User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'main-prefix')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
Antipsychotic tied to dose-related weight gain, higher cholesterol
new research suggests.
Investigators analyzed 1-year data for more than 400 patients who were taking risperidone and/or its metabolite paliperidone (Invega). Results showed increments of 1 mg of risperidone-equivalent doses were associated with an increase of 0.25% of weight within a year of follow-up.
“Although our findings report a positive and statistically significant dose-dependence of weight gain and cholesterol, both total and LDL [cholesterol], the size of the predicted changes of metabolic effects is clinically nonrelevant,” lead author Marianna Piras, PharmD, Centre for Psychiatric Neuroscience, Lausanne (Switzerland) University Hospital, said in an interview.
“Therefore, dose lowering would not have a beneficial effect on attenuating weight gain or cholesterol increases and could lead to psychiatric decompensation,” said Ms. Piras, who is also a PhD candidate in the unit of pharmacogenetics and clinical psychopharmacology at the University of Lausanne.
However, she added that because dose increments could increase risk for significant weight gain in the first month of treatment – the dose can be increased typically in a range of 1-10 grams – and strong dose increments could contribute to metabolic worsening over time, “risperidone minimum effective doses should be preferred.”
The findings were published online in the Journal of Clinical Psychiatry.
‘Serious public health issue’
Compared with the general population, patients with mental illness present with a greater prevalence of metabolic disorders. In addition, several psychotropic medications, including antipsychotics, can induce metabolic alterations such as weight gain, the investigators noted.
Antipsychotic-induced metabolic adverse effects “constitute a serious public health issue” because they are risk factors for cardiovascular diseases such as obesity and/or dyslipidemia, “which have been associated with a 10-year reduced life expectancy in the psychiatric population,” Ms. Piras said.
“The dose-dependence of metabolic adverse effects is a debated subject that needs to be assessed for each psychotropic drug known to induce weight gain,” she added.
Several previous studies have examined whether there is a dose-related effect of antipsychotics on metabolic parameters, “with some results suggesting that [weight gain] seems to develop even when low off-label doses are prescribed,” Ms. Piras noted.
She and her colleagues had already studied dose-related metabolic effects of quetiapine (Seroquel) and olanzapine (Zyprexa).
Risperidone is an antipsychotic with a “medium to high metabolic risk profile,” the researchers note, and few studies have examined the impact of risperidone on metabolic parameters other than weight gain.
For the current analysis, they analyzed data from a longitudinal study that included 438 patients (mean age, 40.7 years; 50.7% men) who started treatment with risperidone and/or paliperidone between 2007 and 2018.
The participants had diagnoses of schizophrenia, schizoaffective disorder, bipolar disorder, depression, “other,” or “unknown.”
Clinical follow-up periods were up to a year, but were no shorter than 3 weeks. The investigators also assessed the data at different time intervals at 1, 3, 6, and 12 months “to appreciate the evolution of the metabolic parameters.”
In addition, they collected demographic and clinical information, such as comorbidities, and measured patients’ weight, height, waist circumference, blood pressure, plasma glucose, and lipids at baseline and at 1, 3, and 12 months and then annually. Weight, waist circumference, and BP were also assessed at 2 and 6 months.
Doses of paliperidone were converted into risperidone-equivalent doses.
Significant weight gain over time
The mean duration of follow-up for the participants, of whom 374 were being treated with risperidone and 64 with paliperidone, was 153 days. Close to half (48.2%) were taking other psychotropic medications known to be associated with some degree of metabolic risk.
Patients were divided into two cohorts based on their daily dose intake (DDI): less than 3 mg/day (n = 201) and at least 3 mg/day (n = 237).
In the overall cohort, a “significant effect of time on weight change was found for each time point,” the investigators reported.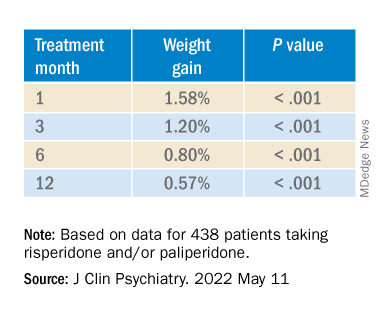
When the researchers looked at the changes according to DDI, they found that each 1-mg dose increase was associated with incremental weight gain at each time point.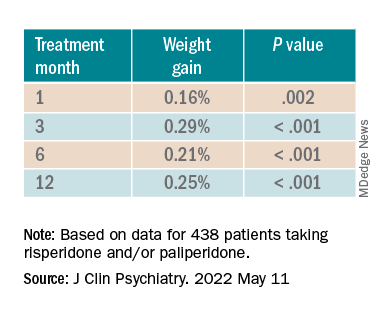
Patients who had 5% or greater weight gain in the first month continued to gain weight more than patients who did not reach that threshold, leading the researchers to call that early threshold a “strong predictor of important weight gain in the long term.” There was a weight gain of 6.68% at 3 months, of 7.36% at 6 months, and of 7.7% at 12 months.
After the patients were stratified by age, there were differences in the effect of DDI on various age groups at different time points.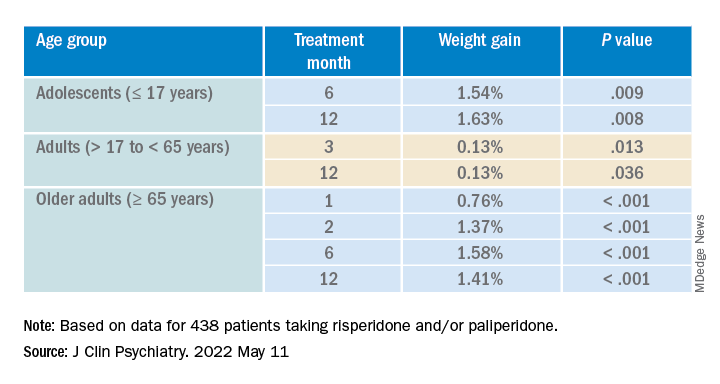
Dose was shown to have a significant effect on weight gain for women at all four time points (P ≥ .001), but for men only at 3 months (P = .003).
For each additional 1-mg dose, there was a 0.05 mmol/L (1.93 mg/dL) increase in total cholesterol (P = .018) after 1 year and a 0.04 mmol/L (1.54 mg/dL) increase in LDL cholesterol (P = .011).
There were no significant effects of time or DDI on triglycerides, HDL cholesterol, glucose levels, and systolic BP, and there was a negative effect of DDI on diastolic BP (P = .001).
The findings “provide evidence for a small dose effect of risperidone” on weight gain and total and LDL cholesterol levels, the investigators note.
Ms. Piras added that because each antipsychotic differs in its metabolic risk profile, “further analyses on other antipsychotics are ongoing in our laboratory, so far confirming our findings.”
Small increases, big changes
Commenting on the study, Erika Nurmi, MD, PhD, associate professor in the department of psychiatry and biobehavioral sciences at the Semel Institute for Neuroscience, University of California, Los Angeles, said the study is “unique in the field.”

It “leverages real-world data from a large patient registry to ask a long-unanswered question: Are weight and metabolic adverse effects proportional to dose? Big data approaches like these are very powerful, given the large number of participants that can be included,” said Dr. Nurmi, who was not involved with the research.
However, she cautioned, the “biggest drawback [is that] these data are by nature much more complex and prone to confounding effects.”
In this case, a “critical confounder” for the study was that the majority of individuals taking higher risperidone doses were also taking other drugs known to cause weight gain, whereas the majority of those on lower risperidone doses were not. “This difference may explain the dose relationship observed,” she said.
Because real-world, big data are “valuable but also messy, conclusions drawn from them must be interpreted with caution,” Dr. Nurmi said.
She added that it is generally wise to use the lowest effective dose possible.
“Clinicians should appreciate that even small doses of antipsychotics can cause big changes in weight. Risks and benefits of medications must be carefully considered in clinical practice,” Dr. Nurmi said.
The research was funded in part by the Swiss National Research Foundation. Piras reports no relevant financial relationships. The other investigators’ disclosures are listed in the original article. Dr. Nurmi reported no relevant financial relationships, but she is an unpaid member of the Tourette Association of America’s medical advisory board and of the Myriad Genetics scientific advisory board.
A version of this article first appeared on Medscape.com.
new research suggests.
Investigators analyzed 1-year data for more than 400 patients who were taking risperidone and/or its metabolite paliperidone (Invega). Results showed increments of 1 mg of risperidone-equivalent doses were associated with an increase of 0.25% of weight within a year of follow-up.
“Although our findings report a positive and statistically significant dose-dependence of weight gain and cholesterol, both total and LDL [cholesterol], the size of the predicted changes of metabolic effects is clinically nonrelevant,” lead author Marianna Piras, PharmD, Centre for Psychiatric Neuroscience, Lausanne (Switzerland) University Hospital, said in an interview.
“Therefore, dose lowering would not have a beneficial effect on attenuating weight gain or cholesterol increases and could lead to psychiatric decompensation,” said Ms. Piras, who is also a PhD candidate in the unit of pharmacogenetics and clinical psychopharmacology at the University of Lausanne.
However, she added that because dose increments could increase risk for significant weight gain in the first month of treatment – the dose can be increased typically in a range of 1-10 grams – and strong dose increments could contribute to metabolic worsening over time, “risperidone minimum effective doses should be preferred.”
The findings were published online in the Journal of Clinical Psychiatry.
‘Serious public health issue’
Compared with the general population, patients with mental illness present with a greater prevalence of metabolic disorders. In addition, several psychotropic medications, including antipsychotics, can induce metabolic alterations such as weight gain, the investigators noted.
Antipsychotic-induced metabolic adverse effects “constitute a serious public health issue” because they are risk factors for cardiovascular diseases such as obesity and/or dyslipidemia, “which have been associated with a 10-year reduced life expectancy in the psychiatric population,” Ms. Piras said.
“The dose-dependence of metabolic adverse effects is a debated subject that needs to be assessed for each psychotropic drug known to induce weight gain,” she added.
Several previous studies have examined whether there is a dose-related effect of antipsychotics on metabolic parameters, “with some results suggesting that [weight gain] seems to develop even when low off-label doses are prescribed,” Ms. Piras noted.
She and her colleagues had already studied dose-related metabolic effects of quetiapine (Seroquel) and olanzapine (Zyprexa).
Risperidone is an antipsychotic with a “medium to high metabolic risk profile,” the researchers note, and few studies have examined the impact of risperidone on metabolic parameters other than weight gain.
For the current analysis, they analyzed data from a longitudinal study that included 438 patients (mean age, 40.7 years; 50.7% men) who started treatment with risperidone and/or paliperidone between 2007 and 2018.
The participants had diagnoses of schizophrenia, schizoaffective disorder, bipolar disorder, depression, “other,” or “unknown.”
Clinical follow-up periods were up to a year, but were no shorter than 3 weeks. The investigators also assessed the data at different time intervals at 1, 3, 6, and 12 months “to appreciate the evolution of the metabolic parameters.”
In addition, they collected demographic and clinical information, such as comorbidities, and measured patients’ weight, height, waist circumference, blood pressure, plasma glucose, and lipids at baseline and at 1, 3, and 12 months and then annually. Weight, waist circumference, and BP were also assessed at 2 and 6 months.
Doses of paliperidone were converted into risperidone-equivalent doses.
Significant weight gain over time
The mean duration of follow-up for the participants, of whom 374 were being treated with risperidone and 64 with paliperidone, was 153 days. Close to half (48.2%) were taking other psychotropic medications known to be associated with some degree of metabolic risk.
Patients were divided into two cohorts based on their daily dose intake (DDI): less than 3 mg/day (n = 201) and at least 3 mg/day (n = 237).
In the overall cohort, a “significant effect of time on weight change was found for each time point,” the investigators reported.
When the researchers looked at the changes according to DDI, they found that each 1-mg dose increase was associated with incremental weight gain at each time point.
Patients who had 5% or greater weight gain in the first month continued to gain weight more than patients who did not reach that threshold, leading the researchers to call that early threshold a “strong predictor of important weight gain in the long term.” There was a weight gain of 6.68% at 3 months, of 7.36% at 6 months, and of 7.7% at 12 months.
After the patients were stratified by age, there were differences in the effect of DDI on various age groups at different time points.
Dose was shown to have a significant effect on weight gain for women at all four time points (P ≥ .001), but for men only at 3 months (P = .003).
For each additional 1-mg dose, there was a 0.05 mmol/L (1.93 mg/dL) increase in total cholesterol (P = .018) after 1 year and a 0.04 mmol/L (1.54 mg/dL) increase in LDL cholesterol (P = .011).
There were no significant effects of time or DDI on triglycerides, HDL cholesterol, glucose levels, and systolic BP, and there was a negative effect of DDI on diastolic BP (P = .001).
The findings “provide evidence for a small dose effect of risperidone” on weight gain and total and LDL cholesterol levels, the investigators note.
Ms. Piras added that because each antipsychotic differs in its metabolic risk profile, “further analyses on other antipsychotics are ongoing in our laboratory, so far confirming our findings.”
Small increases, big changes
Commenting on the study, Erika Nurmi, MD, PhD, associate professor in the department of psychiatry and biobehavioral sciences at the Semel Institute for Neuroscience, University of California, Los Angeles, said the study is “unique in the field.”
It “leverages real-world data from a large patient registry to ask a long-unanswered question: Are weight and metabolic adverse effects proportional to dose? Big data approaches like these are very powerful, given the large number of participants that can be included,” said Dr. Nurmi, who was not involved with the research.
However, she cautioned, the “biggest drawback [is that] these data are by nature much more complex and prone to confounding effects.”
In this case, a “critical confounder” for the study was that the majority of individuals taking higher risperidone doses were also taking other drugs known to cause weight gain, whereas the majority of those on lower risperidone doses were not. “This difference may explain the dose relationship observed,” she said.
Because real-world, big data are “valuable but also messy, conclusions drawn from them must be interpreted with caution,” Dr. Nurmi said.
She added that it is generally wise to use the lowest effective dose possible.
“Clinicians should appreciate that even small doses of antipsychotics can cause big changes in weight. Risks and benefits of medications must be carefully considered in clinical practice,” Dr. Nurmi said.
The research was funded in part by the Swiss National Research Foundation. Piras reports no relevant financial relationships. The other investigators’ disclosures are listed in the original article. Dr. Nurmi reported no relevant financial relationships, but she is an unpaid member of the Tourette Association of America’s medical advisory board and of the Myriad Genetics scientific advisory board.
A version of this article first appeared on Medscape.com.
new research suggests.
Investigators analyzed 1-year data for more than 400 patients who were taking risperidone and/or its metabolite paliperidone (Invega). Results showed increments of 1 mg of risperidone-equivalent doses were associated with an increase of 0.25% of weight within a year of follow-up.
“Although our findings report a positive and statistically significant dose-dependence of weight gain and cholesterol, both total and LDL [cholesterol], the size of the predicted changes of metabolic effects is clinically nonrelevant,” lead author Marianna Piras, PharmD, Centre for Psychiatric Neuroscience, Lausanne (Switzerland) University Hospital, said in an interview.
“Therefore, dose lowering would not have a beneficial effect on attenuating weight gain or cholesterol increases and could lead to psychiatric decompensation,” said Ms. Piras, who is also a PhD candidate in the unit of pharmacogenetics and clinical psychopharmacology at the University of Lausanne.
However, she added that because dose increments could increase risk for significant weight gain in the first month of treatment – the dose can be increased typically in a range of 1-10 grams – and strong dose increments could contribute to metabolic worsening over time, “risperidone minimum effective doses should be preferred.”
The findings were published online in the Journal of Clinical Psychiatry.
‘Serious public health issue’
Compared with the general population, patients with mental illness present with a greater prevalence of metabolic disorders. In addition, several psychotropic medications, including antipsychotics, can induce metabolic alterations such as weight gain, the investigators noted.
Antipsychotic-induced metabolic adverse effects “constitute a serious public health issue” because they are risk factors for cardiovascular diseases such as obesity and/or dyslipidemia, “which have been associated with a 10-year reduced life expectancy in the psychiatric population,” Ms. Piras said.
“The dose-dependence of metabolic adverse effects is a debated subject that needs to be assessed for each psychotropic drug known to induce weight gain,” she added.
Several previous studies have examined whether there is a dose-related effect of antipsychotics on metabolic parameters, “with some results suggesting that [weight gain] seems to develop even when low off-label doses are prescribed,” Ms. Piras noted.
She and her colleagues had already studied dose-related metabolic effects of quetiapine (Seroquel) and olanzapine (Zyprexa).
Risperidone is an antipsychotic with a “medium to high metabolic risk profile,” the researchers note, and few studies have examined the impact of risperidone on metabolic parameters other than weight gain.
For the current analysis, they analyzed data from a longitudinal study that included 438 patients (mean age, 40.7 years; 50.7% men) who started treatment with risperidone and/or paliperidone between 2007 and 2018.
The participants had diagnoses of schizophrenia, schizoaffective disorder, bipolar disorder, depression, “other,” or “unknown.”
Clinical follow-up periods were up to a year, but were no shorter than 3 weeks. The investigators also assessed the data at different time intervals at 1, 3, 6, and 12 months “to appreciate the evolution of the metabolic parameters.”
In addition, they collected demographic and clinical information, such as comorbidities, and measured patients’ weight, height, waist circumference, blood pressure, plasma glucose, and lipids at baseline and at 1, 3, and 12 months and then annually. Weight, waist circumference, and BP were also assessed at 2 and 6 months.
Doses of paliperidone were converted into risperidone-equivalent doses.
Significant weight gain over time
The mean duration of follow-up for the participants, of whom 374 were being treated with risperidone and 64 with paliperidone, was 153 days. Close to half (48.2%) were taking other psychotropic medications known to be associated with some degree of metabolic risk.
Patients were divided into two cohorts based on their daily dose intake (DDI): less than 3 mg/day (n = 201) and at least 3 mg/day (n = 237).
In the overall cohort, a “significant effect of time on weight change was found for each time point,” the investigators reported.
When the researchers looked at the changes according to DDI, they found that each 1-mg dose increase was associated with incremental weight gain at each time point.
Patients who had 5% or greater weight gain in the first month continued to gain weight more than patients who did not reach that threshold, leading the researchers to call that early threshold a “strong predictor of important weight gain in the long term.” There was a weight gain of 6.68% at 3 months, of 7.36% at 6 months, and of 7.7% at 12 months.
After the patients were stratified by age, there were differences in the effect of DDI on various age groups at different time points.
Dose was shown to have a significant effect on weight gain for women at all four time points (P ≥ .001), but for men only at 3 months (P = .003).
For each additional 1-mg dose, there was a 0.05 mmol/L (1.93 mg/dL) increase in total cholesterol (P = .018) after 1 year and a 0.04 mmol/L (1.54 mg/dL) increase in LDL cholesterol (P = .011).
There were no significant effects of time or DDI on triglycerides, HDL cholesterol, glucose levels, and systolic BP, and there was a negative effect of DDI on diastolic BP (P = .001).
The findings “provide evidence for a small dose effect of risperidone” on weight gain and total and LDL cholesterol levels, the investigators note.
Ms. Piras added that because each antipsychotic differs in its metabolic risk profile, “further analyses on other antipsychotics are ongoing in our laboratory, so far confirming our findings.”
Small increases, big changes
Commenting on the study, Erika Nurmi, MD, PhD, associate professor in the department of psychiatry and biobehavioral sciences at the Semel Institute for Neuroscience, University of California, Los Angeles, said the study is “unique in the field.”
It “leverages real-world data from a large patient registry to ask a long-unanswered question: Are weight and metabolic adverse effects proportional to dose? Big data approaches like these are very powerful, given the large number of participants that can be included,” said Dr. Nurmi, who was not involved with the research.
However, she cautioned, the “biggest drawback [is that] these data are by nature much more complex and prone to confounding effects.”
In this case, a “critical confounder” for the study was that the majority of individuals taking higher risperidone doses were also taking other drugs known to cause weight gain, whereas the majority of those on lower risperidone doses were not. “This difference may explain the dose relationship observed,” she said.
Because real-world, big data are “valuable but also messy, conclusions drawn from them must be interpreted with caution,” Dr. Nurmi said.
She added that it is generally wise to use the lowest effective dose possible.
“Clinicians should appreciate that even small doses of antipsychotics can cause big changes in weight. Risks and benefits of medications must be carefully considered in clinical practice,” Dr. Nurmi said.
The research was funded in part by the Swiss National Research Foundation. Piras reports no relevant financial relationships. The other investigators’ disclosures are listed in the original article. Dr. Nurmi reported no relevant financial relationships, but she is an unpaid member of the Tourette Association of America’s medical advisory board and of the Myriad Genetics scientific advisory board.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF CLINICAL PSYCHIATRY
Cannabis may relieve pain as effectively as opioids, but more research is needed
Several other systematic reviews have recently evaluated cannabinoids for treating chronic pain, but the new study’s methodology was “distinct” in “important ways,” leading to “conclusions that differ from other reviews,” according to the authors of the paper published in the Annals of Internal Medicine.

In the new systematic review, synthetic products with high THC:CBD ratios were associated with moderate improvements in pain, whereas plant-based products with comparable THC:CBD ratios offered less relief, said study author Marian S. McDonagh, PharmD, professor of medical informatics and clinical epidemiology, and codirector of the Evidence-based Practice Center at Oregon Health & Science University, Portland, and colleagues.
Specifically, the investigators stratified cannabis-based interventions according to relative content of two key cannabinoids: THC and CBD. Products were sorted into five categories: high THC:CBD ratio (at least 2:1), comparable THC:CBD ratio (less than 2:1 but more than 1:2), low THC:CBD ratio (no more than 1:2), whole-plant cannabis products, and other cannabinoids.
“In preclinical studies, THC and related compounds have demonstrated analgesic properties, although its psychoactive effects and addiction potential may limit its suitability as an analgesic,” the investigators wrote. “CBD and other cannabinoids may also have some analgesic or anti-inflammatory properties and are not believed to be psychoactive or addictive. Given the variation in analgesic effect with THC and CBD, response may differ according to the ratio of THC to CBD in products used to treat pain.”
The final analysis included 18 randomized placebo-controlled trials involving 1,740 individuals and 7 cohort studies involving 13,095 individuals. Most of the studies were short-term, lasting 1-6 months.
Pain was scored on a ten-point scale, with improvements reported as the mean difference from baseline to post treatment. A mean difference in pain score of 0.5-1.0 was considered a “small effect,” an improvement of 1-2 points was considered a “moderate effect,” and an improvement greater than 2 points was considered a “large effect.”
Cannabis-based products with relatively high THC:CBD ratios showed efficacy
Synthetic products with high THC:CBD ratios offered moderate pain relief, based on a mean difference in pain score of –1.15 (95% confidence interval, –1.99 to –0.54), whereas products with comparable THC:CBD ratios were associated with a small effect on pain, with a mean difference of –0.52 (95% CI, –0.95 to –0.19).
According to Dr. McDonagh, treatment response rates were on par with response rates for more conventional treatments, “such as opioids or specific antidepressant drugs,” but data for the cannabis-based products are weaker.
“The amount of evidence available for cannabis-related products is very limited for [response rates], and therefore less certain,” Dr. McDonagh said in an interview. “The average reduction in pain severity is also similar to some other treatments, but we do not have studies directly comparing these treatments to draw conclusions.”
Although the cannabis-based products with relatively high and comparable THC:CBD ratios showed efficacy, they were also associated with “moderate to large increased risk for dizziness, sedation, and nausea,” the investigators wrote, noting that evidence was insufficient to characterize other “key adverse event outcomes” that may occur with long-term use, such as “psychosis, cannabis use disorder, and cognitive deficits.”
For products with low THC:CBD ratios, or without reported THC:CBD ratios, data were too scarce to reach any conclusions at all about safety or efficacy, highlighting the sizable knowledge gaps that remain in the area, the authors said.
“The current evidence on cannabis-related products for chronic pain is quite limited,” Dr. McDonagh said in an interview. “Patients with chronic pain should consult with their doctor to discuss which of the many options for treating chronic pain is best for them to start with.”
Patients may face resistance when asking about cannabis
According to Kevin F. Boehnke, PhD, and Daniel J. Clauw, MD, of the anesthesiology department and Chronic Pain and Fatigue Research Center at the University of Michigan, Ann Arbor, patients with chronic pain may face resistance, or even risk of being reported, when asking about cannabis-based products.
“Some physicians cite lack of data as rationale for not engaging with patients who wish to use or currently use cannabis,” Dr. Boehnke and Dr. Clauw wrote in an accompanying editorial. “Such practices may reflect consideration of cannabis solely as a drug of misuse (even in the 37 states where medical cannabis is legal) and requirements to refer patients who disclose or test positive for cannabis use to addiction services or decline to refill opioid prescriptions.”
Instead of shutting patients out, Dr. Boehnke and Dr. Clauw suggested clinicians engage in an “open information exchange” with their patients that focuses on “pragmatism, patient experience, known cannabinoid effects, and harm reduction.” In these conversations, the editorialists recommend noting that, “as with other analgesics, some persons will benefit, and others will not.”
They also offered some practical guidance: “Clinicians could suggest using tinctures (effect onset, 15-45 minutes) for breakthrough pain and edibles or capsules (which last about 6-8 hours) for extended relief. ... The scientific literature suggests that CBD doses could start at 5-10 mg twice daily and increase to 40-50 mg daily, whereas THC doses could start at 0.5-3 mg (initially at night) and increase to 30-40 mg/day.”
David Copenhaver, MD, MPH, clinical professor and chief of the division of pain medicine at UC Davis Health, Sacramento, shared a similar clinical mindset for patients choosing between opioids and cannabis-based products, specifically, CBD.

Compared with opioids, “the side-effect profile for CBD is less and the risk of mortality is less,” Dr. Copenhaver said in an interview, pointing out that nobody, to his knowledge, has ever died from an overdose of cannabis alone, and that CBD doses up to 1,000 mg/kg have been safely tolerated in people. “You present that, and most patients will say, ‘You know, I’d like to give this a try.’”
If so, Dr. Copenhaver makes sure patients know about a nonmedical risk: “The risk to the pocketbook.” Unlike opioids, which are covered under most insurance policies, most cannabis-based therapies are self-pay.
Buyers may get what they pay for, Dr. Copenhaver said, since products vary in quality, as do the dispensaries, from “very modest,” to highly sophisticated, with some even using chromatographic datasets to support the purity of their products.
Dr. Copenhaver steers his patients toward these more sophisticated retailers. Their expertise appears to be paying off, he said, not only in relief for patients, but also in market share. “Survival of the most fit will occur in the marketplace based on the results,” he said. “Unfortunately, some of that information doesn’t get percolated out into the literature.”
For investigators to fully uncover what cannabis-based products can do for chronic pain, Dr. Copenhaver said they need to get as “granular” as the leading dispensaries, which may first require recognition of the “very expansive opportunity” that less-studied cannabinoids may provide.
The study was supported by the Agency for Healthcare Research and Quality, U.S. Department of Health & Human Services. The investigators, Dr. Boehnke, Dr. Clauw, and Dr. Copenhaver, disclosed no conflicts of interest.
Several other systematic reviews have recently evaluated cannabinoids for treating chronic pain, but the new study’s methodology was “distinct” in “important ways,” leading to “conclusions that differ from other reviews,” according to the authors of the paper published in the Annals of Internal Medicine.
In the new systematic review, synthetic products with high THC:CBD ratios were associated with moderate improvements in pain, whereas plant-based products with comparable THC:CBD ratios offered less relief, said study author Marian S. McDonagh, PharmD, professor of medical informatics and clinical epidemiology, and codirector of the Evidence-based Practice Center at Oregon Health & Science University, Portland, and colleagues.
Specifically, the investigators stratified cannabis-based interventions according to relative content of two key cannabinoids: THC and CBD. Products were sorted into five categories: high THC:CBD ratio (at least 2:1), comparable THC:CBD ratio (less than 2:1 but more than 1:2), low THC:CBD ratio (no more than 1:2), whole-plant cannabis products, and other cannabinoids.
“In preclinical studies, THC and related compounds have demonstrated analgesic properties, although its psychoactive effects and addiction potential may limit its suitability as an analgesic,” the investigators wrote. “CBD and other cannabinoids may also have some analgesic or anti-inflammatory properties and are not believed to be psychoactive or addictive. Given the variation in analgesic effect with THC and CBD, response may differ according to the ratio of THC to CBD in products used to treat pain.”
The final analysis included 18 randomized placebo-controlled trials involving 1,740 individuals and 7 cohort studies involving 13,095 individuals. Most of the studies were short-term, lasting 1-6 months.
Pain was scored on a ten-point scale, with improvements reported as the mean difference from baseline to post treatment. A mean difference in pain score of 0.5-1.0 was considered a “small effect,” an improvement of 1-2 points was considered a “moderate effect,” and an improvement greater than 2 points was considered a “large effect.”
Cannabis-based products with relatively high THC:CBD ratios showed efficacy
Synthetic products with high THC:CBD ratios offered moderate pain relief, based on a mean difference in pain score of –1.15 (95% confidence interval, –1.99 to –0.54), whereas products with comparable THC:CBD ratios were associated with a small effect on pain, with a mean difference of –0.52 (95% CI, –0.95 to –0.19).
According to Dr. McDonagh, treatment response rates were on par with response rates for more conventional treatments, “such as opioids or specific antidepressant drugs,” but data for the cannabis-based products are weaker.
“The amount of evidence available for cannabis-related products is very limited for [response rates], and therefore less certain,” Dr. McDonagh said in an interview. “The average reduction in pain severity is also similar to some other treatments, but we do not have studies directly comparing these treatments to draw conclusions.”
Although the cannabis-based products with relatively high and comparable THC:CBD ratios showed efficacy, they were also associated with “moderate to large increased risk for dizziness, sedation, and nausea,” the investigators wrote, noting that evidence was insufficient to characterize other “key adverse event outcomes” that may occur with long-term use, such as “psychosis, cannabis use disorder, and cognitive deficits.”
For products with low THC:CBD ratios, or without reported THC:CBD ratios, data were too scarce to reach any conclusions at all about safety or efficacy, highlighting the sizable knowledge gaps that remain in the area, the authors said.
“The current evidence on cannabis-related products for chronic pain is quite limited,” Dr. McDonagh said in an interview. “Patients with chronic pain should consult with their doctor to discuss which of the many options for treating chronic pain is best for them to start with.”
Patients may face resistance when asking about cannabis
According to Kevin F. Boehnke, PhD, and Daniel J. Clauw, MD, of the anesthesiology department and Chronic Pain and Fatigue Research Center at the University of Michigan, Ann Arbor, patients with chronic pain may face resistance, or even risk of being reported, when asking about cannabis-based products.
“Some physicians cite lack of data as rationale for not engaging with patients who wish to use or currently use cannabis,” Dr. Boehnke and Dr. Clauw wrote in an accompanying editorial. “Such practices may reflect consideration of cannabis solely as a drug of misuse (even in the 37 states where medical cannabis is legal) and requirements to refer patients who disclose or test positive for cannabis use to addiction services or decline to refill opioid prescriptions.”
Instead of shutting patients out, Dr. Boehnke and Dr. Clauw suggested clinicians engage in an “open information exchange” with their patients that focuses on “pragmatism, patient experience, known cannabinoid effects, and harm reduction.” In these conversations, the editorialists recommend noting that, “as with other analgesics, some persons will benefit, and others will not.”
They also offered some practical guidance: “Clinicians could suggest using tinctures (effect onset, 15-45 minutes) for breakthrough pain and edibles or capsules (which last about 6-8 hours) for extended relief. ... The scientific literature suggests that CBD doses could start at 5-10 mg twice daily and increase to 40-50 mg daily, whereas THC doses could start at 0.5-3 mg (initially at night) and increase to 30-40 mg/day.”
David Copenhaver, MD, MPH, clinical professor and chief of the division of pain medicine at UC Davis Health, Sacramento, shared a similar clinical mindset for patients choosing between opioids and cannabis-based products, specifically, CBD.
Compared with opioids, “the side-effect profile for CBD is less and the risk of mortality is less,” Dr. Copenhaver said in an interview, pointing out that nobody, to his knowledge, has ever died from an overdose of cannabis alone, and that CBD doses up to 1,000 mg/kg have been safely tolerated in people. “You present that, and most patients will say, ‘You know, I’d like to give this a try.’”
If so, Dr. Copenhaver makes sure patients know about a nonmedical risk: “The risk to the pocketbook.” Unlike opioids, which are covered under most insurance policies, most cannabis-based therapies are self-pay.
Buyers may get what they pay for, Dr. Copenhaver said, since products vary in quality, as do the dispensaries, from “very modest,” to highly sophisticated, with some even using chromatographic datasets to support the purity of their products.
Dr. Copenhaver steers his patients toward these more sophisticated retailers. Their expertise appears to be paying off, he said, not only in relief for patients, but also in market share. “Survival of the most fit will occur in the marketplace based on the results,” he said. “Unfortunately, some of that information doesn’t get percolated out into the literature.”
For investigators to fully uncover what cannabis-based products can do for chronic pain, Dr. Copenhaver said they need to get as “granular” as the leading dispensaries, which may first require recognition of the “very expansive opportunity” that less-studied cannabinoids may provide.
The study was supported by the Agency for Healthcare Research and Quality, U.S. Department of Health & Human Services. The investigators, Dr. Boehnke, Dr. Clauw, and Dr. Copenhaver, disclosed no conflicts of interest.
Several other systematic reviews have recently evaluated cannabinoids for treating chronic pain, but the new study’s methodology was “distinct” in “important ways,” leading to “conclusions that differ from other reviews,” according to the authors of the paper published in the Annals of Internal Medicine.
In the new systematic review, synthetic products with high THC:CBD ratios were associated with moderate improvements in pain, whereas plant-based products with comparable THC:CBD ratios offered less relief, said study author Marian S. McDonagh, PharmD, professor of medical informatics and clinical epidemiology, and codirector of the Evidence-based Practice Center at Oregon Health & Science University, Portland, and colleagues.
Specifically, the investigators stratified cannabis-based interventions according to relative content of two key cannabinoids: THC and CBD. Products were sorted into five categories: high THC:CBD ratio (at least 2:1), comparable THC:CBD ratio (less than 2:1 but more than 1:2), low THC:CBD ratio (no more than 1:2), whole-plant cannabis products, and other cannabinoids.
“In preclinical studies, THC and related compounds have demonstrated analgesic properties, although its psychoactive effects and addiction potential may limit its suitability as an analgesic,” the investigators wrote. “CBD and other cannabinoids may also have some analgesic or anti-inflammatory properties and are not believed to be psychoactive or addictive. Given the variation in analgesic effect with THC and CBD, response may differ according to the ratio of THC to CBD in products used to treat pain.”
The final analysis included 18 randomized placebo-controlled trials involving 1,740 individuals and 7 cohort studies involving 13,095 individuals. Most of the studies were short-term, lasting 1-6 months.
Pain was scored on a ten-point scale, with improvements reported as the mean difference from baseline to post treatment. A mean difference in pain score of 0.5-1.0 was considered a “small effect,” an improvement of 1-2 points was considered a “moderate effect,” and an improvement greater than 2 points was considered a “large effect.”
Cannabis-based products with relatively high THC:CBD ratios showed efficacy
Synthetic products with high THC:CBD ratios offered moderate pain relief, based on a mean difference in pain score of –1.15 (95% confidence interval, –1.99 to –0.54), whereas products with comparable THC:CBD ratios were associated with a small effect on pain, with a mean difference of –0.52 (95% CI, –0.95 to –0.19).
According to Dr. McDonagh, treatment response rates were on par with response rates for more conventional treatments, “such as opioids or specific antidepressant drugs,” but data for the cannabis-based products are weaker.
“The amount of evidence available for cannabis-related products is very limited for [response rates], and therefore less certain,” Dr. McDonagh said in an interview. “The average reduction in pain severity is also similar to some other treatments, but we do not have studies directly comparing these treatments to draw conclusions.”
Although the cannabis-based products with relatively high and comparable THC:CBD ratios showed efficacy, they were also associated with “moderate to large increased risk for dizziness, sedation, and nausea,” the investigators wrote, noting that evidence was insufficient to characterize other “key adverse event outcomes” that may occur with long-term use, such as “psychosis, cannabis use disorder, and cognitive deficits.”
For products with low THC:CBD ratios, or without reported THC:CBD ratios, data were too scarce to reach any conclusions at all about safety or efficacy, highlighting the sizable knowledge gaps that remain in the area, the authors said.
“The current evidence on cannabis-related products for chronic pain is quite limited,” Dr. McDonagh said in an interview. “Patients with chronic pain should consult with their doctor to discuss which of the many options for treating chronic pain is best for them to start with.”
Patients may face resistance when asking about cannabis
According to Kevin F. Boehnke, PhD, and Daniel J. Clauw, MD, of the anesthesiology department and Chronic Pain and Fatigue Research Center at the University of Michigan, Ann Arbor, patients with chronic pain may face resistance, or even risk of being reported, when asking about cannabis-based products.
“Some physicians cite lack of data as rationale for not engaging with patients who wish to use or currently use cannabis,” Dr. Boehnke and Dr. Clauw wrote in an accompanying editorial. “Such practices may reflect consideration of cannabis solely as a drug of misuse (even in the 37 states where medical cannabis is legal) and requirements to refer patients who disclose or test positive for cannabis use to addiction services or decline to refill opioid prescriptions.”
Instead of shutting patients out, Dr. Boehnke and Dr. Clauw suggested clinicians engage in an “open information exchange” with their patients that focuses on “pragmatism, patient experience, known cannabinoid effects, and harm reduction.” In these conversations, the editorialists recommend noting that, “as with other analgesics, some persons will benefit, and others will not.”
They also offered some practical guidance: “Clinicians could suggest using tinctures (effect onset, 15-45 minutes) for breakthrough pain and edibles or capsules (which last about 6-8 hours) for extended relief. ... The scientific literature suggests that CBD doses could start at 5-10 mg twice daily and increase to 40-50 mg daily, whereas THC doses could start at 0.5-3 mg (initially at night) and increase to 30-40 mg/day.”
David Copenhaver, MD, MPH, clinical professor and chief of the division of pain medicine at UC Davis Health, Sacramento, shared a similar clinical mindset for patients choosing between opioids and cannabis-based products, specifically, CBD.
Compared with opioids, “the side-effect profile for CBD is less and the risk of mortality is less,” Dr. Copenhaver said in an interview, pointing out that nobody, to his knowledge, has ever died from an overdose of cannabis alone, and that CBD doses up to 1,000 mg/kg have been safely tolerated in people. “You present that, and most patients will say, ‘You know, I’d like to give this a try.’”
If so, Dr. Copenhaver makes sure patients know about a nonmedical risk: “The risk to the pocketbook.” Unlike opioids, which are covered under most insurance policies, most cannabis-based therapies are self-pay.
Buyers may get what they pay for, Dr. Copenhaver said, since products vary in quality, as do the dispensaries, from “very modest,” to highly sophisticated, with some even using chromatographic datasets to support the purity of their products.
Dr. Copenhaver steers his patients toward these more sophisticated retailers. Their expertise appears to be paying off, he said, not only in relief for patients, but also in market share. “Survival of the most fit will occur in the marketplace based on the results,” he said. “Unfortunately, some of that information doesn’t get percolated out into the literature.”
For investigators to fully uncover what cannabis-based products can do for chronic pain, Dr. Copenhaver said they need to get as “granular” as the leading dispensaries, which may first require recognition of the “very expansive opportunity” that less-studied cannabinoids may provide.
The study was supported by the Agency for Healthcare Research and Quality, U.S. Department of Health & Human Services. The investigators, Dr. Boehnke, Dr. Clauw, and Dr. Copenhaver, disclosed no conflicts of interest.
FROM ANNALS OF INTERNAL MEDICINE

The mental health of health care professionals takes center stage
Mental illness has been waiting in the wings for years; ignored, ridiculed, minimized, and stigmatized. Those who succumbed to it tried to lend testimonials, but to no avail. Those who were spared its effects remained in disbelief. So, it stayed on the sidelines, growing in intensity and breadth, yet stifled by the masses, until 2 years ago.
In March 2020, when COVID-19 became a pandemic, the importance of mental health finally became undeniable. As the pandemic’s effects progressed and wreaked havoc on our nation, our mental illness rates simultaneously surged. This surge paralleled that of the COVID-19 pandemic’s and in fact, contributed to a secondary crisis, allowing mental health to finally be addressed and gain center stage status.

But “mental health” is not easily defined, as it takes on many forms and is expressed in a variety of ways and via a myriad of symptoms. It does not discriminate by gender, race, age, socioeconomic status, educational level, profession, religion, or geography. At times, mental health status is consistent but at other times it can fluctuate in intensity, duration, and expression. It can be difficult to manage, yet there are various treatment modalities that can be implemented to lessen the impact of mental illness. Stressful events seem to potentiate its manifestation and yet, there are times it seems to appear spontaneously, much as an uninvited guest.
Mental health has a strong synergistic relationship with physical health, as they are very interdependent and allow us to function at our best only when they are both operating optimally. It should come as no surprise then, that the COVID-19 pandemic contributed to the exponential surge of mental illnesses. Capitalizing on its nondiscriminatory nature, mental illness impacted a large segment of the population – both those suffering from COVID-19 as well as those treating them.
As the nation starts to heal from the immediate and lingering physical and emotional consequences of the COVID-19 pandemic, President Biden has chosen to address and try to meet the needs of the health care heroes, the healers. The signing of H.R. 1667, the Dr. Lorna Breen Health Care Provider Protection Act into law on March 18, 2022, showed dedication to the health care community that has given tirelessly to our nation during the COVID-19 pandemic, and is itself recuperating from that effort.
Taking a top-down approach is essential to assuring the health of the nation. If our healers are not healthy, physically and mentally, they will not be able treat those whom they are dedicated to helping. Openly discussing and acknowledging the mental health problems of health care workers as a community makes it okay to not be okay. It normalizes the need for health care workers to prioritize their own mental health. It can also start to ease the fear of professional backlash or repercussions for practicing self-care.
I, for one, am very grateful for the prioritizing and promoting of the importance of mental health and wellness amongst health care workers. This helps to reduce the stigma of mental illness, helps us understand its impact, and allows us to formulate strategies and solutions to address its effects. The time has come.
Dr. Jarkon is a psychiatrist and director of the Center for Behavioral Health at the New York Institute of Technology College of Osteopathic Medicine in Old Westbury, N.Y.
Mental illness has been waiting in the wings for years; ignored, ridiculed, minimized, and stigmatized. Those who succumbed to it tried to lend testimonials, but to no avail. Those who were spared its effects remained in disbelief. So, it stayed on the sidelines, growing in intensity and breadth, yet stifled by the masses, until 2 years ago.
In March 2020, when COVID-19 became a pandemic, the importance of mental health finally became undeniable. As the pandemic’s effects progressed and wreaked havoc on our nation, our mental illness rates simultaneously surged. This surge paralleled that of the COVID-19 pandemic’s and in fact, contributed to a secondary crisis, allowing mental health to finally be addressed and gain center stage status.
But “mental health” is not easily defined, as it takes on many forms and is expressed in a variety of ways and via a myriad of symptoms. It does not discriminate by gender, race, age, socioeconomic status, educational level, profession, religion, or geography. At times, mental health status is consistent but at other times it can fluctuate in intensity, duration, and expression. It can be difficult to manage, yet there are various treatment modalities that can be implemented to lessen the impact of mental illness. Stressful events seem to potentiate its manifestation and yet, there are times it seems to appear spontaneously, much as an uninvited guest.
Mental health has a strong synergistic relationship with physical health, as they are very interdependent and allow us to function at our best only when they are both operating optimally. It should come as no surprise then, that the COVID-19 pandemic contributed to the exponential surge of mental illnesses. Capitalizing on its nondiscriminatory nature, mental illness impacted a large segment of the population – both those suffering from COVID-19 as well as those treating them.
As the nation starts to heal from the immediate and lingering physical and emotional consequences of the COVID-19 pandemic, President Biden has chosen to address and try to meet the needs of the health care heroes, the healers. The signing of H.R. 1667, the Dr. Lorna Breen Health Care Provider Protection Act into law on March 18, 2022, showed dedication to the health care community that has given tirelessly to our nation during the COVID-19 pandemic, and is itself recuperating from that effort.
Taking a top-down approach is essential to assuring the health of the nation. If our healers are not healthy, physically and mentally, they will not be able treat those whom they are dedicated to helping. Openly discussing and acknowledging the mental health problems of health care workers as a community makes it okay to not be okay. It normalizes the need for health care workers to prioritize their own mental health. It can also start to ease the fear of professional backlash or repercussions for practicing self-care.
I, for one, am very grateful for the prioritizing and promoting of the importance of mental health and wellness amongst health care workers. This helps to reduce the stigma of mental illness, helps us understand its impact, and allows us to formulate strategies and solutions to address its effects. The time has come.
Dr. Jarkon is a psychiatrist and director of the Center for Behavioral Health at the New York Institute of Technology College of Osteopathic Medicine in Old Westbury, N.Y.
Mental illness has been waiting in the wings for years; ignored, ridiculed, minimized, and stigmatized. Those who succumbed to it tried to lend testimonials, but to no avail. Those who were spared its effects remained in disbelief. So, it stayed on the sidelines, growing in intensity and breadth, yet stifled by the masses, until 2 years ago.
In March 2020, when COVID-19 became a pandemic, the importance of mental health finally became undeniable. As the pandemic’s effects progressed and wreaked havoc on our nation, our mental illness rates simultaneously surged. This surge paralleled that of the COVID-19 pandemic’s and in fact, contributed to a secondary crisis, allowing mental health to finally be addressed and gain center stage status.
But “mental health” is not easily defined, as it takes on many forms and is expressed in a variety of ways and via a myriad of symptoms. It does not discriminate by gender, race, age, socioeconomic status, educational level, profession, religion, or geography. At times, mental health status is consistent but at other times it can fluctuate in intensity, duration, and expression. It can be difficult to manage, yet there are various treatment modalities that can be implemented to lessen the impact of mental illness. Stressful events seem to potentiate its manifestation and yet, there are times it seems to appear spontaneously, much as an uninvited guest.
Mental health has a strong synergistic relationship with physical health, as they are very interdependent and allow us to function at our best only when they are both operating optimally. It should come as no surprise then, that the COVID-19 pandemic contributed to the exponential surge of mental illnesses. Capitalizing on its nondiscriminatory nature, mental illness impacted a large segment of the population – both those suffering from COVID-19 as well as those treating them.
As the nation starts to heal from the immediate and lingering physical and emotional consequences of the COVID-19 pandemic, President Biden has chosen to address and try to meet the needs of the health care heroes, the healers. The signing of H.R. 1667, the Dr. Lorna Breen Health Care Provider Protection Act into law on March 18, 2022, showed dedication to the health care community that has given tirelessly to our nation during the COVID-19 pandemic, and is itself recuperating from that effort.
Taking a top-down approach is essential to assuring the health of the nation. If our healers are not healthy, physically and mentally, they will not be able treat those whom they are dedicated to helping. Openly discussing and acknowledging the mental health problems of health care workers as a community makes it okay to not be okay. It normalizes the need for health care workers to prioritize their own mental health. It can also start to ease the fear of professional backlash or repercussions for practicing self-care.
I, for one, am very grateful for the prioritizing and promoting of the importance of mental health and wellness amongst health care workers. This helps to reduce the stigma of mental illness, helps us understand its impact, and allows us to formulate strategies and solutions to address its effects. The time has come.
Dr. Jarkon is a psychiatrist and director of the Center for Behavioral Health at the New York Institute of Technology College of Osteopathic Medicine in Old Westbury, N.Y.
FDA denies petition to disqualify researchers over controversial ketamine studies
The U.S. Food and Drug Administration has declined to take further action against a group of investigators at Hennepin County Medical Center/Hennepin Healthcare (HCMC) who conducted controversial studies involving ketamine and other sedatives on agitated persons without their consent.
A citizen petition filed by Public Citizen, a consumer advocacy group, had asked the FDA to initiate clinical-investigator disqualification proceedings against Jon Cole, MD, and Lauren Klein, MD, along with other researchers who participated in the studies, for “repeatedly and deliberately initiating and conducting clinical investigations of investigational drug products” without having submitted or having in effect the investigational new drug applications (INDs) required by the FDA.
In certain situations, wherein the FDA alleges that a clinical investigator has violated applicable regulations, the agency may initiate clinical investigator disqualification proceedings. The names of the disqualified researchers are then added to a federal database.
The petition, which was filed in November 2021, also requested that the FDA initiate disqualification proceedings against the institutional review board (IRB) at HCMC for repeatedly failing to comply with federal regulations that adversely affected the rights and welfare of the individuals who were enrolled in the study without their consent.
Of note, Public Citizen stated that the FDA should have required the hospital to contact the more than 1,700 patients who “were unwittingly enrolled in unethical experiments” and inform them that their rights had been violated and their health potentially endangered by the research team.
Michael A. Carome, MD, director of Public Citizen’s Health Research Group, told this news organization that it is uncommon for the FDA to disqualify researchers. “It should be more common than it is,” he said. “I think that FDA is just reluctant to take more action.”
The actions of the Hennepin investigators were “repetitive and appeared to be in deliberate violation of regulations,” he added. “The case for the FDA disqualifying the HCMC researchers is overwhelming. The FDA’s slap-on-the-wrist approach to such appalling regulatory and ethical violations risks emboldening other researchers to disregard the rights and welfare of human subjects.”
Carl Elliott, MD, PhD, a bioethicist at the University of Minnesota, Minneapolis, agrees that the researcher from HCMC should be disqualified. “They didn’t just conduct risky, exploitative studies – they conducted them after the FDA had warned them not to proceed,” he said. “The message sent by this slap on the wrist is that investigators can do whatever they want to nonconsenting subjects, and the FDA will look the other way.”
Initial complaint
Public Citizen initially filed a complaint with the FDA in 2018, after learning that researchers affiliated with HCMC were conducting high-risk clinical trials involving ketamine to control agitation outside of the hospital setting. The complaint was cosigned by 64 doctors, bioethicists, and academic researchers and was also submitted to the Office for Human Research Protections.
The FDA typically allows investigational drugs to be used in emergency situation without obtaining informed consent if the therapies are known to carry a minimal risk. The IRB at HCMC had determined that this was the case with ketamine and approved the trials.
But according to Public Citizen’s complaint, prior research had suggested that ketamine could cause more complications and severe adverse events, compared with other sedatives.
The trials were conducted between 2014 and 2018, and in its letter, Public Citizen alleged that the investigators and the IRB had allowed these trials to proceed without obtaining informed consent from patients. The goal was to evaluate how well ketamine worked, compared with other drugs in calming agitated individuals: “The patients were given either ketamine or haloperidol for agitation by paramedics who responded to medical emergencies, and the goal was to see which drug worked faster,” said Dr. Carome. “Patients were only notified afterwards that they had received a sedative. Informed consent had been waived by IRB.”
In the first clinical trial conducted by HCMC, published in 2016, the researchers had hypothesized that 5 mg/kg of intramuscular ketamine would be superior to 10 mg of intramuscular haloperidol for severe prehospital agitation. Time to adequate sedation was the primary outcome measure. The study included 146 people; 64 received ketamine and 82 received haloperidol. They found that ketamine worked far more quickly than haloperidol (5 minutes vs. 17 minutes) but that the risk for complications was much higher. Complications occurred in 49% of patients receiving ketamine, compared with 5%.
“There was a 10-fold risk of adverse events,” said Dr. Carome. “And 39% of patients given ketamine had respiratory problems requiring intubation, compared to 4% who received haloperidol.”
A second study was launched in 2017, wherein ketamine was compared with midazolam in agitated patients. During the first 6-month period of the study, individuals would receive a ketamine-based protocol for prehospital agitation, and during the second 6 months, that would switch to midazolam. However, the study was halted in June 2018 after the local newspaper, the Star Tribune, reported that the city police had encouraged medical personnel to sedate agitated patients. This included individuals who had already been physically restrained.
The report stated that “in many cases, the individual being detained or arrested was not only handcuffed but strapped down on a stretcher in an ambulance before receiving ketamine,” and that it raised a “concerning question” over why these people were given the drug before they were transported to the hospital, “given the immediate effects on breathing and heart function that the drug induces.”
Along with halting the trial, HCMC asked for a review of cases involving its paramedics; an independent investigation led by former U.S. Deputy Attorney General Sally Yates was initiated to assess whether the Minneapolis police had crossed a line and urged paramedics to use ketamine.
“The decision to use ketamine was based on the study’s timeline and not on clinical judgment,” said Dr. Carome.
The FDA acknowledged receipt of the complaint and inspected the IRB records and the clinical trial data. Preliminary reports received by Public Citizen confirmed their allegations. “There were not appropriate protections for vulnerable subjects,” he said. “In 2019, the FDA did further investigations, and those reports had similar findings.”
FDA letters
The FDA had sent warning letters to Dr. Cole and Dr. Klein, citing them for ignoring federal safety laws in experimental research on the public. In their investigations, the FDA cited “objectionable conditions” for the studies led by Dr. Cole and Dr. Klein, according to the letters. Both researchers seemingly ignored FDA regulations and used practices that subjected patients to “significantly increased risk,” and the hospital defended its research with “factually incorrect” statements.
In a letter to Dr. Cole, the FDA noted that he never filed INDs for the trials with the FDA, as required by law, and that he also failed to write appropriate protocols to ensure that children and pregnant women were not enrolled in the research. Individuals under the influence of intoxicants also were not excluded, though the use of ketamine is cautioned in this population.
“Administration of the investigational drugs to these subjects placed them at significantly increased risk of the adverse events associated with the investigational products and decreased the acceptability of those risks,” the FDA said in its letter. “Your failure to exclude, and the lack of any precautions for, subjects under the influence of various intoxicants significantly increased the risks and/or decreased the acceptability of the risks associated with the investigational drugs.”
However, Dr. Cole conducted both studies in the prehospital setting and failed to initiate any specific measures to protect study participants, according to the FDA.
Petition denied
Dr. Carome noted that the researchers had committed repetitive egregious regulatory violations over a 4-year period, which were documented by the FDA in their warning letters to Dr. Cole and Dr. Klein. “We felt that they were so egregious that we need to send a signal to the community that this sort of behavior will not be tolerated,” he said. “The FDA denied our petition, and we think that sends the wrong signal to the research community.”
In their response, the FDA noted that as with judicial enforcement, “the Agency makes decisions regarding whether to pursue administrative enforcement action, including disqualification proceedings, on a case-by-case basis, considering all relevant facts and circumstances.” They added that at this time, they would not be taking further action against Dr. Cole and Dr. Klein.
“However, we intend to continue to consider all the options available to the Agency as we determine whether to pursue additional compliance actions related to this matter,” the FDA concluded.
The FDA declined to comment further on their decision.
Dr. Cole also declined to comment, but Hennepin Healthcare told this news organization that the “decision by the FDA to deny the petition validates the changes we made to strengthen and improve the clinical research program across the institution since the closing of the studies in 2018. We look forward to continuing to work with the FDA to ensure full compliance with the standards in place to protect research subjects.”
A version of this article first appeared on Medscape.com.
The U.S. Food and Drug Administration has declined to take further action against a group of investigators at Hennepin County Medical Center/Hennepin Healthcare (HCMC) who conducted controversial studies involving ketamine and other sedatives on agitated persons without their consent.
A citizen petition filed by Public Citizen, a consumer advocacy group, had asked the FDA to initiate clinical-investigator disqualification proceedings against Jon Cole, MD, and Lauren Klein, MD, along with other researchers who participated in the studies, for “repeatedly and deliberately initiating and conducting clinical investigations of investigational drug products” without having submitted or having in effect the investigational new drug applications (INDs) required by the FDA.
In certain situations, wherein the FDA alleges that a clinical investigator has violated applicable regulations, the agency may initiate clinical investigator disqualification proceedings. The names of the disqualified researchers are then added to a federal database.
The petition, which was filed in November 2021, also requested that the FDA initiate disqualification proceedings against the institutional review board (IRB) at HCMC for repeatedly failing to comply with federal regulations that adversely affected the rights and welfare of the individuals who were enrolled in the study without their consent.
Of note, Public Citizen stated that the FDA should have required the hospital to contact the more than 1,700 patients who “were unwittingly enrolled in unethical experiments” and inform them that their rights had been violated and their health potentially endangered by the research team.
Michael A. Carome, MD, director of Public Citizen’s Health Research Group, told this news organization that it is uncommon for the FDA to disqualify researchers. “It should be more common than it is,” he said. “I think that FDA is just reluctant to take more action.”
The actions of the Hennepin investigators were “repetitive and appeared to be in deliberate violation of regulations,” he added. “The case for the FDA disqualifying the HCMC researchers is overwhelming. The FDA’s slap-on-the-wrist approach to such appalling regulatory and ethical violations risks emboldening other researchers to disregard the rights and welfare of human subjects.”
Carl Elliott, MD, PhD, a bioethicist at the University of Minnesota, Minneapolis, agrees that the researcher from HCMC should be disqualified. “They didn’t just conduct risky, exploitative studies – they conducted them after the FDA had warned them not to proceed,” he said. “The message sent by this slap on the wrist is that investigators can do whatever they want to nonconsenting subjects, and the FDA will look the other way.”
Initial complaint
Public Citizen initially filed a complaint with the FDA in 2018, after learning that researchers affiliated with HCMC were conducting high-risk clinical trials involving ketamine to control agitation outside of the hospital setting. The complaint was cosigned by 64 doctors, bioethicists, and academic researchers and was also submitted to the Office for Human Research Protections.
The FDA typically allows investigational drugs to be used in emergency situation without obtaining informed consent if the therapies are known to carry a minimal risk. The IRB at HCMC had determined that this was the case with ketamine and approved the trials.
But according to Public Citizen’s complaint, prior research had suggested that ketamine could cause more complications and severe adverse events, compared with other sedatives.
The trials were conducted between 2014 and 2018, and in its letter, Public Citizen alleged that the investigators and the IRB had allowed these trials to proceed without obtaining informed consent from patients. The goal was to evaluate how well ketamine worked, compared with other drugs in calming agitated individuals: “The patients were given either ketamine or haloperidol for agitation by paramedics who responded to medical emergencies, and the goal was to see which drug worked faster,” said Dr. Carome. “Patients were only notified afterwards that they had received a sedative. Informed consent had been waived by IRB.”
In the first clinical trial conducted by HCMC, published in 2016, the researchers had hypothesized that 5 mg/kg of intramuscular ketamine would be superior to 10 mg of intramuscular haloperidol for severe prehospital agitation. Time to adequate sedation was the primary outcome measure. The study included 146 people; 64 received ketamine and 82 received haloperidol. They found that ketamine worked far more quickly than haloperidol (5 minutes vs. 17 minutes) but that the risk for complications was much higher. Complications occurred in 49% of patients receiving ketamine, compared with 5%.
“There was a 10-fold risk of adverse events,” said Dr. Carome. “And 39% of patients given ketamine had respiratory problems requiring intubation, compared to 4% who received haloperidol.”
A second study was launched in 2017, wherein ketamine was compared with midazolam in agitated patients. During the first 6-month period of the study, individuals would receive a ketamine-based protocol for prehospital agitation, and during the second 6 months, that would switch to midazolam. However, the study was halted in June 2018 after the local newspaper, the Star Tribune, reported that the city police had encouraged medical personnel to sedate agitated patients. This included individuals who had already been physically restrained.
The report stated that “in many cases, the individual being detained or arrested was not only handcuffed but strapped down on a stretcher in an ambulance before receiving ketamine,” and that it raised a “concerning question” over why these people were given the drug before they were transported to the hospital, “given the immediate effects on breathing and heart function that the drug induces.”
Along with halting the trial, HCMC asked for a review of cases involving its paramedics; an independent investigation led by former U.S. Deputy Attorney General Sally Yates was initiated to assess whether the Minneapolis police had crossed a line and urged paramedics to use ketamine.
“The decision to use ketamine was based on the study’s timeline and not on clinical judgment,” said Dr. Carome.
The FDA acknowledged receipt of the complaint and inspected the IRB records and the clinical trial data. Preliminary reports received by Public Citizen confirmed their allegations. “There were not appropriate protections for vulnerable subjects,” he said. “In 2019, the FDA did further investigations, and those reports had similar findings.”
FDA letters
The FDA had sent warning letters to Dr. Cole and Dr. Klein, citing them for ignoring federal safety laws in experimental research on the public. In their investigations, the FDA cited “objectionable conditions” for the studies led by Dr. Cole and Dr. Klein, according to the letters. Both researchers seemingly ignored FDA regulations and used practices that subjected patients to “significantly increased risk,” and the hospital defended its research with “factually incorrect” statements.
In a letter to Dr. Cole, the FDA noted that he never filed INDs for the trials with the FDA, as required by law, and that he also failed to write appropriate protocols to ensure that children and pregnant women were not enrolled in the research. Individuals under the influence of intoxicants also were not excluded, though the use of ketamine is cautioned in this population.
“Administration of the investigational drugs to these subjects placed them at significantly increased risk of the adverse events associated with the investigational products and decreased the acceptability of those risks,” the FDA said in its letter. “Your failure to exclude, and the lack of any precautions for, subjects under the influence of various intoxicants significantly increased the risks and/or decreased the acceptability of the risks associated with the investigational drugs.”
However, Dr. Cole conducted both studies in the prehospital setting and failed to initiate any specific measures to protect study participants, according to the FDA.
Petition denied
Dr. Carome noted that the researchers had committed repetitive egregious regulatory violations over a 4-year period, which were documented by the FDA in their warning letters to Dr. Cole and Dr. Klein. “We felt that they were so egregious that we need to send a signal to the community that this sort of behavior will not be tolerated,” he said. “The FDA denied our petition, and we think that sends the wrong signal to the research community.”
In their response, the FDA noted that as with judicial enforcement, “the Agency makes decisions regarding whether to pursue administrative enforcement action, including disqualification proceedings, on a case-by-case basis, considering all relevant facts and circumstances.” They added that at this time, they would not be taking further action against Dr. Cole and Dr. Klein.
“However, we intend to continue to consider all the options available to the Agency as we determine whether to pursue additional compliance actions related to this matter,” the FDA concluded.
The FDA declined to comment further on their decision.
Dr. Cole also declined to comment, but Hennepin Healthcare told this news organization that the “decision by the FDA to deny the petition validates the changes we made to strengthen and improve the clinical research program across the institution since the closing of the studies in 2018. We look forward to continuing to work with the FDA to ensure full compliance with the standards in place to protect research subjects.”
A version of this article first appeared on Medscape.com.
The U.S. Food and Drug Administration has declined to take further action against a group of investigators at Hennepin County Medical Center/Hennepin Healthcare (HCMC) who conducted controversial studies involving ketamine and other sedatives on agitated persons without their consent.
A citizen petition filed by Public Citizen, a consumer advocacy group, had asked the FDA to initiate clinical-investigator disqualification proceedings against Jon Cole, MD, and Lauren Klein, MD, along with other researchers who participated in the studies, for “repeatedly and deliberately initiating and conducting clinical investigations of investigational drug products” without having submitted or having in effect the investigational new drug applications (INDs) required by the FDA.
In certain situations, wherein the FDA alleges that a clinical investigator has violated applicable regulations, the agency may initiate clinical investigator disqualification proceedings. The names of the disqualified researchers are then added to a federal database.
The petition, which was filed in November 2021, also requested that the FDA initiate disqualification proceedings against the institutional review board (IRB) at HCMC for repeatedly failing to comply with federal regulations that adversely affected the rights and welfare of the individuals who were enrolled in the study without their consent.
Of note, Public Citizen stated that the FDA should have required the hospital to contact the more than 1,700 patients who “were unwittingly enrolled in unethical experiments” and inform them that their rights had been violated and their health potentially endangered by the research team.
Michael A. Carome, MD, director of Public Citizen’s Health Research Group, told this news organization that it is uncommon for the FDA to disqualify researchers. “It should be more common than it is,” he said. “I think that FDA is just reluctant to take more action.”
The actions of the Hennepin investigators were “repetitive and appeared to be in deliberate violation of regulations,” he added. “The case for the FDA disqualifying the HCMC researchers is overwhelming. The FDA’s slap-on-the-wrist approach to such appalling regulatory and ethical violations risks emboldening other researchers to disregard the rights and welfare of human subjects.”
Carl Elliott, MD, PhD, a bioethicist at the University of Minnesota, Minneapolis, agrees that the researcher from HCMC should be disqualified. “They didn’t just conduct risky, exploitative studies – they conducted them after the FDA had warned them not to proceed,” he said. “The message sent by this slap on the wrist is that investigators can do whatever they want to nonconsenting subjects, and the FDA will look the other way.”
Initial complaint
Public Citizen initially filed a complaint with the FDA in 2018, after learning that researchers affiliated with HCMC were conducting high-risk clinical trials involving ketamine to control agitation outside of the hospital setting. The complaint was cosigned by 64 doctors, bioethicists, and academic researchers and was also submitted to the Office for Human Research Protections.
The FDA typically allows investigational drugs to be used in emergency situation without obtaining informed consent if the therapies are known to carry a minimal risk. The IRB at HCMC had determined that this was the case with ketamine and approved the trials.
But according to Public Citizen’s complaint, prior research had suggested that ketamine could cause more complications and severe adverse events, compared with other sedatives.
The trials were conducted between 2014 and 2018, and in its letter, Public Citizen alleged that the investigators and the IRB had allowed these trials to proceed without obtaining informed consent from patients. The goal was to evaluate how well ketamine worked, compared with other drugs in calming agitated individuals: “The patients were given either ketamine or haloperidol for agitation by paramedics who responded to medical emergencies, and the goal was to see which drug worked faster,” said Dr. Carome. “Patients were only notified afterwards that they had received a sedative. Informed consent had been waived by IRB.”
In the first clinical trial conducted by HCMC, published in 2016, the researchers had hypothesized that 5 mg/kg of intramuscular ketamine would be superior to 10 mg of intramuscular haloperidol for severe prehospital agitation. Time to adequate sedation was the primary outcome measure. The study included 146 people; 64 received ketamine and 82 received haloperidol. They found that ketamine worked far more quickly than haloperidol (5 minutes vs. 17 minutes) but that the risk for complications was much higher. Complications occurred in 49% of patients receiving ketamine, compared with 5%.
“There was a 10-fold risk of adverse events,” said Dr. Carome. “And 39% of patients given ketamine had respiratory problems requiring intubation, compared to 4% who received haloperidol.”
A second study was launched in 2017, wherein ketamine was compared with midazolam in agitated patients. During the first 6-month period of the study, individuals would receive a ketamine-based protocol for prehospital agitation, and during the second 6 months, that would switch to midazolam. However, the study was halted in June 2018 after the local newspaper, the Star Tribune, reported that the city police had encouraged medical personnel to sedate agitated patients. This included individuals who had already been physically restrained.
The report stated that “in many cases, the individual being detained or arrested was not only handcuffed but strapped down on a stretcher in an ambulance before receiving ketamine,” and that it raised a “concerning question” over why these people were given the drug before they were transported to the hospital, “given the immediate effects on breathing and heart function that the drug induces.”
Along with halting the trial, HCMC asked for a review of cases involving its paramedics; an independent investigation led by former U.S. Deputy Attorney General Sally Yates was initiated to assess whether the Minneapolis police had crossed a line and urged paramedics to use ketamine.
“The decision to use ketamine was based on the study’s timeline and not on clinical judgment,” said Dr. Carome.
The FDA acknowledged receipt of the complaint and inspected the IRB records and the clinical trial data. Preliminary reports received by Public Citizen confirmed their allegations. “There were not appropriate protections for vulnerable subjects,” he said. “In 2019, the FDA did further investigations, and those reports had similar findings.”
FDA letters
The FDA had sent warning letters to Dr. Cole and Dr. Klein, citing them for ignoring federal safety laws in experimental research on the public. In their investigations, the FDA cited “objectionable conditions” for the studies led by Dr. Cole and Dr. Klein, according to the letters. Both researchers seemingly ignored FDA regulations and used practices that subjected patients to “significantly increased risk,” and the hospital defended its research with “factually incorrect” statements.
In a letter to Dr. Cole, the FDA noted that he never filed INDs for the trials with the FDA, as required by law, and that he also failed to write appropriate protocols to ensure that children and pregnant women were not enrolled in the research. Individuals under the influence of intoxicants also were not excluded, though the use of ketamine is cautioned in this population.
“Administration of the investigational drugs to these subjects placed them at significantly increased risk of the adverse events associated with the investigational products and decreased the acceptability of those risks,” the FDA said in its letter. “Your failure to exclude, and the lack of any precautions for, subjects under the influence of various intoxicants significantly increased the risks and/or decreased the acceptability of the risks associated with the investigational drugs.”
However, Dr. Cole conducted both studies in the prehospital setting and failed to initiate any specific measures to protect study participants, according to the FDA.
Petition denied
Dr. Carome noted that the researchers had committed repetitive egregious regulatory violations over a 4-year period, which were documented by the FDA in their warning letters to Dr. Cole and Dr. Klein. “We felt that they were so egregious that we need to send a signal to the community that this sort of behavior will not be tolerated,” he said. “The FDA denied our petition, and we think that sends the wrong signal to the research community.”
In their response, the FDA noted that as with judicial enforcement, “the Agency makes decisions regarding whether to pursue administrative enforcement action, including disqualification proceedings, on a case-by-case basis, considering all relevant facts and circumstances.” They added that at this time, they would not be taking further action against Dr. Cole and Dr. Klein.
“However, we intend to continue to consider all the options available to the Agency as we determine whether to pursue additional compliance actions related to this matter,” the FDA concluded.
The FDA declined to comment further on their decision.
Dr. Cole also declined to comment, but Hennepin Healthcare told this news organization that the “decision by the FDA to deny the petition validates the changes we made to strengthen and improve the clinical research program across the institution since the closing of the studies in 2018. We look forward to continuing to work with the FDA to ensure full compliance with the standards in place to protect research subjects.”
A version of this article first appeared on Medscape.com.
Trans teens less likely to commit acts of sexual violence, says new study
Transgender and nonbinary adolescents are twice as likely to experience sexual violence as their cisgendered peers but are less likely to attempt rape or commit sexual assault, researchers have found.
The study, which was published online in JAMA Network Open, is among the first on the sexual violence that trans, nonbinary, and other gender nonconforming adolescents experience. Previous studies have focused on adults.
“In the busy world of clinical care, it is essential that clinicians be aware of potential disparities their patients are navigating,” said Michele Ybarra, PhD, MPH, president and research director of the Center for Innovative Public Health Research, San Clemente, California, who led the study. “This includes sexual violence victimization for gender minority youth and the need to talk about consent and boundaries for youth of all genders.”
Dr. Ybarra said that while clinicians may be aware that transgender young people face stigma, discrimination, and bullying, they may not be aware that trans youth are also the targets of sexual violence.
Studies indicate that health care providers and communities have significant misconceptions about sexually explicit behavior among trans and nonbinary teens. Misconceptions can lead to discrimination, resulting in higher rates of drug abuse, dropping out of school, suicide, and homelessness.
Dr. Ybarra and her colleagues surveyed 911 trans, nonbinary, or questioning youth on Instagram and Facebook through a collaboration with Growing Up With Media, a national longitudinal survey designed to investigate sexual violence during adolescence.
They also surveyed 3,282 cisgender persons aged 14-16 years who were recruited to the study between June 2018 and March 2020. The term “cisgender” refers to youth who identify with their gender at birth.
The questionnaires asked teens about gender identity, race, economic status, and support systems at home. Factors associated with not experiencing sexual violence included having a strong network of friends, family, and educators; involvement in the community; and having people close who affirm their gender identity.
More than three-fourths (78%) of youth surveyed identified as cisgender, 13.9% identified as questioning, and 7.9% identified as transgender.
Roughly two-thirds (67%) of transgender adolescents said they had experienced serious sexual violence, 73% reported experiencing violence in their communities, and 63% said they had been exposed to aggressive behavior. In contrast, 6.7% of trans youth said they had ever committed sexual violence, while 7.4% of cisgender teens surveyed, or 243 students, said they had done so.
“The relative lack of visibility of gender minority youth in sexual violence research is unacceptable,” Dr. Ybarra told this news organization. “To be counted, one needs to be seen. We aimed to start addressing this exclusion with the current study.”
The findings provide a lens into the levels of sexual violence that LGBTQIA+ youth experience and an opportunity to provide more inclusive care, according to Elizabeth Miller, MD, PhD, FSAHM, Distinguished Professor of Pediatrics, director of the Division of Adolescent and Young Adult Medicine, and medical director of community and population health at UPMC Children’s Hospital of Pittsburgh, who was not involved in the study.
“There are unfortunately pervasive and harmful stereotypes in our society about the ‘sexual deviancy’ attributed to LGBTQIA+ individuals,” Dr. Miller told this news organization. “This study adds to the research literature that counters and challenges these harmful – and inaccurate – perceptions.”
Dr. Miller said clinicians can help this population by offering youth accurate information about relevant support and services, including how to help a friend.
Programs that providers could incorporate include gender transformative approaches, which guide youth to examine gender norms and inequities and that develop leadership skills.
Such programs are more common outside the United States and have been shown to decrease LGBTQIA+ youth exposure to sexual violence, she said.
Dr. Miller said more research is needed to understand the contexts in which gender minority youth experience sexual violence to guide prevention efforts: “We need to move beyond individual-focused interventions to considering community-level interventions to create safer and more inclusive spaces for all youth.”
Dr. Miller has received royalties for writing content for UptoDate Wolters Kluwer outside of the current study. Dr. Ybarra has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Transgender and nonbinary adolescents are twice as likely to experience sexual violence as their cisgendered peers but are less likely to attempt rape or commit sexual assault, researchers have found.
The study, which was published online in JAMA Network Open, is among the first on the sexual violence that trans, nonbinary, and other gender nonconforming adolescents experience. Previous studies have focused on adults.
“In the busy world of clinical care, it is essential that clinicians be aware of potential disparities their patients are navigating,” said Michele Ybarra, PhD, MPH, president and research director of the Center for Innovative Public Health Research, San Clemente, California, who led the study. “This includes sexual violence victimization for gender minority youth and the need to talk about consent and boundaries for youth of all genders.”
Dr. Ybarra said that while clinicians may be aware that transgender young people face stigma, discrimination, and bullying, they may not be aware that trans youth are also the targets of sexual violence.
Studies indicate that health care providers and communities have significant misconceptions about sexually explicit behavior among trans and nonbinary teens. Misconceptions can lead to discrimination, resulting in higher rates of drug abuse, dropping out of school, suicide, and homelessness.
Dr. Ybarra and her colleagues surveyed 911 trans, nonbinary, or questioning youth on Instagram and Facebook through a collaboration with Growing Up With Media, a national longitudinal survey designed to investigate sexual violence during adolescence.
They also surveyed 3,282 cisgender persons aged 14-16 years who were recruited to the study between June 2018 and March 2020. The term “cisgender” refers to youth who identify with their gender at birth.
The questionnaires asked teens about gender identity, race, economic status, and support systems at home. Factors associated with not experiencing sexual violence included having a strong network of friends, family, and educators; involvement in the community; and having people close who affirm their gender identity.
More than three-fourths (78%) of youth surveyed identified as cisgender, 13.9% identified as questioning, and 7.9% identified as transgender.
Roughly two-thirds (67%) of transgender adolescents said they had experienced serious sexual violence, 73% reported experiencing violence in their communities, and 63% said they had been exposed to aggressive behavior. In contrast, 6.7% of trans youth said they had ever committed sexual violence, while 7.4% of cisgender teens surveyed, or 243 students, said they had done so.
“The relative lack of visibility of gender minority youth in sexual violence research is unacceptable,” Dr. Ybarra told this news organization. “To be counted, one needs to be seen. We aimed to start addressing this exclusion with the current study.”
The findings provide a lens into the levels of sexual violence that LGBTQIA+ youth experience and an opportunity to provide more inclusive care, according to Elizabeth Miller, MD, PhD, FSAHM, Distinguished Professor of Pediatrics, director of the Division of Adolescent and Young Adult Medicine, and medical director of community and population health at UPMC Children’s Hospital of Pittsburgh, who was not involved in the study.
“There are unfortunately pervasive and harmful stereotypes in our society about the ‘sexual deviancy’ attributed to LGBTQIA+ individuals,” Dr. Miller told this news organization. “This study adds to the research literature that counters and challenges these harmful – and inaccurate – perceptions.”
Dr. Miller said clinicians can help this population by offering youth accurate information about relevant support and services, including how to help a friend.
Programs that providers could incorporate include gender transformative approaches, which guide youth to examine gender norms and inequities and that develop leadership skills.
Such programs are more common outside the United States and have been shown to decrease LGBTQIA+ youth exposure to sexual violence, she said.
Dr. Miller said more research is needed to understand the contexts in which gender minority youth experience sexual violence to guide prevention efforts: “We need to move beyond individual-focused interventions to considering community-level interventions to create safer and more inclusive spaces for all youth.”
Dr. Miller has received royalties for writing content for UptoDate Wolters Kluwer outside of the current study. Dr. Ybarra has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Transgender and nonbinary adolescents are twice as likely to experience sexual violence as their cisgendered peers but are less likely to attempt rape or commit sexual assault, researchers have found.
The study, which was published online in JAMA Network Open, is among the first on the sexual violence that trans, nonbinary, and other gender nonconforming adolescents experience. Previous studies have focused on adults.
“In the busy world of clinical care, it is essential that clinicians be aware of potential disparities their patients are navigating,” said Michele Ybarra, PhD, MPH, president and research director of the Center for Innovative Public Health Research, San Clemente, California, who led the study. “This includes sexual violence victimization for gender minority youth and the need to talk about consent and boundaries for youth of all genders.”
Dr. Ybarra said that while clinicians may be aware that transgender young people face stigma, discrimination, and bullying, they may not be aware that trans youth are also the targets of sexual violence.
Studies indicate that health care providers and communities have significant misconceptions about sexually explicit behavior among trans and nonbinary teens. Misconceptions can lead to discrimination, resulting in higher rates of drug abuse, dropping out of school, suicide, and homelessness.
Dr. Ybarra and her colleagues surveyed 911 trans, nonbinary, or questioning youth on Instagram and Facebook through a collaboration with Growing Up With Media, a national longitudinal survey designed to investigate sexual violence during adolescence.
They also surveyed 3,282 cisgender persons aged 14-16 years who were recruited to the study between June 2018 and March 2020. The term “cisgender” refers to youth who identify with their gender at birth.
The questionnaires asked teens about gender identity, race, economic status, and support systems at home. Factors associated with not experiencing sexual violence included having a strong network of friends, family, and educators; involvement in the community; and having people close who affirm their gender identity.
More than three-fourths (78%) of youth surveyed identified as cisgender, 13.9% identified as questioning, and 7.9% identified as transgender.
Roughly two-thirds (67%) of transgender adolescents said they had experienced serious sexual violence, 73% reported experiencing violence in their communities, and 63% said they had been exposed to aggressive behavior. In contrast, 6.7% of trans youth said they had ever committed sexual violence, while 7.4% of cisgender teens surveyed, or 243 students, said they had done so.
“The relative lack of visibility of gender minority youth in sexual violence research is unacceptable,” Dr. Ybarra told this news organization. “To be counted, one needs to be seen. We aimed to start addressing this exclusion with the current study.”
The findings provide a lens into the levels of sexual violence that LGBTQIA+ youth experience and an opportunity to provide more inclusive care, according to Elizabeth Miller, MD, PhD, FSAHM, Distinguished Professor of Pediatrics, director of the Division of Adolescent and Young Adult Medicine, and medical director of community and population health at UPMC Children’s Hospital of Pittsburgh, who was not involved in the study.
“There are unfortunately pervasive and harmful stereotypes in our society about the ‘sexual deviancy’ attributed to LGBTQIA+ individuals,” Dr. Miller told this news organization. “This study adds to the research literature that counters and challenges these harmful – and inaccurate – perceptions.”
Dr. Miller said clinicians can help this population by offering youth accurate information about relevant support and services, including how to help a friend.
Programs that providers could incorporate include gender transformative approaches, which guide youth to examine gender norms and inequities and that develop leadership skills.
Such programs are more common outside the United States and have been shown to decrease LGBTQIA+ youth exposure to sexual violence, she said.
Dr. Miller said more research is needed to understand the contexts in which gender minority youth experience sexual violence to guide prevention efforts: “We need to move beyond individual-focused interventions to considering community-level interventions to create safer and more inclusive spaces for all youth.”
Dr. Miller has received royalties for writing content for UptoDate Wolters Kluwer outside of the current study. Dr. Ybarra has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Long-term schizophrenia treatment may not always be necessary
NEW ORLEANS – Patients with new-onset schizophrenia often ask psychiatrist Stephen R. Marder, MD, whether they’ll need to be on medications forever to treat the disorder. Now, he said, research is showing that the answer isn’t always yes.
In many cases, “it’s an open question” whether lifelong medical treatment is needed, said Dr. Marder, a professor at the Semel Institute for Neuroscience and Human Behavior at the University of California, Los Angeles, who spoke in a presentation about schizophrenia treatment at the annual meeting of the American Psychiatric Association.

According to Dr. Marder, research about relapses suggests that there may be a subpopulation of patients who can come off antipsychotics and remain in remission or partial remission. “The problem,” he said, “is that group is very hard to identify.”
Indeed, he highlighted a 2017 study that suggested The study noted choosing the best candidates isn’t simple, as “we do not have clinical measures or biomarkers that allow us to identify them prospectively. Because relapses and delays in the treatment of psychosis have been associated with poorer outcomes, there may be risk associated with withholding or discontinuing medication.”
There are more complications. There’s some evidence that antipsychotic drugs reduce brain volume, Dr. Marder said. But on the other hand, each psychotic episode can itself be harmful. “There is clear evidence that for each psychotic episode, they can take longer to improve, and they need higher doses.”
What to do? “My suggestion for most patients is to keep them on a relatively mild dose of an antipsychotic,” Dr. Marder said, “then to have a gradual decrease in the dose. I’ve done it in many patients.”
Which drug is best over the long term – oral or long-acting injectable antipsychotics? “It’s a hard question to answer because if you rely on randomized clinical trials – with patients who signed consent and are willing to be in a study like that – the subjects are sometimes not the ones who benefit the most from the long-acting drugs. So for many of the randomized clinical trials, the data was incomplete, and it was hard to make the case.”
But if you combine meta-analyses and cohort studies, as a 2021 study did, “you come up with a really clear answer: LAIs [long-acting injectables] are superior. They lead to a superior outcomes when it comes to rehospitalization and psychotic relapse,” Dr. Marder said.
That study reported that “LAIs were more beneficial than oral antipsychotics in 60 [18.3%] of 328 comparisons, not different in 252 [76.8%] comparisons, and less beneficial in 16 [4.9%] comparisons.”
More schizophrenia treatment pearls
People with schizophrenia – including those who aren’t on medication – face three times the risk of developing type 2 diabetes as the general population, “maybe because there’s a shared genetic risk for both disorders,” Dr. Marder said. “Those of you who have a lot of schizophrenia patients, I suspect you’re monitoring if they’re treating their type 2 diabetes and their obesity.”
Which antipsychotics are the best option for these patients? He highlighted a 2020 systematic review and meta-analysis that offers helpful insight into connections between 18 drugs and factors like weight and cholesterol.
Dr. Marder added that “if somebody has an elevation in their triglycerides or [hemoglobin] A1c in one single fasting blood glucose during the first 6 weeks of treatment, even if they haven’t been rated, it suggests that they’re developing insulin resistance.” At that point, he said, it’s a good idea to reconsider the medication choice.
Also, he said, keep in mind that “there’s substantial evidence that metformin is the appropriate treatment for patients who begin to demonstrate insulin resistance. It also works sometimes for weight loss.”
Exercise in people with schizophrenia can pay important dividends. A 2016 meta-analysis suggests that “not only does exercise for people with schizophrenia lead to better cardiovascular health, it’s good for the brain and improves cognitive functioning,” Dr. Marder said. “It’s not easy sometimes to get people with schizophrenia to exercise, but it’s many times worth the effort.”
Dr. Marder reported consulting for Boehringer Ingelheim, Lundbeck, Otsuka, Roche, Neurocrine, Sunovion, Newron, Merck, and Biogen; editor of UptoDate and Schizophrenia Bulletin Open; and research support from Boehringer Ingelheim.
NEW ORLEANS – Patients with new-onset schizophrenia often ask psychiatrist Stephen R. Marder, MD, whether they’ll need to be on medications forever to treat the disorder. Now, he said, research is showing that the answer isn’t always yes.
In many cases, “it’s an open question” whether lifelong medical treatment is needed, said Dr. Marder, a professor at the Semel Institute for Neuroscience and Human Behavior at the University of California, Los Angeles, who spoke in a presentation about schizophrenia treatment at the annual meeting of the American Psychiatric Association.
According to Dr. Marder, research about relapses suggests that there may be a subpopulation of patients who can come off antipsychotics and remain in remission or partial remission. “The problem,” he said, “is that group is very hard to identify.”
Indeed, he highlighted a 2017 study that suggested The study noted choosing the best candidates isn’t simple, as “we do not have clinical measures or biomarkers that allow us to identify them prospectively. Because relapses and delays in the treatment of psychosis have been associated with poorer outcomes, there may be risk associated with withholding or discontinuing medication.”
There are more complications. There’s some evidence that antipsychotic drugs reduce brain volume, Dr. Marder said. But on the other hand, each psychotic episode can itself be harmful. “There is clear evidence that for each psychotic episode, they can take longer to improve, and they need higher doses.”
What to do? “My suggestion for most patients is to keep them on a relatively mild dose of an antipsychotic,” Dr. Marder said, “then to have a gradual decrease in the dose. I’ve done it in many patients.”
Which drug is best over the long term – oral or long-acting injectable antipsychotics? “It’s a hard question to answer because if you rely on randomized clinical trials – with patients who signed consent and are willing to be in a study like that – the subjects are sometimes not the ones who benefit the most from the long-acting drugs. So for many of the randomized clinical trials, the data was incomplete, and it was hard to make the case.”
But if you combine meta-analyses and cohort studies, as a 2021 study did, “you come up with a really clear answer: LAIs [long-acting injectables] are superior. They lead to a superior outcomes when it comes to rehospitalization and psychotic relapse,” Dr. Marder said.
That study reported that “LAIs were more beneficial than oral antipsychotics in 60 [18.3%] of 328 comparisons, not different in 252 [76.8%] comparisons, and less beneficial in 16 [4.9%] comparisons.”
More schizophrenia treatment pearls
People with schizophrenia – including those who aren’t on medication – face three times the risk of developing type 2 diabetes as the general population, “maybe because there’s a shared genetic risk for both disorders,” Dr. Marder said. “Those of you who have a lot of schizophrenia patients, I suspect you’re monitoring if they’re treating their type 2 diabetes and their obesity.”
Which antipsychotics are the best option for these patients? He highlighted a 2020 systematic review and meta-analysis that offers helpful insight into connections between 18 drugs and factors like weight and cholesterol.
Dr. Marder added that “if somebody has an elevation in their triglycerides or [hemoglobin] A1c in one single fasting blood glucose during the first 6 weeks of treatment, even if they haven’t been rated, it suggests that they’re developing insulin resistance.” At that point, he said, it’s a good idea to reconsider the medication choice.
Also, he said, keep in mind that “there’s substantial evidence that metformin is the appropriate treatment for patients who begin to demonstrate insulin resistance. It also works sometimes for weight loss.”
Exercise in people with schizophrenia can pay important dividends. A 2016 meta-analysis suggests that “not only does exercise for people with schizophrenia lead to better cardiovascular health, it’s good for the brain and improves cognitive functioning,” Dr. Marder said. “It’s not easy sometimes to get people with schizophrenia to exercise, but it’s many times worth the effort.”
Dr. Marder reported consulting for Boehringer Ingelheim, Lundbeck, Otsuka, Roche, Neurocrine, Sunovion, Newron, Merck, and Biogen; editor of UptoDate and Schizophrenia Bulletin Open; and research support from Boehringer Ingelheim.
NEW ORLEANS – Patients with new-onset schizophrenia often ask psychiatrist Stephen R. Marder, MD, whether they’ll need to be on medications forever to treat the disorder. Now, he said, research is showing that the answer isn’t always yes.
In many cases, “it’s an open question” whether lifelong medical treatment is needed, said Dr. Marder, a professor at the Semel Institute for Neuroscience and Human Behavior at the University of California, Los Angeles, who spoke in a presentation about schizophrenia treatment at the annual meeting of the American Psychiatric Association.
According to Dr. Marder, research about relapses suggests that there may be a subpopulation of patients who can come off antipsychotics and remain in remission or partial remission. “The problem,” he said, “is that group is very hard to identify.”
Indeed, he highlighted a 2017 study that suggested The study noted choosing the best candidates isn’t simple, as “we do not have clinical measures or biomarkers that allow us to identify them prospectively. Because relapses and delays in the treatment of psychosis have been associated with poorer outcomes, there may be risk associated with withholding or discontinuing medication.”
There are more complications. There’s some evidence that antipsychotic drugs reduce brain volume, Dr. Marder said. But on the other hand, each psychotic episode can itself be harmful. “There is clear evidence that for each psychotic episode, they can take longer to improve, and they need higher doses.”
What to do? “My suggestion for most patients is to keep them on a relatively mild dose of an antipsychotic,” Dr. Marder said, “then to have a gradual decrease in the dose. I’ve done it in many patients.”
Which drug is best over the long term – oral or long-acting injectable antipsychotics? “It’s a hard question to answer because if you rely on randomized clinical trials – with patients who signed consent and are willing to be in a study like that – the subjects are sometimes not the ones who benefit the most from the long-acting drugs. So for many of the randomized clinical trials, the data was incomplete, and it was hard to make the case.”
But if you combine meta-analyses and cohort studies, as a 2021 study did, “you come up with a really clear answer: LAIs [long-acting injectables] are superior. They lead to a superior outcomes when it comes to rehospitalization and psychotic relapse,” Dr. Marder said.
That study reported that “LAIs were more beneficial than oral antipsychotics in 60 [18.3%] of 328 comparisons, not different in 252 [76.8%] comparisons, and less beneficial in 16 [4.9%] comparisons.”
More schizophrenia treatment pearls
People with schizophrenia – including those who aren’t on medication – face three times the risk of developing type 2 diabetes as the general population, “maybe because there’s a shared genetic risk for both disorders,” Dr. Marder said. “Those of you who have a lot of schizophrenia patients, I suspect you’re monitoring if they’re treating their type 2 diabetes and their obesity.”
Which antipsychotics are the best option for these patients? He highlighted a 2020 systematic review and meta-analysis that offers helpful insight into connections between 18 drugs and factors like weight and cholesterol.
Dr. Marder added that “if somebody has an elevation in their triglycerides or [hemoglobin] A1c in one single fasting blood glucose during the first 6 weeks of treatment, even if they haven’t been rated, it suggests that they’re developing insulin resistance.” At that point, he said, it’s a good idea to reconsider the medication choice.
Also, he said, keep in mind that “there’s substantial evidence that metformin is the appropriate treatment for patients who begin to demonstrate insulin resistance. It also works sometimes for weight loss.”
Exercise in people with schizophrenia can pay important dividends. A 2016 meta-analysis suggests that “not only does exercise for people with schizophrenia lead to better cardiovascular health, it’s good for the brain and improves cognitive functioning,” Dr. Marder said. “It’s not easy sometimes to get people with schizophrenia to exercise, but it’s many times worth the effort.”
Dr. Marder reported consulting for Boehringer Ingelheim, Lundbeck, Otsuka, Roche, Neurocrine, Sunovion, Newron, Merck, and Biogen; editor of UptoDate and Schizophrenia Bulletin Open; and research support from Boehringer Ingelheim.
AT APA 2022
Surgeons, who see it up close, offer ways to stop gun violence
Their strategies can work regardless of where you stand on the Second Amendment of the Constitution, said Patricia Turner, MD. “Our proposals are embraced by both gun owners and non–gun owners alike, and we are unique in that regard.”
These “implementable solutions” could prevent the next massacre, Dr. Turner, executive director of the American College of Surgeons, said during a news briefing the group sponsored on June 2.
“Our future – indeed all of our futures – depend on our ability to find durable, actionable steps that we can implement tomorrow to save lives,” she said.
Firsthand perspective
“Sadly I’m here today as a trauma surgeon who has cared for two of the largest mass shootings in modern U.S. history,” said Ronald Stewart, MD, chair of the department of surgery at University Hospital in San Antonio, Texas.
Dr. Stewart treated victims of the 2017 Sutherland Springs First Baptist Church shooting – where 27 people died, including the shooter – and the recent Uvalde school shooting, both in Texas.
“The injuries inflicted by high-velocity weapons used at both of these attacks are horrific. A high-capacity, magazine-fed automatic rifle such as the AR-15 causes extremely destructive tissue wounds,” he said.
One of the group’s proposals is to increase the regulation of high-velocity weapons, including AR-15s.
“These wounds are horribly lethal at close range, and sadly, most victims do not survive long enough to make it to a trauma center,” Dr. Stewart said.
On a positive note, “all of our current [Uvalde] patients are improving, which really brings us joy in this dark time,” he said. “But all of them have a long road to deal with recovery with both the physical and emotional impact of their injuries.”
Jeffrey Kerby, MD, agreed.
“Trauma surgeons see the short-term physical effects of these injuries and watch patients struggle with the long-term impact of these wounds,” said Dr. Kerby, director of trauma and acute care surgery at the University of Alabama at Birmingham.
Surgeons feel ‘profound impact’ of shootings
“Firearm violence has a profound impact on surgeons, and we are the undisputed subject matter experts in treating the tragic results,” said Patrick Bailey, MD, medical director for advocacy at the American College of Surgeons.
“This impacts surgeons as well,” said Dr. Kerby, chair of the Committee on Trauma for the surgeons’ group. “We are human, and we can’t help but share in the grief, the pain, and the suffering that our patients endure.
“As a pediatric surgeon ... I have too often witnessed the impact of firearm violence, and obviously, the devastation extends beyond the victims to their families,” he said. “To put it succinctly, in our culture, parents are not supposed to be put in a position of burying their children.”
A public health crisis
“It’s important to recognize that we’ve been talking about a public health approach,” said Eileen Bulger, MD, acting chief of the trauma division at the University of Washington in Seattle. That strategy is important for engaging both firearm owners and communities that have a higher risk for firearm violence, she said.
A committee of the American College of Surgeons developed specific recommendations in 2018, which are still valid today. The group brought together surgeons from across the U.S. including “passionate firearm owners and experts in firearm safety,” Dr. Bulger said.
The committee, for example, agreed on 10 specific recommendations “that we believe are bipartisan and could have an immediate impact in saving lives.”
“I’m a lifelong gun owner,” Dr. Bailey said, emphasizing that the team’s process included participation and perspective from other surgeons “who, like me, are also gun owners, but gun owners who also seek to reduce the impact of firearm violence in our country.”
The recommendations address these areas:
- Gun ownership
- Firearm registration
- Licensure
- Education and training
- Ownership responsibilities
- Mandatory reporting and risk reduction
- Safety innovation and technology
- Research
- The culture of violence
- Social isolation and mental health
For example, “we currently have certain classes of weapons with significant offensive capability,” Dr. Bulger said, “that are appropriately restricted and regulated under the National Firearms Act as Class 3 weapons.”
This group includes fully automatic machine guns, explosive devices, and short-barrel shotguns.
“We recommend a formal reassessment of the firearms designated within each of these national firearms classifications,” Dr. Bulger said.
For example, high-capacity, magazine-fed semiautomatic rifles, such as the AR-15, should be considered for reclassification as NFA Class 3 firearms, or they should get a new designation with tighter regulation.
The ACS endorses formal firearm safety training for all new gun owners. Also, owners who do not provide reasonably safe firearm storage should be held responsible for events related to the discharge of their firearms, Dr. Bulger said. And people who are deemed an imminent threat to themselves or others through firearm ownership should be temporarily or permanently restricted, with due process.
Research and reporting reforms
The ACS is also calling for research on firearm injuries and firearm injury prevention to be federally funded, Dr. Bulger said. The research should be done in a nonpartisan manner, she said.
“We have concerns that the manner and tone in which information is released to the public may lead to copycat mass killers,” she said. “The ACS recommends that law enforcement officials and the press take steps to eliminate the notoriety of the shooter, for example.”
Dr. Bulger also addressed the mental health angle. “We encourage recognition of mental health warning signs and social isolation by teachers, counselors, peers, and parents.” When identified, immediate referral to professionals is needed.
In addition to these recommendations, another team from the American College of Surgeons has published an overview of ways to address the inequities that contribute to violence. “We advocate for federal funding to support the development of hospital-based and community programs for violence intervention and prevention,” Dr. Bulger said.
Dr. Bailey said that as a gun owner himself, he thinks other gun owners would support these recommendations.
“I do not believe that the steps recommended ... pose undue burden on the rights of individual gun owners,” he said.
The time is now
Most firearm injuries are not from mass shooting events, Dr. Kerby said.
“My own trauma center has seen a 40% increase in the number of firearm injuries just in the last 2 years,” he added, “and these numbers continue to grow.”
A version of this article first appeared on WebMD.com.
Their strategies can work regardless of where you stand on the Second Amendment of the Constitution, said Patricia Turner, MD. “Our proposals are embraced by both gun owners and non–gun owners alike, and we are unique in that regard.”
These “implementable solutions” could prevent the next massacre, Dr. Turner, executive director of the American College of Surgeons, said during a news briefing the group sponsored on June 2.
“Our future – indeed all of our futures – depend on our ability to find durable, actionable steps that we can implement tomorrow to save lives,” she said.
Firsthand perspective
“Sadly I’m here today as a trauma surgeon who has cared for two of the largest mass shootings in modern U.S. history,” said Ronald Stewart, MD, chair of the department of surgery at University Hospital in San Antonio, Texas.
Dr. Stewart treated victims of the 2017 Sutherland Springs First Baptist Church shooting – where 27 people died, including the shooter – and the recent Uvalde school shooting, both in Texas.
“The injuries inflicted by high-velocity weapons used at both of these attacks are horrific. A high-capacity, magazine-fed automatic rifle such as the AR-15 causes extremely destructive tissue wounds,” he said.
One of the group’s proposals is to increase the regulation of high-velocity weapons, including AR-15s.
“These wounds are horribly lethal at close range, and sadly, most victims do not survive long enough to make it to a trauma center,” Dr. Stewart said.
On a positive note, “all of our current [Uvalde] patients are improving, which really brings us joy in this dark time,” he said. “But all of them have a long road to deal with recovery with both the physical and emotional impact of their injuries.”
Jeffrey Kerby, MD, agreed.
“Trauma surgeons see the short-term physical effects of these injuries and watch patients struggle with the long-term impact of these wounds,” said Dr. Kerby, director of trauma and acute care surgery at the University of Alabama at Birmingham.
Surgeons feel ‘profound impact’ of shootings
“Firearm violence has a profound impact on surgeons, and we are the undisputed subject matter experts in treating the tragic results,” said Patrick Bailey, MD, medical director for advocacy at the American College of Surgeons.
“This impacts surgeons as well,” said Dr. Kerby, chair of the Committee on Trauma for the surgeons’ group. “We are human, and we can’t help but share in the grief, the pain, and the suffering that our patients endure.
“As a pediatric surgeon ... I have too often witnessed the impact of firearm violence, and obviously, the devastation extends beyond the victims to their families,” he said. “To put it succinctly, in our culture, parents are not supposed to be put in a position of burying their children.”
A public health crisis
“It’s important to recognize that we’ve been talking about a public health approach,” said Eileen Bulger, MD, acting chief of the trauma division at the University of Washington in Seattle. That strategy is important for engaging both firearm owners and communities that have a higher risk for firearm violence, she said.
A committee of the American College of Surgeons developed specific recommendations in 2018, which are still valid today. The group brought together surgeons from across the U.S. including “passionate firearm owners and experts in firearm safety,” Dr. Bulger said.
The committee, for example, agreed on 10 specific recommendations “that we believe are bipartisan and could have an immediate impact in saving lives.”
“I’m a lifelong gun owner,” Dr. Bailey said, emphasizing that the team’s process included participation and perspective from other surgeons “who, like me, are also gun owners, but gun owners who also seek to reduce the impact of firearm violence in our country.”
The recommendations address these areas:
- Gun ownership
- Firearm registration
- Licensure
- Education and training
- Ownership responsibilities
- Mandatory reporting and risk reduction
- Safety innovation and technology
- Research
- The culture of violence
- Social isolation and mental health
For example, “we currently have certain classes of weapons with significant offensive capability,” Dr. Bulger said, “that are appropriately restricted and regulated under the National Firearms Act as Class 3 weapons.”
This group includes fully automatic machine guns, explosive devices, and short-barrel shotguns.
“We recommend a formal reassessment of the firearms designated within each of these national firearms classifications,” Dr. Bulger said.
For example, high-capacity, magazine-fed semiautomatic rifles, such as the AR-15, should be considered for reclassification as NFA Class 3 firearms, or they should get a new designation with tighter regulation.
The ACS endorses formal firearm safety training for all new gun owners. Also, owners who do not provide reasonably safe firearm storage should be held responsible for events related to the discharge of their firearms, Dr. Bulger said. And people who are deemed an imminent threat to themselves or others through firearm ownership should be temporarily or permanently restricted, with due process.
Research and reporting reforms
The ACS is also calling for research on firearm injuries and firearm injury prevention to be federally funded, Dr. Bulger said. The research should be done in a nonpartisan manner, she said.
“We have concerns that the manner and tone in which information is released to the public may lead to copycat mass killers,” she said. “The ACS recommends that law enforcement officials and the press take steps to eliminate the notoriety of the shooter, for example.”
Dr. Bulger also addressed the mental health angle. “We encourage recognition of mental health warning signs and social isolation by teachers, counselors, peers, and parents.” When identified, immediate referral to professionals is needed.
In addition to these recommendations, another team from the American College of Surgeons has published an overview of ways to address the inequities that contribute to violence. “We advocate for federal funding to support the development of hospital-based and community programs for violence intervention and prevention,” Dr. Bulger said.
Dr. Bailey said that as a gun owner himself, he thinks other gun owners would support these recommendations.
“I do not believe that the steps recommended ... pose undue burden on the rights of individual gun owners,” he said.
The time is now
Most firearm injuries are not from mass shooting events, Dr. Kerby said.
“My own trauma center has seen a 40% increase in the number of firearm injuries just in the last 2 years,” he added, “and these numbers continue to grow.”
A version of this article first appeared on WebMD.com.
Their strategies can work regardless of where you stand on the Second Amendment of the Constitution, said Patricia Turner, MD. “Our proposals are embraced by both gun owners and non–gun owners alike, and we are unique in that regard.”
These “implementable solutions” could prevent the next massacre, Dr. Turner, executive director of the American College of Surgeons, said during a news briefing the group sponsored on June 2.
“Our future – indeed all of our futures – depend on our ability to find durable, actionable steps that we can implement tomorrow to save lives,” she said.
Firsthand perspective
“Sadly I’m here today as a trauma surgeon who has cared for two of the largest mass shootings in modern U.S. history,” said Ronald Stewart, MD, chair of the department of surgery at University Hospital in San Antonio, Texas.
Dr. Stewart treated victims of the 2017 Sutherland Springs First Baptist Church shooting – where 27 people died, including the shooter – and the recent Uvalde school shooting, both in Texas.
“The injuries inflicted by high-velocity weapons used at both of these attacks are horrific. A high-capacity, magazine-fed automatic rifle such as the AR-15 causes extremely destructive tissue wounds,” he said.
One of the group’s proposals is to increase the regulation of high-velocity weapons, including AR-15s.
“These wounds are horribly lethal at close range, and sadly, most victims do not survive long enough to make it to a trauma center,” Dr. Stewart said.
On a positive note, “all of our current [Uvalde] patients are improving, which really brings us joy in this dark time,” he said. “But all of them have a long road to deal with recovery with both the physical and emotional impact of their injuries.”
Jeffrey Kerby, MD, agreed.
“Trauma surgeons see the short-term physical effects of these injuries and watch patients struggle with the long-term impact of these wounds,” said Dr. Kerby, director of trauma and acute care surgery at the University of Alabama at Birmingham.
Surgeons feel ‘profound impact’ of shootings
“Firearm violence has a profound impact on surgeons, and we are the undisputed subject matter experts in treating the tragic results,” said Patrick Bailey, MD, medical director for advocacy at the American College of Surgeons.
“This impacts surgeons as well,” said Dr. Kerby, chair of the Committee on Trauma for the surgeons’ group. “We are human, and we can’t help but share in the grief, the pain, and the suffering that our patients endure.
“As a pediatric surgeon ... I have too often witnessed the impact of firearm violence, and obviously, the devastation extends beyond the victims to their families,” he said. “To put it succinctly, in our culture, parents are not supposed to be put in a position of burying their children.”
A public health crisis
“It’s important to recognize that we’ve been talking about a public health approach,” said Eileen Bulger, MD, acting chief of the trauma division at the University of Washington in Seattle. That strategy is important for engaging both firearm owners and communities that have a higher risk for firearm violence, she said.
A committee of the American College of Surgeons developed specific recommendations in 2018, which are still valid today. The group brought together surgeons from across the U.S. including “passionate firearm owners and experts in firearm safety,” Dr. Bulger said.
The committee, for example, agreed on 10 specific recommendations “that we believe are bipartisan and could have an immediate impact in saving lives.”
“I’m a lifelong gun owner,” Dr. Bailey said, emphasizing that the team’s process included participation and perspective from other surgeons “who, like me, are also gun owners, but gun owners who also seek to reduce the impact of firearm violence in our country.”
The recommendations address these areas:
- Gun ownership
- Firearm registration
- Licensure
- Education and training
- Ownership responsibilities
- Mandatory reporting and risk reduction
- Safety innovation and technology
- Research
- The culture of violence
- Social isolation and mental health
For example, “we currently have certain classes of weapons with significant offensive capability,” Dr. Bulger said, “that are appropriately restricted and regulated under the National Firearms Act as Class 3 weapons.”
This group includes fully automatic machine guns, explosive devices, and short-barrel shotguns.
“We recommend a formal reassessment of the firearms designated within each of these national firearms classifications,” Dr. Bulger said.
For example, high-capacity, magazine-fed semiautomatic rifles, such as the AR-15, should be considered for reclassification as NFA Class 3 firearms, or they should get a new designation with tighter regulation.
The ACS endorses formal firearm safety training for all new gun owners. Also, owners who do not provide reasonably safe firearm storage should be held responsible for events related to the discharge of their firearms, Dr. Bulger said. And people who are deemed an imminent threat to themselves or others through firearm ownership should be temporarily or permanently restricted, with due process.
Research and reporting reforms
The ACS is also calling for research on firearm injuries and firearm injury prevention to be federally funded, Dr. Bulger said. The research should be done in a nonpartisan manner, she said.
“We have concerns that the manner and tone in which information is released to the public may lead to copycat mass killers,” she said. “The ACS recommends that law enforcement officials and the press take steps to eliminate the notoriety of the shooter, for example.”
Dr. Bulger also addressed the mental health angle. “We encourage recognition of mental health warning signs and social isolation by teachers, counselors, peers, and parents.” When identified, immediate referral to professionals is needed.
In addition to these recommendations, another team from the American College of Surgeons has published an overview of ways to address the inequities that contribute to violence. “We advocate for federal funding to support the development of hospital-based and community programs for violence intervention and prevention,” Dr. Bulger said.
Dr. Bailey said that as a gun owner himself, he thinks other gun owners would support these recommendations.
“I do not believe that the steps recommended ... pose undue burden on the rights of individual gun owners,” he said.
The time is now
Most firearm injuries are not from mass shooting events, Dr. Kerby said.
“My own trauma center has seen a 40% increase in the number of firearm injuries just in the last 2 years,” he added, “and these numbers continue to grow.”
A version of this article first appeared on WebMD.com.
High-dose antipsychotics show some benefit in treatment-resistant cases
NEW ORLEANS – Patients with severe schizophrenia who fail to respond to treatment with standard doses of second-generation antipsychotics show significant improvement with – and tolerance of – higher maintenance doses of the drugs, new research shows.
“The use of [higher doses of] long-acting injectable second-generation antipsychotics shows improvement not only in treatment adherence, but also in diminished relapses and suicide attempts compared with other previous treatment options used with these severely ill patients,” lead author Juan Jose Fernandez-Miranda, MD, said in an interview.

Dr. Fernandez-Miranda, of the Mental Health Service of the Principality of Asturias, in Gijón, Spain, underscored the tolerability of the novel approach of high doses: “No important side effects were found, and less than occurred with previous treatments,” he said.
While higher doses of second-generation antipsychotics for patients with treatment refractory schizophrenia are sometimes considered necessary, particularly with acute psychosis, evidence of benefits of the approach is lacking, and there are concerns about adverse events such as extrapyramidal symptoms and hyperprolactinemia.
To investigate the effects, the authors evaluated patients in a community-based, case managed program with severe, (CGI-S = 5), resistant schizophrenia.
All had been treated in the previous 3 years with at least two different antipsychotics, including clozapine in a few cases, with poor outcomes when receiving standard doses, and eligibility included being at risk of medication noncompliance, and/or experiencing a lack of effectiveness or adverse effects with previous antipsychotics.
For the second 3 years of the observational study, they were treated with doses of at least 75 mg of risperidone long-acting injectable (n = 60), 175 mg or more of monthly paliperidone palmitate (n = 60), or 600 mg or higher of aripiprazole once monthly (n = 30).
During the study, the average antipsychotic doses were: risperidone 111.2 mg/14 days; paliperidone palmitate 231.2 mg. eq./28 days; and aripiprazole 780 mg/28 days. In addition to the intensive pharmacological intervention, patients received psychosocial integrated intervention, as in the previous 3 years.
Over the 3 years with the higher maintenance doses, significant improvements were observed with all of the injectable treatment groups in terms of decreases on the Clinical Global Impression Scale – Severity score (CGI-S; P < .01) and in the four areas of the World Health Organization Disability Schedule (WHO-DAS), including in self-care, occupational, family, and social measures (P < .01 through P < .001).
Scores on the Medication Adherence Rating Scale (MARS), increased with all of the long-acting injectables (P < .01), particularly with paliperidone palmitate and aripiprazole.
Patients had significant decreases in hospital admissions at the end of the 36-month treatments and reductions in suicide attempts (both P < .001), compared with the previous 3 years, without any differences across the three injectables.
Importantly, tolerability was good for all of the long-acting antidepressants, with reductions in side effects as well as biological parameters compared with previous treatments, notably in the aripiprazole group.
While reductions in weight and prolactin levels were observed in all long-acting treatments, the differences were statistically significant only among patients treated with aripiprazole (P < .05), as was expected.
Two patients treated with aripiprazole discontinued treatment because of side effects from treatment, and the rate was five with paliperidone palmitate and nine with risperidone.
One person in the aripiprazole group discontinued because of a lack of effectiveness, while two discontinued in the paliperidone palmitate group and four with risperidone.
Dr. Fernandez-Miranda noted that “both the intensive case-managed multicomponent treatment and use of high doses of long-acting antipsychotics were in all probability linked to the high adherence and positive clinical outcomes.”
The results provide evidence that “long-acting second-generation antipsychotics are a remarkable option for patients with severe schizophrenia and a background of treatment discontinuation or intolerable adverse effects with other antipsychotics,” Dr. Fernandez-Miranda added.
“We suggest that, in some illness critical conditions, high doses of long-acting second-generation antipsychotics could represent an alternative to clozapine,” he added.
Some hesitation warranted
Commenting on the study, T. Scott Stroup, MD, MPH, professor of psychiatry at Columbia University, New York, noted the key limitations of a lack of randomization and comparison group of clozapine or typical-dose long-acting injectables.

“In addition, pre-post or mirror-image designs may be affected by expectation bias and regression to the mean,” he said in an interview.
“I don’t doubt that some patients do well on relatively high doses of long-acting injectable medications and that some tolerate these doses,” he noted “Most adverse effects are dose related, but without a typical-dose comparison group we cannot assess this.”
Ultimately, Dr. Stroup recommends sticking with standard recommendations – at least to start.
“My take-home message is that clozapine remains the treatment of choice for treatment-resistant schizophrenia, and in most cases clozapine should be tried before considering high-dose long-acting injectables,” he said.
“If there is uncertainty about whether someone is taking a prescribed oral antipsychotic medication, then a trial of a typical dose of a long-acting injectable is a good option to rule out pseudo-treatment resistance.”
Furthermore, “this study doesn’t affect the recommendation that people who need antipsychotic medications should receive the lowest effective dose,” he said.
The authors and Dr. Stroup had no disclosures to report.
NEW ORLEANS – Patients with severe schizophrenia who fail to respond to treatment with standard doses of second-generation antipsychotics show significant improvement with – and tolerance of – higher maintenance doses of the drugs, new research shows.
“The use of [higher doses of] long-acting injectable second-generation antipsychotics shows improvement not only in treatment adherence, but also in diminished relapses and suicide attempts compared with other previous treatment options used with these severely ill patients,” lead author Juan Jose Fernandez-Miranda, MD, said in an interview.
Dr. Fernandez-Miranda, of the Mental Health Service of the Principality of Asturias, in Gijón, Spain, underscored the tolerability of the novel approach of high doses: “No important side effects were found, and less than occurred with previous treatments,” he said.
While higher doses of second-generation antipsychotics for patients with treatment refractory schizophrenia are sometimes considered necessary, particularly with acute psychosis, evidence of benefits of the approach is lacking, and there are concerns about adverse events such as extrapyramidal symptoms and hyperprolactinemia.
To investigate the effects, the authors evaluated patients in a community-based, case managed program with severe, (CGI-S = 5), resistant schizophrenia.
All had been treated in the previous 3 years with at least two different antipsychotics, including clozapine in a few cases, with poor outcomes when receiving standard doses, and eligibility included being at risk of medication noncompliance, and/or experiencing a lack of effectiveness or adverse effects with previous antipsychotics.
For the second 3 years of the observational study, they were treated with doses of at least 75 mg of risperidone long-acting injectable (n = 60), 175 mg or more of monthly paliperidone palmitate (n = 60), or 600 mg or higher of aripiprazole once monthly (n = 30).
During the study, the average antipsychotic doses were: risperidone 111.2 mg/14 days; paliperidone palmitate 231.2 mg. eq./28 days; and aripiprazole 780 mg/28 days. In addition to the intensive pharmacological intervention, patients received psychosocial integrated intervention, as in the previous 3 years.
Over the 3 years with the higher maintenance doses, significant improvements were observed with all of the injectable treatment groups in terms of decreases on the Clinical Global Impression Scale – Severity score (CGI-S; P < .01) and in the four areas of the World Health Organization Disability Schedule (WHO-DAS), including in self-care, occupational, family, and social measures (P < .01 through P < .001).
Scores on the Medication Adherence Rating Scale (MARS), increased with all of the long-acting injectables (P < .01), particularly with paliperidone palmitate and aripiprazole.
Patients had significant decreases in hospital admissions at the end of the 36-month treatments and reductions in suicide attempts (both P < .001), compared with the previous 3 years, without any differences across the three injectables.
Importantly, tolerability was good for all of the long-acting antidepressants, with reductions in side effects as well as biological parameters compared with previous treatments, notably in the aripiprazole group.
While reductions in weight and prolactin levels were observed in all long-acting treatments, the differences were statistically significant only among patients treated with aripiprazole (P < .05), as was expected.
Two patients treated with aripiprazole discontinued treatment because of side effects from treatment, and the rate was five with paliperidone palmitate and nine with risperidone.
One person in the aripiprazole group discontinued because of a lack of effectiveness, while two discontinued in the paliperidone palmitate group and four with risperidone.
Dr. Fernandez-Miranda noted that “both the intensive case-managed multicomponent treatment and use of high doses of long-acting antipsychotics were in all probability linked to the high adherence and positive clinical outcomes.”
The results provide evidence that “long-acting second-generation antipsychotics are a remarkable option for patients with severe schizophrenia and a background of treatment discontinuation or intolerable adverse effects with other antipsychotics,” Dr. Fernandez-Miranda added.
“We suggest that, in some illness critical conditions, high doses of long-acting second-generation antipsychotics could represent an alternative to clozapine,” he added.
Some hesitation warranted
Commenting on the study, T. Scott Stroup, MD, MPH, professor of psychiatry at Columbia University, New York, noted the key limitations of a lack of randomization and comparison group of clozapine or typical-dose long-acting injectables.
“In addition, pre-post or mirror-image designs may be affected by expectation bias and regression to the mean,” he said in an interview.
“I don’t doubt that some patients do well on relatively high doses of long-acting injectable medications and that some tolerate these doses,” he noted “Most adverse effects are dose related, but without a typical-dose comparison group we cannot assess this.”
Ultimately, Dr. Stroup recommends sticking with standard recommendations – at least to start.
“My take-home message is that clozapine remains the treatment of choice for treatment-resistant schizophrenia, and in most cases clozapine should be tried before considering high-dose long-acting injectables,” he said.
“If there is uncertainty about whether someone is taking a prescribed oral antipsychotic medication, then a trial of a typical dose of a long-acting injectable is a good option to rule out pseudo-treatment resistance.”
Furthermore, “this study doesn’t affect the recommendation that people who need antipsychotic medications should receive the lowest effective dose,” he said.
The authors and Dr. Stroup had no disclosures to report.
NEW ORLEANS – Patients with severe schizophrenia who fail to respond to treatment with standard doses of second-generation antipsychotics show significant improvement with – and tolerance of – higher maintenance doses of the drugs, new research shows.
“The use of [higher doses of] long-acting injectable second-generation antipsychotics shows improvement not only in treatment adherence, but also in diminished relapses and suicide attempts compared with other previous treatment options used with these severely ill patients,” lead author Juan Jose Fernandez-Miranda, MD, said in an interview.
Dr. Fernandez-Miranda, of the Mental Health Service of the Principality of Asturias, in Gijón, Spain, underscored the tolerability of the novel approach of high doses: “No important side effects were found, and less than occurred with previous treatments,” he said.
While higher doses of second-generation antipsychotics for patients with treatment refractory schizophrenia are sometimes considered necessary, particularly with acute psychosis, evidence of benefits of the approach is lacking, and there are concerns about adverse events such as extrapyramidal symptoms and hyperprolactinemia.
To investigate the effects, the authors evaluated patients in a community-based, case managed program with severe, (CGI-S = 5), resistant schizophrenia.
All had been treated in the previous 3 years with at least two different antipsychotics, including clozapine in a few cases, with poor outcomes when receiving standard doses, and eligibility included being at risk of medication noncompliance, and/or experiencing a lack of effectiveness or adverse effects with previous antipsychotics.
For the second 3 years of the observational study, they were treated with doses of at least 75 mg of risperidone long-acting injectable (n = 60), 175 mg or more of monthly paliperidone palmitate (n = 60), or 600 mg or higher of aripiprazole once monthly (n = 30).
During the study, the average antipsychotic doses were: risperidone 111.2 mg/14 days; paliperidone palmitate 231.2 mg. eq./28 days; and aripiprazole 780 mg/28 days. In addition to the intensive pharmacological intervention, patients received psychosocial integrated intervention, as in the previous 3 years.
Over the 3 years with the higher maintenance doses, significant improvements were observed with all of the injectable treatment groups in terms of decreases on the Clinical Global Impression Scale – Severity score (CGI-S; P < .01) and in the four areas of the World Health Organization Disability Schedule (WHO-DAS), including in self-care, occupational, family, and social measures (P < .01 through P < .001).
Scores on the Medication Adherence Rating Scale (MARS), increased with all of the long-acting injectables (P < .01), particularly with paliperidone palmitate and aripiprazole.
Patients had significant decreases in hospital admissions at the end of the 36-month treatments and reductions in suicide attempts (both P < .001), compared with the previous 3 years, without any differences across the three injectables.
Importantly, tolerability was good for all of the long-acting antidepressants, with reductions in side effects as well as biological parameters compared with previous treatments, notably in the aripiprazole group.
While reductions in weight and prolactin levels were observed in all long-acting treatments, the differences were statistically significant only among patients treated with aripiprazole (P < .05), as was expected.
Two patients treated with aripiprazole discontinued treatment because of side effects from treatment, and the rate was five with paliperidone palmitate and nine with risperidone.
One person in the aripiprazole group discontinued because of a lack of effectiveness, while two discontinued in the paliperidone palmitate group and four with risperidone.
Dr. Fernandez-Miranda noted that “both the intensive case-managed multicomponent treatment and use of high doses of long-acting antipsychotics were in all probability linked to the high adherence and positive clinical outcomes.”
The results provide evidence that “long-acting second-generation antipsychotics are a remarkable option for patients with severe schizophrenia and a background of treatment discontinuation or intolerable adverse effects with other antipsychotics,” Dr. Fernandez-Miranda added.
“We suggest that, in some illness critical conditions, high doses of long-acting second-generation antipsychotics could represent an alternative to clozapine,” he added.
Some hesitation warranted
Commenting on the study, T. Scott Stroup, MD, MPH, professor of psychiatry at Columbia University, New York, noted the key limitations of a lack of randomization and comparison group of clozapine or typical-dose long-acting injectables.
“In addition, pre-post or mirror-image designs may be affected by expectation bias and regression to the mean,” he said in an interview.
“I don’t doubt that some patients do well on relatively high doses of long-acting injectable medications and that some tolerate these doses,” he noted “Most adverse effects are dose related, but without a typical-dose comparison group we cannot assess this.”
Ultimately, Dr. Stroup recommends sticking with standard recommendations – at least to start.
“My take-home message is that clozapine remains the treatment of choice for treatment-resistant schizophrenia, and in most cases clozapine should be tried before considering high-dose long-acting injectables,” he said.
“If there is uncertainty about whether someone is taking a prescribed oral antipsychotic medication, then a trial of a typical dose of a long-acting injectable is a good option to rule out pseudo-treatment resistance.”
Furthermore, “this study doesn’t affect the recommendation that people who need antipsychotic medications should receive the lowest effective dose,” he said.
The authors and Dr. Stroup had no disclosures to report.
AT APA 2022
High rates of med student burnout during COVID
NEW ORLEANS –
Researchers surveyed 613 medical students representing all years of a medical program during the last week of the Spring semester of 2021.
Based on the Maslach Burnout Inventory-Student Survey (MBI-SS), more than half (54%) of the students had symptoms of burnout.
Eighty percent of students scored high on emotional exhaustion, 57% scored high on cynicism, and 36% scored low on academic effectiveness.
Compared with male medical students, female medical students were more apt to exhibit signs of burnout (60% vs. 44%), emotional exhaustion (80% vs. 73%), and cynicism (62% vs. 49%).
After adjusting for associated factors, female medical students were significantly more likely to suffer from burnout than male students (odds ratio, 1.90; 95% confidence interval, 1.34-2.70; P < .001).
Smoking was also linked to higher likelihood of burnout among medical students (OR, 2.12; 95% CI, 1.18-3.81; P < .05). The death of a family member from COVID-19 also put medical students at heightened risk for burnout (OR, 1.60; 95% CI, 1.08-2.36; P < .05).
The survey results were presented at the American Psychiatric Association (APA) Annual Meeting.
The findings point to the need to study burnout prevalence in universities and develop strategies to promote the mental health of future physicians, presenter Sofia Jezzini-Martínez, fourth-year medical student, Autonomous University of Nuevo Leon, Monterrey, Mexico, wrote in her conference abstract.
In related research presented at the APA meeting, researchers surveyed second-, third-, and fourth-year medical students from California during the pandemic.
Roughly 80% exhibited symptoms of anxiety and 68% exhibited depressive symptoms, of whom about 18% also reported having thoughts of suicide.
Yet only about half of the medical students exhibiting anxiety or depressive symptoms sought help from a mental health professional, and 20% reported using substances to cope with stress.
“Given that the pandemic is ongoing, we hope to draw attention to mental health needs of medical students and influence medical schools to direct appropriate and timely resources to this group,” presenter Sarthak Angal, MD, psychiatry resident, Kaiser Permanente San Jose Medical Center, California, wrote in his conference abstract.
Managing expectations
Weighing in on medical student burnout, Ihuoma Njoku, MD, department of psychiatry and neurobehavioral sciences, University of Virginia, Charlottesville, noted that, “particularly for women in multiple fields, including medicine, there’s a lot of burden placed on them.”
“Women are pulled in a lot of different directions and have increased demands, which may help explain their higher rate of burnout,” Dr. Njoku commented.
She noted that these surveys were conducted during the COVID-19 pandemic, “a period when students’ education experience was a lot different than what they expected and maybe what they wanted.”
Dr. Njoku noted that the challenges of the pandemic are particularly hard on fourth-year medical students.
“A big part of fourth year is applying to residency, and many were doing virtual interviews for residency. That makes it hard to really get an appreciation of the place you will spend the next three to eight years of your life,” she told this news organization.
A version of this article first appeared on Medscape.com.
NEW ORLEANS –
Researchers surveyed 613 medical students representing all years of a medical program during the last week of the Spring semester of 2021.
Based on the Maslach Burnout Inventory-Student Survey (MBI-SS), more than half (54%) of the students had symptoms of burnout.
Eighty percent of students scored high on emotional exhaustion, 57% scored high on cynicism, and 36% scored low on academic effectiveness.
Compared with male medical students, female medical students were more apt to exhibit signs of burnout (60% vs. 44%), emotional exhaustion (80% vs. 73%), and cynicism (62% vs. 49%).
After adjusting for associated factors, female medical students were significantly more likely to suffer from burnout than male students (odds ratio, 1.90; 95% confidence interval, 1.34-2.70; P < .001).
Smoking was also linked to higher likelihood of burnout among medical students (OR, 2.12; 95% CI, 1.18-3.81; P < .05). The death of a family member from COVID-19 also put medical students at heightened risk for burnout (OR, 1.60; 95% CI, 1.08-2.36; P < .05).
The survey results were presented at the American Psychiatric Association (APA) Annual Meeting.
The findings point to the need to study burnout prevalence in universities and develop strategies to promote the mental health of future physicians, presenter Sofia Jezzini-Martínez, fourth-year medical student, Autonomous University of Nuevo Leon, Monterrey, Mexico, wrote in her conference abstract.
In related research presented at the APA meeting, researchers surveyed second-, third-, and fourth-year medical students from California during the pandemic.
Roughly 80% exhibited symptoms of anxiety and 68% exhibited depressive symptoms, of whom about 18% also reported having thoughts of suicide.
Yet only about half of the medical students exhibiting anxiety or depressive symptoms sought help from a mental health professional, and 20% reported using substances to cope with stress.
“Given that the pandemic is ongoing, we hope to draw attention to mental health needs of medical students and influence medical schools to direct appropriate and timely resources to this group,” presenter Sarthak Angal, MD, psychiatry resident, Kaiser Permanente San Jose Medical Center, California, wrote in his conference abstract.
Managing expectations
Weighing in on medical student burnout, Ihuoma Njoku, MD, department of psychiatry and neurobehavioral sciences, University of Virginia, Charlottesville, noted that, “particularly for women in multiple fields, including medicine, there’s a lot of burden placed on them.”
“Women are pulled in a lot of different directions and have increased demands, which may help explain their higher rate of burnout,” Dr. Njoku commented.
She noted that these surveys were conducted during the COVID-19 pandemic, “a period when students’ education experience was a lot different than what they expected and maybe what they wanted.”
Dr. Njoku noted that the challenges of the pandemic are particularly hard on fourth-year medical students.
“A big part of fourth year is applying to residency, and many were doing virtual interviews for residency. That makes it hard to really get an appreciation of the place you will spend the next three to eight years of your life,” she told this news organization.
A version of this article first appeared on Medscape.com.
NEW ORLEANS –
Researchers surveyed 613 medical students representing all years of a medical program during the last week of the Spring semester of 2021.
Based on the Maslach Burnout Inventory-Student Survey (MBI-SS), more than half (54%) of the students had symptoms of burnout.
Eighty percent of students scored high on emotional exhaustion, 57% scored high on cynicism, and 36% scored low on academic effectiveness.
Compared with male medical students, female medical students were more apt to exhibit signs of burnout (60% vs. 44%), emotional exhaustion (80% vs. 73%), and cynicism (62% vs. 49%).
After adjusting for associated factors, female medical students were significantly more likely to suffer from burnout than male students (odds ratio, 1.90; 95% confidence interval, 1.34-2.70; P < .001).
Smoking was also linked to higher likelihood of burnout among medical students (OR, 2.12; 95% CI, 1.18-3.81; P < .05). The death of a family member from COVID-19 also put medical students at heightened risk for burnout (OR, 1.60; 95% CI, 1.08-2.36; P < .05).
The survey results were presented at the American Psychiatric Association (APA) Annual Meeting.
The findings point to the need to study burnout prevalence in universities and develop strategies to promote the mental health of future physicians, presenter Sofia Jezzini-Martínez, fourth-year medical student, Autonomous University of Nuevo Leon, Monterrey, Mexico, wrote in her conference abstract.
In related research presented at the APA meeting, researchers surveyed second-, third-, and fourth-year medical students from California during the pandemic.
Roughly 80% exhibited symptoms of anxiety and 68% exhibited depressive symptoms, of whom about 18% also reported having thoughts of suicide.
Yet only about half of the medical students exhibiting anxiety or depressive symptoms sought help from a mental health professional, and 20% reported using substances to cope with stress.
“Given that the pandemic is ongoing, we hope to draw attention to mental health needs of medical students and influence medical schools to direct appropriate and timely resources to this group,” presenter Sarthak Angal, MD, psychiatry resident, Kaiser Permanente San Jose Medical Center, California, wrote in his conference abstract.
Managing expectations
Weighing in on medical student burnout, Ihuoma Njoku, MD, department of psychiatry and neurobehavioral sciences, University of Virginia, Charlottesville, noted that, “particularly for women in multiple fields, including medicine, there’s a lot of burden placed on them.”
“Women are pulled in a lot of different directions and have increased demands, which may help explain their higher rate of burnout,” Dr. Njoku commented.
She noted that these surveys were conducted during the COVID-19 pandemic, “a period when students’ education experience was a lot different than what they expected and maybe what they wanted.”
Dr. Njoku noted that the challenges of the pandemic are particularly hard on fourth-year medical students.
“A big part of fourth year is applying to residency, and many were doing virtual interviews for residency. That makes it hard to really get an appreciation of the place you will spend the next three to eight years of your life,” she told this news organization.
A version of this article first appeared on Medscape.com.
FROM APA 2022
At-home vagus nerve stimulation promising for postpartum depression
At-home, noninvasive auricular vagus nerve stimulation (aVNS) therapy is well-tolerated and associated with a significant reduction in postpartum depressive and anxiety symptoms, new research suggests.
In a small proof-of-concept pilot study of 25 women with postpartum depression receiving 6 weeks of daily aVNS treatment, results showed that 74% achieved response and 61% achieved remission, as shown in reduced scores on the Hamilton Rating Scale for Depression (HAM-D17).
Although invasive electrical stimulation of the vagus nerve was approved by the U.S. Food and Drug Administration for treatment-resistant depression in 2005, it involves risk for implantation, infection, and significant side effects, coinvestigator Kristina M. Deligiannidis, MD, director, Women’s Behavioral Health, Zucker Hillside Hospital, Northwell Health, Glen Oaks, New York, told this news organization.

“This newer approach, transcutaneous auricular VNS, is non-invasive, is well tolerated, and has shown initial efficacy in major depression in men and women,” she said.
The findings were presented at the virtual American Society of Clinical Psychopharmacology (ASCP) Annual Meeting.
Potential alternative to meds
“Given that aVNS is a non-invasive treatment which can be administered at home, we wanted to test if this approach was safe, feasible, and could reduce depressive symptoms in women with postpartum depression, as many of these women have barriers to accessing current treatments,” Dr. Deligiannidis said.
Auricular VNS uses surface skin electrodes to stimulate nerve endings of a branch of the vagus nerve, located on the surface of the outer ear. Those nerve endings travel to the brain where they have been shown to modulate brain communication in areas important for mood and anxiety regulation, she said.
Dr. Deligiannidis noted that evidence-based treatments for postpartum depression include psychotherapies and antidepressants. However, some women have difficulty accessing weekly psychotherapy, and, when antidepressants are indicated, many are reluctant to take them if they are breastfeeding because of concerns about the medications getting into their breast milk, she said.
Although most antidepressants are safe in lactation, many women postpone antidepressant treatment until they have finished breastfeeding, which can postpone their postpartum depression treatment, Dr. Deligiannidis added.
“At home treatments reduce many barriers women have to current treatments, and this intervention [of aVNS] does not impact breastfeeding, as it is not a medication approach,” she said.
The researchers enrolled 25 women (mean age, 33.7 years) diagnosed with postpartum depression. Ten of the women (40%) were on a stable dose of antidepressant medication.
The participants self-administered 6 weeks of open-label aVNS for 15 minutes daily at home. They were then observed without intervention for an additional 2 weeks. The women also completed medical, psychiatric, and safety interviews throughout the study period.
Promising findings
At baseline, the mean HAM-D17 was 18.4 and was similar for those on (17.8) and off (18.9) antidepressants.
By week 6, the mean HAM-D17 total score decreased by 9.7 points overall, compared with baseline score. For participants on antidepressants, the HAM-D17 decreased by 8.7 points; for women off antidepressants, it decreased by 10.3 points.
In addition, 74% of the women achieved a response to the therapy, and 61% achieved remission of their depressive symptoms.
The most common adverse effects were discomfort (n = 5 patients), headache (n = 3), and dizziness (n = 2). All resolved without intervention.
Commenting on the findings, Anita Clayton, MD, professor and chair, department of psychiatry and neurobehavioral sciences, University of Virginia School of Medicine, Charlottesville, said the study was “quite interesting.”

Dr. Clayton, who was not involved with the research, also noted the “pretty high” response and remission rates.
“So, I think this does have promise, and it would be worth doing a study where you look at placebo versus this treatment,” she said.
“Many women are fearful of taking medicines postpartum, even peripartum, unless they have had pre-existing severe depression. This is not a medicine, and it sounds like it could be useful even in people who are pregnant, although it’s harder to do studies in pregnant women,” Dr. Clayton added.
The study was funded by Nesos Corporation. Dr. Deligiannidis received contracted research funds from Nesos Corporation to conduct this study. She also serves as a consultant to Sage Therapeutics, Brii Biosciences, and GH Research. Dr. Clayton reports financial relationships with Dare Bioscience, Janssen, Praxis Precision Medicines, Relmada Therapeutics, Sage Therapeutics, AbbVie, Brii Biosciences, Fabre-Kramer, Field Trip Health, Mind Cure Health, Ovoca Bio, PureTech Health, S1 Biopharma, Takeda/Lundbeck, Vella Bioscience, WCG MedAvante-ProPhase, Ballantine Books/Random House, Changes in Sexual Functioning Questionnaire, Guilford Publications, Euthymics Bioscience, and Mediflix.
A version of this article first appeared on Medscape.com.
At-home, noninvasive auricular vagus nerve stimulation (aVNS) therapy is well-tolerated and associated with a significant reduction in postpartum depressive and anxiety symptoms, new research suggests.
In a small proof-of-concept pilot study of 25 women with postpartum depression receiving 6 weeks of daily aVNS treatment, results showed that 74% achieved response and 61% achieved remission, as shown in reduced scores on the Hamilton Rating Scale for Depression (HAM-D17).
Although invasive electrical stimulation of the vagus nerve was approved by the U.S. Food and Drug Administration for treatment-resistant depression in 2005, it involves risk for implantation, infection, and significant side effects, coinvestigator Kristina M. Deligiannidis, MD, director, Women’s Behavioral Health, Zucker Hillside Hospital, Northwell Health, Glen Oaks, New York, told this news organization.
“This newer approach, transcutaneous auricular VNS, is non-invasive, is well tolerated, and has shown initial efficacy in major depression in men and women,” she said.
The findings were presented at the virtual American Society of Clinical Psychopharmacology (ASCP) Annual Meeting.
Potential alternative to meds
“Given that aVNS is a non-invasive treatment which can be administered at home, we wanted to test if this approach was safe, feasible, and could reduce depressive symptoms in women with postpartum depression, as many of these women have barriers to accessing current treatments,” Dr. Deligiannidis said.
Auricular VNS uses surface skin electrodes to stimulate nerve endings of a branch of the vagus nerve, located on the surface of the outer ear. Those nerve endings travel to the brain where they have been shown to modulate brain communication in areas important for mood and anxiety regulation, she said.
Dr. Deligiannidis noted that evidence-based treatments for postpartum depression include psychotherapies and antidepressants. However, some women have difficulty accessing weekly psychotherapy, and, when antidepressants are indicated, many are reluctant to take them if they are breastfeeding because of concerns about the medications getting into their breast milk, she said.
Although most antidepressants are safe in lactation, many women postpone antidepressant treatment until they have finished breastfeeding, which can postpone their postpartum depression treatment, Dr. Deligiannidis added.
“At home treatments reduce many barriers women have to current treatments, and this intervention [of aVNS] does not impact breastfeeding, as it is not a medication approach,” she said.
The researchers enrolled 25 women (mean age, 33.7 years) diagnosed with postpartum depression. Ten of the women (40%) were on a stable dose of antidepressant medication.
The participants self-administered 6 weeks of open-label aVNS for 15 minutes daily at home. They were then observed without intervention for an additional 2 weeks. The women also completed medical, psychiatric, and safety interviews throughout the study period.
Promising findings
At baseline, the mean HAM-D17 was 18.4 and was similar for those on (17.8) and off (18.9) antidepressants.
By week 6, the mean HAM-D17 total score decreased by 9.7 points overall, compared with baseline score. For participants on antidepressants, the HAM-D17 decreased by 8.7 points; for women off antidepressants, it decreased by 10.3 points.
In addition, 74% of the women achieved a response to the therapy, and 61% achieved remission of their depressive symptoms.
The most common adverse effects were discomfort (n = 5 patients), headache (n = 3), and dizziness (n = 2). All resolved without intervention.
Commenting on the findings, Anita Clayton, MD, professor and chair, department of psychiatry and neurobehavioral sciences, University of Virginia School of Medicine, Charlottesville, said the study was “quite interesting.”
Dr. Clayton, who was not involved with the research, also noted the “pretty high” response and remission rates.
“So, I think this does have promise, and it would be worth doing a study where you look at placebo versus this treatment,” she said.
“Many women are fearful of taking medicines postpartum, even peripartum, unless they have had pre-existing severe depression. This is not a medicine, and it sounds like it could be useful even in people who are pregnant, although it’s harder to do studies in pregnant women,” Dr. Clayton added.
The study was funded by Nesos Corporation. Dr. Deligiannidis received contracted research funds from Nesos Corporation to conduct this study. She also serves as a consultant to Sage Therapeutics, Brii Biosciences, and GH Research. Dr. Clayton reports financial relationships with Dare Bioscience, Janssen, Praxis Precision Medicines, Relmada Therapeutics, Sage Therapeutics, AbbVie, Brii Biosciences, Fabre-Kramer, Field Trip Health, Mind Cure Health, Ovoca Bio, PureTech Health, S1 Biopharma, Takeda/Lundbeck, Vella Bioscience, WCG MedAvante-ProPhase, Ballantine Books/Random House, Changes in Sexual Functioning Questionnaire, Guilford Publications, Euthymics Bioscience, and Mediflix.
A version of this article first appeared on Medscape.com.
At-home, noninvasive auricular vagus nerve stimulation (aVNS) therapy is well-tolerated and associated with a significant reduction in postpartum depressive and anxiety symptoms, new research suggests.
In a small proof-of-concept pilot study of 25 women with postpartum depression receiving 6 weeks of daily aVNS treatment, results showed that 74% achieved response and 61% achieved remission, as shown in reduced scores on the Hamilton Rating Scale for Depression (HAM-D17).
Although invasive electrical stimulation of the vagus nerve was approved by the U.S. Food and Drug Administration for treatment-resistant depression in 2005, it involves risk for implantation, infection, and significant side effects, coinvestigator Kristina M. Deligiannidis, MD, director, Women’s Behavioral Health, Zucker Hillside Hospital, Northwell Health, Glen Oaks, New York, told this news organization.
“This newer approach, transcutaneous auricular VNS, is non-invasive, is well tolerated, and has shown initial efficacy in major depression in men and women,” she said.
The findings were presented at the virtual American Society of Clinical Psychopharmacology (ASCP) Annual Meeting.
Potential alternative to meds
“Given that aVNS is a non-invasive treatment which can be administered at home, we wanted to test if this approach was safe, feasible, and could reduce depressive symptoms in women with postpartum depression, as many of these women have barriers to accessing current treatments,” Dr. Deligiannidis said.
Auricular VNS uses surface skin electrodes to stimulate nerve endings of a branch of the vagus nerve, located on the surface of the outer ear. Those nerve endings travel to the brain where they have been shown to modulate brain communication in areas important for mood and anxiety regulation, she said.
Dr. Deligiannidis noted that evidence-based treatments for postpartum depression include psychotherapies and antidepressants. However, some women have difficulty accessing weekly psychotherapy, and, when antidepressants are indicated, many are reluctant to take them if they are breastfeeding because of concerns about the medications getting into their breast milk, she said.
Although most antidepressants are safe in lactation, many women postpone antidepressant treatment until they have finished breastfeeding, which can postpone their postpartum depression treatment, Dr. Deligiannidis added.
“At home treatments reduce many barriers women have to current treatments, and this intervention [of aVNS] does not impact breastfeeding, as it is not a medication approach,” she said.
The researchers enrolled 25 women (mean age, 33.7 years) diagnosed with postpartum depression. Ten of the women (40%) were on a stable dose of antidepressant medication.
The participants self-administered 6 weeks of open-label aVNS for 15 minutes daily at home. They were then observed without intervention for an additional 2 weeks. The women also completed medical, psychiatric, and safety interviews throughout the study period.
Promising findings
At baseline, the mean HAM-D17 was 18.4 and was similar for those on (17.8) and off (18.9) antidepressants.
By week 6, the mean HAM-D17 total score decreased by 9.7 points overall, compared with baseline score. For participants on antidepressants, the HAM-D17 decreased by 8.7 points; for women off antidepressants, it decreased by 10.3 points.
In addition, 74% of the women achieved a response to the therapy, and 61% achieved remission of their depressive symptoms.
The most common adverse effects were discomfort (n = 5 patients), headache (n = 3), and dizziness (n = 2). All resolved without intervention.
Commenting on the findings, Anita Clayton, MD, professor and chair, department of psychiatry and neurobehavioral sciences, University of Virginia School of Medicine, Charlottesville, said the study was “quite interesting.”
Dr. Clayton, who was not involved with the research, also noted the “pretty high” response and remission rates.
“So, I think this does have promise, and it would be worth doing a study where you look at placebo versus this treatment,” she said.
“Many women are fearful of taking medicines postpartum, even peripartum, unless they have had pre-existing severe depression. This is not a medicine, and it sounds like it could be useful even in people who are pregnant, although it’s harder to do studies in pregnant women,” Dr. Clayton added.
The study was funded by Nesos Corporation. Dr. Deligiannidis received contracted research funds from Nesos Corporation to conduct this study. She also serves as a consultant to Sage Therapeutics, Brii Biosciences, and GH Research. Dr. Clayton reports financial relationships with Dare Bioscience, Janssen, Praxis Precision Medicines, Relmada Therapeutics, Sage Therapeutics, AbbVie, Brii Biosciences, Fabre-Kramer, Field Trip Health, Mind Cure Health, Ovoca Bio, PureTech Health, S1 Biopharma, Takeda/Lundbeck, Vella Bioscience, WCG MedAvante-ProPhase, Ballantine Books/Random House, Changes in Sexual Functioning Questionnaire, Guilford Publications, Euthymics Bioscience, and Mediflix.
A version of this article first appeared on Medscape.com.