsis team was more likely to intervene on patients with a quick Sepsis-Related Organ Failure Assessment score greater than 1 (33.8% vs. 22.8%), change or initiate antibiotics within 3 hours (64.6% vs. 37.2%), and obtain blood cultures on time (66.4% vs 45.2%). An additional difference between the two groups was that the sepsis team had better compliance with the 3-hour bundle (15.2% vs 8.4%).
Despite the sepsis team’s higher level of compliance with certain protocols, the combined outcome measure of mortality and organ dysfunction within 28 days was not significantly higher for patients treated by the sepsis team (11.3% vs. 9.8%; P = .6). In fact, there was at least one downside to being treated by the sepsis team, which was having a 14% longer hospital stay.
Chhaya Patel, MD, is scheduled to present the abstract on Sun., Oct. 29th, at 2:30-2:45 p.m. in Convention Center – 602B. This research is part of the Sepsis & Septic Shock session at the CHEST annual meeting, which will run from 1:30 to 3:00 p.m.
A sepsis response team did not have a positive effect on mortality or organ dysfunction in septic patients, compared with standard treatment by a primary care team, according to a study abstract scheduled to be presented at CHEST 2017.
Compared with the primary care team, the sepsis team was more likely to intervene on patients with a quick Sepsis-Related Organ Failure Assessment score greater than 1 (33.8% vs. 22.8%), change or initiate antibiotics within 3 hours (64.6% vs. 37.2%), and obtain blood cultures on time (66.4% vs 45.2%). An additional difference between the two groups was that the sepsis team had better compliance with the 3-hour bundle (15.2% vs 8.4%).
Despite the sepsis team’s higher level of compliance with certain protocols, the combined outcome measure of mortality and organ dysfunction within 28 days was not significantly higher for patients treated by the sepsis team (11.3% vs. 9.8%; P = .6). In fact, there was at least one downside to being treated by the sepsis team, which was having a 14% longer hospital stay.
Chhaya Patel, MD, is scheduled to present the abstract on Sun., Oct. 29th, at 2:30-2:45 p.m. in Convention Center – 602B. This research is part of the Sepsis & Septic Shock session at the CHEST annual meeting, which will run from 1:30 to 3:00 p.m.
FROM CHEST 2017