User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
The future of pediatrics
Things will change. That is a constant. The practice of pediatrics will be different in the future. The pandemic has changed some things; mostly it has accelerated changes, advancements, improvements, and losses that were already occurring. Telemedicine will play a more prominent role in the future. The finances of solo and small-group practice have become more difficult.

As I wrote my prior column on the character traits/virtues of an admirable physician, I also began brainstorming this column on the traits of an admirable profession. Then the American Academy of Pediatrics’ virtual National Conference & Exhibition had many presentations encouraging pediatricians to adopt a conglomeration of activities in their offices. I became skeptical. Which should be selected? To make a wise choice, I review the major goals of medicine, which I have evolved to embrace as the quadruple aims.
First and hopefully always foremost, the health professions are dedicated to the health of their patients and, hopefully, the population at large. This trait dates to the Hippocratic Oath.
Second, physicians have a stewardship over a vast collection of knowledge, skills, resources, and funds. When I started my career, U.S. health care had increased from 6% of the gross domestic product to 9%, nearly twice that of other developed nations, and was expanding rapidly, contributing to widespread economic problems including the national debt. The health economists of the 1980’s made dire predictions that the nation was headed up to 12% of the GDP, which would cause the sky to start falling. Last I checked U.S. health care is approaching 18% of the GDP. The sky seems intact, although the oceans are rising and the hillsides are burning.
Managed care of the 1990s became focused on the consumer experience. Evaluations of physicians and nurses became dependent on consumer surveys. I recall one survey about the care I personally had received as day surgery. It was mostly about scheduling, being greeted on arrival, the waiting room, and other fluff. Only 1 of the over 20 questions had any bearing on whether I thought the diagnosis was correct, the treatment was effective, or my physician was competent. As a cancer patient, my priorities were not aligned with that survey’s concept of quality.
From 2008, I recall the Triple Aim: “Improving the U.S. health care system requires simultaneous pursuit of three aims: improving the experience of care, improving the health of populations, and reducing per capita costs of health care.”
Over the ensuing decade, physician wellness has been added to make a quadruple aim. If the system isn’t professionally rewarding, burnout occurs. Skills and experience are lost. The best and brightest are not attracted to the specialty. Quality goes down. So physicians must factor this into decisions about the future of pediatrics.
There are many social determinants of health that have large impacts on the population health of children, and it does not necessarily follow that I should spend my patient care time on those determinants. As a professional, I have a responsibility to ensure that I am treating important problems that match my extensive (and expensive) training, knowledge, skills, and experience.

I recently read a persuasive argument that caring for ADHD is an important and doable part of modern general pediatrics. I agree, but I agreed with the proponent’s idea 25 years ago when I joined a large group and saw my own ADHD patients. Change can be slow.
Pharmacology options for anxiety have become safer, more effective, and better understood in children. General pediatricians may now be able to provide important, earlier, and accessible intervention for pediatric anxiety and other mental health issues.
Food insecurity is a worsening issue during the pandemic, but not one which I have specialized abilities to address. A brochure listing available local resources could be posted in waiting rooms and exam rooms. Is spending time asking about it during a visit the best use of a pediatrician’s time? That is a choice a professional needs to make. It may depend on your patient panel and community resources. In the past, I was more inclined to focus on medical care and donate the extra income to my church’s food bank. But the world has changed. Perhaps the pediatrician’s office of the 2020s is a department store, with social workers, psychologists, and therapists located under the same roof. It reminds me of the Mayo model. Wealthy people would travel to Rochester for an executive physical. That physical would frequently recommend seeing a couple specialists before leaving town. It is an effective model but also luxurious.
Racism causes major harms, both to physical health and mental health. Is asking about it a wise use of limited time for well-child visits? What resources will you offer?
Climate change, hurricanes, and wildfires are harming children. Is debating the issue with your patient’s parents productive? I am zealous about the topic. I spend considerable time and money promoting the credibility of science within various religious organizations, but I try to avoid bringing politics into my interactions with patients.
As a professional, your choices may be different. Many people are telling you what you should care about. The executive well-child visit would be beneficial, but it would also take 2 hours. Don’t be misled into spending too much effort on issues not in your expertise. Choose wisely.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. He has no relevant financial disclosures. Email him at [email protected].
Things will change. That is a constant. The practice of pediatrics will be different in the future. The pandemic has changed some things; mostly it has accelerated changes, advancements, improvements, and losses that were already occurring. Telemedicine will play a more prominent role in the future. The finances of solo and small-group practice have become more difficult.
As I wrote my prior column on the character traits/virtues of an admirable physician, I also began brainstorming this column on the traits of an admirable profession. Then the American Academy of Pediatrics’ virtual National Conference & Exhibition had many presentations encouraging pediatricians to adopt a conglomeration of activities in their offices. I became skeptical. Which should be selected? To make a wise choice, I review the major goals of medicine, which I have evolved to embrace as the quadruple aims.
First and hopefully always foremost, the health professions are dedicated to the health of their patients and, hopefully, the population at large. This trait dates to the Hippocratic Oath.
Second, physicians have a stewardship over a vast collection of knowledge, skills, resources, and funds. When I started my career, U.S. health care had increased from 6% of the gross domestic product to 9%, nearly twice that of other developed nations, and was expanding rapidly, contributing to widespread economic problems including the national debt. The health economists of the 1980’s made dire predictions that the nation was headed up to 12% of the GDP, which would cause the sky to start falling. Last I checked U.S. health care is approaching 18% of the GDP. The sky seems intact, although the oceans are rising and the hillsides are burning.
Managed care of the 1990s became focused on the consumer experience. Evaluations of physicians and nurses became dependent on consumer surveys. I recall one survey about the care I personally had received as day surgery. It was mostly about scheduling, being greeted on arrival, the waiting room, and other fluff. Only 1 of the over 20 questions had any bearing on whether I thought the diagnosis was correct, the treatment was effective, or my physician was competent. As a cancer patient, my priorities were not aligned with that survey’s concept of quality.
From 2008, I recall the Triple Aim: “Improving the U.S. health care system requires simultaneous pursuit of three aims: improving the experience of care, improving the health of populations, and reducing per capita costs of health care.”
Over the ensuing decade, physician wellness has been added to make a quadruple aim. If the system isn’t professionally rewarding, burnout occurs. Skills and experience are lost. The best and brightest are not attracted to the specialty. Quality goes down. So physicians must factor this into decisions about the future of pediatrics.
There are many social determinants of health that have large impacts on the population health of children, and it does not necessarily follow that I should spend my patient care time on those determinants. As a professional, I have a responsibility to ensure that I am treating important problems that match my extensive (and expensive) training, knowledge, skills, and experience.
I recently read a persuasive argument that caring for ADHD is an important and doable part of modern general pediatrics. I agree, but I agreed with the proponent’s idea 25 years ago when I joined a large group and saw my own ADHD patients. Change can be slow.
Pharmacology options for anxiety have become safer, more effective, and better understood in children. General pediatricians may now be able to provide important, earlier, and accessible intervention for pediatric anxiety and other mental health issues.
Food insecurity is a worsening issue during the pandemic, but not one which I have specialized abilities to address. A brochure listing available local resources could be posted in waiting rooms and exam rooms. Is spending time asking about it during a visit the best use of a pediatrician’s time? That is a choice a professional needs to make. It may depend on your patient panel and community resources. In the past, I was more inclined to focus on medical care and donate the extra income to my church’s food bank. But the world has changed. Perhaps the pediatrician’s office of the 2020s is a department store, with social workers, psychologists, and therapists located under the same roof. It reminds me of the Mayo model. Wealthy people would travel to Rochester for an executive physical. That physical would frequently recommend seeing a couple specialists before leaving town. It is an effective model but also luxurious.
Racism causes major harms, both to physical health and mental health. Is asking about it a wise use of limited time for well-child visits? What resources will you offer?
Climate change, hurricanes, and wildfires are harming children. Is debating the issue with your patient’s parents productive? I am zealous about the topic. I spend considerable time and money promoting the credibility of science within various religious organizations, but I try to avoid bringing politics into my interactions with patients.
As a professional, your choices may be different. Many people are telling you what you should care about. The executive well-child visit would be beneficial, but it would also take 2 hours. Don’t be misled into spending too much effort on issues not in your expertise. Choose wisely.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. He has no relevant financial disclosures. Email him at [email protected].
Things will change. That is a constant. The practice of pediatrics will be different in the future. The pandemic has changed some things; mostly it has accelerated changes, advancements, improvements, and losses that were already occurring. Telemedicine will play a more prominent role in the future. The finances of solo and small-group practice have become more difficult.
As I wrote my prior column on the character traits/virtues of an admirable physician, I also began brainstorming this column on the traits of an admirable profession. Then the American Academy of Pediatrics’ virtual National Conference & Exhibition had many presentations encouraging pediatricians to adopt a conglomeration of activities in their offices. I became skeptical. Which should be selected? To make a wise choice, I review the major goals of medicine, which I have evolved to embrace as the quadruple aims.
First and hopefully always foremost, the health professions are dedicated to the health of their patients and, hopefully, the population at large. This trait dates to the Hippocratic Oath.
Second, physicians have a stewardship over a vast collection of knowledge, skills, resources, and funds. When I started my career, U.S. health care had increased from 6% of the gross domestic product to 9%, nearly twice that of other developed nations, and was expanding rapidly, contributing to widespread economic problems including the national debt. The health economists of the 1980’s made dire predictions that the nation was headed up to 12% of the GDP, which would cause the sky to start falling. Last I checked U.S. health care is approaching 18% of the GDP. The sky seems intact, although the oceans are rising and the hillsides are burning.
Managed care of the 1990s became focused on the consumer experience. Evaluations of physicians and nurses became dependent on consumer surveys. I recall one survey about the care I personally had received as day surgery. It was mostly about scheduling, being greeted on arrival, the waiting room, and other fluff. Only 1 of the over 20 questions had any bearing on whether I thought the diagnosis was correct, the treatment was effective, or my physician was competent. As a cancer patient, my priorities were not aligned with that survey’s concept of quality.
From 2008, I recall the Triple Aim: “Improving the U.S. health care system requires simultaneous pursuit of three aims: improving the experience of care, improving the health of populations, and reducing per capita costs of health care.”
Over the ensuing decade, physician wellness has been added to make a quadruple aim. If the system isn’t professionally rewarding, burnout occurs. Skills and experience are lost. The best and brightest are not attracted to the specialty. Quality goes down. So physicians must factor this into decisions about the future of pediatrics.
There are many social determinants of health that have large impacts on the population health of children, and it does not necessarily follow that I should spend my patient care time on those determinants. As a professional, I have a responsibility to ensure that I am treating important problems that match my extensive (and expensive) training, knowledge, skills, and experience.
I recently read a persuasive argument that caring for ADHD is an important and doable part of modern general pediatrics. I agree, but I agreed with the proponent’s idea 25 years ago when I joined a large group and saw my own ADHD patients. Change can be slow.
Pharmacology options for anxiety have become safer, more effective, and better understood in children. General pediatricians may now be able to provide important, earlier, and accessible intervention for pediatric anxiety and other mental health issues.
Food insecurity is a worsening issue during the pandemic, but not one which I have specialized abilities to address. A brochure listing available local resources could be posted in waiting rooms and exam rooms. Is spending time asking about it during a visit the best use of a pediatrician’s time? That is a choice a professional needs to make. It may depend on your patient panel and community resources. In the past, I was more inclined to focus on medical care and donate the extra income to my church’s food bank. But the world has changed. Perhaps the pediatrician’s office of the 2020s is a department store, with social workers, psychologists, and therapists located under the same roof. It reminds me of the Mayo model. Wealthy people would travel to Rochester for an executive physical. That physical would frequently recommend seeing a couple specialists before leaving town. It is an effective model but also luxurious.
Racism causes major harms, both to physical health and mental health. Is asking about it a wise use of limited time for well-child visits? What resources will you offer?
Climate change, hurricanes, and wildfires are harming children. Is debating the issue with your patient’s parents productive? I am zealous about the topic. I spend considerable time and money promoting the credibility of science within various religious organizations, but I try to avoid bringing politics into my interactions with patients.
As a professional, your choices may be different. Many people are telling you what you should care about. The executive well-child visit would be beneficial, but it would also take 2 hours. Don’t be misled into spending too much effort on issues not in your expertise. Choose wisely.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. He has no relevant financial disclosures. Email him at [email protected].
Poverty raises depression risk in patients with cystic fibrosis
Poor people with chronic illness have greater difficulty managing their disease than do their better-off counterparts, and a new study confirms this reality for patients with cystic fibrosis.
and anxiety symptoms, according to a new cross-sectional study. The data were drawn from the Cystic Fibrosis Foundation’s Success with Therapies Research Consortium.
“Assessing the special challenges that individuals with lower SES face, including financial barriers, is essential to understand how we can address the unique combinations of adherence barriers. In other chronic disorders, financial barriers or lower socioeconomic status is associated with nonadherence, but this relationship has not been well established in cystic fibrosis,” said Kimberly Dickinson, MD, MPH, of Johns Hopkins University, Baltimore, during her presentation of the results at the virtual North American Cystic Fibrosis Conference.

“I’ve always thought that my patients in the poorer population were doing worse, and I think this demonstrates that that’s true,” said Robert Giusti, MD, in an interview. Dr. Giusti is a clinical professor of pediatrics at the New York University and director of the Pediatric Cystic Fibrosis Center in New York. He was not involved in the study.
“These are very pertinent issues, especially if you think about the pandemic, and some of the issues related to mental health. It just highlights the importance of socioeconomic status and screening for some of the known risk factors so that we can develop interventions or programs to provide equitable care to all of our cystic fibrosis patients,” said Ryan Perkins, MD, who moderated the session where the study was presented. He is a pediatric and adult pulmonary fellow at Boston Children’s Hospital and Brigham and Women’s Hospital, also in Boston.
The researchers looked retrospectively at 1 year’s worth of pharmacy refill receipts and number of times prescriptions were refilled versus the number of times prescribed, then calculated medicinal possession ratios. This was cross-referenced with annual household income and insurance status of patients with CF at 12 pediatric and 9 adult CF care centers, for a total of 376 patients (128 pediatric and 248 adult).
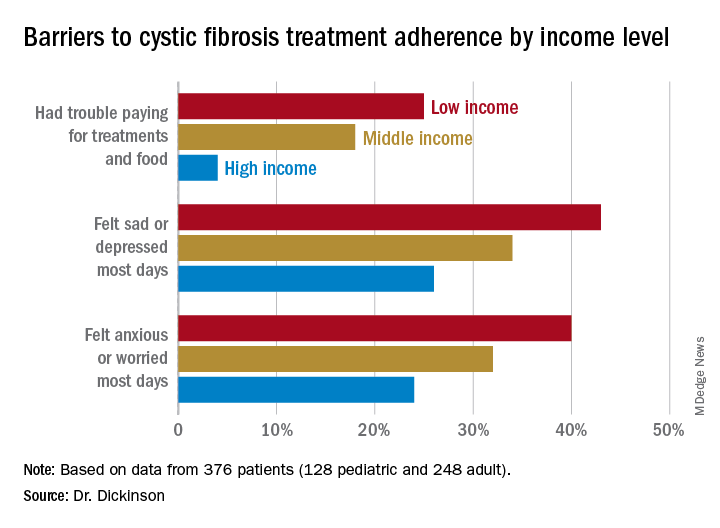
In this population, 32% of participants had public or no insurance, 68% had private or military insurance. The public/no insurance group was more likely than the private/military insurance group to report having trouble paying for treatments, food, or critical expenses related to CF care (23.3% vs. 12.1%, respectively); feeling symptoms on most days of depression (42.5% vs. 31.3%) or anxiety (40.0% vs. 28.5%); and experiencing conflict or stress with loved ones over treatments (30.0% vs. 20.3%) (P < .05 for all).
In all, 35% had a household income less than $40,000 per year, 33% between $44,000 and $100,000, and 32% higher than $100,000. The low-income group had a lower composite medication possession ratio (0.41) than the middle- (0.44) or high-income (0.52) groups, were more likely to have trouble paying for treatments, food, or treatment-related expenses (25%, 18%, 4%, respectively); were more likely most days to report symptoms of depression (43%, 34%, 26%) or anxiety (40%, 32%, 24%), and to have concerns about whether treatments were effective (42%, 27%, 29%). They were more likely to not be able to maintain a daily schedule or routine for treatments (28%, 22%, 14%).
The study showed that adherence barriers and suboptimal adherence are issues that cross all socioeconomic categories, though they were more problematic in the lowest bracket. Greater anxiety and depression among lower income individuals and those with private or no insurance was a key finding, according to Dr. Dickinson. “It highlights the importance of screening for mental health comorbidities that may impact non-adherence,” she said.
The study received funding from the Cystic Fibrosis Foundation. Dr. Dickinson, Dr. Giusti, and Dr. Perkins have no relevant financial disclosures.
Poor people with chronic illness have greater difficulty managing their disease than do their better-off counterparts, and a new study confirms this reality for patients with cystic fibrosis.
and anxiety symptoms, according to a new cross-sectional study. The data were drawn from the Cystic Fibrosis Foundation’s Success with Therapies Research Consortium.
“Assessing the special challenges that individuals with lower SES face, including financial barriers, is essential to understand how we can address the unique combinations of adherence barriers. In other chronic disorders, financial barriers or lower socioeconomic status is associated with nonadherence, but this relationship has not been well established in cystic fibrosis,” said Kimberly Dickinson, MD, MPH, of Johns Hopkins University, Baltimore, during her presentation of the results at the virtual North American Cystic Fibrosis Conference.
“I’ve always thought that my patients in the poorer population were doing worse, and I think this demonstrates that that’s true,” said Robert Giusti, MD, in an interview. Dr. Giusti is a clinical professor of pediatrics at the New York University and director of the Pediatric Cystic Fibrosis Center in New York. He was not involved in the study.
“These are very pertinent issues, especially if you think about the pandemic, and some of the issues related to mental health. It just highlights the importance of socioeconomic status and screening for some of the known risk factors so that we can develop interventions or programs to provide equitable care to all of our cystic fibrosis patients,” said Ryan Perkins, MD, who moderated the session where the study was presented. He is a pediatric and adult pulmonary fellow at Boston Children’s Hospital and Brigham and Women’s Hospital, also in Boston.
The researchers looked retrospectively at 1 year’s worth of pharmacy refill receipts and number of times prescriptions were refilled versus the number of times prescribed, then calculated medicinal possession ratios. This was cross-referenced with annual household income and insurance status of patients with CF at 12 pediatric and 9 adult CF care centers, for a total of 376 patients (128 pediatric and 248 adult).
In this population, 32% of participants had public or no insurance, 68% had private or military insurance. The public/no insurance group was more likely than the private/military insurance group to report having trouble paying for treatments, food, or critical expenses related to CF care (23.3% vs. 12.1%, respectively); feeling symptoms on most days of depression (42.5% vs. 31.3%) or anxiety (40.0% vs. 28.5%); and experiencing conflict or stress with loved ones over treatments (30.0% vs. 20.3%) (P < .05 for all).
In all, 35% had a household income less than $40,000 per year, 33% between $44,000 and $100,000, and 32% higher than $100,000. The low-income group had a lower composite medication possession ratio (0.41) than the middle- (0.44) or high-income (0.52) groups, were more likely to have trouble paying for treatments, food, or treatment-related expenses (25%, 18%, 4%, respectively); were more likely most days to report symptoms of depression (43%, 34%, 26%) or anxiety (40%, 32%, 24%), and to have concerns about whether treatments were effective (42%, 27%, 29%). They were more likely to not be able to maintain a daily schedule or routine for treatments (28%, 22%, 14%).
The study showed that adherence barriers and suboptimal adherence are issues that cross all socioeconomic categories, though they were more problematic in the lowest bracket. Greater anxiety and depression among lower income individuals and those with private or no insurance was a key finding, according to Dr. Dickinson. “It highlights the importance of screening for mental health comorbidities that may impact non-adherence,” she said.
The study received funding from the Cystic Fibrosis Foundation. Dr. Dickinson, Dr. Giusti, and Dr. Perkins have no relevant financial disclosures.
Poor people with chronic illness have greater difficulty managing their disease than do their better-off counterparts, and a new study confirms this reality for patients with cystic fibrosis.
and anxiety symptoms, according to a new cross-sectional study. The data were drawn from the Cystic Fibrosis Foundation’s Success with Therapies Research Consortium.
“Assessing the special challenges that individuals with lower SES face, including financial barriers, is essential to understand how we can address the unique combinations of adherence barriers. In other chronic disorders, financial barriers or lower socioeconomic status is associated with nonadherence, but this relationship has not been well established in cystic fibrosis,” said Kimberly Dickinson, MD, MPH, of Johns Hopkins University, Baltimore, during her presentation of the results at the virtual North American Cystic Fibrosis Conference.
“I’ve always thought that my patients in the poorer population were doing worse, and I think this demonstrates that that’s true,” said Robert Giusti, MD, in an interview. Dr. Giusti is a clinical professor of pediatrics at the New York University and director of the Pediatric Cystic Fibrosis Center in New York. He was not involved in the study.
“These are very pertinent issues, especially if you think about the pandemic, and some of the issues related to mental health. It just highlights the importance of socioeconomic status and screening for some of the known risk factors so that we can develop interventions or programs to provide equitable care to all of our cystic fibrosis patients,” said Ryan Perkins, MD, who moderated the session where the study was presented. He is a pediatric and adult pulmonary fellow at Boston Children’s Hospital and Brigham and Women’s Hospital, also in Boston.
The researchers looked retrospectively at 1 year’s worth of pharmacy refill receipts and number of times prescriptions were refilled versus the number of times prescribed, then calculated medicinal possession ratios. This was cross-referenced with annual household income and insurance status of patients with CF at 12 pediatric and 9 adult CF care centers, for a total of 376 patients (128 pediatric and 248 adult).
In this population, 32% of participants had public or no insurance, 68% had private or military insurance. The public/no insurance group was more likely than the private/military insurance group to report having trouble paying for treatments, food, or critical expenses related to CF care (23.3% vs. 12.1%, respectively); feeling symptoms on most days of depression (42.5% vs. 31.3%) or anxiety (40.0% vs. 28.5%); and experiencing conflict or stress with loved ones over treatments (30.0% vs. 20.3%) (P < .05 for all).
In all, 35% had a household income less than $40,000 per year, 33% between $44,000 and $100,000, and 32% higher than $100,000. The low-income group had a lower composite medication possession ratio (0.41) than the middle- (0.44) or high-income (0.52) groups, were more likely to have trouble paying for treatments, food, or treatment-related expenses (25%, 18%, 4%, respectively); were more likely most days to report symptoms of depression (43%, 34%, 26%) or anxiety (40%, 32%, 24%), and to have concerns about whether treatments were effective (42%, 27%, 29%). They were more likely to not be able to maintain a daily schedule or routine for treatments (28%, 22%, 14%).
The study showed that adherence barriers and suboptimal adherence are issues that cross all socioeconomic categories, though they were more problematic in the lowest bracket. Greater anxiety and depression among lower income individuals and those with private or no insurance was a key finding, according to Dr. Dickinson. “It highlights the importance of screening for mental health comorbidities that may impact non-adherence,” she said.
The study received funding from the Cystic Fibrosis Foundation. Dr. Dickinson, Dr. Giusti, and Dr. Perkins have no relevant financial disclosures.
FROM NACFC 2020
.
Biden plan to lower Medicare eligibility age to 60 faces hostility from hospitals
Of his many plans to expand insurance coverage, President-elect Joe Biden’s simplest strategy is lowering the eligibility age for Medicare from 65 to 60.
But the plan is sure to face long odds, even if the Democrats can snag control of the Senate in January by winning two runoff elections in Georgia.
Republicans, who fought the creation of Medicare in the 1960s and typically oppose expanding government entitlement programs, are not the biggest obstacle. Instead, the nation’s hospitals, a powerful political force, are poised to derail any effort.
“Hospitals certainly are not going to be happy with it,” said Jonathan Oberlander, professor of health policy and management at the University of North Carolina at Chapel Hill.
Medicare reimbursement rates for patients admitted to hospitals average half what commercial or employer-sponsored insurance plans pay.
“It will be a huge lift [in Congress] as the realities of lower Medicare reimbursement rates will activate some powerful interests against this,” said Josh Archambault, a senior fellow with the conservative Foundation for Government Accountability.
Biden, who turns 78 this month, said his plan will help Americans who retire early and those who are unemployed or can’t find jobs with health benefits.
“It reflects the reality that, even after the current crisis ends, older Americans are likely to find it difficult to secure jobs,” Biden wrote in April.
Lowering the Medicare eligibility age is popular. About 85% of Democrats and 69% of Republicans favor allowing those as young as 50 to buy into Medicare, according to a KFF tracking poll from January 2019. (KHN is an editorially independent program of KFF.)
Although opposition from the hospital industry is expected to be fierce, that is not the only obstacle to Biden’s plan.
Critics, especially Republicans on Capitol Hill, will point to the nation’s $3 trillion budget deficit as well as the dim outlook for the Medicare Hospital Insurance Trust Fund. That fund is on track to reach insolvency in 2024. That means there won’t be enough money to fully pay hospitals and nursing homes for inpatient care for Medicare beneficiaries.
Moreover, it’s unclear whether expanding Medicare will fit on the Democrats’ crowded health agenda, which also includes dealing with the COVID-19 pandemic, possibly rescuing the Affordable Care Act if the Supreme Court strikes down part or all of the law in a current case, expanding Obamacare subsidies and lowering drug costs.
Biden’s proposal is a nod to the liberal wing of the Democratic Party, which has advocated for Sen. Bernie Sanders’ (I-Vt.) government-run “Medicare for All” health system that would provide universal coverage. Biden opposed that effort, saying the nation could not afford it. He wanted to retain the private health insurance system, which covers 180 million people.
To expand coverage, Biden has proposed two major initiatives. In addition to the Medicare eligibility change, he wants Congress to approve a government-run health plan that people could buy into instead of purchasing coverage from insurance companies on their own or through the Obamacare marketplaces. Insurers helped beat back this “public option” initiative in 2009 during the congressional debate over the ACA.
The appeal of lowering Medicare eligibility to help those without insurance lies with leveraging a popular government program that has low administrative costs.
“It is hard to find a reform idea that is more popular than opening up Medicare” to people as young as 60, Oberlander said. He said early retirees would like the concept, as would employers, who could save on their health costs as workers gravitate to Medicare.
The eligibility age has been set at 65 since Medicare was created in 1965 as part of President Lyndon Johnson’s Great Society reform package. It was designed to coincide with the age when people at that time qualified for Social Security. Today, people generally qualify for early, reduced Social Security benefits at age 62, though they have to wait until age 66 for full benefits.
While people can qualify on the basis of other criteria, such as having a disability or end-stage renal disease, 85% of the 57 million Medicare enrollees are in the program simply because they’re old enough.
Lowering the age to 60 could add as many as 23 million people to Medicare, according to an analysis by the consulting firm Avalere Health. It’s unclear, however, if everyone who would be eligible would sign up or if Biden would limit the expansion to the 1.7 million people in that age range who are uninsured and the 3.2 million who buy coverage on their own.
Avalere says 3.2 million people in that age group buy coverage on the individual market.
While the 60-to-65 group has the lowest uninsured rate (8%) among adults, it has the highest health costs and pays the highest rates for individual coverage, said Cristina Boccuti, director of health policy at West Health, a nonpartisan research group.
About 13 million of those between 60 and 65 have coverage through their employer, according to Avalere. While they would not have to drop coverage to join Medicare, they could possibly opt to also pay to join the federal program and use it as a wraparound for their existing coverage. Medicare might then pick up costs for some services that the consumers would have to shoulder out-of-pocket.
Some 4 million people between 60 and 65 are enrolled in Medicaid, the state-federal health insurance program for low-income people. Shifting them to Medicare would make that their primary health insurer, a move that would save states money since they split Medicaid costs with the federal government.
Chris Pope, a senior fellow with the conservative Manhattan Institute, said getting health industry support, particularly from hospitals, will be vital for any health coverage expansion. “Hospitals are very aware about generous commercial rates being replaced by lower Medicare rates,” he said.
“Members of Congress, a lot of them are close to their hospitals and do not want to see them with a revenue hole,” he said.
President Barack Obama made a deal with the industry on the way to passing the ACA. In exchange for gaining millions of paying customers and lowering their uncompensated care by billions of dollars, the hospital industry agreed to give up future Medicare funds designed to help them cope with the uninsured. Showing the industry’s prowess on Capitol Hill, Congress has delayed those funding cuts for more than six years.
Jacob Hacker, a Yale University political scientist, noted that expanding Medicare would reduce the number of Americans who rely on employer-sponsored coverage. The pitfalls of the employer system were highlighted in 2020 as millions lost their jobs and workplace health coverage.
Even if they can win the two Georgia seats and take control of the Senate with the vice president breaking any ties, Democrats would be unlikely to pass major legislation without GOP support — unless they are willing to jettison the long-standing filibuster rule so they can pass most legislation with a simple 51-vote majority instead of 60 votes.
Hacker said that slim margin would make it difficult for Democrats to deal with many health issues all at once.
“Congress is not good at parallel processing,” Hacker said, referring to handling multiple priorities at the same time. “And the window is relatively short.”
KHN (Kaiser Health News) is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
Of his many plans to expand insurance coverage, President-elect Joe Biden’s simplest strategy is lowering the eligibility age for Medicare from 65 to 60.
But the plan is sure to face long odds, even if the Democrats can snag control of the Senate in January by winning two runoff elections in Georgia.
Republicans, who fought the creation of Medicare in the 1960s and typically oppose expanding government entitlement programs, are not the biggest obstacle. Instead, the nation’s hospitals, a powerful political force, are poised to derail any effort.
“Hospitals certainly are not going to be happy with it,” said Jonathan Oberlander, professor of health policy and management at the University of North Carolina at Chapel Hill.
Medicare reimbursement rates for patients admitted to hospitals average half what commercial or employer-sponsored insurance plans pay.
“It will be a huge lift [in Congress] as the realities of lower Medicare reimbursement rates will activate some powerful interests against this,” said Josh Archambault, a senior fellow with the conservative Foundation for Government Accountability.
Biden, who turns 78 this month, said his plan will help Americans who retire early and those who are unemployed or can’t find jobs with health benefits.
“It reflects the reality that, even after the current crisis ends, older Americans are likely to find it difficult to secure jobs,” Biden wrote in April.
Lowering the Medicare eligibility age is popular. About 85% of Democrats and 69% of Republicans favor allowing those as young as 50 to buy into Medicare, according to a KFF tracking poll from January 2019. (KHN is an editorially independent program of KFF.)
Although opposition from the hospital industry is expected to be fierce, that is not the only obstacle to Biden’s plan.
Critics, especially Republicans on Capitol Hill, will point to the nation’s $3 trillion budget deficit as well as the dim outlook for the Medicare Hospital Insurance Trust Fund. That fund is on track to reach insolvency in 2024. That means there won’t be enough money to fully pay hospitals and nursing homes for inpatient care for Medicare beneficiaries.
Moreover, it’s unclear whether expanding Medicare will fit on the Democrats’ crowded health agenda, which also includes dealing with the COVID-19 pandemic, possibly rescuing the Affordable Care Act if the Supreme Court strikes down part or all of the law in a current case, expanding Obamacare subsidies and lowering drug costs.
Biden’s proposal is a nod to the liberal wing of the Democratic Party, which has advocated for Sen. Bernie Sanders’ (I-Vt.) government-run “Medicare for All” health system that would provide universal coverage. Biden opposed that effort, saying the nation could not afford it. He wanted to retain the private health insurance system, which covers 180 million people.
To expand coverage, Biden has proposed two major initiatives. In addition to the Medicare eligibility change, he wants Congress to approve a government-run health plan that people could buy into instead of purchasing coverage from insurance companies on their own or through the Obamacare marketplaces. Insurers helped beat back this “public option” initiative in 2009 during the congressional debate over the ACA.
The appeal of lowering Medicare eligibility to help those without insurance lies with leveraging a popular government program that has low administrative costs.
“It is hard to find a reform idea that is more popular than opening up Medicare” to people as young as 60, Oberlander said. He said early retirees would like the concept, as would employers, who could save on their health costs as workers gravitate to Medicare.
The eligibility age has been set at 65 since Medicare was created in 1965 as part of President Lyndon Johnson’s Great Society reform package. It was designed to coincide with the age when people at that time qualified for Social Security. Today, people generally qualify for early, reduced Social Security benefits at age 62, though they have to wait until age 66 for full benefits.
While people can qualify on the basis of other criteria, such as having a disability or end-stage renal disease, 85% of the 57 million Medicare enrollees are in the program simply because they’re old enough.
Lowering the age to 60 could add as many as 23 million people to Medicare, according to an analysis by the consulting firm Avalere Health. It’s unclear, however, if everyone who would be eligible would sign up or if Biden would limit the expansion to the 1.7 million people in that age range who are uninsured and the 3.2 million who buy coverage on their own.
Avalere says 3.2 million people in that age group buy coverage on the individual market.
While the 60-to-65 group has the lowest uninsured rate (8%) among adults, it has the highest health costs and pays the highest rates for individual coverage, said Cristina Boccuti, director of health policy at West Health, a nonpartisan research group.
About 13 million of those between 60 and 65 have coverage through their employer, according to Avalere. While they would not have to drop coverage to join Medicare, they could possibly opt to also pay to join the federal program and use it as a wraparound for their existing coverage. Medicare might then pick up costs for some services that the consumers would have to shoulder out-of-pocket.
Some 4 million people between 60 and 65 are enrolled in Medicaid, the state-federal health insurance program for low-income people. Shifting them to Medicare would make that their primary health insurer, a move that would save states money since they split Medicaid costs with the federal government.
Chris Pope, a senior fellow with the conservative Manhattan Institute, said getting health industry support, particularly from hospitals, will be vital for any health coverage expansion. “Hospitals are very aware about generous commercial rates being replaced by lower Medicare rates,” he said.
“Members of Congress, a lot of them are close to their hospitals and do not want to see them with a revenue hole,” he said.
President Barack Obama made a deal with the industry on the way to passing the ACA. In exchange for gaining millions of paying customers and lowering their uncompensated care by billions of dollars, the hospital industry agreed to give up future Medicare funds designed to help them cope with the uninsured. Showing the industry’s prowess on Capitol Hill, Congress has delayed those funding cuts for more than six years.
Jacob Hacker, a Yale University political scientist, noted that expanding Medicare would reduce the number of Americans who rely on employer-sponsored coverage. The pitfalls of the employer system were highlighted in 2020 as millions lost their jobs and workplace health coverage.
Even if they can win the two Georgia seats and take control of the Senate with the vice president breaking any ties, Democrats would be unlikely to pass major legislation without GOP support — unless they are willing to jettison the long-standing filibuster rule so they can pass most legislation with a simple 51-vote majority instead of 60 votes.
Hacker said that slim margin would make it difficult for Democrats to deal with many health issues all at once.
“Congress is not good at parallel processing,” Hacker said, referring to handling multiple priorities at the same time. “And the window is relatively short.”
KHN (Kaiser Health News) is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
Of his many plans to expand insurance coverage, President-elect Joe Biden’s simplest strategy is lowering the eligibility age for Medicare from 65 to 60.
But the plan is sure to face long odds, even if the Democrats can snag control of the Senate in January by winning two runoff elections in Georgia.
Republicans, who fought the creation of Medicare in the 1960s and typically oppose expanding government entitlement programs, are not the biggest obstacle. Instead, the nation’s hospitals, a powerful political force, are poised to derail any effort.
“Hospitals certainly are not going to be happy with it,” said Jonathan Oberlander, professor of health policy and management at the University of North Carolina at Chapel Hill.
Medicare reimbursement rates for patients admitted to hospitals average half what commercial or employer-sponsored insurance plans pay.
“It will be a huge lift [in Congress] as the realities of lower Medicare reimbursement rates will activate some powerful interests against this,” said Josh Archambault, a senior fellow with the conservative Foundation for Government Accountability.
Biden, who turns 78 this month, said his plan will help Americans who retire early and those who are unemployed or can’t find jobs with health benefits.
“It reflects the reality that, even after the current crisis ends, older Americans are likely to find it difficult to secure jobs,” Biden wrote in April.
Lowering the Medicare eligibility age is popular. About 85% of Democrats and 69% of Republicans favor allowing those as young as 50 to buy into Medicare, according to a KFF tracking poll from January 2019. (KHN is an editorially independent program of KFF.)
Although opposition from the hospital industry is expected to be fierce, that is not the only obstacle to Biden’s plan.
Critics, especially Republicans on Capitol Hill, will point to the nation’s $3 trillion budget deficit as well as the dim outlook for the Medicare Hospital Insurance Trust Fund. That fund is on track to reach insolvency in 2024. That means there won’t be enough money to fully pay hospitals and nursing homes for inpatient care for Medicare beneficiaries.
Moreover, it’s unclear whether expanding Medicare will fit on the Democrats’ crowded health agenda, which also includes dealing with the COVID-19 pandemic, possibly rescuing the Affordable Care Act if the Supreme Court strikes down part or all of the law in a current case, expanding Obamacare subsidies and lowering drug costs.
Biden’s proposal is a nod to the liberal wing of the Democratic Party, which has advocated for Sen. Bernie Sanders’ (I-Vt.) government-run “Medicare for All” health system that would provide universal coverage. Biden opposed that effort, saying the nation could not afford it. He wanted to retain the private health insurance system, which covers 180 million people.
To expand coverage, Biden has proposed two major initiatives. In addition to the Medicare eligibility change, he wants Congress to approve a government-run health plan that people could buy into instead of purchasing coverage from insurance companies on their own or through the Obamacare marketplaces. Insurers helped beat back this “public option” initiative in 2009 during the congressional debate over the ACA.
The appeal of lowering Medicare eligibility to help those without insurance lies with leveraging a popular government program that has low administrative costs.
“It is hard to find a reform idea that is more popular than opening up Medicare” to people as young as 60, Oberlander said. He said early retirees would like the concept, as would employers, who could save on their health costs as workers gravitate to Medicare.
The eligibility age has been set at 65 since Medicare was created in 1965 as part of President Lyndon Johnson’s Great Society reform package. It was designed to coincide with the age when people at that time qualified for Social Security. Today, people generally qualify for early, reduced Social Security benefits at age 62, though they have to wait until age 66 for full benefits.
While people can qualify on the basis of other criteria, such as having a disability or end-stage renal disease, 85% of the 57 million Medicare enrollees are in the program simply because they’re old enough.
Lowering the age to 60 could add as many as 23 million people to Medicare, according to an analysis by the consulting firm Avalere Health. It’s unclear, however, if everyone who would be eligible would sign up or if Biden would limit the expansion to the 1.7 million people in that age range who are uninsured and the 3.2 million who buy coverage on their own.
Avalere says 3.2 million people in that age group buy coverage on the individual market.
While the 60-to-65 group has the lowest uninsured rate (8%) among adults, it has the highest health costs and pays the highest rates for individual coverage, said Cristina Boccuti, director of health policy at West Health, a nonpartisan research group.
About 13 million of those between 60 and 65 have coverage through their employer, according to Avalere. While they would not have to drop coverage to join Medicare, they could possibly opt to also pay to join the federal program and use it as a wraparound for their existing coverage. Medicare might then pick up costs for some services that the consumers would have to shoulder out-of-pocket.
Some 4 million people between 60 and 65 are enrolled in Medicaid, the state-federal health insurance program for low-income people. Shifting them to Medicare would make that their primary health insurer, a move that would save states money since they split Medicaid costs with the federal government.
Chris Pope, a senior fellow with the conservative Manhattan Institute, said getting health industry support, particularly from hospitals, will be vital for any health coverage expansion. “Hospitals are very aware about generous commercial rates being replaced by lower Medicare rates,” he said.
“Members of Congress, a lot of them are close to their hospitals and do not want to see them with a revenue hole,” he said.
President Barack Obama made a deal with the industry on the way to passing the ACA. In exchange for gaining millions of paying customers and lowering their uncompensated care by billions of dollars, the hospital industry agreed to give up future Medicare funds designed to help them cope with the uninsured. Showing the industry’s prowess on Capitol Hill, Congress has delayed those funding cuts for more than six years.
Jacob Hacker, a Yale University political scientist, noted that expanding Medicare would reduce the number of Americans who rely on employer-sponsored coverage. The pitfalls of the employer system were highlighted in 2020 as millions lost their jobs and workplace health coverage.
Even if they can win the two Georgia seats and take control of the Senate with the vice president breaking any ties, Democrats would be unlikely to pass major legislation without GOP support — unless they are willing to jettison the long-standing filibuster rule so they can pass most legislation with a simple 51-vote majority instead of 60 votes.
Hacker said that slim margin would make it difficult for Democrats to deal with many health issues all at once.
“Congress is not good at parallel processing,” Hacker said, referring to handling multiple priorities at the same time. “And the window is relatively short.”
KHN (Kaiser Health News) is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
Dripping, dabbing, and bongs: Can’t tell the players without a scorecard
E-cigarettes may be synonymous with vaping to most physicians, but there are other ways for patients to inhale nicotine or tetrahydrocannabinol-containing aerosols, according to investigators at the Cleveland Clinic. 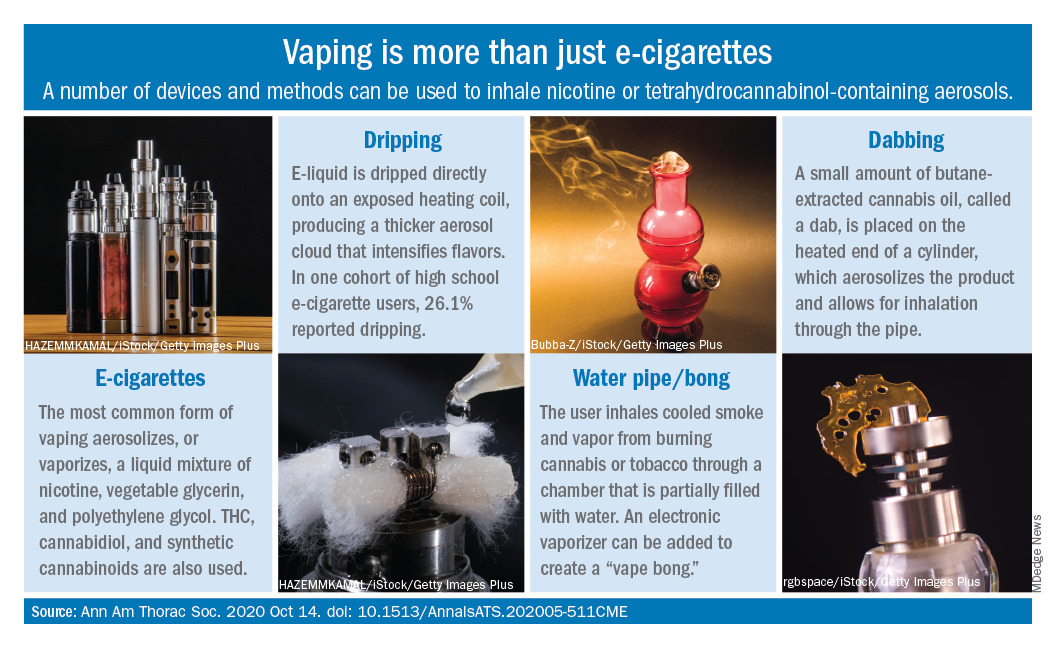
Humberto Choi, MD, and associates wrote in the Annals of the American Thoracic Society.
These “alternate aerosol inhalation methods” have been poorly described thus far, so little is known about their scope of use and potential health impact, they noted.
Dripping involves an e-cigarette modified to expose the heating coil. The e-cigarette liquid is dripped directly onto the hot coil, which produces immediate aerosolization and results in a thicker cloud.
Dripping “may expose users to higher levels of nicotine compared to e-cigarette inhalation” and lead to “increased release of volatile aldehydes as a result of the higher heating potential of direct atomizer exposure,” the investigators suggested.
Water pipes, or bongs, produce both smoke and vapor, although an electronic vaporizer can be attached to create a “vape bong.” About 21% of daily cannabis users report using a bong, but tobacco inhalation is less common. Cases of severe pulmonary infections have been associated with bong use, along with a couple of tuberculosis clusters, Dr. Choi and associates said.
Dabbing uses butane-extracted, concentrated cannabis oil inhaled through a modified water pipe or bong or a smaller device called a “dab pen.” A small amount, or “dab,” of the product is placed on the “nail,” which replaces the bowl of the water pipe, heated with a blowtorch, and inhaled through the pipe, the researchers explained.
The prevalence of dabbing is unknown, but “the most recent Monitoring the Future survey of high school seniors shows that 11.9% of students have used a marijuana vaporizer at some point in their life,” they said.
Besides the fire risks involved in creating the material needed for dabbing – use of heating plates, ovens, and devices for removing butane vapors – inhalation of residual butane vapors could lead to vomiting, cardiac arrhythmias, acute encephalopathy, and respiratory depression, Dr. Choi and associates said.
Nicotine dependence is also a concern, as is the possibility of withdrawal symptoms. “Patients presenting with prolonged and severe vomiting, psychotic symptoms, or other acute neuropsychiatric symptoms should raise the suspicion of [tetrahydrocannabinol]-containing products especially synthetic cannabinoids,” they wrote.
SOURCE: Choi H et al. Ann Am Thorac Soc. 2020 Oct 14. doi: 10.1513/AnnalsATS.202005-511CME.
E-cigarettes may be synonymous with vaping to most physicians, but there are other ways for patients to inhale nicotine or tetrahydrocannabinol-containing aerosols, according to investigators at the Cleveland Clinic.
Humberto Choi, MD, and associates wrote in the Annals of the American Thoracic Society.
These “alternate aerosol inhalation methods” have been poorly described thus far, so little is known about their scope of use and potential health impact, they noted.
Dripping involves an e-cigarette modified to expose the heating coil. The e-cigarette liquid is dripped directly onto the hot coil, which produces immediate aerosolization and results in a thicker cloud.
Dripping “may expose users to higher levels of nicotine compared to e-cigarette inhalation” and lead to “increased release of volatile aldehydes as a result of the higher heating potential of direct atomizer exposure,” the investigators suggested.
Water pipes, or bongs, produce both smoke and vapor, although an electronic vaporizer can be attached to create a “vape bong.” About 21% of daily cannabis users report using a bong, but tobacco inhalation is less common. Cases of severe pulmonary infections have been associated with bong use, along with a couple of tuberculosis clusters, Dr. Choi and associates said.
Dabbing uses butane-extracted, concentrated cannabis oil inhaled through a modified water pipe or bong or a smaller device called a “dab pen.” A small amount, or “dab,” of the product is placed on the “nail,” which replaces the bowl of the water pipe, heated with a blowtorch, and inhaled through the pipe, the researchers explained.
The prevalence of dabbing is unknown, but “the most recent Monitoring the Future survey of high school seniors shows that 11.9% of students have used a marijuana vaporizer at some point in their life,” they said.
Besides the fire risks involved in creating the material needed for dabbing – use of heating plates, ovens, and devices for removing butane vapors – inhalation of residual butane vapors could lead to vomiting, cardiac arrhythmias, acute encephalopathy, and respiratory depression, Dr. Choi and associates said.
Nicotine dependence is also a concern, as is the possibility of withdrawal symptoms. “Patients presenting with prolonged and severe vomiting, psychotic symptoms, or other acute neuropsychiatric symptoms should raise the suspicion of [tetrahydrocannabinol]-containing products especially synthetic cannabinoids,” they wrote.
SOURCE: Choi H et al. Ann Am Thorac Soc. 2020 Oct 14. doi: 10.1513/AnnalsATS.202005-511CME.
E-cigarettes may be synonymous with vaping to most physicians, but there are other ways for patients to inhale nicotine or tetrahydrocannabinol-containing aerosols, according to investigators at the Cleveland Clinic.
Humberto Choi, MD, and associates wrote in the Annals of the American Thoracic Society.
These “alternate aerosol inhalation methods” have been poorly described thus far, so little is known about their scope of use and potential health impact, they noted.
Dripping involves an e-cigarette modified to expose the heating coil. The e-cigarette liquid is dripped directly onto the hot coil, which produces immediate aerosolization and results in a thicker cloud.
Dripping “may expose users to higher levels of nicotine compared to e-cigarette inhalation” and lead to “increased release of volatile aldehydes as a result of the higher heating potential of direct atomizer exposure,” the investigators suggested.
Water pipes, or bongs, produce both smoke and vapor, although an electronic vaporizer can be attached to create a “vape bong.” About 21% of daily cannabis users report using a bong, but tobacco inhalation is less common. Cases of severe pulmonary infections have been associated with bong use, along with a couple of tuberculosis clusters, Dr. Choi and associates said.
Dabbing uses butane-extracted, concentrated cannabis oil inhaled through a modified water pipe or bong or a smaller device called a “dab pen.” A small amount, or “dab,” of the product is placed on the “nail,” which replaces the bowl of the water pipe, heated with a blowtorch, and inhaled through the pipe, the researchers explained.
The prevalence of dabbing is unknown, but “the most recent Monitoring the Future survey of high school seniors shows that 11.9% of students have used a marijuana vaporizer at some point in their life,” they said.
Besides the fire risks involved in creating the material needed for dabbing – use of heating plates, ovens, and devices for removing butane vapors – inhalation of residual butane vapors could lead to vomiting, cardiac arrhythmias, acute encephalopathy, and respiratory depression, Dr. Choi and associates said.
Nicotine dependence is also a concern, as is the possibility of withdrawal symptoms. “Patients presenting with prolonged and severe vomiting, psychotic symptoms, or other acute neuropsychiatric symptoms should raise the suspicion of [tetrahydrocannabinol]-containing products especially synthetic cannabinoids,” they wrote.
SOURCE: Choi H et al. Ann Am Thorac Soc. 2020 Oct 14. doi: 10.1513/AnnalsATS.202005-511CME.
FROM ANNALS OF THE AMERICAN THORACIC SOCIETY
Search for a snakebite drug might lead to a COVID treatment, too
Matthew Lewin, MD, PhD, founder of the Center for Exploration and Travel Health at the California Academy of Sciences, was researching snakebite treatments in rural locations in preparation for an expedition to the Philippines in 2011.
The story of a renowned herpetologist from the academy, Joseph Slowinski, who was bitten by a highly venomous krait in Myanmar and couldn’t get to a hospital in time to save his life a decade earlier, weighed on the emergency room doctor.
“I concluded that I needed something small and compact and that doesn’t care what kind of snake,” Dr. Lewin said.
It didn’t exist. That set Dr. Lewin in pursuit of a modern snakebite drug, a journey that finds his Corte Madera, Calif., company, Ophirex, nearing a promising oral treatment that fits in a pocket; is stable, easy to use, and affordable; and treats the venom from many species. “That’s the holy grail of snakebite treatment,” he said.
His work has gotten a boost with multimillion-dollar grants from a British charity and the U.S. Army. If it works – and it has been shown to work extremely well in mice and pigs – it could save tens of thousands of lives a year.
Dr. Lewin and Ophirex are not alone in their quest. Snakebites kill nearly 140,000 people a year, overwhelmingly in impoverished rural areas of Asia and Africa without adequate medical infrastructure and knowledge to administer antivenom. Though just a few people die each year in the United States from snakebites, the problem has risen to the top of the list of global health concerns in recent years. Funding has soared, and other research groups have also done promising work on new treatments. Herpetologists say deforestation and climate change are increasing human-snake encounters by forcing snakes to move to new habitats.
Dr. Lewin’s research is centered on a drug called varespladib. The enzyme inhibitor has proven itself in in-vitro lab studies and has effectively saved mice and pigs dosed with venom.
Along the way, Dr. Lewin and his team have come across another potential use for the drug. Varespladib has a positive effect on acute respiratory distress syndrome, associated with COVID-19. Next year, Ophirex will conduct human trials for the possible treatment of the condition funded with $9.9 million from the Army.
The link to a snakebite? The inflammation of the lungs caused by the coronavirus produces the sPLA2 enzyme. A more deadly version of the same enzyme is produced by snake venom.
The other companies that have come up with promising approaches to snakebite aren’t as far along as Ophirex. At the University of California-Irvine, chemist Ken Shea and his team created a nanogel – a kind of polymer used in medical applications – that blocks key proteins in the venom that cause cell destruction. At the Technical University of Denmark, Copenhagen, Andreas Laustsen is looking at engineering bacteria to manufacture anti-venom in fermentation tanks.
The days of incising a snakebite and sucking out the poison are long over, but the current treatment for venomous snakebites remains archaic.
Since the early 1900s, antivenom has been made by injecting horses or other animals with venom milked from snakes and diluted. The animals’ immune systems generate antibodies over several months, and blood plasma is taken from the animals and antibodies extracted from it.
It’s extremely expensive. Hospitals in the United States can charge as much as $15,000 a vial – and a single snakebite might require anywhere from 4 to 50 vials. Moreover, antivenom exists for little more than half the world’s species of venomous snakes.
A major problem is the roughly 2 hours it takes on average for a snakebite victim to reach a hospital and begin treatment. The chemical weapon that is venom starts immediately to destroy cells as it digests its next meal, making fast treatment essential to saving lives and preventing tissue loss.
“The two-hour window between fang and needle is where the most damage occurs,” said Leslie Boyer, director of the University of Arizona’s Venom Immunochemistry, Pharmacology and Emergency Response (VIPER) Institute. “We have a saying, ‘Time is tissue.’ ”
That’s why the search for a new snakebite drug has focused on an inexpensive treatment that can be taken into the field. Dr. Lewin’s drug wouldn’t replace antivenom. Instead, he thinks of it as the first line of defense until the victim can reach a hospital for antivenom treatment.
Dr. Lewin said he expects the drug to be inexpensive, so people in regions where snakebites are common can afford it.
Venom is extremely complicated chemically, and Dr. Lewin began his search by sussing out which of its myriad components to block. He zeroed in on the sPLA2 enzyme.
Surveying the literature about drugs that had been clinically tested for other conditions, he came across varespladib. It had been developed jointly by Eli Lilly and Shionogi, a Japanese pharmaceutical company, as a possible treatment for sepsis. They had never taken it to market.
If it worked, Dr. Lewin could license the right to produce the drug, which had already been thoroughly studied and was shown to be safe.
He placed venom in an array of test tubes. Varespladib and other drugs were added to the venom. He then added a reagent. If the venom was still active, the solution would turn yellow; if it was neutralized, it would remain clear.
The vials with varespladib “came up completely blank,” he said. “It was so stunning I said, ‘I must have made a mistake.’ ”
With a small grant, he sent the drug to the Yale Center for Molecular Discovery and found that varespladib effectively neutralized the venom of snakes found on six continents. The results were published in the journal Toxins and sent ripples through the small community of snakebite researchers.
Dr. Lewin then conducted tests on mice and pigs. Both were successful.
Human clinical trials are next, but they have been delayed by the pandemic. They are scheduled to get underway next spring.
Along the way, Dr. Lewin was fortunate enough to make some good connections that led to funding. In 2012, he attended a party at the Mill Valley, Calif., home of Jerry Harrison, the former guitarist and keyboardist for Talking Heads. Mr. Harrison had long been interested in business and start-ups – he said he was the most careful reader of the ’80s band’s contracts – and at the party he asked “if anyone had any ideas lying fallow,” Mr. Harrison said.
“And Matt pipes up and says, ‘I have this idea how to prevent people from dying from snakebites,’ ” Mr. Harrison said.
The musician said he was a bit taken aback by such an unusual and dire problem, but “I thought if it can save lives we have to do it,” he said. He became an investor and cofounder of Ophirex with Dr. Lewin.
Dr. Lewin met Lt. Col. Rebecca Carter, a biochemist who was assigned to lead the Medical Modernization Division of Air Force Special Operations Command, in 2016 when she attended a Venom Week conference in Greenville, N.C. He was presenting the results of his mouse studies. She told him about her first mission: to find a universal antivenom for medics on special operations teams in Africa. She persuaded the Special Operations Command Biomedical Research Advisory Group, which specializes in getting critical projects to production, to grant Ophirex $148,000 in 2017. She later retired from the Air Force and now works for Ophirex as vice president.
More multimillion-dollar grants followed, including the Army’s COVID grant. Clinical trials are scheduled to begin this winter.
Despite the progress and the sudden cash flow, Dr. Lewin tamps down talk of a universal snakebite cure. “There’s enough evidence to say the drug deserves to have its day in clinical trials,” he said.
KHN (Kaiser Health News) is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
Matthew Lewin, MD, PhD, founder of the Center for Exploration and Travel Health at the California Academy of Sciences, was researching snakebite treatments in rural locations in preparation for an expedition to the Philippines in 2011.
The story of a renowned herpetologist from the academy, Joseph Slowinski, who was bitten by a highly venomous krait in Myanmar and couldn’t get to a hospital in time to save his life a decade earlier, weighed on the emergency room doctor.
“I concluded that I needed something small and compact and that doesn’t care what kind of snake,” Dr. Lewin said.
It didn’t exist. That set Dr. Lewin in pursuit of a modern snakebite drug, a journey that finds his Corte Madera, Calif., company, Ophirex, nearing a promising oral treatment that fits in a pocket; is stable, easy to use, and affordable; and treats the venom from many species. “That’s the holy grail of snakebite treatment,” he said.
His work has gotten a boost with multimillion-dollar grants from a British charity and the U.S. Army. If it works – and it has been shown to work extremely well in mice and pigs – it could save tens of thousands of lives a year.
Dr. Lewin and Ophirex are not alone in their quest. Snakebites kill nearly 140,000 people a year, overwhelmingly in impoverished rural areas of Asia and Africa without adequate medical infrastructure and knowledge to administer antivenom. Though just a few people die each year in the United States from snakebites, the problem has risen to the top of the list of global health concerns in recent years. Funding has soared, and other research groups have also done promising work on new treatments. Herpetologists say deforestation and climate change are increasing human-snake encounters by forcing snakes to move to new habitats.
Dr. Lewin’s research is centered on a drug called varespladib. The enzyme inhibitor has proven itself in in-vitro lab studies and has effectively saved mice and pigs dosed with venom.
Along the way, Dr. Lewin and his team have come across another potential use for the drug. Varespladib has a positive effect on acute respiratory distress syndrome, associated with COVID-19. Next year, Ophirex will conduct human trials for the possible treatment of the condition funded with $9.9 million from the Army.
The link to a snakebite? The inflammation of the lungs caused by the coronavirus produces the sPLA2 enzyme. A more deadly version of the same enzyme is produced by snake venom.
The other companies that have come up with promising approaches to snakebite aren’t as far along as Ophirex. At the University of California-Irvine, chemist Ken Shea and his team created a nanogel – a kind of polymer used in medical applications – that blocks key proteins in the venom that cause cell destruction. At the Technical University of Denmark, Copenhagen, Andreas Laustsen is looking at engineering bacteria to manufacture anti-venom in fermentation tanks.
The days of incising a snakebite and sucking out the poison are long over, but the current treatment for venomous snakebites remains archaic.
Since the early 1900s, antivenom has been made by injecting horses or other animals with venom milked from snakes and diluted. The animals’ immune systems generate antibodies over several months, and blood plasma is taken from the animals and antibodies extracted from it.
It’s extremely expensive. Hospitals in the United States can charge as much as $15,000 a vial – and a single snakebite might require anywhere from 4 to 50 vials. Moreover, antivenom exists for little more than half the world’s species of venomous snakes.
A major problem is the roughly 2 hours it takes on average for a snakebite victim to reach a hospital and begin treatment. The chemical weapon that is venom starts immediately to destroy cells as it digests its next meal, making fast treatment essential to saving lives and preventing tissue loss.
“The two-hour window between fang and needle is where the most damage occurs,” said Leslie Boyer, director of the University of Arizona’s Venom Immunochemistry, Pharmacology and Emergency Response (VIPER) Institute. “We have a saying, ‘Time is tissue.’ ”
That’s why the search for a new snakebite drug has focused on an inexpensive treatment that can be taken into the field. Dr. Lewin’s drug wouldn’t replace antivenom. Instead, he thinks of it as the first line of defense until the victim can reach a hospital for antivenom treatment.
Dr. Lewin said he expects the drug to be inexpensive, so people in regions where snakebites are common can afford it.
Venom is extremely complicated chemically, and Dr. Lewin began his search by sussing out which of its myriad components to block. He zeroed in on the sPLA2 enzyme.
Surveying the literature about drugs that had been clinically tested for other conditions, he came across varespladib. It had been developed jointly by Eli Lilly and Shionogi, a Japanese pharmaceutical company, as a possible treatment for sepsis. They had never taken it to market.
If it worked, Dr. Lewin could license the right to produce the drug, which had already been thoroughly studied and was shown to be safe.
He placed venom in an array of test tubes. Varespladib and other drugs were added to the venom. He then added a reagent. If the venom was still active, the solution would turn yellow; if it was neutralized, it would remain clear.
The vials with varespladib “came up completely blank,” he said. “It was so stunning I said, ‘I must have made a mistake.’ ”
With a small grant, he sent the drug to the Yale Center for Molecular Discovery and found that varespladib effectively neutralized the venom of snakes found on six continents. The results were published in the journal Toxins and sent ripples through the small community of snakebite researchers.
Dr. Lewin then conducted tests on mice and pigs. Both were successful.
Human clinical trials are next, but they have been delayed by the pandemic. They are scheduled to get underway next spring.
Along the way, Dr. Lewin was fortunate enough to make some good connections that led to funding. In 2012, he attended a party at the Mill Valley, Calif., home of Jerry Harrison, the former guitarist and keyboardist for Talking Heads. Mr. Harrison had long been interested in business and start-ups – he said he was the most careful reader of the ’80s band’s contracts – and at the party he asked “if anyone had any ideas lying fallow,” Mr. Harrison said.
“And Matt pipes up and says, ‘I have this idea how to prevent people from dying from snakebites,’ ” Mr. Harrison said.
The musician said he was a bit taken aback by such an unusual and dire problem, but “I thought if it can save lives we have to do it,” he said. He became an investor and cofounder of Ophirex with Dr. Lewin.
Dr. Lewin met Lt. Col. Rebecca Carter, a biochemist who was assigned to lead the Medical Modernization Division of Air Force Special Operations Command, in 2016 when she attended a Venom Week conference in Greenville, N.C. He was presenting the results of his mouse studies. She told him about her first mission: to find a universal antivenom for medics on special operations teams in Africa. She persuaded the Special Operations Command Biomedical Research Advisory Group, which specializes in getting critical projects to production, to grant Ophirex $148,000 in 2017. She later retired from the Air Force and now works for Ophirex as vice president.
More multimillion-dollar grants followed, including the Army’s COVID grant. Clinical trials are scheduled to begin this winter.
Despite the progress and the sudden cash flow, Dr. Lewin tamps down talk of a universal snakebite cure. “There’s enough evidence to say the drug deserves to have its day in clinical trials,” he said.
KHN (Kaiser Health News) is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
Matthew Lewin, MD, PhD, founder of the Center for Exploration and Travel Health at the California Academy of Sciences, was researching snakebite treatments in rural locations in preparation for an expedition to the Philippines in 2011.
The story of a renowned herpetologist from the academy, Joseph Slowinski, who was bitten by a highly venomous krait in Myanmar and couldn’t get to a hospital in time to save his life a decade earlier, weighed on the emergency room doctor.
“I concluded that I needed something small and compact and that doesn’t care what kind of snake,” Dr. Lewin said.
It didn’t exist. That set Dr. Lewin in pursuit of a modern snakebite drug, a journey that finds his Corte Madera, Calif., company, Ophirex, nearing a promising oral treatment that fits in a pocket; is stable, easy to use, and affordable; and treats the venom from many species. “That’s the holy grail of snakebite treatment,” he said.
His work has gotten a boost with multimillion-dollar grants from a British charity and the U.S. Army. If it works – and it has been shown to work extremely well in mice and pigs – it could save tens of thousands of lives a year.
Dr. Lewin and Ophirex are not alone in their quest. Snakebites kill nearly 140,000 people a year, overwhelmingly in impoverished rural areas of Asia and Africa without adequate medical infrastructure and knowledge to administer antivenom. Though just a few people die each year in the United States from snakebites, the problem has risen to the top of the list of global health concerns in recent years. Funding has soared, and other research groups have also done promising work on new treatments. Herpetologists say deforestation and climate change are increasing human-snake encounters by forcing snakes to move to new habitats.
Dr. Lewin’s research is centered on a drug called varespladib. The enzyme inhibitor has proven itself in in-vitro lab studies and has effectively saved mice and pigs dosed with venom.
Along the way, Dr. Lewin and his team have come across another potential use for the drug. Varespladib has a positive effect on acute respiratory distress syndrome, associated with COVID-19. Next year, Ophirex will conduct human trials for the possible treatment of the condition funded with $9.9 million from the Army.
The link to a snakebite? The inflammation of the lungs caused by the coronavirus produces the sPLA2 enzyme. A more deadly version of the same enzyme is produced by snake venom.
The other companies that have come up with promising approaches to snakebite aren’t as far along as Ophirex. At the University of California-Irvine, chemist Ken Shea and his team created a nanogel – a kind of polymer used in medical applications – that blocks key proteins in the venom that cause cell destruction. At the Technical University of Denmark, Copenhagen, Andreas Laustsen is looking at engineering bacteria to manufacture anti-venom in fermentation tanks.
The days of incising a snakebite and sucking out the poison are long over, but the current treatment for venomous snakebites remains archaic.
Since the early 1900s, antivenom has been made by injecting horses or other animals with venom milked from snakes and diluted. The animals’ immune systems generate antibodies over several months, and blood plasma is taken from the animals and antibodies extracted from it.
It’s extremely expensive. Hospitals in the United States can charge as much as $15,000 a vial – and a single snakebite might require anywhere from 4 to 50 vials. Moreover, antivenom exists for little more than half the world’s species of venomous snakes.
A major problem is the roughly 2 hours it takes on average for a snakebite victim to reach a hospital and begin treatment. The chemical weapon that is venom starts immediately to destroy cells as it digests its next meal, making fast treatment essential to saving lives and preventing tissue loss.
“The two-hour window between fang and needle is where the most damage occurs,” said Leslie Boyer, director of the University of Arizona’s Venom Immunochemistry, Pharmacology and Emergency Response (VIPER) Institute. “We have a saying, ‘Time is tissue.’ ”
That’s why the search for a new snakebite drug has focused on an inexpensive treatment that can be taken into the field. Dr. Lewin’s drug wouldn’t replace antivenom. Instead, he thinks of it as the first line of defense until the victim can reach a hospital for antivenom treatment.
Dr. Lewin said he expects the drug to be inexpensive, so people in regions where snakebites are common can afford it.
Venom is extremely complicated chemically, and Dr. Lewin began his search by sussing out which of its myriad components to block. He zeroed in on the sPLA2 enzyme.
Surveying the literature about drugs that had been clinically tested for other conditions, he came across varespladib. It had been developed jointly by Eli Lilly and Shionogi, a Japanese pharmaceutical company, as a possible treatment for sepsis. They had never taken it to market.
If it worked, Dr. Lewin could license the right to produce the drug, which had already been thoroughly studied and was shown to be safe.
He placed venom in an array of test tubes. Varespladib and other drugs were added to the venom. He then added a reagent. If the venom was still active, the solution would turn yellow; if it was neutralized, it would remain clear.
The vials with varespladib “came up completely blank,” he said. “It was so stunning I said, ‘I must have made a mistake.’ ”
With a small grant, he sent the drug to the Yale Center for Molecular Discovery and found that varespladib effectively neutralized the venom of snakes found on six continents. The results were published in the journal Toxins and sent ripples through the small community of snakebite researchers.
Dr. Lewin then conducted tests on mice and pigs. Both were successful.
Human clinical trials are next, but they have been delayed by the pandemic. They are scheduled to get underway next spring.
Along the way, Dr. Lewin was fortunate enough to make some good connections that led to funding. In 2012, he attended a party at the Mill Valley, Calif., home of Jerry Harrison, the former guitarist and keyboardist for Talking Heads. Mr. Harrison had long been interested in business and start-ups – he said he was the most careful reader of the ’80s band’s contracts – and at the party he asked “if anyone had any ideas lying fallow,” Mr. Harrison said.
“And Matt pipes up and says, ‘I have this idea how to prevent people from dying from snakebites,’ ” Mr. Harrison said.
The musician said he was a bit taken aback by such an unusual and dire problem, but “I thought if it can save lives we have to do it,” he said. He became an investor and cofounder of Ophirex with Dr. Lewin.
Dr. Lewin met Lt. Col. Rebecca Carter, a biochemist who was assigned to lead the Medical Modernization Division of Air Force Special Operations Command, in 2016 when she attended a Venom Week conference in Greenville, N.C. He was presenting the results of his mouse studies. She told him about her first mission: to find a universal antivenom for medics on special operations teams in Africa. She persuaded the Special Operations Command Biomedical Research Advisory Group, which specializes in getting critical projects to production, to grant Ophirex $148,000 in 2017. She later retired from the Air Force and now works for Ophirex as vice president.
More multimillion-dollar grants followed, including the Army’s COVID grant. Clinical trials are scheduled to begin this winter.
Despite the progress and the sudden cash flow, Dr. Lewin tamps down talk of a universal snakebite cure. “There’s enough evidence to say the drug deserves to have its day in clinical trials,” he said.
KHN (Kaiser Health News) is a nonprofit news service covering health issues. It is an editorially independent program of KFF (Kaiser Family Foundation), which is not affiliated with Kaiser Permanente.
Moral distress: COVID-19 shortages prompt tough decisions at bedside
Choosing which hospitalized COVID-19 patients receive potentially lifesaving care, making urgent calls for ventilators and other equipment, and triaging care based on patient age and comorbidities were among the challenges revealed in new feedback from health care leaders and frontline workers.
Even though many hospitals have contingency plans for how to allocate resources and triage patient care during crisis capacity, for many providers during the real-world COVID-19 trial of these protocols, they fell short.
Many hospital crisis capacity plans, for example, were too general to address all the specific challenges arising during the pandemic, investigators report in a study published online Nov. 6 in JAMA Network Open.
“Our research shows that the types of challenges and approach to resource limitation in real-world clinical settings during the pandemic differed in practice from how we had prepared in theory,” lead author Catherine Butler, MD, told Medscape Medical News. Insufficient dialysis treatment time, staff shortages, and routine supply scarcity are examples “for which there was not an established plan or approach for appropriate allocation.”
“This left frontline clinicians to determine what constituted an acceptable standard of care and to make difficult allocation decisions at the bedside,” added Butler, acting instructor in the Division of Nephrology at the University of Washington in Seattle and a research fellow at the VA Health Services Research and Development Seattle-Denver Center of Innovation.
The investigators conducted semistructured interviews in April and May with 61 clinicians and health leaders. Mean age was 46 years, 63% were women, and participants practiced in 15 states. Most participants hailed from locations hard-hit by the pandemic at the time, including Seattle, New York City, and New Orleans.
Triage tribulations
The qualitative study included comments from respondents on three major themes that emerged: planning for crisis capacity, adapting to resource limitation, and the multiple unprecedented barriers to care delivery.
Overall, planning and support from institutional leaders varied. One provider said, “Talking to administration, and they just seemed really disengaged with the problem. We asked multiple times if there was a triage command center or a plan for what would occur if we got to the point where we had to triage resources. They said there was, but they wouldn’t provide it to us.”
Another had a more positive experience. “The biggest deal in the ethics world in the last 2 months has been preparing in case we need to triage. So, we have a very detailed, elaborate, well thought-out triage policy … that was done at the highest levels of the system.”
Clinicians said they participate on triage teams – despite the moral weight and likely emotional burden – out of a sense of duty.
Interestingly, some providers on these teams also reported a reluctance to reveal their participation to colleagues. “I didn’t feel like I should tell anybody … even some of my close friends who are physicians and nurses here … that I’ve been asked to be on this [triage team],” one respondent said. “I didn’t feel like I should make it known.”
Adapting to scarce resources
Multiple providers said they faced difficult care decisions because of limited dialysis or supply shortages. “They felt that this patient had the greatest likelihood of benefiting from most aggressive therapy. … I think there was probably like 5 or 6 patients in the ICU … and then you had this 35-year-old with no comorbidities,” one respondent said. “That’s who the ICU dialyzed, and I couldn’t really disagree.”
“I emailed all of [my colleagues], and I said ‘Help! We need X, we need CRRT [continuous renal replacement therapy] machines, we need dialysates,’ “ another responded.
“One of the attendings had a tweet when we were running out of CRRT. He had a tweet about, ‘Can anybody give us supplies for CRRT?’ So, it got to that. You do anything. You get really desperate,” the clinician said.
Other providers reported getting innovative under the circumstances. “My partner’s son, he actually borrowed a couple of 3D printers. He printed some of these face shields, and then they got the formula, or the specifics as to how to make this particular connection to connect to a dialysis machine to generate dialysate. So, he also printed some of those from the 3D printer.”
Dire situations with dialysis
Another respondent understood the focus on ventilators and ICU beds throughout the crisis, but said “no one has acknowledged that dialysis has been one of the most, if not the most, limited resources.”
Another clinician expressed surprise at a decision made in the face of limited availability of traditional dialysis. “A month ago, people said we were going to do acute peritoneal dialysis [PD]. And I said, ‘No, we’re not going to do acute PD. PD, it’s not that great for acute patients, sick people in the ICUs. I don’t think we’re going to do PD.’
“Three days later we were doing acute PD. I mean, that was unbelievable!”
Some institutions rationed dialysis therapy. “We went through the entire list at the beginning of the week and [said], this person has to dialyze these days, this person would probably benefit from a dialysis session, a third group person we could probably just string along and medically manage if we needed to,” one provider said.
Another respondent reported a different strategy. “No one was not getting dialysis, but there were a lot of people getting minimal dialysis. Even though people were getting treated, resources were very stretched.”
Changing family dynamics
COVID-19 has naturally changed how clinicians speak with families. One respondent recalled looking at the ICU physician and being like, ‘Have you talked to the son this week?’ And she’s like, ‘Oh my God, no. … Did you talk to the son?’ I’m like, ‘Oh my God, no.’ “
They realized, the respondent added, “that none of us had called the family because it’s just not in your workflow. You’re so used to the family being there.”
Multiple providers also feared a conversation with family regarding necessary changes to care given the limitation of resources during the pandemic.
“Most families have been actually very understanding. This is a crisis, and we’re in a pandemic, and we’re all doing things we wouldn’t normally do.”
Another respondent said, “We were pretty honest about how resources were limited and how we were doing with this COVID-19 surge. And I think we talked about how the usual ability to provide aggressive dialysis was not the case with COVID-19. There was a lot of understanding, sometimes to my surprise. I would think people would be more upset when hearing something like that.”
Many clinicians facing these challenges experience moral distress, the researchers noted.
“Early in the pandemic, it became quickly apparent that possible resource limitation, such as scarce ventilators, was a major ethical concern. There was robust debate and discussion published in medical journals and the popular press about how to appropriately allocate health care resources,” the University of Washington’s Butler said.
“Transparency, accountability, and standardized processes for rationing these resources in ‘crisis capacity’ settings were seen as key to avoiding the impact of implicit bias and moral distress for clinicians,” she added.
Lessons learned
In terms of potential solutions that could mitigate these challenges in the future, health care leaders “could develop standardized protocols or guidelines for allocating a broader range of potentially scarce health care resources even before ‘crisis capacity’ is declared,” Butler said.
Furthermore, no frontline worker should have to go it alone. “Medical ethicists and/or other clinicians familiar with ethical considerations in settings of scarce health care resources might provide bedside consultation and collaborate with frontline providers who must grapple with the impact of more subtle forms of resource limitation on clinical decision-making.”
The study was partially funded by grants from the National Institute of Diabetes and Digestive and Kidney Diseases and a COVID-19 Research Award from the University of Washington Institute of Translational Health Sciences given to Butler.
This article first appeared on Medscape.com.
Choosing which hospitalized COVID-19 patients receive potentially lifesaving care, making urgent calls for ventilators and other equipment, and triaging care based on patient age and comorbidities were among the challenges revealed in new feedback from health care leaders and frontline workers.
Even though many hospitals have contingency plans for how to allocate resources and triage patient care during crisis capacity, for many providers during the real-world COVID-19 trial of these protocols, they fell short.
Many hospital crisis capacity plans, for example, were too general to address all the specific challenges arising during the pandemic, investigators report in a study published online Nov. 6 in JAMA Network Open.
“Our research shows that the types of challenges and approach to resource limitation in real-world clinical settings during the pandemic differed in practice from how we had prepared in theory,” lead author Catherine Butler, MD, told Medscape Medical News. Insufficient dialysis treatment time, staff shortages, and routine supply scarcity are examples “for which there was not an established plan or approach for appropriate allocation.”
“This left frontline clinicians to determine what constituted an acceptable standard of care and to make difficult allocation decisions at the bedside,” added Butler, acting instructor in the Division of Nephrology at the University of Washington in Seattle and a research fellow at the VA Health Services Research and Development Seattle-Denver Center of Innovation.
The investigators conducted semistructured interviews in April and May with 61 clinicians and health leaders. Mean age was 46 years, 63% were women, and participants practiced in 15 states. Most participants hailed from locations hard-hit by the pandemic at the time, including Seattle, New York City, and New Orleans.
Triage tribulations
The qualitative study included comments from respondents on three major themes that emerged: planning for crisis capacity, adapting to resource limitation, and the multiple unprecedented barriers to care delivery.
Overall, planning and support from institutional leaders varied. One provider said, “Talking to administration, and they just seemed really disengaged with the problem. We asked multiple times if there was a triage command center or a plan for what would occur if we got to the point where we had to triage resources. They said there was, but they wouldn’t provide it to us.”
Another had a more positive experience. “The biggest deal in the ethics world in the last 2 months has been preparing in case we need to triage. So, we have a very detailed, elaborate, well thought-out triage policy … that was done at the highest levels of the system.”
Clinicians said they participate on triage teams – despite the moral weight and likely emotional burden – out of a sense of duty.
Interestingly, some providers on these teams also reported a reluctance to reveal their participation to colleagues. “I didn’t feel like I should tell anybody … even some of my close friends who are physicians and nurses here … that I’ve been asked to be on this [triage team],” one respondent said. “I didn’t feel like I should make it known.”
Adapting to scarce resources
Multiple providers said they faced difficult care decisions because of limited dialysis or supply shortages. “They felt that this patient had the greatest likelihood of benefiting from most aggressive therapy. … I think there was probably like 5 or 6 patients in the ICU … and then you had this 35-year-old with no comorbidities,” one respondent said. “That’s who the ICU dialyzed, and I couldn’t really disagree.”
“I emailed all of [my colleagues], and I said ‘Help! We need X, we need CRRT [continuous renal replacement therapy] machines, we need dialysates,’ “ another responded.
“One of the attendings had a tweet when we were running out of CRRT. He had a tweet about, ‘Can anybody give us supplies for CRRT?’ So, it got to that. You do anything. You get really desperate,” the clinician said.
Other providers reported getting innovative under the circumstances. “My partner’s son, he actually borrowed a couple of 3D printers. He printed some of these face shields, and then they got the formula, or the specifics as to how to make this particular connection to connect to a dialysis machine to generate dialysate. So, he also printed some of those from the 3D printer.”
Dire situations with dialysis
Another respondent understood the focus on ventilators and ICU beds throughout the crisis, but said “no one has acknowledged that dialysis has been one of the most, if not the most, limited resources.”
Another clinician expressed surprise at a decision made in the face of limited availability of traditional dialysis. “A month ago, people said we were going to do acute peritoneal dialysis [PD]. And I said, ‘No, we’re not going to do acute PD. PD, it’s not that great for acute patients, sick people in the ICUs. I don’t think we’re going to do PD.’
“Three days later we were doing acute PD. I mean, that was unbelievable!”
Some institutions rationed dialysis therapy. “We went through the entire list at the beginning of the week and [said], this person has to dialyze these days, this person would probably benefit from a dialysis session, a third group person we could probably just string along and medically manage if we needed to,” one provider said.
Another respondent reported a different strategy. “No one was not getting dialysis, but there were a lot of people getting minimal dialysis. Even though people were getting treated, resources were very stretched.”
Changing family dynamics
COVID-19 has naturally changed how clinicians speak with families. One respondent recalled looking at the ICU physician and being like, ‘Have you talked to the son this week?’ And she’s like, ‘Oh my God, no. … Did you talk to the son?’ I’m like, ‘Oh my God, no.’ “
They realized, the respondent added, “that none of us had called the family because it’s just not in your workflow. You’re so used to the family being there.”
Multiple providers also feared a conversation with family regarding necessary changes to care given the limitation of resources during the pandemic.
“Most families have been actually very understanding. This is a crisis, and we’re in a pandemic, and we’re all doing things we wouldn’t normally do.”
Another respondent said, “We were pretty honest about how resources were limited and how we were doing with this COVID-19 surge. And I think we talked about how the usual ability to provide aggressive dialysis was not the case with COVID-19. There was a lot of understanding, sometimes to my surprise. I would think people would be more upset when hearing something like that.”
Many clinicians facing these challenges experience moral distress, the researchers noted.
“Early in the pandemic, it became quickly apparent that possible resource limitation, such as scarce ventilators, was a major ethical concern. There was robust debate and discussion published in medical journals and the popular press about how to appropriately allocate health care resources,” the University of Washington’s Butler said.
“Transparency, accountability, and standardized processes for rationing these resources in ‘crisis capacity’ settings were seen as key to avoiding the impact of implicit bias and moral distress for clinicians,” she added.
Lessons learned
In terms of potential solutions that could mitigate these challenges in the future, health care leaders “could develop standardized protocols or guidelines for allocating a broader range of potentially scarce health care resources even before ‘crisis capacity’ is declared,” Butler said.
Furthermore, no frontline worker should have to go it alone. “Medical ethicists and/or other clinicians familiar with ethical considerations in settings of scarce health care resources might provide bedside consultation and collaborate with frontline providers who must grapple with the impact of more subtle forms of resource limitation on clinical decision-making.”
The study was partially funded by grants from the National Institute of Diabetes and Digestive and Kidney Diseases and a COVID-19 Research Award from the University of Washington Institute of Translational Health Sciences given to Butler.
This article first appeared on Medscape.com.
Choosing which hospitalized COVID-19 patients receive potentially lifesaving care, making urgent calls for ventilators and other equipment, and triaging care based on patient age and comorbidities were among the challenges revealed in new feedback from health care leaders and frontline workers.
Even though many hospitals have contingency plans for how to allocate resources and triage patient care during crisis capacity, for many providers during the real-world COVID-19 trial of these protocols, they fell short.
Many hospital crisis capacity plans, for example, were too general to address all the specific challenges arising during the pandemic, investigators report in a study published online Nov. 6 in JAMA Network Open.
“Our research shows that the types of challenges and approach to resource limitation in real-world clinical settings during the pandemic differed in practice from how we had prepared in theory,” lead author Catherine Butler, MD, told Medscape Medical News. Insufficient dialysis treatment time, staff shortages, and routine supply scarcity are examples “for which there was not an established plan or approach for appropriate allocation.”
“This left frontline clinicians to determine what constituted an acceptable standard of care and to make difficult allocation decisions at the bedside,” added Butler, acting instructor in the Division of Nephrology at the University of Washington in Seattle and a research fellow at the VA Health Services Research and Development Seattle-Denver Center of Innovation.
The investigators conducted semistructured interviews in April and May with 61 clinicians and health leaders. Mean age was 46 years, 63% were women, and participants practiced in 15 states. Most participants hailed from locations hard-hit by the pandemic at the time, including Seattle, New York City, and New Orleans.
Triage tribulations
The qualitative study included comments from respondents on three major themes that emerged: planning for crisis capacity, adapting to resource limitation, and the multiple unprecedented barriers to care delivery.
Overall, planning and support from institutional leaders varied. One provider said, “Talking to administration, and they just seemed really disengaged with the problem. We asked multiple times if there was a triage command center or a plan for what would occur if we got to the point where we had to triage resources. They said there was, but they wouldn’t provide it to us.”
Another had a more positive experience. “The biggest deal in the ethics world in the last 2 months has been preparing in case we need to triage. So, we have a very detailed, elaborate, well thought-out triage policy … that was done at the highest levels of the system.”
Clinicians said they participate on triage teams – despite the moral weight and likely emotional burden – out of a sense of duty.
Interestingly, some providers on these teams also reported a reluctance to reveal their participation to colleagues. “I didn’t feel like I should tell anybody … even some of my close friends who are physicians and nurses here … that I’ve been asked to be on this [triage team],” one respondent said. “I didn’t feel like I should make it known.”
Adapting to scarce resources
Multiple providers said they faced difficult care decisions because of limited dialysis or supply shortages. “They felt that this patient had the greatest likelihood of benefiting from most aggressive therapy. … I think there was probably like 5 or 6 patients in the ICU … and then you had this 35-year-old with no comorbidities,” one respondent said. “That’s who the ICU dialyzed, and I couldn’t really disagree.”
“I emailed all of [my colleagues], and I said ‘Help! We need X, we need CRRT [continuous renal replacement therapy] machines, we need dialysates,’ “ another responded.
“One of the attendings had a tweet when we were running out of CRRT. He had a tweet about, ‘Can anybody give us supplies for CRRT?’ So, it got to that. You do anything. You get really desperate,” the clinician said.
Other providers reported getting innovative under the circumstances. “My partner’s son, he actually borrowed a couple of 3D printers. He printed some of these face shields, and then they got the formula, or the specifics as to how to make this particular connection to connect to a dialysis machine to generate dialysate. So, he also printed some of those from the 3D printer.”
Dire situations with dialysis
Another respondent understood the focus on ventilators and ICU beds throughout the crisis, but said “no one has acknowledged that dialysis has been one of the most, if not the most, limited resources.”
Another clinician expressed surprise at a decision made in the face of limited availability of traditional dialysis. “A month ago, people said we were going to do acute peritoneal dialysis [PD]. And I said, ‘No, we’re not going to do acute PD. PD, it’s not that great for acute patients, sick people in the ICUs. I don’t think we’re going to do PD.’
“Three days later we were doing acute PD. I mean, that was unbelievable!”
Some institutions rationed dialysis therapy. “We went through the entire list at the beginning of the week and [said], this person has to dialyze these days, this person would probably benefit from a dialysis session, a third group person we could probably just string along and medically manage if we needed to,” one provider said.
Another respondent reported a different strategy. “No one was not getting dialysis, but there were a lot of people getting minimal dialysis. Even though people were getting treated, resources were very stretched.”
Changing family dynamics
COVID-19 has naturally changed how clinicians speak with families. One respondent recalled looking at the ICU physician and being like, ‘Have you talked to the son this week?’ And she’s like, ‘Oh my God, no. … Did you talk to the son?’ I’m like, ‘Oh my God, no.’ “
They realized, the respondent added, “that none of us had called the family because it’s just not in your workflow. You’re so used to the family being there.”
Multiple providers also feared a conversation with family regarding necessary changes to care given the limitation of resources during the pandemic.
“Most families have been actually very understanding. This is a crisis, and we’re in a pandemic, and we’re all doing things we wouldn’t normally do.”
Another respondent said, “We were pretty honest about how resources were limited and how we were doing with this COVID-19 surge. And I think we talked about how the usual ability to provide aggressive dialysis was not the case with COVID-19. There was a lot of understanding, sometimes to my surprise. I would think people would be more upset when hearing something like that.”
Many clinicians facing these challenges experience moral distress, the researchers noted.
“Early in the pandemic, it became quickly apparent that possible resource limitation, such as scarce ventilators, was a major ethical concern. There was robust debate and discussion published in medical journals and the popular press about how to appropriately allocate health care resources,” the University of Washington’s Butler said.
“Transparency, accountability, and standardized processes for rationing these resources in ‘crisis capacity’ settings were seen as key to avoiding the impact of implicit bias and moral distress for clinicians,” she added.
Lessons learned
In terms of potential solutions that could mitigate these challenges in the future, health care leaders “could develop standardized protocols or guidelines for allocating a broader range of potentially scarce health care resources even before ‘crisis capacity’ is declared,” Butler said.
Furthermore, no frontline worker should have to go it alone. “Medical ethicists and/or other clinicians familiar with ethical considerations in settings of scarce health care resources might provide bedside consultation and collaborate with frontline providers who must grapple with the impact of more subtle forms of resource limitation on clinical decision-making.”
The study was partially funded by grants from the National Institute of Diabetes and Digestive and Kidney Diseases and a COVID-19 Research Award from the University of Washington Institute of Translational Health Sciences given to Butler.
This article first appeared on Medscape.com.
What happened to melanoma care during COVID-19 sequestration
Initial evidence suggests that the , Rebecca I. Hartman, MD, MPH, said at a virtual forum on cutaneous malignancies jointly presented by Postgraduate Institute for Medicine and Global Academy for Medication Education.

This is not what National Comprehensive Cancer Network officials expected when they issued short-term recommendations on how to manage cutaneous melanoma during the first wave of the COVID-19 pandemic. Those recommendations for restriction of care, which Dr. Hartman characterized as “pretty significant changes from how we typically practice melanoma care in the U.S.,” came at a time when there was justifiable concern that the first COVID-19 surge would strain the U.S. health care system beyond the breaking point.
The rationale given for the NCCN recommendations was that most time-to-treat studies have shown no adverse patient outcomes for 90-day delays in treatment, even for thicker melanomas. But those studies, all retrospective, have been called into question. And the first real-world data on the impact of care restrictions during the lockdown, reported by Italian dermatologists, highlights adverse effects with potentially far-reaching consequences, noted Dr. Hartman, director of melanoma epidemiology at Brigham and Women’s Hospital and a dermatologist, Harvard University, Boston.
Analysis of the impact of lockdown-induced delays in melanoma care is not merely an academic exercise, she added. While everyone hopes that the spring 2020 COVID-19 shelter-in-place was a once-in-a-lifetime event, there’s no guarantee that will be the case. Moreover, the lockdown provides a natural experiment addressing the possible consequences of melanoma care delays on patient outcomes, a topic that for ethical reasons could never be addressed in a randomized trial.
The short-term NCCN recommendations included the use of excisional biopsies for melanoma diagnosis whenever possible; and delay of up to 3 months for wide local excision of in situ melanoma, any invasive melanoma with negative margins, and even T1 melanomas with positive margins provided the bulk of the lesion had been excised. The guidance also suggested delaying sentinel lymph node biopsy (SLNB), along with increased use of neoadjuvant therapy in patients with clinically palpable regional lymph nodes in order to delay surgery for up to 8 weeks. Single-agent systemic therapy at the least-frequent dosing was advised in order to minimize toxicity and reduce the need for additional health care resources: for example, nivolumab (Opdivo) at 480 mg every 4 weeks instead of every 2 weeks, and pembrolizumab (Keytruda) at 400 mg every 6 weeks, rather than every 3 weeks.
So, that’s what the NCCN recommended. Here’s what actually happened during shelter-in-place as captured in Dr. Hartman’s survey of 18 U.S. members of the Melanoma Prevention Working Group, all practicing dermatology in centers particularly hard-hit in the first wave of the pandemic: In-person new melanoma patient visits plunged from an average of 4.83 per week per provider to 0.83 per week. Telemedicine visits with new melanoma patients went from zero prepandemic to 0.67 visits per week per provider, which doesn’t come close to making up for the drop in in-person visits. Interestingly, two respondents reported turning to gene-expression profile testing for patient prognostication because of delays in SLNB.
Wide local excision was delayed by an average of 6 weeks in roughly one-third of melanoma patients with early tumor stage disease, regardless of margin status. For patients with stage T1b disease, wide local excision was typically performed on time during shelter-in-place; however, SLNB was delayed by an average of 5 weeks in 22% of patients with positive margins and 28% of those with negative margins. In contrast, 80% of patients with more advanced T2-T4 melanoma underwent on-schedule definitive management with wide local excision and SLNB, Dr. Hartman reported.
Critics have taken issue with the NCCN’s conclusion that most time-to-treatment studies show no harm arising from 90-day treatment delays. A review of the relevant published literature by Dr. Hartman’s Harvard colleagues, published in July, found that the evidence is mixed. “There is insufficient evidence to definitively conclude that delayed wide resection after gross removal of the primary melanoma is without harm,” they concluded in the review.
Spanish dermatologists performed a modeling study in order to estimate the potential impact of COVID-19 lockdowns on 5- and 10-year survival of melanoma patients. Using the growth rate of a random sample of 1,000 melanomas to model estimates of tumor thickness after various delays, coupled with American Joint Committee on Cancer survival data for different T stages, they estimated that 5-year survival would be reduced from 94.2% to 92.3% with a 90-day delay in diagnosis, and that 10-year survival would drop from 90.0% to 87.6%.
But that’s merely modeling. Francesco Ricci, MD, PhD, and colleagues from the melanoma unit at the Istituto Dermopatico dell’Immacolata, Rome, have provided a first look at the real-world impact of the lockdown. In the prelockdown period of January through March 9th, 2020, the referral center averaged 2.3 new melanoma diagnoses per day. During the Rome lockdown, from March 10th through May 3rd, this figure dropped to a mean of 0.6 melanoma diagnoses per day. Postlockdown, from May 4th to June 6th, the average climbed to 1.3 per day. The rate of newly diagnosed nodular melanoma was 5.5-fold greater postlockdown, compared with prelockdown; the rate of ulcerated melanoma was 4.9-fold greater.
“We can hypothesize that this may have been due to delays in diagnosis and care,” Dr. Hartman commented. “This is important because we know that nodular melanoma as well as ulceration tend to have a worse prognosis in terms of mortality.”
The mean Breslow thickness of newly diagnosed melanomas was 0.88 mm prelockdown, 0.66 mm during lockdown, and 1.96 mm postlockdown. The investigators speculated that the reduced Breslow thickness of melanomas diagnosed during lockdown might be explained by a greater willingness of more health-conscious people to defy the shelter-in-place instructions because of their concern about a suspicious skin lesion. “Though it is way too early to gauge the consequences of such diagnostic delay, should this issue be neglected, dermatologists and their patients may pay a higher price later with increased morbidity, mortality, and financial burden,” according to the investigators.
Dr. Hartman observed that it will be important to learn whether similar experiences occurred elsewhere during lockdown.

Another speaker, John M. Kirkwood, MD, said he has seen several melanoma patients referred from outside centers who had delays of up to 3 months in sentinel lymph node management of T2 and T3 tumors during lockdown who now have widespread metastatic disease.
“Now, is that anecdotal? I don’t know, it’s just worrisome to me,” commented Dr. Kirkwood, professor of medicine, dermatology, and translational science at the University of Pittsburgh.
Merrick Ross, MD, professor of surgical oncology at M.D. Anderson Cancer Center, Houston, recalled, “There was a period of time [during the lockdown] when we weren’t allowed to do certain elective procedures, if you want to call cancer surgery elective.”

“It’s too soon to talk about outcomes because a lot of patients are still in the process of being treated after what I would consider a significant delay in diagnosis,” the surgeon added.
An audience member asked if there will be an opportunity to see data on the damage done by delaying melanoma management as compared to lives saved through the lockdown for COVID-19. Dr. Ross replied that M.D. Anderson is in the midst of an institution-wide study analyzing the delay in diagnosis of a range of cancers.
“In our melanoma center it is absolutely clear, although we’re still collecting data, that the median tumor thickness is much higher since the lockdown,” Dr. Ross commented.
Dr. Hartman said she and her coinvestigators in the Melanoma Prevention Working Group are attempting to tally up the damage done via the lockdown by delaying melanoma diagnosis and treatment. But she agreed with the questioner that the most important thing is overall net lives saved through shelter-in-place.
“I’m sure that, separately, nondermatologists – perhaps infectious disease doctors and internists – are looking at how many lives were saved by the lockdown policy. So I do think all that data will come out,” Dr. Hartman predicted.
She reported having no financial conflicts regarding her presentation.
Global Academy for Medical Education and this news organization are owned by the same company.
SOURCE: Hartman, R. Cutaneous malignancies forum.
Initial evidence suggests that the , Rebecca I. Hartman, MD, MPH, said at a virtual forum on cutaneous malignancies jointly presented by Postgraduate Institute for Medicine and Global Academy for Medication Education.
This is not what National Comprehensive Cancer Network officials expected when they issued short-term recommendations on how to manage cutaneous melanoma during the first wave of the COVID-19 pandemic. Those recommendations for restriction of care, which Dr. Hartman characterized as “pretty significant changes from how we typically practice melanoma care in the U.S.,” came at a time when there was justifiable concern that the first COVID-19 surge would strain the U.S. health care system beyond the breaking point.
The rationale given for the NCCN recommendations was that most time-to-treat studies have shown no adverse patient outcomes for 90-day delays in treatment, even for thicker melanomas. But those studies, all retrospective, have been called into question. And the first real-world data on the impact of care restrictions during the lockdown, reported by Italian dermatologists, highlights adverse effects with potentially far-reaching consequences, noted Dr. Hartman, director of melanoma epidemiology at Brigham and Women’s Hospital and a dermatologist, Harvard University, Boston.
Analysis of the impact of lockdown-induced delays in melanoma care is not merely an academic exercise, she added. While everyone hopes that the spring 2020 COVID-19 shelter-in-place was a once-in-a-lifetime event, there’s no guarantee that will be the case. Moreover, the lockdown provides a natural experiment addressing the possible consequences of melanoma care delays on patient outcomes, a topic that for ethical reasons could never be addressed in a randomized trial.
The short-term NCCN recommendations included the use of excisional biopsies for melanoma diagnosis whenever possible; and delay of up to 3 months for wide local excision of in situ melanoma, any invasive melanoma with negative margins, and even T1 melanomas with positive margins provided the bulk of the lesion had been excised. The guidance also suggested delaying sentinel lymph node biopsy (SLNB), along with increased use of neoadjuvant therapy in patients with clinically palpable regional lymph nodes in order to delay surgery for up to 8 weeks. Single-agent systemic therapy at the least-frequent dosing was advised in order to minimize toxicity and reduce the need for additional health care resources: for example, nivolumab (Opdivo) at 480 mg every 4 weeks instead of every 2 weeks, and pembrolizumab (Keytruda) at 400 mg every 6 weeks, rather than every 3 weeks.
So, that’s what the NCCN recommended. Here’s what actually happened during shelter-in-place as captured in Dr. Hartman’s survey of 18 U.S. members of the Melanoma Prevention Working Group, all practicing dermatology in centers particularly hard-hit in the first wave of the pandemic: In-person new melanoma patient visits plunged from an average of 4.83 per week per provider to 0.83 per week. Telemedicine visits with new melanoma patients went from zero prepandemic to 0.67 visits per week per provider, which doesn’t come close to making up for the drop in in-person visits. Interestingly, two respondents reported turning to gene-expression profile testing for patient prognostication because of delays in SLNB.
Wide local excision was delayed by an average of 6 weeks in roughly one-third of melanoma patients with early tumor stage disease, regardless of margin status. For patients with stage T1b disease, wide local excision was typically performed on time during shelter-in-place; however, SLNB was delayed by an average of 5 weeks in 22% of patients with positive margins and 28% of those with negative margins. In contrast, 80% of patients with more advanced T2-T4 melanoma underwent on-schedule definitive management with wide local excision and SLNB, Dr. Hartman reported.
Critics have taken issue with the NCCN’s conclusion that most time-to-treatment studies show no harm arising from 90-day treatment delays. A review of the relevant published literature by Dr. Hartman’s Harvard colleagues, published in July, found that the evidence is mixed. “There is insufficient evidence to definitively conclude that delayed wide resection after gross removal of the primary melanoma is without harm,” they concluded in the review.
Spanish dermatologists performed a modeling study in order to estimate the potential impact of COVID-19 lockdowns on 5- and 10-year survival of melanoma patients. Using the growth rate of a random sample of 1,000 melanomas to model estimates of tumor thickness after various delays, coupled with American Joint Committee on Cancer survival data for different T stages, they estimated that 5-year survival would be reduced from 94.2% to 92.3% with a 90-day delay in diagnosis, and that 10-year survival would drop from 90.0% to 87.6%.
But that’s merely modeling. Francesco Ricci, MD, PhD, and colleagues from the melanoma unit at the Istituto Dermopatico dell’Immacolata, Rome, have provided a first look at the real-world impact of the lockdown. In the prelockdown period of January through March 9th, 2020, the referral center averaged 2.3 new melanoma diagnoses per day. During the Rome lockdown, from March 10th through May 3rd, this figure dropped to a mean of 0.6 melanoma diagnoses per day. Postlockdown, from May 4th to June 6th, the average climbed to 1.3 per day. The rate of newly diagnosed nodular melanoma was 5.5-fold greater postlockdown, compared with prelockdown; the rate of ulcerated melanoma was 4.9-fold greater.
“We can hypothesize that this may have been due to delays in diagnosis and care,” Dr. Hartman commented. “This is important because we know that nodular melanoma as well as ulceration tend to have a worse prognosis in terms of mortality.”
The mean Breslow thickness of newly diagnosed melanomas was 0.88 mm prelockdown, 0.66 mm during lockdown, and 1.96 mm postlockdown. The investigators speculated that the reduced Breslow thickness of melanomas diagnosed during lockdown might be explained by a greater willingness of more health-conscious people to defy the shelter-in-place instructions because of their concern about a suspicious skin lesion. “Though it is way too early to gauge the consequences of such diagnostic delay, should this issue be neglected, dermatologists and their patients may pay a higher price later with increased morbidity, mortality, and financial burden,” according to the investigators.
Dr. Hartman observed that it will be important to learn whether similar experiences occurred elsewhere during lockdown.
Another speaker, John M. Kirkwood, MD, said he has seen several melanoma patients referred from outside centers who had delays of up to 3 months in sentinel lymph node management of T2 and T3 tumors during lockdown who now have widespread metastatic disease.
“Now, is that anecdotal? I don’t know, it’s just worrisome to me,” commented Dr. Kirkwood, professor of medicine, dermatology, and translational science at the University of Pittsburgh.
Merrick Ross, MD, professor of surgical oncology at M.D. Anderson Cancer Center, Houston, recalled, “There was a period of time [during the lockdown] when we weren’t allowed to do certain elective procedures, if you want to call cancer surgery elective.”
“It’s too soon to talk about outcomes because a lot of patients are still in the process of being treated after what I would consider a significant delay in diagnosis,” the surgeon added.
An audience member asked if there will be an opportunity to see data on the damage done by delaying melanoma management as compared to lives saved through the lockdown for COVID-19. Dr. Ross replied that M.D. Anderson is in the midst of an institution-wide study analyzing the delay in diagnosis of a range of cancers.
“In our melanoma center it is absolutely clear, although we’re still collecting data, that the median tumor thickness is much higher since the lockdown,” Dr. Ross commented.
Dr. Hartman said she and her coinvestigators in the Melanoma Prevention Working Group are attempting to tally up the damage done via the lockdown by delaying melanoma diagnosis and treatment. But she agreed with the questioner that the most important thing is overall net lives saved through shelter-in-place.
“I’m sure that, separately, nondermatologists – perhaps infectious disease doctors and internists – are looking at how many lives were saved by the lockdown policy. So I do think all that data will come out,” Dr. Hartman predicted.
She reported having no financial conflicts regarding her presentation.
Global Academy for Medical Education and this news organization are owned by the same company.
SOURCE: Hartman, R. Cutaneous malignancies forum.
Initial evidence suggests that the , Rebecca I. Hartman, MD, MPH, said at a virtual forum on cutaneous malignancies jointly presented by Postgraduate Institute for Medicine and Global Academy for Medication Education.
This is not what National Comprehensive Cancer Network officials expected when they issued short-term recommendations on how to manage cutaneous melanoma during the first wave of the COVID-19 pandemic. Those recommendations for restriction of care, which Dr. Hartman characterized as “pretty significant changes from how we typically practice melanoma care in the U.S.,” came at a time when there was justifiable concern that the first COVID-19 surge would strain the U.S. health care system beyond the breaking point.
The rationale given for the NCCN recommendations was that most time-to-treat studies have shown no adverse patient outcomes for 90-day delays in treatment, even for thicker melanomas. But those studies, all retrospective, have been called into question. And the first real-world data on the impact of care restrictions during the lockdown, reported by Italian dermatologists, highlights adverse effects with potentially far-reaching consequences, noted Dr. Hartman, director of melanoma epidemiology at Brigham and Women’s Hospital and a dermatologist, Harvard University, Boston.
Analysis of the impact of lockdown-induced delays in melanoma care is not merely an academic exercise, she added. While everyone hopes that the spring 2020 COVID-19 shelter-in-place was a once-in-a-lifetime event, there’s no guarantee that will be the case. Moreover, the lockdown provides a natural experiment addressing the possible consequences of melanoma care delays on patient outcomes, a topic that for ethical reasons could never be addressed in a randomized trial.
The short-term NCCN recommendations included the use of excisional biopsies for melanoma diagnosis whenever possible; and delay of up to 3 months for wide local excision of in situ melanoma, any invasive melanoma with negative margins, and even T1 melanomas with positive margins provided the bulk of the lesion had been excised. The guidance also suggested delaying sentinel lymph node biopsy (SLNB), along with increased use of neoadjuvant therapy in patients with clinically palpable regional lymph nodes in order to delay surgery for up to 8 weeks. Single-agent systemic therapy at the least-frequent dosing was advised in order to minimize toxicity and reduce the need for additional health care resources: for example, nivolumab (Opdivo) at 480 mg every 4 weeks instead of every 2 weeks, and pembrolizumab (Keytruda) at 400 mg every 6 weeks, rather than every 3 weeks.
So, that’s what the NCCN recommended. Here’s what actually happened during shelter-in-place as captured in Dr. Hartman’s survey of 18 U.S. members of the Melanoma Prevention Working Group, all practicing dermatology in centers particularly hard-hit in the first wave of the pandemic: In-person new melanoma patient visits plunged from an average of 4.83 per week per provider to 0.83 per week. Telemedicine visits with new melanoma patients went from zero prepandemic to 0.67 visits per week per provider, which doesn’t come close to making up for the drop in in-person visits. Interestingly, two respondents reported turning to gene-expression profile testing for patient prognostication because of delays in SLNB.
Wide local excision was delayed by an average of 6 weeks in roughly one-third of melanoma patients with early tumor stage disease, regardless of margin status. For patients with stage T1b disease, wide local excision was typically performed on time during shelter-in-place; however, SLNB was delayed by an average of 5 weeks in 22% of patients with positive margins and 28% of those with negative margins. In contrast, 80% of patients with more advanced T2-T4 melanoma underwent on-schedule definitive management with wide local excision and SLNB, Dr. Hartman reported.
Critics have taken issue with the NCCN’s conclusion that most time-to-treatment studies show no harm arising from 90-day treatment delays. A review of the relevant published literature by Dr. Hartman’s Harvard colleagues, published in July, found that the evidence is mixed. “There is insufficient evidence to definitively conclude that delayed wide resection after gross removal of the primary melanoma is without harm,” they concluded in the review.
Spanish dermatologists performed a modeling study in order to estimate the potential impact of COVID-19 lockdowns on 5- and 10-year survival of melanoma patients. Using the growth rate of a random sample of 1,000 melanomas to model estimates of tumor thickness after various delays, coupled with American Joint Committee on Cancer survival data for different T stages, they estimated that 5-year survival would be reduced from 94.2% to 92.3% with a 90-day delay in diagnosis, and that 10-year survival would drop from 90.0% to 87.6%.
But that’s merely modeling. Francesco Ricci, MD, PhD, and colleagues from the melanoma unit at the Istituto Dermopatico dell’Immacolata, Rome, have provided a first look at the real-world impact of the lockdown. In the prelockdown period of January through March 9th, 2020, the referral center averaged 2.3 new melanoma diagnoses per day. During the Rome lockdown, from March 10th through May 3rd, this figure dropped to a mean of 0.6 melanoma diagnoses per day. Postlockdown, from May 4th to June 6th, the average climbed to 1.3 per day. The rate of newly diagnosed nodular melanoma was 5.5-fold greater postlockdown, compared with prelockdown; the rate of ulcerated melanoma was 4.9-fold greater.
“We can hypothesize that this may have been due to delays in diagnosis and care,” Dr. Hartman commented. “This is important because we know that nodular melanoma as well as ulceration tend to have a worse prognosis in terms of mortality.”
The mean Breslow thickness of newly diagnosed melanomas was 0.88 mm prelockdown, 0.66 mm during lockdown, and 1.96 mm postlockdown. The investigators speculated that the reduced Breslow thickness of melanomas diagnosed during lockdown might be explained by a greater willingness of more health-conscious people to defy the shelter-in-place instructions because of their concern about a suspicious skin lesion. “Though it is way too early to gauge the consequences of such diagnostic delay, should this issue be neglected, dermatologists and their patients may pay a higher price later with increased morbidity, mortality, and financial burden,” according to the investigators.
Dr. Hartman observed that it will be important to learn whether similar experiences occurred elsewhere during lockdown.
Another speaker, John M. Kirkwood, MD, said he has seen several melanoma patients referred from outside centers who had delays of up to 3 months in sentinel lymph node management of T2 and T3 tumors during lockdown who now have widespread metastatic disease.
“Now, is that anecdotal? I don’t know, it’s just worrisome to me,” commented Dr. Kirkwood, professor of medicine, dermatology, and translational science at the University of Pittsburgh.
Merrick Ross, MD, professor of surgical oncology at M.D. Anderson Cancer Center, Houston, recalled, “There was a period of time [during the lockdown] when we weren’t allowed to do certain elective procedures, if you want to call cancer surgery elective.”
“It’s too soon to talk about outcomes because a lot of patients are still in the process of being treated after what I would consider a significant delay in diagnosis,” the surgeon added.
An audience member asked if there will be an opportunity to see data on the damage done by delaying melanoma management as compared to lives saved through the lockdown for COVID-19. Dr. Ross replied that M.D. Anderson is in the midst of an institution-wide study analyzing the delay in diagnosis of a range of cancers.
“In our melanoma center it is absolutely clear, although we’re still collecting data, that the median tumor thickness is much higher since the lockdown,” Dr. Ross commented.
Dr. Hartman said she and her coinvestigators in the Melanoma Prevention Working Group are attempting to tally up the damage done via the lockdown by delaying melanoma diagnosis and treatment. But she agreed with the questioner that the most important thing is overall net lives saved through shelter-in-place.
“I’m sure that, separately, nondermatologists – perhaps infectious disease doctors and internists – are looking at how many lives were saved by the lockdown policy. So I do think all that data will come out,” Dr. Hartman predicted.
She reported having no financial conflicts regarding her presentation.
Global Academy for Medical Education and this news organization are owned by the same company.
SOURCE: Hartman, R. Cutaneous malignancies forum.
REPORTING FROM THE CUTANEOUS MALIGNANCIES FORUM
JIA guideline calls for earlier use of targeted therapies
A draft guideline for the management of patients with juvenile idiopathic arthritis reflects changes in therapy away from reliance on NSAIDs and glucocorticoids and toward earlier introduction of biologic disease-modifying antirheumatic drugs (DMARDs).

The guideline, described in an oral session during the virtual annual meeting of the American College of Rheumatology, contains weighted recommendations for the treatment of JIA, including therapeutic approaches for oligoarthritis, tempromandibular joint (TMJ) arthritis, and systemic JIA (sJIA). The recommendations were the result of expert consensus and literature review using GRADE methodology, with input from clinicians, as well as patients and parents.
“Although evidence remains very low and many recommendations are conditional, the inclusion of parents and patients in the decision-making process strengthens their validity,” said project principal investigator Karen Onel, MD, of the Hospital for Special Surgery and Weill Cornell Medicine, both in New York.
She added that “it’s important to remember that these guidelines are meant to be guidelines; clinical care remains in the hands of the provider and the patient, and we endorse the importance of shared decision-making in coming to these agreements.”
Dr. Onel outlined key recommendations for patients for whom a diagnosis of JIA has already been made and who have no contraindications to recommended therapies. The strength of the recommendations (strong or conditional) and evidence levels (high, moderate, low, very low) were also reported.
Oligoarthritis with fewer than five involved joints
For these patients, intra-articular glucocorticoids (IAGC) are recommended as a part of initial therapy (strong, very low evidence).
Triamcinolone acetonide is the preferred agent in this situation (strong, low evidence).
The guideline also has a conditional recommendation (very low evidence) for a trial of consistent NSAIDS as part of initial therapy and a conditional recommendation against oral glucocorticoids for initial therapy (very low evidence).
Patients with no or incomplete responses or intolerance to NSAIDS and/or IAGC may be tried on a nonbiologic DMARD (strong, very low evidence), with methotrexate as the preferred agent (conditional, low evidence).
If the patient has no response or an inadequate response to at least one nonbiologic DMARD, biologic DMARDs are recommended (strong, very low evidence), with no preferred agent.
The guideline also conditionally recommends (all with very low evidence) using risk factors and validated disease activity measures to guide treatment decisions, as well as imaging guidance of joints that are difficult to access or to localize the distribution of inflammation.
TMJ arthritis
For patients with temporomandibular joint arthritis, isolated or not, IAGCs are conditionally recommended as part of initial therapy (very low evidence) with no preferred agents. The guideline also conditionally recommends in favor of a trial of consistent NSAIDs, and against oral glucocorticoids in initial therapy (evidence for both very low).
Recommendations for patients with TMJ with no or an incomplete response to the initial therapy are the same as for patients with oligoarthritis, with no preferred agent.
sJIA without macrophage activation syndrome
For patients with sJIA without macrophage activation syndrome (MAS), NSAIDS are conditionally recommended as initial monotherapy (very low evidence). Biologic DMARDS (including interleukin-1 and IL-6 inhibitors) are also recommended, conditionally, as initial monotherapy, with no preferred agent.
If the patient has an inadequate response or intolerance to NSAIDS and at least one nonbiologic DMARD, a single biologic DMARD is recommended over a combination of nonbiologic therapies (strong, very low evidence).
“However, there have been reports of emergent, highly severe lung disease associated with the use of biologics in children with systemic JIA, especially in those who are young, with chronic macrophage activation syndrome, and those with trisomy 21. More information is needed to clarify the safety of these agents,” Dr. Onel said.
There is a conditional recommendation against oral glucocorticoids as initial monotherapy, and strong recommendation against nonbiologic DMARDs as initial monotherapy (both very low evidence).
sJIA with MAS
“Macrophage activation syndrome is a major cause of morbidity and mortality for children with sJIA. Cytokine storm and secondary hemophagocytic syndrome can be seen with any rheumatic disease, but are most commonly seen with sJIA,” she said.
The features of MAS include fever, high ferritin levels, cytopenias, elevated liver-function test results, and high triglyceride levels.
For these patients, glucocorticoids are recommended as initial monotherapy (conditional, very low evidence). Biologic DMARDs (IL-1 and IL-6 inhibitors) are recommended over calcineurin inhibitors for achieving inactive disease and resolution of MAS (conditional, very low evidence). There is no preferred agent.
For patients with residual arthritis and an incomplete response to IL-1 or IL-6 inhibitors, biologic and nonbiologic DMARDs are recommended over chronic glucocorticoids (strong, very low evidence). There is no preferred agent.
After an MAS inactive disease state has been attained, the guideline recommends tapering and discontinuing glucocorticoids (strong, very low evidence) and the same for biologic DMARDs (conditional, very low evidence).
All children with JIA
In addition to the recommendations on specific clinical situations, the guideline includes recommendations for all children with JIA on medication monitoring, laboratory testing, and infection screening, as well as immunization and nonpharmacologic management.
A rheumatologist who was not involved in development of the guidelines commented on the importance of optimal management of JIA.

“Children are not immune from devastating rheumatic diseases, and the largest group is juvenile idiopathic arthritis. In my clinic, I have patients in their 30s, 40s, and 50s who have adult persistence of their arthritis from JIA who have permanent joint damage and even ongoing hard-to-control disease, and it has to do with the lack of therapies in the 1990s,” said Donald Thomas, MD, from Arthritis and Pain Associates of Prince George’s County (Md.).
“Today when we get a young adult transitioned from the pediatric clinic they’re usually in remission or have low disease activity because these treatments have paralleled those of our adult RA patients. Yet they do [provide clinicians with] unique challenges, with stunting of growth, macrophage activiation syndrome, and having to work with family members of the patient,” he said at a press briefing he moderated following the presentation of RA and JIA guidelines.
Eyal Muscal, MD, associate professor of pediatrics and rheumatology at Baylor College of Medicine, Houston, said in an interview that the guidelines clarify recommendations about earlier use of targeted therapies, primarily biologics.
“This will not change care, but hopefully remind all to adopt such strategies. Yet earlier utilization of often expensive biologic agents is delayed by administrative and insurance hurdles in the U.S. and access to these medications globally. I hope the guidelines will enhance advocacy on a state, national, and global stage,” he said when asked for comment.
The guideline development process is supported by ACR. Dr. Onel, Dr. Thomas, and Dr. Muscal reported no relevant conflicts of interest.
SOURCE: Onel K et al. ACR 2020, Presented November 8.
A draft guideline for the management of patients with juvenile idiopathic arthritis reflects changes in therapy away from reliance on NSAIDs and glucocorticoids and toward earlier introduction of biologic disease-modifying antirheumatic drugs (DMARDs).
The guideline, described in an oral session during the virtual annual meeting of the American College of Rheumatology, contains weighted recommendations for the treatment of JIA, including therapeutic approaches for oligoarthritis, tempromandibular joint (TMJ) arthritis, and systemic JIA (sJIA). The recommendations were the result of expert consensus and literature review using GRADE methodology, with input from clinicians, as well as patients and parents.
“Although evidence remains very low and many recommendations are conditional, the inclusion of parents and patients in the decision-making process strengthens their validity,” said project principal investigator Karen Onel, MD, of the Hospital for Special Surgery and Weill Cornell Medicine, both in New York.
She added that “it’s important to remember that these guidelines are meant to be guidelines; clinical care remains in the hands of the provider and the patient, and we endorse the importance of shared decision-making in coming to these agreements.”
Dr. Onel outlined key recommendations for patients for whom a diagnosis of JIA has already been made and who have no contraindications to recommended therapies. The strength of the recommendations (strong or conditional) and evidence levels (high, moderate, low, very low) were also reported.
Oligoarthritis with fewer than five involved joints
For these patients, intra-articular glucocorticoids (IAGC) are recommended as a part of initial therapy (strong, very low evidence).
Triamcinolone acetonide is the preferred agent in this situation (strong, low evidence).
The guideline also has a conditional recommendation (very low evidence) for a trial of consistent NSAIDS as part of initial therapy and a conditional recommendation against oral glucocorticoids for initial therapy (very low evidence).
Patients with no or incomplete responses or intolerance to NSAIDS and/or IAGC may be tried on a nonbiologic DMARD (strong, very low evidence), with methotrexate as the preferred agent (conditional, low evidence).
If the patient has no response or an inadequate response to at least one nonbiologic DMARD, biologic DMARDs are recommended (strong, very low evidence), with no preferred agent.
The guideline also conditionally recommends (all with very low evidence) using risk factors and validated disease activity measures to guide treatment decisions, as well as imaging guidance of joints that are difficult to access or to localize the distribution of inflammation.
TMJ arthritis
For patients with temporomandibular joint arthritis, isolated or not, IAGCs are conditionally recommended as part of initial therapy (very low evidence) with no preferred agents. The guideline also conditionally recommends in favor of a trial of consistent NSAIDs, and against oral glucocorticoids in initial therapy (evidence for both very low).
Recommendations for patients with TMJ with no or an incomplete response to the initial therapy are the same as for patients with oligoarthritis, with no preferred agent.
sJIA without macrophage activation syndrome
For patients with sJIA without macrophage activation syndrome (MAS), NSAIDS are conditionally recommended as initial monotherapy (very low evidence). Biologic DMARDS (including interleukin-1 and IL-6 inhibitors) are also recommended, conditionally, as initial monotherapy, with no preferred agent.
If the patient has an inadequate response or intolerance to NSAIDS and at least one nonbiologic DMARD, a single biologic DMARD is recommended over a combination of nonbiologic therapies (strong, very low evidence).
“However, there have been reports of emergent, highly severe lung disease associated with the use of biologics in children with systemic JIA, especially in those who are young, with chronic macrophage activation syndrome, and those with trisomy 21. More information is needed to clarify the safety of these agents,” Dr. Onel said.
There is a conditional recommendation against oral glucocorticoids as initial monotherapy, and strong recommendation against nonbiologic DMARDs as initial monotherapy (both very low evidence).
sJIA with MAS
“Macrophage activation syndrome is a major cause of morbidity and mortality for children with sJIA. Cytokine storm and secondary hemophagocytic syndrome can be seen with any rheumatic disease, but are most commonly seen with sJIA,” she said.
The features of MAS include fever, high ferritin levels, cytopenias, elevated liver-function test results, and high triglyceride levels.
For these patients, glucocorticoids are recommended as initial monotherapy (conditional, very low evidence). Biologic DMARDs (IL-1 and IL-6 inhibitors) are recommended over calcineurin inhibitors for achieving inactive disease and resolution of MAS (conditional, very low evidence). There is no preferred agent.
For patients with residual arthritis and an incomplete response to IL-1 or IL-6 inhibitors, biologic and nonbiologic DMARDs are recommended over chronic glucocorticoids (strong, very low evidence). There is no preferred agent.
After an MAS inactive disease state has been attained, the guideline recommends tapering and discontinuing glucocorticoids (strong, very low evidence) and the same for biologic DMARDs (conditional, very low evidence).
All children with JIA
In addition to the recommendations on specific clinical situations, the guideline includes recommendations for all children with JIA on medication monitoring, laboratory testing, and infection screening, as well as immunization and nonpharmacologic management.
A rheumatologist who was not involved in development of the guidelines commented on the importance of optimal management of JIA.
“Children are not immune from devastating rheumatic diseases, and the largest group is juvenile idiopathic arthritis. In my clinic, I have patients in their 30s, 40s, and 50s who have adult persistence of their arthritis from JIA who have permanent joint damage and even ongoing hard-to-control disease, and it has to do with the lack of therapies in the 1990s,” said Donald Thomas, MD, from Arthritis and Pain Associates of Prince George’s County (Md.).
“Today when we get a young adult transitioned from the pediatric clinic they’re usually in remission or have low disease activity because these treatments have paralleled those of our adult RA patients. Yet they do [provide clinicians with] unique challenges, with stunting of growth, macrophage activiation syndrome, and having to work with family members of the patient,” he said at a press briefing he moderated following the presentation of RA and JIA guidelines.
Eyal Muscal, MD, associate professor of pediatrics and rheumatology at Baylor College of Medicine, Houston, said in an interview that the guidelines clarify recommendations about earlier use of targeted therapies, primarily biologics.
“This will not change care, but hopefully remind all to adopt such strategies. Yet earlier utilization of often expensive biologic agents is delayed by administrative and insurance hurdles in the U.S. and access to these medications globally. I hope the guidelines will enhance advocacy on a state, national, and global stage,” he said when asked for comment.
The guideline development process is supported by ACR. Dr. Onel, Dr. Thomas, and Dr. Muscal reported no relevant conflicts of interest.
SOURCE: Onel K et al. ACR 2020, Presented November 8.
A draft guideline for the management of patients with juvenile idiopathic arthritis reflects changes in therapy away from reliance on NSAIDs and glucocorticoids and toward earlier introduction of biologic disease-modifying antirheumatic drugs (DMARDs).
The guideline, described in an oral session during the virtual annual meeting of the American College of Rheumatology, contains weighted recommendations for the treatment of JIA, including therapeutic approaches for oligoarthritis, tempromandibular joint (TMJ) arthritis, and systemic JIA (sJIA). The recommendations were the result of expert consensus and literature review using GRADE methodology, with input from clinicians, as well as patients and parents.
“Although evidence remains very low and many recommendations are conditional, the inclusion of parents and patients in the decision-making process strengthens their validity,” said project principal investigator Karen Onel, MD, of the Hospital for Special Surgery and Weill Cornell Medicine, both in New York.
She added that “it’s important to remember that these guidelines are meant to be guidelines; clinical care remains in the hands of the provider and the patient, and we endorse the importance of shared decision-making in coming to these agreements.”
Dr. Onel outlined key recommendations for patients for whom a diagnosis of JIA has already been made and who have no contraindications to recommended therapies. The strength of the recommendations (strong or conditional) and evidence levels (high, moderate, low, very low) were also reported.
Oligoarthritis with fewer than five involved joints
For these patients, intra-articular glucocorticoids (IAGC) are recommended as a part of initial therapy (strong, very low evidence).
Triamcinolone acetonide is the preferred agent in this situation (strong, low evidence).
The guideline also has a conditional recommendation (very low evidence) for a trial of consistent NSAIDS as part of initial therapy and a conditional recommendation against oral glucocorticoids for initial therapy (very low evidence).
Patients with no or incomplete responses or intolerance to NSAIDS and/or IAGC may be tried on a nonbiologic DMARD (strong, very low evidence), with methotrexate as the preferred agent (conditional, low evidence).
If the patient has no response or an inadequate response to at least one nonbiologic DMARD, biologic DMARDs are recommended (strong, very low evidence), with no preferred agent.
The guideline also conditionally recommends (all with very low evidence) using risk factors and validated disease activity measures to guide treatment decisions, as well as imaging guidance of joints that are difficult to access or to localize the distribution of inflammation.
TMJ arthritis
For patients with temporomandibular joint arthritis, isolated or not, IAGCs are conditionally recommended as part of initial therapy (very low evidence) with no preferred agents. The guideline also conditionally recommends in favor of a trial of consistent NSAIDs, and against oral glucocorticoids in initial therapy (evidence for both very low).
Recommendations for patients with TMJ with no or an incomplete response to the initial therapy are the same as for patients with oligoarthritis, with no preferred agent.
sJIA without macrophage activation syndrome
For patients with sJIA without macrophage activation syndrome (MAS), NSAIDS are conditionally recommended as initial monotherapy (very low evidence). Biologic DMARDS (including interleukin-1 and IL-6 inhibitors) are also recommended, conditionally, as initial monotherapy, with no preferred agent.
If the patient has an inadequate response or intolerance to NSAIDS and at least one nonbiologic DMARD, a single biologic DMARD is recommended over a combination of nonbiologic therapies (strong, very low evidence).
“However, there have been reports of emergent, highly severe lung disease associated with the use of biologics in children with systemic JIA, especially in those who are young, with chronic macrophage activation syndrome, and those with trisomy 21. More information is needed to clarify the safety of these agents,” Dr. Onel said.
There is a conditional recommendation against oral glucocorticoids as initial monotherapy, and strong recommendation against nonbiologic DMARDs as initial monotherapy (both very low evidence).
sJIA with MAS
“Macrophage activation syndrome is a major cause of morbidity and mortality for children with sJIA. Cytokine storm and secondary hemophagocytic syndrome can be seen with any rheumatic disease, but are most commonly seen with sJIA,” she said.
The features of MAS include fever, high ferritin levels, cytopenias, elevated liver-function test results, and high triglyceride levels.
For these patients, glucocorticoids are recommended as initial monotherapy (conditional, very low evidence). Biologic DMARDs (IL-1 and IL-6 inhibitors) are recommended over calcineurin inhibitors for achieving inactive disease and resolution of MAS (conditional, very low evidence). There is no preferred agent.
For patients with residual arthritis and an incomplete response to IL-1 or IL-6 inhibitors, biologic and nonbiologic DMARDs are recommended over chronic glucocorticoids (strong, very low evidence). There is no preferred agent.
After an MAS inactive disease state has been attained, the guideline recommends tapering and discontinuing glucocorticoids (strong, very low evidence) and the same for biologic DMARDs (conditional, very low evidence).
All children with JIA
In addition to the recommendations on specific clinical situations, the guideline includes recommendations for all children with JIA on medication monitoring, laboratory testing, and infection screening, as well as immunization and nonpharmacologic management.
A rheumatologist who was not involved in development of the guidelines commented on the importance of optimal management of JIA.
“Children are not immune from devastating rheumatic diseases, and the largest group is juvenile idiopathic arthritis. In my clinic, I have patients in their 30s, 40s, and 50s who have adult persistence of their arthritis from JIA who have permanent joint damage and even ongoing hard-to-control disease, and it has to do with the lack of therapies in the 1990s,” said Donald Thomas, MD, from Arthritis and Pain Associates of Prince George’s County (Md.).
“Today when we get a young adult transitioned from the pediatric clinic they’re usually in remission or have low disease activity because these treatments have paralleled those of our adult RA patients. Yet they do [provide clinicians with] unique challenges, with stunting of growth, macrophage activiation syndrome, and having to work with family members of the patient,” he said at a press briefing he moderated following the presentation of RA and JIA guidelines.
Eyal Muscal, MD, associate professor of pediatrics and rheumatology at Baylor College of Medicine, Houston, said in an interview that the guidelines clarify recommendations about earlier use of targeted therapies, primarily biologics.
“This will not change care, but hopefully remind all to adopt such strategies. Yet earlier utilization of often expensive biologic agents is delayed by administrative and insurance hurdles in the U.S. and access to these medications globally. I hope the guidelines will enhance advocacy on a state, national, and global stage,” he said when asked for comment.
The guideline development process is supported by ACR. Dr. Onel, Dr. Thomas, and Dr. Muscal reported no relevant conflicts of interest.
SOURCE: Onel K et al. ACR 2020, Presented November 8.
FROM ACR 2020
Trump could clean house at health agencies
Others may soon depart voluntarily. Politico reported in late October that more than two dozen political appointees had already left the U.S. Department Health and Human Services (HHS) since the start of the COVID-19 pandemic in February and that potentially dozens of the more than 100 in the department would leave if Trump was not reelected.
Trump hasn’t conceded, he is challenging the election results, and he has already fired his Defense Secretary, Mark Esper.
Among those possibly in Trump’s sights: HHS Secretary Alex Azar, US Food and Drug Administration (FDA) Commissioner Stephen Hahn, MD, Centers for Disease Control and Prevention (CDC) Director Robert Redfield, MD, and White House Coronavirus Task Force member Anthony Fauci, MD, who is also the director of the National Institutes of Allergy and Infectious Diseases.
Seema Verma, the administrator of the Centers for Medicare & Medicaid Services (CMS), is likely safe. According to Politico, Verma is expected to leave on her own terms.
Azar has had a long run as a Trump appointee. He took office in January 2018 and has been a staunch loyalist. But he’s frequently been the butt of grousing by Trump for not doing enough to help lower drug prices and for his handling of the coronavirus pandemic. Azar was initially in charge of the Trump virus effort but was quickly replaced by Vice President Mike Pence.
It was widely reported in late April that Trump was considering firing Azar, but the president called that “fake news” in a tweet.
Azar has complained about Hahn, who was confirmed in December 2019. According to Politico, Azar was looking into how to remove Hahn as commissioner because of the FDA’s battle with the White House over standards for emergency use authorization of a coronavirus vaccine.
In addition, Trump was infuriated by the agency’s insistence that it stick to the highest bar for an emergency approval. “The deep state, or whoever, over at the FDA is making it very difficult for drug companies to get people in order to test the vaccines and therapeutics. Obviously, they are hoping to delay the answer until after November 3rd,” Trump tweeted at Hahn.
Fauci on the firing line?
Most of the president’s ire has been directed at Fauci. As far back as April, Trump retweeted a call for Fauci’s firing. Twitter removed the original tweet but kept Trump’s comments on the original tweet.
The president has frequently questioned Fauci’s advice, sidelined him from task force meetings, and infrequently met with him. Trump called Fauci a “disaster” during a call with supporters in October, and then, at a campaign rally in November, intimated that he would fire the scientist after the election, according to The Washington Post.
But such a firing cannot be easily done. Some have speculated that Trump could pressure Fauci’s boss, Francis Collins, MD, PhD — the director of the National Institutes of Health (NIH), who is a political appointee — to get rid of him. But Collins would have to come up with a reason to fire Fauci. Because he is not a political appointee, Fauci is afforded a raft of protections given to civil service employees of the federal government.
To demote or fire Fauci, Collins would have to give him 30 days’ notice unless there’s a belief that he committed a crime. Fauci would have at least a week to offer evidence and affidavits in support of his service.
He’d also be entitled to legal representation, a written decision, and the specific reasons for the action being taken quickly. He could also request a hearing, and he’d be able to appeal any action to the Merit Systems Protection Board. The process could take months, if not years.
In late October, Trump issued an executive order that would reclassify certain federal employees so that they wouldn’t have such protections. But agencies have until mid-January to come up with lists of such workers, according to Government Executive.
Collins has been with NIH since 1993, when he headed the Human Genome Project and the National Human Genome Research Institute. Politico has speculated that Collins, 70, might retire if Trump was reelected. It’s unclear what he’ll do now.
Redfield, who has taken heat for his leadership from many in public health — and was asked in October to stand up to Trump by former CDC Director William H. Foege, MD — has been openly contradicted by the president on more than one occasion, according to The New York Times.
In September, The Hill reported that Trump told reporters that he’d chastised Redfield by phone soon after Redfield had told a Senate committee that a coronavirus vaccine would not be available until mid-2021.
This article first appeared on Medscape.com.
Others may soon depart voluntarily. Politico reported in late October that more than two dozen political appointees had already left the U.S. Department Health and Human Services (HHS) since the start of the COVID-19 pandemic in February and that potentially dozens of the more than 100 in the department would leave if Trump was not reelected.
Trump hasn’t conceded, he is challenging the election results, and he has already fired his Defense Secretary, Mark Esper.
Among those possibly in Trump’s sights: HHS Secretary Alex Azar, US Food and Drug Administration (FDA) Commissioner Stephen Hahn, MD, Centers for Disease Control and Prevention (CDC) Director Robert Redfield, MD, and White House Coronavirus Task Force member Anthony Fauci, MD, who is also the director of the National Institutes of Allergy and Infectious Diseases.
Seema Verma, the administrator of the Centers for Medicare & Medicaid Services (CMS), is likely safe. According to Politico, Verma is expected to leave on her own terms.
Azar has had a long run as a Trump appointee. He took office in January 2018 and has been a staunch loyalist. But he’s frequently been the butt of grousing by Trump for not doing enough to help lower drug prices and for his handling of the coronavirus pandemic. Azar was initially in charge of the Trump virus effort but was quickly replaced by Vice President Mike Pence.
It was widely reported in late April that Trump was considering firing Azar, but the president called that “fake news” in a tweet.
Azar has complained about Hahn, who was confirmed in December 2019. According to Politico, Azar was looking into how to remove Hahn as commissioner because of the FDA’s battle with the White House over standards for emergency use authorization of a coronavirus vaccine.
In addition, Trump was infuriated by the agency’s insistence that it stick to the highest bar for an emergency approval. “The deep state, or whoever, over at the FDA is making it very difficult for drug companies to get people in order to test the vaccines and therapeutics. Obviously, they are hoping to delay the answer until after November 3rd,” Trump tweeted at Hahn.
Fauci on the firing line?
Most of the president’s ire has been directed at Fauci. As far back as April, Trump retweeted a call for Fauci’s firing. Twitter removed the original tweet but kept Trump’s comments on the original tweet.
The president has frequently questioned Fauci’s advice, sidelined him from task force meetings, and infrequently met with him. Trump called Fauci a “disaster” during a call with supporters in October, and then, at a campaign rally in November, intimated that he would fire the scientist after the election, according to The Washington Post.
But such a firing cannot be easily done. Some have speculated that Trump could pressure Fauci’s boss, Francis Collins, MD, PhD — the director of the National Institutes of Health (NIH), who is a political appointee — to get rid of him. But Collins would have to come up with a reason to fire Fauci. Because he is not a political appointee, Fauci is afforded a raft of protections given to civil service employees of the federal government.
To demote or fire Fauci, Collins would have to give him 30 days’ notice unless there’s a belief that he committed a crime. Fauci would have at least a week to offer evidence and affidavits in support of his service.
He’d also be entitled to legal representation, a written decision, and the specific reasons for the action being taken quickly. He could also request a hearing, and he’d be able to appeal any action to the Merit Systems Protection Board. The process could take months, if not years.
In late October, Trump issued an executive order that would reclassify certain federal employees so that they wouldn’t have such protections. But agencies have until mid-January to come up with lists of such workers, according to Government Executive.
Collins has been with NIH since 1993, when he headed the Human Genome Project and the National Human Genome Research Institute. Politico has speculated that Collins, 70, might retire if Trump was reelected. It’s unclear what he’ll do now.
Redfield, who has taken heat for his leadership from many in public health — and was asked in October to stand up to Trump by former CDC Director William H. Foege, MD — has been openly contradicted by the president on more than one occasion, according to The New York Times.
In September, The Hill reported that Trump told reporters that he’d chastised Redfield by phone soon after Redfield had told a Senate committee that a coronavirus vaccine would not be available until mid-2021.
This article first appeared on Medscape.com.
Others may soon depart voluntarily. Politico reported in late October that more than two dozen political appointees had already left the U.S. Department Health and Human Services (HHS) since the start of the COVID-19 pandemic in February and that potentially dozens of the more than 100 in the department would leave if Trump was not reelected.
Trump hasn’t conceded, he is challenging the election results, and he has already fired his Defense Secretary, Mark Esper.
Among those possibly in Trump’s sights: HHS Secretary Alex Azar, US Food and Drug Administration (FDA) Commissioner Stephen Hahn, MD, Centers for Disease Control and Prevention (CDC) Director Robert Redfield, MD, and White House Coronavirus Task Force member Anthony Fauci, MD, who is also the director of the National Institutes of Allergy and Infectious Diseases.
Seema Verma, the administrator of the Centers for Medicare & Medicaid Services (CMS), is likely safe. According to Politico, Verma is expected to leave on her own terms.
Azar has had a long run as a Trump appointee. He took office in January 2018 and has been a staunch loyalist. But he’s frequently been the butt of grousing by Trump for not doing enough to help lower drug prices and for his handling of the coronavirus pandemic. Azar was initially in charge of the Trump virus effort but was quickly replaced by Vice President Mike Pence.
It was widely reported in late April that Trump was considering firing Azar, but the president called that “fake news” in a tweet.
Azar has complained about Hahn, who was confirmed in December 2019. According to Politico, Azar was looking into how to remove Hahn as commissioner because of the FDA’s battle with the White House over standards for emergency use authorization of a coronavirus vaccine.
In addition, Trump was infuriated by the agency’s insistence that it stick to the highest bar for an emergency approval. “The deep state, or whoever, over at the FDA is making it very difficult for drug companies to get people in order to test the vaccines and therapeutics. Obviously, they are hoping to delay the answer until after November 3rd,” Trump tweeted at Hahn.
Fauci on the firing line?
Most of the president’s ire has been directed at Fauci. As far back as April, Trump retweeted a call for Fauci’s firing. Twitter removed the original tweet but kept Trump’s comments on the original tweet.
The president has frequently questioned Fauci’s advice, sidelined him from task force meetings, and infrequently met with him. Trump called Fauci a “disaster” during a call with supporters in October, and then, at a campaign rally in November, intimated that he would fire the scientist after the election, according to The Washington Post.
But such a firing cannot be easily done. Some have speculated that Trump could pressure Fauci’s boss, Francis Collins, MD, PhD — the director of the National Institutes of Health (NIH), who is a political appointee — to get rid of him. But Collins would have to come up with a reason to fire Fauci. Because he is not a political appointee, Fauci is afforded a raft of protections given to civil service employees of the federal government.
To demote or fire Fauci, Collins would have to give him 30 days’ notice unless there’s a belief that he committed a crime. Fauci would have at least a week to offer evidence and affidavits in support of his service.
He’d also be entitled to legal representation, a written decision, and the specific reasons for the action being taken quickly. He could also request a hearing, and he’d be able to appeal any action to the Merit Systems Protection Board. The process could take months, if not years.
In late October, Trump issued an executive order that would reclassify certain federal employees so that they wouldn’t have such protections. But agencies have until mid-January to come up with lists of such workers, according to Government Executive.
Collins has been with NIH since 1993, when he headed the Human Genome Project and the National Human Genome Research Institute. Politico has speculated that Collins, 70, might retire if Trump was reelected. It’s unclear what he’ll do now.
Redfield, who has taken heat for his leadership from many in public health — and was asked in October to stand up to Trump by former CDC Director William H. Foege, MD — has been openly contradicted by the president on more than one occasion, according to The New York Times.
In September, The Hill reported that Trump told reporters that he’d chastised Redfield by phone soon after Redfield had told a Senate committee that a coronavirus vaccine would not be available until mid-2021.
This article first appeared on Medscape.com.
Supreme Court Justices seem skeptical of case to overturn ACA
The Justices conducted arguments by telephone in the case, California v Texas (previously California v US), which was brought by 18 Republican state officials and two individual plaintiffs. The Trump administration joined the plaintiffs in June, arguing that the entire law should be overturned. The ACA is being defended by Democratic state officials from 16 states and Washington, D.C.
The Republican plaintiffs have essentially argued that the ACA cannot stand without the individual mandate requirement – that it is not possible to “sever” it from the rest of the Act. In 2017, Congress set the tax penalty to $0 if an individual did not buy insurance. The mandate to buy insurance was left in place, but there were no longer any consequences. The plaintiffs said that congressional act was equivalent to severing the mandate.
But many Justices appeared to take a dim view of that argument.
“It’s a very straightforward case for severability under our precedents,” said Justice Brett Kavanaugh. “Meaning that we would excise the mandate and leave the rest of the Act in play. Congress knows how to write an inseverability clause and that is not the language that they chose here,” he said.
Justice Elena Kagan also questioned how it would jibe with legal precedent to allow the severing of one part of a law when there was no clear instruction from Congress on the issue. She also raised the concern that it would open the door to all sorts of challenges.
“It would seem a big deal to say that, if you can point to injury with respect to one provision and you can concoct some kind of inseverability argument, that allows you to challenge anything else in the statute,” she said.
“Isn’t that something that really cuts against all of our doctrine?” asked Kagan.
“I think it’s hard for you to argue that Congress intended the entire Act to fall if the mandate was struck down when the same Congress that lowered the penalty to zero did not even try to repeal the rest of the act,” said Chief Justice John Roberts.
“I think, frankly, that they wanted the Court to do that but that’s not our job,” he added.
Proof of harm?
To have the standing to sue, the plaintiffs have to prove they have been harmed by the ACA. Texas Solicitor General Kyle Hawkins said that individuals feel compelled to buy insurance – even without a penalty hanging over their heads.
Justice Stephen Breyer argued that many laws include what he called “precatory” language – that is, they seek to compel citizens to do something. But most don’t penalize those who fail to act – just like the ACA currently.
If, as the Texas plaintiffs argued, it’s still unconstitutional to make such a request, “I think there will be an awful lot of language in an awful lot of statutes that will suddenly be the subject of court constitutional challenge,” he said.
Hawkins disagreed. He said the ACA’s mandate “is not some suggestion, not some hortatory statement. It is the law of the United States of America today that you have to purchase health insurance and not just any health insurance, but health insurance that the federal government has decided would be best for you.”
Hawkins said that, if just one additional person signed up for Medicaid, the state of Texas and the other plaintiff states would be harmed. He said people were continuing to enroll in the program because they believed the law required them to get health insurance.
Justice Sonia Sotomayor said that defied common sense. “The problem is that your theory assumes people that people are going to pay a tax and break the law by not buying insurance, but they wouldn’t do it when the tax is zero.”
What’s at stake
It’s unlikely the justices will issue a decision immediately. They have until the end of the term in June to rule.
Katie Keith, JD, MPH, a principal at Keith Policy Solutions, LLC, outlined the potential outcomes in Health Affairs .
“The most likely scenario is that the Court maintains the status quo,” she wrote. They could get there by deciding Texas et al. did not have standing to bring the case. Or they could decide that either the mandate is constitutional or that it is unconstitutional but can be severed from the rest of the ACA.
The Court could alternatively find that some or all of the law’s insurance provisions – such as protections for people with pre-existing conditions – can’t be severed from the mandate. Or the justices could strike down all of the insurance consumer protections, the health insurance marketplaces, premium tax credits, and other provisions, which would force states to come up with the money to help people buy insurance. And states are unlikely to be able to do so, especially with the pandemic stretching their budgets.
Finally, the Court could find that the mandate can’t be separated, which would essentially overturn the law.
If that happens, some 15 million people could lose Medicaid coverage, 11 million who buy on health insurance exchanges could lose coverage, and 2.3 million young adults would no longer be able to stay on parents’ policies, according to the Kaiser Family Foundation. Kaiser also estimates that 54 million people under age 65 who have pre-existing conditions would no longer be guaranteed coverage.
The Urban Institute estimates that 21 million people could lose insurance – 15 million through Medicaid and the Children’s Health Insurance Program (CHIP) and 7.6 million through private nongroup coverage.
Medical societies weigh in
Multiple physicians’ groups, patient advocates, and hospital organizations have filed briefs with the Court in favor of keeping the law intact.
Twenty patient groups representing millions with pre-existing conditions – including the American Cancer Society, American Diabetes Association, American Heart Association, National Alliance on Mental Illness, National Organization for Rare Disorders, and the Kennedy Forum – filed a court brief in May arguing that the law has expanded access to insurance and improved patient outcomes.
“The coronavirus pandemic has only served to underscore the necessity of meaningful coverage – especially for those who are at high risk of being severely affected by the virus – including countless Americans who have pre-existing, acute or chronic conditions like heart disease, cancer, diabetes, lung diseases and multiple sclerosis,” they said in a statement.
Jacqueline W. Fincher, MD, MACP, president of the American College of Physicians, which joined a court brief in support of the law with 19 other medical organizations, said the law has worked.
“The coverage, protections and benefits provided by the ACA are critical to the well-being of millions of Americans,” she said in a statement.
“If the ACA were to be thrown out at the same time that we face the pandemic, it would cause chaos for physicians and our patients, and for the entire health care system,” said Fincher, adding that millions of Americans who have been infected could lose insurance if protections for pre-existing conditions disappeared.
“The ACA has revolutionized access to care for tens of millions of women by helping them obtain meaningful health coverage, ensuring that essential care is covered by insurers, and protecting patients from unfair insurance practices,” said Maureen G. Phipps, MD, MPH, CEO of the American College of Obstetricians and Gynecologists (ACOG), in a statement.
Overturning the ACA “would be one of the most singularly disruptive acts to be committed during this public health crisis,” she said.
American Psychiatric Association President Jeffrey Geller, MD, MPH, also warned of disruptions to care, especially for those with mental health and substance use disorders. “We urge the Supreme Court to preserve the entire Act, including the individual mandate,” he said, in a statement.
“In the midst of COVID is no time to let down the millions who we serve as our patients,” said Chip Kahn, Federation of American Health Systems president and CEO, in a statement.
“As caregivers, the goal of hospitals for our patients is to see increased access to affordable coverage for all Americans – not new obstacles,” he said, adding that the ACA “can accomplish this goal. We hope the Supreme Court will see its way clear to allow it to go forward.”
For the defense
Many legal analysts on social media who listened in to today’s hearing agreed that the tenor of the proceedings seemed to lean toward survival of the ACA.
“At this point I would say it is *extremely* likely that the ACA will be upheld, but the mandate struck down and severed out,” tweeted Raffi Melkonian, an appellate lawyer in Houston, Texas. “A decision on standing (throwing out the case entirely) is also possible. The chance that the ACA is struck down v. low.”
“Both Kavanaugh and Roberts have suggested this morning that they may view the individual mandate as severable from the rest of the law. If those two justices join the court’s three liberals in finding that the mandate is severable, that would be five votes to save the ACA,” tweeted the analysts at SCOTUS Blog.
Sean Marotta, a lawyer with Hogan Lovells’ Supreme Court group, agreed. “Oral argument is always an imperfect measure, but the Act’s defenders should feel good today,” he tweeted.
This article first appeared on Medscape.com.
The Justices conducted arguments by telephone in the case, California v Texas (previously California v US), which was brought by 18 Republican state officials and two individual plaintiffs. The Trump administration joined the plaintiffs in June, arguing that the entire law should be overturned. The ACA is being defended by Democratic state officials from 16 states and Washington, D.C.
The Republican plaintiffs have essentially argued that the ACA cannot stand without the individual mandate requirement – that it is not possible to “sever” it from the rest of the Act. In 2017, Congress set the tax penalty to $0 if an individual did not buy insurance. The mandate to buy insurance was left in place, but there were no longer any consequences. The plaintiffs said that congressional act was equivalent to severing the mandate.
But many Justices appeared to take a dim view of that argument.
“It’s a very straightforward case for severability under our precedents,” said Justice Brett Kavanaugh. “Meaning that we would excise the mandate and leave the rest of the Act in play. Congress knows how to write an inseverability clause and that is not the language that they chose here,” he said.
Justice Elena Kagan also questioned how it would jibe with legal precedent to allow the severing of one part of a law when there was no clear instruction from Congress on the issue. She also raised the concern that it would open the door to all sorts of challenges.
“It would seem a big deal to say that, if you can point to injury with respect to one provision and you can concoct some kind of inseverability argument, that allows you to challenge anything else in the statute,” she said.
“Isn’t that something that really cuts against all of our doctrine?” asked Kagan.
“I think it’s hard for you to argue that Congress intended the entire Act to fall if the mandate was struck down when the same Congress that lowered the penalty to zero did not even try to repeal the rest of the act,” said Chief Justice John Roberts.
“I think, frankly, that they wanted the Court to do that but that’s not our job,” he added.
Proof of harm?
To have the standing to sue, the plaintiffs have to prove they have been harmed by the ACA. Texas Solicitor General Kyle Hawkins said that individuals feel compelled to buy insurance – even without a penalty hanging over their heads.
Justice Stephen Breyer argued that many laws include what he called “precatory” language – that is, they seek to compel citizens to do something. But most don’t penalize those who fail to act – just like the ACA currently.
If, as the Texas plaintiffs argued, it’s still unconstitutional to make such a request, “I think there will be an awful lot of language in an awful lot of statutes that will suddenly be the subject of court constitutional challenge,” he said.
Hawkins disagreed. He said the ACA’s mandate “is not some suggestion, not some hortatory statement. It is the law of the United States of America today that you have to purchase health insurance and not just any health insurance, but health insurance that the federal government has decided would be best for you.”
Hawkins said that, if just one additional person signed up for Medicaid, the state of Texas and the other plaintiff states would be harmed. He said people were continuing to enroll in the program because they believed the law required them to get health insurance.
Justice Sonia Sotomayor said that defied common sense. “The problem is that your theory assumes people that people are going to pay a tax and break the law by not buying insurance, but they wouldn’t do it when the tax is zero.”
What’s at stake
It’s unlikely the justices will issue a decision immediately. They have until the end of the term in June to rule.
Katie Keith, JD, MPH, a principal at Keith Policy Solutions, LLC, outlined the potential outcomes in Health Affairs .
“The most likely scenario is that the Court maintains the status quo,” she wrote. They could get there by deciding Texas et al. did not have standing to bring the case. Or they could decide that either the mandate is constitutional or that it is unconstitutional but can be severed from the rest of the ACA.
The Court could alternatively find that some or all of the law’s insurance provisions – such as protections for people with pre-existing conditions – can’t be severed from the mandate. Or the justices could strike down all of the insurance consumer protections, the health insurance marketplaces, premium tax credits, and other provisions, which would force states to come up with the money to help people buy insurance. And states are unlikely to be able to do so, especially with the pandemic stretching their budgets.
Finally, the Court could find that the mandate can’t be separated, which would essentially overturn the law.
If that happens, some 15 million people could lose Medicaid coverage, 11 million who buy on health insurance exchanges could lose coverage, and 2.3 million young adults would no longer be able to stay on parents’ policies, according to the Kaiser Family Foundation. Kaiser also estimates that 54 million people under age 65 who have pre-existing conditions would no longer be guaranteed coverage.
The Urban Institute estimates that 21 million people could lose insurance – 15 million through Medicaid and the Children’s Health Insurance Program (CHIP) and 7.6 million through private nongroup coverage.
Medical societies weigh in
Multiple physicians’ groups, patient advocates, and hospital organizations have filed briefs with the Court in favor of keeping the law intact.
Twenty patient groups representing millions with pre-existing conditions – including the American Cancer Society, American Diabetes Association, American Heart Association, National Alliance on Mental Illness, National Organization for Rare Disorders, and the Kennedy Forum – filed a court brief in May arguing that the law has expanded access to insurance and improved patient outcomes.
“The coronavirus pandemic has only served to underscore the necessity of meaningful coverage – especially for those who are at high risk of being severely affected by the virus – including countless Americans who have pre-existing, acute or chronic conditions like heart disease, cancer, diabetes, lung diseases and multiple sclerosis,” they said in a statement.
Jacqueline W. Fincher, MD, MACP, president of the American College of Physicians, which joined a court brief in support of the law with 19 other medical organizations, said the law has worked.
“The coverage, protections and benefits provided by the ACA are critical to the well-being of millions of Americans,” she said in a statement.
“If the ACA were to be thrown out at the same time that we face the pandemic, it would cause chaos for physicians and our patients, and for the entire health care system,” said Fincher, adding that millions of Americans who have been infected could lose insurance if protections for pre-existing conditions disappeared.
“The ACA has revolutionized access to care for tens of millions of women by helping them obtain meaningful health coverage, ensuring that essential care is covered by insurers, and protecting patients from unfair insurance practices,” said Maureen G. Phipps, MD, MPH, CEO of the American College of Obstetricians and Gynecologists (ACOG), in a statement.
Overturning the ACA “would be one of the most singularly disruptive acts to be committed during this public health crisis,” she said.
American Psychiatric Association President Jeffrey Geller, MD, MPH, also warned of disruptions to care, especially for those with mental health and substance use disorders. “We urge the Supreme Court to preserve the entire Act, including the individual mandate,” he said, in a statement.
“In the midst of COVID is no time to let down the millions who we serve as our patients,” said Chip Kahn, Federation of American Health Systems president and CEO, in a statement.
“As caregivers, the goal of hospitals for our patients is to see increased access to affordable coverage for all Americans – not new obstacles,” he said, adding that the ACA “can accomplish this goal. We hope the Supreme Court will see its way clear to allow it to go forward.”
For the defense
Many legal analysts on social media who listened in to today’s hearing agreed that the tenor of the proceedings seemed to lean toward survival of the ACA.
“At this point I would say it is *extremely* likely that the ACA will be upheld, but the mandate struck down and severed out,” tweeted Raffi Melkonian, an appellate lawyer in Houston, Texas. “A decision on standing (throwing out the case entirely) is also possible. The chance that the ACA is struck down v. low.”
“Both Kavanaugh and Roberts have suggested this morning that they may view the individual mandate as severable from the rest of the law. If those two justices join the court’s three liberals in finding that the mandate is severable, that would be five votes to save the ACA,” tweeted the analysts at SCOTUS Blog.
Sean Marotta, a lawyer with Hogan Lovells’ Supreme Court group, agreed. “Oral argument is always an imperfect measure, but the Act’s defenders should feel good today,” he tweeted.
This article first appeared on Medscape.com.
The Justices conducted arguments by telephone in the case, California v Texas (previously California v US), which was brought by 18 Republican state officials and two individual plaintiffs. The Trump administration joined the plaintiffs in June, arguing that the entire law should be overturned. The ACA is being defended by Democratic state officials from 16 states and Washington, D.C.
The Republican plaintiffs have essentially argued that the ACA cannot stand without the individual mandate requirement – that it is not possible to “sever” it from the rest of the Act. In 2017, Congress set the tax penalty to $0 if an individual did not buy insurance. The mandate to buy insurance was left in place, but there were no longer any consequences. The plaintiffs said that congressional act was equivalent to severing the mandate.
But many Justices appeared to take a dim view of that argument.
“It’s a very straightforward case for severability under our precedents,” said Justice Brett Kavanaugh. “Meaning that we would excise the mandate and leave the rest of the Act in play. Congress knows how to write an inseverability clause and that is not the language that they chose here,” he said.
Justice Elena Kagan also questioned how it would jibe with legal precedent to allow the severing of one part of a law when there was no clear instruction from Congress on the issue. She also raised the concern that it would open the door to all sorts of challenges.
“It would seem a big deal to say that, if you can point to injury with respect to one provision and you can concoct some kind of inseverability argument, that allows you to challenge anything else in the statute,” she said.
“Isn’t that something that really cuts against all of our doctrine?” asked Kagan.
“I think it’s hard for you to argue that Congress intended the entire Act to fall if the mandate was struck down when the same Congress that lowered the penalty to zero did not even try to repeal the rest of the act,” said Chief Justice John Roberts.
“I think, frankly, that they wanted the Court to do that but that’s not our job,” he added.
Proof of harm?
To have the standing to sue, the plaintiffs have to prove they have been harmed by the ACA. Texas Solicitor General Kyle Hawkins said that individuals feel compelled to buy insurance – even without a penalty hanging over their heads.
Justice Stephen Breyer argued that many laws include what he called “precatory” language – that is, they seek to compel citizens to do something. But most don’t penalize those who fail to act – just like the ACA currently.
If, as the Texas plaintiffs argued, it’s still unconstitutional to make such a request, “I think there will be an awful lot of language in an awful lot of statutes that will suddenly be the subject of court constitutional challenge,” he said.
Hawkins disagreed. He said the ACA’s mandate “is not some suggestion, not some hortatory statement. It is the law of the United States of America today that you have to purchase health insurance and not just any health insurance, but health insurance that the federal government has decided would be best for you.”
Hawkins said that, if just one additional person signed up for Medicaid, the state of Texas and the other plaintiff states would be harmed. He said people were continuing to enroll in the program because they believed the law required them to get health insurance.
Justice Sonia Sotomayor said that defied common sense. “The problem is that your theory assumes people that people are going to pay a tax and break the law by not buying insurance, but they wouldn’t do it when the tax is zero.”
What’s at stake
It’s unlikely the justices will issue a decision immediately. They have until the end of the term in June to rule.
Katie Keith, JD, MPH, a principal at Keith Policy Solutions, LLC, outlined the potential outcomes in Health Affairs .
“The most likely scenario is that the Court maintains the status quo,” she wrote. They could get there by deciding Texas et al. did not have standing to bring the case. Or they could decide that either the mandate is constitutional or that it is unconstitutional but can be severed from the rest of the ACA.
The Court could alternatively find that some or all of the law’s insurance provisions – such as protections for people with pre-existing conditions – can’t be severed from the mandate. Or the justices could strike down all of the insurance consumer protections, the health insurance marketplaces, premium tax credits, and other provisions, which would force states to come up with the money to help people buy insurance. And states are unlikely to be able to do so, especially with the pandemic stretching their budgets.
Finally, the Court could find that the mandate can’t be separated, which would essentially overturn the law.
If that happens, some 15 million people could lose Medicaid coverage, 11 million who buy on health insurance exchanges could lose coverage, and 2.3 million young adults would no longer be able to stay on parents’ policies, according to the Kaiser Family Foundation. Kaiser also estimates that 54 million people under age 65 who have pre-existing conditions would no longer be guaranteed coverage.
The Urban Institute estimates that 21 million people could lose insurance – 15 million through Medicaid and the Children’s Health Insurance Program (CHIP) and 7.6 million through private nongroup coverage.
Medical societies weigh in
Multiple physicians’ groups, patient advocates, and hospital organizations have filed briefs with the Court in favor of keeping the law intact.
Twenty patient groups representing millions with pre-existing conditions – including the American Cancer Society, American Diabetes Association, American Heart Association, National Alliance on Mental Illness, National Organization for Rare Disorders, and the Kennedy Forum – filed a court brief in May arguing that the law has expanded access to insurance and improved patient outcomes.
“The coronavirus pandemic has only served to underscore the necessity of meaningful coverage – especially for those who are at high risk of being severely affected by the virus – including countless Americans who have pre-existing, acute or chronic conditions like heart disease, cancer, diabetes, lung diseases and multiple sclerosis,” they said in a statement.
Jacqueline W. Fincher, MD, MACP, president of the American College of Physicians, which joined a court brief in support of the law with 19 other medical organizations, said the law has worked.
“The coverage, protections and benefits provided by the ACA are critical to the well-being of millions of Americans,” she said in a statement.
“If the ACA were to be thrown out at the same time that we face the pandemic, it would cause chaos for physicians and our patients, and for the entire health care system,” said Fincher, adding that millions of Americans who have been infected could lose insurance if protections for pre-existing conditions disappeared.
“The ACA has revolutionized access to care for tens of millions of women by helping them obtain meaningful health coverage, ensuring that essential care is covered by insurers, and protecting patients from unfair insurance practices,” said Maureen G. Phipps, MD, MPH, CEO of the American College of Obstetricians and Gynecologists (ACOG), in a statement.
Overturning the ACA “would be one of the most singularly disruptive acts to be committed during this public health crisis,” she said.
American Psychiatric Association President Jeffrey Geller, MD, MPH, also warned of disruptions to care, especially for those with mental health and substance use disorders. “We urge the Supreme Court to preserve the entire Act, including the individual mandate,” he said, in a statement.
“In the midst of COVID is no time to let down the millions who we serve as our patients,” said Chip Kahn, Federation of American Health Systems president and CEO, in a statement.
“As caregivers, the goal of hospitals for our patients is to see increased access to affordable coverage for all Americans – not new obstacles,” he said, adding that the ACA “can accomplish this goal. We hope the Supreme Court will see its way clear to allow it to go forward.”
For the defense
Many legal analysts on social media who listened in to today’s hearing agreed that the tenor of the proceedings seemed to lean toward survival of the ACA.
“At this point I would say it is *extremely* likely that the ACA will be upheld, but the mandate struck down and severed out,” tweeted Raffi Melkonian, an appellate lawyer in Houston, Texas. “A decision on standing (throwing out the case entirely) is also possible. The chance that the ACA is struck down v. low.”
“Both Kavanaugh and Roberts have suggested this morning that they may view the individual mandate as severable from the rest of the law. If those two justices join the court’s three liberals in finding that the mandate is severable, that would be five votes to save the ACA,” tweeted the analysts at SCOTUS Blog.
Sean Marotta, a lawyer with Hogan Lovells’ Supreme Court group, agreed. “Oral argument is always an imperfect measure, but the Act’s defenders should feel good today,” he tweeted.
This article first appeared on Medscape.com.