User login
A pacemaker patient’s electrical dilemma
CASE: Relapsing depression
Mrs. A, age 41, presents with worsening depression and suicidal ideation with a plan to take an overdose of her medications. She describes herself as “tense, anxious, and worrying all the time.” She reports worsening mood, loss of interest in previously pleasurable activities, lack of energy and drive, and difficulties performing routine household tasks. She also endorses a combination of initial and middle insomnia. According to her husband, the patient has been slow in movement and speech and has not been taking adequate care of herself.
Mrs. A denies auditory or visual hallucinations, thought insertion, thought withdrawal, thought broadcast, ideas of reference, or paranoid ideation. She also denies recent or past symptoms of mania or hypomania.
Mrs. A has a history of alcohol abuse and major depressive disorder. For her first depressive episode 5 years ago, she was treated with paroxetine, 20 to 80 mg/d, with good results. Following a depressive relapse, she was switched to fluoxetine, 80 mg/d, which improved her depressive symptoms. Approximately 2 years later, she experienced another depressive relapse that resulted in hospitalization. During hospitalization and subsequent outpatient visits, she was treated with citalopram, 20 mg/d, ziprasidone, 80 mg bid, and lorazepam, 1 mg tid. Her depressive symptoms were in partial remission for 2 years until her current relapse.
Her medical history includes syncope of unexplained origin, for which she received an implanted cardiac pacemaker 3 years ago. She takes sertraline, 150 mg/d, methylphenidate, 15 mg/d, and trazodone, 200 mg at night. Laboratory testing is unremarkable.
On mental status examination, Mrs. A’s mood is sad and her affect constricted. Her speech is fluent but slow, and she speaks only when spoken to. We note that Mrs. A has thought blocking but no hallucinations or delusions. She is alert and oriented, but her attention and concentration are impaired. Her insight is fair, and judgment is poor.
The authors’ observations
Somatic therapy for severe major depressive disorders has been limited principally to pharmacotherapy. Despite the availability of effective antidepressants and aggressive treatment, for many patients—such as Mrs. A—the course of depression is characterized by relapse, recurrence, and chronicity.1,2
Because Mrs. A has treatment-refractory depression, we decide to treat her with ECT. ECT has few contraindications and typically is well tolerated. It commonly is used to treat depression in patients with cardiac conditions and generally is quite safe in this population.3,4
ECT in patients with cardiac pacemakers in situ theoretically presents an increased risk of complications, however.5 Specific concerns of administering ECT to pacemaker patients include electrical interference from ECT stimulus and pacemaker sensing of:
- myopotentials that originate from succinylcholine-induced fasciculation (muscular twitching of contiguous groups of muscle fibers)
- muscle contractions that result in incomplete muscle paralysis
- dysrhythmias during the seizure.
Skeletal muscle can generate significant electrical potentials that are well within the sensing capabilities of most newer pulse generators. This happens most frequently in some dual-chamber pacemakers that can automatically perform mode switching or adapt their sensing and pacing thresholds to new situations, which might make them more sensitive to interference by ECT.
Similar concerns apply to administering ECT to patients receiving vagus nerve stimulation (VNS) therapy, as both VNS pulse generators and cardiac pacemakers are battery-powered, electrical signal-producing mechanisms housed in a metal case. The safety of concurrent ECT and VNS therapy is unknown (Box).6,7
Although vagus nerve stimulation (VNS) and electroconvulsive therapy (ECT) are not mutually exclusive, the safety of concurrent use of these 2 therapies is uncertain.6 The manufacturer of the VNS device recommends turning off the VNS pulse generator before administering ECT. In at least 1 case report, however, ECT was administered safely without the VNS pulse generator turned off.7
No case reports describe the safety of VNS in patients with an implanted device such as a pacemaker or automatic cardioverter defibrillator. According to the manufacturer, the VNS system may affect the operation of other devices. For VNS patients who require an implantable pacemaker, defibrillator therapy, or other types of stimulators, the VNS manufacturer advises careful programming of each system and implanting the 2 stimulators at least 10 centimeters (4 inches) apart to avoid communication interference.
What the evidence says
In evidence-based medicine, we tend to say: “In God we trust; all the others have to bring their data.” Unfortunately, it is difficult to conduct a trial of patients with multiple medical issues. Based on anecdotal reports, it appears that ECT use in patients with an implanted cardiac device such as a pacemaker or automatic internal cardioverter-defibrillator (AICD) generally is safe.8-12
One case report describes successful administration of ECT in a treatment-refractory depressed patient with an AICD. The AICD was deactivated during ECT and re-activated immediately upon completion of each treatment. The case report’s authors concluded that the presence of an AICD should not be a contraindication to ECT.13
A chart review of 3 patients with ICDs who received concurrent ECT found treatment was generally uneventful.12 One patient developed tachycardia with a rate-dependent left bundle branch block and hypotension in the recovery room, which responded promptly to esmolol. She did not experience similar events after subsequent ECT treatments.
Minimizing risk
In the absence of controlled data about the use of ECT in patients with implanted cardiac devices, crucial therapeutic decisions depend on the physician’s skill and judgment. Risk strategies can minimize complications (Algorithm).12 An internist or cardiologist experienced in pacemaker management should conduct a device interrogation—evaluating thresholds, lead impedance, and battery voltage and reviewing histograms, mode switch episodes, and stored electrograms—before the first ECT session and after the final one.
Most modern implantable pacemakers work in the synchronous (demand), rate-adaptive mode. In a patient in whom non-cardiac electrical signals cause bradycardia or asystole during ECT, the pacemaker can be reprogrammed to be less sensitive by placing a magnet over the pulse generator, which converts the pacemaker to an asynchronous (fixed), non-sensing mode. It is important to keep in mind that magnet application will not “turn off” a pacemaker; although each pacemaker is programmed to respond to a magnet in a specific fashion, the main response is asynchronous pacing.
Careful cardiac monitoring during ECT is essential (Table). The cardiologist or internist should be available during the first few ECT sessions to monitor for potential pacemaker interference or malfunction. This physician should be familiar with the pacemaker model and type of lead system so he or she can deactivate, reactivate, or reprogram the device.
Algorithm
Reducing risk when administering ECT to cardiac pacemaker patients
| Step 1 | |
| Evaluate the patient to ensure medical suitability for ECT and associated anesthesia | |
| Step 2 | ↓ |
| Conduct pacemaker interrogation (evaluating thresholds, lead impedance, and battery voltage and reviewing histograms, mode switch episodes, and stored electrograms) prior to first ECT treatment and after completion of full ECT course | |
| Step 3 | ↓ |
| Perform cardiac monitoring during and immediately after administering ECT | |
| Step 4 | ↓ |
| Have a magnet available to reprogram the pacemaker in the event of pacemaker inhibition or symptomatic bradycardia during ECT | |
| Step 5 | ↓ |
| Check that all monitoring devices are properly grounded, insulate the patient’s stretcher, and ensure that the patient does not touch anyone who is in contact with the ground during presentation of the ECT electrical stimulus | |
| ECT: electroconvulsive therapy | |
| Source: Reference 12 | |
Guidelines for monitoring cardiac pacemaker patients during ECT
| Use multilead ECG monitoring |
| Have equipment available to rapidly obtain central access (if vasoactive medications or transvenous pacing is needed) |
| Assess the plethysmography tracing of the pulse oximeter (a useful surrogate if the patient experiences dysrhythmias) |
| Have ready an external defibrillator |
TREATMENT: Successful ECT
We seek a medical consultation before initiating ECT. An internist performs device interrogation before the first ECT treatment and is present in the ECT treatment suite to ensure proper pacemaker conversion and to monitor for cardiac complications. The internist conducts another device interrogation after the acute series of ECT treatments.
Mrs. A tolerates the ECT sessions without cardiac complications. Her depressive symptoms respond well to 12 ECT sessions. She is more interactive and reports better attention and concentration. Although Mrs. A still has middle and initial insomnia, she denies thoughts of harming herself or anyone else.
Related resources
- Yarlagadda C. Pacemaker failure. www.emedicine.com/med/TOPIC1704.HTM.
- Atracurium • Tracrium
- Citalopram • Celexa
- Esmolol • Brevibloc
- Fluoxetine • Prozac
- Lorazepam • Ativan
- Methylphenidate • Ritalin, Concerta, others
- Nortriptyline • Aventyl, Pamelor, others
- Paroxetine • Paxil
- Sertraline • Zoloft
- Succinylcholine • Anectine
- Trazodone • Desyrel
- Venlafaxine • Effexor
- Ziprasidone • Geodon
Dr. Romanowicz reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Ramaswamy receives research support from Bristol-Myers Squibb, Shire, and Forest Pharmaceuticals and is a consultant to Dainippon Sumitomo Pharma.
1. American Psychiatric Association Committee on ECT. The practice of electroconvulsive therapy: recommendations for treatment, training, and privileging. 2nd ed. Washington, D.C: American Psychiatric Association; 2001.
2. Russell JC, Rasmussen KG, O’Connor MK, et al. Long-term maintenance ECT: a retrospective review of efficacy and cognitive outcome. J ECT. 2003;19(1):4-9.
3. Alexopoulos GS, Shamoian CJ, Lucas J, et al. Medical problems of geriatric psychiatric patients and younger controls during electroconvulsive therapy. J Am Geriatr Soc. 1984;32(9):651-654.
4. Rasmussen KG, Rummans TA, Richardson JR. Electroconvulsive therapy in the medically ill. Psychiatric Clin North Am. 2002;25:177-193.
5. MacPherson RD, Loo CK, Barrett N. Electroconvulsive therapy in patients with cardiac pacemakers. Anaesth Intensive Care. 2006;34(4):470-474.
6. Burke MJ, Husain MM. Concomitant use of vagus nerve stimulation and electroconvulsive therapy for treatment-resistant depression. J ECT. 2006;22(3):218-222.
7. Husain MM, Montgomery JH, Fernandes P, et al. Safety of vagus nerve stimulation with ECT. Am J Psychiatry. 2002;159:1243.-
8. Alexopoulos GS, Frances RJ. ECT and cardiac patients with pacemakers. Am J Psychiatry. 1980;137(9):1111-1112.
9. Stone KR, McPherson CA. Assessment and management of patients with pacemakers and implantable cardioverter defibrillators. Crit Care Med. 2004;32(4 suppl):S155-S165.
10. Maisel WH, Sweeney MO, Stevenson WG, et al. Recalls and safety alerts involving pacemakers and implantable cardioverter-defibrillator generators. JAMA. 2001;286(7):793-799.
11. Gibson TC, Leaman DM, Devors J, et al. Pacemaker function in relation to electroconvulsive therapy. Chest. 1973;63(6):1025-1027.
12. Dolenc TJ, Barnes RD, Hayes DL, et al. Electroconvulsive therapy in patients with cardiac pacemakers and implantable cardioverter defibrillators. Pacing Clin Electrophysiol. 2004;27(9):1257-1263.
13. Lapid MI, Rummans TA, Hofmann VE, et al. ECT and automatic internal cardioverter-defibrillator. J ECT. 2001;17(2):146-148.
CASE: Relapsing depression
Mrs. A, age 41, presents with worsening depression and suicidal ideation with a plan to take an overdose of her medications. She describes herself as “tense, anxious, and worrying all the time.” She reports worsening mood, loss of interest in previously pleasurable activities, lack of energy and drive, and difficulties performing routine household tasks. She also endorses a combination of initial and middle insomnia. According to her husband, the patient has been slow in movement and speech and has not been taking adequate care of herself.
Mrs. A denies auditory or visual hallucinations, thought insertion, thought withdrawal, thought broadcast, ideas of reference, or paranoid ideation. She also denies recent or past symptoms of mania or hypomania.
Mrs. A has a history of alcohol abuse and major depressive disorder. For her first depressive episode 5 years ago, she was treated with paroxetine, 20 to 80 mg/d, with good results. Following a depressive relapse, she was switched to fluoxetine, 80 mg/d, which improved her depressive symptoms. Approximately 2 years later, she experienced another depressive relapse that resulted in hospitalization. During hospitalization and subsequent outpatient visits, she was treated with citalopram, 20 mg/d, ziprasidone, 80 mg bid, and lorazepam, 1 mg tid. Her depressive symptoms were in partial remission for 2 years until her current relapse.
Her medical history includes syncope of unexplained origin, for which she received an implanted cardiac pacemaker 3 years ago. She takes sertraline, 150 mg/d, methylphenidate, 15 mg/d, and trazodone, 200 mg at night. Laboratory testing is unremarkable.
On mental status examination, Mrs. A’s mood is sad and her affect constricted. Her speech is fluent but slow, and she speaks only when spoken to. We note that Mrs. A has thought blocking but no hallucinations or delusions. She is alert and oriented, but her attention and concentration are impaired. Her insight is fair, and judgment is poor.
The authors’ observations
Somatic therapy for severe major depressive disorders has been limited principally to pharmacotherapy. Despite the availability of effective antidepressants and aggressive treatment, for many patients—such as Mrs. A—the course of depression is characterized by relapse, recurrence, and chronicity.1,2
Because Mrs. A has treatment-refractory depression, we decide to treat her with ECT. ECT has few contraindications and typically is well tolerated. It commonly is used to treat depression in patients with cardiac conditions and generally is quite safe in this population.3,4
ECT in patients with cardiac pacemakers in situ theoretically presents an increased risk of complications, however.5 Specific concerns of administering ECT to pacemaker patients include electrical interference from ECT stimulus and pacemaker sensing of:
- myopotentials that originate from succinylcholine-induced fasciculation (muscular twitching of contiguous groups of muscle fibers)
- muscle contractions that result in incomplete muscle paralysis
- dysrhythmias during the seizure.
Skeletal muscle can generate significant electrical potentials that are well within the sensing capabilities of most newer pulse generators. This happens most frequently in some dual-chamber pacemakers that can automatically perform mode switching or adapt their sensing and pacing thresholds to new situations, which might make them more sensitive to interference by ECT.
Similar concerns apply to administering ECT to patients receiving vagus nerve stimulation (VNS) therapy, as both VNS pulse generators and cardiac pacemakers are battery-powered, electrical signal-producing mechanisms housed in a metal case. The safety of concurrent ECT and VNS therapy is unknown (Box).6,7
Although vagus nerve stimulation (VNS) and electroconvulsive therapy (ECT) are not mutually exclusive, the safety of concurrent use of these 2 therapies is uncertain.6 The manufacturer of the VNS device recommends turning off the VNS pulse generator before administering ECT. In at least 1 case report, however, ECT was administered safely without the VNS pulse generator turned off.7
No case reports describe the safety of VNS in patients with an implanted device such as a pacemaker or automatic cardioverter defibrillator. According to the manufacturer, the VNS system may affect the operation of other devices. For VNS patients who require an implantable pacemaker, defibrillator therapy, or other types of stimulators, the VNS manufacturer advises careful programming of each system and implanting the 2 stimulators at least 10 centimeters (4 inches) apart to avoid communication interference.
What the evidence says
In evidence-based medicine, we tend to say: “In God we trust; all the others have to bring their data.” Unfortunately, it is difficult to conduct a trial of patients with multiple medical issues. Based on anecdotal reports, it appears that ECT use in patients with an implanted cardiac device such as a pacemaker or automatic internal cardioverter-defibrillator (AICD) generally is safe.8-12
One case report describes successful administration of ECT in a treatment-refractory depressed patient with an AICD. The AICD was deactivated during ECT and re-activated immediately upon completion of each treatment. The case report’s authors concluded that the presence of an AICD should not be a contraindication to ECT.13
A chart review of 3 patients with ICDs who received concurrent ECT found treatment was generally uneventful.12 One patient developed tachycardia with a rate-dependent left bundle branch block and hypotension in the recovery room, which responded promptly to esmolol. She did not experience similar events after subsequent ECT treatments.
Minimizing risk
In the absence of controlled data about the use of ECT in patients with implanted cardiac devices, crucial therapeutic decisions depend on the physician’s skill and judgment. Risk strategies can minimize complications (Algorithm).12 An internist or cardiologist experienced in pacemaker management should conduct a device interrogation—evaluating thresholds, lead impedance, and battery voltage and reviewing histograms, mode switch episodes, and stored electrograms—before the first ECT session and after the final one.
Most modern implantable pacemakers work in the synchronous (demand), rate-adaptive mode. In a patient in whom non-cardiac electrical signals cause bradycardia or asystole during ECT, the pacemaker can be reprogrammed to be less sensitive by placing a magnet over the pulse generator, which converts the pacemaker to an asynchronous (fixed), non-sensing mode. It is important to keep in mind that magnet application will not “turn off” a pacemaker; although each pacemaker is programmed to respond to a magnet in a specific fashion, the main response is asynchronous pacing.
Careful cardiac monitoring during ECT is essential (Table). The cardiologist or internist should be available during the first few ECT sessions to monitor for potential pacemaker interference or malfunction. This physician should be familiar with the pacemaker model and type of lead system so he or she can deactivate, reactivate, or reprogram the device.
Algorithm
Reducing risk when administering ECT to cardiac pacemaker patients
| Step 1 | |
| Evaluate the patient to ensure medical suitability for ECT and associated anesthesia | |
| Step 2 | ↓ |
| Conduct pacemaker interrogation (evaluating thresholds, lead impedance, and battery voltage and reviewing histograms, mode switch episodes, and stored electrograms) prior to first ECT treatment and after completion of full ECT course | |
| Step 3 | ↓ |
| Perform cardiac monitoring during and immediately after administering ECT | |
| Step 4 | ↓ |
| Have a magnet available to reprogram the pacemaker in the event of pacemaker inhibition or symptomatic bradycardia during ECT | |
| Step 5 | ↓ |
| Check that all monitoring devices are properly grounded, insulate the patient’s stretcher, and ensure that the patient does not touch anyone who is in contact with the ground during presentation of the ECT electrical stimulus | |
| ECT: electroconvulsive therapy | |
| Source: Reference 12 | |
Guidelines for monitoring cardiac pacemaker patients during ECT
| Use multilead ECG monitoring |
| Have equipment available to rapidly obtain central access (if vasoactive medications or transvenous pacing is needed) |
| Assess the plethysmography tracing of the pulse oximeter (a useful surrogate if the patient experiences dysrhythmias) |
| Have ready an external defibrillator |
TREATMENT: Successful ECT
We seek a medical consultation before initiating ECT. An internist performs device interrogation before the first ECT treatment and is present in the ECT treatment suite to ensure proper pacemaker conversion and to monitor for cardiac complications. The internist conducts another device interrogation after the acute series of ECT treatments.
Mrs. A tolerates the ECT sessions without cardiac complications. Her depressive symptoms respond well to 12 ECT sessions. She is more interactive and reports better attention and concentration. Although Mrs. A still has middle and initial insomnia, she denies thoughts of harming herself or anyone else.
Related resources
- Yarlagadda C. Pacemaker failure. www.emedicine.com/med/TOPIC1704.HTM.
- Atracurium • Tracrium
- Citalopram • Celexa
- Esmolol • Brevibloc
- Fluoxetine • Prozac
- Lorazepam • Ativan
- Methylphenidate • Ritalin, Concerta, others
- Nortriptyline • Aventyl, Pamelor, others
- Paroxetine • Paxil
- Sertraline • Zoloft
- Succinylcholine • Anectine
- Trazodone • Desyrel
- Venlafaxine • Effexor
- Ziprasidone • Geodon
Dr. Romanowicz reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Ramaswamy receives research support from Bristol-Myers Squibb, Shire, and Forest Pharmaceuticals and is a consultant to Dainippon Sumitomo Pharma.
CASE: Relapsing depression
Mrs. A, age 41, presents with worsening depression and suicidal ideation with a plan to take an overdose of her medications. She describes herself as “tense, anxious, and worrying all the time.” She reports worsening mood, loss of interest in previously pleasurable activities, lack of energy and drive, and difficulties performing routine household tasks. She also endorses a combination of initial and middle insomnia. According to her husband, the patient has been slow in movement and speech and has not been taking adequate care of herself.
Mrs. A denies auditory or visual hallucinations, thought insertion, thought withdrawal, thought broadcast, ideas of reference, or paranoid ideation. She also denies recent or past symptoms of mania or hypomania.
Mrs. A has a history of alcohol abuse and major depressive disorder. For her first depressive episode 5 years ago, she was treated with paroxetine, 20 to 80 mg/d, with good results. Following a depressive relapse, she was switched to fluoxetine, 80 mg/d, which improved her depressive symptoms. Approximately 2 years later, she experienced another depressive relapse that resulted in hospitalization. During hospitalization and subsequent outpatient visits, she was treated with citalopram, 20 mg/d, ziprasidone, 80 mg bid, and lorazepam, 1 mg tid. Her depressive symptoms were in partial remission for 2 years until her current relapse.
Her medical history includes syncope of unexplained origin, for which she received an implanted cardiac pacemaker 3 years ago. She takes sertraline, 150 mg/d, methylphenidate, 15 mg/d, and trazodone, 200 mg at night. Laboratory testing is unremarkable.
On mental status examination, Mrs. A’s mood is sad and her affect constricted. Her speech is fluent but slow, and she speaks only when spoken to. We note that Mrs. A has thought blocking but no hallucinations or delusions. She is alert and oriented, but her attention and concentration are impaired. Her insight is fair, and judgment is poor.
The authors’ observations
Somatic therapy for severe major depressive disorders has been limited principally to pharmacotherapy. Despite the availability of effective antidepressants and aggressive treatment, for many patients—such as Mrs. A—the course of depression is characterized by relapse, recurrence, and chronicity.1,2
Because Mrs. A has treatment-refractory depression, we decide to treat her with ECT. ECT has few contraindications and typically is well tolerated. It commonly is used to treat depression in patients with cardiac conditions and generally is quite safe in this population.3,4
ECT in patients with cardiac pacemakers in situ theoretically presents an increased risk of complications, however.5 Specific concerns of administering ECT to pacemaker patients include electrical interference from ECT stimulus and pacemaker sensing of:
- myopotentials that originate from succinylcholine-induced fasciculation (muscular twitching of contiguous groups of muscle fibers)
- muscle contractions that result in incomplete muscle paralysis
- dysrhythmias during the seizure.
Skeletal muscle can generate significant electrical potentials that are well within the sensing capabilities of most newer pulse generators. This happens most frequently in some dual-chamber pacemakers that can automatically perform mode switching or adapt their sensing and pacing thresholds to new situations, which might make them more sensitive to interference by ECT.
Similar concerns apply to administering ECT to patients receiving vagus nerve stimulation (VNS) therapy, as both VNS pulse generators and cardiac pacemakers are battery-powered, electrical signal-producing mechanisms housed in a metal case. The safety of concurrent ECT and VNS therapy is unknown (Box).6,7
Although vagus nerve stimulation (VNS) and electroconvulsive therapy (ECT) are not mutually exclusive, the safety of concurrent use of these 2 therapies is uncertain.6 The manufacturer of the VNS device recommends turning off the VNS pulse generator before administering ECT. In at least 1 case report, however, ECT was administered safely without the VNS pulse generator turned off.7
No case reports describe the safety of VNS in patients with an implanted device such as a pacemaker or automatic cardioverter defibrillator. According to the manufacturer, the VNS system may affect the operation of other devices. For VNS patients who require an implantable pacemaker, defibrillator therapy, or other types of stimulators, the VNS manufacturer advises careful programming of each system and implanting the 2 stimulators at least 10 centimeters (4 inches) apart to avoid communication interference.
What the evidence says
In evidence-based medicine, we tend to say: “In God we trust; all the others have to bring their data.” Unfortunately, it is difficult to conduct a trial of patients with multiple medical issues. Based on anecdotal reports, it appears that ECT use in patients with an implanted cardiac device such as a pacemaker or automatic internal cardioverter-defibrillator (AICD) generally is safe.8-12
One case report describes successful administration of ECT in a treatment-refractory depressed patient with an AICD. The AICD was deactivated during ECT and re-activated immediately upon completion of each treatment. The case report’s authors concluded that the presence of an AICD should not be a contraindication to ECT.13
A chart review of 3 patients with ICDs who received concurrent ECT found treatment was generally uneventful.12 One patient developed tachycardia with a rate-dependent left bundle branch block and hypotension in the recovery room, which responded promptly to esmolol. She did not experience similar events after subsequent ECT treatments.
Minimizing risk
In the absence of controlled data about the use of ECT in patients with implanted cardiac devices, crucial therapeutic decisions depend on the physician’s skill and judgment. Risk strategies can minimize complications (Algorithm).12 An internist or cardiologist experienced in pacemaker management should conduct a device interrogation—evaluating thresholds, lead impedance, and battery voltage and reviewing histograms, mode switch episodes, and stored electrograms—before the first ECT session and after the final one.
Most modern implantable pacemakers work in the synchronous (demand), rate-adaptive mode. In a patient in whom non-cardiac electrical signals cause bradycardia or asystole during ECT, the pacemaker can be reprogrammed to be less sensitive by placing a magnet over the pulse generator, which converts the pacemaker to an asynchronous (fixed), non-sensing mode. It is important to keep in mind that magnet application will not “turn off” a pacemaker; although each pacemaker is programmed to respond to a magnet in a specific fashion, the main response is asynchronous pacing.
Careful cardiac monitoring during ECT is essential (Table). The cardiologist or internist should be available during the first few ECT sessions to monitor for potential pacemaker interference or malfunction. This physician should be familiar with the pacemaker model and type of lead system so he or she can deactivate, reactivate, or reprogram the device.
Algorithm
Reducing risk when administering ECT to cardiac pacemaker patients
| Step 1 | |
| Evaluate the patient to ensure medical suitability for ECT and associated anesthesia | |
| Step 2 | ↓ |
| Conduct pacemaker interrogation (evaluating thresholds, lead impedance, and battery voltage and reviewing histograms, mode switch episodes, and stored electrograms) prior to first ECT treatment and after completion of full ECT course | |
| Step 3 | ↓ |
| Perform cardiac monitoring during and immediately after administering ECT | |
| Step 4 | ↓ |
| Have a magnet available to reprogram the pacemaker in the event of pacemaker inhibition or symptomatic bradycardia during ECT | |
| Step 5 | ↓ |
| Check that all monitoring devices are properly grounded, insulate the patient’s stretcher, and ensure that the patient does not touch anyone who is in contact with the ground during presentation of the ECT electrical stimulus | |
| ECT: electroconvulsive therapy | |
| Source: Reference 12 | |
Guidelines for monitoring cardiac pacemaker patients during ECT
| Use multilead ECG monitoring |
| Have equipment available to rapidly obtain central access (if vasoactive medications or transvenous pacing is needed) |
| Assess the plethysmography tracing of the pulse oximeter (a useful surrogate if the patient experiences dysrhythmias) |
| Have ready an external defibrillator |
TREATMENT: Successful ECT
We seek a medical consultation before initiating ECT. An internist performs device interrogation before the first ECT treatment and is present in the ECT treatment suite to ensure proper pacemaker conversion and to monitor for cardiac complications. The internist conducts another device interrogation after the acute series of ECT treatments.
Mrs. A tolerates the ECT sessions without cardiac complications. Her depressive symptoms respond well to 12 ECT sessions. She is more interactive and reports better attention and concentration. Although Mrs. A still has middle and initial insomnia, she denies thoughts of harming herself or anyone else.
Related resources
- Yarlagadda C. Pacemaker failure. www.emedicine.com/med/TOPIC1704.HTM.
- Atracurium • Tracrium
- Citalopram • Celexa
- Esmolol • Brevibloc
- Fluoxetine • Prozac
- Lorazepam • Ativan
- Methylphenidate • Ritalin, Concerta, others
- Nortriptyline • Aventyl, Pamelor, others
- Paroxetine • Paxil
- Sertraline • Zoloft
- Succinylcholine • Anectine
- Trazodone • Desyrel
- Venlafaxine • Effexor
- Ziprasidone • Geodon
Dr. Romanowicz reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Ramaswamy receives research support from Bristol-Myers Squibb, Shire, and Forest Pharmaceuticals and is a consultant to Dainippon Sumitomo Pharma.
1. American Psychiatric Association Committee on ECT. The practice of electroconvulsive therapy: recommendations for treatment, training, and privileging. 2nd ed. Washington, D.C: American Psychiatric Association; 2001.
2. Russell JC, Rasmussen KG, O’Connor MK, et al. Long-term maintenance ECT: a retrospective review of efficacy and cognitive outcome. J ECT. 2003;19(1):4-9.
3. Alexopoulos GS, Shamoian CJ, Lucas J, et al. Medical problems of geriatric psychiatric patients and younger controls during electroconvulsive therapy. J Am Geriatr Soc. 1984;32(9):651-654.
4. Rasmussen KG, Rummans TA, Richardson JR. Electroconvulsive therapy in the medically ill. Psychiatric Clin North Am. 2002;25:177-193.
5. MacPherson RD, Loo CK, Barrett N. Electroconvulsive therapy in patients with cardiac pacemakers. Anaesth Intensive Care. 2006;34(4):470-474.
6. Burke MJ, Husain MM. Concomitant use of vagus nerve stimulation and electroconvulsive therapy for treatment-resistant depression. J ECT. 2006;22(3):218-222.
7. Husain MM, Montgomery JH, Fernandes P, et al. Safety of vagus nerve stimulation with ECT. Am J Psychiatry. 2002;159:1243.-
8. Alexopoulos GS, Frances RJ. ECT and cardiac patients with pacemakers. Am J Psychiatry. 1980;137(9):1111-1112.
9. Stone KR, McPherson CA. Assessment and management of patients with pacemakers and implantable cardioverter defibrillators. Crit Care Med. 2004;32(4 suppl):S155-S165.
10. Maisel WH, Sweeney MO, Stevenson WG, et al. Recalls and safety alerts involving pacemakers and implantable cardioverter-defibrillator generators. JAMA. 2001;286(7):793-799.
11. Gibson TC, Leaman DM, Devors J, et al. Pacemaker function in relation to electroconvulsive therapy. Chest. 1973;63(6):1025-1027.
12. Dolenc TJ, Barnes RD, Hayes DL, et al. Electroconvulsive therapy in patients with cardiac pacemakers and implantable cardioverter defibrillators. Pacing Clin Electrophysiol. 2004;27(9):1257-1263.
13. Lapid MI, Rummans TA, Hofmann VE, et al. ECT and automatic internal cardioverter-defibrillator. J ECT. 2001;17(2):146-148.
1. American Psychiatric Association Committee on ECT. The practice of electroconvulsive therapy: recommendations for treatment, training, and privileging. 2nd ed. Washington, D.C: American Psychiatric Association; 2001.
2. Russell JC, Rasmussen KG, O’Connor MK, et al. Long-term maintenance ECT: a retrospective review of efficacy and cognitive outcome. J ECT. 2003;19(1):4-9.
3. Alexopoulos GS, Shamoian CJ, Lucas J, et al. Medical problems of geriatric psychiatric patients and younger controls during electroconvulsive therapy. J Am Geriatr Soc. 1984;32(9):651-654.
4. Rasmussen KG, Rummans TA, Richardson JR. Electroconvulsive therapy in the medically ill. Psychiatric Clin North Am. 2002;25:177-193.
5. MacPherson RD, Loo CK, Barrett N. Electroconvulsive therapy in patients with cardiac pacemakers. Anaesth Intensive Care. 2006;34(4):470-474.
6. Burke MJ, Husain MM. Concomitant use of vagus nerve stimulation and electroconvulsive therapy for treatment-resistant depression. J ECT. 2006;22(3):218-222.
7. Husain MM, Montgomery JH, Fernandes P, et al. Safety of vagus nerve stimulation with ECT. Am J Psychiatry. 2002;159:1243.-
8. Alexopoulos GS, Frances RJ. ECT and cardiac patients with pacemakers. Am J Psychiatry. 1980;137(9):1111-1112.
9. Stone KR, McPherson CA. Assessment and management of patients with pacemakers and implantable cardioverter defibrillators. Crit Care Med. 2004;32(4 suppl):S155-S165.
10. Maisel WH, Sweeney MO, Stevenson WG, et al. Recalls and safety alerts involving pacemakers and implantable cardioverter-defibrillator generators. JAMA. 2001;286(7):793-799.
11. Gibson TC, Leaman DM, Devors J, et al. Pacemaker function in relation to electroconvulsive therapy. Chest. 1973;63(6):1025-1027.
12. Dolenc TJ, Barnes RD, Hayes DL, et al. Electroconvulsive therapy in patients with cardiac pacemakers and implantable cardioverter defibrillators. Pacing Clin Electrophysiol. 2004;27(9):1257-1263.
13. Lapid MI, Rummans TA, Hofmann VE, et al. ECT and automatic internal cardioverter-defibrillator. J ECT. 2001;17(2):146-148.
A mysterious physical and mental decline
HISTORY: ‘Not himself’
Mr. C, age 69, presents to the emergency department complaining of intermittent fever of about 100°F, hematuria, headache, weakness, fatigue, and decreased appetite over 2 months. Testing shows acute renal failure, elevated C-reactive protein, and increased sedimentation rate. The attending internist admits Mr. C with a working diagnosis of temporal arteritis and acute renal failure, administers corticosteroids for headache, and orders a right temporal artery biopsy, which shows no signs of vasculitis.
Family members report that Mr. C has not been himself—he has become increasingly withdrawn and “emotionless.” Mr. C’s wife says her husband has needed help with dressing and eating because of short-term memory loss over 9 months. She says he has lost 20 to 30 lb.
The patient’s cognitive function appears to have worsened since he developed these physical symptoms. Mrs. C also reports that he has had weakness and fatigue for 8 months.
One month earlier, the patient was admitted to a different hospital and treated for 2 weeks with IV antibiotics for fever of unknown origin. Results of lumbar puncture and extensive rheumatologic, infectious disease, urologic, and gastroenterologic evaluations were normal.
The internal medicine physician requests a psychiatric consultation. During our interview, Mr. C is cooperative, shows no signs of acute distress, is well groomed and dressed appropriately, and maintains eye contact. Speech rate and volume are low, with normal articulation and coherence, diminished spontaneity, and paucity of language. Mrs. C tells us her husband was lively and talkative before his recent illness. His mood is euthymic, and he is pleasant and cheerful during the evaluation.
The authors’ observations
Initially, we suspect an underlying medical condition is causing Mr. C’s psychiatric symptoms.
Mr. C’s wife reports that her husband stopped drinking 2 years ago after his family expressed concern about his health. Mr. C’s past alcohol use could not be quantified. He has not abused illicit drugs and has no personal or family history of dementia, trauma, or psychiatric or neurologic disorders.
EVALUATION: Impaired memory
Mr. C is afebrile during the initial physical examination, but fever returns within several days. Neurologic examination is normal, and negative rapid plasma reagin rules out syphilis. Vitamin B12 and folate levels are normal, as is thyroid function. Other laboratory findings are outside normal limits (Table).
Urine is cloudy with 2+ protein, 3+ blood, and trace leukocyte esterase. The presence of protein and blood suggests a glomerular disease such as a glomerulonephritis.
A positive leukocyte esterase test results from the presence of white blood cells, either as whole cells or as lysed cells. An abnormal number of leukocytes may appear with upper or lower urinary tract infection or in acute glomerulonephritis.
Chest radiography shows increased bilateral pulmonary vasculature, which can indicate pulmonary hypertension.
Mr. C has fair attention and concentration but impaired recent memory. He cannot recall yesterday’s events without help.
Mr. C’s Mini-Mental State Examination score of 21/30 suggests markedly impaired executive functioning and cognitive deficits. The attending psychiatrist recommends brain MRI.
Table
Mr. C’s laboratory findings
| Value | Normal range | |
|---|---|---|
| WBC | 15.1 | 4.8 to 10.8 cells/μL |
| Hb | 9 | 13.8 to 17.5 g/dL |
| Hct | 25.9% | 40% to 54% |
| MCV | 89.7 | 80 to 94 fL |
| BUN | 119 | 7 to 18 mg/dL |
| Cr | 12.1 | 0.7 to 1.3 mg/dL |
| Na | 125 | 136 to 145 mmol/L |
| K | 6.5 | 3.5 to 5 mEq/dL |
| HCO3 | 13.5 | 22 to 29 mmol/L |
| ECR | 125 | 30 mm/hr |
| WBC: white blood cell; Hb: hemoglobin; Hct: hematocrit; MCV: mean corpuscular volume; BUN: blood urea nitrogen; Cr: creatinine; Na: sodium; K: potassium; HCO3: bicarbonate; ESR: erythrocyte sedimentation rate | ||
The authors’ observations
Mr. C shows markedly impaired cognitive function without significant impairment of attention and concentration despite his progressive deterioration and increasing disability. Urine toxicology shows no illicit substances. Given his lack of a previous mood disorder and his family’s description of him as formerly vibrant and cheerful, he likely does not have a mood disorder.
Based on the history of events, including the symptom pattern, we rule out delirium. We suspect that Mr. C has dementia secondary to a general medical condition. His symptoms seem to be directly related to his medical complaints and do not have a waxing and waning course. The internal medicine physician orders additional laboratory tests.
TESTING: Kidney, lung damage
Over 5 days, Mr. C’s intermittent low-grade fevers continue. Laboratory tests are negative for HIV antibody, hepatitis panel, and antinuclear antibodies (ANA). C-reactive protein is elevated at 27.8 mg/dL (normal range,
Renal ultrasound is normal, but preliminary renal biopsy shows rapidly progressive glomerulonephritis. The internist immediately starts dialysis, cyclophosphamide at 1.5 mg/kg, and prednisone, 1 mg/kg. The pathology report on the renal biopsy describes extensive crescentic glomerular destruction, with inflammatory cells present.
Ten days after admission, Mr. C develops hemoptysis, and chest radiography shows increasing alveolar infiltrates. The attending internist consults pulmonary and critical care services.
The consultant suspects a pulmonary-renal syndrome because of bilateral alveolar infiltrates (diffuse alveolar hemorrhage). The internal medicine team continues high-dose corticosteroids, followed by plasmapheresis.
Brain MRI shows subacute to chronic infarcts involving the right basal ganglia and corona radiate and mild to moderate small vessel ischemic changes. Old areas of hemorrhage are noted within both cerebellar lobes, left temporal lobe, right basal ganglia, right parietal lobe, and right frontal lobe.
During follow-up interviews, Mr. C often cannot recall recent dialysis or plasmapheresis and reports no physical symptoms. His short-term memory continues to deteriorate; he would forget to eat if not cued by family or nursing staff. He shows global cognitive deficits and is increasingly withdrawn and flat.
The authors’ observations
Although few case reports have associated Goodpasture’s syndrome with neurobehavioral changes, the apparent relationship of Mr. C’s medical symptoms with the worsening of his cognitive impairment suggests a link.
Mr. C’s MRI findings also might suggest CNS vasculitis, which affects small arteries of the cerebral and spinal cord leptomeninges and parenchyma, leading to CNS dys-function.6-8 CNS vasculitis can result from primary nervous system involvement or from a secondary systemic process such as Goodpasture’s syndrome.9
We rule out lupus because Mr. C is ANA-negative; this test has 99% sensitivity for lupus.10
Goodpasture’s syndrome, which afflicts 1 Patients typically present with alveolar bleeding, rapidly progressive acute renal failure with proteinuria,1 and pulmonary symptoms such as dyspnea and hemoptysis.2
Possible triggers include:
- viral upper respiratory tract infection (20% to 60% of patients)3
- exposure to hydrocarbon solvents (3,4
Mr. C was exposed to solvents during the 15 years he worked in a factory. Some researchers believe a noxious event among genetically susceptible persons damages basement membrane and exposes an antigen that triggers IgG auto-antibody production.3,4
Malaise, weight loss, and fever are atypical in Goodpasture’s syndrome but could suggest concomitant vasculitis.5
OUTCOME: Ongoing disability
Mr. C is hospitalized for 6 weeks. He receives cyclophosphamide, prednisone, and 10 sessions of plasmapheresis. We prescribe mirtazapine, 15 mg at bedtime, to treat mood symptoms. We chose mirtazapine because of the drug’s sleep-restoring and appetite-stimulating properties.
Mr. C’s fever resolves and pulmonary function soon improves, but his cognitive impairment persists. He has difficulties preparing meals, taking medications, and managing his money.
Mr. C is discharged with a referral to a psychiatrist. He continues taking mirtazapine and a lower dose of prednisone. He requires ongoing hemodialysis and assistance with activities of daily living.
The authors’ observations
Prompt multidisciplinary intervention is critical when patients present with concurrent cognitive and medical symptoms. A thorough psychiatric evaluation can help piece together the illness’ course. The psychiatrist’s role in a multidisciplinary assessment is to:
- document neurocognitive changes
- verify them through collateral information
- correlate these changes with the timing of medical symptoms.
An underlying psychiatric condition can complicate the diagnosis. In these cases, careful interviewing and collateral information can help you discern the chronology of events.
1. Bolton WK. Goodpasture’s syndrome. Kidney Int 1996;50(5):1753-66.
2. Pusey CD. Anti-glomerular basement membrane disease. Kidney Int 2003;64(4):1535-50.
3. Humes HD, DuPont HL. eds. Kelley’s textbook of internal medicine. 4th ed. New York, NY: Lippincott Williams & Wilkins; 2000.
4. Stevenson A, Yaqoob M, Mason H, et al. Biochemical markers of basement membrane disturbances and occupational exposure to hydrocarbons and mixed solvents. QJM 1995;88(1):23-8.
5. Kluth DC, Rees AJ. Anti-glomerular basement membrane disease. J Am Soc Nephrol. 1999;10(11):2446-53.
6. Rydel JJ, Rodby RA. An 18-year-old man with Goodpasture’s syndrome and ANCA-negative central nervous system vasculitis. Am J Kidney Dis 1998;31(2):345-9.
7. Gittins N, Basu A, Eyre J, et al. Cerebral vasculitis in a teenager with Goodpasture’s syndrome. Nephrol Dial Transplant 2004;19(12):3168-71.
8. Garnier P, Deprele C. Cerebral angiitis and Goodpasture’s syndrome. Rev Neurol 2003;159(1):68-70.
9. Calabrese LH, Duna GF, Lie JT. Vasculitis in the central nervous system. Arthritis Rhem 1997;40(7):1189-201.
10. Edworthy SM, Zatarain E, McShane DJ, Bloch DA. Analysis of the 1982 ARA lupus criteria data set by recursive partitioning methodology: new insights into the relative merit of individual criteria. J Rheumatol 1988;15(10):1493-8.
HISTORY: ‘Not himself’
Mr. C, age 69, presents to the emergency department complaining of intermittent fever of about 100°F, hematuria, headache, weakness, fatigue, and decreased appetite over 2 months. Testing shows acute renal failure, elevated C-reactive protein, and increased sedimentation rate. The attending internist admits Mr. C with a working diagnosis of temporal arteritis and acute renal failure, administers corticosteroids for headache, and orders a right temporal artery biopsy, which shows no signs of vasculitis.
Family members report that Mr. C has not been himself—he has become increasingly withdrawn and “emotionless.” Mr. C’s wife says her husband has needed help with dressing and eating because of short-term memory loss over 9 months. She says he has lost 20 to 30 lb.
The patient’s cognitive function appears to have worsened since he developed these physical symptoms. Mrs. C also reports that he has had weakness and fatigue for 8 months.
One month earlier, the patient was admitted to a different hospital and treated for 2 weeks with IV antibiotics for fever of unknown origin. Results of lumbar puncture and extensive rheumatologic, infectious disease, urologic, and gastroenterologic evaluations were normal.
The internal medicine physician requests a psychiatric consultation. During our interview, Mr. C is cooperative, shows no signs of acute distress, is well groomed and dressed appropriately, and maintains eye contact. Speech rate and volume are low, with normal articulation and coherence, diminished spontaneity, and paucity of language. Mrs. C tells us her husband was lively and talkative before his recent illness. His mood is euthymic, and he is pleasant and cheerful during the evaluation.
The authors’ observations
Initially, we suspect an underlying medical condition is causing Mr. C’s psychiatric symptoms.
Mr. C’s wife reports that her husband stopped drinking 2 years ago after his family expressed concern about his health. Mr. C’s past alcohol use could not be quantified. He has not abused illicit drugs and has no personal or family history of dementia, trauma, or psychiatric or neurologic disorders.
EVALUATION: Impaired memory
Mr. C is afebrile during the initial physical examination, but fever returns within several days. Neurologic examination is normal, and negative rapid plasma reagin rules out syphilis. Vitamin B12 and folate levels are normal, as is thyroid function. Other laboratory findings are outside normal limits (Table).
Urine is cloudy with 2+ protein, 3+ blood, and trace leukocyte esterase. The presence of protein and blood suggests a glomerular disease such as a glomerulonephritis.
A positive leukocyte esterase test results from the presence of white blood cells, either as whole cells or as lysed cells. An abnormal number of leukocytes may appear with upper or lower urinary tract infection or in acute glomerulonephritis.
Chest radiography shows increased bilateral pulmonary vasculature, which can indicate pulmonary hypertension.
Mr. C has fair attention and concentration but impaired recent memory. He cannot recall yesterday’s events without help.
Mr. C’s Mini-Mental State Examination score of 21/30 suggests markedly impaired executive functioning and cognitive deficits. The attending psychiatrist recommends brain MRI.
Table
Mr. C’s laboratory findings
| Value | Normal range | |
|---|---|---|
| WBC | 15.1 | 4.8 to 10.8 cells/μL |
| Hb | 9 | 13.8 to 17.5 g/dL |
| Hct | 25.9% | 40% to 54% |
| MCV | 89.7 | 80 to 94 fL |
| BUN | 119 | 7 to 18 mg/dL |
| Cr | 12.1 | 0.7 to 1.3 mg/dL |
| Na | 125 | 136 to 145 mmol/L |
| K | 6.5 | 3.5 to 5 mEq/dL |
| HCO3 | 13.5 | 22 to 29 mmol/L |
| ECR | 125 | 30 mm/hr |
| WBC: white blood cell; Hb: hemoglobin; Hct: hematocrit; MCV: mean corpuscular volume; BUN: blood urea nitrogen; Cr: creatinine; Na: sodium; K: potassium; HCO3: bicarbonate; ESR: erythrocyte sedimentation rate | ||
The authors’ observations
Mr. C shows markedly impaired cognitive function without significant impairment of attention and concentration despite his progressive deterioration and increasing disability. Urine toxicology shows no illicit substances. Given his lack of a previous mood disorder and his family’s description of him as formerly vibrant and cheerful, he likely does not have a mood disorder.
Based on the history of events, including the symptom pattern, we rule out delirium. We suspect that Mr. C has dementia secondary to a general medical condition. His symptoms seem to be directly related to his medical complaints and do not have a waxing and waning course. The internal medicine physician orders additional laboratory tests.
TESTING: Kidney, lung damage
Over 5 days, Mr. C’s intermittent low-grade fevers continue. Laboratory tests are negative for HIV antibody, hepatitis panel, and antinuclear antibodies (ANA). C-reactive protein is elevated at 27.8 mg/dL (normal range,
Renal ultrasound is normal, but preliminary renal biopsy shows rapidly progressive glomerulonephritis. The internist immediately starts dialysis, cyclophosphamide at 1.5 mg/kg, and prednisone, 1 mg/kg. The pathology report on the renal biopsy describes extensive crescentic glomerular destruction, with inflammatory cells present.
Ten days after admission, Mr. C develops hemoptysis, and chest radiography shows increasing alveolar infiltrates. The attending internist consults pulmonary and critical care services.
The consultant suspects a pulmonary-renal syndrome because of bilateral alveolar infiltrates (diffuse alveolar hemorrhage). The internal medicine team continues high-dose corticosteroids, followed by plasmapheresis.
Brain MRI shows subacute to chronic infarcts involving the right basal ganglia and corona radiate and mild to moderate small vessel ischemic changes. Old areas of hemorrhage are noted within both cerebellar lobes, left temporal lobe, right basal ganglia, right parietal lobe, and right frontal lobe.
During follow-up interviews, Mr. C often cannot recall recent dialysis or plasmapheresis and reports no physical symptoms. His short-term memory continues to deteriorate; he would forget to eat if not cued by family or nursing staff. He shows global cognitive deficits and is increasingly withdrawn and flat.
The authors’ observations
Although few case reports have associated Goodpasture’s syndrome with neurobehavioral changes, the apparent relationship of Mr. C’s medical symptoms with the worsening of his cognitive impairment suggests a link.
Mr. C’s MRI findings also might suggest CNS vasculitis, which affects small arteries of the cerebral and spinal cord leptomeninges and parenchyma, leading to CNS dys-function.6-8 CNS vasculitis can result from primary nervous system involvement or from a secondary systemic process such as Goodpasture’s syndrome.9
We rule out lupus because Mr. C is ANA-negative; this test has 99% sensitivity for lupus.10
Goodpasture’s syndrome, which afflicts 1 Patients typically present with alveolar bleeding, rapidly progressive acute renal failure with proteinuria,1 and pulmonary symptoms such as dyspnea and hemoptysis.2
Possible triggers include:
- viral upper respiratory tract infection (20% to 60% of patients)3
- exposure to hydrocarbon solvents (3,4
Mr. C was exposed to solvents during the 15 years he worked in a factory. Some researchers believe a noxious event among genetically susceptible persons damages basement membrane and exposes an antigen that triggers IgG auto-antibody production.3,4
Malaise, weight loss, and fever are atypical in Goodpasture’s syndrome but could suggest concomitant vasculitis.5
OUTCOME: Ongoing disability
Mr. C is hospitalized for 6 weeks. He receives cyclophosphamide, prednisone, and 10 sessions of plasmapheresis. We prescribe mirtazapine, 15 mg at bedtime, to treat mood symptoms. We chose mirtazapine because of the drug’s sleep-restoring and appetite-stimulating properties.
Mr. C’s fever resolves and pulmonary function soon improves, but his cognitive impairment persists. He has difficulties preparing meals, taking medications, and managing his money.
Mr. C is discharged with a referral to a psychiatrist. He continues taking mirtazapine and a lower dose of prednisone. He requires ongoing hemodialysis and assistance with activities of daily living.
The authors’ observations
Prompt multidisciplinary intervention is critical when patients present with concurrent cognitive and medical symptoms. A thorough psychiatric evaluation can help piece together the illness’ course. The psychiatrist’s role in a multidisciplinary assessment is to:
- document neurocognitive changes
- verify them through collateral information
- correlate these changes with the timing of medical symptoms.
An underlying psychiatric condition can complicate the diagnosis. In these cases, careful interviewing and collateral information can help you discern the chronology of events.
HISTORY: ‘Not himself’
Mr. C, age 69, presents to the emergency department complaining of intermittent fever of about 100°F, hematuria, headache, weakness, fatigue, and decreased appetite over 2 months. Testing shows acute renal failure, elevated C-reactive protein, and increased sedimentation rate. The attending internist admits Mr. C with a working diagnosis of temporal arteritis and acute renal failure, administers corticosteroids for headache, and orders a right temporal artery biopsy, which shows no signs of vasculitis.
Family members report that Mr. C has not been himself—he has become increasingly withdrawn and “emotionless.” Mr. C’s wife says her husband has needed help with dressing and eating because of short-term memory loss over 9 months. She says he has lost 20 to 30 lb.
The patient’s cognitive function appears to have worsened since he developed these physical symptoms. Mrs. C also reports that he has had weakness and fatigue for 8 months.
One month earlier, the patient was admitted to a different hospital and treated for 2 weeks with IV antibiotics for fever of unknown origin. Results of lumbar puncture and extensive rheumatologic, infectious disease, urologic, and gastroenterologic evaluations were normal.
The internal medicine physician requests a psychiatric consultation. During our interview, Mr. C is cooperative, shows no signs of acute distress, is well groomed and dressed appropriately, and maintains eye contact. Speech rate and volume are low, with normal articulation and coherence, diminished spontaneity, and paucity of language. Mrs. C tells us her husband was lively and talkative before his recent illness. His mood is euthymic, and he is pleasant and cheerful during the evaluation.
The authors’ observations
Initially, we suspect an underlying medical condition is causing Mr. C’s psychiatric symptoms.
Mr. C’s wife reports that her husband stopped drinking 2 years ago after his family expressed concern about his health. Mr. C’s past alcohol use could not be quantified. He has not abused illicit drugs and has no personal or family history of dementia, trauma, or psychiatric or neurologic disorders.
EVALUATION: Impaired memory
Mr. C is afebrile during the initial physical examination, but fever returns within several days. Neurologic examination is normal, and negative rapid plasma reagin rules out syphilis. Vitamin B12 and folate levels are normal, as is thyroid function. Other laboratory findings are outside normal limits (Table).
Urine is cloudy with 2+ protein, 3+ blood, and trace leukocyte esterase. The presence of protein and blood suggests a glomerular disease such as a glomerulonephritis.
A positive leukocyte esterase test results from the presence of white blood cells, either as whole cells or as lysed cells. An abnormal number of leukocytes may appear with upper or lower urinary tract infection or in acute glomerulonephritis.
Chest radiography shows increased bilateral pulmonary vasculature, which can indicate pulmonary hypertension.
Mr. C has fair attention and concentration but impaired recent memory. He cannot recall yesterday’s events without help.
Mr. C’s Mini-Mental State Examination score of 21/30 suggests markedly impaired executive functioning and cognitive deficits. The attending psychiatrist recommends brain MRI.
Table
Mr. C’s laboratory findings
| Value | Normal range | |
|---|---|---|
| WBC | 15.1 | 4.8 to 10.8 cells/μL |
| Hb | 9 | 13.8 to 17.5 g/dL |
| Hct | 25.9% | 40% to 54% |
| MCV | 89.7 | 80 to 94 fL |
| BUN | 119 | 7 to 18 mg/dL |
| Cr | 12.1 | 0.7 to 1.3 mg/dL |
| Na | 125 | 136 to 145 mmol/L |
| K | 6.5 | 3.5 to 5 mEq/dL |
| HCO3 | 13.5 | 22 to 29 mmol/L |
| ECR | 125 | 30 mm/hr |
| WBC: white blood cell; Hb: hemoglobin; Hct: hematocrit; MCV: mean corpuscular volume; BUN: blood urea nitrogen; Cr: creatinine; Na: sodium; K: potassium; HCO3: bicarbonate; ESR: erythrocyte sedimentation rate | ||
The authors’ observations
Mr. C shows markedly impaired cognitive function without significant impairment of attention and concentration despite his progressive deterioration and increasing disability. Urine toxicology shows no illicit substances. Given his lack of a previous mood disorder and his family’s description of him as formerly vibrant and cheerful, he likely does not have a mood disorder.
Based on the history of events, including the symptom pattern, we rule out delirium. We suspect that Mr. C has dementia secondary to a general medical condition. His symptoms seem to be directly related to his medical complaints and do not have a waxing and waning course. The internal medicine physician orders additional laboratory tests.
TESTING: Kidney, lung damage
Over 5 days, Mr. C’s intermittent low-grade fevers continue. Laboratory tests are negative for HIV antibody, hepatitis panel, and antinuclear antibodies (ANA). C-reactive protein is elevated at 27.8 mg/dL (normal range,
Renal ultrasound is normal, but preliminary renal biopsy shows rapidly progressive glomerulonephritis. The internist immediately starts dialysis, cyclophosphamide at 1.5 mg/kg, and prednisone, 1 mg/kg. The pathology report on the renal biopsy describes extensive crescentic glomerular destruction, with inflammatory cells present.
Ten days after admission, Mr. C develops hemoptysis, and chest radiography shows increasing alveolar infiltrates. The attending internist consults pulmonary and critical care services.
The consultant suspects a pulmonary-renal syndrome because of bilateral alveolar infiltrates (diffuse alveolar hemorrhage). The internal medicine team continues high-dose corticosteroids, followed by plasmapheresis.
Brain MRI shows subacute to chronic infarcts involving the right basal ganglia and corona radiate and mild to moderate small vessel ischemic changes. Old areas of hemorrhage are noted within both cerebellar lobes, left temporal lobe, right basal ganglia, right parietal lobe, and right frontal lobe.
During follow-up interviews, Mr. C often cannot recall recent dialysis or plasmapheresis and reports no physical symptoms. His short-term memory continues to deteriorate; he would forget to eat if not cued by family or nursing staff. He shows global cognitive deficits and is increasingly withdrawn and flat.
The authors’ observations
Although few case reports have associated Goodpasture’s syndrome with neurobehavioral changes, the apparent relationship of Mr. C’s medical symptoms with the worsening of his cognitive impairment suggests a link.
Mr. C’s MRI findings also might suggest CNS vasculitis, which affects small arteries of the cerebral and spinal cord leptomeninges and parenchyma, leading to CNS dys-function.6-8 CNS vasculitis can result from primary nervous system involvement or from a secondary systemic process such as Goodpasture’s syndrome.9
We rule out lupus because Mr. C is ANA-negative; this test has 99% sensitivity for lupus.10
Goodpasture’s syndrome, which afflicts 1 Patients typically present with alveolar bleeding, rapidly progressive acute renal failure with proteinuria,1 and pulmonary symptoms such as dyspnea and hemoptysis.2
Possible triggers include:
- viral upper respiratory tract infection (20% to 60% of patients)3
- exposure to hydrocarbon solvents (3,4
Mr. C was exposed to solvents during the 15 years he worked in a factory. Some researchers believe a noxious event among genetically susceptible persons damages basement membrane and exposes an antigen that triggers IgG auto-antibody production.3,4
Malaise, weight loss, and fever are atypical in Goodpasture’s syndrome but could suggest concomitant vasculitis.5
OUTCOME: Ongoing disability
Mr. C is hospitalized for 6 weeks. He receives cyclophosphamide, prednisone, and 10 sessions of plasmapheresis. We prescribe mirtazapine, 15 mg at bedtime, to treat mood symptoms. We chose mirtazapine because of the drug’s sleep-restoring and appetite-stimulating properties.
Mr. C’s fever resolves and pulmonary function soon improves, but his cognitive impairment persists. He has difficulties preparing meals, taking medications, and managing his money.
Mr. C is discharged with a referral to a psychiatrist. He continues taking mirtazapine and a lower dose of prednisone. He requires ongoing hemodialysis and assistance with activities of daily living.
The authors’ observations
Prompt multidisciplinary intervention is critical when patients present with concurrent cognitive and medical symptoms. A thorough psychiatric evaluation can help piece together the illness’ course. The psychiatrist’s role in a multidisciplinary assessment is to:
- document neurocognitive changes
- verify them through collateral information
- correlate these changes with the timing of medical symptoms.
An underlying psychiatric condition can complicate the diagnosis. In these cases, careful interviewing and collateral information can help you discern the chronology of events.
1. Bolton WK. Goodpasture’s syndrome. Kidney Int 1996;50(5):1753-66.
2. Pusey CD. Anti-glomerular basement membrane disease. Kidney Int 2003;64(4):1535-50.
3. Humes HD, DuPont HL. eds. Kelley’s textbook of internal medicine. 4th ed. New York, NY: Lippincott Williams & Wilkins; 2000.
4. Stevenson A, Yaqoob M, Mason H, et al. Biochemical markers of basement membrane disturbances and occupational exposure to hydrocarbons and mixed solvents. QJM 1995;88(1):23-8.
5. Kluth DC, Rees AJ. Anti-glomerular basement membrane disease. J Am Soc Nephrol. 1999;10(11):2446-53.
6. Rydel JJ, Rodby RA. An 18-year-old man with Goodpasture’s syndrome and ANCA-negative central nervous system vasculitis. Am J Kidney Dis 1998;31(2):345-9.
7. Gittins N, Basu A, Eyre J, et al. Cerebral vasculitis in a teenager with Goodpasture’s syndrome. Nephrol Dial Transplant 2004;19(12):3168-71.
8. Garnier P, Deprele C. Cerebral angiitis and Goodpasture’s syndrome. Rev Neurol 2003;159(1):68-70.
9. Calabrese LH, Duna GF, Lie JT. Vasculitis in the central nervous system. Arthritis Rhem 1997;40(7):1189-201.
10. Edworthy SM, Zatarain E, McShane DJ, Bloch DA. Analysis of the 1982 ARA lupus criteria data set by recursive partitioning methodology: new insights into the relative merit of individual criteria. J Rheumatol 1988;15(10):1493-8.
1. Bolton WK. Goodpasture’s syndrome. Kidney Int 1996;50(5):1753-66.
2. Pusey CD. Anti-glomerular basement membrane disease. Kidney Int 2003;64(4):1535-50.
3. Humes HD, DuPont HL. eds. Kelley’s textbook of internal medicine. 4th ed. New York, NY: Lippincott Williams & Wilkins; 2000.
4. Stevenson A, Yaqoob M, Mason H, et al. Biochemical markers of basement membrane disturbances and occupational exposure to hydrocarbons and mixed solvents. QJM 1995;88(1):23-8.
5. Kluth DC, Rees AJ. Anti-glomerular basement membrane disease. J Am Soc Nephrol. 1999;10(11):2446-53.
6. Rydel JJ, Rodby RA. An 18-year-old man with Goodpasture’s syndrome and ANCA-negative central nervous system vasculitis. Am J Kidney Dis 1998;31(2):345-9.
7. Gittins N, Basu A, Eyre J, et al. Cerebral vasculitis in a teenager with Goodpasture’s syndrome. Nephrol Dial Transplant 2004;19(12):3168-71.
8. Garnier P, Deprele C. Cerebral angiitis and Goodpasture’s syndrome. Rev Neurol 2003;159(1):68-70.
9. Calabrese LH, Duna GF, Lie JT. Vasculitis in the central nervous system. Arthritis Rhem 1997;40(7):1189-201.
10. Edworthy SM, Zatarain E, McShane DJ, Bloch DA. Analysis of the 1982 ARA lupus criteria data set by recursive partitioning methodology: new insights into the relative merit of individual criteria. J Rheumatol 1988;15(10):1493-8.
The inexplicably suicidal patient
CASE: Confused and suicidal
Mr. A, age 39, becomes disoriented while walking and approaches a suspension bridge. He borrows a passerby’s cell phone and calls his sister. His sister later states that he was confused and expressed his final goodbyes, saying, “I will see Mom in heaven.” He gives back the phone and leaps of the bridge. A nearby boat rescues him almost immediately.
Mr. A is brought to the trauma unit, where he is treated for a lacerated liver. After he is stabilized, Mr. A is awake and answering questions appropriately. He is placed on suicide precautions and direct 24-hour, one-to-one supervision. Our psychiatric team evaluates him.
Mr. A reports no history of diabetes, hypertension, cardiac disorders, or neurologic disorders, but does have a history of cognitive developmental delay. He has no history of psychiatric illness, suicide attempts, or self-injurious behavior. He denies a psychiatric family history or using alcohol, tobacco, or illicit drugs; drug screen is negative. He is unemployed, collects disability, and lives with his sister.
The authors’ observations
In our initial evaluation, we find no obvious reason for Mr. A’s confusion or suicide attempt. We decide to closely review Mr. A’s history in the days leading up to his jumping off the bridge.
HISTORY: Otitis media treatment
Mr. A has a history of chronic otitis media and sought treatment for ear pain at a local emergency room (ER) 10 days before his suicide attempt. He was prescribed amoxicillin, 500 mg tid for 10 days, and meclizine, 25 mg every 8 hours as needed for dizziness.
Immediately after his first dose of both drugs, the patient told his family he was feeling “weird,” but denied being dizzy. Thinking the unusual feeling was from meclizine, Mr. A stopped taking it but continued amoxicillin. On the second day of amoxicillin, he noticed bouts of confusion. He could perform his daily activities, but with difficulty. Mr. A’s niece said he had to ask for help with minor tasks, such as opening a can of soup.
On day 3, Mr. A developed prominent auditory hallucinations. He described hearing unrecognizable male and female voices chattering and mumbling throughout the day. The voices and confusion progressively worsened, but Mr. A continued taking the antibiotic and did not mention the voices to his family.
Mr. A’s sister reports that in a phone conversation with her brother on day 7, “he wasn’t himself…he was talking about my sister and mother but what he said didn’t make sense.” She asked a neighbor to check on Mr. A; he reported that Mr. A was “OK.” On the final day of amoxicillin—day 10—Mr. A became increasingly agitated. He says us that shortly before wandering onto the bridge and jumping, he was having a difficult time dealing with the voices and confusion.
We suspect amoxicillin might have been responsible for Mr. A’s psychotic symptoms.
The authors’ observations
Treatment modalities and pharmaceutical approaches used to treat infectious diseases carry many potential adverse effects. When a patient presents with new-onset psychiatric symptoms, explore whether they are related to an underlying mood disorder or medication side effects. Three important considerations are to:
- determine whether the condition is reversible by discontinuing a drug
- identify and characterize previously unrecognized adverse drug effects
- avoid inaccurate diagnosis that leads to nonindicated psychiatric treatment.1
Antibiotic side effects vary, depending on the particular drug and its target bacteria. The most common are gastrointestinal, such as upset stomach and diarrhea. Antibiotics also can induce an anaphylactic reaction ranging from mild (pruritic rash or slight wheezing) to life-threatening (swelling of the throat, difficulty breathing, and hypotension).
Several classes of antibiotics have psychiatric side effects that range from minor confusion and irritability to severe encephalopathy and suicide (Table 1).2 Case reports have described psychotic symptoms associated with cotrimoxazole,3 trimethoprim/sulfamethoxazole,4 and ciprofloxacin.5 An older review found that amoxicillin is among the top 10 most commonly prescribed medications associated with psychiatric side effects.1
Table 1
Potential psychiatric effects of antibiotics
| Medication | Side effects |
|---|---|
| Antibacterials | |
| Penicillins | Encephalopathy, irritability, sedation, anxiety, hallucinations |
| Cephalosporins | Sleep disturbances, hallucinations |
| Cycloserine | Dose-dependent side effects, depression, irritability, psychosis |
| Quinolones | Sleep and mood disorders, psychosis |
| Nitrofurans | Euphoria, psychosis, sleep disturbances |
| Tetracyclines | Decreased concentration, mood and sleep disorders |
| Chloramphenicol | Depression |
| Trimethoprim, sulfonamides | Depression, psychosis |
| Antimycobacterials | |
| Isoniazid | Cognitive impairment, mood disorder, psychosis |
| Clofazimine | Major depression, suicide |
| Rifampin | Sedation |
| Ethionamide | Sedation, irritability, agitation, depression, psychosis |
| Ganciclovir | Sleep disturbances, anxiety, mood disorders, psychosis |
| Antifungals | |
| Amphotericin B | Delirium |
| Ketoconazole | Decreased libido, mood disorders, psychosis |
| Flucytosine | Sedation, hallucinations |
| Griseofulvin | Depression, psychosis, sleep disturbances |
| Source: Turjanski N, Lloyd GG. Psychiatric side effects of medications: recent developments. Advances in Psychiatric Treatment 2005;11:58-70. Reprinted with permission | |
Amoxicillin is a penicillin-based, broad-spectrum antibiotic (Box).1,6 Its potential psychiatric side effects include encephalopathy, irritability, sedation, anxiety, and hallucinations.2 These symptoms usually are managed by reducing the dosage or discontinuing the medication. In some cases, antipsychotics may be used to control the symptoms.
Beta-lactam compounds inhibit bacterial growth by interfering with cell wall synthesis. As a beta-lactam antibiotic, amoxicillin’s chemistry, mechanism of action, pharmacologic and clinical effects, and immunologic characteristics are similar to those of cephalosporins, monobactams, carbapenems, and beta-lactamase inhibitors.6
Amoxicillin is an aminopenicillin. These antibiotics retain the antibacterial spectrum of penicillin but have a broader spectrum against gram-negative organisms because of their enhanced ability to penetrate the gram-negative outer membrane. Amoxicillin causes less gastrointestinal (GI) irritation than penicillin and is stable in an acidic environment.
Amoxicillin is administered 250 to 500 mg every 8 hours for adults and 20 to 40 mg/kg of body weight every 24 hours for pediatric patients.1 Amoxicillin is more stable and better absorbed in the GI tract than most penicillins, so amoxicillin 3 times a day is as effective as 4 daily doses of other penicillins.
A literature search reveals 3 cases of amoxicillin-related psychosis (Table 2).7-9 A 30-year-old woman with a urinary tract infection (UTI) developed “confusional manic symptoms” after 10 days of amoxicillin.7 The patient’s family reported she’d had a similar reaction 14 years earlier following 9 days of ampicillin for a perforated appendix; since then she had received non-aminopenicillins without incident. In both incidents, her psychotic symptoms resolved.
A 55-year-old man developed auditory, visual, and tactile hallucinations within hours of his first dose of amoxicillin for presumed pneumonia. The patient “was able to describe what he had experienced clearly with evidence of subjective terror.”8
Most recently, a 63-year-old woman taking amoxicillin, 250 mg tid, for a UTI developed sleep disturbance after 1 day and auditory and visual hallucinations after 4 days. She had a similar episode that required hospitalization 5 years earlier. In both episodes, psychotic symptoms resolved within 3 days of antibiotic discontinuation, with no psychotropic drug treatment.9
Table 2
Amoxicillin-triggered psychosis: 3 case reports
| Study | Patient | Description |
|---|---|---|
| Beal et al7 | Woman, age 30 | Confusional manic symptoms after 10 days of treatment; symptoms resolved within 12 days of admission; patient had a similar reaction to ampicillin 14 years earlier |
| Stell et al8 | Man, age 55 | Auditory, visual, and tactile hallucinations within hours of first dose |
| Rao9 | Woman, age 63 | Auditory and visual hallucinations 1 week after taking 250 mg tid; patient had a similar reaction to amoxicillin 5 years earlier; in both cases symptoms resolved within 3 days of discontinuing amoxicillin |
Mechanism of psychiatric effects
The mechanisms of antibiotic-related neuropsychiatric sequelae are uncertain and vary with drug class and patient factors.
Hoigné’s syndrome—an acute psychotic reaction to intramuscular procaine penicillin first reported around 1950—is characterized by psychiatric symptoms, predominantly anxiety and hallucinations, almost immediately following injection. Anxiety is marked by a fear of imminent death as well as autonomic hyperactivity. This “pseudoanaphylactic reaction” persists for 5 to 30 minutes and has been noted for its resemblance to temporal lobe and limbic seizures (perceptual disturbance, sympathetic hyperactivity, and “doom anxiety”).
The underlying pathophysiology remains unclear; the reaction was originally attributed to microembolization of procaine crystals to the lungs and brain, later to direct procaine neurotoxicity, and most recently to temporolimbic kindling—the appearance of physiologic and behavioral responses to repetition of a stimulus (procaine) that initially is without effect.10
A potential mechanism for amoxicillin’s neuropsychiatric effects is less clear. Because amoxicillin is an oral medication, hypotheses regarding Hoigné’s syndrome seem inapplicable. In addition, amoxicillin is largely excreted unchanged by the kidneys; the lack of significant P450 metabolism argues against mechanisms mediated by polypharmacy or altered metabolite levels. Furthermore, penicillins are polar molecules with poor CNS penetration.6 Penicillins demonstrate known neurotoxicity, however, most often causing convulsions or myelopathy. Identified risk factors for penicillin neurotoxicity include:
- intravenous/thecal administration
- high doses
- CNS disease
- renal insufficiency
- advanced age
- use of drugs that block antibiotic export from the CNS
- conditions that increase blood-brain barrier permeability.
One hypothesis focuses on penicillins’ inhibition of both the GABAA receptor-chloride ionophore complex and the benzodiazepine receptor, yielding CNS disinhibition and decreasing the seizure threshold. Notably, GABA antagonism is considered a primary facilitator of CNS kindling. Penicillin also has been reported to cause delirium related to allergy-mediated cerebral edema.11 Beal et al7 argue for an immune-mediated cerebritis.
Psychiatric symptoms secondary to antibiotics—particularly penicillins—are likely multifactorial, suggesting certain individuals may be predisposed to “Hoigné’s syndrome” from amoxicillin. In the 3 case reports of amoxicillin-related psychosis, there is variation in duration of exposure until symptom onset, medical indication for the antibiotic, and patient age and gender. Any or all of these factors may be clinically significant. None of these patients, however, had a psychiatric history.
It is not clear whether a single 25-mg dose of meclizine—an H1-receptor antagonist—played a role in Mr. A’s psychotic symptoms. Meclizine overdose can cause extreme drowsiness, seizures, hallucinations, and decreased breathing. This anticholinergic has a half-life of only 6 hours and a duration of action of up to 24 hours, although anticholinergic toxicity from overdose can last for days.10 Mr. A ingested a single 25-mg dose of meclizine, however, and his auditory hallucinations persisted for 9 days. Furthermore, Mr. A’s previous well-tolerated meclizine use and lack of other signs and symptoms of anticholinergic toxicity do not support a substantial role for meclizine in his psychotic symptoms.
OUTCOME: Symptoms resolve
Mr. A’s confusion and auditory hallucinations resolve approximately 36 hours after he completed amoxicillin treatment. When transferred to the psychiatric unit, he denies auditory hallucinations or suicidal ideation. He also denies ear pain, tinnitus, vertigo, or ear tenderness; physical examination of the ear is unremarkable. Throughout the hospital admission, Mr. A experiences no confusion or changes in mental status and he continues to adamantly deny suicidal ideation.
He does not require treatment with anti-psychotics or other psychotropic medications and is discharged in stable condition.
Related resources
- Levenson JL, Schneider RK. Infectious diseases. In: Levenson JL, ed. The American Psychiatric Publishing textbook of psychosomatic medicine. Washington, DC: American Psychiatric Publishing; 2005:577-98.
Drug brand names
- Amoxicillin • Amoxil, Trimox, others
- Amphotericin B • Amphocin, Abelcet
- Ampicillin • Principen
- Chloramphenicol • Chloromycetin
- Ciprofloxacin • Cipro
- Clofazimine • Lamprene
- Cycloserine • Seromycin
- Ethionamide • Trecator
- Flucytosine • Ancobon
- Ganciclovir • Cytovene
- Griseofulvin • Fulvicin U/F, Grifulvin V
- Isoniazid • Nydrazid
- Ketoconazole • Nizoral
- Meclizine • Antivert, Bonine, others
- Rifampin • Rifadin, Rimactane
- Trimethoprim/sulfamethoxazole • Bactrim, Septra
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Hubbard JR, Levenson JL, Patrick GA. Psychiatric side effects associated with the ten most commonly dispensed prescription drugs: a review. J Fam Pract 1991;33(2):177-86.
2. Turjanski N, Lloyd GG. Psychiatric side effects of medications: recent developments. Advances in Psychiatric Treatment 2005;11:58-70.
3. Weis S, Karagülle D, Kornhuber J, Bayerlein K. Cotrimoxazole-induced psychosis: a case report and review of literature. Pharmacopsychiatry 2006;39:236-7.
4. Saidinejad M, Ewald MB, Shannon MW. Transient psychosis in an immune-competent patient after oral trimethoprimsulfamethoxazole administration. Pediatrics 2005;115(6):e739-41.
5. Grimm O, Alm B, Für Seelische Z. A case of ciprofloxacin-induced acute polymorphic psychosis with a distinct deficit in executive functions. Psychosomatics 2007;48(3):269.-
6. Katzung BG. Basic and clinical pharmacology. 7th ed. Stamford, CT: Appleton & Lange; 1998;726-32.
7. Beal DM, Hudson B, Zaiac M. Amoxacillin-induced psychosis? Am J Psychiatry 1986;143(2):255-6.
8. Stell IM, Ojo OA. Amoxycillin-induced hallucinations—a variant of Hoigne’s syndrome? Br J Clin Pract 1996;50(5):279.-
9. Rao R. Penicillin psychosis in later life: Hoigne’s syndrome revisited. J Neuropsychiatry Clin Neurosci 1999;11(4):517-8.
10. Araszkiewicz A, Rybakowski JK. Hoigne’s syndrome, kindling, and panic disorder. Depress Anxiety 1996-1997;4(3):139-43.
11. Sternbach H, State R. Antibiotics: neuropsychiatric effects and psychotropic interactions. Harv Rev Psychiatry 1997;5(4):214-26.
CASE: Confused and suicidal
Mr. A, age 39, becomes disoriented while walking and approaches a suspension bridge. He borrows a passerby’s cell phone and calls his sister. His sister later states that he was confused and expressed his final goodbyes, saying, “I will see Mom in heaven.” He gives back the phone and leaps of the bridge. A nearby boat rescues him almost immediately.
Mr. A is brought to the trauma unit, where he is treated for a lacerated liver. After he is stabilized, Mr. A is awake and answering questions appropriately. He is placed on suicide precautions and direct 24-hour, one-to-one supervision. Our psychiatric team evaluates him.
Mr. A reports no history of diabetes, hypertension, cardiac disorders, or neurologic disorders, but does have a history of cognitive developmental delay. He has no history of psychiatric illness, suicide attempts, or self-injurious behavior. He denies a psychiatric family history or using alcohol, tobacco, or illicit drugs; drug screen is negative. He is unemployed, collects disability, and lives with his sister.
The authors’ observations
In our initial evaluation, we find no obvious reason for Mr. A’s confusion or suicide attempt. We decide to closely review Mr. A’s history in the days leading up to his jumping off the bridge.
HISTORY: Otitis media treatment
Mr. A has a history of chronic otitis media and sought treatment for ear pain at a local emergency room (ER) 10 days before his suicide attempt. He was prescribed amoxicillin, 500 mg tid for 10 days, and meclizine, 25 mg every 8 hours as needed for dizziness.
Immediately after his first dose of both drugs, the patient told his family he was feeling “weird,” but denied being dizzy. Thinking the unusual feeling was from meclizine, Mr. A stopped taking it but continued amoxicillin. On the second day of amoxicillin, he noticed bouts of confusion. He could perform his daily activities, but with difficulty. Mr. A’s niece said he had to ask for help with minor tasks, such as opening a can of soup.
On day 3, Mr. A developed prominent auditory hallucinations. He described hearing unrecognizable male and female voices chattering and mumbling throughout the day. The voices and confusion progressively worsened, but Mr. A continued taking the antibiotic and did not mention the voices to his family.
Mr. A’s sister reports that in a phone conversation with her brother on day 7, “he wasn’t himself…he was talking about my sister and mother but what he said didn’t make sense.” She asked a neighbor to check on Mr. A; he reported that Mr. A was “OK.” On the final day of amoxicillin—day 10—Mr. A became increasingly agitated. He says us that shortly before wandering onto the bridge and jumping, he was having a difficult time dealing with the voices and confusion.
We suspect amoxicillin might have been responsible for Mr. A’s psychotic symptoms.
The authors’ observations
Treatment modalities and pharmaceutical approaches used to treat infectious diseases carry many potential adverse effects. When a patient presents with new-onset psychiatric symptoms, explore whether they are related to an underlying mood disorder or medication side effects. Three important considerations are to:
- determine whether the condition is reversible by discontinuing a drug
- identify and characterize previously unrecognized adverse drug effects
- avoid inaccurate diagnosis that leads to nonindicated psychiatric treatment.1
Antibiotic side effects vary, depending on the particular drug and its target bacteria. The most common are gastrointestinal, such as upset stomach and diarrhea. Antibiotics also can induce an anaphylactic reaction ranging from mild (pruritic rash or slight wheezing) to life-threatening (swelling of the throat, difficulty breathing, and hypotension).
Several classes of antibiotics have psychiatric side effects that range from minor confusion and irritability to severe encephalopathy and suicide (Table 1).2 Case reports have described psychotic symptoms associated with cotrimoxazole,3 trimethoprim/sulfamethoxazole,4 and ciprofloxacin.5 An older review found that amoxicillin is among the top 10 most commonly prescribed medications associated with psychiatric side effects.1
Table 1
Potential psychiatric effects of antibiotics
| Medication | Side effects |
|---|---|
| Antibacterials | |
| Penicillins | Encephalopathy, irritability, sedation, anxiety, hallucinations |
| Cephalosporins | Sleep disturbances, hallucinations |
| Cycloserine | Dose-dependent side effects, depression, irritability, psychosis |
| Quinolones | Sleep and mood disorders, psychosis |
| Nitrofurans | Euphoria, psychosis, sleep disturbances |
| Tetracyclines | Decreased concentration, mood and sleep disorders |
| Chloramphenicol | Depression |
| Trimethoprim, sulfonamides | Depression, psychosis |
| Antimycobacterials | |
| Isoniazid | Cognitive impairment, mood disorder, psychosis |
| Clofazimine | Major depression, suicide |
| Rifampin | Sedation |
| Ethionamide | Sedation, irritability, agitation, depression, psychosis |
| Ganciclovir | Sleep disturbances, anxiety, mood disorders, psychosis |
| Antifungals | |
| Amphotericin B | Delirium |
| Ketoconazole | Decreased libido, mood disorders, psychosis |
| Flucytosine | Sedation, hallucinations |
| Griseofulvin | Depression, psychosis, sleep disturbances |
| Source: Turjanski N, Lloyd GG. Psychiatric side effects of medications: recent developments. Advances in Psychiatric Treatment 2005;11:58-70. Reprinted with permission | |
Amoxicillin is a penicillin-based, broad-spectrum antibiotic (Box).1,6 Its potential psychiatric side effects include encephalopathy, irritability, sedation, anxiety, and hallucinations.2 These symptoms usually are managed by reducing the dosage or discontinuing the medication. In some cases, antipsychotics may be used to control the symptoms.
Beta-lactam compounds inhibit bacterial growth by interfering with cell wall synthesis. As a beta-lactam antibiotic, amoxicillin’s chemistry, mechanism of action, pharmacologic and clinical effects, and immunologic characteristics are similar to those of cephalosporins, monobactams, carbapenems, and beta-lactamase inhibitors.6
Amoxicillin is an aminopenicillin. These antibiotics retain the antibacterial spectrum of penicillin but have a broader spectrum against gram-negative organisms because of their enhanced ability to penetrate the gram-negative outer membrane. Amoxicillin causes less gastrointestinal (GI) irritation than penicillin and is stable in an acidic environment.
Amoxicillin is administered 250 to 500 mg every 8 hours for adults and 20 to 40 mg/kg of body weight every 24 hours for pediatric patients.1 Amoxicillin is more stable and better absorbed in the GI tract than most penicillins, so amoxicillin 3 times a day is as effective as 4 daily doses of other penicillins.
A literature search reveals 3 cases of amoxicillin-related psychosis (Table 2).7-9 A 30-year-old woman with a urinary tract infection (UTI) developed “confusional manic symptoms” after 10 days of amoxicillin.7 The patient’s family reported she’d had a similar reaction 14 years earlier following 9 days of ampicillin for a perforated appendix; since then she had received non-aminopenicillins without incident. In both incidents, her psychotic symptoms resolved.
A 55-year-old man developed auditory, visual, and tactile hallucinations within hours of his first dose of amoxicillin for presumed pneumonia. The patient “was able to describe what he had experienced clearly with evidence of subjective terror.”8
Most recently, a 63-year-old woman taking amoxicillin, 250 mg tid, for a UTI developed sleep disturbance after 1 day and auditory and visual hallucinations after 4 days. She had a similar episode that required hospitalization 5 years earlier. In both episodes, psychotic symptoms resolved within 3 days of antibiotic discontinuation, with no psychotropic drug treatment.9
Table 2
Amoxicillin-triggered psychosis: 3 case reports
| Study | Patient | Description |
|---|---|---|
| Beal et al7 | Woman, age 30 | Confusional manic symptoms after 10 days of treatment; symptoms resolved within 12 days of admission; patient had a similar reaction to ampicillin 14 years earlier |
| Stell et al8 | Man, age 55 | Auditory, visual, and tactile hallucinations within hours of first dose |
| Rao9 | Woman, age 63 | Auditory and visual hallucinations 1 week after taking 250 mg tid; patient had a similar reaction to amoxicillin 5 years earlier; in both cases symptoms resolved within 3 days of discontinuing amoxicillin |
Mechanism of psychiatric effects
The mechanisms of antibiotic-related neuropsychiatric sequelae are uncertain and vary with drug class and patient factors.
Hoigné’s syndrome—an acute psychotic reaction to intramuscular procaine penicillin first reported around 1950—is characterized by psychiatric symptoms, predominantly anxiety and hallucinations, almost immediately following injection. Anxiety is marked by a fear of imminent death as well as autonomic hyperactivity. This “pseudoanaphylactic reaction” persists for 5 to 30 minutes and has been noted for its resemblance to temporal lobe and limbic seizures (perceptual disturbance, sympathetic hyperactivity, and “doom anxiety”).
The underlying pathophysiology remains unclear; the reaction was originally attributed to microembolization of procaine crystals to the lungs and brain, later to direct procaine neurotoxicity, and most recently to temporolimbic kindling—the appearance of physiologic and behavioral responses to repetition of a stimulus (procaine) that initially is without effect.10
A potential mechanism for amoxicillin’s neuropsychiatric effects is less clear. Because amoxicillin is an oral medication, hypotheses regarding Hoigné’s syndrome seem inapplicable. In addition, amoxicillin is largely excreted unchanged by the kidneys; the lack of significant P450 metabolism argues against mechanisms mediated by polypharmacy or altered metabolite levels. Furthermore, penicillins are polar molecules with poor CNS penetration.6 Penicillins demonstrate known neurotoxicity, however, most often causing convulsions or myelopathy. Identified risk factors for penicillin neurotoxicity include:
- intravenous/thecal administration
- high doses
- CNS disease
- renal insufficiency
- advanced age
- use of drugs that block antibiotic export from the CNS
- conditions that increase blood-brain barrier permeability.
One hypothesis focuses on penicillins’ inhibition of both the GABAA receptor-chloride ionophore complex and the benzodiazepine receptor, yielding CNS disinhibition and decreasing the seizure threshold. Notably, GABA antagonism is considered a primary facilitator of CNS kindling. Penicillin also has been reported to cause delirium related to allergy-mediated cerebral edema.11 Beal et al7 argue for an immune-mediated cerebritis.
Psychiatric symptoms secondary to antibiotics—particularly penicillins—are likely multifactorial, suggesting certain individuals may be predisposed to “Hoigné’s syndrome” from amoxicillin. In the 3 case reports of amoxicillin-related psychosis, there is variation in duration of exposure until symptom onset, medical indication for the antibiotic, and patient age and gender. Any or all of these factors may be clinically significant. None of these patients, however, had a psychiatric history.
It is not clear whether a single 25-mg dose of meclizine—an H1-receptor antagonist—played a role in Mr. A’s psychotic symptoms. Meclizine overdose can cause extreme drowsiness, seizures, hallucinations, and decreased breathing. This anticholinergic has a half-life of only 6 hours and a duration of action of up to 24 hours, although anticholinergic toxicity from overdose can last for days.10 Mr. A ingested a single 25-mg dose of meclizine, however, and his auditory hallucinations persisted for 9 days. Furthermore, Mr. A’s previous well-tolerated meclizine use and lack of other signs and symptoms of anticholinergic toxicity do not support a substantial role for meclizine in his psychotic symptoms.
OUTCOME: Symptoms resolve
Mr. A’s confusion and auditory hallucinations resolve approximately 36 hours after he completed amoxicillin treatment. When transferred to the psychiatric unit, he denies auditory hallucinations or suicidal ideation. He also denies ear pain, tinnitus, vertigo, or ear tenderness; physical examination of the ear is unremarkable. Throughout the hospital admission, Mr. A experiences no confusion or changes in mental status and he continues to adamantly deny suicidal ideation.
He does not require treatment with anti-psychotics or other psychotropic medications and is discharged in stable condition.
Related resources
- Levenson JL, Schneider RK. Infectious diseases. In: Levenson JL, ed. The American Psychiatric Publishing textbook of psychosomatic medicine. Washington, DC: American Psychiatric Publishing; 2005:577-98.
Drug brand names
- Amoxicillin • Amoxil, Trimox, others
- Amphotericin B • Amphocin, Abelcet
- Ampicillin • Principen
- Chloramphenicol • Chloromycetin
- Ciprofloxacin • Cipro
- Clofazimine • Lamprene
- Cycloserine • Seromycin
- Ethionamide • Trecator
- Flucytosine • Ancobon
- Ganciclovir • Cytovene
- Griseofulvin • Fulvicin U/F, Grifulvin V
- Isoniazid • Nydrazid
- Ketoconazole • Nizoral
- Meclizine • Antivert, Bonine, others
- Rifampin • Rifadin, Rimactane
- Trimethoprim/sulfamethoxazole • Bactrim, Septra
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: Confused and suicidal
Mr. A, age 39, becomes disoriented while walking and approaches a suspension bridge. He borrows a passerby’s cell phone and calls his sister. His sister later states that he was confused and expressed his final goodbyes, saying, “I will see Mom in heaven.” He gives back the phone and leaps of the bridge. A nearby boat rescues him almost immediately.
Mr. A is brought to the trauma unit, where he is treated for a lacerated liver. After he is stabilized, Mr. A is awake and answering questions appropriately. He is placed on suicide precautions and direct 24-hour, one-to-one supervision. Our psychiatric team evaluates him.
Mr. A reports no history of diabetes, hypertension, cardiac disorders, or neurologic disorders, but does have a history of cognitive developmental delay. He has no history of psychiatric illness, suicide attempts, or self-injurious behavior. He denies a psychiatric family history or using alcohol, tobacco, or illicit drugs; drug screen is negative. He is unemployed, collects disability, and lives with his sister.
The authors’ observations
In our initial evaluation, we find no obvious reason for Mr. A’s confusion or suicide attempt. We decide to closely review Mr. A’s history in the days leading up to his jumping off the bridge.
HISTORY: Otitis media treatment
Mr. A has a history of chronic otitis media and sought treatment for ear pain at a local emergency room (ER) 10 days before his suicide attempt. He was prescribed amoxicillin, 500 mg tid for 10 days, and meclizine, 25 mg every 8 hours as needed for dizziness.
Immediately after his first dose of both drugs, the patient told his family he was feeling “weird,” but denied being dizzy. Thinking the unusual feeling was from meclizine, Mr. A stopped taking it but continued amoxicillin. On the second day of amoxicillin, he noticed bouts of confusion. He could perform his daily activities, but with difficulty. Mr. A’s niece said he had to ask for help with minor tasks, such as opening a can of soup.
On day 3, Mr. A developed prominent auditory hallucinations. He described hearing unrecognizable male and female voices chattering and mumbling throughout the day. The voices and confusion progressively worsened, but Mr. A continued taking the antibiotic and did not mention the voices to his family.
Mr. A’s sister reports that in a phone conversation with her brother on day 7, “he wasn’t himself…he was talking about my sister and mother but what he said didn’t make sense.” She asked a neighbor to check on Mr. A; he reported that Mr. A was “OK.” On the final day of amoxicillin—day 10—Mr. A became increasingly agitated. He says us that shortly before wandering onto the bridge and jumping, he was having a difficult time dealing with the voices and confusion.
We suspect amoxicillin might have been responsible for Mr. A’s psychotic symptoms.
The authors’ observations
Treatment modalities and pharmaceutical approaches used to treat infectious diseases carry many potential adverse effects. When a patient presents with new-onset psychiatric symptoms, explore whether they are related to an underlying mood disorder or medication side effects. Three important considerations are to:
- determine whether the condition is reversible by discontinuing a drug
- identify and characterize previously unrecognized adverse drug effects
- avoid inaccurate diagnosis that leads to nonindicated psychiatric treatment.1
Antibiotic side effects vary, depending on the particular drug and its target bacteria. The most common are gastrointestinal, such as upset stomach and diarrhea. Antibiotics also can induce an anaphylactic reaction ranging from mild (pruritic rash or slight wheezing) to life-threatening (swelling of the throat, difficulty breathing, and hypotension).
Several classes of antibiotics have psychiatric side effects that range from minor confusion and irritability to severe encephalopathy and suicide (Table 1).2 Case reports have described psychotic symptoms associated with cotrimoxazole,3 trimethoprim/sulfamethoxazole,4 and ciprofloxacin.5 An older review found that amoxicillin is among the top 10 most commonly prescribed medications associated with psychiatric side effects.1
Table 1
Potential psychiatric effects of antibiotics
| Medication | Side effects |
|---|---|
| Antibacterials | |
| Penicillins | Encephalopathy, irritability, sedation, anxiety, hallucinations |
| Cephalosporins | Sleep disturbances, hallucinations |
| Cycloserine | Dose-dependent side effects, depression, irritability, psychosis |
| Quinolones | Sleep and mood disorders, psychosis |
| Nitrofurans | Euphoria, psychosis, sleep disturbances |
| Tetracyclines | Decreased concentration, mood and sleep disorders |
| Chloramphenicol | Depression |
| Trimethoprim, sulfonamides | Depression, psychosis |
| Antimycobacterials | |
| Isoniazid | Cognitive impairment, mood disorder, psychosis |
| Clofazimine | Major depression, suicide |
| Rifampin | Sedation |
| Ethionamide | Sedation, irritability, agitation, depression, psychosis |
| Ganciclovir | Sleep disturbances, anxiety, mood disorders, psychosis |
| Antifungals | |
| Amphotericin B | Delirium |
| Ketoconazole | Decreased libido, mood disorders, psychosis |
| Flucytosine | Sedation, hallucinations |
| Griseofulvin | Depression, psychosis, sleep disturbances |
| Source: Turjanski N, Lloyd GG. Psychiatric side effects of medications: recent developments. Advances in Psychiatric Treatment 2005;11:58-70. Reprinted with permission | |
Amoxicillin is a penicillin-based, broad-spectrum antibiotic (Box).1,6 Its potential psychiatric side effects include encephalopathy, irritability, sedation, anxiety, and hallucinations.2 These symptoms usually are managed by reducing the dosage or discontinuing the medication. In some cases, antipsychotics may be used to control the symptoms.
Beta-lactam compounds inhibit bacterial growth by interfering with cell wall synthesis. As a beta-lactam antibiotic, amoxicillin’s chemistry, mechanism of action, pharmacologic and clinical effects, and immunologic characteristics are similar to those of cephalosporins, monobactams, carbapenems, and beta-lactamase inhibitors.6
Amoxicillin is an aminopenicillin. These antibiotics retain the antibacterial spectrum of penicillin but have a broader spectrum against gram-negative organisms because of their enhanced ability to penetrate the gram-negative outer membrane. Amoxicillin causes less gastrointestinal (GI) irritation than penicillin and is stable in an acidic environment.
Amoxicillin is administered 250 to 500 mg every 8 hours for adults and 20 to 40 mg/kg of body weight every 24 hours for pediatric patients.1 Amoxicillin is more stable and better absorbed in the GI tract than most penicillins, so amoxicillin 3 times a day is as effective as 4 daily doses of other penicillins.
A literature search reveals 3 cases of amoxicillin-related psychosis (Table 2).7-9 A 30-year-old woman with a urinary tract infection (UTI) developed “confusional manic symptoms” after 10 days of amoxicillin.7 The patient’s family reported she’d had a similar reaction 14 years earlier following 9 days of ampicillin for a perforated appendix; since then she had received non-aminopenicillins without incident. In both incidents, her psychotic symptoms resolved.
A 55-year-old man developed auditory, visual, and tactile hallucinations within hours of his first dose of amoxicillin for presumed pneumonia. The patient “was able to describe what he had experienced clearly with evidence of subjective terror.”8
Most recently, a 63-year-old woman taking amoxicillin, 250 mg tid, for a UTI developed sleep disturbance after 1 day and auditory and visual hallucinations after 4 days. She had a similar episode that required hospitalization 5 years earlier. In both episodes, psychotic symptoms resolved within 3 days of antibiotic discontinuation, with no psychotropic drug treatment.9
Table 2
Amoxicillin-triggered psychosis: 3 case reports
| Study | Patient | Description |
|---|---|---|
| Beal et al7 | Woman, age 30 | Confusional manic symptoms after 10 days of treatment; symptoms resolved within 12 days of admission; patient had a similar reaction to ampicillin 14 years earlier |
| Stell et al8 | Man, age 55 | Auditory, visual, and tactile hallucinations within hours of first dose |
| Rao9 | Woman, age 63 | Auditory and visual hallucinations 1 week after taking 250 mg tid; patient had a similar reaction to amoxicillin 5 years earlier; in both cases symptoms resolved within 3 days of discontinuing amoxicillin |
Mechanism of psychiatric effects
The mechanisms of antibiotic-related neuropsychiatric sequelae are uncertain and vary with drug class and patient factors.
Hoigné’s syndrome—an acute psychotic reaction to intramuscular procaine penicillin first reported around 1950—is characterized by psychiatric symptoms, predominantly anxiety and hallucinations, almost immediately following injection. Anxiety is marked by a fear of imminent death as well as autonomic hyperactivity. This “pseudoanaphylactic reaction” persists for 5 to 30 minutes and has been noted for its resemblance to temporal lobe and limbic seizures (perceptual disturbance, sympathetic hyperactivity, and “doom anxiety”).
The underlying pathophysiology remains unclear; the reaction was originally attributed to microembolization of procaine crystals to the lungs and brain, later to direct procaine neurotoxicity, and most recently to temporolimbic kindling—the appearance of physiologic and behavioral responses to repetition of a stimulus (procaine) that initially is without effect.10
A potential mechanism for amoxicillin’s neuropsychiatric effects is less clear. Because amoxicillin is an oral medication, hypotheses regarding Hoigné’s syndrome seem inapplicable. In addition, amoxicillin is largely excreted unchanged by the kidneys; the lack of significant P450 metabolism argues against mechanisms mediated by polypharmacy or altered metabolite levels. Furthermore, penicillins are polar molecules with poor CNS penetration.6 Penicillins demonstrate known neurotoxicity, however, most often causing convulsions or myelopathy. Identified risk factors for penicillin neurotoxicity include:
- intravenous/thecal administration
- high doses
- CNS disease
- renal insufficiency
- advanced age
- use of drugs that block antibiotic export from the CNS
- conditions that increase blood-brain barrier permeability.
One hypothesis focuses on penicillins’ inhibition of both the GABAA receptor-chloride ionophore complex and the benzodiazepine receptor, yielding CNS disinhibition and decreasing the seizure threshold. Notably, GABA antagonism is considered a primary facilitator of CNS kindling. Penicillin also has been reported to cause delirium related to allergy-mediated cerebral edema.11 Beal et al7 argue for an immune-mediated cerebritis.
Psychiatric symptoms secondary to antibiotics—particularly penicillins—are likely multifactorial, suggesting certain individuals may be predisposed to “Hoigné’s syndrome” from amoxicillin. In the 3 case reports of amoxicillin-related psychosis, there is variation in duration of exposure until symptom onset, medical indication for the antibiotic, and patient age and gender. Any or all of these factors may be clinically significant. None of these patients, however, had a psychiatric history.
It is not clear whether a single 25-mg dose of meclizine—an H1-receptor antagonist—played a role in Mr. A’s psychotic symptoms. Meclizine overdose can cause extreme drowsiness, seizures, hallucinations, and decreased breathing. This anticholinergic has a half-life of only 6 hours and a duration of action of up to 24 hours, although anticholinergic toxicity from overdose can last for days.10 Mr. A ingested a single 25-mg dose of meclizine, however, and his auditory hallucinations persisted for 9 days. Furthermore, Mr. A’s previous well-tolerated meclizine use and lack of other signs and symptoms of anticholinergic toxicity do not support a substantial role for meclizine in his psychotic symptoms.
OUTCOME: Symptoms resolve
Mr. A’s confusion and auditory hallucinations resolve approximately 36 hours after he completed amoxicillin treatment. When transferred to the psychiatric unit, he denies auditory hallucinations or suicidal ideation. He also denies ear pain, tinnitus, vertigo, or ear tenderness; physical examination of the ear is unremarkable. Throughout the hospital admission, Mr. A experiences no confusion or changes in mental status and he continues to adamantly deny suicidal ideation.
He does not require treatment with anti-psychotics or other psychotropic medications and is discharged in stable condition.
Related resources
- Levenson JL, Schneider RK. Infectious diseases. In: Levenson JL, ed. The American Psychiatric Publishing textbook of psychosomatic medicine. Washington, DC: American Psychiatric Publishing; 2005:577-98.
Drug brand names
- Amoxicillin • Amoxil, Trimox, others
- Amphotericin B • Amphocin, Abelcet
- Ampicillin • Principen
- Chloramphenicol • Chloromycetin
- Ciprofloxacin • Cipro
- Clofazimine • Lamprene
- Cycloserine • Seromycin
- Ethionamide • Trecator
- Flucytosine • Ancobon
- Ganciclovir • Cytovene
- Griseofulvin • Fulvicin U/F, Grifulvin V
- Isoniazid • Nydrazid
- Ketoconazole • Nizoral
- Meclizine • Antivert, Bonine, others
- Rifampin • Rifadin, Rimactane
- Trimethoprim/sulfamethoxazole • Bactrim, Septra
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Hubbard JR, Levenson JL, Patrick GA. Psychiatric side effects associated with the ten most commonly dispensed prescription drugs: a review. J Fam Pract 1991;33(2):177-86.
2. Turjanski N, Lloyd GG. Psychiatric side effects of medications: recent developments. Advances in Psychiatric Treatment 2005;11:58-70.
3. Weis S, Karagülle D, Kornhuber J, Bayerlein K. Cotrimoxazole-induced psychosis: a case report and review of literature. Pharmacopsychiatry 2006;39:236-7.
4. Saidinejad M, Ewald MB, Shannon MW. Transient psychosis in an immune-competent patient after oral trimethoprimsulfamethoxazole administration. Pediatrics 2005;115(6):e739-41.
5. Grimm O, Alm B, Für Seelische Z. A case of ciprofloxacin-induced acute polymorphic psychosis with a distinct deficit in executive functions. Psychosomatics 2007;48(3):269.-
6. Katzung BG. Basic and clinical pharmacology. 7th ed. Stamford, CT: Appleton & Lange; 1998;726-32.
7. Beal DM, Hudson B, Zaiac M. Amoxacillin-induced psychosis? Am J Psychiatry 1986;143(2):255-6.
8. Stell IM, Ojo OA. Amoxycillin-induced hallucinations—a variant of Hoigne’s syndrome? Br J Clin Pract 1996;50(5):279.-
9. Rao R. Penicillin psychosis in later life: Hoigne’s syndrome revisited. J Neuropsychiatry Clin Neurosci 1999;11(4):517-8.
10. Araszkiewicz A, Rybakowski JK. Hoigne’s syndrome, kindling, and panic disorder. Depress Anxiety 1996-1997;4(3):139-43.
11. Sternbach H, State R. Antibiotics: neuropsychiatric effects and psychotropic interactions. Harv Rev Psychiatry 1997;5(4):214-26.
1. Hubbard JR, Levenson JL, Patrick GA. Psychiatric side effects associated with the ten most commonly dispensed prescription drugs: a review. J Fam Pract 1991;33(2):177-86.
2. Turjanski N, Lloyd GG. Psychiatric side effects of medications: recent developments. Advances in Psychiatric Treatment 2005;11:58-70.
3. Weis S, Karagülle D, Kornhuber J, Bayerlein K. Cotrimoxazole-induced psychosis: a case report and review of literature. Pharmacopsychiatry 2006;39:236-7.
4. Saidinejad M, Ewald MB, Shannon MW. Transient psychosis in an immune-competent patient after oral trimethoprimsulfamethoxazole administration. Pediatrics 2005;115(6):e739-41.
5. Grimm O, Alm B, Für Seelische Z. A case of ciprofloxacin-induced acute polymorphic psychosis with a distinct deficit in executive functions. Psychosomatics 2007;48(3):269.-
6. Katzung BG. Basic and clinical pharmacology. 7th ed. Stamford, CT: Appleton & Lange; 1998;726-32.
7. Beal DM, Hudson B, Zaiac M. Amoxacillin-induced psychosis? Am J Psychiatry 1986;143(2):255-6.
8. Stell IM, Ojo OA. Amoxycillin-induced hallucinations—a variant of Hoigne’s syndrome? Br J Clin Pract 1996;50(5):279.-
9. Rao R. Penicillin psychosis in later life: Hoigne’s syndrome revisited. J Neuropsychiatry Clin Neurosci 1999;11(4):517-8.
10. Araszkiewicz A, Rybakowski JK. Hoigne’s syndrome, kindling, and panic disorder. Depress Anxiety 1996-1997;4(3):139-43.
11. Sternbach H, State R. Antibiotics: neuropsychiatric effects and psychotropic interactions. Harv Rev Psychiatry 1997;5(4):214-26.
The sailor who won’t follow orders
CASE: An unlikable patient
Mr. L, age 56, is admitted to the psychiatric unit at our Veterans Affairs Medical Center for active suicidal ideation; he has a history of self-injurious behaviors that include mutilation and overdose. He also has a history of alcohol dependence and multiple inpatient psychiatric admissions. He has never married and conflicts with his siblings—in whose home he has been staying—have led to frequent homelessness.
His affect is silly and shallow. He also shows signs of haughtiness, disinhibition, grandiosity, and confabulation. For example, he says that while in the Navy he had 82 sexual exploits and developed a drug that cured herpes.
We start Mr. L on divalproex, 1,500 mg/d, and quetiapine, titrated to 200 mg/d. After 3 days he is discharged, but this begins a cycle of repeated suicide gestures and readmissions—9 within the next 3 months. Each time he is discharged, Mr. L fails to follow through on treatment recommendations and is indifferent to our staff’s annoyed reactions.
The author’s observations
Some of our staff members regard Mr. L’s suicidal gestures as manipulative and feel angry and demoralized by his poor adherence to outpatient treatment plans. Their negative countertransference might have impacted how they evaluated Mr. L through repeated admissions and discharges. During Mr. L’s ninth admission, we decide to reevaluate his longitudinal history for clues to his noncompliant behavior.
History: Undocumented injury
Mr. L says he began drinking alcohol at age 16. He reports that he has grown marijuana but has not smoked it since 1991. He denies using heroin or other drugs.
Mr. L states that he suffered a head injury in 1975 after falling off a ladder on a Navy ship. He describes losing consciousness for a brief but uncertain duration. He reports that he has developed a seizure disorder since this fall and a history of amnesia secondary to past seizures. His medical records contain no witnessed seizures. Mr. L also says he was hospitalized a few years ago and placed on a ventilator for 7 days for an undetermined reason.
The authors’ observations
Based on Mr. L’s report of a possible traumatic brain injury (TBI), we order a neurologic evaluation. A year earlier, MRI of the brain without contrast demonstrated minimal, nonspecific periventricular and subcortical, punctuate hyperintensities on flair and T2 weighted sequences that are nonspecific. Overall, the impression was “diffuse involutional changes and mild nonspecific periventricular and subcortical white matter hyperintensities,” which might reflect covert vascular brain injury.
Our frustration over Mr. L’s repeated readmissions for suicidal gestures led us to seek outside evaluation and consultation from a senior psychiatrist for assistance with discharge and treatment planning. Unlike our staff, the consulting psychiatrist did not harbor strong negative feelings toward the patient.
Mr. L’s history of deterioration in psychosocial functioning prompted this psychiatrist to perform a thorough mental status examination that focused on cognitive elements and request formal neuropsychological testing.
Evalutation: Cognitive Deficits
During mental status examination, Mr. L has difficulty recalling 3 items and uses a memory strategy to assist himself. He fails to recollect in reverse order the last 5 U.S. presidents. He spells “world” backward, but has difficulty repeating 6 digits forward and 4 backward. He is unable to do serial 7 subtractions from 93 to 65 correctly. He adequately copies interlocking pentagons and draws a clock with the correct time. He achieves a score of 28/30 on the Folstein Mini Mental State Exam, missing the date by 4 days and recalling 2 of 3 words.
These results suggest Mr. L has difficulty with attention and working memory, short-term memory, fund of general information and long-term memory, and ability to perform simple calculations. Most important, they indicate the need for further study, especially a neuropsychological test battery.
Mr. L’s abnormal neuropsychological test results are summarized in the Table. He manifests concretization of thought. His loss of conceptual fluidity is documented formally by measures of perseverative errors and categories completed on the Wisconsin Card Sorting Test (WCST). These findings support a diagnosis of acquired dementia.
Table
Abnormal findings on Mr. L’s neuropsychological testing
| Cognitive domain | Test | Score | Interpretation |
|---|---|---|---|
| Mental status and effort | |||
| Mental status | MMSE total score | 28/30 | 2 of 3 items recalled after delay |
| Orientation | MMSE orientation questions | 9/10 | Date off by 4 days |
| Premorbid IQ estimate | WRAT-4 Reading Standard | 66th percentile | Within normal limits. Inconsistent with educational attainment, but could be impacted by temporal lobe findings |
| Verbal memory | |||
| Immediate memory | RBANS Immediate Memory Index (List and Story Learning) | 1st percentile | Severe impairment |
| Delayed memory | RBANS Delayed Memory Index | 1st percentile | Severe impairment |
| Recognition memory | List Learning | Severe impairment | |
| Visuospatial memory | |||
| Delayed memory | RBANS Figure Recall | 3rd percentile | Severe impairment |
| Executive functioning | |||
| Cognitive flexibility | Trails B | 10th percentile | Severe impairment based on educational attainment |
| WCST | Low scores: Nonperseverative errors, perseverative errors, and categories completed | ||
| * Tests of mental status effort, visuomotor processing speed, confrontation naming, visuospatial function, attention, and executive functioning fluency/initiation were within normal limits | |||
| MMSE: Mini Mental State Exam; WRAT: Wide Range Achievement Test; RBANS: Repeatable Battery for the Assessment of Neuropsychological Status; WCST: Wisconsin Card Sorting Test | |||
The authors’ observations
Mr. L’s history, cognitive testing, head imaging, and behavioral observations suggest that several pathogenic factors contribute to his impaired functioning. First, he describes a TBI of unknown severity occurring in 1975. Although brain scans did not show evidence of midline shift or encephalomalacia, a direct blow to the head after falling from a height combined with possible post-injury seizures suggests a TBI of at least moderate severity.
Second, Mr. L describes an incident in which he required inpatient respiratory assistance. Although the precipitating medical event was unclear, anoxia or hypoxia is likely. A recent CT revealed low attenuation in the left temporal region that could represent an infarct.
Mr. L’s severe memory impairment and moderate to severe impairment in cognitive flexibility are commonly reported after a TBI of moderate severity. If an ischemic incident were the primary contributor, a lateralized pattern of cognitive dysfunction—which Mr. L does not exhibit—would be expected.
Although Mr. L likely has vascular dementia, his MRI findings do not indicate sufficient disease to account for his memory scores. Vascular dementia is associated with slow, stepwise cognitive deterioration, which is not consistent with severely impaired memory in a 56-year-old patient.
Finally, alcoholism is associated with cognitive difficulty in memory, visuospatial functioning, and abstract reasoning. Mr. L demonstrated significant difficulty in memory and abstract reasoning, but his visuospatial functioning was largely intact. In the absence of Wernicke’s encephalopathy, chronic alcoholics generally do not show memory decrements in line with Mr. L’s. His MRI results indicated only minimal ventricular and sulcal enlargement. Because atrophy is present in approximately 60% of chronic alcoholics, this finding provides evidence of a contribution, but the other contributory factors are associated with more definitive medical outcomes. Thus, alcoholism must be viewed as a secondary contributor to Mr. L’s impaired functioning.
Taking into account all known contributors, TBI emerges as the primary diagnosis.
Consider neurologic injury
Recognizing and characterizing personality changes related to neurologic injury and disease is often problematic and unreliable, even when psychometrically validated instruments and structured diagnostic interviews are used (Box 1).1-5 Mr. L’s presentation differed from the more commonly reported “impulsive aggression” associated with closed head injury. Sequelae from TBI were contributing to his clinical presentation but was obscured by his shallow and silly affect, inability to accurately assess social cues, and lack of empathy.
Mr. L reported suffering a head injury from falling off a ladder. Personality changes that result from traumatic brain injury (TBI) of the sudden deceleration type—even when mild—are frequently referable to the frontal lobe, especially focal orbital and/or ventromedial damage of the prefrontal cortex.1-5 This is because of the physical proximity of the sphenoid wing to the orbitofrontal region and effects of shearing.
As a result of this damage, patients lack insight into their accompanying cognitive and behavioral abnormalities, such as the egocentricity and impaired empathy shown by Mr. L. These changes might not be detected in clinical interviews and over brief periods.2 Appreciating an acquired personality disturbance may require evaluating the patient’s behavior over months or years.2
In retrospect, Mr. L’s seeking repeated inpatient psychiatric hospitalizations is consistent with poor planning and problem-solving skills. He has a limited repertoire of adaptive behaviors and has learned that suicidal gestures lead to admission and caretaking. These are important to him because he is frequently homeless. His lack of insight is seen in his unrealistic plans for employment in jobs requiring specialized technical skills.
Mr. L’s case emphasizes the importance of considering brain injury as an etiologic factor in personality changes. It also highlights the complex—and seemingly nonoverlapping—functions and dysfunctions of the frontal lobe, including:
- source memory
- working memory
- sustained attention
- conceptual fluidity
- imaginative thinking
- impulse regulation
- planning and problem-solving skills.
Documenting Mr. L’s cognitive deficits and acquired dementia diagnosis changed our staff’s perception of his behavior, enabling us to overcome negative countertransference (Box 2). We no longer regarded him as deliberately manipulative and refer him for appropriate treatment.
Countertransference can interfere with optimal workup and treatment of patients with character changes related to traumatic brain injury and neurodegenerative processes. When we interpreted Mr. L’s suicidal gestures and hospitalizations as manipulative and deliberate, we failed to appreciate the limited number of things he could do to obtain a safe and protective environment. We also failed to recognize that his poor planning and problem-solving skills—as well as lack of insight into his illness—prevented him from adhering to outpatient treatment.
Originally, we attributed Mr. L’s egocentricity, lack of empathy, and lack of adherence to axis II pathology.
Our staff’s hostile feelings toward Mr. L led us to insufficiently consider his history—which is consistent with cognitive decline—during biopsychosocial evaluation and treatment planning. Mr. L’s status as a frequently homeless, unemployed person reflects a sharp decline for a highly educated person who served as a Navy officer and performed radiation inspections on nuclear-powered vessels.
Outome: Residential placement
We realize Mr. L needs cognitive rehabilitation—including assistance with planning and problem solving—and arrange for his placement in a residential facility for this specialized rehabilitation. Mr. L receives supportive psychotherapy and cognitive remediation from a psychologist. He also is involved in incentive work therapy with a vocational rehabilitation specialist.
Related resource
- Silver, JM, McAllister TW, Yudofsky SC, eds. Textbook of traumatic brain injury. Washington, DC: American Psychiatric Publishing; 2005.
- Divalproex • Depakote
- Quetiapine • Seroquel
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Tranel D. Functional neuroanatomy: neuropsychological correlates of cortical and subcortical damage. In: Yudofsky SC, Hales RE, eds. The American Psychiatric Publishing textbook of neuropsychiatry and clinical neurosciences. 4th ed. Washington, DC: American Psychiatric Publishing; 2002:71-113.
2. Barrash J, Tranel D, Anderson SW. Acquired personality disturbances associated with bilateral damage to the ventromedial prefrontal region. Dev Neuropsychol 2000;18(3):355-81.
3. Silver JM, Hales RE, Yudofsky SC. Neuropsychiatric aspects of traumatic brain injury. In: Yudofsky SC, Hales RE, eds. The American Psychiatric Publishing textbook of neuropsychiatry and clinical neurosciences. 4th ed. Washington, DC: American Psychiatric Publishing; 2002:625-72.
4. Damasio AR, Tranel D, Damasio HC. Somatic markers and the guidance of behavior: theory and preliminary testing. In: Levin HS, Eisenberg HM, Benton AL, eds. Frontal lobe function and dysfunction. Oxford, UK: Oxford University Press; 1991:217-29.
5. Prigatano GP. The relationship of frontal lobe damage to diminished awareness: studies in rehabilitation. In: Levin HS, Eisenberg HM, Benton AL, eds. Frontal lobe function and dysfunction. Oxford, UK: Oxford University Press; 1991:381-97.
CASE: An unlikable patient
Mr. L, age 56, is admitted to the psychiatric unit at our Veterans Affairs Medical Center for active suicidal ideation; he has a history of self-injurious behaviors that include mutilation and overdose. He also has a history of alcohol dependence and multiple inpatient psychiatric admissions. He has never married and conflicts with his siblings—in whose home he has been staying—have led to frequent homelessness.
His affect is silly and shallow. He also shows signs of haughtiness, disinhibition, grandiosity, and confabulation. For example, he says that while in the Navy he had 82 sexual exploits and developed a drug that cured herpes.
We start Mr. L on divalproex, 1,500 mg/d, and quetiapine, titrated to 200 mg/d. After 3 days he is discharged, but this begins a cycle of repeated suicide gestures and readmissions—9 within the next 3 months. Each time he is discharged, Mr. L fails to follow through on treatment recommendations and is indifferent to our staff’s annoyed reactions.
The author’s observations
Some of our staff members regard Mr. L’s suicidal gestures as manipulative and feel angry and demoralized by his poor adherence to outpatient treatment plans. Their negative countertransference might have impacted how they evaluated Mr. L through repeated admissions and discharges. During Mr. L’s ninth admission, we decide to reevaluate his longitudinal history for clues to his noncompliant behavior.
History: Undocumented injury
Mr. L says he began drinking alcohol at age 16. He reports that he has grown marijuana but has not smoked it since 1991. He denies using heroin or other drugs.
Mr. L states that he suffered a head injury in 1975 after falling off a ladder on a Navy ship. He describes losing consciousness for a brief but uncertain duration. He reports that he has developed a seizure disorder since this fall and a history of amnesia secondary to past seizures. His medical records contain no witnessed seizures. Mr. L also says he was hospitalized a few years ago and placed on a ventilator for 7 days for an undetermined reason.
The authors’ observations
Based on Mr. L’s report of a possible traumatic brain injury (TBI), we order a neurologic evaluation. A year earlier, MRI of the brain without contrast demonstrated minimal, nonspecific periventricular and subcortical, punctuate hyperintensities on flair and T2 weighted sequences that are nonspecific. Overall, the impression was “diffuse involutional changes and mild nonspecific periventricular and subcortical white matter hyperintensities,” which might reflect covert vascular brain injury.
Our frustration over Mr. L’s repeated readmissions for suicidal gestures led us to seek outside evaluation and consultation from a senior psychiatrist for assistance with discharge and treatment planning. Unlike our staff, the consulting psychiatrist did not harbor strong negative feelings toward the patient.
Mr. L’s history of deterioration in psychosocial functioning prompted this psychiatrist to perform a thorough mental status examination that focused on cognitive elements and request formal neuropsychological testing.
Evalutation: Cognitive Deficits
During mental status examination, Mr. L has difficulty recalling 3 items and uses a memory strategy to assist himself. He fails to recollect in reverse order the last 5 U.S. presidents. He spells “world” backward, but has difficulty repeating 6 digits forward and 4 backward. He is unable to do serial 7 subtractions from 93 to 65 correctly. He adequately copies interlocking pentagons and draws a clock with the correct time. He achieves a score of 28/30 on the Folstein Mini Mental State Exam, missing the date by 4 days and recalling 2 of 3 words.
These results suggest Mr. L has difficulty with attention and working memory, short-term memory, fund of general information and long-term memory, and ability to perform simple calculations. Most important, they indicate the need for further study, especially a neuropsychological test battery.
Mr. L’s abnormal neuropsychological test results are summarized in the Table. He manifests concretization of thought. His loss of conceptual fluidity is documented formally by measures of perseverative errors and categories completed on the Wisconsin Card Sorting Test (WCST). These findings support a diagnosis of acquired dementia.
Table
Abnormal findings on Mr. L’s neuropsychological testing
| Cognitive domain | Test | Score | Interpretation |
|---|---|---|---|
| Mental status and effort | |||
| Mental status | MMSE total score | 28/30 | 2 of 3 items recalled after delay |
| Orientation | MMSE orientation questions | 9/10 | Date off by 4 days |
| Premorbid IQ estimate | WRAT-4 Reading Standard | 66th percentile | Within normal limits. Inconsistent with educational attainment, but could be impacted by temporal lobe findings |
| Verbal memory | |||
| Immediate memory | RBANS Immediate Memory Index (List and Story Learning) | 1st percentile | Severe impairment |
| Delayed memory | RBANS Delayed Memory Index | 1st percentile | Severe impairment |
| Recognition memory | List Learning | Severe impairment | |
| Visuospatial memory | |||
| Delayed memory | RBANS Figure Recall | 3rd percentile | Severe impairment |
| Executive functioning | |||
| Cognitive flexibility | Trails B | 10th percentile | Severe impairment based on educational attainment |
| WCST | Low scores: Nonperseverative errors, perseverative errors, and categories completed | ||
| * Tests of mental status effort, visuomotor processing speed, confrontation naming, visuospatial function, attention, and executive functioning fluency/initiation were within normal limits | |||
| MMSE: Mini Mental State Exam; WRAT: Wide Range Achievement Test; RBANS: Repeatable Battery for the Assessment of Neuropsychological Status; WCST: Wisconsin Card Sorting Test | |||
The authors’ observations
Mr. L’s history, cognitive testing, head imaging, and behavioral observations suggest that several pathogenic factors contribute to his impaired functioning. First, he describes a TBI of unknown severity occurring in 1975. Although brain scans did not show evidence of midline shift or encephalomalacia, a direct blow to the head after falling from a height combined with possible post-injury seizures suggests a TBI of at least moderate severity.
Second, Mr. L describes an incident in which he required inpatient respiratory assistance. Although the precipitating medical event was unclear, anoxia or hypoxia is likely. A recent CT revealed low attenuation in the left temporal region that could represent an infarct.
Mr. L’s severe memory impairment and moderate to severe impairment in cognitive flexibility are commonly reported after a TBI of moderate severity. If an ischemic incident were the primary contributor, a lateralized pattern of cognitive dysfunction—which Mr. L does not exhibit—would be expected.
Although Mr. L likely has vascular dementia, his MRI findings do not indicate sufficient disease to account for his memory scores. Vascular dementia is associated with slow, stepwise cognitive deterioration, which is not consistent with severely impaired memory in a 56-year-old patient.
Finally, alcoholism is associated with cognitive difficulty in memory, visuospatial functioning, and abstract reasoning. Mr. L demonstrated significant difficulty in memory and abstract reasoning, but his visuospatial functioning was largely intact. In the absence of Wernicke’s encephalopathy, chronic alcoholics generally do not show memory decrements in line with Mr. L’s. His MRI results indicated only minimal ventricular and sulcal enlargement. Because atrophy is present in approximately 60% of chronic alcoholics, this finding provides evidence of a contribution, but the other contributory factors are associated with more definitive medical outcomes. Thus, alcoholism must be viewed as a secondary contributor to Mr. L’s impaired functioning.
Taking into account all known contributors, TBI emerges as the primary diagnosis.
Consider neurologic injury
Recognizing and characterizing personality changes related to neurologic injury and disease is often problematic and unreliable, even when psychometrically validated instruments and structured diagnostic interviews are used (Box 1).1-5 Mr. L’s presentation differed from the more commonly reported “impulsive aggression” associated with closed head injury. Sequelae from TBI were contributing to his clinical presentation but was obscured by his shallow and silly affect, inability to accurately assess social cues, and lack of empathy.
Mr. L reported suffering a head injury from falling off a ladder. Personality changes that result from traumatic brain injury (TBI) of the sudden deceleration type—even when mild—are frequently referable to the frontal lobe, especially focal orbital and/or ventromedial damage of the prefrontal cortex.1-5 This is because of the physical proximity of the sphenoid wing to the orbitofrontal region and effects of shearing.
As a result of this damage, patients lack insight into their accompanying cognitive and behavioral abnormalities, such as the egocentricity and impaired empathy shown by Mr. L. These changes might not be detected in clinical interviews and over brief periods.2 Appreciating an acquired personality disturbance may require evaluating the patient’s behavior over months or years.2
In retrospect, Mr. L’s seeking repeated inpatient psychiatric hospitalizations is consistent with poor planning and problem-solving skills. He has a limited repertoire of adaptive behaviors and has learned that suicidal gestures lead to admission and caretaking. These are important to him because he is frequently homeless. His lack of insight is seen in his unrealistic plans for employment in jobs requiring specialized technical skills.
Mr. L’s case emphasizes the importance of considering brain injury as an etiologic factor in personality changes. It also highlights the complex—and seemingly nonoverlapping—functions and dysfunctions of the frontal lobe, including:
- source memory
- working memory
- sustained attention
- conceptual fluidity
- imaginative thinking
- impulse regulation
- planning and problem-solving skills.
Documenting Mr. L’s cognitive deficits and acquired dementia diagnosis changed our staff’s perception of his behavior, enabling us to overcome negative countertransference (Box 2). We no longer regarded him as deliberately manipulative and refer him for appropriate treatment.
Countertransference can interfere with optimal workup and treatment of patients with character changes related to traumatic brain injury and neurodegenerative processes. When we interpreted Mr. L’s suicidal gestures and hospitalizations as manipulative and deliberate, we failed to appreciate the limited number of things he could do to obtain a safe and protective environment. We also failed to recognize that his poor planning and problem-solving skills—as well as lack of insight into his illness—prevented him from adhering to outpatient treatment.
Originally, we attributed Mr. L’s egocentricity, lack of empathy, and lack of adherence to axis II pathology.
Our staff’s hostile feelings toward Mr. L led us to insufficiently consider his history—which is consistent with cognitive decline—during biopsychosocial evaluation and treatment planning. Mr. L’s status as a frequently homeless, unemployed person reflects a sharp decline for a highly educated person who served as a Navy officer and performed radiation inspections on nuclear-powered vessels.
Outome: Residential placement
We realize Mr. L needs cognitive rehabilitation—including assistance with planning and problem solving—and arrange for his placement in a residential facility for this specialized rehabilitation. Mr. L receives supportive psychotherapy and cognitive remediation from a psychologist. He also is involved in incentive work therapy with a vocational rehabilitation specialist.
Related resource
- Silver, JM, McAllister TW, Yudofsky SC, eds. Textbook of traumatic brain injury. Washington, DC: American Psychiatric Publishing; 2005.
- Divalproex • Depakote
- Quetiapine • Seroquel
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: An unlikable patient
Mr. L, age 56, is admitted to the psychiatric unit at our Veterans Affairs Medical Center for active suicidal ideation; he has a history of self-injurious behaviors that include mutilation and overdose. He also has a history of alcohol dependence and multiple inpatient psychiatric admissions. He has never married and conflicts with his siblings—in whose home he has been staying—have led to frequent homelessness.
His affect is silly and shallow. He also shows signs of haughtiness, disinhibition, grandiosity, and confabulation. For example, he says that while in the Navy he had 82 sexual exploits and developed a drug that cured herpes.
We start Mr. L on divalproex, 1,500 mg/d, and quetiapine, titrated to 200 mg/d. After 3 days he is discharged, but this begins a cycle of repeated suicide gestures and readmissions—9 within the next 3 months. Each time he is discharged, Mr. L fails to follow through on treatment recommendations and is indifferent to our staff’s annoyed reactions.
The author’s observations
Some of our staff members regard Mr. L’s suicidal gestures as manipulative and feel angry and demoralized by his poor adherence to outpatient treatment plans. Their negative countertransference might have impacted how they evaluated Mr. L through repeated admissions and discharges. During Mr. L’s ninth admission, we decide to reevaluate his longitudinal history for clues to his noncompliant behavior.
History: Undocumented injury
Mr. L says he began drinking alcohol at age 16. He reports that he has grown marijuana but has not smoked it since 1991. He denies using heroin or other drugs.
Mr. L states that he suffered a head injury in 1975 after falling off a ladder on a Navy ship. He describes losing consciousness for a brief but uncertain duration. He reports that he has developed a seizure disorder since this fall and a history of amnesia secondary to past seizures. His medical records contain no witnessed seizures. Mr. L also says he was hospitalized a few years ago and placed on a ventilator for 7 days for an undetermined reason.
The authors’ observations
Based on Mr. L’s report of a possible traumatic brain injury (TBI), we order a neurologic evaluation. A year earlier, MRI of the brain without contrast demonstrated minimal, nonspecific periventricular and subcortical, punctuate hyperintensities on flair and T2 weighted sequences that are nonspecific. Overall, the impression was “diffuse involutional changes and mild nonspecific periventricular and subcortical white matter hyperintensities,” which might reflect covert vascular brain injury.
Our frustration over Mr. L’s repeated readmissions for suicidal gestures led us to seek outside evaluation and consultation from a senior psychiatrist for assistance with discharge and treatment planning. Unlike our staff, the consulting psychiatrist did not harbor strong negative feelings toward the patient.
Mr. L’s history of deterioration in psychosocial functioning prompted this psychiatrist to perform a thorough mental status examination that focused on cognitive elements and request formal neuropsychological testing.
Evalutation: Cognitive Deficits
During mental status examination, Mr. L has difficulty recalling 3 items and uses a memory strategy to assist himself. He fails to recollect in reverse order the last 5 U.S. presidents. He spells “world” backward, but has difficulty repeating 6 digits forward and 4 backward. He is unable to do serial 7 subtractions from 93 to 65 correctly. He adequately copies interlocking pentagons and draws a clock with the correct time. He achieves a score of 28/30 on the Folstein Mini Mental State Exam, missing the date by 4 days and recalling 2 of 3 words.
These results suggest Mr. L has difficulty with attention and working memory, short-term memory, fund of general information and long-term memory, and ability to perform simple calculations. Most important, they indicate the need for further study, especially a neuropsychological test battery.
Mr. L’s abnormal neuropsychological test results are summarized in the Table. He manifests concretization of thought. His loss of conceptual fluidity is documented formally by measures of perseverative errors and categories completed on the Wisconsin Card Sorting Test (WCST). These findings support a diagnosis of acquired dementia.
Table
Abnormal findings on Mr. L’s neuropsychological testing
| Cognitive domain | Test | Score | Interpretation |
|---|---|---|---|
| Mental status and effort | |||
| Mental status | MMSE total score | 28/30 | 2 of 3 items recalled after delay |
| Orientation | MMSE orientation questions | 9/10 | Date off by 4 days |
| Premorbid IQ estimate | WRAT-4 Reading Standard | 66th percentile | Within normal limits. Inconsistent with educational attainment, but could be impacted by temporal lobe findings |
| Verbal memory | |||
| Immediate memory | RBANS Immediate Memory Index (List and Story Learning) | 1st percentile | Severe impairment |
| Delayed memory | RBANS Delayed Memory Index | 1st percentile | Severe impairment |
| Recognition memory | List Learning | Severe impairment | |
| Visuospatial memory | |||
| Delayed memory | RBANS Figure Recall | 3rd percentile | Severe impairment |
| Executive functioning | |||
| Cognitive flexibility | Trails B | 10th percentile | Severe impairment based on educational attainment |
| WCST | Low scores: Nonperseverative errors, perseverative errors, and categories completed | ||
| * Tests of mental status effort, visuomotor processing speed, confrontation naming, visuospatial function, attention, and executive functioning fluency/initiation were within normal limits | |||
| MMSE: Mini Mental State Exam; WRAT: Wide Range Achievement Test; RBANS: Repeatable Battery for the Assessment of Neuropsychological Status; WCST: Wisconsin Card Sorting Test | |||
The authors’ observations
Mr. L’s history, cognitive testing, head imaging, and behavioral observations suggest that several pathogenic factors contribute to his impaired functioning. First, he describes a TBI of unknown severity occurring in 1975. Although brain scans did not show evidence of midline shift or encephalomalacia, a direct blow to the head after falling from a height combined with possible post-injury seizures suggests a TBI of at least moderate severity.
Second, Mr. L describes an incident in which he required inpatient respiratory assistance. Although the precipitating medical event was unclear, anoxia or hypoxia is likely. A recent CT revealed low attenuation in the left temporal region that could represent an infarct.
Mr. L’s severe memory impairment and moderate to severe impairment in cognitive flexibility are commonly reported after a TBI of moderate severity. If an ischemic incident were the primary contributor, a lateralized pattern of cognitive dysfunction—which Mr. L does not exhibit—would be expected.
Although Mr. L likely has vascular dementia, his MRI findings do not indicate sufficient disease to account for his memory scores. Vascular dementia is associated with slow, stepwise cognitive deterioration, which is not consistent with severely impaired memory in a 56-year-old patient.
Finally, alcoholism is associated with cognitive difficulty in memory, visuospatial functioning, and abstract reasoning. Mr. L demonstrated significant difficulty in memory and abstract reasoning, but his visuospatial functioning was largely intact. In the absence of Wernicke’s encephalopathy, chronic alcoholics generally do not show memory decrements in line with Mr. L’s. His MRI results indicated only minimal ventricular and sulcal enlargement. Because atrophy is present in approximately 60% of chronic alcoholics, this finding provides evidence of a contribution, but the other contributory factors are associated with more definitive medical outcomes. Thus, alcoholism must be viewed as a secondary contributor to Mr. L’s impaired functioning.
Taking into account all known contributors, TBI emerges as the primary diagnosis.
Consider neurologic injury
Recognizing and characterizing personality changes related to neurologic injury and disease is often problematic and unreliable, even when psychometrically validated instruments and structured diagnostic interviews are used (Box 1).1-5 Mr. L’s presentation differed from the more commonly reported “impulsive aggression” associated with closed head injury. Sequelae from TBI were contributing to his clinical presentation but was obscured by his shallow and silly affect, inability to accurately assess social cues, and lack of empathy.
Mr. L reported suffering a head injury from falling off a ladder. Personality changes that result from traumatic brain injury (TBI) of the sudden deceleration type—even when mild—are frequently referable to the frontal lobe, especially focal orbital and/or ventromedial damage of the prefrontal cortex.1-5 This is because of the physical proximity of the sphenoid wing to the orbitofrontal region and effects of shearing.
As a result of this damage, patients lack insight into their accompanying cognitive and behavioral abnormalities, such as the egocentricity and impaired empathy shown by Mr. L. These changes might not be detected in clinical interviews and over brief periods.2 Appreciating an acquired personality disturbance may require evaluating the patient’s behavior over months or years.2
In retrospect, Mr. L’s seeking repeated inpatient psychiatric hospitalizations is consistent with poor planning and problem-solving skills. He has a limited repertoire of adaptive behaviors and has learned that suicidal gestures lead to admission and caretaking. These are important to him because he is frequently homeless. His lack of insight is seen in his unrealistic plans for employment in jobs requiring specialized technical skills.
Mr. L’s case emphasizes the importance of considering brain injury as an etiologic factor in personality changes. It also highlights the complex—and seemingly nonoverlapping—functions and dysfunctions of the frontal lobe, including:
- source memory
- working memory
- sustained attention
- conceptual fluidity
- imaginative thinking
- impulse regulation
- planning and problem-solving skills.
Documenting Mr. L’s cognitive deficits and acquired dementia diagnosis changed our staff’s perception of his behavior, enabling us to overcome negative countertransference (Box 2). We no longer regarded him as deliberately manipulative and refer him for appropriate treatment.
Countertransference can interfere with optimal workup and treatment of patients with character changes related to traumatic brain injury and neurodegenerative processes. When we interpreted Mr. L’s suicidal gestures and hospitalizations as manipulative and deliberate, we failed to appreciate the limited number of things he could do to obtain a safe and protective environment. We also failed to recognize that his poor planning and problem-solving skills—as well as lack of insight into his illness—prevented him from adhering to outpatient treatment.
Originally, we attributed Mr. L’s egocentricity, lack of empathy, and lack of adherence to axis II pathology.
Our staff’s hostile feelings toward Mr. L led us to insufficiently consider his history—which is consistent with cognitive decline—during biopsychosocial evaluation and treatment planning. Mr. L’s status as a frequently homeless, unemployed person reflects a sharp decline for a highly educated person who served as a Navy officer and performed radiation inspections on nuclear-powered vessels.
Outome: Residential placement
We realize Mr. L needs cognitive rehabilitation—including assistance with planning and problem solving—and arrange for his placement in a residential facility for this specialized rehabilitation. Mr. L receives supportive psychotherapy and cognitive remediation from a psychologist. He also is involved in incentive work therapy with a vocational rehabilitation specialist.
Related resource
- Silver, JM, McAllister TW, Yudofsky SC, eds. Textbook of traumatic brain injury. Washington, DC: American Psychiatric Publishing; 2005.
- Divalproex • Depakote
- Quetiapine • Seroquel
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Tranel D. Functional neuroanatomy: neuropsychological correlates of cortical and subcortical damage. In: Yudofsky SC, Hales RE, eds. The American Psychiatric Publishing textbook of neuropsychiatry and clinical neurosciences. 4th ed. Washington, DC: American Psychiatric Publishing; 2002:71-113.
2. Barrash J, Tranel D, Anderson SW. Acquired personality disturbances associated with bilateral damage to the ventromedial prefrontal region. Dev Neuropsychol 2000;18(3):355-81.
3. Silver JM, Hales RE, Yudofsky SC. Neuropsychiatric aspects of traumatic brain injury. In: Yudofsky SC, Hales RE, eds. The American Psychiatric Publishing textbook of neuropsychiatry and clinical neurosciences. 4th ed. Washington, DC: American Psychiatric Publishing; 2002:625-72.
4. Damasio AR, Tranel D, Damasio HC. Somatic markers and the guidance of behavior: theory and preliminary testing. In: Levin HS, Eisenberg HM, Benton AL, eds. Frontal lobe function and dysfunction. Oxford, UK: Oxford University Press; 1991:217-29.
5. Prigatano GP. The relationship of frontal lobe damage to diminished awareness: studies in rehabilitation. In: Levin HS, Eisenberg HM, Benton AL, eds. Frontal lobe function and dysfunction. Oxford, UK: Oxford University Press; 1991:381-97.
1. Tranel D. Functional neuroanatomy: neuropsychological correlates of cortical and subcortical damage. In: Yudofsky SC, Hales RE, eds. The American Psychiatric Publishing textbook of neuropsychiatry and clinical neurosciences. 4th ed. Washington, DC: American Psychiatric Publishing; 2002:71-113.
2. Barrash J, Tranel D, Anderson SW. Acquired personality disturbances associated with bilateral damage to the ventromedial prefrontal region. Dev Neuropsychol 2000;18(3):355-81.
3. Silver JM, Hales RE, Yudofsky SC. Neuropsychiatric aspects of traumatic brain injury. In: Yudofsky SC, Hales RE, eds. The American Psychiatric Publishing textbook of neuropsychiatry and clinical neurosciences. 4th ed. Washington, DC: American Psychiatric Publishing; 2002:625-72.
4. Damasio AR, Tranel D, Damasio HC. Somatic markers and the guidance of behavior: theory and preliminary testing. In: Levin HS, Eisenberg HM, Benton AL, eds. Frontal lobe function and dysfunction. Oxford, UK: Oxford University Press; 1991:217-29.
5. Prigatano GP. The relationship of frontal lobe damage to diminished awareness: studies in rehabilitation. In: Levin HS, Eisenberg HM, Benton AL, eds. Frontal lobe function and dysfunction. Oxford, UK: Oxford University Press; 1991:381-97.
The puzzling self-poisoner
CASE: Unusual suicide attempt
After a friend calls 911, Ms. M, age 20, is brought to an emergency room (ER) complaining of severe leg and abdominal pain. The ER physician finds she is bleeding from her vagina and nose and has severe ecchymosis anemia. After Ms. M is admitted, clinicians discover these conditions are secondary to a suicide attempt—she ingested 15 to 16 pellets of rat poison daily for approximately 2 months.
While hospitalized, Ms. M is treated with several transfusions of fresh frozen plasma, packed red blood cells, and phytonadione (vitamin K). A consultation-liaison psychiatrist diagnoses bipolar disorder and starts Ms. M on lamotrigine, 25 mg once daily. (The justification for this diagnosis was not documented.) After physicians judge her to be medically stable, Ms. M is involuntarily committed to a short-term psychiatric care facility. Her vital signs and coagulation values are stable.
At the psychiatric facility, our team determines that her symptoms and history are consistent with major depressive disorder, recurrent. For 5 months, Ms. M had depressed mood for most of the day, diminished interest in activities, and feelings of worthlessness. She also experienced weight loss—10 lbs in 2 months—with decreased appetite and low energy for most of the day. She denies past symptoms of mania or psychosis. She says she does not know why she was diagnosed with bipolar disorder. She admits to multiple previous suicide attempts via hanging and ingesting cleaning fluid or rat poison.
We place Ms. M on suicide precautions and prescribe escitalopram, 10 mg/d, in addition to lamotrigine, 50 mg once daily. We continue lamotrigine despite a lack of documentation for Ms. M’s bipolar diagnosis because evidence suggests the drug may be an effective augmentation to antidepressants in patients with treatment-resistant depression.1
The author’s observations
Any patient transferred from a medical floor to a psychiatric inpatient unit should have documentation that clarifies any need for further medical treatment. Ms. M’s physicians told us that she was medically stable and should require little if any further treatment for her ingestion of rat poison.
TREATMENT: Coagulation concerns
We request a medical consult to monitor possible complications from the rat poison. The physician advises that rat poison essentially is the same as the anticoagulant warfarin and its effects should steadily decrease over time because its half-life is 20 to 60 hours. However, for safety reasons, we closely follow Ms. M’s coagulation values and order daily vitamin K injections, 5 mg SC.
Further medical investigation shows no evidence of complications, but Ms. M continues to request medication for pain in her left leg. The physician prescribes acetaminophen, 650 mg every 6 hours as needed for pain, which the patient takes at almost every opportunity, often 4 times a day. The physician does not choose a nonsteroidal anti-inflammatory drug (NSAID) for pain to avoid the possibility of gastrointestinal (GI) irritation that could lead to bleeding.
In the psychiatric facility, the patient’s international normalized ratio (INR) is found to be rising, indicating a lack of clotting and a risk of uncontrolled bleeding. The physician states that given the half-life of warfarin, Ms. M’s INR should be decreasing. Liver function testing does not show that liver dysfunction is contributing to the increasing INR.
Because we assume the vitamin K the patient received has been absorbed, we hypothesize that Ms. M has continued to surreptitiously ingest rat poison or another anticoagulant, which she denies. We search Ms. M and her room. She is placed on 1-to-1 observation 24 hours a day. Ms. M’s visitors also are searched, and visits are observed. We find no evidence of an anticoagulant agent.
Ms. M’s INR continues to rise. We search the facility to rule out the possibility that the patient had hidden a supply of anticoagulant outside her room. The search finds nothing. At this point we consider performing an abdominal x-ray to rule out the possibility that Ms. M may have a supply of medication hidden in her gastrointestinal tract.
The author’s observations
Patients hiding and using contraband is a common problem in involuntary inpatient units. It seemed that Ms. M was secretly ingesting rat poison. Her history showed she was determined to end her life, and she ingested rat poison daily for months. However, because an exhaustive search for contraband and 1-to-1 observation yielded no positive results, the evidence did not support this theory. Some team members thought we were not searching hard enough. I decided we needed to pursue other theories.
I was skeptical that escitalopram could be contributing to Ms. M’s rising anticoagulation values. Selective serotonin reuptake inhibitors have antiplatelet effects, but platelet function does not affect INR to the degree we were observing.
‘Superwarfarins’
Physicians had advised us that Ms. M’s INR should decrease under the assumption that rat poison is for all practical purposes the same as warfarin, but we had not investigated distinctions between the 2 compounds. A literature search revealed that several rat poisons are not simply warfarin repackaged as a pesticide. Most are “superwarfarins”—chemicals similar to warfarin but more potent and with a much longer half-life.2 Case report data suggest the plasma half-life of these chemicals is 20 to 62 days.3
Most commercial rat poisons are made of brodifacoum, which has a chemical structure similar to warfarin but with an additional long polycyclic hydrocarbon side chain (Figure 1). The potency of brodifacoum compared with warfarin is approximately 100 to 1.4-6 The chemical is highly lipophilic and can stay in the body for an extended period.4-6 Lab tests can measure serum brodifacoum levels.3
After Ms. M identifies the brand name of the rat poison she ingested, we contact the American Association of Poison Control Centers and verify the agent she used was brodifacoum. This explains why her INR was not decreasing—but does not explain the increase.
A drug interaction? Because Ms. M’s liver function is within normal limits, the next theory to investigate is if brodifacoum is interacting with any medications she is taking. I could not find any medical journal articles, programs, or Web sites describing brodifacoum’s interactions with medications. After all, brodifacoum is a pesticide, not a medication.
I considered that because brodifacoum and warfarin have a similar structure and function, they may interact with medications in a similar manner. After another literature search, only acetaminophen had evidence of interaction with warfarin that could explain her rising INR.
Documentation of interactions between warfarin and acetaminophen are sparse. In one case, a 74-year-old man receiving warfarin for atrial fibrillation experienced an abrupt increase in INR after taking acetaminophen.7 In a double-blind, placebo controlled, randomized trial of patients taking warfarin, INR rose rapidly after the start of acetaminophen and was significantly increased within 1 week compared with patients receiving placebo.8
Figure 1 Chemical structures of warfarin and rat poison
Most commercial rat poisons are made of brodifacoum, which is chemically similar to warfarin but has an additional long polycyclic hydrocarbon side chain.
FOLLOW-UP: Analgesic substitution
We suggest to the physician that Ms. M’s INR may be increasing because of an interaction between brodifacoum and acetaminophen, which she took several times a day. On day 8 of Ms. M’s hospitalization, the physician discontinues acetaminophen and prescribes ibuprofen, 400 mg tid as needed for pain, and pantoprazole, 40 mg/d, to prevent GI bleeding from possible irritation caused by ibuprofen. The team continues to monitor Ms. M’s coagulation values.
Within a day of discontinuing acetaminophen, Ms. M’s INR decreased as expected (Figure 2). The rest of her medication regimen is continued, and her INR levels continued to decrease.
One-to-one observation is discontinued. However, because of the patient’s continued determination to end her life and no significant improvement in her depression, Ms. M is considered a danger to herself and involuntary inpatient hospitalization is continued.
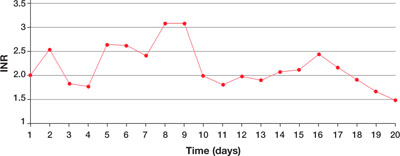
Figure 2 Ms. M’s INR values during hospitalization
The patient’s INR values began to rise mysteriously after she was transferred to the inpatient psychiatric unit. Acetaminophen was discontinued on day 8, and within a day her INR values began to drop.
INR: International normalized ratio
The author’s observations
Poisoning is a common method of attempting suicide, patients may use substances that clinicians rarely encounter. For most toxic, nonmedication substances, data on interactions with medications are sparse. if you suspect your patient has ingested a toxic substance with which the treatment team has little experience, contact the American Association of Poison Control Centers at 800-222-1222.
Suspect superwarfarin poisoning in suicidal patients with coagulopathy, prolonged prothrombin time, and elevated INR that does not respond to large amounts of vitamin K.9,10 These patients are at high risk of successfully completing suicide because of superwarfarins’ long half-life and daily maintenance required to keep coagulation levels within a safe range for at least several weeks.
The most serious complication these patients face is intracranial hemorrhage, which occurs in 2% of patients with excessive warfarin-based coagulation and is associated with a 77% mortality rate.11 GI bleeding occurs in 67% of these patients.2
Also take into account medical conditions—such as hypertension or hepatic disease—and medication side effects that can increase bleeding risk. When treating pain in these patients, consider avoiding acetaminophen but be aware of the risks of NSAIDs, such as gastritis or GI bleeding.
Related resource
- The American Association of Poison Control Centers. 800-222-1222; www.aapcc.org.
Drug brand names
- Escitalopram • Lexapro
- Lamotrigine • Lamictal
- Pantoprazole • Protonix
- Warfarin • Coumadin
Disclosure
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Sharma V, Khan M, Corpse C. Role of lamotrigine in the management of treatment-resistant bipolar II depression: a chart review. J Affect Disord Epub 2008 Mar 1.
2. Su M, Hoffman R. Anticoagulants. In: Flomenbaum NE, Goldfrank LR, Hoffman RS, et al, eds. Goldfrank’s toxicologic emergencies. 8th ed. New York, NY: McGraw-Hill Medical Publishing; 2006:891-4.
3. Chua JD, Friedenberg WR. Superwarfarin poisoning. Anaesth Intensive Care 1997;25:707-9.
4. Leck JB, Park BK. A comparative study of the effect of warfarin and brodifacoum on the relationship between vitamin K1 metabolism and clotting factor activity in warfarin susceptible and warfarin resistant rats. Biochem Pharmacol 1981;30:123-9.
5. Lund M. Comparative effect of the three rodenticides warfarin, difenacoum and brodifacoum on eight rodent species in short feeding periods. J Hyg 1981;87:101-7.
6. Park BK, Scott AK, Wilson AC, et al. Plasma disposition of vitamin K antagonism by warfarin, difenacoum and brodifacoum in the rabbit. Biochem Pharmacol 1982;31:3535-639.
7. Gebauer MG, Nyfort-Hansen K, Henschke PJ, Gallus AS. Warfarin and acetaminophen interaction. Pharmacotherapy 2003;23(1):109-12.
8. Mahe I, Bertrand N, Drouet L, et al. Interaction between paracetamol and warfarin in patients: a double-blind, placebo-controlled, randomized study. Haematologica 2006;91(12):1621-7.
9. Sharma P, Bentley P. Of rats and men: superwarfarin toxicity. Lancet 2005;365:552-3.
10. Scully M. Warfarin therapy: rat poison and the prevention of thrombosis. Biochemist 2002;24:15-7.
11. Mathiesen T, Benediktsdottir K, Johnsson H, Lindqvist M. Intracranial traumatic and nontraumatic haemorrhagic complications of warfarin treatment. Acta Neurol Scan 1995;91:208-14.
CASE: Unusual suicide attempt
After a friend calls 911, Ms. M, age 20, is brought to an emergency room (ER) complaining of severe leg and abdominal pain. The ER physician finds she is bleeding from her vagina and nose and has severe ecchymosis anemia. After Ms. M is admitted, clinicians discover these conditions are secondary to a suicide attempt—she ingested 15 to 16 pellets of rat poison daily for approximately 2 months.
While hospitalized, Ms. M is treated with several transfusions of fresh frozen plasma, packed red blood cells, and phytonadione (vitamin K). A consultation-liaison psychiatrist diagnoses bipolar disorder and starts Ms. M on lamotrigine, 25 mg once daily. (The justification for this diagnosis was not documented.) After physicians judge her to be medically stable, Ms. M is involuntarily committed to a short-term psychiatric care facility. Her vital signs and coagulation values are stable.
At the psychiatric facility, our team determines that her symptoms and history are consistent with major depressive disorder, recurrent. For 5 months, Ms. M had depressed mood for most of the day, diminished interest in activities, and feelings of worthlessness. She also experienced weight loss—10 lbs in 2 months—with decreased appetite and low energy for most of the day. She denies past symptoms of mania or psychosis. She says she does not know why she was diagnosed with bipolar disorder. She admits to multiple previous suicide attempts via hanging and ingesting cleaning fluid or rat poison.
We place Ms. M on suicide precautions and prescribe escitalopram, 10 mg/d, in addition to lamotrigine, 50 mg once daily. We continue lamotrigine despite a lack of documentation for Ms. M’s bipolar diagnosis because evidence suggests the drug may be an effective augmentation to antidepressants in patients with treatment-resistant depression.1
The author’s observations
Any patient transferred from a medical floor to a psychiatric inpatient unit should have documentation that clarifies any need for further medical treatment. Ms. M’s physicians told us that she was medically stable and should require little if any further treatment for her ingestion of rat poison.
TREATMENT: Coagulation concerns
We request a medical consult to monitor possible complications from the rat poison. The physician advises that rat poison essentially is the same as the anticoagulant warfarin and its effects should steadily decrease over time because its half-life is 20 to 60 hours. However, for safety reasons, we closely follow Ms. M’s coagulation values and order daily vitamin K injections, 5 mg SC.
Further medical investigation shows no evidence of complications, but Ms. M continues to request medication for pain in her left leg. The physician prescribes acetaminophen, 650 mg every 6 hours as needed for pain, which the patient takes at almost every opportunity, often 4 times a day. The physician does not choose a nonsteroidal anti-inflammatory drug (NSAID) for pain to avoid the possibility of gastrointestinal (GI) irritation that could lead to bleeding.
In the psychiatric facility, the patient’s international normalized ratio (INR) is found to be rising, indicating a lack of clotting and a risk of uncontrolled bleeding. The physician states that given the half-life of warfarin, Ms. M’s INR should be decreasing. Liver function testing does not show that liver dysfunction is contributing to the increasing INR.
Because we assume the vitamin K the patient received has been absorbed, we hypothesize that Ms. M has continued to surreptitiously ingest rat poison or another anticoagulant, which she denies. We search Ms. M and her room. She is placed on 1-to-1 observation 24 hours a day. Ms. M’s visitors also are searched, and visits are observed. We find no evidence of an anticoagulant agent.
Ms. M’s INR continues to rise. We search the facility to rule out the possibility that the patient had hidden a supply of anticoagulant outside her room. The search finds nothing. At this point we consider performing an abdominal x-ray to rule out the possibility that Ms. M may have a supply of medication hidden in her gastrointestinal tract.
The author’s observations
Patients hiding and using contraband is a common problem in involuntary inpatient units. It seemed that Ms. M was secretly ingesting rat poison. Her history showed she was determined to end her life, and she ingested rat poison daily for months. However, because an exhaustive search for contraband and 1-to-1 observation yielded no positive results, the evidence did not support this theory. Some team members thought we were not searching hard enough. I decided we needed to pursue other theories.
I was skeptical that escitalopram could be contributing to Ms. M’s rising anticoagulation values. Selective serotonin reuptake inhibitors have antiplatelet effects, but platelet function does not affect INR to the degree we were observing.
‘Superwarfarins’
Physicians had advised us that Ms. M’s INR should decrease under the assumption that rat poison is for all practical purposes the same as warfarin, but we had not investigated distinctions between the 2 compounds. A literature search revealed that several rat poisons are not simply warfarin repackaged as a pesticide. Most are “superwarfarins”—chemicals similar to warfarin but more potent and with a much longer half-life.2 Case report data suggest the plasma half-life of these chemicals is 20 to 62 days.3
Most commercial rat poisons are made of brodifacoum, which has a chemical structure similar to warfarin but with an additional long polycyclic hydrocarbon side chain (Figure 1). The potency of brodifacoum compared with warfarin is approximately 100 to 1.4-6 The chemical is highly lipophilic and can stay in the body for an extended period.4-6 Lab tests can measure serum brodifacoum levels.3
After Ms. M identifies the brand name of the rat poison she ingested, we contact the American Association of Poison Control Centers and verify the agent she used was brodifacoum. This explains why her INR was not decreasing—but does not explain the increase.
A drug interaction? Because Ms. M’s liver function is within normal limits, the next theory to investigate is if brodifacoum is interacting with any medications she is taking. I could not find any medical journal articles, programs, or Web sites describing brodifacoum’s interactions with medications. After all, brodifacoum is a pesticide, not a medication.
I considered that because brodifacoum and warfarin have a similar structure and function, they may interact with medications in a similar manner. After another literature search, only acetaminophen had evidence of interaction with warfarin that could explain her rising INR.
Documentation of interactions between warfarin and acetaminophen are sparse. In one case, a 74-year-old man receiving warfarin for atrial fibrillation experienced an abrupt increase in INR after taking acetaminophen.7 In a double-blind, placebo controlled, randomized trial of patients taking warfarin, INR rose rapidly after the start of acetaminophen and was significantly increased within 1 week compared with patients receiving placebo.8
Figure 1 Chemical structures of warfarin and rat poison
Most commercial rat poisons are made of brodifacoum, which is chemically similar to warfarin but has an additional long polycyclic hydrocarbon side chain.
FOLLOW-UP: Analgesic substitution
We suggest to the physician that Ms. M’s INR may be increasing because of an interaction between brodifacoum and acetaminophen, which she took several times a day. On day 8 of Ms. M’s hospitalization, the physician discontinues acetaminophen and prescribes ibuprofen, 400 mg tid as needed for pain, and pantoprazole, 40 mg/d, to prevent GI bleeding from possible irritation caused by ibuprofen. The team continues to monitor Ms. M’s coagulation values.
Within a day of discontinuing acetaminophen, Ms. M’s INR decreased as expected (Figure 2). The rest of her medication regimen is continued, and her INR levels continued to decrease.
One-to-one observation is discontinued. However, because of the patient’s continued determination to end her life and no significant improvement in her depression, Ms. M is considered a danger to herself and involuntary inpatient hospitalization is continued.
Figure 2 Ms. M’s INR values during hospitalization
The patient’s INR values began to rise mysteriously after she was transferred to the inpatient psychiatric unit. Acetaminophen was discontinued on day 8, and within a day her INR values began to drop.
INR: International normalized ratio
The author’s observations
Poisoning is a common method of attempting suicide, patients may use substances that clinicians rarely encounter. For most toxic, nonmedication substances, data on interactions with medications are sparse. if you suspect your patient has ingested a toxic substance with which the treatment team has little experience, contact the American Association of Poison Control Centers at 800-222-1222.
Suspect superwarfarin poisoning in suicidal patients with coagulopathy, prolonged prothrombin time, and elevated INR that does not respond to large amounts of vitamin K.9,10 These patients are at high risk of successfully completing suicide because of superwarfarins’ long half-life and daily maintenance required to keep coagulation levels within a safe range for at least several weeks.
The most serious complication these patients face is intracranial hemorrhage, which occurs in 2% of patients with excessive warfarin-based coagulation and is associated with a 77% mortality rate.11 GI bleeding occurs in 67% of these patients.2
Also take into account medical conditions—such as hypertension or hepatic disease—and medication side effects that can increase bleeding risk. When treating pain in these patients, consider avoiding acetaminophen but be aware of the risks of NSAIDs, such as gastritis or GI bleeding.
Related resource
- The American Association of Poison Control Centers. 800-222-1222; www.aapcc.org.
Drug brand names
- Escitalopram • Lexapro
- Lamotrigine • Lamictal
- Pantoprazole • Protonix
- Warfarin • Coumadin
Disclosure
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: Unusual suicide attempt
After a friend calls 911, Ms. M, age 20, is brought to an emergency room (ER) complaining of severe leg and abdominal pain. The ER physician finds she is bleeding from her vagina and nose and has severe ecchymosis anemia. After Ms. M is admitted, clinicians discover these conditions are secondary to a suicide attempt—she ingested 15 to 16 pellets of rat poison daily for approximately 2 months.
While hospitalized, Ms. M is treated with several transfusions of fresh frozen plasma, packed red blood cells, and phytonadione (vitamin K). A consultation-liaison psychiatrist diagnoses bipolar disorder and starts Ms. M on lamotrigine, 25 mg once daily. (The justification for this diagnosis was not documented.) After physicians judge her to be medically stable, Ms. M is involuntarily committed to a short-term psychiatric care facility. Her vital signs and coagulation values are stable.
At the psychiatric facility, our team determines that her symptoms and history are consistent with major depressive disorder, recurrent. For 5 months, Ms. M had depressed mood for most of the day, diminished interest in activities, and feelings of worthlessness. She also experienced weight loss—10 lbs in 2 months—with decreased appetite and low energy for most of the day. She denies past symptoms of mania or psychosis. She says she does not know why she was diagnosed with bipolar disorder. She admits to multiple previous suicide attempts via hanging and ingesting cleaning fluid or rat poison.
We place Ms. M on suicide precautions and prescribe escitalopram, 10 mg/d, in addition to lamotrigine, 50 mg once daily. We continue lamotrigine despite a lack of documentation for Ms. M’s bipolar diagnosis because evidence suggests the drug may be an effective augmentation to antidepressants in patients with treatment-resistant depression.1
The author’s observations
Any patient transferred from a medical floor to a psychiatric inpatient unit should have documentation that clarifies any need for further medical treatment. Ms. M’s physicians told us that she was medically stable and should require little if any further treatment for her ingestion of rat poison.
TREATMENT: Coagulation concerns
We request a medical consult to monitor possible complications from the rat poison. The physician advises that rat poison essentially is the same as the anticoagulant warfarin and its effects should steadily decrease over time because its half-life is 20 to 60 hours. However, for safety reasons, we closely follow Ms. M’s coagulation values and order daily vitamin K injections, 5 mg SC.
Further medical investigation shows no evidence of complications, but Ms. M continues to request medication for pain in her left leg. The physician prescribes acetaminophen, 650 mg every 6 hours as needed for pain, which the patient takes at almost every opportunity, often 4 times a day. The physician does not choose a nonsteroidal anti-inflammatory drug (NSAID) for pain to avoid the possibility of gastrointestinal (GI) irritation that could lead to bleeding.
In the psychiatric facility, the patient’s international normalized ratio (INR) is found to be rising, indicating a lack of clotting and a risk of uncontrolled bleeding. The physician states that given the half-life of warfarin, Ms. M’s INR should be decreasing. Liver function testing does not show that liver dysfunction is contributing to the increasing INR.
Because we assume the vitamin K the patient received has been absorbed, we hypothesize that Ms. M has continued to surreptitiously ingest rat poison or another anticoagulant, which she denies. We search Ms. M and her room. She is placed on 1-to-1 observation 24 hours a day. Ms. M’s visitors also are searched, and visits are observed. We find no evidence of an anticoagulant agent.
Ms. M’s INR continues to rise. We search the facility to rule out the possibility that the patient had hidden a supply of anticoagulant outside her room. The search finds nothing. At this point we consider performing an abdominal x-ray to rule out the possibility that Ms. M may have a supply of medication hidden in her gastrointestinal tract.
The author’s observations
Patients hiding and using contraband is a common problem in involuntary inpatient units. It seemed that Ms. M was secretly ingesting rat poison. Her history showed she was determined to end her life, and she ingested rat poison daily for months. However, because an exhaustive search for contraband and 1-to-1 observation yielded no positive results, the evidence did not support this theory. Some team members thought we were not searching hard enough. I decided we needed to pursue other theories.
I was skeptical that escitalopram could be contributing to Ms. M’s rising anticoagulation values. Selective serotonin reuptake inhibitors have antiplatelet effects, but platelet function does not affect INR to the degree we were observing.
‘Superwarfarins’
Physicians had advised us that Ms. M’s INR should decrease under the assumption that rat poison is for all practical purposes the same as warfarin, but we had not investigated distinctions between the 2 compounds. A literature search revealed that several rat poisons are not simply warfarin repackaged as a pesticide. Most are “superwarfarins”—chemicals similar to warfarin but more potent and with a much longer half-life.2 Case report data suggest the plasma half-life of these chemicals is 20 to 62 days.3
Most commercial rat poisons are made of brodifacoum, which has a chemical structure similar to warfarin but with an additional long polycyclic hydrocarbon side chain (Figure 1). The potency of brodifacoum compared with warfarin is approximately 100 to 1.4-6 The chemical is highly lipophilic and can stay in the body for an extended period.4-6 Lab tests can measure serum brodifacoum levels.3
After Ms. M identifies the brand name of the rat poison she ingested, we contact the American Association of Poison Control Centers and verify the agent she used was brodifacoum. This explains why her INR was not decreasing—but does not explain the increase.
A drug interaction? Because Ms. M’s liver function is within normal limits, the next theory to investigate is if brodifacoum is interacting with any medications she is taking. I could not find any medical journal articles, programs, or Web sites describing brodifacoum’s interactions with medications. After all, brodifacoum is a pesticide, not a medication.
I considered that because brodifacoum and warfarin have a similar structure and function, they may interact with medications in a similar manner. After another literature search, only acetaminophen had evidence of interaction with warfarin that could explain her rising INR.
Documentation of interactions between warfarin and acetaminophen are sparse. In one case, a 74-year-old man receiving warfarin for atrial fibrillation experienced an abrupt increase in INR after taking acetaminophen.7 In a double-blind, placebo controlled, randomized trial of patients taking warfarin, INR rose rapidly after the start of acetaminophen and was significantly increased within 1 week compared with patients receiving placebo.8
Figure 1 Chemical structures of warfarin and rat poison
Most commercial rat poisons are made of brodifacoum, which is chemically similar to warfarin but has an additional long polycyclic hydrocarbon side chain.
FOLLOW-UP: Analgesic substitution
We suggest to the physician that Ms. M’s INR may be increasing because of an interaction between brodifacoum and acetaminophen, which she took several times a day. On day 8 of Ms. M’s hospitalization, the physician discontinues acetaminophen and prescribes ibuprofen, 400 mg tid as needed for pain, and pantoprazole, 40 mg/d, to prevent GI bleeding from possible irritation caused by ibuprofen. The team continues to monitor Ms. M’s coagulation values.
Within a day of discontinuing acetaminophen, Ms. M’s INR decreased as expected (Figure 2). The rest of her medication regimen is continued, and her INR levels continued to decrease.
One-to-one observation is discontinued. However, because of the patient’s continued determination to end her life and no significant improvement in her depression, Ms. M is considered a danger to herself and involuntary inpatient hospitalization is continued.
Figure 2 Ms. M’s INR values during hospitalization
The patient’s INR values began to rise mysteriously after she was transferred to the inpatient psychiatric unit. Acetaminophen was discontinued on day 8, and within a day her INR values began to drop.
INR: International normalized ratio
The author’s observations
Poisoning is a common method of attempting suicide, patients may use substances that clinicians rarely encounter. For most toxic, nonmedication substances, data on interactions with medications are sparse. if you suspect your patient has ingested a toxic substance with which the treatment team has little experience, contact the American Association of Poison Control Centers at 800-222-1222.
Suspect superwarfarin poisoning in suicidal patients with coagulopathy, prolonged prothrombin time, and elevated INR that does not respond to large amounts of vitamin K.9,10 These patients are at high risk of successfully completing suicide because of superwarfarins’ long half-life and daily maintenance required to keep coagulation levels within a safe range for at least several weeks.
The most serious complication these patients face is intracranial hemorrhage, which occurs in 2% of patients with excessive warfarin-based coagulation and is associated with a 77% mortality rate.11 GI bleeding occurs in 67% of these patients.2
Also take into account medical conditions—such as hypertension or hepatic disease—and medication side effects that can increase bleeding risk. When treating pain in these patients, consider avoiding acetaminophen but be aware of the risks of NSAIDs, such as gastritis or GI bleeding.
Related resource
- The American Association of Poison Control Centers. 800-222-1222; www.aapcc.org.
Drug brand names
- Escitalopram • Lexapro
- Lamotrigine • Lamictal
- Pantoprazole • Protonix
- Warfarin • Coumadin
Disclosure
The author reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Sharma V, Khan M, Corpse C. Role of lamotrigine in the management of treatment-resistant bipolar II depression: a chart review. J Affect Disord Epub 2008 Mar 1.
2. Su M, Hoffman R. Anticoagulants. In: Flomenbaum NE, Goldfrank LR, Hoffman RS, et al, eds. Goldfrank’s toxicologic emergencies. 8th ed. New York, NY: McGraw-Hill Medical Publishing; 2006:891-4.
3. Chua JD, Friedenberg WR. Superwarfarin poisoning. Anaesth Intensive Care 1997;25:707-9.
4. Leck JB, Park BK. A comparative study of the effect of warfarin and brodifacoum on the relationship between vitamin K1 metabolism and clotting factor activity in warfarin susceptible and warfarin resistant rats. Biochem Pharmacol 1981;30:123-9.
5. Lund M. Comparative effect of the three rodenticides warfarin, difenacoum and brodifacoum on eight rodent species in short feeding periods. J Hyg 1981;87:101-7.
6. Park BK, Scott AK, Wilson AC, et al. Plasma disposition of vitamin K antagonism by warfarin, difenacoum and brodifacoum in the rabbit. Biochem Pharmacol 1982;31:3535-639.
7. Gebauer MG, Nyfort-Hansen K, Henschke PJ, Gallus AS. Warfarin and acetaminophen interaction. Pharmacotherapy 2003;23(1):109-12.
8. Mahe I, Bertrand N, Drouet L, et al. Interaction between paracetamol and warfarin in patients: a double-blind, placebo-controlled, randomized study. Haematologica 2006;91(12):1621-7.
9. Sharma P, Bentley P. Of rats and men: superwarfarin toxicity. Lancet 2005;365:552-3.
10. Scully M. Warfarin therapy: rat poison and the prevention of thrombosis. Biochemist 2002;24:15-7.
11. Mathiesen T, Benediktsdottir K, Johnsson H, Lindqvist M. Intracranial traumatic and nontraumatic haemorrhagic complications of warfarin treatment. Acta Neurol Scan 1995;91:208-14.
1. Sharma V, Khan M, Corpse C. Role of lamotrigine in the management of treatment-resistant bipolar II depression: a chart review. J Affect Disord Epub 2008 Mar 1.
2. Su M, Hoffman R. Anticoagulants. In: Flomenbaum NE, Goldfrank LR, Hoffman RS, et al, eds. Goldfrank’s toxicologic emergencies. 8th ed. New York, NY: McGraw-Hill Medical Publishing; 2006:891-4.
3. Chua JD, Friedenberg WR. Superwarfarin poisoning. Anaesth Intensive Care 1997;25:707-9.
4. Leck JB, Park BK. A comparative study of the effect of warfarin and brodifacoum on the relationship between vitamin K1 metabolism and clotting factor activity in warfarin susceptible and warfarin resistant rats. Biochem Pharmacol 1981;30:123-9.
5. Lund M. Comparative effect of the three rodenticides warfarin, difenacoum and brodifacoum on eight rodent species in short feeding periods. J Hyg 1981;87:101-7.
6. Park BK, Scott AK, Wilson AC, et al. Plasma disposition of vitamin K antagonism by warfarin, difenacoum and brodifacoum in the rabbit. Biochem Pharmacol 1982;31:3535-639.
7. Gebauer MG, Nyfort-Hansen K, Henschke PJ, Gallus AS. Warfarin and acetaminophen interaction. Pharmacotherapy 2003;23(1):109-12.
8. Mahe I, Bertrand N, Drouet L, et al. Interaction between paracetamol and warfarin in patients: a double-blind, placebo-controlled, randomized study. Haematologica 2006;91(12):1621-7.
9. Sharma P, Bentley P. Of rats and men: superwarfarin toxicity. Lancet 2005;365:552-3.
10. Scully M. Warfarin therapy: rat poison and the prevention of thrombosis. Biochemist 2002;24:15-7.
11. Mathiesen T, Benediktsdottir K, Johnsson H, Lindqvist M. Intracranial traumatic and nontraumatic haemorrhagic complications of warfarin treatment. Acta Neurol Scan 1995;91:208-14.
The wilting widow’s masquerading illness
CASE: Unexplained unresponsiveness
One month after being hospitalized with E coli sepsis—and just after completing a course of ciprofloxacin—Mrs. D, a 79-year-old widow, becomes withdrawn and has several days of worsening fatigue, weakness, and somnolence. Within 2 hours of being admitted to the hospital, she becomes flaccid and unresponsive, although she seems to be awake. She has decreased respirations and is intubated.
The neurology team finds her unresponsive to verbal and noxious stimuli, with some resistance to eye opening. Neurologic exam is nonfocal. Cranial nerve testing is intact, muscle strength and reflexes are normal and symmetrical, and sensory function is intact to light touch. MRI, ECG, chest radiography, and laboratory tests—including metabolic and infectious screenings—do not reveal acute pathology. Within hours, Mrs. D becomes much more responsive and is successfully extubated. Her rapid improvement rules out locked-in syndrome.
The next day, Mrs. D has another episode of reduced responsiveness that lasts several minutes and resolves quickly. The neurologist observes this episode—which occurred when Mrs. D’s daughter entered the room—and recommends a psychiatric consultation.
For the past 3 weeks Mrs. D has experienced depressed mood, low energy, poor sleep, memory complaints, and feeling as if her mind was “scattered.” She has stopped attending church, is isolating to her home, and has been hiding valuables because of an irrational fear that she would lose possessions from her estate. Her primary care physician noted markedly reduced speech during recent office visits and agrees with the family that Mrs. D seems depressed.
On psychiatric exam, Mrs. D’s speech is quiet and slow but coherent. Her mood is depressed with a flat affect. Her thought process is goal-directed, and her Mini-Mental State Examination (MMSE) score is 27/30, indicating her cognition is grossly intact.
Mrs. D develops a low-grade fever. Although the physician does not suspect an infection, he prescribes a prophylactic course of levofloxacin, 500 mg/d. After 2 days of monitoring and assessments, the psychiatrist attributes Mrs. D’s presentation to depression, prescribes bupropion, 100 mg/d, and zolpidem, 5 mg at bedtime, and refers her for psychiatric follow-up.
Six days after discharge, Mrs. D’s family brings her to the psychiatric emergency room. They report that since discharge she has remained fatigued and seems confused intermittently. Her depressive symptoms—decreased appetite, anhedonia, poor sleep, and agitation—persist, and her personal care has deteriorated.
The authors’ observations
The psychiatrist attributes Mrs. D’s declining functioning to a worsening mood disorder. Major depression with psychotic features can include:
- fearfulness
- suspiciousness
- delusions of poverty.
Mrs. D’s cognitive and behavioral status fluctuated during her initial medical hospitalization, and on 1 occasion she required intubation. Her confusion worsened after discharge. These aspects of her history, along with worsening psychosis, can indicate seizures.
Psychiatric manifestations of seizures have been recognized for centuries. Partial complex seizures—one of the most common seizure types—have been called “psychosensory” or “psychomotor” seizures because they often include psychiatric symptoms.1
Psychiatric symptoms most often occur with seizures involving the temporal lobe, and limbic system activation adds an affective dimension to perceptual data processed by the temporal neocortex.2 Frontal and parietal lobe seizure foci also are associated with behavior change.
Psychiatric manifestations of seizures can include:
- cognitive problems
- anxiety
- mood/affect, psychotic, and dissociative symptoms
- personality changes (Table 1).2-6
As many as 30% of patients with seizures experience prominent psychiatric symptoms.7 Approximately one-half have comorbid psychiatric syndromes.8
Table 1
Seizure-related psychiatric symptoms: What to look for
| Symptom type | Characteristic features with seizures |
|---|---|
| Cognitive: intellectual function, memory, orientation | Episodic, fluctuating course of changes Amnesia occurs with complex—but not simple—seizures |
| Anxiety | Occurs most often with temporal lobe seizures May appear as full-blown panic attack Agoraphobia is rare Associated seizure features may include disturbed consciousness, automatisms, and hallucinations |
| Mood and affect | Change in affect is often episodic and profound, without many other symptoms associated with major depression or mania |
| Psychotic | Usually manifests as a single symptom, often described as incongruous, fragmentary, or out of context2 Occurs most often with temporal lobe seizures3 Delusions (paranoid, grandiose), forced thinking Hallucinations: auditory, visual, olfactory, tactile, gustatory Negative symptoms (emotional withdrawal, blunted affect) may be more common in frontal lobe seizures4 |
| Dissociative: depersonalization, déjà vu, jamais vu | Symptoms tend to be less extreme than in patients with dissociative identity disorder or PTSD May occur more often in context of panic symptoms with temporal lobe seizures5 |
| Personality changes (in epilepsy) | May be due to underlying frontal or temporal lobe damage Includes anancastic personality, emotionally unstable personality, and Geschwind syndrome (hypergraphia, hyperreligiosity, hyposexuality, and viscous personality style—perseverative and difficult to disengage from conversation)6 |
| PTSD: posttraumatic stress disorder | |
EVALUATION: Continuing decline
The emergency room staff learns Mrs. D has a history of vague auditory hallucinations and has developed more overt paranoia, including thoughts that police may be out to harm her. She has difficulty responding to questions and can not offer details of her history; her speech is soft and her thought process appears slowed.
Mrs. D is admitted to the inpatient psychiatry service. Her family reports that she has episodes of disorientation, poor memory, staring, and paranoia about the police that last minutes to 1 hour.
On a subsequent examination 1 hour later, her speech difficulties are variable. She cannot speak fluently, has limited ability to repeat phrases, and cannot follow simple verbal commands. These symptoms persist only minutes. Mrs. D slowly becomes more conversant but appears tired. During the next few hours she is disoriented and tries to walk into the nursing station. Other repetitive activity includes putting on/taking offmultiple layers of clothing.
The authors’ observations
- A normal EEG does not guarantee the absence of recent seizures; a standard scalp EEG can miss epileptiform changes that may occur earlier in the ictal phase.9
- EEG abnormalities may occur in normal subjects.
- visual, olfactory, or tactile hallucinations
- mutism
- catatonia
- poor memory not due to inattention
- episodic aphasia, apraxia, or agnosia.
Mrs. D’s confusion level and speech abnormalities varied over time. Her speech arrest early in the admission appeared to be a Broca’s or expressive aphasia because she comprehended commands but was unable to speak. Later, her speech exhibited a mixed transcortical aphasia pattern—she was unable to speak or comprehend, but retained some ability to repeat. The changing aphasia patterns and the often abrupt starting and stopping of these symptoms were the clues that an active process was occurring, suggesting that seizures should be considered.
DIAGNOSIS: Irrefutable EEG evidence
Mrs. D receives another neurology consult. An EEG shows spike and wave discharges in both frontal lobes consistent with nonconvulsive status epilepticus (NCSE). During these bursts, the neurologist notes speech arrest and altered alertness. Phenytoin loading is administered as a single 800-mg oral dose followed by 100 mg twice daily, and Mrs. D is transferred to the neurology unit for further stabilization.
The authors’ observations
When evaluating whether a psychiatric presentation reflects an underlying general medical or neurologic disorder—including seizures—consider the clinical features outlined in Table 2.12
In Mrs. D’s case, several factors supported the diagnosis of depression. She had numerous depressive symptoms, including depressed mood, social withdrawal, low energy, poor sleep, and “scattered mind,” which the psychiatrist interpreted as poor concentration. Interestingly, she attributed her dramatic episode of mutism and unresponsiveness in the hospital to being depressed. Mrs. D also had a personal and family history of depression; she had experienced a possible major depressive episode in her late 20s but was never treated, and her brother had depression.
Several features of her presentation were atypical, however, and suggested a medical etiology. Her family described the onset of her symptoms as abrupt, and she declined rapidly. Mrs. D’s concern about her estate had no connection with reality, and she became more psychotic. The dramatic episode of decreased responsiveness that led to her intubation was both peculiar and brief.
Mrs. D’s symptoms had an episodic quality with sudden onset, were repeatedly associated with aphasia, and included some automatic behavior (including dressing and undressing) suggestive of seizures. Symptoms of depression should not be surprising in this context because depression may be the most common comorbid psychiatric condition in elderly persons with epilepsy.13 Indeed, Mrs. D’s ultimate diagnosis—NCSE—is characterized by great variability in presentation, ranging from mildly impaired attention and orientation to mood disturbance, speech disturbance, and psychosis. All of these symptoms are seen with seizures.
Further, NCSE can have gradual or sudden onset, varying intensity and duration of symptoms, and fluctuating responsiveness.14 At least 10% of patients presenting with NCSE have no history of seizures.15 Precipitating factors include infection and drug toxicity.14
OUTCOME: Dual treatment
During a one-week neurology hospitalization, Mrs. D continues to receive phenytoin. Long-term EEG monitoring reveals she is no longer in status epilepticus. The patient is prescribed citalopram, 10 mg/d, and olanzapine, 2.5 mg at bedtime, to resolve mild depressive symptoms and hallucinosis. Mrs. D is referred for both neurology and psychiatry outpatient follow-up.
Table 2
Is the patient’s disorder psychiatric or medical/neurologic?
| Are the symptoms typical of a psychiatric disorder, including the severity? |
| Are the onset and course of symptoms usual? |
| Does the patient have risk factors for psychiatric illness, such as a personal or family history of psychiatric illness? |
| Are psychiatric symptoms responding poorly to treatment? |
| Does the patient have a general medical or neurologic condition commonly associated with psychiatric symptoms? |
| Does the patient exhibit abnormal cognitive functioning, including memory impairment or altered level of consciousness? |
| Did the psychiatric symptoms emerge after an abrupt change in personality? |
| Source: Reference 12 |
- Ettinger AB, Kanner AM, eds. Psychiatric issues in epilepsy: a practical guide to diagnosis and treatment. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2006.
- Bupropion • Wellbutrin
- Ciprofloxacin • Cipro
- Citalopram • Celexa
- Levofloxacin • Levaquin
- Olanzapine • Zyprexa
- Phenytoin • Dilantin
- Zolpidem • Ambien
Dr. Saragoza reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Maixner receives research/grant support from Neuronetics Inc., and is a speaker for Pfizer Inc., Bristol-Meyers Squibb, Janssen LP, and AstraZeneca.
1. Taylor M. The fundamentals of clinical neuropsychiatry. New York, NY: Oxford University Press; 1999:298-324.
2. Gloor P. The role of the limbic system in experiential phenomena of temporal lobe epilepsy. Ann Neurol 1982;12(2):129-44.
3. Scheepers M. Epilepsy and behaviour. Curr Opin Neurol 2003;16:183-7.
4. Adachi N. Inter-ictal and post-ictal psychoses in frontal lobe epilepsy: a retrospective comparison with psychoses in temporal lobe epilepsy. Seizure 2000;9:328-35.
5. Toni C. Psychosensorial and related phenomena in panic disorder and in temporal lobe epilepsy. Compr Psychiatry 1996;37(2):125-33.
6. Tucker G. Seizure disorders presenting with psychiatric symptomatology. Psychiatr Clin North Am 1998;21(3):626-35.
7. Onuma T. Classification of psychiatric symptoms in patients with epilepsy. Epilepsia 2000;41(suppl 9):43-8.
8. Marsh L, Rao V. Psychiatric complications in patients with epilepsy: a review. Epilepsy Res 2002;49(1):11-33.
9. Stern T. ed. Massachusetts General Hospital handbook of general hospital psychiatry. 5th ed. St. Louis, MO: Mosby; 2004;457-62.
10. O’Sullivan S. The role of the standard EEG in clinical psychiatry. Human Psychopharmacol Clin Exp 2006;21:265-71.
11. Gelb D. Introduction to clinical neurology. 2nd ed. London, UK: Butterworth Heinemann; 2000;133-4.
12. Marsh CM. Psychiatric presentations of medical illness. Psychiatr Clin North Am 1997;20(1):181-2.
13. Cloyd J, Hauser W, Towne A, et al. Epidemiological and medical aspects of epilepsy in the elderly. Epilepsy Res 2006;68(suppl 1):S39-48.
14. Riggio S. Nonconvulsive status epilepticus: clinical features and diagnostic challenges. Psychiatr Clin North Am 2005;28:653-64.
15. Mehlhorn AJ, Brown DA. Safety concerns with fluoroquinolones. Ann Pharmacother 2007;41:1859-66.
CASE: Unexplained unresponsiveness
One month after being hospitalized with E coli sepsis—and just after completing a course of ciprofloxacin—Mrs. D, a 79-year-old widow, becomes withdrawn and has several days of worsening fatigue, weakness, and somnolence. Within 2 hours of being admitted to the hospital, she becomes flaccid and unresponsive, although she seems to be awake. She has decreased respirations and is intubated.
The neurology team finds her unresponsive to verbal and noxious stimuli, with some resistance to eye opening. Neurologic exam is nonfocal. Cranial nerve testing is intact, muscle strength and reflexes are normal and symmetrical, and sensory function is intact to light touch. MRI, ECG, chest radiography, and laboratory tests—including metabolic and infectious screenings—do not reveal acute pathology. Within hours, Mrs. D becomes much more responsive and is successfully extubated. Her rapid improvement rules out locked-in syndrome.
The next day, Mrs. D has another episode of reduced responsiveness that lasts several minutes and resolves quickly. The neurologist observes this episode—which occurred when Mrs. D’s daughter entered the room—and recommends a psychiatric consultation.
For the past 3 weeks Mrs. D has experienced depressed mood, low energy, poor sleep, memory complaints, and feeling as if her mind was “scattered.” She has stopped attending church, is isolating to her home, and has been hiding valuables because of an irrational fear that she would lose possessions from her estate. Her primary care physician noted markedly reduced speech during recent office visits and agrees with the family that Mrs. D seems depressed.
On psychiatric exam, Mrs. D’s speech is quiet and slow but coherent. Her mood is depressed with a flat affect. Her thought process is goal-directed, and her Mini-Mental State Examination (MMSE) score is 27/30, indicating her cognition is grossly intact.
Mrs. D develops a low-grade fever. Although the physician does not suspect an infection, he prescribes a prophylactic course of levofloxacin, 500 mg/d. After 2 days of monitoring and assessments, the psychiatrist attributes Mrs. D’s presentation to depression, prescribes bupropion, 100 mg/d, and zolpidem, 5 mg at bedtime, and refers her for psychiatric follow-up.
Six days after discharge, Mrs. D’s family brings her to the psychiatric emergency room. They report that since discharge she has remained fatigued and seems confused intermittently. Her depressive symptoms—decreased appetite, anhedonia, poor sleep, and agitation—persist, and her personal care has deteriorated.
The authors’ observations
The psychiatrist attributes Mrs. D’s declining functioning to a worsening mood disorder. Major depression with psychotic features can include:
- fearfulness
- suspiciousness
- delusions of poverty.
Mrs. D’s cognitive and behavioral status fluctuated during her initial medical hospitalization, and on 1 occasion she required intubation. Her confusion worsened after discharge. These aspects of her history, along with worsening psychosis, can indicate seizures.
Psychiatric manifestations of seizures have been recognized for centuries. Partial complex seizures—one of the most common seizure types—have been called “psychosensory” or “psychomotor” seizures because they often include psychiatric symptoms.1
Psychiatric symptoms most often occur with seizures involving the temporal lobe, and limbic system activation adds an affective dimension to perceptual data processed by the temporal neocortex.2 Frontal and parietal lobe seizure foci also are associated with behavior change.
Psychiatric manifestations of seizures can include:
- cognitive problems
- anxiety
- mood/affect, psychotic, and dissociative symptoms
- personality changes (Table 1).2-6
As many as 30% of patients with seizures experience prominent psychiatric symptoms.7 Approximately one-half have comorbid psychiatric syndromes.8
Table 1
Seizure-related psychiatric symptoms: What to look for
| Symptom type | Characteristic features with seizures |
|---|---|
| Cognitive: intellectual function, memory, orientation | Episodic, fluctuating course of changes Amnesia occurs with complex—but not simple—seizures |
| Anxiety | Occurs most often with temporal lobe seizures May appear as full-blown panic attack Agoraphobia is rare Associated seizure features may include disturbed consciousness, automatisms, and hallucinations |
| Mood and affect | Change in affect is often episodic and profound, without many other symptoms associated with major depression or mania |
| Psychotic | Usually manifests as a single symptom, often described as incongruous, fragmentary, or out of context2 Occurs most often with temporal lobe seizures3 Delusions (paranoid, grandiose), forced thinking Hallucinations: auditory, visual, olfactory, tactile, gustatory Negative symptoms (emotional withdrawal, blunted affect) may be more common in frontal lobe seizures4 |
| Dissociative: depersonalization, déjà vu, jamais vu | Symptoms tend to be less extreme than in patients with dissociative identity disorder or PTSD May occur more often in context of panic symptoms with temporal lobe seizures5 |
| Personality changes (in epilepsy) | May be due to underlying frontal or temporal lobe damage Includes anancastic personality, emotionally unstable personality, and Geschwind syndrome (hypergraphia, hyperreligiosity, hyposexuality, and viscous personality style—perseverative and difficult to disengage from conversation)6 |
| PTSD: posttraumatic stress disorder | |
EVALUATION: Continuing decline
The emergency room staff learns Mrs. D has a history of vague auditory hallucinations and has developed more overt paranoia, including thoughts that police may be out to harm her. She has difficulty responding to questions and can not offer details of her history; her speech is soft and her thought process appears slowed.
Mrs. D is admitted to the inpatient psychiatry service. Her family reports that she has episodes of disorientation, poor memory, staring, and paranoia about the police that last minutes to 1 hour.
On a subsequent examination 1 hour later, her speech difficulties are variable. She cannot speak fluently, has limited ability to repeat phrases, and cannot follow simple verbal commands. These symptoms persist only minutes. Mrs. D slowly becomes more conversant but appears tired. During the next few hours she is disoriented and tries to walk into the nursing station. Other repetitive activity includes putting on/taking offmultiple layers of clothing.
The authors’ observations
- A normal EEG does not guarantee the absence of recent seizures; a standard scalp EEG can miss epileptiform changes that may occur earlier in the ictal phase.9
- EEG abnormalities may occur in normal subjects.
- visual, olfactory, or tactile hallucinations
- mutism
- catatonia
- poor memory not due to inattention
- episodic aphasia, apraxia, or agnosia.
Mrs. D’s confusion level and speech abnormalities varied over time. Her speech arrest early in the admission appeared to be a Broca’s or expressive aphasia because she comprehended commands but was unable to speak. Later, her speech exhibited a mixed transcortical aphasia pattern—she was unable to speak or comprehend, but retained some ability to repeat. The changing aphasia patterns and the often abrupt starting and stopping of these symptoms were the clues that an active process was occurring, suggesting that seizures should be considered.
DIAGNOSIS: Irrefutable EEG evidence
Mrs. D receives another neurology consult. An EEG shows spike and wave discharges in both frontal lobes consistent with nonconvulsive status epilepticus (NCSE). During these bursts, the neurologist notes speech arrest and altered alertness. Phenytoin loading is administered as a single 800-mg oral dose followed by 100 mg twice daily, and Mrs. D is transferred to the neurology unit for further stabilization.
The authors’ observations
When evaluating whether a psychiatric presentation reflects an underlying general medical or neurologic disorder—including seizures—consider the clinical features outlined in Table 2.12
In Mrs. D’s case, several factors supported the diagnosis of depression. She had numerous depressive symptoms, including depressed mood, social withdrawal, low energy, poor sleep, and “scattered mind,” which the psychiatrist interpreted as poor concentration. Interestingly, she attributed her dramatic episode of mutism and unresponsiveness in the hospital to being depressed. Mrs. D also had a personal and family history of depression; she had experienced a possible major depressive episode in her late 20s but was never treated, and her brother had depression.
Several features of her presentation were atypical, however, and suggested a medical etiology. Her family described the onset of her symptoms as abrupt, and she declined rapidly. Mrs. D’s concern about her estate had no connection with reality, and she became more psychotic. The dramatic episode of decreased responsiveness that led to her intubation was both peculiar and brief.
Mrs. D’s symptoms had an episodic quality with sudden onset, were repeatedly associated with aphasia, and included some automatic behavior (including dressing and undressing) suggestive of seizures. Symptoms of depression should not be surprising in this context because depression may be the most common comorbid psychiatric condition in elderly persons with epilepsy.13 Indeed, Mrs. D’s ultimate diagnosis—NCSE—is characterized by great variability in presentation, ranging from mildly impaired attention and orientation to mood disturbance, speech disturbance, and psychosis. All of these symptoms are seen with seizures.
Further, NCSE can have gradual or sudden onset, varying intensity and duration of symptoms, and fluctuating responsiveness.14 At least 10% of patients presenting with NCSE have no history of seizures.15 Precipitating factors include infection and drug toxicity.14
OUTCOME: Dual treatment
During a one-week neurology hospitalization, Mrs. D continues to receive phenytoin. Long-term EEG monitoring reveals she is no longer in status epilepticus. The patient is prescribed citalopram, 10 mg/d, and olanzapine, 2.5 mg at bedtime, to resolve mild depressive symptoms and hallucinosis. Mrs. D is referred for both neurology and psychiatry outpatient follow-up.
Table 2
Is the patient’s disorder psychiatric or medical/neurologic?
| Are the symptoms typical of a psychiatric disorder, including the severity? |
| Are the onset and course of symptoms usual? |
| Does the patient have risk factors for psychiatric illness, such as a personal or family history of psychiatric illness? |
| Are psychiatric symptoms responding poorly to treatment? |
| Does the patient have a general medical or neurologic condition commonly associated with psychiatric symptoms? |
| Does the patient exhibit abnormal cognitive functioning, including memory impairment or altered level of consciousness? |
| Did the psychiatric symptoms emerge after an abrupt change in personality? |
| Source: Reference 12 |
- Ettinger AB, Kanner AM, eds. Psychiatric issues in epilepsy: a practical guide to diagnosis and treatment. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2006.
- Bupropion • Wellbutrin
- Ciprofloxacin • Cipro
- Citalopram • Celexa
- Levofloxacin • Levaquin
- Olanzapine • Zyprexa
- Phenytoin • Dilantin
- Zolpidem • Ambien
Dr. Saragoza reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Maixner receives research/grant support from Neuronetics Inc., and is a speaker for Pfizer Inc., Bristol-Meyers Squibb, Janssen LP, and AstraZeneca.
CASE: Unexplained unresponsiveness
One month after being hospitalized with E coli sepsis—and just after completing a course of ciprofloxacin—Mrs. D, a 79-year-old widow, becomes withdrawn and has several days of worsening fatigue, weakness, and somnolence. Within 2 hours of being admitted to the hospital, she becomes flaccid and unresponsive, although she seems to be awake. She has decreased respirations and is intubated.
The neurology team finds her unresponsive to verbal and noxious stimuli, with some resistance to eye opening. Neurologic exam is nonfocal. Cranial nerve testing is intact, muscle strength and reflexes are normal and symmetrical, and sensory function is intact to light touch. MRI, ECG, chest radiography, and laboratory tests—including metabolic and infectious screenings—do not reveal acute pathology. Within hours, Mrs. D becomes much more responsive and is successfully extubated. Her rapid improvement rules out locked-in syndrome.
The next day, Mrs. D has another episode of reduced responsiveness that lasts several minutes and resolves quickly. The neurologist observes this episode—which occurred when Mrs. D’s daughter entered the room—and recommends a psychiatric consultation.
For the past 3 weeks Mrs. D has experienced depressed mood, low energy, poor sleep, memory complaints, and feeling as if her mind was “scattered.” She has stopped attending church, is isolating to her home, and has been hiding valuables because of an irrational fear that she would lose possessions from her estate. Her primary care physician noted markedly reduced speech during recent office visits and agrees with the family that Mrs. D seems depressed.
On psychiatric exam, Mrs. D’s speech is quiet and slow but coherent. Her mood is depressed with a flat affect. Her thought process is goal-directed, and her Mini-Mental State Examination (MMSE) score is 27/30, indicating her cognition is grossly intact.
Mrs. D develops a low-grade fever. Although the physician does not suspect an infection, he prescribes a prophylactic course of levofloxacin, 500 mg/d. After 2 days of monitoring and assessments, the psychiatrist attributes Mrs. D’s presentation to depression, prescribes bupropion, 100 mg/d, and zolpidem, 5 mg at bedtime, and refers her for psychiatric follow-up.
Six days after discharge, Mrs. D’s family brings her to the psychiatric emergency room. They report that since discharge she has remained fatigued and seems confused intermittently. Her depressive symptoms—decreased appetite, anhedonia, poor sleep, and agitation—persist, and her personal care has deteriorated.
The authors’ observations
The psychiatrist attributes Mrs. D’s declining functioning to a worsening mood disorder. Major depression with psychotic features can include:
- fearfulness
- suspiciousness
- delusions of poverty.
Mrs. D’s cognitive and behavioral status fluctuated during her initial medical hospitalization, and on 1 occasion she required intubation. Her confusion worsened after discharge. These aspects of her history, along with worsening psychosis, can indicate seizures.
Psychiatric manifestations of seizures have been recognized for centuries. Partial complex seizures—one of the most common seizure types—have been called “psychosensory” or “psychomotor” seizures because they often include psychiatric symptoms.1
Psychiatric symptoms most often occur with seizures involving the temporal lobe, and limbic system activation adds an affective dimension to perceptual data processed by the temporal neocortex.2 Frontal and parietal lobe seizure foci also are associated with behavior change.
Psychiatric manifestations of seizures can include:
- cognitive problems
- anxiety
- mood/affect, psychotic, and dissociative symptoms
- personality changes (Table 1).2-6
As many as 30% of patients with seizures experience prominent psychiatric symptoms.7 Approximately one-half have comorbid psychiatric syndromes.8
Table 1
Seizure-related psychiatric symptoms: What to look for
| Symptom type | Characteristic features with seizures |
|---|---|
| Cognitive: intellectual function, memory, orientation | Episodic, fluctuating course of changes Amnesia occurs with complex—but not simple—seizures |
| Anxiety | Occurs most often with temporal lobe seizures May appear as full-blown panic attack Agoraphobia is rare Associated seizure features may include disturbed consciousness, automatisms, and hallucinations |
| Mood and affect | Change in affect is often episodic and profound, without many other symptoms associated with major depression or mania |
| Psychotic | Usually manifests as a single symptom, often described as incongruous, fragmentary, or out of context2 Occurs most often with temporal lobe seizures3 Delusions (paranoid, grandiose), forced thinking Hallucinations: auditory, visual, olfactory, tactile, gustatory Negative symptoms (emotional withdrawal, blunted affect) may be more common in frontal lobe seizures4 |
| Dissociative: depersonalization, déjà vu, jamais vu | Symptoms tend to be less extreme than in patients with dissociative identity disorder or PTSD May occur more often in context of panic symptoms with temporal lobe seizures5 |
| Personality changes (in epilepsy) | May be due to underlying frontal or temporal lobe damage Includes anancastic personality, emotionally unstable personality, and Geschwind syndrome (hypergraphia, hyperreligiosity, hyposexuality, and viscous personality style—perseverative and difficult to disengage from conversation)6 |
| PTSD: posttraumatic stress disorder | |
EVALUATION: Continuing decline
The emergency room staff learns Mrs. D has a history of vague auditory hallucinations and has developed more overt paranoia, including thoughts that police may be out to harm her. She has difficulty responding to questions and can not offer details of her history; her speech is soft and her thought process appears slowed.
Mrs. D is admitted to the inpatient psychiatry service. Her family reports that she has episodes of disorientation, poor memory, staring, and paranoia about the police that last minutes to 1 hour.
On a subsequent examination 1 hour later, her speech difficulties are variable. She cannot speak fluently, has limited ability to repeat phrases, and cannot follow simple verbal commands. These symptoms persist only minutes. Mrs. D slowly becomes more conversant but appears tired. During the next few hours she is disoriented and tries to walk into the nursing station. Other repetitive activity includes putting on/taking offmultiple layers of clothing.
The authors’ observations
- A normal EEG does not guarantee the absence of recent seizures; a standard scalp EEG can miss epileptiform changes that may occur earlier in the ictal phase.9
- EEG abnormalities may occur in normal subjects.
- visual, olfactory, or tactile hallucinations
- mutism
- catatonia
- poor memory not due to inattention
- episodic aphasia, apraxia, or agnosia.
Mrs. D’s confusion level and speech abnormalities varied over time. Her speech arrest early in the admission appeared to be a Broca’s or expressive aphasia because she comprehended commands but was unable to speak. Later, her speech exhibited a mixed transcortical aphasia pattern—she was unable to speak or comprehend, but retained some ability to repeat. The changing aphasia patterns and the often abrupt starting and stopping of these symptoms were the clues that an active process was occurring, suggesting that seizures should be considered.
DIAGNOSIS: Irrefutable EEG evidence
Mrs. D receives another neurology consult. An EEG shows spike and wave discharges in both frontal lobes consistent with nonconvulsive status epilepticus (NCSE). During these bursts, the neurologist notes speech arrest and altered alertness. Phenytoin loading is administered as a single 800-mg oral dose followed by 100 mg twice daily, and Mrs. D is transferred to the neurology unit for further stabilization.
The authors’ observations
When evaluating whether a psychiatric presentation reflects an underlying general medical or neurologic disorder—including seizures—consider the clinical features outlined in Table 2.12
In Mrs. D’s case, several factors supported the diagnosis of depression. She had numerous depressive symptoms, including depressed mood, social withdrawal, low energy, poor sleep, and “scattered mind,” which the psychiatrist interpreted as poor concentration. Interestingly, she attributed her dramatic episode of mutism and unresponsiveness in the hospital to being depressed. Mrs. D also had a personal and family history of depression; she had experienced a possible major depressive episode in her late 20s but was never treated, and her brother had depression.
Several features of her presentation were atypical, however, and suggested a medical etiology. Her family described the onset of her symptoms as abrupt, and she declined rapidly. Mrs. D’s concern about her estate had no connection with reality, and she became more psychotic. The dramatic episode of decreased responsiveness that led to her intubation was both peculiar and brief.
Mrs. D’s symptoms had an episodic quality with sudden onset, were repeatedly associated with aphasia, and included some automatic behavior (including dressing and undressing) suggestive of seizures. Symptoms of depression should not be surprising in this context because depression may be the most common comorbid psychiatric condition in elderly persons with epilepsy.13 Indeed, Mrs. D’s ultimate diagnosis—NCSE—is characterized by great variability in presentation, ranging from mildly impaired attention and orientation to mood disturbance, speech disturbance, and psychosis. All of these symptoms are seen with seizures.
Further, NCSE can have gradual or sudden onset, varying intensity and duration of symptoms, and fluctuating responsiveness.14 At least 10% of patients presenting with NCSE have no history of seizures.15 Precipitating factors include infection and drug toxicity.14
OUTCOME: Dual treatment
During a one-week neurology hospitalization, Mrs. D continues to receive phenytoin. Long-term EEG monitoring reveals she is no longer in status epilepticus. The patient is prescribed citalopram, 10 mg/d, and olanzapine, 2.5 mg at bedtime, to resolve mild depressive symptoms and hallucinosis. Mrs. D is referred for both neurology and psychiatry outpatient follow-up.
Table 2
Is the patient’s disorder psychiatric or medical/neurologic?
| Are the symptoms typical of a psychiatric disorder, including the severity? |
| Are the onset and course of symptoms usual? |
| Does the patient have risk factors for psychiatric illness, such as a personal or family history of psychiatric illness? |
| Are psychiatric symptoms responding poorly to treatment? |
| Does the patient have a general medical or neurologic condition commonly associated with psychiatric symptoms? |
| Does the patient exhibit abnormal cognitive functioning, including memory impairment or altered level of consciousness? |
| Did the psychiatric symptoms emerge after an abrupt change in personality? |
| Source: Reference 12 |
- Ettinger AB, Kanner AM, eds. Psychiatric issues in epilepsy: a practical guide to diagnosis and treatment. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2006.
- Bupropion • Wellbutrin
- Ciprofloxacin • Cipro
- Citalopram • Celexa
- Levofloxacin • Levaquin
- Olanzapine • Zyprexa
- Phenytoin • Dilantin
- Zolpidem • Ambien
Dr. Saragoza reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Maixner receives research/grant support from Neuronetics Inc., and is a speaker for Pfizer Inc., Bristol-Meyers Squibb, Janssen LP, and AstraZeneca.
1. Taylor M. The fundamentals of clinical neuropsychiatry. New York, NY: Oxford University Press; 1999:298-324.
2. Gloor P. The role of the limbic system in experiential phenomena of temporal lobe epilepsy. Ann Neurol 1982;12(2):129-44.
3. Scheepers M. Epilepsy and behaviour. Curr Opin Neurol 2003;16:183-7.
4. Adachi N. Inter-ictal and post-ictal psychoses in frontal lobe epilepsy: a retrospective comparison with psychoses in temporal lobe epilepsy. Seizure 2000;9:328-35.
5. Toni C. Psychosensorial and related phenomena in panic disorder and in temporal lobe epilepsy. Compr Psychiatry 1996;37(2):125-33.
6. Tucker G. Seizure disorders presenting with psychiatric symptomatology. Psychiatr Clin North Am 1998;21(3):626-35.
7. Onuma T. Classification of psychiatric symptoms in patients with epilepsy. Epilepsia 2000;41(suppl 9):43-8.
8. Marsh L, Rao V. Psychiatric complications in patients with epilepsy: a review. Epilepsy Res 2002;49(1):11-33.
9. Stern T. ed. Massachusetts General Hospital handbook of general hospital psychiatry. 5th ed. St. Louis, MO: Mosby; 2004;457-62.
10. O’Sullivan S. The role of the standard EEG in clinical psychiatry. Human Psychopharmacol Clin Exp 2006;21:265-71.
11. Gelb D. Introduction to clinical neurology. 2nd ed. London, UK: Butterworth Heinemann; 2000;133-4.
12. Marsh CM. Psychiatric presentations of medical illness. Psychiatr Clin North Am 1997;20(1):181-2.
13. Cloyd J, Hauser W, Towne A, et al. Epidemiological and medical aspects of epilepsy in the elderly. Epilepsy Res 2006;68(suppl 1):S39-48.
14. Riggio S. Nonconvulsive status epilepticus: clinical features and diagnostic challenges. Psychiatr Clin North Am 2005;28:653-64.
15. Mehlhorn AJ, Brown DA. Safety concerns with fluoroquinolones. Ann Pharmacother 2007;41:1859-66.
1. Taylor M. The fundamentals of clinical neuropsychiatry. New York, NY: Oxford University Press; 1999:298-324.
2. Gloor P. The role of the limbic system in experiential phenomena of temporal lobe epilepsy. Ann Neurol 1982;12(2):129-44.
3. Scheepers M. Epilepsy and behaviour. Curr Opin Neurol 2003;16:183-7.
4. Adachi N. Inter-ictal and post-ictal psychoses in frontal lobe epilepsy: a retrospective comparison with psychoses in temporal lobe epilepsy. Seizure 2000;9:328-35.
5. Toni C. Psychosensorial and related phenomena in panic disorder and in temporal lobe epilepsy. Compr Psychiatry 1996;37(2):125-33.
6. Tucker G. Seizure disorders presenting with psychiatric symptomatology. Psychiatr Clin North Am 1998;21(3):626-35.
7. Onuma T. Classification of psychiatric symptoms in patients with epilepsy. Epilepsia 2000;41(suppl 9):43-8.
8. Marsh L, Rao V. Psychiatric complications in patients with epilepsy: a review. Epilepsy Res 2002;49(1):11-33.
9. Stern T. ed. Massachusetts General Hospital handbook of general hospital psychiatry. 5th ed. St. Louis, MO: Mosby; 2004;457-62.
10. O’Sullivan S. The role of the standard EEG in clinical psychiatry. Human Psychopharmacol Clin Exp 2006;21:265-71.
11. Gelb D. Introduction to clinical neurology. 2nd ed. London, UK: Butterworth Heinemann; 2000;133-4.
12. Marsh CM. Psychiatric presentations of medical illness. Psychiatr Clin North Am 1997;20(1):181-2.
13. Cloyd J, Hauser W, Towne A, et al. Epidemiological and medical aspects of epilepsy in the elderly. Epilepsy Res 2006;68(suppl 1):S39-48.
14. Riggio S. Nonconvulsive status epilepticus: clinical features and diagnostic challenges. Psychiatr Clin North Am 2005;28:653-64.
15. Mehlhorn AJ, Brown DA. Safety concerns with fluoroquinolones. Ann Pharmacother 2007;41:1859-66.
‘I’ve been abducted by aliens’
CASE: ’I’m not crazy’
Ms. S, age 55, presents for treatment because she is feeling depressed and anxious. Her symptoms include decreased concentration, intermittent irritability, hoarding, and difficulty starting and completing tasks. She also has chronic sleep difficulties that often keep her awake until dawn.
Fatigue, lack of focus, and poor comprehension and motivation have left her unemployed. She and her teenage daughter live with Ms. S’s elderly mother. Ms. S feels tremendous guilt because she cannot be the mother and daughter she wants to be.
Initially, I (PK) diagnose Ms. S with major depressive disorder and prescribe sertraline, 100 mg/d, which improves her mood and energy. However, her inability to stay organized results in her being “let go” from job training.
Ms. S reports similar difficulties in school as a child. I determine that she meets DSM-IV-TR criteria for attention-deficit/hyperactivity disorder (ADHD). Adding methylphenidate, 10 mg bid, improves her concentration and ability to complete tasks. It also reduces the impulsivity that has disrupted her relationships.
Despite a strong desire to normalize her sleep schedule, Ms. S continues to have difficulty falling asleep, so I add melatonin, 3 to 6 mg at bedtime. Her sleeping pattern is improved, but still variable. She also tries quetiapine, 25 mg at bedtime, but soon discontinues it due to intolerance.
As our rapport strengthens, Ms. S reveals that she has had multiple encounters with aliens beginning at age 3. Although she has not had an “alien experience” for about 5 years, she does not feel safe sleeping at night and instead sleeps during the day. Her efforts to stay awake at night strain her relationship with her mother.
The authors’ observations
Approximately 1% of the U.S. population report alien abduction experiences (AAE)—an umbrella term that includes alleged contact with aliens ranging from sightings to abductions.1 Patients rarely report AAE to mental health professionals. In our society, claiming to be an “abductee” implies that one might be insane. A survey of 398 Canadian students that assessed attitudes, beliefs, and experiences regarding alien abductions found that 79% of respondents believed they would have mostly negative consequences—such as being laughed at or socially isolated—if they claimed to have encountered aliens.1
Persons who have AAE may attend support groups of fellow “abductees” to accumulate behavior-consonant information (hearing other people’s abduction stories) and reduce dissonance by being surrounded by others who share a questionable belief.2 A survey of “abductees” found that 88% report at least some positive aspects of the experience, such as a sense of importance or feeling as though they were chosen to bridge communication between extraterrestrials and humans.3
- high levels of psychic energy
- self-sufficiency
- resourcefulness
- a tendency to question authority and to be exposed to situational conflicts.1
After Ms. S reveals her alien experiences, I reassure her in a nonjudgmental manner that we will explore her experiences and determine ways to help her cope with them.
HISTORY: Terrifying experiences
Ms. S elaborates on her alien experiences, relating a particularly terrifying example from her teen years. She was lying awake in bed, looking at the ceiling, where she saw a jeweled spider with a drill. As the spider descended from the ceiling and spread its legs, she recalled a noise like a dentist’s drill. As the spider neared her face, it grew larger and larger. Terrified, Ms. S was unable to scream for help or move anything except her eyes as the spider clamped its legs around her head and bored into her skull. She reported that although she could feel the drill go in, it wasn’t painful.
Other experiences included giving birth, undergoing examinations or probes, and communicating with aliens. Although she is very distressed by most memories, she feels she benefited from others. For example, as a child, Ms. S’s math skills improved dramatically after an AAE episode; she believes this was a gift from the aliens. Ms. S’s AAE memories are as vivid to her as memories of her college graduation. She had been reluctant to discuss these events with anyone outside her family out of fear of being perceived as “crazy.”
Ms. S says she was a shy child who had difficulty making friends. She was plagued with fatigue and worry about family members. She believed that aliens might attack her sisters and felt obligated to stay awake at night to protect them. Aside from alien experiences, Ms. S reports a happy childhood.
She has always been an avid reader. At age 8 or 9, after reading a book on alien abduction, she concluded that she had been abducted. Later, she joined a group of professed alien abductees. She feels accepted and validated by this group and has a forum for discussing her experiences without fear of ridicule or rejection.
Ms. S remains frightened by things that remind her of aliens. Although she wrote a summary of her alien experiences, she cannot draw a picture of an alien, and thoughts or images of the prototypical “grey” alien trigger panic. She also feels somewhat “different,” nervous, and distant from others.
The authors’ observations
Reviewing AAE literature led me to consider several diagnoses, including:
- psychosis
- seizures
- false memory (sexual abuse, trauma)
- narcolepsy
- sleep paralysis.
Electroencephalography (during drowsiness) revealed abnormal activity (occurrences of widely scattered bursts of nonspecific, round, sharply contoured slow waves in the left frontal region) only in the F7 electrode. In the absence of clinical symptoms and when found in a single lead, this is considered a normal variant.
Diagnostic testing ruled out hallucinosis related to seizures. I also ruled out false memory related to sexual abuse or trauma, which is commonly found in patients who present with AAE.
Collaborative information from relatives did not uncover a history of psychosis. She and family members reported, however, that Ms. S’s father and 1 sister had periodic sleep disturbances with associated hallucinations. I began to suspect sleep paralysis.
The authors’ observations
Full-body paralysis normally accompanies rapid eye movement (REM) sleep, which occurs several times a night.4 Sleep paralysis is a transient state that occurs when an individual becomes conscious of this immobility, typically while falling asleep or awakening.5 These experiences can be accompanied by hypnagogic (while falling asleep) or hypnopompic (while awakening) hallucinations. An estimated 30% of the population has had at least one sleep paralysis episode.6 In one study, 5% of sleep paralysis patients had episodes that were accompanied by hallucinations.7
Although individuals cannot make gross body movements during sleep paralysis, they can open their eyes and are able to report events that occurred around them during the episode.8 Patients interpret sleep paralysis experiences in subjective terms. Common descriptions include intense fear, breathing difficulties, feeling of bodily pressure—especially on the chest—and sensations of floating, flying, or falling (Table 1).7,9
During sleep paralysis episodes, individuals typically sense a threatening presence.6 Patients have reported beastly and demonic figures of doom: devils, demons, witches, aliens, and even cinematic villains such as Darth Vader and Freddy Kruger.6 Others have described this presence in terms of alien visitations or abductions.
Table 1
4 types of sleep paralysis-related hallucinations
| Intruder | Vague sense of a threatening presence accompanied by visual, auditory, and tactile hallucinations—noises, footsteps, gibbering voices, humanoid apparitions, and sensation of being touched or grabbed |
| Incubus | Breathing difficulties, feelings of suffocation, bodily pressure (particularly on the chest, as if someone were sitting or standing on it), pain, and thoughts of impending death |
| Vestibular-motor | Sensations of floating (levitation), flying, and falling |
| Other | Out-of-body experiences, autoscopy (seeing oneself from an external point), and fictive motor movements, ranging from simple arm movements to sitting up to apparent locomotion through the environment |
| Source: References 7,9 | |
A Harvard University study of 11 individuals who reported alien abductions found that all participants experienced a similar sequence of events:
- They suspected abduction after sleep episodes characterized by awakening, full-body paralysis, intense fear, and a feeling of a presence. Several reported tactile or visual sensations strikingly similar to descriptions of sleep paralysis, such as levitating, being touched, and seeing shadowy figures.
- They sought explanations for what they perceived as anomalous experiences.
- They “recovered” abduction memories in therapy (with the help of techniques such as hypnosis) or spontaneously (after reading books or seeing movies or television shows depicting similar episodes).4
Ms. S reported no daytime sleep attacks, cataplexy, or rapid onset of dreaming. Because her reported AAEs were spread out and the last occurred approximately 5 years ago, I decided against conducting a sleep study because it likely would be low yield and costly. I reached a diagnosis of sleep paralysis-familial type, chronic based on:
- an absence of organic or psychiatric dysfunction
- a familial pattern of sleep disturbances
- the temporal pattern and description of her symptoms (Table 2).11
Table 2
Diagnostic criteria for sleep paralysis
| A. Patient complains of inability to move the trunk or limbs at sleep onset or upon awakening |
| B. Brief episodes of partial or complete skeletal muscle paralysis |
| C. Episodes can be associated with hypnagogic (preceding sleep) hallucinations or dreamlike mentation |
D. Polysomnographic monitoring demonstrates at least 1 of the following:
|
| E. Symptoms are not associated with other medical or mental disorders, such as hysteria or hypokalemic paralysis |
| Minimal criteria are A plus B plus E |
| Note: If symptoms are associated with a familial history, the diagnosis is sleep paralysis-familial type. If symptoms are not associated with a familial history, the diagnosis is sleep paralysis-isolated type |
| Severity criteria Mild: Moderate: >1 episode per month but Severe: ≥1 episode per week |
| Duration criteria Acute: ≤1 month Subacute: >1 month but Chronic: ≥6 months |
| REM: rapid eye movement |
| Source: Reference 11 |
TREATMENT: Reassurance, therapy
Effective treatment for Ms. S required helping her to understand that an organic condition was the foundation of her experiences. I began by conveying the sleep paralysis diagnosis and my understanding of the occupational and personal consequences that this condition had had for her. I explained the physiology of sleep paralysis and that memories or hallucinations (dreamlike mentation) are preserved in an extremely vivid fashion because her eyes are open. I acknowledged the realistic character of her experiences and the resulting symptoms of posttraumatic stress disorder (PTSD).
I refer Ms. S to a therapist for psychotherapy. The therapist begins by using trauma informed techniques to address Ms. S’s PTSD. As she improves, her therapy evolves into a combination of narrative and supportive psychotherapy, and then family systems therapy to address issues with her daughter and mother.
In a follow-up visit 1 year after beginning treatment, Ms. S cites multiple improvements, with no recurrence of sleep paralysis episodes. She continues to take sertraline, which relieves her depression and anxiety, and methylphenidate to improve her attention and concentration. She has taken on more responsibility at home, cleaning, preparing meals, helping her daughter choose a college, and attending to her mother’s health issues. Ms. S still has difficulties with her sleep patterns, and her new psychiatrist is exploring the possibility of a bipolar component to her mood disorder.
The authors’ observations
Like other traumas, AAE can induce symptoms of acute or chronic PTSD. The various psychoses, personality disorders, and dissociative disorders that could account for abduction experiences are characterized by delusions, so conduct ongoing assessment for these conditions in patients who report AAE. However, evidence suggests that serious psychopathology is no more common among “abductees” than among the general population.12
Persons reporting AAE exhibit physiologic reactivity as profound as that of survivors of combat or sexual assault.13 This reactivity confirms that the emotional power of the memory is as evocative and problematic as the physiologic reactions attributable to genuine (documented) traumatic events. Because patients have difficulty differentiating these hallucinations from actual events, they experience emotional pain and suffering. Fifty-seven percent of sleep paralysis patients who report AAE attempt suicide.14
There are no FDA-approved medications for treating sleep paralysis. Pharmacotherapy can be used to address psychiatric symptoms such as the depression and anxiety Ms. S exhibited.
Related resources
- American Academy of Sleep Medicine. International classification of sleep disorders, revised: diagnostic and coding manual. Chicago, IL: American Academy of Sleep Medicine; 2001:166-9.
- Cheyne JA. Sleep paralysis and associated hypnagogic and hypnopompic experiences. http://watarts.uwaterloo.ca/~acheyne/S_P.html.
- Methylphenidate • Ritalin
- Quetiapine • Seroquel
- Sertraline • Zoloft
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Patry AL, Pelletier LG. Extraterrestrial beliefs and experiences: an application of the theory of reasoned action. J Soc Psychol 2001;141(2):199-217.
2. Newman LS, Baumeister RF. Toward an explanation of the UFO abduction phenomenon: hypnotic elaboration, extraterrestrial sadomasochism, and spurious memories. Psychol Inq 1996;7(2):99-126.
3. Bader CD. Supernatural support groups: who are the UFO abductees and ritual-abuse survivors? J Sci Study Relig 2003;42(4):669-78.
4. Clancy SA, McNally RJ, Schacter DL, et al. Memory distortion in people reporting abduction by aliens. J Abnorm Psychol 2002;111(3):455-61.
5. Girard TA, Cheyne JA. Individual differences in lateralization of hallucinations associated with sleep paralysis. Laterality 2004;9(1):93-111.
6. Cheyne JA. The ominous numinous: sensed presence and “other” hallucinations. Journal of Consciousness Studies 2001;8(5-7):133-50.
7. Cheyne JA, Newby-Clark IR, Rueffer SD. Relations among hypnagogic and hypnopompic experiences associated with sleep paralysis. J Sleep Res 1999;8:313-7.
8. Cheyne JA, Rueffer SD, Newby-Clark IR. Hypnagogic and hypnopompic hallucinations during sleep paralysis: neurological and cultural construction of the night-mare. Conscious Cogn 1999;8(3):319-37.
9. Cheyne JA. Sleep paralysis and the structure of waking-nightmare hallucinations. Dreaming 2003;13(3):163-79.
10. Spanos NP, Cross PA, Dickson K, et al. Close encounters: an examination of UFO experiences. J Abnorm Psychol 1993;102(4):624-32.
11. American Academy of Sleep Medicine. International classification of sleep disorders, revised: diagnostic and coding manual. Chicago, IL: American Academy of Sleep Medicine. 2001;166-9.
12. Holden KJ, French CC. Alien abduction experiences: some clues from neuropsychology and neuropsychiatry. Cognit Neuropsychiatry 2002;7(3):163-78.
13. McNally RJ. Applying biological data in forensic and policy arenas. Ann N Y Acad Sci 2006;1071:267-76.
14. Stone-Carmen J. A descriptive study of people reporting abduction by unidentified flying objects (UFOs). In: Pritchard A, Pritchard DE, Mack JE, et al, eds. Alien discussions: proceedings of the abduction study conference held at MIT. Cambridge, MA: North Cambridge Press; 1994:309-15
CASE: ’I’m not crazy’
Ms. S, age 55, presents for treatment because she is feeling depressed and anxious. Her symptoms include decreased concentration, intermittent irritability, hoarding, and difficulty starting and completing tasks. She also has chronic sleep difficulties that often keep her awake until dawn.
Fatigue, lack of focus, and poor comprehension and motivation have left her unemployed. She and her teenage daughter live with Ms. S’s elderly mother. Ms. S feels tremendous guilt because she cannot be the mother and daughter she wants to be.
Initially, I (PK) diagnose Ms. S with major depressive disorder and prescribe sertraline, 100 mg/d, which improves her mood and energy. However, her inability to stay organized results in her being “let go” from job training.
Ms. S reports similar difficulties in school as a child. I determine that she meets DSM-IV-TR criteria for attention-deficit/hyperactivity disorder (ADHD). Adding methylphenidate, 10 mg bid, improves her concentration and ability to complete tasks. It also reduces the impulsivity that has disrupted her relationships.
Despite a strong desire to normalize her sleep schedule, Ms. S continues to have difficulty falling asleep, so I add melatonin, 3 to 6 mg at bedtime. Her sleeping pattern is improved, but still variable. She also tries quetiapine, 25 mg at bedtime, but soon discontinues it due to intolerance.
As our rapport strengthens, Ms. S reveals that she has had multiple encounters with aliens beginning at age 3. Although she has not had an “alien experience” for about 5 years, she does not feel safe sleeping at night and instead sleeps during the day. Her efforts to stay awake at night strain her relationship with her mother.
The authors’ observations
Approximately 1% of the U.S. population report alien abduction experiences (AAE)—an umbrella term that includes alleged contact with aliens ranging from sightings to abductions.1 Patients rarely report AAE to mental health professionals. In our society, claiming to be an “abductee” implies that one might be insane. A survey of 398 Canadian students that assessed attitudes, beliefs, and experiences regarding alien abductions found that 79% of respondents believed they would have mostly negative consequences—such as being laughed at or socially isolated—if they claimed to have encountered aliens.1
Persons who have AAE may attend support groups of fellow “abductees” to accumulate behavior-consonant information (hearing other people’s abduction stories) and reduce dissonance by being surrounded by others who share a questionable belief.2 A survey of “abductees” found that 88% report at least some positive aspects of the experience, such as a sense of importance or feeling as though they were chosen to bridge communication between extraterrestrials and humans.3
- high levels of psychic energy
- self-sufficiency
- resourcefulness
- a tendency to question authority and to be exposed to situational conflicts.1
After Ms. S reveals her alien experiences, I reassure her in a nonjudgmental manner that we will explore her experiences and determine ways to help her cope with them.
HISTORY: Terrifying experiences
Ms. S elaborates on her alien experiences, relating a particularly terrifying example from her teen years. She was lying awake in bed, looking at the ceiling, where she saw a jeweled spider with a drill. As the spider descended from the ceiling and spread its legs, she recalled a noise like a dentist’s drill. As the spider neared her face, it grew larger and larger. Terrified, Ms. S was unable to scream for help or move anything except her eyes as the spider clamped its legs around her head and bored into her skull. She reported that although she could feel the drill go in, it wasn’t painful.
Other experiences included giving birth, undergoing examinations or probes, and communicating with aliens. Although she is very distressed by most memories, she feels she benefited from others. For example, as a child, Ms. S’s math skills improved dramatically after an AAE episode; she believes this was a gift from the aliens. Ms. S’s AAE memories are as vivid to her as memories of her college graduation. She had been reluctant to discuss these events with anyone outside her family out of fear of being perceived as “crazy.”
Ms. S says she was a shy child who had difficulty making friends. She was plagued with fatigue and worry about family members. She believed that aliens might attack her sisters and felt obligated to stay awake at night to protect them. Aside from alien experiences, Ms. S reports a happy childhood.
She has always been an avid reader. At age 8 or 9, after reading a book on alien abduction, she concluded that she had been abducted. Later, she joined a group of professed alien abductees. She feels accepted and validated by this group and has a forum for discussing her experiences without fear of ridicule or rejection.
Ms. S remains frightened by things that remind her of aliens. Although she wrote a summary of her alien experiences, she cannot draw a picture of an alien, and thoughts or images of the prototypical “grey” alien trigger panic. She also feels somewhat “different,” nervous, and distant from others.
The authors’ observations
Reviewing AAE literature led me to consider several diagnoses, including:
- psychosis
- seizures
- false memory (sexual abuse, trauma)
- narcolepsy
- sleep paralysis.
Electroencephalography (during drowsiness) revealed abnormal activity (occurrences of widely scattered bursts of nonspecific, round, sharply contoured slow waves in the left frontal region) only in the F7 electrode. In the absence of clinical symptoms and when found in a single lead, this is considered a normal variant.
Diagnostic testing ruled out hallucinosis related to seizures. I also ruled out false memory related to sexual abuse or trauma, which is commonly found in patients who present with AAE.
Collaborative information from relatives did not uncover a history of psychosis. She and family members reported, however, that Ms. S’s father and 1 sister had periodic sleep disturbances with associated hallucinations. I began to suspect sleep paralysis.
The authors’ observations
Full-body paralysis normally accompanies rapid eye movement (REM) sleep, which occurs several times a night.4 Sleep paralysis is a transient state that occurs when an individual becomes conscious of this immobility, typically while falling asleep or awakening.5 These experiences can be accompanied by hypnagogic (while falling asleep) or hypnopompic (while awakening) hallucinations. An estimated 30% of the population has had at least one sleep paralysis episode.6 In one study, 5% of sleep paralysis patients had episodes that were accompanied by hallucinations.7
Although individuals cannot make gross body movements during sleep paralysis, they can open their eyes and are able to report events that occurred around them during the episode.8 Patients interpret sleep paralysis experiences in subjective terms. Common descriptions include intense fear, breathing difficulties, feeling of bodily pressure—especially on the chest—and sensations of floating, flying, or falling (Table 1).7,9
During sleep paralysis episodes, individuals typically sense a threatening presence.6 Patients have reported beastly and demonic figures of doom: devils, demons, witches, aliens, and even cinematic villains such as Darth Vader and Freddy Kruger.6 Others have described this presence in terms of alien visitations or abductions.
Table 1
4 types of sleep paralysis-related hallucinations
| Intruder | Vague sense of a threatening presence accompanied by visual, auditory, and tactile hallucinations—noises, footsteps, gibbering voices, humanoid apparitions, and sensation of being touched or grabbed |
| Incubus | Breathing difficulties, feelings of suffocation, bodily pressure (particularly on the chest, as if someone were sitting or standing on it), pain, and thoughts of impending death |
| Vestibular-motor | Sensations of floating (levitation), flying, and falling |
| Other | Out-of-body experiences, autoscopy (seeing oneself from an external point), and fictive motor movements, ranging from simple arm movements to sitting up to apparent locomotion through the environment |
| Source: References 7,9 | |
A Harvard University study of 11 individuals who reported alien abductions found that all participants experienced a similar sequence of events:
- They suspected abduction after sleep episodes characterized by awakening, full-body paralysis, intense fear, and a feeling of a presence. Several reported tactile or visual sensations strikingly similar to descriptions of sleep paralysis, such as levitating, being touched, and seeing shadowy figures.
- They sought explanations for what they perceived as anomalous experiences.
- They “recovered” abduction memories in therapy (with the help of techniques such as hypnosis) or spontaneously (after reading books or seeing movies or television shows depicting similar episodes).4
Ms. S reported no daytime sleep attacks, cataplexy, or rapid onset of dreaming. Because her reported AAEs were spread out and the last occurred approximately 5 years ago, I decided against conducting a sleep study because it likely would be low yield and costly. I reached a diagnosis of sleep paralysis-familial type, chronic based on:
- an absence of organic or psychiatric dysfunction
- a familial pattern of sleep disturbances
- the temporal pattern and description of her symptoms (Table 2).11
Table 2
Diagnostic criteria for sleep paralysis
| A. Patient complains of inability to move the trunk or limbs at sleep onset or upon awakening |
| B. Brief episodes of partial or complete skeletal muscle paralysis |
| C. Episodes can be associated with hypnagogic (preceding sleep) hallucinations or dreamlike mentation |
D. Polysomnographic monitoring demonstrates at least 1 of the following:
|
| E. Symptoms are not associated with other medical or mental disorders, such as hysteria or hypokalemic paralysis |
| Minimal criteria are A plus B plus E |
| Note: If symptoms are associated with a familial history, the diagnosis is sleep paralysis-familial type. If symptoms are not associated with a familial history, the diagnosis is sleep paralysis-isolated type |
| Severity criteria Mild: Moderate: >1 episode per month but Severe: ≥1 episode per week |
| Duration criteria Acute: ≤1 month Subacute: >1 month but Chronic: ≥6 months |
| REM: rapid eye movement |
| Source: Reference 11 |
TREATMENT: Reassurance, therapy
Effective treatment for Ms. S required helping her to understand that an organic condition was the foundation of her experiences. I began by conveying the sleep paralysis diagnosis and my understanding of the occupational and personal consequences that this condition had had for her. I explained the physiology of sleep paralysis and that memories or hallucinations (dreamlike mentation) are preserved in an extremely vivid fashion because her eyes are open. I acknowledged the realistic character of her experiences and the resulting symptoms of posttraumatic stress disorder (PTSD).
I refer Ms. S to a therapist for psychotherapy. The therapist begins by using trauma informed techniques to address Ms. S’s PTSD. As she improves, her therapy evolves into a combination of narrative and supportive psychotherapy, and then family systems therapy to address issues with her daughter and mother.
In a follow-up visit 1 year after beginning treatment, Ms. S cites multiple improvements, with no recurrence of sleep paralysis episodes. She continues to take sertraline, which relieves her depression and anxiety, and methylphenidate to improve her attention and concentration. She has taken on more responsibility at home, cleaning, preparing meals, helping her daughter choose a college, and attending to her mother’s health issues. Ms. S still has difficulties with her sleep patterns, and her new psychiatrist is exploring the possibility of a bipolar component to her mood disorder.
The authors’ observations
Like other traumas, AAE can induce symptoms of acute or chronic PTSD. The various psychoses, personality disorders, and dissociative disorders that could account for abduction experiences are characterized by delusions, so conduct ongoing assessment for these conditions in patients who report AAE. However, evidence suggests that serious psychopathology is no more common among “abductees” than among the general population.12
Persons reporting AAE exhibit physiologic reactivity as profound as that of survivors of combat or sexual assault.13 This reactivity confirms that the emotional power of the memory is as evocative and problematic as the physiologic reactions attributable to genuine (documented) traumatic events. Because patients have difficulty differentiating these hallucinations from actual events, they experience emotional pain and suffering. Fifty-seven percent of sleep paralysis patients who report AAE attempt suicide.14
There are no FDA-approved medications for treating sleep paralysis. Pharmacotherapy can be used to address psychiatric symptoms such as the depression and anxiety Ms. S exhibited.
Related resources
- American Academy of Sleep Medicine. International classification of sleep disorders, revised: diagnostic and coding manual. Chicago, IL: American Academy of Sleep Medicine; 2001:166-9.
- Cheyne JA. Sleep paralysis and associated hypnagogic and hypnopompic experiences. http://watarts.uwaterloo.ca/~acheyne/S_P.html.
- Methylphenidate • Ritalin
- Quetiapine • Seroquel
- Sertraline • Zoloft
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: ’I’m not crazy’
Ms. S, age 55, presents for treatment because she is feeling depressed and anxious. Her symptoms include decreased concentration, intermittent irritability, hoarding, and difficulty starting and completing tasks. She also has chronic sleep difficulties that often keep her awake until dawn.
Fatigue, lack of focus, and poor comprehension and motivation have left her unemployed. She and her teenage daughter live with Ms. S’s elderly mother. Ms. S feels tremendous guilt because she cannot be the mother and daughter she wants to be.
Initially, I (PK) diagnose Ms. S with major depressive disorder and prescribe sertraline, 100 mg/d, which improves her mood and energy. However, her inability to stay organized results in her being “let go” from job training.
Ms. S reports similar difficulties in school as a child. I determine that she meets DSM-IV-TR criteria for attention-deficit/hyperactivity disorder (ADHD). Adding methylphenidate, 10 mg bid, improves her concentration and ability to complete tasks. It also reduces the impulsivity that has disrupted her relationships.
Despite a strong desire to normalize her sleep schedule, Ms. S continues to have difficulty falling asleep, so I add melatonin, 3 to 6 mg at bedtime. Her sleeping pattern is improved, but still variable. She also tries quetiapine, 25 mg at bedtime, but soon discontinues it due to intolerance.
As our rapport strengthens, Ms. S reveals that she has had multiple encounters with aliens beginning at age 3. Although she has not had an “alien experience” for about 5 years, she does not feel safe sleeping at night and instead sleeps during the day. Her efforts to stay awake at night strain her relationship with her mother.
The authors’ observations
Approximately 1% of the U.S. population report alien abduction experiences (AAE)—an umbrella term that includes alleged contact with aliens ranging from sightings to abductions.1 Patients rarely report AAE to mental health professionals. In our society, claiming to be an “abductee” implies that one might be insane. A survey of 398 Canadian students that assessed attitudes, beliefs, and experiences regarding alien abductions found that 79% of respondents believed they would have mostly negative consequences—such as being laughed at or socially isolated—if they claimed to have encountered aliens.1
Persons who have AAE may attend support groups of fellow “abductees” to accumulate behavior-consonant information (hearing other people’s abduction stories) and reduce dissonance by being surrounded by others who share a questionable belief.2 A survey of “abductees” found that 88% report at least some positive aspects of the experience, such as a sense of importance or feeling as though they were chosen to bridge communication between extraterrestrials and humans.3
- high levels of psychic energy
- self-sufficiency
- resourcefulness
- a tendency to question authority and to be exposed to situational conflicts.1
After Ms. S reveals her alien experiences, I reassure her in a nonjudgmental manner that we will explore her experiences and determine ways to help her cope with them.
HISTORY: Terrifying experiences
Ms. S elaborates on her alien experiences, relating a particularly terrifying example from her teen years. She was lying awake in bed, looking at the ceiling, where she saw a jeweled spider with a drill. As the spider descended from the ceiling and spread its legs, she recalled a noise like a dentist’s drill. As the spider neared her face, it grew larger and larger. Terrified, Ms. S was unable to scream for help or move anything except her eyes as the spider clamped its legs around her head and bored into her skull. She reported that although she could feel the drill go in, it wasn’t painful.
Other experiences included giving birth, undergoing examinations or probes, and communicating with aliens. Although she is very distressed by most memories, she feels she benefited from others. For example, as a child, Ms. S’s math skills improved dramatically after an AAE episode; she believes this was a gift from the aliens. Ms. S’s AAE memories are as vivid to her as memories of her college graduation. She had been reluctant to discuss these events with anyone outside her family out of fear of being perceived as “crazy.”
Ms. S says she was a shy child who had difficulty making friends. She was plagued with fatigue and worry about family members. She believed that aliens might attack her sisters and felt obligated to stay awake at night to protect them. Aside from alien experiences, Ms. S reports a happy childhood.
She has always been an avid reader. At age 8 or 9, after reading a book on alien abduction, she concluded that she had been abducted. Later, she joined a group of professed alien abductees. She feels accepted and validated by this group and has a forum for discussing her experiences without fear of ridicule or rejection.
Ms. S remains frightened by things that remind her of aliens. Although she wrote a summary of her alien experiences, she cannot draw a picture of an alien, and thoughts or images of the prototypical “grey” alien trigger panic. She also feels somewhat “different,” nervous, and distant from others.
The authors’ observations
Reviewing AAE literature led me to consider several diagnoses, including:
- psychosis
- seizures
- false memory (sexual abuse, trauma)
- narcolepsy
- sleep paralysis.
Electroencephalography (during drowsiness) revealed abnormal activity (occurrences of widely scattered bursts of nonspecific, round, sharply contoured slow waves in the left frontal region) only in the F7 electrode. In the absence of clinical symptoms and when found in a single lead, this is considered a normal variant.
Diagnostic testing ruled out hallucinosis related to seizures. I also ruled out false memory related to sexual abuse or trauma, which is commonly found in patients who present with AAE.
Collaborative information from relatives did not uncover a history of psychosis. She and family members reported, however, that Ms. S’s father and 1 sister had periodic sleep disturbances with associated hallucinations. I began to suspect sleep paralysis.
The authors’ observations
Full-body paralysis normally accompanies rapid eye movement (REM) sleep, which occurs several times a night.4 Sleep paralysis is a transient state that occurs when an individual becomes conscious of this immobility, typically while falling asleep or awakening.5 These experiences can be accompanied by hypnagogic (while falling asleep) or hypnopompic (while awakening) hallucinations. An estimated 30% of the population has had at least one sleep paralysis episode.6 In one study, 5% of sleep paralysis patients had episodes that were accompanied by hallucinations.7
Although individuals cannot make gross body movements during sleep paralysis, they can open their eyes and are able to report events that occurred around them during the episode.8 Patients interpret sleep paralysis experiences in subjective terms. Common descriptions include intense fear, breathing difficulties, feeling of bodily pressure—especially on the chest—and sensations of floating, flying, or falling (Table 1).7,9
During sleep paralysis episodes, individuals typically sense a threatening presence.6 Patients have reported beastly and demonic figures of doom: devils, demons, witches, aliens, and even cinematic villains such as Darth Vader and Freddy Kruger.6 Others have described this presence in terms of alien visitations or abductions.
Table 1
4 types of sleep paralysis-related hallucinations
| Intruder | Vague sense of a threatening presence accompanied by visual, auditory, and tactile hallucinations—noises, footsteps, gibbering voices, humanoid apparitions, and sensation of being touched or grabbed |
| Incubus | Breathing difficulties, feelings of suffocation, bodily pressure (particularly on the chest, as if someone were sitting or standing on it), pain, and thoughts of impending death |
| Vestibular-motor | Sensations of floating (levitation), flying, and falling |
| Other | Out-of-body experiences, autoscopy (seeing oneself from an external point), and fictive motor movements, ranging from simple arm movements to sitting up to apparent locomotion through the environment |
| Source: References 7,9 | |
A Harvard University study of 11 individuals who reported alien abductions found that all participants experienced a similar sequence of events:
- They suspected abduction after sleep episodes characterized by awakening, full-body paralysis, intense fear, and a feeling of a presence. Several reported tactile or visual sensations strikingly similar to descriptions of sleep paralysis, such as levitating, being touched, and seeing shadowy figures.
- They sought explanations for what they perceived as anomalous experiences.
- They “recovered” abduction memories in therapy (with the help of techniques such as hypnosis) or spontaneously (after reading books or seeing movies or television shows depicting similar episodes).4
Ms. S reported no daytime sleep attacks, cataplexy, or rapid onset of dreaming. Because her reported AAEs were spread out and the last occurred approximately 5 years ago, I decided against conducting a sleep study because it likely would be low yield and costly. I reached a diagnosis of sleep paralysis-familial type, chronic based on:
- an absence of organic or psychiatric dysfunction
- a familial pattern of sleep disturbances
- the temporal pattern and description of her symptoms (Table 2).11
Table 2
Diagnostic criteria for sleep paralysis
| A. Patient complains of inability to move the trunk or limbs at sleep onset or upon awakening |
| B. Brief episodes of partial or complete skeletal muscle paralysis |
| C. Episodes can be associated with hypnagogic (preceding sleep) hallucinations or dreamlike mentation |
D. Polysomnographic monitoring demonstrates at least 1 of the following:
|
| E. Symptoms are not associated with other medical or mental disorders, such as hysteria or hypokalemic paralysis |
| Minimal criteria are A plus B plus E |
| Note: If symptoms are associated with a familial history, the diagnosis is sleep paralysis-familial type. If symptoms are not associated with a familial history, the diagnosis is sleep paralysis-isolated type |
| Severity criteria Mild: Moderate: >1 episode per month but Severe: ≥1 episode per week |
| Duration criteria Acute: ≤1 month Subacute: >1 month but Chronic: ≥6 months |
| REM: rapid eye movement |
| Source: Reference 11 |
TREATMENT: Reassurance, therapy
Effective treatment for Ms. S required helping her to understand that an organic condition was the foundation of her experiences. I began by conveying the sleep paralysis diagnosis and my understanding of the occupational and personal consequences that this condition had had for her. I explained the physiology of sleep paralysis and that memories or hallucinations (dreamlike mentation) are preserved in an extremely vivid fashion because her eyes are open. I acknowledged the realistic character of her experiences and the resulting symptoms of posttraumatic stress disorder (PTSD).
I refer Ms. S to a therapist for psychotherapy. The therapist begins by using trauma informed techniques to address Ms. S’s PTSD. As she improves, her therapy evolves into a combination of narrative and supportive psychotherapy, and then family systems therapy to address issues with her daughter and mother.
In a follow-up visit 1 year after beginning treatment, Ms. S cites multiple improvements, with no recurrence of sleep paralysis episodes. She continues to take sertraline, which relieves her depression and anxiety, and methylphenidate to improve her attention and concentration. She has taken on more responsibility at home, cleaning, preparing meals, helping her daughter choose a college, and attending to her mother’s health issues. Ms. S still has difficulties with her sleep patterns, and her new psychiatrist is exploring the possibility of a bipolar component to her mood disorder.
The authors’ observations
Like other traumas, AAE can induce symptoms of acute or chronic PTSD. The various psychoses, personality disorders, and dissociative disorders that could account for abduction experiences are characterized by delusions, so conduct ongoing assessment for these conditions in patients who report AAE. However, evidence suggests that serious psychopathology is no more common among “abductees” than among the general population.12
Persons reporting AAE exhibit physiologic reactivity as profound as that of survivors of combat or sexual assault.13 This reactivity confirms that the emotional power of the memory is as evocative and problematic as the physiologic reactions attributable to genuine (documented) traumatic events. Because patients have difficulty differentiating these hallucinations from actual events, they experience emotional pain and suffering. Fifty-seven percent of sleep paralysis patients who report AAE attempt suicide.14
There are no FDA-approved medications for treating sleep paralysis. Pharmacotherapy can be used to address psychiatric symptoms such as the depression and anxiety Ms. S exhibited.
Related resources
- American Academy of Sleep Medicine. International classification of sleep disorders, revised: diagnostic and coding manual. Chicago, IL: American Academy of Sleep Medicine; 2001:166-9.
- Cheyne JA. Sleep paralysis and associated hypnagogic and hypnopompic experiences. http://watarts.uwaterloo.ca/~acheyne/S_P.html.
- Methylphenidate • Ritalin
- Quetiapine • Seroquel
- Sertraline • Zoloft
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Patry AL, Pelletier LG. Extraterrestrial beliefs and experiences: an application of the theory of reasoned action. J Soc Psychol 2001;141(2):199-217.
2. Newman LS, Baumeister RF. Toward an explanation of the UFO abduction phenomenon: hypnotic elaboration, extraterrestrial sadomasochism, and spurious memories. Psychol Inq 1996;7(2):99-126.
3. Bader CD. Supernatural support groups: who are the UFO abductees and ritual-abuse survivors? J Sci Study Relig 2003;42(4):669-78.
4. Clancy SA, McNally RJ, Schacter DL, et al. Memory distortion in people reporting abduction by aliens. J Abnorm Psychol 2002;111(3):455-61.
5. Girard TA, Cheyne JA. Individual differences in lateralization of hallucinations associated with sleep paralysis. Laterality 2004;9(1):93-111.
6. Cheyne JA. The ominous numinous: sensed presence and “other” hallucinations. Journal of Consciousness Studies 2001;8(5-7):133-50.
7. Cheyne JA, Newby-Clark IR, Rueffer SD. Relations among hypnagogic and hypnopompic experiences associated with sleep paralysis. J Sleep Res 1999;8:313-7.
8. Cheyne JA, Rueffer SD, Newby-Clark IR. Hypnagogic and hypnopompic hallucinations during sleep paralysis: neurological and cultural construction of the night-mare. Conscious Cogn 1999;8(3):319-37.
9. Cheyne JA. Sleep paralysis and the structure of waking-nightmare hallucinations. Dreaming 2003;13(3):163-79.
10. Spanos NP, Cross PA, Dickson K, et al. Close encounters: an examination of UFO experiences. J Abnorm Psychol 1993;102(4):624-32.
11. American Academy of Sleep Medicine. International classification of sleep disorders, revised: diagnostic and coding manual. Chicago, IL: American Academy of Sleep Medicine. 2001;166-9.
12. Holden KJ, French CC. Alien abduction experiences: some clues from neuropsychology and neuropsychiatry. Cognit Neuropsychiatry 2002;7(3):163-78.
13. McNally RJ. Applying biological data in forensic and policy arenas. Ann N Y Acad Sci 2006;1071:267-76.
14. Stone-Carmen J. A descriptive study of people reporting abduction by unidentified flying objects (UFOs). In: Pritchard A, Pritchard DE, Mack JE, et al, eds. Alien discussions: proceedings of the abduction study conference held at MIT. Cambridge, MA: North Cambridge Press; 1994:309-15
1. Patry AL, Pelletier LG. Extraterrestrial beliefs and experiences: an application of the theory of reasoned action. J Soc Psychol 2001;141(2):199-217.
2. Newman LS, Baumeister RF. Toward an explanation of the UFO abduction phenomenon: hypnotic elaboration, extraterrestrial sadomasochism, and spurious memories. Psychol Inq 1996;7(2):99-126.
3. Bader CD. Supernatural support groups: who are the UFO abductees and ritual-abuse survivors? J Sci Study Relig 2003;42(4):669-78.
4. Clancy SA, McNally RJ, Schacter DL, et al. Memory distortion in people reporting abduction by aliens. J Abnorm Psychol 2002;111(3):455-61.
5. Girard TA, Cheyne JA. Individual differences in lateralization of hallucinations associated with sleep paralysis. Laterality 2004;9(1):93-111.
6. Cheyne JA. The ominous numinous: sensed presence and “other” hallucinations. Journal of Consciousness Studies 2001;8(5-7):133-50.
7. Cheyne JA, Newby-Clark IR, Rueffer SD. Relations among hypnagogic and hypnopompic experiences associated with sleep paralysis. J Sleep Res 1999;8:313-7.
8. Cheyne JA, Rueffer SD, Newby-Clark IR. Hypnagogic and hypnopompic hallucinations during sleep paralysis: neurological and cultural construction of the night-mare. Conscious Cogn 1999;8(3):319-37.
9. Cheyne JA. Sleep paralysis and the structure of waking-nightmare hallucinations. Dreaming 2003;13(3):163-79.
10. Spanos NP, Cross PA, Dickson K, et al. Close encounters: an examination of UFO experiences. J Abnorm Psychol 1993;102(4):624-32.
11. American Academy of Sleep Medicine. International classification of sleep disorders, revised: diagnostic and coding manual. Chicago, IL: American Academy of Sleep Medicine. 2001;166-9.
12. Holden KJ, French CC. Alien abduction experiences: some clues from neuropsychology and neuropsychiatry. Cognit Neuropsychiatry 2002;7(3):163-78.
13. McNally RJ. Applying biological data in forensic and policy arenas. Ann N Y Acad Sci 2006;1071:267-76.
14. Stone-Carmen J. A descriptive study of people reporting abduction by unidentified flying objects (UFOs). In: Pritchard A, Pritchard DE, Mack JE, et al, eds. Alien discussions: proceedings of the abduction study conference held at MIT. Cambridge, MA: North Cambridge Press; 1994:309-15
The patient who ‘spilled salt’
HISTORY: ‘They’re out to get me’
Mrs. V, age 64, tells her primary care physician she has felt “bad” for 2 weeks. She complains of depressed mood, middle insomnia, diminished appetite, poor concentration, and poor energy. She denies suicidal thoughts but reports feeling alone, overwhelmed, and unable to manage her daily life.
Mrs. V is very concerned about losing her job because she cannot function at work. She believes her coworkers may be plotting to get her fired. The primary care physician refers Mrs. V to us to evaluate her mood.
According to her daughter, Mrs. V has had multiple psychiatric hospitalizations; the most recent occurred 2 years ago when she was admitted for paranoia and disorganized behavior. The daughter also mentions that her mother has a remote history of daily alcohol use, drinking until she was intoxicated. Mrs. V says she occasionally drinks beer and she scores 2 out of 4 on the CAGE questionnaire, which may indicate alcohol dependence.
During mental status examination, Mrs. V is alert and oriented to person, place, and date. She is pleasant and cooperative but shows apparent thought blocking and some tangentiality. She has substantial difficulty answering questions and articulating symptoms. Speech is slow in rate and rhythm. Mrs. V’s mood is severely depressed and her affect constricted.
She denies suicidal or homicidal ideations or visual or auditory hallucinations. Cognitive testing reveals mild deficits in recall memory and poor concentration. Her insight is limited and her judgment fair.
Her medical history includes hypertension, hyperlipidemia, coronary artery disease, cardiac catheterization, and hyponatremia. Her medication regimen consists of aripiprazole, 15 mg/d; diltiazem, 180 mg/d; atenolol, 25 mg/d; aspirin, 325 mg/d; atorvastatin, 10 mg/d; sertraline, 50 mg/d; and ibuprofen, 600 mg as needed for hip pain. She also reports taking diuretics in the past.
Vital signs include blood pressure, 125/95 mm Hg; respirations, 16/min; temperature, 98.2° F; and pulse rate, 72/min. Serum investigations reveal sodium, 119 mEq/L (normal range: 135 to 145 mEq/L) and random blood sugar, 160 mg/dL (normal range: 60 to 114 mg/dL).
The authors’ observations
The combination of major depression with psychosis and hyponatremia makes Mrs. V’s case challenging. Hyponatremia in psychiatric inpatients can prompt medical consultation, thus possibly halting or delaying psychiatric treatment.
Hyponatremia has been associated with the use of:
- diuretics
- selective serotonin reuptake inhibitors (SSRIs)
- serotonin-norepinephrine reuptake inhibitors (SNRIs)
- tricyclic antidepressants
- calcium antagonists.
Among psychiatric inpatients, the risk of hyponatremia is doubled in women.1 It is unclear, however, if female gender is an independent risk factor for hyponatremia. Sharabi et al2 reported that patients of both sexes age >65 have a 9-fold greater risk of developing hyponatremia than younger counterparts.
In addition, hyponatremia risk during any antidepressant treatment is highest:
- in the summer
- during the first weeks of treatment
- with concomitant drug use, especially with diuretics.3
The authors’ observations
Based on Mrs. V’s initial lab results (Table 1), we classify her hyponatremia as euvolemic, with high urine osmolarity (≥100 mOsm/L). That helps narrow our differential diagnosis to glucocorticoid deficiency, hypothyroidism, and SIADH (Table 2).5 We exclude psychogenic polydipsia, “tea and toast” syndrome, or beer potomania because they usually present as euvolemic hyponatremia with low urinary osmolality.
SSRI use in elderly persons has been associated with hyponatremia, which in some cases may be consistent with SIADH. Unfortunately, few psychiatrists are aware of this potentially fatal side effect.
SIADH occurs in association with reduced serum osmolality. It is characterized by:
- hypotonic hyponatremia (serum sodium
- inappropriately elevated urine osmolarity (>200 mOsm/L) relative to plasma osmolarity
- elevated urine sodium (typically >20 mEq/L).4
The key to the pathophysiology, signs, symptoms, and treatment of SIADH is understanding that the hyponatremia is a result of excess water and not a sodium deficiency. Hyponatremia’s signs and symptoms primarily are related to CNS dysfunction and correlate with how rapidly and severely the condition develops.
We monitor Mrs. V for anorexia, nausea, and malaise because they would be the earliest findings, followed by headache, irritability, confusion, muscle cramps, weakness, obtundation, seizures, and coma. These occur as osmotic fluid shifts and results in cerebral edema and increased intracranial pressure. When sodium concentration drops below 105 mEq/L, life-threatening complications are likely.
Table 1
Mrs. V’s laboratory results
| Mrs. V’s results | |||
|---|---|---|---|
| Normal range | Before Tx | After Tx | |
| Serum sodium (mEq/L) | 135 to 145 | 119 | 127 |
| Serum potassium (mEq/L) | 3.5 to 5.0 | 3.6 | 3.8 |
| Creatinine (mg/dL) | 0.5 to 1.7 | 0.74 | 0.84 |
| Glucose (mg/dL) | 60 to 114 | 160 | 150 |
| Osmolarity | |||
| Serum (measured; mOsm/L) | 275 to 300 | 258 | 242 |
| Urine (mOsm/L) | 257 | 180 | |
| Urine sodium (mEq/L) | 20 to 40 | 48 | 42 |
Mrs. V’s laboratory results
| Hypovolemic hyponatremia | Euvolemic hyponatremia | Hypervolemic hyponatremia |
|---|---|---|
| Vomiting Diarrhea Laxative abuse Renal disease Nasogastric suction Salt-wasting nephropathy Addison’s disease | Normal urinary sodium Glucocorticoid deficiency Hypothyroidism Certain drugs SIADH | Congestive heart failure Nephrotic syndrome Cirrhosis |
| Low urinary osmolality Psychogenic polydipsia ‘Tea and toast’ syndrome Beer potomania | ||
| SIADH: syndrome of inappropriate antidiuretic hormone | ||
| Source: Reference 5 | ||
SSRIs and SIADH
Bouman et al6 estimated that the incidence of SSRI-induced SIADH in elderly patients is 12%. Liu et al7 described 706 cases of hyponatremia associated with SSRI use in unpublished reports. Fluoxetine was most commonly the cause (75.3% cases), followed by paroxetine (12.4%), sertraline (11.7%), and fluvoxamine (1.5%). Resuming the same drug resulted in hyponatremia in 16 of 24 of these cases (66.7%).
Kirby et al,8 however, found no clear advantages in different SSRIs’ propensity to cause hyponatremia. Seventy-one percent of patients treated with the SNRI venlafaxine developed hyponatremia, compared with 32% taking paroxetine and 29% receiving sertraline. It is unclear whether a specific SSRI or venlafaxine has a stronger association with hyponatremia than any other antidepressant.
Hyponatremia’s nonspecific symptoms and wide range of time to detection (1 to 253 days) suggest clinicians usually detect the condition by chance rather than specifically assessing for it.9
TREATMENT: Medication change?
Coordinating Mrs. V’s depression and hyponatremia treatment is critical. We propose discontinuing sertraline and treating Mrs. V’s symptoms with electroconvulsive therapy (ECT). She refuses ECT, stating “I don’t feel that bad. My father was treated with ECT and I am scared of it.”
The authors’ observations
SSRI-induced hyponatremia can be transient or persistent and recurrent. The usual approach is to discontinue the SSRI and try a different antidepressant. Because hyponatremia has been associated with all SSRIs and SNRIs, it would be prudent to choose an alternate antidepressant agent outside these classes. If patients must continue taking an antidepressant that causes hyponatremia, avoid concurrent use of drugs that cause hyponatremia, restrict fluid intake, and consider adding a medication that prevents hyponatremia, such as demeclocycline or fludrocortisone.
SSRI-induced hyponatremia may resolve:
- with SSRI discontinuation alone11
- with fluid restriction and without discontinuation of the SSRI11
- with drug discontinuation, fluid restriction, and sodium chloride and potassium supplementation.12
FOLLOW-UP: Analysis error?
Despite modifications to Mrs. V’s diet, her fasting serum glucose level remains >100. She is diagnosed with diabetes mellitus type 2 and treated with metformin. We continue mirtazapine, which has successfully controlled Mrs. V’s depressive symptoms. Her serum sodium levels start normalizing.
The authors’ observations
Related resources
- Siegel AJ. Hyponatremia in psychiatric patients: update on evaluation and management. Harv Rev Psychiatry 2008;16(1):13-24.
- Atalay A, Turhan N, Aki OE. A challenging case of syndrome of inappropriate secretion of antidiuretic hormone in an elderly patient secondary to quetiapine. South Med J 2007;100(8):832-3.
- Aripiprazole • Abilify
- Atenolol • Tenormin
- Atorvastatin • Lipitor
- Demeclocycline • Declomycin, Declostatin, others
- Diltiazem • Cardizem, Dilacor, others
- Fludrocortisone • Florinef
- Fluvoxamine • Luvox
- Ibuprofen • Advil, Motrin, others
- Metformin • Glucophage, Diabex, others
- Mirtazapine • Remeron
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosures
Dr. Romanowicz reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Ramaswamy receives research support from Bristol-Myers Squibb, Shire, and Forest Pharmaceuticals and is a consultant to Dainippon Sumitomo Pharma.
Dr. Wilson receives research support from the National Institute of Mental Health, the Veterans Administration, the State of Nebraska, Health Futures Foundation, Inc., AstraZeneca, Dainippon Sumitomo Pharma, Eli Lilly and Company, and Pfizer Inc. and serves as a consultant to the Substance Abuse and Mental Health Services Administration and the State of Nebraska.
Reference
1. Siegler EL, Tamres D, Berlin JA, et al. Risk factors for the development of hyponatremia in psychiatric inpatients. Arch Intern Med 1995;155(9):953-7.
2. Sharabi Y, Illan R, Kamari Y, et al. Diuretic induced hyponatraemia in elderly hypertensive women. J Hum Hypertens 2002;16(9):631-5.
3. Rosner MH. Severe hyponatremia associated with the combined use of thiazide diuretics and selective serotonin reuptake inhibitors. Am J Med Sci 2004;327(2):109-11.
4. Buff DD, Markowitz S. Hyponatremia in the psychiatric patient: a review of diagnostic and management strategies. Psychiatr Ann 2003;33(5):318-25.
5. Levitan A. Hyponatremia: how to recognize the cause promptly—and avoid treatment pitfalls. Consultant 2003;43(7):861-70.
6. Bouman WP, Pinner G, Johnson H. Incidence of selective serotonin reuptake inhibitor (SSRI) induced hyponatraemia due to the syndrome of inappropriate antidiuretic hormone (SIADH) secretion in the elderly. Int J Geriatr Psychiatry 1998;13(1):12-5
7. Liu BA, Mittmann N, Knowles SR, et al. Hyponatremia and the syndrome of inappropriate secretion of antidiuretic hormone associated with the use of selective serotonin reuptake inhibitors: a review of spontaneous reports. CMAJ 1996;155(5):519-27
8. Kirby D, Ames D. Hyponatraemia and selective serotonin re-uptake inhibitors in elderly patients. Int J Geriatr Psychiatry 2001;16(5):484-93
9. Kirchner V, Silver LE, Kelly CA. Selective serotonin reuptake inhibitors and hyponatraemia: review and proposed mechanisms in the elderly. J Psychopharmacol 1998;12(4):396-400.
10. Jagsch C, Marksteiner J, Seiringer E, Windhager E. Successful mirtazapine treatment of an 81-year-old patient with syndrome of inappropriate antidiuretic hormone secretion. Pharmacopsychiatry 2007;40(3):129-31.
11. Bigaillon C, El Jahiri Y, Garcia C, et al. Inappropriate ADH secretion-induced hyponatremia and associated with paroxetine use. Rev Med Interne 2007;28(9):642-4.
12. Blacksten JV, Birt JA. Syndrome of inappropriate secretion of antidiuretic hormone secondary to fluoxetine. Ann Pharmacother 1993;27(6):723-4.
HISTORY: ‘They’re out to get me’
Mrs. V, age 64, tells her primary care physician she has felt “bad” for 2 weeks. She complains of depressed mood, middle insomnia, diminished appetite, poor concentration, and poor energy. She denies suicidal thoughts but reports feeling alone, overwhelmed, and unable to manage her daily life.
Mrs. V is very concerned about losing her job because she cannot function at work. She believes her coworkers may be plotting to get her fired. The primary care physician refers Mrs. V to us to evaluate her mood.
According to her daughter, Mrs. V has had multiple psychiatric hospitalizations; the most recent occurred 2 years ago when she was admitted for paranoia and disorganized behavior. The daughter also mentions that her mother has a remote history of daily alcohol use, drinking until she was intoxicated. Mrs. V says she occasionally drinks beer and she scores 2 out of 4 on the CAGE questionnaire, which may indicate alcohol dependence.
During mental status examination, Mrs. V is alert and oriented to person, place, and date. She is pleasant and cooperative but shows apparent thought blocking and some tangentiality. She has substantial difficulty answering questions and articulating symptoms. Speech is slow in rate and rhythm. Mrs. V’s mood is severely depressed and her affect constricted.
She denies suicidal or homicidal ideations or visual or auditory hallucinations. Cognitive testing reveals mild deficits in recall memory and poor concentration. Her insight is limited and her judgment fair.
Her medical history includes hypertension, hyperlipidemia, coronary artery disease, cardiac catheterization, and hyponatremia. Her medication regimen consists of aripiprazole, 15 mg/d; diltiazem, 180 mg/d; atenolol, 25 mg/d; aspirin, 325 mg/d; atorvastatin, 10 mg/d; sertraline, 50 mg/d; and ibuprofen, 600 mg as needed for hip pain. She also reports taking diuretics in the past.
Vital signs include blood pressure, 125/95 mm Hg; respirations, 16/min; temperature, 98.2° F; and pulse rate, 72/min. Serum investigations reveal sodium, 119 mEq/L (normal range: 135 to 145 mEq/L) and random blood sugar, 160 mg/dL (normal range: 60 to 114 mg/dL).
The authors’ observations
The combination of major depression with psychosis and hyponatremia makes Mrs. V’s case challenging. Hyponatremia in psychiatric inpatients can prompt medical consultation, thus possibly halting or delaying psychiatric treatment.
Hyponatremia has been associated with the use of:
- diuretics
- selective serotonin reuptake inhibitors (SSRIs)
- serotonin-norepinephrine reuptake inhibitors (SNRIs)
- tricyclic antidepressants
- calcium antagonists.
Among psychiatric inpatients, the risk of hyponatremia is doubled in women.1 It is unclear, however, if female gender is an independent risk factor for hyponatremia. Sharabi et al2 reported that patients of both sexes age >65 have a 9-fold greater risk of developing hyponatremia than younger counterparts.
In addition, hyponatremia risk during any antidepressant treatment is highest:
- in the summer
- during the first weeks of treatment
- with concomitant drug use, especially with diuretics.3
The authors’ observations
Based on Mrs. V’s initial lab results (Table 1), we classify her hyponatremia as euvolemic, with high urine osmolarity (≥100 mOsm/L). That helps narrow our differential diagnosis to glucocorticoid deficiency, hypothyroidism, and SIADH (Table 2).5 We exclude psychogenic polydipsia, “tea and toast” syndrome, or beer potomania because they usually present as euvolemic hyponatremia with low urinary osmolality.
SSRI use in elderly persons has been associated with hyponatremia, which in some cases may be consistent with SIADH. Unfortunately, few psychiatrists are aware of this potentially fatal side effect.
SIADH occurs in association with reduced serum osmolality. It is characterized by:
- hypotonic hyponatremia (serum sodium
- inappropriately elevated urine osmolarity (>200 mOsm/L) relative to plasma osmolarity
- elevated urine sodium (typically >20 mEq/L).4
The key to the pathophysiology, signs, symptoms, and treatment of SIADH is understanding that the hyponatremia is a result of excess water and not a sodium deficiency. Hyponatremia’s signs and symptoms primarily are related to CNS dysfunction and correlate with how rapidly and severely the condition develops.
We monitor Mrs. V for anorexia, nausea, and malaise because they would be the earliest findings, followed by headache, irritability, confusion, muscle cramps, weakness, obtundation, seizures, and coma. These occur as osmotic fluid shifts and results in cerebral edema and increased intracranial pressure. When sodium concentration drops below 105 mEq/L, life-threatening complications are likely.
Table 1
Mrs. V’s laboratory results
| Mrs. V’s results | |||
|---|---|---|---|
| Normal range | Before Tx | After Tx | |
| Serum sodium (mEq/L) | 135 to 145 | 119 | 127 |
| Serum potassium (mEq/L) | 3.5 to 5.0 | 3.6 | 3.8 |
| Creatinine (mg/dL) | 0.5 to 1.7 | 0.74 | 0.84 |
| Glucose (mg/dL) | 60 to 114 | 160 | 150 |
| Osmolarity | |||
| Serum (measured; mOsm/L) | 275 to 300 | 258 | 242 |
| Urine (mOsm/L) | 257 | 180 | |
| Urine sodium (mEq/L) | 20 to 40 | 48 | 42 |
Mrs. V’s laboratory results
| Hypovolemic hyponatremia | Euvolemic hyponatremia | Hypervolemic hyponatremia |
|---|---|---|
| Vomiting Diarrhea Laxative abuse Renal disease Nasogastric suction Salt-wasting nephropathy Addison’s disease | Normal urinary sodium Glucocorticoid deficiency Hypothyroidism Certain drugs SIADH | Congestive heart failure Nephrotic syndrome Cirrhosis |
| Low urinary osmolality Psychogenic polydipsia ‘Tea and toast’ syndrome Beer potomania | ||
| SIADH: syndrome of inappropriate antidiuretic hormone | ||
| Source: Reference 5 | ||
SSRIs and SIADH
Bouman et al6 estimated that the incidence of SSRI-induced SIADH in elderly patients is 12%. Liu et al7 described 706 cases of hyponatremia associated with SSRI use in unpublished reports. Fluoxetine was most commonly the cause (75.3% cases), followed by paroxetine (12.4%), sertraline (11.7%), and fluvoxamine (1.5%). Resuming the same drug resulted in hyponatremia in 16 of 24 of these cases (66.7%).
Kirby et al,8 however, found no clear advantages in different SSRIs’ propensity to cause hyponatremia. Seventy-one percent of patients treated with the SNRI venlafaxine developed hyponatremia, compared with 32% taking paroxetine and 29% receiving sertraline. It is unclear whether a specific SSRI or venlafaxine has a stronger association with hyponatremia than any other antidepressant.
Hyponatremia’s nonspecific symptoms and wide range of time to detection (1 to 253 days) suggest clinicians usually detect the condition by chance rather than specifically assessing for it.9
TREATMENT: Medication change?
Coordinating Mrs. V’s depression and hyponatremia treatment is critical. We propose discontinuing sertraline and treating Mrs. V’s symptoms with electroconvulsive therapy (ECT). She refuses ECT, stating “I don’t feel that bad. My father was treated with ECT and I am scared of it.”
The authors’ observations
SSRI-induced hyponatremia can be transient or persistent and recurrent. The usual approach is to discontinue the SSRI and try a different antidepressant. Because hyponatremia has been associated with all SSRIs and SNRIs, it would be prudent to choose an alternate antidepressant agent outside these classes. If patients must continue taking an antidepressant that causes hyponatremia, avoid concurrent use of drugs that cause hyponatremia, restrict fluid intake, and consider adding a medication that prevents hyponatremia, such as demeclocycline or fludrocortisone.
SSRI-induced hyponatremia may resolve:
- with SSRI discontinuation alone11
- with fluid restriction and without discontinuation of the SSRI11
- with drug discontinuation, fluid restriction, and sodium chloride and potassium supplementation.12
FOLLOW-UP: Analysis error?
Despite modifications to Mrs. V’s diet, her fasting serum glucose level remains >100. She is diagnosed with diabetes mellitus type 2 and treated with metformin. We continue mirtazapine, which has successfully controlled Mrs. V’s depressive symptoms. Her serum sodium levels start normalizing.
The authors’ observations
Related resources
- Siegel AJ. Hyponatremia in psychiatric patients: update on evaluation and management. Harv Rev Psychiatry 2008;16(1):13-24.
- Atalay A, Turhan N, Aki OE. A challenging case of syndrome of inappropriate secretion of antidiuretic hormone in an elderly patient secondary to quetiapine. South Med J 2007;100(8):832-3.
- Aripiprazole • Abilify
- Atenolol • Tenormin
- Atorvastatin • Lipitor
- Demeclocycline • Declomycin, Declostatin, others
- Diltiazem • Cardizem, Dilacor, others
- Fludrocortisone • Florinef
- Fluvoxamine • Luvox
- Ibuprofen • Advil, Motrin, others
- Metformin • Glucophage, Diabex, others
- Mirtazapine • Remeron
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosures
Dr. Romanowicz reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Ramaswamy receives research support from Bristol-Myers Squibb, Shire, and Forest Pharmaceuticals and is a consultant to Dainippon Sumitomo Pharma.
Dr. Wilson receives research support from the National Institute of Mental Health, the Veterans Administration, the State of Nebraska, Health Futures Foundation, Inc., AstraZeneca, Dainippon Sumitomo Pharma, Eli Lilly and Company, and Pfizer Inc. and serves as a consultant to the Substance Abuse and Mental Health Services Administration and the State of Nebraska.
HISTORY: ‘They’re out to get me’
Mrs. V, age 64, tells her primary care physician she has felt “bad” for 2 weeks. She complains of depressed mood, middle insomnia, diminished appetite, poor concentration, and poor energy. She denies suicidal thoughts but reports feeling alone, overwhelmed, and unable to manage her daily life.
Mrs. V is very concerned about losing her job because she cannot function at work. She believes her coworkers may be plotting to get her fired. The primary care physician refers Mrs. V to us to evaluate her mood.
According to her daughter, Mrs. V has had multiple psychiatric hospitalizations; the most recent occurred 2 years ago when she was admitted for paranoia and disorganized behavior. The daughter also mentions that her mother has a remote history of daily alcohol use, drinking until she was intoxicated. Mrs. V says she occasionally drinks beer and she scores 2 out of 4 on the CAGE questionnaire, which may indicate alcohol dependence.
During mental status examination, Mrs. V is alert and oriented to person, place, and date. She is pleasant and cooperative but shows apparent thought blocking and some tangentiality. She has substantial difficulty answering questions and articulating symptoms. Speech is slow in rate and rhythm. Mrs. V’s mood is severely depressed and her affect constricted.
She denies suicidal or homicidal ideations or visual or auditory hallucinations. Cognitive testing reveals mild deficits in recall memory and poor concentration. Her insight is limited and her judgment fair.
Her medical history includes hypertension, hyperlipidemia, coronary artery disease, cardiac catheterization, and hyponatremia. Her medication regimen consists of aripiprazole, 15 mg/d; diltiazem, 180 mg/d; atenolol, 25 mg/d; aspirin, 325 mg/d; atorvastatin, 10 mg/d; sertraline, 50 mg/d; and ibuprofen, 600 mg as needed for hip pain. She also reports taking diuretics in the past.
Vital signs include blood pressure, 125/95 mm Hg; respirations, 16/min; temperature, 98.2° F; and pulse rate, 72/min. Serum investigations reveal sodium, 119 mEq/L (normal range: 135 to 145 mEq/L) and random blood sugar, 160 mg/dL (normal range: 60 to 114 mg/dL).
The authors’ observations
The combination of major depression with psychosis and hyponatremia makes Mrs. V’s case challenging. Hyponatremia in psychiatric inpatients can prompt medical consultation, thus possibly halting or delaying psychiatric treatment.
Hyponatremia has been associated with the use of:
- diuretics
- selective serotonin reuptake inhibitors (SSRIs)
- serotonin-norepinephrine reuptake inhibitors (SNRIs)
- tricyclic antidepressants
- calcium antagonists.
Among psychiatric inpatients, the risk of hyponatremia is doubled in women.1 It is unclear, however, if female gender is an independent risk factor for hyponatremia. Sharabi et al2 reported that patients of both sexes age >65 have a 9-fold greater risk of developing hyponatremia than younger counterparts.
In addition, hyponatremia risk during any antidepressant treatment is highest:
- in the summer
- during the first weeks of treatment
- with concomitant drug use, especially with diuretics.3
The authors’ observations
Based on Mrs. V’s initial lab results (Table 1), we classify her hyponatremia as euvolemic, with high urine osmolarity (≥100 mOsm/L). That helps narrow our differential diagnosis to glucocorticoid deficiency, hypothyroidism, and SIADH (Table 2).5 We exclude psychogenic polydipsia, “tea and toast” syndrome, or beer potomania because they usually present as euvolemic hyponatremia with low urinary osmolality.
SSRI use in elderly persons has been associated with hyponatremia, which in some cases may be consistent with SIADH. Unfortunately, few psychiatrists are aware of this potentially fatal side effect.
SIADH occurs in association with reduced serum osmolality. It is characterized by:
- hypotonic hyponatremia (serum sodium
- inappropriately elevated urine osmolarity (>200 mOsm/L) relative to plasma osmolarity
- elevated urine sodium (typically >20 mEq/L).4
The key to the pathophysiology, signs, symptoms, and treatment of SIADH is understanding that the hyponatremia is a result of excess water and not a sodium deficiency. Hyponatremia’s signs and symptoms primarily are related to CNS dysfunction and correlate with how rapidly and severely the condition develops.
We monitor Mrs. V for anorexia, nausea, and malaise because they would be the earliest findings, followed by headache, irritability, confusion, muscle cramps, weakness, obtundation, seizures, and coma. These occur as osmotic fluid shifts and results in cerebral edema and increased intracranial pressure. When sodium concentration drops below 105 mEq/L, life-threatening complications are likely.
Table 1
Mrs. V’s laboratory results
| Mrs. V’s results | |||
|---|---|---|---|
| Normal range | Before Tx | After Tx | |
| Serum sodium (mEq/L) | 135 to 145 | 119 | 127 |
| Serum potassium (mEq/L) | 3.5 to 5.0 | 3.6 | 3.8 |
| Creatinine (mg/dL) | 0.5 to 1.7 | 0.74 | 0.84 |
| Glucose (mg/dL) | 60 to 114 | 160 | 150 |
| Osmolarity | |||
| Serum (measured; mOsm/L) | 275 to 300 | 258 | 242 |
| Urine (mOsm/L) | 257 | 180 | |
| Urine sodium (mEq/L) | 20 to 40 | 48 | 42 |
Mrs. V’s laboratory results
| Hypovolemic hyponatremia | Euvolemic hyponatremia | Hypervolemic hyponatremia |
|---|---|---|
| Vomiting Diarrhea Laxative abuse Renal disease Nasogastric suction Salt-wasting nephropathy Addison’s disease | Normal urinary sodium Glucocorticoid deficiency Hypothyroidism Certain drugs SIADH | Congestive heart failure Nephrotic syndrome Cirrhosis |
| Low urinary osmolality Psychogenic polydipsia ‘Tea and toast’ syndrome Beer potomania | ||
| SIADH: syndrome of inappropriate antidiuretic hormone | ||
| Source: Reference 5 | ||
SSRIs and SIADH
Bouman et al6 estimated that the incidence of SSRI-induced SIADH in elderly patients is 12%. Liu et al7 described 706 cases of hyponatremia associated with SSRI use in unpublished reports. Fluoxetine was most commonly the cause (75.3% cases), followed by paroxetine (12.4%), sertraline (11.7%), and fluvoxamine (1.5%). Resuming the same drug resulted in hyponatremia in 16 of 24 of these cases (66.7%).
Kirby et al,8 however, found no clear advantages in different SSRIs’ propensity to cause hyponatremia. Seventy-one percent of patients treated with the SNRI venlafaxine developed hyponatremia, compared with 32% taking paroxetine and 29% receiving sertraline. It is unclear whether a specific SSRI or venlafaxine has a stronger association with hyponatremia than any other antidepressant.
Hyponatremia’s nonspecific symptoms and wide range of time to detection (1 to 253 days) suggest clinicians usually detect the condition by chance rather than specifically assessing for it.9
TREATMENT: Medication change?
Coordinating Mrs. V’s depression and hyponatremia treatment is critical. We propose discontinuing sertraline and treating Mrs. V’s symptoms with electroconvulsive therapy (ECT). She refuses ECT, stating “I don’t feel that bad. My father was treated with ECT and I am scared of it.”
The authors’ observations
SSRI-induced hyponatremia can be transient or persistent and recurrent. The usual approach is to discontinue the SSRI and try a different antidepressant. Because hyponatremia has been associated with all SSRIs and SNRIs, it would be prudent to choose an alternate antidepressant agent outside these classes. If patients must continue taking an antidepressant that causes hyponatremia, avoid concurrent use of drugs that cause hyponatremia, restrict fluid intake, and consider adding a medication that prevents hyponatremia, such as demeclocycline or fludrocortisone.
SSRI-induced hyponatremia may resolve:
- with SSRI discontinuation alone11
- with fluid restriction and without discontinuation of the SSRI11
- with drug discontinuation, fluid restriction, and sodium chloride and potassium supplementation.12
FOLLOW-UP: Analysis error?
Despite modifications to Mrs. V’s diet, her fasting serum glucose level remains >100. She is diagnosed with diabetes mellitus type 2 and treated with metformin. We continue mirtazapine, which has successfully controlled Mrs. V’s depressive symptoms. Her serum sodium levels start normalizing.
The authors’ observations
Related resources
- Siegel AJ. Hyponatremia in psychiatric patients: update on evaluation and management. Harv Rev Psychiatry 2008;16(1):13-24.
- Atalay A, Turhan N, Aki OE. A challenging case of syndrome of inappropriate secretion of antidiuretic hormone in an elderly patient secondary to quetiapine. South Med J 2007;100(8):832-3.
- Aripiprazole • Abilify
- Atenolol • Tenormin
- Atorvastatin • Lipitor
- Demeclocycline • Declomycin, Declostatin, others
- Diltiazem • Cardizem, Dilacor, others
- Fludrocortisone • Florinef
- Fluvoxamine • Luvox
- Ibuprofen • Advil, Motrin, others
- Metformin • Glucophage, Diabex, others
- Mirtazapine • Remeron
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosures
Dr. Romanowicz reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Ramaswamy receives research support from Bristol-Myers Squibb, Shire, and Forest Pharmaceuticals and is a consultant to Dainippon Sumitomo Pharma.
Dr. Wilson receives research support from the National Institute of Mental Health, the Veterans Administration, the State of Nebraska, Health Futures Foundation, Inc., AstraZeneca, Dainippon Sumitomo Pharma, Eli Lilly and Company, and Pfizer Inc. and serves as a consultant to the Substance Abuse and Mental Health Services Administration and the State of Nebraska.
Reference
1. Siegler EL, Tamres D, Berlin JA, et al. Risk factors for the development of hyponatremia in psychiatric inpatients. Arch Intern Med 1995;155(9):953-7.
2. Sharabi Y, Illan R, Kamari Y, et al. Diuretic induced hyponatraemia in elderly hypertensive women. J Hum Hypertens 2002;16(9):631-5.
3. Rosner MH. Severe hyponatremia associated with the combined use of thiazide diuretics and selective serotonin reuptake inhibitors. Am J Med Sci 2004;327(2):109-11.
4. Buff DD, Markowitz S. Hyponatremia in the psychiatric patient: a review of diagnostic and management strategies. Psychiatr Ann 2003;33(5):318-25.
5. Levitan A. Hyponatremia: how to recognize the cause promptly—and avoid treatment pitfalls. Consultant 2003;43(7):861-70.
6. Bouman WP, Pinner G, Johnson H. Incidence of selective serotonin reuptake inhibitor (SSRI) induced hyponatraemia due to the syndrome of inappropriate antidiuretic hormone (SIADH) secretion in the elderly. Int J Geriatr Psychiatry 1998;13(1):12-5
7. Liu BA, Mittmann N, Knowles SR, et al. Hyponatremia and the syndrome of inappropriate secretion of antidiuretic hormone associated with the use of selective serotonin reuptake inhibitors: a review of spontaneous reports. CMAJ 1996;155(5):519-27
8. Kirby D, Ames D. Hyponatraemia and selective serotonin re-uptake inhibitors in elderly patients. Int J Geriatr Psychiatry 2001;16(5):484-93
9. Kirchner V, Silver LE, Kelly CA. Selective serotonin reuptake inhibitors and hyponatraemia: review and proposed mechanisms in the elderly. J Psychopharmacol 1998;12(4):396-400.
10. Jagsch C, Marksteiner J, Seiringer E, Windhager E. Successful mirtazapine treatment of an 81-year-old patient with syndrome of inappropriate antidiuretic hormone secretion. Pharmacopsychiatry 2007;40(3):129-31.
11. Bigaillon C, El Jahiri Y, Garcia C, et al. Inappropriate ADH secretion-induced hyponatremia and associated with paroxetine use. Rev Med Interne 2007;28(9):642-4.
12. Blacksten JV, Birt JA. Syndrome of inappropriate secretion of antidiuretic hormone secondary to fluoxetine. Ann Pharmacother 1993;27(6):723-4.
Reference
1. Siegler EL, Tamres D, Berlin JA, et al. Risk factors for the development of hyponatremia in psychiatric inpatients. Arch Intern Med 1995;155(9):953-7.
2. Sharabi Y, Illan R, Kamari Y, et al. Diuretic induced hyponatraemia in elderly hypertensive women. J Hum Hypertens 2002;16(9):631-5.
3. Rosner MH. Severe hyponatremia associated with the combined use of thiazide diuretics and selective serotonin reuptake inhibitors. Am J Med Sci 2004;327(2):109-11.
4. Buff DD, Markowitz S. Hyponatremia in the psychiatric patient: a review of diagnostic and management strategies. Psychiatr Ann 2003;33(5):318-25.
5. Levitan A. Hyponatremia: how to recognize the cause promptly—and avoid treatment pitfalls. Consultant 2003;43(7):861-70.
6. Bouman WP, Pinner G, Johnson H. Incidence of selective serotonin reuptake inhibitor (SSRI) induced hyponatraemia due to the syndrome of inappropriate antidiuretic hormone (SIADH) secretion in the elderly. Int J Geriatr Psychiatry 1998;13(1):12-5
7. Liu BA, Mittmann N, Knowles SR, et al. Hyponatremia and the syndrome of inappropriate secretion of antidiuretic hormone associated with the use of selective serotonin reuptake inhibitors: a review of spontaneous reports. CMAJ 1996;155(5):519-27
8. Kirby D, Ames D. Hyponatraemia and selective serotonin re-uptake inhibitors in elderly patients. Int J Geriatr Psychiatry 2001;16(5):484-93
9. Kirchner V, Silver LE, Kelly CA. Selective serotonin reuptake inhibitors and hyponatraemia: review and proposed mechanisms in the elderly. J Psychopharmacol 1998;12(4):396-400.
10. Jagsch C, Marksteiner J, Seiringer E, Windhager E. Successful mirtazapine treatment of an 81-year-old patient with syndrome of inappropriate antidiuretic hormone secretion. Pharmacopsychiatry 2007;40(3):129-31.
11. Bigaillon C, El Jahiri Y, Garcia C, et al. Inappropriate ADH secretion-induced hyponatremia and associated with paroxetine use. Rev Med Interne 2007;28(9):642-4.
12. Blacksten JV, Birt JA. Syndrome of inappropriate secretion of antidiuretic hormone secondary to fluoxetine. Ann Pharmacother 1993;27(6):723-4.
A Reverend’s tale: Too tragic to be true?
CASE: A tragic tale
Reverend R, a 62-year-old Methodist minister, is admitted to a general surgical service for abdominal pain secondary to a recurring bowel obstruction. While there, he learns that his pregnant 24-year-old fiancée was struck and killed by a drunk driver as she was driving to visit him. Her medical team was not able to save her child. The surgical service requests a psychiatric consultation for Reverend R to assist him with grieving.
Our team interviews Reverend R 3 days after his fiancée’s death. We did not have access to his psychiatric records before our evaluation, but his chart indicates Reverend R had been hospitalized for nearly 3 months after being transferred from another hospital. He has a history of colon cancer and cerebral palsy and has struggled with depression since college. He had 1 psychiatric hospitalization 26 years earlier and no history of suicide attempts. He has responded to pharmacotherapy and is taking sertraline, 100 mg daily.
Reverend R expresses grief, stating he has lost the love of his life. With prompting, he provides a few details about his fiancée but does not say much about the accident. He says he feels guilty and frustrated that he can’t attend his fiancée’s funeral because “I have a nasogastric tube.” He claims he has cried excessively in the last few days, repeatedly stating, “I soaked 4 towels.” He is profusely apologetic for expressing his grief, as if doing so was inappropriate.
Reverend R acknowledges feeling sad but denies pervasively depressed mood or anhedonia, excessive guilt, or feelings of hopelessness, helplessness, or worthlessness. His affect ranges from mildly dysphoric to jovial and witty. His thought form and content are logical, linear, and goal-oriented. He denies having preoccupations, obsessions, delusions, or hallucinations. Attention and concentration are intact without evidence of waxing and waning. Cognition and memory also are intact. His Folstein Mini-Mental State Exam (MMSE) score is 29/30. Insight and judgment are assessed to be good, and intellect is above average.
We end our interview by asking Reverend R for permission to contact his psychiatrist for additional information. He stops making eye contact, begins to stammer, and tells us he is acutely short of breath. We seek out his nurse to check him, and within a few minutes his shortness of breath resolves without intervention.
The authors’ observations
Reverend R’s presentation does not suggest that his fiancée died 3 days ago. Without prompting, he says little about her or the accident, but he provides a great deal of information about himself. He clearly enjoys our attention, several times enthusiastically asking, “What else would you like to know about me?” At times he focuses on irrelevant topics.
He does not appear depressed and, although Reverend R’s voice breaks at times, we do not observe tears. His intermittent jovial, witty manner is inappropriate, but he is oriented and his MMSE provides no evidence of delirium. He does not elaborate on his frustration at being unable to attend the funeral and seems satisfied with the possibility of watching a video of the service.
Reverend R does not meet DSM-IV-TR criteria for major depressive disorder. We feel his emotions and conduct are unusual in response to the stress and therefore, based on what we have learned so far, we believe he best meets criteria for an adjustment disorder.
HISTORY: A series of traumas
During our initial interview, Reverend R explains that his life has been characterized by a series of traumatic events (Table 1). He had been sexually assaulted twice: by an uncle during childhood and by a male nurse while hospitalized for depression 26 years ago. The nurse had HIV, but the Reverend tested negative.
The day before our visit was not only the Reverend’s birthday but also was to be his wedding day. The Reverend had met his fiancée, a nurse, at the nursing home where he lives. At times, she took him on outings for dinner and other activities.
We ask the Reverend precisely why he needed 24-hour care and why he had been in the nursing home for 15 years. He is not able to provide a reasonable explanation.
Table 1
Reverend R’s life story: A series of traumatic events
| Period | Event |
|---|---|
| Childhood | Sexually assaulted by an uncle |
| Young adulthood | Develops depression; 1 hospitalization in his 30s; sexually assaulted by male nurse while hospitalized |
| Adulthood | Motor vehicle accident results in traumatic brain injury and leads to nursing home placement in his late 40s |
| 3 months ago | Hospitalized for abdominal pain secondary to recurring bowel obstruction; medical history includes colon cancer, cerebral palsy |
| Presently | Loses pregnant, 24-year-old fiancée in a traffic accident |
The authors’ observations
Reverend R talks almost incessantly about the atrocities he suffered throughout his life. Times of happiness and success are the exception.
We begin to doubt the veracity of certain details of his story. We question the plausibility of a young nurse having an intimate relationship with and becoming pregnant by a 62-year-old nursing home patient who was an ordained minister. Reverend R’s claim of being the nursing home’s public relations director and performing sermons there seems unlikely. His stories are inconsistent; whenever we question him, he creates a reply that he is convinced seems believable. A collateral history is imperative for us to establish a diagnosis.
FOLLOW-UP: His story starts to fray
At a follow-up visit the next day, the Reverend states that he has been sad and at times he will “fall apart” in response to his fiancée’s death. He says that a video of the memorial service his fiancée’s father gave him had been “hard to watch.” We ask if he has the video; he says that he sent it back to the nursing home.
The authors’ observations
It seems strange that Reverend R is concerned that talking with us could compromise his return to the nursing home. His questions and behavior are paranoid; we did not observe this type of behavior during our initial interview.
We investigate Reverend R’s claims. A hospital dismissal summary from 13 years ago documents that Reverend R had been caught pulling out his NG tube. Additionally, he was observed drinking out of the sink when he was advised to take nothing by mouth.
Within days of that hospitalization, he presented to our outpatient gastrointestinal clinic for a second opinion regarding his abdominal pain. His father demanded that the Reverend be admitted. When told that hospitalization was not warranted, Reverend R and his father became angry and abruptly left the office.
Our hospital’s nursing staff is a vital source of information because they observed Reverend R often during his 3-month stay. They are suspicious of his history because they noticed discrepancies, such as Reverend R telling one nurse his fiancée died on a Thursday and another she died on a Friday. He spoke of people visiting him, but the staff never saw any visitors.
The nursing staff reports that at times he would use profanity and was quite hostile. A member of our team saw him yelling at a female chaplain. In our initial interview he told our team that the chaplain had reprimanded him for having premarital relations with his fiancée.
We find no evidence of an accident that resulted in the death of a 24-year-old pregnant female. Obviously, there was never a funeral or visits from the fictitious fiancée’s father. The sexual assault by the male nurse while hospitalized is possible but not probable, given the other falsehoods Reverend R told.
The seminary Reverend R told us he attended exists, but we are not able to determine if he was educated there. He told some staff members he had obtained a Master’s degree and others a PhD.
Reverend R refuses to sign a release of information form for the nursing home. We speak with the nurse who worked with Reverend R’s psychiatrist, who confirms that the patient’s diagnosis was depression. She tells us that the Reverend said he relocated to that area to live closer to a man with whom he had a romantic relationship. Reverend R confided to her that his father never approved of the relationship, but his mother accepted it.
DIAGNOSIS: A rarely seen symptom
Reverend R meets the DSM-IV-TR criteria for factitious disorder (Table 2).1 The presentation of a patient with this disorder may include:
- fabrication of subjective complaints
- self-inflicted conditions
- exaggeration or exacerbation of pre-existing conditions
- any combination of these.
Differential diagnosis for pseudologia fantastica includes dementia, delusional disorder, antisocial personality disorder, borderline personality disorder, factitious disorder, malingering, hypochondriasis, substance abuse/dependence, and schizophrenia/schizophreniform disorder.3
Table 2
DSM-IV-TR criteria for factitious disorder*
| Intentional production or feigning of physical or psychological signs and symptoms |
| Motivation for the behavior is to assume the sick role |
| External incentives such as economic gain, avoiding legal responsibility, or improving physical well-being are absent |
| * Specifiers include with predominantly psychological signs and symptoms, with predominantly physical signs and symptoms, or a combination of both |
| Source: Reference 1 |
Characteristics of stories told by patients with pseudologia fantastica
|
|
|
|
|
| Source: Reference 2 |
Because of an unstable self image, the pseudologia fantastica patient constantly battles to regulate his or her sense of self. The dramatic production of symptoms due to this constant battle is thought to be a way for the patient to stabilize the self by making the experience of distress concrete and legitimate.5 It was fascinating to see Reverend R’s defense mechanisms work.
Confronting patients such as Reverend R likely is not the best approach. Showing them respect and empathy is important. Creating a safe, supportive environment in which they can express themselves will encourage them to consider ongoing psychiatric care.3,6
OUTCOME: Return to nursing home
Approximately 1 week after our follow-up visit, Reverend R was discharged to the nursing home where he had resided prior to the hospitalization. Several attempts to contact him to obtain additional information and collateral history were unsuccessful, but clearly we had enough information to refute the reason we were asked to evaluate him.
Related resources
- Epstein LA, Stern TA. Factitious illness: a 3-step consultation-liaison approach. Current Psychiatry 2007;6(4):54-58.
- Birch CD, Kelln BRC, Aquino EPB. A review and case report of pseudologia fantastica. Journal of Forensic Psychiatry and Psychology 2006;17(2):299-320.
- Sertraline • Zoloft
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Diagnostic and statistical manual of mental disorders. 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
2. King BH, Ford CV. Pseudologia fantastica. Acta Psychiatr Scand 1988;77(1):1-6.
3. Newmark N, Adityanjee, Kay J. Pseudologia fantastica and factitious disorder: review of the literature and a case report. Compr Psychiatry 1999;40(2):89-95.
4. Levenson JL. Deception syndromes: factitious disorders and malingering. In: Ford CV, ed. Textbook of psychosomatic medicine. Washington, DC: American Psychiatric Publishing; 2005:297-309.
5. Spivak H, Rodin G, Sutherland A. The psychology of factitious disorders. A reconsideration. Psychosomatics 1994;35:25-34.
6. Hoyer TV. Pseudologia fantastica: a consideration of “the lie” and a case presentation. Psychiatr Q 1959;33:203-20.
CASE: A tragic tale
Reverend R, a 62-year-old Methodist minister, is admitted to a general surgical service for abdominal pain secondary to a recurring bowel obstruction. While there, he learns that his pregnant 24-year-old fiancée was struck and killed by a drunk driver as she was driving to visit him. Her medical team was not able to save her child. The surgical service requests a psychiatric consultation for Reverend R to assist him with grieving.
Our team interviews Reverend R 3 days after his fiancée’s death. We did not have access to his psychiatric records before our evaluation, but his chart indicates Reverend R had been hospitalized for nearly 3 months after being transferred from another hospital. He has a history of colon cancer and cerebral palsy and has struggled with depression since college. He had 1 psychiatric hospitalization 26 years earlier and no history of suicide attempts. He has responded to pharmacotherapy and is taking sertraline, 100 mg daily.
Reverend R expresses grief, stating he has lost the love of his life. With prompting, he provides a few details about his fiancée but does not say much about the accident. He says he feels guilty and frustrated that he can’t attend his fiancée’s funeral because “I have a nasogastric tube.” He claims he has cried excessively in the last few days, repeatedly stating, “I soaked 4 towels.” He is profusely apologetic for expressing his grief, as if doing so was inappropriate.
Reverend R acknowledges feeling sad but denies pervasively depressed mood or anhedonia, excessive guilt, or feelings of hopelessness, helplessness, or worthlessness. His affect ranges from mildly dysphoric to jovial and witty. His thought form and content are logical, linear, and goal-oriented. He denies having preoccupations, obsessions, delusions, or hallucinations. Attention and concentration are intact without evidence of waxing and waning. Cognition and memory also are intact. His Folstein Mini-Mental State Exam (MMSE) score is 29/30. Insight and judgment are assessed to be good, and intellect is above average.
We end our interview by asking Reverend R for permission to contact his psychiatrist for additional information. He stops making eye contact, begins to stammer, and tells us he is acutely short of breath. We seek out his nurse to check him, and within a few minutes his shortness of breath resolves without intervention.
The authors’ observations
Reverend R’s presentation does not suggest that his fiancée died 3 days ago. Without prompting, he says little about her or the accident, but he provides a great deal of information about himself. He clearly enjoys our attention, several times enthusiastically asking, “What else would you like to know about me?” At times he focuses on irrelevant topics.
He does not appear depressed and, although Reverend R’s voice breaks at times, we do not observe tears. His intermittent jovial, witty manner is inappropriate, but he is oriented and his MMSE provides no evidence of delirium. He does not elaborate on his frustration at being unable to attend the funeral and seems satisfied with the possibility of watching a video of the service.
Reverend R does not meet DSM-IV-TR criteria for major depressive disorder. We feel his emotions and conduct are unusual in response to the stress and therefore, based on what we have learned so far, we believe he best meets criteria for an adjustment disorder.
HISTORY: A series of traumas
During our initial interview, Reverend R explains that his life has been characterized by a series of traumatic events (Table 1). He had been sexually assaulted twice: by an uncle during childhood and by a male nurse while hospitalized for depression 26 years ago. The nurse had HIV, but the Reverend tested negative.
The day before our visit was not only the Reverend’s birthday but also was to be his wedding day. The Reverend had met his fiancée, a nurse, at the nursing home where he lives. At times, she took him on outings for dinner and other activities.
We ask the Reverend precisely why he needed 24-hour care and why he had been in the nursing home for 15 years. He is not able to provide a reasonable explanation.
Table 1
Reverend R’s life story: A series of traumatic events
| Period | Event |
|---|---|
| Childhood | Sexually assaulted by an uncle |
| Young adulthood | Develops depression; 1 hospitalization in his 30s; sexually assaulted by male nurse while hospitalized |
| Adulthood | Motor vehicle accident results in traumatic brain injury and leads to nursing home placement in his late 40s |
| 3 months ago | Hospitalized for abdominal pain secondary to recurring bowel obstruction; medical history includes colon cancer, cerebral palsy |
| Presently | Loses pregnant, 24-year-old fiancée in a traffic accident |
The authors’ observations
Reverend R talks almost incessantly about the atrocities he suffered throughout his life. Times of happiness and success are the exception.
We begin to doubt the veracity of certain details of his story. We question the plausibility of a young nurse having an intimate relationship with and becoming pregnant by a 62-year-old nursing home patient who was an ordained minister. Reverend R’s claim of being the nursing home’s public relations director and performing sermons there seems unlikely. His stories are inconsistent; whenever we question him, he creates a reply that he is convinced seems believable. A collateral history is imperative for us to establish a diagnosis.
FOLLOW-UP: His story starts to fray
At a follow-up visit the next day, the Reverend states that he has been sad and at times he will “fall apart” in response to his fiancée’s death. He says that a video of the memorial service his fiancée’s father gave him had been “hard to watch.” We ask if he has the video; he says that he sent it back to the nursing home.
The authors’ observations
It seems strange that Reverend R is concerned that talking with us could compromise his return to the nursing home. His questions and behavior are paranoid; we did not observe this type of behavior during our initial interview.
We investigate Reverend R’s claims. A hospital dismissal summary from 13 years ago documents that Reverend R had been caught pulling out his NG tube. Additionally, he was observed drinking out of the sink when he was advised to take nothing by mouth.
Within days of that hospitalization, he presented to our outpatient gastrointestinal clinic for a second opinion regarding his abdominal pain. His father demanded that the Reverend be admitted. When told that hospitalization was not warranted, Reverend R and his father became angry and abruptly left the office.
Our hospital’s nursing staff is a vital source of information because they observed Reverend R often during his 3-month stay. They are suspicious of his history because they noticed discrepancies, such as Reverend R telling one nurse his fiancée died on a Thursday and another she died on a Friday. He spoke of people visiting him, but the staff never saw any visitors.
The nursing staff reports that at times he would use profanity and was quite hostile. A member of our team saw him yelling at a female chaplain. In our initial interview he told our team that the chaplain had reprimanded him for having premarital relations with his fiancée.
We find no evidence of an accident that resulted in the death of a 24-year-old pregnant female. Obviously, there was never a funeral or visits from the fictitious fiancée’s father. The sexual assault by the male nurse while hospitalized is possible but not probable, given the other falsehoods Reverend R told.
The seminary Reverend R told us he attended exists, but we are not able to determine if he was educated there. He told some staff members he had obtained a Master’s degree and others a PhD.
Reverend R refuses to sign a release of information form for the nursing home. We speak with the nurse who worked with Reverend R’s psychiatrist, who confirms that the patient’s diagnosis was depression. She tells us that the Reverend said he relocated to that area to live closer to a man with whom he had a romantic relationship. Reverend R confided to her that his father never approved of the relationship, but his mother accepted it.
DIAGNOSIS: A rarely seen symptom
Reverend R meets the DSM-IV-TR criteria for factitious disorder (Table 2).1 The presentation of a patient with this disorder may include:
- fabrication of subjective complaints
- self-inflicted conditions
- exaggeration or exacerbation of pre-existing conditions
- any combination of these.
Differential diagnosis for pseudologia fantastica includes dementia, delusional disorder, antisocial personality disorder, borderline personality disorder, factitious disorder, malingering, hypochondriasis, substance abuse/dependence, and schizophrenia/schizophreniform disorder.3
Table 2
DSM-IV-TR criteria for factitious disorder*
| Intentional production or feigning of physical or psychological signs and symptoms |
| Motivation for the behavior is to assume the sick role |
| External incentives such as economic gain, avoiding legal responsibility, or improving physical well-being are absent |
| * Specifiers include with predominantly psychological signs and symptoms, with predominantly physical signs and symptoms, or a combination of both |
| Source: Reference 1 |
Characteristics of stories told by patients with pseudologia fantastica
|
|
|
|
|
| Source: Reference 2 |
Because of an unstable self image, the pseudologia fantastica patient constantly battles to regulate his or her sense of self. The dramatic production of symptoms due to this constant battle is thought to be a way for the patient to stabilize the self by making the experience of distress concrete and legitimate.5 It was fascinating to see Reverend R’s defense mechanisms work.
Confronting patients such as Reverend R likely is not the best approach. Showing them respect and empathy is important. Creating a safe, supportive environment in which they can express themselves will encourage them to consider ongoing psychiatric care.3,6
OUTCOME: Return to nursing home
Approximately 1 week after our follow-up visit, Reverend R was discharged to the nursing home where he had resided prior to the hospitalization. Several attempts to contact him to obtain additional information and collateral history were unsuccessful, but clearly we had enough information to refute the reason we were asked to evaluate him.
Related resources
- Epstein LA, Stern TA. Factitious illness: a 3-step consultation-liaison approach. Current Psychiatry 2007;6(4):54-58.
- Birch CD, Kelln BRC, Aquino EPB. A review and case report of pseudologia fantastica. Journal of Forensic Psychiatry and Psychology 2006;17(2):299-320.
- Sertraline • Zoloft
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: A tragic tale
Reverend R, a 62-year-old Methodist minister, is admitted to a general surgical service for abdominal pain secondary to a recurring bowel obstruction. While there, he learns that his pregnant 24-year-old fiancée was struck and killed by a drunk driver as she was driving to visit him. Her medical team was not able to save her child. The surgical service requests a psychiatric consultation for Reverend R to assist him with grieving.
Our team interviews Reverend R 3 days after his fiancée’s death. We did not have access to his psychiatric records before our evaluation, but his chart indicates Reverend R had been hospitalized for nearly 3 months after being transferred from another hospital. He has a history of colon cancer and cerebral palsy and has struggled with depression since college. He had 1 psychiatric hospitalization 26 years earlier and no history of suicide attempts. He has responded to pharmacotherapy and is taking sertraline, 100 mg daily.
Reverend R expresses grief, stating he has lost the love of his life. With prompting, he provides a few details about his fiancée but does not say much about the accident. He says he feels guilty and frustrated that he can’t attend his fiancée’s funeral because “I have a nasogastric tube.” He claims he has cried excessively in the last few days, repeatedly stating, “I soaked 4 towels.” He is profusely apologetic for expressing his grief, as if doing so was inappropriate.
Reverend R acknowledges feeling sad but denies pervasively depressed mood or anhedonia, excessive guilt, or feelings of hopelessness, helplessness, or worthlessness. His affect ranges from mildly dysphoric to jovial and witty. His thought form and content are logical, linear, and goal-oriented. He denies having preoccupations, obsessions, delusions, or hallucinations. Attention and concentration are intact without evidence of waxing and waning. Cognition and memory also are intact. His Folstein Mini-Mental State Exam (MMSE) score is 29/30. Insight and judgment are assessed to be good, and intellect is above average.
We end our interview by asking Reverend R for permission to contact his psychiatrist for additional information. He stops making eye contact, begins to stammer, and tells us he is acutely short of breath. We seek out his nurse to check him, and within a few minutes his shortness of breath resolves without intervention.
The authors’ observations
Reverend R’s presentation does not suggest that his fiancée died 3 days ago. Without prompting, he says little about her or the accident, but he provides a great deal of information about himself. He clearly enjoys our attention, several times enthusiastically asking, “What else would you like to know about me?” At times he focuses on irrelevant topics.
He does not appear depressed and, although Reverend R’s voice breaks at times, we do not observe tears. His intermittent jovial, witty manner is inappropriate, but he is oriented and his MMSE provides no evidence of delirium. He does not elaborate on his frustration at being unable to attend the funeral and seems satisfied with the possibility of watching a video of the service.
Reverend R does not meet DSM-IV-TR criteria for major depressive disorder. We feel his emotions and conduct are unusual in response to the stress and therefore, based on what we have learned so far, we believe he best meets criteria for an adjustment disorder.
HISTORY: A series of traumas
During our initial interview, Reverend R explains that his life has been characterized by a series of traumatic events (Table 1). He had been sexually assaulted twice: by an uncle during childhood and by a male nurse while hospitalized for depression 26 years ago. The nurse had HIV, but the Reverend tested negative.
The day before our visit was not only the Reverend’s birthday but also was to be his wedding day. The Reverend had met his fiancée, a nurse, at the nursing home where he lives. At times, she took him on outings for dinner and other activities.
We ask the Reverend precisely why he needed 24-hour care and why he had been in the nursing home for 15 years. He is not able to provide a reasonable explanation.
Table 1
Reverend R’s life story: A series of traumatic events
| Period | Event |
|---|---|
| Childhood | Sexually assaulted by an uncle |
| Young adulthood | Develops depression; 1 hospitalization in his 30s; sexually assaulted by male nurse while hospitalized |
| Adulthood | Motor vehicle accident results in traumatic brain injury and leads to nursing home placement in his late 40s |
| 3 months ago | Hospitalized for abdominal pain secondary to recurring bowel obstruction; medical history includes colon cancer, cerebral palsy |
| Presently | Loses pregnant, 24-year-old fiancée in a traffic accident |
The authors’ observations
Reverend R talks almost incessantly about the atrocities he suffered throughout his life. Times of happiness and success are the exception.
We begin to doubt the veracity of certain details of his story. We question the plausibility of a young nurse having an intimate relationship with and becoming pregnant by a 62-year-old nursing home patient who was an ordained minister. Reverend R’s claim of being the nursing home’s public relations director and performing sermons there seems unlikely. His stories are inconsistent; whenever we question him, he creates a reply that he is convinced seems believable. A collateral history is imperative for us to establish a diagnosis.
FOLLOW-UP: His story starts to fray
At a follow-up visit the next day, the Reverend states that he has been sad and at times he will “fall apart” in response to his fiancée’s death. He says that a video of the memorial service his fiancée’s father gave him had been “hard to watch.” We ask if he has the video; he says that he sent it back to the nursing home.
The authors’ observations
It seems strange that Reverend R is concerned that talking with us could compromise his return to the nursing home. His questions and behavior are paranoid; we did not observe this type of behavior during our initial interview.
We investigate Reverend R’s claims. A hospital dismissal summary from 13 years ago documents that Reverend R had been caught pulling out his NG tube. Additionally, he was observed drinking out of the sink when he was advised to take nothing by mouth.
Within days of that hospitalization, he presented to our outpatient gastrointestinal clinic for a second opinion regarding his abdominal pain. His father demanded that the Reverend be admitted. When told that hospitalization was not warranted, Reverend R and his father became angry and abruptly left the office.
Our hospital’s nursing staff is a vital source of information because they observed Reverend R often during his 3-month stay. They are suspicious of his history because they noticed discrepancies, such as Reverend R telling one nurse his fiancée died on a Thursday and another she died on a Friday. He spoke of people visiting him, but the staff never saw any visitors.
The nursing staff reports that at times he would use profanity and was quite hostile. A member of our team saw him yelling at a female chaplain. In our initial interview he told our team that the chaplain had reprimanded him for having premarital relations with his fiancée.
We find no evidence of an accident that resulted in the death of a 24-year-old pregnant female. Obviously, there was never a funeral or visits from the fictitious fiancée’s father. The sexual assault by the male nurse while hospitalized is possible but not probable, given the other falsehoods Reverend R told.
The seminary Reverend R told us he attended exists, but we are not able to determine if he was educated there. He told some staff members he had obtained a Master’s degree and others a PhD.
Reverend R refuses to sign a release of information form for the nursing home. We speak with the nurse who worked with Reverend R’s psychiatrist, who confirms that the patient’s diagnosis was depression. She tells us that the Reverend said he relocated to that area to live closer to a man with whom he had a romantic relationship. Reverend R confided to her that his father never approved of the relationship, but his mother accepted it.
DIAGNOSIS: A rarely seen symptom
Reverend R meets the DSM-IV-TR criteria for factitious disorder (Table 2).1 The presentation of a patient with this disorder may include:
- fabrication of subjective complaints
- self-inflicted conditions
- exaggeration or exacerbation of pre-existing conditions
- any combination of these.
Differential diagnosis for pseudologia fantastica includes dementia, delusional disorder, antisocial personality disorder, borderline personality disorder, factitious disorder, malingering, hypochondriasis, substance abuse/dependence, and schizophrenia/schizophreniform disorder.3
Table 2
DSM-IV-TR criteria for factitious disorder*
| Intentional production or feigning of physical or psychological signs and symptoms |
| Motivation for the behavior is to assume the sick role |
| External incentives such as economic gain, avoiding legal responsibility, or improving physical well-being are absent |
| * Specifiers include with predominantly psychological signs and symptoms, with predominantly physical signs and symptoms, or a combination of both |
| Source: Reference 1 |
Characteristics of stories told by patients with pseudologia fantastica
|
|
|
|
|
| Source: Reference 2 |
Because of an unstable self image, the pseudologia fantastica patient constantly battles to regulate his or her sense of self. The dramatic production of symptoms due to this constant battle is thought to be a way for the patient to stabilize the self by making the experience of distress concrete and legitimate.5 It was fascinating to see Reverend R’s defense mechanisms work.
Confronting patients such as Reverend R likely is not the best approach. Showing them respect and empathy is important. Creating a safe, supportive environment in which they can express themselves will encourage them to consider ongoing psychiatric care.3,6
OUTCOME: Return to nursing home
Approximately 1 week after our follow-up visit, Reverend R was discharged to the nursing home where he had resided prior to the hospitalization. Several attempts to contact him to obtain additional information and collateral history were unsuccessful, but clearly we had enough information to refute the reason we were asked to evaluate him.
Related resources
- Epstein LA, Stern TA. Factitious illness: a 3-step consultation-liaison approach. Current Psychiatry 2007;6(4):54-58.
- Birch CD, Kelln BRC, Aquino EPB. A review and case report of pseudologia fantastica. Journal of Forensic Psychiatry and Psychology 2006;17(2):299-320.
- Sertraline • Zoloft
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Diagnostic and statistical manual of mental disorders. 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
2. King BH, Ford CV. Pseudologia fantastica. Acta Psychiatr Scand 1988;77(1):1-6.
3. Newmark N, Adityanjee, Kay J. Pseudologia fantastica and factitious disorder: review of the literature and a case report. Compr Psychiatry 1999;40(2):89-95.
4. Levenson JL. Deception syndromes: factitious disorders and malingering. In: Ford CV, ed. Textbook of psychosomatic medicine. Washington, DC: American Psychiatric Publishing; 2005:297-309.
5. Spivak H, Rodin G, Sutherland A. The psychology of factitious disorders. A reconsideration. Psychosomatics 1994;35:25-34.
6. Hoyer TV. Pseudologia fantastica: a consideration of “the lie” and a case presentation. Psychiatr Q 1959;33:203-20.
1. Diagnostic and statistical manual of mental disorders. 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
2. King BH, Ford CV. Pseudologia fantastica. Acta Psychiatr Scand 1988;77(1):1-6.
3. Newmark N, Adityanjee, Kay J. Pseudologia fantastica and factitious disorder: review of the literature and a case report. Compr Psychiatry 1999;40(2):89-95.
4. Levenson JL. Deception syndromes: factitious disorders and malingering. In: Ford CV, ed. Textbook of psychosomatic medicine. Washington, DC: American Psychiatric Publishing; 2005:297-309.
5. Spivak H, Rodin G, Sutherland A. The psychology of factitious disorders. A reconsideration. Psychosomatics 1994;35:25-34.
6. Hoyer TV. Pseudologia fantastica: a consideration of “the lie” and a case presentation. Psychiatr Q 1959;33:203-20.
When the pain decreased, her troubles began
CASE: She’s not herself
Mrs. M, age 74, is brought to the ER by her husband after he finds her lying on their bedroom floor, incoherent and extremely drowsy. He reports that his wife, who suffers chronic arthritic back and joint pain, might have overdosed on pain medications.
According to her husband, Mrs. M has been taking combination oxycodone/acetaminophen and transdermal fentanyl at unknown dosages, but he is unsure when she started using these medications or if she is taking others. Serum toxicology screening shows twice the normal values for opioids and benzodiazepines; other laboratory results are normal.
Mrs. M is medically stable but her mental status is altered. She is oblivious to time, place and person, speaks to no one, and seems lost in her own world. The hospital’s medical service admits Mrs. M for stabilization and to determine whether the overdose was intentional.
Two days later, we evaluate Mrs. M’s mental status at the attending physician’s request. She appears confused and cannot answer our questions. Her husband tells us she was “doing fine” until approximately 4 months ago, when she started becoming increasingly forgetful and lethargic. He says she has been forgetting routine chores such as paying bills and grocery shopping. Recently, she has been getting lost during her evening walk; neighbors often help her find her way home.
The authors’ observations
Two opioid medications—oxycodone/acetaminophen combination and transdermal fentanyl—are commonly used to manage moderate or severe pain from any type of chronic arthritis.
- Oxycodone, a semisynthetic opioid analgesic indicated for moderate to moderately severe pain, is used when nondrug measures and nonnarcotic medications do not control the pain.
- Transdermal fentanyl, a potent analgesic indicated for persistent moderate to severe chronic pain, typically is prescribed to patients who tolerate oral oxycodone, 30 mg/d; morphine, 60 mg; hydromorphone, 8 mg; or an equianalgesic dosage of another opioid for ≥1 week.
Mrs. M also was taking a benzodiazepine, but which medication—and why she was taking it—were unclear. She had no psychiatric diagnosis, and her husband could not recall her medication history.
We also cannot explain Mrs. M’s negative cognitive and behavioral changes. Opioid overuse and onset of dementia-related cognitive decline are possibilities.
TRANSFER Why is she confused?
Based on information from the pharmacy department, doctors at the medical unit restart oxycodone/acetaminophen, 7.5/325 mg tid, and transdermal fentanyl, 25 mcg/hr every 3 days. After discussing how to treat Mrs. M, the psychiatric and medical services transfer her to the geriatric psychiatric inpatient unit 3 days after admission.
We visit Mrs. M hours after her transfer. She seems lethargic but not confused, although Mini-Mental State Examination (MMSE) score of 15 suggests moderate cognitive impairment. Vitamin B12 and thyroid levels, erythrocyte sedimentation rate, and syphilis test results are normal, allowing us to rule out organic causes for her dementia. Brain MRI shows no neurologic damage. On a scale of 1 to 5 with 5 being most severe, Mrs. M scores her pain as 2 (mild) and her sedation as 3 (moderate).
With Mrs. M’s permission, we call her primary care physician for collateral information. The physician tells us Mrs. M has suffered severe joint pain for 2 years. Nonnarcotic medications and treatments—including counseling, support groups, massage, yoga, exercise, biofeedback, relaxation therapy, and physical therapy—were ineffective.
Approximately 10 months ago, the physician started oxycodone/acetaminophen at 2.5/325 mg bid and titrated it over 6 weeks to 7.5/325 mg tid for Mrs. M’s persistent joint pain. Four months ago, with her pain still severe, the physician added transdermal fentanyl, 25 mcg/hr every 3 days, after which the patient reported mild improvement.
One month after starting the fentanyl patch, Mrs. M complained of sudden forgetfulness, low energy, poor concentration, and increased sleep. The physician suspected depression with possible comorbid anxiety and prescribed sertraline, 50 mg/d, and alprazolam, 0.5 mg bid. Mrs. M stopped sertraline after 3 days because it was causing diarrhea but kept taking alprazolam.
Mrs. M saw her primary care physician once after starting alprazolam and sertraline but missed her most recent appointment last month. The physician says he inadvertently approved at least 1 premature request for an alprazolam refill.
Six days after admission, Mrs. M’s sedation, cognitive impairment, and lethargy persist. She reports no mood and anxiety problems, and we have not restarted alprazolam.
The authors’ observations
The fentanyl patch most likely began to diminish Mrs. M’s alertness soon after she started using it. The doctor, however, mistook cognitive slowing for new-onset depression or anxiety. Depressive symptoms can imitate dementia, but Mrs. M’s severe sedation and denial of depressive symptoms suggest a medication side effect.
The primary care physician’s reconstruction of Mrs. M’s history explained her positive benzodiazepine reading, and her use of the short-acting benzodiazepine alprazolam could account for her sudden-onset paranoia and cognitive decline (Box). Benzodiazepines can cause behavioral side effects such as disinhibition, agitation, or paranoia, and patients age ≥65 are at increased risk for these side effects.4 In particular, benzodiazepines with half-lives ≥6 to 8 hours such as clonazepam and oxazepam can cause short-term memory impairment, confusion, and delirium.5-7
Reconstructing treatment history is critical if the patient or family members cannot recall past treatments or if the patient cannot communicate.
Get permission from the patient or family as required under the Health Insurance Portability and Accountability Act. Then contact the primary care or other prescribing physician to obtain:
- a copy of the physician’s last progress note and initial evaluation
- notes about adverse reactions to current or past medications
- trials of medications and other treatments relevant to the current complaint.
In emergent cases when the patient is unresponsive or mentally incapacitated and no family members are available, follow the above steps and initiate treatment. Carefully document that the patient was incoherent, his life was in danger, and you could not reach a family member for permission to treat.
If you cannot communicate with the patient or contact a family member but care is less emergent, consult the hospital’s ethics committee to see if a guardian has been appointed. Contact the primary care physician only after the guardian grants permission.
When prescribing benzodiazepines (especially in older patients) watch for signs of overuse or abuse, such as early requests for refills, unkempt appearance, excessive sleepiness, or agitation (Table 1).
Warning signs of opioid, benzodiazepine overuse
| Frequent requests for early refills |
| Patient exceeds prescribed dosage without authorization |
| Patient reports lost/stolen prescription; if patient has history of substance abuse/dependence or legal problems, even 1 report should raise a red flag |
| Patient increasingly unkempt or impaired |
| Negative mood change |
| Agitation |
| Patient involved in car or other accidents |
| Sedation |
| Purposeful oversedation, particularly when patient has an apparent secondary gain from opioid use (such as qualifying for disability benefits or escaping from work) |
| New-onset cognitive impairment |
| Patient abusing alcohol or other illicit CNS depressants |
The authors’ observations
Persistent chronic pain in the elderly can diminish health and quality of life, resulting in depression, social isolation, immobility, and sleep disturbance.
Managing an older patient’s pain can be challenging (Table 2). Opioids are effective painkillers, but even at relatively low dosages they can diminish function and cognition and increase risk of delirium. Also, patients’ ability to tolerate different opioids at different dosages varies widely.
Mrs. M’s opioid regimen was intolerable and numerous other treatments did not alleviate her pain. At this point, replacing fentanyl with another opioid was our best option.8
We decided to try methadone, which is indicated for moderate to severe pain that does not respond to nonnarcotic treatments. Methadone often is used for chronic pain associated with arthritis or malignancy.
Methadone is less sedating, more tolerable, and carries a lower risk of cognitive side effects than other opioids. Methadone also is fast- and long-acting—its analgesic effects begin within 30 minutes to 1 hour of oral administration9 and last approximately 12 hours, thus reducing the risk of breakthrough pain. Methadone also:
- has no active metabolites, which decreases the risk of hepatic side effects
- offers a high volume of distribution, thus allowing clinical effect with minimal dosing.
Beware the potential for addiction when prescribing opioids to any patient.13,14 The U.S. Drug Enforcement Agency classifies both methadone and fentanyl as schedule II substances, which applies to highly addictive medications with FDA-approved indications. See patients at least biweekly, especially when switching or titrating pain medications, and watch closely for signs of overuse or addiction. Inform patients to:
- watch for symptoms such as oversedation, memory and concentration problems, and sudden changes in personality
- call you to clarify if these symptoms are methadone side effects.
Watch for other potential side effects of methadone, such as constipation, sedation, breakthrough pain, sexual dysfunction, decreased immunity, respiratory depression, or prolonged corrected QT intervals.
Patients usually tolerate an immediate switch from transdermal fentanyl to methadone, but a sudden switch from high-dose fentanyl can reduce methadone’s effectiveness. Starting methadone at a high dosage to compensate for loss of effectiveness could increase side effect risk. If the fentanyl dosage exceeds 100 mcg/hr, taper by 25 mcg weekly. Simultaneously start methadone at a low dosage and titrate by 5 to 10 mg weekly as needed.
Table 2
Chronic pain management in the elderly: Dos and don’ts
| DO |
| Use self rating scales, as patient can gauge his/her own pain most accurately |
| Consider nonpharmacologic treatments and nonnarcotic analgesics first |
| Watch closely for side effects and drug-drug/drug-disease interactions in patients receiving analgesics long-term |
| Monitor patients receiving opioids long-term for oversedation, changes in cognition and function |
| Consider switching to methadone or another opioid if patient cannot tolerate current opioid regimen |
| DO NOT |
| Prescribe propoxyphene or meperidine—which carry a higher risk of adverse effects than other opioids—to older patient |
| Prescribe opioids if the medical history is unclear |
| Increase opioid dosages without seeing the patient |
TREATMENT Medication change
We stop transdermal fentanyl and start oral methadone, 5 mg bid, while continuing oxycodone/acetaminophen at the previous dosage.
Two days later, Mrs. M is much more alert. Since admission 1 week ago, her sedation rating has improved from 3 (mildly sedated) to 4 (almost fully alert). She rates her pain as mild and reports no breakthrough pain or other side effects from methadone. Her MMSE score has improved to 24—suggesting close to normal cognition—and she is much more interactive with staff and family.
Eight days after we start methadone, we stop oxycodone/acetaminophen and increase methadone to 10 mg bid to further improve cognition and alertness and to see if 1 pain medication is suffcient. Two days later, we discharge Mrs. M. She is fully alert, feels little or no joint pain, and is tolerating the methadone increase.
At outpatient follow-up 4 weeks later, Mrs. M remains pain-free and her MMSE score is 29, suggesting normal cognition. Over 8 months, we continue to see her monthly and then bi-monthly, after which we refer her to her primary care physician.
Related resources
- American Association for Geriatric Psychiatry. www.aagponline.org.
- American Pain Society. www.ampainsoc.org.
- Alprazolam • Xanax
- Clonazepam • Klonopin
- Fentanyl (transdermal) • Duragesic
- Hydromorphone • Dilaudid
- Meperidine • Demerol
- Methadone • Dolophine
- Oxazepam • Serax
- Oxycodone • OxyContin, Roxicodone
- Oxycodone/acetaminophen • Percocet
- Propoxyphene • Darvon
- Sertraline • Zoloft
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Edinboro LE, Poklis A, Trautman D, et al. Fatal fentanyl intoxication following excessive transdermal application. J Forenscic Sci 1997;42:741-3.
2. Rose PG, Macfee MS, Boswell MV. Fentanyl transdermal system overdose secondary to cutaneous hyperthermia. Anesth Analg 1993;77:390-1.
3. Lawlor PG, Bruera E. Side effects of opioids in chronic pain treatment. Curr Opin Anaesthesiol 1998;5:539-45.
4. Lechin F, Van der Dijs B, Benaim M. Benzodiazepines; tolerability in elderly patients. Psychother Psychosom 1996;65:171-82.
5. Hall RC, Zisook S. Paradoxical reactions to benzodiazepines. Br J Clin Pharmacology 1981;11(suppl 1):99S-104S.
6. Cole JO, Kando JC. Adverse behavioral events reported in patients taking alprazolam and other benzodiazepines. J Clin Psychiatry 1993;54(suppl):49-61.
7. Paton P. Benzodiazepines and disinhibition. Psychiatr Bull 2002;26:460-2.
8. Quigley C. Opioid switching to improve pain relief and drug tolerability (review). Cochrane Database Syst Rev 2004(3);CD004847.-
9. National Highway Traffic Safety Administration. Methadone. Available at: http://www.nhtsa.dot.gov/PEOPLE/INJURY/research/job185drugs/methadone.htm. Accessed February 14, 2008.
10. Manzini I, Lossignol DA, Body JJ. Opioid switch to oral methadone in cancer pain. Curr Opin Oncol 2000;12:308-13.
11. Layson-Wolf C, Goode JV, Small R. Clinical use of methadone. J Pain Palliat Care 2002;16:29-59.
12. Krantz MJ, Lewkowiez L, Hays H, et al. Torsades de pointes associated with high dose methadone. Ann Intern Med 2002;139:501-4.
13. Fishbain D, Rosomoff H, Rosomoff RS. Drug abuse, dependence, and addiction in chronic patients. Clin J Pain 1992;8:77-85.
14. Hoffmann NG, Olofsson O, Salen B, Wickstrom L. Prevalence of abuse and dependency in chronic pain patients. Int J Addict 1995;30:919-27.
CASE: She’s not herself
Mrs. M, age 74, is brought to the ER by her husband after he finds her lying on their bedroom floor, incoherent and extremely drowsy. He reports that his wife, who suffers chronic arthritic back and joint pain, might have overdosed on pain medications.
According to her husband, Mrs. M has been taking combination oxycodone/acetaminophen and transdermal fentanyl at unknown dosages, but he is unsure when she started using these medications or if she is taking others. Serum toxicology screening shows twice the normal values for opioids and benzodiazepines; other laboratory results are normal.
Mrs. M is medically stable but her mental status is altered. She is oblivious to time, place and person, speaks to no one, and seems lost in her own world. The hospital’s medical service admits Mrs. M for stabilization and to determine whether the overdose was intentional.
Two days later, we evaluate Mrs. M’s mental status at the attending physician’s request. She appears confused and cannot answer our questions. Her husband tells us she was “doing fine” until approximately 4 months ago, when she started becoming increasingly forgetful and lethargic. He says she has been forgetting routine chores such as paying bills and grocery shopping. Recently, she has been getting lost during her evening walk; neighbors often help her find her way home.
The authors’ observations
Two opioid medications—oxycodone/acetaminophen combination and transdermal fentanyl—are commonly used to manage moderate or severe pain from any type of chronic arthritis.
- Oxycodone, a semisynthetic opioid analgesic indicated for moderate to moderately severe pain, is used when nondrug measures and nonnarcotic medications do not control the pain.
- Transdermal fentanyl, a potent analgesic indicated for persistent moderate to severe chronic pain, typically is prescribed to patients who tolerate oral oxycodone, 30 mg/d; morphine, 60 mg; hydromorphone, 8 mg; or an equianalgesic dosage of another opioid for ≥1 week.
Mrs. M also was taking a benzodiazepine, but which medication—and why she was taking it—were unclear. She had no psychiatric diagnosis, and her husband could not recall her medication history.
We also cannot explain Mrs. M’s negative cognitive and behavioral changes. Opioid overuse and onset of dementia-related cognitive decline are possibilities.
TRANSFER Why is she confused?
Based on information from the pharmacy department, doctors at the medical unit restart oxycodone/acetaminophen, 7.5/325 mg tid, and transdermal fentanyl, 25 mcg/hr every 3 days. After discussing how to treat Mrs. M, the psychiatric and medical services transfer her to the geriatric psychiatric inpatient unit 3 days after admission.
We visit Mrs. M hours after her transfer. She seems lethargic but not confused, although Mini-Mental State Examination (MMSE) score of 15 suggests moderate cognitive impairment. Vitamin B12 and thyroid levels, erythrocyte sedimentation rate, and syphilis test results are normal, allowing us to rule out organic causes for her dementia. Brain MRI shows no neurologic damage. On a scale of 1 to 5 with 5 being most severe, Mrs. M scores her pain as 2 (mild) and her sedation as 3 (moderate).
With Mrs. M’s permission, we call her primary care physician for collateral information. The physician tells us Mrs. M has suffered severe joint pain for 2 years. Nonnarcotic medications and treatments—including counseling, support groups, massage, yoga, exercise, biofeedback, relaxation therapy, and physical therapy—were ineffective.
Approximately 10 months ago, the physician started oxycodone/acetaminophen at 2.5/325 mg bid and titrated it over 6 weeks to 7.5/325 mg tid for Mrs. M’s persistent joint pain. Four months ago, with her pain still severe, the physician added transdermal fentanyl, 25 mcg/hr every 3 days, after which the patient reported mild improvement.
One month after starting the fentanyl patch, Mrs. M complained of sudden forgetfulness, low energy, poor concentration, and increased sleep. The physician suspected depression with possible comorbid anxiety and prescribed sertraline, 50 mg/d, and alprazolam, 0.5 mg bid. Mrs. M stopped sertraline after 3 days because it was causing diarrhea but kept taking alprazolam.
Mrs. M saw her primary care physician once after starting alprazolam and sertraline but missed her most recent appointment last month. The physician says he inadvertently approved at least 1 premature request for an alprazolam refill.
Six days after admission, Mrs. M’s sedation, cognitive impairment, and lethargy persist. She reports no mood and anxiety problems, and we have not restarted alprazolam.
The authors’ observations
The fentanyl patch most likely began to diminish Mrs. M’s alertness soon after she started using it. The doctor, however, mistook cognitive slowing for new-onset depression or anxiety. Depressive symptoms can imitate dementia, but Mrs. M’s severe sedation and denial of depressive symptoms suggest a medication side effect.
The primary care physician’s reconstruction of Mrs. M’s history explained her positive benzodiazepine reading, and her use of the short-acting benzodiazepine alprazolam could account for her sudden-onset paranoia and cognitive decline (Box). Benzodiazepines can cause behavioral side effects such as disinhibition, agitation, or paranoia, and patients age ≥65 are at increased risk for these side effects.4 In particular, benzodiazepines with half-lives ≥6 to 8 hours such as clonazepam and oxazepam can cause short-term memory impairment, confusion, and delirium.5-7
Reconstructing treatment history is critical if the patient or family members cannot recall past treatments or if the patient cannot communicate.
Get permission from the patient or family as required under the Health Insurance Portability and Accountability Act. Then contact the primary care or other prescribing physician to obtain:
- a copy of the physician’s last progress note and initial evaluation
- notes about adverse reactions to current or past medications
- trials of medications and other treatments relevant to the current complaint.
In emergent cases when the patient is unresponsive or mentally incapacitated and no family members are available, follow the above steps and initiate treatment. Carefully document that the patient was incoherent, his life was in danger, and you could not reach a family member for permission to treat.
If you cannot communicate with the patient or contact a family member but care is less emergent, consult the hospital’s ethics committee to see if a guardian has been appointed. Contact the primary care physician only after the guardian grants permission.
When prescribing benzodiazepines (especially in older patients) watch for signs of overuse or abuse, such as early requests for refills, unkempt appearance, excessive sleepiness, or agitation (Table 1).
Warning signs of opioid, benzodiazepine overuse
| Frequent requests for early refills |
| Patient exceeds prescribed dosage without authorization |
| Patient reports lost/stolen prescription; if patient has history of substance abuse/dependence or legal problems, even 1 report should raise a red flag |
| Patient increasingly unkempt or impaired |
| Negative mood change |
| Agitation |
| Patient involved in car or other accidents |
| Sedation |
| Purposeful oversedation, particularly when patient has an apparent secondary gain from opioid use (such as qualifying for disability benefits or escaping from work) |
| New-onset cognitive impairment |
| Patient abusing alcohol or other illicit CNS depressants |
The authors’ observations
Persistent chronic pain in the elderly can diminish health and quality of life, resulting in depression, social isolation, immobility, and sleep disturbance.
Managing an older patient’s pain can be challenging (Table 2). Opioids are effective painkillers, but even at relatively low dosages they can diminish function and cognition and increase risk of delirium. Also, patients’ ability to tolerate different opioids at different dosages varies widely.
Mrs. M’s opioid regimen was intolerable and numerous other treatments did not alleviate her pain. At this point, replacing fentanyl with another opioid was our best option.8
We decided to try methadone, which is indicated for moderate to severe pain that does not respond to nonnarcotic treatments. Methadone often is used for chronic pain associated with arthritis or malignancy.
Methadone is less sedating, more tolerable, and carries a lower risk of cognitive side effects than other opioids. Methadone also is fast- and long-acting—its analgesic effects begin within 30 minutes to 1 hour of oral administration9 and last approximately 12 hours, thus reducing the risk of breakthrough pain. Methadone also:
- has no active metabolites, which decreases the risk of hepatic side effects
- offers a high volume of distribution, thus allowing clinical effect with minimal dosing.
Beware the potential for addiction when prescribing opioids to any patient.13,14 The U.S. Drug Enforcement Agency classifies both methadone and fentanyl as schedule II substances, which applies to highly addictive medications with FDA-approved indications. See patients at least biweekly, especially when switching or titrating pain medications, and watch closely for signs of overuse or addiction. Inform patients to:
- watch for symptoms such as oversedation, memory and concentration problems, and sudden changes in personality
- call you to clarify if these symptoms are methadone side effects.
Watch for other potential side effects of methadone, such as constipation, sedation, breakthrough pain, sexual dysfunction, decreased immunity, respiratory depression, or prolonged corrected QT intervals.
Patients usually tolerate an immediate switch from transdermal fentanyl to methadone, but a sudden switch from high-dose fentanyl can reduce methadone’s effectiveness. Starting methadone at a high dosage to compensate for loss of effectiveness could increase side effect risk. If the fentanyl dosage exceeds 100 mcg/hr, taper by 25 mcg weekly. Simultaneously start methadone at a low dosage and titrate by 5 to 10 mg weekly as needed.
Table 2
Chronic pain management in the elderly: Dos and don’ts
| DO |
| Use self rating scales, as patient can gauge his/her own pain most accurately |
| Consider nonpharmacologic treatments and nonnarcotic analgesics first |
| Watch closely for side effects and drug-drug/drug-disease interactions in patients receiving analgesics long-term |
| Monitor patients receiving opioids long-term for oversedation, changes in cognition and function |
| Consider switching to methadone or another opioid if patient cannot tolerate current opioid regimen |
| DO NOT |
| Prescribe propoxyphene or meperidine—which carry a higher risk of adverse effects than other opioids—to older patient |
| Prescribe opioids if the medical history is unclear |
| Increase opioid dosages without seeing the patient |
TREATMENT Medication change
We stop transdermal fentanyl and start oral methadone, 5 mg bid, while continuing oxycodone/acetaminophen at the previous dosage.
Two days later, Mrs. M is much more alert. Since admission 1 week ago, her sedation rating has improved from 3 (mildly sedated) to 4 (almost fully alert). She rates her pain as mild and reports no breakthrough pain or other side effects from methadone. Her MMSE score has improved to 24—suggesting close to normal cognition—and she is much more interactive with staff and family.
Eight days after we start methadone, we stop oxycodone/acetaminophen and increase methadone to 10 mg bid to further improve cognition and alertness and to see if 1 pain medication is suffcient. Two days later, we discharge Mrs. M. She is fully alert, feels little or no joint pain, and is tolerating the methadone increase.
At outpatient follow-up 4 weeks later, Mrs. M remains pain-free and her MMSE score is 29, suggesting normal cognition. Over 8 months, we continue to see her monthly and then bi-monthly, after which we refer her to her primary care physician.
Related resources
- American Association for Geriatric Psychiatry. www.aagponline.org.
- American Pain Society. www.ampainsoc.org.
- Alprazolam • Xanax
- Clonazepam • Klonopin
- Fentanyl (transdermal) • Duragesic
- Hydromorphone • Dilaudid
- Meperidine • Demerol
- Methadone • Dolophine
- Oxazepam • Serax
- Oxycodone • OxyContin, Roxicodone
- Oxycodone/acetaminophen • Percocet
- Propoxyphene • Darvon
- Sertraline • Zoloft
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
CASE: She’s not herself
Mrs. M, age 74, is brought to the ER by her husband after he finds her lying on their bedroom floor, incoherent and extremely drowsy. He reports that his wife, who suffers chronic arthritic back and joint pain, might have overdosed on pain medications.
According to her husband, Mrs. M has been taking combination oxycodone/acetaminophen and transdermal fentanyl at unknown dosages, but he is unsure when she started using these medications or if she is taking others. Serum toxicology screening shows twice the normal values for opioids and benzodiazepines; other laboratory results are normal.
Mrs. M is medically stable but her mental status is altered. She is oblivious to time, place and person, speaks to no one, and seems lost in her own world. The hospital’s medical service admits Mrs. M for stabilization and to determine whether the overdose was intentional.
Two days later, we evaluate Mrs. M’s mental status at the attending physician’s request. She appears confused and cannot answer our questions. Her husband tells us she was “doing fine” until approximately 4 months ago, when she started becoming increasingly forgetful and lethargic. He says she has been forgetting routine chores such as paying bills and grocery shopping. Recently, she has been getting lost during her evening walk; neighbors often help her find her way home.
The authors’ observations
Two opioid medications—oxycodone/acetaminophen combination and transdermal fentanyl—are commonly used to manage moderate or severe pain from any type of chronic arthritis.
- Oxycodone, a semisynthetic opioid analgesic indicated for moderate to moderately severe pain, is used when nondrug measures and nonnarcotic medications do not control the pain.
- Transdermal fentanyl, a potent analgesic indicated for persistent moderate to severe chronic pain, typically is prescribed to patients who tolerate oral oxycodone, 30 mg/d; morphine, 60 mg; hydromorphone, 8 mg; or an equianalgesic dosage of another opioid for ≥1 week.
Mrs. M also was taking a benzodiazepine, but which medication—and why she was taking it—were unclear. She had no psychiatric diagnosis, and her husband could not recall her medication history.
We also cannot explain Mrs. M’s negative cognitive and behavioral changes. Opioid overuse and onset of dementia-related cognitive decline are possibilities.
TRANSFER Why is she confused?
Based on information from the pharmacy department, doctors at the medical unit restart oxycodone/acetaminophen, 7.5/325 mg tid, and transdermal fentanyl, 25 mcg/hr every 3 days. After discussing how to treat Mrs. M, the psychiatric and medical services transfer her to the geriatric psychiatric inpatient unit 3 days after admission.
We visit Mrs. M hours after her transfer. She seems lethargic but not confused, although Mini-Mental State Examination (MMSE) score of 15 suggests moderate cognitive impairment. Vitamin B12 and thyroid levels, erythrocyte sedimentation rate, and syphilis test results are normal, allowing us to rule out organic causes for her dementia. Brain MRI shows no neurologic damage. On a scale of 1 to 5 with 5 being most severe, Mrs. M scores her pain as 2 (mild) and her sedation as 3 (moderate).
With Mrs. M’s permission, we call her primary care physician for collateral information. The physician tells us Mrs. M has suffered severe joint pain for 2 years. Nonnarcotic medications and treatments—including counseling, support groups, massage, yoga, exercise, biofeedback, relaxation therapy, and physical therapy—were ineffective.
Approximately 10 months ago, the physician started oxycodone/acetaminophen at 2.5/325 mg bid and titrated it over 6 weeks to 7.5/325 mg tid for Mrs. M’s persistent joint pain. Four months ago, with her pain still severe, the physician added transdermal fentanyl, 25 mcg/hr every 3 days, after which the patient reported mild improvement.
One month after starting the fentanyl patch, Mrs. M complained of sudden forgetfulness, low energy, poor concentration, and increased sleep. The physician suspected depression with possible comorbid anxiety and prescribed sertraline, 50 mg/d, and alprazolam, 0.5 mg bid. Mrs. M stopped sertraline after 3 days because it was causing diarrhea but kept taking alprazolam.
Mrs. M saw her primary care physician once after starting alprazolam and sertraline but missed her most recent appointment last month. The physician says he inadvertently approved at least 1 premature request for an alprazolam refill.
Six days after admission, Mrs. M’s sedation, cognitive impairment, and lethargy persist. She reports no mood and anxiety problems, and we have not restarted alprazolam.
The authors’ observations
The fentanyl patch most likely began to diminish Mrs. M’s alertness soon after she started using it. The doctor, however, mistook cognitive slowing for new-onset depression or anxiety. Depressive symptoms can imitate dementia, but Mrs. M’s severe sedation and denial of depressive symptoms suggest a medication side effect.
The primary care physician’s reconstruction of Mrs. M’s history explained her positive benzodiazepine reading, and her use of the short-acting benzodiazepine alprazolam could account for her sudden-onset paranoia and cognitive decline (Box). Benzodiazepines can cause behavioral side effects such as disinhibition, agitation, or paranoia, and patients age ≥65 are at increased risk for these side effects.4 In particular, benzodiazepines with half-lives ≥6 to 8 hours such as clonazepam and oxazepam can cause short-term memory impairment, confusion, and delirium.5-7
Reconstructing treatment history is critical if the patient or family members cannot recall past treatments or if the patient cannot communicate.
Get permission from the patient or family as required under the Health Insurance Portability and Accountability Act. Then contact the primary care or other prescribing physician to obtain:
- a copy of the physician’s last progress note and initial evaluation
- notes about adverse reactions to current or past medications
- trials of medications and other treatments relevant to the current complaint.
In emergent cases when the patient is unresponsive or mentally incapacitated and no family members are available, follow the above steps and initiate treatment. Carefully document that the patient was incoherent, his life was in danger, and you could not reach a family member for permission to treat.
If you cannot communicate with the patient or contact a family member but care is less emergent, consult the hospital’s ethics committee to see if a guardian has been appointed. Contact the primary care physician only after the guardian grants permission.
When prescribing benzodiazepines (especially in older patients) watch for signs of overuse or abuse, such as early requests for refills, unkempt appearance, excessive sleepiness, or agitation (Table 1).
Warning signs of opioid, benzodiazepine overuse
| Frequent requests for early refills |
| Patient exceeds prescribed dosage without authorization |
| Patient reports lost/stolen prescription; if patient has history of substance abuse/dependence or legal problems, even 1 report should raise a red flag |
| Patient increasingly unkempt or impaired |
| Negative mood change |
| Agitation |
| Patient involved in car or other accidents |
| Sedation |
| Purposeful oversedation, particularly when patient has an apparent secondary gain from opioid use (such as qualifying for disability benefits or escaping from work) |
| New-onset cognitive impairment |
| Patient abusing alcohol or other illicit CNS depressants |
The authors’ observations
Persistent chronic pain in the elderly can diminish health and quality of life, resulting in depression, social isolation, immobility, and sleep disturbance.
Managing an older patient’s pain can be challenging (Table 2). Opioids are effective painkillers, but even at relatively low dosages they can diminish function and cognition and increase risk of delirium. Also, patients’ ability to tolerate different opioids at different dosages varies widely.
Mrs. M’s opioid regimen was intolerable and numerous other treatments did not alleviate her pain. At this point, replacing fentanyl with another opioid was our best option.8
We decided to try methadone, which is indicated for moderate to severe pain that does not respond to nonnarcotic treatments. Methadone often is used for chronic pain associated with arthritis or malignancy.
Methadone is less sedating, more tolerable, and carries a lower risk of cognitive side effects than other opioids. Methadone also is fast- and long-acting—its analgesic effects begin within 30 minutes to 1 hour of oral administration9 and last approximately 12 hours, thus reducing the risk of breakthrough pain. Methadone also:
- has no active metabolites, which decreases the risk of hepatic side effects
- offers a high volume of distribution, thus allowing clinical effect with minimal dosing.
Beware the potential for addiction when prescribing opioids to any patient.13,14 The U.S. Drug Enforcement Agency classifies both methadone and fentanyl as schedule II substances, which applies to highly addictive medications with FDA-approved indications. See patients at least biweekly, especially when switching or titrating pain medications, and watch closely for signs of overuse or addiction. Inform patients to:
- watch for symptoms such as oversedation, memory and concentration problems, and sudden changes in personality
- call you to clarify if these symptoms are methadone side effects.
Watch for other potential side effects of methadone, such as constipation, sedation, breakthrough pain, sexual dysfunction, decreased immunity, respiratory depression, or prolonged corrected QT intervals.
Patients usually tolerate an immediate switch from transdermal fentanyl to methadone, but a sudden switch from high-dose fentanyl can reduce methadone’s effectiveness. Starting methadone at a high dosage to compensate for loss of effectiveness could increase side effect risk. If the fentanyl dosage exceeds 100 mcg/hr, taper by 25 mcg weekly. Simultaneously start methadone at a low dosage and titrate by 5 to 10 mg weekly as needed.
Table 2
Chronic pain management in the elderly: Dos and don’ts
| DO |
| Use self rating scales, as patient can gauge his/her own pain most accurately |
| Consider nonpharmacologic treatments and nonnarcotic analgesics first |
| Watch closely for side effects and drug-drug/drug-disease interactions in patients receiving analgesics long-term |
| Monitor patients receiving opioids long-term for oversedation, changes in cognition and function |
| Consider switching to methadone or another opioid if patient cannot tolerate current opioid regimen |
| DO NOT |
| Prescribe propoxyphene or meperidine—which carry a higher risk of adverse effects than other opioids—to older patient |
| Prescribe opioids if the medical history is unclear |
| Increase opioid dosages without seeing the patient |
TREATMENT Medication change
We stop transdermal fentanyl and start oral methadone, 5 mg bid, while continuing oxycodone/acetaminophen at the previous dosage.
Two days later, Mrs. M is much more alert. Since admission 1 week ago, her sedation rating has improved from 3 (mildly sedated) to 4 (almost fully alert). She rates her pain as mild and reports no breakthrough pain or other side effects from methadone. Her MMSE score has improved to 24—suggesting close to normal cognition—and she is much more interactive with staff and family.
Eight days after we start methadone, we stop oxycodone/acetaminophen and increase methadone to 10 mg bid to further improve cognition and alertness and to see if 1 pain medication is suffcient. Two days later, we discharge Mrs. M. She is fully alert, feels little or no joint pain, and is tolerating the methadone increase.
At outpatient follow-up 4 weeks later, Mrs. M remains pain-free and her MMSE score is 29, suggesting normal cognition. Over 8 months, we continue to see her monthly and then bi-monthly, after which we refer her to her primary care physician.
Related resources
- American Association for Geriatric Psychiatry. www.aagponline.org.
- American Pain Society. www.ampainsoc.org.
- Alprazolam • Xanax
- Clonazepam • Klonopin
- Fentanyl (transdermal) • Duragesic
- Hydromorphone • Dilaudid
- Meperidine • Demerol
- Methadone • Dolophine
- Oxazepam • Serax
- Oxycodone • OxyContin, Roxicodone
- Oxycodone/acetaminophen • Percocet
- Propoxyphene • Darvon
- Sertraline • Zoloft
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Edinboro LE, Poklis A, Trautman D, et al. Fatal fentanyl intoxication following excessive transdermal application. J Forenscic Sci 1997;42:741-3.
2. Rose PG, Macfee MS, Boswell MV. Fentanyl transdermal system overdose secondary to cutaneous hyperthermia. Anesth Analg 1993;77:390-1.
3. Lawlor PG, Bruera E. Side effects of opioids in chronic pain treatment. Curr Opin Anaesthesiol 1998;5:539-45.
4. Lechin F, Van der Dijs B, Benaim M. Benzodiazepines; tolerability in elderly patients. Psychother Psychosom 1996;65:171-82.
5. Hall RC, Zisook S. Paradoxical reactions to benzodiazepines. Br J Clin Pharmacology 1981;11(suppl 1):99S-104S.
6. Cole JO, Kando JC. Adverse behavioral events reported in patients taking alprazolam and other benzodiazepines. J Clin Psychiatry 1993;54(suppl):49-61.
7. Paton P. Benzodiazepines and disinhibition. Psychiatr Bull 2002;26:460-2.
8. Quigley C. Opioid switching to improve pain relief and drug tolerability (review). Cochrane Database Syst Rev 2004(3);CD004847.-
9. National Highway Traffic Safety Administration. Methadone. Available at: http://www.nhtsa.dot.gov/PEOPLE/INJURY/research/job185drugs/methadone.htm. Accessed February 14, 2008.
10. Manzini I, Lossignol DA, Body JJ. Opioid switch to oral methadone in cancer pain. Curr Opin Oncol 2000;12:308-13.
11. Layson-Wolf C, Goode JV, Small R. Clinical use of methadone. J Pain Palliat Care 2002;16:29-59.
12. Krantz MJ, Lewkowiez L, Hays H, et al. Torsades de pointes associated with high dose methadone. Ann Intern Med 2002;139:501-4.
13. Fishbain D, Rosomoff H, Rosomoff RS. Drug abuse, dependence, and addiction in chronic patients. Clin J Pain 1992;8:77-85.
14. Hoffmann NG, Olofsson O, Salen B, Wickstrom L. Prevalence of abuse and dependency in chronic pain patients. Int J Addict 1995;30:919-27.
1. Edinboro LE, Poklis A, Trautman D, et al. Fatal fentanyl intoxication following excessive transdermal application. J Forenscic Sci 1997;42:741-3.
2. Rose PG, Macfee MS, Boswell MV. Fentanyl transdermal system overdose secondary to cutaneous hyperthermia. Anesth Analg 1993;77:390-1.
3. Lawlor PG, Bruera E. Side effects of opioids in chronic pain treatment. Curr Opin Anaesthesiol 1998;5:539-45.
4. Lechin F, Van der Dijs B, Benaim M. Benzodiazepines; tolerability in elderly patients. Psychother Psychosom 1996;65:171-82.
5. Hall RC, Zisook S. Paradoxical reactions to benzodiazepines. Br J Clin Pharmacology 1981;11(suppl 1):99S-104S.
6. Cole JO, Kando JC. Adverse behavioral events reported in patients taking alprazolam and other benzodiazepines. J Clin Psychiatry 1993;54(suppl):49-61.
7. Paton P. Benzodiazepines and disinhibition. Psychiatr Bull 2002;26:460-2.
8. Quigley C. Opioid switching to improve pain relief and drug tolerability (review). Cochrane Database Syst Rev 2004(3);CD004847.-
9. National Highway Traffic Safety Administration. Methadone. Available at: http://www.nhtsa.dot.gov/PEOPLE/INJURY/research/job185drugs/methadone.htm. Accessed February 14, 2008.
10. Manzini I, Lossignol DA, Body JJ. Opioid switch to oral methadone in cancer pain. Curr Opin Oncol 2000;12:308-13.
11. Layson-Wolf C, Goode JV, Small R. Clinical use of methadone. J Pain Palliat Care 2002;16:29-59.
12. Krantz MJ, Lewkowiez L, Hays H, et al. Torsades de pointes associated with high dose methadone. Ann Intern Med 2002;139:501-4.
13. Fishbain D, Rosomoff H, Rosomoff RS. Drug abuse, dependence, and addiction in chronic patients. Clin J Pain 1992;8:77-85.
14. Hoffmann NG, Olofsson O, Salen B, Wickstrom L. Prevalence of abuse and dependency in chronic pain patients. Int J Addict 1995;30:919-27.