User login
A case of sudden psychosis
CASE: New-onset psychosis
Ms. T, age 26, presents to the psychiatric emergency room after a 1-week change in behavior. According to her family, Ms. T began to experience hyperactivity, increased rate of speech, and decreased sleep after her mother passed away 1 week ago. On the day of presentation, Ms. T had returned to work after a week’s hiatus. Coworkers brought her to the hospital when Ms. T threw herself on the floor and flailed about. Family members report that Ms. T had been complaining of headache that day and during the preceding week. In the emergency room, the patient is intrusive and easily distractible, although able to give a history.
Ms. T has no psychiatric history. Her family history is positive for bipolar spectrum illness. Our initial consideration is that Ms. T is experiencing mania or psychotic symptoms triggered by the recent loss of her mother. Ms. T is evaluated in the medical emergency room to rule out a primary medical illness. Standard labs and head CT are normal, so she is returned to the psychiatric emergency room. She becomes severely agitated and requires multiple IM antipsychotics—2 courses of haloperidol, 10 mg; 2 courses of ziprasidone, 20 mg; and olanzapine, 10 mg. She is admitted to the inpatient psychiatric service with a diagnosis of psychosis not otherwise specified.
Soon after admission, Ms. T suffers a witnessed generalized tonic-clonic seizure and is transferred to the internal medicine service. After the seizure she is awake but minimally responsive. She does not display purposeful movements, opens her eyes but can follow the examiner only on occasion, and displays periodic facial grimacing. In addition, Ms. T is intermittently hypoxic—requiring supplemental oxygen via nasal cannula—and febrile, with persistent tachycardia. Electroencephalography (EEG) shows nonconvulsive status epilepticus involving the bilateral temporal regions.
Ms. T is transferred to the neurosurgical intensive care unit for monitoring and IV anticonvulsants. Subsequent EEGs demonstrate generalized slowing but no epileptiform activity. An infectious workup is negative. Head MRI shows bilateral cerebellar T2/FLAIR increased signal, which is a nonspecific finding. Cerebrospinal fluid (CSF) studies show lymphocytic pleocytosis and oligoclonal bands. These findings suggest a CSF humoral immune response; an extensive laboratory workup is otherwise largely unremarkable ( Table 1 ).
The authors’ observations
We consider that Ms. T may have schizophrenia. Schizophrenia onset is insidious, often with prodromal symptoms occurring months to years before diagnosis.1,2 In Ms. T, the onset of the disturbance was brief; her family noted a change in behavior for only 1 week before presentation. Given this history, brief psychotic disorder remains high on the differential diagnosis because Ms. T’s disorganized speech and behavior occurred seeming in relation to her mother’s death.
Bipolar disorder is characterized by strong heritability, with risks increasing if there is a first-degree relative with the illness. The hallmark of bipolar I disorder is a manic episode, which presents as:
- decreased need for sleep
- grandiosity
- flight of ideas
- reckless or thoughtless behaviors
- increased energy
- increased productivity
- expansive or irritable mood.
Psychiatric symptoms secondary to seizure disorder are well documented. Cognitive, mood, anxiety, and psychotic phenomena may occur in up to 50% of patients with seizures.3 Typically, these symptoms are categorized as occurring during a seizure, after a seizure (post-ictal), or between seizures (interictal).
Manic syndromes secondary to seizure disorders present in an atypical manner with irritability and hyperactivity. Psychotic syndromes, on the other hand, appear with more classic schizophrenia-type symptoms:
- paranoia and persecutory delusions
- auditory and visual hallucinations
- amotivation
- apathy
- flattened affect
- disorganization.3
Paraneoplastic syndromes may be associated with mood changes and other psychiatric symptoms.4-6 Diagnosis is contingent on discovering the primary neoplasm, with or without specific paraneoplastic antibodies. Treatment is tailored to the oncologic process.
Table 1
Ms. T’s laboratory workup*
| Test | Result |
|---|---|
| C-reactive protein | 0.7 |
| Erythrocyte sedimentation rate | 5 |
| Cryptococcal antigen (serum) | Negative |
| Antinuclear antibody | Negative |
| CSF lymphocytes | 88 |
| CSF nucleated cells | 200 |
| CSF RBC | 33 |
| CSF glucose | 44 |
| CSF protein | 45 |
| CSF igG index | 1.2 |
| CSF oligoclonal bands | Present |
| CSF: cerebrospinal fluid; igG: immunoglobulin G; RBC: red blood cell | |
| *Results were negative for gonorrhea, chlamydia, lupus, human immunodeficiency virus, syphilis, Lyme disease, varicella zoster virus, West Nile virus, herpes simplex virus, Epstein-Barr virus, cytomegalovirus, tuberculosis, and California, St. Louis, eastern equine, and western equine encephalitis | |
EVALUATION: A medical cause
The psychiatry consultation-liaison service is asked to further evaluate Ms. T for psychiatric contributions to her continued altered mental status. Ms. T remains in restraints and receives fosphenytoin, 200 mg bid; levetiracetam, 1,000 mg bid; and lorazepam as needed for agitation. Following consultation, the team considers a working diagnosis of an autoimmune encephalopathy based on the negative infectious workup, the patient’s demographics, and the clinical picture (psychiatric symptoms, seizure, and encephalopathy). Ms. T undergoes 5 courses of plasma exchange with no effect. Catatonia is considered, but the patient does not demonstrate significant change with numerous doses of lorazepam.
Because Ms. T does not improve, the team starts a more specific paraneoplastic workup. MRI reveals a 9-mm lesion on her right ovary. Corticosteroids, including IV methylprednisolone, 1 g/d, are started. Ms. T’s clinical presentation improves; soon after scheduled corticosteroid dosing, she is taken to the operating room for right salpingo-oophorectomy. Surgical pathology later confirms the lesion as a mature teratoma. A standard paraneoplastic panel is negative; a separate test for anti-NMDA (N-methyl-D-aspartate) receptor antibodies is positive, however, and confirms the diagnosis of ovarian mass-associated anti-NMDA receptor limbic encephalitis.
Paraneoplastic syndromes
This case represents the interface between a complicated medical phenomenon and psychiatric symptomatology. Mood changes (typically depression), memory problems, paranoia, hypersomnolence, aggressive behavior, agitation, and catatonia have been associated with paraneoplastic syndromes.4-6
Common malignant associations include small cell lung carcinoma (most common) and breast, stomach, colon, renal, bladder, ovarian, uterine, testicular, cell line, and thymic cancers. Research strongly suggests an autoimmune mechanism: tumor-related antibodies cross-react with similar antigens in the neurologic system. Paraneoplastic symptoms often precede symptoms of the malignancy, and the diagnosis is suggested by positive imaging and a paraneoplastic panel.
Anti-NMDA receptor limbic encephalitis is a paraneoplastic syndrome associated with ovarian teratomas and antibodies specific to the glutamate receptor. It is thought to be an autoimmune phenomenon whereby tumor-related antibodies elicit an immune response within certain parts of the neurologic system. Ms. T represents a typical clinical presentation of this syndrome—she is a young, otherwise healthy woman with:
- preceding headache
- new-onset psychotic symptoms
- seizure activity (particularly in the temporal lobes)
- central hypoventilation
- hyperthermia and tachycardia
- dyskinesia and catatonia-like symptoms.5
TREATMENT: Rapid improvement
After removal of the dermoid lesion and IV corticosteroids, Ms. T exhibits rapid improvement. She begins acknowledging others in the room, making eye contact for nearly the first time during this hospitalization, and starts recognizing family members. She also begins verbalizing, responding appropriately to questions in 1 or 2 words. After a 34-day hospital stay, Ms. T is transferred to another facility for rehabilitation; her medication list consists of a corticosteroid taper from prednisone, 20 mg/d, over 2 weeks; fosphenytoin, 200 mg bid; and levetiracetam, 1,000 mg bid.
She eventually is discharged from the rehabilitation facility with noted improvement in multiple domains: she demonstrates cognitive improvement and can walk short distances. She continues to require 24-hour care and exhibits intermittent agitation.
The authors’ observations
We present the case of a patient with a specific paraneoplastic disorder—anti-NMDA receptor limbic encephalitis—with symptoms mimicking those seen in psychiatric disorders such as schizophrenia and bipolar disorder. These similarities complicate recognition and treatment of the underlying disorder.
Ms. T had a complicated yet typical presentation of anti-NMDA receptor limbic encephalitis ( Table 2 ) that was initially mistaken for a manic episode with psychotic features. The diagnosis was made more complex by the death of her mother 1 week before presentation, which could have precipitated her symptom onset. Similar case reports have appeared in neurologic and—less frequently—psychiatric literature ( Box ).5,7-10
5 Ms. T spent time on psychiatric, internal medicine, and neurologic services before her team established a definitive diagnosis.
Because neurobehavioral symptoms predominate early in the course of paraneoplastic illness,5 psychiatrists should prepare to be the first medical point of contact for these patients.
Table 2
Anti-NMDA receptor encephalitis: Symptoms, findings, and treatment
| Typical presentation |
| Young female Prodromal symptoms New onset psychosis, anxiety, or mood symptoms Catatonia Coma Seizure activity (typically bilateral temporal lobe activity on EEG) Hypoventilation Autonomic instability Dyskinesia |
| Laboratory and radiologic findings |
| CSF or serum antibodies CSF pleocytosis and elevated protein, normal glucose Background slowing or sharp-wave activity on EEG Temporal lobe abnormalities |
| Treatment |
| Tumor resection Immunosuppressants (typically corticosteroids) Intravenous immunoglobulin Plasmapheresis |
| CSF: cerebrospinal fluid; EEG: electroencephalography; NMDA: N-methyl-D-aspartate |
Box
Neurology. Several case reports in neurologic literature describe presentations similar to Ms. T’s.
Sansing et al8 described a 34-year-old woman with prominent psychiatric symptoms who had an immature ovarian teratoma with positive anti-NMDA (N-methyl-D-aspartate) receptor antibody. She was treated with tumor resection, plasmapheresis, and corticosteroids and experienced significant improvement.
Nasky et al7 describe a 23-year-old woman with paranoia, agitation, and delusions. A neoplasm was not identified, but she was anti-NMDA receptor antibody positive and improved with IV corticosteroids and IV immunoglobulin.
Dalmau et al5 compiled a case series analysis of 100 cases of anti-NMDA receptor encephalitis. Tumor removal with IV corticosteroids, IV immunoglobulin, and plasma exchange were the most common treatments. Patients with tumors that were identified and resected had better functional recovery than those without tumor resection.5
Psychiatry. A search of psychiatric literature yielded only 2 pertinent case reports. Lee et al9 described an 11-year-old girl with acute confusion, agitation, paranoia, hallucinations, and later malignant catatonia that improved after removal of an ovarian teratoma. Seki et al10 reported on an 18-year-old woman who presented with schizophrenia-like symptoms of disorganization and loss of self awareness. This patient’s symptoms resolved almost completely after unilateral salpingo-oophorectomy, corticosteroid administration, and plasma exchange.
- Dalmau J, Rosenfeld MR. Paraneoplastic syndromes of the CNS. Lancet Neurol. 2008;7(4):327-340.
- Fosphenytoin • Cerebyx
- Haloperidol • Haldol
- Levetiracetam • Keppra
- Lorazepam • Ativan
- Methylprednisolone • Medrol, Depo-Medrol, others
- Olanzapine • Zyprexa
- Prednisone • Deltasone, Meticorten
- Ziprasidone • Geodon
Drs. Cavalieri and Southammakosane report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. White is a consultant for Pfizer Inc.
1. Buckley PF. Update on the etiology and treatment of schizophrenia and bipolar disorder. CNS Spectr. 2008;13 (2 suppl 1):1-12.
2. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
3. Lyketsos CG, Kozauer N, Rabins PV. Psychiatric manifestations of neurologic disease: where are we headed? Dialogues Clin Neurosci. 2007;9:111-124.
4. Foster AR, Caplan JP. Paraneoplastic limbic encephalitis. Psychosomatics. 2009;50:108-113.
5. Dalmau J, Gleichman AJ, Hughes EG, et al. Anti-NMDA-receptor encephalitis: case series and analysis of the effects of antibodies. Lancet Neurol. 2008;7:1091-1098.
6. Dalmau J, Tuzun E, Hai-Yan W, et al. Paraneoplastic anti-N-methyl-D-aspartate receptor encephalitis associated with ovarian teratoma. Ann Neurol. 2007;61:25-36.
7. Nasky KM, Knittel D, Manos GH. Psychosis associated with anti-N-methyl-D-aspartate receptor antibodies. CNS Spectr. 2008;13(8):699-703.
8. Sansing LH, Tuzun E, Ko MW, et al. A patient with encephalitis associated with NMDA receptor antibodies. Nat Clin Pract Neurol. 2007;3(5):291-296.
9. Lee A, Glick DB, Dinwiddie SH. Electroconvulsive therapy in a pediatric patient with malignant catatonia and paraneoplastic limbic encephalitis. J ECT. 2006;22:267-270.
10. Seki M, Suzuki S, Iizuka T, et al. Neurological response to early removal of ovarian teratoma in anti-NMDAR encephalitis. J Neurol Neurosurg Psychiatry. 2008;79:324-326.
CASE: New-onset psychosis
Ms. T, age 26, presents to the psychiatric emergency room after a 1-week change in behavior. According to her family, Ms. T began to experience hyperactivity, increased rate of speech, and decreased sleep after her mother passed away 1 week ago. On the day of presentation, Ms. T had returned to work after a week’s hiatus. Coworkers brought her to the hospital when Ms. T threw herself on the floor and flailed about. Family members report that Ms. T had been complaining of headache that day and during the preceding week. In the emergency room, the patient is intrusive and easily distractible, although able to give a history.
Ms. T has no psychiatric history. Her family history is positive for bipolar spectrum illness. Our initial consideration is that Ms. T is experiencing mania or psychotic symptoms triggered by the recent loss of her mother. Ms. T is evaluated in the medical emergency room to rule out a primary medical illness. Standard labs and head CT are normal, so she is returned to the psychiatric emergency room. She becomes severely agitated and requires multiple IM antipsychotics—2 courses of haloperidol, 10 mg; 2 courses of ziprasidone, 20 mg; and olanzapine, 10 mg. She is admitted to the inpatient psychiatric service with a diagnosis of psychosis not otherwise specified.
Soon after admission, Ms. T suffers a witnessed generalized tonic-clonic seizure and is transferred to the internal medicine service. After the seizure she is awake but minimally responsive. She does not display purposeful movements, opens her eyes but can follow the examiner only on occasion, and displays periodic facial grimacing. In addition, Ms. T is intermittently hypoxic—requiring supplemental oxygen via nasal cannula—and febrile, with persistent tachycardia. Electroencephalography (EEG) shows nonconvulsive status epilepticus involving the bilateral temporal regions.
Ms. T is transferred to the neurosurgical intensive care unit for monitoring and IV anticonvulsants. Subsequent EEGs demonstrate generalized slowing but no epileptiform activity. An infectious workup is negative. Head MRI shows bilateral cerebellar T2/FLAIR increased signal, which is a nonspecific finding. Cerebrospinal fluid (CSF) studies show lymphocytic pleocytosis and oligoclonal bands. These findings suggest a CSF humoral immune response; an extensive laboratory workup is otherwise largely unremarkable ( Table 1 ).
The authors’ observations
We consider that Ms. T may have schizophrenia. Schizophrenia onset is insidious, often with prodromal symptoms occurring months to years before diagnosis.1,2 In Ms. T, the onset of the disturbance was brief; her family noted a change in behavior for only 1 week before presentation. Given this history, brief psychotic disorder remains high on the differential diagnosis because Ms. T’s disorganized speech and behavior occurred seeming in relation to her mother’s death.
Bipolar disorder is characterized by strong heritability, with risks increasing if there is a first-degree relative with the illness. The hallmark of bipolar I disorder is a manic episode, which presents as:
- decreased need for sleep
- grandiosity
- flight of ideas
- reckless or thoughtless behaviors
- increased energy
- increased productivity
- expansive or irritable mood.
Psychiatric symptoms secondary to seizure disorder are well documented. Cognitive, mood, anxiety, and psychotic phenomena may occur in up to 50% of patients with seizures.3 Typically, these symptoms are categorized as occurring during a seizure, after a seizure (post-ictal), or between seizures (interictal).
Manic syndromes secondary to seizure disorders present in an atypical manner with irritability and hyperactivity. Psychotic syndromes, on the other hand, appear with more classic schizophrenia-type symptoms:
- paranoia and persecutory delusions
- auditory and visual hallucinations
- amotivation
- apathy
- flattened affect
- disorganization.3
Paraneoplastic syndromes may be associated with mood changes and other psychiatric symptoms.4-6 Diagnosis is contingent on discovering the primary neoplasm, with or without specific paraneoplastic antibodies. Treatment is tailored to the oncologic process.
Table 1
Ms. T’s laboratory workup*
| Test | Result |
|---|---|
| C-reactive protein | 0.7 |
| Erythrocyte sedimentation rate | 5 |
| Cryptococcal antigen (serum) | Negative |
| Antinuclear antibody | Negative |
| CSF lymphocytes | 88 |
| CSF nucleated cells | 200 |
| CSF RBC | 33 |
| CSF glucose | 44 |
| CSF protein | 45 |
| CSF igG index | 1.2 |
| CSF oligoclonal bands | Present |
| CSF: cerebrospinal fluid; igG: immunoglobulin G; RBC: red blood cell | |
| *Results were negative for gonorrhea, chlamydia, lupus, human immunodeficiency virus, syphilis, Lyme disease, varicella zoster virus, West Nile virus, herpes simplex virus, Epstein-Barr virus, cytomegalovirus, tuberculosis, and California, St. Louis, eastern equine, and western equine encephalitis | |
EVALUATION: A medical cause
The psychiatry consultation-liaison service is asked to further evaluate Ms. T for psychiatric contributions to her continued altered mental status. Ms. T remains in restraints and receives fosphenytoin, 200 mg bid; levetiracetam, 1,000 mg bid; and lorazepam as needed for agitation. Following consultation, the team considers a working diagnosis of an autoimmune encephalopathy based on the negative infectious workup, the patient’s demographics, and the clinical picture (psychiatric symptoms, seizure, and encephalopathy). Ms. T undergoes 5 courses of plasma exchange with no effect. Catatonia is considered, but the patient does not demonstrate significant change with numerous doses of lorazepam.
Because Ms. T does not improve, the team starts a more specific paraneoplastic workup. MRI reveals a 9-mm lesion on her right ovary. Corticosteroids, including IV methylprednisolone, 1 g/d, are started. Ms. T’s clinical presentation improves; soon after scheduled corticosteroid dosing, she is taken to the operating room for right salpingo-oophorectomy. Surgical pathology later confirms the lesion as a mature teratoma. A standard paraneoplastic panel is negative; a separate test for anti-NMDA (N-methyl-D-aspartate) receptor antibodies is positive, however, and confirms the diagnosis of ovarian mass-associated anti-NMDA receptor limbic encephalitis.
Paraneoplastic syndromes
This case represents the interface between a complicated medical phenomenon and psychiatric symptomatology. Mood changes (typically depression), memory problems, paranoia, hypersomnolence, aggressive behavior, agitation, and catatonia have been associated with paraneoplastic syndromes.4-6
Common malignant associations include small cell lung carcinoma (most common) and breast, stomach, colon, renal, bladder, ovarian, uterine, testicular, cell line, and thymic cancers. Research strongly suggests an autoimmune mechanism: tumor-related antibodies cross-react with similar antigens in the neurologic system. Paraneoplastic symptoms often precede symptoms of the malignancy, and the diagnosis is suggested by positive imaging and a paraneoplastic panel.
Anti-NMDA receptor limbic encephalitis is a paraneoplastic syndrome associated with ovarian teratomas and antibodies specific to the glutamate receptor. It is thought to be an autoimmune phenomenon whereby tumor-related antibodies elicit an immune response within certain parts of the neurologic system. Ms. T represents a typical clinical presentation of this syndrome—she is a young, otherwise healthy woman with:
- preceding headache
- new-onset psychotic symptoms
- seizure activity (particularly in the temporal lobes)
- central hypoventilation
- hyperthermia and tachycardia
- dyskinesia and catatonia-like symptoms.5
TREATMENT: Rapid improvement
After removal of the dermoid lesion and IV corticosteroids, Ms. T exhibits rapid improvement. She begins acknowledging others in the room, making eye contact for nearly the first time during this hospitalization, and starts recognizing family members. She also begins verbalizing, responding appropriately to questions in 1 or 2 words. After a 34-day hospital stay, Ms. T is transferred to another facility for rehabilitation; her medication list consists of a corticosteroid taper from prednisone, 20 mg/d, over 2 weeks; fosphenytoin, 200 mg bid; and levetiracetam, 1,000 mg bid.
She eventually is discharged from the rehabilitation facility with noted improvement in multiple domains: she demonstrates cognitive improvement and can walk short distances. She continues to require 24-hour care and exhibits intermittent agitation.
The authors’ observations
We present the case of a patient with a specific paraneoplastic disorder—anti-NMDA receptor limbic encephalitis—with symptoms mimicking those seen in psychiatric disorders such as schizophrenia and bipolar disorder. These similarities complicate recognition and treatment of the underlying disorder.
Ms. T had a complicated yet typical presentation of anti-NMDA receptor limbic encephalitis ( Table 2 ) that was initially mistaken for a manic episode with psychotic features. The diagnosis was made more complex by the death of her mother 1 week before presentation, which could have precipitated her symptom onset. Similar case reports have appeared in neurologic and—less frequently—psychiatric literature ( Box ).5,7-10
5 Ms. T spent time on psychiatric, internal medicine, and neurologic services before her team established a definitive diagnosis.
Because neurobehavioral symptoms predominate early in the course of paraneoplastic illness,5 psychiatrists should prepare to be the first medical point of contact for these patients.
Table 2
Anti-NMDA receptor encephalitis: Symptoms, findings, and treatment
| Typical presentation |
| Young female Prodromal symptoms New onset psychosis, anxiety, or mood symptoms Catatonia Coma Seizure activity (typically bilateral temporal lobe activity on EEG) Hypoventilation Autonomic instability Dyskinesia |
| Laboratory and radiologic findings |
| CSF or serum antibodies CSF pleocytosis and elevated protein, normal glucose Background slowing or sharp-wave activity on EEG Temporal lobe abnormalities |
| Treatment |
| Tumor resection Immunosuppressants (typically corticosteroids) Intravenous immunoglobulin Plasmapheresis |
| CSF: cerebrospinal fluid; EEG: electroencephalography; NMDA: N-methyl-D-aspartate |
Box
Neurology. Several case reports in neurologic literature describe presentations similar to Ms. T’s.
Sansing et al8 described a 34-year-old woman with prominent psychiatric symptoms who had an immature ovarian teratoma with positive anti-NMDA (N-methyl-D-aspartate) receptor antibody. She was treated with tumor resection, plasmapheresis, and corticosteroids and experienced significant improvement.
Nasky et al7 describe a 23-year-old woman with paranoia, agitation, and delusions. A neoplasm was not identified, but she was anti-NMDA receptor antibody positive and improved with IV corticosteroids and IV immunoglobulin.
Dalmau et al5 compiled a case series analysis of 100 cases of anti-NMDA receptor encephalitis. Tumor removal with IV corticosteroids, IV immunoglobulin, and plasma exchange were the most common treatments. Patients with tumors that were identified and resected had better functional recovery than those without tumor resection.5
Psychiatry. A search of psychiatric literature yielded only 2 pertinent case reports. Lee et al9 described an 11-year-old girl with acute confusion, agitation, paranoia, hallucinations, and later malignant catatonia that improved after removal of an ovarian teratoma. Seki et al10 reported on an 18-year-old woman who presented with schizophrenia-like symptoms of disorganization and loss of self awareness. This patient’s symptoms resolved almost completely after unilateral salpingo-oophorectomy, corticosteroid administration, and plasma exchange.
- Dalmau J, Rosenfeld MR. Paraneoplastic syndromes of the CNS. Lancet Neurol. 2008;7(4):327-340.
- Fosphenytoin • Cerebyx
- Haloperidol • Haldol
- Levetiracetam • Keppra
- Lorazepam • Ativan
- Methylprednisolone • Medrol, Depo-Medrol, others
- Olanzapine • Zyprexa
- Prednisone • Deltasone, Meticorten
- Ziprasidone • Geodon
Drs. Cavalieri and Southammakosane report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. White is a consultant for Pfizer Inc.
CASE: New-onset psychosis
Ms. T, age 26, presents to the psychiatric emergency room after a 1-week change in behavior. According to her family, Ms. T began to experience hyperactivity, increased rate of speech, and decreased sleep after her mother passed away 1 week ago. On the day of presentation, Ms. T had returned to work after a week’s hiatus. Coworkers brought her to the hospital when Ms. T threw herself on the floor and flailed about. Family members report that Ms. T had been complaining of headache that day and during the preceding week. In the emergency room, the patient is intrusive and easily distractible, although able to give a history.
Ms. T has no psychiatric history. Her family history is positive for bipolar spectrum illness. Our initial consideration is that Ms. T is experiencing mania or psychotic symptoms triggered by the recent loss of her mother. Ms. T is evaluated in the medical emergency room to rule out a primary medical illness. Standard labs and head CT are normal, so she is returned to the psychiatric emergency room. She becomes severely agitated and requires multiple IM antipsychotics—2 courses of haloperidol, 10 mg; 2 courses of ziprasidone, 20 mg; and olanzapine, 10 mg. She is admitted to the inpatient psychiatric service with a diagnosis of psychosis not otherwise specified.
Soon after admission, Ms. T suffers a witnessed generalized tonic-clonic seizure and is transferred to the internal medicine service. After the seizure she is awake but minimally responsive. She does not display purposeful movements, opens her eyes but can follow the examiner only on occasion, and displays periodic facial grimacing. In addition, Ms. T is intermittently hypoxic—requiring supplemental oxygen via nasal cannula—and febrile, with persistent tachycardia. Electroencephalography (EEG) shows nonconvulsive status epilepticus involving the bilateral temporal regions.
Ms. T is transferred to the neurosurgical intensive care unit for monitoring and IV anticonvulsants. Subsequent EEGs demonstrate generalized slowing but no epileptiform activity. An infectious workup is negative. Head MRI shows bilateral cerebellar T2/FLAIR increased signal, which is a nonspecific finding. Cerebrospinal fluid (CSF) studies show lymphocytic pleocytosis and oligoclonal bands. These findings suggest a CSF humoral immune response; an extensive laboratory workup is otherwise largely unremarkable ( Table 1 ).
The authors’ observations
We consider that Ms. T may have schizophrenia. Schizophrenia onset is insidious, often with prodromal symptoms occurring months to years before diagnosis.1,2 In Ms. T, the onset of the disturbance was brief; her family noted a change in behavior for only 1 week before presentation. Given this history, brief psychotic disorder remains high on the differential diagnosis because Ms. T’s disorganized speech and behavior occurred seeming in relation to her mother’s death.
Bipolar disorder is characterized by strong heritability, with risks increasing if there is a first-degree relative with the illness. The hallmark of bipolar I disorder is a manic episode, which presents as:
- decreased need for sleep
- grandiosity
- flight of ideas
- reckless or thoughtless behaviors
- increased energy
- increased productivity
- expansive or irritable mood.
Psychiatric symptoms secondary to seizure disorder are well documented. Cognitive, mood, anxiety, and psychotic phenomena may occur in up to 50% of patients with seizures.3 Typically, these symptoms are categorized as occurring during a seizure, after a seizure (post-ictal), or between seizures (interictal).
Manic syndromes secondary to seizure disorders present in an atypical manner with irritability and hyperactivity. Psychotic syndromes, on the other hand, appear with more classic schizophrenia-type symptoms:
- paranoia and persecutory delusions
- auditory and visual hallucinations
- amotivation
- apathy
- flattened affect
- disorganization.3
Paraneoplastic syndromes may be associated with mood changes and other psychiatric symptoms.4-6 Diagnosis is contingent on discovering the primary neoplasm, with or without specific paraneoplastic antibodies. Treatment is tailored to the oncologic process.
Table 1
Ms. T’s laboratory workup*
| Test | Result |
|---|---|
| C-reactive protein | 0.7 |
| Erythrocyte sedimentation rate | 5 |
| Cryptococcal antigen (serum) | Negative |
| Antinuclear antibody | Negative |
| CSF lymphocytes | 88 |
| CSF nucleated cells | 200 |
| CSF RBC | 33 |
| CSF glucose | 44 |
| CSF protein | 45 |
| CSF igG index | 1.2 |
| CSF oligoclonal bands | Present |
| CSF: cerebrospinal fluid; igG: immunoglobulin G; RBC: red blood cell | |
| *Results were negative for gonorrhea, chlamydia, lupus, human immunodeficiency virus, syphilis, Lyme disease, varicella zoster virus, West Nile virus, herpes simplex virus, Epstein-Barr virus, cytomegalovirus, tuberculosis, and California, St. Louis, eastern equine, and western equine encephalitis | |
EVALUATION: A medical cause
The psychiatry consultation-liaison service is asked to further evaluate Ms. T for psychiatric contributions to her continued altered mental status. Ms. T remains in restraints and receives fosphenytoin, 200 mg bid; levetiracetam, 1,000 mg bid; and lorazepam as needed for agitation. Following consultation, the team considers a working diagnosis of an autoimmune encephalopathy based on the negative infectious workup, the patient’s demographics, and the clinical picture (psychiatric symptoms, seizure, and encephalopathy). Ms. T undergoes 5 courses of plasma exchange with no effect. Catatonia is considered, but the patient does not demonstrate significant change with numerous doses of lorazepam.
Because Ms. T does not improve, the team starts a more specific paraneoplastic workup. MRI reveals a 9-mm lesion on her right ovary. Corticosteroids, including IV methylprednisolone, 1 g/d, are started. Ms. T’s clinical presentation improves; soon after scheduled corticosteroid dosing, she is taken to the operating room for right salpingo-oophorectomy. Surgical pathology later confirms the lesion as a mature teratoma. A standard paraneoplastic panel is negative; a separate test for anti-NMDA (N-methyl-D-aspartate) receptor antibodies is positive, however, and confirms the diagnosis of ovarian mass-associated anti-NMDA receptor limbic encephalitis.
Paraneoplastic syndromes
This case represents the interface between a complicated medical phenomenon and psychiatric symptomatology. Mood changes (typically depression), memory problems, paranoia, hypersomnolence, aggressive behavior, agitation, and catatonia have been associated with paraneoplastic syndromes.4-6
Common malignant associations include small cell lung carcinoma (most common) and breast, stomach, colon, renal, bladder, ovarian, uterine, testicular, cell line, and thymic cancers. Research strongly suggests an autoimmune mechanism: tumor-related antibodies cross-react with similar antigens in the neurologic system. Paraneoplastic symptoms often precede symptoms of the malignancy, and the diagnosis is suggested by positive imaging and a paraneoplastic panel.
Anti-NMDA receptor limbic encephalitis is a paraneoplastic syndrome associated with ovarian teratomas and antibodies specific to the glutamate receptor. It is thought to be an autoimmune phenomenon whereby tumor-related antibodies elicit an immune response within certain parts of the neurologic system. Ms. T represents a typical clinical presentation of this syndrome—she is a young, otherwise healthy woman with:
- preceding headache
- new-onset psychotic symptoms
- seizure activity (particularly in the temporal lobes)
- central hypoventilation
- hyperthermia and tachycardia
- dyskinesia and catatonia-like symptoms.5
TREATMENT: Rapid improvement
After removal of the dermoid lesion and IV corticosteroids, Ms. T exhibits rapid improvement. She begins acknowledging others in the room, making eye contact for nearly the first time during this hospitalization, and starts recognizing family members. She also begins verbalizing, responding appropriately to questions in 1 or 2 words. After a 34-day hospital stay, Ms. T is transferred to another facility for rehabilitation; her medication list consists of a corticosteroid taper from prednisone, 20 mg/d, over 2 weeks; fosphenytoin, 200 mg bid; and levetiracetam, 1,000 mg bid.
She eventually is discharged from the rehabilitation facility with noted improvement in multiple domains: she demonstrates cognitive improvement and can walk short distances. She continues to require 24-hour care and exhibits intermittent agitation.
The authors’ observations
We present the case of a patient with a specific paraneoplastic disorder—anti-NMDA receptor limbic encephalitis—with symptoms mimicking those seen in psychiatric disorders such as schizophrenia and bipolar disorder. These similarities complicate recognition and treatment of the underlying disorder.
Ms. T had a complicated yet typical presentation of anti-NMDA receptor limbic encephalitis ( Table 2 ) that was initially mistaken for a manic episode with psychotic features. The diagnosis was made more complex by the death of her mother 1 week before presentation, which could have precipitated her symptom onset. Similar case reports have appeared in neurologic and—less frequently—psychiatric literature ( Box ).5,7-10
5 Ms. T spent time on psychiatric, internal medicine, and neurologic services before her team established a definitive diagnosis.
Because neurobehavioral symptoms predominate early in the course of paraneoplastic illness,5 psychiatrists should prepare to be the first medical point of contact for these patients.
Table 2
Anti-NMDA receptor encephalitis: Symptoms, findings, and treatment
| Typical presentation |
| Young female Prodromal symptoms New onset psychosis, anxiety, or mood symptoms Catatonia Coma Seizure activity (typically bilateral temporal lobe activity on EEG) Hypoventilation Autonomic instability Dyskinesia |
| Laboratory and radiologic findings |
| CSF or serum antibodies CSF pleocytosis and elevated protein, normal glucose Background slowing or sharp-wave activity on EEG Temporal lobe abnormalities |
| Treatment |
| Tumor resection Immunosuppressants (typically corticosteroids) Intravenous immunoglobulin Plasmapheresis |
| CSF: cerebrospinal fluid; EEG: electroencephalography; NMDA: N-methyl-D-aspartate |
Box
Neurology. Several case reports in neurologic literature describe presentations similar to Ms. T’s.
Sansing et al8 described a 34-year-old woman with prominent psychiatric symptoms who had an immature ovarian teratoma with positive anti-NMDA (N-methyl-D-aspartate) receptor antibody. She was treated with tumor resection, plasmapheresis, and corticosteroids and experienced significant improvement.
Nasky et al7 describe a 23-year-old woman with paranoia, agitation, and delusions. A neoplasm was not identified, but she was anti-NMDA receptor antibody positive and improved with IV corticosteroids and IV immunoglobulin.
Dalmau et al5 compiled a case series analysis of 100 cases of anti-NMDA receptor encephalitis. Tumor removal with IV corticosteroids, IV immunoglobulin, and plasma exchange were the most common treatments. Patients with tumors that were identified and resected had better functional recovery than those without tumor resection.5
Psychiatry. A search of psychiatric literature yielded only 2 pertinent case reports. Lee et al9 described an 11-year-old girl with acute confusion, agitation, paranoia, hallucinations, and later malignant catatonia that improved after removal of an ovarian teratoma. Seki et al10 reported on an 18-year-old woman who presented with schizophrenia-like symptoms of disorganization and loss of self awareness. This patient’s symptoms resolved almost completely after unilateral salpingo-oophorectomy, corticosteroid administration, and plasma exchange.
- Dalmau J, Rosenfeld MR. Paraneoplastic syndromes of the CNS. Lancet Neurol. 2008;7(4):327-340.
- Fosphenytoin • Cerebyx
- Haloperidol • Haldol
- Levetiracetam • Keppra
- Lorazepam • Ativan
- Methylprednisolone • Medrol, Depo-Medrol, others
- Olanzapine • Zyprexa
- Prednisone • Deltasone, Meticorten
- Ziprasidone • Geodon
Drs. Cavalieri and Southammakosane report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. White is a consultant for Pfizer Inc.
1. Buckley PF. Update on the etiology and treatment of schizophrenia and bipolar disorder. CNS Spectr. 2008;13 (2 suppl 1):1-12.
2. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
3. Lyketsos CG, Kozauer N, Rabins PV. Psychiatric manifestations of neurologic disease: where are we headed? Dialogues Clin Neurosci. 2007;9:111-124.
4. Foster AR, Caplan JP. Paraneoplastic limbic encephalitis. Psychosomatics. 2009;50:108-113.
5. Dalmau J, Gleichman AJ, Hughes EG, et al. Anti-NMDA-receptor encephalitis: case series and analysis of the effects of antibodies. Lancet Neurol. 2008;7:1091-1098.
6. Dalmau J, Tuzun E, Hai-Yan W, et al. Paraneoplastic anti-N-methyl-D-aspartate receptor encephalitis associated with ovarian teratoma. Ann Neurol. 2007;61:25-36.
7. Nasky KM, Knittel D, Manos GH. Psychosis associated with anti-N-methyl-D-aspartate receptor antibodies. CNS Spectr. 2008;13(8):699-703.
8. Sansing LH, Tuzun E, Ko MW, et al. A patient with encephalitis associated with NMDA receptor antibodies. Nat Clin Pract Neurol. 2007;3(5):291-296.
9. Lee A, Glick DB, Dinwiddie SH. Electroconvulsive therapy in a pediatric patient with malignant catatonia and paraneoplastic limbic encephalitis. J ECT. 2006;22:267-270.
10. Seki M, Suzuki S, Iizuka T, et al. Neurological response to early removal of ovarian teratoma in anti-NMDAR encephalitis. J Neurol Neurosurg Psychiatry. 2008;79:324-326.
1. Buckley PF. Update on the etiology and treatment of schizophrenia and bipolar disorder. CNS Spectr. 2008;13 (2 suppl 1):1-12.
2. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
3. Lyketsos CG, Kozauer N, Rabins PV. Psychiatric manifestations of neurologic disease: where are we headed? Dialogues Clin Neurosci. 2007;9:111-124.
4. Foster AR, Caplan JP. Paraneoplastic limbic encephalitis. Psychosomatics. 2009;50:108-113.
5. Dalmau J, Gleichman AJ, Hughes EG, et al. Anti-NMDA-receptor encephalitis: case series and analysis of the effects of antibodies. Lancet Neurol. 2008;7:1091-1098.
6. Dalmau J, Tuzun E, Hai-Yan W, et al. Paraneoplastic anti-N-methyl-D-aspartate receptor encephalitis associated with ovarian teratoma. Ann Neurol. 2007;61:25-36.
7. Nasky KM, Knittel D, Manos GH. Psychosis associated with anti-N-methyl-D-aspartate receptor antibodies. CNS Spectr. 2008;13(8):699-703.
8. Sansing LH, Tuzun E, Ko MW, et al. A patient with encephalitis associated with NMDA receptor antibodies. Nat Clin Pract Neurol. 2007;3(5):291-296.
9. Lee A, Glick DB, Dinwiddie SH. Electroconvulsive therapy in a pediatric patient with malignant catatonia and paraneoplastic limbic encephalitis. J ECT. 2006;22:267-270.
10. Seki M, Suzuki S, Iizuka T, et al. Neurological response to early removal of ovarian teratoma in anti-NMDAR encephalitis. J Neurol Neurosurg Psychiatry. 2008;79:324-326.
A mysterious case of mania
CASE: First-episode mania
Mrs. P, age 47, is brought to the emergency department (ED) because her family is concerned about her behavioral changes over the last week. Her husband reports that Mrs. P has become hyper-religious and talkative. She has been perseverating on numbers and dates and incessantly calling people. Mrs. P reports increased energy and decreased need for sleep. On examination, she has pressured speech. She has no psychiatric history; however, for the past year, she has been taking sertraline, 100 mg/d, and desipramine, 25 mg/d, which her primary care physician prescribed for unknown reasons.
Mrs. P has struggled with chronic back pain for years, but an MRI of her spine is negative. Her family strongly believes that for the past 3 years Mrs. P has been receiving too many medications from her pain management specialist. Six weeks before her current presentation, she was receiving methadone, 40 mg/d, hydrocodone, at least 20 mg/d, and tramadol, 400 mg/d in divided doses. She also was taking an unknown dose of at least 1 benzodiazepine.
Mrs. P’s husband notes she stopped taking methadone abruptly approximately 5 weeks ago. However, about 3 weeks ago, Mrs. P accidentally overdosed on opioids and was hospitalized for several days. Urine drug screen at the time was positive for acetaminophen, salicylate, propoxyphene, opiate, benzodiazepine, and tricyclic antidepressant.
Mrs. P’s medical history includes auditory nerve loss from birth; her mother had German measles (rubella). Mrs. P never learned American Sign Language. She underwent cochlear implant surgery 1 year ago and now has only mild difficulties speaking.
The authors’ observations
Manic symptoms are common in patients with comorbid medical disorders and present a diagnostic challenge. Obtaining an accurate history from the patient may be difficult. Such evaluations often require extensive investigation and collection of data from multiple sources, including:
- medical records
- family members
- patient observation.
Mrs. P’s history is marked by contradicting data from these sources. For example, her family says she stopped taking “pain medications” 5 weeks ago, but 2 weeks later her urine drug screen showed opioids.
Both illicit drugs and prescribed medications can precipitate manic symptoms. From medical records and drug testing, it was evident that Mrs. P had a history of medication abuse/overdose/misuse.
Mania also has been associated with substance withdrawal. Mrs. P allegedly stopped taking methadone 4 weeks before the onset of manic symptoms. Methadone is a synthetic opioid with a pharmacokinetic and pharmacodynamic profile that presents clinical challenges, including:
- large interindividual variability in methadone pharmacokinetics
- lack of reliable equianalgesic conversion ratio to and from other opioids
- potential for multiple drug interactions and complex pharmacodynamics.
An opioid’s half-life determines the onset and duration of withdrawal syndrome symptoms.1 Methadone metabolism is predominantly mediated by CYP3A4, CYP2B6, CYP2D6, and to some extent by CYP2C19.1 We performed genetic testing to help evaluate how Mrs. P metabolized medications. Mrs. P had a normal genotype for CYP2D6, which meant that she should process opioids at a normal rate; however, she was heterozygous for CYP2C19*2 polymorphism, so it is possible that methadone stayed in her system longer than average.
Evidence documenting methadone drug interactions is limited (Table 1).1 Mrs. P was taking sertraline and desipramine; both have potent effects via 2D6 inhibition that could increase plasma methadone concentration. Other evidence indicates that benzodiazepines and methadone may have synergistic interactions that could increase opioid sedation or respiratory depression.1
Table 1
Is a drug interaction with methadone causing Mrs. P’s mania?
| Medication class/agent | Effect on methadone level | Effect on methadone metabolism | Additional effects of interaction |
|---|---|---|---|
| Selective serotonin reuptake inhibitors | |||
| Fluvoxamine | Increase | Inhibition | Opioid toxicity |
| Fluoxetine | Increase | Inhibition | Torsades de pointes |
| Paroxetine | Increase | Inhibition | Decreased hepatic metabolism |
| Sertraline* | Increase | Autoinduction | Torsades de pointes |
| Citalopram | — | — | Torsades de pointes |
| Tricyclic antidepressants | |||
| Desipramine* | — | Inhibition | Increased desipramine levels/inhibition of desipramine metabolism |
| Amitriptyline | Increase methadone clearance | — | Torsades de pointes/prolonged QT interval |
| Anti-inflammatory drugs | |||
| NSAIDs* | — | — | Enhanced analgesia/opioid-sparing effect |
| Aspirin* | — | — | Paradoxical activation of platelet receptors |
| Benzodiazepines | |||
| Alprazolam | — | — | CNS depression/sedation/overdose |
| Diazepam* | — | Inhibition | Additive depressant effects |
| Opioid agonists | |||
| Dextromethorphan | — | Inhibition (not significant) | Increased side effects, especially sleepiness and drowsiness |
| Tramadol* | — | — | Well tolerated |
| Nicotine | Decrease | Can increase smoking rate | |
| *Medications taken by Mrs. P | |||
| NSAIDs: nonsteroidal anti-inflammatory drugs | |||
| Source: Reference 1 | |||
EVALUATION: Few clues
In our ED, Mrs. P’s urine drug abuse screen is positive for salicylate and benzodiazepine only. Findings from physical examination, vital signs, ECG, and chest radiography are within normal limits. Internal medicine consultation is unremarkable. Mrs. P’s laboratory investigation is notable for an elevated white blood cell count, but this normalizes over a week.
Mrs. P shows no evidence of infection and is normoglycemic. B12 and folate are within normal limits. Serum electrolytes, liver function testing, sensitive thyroid stimulating hormone, and C-reactive protein are within normal limits. Urinalysis is negative except for a small amount of hemoglobin. Her creatine kinase (CK) is in the upper normal range. Human immunodeficiency virus (HIV) and syphilis testing is negative. Ceruloplasmin level also is normal. Heavy metal screen is negative. Head MRI and CT from previous hospitalizations were unremarkable.
The authors’ observations
Our first step was to clarify Mrs. P’s diagnosis. In reviewing differential diagnoses, we considered:
- serotonin syndrome
- benzodiazepine withdrawal syndrome
- antidepressant-induced mania
- adrenergic toxicity
- malignant hyperthermia
- heat stroke
- infectious causes.
Our index of suspicion for serotonin syndrome was low because Mrs. P didn’t meet criteria required for diagnosis. Relevant signs and symptoms included confusion, elevated mood (major) and agitation, nervousness, insomnia, and low blood pressure (minor).
Based on concerns about medication interactions, we discontinued sertraline and desipramine. According to the patient’s sister, Mrs. P’s manic symptoms markedly responded to PRN doses of lorazepam. We prescribed lorazepam, 1 mg every 6 hours, and observed Mrs. P for signs and symptoms of benzodiazepine withdrawal.
HISTORY: OTC drug use
According to Mrs. P’s mother, after her daughter abruptly discontinued methadone, she began to have very strong headaches, which she treated with Excedrin or Excedrin Sinus. The mother said that 4 days before Mrs. P came to the ED, she found her daughter holding 4 tablets of Excedrin and an empty bottle. Unfortunately her mother was unable to say what type of Excedrin it was. When the treatment team asks Mrs. P how many pills she usually takes, she says she doesn’t know but usually until the pain stops.
The authors’ observations
Management of secondary mania should focus on treating the underlying condition (Algorithm). Neurology categorizes mania into 3 categories:2
- confusional-delirious states
- manic symptoms associated with focal or multifocal cerebral lesions
- affective disorders (manic-depressive and depressive psychoses).
Medical workup ruled out common secondary causes of psychosis. Collaborative information from relatives revealed no family history of mental illness.
Patients with hearing loss and deafness have been shown to be at increased risk for psychotic disorders compared with the general population. Severe sensory deficits early in Mrs. P’s life may have influenced the orderly development of neural connections in her sensory cortex and association areas.3 Mrs. P was deaf for the first 45 years of life. It could be hypothesized that her sensory deficits significantly influenced her ability to reality test. After receiving a cochlear implant, Mrs. P rapidly went from no auditory stimulation to marked improvement. This stressor might precipitate psychotic symptoms. However, her presentation seemed to be characterized more by manic symptoms or an agitated delirium. It also did not fit temporally with her presentation.
We begin to suspect that Mrs. P’s mania is substance-induced. Excedrin, an over-the-counter medication, contains aspirin and caffeine. Excedrin Sinus also contains phenylephrine. Amphetamines, caffeine, ephedrine, pseudoephedrine, and phenylpropanolamine have all been linked to manic-like psychotic episodes.
Concerns about the illicit conversion of pseudoephedrine into methamphetamine obliged pharmaceutical companies in the United States to switch product formulations to phenylephrine in 2005,4 although some “behind-the-counter” medications may contain pseudoephedrine. Phenylephrine is a relatively selective α1 agonist with weak α2 adrenoceptor agonist activity and low β agonist activity. It is very similar to pseudo-ephedrine, which is known to be implicated in the development of manic symptoms.5,6
Pseudoephedrine can raise CK levels and cause rhabdomyolysis.7,8 Mrs. P’s CK level was 176 (normal range 36 to 176 U/L) 4 days after her initial presentation, and she had a moderate amount of myoglobin in her urine. Her creatinine was normal. The patient was taking excessive amounts of caffeine and—if she was using Excedrin Sinus—pseudoephedrine or phenylephrine. We were unable to determine whether her Excedrin contained pseudoephedrine or phenylephrine. In addition, she was going through opioid withdrawal and reported problems with her sleep. There was also a question of Mrs. P’s unknown methadone use combined with its decreased clearance secondary to medication interactions.
While previously hospitalized for overdose, Mrs. P tested positive for propoxyphene. Excessive use of propoxyphene also can cause numerous adverse reactions. Some of that could have explained why Mrs. P’s presentation includes nervousness, CNS stimulation, excitement, insomnia, and restlessness.5
Based on multiple factors, we believe Mrs. P meets DSM-IV-TR criteria for substance-induced mood disorder (Table 2).9 This diagnosis is supported by Mrs. P’s history of complex polypharmacy, excessive caffeine use, sleep deprivation, and possible opioid withdrawal.
Algorithm: Managing substance-induced manic disorder
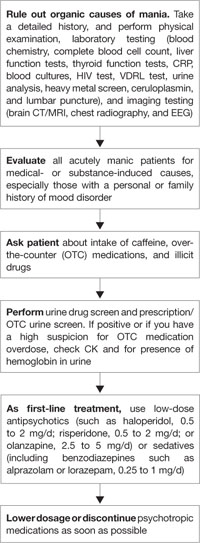
CK: creatine kinase; CRP: C-reactive protein; CT: computed tomography; EEG: electroencephalogram; HIV: human immunodeficiency virus; MRI: magnetic resonance imaging; VDRL: venereal disease research laboratoryTable 2
DSM-IV-TR criteria for substance-induced mood disorder*
| A. A prominent and persistent disturbance in mood predominates in the clinical picture and is characterized by either (or both) of the following: 1. depressed mood or markedly diminished interest or pleasure in all, or almost all, activities 2. elevated, expansive, or irritable mood |
| B. There is evidence from the history, physical examination, or laboratory findings of: 1. the symptoms in Criterion A developed during, or within 1 month of, substance intoxication or withdrawal, or 2. medication use is etiologically related to the disturbance |
| C. The disturbance is not better accounted for by a mood disorder that is not substance-induced |
| D. The disturbance does not occur exclusively during the course of a delirium |
| E. The symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning |
| Minimal criteria are A plus B plus E |
| *Make this diagnosis only when mood symptoms are in excess of those usually associated with substance intoxication or substance withdrawal syndrome and when symptoms are sufficiently severe to warrant independent clinical attention |
| Source: Reference 9 |
TREATMENT: Escalating symptoms
While hospitalized, Mrs. P focuses solely on receiving pain medication. She does not know why she is in the hospital. She is easily distractible, intermittently intrusive, and disorganized and tangential in her thought process.
Two days after admission, her uncontrolled behavior escalates and she has marked psychomotor agitation. She is confused but remains oriented to time, place, and person. We start treatment with risperidone, 0.5 mg each morning and 1 mg at bedtime, because this agent is well tolerated, efficacious, and easily titrated to symptom response. Mrs. P’s symptoms improve, but she does not return to her reported baseline. Two days later, we increase risperidone to 1 mg every morning and 2 mg at bedtime. On the 6th day of hospitalization, Mrs. P is more organized and able to follow simple commands. She denies auditory or visual hallucinations. On the 10th day, she improves markedly and is back to her baseline level of functioning.
We perform psychological testing, including the Wechsler Adult Intelligence Scale (WAIS III) and the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS, Form A). The results show global neurocognitive deficits. Mrs. P’s intellectual skill is significantly below average, with verbal abilities reflecting functioning in the mildly retarded range. Nonverbal skills were stronger but still below average. Mrs. P’s capacity to learn and retain new information and to understand even modestly complex concepts is quite limited.
Because of Mrs. P’s long history of poly-substance abuse, inability to process information, and chronic back pain, we judge her to be at high risk for relapse. However, Mrs. P and her family are not interested in chemical dependence treatment.
This left us facing a difficult clinical situation. Mrs. P had a pattern of presenting to multiple physicians and eventually receiving narcotics. Her family provided transportation for her to these appointments but also was concerned about her drug use. With the patient and her family, we carefully outline Mrs. P’s treatment needs, including:
- medication monitoring by a psychiatrist after discharge
- a single, consistent primary care physician to manage her care
- a treatment plan shared by all clinicians involved in her care.
We review with Mrs. P and her family the benefits of behavioral approaches to chronic pain management. They agree to our recommendation that the family control Mrs. P’s medication supply. We discharge her on risperidone, 0.5 mg each morning and 1 mg at bedtime, and she is scheduled for follow-up with a local psychiatrist.
Related resource
- Krauthammer C, Klerman GL. Manic syndromes associated with antecedent physical illness or drugs. Arch Gen Psychiatry. 1978;35(11):1333-1339.
Drug brand names
- Alprazolam • Xanax
- Amitriptyline • Elavil
- Citalopram • Celexa
- Desipramine • Norpramin
- Diazepam • Valium
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Hydrocodone • Vicodin, Lortab, others
- Lorazepam • Ativan
- Methadone • Dolophine, Methadose
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Propoxyphene • Darvon, Darvocet, others
- Risperidone • Risperdal
- Sertraline • Zoloft
- Tramadol • Ultram
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. De Fazio S, Gallelli L, De Siena A, et al. Role of CYP3A5 in abnormal clearance methadone. Ann Pharmacother. 2008;42(6):893-897.
2. Ropper AH, Brown RH. Adams and Victor’s principles of neurology. 8th ed. New York, NY: McGraw-Hill Professional; 2005.
3. Thewissen V, Myin-Germeys I, Bentall R, et al. Hearing impairment and psychosis revisited. Schizophr Res. 2005;76(1):99-103.
4. Eccles R. Substitution of phenylephrine for pseudoephedrine as a nasal decongeststant. An illogical way to control methamphetamine abuse. Br J Clin Pharmacol. 2007;63(1):10-14.
5. Wilson H, Woods D. Pseudoephedrine causing mania-like symptoms. N Z Med J. 2002;115(1148):86.-
6. Dalton R. Mixed bipolar disorder precipitated by pseudoephedrine hydrochloride. South Med J. 1990;83(1):64-65.
7. Mansi IA, Huang J. Rhabdomyolysis in response to weight-loss herbal medicine. Am J Med Sci. 2004;327:356-357.
8. Sandhu RS, Como JJ, Scalea TS. Renal failure and exercise-induced rhabdomyolysis in patients taking performance-enhancing compounds. J Trauma. 2002;53:761-764.
9. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
CASE: First-episode mania
Mrs. P, age 47, is brought to the emergency department (ED) because her family is concerned about her behavioral changes over the last week. Her husband reports that Mrs. P has become hyper-religious and talkative. She has been perseverating on numbers and dates and incessantly calling people. Mrs. P reports increased energy and decreased need for sleep. On examination, she has pressured speech. She has no psychiatric history; however, for the past year, she has been taking sertraline, 100 mg/d, and desipramine, 25 mg/d, which her primary care physician prescribed for unknown reasons.
Mrs. P has struggled with chronic back pain for years, but an MRI of her spine is negative. Her family strongly believes that for the past 3 years Mrs. P has been receiving too many medications from her pain management specialist. Six weeks before her current presentation, she was receiving methadone, 40 mg/d, hydrocodone, at least 20 mg/d, and tramadol, 400 mg/d in divided doses. She also was taking an unknown dose of at least 1 benzodiazepine.
Mrs. P’s husband notes she stopped taking methadone abruptly approximately 5 weeks ago. However, about 3 weeks ago, Mrs. P accidentally overdosed on opioids and was hospitalized for several days. Urine drug screen at the time was positive for acetaminophen, salicylate, propoxyphene, opiate, benzodiazepine, and tricyclic antidepressant.
Mrs. P’s medical history includes auditory nerve loss from birth; her mother had German measles (rubella). Mrs. P never learned American Sign Language. She underwent cochlear implant surgery 1 year ago and now has only mild difficulties speaking.
The authors’ observations
Manic symptoms are common in patients with comorbid medical disorders and present a diagnostic challenge. Obtaining an accurate history from the patient may be difficult. Such evaluations often require extensive investigation and collection of data from multiple sources, including:
- medical records
- family members
- patient observation.
Mrs. P’s history is marked by contradicting data from these sources. For example, her family says she stopped taking “pain medications” 5 weeks ago, but 2 weeks later her urine drug screen showed opioids.
Both illicit drugs and prescribed medications can precipitate manic symptoms. From medical records and drug testing, it was evident that Mrs. P had a history of medication abuse/overdose/misuse.
Mania also has been associated with substance withdrawal. Mrs. P allegedly stopped taking methadone 4 weeks before the onset of manic symptoms. Methadone is a synthetic opioid with a pharmacokinetic and pharmacodynamic profile that presents clinical challenges, including:
- large interindividual variability in methadone pharmacokinetics
- lack of reliable equianalgesic conversion ratio to and from other opioids
- potential for multiple drug interactions and complex pharmacodynamics.
An opioid’s half-life determines the onset and duration of withdrawal syndrome symptoms.1 Methadone metabolism is predominantly mediated by CYP3A4, CYP2B6, CYP2D6, and to some extent by CYP2C19.1 We performed genetic testing to help evaluate how Mrs. P metabolized medications. Mrs. P had a normal genotype for CYP2D6, which meant that she should process opioids at a normal rate; however, she was heterozygous for CYP2C19*2 polymorphism, so it is possible that methadone stayed in her system longer than average.
Evidence documenting methadone drug interactions is limited (Table 1).1 Mrs. P was taking sertraline and desipramine; both have potent effects via 2D6 inhibition that could increase plasma methadone concentration. Other evidence indicates that benzodiazepines and methadone may have synergistic interactions that could increase opioid sedation or respiratory depression.1
Table 1
Is a drug interaction with methadone causing Mrs. P’s mania?
| Medication class/agent | Effect on methadone level | Effect on methadone metabolism | Additional effects of interaction |
|---|---|---|---|
| Selective serotonin reuptake inhibitors | |||
| Fluvoxamine | Increase | Inhibition | Opioid toxicity |
| Fluoxetine | Increase | Inhibition | Torsades de pointes |
| Paroxetine | Increase | Inhibition | Decreased hepatic metabolism |
| Sertraline* | Increase | Autoinduction | Torsades de pointes |
| Citalopram | — | — | Torsades de pointes |
| Tricyclic antidepressants | |||
| Desipramine* | — | Inhibition | Increased desipramine levels/inhibition of desipramine metabolism |
| Amitriptyline | Increase methadone clearance | — | Torsades de pointes/prolonged QT interval |
| Anti-inflammatory drugs | |||
| NSAIDs* | — | — | Enhanced analgesia/opioid-sparing effect |
| Aspirin* | — | — | Paradoxical activation of platelet receptors |
| Benzodiazepines | |||
| Alprazolam | — | — | CNS depression/sedation/overdose |
| Diazepam* | — | Inhibition | Additive depressant effects |
| Opioid agonists | |||
| Dextromethorphan | — | Inhibition (not significant) | Increased side effects, especially sleepiness and drowsiness |
| Tramadol* | — | — | Well tolerated |
| Nicotine | Decrease | Can increase smoking rate | |
| *Medications taken by Mrs. P | |||
| NSAIDs: nonsteroidal anti-inflammatory drugs | |||
| Source: Reference 1 | |||
EVALUATION: Few clues
In our ED, Mrs. P’s urine drug abuse screen is positive for salicylate and benzodiazepine only. Findings from physical examination, vital signs, ECG, and chest radiography are within normal limits. Internal medicine consultation is unremarkable. Mrs. P’s laboratory investigation is notable for an elevated white blood cell count, but this normalizes over a week.
Mrs. P shows no evidence of infection and is normoglycemic. B12 and folate are within normal limits. Serum electrolytes, liver function testing, sensitive thyroid stimulating hormone, and C-reactive protein are within normal limits. Urinalysis is negative except for a small amount of hemoglobin. Her creatine kinase (CK) is in the upper normal range. Human immunodeficiency virus (HIV) and syphilis testing is negative. Ceruloplasmin level also is normal. Heavy metal screen is negative. Head MRI and CT from previous hospitalizations were unremarkable.
The authors’ observations
Our first step was to clarify Mrs. P’s diagnosis. In reviewing differential diagnoses, we considered:
- serotonin syndrome
- benzodiazepine withdrawal syndrome
- antidepressant-induced mania
- adrenergic toxicity
- malignant hyperthermia
- heat stroke
- infectious causes.
Our index of suspicion for serotonin syndrome was low because Mrs. P didn’t meet criteria required for diagnosis. Relevant signs and symptoms included confusion, elevated mood (major) and agitation, nervousness, insomnia, and low blood pressure (minor).
Based on concerns about medication interactions, we discontinued sertraline and desipramine. According to the patient’s sister, Mrs. P’s manic symptoms markedly responded to PRN doses of lorazepam. We prescribed lorazepam, 1 mg every 6 hours, and observed Mrs. P for signs and symptoms of benzodiazepine withdrawal.
HISTORY: OTC drug use
According to Mrs. P’s mother, after her daughter abruptly discontinued methadone, she began to have very strong headaches, which she treated with Excedrin or Excedrin Sinus. The mother said that 4 days before Mrs. P came to the ED, she found her daughter holding 4 tablets of Excedrin and an empty bottle. Unfortunately her mother was unable to say what type of Excedrin it was. When the treatment team asks Mrs. P how many pills she usually takes, she says she doesn’t know but usually until the pain stops.
The authors’ observations
Management of secondary mania should focus on treating the underlying condition (Algorithm). Neurology categorizes mania into 3 categories:2
- confusional-delirious states
- manic symptoms associated with focal or multifocal cerebral lesions
- affective disorders (manic-depressive and depressive psychoses).
Medical workup ruled out common secondary causes of psychosis. Collaborative information from relatives revealed no family history of mental illness.
Patients with hearing loss and deafness have been shown to be at increased risk for psychotic disorders compared with the general population. Severe sensory deficits early in Mrs. P’s life may have influenced the orderly development of neural connections in her sensory cortex and association areas.3 Mrs. P was deaf for the first 45 years of life. It could be hypothesized that her sensory deficits significantly influenced her ability to reality test. After receiving a cochlear implant, Mrs. P rapidly went from no auditory stimulation to marked improvement. This stressor might precipitate psychotic symptoms. However, her presentation seemed to be characterized more by manic symptoms or an agitated delirium. It also did not fit temporally with her presentation.
We begin to suspect that Mrs. P’s mania is substance-induced. Excedrin, an over-the-counter medication, contains aspirin and caffeine. Excedrin Sinus also contains phenylephrine. Amphetamines, caffeine, ephedrine, pseudoephedrine, and phenylpropanolamine have all been linked to manic-like psychotic episodes.
Concerns about the illicit conversion of pseudoephedrine into methamphetamine obliged pharmaceutical companies in the United States to switch product formulations to phenylephrine in 2005,4 although some “behind-the-counter” medications may contain pseudoephedrine. Phenylephrine is a relatively selective α1 agonist with weak α2 adrenoceptor agonist activity and low β agonist activity. It is very similar to pseudo-ephedrine, which is known to be implicated in the development of manic symptoms.5,6
Pseudoephedrine can raise CK levels and cause rhabdomyolysis.7,8 Mrs. P’s CK level was 176 (normal range 36 to 176 U/L) 4 days after her initial presentation, and she had a moderate amount of myoglobin in her urine. Her creatinine was normal. The patient was taking excessive amounts of caffeine and—if she was using Excedrin Sinus—pseudoephedrine or phenylephrine. We were unable to determine whether her Excedrin contained pseudoephedrine or phenylephrine. In addition, she was going through opioid withdrawal and reported problems with her sleep. There was also a question of Mrs. P’s unknown methadone use combined with its decreased clearance secondary to medication interactions.
While previously hospitalized for overdose, Mrs. P tested positive for propoxyphene. Excessive use of propoxyphene also can cause numerous adverse reactions. Some of that could have explained why Mrs. P’s presentation includes nervousness, CNS stimulation, excitement, insomnia, and restlessness.5
Based on multiple factors, we believe Mrs. P meets DSM-IV-TR criteria for substance-induced mood disorder (Table 2).9 This diagnosis is supported by Mrs. P’s history of complex polypharmacy, excessive caffeine use, sleep deprivation, and possible opioid withdrawal.
Algorithm: Managing substance-induced manic disorder
CK: creatine kinase; CRP: C-reactive protein; CT: computed tomography; EEG: electroencephalogram; HIV: human immunodeficiency virus; MRI: magnetic resonance imaging; VDRL: venereal disease research laboratoryTable 2
DSM-IV-TR criteria for substance-induced mood disorder*
| A. A prominent and persistent disturbance in mood predominates in the clinical picture and is characterized by either (or both) of the following: 1. depressed mood or markedly diminished interest or pleasure in all, or almost all, activities 2. elevated, expansive, or irritable mood |
| B. There is evidence from the history, physical examination, or laboratory findings of: 1. the symptoms in Criterion A developed during, or within 1 month of, substance intoxication or withdrawal, or 2. medication use is etiologically related to the disturbance |
| C. The disturbance is not better accounted for by a mood disorder that is not substance-induced |
| D. The disturbance does not occur exclusively during the course of a delirium |
| E. The symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning |
| Minimal criteria are A plus B plus E |
| *Make this diagnosis only when mood symptoms are in excess of those usually associated with substance intoxication or substance withdrawal syndrome and when symptoms are sufficiently severe to warrant independent clinical attention |
| Source: Reference 9 |
TREATMENT: Escalating symptoms
While hospitalized, Mrs. P focuses solely on receiving pain medication. She does not know why she is in the hospital. She is easily distractible, intermittently intrusive, and disorganized and tangential in her thought process.
Two days after admission, her uncontrolled behavior escalates and she has marked psychomotor agitation. She is confused but remains oriented to time, place, and person. We start treatment with risperidone, 0.5 mg each morning and 1 mg at bedtime, because this agent is well tolerated, efficacious, and easily titrated to symptom response. Mrs. P’s symptoms improve, but she does not return to her reported baseline. Two days later, we increase risperidone to 1 mg every morning and 2 mg at bedtime. On the 6th day of hospitalization, Mrs. P is more organized and able to follow simple commands. She denies auditory or visual hallucinations. On the 10th day, she improves markedly and is back to her baseline level of functioning.
We perform psychological testing, including the Wechsler Adult Intelligence Scale (WAIS III) and the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS, Form A). The results show global neurocognitive deficits. Mrs. P’s intellectual skill is significantly below average, with verbal abilities reflecting functioning in the mildly retarded range. Nonverbal skills were stronger but still below average. Mrs. P’s capacity to learn and retain new information and to understand even modestly complex concepts is quite limited.
Because of Mrs. P’s long history of poly-substance abuse, inability to process information, and chronic back pain, we judge her to be at high risk for relapse. However, Mrs. P and her family are not interested in chemical dependence treatment.
This left us facing a difficult clinical situation. Mrs. P had a pattern of presenting to multiple physicians and eventually receiving narcotics. Her family provided transportation for her to these appointments but also was concerned about her drug use. With the patient and her family, we carefully outline Mrs. P’s treatment needs, including:
- medication monitoring by a psychiatrist after discharge
- a single, consistent primary care physician to manage her care
- a treatment plan shared by all clinicians involved in her care.
We review with Mrs. P and her family the benefits of behavioral approaches to chronic pain management. They agree to our recommendation that the family control Mrs. P’s medication supply. We discharge her on risperidone, 0.5 mg each morning and 1 mg at bedtime, and she is scheduled for follow-up with a local psychiatrist.
Related resource
- Krauthammer C, Klerman GL. Manic syndromes associated with antecedent physical illness or drugs. Arch Gen Psychiatry. 1978;35(11):1333-1339.
Drug brand names
- Alprazolam • Xanax
- Amitriptyline • Elavil
- Citalopram • Celexa
- Desipramine • Norpramin
- Diazepam • Valium
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Hydrocodone • Vicodin, Lortab, others
- Lorazepam • Ativan
- Methadone • Dolophine, Methadose
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Propoxyphene • Darvon, Darvocet, others
- Risperidone • Risperdal
- Sertraline • Zoloft
- Tramadol • Ultram
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: First-episode mania
Mrs. P, age 47, is brought to the emergency department (ED) because her family is concerned about her behavioral changes over the last week. Her husband reports that Mrs. P has become hyper-religious and talkative. She has been perseverating on numbers and dates and incessantly calling people. Mrs. P reports increased energy and decreased need for sleep. On examination, she has pressured speech. She has no psychiatric history; however, for the past year, she has been taking sertraline, 100 mg/d, and desipramine, 25 mg/d, which her primary care physician prescribed for unknown reasons.
Mrs. P has struggled with chronic back pain for years, but an MRI of her spine is negative. Her family strongly believes that for the past 3 years Mrs. P has been receiving too many medications from her pain management specialist. Six weeks before her current presentation, she was receiving methadone, 40 mg/d, hydrocodone, at least 20 mg/d, and tramadol, 400 mg/d in divided doses. She also was taking an unknown dose of at least 1 benzodiazepine.
Mrs. P’s husband notes she stopped taking methadone abruptly approximately 5 weeks ago. However, about 3 weeks ago, Mrs. P accidentally overdosed on opioids and was hospitalized for several days. Urine drug screen at the time was positive for acetaminophen, salicylate, propoxyphene, opiate, benzodiazepine, and tricyclic antidepressant.
Mrs. P’s medical history includes auditory nerve loss from birth; her mother had German measles (rubella). Mrs. P never learned American Sign Language. She underwent cochlear implant surgery 1 year ago and now has only mild difficulties speaking.
The authors’ observations
Manic symptoms are common in patients with comorbid medical disorders and present a diagnostic challenge. Obtaining an accurate history from the patient may be difficult. Such evaluations often require extensive investigation and collection of data from multiple sources, including:
- medical records
- family members
- patient observation.
Mrs. P’s history is marked by contradicting data from these sources. For example, her family says she stopped taking “pain medications” 5 weeks ago, but 2 weeks later her urine drug screen showed opioids.
Both illicit drugs and prescribed medications can precipitate manic symptoms. From medical records and drug testing, it was evident that Mrs. P had a history of medication abuse/overdose/misuse.
Mania also has been associated with substance withdrawal. Mrs. P allegedly stopped taking methadone 4 weeks before the onset of manic symptoms. Methadone is a synthetic opioid with a pharmacokinetic and pharmacodynamic profile that presents clinical challenges, including:
- large interindividual variability in methadone pharmacokinetics
- lack of reliable equianalgesic conversion ratio to and from other opioids
- potential for multiple drug interactions and complex pharmacodynamics.
An opioid’s half-life determines the onset and duration of withdrawal syndrome symptoms.1 Methadone metabolism is predominantly mediated by CYP3A4, CYP2B6, CYP2D6, and to some extent by CYP2C19.1 We performed genetic testing to help evaluate how Mrs. P metabolized medications. Mrs. P had a normal genotype for CYP2D6, which meant that she should process opioids at a normal rate; however, she was heterozygous for CYP2C19*2 polymorphism, so it is possible that methadone stayed in her system longer than average.
Evidence documenting methadone drug interactions is limited (Table 1).1 Mrs. P was taking sertraline and desipramine; both have potent effects via 2D6 inhibition that could increase plasma methadone concentration. Other evidence indicates that benzodiazepines and methadone may have synergistic interactions that could increase opioid sedation or respiratory depression.1
Table 1
Is a drug interaction with methadone causing Mrs. P’s mania?
| Medication class/agent | Effect on methadone level | Effect on methadone metabolism | Additional effects of interaction |
|---|---|---|---|
| Selective serotonin reuptake inhibitors | |||
| Fluvoxamine | Increase | Inhibition | Opioid toxicity |
| Fluoxetine | Increase | Inhibition | Torsades de pointes |
| Paroxetine | Increase | Inhibition | Decreased hepatic metabolism |
| Sertraline* | Increase | Autoinduction | Torsades de pointes |
| Citalopram | — | — | Torsades de pointes |
| Tricyclic antidepressants | |||
| Desipramine* | — | Inhibition | Increased desipramine levels/inhibition of desipramine metabolism |
| Amitriptyline | Increase methadone clearance | — | Torsades de pointes/prolonged QT interval |
| Anti-inflammatory drugs | |||
| NSAIDs* | — | — | Enhanced analgesia/opioid-sparing effect |
| Aspirin* | — | — | Paradoxical activation of platelet receptors |
| Benzodiazepines | |||
| Alprazolam | — | — | CNS depression/sedation/overdose |
| Diazepam* | — | Inhibition | Additive depressant effects |
| Opioid agonists | |||
| Dextromethorphan | — | Inhibition (not significant) | Increased side effects, especially sleepiness and drowsiness |
| Tramadol* | — | — | Well tolerated |
| Nicotine | Decrease | Can increase smoking rate | |
| *Medications taken by Mrs. P | |||
| NSAIDs: nonsteroidal anti-inflammatory drugs | |||
| Source: Reference 1 | |||
EVALUATION: Few clues
In our ED, Mrs. P’s urine drug abuse screen is positive for salicylate and benzodiazepine only. Findings from physical examination, vital signs, ECG, and chest radiography are within normal limits. Internal medicine consultation is unremarkable. Mrs. P’s laboratory investigation is notable for an elevated white blood cell count, but this normalizes over a week.
Mrs. P shows no evidence of infection and is normoglycemic. B12 and folate are within normal limits. Serum electrolytes, liver function testing, sensitive thyroid stimulating hormone, and C-reactive protein are within normal limits. Urinalysis is negative except for a small amount of hemoglobin. Her creatine kinase (CK) is in the upper normal range. Human immunodeficiency virus (HIV) and syphilis testing is negative. Ceruloplasmin level also is normal. Heavy metal screen is negative. Head MRI and CT from previous hospitalizations were unremarkable.
The authors’ observations
Our first step was to clarify Mrs. P’s diagnosis. In reviewing differential diagnoses, we considered:
- serotonin syndrome
- benzodiazepine withdrawal syndrome
- antidepressant-induced mania
- adrenergic toxicity
- malignant hyperthermia
- heat stroke
- infectious causes.
Our index of suspicion for serotonin syndrome was low because Mrs. P didn’t meet criteria required for diagnosis. Relevant signs and symptoms included confusion, elevated mood (major) and agitation, nervousness, insomnia, and low blood pressure (minor).
Based on concerns about medication interactions, we discontinued sertraline and desipramine. According to the patient’s sister, Mrs. P’s manic symptoms markedly responded to PRN doses of lorazepam. We prescribed lorazepam, 1 mg every 6 hours, and observed Mrs. P for signs and symptoms of benzodiazepine withdrawal.
HISTORY: OTC drug use
According to Mrs. P’s mother, after her daughter abruptly discontinued methadone, she began to have very strong headaches, which she treated with Excedrin or Excedrin Sinus. The mother said that 4 days before Mrs. P came to the ED, she found her daughter holding 4 tablets of Excedrin and an empty bottle. Unfortunately her mother was unable to say what type of Excedrin it was. When the treatment team asks Mrs. P how many pills she usually takes, she says she doesn’t know but usually until the pain stops.
The authors’ observations
Management of secondary mania should focus on treating the underlying condition (Algorithm). Neurology categorizes mania into 3 categories:2
- confusional-delirious states
- manic symptoms associated with focal or multifocal cerebral lesions
- affective disorders (manic-depressive and depressive psychoses).
Medical workup ruled out common secondary causes of psychosis. Collaborative information from relatives revealed no family history of mental illness.
Patients with hearing loss and deafness have been shown to be at increased risk for psychotic disorders compared with the general population. Severe sensory deficits early in Mrs. P’s life may have influenced the orderly development of neural connections in her sensory cortex and association areas.3 Mrs. P was deaf for the first 45 years of life. It could be hypothesized that her sensory deficits significantly influenced her ability to reality test. After receiving a cochlear implant, Mrs. P rapidly went from no auditory stimulation to marked improvement. This stressor might precipitate psychotic symptoms. However, her presentation seemed to be characterized more by manic symptoms or an agitated delirium. It also did not fit temporally with her presentation.
We begin to suspect that Mrs. P’s mania is substance-induced. Excedrin, an over-the-counter medication, contains aspirin and caffeine. Excedrin Sinus also contains phenylephrine. Amphetamines, caffeine, ephedrine, pseudoephedrine, and phenylpropanolamine have all been linked to manic-like psychotic episodes.
Concerns about the illicit conversion of pseudoephedrine into methamphetamine obliged pharmaceutical companies in the United States to switch product formulations to phenylephrine in 2005,4 although some “behind-the-counter” medications may contain pseudoephedrine. Phenylephrine is a relatively selective α1 agonist with weak α2 adrenoceptor agonist activity and low β agonist activity. It is very similar to pseudo-ephedrine, which is known to be implicated in the development of manic symptoms.5,6
Pseudoephedrine can raise CK levels and cause rhabdomyolysis.7,8 Mrs. P’s CK level was 176 (normal range 36 to 176 U/L) 4 days after her initial presentation, and she had a moderate amount of myoglobin in her urine. Her creatinine was normal. The patient was taking excessive amounts of caffeine and—if she was using Excedrin Sinus—pseudoephedrine or phenylephrine. We were unable to determine whether her Excedrin contained pseudoephedrine or phenylephrine. In addition, she was going through opioid withdrawal and reported problems with her sleep. There was also a question of Mrs. P’s unknown methadone use combined with its decreased clearance secondary to medication interactions.
While previously hospitalized for overdose, Mrs. P tested positive for propoxyphene. Excessive use of propoxyphene also can cause numerous adverse reactions. Some of that could have explained why Mrs. P’s presentation includes nervousness, CNS stimulation, excitement, insomnia, and restlessness.5
Based on multiple factors, we believe Mrs. P meets DSM-IV-TR criteria for substance-induced mood disorder (Table 2).9 This diagnosis is supported by Mrs. P’s history of complex polypharmacy, excessive caffeine use, sleep deprivation, and possible opioid withdrawal.
Algorithm: Managing substance-induced manic disorder
CK: creatine kinase; CRP: C-reactive protein; CT: computed tomography; EEG: electroencephalogram; HIV: human immunodeficiency virus; MRI: magnetic resonance imaging; VDRL: venereal disease research laboratoryTable 2
DSM-IV-TR criteria for substance-induced mood disorder*
| A. A prominent and persistent disturbance in mood predominates in the clinical picture and is characterized by either (or both) of the following: 1. depressed mood or markedly diminished interest or pleasure in all, or almost all, activities 2. elevated, expansive, or irritable mood |
| B. There is evidence from the history, physical examination, or laboratory findings of: 1. the symptoms in Criterion A developed during, or within 1 month of, substance intoxication or withdrawal, or 2. medication use is etiologically related to the disturbance |
| C. The disturbance is not better accounted for by a mood disorder that is not substance-induced |
| D. The disturbance does not occur exclusively during the course of a delirium |
| E. The symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning |
| Minimal criteria are A plus B plus E |
| *Make this diagnosis only when mood symptoms are in excess of those usually associated with substance intoxication or substance withdrawal syndrome and when symptoms are sufficiently severe to warrant independent clinical attention |
| Source: Reference 9 |
TREATMENT: Escalating symptoms
While hospitalized, Mrs. P focuses solely on receiving pain medication. She does not know why she is in the hospital. She is easily distractible, intermittently intrusive, and disorganized and tangential in her thought process.
Two days after admission, her uncontrolled behavior escalates and she has marked psychomotor agitation. She is confused but remains oriented to time, place, and person. We start treatment with risperidone, 0.5 mg each morning and 1 mg at bedtime, because this agent is well tolerated, efficacious, and easily titrated to symptom response. Mrs. P’s symptoms improve, but she does not return to her reported baseline. Two days later, we increase risperidone to 1 mg every morning and 2 mg at bedtime. On the 6th day of hospitalization, Mrs. P is more organized and able to follow simple commands. She denies auditory or visual hallucinations. On the 10th day, she improves markedly and is back to her baseline level of functioning.
We perform psychological testing, including the Wechsler Adult Intelligence Scale (WAIS III) and the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS, Form A). The results show global neurocognitive deficits. Mrs. P’s intellectual skill is significantly below average, with verbal abilities reflecting functioning in the mildly retarded range. Nonverbal skills were stronger but still below average. Mrs. P’s capacity to learn and retain new information and to understand even modestly complex concepts is quite limited.
Because of Mrs. P’s long history of poly-substance abuse, inability to process information, and chronic back pain, we judge her to be at high risk for relapse. However, Mrs. P and her family are not interested in chemical dependence treatment.
This left us facing a difficult clinical situation. Mrs. P had a pattern of presenting to multiple physicians and eventually receiving narcotics. Her family provided transportation for her to these appointments but also was concerned about her drug use. With the patient and her family, we carefully outline Mrs. P’s treatment needs, including:
- medication monitoring by a psychiatrist after discharge
- a single, consistent primary care physician to manage her care
- a treatment plan shared by all clinicians involved in her care.
We review with Mrs. P and her family the benefits of behavioral approaches to chronic pain management. They agree to our recommendation that the family control Mrs. P’s medication supply. We discharge her on risperidone, 0.5 mg each morning and 1 mg at bedtime, and she is scheduled for follow-up with a local psychiatrist.
Related resource
- Krauthammer C, Klerman GL. Manic syndromes associated with antecedent physical illness or drugs. Arch Gen Psychiatry. 1978;35(11):1333-1339.
Drug brand names
- Alprazolam • Xanax
- Amitriptyline • Elavil
- Citalopram • Celexa
- Desipramine • Norpramin
- Diazepam • Valium
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Hydrocodone • Vicodin, Lortab, others
- Lorazepam • Ativan
- Methadone • Dolophine, Methadose
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Propoxyphene • Darvon, Darvocet, others
- Risperidone • Risperdal
- Sertraline • Zoloft
- Tramadol • Ultram
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. De Fazio S, Gallelli L, De Siena A, et al. Role of CYP3A5 in abnormal clearance methadone. Ann Pharmacother. 2008;42(6):893-897.
2. Ropper AH, Brown RH. Adams and Victor’s principles of neurology. 8th ed. New York, NY: McGraw-Hill Professional; 2005.
3. Thewissen V, Myin-Germeys I, Bentall R, et al. Hearing impairment and psychosis revisited. Schizophr Res. 2005;76(1):99-103.
4. Eccles R. Substitution of phenylephrine for pseudoephedrine as a nasal decongeststant. An illogical way to control methamphetamine abuse. Br J Clin Pharmacol. 2007;63(1):10-14.
5. Wilson H, Woods D. Pseudoephedrine causing mania-like symptoms. N Z Med J. 2002;115(1148):86.-
6. Dalton R. Mixed bipolar disorder precipitated by pseudoephedrine hydrochloride. South Med J. 1990;83(1):64-65.
7. Mansi IA, Huang J. Rhabdomyolysis in response to weight-loss herbal medicine. Am J Med Sci. 2004;327:356-357.
8. Sandhu RS, Como JJ, Scalea TS. Renal failure and exercise-induced rhabdomyolysis in patients taking performance-enhancing compounds. J Trauma. 2002;53:761-764.
9. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
1. De Fazio S, Gallelli L, De Siena A, et al. Role of CYP3A5 in abnormal clearance methadone. Ann Pharmacother. 2008;42(6):893-897.
2. Ropper AH, Brown RH. Adams and Victor’s principles of neurology. 8th ed. New York, NY: McGraw-Hill Professional; 2005.
3. Thewissen V, Myin-Germeys I, Bentall R, et al. Hearing impairment and psychosis revisited. Schizophr Res. 2005;76(1):99-103.
4. Eccles R. Substitution of phenylephrine for pseudoephedrine as a nasal decongeststant. An illogical way to control methamphetamine abuse. Br J Clin Pharmacol. 2007;63(1):10-14.
5. Wilson H, Woods D. Pseudoephedrine causing mania-like symptoms. N Z Med J. 2002;115(1148):86.-
6. Dalton R. Mixed bipolar disorder precipitated by pseudoephedrine hydrochloride. South Med J. 1990;83(1):64-65.
7. Mansi IA, Huang J. Rhabdomyolysis in response to weight-loss herbal medicine. Am J Med Sci. 2004;327:356-357.
8. Sandhu RS, Como JJ, Scalea TS. Renal failure and exercise-induced rhabdomyolysis in patients taking performance-enhancing compounds. J Trauma. 2002;53:761-764.
9. Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
The patient who didn’t know
CASE: Unable to communicate
Mrs. A, age 44, is airlifted to the emergency room after a motor vehicle accident in which she was the restrained front seat passenger. She was on the way to a mental health follow-up appointment with her husband, who died on the scene, and 24-year-old son, who sustained multiple injuries. At the accident scene, Mrs. A was awake and responded to all questions by saying, “I don’t know.” No other history could be obtained. She was carrying documents from a local psychiatric facility that stated she had been discharged 1 month ago with a diagnosis of psychotic disorder, not otherwise specified (NOS). Her discharge medications were olanzapine, 15 mg at bedtime; escitalopram, 20 mg/d; lamotrigine, 100 mg/d; zolpidem, 10 mg as needed at bedtime; and diazepam, 5 mg tid.
Initial assessment reveals mild concussion, nondisplaced fractures of the left C7 and T1 transverse processes, and fracture of the posterior left first rib. Mrs. A is admitted to the trauma surgery service. Soon after, nurses report that Mrs. A is not able to report symptoms. Psychiatry service is consulted to evaluate her continued confusion and inability to communicate.
The authors’ observations
Mrs. A seems anxious because of my repeated attempts to communicate. Her affect is restricted, and her speech is limited to “I don’t know” but fluent. She does not appear to be responding to internal stimuli. Neurologic examination, including cranial nerves and reflexes, is normal. A chart review reveals that her psychiatric medications have been continued upon admission.
HISTORY: Always nervous
We contact Mrs. A’s son, who also was admitted to the hospital, for more information. He reports that his mother has a long history of “nerve problems,” which he describes as “crying and feeling sad and nervous.” He says Mrs. A’s mother also had these problems, and Mrs. A’s childhood was difficult (Table 1). Because of this condition, Mrs. A lives alone in a trailer next to the house where her husband and children live.
Mrs. A’s son said that she had a “nervous breakdown” a few months ago, was admitted to the local psychiatric facility, and since then had been saying only, “I don’t know.” She can communicate her wishes by pointing at “Yes” or “No” written on paper. At home, she can perform all activities of daily living (ADLs), including paying bills. He denies that his mother engages in drug abuse.
We obtain Mrs. A’s treatment records from the psychiatric facility and learn she was admitted with a history of confusion, auditory and visual hallucinations, and crying episodes. She had a history of noncompliance with outpatient medications, which included diazepam, duloxetine, and ziprasidone. Upon admission to that facility, Mrs. A was alert but disoriented to place and time. She answered questions slowly but was brief, sometimes incoherent, and having auditory and visual hallucinations.
During that hospitalization, clinicians established a working diagnosis of psychotic disorder, NOS. Mrs. A was noted to have a urinary tract infection, which they treated with amoxicillin/clavulanate. Ziprasidone was discontinued and olanzapine was started. Escitalopram and lamotrigine were added. Mrs. A’s hallucinations gradually resolved, and she was able to perform ADLs. However, she did not communicate much and started answering most questions with “I don’t know.” At discharge, she was sent home to the care of her sister and husband.
Since then, Mrs. A had been taking her medications regularly but did not show improvement in her speech or methods of communication.
The authors’ observations
7 and frontotemporal8 and stroke-related9 speech disorder. Neuroimaging studies may be helpful in differentiating language disorders from psychosis. For example, evidence of lesions in the language centers of the brain is found in some cases of aphasia, and enlarged ventricles is a common finding in patients with schizophrenia. We considered all of these possibilities when evaluating Mrs. A (Table 2).
Table 1
Mrs. A’s family and personal history of ‘nerve problems’
| Childhood | Mrs. A’s mother had ‘nerve problems.’ Her father physically abused Mrs. A. She received a ninth-grade education |
| Adult life | Married at age 17, Mrs. A had her first child at age 19, second child at age 20, and third child at age 21. She never obtained employment but raised her children with her husband |
| Last 2 years | Mrs. A lived in a trailer next to the house where her husband lived with 2 of their children. Family reports Mrs. A’s ’nerve problems’ were the reason for the separation. They state they took care of her needs and made sure she took her medications |
| Last 2 months | Mrs. A was admitted to a local psychiatric facility with confusion, hallucinations, crying spells, and decreased speech. After discharge, she could perform activities of daily living, but her speech did not improve |
| Present | Mrs. A is a passenger in a motor vehicle accident that results in her husband’s death and multiple injuries to her son. She is admitted to our hospital |
What is the cause of Mrs. A’s speech difficulties?
| Possible diagnosis | Finding that ruled it out |
|---|---|
| Primary progressive aphasia | Subacute onset with rapid progression |
| Frontotemporal dementia | Inconclusive mild frontotemporal atrophy on brain MRI |
| Nonconvulsive status epilepticus | Normal EEG |
| Conversion disorder | Uncommon presentation: Mrs. A is beyond usual age of onset, and symptoms have lasted >1 month |
| Broca’s aphasia/CVA | No corresponding organic lesions on MRI |
| Factitious disorder | No motivation to assume the sick role |
| Psychotic speech | No other evidence of psychosis |
| CVA: cerebrovascular accident; EEG: electroencephalography; MRI: magnetic resonance imaging | |
TREATMENT: An abbreviated stay
A week after admission, Mrs. A is deemed medically stable. Head CT reveals a small, calcified left parietal meningioma that did not correlate with her symptoms (Table 3). Brain MRI shows mild frontotemporal atrophy that was considered inconclusive evidence for a diagnosis of frontotemporal dementia; there is no evidence of infarction, tumors, or other enhancing lesions that may have explained Mrs. A’s symptoms. A 12-lead EEG shows no abnormalities, which rules out a seizure disorder.
Neurology consult rules out concussion syndrome. Over several different evaluations, Mrs. A is noted to follow commands, perform ADLs, and walk. She is able to write her name legibly but is unable to write anything else or to perform a clock-drawing test.
A speech pathology evaluation is requested. A speech pathologist diagnoses Mrs. A with expressive aphasia—impaired ability to speak and write—with some receptive component, meaning her ability to comprehend spoken words also is impaired.
Mrs. A’s speech status does not change, and she remains unable to communicate. She is discharged 10 days after admission with scheduled outpatient follow-up.
Table 3
Findings of Mrs. A’s neurologic testing
| Test | Result |
|---|---|
| Head CT | 1-cm dural-based lesion in the left posterior parietal region |
| Brain MRI | Mild, inconclusive frontotemporal atrophy |
| EEG | Normal |
| CT: computed tomography; EEG: electroencephalography; MRI: magnetic resonance imaging | |
The authors’ observations
At discharge, it seemed likely that Mrs. A may have early symptoms of a neurodegenerative illness, such as frontotemporal dementia, or the aphasia may be a manifestation of chronic psychotic depression. We wanted to follow up with neuropsychological testing and PET scan before establishing a definitive psychiatric diagnosis and modifying the treatment plan.
Related resources
- The Academy of Aphasia. www.academyofaphasia.org.
- The National Aphasia Association. www.aphasia.org.
- Amoxicillin/clavulanate • Augmentin
- Diazepam • Valium
- Duloxetine • Cymbalta
- Escitalopram • Lexapro
- Lamotrigine • Lamictal
- Olanzapine • Zyprexa
- Ziprasidone • Geodon
- Zolpidem • Ambien
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Jodzio K, Gasecki D, Drumm DA, et al. Neuroanatomical correlates of the post-stroke aphasias studied with cerebral blood flow SPECT scanning. Med Sci Monit. 2003;9(3):MT32-41.
2. Stein M, Cantrell SB. Nonfluent aphasia after closed head trauma: report of a case. J Oral Maxillofac Surg. 1999;57(6):745-748.
3. Piñol-Ripoll G, Pérez-Lázaro C, Beltrán-Marín I, et al. Aphasia as the sole symptom of partial status epilepticus [in Spanish]. Rev Neurol. 2004;39(11):1096-1097.
4. Balafouta MJ, Kouvaris JR, Miliadou AC, et al. Primitive neuroectodermal tumour in a 60-year-old man: a case report and literature review. Br J Radiol. 2003;76(901):62-65.
5. Kuramoto S, Hirano T, Uyama E, et al. A case of slowly progressive aphasia accompanied with auditory agnosia [in Japanese]. Rinsho Shinkeigaku. 2002;42(4):299-303.
6. Bulandra R, Medvighi O, Ninosu N. Aphasia or psychotic speech (discussion of a case) [in Romanian]. Neurol Psihiatr Neurochir. 1970;15(6):553-558.
7. Lawson B, Quintana JC. Non convulsive status epilepticus: an heterogeneous disease with a difficult diagnosis. Report of 2 cases with unusual presentation [in Spanish]. Rev Med Chil. 2003;131(9):1045-1050.
8. Vanderzeypen F, Bier JC, Genevrois C, et al. Frontal dementia or dementia praecox? A case report of a psychotic disorder with a severe decline [in French]. Encephale. 2003;29(2):172-180.
9. Sambunaris A, Hyde TM. Stroke-related aphasias mistaken for psychotic speech: two case reports. J Geriatr Psychiatry Neurol. 1994;7(3):144-147.
CASE: Unable to communicate
Mrs. A, age 44, is airlifted to the emergency room after a motor vehicle accident in which she was the restrained front seat passenger. She was on the way to a mental health follow-up appointment with her husband, who died on the scene, and 24-year-old son, who sustained multiple injuries. At the accident scene, Mrs. A was awake and responded to all questions by saying, “I don’t know.” No other history could be obtained. She was carrying documents from a local psychiatric facility that stated she had been discharged 1 month ago with a diagnosis of psychotic disorder, not otherwise specified (NOS). Her discharge medications were olanzapine, 15 mg at bedtime; escitalopram, 20 mg/d; lamotrigine, 100 mg/d; zolpidem, 10 mg as needed at bedtime; and diazepam, 5 mg tid.
Initial assessment reveals mild concussion, nondisplaced fractures of the left C7 and T1 transverse processes, and fracture of the posterior left first rib. Mrs. A is admitted to the trauma surgery service. Soon after, nurses report that Mrs. A is not able to report symptoms. Psychiatry service is consulted to evaluate her continued confusion and inability to communicate.
The authors’ observations
Mrs. A seems anxious because of my repeated attempts to communicate. Her affect is restricted, and her speech is limited to “I don’t know” but fluent. She does not appear to be responding to internal stimuli. Neurologic examination, including cranial nerves and reflexes, is normal. A chart review reveals that her psychiatric medications have been continued upon admission.
HISTORY: Always nervous
We contact Mrs. A’s son, who also was admitted to the hospital, for more information. He reports that his mother has a long history of “nerve problems,” which he describes as “crying and feeling sad and nervous.” He says Mrs. A’s mother also had these problems, and Mrs. A’s childhood was difficult (Table 1). Because of this condition, Mrs. A lives alone in a trailer next to the house where her husband and children live.
Mrs. A’s son said that she had a “nervous breakdown” a few months ago, was admitted to the local psychiatric facility, and since then had been saying only, “I don’t know.” She can communicate her wishes by pointing at “Yes” or “No” written on paper. At home, she can perform all activities of daily living (ADLs), including paying bills. He denies that his mother engages in drug abuse.
We obtain Mrs. A’s treatment records from the psychiatric facility and learn she was admitted with a history of confusion, auditory and visual hallucinations, and crying episodes. She had a history of noncompliance with outpatient medications, which included diazepam, duloxetine, and ziprasidone. Upon admission to that facility, Mrs. A was alert but disoriented to place and time. She answered questions slowly but was brief, sometimes incoherent, and having auditory and visual hallucinations.
During that hospitalization, clinicians established a working diagnosis of psychotic disorder, NOS. Mrs. A was noted to have a urinary tract infection, which they treated with amoxicillin/clavulanate. Ziprasidone was discontinued and olanzapine was started. Escitalopram and lamotrigine were added. Mrs. A’s hallucinations gradually resolved, and she was able to perform ADLs. However, she did not communicate much and started answering most questions with “I don’t know.” At discharge, she was sent home to the care of her sister and husband.
Since then, Mrs. A had been taking her medications regularly but did not show improvement in her speech or methods of communication.
The authors’ observations
7 and frontotemporal8 and stroke-related9 speech disorder. Neuroimaging studies may be helpful in differentiating language disorders from psychosis. For example, evidence of lesions in the language centers of the brain is found in some cases of aphasia, and enlarged ventricles is a common finding in patients with schizophrenia. We considered all of these possibilities when evaluating Mrs. A (Table 2).
Table 1
Mrs. A’s family and personal history of ‘nerve problems’
| Childhood | Mrs. A’s mother had ‘nerve problems.’ Her father physically abused Mrs. A. She received a ninth-grade education |
| Adult life | Married at age 17, Mrs. A had her first child at age 19, second child at age 20, and third child at age 21. She never obtained employment but raised her children with her husband |
| Last 2 years | Mrs. A lived in a trailer next to the house where her husband lived with 2 of their children. Family reports Mrs. A’s ’nerve problems’ were the reason for the separation. They state they took care of her needs and made sure she took her medications |
| Last 2 months | Mrs. A was admitted to a local psychiatric facility with confusion, hallucinations, crying spells, and decreased speech. After discharge, she could perform activities of daily living, but her speech did not improve |
| Present | Mrs. A is a passenger in a motor vehicle accident that results in her husband’s death and multiple injuries to her son. She is admitted to our hospital |
What is the cause of Mrs. A’s speech difficulties?
| Possible diagnosis | Finding that ruled it out |
|---|---|
| Primary progressive aphasia | Subacute onset with rapid progression |
| Frontotemporal dementia | Inconclusive mild frontotemporal atrophy on brain MRI |
| Nonconvulsive status epilepticus | Normal EEG |
| Conversion disorder | Uncommon presentation: Mrs. A is beyond usual age of onset, and symptoms have lasted >1 month |
| Broca’s aphasia/CVA | No corresponding organic lesions on MRI |
| Factitious disorder | No motivation to assume the sick role |
| Psychotic speech | No other evidence of psychosis |
| CVA: cerebrovascular accident; EEG: electroencephalography; MRI: magnetic resonance imaging | |
TREATMENT: An abbreviated stay
A week after admission, Mrs. A is deemed medically stable. Head CT reveals a small, calcified left parietal meningioma that did not correlate with her symptoms (Table 3). Brain MRI shows mild frontotemporal atrophy that was considered inconclusive evidence for a diagnosis of frontotemporal dementia; there is no evidence of infarction, tumors, or other enhancing lesions that may have explained Mrs. A’s symptoms. A 12-lead EEG shows no abnormalities, which rules out a seizure disorder.
Neurology consult rules out concussion syndrome. Over several different evaluations, Mrs. A is noted to follow commands, perform ADLs, and walk. She is able to write her name legibly but is unable to write anything else or to perform a clock-drawing test.
A speech pathology evaluation is requested. A speech pathologist diagnoses Mrs. A with expressive aphasia—impaired ability to speak and write—with some receptive component, meaning her ability to comprehend spoken words also is impaired.
Mrs. A’s speech status does not change, and she remains unable to communicate. She is discharged 10 days after admission with scheduled outpatient follow-up.
Table 3
Findings of Mrs. A’s neurologic testing
| Test | Result |
|---|---|
| Head CT | 1-cm dural-based lesion in the left posterior parietal region |
| Brain MRI | Mild, inconclusive frontotemporal atrophy |
| EEG | Normal |
| CT: computed tomography; EEG: electroencephalography; MRI: magnetic resonance imaging | |
The authors’ observations
At discharge, it seemed likely that Mrs. A may have early symptoms of a neurodegenerative illness, such as frontotemporal dementia, or the aphasia may be a manifestation of chronic psychotic depression. We wanted to follow up with neuropsychological testing and PET scan before establishing a definitive psychiatric diagnosis and modifying the treatment plan.
Related resources
- The Academy of Aphasia. www.academyofaphasia.org.
- The National Aphasia Association. www.aphasia.org.
- Amoxicillin/clavulanate • Augmentin
- Diazepam • Valium
- Duloxetine • Cymbalta
- Escitalopram • Lexapro
- Lamotrigine • Lamictal
- Olanzapine • Zyprexa
- Ziprasidone • Geodon
- Zolpidem • Ambien
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: Unable to communicate
Mrs. A, age 44, is airlifted to the emergency room after a motor vehicle accident in which she was the restrained front seat passenger. She was on the way to a mental health follow-up appointment with her husband, who died on the scene, and 24-year-old son, who sustained multiple injuries. At the accident scene, Mrs. A was awake and responded to all questions by saying, “I don’t know.” No other history could be obtained. She was carrying documents from a local psychiatric facility that stated she had been discharged 1 month ago with a diagnosis of psychotic disorder, not otherwise specified (NOS). Her discharge medications were olanzapine, 15 mg at bedtime; escitalopram, 20 mg/d; lamotrigine, 100 mg/d; zolpidem, 10 mg as needed at bedtime; and diazepam, 5 mg tid.
Initial assessment reveals mild concussion, nondisplaced fractures of the left C7 and T1 transverse processes, and fracture of the posterior left first rib. Mrs. A is admitted to the trauma surgery service. Soon after, nurses report that Mrs. A is not able to report symptoms. Psychiatry service is consulted to evaluate her continued confusion and inability to communicate.
The authors’ observations
Mrs. A seems anxious because of my repeated attempts to communicate. Her affect is restricted, and her speech is limited to “I don’t know” but fluent. She does not appear to be responding to internal stimuli. Neurologic examination, including cranial nerves and reflexes, is normal. A chart review reveals that her psychiatric medications have been continued upon admission.
HISTORY: Always nervous
We contact Mrs. A’s son, who also was admitted to the hospital, for more information. He reports that his mother has a long history of “nerve problems,” which he describes as “crying and feeling sad and nervous.” He says Mrs. A’s mother also had these problems, and Mrs. A’s childhood was difficult (Table 1). Because of this condition, Mrs. A lives alone in a trailer next to the house where her husband and children live.
Mrs. A’s son said that she had a “nervous breakdown” a few months ago, was admitted to the local psychiatric facility, and since then had been saying only, “I don’t know.” She can communicate her wishes by pointing at “Yes” or “No” written on paper. At home, she can perform all activities of daily living (ADLs), including paying bills. He denies that his mother engages in drug abuse.
We obtain Mrs. A’s treatment records from the psychiatric facility and learn she was admitted with a history of confusion, auditory and visual hallucinations, and crying episodes. She had a history of noncompliance with outpatient medications, which included diazepam, duloxetine, and ziprasidone. Upon admission to that facility, Mrs. A was alert but disoriented to place and time. She answered questions slowly but was brief, sometimes incoherent, and having auditory and visual hallucinations.
During that hospitalization, clinicians established a working diagnosis of psychotic disorder, NOS. Mrs. A was noted to have a urinary tract infection, which they treated with amoxicillin/clavulanate. Ziprasidone was discontinued and olanzapine was started. Escitalopram and lamotrigine were added. Mrs. A’s hallucinations gradually resolved, and she was able to perform ADLs. However, she did not communicate much and started answering most questions with “I don’t know.” At discharge, she was sent home to the care of her sister and husband.
Since then, Mrs. A had been taking her medications regularly but did not show improvement in her speech or methods of communication.
The authors’ observations
7 and frontotemporal8 and stroke-related9 speech disorder. Neuroimaging studies may be helpful in differentiating language disorders from psychosis. For example, evidence of lesions in the language centers of the brain is found in some cases of aphasia, and enlarged ventricles is a common finding in patients with schizophrenia. We considered all of these possibilities when evaluating Mrs. A (Table 2).
Table 1
Mrs. A’s family and personal history of ‘nerve problems’
| Childhood | Mrs. A’s mother had ‘nerve problems.’ Her father physically abused Mrs. A. She received a ninth-grade education |
| Adult life | Married at age 17, Mrs. A had her first child at age 19, second child at age 20, and third child at age 21. She never obtained employment but raised her children with her husband |
| Last 2 years | Mrs. A lived in a trailer next to the house where her husband lived with 2 of their children. Family reports Mrs. A’s ’nerve problems’ were the reason for the separation. They state they took care of her needs and made sure she took her medications |
| Last 2 months | Mrs. A was admitted to a local psychiatric facility with confusion, hallucinations, crying spells, and decreased speech. After discharge, she could perform activities of daily living, but her speech did not improve |
| Present | Mrs. A is a passenger in a motor vehicle accident that results in her husband’s death and multiple injuries to her son. She is admitted to our hospital |
What is the cause of Mrs. A’s speech difficulties?
| Possible diagnosis | Finding that ruled it out |
|---|---|
| Primary progressive aphasia | Subacute onset with rapid progression |
| Frontotemporal dementia | Inconclusive mild frontotemporal atrophy on brain MRI |
| Nonconvulsive status epilepticus | Normal EEG |
| Conversion disorder | Uncommon presentation: Mrs. A is beyond usual age of onset, and symptoms have lasted >1 month |
| Broca’s aphasia/CVA | No corresponding organic lesions on MRI |
| Factitious disorder | No motivation to assume the sick role |
| Psychotic speech | No other evidence of psychosis |
| CVA: cerebrovascular accident; EEG: electroencephalography; MRI: magnetic resonance imaging | |
TREATMENT: An abbreviated stay
A week after admission, Mrs. A is deemed medically stable. Head CT reveals a small, calcified left parietal meningioma that did not correlate with her symptoms (Table 3). Brain MRI shows mild frontotemporal atrophy that was considered inconclusive evidence for a diagnosis of frontotemporal dementia; there is no evidence of infarction, tumors, or other enhancing lesions that may have explained Mrs. A’s symptoms. A 12-lead EEG shows no abnormalities, which rules out a seizure disorder.
Neurology consult rules out concussion syndrome. Over several different evaluations, Mrs. A is noted to follow commands, perform ADLs, and walk. She is able to write her name legibly but is unable to write anything else or to perform a clock-drawing test.
A speech pathology evaluation is requested. A speech pathologist diagnoses Mrs. A with expressive aphasia—impaired ability to speak and write—with some receptive component, meaning her ability to comprehend spoken words also is impaired.
Mrs. A’s speech status does not change, and she remains unable to communicate. She is discharged 10 days after admission with scheduled outpatient follow-up.
Table 3
Findings of Mrs. A’s neurologic testing
| Test | Result |
|---|---|
| Head CT | 1-cm dural-based lesion in the left posterior parietal region |
| Brain MRI | Mild, inconclusive frontotemporal atrophy |
| EEG | Normal |
| CT: computed tomography; EEG: electroencephalography; MRI: magnetic resonance imaging | |
The authors’ observations
At discharge, it seemed likely that Mrs. A may have early symptoms of a neurodegenerative illness, such as frontotemporal dementia, or the aphasia may be a manifestation of chronic psychotic depression. We wanted to follow up with neuropsychological testing and PET scan before establishing a definitive psychiatric diagnosis and modifying the treatment plan.
Related resources
- The Academy of Aphasia. www.academyofaphasia.org.
- The National Aphasia Association. www.aphasia.org.
- Amoxicillin/clavulanate • Augmentin
- Diazepam • Valium
- Duloxetine • Cymbalta
- Escitalopram • Lexapro
- Lamotrigine • Lamictal
- Olanzapine • Zyprexa
- Ziprasidone • Geodon
- Zolpidem • Ambien
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Jodzio K, Gasecki D, Drumm DA, et al. Neuroanatomical correlates of the post-stroke aphasias studied with cerebral blood flow SPECT scanning. Med Sci Monit. 2003;9(3):MT32-41.
2. Stein M, Cantrell SB. Nonfluent aphasia after closed head trauma: report of a case. J Oral Maxillofac Surg. 1999;57(6):745-748.
3. Piñol-Ripoll G, Pérez-Lázaro C, Beltrán-Marín I, et al. Aphasia as the sole symptom of partial status epilepticus [in Spanish]. Rev Neurol. 2004;39(11):1096-1097.
4. Balafouta MJ, Kouvaris JR, Miliadou AC, et al. Primitive neuroectodermal tumour in a 60-year-old man: a case report and literature review. Br J Radiol. 2003;76(901):62-65.
5. Kuramoto S, Hirano T, Uyama E, et al. A case of slowly progressive aphasia accompanied with auditory agnosia [in Japanese]. Rinsho Shinkeigaku. 2002;42(4):299-303.
6. Bulandra R, Medvighi O, Ninosu N. Aphasia or psychotic speech (discussion of a case) [in Romanian]. Neurol Psihiatr Neurochir. 1970;15(6):553-558.
7. Lawson B, Quintana JC. Non convulsive status epilepticus: an heterogeneous disease with a difficult diagnosis. Report of 2 cases with unusual presentation [in Spanish]. Rev Med Chil. 2003;131(9):1045-1050.
8. Vanderzeypen F, Bier JC, Genevrois C, et al. Frontal dementia or dementia praecox? A case report of a psychotic disorder with a severe decline [in French]. Encephale. 2003;29(2):172-180.
9. Sambunaris A, Hyde TM. Stroke-related aphasias mistaken for psychotic speech: two case reports. J Geriatr Psychiatry Neurol. 1994;7(3):144-147.
1. Jodzio K, Gasecki D, Drumm DA, et al. Neuroanatomical correlates of the post-stroke aphasias studied with cerebral blood flow SPECT scanning. Med Sci Monit. 2003;9(3):MT32-41.
2. Stein M, Cantrell SB. Nonfluent aphasia after closed head trauma: report of a case. J Oral Maxillofac Surg. 1999;57(6):745-748.
3. Piñol-Ripoll G, Pérez-Lázaro C, Beltrán-Marín I, et al. Aphasia as the sole symptom of partial status epilepticus [in Spanish]. Rev Neurol. 2004;39(11):1096-1097.
4. Balafouta MJ, Kouvaris JR, Miliadou AC, et al. Primitive neuroectodermal tumour in a 60-year-old man: a case report and literature review. Br J Radiol. 2003;76(901):62-65.
5. Kuramoto S, Hirano T, Uyama E, et al. A case of slowly progressive aphasia accompanied with auditory agnosia [in Japanese]. Rinsho Shinkeigaku. 2002;42(4):299-303.
6. Bulandra R, Medvighi O, Ninosu N. Aphasia or psychotic speech (discussion of a case) [in Romanian]. Neurol Psihiatr Neurochir. 1970;15(6):553-558.
7. Lawson B, Quintana JC. Non convulsive status epilepticus: an heterogeneous disease with a difficult diagnosis. Report of 2 cases with unusual presentation [in Spanish]. Rev Med Chil. 2003;131(9):1045-1050.
8. Vanderzeypen F, Bier JC, Genevrois C, et al. Frontal dementia or dementia praecox? A case report of a psychotic disorder with a severe decline [in French]. Encephale. 2003;29(2):172-180.
9. Sambunaris A, Hyde TM. Stroke-related aphasias mistaken for psychotic speech: two case reports. J Geriatr Psychiatry Neurol. 1994;7(3):144-147.
A case of the body snatchers
CASE: Spirits replacing body parts
Mrs. P, age 63, is admitted involuntarily to our inpatient unit after elopement from another emergency room the prior day. For several weeks she had been leaving her house multiple times and wandering the streets in the middle of each night.
Mrs. P is experiencing auditory and visual hallucinations of evil spirits and religious and hypersexual delusions. She cannot recognize her face and believes her voice has been replaced by another’s. She also thinks that her face, nose, lips, voice, and abdomen are not her own. She believes evil spirits that reside within her body are continuously replacing her body parts. She claims these spirits inhabit her left vaginal wall, deposit money there, and are sexually assaulting her each night. She feels that a constant battle between good and evil spirits occurs within her body. She is very angry and states she does not need medication but rather an exorcism.
During her admission, Mrs. P continues to display psychomotor agitation, pressured speech, disorganized thought, religious and hypersexual delusions, grandiosity, and auditory and visual hallucinations. A workup that included a basic metabolic panel, complete blood count, thyroid tests, and abdominal/pelvic CT finds no medical causes for her symptoms. Ob/Gyn is consulted, but Mrs. P refuses a vaginal ultrasound.
The author’s observations
Mrs. P demonstrated symptoms consistent with both mood and thought disorders. Her symptoms of pressured speech, grandiosity, hypersexuality, and decreased need for sleep suggest a manic episode in bipolar disorder. The thought disorganization, delusions, and hallucinations were in line with psychosis.
HISTORY: Failed medications
Mrs. P was first hospitalized at age 29 and has had multiple inpatient admissions for mania, depression, and psychosis. As an outpatient, she was noncompliant with her medications and regularly decompensated and required acute inpatient admission.
Past failed medication trials include risperidone, risperidone long-acting injection, paliperidone, ziprasidone, quetiapine, haloperidol, lamotrigine, and valproic acid. These trials failed because of intolerable side effects or lack of efficacy. She takes lithium, 600 mg every morning and 900 mg at bedtime, for mood stabilization but refuses to try antipsychotics again because she feels the devil is going to attack her through the medications.
The authors’ observations
During her initial hospitalization at age 29, Mrs. P was diagnosed with schizophrenia. In subsequent years she appeared more manic, so her diagnosis was changed to schizoaffective disorder-bipolar type.
Based on our clinical interview, we decide that Mrs. P exhibits a variant of Capgras syndrome, a type of delusional misidentification syndrome in which a person believes other people are not their true selves but have been replaced by identical imposters ( Table ).1 Patients will at some level recognize a person, but they cannot experience the familiarity that is usually felt when seeing that person. Mrs. P’s case was unusual because instead of believing her loved ones were imposters, she could not recognize herself—her body, face, and voice were foreign to her.
We consider and rule out other misidentification syndromes, including mirrored-self misidentification, a condition in which patients cannot recognize themselves (and sometimes others) in a mirror. Mrs. P’s inability to recognize herself is not limited to her reflection. She is adamant that her hands and a part of her abdomen are not her own but another woman’s. She maintains this delusion even when looking directly at herself.
Breen2 argued that a face-processing deficit alone may not account for a mirror delusion; an inability to understand mirror spatial relations in reflections also may be present. Similar to Capgras, in mirrored-self misidentification there may be a perceptual deficit as well as a reasoning deficit that allows the patient to hold on to the delusion. In both delusions, there is a failure of reality testing.3
Table
4 types of delusional misidentification syndromes
| Syndrome | Delusion |
|---|---|
| Capgras syndrome | Belief that a loved one has been replaced by an identical impostor |
| Fregoli delusion | Belief that different people are actually the same person in disguise |
| Intermetamorphosis | Belief that one has switched identities with another individual or that others believe the afflicted to be someone else |
| Subjective doubles | Belief there exists a double of oneself living a separate life |
| Source: Reference 1 | |
Capgras syndrome
4
Capgras syndrome can be triggered by systemic infections, thyroid dysfunction, concussion, or intoxication. It is seen with head injury, toxic encephalopathy, and dementia.5
Joseph Capgras first described this syndrome in 1923. He discovered it by studying brain-injured patients who had prosopagnosia—the inability to recognize familiar faces. Patients with prosopagnosia are not delusional and understand that their inability to recognize faces is an impairment. Brain-injured patients with prosopagnosia had an autonomic arousal (measured by galvanic skin response) with familiar faces and thus unconscious face recognition was intact.5
Ellis et al6 described Capgras syndrome as being a “reverse” of prosopagnosia. They felt that in patients with Capgras, the conscious ability to recognize a face is intact, but the patient cannot produce an emotional response that usually occurs when seeing a familiar face. Thus, patients can recognize a person but feel that something is “off” or “wrong” and believe that the person must be an “imposter.” This hypothesis was supported by a 1997 study of 5 patients with schizophrenia who had Capgras.7
Breen2 reviewed 69 case reports of Capgras that had brain imaging results. Twenty-seven had normal brain imaging, 31 had global atrophy or bilateral brain damage, 2 had global atrophy and a right focal lesion, and 6 had a right hemispheric lesion. Thus, Capgras can occur in patients with normal or abnormal brain imaging.
Young9 developed an interactionist model of Capgras syndrome, in which a patient’s delusional belief allows the patient to explain his or her confusion and give the experience meaning. The experience then validates the belief, which makes the belief resistant to revision.
The main treatment of Capgras syndrome is pharmacotherapy with antipsychotics and cognitive-behavioral therapy (CBT) to help with fixed delusions.
Patients with Capgras syndrome believe people whom they know well have been replaced by identical imposters. One of the intriguing aspects of Capgras is that the patient to some extent must recognize a person’s face to be able to identify the person as an imposter.
A Capgras patient’s conscious ability to recognize a face is intact; however, the patient cannot produce the emotional response that usually occurs when seeing a familiar face. There is a disconnect between the areas in the brain that are responsible for facial recognition and those involved in emotions and memory. In patients with neurologic damage, this disconnect is believed to occur by:
- damage to the ventromedial frontal cortex, which causes impairment of automatic arousal responses and
- damage to the right frontal lobe, which causes inability to evaluate beliefs and impairs reasoning.
To rationalize the strange feeling produced by the inability to recognize a face, the patient develops a delusion that the loved one is an imposter.
TREATMENT: Pharmacotherapy
At admission, Mrs. P was taking only lithium for mood stabilization because she refused to take antipsychotics. During her stay, she reluctantly agrees to start haloperidol, which is titrated up to 20 mg bid. She experiences delusions related to the Devil attacking her via the haloperidol and thus is switched to fluphenazine, titrated up to 20 mg bid. She feels that liquid fluphenazine agrees with her the most, so she is stabilized and eventually discharged with this formulation. Switching to a depot formulation would have improved compliance, but Mrs. P adamantly resists this.
As her psychotic symptoms begin to resolve, Mrs. P begins to feel she is getting her body parts back. For example, she feels her face is her own but her nose is still not hers. During Mrs. P’s hospitalization, these bodily delusions lessen and eventually clear.
Other aspects of her psychosis and mania also resolve. She has some residual religious delusions at discharge but feels she has her body back and overall is much improved. Upon discharge Mrs. P is encouraged to follow up with a therapist for CBT, but she feels she does not need therapy and wants only to speak with her priest, even after most of her symptoms resolve. She also declines neuropsychological counseling.
Related resources
- Denes G. Capgras delusion. Neurol Sci. 2007;28:163-164.
- Coltheart M, Langdon R, McKay R. Schizophrenia and monothematic delusions. Schizophr Bull. 2007;33:642-647. http://schizophreniabulletin.oxfordjournals.org/cgi/content/full/33/3/642.
- Fluphenazine • Prolixin
- Haloperidol • Haldol
- Lamotrigine • Lamictal
- Lithium • Eskalith, Lithobid
- Paliperidone • Invega
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Risperidone long-acting injection • Risperdal Consta
- Valproic acid • Depakote
- Ziprasidone • Geodon
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Ellis HD, Luauté JP, Retterstøl N. Delusional misidentification syndromes. Psychopathology. 1994;27(3-5):117-120.
2. Breen N, Caine D, Coltheart M. Mirrored-self misidentification: two cases of focal onset dementia. Neurocase. 2001;7:239-254.
3. Brédart S, Young A. Self-recognition in everyday life. Cogn Neuropsychiatry. 2004;9:183-197.
4. Tamam L, Karatas G, Zeren T, et al. The prevalence of Capgras syndrome in a university hospital setting. Acta Neuropsychiatrica. 2003;15:290-295.
5. Barton J. Disorders of face perception and recognition. Neurol Clin. 2003;21:521-548.
6. Ellis H, Young AW. Accounting for delusional misidentifications. Br J Psychiatry. 1990;157:239-248.
7. Ellis HD, Young AW, Quayle AH, et al. Reduced autonomic responses to faces in Capgras delusion. Proc Biol Sci. 1997;264(1384):1085-1092.
8. Hirstein W, Ramachandran V. Capgras syndrome: a novel probe for understanding the neural representation of identity and familiarity of persons. Proc Biol Sci. 1997;264(1380):437-444.
9. Young G. Capgras delusion: an interactionist model. Conscious Cogn. 2008;17:863-876.
10. Feinberg T, Keenan J. Where in the brain is the self? Conscious Cogn. 2005;14:661-678.
CASE: Spirits replacing body parts
Mrs. P, age 63, is admitted involuntarily to our inpatient unit after elopement from another emergency room the prior day. For several weeks she had been leaving her house multiple times and wandering the streets in the middle of each night.
Mrs. P is experiencing auditory and visual hallucinations of evil spirits and religious and hypersexual delusions. She cannot recognize her face and believes her voice has been replaced by another’s. She also thinks that her face, nose, lips, voice, and abdomen are not her own. She believes evil spirits that reside within her body are continuously replacing her body parts. She claims these spirits inhabit her left vaginal wall, deposit money there, and are sexually assaulting her each night. She feels that a constant battle between good and evil spirits occurs within her body. She is very angry and states she does not need medication but rather an exorcism.
During her admission, Mrs. P continues to display psychomotor agitation, pressured speech, disorganized thought, religious and hypersexual delusions, grandiosity, and auditory and visual hallucinations. A workup that included a basic metabolic panel, complete blood count, thyroid tests, and abdominal/pelvic CT finds no medical causes for her symptoms. Ob/Gyn is consulted, but Mrs. P refuses a vaginal ultrasound.
The author’s observations
Mrs. P demonstrated symptoms consistent with both mood and thought disorders. Her symptoms of pressured speech, grandiosity, hypersexuality, and decreased need for sleep suggest a manic episode in bipolar disorder. The thought disorganization, delusions, and hallucinations were in line with psychosis.
HISTORY: Failed medications
Mrs. P was first hospitalized at age 29 and has had multiple inpatient admissions for mania, depression, and psychosis. As an outpatient, she was noncompliant with her medications and regularly decompensated and required acute inpatient admission.
Past failed medication trials include risperidone, risperidone long-acting injection, paliperidone, ziprasidone, quetiapine, haloperidol, lamotrigine, and valproic acid. These trials failed because of intolerable side effects or lack of efficacy. She takes lithium, 600 mg every morning and 900 mg at bedtime, for mood stabilization but refuses to try antipsychotics again because she feels the devil is going to attack her through the medications.
The authors’ observations
During her initial hospitalization at age 29, Mrs. P was diagnosed with schizophrenia. In subsequent years she appeared more manic, so her diagnosis was changed to schizoaffective disorder-bipolar type.
Based on our clinical interview, we decide that Mrs. P exhibits a variant of Capgras syndrome, a type of delusional misidentification syndrome in which a person believes other people are not their true selves but have been replaced by identical imposters ( Table ).1 Patients will at some level recognize a person, but they cannot experience the familiarity that is usually felt when seeing that person. Mrs. P’s case was unusual because instead of believing her loved ones were imposters, she could not recognize herself—her body, face, and voice were foreign to her.
We consider and rule out other misidentification syndromes, including mirrored-self misidentification, a condition in which patients cannot recognize themselves (and sometimes others) in a mirror. Mrs. P’s inability to recognize herself is not limited to her reflection. She is adamant that her hands and a part of her abdomen are not her own but another woman’s. She maintains this delusion even when looking directly at herself.
Breen2 argued that a face-processing deficit alone may not account for a mirror delusion; an inability to understand mirror spatial relations in reflections also may be present. Similar to Capgras, in mirrored-self misidentification there may be a perceptual deficit as well as a reasoning deficit that allows the patient to hold on to the delusion. In both delusions, there is a failure of reality testing.3
Table
4 types of delusional misidentification syndromes
| Syndrome | Delusion |
|---|---|
| Capgras syndrome | Belief that a loved one has been replaced by an identical impostor |
| Fregoli delusion | Belief that different people are actually the same person in disguise |
| Intermetamorphosis | Belief that one has switched identities with another individual or that others believe the afflicted to be someone else |
| Subjective doubles | Belief there exists a double of oneself living a separate life |
| Source: Reference 1 | |
Capgras syndrome
4
Capgras syndrome can be triggered by systemic infections, thyroid dysfunction, concussion, or intoxication. It is seen with head injury, toxic encephalopathy, and dementia.5
Joseph Capgras first described this syndrome in 1923. He discovered it by studying brain-injured patients who had prosopagnosia—the inability to recognize familiar faces. Patients with prosopagnosia are not delusional and understand that their inability to recognize faces is an impairment. Brain-injured patients with prosopagnosia had an autonomic arousal (measured by galvanic skin response) with familiar faces and thus unconscious face recognition was intact.5
Ellis et al6 described Capgras syndrome as being a “reverse” of prosopagnosia. They felt that in patients with Capgras, the conscious ability to recognize a face is intact, but the patient cannot produce an emotional response that usually occurs when seeing a familiar face. Thus, patients can recognize a person but feel that something is “off” or “wrong” and believe that the person must be an “imposter.” This hypothesis was supported by a 1997 study of 5 patients with schizophrenia who had Capgras.7
Breen2 reviewed 69 case reports of Capgras that had brain imaging results. Twenty-seven had normal brain imaging, 31 had global atrophy or bilateral brain damage, 2 had global atrophy and a right focal lesion, and 6 had a right hemispheric lesion. Thus, Capgras can occur in patients with normal or abnormal brain imaging.
Young9 developed an interactionist model of Capgras syndrome, in which a patient’s delusional belief allows the patient to explain his or her confusion and give the experience meaning. The experience then validates the belief, which makes the belief resistant to revision.
The main treatment of Capgras syndrome is pharmacotherapy with antipsychotics and cognitive-behavioral therapy (CBT) to help with fixed delusions.
Patients with Capgras syndrome believe people whom they know well have been replaced by identical imposters. One of the intriguing aspects of Capgras is that the patient to some extent must recognize a person’s face to be able to identify the person as an imposter.
A Capgras patient’s conscious ability to recognize a face is intact; however, the patient cannot produce the emotional response that usually occurs when seeing a familiar face. There is a disconnect between the areas in the brain that are responsible for facial recognition and those involved in emotions and memory. In patients with neurologic damage, this disconnect is believed to occur by:
- damage to the ventromedial frontal cortex, which causes impairment of automatic arousal responses and
- damage to the right frontal lobe, which causes inability to evaluate beliefs and impairs reasoning.
To rationalize the strange feeling produced by the inability to recognize a face, the patient develops a delusion that the loved one is an imposter.
TREATMENT: Pharmacotherapy
At admission, Mrs. P was taking only lithium for mood stabilization because she refused to take antipsychotics. During her stay, she reluctantly agrees to start haloperidol, which is titrated up to 20 mg bid. She experiences delusions related to the Devil attacking her via the haloperidol and thus is switched to fluphenazine, titrated up to 20 mg bid. She feels that liquid fluphenazine agrees with her the most, so she is stabilized and eventually discharged with this formulation. Switching to a depot formulation would have improved compliance, but Mrs. P adamantly resists this.
As her psychotic symptoms begin to resolve, Mrs. P begins to feel she is getting her body parts back. For example, she feels her face is her own but her nose is still not hers. During Mrs. P’s hospitalization, these bodily delusions lessen and eventually clear.
Other aspects of her psychosis and mania also resolve. She has some residual religious delusions at discharge but feels she has her body back and overall is much improved. Upon discharge Mrs. P is encouraged to follow up with a therapist for CBT, but she feels she does not need therapy and wants only to speak with her priest, even after most of her symptoms resolve. She also declines neuropsychological counseling.
Related resources
- Denes G. Capgras delusion. Neurol Sci. 2007;28:163-164.
- Coltheart M, Langdon R, McKay R. Schizophrenia and monothematic delusions. Schizophr Bull. 2007;33:642-647. http://schizophreniabulletin.oxfordjournals.org/cgi/content/full/33/3/642.
- Fluphenazine • Prolixin
- Haloperidol • Haldol
- Lamotrigine • Lamictal
- Lithium • Eskalith, Lithobid
- Paliperidone • Invega
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Risperidone long-acting injection • Risperdal Consta
- Valproic acid • Depakote
- Ziprasidone • Geodon
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: Spirits replacing body parts
Mrs. P, age 63, is admitted involuntarily to our inpatient unit after elopement from another emergency room the prior day. For several weeks she had been leaving her house multiple times and wandering the streets in the middle of each night.
Mrs. P is experiencing auditory and visual hallucinations of evil spirits and religious and hypersexual delusions. She cannot recognize her face and believes her voice has been replaced by another’s. She also thinks that her face, nose, lips, voice, and abdomen are not her own. She believes evil spirits that reside within her body are continuously replacing her body parts. She claims these spirits inhabit her left vaginal wall, deposit money there, and are sexually assaulting her each night. She feels that a constant battle between good and evil spirits occurs within her body. She is very angry and states she does not need medication but rather an exorcism.
During her admission, Mrs. P continues to display psychomotor agitation, pressured speech, disorganized thought, religious and hypersexual delusions, grandiosity, and auditory and visual hallucinations. A workup that included a basic metabolic panel, complete blood count, thyroid tests, and abdominal/pelvic CT finds no medical causes for her symptoms. Ob/Gyn is consulted, but Mrs. P refuses a vaginal ultrasound.
The author’s observations
Mrs. P demonstrated symptoms consistent with both mood and thought disorders. Her symptoms of pressured speech, grandiosity, hypersexuality, and decreased need for sleep suggest a manic episode in bipolar disorder. The thought disorganization, delusions, and hallucinations were in line with psychosis.
HISTORY: Failed medications
Mrs. P was first hospitalized at age 29 and has had multiple inpatient admissions for mania, depression, and psychosis. As an outpatient, she was noncompliant with her medications and regularly decompensated and required acute inpatient admission.
Past failed medication trials include risperidone, risperidone long-acting injection, paliperidone, ziprasidone, quetiapine, haloperidol, lamotrigine, and valproic acid. These trials failed because of intolerable side effects or lack of efficacy. She takes lithium, 600 mg every morning and 900 mg at bedtime, for mood stabilization but refuses to try antipsychotics again because she feels the devil is going to attack her through the medications.
The authors’ observations
During her initial hospitalization at age 29, Mrs. P was diagnosed with schizophrenia. In subsequent years she appeared more manic, so her diagnosis was changed to schizoaffective disorder-bipolar type.
Based on our clinical interview, we decide that Mrs. P exhibits a variant of Capgras syndrome, a type of delusional misidentification syndrome in which a person believes other people are not their true selves but have been replaced by identical imposters ( Table ).1 Patients will at some level recognize a person, but they cannot experience the familiarity that is usually felt when seeing that person. Mrs. P’s case was unusual because instead of believing her loved ones were imposters, she could not recognize herself—her body, face, and voice were foreign to her.
We consider and rule out other misidentification syndromes, including mirrored-self misidentification, a condition in which patients cannot recognize themselves (and sometimes others) in a mirror. Mrs. P’s inability to recognize herself is not limited to her reflection. She is adamant that her hands and a part of her abdomen are not her own but another woman’s. She maintains this delusion even when looking directly at herself.
Breen2 argued that a face-processing deficit alone may not account for a mirror delusion; an inability to understand mirror spatial relations in reflections also may be present. Similar to Capgras, in mirrored-self misidentification there may be a perceptual deficit as well as a reasoning deficit that allows the patient to hold on to the delusion. In both delusions, there is a failure of reality testing.3
Table
4 types of delusional misidentification syndromes
| Syndrome | Delusion |
|---|---|
| Capgras syndrome | Belief that a loved one has been replaced by an identical impostor |
| Fregoli delusion | Belief that different people are actually the same person in disguise |
| Intermetamorphosis | Belief that one has switched identities with another individual or that others believe the afflicted to be someone else |
| Subjective doubles | Belief there exists a double of oneself living a separate life |
| Source: Reference 1 | |
Capgras syndrome
4
Capgras syndrome can be triggered by systemic infections, thyroid dysfunction, concussion, or intoxication. It is seen with head injury, toxic encephalopathy, and dementia.5
Joseph Capgras first described this syndrome in 1923. He discovered it by studying brain-injured patients who had prosopagnosia—the inability to recognize familiar faces. Patients with prosopagnosia are not delusional and understand that their inability to recognize faces is an impairment. Brain-injured patients with prosopagnosia had an autonomic arousal (measured by galvanic skin response) with familiar faces and thus unconscious face recognition was intact.5
Ellis et al6 described Capgras syndrome as being a “reverse” of prosopagnosia. They felt that in patients with Capgras, the conscious ability to recognize a face is intact, but the patient cannot produce an emotional response that usually occurs when seeing a familiar face. Thus, patients can recognize a person but feel that something is “off” or “wrong” and believe that the person must be an “imposter.” This hypothesis was supported by a 1997 study of 5 patients with schizophrenia who had Capgras.7
Breen2 reviewed 69 case reports of Capgras that had brain imaging results. Twenty-seven had normal brain imaging, 31 had global atrophy or bilateral brain damage, 2 had global atrophy and a right focal lesion, and 6 had a right hemispheric lesion. Thus, Capgras can occur in patients with normal or abnormal brain imaging.
Young9 developed an interactionist model of Capgras syndrome, in which a patient’s delusional belief allows the patient to explain his or her confusion and give the experience meaning. The experience then validates the belief, which makes the belief resistant to revision.
The main treatment of Capgras syndrome is pharmacotherapy with antipsychotics and cognitive-behavioral therapy (CBT) to help with fixed delusions.
Patients with Capgras syndrome believe people whom they know well have been replaced by identical imposters. One of the intriguing aspects of Capgras is that the patient to some extent must recognize a person’s face to be able to identify the person as an imposter.
A Capgras patient’s conscious ability to recognize a face is intact; however, the patient cannot produce the emotional response that usually occurs when seeing a familiar face. There is a disconnect between the areas in the brain that are responsible for facial recognition and those involved in emotions and memory. In patients with neurologic damage, this disconnect is believed to occur by:
- damage to the ventromedial frontal cortex, which causes impairment of automatic arousal responses and
- damage to the right frontal lobe, which causes inability to evaluate beliefs and impairs reasoning.
To rationalize the strange feeling produced by the inability to recognize a face, the patient develops a delusion that the loved one is an imposter.
TREATMENT: Pharmacotherapy
At admission, Mrs. P was taking only lithium for mood stabilization because she refused to take antipsychotics. During her stay, she reluctantly agrees to start haloperidol, which is titrated up to 20 mg bid. She experiences delusions related to the Devil attacking her via the haloperidol and thus is switched to fluphenazine, titrated up to 20 mg bid. She feels that liquid fluphenazine agrees with her the most, so she is stabilized and eventually discharged with this formulation. Switching to a depot formulation would have improved compliance, but Mrs. P adamantly resists this.
As her psychotic symptoms begin to resolve, Mrs. P begins to feel she is getting her body parts back. For example, she feels her face is her own but her nose is still not hers. During Mrs. P’s hospitalization, these bodily delusions lessen and eventually clear.
Other aspects of her psychosis and mania also resolve. She has some residual religious delusions at discharge but feels she has her body back and overall is much improved. Upon discharge Mrs. P is encouraged to follow up with a therapist for CBT, but she feels she does not need therapy and wants only to speak with her priest, even after most of her symptoms resolve. She also declines neuropsychological counseling.
Related resources
- Denes G. Capgras delusion. Neurol Sci. 2007;28:163-164.
- Coltheart M, Langdon R, McKay R. Schizophrenia and monothematic delusions. Schizophr Bull. 2007;33:642-647. http://schizophreniabulletin.oxfordjournals.org/cgi/content/full/33/3/642.
- Fluphenazine • Prolixin
- Haloperidol • Haldol
- Lamotrigine • Lamictal
- Lithium • Eskalith, Lithobid
- Paliperidone • Invega
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Risperidone long-acting injection • Risperdal Consta
- Valproic acid • Depakote
- Ziprasidone • Geodon
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Ellis HD, Luauté JP, Retterstøl N. Delusional misidentification syndromes. Psychopathology. 1994;27(3-5):117-120.
2. Breen N, Caine D, Coltheart M. Mirrored-self misidentification: two cases of focal onset dementia. Neurocase. 2001;7:239-254.
3. Brédart S, Young A. Self-recognition in everyday life. Cogn Neuropsychiatry. 2004;9:183-197.
4. Tamam L, Karatas G, Zeren T, et al. The prevalence of Capgras syndrome in a university hospital setting. Acta Neuropsychiatrica. 2003;15:290-295.
5. Barton J. Disorders of face perception and recognition. Neurol Clin. 2003;21:521-548.
6. Ellis H, Young AW. Accounting for delusional misidentifications. Br J Psychiatry. 1990;157:239-248.
7. Ellis HD, Young AW, Quayle AH, et al. Reduced autonomic responses to faces in Capgras delusion. Proc Biol Sci. 1997;264(1384):1085-1092.
8. Hirstein W, Ramachandran V. Capgras syndrome: a novel probe for understanding the neural representation of identity and familiarity of persons. Proc Biol Sci. 1997;264(1380):437-444.
9. Young G. Capgras delusion: an interactionist model. Conscious Cogn. 2008;17:863-876.
10. Feinberg T, Keenan J. Where in the brain is the self? Conscious Cogn. 2005;14:661-678.
1. Ellis HD, Luauté JP, Retterstøl N. Delusional misidentification syndromes. Psychopathology. 1994;27(3-5):117-120.
2. Breen N, Caine D, Coltheart M. Mirrored-self misidentification: two cases of focal onset dementia. Neurocase. 2001;7:239-254.
3. Brédart S, Young A. Self-recognition in everyday life. Cogn Neuropsychiatry. 2004;9:183-197.
4. Tamam L, Karatas G, Zeren T, et al. The prevalence of Capgras syndrome in a university hospital setting. Acta Neuropsychiatrica. 2003;15:290-295.
5. Barton J. Disorders of face perception and recognition. Neurol Clin. 2003;21:521-548.
6. Ellis H, Young AW. Accounting for delusional misidentifications. Br J Psychiatry. 1990;157:239-248.
7. Ellis HD, Young AW, Quayle AH, et al. Reduced autonomic responses to faces in Capgras delusion. Proc Biol Sci. 1997;264(1384):1085-1092.
8. Hirstein W, Ramachandran V. Capgras syndrome: a novel probe for understanding the neural representation of identity and familiarity of persons. Proc Biol Sci. 1997;264(1380):437-444.
9. Young G. Capgras delusion: an interactionist model. Conscious Cogn. 2008;17:863-876.
10. Feinberg T, Keenan J. Where in the brain is the self? Conscious Cogn. 2005;14:661-678.
The nurse who worked the system
CASE: A ‘high utilizer’
Ms. Y, a 49-year-old intensive care registered nurse, is admitted to the psychiatric hospital for suicidal ideation for the eighth time in 1 year. Ms. Y has chronic suicidal ideation with multiple attempts and has been on disability for 3 years for treatment of severe depression. She has been hospitalized for depression with suicide ideation 49 times since her divorce 6 years ago. She is prescribed fluoxetine, 60 mg/d, quetiapine, 400 mg/d, and clonazepam, 2 mg/d.
The authors’ observations
Ms. Y possesses 7 of the 11 characteristics of a high utilizer of psychiatric services (Table 1),1,2 defined as a patient who is:
- 2 standard deviations above the mean number of visits to an urban psychiatric emergency service in 6 months or
- has 4 inpatient admissions in a quarter or 6 inpatient admissions in 1 year.
Table 1
Common characteristics of high utilizers* of psychiatric services
| Homelessness |
| Developmental delays |
| Enrolled in a mental health plan |
| History of voluntary and involuntary hospitalization |
| Personality disorders |
| Likely to be uncooperative |
| Substance abuse or dependence (or history) |
| History of incarceration |
| Unreliable social support |
| Young Caucasian women |
| * Defined as having either 2 standard deviations above the mean number of visits to an urban psychiatric emergency service in 6 months or 4 inpatient admissions in a quarter or 6 inpatient admissions in 1 year |
| Source: References 1,2 |
The author’s observations
Because previous hospitalizations and courses of ECT have provided Ms. Y with only minimal, short-lived improvement, the treatment team decides to reconsider her diagnosis and treatment plan. Ms. Y’s first psychiatrist diagnosed her with major depressive disorder. After thoroughly interviewing Ms. Y and reviewing her history, the hospital psychiatrist determines that she meets criteria for borderline personality disorder (BPD) in addition to major depression. The psychiatrist explains this diagnosis to Ms. Y, provides her with education and support, and recommends dialectical behavioral therapy (DBT) and case management. She rejects the new diagnosis and treatment plan and pleads for help establishing treatment with a new psychiatrist.
The team at the psychiatric hospital feels Ms. Y needs to receive ongoing treatment from a psychiatrist. In the hope that she will be able to establish a therapeutic alliance with a new psychiatrist and therapist, they decide to continue working with Ms. Y if she accepts the BPD diagnosis and agrees to undergo DBT.
EVALUATION: A troubling pattern
Before Ms. Y’s husband divorced her, she had not received psychiatric care and had no psychiatric diagnosis. During the contentious divorce, she experienced depressive symptoms that later intensified, and she was unable to return to her previous high level of functioning.
Ms. Y became suicidal and was hospitalized for the first time shortly after the divorce was finalized and her ex-husband remarried. She began treatment with a psychiatrist, whom she idealized and saw for 5 years.
When this psychiatrist—who had been one of the few stable relationships in Ms. Y’s life—moved to another state, Ms. Y experienced a rapid recurrence of depression. She began treatment with 3 other psychiatrists but fired them because they “never understand me” like her first psychiatrist did, and she never felt she received the consistent, supportive care she deserved. She become suicidal and again required psychiatric hospitalization. This pattern continued up to her current admission.
The authors’ observations
Ms. Y briefly returns to work between hospitalizations but is not able to tolerate the stress. At one point she was admitted to an out-of-state facility; after this 2-month stay, she remained out of the local psychiatric hospital for 6 months but then became unable to function and was readmitted to the local psychiatric hospital.
When interviewed, Ms. Y describes feeling hopeless, empty, and alone each time 2 of her 3 children return to college after summer break. Her youngest child lives at home but is involved in extracurricular high school activities, and doesn’t seem to need her. Ms. Y is estranged from both parents. Her social support is unreliable because she tends to push others away and isolate herself.
The authors’ observations
Because she has no history of mania, Ms. Y does not meet criteria for bipolar affective disorder. Her multidisciplinary treatment team feels she is too fragile to transfer care to new providers or to foster care, so we schedule a care conference and carefully compose a 6-month contract to formally articulate limits and boundaries within which we will continue to treat her.
The contract specifies that Ms. Y will participate in DBT, take her medications exactly as prescribed, and not receive any early refills of her prescriptions. We arrange with Ms. Y’s health plan to have a home healthcare agency provide her medications weekly. This benefit was not available to other health plan members. Ms. Y signs the contract.
TREATMENT: Contract violation
Ms. Y complies with the contract for 2 months, then abruptly fires her long-term therapist, whom she claims violated confidentiality by giving false information to another provider. At her next session, Ms. Y will not provide details about the alleged incident, and the issue never is resolved. She admits she did not start DBT and is not taking her medications as prescribed.
Ms. Y expresses her disagreement with the terms of the contract. She becomes very upset and asks for her care to be transferred to another psychiatrist. She demands to be followed at the current clinic because “I was born here.” She denies being actively suicidal and terminates the session early. That afternoon, she calls 1 of the inpatient psychiatrists and asks if he would treat her. She also calls the first psychiatrist she had seen to enlist help in obtaining care.
The authors’ observations
In Groves’ description of 4 types of “hateful patients,” Ms. Y represents a combination of an entitled demander and a manipulative help-rejecter. The behaviors and personality disorders associated with these types of patients—and effective management strategies—are listed in (Table 2).3 (Table 3) offers tips for successfully dealing with high utilizers of psychiatric services. High utilizers of medical services other than psychiatry are more likely than patients who are not high utilizers to have a psychiatric disorder (Box).4-9
Patients who are high utilizers of medical services other than psychiatry have up to 50% higher rates of psychiatric disorders—particularly depression—compared with less-frequent utilizers.4-6 Screening medical patients for depression helps ensure that these patients are correctly diagnosed and treated.
Depression is a risk factor for nonadherence with medical treatment, and treating depression leads to decreased utilization of medical services.7,8 Patients with successfully treated depression may have reduced functional disability as well.9
Some members of our treatment team began to experience countertransference, which also interfered with Ms. Y’s treatment. They viewed her behavior as entitled, demanding, and manipulative and dreaded caring for her. Failing to recognize such defenses can lead to consequences such as malignant alienation—a progressive deterioration in the patient’s relationship with others that includes loss of sympathy and support from staff members—which can put a patient at high risk for suicide.10
After a lengthy discussion among several psychiatrists, therapists, nurses, and attorneys, the treatment team decided to terminate outpatient care for Ms. Y at our facility because of her chronic nonadherence to treatment recommendations. Ms. Y had manipulated numerous providers in our department, called multiple doctors in our facility to ask them to care for her, and asked her ex-husband to contact the department administration on her behalf. Her behavior bordered on harassment. In addition, the interventions we provided were making her worse, not better. Factors that influenced our decision included:
- fear of Ms. Y committing suicide
- fear of setting limits
- fear of being reported to the Medical Board
- fear of a lawsuit.
Table 2
Strategies for helping 4 types of ‘hateful patients’
| Dependent clinger | |
| Behaviors | Shows extreme gratitude with flattery |
| Associated personality traits/disorders | Codependent |
| Management strategies | As early and as tactfully as possible, set firm limits on the patient’s expectations for an intense doctor-patient relationship. Tell the patient that you have limits not only on knowledge and skill but also on time and stamina |
| Entitled demander | |
| Behaviors | Intimidates, devalues, induces guilt, may try to control with threats; terrified of abandonment |
| Associated personality traits/disorders | Narcissistic, borderline personality disorder |
| Management strategies | Try to rechannel your patient’s feelings of entitlement into a partnership that acknowledges his or her entitlement not to unrealistic demands but to good medical care. Help your patient stop directing anger at the healthcare team |
| Manipulative help-rejecter | |
| Behaviors | Resists treatment; may seem happy with treatment failures |
| Associated personality traits/disorders | Psychopathy, paranoia, borderline personality disorder, negativistic, passive/aggressive |
| Management strategies | Diminish your patient’s notion that losing the symptom or illness implies losing the doctor by ‘sharing’ your patient’s pessimism. Tell your patient that treatment may not cure the illness. Schedule regular follow-up visits |
| Self-destructive denier | |
| Behaviors | Denial helps them survive |
| Associated personality traits/disorders | Borderline personality disorder, histrionic, schizoid, schizotypal |
| Management strategies | Recognize that this type of patient can make clinicians wish the patient would die and that the chance of helping a self-destructive denier is minimal. Lower unrealistic expectations of delivering perfect care. Evaluate the patient for a treatable mental illness, such as depression, anxiety, etc. |
| Source: Reference 3 | |
Table 3
Tips for managing high utilizers
Establish a collaborative treatment plan with firm limits and expectations
|
Acknowledge your feelings and countertransference
|
Explore your patient’s expectations and commitment to treatment by asking:
|
Practice safely and proactively
|
OUTCOME: The pattern continues
Ms. Y continues to receive treatment with a different outpatient psychiatrist and therapist in the area. She has not been hospitalized for almost 2 years but her financial state has deteriorated and she has had a recurrence of depression. Ms. Y’s psychiatrist recently called the hospital to ask for direct admission on the patient’s behalf, stating that Ms. Y did not want to wait hours to be seen in the ER. Hospital staff explained that she needs to first come to the ER for evaluation. Ms. Y refused to come to the ER and was not admitted. About 1 month later, Ms. Y’s psychiatrist called again, and she was directly admitted to the psychiatric hospital.
Related resource
- National Suicide Prevention Lifeline. 1-800-273-TALK (8255). www.suicidepreventionlifeline.org.
- Clonazepam • Klonopin
- Fluoxetine • Prozac
- Quetiapine • Seroquel
The authors report no financial relationship with any company whose products are mentioned in this article or manufacturers of competing products.
1. Pasic J, Russo J, Roy-Byrne P. High utilizers of psychiatric emergency services. Psychiatr Serv. 2005;56(6):678-684.
2. Geller J, Fisher W, McDermeit M, et al. The effects of public managed care on patterns of intensive use of inpatient psychiatric services. Psychiatr Serv. 1998;49:327-332.
3. Groves JE. Taking care of the hateful patient. N Engl J Med. 1978;298(16):883-887.
4. Karlsson H, Lehtinen V, Joukamaa M. Are frequent attenders of primary health care distressed? Scan J Health Care. 1995;13:32-38.
5. Karlsson H, Lehtinen V, Joukamaa M. Psychiatric morbidity among frequent attenders in primary care. Gen Hosp Psychiatry. 1995;17:19-25.
6. Lefevre F, Refiler D, Lee P, et al. Screening for undetected mental disorders in high utilizers of primary care services. J Gen Int Med. 1999;14:425-431.
7. Pearson S, Katzelnick D, Simon G, et al. Depression among high utilizers of medical care. J Gen Intern Med. 1999;14:461-468.
8. DiMatteo MR, Lepper HS, Croghan TW. Depression is a risk factor for noncompliance with medical treatment: meta-analysis of the effects of anxiety and depression on medical adherence. Arch Intern Med. 2000;160:2101-2107.
9. Von Korff M, Ormel J, Katon W, et al. Disability and depression among high utilizers of health care. A longitudinal analysis. Arch Gen Psychiatry. 1992;49(2):91-100.
10. Watts D, Morgan G. Malignant alienation dangers for patients who are hard to like. Br J Psychiatry. 1994;164:11-15.
CASE: A ‘high utilizer’
Ms. Y, a 49-year-old intensive care registered nurse, is admitted to the psychiatric hospital for suicidal ideation for the eighth time in 1 year. Ms. Y has chronic suicidal ideation with multiple attempts and has been on disability for 3 years for treatment of severe depression. She has been hospitalized for depression with suicide ideation 49 times since her divorce 6 years ago. She is prescribed fluoxetine, 60 mg/d, quetiapine, 400 mg/d, and clonazepam, 2 mg/d.
The authors’ observations
Ms. Y possesses 7 of the 11 characteristics of a high utilizer of psychiatric services (Table 1),1,2 defined as a patient who is:
- 2 standard deviations above the mean number of visits to an urban psychiatric emergency service in 6 months or
- has 4 inpatient admissions in a quarter or 6 inpatient admissions in 1 year.
Table 1
Common characteristics of high utilizers* of psychiatric services
| Homelessness |
| Developmental delays |
| Enrolled in a mental health plan |
| History of voluntary and involuntary hospitalization |
| Personality disorders |
| Likely to be uncooperative |
| Substance abuse or dependence (or history) |
| History of incarceration |
| Unreliable social support |
| Young Caucasian women |
| * Defined as having either 2 standard deviations above the mean number of visits to an urban psychiatric emergency service in 6 months or 4 inpatient admissions in a quarter or 6 inpatient admissions in 1 year |
| Source: References 1,2 |
The author’s observations
Because previous hospitalizations and courses of ECT have provided Ms. Y with only minimal, short-lived improvement, the treatment team decides to reconsider her diagnosis and treatment plan. Ms. Y’s first psychiatrist diagnosed her with major depressive disorder. After thoroughly interviewing Ms. Y and reviewing her history, the hospital psychiatrist determines that she meets criteria for borderline personality disorder (BPD) in addition to major depression. The psychiatrist explains this diagnosis to Ms. Y, provides her with education and support, and recommends dialectical behavioral therapy (DBT) and case management. She rejects the new diagnosis and treatment plan and pleads for help establishing treatment with a new psychiatrist.
The team at the psychiatric hospital feels Ms. Y needs to receive ongoing treatment from a psychiatrist. In the hope that she will be able to establish a therapeutic alliance with a new psychiatrist and therapist, they decide to continue working with Ms. Y if she accepts the BPD diagnosis and agrees to undergo DBT.
EVALUATION: A troubling pattern
Before Ms. Y’s husband divorced her, she had not received psychiatric care and had no psychiatric diagnosis. During the contentious divorce, she experienced depressive symptoms that later intensified, and she was unable to return to her previous high level of functioning.
Ms. Y became suicidal and was hospitalized for the first time shortly after the divorce was finalized and her ex-husband remarried. She began treatment with a psychiatrist, whom she idealized and saw for 5 years.
When this psychiatrist—who had been one of the few stable relationships in Ms. Y’s life—moved to another state, Ms. Y experienced a rapid recurrence of depression. She began treatment with 3 other psychiatrists but fired them because they “never understand me” like her first psychiatrist did, and she never felt she received the consistent, supportive care she deserved. She become suicidal and again required psychiatric hospitalization. This pattern continued up to her current admission.
The authors’ observations
Ms. Y briefly returns to work between hospitalizations but is not able to tolerate the stress. At one point she was admitted to an out-of-state facility; after this 2-month stay, she remained out of the local psychiatric hospital for 6 months but then became unable to function and was readmitted to the local psychiatric hospital.
When interviewed, Ms. Y describes feeling hopeless, empty, and alone each time 2 of her 3 children return to college after summer break. Her youngest child lives at home but is involved in extracurricular high school activities, and doesn’t seem to need her. Ms. Y is estranged from both parents. Her social support is unreliable because she tends to push others away and isolate herself.
The authors’ observations
Because she has no history of mania, Ms. Y does not meet criteria for bipolar affective disorder. Her multidisciplinary treatment team feels she is too fragile to transfer care to new providers or to foster care, so we schedule a care conference and carefully compose a 6-month contract to formally articulate limits and boundaries within which we will continue to treat her.
The contract specifies that Ms. Y will participate in DBT, take her medications exactly as prescribed, and not receive any early refills of her prescriptions. We arrange with Ms. Y’s health plan to have a home healthcare agency provide her medications weekly. This benefit was not available to other health plan members. Ms. Y signs the contract.
TREATMENT: Contract violation
Ms. Y complies with the contract for 2 months, then abruptly fires her long-term therapist, whom she claims violated confidentiality by giving false information to another provider. At her next session, Ms. Y will not provide details about the alleged incident, and the issue never is resolved. She admits she did not start DBT and is not taking her medications as prescribed.
Ms. Y expresses her disagreement with the terms of the contract. She becomes very upset and asks for her care to be transferred to another psychiatrist. She demands to be followed at the current clinic because “I was born here.” She denies being actively suicidal and terminates the session early. That afternoon, she calls 1 of the inpatient psychiatrists and asks if he would treat her. She also calls the first psychiatrist she had seen to enlist help in obtaining care.
The authors’ observations
In Groves’ description of 4 types of “hateful patients,” Ms. Y represents a combination of an entitled demander and a manipulative help-rejecter. The behaviors and personality disorders associated with these types of patients—and effective management strategies—are listed in (Table 2).3 (Table 3) offers tips for successfully dealing with high utilizers of psychiatric services. High utilizers of medical services other than psychiatry are more likely than patients who are not high utilizers to have a psychiatric disorder (Box).4-9
Patients who are high utilizers of medical services other than psychiatry have up to 50% higher rates of psychiatric disorders—particularly depression—compared with less-frequent utilizers.4-6 Screening medical patients for depression helps ensure that these patients are correctly diagnosed and treated.
Depression is a risk factor for nonadherence with medical treatment, and treating depression leads to decreased utilization of medical services.7,8 Patients with successfully treated depression may have reduced functional disability as well.9
Some members of our treatment team began to experience countertransference, which also interfered with Ms. Y’s treatment. They viewed her behavior as entitled, demanding, and manipulative and dreaded caring for her. Failing to recognize such defenses can lead to consequences such as malignant alienation—a progressive deterioration in the patient’s relationship with others that includes loss of sympathy and support from staff members—which can put a patient at high risk for suicide.10
After a lengthy discussion among several psychiatrists, therapists, nurses, and attorneys, the treatment team decided to terminate outpatient care for Ms. Y at our facility because of her chronic nonadherence to treatment recommendations. Ms. Y had manipulated numerous providers in our department, called multiple doctors in our facility to ask them to care for her, and asked her ex-husband to contact the department administration on her behalf. Her behavior bordered on harassment. In addition, the interventions we provided were making her worse, not better. Factors that influenced our decision included:
- fear of Ms. Y committing suicide
- fear of setting limits
- fear of being reported to the Medical Board
- fear of a lawsuit.
Table 2
Strategies for helping 4 types of ‘hateful patients’
| Dependent clinger | |
| Behaviors | Shows extreme gratitude with flattery |
| Associated personality traits/disorders | Codependent |
| Management strategies | As early and as tactfully as possible, set firm limits on the patient’s expectations for an intense doctor-patient relationship. Tell the patient that you have limits not only on knowledge and skill but also on time and stamina |
| Entitled demander | |
| Behaviors | Intimidates, devalues, induces guilt, may try to control with threats; terrified of abandonment |
| Associated personality traits/disorders | Narcissistic, borderline personality disorder |
| Management strategies | Try to rechannel your patient’s feelings of entitlement into a partnership that acknowledges his or her entitlement not to unrealistic demands but to good medical care. Help your patient stop directing anger at the healthcare team |
| Manipulative help-rejecter | |
| Behaviors | Resists treatment; may seem happy with treatment failures |
| Associated personality traits/disorders | Psychopathy, paranoia, borderline personality disorder, negativistic, passive/aggressive |
| Management strategies | Diminish your patient’s notion that losing the symptom or illness implies losing the doctor by ‘sharing’ your patient’s pessimism. Tell your patient that treatment may not cure the illness. Schedule regular follow-up visits |
| Self-destructive denier | |
| Behaviors | Denial helps them survive |
| Associated personality traits/disorders | Borderline personality disorder, histrionic, schizoid, schizotypal |
| Management strategies | Recognize that this type of patient can make clinicians wish the patient would die and that the chance of helping a self-destructive denier is minimal. Lower unrealistic expectations of delivering perfect care. Evaluate the patient for a treatable mental illness, such as depression, anxiety, etc. |
| Source: Reference 3 | |
Table 3
Tips for managing high utilizers
Establish a collaborative treatment plan with firm limits and expectations
|
Acknowledge your feelings and countertransference
|
Explore your patient’s expectations and commitment to treatment by asking:
|
Practice safely and proactively
|
OUTCOME: The pattern continues
Ms. Y continues to receive treatment with a different outpatient psychiatrist and therapist in the area. She has not been hospitalized for almost 2 years but her financial state has deteriorated and she has had a recurrence of depression. Ms. Y’s psychiatrist recently called the hospital to ask for direct admission on the patient’s behalf, stating that Ms. Y did not want to wait hours to be seen in the ER. Hospital staff explained that she needs to first come to the ER for evaluation. Ms. Y refused to come to the ER and was not admitted. About 1 month later, Ms. Y’s psychiatrist called again, and she was directly admitted to the psychiatric hospital.
Related resource
- National Suicide Prevention Lifeline. 1-800-273-TALK (8255). www.suicidepreventionlifeline.org.
- Clonazepam • Klonopin
- Fluoxetine • Prozac
- Quetiapine • Seroquel
The authors report no financial relationship with any company whose products are mentioned in this article or manufacturers of competing products.
CASE: A ‘high utilizer’
Ms. Y, a 49-year-old intensive care registered nurse, is admitted to the psychiatric hospital for suicidal ideation for the eighth time in 1 year. Ms. Y has chronic suicidal ideation with multiple attempts and has been on disability for 3 years for treatment of severe depression. She has been hospitalized for depression with suicide ideation 49 times since her divorce 6 years ago. She is prescribed fluoxetine, 60 mg/d, quetiapine, 400 mg/d, and clonazepam, 2 mg/d.
The authors’ observations
Ms. Y possesses 7 of the 11 characteristics of a high utilizer of psychiatric services (Table 1),1,2 defined as a patient who is:
- 2 standard deviations above the mean number of visits to an urban psychiatric emergency service in 6 months or
- has 4 inpatient admissions in a quarter or 6 inpatient admissions in 1 year.
Table 1
Common characteristics of high utilizers* of psychiatric services
| Homelessness |
| Developmental delays |
| Enrolled in a mental health plan |
| History of voluntary and involuntary hospitalization |
| Personality disorders |
| Likely to be uncooperative |
| Substance abuse or dependence (or history) |
| History of incarceration |
| Unreliable social support |
| Young Caucasian women |
| * Defined as having either 2 standard deviations above the mean number of visits to an urban psychiatric emergency service in 6 months or 4 inpatient admissions in a quarter or 6 inpatient admissions in 1 year |
| Source: References 1,2 |
The author’s observations
Because previous hospitalizations and courses of ECT have provided Ms. Y with only minimal, short-lived improvement, the treatment team decides to reconsider her diagnosis and treatment plan. Ms. Y’s first psychiatrist diagnosed her with major depressive disorder. After thoroughly interviewing Ms. Y and reviewing her history, the hospital psychiatrist determines that she meets criteria for borderline personality disorder (BPD) in addition to major depression. The psychiatrist explains this diagnosis to Ms. Y, provides her with education and support, and recommends dialectical behavioral therapy (DBT) and case management. She rejects the new diagnosis and treatment plan and pleads for help establishing treatment with a new psychiatrist.
The team at the psychiatric hospital feels Ms. Y needs to receive ongoing treatment from a psychiatrist. In the hope that she will be able to establish a therapeutic alliance with a new psychiatrist and therapist, they decide to continue working with Ms. Y if she accepts the BPD diagnosis and agrees to undergo DBT.
EVALUATION: A troubling pattern
Before Ms. Y’s husband divorced her, she had not received psychiatric care and had no psychiatric diagnosis. During the contentious divorce, she experienced depressive symptoms that later intensified, and she was unable to return to her previous high level of functioning.
Ms. Y became suicidal and was hospitalized for the first time shortly after the divorce was finalized and her ex-husband remarried. She began treatment with a psychiatrist, whom she idealized and saw for 5 years.
When this psychiatrist—who had been one of the few stable relationships in Ms. Y’s life—moved to another state, Ms. Y experienced a rapid recurrence of depression. She began treatment with 3 other psychiatrists but fired them because they “never understand me” like her first psychiatrist did, and she never felt she received the consistent, supportive care she deserved. She become suicidal and again required psychiatric hospitalization. This pattern continued up to her current admission.
The authors’ observations
Ms. Y briefly returns to work between hospitalizations but is not able to tolerate the stress. At one point she was admitted to an out-of-state facility; after this 2-month stay, she remained out of the local psychiatric hospital for 6 months but then became unable to function and was readmitted to the local psychiatric hospital.
When interviewed, Ms. Y describes feeling hopeless, empty, and alone each time 2 of her 3 children return to college after summer break. Her youngest child lives at home but is involved in extracurricular high school activities, and doesn’t seem to need her. Ms. Y is estranged from both parents. Her social support is unreliable because she tends to push others away and isolate herself.
The authors’ observations
Because she has no history of mania, Ms. Y does not meet criteria for bipolar affective disorder. Her multidisciplinary treatment team feels she is too fragile to transfer care to new providers or to foster care, so we schedule a care conference and carefully compose a 6-month contract to formally articulate limits and boundaries within which we will continue to treat her.
The contract specifies that Ms. Y will participate in DBT, take her medications exactly as prescribed, and not receive any early refills of her prescriptions. We arrange with Ms. Y’s health plan to have a home healthcare agency provide her medications weekly. This benefit was not available to other health plan members. Ms. Y signs the contract.
TREATMENT: Contract violation
Ms. Y complies with the contract for 2 months, then abruptly fires her long-term therapist, whom she claims violated confidentiality by giving false information to another provider. At her next session, Ms. Y will not provide details about the alleged incident, and the issue never is resolved. She admits she did not start DBT and is not taking her medications as prescribed.
Ms. Y expresses her disagreement with the terms of the contract. She becomes very upset and asks for her care to be transferred to another psychiatrist. She demands to be followed at the current clinic because “I was born here.” She denies being actively suicidal and terminates the session early. That afternoon, she calls 1 of the inpatient psychiatrists and asks if he would treat her. She also calls the first psychiatrist she had seen to enlist help in obtaining care.
The authors’ observations
In Groves’ description of 4 types of “hateful patients,” Ms. Y represents a combination of an entitled demander and a manipulative help-rejecter. The behaviors and personality disorders associated with these types of patients—and effective management strategies—are listed in (Table 2).3 (Table 3) offers tips for successfully dealing with high utilizers of psychiatric services. High utilizers of medical services other than psychiatry are more likely than patients who are not high utilizers to have a psychiatric disorder (Box).4-9
Patients who are high utilizers of medical services other than psychiatry have up to 50% higher rates of psychiatric disorders—particularly depression—compared with less-frequent utilizers.4-6 Screening medical patients for depression helps ensure that these patients are correctly diagnosed and treated.
Depression is a risk factor for nonadherence with medical treatment, and treating depression leads to decreased utilization of medical services.7,8 Patients with successfully treated depression may have reduced functional disability as well.9
Some members of our treatment team began to experience countertransference, which also interfered with Ms. Y’s treatment. They viewed her behavior as entitled, demanding, and manipulative and dreaded caring for her. Failing to recognize such defenses can lead to consequences such as malignant alienation—a progressive deterioration in the patient’s relationship with others that includes loss of sympathy and support from staff members—which can put a patient at high risk for suicide.10
After a lengthy discussion among several psychiatrists, therapists, nurses, and attorneys, the treatment team decided to terminate outpatient care for Ms. Y at our facility because of her chronic nonadherence to treatment recommendations. Ms. Y had manipulated numerous providers in our department, called multiple doctors in our facility to ask them to care for her, and asked her ex-husband to contact the department administration on her behalf. Her behavior bordered on harassment. In addition, the interventions we provided were making her worse, not better. Factors that influenced our decision included:
- fear of Ms. Y committing suicide
- fear of setting limits
- fear of being reported to the Medical Board
- fear of a lawsuit.
Table 2
Strategies for helping 4 types of ‘hateful patients’
| Dependent clinger | |
| Behaviors | Shows extreme gratitude with flattery |
| Associated personality traits/disorders | Codependent |
| Management strategies | As early and as tactfully as possible, set firm limits on the patient’s expectations for an intense doctor-patient relationship. Tell the patient that you have limits not only on knowledge and skill but also on time and stamina |
| Entitled demander | |
| Behaviors | Intimidates, devalues, induces guilt, may try to control with threats; terrified of abandonment |
| Associated personality traits/disorders | Narcissistic, borderline personality disorder |
| Management strategies | Try to rechannel your patient’s feelings of entitlement into a partnership that acknowledges his or her entitlement not to unrealistic demands but to good medical care. Help your patient stop directing anger at the healthcare team |
| Manipulative help-rejecter | |
| Behaviors | Resists treatment; may seem happy with treatment failures |
| Associated personality traits/disorders | Psychopathy, paranoia, borderline personality disorder, negativistic, passive/aggressive |
| Management strategies | Diminish your patient’s notion that losing the symptom or illness implies losing the doctor by ‘sharing’ your patient’s pessimism. Tell your patient that treatment may not cure the illness. Schedule regular follow-up visits |
| Self-destructive denier | |
| Behaviors | Denial helps them survive |
| Associated personality traits/disorders | Borderline personality disorder, histrionic, schizoid, schizotypal |
| Management strategies | Recognize that this type of patient can make clinicians wish the patient would die and that the chance of helping a self-destructive denier is minimal. Lower unrealistic expectations of delivering perfect care. Evaluate the patient for a treatable mental illness, such as depression, anxiety, etc. |
| Source: Reference 3 | |
Table 3
Tips for managing high utilizers
Establish a collaborative treatment plan with firm limits and expectations
|
Acknowledge your feelings and countertransference
|
Explore your patient’s expectations and commitment to treatment by asking:
|
Practice safely and proactively
|
OUTCOME: The pattern continues
Ms. Y continues to receive treatment with a different outpatient psychiatrist and therapist in the area. She has not been hospitalized for almost 2 years but her financial state has deteriorated and she has had a recurrence of depression. Ms. Y’s psychiatrist recently called the hospital to ask for direct admission on the patient’s behalf, stating that Ms. Y did not want to wait hours to be seen in the ER. Hospital staff explained that she needs to first come to the ER for evaluation. Ms. Y refused to come to the ER and was not admitted. About 1 month later, Ms. Y’s psychiatrist called again, and she was directly admitted to the psychiatric hospital.
Related resource
- National Suicide Prevention Lifeline. 1-800-273-TALK (8255). www.suicidepreventionlifeline.org.
- Clonazepam • Klonopin
- Fluoxetine • Prozac
- Quetiapine • Seroquel
The authors report no financial relationship with any company whose products are mentioned in this article or manufacturers of competing products.
1. Pasic J, Russo J, Roy-Byrne P. High utilizers of psychiatric emergency services. Psychiatr Serv. 2005;56(6):678-684.
2. Geller J, Fisher W, McDermeit M, et al. The effects of public managed care on patterns of intensive use of inpatient psychiatric services. Psychiatr Serv. 1998;49:327-332.
3. Groves JE. Taking care of the hateful patient. N Engl J Med. 1978;298(16):883-887.
4. Karlsson H, Lehtinen V, Joukamaa M. Are frequent attenders of primary health care distressed? Scan J Health Care. 1995;13:32-38.
5. Karlsson H, Lehtinen V, Joukamaa M. Psychiatric morbidity among frequent attenders in primary care. Gen Hosp Psychiatry. 1995;17:19-25.
6. Lefevre F, Refiler D, Lee P, et al. Screening for undetected mental disorders in high utilizers of primary care services. J Gen Int Med. 1999;14:425-431.
7. Pearson S, Katzelnick D, Simon G, et al. Depression among high utilizers of medical care. J Gen Intern Med. 1999;14:461-468.
8. DiMatteo MR, Lepper HS, Croghan TW. Depression is a risk factor for noncompliance with medical treatment: meta-analysis of the effects of anxiety and depression on medical adherence. Arch Intern Med. 2000;160:2101-2107.
9. Von Korff M, Ormel J, Katon W, et al. Disability and depression among high utilizers of health care. A longitudinal analysis. Arch Gen Psychiatry. 1992;49(2):91-100.
10. Watts D, Morgan G. Malignant alienation dangers for patients who are hard to like. Br J Psychiatry. 1994;164:11-15.
1. Pasic J, Russo J, Roy-Byrne P. High utilizers of psychiatric emergency services. Psychiatr Serv. 2005;56(6):678-684.
2. Geller J, Fisher W, McDermeit M, et al. The effects of public managed care on patterns of intensive use of inpatient psychiatric services. Psychiatr Serv. 1998;49:327-332.
3. Groves JE. Taking care of the hateful patient. N Engl J Med. 1978;298(16):883-887.
4. Karlsson H, Lehtinen V, Joukamaa M. Are frequent attenders of primary health care distressed? Scan J Health Care. 1995;13:32-38.
5. Karlsson H, Lehtinen V, Joukamaa M. Psychiatric morbidity among frequent attenders in primary care. Gen Hosp Psychiatry. 1995;17:19-25.
6. Lefevre F, Refiler D, Lee P, et al. Screening for undetected mental disorders in high utilizers of primary care services. J Gen Int Med. 1999;14:425-431.
7. Pearson S, Katzelnick D, Simon G, et al. Depression among high utilizers of medical care. J Gen Intern Med. 1999;14:461-468.
8. DiMatteo MR, Lepper HS, Croghan TW. Depression is a risk factor for noncompliance with medical treatment: meta-analysis of the effects of anxiety and depression on medical adherence. Arch Intern Med. 2000;160:2101-2107.
9. Von Korff M, Ormel J, Katon W, et al. Disability and depression among high utilizers of health care. A longitudinal analysis. Arch Gen Psychiatry. 1992;49(2):91-100.
10. Watts D, Morgan G. Malignant alienation dangers for patients who are hard to like. Br J Psychiatry. 1994;164:11-15.
Afraid to leave home
CASE: Disabling anxiety
Mr. B, age 35, has a history of schizophrenia, chronic paranoid type and has been hospitalized more than 12 times since its onset 10 years ago. He received clozapine during his most recent hospitalization approximately 5 years ago and experienced full symptom response without the motor side effects he developed in response to other medications. He visits a psychiatrist monthly for medications and supportive psychotherapy, and he receives intensive case management and housing from a community mental health center.
When Mr. B is assigned to my (CK) care, his psychotic symptoms are in remission, but he complains of anxiety that leaves him almost homebound. He has intense fear of bridges, upper-floor windows, express buses, subways, riding in speeding vehicles, and having a seizure.
If Mr. B faces any of these triggers, he experiences harmful thoughts—such as jumping out a window or off a bridge—even though he does not endorse suicidality. These thoughts are intrusive, ego-dystonic, and ruminative. He avoids these triggers at all costs, which compromises his housing and employment opportunities. He experienced a single panic attack in the subway 1 year earlier. Mr. B firmly believes that any intense anxiety he experiences will trigger a psychotic episode. When faced with sudden urges, he believes his illness would interfere with his ability to control his impulses.
He reports that these symptoms started when he began clozapine and have worsened. Mr. B says he experiences a feeling of “uneasiness” approximately 2 hours after taking clozapine that is exacerbated if he faces a trigger. He describes the uneasiness as “the feeling of being about to have a seizure” during which he would “lose control” of his body.
When I begin treating Mr. B, he is receiving clozapine, 125 mg bid. In an effort to combat Mr. B’s anxiety, a previous psychiatrist had titrated clonazepam up to 5 mg/d as needed. Mr. B is compliant with his medications and appointments but refuses to change his psychotropic or psychotherapy regimen.
The authors’ observations
Approximately 50% of patients with schizophrenia have at least 1 anxiety disorder, and close to 30% meet criteria for >1 anxiety disorder.1 Social anxiety disorder (SAD), generalized anxiety disorder, panic disorder, posttraumatic stress disorder, and obsessive-compulsive disorder (OCD) have been found comorbid with schizophrenia, with rates as high as 30% for each.1
Possible causes of unusually high rates of anxiety disorders in schizophrenia include trauma history, delusional conviction and inflexibility of abstract thought,2 and passive coping mechanisms.
Schizophrenic illnesses may be linked to anxiety antecedents such as panic or social phobia that:
- develop into more profound psychopathology
- or bring about anxiety symptoms, given the severity of the subjective psychotic experience.
Comorbid OCD, panic disorder, and SAD frequently persist after remission of psychotic symptoms. Comorbid anxiety disorders may play a role in the psychotic symptoms themselves (such as panic and social anxiety related to paranoia, OCD, and bizarre behavior) and negatively impact quality of life.4
- increased hallucinations
- poor psychosocial function
- hopelessness.5
Table 1
Treatment options for comorbid schizophrenia and anxiety
| Modality | Options | Comments |
|---|---|---|
| Psychopharmacology | Antipsychotics
| Favor monotherapy at full dose for full trial period before considering adjunct therapy with a second antipsychotic, for which evidence is still equivocal |
Antidepressants
| Avoid bupropion because of possible dopamine agonism | |
| Benzodiazepines | Weigh risks of sedation and potential for addiction vs benefits of immediate relief | |
| Gabapentin | Use high doses to obtain symptomatic response | |
| Psychotherapy | CBT (for psychosis and anxiety) Supportive (for decompensating psychosis) Behavioral Activity and vocational | |
| CBT: cognitive-behavioral therapy; SSRI: selective serotonin reuptake inhibitor; SNRI: serotonin-norepinephrine reuptake inhibitor | ||
HISTORY: Propensity for violence
Mr. B was born in a large city and raised by his single mother. He denies childhood physical or sexual abuse. Mr. B reports engaging in violent activity since he was an adolescent, but this activity is undocumented because he has never been arrested. Mr. B still belongs to a gang he joined after being assaulted at age 16.
Mr. B was diagnosed with schizophrenia at age 20 following an overt psychotic episode and suicide attempt by hanging. During his psychotic episodes, he thinks groups of people are plotting to kill him. He hears people talking about him or voices telling him about others’ plots against him. Mr. B probably has experienced these symptoms since early childhood, as evidenced by reports of attention-deficit/hyperactivity disorder, oppositional defiant disorder, conduct disorder, and tics.
Numerous medication trials failed. Antipsychotics were ineffective or poorly tolerated because of motor side effects or intense sedation. Mr. B did not tolerate selective serotonin reuptake inhibitors (SSRIs) because of akathisia or sexual side effects. Mr. B had a history of poor medication compliance until he began clozapine treatment.
Mr. B used cannabis daily until 10 years ago. He smokes cigarettes and reports occasional alcohol use. He has no history of chronic substance or alcohol use, withdrawal symptoms, or complications from intoxication.
Mr. B is unemployed and receives Supplemental Security Income. He has never married or had children.
Medical comorbidities include a white blood cell count and absolute neutrophil count that have been chronically in the lower limit range, and dyslipidemia and diabetes, for which Mr. B receives statins and oral hypoglycemics. He has no history of seizures or brain trauma. His family history includes substance dependence on his mother’s side and schizophrenia in 2 paternal cousins.
The authors’ observations
Mr. B’s anxiety disorder has not been clearly elucidated. He does not seem to meet criteria for:
- panic disorder (only 1 panic attack)
- OCD (no compulsions to diminish anxiety)
- specific phobia (phobias were too broad and lacked fear of an object itself).
Clozapine has been associated with the emergence or worsening of obsessive-compulsive symptoms, although conclusions of studies that investigated this link are equivocal.7 Most of the literature consists of isolated case reports, some of which advocate clozapine for treating obsessive-compulsive disorder rather than for its role as a causative agent.
A case report has associated clozapine with the development of panic disorder in a 34-year-old woman receiving 400 mg/d for paranoid schizophrenia.8 She developed daily attacks of sudden chest compression, dizziness, fear of dying, and intense anxiety. These symptoms progressively improved and eventually resolved after she was switched to olanzapine, 10 mg/d. Clozapine also has been associated with cardiomyopathy presenting as panic attacks.9
The phenomenology of his symptoms appears to be linked to his psychodynamic development, but previous therapists had not explored this. In addition, his relationships with his therapists, illness, and medications are complex. Mr. B is poorly engaged, lacks motivation toward recovery goals, and does not trust me. However, he holds high expectations of the potential damage or benefits of medication.
Table 2
Anxiety: How to differentiate disorders and symptoms
| Disorder/symptom | Keys to differential diagnosis |
|---|---|
| Panic disorder | ≥2 panic attacks |
| Agoraphobia | Fear of ‘no escape,’ ‘no options,’ ‘loss of control’ |
| Generalized anxiety disorder | Constant worriers |
| Specific phobias | Fear of an object itself, not the response it will elicit within the patient |
| Obsessive-compulsive disorder | Patterns of intrusive thoughts followed by an action to undo or avoid anxiety |
| Residual paranoia | Feeling of insecurity associated with episodes of decompensation that have remained inter-episode |
| Drug-seeking behaviors | Secondary gain, in direct relationship to request for medication |
| Akathisia, other side effects | Inner restlessness that is constant, without trigger |
Mr. B was taking clonazepam when our work began, and discontinuing it would have increased his risk for seizures and the possibility of him seeking illicit benzodiazepines. Furthermore, discontinuing clonazepam might have thwarted an emerging therapeutic relationship that would become key to enhancing his motivation and exploring the antisocial and narcissistic traits that were limiting his recovery.
I slowly increase the frequency of my sessions with Mr. B from monthly to biweekly to weekly. We focus on strengthening the therapeutic alliance, motivational enhancement, emotional expression, and verbal identification of feeling states. We explore anxiety symptoms and psychosis using cognitive-behavioral therapy techniques informed by psychodynamic aspects of his experience, with the goal of resuming his prior level of functionality, including employment.
I carefully and slowly change Mr. B’s medications. First I increase his clozapine to 300 mg/d in 150 mg divided doses in an attempt to cover the possibility of residual paranoia, and for anxiolytic sedation without introducing a new medication. However, Mr. B’s anxiety symptoms worsen, so I resume the baseline dosage (125 mg bid). I choose not to switch to another antipsychotic because the risk for psychotic decompensation outweighs the potential benefits. I lower clonazepam to 2 mg/d in split doses. I teach Mr. B anxiety management techniques, including distraction, exposure, and anxiety tolerance training.
Because Mr. B refuses to start an SSRI for his anxiety symptoms, I prescribe bupropion and monitor him closely for dopamine agonism as evidenced by a re-emergence of psychosis. Once again, his anxiety symptoms worsen.
I stop bupropion and switch Mr. B to gabapentin, titrated to 400 mg tid. I chose this medication because of its sedation properties and relatively safe side effect profile. Mr. B was willing to try gabapentin—which was first approved to treat epilepsy—because he was afraid of having a seizure and also because it is not associated with sexual side effects. Furthermore, its GABA-mimetic actions made it a plausible alternative to replicate the benefits he was getting from clonazepam.
TREATMENT: An effective drug
Mr. B tolerates gabapentin well and his anxiety symptoms are much more sporadic, shorter, and more easily controlled by conscious exercise. The content of his thoughts is less disastrous and less ego-dystonic. He feels less dysphoria associated with clozapine and does not need as much clonazepam. He overcomes his avoidance of all fear-provoking triggers except walking across bridges.
Mr. B continues his regimen of clozapine, clonazepam, and gabapentin. He moves to independent housing and applies for employment.
Related resource
- Garrett M, Lerman M. CBT for psychosis for long-term inpatients with a forensic history. Psychiatr Serv. 2007;58(5):712-713.
- Aripiprazole • Abilify
- Bupropion • Wellbutrin
- Clonazepam • Klonopin
- Clozapine • Clozaril
- Gabapentin • Neurontin
- Olanzapine • Zyprexa
- Ziprasidone • Geodon
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Ciapparelli A, Paggini R, Marazziti D, et al. Comorbidity with axis I anxiety disorders in remitted psychotic patients 1 year after hospitalization. CNS Spectr. 2007;12(12):913-919.
2. Lysaker PH, Hammersley J. Association of delusions and lack of cognitive flexibility with social anxiety in schizophrenia spectrum disorders. Schizophr Res. 2006;86(1-3):147-153.
3. Lyons MJ, Huppert J, Toomey R, et al. Lifetime prevalence of mood and anxiety disorders in twin pairs discordant for schizophrenia. Twin Res. 2000;3(1):28-32.
4. Braga RJ, Mendlowicz MV, Marrocos RP, et al. Anxiety disorders in outpatients with schizophrenia: prevalence and impact on the subjective quality of life. J Psychiatr Res. 2005;39(4):409-414.
5. Lysaker PH, Salyers MP. Anxiety symptoms in schizophrenia spectrum disorders: associations with social function, positive and negative symptoms, hope and trauma history. Acta Psychiatr Scand. 2007;116(4):290-298.
6. Seedat S, Fritelli V, Oosthuizen P, et al. Measuring anxiety in patients with schizophrenia. J Nerv Ment Dis. 2007;195(4):320-324.
7. Ke CL, Yen CF, Chen CC, et al. Obsessive-compulsive symptoms associated with clozapine and risperidone treatment: three case reports and review of the literature. Kaohsiung J Med Sci. 2004;20(6):295-301.
8. Bressan RA, Monteiro VB, Dias CC. Panic disorder associated with clozapine. Am J Psychiatry. 2000;157(12):2056.-
9. Sagar R, Berry N, Sadhu R, et al. Clozapine-induced cardiomyopathy presenting as panic attacks. J Psychiatr Pract. 2008;14(3):182-185.
CASE: Disabling anxiety
Mr. B, age 35, has a history of schizophrenia, chronic paranoid type and has been hospitalized more than 12 times since its onset 10 years ago. He received clozapine during his most recent hospitalization approximately 5 years ago and experienced full symptom response without the motor side effects he developed in response to other medications. He visits a psychiatrist monthly for medications and supportive psychotherapy, and he receives intensive case management and housing from a community mental health center.
When Mr. B is assigned to my (CK) care, his psychotic symptoms are in remission, but he complains of anxiety that leaves him almost homebound. He has intense fear of bridges, upper-floor windows, express buses, subways, riding in speeding vehicles, and having a seizure.
If Mr. B faces any of these triggers, he experiences harmful thoughts—such as jumping out a window or off a bridge—even though he does not endorse suicidality. These thoughts are intrusive, ego-dystonic, and ruminative. He avoids these triggers at all costs, which compromises his housing and employment opportunities. He experienced a single panic attack in the subway 1 year earlier. Mr. B firmly believes that any intense anxiety he experiences will trigger a psychotic episode. When faced with sudden urges, he believes his illness would interfere with his ability to control his impulses.
He reports that these symptoms started when he began clozapine and have worsened. Mr. B says he experiences a feeling of “uneasiness” approximately 2 hours after taking clozapine that is exacerbated if he faces a trigger. He describes the uneasiness as “the feeling of being about to have a seizure” during which he would “lose control” of his body.
When I begin treating Mr. B, he is receiving clozapine, 125 mg bid. In an effort to combat Mr. B’s anxiety, a previous psychiatrist had titrated clonazepam up to 5 mg/d as needed. Mr. B is compliant with his medications and appointments but refuses to change his psychotropic or psychotherapy regimen.
The authors’ observations
Approximately 50% of patients with schizophrenia have at least 1 anxiety disorder, and close to 30% meet criteria for >1 anxiety disorder.1 Social anxiety disorder (SAD), generalized anxiety disorder, panic disorder, posttraumatic stress disorder, and obsessive-compulsive disorder (OCD) have been found comorbid with schizophrenia, with rates as high as 30% for each.1
Possible causes of unusually high rates of anxiety disorders in schizophrenia include trauma history, delusional conviction and inflexibility of abstract thought,2 and passive coping mechanisms.
Schizophrenic illnesses may be linked to anxiety antecedents such as panic or social phobia that:
- develop into more profound psychopathology
- or bring about anxiety symptoms, given the severity of the subjective psychotic experience.
Comorbid OCD, panic disorder, and SAD frequently persist after remission of psychotic symptoms. Comorbid anxiety disorders may play a role in the psychotic symptoms themselves (such as panic and social anxiety related to paranoia, OCD, and bizarre behavior) and negatively impact quality of life.4
- increased hallucinations
- poor psychosocial function
- hopelessness.5
Table 1
Treatment options for comorbid schizophrenia and anxiety
| Modality | Options | Comments |
|---|---|---|
| Psychopharmacology | Antipsychotics
| Favor monotherapy at full dose for full trial period before considering adjunct therapy with a second antipsychotic, for which evidence is still equivocal |
Antidepressants
| Avoid bupropion because of possible dopamine agonism | |
| Benzodiazepines | Weigh risks of sedation and potential for addiction vs benefits of immediate relief | |
| Gabapentin | Use high doses to obtain symptomatic response | |
| Psychotherapy | CBT (for psychosis and anxiety) Supportive (for decompensating psychosis) Behavioral Activity and vocational | |
| CBT: cognitive-behavioral therapy; SSRI: selective serotonin reuptake inhibitor; SNRI: serotonin-norepinephrine reuptake inhibitor | ||
HISTORY: Propensity for violence
Mr. B was born in a large city and raised by his single mother. He denies childhood physical or sexual abuse. Mr. B reports engaging in violent activity since he was an adolescent, but this activity is undocumented because he has never been arrested. Mr. B still belongs to a gang he joined after being assaulted at age 16.
Mr. B was diagnosed with schizophrenia at age 20 following an overt psychotic episode and suicide attempt by hanging. During his psychotic episodes, he thinks groups of people are plotting to kill him. He hears people talking about him or voices telling him about others’ plots against him. Mr. B probably has experienced these symptoms since early childhood, as evidenced by reports of attention-deficit/hyperactivity disorder, oppositional defiant disorder, conduct disorder, and tics.
Numerous medication trials failed. Antipsychotics were ineffective or poorly tolerated because of motor side effects or intense sedation. Mr. B did not tolerate selective serotonin reuptake inhibitors (SSRIs) because of akathisia or sexual side effects. Mr. B had a history of poor medication compliance until he began clozapine treatment.
Mr. B used cannabis daily until 10 years ago. He smokes cigarettes and reports occasional alcohol use. He has no history of chronic substance or alcohol use, withdrawal symptoms, or complications from intoxication.
Mr. B is unemployed and receives Supplemental Security Income. He has never married or had children.
Medical comorbidities include a white blood cell count and absolute neutrophil count that have been chronically in the lower limit range, and dyslipidemia and diabetes, for which Mr. B receives statins and oral hypoglycemics. He has no history of seizures or brain trauma. His family history includes substance dependence on his mother’s side and schizophrenia in 2 paternal cousins.
The authors’ observations
Mr. B’s anxiety disorder has not been clearly elucidated. He does not seem to meet criteria for:
- panic disorder (only 1 panic attack)
- OCD (no compulsions to diminish anxiety)
- specific phobia (phobias were too broad and lacked fear of an object itself).
Clozapine has been associated with the emergence or worsening of obsessive-compulsive symptoms, although conclusions of studies that investigated this link are equivocal.7 Most of the literature consists of isolated case reports, some of which advocate clozapine for treating obsessive-compulsive disorder rather than for its role as a causative agent.
A case report has associated clozapine with the development of panic disorder in a 34-year-old woman receiving 400 mg/d for paranoid schizophrenia.8 She developed daily attacks of sudden chest compression, dizziness, fear of dying, and intense anxiety. These symptoms progressively improved and eventually resolved after she was switched to olanzapine, 10 mg/d. Clozapine also has been associated with cardiomyopathy presenting as panic attacks.9
The phenomenology of his symptoms appears to be linked to his psychodynamic development, but previous therapists had not explored this. In addition, his relationships with his therapists, illness, and medications are complex. Mr. B is poorly engaged, lacks motivation toward recovery goals, and does not trust me. However, he holds high expectations of the potential damage or benefits of medication.
Table 2
Anxiety: How to differentiate disorders and symptoms
| Disorder/symptom | Keys to differential diagnosis |
|---|---|
| Panic disorder | ≥2 panic attacks |
| Agoraphobia | Fear of ‘no escape,’ ‘no options,’ ‘loss of control’ |
| Generalized anxiety disorder | Constant worriers |
| Specific phobias | Fear of an object itself, not the response it will elicit within the patient |
| Obsessive-compulsive disorder | Patterns of intrusive thoughts followed by an action to undo or avoid anxiety |
| Residual paranoia | Feeling of insecurity associated with episodes of decompensation that have remained inter-episode |
| Drug-seeking behaviors | Secondary gain, in direct relationship to request for medication |
| Akathisia, other side effects | Inner restlessness that is constant, without trigger |
Mr. B was taking clonazepam when our work began, and discontinuing it would have increased his risk for seizures and the possibility of him seeking illicit benzodiazepines. Furthermore, discontinuing clonazepam might have thwarted an emerging therapeutic relationship that would become key to enhancing his motivation and exploring the antisocial and narcissistic traits that were limiting his recovery.
I slowly increase the frequency of my sessions with Mr. B from monthly to biweekly to weekly. We focus on strengthening the therapeutic alliance, motivational enhancement, emotional expression, and verbal identification of feeling states. We explore anxiety symptoms and psychosis using cognitive-behavioral therapy techniques informed by psychodynamic aspects of his experience, with the goal of resuming his prior level of functionality, including employment.
I carefully and slowly change Mr. B’s medications. First I increase his clozapine to 300 mg/d in 150 mg divided doses in an attempt to cover the possibility of residual paranoia, and for anxiolytic sedation without introducing a new medication. However, Mr. B’s anxiety symptoms worsen, so I resume the baseline dosage (125 mg bid). I choose not to switch to another antipsychotic because the risk for psychotic decompensation outweighs the potential benefits. I lower clonazepam to 2 mg/d in split doses. I teach Mr. B anxiety management techniques, including distraction, exposure, and anxiety tolerance training.
Because Mr. B refuses to start an SSRI for his anxiety symptoms, I prescribe bupropion and monitor him closely for dopamine agonism as evidenced by a re-emergence of psychosis. Once again, his anxiety symptoms worsen.
I stop bupropion and switch Mr. B to gabapentin, titrated to 400 mg tid. I chose this medication because of its sedation properties and relatively safe side effect profile. Mr. B was willing to try gabapentin—which was first approved to treat epilepsy—because he was afraid of having a seizure and also because it is not associated with sexual side effects. Furthermore, its GABA-mimetic actions made it a plausible alternative to replicate the benefits he was getting from clonazepam.
TREATMENT: An effective drug
Mr. B tolerates gabapentin well and his anxiety symptoms are much more sporadic, shorter, and more easily controlled by conscious exercise. The content of his thoughts is less disastrous and less ego-dystonic. He feels less dysphoria associated with clozapine and does not need as much clonazepam. He overcomes his avoidance of all fear-provoking triggers except walking across bridges.
Mr. B continues his regimen of clozapine, clonazepam, and gabapentin. He moves to independent housing and applies for employment.
Related resource
- Garrett M, Lerman M. CBT for psychosis for long-term inpatients with a forensic history. Psychiatr Serv. 2007;58(5):712-713.
- Aripiprazole • Abilify
- Bupropion • Wellbutrin
- Clonazepam • Klonopin
- Clozapine • Clozaril
- Gabapentin • Neurontin
- Olanzapine • Zyprexa
- Ziprasidone • Geodon
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: Disabling anxiety
Mr. B, age 35, has a history of schizophrenia, chronic paranoid type and has been hospitalized more than 12 times since its onset 10 years ago. He received clozapine during his most recent hospitalization approximately 5 years ago and experienced full symptom response without the motor side effects he developed in response to other medications. He visits a psychiatrist monthly for medications and supportive psychotherapy, and he receives intensive case management and housing from a community mental health center.
When Mr. B is assigned to my (CK) care, his psychotic symptoms are in remission, but he complains of anxiety that leaves him almost homebound. He has intense fear of bridges, upper-floor windows, express buses, subways, riding in speeding vehicles, and having a seizure.
If Mr. B faces any of these triggers, he experiences harmful thoughts—such as jumping out a window or off a bridge—even though he does not endorse suicidality. These thoughts are intrusive, ego-dystonic, and ruminative. He avoids these triggers at all costs, which compromises his housing and employment opportunities. He experienced a single panic attack in the subway 1 year earlier. Mr. B firmly believes that any intense anxiety he experiences will trigger a psychotic episode. When faced with sudden urges, he believes his illness would interfere with his ability to control his impulses.
He reports that these symptoms started when he began clozapine and have worsened. Mr. B says he experiences a feeling of “uneasiness” approximately 2 hours after taking clozapine that is exacerbated if he faces a trigger. He describes the uneasiness as “the feeling of being about to have a seizure” during which he would “lose control” of his body.
When I begin treating Mr. B, he is receiving clozapine, 125 mg bid. In an effort to combat Mr. B’s anxiety, a previous psychiatrist had titrated clonazepam up to 5 mg/d as needed. Mr. B is compliant with his medications and appointments but refuses to change his psychotropic or psychotherapy regimen.
The authors’ observations
Approximately 50% of patients with schizophrenia have at least 1 anxiety disorder, and close to 30% meet criteria for >1 anxiety disorder.1 Social anxiety disorder (SAD), generalized anxiety disorder, panic disorder, posttraumatic stress disorder, and obsessive-compulsive disorder (OCD) have been found comorbid with schizophrenia, with rates as high as 30% for each.1
Possible causes of unusually high rates of anxiety disorders in schizophrenia include trauma history, delusional conviction and inflexibility of abstract thought,2 and passive coping mechanisms.
Schizophrenic illnesses may be linked to anxiety antecedents such as panic or social phobia that:
- develop into more profound psychopathology
- or bring about anxiety symptoms, given the severity of the subjective psychotic experience.
Comorbid OCD, panic disorder, and SAD frequently persist after remission of psychotic symptoms. Comorbid anxiety disorders may play a role in the psychotic symptoms themselves (such as panic and social anxiety related to paranoia, OCD, and bizarre behavior) and negatively impact quality of life.4
- increased hallucinations
- poor psychosocial function
- hopelessness.5
Table 1
Treatment options for comorbid schizophrenia and anxiety
| Modality | Options | Comments |
|---|---|---|
| Psychopharmacology | Antipsychotics
| Favor monotherapy at full dose for full trial period before considering adjunct therapy with a second antipsychotic, for which evidence is still equivocal |
Antidepressants
| Avoid bupropion because of possible dopamine agonism | |
| Benzodiazepines | Weigh risks of sedation and potential for addiction vs benefits of immediate relief | |
| Gabapentin | Use high doses to obtain symptomatic response | |
| Psychotherapy | CBT (for psychosis and anxiety) Supportive (for decompensating psychosis) Behavioral Activity and vocational | |
| CBT: cognitive-behavioral therapy; SSRI: selective serotonin reuptake inhibitor; SNRI: serotonin-norepinephrine reuptake inhibitor | ||
HISTORY: Propensity for violence
Mr. B was born in a large city and raised by his single mother. He denies childhood physical or sexual abuse. Mr. B reports engaging in violent activity since he was an adolescent, but this activity is undocumented because he has never been arrested. Mr. B still belongs to a gang he joined after being assaulted at age 16.
Mr. B was diagnosed with schizophrenia at age 20 following an overt psychotic episode and suicide attempt by hanging. During his psychotic episodes, he thinks groups of people are plotting to kill him. He hears people talking about him or voices telling him about others’ plots against him. Mr. B probably has experienced these symptoms since early childhood, as evidenced by reports of attention-deficit/hyperactivity disorder, oppositional defiant disorder, conduct disorder, and tics.
Numerous medication trials failed. Antipsychotics were ineffective or poorly tolerated because of motor side effects or intense sedation. Mr. B did not tolerate selective serotonin reuptake inhibitors (SSRIs) because of akathisia or sexual side effects. Mr. B had a history of poor medication compliance until he began clozapine treatment.
Mr. B used cannabis daily until 10 years ago. He smokes cigarettes and reports occasional alcohol use. He has no history of chronic substance or alcohol use, withdrawal symptoms, or complications from intoxication.
Mr. B is unemployed and receives Supplemental Security Income. He has never married or had children.
Medical comorbidities include a white blood cell count and absolute neutrophil count that have been chronically in the lower limit range, and dyslipidemia and diabetes, for which Mr. B receives statins and oral hypoglycemics. He has no history of seizures or brain trauma. His family history includes substance dependence on his mother’s side and schizophrenia in 2 paternal cousins.
The authors’ observations
Mr. B’s anxiety disorder has not been clearly elucidated. He does not seem to meet criteria for:
- panic disorder (only 1 panic attack)
- OCD (no compulsions to diminish anxiety)
- specific phobia (phobias were too broad and lacked fear of an object itself).
Clozapine has been associated with the emergence or worsening of obsessive-compulsive symptoms, although conclusions of studies that investigated this link are equivocal.7 Most of the literature consists of isolated case reports, some of which advocate clozapine for treating obsessive-compulsive disorder rather than for its role as a causative agent.
A case report has associated clozapine with the development of panic disorder in a 34-year-old woman receiving 400 mg/d for paranoid schizophrenia.8 She developed daily attacks of sudden chest compression, dizziness, fear of dying, and intense anxiety. These symptoms progressively improved and eventually resolved after she was switched to olanzapine, 10 mg/d. Clozapine also has been associated with cardiomyopathy presenting as panic attacks.9
The phenomenology of his symptoms appears to be linked to his psychodynamic development, but previous therapists had not explored this. In addition, his relationships with his therapists, illness, and medications are complex. Mr. B is poorly engaged, lacks motivation toward recovery goals, and does not trust me. However, he holds high expectations of the potential damage or benefits of medication.
Table 2
Anxiety: How to differentiate disorders and symptoms
| Disorder/symptom | Keys to differential diagnosis |
|---|---|
| Panic disorder | ≥2 panic attacks |
| Agoraphobia | Fear of ‘no escape,’ ‘no options,’ ‘loss of control’ |
| Generalized anxiety disorder | Constant worriers |
| Specific phobias | Fear of an object itself, not the response it will elicit within the patient |
| Obsessive-compulsive disorder | Patterns of intrusive thoughts followed by an action to undo or avoid anxiety |
| Residual paranoia | Feeling of insecurity associated with episodes of decompensation that have remained inter-episode |
| Drug-seeking behaviors | Secondary gain, in direct relationship to request for medication |
| Akathisia, other side effects | Inner restlessness that is constant, without trigger |
Mr. B was taking clonazepam when our work began, and discontinuing it would have increased his risk for seizures and the possibility of him seeking illicit benzodiazepines. Furthermore, discontinuing clonazepam might have thwarted an emerging therapeutic relationship that would become key to enhancing his motivation and exploring the antisocial and narcissistic traits that were limiting his recovery.
I slowly increase the frequency of my sessions with Mr. B from monthly to biweekly to weekly. We focus on strengthening the therapeutic alliance, motivational enhancement, emotional expression, and verbal identification of feeling states. We explore anxiety symptoms and psychosis using cognitive-behavioral therapy techniques informed by psychodynamic aspects of his experience, with the goal of resuming his prior level of functionality, including employment.
I carefully and slowly change Mr. B’s medications. First I increase his clozapine to 300 mg/d in 150 mg divided doses in an attempt to cover the possibility of residual paranoia, and for anxiolytic sedation without introducing a new medication. However, Mr. B’s anxiety symptoms worsen, so I resume the baseline dosage (125 mg bid). I choose not to switch to another antipsychotic because the risk for psychotic decompensation outweighs the potential benefits. I lower clonazepam to 2 mg/d in split doses. I teach Mr. B anxiety management techniques, including distraction, exposure, and anxiety tolerance training.
Because Mr. B refuses to start an SSRI for his anxiety symptoms, I prescribe bupropion and monitor him closely for dopamine agonism as evidenced by a re-emergence of psychosis. Once again, his anxiety symptoms worsen.
I stop bupropion and switch Mr. B to gabapentin, titrated to 400 mg tid. I chose this medication because of its sedation properties and relatively safe side effect profile. Mr. B was willing to try gabapentin—which was first approved to treat epilepsy—because he was afraid of having a seizure and also because it is not associated with sexual side effects. Furthermore, its GABA-mimetic actions made it a plausible alternative to replicate the benefits he was getting from clonazepam.
TREATMENT: An effective drug
Mr. B tolerates gabapentin well and his anxiety symptoms are much more sporadic, shorter, and more easily controlled by conscious exercise. The content of his thoughts is less disastrous and less ego-dystonic. He feels less dysphoria associated with clozapine and does not need as much clonazepam. He overcomes his avoidance of all fear-provoking triggers except walking across bridges.
Mr. B continues his regimen of clozapine, clonazepam, and gabapentin. He moves to independent housing and applies for employment.
Related resource
- Garrett M, Lerman M. CBT for psychosis for long-term inpatients with a forensic history. Psychiatr Serv. 2007;58(5):712-713.
- Aripiprazole • Abilify
- Bupropion • Wellbutrin
- Clonazepam • Klonopin
- Clozapine • Clozaril
- Gabapentin • Neurontin
- Olanzapine • Zyprexa
- Ziprasidone • Geodon
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Ciapparelli A, Paggini R, Marazziti D, et al. Comorbidity with axis I anxiety disorders in remitted psychotic patients 1 year after hospitalization. CNS Spectr. 2007;12(12):913-919.
2. Lysaker PH, Hammersley J. Association of delusions and lack of cognitive flexibility with social anxiety in schizophrenia spectrum disorders. Schizophr Res. 2006;86(1-3):147-153.
3. Lyons MJ, Huppert J, Toomey R, et al. Lifetime prevalence of mood and anxiety disorders in twin pairs discordant for schizophrenia. Twin Res. 2000;3(1):28-32.
4. Braga RJ, Mendlowicz MV, Marrocos RP, et al. Anxiety disorders in outpatients with schizophrenia: prevalence and impact on the subjective quality of life. J Psychiatr Res. 2005;39(4):409-414.
5. Lysaker PH, Salyers MP. Anxiety symptoms in schizophrenia spectrum disorders: associations with social function, positive and negative symptoms, hope and trauma history. Acta Psychiatr Scand. 2007;116(4):290-298.
6. Seedat S, Fritelli V, Oosthuizen P, et al. Measuring anxiety in patients with schizophrenia. J Nerv Ment Dis. 2007;195(4):320-324.
7. Ke CL, Yen CF, Chen CC, et al. Obsessive-compulsive symptoms associated with clozapine and risperidone treatment: three case reports and review of the literature. Kaohsiung J Med Sci. 2004;20(6):295-301.
8. Bressan RA, Monteiro VB, Dias CC. Panic disorder associated with clozapine. Am J Psychiatry. 2000;157(12):2056.-
9. Sagar R, Berry N, Sadhu R, et al. Clozapine-induced cardiomyopathy presenting as panic attacks. J Psychiatr Pract. 2008;14(3):182-185.
1. Ciapparelli A, Paggini R, Marazziti D, et al. Comorbidity with axis I anxiety disorders in remitted psychotic patients 1 year after hospitalization. CNS Spectr. 2007;12(12):913-919.
2. Lysaker PH, Hammersley J. Association of delusions and lack of cognitive flexibility with social anxiety in schizophrenia spectrum disorders. Schizophr Res. 2006;86(1-3):147-153.
3. Lyons MJ, Huppert J, Toomey R, et al. Lifetime prevalence of mood and anxiety disorders in twin pairs discordant for schizophrenia. Twin Res. 2000;3(1):28-32.
4. Braga RJ, Mendlowicz MV, Marrocos RP, et al. Anxiety disorders in outpatients with schizophrenia: prevalence and impact on the subjective quality of life. J Psychiatr Res. 2005;39(4):409-414.
5. Lysaker PH, Salyers MP. Anxiety symptoms in schizophrenia spectrum disorders: associations with social function, positive and negative symptoms, hope and trauma history. Acta Psychiatr Scand. 2007;116(4):290-298.
6. Seedat S, Fritelli V, Oosthuizen P, et al. Measuring anxiety in patients with schizophrenia. J Nerv Ment Dis. 2007;195(4):320-324.
7. Ke CL, Yen CF, Chen CC, et al. Obsessive-compulsive symptoms associated with clozapine and risperidone treatment: three case reports and review of the literature. Kaohsiung J Med Sci. 2004;20(6):295-301.
8. Bressan RA, Monteiro VB, Dias CC. Panic disorder associated with clozapine. Am J Psychiatry. 2000;157(12):2056.-
9. Sagar R, Berry N, Sadhu R, et al. Clozapine-induced cardiomyopathy presenting as panic attacks. J Psychiatr Pract. 2008;14(3):182-185.
A chilling complication
CASE: Hypothermic and confused
Mr. S, age 38, is brought to the emergency room after being found unresponsive. He has a history of poorly controlled type I diabetes. On admission his core body temperature is 35.5°C (95.9°F), blood pressure is 98/70 mm Hg, respiration is 12 breaths per minute, and pulse is 88 beats per minute. The emergency room physician believes Mr. S has syndrome of inappropriate antidiuretic hormone of unknown cause and a urinary tract infection. As emergency room clinicians address these problems, Mr. S becomes increasingly confused and his responses to questioning do not make sense. His Mini-Mental State Examination score is 7/30, indicating severe cognitive impairment.
Further workup includes a brain MRI, which shows mild cerebral atrophy; HIV testing, which is negative; cosyntropin stimulation test, which indicates normal adrenal function; and a lumbar puncture, which indicates non-polio enterovirus. The hospital’s infectious disease service is consulted, but because Mr. S is not exhibiting encephalitis no intervention is recommended.
The psychiatrist decides the patient’s symptoms are the result of a long course of delirium secondary to his medical condition. He starts oral risperidone, 1 mg bid. Mr. S’ temperature at this time is 36.8°C. Mr. S fails to improve, so the psychiatrist initiates quetiapine, 100 mg qhs. Two days after starting the combination of risperidone and quetiapine, Mr. S’ temperature is 35.2°C.
The author’s observations
Body temperature dysregulation as a result of antipsychotic use can manifest as hyperthermia in the case of neuroleptic malignant syndrome or, less commonly, hypothermia.1 Symptoms of hypothermia—defined as a core body temperature of Table 1).2 However, a hypothermic patient can be asymptomatic.
A recent literature review3 evaluated hypothermia cases following antipsychotic use reported in the PubMed and Embase databases (43 case reports) and the World Health Organization’s database of adverse drug reactions (480 reports). In this sample:
- More than one-half of patients had schizophrenia, 41% were male, and the mean age was 49.
- The reported mean body temperature was 32.6°C, with a range of 20°C to 36.1°C.
- 80% of hypothermia episodes occurred during an antipsychotic start, change, or dosage increase.
- 57% occurred within 2 days of a start, change, or dosage increase, and 16% occurred between days 2 to 7.
Hypothermia symptoms
| Delirium |
| Slurred speech |
| Ataxia |
| Fatigue |
| Incoordination |
| Subjective coldness |
| Shivering |
| Bradycardia |
| Source: Reference 2 |
TREATMENT: Antipsychotic changes
Mr. S’ disorganized behavior continues, but a workup for delirium is negative. Because the patient experiences cogwheel rigidity, the psychiatrist decreases risperidone and titrates quetiapine to 150 mg bid. Mr. S’ temperature rises to 36.8°C, and risperidone is stopped. Because of Mr. S’ continued disorganized behavior and low blood pressure, the psychiatrist changes the antipsychotic to ziprasidone, 40 mg bid. Within 5 days of this switch, Mr. S’ temperature drops from 36.4°C to 35.4°C, and then slowly returns to normal.
The psychiatrist increases aripiprazole to 15 mg/d. Within 2 days Mr. S’ temperature drops to 34.7°C, then gradually normalizes over the next 7 days. Aripiprazole is increased to 20 mg. Mr. S’ mental status improves and he is fully oriented, but his temperature drops to 34.1°C. His blood glucose continues to fluctuate despite normal dietary intake.
The author’s observations
Antipsychotics can influence thermoregulation by effects on the anterior preoptic hypothalamus. One possible mechanism is related to effects on the serotonin system. Atypical antipsychotics—which have a strong affinity for 5-HT2A—seem to be implicated in this reaction.
Another possible mechanism is action on alpha-2 adrenergic receptors, which may increase the hypothermic effects by inhibiting peripheral responses to cooling such as vasoconstriction and shivering. In addition, mixing atypical antipsychotics with mood stabilizers and benzodiazepines contributes to this reaction.4
GABA may have a role in hypothermia. Experiments with rats have shown that L-methionine-DL-sulfoximine infusions into the dorsal raphe nucleus of rats slows serotonin turnover, which decreases the release of GABA synthesis, and both induce hypothermia.5
Other neurotransmitter systems involved include dopamine and norepinephrine and their increased metabolism. One study compared clozapine with risperidone, quetiapine, and olanzapine with regard to dopamine receptor affinity in rats.5 Clozapine had a greater affinity for D1 compared with D2 receptors. Researchers used antipsychotic-induced hypothermia to measure this. Clozapine, olanzapine, and risperidone produced dose-dependent hypothermia, which researchers were able to prevent by blocking the D1 receptor.
Other factors can contribute to hypothermia in patients taking antipsychotics, including:
- pre-existing brain damage
- lesions of the preoptic anterior hypothalamic region
- neurotensin, a thermoregulatory neuropeptide
- ambient temperature
- apathy and indifference resulting from antipsychotic use, which may dampen behavior aimed toward thermoregulation, such as using blankets when sleeping.
OUTCOME: Multiple infections
Mr. S remains hospitalized because of complications related to his diabetes, which contribute to fluctuations in mental status consistent with delirium. Two months into Mr. S’ hospital stay, the psychiatrist decides to address these symptoms by restarting risperidone, 0.5 mg in the morning and 1 mg in the evening. Within several days of restarting risperidone, Mr. S’ temperature drops from 37°C to 35.1°C. One day after another dose of risperidone, 0.5 mg, is added at noon, the patient’s temperature drops to 33.1°C. Mr. S continues to be lethargic and confused and is hypoglycemic.
Mr. S eventually decompensates and is admitted to the ICU, where he is intubated. There, the patient has positive cultures for methicillin-resistant Staphylococcus aureus and vancomycin-resistant enterococci. While in the ICU Mr. S continues to receive risperidone, and his temperature drops to 30.5°C.
Mr. S improves and he is subsequently sent to the medical floor, then he is discharged to a long-term acute care facility. His temperature continues to range between 33°C and 34°C for 2 weeks, then returns to normal after all antipsychotics are discontinued.
The author’s observations
This case report documents periods of hypothermia in a male patient who received various antipsychotics during treatment. It appears that his hypothermia occurred in conjunction with starting and changing antipsychotics and increasing dosages (Table 2).
Mr. S’ case is unique in that it involves hypothermia apparently in response to multiple atypical antipsychotics in 1 patient over a prolonged time; to our knowledge, no other such cases exist. This was a complicated case of a patient with multiple serious comorbidities. We feel, however, that antipsychotics were the major contributor to Mr. S’ hypothermia because the drops in temperature occurred as discrete periods tied to times of antipsychotic use.
Close monitoring of drug serum levels—particularly when starting, changing, or increasing a dosage—may help prevent antipsychotic-induced hypothermia. Be vigilant for behavioral changes and problems that could contribute to hypothermia, such as social isolation and inappropriate dress, as well as comorbidities such as infection. It is unclear at what core body temperature to consider stopping an antipsychotic or decreasing the dosage.
Table 2
Mr. S’ temperature during hospitalization
| Hospitalized day | Core body temperature (°C)* | Antipsychotic |
|---|---|---|
| Admission | 35.5 | None |
| 8 | 36.8 | Started risperidone, 1 mg bid |
| 11 | 35.2 | Added quetiapine, 100 mg po qhs |
| 14 | 36.8 | Stopped risperidone, increased quetiapine to 150 mg bid |
| 18 | 35.4 | Switched to ziprasidone, 40 mg bid |
| 23 | 35.7 | Switched to aripiprazole, 10 mg/d |
| 30 | 34.7 | Increased aripiprazole to 15 mg/d |
| 38 | 34.1 | Increased aripiprazole to 20 mg/d |
| 76 | 33.1 | Switched to risperidone, 0.5 mg am and noon and 1 mg qhs |
| 107 | 37.0 | None |
| *Normal core body temperature is 37°C (98.6°F) | ||
- Gibbons GM, Wein DA, Paula R. Profound hypothermia secondary to normal ziprasidone use. Am J Emerg Med. 2008;26(6):737.
- Aripiprazole • Abilify
- Clozapine • Clozaril
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Vancomycin • Vancocin
- Ziprasidone • Geodon
The authors report no financial relationship with an company whose products are mentioned in this article or with manufacturers of competing products.
1. Blass DM, Chuen M. Olanzapine-associated hypothermia. Psychosomatics. 2004;45(2):135-139.
2. Mayo Foundation for Medical Education and Research. Hypothermia: first aid. Available at: http://www.mayoclinic.com/health/first-aid-hypothermia/FA00017. Accessed March 31, 2008.
3. van Marum RJ, Wegewijs MA, Loonene AJ, et al. Hypothermia following antipsychotic drug use. Eur J Clin Pharmacol. 2007;63(6):627-631.
4. Chen KC, Yang YK, Chen PS, et al. Two case studies of hypothermia induced by an increased dosage of zotepine in a combination therapy. Psychiatry Clin Neurosci. 2003;57(4):369-371.
5. Oerther S, Ahlenius S. Atypical antipsychotics and dopamine D1 receptor agonism: an in vivo experimental study using core temperature measurements in the rat. J Pharmacol Exp Ther. 2000;292(2):731-736.
CASE: Hypothermic and confused
Mr. S, age 38, is brought to the emergency room after being found unresponsive. He has a history of poorly controlled type I diabetes. On admission his core body temperature is 35.5°C (95.9°F), blood pressure is 98/70 mm Hg, respiration is 12 breaths per minute, and pulse is 88 beats per minute. The emergency room physician believes Mr. S has syndrome of inappropriate antidiuretic hormone of unknown cause and a urinary tract infection. As emergency room clinicians address these problems, Mr. S becomes increasingly confused and his responses to questioning do not make sense. His Mini-Mental State Examination score is 7/30, indicating severe cognitive impairment.
Further workup includes a brain MRI, which shows mild cerebral atrophy; HIV testing, which is negative; cosyntropin stimulation test, which indicates normal adrenal function; and a lumbar puncture, which indicates non-polio enterovirus. The hospital’s infectious disease service is consulted, but because Mr. S is not exhibiting encephalitis no intervention is recommended.
The psychiatrist decides the patient’s symptoms are the result of a long course of delirium secondary to his medical condition. He starts oral risperidone, 1 mg bid. Mr. S’ temperature at this time is 36.8°C. Mr. S fails to improve, so the psychiatrist initiates quetiapine, 100 mg qhs. Two days after starting the combination of risperidone and quetiapine, Mr. S’ temperature is 35.2°C.
The author’s observations
Body temperature dysregulation as a result of antipsychotic use can manifest as hyperthermia in the case of neuroleptic malignant syndrome or, less commonly, hypothermia.1 Symptoms of hypothermia—defined as a core body temperature of Table 1).2 However, a hypothermic patient can be asymptomatic.
A recent literature review3 evaluated hypothermia cases following antipsychotic use reported in the PubMed and Embase databases (43 case reports) and the World Health Organization’s database of adverse drug reactions (480 reports). In this sample:
- More than one-half of patients had schizophrenia, 41% were male, and the mean age was 49.
- The reported mean body temperature was 32.6°C, with a range of 20°C to 36.1°C.
- 80% of hypothermia episodes occurred during an antipsychotic start, change, or dosage increase.
- 57% occurred within 2 days of a start, change, or dosage increase, and 16% occurred between days 2 to 7.
Hypothermia symptoms
| Delirium |
| Slurred speech |
| Ataxia |
| Fatigue |
| Incoordination |
| Subjective coldness |
| Shivering |
| Bradycardia |
| Source: Reference 2 |
TREATMENT: Antipsychotic changes
Mr. S’ disorganized behavior continues, but a workup for delirium is negative. Because the patient experiences cogwheel rigidity, the psychiatrist decreases risperidone and titrates quetiapine to 150 mg bid. Mr. S’ temperature rises to 36.8°C, and risperidone is stopped. Because of Mr. S’ continued disorganized behavior and low blood pressure, the psychiatrist changes the antipsychotic to ziprasidone, 40 mg bid. Within 5 days of this switch, Mr. S’ temperature drops from 36.4°C to 35.4°C, and then slowly returns to normal.
The psychiatrist increases aripiprazole to 15 mg/d. Within 2 days Mr. S’ temperature drops to 34.7°C, then gradually normalizes over the next 7 days. Aripiprazole is increased to 20 mg. Mr. S’ mental status improves and he is fully oriented, but his temperature drops to 34.1°C. His blood glucose continues to fluctuate despite normal dietary intake.
The author’s observations
Antipsychotics can influence thermoregulation by effects on the anterior preoptic hypothalamus. One possible mechanism is related to effects on the serotonin system. Atypical antipsychotics—which have a strong affinity for 5-HT2A—seem to be implicated in this reaction.
Another possible mechanism is action on alpha-2 adrenergic receptors, which may increase the hypothermic effects by inhibiting peripheral responses to cooling such as vasoconstriction and shivering. In addition, mixing atypical antipsychotics with mood stabilizers and benzodiazepines contributes to this reaction.4
GABA may have a role in hypothermia. Experiments with rats have shown that L-methionine-DL-sulfoximine infusions into the dorsal raphe nucleus of rats slows serotonin turnover, which decreases the release of GABA synthesis, and both induce hypothermia.5
Other neurotransmitter systems involved include dopamine and norepinephrine and their increased metabolism. One study compared clozapine with risperidone, quetiapine, and olanzapine with regard to dopamine receptor affinity in rats.5 Clozapine had a greater affinity for D1 compared with D2 receptors. Researchers used antipsychotic-induced hypothermia to measure this. Clozapine, olanzapine, and risperidone produced dose-dependent hypothermia, which researchers were able to prevent by blocking the D1 receptor.
Other factors can contribute to hypothermia in patients taking antipsychotics, including:
- pre-existing brain damage
- lesions of the preoptic anterior hypothalamic region
- neurotensin, a thermoregulatory neuropeptide
- ambient temperature
- apathy and indifference resulting from antipsychotic use, which may dampen behavior aimed toward thermoregulation, such as using blankets when sleeping.
OUTCOME: Multiple infections
Mr. S remains hospitalized because of complications related to his diabetes, which contribute to fluctuations in mental status consistent with delirium. Two months into Mr. S’ hospital stay, the psychiatrist decides to address these symptoms by restarting risperidone, 0.5 mg in the morning and 1 mg in the evening. Within several days of restarting risperidone, Mr. S’ temperature drops from 37°C to 35.1°C. One day after another dose of risperidone, 0.5 mg, is added at noon, the patient’s temperature drops to 33.1°C. Mr. S continues to be lethargic and confused and is hypoglycemic.
Mr. S eventually decompensates and is admitted to the ICU, where he is intubated. There, the patient has positive cultures for methicillin-resistant Staphylococcus aureus and vancomycin-resistant enterococci. While in the ICU Mr. S continues to receive risperidone, and his temperature drops to 30.5°C.
Mr. S improves and he is subsequently sent to the medical floor, then he is discharged to a long-term acute care facility. His temperature continues to range between 33°C and 34°C for 2 weeks, then returns to normal after all antipsychotics are discontinued.
The author’s observations
This case report documents periods of hypothermia in a male patient who received various antipsychotics during treatment. It appears that his hypothermia occurred in conjunction with starting and changing antipsychotics and increasing dosages (Table 2).
Mr. S’ case is unique in that it involves hypothermia apparently in response to multiple atypical antipsychotics in 1 patient over a prolonged time; to our knowledge, no other such cases exist. This was a complicated case of a patient with multiple serious comorbidities. We feel, however, that antipsychotics were the major contributor to Mr. S’ hypothermia because the drops in temperature occurred as discrete periods tied to times of antipsychotic use.
Close monitoring of drug serum levels—particularly when starting, changing, or increasing a dosage—may help prevent antipsychotic-induced hypothermia. Be vigilant for behavioral changes and problems that could contribute to hypothermia, such as social isolation and inappropriate dress, as well as comorbidities such as infection. It is unclear at what core body temperature to consider stopping an antipsychotic or decreasing the dosage.
Table 2
Mr. S’ temperature during hospitalization
| Hospitalized day | Core body temperature (°C)* | Antipsychotic |
|---|---|---|
| Admission | 35.5 | None |
| 8 | 36.8 | Started risperidone, 1 mg bid |
| 11 | 35.2 | Added quetiapine, 100 mg po qhs |
| 14 | 36.8 | Stopped risperidone, increased quetiapine to 150 mg bid |
| 18 | 35.4 | Switched to ziprasidone, 40 mg bid |
| 23 | 35.7 | Switched to aripiprazole, 10 mg/d |
| 30 | 34.7 | Increased aripiprazole to 15 mg/d |
| 38 | 34.1 | Increased aripiprazole to 20 mg/d |
| 76 | 33.1 | Switched to risperidone, 0.5 mg am and noon and 1 mg qhs |
| 107 | 37.0 | None |
| *Normal core body temperature is 37°C (98.6°F) | ||
- Gibbons GM, Wein DA, Paula R. Profound hypothermia secondary to normal ziprasidone use. Am J Emerg Med. 2008;26(6):737.
- Aripiprazole • Abilify
- Clozapine • Clozaril
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Vancomycin • Vancocin
- Ziprasidone • Geodon
The authors report no financial relationship with an company whose products are mentioned in this article or with manufacturers of competing products.
CASE: Hypothermic and confused
Mr. S, age 38, is brought to the emergency room after being found unresponsive. He has a history of poorly controlled type I diabetes. On admission his core body temperature is 35.5°C (95.9°F), blood pressure is 98/70 mm Hg, respiration is 12 breaths per minute, and pulse is 88 beats per minute. The emergency room physician believes Mr. S has syndrome of inappropriate antidiuretic hormone of unknown cause and a urinary tract infection. As emergency room clinicians address these problems, Mr. S becomes increasingly confused and his responses to questioning do not make sense. His Mini-Mental State Examination score is 7/30, indicating severe cognitive impairment.
Further workup includes a brain MRI, which shows mild cerebral atrophy; HIV testing, which is negative; cosyntropin stimulation test, which indicates normal adrenal function; and a lumbar puncture, which indicates non-polio enterovirus. The hospital’s infectious disease service is consulted, but because Mr. S is not exhibiting encephalitis no intervention is recommended.
The psychiatrist decides the patient’s symptoms are the result of a long course of delirium secondary to his medical condition. He starts oral risperidone, 1 mg bid. Mr. S’ temperature at this time is 36.8°C. Mr. S fails to improve, so the psychiatrist initiates quetiapine, 100 mg qhs. Two days after starting the combination of risperidone and quetiapine, Mr. S’ temperature is 35.2°C.
The author’s observations
Body temperature dysregulation as a result of antipsychotic use can manifest as hyperthermia in the case of neuroleptic malignant syndrome or, less commonly, hypothermia.1 Symptoms of hypothermia—defined as a core body temperature of Table 1).2 However, a hypothermic patient can be asymptomatic.
A recent literature review3 evaluated hypothermia cases following antipsychotic use reported in the PubMed and Embase databases (43 case reports) and the World Health Organization’s database of adverse drug reactions (480 reports). In this sample:
- More than one-half of patients had schizophrenia, 41% were male, and the mean age was 49.
- The reported mean body temperature was 32.6°C, with a range of 20°C to 36.1°C.
- 80% of hypothermia episodes occurred during an antipsychotic start, change, or dosage increase.
- 57% occurred within 2 days of a start, change, or dosage increase, and 16% occurred between days 2 to 7.
Hypothermia symptoms
| Delirium |
| Slurred speech |
| Ataxia |
| Fatigue |
| Incoordination |
| Subjective coldness |
| Shivering |
| Bradycardia |
| Source: Reference 2 |
TREATMENT: Antipsychotic changes
Mr. S’ disorganized behavior continues, but a workup for delirium is negative. Because the patient experiences cogwheel rigidity, the psychiatrist decreases risperidone and titrates quetiapine to 150 mg bid. Mr. S’ temperature rises to 36.8°C, and risperidone is stopped. Because of Mr. S’ continued disorganized behavior and low blood pressure, the psychiatrist changes the antipsychotic to ziprasidone, 40 mg bid. Within 5 days of this switch, Mr. S’ temperature drops from 36.4°C to 35.4°C, and then slowly returns to normal.
The psychiatrist increases aripiprazole to 15 mg/d. Within 2 days Mr. S’ temperature drops to 34.7°C, then gradually normalizes over the next 7 days. Aripiprazole is increased to 20 mg. Mr. S’ mental status improves and he is fully oriented, but his temperature drops to 34.1°C. His blood glucose continues to fluctuate despite normal dietary intake.
The author’s observations
Antipsychotics can influence thermoregulation by effects on the anterior preoptic hypothalamus. One possible mechanism is related to effects on the serotonin system. Atypical antipsychotics—which have a strong affinity for 5-HT2A—seem to be implicated in this reaction.
Another possible mechanism is action on alpha-2 adrenergic receptors, which may increase the hypothermic effects by inhibiting peripheral responses to cooling such as vasoconstriction and shivering. In addition, mixing atypical antipsychotics with mood stabilizers and benzodiazepines contributes to this reaction.4
GABA may have a role in hypothermia. Experiments with rats have shown that L-methionine-DL-sulfoximine infusions into the dorsal raphe nucleus of rats slows serotonin turnover, which decreases the release of GABA synthesis, and both induce hypothermia.5
Other neurotransmitter systems involved include dopamine and norepinephrine and their increased metabolism. One study compared clozapine with risperidone, quetiapine, and olanzapine with regard to dopamine receptor affinity in rats.5 Clozapine had a greater affinity for D1 compared with D2 receptors. Researchers used antipsychotic-induced hypothermia to measure this. Clozapine, olanzapine, and risperidone produced dose-dependent hypothermia, which researchers were able to prevent by blocking the D1 receptor.
Other factors can contribute to hypothermia in patients taking antipsychotics, including:
- pre-existing brain damage
- lesions of the preoptic anterior hypothalamic region
- neurotensin, a thermoregulatory neuropeptide
- ambient temperature
- apathy and indifference resulting from antipsychotic use, which may dampen behavior aimed toward thermoregulation, such as using blankets when sleeping.
OUTCOME: Multiple infections
Mr. S remains hospitalized because of complications related to his diabetes, which contribute to fluctuations in mental status consistent with delirium. Two months into Mr. S’ hospital stay, the psychiatrist decides to address these symptoms by restarting risperidone, 0.5 mg in the morning and 1 mg in the evening. Within several days of restarting risperidone, Mr. S’ temperature drops from 37°C to 35.1°C. One day after another dose of risperidone, 0.5 mg, is added at noon, the patient’s temperature drops to 33.1°C. Mr. S continues to be lethargic and confused and is hypoglycemic.
Mr. S eventually decompensates and is admitted to the ICU, where he is intubated. There, the patient has positive cultures for methicillin-resistant Staphylococcus aureus and vancomycin-resistant enterococci. While in the ICU Mr. S continues to receive risperidone, and his temperature drops to 30.5°C.
Mr. S improves and he is subsequently sent to the medical floor, then he is discharged to a long-term acute care facility. His temperature continues to range between 33°C and 34°C for 2 weeks, then returns to normal after all antipsychotics are discontinued.
The author’s observations
This case report documents periods of hypothermia in a male patient who received various antipsychotics during treatment. It appears that his hypothermia occurred in conjunction with starting and changing antipsychotics and increasing dosages (Table 2).
Mr. S’ case is unique in that it involves hypothermia apparently in response to multiple atypical antipsychotics in 1 patient over a prolonged time; to our knowledge, no other such cases exist. This was a complicated case of a patient with multiple serious comorbidities. We feel, however, that antipsychotics were the major contributor to Mr. S’ hypothermia because the drops in temperature occurred as discrete periods tied to times of antipsychotic use.
Close monitoring of drug serum levels—particularly when starting, changing, or increasing a dosage—may help prevent antipsychotic-induced hypothermia. Be vigilant for behavioral changes and problems that could contribute to hypothermia, such as social isolation and inappropriate dress, as well as comorbidities such as infection. It is unclear at what core body temperature to consider stopping an antipsychotic or decreasing the dosage.
Table 2
Mr. S’ temperature during hospitalization
| Hospitalized day | Core body temperature (°C)* | Antipsychotic |
|---|---|---|
| Admission | 35.5 | None |
| 8 | 36.8 | Started risperidone, 1 mg bid |
| 11 | 35.2 | Added quetiapine, 100 mg po qhs |
| 14 | 36.8 | Stopped risperidone, increased quetiapine to 150 mg bid |
| 18 | 35.4 | Switched to ziprasidone, 40 mg bid |
| 23 | 35.7 | Switched to aripiprazole, 10 mg/d |
| 30 | 34.7 | Increased aripiprazole to 15 mg/d |
| 38 | 34.1 | Increased aripiprazole to 20 mg/d |
| 76 | 33.1 | Switched to risperidone, 0.5 mg am and noon and 1 mg qhs |
| 107 | 37.0 | None |
| *Normal core body temperature is 37°C (98.6°F) | ||
- Gibbons GM, Wein DA, Paula R. Profound hypothermia secondary to normal ziprasidone use. Am J Emerg Med. 2008;26(6):737.
- Aripiprazole • Abilify
- Clozapine • Clozaril
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Vancomycin • Vancocin
- Ziprasidone • Geodon
The authors report no financial relationship with an company whose products are mentioned in this article or with manufacturers of competing products.
1. Blass DM, Chuen M. Olanzapine-associated hypothermia. Psychosomatics. 2004;45(2):135-139.
2. Mayo Foundation for Medical Education and Research. Hypothermia: first aid. Available at: http://www.mayoclinic.com/health/first-aid-hypothermia/FA00017. Accessed March 31, 2008.
3. van Marum RJ, Wegewijs MA, Loonene AJ, et al. Hypothermia following antipsychotic drug use. Eur J Clin Pharmacol. 2007;63(6):627-631.
4. Chen KC, Yang YK, Chen PS, et al. Two case studies of hypothermia induced by an increased dosage of zotepine in a combination therapy. Psychiatry Clin Neurosci. 2003;57(4):369-371.
5. Oerther S, Ahlenius S. Atypical antipsychotics and dopamine D1 receptor agonism: an in vivo experimental study using core temperature measurements in the rat. J Pharmacol Exp Ther. 2000;292(2):731-736.
1. Blass DM, Chuen M. Olanzapine-associated hypothermia. Psychosomatics. 2004;45(2):135-139.
2. Mayo Foundation for Medical Education and Research. Hypothermia: first aid. Available at: http://www.mayoclinic.com/health/first-aid-hypothermia/FA00017. Accessed March 31, 2008.
3. van Marum RJ, Wegewijs MA, Loonene AJ, et al. Hypothermia following antipsychotic drug use. Eur J Clin Pharmacol. 2007;63(6):627-631.
4. Chen KC, Yang YK, Chen PS, et al. Two case studies of hypothermia induced by an increased dosage of zotepine in a combination therapy. Psychiatry Clin Neurosci. 2003;57(4):369-371.
5. Oerther S, Ahlenius S. Atypical antipsychotics and dopamine D1 receptor agonism: an in vivo experimental study using core temperature measurements in the rat. J Pharmacol Exp Ther. 2000;292(2):731-736.
A mysterious loss of memory
Case: Worsening memory
Mrs. K, age 46, is being treated by a neurologist for stable relapsing-remitting multiple sclerosis (MS) and migraine headaches when she complains of worsening memory over the past 5 years. She reports having difficulty recalling details of recent events and conversations. She describes occasional word-finding difficulties and problems maintaining her train of thought. She forgets where she places things and has gotten lost while driving, even on familiar routes. Her husband reports she takes more time to process things in general.
Mrs. K’s cognitive decline has affected her daily life and ability to work. For 4 years, she has been an office assistant at a campground, where she takes phone reservations and keeps a site schedule. Formerly simple tasks—such as taking a phone number—have become increasingly difficult, and she cannot recall a list of 3 things to buy at the supermarket without writing them down.
As a teenager, Mrs. K suffered migraines but did not seek treatment, and her headaches remitted for about 10 years. At age 29, she started to experience tunnel vision. Three years later she reported bilateral foot numbness and was diagnosed with MS. She responded well to interferon beta-1b but her migraines returned, occurring several times a week. Her migraines are successfully treated with topiramate, 75 mg/d, for prophylactic therapy and rizatriptan, 10 mg, as needed for abortive therapy. Her medication regimen also includes:
- eszopiclone, 2 mg/d, and amitriptyline, 10 mg/d, for insomnia
- butalbital/aspirin/caffeine, 50/325/40 mg, as needed for tension headaches
- fexofenadine, 12 mg/d, and budesonide, 32 mcg, 4 sprays/d, for allergy symptoms
- esomeprazole, 80 mg/d, and famotidine, 20 mg/d, as needed for dyspepsia
- propranolol, 120 mg/d, for hypertension
- levothyroxine, 75 mcg/d, for hypothyroidism
- conjugatedestrogens, 0.45 mg/d, for hypoestrogenemia
- alprazolam, 0.25 mg/d, aspirin, 81 mg/d, vitamin E, 800 IU/d, and a multivitamin.
The neurologist orders neuropsychological testing. Mrs. K demonstrates some depressive symptoms but is within normal limits across all aspects of neurocognition, including basic and complex attention, memory, bilateral motor functioning, expressive and receptive language, visuospatial/constructional function, and self-regulatory/executive functioning. The neurologist refers Mrs. K for psychiatric evaluation of her depressive symptoms.
The author’s observations
Many neuropsychiatric abnormalities may accompany MS (Table).1 These can be classified as cognitive dysfunction or disturbances in mood, affect, and behavior.
Although the cause of cognitive impairment in patients with MS is unclear, its extent and profound impact on functioning has become widely recognized over the past 20 years.2
An estimated 40% to 65% of patients with MS suffer from cognitive dysfunction.1,3 Testing indicates deficiencies most often in:
- attention
- information processing speed
- working memory
- verbal memory
- visuospatial function
- executive functions.4
- reduced social interactions
- increased sexual dysfunction
- greater difficulty with household tasks.6
Long-term interferon beta-1b treatment prevents MS relapses, but a recent study found that interferon beta-1b had a negative impact on patients’ mental health composite score and in most quality-of-life subscales over 2 years.8 Nevertheless, Mrs. K received interferon beta-1b therapy for at least 9 years without noticing cognitive decline.
Table
Neuropsychiatric conditions associated with MS
| Disorder | Prevalence |
|---|---|
| Major depression | Lifetime prevalence: 50% |
| Bipolar disorder | Estimated prevalence is 10%, twice that of the general population |
| Euphoria | 25% |
| Pseudobulbar affect | Pathological laughing or crying, emotional incontinence; affects 10% of patients |
| Psychosis | 2% to 3% vs 0.5% to 1% in general population |
| Cognitive impairment | 40% to 60% |
| Source: Reference 1 | |
EVALUATION: Dysthymia
Mrs. K reports memory problems as her chief complaint. She also complains of a depressed mood, irritability, distractibility, and insomnia since her memory problems began, and admits being readily tearful. Mrs. K has difficulty “turning off her thinking” at night, which leads to delayed sleep onset, but denies sleeplessness, racing thoughts, or feelings of euphoria.
Her thought process is coherent and goal-directed, and she denies having auditory or visual hallucinations or active or passive suicidal or homicidal ideation. She scores 29/30 on the Mini-Mental State Exam, but by interview she appears to have impaired remote memory. Mrs. K demonstrates unimpaired judgment and good insight.
The author’s observations
Mrs. K meets DSM-IV-TR criteria for dysthymic disorder and agrees to start mirtazapine, 15 mg at bedtime. I chose this antidepressant because Mrs. K continues to complain of difficulty falling asleep, and mirtazapine is known to significantly decrease sleep latency and increase total sleep time. Approximately one-half of patients with MS will experience depression.1,9 In a recent study of 245 MS patients followed in a neurology clinic, two-thirds of those who met criteria for major depressive disorder did not receive antidepressants.10
TREATMENT: A new strategy
After 2 more months Mrs. K’s mood is euthymic and she demonstrates a bright affect, but she experiences continued decline in short- and long-term memory and reports increasing frustration with simple tasks. The rest of her mental status exam is unremarkable. I instruct her to reduce the mirtazapine dosage to 15 mg/d.
At the next visit 10 weeks later, she again presents with a euthymic mood and a bright affect. She says she attempted to decrease mirtazapine but experienced increased irritability so she remained on the 30-mg dose, with a positive effect on her mood and reduced irritability. Unfortunately, her memory problems persist.
Approximately 2 years after Mrs. K’s first visit, I devise a new pharmacologic strategy. Mrs. K believes that she no longer is depressed and that her only problem is her inability to recall events. To address this, I decide to try memantine, which has been shown to cause modest improvement in clinical symptoms in severe stages of Alzheimer’s disease11 and also has been reported to be useful in the treatment of cognitive impairment in some bipolar disorder patients.12 I start memantine at 10 mg/d and titrate up to 20 mg/d in 3 months.
The author’s observations
Mrs. K’s substantial memory improvement while receiving memantine warrants considering the drug for patients with cognitive dysfunction attributable to MS. Memantine is an uncompetitive NMDA receptor antagonist that the FDA approved in 2003 to treat moderate-to-severe Alzheimer’s disease (Box).11,13 It is generally well tolerated and safe, with a low potential for drug-drug interactions. In clinical trials of patients receiving memantine for Alzheimer’s disease and vascular dementia, the most commonly reported side effects were dizziness, headache, constipation, and confusion.14
A recent trial of memantine therapy for MS at the University of Navarra was suspended for reversible mild-to-moderate neurologic side effects.15 A phase II/phase III double-blind placebo-controlled trial at the University of Oregon designed to determine whether memantine is an effective treatment for memory and cognitive problems associated with MS is recruiting participants.16
Memantine has been reported to successfully treat other MS symptoms. A 1997 retrospective study found that 11 patients with acquired pendular nystagmus (APN) secondary to MS experienced complete resolution of APN when given memantine.17
Memantine was FDA-approved in 2003 to treat moderate-to-severe Alzheimer’s disease dementia. The drug also has been used off-label to treat vascular dementia, dementia of Wernicke-Korsakoff syndrome, and acquired pendular nystagmus.11
Although the neurobiologic basis for memantine’s therapeutic activity in patients with dementia is not fully understood, it is thought to reduce glutamatergic excitotoxicity. The mechanism of action is voltage-dependent, uncompetitive N-methyl-D-aspartate (NMDA) receptor antagonism with low-to-moderate affinity and fast blocking/unblocking kinetics.12 Its kinetic profile is beneficial because it allows memantine to occupy the receptor for a sufficient time to prevent pathologic activation of glutamate receptors. However, it dissociates when the physiologic activation of glutamate receptors is necessary, thus preserving normal NMDA receptor activity required for learning and memory. By blocking the effects of abnormal glutamate activity, memantine may prevent abnormal neuronal cell death and cognitive dysfunction.
- Parsons CG, Stöffler A, Danysz W. Memantine: a NMDA receptor antagonist that improves memory by restoration of homeostasis in the glutamatergic system—too little activation is bad, too much is even worse. Neuropharmacology. 2007;53(6):699-723.
- Alprazolam • Xanax
- Amitriptyline • Elavil
- Budesonide • Rhinocort
- Butalbital/Aspirin/Caffeine • Fiorinal
- Conjugated Estrogens • Premarin
- Esomeprazole • Nexium
- Eszopiclone • Lunesta
- Famotidine • Pepcid
- Fexofenadine • Allegra
- Interferon beta-1b • Betaseron
- Levothyroxine • Synthroid
- Memantine • Namenda
- Propranolol • Inderal
- Rizatriptan • Maxalt
- Topiramate • Topamax
Dr. Rao is a speaker for Forest Pharmaceuticals.
Acknowledgement
The author thanks Alexander M. Timchak, MS-IV, Stritch School of Medicine, Loyola University, Chicago, for his assistance with this article.
1. Ghaffar O, Feinstein A. The neuropsychiatry of multiple sclerosis: a review of recent developments. Curr Opin Psychiatry. 2007;20(3):278-285.
2. Amato MP, Portaccio E, Zipoli V. Are there protective treatments for cognitive decline in MS? J Neurol Sci. 2006;245(1-2):183-186.
3. Bobholz JA, Rao SM. Cognitive dysfunction in multiple sclerosis: a review of recent developments. Curr Opin Neurol. 2003;16(3):283-288.
4. Hoffmann S, Tittgemeyer M, von Cramon DY. Cognitive impairment in multiple sclerosis. Curr Opin Neurol. 2007;20(3):275-280.
5. Pierson SH, Griffith N. Treatment of cognitive impairment in multiple sclerosis. Behav Neurol. 2006;17(1):53-67.
6. Bagert B, Camplair P, Bourdette D. Cognitive dysfunction in multiple sclerosis: natural history, pathophysiology and management. CNS Drugs. 2002;16(7):445-455.
7. Martin R, Kuzniecky R, Ho S, et al. Cognitive effects of topiramate, gabapentin, and lamotrigine in healthy young adults. Neurology. 1999;52(2):321-327.
8. Simone IL, Ceccarelli A, Tortorella C, et al. Influence of Interferon beta treatment on quality of life in multiple sclerosis patients. Health Qual Life Outcomes. 2006;4:96.-
9. Siegert RJ, Abernethy DA. Depression in multiple sclerosis: a review. J Neurol Neurosurg Psychiatry. 2005;76(4):469-475.
10. Mohr DC, Hart SL, Fonareva I, et al. Treatment of depression for patients with multiple sclerosis in neurology clinics. Mult Scler. 2006;12(2):204-208.
11. Kumar S. Memantine: pharmacological properties and clinical uses. Neurol India. 2004;52(3):307-309.
12. Teng CT, Demetrio FN. Memantine may acutely improve cognition and have a mood stabilizing effect in treatment-resistant bipolar disorder. Rev Bras Psiquiatr. 2006;28(3):252-4.
13. Danysz W, Parsons CG, Mobius HJ, et al. Neuroprotective and symptomatological action of memantine relevant for Alzheimer’s disease: a unified glutamatergic hypothesis on the mechanism of action. Neurotox Res. 2000;2(2-3):85-97.
14. Namenda [package insert] St. Louis, MO: Forest Pharmaceuticals; 2007.
15. Memantine therapy for multiple sclerosis (NCT00638833) Available at: http://www.clinicaltrials.gov/ct2/show/NCT00638833. Accessed February 17, 2009.
16. Trial of memantine for cognitive impairment in multiple sclerosis (NCT00300716) Available at: http://www.clinicaltrials.gov/ct2/show/NCT00300716. Accessed February 17, 2009.
17. Starck M, Albrecht H, Pöllmann W, et al. Drug therapy for acquired pendular nystagmus in multiple sclerosis. J Neurol. 1997;244(1):9-16.
Case: Worsening memory
Mrs. K, age 46, is being treated by a neurologist for stable relapsing-remitting multiple sclerosis (MS) and migraine headaches when she complains of worsening memory over the past 5 years. She reports having difficulty recalling details of recent events and conversations. She describes occasional word-finding difficulties and problems maintaining her train of thought. She forgets where she places things and has gotten lost while driving, even on familiar routes. Her husband reports she takes more time to process things in general.
Mrs. K’s cognitive decline has affected her daily life and ability to work. For 4 years, she has been an office assistant at a campground, where she takes phone reservations and keeps a site schedule. Formerly simple tasks—such as taking a phone number—have become increasingly difficult, and she cannot recall a list of 3 things to buy at the supermarket without writing them down.
As a teenager, Mrs. K suffered migraines but did not seek treatment, and her headaches remitted for about 10 years. At age 29, she started to experience tunnel vision. Three years later she reported bilateral foot numbness and was diagnosed with MS. She responded well to interferon beta-1b but her migraines returned, occurring several times a week. Her migraines are successfully treated with topiramate, 75 mg/d, for prophylactic therapy and rizatriptan, 10 mg, as needed for abortive therapy. Her medication regimen also includes:
- eszopiclone, 2 mg/d, and amitriptyline, 10 mg/d, for insomnia
- butalbital/aspirin/caffeine, 50/325/40 mg, as needed for tension headaches
- fexofenadine, 12 mg/d, and budesonide, 32 mcg, 4 sprays/d, for allergy symptoms
- esomeprazole, 80 mg/d, and famotidine, 20 mg/d, as needed for dyspepsia
- propranolol, 120 mg/d, for hypertension
- levothyroxine, 75 mcg/d, for hypothyroidism
- conjugatedestrogens, 0.45 mg/d, for hypoestrogenemia
- alprazolam, 0.25 mg/d, aspirin, 81 mg/d, vitamin E, 800 IU/d, and a multivitamin.
The neurologist orders neuropsychological testing. Mrs. K demonstrates some depressive symptoms but is within normal limits across all aspects of neurocognition, including basic and complex attention, memory, bilateral motor functioning, expressive and receptive language, visuospatial/constructional function, and self-regulatory/executive functioning. The neurologist refers Mrs. K for psychiatric evaluation of her depressive symptoms.
The author’s observations
Many neuropsychiatric abnormalities may accompany MS (Table).1 These can be classified as cognitive dysfunction or disturbances in mood, affect, and behavior.
Although the cause of cognitive impairment in patients with MS is unclear, its extent and profound impact on functioning has become widely recognized over the past 20 years.2
An estimated 40% to 65% of patients with MS suffer from cognitive dysfunction.1,3 Testing indicates deficiencies most often in:
- attention
- information processing speed
- working memory
- verbal memory
- visuospatial function
- executive functions.4
- reduced social interactions
- increased sexual dysfunction
- greater difficulty with household tasks.6
Long-term interferon beta-1b treatment prevents MS relapses, but a recent study found that interferon beta-1b had a negative impact on patients’ mental health composite score and in most quality-of-life subscales over 2 years.8 Nevertheless, Mrs. K received interferon beta-1b therapy for at least 9 years without noticing cognitive decline.
Table
Neuropsychiatric conditions associated with MS
| Disorder | Prevalence |
|---|---|
| Major depression | Lifetime prevalence: 50% |
| Bipolar disorder | Estimated prevalence is 10%, twice that of the general population |
| Euphoria | 25% |
| Pseudobulbar affect | Pathological laughing or crying, emotional incontinence; affects 10% of patients |
| Psychosis | 2% to 3% vs 0.5% to 1% in general population |
| Cognitive impairment | 40% to 60% |
| Source: Reference 1 | |
EVALUATION: Dysthymia
Mrs. K reports memory problems as her chief complaint. She also complains of a depressed mood, irritability, distractibility, and insomnia since her memory problems began, and admits being readily tearful. Mrs. K has difficulty “turning off her thinking” at night, which leads to delayed sleep onset, but denies sleeplessness, racing thoughts, or feelings of euphoria.
Her thought process is coherent and goal-directed, and she denies having auditory or visual hallucinations or active or passive suicidal or homicidal ideation. She scores 29/30 on the Mini-Mental State Exam, but by interview she appears to have impaired remote memory. Mrs. K demonstrates unimpaired judgment and good insight.
The author’s observations
Mrs. K meets DSM-IV-TR criteria for dysthymic disorder and agrees to start mirtazapine, 15 mg at bedtime. I chose this antidepressant because Mrs. K continues to complain of difficulty falling asleep, and mirtazapine is known to significantly decrease sleep latency and increase total sleep time. Approximately one-half of patients with MS will experience depression.1,9 In a recent study of 245 MS patients followed in a neurology clinic, two-thirds of those who met criteria for major depressive disorder did not receive antidepressants.10
TREATMENT: A new strategy
After 2 more months Mrs. K’s mood is euthymic and she demonstrates a bright affect, but she experiences continued decline in short- and long-term memory and reports increasing frustration with simple tasks. The rest of her mental status exam is unremarkable. I instruct her to reduce the mirtazapine dosage to 15 mg/d.
At the next visit 10 weeks later, she again presents with a euthymic mood and a bright affect. She says she attempted to decrease mirtazapine but experienced increased irritability so she remained on the 30-mg dose, with a positive effect on her mood and reduced irritability. Unfortunately, her memory problems persist.
Approximately 2 years after Mrs. K’s first visit, I devise a new pharmacologic strategy. Mrs. K believes that she no longer is depressed and that her only problem is her inability to recall events. To address this, I decide to try memantine, which has been shown to cause modest improvement in clinical symptoms in severe stages of Alzheimer’s disease11 and also has been reported to be useful in the treatment of cognitive impairment in some bipolar disorder patients.12 I start memantine at 10 mg/d and titrate up to 20 mg/d in 3 months.
The author’s observations
Mrs. K’s substantial memory improvement while receiving memantine warrants considering the drug for patients with cognitive dysfunction attributable to MS. Memantine is an uncompetitive NMDA receptor antagonist that the FDA approved in 2003 to treat moderate-to-severe Alzheimer’s disease (Box).11,13 It is generally well tolerated and safe, with a low potential for drug-drug interactions. In clinical trials of patients receiving memantine for Alzheimer’s disease and vascular dementia, the most commonly reported side effects were dizziness, headache, constipation, and confusion.14
A recent trial of memantine therapy for MS at the University of Navarra was suspended for reversible mild-to-moderate neurologic side effects.15 A phase II/phase III double-blind placebo-controlled trial at the University of Oregon designed to determine whether memantine is an effective treatment for memory and cognitive problems associated with MS is recruiting participants.16
Memantine has been reported to successfully treat other MS symptoms. A 1997 retrospective study found that 11 patients with acquired pendular nystagmus (APN) secondary to MS experienced complete resolution of APN when given memantine.17
Memantine was FDA-approved in 2003 to treat moderate-to-severe Alzheimer’s disease dementia. The drug also has been used off-label to treat vascular dementia, dementia of Wernicke-Korsakoff syndrome, and acquired pendular nystagmus.11
Although the neurobiologic basis for memantine’s therapeutic activity in patients with dementia is not fully understood, it is thought to reduce glutamatergic excitotoxicity. The mechanism of action is voltage-dependent, uncompetitive N-methyl-D-aspartate (NMDA) receptor antagonism with low-to-moderate affinity and fast blocking/unblocking kinetics.12 Its kinetic profile is beneficial because it allows memantine to occupy the receptor for a sufficient time to prevent pathologic activation of glutamate receptors. However, it dissociates when the physiologic activation of glutamate receptors is necessary, thus preserving normal NMDA receptor activity required for learning and memory. By blocking the effects of abnormal glutamate activity, memantine may prevent abnormal neuronal cell death and cognitive dysfunction.
- Parsons CG, Stöffler A, Danysz W. Memantine: a NMDA receptor antagonist that improves memory by restoration of homeostasis in the glutamatergic system—too little activation is bad, too much is even worse. Neuropharmacology. 2007;53(6):699-723.
- Alprazolam • Xanax
- Amitriptyline • Elavil
- Budesonide • Rhinocort
- Butalbital/Aspirin/Caffeine • Fiorinal
- Conjugated Estrogens • Premarin
- Esomeprazole • Nexium
- Eszopiclone • Lunesta
- Famotidine • Pepcid
- Fexofenadine • Allegra
- Interferon beta-1b • Betaseron
- Levothyroxine • Synthroid
- Memantine • Namenda
- Propranolol • Inderal
- Rizatriptan • Maxalt
- Topiramate • Topamax
Dr. Rao is a speaker for Forest Pharmaceuticals.
Acknowledgement
The author thanks Alexander M. Timchak, MS-IV, Stritch School of Medicine, Loyola University, Chicago, for his assistance with this article.
Case: Worsening memory
Mrs. K, age 46, is being treated by a neurologist for stable relapsing-remitting multiple sclerosis (MS) and migraine headaches when she complains of worsening memory over the past 5 years. She reports having difficulty recalling details of recent events and conversations. She describes occasional word-finding difficulties and problems maintaining her train of thought. She forgets where she places things and has gotten lost while driving, even on familiar routes. Her husband reports she takes more time to process things in general.
Mrs. K’s cognitive decline has affected her daily life and ability to work. For 4 years, she has been an office assistant at a campground, where she takes phone reservations and keeps a site schedule. Formerly simple tasks—such as taking a phone number—have become increasingly difficult, and she cannot recall a list of 3 things to buy at the supermarket without writing them down.
As a teenager, Mrs. K suffered migraines but did not seek treatment, and her headaches remitted for about 10 years. At age 29, she started to experience tunnel vision. Three years later she reported bilateral foot numbness and was diagnosed with MS. She responded well to interferon beta-1b but her migraines returned, occurring several times a week. Her migraines are successfully treated with topiramate, 75 mg/d, for prophylactic therapy and rizatriptan, 10 mg, as needed for abortive therapy. Her medication regimen also includes:
- eszopiclone, 2 mg/d, and amitriptyline, 10 mg/d, for insomnia
- butalbital/aspirin/caffeine, 50/325/40 mg, as needed for tension headaches
- fexofenadine, 12 mg/d, and budesonide, 32 mcg, 4 sprays/d, for allergy symptoms
- esomeprazole, 80 mg/d, and famotidine, 20 mg/d, as needed for dyspepsia
- propranolol, 120 mg/d, for hypertension
- levothyroxine, 75 mcg/d, for hypothyroidism
- conjugatedestrogens, 0.45 mg/d, for hypoestrogenemia
- alprazolam, 0.25 mg/d, aspirin, 81 mg/d, vitamin E, 800 IU/d, and a multivitamin.
The neurologist orders neuropsychological testing. Mrs. K demonstrates some depressive symptoms but is within normal limits across all aspects of neurocognition, including basic and complex attention, memory, bilateral motor functioning, expressive and receptive language, visuospatial/constructional function, and self-regulatory/executive functioning. The neurologist refers Mrs. K for psychiatric evaluation of her depressive symptoms.
The author’s observations
Many neuropsychiatric abnormalities may accompany MS (Table).1 These can be classified as cognitive dysfunction or disturbances in mood, affect, and behavior.
Although the cause of cognitive impairment in patients with MS is unclear, its extent and profound impact on functioning has become widely recognized over the past 20 years.2
An estimated 40% to 65% of patients with MS suffer from cognitive dysfunction.1,3 Testing indicates deficiencies most often in:
- attention
- information processing speed
- working memory
- verbal memory
- visuospatial function
- executive functions.4
- reduced social interactions
- increased sexual dysfunction
- greater difficulty with household tasks.6
Long-term interferon beta-1b treatment prevents MS relapses, but a recent study found that interferon beta-1b had a negative impact on patients’ mental health composite score and in most quality-of-life subscales over 2 years.8 Nevertheless, Mrs. K received interferon beta-1b therapy for at least 9 years without noticing cognitive decline.
Table
Neuropsychiatric conditions associated with MS
| Disorder | Prevalence |
|---|---|
| Major depression | Lifetime prevalence: 50% |
| Bipolar disorder | Estimated prevalence is 10%, twice that of the general population |
| Euphoria | 25% |
| Pseudobulbar affect | Pathological laughing or crying, emotional incontinence; affects 10% of patients |
| Psychosis | 2% to 3% vs 0.5% to 1% in general population |
| Cognitive impairment | 40% to 60% |
| Source: Reference 1 | |
EVALUATION: Dysthymia
Mrs. K reports memory problems as her chief complaint. She also complains of a depressed mood, irritability, distractibility, and insomnia since her memory problems began, and admits being readily tearful. Mrs. K has difficulty “turning off her thinking” at night, which leads to delayed sleep onset, but denies sleeplessness, racing thoughts, or feelings of euphoria.
Her thought process is coherent and goal-directed, and she denies having auditory or visual hallucinations or active or passive suicidal or homicidal ideation. She scores 29/30 on the Mini-Mental State Exam, but by interview she appears to have impaired remote memory. Mrs. K demonstrates unimpaired judgment and good insight.
The author’s observations
Mrs. K meets DSM-IV-TR criteria for dysthymic disorder and agrees to start mirtazapine, 15 mg at bedtime. I chose this antidepressant because Mrs. K continues to complain of difficulty falling asleep, and mirtazapine is known to significantly decrease sleep latency and increase total sleep time. Approximately one-half of patients with MS will experience depression.1,9 In a recent study of 245 MS patients followed in a neurology clinic, two-thirds of those who met criteria for major depressive disorder did not receive antidepressants.10
TREATMENT: A new strategy
After 2 more months Mrs. K’s mood is euthymic and she demonstrates a bright affect, but she experiences continued decline in short- and long-term memory and reports increasing frustration with simple tasks. The rest of her mental status exam is unremarkable. I instruct her to reduce the mirtazapine dosage to 15 mg/d.
At the next visit 10 weeks later, she again presents with a euthymic mood and a bright affect. She says she attempted to decrease mirtazapine but experienced increased irritability so she remained on the 30-mg dose, with a positive effect on her mood and reduced irritability. Unfortunately, her memory problems persist.
Approximately 2 years after Mrs. K’s first visit, I devise a new pharmacologic strategy. Mrs. K believes that she no longer is depressed and that her only problem is her inability to recall events. To address this, I decide to try memantine, which has been shown to cause modest improvement in clinical symptoms in severe stages of Alzheimer’s disease11 and also has been reported to be useful in the treatment of cognitive impairment in some bipolar disorder patients.12 I start memantine at 10 mg/d and titrate up to 20 mg/d in 3 months.
The author’s observations
Mrs. K’s substantial memory improvement while receiving memantine warrants considering the drug for patients with cognitive dysfunction attributable to MS. Memantine is an uncompetitive NMDA receptor antagonist that the FDA approved in 2003 to treat moderate-to-severe Alzheimer’s disease (Box).11,13 It is generally well tolerated and safe, with a low potential for drug-drug interactions. In clinical trials of patients receiving memantine for Alzheimer’s disease and vascular dementia, the most commonly reported side effects were dizziness, headache, constipation, and confusion.14
A recent trial of memantine therapy for MS at the University of Navarra was suspended for reversible mild-to-moderate neurologic side effects.15 A phase II/phase III double-blind placebo-controlled trial at the University of Oregon designed to determine whether memantine is an effective treatment for memory and cognitive problems associated with MS is recruiting participants.16
Memantine has been reported to successfully treat other MS symptoms. A 1997 retrospective study found that 11 patients with acquired pendular nystagmus (APN) secondary to MS experienced complete resolution of APN when given memantine.17
Memantine was FDA-approved in 2003 to treat moderate-to-severe Alzheimer’s disease dementia. The drug also has been used off-label to treat vascular dementia, dementia of Wernicke-Korsakoff syndrome, and acquired pendular nystagmus.11
Although the neurobiologic basis for memantine’s therapeutic activity in patients with dementia is not fully understood, it is thought to reduce glutamatergic excitotoxicity. The mechanism of action is voltage-dependent, uncompetitive N-methyl-D-aspartate (NMDA) receptor antagonism with low-to-moderate affinity and fast blocking/unblocking kinetics.12 Its kinetic profile is beneficial because it allows memantine to occupy the receptor for a sufficient time to prevent pathologic activation of glutamate receptors. However, it dissociates when the physiologic activation of glutamate receptors is necessary, thus preserving normal NMDA receptor activity required for learning and memory. By blocking the effects of abnormal glutamate activity, memantine may prevent abnormal neuronal cell death and cognitive dysfunction.
- Parsons CG, Stöffler A, Danysz W. Memantine: a NMDA receptor antagonist that improves memory by restoration of homeostasis in the glutamatergic system—too little activation is bad, too much is even worse. Neuropharmacology. 2007;53(6):699-723.
- Alprazolam • Xanax
- Amitriptyline • Elavil
- Budesonide • Rhinocort
- Butalbital/Aspirin/Caffeine • Fiorinal
- Conjugated Estrogens • Premarin
- Esomeprazole • Nexium
- Eszopiclone • Lunesta
- Famotidine • Pepcid
- Fexofenadine • Allegra
- Interferon beta-1b • Betaseron
- Levothyroxine • Synthroid
- Memantine • Namenda
- Propranolol • Inderal
- Rizatriptan • Maxalt
- Topiramate • Topamax
Dr. Rao is a speaker for Forest Pharmaceuticals.
Acknowledgement
The author thanks Alexander M. Timchak, MS-IV, Stritch School of Medicine, Loyola University, Chicago, for his assistance with this article.
1. Ghaffar O, Feinstein A. The neuropsychiatry of multiple sclerosis: a review of recent developments. Curr Opin Psychiatry. 2007;20(3):278-285.
2. Amato MP, Portaccio E, Zipoli V. Are there protective treatments for cognitive decline in MS? J Neurol Sci. 2006;245(1-2):183-186.
3. Bobholz JA, Rao SM. Cognitive dysfunction in multiple sclerosis: a review of recent developments. Curr Opin Neurol. 2003;16(3):283-288.
4. Hoffmann S, Tittgemeyer M, von Cramon DY. Cognitive impairment in multiple sclerosis. Curr Opin Neurol. 2007;20(3):275-280.
5. Pierson SH, Griffith N. Treatment of cognitive impairment in multiple sclerosis. Behav Neurol. 2006;17(1):53-67.
6. Bagert B, Camplair P, Bourdette D. Cognitive dysfunction in multiple sclerosis: natural history, pathophysiology and management. CNS Drugs. 2002;16(7):445-455.
7. Martin R, Kuzniecky R, Ho S, et al. Cognitive effects of topiramate, gabapentin, and lamotrigine in healthy young adults. Neurology. 1999;52(2):321-327.
8. Simone IL, Ceccarelli A, Tortorella C, et al. Influence of Interferon beta treatment on quality of life in multiple sclerosis patients. Health Qual Life Outcomes. 2006;4:96.-
9. Siegert RJ, Abernethy DA. Depression in multiple sclerosis: a review. J Neurol Neurosurg Psychiatry. 2005;76(4):469-475.
10. Mohr DC, Hart SL, Fonareva I, et al. Treatment of depression for patients with multiple sclerosis in neurology clinics. Mult Scler. 2006;12(2):204-208.
11. Kumar S. Memantine: pharmacological properties and clinical uses. Neurol India. 2004;52(3):307-309.
12. Teng CT, Demetrio FN. Memantine may acutely improve cognition and have a mood stabilizing effect in treatment-resistant bipolar disorder. Rev Bras Psiquiatr. 2006;28(3):252-4.
13. Danysz W, Parsons CG, Mobius HJ, et al. Neuroprotective and symptomatological action of memantine relevant for Alzheimer’s disease: a unified glutamatergic hypothesis on the mechanism of action. Neurotox Res. 2000;2(2-3):85-97.
14. Namenda [package insert] St. Louis, MO: Forest Pharmaceuticals; 2007.
15. Memantine therapy for multiple sclerosis (NCT00638833) Available at: http://www.clinicaltrials.gov/ct2/show/NCT00638833. Accessed February 17, 2009.
16. Trial of memantine for cognitive impairment in multiple sclerosis (NCT00300716) Available at: http://www.clinicaltrials.gov/ct2/show/NCT00300716. Accessed February 17, 2009.
17. Starck M, Albrecht H, Pöllmann W, et al. Drug therapy for acquired pendular nystagmus in multiple sclerosis. J Neurol. 1997;244(1):9-16.
1. Ghaffar O, Feinstein A. The neuropsychiatry of multiple sclerosis: a review of recent developments. Curr Opin Psychiatry. 2007;20(3):278-285.
2. Amato MP, Portaccio E, Zipoli V. Are there protective treatments for cognitive decline in MS? J Neurol Sci. 2006;245(1-2):183-186.
3. Bobholz JA, Rao SM. Cognitive dysfunction in multiple sclerosis: a review of recent developments. Curr Opin Neurol. 2003;16(3):283-288.
4. Hoffmann S, Tittgemeyer M, von Cramon DY. Cognitive impairment in multiple sclerosis. Curr Opin Neurol. 2007;20(3):275-280.
5. Pierson SH, Griffith N. Treatment of cognitive impairment in multiple sclerosis. Behav Neurol. 2006;17(1):53-67.
6. Bagert B, Camplair P, Bourdette D. Cognitive dysfunction in multiple sclerosis: natural history, pathophysiology and management. CNS Drugs. 2002;16(7):445-455.
7. Martin R, Kuzniecky R, Ho S, et al. Cognitive effects of topiramate, gabapentin, and lamotrigine in healthy young adults. Neurology. 1999;52(2):321-327.
8. Simone IL, Ceccarelli A, Tortorella C, et al. Influence of Interferon beta treatment on quality of life in multiple sclerosis patients. Health Qual Life Outcomes. 2006;4:96.-
9. Siegert RJ, Abernethy DA. Depression in multiple sclerosis: a review. J Neurol Neurosurg Psychiatry. 2005;76(4):469-475.
10. Mohr DC, Hart SL, Fonareva I, et al. Treatment of depression for patients with multiple sclerosis in neurology clinics. Mult Scler. 2006;12(2):204-208.
11. Kumar S. Memantine: pharmacological properties and clinical uses. Neurol India. 2004;52(3):307-309.
12. Teng CT, Demetrio FN. Memantine may acutely improve cognition and have a mood stabilizing effect in treatment-resistant bipolar disorder. Rev Bras Psiquiatr. 2006;28(3):252-4.
13. Danysz W, Parsons CG, Mobius HJ, et al. Neuroprotective and symptomatological action of memantine relevant for Alzheimer’s disease: a unified glutamatergic hypothesis on the mechanism of action. Neurotox Res. 2000;2(2-3):85-97.
14. Namenda [package insert] St. Louis, MO: Forest Pharmaceuticals; 2007.
15. Memantine therapy for multiple sclerosis (NCT00638833) Available at: http://www.clinicaltrials.gov/ct2/show/NCT00638833. Accessed February 17, 2009.
16. Trial of memantine for cognitive impairment in multiple sclerosis (NCT00300716) Available at: http://www.clinicaltrials.gov/ct2/show/NCT00300716. Accessed February 17, 2009.
17. Starck M, Albrecht H, Pöllmann W, et al. Drug therapy for acquired pendular nystagmus in multiple sclerosis. J Neurol. 1997;244(1):9-16.
The treatment-resistant catatonia patient
Case: Worsening psychosis
Ms. R, age 21, is admitted to our psychiatric facility while experiencing paranoid delusions and auditory hallucinations. Upon admission, she is agitated and her mood is labile.
Ms. R has 4 previous brief psychiatric admissions and was diagnosed with schizoaffective disorder, bipolar type and moderate mental retardation. Her family history is positive for psychiatric illness, as her mother was diagnosed with schizophrenia. Prior to admission, Ms. R was taking ziprasidone, 160 mg/d, and lithium, 450 mg/d, for 11 months. Both were discontinued during the first week of admission because Ms. R was not responding.
During this admission, the treating psychiatrist assesses Ms. R using the Schedules for Clinicians’ Interview in Psychiatry (SCIP), an instrument developed by the lead author (AA) for psychiatrists to use in conjunction with their routine clinical interviews in inpatient and outpatient settings (see Related Resources). The SCIP includes a 25-question screening section and a diagnostic section that consists of 7 modules that represent major psychiatric diagnoses defined by DSM and International Classification of Diseases criteria.1
During the first week of admission, we monitor Ms. R and administer haloperidol as needed, 10 mg total. Eight days after admission, she develops severe catatonia. On the catatonia scale of the SCIP, Ms. R scores the maximum on measures of immobility, catalepsy/waxy flexibility, and mutism (Table).
How would you treat Ms. R’s catatonia?
Table
Patient’s catatonia symptoms: Response to pharmacotherapy
| Lorazepam only | Lorazepam + risperidone | Risperidone oral only | Risperidone long-acting injection only | |
|---|---|---|---|---|
| Dosage(s) | 7 mg total over 7 days | Lorazepam: 4 mg/d Risperidone: 4 mg/d | 8 mg/d | 37.5 mg every 2 weeks |
| Scores on SCIP catatonia scale:* | ||||
| Immobility | 2 | 1 | 0 | 0 |
| Catalepsy/waxy flexibility† | 2 | 1 | 0 | 0 |
| Mutism | 2 | 0 | 0 | 0 |
| Total score | 6 | 2 | 0 | 0 |
| *Scale of 0 to 2, with 0=none, 1=less than half the time, and 2=more than half the time. Symptoms are evaluated over a 1-day period | ||||
| †For this category, 0=none, 1=brief (usually 1 minute | ||||
| SCIP: Schedules for Clinicians’ Interview in Psychiatry | ||||
The authors’ observations
DSM-IV-TR recognizes catatonia as a schizophrenia subtype, as a descriptor for mania and major depression, and as being caused by various medical conditions, such as neuroleptic malignant syndrome, encephalopathy, or renal failure.2 Kahlbaum initially described catatonia in 1873 as a brain disease characterized by motor abnormalities such as akinesia, rigidity, negativism, mutism, grimacing, posturing, catalepsy, waxy flexibility, and verbigerations.3 Catatonia is characterized by hypo- and hyperkinetic features. Catalepsy, stupor, rigidity, and catatonic posturing with waxy flexibility might alternate with violent catatonic excitement.4
Catatonia can be life-threatening; patients might not be able to eat or chew food, which puts them at risk for aspiration. Those with immobility might not move to urinate or defecate. During the first half of the 20th century, catatonia was documented in up to 50% of patients with schizophrenia.5 Since then, the incidence of catatonia has decreased, possibly the result of advances in psychopharmacology.6
Two days after Ms. R develops catatonia, we transfer her to a local hospital for evaluation to rule out a medical cause of her catatonic symptoms.
EVALUATION: No medical cause
At the hospital, physical examination, electroencephalography, drug screening, and liver and thyroid function tests are within normal limits, eliminating an organic cause of Ms. R’s catatonia. MRI of the head shows a 3-mm mass at the base of the infundibulum, which is unchanged from a prior MRI. Ms. R received 7 mg total of lorazepam over 4 days without relief of her catatonia. She is transferred back to our facility.
The authors’ observations
Benzodiazepines and ECT are effective treatments for catatonia.7 Benzodiazepines are considered first-line treatment because of their efficacy and favorable side-effect profile.7 Lorazepam frequently is used to treat catatonia in the short term.8 Long-term use of benzodiazepines, however, is associated with tolerance, addiction, and rebound phenomena.8,9
Patients with catatonia who do not respond to benzodiazepines may benefit from ECT.9 ECT can cause serious side effects, however, including memory impairment, confusion, delirium, and cardiac arrhythmias.10
Atypical antipsychotics may alleviate motor symptoms of catatonia by virtue of their 5-HT2A receptor antagonistic action.9 In 2 case reports, risperidone successfully treated catatonia.4,11 Kopala et al11 found risperidone, 4 mg/d, was effective in treating severe, first-episode catatonic schizophrenia in a neuroleptic-naive young man. This efficacy was sustained over a 3.5-year outpatient follow-up.
In another report, risperidone, 6 mg/d, effectively treated catatonia and prevented further episodes in a patient with schizophrenia who developed severe catatonia after receiving adequate treatment for Lyme disease with encephalitis.4 Two relapses of catatonic syndrome occurred when risperidone was reduced to 2 mg/d, and remission occurred after risperidone was increased to 6 mg/d. Risperidone’s antagonistic activity of the 5-HT2/D2 receptors may be relevant to its anticatatonic effect.12
Other atypical antipsychotics—ziprasidone and olanzapine—also have been shown to be effective in treating catatonia. Levy et al13 reported successful treatment of a catatonic state (with catalepsy, stupor, and mutism) using intramuscular ziprasidone followed by oral ziprasidone. A data analysis by Martenyi et al14 showed olanzapine to be effective in treating nonspecific signs and symptoms of catatonia, as measured by the Positive and Negative Syndrome Scale.
TREATMENT: Trying risperidone
Based on case reports showing risperidone’s efficacy for catatonia, we start Ms. R on risperidone, 4 mg/d, and lorazepam, 4 mg/d. Eight days later, her catatonic symptoms decrease substantially—she scores 2/6 on the SCIP catatonia scale (Table)—and she starts to talk with the staff.
We continue this regimen for 30 days, then discontinue lorazepam to avoid long-term side effects—such as dependence—and titrate risperidone to 8 mg/d. Ms. R continues to improve while taking risperidone only. Twenty-three days after stopping lorazepam, she is free of catatonic symptoms, scoring 0/6 on the SCIP catatonia scale.
We discharge Ms. R on risperidone. Because she has a history of medication nonadherence, we prescribe risperidone long-acting injection, 37.5 mg every 2 weeks, while continuing oral risperidone for 3 weeks after the first injection. She does well on this medication, experiencing no catatonic symptoms or adverse effects over the next 15 months as measured by the SCIP assessment.
The authors’ observations
This is the third case report in the literature to show that risperidone is effective in short- and long-term treatment of catatonia.4,11 Although Ms. R’s initial response can be attributed at least partially to lorazepam—which is known to be effective in treating catatonia—she continued to show improvement while taking risperidone only and remained free from catatonic symptoms for 15 months, until she was readmitted for reasons unrelated to catatonia.
We recommend using risperidone to treat catatonia in patients who do not respond to a benzodiazepine, especially those with other psychotic symptoms such as delusions or hallucinations. While administering risperidone, watch for long-term side effects, such as hyperlipidemia, weight gain, and diabetes. For catatonia in patients who cannot tolerate risperidone, consider olanzapine or ziprasidone.
- Schedules for Clinicians’ Interview in Psychiatry (SCIP). Available from Ahmed Aboraya, [email protected].
- Valevski A, Loebl T, Keren T, et al. Response of catatonia to risperidone: two case reports. Clin Neuropharmacol. 2001;24(4):228-231.
- Van Den Eede F, Van Hecke J, Van Dalfsen A, et al. The use of atypical antipsychotics in the treatment of catatonia. Eur Psychiatry. 2005;20(5-6):422-429.
- Haloperidol • Haldol
- Lithium • Eskalith, Lithobid
- Lorazepam • Ativan
- Olanzapine • Zyprexa
- Risperidone • Risperdal
- Risperidone long-acting injection • Risperdal Consta
- Ziprasidone • Geodon
The authors have no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Aboraya A, Tien A. Schedules for Clinicians’ Interviews in Psychiatry (SCIP): work in progress. International Journal of Mental Health and Addiction. Available at: http://www.ijma-journal.com/pdf/c01a09.pdf. Accessed February 4, 2009.
2. Diagnostic and statistical manual of disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
3. Kahlbaum KL. In: Levi Y, Pridon T, trans. Catatonia. Baltimore, MD: Johns Hopkins University Press; 1973.
4. Hesslinger B, Walden J, Normann C. Acute and long-term treatment of catatonia with risperidone. Pharmacopsychiatry. 2001;34(1):25-26.
5. Bleuler E. Dementia praecox. New York, NY: International University Press; 1950.
6. Blumer D. Catatonia and the neuroleptics: psychobiologic significance of remote and recent findings. Compr Psychiatry. 1997;38(4):193-201.
7. Bush G, Fink M, Petrides G, et al. Catatonia. II Treatment with lorazepam and electroconvulsive therapy. Acta Psychiatr Scand. 1996;93(2):137-143.
8. Duggal HS, Gandotra G. Risperidone treatment of periodic catatonia. Can J Psychiatry. 2005;50(4):241-242.
9. Duggal HS. Risperidone treatment of febrile catatonia in first-episode psychosis. Gen Hosp Psychiatry. 2005;27(1):80-81.
10. Rudorfer M, Henry M, Sackeim H. Electroconvulsive therapy. In: Tasman A, Kay J, Lieberman JA, eds. Psychiatry: therapeutics. London, UK: John Wiley & Sons; 2003:167-203.
11. Kopala LC, Caudle C. Acute and longer-term effects of risperidone in a case of first-episode catatonic schizophrenia. J Psychopharmacol. 1998;12(3):314-317.
12. Poyurousky M, Bergman J, Weizman A. Risperidone in the treatment of catatonia in a schizophrenic patient. Isr J Psychiatry Relat Sci. 1997;34(4):323-324.
13. Levy WO, Nunez CY. Use of ziprasidone to treat bipolar-associated catatonia. Bipolar Disord. 2004;6(2):166-167.
14. Martenyi F, Metcalfe S, Schausberger B, et al. An efficacy analysis of olanzapine treatment data in schizophrenia patients with catatonic signs and symptoms. J Clin Psychiatry. 2001;62(suppl 2):225-227.
Case: Worsening psychosis
Ms. R, age 21, is admitted to our psychiatric facility while experiencing paranoid delusions and auditory hallucinations. Upon admission, she is agitated and her mood is labile.
Ms. R has 4 previous brief psychiatric admissions and was diagnosed with schizoaffective disorder, bipolar type and moderate mental retardation. Her family history is positive for psychiatric illness, as her mother was diagnosed with schizophrenia. Prior to admission, Ms. R was taking ziprasidone, 160 mg/d, and lithium, 450 mg/d, for 11 months. Both were discontinued during the first week of admission because Ms. R was not responding.
During this admission, the treating psychiatrist assesses Ms. R using the Schedules for Clinicians’ Interview in Psychiatry (SCIP), an instrument developed by the lead author (AA) for psychiatrists to use in conjunction with their routine clinical interviews in inpatient and outpatient settings (see Related Resources). The SCIP includes a 25-question screening section and a diagnostic section that consists of 7 modules that represent major psychiatric diagnoses defined by DSM and International Classification of Diseases criteria.1
During the first week of admission, we monitor Ms. R and administer haloperidol as needed, 10 mg total. Eight days after admission, she develops severe catatonia. On the catatonia scale of the SCIP, Ms. R scores the maximum on measures of immobility, catalepsy/waxy flexibility, and mutism (Table).
How would you treat Ms. R’s catatonia?
Table
Patient’s catatonia symptoms: Response to pharmacotherapy
| Lorazepam only | Lorazepam + risperidone | Risperidone oral only | Risperidone long-acting injection only | |
|---|---|---|---|---|
| Dosage(s) | 7 mg total over 7 days | Lorazepam: 4 mg/d Risperidone: 4 mg/d | 8 mg/d | 37.5 mg every 2 weeks |
| Scores on SCIP catatonia scale:* | ||||
| Immobility | 2 | 1 | 0 | 0 |
| Catalepsy/waxy flexibility† | 2 | 1 | 0 | 0 |
| Mutism | 2 | 0 | 0 | 0 |
| Total score | 6 | 2 | 0 | 0 |
| *Scale of 0 to 2, with 0=none, 1=less than half the time, and 2=more than half the time. Symptoms are evaluated over a 1-day period | ||||
| †For this category, 0=none, 1=brief (usually 1 minute | ||||
| SCIP: Schedules for Clinicians’ Interview in Psychiatry | ||||
The authors’ observations
DSM-IV-TR recognizes catatonia as a schizophrenia subtype, as a descriptor for mania and major depression, and as being caused by various medical conditions, such as neuroleptic malignant syndrome, encephalopathy, or renal failure.2 Kahlbaum initially described catatonia in 1873 as a brain disease characterized by motor abnormalities such as akinesia, rigidity, negativism, mutism, grimacing, posturing, catalepsy, waxy flexibility, and verbigerations.3 Catatonia is characterized by hypo- and hyperkinetic features. Catalepsy, stupor, rigidity, and catatonic posturing with waxy flexibility might alternate with violent catatonic excitement.4
Catatonia can be life-threatening; patients might not be able to eat or chew food, which puts them at risk for aspiration. Those with immobility might not move to urinate or defecate. During the first half of the 20th century, catatonia was documented in up to 50% of patients with schizophrenia.5 Since then, the incidence of catatonia has decreased, possibly the result of advances in psychopharmacology.6
Two days after Ms. R develops catatonia, we transfer her to a local hospital for evaluation to rule out a medical cause of her catatonic symptoms.
EVALUATION: No medical cause
At the hospital, physical examination, electroencephalography, drug screening, and liver and thyroid function tests are within normal limits, eliminating an organic cause of Ms. R’s catatonia. MRI of the head shows a 3-mm mass at the base of the infundibulum, which is unchanged from a prior MRI. Ms. R received 7 mg total of lorazepam over 4 days without relief of her catatonia. She is transferred back to our facility.
The authors’ observations
Benzodiazepines and ECT are effective treatments for catatonia.7 Benzodiazepines are considered first-line treatment because of their efficacy and favorable side-effect profile.7 Lorazepam frequently is used to treat catatonia in the short term.8 Long-term use of benzodiazepines, however, is associated with tolerance, addiction, and rebound phenomena.8,9
Patients with catatonia who do not respond to benzodiazepines may benefit from ECT.9 ECT can cause serious side effects, however, including memory impairment, confusion, delirium, and cardiac arrhythmias.10
Atypical antipsychotics may alleviate motor symptoms of catatonia by virtue of their 5-HT2A receptor antagonistic action.9 In 2 case reports, risperidone successfully treated catatonia.4,11 Kopala et al11 found risperidone, 4 mg/d, was effective in treating severe, first-episode catatonic schizophrenia in a neuroleptic-naive young man. This efficacy was sustained over a 3.5-year outpatient follow-up.
In another report, risperidone, 6 mg/d, effectively treated catatonia and prevented further episodes in a patient with schizophrenia who developed severe catatonia after receiving adequate treatment for Lyme disease with encephalitis.4 Two relapses of catatonic syndrome occurred when risperidone was reduced to 2 mg/d, and remission occurred after risperidone was increased to 6 mg/d. Risperidone’s antagonistic activity of the 5-HT2/D2 receptors may be relevant to its anticatatonic effect.12
Other atypical antipsychotics—ziprasidone and olanzapine—also have been shown to be effective in treating catatonia. Levy et al13 reported successful treatment of a catatonic state (with catalepsy, stupor, and mutism) using intramuscular ziprasidone followed by oral ziprasidone. A data analysis by Martenyi et al14 showed olanzapine to be effective in treating nonspecific signs and symptoms of catatonia, as measured by the Positive and Negative Syndrome Scale.
TREATMENT: Trying risperidone
Based on case reports showing risperidone’s efficacy for catatonia, we start Ms. R on risperidone, 4 mg/d, and lorazepam, 4 mg/d. Eight days later, her catatonic symptoms decrease substantially—she scores 2/6 on the SCIP catatonia scale (Table)—and she starts to talk with the staff.
We continue this regimen for 30 days, then discontinue lorazepam to avoid long-term side effects—such as dependence—and titrate risperidone to 8 mg/d. Ms. R continues to improve while taking risperidone only. Twenty-three days after stopping lorazepam, she is free of catatonic symptoms, scoring 0/6 on the SCIP catatonia scale.
We discharge Ms. R on risperidone. Because she has a history of medication nonadherence, we prescribe risperidone long-acting injection, 37.5 mg every 2 weeks, while continuing oral risperidone for 3 weeks after the first injection. She does well on this medication, experiencing no catatonic symptoms or adverse effects over the next 15 months as measured by the SCIP assessment.
The authors’ observations
This is the third case report in the literature to show that risperidone is effective in short- and long-term treatment of catatonia.4,11 Although Ms. R’s initial response can be attributed at least partially to lorazepam—which is known to be effective in treating catatonia—she continued to show improvement while taking risperidone only and remained free from catatonic symptoms for 15 months, until she was readmitted for reasons unrelated to catatonia.
We recommend using risperidone to treat catatonia in patients who do not respond to a benzodiazepine, especially those with other psychotic symptoms such as delusions or hallucinations. While administering risperidone, watch for long-term side effects, such as hyperlipidemia, weight gain, and diabetes. For catatonia in patients who cannot tolerate risperidone, consider olanzapine or ziprasidone.
- Schedules for Clinicians’ Interview in Psychiatry (SCIP). Available from Ahmed Aboraya, [email protected].
- Valevski A, Loebl T, Keren T, et al. Response of catatonia to risperidone: two case reports. Clin Neuropharmacol. 2001;24(4):228-231.
- Van Den Eede F, Van Hecke J, Van Dalfsen A, et al. The use of atypical antipsychotics in the treatment of catatonia. Eur Psychiatry. 2005;20(5-6):422-429.
- Haloperidol • Haldol
- Lithium • Eskalith, Lithobid
- Lorazepam • Ativan
- Olanzapine • Zyprexa
- Risperidone • Risperdal
- Risperidone long-acting injection • Risperdal Consta
- Ziprasidone • Geodon
The authors have no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Case: Worsening psychosis
Ms. R, age 21, is admitted to our psychiatric facility while experiencing paranoid delusions and auditory hallucinations. Upon admission, she is agitated and her mood is labile.
Ms. R has 4 previous brief psychiatric admissions and was diagnosed with schizoaffective disorder, bipolar type and moderate mental retardation. Her family history is positive for psychiatric illness, as her mother was diagnosed with schizophrenia. Prior to admission, Ms. R was taking ziprasidone, 160 mg/d, and lithium, 450 mg/d, for 11 months. Both were discontinued during the first week of admission because Ms. R was not responding.
During this admission, the treating psychiatrist assesses Ms. R using the Schedules for Clinicians’ Interview in Psychiatry (SCIP), an instrument developed by the lead author (AA) for psychiatrists to use in conjunction with their routine clinical interviews in inpatient and outpatient settings (see Related Resources). The SCIP includes a 25-question screening section and a diagnostic section that consists of 7 modules that represent major psychiatric diagnoses defined by DSM and International Classification of Diseases criteria.1
During the first week of admission, we monitor Ms. R and administer haloperidol as needed, 10 mg total. Eight days after admission, she develops severe catatonia. On the catatonia scale of the SCIP, Ms. R scores the maximum on measures of immobility, catalepsy/waxy flexibility, and mutism (Table).
How would you treat Ms. R’s catatonia?
Table
Patient’s catatonia symptoms: Response to pharmacotherapy
| Lorazepam only | Lorazepam + risperidone | Risperidone oral only | Risperidone long-acting injection only | |
|---|---|---|---|---|
| Dosage(s) | 7 mg total over 7 days | Lorazepam: 4 mg/d Risperidone: 4 mg/d | 8 mg/d | 37.5 mg every 2 weeks |
| Scores on SCIP catatonia scale:* | ||||
| Immobility | 2 | 1 | 0 | 0 |
| Catalepsy/waxy flexibility† | 2 | 1 | 0 | 0 |
| Mutism | 2 | 0 | 0 | 0 |
| Total score | 6 | 2 | 0 | 0 |
| *Scale of 0 to 2, with 0=none, 1=less than half the time, and 2=more than half the time. Symptoms are evaluated over a 1-day period | ||||
| †For this category, 0=none, 1=brief (usually 1 minute | ||||
| SCIP: Schedules for Clinicians’ Interview in Psychiatry | ||||
The authors’ observations
DSM-IV-TR recognizes catatonia as a schizophrenia subtype, as a descriptor for mania and major depression, and as being caused by various medical conditions, such as neuroleptic malignant syndrome, encephalopathy, or renal failure.2 Kahlbaum initially described catatonia in 1873 as a brain disease characterized by motor abnormalities such as akinesia, rigidity, negativism, mutism, grimacing, posturing, catalepsy, waxy flexibility, and verbigerations.3 Catatonia is characterized by hypo- and hyperkinetic features. Catalepsy, stupor, rigidity, and catatonic posturing with waxy flexibility might alternate with violent catatonic excitement.4
Catatonia can be life-threatening; patients might not be able to eat or chew food, which puts them at risk for aspiration. Those with immobility might not move to urinate or defecate. During the first half of the 20th century, catatonia was documented in up to 50% of patients with schizophrenia.5 Since then, the incidence of catatonia has decreased, possibly the result of advances in psychopharmacology.6
Two days after Ms. R develops catatonia, we transfer her to a local hospital for evaluation to rule out a medical cause of her catatonic symptoms.
EVALUATION: No medical cause
At the hospital, physical examination, electroencephalography, drug screening, and liver and thyroid function tests are within normal limits, eliminating an organic cause of Ms. R’s catatonia. MRI of the head shows a 3-mm mass at the base of the infundibulum, which is unchanged from a prior MRI. Ms. R received 7 mg total of lorazepam over 4 days without relief of her catatonia. She is transferred back to our facility.
The authors’ observations
Benzodiazepines and ECT are effective treatments for catatonia.7 Benzodiazepines are considered first-line treatment because of their efficacy and favorable side-effect profile.7 Lorazepam frequently is used to treat catatonia in the short term.8 Long-term use of benzodiazepines, however, is associated with tolerance, addiction, and rebound phenomena.8,9
Patients with catatonia who do not respond to benzodiazepines may benefit from ECT.9 ECT can cause serious side effects, however, including memory impairment, confusion, delirium, and cardiac arrhythmias.10
Atypical antipsychotics may alleviate motor symptoms of catatonia by virtue of their 5-HT2A receptor antagonistic action.9 In 2 case reports, risperidone successfully treated catatonia.4,11 Kopala et al11 found risperidone, 4 mg/d, was effective in treating severe, first-episode catatonic schizophrenia in a neuroleptic-naive young man. This efficacy was sustained over a 3.5-year outpatient follow-up.
In another report, risperidone, 6 mg/d, effectively treated catatonia and prevented further episodes in a patient with schizophrenia who developed severe catatonia after receiving adequate treatment for Lyme disease with encephalitis.4 Two relapses of catatonic syndrome occurred when risperidone was reduced to 2 mg/d, and remission occurred after risperidone was increased to 6 mg/d. Risperidone’s antagonistic activity of the 5-HT2/D2 receptors may be relevant to its anticatatonic effect.12
Other atypical antipsychotics—ziprasidone and olanzapine—also have been shown to be effective in treating catatonia. Levy et al13 reported successful treatment of a catatonic state (with catalepsy, stupor, and mutism) using intramuscular ziprasidone followed by oral ziprasidone. A data analysis by Martenyi et al14 showed olanzapine to be effective in treating nonspecific signs and symptoms of catatonia, as measured by the Positive and Negative Syndrome Scale.
TREATMENT: Trying risperidone
Based on case reports showing risperidone’s efficacy for catatonia, we start Ms. R on risperidone, 4 mg/d, and lorazepam, 4 mg/d. Eight days later, her catatonic symptoms decrease substantially—she scores 2/6 on the SCIP catatonia scale (Table)—and she starts to talk with the staff.
We continue this regimen for 30 days, then discontinue lorazepam to avoid long-term side effects—such as dependence—and titrate risperidone to 8 mg/d. Ms. R continues to improve while taking risperidone only. Twenty-three days after stopping lorazepam, she is free of catatonic symptoms, scoring 0/6 on the SCIP catatonia scale.
We discharge Ms. R on risperidone. Because she has a history of medication nonadherence, we prescribe risperidone long-acting injection, 37.5 mg every 2 weeks, while continuing oral risperidone for 3 weeks after the first injection. She does well on this medication, experiencing no catatonic symptoms or adverse effects over the next 15 months as measured by the SCIP assessment.
The authors’ observations
This is the third case report in the literature to show that risperidone is effective in short- and long-term treatment of catatonia.4,11 Although Ms. R’s initial response can be attributed at least partially to lorazepam—which is known to be effective in treating catatonia—she continued to show improvement while taking risperidone only and remained free from catatonic symptoms for 15 months, until she was readmitted for reasons unrelated to catatonia.
We recommend using risperidone to treat catatonia in patients who do not respond to a benzodiazepine, especially those with other psychotic symptoms such as delusions or hallucinations. While administering risperidone, watch for long-term side effects, such as hyperlipidemia, weight gain, and diabetes. For catatonia in patients who cannot tolerate risperidone, consider olanzapine or ziprasidone.
- Schedules for Clinicians’ Interview in Psychiatry (SCIP). Available from Ahmed Aboraya, [email protected].
- Valevski A, Loebl T, Keren T, et al. Response of catatonia to risperidone: two case reports. Clin Neuropharmacol. 2001;24(4):228-231.
- Van Den Eede F, Van Hecke J, Van Dalfsen A, et al. The use of atypical antipsychotics in the treatment of catatonia. Eur Psychiatry. 2005;20(5-6):422-429.
- Haloperidol • Haldol
- Lithium • Eskalith, Lithobid
- Lorazepam • Ativan
- Olanzapine • Zyprexa
- Risperidone • Risperdal
- Risperidone long-acting injection • Risperdal Consta
- Ziprasidone • Geodon
The authors have no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Aboraya A, Tien A. Schedules for Clinicians’ Interviews in Psychiatry (SCIP): work in progress. International Journal of Mental Health and Addiction. Available at: http://www.ijma-journal.com/pdf/c01a09.pdf. Accessed February 4, 2009.
2. Diagnostic and statistical manual of disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
3. Kahlbaum KL. In: Levi Y, Pridon T, trans. Catatonia. Baltimore, MD: Johns Hopkins University Press; 1973.
4. Hesslinger B, Walden J, Normann C. Acute and long-term treatment of catatonia with risperidone. Pharmacopsychiatry. 2001;34(1):25-26.
5. Bleuler E. Dementia praecox. New York, NY: International University Press; 1950.
6. Blumer D. Catatonia and the neuroleptics: psychobiologic significance of remote and recent findings. Compr Psychiatry. 1997;38(4):193-201.
7. Bush G, Fink M, Petrides G, et al. Catatonia. II Treatment with lorazepam and electroconvulsive therapy. Acta Psychiatr Scand. 1996;93(2):137-143.
8. Duggal HS, Gandotra G. Risperidone treatment of periodic catatonia. Can J Psychiatry. 2005;50(4):241-242.
9. Duggal HS. Risperidone treatment of febrile catatonia in first-episode psychosis. Gen Hosp Psychiatry. 2005;27(1):80-81.
10. Rudorfer M, Henry M, Sackeim H. Electroconvulsive therapy. In: Tasman A, Kay J, Lieberman JA, eds. Psychiatry: therapeutics. London, UK: John Wiley & Sons; 2003:167-203.
11. Kopala LC, Caudle C. Acute and longer-term effects of risperidone in a case of first-episode catatonic schizophrenia. J Psychopharmacol. 1998;12(3):314-317.
12. Poyurousky M, Bergman J, Weizman A. Risperidone in the treatment of catatonia in a schizophrenic patient. Isr J Psychiatry Relat Sci. 1997;34(4):323-324.
13. Levy WO, Nunez CY. Use of ziprasidone to treat bipolar-associated catatonia. Bipolar Disord. 2004;6(2):166-167.
14. Martenyi F, Metcalfe S, Schausberger B, et al. An efficacy analysis of olanzapine treatment data in schizophrenia patients with catatonic signs and symptoms. J Clin Psychiatry. 2001;62(suppl 2):225-227.
1. Aboraya A, Tien A. Schedules for Clinicians’ Interviews in Psychiatry (SCIP): work in progress. International Journal of Mental Health and Addiction. Available at: http://www.ijma-journal.com/pdf/c01a09.pdf. Accessed February 4, 2009.
2. Diagnostic and statistical manual of disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
3. Kahlbaum KL. In: Levi Y, Pridon T, trans. Catatonia. Baltimore, MD: Johns Hopkins University Press; 1973.
4. Hesslinger B, Walden J, Normann C. Acute and long-term treatment of catatonia with risperidone. Pharmacopsychiatry. 2001;34(1):25-26.
5. Bleuler E. Dementia praecox. New York, NY: International University Press; 1950.
6. Blumer D. Catatonia and the neuroleptics: psychobiologic significance of remote and recent findings. Compr Psychiatry. 1997;38(4):193-201.
7. Bush G, Fink M, Petrides G, et al. Catatonia. II Treatment with lorazepam and electroconvulsive therapy. Acta Psychiatr Scand. 1996;93(2):137-143.
8. Duggal HS, Gandotra G. Risperidone treatment of periodic catatonia. Can J Psychiatry. 2005;50(4):241-242.
9. Duggal HS. Risperidone treatment of febrile catatonia in first-episode psychosis. Gen Hosp Psychiatry. 2005;27(1):80-81.
10. Rudorfer M, Henry M, Sackeim H. Electroconvulsive therapy. In: Tasman A, Kay J, Lieberman JA, eds. Psychiatry: therapeutics. London, UK: John Wiley & Sons; 2003:167-203.
11. Kopala LC, Caudle C. Acute and longer-term effects of risperidone in a case of first-episode catatonic schizophrenia. J Psychopharmacol. 1998;12(3):314-317.
12. Poyurousky M, Bergman J, Weizman A. Risperidone in the treatment of catatonia in a schizophrenic patient. Isr J Psychiatry Relat Sci. 1997;34(4):323-324.
13. Levy WO, Nunez CY. Use of ziprasidone to treat bipolar-associated catatonia. Bipolar Disord. 2004;6(2):166-167.
14. Martenyi F, Metcalfe S, Schausberger B, et al. An efficacy analysis of olanzapine treatment data in schizophrenia patients with catatonic signs and symptoms. J Clin Psychiatry. 2001;62(suppl 2):225-227.
The angry patient with Asperger’s
CASE ‘Sad, worried, and angry’
Mr. A, age 24, is referred to our university psychiatric clinic. He reports that he’s sad, worried, angry, and wants to hurt people. He endorses having chronic depressive episodes that last >2 weeks and consist of poor sleep, low energy, anhedonia, poor concentration, and psychomotor retardation.
He is developmentally disabled and has been living in a group home for almost 1 year. In former group homes, Mr. A threatened and assaulted other patients and staff. In 1 incident Mr. A broke a patient’s nose and was incarcerated for 4 days. With the help of a job coach, Mr. A has been working in a department store for 8 months. He was fired from other jobs because he threatened co-workers.
The author’s observations
Problem behaviors in patients with pervasive developmental disorders include aggression and self-injury. These behaviors may improve with behavioral or pharmacologic interventions.1 For example, risperidone is FDA-approved to treat irritability associated with autistic disorder in children and adolescents age 5 to 16 years.2 Violence has been reported in patients with pervasive developmental disorders, and such symptoms can lead to psychiatric referral.1
HISTORY Difficult childhood
Mr. A’s medical history is unremarkable. He has no history of hypomania, mania, psychosis, substance use, tics, seizures, genetic illnesses, head trauma, or physical or sexual abuse. He has never attempted suicide nor been hospitalized for psychiatric illness.
With Mr. A’s permission, his mother is consulted. She says that as a child Mr. A would become extremely interested in various topics—including Pokémon, Magic cards, and video games—and had a strong desire to tell everyone the details of each. However, he rocked back and forth, had few friends, and would bite other children.
Mr. A has no history of language delay but received speech therapy during his childhood to help him “work on eye contact and social skills.” He is estranged from and angry with his father, who has difficulty accepting his son’s developmental disability.
At the time of referral, Mr. A is receiving paroxetine, 30 mg/d, for depression, risperidone, 1.5 mg/d, for aggression, and dextroamphetamine/amphetamine extended-release, 30 mg/d, for hyperactivity/inattention. The efficacy of these medications, which were prescribed by an outside psychiatrist, is unclear.
Table 1
Diagnostic criteria for Asperger’s disorder
A. Qualitative impairment in social interaction, as manifested by ≥2 of the following:
|
B. Restricted repetitive and stereotyped patterns of behavior, interests, and activities, as manifested by ≥1 of the following:
|
| C. The disturbance causes clinically significant impairment in social, occupational, or other important areas of functioning. |
| D. There is no clinically significant general delay in language (eg, single words used by age 2 years, communicative phrases used by age 3 years). |
| E. There is no clinically significant delay in cognitive development or in the development of age-appropriate self-help skills, adaptive behavior (other than in social interaction), and curiosity about the environment in childhood. |
| F. Criteria are not met for another specific pervasive developmental disorder or schizophrenia. |
| Source: Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000 |
Based on Mr. A’s impaired social interaction, repetitive interests and behaviors, and lack of language delay, Mr. A meets criteria for Asperger’s disorder (Table 1). He also meets criteria for major depressive disorder, recurrent, moderate.
The author’s observations
Psychosocial interventions for patients with an autism-spectrum disorder consist of educational, vocational, behavioral, and family interventions. Individual, group, and family psychotherapy may benefit patients with Asperger’s disorder who have comorbid depression.1
TREATMENT A rocky start
At Mr. A’s initial assessment, the clinic psychiatrist increases risperidone to 1 mg twice daily to target aggression. Even after receiving this dosage for 1 month, however, Mr. A continues to display physical aggression toward peers in the group home whenever he becomes angry.
The psychiatrist refers Mr. A to a social worker for supportive therapy to help him cope with worry and chronic sadness. The social worker uses general cognitive-behavioral strategies for anxiety and aggression for 12 sessions over 8 months until scheduling conflicts end therapy. The efficacy of this therapy is minimal; Mr. A remains depressed, anxious, and aggressive. During this time, the psychiatrist increases paroxetine to 40 mg/d, but Mr. A continues to feel depressed after 1 month. Mr. A is cross-tapered to duloxetine, but continues to feel depressed after receiving duloxetine, 60 mg/d, for 1 month.
My first visit with Mr. A occurs 3 months after his last visit with the social worker. He states he does not remember anything from those sessions. Mr. A’s goals for therapy are to reduce anxiety, manage anger, and improve relationship skills.
I begin the first 4 months of Mr. A’s therapy with cognitive-behavioral interventions based on the Treatment of Adolescents Depression Study (TADS) manual.3 Although Mr. A is an adult, I choose a manual that targets adolescents because my clinical impression is that his cognitive developmental level is more like an adolescent’s than an adult’s.
I assign homework such as mood monitoring. I ask him to use a form from the TADS manual to rate his mood on a scale of 0 to 10 every morning, afternoon, and evening, and write down what he is doing that makes him feel that way at the time he rates his mood. Mr. A never completes any homework; during each session he states he “just forgot to do it.”
I discuss concepts such as goal setting, for a novel Mr. A says he wants to write, and relaxation strategies to address anger; in session, I work with him on filling out the “What Helps Me to Relax?” form from the TADS manual. Mr. A lists “play games,” “write my book,” “listen to music,” “go outside,” and “exercise” as strategies to help him relax. We also work on visual handouts—such as “Safety Plan” and “What Can I Do to Relax”—to post in his room.
Mr. A does not show up for 3 sessions. When I call the group home, a staff member tells me they were busy with other patients and forgot about Mr. A. I decide to call the group home the day before each appointment as a reminder. This increases Mr. A’s attendance rate.
During each session, Mr. A complains about the quality of the group home, the staff, and other patients. To get my own perspective of Mr. A’s living environment, I consider visiting his group home, similar to how a geriatric psychiatrist sees patients in a nursing home or an assertive community treatment team psychiatrist sees patients in their home environments. Because I am concerned about boundary crossings/violations, I first discuss this action with 2 psychotherapists not involved in Mr. A’s treatment. They recommend that I limit this action to a one-time visit.
I visit Mr. A’s group home 2 months after my first session with him. Located in front of a dairy farm in a rural part of the state about 1 hour from our clinic, the isolated facility has a secured keypad entry. When I meet Mr. A there, he says he feels as if he is in jail. I meet the staff and find them willing to help with various aspects of Mr. A’s treatment, such as discussing events, reporting behaviors, and helping carry out interventions.
For example, I ask staff to remind Mr. A of his relaxation strategies when he becomes angry. On the “Safety Plan” handout, I had Mr. A identify 5 people he could talk to when he becomes angry; I ask staff to remind him of those people when Mr. A becomes angry. I also ask staff to ask Mr. A every day if he is writing the novel he wants to complete. After my visit, Mr. A starts putting more effort into therapy. When I set a daily goal of working on his novel for 15 minutes, he starts bringing pages of his writings to sessions.
Table 2
Social skills training for patients with Asperger’s disorde
| Starting a conversation: “Hi, how was your day?” |
| Staying on topic: “Oh, that sounds interesting. Tell me more about…” |
| Making eye contact: Look at people’s eyes when talking to them |
| Greetings: “Hi, how are you?” |
| Ending a conversation: “Well, I have to go now. I’ll see you later!” |
| Shifting topics: “Speaking of…, did you hear about…?” |
| Source:Reference 7 |
The author’s observations
In a study in rural Appalachia, telephone reminders increased attendance at psychiatric intake appointments.4 Calling the group home before each of Mr. A’s appointments took extra time out of my schedule but improved Mr. A’s attendance rate.
In residential treatment of children, Monahan notes that childcare workers could contribute useful observations and benefit from the therapist’s advice.5 Establishing rapport with the staff at Mr. A’s group home helped me proceed with therapy.
TREATMENT Social skills training
In the second 4 months of therapy, Mr. A changes jobs to become a greeter in a local video game store. He is happy, and group home staff members are pleased they no longer spend 2 hours each day transporting him to his previous job.
Soon after, during a reminder phone call, a staff member tells me that Mr. A’s brother and father were murdered the prior week. Three staff members attend Mr. A’s brother’s funeral, which he appreciates. Mr. A refuses to attend his father’s funeral because of continued anger toward him.
When I ask Mr. A if he wants to talk about the deaths, he declines. I subsequently spend half a session discussing strategies to address grief,6 such as imagining a conversation with his deceased brother.
I decide to review Mr. A’s therapy goals because he still has a lot of anger toward his recently deceased father. I am concerned he might discharge this anger onto a staff member, coworker, or fellow patient. Mr. A states he wants to focus on relationships, especially his anxiety around women. He discusses his anxiety with starting and maintaining conversations with women.
I begin role-playing in sessions by pretending to be a woman for Mr. A to speak with, but he feels this is silly. I teach him exercises from a social skills training workbook developed for patients with Asperger’s, such as “Starting a conversation,” “Staying on topic,” and “Making eye contact” (Table 2).7 Mr. A says group home staff members occasionally take him out to a nearby nightclub and encourage him to talk to women.
To see how Mr. A behaves in public, during our sessions I take him to different parts of the hospital, such as the gift shop, library, and deli. I instruct him to ask various women non-threatening questions, such as how much a certain entrée costs. I note his body language, such as tilting his head down and fidgeting during conversations. I provide him with immediate feedback, which slowly increases his awareness of these behaviors.
With Mr. A’s permission, I educate the group home staff about how to point out these behaviors when Mr. A is in public. I ask them to focus on body language and emphasize that Mr. A needs to apply what I teach him to other settings.
The author’s observations
Patients with Asperger’s disorder need specific training to build a repertoire of social skills.7 Teaching in real-life settings helps patients generalize these skills.1
Zimmerman8 discusses how caregivers might have an unrealistic, “magical” view of psychotherapy and feel suspicious of the process. With Mr. A’s permission, I ask group home staff members to meet with me for 10 minutes at the end of each of Mr. A’s sessions to make them aware of what is happening with his therapy. I want them to feel that they are an important part of Mr. A’s therapy. These meetings may have alleviated staff members’ fears about my time with him. Even though Mr. A granted me permission to disclose all details of our sessions with the staff, I was careful to not disclose sensitive issues, such as the patient’s dreams and fantasies.
TREATMENT ‘Fear’
Mr. A rates his anxiety as a 4/10 whenever he speaks with women. To more specifically understand his underlying cognitions, I use Kendall’s FEAR plan (Table 3).9
I ask him to divide his automatic “E” thoughts into “she” and “I” thoughts. Examples of automatic “she” thoughts include “She probably won’t like me” and “She thinks I’m not cute.” Examples of automatic “I” thoughts include “I’m probably not smart enough for her” and “I think we won’t have anything in common.”
Table 3
The FEAR plan*
| F=feeling anxious | |
| E=expecting bad things to happen | |
| A=attitudes and actions that can help | |
| R=results and rewards | |
| Developed to help anxious children and adolescents recognize signs of anxiety, relax, and modify anxious self-talk and thinking. | |
| Source:Reference 9 | |
The author’s observations
Schwartz10 discusses countertransference challenges in nursing home patients, where therapists identify with patients’ hopelessness. Schwartz recommends addressing these challenges by thinking of realistic expectations. Even though a facility might be far from perfect, it may be “good enough.”
Mr. A’s group home was far from perfect and located in an isolated setting. Even so, I was able to help him complete psychotherapy at our clinic by adapting my practice to his needs, including:
- making reminder phone calls for appointments
- visiting the group home
- enlisting the help of caregivers with therapeutic techniques.
OUTCOME Improving
In the final 4 months of therapy, we continue to work on social skills lessons, practice exercises in the hospital, and the FEAR acronym. I continue to include caregivers in these efforts.
During 1 session, I tell Mr. A I will be leaving at the end of my fellowship. In the final month, I gradually transition him to a new therapist. I decided to transition him to a male therapist so Mr. A will continue to feel comfortable sharing his feelings, rather than shutting down from anxiety with a female therapist. As I end therapy, Mr. A is promoted to a cashier at the video game store and enrolls in classes to study for a General Education Development (GED) certificate.
Related resource
- National Institute of Mental Health. Autism spectrum disorders. www.nimh.nih.gov/health/publications/autism/complete-publication.shtml.
- Bupropion extended-release • Wellbutrin XL
- Dextroamphetamine/amphetamine extended-release • Adderall XR
- Duloxetine • Cymbalta
- Paroxetine • Paxil
- Risperidone • Risperdal
- Ziprasidone • Geodon
The author reports no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgment
The author thanks Dr. Ann Lagges, PhD, for her assistance with this patient’s treatment.
1. American Association of Child and Adolescent Psychiatry. Practice parameters for autism in children, adolescents, and adults. Available at: http://www.aacap.org/galleries/PracticeParameters/Autism.pdf. Accessed December 25, 2008.
2. Risperdal [package insert]. Titusville, NJ: Janssen Pharmaceuticals, Inc; 2008. Available at: http://www.risperdal.com/risperdal/shared/pi/risperdal.pdf. Accessed December 25, 2008.
3. Curry JF, Wells KC, Brent DA, et al. Treatment for adolescents with depression study (TADS): cognitive behavior therapy manual. Available at: https://trialweb.dcri.duke.edu/tads/tad/manuals/TADS_CBT.pdf. Accessed August 2, 2007.
4. Shoffner J, Staudt M, Marcus S, et al. Using telephone reminders to increase attendance at psychiatric appointments: findings of a pilot study in rural Appalachia. Psychiatr Serv. 2007;58(6):872-875.
5. Monahan RT. Individual and group psychotherapy. In: Lyman RD, Prentice-Dunn S, Gabel S, eds. Residential and inpatient treatment of children and adolescents. New York, NY: Plenum Publishing; 1989:192.
6. Shear K, Frank E, Houck PR, et al. Treatment of complicated grief: a randomized controlled trial. JAMA. 2005;293(1):2601-2608.
7. Baker JE. Social skills training for children and adolescents with Asperger syndrome and social-communication problems. Shawnee Mission, KS: Autism Asperger Publishing Company; 2003.
8. Zimmerman DP. Psychotherapy in residential treatment: historical development and critical issues. Child Adolesc Psychiatr Clin N Am. 2004;13(2):347-361.
9. Kendall PC, Hedtke A. Coping cat workbook. 2nd ed. Ardmore, PA: Workbook Publishing; 2006.
10. Schwartz K. Remembering the forgotten: psychotherapy groups for the nursing home resident. Int J Group Psychother. 2007;57(4):497-514.
CASE ‘Sad, worried, and angry’
Mr. A, age 24, is referred to our university psychiatric clinic. He reports that he’s sad, worried, angry, and wants to hurt people. He endorses having chronic depressive episodes that last >2 weeks and consist of poor sleep, low energy, anhedonia, poor concentration, and psychomotor retardation.
He is developmentally disabled and has been living in a group home for almost 1 year. In former group homes, Mr. A threatened and assaulted other patients and staff. In 1 incident Mr. A broke a patient’s nose and was incarcerated for 4 days. With the help of a job coach, Mr. A has been working in a department store for 8 months. He was fired from other jobs because he threatened co-workers.
The author’s observations
Problem behaviors in patients with pervasive developmental disorders include aggression and self-injury. These behaviors may improve with behavioral or pharmacologic interventions.1 For example, risperidone is FDA-approved to treat irritability associated with autistic disorder in children and adolescents age 5 to 16 years.2 Violence has been reported in patients with pervasive developmental disorders, and such symptoms can lead to psychiatric referral.1
HISTORY Difficult childhood
Mr. A’s medical history is unremarkable. He has no history of hypomania, mania, psychosis, substance use, tics, seizures, genetic illnesses, head trauma, or physical or sexual abuse. He has never attempted suicide nor been hospitalized for psychiatric illness.
With Mr. A’s permission, his mother is consulted. She says that as a child Mr. A would become extremely interested in various topics—including Pokémon, Magic cards, and video games—and had a strong desire to tell everyone the details of each. However, he rocked back and forth, had few friends, and would bite other children.
Mr. A has no history of language delay but received speech therapy during his childhood to help him “work on eye contact and social skills.” He is estranged from and angry with his father, who has difficulty accepting his son’s developmental disability.
At the time of referral, Mr. A is receiving paroxetine, 30 mg/d, for depression, risperidone, 1.5 mg/d, for aggression, and dextroamphetamine/amphetamine extended-release, 30 mg/d, for hyperactivity/inattention. The efficacy of these medications, which were prescribed by an outside psychiatrist, is unclear.
Table 1
Diagnostic criteria for Asperger’s disorder
A. Qualitative impairment in social interaction, as manifested by ≥2 of the following:
|
B. Restricted repetitive and stereotyped patterns of behavior, interests, and activities, as manifested by ≥1 of the following:
|
| C. The disturbance causes clinically significant impairment in social, occupational, or other important areas of functioning. |
| D. There is no clinically significant general delay in language (eg, single words used by age 2 years, communicative phrases used by age 3 years). |
| E. There is no clinically significant delay in cognitive development or in the development of age-appropriate self-help skills, adaptive behavior (other than in social interaction), and curiosity about the environment in childhood. |
| F. Criteria are not met for another specific pervasive developmental disorder or schizophrenia. |
| Source: Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000 |
Based on Mr. A’s impaired social interaction, repetitive interests and behaviors, and lack of language delay, Mr. A meets criteria for Asperger’s disorder (Table 1). He also meets criteria for major depressive disorder, recurrent, moderate.
The author’s observations
Psychosocial interventions for patients with an autism-spectrum disorder consist of educational, vocational, behavioral, and family interventions. Individual, group, and family psychotherapy may benefit patients with Asperger’s disorder who have comorbid depression.1
TREATMENT A rocky start
At Mr. A’s initial assessment, the clinic psychiatrist increases risperidone to 1 mg twice daily to target aggression. Even after receiving this dosage for 1 month, however, Mr. A continues to display physical aggression toward peers in the group home whenever he becomes angry.
The psychiatrist refers Mr. A to a social worker for supportive therapy to help him cope with worry and chronic sadness. The social worker uses general cognitive-behavioral strategies for anxiety and aggression for 12 sessions over 8 months until scheduling conflicts end therapy. The efficacy of this therapy is minimal; Mr. A remains depressed, anxious, and aggressive. During this time, the psychiatrist increases paroxetine to 40 mg/d, but Mr. A continues to feel depressed after 1 month. Mr. A is cross-tapered to duloxetine, but continues to feel depressed after receiving duloxetine, 60 mg/d, for 1 month.
My first visit with Mr. A occurs 3 months after his last visit with the social worker. He states he does not remember anything from those sessions. Mr. A’s goals for therapy are to reduce anxiety, manage anger, and improve relationship skills.
I begin the first 4 months of Mr. A’s therapy with cognitive-behavioral interventions based on the Treatment of Adolescents Depression Study (TADS) manual.3 Although Mr. A is an adult, I choose a manual that targets adolescents because my clinical impression is that his cognitive developmental level is more like an adolescent’s than an adult’s.
I assign homework such as mood monitoring. I ask him to use a form from the TADS manual to rate his mood on a scale of 0 to 10 every morning, afternoon, and evening, and write down what he is doing that makes him feel that way at the time he rates his mood. Mr. A never completes any homework; during each session he states he “just forgot to do it.”
I discuss concepts such as goal setting, for a novel Mr. A says he wants to write, and relaxation strategies to address anger; in session, I work with him on filling out the “What Helps Me to Relax?” form from the TADS manual. Mr. A lists “play games,” “write my book,” “listen to music,” “go outside,” and “exercise” as strategies to help him relax. We also work on visual handouts—such as “Safety Plan” and “What Can I Do to Relax”—to post in his room.
Mr. A does not show up for 3 sessions. When I call the group home, a staff member tells me they were busy with other patients and forgot about Mr. A. I decide to call the group home the day before each appointment as a reminder. This increases Mr. A’s attendance rate.
During each session, Mr. A complains about the quality of the group home, the staff, and other patients. To get my own perspective of Mr. A’s living environment, I consider visiting his group home, similar to how a geriatric psychiatrist sees patients in a nursing home or an assertive community treatment team psychiatrist sees patients in their home environments. Because I am concerned about boundary crossings/violations, I first discuss this action with 2 psychotherapists not involved in Mr. A’s treatment. They recommend that I limit this action to a one-time visit.
I visit Mr. A’s group home 2 months after my first session with him. Located in front of a dairy farm in a rural part of the state about 1 hour from our clinic, the isolated facility has a secured keypad entry. When I meet Mr. A there, he says he feels as if he is in jail. I meet the staff and find them willing to help with various aspects of Mr. A’s treatment, such as discussing events, reporting behaviors, and helping carry out interventions.
For example, I ask staff to remind Mr. A of his relaxation strategies when he becomes angry. On the “Safety Plan” handout, I had Mr. A identify 5 people he could talk to when he becomes angry; I ask staff to remind him of those people when Mr. A becomes angry. I also ask staff to ask Mr. A every day if he is writing the novel he wants to complete. After my visit, Mr. A starts putting more effort into therapy. When I set a daily goal of working on his novel for 15 minutes, he starts bringing pages of his writings to sessions.
Table 2
Social skills training for patients with Asperger’s disorde
| Starting a conversation: “Hi, how was your day?” |
| Staying on topic: “Oh, that sounds interesting. Tell me more about…” |
| Making eye contact: Look at people’s eyes when talking to them |
| Greetings: “Hi, how are you?” |
| Ending a conversation: “Well, I have to go now. I’ll see you later!” |
| Shifting topics: “Speaking of…, did you hear about…?” |
| Source:Reference 7 |
The author’s observations
In a study in rural Appalachia, telephone reminders increased attendance at psychiatric intake appointments.4 Calling the group home before each of Mr. A’s appointments took extra time out of my schedule but improved Mr. A’s attendance rate.
In residential treatment of children, Monahan notes that childcare workers could contribute useful observations and benefit from the therapist’s advice.5 Establishing rapport with the staff at Mr. A’s group home helped me proceed with therapy.
TREATMENT Social skills training
In the second 4 months of therapy, Mr. A changes jobs to become a greeter in a local video game store. He is happy, and group home staff members are pleased they no longer spend 2 hours each day transporting him to his previous job.
Soon after, during a reminder phone call, a staff member tells me that Mr. A’s brother and father were murdered the prior week. Three staff members attend Mr. A’s brother’s funeral, which he appreciates. Mr. A refuses to attend his father’s funeral because of continued anger toward him.
When I ask Mr. A if he wants to talk about the deaths, he declines. I subsequently spend half a session discussing strategies to address grief,6 such as imagining a conversation with his deceased brother.
I decide to review Mr. A’s therapy goals because he still has a lot of anger toward his recently deceased father. I am concerned he might discharge this anger onto a staff member, coworker, or fellow patient. Mr. A states he wants to focus on relationships, especially his anxiety around women. He discusses his anxiety with starting and maintaining conversations with women.
I begin role-playing in sessions by pretending to be a woman for Mr. A to speak with, but he feels this is silly. I teach him exercises from a social skills training workbook developed for patients with Asperger’s, such as “Starting a conversation,” “Staying on topic,” and “Making eye contact” (Table 2).7 Mr. A says group home staff members occasionally take him out to a nearby nightclub and encourage him to talk to women.
To see how Mr. A behaves in public, during our sessions I take him to different parts of the hospital, such as the gift shop, library, and deli. I instruct him to ask various women non-threatening questions, such as how much a certain entrée costs. I note his body language, such as tilting his head down and fidgeting during conversations. I provide him with immediate feedback, which slowly increases his awareness of these behaviors.
With Mr. A’s permission, I educate the group home staff about how to point out these behaviors when Mr. A is in public. I ask them to focus on body language and emphasize that Mr. A needs to apply what I teach him to other settings.
The author’s observations
Patients with Asperger’s disorder need specific training to build a repertoire of social skills.7 Teaching in real-life settings helps patients generalize these skills.1
Zimmerman8 discusses how caregivers might have an unrealistic, “magical” view of psychotherapy and feel suspicious of the process. With Mr. A’s permission, I ask group home staff members to meet with me for 10 minutes at the end of each of Mr. A’s sessions to make them aware of what is happening with his therapy. I want them to feel that they are an important part of Mr. A’s therapy. These meetings may have alleviated staff members’ fears about my time with him. Even though Mr. A granted me permission to disclose all details of our sessions with the staff, I was careful to not disclose sensitive issues, such as the patient’s dreams and fantasies.
TREATMENT ‘Fear’
Mr. A rates his anxiety as a 4/10 whenever he speaks with women. To more specifically understand his underlying cognitions, I use Kendall’s FEAR plan (Table 3).9
I ask him to divide his automatic “E” thoughts into “she” and “I” thoughts. Examples of automatic “she” thoughts include “She probably won’t like me” and “She thinks I’m not cute.” Examples of automatic “I” thoughts include “I’m probably not smart enough for her” and “I think we won’t have anything in common.”
Table 3
The FEAR plan*
| F=feeling anxious | |
| E=expecting bad things to happen | |
| A=attitudes and actions that can help | |
| R=results and rewards | |
| Developed to help anxious children and adolescents recognize signs of anxiety, relax, and modify anxious self-talk and thinking. | |
| Source:Reference 9 | |
The author’s observations
Schwartz10 discusses countertransference challenges in nursing home patients, where therapists identify with patients’ hopelessness. Schwartz recommends addressing these challenges by thinking of realistic expectations. Even though a facility might be far from perfect, it may be “good enough.”
Mr. A’s group home was far from perfect and located in an isolated setting. Even so, I was able to help him complete psychotherapy at our clinic by adapting my practice to his needs, including:
- making reminder phone calls for appointments
- visiting the group home
- enlisting the help of caregivers with therapeutic techniques.
OUTCOME Improving
In the final 4 months of therapy, we continue to work on social skills lessons, practice exercises in the hospital, and the FEAR acronym. I continue to include caregivers in these efforts.
During 1 session, I tell Mr. A I will be leaving at the end of my fellowship. In the final month, I gradually transition him to a new therapist. I decided to transition him to a male therapist so Mr. A will continue to feel comfortable sharing his feelings, rather than shutting down from anxiety with a female therapist. As I end therapy, Mr. A is promoted to a cashier at the video game store and enrolls in classes to study for a General Education Development (GED) certificate.
Related resource
- National Institute of Mental Health. Autism spectrum disorders. www.nimh.nih.gov/health/publications/autism/complete-publication.shtml.
- Bupropion extended-release • Wellbutrin XL
- Dextroamphetamine/amphetamine extended-release • Adderall XR
- Duloxetine • Cymbalta
- Paroxetine • Paxil
- Risperidone • Risperdal
- Ziprasidone • Geodon
The author reports no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgment
The author thanks Dr. Ann Lagges, PhD, for her assistance with this patient’s treatment.
CASE ‘Sad, worried, and angry’
Mr. A, age 24, is referred to our university psychiatric clinic. He reports that he’s sad, worried, angry, and wants to hurt people. He endorses having chronic depressive episodes that last >2 weeks and consist of poor sleep, low energy, anhedonia, poor concentration, and psychomotor retardation.
He is developmentally disabled and has been living in a group home for almost 1 year. In former group homes, Mr. A threatened and assaulted other patients and staff. In 1 incident Mr. A broke a patient’s nose and was incarcerated for 4 days. With the help of a job coach, Mr. A has been working in a department store for 8 months. He was fired from other jobs because he threatened co-workers.
The author’s observations
Problem behaviors in patients with pervasive developmental disorders include aggression and self-injury. These behaviors may improve with behavioral or pharmacologic interventions.1 For example, risperidone is FDA-approved to treat irritability associated with autistic disorder in children and adolescents age 5 to 16 years.2 Violence has been reported in patients with pervasive developmental disorders, and such symptoms can lead to psychiatric referral.1
HISTORY Difficult childhood
Mr. A’s medical history is unremarkable. He has no history of hypomania, mania, psychosis, substance use, tics, seizures, genetic illnesses, head trauma, or physical or sexual abuse. He has never attempted suicide nor been hospitalized for psychiatric illness.
With Mr. A’s permission, his mother is consulted. She says that as a child Mr. A would become extremely interested in various topics—including Pokémon, Magic cards, and video games—and had a strong desire to tell everyone the details of each. However, he rocked back and forth, had few friends, and would bite other children.
Mr. A has no history of language delay but received speech therapy during his childhood to help him “work on eye contact and social skills.” He is estranged from and angry with his father, who has difficulty accepting his son’s developmental disability.
At the time of referral, Mr. A is receiving paroxetine, 30 mg/d, for depression, risperidone, 1.5 mg/d, for aggression, and dextroamphetamine/amphetamine extended-release, 30 mg/d, for hyperactivity/inattention. The efficacy of these medications, which were prescribed by an outside psychiatrist, is unclear.
Table 1
Diagnostic criteria for Asperger’s disorder
A. Qualitative impairment in social interaction, as manifested by ≥2 of the following:
|
B. Restricted repetitive and stereotyped patterns of behavior, interests, and activities, as manifested by ≥1 of the following:
|
| C. The disturbance causes clinically significant impairment in social, occupational, or other important areas of functioning. |
| D. There is no clinically significant general delay in language (eg, single words used by age 2 years, communicative phrases used by age 3 years). |
| E. There is no clinically significant delay in cognitive development or in the development of age-appropriate self-help skills, adaptive behavior (other than in social interaction), and curiosity about the environment in childhood. |
| F. Criteria are not met for another specific pervasive developmental disorder or schizophrenia. |
| Source: Diagnostic and statistical manual of mental disorders, 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000 |
Based on Mr. A’s impaired social interaction, repetitive interests and behaviors, and lack of language delay, Mr. A meets criteria for Asperger’s disorder (Table 1). He also meets criteria for major depressive disorder, recurrent, moderate.
The author’s observations
Psychosocial interventions for patients with an autism-spectrum disorder consist of educational, vocational, behavioral, and family interventions. Individual, group, and family psychotherapy may benefit patients with Asperger’s disorder who have comorbid depression.1
TREATMENT A rocky start
At Mr. A’s initial assessment, the clinic psychiatrist increases risperidone to 1 mg twice daily to target aggression. Even after receiving this dosage for 1 month, however, Mr. A continues to display physical aggression toward peers in the group home whenever he becomes angry.
The psychiatrist refers Mr. A to a social worker for supportive therapy to help him cope with worry and chronic sadness. The social worker uses general cognitive-behavioral strategies for anxiety and aggression for 12 sessions over 8 months until scheduling conflicts end therapy. The efficacy of this therapy is minimal; Mr. A remains depressed, anxious, and aggressive. During this time, the psychiatrist increases paroxetine to 40 mg/d, but Mr. A continues to feel depressed after 1 month. Mr. A is cross-tapered to duloxetine, but continues to feel depressed after receiving duloxetine, 60 mg/d, for 1 month.
My first visit with Mr. A occurs 3 months after his last visit with the social worker. He states he does not remember anything from those sessions. Mr. A’s goals for therapy are to reduce anxiety, manage anger, and improve relationship skills.
I begin the first 4 months of Mr. A’s therapy with cognitive-behavioral interventions based on the Treatment of Adolescents Depression Study (TADS) manual.3 Although Mr. A is an adult, I choose a manual that targets adolescents because my clinical impression is that his cognitive developmental level is more like an adolescent’s than an adult’s.
I assign homework such as mood monitoring. I ask him to use a form from the TADS manual to rate his mood on a scale of 0 to 10 every morning, afternoon, and evening, and write down what he is doing that makes him feel that way at the time he rates his mood. Mr. A never completes any homework; during each session he states he “just forgot to do it.”
I discuss concepts such as goal setting, for a novel Mr. A says he wants to write, and relaxation strategies to address anger; in session, I work with him on filling out the “What Helps Me to Relax?” form from the TADS manual. Mr. A lists “play games,” “write my book,” “listen to music,” “go outside,” and “exercise” as strategies to help him relax. We also work on visual handouts—such as “Safety Plan” and “What Can I Do to Relax”—to post in his room.
Mr. A does not show up for 3 sessions. When I call the group home, a staff member tells me they were busy with other patients and forgot about Mr. A. I decide to call the group home the day before each appointment as a reminder. This increases Mr. A’s attendance rate.
During each session, Mr. A complains about the quality of the group home, the staff, and other patients. To get my own perspective of Mr. A’s living environment, I consider visiting his group home, similar to how a geriatric psychiatrist sees patients in a nursing home or an assertive community treatment team psychiatrist sees patients in their home environments. Because I am concerned about boundary crossings/violations, I first discuss this action with 2 psychotherapists not involved in Mr. A’s treatment. They recommend that I limit this action to a one-time visit.
I visit Mr. A’s group home 2 months after my first session with him. Located in front of a dairy farm in a rural part of the state about 1 hour from our clinic, the isolated facility has a secured keypad entry. When I meet Mr. A there, he says he feels as if he is in jail. I meet the staff and find them willing to help with various aspects of Mr. A’s treatment, such as discussing events, reporting behaviors, and helping carry out interventions.
For example, I ask staff to remind Mr. A of his relaxation strategies when he becomes angry. On the “Safety Plan” handout, I had Mr. A identify 5 people he could talk to when he becomes angry; I ask staff to remind him of those people when Mr. A becomes angry. I also ask staff to ask Mr. A every day if he is writing the novel he wants to complete. After my visit, Mr. A starts putting more effort into therapy. When I set a daily goal of working on his novel for 15 minutes, he starts bringing pages of his writings to sessions.
Table 2
Social skills training for patients with Asperger’s disorde
| Starting a conversation: “Hi, how was your day?” |
| Staying on topic: “Oh, that sounds interesting. Tell me more about…” |
| Making eye contact: Look at people’s eyes when talking to them |
| Greetings: “Hi, how are you?” |
| Ending a conversation: “Well, I have to go now. I’ll see you later!” |
| Shifting topics: “Speaking of…, did you hear about…?” |
| Source:Reference 7 |
The author’s observations
In a study in rural Appalachia, telephone reminders increased attendance at psychiatric intake appointments.4 Calling the group home before each of Mr. A’s appointments took extra time out of my schedule but improved Mr. A’s attendance rate.
In residential treatment of children, Monahan notes that childcare workers could contribute useful observations and benefit from the therapist’s advice.5 Establishing rapport with the staff at Mr. A’s group home helped me proceed with therapy.
TREATMENT Social skills training
In the second 4 months of therapy, Mr. A changes jobs to become a greeter in a local video game store. He is happy, and group home staff members are pleased they no longer spend 2 hours each day transporting him to his previous job.
Soon after, during a reminder phone call, a staff member tells me that Mr. A’s brother and father were murdered the prior week. Three staff members attend Mr. A’s brother’s funeral, which he appreciates. Mr. A refuses to attend his father’s funeral because of continued anger toward him.
When I ask Mr. A if he wants to talk about the deaths, he declines. I subsequently spend half a session discussing strategies to address grief,6 such as imagining a conversation with his deceased brother.
I decide to review Mr. A’s therapy goals because he still has a lot of anger toward his recently deceased father. I am concerned he might discharge this anger onto a staff member, coworker, or fellow patient. Mr. A states he wants to focus on relationships, especially his anxiety around women. He discusses his anxiety with starting and maintaining conversations with women.
I begin role-playing in sessions by pretending to be a woman for Mr. A to speak with, but he feels this is silly. I teach him exercises from a social skills training workbook developed for patients with Asperger’s, such as “Starting a conversation,” “Staying on topic,” and “Making eye contact” (Table 2).7 Mr. A says group home staff members occasionally take him out to a nearby nightclub and encourage him to talk to women.
To see how Mr. A behaves in public, during our sessions I take him to different parts of the hospital, such as the gift shop, library, and deli. I instruct him to ask various women non-threatening questions, such as how much a certain entrée costs. I note his body language, such as tilting his head down and fidgeting during conversations. I provide him with immediate feedback, which slowly increases his awareness of these behaviors.
With Mr. A’s permission, I educate the group home staff about how to point out these behaviors when Mr. A is in public. I ask them to focus on body language and emphasize that Mr. A needs to apply what I teach him to other settings.
The author’s observations
Patients with Asperger’s disorder need specific training to build a repertoire of social skills.7 Teaching in real-life settings helps patients generalize these skills.1
Zimmerman8 discusses how caregivers might have an unrealistic, “magical” view of psychotherapy and feel suspicious of the process. With Mr. A’s permission, I ask group home staff members to meet with me for 10 minutes at the end of each of Mr. A’s sessions to make them aware of what is happening with his therapy. I want them to feel that they are an important part of Mr. A’s therapy. These meetings may have alleviated staff members’ fears about my time with him. Even though Mr. A granted me permission to disclose all details of our sessions with the staff, I was careful to not disclose sensitive issues, such as the patient’s dreams and fantasies.
TREATMENT ‘Fear’
Mr. A rates his anxiety as a 4/10 whenever he speaks with women. To more specifically understand his underlying cognitions, I use Kendall’s FEAR plan (Table 3).9
I ask him to divide his automatic “E” thoughts into “she” and “I” thoughts. Examples of automatic “she” thoughts include “She probably won’t like me” and “She thinks I’m not cute.” Examples of automatic “I” thoughts include “I’m probably not smart enough for her” and “I think we won’t have anything in common.”
Table 3
The FEAR plan*
| F=feeling anxious | |
| E=expecting bad things to happen | |
| A=attitudes and actions that can help | |
| R=results and rewards | |
| Developed to help anxious children and adolescents recognize signs of anxiety, relax, and modify anxious self-talk and thinking. | |
| Source:Reference 9 | |
The author’s observations
Schwartz10 discusses countertransference challenges in nursing home patients, where therapists identify with patients’ hopelessness. Schwartz recommends addressing these challenges by thinking of realistic expectations. Even though a facility might be far from perfect, it may be “good enough.”
Mr. A’s group home was far from perfect and located in an isolated setting. Even so, I was able to help him complete psychotherapy at our clinic by adapting my practice to his needs, including:
- making reminder phone calls for appointments
- visiting the group home
- enlisting the help of caregivers with therapeutic techniques.
OUTCOME Improving
In the final 4 months of therapy, we continue to work on social skills lessons, practice exercises in the hospital, and the FEAR acronym. I continue to include caregivers in these efforts.
During 1 session, I tell Mr. A I will be leaving at the end of my fellowship. In the final month, I gradually transition him to a new therapist. I decided to transition him to a male therapist so Mr. A will continue to feel comfortable sharing his feelings, rather than shutting down from anxiety with a female therapist. As I end therapy, Mr. A is promoted to a cashier at the video game store and enrolls in classes to study for a General Education Development (GED) certificate.
Related resource
- National Institute of Mental Health. Autism spectrum disorders. www.nimh.nih.gov/health/publications/autism/complete-publication.shtml.
- Bupropion extended-release • Wellbutrin XL
- Dextroamphetamine/amphetamine extended-release • Adderall XR
- Duloxetine • Cymbalta
- Paroxetine • Paxil
- Risperidone • Risperdal
- Ziprasidone • Geodon
The author reports no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgment
The author thanks Dr. Ann Lagges, PhD, for her assistance with this patient’s treatment.
1. American Association of Child and Adolescent Psychiatry. Practice parameters for autism in children, adolescents, and adults. Available at: http://www.aacap.org/galleries/PracticeParameters/Autism.pdf. Accessed December 25, 2008.
2. Risperdal [package insert]. Titusville, NJ: Janssen Pharmaceuticals, Inc; 2008. Available at: http://www.risperdal.com/risperdal/shared/pi/risperdal.pdf. Accessed December 25, 2008.
3. Curry JF, Wells KC, Brent DA, et al. Treatment for adolescents with depression study (TADS): cognitive behavior therapy manual. Available at: https://trialweb.dcri.duke.edu/tads/tad/manuals/TADS_CBT.pdf. Accessed August 2, 2007.
4. Shoffner J, Staudt M, Marcus S, et al. Using telephone reminders to increase attendance at psychiatric appointments: findings of a pilot study in rural Appalachia. Psychiatr Serv. 2007;58(6):872-875.
5. Monahan RT. Individual and group psychotherapy. In: Lyman RD, Prentice-Dunn S, Gabel S, eds. Residential and inpatient treatment of children and adolescents. New York, NY: Plenum Publishing; 1989:192.
6. Shear K, Frank E, Houck PR, et al. Treatment of complicated grief: a randomized controlled trial. JAMA. 2005;293(1):2601-2608.
7. Baker JE. Social skills training for children and adolescents with Asperger syndrome and social-communication problems. Shawnee Mission, KS: Autism Asperger Publishing Company; 2003.
8. Zimmerman DP. Psychotherapy in residential treatment: historical development and critical issues. Child Adolesc Psychiatr Clin N Am. 2004;13(2):347-361.
9. Kendall PC, Hedtke A. Coping cat workbook. 2nd ed. Ardmore, PA: Workbook Publishing; 2006.
10. Schwartz K. Remembering the forgotten: psychotherapy groups for the nursing home resident. Int J Group Psychother. 2007;57(4):497-514.
1. American Association of Child and Adolescent Psychiatry. Practice parameters for autism in children, adolescents, and adults. Available at: http://www.aacap.org/galleries/PracticeParameters/Autism.pdf. Accessed December 25, 2008.
2. Risperdal [package insert]. Titusville, NJ: Janssen Pharmaceuticals, Inc; 2008. Available at: http://www.risperdal.com/risperdal/shared/pi/risperdal.pdf. Accessed December 25, 2008.
3. Curry JF, Wells KC, Brent DA, et al. Treatment for adolescents with depression study (TADS): cognitive behavior therapy manual. Available at: https://trialweb.dcri.duke.edu/tads/tad/manuals/TADS_CBT.pdf. Accessed August 2, 2007.
4. Shoffner J, Staudt M, Marcus S, et al. Using telephone reminders to increase attendance at psychiatric appointments: findings of a pilot study in rural Appalachia. Psychiatr Serv. 2007;58(6):872-875.
5. Monahan RT. Individual and group psychotherapy. In: Lyman RD, Prentice-Dunn S, Gabel S, eds. Residential and inpatient treatment of children and adolescents. New York, NY: Plenum Publishing; 1989:192.
6. Shear K, Frank E, Houck PR, et al. Treatment of complicated grief: a randomized controlled trial. JAMA. 2005;293(1):2601-2608.
7. Baker JE. Social skills training for children and adolescents with Asperger syndrome and social-communication problems. Shawnee Mission, KS: Autism Asperger Publishing Company; 2003.
8. Zimmerman DP. Psychotherapy in residential treatment: historical development and critical issues. Child Adolesc Psychiatr Clin N Am. 2004;13(2):347-361.
9. Kendall PC, Hedtke A. Coping cat workbook. 2nd ed. Ardmore, PA: Workbook Publishing; 2006.
10. Schwartz K. Remembering the forgotten: psychotherapy groups for the nursing home resident. Int J Group Psychother. 2007;57(4):497-514.