User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Suicide often associated with bullying in LGBTQ youth
based on analysis of a national database.
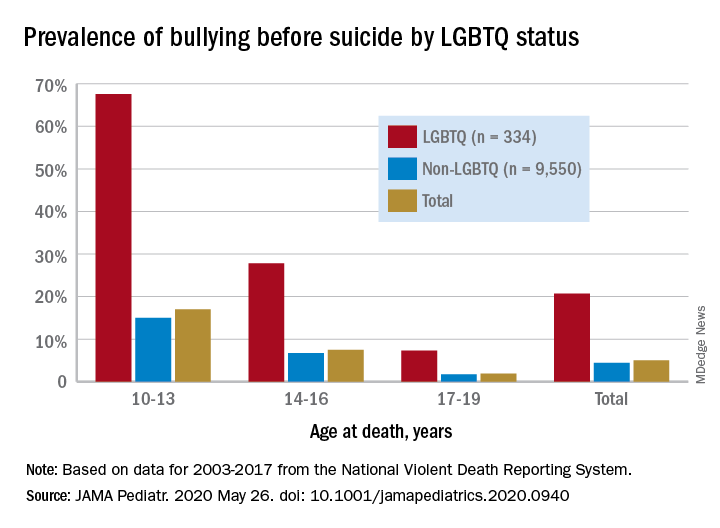
Among suicide decedents aged 10-19 years who were classified as LGBTQ, 21% had been bullied, compared with 4% of non-LGBTQ youths, and the discrepancy increased among younger individuals, Kirsty A. Clark, PhD, of Yale University, New Haven, Conn., and associates wrote in JAMA Pediatrics.
Here’s how the presence of bullying broke down by age group by LGBTQ/non-LGBTQ status: 68%/15% among 10- to 13-year-olds, 28%/7% for 14- to-16-year-olds, and 7%/2% among 17- to 19-year-olds, based on data for 2003-2017 from the National Violent Death Reporting System.
Postmortem records from that reporting system include “two narratives summarizing the coroner or medical examiner records and law enforcement reports describing suicide antecedents as reported by the decedent’s family or friends; the decedent’s diary, social media, and text or email messages; and any suicide note,” the investigators noted.
Although prevalence of bullying was higher among LGBTQ youth, non-LGBTQ individuals represented 97% of the 9,884 suicide decedents and 86% of the 490 bullying-associated deaths in the study, they wrote.
Other suicide antecedents also were more prevalent in the LGBTQ group: depressed mood (46% vs. 35%), suicide-thought history (37% vs. 21%), suicide-attempt history (28% vs. 21%), and school-related problem (27% vs. 18%), Dr. Clark and associates reported.
“Bullying can be a deadly antecedent to suicide, especially among LGBTQ youth,” the investigators wrote. “Pediatricians can help to reduce this risk through adopting clinical practice approaches sensitive to the vulnerabilities of LGBTQ youth.”
SOURCE: Clark KA et al. JAMA Pediatr. 2020 May 26. doi: 10.1001/jamapediatrics.2020.0940.
based on analysis of a national database.
Among suicide decedents aged 10-19 years who were classified as LGBTQ, 21% had been bullied, compared with 4% of non-LGBTQ youths, and the discrepancy increased among younger individuals, Kirsty A. Clark, PhD, of Yale University, New Haven, Conn., and associates wrote in JAMA Pediatrics.
Here’s how the presence of bullying broke down by age group by LGBTQ/non-LGBTQ status: 68%/15% among 10- to 13-year-olds, 28%/7% for 14- to-16-year-olds, and 7%/2% among 17- to 19-year-olds, based on data for 2003-2017 from the National Violent Death Reporting System.
Postmortem records from that reporting system include “two narratives summarizing the coroner or medical examiner records and law enforcement reports describing suicide antecedents as reported by the decedent’s family or friends; the decedent’s diary, social media, and text or email messages; and any suicide note,” the investigators noted.
Although prevalence of bullying was higher among LGBTQ youth, non-LGBTQ individuals represented 97% of the 9,884 suicide decedents and 86% of the 490 bullying-associated deaths in the study, they wrote.
Other suicide antecedents also were more prevalent in the LGBTQ group: depressed mood (46% vs. 35%), suicide-thought history (37% vs. 21%), suicide-attempt history (28% vs. 21%), and school-related problem (27% vs. 18%), Dr. Clark and associates reported.
“Bullying can be a deadly antecedent to suicide, especially among LGBTQ youth,” the investigators wrote. “Pediatricians can help to reduce this risk through adopting clinical practice approaches sensitive to the vulnerabilities of LGBTQ youth.”
SOURCE: Clark KA et al. JAMA Pediatr. 2020 May 26. doi: 10.1001/jamapediatrics.2020.0940.
based on analysis of a national database.
Among suicide decedents aged 10-19 years who were classified as LGBTQ, 21% had been bullied, compared with 4% of non-LGBTQ youths, and the discrepancy increased among younger individuals, Kirsty A. Clark, PhD, of Yale University, New Haven, Conn., and associates wrote in JAMA Pediatrics.
Here’s how the presence of bullying broke down by age group by LGBTQ/non-LGBTQ status: 68%/15% among 10- to 13-year-olds, 28%/7% for 14- to-16-year-olds, and 7%/2% among 17- to 19-year-olds, based on data for 2003-2017 from the National Violent Death Reporting System.
Postmortem records from that reporting system include “two narratives summarizing the coroner or medical examiner records and law enforcement reports describing suicide antecedents as reported by the decedent’s family or friends; the decedent’s diary, social media, and text or email messages; and any suicide note,” the investigators noted.
Although prevalence of bullying was higher among LGBTQ youth, non-LGBTQ individuals represented 97% of the 9,884 suicide decedents and 86% of the 490 bullying-associated deaths in the study, they wrote.
Other suicide antecedents also were more prevalent in the LGBTQ group: depressed mood (46% vs. 35%), suicide-thought history (37% vs. 21%), suicide-attempt history (28% vs. 21%), and school-related problem (27% vs. 18%), Dr. Clark and associates reported.
“Bullying can be a deadly antecedent to suicide, especially among LGBTQ youth,” the investigators wrote. “Pediatricians can help to reduce this risk through adopting clinical practice approaches sensitive to the vulnerabilities of LGBTQ youth.”
SOURCE: Clark KA et al. JAMA Pediatr. 2020 May 26. doi: 10.1001/jamapediatrics.2020.0940.
FROM JAMA PEDIATRICS
Primary care practices struggle to survive despite visit rebound
Primary care practices are facing an existential threat, and they need government help now if they are to survive.
That was the main message at a teleconference held on May 20 to announce the results of a study showing that outpatient visits have rebounded across the United States. Having dropped 60% from their prepandemic level in early April, office visits are now significantly higher but are still 30% less than the baseline, on average, according to new data from the Commonwealth Fund, Harvard University, and Phreesia, a health information technology firm.
The outpatient visits study shows that most of the recovery was attributable to a rise in in-person visits, not telehealth encounters, which have plateaued. The rebound was more pronounced in some regions, like the South and Southwest, than in others, such as New England and the Mid-Atlantic.
the study shows. While some other specialties have seen a greater drop-off in visits, speakers at the news conference drew reporters’ attention to the financial plight of primary care.
“Primary care practices are in dire straits, and their ability to treat patients is under threat,” said Melinda Abrams, MS, senior vice president of delivery system reform and international innovations for the Commonwealth Fund. “In the long term, an investment in primary care will ensure we have primary care, because we are concerned about its collapse.”
Health policy experts from the Commonwealth Fund and other organizations, she said, propose that the next round of federal economic stimulus funding include recovery resources dedicated to primary care practices, especially small practices and those in underserved areas. She said the money should be distributed immediately through Medicare and Medicaid in supplemental monthly payments.
Up to now, Ms. Abrams said, no money in any of the federal rescue packages has been specifically earmarked for primary care.
Close permanently?
Farzad Mostashari, MD, CEO of Aledade and former national coordinator for health information technology at the U.S. Department of Health & Human Services, agreed primary care needs immediate help.
Aledade’s customers for population health management services, he noted, are some of the most forward-looking and technologically savvy primary care groups. “Nevertheless, those practices are suffering,” Dr. Mostashari said. “Many of them are at risk financially. There has been a massive 60%-70% drop in face-to-face visits. About 40% of visits are telehealth, but the practices are still down 30% or more in visits. And they’re losing ancillary revenues from procedures and labs.”
The financial devastation of the pandemic is causing some physicians to question whether they will be able to stay in practice. A recent survey from the California Healthcare Foundation found that a third of California primary care doctors are worried their practices will be forced to close permanently because of the financial impact of COVID-19. Many doctors said their practices had furloughed or laid off staff or that they’d been forced to take pay cuts.
Similarly, a recent survey by the Patient-Centered Primary Care Collaborative found that 13% of practices predicted closure within the next month and that 20% have already had temporary closures. Forty-two percent of the practices have laid off or furloughed staff, and 51% are uncertain about their financial future through June.
Primary care is essential
A pandemic-related reduction in the number of primary care physicians would exacerbate what many observers view as a nationwide shortage of primary care. Right now, the health care system badly needs all the primary care doctors it has, Ms. Abrams and Dr. Mostashari said.
Decades of research have shown that strong primary care is associated with better outcomes, lower per capita costs, and greater equity, Ms. Abrams noted. In addition, she said, dedicated support for primary care during the pandemic will help ensure that doctors meet the needs of patients with chronic diseases so they don’t have to be hospitalized.
Moreover, with proper support, primary care physicians can expand COVID-19 testing “so we can reopen the economy and perhaps prevent or contain the second wave of the virus,” she said.
Dr. Mostashari pointed out that primary care providers are on the front line of the pandemic. Although much attention has been rightfully given to those who treat COVID-19 patients in hospitals, he observed, “before those patients are admitted, they need to see primary care physicians. ... We have to maintain the primary care first line of defense. When the CDC says if you’re having symptoms, call your doctor, someone has to pick up the phone at the other end.”
In addition, he said, “there’s a hidden pandemic of untreated chronic conditions we should all be worried about. We know primary care is important because if you don’t do prevention, you’ll pay the price in heart attacks and strokes and kidney failure, and we’ve seen a dramatic decline in primary care services. In New York City, some people who have avoided necessary care have had bad outcomes, including in-home cardiac death.”
Dr. Mostashari also argued that the negative financial impact of COVID-19 could lead to a further consolidation of the industry as health systems and private equity investors take over failing practices. Past experience suggests that that would result in “a lack of choice, a lack of competition, and a lack of access” in many cases, he said.
The best long-term solution, he said, is to pay primary care physicians capitation instead of on a fee-for-service basis so that they’re not dependent on income from face-to-face visits.
In the short term, however, they need direct cash payments, Dr. Mostashari said. He called on Congress to allocate at least $15 billion to bolster the viability of primary care practices.
Telehealth levels off
One of the key findings of the outpatient visits study is that telehealth encounters, after soaring in the early days of the pandemic, have leveled off. After hitting a peak of 14% of all visits in mid-April, telehealth visits now make up about 12% of the total.
Study coauthor Ateev Mehrotra, MD, MPH, an associate professor of health policy and medicine at Harvard Medical School, Boston, said he’d expected the use of telehealth to continue rising. The fact that it hasn’t, he told reporters at the news conference, may be related to the different ways in which practices conduct virtual encounters.
“Some practices are using HIPAA-compliant [telehealth] platforms and training their patients on how to use those platforms,” Dr. Mehrotra noted. “Other clinics are mainly just phoning patients. You could envision those practices could easily revert back to in-person visits, because a phone call is going to be limited in many cases. Also, practices need to know whether payers will keep covering telehealth after the pandemic is over.”
The study shows that in-person visits, which declined more than total visits in March and early April, are now increasing at about the same rate as total visits. However, in-person visits are still down by more than 40%.
Asked whether financially vulnerable practices will be able to afford the safeguards that medical societies recommend to resume in-person visits, Dr. Mostashari pointed out that Medicare is now paying $28 to collect a COVID-19 specimen from a patient.
“Just the cost of changing PPE, plus disinfecting the room or setting up a separate room or testing facility: Those expenses are not included. We should have better accounting on what it actually costs to run a practice in the time of COVID. It’s not the same as their earlier operating costs.”
Dr. Mehrotra agreed. “You also can’t have 20 people in your waiting room or the throughput you had previously. So the number of patients you’ll be able to see will be lower because of appropriate restrictions.”
A version of this article originally appeared on Medscape.com.
Primary care practices are facing an existential threat, and they need government help now if they are to survive.
That was the main message at a teleconference held on May 20 to announce the results of a study showing that outpatient visits have rebounded across the United States. Having dropped 60% from their prepandemic level in early April, office visits are now significantly higher but are still 30% less than the baseline, on average, according to new data from the Commonwealth Fund, Harvard University, and Phreesia, a health information technology firm.
The outpatient visits study shows that most of the recovery was attributable to a rise in in-person visits, not telehealth encounters, which have plateaued. The rebound was more pronounced in some regions, like the South and Southwest, than in others, such as New England and the Mid-Atlantic.
the study shows. While some other specialties have seen a greater drop-off in visits, speakers at the news conference drew reporters’ attention to the financial plight of primary care.
“Primary care practices are in dire straits, and their ability to treat patients is under threat,” said Melinda Abrams, MS, senior vice president of delivery system reform and international innovations for the Commonwealth Fund. “In the long term, an investment in primary care will ensure we have primary care, because we are concerned about its collapse.”
Health policy experts from the Commonwealth Fund and other organizations, she said, propose that the next round of federal economic stimulus funding include recovery resources dedicated to primary care practices, especially small practices and those in underserved areas. She said the money should be distributed immediately through Medicare and Medicaid in supplemental monthly payments.
Up to now, Ms. Abrams said, no money in any of the federal rescue packages has been specifically earmarked for primary care.
Close permanently?
Farzad Mostashari, MD, CEO of Aledade and former national coordinator for health information technology at the U.S. Department of Health & Human Services, agreed primary care needs immediate help.
Aledade’s customers for population health management services, he noted, are some of the most forward-looking and technologically savvy primary care groups. “Nevertheless, those practices are suffering,” Dr. Mostashari said. “Many of them are at risk financially. There has been a massive 60%-70% drop in face-to-face visits. About 40% of visits are telehealth, but the practices are still down 30% or more in visits. And they’re losing ancillary revenues from procedures and labs.”
The financial devastation of the pandemic is causing some physicians to question whether they will be able to stay in practice. A recent survey from the California Healthcare Foundation found that a third of California primary care doctors are worried their practices will be forced to close permanently because of the financial impact of COVID-19. Many doctors said their practices had furloughed or laid off staff or that they’d been forced to take pay cuts.
Similarly, a recent survey by the Patient-Centered Primary Care Collaborative found that 13% of practices predicted closure within the next month and that 20% have already had temporary closures. Forty-two percent of the practices have laid off or furloughed staff, and 51% are uncertain about their financial future through June.
Primary care is essential
A pandemic-related reduction in the number of primary care physicians would exacerbate what many observers view as a nationwide shortage of primary care. Right now, the health care system badly needs all the primary care doctors it has, Ms. Abrams and Dr. Mostashari said.
Decades of research have shown that strong primary care is associated with better outcomes, lower per capita costs, and greater equity, Ms. Abrams noted. In addition, she said, dedicated support for primary care during the pandemic will help ensure that doctors meet the needs of patients with chronic diseases so they don’t have to be hospitalized.
Moreover, with proper support, primary care physicians can expand COVID-19 testing “so we can reopen the economy and perhaps prevent or contain the second wave of the virus,” she said.
Dr. Mostashari pointed out that primary care providers are on the front line of the pandemic. Although much attention has been rightfully given to those who treat COVID-19 patients in hospitals, he observed, “before those patients are admitted, they need to see primary care physicians. ... We have to maintain the primary care first line of defense. When the CDC says if you’re having symptoms, call your doctor, someone has to pick up the phone at the other end.”
In addition, he said, “there’s a hidden pandemic of untreated chronic conditions we should all be worried about. We know primary care is important because if you don’t do prevention, you’ll pay the price in heart attacks and strokes and kidney failure, and we’ve seen a dramatic decline in primary care services. In New York City, some people who have avoided necessary care have had bad outcomes, including in-home cardiac death.”
Dr. Mostashari also argued that the negative financial impact of COVID-19 could lead to a further consolidation of the industry as health systems and private equity investors take over failing practices. Past experience suggests that that would result in “a lack of choice, a lack of competition, and a lack of access” in many cases, he said.
The best long-term solution, he said, is to pay primary care physicians capitation instead of on a fee-for-service basis so that they’re not dependent on income from face-to-face visits.
In the short term, however, they need direct cash payments, Dr. Mostashari said. He called on Congress to allocate at least $15 billion to bolster the viability of primary care practices.
Telehealth levels off
One of the key findings of the outpatient visits study is that telehealth encounters, after soaring in the early days of the pandemic, have leveled off. After hitting a peak of 14% of all visits in mid-April, telehealth visits now make up about 12% of the total.
Study coauthor Ateev Mehrotra, MD, MPH, an associate professor of health policy and medicine at Harvard Medical School, Boston, said he’d expected the use of telehealth to continue rising. The fact that it hasn’t, he told reporters at the news conference, may be related to the different ways in which practices conduct virtual encounters.
“Some practices are using HIPAA-compliant [telehealth] platforms and training their patients on how to use those platforms,” Dr. Mehrotra noted. “Other clinics are mainly just phoning patients. You could envision those practices could easily revert back to in-person visits, because a phone call is going to be limited in many cases. Also, practices need to know whether payers will keep covering telehealth after the pandemic is over.”
The study shows that in-person visits, which declined more than total visits in March and early April, are now increasing at about the same rate as total visits. However, in-person visits are still down by more than 40%.
Asked whether financially vulnerable practices will be able to afford the safeguards that medical societies recommend to resume in-person visits, Dr. Mostashari pointed out that Medicare is now paying $28 to collect a COVID-19 specimen from a patient.
“Just the cost of changing PPE, plus disinfecting the room or setting up a separate room or testing facility: Those expenses are not included. We should have better accounting on what it actually costs to run a practice in the time of COVID. It’s not the same as their earlier operating costs.”
Dr. Mehrotra agreed. “You also can’t have 20 people in your waiting room or the throughput you had previously. So the number of patients you’ll be able to see will be lower because of appropriate restrictions.”
A version of this article originally appeared on Medscape.com.
Primary care practices are facing an existential threat, and they need government help now if they are to survive.
That was the main message at a teleconference held on May 20 to announce the results of a study showing that outpatient visits have rebounded across the United States. Having dropped 60% from their prepandemic level in early April, office visits are now significantly higher but are still 30% less than the baseline, on average, according to new data from the Commonwealth Fund, Harvard University, and Phreesia, a health information technology firm.
The outpatient visits study shows that most of the recovery was attributable to a rise in in-person visits, not telehealth encounters, which have plateaued. The rebound was more pronounced in some regions, like the South and Southwest, than in others, such as New England and the Mid-Atlantic.
the study shows. While some other specialties have seen a greater drop-off in visits, speakers at the news conference drew reporters’ attention to the financial plight of primary care.
“Primary care practices are in dire straits, and their ability to treat patients is under threat,” said Melinda Abrams, MS, senior vice president of delivery system reform and international innovations for the Commonwealth Fund. “In the long term, an investment in primary care will ensure we have primary care, because we are concerned about its collapse.”
Health policy experts from the Commonwealth Fund and other organizations, she said, propose that the next round of federal economic stimulus funding include recovery resources dedicated to primary care practices, especially small practices and those in underserved areas. She said the money should be distributed immediately through Medicare and Medicaid in supplemental monthly payments.
Up to now, Ms. Abrams said, no money in any of the federal rescue packages has been specifically earmarked for primary care.
Close permanently?
Farzad Mostashari, MD, CEO of Aledade and former national coordinator for health information technology at the U.S. Department of Health & Human Services, agreed primary care needs immediate help.
Aledade’s customers for population health management services, he noted, are some of the most forward-looking and technologically savvy primary care groups. “Nevertheless, those practices are suffering,” Dr. Mostashari said. “Many of them are at risk financially. There has been a massive 60%-70% drop in face-to-face visits. About 40% of visits are telehealth, but the practices are still down 30% or more in visits. And they’re losing ancillary revenues from procedures and labs.”
The financial devastation of the pandemic is causing some physicians to question whether they will be able to stay in practice. A recent survey from the California Healthcare Foundation found that a third of California primary care doctors are worried their practices will be forced to close permanently because of the financial impact of COVID-19. Many doctors said their practices had furloughed or laid off staff or that they’d been forced to take pay cuts.
Similarly, a recent survey by the Patient-Centered Primary Care Collaborative found that 13% of practices predicted closure within the next month and that 20% have already had temporary closures. Forty-two percent of the practices have laid off or furloughed staff, and 51% are uncertain about their financial future through June.
Primary care is essential
A pandemic-related reduction in the number of primary care physicians would exacerbate what many observers view as a nationwide shortage of primary care. Right now, the health care system badly needs all the primary care doctors it has, Ms. Abrams and Dr. Mostashari said.
Decades of research have shown that strong primary care is associated with better outcomes, lower per capita costs, and greater equity, Ms. Abrams noted. In addition, she said, dedicated support for primary care during the pandemic will help ensure that doctors meet the needs of patients with chronic diseases so they don’t have to be hospitalized.
Moreover, with proper support, primary care physicians can expand COVID-19 testing “so we can reopen the economy and perhaps prevent or contain the second wave of the virus,” she said.
Dr. Mostashari pointed out that primary care providers are on the front line of the pandemic. Although much attention has been rightfully given to those who treat COVID-19 patients in hospitals, he observed, “before those patients are admitted, they need to see primary care physicians. ... We have to maintain the primary care first line of defense. When the CDC says if you’re having symptoms, call your doctor, someone has to pick up the phone at the other end.”
In addition, he said, “there’s a hidden pandemic of untreated chronic conditions we should all be worried about. We know primary care is important because if you don’t do prevention, you’ll pay the price in heart attacks and strokes and kidney failure, and we’ve seen a dramatic decline in primary care services. In New York City, some people who have avoided necessary care have had bad outcomes, including in-home cardiac death.”
Dr. Mostashari also argued that the negative financial impact of COVID-19 could lead to a further consolidation of the industry as health systems and private equity investors take over failing practices. Past experience suggests that that would result in “a lack of choice, a lack of competition, and a lack of access” in many cases, he said.
The best long-term solution, he said, is to pay primary care physicians capitation instead of on a fee-for-service basis so that they’re not dependent on income from face-to-face visits.
In the short term, however, they need direct cash payments, Dr. Mostashari said. He called on Congress to allocate at least $15 billion to bolster the viability of primary care practices.
Telehealth levels off
One of the key findings of the outpatient visits study is that telehealth encounters, after soaring in the early days of the pandemic, have leveled off. After hitting a peak of 14% of all visits in mid-April, telehealth visits now make up about 12% of the total.
Study coauthor Ateev Mehrotra, MD, MPH, an associate professor of health policy and medicine at Harvard Medical School, Boston, said he’d expected the use of telehealth to continue rising. The fact that it hasn’t, he told reporters at the news conference, may be related to the different ways in which practices conduct virtual encounters.
“Some practices are using HIPAA-compliant [telehealth] platforms and training their patients on how to use those platforms,” Dr. Mehrotra noted. “Other clinics are mainly just phoning patients. You could envision those practices could easily revert back to in-person visits, because a phone call is going to be limited in many cases. Also, practices need to know whether payers will keep covering telehealth after the pandemic is over.”
The study shows that in-person visits, which declined more than total visits in March and early April, are now increasing at about the same rate as total visits. However, in-person visits are still down by more than 40%.
Asked whether financially vulnerable practices will be able to afford the safeguards that medical societies recommend to resume in-person visits, Dr. Mostashari pointed out that Medicare is now paying $28 to collect a COVID-19 specimen from a patient.
“Just the cost of changing PPE, plus disinfecting the room or setting up a separate room or testing facility: Those expenses are not included. We should have better accounting on what it actually costs to run a practice in the time of COVID. It’s not the same as their earlier operating costs.”
Dr. Mehrotra agreed. “You also can’t have 20 people in your waiting room or the throughput you had previously. So the number of patients you’ll be able to see will be lower because of appropriate restrictions.”
A version of this article originally appeared on Medscape.com.
Biologic approved for atopic dermatitis in children
The Food and Drug Administration has approved dupilumab for children aged 6-11 years with moderate to severe atopic dermatitis, the manufacturers announced.
The new indication is for children “whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable,” Regeneron and Sanofi said in a press release, which points out that this is the first biologic approved for AD in this age group.
For children aged 6-11, the two available dupilumab (Dupixent) doses in prefilled syringes are given based on weight – 300 mg every 4 weeks for children between 15 to 29 kg and 200 mg every 2 weeks for children 30 to 59 kg – following an initial loading dose.
In phase 3 trials, children with severe AD who received dupilumab and topical corticosteroids improved significantly in overall disease severity, skin clearance, and itch, compared with those getting steroids alone. Eczema Area and Severity Index-75, for example, was reached by 75% of patients on either dupilumab dose, compared with 28% and 26% , respectively, for those receiving steroids alone every 4 and every 2 weeks, the statement said.
Over the 16-week treatment period, overall rates of adverse events were 65% for those getting dupilumab every 4 weeks and 61% for every 2 weeks – compared with steroids alone (72% and 75%, respectively), the statement said.
The fully human monoclonal antibody inhibits signaling of the interleukin-4 and interleukin-13 proteins and is already approved as an add-on maintenance treatment in children aged 12 years and older with moderate to severe asthma (eosinophilic phenotype or oral-corticosteroid dependent) and in adults with inadequately controlled chronic rhinosinusitis with nasal polyposis, according to the prescribing information.
The Food and Drug Administration has approved dupilumab for children aged 6-11 years with moderate to severe atopic dermatitis, the manufacturers announced.
The new indication is for children “whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable,” Regeneron and Sanofi said in a press release, which points out that this is the first biologic approved for AD in this age group.
For children aged 6-11, the two available dupilumab (Dupixent) doses in prefilled syringes are given based on weight – 300 mg every 4 weeks for children between 15 to 29 kg and 200 mg every 2 weeks for children 30 to 59 kg – following an initial loading dose.
In phase 3 trials, children with severe AD who received dupilumab and topical corticosteroids improved significantly in overall disease severity, skin clearance, and itch, compared with those getting steroids alone. Eczema Area and Severity Index-75, for example, was reached by 75% of patients on either dupilumab dose, compared with 28% and 26% , respectively, for those receiving steroids alone every 4 and every 2 weeks, the statement said.
Over the 16-week treatment period, overall rates of adverse events were 65% for those getting dupilumab every 4 weeks and 61% for every 2 weeks – compared with steroids alone (72% and 75%, respectively), the statement said.
The fully human monoclonal antibody inhibits signaling of the interleukin-4 and interleukin-13 proteins and is already approved as an add-on maintenance treatment in children aged 12 years and older with moderate to severe asthma (eosinophilic phenotype or oral-corticosteroid dependent) and in adults with inadequately controlled chronic rhinosinusitis with nasal polyposis, according to the prescribing information.
The Food and Drug Administration has approved dupilumab for children aged 6-11 years with moderate to severe atopic dermatitis, the manufacturers announced.
The new indication is for children “whose disease is not adequately controlled with topical prescription therapies or when those therapies are not advisable,” Regeneron and Sanofi said in a press release, which points out that this is the first biologic approved for AD in this age group.
For children aged 6-11, the two available dupilumab (Dupixent) doses in prefilled syringes are given based on weight – 300 mg every 4 weeks for children between 15 to 29 kg and 200 mg every 2 weeks for children 30 to 59 kg – following an initial loading dose.
In phase 3 trials, children with severe AD who received dupilumab and topical corticosteroids improved significantly in overall disease severity, skin clearance, and itch, compared with those getting steroids alone. Eczema Area and Severity Index-75, for example, was reached by 75% of patients on either dupilumab dose, compared with 28% and 26% , respectively, for those receiving steroids alone every 4 and every 2 weeks, the statement said.
Over the 16-week treatment period, overall rates of adverse events were 65% for those getting dupilumab every 4 weeks and 61% for every 2 weeks – compared with steroids alone (72% and 75%, respectively), the statement said.
The fully human monoclonal antibody inhibits signaling of the interleukin-4 and interleukin-13 proteins and is already approved as an add-on maintenance treatment in children aged 12 years and older with moderate to severe asthma (eosinophilic phenotype or oral-corticosteroid dependent) and in adults with inadequately controlled chronic rhinosinusitis with nasal polyposis, according to the prescribing information.
Family physicians have lowest incentive bonuses, survey finds
according to the Medscape Family Medicine Physician Compensation Report 2020.
This year’s survey was the first to ask about bonuses, and it showed strong contrasts between specialties. Family physicians’ bonuses averaged $24,000, whereas orthopedists’ were four times higher, at $96,000.
Two-thirds of family physicians (67%), similar to physicians overall, reported that bonuses had no influence on the number of hours worked.
More than half of all physicians in the survey (56%) said they got such bonuses.
Family physicians’ pay was up $3,000 from last year, to $234,000, but still ranked near the bottom in comparison with other specialties. Only physicians in public health/preventive medicine and pediatrics made less, both at $232,000.
The top four specialties in pay were the same this year as they were last year and ranked in the same order: Orthopedists made the most, at $511,000, followed by plastic surgeons ($479,000), otolaryngologists ($455,000), and cardiologists ($438,000).
However, the compensation picture is changing for all physicians. This report reflects data gathered between Oct. 4, 2019, and Feb. 10, 2020. Since that time, the COVID-19 crisis has reversed income gains for physicians overall. In a study from the Medical Group Management Association, researchers estimated that more than half of medical practices reported a drop in revenue by early April of 55% and a drop in patient volume of 60%.
Male family physicians continue to make more than their female colleagues, with this year’s difference at 26% ($257,000 vs. $205,000). Male specialists overall in the survey made 31% more than their female counterparts.
Few claims denied
A bright spot in compensation was that family physicians have among the lowest rates (14%) of claims that are denied or that need to be resubmitted. Plastic surgeons have twice that rate (28%) of rejected claims.
The survey authors noted, “One study found that, on average, 63% of denied claims are recoverable, but health care professionals spend about $118 per claim on appeals.”
Family physicians were in the middle of the pack as far as how much time was spent on paperwork. On average, they spent 15.9 hours a week on the tasks. Intensivists spent the most, at 19.1 hours each week, and ophthalmologists spent the least, at 9.8 hours per week.
Although 73% of physicians overall said they had no plans to stop accepting new and current Medicare and Medicaid patients, only 65% of family physicians answered that way. Seventeen percent said they would stop taking new Medicare patients, and 9% said they wouldn’t take new Medicaid patients; 15% had not made those decisions yet.
Rules and regulations are the biggest challenges
Asked about their biggest challenges, 29% of family physicians put “having so many rules and regulations” at the top. Next came working with an electronic health records system, followed by dealing with difficult patients.
The biggest reward, they said again this year, was “gratitude/relationships with patients” (34% ranked it at the top), followed by “knowing I’m making the world a better place” (25%), “being very good at what I do/finding answers, diagnoses” (18%), and “making good money at a job that I like” (10%).
Most family practices employ advanced practice providers (62% employed NPs, and 43% employed PAs). Fewer than one-third employed neither.
Of the family medicine physicians who did work with advanced practice providers in their offices, half (50%) said they improved profitability, 45% said they had no effect, and 5% said they decreased profitability.
A version of this article originally appeared on Medscape.com.
according to the Medscape Family Medicine Physician Compensation Report 2020.
This year’s survey was the first to ask about bonuses, and it showed strong contrasts between specialties. Family physicians’ bonuses averaged $24,000, whereas orthopedists’ were four times higher, at $96,000.
Two-thirds of family physicians (67%), similar to physicians overall, reported that bonuses had no influence on the number of hours worked.
More than half of all physicians in the survey (56%) said they got such bonuses.
Family physicians’ pay was up $3,000 from last year, to $234,000, but still ranked near the bottom in comparison with other specialties. Only physicians in public health/preventive medicine and pediatrics made less, both at $232,000.
The top four specialties in pay were the same this year as they were last year and ranked in the same order: Orthopedists made the most, at $511,000, followed by plastic surgeons ($479,000), otolaryngologists ($455,000), and cardiologists ($438,000).
However, the compensation picture is changing for all physicians. This report reflects data gathered between Oct. 4, 2019, and Feb. 10, 2020. Since that time, the COVID-19 crisis has reversed income gains for physicians overall. In a study from the Medical Group Management Association, researchers estimated that more than half of medical practices reported a drop in revenue by early April of 55% and a drop in patient volume of 60%.
Male family physicians continue to make more than their female colleagues, with this year’s difference at 26% ($257,000 vs. $205,000). Male specialists overall in the survey made 31% more than their female counterparts.
Few claims denied
A bright spot in compensation was that family physicians have among the lowest rates (14%) of claims that are denied or that need to be resubmitted. Plastic surgeons have twice that rate (28%) of rejected claims.
The survey authors noted, “One study found that, on average, 63% of denied claims are recoverable, but health care professionals spend about $118 per claim on appeals.”
Family physicians were in the middle of the pack as far as how much time was spent on paperwork. On average, they spent 15.9 hours a week on the tasks. Intensivists spent the most, at 19.1 hours each week, and ophthalmologists spent the least, at 9.8 hours per week.
Although 73% of physicians overall said they had no plans to stop accepting new and current Medicare and Medicaid patients, only 65% of family physicians answered that way. Seventeen percent said they would stop taking new Medicare patients, and 9% said they wouldn’t take new Medicaid patients; 15% had not made those decisions yet.
Rules and regulations are the biggest challenges
Asked about their biggest challenges, 29% of family physicians put “having so many rules and regulations” at the top. Next came working with an electronic health records system, followed by dealing with difficult patients.
The biggest reward, they said again this year, was “gratitude/relationships with patients” (34% ranked it at the top), followed by “knowing I’m making the world a better place” (25%), “being very good at what I do/finding answers, diagnoses” (18%), and “making good money at a job that I like” (10%).
Most family practices employ advanced practice providers (62% employed NPs, and 43% employed PAs). Fewer than one-third employed neither.
Of the family medicine physicians who did work with advanced practice providers in their offices, half (50%) said they improved profitability, 45% said they had no effect, and 5% said they decreased profitability.
A version of this article originally appeared on Medscape.com.
according to the Medscape Family Medicine Physician Compensation Report 2020.
This year’s survey was the first to ask about bonuses, and it showed strong contrasts between specialties. Family physicians’ bonuses averaged $24,000, whereas orthopedists’ were four times higher, at $96,000.
Two-thirds of family physicians (67%), similar to physicians overall, reported that bonuses had no influence on the number of hours worked.
More than half of all physicians in the survey (56%) said they got such bonuses.
Family physicians’ pay was up $3,000 from last year, to $234,000, but still ranked near the bottom in comparison with other specialties. Only physicians in public health/preventive medicine and pediatrics made less, both at $232,000.
The top four specialties in pay were the same this year as they were last year and ranked in the same order: Orthopedists made the most, at $511,000, followed by plastic surgeons ($479,000), otolaryngologists ($455,000), and cardiologists ($438,000).
However, the compensation picture is changing for all physicians. This report reflects data gathered between Oct. 4, 2019, and Feb. 10, 2020. Since that time, the COVID-19 crisis has reversed income gains for physicians overall. In a study from the Medical Group Management Association, researchers estimated that more than half of medical practices reported a drop in revenue by early April of 55% and a drop in patient volume of 60%.
Male family physicians continue to make more than their female colleagues, with this year’s difference at 26% ($257,000 vs. $205,000). Male specialists overall in the survey made 31% more than their female counterparts.
Few claims denied
A bright spot in compensation was that family physicians have among the lowest rates (14%) of claims that are denied or that need to be resubmitted. Plastic surgeons have twice that rate (28%) of rejected claims.
The survey authors noted, “One study found that, on average, 63% of denied claims are recoverable, but health care professionals spend about $118 per claim on appeals.”
Family physicians were in the middle of the pack as far as how much time was spent on paperwork. On average, they spent 15.9 hours a week on the tasks. Intensivists spent the most, at 19.1 hours each week, and ophthalmologists spent the least, at 9.8 hours per week.
Although 73% of physicians overall said they had no plans to stop accepting new and current Medicare and Medicaid patients, only 65% of family physicians answered that way. Seventeen percent said they would stop taking new Medicare patients, and 9% said they wouldn’t take new Medicaid patients; 15% had not made those decisions yet.
Rules and regulations are the biggest challenges
Asked about their biggest challenges, 29% of family physicians put “having so many rules and regulations” at the top. Next came working with an electronic health records system, followed by dealing with difficult patients.
The biggest reward, they said again this year, was “gratitude/relationships with patients” (34% ranked it at the top), followed by “knowing I’m making the world a better place” (25%), “being very good at what I do/finding answers, diagnoses” (18%), and “making good money at a job that I like” (10%).
Most family practices employ advanced practice providers (62% employed NPs, and 43% employed PAs). Fewer than one-third employed neither.
Of the family medicine physicians who did work with advanced practice providers in their offices, half (50%) said they improved profitability, 45% said they had no effect, and 5% said they decreased profitability.
A version of this article originally appeared on Medscape.com.
More evidence hydroxychloroquine is ineffective, harmful in COVID-19
Hydroxychloroquine and chloroquine, with or without azithromycin or clarithromycin, offer no benefit in treating patients with COVID-19 and, instead, are associated with ventricular arrhythmias and higher rates of mortality, according to a major new international study.

In the largest observational study of its kind, including close to 100,000 people in 671 hospitals on six continents, investigators compared outcomes in 15,000 patients with COVID-19 treated with hydroxychloroquine and chloroquine alone or in combination with a macrolide with 80,000 control patients with COVID-19 not receiving these agents.
Treatment with any of these medications, either alone or in combination, was associated with increased death during hospitalization; compared with about 10% in control group patients, mortality rates ranged from more than 16% to almost 24% in the treated groups.
Patients treated with hydroxychloroquine plus a macrolide showed the highest rates of serious cardiac arrhythmias, and, even after accounting for demographic factors and comorbidities, this combination was found to be associated with a more than 5-fold increase in the risk of developing a serious arrhythmia while in the hospital.
“In this real-world study, the biggest yet, we looked at 100,000 patients [with COVID-19] across six continents and found not the slightest hint of benefits and only risks, and the data is pretty straightforward,” study coauthor Frank Ruschitzka, MD, director of the Heart Center at University Hospital, Zürich, said in an interview. The study was published online May 22 in The Lancet.
‘Inconclusive’ evidence
The absence of an effective treatment for COVID-19 has led to the “repurposing” of the antimalarial drug chloroquine and its analogue hydroxychloroquine, which is used for treating autoimmune disease, but this approach is based on anecdotal evidence or open-label randomized trials that have been “largely inconclusive,” the authors wrote.
Additional agents used to treat COVID-19 are second-generation macrolides (azithromycin or clarithromycin), in combination with chloroquine or hydroxychloroquine, “despite limited evidence” and the risk for ventricular arrhythmias, the authors noted.
“Our primary question was whether there was any associated benefits of the use of hydroxychloroquine, chloroquine, or a combined regimen with macrolides in treating COVID-19, and — if there was no benefit — would there be harm?” lead author Mandeep R. Mehra, MD, MSc, William Harvey Distinguished Chair in Advanced Cardiovascular Medicine, Brigham and Women’s Hospital, Boston, said in an interview.
The investigators used data from a multinational registry comprising 671 hospitals that included patients (n = 96,032; mean age 53.8 years; 46.3% female) who had been hospitalized between Dec. 20, 2019, and April 14, 2020, with confirmed COVID-19 infection.
They also collected data about demographics, underlying comorbidities, and medical history, and medications that patients were taking at baseline.
Patients receiving treatment (n = 14,888) were divided into four groups: those receiving chloroquine alone (n = 1,868), those receiving chloroquine with a macrolide (n = 3,783), those receiving hydroxychloroquine alone (n = 3,016) and those receiving hydroxychloroquine with a macrolide (n = 6,221).
The remaining patients not treated with these regimens (n = 81,144) were regarded as the control group.
Most patients (65.9%) came from North America, followed by Europe (17.39%), Asia (7.9%), Africa (4.6%), South America (3.7%), and Australia (0.6%). Most (66.9%) were white, followed by patients of Asian origin (14.1%), black patients (9.4%), and Hispanic patients (6.2%).
Comorbidities and underlying conditions included obesity, hyperlipidemia, and hypertension in about 30%.
Comorbidities and underlying conditions
The investigators conducted multiple analyses to control for confounding variables, including Cox proportional hazards regression and propensity score matching analyses.
“In an observational study, there is always a chance of residual confounding, which is why we did propensity score based matched analyses,” Dr. Ruschitzka explained.
No significant differences were found in distribution of demographics and comorbidities between the groups.
As good as it gets
“We found no benefit in any of the four treatment regimens for hospitalized patients with COVID-19, but we did notice higher rates of death and serious ventricular arrhythmias in these patients, compared to the controls,” Dr. Mehra reported.
Of the patients in the control group, roughly 9.3% died during their hospitalization, compared with 16.4% of patients treated with chloroquine alone, 18.0% of those treated with hydroxychloroquine alone, 22.2% of those treated with chloroquine and a macrolide, and 23.8% of those treated with hydroxychloroquine and a macrolide.
After accounting for confounding variables, the researchers estimated that the excess mortality risk attributable to use of the drug regimen ranged from 34% to 45%.
Patients treated with any of the four regimens sustained more serious arrhythmias, compared with those in the control group (0.35), with the biggest increase seen in the group treated with the combination of hydroxychloroquine plus a macrolide (8.1%), followed by chloroquine with a macrolide (6.5%), hydroxychloroquine alone (6.1%), and chloroquine alone (4.3%).
“We were fairly reassured that, although the study was observational, the signals were robust and consistent across all regions of the world in diverse populations, and we did not see any muting of that signal, depending on region,” Dr. Mehra said.
“Two months ago, we were all scratching our heads about how to treat patients with COVID-19, and then came a drug [hydroxychloroquine] with some anecdotal evidence, but now we have 2 months more experience, and we looked to science to provide some answer,” Dr. Ruschitzka said.
“Although this was not a randomized, controlled trial, so we do not have a definite answer, the data provided in this [large, multinational] real-world study is as good as it gets and the best data we have,” he concluded.
“Let the science speak for itself”
Commenting on the study in an interview, Christian Funck-Brentano, MD, from the Hospital Pitié-Salpêtrière and Sorbonne University, both in Paris, said that, although the study is observational and therefore not as reliable as a randomized controlled trial, it is “nevertheless well-documented, studied a huge amount of people, and utilized several sensitivity methods, all of which showed the same results.”
Dr. Funck-Brentano, who is the coauthor of an accompanying editorial in The Lancet and was not involved with the study, said that “we now have no evidence that hydroxychloroquine and chloroquine alone or in combination with a macrolide do any good and we have potential evidence that they do harm and kill people.”
Also commenting on the study in an interview, David Holtgrave, PhD, dean of the School of Public Health at the State University of New York at Albany, said that, “while no one observational study alone would lead to a firm clinical recommendation, I think it is helpful for physicians and public health officials to be aware of the findings of the peer-reviewed observational studies to date and the National Institutes of Health COVID-19 treatment guidelines and the Food and Drug Administration’s statement of drug safety concern about hydroxychloroquine to inform their decision-making as we await the results of randomized clinical trials of these drugs for the treatment of COVID-19,” said Dr. Holtgrave, who was not involved with the study.
He added that, to his knowledge, there are “still no published studies of prophylactic use of these drugs to prevent COVID-19.”
Dr. Mehra emphasized that a cardinal principle of practicing medicine is “first do no harm” and “even in situations where you believe a desperate disease calls for desperate measures, responsible physicians should take a step back and ask if we are doing harm, and until we can say we aren’t, I don’t think it’s wise to push something like this in the absence of good efficacy data.”
Dr. Ruschitzka added that those who are encouraging the use of these agents “should review their decision based on today’s data and let the science speak for itself.”
The study was supported by the William Harvey Distinguished Chair in Advanced Cardiovascular Medicine at Brigham and Women’s Hospital, Boston. Dr. Mehra reported personal fees from Abbott, Medtronic, Janssen, Mesoblast, Portola, Bayer, Baim Institute for Clinical Research, NuPulseCV, FineHeart, Leviticus, Roivant, and Triple Gene. Dr. Ruschitzka was paid for time spent as a committee member for clinical trials, advisory boards, other forms of consulting, and lectures or presentations; these payments were made directly to the University of Zürich and no personal payments were received in relation to these trials or other activities. Dr. Funck-Brentano, his coauthor, and Dr. Holtgrave declared no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Hydroxychloroquine and chloroquine, with or without azithromycin or clarithromycin, offer no benefit in treating patients with COVID-19 and, instead, are associated with ventricular arrhythmias and higher rates of mortality, according to a major new international study.
In the largest observational study of its kind, including close to 100,000 people in 671 hospitals on six continents, investigators compared outcomes in 15,000 patients with COVID-19 treated with hydroxychloroquine and chloroquine alone or in combination with a macrolide with 80,000 control patients with COVID-19 not receiving these agents.
Treatment with any of these medications, either alone or in combination, was associated with increased death during hospitalization; compared with about 10% in control group patients, mortality rates ranged from more than 16% to almost 24% in the treated groups.
Patients treated with hydroxychloroquine plus a macrolide showed the highest rates of serious cardiac arrhythmias, and, even after accounting for demographic factors and comorbidities, this combination was found to be associated with a more than 5-fold increase in the risk of developing a serious arrhythmia while in the hospital.
“In this real-world study, the biggest yet, we looked at 100,000 patients [with COVID-19] across six continents and found not the slightest hint of benefits and only risks, and the data is pretty straightforward,” study coauthor Frank Ruschitzka, MD, director of the Heart Center at University Hospital, Zürich, said in an interview. The study was published online May 22 in The Lancet.
‘Inconclusive’ evidence
The absence of an effective treatment for COVID-19 has led to the “repurposing” of the antimalarial drug chloroquine and its analogue hydroxychloroquine, which is used for treating autoimmune disease, but this approach is based on anecdotal evidence or open-label randomized trials that have been “largely inconclusive,” the authors wrote.
Additional agents used to treat COVID-19 are second-generation macrolides (azithromycin or clarithromycin), in combination with chloroquine or hydroxychloroquine, “despite limited evidence” and the risk for ventricular arrhythmias, the authors noted.
“Our primary question was whether there was any associated benefits of the use of hydroxychloroquine, chloroquine, or a combined regimen with macrolides in treating COVID-19, and — if there was no benefit — would there be harm?” lead author Mandeep R. Mehra, MD, MSc, William Harvey Distinguished Chair in Advanced Cardiovascular Medicine, Brigham and Women’s Hospital, Boston, said in an interview.
The investigators used data from a multinational registry comprising 671 hospitals that included patients (n = 96,032; mean age 53.8 years; 46.3% female) who had been hospitalized between Dec. 20, 2019, and April 14, 2020, with confirmed COVID-19 infection.
They also collected data about demographics, underlying comorbidities, and medical history, and medications that patients were taking at baseline.
Patients receiving treatment (n = 14,888) were divided into four groups: those receiving chloroquine alone (n = 1,868), those receiving chloroquine with a macrolide (n = 3,783), those receiving hydroxychloroquine alone (n = 3,016) and those receiving hydroxychloroquine with a macrolide (n = 6,221).
The remaining patients not treated with these regimens (n = 81,144) were regarded as the control group.
Most patients (65.9%) came from North America, followed by Europe (17.39%), Asia (7.9%), Africa (4.6%), South America (3.7%), and Australia (0.6%). Most (66.9%) were white, followed by patients of Asian origin (14.1%), black patients (9.4%), and Hispanic patients (6.2%).
Comorbidities and underlying conditions included obesity, hyperlipidemia, and hypertension in about 30%.
Comorbidities and underlying conditions
The investigators conducted multiple analyses to control for confounding variables, including Cox proportional hazards regression and propensity score matching analyses.
“In an observational study, there is always a chance of residual confounding, which is why we did propensity score based matched analyses,” Dr. Ruschitzka explained.
No significant differences were found in distribution of demographics and comorbidities between the groups.
As good as it gets
“We found no benefit in any of the four treatment regimens for hospitalized patients with COVID-19, but we did notice higher rates of death and serious ventricular arrhythmias in these patients, compared to the controls,” Dr. Mehra reported.
Of the patients in the control group, roughly 9.3% died during their hospitalization, compared with 16.4% of patients treated with chloroquine alone, 18.0% of those treated with hydroxychloroquine alone, 22.2% of those treated with chloroquine and a macrolide, and 23.8% of those treated with hydroxychloroquine and a macrolide.
After accounting for confounding variables, the researchers estimated that the excess mortality risk attributable to use of the drug regimen ranged from 34% to 45%.
Patients treated with any of the four regimens sustained more serious arrhythmias, compared with those in the control group (0.35), with the biggest increase seen in the group treated with the combination of hydroxychloroquine plus a macrolide (8.1%), followed by chloroquine with a macrolide (6.5%), hydroxychloroquine alone (6.1%), and chloroquine alone (4.3%).
“We were fairly reassured that, although the study was observational, the signals were robust and consistent across all regions of the world in diverse populations, and we did not see any muting of that signal, depending on region,” Dr. Mehra said.
“Two months ago, we were all scratching our heads about how to treat patients with COVID-19, and then came a drug [hydroxychloroquine] with some anecdotal evidence, but now we have 2 months more experience, and we looked to science to provide some answer,” Dr. Ruschitzka said.
“Although this was not a randomized, controlled trial, so we do not have a definite answer, the data provided in this [large, multinational] real-world study is as good as it gets and the best data we have,” he concluded.
“Let the science speak for itself”
Commenting on the study in an interview, Christian Funck-Brentano, MD, from the Hospital Pitié-Salpêtrière and Sorbonne University, both in Paris, said that, although the study is observational and therefore not as reliable as a randomized controlled trial, it is “nevertheless well-documented, studied a huge amount of people, and utilized several sensitivity methods, all of which showed the same results.”
Dr. Funck-Brentano, who is the coauthor of an accompanying editorial in The Lancet and was not involved with the study, said that “we now have no evidence that hydroxychloroquine and chloroquine alone or in combination with a macrolide do any good and we have potential evidence that they do harm and kill people.”
Also commenting on the study in an interview, David Holtgrave, PhD, dean of the School of Public Health at the State University of New York at Albany, said that, “while no one observational study alone would lead to a firm clinical recommendation, I think it is helpful for physicians and public health officials to be aware of the findings of the peer-reviewed observational studies to date and the National Institutes of Health COVID-19 treatment guidelines and the Food and Drug Administration’s statement of drug safety concern about hydroxychloroquine to inform their decision-making as we await the results of randomized clinical trials of these drugs for the treatment of COVID-19,” said Dr. Holtgrave, who was not involved with the study.
He added that, to his knowledge, there are “still no published studies of prophylactic use of these drugs to prevent COVID-19.”
Dr. Mehra emphasized that a cardinal principle of practicing medicine is “first do no harm” and “even in situations where you believe a desperate disease calls for desperate measures, responsible physicians should take a step back and ask if we are doing harm, and until we can say we aren’t, I don’t think it’s wise to push something like this in the absence of good efficacy data.”
Dr. Ruschitzka added that those who are encouraging the use of these agents “should review their decision based on today’s data and let the science speak for itself.”
The study was supported by the William Harvey Distinguished Chair in Advanced Cardiovascular Medicine at Brigham and Women’s Hospital, Boston. Dr. Mehra reported personal fees from Abbott, Medtronic, Janssen, Mesoblast, Portola, Bayer, Baim Institute for Clinical Research, NuPulseCV, FineHeart, Leviticus, Roivant, and Triple Gene. Dr. Ruschitzka was paid for time spent as a committee member for clinical trials, advisory boards, other forms of consulting, and lectures or presentations; these payments were made directly to the University of Zürich and no personal payments were received in relation to these trials or other activities. Dr. Funck-Brentano, his coauthor, and Dr. Holtgrave declared no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Hydroxychloroquine and chloroquine, with or without azithromycin or clarithromycin, offer no benefit in treating patients with COVID-19 and, instead, are associated with ventricular arrhythmias and higher rates of mortality, according to a major new international study.
In the largest observational study of its kind, including close to 100,000 people in 671 hospitals on six continents, investigators compared outcomes in 15,000 patients with COVID-19 treated with hydroxychloroquine and chloroquine alone or in combination with a macrolide with 80,000 control patients with COVID-19 not receiving these agents.
Treatment with any of these medications, either alone or in combination, was associated with increased death during hospitalization; compared with about 10% in control group patients, mortality rates ranged from more than 16% to almost 24% in the treated groups.
Patients treated with hydroxychloroquine plus a macrolide showed the highest rates of serious cardiac arrhythmias, and, even after accounting for demographic factors and comorbidities, this combination was found to be associated with a more than 5-fold increase in the risk of developing a serious arrhythmia while in the hospital.
“In this real-world study, the biggest yet, we looked at 100,000 patients [with COVID-19] across six continents and found not the slightest hint of benefits and only risks, and the data is pretty straightforward,” study coauthor Frank Ruschitzka, MD, director of the Heart Center at University Hospital, Zürich, said in an interview. The study was published online May 22 in The Lancet.
‘Inconclusive’ evidence
The absence of an effective treatment for COVID-19 has led to the “repurposing” of the antimalarial drug chloroquine and its analogue hydroxychloroquine, which is used for treating autoimmune disease, but this approach is based on anecdotal evidence or open-label randomized trials that have been “largely inconclusive,” the authors wrote.
Additional agents used to treat COVID-19 are second-generation macrolides (azithromycin or clarithromycin), in combination with chloroquine or hydroxychloroquine, “despite limited evidence” and the risk for ventricular arrhythmias, the authors noted.
“Our primary question was whether there was any associated benefits of the use of hydroxychloroquine, chloroquine, or a combined regimen with macrolides in treating COVID-19, and — if there was no benefit — would there be harm?” lead author Mandeep R. Mehra, MD, MSc, William Harvey Distinguished Chair in Advanced Cardiovascular Medicine, Brigham and Women’s Hospital, Boston, said in an interview.
The investigators used data from a multinational registry comprising 671 hospitals that included patients (n = 96,032; mean age 53.8 years; 46.3% female) who had been hospitalized between Dec. 20, 2019, and April 14, 2020, with confirmed COVID-19 infection.
They also collected data about demographics, underlying comorbidities, and medical history, and medications that patients were taking at baseline.
Patients receiving treatment (n = 14,888) were divided into four groups: those receiving chloroquine alone (n = 1,868), those receiving chloroquine with a macrolide (n = 3,783), those receiving hydroxychloroquine alone (n = 3,016) and those receiving hydroxychloroquine with a macrolide (n = 6,221).
The remaining patients not treated with these regimens (n = 81,144) were regarded as the control group.
Most patients (65.9%) came from North America, followed by Europe (17.39%), Asia (7.9%), Africa (4.6%), South America (3.7%), and Australia (0.6%). Most (66.9%) were white, followed by patients of Asian origin (14.1%), black patients (9.4%), and Hispanic patients (6.2%).
Comorbidities and underlying conditions included obesity, hyperlipidemia, and hypertension in about 30%.
Comorbidities and underlying conditions
The investigators conducted multiple analyses to control for confounding variables, including Cox proportional hazards regression and propensity score matching analyses.
“In an observational study, there is always a chance of residual confounding, which is why we did propensity score based matched analyses,” Dr. Ruschitzka explained.
No significant differences were found in distribution of demographics and comorbidities between the groups.
As good as it gets
“We found no benefit in any of the four treatment regimens for hospitalized patients with COVID-19, but we did notice higher rates of death and serious ventricular arrhythmias in these patients, compared to the controls,” Dr. Mehra reported.
Of the patients in the control group, roughly 9.3% died during their hospitalization, compared with 16.4% of patients treated with chloroquine alone, 18.0% of those treated with hydroxychloroquine alone, 22.2% of those treated with chloroquine and a macrolide, and 23.8% of those treated with hydroxychloroquine and a macrolide.
After accounting for confounding variables, the researchers estimated that the excess mortality risk attributable to use of the drug regimen ranged from 34% to 45%.
Patients treated with any of the four regimens sustained more serious arrhythmias, compared with those in the control group (0.35), with the biggest increase seen in the group treated with the combination of hydroxychloroquine plus a macrolide (8.1%), followed by chloroquine with a macrolide (6.5%), hydroxychloroquine alone (6.1%), and chloroquine alone (4.3%).
“We were fairly reassured that, although the study was observational, the signals were robust and consistent across all regions of the world in diverse populations, and we did not see any muting of that signal, depending on region,” Dr. Mehra said.
“Two months ago, we were all scratching our heads about how to treat patients with COVID-19, and then came a drug [hydroxychloroquine] with some anecdotal evidence, but now we have 2 months more experience, and we looked to science to provide some answer,” Dr. Ruschitzka said.
“Although this was not a randomized, controlled trial, so we do not have a definite answer, the data provided in this [large, multinational] real-world study is as good as it gets and the best data we have,” he concluded.
“Let the science speak for itself”
Commenting on the study in an interview, Christian Funck-Brentano, MD, from the Hospital Pitié-Salpêtrière and Sorbonne University, both in Paris, said that, although the study is observational and therefore not as reliable as a randomized controlled trial, it is “nevertheless well-documented, studied a huge amount of people, and utilized several sensitivity methods, all of which showed the same results.”
Dr. Funck-Brentano, who is the coauthor of an accompanying editorial in The Lancet and was not involved with the study, said that “we now have no evidence that hydroxychloroquine and chloroquine alone or in combination with a macrolide do any good and we have potential evidence that they do harm and kill people.”
Also commenting on the study in an interview, David Holtgrave, PhD, dean of the School of Public Health at the State University of New York at Albany, said that, “while no one observational study alone would lead to a firm clinical recommendation, I think it is helpful for physicians and public health officials to be aware of the findings of the peer-reviewed observational studies to date and the National Institutes of Health COVID-19 treatment guidelines and the Food and Drug Administration’s statement of drug safety concern about hydroxychloroquine to inform their decision-making as we await the results of randomized clinical trials of these drugs for the treatment of COVID-19,” said Dr. Holtgrave, who was not involved with the study.
He added that, to his knowledge, there are “still no published studies of prophylactic use of these drugs to prevent COVID-19.”
Dr. Mehra emphasized that a cardinal principle of practicing medicine is “first do no harm” and “even in situations where you believe a desperate disease calls for desperate measures, responsible physicians should take a step back and ask if we are doing harm, and until we can say we aren’t, I don’t think it’s wise to push something like this in the absence of good efficacy data.”
Dr. Ruschitzka added that those who are encouraging the use of these agents “should review their decision based on today’s data and let the science speak for itself.”
The study was supported by the William Harvey Distinguished Chair in Advanced Cardiovascular Medicine at Brigham and Women’s Hospital, Boston. Dr. Mehra reported personal fees from Abbott, Medtronic, Janssen, Mesoblast, Portola, Bayer, Baim Institute for Clinical Research, NuPulseCV, FineHeart, Leviticus, Roivant, and Triple Gene. Dr. Ruschitzka was paid for time spent as a committee member for clinical trials, advisory boards, other forms of consulting, and lectures or presentations; these payments were made directly to the University of Zürich and no personal payments were received in relation to these trials or other activities. Dr. Funck-Brentano, his coauthor, and Dr. Holtgrave declared no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Immunotherapy, steroids had positive outcomes in COVID-19–associated multisystem inflammatory syndrome
According to study of a cluster of patients in France and Switzerland, children may experience an acute cardiac decompensation from the severe inflammatory state following SARS-CoV-2 infection, termed multisystem inflammatory syndrome in children (MIS-C). Treatment with immunoglobulin appears to be associated with recovery of left ventricular systolic function.
“The pediatric and cardiology communities should be acutely aware of this new disease probably related to SARS-CoV-2 infection (MIS-C), that shares similarities with Kawasaki disease but has specificities in its presentation,” researchers led by Zahra Belhadjer, MD, of Necker-Enfants Malades Hospital in Paris, wrote in a cases series report published online in Circulation “Early diagnosis and management appear to lead to favorable outcome using classical therapies. Elucidating the immune mechanisms of this disease will afford further insights for treatment and potential global prevention of severe forms.”
Over a 2-month period that coincided with the SARS-CoV-2 pandemic in France and Switzerland, the researchers retrospectively collected clinical, biological, therapeutic, and early-outcomes data in 35 children who were admitted to pediatric ICUs in 14 centers for cardiogenic shock, left ventricular dysfunction, and severe inflammatory state. Their median age was 10 years, all presented with a fever, 80% had gastrointestinal symptoms of abdominal pain, vomiting, or diarrhea, and 28% had comorbidities that included body mass index of greater than 25 kg/m2 (17%), asthma (9%), and lupus (3%), and overweight. Only 17% presented with chest pain. The researchers observed that left ventricular ejection fraction was less than 30% in 28% of patients, and 80% required inotropic support with 28% treated with extracorporeal membrane oxygenation (ECMO). All patients presented with a severe inflammatory state evidenced by elevated C-reactive protein and d-dimer. Interleukin 6 was elevated to a median of 135 pg/mL in 13 of the patients. Elevation of troponin I was constant but mild to moderate, and NT-proBNP or BNP elevation was present in all children.
Nearly all patients 35 (88%) patients tested positive for SARS-CoV-2 infection by polymerase chain reaction of nasopharyngeal swab or serology. Most patients (80%) received IV inotropic support, 71% received first-line IV immunoglobulin, 65% received anticoagulation with heparin, 34% received IV steroids having been considered high-risk patients with symptoms similar to an incomplete form of Kawasaki disease, and 8% received treatment with an interleukin-1 receptor antagonist because of a persistent severe inflammatory state. Left ventricular function was restored in 71% of those discharged from the intensive care unit. No patient died, and all patients treated with ECMO were successfully weaned after a median of 4.5 days.
“Some aspects of this emerging pediatric disease (MIS-C) are similar to those of Kawasaki disease: prolonged fever, multisystem inflammation with skin rash, lymphadenopathy, diarrhea, meningism, and high levels of inflammatory biomarkers,” the researchers wrote. “But differences are important and raise the question as to whether this syndrome is Kawasaki disease with SARS-CoV-2 as the triggering agent, or represents a different syndrome (MIS-C). Kawasaki disease predominantly affects young children younger than 5 years, whereas the median age in our series is 10 years. Incomplete forms of Kawasaki disease occur in infants who may have fever as the sole clinical finding, whereas older patients are more prone to exhibit the complete form.”
They went on to note that the overlapping features between MIS-C and Kawasaki disease “may be due to similar pathophysiology. The etiologic agent of Kawasaki disease is unknown but likely to be ubiquitous, causing asymptomatic childhood infection but triggering the immunologic cascade of Kawasaki disease in genetically susceptible individuals. Please note that infection with a novel RNA virus that enters through the upper respiratory tract has been proposed to be the cause of the disease (see PLoS One. 2008 Feb 13;3:e1582 and J Infect Dis. 2011 Apr 1;203:1021-30).”
Based on the work of authors, it appears that a high index of suspicion for MIS-C is important for children who develop Kawasaki-like symptoms, David J. Goldberg, MD, said in an interview. “Although children have largely been spared from the acute respiratory presentation of the SARS-CoV-2 pandemic, the recognition and understanding of what appears to be a postviral inflammatory response is a critical first step in developing treatment algorithms for this disease process,” said Dr. Goldberg, a board-certified attending cardiologist in the cardiac center and fetal heart program at Children’s Hospital of Philadelphia. “If inflammatory markers are elevated, particularly if there are accompanying gastrointestinal symptoms, the possibility of cardiac involvement suggests the utility of screening echocardiography. Given the potential need for inotropic or mechanical circulatory support, the presence of myocardial dysfunction dictates care in an intensive care unit capable of providing advanced therapies. While the evidence from Dr. Belhadjer’s cohort suggests that full recovery is probable, there is still much to be learned about this unique inflammatory syndrome and the alarm has rightly been sounded.”
The researchers and Dr. Goldberg reported having no disclosures.
SOURCE: Belhadjer Z et al. Circulation 2020 May 17; doi: 10.1161/circulationaha.120.048360.
According to study of a cluster of patients in France and Switzerland, children may experience an acute cardiac decompensation from the severe inflammatory state following SARS-CoV-2 infection, termed multisystem inflammatory syndrome in children (MIS-C). Treatment with immunoglobulin appears to be associated with recovery of left ventricular systolic function.
“The pediatric and cardiology communities should be acutely aware of this new disease probably related to SARS-CoV-2 infection (MIS-C), that shares similarities with Kawasaki disease but has specificities in its presentation,” researchers led by Zahra Belhadjer, MD, of Necker-Enfants Malades Hospital in Paris, wrote in a cases series report published online in Circulation “Early diagnosis and management appear to lead to favorable outcome using classical therapies. Elucidating the immune mechanisms of this disease will afford further insights for treatment and potential global prevention of severe forms.”
Over a 2-month period that coincided with the SARS-CoV-2 pandemic in France and Switzerland, the researchers retrospectively collected clinical, biological, therapeutic, and early-outcomes data in 35 children who were admitted to pediatric ICUs in 14 centers for cardiogenic shock, left ventricular dysfunction, and severe inflammatory state. Their median age was 10 years, all presented with a fever, 80% had gastrointestinal symptoms of abdominal pain, vomiting, or diarrhea, and 28% had comorbidities that included body mass index of greater than 25 kg/m2 (17%), asthma (9%), and lupus (3%), and overweight. Only 17% presented with chest pain. The researchers observed that left ventricular ejection fraction was less than 30% in 28% of patients, and 80% required inotropic support with 28% treated with extracorporeal membrane oxygenation (ECMO). All patients presented with a severe inflammatory state evidenced by elevated C-reactive protein and d-dimer. Interleukin 6 was elevated to a median of 135 pg/mL in 13 of the patients. Elevation of troponin I was constant but mild to moderate, and NT-proBNP or BNP elevation was present in all children.
Nearly all patients 35 (88%) patients tested positive for SARS-CoV-2 infection by polymerase chain reaction of nasopharyngeal swab or serology. Most patients (80%) received IV inotropic support, 71% received first-line IV immunoglobulin, 65% received anticoagulation with heparin, 34% received IV steroids having been considered high-risk patients with symptoms similar to an incomplete form of Kawasaki disease, and 8% received treatment with an interleukin-1 receptor antagonist because of a persistent severe inflammatory state. Left ventricular function was restored in 71% of those discharged from the intensive care unit. No patient died, and all patients treated with ECMO were successfully weaned after a median of 4.5 days.
“Some aspects of this emerging pediatric disease (MIS-C) are similar to those of Kawasaki disease: prolonged fever, multisystem inflammation with skin rash, lymphadenopathy, diarrhea, meningism, and high levels of inflammatory biomarkers,” the researchers wrote. “But differences are important and raise the question as to whether this syndrome is Kawasaki disease with SARS-CoV-2 as the triggering agent, or represents a different syndrome (MIS-C). Kawasaki disease predominantly affects young children younger than 5 years, whereas the median age in our series is 10 years. Incomplete forms of Kawasaki disease occur in infants who may have fever as the sole clinical finding, whereas older patients are more prone to exhibit the complete form.”
They went on to note that the overlapping features between MIS-C and Kawasaki disease “may be due to similar pathophysiology. The etiologic agent of Kawasaki disease is unknown but likely to be ubiquitous, causing asymptomatic childhood infection but triggering the immunologic cascade of Kawasaki disease in genetically susceptible individuals. Please note that infection with a novel RNA virus that enters through the upper respiratory tract has been proposed to be the cause of the disease (see PLoS One. 2008 Feb 13;3:e1582 and J Infect Dis. 2011 Apr 1;203:1021-30).”
Based on the work of authors, it appears that a high index of suspicion for MIS-C is important for children who develop Kawasaki-like symptoms, David J. Goldberg, MD, said in an interview. “Although children have largely been spared from the acute respiratory presentation of the SARS-CoV-2 pandemic, the recognition and understanding of what appears to be a postviral inflammatory response is a critical first step in developing treatment algorithms for this disease process,” said Dr. Goldberg, a board-certified attending cardiologist in the cardiac center and fetal heart program at Children’s Hospital of Philadelphia. “If inflammatory markers are elevated, particularly if there are accompanying gastrointestinal symptoms, the possibility of cardiac involvement suggests the utility of screening echocardiography. Given the potential need for inotropic or mechanical circulatory support, the presence of myocardial dysfunction dictates care in an intensive care unit capable of providing advanced therapies. While the evidence from Dr. Belhadjer’s cohort suggests that full recovery is probable, there is still much to be learned about this unique inflammatory syndrome and the alarm has rightly been sounded.”
The researchers and Dr. Goldberg reported having no disclosures.
SOURCE: Belhadjer Z et al. Circulation 2020 May 17; doi: 10.1161/circulationaha.120.048360.
According to study of a cluster of patients in France and Switzerland, children may experience an acute cardiac decompensation from the severe inflammatory state following SARS-CoV-2 infection, termed multisystem inflammatory syndrome in children (MIS-C). Treatment with immunoglobulin appears to be associated with recovery of left ventricular systolic function.
“The pediatric and cardiology communities should be acutely aware of this new disease probably related to SARS-CoV-2 infection (MIS-C), that shares similarities with Kawasaki disease but has specificities in its presentation,” researchers led by Zahra Belhadjer, MD, of Necker-Enfants Malades Hospital in Paris, wrote in a cases series report published online in Circulation “Early diagnosis and management appear to lead to favorable outcome using classical therapies. Elucidating the immune mechanisms of this disease will afford further insights for treatment and potential global prevention of severe forms.”
Over a 2-month period that coincided with the SARS-CoV-2 pandemic in France and Switzerland, the researchers retrospectively collected clinical, biological, therapeutic, and early-outcomes data in 35 children who were admitted to pediatric ICUs in 14 centers for cardiogenic shock, left ventricular dysfunction, and severe inflammatory state. Their median age was 10 years, all presented with a fever, 80% had gastrointestinal symptoms of abdominal pain, vomiting, or diarrhea, and 28% had comorbidities that included body mass index of greater than 25 kg/m2 (17%), asthma (9%), and lupus (3%), and overweight. Only 17% presented with chest pain. The researchers observed that left ventricular ejection fraction was less than 30% in 28% of patients, and 80% required inotropic support with 28% treated with extracorporeal membrane oxygenation (ECMO). All patients presented with a severe inflammatory state evidenced by elevated C-reactive protein and d-dimer. Interleukin 6 was elevated to a median of 135 pg/mL in 13 of the patients. Elevation of troponin I was constant but mild to moderate, and NT-proBNP or BNP elevation was present in all children.
Nearly all patients 35 (88%) patients tested positive for SARS-CoV-2 infection by polymerase chain reaction of nasopharyngeal swab or serology. Most patients (80%) received IV inotropic support, 71% received first-line IV immunoglobulin, 65% received anticoagulation with heparin, 34% received IV steroids having been considered high-risk patients with symptoms similar to an incomplete form of Kawasaki disease, and 8% received treatment with an interleukin-1 receptor antagonist because of a persistent severe inflammatory state. Left ventricular function was restored in 71% of those discharged from the intensive care unit. No patient died, and all patients treated with ECMO were successfully weaned after a median of 4.5 days.
“Some aspects of this emerging pediatric disease (MIS-C) are similar to those of Kawasaki disease: prolonged fever, multisystem inflammation with skin rash, lymphadenopathy, diarrhea, meningism, and high levels of inflammatory biomarkers,” the researchers wrote. “But differences are important and raise the question as to whether this syndrome is Kawasaki disease with SARS-CoV-2 as the triggering agent, or represents a different syndrome (MIS-C). Kawasaki disease predominantly affects young children younger than 5 years, whereas the median age in our series is 10 years. Incomplete forms of Kawasaki disease occur in infants who may have fever as the sole clinical finding, whereas older patients are more prone to exhibit the complete form.”
They went on to note that the overlapping features between MIS-C and Kawasaki disease “may be due to similar pathophysiology. The etiologic agent of Kawasaki disease is unknown but likely to be ubiquitous, causing asymptomatic childhood infection but triggering the immunologic cascade of Kawasaki disease in genetically susceptible individuals. Please note that infection with a novel RNA virus that enters through the upper respiratory tract has been proposed to be the cause of the disease (see PLoS One. 2008 Feb 13;3:e1582 and J Infect Dis. 2011 Apr 1;203:1021-30).”
Based on the work of authors, it appears that a high index of suspicion for MIS-C is important for children who develop Kawasaki-like symptoms, David J. Goldberg, MD, said in an interview. “Although children have largely been spared from the acute respiratory presentation of the SARS-CoV-2 pandemic, the recognition and understanding of what appears to be a postviral inflammatory response is a critical first step in developing treatment algorithms for this disease process,” said Dr. Goldberg, a board-certified attending cardiologist in the cardiac center and fetal heart program at Children’s Hospital of Philadelphia. “If inflammatory markers are elevated, particularly if there are accompanying gastrointestinal symptoms, the possibility of cardiac involvement suggests the utility of screening echocardiography. Given the potential need for inotropic or mechanical circulatory support, the presence of myocardial dysfunction dictates care in an intensive care unit capable of providing advanced therapies. While the evidence from Dr. Belhadjer’s cohort suggests that full recovery is probable, there is still much to be learned about this unique inflammatory syndrome and the alarm has rightly been sounded.”
The researchers and Dr. Goldberg reported having no disclosures.
SOURCE: Belhadjer Z et al. Circulation 2020 May 17; doi: 10.1161/circulationaha.120.048360.
FROM CIRCULATION
Today’s top news highlights: Remdesivir data dive, FDA approves contraceptive gel
:
Remdesivir trial data published
Weeks after topline remdesivir data appeared in the press, investigators published their full experience using the drug to treat COVID-19 patients. The study, published in the New England Journal of Medicine, showed the drug reduced recovery time from 15 to 11 days, compared with placebo. Patients receiving oxygen seemed to fare best from treatment with remdesivir. “There is clear and consistent evidence of clinically significant benefit for those hospitalized on oxygen but not yet requiring mechanical ventilation,” Daniel Kaul, MD, a professor of infectious diseases at the University of Michigan, Ann Arbor, said after seeing the published results. “Surprisingly, early dosing as measured from time to onset of symptoms did not seem to make a difference.” READ MORE.
FDA approves contraceptive gel
The Food and Drug Administration approved Phexxi (lactic acid, citric acid, and potassium bitartrate) vaginal gel to prevent pregnancy in women of reproductive potential. It’s the first nonhormonal, on-demand, vaginal pH regulator contraceptive designed to maintain vaginal pH within the range of 3.5-4.5. READ MORE.
COVID-19 lessons from one cancer center
Physicians at Levine Cancer Institute in Charlotte, N.C., largely have been able to keep hematologic oncology patients on their treatment regimens and continue to care for inpatients during the early months of the COVID-19 pandemic. How have they kept the situation managable? Strict infection control, liberal testing, and a proactive plan to defer and temporarily replace infusion care when medically appropriate were all part of the strategy. “My impression is that the incidence has been low partly because our patients, especially those with hematologic malignancies including those on active chemotherapy, were already getting warned to be cautious, even before the coronavirus, using distancing, masking, and meticulous hand hygiene,” said Peter Voorhees, MD, professor of medicine and director of Medical Operations and Outreach Services in Levine Cancer Institute’s Department of Hematologic Oncology and Blood Disorders. READ MORE.
Convalescent plasma: Hope or hype?
There are currently more than two dozen trials of convalescent plasma in the United States and elsewhere but most are single-arm trials to determine if one infusion can decrease the need for intubation or help patients on a ventilator to improve. Others researchers are investigating whether convalescent plasma might be used before severe disease sets in. Meanwhile, about 2,200 hospitals are participating in an expanded access program being led by the Mayo Clinic nationwide. The National Institutes of Health recently said that “there are insufficient clinical data to recommend either for or against” its use for COVID-19. READ MORE.
New rosacea treatment guidelines
Patients with rosacea should receive treatments based on their phenotype and specific symptoms, rather than being assigned into distinct subtype categories, according to updated guidance published in the Journal of the American Academy of Dermatology. The update comes from the National Rosacea Society Expert Committee and is based on a review of the evidence. Patients “shouldn’t be classified as having a certain subtype of rosacea” since “many patients have features that overlap more than one subtype,” said Diane Thiboutot, MD, lead author of the update and a professor of dermatology and associate dean of clinical and translational research education at Penn State University, Hershey. READ MORE.
For more on COVID-19, visit our Resource Center. All of our latest news is available on MDedge.com.
:
Remdesivir trial data published
Weeks after topline remdesivir data appeared in the press, investigators published their full experience using the drug to treat COVID-19 patients. The study, published in the New England Journal of Medicine, showed the drug reduced recovery time from 15 to 11 days, compared with placebo. Patients receiving oxygen seemed to fare best from treatment with remdesivir. “There is clear and consistent evidence of clinically significant benefit for those hospitalized on oxygen but not yet requiring mechanical ventilation,” Daniel Kaul, MD, a professor of infectious diseases at the University of Michigan, Ann Arbor, said after seeing the published results. “Surprisingly, early dosing as measured from time to onset of symptoms did not seem to make a difference.” READ MORE.
FDA approves contraceptive gel
The Food and Drug Administration approved Phexxi (lactic acid, citric acid, and potassium bitartrate) vaginal gel to prevent pregnancy in women of reproductive potential. It’s the first nonhormonal, on-demand, vaginal pH regulator contraceptive designed to maintain vaginal pH within the range of 3.5-4.5. READ MORE.
COVID-19 lessons from one cancer center
Physicians at Levine Cancer Institute in Charlotte, N.C., largely have been able to keep hematologic oncology patients on their treatment regimens and continue to care for inpatients during the early months of the COVID-19 pandemic. How have they kept the situation managable? Strict infection control, liberal testing, and a proactive plan to defer and temporarily replace infusion care when medically appropriate were all part of the strategy. “My impression is that the incidence has been low partly because our patients, especially those with hematologic malignancies including those on active chemotherapy, were already getting warned to be cautious, even before the coronavirus, using distancing, masking, and meticulous hand hygiene,” said Peter Voorhees, MD, professor of medicine and director of Medical Operations and Outreach Services in Levine Cancer Institute’s Department of Hematologic Oncology and Blood Disorders. READ MORE.
Convalescent plasma: Hope or hype?
There are currently more than two dozen trials of convalescent plasma in the United States and elsewhere but most are single-arm trials to determine if one infusion can decrease the need for intubation or help patients on a ventilator to improve. Others researchers are investigating whether convalescent plasma might be used before severe disease sets in. Meanwhile, about 2,200 hospitals are participating in an expanded access program being led by the Mayo Clinic nationwide. The National Institutes of Health recently said that “there are insufficient clinical data to recommend either for or against” its use for COVID-19. READ MORE.
New rosacea treatment guidelines
Patients with rosacea should receive treatments based on their phenotype and specific symptoms, rather than being assigned into distinct subtype categories, according to updated guidance published in the Journal of the American Academy of Dermatology. The update comes from the National Rosacea Society Expert Committee and is based on a review of the evidence. Patients “shouldn’t be classified as having a certain subtype of rosacea” since “many patients have features that overlap more than one subtype,” said Diane Thiboutot, MD, lead author of the update and a professor of dermatology and associate dean of clinical and translational research education at Penn State University, Hershey. READ MORE.
For more on COVID-19, visit our Resource Center. All of our latest news is available on MDedge.com.
:
Remdesivir trial data published
Weeks after topline remdesivir data appeared in the press, investigators published their full experience using the drug to treat COVID-19 patients. The study, published in the New England Journal of Medicine, showed the drug reduced recovery time from 15 to 11 days, compared with placebo. Patients receiving oxygen seemed to fare best from treatment with remdesivir. “There is clear and consistent evidence of clinically significant benefit for those hospitalized on oxygen but not yet requiring mechanical ventilation,” Daniel Kaul, MD, a professor of infectious diseases at the University of Michigan, Ann Arbor, said after seeing the published results. “Surprisingly, early dosing as measured from time to onset of symptoms did not seem to make a difference.” READ MORE.
FDA approves contraceptive gel
The Food and Drug Administration approved Phexxi (lactic acid, citric acid, and potassium bitartrate) vaginal gel to prevent pregnancy in women of reproductive potential. It’s the first nonhormonal, on-demand, vaginal pH regulator contraceptive designed to maintain vaginal pH within the range of 3.5-4.5. READ MORE.
COVID-19 lessons from one cancer center
Physicians at Levine Cancer Institute in Charlotte, N.C., largely have been able to keep hematologic oncology patients on their treatment regimens and continue to care for inpatients during the early months of the COVID-19 pandemic. How have they kept the situation managable? Strict infection control, liberal testing, and a proactive plan to defer and temporarily replace infusion care when medically appropriate were all part of the strategy. “My impression is that the incidence has been low partly because our patients, especially those with hematologic malignancies including those on active chemotherapy, were already getting warned to be cautious, even before the coronavirus, using distancing, masking, and meticulous hand hygiene,” said Peter Voorhees, MD, professor of medicine and director of Medical Operations and Outreach Services in Levine Cancer Institute’s Department of Hematologic Oncology and Blood Disorders. READ MORE.
Convalescent plasma: Hope or hype?
There are currently more than two dozen trials of convalescent plasma in the United States and elsewhere but most are single-arm trials to determine if one infusion can decrease the need for intubation or help patients on a ventilator to improve. Others researchers are investigating whether convalescent plasma might be used before severe disease sets in. Meanwhile, about 2,200 hospitals are participating in an expanded access program being led by the Mayo Clinic nationwide. The National Institutes of Health recently said that “there are insufficient clinical data to recommend either for or against” its use for COVID-19. READ MORE.
New rosacea treatment guidelines
Patients with rosacea should receive treatments based on their phenotype and specific symptoms, rather than being assigned into distinct subtype categories, according to updated guidance published in the Journal of the American Academy of Dermatology. The update comes from the National Rosacea Society Expert Committee and is based on a review of the evidence. Patients “shouldn’t be classified as having a certain subtype of rosacea” since “many patients have features that overlap more than one subtype,” said Diane Thiboutot, MD, lead author of the update and a professor of dermatology and associate dean of clinical and translational research education at Penn State University, Hershey. READ MORE.
For more on COVID-19, visit our Resource Center. All of our latest news is available on MDedge.com.
Picky eating is stable in childhood, correlates with lower BMI
Picky eating at age 4 years is stable over an approximately 4-year period, research published in Pediatrics suggests.

In addition, picky eating is associated with lower body mass index (BMI). said Carmen Fernandez, MPH, a researcher and medical student at University of Michigan in Ann Arbor, and colleagues.
Whether picky eating is a stable trait and how it relates to weight status has been unclear. Furthermore, “previous longitudinal studies have not focused on low-income children, who are at elevated risk for being both overweight and picky,” said Ms. Fernandez and associates.
A stable trait
To examine trajectories of picky eating in a low-income population of children and how picky eating relates to BMI z score (BMIz) and maternal behavior, the researchers conducted a longitudinal cohort study. They recruited more than 300 mother-child dyads from Head Start programs in Southeastern Michigan between 2009 and 2011. Children were 3-4 years old at recruitment, and researchers collected data at five time points. Children had an average age of 4 years at the first time point and 9 years at the fifth time point. Investigators collected child BMIz scores at all time points, Children’s Eating Behavior Questionnaire (CEBQ) scores at four time points, and Child Feeding Questionnaire and Caregiver’s Feeding Styles Questionnaire scores at three time points. Mothers completed the Emotion Regulation Checklist at baseline.
Among 317 children, an analysis identified three trajectories of picky eating severity as measured by the CEBQ Food Fussiness subscale: persistently low (29% of the children), persistently medium (57%), and persistently high (14%). “Maternal feeding behaviors characterized by restriction and demandingness were associated with picky eating,” the authors said. In post hoc analyses, emotional regulation was higher and emotional lability was lower among children with low levels of picky eating, compared with children with medium and high levels of picky eating.
“High and medium picky eating was associated with lower average BMIz, in the healthy BMIz range, suggesting that picky eating could be protective against overweight and obesity, as others have proposed,” Ms. Fernandez and colleagues said. “We did not find evidence that picky eating was associated with being underweight, which is consistent with previous studies. ... Little is known, however, about the long-term weight gain trajectories of picky eaters into adulthood, and this is an important area for future research.”
The results from this cohort may not apply to other populations, the authors noted.
What to do about picky eating
“Health providers, researchers, and parents do not yet have a handle on the management and messaging of picky eating in children,” said Nancy L. Zucker, PhD, and Sheryl O. Hughes, PhD, in an accompanying editorial. “When a parent describes a child as often or always selective, it is beyond normative. … Roughly only 14% were described this way.”
The results suggest a need for early intervention, and age 24 months and younger may be when “children are more receptive to the exploration of new tastes,” said Dr. Zucker of the department of psychiatry and behavioral sciences and the department of psychology and neuroscience at Duke University in Durham, NC., and Dr. Hughes of the Children’s Nutrition Research Center at Baylor College of Medicine in Houston.
Researchers should examine the impact of an authoritative feeding style, which combines elements of authoritarian and indulgent feeding styles, on a child’s willingness to explore foods, said Dr. Zucker and Dr. Hughes. This feeding style incorporates “structure and guidance while being sensitive to the child’s needs without being punitive,” they said. “According to theories of inhibitory learning ... we can think of children with elevated picky eating as having thousands of negative memories about food (e.g., conflict, unexpected tastes, discomfort). Thus, caregivers can work to create positive memories and experiences around food (e.g., cooking, gardening) to help picky eaters expand their preferences. However, in doing so, it is critical that caregivers let go of their need for a child to taste something and instead focus on accumulating pleasant experiences.”
Whether this approach reduces pickiness is unknown, but it may improve shared eating experiences, Dr. Zucker and Dr. Hughes said.
Ms. Fernandez and coauthors had no relevant financial disclosures. The study was supported by the American Heart Association, the Eunice Kennedy Shriver National Institute of Child Health and Human Development, and the National Institutes of Health. Dr. Zucker received funding from the National Science Foundation and National Institute of Mental Health; Dr. Hughes had no relevant financial disclosures. The editorial was funded by the National Institutes of Health.
SOURCES: Fernandez C et al. Pediatrics. 2020 May 26. doi: 10.1542/peds.2019-2018; Zucker NL and Hughes SO. Pediatrics. 2020 May 26. doi: 10.1542/peds.2020-0893.
Picky eating at age 4 years is stable over an approximately 4-year period, research published in Pediatrics suggests.
In addition, picky eating is associated with lower body mass index (BMI). said Carmen Fernandez, MPH, a researcher and medical student at University of Michigan in Ann Arbor, and colleagues.
Whether picky eating is a stable trait and how it relates to weight status has been unclear. Furthermore, “previous longitudinal studies have not focused on low-income children, who are at elevated risk for being both overweight and picky,” said Ms. Fernandez and associates.
A stable trait
To examine trajectories of picky eating in a low-income population of children and how picky eating relates to BMI z score (BMIz) and maternal behavior, the researchers conducted a longitudinal cohort study. They recruited more than 300 mother-child dyads from Head Start programs in Southeastern Michigan between 2009 and 2011. Children were 3-4 years old at recruitment, and researchers collected data at five time points. Children had an average age of 4 years at the first time point and 9 years at the fifth time point. Investigators collected child BMIz scores at all time points, Children’s Eating Behavior Questionnaire (CEBQ) scores at four time points, and Child Feeding Questionnaire and Caregiver’s Feeding Styles Questionnaire scores at three time points. Mothers completed the Emotion Regulation Checklist at baseline.
Among 317 children, an analysis identified three trajectories of picky eating severity as measured by the CEBQ Food Fussiness subscale: persistently low (29% of the children), persistently medium (57%), and persistently high (14%). “Maternal feeding behaviors characterized by restriction and demandingness were associated with picky eating,” the authors said. In post hoc analyses, emotional regulation was higher and emotional lability was lower among children with low levels of picky eating, compared with children with medium and high levels of picky eating.
“High and medium picky eating was associated with lower average BMIz, in the healthy BMIz range, suggesting that picky eating could be protective against overweight and obesity, as others have proposed,” Ms. Fernandez and colleagues said. “We did not find evidence that picky eating was associated with being underweight, which is consistent with previous studies. ... Little is known, however, about the long-term weight gain trajectories of picky eaters into adulthood, and this is an important area for future research.”
The results from this cohort may not apply to other populations, the authors noted.
What to do about picky eating
“Health providers, researchers, and parents do not yet have a handle on the management and messaging of picky eating in children,” said Nancy L. Zucker, PhD, and Sheryl O. Hughes, PhD, in an accompanying editorial. “When a parent describes a child as often or always selective, it is beyond normative. … Roughly only 14% were described this way.”
The results suggest a need for early intervention, and age 24 months and younger may be when “children are more receptive to the exploration of new tastes,” said Dr. Zucker of the department of psychiatry and behavioral sciences and the department of psychology and neuroscience at Duke University in Durham, NC., and Dr. Hughes of the Children’s Nutrition Research Center at Baylor College of Medicine in Houston.
Researchers should examine the impact of an authoritative feeding style, which combines elements of authoritarian and indulgent feeding styles, on a child’s willingness to explore foods, said Dr. Zucker and Dr. Hughes. This feeding style incorporates “structure and guidance while being sensitive to the child’s needs without being punitive,” they said. “According to theories of inhibitory learning ... we can think of children with elevated picky eating as having thousands of negative memories about food (e.g., conflict, unexpected tastes, discomfort). Thus, caregivers can work to create positive memories and experiences around food (e.g., cooking, gardening) to help picky eaters expand their preferences. However, in doing so, it is critical that caregivers let go of their need for a child to taste something and instead focus on accumulating pleasant experiences.”
Whether this approach reduces pickiness is unknown, but it may improve shared eating experiences, Dr. Zucker and Dr. Hughes said.
Ms. Fernandez and coauthors had no relevant financial disclosures. The study was supported by the American Heart Association, the Eunice Kennedy Shriver National Institute of Child Health and Human Development, and the National Institutes of Health. Dr. Zucker received funding from the National Science Foundation and National Institute of Mental Health; Dr. Hughes had no relevant financial disclosures. The editorial was funded by the National Institutes of Health.
SOURCES: Fernandez C et al. Pediatrics. 2020 May 26. doi: 10.1542/peds.2019-2018; Zucker NL and Hughes SO. Pediatrics. 2020 May 26. doi: 10.1542/peds.2020-0893.
Picky eating at age 4 years is stable over an approximately 4-year period, research published in Pediatrics suggests.
In addition, picky eating is associated with lower body mass index (BMI). said Carmen Fernandez, MPH, a researcher and medical student at University of Michigan in Ann Arbor, and colleagues.
Whether picky eating is a stable trait and how it relates to weight status has been unclear. Furthermore, “previous longitudinal studies have not focused on low-income children, who are at elevated risk for being both overweight and picky,” said Ms. Fernandez and associates.
A stable trait
To examine trajectories of picky eating in a low-income population of children and how picky eating relates to BMI z score (BMIz) and maternal behavior, the researchers conducted a longitudinal cohort study. They recruited more than 300 mother-child dyads from Head Start programs in Southeastern Michigan between 2009 and 2011. Children were 3-4 years old at recruitment, and researchers collected data at five time points. Children had an average age of 4 years at the first time point and 9 years at the fifth time point. Investigators collected child BMIz scores at all time points, Children’s Eating Behavior Questionnaire (CEBQ) scores at four time points, and Child Feeding Questionnaire and Caregiver’s Feeding Styles Questionnaire scores at three time points. Mothers completed the Emotion Regulation Checklist at baseline.
Among 317 children, an analysis identified three trajectories of picky eating severity as measured by the CEBQ Food Fussiness subscale: persistently low (29% of the children), persistently medium (57%), and persistently high (14%). “Maternal feeding behaviors characterized by restriction and demandingness were associated with picky eating,” the authors said. In post hoc analyses, emotional regulation was higher and emotional lability was lower among children with low levels of picky eating, compared with children with medium and high levels of picky eating.
“High and medium picky eating was associated with lower average BMIz, in the healthy BMIz range, suggesting that picky eating could be protective against overweight and obesity, as others have proposed,” Ms. Fernandez and colleagues said. “We did not find evidence that picky eating was associated with being underweight, which is consistent with previous studies. ... Little is known, however, about the long-term weight gain trajectories of picky eaters into adulthood, and this is an important area for future research.”
The results from this cohort may not apply to other populations, the authors noted.
What to do about picky eating
“Health providers, researchers, and parents do not yet have a handle on the management and messaging of picky eating in children,” said Nancy L. Zucker, PhD, and Sheryl O. Hughes, PhD, in an accompanying editorial. “When a parent describes a child as often or always selective, it is beyond normative. … Roughly only 14% were described this way.”
The results suggest a need for early intervention, and age 24 months and younger may be when “children are more receptive to the exploration of new tastes,” said Dr. Zucker of the department of psychiatry and behavioral sciences and the department of psychology and neuroscience at Duke University in Durham, NC., and Dr. Hughes of the Children’s Nutrition Research Center at Baylor College of Medicine in Houston.
Researchers should examine the impact of an authoritative feeding style, which combines elements of authoritarian and indulgent feeding styles, on a child’s willingness to explore foods, said Dr. Zucker and Dr. Hughes. This feeding style incorporates “structure and guidance while being sensitive to the child’s needs without being punitive,” they said. “According to theories of inhibitory learning ... we can think of children with elevated picky eating as having thousands of negative memories about food (e.g., conflict, unexpected tastes, discomfort). Thus, caregivers can work to create positive memories and experiences around food (e.g., cooking, gardening) to help picky eaters expand their preferences. However, in doing so, it is critical that caregivers let go of their need for a child to taste something and instead focus on accumulating pleasant experiences.”
Whether this approach reduces pickiness is unknown, but it may improve shared eating experiences, Dr. Zucker and Dr. Hughes said.
Ms. Fernandez and coauthors had no relevant financial disclosures. The study was supported by the American Heart Association, the Eunice Kennedy Shriver National Institute of Child Health and Human Development, and the National Institutes of Health. Dr. Zucker received funding from the National Science Foundation and National Institute of Mental Health; Dr. Hughes had no relevant financial disclosures. The editorial was funded by the National Institutes of Health.
SOURCES: Fernandez C et al. Pediatrics. 2020 May 26. doi: 10.1542/peds.2019-2018; Zucker NL and Hughes SO. Pediatrics. 2020 May 26. doi: 10.1542/peds.2020-0893.
FROM PEDIATRICS
Is HIPAA critical?
Ignorance may be bliss for some. But as I sit here in my scenic social isolation on the Maine coast I find that, like most people, what I don’t know unsettles me. How is the COVID-19 virus spread? Does my wife’s wipe down of the doorknobs after I return from the grocery store really make us any less likely to contract the virus? Is wearing my homemade bandana face mask doing anything to protect me? I suspect not, but I wear it as a statement of courtesy and solidarity to my fellow community members.
Does the 6-foot rule make any sense? I’ve read that it is based on a study dating back to the 1930s. I’ve seen images of the 25-foot droplet plume blasting out from a sneeze and understand that, as a bicyclist, I may be generating a shower of droplets in my wake. But, are those droplets a threat to anyone I pedal by if I am symptom free? What does being a carrier mean when we are talking about COVID-19?
What makes me more vulnerable to this particular virus as an apparently healthy septuagenarian? What collection of misfortunes have fallen on those younger victims of the pandemic? How often was it genetic?
Of course, none of us has the information yet that can provide us answers. This vacuum has attracted scores of “experts” bold enough or careless enough to venture an opinion. They may have also issued a caveat, but how often have the media failed to include it in the report or buried it in the fine print at the end of the story?
My discomfort with this information void has left me and you and everyone else to our imaginations to craft our own explanations. So, I try to piece together a construct based on what I can glean from what I read and see in the news because like most people I fortunately have no first-hand information about even a single case. The number of deaths is horrifying, but may not have hit close to home and given most of us a real personal sense of the illness and its character.
Maine is a small state with just over a million inhabitants, and most of us have some connection to one another. It may be that a person is the second cousin of someone who used to live 2 miles down the road. But, there is some feeling of familiarity. We have had deaths related to COVID-19, but very scanty information other than the county about where they occurred and whether the victim was a resident of an extended care facility. We are told very little if any details about exposure as officials invoke HIPAA regulations that leave us in the dark. Other than one vague reference to a “traveling salesman” who may have introduced the virus to several nursing homes, there has been very little information about how the virus may have been spread here in Maine. Even national reports of the deaths of high-profile entertainers and retired athletes are usually draped in the same haze of privacy.
Most of us don’t need to know the names and street addresses of the victims but a few anonymous narratives that include some general information on how epidemiologists believe clusters began and propagated would help us understand our risks with just a glimmer of clarity.
Of course the epidemiologists may not have the answers we are seeking because they too are struggling to untangle connections hampered by concerns of privacy. There is no question that privacy must remain an important part of the physician-patient relationship. But a pandemic has thrown us into a situation where common sense demands that HIPAA be interpreted with an emphasis on the greater good. Finding that balance between privacy and public knowledge will continue to be one of our greatest challenges.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at [email protected].
Ignorance may be bliss for some. But as I sit here in my scenic social isolation on the Maine coast I find that, like most people, what I don’t know unsettles me. How is the COVID-19 virus spread? Does my wife’s wipe down of the doorknobs after I return from the grocery store really make us any less likely to contract the virus? Is wearing my homemade bandana face mask doing anything to protect me? I suspect not, but I wear it as a statement of courtesy and solidarity to my fellow community members.
Does the 6-foot rule make any sense? I’ve read that it is based on a study dating back to the 1930s. I’ve seen images of the 25-foot droplet plume blasting out from a sneeze and understand that, as a bicyclist, I may be generating a shower of droplets in my wake. But, are those droplets a threat to anyone I pedal by if I am symptom free? What does being a carrier mean when we are talking about COVID-19?
What makes me more vulnerable to this particular virus as an apparently healthy septuagenarian? What collection of misfortunes have fallen on those younger victims of the pandemic? How often was it genetic?
Of course, none of us has the information yet that can provide us answers. This vacuum has attracted scores of “experts” bold enough or careless enough to venture an opinion. They may have also issued a caveat, but how often have the media failed to include it in the report or buried it in the fine print at the end of the story?
My discomfort with this information void has left me and you and everyone else to our imaginations to craft our own explanations. So, I try to piece together a construct based on what I can glean from what I read and see in the news because like most people I fortunately have no first-hand information about even a single case. The number of deaths is horrifying, but may not have hit close to home and given most of us a real personal sense of the illness and its character.
Maine is a small state with just over a million inhabitants, and most of us have some connection to one another. It may be that a person is the second cousin of someone who used to live 2 miles down the road. But, there is some feeling of familiarity. We have had deaths related to COVID-19, but very scanty information other than the county about where they occurred and whether the victim was a resident of an extended care facility. We are told very little if any details about exposure as officials invoke HIPAA regulations that leave us in the dark. Other than one vague reference to a “traveling salesman” who may have introduced the virus to several nursing homes, there has been very little information about how the virus may have been spread here in Maine. Even national reports of the deaths of high-profile entertainers and retired athletes are usually draped in the same haze of privacy.
Most of us don’t need to know the names and street addresses of the victims but a few anonymous narratives that include some general information on how epidemiologists believe clusters began and propagated would help us understand our risks with just a glimmer of clarity.
Of course the epidemiologists may not have the answers we are seeking because they too are struggling to untangle connections hampered by concerns of privacy. There is no question that privacy must remain an important part of the physician-patient relationship. But a pandemic has thrown us into a situation where common sense demands that HIPAA be interpreted with an emphasis on the greater good. Finding that balance between privacy and public knowledge will continue to be one of our greatest challenges.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at [email protected].
Ignorance may be bliss for some. But as I sit here in my scenic social isolation on the Maine coast I find that, like most people, what I don’t know unsettles me. How is the COVID-19 virus spread? Does my wife’s wipe down of the doorknobs after I return from the grocery store really make us any less likely to contract the virus? Is wearing my homemade bandana face mask doing anything to protect me? I suspect not, but I wear it as a statement of courtesy and solidarity to my fellow community members.
Does the 6-foot rule make any sense? I’ve read that it is based on a study dating back to the 1930s. I’ve seen images of the 25-foot droplet plume blasting out from a sneeze and understand that, as a bicyclist, I may be generating a shower of droplets in my wake. But, are those droplets a threat to anyone I pedal by if I am symptom free? What does being a carrier mean when we are talking about COVID-19?
What makes me more vulnerable to this particular virus as an apparently healthy septuagenarian? What collection of misfortunes have fallen on those younger victims of the pandemic? How often was it genetic?
Of course, none of us has the information yet that can provide us answers. This vacuum has attracted scores of “experts” bold enough or careless enough to venture an opinion. They may have also issued a caveat, but how often have the media failed to include it in the report or buried it in the fine print at the end of the story?
My discomfort with this information void has left me and you and everyone else to our imaginations to craft our own explanations. So, I try to piece together a construct based on what I can glean from what I read and see in the news because like most people I fortunately have no first-hand information about even a single case. The number of deaths is horrifying, but may not have hit close to home and given most of us a real personal sense of the illness and its character.
Maine is a small state with just over a million inhabitants, and most of us have some connection to one another. It may be that a person is the second cousin of someone who used to live 2 miles down the road. But, there is some feeling of familiarity. We have had deaths related to COVID-19, but very scanty information other than the county about where they occurred and whether the victim was a resident of an extended care facility. We are told very little if any details about exposure as officials invoke HIPAA regulations that leave us in the dark. Other than one vague reference to a “traveling salesman” who may have introduced the virus to several nursing homes, there has been very little information about how the virus may have been spread here in Maine. Even national reports of the deaths of high-profile entertainers and retired athletes are usually draped in the same haze of privacy.
Most of us don’t need to know the names and street addresses of the victims but a few anonymous narratives that include some general information on how epidemiologists believe clusters began and propagated would help us understand our risks with just a glimmer of clarity.
Of course the epidemiologists may not have the answers we are seeking because they too are struggling to untangle connections hampered by concerns of privacy. There is no question that privacy must remain an important part of the physician-patient relationship. But a pandemic has thrown us into a situation where common sense demands that HIPAA be interpreted with an emphasis on the greater good. Finding that balance between privacy and public knowledge will continue to be one of our greatest challenges.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at [email protected].
FDA approves Phexxi for use as an on-demand contraceptive

Evofem Biosciences expects to release Phexxi – the first nonhormonal, on-demand, vaginal pH regulator contraceptive designed to maintain vaginal pH within the range of 3.5-4.5 – in September 2020 alongside the Phexxi Concierge Experience, a comprehensive patient and health care provider telemedicine support system, according to the company’s press release. The service is designed to provide physicians with on-demand educational support, and to speed and simplify women’s access to Phexxi.
In an open-label multicenter trial, women aged 18-35 with regular menstrual cycles intravaginally administered a 5-gram dose of Phexxi vaginal gel up to 1 hour prior to intercourse; they did so for up to seven cycles. There were 101 pregnancies in 1,183 subjects during 4,769 cycles. The 7-cycle cumulative pregnancy rate was 14% (95% confidence interval: 10.0%, 17.5%).
The most common adverse events associated with Phexxi were vulvovaginal burning sensation, vulvovaginal pruritus, vulvovaginal mycotic infection, urinary tract infection, bacterial vaginosis, vaginal discharge, dysuria, and vulvovaginal pain.
Evofem Biosciences expects to release Phexxi – the first nonhormonal, on-demand, vaginal pH regulator contraceptive designed to maintain vaginal pH within the range of 3.5-4.5 – in September 2020 alongside the Phexxi Concierge Experience, a comprehensive patient and health care provider telemedicine support system, according to the company’s press release. The service is designed to provide physicians with on-demand educational support, and to speed and simplify women’s access to Phexxi.
In an open-label multicenter trial, women aged 18-35 with regular menstrual cycles intravaginally administered a 5-gram dose of Phexxi vaginal gel up to 1 hour prior to intercourse; they did so for up to seven cycles. There were 101 pregnancies in 1,183 subjects during 4,769 cycles. The 7-cycle cumulative pregnancy rate was 14% (95% confidence interval: 10.0%, 17.5%).
The most common adverse events associated with Phexxi were vulvovaginal burning sensation, vulvovaginal pruritus, vulvovaginal mycotic infection, urinary tract infection, bacterial vaginosis, vaginal discharge, dysuria, and vulvovaginal pain.
Evofem Biosciences expects to release Phexxi – the first nonhormonal, on-demand, vaginal pH regulator contraceptive designed to maintain vaginal pH within the range of 3.5-4.5 – in September 2020 alongside the Phexxi Concierge Experience, a comprehensive patient and health care provider telemedicine support system, according to the company’s press release. The service is designed to provide physicians with on-demand educational support, and to speed and simplify women’s access to Phexxi.
In an open-label multicenter trial, women aged 18-35 with regular menstrual cycles intravaginally administered a 5-gram dose of Phexxi vaginal gel up to 1 hour prior to intercourse; they did so for up to seven cycles. There were 101 pregnancies in 1,183 subjects during 4,769 cycles. The 7-cycle cumulative pregnancy rate was 14% (95% confidence interval: 10.0%, 17.5%).
The most common adverse events associated with Phexxi were vulvovaginal burning sensation, vulvovaginal pruritus, vulvovaginal mycotic infection, urinary tract infection, bacterial vaginosis, vaginal discharge, dysuria, and vulvovaginal pain.