User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Parkinson’s disease could be hiding behind those nightmares
Living the dream, diagnosing the nightmare
Does a bad dream mean you should be consulting your doctor about an impending neurologic disease? Maybe.
New research published in eClinicalMedicine suggests that, for some people, bad dreams and nightmares have been associated with developing Parkinson’s disease later in life. Dr. Abidemi I. Otaiku of the University of Birmingham (England) analyzed data from a cohort study involving 3,818 older men, of whom 2.3% were diagnosed with Parkinson’s during the 12 years of follow-up.
Dr. Otaiku found those with frequent nightmares – at least once per week – were twice as likely to develop Parkinson’s than were those without, with most of the diagnoses coming in the first 5 years.
Although more research needs to be done, “identifying the significance of bad dreams and nightmares could indicate that individuals who experience changes to their dreams in older age – without any obvious trigger – should seek medical advice,” he said in a Eurekalert statement.
Dr. Otaiku pointed out that studying dreams can tell us a lot about how our brains work and are structured. By using electroencephalography, Dr. Otaiku plans to look into the biological reasons for why we dream the way we do.
So could it be that those killer clowns are actually giving you a heads up on your health?
Maybe next time try a paper route
There’s just no winning with teenagers sometimes. You tell them to go outside, they’ll sit in the dark playing video games all night. You tell them to get better grades, they’ll skip school. You tell them to get a hobby, they’ll scam the German government for millions of euros.
The COVID-19 pandemic has been tricky for governments to manage. Massive amounts of infrastructure needed to be set up, and that means corners got cut. Germany was no exception in this regard; the government entrusted the Kassenärztlichen Vereinigung, a doctor’s association, with overseeing COVID testing and payment at private test centers. To make things a bit easier, all they required private test centers to provide to receive reimbursement was an invoice.
This is where our 17-year-old from Freiburg comes in. In a spark of entrepreneurial genius, he decided to falsify documents and create an entirely fictional COVID test center. The KV approved it, and between March and July of 2021, he sent in thousands of fake invoices. Over that 4-month period, he submitted 500,000 invoices and received 5.7 million euros as compensation. That’s a few thousand tests per day, which was absolutely absurd, but he avoided scrutiny for months.
In the end, it wasn’t even the KV that noticed the fraud, but the bank. A bank employee noticed millions flowing into the account of a teenager and suspected money laundering, alerting the government. Fortunately for our young friend, since he was under 18 when he hatched his scheme, he was tried as a minor, avoiding jail time. His ill-gotten gains were confiscated, he has to pay a relatively minimal fine, and he will be on probation for 1 year. And presumably, he’ll be on the receiving end of the grounding of a lifetime.
You look like I need more sleep
Like most people, not getting our beauty sleep can make us look tired and feel less attractive, but a new study from Sweden shows that the sleep deprived also are more likely to find others less attractive. That’s probably not a good finding for singles who often go out trying to meet someone after a long day of work.

For the study, 45 young men and women were required to spend one night with no sleep and then another night with the possibility of 8 hours of sleep. The following mornings, eye-tracking technology was used as they looked at images of happy, angry, fearful, and neutral faces. The subjects then rated the faces for attractiveness, trustworthiness, and healthiness.
“The finding that sleep-deprived subjects in our experiment rated angry faces as less trustworthy and healthy-looking and neutral and fearful faces as less attractive indicates that sleep loss is associated with more negative social impressions of others,” senior author Christian Benedict of Uppsala University said in a statement.
When we are sleep deprived, the researchers added, we might not stop to really look at someone else, which has a negative impact on how we perceive people because we are not focusing on what their facial expressions are really telling us.
We already knew that not sleeping well has many negative effects on us, but now – thank you very much, science – we have something else to think about. Better hope your crush at work gets enough sleep so you’ll be accurately noticed.
The expanding-hole illusion of science
Time for a LOTME-style reality check: I think, therefore I am.
So far, so good. Next step: I think, therefore I am. I think.
Works for us. Now for the biggie: I think I am seeing the black hole in the middle of this image expanding.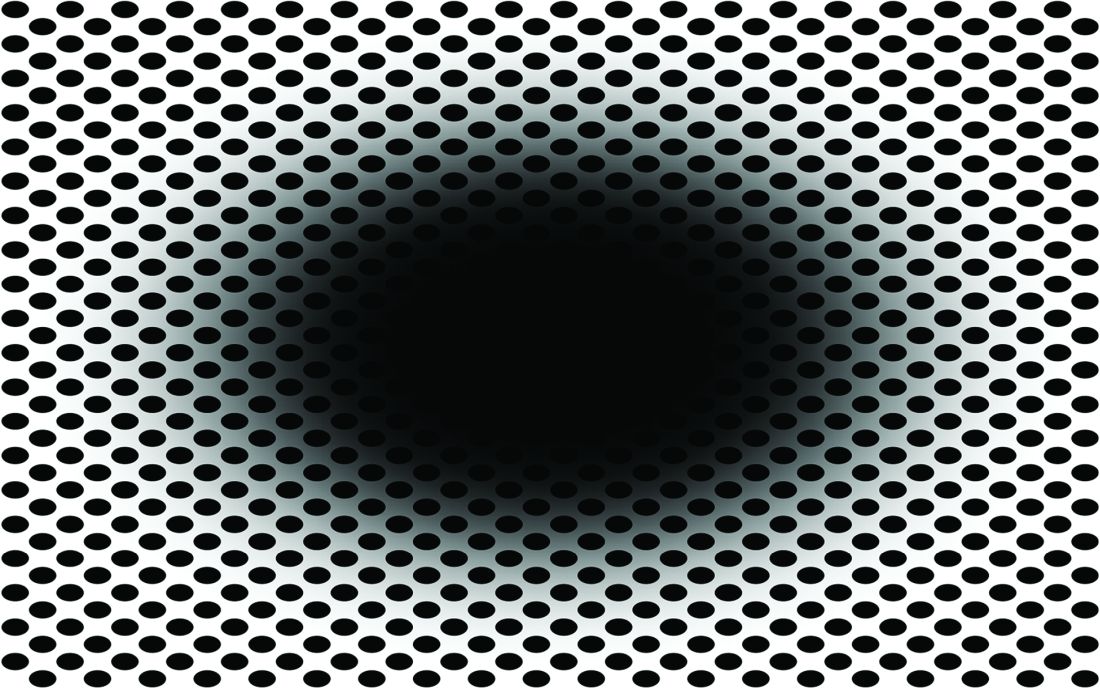
Does that work for you? Do you perceive the black hole as expanding? If you do, then you fit in with the 86% of subjects in a recent study who perceived the same thing.
Lead author Bruno Laeng of the University of Oslo explained the effect in a statement from Frontiers Science News. “The circular smear or shadow gradient of the central black hole evokes a marked impression of optic flow, as if the observer were heading forward into a hole or tunnel. ... The pupil reacts to how we perceive light – even if this ‘light’ is imaginary like in the illusion – and not just to the amount of light energy that actually enters the eye.”
The illusion is so good at deceiving the brain “that it even prompts a dilation reflex of the pupils to let in more light, just as would happen if we were really moving into a dark area,” the investigators said.
Of the 50 men and women who had their eye movements measured while looking at the illusion, only 14% didn’t perceive the illusion when the hole was black. When the hole was a color, that figure went up to 20%. There also was a strong dilation reflex with black holes, but colored holes caused the subjects’ pupils to constrict, they noted.
Dr. Laeng and his associates can’t explain why some people don’t see the movement, but they did offer this: “Pupils’ dilation or contraction reflex is not a closed-loop mechanism, like a photocell opening a door, impervious to any other information than the actual amount of light stimulating the photoreceptor. Rather, the eye adjusts to perceived and even imagined light, not simply to physical energy.”
And now, back to our reality check: We think we perceive the light of a cheeseburger, therefore it’s time for lunch.
Living the dream, diagnosing the nightmare
Does a bad dream mean you should be consulting your doctor about an impending neurologic disease? Maybe.
New research published in eClinicalMedicine suggests that, for some people, bad dreams and nightmares have been associated with developing Parkinson’s disease later in life. Dr. Abidemi I. Otaiku of the University of Birmingham (England) analyzed data from a cohort study involving 3,818 older men, of whom 2.3% were diagnosed with Parkinson’s during the 12 years of follow-up.
Dr. Otaiku found those with frequent nightmares – at least once per week – were twice as likely to develop Parkinson’s than were those without, with most of the diagnoses coming in the first 5 years.
Although more research needs to be done, “identifying the significance of bad dreams and nightmares could indicate that individuals who experience changes to their dreams in older age – without any obvious trigger – should seek medical advice,” he said in a Eurekalert statement.
Dr. Otaiku pointed out that studying dreams can tell us a lot about how our brains work and are structured. By using electroencephalography, Dr. Otaiku plans to look into the biological reasons for why we dream the way we do.
So could it be that those killer clowns are actually giving you a heads up on your health?
Maybe next time try a paper route
There’s just no winning with teenagers sometimes. You tell them to go outside, they’ll sit in the dark playing video games all night. You tell them to get better grades, they’ll skip school. You tell them to get a hobby, they’ll scam the German government for millions of euros.
The COVID-19 pandemic has been tricky for governments to manage. Massive amounts of infrastructure needed to be set up, and that means corners got cut. Germany was no exception in this regard; the government entrusted the Kassenärztlichen Vereinigung, a doctor’s association, with overseeing COVID testing and payment at private test centers. To make things a bit easier, all they required private test centers to provide to receive reimbursement was an invoice.
This is where our 17-year-old from Freiburg comes in. In a spark of entrepreneurial genius, he decided to falsify documents and create an entirely fictional COVID test center. The KV approved it, and between March and July of 2021, he sent in thousands of fake invoices. Over that 4-month period, he submitted 500,000 invoices and received 5.7 million euros as compensation. That’s a few thousand tests per day, which was absolutely absurd, but he avoided scrutiny for months.
In the end, it wasn’t even the KV that noticed the fraud, but the bank. A bank employee noticed millions flowing into the account of a teenager and suspected money laundering, alerting the government. Fortunately for our young friend, since he was under 18 when he hatched his scheme, he was tried as a minor, avoiding jail time. His ill-gotten gains were confiscated, he has to pay a relatively minimal fine, and he will be on probation for 1 year. And presumably, he’ll be on the receiving end of the grounding of a lifetime.
You look like I need more sleep
Like most people, not getting our beauty sleep can make us look tired and feel less attractive, but a new study from Sweden shows that the sleep deprived also are more likely to find others less attractive. That’s probably not a good finding for singles who often go out trying to meet someone after a long day of work.
For the study, 45 young men and women were required to spend one night with no sleep and then another night with the possibility of 8 hours of sleep. The following mornings, eye-tracking technology was used as they looked at images of happy, angry, fearful, and neutral faces. The subjects then rated the faces for attractiveness, trustworthiness, and healthiness.
“The finding that sleep-deprived subjects in our experiment rated angry faces as less trustworthy and healthy-looking and neutral and fearful faces as less attractive indicates that sleep loss is associated with more negative social impressions of others,” senior author Christian Benedict of Uppsala University said in a statement.
When we are sleep deprived, the researchers added, we might not stop to really look at someone else, which has a negative impact on how we perceive people because we are not focusing on what their facial expressions are really telling us.
We already knew that not sleeping well has many negative effects on us, but now – thank you very much, science – we have something else to think about. Better hope your crush at work gets enough sleep so you’ll be accurately noticed.
The expanding-hole illusion of science
Time for a LOTME-style reality check: I think, therefore I am.
So far, so good. Next step: I think, therefore I am. I think.
Works for us. Now for the biggie: I think I am seeing the black hole in the middle of this image expanding.
Does that work for you? Do you perceive the black hole as expanding? If you do, then you fit in with the 86% of subjects in a recent study who perceived the same thing.
Lead author Bruno Laeng of the University of Oslo explained the effect in a statement from Frontiers Science News. “The circular smear or shadow gradient of the central black hole evokes a marked impression of optic flow, as if the observer were heading forward into a hole or tunnel. ... The pupil reacts to how we perceive light – even if this ‘light’ is imaginary like in the illusion – and not just to the amount of light energy that actually enters the eye.”
The illusion is so good at deceiving the brain “that it even prompts a dilation reflex of the pupils to let in more light, just as would happen if we were really moving into a dark area,” the investigators said.
Of the 50 men and women who had their eye movements measured while looking at the illusion, only 14% didn’t perceive the illusion when the hole was black. When the hole was a color, that figure went up to 20%. There also was a strong dilation reflex with black holes, but colored holes caused the subjects’ pupils to constrict, they noted.
Dr. Laeng and his associates can’t explain why some people don’t see the movement, but they did offer this: “Pupils’ dilation or contraction reflex is not a closed-loop mechanism, like a photocell opening a door, impervious to any other information than the actual amount of light stimulating the photoreceptor. Rather, the eye adjusts to perceived and even imagined light, not simply to physical energy.”
And now, back to our reality check: We think we perceive the light of a cheeseburger, therefore it’s time for lunch.
Living the dream, diagnosing the nightmare
Does a bad dream mean you should be consulting your doctor about an impending neurologic disease? Maybe.
New research published in eClinicalMedicine suggests that, for some people, bad dreams and nightmares have been associated with developing Parkinson’s disease later in life. Dr. Abidemi I. Otaiku of the University of Birmingham (England) analyzed data from a cohort study involving 3,818 older men, of whom 2.3% were diagnosed with Parkinson’s during the 12 years of follow-up.
Dr. Otaiku found those with frequent nightmares – at least once per week – were twice as likely to develop Parkinson’s than were those without, with most of the diagnoses coming in the first 5 years.
Although more research needs to be done, “identifying the significance of bad dreams and nightmares could indicate that individuals who experience changes to their dreams in older age – without any obvious trigger – should seek medical advice,” he said in a Eurekalert statement.
Dr. Otaiku pointed out that studying dreams can tell us a lot about how our brains work and are structured. By using electroencephalography, Dr. Otaiku plans to look into the biological reasons for why we dream the way we do.
So could it be that those killer clowns are actually giving you a heads up on your health?
Maybe next time try a paper route
There’s just no winning with teenagers sometimes. You tell them to go outside, they’ll sit in the dark playing video games all night. You tell them to get better grades, they’ll skip school. You tell them to get a hobby, they’ll scam the German government for millions of euros.
The COVID-19 pandemic has been tricky for governments to manage. Massive amounts of infrastructure needed to be set up, and that means corners got cut. Germany was no exception in this regard; the government entrusted the Kassenärztlichen Vereinigung, a doctor’s association, with overseeing COVID testing and payment at private test centers. To make things a bit easier, all they required private test centers to provide to receive reimbursement was an invoice.
This is where our 17-year-old from Freiburg comes in. In a spark of entrepreneurial genius, he decided to falsify documents and create an entirely fictional COVID test center. The KV approved it, and between March and July of 2021, he sent in thousands of fake invoices. Over that 4-month period, he submitted 500,000 invoices and received 5.7 million euros as compensation. That’s a few thousand tests per day, which was absolutely absurd, but he avoided scrutiny for months.
In the end, it wasn’t even the KV that noticed the fraud, but the bank. A bank employee noticed millions flowing into the account of a teenager and suspected money laundering, alerting the government. Fortunately for our young friend, since he was under 18 when he hatched his scheme, he was tried as a minor, avoiding jail time. His ill-gotten gains were confiscated, he has to pay a relatively minimal fine, and he will be on probation for 1 year. And presumably, he’ll be on the receiving end of the grounding of a lifetime.
You look like I need more sleep
Like most people, not getting our beauty sleep can make us look tired and feel less attractive, but a new study from Sweden shows that the sleep deprived also are more likely to find others less attractive. That’s probably not a good finding for singles who often go out trying to meet someone after a long day of work.
For the study, 45 young men and women were required to spend one night with no sleep and then another night with the possibility of 8 hours of sleep. The following mornings, eye-tracking technology was used as they looked at images of happy, angry, fearful, and neutral faces. The subjects then rated the faces for attractiveness, trustworthiness, and healthiness.
“The finding that sleep-deprived subjects in our experiment rated angry faces as less trustworthy and healthy-looking and neutral and fearful faces as less attractive indicates that sleep loss is associated with more negative social impressions of others,” senior author Christian Benedict of Uppsala University said in a statement.
When we are sleep deprived, the researchers added, we might not stop to really look at someone else, which has a negative impact on how we perceive people because we are not focusing on what their facial expressions are really telling us.
We already knew that not sleeping well has many negative effects on us, but now – thank you very much, science – we have something else to think about. Better hope your crush at work gets enough sleep so you’ll be accurately noticed.
The expanding-hole illusion of science
Time for a LOTME-style reality check: I think, therefore I am.
So far, so good. Next step: I think, therefore I am. I think.
Works for us. Now for the biggie: I think I am seeing the black hole in the middle of this image expanding.
Does that work for you? Do you perceive the black hole as expanding? If you do, then you fit in with the 86% of subjects in a recent study who perceived the same thing.
Lead author Bruno Laeng of the University of Oslo explained the effect in a statement from Frontiers Science News. “The circular smear or shadow gradient of the central black hole evokes a marked impression of optic flow, as if the observer were heading forward into a hole or tunnel. ... The pupil reacts to how we perceive light – even if this ‘light’ is imaginary like in the illusion – and not just to the amount of light energy that actually enters the eye.”
The illusion is so good at deceiving the brain “that it even prompts a dilation reflex of the pupils to let in more light, just as would happen if we were really moving into a dark area,” the investigators said.
Of the 50 men and women who had their eye movements measured while looking at the illusion, only 14% didn’t perceive the illusion when the hole was black. When the hole was a color, that figure went up to 20%. There also was a strong dilation reflex with black holes, but colored holes caused the subjects’ pupils to constrict, they noted.
Dr. Laeng and his associates can’t explain why some people don’t see the movement, but they did offer this: “Pupils’ dilation or contraction reflex is not a closed-loop mechanism, like a photocell opening a door, impervious to any other information than the actual amount of light stimulating the photoreceptor. Rather, the eye adjusts to perceived and even imagined light, not simply to physical energy.”
And now, back to our reality check: We think we perceive the light of a cheeseburger, therefore it’s time for lunch.
PCOS comes with high morbidity, medication use into late 40s
Women with polycystic ovary syndrome (PCOS) have an increased risk for several diseases and symptoms, many independent of body mass index (BMI), new research indicates.
Some diseases are linked for the first time to PCOS in this study, the authors wrote.
Researchers, led by Linda Kujanpää, MD, of the research unit for pediatrics, dermatology, clinical genetics, obstetrics, and gynecology at University of Oulu (Finland), found the morbidity risk is evident through the late reproductive years.
The paper was published online in Acta Obstetricia et Gynecologica Scandinavica.
This population-based follow-up study investigated comorbidities and medication and health care services use among women with PCOS in Finland at age 46 years via answers to a questionnaire.
The whole PCOS population (n = 280) consisted of women who reported both hirsutism and oligo/amenorrhea at age 31 (4.1%) and/or polycystic ovary morphology/PCOS at age 46 (3.1%), of which 246 replied to the 46-year questionnaire. They were compared with a control group of 1,573 women without PCOS.
Overall morbidity risk was 35% higher than for women without PCOS (risk ratio, 1.35; 95% confidence interval, 1.16-1.57). Medication use was 27% higher (RR, 1.27; 95% CI, 1.08-1.50), and the risk remained after adjusting for BMI.
Diagnoses with increased prevalence in women with PCOS were osteoarthritis, migraine, hypertension, tendinitis, and endometriosis. PCOS was also associated with autoimmune diseases and recurrent upper respiratory tract infections.
“BMI seems not to be solely responsible for the increased morbidity,” the researchers found. The average morbidity score of women with PCOS with a BMI of 25 kg/m2 or higher was similar to that of women with PCOS and lower BMI.
Mindy Christianson, MD, medical director at Johns Hopkins Fertility Center and associate professor of gynecology and obstetrics at Johns Hopkins University, both in Baltimore, said in an interview that the links to diseases independent of BMI are interesting because there’s so much focus on counseling women with PCOS to lose weight.
While that message is still important, it’s important to realize that some related diseases and conditions – such as autoimmune diseases and migraine – are not driven by BMI.
“It really drives home the point that polycystic ovary syndrome is really a chronic medical condition and puts patients at risk for a number of health conditions,” she said. “Having a good primary care physician is important to help them with their overall health.”
Women with PCOS said their health was poor or very poor almost three times more often than did women in the control group.
Surprisingly few studies have looked at overall comorbidity in women with PCOS, the authors wrote.
“This should be of high priority given the high cost to society resulting from PCOS-related morbidity,” they added. As an example, they pointed out that PCOS-related type 2 diabetes alone costs an estimated $1.77 billion in the United States and £237 million ($310 million) each year in the United Kingdom.
Additionally, the focus in previous research has typically been on women in their early or mid-reproductive years, and morbidity burden data in late reproductive years are scarce.
The study population was pulled from the longitudinal Northern Finland Birth Cohort 1966 and included all pregnancies with estimated date of delivery during 1966 in two provinces of Finland (5,889 women).
Dr. Christianson said she hopes this study will spur more research on PCOS, which has been severely underfunded, especially in the United States.
Part of the reason for that is there is a limited number of subspecialists in the country who work with patients with PCOS and do research in the area. PCOS often gets lost in the research priorities of infertility, diabetes, and thyroid disease.
The message in this study that PCOS is not just a fertility issue or an obesity issue but an overall health issue with a substantial cost to the health system may help raise awareness, Dr. Christianson said.
This study was supported by grants from The Finnish Medical Foundation, The Academy of Finland, The Sigrid Juselius Foundation, The Finnish Cultural Foundation, The Jalmari and Rauha Ahokas Foundation, The Päivikki and Sakari Sohlberg Foundation, Genesis Research Trust, The Medical Research Council, University of Oulu, Oulu University Hospital, Ministry of Health and Social Affairs, National Institute for Health and Welfare, Regional Institute of Occupational Health, and the European Regional Development Fund. The Study authors and Dr. Christianson reported no relevant financial relationships.
Women with polycystic ovary syndrome (PCOS) have an increased risk for several diseases and symptoms, many independent of body mass index (BMI), new research indicates.
Some diseases are linked for the first time to PCOS in this study, the authors wrote.
Researchers, led by Linda Kujanpää, MD, of the research unit for pediatrics, dermatology, clinical genetics, obstetrics, and gynecology at University of Oulu (Finland), found the morbidity risk is evident through the late reproductive years.
The paper was published online in Acta Obstetricia et Gynecologica Scandinavica.
This population-based follow-up study investigated comorbidities and medication and health care services use among women with PCOS in Finland at age 46 years via answers to a questionnaire.
The whole PCOS population (n = 280) consisted of women who reported both hirsutism and oligo/amenorrhea at age 31 (4.1%) and/or polycystic ovary morphology/PCOS at age 46 (3.1%), of which 246 replied to the 46-year questionnaire. They were compared with a control group of 1,573 women without PCOS.
Overall morbidity risk was 35% higher than for women without PCOS (risk ratio, 1.35; 95% confidence interval, 1.16-1.57). Medication use was 27% higher (RR, 1.27; 95% CI, 1.08-1.50), and the risk remained after adjusting for BMI.
Diagnoses with increased prevalence in women with PCOS were osteoarthritis, migraine, hypertension, tendinitis, and endometriosis. PCOS was also associated with autoimmune diseases and recurrent upper respiratory tract infections.
“BMI seems not to be solely responsible for the increased morbidity,” the researchers found. The average morbidity score of women with PCOS with a BMI of 25 kg/m2 or higher was similar to that of women with PCOS and lower BMI.
Mindy Christianson, MD, medical director at Johns Hopkins Fertility Center and associate professor of gynecology and obstetrics at Johns Hopkins University, both in Baltimore, said in an interview that the links to diseases independent of BMI are interesting because there’s so much focus on counseling women with PCOS to lose weight.
While that message is still important, it’s important to realize that some related diseases and conditions – such as autoimmune diseases and migraine – are not driven by BMI.
“It really drives home the point that polycystic ovary syndrome is really a chronic medical condition and puts patients at risk for a number of health conditions,” she said. “Having a good primary care physician is important to help them with their overall health.”
Women with PCOS said their health was poor or very poor almost three times more often than did women in the control group.
Surprisingly few studies have looked at overall comorbidity in women with PCOS, the authors wrote.
“This should be of high priority given the high cost to society resulting from PCOS-related morbidity,” they added. As an example, they pointed out that PCOS-related type 2 diabetes alone costs an estimated $1.77 billion in the United States and £237 million ($310 million) each year in the United Kingdom.
Additionally, the focus in previous research has typically been on women in their early or mid-reproductive years, and morbidity burden data in late reproductive years are scarce.
The study population was pulled from the longitudinal Northern Finland Birth Cohort 1966 and included all pregnancies with estimated date of delivery during 1966 in two provinces of Finland (5,889 women).
Dr. Christianson said she hopes this study will spur more research on PCOS, which has been severely underfunded, especially in the United States.
Part of the reason for that is there is a limited number of subspecialists in the country who work with patients with PCOS and do research in the area. PCOS often gets lost in the research priorities of infertility, diabetes, and thyroid disease.
The message in this study that PCOS is not just a fertility issue or an obesity issue but an overall health issue with a substantial cost to the health system may help raise awareness, Dr. Christianson said.
This study was supported by grants from The Finnish Medical Foundation, The Academy of Finland, The Sigrid Juselius Foundation, The Finnish Cultural Foundation, The Jalmari and Rauha Ahokas Foundation, The Päivikki and Sakari Sohlberg Foundation, Genesis Research Trust, The Medical Research Council, University of Oulu, Oulu University Hospital, Ministry of Health and Social Affairs, National Institute for Health and Welfare, Regional Institute of Occupational Health, and the European Regional Development Fund. The Study authors and Dr. Christianson reported no relevant financial relationships.
Women with polycystic ovary syndrome (PCOS) have an increased risk for several diseases and symptoms, many independent of body mass index (BMI), new research indicates.
Some diseases are linked for the first time to PCOS in this study, the authors wrote.
Researchers, led by Linda Kujanpää, MD, of the research unit for pediatrics, dermatology, clinical genetics, obstetrics, and gynecology at University of Oulu (Finland), found the morbidity risk is evident through the late reproductive years.
The paper was published online in Acta Obstetricia et Gynecologica Scandinavica.
This population-based follow-up study investigated comorbidities and medication and health care services use among women with PCOS in Finland at age 46 years via answers to a questionnaire.
The whole PCOS population (n = 280) consisted of women who reported both hirsutism and oligo/amenorrhea at age 31 (4.1%) and/or polycystic ovary morphology/PCOS at age 46 (3.1%), of which 246 replied to the 46-year questionnaire. They were compared with a control group of 1,573 women without PCOS.
Overall morbidity risk was 35% higher than for women without PCOS (risk ratio, 1.35; 95% confidence interval, 1.16-1.57). Medication use was 27% higher (RR, 1.27; 95% CI, 1.08-1.50), and the risk remained after adjusting for BMI.
Diagnoses with increased prevalence in women with PCOS were osteoarthritis, migraine, hypertension, tendinitis, and endometriosis. PCOS was also associated with autoimmune diseases and recurrent upper respiratory tract infections.
“BMI seems not to be solely responsible for the increased morbidity,” the researchers found. The average morbidity score of women with PCOS with a BMI of 25 kg/m2 or higher was similar to that of women with PCOS and lower BMI.
Mindy Christianson, MD, medical director at Johns Hopkins Fertility Center and associate professor of gynecology and obstetrics at Johns Hopkins University, both in Baltimore, said in an interview that the links to diseases independent of BMI are interesting because there’s so much focus on counseling women with PCOS to lose weight.
While that message is still important, it’s important to realize that some related diseases and conditions – such as autoimmune diseases and migraine – are not driven by BMI.
“It really drives home the point that polycystic ovary syndrome is really a chronic medical condition and puts patients at risk for a number of health conditions,” she said. “Having a good primary care physician is important to help them with their overall health.”
Women with PCOS said their health was poor or very poor almost three times more often than did women in the control group.
Surprisingly few studies have looked at overall comorbidity in women with PCOS, the authors wrote.
“This should be of high priority given the high cost to society resulting from PCOS-related morbidity,” they added. As an example, they pointed out that PCOS-related type 2 diabetes alone costs an estimated $1.77 billion in the United States and £237 million ($310 million) each year in the United Kingdom.
Additionally, the focus in previous research has typically been on women in their early or mid-reproductive years, and morbidity burden data in late reproductive years are scarce.
The study population was pulled from the longitudinal Northern Finland Birth Cohort 1966 and included all pregnancies with estimated date of delivery during 1966 in two provinces of Finland (5,889 women).
Dr. Christianson said she hopes this study will spur more research on PCOS, which has been severely underfunded, especially in the United States.
Part of the reason for that is there is a limited number of subspecialists in the country who work with patients with PCOS and do research in the area. PCOS often gets lost in the research priorities of infertility, diabetes, and thyroid disease.
The message in this study that PCOS is not just a fertility issue or an obesity issue but an overall health issue with a substantial cost to the health system may help raise awareness, Dr. Christianson said.
This study was supported by grants from The Finnish Medical Foundation, The Academy of Finland, The Sigrid Juselius Foundation, The Finnish Cultural Foundation, The Jalmari and Rauha Ahokas Foundation, The Päivikki and Sakari Sohlberg Foundation, Genesis Research Trust, The Medical Research Council, University of Oulu, Oulu University Hospital, Ministry of Health and Social Affairs, National Institute for Health and Welfare, Regional Institute of Occupational Health, and the European Regional Development Fund. The Study authors and Dr. Christianson reported no relevant financial relationships.
FROM ACTA OBSTETRICIA ET GYNECOLOGICA SCANDINAVICA
Pregnant women with monkeypox advised to have C-section
The risk of monkeypox infection remains low for the general public, the authors wrote, though cases continue to grow worldwide, particularly in the United Kingdom.
“We are aware infants and children are at greater risk of becoming seriously ill if they do catch monkeypox,” Edward Morris, MBBS, one of the authors and president of the Royal College of Obstetricians and Gynecologists, said in a statement.
“Therefore, to minimize the risk of a baby contracting the virus, we recommend health care professionals discuss the benefits and risks of having a cesarean birth with a pregnant woman or person who has or is suspected of having the virus,” he said.
Dr. Morris and colleagues pulled together existing evidence on monkeypox diagnosis, treatment, and recommended modes of birth for mothers and babies.
“The World Health Organization states there could be adverse consequences for pregnant women and babies if they become infected, including congenital monkeypox, miscarriage, or stillbirth, which is why we have provided clear guidance for health care professionals in this paper,” Dr. Morris said.
The monkeypox virus typically spreads through direct contact, droplets, or contaminated surfaces and objects. But some limited evidence shows that the virus can be passed from a mother to a baby via the placenta, which can lead to congenital monkeypox.
What’s more, mothers may be able to transmit the virus during or after birth. Although no evidence exists around the optimal mode of birth, a pregnant woman with an active monkeypox infection may choose to avoid vaginal delivery to reduce direct contact.
“If genital lesions are identified on a pregnant woman, then a cesarean birth will be recommended,” the authors wrote. “If a pregnant woman or person has suspected or confirmed monkeypox, a caesarean birth will be offered following discussion of the possible risk of neonatal infection, which may be serious.”
After giving birth, close contact can spread the virus as well. To minimize the risk, the authors recommend isolating the baby from family members who have confirmed or suspected monkeypox and carefully monitoring for infection.
Mothers with an active monkeypox infection should also avoid breastfeeding to lower the risk of spreading the virus to their newborn, the authors wrote. But to support breastfeeding after infection, mothers can express and discard milk until the isolation period has passed.
Pregnant women who become infected may also consider getting vaccinated, the authors wrote. Vaccination up to 14 days after exposure doesn’t prevent the disease but can reduce the severity of symptoms. In the current outbreak, public health organizations advised doctors to vaccinate contacts of confirmed cases, including pregnant people.
The data for monkeypox vaccine use in pregnant women is small, the authors wrote, including fewer than 300 women. In previous studies, no adverse outcomes were found. The vaccine is also considered safe for breastfeeding.
“The decision whether to have the vaccine in pregnancy should be a personal choice,” the authors wrote. “Pregnant women and people should be encouraged to discuss the risks and benefits of vaccination, including possible side effects, with a health care professional before making their final decision.”
A version of this article first appeared on Medscape.com.
The risk of monkeypox infection remains low for the general public, the authors wrote, though cases continue to grow worldwide, particularly in the United Kingdom.
“We are aware infants and children are at greater risk of becoming seriously ill if they do catch monkeypox,” Edward Morris, MBBS, one of the authors and president of the Royal College of Obstetricians and Gynecologists, said in a statement.
“Therefore, to minimize the risk of a baby contracting the virus, we recommend health care professionals discuss the benefits and risks of having a cesarean birth with a pregnant woman or person who has or is suspected of having the virus,” he said.
Dr. Morris and colleagues pulled together existing evidence on monkeypox diagnosis, treatment, and recommended modes of birth for mothers and babies.
“The World Health Organization states there could be adverse consequences for pregnant women and babies if they become infected, including congenital monkeypox, miscarriage, or stillbirth, which is why we have provided clear guidance for health care professionals in this paper,” Dr. Morris said.
The monkeypox virus typically spreads through direct contact, droplets, or contaminated surfaces and objects. But some limited evidence shows that the virus can be passed from a mother to a baby via the placenta, which can lead to congenital monkeypox.
What’s more, mothers may be able to transmit the virus during or after birth. Although no evidence exists around the optimal mode of birth, a pregnant woman with an active monkeypox infection may choose to avoid vaginal delivery to reduce direct contact.
“If genital lesions are identified on a pregnant woman, then a cesarean birth will be recommended,” the authors wrote. “If a pregnant woman or person has suspected or confirmed monkeypox, a caesarean birth will be offered following discussion of the possible risk of neonatal infection, which may be serious.”
After giving birth, close contact can spread the virus as well. To minimize the risk, the authors recommend isolating the baby from family members who have confirmed or suspected monkeypox and carefully monitoring for infection.
Mothers with an active monkeypox infection should also avoid breastfeeding to lower the risk of spreading the virus to their newborn, the authors wrote. But to support breastfeeding after infection, mothers can express and discard milk until the isolation period has passed.
Pregnant women who become infected may also consider getting vaccinated, the authors wrote. Vaccination up to 14 days after exposure doesn’t prevent the disease but can reduce the severity of symptoms. In the current outbreak, public health organizations advised doctors to vaccinate contacts of confirmed cases, including pregnant people.
The data for monkeypox vaccine use in pregnant women is small, the authors wrote, including fewer than 300 women. In previous studies, no adverse outcomes were found. The vaccine is also considered safe for breastfeeding.
“The decision whether to have the vaccine in pregnancy should be a personal choice,” the authors wrote. “Pregnant women and people should be encouraged to discuss the risks and benefits of vaccination, including possible side effects, with a health care professional before making their final decision.”
A version of this article first appeared on Medscape.com.
The risk of monkeypox infection remains low for the general public, the authors wrote, though cases continue to grow worldwide, particularly in the United Kingdom.
“We are aware infants and children are at greater risk of becoming seriously ill if they do catch monkeypox,” Edward Morris, MBBS, one of the authors and president of the Royal College of Obstetricians and Gynecologists, said in a statement.
“Therefore, to minimize the risk of a baby contracting the virus, we recommend health care professionals discuss the benefits and risks of having a cesarean birth with a pregnant woman or person who has or is suspected of having the virus,” he said.
Dr. Morris and colleagues pulled together existing evidence on monkeypox diagnosis, treatment, and recommended modes of birth for mothers and babies.
“The World Health Organization states there could be adverse consequences for pregnant women and babies if they become infected, including congenital monkeypox, miscarriage, or stillbirth, which is why we have provided clear guidance for health care professionals in this paper,” Dr. Morris said.
The monkeypox virus typically spreads through direct contact, droplets, or contaminated surfaces and objects. But some limited evidence shows that the virus can be passed from a mother to a baby via the placenta, which can lead to congenital monkeypox.
What’s more, mothers may be able to transmit the virus during or after birth. Although no evidence exists around the optimal mode of birth, a pregnant woman with an active monkeypox infection may choose to avoid vaginal delivery to reduce direct contact.
“If genital lesions are identified on a pregnant woman, then a cesarean birth will be recommended,” the authors wrote. “If a pregnant woman or person has suspected or confirmed monkeypox, a caesarean birth will be offered following discussion of the possible risk of neonatal infection, which may be serious.”
After giving birth, close contact can spread the virus as well. To minimize the risk, the authors recommend isolating the baby from family members who have confirmed or suspected monkeypox and carefully monitoring for infection.
Mothers with an active monkeypox infection should also avoid breastfeeding to lower the risk of spreading the virus to their newborn, the authors wrote. But to support breastfeeding after infection, mothers can express and discard milk until the isolation period has passed.
Pregnant women who become infected may also consider getting vaccinated, the authors wrote. Vaccination up to 14 days after exposure doesn’t prevent the disease but can reduce the severity of symptoms. In the current outbreak, public health organizations advised doctors to vaccinate contacts of confirmed cases, including pregnant people.
The data for monkeypox vaccine use in pregnant women is small, the authors wrote, including fewer than 300 women. In previous studies, no adverse outcomes were found. The vaccine is also considered safe for breastfeeding.
“The decision whether to have the vaccine in pregnancy should be a personal choice,” the authors wrote. “Pregnant women and people should be encouraged to discuss the risks and benefits of vaccination, including possible side effects, with a health care professional before making their final decision.”
A version of this article first appeared on Medscape.com.
FROM ULTRASOUND IN OBSTETRICS & GYNECOLOGY
Biologics, Women, and Pregnancy: What’s Known?
As the and the child’s development.
“I get asked a lot about fertility,” Vivian Shi, MD, associate professor of dermatology at the University of Arkansas, Little Rock, said at MedscapeLive’s Women’s and Pediatric Dermatology Seminar. Patients want to know, she said, if they go on a specific drug, whether it will affect their chances of conceiving and what else they need to know about safety.
She told the audience what she tells her patients: The answers are not complete but are evolving at a steady pace.
“Putting this talk together was kind of like a scavenger hunt,” said Dr. Shi, who gathered data from pregnancy exposure registries, published research, the Food and Drug Administration, and other sources on biologics. As more studies emerge each year, she said, recommendations will become stronger for considering treatment by certain biological drugs, taking into account effects on fertility, pregnancy, lactation, and the infant.
Among the biologics commonly used in dermatology are:
- Tumor necrosis factor (TNF) inhibitors (etanercept, adalimumab, infliximab, certolizumab).
- Interleukin (IL)–12 and -23 antagonist (ustekinumab).
- IL-17 antagonists (ixekizumab, secukinumab, brodalumab).
- IL-23 antagonists (risankizumab, tildrakizumab, guselkumab).
- IL-4, -13 antagonist (dupilumab) and IL-13 antagonist (tralokinumab).
- CD20-directed cytolytic antibody (rituximab).
To help with decision-making, Dr. Shi discussed the relatively new FDA labeling regulations as well as pregnancy exposure registries, research studies, and recommendations.
FDA pregnancy risk summaries
Under the previous system of classification of drugs in pregnancy, the FDA rated drugs as A, B, C, D, X. These categories ranged from showing no risks to the fetus to clear risk, but were oversimplistic and confusing, Dr. Shi said. Category C was especially confusing, as a drug with no animal or human data was put in the same category as a drug with adverse fetal effects on animals, she noted.
However, effective June 30, 2015, the FDA replaced pregnancy categories with risk summaries by medication. As of June, 2020, all prescription drugs were to remove pregnancy letter labeling. The risk summaries note human data when they are available and also note when no data are available. This information, Dr. Shi said, originates from many sources, including studies published in the medical literature, postmarketing studies conducted by companies, and pregnancy exposure registries, conducted by some companies and others. The FDA does not endorse any specific registries, but does post a list of such registries. Another helpful resource, she said, is Mother to Baby, a service of the nonprofit Organization of Teratology Information Specialists (OTIS).
Known, not known
Citing published literature, Dr. Shi said that TNF inhibitors have the most robust safety data from preconception to after birth. Less is known, she said, about the reproductive safety effects of other biologics used for dermatologic conditions, as they are newer than the anti-TNF medicines.
She reviewed a variety of research studies evaluating the safety of biologics during pregnancy and beyond. Highlights include results from a large registry, the Psoriasis Longitudinal Assessment and Registry (PSOLAR), of 298 pregnancies in about 220 women from 2007 to 2019, looking at 13 different biologics. The overall and live-birth outcomes in the women on biologics for psoriasis were similar to those for the general population and the rate of congenital anomalies was 0.8%, researchers reported in 2021, lower than the generally cited annual figure of U.S. births.
Studies evaluating biologics for nondermatologic conditions suggest safety. A prospective cohort study of women who took adalimumab in pregnancy (for rheumatoid arthritis or Crohn’s disease) found no increased risk for birth defects. In another study looking at women who were breastfeeding, researchers found no increased risk of infections or delay in developmental milestones in the children of women taking biologics for inflammatory bowel disease, compared with those not on the medications.
A report using data from the World Health Organization concludes that dupilumab appears to be safe during pregnancy, based on an evaluation of 36 pregnancy-related reports among more than 37,000 unique adverse event reports related to dupilumab in a global database.
Recommendations about biologic use from different organizations don’t always mesh, Dr. Shi said, noting that European guidelines tend to be stricter, as some reviews show.
If a mother is exposed to any biologic therapy other than certolizumab during the third trimester, after 27 weeks, Dr. Shi said, “you want to consider avoiding a live vaccine for the first 6 months of the baby’s life.” It turns out, she said, the only recommended live vaccine during that period is the rotavirus vaccine, and she suggests doctors recommend postponing that one until the babies are older if women have been on biologics other than certolizumab.
Her other take-home messages: TNF inhibitors have the most robust safety data from before conception through lactation. Under current guidelines, certolizumab is viewed as the safest to use throughout pregnancy. Dr. Shi’s message to her colleagues fielding the same questions she gets from patients: “There is more data coming out every year. Ultimately, we will have better information to inform our patients.”
At the conference, Lawrence F. Eichenfield, MD, a course director and professor of dermatology and pediatrics at the University of California, San Diego and Rady Children’s Hospital San Diego, encouraged Dr. Shi to write up her presentation as a resource for other dermatologists – which she said is in progress.
Medscape Live and this news organization are owned by the same parent company. Dr. Shi disclosed consulting and investigative and research funding from several pharmaceutical firms, but not directly related to the content of her presentation.
As the and the child’s development.
“I get asked a lot about fertility,” Vivian Shi, MD, associate professor of dermatology at the University of Arkansas, Little Rock, said at MedscapeLive’s Women’s and Pediatric Dermatology Seminar. Patients want to know, she said, if they go on a specific drug, whether it will affect their chances of conceiving and what else they need to know about safety.
She told the audience what she tells her patients: The answers are not complete but are evolving at a steady pace.
“Putting this talk together was kind of like a scavenger hunt,” said Dr. Shi, who gathered data from pregnancy exposure registries, published research, the Food and Drug Administration, and other sources on biologics. As more studies emerge each year, she said, recommendations will become stronger for considering treatment by certain biological drugs, taking into account effects on fertility, pregnancy, lactation, and the infant.
Among the biologics commonly used in dermatology are:
- Tumor necrosis factor (TNF) inhibitors (etanercept, adalimumab, infliximab, certolizumab).
- Interleukin (IL)–12 and -23 antagonist (ustekinumab).
- IL-17 antagonists (ixekizumab, secukinumab, brodalumab).
- IL-23 antagonists (risankizumab, tildrakizumab, guselkumab).
- IL-4, -13 antagonist (dupilumab) and IL-13 antagonist (tralokinumab).
- CD20-directed cytolytic antibody (rituximab).
To help with decision-making, Dr. Shi discussed the relatively new FDA labeling regulations as well as pregnancy exposure registries, research studies, and recommendations.
FDA pregnancy risk summaries
Under the previous system of classification of drugs in pregnancy, the FDA rated drugs as A, B, C, D, X. These categories ranged from showing no risks to the fetus to clear risk, but were oversimplistic and confusing, Dr. Shi said. Category C was especially confusing, as a drug with no animal or human data was put in the same category as a drug with adverse fetal effects on animals, she noted.
However, effective June 30, 2015, the FDA replaced pregnancy categories with risk summaries by medication. As of June, 2020, all prescription drugs were to remove pregnancy letter labeling. The risk summaries note human data when they are available and also note when no data are available. This information, Dr. Shi said, originates from many sources, including studies published in the medical literature, postmarketing studies conducted by companies, and pregnancy exposure registries, conducted by some companies and others. The FDA does not endorse any specific registries, but does post a list of such registries. Another helpful resource, she said, is Mother to Baby, a service of the nonprofit Organization of Teratology Information Specialists (OTIS).
Known, not known
Citing published literature, Dr. Shi said that TNF inhibitors have the most robust safety data from preconception to after birth. Less is known, she said, about the reproductive safety effects of other biologics used for dermatologic conditions, as they are newer than the anti-TNF medicines.
She reviewed a variety of research studies evaluating the safety of biologics during pregnancy and beyond. Highlights include results from a large registry, the Psoriasis Longitudinal Assessment and Registry (PSOLAR), of 298 pregnancies in about 220 women from 2007 to 2019, looking at 13 different biologics. The overall and live-birth outcomes in the women on biologics for psoriasis were similar to those for the general population and the rate of congenital anomalies was 0.8%, researchers reported in 2021, lower than the generally cited annual figure of U.S. births.
Studies evaluating biologics for nondermatologic conditions suggest safety. A prospective cohort study of women who took adalimumab in pregnancy (for rheumatoid arthritis or Crohn’s disease) found no increased risk for birth defects. In another study looking at women who were breastfeeding, researchers found no increased risk of infections or delay in developmental milestones in the children of women taking biologics for inflammatory bowel disease, compared with those not on the medications.
A report using data from the World Health Organization concludes that dupilumab appears to be safe during pregnancy, based on an evaluation of 36 pregnancy-related reports among more than 37,000 unique adverse event reports related to dupilumab in a global database.
Recommendations about biologic use from different organizations don’t always mesh, Dr. Shi said, noting that European guidelines tend to be stricter, as some reviews show.
If a mother is exposed to any biologic therapy other than certolizumab during the third trimester, after 27 weeks, Dr. Shi said, “you want to consider avoiding a live vaccine for the first 6 months of the baby’s life.” It turns out, she said, the only recommended live vaccine during that period is the rotavirus vaccine, and she suggests doctors recommend postponing that one until the babies are older if women have been on biologics other than certolizumab.
Her other take-home messages: TNF inhibitors have the most robust safety data from before conception through lactation. Under current guidelines, certolizumab is viewed as the safest to use throughout pregnancy. Dr. Shi’s message to her colleagues fielding the same questions she gets from patients: “There is more data coming out every year. Ultimately, we will have better information to inform our patients.”
At the conference, Lawrence F. Eichenfield, MD, a course director and professor of dermatology and pediatrics at the University of California, San Diego and Rady Children’s Hospital San Diego, encouraged Dr. Shi to write up her presentation as a resource for other dermatologists – which she said is in progress.
Medscape Live and this news organization are owned by the same parent company. Dr. Shi disclosed consulting and investigative and research funding from several pharmaceutical firms, but not directly related to the content of her presentation.
As the and the child’s development.
“I get asked a lot about fertility,” Vivian Shi, MD, associate professor of dermatology at the University of Arkansas, Little Rock, said at MedscapeLive’s Women’s and Pediatric Dermatology Seminar. Patients want to know, she said, if they go on a specific drug, whether it will affect their chances of conceiving and what else they need to know about safety.
She told the audience what she tells her patients: The answers are not complete but are evolving at a steady pace.
“Putting this talk together was kind of like a scavenger hunt,” said Dr. Shi, who gathered data from pregnancy exposure registries, published research, the Food and Drug Administration, and other sources on biologics. As more studies emerge each year, she said, recommendations will become stronger for considering treatment by certain biological drugs, taking into account effects on fertility, pregnancy, lactation, and the infant.
Among the biologics commonly used in dermatology are:
- Tumor necrosis factor (TNF) inhibitors (etanercept, adalimumab, infliximab, certolizumab).
- Interleukin (IL)–12 and -23 antagonist (ustekinumab).
- IL-17 antagonists (ixekizumab, secukinumab, brodalumab).
- IL-23 antagonists (risankizumab, tildrakizumab, guselkumab).
- IL-4, -13 antagonist (dupilumab) and IL-13 antagonist (tralokinumab).
- CD20-directed cytolytic antibody (rituximab).
To help with decision-making, Dr. Shi discussed the relatively new FDA labeling regulations as well as pregnancy exposure registries, research studies, and recommendations.
FDA pregnancy risk summaries
Under the previous system of classification of drugs in pregnancy, the FDA rated drugs as A, B, C, D, X. These categories ranged from showing no risks to the fetus to clear risk, but were oversimplistic and confusing, Dr. Shi said. Category C was especially confusing, as a drug with no animal or human data was put in the same category as a drug with adverse fetal effects on animals, she noted.
However, effective June 30, 2015, the FDA replaced pregnancy categories with risk summaries by medication. As of June, 2020, all prescription drugs were to remove pregnancy letter labeling. The risk summaries note human data when they are available and also note when no data are available. This information, Dr. Shi said, originates from many sources, including studies published in the medical literature, postmarketing studies conducted by companies, and pregnancy exposure registries, conducted by some companies and others. The FDA does not endorse any specific registries, but does post a list of such registries. Another helpful resource, she said, is Mother to Baby, a service of the nonprofit Organization of Teratology Information Specialists (OTIS).
Known, not known
Citing published literature, Dr. Shi said that TNF inhibitors have the most robust safety data from preconception to after birth. Less is known, she said, about the reproductive safety effects of other biologics used for dermatologic conditions, as they are newer than the anti-TNF medicines.
She reviewed a variety of research studies evaluating the safety of biologics during pregnancy and beyond. Highlights include results from a large registry, the Psoriasis Longitudinal Assessment and Registry (PSOLAR), of 298 pregnancies in about 220 women from 2007 to 2019, looking at 13 different biologics. The overall and live-birth outcomes in the women on biologics for psoriasis were similar to those for the general population and the rate of congenital anomalies was 0.8%, researchers reported in 2021, lower than the generally cited annual figure of U.S. births.
Studies evaluating biologics for nondermatologic conditions suggest safety. A prospective cohort study of women who took adalimumab in pregnancy (for rheumatoid arthritis or Crohn’s disease) found no increased risk for birth defects. In another study looking at women who were breastfeeding, researchers found no increased risk of infections or delay in developmental milestones in the children of women taking biologics for inflammatory bowel disease, compared with those not on the medications.
A report using data from the World Health Organization concludes that dupilumab appears to be safe during pregnancy, based on an evaluation of 36 pregnancy-related reports among more than 37,000 unique adverse event reports related to dupilumab in a global database.
Recommendations about biologic use from different organizations don’t always mesh, Dr. Shi said, noting that European guidelines tend to be stricter, as some reviews show.
If a mother is exposed to any biologic therapy other than certolizumab during the third trimester, after 27 weeks, Dr. Shi said, “you want to consider avoiding a live vaccine for the first 6 months of the baby’s life.” It turns out, she said, the only recommended live vaccine during that period is the rotavirus vaccine, and she suggests doctors recommend postponing that one until the babies are older if women have been on biologics other than certolizumab.
Her other take-home messages: TNF inhibitors have the most robust safety data from before conception through lactation. Under current guidelines, certolizumab is viewed as the safest to use throughout pregnancy. Dr. Shi’s message to her colleagues fielding the same questions she gets from patients: “There is more data coming out every year. Ultimately, we will have better information to inform our patients.”
At the conference, Lawrence F. Eichenfield, MD, a course director and professor of dermatology and pediatrics at the University of California, San Diego and Rady Children’s Hospital San Diego, encouraged Dr. Shi to write up her presentation as a resource for other dermatologists – which she said is in progress.
Medscape Live and this news organization are owned by the same parent company. Dr. Shi disclosed consulting and investigative and research funding from several pharmaceutical firms, but not directly related to the content of her presentation.
FROM MEDSCAPELIVE WOMEN’S & PEDIATRIC DERMATOLOGY SEMINAR
‘Medical maximizers’ dole out unneeded antibiotics for ASB
So why did you get that prescription?
The Infectious Diseases Society of America recommends against antibiotics in this scenario, with exceptions for patients who are pregnant or undergoing certain urologic procedures.
Antibiotics for asymptomatic bacteriuria (ASB) generally do not help; are costly; and can cause side effects, Clostridioides difficile infection, and antibiotic resistance.
Still, antibiotic treatment for asymptomatic bacteriuria remains common, despite guidelines.
And when researchers recently surveyed 551 primary care clinicians to see which ones would inappropriately prescribe antibiotics for a positive urine culture, the answer was most of them: 71%.
“Regardless of years in practice, training background, or professional degree, most clinicians indicated that they would prescribe antibiotics for asymptomatic bacteriuria,” the researchers reported in JAMA Network Open.
Some groups of clinicians seemed especially likely to prescribe antibiotics unnecessarily.
“Medical maximizers” – clinicians who prefer treatment even when its value is ambiguous – and family medicine clinicians were more likely to prescribe antibiotics in response to a hypothetical case.
On the other hand, resident physicians and clinicians in the U.S. Pacific Northwest were less likely to provide antibiotics inappropriately, the researchers found.
Study author Jonathan D. Baghdadi, MD, PhD, with the department of epidemiology and public health at the University of Maryland and the Veterans Affairs Maryland Healthcare System in Baltimore, summed up the findings on Twitter: “ ... who prescribes antibiotics for asymptomatic bacteriuria? The answer is most primary care clinicians in every category, but it’s more common among clinicians who want to ‘do everything.’ ”
Dr. Baghdadi said the gaps reflect problems with the medical system rather than individual clinicians.
“I don’t believe that individual clinicians knowingly choose to prescribe inappropriate antibiotics in defiance of guidelines,” Dr. Baghdadi told this news organization. “Clinical decision-making is complicated, and the decision to prescribe inappropriate antibiotics depends on patient expectations, clinician perception of patient expectations, time pressure in the clinic, regional variation in medical practice, the culture of antibiotic use, and likely in some cases the perception that doing more is better.”
In addition, researchers have used various definitions of ASB over time and in different contexts, he said.
What to do for Mr. Williams?
To examine clinician attitudes and characteristics associated with prescribing antibiotics for asymptomatic bacteriuria, Dr. Baghdadi and his colleagues analyzed survey responses from 490 physicians and 61 advanced practice clinicians.
Study participants completed tests that measure numeracy, risk-taking preferences, burnout, and tendency to maximize care. They were presented with four hypothetical clinical scenarios, including a case of asymptomatic bacteriuria: “Mr. Williams, a 65-year-old man, comes to the office for follow-up of his osteoarthritis. He has noted foul-smelling urine and no pain or difficulty with urination. A urine dipstick shows trace blood. He has no particular preference for testing and wants your advice.”
Clinicians who had been in practice for at least 10 years were more likely to prescribe antibiotics (82%) to “Mr. Williams” than were those with 3-9 years in practice (73%) or less than 3 years in practice (64%).
Of 120 clinicians with a background in family medicine, 85% said they would have prescribed antibiotics, versus 62% of 207 clinicians with a background in internal medicine.
Nurse practitioners and physician assistants were more likely to prescribe antibiotics (90%) than were attending (78%) and resident physicians (63%).
In one analysis, a background in family medicine was associated with nearly three times higher odds of prescribing antibiotics. And a high “medical maximizer” score was associated with about twice the odds of prescribing the medications.
Meanwhile, resident physicians and clinicians in the Pacific Northwest had a lower likelihood of prescribing antibiotics, with odds ratios of 0.57 and 0.49, respectively.
The respondents who prescribed antibiotics estimated a 90% probability of UTI, whereas those who did not prescribe antibiotics estimated a 15% probability of the condition.
Breaking a habit
Some prescribers may know not to treat asymptomatic bacteriuria but mistakenly consider certain findings to be symptoms of UTI.
Bradley Langford, PharmD, an antimicrobial stewardship expert with Public Health Ontario, said in his experience, most clinicians who say they know not to treat ASB incorrectly believe that cloudy urine, altered cognition, and other nonspecific symptoms indicate a UTI.
“The fact that most clinicians would treat ASB suggests that there is still a lot of work to do to improve antimicrobial stewardship, particularly outside of the hospital setting,” Dr. Langford told this news organization.
Avoiding unnecessary antibiotics is important not just because of the lack of benefit, but also because of the potential harms, said Dr. Langford. He has created a list of rebuttals for commonly given reasons for testing and treating asymptomatic bacteriuria.
“Using antibiotics for ASB can counterintuitively increase the risk for symptomatic UTI due to the disruption of protective local microflora, allowing for the growth of more pathogenic/resistant organisms,” he said.
One approach to addressing the problem: Don’t test urine in the first place if patients are asymptomatic. Virtual learning sessions have been shown to reduce urine culturing and urinary antibiotic prescribing in long-term care homes, Dr. Langford noted.
Updated training for health care professionals from the outset may also be key, and the lower rate of prescribing intent among resident physicians is reassuring, he said.
A role for patients
Patients could also help decrease the inappropriate use of antibiotics.
“Be clear with your doctor about your expectations for the health care interaction, including whether you are expecting to receive antibiotics,” Dr. Baghdadi said. “Your doctor may assume you contacted them because you wanted a prescription. If you are not expecting antibiotics, you should feel free to say so. And if you are asymptomatic, you may not need antibiotics, even if the urine culture is positive.”
The study was funded by a grant from the National Institutes of Health, and Dr. Baghdadi received grant support from the University of Maryland, Baltimore Institute for Clinical and Translational Research. Coauthors disclosed government grants and ties to Memorial Sloan Kettering Cancer Center, Vedanta Biosciences, Opentrons, and Fimbrion. Dr. Langford reported no relevant financial conflicts of interest.
A version of this article first appeared on Medscape.com.
So why did you get that prescription?
The Infectious Diseases Society of America recommends against antibiotics in this scenario, with exceptions for patients who are pregnant or undergoing certain urologic procedures.
Antibiotics for asymptomatic bacteriuria (ASB) generally do not help; are costly; and can cause side effects, Clostridioides difficile infection, and antibiotic resistance.
Still, antibiotic treatment for asymptomatic bacteriuria remains common, despite guidelines.
And when researchers recently surveyed 551 primary care clinicians to see which ones would inappropriately prescribe antibiotics for a positive urine culture, the answer was most of them: 71%.
“Regardless of years in practice, training background, or professional degree, most clinicians indicated that they would prescribe antibiotics for asymptomatic bacteriuria,” the researchers reported in JAMA Network Open.
Some groups of clinicians seemed especially likely to prescribe antibiotics unnecessarily.
“Medical maximizers” – clinicians who prefer treatment even when its value is ambiguous – and family medicine clinicians were more likely to prescribe antibiotics in response to a hypothetical case.
On the other hand, resident physicians and clinicians in the U.S. Pacific Northwest were less likely to provide antibiotics inappropriately, the researchers found.
Study author Jonathan D. Baghdadi, MD, PhD, with the department of epidemiology and public health at the University of Maryland and the Veterans Affairs Maryland Healthcare System in Baltimore, summed up the findings on Twitter: “ ... who prescribes antibiotics for asymptomatic bacteriuria? The answer is most primary care clinicians in every category, but it’s more common among clinicians who want to ‘do everything.’ ”
Dr. Baghdadi said the gaps reflect problems with the medical system rather than individual clinicians.
“I don’t believe that individual clinicians knowingly choose to prescribe inappropriate antibiotics in defiance of guidelines,” Dr. Baghdadi told this news organization. “Clinical decision-making is complicated, and the decision to prescribe inappropriate antibiotics depends on patient expectations, clinician perception of patient expectations, time pressure in the clinic, regional variation in medical practice, the culture of antibiotic use, and likely in some cases the perception that doing more is better.”
In addition, researchers have used various definitions of ASB over time and in different contexts, he said.
What to do for Mr. Williams?
To examine clinician attitudes and characteristics associated with prescribing antibiotics for asymptomatic bacteriuria, Dr. Baghdadi and his colleagues analyzed survey responses from 490 physicians and 61 advanced practice clinicians.
Study participants completed tests that measure numeracy, risk-taking preferences, burnout, and tendency to maximize care. They were presented with four hypothetical clinical scenarios, including a case of asymptomatic bacteriuria: “Mr. Williams, a 65-year-old man, comes to the office for follow-up of his osteoarthritis. He has noted foul-smelling urine and no pain or difficulty with urination. A urine dipstick shows trace blood. He has no particular preference for testing and wants your advice.”
Clinicians who had been in practice for at least 10 years were more likely to prescribe antibiotics (82%) to “Mr. Williams” than were those with 3-9 years in practice (73%) or less than 3 years in practice (64%).
Of 120 clinicians with a background in family medicine, 85% said they would have prescribed antibiotics, versus 62% of 207 clinicians with a background in internal medicine.
Nurse practitioners and physician assistants were more likely to prescribe antibiotics (90%) than were attending (78%) and resident physicians (63%).
In one analysis, a background in family medicine was associated with nearly three times higher odds of prescribing antibiotics. And a high “medical maximizer” score was associated with about twice the odds of prescribing the medications.
Meanwhile, resident physicians and clinicians in the Pacific Northwest had a lower likelihood of prescribing antibiotics, with odds ratios of 0.57 and 0.49, respectively.
The respondents who prescribed antibiotics estimated a 90% probability of UTI, whereas those who did not prescribe antibiotics estimated a 15% probability of the condition.
Breaking a habit
Some prescribers may know not to treat asymptomatic bacteriuria but mistakenly consider certain findings to be symptoms of UTI.
Bradley Langford, PharmD, an antimicrobial stewardship expert with Public Health Ontario, said in his experience, most clinicians who say they know not to treat ASB incorrectly believe that cloudy urine, altered cognition, and other nonspecific symptoms indicate a UTI.
“The fact that most clinicians would treat ASB suggests that there is still a lot of work to do to improve antimicrobial stewardship, particularly outside of the hospital setting,” Dr. Langford told this news organization.
Avoiding unnecessary antibiotics is important not just because of the lack of benefit, but also because of the potential harms, said Dr. Langford. He has created a list of rebuttals for commonly given reasons for testing and treating asymptomatic bacteriuria.
“Using antibiotics for ASB can counterintuitively increase the risk for symptomatic UTI due to the disruption of protective local microflora, allowing for the growth of more pathogenic/resistant organisms,” he said.
One approach to addressing the problem: Don’t test urine in the first place if patients are asymptomatic. Virtual learning sessions have been shown to reduce urine culturing and urinary antibiotic prescribing in long-term care homes, Dr. Langford noted.
Updated training for health care professionals from the outset may also be key, and the lower rate of prescribing intent among resident physicians is reassuring, he said.
A role for patients
Patients could also help decrease the inappropriate use of antibiotics.
“Be clear with your doctor about your expectations for the health care interaction, including whether you are expecting to receive antibiotics,” Dr. Baghdadi said. “Your doctor may assume you contacted them because you wanted a prescription. If you are not expecting antibiotics, you should feel free to say so. And if you are asymptomatic, you may not need antibiotics, even if the urine culture is positive.”
The study was funded by a grant from the National Institutes of Health, and Dr. Baghdadi received grant support from the University of Maryland, Baltimore Institute for Clinical and Translational Research. Coauthors disclosed government grants and ties to Memorial Sloan Kettering Cancer Center, Vedanta Biosciences, Opentrons, and Fimbrion. Dr. Langford reported no relevant financial conflicts of interest.
A version of this article first appeared on Medscape.com.
So why did you get that prescription?
The Infectious Diseases Society of America recommends against antibiotics in this scenario, with exceptions for patients who are pregnant or undergoing certain urologic procedures.
Antibiotics for asymptomatic bacteriuria (ASB) generally do not help; are costly; and can cause side effects, Clostridioides difficile infection, and antibiotic resistance.
Still, antibiotic treatment for asymptomatic bacteriuria remains common, despite guidelines.
And when researchers recently surveyed 551 primary care clinicians to see which ones would inappropriately prescribe antibiotics for a positive urine culture, the answer was most of them: 71%.
“Regardless of years in practice, training background, or professional degree, most clinicians indicated that they would prescribe antibiotics for asymptomatic bacteriuria,” the researchers reported in JAMA Network Open.
Some groups of clinicians seemed especially likely to prescribe antibiotics unnecessarily.
“Medical maximizers” – clinicians who prefer treatment even when its value is ambiguous – and family medicine clinicians were more likely to prescribe antibiotics in response to a hypothetical case.
On the other hand, resident physicians and clinicians in the U.S. Pacific Northwest were less likely to provide antibiotics inappropriately, the researchers found.
Study author Jonathan D. Baghdadi, MD, PhD, with the department of epidemiology and public health at the University of Maryland and the Veterans Affairs Maryland Healthcare System in Baltimore, summed up the findings on Twitter: “ ... who prescribes antibiotics for asymptomatic bacteriuria? The answer is most primary care clinicians in every category, but it’s more common among clinicians who want to ‘do everything.’ ”
Dr. Baghdadi said the gaps reflect problems with the medical system rather than individual clinicians.
“I don’t believe that individual clinicians knowingly choose to prescribe inappropriate antibiotics in defiance of guidelines,” Dr. Baghdadi told this news organization. “Clinical decision-making is complicated, and the decision to prescribe inappropriate antibiotics depends on patient expectations, clinician perception of patient expectations, time pressure in the clinic, regional variation in medical practice, the culture of antibiotic use, and likely in some cases the perception that doing more is better.”
In addition, researchers have used various definitions of ASB over time and in different contexts, he said.
What to do for Mr. Williams?
To examine clinician attitudes and characteristics associated with prescribing antibiotics for asymptomatic bacteriuria, Dr. Baghdadi and his colleagues analyzed survey responses from 490 physicians and 61 advanced practice clinicians.
Study participants completed tests that measure numeracy, risk-taking preferences, burnout, and tendency to maximize care. They were presented with four hypothetical clinical scenarios, including a case of asymptomatic bacteriuria: “Mr. Williams, a 65-year-old man, comes to the office for follow-up of his osteoarthritis. He has noted foul-smelling urine and no pain or difficulty with urination. A urine dipstick shows trace blood. He has no particular preference for testing and wants your advice.”
Clinicians who had been in practice for at least 10 years were more likely to prescribe antibiotics (82%) to “Mr. Williams” than were those with 3-9 years in practice (73%) or less than 3 years in practice (64%).
Of 120 clinicians with a background in family medicine, 85% said they would have prescribed antibiotics, versus 62% of 207 clinicians with a background in internal medicine.
Nurse practitioners and physician assistants were more likely to prescribe antibiotics (90%) than were attending (78%) and resident physicians (63%).
In one analysis, a background in family medicine was associated with nearly three times higher odds of prescribing antibiotics. And a high “medical maximizer” score was associated with about twice the odds of prescribing the medications.
Meanwhile, resident physicians and clinicians in the Pacific Northwest had a lower likelihood of prescribing antibiotics, with odds ratios of 0.57 and 0.49, respectively.
The respondents who prescribed antibiotics estimated a 90% probability of UTI, whereas those who did not prescribe antibiotics estimated a 15% probability of the condition.
Breaking a habit
Some prescribers may know not to treat asymptomatic bacteriuria but mistakenly consider certain findings to be symptoms of UTI.
Bradley Langford, PharmD, an antimicrobial stewardship expert with Public Health Ontario, said in his experience, most clinicians who say they know not to treat ASB incorrectly believe that cloudy urine, altered cognition, and other nonspecific symptoms indicate a UTI.
“The fact that most clinicians would treat ASB suggests that there is still a lot of work to do to improve antimicrobial stewardship, particularly outside of the hospital setting,” Dr. Langford told this news organization.
Avoiding unnecessary antibiotics is important not just because of the lack of benefit, but also because of the potential harms, said Dr. Langford. He has created a list of rebuttals for commonly given reasons for testing and treating asymptomatic bacteriuria.
“Using antibiotics for ASB can counterintuitively increase the risk for symptomatic UTI due to the disruption of protective local microflora, allowing for the growth of more pathogenic/resistant organisms,” he said.
One approach to addressing the problem: Don’t test urine in the first place if patients are asymptomatic. Virtual learning sessions have been shown to reduce urine culturing and urinary antibiotic prescribing in long-term care homes, Dr. Langford noted.
Updated training for health care professionals from the outset may also be key, and the lower rate of prescribing intent among resident physicians is reassuring, he said.
A role for patients
Patients could also help decrease the inappropriate use of antibiotics.
“Be clear with your doctor about your expectations for the health care interaction, including whether you are expecting to receive antibiotics,” Dr. Baghdadi said. “Your doctor may assume you contacted them because you wanted a prescription. If you are not expecting antibiotics, you should feel free to say so. And if you are asymptomatic, you may not need antibiotics, even if the urine culture is positive.”
The study was funded by a grant from the National Institutes of Health, and Dr. Baghdadi received grant support from the University of Maryland, Baltimore Institute for Clinical and Translational Research. Coauthors disclosed government grants and ties to Memorial Sloan Kettering Cancer Center, Vedanta Biosciences, Opentrons, and Fimbrion. Dr. Langford reported no relevant financial conflicts of interest.
A version of this article first appeared on Medscape.com.
Substance use the main cause of physician license actions
Despite a sharp uptick in 2011, substance use–specific license actions taken against physicians dropped in frequency between 2004 and 2020.
More than three fourths (76.3%) of license actions taken against physicians were related to substance use, according to a recent study published in JAMA. Psychological impairment was the reason associated with more than 1 in 10 (11.5%) actions taken against physicians’ licenses, while physical impairment was the reason behind approximately 12% of such actions, per the study.
Researchers analyzed 5032 actions taken against the licenses of U.S. physicians. The actions were reported to the National Practitioner Data Bank and were related to substance use, psychological impairment, and physical impairment. The National Practitioner Data Bank is a web-based repository of reports with information on medical malpractice payments and certain adverse actions related to healthcare practitioners, providers, and suppliers. It is provided by the Department of Health & Human Services.
“While there has been increased attention [on] the mental health of physicians, we wanted to understand the extent to which changes in attitudes and practices were reflected in actions taken by hospitals or licensing boards, which are reported in the National Practitioner Data Bank,” Lisa Rotenstein, MD, a primary care physician at Boston’s Brigham and Women’s Hospital and lead author of the study, told this news organization.
Dr. Rotenstein, who is an assistant professor at Harvard Medical School, Boston, studies issues of mental health among physicians and trainees. Dr. Rotenstein was the lead author of a 2016 study that found that more than a quarter (27.2%) of medical students have depressive symptoms. She was also lead author of a 2018 study published in JAMA on the prevalence of burnout among attending physicians.
Actions against physicians trending downward
2011 marked the peak in actions taken against physicians’ licenses for substance use, per the study, but actions related to substance use have otherwise maintained a steady decline over the past 17 years. Researchers found that physicians with license actions as a result of substance use or psychological impairment were more likely to receive indefinite penalties, while also having emergency action taken against their license to practice.
In addition, physicians who had actions taken against their licenses because of substance use or psychological impairment were more likely to accrue a greater number of actions over the course of their careers, according to the study.
About 47% of physicians reported experiencing burnout per Medscape’s Physician Burnout and Depression Report 2022: Stress, Anxiety, and Anger report. Burnout among emergency physicians spiked from 43% in 2020 to 60% in 2021, according to the report.
More than one quarter (26%) of physicians reported drinking alcohol to cope with burnout in 2020, according to Medscape’s 2021 Physician Burnout and Suicide Report. Per the 2021 report, 48% of physicians chose exercise to deal with burnout, while 35% indulged in eating junk food.
Peter Grinspoon, MD, a Boston-based primary care physician, wrote in The Los Angeles Times in 2016 that the rate of substance abuse among physicians starts at 10% and can go as high as 15%; by comparison, rates of substance use among the general population are 8%-10%. “What appears to account for the difference is physician distress, and in the case of drug abuse, plentiful access,” he added.
Dr. Grinspoon wrote a 2016 book called “Free Refills: A Doctor Confronts His Addiction,” which chronicles his experience in recovery and relapse as a physician who was dependent on opioid painkillers.
The findings from the recent study in JAMA “suggest we have made some progress in addressing issues related to substance use in ways that don’t result in license actions or even in meeting physicians’ need for support related to substance use,” said Dr. Rotenstein.
Still, she insists that there’s “substantial opportunity to improve mental health and support offerings for physicians and to reduce stigma related to seeking and receiving mental health support, ideally averting the need for license actions.”
According to Dr. Rotenstein, the cases listed in the National Practitioner Data Bank represent the most severe cases; these reports have risen to a high level of attention or concern and are the result of adverse action reports submitted by healthcare institutions and state licensing boards.
“There are many, many more physicians whose cases are not represented here but who struggle with depression, anxiety, substance use, and more,” said Dr. Rotenstein.
A version of this article first appeared on Medscape.com.
Despite a sharp uptick in 2011, substance use–specific license actions taken against physicians dropped in frequency between 2004 and 2020.
More than three fourths (76.3%) of license actions taken against physicians were related to substance use, according to a recent study published in JAMA. Psychological impairment was the reason associated with more than 1 in 10 (11.5%) actions taken against physicians’ licenses, while physical impairment was the reason behind approximately 12% of such actions, per the study.
Researchers analyzed 5032 actions taken against the licenses of U.S. physicians. The actions were reported to the National Practitioner Data Bank and were related to substance use, psychological impairment, and physical impairment. The National Practitioner Data Bank is a web-based repository of reports with information on medical malpractice payments and certain adverse actions related to healthcare practitioners, providers, and suppliers. It is provided by the Department of Health & Human Services.
“While there has been increased attention [on] the mental health of physicians, we wanted to understand the extent to which changes in attitudes and practices were reflected in actions taken by hospitals or licensing boards, which are reported in the National Practitioner Data Bank,” Lisa Rotenstein, MD, a primary care physician at Boston’s Brigham and Women’s Hospital and lead author of the study, told this news organization.
Dr. Rotenstein, who is an assistant professor at Harvard Medical School, Boston, studies issues of mental health among physicians and trainees. Dr. Rotenstein was the lead author of a 2016 study that found that more than a quarter (27.2%) of medical students have depressive symptoms. She was also lead author of a 2018 study published in JAMA on the prevalence of burnout among attending physicians.
Actions against physicians trending downward
2011 marked the peak in actions taken against physicians’ licenses for substance use, per the study, but actions related to substance use have otherwise maintained a steady decline over the past 17 years. Researchers found that physicians with license actions as a result of substance use or psychological impairment were more likely to receive indefinite penalties, while also having emergency action taken against their license to practice.
In addition, physicians who had actions taken against their licenses because of substance use or psychological impairment were more likely to accrue a greater number of actions over the course of their careers, according to the study.
About 47% of physicians reported experiencing burnout per Medscape’s Physician Burnout and Depression Report 2022: Stress, Anxiety, and Anger report. Burnout among emergency physicians spiked from 43% in 2020 to 60% in 2021, according to the report.
More than one quarter (26%) of physicians reported drinking alcohol to cope with burnout in 2020, according to Medscape’s 2021 Physician Burnout and Suicide Report. Per the 2021 report, 48% of physicians chose exercise to deal with burnout, while 35% indulged in eating junk food.
Peter Grinspoon, MD, a Boston-based primary care physician, wrote in The Los Angeles Times in 2016 that the rate of substance abuse among physicians starts at 10% and can go as high as 15%; by comparison, rates of substance use among the general population are 8%-10%. “What appears to account for the difference is physician distress, and in the case of drug abuse, plentiful access,” he added.
Dr. Grinspoon wrote a 2016 book called “Free Refills: A Doctor Confronts His Addiction,” which chronicles his experience in recovery and relapse as a physician who was dependent on opioid painkillers.
The findings from the recent study in JAMA “suggest we have made some progress in addressing issues related to substance use in ways that don’t result in license actions or even in meeting physicians’ need for support related to substance use,” said Dr. Rotenstein.
Still, she insists that there’s “substantial opportunity to improve mental health and support offerings for physicians and to reduce stigma related to seeking and receiving mental health support, ideally averting the need for license actions.”
According to Dr. Rotenstein, the cases listed in the National Practitioner Data Bank represent the most severe cases; these reports have risen to a high level of attention or concern and are the result of adverse action reports submitted by healthcare institutions and state licensing boards.
“There are many, many more physicians whose cases are not represented here but who struggle with depression, anxiety, substance use, and more,” said Dr. Rotenstein.
A version of this article first appeared on Medscape.com.
Despite a sharp uptick in 2011, substance use–specific license actions taken against physicians dropped in frequency between 2004 and 2020.
More than three fourths (76.3%) of license actions taken against physicians were related to substance use, according to a recent study published in JAMA. Psychological impairment was the reason associated with more than 1 in 10 (11.5%) actions taken against physicians’ licenses, while physical impairment was the reason behind approximately 12% of such actions, per the study.
Researchers analyzed 5032 actions taken against the licenses of U.S. physicians. The actions were reported to the National Practitioner Data Bank and were related to substance use, psychological impairment, and physical impairment. The National Practitioner Data Bank is a web-based repository of reports with information on medical malpractice payments and certain adverse actions related to healthcare practitioners, providers, and suppliers. It is provided by the Department of Health & Human Services.
“While there has been increased attention [on] the mental health of physicians, we wanted to understand the extent to which changes in attitudes and practices were reflected in actions taken by hospitals or licensing boards, which are reported in the National Practitioner Data Bank,” Lisa Rotenstein, MD, a primary care physician at Boston’s Brigham and Women’s Hospital and lead author of the study, told this news organization.
Dr. Rotenstein, who is an assistant professor at Harvard Medical School, Boston, studies issues of mental health among physicians and trainees. Dr. Rotenstein was the lead author of a 2016 study that found that more than a quarter (27.2%) of medical students have depressive symptoms. She was also lead author of a 2018 study published in JAMA on the prevalence of burnout among attending physicians.
Actions against physicians trending downward
2011 marked the peak in actions taken against physicians’ licenses for substance use, per the study, but actions related to substance use have otherwise maintained a steady decline over the past 17 years. Researchers found that physicians with license actions as a result of substance use or psychological impairment were more likely to receive indefinite penalties, while also having emergency action taken against their license to practice.
In addition, physicians who had actions taken against their licenses because of substance use or psychological impairment were more likely to accrue a greater number of actions over the course of their careers, according to the study.
About 47% of physicians reported experiencing burnout per Medscape’s Physician Burnout and Depression Report 2022: Stress, Anxiety, and Anger report. Burnout among emergency physicians spiked from 43% in 2020 to 60% in 2021, according to the report.
More than one quarter (26%) of physicians reported drinking alcohol to cope with burnout in 2020, according to Medscape’s 2021 Physician Burnout and Suicide Report. Per the 2021 report, 48% of physicians chose exercise to deal with burnout, while 35% indulged in eating junk food.
Peter Grinspoon, MD, a Boston-based primary care physician, wrote in The Los Angeles Times in 2016 that the rate of substance abuse among physicians starts at 10% and can go as high as 15%; by comparison, rates of substance use among the general population are 8%-10%. “What appears to account for the difference is physician distress, and in the case of drug abuse, plentiful access,” he added.
Dr. Grinspoon wrote a 2016 book called “Free Refills: A Doctor Confronts His Addiction,” which chronicles his experience in recovery and relapse as a physician who was dependent on opioid painkillers.
The findings from the recent study in JAMA “suggest we have made some progress in addressing issues related to substance use in ways that don’t result in license actions or even in meeting physicians’ need for support related to substance use,” said Dr. Rotenstein.
Still, she insists that there’s “substantial opportunity to improve mental health and support offerings for physicians and to reduce stigma related to seeking and receiving mental health support, ideally averting the need for license actions.”
According to Dr. Rotenstein, the cases listed in the National Practitioner Data Bank represent the most severe cases; these reports have risen to a high level of attention or concern and are the result of adverse action reports submitted by healthcare institutions and state licensing boards.
“There are many, many more physicians whose cases are not represented here but who struggle with depression, anxiety, substance use, and more,” said Dr. Rotenstein.
A version of this article first appeared on Medscape.com.
FROM JAMA
FDA panel strongly backs protein-based Novavax COVID-19 vaccine
than the cutting-edge technology used in mRNA-based shots.
The Vaccines and Related Biological Products Advisory Committee of the Food and Drug Administration voted almost unanimously June 7 in favor of Novavax’s two-dose COVID-19 vaccine for those 18 or older – despite some concerns over rare events of myocarditis and pericarditis.
The tally was 21 “yes” votes, without any “no” votes, but one abstention from a panelist who then offered a largely positive take on this vaccine.
Panelist Bruce Gellin, MD, explained at the end of the meeting that he would have cast a conditional vote in favor of the Novavax vaccine, called NVX-CoV2373, had that been an option. Dr. Gellin, chief of global public health strategy for the Rockefeller Foundation and a vaccine expert, said he didn’t want his abstention to be considered as signaling opposition to the Novavax shot.
Instead, he said, he expects FDA officials will gather more data and evidence about the Novavax vaccine, especially in relation to certain manufacturing issues, before making its decision on the company’s application.
Earlier in the day, a top FDA vaccine reviewer, Doran Fink, MD, PhD, noted that there were important manufacturing differences between the Novavax vaccine supply used in different projects, complicating efforts to assess the company’s application for emergency use authorization (EUA).
But Dr. Fink noted that the FDA staff already had made a convincing case in its briefing document, with enough evidence for an initial conditional clearance to be found in available data.
The FDA is not bound to follow the suggestions of its advisory committees but it often does.
Using the ‘bully pulpit’
At the beginning of the meeting, Peter Marks, MD, PhD, director of the FDA’s Center for Biologics Evaluation and Research, said he was seizing the “bully pulpit” in addressing the need to persuade more people in the United States to take shots against COVID-19.
About 67% of people in the United States aged 18 and older are fully vaccinated, but only about 50% of those in this group have had a first booster, according to the Centers for Disease Control and Prevention.
The two-dose mRNA vaccines from Pfizer and Moderna have been the subject of intense misinformation campaigns on social media, despite efforts by the FDA and other public health officials to convey the message about their strong benefit-risk profile. The FDA in May limited the authorized use of Johnson & Johnson’s single-dose COVID-19 shot, which is based on a different technology, because of concerns about rare and potentially life-threatening blood clots.
Novavax has been described as a more traditional vaccine – a protein subunit shot similar to one people have long received for protection against influenza, pertussis (whooping cough), diphtheria, and tetanus.
“Having a protein-based alternative may be more comfortable for some in terms of their acceptance of vaccines,” Dr. Marks said. “We do have a problem with vaccine uptake that is very serious in the United States. And anything we can do to get people more comfortable to be able to accept these potentially life-saving medical products is something that we feel we are compelled to do.”
Dr. Marks offered these remarks in answer to an FDA panelist’s question about the need to consider an EUA for yet another vaccine.
EUAs are special clearances the FDA can grant in connection with public health emergencies such as the pandemic. The FDA used EUAs for the initial December 2020 clearances of the Pfizer-BioNTech and Moderna vaccines. It has since granted normal approvals for both of these mRNA-based vaccines, based on larger bodies of evidence gathered and submitted by their developers.
During the meeting, the FDA panelists in general appeared comfortable with the idea of granting another EUA for a vaccine. There was agreement that the shot appeared to work in key tests, although these were done before the rise of the Omicron variant.
In a key test, known as study 301, the Novavax vaccine was judged to be 90.4% effective. In the study, 17 of the 17,272 people who got the Novavax vaccine developed COVID-19, compared with 79 of the 8,385 in the placebo group.
Panelists expressed disappointment with the lack of information about how the shot would work now.
“We’re looking at the efficacy against strains that don’t exist any longer,” said panelist Eric J. Rubin, MD, PhD, a Harvard professor and editor of the New England Journal of Medicine.
Still, Dr. Rubin added that he agreed with the argument the FDA’s Dr. Marks had made earlier for an EUA for the Novavax vaccine.
“If there really is a population of patients who are willing to take this and not willing to take the existing vaccines, I think it’s pretty compelling,” Dr. Rubin said.
Other FDA panelists were skeptical of this argument. Jay Portnoy, MD, who was listed on the FDA roster as the panel’s consumer representative, said he has close friends who are vaccine skeptics.
“Their hesitancy is more ideological than technological,” said Dr. Portnoy of Children’s Mercy Hospital, Kansas City, Mo. “So I really doubt that this vaccine is going to crack that nut, but perhaps some individuals would get this when they wouldn’t get the other ones.”
Myocarditis, pericarditis
The Novavax vaccine is already authorized in other countries, including Canada. Novavax in February announced that it had begun shipping its first doses of the vaccine to European Union member states. The vaccine can be moved through existing vaccine supply and cold chain channels instead of requiring complex new delivery procedures.
That could prove an advantage in time, said FDA panelist Michael Nelson, MD, PhD, of the University of Virginia, Charlottesville.
“Who knows even with supply chain challenges down the road, it will be nice to have options going forward,” Dr. Nelson said.
As with other COVID-19 vaccines, clinicians and researchers are still working to understand the potential risk for inflammation of heart muscle and nearby tissue with vaccination. Most patients with myocarditis or pericarditis who sought medical care for these conditions responded well to medicine and rest and felt better quickly, the CDC says on its website. They usually return to their normal daily activities after their symptoms improve.
At the June 7 meeting, Dr. Nelson said there may be cases of myocarditis that go undetected.
“Our signals are those who get admitted to the emergency room and the hospital,” he said. “I’m quite convinced that there are others who are experiencing cardiac events of lesser severity that are worthy of being studied, both from mechanistic and outcomes standpoints. So we have a lot of work to do.”
In looking at results for an initial pool of 40,000 people who received the Novavax vaccine, there were five reported cases of myocarditis or pericarditis developing within 20 days of people getting the shot, the FDA staff said in its presentation on safety.
In a briefing document released ahead of the advisory committee meeting, the FDA staff flagged this number of cases in a relatively small database as a concern, noting it “could be higher than reported during postauthorization use of mRNA COVID-19 vaccines (for which no cases were identified in preauthorization evaluation).”
Novavax officials took a somewhat unusual step of responding in public. The Gaithersburg, Md.–based company on June 3 issued a statement saying researchers had come to “expect to see natural background events of myocarditis in any sufficiently large database, and that young males are at higher risk.”
The data from the company’s placebo-controlled studies show that, overall, in its clinical development program, the rate of myocarditis was balanced between the vaccine and placebo arms (0.007% and 0.005%), Novavax said.
At the June 7 meeting, FDA panelists including Dr. Nelson, and Paul A. Offit, MD, of Children’s Hospital of Philadelphia, urged continued study to try to determine whether and how the vaccines could trigger myocarditis. Investments made now in pursuing these questions related to COVID-19 shots may pay off later, Dr. Offit said.
“We can use that knowledge to make safer vaccines for a disease that is going to be with us for decades, if not longer,” he said.
A version of this article first appeared on Medscape.com.
than the cutting-edge technology used in mRNA-based shots.
The Vaccines and Related Biological Products Advisory Committee of the Food and Drug Administration voted almost unanimously June 7 in favor of Novavax’s two-dose COVID-19 vaccine for those 18 or older – despite some concerns over rare events of myocarditis and pericarditis.
The tally was 21 “yes” votes, without any “no” votes, but one abstention from a panelist who then offered a largely positive take on this vaccine.
Panelist Bruce Gellin, MD, explained at the end of the meeting that he would have cast a conditional vote in favor of the Novavax vaccine, called NVX-CoV2373, had that been an option. Dr. Gellin, chief of global public health strategy for the Rockefeller Foundation and a vaccine expert, said he didn’t want his abstention to be considered as signaling opposition to the Novavax shot.
Instead, he said, he expects FDA officials will gather more data and evidence about the Novavax vaccine, especially in relation to certain manufacturing issues, before making its decision on the company’s application.
Earlier in the day, a top FDA vaccine reviewer, Doran Fink, MD, PhD, noted that there were important manufacturing differences between the Novavax vaccine supply used in different projects, complicating efforts to assess the company’s application for emergency use authorization (EUA).
But Dr. Fink noted that the FDA staff already had made a convincing case in its briefing document, with enough evidence for an initial conditional clearance to be found in available data.
The FDA is not bound to follow the suggestions of its advisory committees but it often does.
Using the ‘bully pulpit’
At the beginning of the meeting, Peter Marks, MD, PhD, director of the FDA’s Center for Biologics Evaluation and Research, said he was seizing the “bully pulpit” in addressing the need to persuade more people in the United States to take shots against COVID-19.
About 67% of people in the United States aged 18 and older are fully vaccinated, but only about 50% of those in this group have had a first booster, according to the Centers for Disease Control and Prevention.
The two-dose mRNA vaccines from Pfizer and Moderna have been the subject of intense misinformation campaigns on social media, despite efforts by the FDA and other public health officials to convey the message about their strong benefit-risk profile. The FDA in May limited the authorized use of Johnson & Johnson’s single-dose COVID-19 shot, which is based on a different technology, because of concerns about rare and potentially life-threatening blood clots.
Novavax has been described as a more traditional vaccine – a protein subunit shot similar to one people have long received for protection against influenza, pertussis (whooping cough), diphtheria, and tetanus.
“Having a protein-based alternative may be more comfortable for some in terms of their acceptance of vaccines,” Dr. Marks said. “We do have a problem with vaccine uptake that is very serious in the United States. And anything we can do to get people more comfortable to be able to accept these potentially life-saving medical products is something that we feel we are compelled to do.”
Dr. Marks offered these remarks in answer to an FDA panelist’s question about the need to consider an EUA for yet another vaccine.
EUAs are special clearances the FDA can grant in connection with public health emergencies such as the pandemic. The FDA used EUAs for the initial December 2020 clearances of the Pfizer-BioNTech and Moderna vaccines. It has since granted normal approvals for both of these mRNA-based vaccines, based on larger bodies of evidence gathered and submitted by their developers.
During the meeting, the FDA panelists in general appeared comfortable with the idea of granting another EUA for a vaccine. There was agreement that the shot appeared to work in key tests, although these were done before the rise of the Omicron variant.
In a key test, known as study 301, the Novavax vaccine was judged to be 90.4% effective. In the study, 17 of the 17,272 people who got the Novavax vaccine developed COVID-19, compared with 79 of the 8,385 in the placebo group.
Panelists expressed disappointment with the lack of information about how the shot would work now.
“We’re looking at the efficacy against strains that don’t exist any longer,” said panelist Eric J. Rubin, MD, PhD, a Harvard professor and editor of the New England Journal of Medicine.
Still, Dr. Rubin added that he agreed with the argument the FDA’s Dr. Marks had made earlier for an EUA for the Novavax vaccine.
“If there really is a population of patients who are willing to take this and not willing to take the existing vaccines, I think it’s pretty compelling,” Dr. Rubin said.
Other FDA panelists were skeptical of this argument. Jay Portnoy, MD, who was listed on the FDA roster as the panel’s consumer representative, said he has close friends who are vaccine skeptics.
“Their hesitancy is more ideological than technological,” said Dr. Portnoy of Children’s Mercy Hospital, Kansas City, Mo. “So I really doubt that this vaccine is going to crack that nut, but perhaps some individuals would get this when they wouldn’t get the other ones.”
Myocarditis, pericarditis
The Novavax vaccine is already authorized in other countries, including Canada. Novavax in February announced that it had begun shipping its first doses of the vaccine to European Union member states. The vaccine can be moved through existing vaccine supply and cold chain channels instead of requiring complex new delivery procedures.
That could prove an advantage in time, said FDA panelist Michael Nelson, MD, PhD, of the University of Virginia, Charlottesville.
“Who knows even with supply chain challenges down the road, it will be nice to have options going forward,” Dr. Nelson said.
As with other COVID-19 vaccines, clinicians and researchers are still working to understand the potential risk for inflammation of heart muscle and nearby tissue with vaccination. Most patients with myocarditis or pericarditis who sought medical care for these conditions responded well to medicine and rest and felt better quickly, the CDC says on its website. They usually return to their normal daily activities after their symptoms improve.
At the June 7 meeting, Dr. Nelson said there may be cases of myocarditis that go undetected.
“Our signals are those who get admitted to the emergency room and the hospital,” he said. “I’m quite convinced that there are others who are experiencing cardiac events of lesser severity that are worthy of being studied, both from mechanistic and outcomes standpoints. So we have a lot of work to do.”
In looking at results for an initial pool of 40,000 people who received the Novavax vaccine, there were five reported cases of myocarditis or pericarditis developing within 20 days of people getting the shot, the FDA staff said in its presentation on safety.
In a briefing document released ahead of the advisory committee meeting, the FDA staff flagged this number of cases in a relatively small database as a concern, noting it “could be higher than reported during postauthorization use of mRNA COVID-19 vaccines (for which no cases were identified in preauthorization evaluation).”
Novavax officials took a somewhat unusual step of responding in public. The Gaithersburg, Md.–based company on June 3 issued a statement saying researchers had come to “expect to see natural background events of myocarditis in any sufficiently large database, and that young males are at higher risk.”
The data from the company’s placebo-controlled studies show that, overall, in its clinical development program, the rate of myocarditis was balanced between the vaccine and placebo arms (0.007% and 0.005%), Novavax said.
At the June 7 meeting, FDA panelists including Dr. Nelson, and Paul A. Offit, MD, of Children’s Hospital of Philadelphia, urged continued study to try to determine whether and how the vaccines could trigger myocarditis. Investments made now in pursuing these questions related to COVID-19 shots may pay off later, Dr. Offit said.
“We can use that knowledge to make safer vaccines for a disease that is going to be with us for decades, if not longer,” he said.
A version of this article first appeared on Medscape.com.
than the cutting-edge technology used in mRNA-based shots.
The Vaccines and Related Biological Products Advisory Committee of the Food and Drug Administration voted almost unanimously June 7 in favor of Novavax’s two-dose COVID-19 vaccine for those 18 or older – despite some concerns over rare events of myocarditis and pericarditis.
The tally was 21 “yes” votes, without any “no” votes, but one abstention from a panelist who then offered a largely positive take on this vaccine.
Panelist Bruce Gellin, MD, explained at the end of the meeting that he would have cast a conditional vote in favor of the Novavax vaccine, called NVX-CoV2373, had that been an option. Dr. Gellin, chief of global public health strategy for the Rockefeller Foundation and a vaccine expert, said he didn’t want his abstention to be considered as signaling opposition to the Novavax shot.
Instead, he said, he expects FDA officials will gather more data and evidence about the Novavax vaccine, especially in relation to certain manufacturing issues, before making its decision on the company’s application.
Earlier in the day, a top FDA vaccine reviewer, Doran Fink, MD, PhD, noted that there were important manufacturing differences between the Novavax vaccine supply used in different projects, complicating efforts to assess the company’s application for emergency use authorization (EUA).
But Dr. Fink noted that the FDA staff already had made a convincing case in its briefing document, with enough evidence for an initial conditional clearance to be found in available data.
The FDA is not bound to follow the suggestions of its advisory committees but it often does.
Using the ‘bully pulpit’
At the beginning of the meeting, Peter Marks, MD, PhD, director of the FDA’s Center for Biologics Evaluation and Research, said he was seizing the “bully pulpit” in addressing the need to persuade more people in the United States to take shots against COVID-19.
About 67% of people in the United States aged 18 and older are fully vaccinated, but only about 50% of those in this group have had a first booster, according to the Centers for Disease Control and Prevention.
The two-dose mRNA vaccines from Pfizer and Moderna have been the subject of intense misinformation campaigns on social media, despite efforts by the FDA and other public health officials to convey the message about their strong benefit-risk profile. The FDA in May limited the authorized use of Johnson & Johnson’s single-dose COVID-19 shot, which is based on a different technology, because of concerns about rare and potentially life-threatening blood clots.
Novavax has been described as a more traditional vaccine – a protein subunit shot similar to one people have long received for protection against influenza, pertussis (whooping cough), diphtheria, and tetanus.
“Having a protein-based alternative may be more comfortable for some in terms of their acceptance of vaccines,” Dr. Marks said. “We do have a problem with vaccine uptake that is very serious in the United States. And anything we can do to get people more comfortable to be able to accept these potentially life-saving medical products is something that we feel we are compelled to do.”
Dr. Marks offered these remarks in answer to an FDA panelist’s question about the need to consider an EUA for yet another vaccine.
EUAs are special clearances the FDA can grant in connection with public health emergencies such as the pandemic. The FDA used EUAs for the initial December 2020 clearances of the Pfizer-BioNTech and Moderna vaccines. It has since granted normal approvals for both of these mRNA-based vaccines, based on larger bodies of evidence gathered and submitted by their developers.
During the meeting, the FDA panelists in general appeared comfortable with the idea of granting another EUA for a vaccine. There was agreement that the shot appeared to work in key tests, although these were done before the rise of the Omicron variant.
In a key test, known as study 301, the Novavax vaccine was judged to be 90.4% effective. In the study, 17 of the 17,272 people who got the Novavax vaccine developed COVID-19, compared with 79 of the 8,385 in the placebo group.
Panelists expressed disappointment with the lack of information about how the shot would work now.
“We’re looking at the efficacy against strains that don’t exist any longer,” said panelist Eric J. Rubin, MD, PhD, a Harvard professor and editor of the New England Journal of Medicine.
Still, Dr. Rubin added that he agreed with the argument the FDA’s Dr. Marks had made earlier for an EUA for the Novavax vaccine.
“If there really is a population of patients who are willing to take this and not willing to take the existing vaccines, I think it’s pretty compelling,” Dr. Rubin said.
Other FDA panelists were skeptical of this argument. Jay Portnoy, MD, who was listed on the FDA roster as the panel’s consumer representative, said he has close friends who are vaccine skeptics.
“Their hesitancy is more ideological than technological,” said Dr. Portnoy of Children’s Mercy Hospital, Kansas City, Mo. “So I really doubt that this vaccine is going to crack that nut, but perhaps some individuals would get this when they wouldn’t get the other ones.”
Myocarditis, pericarditis
The Novavax vaccine is already authorized in other countries, including Canada. Novavax in February announced that it had begun shipping its first doses of the vaccine to European Union member states. The vaccine can be moved through existing vaccine supply and cold chain channels instead of requiring complex new delivery procedures.
That could prove an advantage in time, said FDA panelist Michael Nelson, MD, PhD, of the University of Virginia, Charlottesville.
“Who knows even with supply chain challenges down the road, it will be nice to have options going forward,” Dr. Nelson said.
As with other COVID-19 vaccines, clinicians and researchers are still working to understand the potential risk for inflammation of heart muscle and nearby tissue with vaccination. Most patients with myocarditis or pericarditis who sought medical care for these conditions responded well to medicine and rest and felt better quickly, the CDC says on its website. They usually return to their normal daily activities after their symptoms improve.
At the June 7 meeting, Dr. Nelson said there may be cases of myocarditis that go undetected.
“Our signals are those who get admitted to the emergency room and the hospital,” he said. “I’m quite convinced that there are others who are experiencing cardiac events of lesser severity that are worthy of being studied, both from mechanistic and outcomes standpoints. So we have a lot of work to do.”
In looking at results for an initial pool of 40,000 people who received the Novavax vaccine, there were five reported cases of myocarditis or pericarditis developing within 20 days of people getting the shot, the FDA staff said in its presentation on safety.
In a briefing document released ahead of the advisory committee meeting, the FDA staff flagged this number of cases in a relatively small database as a concern, noting it “could be higher than reported during postauthorization use of mRNA COVID-19 vaccines (for which no cases were identified in preauthorization evaluation).”
Novavax officials took a somewhat unusual step of responding in public. The Gaithersburg, Md.–based company on June 3 issued a statement saying researchers had come to “expect to see natural background events of myocarditis in any sufficiently large database, and that young males are at higher risk.”
The data from the company’s placebo-controlled studies show that, overall, in its clinical development program, the rate of myocarditis was balanced between the vaccine and placebo arms (0.007% and 0.005%), Novavax said.
At the June 7 meeting, FDA panelists including Dr. Nelson, and Paul A. Offit, MD, of Children’s Hospital of Philadelphia, urged continued study to try to determine whether and how the vaccines could trigger myocarditis. Investments made now in pursuing these questions related to COVID-19 shots may pay off later, Dr. Offit said.
“We can use that knowledge to make safer vaccines for a disease that is going to be with us for decades, if not longer,” he said.
A version of this article first appeared on Medscape.com.
Endometriosis: Diagnosis, Surgical Management, and Overlapping Diagnosis.
As a gynecologist specializing in minimally invasive surgical techniques, what is your involvement in the process for diagnosing endometriosis?
Dr. Lager: At our multidisciplinary endometriosis center, we receive a range of referrals from excellent providers near San Francisco and beyond. As a result, patients will often have had extensive evaluations and multiple treatments. Nonetheless, it is important to take a thorough history, to gain an understanding of the progress of their disease, treatments they have taken and the results or side effects of those treatments, and the goals of the patient in order to guide next steps.
Reviewing previous operative reports, pathology, and surgical photos can also be helpful to guide next steps. Commonly, patients will present with dysmenorrhea, and depending on the severity of associated symptoms, such as dysuria, dyschezia, hematuria, or hematochezia, I may refer patients to our colleagues in urology or GI for further evaluation.
Patients will often have previous imaging such as an ultrasound or CT to evaluate anatomic etiology of the pain, but those studies are often negative. Depending on their history, I may order additional imaging, such as an MRI pelvis, and consideration of vaginal or rectal gel. We have worked closely with our radiologists who have developed a specific endometriosis protocol for deeply infiltrative endometriosis and have a multidisciplinary review committee to discuss complex cases.
Although the gold standard for diagnosis of endometriosis is surgical, this leads to a delay in treatment of 7 to 12 years.[1] So, if a patient presents with symptoms of endometriosis, I will discuss the likely diagnosis and start treatment.
Are there specific techniques that you prefer in your standard practice once a clear diagnosis is determined?
Dr. Lager: As I mentioned, although endometriosis is a surgical diagnosis, there may be findings on imaging which will lead to a diagnosis of endometriosis, including endometriomas, uterosacral thickening, a “kissing ovary” appearance, or hematosalpinx for example.
I discuss a broad range of treatment options based on the patient’s goals, from least invasive treatments to definitive surgery. I discuss dietary changes, integrative medicine (we are fortunate to have an integrative medicine gynecologist here at UCSF Osher Center), and pain psychology. Additionally, I review first-line hormonal management options such as: birth control pills, progestin-only pills, levenogestrol IUD, etonogestrel implant, and medroxyprogesterone acetate injection. In my practice, most patients have already tried initial treatment options, and are most interested in other options. I then review second-line options such as GnRH agonists, antagonists, danazol, and aromatase inhibitors. For patients that have had chronic pelvic pain, I also discuss peripheral and central sensitization, and overlapping diagnoses. Surgical management includes diagnostic laparoscopy and excision or ablation of endometriosis, hysterectomy, and oophorectomy.
Are there specific factors that you look for to help you decide whether surgical management is necessary?
Dr. Lager: There are several reasons why patients decide to proceed with surgical management. First, some patients are reticent to start treatment, particularly if they have had negative experiences with hormonal medications and desire a definitive diagnosis. Other patients choose to proceed with surgery for fertility reasons, and others have severe symptoms that are not managed by medications.
The goal of surgery is to remove all visible endometriotic lesions, restore normal anatomy and for pathologic diagnosis if there is atypical characteristics of an endometrial mass. The pelvic exam and imaging can often be helpful surgical planning. If there is a deeply infiltrative lesion in the bowel or bladder, I consult my urology and colorectal colleagues for surgical planning.
Endometriotic lesions are heterogenous, and can include superficial peritoneal lesions, clear vesicular lesions, “powder burn lesions”, endometriomas, and deep infiltrative lesions.
Additionally, I counsel patients on surgical options depending on the fertility desires. For patients with infertility and symptoms of endometriosis, primary surgery with excision or ablation increases pregnancy rates. One meta-analysis showed that operative laparoscopy improved live births and ongoing pregnancy rates.[2] This was found for the first laparoscopic surgery and not repeat surgery.
Can you talk a little bit more about some of the advancements and the controversies in surgical management, and how that impacts your practice or your treatment?
Dr. Lager: Controversy in surgical management includes excision versus ablation in surgical management of endometriosis. One randomized controlled trial showed an improvement with dyspareunia with excision versus ablation after 5 year follow up.[3] However, a recent meta-analysis from 2021 showed no difference in dysmenorrhea between excision and ablation.[4] I generally perform excision of endometriosis as it can provide a tissue for diagnosis and may allow for complete excision of a lesion that may have an underlying component not easily seen.
We also discussed some of the controversy related to fertility and endometriosis. Management of endometriomas in the face of desired fertility is unclear. Endometriomas that are >3 cm in diameter are associated with decreased anti-Mullerian hormone (AMH) levels, but ovarian cystectomy for endometriomas is also associated with decreased AMH levels. I will counsel patients regarding the risks and benefits of ovarian cystectomy and discuss with the reproductive endocrinologists if they recommend removal to improve oocyte retrieval.
Lastly, conservative versus definitive treatment is an important issue to discuss. Depending on a patient’s goals, conservative surgical management of endometriosis may be the most appropriate procedure. However, if a patient has multiple surgeries, does not desire to have children or has completed childbearing regardless of age and wants to decrease the risk of need for repeat surgery, I will discuss with patients that the risk of reoperation after hysterectomy versus conservative surgery is 8% vs 21% in 2 years and 59% vs 22% after 7 years, respectively.[5] Additionally, the patient may have an overlapping gynecological condition, such as adenomyosis or fibroids, and desire surgical management for those conditions as well. Management ultimately will depend on shared decision making,
You mentioned overlapping diagnosis. What are the impacts and barriers related to misdiagnosis or overlapping diagnosis, and what is your approach to recognizing those signs and symptoms?
Dr. Lager: The classic symptoms of endometriosis can overlap with several medical conditions. In addition to gynecologic issues such as adenomyosis and fibroids that I mentioned previously, symptoms such as pelvic pain, bloating, and dysuria can be associated with gastrointestinal conditions, painful bladder syndrome, neurologic, and musculoskeletal pain conditions. This is complex because the overlapping diagnoses can lead to misdiagnosis, and delay in diagnosis and missing an associated diagnosis can lead to inadequate treatment.
I approach the possibility of overlapping diagnoses in consultation with my colleagues who may recommend further testing, such as endoscopy and colonoscopy. Depending on the diagnoses, several treatments can be started concomitantly to address the multifactorial components of pain. For example, pelvic floor dysfunction related to pelvic pain can affect bowel habits, even without a diagnosis of IBS. Pelvic floor physical therapy can address one component of this. Similarly, even if we surgically or medically manage symptoms of endometriosis, the musculoskeletal pain can lead to persistent or worsening pain. The same goes for pain medicine and peripheral or central pain sensitization or neurological pain.
Was there anything else you’d like to share with your colleagues?
Dr. Lager: Endometriosis is a complex condition that requires a multifactorial approach that takes into consideration a patient’s goals. There is not a one-size fit for all patients with endometriosis due to all the issues we discussed. It will take time to address the varied components of pain and is an iterative process. Minimally invasive surgery has an important role in diagnosis and management of endometriosis but is one of several approaches to treat this complex condition. Thanks for taking the time to discuss this important condition that affects at least 10% of gynecological patients, and potentially more due to delayed and undiagnosed disease.
- Staal AH, van der Zanden M, Nap AW. Diagnostic delay of endometriosis in the Netherlands. Gynecol Obstet Invest. 2016;81(4):321-4. doi: 10.1159/000441911
- Duffy JM, Arambage K, Correa FJ, et al. Laparoscopic surgery for endometriosis. Cochrane Database Syst Rev. 2014;(4):CD011031. Update in: Cochrane Database Syst Rev. 2020;10:CD011031. doi:10.1002/14651858.CD011031.pub2
- Healey M, Cheng C, Kaur H. To excise or ablate endometriosis? A prospective randomized double-blinded trial after 5-year follow-up. J Minim Invasive Gynecol. 2014;21(6):999-1004. doi: 10.1016/j.jmig.2014.04.002
- Burks C, Lee M, DeSarno M, Findley J, Flyckt R. Excision versus ablation for management of minimal to mild endometriosis: a systematic review and meta-analysis. J Minim Invasive Gynecol. 2021;28(3):587-597. doi:10.1016/j.jmig.2020.11.028
- Shakiba K, Bena JF, McGill KM, Minger J, Falcone T. Surgical treatment of endometriosis: a 7-year follow-up on the requirement for further surgery. Obstet Gynecol. 2008;111(6):1285-92. Erratum in: Obstet Gynecol. 2008;112(3):710. doi:10.1097/AOG.0b013e3181758ec6
As a gynecologist specializing in minimally invasive surgical techniques, what is your involvement in the process for diagnosing endometriosis?
Dr. Lager: At our multidisciplinary endometriosis center, we receive a range of referrals from excellent providers near San Francisco and beyond. As a result, patients will often have had extensive evaluations and multiple treatments. Nonetheless, it is important to take a thorough history, to gain an understanding of the progress of their disease, treatments they have taken and the results or side effects of those treatments, and the goals of the patient in order to guide next steps.
Reviewing previous operative reports, pathology, and surgical photos can also be helpful to guide next steps. Commonly, patients will present with dysmenorrhea, and depending on the severity of associated symptoms, such as dysuria, dyschezia, hematuria, or hematochezia, I may refer patients to our colleagues in urology or GI for further evaluation.
Patients will often have previous imaging such as an ultrasound or CT to evaluate anatomic etiology of the pain, but those studies are often negative. Depending on their history, I may order additional imaging, such as an MRI pelvis, and consideration of vaginal or rectal gel. We have worked closely with our radiologists who have developed a specific endometriosis protocol for deeply infiltrative endometriosis and have a multidisciplinary review committee to discuss complex cases.
Although the gold standard for diagnosis of endometriosis is surgical, this leads to a delay in treatment of 7 to 12 years.[1] So, if a patient presents with symptoms of endometriosis, I will discuss the likely diagnosis and start treatment.
Are there specific techniques that you prefer in your standard practice once a clear diagnosis is determined?
Dr. Lager: As I mentioned, although endometriosis is a surgical diagnosis, there may be findings on imaging which will lead to a diagnosis of endometriosis, including endometriomas, uterosacral thickening, a “kissing ovary” appearance, or hematosalpinx for example.
I discuss a broad range of treatment options based on the patient’s goals, from least invasive treatments to definitive surgery. I discuss dietary changes, integrative medicine (we are fortunate to have an integrative medicine gynecologist here at UCSF Osher Center), and pain psychology. Additionally, I review first-line hormonal management options such as: birth control pills, progestin-only pills, levenogestrol IUD, etonogestrel implant, and medroxyprogesterone acetate injection. In my practice, most patients have already tried initial treatment options, and are most interested in other options. I then review second-line options such as GnRH agonists, antagonists, danazol, and aromatase inhibitors. For patients that have had chronic pelvic pain, I also discuss peripheral and central sensitization, and overlapping diagnoses. Surgical management includes diagnostic laparoscopy and excision or ablation of endometriosis, hysterectomy, and oophorectomy.
Are there specific factors that you look for to help you decide whether surgical management is necessary?
Dr. Lager: There are several reasons why patients decide to proceed with surgical management. First, some patients are reticent to start treatment, particularly if they have had negative experiences with hormonal medications and desire a definitive diagnosis. Other patients choose to proceed with surgery for fertility reasons, and others have severe symptoms that are not managed by medications.
The goal of surgery is to remove all visible endometriotic lesions, restore normal anatomy and for pathologic diagnosis if there is atypical characteristics of an endometrial mass. The pelvic exam and imaging can often be helpful surgical planning. If there is a deeply infiltrative lesion in the bowel or bladder, I consult my urology and colorectal colleagues for surgical planning.
Endometriotic lesions are heterogenous, and can include superficial peritoneal lesions, clear vesicular lesions, “powder burn lesions”, endometriomas, and deep infiltrative lesions.
Additionally, I counsel patients on surgical options depending on the fertility desires. For patients with infertility and symptoms of endometriosis, primary surgery with excision or ablation increases pregnancy rates. One meta-analysis showed that operative laparoscopy improved live births and ongoing pregnancy rates.[2] This was found for the first laparoscopic surgery and not repeat surgery.
Can you talk a little bit more about some of the advancements and the controversies in surgical management, and how that impacts your practice or your treatment?
Dr. Lager: Controversy in surgical management includes excision versus ablation in surgical management of endometriosis. One randomized controlled trial showed an improvement with dyspareunia with excision versus ablation after 5 year follow up.[3] However, a recent meta-analysis from 2021 showed no difference in dysmenorrhea between excision and ablation.[4] I generally perform excision of endometriosis as it can provide a tissue for diagnosis and may allow for complete excision of a lesion that may have an underlying component not easily seen.
We also discussed some of the controversy related to fertility and endometriosis. Management of endometriomas in the face of desired fertility is unclear. Endometriomas that are >3 cm in diameter are associated with decreased anti-Mullerian hormone (AMH) levels, but ovarian cystectomy for endometriomas is also associated with decreased AMH levels. I will counsel patients regarding the risks and benefits of ovarian cystectomy and discuss with the reproductive endocrinologists if they recommend removal to improve oocyte retrieval.
Lastly, conservative versus definitive treatment is an important issue to discuss. Depending on a patient’s goals, conservative surgical management of endometriosis may be the most appropriate procedure. However, if a patient has multiple surgeries, does not desire to have children or has completed childbearing regardless of age and wants to decrease the risk of need for repeat surgery, I will discuss with patients that the risk of reoperation after hysterectomy versus conservative surgery is 8% vs 21% in 2 years and 59% vs 22% after 7 years, respectively.[5] Additionally, the patient may have an overlapping gynecological condition, such as adenomyosis or fibroids, and desire surgical management for those conditions as well. Management ultimately will depend on shared decision making,
You mentioned overlapping diagnosis. What are the impacts and barriers related to misdiagnosis or overlapping diagnosis, and what is your approach to recognizing those signs and symptoms?
Dr. Lager: The classic symptoms of endometriosis can overlap with several medical conditions. In addition to gynecologic issues such as adenomyosis and fibroids that I mentioned previously, symptoms such as pelvic pain, bloating, and dysuria can be associated with gastrointestinal conditions, painful bladder syndrome, neurologic, and musculoskeletal pain conditions. This is complex because the overlapping diagnoses can lead to misdiagnosis, and delay in diagnosis and missing an associated diagnosis can lead to inadequate treatment.
I approach the possibility of overlapping diagnoses in consultation with my colleagues who may recommend further testing, such as endoscopy and colonoscopy. Depending on the diagnoses, several treatments can be started concomitantly to address the multifactorial components of pain. For example, pelvic floor dysfunction related to pelvic pain can affect bowel habits, even without a diagnosis of IBS. Pelvic floor physical therapy can address one component of this. Similarly, even if we surgically or medically manage symptoms of endometriosis, the musculoskeletal pain can lead to persistent or worsening pain. The same goes for pain medicine and peripheral or central pain sensitization or neurological pain.
Was there anything else you’d like to share with your colleagues?
Dr. Lager: Endometriosis is a complex condition that requires a multifactorial approach that takes into consideration a patient’s goals. There is not a one-size fit for all patients with endometriosis due to all the issues we discussed. It will take time to address the varied components of pain and is an iterative process. Minimally invasive surgery has an important role in diagnosis and management of endometriosis but is one of several approaches to treat this complex condition. Thanks for taking the time to discuss this important condition that affects at least 10% of gynecological patients, and potentially more due to delayed and undiagnosed disease.
As a gynecologist specializing in minimally invasive surgical techniques, what is your involvement in the process for diagnosing endometriosis?
Dr. Lager: At our multidisciplinary endometriosis center, we receive a range of referrals from excellent providers near San Francisco and beyond. As a result, patients will often have had extensive evaluations and multiple treatments. Nonetheless, it is important to take a thorough history, to gain an understanding of the progress of their disease, treatments they have taken and the results or side effects of those treatments, and the goals of the patient in order to guide next steps.
Reviewing previous operative reports, pathology, and surgical photos can also be helpful to guide next steps. Commonly, patients will present with dysmenorrhea, and depending on the severity of associated symptoms, such as dysuria, dyschezia, hematuria, or hematochezia, I may refer patients to our colleagues in urology or GI for further evaluation.
Patients will often have previous imaging such as an ultrasound or CT to evaluate anatomic etiology of the pain, but those studies are often negative. Depending on their history, I may order additional imaging, such as an MRI pelvis, and consideration of vaginal or rectal gel. We have worked closely with our radiologists who have developed a specific endometriosis protocol for deeply infiltrative endometriosis and have a multidisciplinary review committee to discuss complex cases.
Although the gold standard for diagnosis of endometriosis is surgical, this leads to a delay in treatment of 7 to 12 years.[1] So, if a patient presents with symptoms of endometriosis, I will discuss the likely diagnosis and start treatment.
Are there specific techniques that you prefer in your standard practice once a clear diagnosis is determined?
Dr. Lager: As I mentioned, although endometriosis is a surgical diagnosis, there may be findings on imaging which will lead to a diagnosis of endometriosis, including endometriomas, uterosacral thickening, a “kissing ovary” appearance, or hematosalpinx for example.
I discuss a broad range of treatment options based on the patient’s goals, from least invasive treatments to definitive surgery. I discuss dietary changes, integrative medicine (we are fortunate to have an integrative medicine gynecologist here at UCSF Osher Center), and pain psychology. Additionally, I review first-line hormonal management options such as: birth control pills, progestin-only pills, levenogestrol IUD, etonogestrel implant, and medroxyprogesterone acetate injection. In my practice, most patients have already tried initial treatment options, and are most interested in other options. I then review second-line options such as GnRH agonists, antagonists, danazol, and aromatase inhibitors. For patients that have had chronic pelvic pain, I also discuss peripheral and central sensitization, and overlapping diagnoses. Surgical management includes diagnostic laparoscopy and excision or ablation of endometriosis, hysterectomy, and oophorectomy.
Are there specific factors that you look for to help you decide whether surgical management is necessary?
Dr. Lager: There are several reasons why patients decide to proceed with surgical management. First, some patients are reticent to start treatment, particularly if they have had negative experiences with hormonal medications and desire a definitive diagnosis. Other patients choose to proceed with surgery for fertility reasons, and others have severe symptoms that are not managed by medications.
The goal of surgery is to remove all visible endometriotic lesions, restore normal anatomy and for pathologic diagnosis if there is atypical characteristics of an endometrial mass. The pelvic exam and imaging can often be helpful surgical planning. If there is a deeply infiltrative lesion in the bowel or bladder, I consult my urology and colorectal colleagues for surgical planning.
Endometriotic lesions are heterogenous, and can include superficial peritoneal lesions, clear vesicular lesions, “powder burn lesions”, endometriomas, and deep infiltrative lesions.
Additionally, I counsel patients on surgical options depending on the fertility desires. For patients with infertility and symptoms of endometriosis, primary surgery with excision or ablation increases pregnancy rates. One meta-analysis showed that operative laparoscopy improved live births and ongoing pregnancy rates.[2] This was found for the first laparoscopic surgery and not repeat surgery.
Can you talk a little bit more about some of the advancements and the controversies in surgical management, and how that impacts your practice or your treatment?
Dr. Lager: Controversy in surgical management includes excision versus ablation in surgical management of endometriosis. One randomized controlled trial showed an improvement with dyspareunia with excision versus ablation after 5 year follow up.[3] However, a recent meta-analysis from 2021 showed no difference in dysmenorrhea between excision and ablation.[4] I generally perform excision of endometriosis as it can provide a tissue for diagnosis and may allow for complete excision of a lesion that may have an underlying component not easily seen.
We also discussed some of the controversy related to fertility and endometriosis. Management of endometriomas in the face of desired fertility is unclear. Endometriomas that are >3 cm in diameter are associated with decreased anti-Mullerian hormone (AMH) levels, but ovarian cystectomy for endometriomas is also associated with decreased AMH levels. I will counsel patients regarding the risks and benefits of ovarian cystectomy and discuss with the reproductive endocrinologists if they recommend removal to improve oocyte retrieval.
Lastly, conservative versus definitive treatment is an important issue to discuss. Depending on a patient’s goals, conservative surgical management of endometriosis may be the most appropriate procedure. However, if a patient has multiple surgeries, does not desire to have children or has completed childbearing regardless of age and wants to decrease the risk of need for repeat surgery, I will discuss with patients that the risk of reoperation after hysterectomy versus conservative surgery is 8% vs 21% in 2 years and 59% vs 22% after 7 years, respectively.[5] Additionally, the patient may have an overlapping gynecological condition, such as adenomyosis or fibroids, and desire surgical management for those conditions as well. Management ultimately will depend on shared decision making,
You mentioned overlapping diagnosis. What are the impacts and barriers related to misdiagnosis or overlapping diagnosis, and what is your approach to recognizing those signs and symptoms?
Dr. Lager: The classic symptoms of endometriosis can overlap with several medical conditions. In addition to gynecologic issues such as adenomyosis and fibroids that I mentioned previously, symptoms such as pelvic pain, bloating, and dysuria can be associated with gastrointestinal conditions, painful bladder syndrome, neurologic, and musculoskeletal pain conditions. This is complex because the overlapping diagnoses can lead to misdiagnosis, and delay in diagnosis and missing an associated diagnosis can lead to inadequate treatment.
I approach the possibility of overlapping diagnoses in consultation with my colleagues who may recommend further testing, such as endoscopy and colonoscopy. Depending on the diagnoses, several treatments can be started concomitantly to address the multifactorial components of pain. For example, pelvic floor dysfunction related to pelvic pain can affect bowel habits, even without a diagnosis of IBS. Pelvic floor physical therapy can address one component of this. Similarly, even if we surgically or medically manage symptoms of endometriosis, the musculoskeletal pain can lead to persistent or worsening pain. The same goes for pain medicine and peripheral or central pain sensitization or neurological pain.
Was there anything else you’d like to share with your colleagues?
Dr. Lager: Endometriosis is a complex condition that requires a multifactorial approach that takes into consideration a patient’s goals. There is not a one-size fit for all patients with endometriosis due to all the issues we discussed. It will take time to address the varied components of pain and is an iterative process. Minimally invasive surgery has an important role in diagnosis and management of endometriosis but is one of several approaches to treat this complex condition. Thanks for taking the time to discuss this important condition that affects at least 10% of gynecological patients, and potentially more due to delayed and undiagnosed disease.
- Staal AH, van der Zanden M, Nap AW. Diagnostic delay of endometriosis in the Netherlands. Gynecol Obstet Invest. 2016;81(4):321-4. doi: 10.1159/000441911
- Duffy JM, Arambage K, Correa FJ, et al. Laparoscopic surgery for endometriosis. Cochrane Database Syst Rev. 2014;(4):CD011031. Update in: Cochrane Database Syst Rev. 2020;10:CD011031. doi:10.1002/14651858.CD011031.pub2
- Healey M, Cheng C, Kaur H. To excise or ablate endometriosis? A prospective randomized double-blinded trial after 5-year follow-up. J Minim Invasive Gynecol. 2014;21(6):999-1004. doi: 10.1016/j.jmig.2014.04.002
- Burks C, Lee M, DeSarno M, Findley J, Flyckt R. Excision versus ablation for management of minimal to mild endometriosis: a systematic review and meta-analysis. J Minim Invasive Gynecol. 2021;28(3):587-597. doi:10.1016/j.jmig.2020.11.028
- Shakiba K, Bena JF, McGill KM, Minger J, Falcone T. Surgical treatment of endometriosis: a 7-year follow-up on the requirement for further surgery. Obstet Gynecol. 2008;111(6):1285-92. Erratum in: Obstet Gynecol. 2008;112(3):710. doi:10.1097/AOG.0b013e3181758ec6
- Staal AH, van der Zanden M, Nap AW. Diagnostic delay of endometriosis in the Netherlands. Gynecol Obstet Invest. 2016;81(4):321-4. doi: 10.1159/000441911
- Duffy JM, Arambage K, Correa FJ, et al. Laparoscopic surgery for endometriosis. Cochrane Database Syst Rev. 2014;(4):CD011031. Update in: Cochrane Database Syst Rev. 2020;10:CD011031. doi:10.1002/14651858.CD011031.pub2
- Healey M, Cheng C, Kaur H. To excise or ablate endometriosis? A prospective randomized double-blinded trial after 5-year follow-up. J Minim Invasive Gynecol. 2014;21(6):999-1004. doi: 10.1016/j.jmig.2014.04.002
- Burks C, Lee M, DeSarno M, Findley J, Flyckt R. Excision versus ablation for management of minimal to mild endometriosis: a systematic review and meta-analysis. J Minim Invasive Gynecol. 2021;28(3):587-597. doi:10.1016/j.jmig.2020.11.028
- Shakiba K, Bena JF, McGill KM, Minger J, Falcone T. Surgical treatment of endometriosis: a 7-year follow-up on the requirement for further surgery. Obstet Gynecol. 2008;111(6):1285-92. Erratum in: Obstet Gynecol. 2008;112(3):710. doi:10.1097/AOG.0b013e3181758ec6
Hope for quicker and more accurate endometriosis diagnosis
A new imaging study hopes to make diagnosing endometriosis quicker, more accurate and reduce the need for invasive surgery.
In October 2020 the All Party Parliamentary Group on Endometriosis published a report that included within its recommendations “a commitment to drive down diagnosis times” for women with the condition. On average, it takes around 8 years for a woman to get a diagnosis of endometriosis, a figure, said the authors of the report, that had “not improved in the last decade.”
Indeed, in its report the APPG said that it was seeking a commitment from Governments in all four nations to reduce average diagnosis times with “targets of 4 years or less by 2025, and a year or less by 2030.”
Surgery often needed for endometriosis diagnosis
Endometriosis affects 1 in 10 women between puberty and menopause – 1.5 million in the United Kingdom – often results in multiple general practitioner and accident and emergency department visits, multiple scans, and often laparoscopic surgery to confirm the diagnosis, as there is currently no simple diagnostic test for the condition. One of the main reasons for the delay in diagnosis is the lack of noninvasive tests capable of detecting all endometriosis subtypes – ovarian, superficial, and deep disease.
Now, experts at the Endometriosis CaRe Centre and Nuffield Department of Women’s and Reproductive Health, University of Oxford (England), in collaboration with British life sciences company Serac Healthcare, hope to establish a faster process for diagnosing endometriosis.
Christian Becker, codirector of the Endometriosis CaRe Centre in Oxford, and a study lead, said: “There is an urgent unmet clinical need for a noninvasive marker to identify or rule out endometriosis as it is such a very common disease affecting more than 190 million women worldwide.”
In the study, researchers will investigate whether a 20-minute imaging scan can detect the most common types of endometriosis, which currently require surgery to diagnose. In turn, they hope that earlier diagnosis of the condition will allow women to seek appropriate treatment sooner. They will use an experimental imaging marker – 99mTc-maraciclatide – that binds to areas of inflammation and that can be used in endometriosis to visualize the disease on a scan. The imaging marker has already been used for detecting inflammation in conditions such as rheumatoid arthritis.
Between 2 and 7 days before planned surgery for suspected endometriosis, participants will be invited for an imaging scan, and the team will compare the suspected locations of disease detected on the scan with those seen during surgery to confirm whether this imaging test could be an effective noninvasive method of detecting all endometriosis subtypes.
Doctor visits and repeated investigations reduced
The researchers commented that the potential strengths of the scan lie in the way the imaging marker binds to areas of inflammation, which may allow doctors to distinguish between new and old lesions and detect endometriosis in areas not easily seen during surgery, such as the lung.
They added that the development of a 20-minute imaging test would reduce the need for repeated visits to doctors, for repeated investigations, and for invasive surgery to obtain a diagnosis. This would ultimately “reduce the time taken to confirm or exclude endometriosis,” they pointed out.
Following the publication of the APPG report in October 2020 the group’s then chair, the late Sir David Amess, said: “Without investment in research, a reduction in diagnosis time, and appropriate NHS pathways, those with endometriosis will continue to face huge barriers in accessing the appropriate support at the right time.”
Krina Zondervan, head of department at the Nuffield Department of Women’s and Reproductive Health, University of Oxford, and a study lead, said: “This study highlights that close collaborations between academics, clinicians and industry are important to combine and accelerate discovery and innovation in addressing high-priority areas in women’s health such as endometriosis.”
David Hail, CEO of Serac Healthcare, said: “We are excited about the potential of 99mTc-maraciclatide to diagnose endometriosis noninvasively and delighted to be working with the internationally renowned team at Oxford on this important first study.”
A version of this article first appeared on Medscape UK.
A new imaging study hopes to make diagnosing endometriosis quicker, more accurate and reduce the need for invasive surgery.
In October 2020 the All Party Parliamentary Group on Endometriosis published a report that included within its recommendations “a commitment to drive down diagnosis times” for women with the condition. On average, it takes around 8 years for a woman to get a diagnosis of endometriosis, a figure, said the authors of the report, that had “not improved in the last decade.”
Indeed, in its report the APPG said that it was seeking a commitment from Governments in all four nations to reduce average diagnosis times with “targets of 4 years or less by 2025, and a year or less by 2030.”
Surgery often needed for endometriosis diagnosis
Endometriosis affects 1 in 10 women between puberty and menopause – 1.5 million in the United Kingdom – often results in multiple general practitioner and accident and emergency department visits, multiple scans, and often laparoscopic surgery to confirm the diagnosis, as there is currently no simple diagnostic test for the condition. One of the main reasons for the delay in diagnosis is the lack of noninvasive tests capable of detecting all endometriosis subtypes – ovarian, superficial, and deep disease.
Now, experts at the Endometriosis CaRe Centre and Nuffield Department of Women’s and Reproductive Health, University of Oxford (England), in collaboration with British life sciences company Serac Healthcare, hope to establish a faster process for diagnosing endometriosis.
Christian Becker, codirector of the Endometriosis CaRe Centre in Oxford, and a study lead, said: “There is an urgent unmet clinical need for a noninvasive marker to identify or rule out endometriosis as it is such a very common disease affecting more than 190 million women worldwide.”
In the study, researchers will investigate whether a 20-minute imaging scan can detect the most common types of endometriosis, which currently require surgery to diagnose. In turn, they hope that earlier diagnosis of the condition will allow women to seek appropriate treatment sooner. They will use an experimental imaging marker – 99mTc-maraciclatide – that binds to areas of inflammation and that can be used in endometriosis to visualize the disease on a scan. The imaging marker has already been used for detecting inflammation in conditions such as rheumatoid arthritis.
Between 2 and 7 days before planned surgery for suspected endometriosis, participants will be invited for an imaging scan, and the team will compare the suspected locations of disease detected on the scan with those seen during surgery to confirm whether this imaging test could be an effective noninvasive method of detecting all endometriosis subtypes.
Doctor visits and repeated investigations reduced
The researchers commented that the potential strengths of the scan lie in the way the imaging marker binds to areas of inflammation, which may allow doctors to distinguish between new and old lesions and detect endometriosis in areas not easily seen during surgery, such as the lung.
They added that the development of a 20-minute imaging test would reduce the need for repeated visits to doctors, for repeated investigations, and for invasive surgery to obtain a diagnosis. This would ultimately “reduce the time taken to confirm or exclude endometriosis,” they pointed out.
Following the publication of the APPG report in October 2020 the group’s then chair, the late Sir David Amess, said: “Without investment in research, a reduction in diagnosis time, and appropriate NHS pathways, those with endometriosis will continue to face huge barriers in accessing the appropriate support at the right time.”
Krina Zondervan, head of department at the Nuffield Department of Women’s and Reproductive Health, University of Oxford, and a study lead, said: “This study highlights that close collaborations between academics, clinicians and industry are important to combine and accelerate discovery and innovation in addressing high-priority areas in women’s health such as endometriosis.”
David Hail, CEO of Serac Healthcare, said: “We are excited about the potential of 99mTc-maraciclatide to diagnose endometriosis noninvasively and delighted to be working with the internationally renowned team at Oxford on this important first study.”
A version of this article first appeared on Medscape UK.
A new imaging study hopes to make diagnosing endometriosis quicker, more accurate and reduce the need for invasive surgery.
In October 2020 the All Party Parliamentary Group on Endometriosis published a report that included within its recommendations “a commitment to drive down diagnosis times” for women with the condition. On average, it takes around 8 years for a woman to get a diagnosis of endometriosis, a figure, said the authors of the report, that had “not improved in the last decade.”
Indeed, in its report the APPG said that it was seeking a commitment from Governments in all four nations to reduce average diagnosis times with “targets of 4 years or less by 2025, and a year or less by 2030.”
Surgery often needed for endometriosis diagnosis
Endometriosis affects 1 in 10 women between puberty and menopause – 1.5 million in the United Kingdom – often results in multiple general practitioner and accident and emergency department visits, multiple scans, and often laparoscopic surgery to confirm the diagnosis, as there is currently no simple diagnostic test for the condition. One of the main reasons for the delay in diagnosis is the lack of noninvasive tests capable of detecting all endometriosis subtypes – ovarian, superficial, and deep disease.
Now, experts at the Endometriosis CaRe Centre and Nuffield Department of Women’s and Reproductive Health, University of Oxford (England), in collaboration with British life sciences company Serac Healthcare, hope to establish a faster process for diagnosing endometriosis.
Christian Becker, codirector of the Endometriosis CaRe Centre in Oxford, and a study lead, said: “There is an urgent unmet clinical need for a noninvasive marker to identify or rule out endometriosis as it is such a very common disease affecting more than 190 million women worldwide.”
In the study, researchers will investigate whether a 20-minute imaging scan can detect the most common types of endometriosis, which currently require surgery to diagnose. In turn, they hope that earlier diagnosis of the condition will allow women to seek appropriate treatment sooner. They will use an experimental imaging marker – 99mTc-maraciclatide – that binds to areas of inflammation and that can be used in endometriosis to visualize the disease on a scan. The imaging marker has already been used for detecting inflammation in conditions such as rheumatoid arthritis.
Between 2 and 7 days before planned surgery for suspected endometriosis, participants will be invited for an imaging scan, and the team will compare the suspected locations of disease detected on the scan with those seen during surgery to confirm whether this imaging test could be an effective noninvasive method of detecting all endometriosis subtypes.
Doctor visits and repeated investigations reduced
The researchers commented that the potential strengths of the scan lie in the way the imaging marker binds to areas of inflammation, which may allow doctors to distinguish between new and old lesions and detect endometriosis in areas not easily seen during surgery, such as the lung.
They added that the development of a 20-minute imaging test would reduce the need for repeated visits to doctors, for repeated investigations, and for invasive surgery to obtain a diagnosis. This would ultimately “reduce the time taken to confirm or exclude endometriosis,” they pointed out.
Following the publication of the APPG report in October 2020 the group’s then chair, the late Sir David Amess, said: “Without investment in research, a reduction in diagnosis time, and appropriate NHS pathways, those with endometriosis will continue to face huge barriers in accessing the appropriate support at the right time.”
Krina Zondervan, head of department at the Nuffield Department of Women’s and Reproductive Health, University of Oxford, and a study lead, said: “This study highlights that close collaborations between academics, clinicians and industry are important to combine and accelerate discovery and innovation in addressing high-priority areas in women’s health such as endometriosis.”
David Hail, CEO of Serac Healthcare, said: “We are excited about the potential of 99mTc-maraciclatide to diagnose endometriosis noninvasively and delighted to be working with the internationally renowned team at Oxford on this important first study.”
A version of this article first appeared on Medscape UK.
Women are not being warned that anesthetic may reduce birth pill efficacy
The effectiveness of hormonal contraceptives, including the pill and mini-pill, may be compromised by sugammadex, a drug widely used in anesthesia for reversing neuromuscular blockade induced by rocuronium or vecuronium.
Yet women are not routinely informed that the drug may make their contraception less effective, delegates at Euroanaesthesia, the annual meeting of the European Society of Anaesthesiology and Intensive Care in Milan were told.
New research presented at the meeting supports the authors’ experience that “robust methods for identifying at-risk patients and informing them of the associated risk of contraceptive failures is not common practice across anesthetic departments within the United Kingdom, and likely further afield.”
This is according to a survey of almost 150 anesthetic professionals, including consultants, junior doctors, and physician assistants, working at University College London Hospitals NHS Foundation Trust.
Dr. Neha Passi, Dr. Matt Oliver, and colleagues at the trust’s department of anesthesiology sent out a seven-question survey to their 150 colleagues and received 82 responses, 94% of which claimed awareness of the risk of contraceptive failure with sugammadex. However, 70% of the respondents admitted that they do not routinely discuss this with patients who have received the drug.
Risk with all forms of hormonal contraceptive
Yet current guidance is to inform women of child-bearing age that they have received the drug and, because of increased risk of contraceptive failure, advise those taking oral hormonal contraceptives to follow the missed pill advice in the leaflet that comes with their contraceptives. It also counsels that clinicians should advise women using other types of hormonal contraceptive to use an additional nonhormonal means of contraception for 7 days.
The study authors also carried out a retrospective audit of sugammadex use in the trust and reported that during the 6 weeks covered by the audit, 234 patients were administered sugammadex of whom 65 (28%) were women of childbearing age. Of these, 17 had a medical history that meant they weren’t at risk of pregnancy, but the other 48 should have received advice on the risks of contraceptive failure – however there was no record in the medical notes of such advice having been given for any of the at-risk 48 women.
While sugammadex is the only anesthetic drug known to have this effect, it is recognized to interact with progesterone and so may reduce the effectiveness of hormonal contraceptives, including the progesterone-only pill, combined pill, vaginal rings, implants, and intrauterine devices.
Dr. Passi said: “It is concerning that we are so seldom informing patients of the risk of contraceptive failure following sugammadex use.
“Use of sugammadex is expected to rise as it becomes cheaper in the future, and ensuring that women receiving this medicine are aware it may increase their risk of unwanted pregnancy must be a priority.”
She added: “It is important to note, however, that most patients receiving an anesthetic do not need a muscle relaxant and that sugammadex is one of several drugs available to reverse muscle relaxation.”
Dr. Oliver said: “We only studied one hospital trust but we expect the results to be similar in elsewhere in the U.K.”
In response to their findings, the study’s authors have created patient information leaflets and letters and programmed the trust’s electronic patient record system to identify “at-risk” patients and deliver electronic prompts to the anesthetists caring for them in the perioperative period.
A version of this article first appeared on Medscape UK.
The effectiveness of hormonal contraceptives, including the pill and mini-pill, may be compromised by sugammadex, a drug widely used in anesthesia for reversing neuromuscular blockade induced by rocuronium or vecuronium.
Yet women are not routinely informed that the drug may make their contraception less effective, delegates at Euroanaesthesia, the annual meeting of the European Society of Anaesthesiology and Intensive Care in Milan were told.
New research presented at the meeting supports the authors’ experience that “robust methods for identifying at-risk patients and informing them of the associated risk of contraceptive failures is not common practice across anesthetic departments within the United Kingdom, and likely further afield.”
This is according to a survey of almost 150 anesthetic professionals, including consultants, junior doctors, and physician assistants, working at University College London Hospitals NHS Foundation Trust.
Dr. Neha Passi, Dr. Matt Oliver, and colleagues at the trust’s department of anesthesiology sent out a seven-question survey to their 150 colleagues and received 82 responses, 94% of which claimed awareness of the risk of contraceptive failure with sugammadex. However, 70% of the respondents admitted that they do not routinely discuss this with patients who have received the drug.
Risk with all forms of hormonal contraceptive
Yet current guidance is to inform women of child-bearing age that they have received the drug and, because of increased risk of contraceptive failure, advise those taking oral hormonal contraceptives to follow the missed pill advice in the leaflet that comes with their contraceptives. It also counsels that clinicians should advise women using other types of hormonal contraceptive to use an additional nonhormonal means of contraception for 7 days.
The study authors also carried out a retrospective audit of sugammadex use in the trust and reported that during the 6 weeks covered by the audit, 234 patients were administered sugammadex of whom 65 (28%) were women of childbearing age. Of these, 17 had a medical history that meant they weren’t at risk of pregnancy, but the other 48 should have received advice on the risks of contraceptive failure – however there was no record in the medical notes of such advice having been given for any of the at-risk 48 women.
While sugammadex is the only anesthetic drug known to have this effect, it is recognized to interact with progesterone and so may reduce the effectiveness of hormonal contraceptives, including the progesterone-only pill, combined pill, vaginal rings, implants, and intrauterine devices.
Dr. Passi said: “It is concerning that we are so seldom informing patients of the risk of contraceptive failure following sugammadex use.
“Use of sugammadex is expected to rise as it becomes cheaper in the future, and ensuring that women receiving this medicine are aware it may increase their risk of unwanted pregnancy must be a priority.”
She added: “It is important to note, however, that most patients receiving an anesthetic do not need a muscle relaxant and that sugammadex is one of several drugs available to reverse muscle relaxation.”
Dr. Oliver said: “We only studied one hospital trust but we expect the results to be similar in elsewhere in the U.K.”
In response to their findings, the study’s authors have created patient information leaflets and letters and programmed the trust’s electronic patient record system to identify “at-risk” patients and deliver electronic prompts to the anesthetists caring for them in the perioperative period.
A version of this article first appeared on Medscape UK.
The effectiveness of hormonal contraceptives, including the pill and mini-pill, may be compromised by sugammadex, a drug widely used in anesthesia for reversing neuromuscular blockade induced by rocuronium or vecuronium.
Yet women are not routinely informed that the drug may make their contraception less effective, delegates at Euroanaesthesia, the annual meeting of the European Society of Anaesthesiology and Intensive Care in Milan were told.
New research presented at the meeting supports the authors’ experience that “robust methods for identifying at-risk patients and informing them of the associated risk of contraceptive failures is not common practice across anesthetic departments within the United Kingdom, and likely further afield.”
This is according to a survey of almost 150 anesthetic professionals, including consultants, junior doctors, and physician assistants, working at University College London Hospitals NHS Foundation Trust.
Dr. Neha Passi, Dr. Matt Oliver, and colleagues at the trust’s department of anesthesiology sent out a seven-question survey to their 150 colleagues and received 82 responses, 94% of which claimed awareness of the risk of contraceptive failure with sugammadex. However, 70% of the respondents admitted that they do not routinely discuss this with patients who have received the drug.
Risk with all forms of hormonal contraceptive
Yet current guidance is to inform women of child-bearing age that they have received the drug and, because of increased risk of contraceptive failure, advise those taking oral hormonal contraceptives to follow the missed pill advice in the leaflet that comes with their contraceptives. It also counsels that clinicians should advise women using other types of hormonal contraceptive to use an additional nonhormonal means of contraception for 7 days.
The study authors also carried out a retrospective audit of sugammadex use in the trust and reported that during the 6 weeks covered by the audit, 234 patients were administered sugammadex of whom 65 (28%) were women of childbearing age. Of these, 17 had a medical history that meant they weren’t at risk of pregnancy, but the other 48 should have received advice on the risks of contraceptive failure – however there was no record in the medical notes of such advice having been given for any of the at-risk 48 women.
While sugammadex is the only anesthetic drug known to have this effect, it is recognized to interact with progesterone and so may reduce the effectiveness of hormonal contraceptives, including the progesterone-only pill, combined pill, vaginal rings, implants, and intrauterine devices.
Dr. Passi said: “It is concerning that we are so seldom informing patients of the risk of contraceptive failure following sugammadex use.
“Use of sugammadex is expected to rise as it becomes cheaper in the future, and ensuring that women receiving this medicine are aware it may increase their risk of unwanted pregnancy must be a priority.”
She added: “It is important to note, however, that most patients receiving an anesthetic do not need a muscle relaxant and that sugammadex is one of several drugs available to reverse muscle relaxation.”
Dr. Oliver said: “We only studied one hospital trust but we expect the results to be similar in elsewhere in the U.K.”
In response to their findings, the study’s authors have created patient information leaflets and letters and programmed the trust’s electronic patient record system to identify “at-risk” patients and deliver electronic prompts to the anesthetists caring for them in the perioperative period.
A version of this article first appeared on Medscape UK.
FROM EUROANAESTHESIA