User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
CDC panel recommends Pfizer COVID-19 boosters for ages 12-15
The CDC had already said 16- and 17-year-olds “may” receive a Pfizer booster but the new recommendation adds the 12- to 15-year-old group and strengthens the “may” to “should” for 16- and 17-year-olds.
The committee voted 13-1 to recommend the booster for ages 12-17. CDC Director Rochelle Walensky, MD, must still approve the recommendation for it to take effect.
The vote comes after the FDA on Jan. 3 authorized the Pfizer vaccine booster dose for 12- to 15-year-olds.
The FDA action updated the authorization for the Pfizer vaccine, and the agency also shortened the recommended time between a second dose and the booster to 5 months or more (from 6 months). A third primary series dose is also now authorized for certain immunocompromised children between 5 and 11 years old. Full details are available in an FDA news release.
The CDC on Jan. 4 also backed the shortened time frame and a third primary series dose for some immunocompromised children 5-11 years old. But the CDC delayed a decision on a booster for 12- to 15-year-olds until it heard from its Advisory Committee on Immunization Practices on Jan. 5.
The decision came as school districts nationwide are wrestling with decisions of whether to keep schools open or revert to a virtual format as cases surge, and as pediatric COVID-19 cases and hospitalizations reach new highs.
The only dissenting vote came from Helen Keipp Talbot, MD, associate professor of medicine at Vanderbilt University in Nashville, Tenn.
She said after the vote, “I am just fine with kids getting a booster. This is not me against all boosters. I just really want the U.S. to move forward with all kids.”
Dr. Talbot said earlier in the comment period, “If we divert our public health from the unvaccinated to the vaccinated, we are not going to make a big impact. Boosters are incredibly important but they won’t solve this problem of the crowded hospitals.”
She said vaccinating the unvaccinated must be the priority.
“If you are a parent out there who has not yet vaccinated your child because you have questions, please, please talk to a health care provider,” she said.
Among the 13 supporters of the recommendation was Oliver Brooks, MD, chief medical officer of Watts HealthCare Corporation in Los Angeles.
Dr. Brooks said extending the population for boosters is another tool in the toolbox.
“If it’s a hammer, we should hit that nail hard,” he said.
Sara Oliver, MD, ACIP’s lead for the COVID-19 work group, presented the case behind the recommendation.
She noted the soaring Omicron cases.
“As of Jan. 3, the 7-day average had reached an all-time high of nearly 500,000 cases,” Dr. Oliver noted.
Since this summer, she said, adolescents have had a higher rate of incidence than that of adults.
“The majority of COVID cases continue to occur among the unvaccinated,” she said, “with unvaccinated 12- to 17-year-olds having a 7-times-higher risk of testing positive for SARS-CoV-2 compared to vaccinated 12- to 17-year-olds. Unvaccinated 12- to 17-year-olds have around 11 times higher risk of hospitalization than vaccinated 12- to 17-year-olds.
“Vaccine effectiveness in adolescents 12-15 years old remains high,” Dr. Oliver said, but evidence shows there may be “some waning over time.”
Discussion of risk centered on myocarditis.
Dr. Oliver said myocarditis rates reported after the Pfizer vaccine in Israel across all populations as of Dec. 15 show that “the rates of myocarditis after a third dose are lower than what is seen after the second dose.”
A version of this article first appeared on WebMD.com.
The CDC had already said 16- and 17-year-olds “may” receive a Pfizer booster but the new recommendation adds the 12- to 15-year-old group and strengthens the “may” to “should” for 16- and 17-year-olds.
The committee voted 13-1 to recommend the booster for ages 12-17. CDC Director Rochelle Walensky, MD, must still approve the recommendation for it to take effect.
The vote comes after the FDA on Jan. 3 authorized the Pfizer vaccine booster dose for 12- to 15-year-olds.
The FDA action updated the authorization for the Pfizer vaccine, and the agency also shortened the recommended time between a second dose and the booster to 5 months or more (from 6 months). A third primary series dose is also now authorized for certain immunocompromised children between 5 and 11 years old. Full details are available in an FDA news release.
The CDC on Jan. 4 also backed the shortened time frame and a third primary series dose for some immunocompromised children 5-11 years old. But the CDC delayed a decision on a booster for 12- to 15-year-olds until it heard from its Advisory Committee on Immunization Practices on Jan. 5.
The decision came as school districts nationwide are wrestling with decisions of whether to keep schools open or revert to a virtual format as cases surge, and as pediatric COVID-19 cases and hospitalizations reach new highs.
The only dissenting vote came from Helen Keipp Talbot, MD, associate professor of medicine at Vanderbilt University in Nashville, Tenn.
She said after the vote, “I am just fine with kids getting a booster. This is not me against all boosters. I just really want the U.S. to move forward with all kids.”
Dr. Talbot said earlier in the comment period, “If we divert our public health from the unvaccinated to the vaccinated, we are not going to make a big impact. Boosters are incredibly important but they won’t solve this problem of the crowded hospitals.”
She said vaccinating the unvaccinated must be the priority.
“If you are a parent out there who has not yet vaccinated your child because you have questions, please, please talk to a health care provider,” she said.
Among the 13 supporters of the recommendation was Oliver Brooks, MD, chief medical officer of Watts HealthCare Corporation in Los Angeles.
Dr. Brooks said extending the population for boosters is another tool in the toolbox.
“If it’s a hammer, we should hit that nail hard,” he said.
Sara Oliver, MD, ACIP’s lead for the COVID-19 work group, presented the case behind the recommendation.
She noted the soaring Omicron cases.
“As of Jan. 3, the 7-day average had reached an all-time high of nearly 500,000 cases,” Dr. Oliver noted.
Since this summer, she said, adolescents have had a higher rate of incidence than that of adults.
“The majority of COVID cases continue to occur among the unvaccinated,” she said, “with unvaccinated 12- to 17-year-olds having a 7-times-higher risk of testing positive for SARS-CoV-2 compared to vaccinated 12- to 17-year-olds. Unvaccinated 12- to 17-year-olds have around 11 times higher risk of hospitalization than vaccinated 12- to 17-year-olds.
“Vaccine effectiveness in adolescents 12-15 years old remains high,” Dr. Oliver said, but evidence shows there may be “some waning over time.”
Discussion of risk centered on myocarditis.
Dr. Oliver said myocarditis rates reported after the Pfizer vaccine in Israel across all populations as of Dec. 15 show that “the rates of myocarditis after a third dose are lower than what is seen after the second dose.”
A version of this article first appeared on WebMD.com.
The CDC had already said 16- and 17-year-olds “may” receive a Pfizer booster but the new recommendation adds the 12- to 15-year-old group and strengthens the “may” to “should” for 16- and 17-year-olds.
The committee voted 13-1 to recommend the booster for ages 12-17. CDC Director Rochelle Walensky, MD, must still approve the recommendation for it to take effect.
The vote comes after the FDA on Jan. 3 authorized the Pfizer vaccine booster dose for 12- to 15-year-olds.
The FDA action updated the authorization for the Pfizer vaccine, and the agency also shortened the recommended time between a second dose and the booster to 5 months or more (from 6 months). A third primary series dose is also now authorized for certain immunocompromised children between 5 and 11 years old. Full details are available in an FDA news release.
The CDC on Jan. 4 also backed the shortened time frame and a third primary series dose for some immunocompromised children 5-11 years old. But the CDC delayed a decision on a booster for 12- to 15-year-olds until it heard from its Advisory Committee on Immunization Practices on Jan. 5.
The decision came as school districts nationwide are wrestling with decisions of whether to keep schools open or revert to a virtual format as cases surge, and as pediatric COVID-19 cases and hospitalizations reach new highs.
The only dissenting vote came from Helen Keipp Talbot, MD, associate professor of medicine at Vanderbilt University in Nashville, Tenn.
She said after the vote, “I am just fine with kids getting a booster. This is not me against all boosters. I just really want the U.S. to move forward with all kids.”
Dr. Talbot said earlier in the comment period, “If we divert our public health from the unvaccinated to the vaccinated, we are not going to make a big impact. Boosters are incredibly important but they won’t solve this problem of the crowded hospitals.”
She said vaccinating the unvaccinated must be the priority.
“If you are a parent out there who has not yet vaccinated your child because you have questions, please, please talk to a health care provider,” she said.
Among the 13 supporters of the recommendation was Oliver Brooks, MD, chief medical officer of Watts HealthCare Corporation in Los Angeles.
Dr. Brooks said extending the population for boosters is another tool in the toolbox.
“If it’s a hammer, we should hit that nail hard,” he said.
Sara Oliver, MD, ACIP’s lead for the COVID-19 work group, presented the case behind the recommendation.
She noted the soaring Omicron cases.
“As of Jan. 3, the 7-day average had reached an all-time high of nearly 500,000 cases,” Dr. Oliver noted.
Since this summer, she said, adolescents have had a higher rate of incidence than that of adults.
“The majority of COVID cases continue to occur among the unvaccinated,” she said, “with unvaccinated 12- to 17-year-olds having a 7-times-higher risk of testing positive for SARS-CoV-2 compared to vaccinated 12- to 17-year-olds. Unvaccinated 12- to 17-year-olds have around 11 times higher risk of hospitalization than vaccinated 12- to 17-year-olds.
“Vaccine effectiveness in adolescents 12-15 years old remains high,” Dr. Oliver said, but evidence shows there may be “some waning over time.”
Discussion of risk centered on myocarditis.
Dr. Oliver said myocarditis rates reported after the Pfizer vaccine in Israel across all populations as of Dec. 15 show that “the rates of myocarditis after a third dose are lower than what is seen after the second dose.”
A version of this article first appeared on WebMD.com.
Who needs self-driving cars when we’ve got goldfish?
If a fish can drive …
Have you ever seen a sparrow swim? Have you ever seen an elephant fly? How about a goldfish driving a car? Well, one of these is not just something out of a children’s book.
In a recent study, investigators from Ben-Gurion University did the impossible and got a fish to drive a robotic car on land. How?
No, there wasn’t a tiny steering wheel inside the tank. The researchers created a tank with video recognition ability to sync with the fish. This video shows that the car, on which the tank sat, would navigate in the direction that the fish swam. The goal was to get the fish to “drive” toward a visual target, and with a little training the fish was successful regardless of start point, the researchers explained.
So what does that tell us about the brain and behavior? Shachar Givon, who was part of the research team, said the “study hints that navigational ability is universal rather than specific to the environment.”
The study’s domain transfer methodology (putting one species in the environment of another and have them cope with an unfamiliar task) shows that other animals also have the cognitive ability to transfer skills from one terrestrial environment to another.
That leads us to lesson two. Goldfish are much smarter than we think. So please don’t tap on the glass.
We prefer ‘It’s not writing a funny LOTME article’!
So many medical journals spend all their time grappling with such silly dilemmas as curing cancer or beating COVID-19. Boring! Fortunately, the BMJ dares to stand above the rest by dedicating its Christmas issue to answering the real issues in medicine. And what was the biggest question? Which is the more accurate idiom: “It’s not rocket science,” or “It’s not brain surgery”?

English researchers collected data from 329 aerospace engineers and 72 neurosurgeons who took the Great British Intelligence Test and compared the results against 18,000 people in the general public.
The engineers and neurosurgeons were basically identical in four of the six domains, but neurosurgeons had the advantage when it came to semantic problem solving and engineers had an edge at mental manipulation and attention. The aerospace engineers were identical to the public in all domains, but neurosurgeons held an advantage in problem-solving speed and a disadvantage in memory recall speed.
The researchers noted that exposure to Latin and Greek etymologies during their education gave neurosurgeons the advantage in semantic problem solving, while the aerospace engineers’ advantage in mental manipulation stems from skills taught during engineering training.
But is there a definitive answer to the question? If you’ve got an easy task in front of you, which is more accurate to say: “It’s not rocket science” or “It’s not brain surgery”? Can we get a drum roll?
It’s not brain surgery! At least, as long as the task doesn’t involve rapid problem solving. The investigators hedged further by saying that “It’s a walk in the park” is probably more accurate. Plus, “other specialties might deserve to be on that pedestal, and future work should aim to determine the most deserving profession,” they wrote. Well, at least we’ve got something to look forward to in BMJ’s next Christmas issue.
For COVID-19, a syringe is the sheep of things to come
The logical approach to fighting COVID-19 hasn’t really worked with a lot of people, so how about something more emotional?

People love animals, so they might be a good way to promote the use of vaccines and masks. Puppies are awfully cute, and so are koalas and pandas. And who can say no to a sea otter?
Well, forget it. Instead, we’ve got elephants … and sheep … and goats. Oh my.
First, elephant Santas. The Jirasartwitthaya school in Ayutthaya, Thailand, was recently visited by five elephants in Santa Claus costumes who handed out hand sanitizer and face masks to the students, Reuters said.
“I’m so glad that I got a balloon from the elephant. My heart is pounding very fast,” student Biuon Greham said. And balloons. The elephants handed out sanitizer and masks and balloons. There’s a sentence we never thought we’d write.
And those sheep and goats we mentioned? That was a different party.
Hanspeter Etzold, who “works with shepherds, companies, and animals to run team-building events in the northern German town of Schneverdingen,” according to Reuters, had an idea to promote the use of the COVID-19 vaccine. And yes, it involved sheep and goats.
Mr. Etzold worked with shepherd Wiebke Schmidt-Kochan, who arranged her 700 goats and sheep into the shape of a 100-meter-long syringe using bits of bread laying on the ground. “Sheep are such likable animals – maybe they can get the message over better,” Mr. Etzold told AP.
If those are the carrots in an animals-as-carrots-and-sticks approach, then maybe this golf-club-chomping crab could be the stick. We’re certainly not going to argue with it.
To be or not to be … seen
Increased Zoom meetings have been another side effect of the COVID-19 pandemic as more and more people have been working and learning from home.

A recent study from Washington State University looked at two groups of people who Zoomed on a regular basis: employees and students. Individuals who made the change to remote work/learning were surveyed in the summer and fall of 2020. They completed assessments with questions on their work/classes and their level of self-consciousness.
Those with low self-esteem did not enjoy having to see themselves on camera, and those with higher self-esteem actually enjoyed it more. “Most people believe that seeing yourself during virtual meetings contributes to making the overall experience worse, but that’s not what showed up in my data,” said Kristine Kuhn, PhD, the study’s author.
Dr. Kuhn found that having the choice of whether to have the camera on made a big difference in how the participants felt. Having that control made it a more positive experience. Most professors/bosses would probably like to see the faces of those in the Zoom meetings, but it might be better to let people choose for themselves. The unbrushed-hair club would certainly agree.
If a fish can drive …
Have you ever seen a sparrow swim? Have you ever seen an elephant fly? How about a goldfish driving a car? Well, one of these is not just something out of a children’s book.
In a recent study, investigators from Ben-Gurion University did the impossible and got a fish to drive a robotic car on land. How?
No, there wasn’t a tiny steering wheel inside the tank. The researchers created a tank with video recognition ability to sync with the fish. This video shows that the car, on which the tank sat, would navigate in the direction that the fish swam. The goal was to get the fish to “drive” toward a visual target, and with a little training the fish was successful regardless of start point, the researchers explained.
So what does that tell us about the brain and behavior? Shachar Givon, who was part of the research team, said the “study hints that navigational ability is universal rather than specific to the environment.”
The study’s domain transfer methodology (putting one species in the environment of another and have them cope with an unfamiliar task) shows that other animals also have the cognitive ability to transfer skills from one terrestrial environment to another.
That leads us to lesson two. Goldfish are much smarter than we think. So please don’t tap on the glass.
We prefer ‘It’s not writing a funny LOTME article’!
So many medical journals spend all their time grappling with such silly dilemmas as curing cancer or beating COVID-19. Boring! Fortunately, the BMJ dares to stand above the rest by dedicating its Christmas issue to answering the real issues in medicine. And what was the biggest question? Which is the more accurate idiom: “It’s not rocket science,” or “It’s not brain surgery”?
English researchers collected data from 329 aerospace engineers and 72 neurosurgeons who took the Great British Intelligence Test and compared the results against 18,000 people in the general public.
The engineers and neurosurgeons were basically identical in four of the six domains, but neurosurgeons had the advantage when it came to semantic problem solving and engineers had an edge at mental manipulation and attention. The aerospace engineers were identical to the public in all domains, but neurosurgeons held an advantage in problem-solving speed and a disadvantage in memory recall speed.
The researchers noted that exposure to Latin and Greek etymologies during their education gave neurosurgeons the advantage in semantic problem solving, while the aerospace engineers’ advantage in mental manipulation stems from skills taught during engineering training.
But is there a definitive answer to the question? If you’ve got an easy task in front of you, which is more accurate to say: “It’s not rocket science” or “It’s not brain surgery”? Can we get a drum roll?
It’s not brain surgery! At least, as long as the task doesn’t involve rapid problem solving. The investigators hedged further by saying that “It’s a walk in the park” is probably more accurate. Plus, “other specialties might deserve to be on that pedestal, and future work should aim to determine the most deserving profession,” they wrote. Well, at least we’ve got something to look forward to in BMJ’s next Christmas issue.
For COVID-19, a syringe is the sheep of things to come
The logical approach to fighting COVID-19 hasn’t really worked with a lot of people, so how about something more emotional?
People love animals, so they might be a good way to promote the use of vaccines and masks. Puppies are awfully cute, and so are koalas and pandas. And who can say no to a sea otter?
Well, forget it. Instead, we’ve got elephants … and sheep … and goats. Oh my.
First, elephant Santas. The Jirasartwitthaya school in Ayutthaya, Thailand, was recently visited by five elephants in Santa Claus costumes who handed out hand sanitizer and face masks to the students, Reuters said.
“I’m so glad that I got a balloon from the elephant. My heart is pounding very fast,” student Biuon Greham said. And balloons. The elephants handed out sanitizer and masks and balloons. There’s a sentence we never thought we’d write.
And those sheep and goats we mentioned? That was a different party.
Hanspeter Etzold, who “works with shepherds, companies, and animals to run team-building events in the northern German town of Schneverdingen,” according to Reuters, had an idea to promote the use of the COVID-19 vaccine. And yes, it involved sheep and goats.
Mr. Etzold worked with shepherd Wiebke Schmidt-Kochan, who arranged her 700 goats and sheep into the shape of a 100-meter-long syringe using bits of bread laying on the ground. “Sheep are such likable animals – maybe they can get the message over better,” Mr. Etzold told AP.
If those are the carrots in an animals-as-carrots-and-sticks approach, then maybe this golf-club-chomping crab could be the stick. We’re certainly not going to argue with it.
To be or not to be … seen
Increased Zoom meetings have been another side effect of the COVID-19 pandemic as more and more people have been working and learning from home.
A recent study from Washington State University looked at two groups of people who Zoomed on a regular basis: employees and students. Individuals who made the change to remote work/learning were surveyed in the summer and fall of 2020. They completed assessments with questions on their work/classes and their level of self-consciousness.
Those with low self-esteem did not enjoy having to see themselves on camera, and those with higher self-esteem actually enjoyed it more. “Most people believe that seeing yourself during virtual meetings contributes to making the overall experience worse, but that’s not what showed up in my data,” said Kristine Kuhn, PhD, the study’s author.
Dr. Kuhn found that having the choice of whether to have the camera on made a big difference in how the participants felt. Having that control made it a more positive experience. Most professors/bosses would probably like to see the faces of those in the Zoom meetings, but it might be better to let people choose for themselves. The unbrushed-hair club would certainly agree.
If a fish can drive …
Have you ever seen a sparrow swim? Have you ever seen an elephant fly? How about a goldfish driving a car? Well, one of these is not just something out of a children’s book.
In a recent study, investigators from Ben-Gurion University did the impossible and got a fish to drive a robotic car on land. How?
No, there wasn’t a tiny steering wheel inside the tank. The researchers created a tank with video recognition ability to sync with the fish. This video shows that the car, on which the tank sat, would navigate in the direction that the fish swam. The goal was to get the fish to “drive” toward a visual target, and with a little training the fish was successful regardless of start point, the researchers explained.
So what does that tell us about the brain and behavior? Shachar Givon, who was part of the research team, said the “study hints that navigational ability is universal rather than specific to the environment.”
The study’s domain transfer methodology (putting one species in the environment of another and have them cope with an unfamiliar task) shows that other animals also have the cognitive ability to transfer skills from one terrestrial environment to another.
That leads us to lesson two. Goldfish are much smarter than we think. So please don’t tap on the glass.
We prefer ‘It’s not writing a funny LOTME article’!
So many medical journals spend all their time grappling with such silly dilemmas as curing cancer or beating COVID-19. Boring! Fortunately, the BMJ dares to stand above the rest by dedicating its Christmas issue to answering the real issues in medicine. And what was the biggest question? Which is the more accurate idiom: “It’s not rocket science,” or “It’s not brain surgery”?
English researchers collected data from 329 aerospace engineers and 72 neurosurgeons who took the Great British Intelligence Test and compared the results against 18,000 people in the general public.
The engineers and neurosurgeons were basically identical in four of the six domains, but neurosurgeons had the advantage when it came to semantic problem solving and engineers had an edge at mental manipulation and attention. The aerospace engineers were identical to the public in all domains, but neurosurgeons held an advantage in problem-solving speed and a disadvantage in memory recall speed.
The researchers noted that exposure to Latin and Greek etymologies during their education gave neurosurgeons the advantage in semantic problem solving, while the aerospace engineers’ advantage in mental manipulation stems from skills taught during engineering training.
But is there a definitive answer to the question? If you’ve got an easy task in front of you, which is more accurate to say: “It’s not rocket science” or “It’s not brain surgery”? Can we get a drum roll?
It’s not brain surgery! At least, as long as the task doesn’t involve rapid problem solving. The investigators hedged further by saying that “It’s a walk in the park” is probably more accurate. Plus, “other specialties might deserve to be on that pedestal, and future work should aim to determine the most deserving profession,” they wrote. Well, at least we’ve got something to look forward to in BMJ’s next Christmas issue.
For COVID-19, a syringe is the sheep of things to come
The logical approach to fighting COVID-19 hasn’t really worked with a lot of people, so how about something more emotional?
People love animals, so they might be a good way to promote the use of vaccines and masks. Puppies are awfully cute, and so are koalas and pandas. And who can say no to a sea otter?
Well, forget it. Instead, we’ve got elephants … and sheep … and goats. Oh my.
First, elephant Santas. The Jirasartwitthaya school in Ayutthaya, Thailand, was recently visited by five elephants in Santa Claus costumes who handed out hand sanitizer and face masks to the students, Reuters said.
“I’m so glad that I got a balloon from the elephant. My heart is pounding very fast,” student Biuon Greham said. And balloons. The elephants handed out sanitizer and masks and balloons. There’s a sentence we never thought we’d write.
And those sheep and goats we mentioned? That was a different party.
Hanspeter Etzold, who “works with shepherds, companies, and animals to run team-building events in the northern German town of Schneverdingen,” according to Reuters, had an idea to promote the use of the COVID-19 vaccine. And yes, it involved sheep and goats.
Mr. Etzold worked with shepherd Wiebke Schmidt-Kochan, who arranged her 700 goats and sheep into the shape of a 100-meter-long syringe using bits of bread laying on the ground. “Sheep are such likable animals – maybe they can get the message over better,” Mr. Etzold told AP.
If those are the carrots in an animals-as-carrots-and-sticks approach, then maybe this golf-club-chomping crab could be the stick. We’re certainly not going to argue with it.
To be or not to be … seen
Increased Zoom meetings have been another side effect of the COVID-19 pandemic as more and more people have been working and learning from home.
A recent study from Washington State University looked at two groups of people who Zoomed on a regular basis: employees and students. Individuals who made the change to remote work/learning were surveyed in the summer and fall of 2020. They completed assessments with questions on their work/classes and their level of self-consciousness.
Those with low self-esteem did not enjoy having to see themselves on camera, and those with higher self-esteem actually enjoyed it more. “Most people believe that seeing yourself during virtual meetings contributes to making the overall experience worse, but that’s not what showed up in my data,” said Kristine Kuhn, PhD, the study’s author.
Dr. Kuhn found that having the choice of whether to have the camera on made a big difference in how the participants felt. Having that control made it a more positive experience. Most professors/bosses would probably like to see the faces of those in the Zoom meetings, but it might be better to let people choose for themselves. The unbrushed-hair club would certainly agree.
Gene mutations may drive sudden unexplained deaths in children
, researchers have found.
Previous studies have found de novo genetic variants – those not found in either parent but which occur for the first time in their offspring – that increase the risk of cardiac and seizure disorders, but research on sudden unexplained deaths in children (SUDC) is limited, according to Matthew Halvorsen, PhD, of the University of North Carolina at Chapel Hill, and colleagues. Most cases of SUDC occur in children aged 1-4 years, and a lack of standardized investigation systems likely leads to misclassification of these deaths, they said.
Compared with sudden infant death syndrome (SIDS), which occurs in approximately 1,400 children in the United States each year, approximately 400 children aged 1 year and older die from SUDC annually. A major obstacle to studying these cases is that so-called molecular autopsies – which incorporate genetic analysis into the postmortem examination – typically do not assess the parents’ genetic information and thus limit the ability to identify de novo mutations, they added.
In a study published in the Proceedings of the National Academy of Sciences, Dr. Halvorsen’s group obtained whole exome sequence data from 124 “trios,” meaning a dead child and two living parents. They tested for excessive de novo mutations for different genes involved in conditions that included cardiac arrhythmias and epilepsy. The average age at the time of death for the children was 34.2 months; 54% were male, and 82% were White.
Children who died of SUDC were nearly 10 times as likely to have de novo mutations in genes associated with cardiac and seizure disorders as were unrelated healthy controls (odds ratio, 9.76). Most pathogenic variants were de novo, which highlights the importance of trio studies, the researchers noted.
The researchers identified 11 variants associated with increased risk of SUDC, 7 of which were de novo. Three of the 124 cases carried mutations (two for RYR2 and 1 for TNNI3) affecting genes in the CardiacEpilepsy dataset proposed by the American College of Medical Genetics and Genomics, strengthening the connection to seizure disorders.
Another notable finding was the identification of six de novo mutations involved in altering calcium-related regulation, which suggests a cardiac susceptibility to sudden death.
The data support “novel genetic causes of pediatric sudden deaths that could be discovered with larger cohorts,” the researchers noted. Taken together, they say, the gene mutations could play a role in approximately 9% of SUDC cases.
The study findings were limited by several factors, including lack of population-based case ascertainment, exclusive focus on unexplained deaths, potentially missed mutations, and use of DNA from blood as opposed to organs, the researchers noted.
However, they concluded, “the data indicate that deleterious de novo mutations are significant genetic risk factors for childhood sudden unexplained death, and that their identification may lead to medical intervention that ultimately saves lives.”
Findings highlight impact of SUDC
“This study is important because SUDC is a much more pressing medical need than most people realize,” said Richard Tsien, PhD, of New York University Langone Medical Center, and the corresponding author of the study.
Although SUDC is less common than SIDS, SUDC has essentially no targeted research funding, Dr. Tsien said. Study coauthor Laura Gould, MA, a researcher and mother who lost a young child to SUDC, worked with Orrin Devinsky, MD, to create a registry for families with cases of SUDC. This registry was instrumental in allowing the researchers to “do the molecular detective work we need to do” to see whether a genetic basis exists for SUDC, Dr. Tsien said.
“The detective work comes up with a consistent story,” he said. “More than half of the genes that we found are involved in the normal function of the heart and brain,” performing such functions as delivering calcium ions to the inside of the heart cells and nerve cells.
The study “is the first of its kind,” given the difficulty of acquiring DNA from the child and two parents in SUDC cases, Dr. Tsien said.
Overall, approximately 10% of the cases have a compelling explanation based on the coding of DNA, Dr. Tsien said. From a clinical standpoint, that information might affect what a clinician says to a parent.
A key takeaway is that most of the genetic mutations are spontaneous and are not inherited from the parents, Dr. Tsien said. The study findings indicate that parents who suffer an SUDC loss need not be discouraged from having children, he added.
For the long term, “the more we understand about these disorders, the more information we can offer to families,” he said. Eventually, clinicians might be able to use genetics to identify signs of when SUDC might be more likely. “For example, if a child shows a very mild seizure, this would alert them that there might be potential for a more drastic outcome.”
Meanwhile, families with SUDC cases may find support and benefit in signing up for the registry and knowing that other families have been through a similar experience, Dr. Tsien said.
Genetic studies create opportunities
A significant portion of pediatric mortality remains unexplained, according to Richard D. Goldstein, MD, of Boston Children’s Hospital. One reason is the lack of a formal diagnostic code to identify these deaths.
Research to date has suggested links between SUDC and a family history of febrile seizures, as well as differences in brain structure associated with epilepsy, Dr. Goldstein said.
“An important hypothesis is that these deaths are part of a continuum that also includes stillbirths, SIDS, and sudden unexpected death in epilepsy [SUDEP],” Dr. Goldstein said. “By mandate, investigations of these deaths occur under the jurisdiction of medical examiners and coroners and have, for the most part, been insulated from developments in modern medicine like genomics and proteomics, elements of what are referred to as the molecular autopsy, and studies such as the current study bring attention to what is being missed.”
Dr. Goldstein said the new study buttresses the “conventional clinical suspicion” about the likely causes of SUDC, “but also strengthens the association between sudden unexpected death in pediatrics (SUDP) and SUDEP that we and others have been positing. I think the researchers very nicely make the point that epilepsy and cardiac arrhythmia genes are not as separated in their effects as many would believe.”
As for the clinical applicability of the findings, Dr. Goldstein said medicine needs to offer parents more: “Pediatric deaths without explanation deserve more than a forensic investigation that concerns itself mostly with whether there has been foul play,” he said. “We need to figure out how to engage families, at an incredibly vulnerable time, in helping find the cause of the child’s death and also contributing to needed research. Most of the reported variants were de novo, which means that parent participation is needed to figure out these genetic factors but also that we can offer reassurance to families that other children are not at risk.”
The study was supported by the SUDC Foundation and Finding a Cure for Epilepsy and Seizures (New York University). Dr. Tsien disclosed support from the National Institutes of Health and a grant from FACES. Dr. Goldstein reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, researchers have found.
Previous studies have found de novo genetic variants – those not found in either parent but which occur for the first time in their offspring – that increase the risk of cardiac and seizure disorders, but research on sudden unexplained deaths in children (SUDC) is limited, according to Matthew Halvorsen, PhD, of the University of North Carolina at Chapel Hill, and colleagues. Most cases of SUDC occur in children aged 1-4 years, and a lack of standardized investigation systems likely leads to misclassification of these deaths, they said.
Compared with sudden infant death syndrome (SIDS), which occurs in approximately 1,400 children in the United States each year, approximately 400 children aged 1 year and older die from SUDC annually. A major obstacle to studying these cases is that so-called molecular autopsies – which incorporate genetic analysis into the postmortem examination – typically do not assess the parents’ genetic information and thus limit the ability to identify de novo mutations, they added.
In a study published in the Proceedings of the National Academy of Sciences, Dr. Halvorsen’s group obtained whole exome sequence data from 124 “trios,” meaning a dead child and two living parents. They tested for excessive de novo mutations for different genes involved in conditions that included cardiac arrhythmias and epilepsy. The average age at the time of death for the children was 34.2 months; 54% were male, and 82% were White.
Children who died of SUDC were nearly 10 times as likely to have de novo mutations in genes associated with cardiac and seizure disorders as were unrelated healthy controls (odds ratio, 9.76). Most pathogenic variants were de novo, which highlights the importance of trio studies, the researchers noted.
The researchers identified 11 variants associated with increased risk of SUDC, 7 of which were de novo. Three of the 124 cases carried mutations (two for RYR2 and 1 for TNNI3) affecting genes in the CardiacEpilepsy dataset proposed by the American College of Medical Genetics and Genomics, strengthening the connection to seizure disorders.
Another notable finding was the identification of six de novo mutations involved in altering calcium-related regulation, which suggests a cardiac susceptibility to sudden death.
The data support “novel genetic causes of pediatric sudden deaths that could be discovered with larger cohorts,” the researchers noted. Taken together, they say, the gene mutations could play a role in approximately 9% of SUDC cases.
The study findings were limited by several factors, including lack of population-based case ascertainment, exclusive focus on unexplained deaths, potentially missed mutations, and use of DNA from blood as opposed to organs, the researchers noted.
However, they concluded, “the data indicate that deleterious de novo mutations are significant genetic risk factors for childhood sudden unexplained death, and that their identification may lead to medical intervention that ultimately saves lives.”
Findings highlight impact of SUDC
“This study is important because SUDC is a much more pressing medical need than most people realize,” said Richard Tsien, PhD, of New York University Langone Medical Center, and the corresponding author of the study.
Although SUDC is less common than SIDS, SUDC has essentially no targeted research funding, Dr. Tsien said. Study coauthor Laura Gould, MA, a researcher and mother who lost a young child to SUDC, worked with Orrin Devinsky, MD, to create a registry for families with cases of SUDC. This registry was instrumental in allowing the researchers to “do the molecular detective work we need to do” to see whether a genetic basis exists for SUDC, Dr. Tsien said.
“The detective work comes up with a consistent story,” he said. “More than half of the genes that we found are involved in the normal function of the heart and brain,” performing such functions as delivering calcium ions to the inside of the heart cells and nerve cells.
The study “is the first of its kind,” given the difficulty of acquiring DNA from the child and two parents in SUDC cases, Dr. Tsien said.
Overall, approximately 10% of the cases have a compelling explanation based on the coding of DNA, Dr. Tsien said. From a clinical standpoint, that information might affect what a clinician says to a parent.
A key takeaway is that most of the genetic mutations are spontaneous and are not inherited from the parents, Dr. Tsien said. The study findings indicate that parents who suffer an SUDC loss need not be discouraged from having children, he added.
For the long term, “the more we understand about these disorders, the more information we can offer to families,” he said. Eventually, clinicians might be able to use genetics to identify signs of when SUDC might be more likely. “For example, if a child shows a very mild seizure, this would alert them that there might be potential for a more drastic outcome.”
Meanwhile, families with SUDC cases may find support and benefit in signing up for the registry and knowing that other families have been through a similar experience, Dr. Tsien said.
Genetic studies create opportunities
A significant portion of pediatric mortality remains unexplained, according to Richard D. Goldstein, MD, of Boston Children’s Hospital. One reason is the lack of a formal diagnostic code to identify these deaths.
Research to date has suggested links between SUDC and a family history of febrile seizures, as well as differences in brain structure associated with epilepsy, Dr. Goldstein said.
“An important hypothesis is that these deaths are part of a continuum that also includes stillbirths, SIDS, and sudden unexpected death in epilepsy [SUDEP],” Dr. Goldstein said. “By mandate, investigations of these deaths occur under the jurisdiction of medical examiners and coroners and have, for the most part, been insulated from developments in modern medicine like genomics and proteomics, elements of what are referred to as the molecular autopsy, and studies such as the current study bring attention to what is being missed.”
Dr. Goldstein said the new study buttresses the “conventional clinical suspicion” about the likely causes of SUDC, “but also strengthens the association between sudden unexpected death in pediatrics (SUDP) and SUDEP that we and others have been positing. I think the researchers very nicely make the point that epilepsy and cardiac arrhythmia genes are not as separated in their effects as many would believe.”
As for the clinical applicability of the findings, Dr. Goldstein said medicine needs to offer parents more: “Pediatric deaths without explanation deserve more than a forensic investigation that concerns itself mostly with whether there has been foul play,” he said. “We need to figure out how to engage families, at an incredibly vulnerable time, in helping find the cause of the child’s death and also contributing to needed research. Most of the reported variants were de novo, which means that parent participation is needed to figure out these genetic factors but also that we can offer reassurance to families that other children are not at risk.”
The study was supported by the SUDC Foundation and Finding a Cure for Epilepsy and Seizures (New York University). Dr. Tsien disclosed support from the National Institutes of Health and a grant from FACES. Dr. Goldstein reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, researchers have found.
Previous studies have found de novo genetic variants – those not found in either parent but which occur for the first time in their offspring – that increase the risk of cardiac and seizure disorders, but research on sudden unexplained deaths in children (SUDC) is limited, according to Matthew Halvorsen, PhD, of the University of North Carolina at Chapel Hill, and colleagues. Most cases of SUDC occur in children aged 1-4 years, and a lack of standardized investigation systems likely leads to misclassification of these deaths, they said.
Compared with sudden infant death syndrome (SIDS), which occurs in approximately 1,400 children in the United States each year, approximately 400 children aged 1 year and older die from SUDC annually. A major obstacle to studying these cases is that so-called molecular autopsies – which incorporate genetic analysis into the postmortem examination – typically do not assess the parents’ genetic information and thus limit the ability to identify de novo mutations, they added.
In a study published in the Proceedings of the National Academy of Sciences, Dr. Halvorsen’s group obtained whole exome sequence data from 124 “trios,” meaning a dead child and two living parents. They tested for excessive de novo mutations for different genes involved in conditions that included cardiac arrhythmias and epilepsy. The average age at the time of death for the children was 34.2 months; 54% were male, and 82% were White.
Children who died of SUDC were nearly 10 times as likely to have de novo mutations in genes associated with cardiac and seizure disorders as were unrelated healthy controls (odds ratio, 9.76). Most pathogenic variants were de novo, which highlights the importance of trio studies, the researchers noted.
The researchers identified 11 variants associated with increased risk of SUDC, 7 of which were de novo. Three of the 124 cases carried mutations (two for RYR2 and 1 for TNNI3) affecting genes in the CardiacEpilepsy dataset proposed by the American College of Medical Genetics and Genomics, strengthening the connection to seizure disorders.
Another notable finding was the identification of six de novo mutations involved in altering calcium-related regulation, which suggests a cardiac susceptibility to sudden death.
The data support “novel genetic causes of pediatric sudden deaths that could be discovered with larger cohorts,” the researchers noted. Taken together, they say, the gene mutations could play a role in approximately 9% of SUDC cases.
The study findings were limited by several factors, including lack of population-based case ascertainment, exclusive focus on unexplained deaths, potentially missed mutations, and use of DNA from blood as opposed to organs, the researchers noted.
However, they concluded, “the data indicate that deleterious de novo mutations are significant genetic risk factors for childhood sudden unexplained death, and that their identification may lead to medical intervention that ultimately saves lives.”
Findings highlight impact of SUDC
“This study is important because SUDC is a much more pressing medical need than most people realize,” said Richard Tsien, PhD, of New York University Langone Medical Center, and the corresponding author of the study.
Although SUDC is less common than SIDS, SUDC has essentially no targeted research funding, Dr. Tsien said. Study coauthor Laura Gould, MA, a researcher and mother who lost a young child to SUDC, worked with Orrin Devinsky, MD, to create a registry for families with cases of SUDC. This registry was instrumental in allowing the researchers to “do the molecular detective work we need to do” to see whether a genetic basis exists for SUDC, Dr. Tsien said.
“The detective work comes up with a consistent story,” he said. “More than half of the genes that we found are involved in the normal function of the heart and brain,” performing such functions as delivering calcium ions to the inside of the heart cells and nerve cells.
The study “is the first of its kind,” given the difficulty of acquiring DNA from the child and two parents in SUDC cases, Dr. Tsien said.
Overall, approximately 10% of the cases have a compelling explanation based on the coding of DNA, Dr. Tsien said. From a clinical standpoint, that information might affect what a clinician says to a parent.
A key takeaway is that most of the genetic mutations are spontaneous and are not inherited from the parents, Dr. Tsien said. The study findings indicate that parents who suffer an SUDC loss need not be discouraged from having children, he added.
For the long term, “the more we understand about these disorders, the more information we can offer to families,” he said. Eventually, clinicians might be able to use genetics to identify signs of when SUDC might be more likely. “For example, if a child shows a very mild seizure, this would alert them that there might be potential for a more drastic outcome.”
Meanwhile, families with SUDC cases may find support and benefit in signing up for the registry and knowing that other families have been through a similar experience, Dr. Tsien said.
Genetic studies create opportunities
A significant portion of pediatric mortality remains unexplained, according to Richard D. Goldstein, MD, of Boston Children’s Hospital. One reason is the lack of a formal diagnostic code to identify these deaths.
Research to date has suggested links between SUDC and a family history of febrile seizures, as well as differences in brain structure associated with epilepsy, Dr. Goldstein said.
“An important hypothesis is that these deaths are part of a continuum that also includes stillbirths, SIDS, and sudden unexpected death in epilepsy [SUDEP],” Dr. Goldstein said. “By mandate, investigations of these deaths occur under the jurisdiction of medical examiners and coroners and have, for the most part, been insulated from developments in modern medicine like genomics and proteomics, elements of what are referred to as the molecular autopsy, and studies such as the current study bring attention to what is being missed.”
Dr. Goldstein said the new study buttresses the “conventional clinical suspicion” about the likely causes of SUDC, “but also strengthens the association between sudden unexpected death in pediatrics (SUDP) and SUDEP that we and others have been positing. I think the researchers very nicely make the point that epilepsy and cardiac arrhythmia genes are not as separated in their effects as many would believe.”
As for the clinical applicability of the findings, Dr. Goldstein said medicine needs to offer parents more: “Pediatric deaths without explanation deserve more than a forensic investigation that concerns itself mostly with whether there has been foul play,” he said. “We need to figure out how to engage families, at an incredibly vulnerable time, in helping find the cause of the child’s death and also contributing to needed research. Most of the reported variants were de novo, which means that parent participation is needed to figure out these genetic factors but also that we can offer reassurance to families that other children are not at risk.”
The study was supported by the SUDC Foundation and Finding a Cure for Epilepsy and Seizures (New York University). Dr. Tsien disclosed support from the National Institutes of Health and a grant from FACES. Dr. Goldstein reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
No link between mother’s pill use and CNS tumors in offspring
The study was based on population-based registry data and included 1.1 million children age 19 or younger born in Denmark between 1996 and 2014.
The study, by Marie Hargreave, PhD, Danish Cancer Society Research Center, and colleagues, was published online Jan. 4 in the Journal of the American Medical Association.
Exposure to sex hormones in utero is a recognized cause of cancer in affected offspring, note the authors. Also, the incidence of CNS tumors, among the most common and lethal childhood cancer types, appears to be increasing. Hence, they sought to investigate if there may be a relationship between the two.
During a mean follow-up of 12.9 years, the team found that 725 children were diagnosed with a CNS tumor (47.2% female). Mean age at diagnosis was 7 years. The team noted that 11.5%, 65.7%, and 22.8% of diagnosed children were born to mothers with recent, previous, or no use of hormonal contraception, respectively.
The adjusted incidence rate of CNS tumors was 5.0 per 100,000 person-years for children born to mothers with recent hormonal contraception use (hazard ratio, 0.95), 4.5 per 100,000 person-years for children born to mothers with previous use (HR, 0.86), and 5.3 per 100,000 person-years for children born to mothers with no use.
While recent use of implants (HR, 0.9) and intrauterine devices (HR, 1.5) showed no statistically significant associations for the subgroups of nonoral progestin-only hormonal contraception assessed, the team found that progestin-only injections were significantly associated with an increased risk compared with no use (HR, 6.7). Also, in all post hoc sensitivity analyses, recent use of the main group of nonoral progestin-only products was significantly associated with CNS tumors.
The authors observe that an association between maternal use of injectable contraceptives and increased risk of chromosomal anomalies and major malformations in children has previously been reported. Those results for injections, however, were based on a small number of cases, the result of the likelihood test was null, and adjustments for multiple comparisons were not made. Even if the results for this subgroup are confirmed, the authors point out, because CNS tumors in children are uncommon, the high relative risk estimates would translate to low absolute risk increases.
Although the large number of person-years and cancers increases the statistical precision, and the population-based nationwide design increases the generalizability of the results, the authors caution that uncommonness of CNS tumors in children and the small number of cases in the studied cohort limit subgroup analyses and the statistical precision of certain estimates.
In an accompanying editorial, Logan G. Spector, PhD, and Christopher L. Moertel, MD, from the University of Minnesota Medical School, and H. Irene Su, MD, from the University of California, San Diego, echo the authors’ conclusions, and state: “Thus, women should be reassured about the use of hormonal contraception, including progestin-only injections, and the lack of any increased risk of CNS tumors in their offspring.”
The study was supported by the Danish Cancer Research Foundation, the Arvid Nilssons Foundation, the Gangsted Foundation, the Harboe Foundation, and the Johannes Clemmesens Foundation. Co-author Lina S. Mørch, PhD, reported receiving personal fees from Novo Nordisk as an employee from 2017 to 2019 and grants from Novo Nordisk for a collaborative research project outside the submitted work. Editorialist Christopher Moertel, MD, reported receiving personal fees from OX2 Therapeutics, a spin-off of the University of Minnesota that is involved in the development of brain tumor therapeutics.
A version of this article first appeared on Medscape.com.
The study was based on population-based registry data and included 1.1 million children age 19 or younger born in Denmark between 1996 and 2014.
The study, by Marie Hargreave, PhD, Danish Cancer Society Research Center, and colleagues, was published online Jan. 4 in the Journal of the American Medical Association.
Exposure to sex hormones in utero is a recognized cause of cancer in affected offspring, note the authors. Also, the incidence of CNS tumors, among the most common and lethal childhood cancer types, appears to be increasing. Hence, they sought to investigate if there may be a relationship between the two.
During a mean follow-up of 12.9 years, the team found that 725 children were diagnosed with a CNS tumor (47.2% female). Mean age at diagnosis was 7 years. The team noted that 11.5%, 65.7%, and 22.8% of diagnosed children were born to mothers with recent, previous, or no use of hormonal contraception, respectively.
The adjusted incidence rate of CNS tumors was 5.0 per 100,000 person-years for children born to mothers with recent hormonal contraception use (hazard ratio, 0.95), 4.5 per 100,000 person-years for children born to mothers with previous use (HR, 0.86), and 5.3 per 100,000 person-years for children born to mothers with no use.
While recent use of implants (HR, 0.9) and intrauterine devices (HR, 1.5) showed no statistically significant associations for the subgroups of nonoral progestin-only hormonal contraception assessed, the team found that progestin-only injections were significantly associated with an increased risk compared with no use (HR, 6.7). Also, in all post hoc sensitivity analyses, recent use of the main group of nonoral progestin-only products was significantly associated with CNS tumors.
The authors observe that an association between maternal use of injectable contraceptives and increased risk of chromosomal anomalies and major malformations in children has previously been reported. Those results for injections, however, were based on a small number of cases, the result of the likelihood test was null, and adjustments for multiple comparisons were not made. Even if the results for this subgroup are confirmed, the authors point out, because CNS tumors in children are uncommon, the high relative risk estimates would translate to low absolute risk increases.
Although the large number of person-years and cancers increases the statistical precision, and the population-based nationwide design increases the generalizability of the results, the authors caution that uncommonness of CNS tumors in children and the small number of cases in the studied cohort limit subgroup analyses and the statistical precision of certain estimates.
In an accompanying editorial, Logan G. Spector, PhD, and Christopher L. Moertel, MD, from the University of Minnesota Medical School, and H. Irene Su, MD, from the University of California, San Diego, echo the authors’ conclusions, and state: “Thus, women should be reassured about the use of hormonal contraception, including progestin-only injections, and the lack of any increased risk of CNS tumors in their offspring.”
The study was supported by the Danish Cancer Research Foundation, the Arvid Nilssons Foundation, the Gangsted Foundation, the Harboe Foundation, and the Johannes Clemmesens Foundation. Co-author Lina S. Mørch, PhD, reported receiving personal fees from Novo Nordisk as an employee from 2017 to 2019 and grants from Novo Nordisk for a collaborative research project outside the submitted work. Editorialist Christopher Moertel, MD, reported receiving personal fees from OX2 Therapeutics, a spin-off of the University of Minnesota that is involved in the development of brain tumor therapeutics.
A version of this article first appeared on Medscape.com.
The study was based on population-based registry data and included 1.1 million children age 19 or younger born in Denmark between 1996 and 2014.
The study, by Marie Hargreave, PhD, Danish Cancer Society Research Center, and colleagues, was published online Jan. 4 in the Journal of the American Medical Association.
Exposure to sex hormones in utero is a recognized cause of cancer in affected offspring, note the authors. Also, the incidence of CNS tumors, among the most common and lethal childhood cancer types, appears to be increasing. Hence, they sought to investigate if there may be a relationship between the two.
During a mean follow-up of 12.9 years, the team found that 725 children were diagnosed with a CNS tumor (47.2% female). Mean age at diagnosis was 7 years. The team noted that 11.5%, 65.7%, and 22.8% of diagnosed children were born to mothers with recent, previous, or no use of hormonal contraception, respectively.
The adjusted incidence rate of CNS tumors was 5.0 per 100,000 person-years for children born to mothers with recent hormonal contraception use (hazard ratio, 0.95), 4.5 per 100,000 person-years for children born to mothers with previous use (HR, 0.86), and 5.3 per 100,000 person-years for children born to mothers with no use.
While recent use of implants (HR, 0.9) and intrauterine devices (HR, 1.5) showed no statistically significant associations for the subgroups of nonoral progestin-only hormonal contraception assessed, the team found that progestin-only injections were significantly associated with an increased risk compared with no use (HR, 6.7). Also, in all post hoc sensitivity analyses, recent use of the main group of nonoral progestin-only products was significantly associated with CNS tumors.
The authors observe that an association between maternal use of injectable contraceptives and increased risk of chromosomal anomalies and major malformations in children has previously been reported. Those results for injections, however, were based on a small number of cases, the result of the likelihood test was null, and adjustments for multiple comparisons were not made. Even if the results for this subgroup are confirmed, the authors point out, because CNS tumors in children are uncommon, the high relative risk estimates would translate to low absolute risk increases.
Although the large number of person-years and cancers increases the statistical precision, and the population-based nationwide design increases the generalizability of the results, the authors caution that uncommonness of CNS tumors in children and the small number of cases in the studied cohort limit subgroup analyses and the statistical precision of certain estimates.
In an accompanying editorial, Logan G. Spector, PhD, and Christopher L. Moertel, MD, from the University of Minnesota Medical School, and H. Irene Su, MD, from the University of California, San Diego, echo the authors’ conclusions, and state: “Thus, women should be reassured about the use of hormonal contraception, including progestin-only injections, and the lack of any increased risk of CNS tumors in their offspring.”
The study was supported by the Danish Cancer Research Foundation, the Arvid Nilssons Foundation, the Gangsted Foundation, the Harboe Foundation, and the Johannes Clemmesens Foundation. Co-author Lina S. Mørch, PhD, reported receiving personal fees from Novo Nordisk as an employee from 2017 to 2019 and grants from Novo Nordisk for a collaborative research project outside the submitted work. Editorialist Christopher Moertel, MD, reported receiving personal fees from OX2 Therapeutics, a spin-off of the University of Minnesota that is involved in the development of brain tumor therapeutics.
A version of this article first appeared on Medscape.com.
CDC defends new COVID guidance as doctors raise concerns
, Director Rochelle Walenksy, MD, said during a White House briefing Jan. 5.
Health officials recently shortened the recommended COVID-19 isolation and quarantine period from 10 days to 5, creating confusion amid an outbreak of the highly transmissible Omicron variant, which now accounts for 95% of cases in the United States.
Then, in slightly updated guidance, the CDC recommended using an at-home antigen test after 5 days of isolation if possible, even though these tests having aren’t as sensitive to the Omicron variant, according to the FDA.
“After we released our recs early last week, it became very clear people were interested in using the rapid test, though not authorized for this purpose after the end of their isolation period,” Dr. Walensky said. “We then provided guidance on how they should be used.”
“If that test is negative, people really do need to understand they must continue to wear their mask for those 5 days,” Dr. Walensky said.
But for many, the CDC guidelines are murky and seem to always change.
“Nearly 2 years into this pandemic, with Omicron cases surging across the country, the American people should be able to count on the Centers for Disease Control and Prevention for timely, accurate, clear guidance to protect themselves, their loved ones, and their communities,” American Medical Association president Gerald Harmon, MD, said in a statement. “Instead, the new recommendations on quarantine and isolation are not only confusing, but are risking further spread of the virus.”
About 31% of people remain infectious 5 days after a positive COVID-19 test, Dr. Harmon said, quoting the CDC’s own rationale for changing its guidance.
“With hundreds of thousands of new cases daily and more than a million positive reported cases on January 3, tens of thousands – potentially hundreds of thousands of people – could return to work and school infectious if they follow the CDC’s new guidance on ending isolation after 5 days without a negative test,” he said. “Physicians are concerned that these recommendations put our patients at risk and could further overwhelm our health care system.”
Instead, Dr. Harmon said a negative test should be required for ending isolation.
“Reemerging without knowing one’s status unnecessarily risks further transmission of the virus,” he said.
Meanwhile, also during the White House briefing, officials said that early data continue to show that Omicron infections are less severe than those from other variants, but skyrocketing cases will still put a strain on the health care system.
“The big caveat is we should not be complacent,” presidential Chief Medical Adviser Anthony Fauci, MD, said a White House briefing Jan. 5.
He added that Omicron “could still stress our hospital system because a certain proportion of a large volume of cases, no matter what, are going to be severe.”
Cases continue to increase greatly. This week’s 7-day daily average of infections is 491,700 -- an increase of 98% over last week, Dr. Walensky said. Hospitalizations, while lagging behind case numbers, are still rising significantly: The daily average is 14,800 admissions, up 63% from last week. Daily deaths this week are 1,200, an increase of only 5%.
Dr. Walensky continues to encourage vaccinations, boosters, and other precautions.
“Vaccines and boosters are protecting people from the severe and tragic outcomes that can occur from COVID-19 infection,” she said. “Get vaccinated and get boosted if eligible, wear a mask, stay home when you’re sick, and take a test if you have symptoms or are looking for greater reassurance before you gather with others.”
A version of this article first appeared on WebMD.com.
, Director Rochelle Walenksy, MD, said during a White House briefing Jan. 5.
Health officials recently shortened the recommended COVID-19 isolation and quarantine period from 10 days to 5, creating confusion amid an outbreak of the highly transmissible Omicron variant, which now accounts for 95% of cases in the United States.
Then, in slightly updated guidance, the CDC recommended using an at-home antigen test after 5 days of isolation if possible, even though these tests having aren’t as sensitive to the Omicron variant, according to the FDA.
“After we released our recs early last week, it became very clear people were interested in using the rapid test, though not authorized for this purpose after the end of their isolation period,” Dr. Walensky said. “We then provided guidance on how they should be used.”
“If that test is negative, people really do need to understand they must continue to wear their mask for those 5 days,” Dr. Walensky said.
But for many, the CDC guidelines are murky and seem to always change.
“Nearly 2 years into this pandemic, with Omicron cases surging across the country, the American people should be able to count on the Centers for Disease Control and Prevention for timely, accurate, clear guidance to protect themselves, their loved ones, and their communities,” American Medical Association president Gerald Harmon, MD, said in a statement. “Instead, the new recommendations on quarantine and isolation are not only confusing, but are risking further spread of the virus.”
About 31% of people remain infectious 5 days after a positive COVID-19 test, Dr. Harmon said, quoting the CDC’s own rationale for changing its guidance.
“With hundreds of thousands of new cases daily and more than a million positive reported cases on January 3, tens of thousands – potentially hundreds of thousands of people – could return to work and school infectious if they follow the CDC’s new guidance on ending isolation after 5 days without a negative test,” he said. “Physicians are concerned that these recommendations put our patients at risk and could further overwhelm our health care system.”
Instead, Dr. Harmon said a negative test should be required for ending isolation.
“Reemerging without knowing one’s status unnecessarily risks further transmission of the virus,” he said.
Meanwhile, also during the White House briefing, officials said that early data continue to show that Omicron infections are less severe than those from other variants, but skyrocketing cases will still put a strain on the health care system.
“The big caveat is we should not be complacent,” presidential Chief Medical Adviser Anthony Fauci, MD, said a White House briefing Jan. 5.
He added that Omicron “could still stress our hospital system because a certain proportion of a large volume of cases, no matter what, are going to be severe.”
Cases continue to increase greatly. This week’s 7-day daily average of infections is 491,700 -- an increase of 98% over last week, Dr. Walensky said. Hospitalizations, while lagging behind case numbers, are still rising significantly: The daily average is 14,800 admissions, up 63% from last week. Daily deaths this week are 1,200, an increase of only 5%.
Dr. Walensky continues to encourage vaccinations, boosters, and other precautions.
“Vaccines and boosters are protecting people from the severe and tragic outcomes that can occur from COVID-19 infection,” she said. “Get vaccinated and get boosted if eligible, wear a mask, stay home when you’re sick, and take a test if you have symptoms or are looking for greater reassurance before you gather with others.”
A version of this article first appeared on WebMD.com.
, Director Rochelle Walenksy, MD, said during a White House briefing Jan. 5.
Health officials recently shortened the recommended COVID-19 isolation and quarantine period from 10 days to 5, creating confusion amid an outbreak of the highly transmissible Omicron variant, which now accounts for 95% of cases in the United States.
Then, in slightly updated guidance, the CDC recommended using an at-home antigen test after 5 days of isolation if possible, even though these tests having aren’t as sensitive to the Omicron variant, according to the FDA.
“After we released our recs early last week, it became very clear people were interested in using the rapid test, though not authorized for this purpose after the end of their isolation period,” Dr. Walensky said. “We then provided guidance on how they should be used.”
“If that test is negative, people really do need to understand they must continue to wear their mask for those 5 days,” Dr. Walensky said.
But for many, the CDC guidelines are murky and seem to always change.
“Nearly 2 years into this pandemic, with Omicron cases surging across the country, the American people should be able to count on the Centers for Disease Control and Prevention for timely, accurate, clear guidance to protect themselves, their loved ones, and their communities,” American Medical Association president Gerald Harmon, MD, said in a statement. “Instead, the new recommendations on quarantine and isolation are not only confusing, but are risking further spread of the virus.”
About 31% of people remain infectious 5 days after a positive COVID-19 test, Dr. Harmon said, quoting the CDC’s own rationale for changing its guidance.
“With hundreds of thousands of new cases daily and more than a million positive reported cases on January 3, tens of thousands – potentially hundreds of thousands of people – could return to work and school infectious if they follow the CDC’s new guidance on ending isolation after 5 days without a negative test,” he said. “Physicians are concerned that these recommendations put our patients at risk and could further overwhelm our health care system.”
Instead, Dr. Harmon said a negative test should be required for ending isolation.
“Reemerging without knowing one’s status unnecessarily risks further transmission of the virus,” he said.
Meanwhile, also during the White House briefing, officials said that early data continue to show that Omicron infections are less severe than those from other variants, but skyrocketing cases will still put a strain on the health care system.
“The big caveat is we should not be complacent,” presidential Chief Medical Adviser Anthony Fauci, MD, said a White House briefing Jan. 5.
He added that Omicron “could still stress our hospital system because a certain proportion of a large volume of cases, no matter what, are going to be severe.”
Cases continue to increase greatly. This week’s 7-day daily average of infections is 491,700 -- an increase of 98% over last week, Dr. Walensky said. Hospitalizations, while lagging behind case numbers, are still rising significantly: The daily average is 14,800 admissions, up 63% from last week. Daily deaths this week are 1,200, an increase of only 5%.
Dr. Walensky continues to encourage vaccinations, boosters, and other precautions.
“Vaccines and boosters are protecting people from the severe and tragic outcomes that can occur from COVID-19 infection,” she said. “Get vaccinated and get boosted if eligible, wear a mask, stay home when you’re sick, and take a test if you have symptoms or are looking for greater reassurance before you gather with others.”
A version of this article first appeared on WebMD.com.
Freshwater aquarium provides source for melioidosis infection
A Maryland woman came down with a severe tropical infection called melioidosis from her freshwater home aquarium, says a report in Emerging Infectious Diseases describing a new route of transmission. Melioidosis is caused by the bacteria Burkholderia pseudomallei in soil or water.
Until last year, almost all U.S. cases of melioidosis were from people who lived or traveled to disease-endemic areas. It has been a rare infection in the United States.
But this is not the first case of melioidosis from an unusual source. Earlier in 2021, CDC and state epidemiologists traced an outbreak of melioidosis in Georgia, Kansas, Minnesota, and Texas to B pseudomallei in a bottle of “Better Homes & Gardens Lavender & Chamomile Essential Oil Infused Aromatherapy Room Spray with Gemstones.”
In the aquarium case, the patient was a 56-year-old woman with diabetes and rheumatologic disease. She had been on immunosuppressives (methotrexate, azathioprine, and prednisone) until 1 month before she became symptomatic. She was hospitalized for fever and pneumonia.
Multiple blood cultures obtained on days 1-4 grew B. pseudomallei, but she had no evidence of endocarditis or intravascular seeding. Despite weeks of meropenem (Merrem), she developed evidence of a lung abscess, and trimethoprim/sulfamethoxazole (Bactrim) was added. Ultimately, the patient required a 12-week course of antibiotics.
CDC epidemiologist Patrick Dawson, PhD, first author of the report, told this news organization that although outbreak investigators always ask about pet ownership, they have not explicitly asked about fish. In this case, the patient did not volunteer exposure to the fish.
When state epidemiologists visited the patient’s home, “one of the first things they saw was a few aquariums,” Dr. Dawson said. Seeing the water and knowing “that most freshwater tropical fish in the U.S. are imported from Southeast Asia” led them to culture specifically for B. pseudomallei, which can be difficult for the microbiology lab to identify.
From there, Dr. Dawson explained, “The Maryland Department of Health sent a team to the local pet store” but did not find any of the bacteria there. (The patient had bought her fish 6 months earlier.) The investigators then worked with the national brand “to identify where they had actually sourced the fish from.”
Two retailers supply almost all of U.S. guppies and plants. While investigators could not find an exact matching isolate after so many months had elapsed, they found a positive PCR for B. pseudomallei in a water sample from imported fish in Los Angeles.
Dr. Dawson said tropical fish are imported from southeast Asia and typically come from small family fish farms. The fish import industry has “certain products that they add to the water to hopefully kill any bacteria.” He was unaware whether this included antibiotics but suggested, “we would have seen many more cases [of antibiotic resistance] by now” if it did.
In general advice for the public, Dr. Dawson said, “I would recommend washing hands before and after contact with the aquarium. If you have cuts or wounds on your hands, it’s really important to wear gloves if you have to go clean or maintain the aquarium and you’re putting your hands in the water, just for that extra layer of protection. It’s probably a strong idea to just avoid that altogether if someone’s immunocompromised. And not letting young children under 5 years old clean aquariums.” These are the “simplest things to do to protect yourself.”
Stephen A. Smith, DVM, PhD, a professor in the Aquatic Medicine Program at Virginia-Maryland College of Veterinary Medicine, Blacksburg, also stressed the importance of careful hand hygiene when caring for aquariums. He said that the filter, filter floss, biofilm, charcoal, and gravel might have exceptionally high concentrations of bacteria. Dr. Smith also recommended gloves when cleaning aquariums and not doing this task if immunocompromised.
Dr. Smith, who was not involved in the CDC study, shared a broader perspective, noting that “the reason why it’s important to federal regulators is that [B. pseudomallei] is a tier 1 select agent. And so, when that was isolated, it sent up all the red flags.” The far more common Mycobacterium marinum, or fish handler’s disease, is not reportable.
Mycobacterium marinum is another pathogen of concern that can be acquired from aquariums. These infections typically occur as nodular lesions on the arms and require months of therapy.
Dr. Smith stressed the importance of physicians eliciting a careful exposure history as the key to diagnosing zoonoses. For most exotic aquarium animals, he noted, “They’re caught in the wild wherever they are. They’re transported to a major hub to transport to the U.S., and a lot of times, we don’t have quarantine for those animals.”
Dr. Smith said.
Many infections also occur in the course of water sports – or even hiking and getting a cut or abrasion wet from a stream or lake. Aeromonas hydrophila can cause life-threatening infections. Vibrio vulnificus infections from salt-water injuries can cause sepsis and characteristic hemorrhagic bullae – large, discolored blisters filled with body fluid – during the summer. And eating contaminated shellfish has a 50%-60% death rate.
Other exposures to water-loving bacteria happen during fishing or cleaning/preparing fish. For example, Streptococcus iniae has caused cellulitis, arthritis, endocarditis, and meningitis following superficial or puncture injuries, notably from cleaning tilapia.
Other infections from contact with fish include Erysipelothrix rhusiopathiae (primarily skin infections) and gastroenteritis from Plesiomonas shigelloides, Campylobacter spp, and Salmonella spp.
Each of these zoonoses illustrates the importance of a careful exposure history when there’s an atypical presentation or an infection that is not responding promptly to empiric treatment. The aquarium case broadens the differential to include melioidosis, a serious disease from southeast Asia.
Dr. Dawson and Dr. Smith have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A Maryland woman came down with a severe tropical infection called melioidosis from her freshwater home aquarium, says a report in Emerging Infectious Diseases describing a new route of transmission. Melioidosis is caused by the bacteria Burkholderia pseudomallei in soil or water.
Until last year, almost all U.S. cases of melioidosis were from people who lived or traveled to disease-endemic areas. It has been a rare infection in the United States.
But this is not the first case of melioidosis from an unusual source. Earlier in 2021, CDC and state epidemiologists traced an outbreak of melioidosis in Georgia, Kansas, Minnesota, and Texas to B pseudomallei in a bottle of “Better Homes & Gardens Lavender & Chamomile Essential Oil Infused Aromatherapy Room Spray with Gemstones.”
In the aquarium case, the patient was a 56-year-old woman with diabetes and rheumatologic disease. She had been on immunosuppressives (methotrexate, azathioprine, and prednisone) until 1 month before she became symptomatic. She was hospitalized for fever and pneumonia.
Multiple blood cultures obtained on days 1-4 grew B. pseudomallei, but she had no evidence of endocarditis or intravascular seeding. Despite weeks of meropenem (Merrem), she developed evidence of a lung abscess, and trimethoprim/sulfamethoxazole (Bactrim) was added. Ultimately, the patient required a 12-week course of antibiotics.
CDC epidemiologist Patrick Dawson, PhD, first author of the report, told this news organization that although outbreak investigators always ask about pet ownership, they have not explicitly asked about fish. In this case, the patient did not volunteer exposure to the fish.
When state epidemiologists visited the patient’s home, “one of the first things they saw was a few aquariums,” Dr. Dawson said. Seeing the water and knowing “that most freshwater tropical fish in the U.S. are imported from Southeast Asia” led them to culture specifically for B. pseudomallei, which can be difficult for the microbiology lab to identify.
From there, Dr. Dawson explained, “The Maryland Department of Health sent a team to the local pet store” but did not find any of the bacteria there. (The patient had bought her fish 6 months earlier.) The investigators then worked with the national brand “to identify where they had actually sourced the fish from.”
Two retailers supply almost all of U.S. guppies and plants. While investigators could not find an exact matching isolate after so many months had elapsed, they found a positive PCR for B. pseudomallei in a water sample from imported fish in Los Angeles.
Dr. Dawson said tropical fish are imported from southeast Asia and typically come from small family fish farms. The fish import industry has “certain products that they add to the water to hopefully kill any bacteria.” He was unaware whether this included antibiotics but suggested, “we would have seen many more cases [of antibiotic resistance] by now” if it did.
In general advice for the public, Dr. Dawson said, “I would recommend washing hands before and after contact with the aquarium. If you have cuts or wounds on your hands, it’s really important to wear gloves if you have to go clean or maintain the aquarium and you’re putting your hands in the water, just for that extra layer of protection. It’s probably a strong idea to just avoid that altogether if someone’s immunocompromised. And not letting young children under 5 years old clean aquariums.” These are the “simplest things to do to protect yourself.”
Stephen A. Smith, DVM, PhD, a professor in the Aquatic Medicine Program at Virginia-Maryland College of Veterinary Medicine, Blacksburg, also stressed the importance of careful hand hygiene when caring for aquariums. He said that the filter, filter floss, biofilm, charcoal, and gravel might have exceptionally high concentrations of bacteria. Dr. Smith also recommended gloves when cleaning aquariums and not doing this task if immunocompromised.
Dr. Smith, who was not involved in the CDC study, shared a broader perspective, noting that “the reason why it’s important to federal regulators is that [B. pseudomallei] is a tier 1 select agent. And so, when that was isolated, it sent up all the red flags.” The far more common Mycobacterium marinum, or fish handler’s disease, is not reportable.
Mycobacterium marinum is another pathogen of concern that can be acquired from aquariums. These infections typically occur as nodular lesions on the arms and require months of therapy.
Dr. Smith stressed the importance of physicians eliciting a careful exposure history as the key to diagnosing zoonoses. For most exotic aquarium animals, he noted, “They’re caught in the wild wherever they are. They’re transported to a major hub to transport to the U.S., and a lot of times, we don’t have quarantine for those animals.”
Dr. Smith said.
Many infections also occur in the course of water sports – or even hiking and getting a cut or abrasion wet from a stream or lake. Aeromonas hydrophila can cause life-threatening infections. Vibrio vulnificus infections from salt-water injuries can cause sepsis and characteristic hemorrhagic bullae – large, discolored blisters filled with body fluid – during the summer. And eating contaminated shellfish has a 50%-60% death rate.
Other exposures to water-loving bacteria happen during fishing or cleaning/preparing fish. For example, Streptococcus iniae has caused cellulitis, arthritis, endocarditis, and meningitis following superficial or puncture injuries, notably from cleaning tilapia.
Other infections from contact with fish include Erysipelothrix rhusiopathiae (primarily skin infections) and gastroenteritis from Plesiomonas shigelloides, Campylobacter spp, and Salmonella spp.
Each of these zoonoses illustrates the importance of a careful exposure history when there’s an atypical presentation or an infection that is not responding promptly to empiric treatment. The aquarium case broadens the differential to include melioidosis, a serious disease from southeast Asia.
Dr. Dawson and Dr. Smith have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A Maryland woman came down with a severe tropical infection called melioidosis from her freshwater home aquarium, says a report in Emerging Infectious Diseases describing a new route of transmission. Melioidosis is caused by the bacteria Burkholderia pseudomallei in soil or water.
Until last year, almost all U.S. cases of melioidosis were from people who lived or traveled to disease-endemic areas. It has been a rare infection in the United States.
But this is not the first case of melioidosis from an unusual source. Earlier in 2021, CDC and state epidemiologists traced an outbreak of melioidosis in Georgia, Kansas, Minnesota, and Texas to B pseudomallei in a bottle of “Better Homes & Gardens Lavender & Chamomile Essential Oil Infused Aromatherapy Room Spray with Gemstones.”
In the aquarium case, the patient was a 56-year-old woman with diabetes and rheumatologic disease. She had been on immunosuppressives (methotrexate, azathioprine, and prednisone) until 1 month before she became symptomatic. She was hospitalized for fever and pneumonia.
Multiple blood cultures obtained on days 1-4 grew B. pseudomallei, but she had no evidence of endocarditis or intravascular seeding. Despite weeks of meropenem (Merrem), she developed evidence of a lung abscess, and trimethoprim/sulfamethoxazole (Bactrim) was added. Ultimately, the patient required a 12-week course of antibiotics.
CDC epidemiologist Patrick Dawson, PhD, first author of the report, told this news organization that although outbreak investigators always ask about pet ownership, they have not explicitly asked about fish. In this case, the patient did not volunteer exposure to the fish.
When state epidemiologists visited the patient’s home, “one of the first things they saw was a few aquariums,” Dr. Dawson said. Seeing the water and knowing “that most freshwater tropical fish in the U.S. are imported from Southeast Asia” led them to culture specifically for B. pseudomallei, which can be difficult for the microbiology lab to identify.
From there, Dr. Dawson explained, “The Maryland Department of Health sent a team to the local pet store” but did not find any of the bacteria there. (The patient had bought her fish 6 months earlier.) The investigators then worked with the national brand “to identify where they had actually sourced the fish from.”
Two retailers supply almost all of U.S. guppies and plants. While investigators could not find an exact matching isolate after so many months had elapsed, they found a positive PCR for B. pseudomallei in a water sample from imported fish in Los Angeles.
Dr. Dawson said tropical fish are imported from southeast Asia and typically come from small family fish farms. The fish import industry has “certain products that they add to the water to hopefully kill any bacteria.” He was unaware whether this included antibiotics but suggested, “we would have seen many more cases [of antibiotic resistance] by now” if it did.
In general advice for the public, Dr. Dawson said, “I would recommend washing hands before and after contact with the aquarium. If you have cuts or wounds on your hands, it’s really important to wear gloves if you have to go clean or maintain the aquarium and you’re putting your hands in the water, just for that extra layer of protection. It’s probably a strong idea to just avoid that altogether if someone’s immunocompromised. And not letting young children under 5 years old clean aquariums.” These are the “simplest things to do to protect yourself.”
Stephen A. Smith, DVM, PhD, a professor in the Aquatic Medicine Program at Virginia-Maryland College of Veterinary Medicine, Blacksburg, also stressed the importance of careful hand hygiene when caring for aquariums. He said that the filter, filter floss, biofilm, charcoal, and gravel might have exceptionally high concentrations of bacteria. Dr. Smith also recommended gloves when cleaning aquariums and not doing this task if immunocompromised.
Dr. Smith, who was not involved in the CDC study, shared a broader perspective, noting that “the reason why it’s important to federal regulators is that [B. pseudomallei] is a tier 1 select agent. And so, when that was isolated, it sent up all the red flags.” The far more common Mycobacterium marinum, or fish handler’s disease, is not reportable.
Mycobacterium marinum is another pathogen of concern that can be acquired from aquariums. These infections typically occur as nodular lesions on the arms and require months of therapy.
Dr. Smith stressed the importance of physicians eliciting a careful exposure history as the key to diagnosing zoonoses. For most exotic aquarium animals, he noted, “They’re caught in the wild wherever they are. They’re transported to a major hub to transport to the U.S., and a lot of times, we don’t have quarantine for those animals.”
Dr. Smith said.
Many infections also occur in the course of water sports – or even hiking and getting a cut or abrasion wet from a stream or lake. Aeromonas hydrophila can cause life-threatening infections. Vibrio vulnificus infections from salt-water injuries can cause sepsis and characteristic hemorrhagic bullae – large, discolored blisters filled with body fluid – during the summer. And eating contaminated shellfish has a 50%-60% death rate.
Other exposures to water-loving bacteria happen during fishing or cleaning/preparing fish. For example, Streptococcus iniae has caused cellulitis, arthritis, endocarditis, and meningitis following superficial or puncture injuries, notably from cleaning tilapia.
Other infections from contact with fish include Erysipelothrix rhusiopathiae (primarily skin infections) and gastroenteritis from Plesiomonas shigelloides, Campylobacter spp, and Salmonella spp.
Each of these zoonoses illustrates the importance of a careful exposure history when there’s an atypical presentation or an infection that is not responding promptly to empiric treatment. The aquarium case broadens the differential to include melioidosis, a serious disease from southeast Asia.
Dr. Dawson and Dr. Smith have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Obesity prevention in infants benefits second-born too
According to a statement from the National Institutes of Health, who funded the study, it is the first such infant obesity intervention to show the spillover effect. Findings were published online Dec. 21, 2021, in Obesity.
The program is called Infants Growing on Healthy Trajectories (INSIGHT) responsive parenting (RP) intervention, and it included guidance on feeding, sleep, interactive play, and regulating emotion.
Parents were given guidance by nurses who came to their homes on how to respond when their child is drowsy, sleeping, fussy, and alert. They also learned how to put infants to bed drowsy, but awake, and avoid feeding infants to get them to sleep; how to respond to infants waking up at night; when to start solid foods; how to limit inactive time; and how to use growth charts.
The control group program focused on safety and matched the guidance categories. For example, early visits included information on prevention of sudden infant death syndrome for sleep, breast milk storage and formula for feeding, and safe bathing.
Jennifer S. Savage, Center for Childhood Obesity Research, Penn State University, University Park, led the study that enrolled 117 infants in a randomized controlled trial. Mother and firstborn children were randomized to the RP or home safety intervention (control) group 10-14 days after delivery. Their second-born siblings were enrolled in an observation-only ancillary study.
Second-born children were delivered 2.5 (standard deviation, 0.9) years after firstborns. Anthropometrics were measured in both siblings at ages 3, 16, 28, and 52 weeks.
Firstborn children at 1 year had a body mass index (BMI) that was 0.44 kg/m2 lower than the control group (95% confidence interval, −0.82 to −0.06), and second-born children whose parents received the RP intervention with their first child had BMI that was 0.36 kg/m2 lower.
“What we saw here is that it worked again,” coauthor Ian Paul, MD, MSc, professor of pediatrics and public health sciences at Penn State University, Hershey, said in an interview.
“Once we imprint them with a certain approach to parenting with the first child, they’re doing the same thing with the second child, which is wonderful to see,” he said.
He noted that this happened with second children without any reinforcements or booster information.
Dr. Paul said it’s still not clear which of the interventions – whether related to feeding techniques or sleeping or activity – helps most. And for each family the problematic behaviors may be different.
Responsive parenting programs have shown success previously among firstborns, the authors wrote, but 80% of those children grow up with younger siblings, so an intervention that also benefits them is important.
Weighing the costs of the intervention
The intervention was extensive. It involved four hour-plus nurse visits a year, often by the same nurse who built a relationship with the family.
But Ms. Savage said that it is possible to replicate INSIGHT on a larger scale in the United States with the dozens of home visitation models.
“Currently, 21 home visitation models meet the U.S. Department of Health & Human Services criteria for evidence of effectiveness, such as Nurse Family Partnership, Family Check-up, and Early Head Start Home Based Option. There is an opportunity to use home visitation models at the national scale to potentially interrupt the cycle of poor multigenerational outcomes such as obesity,” she said.
Dr. Paul said the initial investment “can save money in the long term,” given what’s at stake. “We know that 20%-25% of 2- to 5-year-olds are already overweight or obese and if they are already overweight or obese at that age, that;’s likely to persist.”
However, he acknowledged that staff shortages and costs are a challenge.
“Other countries have made that investment in their health care system,” he said. “In the U.S. only a fraction of new mothers and babies get home visitation. The kind of work that we did for obesity prevention has not yet been incorporated into evidence-based models of home visitation, though it certainly could be.”
Dr. Paul said his team is hoping to collaborate with others in the near future on expanding this program to such models of home visitation.
Telehealth, though a less desirable option, compared with in-home visits, could also be utilized, he said.
Short of the comprehensive intervention, he said, many of the concepts can be put into practice by pediatricians and parents.
Dr. Paul noted that the Robert Wood Johnson Foundation has endorsed “responsive feeding” as the preferred approach to feeding infants and toddlers. Responsive feeding – helping parents recognize hunger and satiety cues as opposed to other distress cues – is a big part of the intervention.
“Feeding to soothe is not the preferred approach,” he said. “Food and milk and formula should be used for hunger.” That’s something pediatricians may not be stressing to parents, he said.
Pediatricians can also counsel parents on not using food as a reward. “We shouldn’t be giving kids M&Ms to teach them how to potty train,” he said.
‘Promising’ findings
Charles Wood, MD, a childhood obesity specialist at Duke University, Durham, N.C., who was not part of the study, called the findings “very promising.”
It also makes sense that the “aha moments” of first-time parents learning from the INSIGHT intervention would carry over to the second sibling, he said.
Dr. Wood agreed costs are a big factor. However, he said, the potential downstream costs of not preventing obesity are worse. And this study indicates the benefits may keep spreading with future siblings.
Dr. Wood said accessing obesity interventions outside the pediatrician visit can also help. Connecting patients with support groups or dietitians or with a counselor from Women, Infants, and Children can help. However, consistent messaging among the providers is key, he noted.
Dr. Wood’s research group is investigating text messaging platforms so parents can get answer to real-time questions, such as those about feeding behaviors.
He pointed to a limitation the authors mention, which is that the study was done in mostly White, highly educated, higher-income families.
“There’s a big problem with racial disparities and obesity,” Dr. Wood noted. “We definitely need solutions that address disparities as well.”
Mothers included in the study had given birth for the first time and their infants were enrolled after birth from a single maternity ward between January 2012 and March 2014. Major eligibility criteria were that the babies were full term (at least 37 weeks’ gestation), single births, and delivered to English-speaking mothers at least 20 years of age. Infants who weighed less than 2,500 g at birth were excluded.
The paper’s authors and Dr. Wood declared no relevant financial relationships.
This research was supported by the National Institutes of Health, the National Institute of Diabetes and Digestive and Kidney Diseases; and the Department of Agriculture.
According to a statement from the National Institutes of Health, who funded the study, it is the first such infant obesity intervention to show the spillover effect. Findings were published online Dec. 21, 2021, in Obesity.
The program is called Infants Growing on Healthy Trajectories (INSIGHT) responsive parenting (RP) intervention, and it included guidance on feeding, sleep, interactive play, and regulating emotion.
Parents were given guidance by nurses who came to their homes on how to respond when their child is drowsy, sleeping, fussy, and alert. They also learned how to put infants to bed drowsy, but awake, and avoid feeding infants to get them to sleep; how to respond to infants waking up at night; when to start solid foods; how to limit inactive time; and how to use growth charts.
The control group program focused on safety and matched the guidance categories. For example, early visits included information on prevention of sudden infant death syndrome for sleep, breast milk storage and formula for feeding, and safe bathing.
Jennifer S. Savage, Center for Childhood Obesity Research, Penn State University, University Park, led the study that enrolled 117 infants in a randomized controlled trial. Mother and firstborn children were randomized to the RP or home safety intervention (control) group 10-14 days after delivery. Their second-born siblings were enrolled in an observation-only ancillary study.
Second-born children were delivered 2.5 (standard deviation, 0.9) years after firstborns. Anthropometrics were measured in both siblings at ages 3, 16, 28, and 52 weeks.
Firstborn children at 1 year had a body mass index (BMI) that was 0.44 kg/m2 lower than the control group (95% confidence interval, −0.82 to −0.06), and second-born children whose parents received the RP intervention with their first child had BMI that was 0.36 kg/m2 lower.
“What we saw here is that it worked again,” coauthor Ian Paul, MD, MSc, professor of pediatrics and public health sciences at Penn State University, Hershey, said in an interview.
“Once we imprint them with a certain approach to parenting with the first child, they’re doing the same thing with the second child, which is wonderful to see,” he said.
He noted that this happened with second children without any reinforcements or booster information.
Dr. Paul said it’s still not clear which of the interventions – whether related to feeding techniques or sleeping or activity – helps most. And for each family the problematic behaviors may be different.
Responsive parenting programs have shown success previously among firstborns, the authors wrote, but 80% of those children grow up with younger siblings, so an intervention that also benefits them is important.
Weighing the costs of the intervention
The intervention was extensive. It involved four hour-plus nurse visits a year, often by the same nurse who built a relationship with the family.
But Ms. Savage said that it is possible to replicate INSIGHT on a larger scale in the United States with the dozens of home visitation models.
“Currently, 21 home visitation models meet the U.S. Department of Health & Human Services criteria for evidence of effectiveness, such as Nurse Family Partnership, Family Check-up, and Early Head Start Home Based Option. There is an opportunity to use home visitation models at the national scale to potentially interrupt the cycle of poor multigenerational outcomes such as obesity,” she said.
Dr. Paul said the initial investment “can save money in the long term,” given what’s at stake. “We know that 20%-25% of 2- to 5-year-olds are already overweight or obese and if they are already overweight or obese at that age, that;’s likely to persist.”
However, he acknowledged that staff shortages and costs are a challenge.
“Other countries have made that investment in their health care system,” he said. “In the U.S. only a fraction of new mothers and babies get home visitation. The kind of work that we did for obesity prevention has not yet been incorporated into evidence-based models of home visitation, though it certainly could be.”
Dr. Paul said his team is hoping to collaborate with others in the near future on expanding this program to such models of home visitation.
Telehealth, though a less desirable option, compared with in-home visits, could also be utilized, he said.
Short of the comprehensive intervention, he said, many of the concepts can be put into practice by pediatricians and parents.
Dr. Paul noted that the Robert Wood Johnson Foundation has endorsed “responsive feeding” as the preferred approach to feeding infants and toddlers. Responsive feeding – helping parents recognize hunger and satiety cues as opposed to other distress cues – is a big part of the intervention.
“Feeding to soothe is not the preferred approach,” he said. “Food and milk and formula should be used for hunger.” That’s something pediatricians may not be stressing to parents, he said.
Pediatricians can also counsel parents on not using food as a reward. “We shouldn’t be giving kids M&Ms to teach them how to potty train,” he said.
‘Promising’ findings
Charles Wood, MD, a childhood obesity specialist at Duke University, Durham, N.C., who was not part of the study, called the findings “very promising.”
It also makes sense that the “aha moments” of first-time parents learning from the INSIGHT intervention would carry over to the second sibling, he said.
Dr. Wood agreed costs are a big factor. However, he said, the potential downstream costs of not preventing obesity are worse. And this study indicates the benefits may keep spreading with future siblings.
Dr. Wood said accessing obesity interventions outside the pediatrician visit can also help. Connecting patients with support groups or dietitians or with a counselor from Women, Infants, and Children can help. However, consistent messaging among the providers is key, he noted.
Dr. Wood’s research group is investigating text messaging platforms so parents can get answer to real-time questions, such as those about feeding behaviors.
He pointed to a limitation the authors mention, which is that the study was done in mostly White, highly educated, higher-income families.
“There’s a big problem with racial disparities and obesity,” Dr. Wood noted. “We definitely need solutions that address disparities as well.”
Mothers included in the study had given birth for the first time and their infants were enrolled after birth from a single maternity ward between January 2012 and March 2014. Major eligibility criteria were that the babies were full term (at least 37 weeks’ gestation), single births, and delivered to English-speaking mothers at least 20 years of age. Infants who weighed less than 2,500 g at birth were excluded.
The paper’s authors and Dr. Wood declared no relevant financial relationships.
This research was supported by the National Institutes of Health, the National Institute of Diabetes and Digestive and Kidney Diseases; and the Department of Agriculture.
According to a statement from the National Institutes of Health, who funded the study, it is the first such infant obesity intervention to show the spillover effect. Findings were published online Dec. 21, 2021, in Obesity.
The program is called Infants Growing on Healthy Trajectories (INSIGHT) responsive parenting (RP) intervention, and it included guidance on feeding, sleep, interactive play, and regulating emotion.
Parents were given guidance by nurses who came to their homes on how to respond when their child is drowsy, sleeping, fussy, and alert. They also learned how to put infants to bed drowsy, but awake, and avoid feeding infants to get them to sleep; how to respond to infants waking up at night; when to start solid foods; how to limit inactive time; and how to use growth charts.
The control group program focused on safety and matched the guidance categories. For example, early visits included information on prevention of sudden infant death syndrome for sleep, breast milk storage and formula for feeding, and safe bathing.
Jennifer S. Savage, Center for Childhood Obesity Research, Penn State University, University Park, led the study that enrolled 117 infants in a randomized controlled trial. Mother and firstborn children were randomized to the RP or home safety intervention (control) group 10-14 days after delivery. Their second-born siblings were enrolled in an observation-only ancillary study.
Second-born children were delivered 2.5 (standard deviation, 0.9) years after firstborns. Anthropometrics were measured in both siblings at ages 3, 16, 28, and 52 weeks.
Firstborn children at 1 year had a body mass index (BMI) that was 0.44 kg/m2 lower than the control group (95% confidence interval, −0.82 to −0.06), and second-born children whose parents received the RP intervention with their first child had BMI that was 0.36 kg/m2 lower.
“What we saw here is that it worked again,” coauthor Ian Paul, MD, MSc, professor of pediatrics and public health sciences at Penn State University, Hershey, said in an interview.
“Once we imprint them with a certain approach to parenting with the first child, they’re doing the same thing with the second child, which is wonderful to see,” he said.
He noted that this happened with second children without any reinforcements or booster information.
Dr. Paul said it’s still not clear which of the interventions – whether related to feeding techniques or sleeping or activity – helps most. And for each family the problematic behaviors may be different.
Responsive parenting programs have shown success previously among firstborns, the authors wrote, but 80% of those children grow up with younger siblings, so an intervention that also benefits them is important.
Weighing the costs of the intervention
The intervention was extensive. It involved four hour-plus nurse visits a year, often by the same nurse who built a relationship with the family.
But Ms. Savage said that it is possible to replicate INSIGHT on a larger scale in the United States with the dozens of home visitation models.
“Currently, 21 home visitation models meet the U.S. Department of Health & Human Services criteria for evidence of effectiveness, such as Nurse Family Partnership, Family Check-up, and Early Head Start Home Based Option. There is an opportunity to use home visitation models at the national scale to potentially interrupt the cycle of poor multigenerational outcomes such as obesity,” she said.
Dr. Paul said the initial investment “can save money in the long term,” given what’s at stake. “We know that 20%-25% of 2- to 5-year-olds are already overweight or obese and if they are already overweight or obese at that age, that;’s likely to persist.”
However, he acknowledged that staff shortages and costs are a challenge.
“Other countries have made that investment in their health care system,” he said. “In the U.S. only a fraction of new mothers and babies get home visitation. The kind of work that we did for obesity prevention has not yet been incorporated into evidence-based models of home visitation, though it certainly could be.”
Dr. Paul said his team is hoping to collaborate with others in the near future on expanding this program to such models of home visitation.
Telehealth, though a less desirable option, compared with in-home visits, could also be utilized, he said.
Short of the comprehensive intervention, he said, many of the concepts can be put into practice by pediatricians and parents.
Dr. Paul noted that the Robert Wood Johnson Foundation has endorsed “responsive feeding” as the preferred approach to feeding infants and toddlers. Responsive feeding – helping parents recognize hunger and satiety cues as opposed to other distress cues – is a big part of the intervention.
“Feeding to soothe is not the preferred approach,” he said. “Food and milk and formula should be used for hunger.” That’s something pediatricians may not be stressing to parents, he said.
Pediatricians can also counsel parents on not using food as a reward. “We shouldn’t be giving kids M&Ms to teach them how to potty train,” he said.
‘Promising’ findings
Charles Wood, MD, a childhood obesity specialist at Duke University, Durham, N.C., who was not part of the study, called the findings “very promising.”
It also makes sense that the “aha moments” of first-time parents learning from the INSIGHT intervention would carry over to the second sibling, he said.
Dr. Wood agreed costs are a big factor. However, he said, the potential downstream costs of not preventing obesity are worse. And this study indicates the benefits may keep spreading with future siblings.
Dr. Wood said accessing obesity interventions outside the pediatrician visit can also help. Connecting patients with support groups or dietitians or with a counselor from Women, Infants, and Children can help. However, consistent messaging among the providers is key, he noted.
Dr. Wood’s research group is investigating text messaging platforms so parents can get answer to real-time questions, such as those about feeding behaviors.
He pointed to a limitation the authors mention, which is that the study was done in mostly White, highly educated, higher-income families.
“There’s a big problem with racial disparities and obesity,” Dr. Wood noted. “We definitely need solutions that address disparities as well.”
Mothers included in the study had given birth for the first time and their infants were enrolled after birth from a single maternity ward between January 2012 and March 2014. Major eligibility criteria were that the babies were full term (at least 37 weeks’ gestation), single births, and delivered to English-speaking mothers at least 20 years of age. Infants who weighed less than 2,500 g at birth were excluded.
The paper’s authors and Dr. Wood declared no relevant financial relationships.
This research was supported by the National Institutes of Health, the National Institute of Diabetes and Digestive and Kidney Diseases; and the Department of Agriculture.
FROM OBESITY
Helping teens make the switch from pediatrics to gynecology
For many adolescents, the first visit to a gynecologist can be intimidating. The prospect of meeting a new doctor who will ask prying, deeply personal questions about sex and menstruation is scary. And, in all likelihood, a parent, older sibling, or friend has warned them about the notorious pelvic exam.
The exact timing of when adolescent patients should start seeing a gynecologist varies based on when a patient starts puberty. Primary care physicians and pediatricians can help teens transition by referring patients to an adolescent-friendly practice and clearing up some of the misconceptions that surround the first gynecology visit. Gynecologists, on the other side of the referral, can help patients transition by guaranteeing confidentiality and creating a safe space for young patients.
This news organization interviewed three experts in adolescent health about when teens should start having their gynecological needs addressed and how their physicians can help them undergo that transition.
Age-appropriate care
“Most people get very limited information about their reproductive health,” said Anne-Marie E. Amies Oelschlager, MD, a pediatric and adolescent gynecologist at Seattle Children’s, Seattle, and a member of the American College of Obstetricians and Gynecologists (ACOG) clinical consensus committee on gynecology.
Official guidelines from ACOG call for the initial reproductive health visit to take place between the ages of 13 and 15 years. The exact age may vary, however, depending on the specific needs of the patient.
For example, some patients begin menstruating early, at age 9 or 10, said Mary Romano, MD, MPH, a pediatrician and adolescent medicine specialist at Vanderbilt Children’s Hospital, Nashville, Tenn. Pediatricians who are uncomfortable educating young patients about menstruation should refer the patient to a gynecologist or a pediatric gynecologist for whom such discussions are routine.
If a patient does not have a menstrual cycle by age 14 or 15, that also should be addressed by a family physician or gynecologist, Dr. Romano added.
“The importance here is addressing the reproductive health of the teen starting really at the age of 10 or 12, or once puberty starts,” said Patricia S. Huguelet, MD, a pediatric and adolescent gynecologist at Children’s Hospital Colorado, Aurora. In those early visits, the physician can provide “anticipatory guidance,” counseling the teen on what is normal in terms of menstruation, sex, and relationships, and addressing what is not, she said.
Ideally, patients who were designated female at birth but now identify as male or nonbinary will meet with a gynecologist early on in the gender affirmation process and a gynecologist will continue to consult as part of the patient’s interdisciplinary care team, added Dr. Romano, who counsels LGBTQ+ youth as part of her practice. A gynecologist may support these patients in myriad ways, including helping those who are considering or using puberty blockers and providing reproductive and health education to patients in a way that is sensitive to the patient’s gender identity.
Patient referrals
Some pediatricians and family practice physicians may be talking with their patients about topics such as menstrual cycles and contraception. But those who are uncomfortable asking adolescent patients about their reproductive and sexual health should refer them to a gynecologist or specialist in adolescent medicine, Dr. Romano advised.
“The biggest benefit I’ve noticed is often [patients] come from a pediatrician or family medicine provider and they often appreciate the opportunity to talk to a doctor they haven’t met before about the more personal questions they may have,” Dr. Amies Oelschlager said.
Referring adolescents to a specialist who has either trained in adolescent medicine or has experience treating that age group has benefits, Dr. Romano said. Clinicians with that experience understand adolescents are not “mini-adults” but have unique developmental and medical issues. How to counsel and educate them carries unique challenges, she said.
For example, heavy menstrual bleeding is a leading reason a patient – either an adult or an adolescent – presents to a gynecologist, Dr. Huguelet said. But the pathology differs vastly for those two age groups. For patients in their 30s and 40s, polyps and fibroids are common problems associated with heavy bleeding. Those conditions are rare in adolescents, whereas bleeding disorders are common, she said.
Most patients will continue to see their pediatricians and primary care providers for other issues. And in some areas, gynecologists can reinforce advice from pediatricians, such as encouraging patients to get the HPV vaccine, Dr. Amies Oelschlager said.
Common misconceptions
Primary care physicians can also dispel common misconceptions teens – and their parents – have about gynecology. Some parents may believe that certain methods of birth control cause cancer or infertility, have concerns about the HPV vaccine, or think hormonal therapies are harmful, Dr. Amies Oelschlager said. But the biggest misconception involves the infamous pelvic exam.
“Lots of patients assume that every time they go to the gynecologist they are going to have a pelvic exam,” she said. “When I say, ‘We don’t have to do that,’ they are so relieved.”
Guidelines have changed since the parents of today’s teens were going to the gynecologist for the first time. Many patients now do not need an initial Pap smear until age 25, following a recent guideline change by the American Cancer Society. (ACOG is considering adopting the same stance but still recommends screening start at 21.) “Most patients do not need an exam, even when it comes to sexual health and screening [for sexually transmitted infections], that can be done without an exam,” Dr. Huguelet said.
Confidentiality and comfort
On the other side of the referral, gynecologists should follow several best practices to treat adolescent patients. Arguably the most important part of the initial gynecologic visit is to give patients the option of one-on-one time with the physician with no parent in the room. During that time, the physician should make it clear that what they discuss is confidential and will not be shared with their parent or guardian, Dr. Huguelet said. Patients should also have the option of having a friend or another nonparent individual in the room with them during this one-on-one time with the physician, particularly if the patient does not feel comfortable discussing sensitive subjects completely on her own.
Adolescents receive better care, disclose more, and perceive they are getting better care when the process is confidential, Dr. Romano said. Confidentiality does have limits, however, which physicians should also make sure their patients understand, according to the ACOG guidelines for the initial reproductive visit. These limitations can vary by state depending on issues related to mandatory reporting, insurance billing, and legal requirements of patient notifications of specific services such as abortion.
The use of electronic medical records has raised additional challenges when it comes to communicating privately with adolescent patients, Dr. Amies Oelschlager said. In her practice, she tries to ensure the adolescent is the one with the login information for their records. If not, her office will have the patient’s cell number to text or call securely.
“We feel strongly adolescents should be able to access reproductive health care, mental health care, and care for substance abuse disorders without parental notification,” Dr. Amies Oelschlager said.
Telehealth visits can also be helpful for adolescents coming to gynecology for the first time. And taking the time to establish a rapport with patients at the start of the visit is key, Dr. Huguelet said. By directing questions to the adolescent patient rather than the parent, Dr. Huguelet said, the physician demonstrates that the teen’s treatment needs come first.
ACOG has guidelines on other steps gynecology practices, including those that see both adults and teens, can take to make their offices and visits adolescent-friendly. These steps include asking patients about their preferred names and pronouns at the start of the visit or as part of the initial intake form, training office staff to be comfortable with issues related to adolescent sexuality and gender and sexual diversity among patients, providing a place for teens to wait separately from obstetrics patients, and having age-appropriate literature on hand for adolescents to learn about reproductive health.
After that first reproductive health visit, gynecologists and primary care providers should partner to ensure the whole health of their patients is being addressed, Dr. Huguelet said.
“Collaboration is always going to better serve patients in any area,” said Dr. Romano, “and certainly this area is no different.”
Dr. Amies Oelschlager, Dr. Romano, and Dr. Huguelet have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
For many adolescents, the first visit to a gynecologist can be intimidating. The prospect of meeting a new doctor who will ask prying, deeply personal questions about sex and menstruation is scary. And, in all likelihood, a parent, older sibling, or friend has warned them about the notorious pelvic exam.
The exact timing of when adolescent patients should start seeing a gynecologist varies based on when a patient starts puberty. Primary care physicians and pediatricians can help teens transition by referring patients to an adolescent-friendly practice and clearing up some of the misconceptions that surround the first gynecology visit. Gynecologists, on the other side of the referral, can help patients transition by guaranteeing confidentiality and creating a safe space for young patients.
This news organization interviewed three experts in adolescent health about when teens should start having their gynecological needs addressed and how their physicians can help them undergo that transition.
Age-appropriate care
“Most people get very limited information about their reproductive health,” said Anne-Marie E. Amies Oelschlager, MD, a pediatric and adolescent gynecologist at Seattle Children’s, Seattle, and a member of the American College of Obstetricians and Gynecologists (ACOG) clinical consensus committee on gynecology.
Official guidelines from ACOG call for the initial reproductive health visit to take place between the ages of 13 and 15 years. The exact age may vary, however, depending on the specific needs of the patient.
For example, some patients begin menstruating early, at age 9 or 10, said Mary Romano, MD, MPH, a pediatrician and adolescent medicine specialist at Vanderbilt Children’s Hospital, Nashville, Tenn. Pediatricians who are uncomfortable educating young patients about menstruation should refer the patient to a gynecologist or a pediatric gynecologist for whom such discussions are routine.
If a patient does not have a menstrual cycle by age 14 or 15, that also should be addressed by a family physician or gynecologist, Dr. Romano added.
“The importance here is addressing the reproductive health of the teen starting really at the age of 10 or 12, or once puberty starts,” said Patricia S. Huguelet, MD, a pediatric and adolescent gynecologist at Children’s Hospital Colorado, Aurora. In those early visits, the physician can provide “anticipatory guidance,” counseling the teen on what is normal in terms of menstruation, sex, and relationships, and addressing what is not, she said.
Ideally, patients who were designated female at birth but now identify as male or nonbinary will meet with a gynecologist early on in the gender affirmation process and a gynecologist will continue to consult as part of the patient’s interdisciplinary care team, added Dr. Romano, who counsels LGBTQ+ youth as part of her practice. A gynecologist may support these patients in myriad ways, including helping those who are considering or using puberty blockers and providing reproductive and health education to patients in a way that is sensitive to the patient’s gender identity.
Patient referrals
Some pediatricians and family practice physicians may be talking with their patients about topics such as menstrual cycles and contraception. But those who are uncomfortable asking adolescent patients about their reproductive and sexual health should refer them to a gynecologist or specialist in adolescent medicine, Dr. Romano advised.
“The biggest benefit I’ve noticed is often [patients] come from a pediatrician or family medicine provider and they often appreciate the opportunity to talk to a doctor they haven’t met before about the more personal questions they may have,” Dr. Amies Oelschlager said.
Referring adolescents to a specialist who has either trained in adolescent medicine or has experience treating that age group has benefits, Dr. Romano said. Clinicians with that experience understand adolescents are not “mini-adults” but have unique developmental and medical issues. How to counsel and educate them carries unique challenges, she said.
For example, heavy menstrual bleeding is a leading reason a patient – either an adult or an adolescent – presents to a gynecologist, Dr. Huguelet said. But the pathology differs vastly for those two age groups. For patients in their 30s and 40s, polyps and fibroids are common problems associated with heavy bleeding. Those conditions are rare in adolescents, whereas bleeding disorders are common, she said.
Most patients will continue to see their pediatricians and primary care providers for other issues. And in some areas, gynecologists can reinforce advice from pediatricians, such as encouraging patients to get the HPV vaccine, Dr. Amies Oelschlager said.
Common misconceptions
Primary care physicians can also dispel common misconceptions teens – and their parents – have about gynecology. Some parents may believe that certain methods of birth control cause cancer or infertility, have concerns about the HPV vaccine, or think hormonal therapies are harmful, Dr. Amies Oelschlager said. But the biggest misconception involves the infamous pelvic exam.
“Lots of patients assume that every time they go to the gynecologist they are going to have a pelvic exam,” she said. “When I say, ‘We don’t have to do that,’ they are so relieved.”
Guidelines have changed since the parents of today’s teens were going to the gynecologist for the first time. Many patients now do not need an initial Pap smear until age 25, following a recent guideline change by the American Cancer Society. (ACOG is considering adopting the same stance but still recommends screening start at 21.) “Most patients do not need an exam, even when it comes to sexual health and screening [for sexually transmitted infections], that can be done without an exam,” Dr. Huguelet said.
Confidentiality and comfort
On the other side of the referral, gynecologists should follow several best practices to treat adolescent patients. Arguably the most important part of the initial gynecologic visit is to give patients the option of one-on-one time with the physician with no parent in the room. During that time, the physician should make it clear that what they discuss is confidential and will not be shared with their parent or guardian, Dr. Huguelet said. Patients should also have the option of having a friend or another nonparent individual in the room with them during this one-on-one time with the physician, particularly if the patient does not feel comfortable discussing sensitive subjects completely on her own.
Adolescents receive better care, disclose more, and perceive they are getting better care when the process is confidential, Dr. Romano said. Confidentiality does have limits, however, which physicians should also make sure their patients understand, according to the ACOG guidelines for the initial reproductive visit. These limitations can vary by state depending on issues related to mandatory reporting, insurance billing, and legal requirements of patient notifications of specific services such as abortion.
The use of electronic medical records has raised additional challenges when it comes to communicating privately with adolescent patients, Dr. Amies Oelschlager said. In her practice, she tries to ensure the adolescent is the one with the login information for their records. If not, her office will have the patient’s cell number to text or call securely.
“We feel strongly adolescents should be able to access reproductive health care, mental health care, and care for substance abuse disorders without parental notification,” Dr. Amies Oelschlager said.
Telehealth visits can also be helpful for adolescents coming to gynecology for the first time. And taking the time to establish a rapport with patients at the start of the visit is key, Dr. Huguelet said. By directing questions to the adolescent patient rather than the parent, Dr. Huguelet said, the physician demonstrates that the teen’s treatment needs come first.
ACOG has guidelines on other steps gynecology practices, including those that see both adults and teens, can take to make their offices and visits adolescent-friendly. These steps include asking patients about their preferred names and pronouns at the start of the visit or as part of the initial intake form, training office staff to be comfortable with issues related to adolescent sexuality and gender and sexual diversity among patients, providing a place for teens to wait separately from obstetrics patients, and having age-appropriate literature on hand for adolescents to learn about reproductive health.
After that first reproductive health visit, gynecologists and primary care providers should partner to ensure the whole health of their patients is being addressed, Dr. Huguelet said.
“Collaboration is always going to better serve patients in any area,” said Dr. Romano, “and certainly this area is no different.”
Dr. Amies Oelschlager, Dr. Romano, and Dr. Huguelet have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
For many adolescents, the first visit to a gynecologist can be intimidating. The prospect of meeting a new doctor who will ask prying, deeply personal questions about sex and menstruation is scary. And, in all likelihood, a parent, older sibling, or friend has warned them about the notorious pelvic exam.
The exact timing of when adolescent patients should start seeing a gynecologist varies based on when a patient starts puberty. Primary care physicians and pediatricians can help teens transition by referring patients to an adolescent-friendly practice and clearing up some of the misconceptions that surround the first gynecology visit. Gynecologists, on the other side of the referral, can help patients transition by guaranteeing confidentiality and creating a safe space for young patients.
This news organization interviewed three experts in adolescent health about when teens should start having their gynecological needs addressed and how their physicians can help them undergo that transition.
Age-appropriate care
“Most people get very limited information about their reproductive health,” said Anne-Marie E. Amies Oelschlager, MD, a pediatric and adolescent gynecologist at Seattle Children’s, Seattle, and a member of the American College of Obstetricians and Gynecologists (ACOG) clinical consensus committee on gynecology.
Official guidelines from ACOG call for the initial reproductive health visit to take place between the ages of 13 and 15 years. The exact age may vary, however, depending on the specific needs of the patient.
For example, some patients begin menstruating early, at age 9 or 10, said Mary Romano, MD, MPH, a pediatrician and adolescent medicine specialist at Vanderbilt Children’s Hospital, Nashville, Tenn. Pediatricians who are uncomfortable educating young patients about menstruation should refer the patient to a gynecologist or a pediatric gynecologist for whom such discussions are routine.
If a patient does not have a menstrual cycle by age 14 or 15, that also should be addressed by a family physician or gynecologist, Dr. Romano added.
“The importance here is addressing the reproductive health of the teen starting really at the age of 10 or 12, or once puberty starts,” said Patricia S. Huguelet, MD, a pediatric and adolescent gynecologist at Children’s Hospital Colorado, Aurora. In those early visits, the physician can provide “anticipatory guidance,” counseling the teen on what is normal in terms of menstruation, sex, and relationships, and addressing what is not, she said.
Ideally, patients who were designated female at birth but now identify as male or nonbinary will meet with a gynecologist early on in the gender affirmation process and a gynecologist will continue to consult as part of the patient’s interdisciplinary care team, added Dr. Romano, who counsels LGBTQ+ youth as part of her practice. A gynecologist may support these patients in myriad ways, including helping those who are considering or using puberty blockers and providing reproductive and health education to patients in a way that is sensitive to the patient’s gender identity.
Patient referrals
Some pediatricians and family practice physicians may be talking with their patients about topics such as menstrual cycles and contraception. But those who are uncomfortable asking adolescent patients about their reproductive and sexual health should refer them to a gynecologist or specialist in adolescent medicine, Dr. Romano advised.
“The biggest benefit I’ve noticed is often [patients] come from a pediatrician or family medicine provider and they often appreciate the opportunity to talk to a doctor they haven’t met before about the more personal questions they may have,” Dr. Amies Oelschlager said.
Referring adolescents to a specialist who has either trained in adolescent medicine or has experience treating that age group has benefits, Dr. Romano said. Clinicians with that experience understand adolescents are not “mini-adults” but have unique developmental and medical issues. How to counsel and educate them carries unique challenges, she said.
For example, heavy menstrual bleeding is a leading reason a patient – either an adult or an adolescent – presents to a gynecologist, Dr. Huguelet said. But the pathology differs vastly for those two age groups. For patients in their 30s and 40s, polyps and fibroids are common problems associated with heavy bleeding. Those conditions are rare in adolescents, whereas bleeding disorders are common, she said.
Most patients will continue to see their pediatricians and primary care providers for other issues. And in some areas, gynecologists can reinforce advice from pediatricians, such as encouraging patients to get the HPV vaccine, Dr. Amies Oelschlager said.
Common misconceptions
Primary care physicians can also dispel common misconceptions teens – and their parents – have about gynecology. Some parents may believe that certain methods of birth control cause cancer or infertility, have concerns about the HPV vaccine, or think hormonal therapies are harmful, Dr. Amies Oelschlager said. But the biggest misconception involves the infamous pelvic exam.
“Lots of patients assume that every time they go to the gynecologist they are going to have a pelvic exam,” she said. “When I say, ‘We don’t have to do that,’ they are so relieved.”
Guidelines have changed since the parents of today’s teens were going to the gynecologist for the first time. Many patients now do not need an initial Pap smear until age 25, following a recent guideline change by the American Cancer Society. (ACOG is considering adopting the same stance but still recommends screening start at 21.) “Most patients do not need an exam, even when it comes to sexual health and screening [for sexually transmitted infections], that can be done without an exam,” Dr. Huguelet said.
Confidentiality and comfort
On the other side of the referral, gynecologists should follow several best practices to treat adolescent patients. Arguably the most important part of the initial gynecologic visit is to give patients the option of one-on-one time with the physician with no parent in the room. During that time, the physician should make it clear that what they discuss is confidential and will not be shared with their parent or guardian, Dr. Huguelet said. Patients should also have the option of having a friend or another nonparent individual in the room with them during this one-on-one time with the physician, particularly if the patient does not feel comfortable discussing sensitive subjects completely on her own.
Adolescents receive better care, disclose more, and perceive they are getting better care when the process is confidential, Dr. Romano said. Confidentiality does have limits, however, which physicians should also make sure their patients understand, according to the ACOG guidelines for the initial reproductive visit. These limitations can vary by state depending on issues related to mandatory reporting, insurance billing, and legal requirements of patient notifications of specific services such as abortion.
The use of electronic medical records has raised additional challenges when it comes to communicating privately with adolescent patients, Dr. Amies Oelschlager said. In her practice, she tries to ensure the adolescent is the one with the login information for their records. If not, her office will have the patient’s cell number to text or call securely.
“We feel strongly adolescents should be able to access reproductive health care, mental health care, and care for substance abuse disorders without parental notification,” Dr. Amies Oelschlager said.
Telehealth visits can also be helpful for adolescents coming to gynecology for the first time. And taking the time to establish a rapport with patients at the start of the visit is key, Dr. Huguelet said. By directing questions to the adolescent patient rather than the parent, Dr. Huguelet said, the physician demonstrates that the teen’s treatment needs come first.
ACOG has guidelines on other steps gynecology practices, including those that see both adults and teens, can take to make their offices and visits adolescent-friendly. These steps include asking patients about their preferred names and pronouns at the start of the visit or as part of the initial intake form, training office staff to be comfortable with issues related to adolescent sexuality and gender and sexual diversity among patients, providing a place for teens to wait separately from obstetrics patients, and having age-appropriate literature on hand for adolescents to learn about reproductive health.
After that first reproductive health visit, gynecologists and primary care providers should partner to ensure the whole health of their patients is being addressed, Dr. Huguelet said.
“Collaboration is always going to better serve patients in any area,” said Dr. Romano, “and certainly this area is no different.”
Dr. Amies Oelschlager, Dr. Romano, and Dr. Huguelet have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Surgeon General releases child mental health call to action
The nation’s Surgeon General, Vice Admiral Vivek H. Murthy, MD, MBA, recently released an advisory report on the current state of youth mental health and recommendations to improve well-being. This action follows a number of emergency declarations that have been made by professional organizations such as the American Academy of Child and Adolescent Psychiatry (AACAP), the American Academy of Pediatrics (AAP), and other health care groups to raise awareness about the alarming increase of depression, suicide, anxiety, and other mental health problems in youth.
These reports can be helpful in focusing attention and resources for important public health problems. Many still reference the 1999 report from former Surgeon General David Satcher, MD, PhD, which offered a number of eye-opening statistics regarding the prevalence of mental health conditions and the amount of disability associated with them.

Sadly, the present report indicates that many of these indices have grown worse in the past 20 years. For example, the advisory notes that, even before COVID-19, fully half of female high school students reported persistent feelings of sadness or hopelessness (up 40% from 2009). The report then goes on to cite a number of studies documenting even further rises in youth mental health problems associated with the pandemic.
Most of the advisory, however, is devoted to actions that can be taken by different groups, including young people themselves, parents, educators, the government, and even social media and video game companies, to support mental health and well-being. Multiple online resources are provided at the end of each of these sections.
One of the segments is aimed at health care organizations and professionals. While first making a fairly sweeping statement that “our health care system today is not set up optimally to support the mental health and well-being of children and youth,” this part then outlines five broad recommendations that might help improve the fit. These include the following.
- Increase prevention efforts, such as coordination to enrichment programs and referrals for economic and legal supports for families in need.
- Screen routinely for mental health conditions and link those who screen in with appropriate care.
- Identify mental health needs in parents and caregivers such as depression and substance use that can have negative effects on children.
- Increase partnerships between health care groups and community organizations.
- Build multidisciplinary teams that are culturally appropriate and maximally engage children and caretakers in the decision-making process.
The current report is downloadable for free (see reference below) and it is certainly worthwhile for pediatricians to take a look. Dr. Murthy writes, regarding the current state of mental health, that “it would be a tragedy if we beat back one public health crisis only to allow another to grow in its place.”
The report also outlines specific areas where additional research is needed, such as data on racial and sexual minorities and research on innovative and scalable therapies. In addition to the online resources that are provided, the report is backed by over 250 references.
Since its release, the report has generally been well received, and, indeed, there is much to support. The well-known Child Mind Institute in New York tweeted that “this document is a wake-up call for the country and a long-overdue statement of leadership from the federal government.”
Many of the recommendations are admittedly somewhat commons sense, but there are some that are much less so. For example, one recommendation to youth themselves is to serve others – something that may first come across as counterintuitive but can indeed help children and adolescents develop a sense of purpose and self-worth. The call for pediatric health care professionals to screen parents in addition to the patients themselves will likely result in some debate as well. The recommendation to reduce access to lethal means, including the specific naming of firearms, is also a welcome addition. This report also rightly puts a spotlight on the role of societal factors such as racism and poverty in the development of mental health problems and in getting access to quality treatment.
Also worth noting is how much of the advisory examined the role of media in both the problem and the solution. While recognizing that technology, smartphones, and social media are here to stay, a number of suggestions were given to parents, media organizations, journalists, and entertainment companies to reduce the negative impacts these mediums can have. Explicitly recognized in the report is that “there can be tension between what’s best for the technology company and what’s best for the individual user or society.” Also acknowledged was that the link between media of various types and mental health is complex and inconsistent with there being a strong need for additional work in this area when it comes to academic research as well as product development within these companies themselves.
Yet while there is much to like about the advisory, there remain some areas that seem lacking. For example, the text about what causes mental health conditions gets a little dualistic in mentioning biological and environmental factors without much appreciation that these are hardly independent domains. Perhaps more substantially, there was surprisingly little airtime devoted to an enormous issue that underlies so many other challenges related to mental health care – namely an inadequate workforce that gets smaller by the minute. The topic was treated much too superficially with lots of vague calls to “expand” the workforce that lacked substance or detail.
Overall, however, the new Surgeon General’s Advisory is a welcome document that offers updated knowledge of our current challenges and provides practical responses that truly could make a difference. Now all we have to do is put these recommendations into action.
Dr. Rettew is a child and adolescent psychiatrist and medical director of Lane County Behavioral Health in Eugene, Ore. His latest book is “Parenting Made Complicated: What Science Really Knows About the Greatest Debates of Early Childhood.” You can follow him on Twitter and Facebook @PediPsych.
Reference
“Protecting Youth Mental Health – The U.S. Surgeon General’s Advisory,” U.S. Department of Health & Human Services (2021).
The nation’s Surgeon General, Vice Admiral Vivek H. Murthy, MD, MBA, recently released an advisory report on the current state of youth mental health and recommendations to improve well-being. This action follows a number of emergency declarations that have been made by professional organizations such as the American Academy of Child and Adolescent Psychiatry (AACAP), the American Academy of Pediatrics (AAP), and other health care groups to raise awareness about the alarming increase of depression, suicide, anxiety, and other mental health problems in youth.
These reports can be helpful in focusing attention and resources for important public health problems. Many still reference the 1999 report from former Surgeon General David Satcher, MD, PhD, which offered a number of eye-opening statistics regarding the prevalence of mental health conditions and the amount of disability associated with them.
Sadly, the present report indicates that many of these indices have grown worse in the past 20 years. For example, the advisory notes that, even before COVID-19, fully half of female high school students reported persistent feelings of sadness or hopelessness (up 40% from 2009). The report then goes on to cite a number of studies documenting even further rises in youth mental health problems associated with the pandemic.
Most of the advisory, however, is devoted to actions that can be taken by different groups, including young people themselves, parents, educators, the government, and even social media and video game companies, to support mental health and well-being. Multiple online resources are provided at the end of each of these sections.
One of the segments is aimed at health care organizations and professionals. While first making a fairly sweeping statement that “our health care system today is not set up optimally to support the mental health and well-being of children and youth,” this part then outlines five broad recommendations that might help improve the fit. These include the following.
- Increase prevention efforts, such as coordination to enrichment programs and referrals for economic and legal supports for families in need.
- Screen routinely for mental health conditions and link those who screen in with appropriate care.
- Identify mental health needs in parents and caregivers such as depression and substance use that can have negative effects on children.
- Increase partnerships between health care groups and community organizations.
- Build multidisciplinary teams that are culturally appropriate and maximally engage children and caretakers in the decision-making process.
The current report is downloadable for free (see reference below) and it is certainly worthwhile for pediatricians to take a look. Dr. Murthy writes, regarding the current state of mental health, that “it would be a tragedy if we beat back one public health crisis only to allow another to grow in its place.”
The report also outlines specific areas where additional research is needed, such as data on racial and sexual minorities and research on innovative and scalable therapies. In addition to the online resources that are provided, the report is backed by over 250 references.
Since its release, the report has generally been well received, and, indeed, there is much to support. The well-known Child Mind Institute in New York tweeted that “this document is a wake-up call for the country and a long-overdue statement of leadership from the federal government.”
Many of the recommendations are admittedly somewhat commons sense, but there are some that are much less so. For example, one recommendation to youth themselves is to serve others – something that may first come across as counterintuitive but can indeed help children and adolescents develop a sense of purpose and self-worth. The call for pediatric health care professionals to screen parents in addition to the patients themselves will likely result in some debate as well. The recommendation to reduce access to lethal means, including the specific naming of firearms, is also a welcome addition. This report also rightly puts a spotlight on the role of societal factors such as racism and poverty in the development of mental health problems and in getting access to quality treatment.
Also worth noting is how much of the advisory examined the role of media in both the problem and the solution. While recognizing that technology, smartphones, and social media are here to stay, a number of suggestions were given to parents, media organizations, journalists, and entertainment companies to reduce the negative impacts these mediums can have. Explicitly recognized in the report is that “there can be tension between what’s best for the technology company and what’s best for the individual user or society.” Also acknowledged was that the link between media of various types and mental health is complex and inconsistent with there being a strong need for additional work in this area when it comes to academic research as well as product development within these companies themselves.
Yet while there is much to like about the advisory, there remain some areas that seem lacking. For example, the text about what causes mental health conditions gets a little dualistic in mentioning biological and environmental factors without much appreciation that these are hardly independent domains. Perhaps more substantially, there was surprisingly little airtime devoted to an enormous issue that underlies so many other challenges related to mental health care – namely an inadequate workforce that gets smaller by the minute. The topic was treated much too superficially with lots of vague calls to “expand” the workforce that lacked substance or detail.
Overall, however, the new Surgeon General’s Advisory is a welcome document that offers updated knowledge of our current challenges and provides practical responses that truly could make a difference. Now all we have to do is put these recommendations into action.
Dr. Rettew is a child and adolescent psychiatrist and medical director of Lane County Behavioral Health in Eugene, Ore. His latest book is “Parenting Made Complicated: What Science Really Knows About the Greatest Debates of Early Childhood.” You can follow him on Twitter and Facebook @PediPsych.
Reference
“Protecting Youth Mental Health – The U.S. Surgeon General’s Advisory,” U.S. Department of Health & Human Services (2021).
The nation’s Surgeon General, Vice Admiral Vivek H. Murthy, MD, MBA, recently released an advisory report on the current state of youth mental health and recommendations to improve well-being. This action follows a number of emergency declarations that have been made by professional organizations such as the American Academy of Child and Adolescent Psychiatry (AACAP), the American Academy of Pediatrics (AAP), and other health care groups to raise awareness about the alarming increase of depression, suicide, anxiety, and other mental health problems in youth.
These reports can be helpful in focusing attention and resources for important public health problems. Many still reference the 1999 report from former Surgeon General David Satcher, MD, PhD, which offered a number of eye-opening statistics regarding the prevalence of mental health conditions and the amount of disability associated with them.
Sadly, the present report indicates that many of these indices have grown worse in the past 20 years. For example, the advisory notes that, even before COVID-19, fully half of female high school students reported persistent feelings of sadness or hopelessness (up 40% from 2009). The report then goes on to cite a number of studies documenting even further rises in youth mental health problems associated with the pandemic.
Most of the advisory, however, is devoted to actions that can be taken by different groups, including young people themselves, parents, educators, the government, and even social media and video game companies, to support mental health and well-being. Multiple online resources are provided at the end of each of these sections.
One of the segments is aimed at health care organizations and professionals. While first making a fairly sweeping statement that “our health care system today is not set up optimally to support the mental health and well-being of children and youth,” this part then outlines five broad recommendations that might help improve the fit. These include the following.
- Increase prevention efforts, such as coordination to enrichment programs and referrals for economic and legal supports for families in need.
- Screen routinely for mental health conditions and link those who screen in with appropriate care.
- Identify mental health needs in parents and caregivers such as depression and substance use that can have negative effects on children.
- Increase partnerships between health care groups and community organizations.
- Build multidisciplinary teams that are culturally appropriate and maximally engage children and caretakers in the decision-making process.
The current report is downloadable for free (see reference below) and it is certainly worthwhile for pediatricians to take a look. Dr. Murthy writes, regarding the current state of mental health, that “it would be a tragedy if we beat back one public health crisis only to allow another to grow in its place.”
The report also outlines specific areas where additional research is needed, such as data on racial and sexual minorities and research on innovative and scalable therapies. In addition to the online resources that are provided, the report is backed by over 250 references.
Since its release, the report has generally been well received, and, indeed, there is much to support. The well-known Child Mind Institute in New York tweeted that “this document is a wake-up call for the country and a long-overdue statement of leadership from the federal government.”
Many of the recommendations are admittedly somewhat commons sense, but there are some that are much less so. For example, one recommendation to youth themselves is to serve others – something that may first come across as counterintuitive but can indeed help children and adolescents develop a sense of purpose and self-worth. The call for pediatric health care professionals to screen parents in addition to the patients themselves will likely result in some debate as well. The recommendation to reduce access to lethal means, including the specific naming of firearms, is also a welcome addition. This report also rightly puts a spotlight on the role of societal factors such as racism and poverty in the development of mental health problems and in getting access to quality treatment.
Also worth noting is how much of the advisory examined the role of media in both the problem and the solution. While recognizing that technology, smartphones, and social media are here to stay, a number of suggestions were given to parents, media organizations, journalists, and entertainment companies to reduce the negative impacts these mediums can have. Explicitly recognized in the report is that “there can be tension between what’s best for the technology company and what’s best for the individual user or society.” Also acknowledged was that the link between media of various types and mental health is complex and inconsistent with there being a strong need for additional work in this area when it comes to academic research as well as product development within these companies themselves.
Yet while there is much to like about the advisory, there remain some areas that seem lacking. For example, the text about what causes mental health conditions gets a little dualistic in mentioning biological and environmental factors without much appreciation that these are hardly independent domains. Perhaps more substantially, there was surprisingly little airtime devoted to an enormous issue that underlies so many other challenges related to mental health care – namely an inadequate workforce that gets smaller by the minute. The topic was treated much too superficially with lots of vague calls to “expand” the workforce that lacked substance or detail.
Overall, however, the new Surgeon General’s Advisory is a welcome document that offers updated knowledge of our current challenges and provides practical responses that truly could make a difference. Now all we have to do is put these recommendations into action.
Dr. Rettew is a child and adolescent psychiatrist and medical director of Lane County Behavioral Health in Eugene, Ore. His latest book is “Parenting Made Complicated: What Science Really Knows About the Greatest Debates of Early Childhood.” You can follow him on Twitter and Facebook @PediPsych.
Reference
“Protecting Youth Mental Health – The U.S. Surgeon General’s Advisory,” U.S. Department of Health & Human Services (2021).
Children and COVID: New cases, admissions are higher than ever
Weekly COVID-19 cases in children passed 300,000 for the first time since the pandemic started, according to the American Academy of Pediatrics and the Children’s Hospital Association.
The rate of new COVID-related hospital admissions also reached a new high of 0.74 per 100,000 children as of Dec. 31. The highest rate seen before the current Omicron-fueled surge was 0.47 per 100,000 in early September, data from the Centers for Disease Control and Prevention show.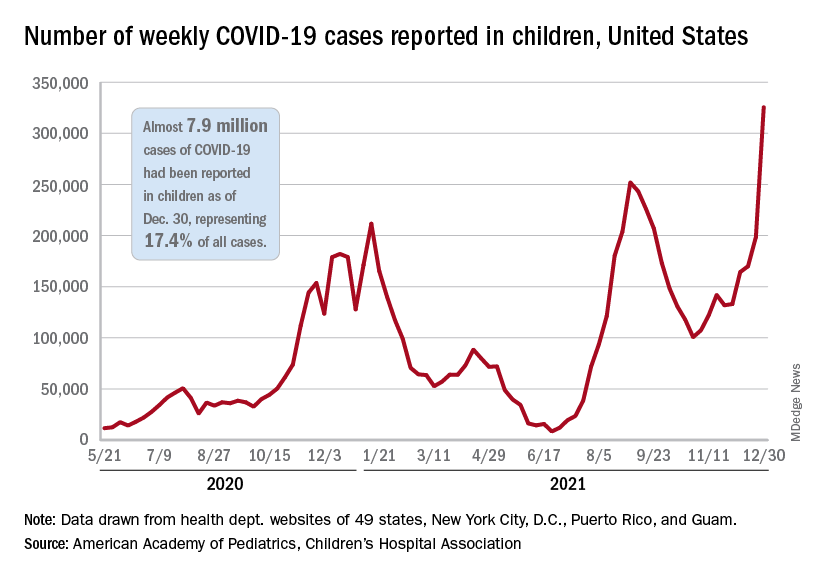
and exceeding the previous week’s count by almost 64%, the AAP and CHA said in their weekly COVID report.
New cases were up in all four regions of the United States, with the Northeast adding the most newly infected children while setting a new high for the fifth consecutive week. The South was just behind for the week but still well off the record it reached in September, the Midwest was third but recorded its busiest week ever, and the West was fourth and nowhere near its previous high, the AAP/CHA report indicated.
The total number of child cases since the pandemic began is almost 7.9 million, they said based on data collected from 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam. That figure represents 17.4% of all cases reported in the United States, and the cumulative rate of COVID infection is up to almost 10,500 per 100,000 children, meaning that 1 in 10 children have been infected.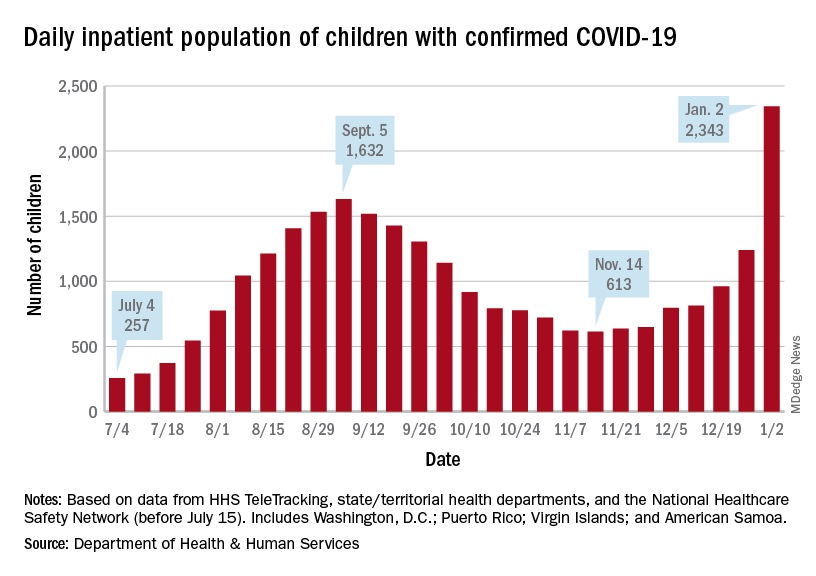
Children are still less likely to be hospitalized than adults, but the gap appears to be closing. On Jan. 2 there were 2,343 children and 87,690 adults in the hospital with confirmed COVID, a ratio of 37 adults for each child, but on Sept. 5, at the height of the previous surge, the ratio of hospitalized adults (93,647) to children (1,632) was 57:1, according to data from the Department of Health & Human Services.
New admissions show a similar pattern: The 0.74 admissions per 100,000 children recorded on Dec. 31 was lower than, for example, adults aged 30-39 years (2.7 per 100,000) or 50-59 years (4.25 per 100,000), but on Sept. 5 the corresponding figures were 0.46 (children), 2.74 (ages 30-39), and 5.03 (aged 50-59), based on the HHS data.
A look at vaccinations
The vaccination response to Omicron, however, has been more subdued and somewhat inconsistent. Vaccine initiation, not surprisingly, was down among eligible children for the week of Dec. 23-29. Before that, both the 5- to 11-year-olds and 12- to 15-year-olds were down for the second week of December and then up a bit (5.6% and 14.3%, respectively) during the third week, while the 16- to 17-year-olds, increased initiation by 63.2%, CDC’s COVID Data Tracker shows.
Less than a quarter (23.5%) of children aged 5-11 received at least one dose of the vaccine in the first 2 months of their eligibility, and only 14.7% are fully vaccinated. Among the older children, coverage looks like this: at least one dose for 61.2% of 12- to 15-year-olds and 67.4% of 16- to 17-year-olds and full vaccination for 51.3% and 57.6%, respectively, the CDC said.
At the state level, Massachusetts and Hawaii have the highest rates for children aged 12-17 years, with 86% having received a least one dose, and Vermont is highest for children aged 5-11 at 56%. The lowest rates can be found in Wyoming (38%) for 12- to 17-year-olds and in Mississippi (6%) for 5- to 11-year-olds, the AAP said in a separate report.
Weekly COVID-19 cases in children passed 300,000 for the first time since the pandemic started, according to the American Academy of Pediatrics and the Children’s Hospital Association.
The rate of new COVID-related hospital admissions also reached a new high of 0.74 per 100,000 children as of Dec. 31. The highest rate seen before the current Omicron-fueled surge was 0.47 per 100,000 in early September, data from the Centers for Disease Control and Prevention show.
and exceeding the previous week’s count by almost 64%, the AAP and CHA said in their weekly COVID report.
New cases were up in all four regions of the United States, with the Northeast adding the most newly infected children while setting a new high for the fifth consecutive week. The South was just behind for the week but still well off the record it reached in September, the Midwest was third but recorded its busiest week ever, and the West was fourth and nowhere near its previous high, the AAP/CHA report indicated.
The total number of child cases since the pandemic began is almost 7.9 million, they said based on data collected from 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam. That figure represents 17.4% of all cases reported in the United States, and the cumulative rate of COVID infection is up to almost 10,500 per 100,000 children, meaning that 1 in 10 children have been infected.
Children are still less likely to be hospitalized than adults, but the gap appears to be closing. On Jan. 2 there were 2,343 children and 87,690 adults in the hospital with confirmed COVID, a ratio of 37 adults for each child, but on Sept. 5, at the height of the previous surge, the ratio of hospitalized adults (93,647) to children (1,632) was 57:1, according to data from the Department of Health & Human Services.
New admissions show a similar pattern: The 0.74 admissions per 100,000 children recorded on Dec. 31 was lower than, for example, adults aged 30-39 years (2.7 per 100,000) or 50-59 years (4.25 per 100,000), but on Sept. 5 the corresponding figures were 0.46 (children), 2.74 (ages 30-39), and 5.03 (aged 50-59), based on the HHS data.
A look at vaccinations
The vaccination response to Omicron, however, has been more subdued and somewhat inconsistent. Vaccine initiation, not surprisingly, was down among eligible children for the week of Dec. 23-29. Before that, both the 5- to 11-year-olds and 12- to 15-year-olds were down for the second week of December and then up a bit (5.6% and 14.3%, respectively) during the third week, while the 16- to 17-year-olds, increased initiation by 63.2%, CDC’s COVID Data Tracker shows.
Less than a quarter (23.5%) of children aged 5-11 received at least one dose of the vaccine in the first 2 months of their eligibility, and only 14.7% are fully vaccinated. Among the older children, coverage looks like this: at least one dose for 61.2% of 12- to 15-year-olds and 67.4% of 16- to 17-year-olds and full vaccination for 51.3% and 57.6%, respectively, the CDC said.
At the state level, Massachusetts and Hawaii have the highest rates for children aged 12-17 years, with 86% having received a least one dose, and Vermont is highest for children aged 5-11 at 56%. The lowest rates can be found in Wyoming (38%) for 12- to 17-year-olds and in Mississippi (6%) for 5- to 11-year-olds, the AAP said in a separate report.
Weekly COVID-19 cases in children passed 300,000 for the first time since the pandemic started, according to the American Academy of Pediatrics and the Children’s Hospital Association.
The rate of new COVID-related hospital admissions also reached a new high of 0.74 per 100,000 children as of Dec. 31. The highest rate seen before the current Omicron-fueled surge was 0.47 per 100,000 in early September, data from the Centers for Disease Control and Prevention show.
and exceeding the previous week’s count by almost 64%, the AAP and CHA said in their weekly COVID report.
New cases were up in all four regions of the United States, with the Northeast adding the most newly infected children while setting a new high for the fifth consecutive week. The South was just behind for the week but still well off the record it reached in September, the Midwest was third but recorded its busiest week ever, and the West was fourth and nowhere near its previous high, the AAP/CHA report indicated.
The total number of child cases since the pandemic began is almost 7.9 million, they said based on data collected from 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam. That figure represents 17.4% of all cases reported in the United States, and the cumulative rate of COVID infection is up to almost 10,500 per 100,000 children, meaning that 1 in 10 children have been infected.
Children are still less likely to be hospitalized than adults, but the gap appears to be closing. On Jan. 2 there were 2,343 children and 87,690 adults in the hospital with confirmed COVID, a ratio of 37 adults for each child, but on Sept. 5, at the height of the previous surge, the ratio of hospitalized adults (93,647) to children (1,632) was 57:1, according to data from the Department of Health & Human Services.
New admissions show a similar pattern: The 0.74 admissions per 100,000 children recorded on Dec. 31 was lower than, for example, adults aged 30-39 years (2.7 per 100,000) or 50-59 years (4.25 per 100,000), but on Sept. 5 the corresponding figures were 0.46 (children), 2.74 (ages 30-39), and 5.03 (aged 50-59), based on the HHS data.
A look at vaccinations
The vaccination response to Omicron, however, has been more subdued and somewhat inconsistent. Vaccine initiation, not surprisingly, was down among eligible children for the week of Dec. 23-29. Before that, both the 5- to 11-year-olds and 12- to 15-year-olds were down for the second week of December and then up a bit (5.6% and 14.3%, respectively) during the third week, while the 16- to 17-year-olds, increased initiation by 63.2%, CDC’s COVID Data Tracker shows.
Less than a quarter (23.5%) of children aged 5-11 received at least one dose of the vaccine in the first 2 months of their eligibility, and only 14.7% are fully vaccinated. Among the older children, coverage looks like this: at least one dose for 61.2% of 12- to 15-year-olds and 67.4% of 16- to 17-year-olds and full vaccination for 51.3% and 57.6%, respectively, the CDC said.
At the state level, Massachusetts and Hawaii have the highest rates for children aged 12-17 years, with 86% having received a least one dose, and Vermont is highest for children aged 5-11 at 56%. The lowest rates can be found in Wyoming (38%) for 12- to 17-year-olds and in Mississippi (6%) for 5- to 11-year-olds, the AAP said in a separate report.