User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'main-prefix')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
U.S. docs at double the risk of postpartum depression
One in four new mothers who are physicians report experiencing postpartum depression, a rate twice that of the general population, according to new survey findings presented at the American College of Obstetricians and Gynecologists (ACOG) 2022 Annual Meeting.
The survey results weren’t all grim. More than three-fourths (78%) of new mothers reported meeting their own breastfeeding goals. Still, Alison Stuebe, MD, director of maternal-fetal medicine, University of North Carolina School of Medicine, Chapel Hill, said the high postpartum depression rates among physicians might be associated with worse patient care.
“Physicians who have had postpartum depression and provide clinical care for children and birthing people can bring their negative experiences to their clinical work, potentially impacting how they counsel and support their patients,” Dr. Stuebe, who was not involved in the study, told this news organization.
For the study, Emily Eischen, a fourth-year medical student at the University of South Florida Morsani College of Medicine, Tampa, and her colleagues sought to learn how physicians and physician trainee mothers fared in the face of the unique stressors of their jobs, including “strenuous work hours, pressures to get back to work, and limited maternity leave.”
The researchers recruited 637 physicians and medical students with a singleton pregnancy to respond to a survey adapted largely from the U.S. Centers for Disease Control and Prevention’s Infant Feeding Practices Study and the CDC’s Pregnancy Risk Assessment Monitoring System.
Most of the respondents, who were enrolled through social media physician groups and email list-serves, were married non-Hispanic White persons; 71% were practicing or training in pediatrics, family medicine, or obstetrics/gynecology, and 2% were medical students.
Data showed that 25% of participants reported postpartum depression. The highest rates were seen among Hispanic/Latino respondents (31%), Black persons (30%), and non-Hispanic White persons (25%). The lowest rates of postpartum depression were for respondents identifying as Asian (15%).
Guilt a driver
Most respondents (80%) with symptoms of postpartum depression attributed their condition to sleep deprivation. Other frequently cited reasons were problems related to infant feeding (44%), lack of adequate maternity leave (41%), and lack of support at work (33%).
“Feeling guilty for not fulfilling work responsibilities, especially for residents, who are in the most difficult time in their careers and have to hand the workload off to others, can be very stressful,” Ms. Eischen said.
Despite the high rates of postpartum depression in the survey, the investigators found that 99% of respondents had initiated breastfeeding, 72% were exclusively breastfeeding, and 78% said they were meeting their personal breastfeeding goals. All of those rates are higher than what is seen in the general population.
Rates of self-reported postpartum depression were higher among those who did not meet their breastfeeding goals than among those who did (36% vs. 23%; P = .003), the researchers found.
Adetola Louis-Jacques, MD, an assistant professor of medicine, USF Health Obstetrics and Gynecology, and the senior author of the study, said the high breastfeeding rates can be attributed partly to an increased appreciation among physicians that lactation and breastfeeding have proven benefits for women and infant health.
“We still have work to do, but at least the journey has started in supporting birthing and lactating physicians,” she said.
However, Dr. Stuebe wondered whether the survey captured a group of respondents more likely to meet breastfeeding goals. She said she was surprised by the high proportion of respondents who did so.
“When surveys are distributed via social media, we don’t have a clear sense of who chooses to participate and who opts out,” she said in an interview. “If the survey was shared through social media groups that focus on supporting breastfeeding among physicians, it could have affected the results.”
No relevant financial relationships have been reported.
A version of this article first appeared on Medscape.com.
One in four new mothers who are physicians report experiencing postpartum depression, a rate twice that of the general population, according to new survey findings presented at the American College of Obstetricians and Gynecologists (ACOG) 2022 Annual Meeting.
The survey results weren’t all grim. More than three-fourths (78%) of new mothers reported meeting their own breastfeeding goals. Still, Alison Stuebe, MD, director of maternal-fetal medicine, University of North Carolina School of Medicine, Chapel Hill, said the high postpartum depression rates among physicians might be associated with worse patient care.
“Physicians who have had postpartum depression and provide clinical care for children and birthing people can bring their negative experiences to their clinical work, potentially impacting how they counsel and support their patients,” Dr. Stuebe, who was not involved in the study, told this news organization.
For the study, Emily Eischen, a fourth-year medical student at the University of South Florida Morsani College of Medicine, Tampa, and her colleagues sought to learn how physicians and physician trainee mothers fared in the face of the unique stressors of their jobs, including “strenuous work hours, pressures to get back to work, and limited maternity leave.”
The researchers recruited 637 physicians and medical students with a singleton pregnancy to respond to a survey adapted largely from the U.S. Centers for Disease Control and Prevention’s Infant Feeding Practices Study and the CDC’s Pregnancy Risk Assessment Monitoring System.
Most of the respondents, who were enrolled through social media physician groups and email list-serves, were married non-Hispanic White persons; 71% were practicing or training in pediatrics, family medicine, or obstetrics/gynecology, and 2% were medical students.
Data showed that 25% of participants reported postpartum depression. The highest rates were seen among Hispanic/Latino respondents (31%), Black persons (30%), and non-Hispanic White persons (25%). The lowest rates of postpartum depression were for respondents identifying as Asian (15%).
Guilt a driver
Most respondents (80%) with symptoms of postpartum depression attributed their condition to sleep deprivation. Other frequently cited reasons were problems related to infant feeding (44%), lack of adequate maternity leave (41%), and lack of support at work (33%).
“Feeling guilty for not fulfilling work responsibilities, especially for residents, who are in the most difficult time in their careers and have to hand the workload off to others, can be very stressful,” Ms. Eischen said.
Despite the high rates of postpartum depression in the survey, the investigators found that 99% of respondents had initiated breastfeeding, 72% were exclusively breastfeeding, and 78% said they were meeting their personal breastfeeding goals. All of those rates are higher than what is seen in the general population.
Rates of self-reported postpartum depression were higher among those who did not meet their breastfeeding goals than among those who did (36% vs. 23%; P = .003), the researchers found.
Adetola Louis-Jacques, MD, an assistant professor of medicine, USF Health Obstetrics and Gynecology, and the senior author of the study, said the high breastfeeding rates can be attributed partly to an increased appreciation among physicians that lactation and breastfeeding have proven benefits for women and infant health.
“We still have work to do, but at least the journey has started in supporting birthing and lactating physicians,” she said.
However, Dr. Stuebe wondered whether the survey captured a group of respondents more likely to meet breastfeeding goals. She said she was surprised by the high proportion of respondents who did so.
“When surveys are distributed via social media, we don’t have a clear sense of who chooses to participate and who opts out,” she said in an interview. “If the survey was shared through social media groups that focus on supporting breastfeeding among physicians, it could have affected the results.”
No relevant financial relationships have been reported.
A version of this article first appeared on Medscape.com.
One in four new mothers who are physicians report experiencing postpartum depression, a rate twice that of the general population, according to new survey findings presented at the American College of Obstetricians and Gynecologists (ACOG) 2022 Annual Meeting.
The survey results weren’t all grim. More than three-fourths (78%) of new mothers reported meeting their own breastfeeding goals. Still, Alison Stuebe, MD, director of maternal-fetal medicine, University of North Carolina School of Medicine, Chapel Hill, said the high postpartum depression rates among physicians might be associated with worse patient care.
“Physicians who have had postpartum depression and provide clinical care for children and birthing people can bring their negative experiences to their clinical work, potentially impacting how they counsel and support their patients,” Dr. Stuebe, who was not involved in the study, told this news organization.
For the study, Emily Eischen, a fourth-year medical student at the University of South Florida Morsani College of Medicine, Tampa, and her colleagues sought to learn how physicians and physician trainee mothers fared in the face of the unique stressors of their jobs, including “strenuous work hours, pressures to get back to work, and limited maternity leave.”
The researchers recruited 637 physicians and medical students with a singleton pregnancy to respond to a survey adapted largely from the U.S. Centers for Disease Control and Prevention’s Infant Feeding Practices Study and the CDC’s Pregnancy Risk Assessment Monitoring System.
Most of the respondents, who were enrolled through social media physician groups and email list-serves, were married non-Hispanic White persons; 71% were practicing or training in pediatrics, family medicine, or obstetrics/gynecology, and 2% were medical students.
Data showed that 25% of participants reported postpartum depression. The highest rates were seen among Hispanic/Latino respondents (31%), Black persons (30%), and non-Hispanic White persons (25%). The lowest rates of postpartum depression were for respondents identifying as Asian (15%).
Guilt a driver
Most respondents (80%) with symptoms of postpartum depression attributed their condition to sleep deprivation. Other frequently cited reasons were problems related to infant feeding (44%), lack of adequate maternity leave (41%), and lack of support at work (33%).
“Feeling guilty for not fulfilling work responsibilities, especially for residents, who are in the most difficult time in their careers and have to hand the workload off to others, can be very stressful,” Ms. Eischen said.
Despite the high rates of postpartum depression in the survey, the investigators found that 99% of respondents had initiated breastfeeding, 72% were exclusively breastfeeding, and 78% said they were meeting their personal breastfeeding goals. All of those rates are higher than what is seen in the general population.
Rates of self-reported postpartum depression were higher among those who did not meet their breastfeeding goals than among those who did (36% vs. 23%; P = .003), the researchers found.
Adetola Louis-Jacques, MD, an assistant professor of medicine, USF Health Obstetrics and Gynecology, and the senior author of the study, said the high breastfeeding rates can be attributed partly to an increased appreciation among physicians that lactation and breastfeeding have proven benefits for women and infant health.
“We still have work to do, but at least the journey has started in supporting birthing and lactating physicians,” she said.
However, Dr. Stuebe wondered whether the survey captured a group of respondents more likely to meet breastfeeding goals. She said she was surprised by the high proportion of respondents who did so.
“When surveys are distributed via social media, we don’t have a clear sense of who chooses to participate and who opts out,” she said in an interview. “If the survey was shared through social media groups that focus on supporting breastfeeding among physicians, it could have affected the results.”
No relevant financial relationships have been reported.
A version of this article first appeared on Medscape.com.
Innocent doc sued after 'secret' medical expert says claim has merit
When the hospital’s trauma team could not get an IV inserted into an accident victim, they called Illinois emergency physician William Sullivan, DO, JD, for help. Dr. Sullivan, who is based in the Chicago suburb of Frankfort, inserted a central line into the patient’s leg on his first attempt – a task that took about 20 minutes.
A year later, Dr. Sullivan was shocked and angry to learn he was being sued by the trauma patient’s family. Inserting the line was his only interaction with the woman, and he had no role in her care management, he said. Yet, the suit claimed he was negligent for failing to diagnose the patient with internal bleeding and for not performing surgery.
“The lawsuit put a lot of stress on our family,” Dr. Sullivan recalled. “At the time my wife was pregnant. I was in law school, and I was also working full time in the ER to support our family. I remember my wife crying on the couch after reading the complaint and asking how the plaintiff’s attorney could get away with making the allegations he made.”
Dr. Sullivan soon learned that 15 medical providers in the patient’s medical record were named as defendants. This included the director of the radiology department, whose name was on a radiology report as “director” but who was actually out of the country when the incident occurred.
Despite some of the accusations being impossible, a medical expert had claimed there was a “meritorious claim” against every health professional named in the suit. Illinois is among the 28 states that require plaintiffs’ attorneys to file an affidavit of merit for medical malpractice claims to move forward.
Dr. Sullivan wondered who would endorse such outlandish accusations, but the expert’s identity was a mystery. According to Illinois law, About one-third of states with merit requirements permit anonymous experts, according to research and attorneys familiar with the issue.
Because the expert’s identity remains hidden, physicians have no way of knowing whether they were qualified to render an opinion, Dr. Sullivan said. The loopholes can drag out frivolous claims and waste significant time and expense, say legal experts. Frequently, it takes a year or more before innocent physicians are dismissed from unfounded lawsuits by the court or dropped when plaintiffs can’t support the claim.
“It’s hugely frustrating,” said Bruce Montoya, JD, a Colorado medical liability defense attorney. “You have an expert who is not disclosed. Further down the road, when experts are being deposed, the plaintiff does not have to reveal whether any of those testifying experts is the same one who certified the case. You never get to determine whether they, in fact, had a certificate reviewer who was legitimate.”
The laws have led to a recent outcry among physicians and fueled a revised resolution by the American College of Emergency Physicians (ACEP) denouncing anonymous affidavits of merit. (The revision has not yet been published online.)
“The minute experts are identified, they can be vetted,” said Rade B. Vukmir, MD, JD, chair of ACEP’s Medical Legal Committee. “There are reasons that you want to clarify the qualification and veracity of the witness. [Anonymous affidavits of merit] don’t allow that, and there’s something inherently wrong with that.”
Because the identities of consulting experts are unknown, it’s hard to know how many are unqualified. Expert witnesses who testify during trials, on the other hand, have long come under scrutiny for questionable qualifications. Some have come under fire for allegedly lying under oath about their experience, misrepresenting their credentials, and falsely representing their knowledge.
“Considering the known problem of potentially unethical expert witness testimony at trial, there’s is the potential likelihood that experts in anonymous affidavits of merit may sometimes lack the qualifications to give opinions,” said Dr. Vukmir, an emergency care physician in Pittsburgh.
Attorneys: Hidden experts increase costs, waste time
In Colorado, Mr. Montoya has seen firsthand how anonymous experts can prolong questionable claims and burden defendants.
Like Illinois, Colorado does not require attorneys to identify the medical experts used to fulfill its certificate of review statute. The expert consulted must have expertise in the same area of the alleged negligence, but does not have to practice in the same specialty, and the statute allows one expert to certify a lawsuit against multiple doctors.
In a recent case, Mr. Montoya represented a Denver neurosurgeon who was sued along with multiple other health care professionals. From the outset, Mr. Montoya argued the claim had no merit against the neurosurgeon, but the plaintiff’s attorney refused to dismiss the physician. Mr. Montoya asked whether the expert consulted for the certificate of merit was a neurosurgeon, but the attorney declined to disclose that information, he said.
The case progressed and Mr. Montoya eventually asked the judge to review the certificate of merit. By law, a judge can confidentially review the certificate of merit and decide whether it aligns with the state statute, but without disclosing the expert’s identity to the defense. The judge ruled the certificate appeared to conform with state law, and the case continued.
A year later, as both sides were getting ready to disclose their experts who would testify, Mr. Montoya again argued the neurosurgeon should be dropped from the suit. This time, he warned if the claim continued against the neurosurgeon, the defense would be filing a motion for summary judgment and pursuing attorney fees and costs. Colorado law allows for such fees if the filing or pursuit of an action is frivolous.
“Boom, my client was dismissed,” Mr. Montoya said. “This is a year later, after multiple conferences among the attorneys, multiple pleadings filed, expert witnesses retained to review the care, discovery exchanged, and records obtained. If we had [a stronger] certificate of review statute, it would have been a different ballgame. It’s never going to get a year down the road.”
In New York, physician defendants have experienced similar woes. The state’s law requires plaintiffs’ attorneys to certify that they consulted with a physician prior to filing the claim, and that they believe based on that discussion, there’s a reasonable basis for the claim to move forward. Attorneys are not required to disclose the expert’s identity.
The law also allows “an out,” explained Morris Auster, JD, senior vice president and chief legislative counsel for the Medical Society of the State of New York. If the attorney made three separate attempts to obtain a consultation, and all three experts would not agree to the consultation, the lawsuit can be filed anyway, he said.
“From our standpoint, it’s important to have an affidavit of merit requirement; it’s better than not having it,” Mr. Auster said. “But its effectiveness in providing control over the filing of lawsuits in New York has never been as strong as it could’ve been.”
Mr. Auster notes that New York has some of the highest liability costs in the country in addition to doctors paying some of the steepest medical liability insurance premiums.
“This really affects a lot of physicians and it’s driving physicians into employment arrangements, so they don’t have to deal with it on their own,” he said. “We support a number of measures to address these significantly high costs, and stronger certificate of merit requirements would certainly be one of those advocacy goals.”
Why are anonymous experts allowed?
Certificates of merit that shield the identity of consultants encourage a greater pool of physicians willing to review cases, said J. Matthew Dudley, JD, president of the Illinois Trial Lawyers Association. When the requirements first went into effect in Illinois, there was significant animosity among physicians toward doctors who testified in medical malpractice cases for patients, Mr. Dudley explained.
“Sometimes they would be ostracized from their professional societies, or it would hurt a referral relationship.” he said. “Over time, that animosity has lessened, but there was a concern that if the identity of physicians in certificates of merit weren’t protected, then doctors would not look at cases for patients.”
This would result in additional barriers for patients and their attorneys in pursuing their legal rights, Mr. Dudley said. He said Illinois’ certificate of merit statute is successful in fulfilling its intended purpose, and he has not seen any statistical evidence to suggest otherwise.
“It has proven effective at decreasing filings in medical malpractice and effectively screening medical malpractice cases,” he said. “Certificates of merit help to decrease filings by firms that aren’t that experienced in dealing with those kinds of cases.”
Kentucky is another state that does not require attorneys to identity the experts consulted for certificates of merit. Malpractice defense attorney Andrew DeSimone, JD, who practices in Kentucky, said this isn’t a problem since attorneys eventually must disclose the expert witnesses who will testify at trial.
“Knowing the name behind the certificate of merit is not that pertinent,” Mr. DeSimone said. “Physicians and their attorneys will ultimately have the chance to question and evaluate the expert witnesses used at trial. The certificate of merit is designed to weed out totally frivolous cases that do not have expert support. It’s not designed to be a trial on the merits.”
The belief that plaintiffs’ attorneys frequently bring weak cases and use unqualified experts to certify claims is not realistic or logical, added Sean Domnick, JD, a Florida medical malpractice attorney and vice president for the American Association for Justice. Medical malpractice cases are extremely challenging for plaintiffs – and they’re expensive, Mr. Domnick said.
“We can’t afford to take bad cases,” he said. “For me to take on a medical malpractice case, it’s not unusual for me to spend well over $100,000. Remember, if we lose, I don’t get that money back and I don’t get paid. Why in the world would a plaintiff take on that type of a burden for a case they didn’t believe in? The logic escapes me.”
In Florida, where Mr. Domnick practices, plaintiffs’ attorneys must send their certificates of merit to the defense with the expert identified. Domnick believes the requirement is a hindrance.
“It creates a delay that is unnecessary in a system that is already designed to wear our clients down,” he said. “It’s just another component that makes it harder on them.”
Hidden experts may insulate plaintiffs’ attorneys from liability
Dr. Sullivan, the Illinois emergency physician, was ultimately dismissed from the multiparty lawsuit, but not for roughly 18 months. After the dismissal, he fought back. He sued the plaintiff’s law firm for malicious prosecution, negligence in hiring, and relying on the opinion of an expert who was unqualified to render an opinion against an emergency physician.
The law firm, however, argued that it was immune from liability because it reasonably relied on the expert’s opinion as required by Illinois law. A trial court agreed with the plaintiffs’ firm. The judge denied Dr. Sullivan’s request to identify the expert, ruling there was no finding that the affidavit was untrue or made without reasonable cause. Dr. Sullivan appealed, and the appellate court upheld the trial’s court decision.
“As happened with my case, law firms can use the affidavit as a defense against countersuits or motions for sanctions,” Dr. Sullivan said. “Although the certificate of merit is intended to prevent attorneys from filing frivolous cases, it can also have the opposite effect of helping to insulate plaintiff attorneys from liability for filing a frivolous lawsuit.”
In Colorado, complaints about the state’s certificate of merit statute have gone before the Colorado Supreme Court. In one case, a lower court ruled that a certificate of merit was deficient because the consultants were not chiropractors. In another case, a nurse defendant argued the claim’s certificate of review was insufficient because the consulting expert was a physician.
In both instances, Colorado judges held the state’s statute does not require consultants to be in the same profession or the same specialty as the health professional defendant.
In New York, meanwhile, Mr. Auster said several bills to strengthen the state’s certificate of merit requirements have failed in recent years.
“It’s hard to say whether it will improve anytime soon,” he said. “The trial lawyers are a very powerful advocacy force in the state, and they tend to oppose even the slightest of changes in civil liability. [In addition], some of these issues have been put on a lower tier because of trying to manage the pandemic.”
Ultimately, Dr. Sullivan said that courts and legislatures need to strongly consider the ethics of allowing anonymous experts to provide testimony against defendant physicians.
“I also think we need to consider how the notion of a secret expert comports with a defendant physician’s due process,” he said. “If an expert’s opinion is appropriate, why would there be a need to shroud one’s identity in a veil of secrecy?”
A version of this article first appeared on Medscape.com.
When the hospital’s trauma team could not get an IV inserted into an accident victim, they called Illinois emergency physician William Sullivan, DO, JD, for help. Dr. Sullivan, who is based in the Chicago suburb of Frankfort, inserted a central line into the patient’s leg on his first attempt – a task that took about 20 minutes.
A year later, Dr. Sullivan was shocked and angry to learn he was being sued by the trauma patient’s family. Inserting the line was his only interaction with the woman, and he had no role in her care management, he said. Yet, the suit claimed he was negligent for failing to diagnose the patient with internal bleeding and for not performing surgery.
“The lawsuit put a lot of stress on our family,” Dr. Sullivan recalled. “At the time my wife was pregnant. I was in law school, and I was also working full time in the ER to support our family. I remember my wife crying on the couch after reading the complaint and asking how the plaintiff’s attorney could get away with making the allegations he made.”
Dr. Sullivan soon learned that 15 medical providers in the patient’s medical record were named as defendants. This included the director of the radiology department, whose name was on a radiology report as “director” but who was actually out of the country when the incident occurred.
Despite some of the accusations being impossible, a medical expert had claimed there was a “meritorious claim” against every health professional named in the suit. Illinois is among the 28 states that require plaintiffs’ attorneys to file an affidavit of merit for medical malpractice claims to move forward.
Dr. Sullivan wondered who would endorse such outlandish accusations, but the expert’s identity was a mystery. According to Illinois law, About one-third of states with merit requirements permit anonymous experts, according to research and attorneys familiar with the issue.
Because the expert’s identity remains hidden, physicians have no way of knowing whether they were qualified to render an opinion, Dr. Sullivan said. The loopholes can drag out frivolous claims and waste significant time and expense, say legal experts. Frequently, it takes a year or more before innocent physicians are dismissed from unfounded lawsuits by the court or dropped when plaintiffs can’t support the claim.
“It’s hugely frustrating,” said Bruce Montoya, JD, a Colorado medical liability defense attorney. “You have an expert who is not disclosed. Further down the road, when experts are being deposed, the plaintiff does not have to reveal whether any of those testifying experts is the same one who certified the case. You never get to determine whether they, in fact, had a certificate reviewer who was legitimate.”
The laws have led to a recent outcry among physicians and fueled a revised resolution by the American College of Emergency Physicians (ACEP) denouncing anonymous affidavits of merit. (The revision has not yet been published online.)
“The minute experts are identified, they can be vetted,” said Rade B. Vukmir, MD, JD, chair of ACEP’s Medical Legal Committee. “There are reasons that you want to clarify the qualification and veracity of the witness. [Anonymous affidavits of merit] don’t allow that, and there’s something inherently wrong with that.”
Because the identities of consulting experts are unknown, it’s hard to know how many are unqualified. Expert witnesses who testify during trials, on the other hand, have long come under scrutiny for questionable qualifications. Some have come under fire for allegedly lying under oath about their experience, misrepresenting their credentials, and falsely representing their knowledge.
“Considering the known problem of potentially unethical expert witness testimony at trial, there’s is the potential likelihood that experts in anonymous affidavits of merit may sometimes lack the qualifications to give opinions,” said Dr. Vukmir, an emergency care physician in Pittsburgh.
Attorneys: Hidden experts increase costs, waste time
In Colorado, Mr. Montoya has seen firsthand how anonymous experts can prolong questionable claims and burden defendants.
Like Illinois, Colorado does not require attorneys to identify the medical experts used to fulfill its certificate of review statute. The expert consulted must have expertise in the same area of the alleged negligence, but does not have to practice in the same specialty, and the statute allows one expert to certify a lawsuit against multiple doctors.
In a recent case, Mr. Montoya represented a Denver neurosurgeon who was sued along with multiple other health care professionals. From the outset, Mr. Montoya argued the claim had no merit against the neurosurgeon, but the plaintiff’s attorney refused to dismiss the physician. Mr. Montoya asked whether the expert consulted for the certificate of merit was a neurosurgeon, but the attorney declined to disclose that information, he said.
The case progressed and Mr. Montoya eventually asked the judge to review the certificate of merit. By law, a judge can confidentially review the certificate of merit and decide whether it aligns with the state statute, but without disclosing the expert’s identity to the defense. The judge ruled the certificate appeared to conform with state law, and the case continued.
A year later, as both sides were getting ready to disclose their experts who would testify, Mr. Montoya again argued the neurosurgeon should be dropped from the suit. This time, he warned if the claim continued against the neurosurgeon, the defense would be filing a motion for summary judgment and pursuing attorney fees and costs. Colorado law allows for such fees if the filing or pursuit of an action is frivolous.
“Boom, my client was dismissed,” Mr. Montoya said. “This is a year later, after multiple conferences among the attorneys, multiple pleadings filed, expert witnesses retained to review the care, discovery exchanged, and records obtained. If we had [a stronger] certificate of review statute, it would have been a different ballgame. It’s never going to get a year down the road.”
In New York, physician defendants have experienced similar woes. The state’s law requires plaintiffs’ attorneys to certify that they consulted with a physician prior to filing the claim, and that they believe based on that discussion, there’s a reasonable basis for the claim to move forward. Attorneys are not required to disclose the expert’s identity.
The law also allows “an out,” explained Morris Auster, JD, senior vice president and chief legislative counsel for the Medical Society of the State of New York. If the attorney made three separate attempts to obtain a consultation, and all three experts would not agree to the consultation, the lawsuit can be filed anyway, he said.
“From our standpoint, it’s important to have an affidavit of merit requirement; it’s better than not having it,” Mr. Auster said. “But its effectiveness in providing control over the filing of lawsuits in New York has never been as strong as it could’ve been.”
Mr. Auster notes that New York has some of the highest liability costs in the country in addition to doctors paying some of the steepest medical liability insurance premiums.
“This really affects a lot of physicians and it’s driving physicians into employment arrangements, so they don’t have to deal with it on their own,” he said. “We support a number of measures to address these significantly high costs, and stronger certificate of merit requirements would certainly be one of those advocacy goals.”
Why are anonymous experts allowed?
Certificates of merit that shield the identity of consultants encourage a greater pool of physicians willing to review cases, said J. Matthew Dudley, JD, president of the Illinois Trial Lawyers Association. When the requirements first went into effect in Illinois, there was significant animosity among physicians toward doctors who testified in medical malpractice cases for patients, Mr. Dudley explained.
“Sometimes they would be ostracized from their professional societies, or it would hurt a referral relationship.” he said. “Over time, that animosity has lessened, but there was a concern that if the identity of physicians in certificates of merit weren’t protected, then doctors would not look at cases for patients.”
This would result in additional barriers for patients and their attorneys in pursuing their legal rights, Mr. Dudley said. He said Illinois’ certificate of merit statute is successful in fulfilling its intended purpose, and he has not seen any statistical evidence to suggest otherwise.
“It has proven effective at decreasing filings in medical malpractice and effectively screening medical malpractice cases,” he said. “Certificates of merit help to decrease filings by firms that aren’t that experienced in dealing with those kinds of cases.”
Kentucky is another state that does not require attorneys to identity the experts consulted for certificates of merit. Malpractice defense attorney Andrew DeSimone, JD, who practices in Kentucky, said this isn’t a problem since attorneys eventually must disclose the expert witnesses who will testify at trial.
“Knowing the name behind the certificate of merit is not that pertinent,” Mr. DeSimone said. “Physicians and their attorneys will ultimately have the chance to question and evaluate the expert witnesses used at trial. The certificate of merit is designed to weed out totally frivolous cases that do not have expert support. It’s not designed to be a trial on the merits.”
The belief that plaintiffs’ attorneys frequently bring weak cases and use unqualified experts to certify claims is not realistic or logical, added Sean Domnick, JD, a Florida medical malpractice attorney and vice president for the American Association for Justice. Medical malpractice cases are extremely challenging for plaintiffs – and they’re expensive, Mr. Domnick said.
“We can’t afford to take bad cases,” he said. “For me to take on a medical malpractice case, it’s not unusual for me to spend well over $100,000. Remember, if we lose, I don’t get that money back and I don’t get paid. Why in the world would a plaintiff take on that type of a burden for a case they didn’t believe in? The logic escapes me.”
In Florida, where Mr. Domnick practices, plaintiffs’ attorneys must send their certificates of merit to the defense with the expert identified. Domnick believes the requirement is a hindrance.
“It creates a delay that is unnecessary in a system that is already designed to wear our clients down,” he said. “It’s just another component that makes it harder on them.”
Hidden experts may insulate plaintiffs’ attorneys from liability
Dr. Sullivan, the Illinois emergency physician, was ultimately dismissed from the multiparty lawsuit, but not for roughly 18 months. After the dismissal, he fought back. He sued the plaintiff’s law firm for malicious prosecution, negligence in hiring, and relying on the opinion of an expert who was unqualified to render an opinion against an emergency physician.
The law firm, however, argued that it was immune from liability because it reasonably relied on the expert’s opinion as required by Illinois law. A trial court agreed with the plaintiffs’ firm. The judge denied Dr. Sullivan’s request to identify the expert, ruling there was no finding that the affidavit was untrue or made without reasonable cause. Dr. Sullivan appealed, and the appellate court upheld the trial’s court decision.
“As happened with my case, law firms can use the affidavit as a defense against countersuits or motions for sanctions,” Dr. Sullivan said. “Although the certificate of merit is intended to prevent attorneys from filing frivolous cases, it can also have the opposite effect of helping to insulate plaintiff attorneys from liability for filing a frivolous lawsuit.”
In Colorado, complaints about the state’s certificate of merit statute have gone before the Colorado Supreme Court. In one case, a lower court ruled that a certificate of merit was deficient because the consultants were not chiropractors. In another case, a nurse defendant argued the claim’s certificate of review was insufficient because the consulting expert was a physician.
In both instances, Colorado judges held the state’s statute does not require consultants to be in the same profession or the same specialty as the health professional defendant.
In New York, meanwhile, Mr. Auster said several bills to strengthen the state’s certificate of merit requirements have failed in recent years.
“It’s hard to say whether it will improve anytime soon,” he said. “The trial lawyers are a very powerful advocacy force in the state, and they tend to oppose even the slightest of changes in civil liability. [In addition], some of these issues have been put on a lower tier because of trying to manage the pandemic.”
Ultimately, Dr. Sullivan said that courts and legislatures need to strongly consider the ethics of allowing anonymous experts to provide testimony against defendant physicians.
“I also think we need to consider how the notion of a secret expert comports with a defendant physician’s due process,” he said. “If an expert’s opinion is appropriate, why would there be a need to shroud one’s identity in a veil of secrecy?”
A version of this article first appeared on Medscape.com.
When the hospital’s trauma team could not get an IV inserted into an accident victim, they called Illinois emergency physician William Sullivan, DO, JD, for help. Dr. Sullivan, who is based in the Chicago suburb of Frankfort, inserted a central line into the patient’s leg on his first attempt – a task that took about 20 minutes.
A year later, Dr. Sullivan was shocked and angry to learn he was being sued by the trauma patient’s family. Inserting the line was his only interaction with the woman, and he had no role in her care management, he said. Yet, the suit claimed he was negligent for failing to diagnose the patient with internal bleeding and for not performing surgery.
“The lawsuit put a lot of stress on our family,” Dr. Sullivan recalled. “At the time my wife was pregnant. I was in law school, and I was also working full time in the ER to support our family. I remember my wife crying on the couch after reading the complaint and asking how the plaintiff’s attorney could get away with making the allegations he made.”
Dr. Sullivan soon learned that 15 medical providers in the patient’s medical record were named as defendants. This included the director of the radiology department, whose name was on a radiology report as “director” but who was actually out of the country when the incident occurred.
Despite some of the accusations being impossible, a medical expert had claimed there was a “meritorious claim” against every health professional named in the suit. Illinois is among the 28 states that require plaintiffs’ attorneys to file an affidavit of merit for medical malpractice claims to move forward.
Dr. Sullivan wondered who would endorse such outlandish accusations, but the expert’s identity was a mystery. According to Illinois law, About one-third of states with merit requirements permit anonymous experts, according to research and attorneys familiar with the issue.
Because the expert’s identity remains hidden, physicians have no way of knowing whether they were qualified to render an opinion, Dr. Sullivan said. The loopholes can drag out frivolous claims and waste significant time and expense, say legal experts. Frequently, it takes a year or more before innocent physicians are dismissed from unfounded lawsuits by the court or dropped when plaintiffs can’t support the claim.
“It’s hugely frustrating,” said Bruce Montoya, JD, a Colorado medical liability defense attorney. “You have an expert who is not disclosed. Further down the road, when experts are being deposed, the plaintiff does not have to reveal whether any of those testifying experts is the same one who certified the case. You never get to determine whether they, in fact, had a certificate reviewer who was legitimate.”
The laws have led to a recent outcry among physicians and fueled a revised resolution by the American College of Emergency Physicians (ACEP) denouncing anonymous affidavits of merit. (The revision has not yet been published online.)
“The minute experts are identified, they can be vetted,” said Rade B. Vukmir, MD, JD, chair of ACEP’s Medical Legal Committee. “There are reasons that you want to clarify the qualification and veracity of the witness. [Anonymous affidavits of merit] don’t allow that, and there’s something inherently wrong with that.”
Because the identities of consulting experts are unknown, it’s hard to know how many are unqualified. Expert witnesses who testify during trials, on the other hand, have long come under scrutiny for questionable qualifications. Some have come under fire for allegedly lying under oath about their experience, misrepresenting their credentials, and falsely representing their knowledge.
“Considering the known problem of potentially unethical expert witness testimony at trial, there’s is the potential likelihood that experts in anonymous affidavits of merit may sometimes lack the qualifications to give opinions,” said Dr. Vukmir, an emergency care physician in Pittsburgh.
Attorneys: Hidden experts increase costs, waste time
In Colorado, Mr. Montoya has seen firsthand how anonymous experts can prolong questionable claims and burden defendants.
Like Illinois, Colorado does not require attorneys to identify the medical experts used to fulfill its certificate of review statute. The expert consulted must have expertise in the same area of the alleged negligence, but does not have to practice in the same specialty, and the statute allows one expert to certify a lawsuit against multiple doctors.
In a recent case, Mr. Montoya represented a Denver neurosurgeon who was sued along with multiple other health care professionals. From the outset, Mr. Montoya argued the claim had no merit against the neurosurgeon, but the plaintiff’s attorney refused to dismiss the physician. Mr. Montoya asked whether the expert consulted for the certificate of merit was a neurosurgeon, but the attorney declined to disclose that information, he said.
The case progressed and Mr. Montoya eventually asked the judge to review the certificate of merit. By law, a judge can confidentially review the certificate of merit and decide whether it aligns with the state statute, but without disclosing the expert’s identity to the defense. The judge ruled the certificate appeared to conform with state law, and the case continued.
A year later, as both sides were getting ready to disclose their experts who would testify, Mr. Montoya again argued the neurosurgeon should be dropped from the suit. This time, he warned if the claim continued against the neurosurgeon, the defense would be filing a motion for summary judgment and pursuing attorney fees and costs. Colorado law allows for such fees if the filing or pursuit of an action is frivolous.
“Boom, my client was dismissed,” Mr. Montoya said. “This is a year later, after multiple conferences among the attorneys, multiple pleadings filed, expert witnesses retained to review the care, discovery exchanged, and records obtained. If we had [a stronger] certificate of review statute, it would have been a different ballgame. It’s never going to get a year down the road.”
In New York, physician defendants have experienced similar woes. The state’s law requires plaintiffs’ attorneys to certify that they consulted with a physician prior to filing the claim, and that they believe based on that discussion, there’s a reasonable basis for the claim to move forward. Attorneys are not required to disclose the expert’s identity.
The law also allows “an out,” explained Morris Auster, JD, senior vice president and chief legislative counsel for the Medical Society of the State of New York. If the attorney made three separate attempts to obtain a consultation, and all three experts would not agree to the consultation, the lawsuit can be filed anyway, he said.
“From our standpoint, it’s important to have an affidavit of merit requirement; it’s better than not having it,” Mr. Auster said. “But its effectiveness in providing control over the filing of lawsuits in New York has never been as strong as it could’ve been.”
Mr. Auster notes that New York has some of the highest liability costs in the country in addition to doctors paying some of the steepest medical liability insurance premiums.
“This really affects a lot of physicians and it’s driving physicians into employment arrangements, so they don’t have to deal with it on their own,” he said. “We support a number of measures to address these significantly high costs, and stronger certificate of merit requirements would certainly be one of those advocacy goals.”
Why are anonymous experts allowed?
Certificates of merit that shield the identity of consultants encourage a greater pool of physicians willing to review cases, said J. Matthew Dudley, JD, president of the Illinois Trial Lawyers Association. When the requirements first went into effect in Illinois, there was significant animosity among physicians toward doctors who testified in medical malpractice cases for patients, Mr. Dudley explained.
“Sometimes they would be ostracized from their professional societies, or it would hurt a referral relationship.” he said. “Over time, that animosity has lessened, but there was a concern that if the identity of physicians in certificates of merit weren’t protected, then doctors would not look at cases for patients.”
This would result in additional barriers for patients and their attorneys in pursuing their legal rights, Mr. Dudley said. He said Illinois’ certificate of merit statute is successful in fulfilling its intended purpose, and he has not seen any statistical evidence to suggest otherwise.
“It has proven effective at decreasing filings in medical malpractice and effectively screening medical malpractice cases,” he said. “Certificates of merit help to decrease filings by firms that aren’t that experienced in dealing with those kinds of cases.”
Kentucky is another state that does not require attorneys to identity the experts consulted for certificates of merit. Malpractice defense attorney Andrew DeSimone, JD, who practices in Kentucky, said this isn’t a problem since attorneys eventually must disclose the expert witnesses who will testify at trial.
“Knowing the name behind the certificate of merit is not that pertinent,” Mr. DeSimone said. “Physicians and their attorneys will ultimately have the chance to question and evaluate the expert witnesses used at trial. The certificate of merit is designed to weed out totally frivolous cases that do not have expert support. It’s not designed to be a trial on the merits.”
The belief that plaintiffs’ attorneys frequently bring weak cases and use unqualified experts to certify claims is not realistic or logical, added Sean Domnick, JD, a Florida medical malpractice attorney and vice president for the American Association for Justice. Medical malpractice cases are extremely challenging for plaintiffs – and they’re expensive, Mr. Domnick said.
“We can’t afford to take bad cases,” he said. “For me to take on a medical malpractice case, it’s not unusual for me to spend well over $100,000. Remember, if we lose, I don’t get that money back and I don’t get paid. Why in the world would a plaintiff take on that type of a burden for a case they didn’t believe in? The logic escapes me.”
In Florida, where Mr. Domnick practices, plaintiffs’ attorneys must send their certificates of merit to the defense with the expert identified. Domnick believes the requirement is a hindrance.
“It creates a delay that is unnecessary in a system that is already designed to wear our clients down,” he said. “It’s just another component that makes it harder on them.”
Hidden experts may insulate plaintiffs’ attorneys from liability
Dr. Sullivan, the Illinois emergency physician, was ultimately dismissed from the multiparty lawsuit, but not for roughly 18 months. After the dismissal, he fought back. He sued the plaintiff’s law firm for malicious prosecution, negligence in hiring, and relying on the opinion of an expert who was unqualified to render an opinion against an emergency physician.
The law firm, however, argued that it was immune from liability because it reasonably relied on the expert’s opinion as required by Illinois law. A trial court agreed with the plaintiffs’ firm. The judge denied Dr. Sullivan’s request to identify the expert, ruling there was no finding that the affidavit was untrue or made without reasonable cause. Dr. Sullivan appealed, and the appellate court upheld the trial’s court decision.
“As happened with my case, law firms can use the affidavit as a defense against countersuits or motions for sanctions,” Dr. Sullivan said. “Although the certificate of merit is intended to prevent attorneys from filing frivolous cases, it can also have the opposite effect of helping to insulate plaintiff attorneys from liability for filing a frivolous lawsuit.”
In Colorado, complaints about the state’s certificate of merit statute have gone before the Colorado Supreme Court. In one case, a lower court ruled that a certificate of merit was deficient because the consultants were not chiropractors. In another case, a nurse defendant argued the claim’s certificate of review was insufficient because the consulting expert was a physician.
In both instances, Colorado judges held the state’s statute does not require consultants to be in the same profession or the same specialty as the health professional defendant.
In New York, meanwhile, Mr. Auster said several bills to strengthen the state’s certificate of merit requirements have failed in recent years.
“It’s hard to say whether it will improve anytime soon,” he said. “The trial lawyers are a very powerful advocacy force in the state, and they tend to oppose even the slightest of changes in civil liability. [In addition], some of these issues have been put on a lower tier because of trying to manage the pandemic.”
Ultimately, Dr. Sullivan said that courts and legislatures need to strongly consider the ethics of allowing anonymous experts to provide testimony against defendant physicians.
“I also think we need to consider how the notion of a secret expert comports with a defendant physician’s due process,” he said. “If an expert’s opinion is appropriate, why would there be a need to shroud one’s identity in a veil of secrecy?”
A version of this article first appeared on Medscape.com.
‘Together, we can demand improvements’: Stanford Health Care’s residents vote to join union
More than 81% of the health system’s resident physicians voted to join the union; the decision garnered 835 yes votes and 214 no votes, according to a CIR-SEIU announcement. The largest housestaff union in the United States and a local of the Service Employees International Union (SEIU), CIR-SEIU represents more than 20,000 resident physicians and fellows.
“With its successful representation with the Committee of Interns and Residents, Stanford housestaff now join the strong community of allied unions and fellow health care workers such as the Committee for Recognition of Nursing Achievement (CRONA), an independent union of Stanford nurses,” according to CIR-SEIU.
“We are organizing not only for a new economic contract that enables all potential housestaff and their families to afford living in the Bay Area but also for a new social contract that redefines how we are valued by the hospital system,” Ben Solomon, MD, PhD, a third-year resident physician in pediatrics at Stanford Medicine and a member of CIR-SEIU, said in an interview.
“This includes advocating for more humane working hours, reasonable parental leave, and childcare support, as well as resources to combat burnout in young physicians,” he added.
Lisa Kim, a spokesperson for Stanford Health Care, told this news organization that “a majority of residents and fellows at Stanford Health Care voted in favor of unionization. Of 1,478 total residents and fellows, 835 voted in favor. CIR/SEIU will be certified as the exclusive bargaining representative for all residents and fellows. Stanford Health Care does not plan to contest the election results.”
“As we begin the collective bargaining process, our goal remains unchanged: providing our residents and fellows with a world-class training experience. We will bring this same focus to negotiations as we strive to support their development as physician leaders,” she added.
The National Labor Relations Board (NLRB) must certify the election results before they are considered final, per CIR-SEIU. An independent federal agency, the NLRB safeguards employees’ rights to organize and determines whether union participation is appropriate while also preventing and remedying unfair labor practices committed by private sector employers and unions.
Concerns date back to initial COVID-19 vaccine rollout
The residents delivered a formal demand to Stanford Health Care to recognize the union in February; their request was not accepted by the health system. The residents’ concerns date as far back as the availability of the COVID-19 vaccines at the end of 2020.
Of the health system’s 5,000 doses, only seven residents and fellows were included in the initial round.
Niraj Sehgal, MD, chief medical officer for Stanford Health Care, apologized in a letter to the graduate medical education community, posted by Palo Alto Weekly, which revealed the root causes to be an algorithm used by the hospital and the age of the residents.
The vote by Stanford Health Care’s residents comes a day after nurses at Stanford and Lucile Packard Children’s hospitals ratified a new contract with their union after a strike for better working conditions and higher pay stretched on for a week, reported Palo Alto Online.
Part of a growing trend
Dr. Solomon got involved in the unionization effort at Stanford Health Care “to have a say in working conditions for residents and fellows,” he said. “As individuals, it’s virtually impossible to make demands to our hospital without risking our careers, but together we can demand improvements on the job and in patient care.”
The health system’s inability to extend COVID-19 vaccines during the initial rollout, “despite our role working with COVID patients on the frontlines,” spurred his involvement in the union effort, said Dr. Solomon.
In the short term, the union will be involved in negotiating its first contract, he said. “However, in the long term, we are committed to supporting the unionization efforts of residents and fellows across the country, including partnering with many housestaff unions here in California.”
Stanford Health Care’s residents are participating in a growing trend. In Worcester, Mass., UMass Medical School’s 613 residents and fellow physicians, who are also represented by CIR-SEIU, had their union certified by the Massachusetts Department of Labor Relations in March 2021, reported the (Worcester) Telegram & Gazette.
Other unionization efforts across the country include a supermajority of 85 interns, residents, and fellows employed by Keck School of Medicine of University of Southern California , who requested that Los Angeles County+USC Medical Center recognize their union, per an announcement. That’s in addition to residents at University of Vermont Medical Center, who announced their intention to unionize in March, reported VTDigger.org.
A version of this article first appeared on Medscape.com.
More than 81% of the health system’s resident physicians voted to join the union; the decision garnered 835 yes votes and 214 no votes, according to a CIR-SEIU announcement. The largest housestaff union in the United States and a local of the Service Employees International Union (SEIU), CIR-SEIU represents more than 20,000 resident physicians and fellows.
“With its successful representation with the Committee of Interns and Residents, Stanford housestaff now join the strong community of allied unions and fellow health care workers such as the Committee for Recognition of Nursing Achievement (CRONA), an independent union of Stanford nurses,” according to CIR-SEIU.
“We are organizing not only for a new economic contract that enables all potential housestaff and their families to afford living in the Bay Area but also for a new social contract that redefines how we are valued by the hospital system,” Ben Solomon, MD, PhD, a third-year resident physician in pediatrics at Stanford Medicine and a member of CIR-SEIU, said in an interview.
“This includes advocating for more humane working hours, reasonable parental leave, and childcare support, as well as resources to combat burnout in young physicians,” he added.
Lisa Kim, a spokesperson for Stanford Health Care, told this news organization that “a majority of residents and fellows at Stanford Health Care voted in favor of unionization. Of 1,478 total residents and fellows, 835 voted in favor. CIR/SEIU will be certified as the exclusive bargaining representative for all residents and fellows. Stanford Health Care does not plan to contest the election results.”
“As we begin the collective bargaining process, our goal remains unchanged: providing our residents and fellows with a world-class training experience. We will bring this same focus to negotiations as we strive to support their development as physician leaders,” she added.
The National Labor Relations Board (NLRB) must certify the election results before they are considered final, per CIR-SEIU. An independent federal agency, the NLRB safeguards employees’ rights to organize and determines whether union participation is appropriate while also preventing and remedying unfair labor practices committed by private sector employers and unions.
Concerns date back to initial COVID-19 vaccine rollout
The residents delivered a formal demand to Stanford Health Care to recognize the union in February; their request was not accepted by the health system. The residents’ concerns date as far back as the availability of the COVID-19 vaccines at the end of 2020.
Of the health system’s 5,000 doses, only seven residents and fellows were included in the initial round.
Niraj Sehgal, MD, chief medical officer for Stanford Health Care, apologized in a letter to the graduate medical education community, posted by Palo Alto Weekly, which revealed the root causes to be an algorithm used by the hospital and the age of the residents.
The vote by Stanford Health Care’s residents comes a day after nurses at Stanford and Lucile Packard Children’s hospitals ratified a new contract with their union after a strike for better working conditions and higher pay stretched on for a week, reported Palo Alto Online.
Part of a growing trend
Dr. Solomon got involved in the unionization effort at Stanford Health Care “to have a say in working conditions for residents and fellows,” he said. “As individuals, it’s virtually impossible to make demands to our hospital without risking our careers, but together we can demand improvements on the job and in patient care.”
The health system’s inability to extend COVID-19 vaccines during the initial rollout, “despite our role working with COVID patients on the frontlines,” spurred his involvement in the union effort, said Dr. Solomon.
In the short term, the union will be involved in negotiating its first contract, he said. “However, in the long term, we are committed to supporting the unionization efforts of residents and fellows across the country, including partnering with many housestaff unions here in California.”
Stanford Health Care’s residents are participating in a growing trend. In Worcester, Mass., UMass Medical School’s 613 residents and fellow physicians, who are also represented by CIR-SEIU, had their union certified by the Massachusetts Department of Labor Relations in March 2021, reported the (Worcester) Telegram & Gazette.
Other unionization efforts across the country include a supermajority of 85 interns, residents, and fellows employed by Keck School of Medicine of University of Southern California , who requested that Los Angeles County+USC Medical Center recognize their union, per an announcement. That’s in addition to residents at University of Vermont Medical Center, who announced their intention to unionize in March, reported VTDigger.org.
A version of this article first appeared on Medscape.com.
More than 81% of the health system’s resident physicians voted to join the union; the decision garnered 835 yes votes and 214 no votes, according to a CIR-SEIU announcement. The largest housestaff union in the United States and a local of the Service Employees International Union (SEIU), CIR-SEIU represents more than 20,000 resident physicians and fellows.
“With its successful representation with the Committee of Interns and Residents, Stanford housestaff now join the strong community of allied unions and fellow health care workers such as the Committee for Recognition of Nursing Achievement (CRONA), an independent union of Stanford nurses,” according to CIR-SEIU.
“We are organizing not only for a new economic contract that enables all potential housestaff and their families to afford living in the Bay Area but also for a new social contract that redefines how we are valued by the hospital system,” Ben Solomon, MD, PhD, a third-year resident physician in pediatrics at Stanford Medicine and a member of CIR-SEIU, said in an interview.
“This includes advocating for more humane working hours, reasonable parental leave, and childcare support, as well as resources to combat burnout in young physicians,” he added.
Lisa Kim, a spokesperson for Stanford Health Care, told this news organization that “a majority of residents and fellows at Stanford Health Care voted in favor of unionization. Of 1,478 total residents and fellows, 835 voted in favor. CIR/SEIU will be certified as the exclusive bargaining representative for all residents and fellows. Stanford Health Care does not plan to contest the election results.”
“As we begin the collective bargaining process, our goal remains unchanged: providing our residents and fellows with a world-class training experience. We will bring this same focus to negotiations as we strive to support their development as physician leaders,” she added.
The National Labor Relations Board (NLRB) must certify the election results before they are considered final, per CIR-SEIU. An independent federal agency, the NLRB safeguards employees’ rights to organize and determines whether union participation is appropriate while also preventing and remedying unfair labor practices committed by private sector employers and unions.
Concerns date back to initial COVID-19 vaccine rollout
The residents delivered a formal demand to Stanford Health Care to recognize the union in February; their request was not accepted by the health system. The residents’ concerns date as far back as the availability of the COVID-19 vaccines at the end of 2020.
Of the health system’s 5,000 doses, only seven residents and fellows were included in the initial round.
Niraj Sehgal, MD, chief medical officer for Stanford Health Care, apologized in a letter to the graduate medical education community, posted by Palo Alto Weekly, which revealed the root causes to be an algorithm used by the hospital and the age of the residents.
The vote by Stanford Health Care’s residents comes a day after nurses at Stanford and Lucile Packard Children’s hospitals ratified a new contract with their union after a strike for better working conditions and higher pay stretched on for a week, reported Palo Alto Online.
Part of a growing trend
Dr. Solomon got involved in the unionization effort at Stanford Health Care “to have a say in working conditions for residents and fellows,” he said. “As individuals, it’s virtually impossible to make demands to our hospital without risking our careers, but together we can demand improvements on the job and in patient care.”
The health system’s inability to extend COVID-19 vaccines during the initial rollout, “despite our role working with COVID patients on the frontlines,” spurred his involvement in the union effort, said Dr. Solomon.
In the short term, the union will be involved in negotiating its first contract, he said. “However, in the long term, we are committed to supporting the unionization efforts of residents and fellows across the country, including partnering with many housestaff unions here in California.”
Stanford Health Care’s residents are participating in a growing trend. In Worcester, Mass., UMass Medical School’s 613 residents and fellow physicians, who are also represented by CIR-SEIU, had their union certified by the Massachusetts Department of Labor Relations in March 2021, reported the (Worcester) Telegram & Gazette.
Other unionization efforts across the country include a supermajority of 85 interns, residents, and fellows employed by Keck School of Medicine of University of Southern California , who requested that Los Angeles County+USC Medical Center recognize their union, per an announcement. That’s in addition to residents at University of Vermont Medical Center, who announced their intention to unionize in March, reported VTDigger.org.
A version of this article first appeared on Medscape.com.
Telehealth continues to loom large, say experts
This physician, Brian Hasselfeld, MD, said his university’s health system did 50-80 telemedicine visits a month before COVID, during a presentation at the annual meeting of the American College of Physicians. This soared to close to 100,000 a month in the pandemic, and now the health system does close to 40,000 a month, he continued.
“Life is definitely different in how we engage with our patients on a day-to-day basis,” said Dr. Hasselfeld, who oversees the telehealth for six hospitals and 50 ambulatory-care locations in Maryland and three other states.
Attitudes gauged in Johns Hopkins surveys suggest that a lot of medical care will continue to be provided by telemedicine. Nine out of 10 patients said they would likely recommend telemedicine to friends and family, and 88% said it would be either moderately, very, or extremely important to have video visit options in the future, he said.
A survey of the Hopkins system’s 3,600 physicians, which generated about 1,300 responses, found that physicians would like to have a considerable chunk of time set aside for telemedicine visits – the median response was 30%.
Virtual care is in ‘early-adopter phase’
But Dr. Hasselfeld said virtual care is still in the “early-adopter phase.” While many physicians said they would like more than half of their time devoted to telehealth, a larger proportion was more likely to say they wanted very little time devoted to it, Dr. Hasselfeld said. Among those wanting to do it are some who want to do all of their visits virtually, he said.
Those who are eager to do it will be those guiding the change, Dr. Hasselfeld said.
“As we move forward – and thinking about how to optimize virtual-care options for your patients – it’s not going to be a forced issue,” he said.
Providing better access to certain patient groups continues to be a challenge. A dashboard developed at Hopkins to identify groups who are at a technological disadvantage and don’t have ready access to telemedicine found that those living in low-income zip codes, African-Americans, and those on Medicaid and Medicare tend to have higher percentages of “audio-only” visits, mainly because of lack of connectivity allowing video visits, Dr. Hasselfeld said.
The lower share of video visits in the inner city suggests that access to telemedicine isn’t just a problem in remote rural areas, as the conventional wisdom has gone, he said.
“It doesn’t matter how many towers we have in downtown Baltimore, or how much fiber we have in the ground,” he said. “If you can’t have a data plan to access that high-speed Internet, or have a home with high-speed Internet, it doesn’t matter.”
Hopkins has developed a tool to assess how likely it is that someone will have trouble connecting for a telemedicine visit – if they’ve previously had an audio-only visit, for instance – and try to get in touch with those patients shortly before a visit so that it runs smoothly, Dr. Hasselfeld said.
The explosion of telemedicine has led to the rise of companies providing care through apps on phones and tablets, he said.
“This is real care being provided to our patients through nontraditional routes, and this is a new force, one our patients see out in the marketplace,” he said. “We have to acknowledge and wrestle with the fact that convenience is a new part of what it means to [provide] access [to] care for patients.”
Heather Hirsch, MD, an internist with Brigham and Women’s Hospital in Boston, said in an interview after the session that telemedicine is poised to improve care.
“I think the good is definitely going to outweigh the bad so long as the infrastructure and the legislation will allow it,” said Dr. Hirsch, who does about half of her visits in person and half through telemedicine, which she performs while at the office. “It does allow for a lot of flexibility for both patients and providers.”
But health care at academic medical centers, she said, needs to adjust to the times.
“We need [academic medicine] for so many reasons,” she said, “but the reality is that it moves very slowly, and the old infrastructure and the slowness to catch up with technology is the worry.”
Dr. Hasselfeld reported financial relationships with Humana and TRUE-See Systems.
This physician, Brian Hasselfeld, MD, said his university’s health system did 50-80 telemedicine visits a month before COVID, during a presentation at the annual meeting of the American College of Physicians. This soared to close to 100,000 a month in the pandemic, and now the health system does close to 40,000 a month, he continued.
“Life is definitely different in how we engage with our patients on a day-to-day basis,” said Dr. Hasselfeld, who oversees the telehealth for six hospitals and 50 ambulatory-care locations in Maryland and three other states.
Attitudes gauged in Johns Hopkins surveys suggest that a lot of medical care will continue to be provided by telemedicine. Nine out of 10 patients said they would likely recommend telemedicine to friends and family, and 88% said it would be either moderately, very, or extremely important to have video visit options in the future, he said.
A survey of the Hopkins system’s 3,600 physicians, which generated about 1,300 responses, found that physicians would like to have a considerable chunk of time set aside for telemedicine visits – the median response was 30%.
Virtual care is in ‘early-adopter phase’
But Dr. Hasselfeld said virtual care is still in the “early-adopter phase.” While many physicians said they would like more than half of their time devoted to telehealth, a larger proportion was more likely to say they wanted very little time devoted to it, Dr. Hasselfeld said. Among those wanting to do it are some who want to do all of their visits virtually, he said.
Those who are eager to do it will be those guiding the change, Dr. Hasselfeld said.
“As we move forward – and thinking about how to optimize virtual-care options for your patients – it’s not going to be a forced issue,” he said.
Providing better access to certain patient groups continues to be a challenge. A dashboard developed at Hopkins to identify groups who are at a technological disadvantage and don’t have ready access to telemedicine found that those living in low-income zip codes, African-Americans, and those on Medicaid and Medicare tend to have higher percentages of “audio-only” visits, mainly because of lack of connectivity allowing video visits, Dr. Hasselfeld said.
The lower share of video visits in the inner city suggests that access to telemedicine isn’t just a problem in remote rural areas, as the conventional wisdom has gone, he said.
“It doesn’t matter how many towers we have in downtown Baltimore, or how much fiber we have in the ground,” he said. “If you can’t have a data plan to access that high-speed Internet, or have a home with high-speed Internet, it doesn’t matter.”
Hopkins has developed a tool to assess how likely it is that someone will have trouble connecting for a telemedicine visit – if they’ve previously had an audio-only visit, for instance – and try to get in touch with those patients shortly before a visit so that it runs smoothly, Dr. Hasselfeld said.
The explosion of telemedicine has led to the rise of companies providing care through apps on phones and tablets, he said.
“This is real care being provided to our patients through nontraditional routes, and this is a new force, one our patients see out in the marketplace,” he said. “We have to acknowledge and wrestle with the fact that convenience is a new part of what it means to [provide] access [to] care for patients.”
Heather Hirsch, MD, an internist with Brigham and Women’s Hospital in Boston, said in an interview after the session that telemedicine is poised to improve care.
“I think the good is definitely going to outweigh the bad so long as the infrastructure and the legislation will allow it,” said Dr. Hirsch, who does about half of her visits in person and half through telemedicine, which she performs while at the office. “It does allow for a lot of flexibility for both patients and providers.”
But health care at academic medical centers, she said, needs to adjust to the times.
“We need [academic medicine] for so many reasons,” she said, “but the reality is that it moves very slowly, and the old infrastructure and the slowness to catch up with technology is the worry.”
Dr. Hasselfeld reported financial relationships with Humana and TRUE-See Systems.
This physician, Brian Hasselfeld, MD, said his university’s health system did 50-80 telemedicine visits a month before COVID, during a presentation at the annual meeting of the American College of Physicians. This soared to close to 100,000 a month in the pandemic, and now the health system does close to 40,000 a month, he continued.
“Life is definitely different in how we engage with our patients on a day-to-day basis,” said Dr. Hasselfeld, who oversees the telehealth for six hospitals and 50 ambulatory-care locations in Maryland and three other states.
Attitudes gauged in Johns Hopkins surveys suggest that a lot of medical care will continue to be provided by telemedicine. Nine out of 10 patients said they would likely recommend telemedicine to friends and family, and 88% said it would be either moderately, very, or extremely important to have video visit options in the future, he said.
A survey of the Hopkins system’s 3,600 physicians, which generated about 1,300 responses, found that physicians would like to have a considerable chunk of time set aside for telemedicine visits – the median response was 30%.
Virtual care is in ‘early-adopter phase’
But Dr. Hasselfeld said virtual care is still in the “early-adopter phase.” While many physicians said they would like more than half of their time devoted to telehealth, a larger proportion was more likely to say they wanted very little time devoted to it, Dr. Hasselfeld said. Among those wanting to do it are some who want to do all of their visits virtually, he said.
Those who are eager to do it will be those guiding the change, Dr. Hasselfeld said.
“As we move forward – and thinking about how to optimize virtual-care options for your patients – it’s not going to be a forced issue,” he said.
Providing better access to certain patient groups continues to be a challenge. A dashboard developed at Hopkins to identify groups who are at a technological disadvantage and don’t have ready access to telemedicine found that those living in low-income zip codes, African-Americans, and those on Medicaid and Medicare tend to have higher percentages of “audio-only” visits, mainly because of lack of connectivity allowing video visits, Dr. Hasselfeld said.
The lower share of video visits in the inner city suggests that access to telemedicine isn’t just a problem in remote rural areas, as the conventional wisdom has gone, he said.
“It doesn’t matter how many towers we have in downtown Baltimore, or how much fiber we have in the ground,” he said. “If you can’t have a data plan to access that high-speed Internet, or have a home with high-speed Internet, it doesn’t matter.”
Hopkins has developed a tool to assess how likely it is that someone will have trouble connecting for a telemedicine visit – if they’ve previously had an audio-only visit, for instance – and try to get in touch with those patients shortly before a visit so that it runs smoothly, Dr. Hasselfeld said.
The explosion of telemedicine has led to the rise of companies providing care through apps on phones and tablets, he said.
“This is real care being provided to our patients through nontraditional routes, and this is a new force, one our patients see out in the marketplace,” he said. “We have to acknowledge and wrestle with the fact that convenience is a new part of what it means to [provide] access [to] care for patients.”
Heather Hirsch, MD, an internist with Brigham and Women’s Hospital in Boston, said in an interview after the session that telemedicine is poised to improve care.
“I think the good is definitely going to outweigh the bad so long as the infrastructure and the legislation will allow it,” said Dr. Hirsch, who does about half of her visits in person and half through telemedicine, which she performs while at the office. “It does allow for a lot of flexibility for both patients and providers.”
But health care at academic medical centers, she said, needs to adjust to the times.
“We need [academic medicine] for so many reasons,” she said, “but the reality is that it moves very slowly, and the old infrastructure and the slowness to catch up with technology is the worry.”
Dr. Hasselfeld reported financial relationships with Humana and TRUE-See Systems.
AT INTERNAL MEDICINE 2022
New toolkit offers help for climate change anxiety
These strategies include volunteering, building a community, discussing emotions with others, practicing mindfulness, and seeking therapy.
The toolkit, which was developed by nursing experts at the University of British Columbia in Vancouver, also offers reflection questions and a film with diverse voices for people to examine their values, emotions, and behaviors in relation to the environment.

“Many people have a hard time understanding the relationship between climate change and mental health and are experiencing high levels of stress about climate change,” Natania Abebe, MSN/MPH, RN, a registered nurse and graduate student at UBC who developed the toolkit, told this news organization.
“Youth, in particular, appear to have higher levels of consciousness regarding climate change because they’re the ones who are going to inherit the planet,” she said. “A big part of why they have mental health issues is that they feel trapped in sociopolitical structures that they didn’t agree to and didn’t necessarily create.”
The toolkit was published online on April 20.
Empowering agents for change
Ms. Abebe was inspired to create the toolkit after giving guest lectures on climate change and mental health as part of UBC’s Nursing 290 course. Her faculty advisor, Raluca Radu, MSN, a lecturer in the School of Nursing at UBC, developed the course in 2020 to teach students about the broad impacts of climate change on communities.

As the course has grown during the past 2 years, Ms. Abebe wanted to create a coping framework and engaging film for health educators to use with students, as well as for everyday people.
The toolkit includes contributions from three Canadian climate change experts, as well as six students from different backgrounds who have taken the course.
“I wanted to center the voices of youth and empower them to think they can be agents for change,” Ms. Abebe said. “I also wanted to highlight diverse voices and take a collaborative approach because climate change is such a big problem that we have to come together to address it.”
Ms. Abebe and Ms. Radu also noticed an increase in climate anxiety in recent years because of the pandemic, worldwide food and energy shortages, and extreme weather events that hit close to home, such as wildfires and floods in British Columbia.
“With the pandemic, people have been spending more time online and thinking about our world at large,” Ms. Abebe said. “At the same time that they’re thinking about it, climate change events are happening simultaneously – not in the future, but right now.”
Economic, social, and political shifts during the past 2 years have also prompted people to question standard practices and institutions, which has created an opportunity to discuss change, Ms. Radu told this news organization.
“It’s a pivotal time to question our values and highly consumerist society,” she said. “We’re at a point in time where, if we don’t take action, the planetary health will be in an irreversible state, and we won’t be able to turn back time and make changes.”
Our psyches and nature
The toolkit includes three main sections that feature video clips and reflective questions around eco-anxiety, eco-paralysis, and ecological grief.
In the first section, eco-anxiety is defined as a “chronic fear of environmental doom,” which could include anxiousness around the likelihood of a severe weather event because of ongoing news coverage and social media. The reflective questions prompt readers to discuss eco-anxiety in their life, work through their emotions, understand their beliefs and values, and determine how to use them to address climate change anxiety.
The second section defines eco-paralysis as the powerlessness that people may feel when they don’t believe they can do anything meaningful on an individual level to address climate change. Paralysis can look like apathy, complacency, or disengagement. The questions prompt readers to observe how paralysis may show up in their lives, explore the tension between individual versus collective responsibility, and consider ways to address their sense of helplessness about climate change.
In the third section, ecological grief centers around “experienced or anticipated ecological losses,” which could include the loss of species, ecosystems, and landscapes because of short- or long-term environmental change. The questions prompt readers to explore their feelings, beliefs, and values and feel empowered to address their ecological grief over climate change.
The toolkit also includes recommendations for books, journal articles, websites, podcasts, and meditations around mental health and climate change, as well as ways to get involved with others. For instance, health care practitioners can register with PaRx, a program in British Columbia that allows providers to prescribe time in nature to improve a client’s health. The program is being adopted across Canada, and people with a prescription can visit local and national parks, historic sites, and marine conservation areas for free.
“This is about recognizing that there is a connection between our psyches and nature, and by talking about it, we can name what we’re feeling,” Ms. Abebe said. “We can take action not only to handle our emotions, but also to live kinder and more sustainable lifestyles.”

Future work will need to focus on population-level approaches to climate change and mental health as well, including policy and financial support to address environmental changes directly.
“We need to start thinking beyond individualized approaches and focus on how to create supportive and resilient communities to respond to climate change,” Kiffer Card, PhD, executive director of the Mental Health and Climate Change Alliance and an assistant professor of health sciences at Simon Fraser University, Burnaby, B.C., told this news organization.
Dr. Card, who wasn’t involved in developing the toolkit, has researched recent trends around climate change anxiety in Canada and fielded questions from health care practitioners and mental health professionals who are looking for ways to help their patients.
“Communities need to be ready to stand up and respond to acute emergency disasters, and government leaders need to take this seriously,” he said. “Those who are experiencing climate anxiety now are the canaries in the coal mine for the severe weather events and consequences to come.”
The toolkit was developed with funding from the Alma Mater Society of the University of British Columbia, Vancouver. Ms. Abebe, Ms. Radu, and Dr. Card reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
These strategies include volunteering, building a community, discussing emotions with others, practicing mindfulness, and seeking therapy.
The toolkit, which was developed by nursing experts at the University of British Columbia in Vancouver, also offers reflection questions and a film with diverse voices for people to examine their values, emotions, and behaviors in relation to the environment.
“Many people have a hard time understanding the relationship between climate change and mental health and are experiencing high levels of stress about climate change,” Natania Abebe, MSN/MPH, RN, a registered nurse and graduate student at UBC who developed the toolkit, told this news organization.
“Youth, in particular, appear to have higher levels of consciousness regarding climate change because they’re the ones who are going to inherit the planet,” she said. “A big part of why they have mental health issues is that they feel trapped in sociopolitical structures that they didn’t agree to and didn’t necessarily create.”
The toolkit was published online on April 20.
Empowering agents for change
Ms. Abebe was inspired to create the toolkit after giving guest lectures on climate change and mental health as part of UBC’s Nursing 290 course. Her faculty advisor, Raluca Radu, MSN, a lecturer in the School of Nursing at UBC, developed the course in 2020 to teach students about the broad impacts of climate change on communities.
As the course has grown during the past 2 years, Ms. Abebe wanted to create a coping framework and engaging film for health educators to use with students, as well as for everyday people.
The toolkit includes contributions from three Canadian climate change experts, as well as six students from different backgrounds who have taken the course.
“I wanted to center the voices of youth and empower them to think they can be agents for change,” Ms. Abebe said. “I also wanted to highlight diverse voices and take a collaborative approach because climate change is such a big problem that we have to come together to address it.”
Ms. Abebe and Ms. Radu also noticed an increase in climate anxiety in recent years because of the pandemic, worldwide food and energy shortages, and extreme weather events that hit close to home, such as wildfires and floods in British Columbia.
“With the pandemic, people have been spending more time online and thinking about our world at large,” Ms. Abebe said. “At the same time that they’re thinking about it, climate change events are happening simultaneously – not in the future, but right now.”
Economic, social, and political shifts during the past 2 years have also prompted people to question standard practices and institutions, which has created an opportunity to discuss change, Ms. Radu told this news organization.
“It’s a pivotal time to question our values and highly consumerist society,” she said. “We’re at a point in time where, if we don’t take action, the planetary health will be in an irreversible state, and we won’t be able to turn back time and make changes.”
Our psyches and nature
The toolkit includes three main sections that feature video clips and reflective questions around eco-anxiety, eco-paralysis, and ecological grief.
In the first section, eco-anxiety is defined as a “chronic fear of environmental doom,” which could include anxiousness around the likelihood of a severe weather event because of ongoing news coverage and social media. The reflective questions prompt readers to discuss eco-anxiety in their life, work through their emotions, understand their beliefs and values, and determine how to use them to address climate change anxiety.
The second section defines eco-paralysis as the powerlessness that people may feel when they don’t believe they can do anything meaningful on an individual level to address climate change. Paralysis can look like apathy, complacency, or disengagement. The questions prompt readers to observe how paralysis may show up in their lives, explore the tension between individual versus collective responsibility, and consider ways to address their sense of helplessness about climate change.
In the third section, ecological grief centers around “experienced or anticipated ecological losses,” which could include the loss of species, ecosystems, and landscapes because of short- or long-term environmental change. The questions prompt readers to explore their feelings, beliefs, and values and feel empowered to address their ecological grief over climate change.
The toolkit also includes recommendations for books, journal articles, websites, podcasts, and meditations around mental health and climate change, as well as ways to get involved with others. For instance, health care practitioners can register with PaRx, a program in British Columbia that allows providers to prescribe time in nature to improve a client’s health. The program is being adopted across Canada, and people with a prescription can visit local and national parks, historic sites, and marine conservation areas for free.
“This is about recognizing that there is a connection between our psyches and nature, and by talking about it, we can name what we’re feeling,” Ms. Abebe said. “We can take action not only to handle our emotions, but also to live kinder and more sustainable lifestyles.”
Future work will need to focus on population-level approaches to climate change and mental health as well, including policy and financial support to address environmental changes directly.
“We need to start thinking beyond individualized approaches and focus on how to create supportive and resilient communities to respond to climate change,” Kiffer Card, PhD, executive director of the Mental Health and Climate Change Alliance and an assistant professor of health sciences at Simon Fraser University, Burnaby, B.C., told this news organization.
Dr. Card, who wasn’t involved in developing the toolkit, has researched recent trends around climate change anxiety in Canada and fielded questions from health care practitioners and mental health professionals who are looking for ways to help their patients.
“Communities need to be ready to stand up and respond to acute emergency disasters, and government leaders need to take this seriously,” he said. “Those who are experiencing climate anxiety now are the canaries in the coal mine for the severe weather events and consequences to come.”
The toolkit was developed with funding from the Alma Mater Society of the University of British Columbia, Vancouver. Ms. Abebe, Ms. Radu, and Dr. Card reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
These strategies include volunteering, building a community, discussing emotions with others, practicing mindfulness, and seeking therapy.
The toolkit, which was developed by nursing experts at the University of British Columbia in Vancouver, also offers reflection questions and a film with diverse voices for people to examine their values, emotions, and behaviors in relation to the environment.
“Many people have a hard time understanding the relationship between climate change and mental health and are experiencing high levels of stress about climate change,” Natania Abebe, MSN/MPH, RN, a registered nurse and graduate student at UBC who developed the toolkit, told this news organization.
“Youth, in particular, appear to have higher levels of consciousness regarding climate change because they’re the ones who are going to inherit the planet,” she said. “A big part of why they have mental health issues is that they feel trapped in sociopolitical structures that they didn’t agree to and didn’t necessarily create.”
The toolkit was published online on April 20.
Empowering agents for change
Ms. Abebe was inspired to create the toolkit after giving guest lectures on climate change and mental health as part of UBC’s Nursing 290 course. Her faculty advisor, Raluca Radu, MSN, a lecturer in the School of Nursing at UBC, developed the course in 2020 to teach students about the broad impacts of climate change on communities.
As the course has grown during the past 2 years, Ms. Abebe wanted to create a coping framework and engaging film for health educators to use with students, as well as for everyday people.
The toolkit includes contributions from three Canadian climate change experts, as well as six students from different backgrounds who have taken the course.
“I wanted to center the voices of youth and empower them to think they can be agents for change,” Ms. Abebe said. “I also wanted to highlight diverse voices and take a collaborative approach because climate change is such a big problem that we have to come together to address it.”
Ms. Abebe and Ms. Radu also noticed an increase in climate anxiety in recent years because of the pandemic, worldwide food and energy shortages, and extreme weather events that hit close to home, such as wildfires and floods in British Columbia.
“With the pandemic, people have been spending more time online and thinking about our world at large,” Ms. Abebe said. “At the same time that they’re thinking about it, climate change events are happening simultaneously – not in the future, but right now.”
Economic, social, and political shifts during the past 2 years have also prompted people to question standard practices and institutions, which has created an opportunity to discuss change, Ms. Radu told this news organization.
“It’s a pivotal time to question our values and highly consumerist society,” she said. “We’re at a point in time where, if we don’t take action, the planetary health will be in an irreversible state, and we won’t be able to turn back time and make changes.”
Our psyches and nature
The toolkit includes three main sections that feature video clips and reflective questions around eco-anxiety, eco-paralysis, and ecological grief.
In the first section, eco-anxiety is defined as a “chronic fear of environmental doom,” which could include anxiousness around the likelihood of a severe weather event because of ongoing news coverage and social media. The reflective questions prompt readers to discuss eco-anxiety in their life, work through their emotions, understand their beliefs and values, and determine how to use them to address climate change anxiety.
The second section defines eco-paralysis as the powerlessness that people may feel when they don’t believe they can do anything meaningful on an individual level to address climate change. Paralysis can look like apathy, complacency, or disengagement. The questions prompt readers to observe how paralysis may show up in their lives, explore the tension between individual versus collective responsibility, and consider ways to address their sense of helplessness about climate change.
In the third section, ecological grief centers around “experienced or anticipated ecological losses,” which could include the loss of species, ecosystems, and landscapes because of short- or long-term environmental change. The questions prompt readers to explore their feelings, beliefs, and values and feel empowered to address their ecological grief over climate change.
The toolkit also includes recommendations for books, journal articles, websites, podcasts, and meditations around mental health and climate change, as well as ways to get involved with others. For instance, health care practitioners can register with PaRx, a program in British Columbia that allows providers to prescribe time in nature to improve a client’s health. The program is being adopted across Canada, and people with a prescription can visit local and national parks, historic sites, and marine conservation areas for free.
“This is about recognizing that there is a connection between our psyches and nature, and by talking about it, we can name what we’re feeling,” Ms. Abebe said. “We can take action not only to handle our emotions, but also to live kinder and more sustainable lifestyles.”
Future work will need to focus on population-level approaches to climate change and mental health as well, including policy and financial support to address environmental changes directly.
“We need to start thinking beyond individualized approaches and focus on how to create supportive and resilient communities to respond to climate change,” Kiffer Card, PhD, executive director of the Mental Health and Climate Change Alliance and an assistant professor of health sciences at Simon Fraser University, Burnaby, B.C., told this news organization.
Dr. Card, who wasn’t involved in developing the toolkit, has researched recent trends around climate change anxiety in Canada and fielded questions from health care practitioners and mental health professionals who are looking for ways to help their patients.
“Communities need to be ready to stand up and respond to acute emergency disasters, and government leaders need to take this seriously,” he said. “Those who are experiencing climate anxiety now are the canaries in the coal mine for the severe weather events and consequences to come.”
The toolkit was developed with funding from the Alma Mater Society of the University of British Columbia, Vancouver. Ms. Abebe, Ms. Radu, and Dr. Card reported no relevant disclosures.
A version of this article first appeared on Medscape.com.
Best antioxidants to prevent age-related dementia identified?
Investigators found that individuals with the highest serum levels of lutein + zeaxanthin and beta-cryptoxanthin at baseline were less likely to have dementia decades later than were their peers with lower levels of these antioxidants.
Lutein and zeaxanthin are found in green leafy vegetables such as kale, spinach, broccoli, and peas. Beta-cryptoxanthin is found in fruits such as oranges, papaya, tangerines, and persimmons.
“Antioxidants may help protect the brain from oxidative stress, which can cause cell damage,” first author May A. Beydoun, PhD, with the National Institute on Aging (NIA), said in a news release.
“This is the first nationally representative study to analyze blood levels of antioxidants in relation to dementia risk,” NIA scientific director Luigi Ferrucci, MD, said in an interview.
“Blood test results may be more representative of the actual antioxidant level than a person’s report of what kind of foods they regularly consume,” Dr. Ferrucci added.
The study was published online in Neurology.
Reduced dementia risk
The researchers tested associations and interactions of serum vitamins A, C and E, and total and individual serum carotenoids and interactions with incident Alzheimer’s disease (AD) and all-cause dementia.
They analyzed data from 7,283 participants in the Third National Health and Nutrition Examination Survey (NHANES III) who were at least 45 years old at baseline and followed for an average of 16-17 years.
They found serum levels of lutein + zeaxanthin were associated with reduced risk of all-cause dementia among people aged 65 and older in models adjusted for lifestyle.
For lutein + zeaxanthin, every standard deviation (SD) increase (roughly 15.4 µmol/liter) was associated with a 7% decrease in risk for dementia (hazard ratio [HR] 0.93; 95% confidence interval [CI], 0.87-0.99, P = .037). This association was attenuated somewhat after adjustment for socioeconomic status.
Serum levels of beta-cryptoxanthin showed a “strong” inverse relationship with all-cause dementia in age- and sex-adjusted models.
For beta-cryptoxanthin, every SD increase (roughly 8.6 µmol/liter) was associated with a 14% reduced risk for dementia in people aged 45 and older (HR, 0.86; 95% CI, 0.80-0.93, P < .001) and 65 and older (HR, 0.86; 95% CI, 0.80-0.93, P = .001).
This relationship remained strong in models adjusted for sociodemographic and socioeconomic factors but attenuated in subsequent models.
No associations were found for lycopene, alpha-carotene, beta-carotene, or vitamins A, C, or E in the fully adjusted models.
Antagonistic interactions were observed for vitamin A and alpha-carotene, vitamin A and beta-carotene, vitamin E and lycopene, and lycopene and beta-carotene, suggesting putative protective effects of one antioxidant at lower levels of the other, the researchers noted.
“This analysis of an observational study found that the most important carotenoids in potentially protecting the brain may be lutein + zeaxanthin and beta-cryptoxanthin. However, randomized controlled trials are needed to prove causality,” said Dr. Ferrucci.
“Experts do not yet know the daily level of antioxidant intake to promote healthy aging of the brain. More research is needed to establish the necessary level of antioxidant intake – through the diet and/or supplements – to promote brain health and healthy aging,” he added.
An important step forward
In an accompanying editorial, Babak Hooshmand, MD, PhD, and Miia Kivipelto, MD, PhD, with Karolinska Institute, Stockholm, noted that while nutrition and dietary components are “potential targets” for dementia risk reduction, observational studies to date have reported “inconsistent findings.”
This study is “an important step towards exploring the complex relationship between antioxidants and dementia because it accounts for factors that could possibly influence the associations and considers interactions between different components,” they wrote.
The findings are “challenging,” they added, because they may lead to the hypothesis that inhibition of oxidative damage by antioxidants might have beneficial effects on preventing dementia.
However, clinical trials of antioxidant supplementation have been mainly “disappointing” and a recent Cochrane review found a lack of evidence for supplement use to preserve cognitive function or prevent dementia, Dr. Hooshmand and Dr. Kivipelto noted.
They added that the study contributes to the belief that antioxidants don’t act independently of each other or other factors, including socioeconomic status and lifestyle, in the mediation of dementia risk.
“A careful examination of the evidence is required to learn how antioxidants influence the complex pathology of dementia, because it appears to be more to it than meets the eye,”they concluded.
The research was supported in part by the Intramural Research Program of the National Institutes of Health and the National Institute on Aging. Dr. Beydoun, Dr. Ferrucci, and Dr. Hooshmand report no relevant disclosures. Dr. Kivipelto has supported advisory boards for Combinostics, Roche, and Biogen.
A version of this article first appeared on Medscape.com.
Investigators found that individuals with the highest serum levels of lutein + zeaxanthin and beta-cryptoxanthin at baseline were less likely to have dementia decades later than were their peers with lower levels of these antioxidants.
Lutein and zeaxanthin are found in green leafy vegetables such as kale, spinach, broccoli, and peas. Beta-cryptoxanthin is found in fruits such as oranges, papaya, tangerines, and persimmons.
“Antioxidants may help protect the brain from oxidative stress, which can cause cell damage,” first author May A. Beydoun, PhD, with the National Institute on Aging (NIA), said in a news release.
“This is the first nationally representative study to analyze blood levels of antioxidants in relation to dementia risk,” NIA scientific director Luigi Ferrucci, MD, said in an interview.
“Blood test results may be more representative of the actual antioxidant level than a person’s report of what kind of foods they regularly consume,” Dr. Ferrucci added.
The study was published online in Neurology.
Reduced dementia risk
The researchers tested associations and interactions of serum vitamins A, C and E, and total and individual serum carotenoids and interactions with incident Alzheimer’s disease (AD) and all-cause dementia.
They analyzed data from 7,283 participants in the Third National Health and Nutrition Examination Survey (NHANES III) who were at least 45 years old at baseline and followed for an average of 16-17 years.
They found serum levels of lutein + zeaxanthin were associated with reduced risk of all-cause dementia among people aged 65 and older in models adjusted for lifestyle.
For lutein + zeaxanthin, every standard deviation (SD) increase (roughly 15.4 µmol/liter) was associated with a 7% decrease in risk for dementia (hazard ratio [HR] 0.93; 95% confidence interval [CI], 0.87-0.99, P = .037). This association was attenuated somewhat after adjustment for socioeconomic status.
Serum levels of beta-cryptoxanthin showed a “strong” inverse relationship with all-cause dementia in age- and sex-adjusted models.
For beta-cryptoxanthin, every SD increase (roughly 8.6 µmol/liter) was associated with a 14% reduced risk for dementia in people aged 45 and older (HR, 0.86; 95% CI, 0.80-0.93, P < .001) and 65 and older (HR, 0.86; 95% CI, 0.80-0.93, P = .001).
This relationship remained strong in models adjusted for sociodemographic and socioeconomic factors but attenuated in subsequent models.
No associations were found for lycopene, alpha-carotene, beta-carotene, or vitamins A, C, or E in the fully adjusted models.
Antagonistic interactions were observed for vitamin A and alpha-carotene, vitamin A and beta-carotene, vitamin E and lycopene, and lycopene and beta-carotene, suggesting putative protective effects of one antioxidant at lower levels of the other, the researchers noted.
“This analysis of an observational study found that the most important carotenoids in potentially protecting the brain may be lutein + zeaxanthin and beta-cryptoxanthin. However, randomized controlled trials are needed to prove causality,” said Dr. Ferrucci.
“Experts do not yet know the daily level of antioxidant intake to promote healthy aging of the brain. More research is needed to establish the necessary level of antioxidant intake – through the diet and/or supplements – to promote brain health and healthy aging,” he added.
An important step forward
In an accompanying editorial, Babak Hooshmand, MD, PhD, and Miia Kivipelto, MD, PhD, with Karolinska Institute, Stockholm, noted that while nutrition and dietary components are “potential targets” for dementia risk reduction, observational studies to date have reported “inconsistent findings.”
This study is “an important step towards exploring the complex relationship between antioxidants and dementia because it accounts for factors that could possibly influence the associations and considers interactions between different components,” they wrote.
The findings are “challenging,” they added, because they may lead to the hypothesis that inhibition of oxidative damage by antioxidants might have beneficial effects on preventing dementia.
However, clinical trials of antioxidant supplementation have been mainly “disappointing” and a recent Cochrane review found a lack of evidence for supplement use to preserve cognitive function or prevent dementia, Dr. Hooshmand and Dr. Kivipelto noted.
They added that the study contributes to the belief that antioxidants don’t act independently of each other or other factors, including socioeconomic status and lifestyle, in the mediation of dementia risk.
“A careful examination of the evidence is required to learn how antioxidants influence the complex pathology of dementia, because it appears to be more to it than meets the eye,”they concluded.
The research was supported in part by the Intramural Research Program of the National Institutes of Health and the National Institute on Aging. Dr. Beydoun, Dr. Ferrucci, and Dr. Hooshmand report no relevant disclosures. Dr. Kivipelto has supported advisory boards for Combinostics, Roche, and Biogen.
A version of this article first appeared on Medscape.com.
Investigators found that individuals with the highest serum levels of lutein + zeaxanthin and beta-cryptoxanthin at baseline were less likely to have dementia decades later than were their peers with lower levels of these antioxidants.
Lutein and zeaxanthin are found in green leafy vegetables such as kale, spinach, broccoli, and peas. Beta-cryptoxanthin is found in fruits such as oranges, papaya, tangerines, and persimmons.
“Antioxidants may help protect the brain from oxidative stress, which can cause cell damage,” first author May A. Beydoun, PhD, with the National Institute on Aging (NIA), said in a news release.
“This is the first nationally representative study to analyze blood levels of antioxidants in relation to dementia risk,” NIA scientific director Luigi Ferrucci, MD, said in an interview.
“Blood test results may be more representative of the actual antioxidant level than a person’s report of what kind of foods they regularly consume,” Dr. Ferrucci added.
The study was published online in Neurology.
Reduced dementia risk
The researchers tested associations and interactions of serum vitamins A, C and E, and total and individual serum carotenoids and interactions with incident Alzheimer’s disease (AD) and all-cause dementia.
They analyzed data from 7,283 participants in the Third National Health and Nutrition Examination Survey (NHANES III) who were at least 45 years old at baseline and followed for an average of 16-17 years.
They found serum levels of lutein + zeaxanthin were associated with reduced risk of all-cause dementia among people aged 65 and older in models adjusted for lifestyle.
For lutein + zeaxanthin, every standard deviation (SD) increase (roughly 15.4 µmol/liter) was associated with a 7% decrease in risk for dementia (hazard ratio [HR] 0.93; 95% confidence interval [CI], 0.87-0.99, P = .037). This association was attenuated somewhat after adjustment for socioeconomic status.
Serum levels of beta-cryptoxanthin showed a “strong” inverse relationship with all-cause dementia in age- and sex-adjusted models.
For beta-cryptoxanthin, every SD increase (roughly 8.6 µmol/liter) was associated with a 14% reduced risk for dementia in people aged 45 and older (HR, 0.86; 95% CI, 0.80-0.93, P < .001) and 65 and older (HR, 0.86; 95% CI, 0.80-0.93, P = .001).
This relationship remained strong in models adjusted for sociodemographic and socioeconomic factors but attenuated in subsequent models.
No associations were found for lycopene, alpha-carotene, beta-carotene, or vitamins A, C, or E in the fully adjusted models.
Antagonistic interactions were observed for vitamin A and alpha-carotene, vitamin A and beta-carotene, vitamin E and lycopene, and lycopene and beta-carotene, suggesting putative protective effects of one antioxidant at lower levels of the other, the researchers noted.
“This analysis of an observational study found that the most important carotenoids in potentially protecting the brain may be lutein + zeaxanthin and beta-cryptoxanthin. However, randomized controlled trials are needed to prove causality,” said Dr. Ferrucci.
“Experts do not yet know the daily level of antioxidant intake to promote healthy aging of the brain. More research is needed to establish the necessary level of antioxidant intake – through the diet and/or supplements – to promote brain health and healthy aging,” he added.
An important step forward
In an accompanying editorial, Babak Hooshmand, MD, PhD, and Miia Kivipelto, MD, PhD, with Karolinska Institute, Stockholm, noted that while nutrition and dietary components are “potential targets” for dementia risk reduction, observational studies to date have reported “inconsistent findings.”
This study is “an important step towards exploring the complex relationship between antioxidants and dementia because it accounts for factors that could possibly influence the associations and considers interactions between different components,” they wrote.
The findings are “challenging,” they added, because they may lead to the hypothesis that inhibition of oxidative damage by antioxidants might have beneficial effects on preventing dementia.
However, clinical trials of antioxidant supplementation have been mainly “disappointing” and a recent Cochrane review found a lack of evidence for supplement use to preserve cognitive function or prevent dementia, Dr. Hooshmand and Dr. Kivipelto noted.
They added that the study contributes to the belief that antioxidants don’t act independently of each other or other factors, including socioeconomic status and lifestyle, in the mediation of dementia risk.
“A careful examination of the evidence is required to learn how antioxidants influence the complex pathology of dementia, because it appears to be more to it than meets the eye,”they concluded.
The research was supported in part by the Intramural Research Program of the National Institutes of Health and the National Institute on Aging. Dr. Beydoun, Dr. Ferrucci, and Dr. Hooshmand report no relevant disclosures. Dr. Kivipelto has supported advisory boards for Combinostics, Roche, and Biogen.
A version of this article first appeared on Medscape.com.
FROM NEUROLOGY
Vagus nerve stimulation: A little-known option for depression
Standard therapies for depression are antidepressants and psychotherapy. In particularly severe cases, electroconvulsive therapy (ECT) or vagus nerve stimulation (VNS) may also be indicated. VNS is an approved, effective, well-tolerated, long-term therapy for chronic and therapy-resistant depression, wrote Christine Reif-Leonhardt, MD, and associates from the University Hospital Frankfurt am Main (Germany), in a recent journal article. The cost of VNS is covered by health insurance funds in Germany.
Available since 1994
As the authors reported, invasive VNS was approved in the European Union in 1994 and in the United States in 1997 for the treatment of children with medicinal therapy–refractory epilepsy. Because positive and lasting effects on mood could be seen in adults after around 3 months of VNS, irrespective of the effectiveness of anticonvulsive medication, “a genuinely antidepressant effect of VNS [was] postulated,” and therefore it was further developed as an antidepressant therapy.
A VNS system first received a CE certification in 2001 in the European Union for the treatment of patients with chronic or relapsing depression who had therapy-resistant depression or who were intolerant of the current depression therapy. In 2005, VNS was approved in the United States for the treatment of patients aged 18 years or older with therapy-resistant major depression for which at least four antidepressant therapies had not helped sufficiently.
Few sham-controlled studies
According to Dr. Reif-Leonhardt and colleagues, there have been multiple studies and case series on VNS in patients with therapy-resistant depression in the past 20 years. Many of the studies highlighted the additional benefits of VNS as an adjuvant procedure, but they were observational studies. Sham-controlled studies are in short supply because of methodologic difficulties and ethical problems.
The largest long-term study is a registry study in which 494 patients with therapy-resistant depression received the combination of the usual antidepressant therapy and VNS. The study lasted 5 years; 301 patients served as a control group and received the usual therapy. The cumulative response to the therapy (68% vs. 41%) and the remission rate (43% vs. 26%) were significantly greater in the group that received VNS, according to the authors. Patients who underwent at least one ECT series of at least seven sessions responded particularly well to VNS. The combined therapy was also more effective in ECT nonresponders than the usual therapy alone.
To date, only one sham-controlled study of VNS treatment for therapy-resistant depression has been conducted. In it, VNS was not significantly superior to a sham stimulation over an observation period of 10 weeks. However, observational studies have provided evidence that the antidepressant effect of VNS only develops after at least 12 months of treatment. According to Dr. Reif-Leonhardt and colleagues, the data indicate that differences in response rate and therapy effect can only be observed in the longer term after 3-12 months and that as the therapy duration increases, so do the effects of VNS. From this, it can be assumed “that the VNS mechanism of action can be attributed to neuroplastic and adaptive phenomena.”
The typical, common side effects of surgery are pain and paresthesia. Through irritation of the nerve, approximately every third patient experiences postoperative hoarseness and a voice change. Serious side effects and complications, such as temporary swallowing disorders, are rare. By reducing the stimulation intensity or lowering the stimulation frequency or impulse width, the side effects associated with stimulation can be alleviated or even eliminated. A second small surgical intervention may become necessary to replace broken cables or the battery (life span, 3-8 years).
Criteria for VNS therapy
When should VNS be considered? The authors specified the following criteria:
- An insufficient response to at least two antidepressants from different substance classes (ideally including one tricyclic) at a sufficient dosage and duration, as well as to two augmentation agents (such as lithium and quetiapine) in combination with guideline psychotherapy
- Intolerable side effects from pharmacotherapy or contraindications to medicinal therapy
- For patients who respond to ECT, the occurrence of relapses or residual symptoms after cessation of (maintenance) ECT, intolerable ECT side effects, or the need for maintenance ECT
- Repeated or long hospital treatments because of depression
This article is a translation of an article from Univadis Germany and first appeared on Medscape.com.
Standard therapies for depression are antidepressants and psychotherapy. In particularly severe cases, electroconvulsive therapy (ECT) or vagus nerve stimulation (VNS) may also be indicated. VNS is an approved, effective, well-tolerated, long-term therapy for chronic and therapy-resistant depression, wrote Christine Reif-Leonhardt, MD, and associates from the University Hospital Frankfurt am Main (Germany), in a recent journal article. The cost of VNS is covered by health insurance funds in Germany.
Available since 1994
As the authors reported, invasive VNS was approved in the European Union in 1994 and in the United States in 1997 for the treatment of children with medicinal therapy–refractory epilepsy. Because positive and lasting effects on mood could be seen in adults after around 3 months of VNS, irrespective of the effectiveness of anticonvulsive medication, “a genuinely antidepressant effect of VNS [was] postulated,” and therefore it was further developed as an antidepressant therapy.
A VNS system first received a CE certification in 2001 in the European Union for the treatment of patients with chronic or relapsing depression who had therapy-resistant depression or who were intolerant of the current depression therapy. In 2005, VNS was approved in the United States for the treatment of patients aged 18 years or older with therapy-resistant major depression for which at least four antidepressant therapies had not helped sufficiently.
Few sham-controlled studies
According to Dr. Reif-Leonhardt and colleagues, there have been multiple studies and case series on VNS in patients with therapy-resistant depression in the past 20 years. Many of the studies highlighted the additional benefits of VNS as an adjuvant procedure, but they were observational studies. Sham-controlled studies are in short supply because of methodologic difficulties and ethical problems.
The largest long-term study is a registry study in which 494 patients with therapy-resistant depression received the combination of the usual antidepressant therapy and VNS. The study lasted 5 years; 301 patients served as a control group and received the usual therapy. The cumulative response to the therapy (68% vs. 41%) and the remission rate (43% vs. 26%) were significantly greater in the group that received VNS, according to the authors. Patients who underwent at least one ECT series of at least seven sessions responded particularly well to VNS. The combined therapy was also more effective in ECT nonresponders than the usual therapy alone.
To date, only one sham-controlled study of VNS treatment for therapy-resistant depression has been conducted. In it, VNS was not significantly superior to a sham stimulation over an observation period of 10 weeks. However, observational studies have provided evidence that the antidepressant effect of VNS only develops after at least 12 months of treatment. According to Dr. Reif-Leonhardt and colleagues, the data indicate that differences in response rate and therapy effect can only be observed in the longer term after 3-12 months and that as the therapy duration increases, so do the effects of VNS. From this, it can be assumed “that the VNS mechanism of action can be attributed to neuroplastic and adaptive phenomena.”
The typical, common side effects of surgery are pain and paresthesia. Through irritation of the nerve, approximately every third patient experiences postoperative hoarseness and a voice change. Serious side effects and complications, such as temporary swallowing disorders, are rare. By reducing the stimulation intensity or lowering the stimulation frequency or impulse width, the side effects associated with stimulation can be alleviated or even eliminated. A second small surgical intervention may become necessary to replace broken cables or the battery (life span, 3-8 years).
Criteria for VNS therapy
When should VNS be considered? The authors specified the following criteria:
- An insufficient response to at least two antidepressants from different substance classes (ideally including one tricyclic) at a sufficient dosage and duration, as well as to two augmentation agents (such as lithium and quetiapine) in combination with guideline psychotherapy
- Intolerable side effects from pharmacotherapy or contraindications to medicinal therapy
- For patients who respond to ECT, the occurrence of relapses or residual symptoms after cessation of (maintenance) ECT, intolerable ECT side effects, or the need for maintenance ECT
- Repeated or long hospital treatments because of depression
This article is a translation of an article from Univadis Germany and first appeared on Medscape.com.
Standard therapies for depression are antidepressants and psychotherapy. In particularly severe cases, electroconvulsive therapy (ECT) or vagus nerve stimulation (VNS) may also be indicated. VNS is an approved, effective, well-tolerated, long-term therapy for chronic and therapy-resistant depression, wrote Christine Reif-Leonhardt, MD, and associates from the University Hospital Frankfurt am Main (Germany), in a recent journal article. The cost of VNS is covered by health insurance funds in Germany.
Available since 1994
As the authors reported, invasive VNS was approved in the European Union in 1994 and in the United States in 1997 for the treatment of children with medicinal therapy–refractory epilepsy. Because positive and lasting effects on mood could be seen in adults after around 3 months of VNS, irrespective of the effectiveness of anticonvulsive medication, “a genuinely antidepressant effect of VNS [was] postulated,” and therefore it was further developed as an antidepressant therapy.
A VNS system first received a CE certification in 2001 in the European Union for the treatment of patients with chronic or relapsing depression who had therapy-resistant depression or who were intolerant of the current depression therapy. In 2005, VNS was approved in the United States for the treatment of patients aged 18 years or older with therapy-resistant major depression for which at least four antidepressant therapies had not helped sufficiently.
Few sham-controlled studies
According to Dr. Reif-Leonhardt and colleagues, there have been multiple studies and case series on VNS in patients with therapy-resistant depression in the past 20 years. Many of the studies highlighted the additional benefits of VNS as an adjuvant procedure, but they were observational studies. Sham-controlled studies are in short supply because of methodologic difficulties and ethical problems.
The largest long-term study is a registry study in which 494 patients with therapy-resistant depression received the combination of the usual antidepressant therapy and VNS. The study lasted 5 years; 301 patients served as a control group and received the usual therapy. The cumulative response to the therapy (68% vs. 41%) and the remission rate (43% vs. 26%) were significantly greater in the group that received VNS, according to the authors. Patients who underwent at least one ECT series of at least seven sessions responded particularly well to VNS. The combined therapy was also more effective in ECT nonresponders than the usual therapy alone.
To date, only one sham-controlled study of VNS treatment for therapy-resistant depression has been conducted. In it, VNS was not significantly superior to a sham stimulation over an observation period of 10 weeks. However, observational studies have provided evidence that the antidepressant effect of VNS only develops after at least 12 months of treatment. According to Dr. Reif-Leonhardt and colleagues, the data indicate that differences in response rate and therapy effect can only be observed in the longer term after 3-12 months and that as the therapy duration increases, so do the effects of VNS. From this, it can be assumed “that the VNS mechanism of action can be attributed to neuroplastic and adaptive phenomena.”
The typical, common side effects of surgery are pain and paresthesia. Through irritation of the nerve, approximately every third patient experiences postoperative hoarseness and a voice change. Serious side effects and complications, such as temporary swallowing disorders, are rare. By reducing the stimulation intensity or lowering the stimulation frequency or impulse width, the side effects associated with stimulation can be alleviated or even eliminated. A second small surgical intervention may become necessary to replace broken cables or the battery (life span, 3-8 years).
Criteria for VNS therapy
When should VNS be considered? The authors specified the following criteria:
- An insufficient response to at least two antidepressants from different substance classes (ideally including one tricyclic) at a sufficient dosage and duration, as well as to two augmentation agents (such as lithium and quetiapine) in combination with guideline psychotherapy
- Intolerable side effects from pharmacotherapy or contraindications to medicinal therapy
- For patients who respond to ECT, the occurrence of relapses or residual symptoms after cessation of (maintenance) ECT, intolerable ECT side effects, or the need for maintenance ECT
- Repeated or long hospital treatments because of depression
This article is a translation of an article from Univadis Germany and first appeared on Medscape.com.
FROM DER NERVENARZT
Residential green space linked to better cognitive function
Exposure to green space may boost cognitive function, new research suggests.
This association may be explained by a reduction in depression, researchers note. Scores for overall cognition and psychomotor speed/attention among women with high green-space exposure were equivalent to those of women an average of 1.2 years younger, they add.
“Despite the fact that the women in our study were relatively younger than those in previous studies, we were still able to detect protective associations between green space and cognition,” lead author Marcia Pescador Jimenez, PhD, assistant professor of epidemiology, Boston University School of Public Health, told this news organization.
“This may signal the public health importance of green space and the important clinical implications at the population level,” she said.

The findings were published online in JAMA Network Open.
Better psychomotor speed, attention
Recent studies on the benefits of green space have shown a link between higher exposure and reduced risks for schizophrenia and ischemic stroke. Other studies have explored the link between green space and dementia and Alzheimer’s disease.
Cognitive function in middle age is associated with subsequent dementia, so Dr. Jimenez said she and her colleagues wanted to analyze the effect of residential green space on cognitive function in middle-aged women.
The study included 13,594 women (median age, 61.2 years) who are participants in the ongoing Nurses’ Health Study II, one of the largest studies to examine risk factors for chronic illness in women.
To calculate the amount of green space, researchers used the Normalized Difference Vegetation Index (NDVI), a satellite-based indicator of green vegetation around a residential address. The data were based on each participant’s 2013 residence.
After adjusting for age at assessment, race, and childhood, adulthood, and neighborhood socioeconomic status, green space was associated with higher scores on the global CogState composite (mean difference per interquartile range in green space, 0.05; 95% confidence interval, .02-.07) and psychomotor speed and attention (mean difference in score, 0.05 standard units; 95% CI, .02-.08) scales.
There was no association between green-space exposure and learning and working memory. Investigators also found no differences based on urbanicity, suggesting the benefits were similar for urban versus rural settings.
Specific to cognitive domains
“We were surprised to see that while our study found that higher levels of residential green space were associated with higher scores on processing speed and attention and on overall cognition, we also found that higher levels of residential green space were not associated with learning/working memory battery scores,” Dr. Jimenez said.
“This is actually in-line with previous research suggesting differing associations between green space and cognition based on the cognitive domain examined,” she added.
About 98% of participants were White, limiting the generalizability of the findings, the researchers note. There was also no information on proximity to or size of green space, or how much time individuals spent in the green space and what kinds of activities they engaged in.
Dr. Jimenez said projects examining the amount of time of green-space exposure are underway.
In addition, the researchers found lower rates of depression might contribute to the cognitive benefits associated with green-space exposure, explaining 3.95% (95% CI, .35%-7.55%) of the association between green space and psychomotor speed/attention and 6.3% (95% CI, .77%-11.81%) of the association between green space and overall cognition.
Reduced air pollution and increased physical activity, which are other factors often thought to contribute to the cognitive benefits of green space, were not significant in this study.
‘Interesting and novel’
Commenting on the findings, Payam Dadvand, MD, PhD, associate research professor, Barcelona Institute for Global Health, called the finding that depression may mediate green-space benefits “quite interesting and novel.”
“The results of this study, given its large sample size and its geographical coverage, adds to an emerging body of evidence on the beneficial association of exposure to green space on aging, and in particular, cognitive aging in older adults,” said Dr. Dadvand, who was not involved with the research.
The study was funded by the National Institutes of Health. Dr. Jimenez and Dr. Dadvand have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Exposure to green space may boost cognitive function, new research suggests.
This association may be explained by a reduction in depression, researchers note. Scores for overall cognition and psychomotor speed/attention among women with high green-space exposure were equivalent to those of women an average of 1.2 years younger, they add.
“Despite the fact that the women in our study were relatively younger than those in previous studies, we were still able to detect protective associations between green space and cognition,” lead author Marcia Pescador Jimenez, PhD, assistant professor of epidemiology, Boston University School of Public Health, told this news organization.
“This may signal the public health importance of green space and the important clinical implications at the population level,” she said.
The findings were published online in JAMA Network Open.
Better psychomotor speed, attention
Recent studies on the benefits of green space have shown a link between higher exposure and reduced risks for schizophrenia and ischemic stroke. Other studies have explored the link between green space and dementia and Alzheimer’s disease.
Cognitive function in middle age is associated with subsequent dementia, so Dr. Jimenez said she and her colleagues wanted to analyze the effect of residential green space on cognitive function in middle-aged women.
The study included 13,594 women (median age, 61.2 years) who are participants in the ongoing Nurses’ Health Study II, one of the largest studies to examine risk factors for chronic illness in women.
To calculate the amount of green space, researchers used the Normalized Difference Vegetation Index (NDVI), a satellite-based indicator of green vegetation around a residential address. The data were based on each participant’s 2013 residence.
After adjusting for age at assessment, race, and childhood, adulthood, and neighborhood socioeconomic status, green space was associated with higher scores on the global CogState composite (mean difference per interquartile range in green space, 0.05; 95% confidence interval, .02-.07) and psychomotor speed and attention (mean difference in score, 0.05 standard units; 95% CI, .02-.08) scales.
There was no association between green-space exposure and learning and working memory. Investigators also found no differences based on urbanicity, suggesting the benefits were similar for urban versus rural settings.
Specific to cognitive domains
“We were surprised to see that while our study found that higher levels of residential green space were associated with higher scores on processing speed and attention and on overall cognition, we also found that higher levels of residential green space were not associated with learning/working memory battery scores,” Dr. Jimenez said.
“This is actually in-line with previous research suggesting differing associations between green space and cognition based on the cognitive domain examined,” she added.
About 98% of participants were White, limiting the generalizability of the findings, the researchers note. There was also no information on proximity to or size of green space, or how much time individuals spent in the green space and what kinds of activities they engaged in.
Dr. Jimenez said projects examining the amount of time of green-space exposure are underway.
In addition, the researchers found lower rates of depression might contribute to the cognitive benefits associated with green-space exposure, explaining 3.95% (95% CI, .35%-7.55%) of the association between green space and psychomotor speed/attention and 6.3% (95% CI, .77%-11.81%) of the association between green space and overall cognition.
Reduced air pollution and increased physical activity, which are other factors often thought to contribute to the cognitive benefits of green space, were not significant in this study.
‘Interesting and novel’
Commenting on the findings, Payam Dadvand, MD, PhD, associate research professor, Barcelona Institute for Global Health, called the finding that depression may mediate green-space benefits “quite interesting and novel.”
“The results of this study, given its large sample size and its geographical coverage, adds to an emerging body of evidence on the beneficial association of exposure to green space on aging, and in particular, cognitive aging in older adults,” said Dr. Dadvand, who was not involved with the research.
The study was funded by the National Institutes of Health. Dr. Jimenez and Dr. Dadvand have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Exposure to green space may boost cognitive function, new research suggests.
This association may be explained by a reduction in depression, researchers note. Scores for overall cognition and psychomotor speed/attention among women with high green-space exposure were equivalent to those of women an average of 1.2 years younger, they add.
“Despite the fact that the women in our study were relatively younger than those in previous studies, we were still able to detect protective associations between green space and cognition,” lead author Marcia Pescador Jimenez, PhD, assistant professor of epidemiology, Boston University School of Public Health, told this news organization.
“This may signal the public health importance of green space and the important clinical implications at the population level,” she said.
The findings were published online in JAMA Network Open.
Better psychomotor speed, attention
Recent studies on the benefits of green space have shown a link between higher exposure and reduced risks for schizophrenia and ischemic stroke. Other studies have explored the link between green space and dementia and Alzheimer’s disease.
Cognitive function in middle age is associated with subsequent dementia, so Dr. Jimenez said she and her colleagues wanted to analyze the effect of residential green space on cognitive function in middle-aged women.
The study included 13,594 women (median age, 61.2 years) who are participants in the ongoing Nurses’ Health Study II, one of the largest studies to examine risk factors for chronic illness in women.
To calculate the amount of green space, researchers used the Normalized Difference Vegetation Index (NDVI), a satellite-based indicator of green vegetation around a residential address. The data were based on each participant’s 2013 residence.
After adjusting for age at assessment, race, and childhood, adulthood, and neighborhood socioeconomic status, green space was associated with higher scores on the global CogState composite (mean difference per interquartile range in green space, 0.05; 95% confidence interval, .02-.07) and psychomotor speed and attention (mean difference in score, 0.05 standard units; 95% CI, .02-.08) scales.
There was no association between green-space exposure and learning and working memory. Investigators also found no differences based on urbanicity, suggesting the benefits were similar for urban versus rural settings.
Specific to cognitive domains
“We were surprised to see that while our study found that higher levels of residential green space were associated with higher scores on processing speed and attention and on overall cognition, we also found that higher levels of residential green space were not associated with learning/working memory battery scores,” Dr. Jimenez said.
“This is actually in-line with previous research suggesting differing associations between green space and cognition based on the cognitive domain examined,” she added.
About 98% of participants were White, limiting the generalizability of the findings, the researchers note. There was also no information on proximity to or size of green space, or how much time individuals spent in the green space and what kinds of activities they engaged in.
Dr. Jimenez said projects examining the amount of time of green-space exposure are underway.
In addition, the researchers found lower rates of depression might contribute to the cognitive benefits associated with green-space exposure, explaining 3.95% (95% CI, .35%-7.55%) of the association between green space and psychomotor speed/attention and 6.3% (95% CI, .77%-11.81%) of the association between green space and overall cognition.
Reduced air pollution and increased physical activity, which are other factors often thought to contribute to the cognitive benefits of green space, were not significant in this study.
‘Interesting and novel’
Commenting on the findings, Payam Dadvand, MD, PhD, associate research professor, Barcelona Institute for Global Health, called the finding that depression may mediate green-space benefits “quite interesting and novel.”
“The results of this study, given its large sample size and its geographical coverage, adds to an emerging body of evidence on the beneficial association of exposure to green space on aging, and in particular, cognitive aging in older adults,” said Dr. Dadvand, who was not involved with the research.
The study was funded by the National Institutes of Health. Dr. Jimenez and Dr. Dadvand have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Adherence to ADHD meds may lower unemployment risk
Investigators analyzed data for almost 13,000 working-age adults with ADHD and found ADHD medication use during the previous 2 years was associated with a 10% lower risk for long-term unemployment in the following year.
In addition, among the female participants, longer treatment duration was associated with a lower risk for subsequent long-term unemployment. In both genders, within-individual comparisons showed long-term unemployment was lower during periods of ADHD medication treatment, compared with nontreatment periods.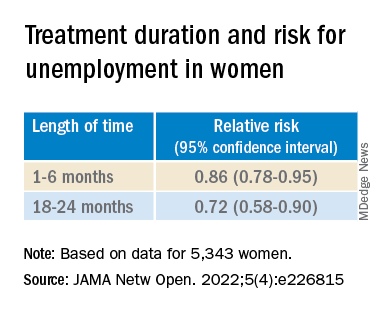
“This evidence should be considered together with the existing knowledge of risks and benefits of ADHD medications when developing treatment plans for working-aged adults,” lead author Lin Li, MSc, a doctoral candidate at the School of Medical Science, Örebro University, Sweden, told this news organization.
“However, the effect size is relatively small in magnitude, indicating that other treatment programs, such as psychotherapy, are also needed to help individuals with ADHD in work-related settings,” Ms. Li said.
The findings were published online in JAMA Network Open.
Evidence gap
Adults with ADHD “have occupational impairments, such as poor work performance, less job stability, financial problems, and increased risk for unemployment,” the investigators write.
However, “less is known about the extent to which pharmacological treatment of ADHD is associated with reductions in unemployment rates,” they add.
“People with ADHD have been reported to have problems in work-related performance,” Ms. Li noted. “ADHD medications could reduce ADHD symptoms and also help with academic achievement, but there is limited evidence on the association between ADHD medication and occupational outcomes.”
To address this gap in evidence, the researchers turned to several major Swedish registries to identify 25,358 individuals with ADHD born between 1958 and 1978 who were aged 30 to 55 years during the study period of Jan. 1, 2008, through Dec. 31, 2013).
Of these, 12,875 (41.5% women; mean age, 37.9 years) were included in the analysis. Most participants (81.19%) had more than 9 years of education.
The registers provided information not only about diagnosis, but also about prescription medications these individuals took for ADHD, including methylphenidate, amphetamine, dexamphetamine, lisdexamfetamine, and atomoxetine.
Administrative records provided data about yearly accumulated unemployment days, with long-term unemployment defined as having at least 90 days of unemployment in a calendar year.
Covariates included age at baseline, sex, country of birth, highest educational level, crime records, and psychiatric comorbidities.
Most patients (69.34%) had at least one psychiatric comorbidity, with depressive, anxiety, and substance use disorders being the most common (in 40.28%, 35.27%, and 28.77%, respectively).
Symptom reduction
The mean length of medication use was 49 days (range, 0-366 days) per year. Of participants in whom these data were available, 31.29% of women and 31.03% of men never used ADHD medications. Among participants treated with ADHD medication (68.71%), only 3.23% of the women and 3.46% of the men had persistent use during the follow-up period.
Among women and men in whom these data were available, (38.85% of the total sample), 35.70% and 41.08%, respectively, were recorded as having one or more long-term unemployment stretches across the study period. In addition, 0.15% and 0.4%, respectively, had long-term unemployment during each of those years.
Use of ADHD medications during the previous 2 years was associated with a 10% lower risk for long-term unemployment in the following year (adjusted relative risk, 0.90; 95% confidence interval, 0.87-0.95).
The researchers also found an association between use of ADHD medications and long-term unemployment among women (RR, 0.82; 95% CI, 0.76-0.89) but not among men (RR, 0.96; 95% CI, 0.91-1.01).
Among women in particular, longer treatment duration was associated with a lower risk of subsequent long-term unemployment (P < .001 for trend).
Within-individual comparisons showed the long-term unemployment rate was lower during periods when individuals were being treated with ADHD medication vs. periods of nontreatment (RR, 0.89; 95% CI, 0.85-0.94).
“Among 12,875 working-aged adults with ADHD in Sweden, we found the use of ADHD medication is associated with a lower risk of long-term unemployment, especially for women,” Ms. Li said.
“The hypothesis of this study is that ADHD medications are effective in reducing ADHD symptoms, which may in turn help to improve work performance among individuals with ADHD,” she added.
However, Ms. Li cautioned, “the information on ADHD symptoms is not available in Swedish National Registers, so more research is needed to test the hypothesis.”
The investigators also suggest that future research “should further explore the effectiveness of stimulant and nonstimulant ADHD medications” and replicate their findings in other settings.
Findings ‘make sense’
Commenting on the study, Ari Tuckman PsyD, expert spokesman for Children and Adults with Attention-Deficit/Hyperactivity Disorder, said, there is “a lot to like about this study, specifically the large sample size and within-individual comparisons that the Scandinavians’ databases allow.”
“We know that ADHD can impact both finding and keeping a job, so it absolutely makes sense that medication use would reduce duration of unemployment,” said Dr. Tuckman, who is in private practice in West Chester, Pa., and was not involved with the research.
However, “I would venture that the results would have been more robust if the authors had been able to only look at those on optimized medication regimens, which is far too few,” he added. “This lack of optimization would have been even more true 10 years ago, which is when the data was from.”
The study was supported by a grant from the Swedish Council for Health, Working Life, and Welfare, an award from the Swedish Research Council, and a grant from Shire International GmbH, a member of the Takeda group of companies. Ms. Li and Dr. Tuckman have disclosed no relevant financial relationships. The other authors’ disclosures are listed in the original paper.
A version of this article first appeared on Medscape.com.
Investigators analyzed data for almost 13,000 working-age adults with ADHD and found ADHD medication use during the previous 2 years was associated with a 10% lower risk for long-term unemployment in the following year.
In addition, among the female participants, longer treatment duration was associated with a lower risk for subsequent long-term unemployment. In both genders, within-individual comparisons showed long-term unemployment was lower during periods of ADHD medication treatment, compared with nontreatment periods.
“This evidence should be considered together with the existing knowledge of risks and benefits of ADHD medications when developing treatment plans for working-aged adults,” lead author Lin Li, MSc, a doctoral candidate at the School of Medical Science, Örebro University, Sweden, told this news organization.
“However, the effect size is relatively small in magnitude, indicating that other treatment programs, such as psychotherapy, are also needed to help individuals with ADHD in work-related settings,” Ms. Li said.
The findings were published online in JAMA Network Open.
Evidence gap
Adults with ADHD “have occupational impairments, such as poor work performance, less job stability, financial problems, and increased risk for unemployment,” the investigators write.
However, “less is known about the extent to which pharmacological treatment of ADHD is associated with reductions in unemployment rates,” they add.
“People with ADHD have been reported to have problems in work-related performance,” Ms. Li noted. “ADHD medications could reduce ADHD symptoms and also help with academic achievement, but there is limited evidence on the association between ADHD medication and occupational outcomes.”
To address this gap in evidence, the researchers turned to several major Swedish registries to identify 25,358 individuals with ADHD born between 1958 and 1978 who were aged 30 to 55 years during the study period of Jan. 1, 2008, through Dec. 31, 2013).
Of these, 12,875 (41.5% women; mean age, 37.9 years) were included in the analysis. Most participants (81.19%) had more than 9 years of education.
The registers provided information not only about diagnosis, but also about prescription medications these individuals took for ADHD, including methylphenidate, amphetamine, dexamphetamine, lisdexamfetamine, and atomoxetine.
Administrative records provided data about yearly accumulated unemployment days, with long-term unemployment defined as having at least 90 days of unemployment in a calendar year.
Covariates included age at baseline, sex, country of birth, highest educational level, crime records, and psychiatric comorbidities.
Most patients (69.34%) had at least one psychiatric comorbidity, with depressive, anxiety, and substance use disorders being the most common (in 40.28%, 35.27%, and 28.77%, respectively).
Symptom reduction
The mean length of medication use was 49 days (range, 0-366 days) per year. Of participants in whom these data were available, 31.29% of women and 31.03% of men never used ADHD medications. Among participants treated with ADHD medication (68.71%), only 3.23% of the women and 3.46% of the men had persistent use during the follow-up period.
Among women and men in whom these data were available, (38.85% of the total sample), 35.70% and 41.08%, respectively, were recorded as having one or more long-term unemployment stretches across the study period. In addition, 0.15% and 0.4%, respectively, had long-term unemployment during each of those years.
Use of ADHD medications during the previous 2 years was associated with a 10% lower risk for long-term unemployment in the following year (adjusted relative risk, 0.90; 95% confidence interval, 0.87-0.95).
The researchers also found an association between use of ADHD medications and long-term unemployment among women (RR, 0.82; 95% CI, 0.76-0.89) but not among men (RR, 0.96; 95% CI, 0.91-1.01).
Among women in particular, longer treatment duration was associated with a lower risk of subsequent long-term unemployment (P < .001 for trend).
Within-individual comparisons showed the long-term unemployment rate was lower during periods when individuals were being treated with ADHD medication vs. periods of nontreatment (RR, 0.89; 95% CI, 0.85-0.94).
“Among 12,875 working-aged adults with ADHD in Sweden, we found the use of ADHD medication is associated with a lower risk of long-term unemployment, especially for women,” Ms. Li said.
“The hypothesis of this study is that ADHD medications are effective in reducing ADHD symptoms, which may in turn help to improve work performance among individuals with ADHD,” she added.
However, Ms. Li cautioned, “the information on ADHD symptoms is not available in Swedish National Registers, so more research is needed to test the hypothesis.”
The investigators also suggest that future research “should further explore the effectiveness of stimulant and nonstimulant ADHD medications” and replicate their findings in other settings.
Findings ‘make sense’
Commenting on the study, Ari Tuckman PsyD, expert spokesman for Children and Adults with Attention-Deficit/Hyperactivity Disorder, said, there is “a lot to like about this study, specifically the large sample size and within-individual comparisons that the Scandinavians’ databases allow.”
“We know that ADHD can impact both finding and keeping a job, so it absolutely makes sense that medication use would reduce duration of unemployment,” said Dr. Tuckman, who is in private practice in West Chester, Pa., and was not involved with the research.
However, “I would venture that the results would have been more robust if the authors had been able to only look at those on optimized medication regimens, which is far too few,” he added. “This lack of optimization would have been even more true 10 years ago, which is when the data was from.”
The study was supported by a grant from the Swedish Council for Health, Working Life, and Welfare, an award from the Swedish Research Council, and a grant from Shire International GmbH, a member of the Takeda group of companies. Ms. Li and Dr. Tuckman have disclosed no relevant financial relationships. The other authors’ disclosures are listed in the original paper.
A version of this article first appeared on Medscape.com.
Investigators analyzed data for almost 13,000 working-age adults with ADHD and found ADHD medication use during the previous 2 years was associated with a 10% lower risk for long-term unemployment in the following year.
In addition, among the female participants, longer treatment duration was associated with a lower risk for subsequent long-term unemployment. In both genders, within-individual comparisons showed long-term unemployment was lower during periods of ADHD medication treatment, compared with nontreatment periods.
“This evidence should be considered together with the existing knowledge of risks and benefits of ADHD medications when developing treatment plans for working-aged adults,” lead author Lin Li, MSc, a doctoral candidate at the School of Medical Science, Örebro University, Sweden, told this news organization.
“However, the effect size is relatively small in magnitude, indicating that other treatment programs, such as psychotherapy, are also needed to help individuals with ADHD in work-related settings,” Ms. Li said.
The findings were published online in JAMA Network Open.
Evidence gap
Adults with ADHD “have occupational impairments, such as poor work performance, less job stability, financial problems, and increased risk for unemployment,” the investigators write.
However, “less is known about the extent to which pharmacological treatment of ADHD is associated with reductions in unemployment rates,” they add.
“People with ADHD have been reported to have problems in work-related performance,” Ms. Li noted. “ADHD medications could reduce ADHD symptoms and also help with academic achievement, but there is limited evidence on the association between ADHD medication and occupational outcomes.”
To address this gap in evidence, the researchers turned to several major Swedish registries to identify 25,358 individuals with ADHD born between 1958 and 1978 who were aged 30 to 55 years during the study period of Jan. 1, 2008, through Dec. 31, 2013).
Of these, 12,875 (41.5% women; mean age, 37.9 years) were included in the analysis. Most participants (81.19%) had more than 9 years of education.
The registers provided information not only about diagnosis, but also about prescription medications these individuals took for ADHD, including methylphenidate, amphetamine, dexamphetamine, lisdexamfetamine, and atomoxetine.
Administrative records provided data about yearly accumulated unemployment days, with long-term unemployment defined as having at least 90 days of unemployment in a calendar year.
Covariates included age at baseline, sex, country of birth, highest educational level, crime records, and psychiatric comorbidities.
Most patients (69.34%) had at least one psychiatric comorbidity, with depressive, anxiety, and substance use disorders being the most common (in 40.28%, 35.27%, and 28.77%, respectively).
Symptom reduction
The mean length of medication use was 49 days (range, 0-366 days) per year. Of participants in whom these data were available, 31.29% of women and 31.03% of men never used ADHD medications. Among participants treated with ADHD medication (68.71%), only 3.23% of the women and 3.46% of the men had persistent use during the follow-up period.
Among women and men in whom these data were available, (38.85% of the total sample), 35.70% and 41.08%, respectively, were recorded as having one or more long-term unemployment stretches across the study period. In addition, 0.15% and 0.4%, respectively, had long-term unemployment during each of those years.
Use of ADHD medications during the previous 2 years was associated with a 10% lower risk for long-term unemployment in the following year (adjusted relative risk, 0.90; 95% confidence interval, 0.87-0.95).
The researchers also found an association between use of ADHD medications and long-term unemployment among women (RR, 0.82; 95% CI, 0.76-0.89) but not among men (RR, 0.96; 95% CI, 0.91-1.01).
Among women in particular, longer treatment duration was associated with a lower risk of subsequent long-term unemployment (P < .001 for trend).
Within-individual comparisons showed the long-term unemployment rate was lower during periods when individuals were being treated with ADHD medication vs. periods of nontreatment (RR, 0.89; 95% CI, 0.85-0.94).
“Among 12,875 working-aged adults with ADHD in Sweden, we found the use of ADHD medication is associated with a lower risk of long-term unemployment, especially for women,” Ms. Li said.
“The hypothesis of this study is that ADHD medications are effective in reducing ADHD symptoms, which may in turn help to improve work performance among individuals with ADHD,” she added.
However, Ms. Li cautioned, “the information on ADHD symptoms is not available in Swedish National Registers, so more research is needed to test the hypothesis.”
The investigators also suggest that future research “should further explore the effectiveness of stimulant and nonstimulant ADHD medications” and replicate their findings in other settings.
Findings ‘make sense’
Commenting on the study, Ari Tuckman PsyD, expert spokesman for Children and Adults with Attention-Deficit/Hyperactivity Disorder, said, there is “a lot to like about this study, specifically the large sample size and within-individual comparisons that the Scandinavians’ databases allow.”
“We know that ADHD can impact both finding and keeping a job, so it absolutely makes sense that medication use would reduce duration of unemployment,” said Dr. Tuckman, who is in private practice in West Chester, Pa., and was not involved with the research.
However, “I would venture that the results would have been more robust if the authors had been able to only look at those on optimized medication regimens, which is far too few,” he added. “This lack of optimization would have been even more true 10 years ago, which is when the data was from.”
The study was supported by a grant from the Swedish Council for Health, Working Life, and Welfare, an award from the Swedish Research Council, and a grant from Shire International GmbH, a member of the Takeda group of companies. Ms. Li and Dr. Tuckman have disclosed no relevant financial relationships. The other authors’ disclosures are listed in the original paper.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Multistate opioid crackdown nets indictment against seven physicians
In coordination with federal and state law enforcement, the DOJ charged the defendants for their involvement in the illegal distribution of opioids. At the time that they were charged with the alleged offenses, 12 of the defendants were medical professionals.
The 12 persons in eight federal districts across the country distributed more than 115 million controlled substances, including buprenorphine, clonazepam, dextroamphetamine-amphetamine, hydrocodone, morphine sulfate, oxycodone, oxymorphone, and Suboxone, per the DOJ.
“Doctors and health care professionals are entrusted with prescribing medicine responsibly and in the best interests of their patients. Today’s takedown targets medical providers across the country whose greed drove them to abandon this responsibility in favor of criminal profits,” said Anne Milgram, administrator of the Drug Enforcement Administration.
Medical professionals, others across six states charged
One former nurse, one business manager, and one individual who practiced medicine without a medical credential are among those listed in the indictment. These include the following:
- Eskender Getachew, MD, a Columbus, Ohio, sleep medicine specialist, was charged with unlawful distribution of controlled substances outside the use of professional practice and not for a legitimate medical practice.
- Charles Kistler, DO, an Upper Arlington, Ohio, family practice physician, was charged with unlawful distribution of controlled substances for unlawful prescribing at Midtown Family Practice Clinic in Columbus.
- Yogeshwar Gil, MBBS, a Manchester, Tenn., family medicine doctor and owner of a medical practice, was charged with conspiracy to unlawfully distribute controlled substances and maintaining a drug-involved premises. Dr. Gil was charged in connection with an alleged scheme to distribute opioids and Suboxone outside the usual course of professional practice and without a legitimate medical purpose.
- Contessa Holley, RN, a Pulaski, Tenn., former nurse and clinical director, was charged with wire fraud, aggravated identity theft, and possession of a controlled substance with intent to distribute. She’s alleged to be connected with a scheme to unlawfully obtain opioids by filling fraudulent prescriptions in the names of current and former patients who were in hospice. The indictment alleged that Ms. Holley used the patients’ hospice benefits to cover the opioids’ costs while keeping the drugs for her own use and for further distribution.
- Francene Aretha Gayle, MD, an Orlando, Fla., physician, was charged with conspiracy to unlawfully distribute controlled substances, conspiracy to commit health care fraud, health care fraud, and several substantive counts of illegally issuing opioid prescriptions. Dr. Gayle was charged along with Schara Monique Davis, a Huntsville, Ala.–based business manager. Per the indictment, Dr. Gayle and Ms. Davis operated three medical clinics in Alabama, where Dr. Gayle was the sole physician. The medical clinics billed health insurers for millions of dollars in patient visits that Dr. Gayle had supposedly conducted but during which she was allegedly absent from the clinics; other staff members conducted the visits instead. It’s alleged that Dr. Gayle presigned prescriptions for opioids that were given to patients.
- Robert Taffet, MD, a Haddonfield, N.J., orthopedic surgeon and owner of a medical practice in Sicklerville, N.J., was charged with conspiracy to unlawfully distribute controlled substances. The indictment alleges that he falsified patient files to state that he interacted with patients when he didn’t and that he issued prescriptions for opioids and other controlled substances without assessing the patients in person or by telemedicine. It’s alleged that Dr. Taffett issued prescriptions for more than 179,000 pills that were dispensed by New Jersey pharmacies between April 2020 and December 2021.
- Hau La, MD, a Brentwood, Tenn., family medicine physician and the operator of Absolute Medical Care in Smyrna, Tenn., was charged with sixteen counts of unlawful distribution of a controlled substance. The physician is alleged to have unlawfully prescribed opioids to eight patients outside the usual course of practice and without a legitimate medical purpose.
- Frederick De Mesa, of War, W.Va., practiced as a physician and used a DEA registration number that allowed him to prescribe controlled substances. Mr. De Mesa prescribed these substances without a medical license and didn’t have an active DEA registration number, according to the indictment.
- Loey Kousa, a former internist from Paintsville, Ky., was charged with unlawful distribution of controlled substances, healthcare fraud, and making false statements in connection with the delivery of health care services. The indictment alleges that the former physician issued prescriptions for opioids outside the usual course of professional practice and without a legitimate medical purpose in his capacity as owner and operator of East KY Clinic in Paintsville. He is alleged to have issued the unlawful prescriptions for patients whose treatments were covered by taxpayer-funded programs such as Medicare and Medicaid; he also billed these programs for medically unnecessary procedures for these patients.
Also included in the indictment were Jay Sadrinia, DMD, a Villa Hills, Ky., dentist, who was charged with four counts of illegal distribution of oxycodone and morphine sulfate and one count of illegal distribution of morphine sulfate that resulted in death or serious bodily injury; and Casey Kelleher, an owner-operator of Neighborhood Pharmacy in Boynton Beach, Fla., who allegedly sold large amounts of oxycodone and hydromorphone on the black market.
The Centers for Medicare & Medicaid Services’ Center for Program Integrity has taken six administrative actions against health care providers for their alleged involvement in these offenses, per the DOJ’s announcement.
“Patient care and safety are top priorities for us, and CMS has taken administrative action against six providers to protect critical resources entrusted to Medicare while also safeguarding people with Medicare,” said CMS Administrator Chiquita Brooks-LaSure.
“These actions to combat fraud, waste, and abuse in our federal programs would not be possible without the close and successful partnership of the Centers for Medicare & Medicaid Services, the Department of Justice, and the U.S. Department of Health and Human Services Office of Inspector General,” she added.
A version of this article first appeared on Medscape.com.
In coordination with federal and state law enforcement, the DOJ charged the defendants for their involvement in the illegal distribution of opioids. At the time that they were charged with the alleged offenses, 12 of the defendants were medical professionals.
The 12 persons in eight federal districts across the country distributed more than 115 million controlled substances, including buprenorphine, clonazepam, dextroamphetamine-amphetamine, hydrocodone, morphine sulfate, oxycodone, oxymorphone, and Suboxone, per the DOJ.
“Doctors and health care professionals are entrusted with prescribing medicine responsibly and in the best interests of their patients. Today’s takedown targets medical providers across the country whose greed drove them to abandon this responsibility in favor of criminal profits,” said Anne Milgram, administrator of the Drug Enforcement Administration.
Medical professionals, others across six states charged
One former nurse, one business manager, and one individual who practiced medicine without a medical credential are among those listed in the indictment. These include the following:
- Eskender Getachew, MD, a Columbus, Ohio, sleep medicine specialist, was charged with unlawful distribution of controlled substances outside the use of professional practice and not for a legitimate medical practice.
- Charles Kistler, DO, an Upper Arlington, Ohio, family practice physician, was charged with unlawful distribution of controlled substances for unlawful prescribing at Midtown Family Practice Clinic in Columbus.
- Yogeshwar Gil, MBBS, a Manchester, Tenn., family medicine doctor and owner of a medical practice, was charged with conspiracy to unlawfully distribute controlled substances and maintaining a drug-involved premises. Dr. Gil was charged in connection with an alleged scheme to distribute opioids and Suboxone outside the usual course of professional practice and without a legitimate medical purpose.
- Contessa Holley, RN, a Pulaski, Tenn., former nurse and clinical director, was charged with wire fraud, aggravated identity theft, and possession of a controlled substance with intent to distribute. She’s alleged to be connected with a scheme to unlawfully obtain opioids by filling fraudulent prescriptions in the names of current and former patients who were in hospice. The indictment alleged that Ms. Holley used the patients’ hospice benefits to cover the opioids’ costs while keeping the drugs for her own use and for further distribution.
- Francene Aretha Gayle, MD, an Orlando, Fla., physician, was charged with conspiracy to unlawfully distribute controlled substances, conspiracy to commit health care fraud, health care fraud, and several substantive counts of illegally issuing opioid prescriptions. Dr. Gayle was charged along with Schara Monique Davis, a Huntsville, Ala.–based business manager. Per the indictment, Dr. Gayle and Ms. Davis operated three medical clinics in Alabama, where Dr. Gayle was the sole physician. The medical clinics billed health insurers for millions of dollars in patient visits that Dr. Gayle had supposedly conducted but during which she was allegedly absent from the clinics; other staff members conducted the visits instead. It’s alleged that Dr. Gayle presigned prescriptions for opioids that were given to patients.
- Robert Taffet, MD, a Haddonfield, N.J., orthopedic surgeon and owner of a medical practice in Sicklerville, N.J., was charged with conspiracy to unlawfully distribute controlled substances. The indictment alleges that he falsified patient files to state that he interacted with patients when he didn’t and that he issued prescriptions for opioids and other controlled substances without assessing the patients in person or by telemedicine. It’s alleged that Dr. Taffett issued prescriptions for more than 179,000 pills that were dispensed by New Jersey pharmacies between April 2020 and December 2021.
- Hau La, MD, a Brentwood, Tenn., family medicine physician and the operator of Absolute Medical Care in Smyrna, Tenn., was charged with sixteen counts of unlawful distribution of a controlled substance. The physician is alleged to have unlawfully prescribed opioids to eight patients outside the usual course of practice and without a legitimate medical purpose.
- Frederick De Mesa, of War, W.Va., practiced as a physician and used a DEA registration number that allowed him to prescribe controlled substances. Mr. De Mesa prescribed these substances without a medical license and didn’t have an active DEA registration number, according to the indictment.
- Loey Kousa, a former internist from Paintsville, Ky., was charged with unlawful distribution of controlled substances, healthcare fraud, and making false statements in connection with the delivery of health care services. The indictment alleges that the former physician issued prescriptions for opioids outside the usual course of professional practice and without a legitimate medical purpose in his capacity as owner and operator of East KY Clinic in Paintsville. He is alleged to have issued the unlawful prescriptions for patients whose treatments were covered by taxpayer-funded programs such as Medicare and Medicaid; he also billed these programs for medically unnecessary procedures for these patients.
Also included in the indictment were Jay Sadrinia, DMD, a Villa Hills, Ky., dentist, who was charged with four counts of illegal distribution of oxycodone and morphine sulfate and one count of illegal distribution of morphine sulfate that resulted in death or serious bodily injury; and Casey Kelleher, an owner-operator of Neighborhood Pharmacy in Boynton Beach, Fla., who allegedly sold large amounts of oxycodone and hydromorphone on the black market.
The Centers for Medicare & Medicaid Services’ Center for Program Integrity has taken six administrative actions against health care providers for their alleged involvement in these offenses, per the DOJ’s announcement.
“Patient care and safety are top priorities for us, and CMS has taken administrative action against six providers to protect critical resources entrusted to Medicare while also safeguarding people with Medicare,” said CMS Administrator Chiquita Brooks-LaSure.
“These actions to combat fraud, waste, and abuse in our federal programs would not be possible without the close and successful partnership of the Centers for Medicare & Medicaid Services, the Department of Justice, and the U.S. Department of Health and Human Services Office of Inspector General,” she added.
A version of this article first appeared on Medscape.com.
In coordination with federal and state law enforcement, the DOJ charged the defendants for their involvement in the illegal distribution of opioids. At the time that they were charged with the alleged offenses, 12 of the defendants were medical professionals.
The 12 persons in eight federal districts across the country distributed more than 115 million controlled substances, including buprenorphine, clonazepam, dextroamphetamine-amphetamine, hydrocodone, morphine sulfate, oxycodone, oxymorphone, and Suboxone, per the DOJ.
“Doctors and health care professionals are entrusted with prescribing medicine responsibly and in the best interests of their patients. Today’s takedown targets medical providers across the country whose greed drove them to abandon this responsibility in favor of criminal profits,” said Anne Milgram, administrator of the Drug Enforcement Administration.
Medical professionals, others across six states charged
One former nurse, one business manager, and one individual who practiced medicine without a medical credential are among those listed in the indictment. These include the following:
- Eskender Getachew, MD, a Columbus, Ohio, sleep medicine specialist, was charged with unlawful distribution of controlled substances outside the use of professional practice and not for a legitimate medical practice.
- Charles Kistler, DO, an Upper Arlington, Ohio, family practice physician, was charged with unlawful distribution of controlled substances for unlawful prescribing at Midtown Family Practice Clinic in Columbus.
- Yogeshwar Gil, MBBS, a Manchester, Tenn., family medicine doctor and owner of a medical practice, was charged with conspiracy to unlawfully distribute controlled substances and maintaining a drug-involved premises. Dr. Gil was charged in connection with an alleged scheme to distribute opioids and Suboxone outside the usual course of professional practice and without a legitimate medical purpose.
- Contessa Holley, RN, a Pulaski, Tenn., former nurse and clinical director, was charged with wire fraud, aggravated identity theft, and possession of a controlled substance with intent to distribute. She’s alleged to be connected with a scheme to unlawfully obtain opioids by filling fraudulent prescriptions in the names of current and former patients who were in hospice. The indictment alleged that Ms. Holley used the patients’ hospice benefits to cover the opioids’ costs while keeping the drugs for her own use and for further distribution.
- Francene Aretha Gayle, MD, an Orlando, Fla., physician, was charged with conspiracy to unlawfully distribute controlled substances, conspiracy to commit health care fraud, health care fraud, and several substantive counts of illegally issuing opioid prescriptions. Dr. Gayle was charged along with Schara Monique Davis, a Huntsville, Ala.–based business manager. Per the indictment, Dr. Gayle and Ms. Davis operated three medical clinics in Alabama, where Dr. Gayle was the sole physician. The medical clinics billed health insurers for millions of dollars in patient visits that Dr. Gayle had supposedly conducted but during which she was allegedly absent from the clinics; other staff members conducted the visits instead. It’s alleged that Dr. Gayle presigned prescriptions for opioids that were given to patients.
- Robert Taffet, MD, a Haddonfield, N.J., orthopedic surgeon and owner of a medical practice in Sicklerville, N.J., was charged with conspiracy to unlawfully distribute controlled substances. The indictment alleges that he falsified patient files to state that he interacted with patients when he didn’t and that he issued prescriptions for opioids and other controlled substances without assessing the patients in person or by telemedicine. It’s alleged that Dr. Taffett issued prescriptions for more than 179,000 pills that were dispensed by New Jersey pharmacies between April 2020 and December 2021.
- Hau La, MD, a Brentwood, Tenn., family medicine physician and the operator of Absolute Medical Care in Smyrna, Tenn., was charged with sixteen counts of unlawful distribution of a controlled substance. The physician is alleged to have unlawfully prescribed opioids to eight patients outside the usual course of practice and without a legitimate medical purpose.
- Frederick De Mesa, of War, W.Va., practiced as a physician and used a DEA registration number that allowed him to prescribe controlled substances. Mr. De Mesa prescribed these substances without a medical license and didn’t have an active DEA registration number, according to the indictment.
- Loey Kousa, a former internist from Paintsville, Ky., was charged with unlawful distribution of controlled substances, healthcare fraud, and making false statements in connection with the delivery of health care services. The indictment alleges that the former physician issued prescriptions for opioids outside the usual course of professional practice and without a legitimate medical purpose in his capacity as owner and operator of East KY Clinic in Paintsville. He is alleged to have issued the unlawful prescriptions for patients whose treatments were covered by taxpayer-funded programs such as Medicare and Medicaid; he also billed these programs for medically unnecessary procedures for these patients.
Also included in the indictment were Jay Sadrinia, DMD, a Villa Hills, Ky., dentist, who was charged with four counts of illegal distribution of oxycodone and morphine sulfate and one count of illegal distribution of morphine sulfate that resulted in death or serious bodily injury; and Casey Kelleher, an owner-operator of Neighborhood Pharmacy in Boynton Beach, Fla., who allegedly sold large amounts of oxycodone and hydromorphone on the black market.
The Centers for Medicare & Medicaid Services’ Center for Program Integrity has taken six administrative actions against health care providers for their alleged involvement in these offenses, per the DOJ’s announcement.
“Patient care and safety are top priorities for us, and CMS has taken administrative action against six providers to protect critical resources entrusted to Medicare while also safeguarding people with Medicare,” said CMS Administrator Chiquita Brooks-LaSure.
“These actions to combat fraud, waste, and abuse in our federal programs would not be possible without the close and successful partnership of the Centers for Medicare & Medicaid Services, the Department of Justice, and the U.S. Department of Health and Human Services Office of Inspector General,” she added.
A version of this article first appeared on Medscape.com.