User login
Take Research Initiative
Hospitalists should consider the hospital their research laboratory,” says Mark V. Williams, MD, FACP, professor of medicine, director, Emory Hospital Medicine Unit, and editor-in-chief of the Journal of Hospital Medicine. “Just as research scientists consider beakers, pipettes, and spectrometers as some of their research tools, we can consider computerized information databases, chart review, and QI projects the tools we use to figure out how we can best deliver care to patients.”
But what are the best ways for hospitalists to conduct research in their institutions? The challenge, says Jeffrey L. Schnipper, MD, MPH, director of clinical research, Brigham and Women’s/Faulkner Hospitalist Service (Boston), and associate physician, Division of General Medicine at Brigham and Women’s Hospital, is that hospitalists are tied to processes—not single interventions.
“The goal of my research,” says Dr. Schnipper, “is to move beyond ‘I got it to work at my hospital’ to ‘this works, in general, at any hospital.’ The vast majority of my projects are related to inpatient quality improvement. Unfortunately, that is not a ‘blue pill.’ If I prove that my quality improvement method improves diabetes control, you still have a lot of work to do to implement it at your hospital.”
How can hospitalists parlay their natural inclinations to improving systems into research that is publishable and generalizable? Healthcare researchers interviewed for this article maintain that savvy use of tools generated from quality improvement research combined with traditional scientific methods can help busy hospitalists streamline their approach to identifying, designing, and conducting valid research projects with publishable results.
Missions Interlaced
Those interviewed for this article agree that the push for quality improvement dovetails with hospitalists’ mission and approach to patient care. “Hospitalists are very systems-oriented,” says Dr. Schnipper. “They are trying to improve not just the care of their individual patients, but the way the whole system works and runs. Frankly, in any environment in which we work, we have a vested interest in making it run better.”
Hospitalists provide a valuable link in the quality improvement chain, agrees Brent James, MD, executive director of the Institute for Healthcare Delivery Research, at Intermountain Healthcare, an integrated delivery system serving 1.2 million patients in Utah, and a leading QI researcher. “Any time you have a group of people who are trying to deliver coordinated care together, and who rely heavily on being able to support each other as a team, this is just an absolute natural model [for conducting QI studies],” he says.

Dr. James was a member of the Institute of Medicine’s National Roundtable on Quality and its subsequent Committee on Quality of Health Care in America that published Crossing the Quality Chasm in 2001. He also just finished a three-year project with the Hastings Center, Garrison, N.Y., funded by an Agency for Healthcare Research and Quality (AHRQ) grant, to examine the ethics of quality improvement.
“Given the quality chasm,” he says, “there is an ethical obligation for physicians, nurses and health professionals to do quality improvement. It surely shouldn’t be a choice—it’s a way of rigorously learning from your own practice.”
Dr. Williams explains that hospitals will increasingly undertake quality improvement initiatives, not just to improve care delivery in their facilities, but in response to pay-for-performance requirements being set up by the federal government and insurers.
“I strongly believe that hospitalists are going to be seen by many hospital administrators as not only collaborators but the leaders of these initiatives,” says Dr. Williams. “And those initiatives can be a form of research if conducted properly. It does require having sufficient resources from the hospital. I don’t think it’s something you can do on Saturday and Sunday nights.”
Steps to the Research
Dr. James has collaborated with Theodore Speroff, PhD, of the Veterans Affairs Health Services Research Center in Nashville, Tenn., and others on many articles delineating the use of PDSA (plan, do, study, act) methodology—also known as rapid cycle of change methodology—to improve the rigor of quality improvement initiatives.1,2
In a nutshell, says Dr. James, the PDSA model consists of several important steps encompassing a study cycle:
- Establish key clinical processes at your institution that warrant studying, and build an evidence-based best practices guideline. For instance, at Intermountain Healthcare 10% of the system’s processes accounted for 90% of clinicians’ work. Hospitalists pick the most prominent care process (DVT prophylaxis, for example) and build an evidence-based best practice guideline;
- Build best practice guidelines into a workflow format (in the form of standing order sets, data, and decision support) to directly support care at the work flow level;
- Build outcomes data comprising three major sub-categories: medical outcomes, service outcomes, and cost outcomes. Each category is further divided into smaller units. For instance, medical outcomes would include indications for appropriateness, condition-specific complication rates, and achieving therapeutic goals;
- Use electronic medical records to develop a system of decision support that ties together best practices, work flow and outcomes tracking; and
- Build educational materials for patients and for the team of professionals delivering the care.
The beauty of rapid cycle of change methodology, says Dr. James, is that it quickly allows teams to correctly identify worthwhile research projects. The team asks: What is our aim or target? How will we know if the target changes or improves (implying a parallel qualitative or quantitative measurement system)? And finally, what might we change to make things work better? “Rapid cycle” connotes a series of PDSA cycles performed one after another in the context of a measurement system.

Increase the Rigor of Studies
Dr. Schnipper believes that continuous quality improvement methods give researchers a toolkit for conducting successful interventional studies. But to use quality improvement methods (e.g., rapid cycle of change—PDSA—methodology) alone may yield less externally valid study results. For example, he says, using QI methods alone, a researcher might continuously change the intervention (for glucose management, for example), watching the results improve over time. This might be the most effective method for improving glucose control in a specific institution, but this renders results “less generalizable to any other institution. It’s never really a before/after study, much less a concurrent randomized controlled trial,” he says. “Many people believe that if you want to conduct research, you have to ‘hold the intervention still’ for at least a certain amount of time so that it’s describable to other people. You may also decide, in the name of generalizability, not to maximally customize your QI intervention to your institution.”
Dr. Schnipper cites a recent Annals of Internal Medicine study that used a combined methodology. The study, by Fine and colleagues at the University of Pittsburgh in conjunction with the Veterans Affairs Center for Health Equity Research and Promotion, compared three intervention strategies (low, moderate, and high intensity) to improve pneumonia care in emergency departments and assessed the performance in institutions assigned to each strategy.3 The high intensity arm used a continuous quality improvement method, allowing each institution to design an intervention that worked best for it. “It was encouraging to see Annals publish an article of this type,” says Dr. Schnipper. “But the question remains: Is this the best way to publish research, such that it’s most useful for other hospitalists who want to improve care at their institutions? Do you include a 20-page online appendix so other people can see exactly what you did?”
QI methodology, Dr. James concedes, is “inherently an observational study design in the hierarchy of evidence because of the way data is collected.” He maintains that researchers can increase the reliability of quality improvement initiatives “by incorporating prospective non-randomized controlled trials designs, or quasi-experiments, the pinnacle of observational study designs. Staggered implementation, risk adjustment, and case matching can bring a quasi-experimental study design within a hair’s breadth of the same evidence reliability of a full randomized controlled trial.”
Once routine care processes are standardized at an institution, other opportunities for controlled studies will appear. Dr. James cites work done at LDS Hospital, Salt Lake City, Utah, by Allen Morris to produce a best practices guideline for treating acute respiratory distress syndrome (ARDS). Now disseminated via ARDSnet (www.ardsnet.org/clinicalnetwork/; Dublin, Calif.), a national research collaborative, these best practices guidelines are now routine care for ARDS at 16 major academic centers. Because routine care is standardized, says Dr. James, that routine care—with Institutional Review Board (IRB) approval and oversight—can become the control arm for comparing new interventions in additional clinical studies. Also, because researchers do not have to initiate a new control arm, operational overhead for new scientific trials is reduced.
“There are definitely ways in which the two fields [quality improvement and rigorous scientific research] make each other better,” says Dr. Schnipper. For his study of glycemic management of diabetic patients in a non-ICU setting (at press time scheduled to publish in a forthcoming issue of the Journal of Hospital Medicine), Dr. Schnipper and his team conducted rigorous prospective data collection, identifying every diabetic on the general medicine service at the time of admission. Using the APACHE III, the team then assessed each patient’s severity of disease, a known confounder of glucose control in hospitalized diabetics. They conducted a detailed chart review to assess the quality of insulin orders for the diabetic patients. Finally, they used a novel statistical technique (marginal structural models) to remove the confounding by indication that occurs when hyperglycemia results in more intensive insulin therapy. They revealed that better quality insulin orders resulted in better glucose control.
“There’s a lot to be said for designing this research so that it is maximally useful for its consumers—hospitalists and others—who want to improve care in their own hospitals. I think we need to move toward multi-center quality improvement studies. If you can get [an intervention] to work at 10 hospitals, then you’ve gone a long way to say this works, in general. As long as you can answer that question—is there knowledge to be gained—then it’s worth doing a study well, with good methods, and it’s worth publishing.”
In Academia Alone?
Dr. Williams hopes the new emphasis on quality improvement, evidenced in such publications as the AHRQ’s August 2004 technical review, “Closing the Quality Gap: A Critical Analysis of Quality Improvement Strategies,” can become a springboard for new areas of research.4 He reports that the Journal of Hospital Medicine has already received article submissions detailing quality improvement initiatives. “We would love to see more,” he says.
It may not always be possible to clear the time for the additional duties of conducting research. Community-based hospitalists do not usually enjoy the same degree of funding and research support infrastructure found in the academic setting. SHM’s “Authoritative Source on the State of the Hospital Medicine Movement” reveals that the majority of hospitalists involved in research are affiliated with universities and medical schools.5 Dr. Williams admits that fitting in research projects can often be a challenge for other busy hospitalists.
“I don’t think it’s something you can just do on nights and weekends. The only way, honestly, that hospitalists can fit research into what they’re doing is if [research] becomes part of their job description,” says Dr. Williams. “And I think the appropriate avenue is through quality improvement initiatives.”
His advice to young hospitalists who want to undertake research projects? Identify existing resources at their institution and find out how they can collaborate with other members of the healthcare team, including nurses and pharmacists.
Community-based hospitalists will most likely benefit, surmises Dr. Schnipper, from emerging initiatives for public reporting and pay for performance, an offshoot of which will yield more useful data sets. “I think they will probably do more collaborative research. Community hospitalists may not have fellowship training in research and protected time to become independent investigators with federal funding,” he says. “What they do have is incredible clinical insight and exact knowledge of the problems in their hospital. I would love to see more academic-community partnerships, where we could do studies in real-world hospitals, not just my ivory tower. Then, we could get some really good, generalizable, multi-center research – which would make everybody happy.” TH
Gretchen Henkel writes regularly for The Hospitalist.
References
- Speroff T, James BC, Nelson EC, et al. Guidelines for appraisal and publication of PDSA quality improvement. Qual Manag Health Care. 2004 Jan-Mar;13(1); 33-39.
- Speroff T, O’Connor GT. Study designs for PDSA quality improvement research. Qual Manag Health Care. 2004 Jan-Mar;13(1);17-32.
- Yealy DM, Auble TE, Stone RA, et al. Effect of increasing the intensity of implementing pneumonia guidelines: a randomized, controlled trial. Ann Intern Med. 2005 Dec 20;143(12):881-894.
- Shojani, KG, McDonald KM, Wachter RM, et al. Closing the quality gap: a critical analysis of quality improvement strategies. Vol. 1, Agency for Healthcare Research and Quality Technical Review; August, 2004. Publication No. 04-0051-1. Available online at www.ahrq.gov/downloads/pub/evidence/pdf/qualgap2/qualgap2.pdf. Last accessed May 30, 2006.
- The Society of Hospital Medicine 2005-2006 Survey. The Authoritative Source on the State of the Hospital Medicine Movement, May, 2006. Philadelphia.
Hospitalists should consider the hospital their research laboratory,” says Mark V. Williams, MD, FACP, professor of medicine, director, Emory Hospital Medicine Unit, and editor-in-chief of the Journal of Hospital Medicine. “Just as research scientists consider beakers, pipettes, and spectrometers as some of their research tools, we can consider computerized information databases, chart review, and QI projects the tools we use to figure out how we can best deliver care to patients.”
But what are the best ways for hospitalists to conduct research in their institutions? The challenge, says Jeffrey L. Schnipper, MD, MPH, director of clinical research, Brigham and Women’s/Faulkner Hospitalist Service (Boston), and associate physician, Division of General Medicine at Brigham and Women’s Hospital, is that hospitalists are tied to processes—not single interventions.
“The goal of my research,” says Dr. Schnipper, “is to move beyond ‘I got it to work at my hospital’ to ‘this works, in general, at any hospital.’ The vast majority of my projects are related to inpatient quality improvement. Unfortunately, that is not a ‘blue pill.’ If I prove that my quality improvement method improves diabetes control, you still have a lot of work to do to implement it at your hospital.”
How can hospitalists parlay their natural inclinations to improving systems into research that is publishable and generalizable? Healthcare researchers interviewed for this article maintain that savvy use of tools generated from quality improvement research combined with traditional scientific methods can help busy hospitalists streamline their approach to identifying, designing, and conducting valid research projects with publishable results.
Missions Interlaced
Those interviewed for this article agree that the push for quality improvement dovetails with hospitalists’ mission and approach to patient care. “Hospitalists are very systems-oriented,” says Dr. Schnipper. “They are trying to improve not just the care of their individual patients, but the way the whole system works and runs. Frankly, in any environment in which we work, we have a vested interest in making it run better.”
Hospitalists provide a valuable link in the quality improvement chain, agrees Brent James, MD, executive director of the Institute for Healthcare Delivery Research, at Intermountain Healthcare, an integrated delivery system serving 1.2 million patients in Utah, and a leading QI researcher. “Any time you have a group of people who are trying to deliver coordinated care together, and who rely heavily on being able to support each other as a team, this is just an absolute natural model [for conducting QI studies],” he says.
Dr. James was a member of the Institute of Medicine’s National Roundtable on Quality and its subsequent Committee on Quality of Health Care in America that published Crossing the Quality Chasm in 2001. He also just finished a three-year project with the Hastings Center, Garrison, N.Y., funded by an Agency for Healthcare Research and Quality (AHRQ) grant, to examine the ethics of quality improvement.
“Given the quality chasm,” he says, “there is an ethical obligation for physicians, nurses and health professionals to do quality improvement. It surely shouldn’t be a choice—it’s a way of rigorously learning from your own practice.”
Dr. Williams explains that hospitals will increasingly undertake quality improvement initiatives, not just to improve care delivery in their facilities, but in response to pay-for-performance requirements being set up by the federal government and insurers.
“I strongly believe that hospitalists are going to be seen by many hospital administrators as not only collaborators but the leaders of these initiatives,” says Dr. Williams. “And those initiatives can be a form of research if conducted properly. It does require having sufficient resources from the hospital. I don’t think it’s something you can do on Saturday and Sunday nights.”
Steps to the Research
Dr. James has collaborated with Theodore Speroff, PhD, of the Veterans Affairs Health Services Research Center in Nashville, Tenn., and others on many articles delineating the use of PDSA (plan, do, study, act) methodology—also known as rapid cycle of change methodology—to improve the rigor of quality improvement initiatives.1,2
In a nutshell, says Dr. James, the PDSA model consists of several important steps encompassing a study cycle:
- Establish key clinical processes at your institution that warrant studying, and build an evidence-based best practices guideline. For instance, at Intermountain Healthcare 10% of the system’s processes accounted for 90% of clinicians’ work. Hospitalists pick the most prominent care process (DVT prophylaxis, for example) and build an evidence-based best practice guideline;
- Build best practice guidelines into a workflow format (in the form of standing order sets, data, and decision support) to directly support care at the work flow level;
- Build outcomes data comprising three major sub-categories: medical outcomes, service outcomes, and cost outcomes. Each category is further divided into smaller units. For instance, medical outcomes would include indications for appropriateness, condition-specific complication rates, and achieving therapeutic goals;
- Use electronic medical records to develop a system of decision support that ties together best practices, work flow and outcomes tracking; and
- Build educational materials for patients and for the team of professionals delivering the care.
The beauty of rapid cycle of change methodology, says Dr. James, is that it quickly allows teams to correctly identify worthwhile research projects. The team asks: What is our aim or target? How will we know if the target changes or improves (implying a parallel qualitative or quantitative measurement system)? And finally, what might we change to make things work better? “Rapid cycle” connotes a series of PDSA cycles performed one after another in the context of a measurement system.
Increase the Rigor of Studies
Dr. Schnipper believes that continuous quality improvement methods give researchers a toolkit for conducting successful interventional studies. But to use quality improvement methods (e.g., rapid cycle of change—PDSA—methodology) alone may yield less externally valid study results. For example, he says, using QI methods alone, a researcher might continuously change the intervention (for glucose management, for example), watching the results improve over time. This might be the most effective method for improving glucose control in a specific institution, but this renders results “less generalizable to any other institution. It’s never really a before/after study, much less a concurrent randomized controlled trial,” he says. “Many people believe that if you want to conduct research, you have to ‘hold the intervention still’ for at least a certain amount of time so that it’s describable to other people. You may also decide, in the name of generalizability, not to maximally customize your QI intervention to your institution.”
Dr. Schnipper cites a recent Annals of Internal Medicine study that used a combined methodology. The study, by Fine and colleagues at the University of Pittsburgh in conjunction with the Veterans Affairs Center for Health Equity Research and Promotion, compared three intervention strategies (low, moderate, and high intensity) to improve pneumonia care in emergency departments and assessed the performance in institutions assigned to each strategy.3 The high intensity arm used a continuous quality improvement method, allowing each institution to design an intervention that worked best for it. “It was encouraging to see Annals publish an article of this type,” says Dr. Schnipper. “But the question remains: Is this the best way to publish research, such that it’s most useful for other hospitalists who want to improve care at their institutions? Do you include a 20-page online appendix so other people can see exactly what you did?”
QI methodology, Dr. James concedes, is “inherently an observational study design in the hierarchy of evidence because of the way data is collected.” He maintains that researchers can increase the reliability of quality improvement initiatives “by incorporating prospective non-randomized controlled trials designs, or quasi-experiments, the pinnacle of observational study designs. Staggered implementation, risk adjustment, and case matching can bring a quasi-experimental study design within a hair’s breadth of the same evidence reliability of a full randomized controlled trial.”
Once routine care processes are standardized at an institution, other opportunities for controlled studies will appear. Dr. James cites work done at LDS Hospital, Salt Lake City, Utah, by Allen Morris to produce a best practices guideline for treating acute respiratory distress syndrome (ARDS). Now disseminated via ARDSnet (www.ardsnet.org/clinicalnetwork/; Dublin, Calif.), a national research collaborative, these best practices guidelines are now routine care for ARDS at 16 major academic centers. Because routine care is standardized, says Dr. James, that routine care—with Institutional Review Board (IRB) approval and oversight—can become the control arm for comparing new interventions in additional clinical studies. Also, because researchers do not have to initiate a new control arm, operational overhead for new scientific trials is reduced.
“There are definitely ways in which the two fields [quality improvement and rigorous scientific research] make each other better,” says Dr. Schnipper. For his study of glycemic management of diabetic patients in a non-ICU setting (at press time scheduled to publish in a forthcoming issue of the Journal of Hospital Medicine), Dr. Schnipper and his team conducted rigorous prospective data collection, identifying every diabetic on the general medicine service at the time of admission. Using the APACHE III, the team then assessed each patient’s severity of disease, a known confounder of glucose control in hospitalized diabetics. They conducted a detailed chart review to assess the quality of insulin orders for the diabetic patients. Finally, they used a novel statistical technique (marginal structural models) to remove the confounding by indication that occurs when hyperglycemia results in more intensive insulin therapy. They revealed that better quality insulin orders resulted in better glucose control.
“There’s a lot to be said for designing this research so that it is maximally useful for its consumers—hospitalists and others—who want to improve care in their own hospitals. I think we need to move toward multi-center quality improvement studies. If you can get [an intervention] to work at 10 hospitals, then you’ve gone a long way to say this works, in general. As long as you can answer that question—is there knowledge to be gained—then it’s worth doing a study well, with good methods, and it’s worth publishing.”
In Academia Alone?
Dr. Williams hopes the new emphasis on quality improvement, evidenced in such publications as the AHRQ’s August 2004 technical review, “Closing the Quality Gap: A Critical Analysis of Quality Improvement Strategies,” can become a springboard for new areas of research.4 He reports that the Journal of Hospital Medicine has already received article submissions detailing quality improvement initiatives. “We would love to see more,” he says.
It may not always be possible to clear the time for the additional duties of conducting research. Community-based hospitalists do not usually enjoy the same degree of funding and research support infrastructure found in the academic setting. SHM’s “Authoritative Source on the State of the Hospital Medicine Movement” reveals that the majority of hospitalists involved in research are affiliated with universities and medical schools.5 Dr. Williams admits that fitting in research projects can often be a challenge for other busy hospitalists.
“I don’t think it’s something you can just do on nights and weekends. The only way, honestly, that hospitalists can fit research into what they’re doing is if [research] becomes part of their job description,” says Dr. Williams. “And I think the appropriate avenue is through quality improvement initiatives.”
His advice to young hospitalists who want to undertake research projects? Identify existing resources at their institution and find out how they can collaborate with other members of the healthcare team, including nurses and pharmacists.
Community-based hospitalists will most likely benefit, surmises Dr. Schnipper, from emerging initiatives for public reporting and pay for performance, an offshoot of which will yield more useful data sets. “I think they will probably do more collaborative research. Community hospitalists may not have fellowship training in research and protected time to become independent investigators with federal funding,” he says. “What they do have is incredible clinical insight and exact knowledge of the problems in their hospital. I would love to see more academic-community partnerships, where we could do studies in real-world hospitals, not just my ivory tower. Then, we could get some really good, generalizable, multi-center research – which would make everybody happy.” TH
Gretchen Henkel writes regularly for The Hospitalist.
References
- Speroff T, James BC, Nelson EC, et al. Guidelines for appraisal and publication of PDSA quality improvement. Qual Manag Health Care. 2004 Jan-Mar;13(1); 33-39.
- Speroff T, O’Connor GT. Study designs for PDSA quality improvement research. Qual Manag Health Care. 2004 Jan-Mar;13(1);17-32.
- Yealy DM, Auble TE, Stone RA, et al. Effect of increasing the intensity of implementing pneumonia guidelines: a randomized, controlled trial. Ann Intern Med. 2005 Dec 20;143(12):881-894.
- Shojani, KG, McDonald KM, Wachter RM, et al. Closing the quality gap: a critical analysis of quality improvement strategies. Vol. 1, Agency for Healthcare Research and Quality Technical Review; August, 2004. Publication No. 04-0051-1. Available online at www.ahrq.gov/downloads/pub/evidence/pdf/qualgap2/qualgap2.pdf. Last accessed May 30, 2006.
- The Society of Hospital Medicine 2005-2006 Survey. The Authoritative Source on the State of the Hospital Medicine Movement, May, 2006. Philadelphia.
Hospitalists should consider the hospital their research laboratory,” says Mark V. Williams, MD, FACP, professor of medicine, director, Emory Hospital Medicine Unit, and editor-in-chief of the Journal of Hospital Medicine. “Just as research scientists consider beakers, pipettes, and spectrometers as some of their research tools, we can consider computerized information databases, chart review, and QI projects the tools we use to figure out how we can best deliver care to patients.”
But what are the best ways for hospitalists to conduct research in their institutions? The challenge, says Jeffrey L. Schnipper, MD, MPH, director of clinical research, Brigham and Women’s/Faulkner Hospitalist Service (Boston), and associate physician, Division of General Medicine at Brigham and Women’s Hospital, is that hospitalists are tied to processes—not single interventions.
“The goal of my research,” says Dr. Schnipper, “is to move beyond ‘I got it to work at my hospital’ to ‘this works, in general, at any hospital.’ The vast majority of my projects are related to inpatient quality improvement. Unfortunately, that is not a ‘blue pill.’ If I prove that my quality improvement method improves diabetes control, you still have a lot of work to do to implement it at your hospital.”
How can hospitalists parlay their natural inclinations to improving systems into research that is publishable and generalizable? Healthcare researchers interviewed for this article maintain that savvy use of tools generated from quality improvement research combined with traditional scientific methods can help busy hospitalists streamline their approach to identifying, designing, and conducting valid research projects with publishable results.
Missions Interlaced
Those interviewed for this article agree that the push for quality improvement dovetails with hospitalists’ mission and approach to patient care. “Hospitalists are very systems-oriented,” says Dr. Schnipper. “They are trying to improve not just the care of their individual patients, but the way the whole system works and runs. Frankly, in any environment in which we work, we have a vested interest in making it run better.”
Hospitalists provide a valuable link in the quality improvement chain, agrees Brent James, MD, executive director of the Institute for Healthcare Delivery Research, at Intermountain Healthcare, an integrated delivery system serving 1.2 million patients in Utah, and a leading QI researcher. “Any time you have a group of people who are trying to deliver coordinated care together, and who rely heavily on being able to support each other as a team, this is just an absolute natural model [for conducting QI studies],” he says.
Dr. James was a member of the Institute of Medicine’s National Roundtable on Quality and its subsequent Committee on Quality of Health Care in America that published Crossing the Quality Chasm in 2001. He also just finished a three-year project with the Hastings Center, Garrison, N.Y., funded by an Agency for Healthcare Research and Quality (AHRQ) grant, to examine the ethics of quality improvement.
“Given the quality chasm,” he says, “there is an ethical obligation for physicians, nurses and health professionals to do quality improvement. It surely shouldn’t be a choice—it’s a way of rigorously learning from your own practice.”
Dr. Williams explains that hospitals will increasingly undertake quality improvement initiatives, not just to improve care delivery in their facilities, but in response to pay-for-performance requirements being set up by the federal government and insurers.
“I strongly believe that hospitalists are going to be seen by many hospital administrators as not only collaborators but the leaders of these initiatives,” says Dr. Williams. “And those initiatives can be a form of research if conducted properly. It does require having sufficient resources from the hospital. I don’t think it’s something you can do on Saturday and Sunday nights.”
Steps to the Research
Dr. James has collaborated with Theodore Speroff, PhD, of the Veterans Affairs Health Services Research Center in Nashville, Tenn., and others on many articles delineating the use of PDSA (plan, do, study, act) methodology—also known as rapid cycle of change methodology—to improve the rigor of quality improvement initiatives.1,2
In a nutshell, says Dr. James, the PDSA model consists of several important steps encompassing a study cycle:
- Establish key clinical processes at your institution that warrant studying, and build an evidence-based best practices guideline. For instance, at Intermountain Healthcare 10% of the system’s processes accounted for 90% of clinicians’ work. Hospitalists pick the most prominent care process (DVT prophylaxis, for example) and build an evidence-based best practice guideline;
- Build best practice guidelines into a workflow format (in the form of standing order sets, data, and decision support) to directly support care at the work flow level;
- Build outcomes data comprising three major sub-categories: medical outcomes, service outcomes, and cost outcomes. Each category is further divided into smaller units. For instance, medical outcomes would include indications for appropriateness, condition-specific complication rates, and achieving therapeutic goals;
- Use electronic medical records to develop a system of decision support that ties together best practices, work flow and outcomes tracking; and
- Build educational materials for patients and for the team of professionals delivering the care.
The beauty of rapid cycle of change methodology, says Dr. James, is that it quickly allows teams to correctly identify worthwhile research projects. The team asks: What is our aim or target? How will we know if the target changes or improves (implying a parallel qualitative or quantitative measurement system)? And finally, what might we change to make things work better? “Rapid cycle” connotes a series of PDSA cycles performed one after another in the context of a measurement system.
Increase the Rigor of Studies
Dr. Schnipper believes that continuous quality improvement methods give researchers a toolkit for conducting successful interventional studies. But to use quality improvement methods (e.g., rapid cycle of change—PDSA—methodology) alone may yield less externally valid study results. For example, he says, using QI methods alone, a researcher might continuously change the intervention (for glucose management, for example), watching the results improve over time. This might be the most effective method for improving glucose control in a specific institution, but this renders results “less generalizable to any other institution. It’s never really a before/after study, much less a concurrent randomized controlled trial,” he says. “Many people believe that if you want to conduct research, you have to ‘hold the intervention still’ for at least a certain amount of time so that it’s describable to other people. You may also decide, in the name of generalizability, not to maximally customize your QI intervention to your institution.”
Dr. Schnipper cites a recent Annals of Internal Medicine study that used a combined methodology. The study, by Fine and colleagues at the University of Pittsburgh in conjunction with the Veterans Affairs Center for Health Equity Research and Promotion, compared three intervention strategies (low, moderate, and high intensity) to improve pneumonia care in emergency departments and assessed the performance in institutions assigned to each strategy.3 The high intensity arm used a continuous quality improvement method, allowing each institution to design an intervention that worked best for it. “It was encouraging to see Annals publish an article of this type,” says Dr. Schnipper. “But the question remains: Is this the best way to publish research, such that it’s most useful for other hospitalists who want to improve care at their institutions? Do you include a 20-page online appendix so other people can see exactly what you did?”
QI methodology, Dr. James concedes, is “inherently an observational study design in the hierarchy of evidence because of the way data is collected.” He maintains that researchers can increase the reliability of quality improvement initiatives “by incorporating prospective non-randomized controlled trials designs, or quasi-experiments, the pinnacle of observational study designs. Staggered implementation, risk adjustment, and case matching can bring a quasi-experimental study design within a hair’s breadth of the same evidence reliability of a full randomized controlled trial.”
Once routine care processes are standardized at an institution, other opportunities for controlled studies will appear. Dr. James cites work done at LDS Hospital, Salt Lake City, Utah, by Allen Morris to produce a best practices guideline for treating acute respiratory distress syndrome (ARDS). Now disseminated via ARDSnet (www.ardsnet.org/clinicalnetwork/; Dublin, Calif.), a national research collaborative, these best practices guidelines are now routine care for ARDS at 16 major academic centers. Because routine care is standardized, says Dr. James, that routine care—with Institutional Review Board (IRB) approval and oversight—can become the control arm for comparing new interventions in additional clinical studies. Also, because researchers do not have to initiate a new control arm, operational overhead for new scientific trials is reduced.
“There are definitely ways in which the two fields [quality improvement and rigorous scientific research] make each other better,” says Dr. Schnipper. For his study of glycemic management of diabetic patients in a non-ICU setting (at press time scheduled to publish in a forthcoming issue of the Journal of Hospital Medicine), Dr. Schnipper and his team conducted rigorous prospective data collection, identifying every diabetic on the general medicine service at the time of admission. Using the APACHE III, the team then assessed each patient’s severity of disease, a known confounder of glucose control in hospitalized diabetics. They conducted a detailed chart review to assess the quality of insulin orders for the diabetic patients. Finally, they used a novel statistical technique (marginal structural models) to remove the confounding by indication that occurs when hyperglycemia results in more intensive insulin therapy. They revealed that better quality insulin orders resulted in better glucose control.
“There’s a lot to be said for designing this research so that it is maximally useful for its consumers—hospitalists and others—who want to improve care in their own hospitals. I think we need to move toward multi-center quality improvement studies. If you can get [an intervention] to work at 10 hospitals, then you’ve gone a long way to say this works, in general. As long as you can answer that question—is there knowledge to be gained—then it’s worth doing a study well, with good methods, and it’s worth publishing.”
In Academia Alone?
Dr. Williams hopes the new emphasis on quality improvement, evidenced in such publications as the AHRQ’s August 2004 technical review, “Closing the Quality Gap: A Critical Analysis of Quality Improvement Strategies,” can become a springboard for new areas of research.4 He reports that the Journal of Hospital Medicine has already received article submissions detailing quality improvement initiatives. “We would love to see more,” he says.
It may not always be possible to clear the time for the additional duties of conducting research. Community-based hospitalists do not usually enjoy the same degree of funding and research support infrastructure found in the academic setting. SHM’s “Authoritative Source on the State of the Hospital Medicine Movement” reveals that the majority of hospitalists involved in research are affiliated with universities and medical schools.5 Dr. Williams admits that fitting in research projects can often be a challenge for other busy hospitalists.
“I don’t think it’s something you can just do on nights and weekends. The only way, honestly, that hospitalists can fit research into what they’re doing is if [research] becomes part of their job description,” says Dr. Williams. “And I think the appropriate avenue is through quality improvement initiatives.”
His advice to young hospitalists who want to undertake research projects? Identify existing resources at their institution and find out how they can collaborate with other members of the healthcare team, including nurses and pharmacists.
Community-based hospitalists will most likely benefit, surmises Dr. Schnipper, from emerging initiatives for public reporting and pay for performance, an offshoot of which will yield more useful data sets. “I think they will probably do more collaborative research. Community hospitalists may not have fellowship training in research and protected time to become independent investigators with federal funding,” he says. “What they do have is incredible clinical insight and exact knowledge of the problems in their hospital. I would love to see more academic-community partnerships, where we could do studies in real-world hospitals, not just my ivory tower. Then, we could get some really good, generalizable, multi-center research – which would make everybody happy.” TH
Gretchen Henkel writes regularly for The Hospitalist.
References
- Speroff T, James BC, Nelson EC, et al. Guidelines for appraisal and publication of PDSA quality improvement. Qual Manag Health Care. 2004 Jan-Mar;13(1); 33-39.
- Speroff T, O’Connor GT. Study designs for PDSA quality improvement research. Qual Manag Health Care. 2004 Jan-Mar;13(1);17-32.
- Yealy DM, Auble TE, Stone RA, et al. Effect of increasing the intensity of implementing pneumonia guidelines: a randomized, controlled trial. Ann Intern Med. 2005 Dec 20;143(12):881-894.
- Shojani, KG, McDonald KM, Wachter RM, et al. Closing the quality gap: a critical analysis of quality improvement strategies. Vol. 1, Agency for Healthcare Research and Quality Technical Review; August, 2004. Publication No. 04-0051-1. Available online at www.ahrq.gov/downloads/pub/evidence/pdf/qualgap2/qualgap2.pdf. Last accessed May 30, 2006.
- The Society of Hospital Medicine 2005-2006 Survey. The Authoritative Source on the State of the Hospital Medicine Movement, May, 2006. Philadelphia.
To Tube or Not to Tube
The ability to maintain nutrition and hydration is essential when caring for hospitalized older adults. When physicians recognize that long-term nutrition and hydration cannot be maintained through an oral route, percutaneous endoscopic gastrostomy (PEG) tube placement may need to be considered for long-term nutritional support. This decision is often distressing for the patient, family, and physician for several reasons.
First, the significant number of competing benefits, risks, and burdens of long-term enteral feeding that have to be considered can be overwhelming. The second reason is the lack of clinical data regarding outcomes of PEG tubes for many patients. The last and usually most distressing reason in the decision of PEG tube feeding involves the cultural, ethical, and religious beliefs involved in this decision.
For many families and physicians providing nutrition, including enteral nutrition, using a PEG tube symbolizes compassion, love, and care. This is because eating represents one of the most basic of human needs. For some, not providing nutrition with a PEG tube is morally and ethically wrong. Withholding PEG tube placement can be perceived as assisted suicide or murder. Some physicians also fear legal, ethical, or religious misconduct should they decide against tube feeding.
Physicians need not fear the legal consequences of discontinuing life-sustaining treatment if an appropriate decision-making process has been followed.1 An adult patient who has decision-making capacity and is appropriately informed has the right to forego any forms of medical therapy including life-sustaining therapy such as PEG tube feeding.2
Deciding whether or not to recommend PEG tube feeding can be accomplished in a series of steps. The first step is to evaluate the clinical benefits, risks, and burdens of long-term nutrition for the individual patient. The second step involves discussing the patient’s life goals with them and their family. On many occasions, the decision to place a PEG tube will be made by a surrogate decision-maker such as the patient’s spouse or child. Usually discussions about nutrition and hydration by PEG tube will occur between patients, families, and physicians when the overall end-of-life goals are reviewed. A physician’s role includes assisting patients and their families by providing information and a clear recommendation for or against the use of a feeding tube, giving alternative options, and ensuring there is true informed consent prior to feeding tube insertion.
The most frequent indication for long-term PEG tube feeding is a neurological disorder such as a stroke.3 PEG tube feeding has been developed as a practical alternative to parental feeding for patients with a functioning gastrointestinal (GI) tract who lack the ability to take food by mouth. PEG tube feeding is considered a medical intervention and, like any other intervention, has to be considered according to specific patient situations.
Why Are Older Adults at Risk?
With advancing age comes a linear decline in food intake. Involuntary weight loss is common among older adults, especially in those who are chronically ill. Poor caloric intake and weight loss can lead to multiple problems such as muscle wasting, anemia, and depression. There is a strong correlation between weight loss and morbidity and mortality.4 Even with mild weight loss of 5% of their body weight in one month, institutionalized older adults are four times more likely to die within one year.5 Similarly, community-dwelling older adults who have mild weight loss are at a higher risk of death after adjusting for multiple variables.6
Age-related changes can negatively affect the body’s ability to regulate energy intake and puts older adults at risk for negative energy balance.7 Older adults are more likely to have additional medical problems, use more medications, and experience psychosocial issues that can lead to weight loss and poor nutrition.8 Common causes of weight loss in older hospitalized adults include cancer, gastrointestinal disorder, and depression.9
Mechanical problems, such as dysphagia secondary to cerebrovascular accidents or degenerative brain diseases that affect swallowing are frequently encountered in the hospitalized older patient. Also, diseases that affect appetite and feeding increase the risk for negative energy balance such as GI diseases, endocrine diseases, infections, COPD, and others.
Many drugs have been associated with weight loss, especially in frail older adults. Drugs can cause a decrease in appetite, changes in food tastes and adsorption, and increase the body’s metabolism, making the patients unable to meet their caloric needs. Drugs implicated in malnutrition and weight loss in older persons include digoxin, amiodarone, methotrexate, lithium, and amitriptyline (to name a few).
Often the patient has poor oral intake for weeks—even months—prior to hospitalization. The duration of poor intake or weight loss may affect the patient’s prognosis and treatment. The inability to meet the calories needed by mouth can be a potential marker for a serious disease. Social factors such as isolation, poverty, and lack of transportation may also play a role in poor oral intake and even weight loss. Therefore, the mechanisms of poor nutrition or weight loss have to be identified before PEG tube placement is recommended.
The Clinical Case of Mrs. H
Mrs. H is an 88-year-old, 90-pound white woman admitted to the hospital for the third time this year secondary to aspiration pneumonia. She has a significant past medical history of 20-pound weight loss in the past year and advanced Alzheimer’s disease with severe aphasia. Her functional status is poor. She has been unable to walk or feed herself for at least a year.
Situations like this often arise in the acute care setting. The practitioner may ask how much and what kind of care makes sense for someone like Mrs. H with a limited life expectancy. She has advanced dementia with possible dysphasia and aspiration pneumonia that can explain her poor oral intake. In Mrs. H’s case, other factors can cause her poor oral intake, such as medications, malignancy, delirium, and psychosocial issues.
In this case, the first goal is to identify the cause(s) of poor oral intake and weight loss for future treatment and prognosis. Target your diagnostic investigation at the most probable explanation. “Shotgun” investigations have low yields and should be avoided. In Mrs. H’s case, discontinue medications that can affect her oral intake such as anticholinergic drugs if possible.
If Mrs. H can swallow, the next step is to provide frequent, small meals with liquid oral supplements between meals (60 to 90 minutes before meals). Oral protein and energy supplements have been shown to reduce all-cause mortality in older patients.10 You might consider the use of orexigenic medications, but they usually take significant time to work and their benefit in Mrs. H’s case is questionable. If she is diagnosed as depressed, a trial with mirtazapine may help both her depression and weight loss.
Other effective strategies to promote oral intake in older adults involve eliminating dietary restrictions and allowing unlimited intake of favorite foods. However, in Mrs. H’s case, poor intake may not improve due to the acute medical problems of aspiration pneumonia and the severity of her dementia with dysphagia. Often, a short course of tube feeding through a nasogastric tube can be tried until the patient’s acute illness improves. In Mrs. H’s case though, she has received nasogastric nutrition during her two recent hospitalizations, and her clinical situation has continued to worsen.
Mrs. H’s two daughters want to discuss PEG placement to improve her nutritional status. She had a recent modified barium swallowing study that showed dysphagia with high risk for aspiration of solids and liquids.
Mortality is high in patients with severely abnormal swallowing studies.11 The reasons commonly used to start tube feeding—preventing aspiration pneumonia, to improve quality of life, and to improve functional status—have not been proven in patients with severe dementia.12 In addition, PEG tube feeding does not provide survival benefits in this group of patients, either.13 Therefore, carefully consider tube feeding in older adults with advanced dementia. Some authorities even discourage the widespread use of PEG tubes for patients who suffer from advance dementia.12
For Mrs. H, additional resources that can be used to facilitate her care include geriatric or palliative consult services, chaplaincy, or ethics committee consultations. If the decision is made to place a PEG tube, a time-limited trial with functional and cognitive goals can follow. On the other hand, if the decision of not placing a PEG tube is reached, allowing Mrs. H to eat and drink freely—even if aspiration risk is present—is an alternative. Comfort measures independent of the decision can always be provided. Families who decide against PEG tube placement can be expected to second-guess their decision and will need continued team support.
PEG Indications and Benefits
A PEG tube should be considered for older adults who have a functional gastrointestinal tract but are unable to consume sufficient oral intake to meet their nutritional needs. Frequent indications for PEG placement include impaired swallowing associated with neurological conditions such as cerebrovascular accident and neoplastic diseases or trauma of the oropharynx, larynx, and esophagus. Other but infrequent use of PEG tube is for gastric decompression in selected patients with gastrointestinal tract obstruction.
For some older adults, PEG tube feeding can provide long-term enteral nutrition and hydration with low risk for complications. It can also provide psychological benefits for patients and family members. These benefits include helping them to avoid guilt about deciding to withhold non-oral feedings and by providing hope for future clinical improvement.
PEG tubes appear to be beneficial as a nutritional treatment of choice for patients with acute dysphagic stroke and for some older adults with neoplastic diseases of the oropharynx, larynx, and esophagus. PEG tubes appear inappropriate for patients with a rapidly progressing incurable illness. PEG tube feeding has not been proven to improve quality of life, symptoms of thirst, or survival across the population of older adults at the end of life.
Burdens and Risks of PEG Tube Nutrition
Adverse effects of PEG tubes include wound infections, abdominal pain, aspiration, obstruction of the feeding tube, and agitation. After PEG tube feeding begins, some older adults become agitated and attempt to remove the tube. They may even require chemical and physical restraints for behavioral control.14 A nursing home study found that after PEG tube placement, older adults did not experience functional improvement. PEG-related complications occurred in close to 30% of the patients and the one-year mortality rate was 50% after tube placement.15
About a quarter of patients will have a complication, such as tube occlusion, wound infection, pain, aspiration pneumonitis, and peritonitis, after the PEG tube is placed.16 Aspiration occurs frequently after PEG tube placement and can occur in up to half of older patients with feeding tubes regardless of whether nasogastric or gastric tubes are used.14,17 Some predictors of early mortality after PEG tube placement are age (75 and older), diabetes mellitus, low body mass index, low albumin, COPD, confusion, and advanced cancer.18,19
In a study of Medicare beneficiaries following gastrostomy placement, the in-hospital mortality rate was 15.3%, and the one-year mortality rate was close to 60%.19 In patients after dysphagic stroke, the in-hospital mortality and one-year mortality rates were close to 25% and 50%, respectively after PEG tube placement.20 The mortality rate and the rate of complications, however, will mainly depend on the primary disease. For example, Mrs. H has a poor prognosis independent of PEG tube placement. For some older adults, PEG tubes have shown to have more benefits—especially for those with good functional status, and proximal GI obstruction due to cancer.
Conclusion
Many patients come to the hospital with poor oral intake and weight loss. Clinicians, patients, and families should think carefully about the benefits, risks, and burdens of PEG tube use before initiating placement. The goals should be in concert with patients’ previously expressed wishes and values.
Deciding against PEG tube placement and focusing on comfort and palliative care can always play a role in the care of acutely and chronically ill older adults. PEG tube placement remains an ethically complex, emotionally charged, and difficult area for the managing physician, the patient, and the family. Further research is required in this area to assist these individuals in making the most appropriate decision. TH
Dr. Amador works in the Division of Geriatrics University of Texas Medical Center. His work is supported by the Geriatric Academic Career Award 1 K01 HP 00056-01 by the Bureau of Health Professions.
References
- Weir RF, Gostin L. Decisions to abate life-sustaining treatment for nonautonomous patients. Ethical standards and legal liability for physicians after Cruzan. JAMA. 1990 Oct 10;264(14):1846-1853.
- American Thoracic Society Bioethics Task Force. Withholding and withdrawing life-sustaining therapy. Am Rev Respir Dis. 1991 Sept;144: 726-731.
- Nicholson FB, Korman MG, Richardson MA. Percutaneous endoscopic gastrostomy: a review of indications, complications and outcome. J Gastroenterol Hepatol. 2000 Jan;15(1):21-25.
- Sullivan DH, Patch GA, Walls RC, et al. Impact of nutrition status on morbidity and mortality in a select population of geriatric rehabilitation patients. Am J Clin Nutr. 1990 May;51(5):749–758.
- Ryan C, Bryant E, Eleazer P, et al. Unintentional weight loss in long-term care: predictor of mortality in the elderly. South Med J. 1995 Jul;88(7):721-724.
- Newman AB, Yanez D, Harris T et al. Weight change in old age and its association with mortality. J Am Geriatr Soc. 2001;49:1309-1318.
- Morley JE. Anorexia of aging. Am J Clin Nutr. 1997;66:760-773.
- Bouras EP, Lange SM, Scolapio JS. Rational approach to patients with unintentional weight loss. Mayo Clin Proc. 2001;76:923-929.
- Rabinovitz M, Pitlik SD, Leifer M, et al. Unintentional weight loss: a retrospective analysis of 154 cases. Arch Intern Med. 1986;146(1):186-187.
- Milne AC, Potter J, Avenell A. Protein and energy supplementation in elderly people at risk from malnutrition. Cochrane Database Syst Rev. 2005 Apr 18;(2):CD003288.
- Cowen ME, Simpson SL, Vettese TE. Survival estimates for patients with abnormal swallowing studies. J Gen Intern Med. 1997 Feb;12(2):88-94.
- Finucane TE, Christmas C, Travis K. Tube feeding in patients with advanced dementia: a review of the evidence. JAMA. 1999 (Oct);282(14):1365-1370.
- Murphy LM, Lipman TO. Percutaneous endoscopic gastrostomy does not prolong survival in patients with dementia. Arch Intern Med. 2003 Jun 9;163 (11):1351-1353.
- Quill T. Utilization of nasogastric feeding tubes in a group of chronically ill, elderly patients in a community hospital. Arch Intern Med. 1989 Sep;149(9):1937-1941.
- Kaw M, Sekas G. Long-term follow-up of consequences of percutaneous endoscopic gastrostomy (PEG) tubes in nursing home patients. Dig Dis Sci. 1994 Apr;39(4):738-743.
- Erdil A, Saka M, Ates Y, et al. Enteral nutrition via percutaneous endoscopic gastrostomy and nutritional status of patients: Five-year prospective study. J Gastroenterol Hepatol. 2005 Jul;20(7):1002-1007.
- Ciocon JO, Silverstone FA, Graver LM, et al. Tube feedings in elderly patients. Arch Intern Med. 1988 Feb;148(2):429-433.
- Mitchell SL, Tetroe JM. Survival after percutaneous endoscopic gastrostomy placement in older persons. J Gerontol A Biol Sci Med Sci. 2000 Dec;55:M735-M739.
- Grant MD, Rudberg MA, Brody JA. Gastrostomy placement and mortality among hospitalized Medicare beneficiaries. JAMA. 1998 Jun 24;279(24):1973-1976.
- James A, Kapur K, Hawthorne AB. Long-term outcome of percutaneous endoscopic gastrostomy feeding in patients with dysphagic stroke. Age and Ageing. 1998 Nov; 27(6):671-676.
The ability to maintain nutrition and hydration is essential when caring for hospitalized older adults. When physicians recognize that long-term nutrition and hydration cannot be maintained through an oral route, percutaneous endoscopic gastrostomy (PEG) tube placement may need to be considered for long-term nutritional support. This decision is often distressing for the patient, family, and physician for several reasons.
First, the significant number of competing benefits, risks, and burdens of long-term enteral feeding that have to be considered can be overwhelming. The second reason is the lack of clinical data regarding outcomes of PEG tubes for many patients. The last and usually most distressing reason in the decision of PEG tube feeding involves the cultural, ethical, and religious beliefs involved in this decision.
For many families and physicians providing nutrition, including enteral nutrition, using a PEG tube symbolizes compassion, love, and care. This is because eating represents one of the most basic of human needs. For some, not providing nutrition with a PEG tube is morally and ethically wrong. Withholding PEG tube placement can be perceived as assisted suicide or murder. Some physicians also fear legal, ethical, or religious misconduct should they decide against tube feeding.
Physicians need not fear the legal consequences of discontinuing life-sustaining treatment if an appropriate decision-making process has been followed.1 An adult patient who has decision-making capacity and is appropriately informed has the right to forego any forms of medical therapy including life-sustaining therapy such as PEG tube feeding.2
Deciding whether or not to recommend PEG tube feeding can be accomplished in a series of steps. The first step is to evaluate the clinical benefits, risks, and burdens of long-term nutrition for the individual patient. The second step involves discussing the patient’s life goals with them and their family. On many occasions, the decision to place a PEG tube will be made by a surrogate decision-maker such as the patient’s spouse or child. Usually discussions about nutrition and hydration by PEG tube will occur between patients, families, and physicians when the overall end-of-life goals are reviewed. A physician’s role includes assisting patients and their families by providing information and a clear recommendation for or against the use of a feeding tube, giving alternative options, and ensuring there is true informed consent prior to feeding tube insertion.
The most frequent indication for long-term PEG tube feeding is a neurological disorder such as a stroke.3 PEG tube feeding has been developed as a practical alternative to parental feeding for patients with a functioning gastrointestinal (GI) tract who lack the ability to take food by mouth. PEG tube feeding is considered a medical intervention and, like any other intervention, has to be considered according to specific patient situations.
Why Are Older Adults at Risk?
With advancing age comes a linear decline in food intake. Involuntary weight loss is common among older adults, especially in those who are chronically ill. Poor caloric intake and weight loss can lead to multiple problems such as muscle wasting, anemia, and depression. There is a strong correlation between weight loss and morbidity and mortality.4 Even with mild weight loss of 5% of their body weight in one month, institutionalized older adults are four times more likely to die within one year.5 Similarly, community-dwelling older adults who have mild weight loss are at a higher risk of death after adjusting for multiple variables.6
Age-related changes can negatively affect the body’s ability to regulate energy intake and puts older adults at risk for negative energy balance.7 Older adults are more likely to have additional medical problems, use more medications, and experience psychosocial issues that can lead to weight loss and poor nutrition.8 Common causes of weight loss in older hospitalized adults include cancer, gastrointestinal disorder, and depression.9
Mechanical problems, such as dysphagia secondary to cerebrovascular accidents or degenerative brain diseases that affect swallowing are frequently encountered in the hospitalized older patient. Also, diseases that affect appetite and feeding increase the risk for negative energy balance such as GI diseases, endocrine diseases, infections, COPD, and others.
Many drugs have been associated with weight loss, especially in frail older adults. Drugs can cause a decrease in appetite, changes in food tastes and adsorption, and increase the body’s metabolism, making the patients unable to meet their caloric needs. Drugs implicated in malnutrition and weight loss in older persons include digoxin, amiodarone, methotrexate, lithium, and amitriptyline (to name a few).
Often the patient has poor oral intake for weeks—even months—prior to hospitalization. The duration of poor intake or weight loss may affect the patient’s prognosis and treatment. The inability to meet the calories needed by mouth can be a potential marker for a serious disease. Social factors such as isolation, poverty, and lack of transportation may also play a role in poor oral intake and even weight loss. Therefore, the mechanisms of poor nutrition or weight loss have to be identified before PEG tube placement is recommended.
The Clinical Case of Mrs. H
Mrs. H is an 88-year-old, 90-pound white woman admitted to the hospital for the third time this year secondary to aspiration pneumonia. She has a significant past medical history of 20-pound weight loss in the past year and advanced Alzheimer’s disease with severe aphasia. Her functional status is poor. She has been unable to walk or feed herself for at least a year.
Situations like this often arise in the acute care setting. The practitioner may ask how much and what kind of care makes sense for someone like Mrs. H with a limited life expectancy. She has advanced dementia with possible dysphasia and aspiration pneumonia that can explain her poor oral intake. In Mrs. H’s case, other factors can cause her poor oral intake, such as medications, malignancy, delirium, and psychosocial issues.
In this case, the first goal is to identify the cause(s) of poor oral intake and weight loss for future treatment and prognosis. Target your diagnostic investigation at the most probable explanation. “Shotgun” investigations have low yields and should be avoided. In Mrs. H’s case, discontinue medications that can affect her oral intake such as anticholinergic drugs if possible.
If Mrs. H can swallow, the next step is to provide frequent, small meals with liquid oral supplements between meals (60 to 90 minutes before meals). Oral protein and energy supplements have been shown to reduce all-cause mortality in older patients.10 You might consider the use of orexigenic medications, but they usually take significant time to work and their benefit in Mrs. H’s case is questionable. If she is diagnosed as depressed, a trial with mirtazapine may help both her depression and weight loss.
Other effective strategies to promote oral intake in older adults involve eliminating dietary restrictions and allowing unlimited intake of favorite foods. However, in Mrs. H’s case, poor intake may not improve due to the acute medical problems of aspiration pneumonia and the severity of her dementia with dysphagia. Often, a short course of tube feeding through a nasogastric tube can be tried until the patient’s acute illness improves. In Mrs. H’s case though, she has received nasogastric nutrition during her two recent hospitalizations, and her clinical situation has continued to worsen.
Mrs. H’s two daughters want to discuss PEG placement to improve her nutritional status. She had a recent modified barium swallowing study that showed dysphagia with high risk for aspiration of solids and liquids.
Mortality is high in patients with severely abnormal swallowing studies.11 The reasons commonly used to start tube feeding—preventing aspiration pneumonia, to improve quality of life, and to improve functional status—have not been proven in patients with severe dementia.12 In addition, PEG tube feeding does not provide survival benefits in this group of patients, either.13 Therefore, carefully consider tube feeding in older adults with advanced dementia. Some authorities even discourage the widespread use of PEG tubes for patients who suffer from advance dementia.12
For Mrs. H, additional resources that can be used to facilitate her care include geriatric or palliative consult services, chaplaincy, or ethics committee consultations. If the decision is made to place a PEG tube, a time-limited trial with functional and cognitive goals can follow. On the other hand, if the decision of not placing a PEG tube is reached, allowing Mrs. H to eat and drink freely—even if aspiration risk is present—is an alternative. Comfort measures independent of the decision can always be provided. Families who decide against PEG tube placement can be expected to second-guess their decision and will need continued team support.
PEG Indications and Benefits
A PEG tube should be considered for older adults who have a functional gastrointestinal tract but are unable to consume sufficient oral intake to meet their nutritional needs. Frequent indications for PEG placement include impaired swallowing associated with neurological conditions such as cerebrovascular accident and neoplastic diseases or trauma of the oropharynx, larynx, and esophagus. Other but infrequent use of PEG tube is for gastric decompression in selected patients with gastrointestinal tract obstruction.
For some older adults, PEG tube feeding can provide long-term enteral nutrition and hydration with low risk for complications. It can also provide psychological benefits for patients and family members. These benefits include helping them to avoid guilt about deciding to withhold non-oral feedings and by providing hope for future clinical improvement.
PEG tubes appear to be beneficial as a nutritional treatment of choice for patients with acute dysphagic stroke and for some older adults with neoplastic diseases of the oropharynx, larynx, and esophagus. PEG tubes appear inappropriate for patients with a rapidly progressing incurable illness. PEG tube feeding has not been proven to improve quality of life, symptoms of thirst, or survival across the population of older adults at the end of life.
Burdens and Risks of PEG Tube Nutrition
Adverse effects of PEG tubes include wound infections, abdominal pain, aspiration, obstruction of the feeding tube, and agitation. After PEG tube feeding begins, some older adults become agitated and attempt to remove the tube. They may even require chemical and physical restraints for behavioral control.14 A nursing home study found that after PEG tube placement, older adults did not experience functional improvement. PEG-related complications occurred in close to 30% of the patients and the one-year mortality rate was 50% after tube placement.15
About a quarter of patients will have a complication, such as tube occlusion, wound infection, pain, aspiration pneumonitis, and peritonitis, after the PEG tube is placed.16 Aspiration occurs frequently after PEG tube placement and can occur in up to half of older patients with feeding tubes regardless of whether nasogastric or gastric tubes are used.14,17 Some predictors of early mortality after PEG tube placement are age (75 and older), diabetes mellitus, low body mass index, low albumin, COPD, confusion, and advanced cancer.18,19
In a study of Medicare beneficiaries following gastrostomy placement, the in-hospital mortality rate was 15.3%, and the one-year mortality rate was close to 60%.19 In patients after dysphagic stroke, the in-hospital mortality and one-year mortality rates were close to 25% and 50%, respectively after PEG tube placement.20 The mortality rate and the rate of complications, however, will mainly depend on the primary disease. For example, Mrs. H has a poor prognosis independent of PEG tube placement. For some older adults, PEG tubes have shown to have more benefits—especially for those with good functional status, and proximal GI obstruction due to cancer.
Conclusion
Many patients come to the hospital with poor oral intake and weight loss. Clinicians, patients, and families should think carefully about the benefits, risks, and burdens of PEG tube use before initiating placement. The goals should be in concert with patients’ previously expressed wishes and values.
Deciding against PEG tube placement and focusing on comfort and palliative care can always play a role in the care of acutely and chronically ill older adults. PEG tube placement remains an ethically complex, emotionally charged, and difficult area for the managing physician, the patient, and the family. Further research is required in this area to assist these individuals in making the most appropriate decision. TH
Dr. Amador works in the Division of Geriatrics University of Texas Medical Center. His work is supported by the Geriatric Academic Career Award 1 K01 HP 00056-01 by the Bureau of Health Professions.
References
- Weir RF, Gostin L. Decisions to abate life-sustaining treatment for nonautonomous patients. Ethical standards and legal liability for physicians after Cruzan. JAMA. 1990 Oct 10;264(14):1846-1853.
- American Thoracic Society Bioethics Task Force. Withholding and withdrawing life-sustaining therapy. Am Rev Respir Dis. 1991 Sept;144: 726-731.
- Nicholson FB, Korman MG, Richardson MA. Percutaneous endoscopic gastrostomy: a review of indications, complications and outcome. J Gastroenterol Hepatol. 2000 Jan;15(1):21-25.
- Sullivan DH, Patch GA, Walls RC, et al. Impact of nutrition status on morbidity and mortality in a select population of geriatric rehabilitation patients. Am J Clin Nutr. 1990 May;51(5):749–758.
- Ryan C, Bryant E, Eleazer P, et al. Unintentional weight loss in long-term care: predictor of mortality in the elderly. South Med J. 1995 Jul;88(7):721-724.
- Newman AB, Yanez D, Harris T et al. Weight change in old age and its association with mortality. J Am Geriatr Soc. 2001;49:1309-1318.
- Morley JE. Anorexia of aging. Am J Clin Nutr. 1997;66:760-773.
- Bouras EP, Lange SM, Scolapio JS. Rational approach to patients with unintentional weight loss. Mayo Clin Proc. 2001;76:923-929.
- Rabinovitz M, Pitlik SD, Leifer M, et al. Unintentional weight loss: a retrospective analysis of 154 cases. Arch Intern Med. 1986;146(1):186-187.
- Milne AC, Potter J, Avenell A. Protein and energy supplementation in elderly people at risk from malnutrition. Cochrane Database Syst Rev. 2005 Apr 18;(2):CD003288.
- Cowen ME, Simpson SL, Vettese TE. Survival estimates for patients with abnormal swallowing studies. J Gen Intern Med. 1997 Feb;12(2):88-94.
- Finucane TE, Christmas C, Travis K. Tube feeding in patients with advanced dementia: a review of the evidence. JAMA. 1999 (Oct);282(14):1365-1370.
- Murphy LM, Lipman TO. Percutaneous endoscopic gastrostomy does not prolong survival in patients with dementia. Arch Intern Med. 2003 Jun 9;163 (11):1351-1353.
- Quill T. Utilization of nasogastric feeding tubes in a group of chronically ill, elderly patients in a community hospital. Arch Intern Med. 1989 Sep;149(9):1937-1941.
- Kaw M, Sekas G. Long-term follow-up of consequences of percutaneous endoscopic gastrostomy (PEG) tubes in nursing home patients. Dig Dis Sci. 1994 Apr;39(4):738-743.
- Erdil A, Saka M, Ates Y, et al. Enteral nutrition via percutaneous endoscopic gastrostomy and nutritional status of patients: Five-year prospective study. J Gastroenterol Hepatol. 2005 Jul;20(7):1002-1007.
- Ciocon JO, Silverstone FA, Graver LM, et al. Tube feedings in elderly patients. Arch Intern Med. 1988 Feb;148(2):429-433.
- Mitchell SL, Tetroe JM. Survival after percutaneous endoscopic gastrostomy placement in older persons. J Gerontol A Biol Sci Med Sci. 2000 Dec;55:M735-M739.
- Grant MD, Rudberg MA, Brody JA. Gastrostomy placement and mortality among hospitalized Medicare beneficiaries. JAMA. 1998 Jun 24;279(24):1973-1976.
- James A, Kapur K, Hawthorne AB. Long-term outcome of percutaneous endoscopic gastrostomy feeding in patients with dysphagic stroke. Age and Ageing. 1998 Nov; 27(6):671-676.
The ability to maintain nutrition and hydration is essential when caring for hospitalized older adults. When physicians recognize that long-term nutrition and hydration cannot be maintained through an oral route, percutaneous endoscopic gastrostomy (PEG) tube placement may need to be considered for long-term nutritional support. This decision is often distressing for the patient, family, and physician for several reasons.
First, the significant number of competing benefits, risks, and burdens of long-term enteral feeding that have to be considered can be overwhelming. The second reason is the lack of clinical data regarding outcomes of PEG tubes for many patients. The last and usually most distressing reason in the decision of PEG tube feeding involves the cultural, ethical, and religious beliefs involved in this decision.
For many families and physicians providing nutrition, including enteral nutrition, using a PEG tube symbolizes compassion, love, and care. This is because eating represents one of the most basic of human needs. For some, not providing nutrition with a PEG tube is morally and ethically wrong. Withholding PEG tube placement can be perceived as assisted suicide or murder. Some physicians also fear legal, ethical, or religious misconduct should they decide against tube feeding.
Physicians need not fear the legal consequences of discontinuing life-sustaining treatment if an appropriate decision-making process has been followed.1 An adult patient who has decision-making capacity and is appropriately informed has the right to forego any forms of medical therapy including life-sustaining therapy such as PEG tube feeding.2
Deciding whether or not to recommend PEG tube feeding can be accomplished in a series of steps. The first step is to evaluate the clinical benefits, risks, and burdens of long-term nutrition for the individual patient. The second step involves discussing the patient’s life goals with them and their family. On many occasions, the decision to place a PEG tube will be made by a surrogate decision-maker such as the patient’s spouse or child. Usually discussions about nutrition and hydration by PEG tube will occur between patients, families, and physicians when the overall end-of-life goals are reviewed. A physician’s role includes assisting patients and their families by providing information and a clear recommendation for or against the use of a feeding tube, giving alternative options, and ensuring there is true informed consent prior to feeding tube insertion.
The most frequent indication for long-term PEG tube feeding is a neurological disorder such as a stroke.3 PEG tube feeding has been developed as a practical alternative to parental feeding for patients with a functioning gastrointestinal (GI) tract who lack the ability to take food by mouth. PEG tube feeding is considered a medical intervention and, like any other intervention, has to be considered according to specific patient situations.
Why Are Older Adults at Risk?
With advancing age comes a linear decline in food intake. Involuntary weight loss is common among older adults, especially in those who are chronically ill. Poor caloric intake and weight loss can lead to multiple problems such as muscle wasting, anemia, and depression. There is a strong correlation between weight loss and morbidity and mortality.4 Even with mild weight loss of 5% of their body weight in one month, institutionalized older adults are four times more likely to die within one year.5 Similarly, community-dwelling older adults who have mild weight loss are at a higher risk of death after adjusting for multiple variables.6
Age-related changes can negatively affect the body’s ability to regulate energy intake and puts older adults at risk for negative energy balance.7 Older adults are more likely to have additional medical problems, use more medications, and experience psychosocial issues that can lead to weight loss and poor nutrition.8 Common causes of weight loss in older hospitalized adults include cancer, gastrointestinal disorder, and depression.9
Mechanical problems, such as dysphagia secondary to cerebrovascular accidents or degenerative brain diseases that affect swallowing are frequently encountered in the hospitalized older patient. Also, diseases that affect appetite and feeding increase the risk for negative energy balance such as GI diseases, endocrine diseases, infections, COPD, and others.
Many drugs have been associated with weight loss, especially in frail older adults. Drugs can cause a decrease in appetite, changes in food tastes and adsorption, and increase the body’s metabolism, making the patients unable to meet their caloric needs. Drugs implicated in malnutrition and weight loss in older persons include digoxin, amiodarone, methotrexate, lithium, and amitriptyline (to name a few).
Often the patient has poor oral intake for weeks—even months—prior to hospitalization. The duration of poor intake or weight loss may affect the patient’s prognosis and treatment. The inability to meet the calories needed by mouth can be a potential marker for a serious disease. Social factors such as isolation, poverty, and lack of transportation may also play a role in poor oral intake and even weight loss. Therefore, the mechanisms of poor nutrition or weight loss have to be identified before PEG tube placement is recommended.
The Clinical Case of Mrs. H
Mrs. H is an 88-year-old, 90-pound white woman admitted to the hospital for the third time this year secondary to aspiration pneumonia. She has a significant past medical history of 20-pound weight loss in the past year and advanced Alzheimer’s disease with severe aphasia. Her functional status is poor. She has been unable to walk or feed herself for at least a year.
Situations like this often arise in the acute care setting. The practitioner may ask how much and what kind of care makes sense for someone like Mrs. H with a limited life expectancy. She has advanced dementia with possible dysphasia and aspiration pneumonia that can explain her poor oral intake. In Mrs. H’s case, other factors can cause her poor oral intake, such as medications, malignancy, delirium, and psychosocial issues.
In this case, the first goal is to identify the cause(s) of poor oral intake and weight loss for future treatment and prognosis. Target your diagnostic investigation at the most probable explanation. “Shotgun” investigations have low yields and should be avoided. In Mrs. H’s case, discontinue medications that can affect her oral intake such as anticholinergic drugs if possible.
If Mrs. H can swallow, the next step is to provide frequent, small meals with liquid oral supplements between meals (60 to 90 minutes before meals). Oral protein and energy supplements have been shown to reduce all-cause mortality in older patients.10 You might consider the use of orexigenic medications, but they usually take significant time to work and their benefit in Mrs. H’s case is questionable. If she is diagnosed as depressed, a trial with mirtazapine may help both her depression and weight loss.
Other effective strategies to promote oral intake in older adults involve eliminating dietary restrictions and allowing unlimited intake of favorite foods. However, in Mrs. H’s case, poor intake may not improve due to the acute medical problems of aspiration pneumonia and the severity of her dementia with dysphagia. Often, a short course of tube feeding through a nasogastric tube can be tried until the patient’s acute illness improves. In Mrs. H’s case though, she has received nasogastric nutrition during her two recent hospitalizations, and her clinical situation has continued to worsen.
Mrs. H’s two daughters want to discuss PEG placement to improve her nutritional status. She had a recent modified barium swallowing study that showed dysphagia with high risk for aspiration of solids and liquids.
Mortality is high in patients with severely abnormal swallowing studies.11 The reasons commonly used to start tube feeding—preventing aspiration pneumonia, to improve quality of life, and to improve functional status—have not been proven in patients with severe dementia.12 In addition, PEG tube feeding does not provide survival benefits in this group of patients, either.13 Therefore, carefully consider tube feeding in older adults with advanced dementia. Some authorities even discourage the widespread use of PEG tubes for patients who suffer from advance dementia.12
For Mrs. H, additional resources that can be used to facilitate her care include geriatric or palliative consult services, chaplaincy, or ethics committee consultations. If the decision is made to place a PEG tube, a time-limited trial with functional and cognitive goals can follow. On the other hand, if the decision of not placing a PEG tube is reached, allowing Mrs. H to eat and drink freely—even if aspiration risk is present—is an alternative. Comfort measures independent of the decision can always be provided. Families who decide against PEG tube placement can be expected to second-guess their decision and will need continued team support.
PEG Indications and Benefits
A PEG tube should be considered for older adults who have a functional gastrointestinal tract but are unable to consume sufficient oral intake to meet their nutritional needs. Frequent indications for PEG placement include impaired swallowing associated with neurological conditions such as cerebrovascular accident and neoplastic diseases or trauma of the oropharynx, larynx, and esophagus. Other but infrequent use of PEG tube is for gastric decompression in selected patients with gastrointestinal tract obstruction.
For some older adults, PEG tube feeding can provide long-term enteral nutrition and hydration with low risk for complications. It can also provide psychological benefits for patients and family members. These benefits include helping them to avoid guilt about deciding to withhold non-oral feedings and by providing hope for future clinical improvement.
PEG tubes appear to be beneficial as a nutritional treatment of choice for patients with acute dysphagic stroke and for some older adults with neoplastic diseases of the oropharynx, larynx, and esophagus. PEG tubes appear inappropriate for patients with a rapidly progressing incurable illness. PEG tube feeding has not been proven to improve quality of life, symptoms of thirst, or survival across the population of older adults at the end of life.
Burdens and Risks of PEG Tube Nutrition
Adverse effects of PEG tubes include wound infections, abdominal pain, aspiration, obstruction of the feeding tube, and agitation. After PEG tube feeding begins, some older adults become agitated and attempt to remove the tube. They may even require chemical and physical restraints for behavioral control.14 A nursing home study found that after PEG tube placement, older adults did not experience functional improvement. PEG-related complications occurred in close to 30% of the patients and the one-year mortality rate was 50% after tube placement.15
About a quarter of patients will have a complication, such as tube occlusion, wound infection, pain, aspiration pneumonitis, and peritonitis, after the PEG tube is placed.16 Aspiration occurs frequently after PEG tube placement and can occur in up to half of older patients with feeding tubes regardless of whether nasogastric or gastric tubes are used.14,17 Some predictors of early mortality after PEG tube placement are age (75 and older), diabetes mellitus, low body mass index, low albumin, COPD, confusion, and advanced cancer.18,19
In a study of Medicare beneficiaries following gastrostomy placement, the in-hospital mortality rate was 15.3%, and the one-year mortality rate was close to 60%.19 In patients after dysphagic stroke, the in-hospital mortality and one-year mortality rates were close to 25% and 50%, respectively after PEG tube placement.20 The mortality rate and the rate of complications, however, will mainly depend on the primary disease. For example, Mrs. H has a poor prognosis independent of PEG tube placement. For some older adults, PEG tubes have shown to have more benefits—especially for those with good functional status, and proximal GI obstruction due to cancer.
Conclusion
Many patients come to the hospital with poor oral intake and weight loss. Clinicians, patients, and families should think carefully about the benefits, risks, and burdens of PEG tube use before initiating placement. The goals should be in concert with patients’ previously expressed wishes and values.
Deciding against PEG tube placement and focusing on comfort and palliative care can always play a role in the care of acutely and chronically ill older adults. PEG tube placement remains an ethically complex, emotionally charged, and difficult area for the managing physician, the patient, and the family. Further research is required in this area to assist these individuals in making the most appropriate decision. TH
Dr. Amador works in the Division of Geriatrics University of Texas Medical Center. His work is supported by the Geriatric Academic Career Award 1 K01 HP 00056-01 by the Bureau of Health Professions.
References
- Weir RF, Gostin L. Decisions to abate life-sustaining treatment for nonautonomous patients. Ethical standards and legal liability for physicians after Cruzan. JAMA. 1990 Oct 10;264(14):1846-1853.
- American Thoracic Society Bioethics Task Force. Withholding and withdrawing life-sustaining therapy. Am Rev Respir Dis. 1991 Sept;144: 726-731.
- Nicholson FB, Korman MG, Richardson MA. Percutaneous endoscopic gastrostomy: a review of indications, complications and outcome. J Gastroenterol Hepatol. 2000 Jan;15(1):21-25.
- Sullivan DH, Patch GA, Walls RC, et al. Impact of nutrition status on morbidity and mortality in a select population of geriatric rehabilitation patients. Am J Clin Nutr. 1990 May;51(5):749–758.
- Ryan C, Bryant E, Eleazer P, et al. Unintentional weight loss in long-term care: predictor of mortality in the elderly. South Med J. 1995 Jul;88(7):721-724.
- Newman AB, Yanez D, Harris T et al. Weight change in old age and its association with mortality. J Am Geriatr Soc. 2001;49:1309-1318.
- Morley JE. Anorexia of aging. Am J Clin Nutr. 1997;66:760-773.
- Bouras EP, Lange SM, Scolapio JS. Rational approach to patients with unintentional weight loss. Mayo Clin Proc. 2001;76:923-929.
- Rabinovitz M, Pitlik SD, Leifer M, et al. Unintentional weight loss: a retrospective analysis of 154 cases. Arch Intern Med. 1986;146(1):186-187.
- Milne AC, Potter J, Avenell A. Protein and energy supplementation in elderly people at risk from malnutrition. Cochrane Database Syst Rev. 2005 Apr 18;(2):CD003288.
- Cowen ME, Simpson SL, Vettese TE. Survival estimates for patients with abnormal swallowing studies. J Gen Intern Med. 1997 Feb;12(2):88-94.
- Finucane TE, Christmas C, Travis K. Tube feeding in patients with advanced dementia: a review of the evidence. JAMA. 1999 (Oct);282(14):1365-1370.
- Murphy LM, Lipman TO. Percutaneous endoscopic gastrostomy does not prolong survival in patients with dementia. Arch Intern Med. 2003 Jun 9;163 (11):1351-1353.
- Quill T. Utilization of nasogastric feeding tubes in a group of chronically ill, elderly patients in a community hospital. Arch Intern Med. 1989 Sep;149(9):1937-1941.
- Kaw M, Sekas G. Long-term follow-up of consequences of percutaneous endoscopic gastrostomy (PEG) tubes in nursing home patients. Dig Dis Sci. 1994 Apr;39(4):738-743.
- Erdil A, Saka M, Ates Y, et al. Enteral nutrition via percutaneous endoscopic gastrostomy and nutritional status of patients: Five-year prospective study. J Gastroenterol Hepatol. 2005 Jul;20(7):1002-1007.
- Ciocon JO, Silverstone FA, Graver LM, et al. Tube feedings in elderly patients. Arch Intern Med. 1988 Feb;148(2):429-433.
- Mitchell SL, Tetroe JM. Survival after percutaneous endoscopic gastrostomy placement in older persons. J Gerontol A Biol Sci Med Sci. 2000 Dec;55:M735-M739.
- Grant MD, Rudberg MA, Brody JA. Gastrostomy placement and mortality among hospitalized Medicare beneficiaries. JAMA. 1998 Jun 24;279(24):1973-1976.
- James A, Kapur K, Hawthorne AB. Long-term outcome of percutaneous endoscopic gastrostomy feeding in patients with dysphagic stroke. Age and Ageing. 1998 Nov; 27(6):671-676.
Team Rapid
The origin of the RRT can be found in medical emergency teams (METs). METs began in Australia as a result of the realization that earlier intervention could lead to better outcomes.1 In December 2004, in response to persistent problems with patient safety, the Institute for Healthcare Improvement launched its “100,000 Lives Campaign.”2 The Institute’s key plan for saving some of these 100,000 lives was to create RRTs at every participating medical center. Participating facilities would also submit data on mortality.
Olive View-UCLA Medical Center (OV-UCLA) signed on to participate in the campaign, and part of that effort was the creation and implementation of an RRT. We joined a University Health Consortium “Commit to Action” team, which assisted us by providing support as we began the creation and implementation of the RRT. What follows is the story of how we created an RRT.
We chose team members from all disciplines that were to be part of the RRT response—both at and behind the scenes: RNs, nursing administrators, hospital administrators, ICU attendings, house staff, laboratory personnel, nursing educators, radiology technicians, and hospital operators. The group was further organized into specific teams to solve problems and present solutions. At this point we learned our first important lesson: We needed to meet individually with all inpatient department chairs to discuss the effect of RRTs.
Activation and Notification
How would the RRT call be activated—overhead or beeper? Who could call, and what would the indications be? The OV-UCLA activation and notification team decided that the RRT could be activated by any staff member. Criteria, including vital signs, mental status, or simply “concern about the patient,” were created and posted. A telephone line in the ICU (X4415) was dedicated for RRT calls, and all other activation was overhead due to the lack of an adequate beeper system. (Other than code pagers, our beeper system can’t be simultaneously activated, and ancillaries don’t have beepers.)
The primary nurse’s responsibilities included calling the primary team or cross-covering team and obtaining a fingerstick glucose on all patients while waiting for the team. In discussions the primary team, we learned our second important lesson: As we presented the RRT to the hospital staff, everyone was concerned about the primary team. Ensuring that a mechanism for notifying the primary team was in place and reassuring staff that the primary team would be involved emerged as essential tasks. It was also imperative to identify the chain of command.
With this need in mind, we decided the primary team would always be the captain and would, therefore, have the authority to dismiss whomever they wanted from the RRT. An ICU attending was assigned to RRT call as supervision for the ICU resident responder. At OV-UCLA, our attending is not in-house and, to date, has not been called.
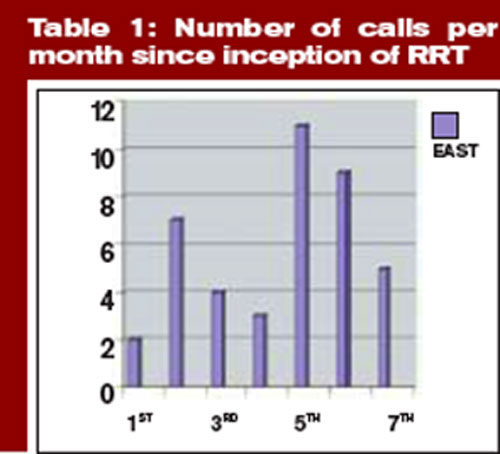
Documentation
The OV-UCLA documentation team was called on to answer the following questions: How would the RRT call be documented? How would medication orders be sent to the pharmacy? How would quality indicators (QI) and data be collected on the calls?
The team’s solution involved creating a one-page, primarily check-based document. The ICU nurse who answered the X4415 telephone in the ICU would begin documentation, which included the time of the call and the chief complaint. When the RRT reached the patient, however, the documentation duties were transferred to the primary RN. All providers were to document on the same page—similar to a code sheet. The RRT nurse and the attending doctor were to check vitals and perform the physical exam, as all information was called out to the documenter.
Medications were to be verbally ordered by the doctor, then read back and verified by the nurses documenting and administering for the RRT. For the most part, medication orders were restricted to what was carried in the RRT bag. The document was eventually copied three times: The original was placed in the chart, one copy was sent to the pharmacy for a record of medication, and the other was saved for QI. The primary team was expected to write a note in the chart’s disposition and time of disposition were to be included in this message.
Equipment
The OV-UCLA equipment team had one important question to answer: What supplies did we need at the bedside?
Although equipment and medications are readily available outside the ICU, the team didn’t want to spend time looking for equipment during an RRT call. “I don’t want a quick RRT call to evolve into a three-hour scavenger hunt,” says one team member.
Because OV-UCLA does not have a 24-hour pharmacist, the group felt it essential to bring medications to the bedside to avoid delays. Our solution to this potential problem was simple. The medication box is prepared by the pharmacy and sealed with one expiration date. Once the box is opened, it is exchanged for a new sealed box. The team chose a rolling duffle to store and transport the supplies, which are compartmentalized into the following sections: infection control, medications, airway and respiratory, IV access and blood draw, and IV start. Medications include respiratory treatments, antibiotics, furosemide, nitroglycerin, metoprolol, heparin and low molecular weight heparin, naloxone, ephedrine, dopamine, glucose, glucagons, and so on. The bag is restocked upon its return to the ICU.
Because of the stress involved in maintaining emergency equipment, we opted to call the supplies a “convenience bag.” This label ensured that only the sealed medication box would require a mandatory check; the rest of the equipment would be monitored on a more informal basis. Because all equipment is available on every floor, and because any RRT call can be converted to a code blue, the team felt that this was reasonable. The committee also purchased a five-pound patient monitor that has a screen for a cardiac tracing, a pulse oximeter, a noninvasive blood pressure monitor, and a temperature probe. This monitor fits easily in a pocket of the duffle.
Education and Publicity
How would staff know to call the RRT? The OV-UCLA team, anticipating that the majority of RRT calls would be activated by the primary RNs, decided that educating all nursing staff was essential.
The hospital nursing education office trained all nurses on all shifts in a short period of time. All nursing staff were taught to use SBAR (situation, background, assessment, and recommendation) communication and to identify early warning signs.1 The importance of recognizing the early warning signs was stressed during the nursing and physician training sessions. Staff were reassured that they didn’t have to know what was wrong with the patient to know that something was wrong and that help was required.
Publicity was accomplished in a variety of ways. The facility purchased pencils in our official color—lime green—that said “Rapid Response Team X4415.” The duffle was wheeled to all nursing stations so that staff could see it. We also ordered custom green-and-white M&M candy (available at www.mms.com) labeled “RRT X4415” to give as a promotional gift when an RRT was called.
Staffing
One last question remained for our team members: Who would respond to the RRT?
The committee felt strongly that an ICU nurse, an ICU resident, and a respiratory therapist should respond. Many physicians on the team did not want a doctor to respond, mostly due to concerns over chain of command. Who would be responsible for decisions made by the RRT? What if an ICU R2 disagreed with a surgery R4? Could they write a “do not call RRT order?” Nursing, on the other hand, wanted physician response; they wanted to be able to stabilize the patient.
Standardized protocols were discussed, but the team felt that the they would unreasonably delay the start. Radiology, which has no code blue response, volunteered to respond to all calls and hand-deliver the film to a computerized viewing system. The lab volunteered to run all RRT labs—designated with a lime green sticker—as quickly as possible.
The medical staff wanted to pilot the RRT, but because we are a small facility (220 beds) and to avoid confusion we launched the RRT for all inpatients. We went live in October 2005. The original plan was to staff an ICU nurse/RRT position. This RRT RN would relieve ICU nurses for breaks to maintain staffing ratios and provide RRT coverage. Because of the omnipresent nursing shortage, however, the RRT position is often pulled and the charge nurse must cover calls. Nurses sign up for RRT overtime and get pulled for patient care duties.
Mock RRT Calls
We performed three RRT drills to determine problem areas. For the first call, we involved a physician who had been vocal about the need for an RRT. The call was for a patient with shortness of breath. Two problems occurred during this drill: The primary team was never called, and there was no overhead page. So a member of our team worked with the hospital operator on our committee and clarified our protocols.
At the second drill, the main problem was documentation. The ICU nurse was so busy documenting that he wasn’t involved with the patient. Because the expertise of the ICU nurse is essential (in fact, there are times when this RN is the most experienced person on the team) we restructured the response so that the primary nurse would document and the ICU nurse was free to provide the hands-on care required.
At the final mock RRT, the major problem was again communication; that is, everyone spoke at once. The team members were encouraged to direct all comments to the team leader and keep any other conversation to a minimum.
A Successful RRT
The following case example, which describes the successful use of our OV-UCLA’s RRT, provides an illuminating look at its effectiveness. In this case, the RRT comprised the ICU nurse, the ICU physician, and the respiratory therapist. The team carried the following equipment: a patient monitor, medications, an IV start, blood sampling tubes, a central line, oxygen masks, and suctioning equipment.
The case began when the primary nurse activated the call. The patient—a 36-year-old HIV-positive male with acute rectal bleeding—was found to have a systolic blood pressure (SBP) reading of 70 and a heart rate of 144. The patient was admitted for anal warts but was noted to have acute bright red blood per rectum. The primary physician team had been called, but had not yet arrived. The primary nurse used the bedside phone to call X4415, and the RRT arrived within three minutes.
Upon arrival, the RRT started a wide bore IV and a central line. The team then called for O-negative blood from the blood bank. The transfusion began seven minutes after the team’s arrival in the patient’s room. The patient was transferred to the ICU and was discharged to the floor the following day.
Results
In four-and-a-half months, we have had 43 calls. The warning signs that precipitated the calls include:
- Respiratory distress: 14 (resulting in eight intubations);
- Cardiac problems: six;
- Altered mental status: four;
- Hypotension: four;
- Post-procedure oversedation: three;
- Vomiting: two;
- Bleeding: two;
- Gastrointestinal: one;
- Mouth bleeding: one;
- Hypoglycemia: one; and
- Unclear etiology: five. TH
Dr. Stein is the medical director, Intensive Care Unit/SDU, at Olive View UCLA Medical Center.
References
- Bellomo R, Goldsmith D, Uchino S, et al. A prospective before-and-after trial of a medical emergency team. Med J Aust. 2003 Sep 15:179(6):283-287
- The Institute for Healthcare Improvement’s 100,000 Lives Campaign. Available at: www.ihi.org. Last accessed July 10, 2006.
- Leonard MS, Graham S, Taggart B. The human factor: effective teamwork and communication in patient strategy. In: Leonard M, Frankel A, Simmonds T, eds. Achieving safe and reliable health care strategies and solutions. 1st ed. ACHE Management Series; 2004. p.37-65.
- Schein RM, Hazday N, Pena M, et al. Clinical antecedents to in-hospital cardiopulmonary arrests. Chest. 1990;98:1388-1392.
- Franklin C, Matthew J. Developing strategies to prevent-in hospital cardiac arrest: analyzing responses of physicians and nurses in the hours before the event. Crit Care Med. 1994;22(2):244-247.
The origin of the RRT can be found in medical emergency teams (METs). METs began in Australia as a result of the realization that earlier intervention could lead to better outcomes.1 In December 2004, in response to persistent problems with patient safety, the Institute for Healthcare Improvement launched its “100,000 Lives Campaign.”2 The Institute’s key plan for saving some of these 100,000 lives was to create RRTs at every participating medical center. Participating facilities would also submit data on mortality.
Olive View-UCLA Medical Center (OV-UCLA) signed on to participate in the campaign, and part of that effort was the creation and implementation of an RRT. We joined a University Health Consortium “Commit to Action” team, which assisted us by providing support as we began the creation and implementation of the RRT. What follows is the story of how we created an RRT.
We chose team members from all disciplines that were to be part of the RRT response—both at and behind the scenes: RNs, nursing administrators, hospital administrators, ICU attendings, house staff, laboratory personnel, nursing educators, radiology technicians, and hospital operators. The group was further organized into specific teams to solve problems and present solutions. At this point we learned our first important lesson: We needed to meet individually with all inpatient department chairs to discuss the effect of RRTs.
Activation and Notification
How would the RRT call be activated—overhead or beeper? Who could call, and what would the indications be? The OV-UCLA activation and notification team decided that the RRT could be activated by any staff member. Criteria, including vital signs, mental status, or simply “concern about the patient,” were created and posted. A telephone line in the ICU (X4415) was dedicated for RRT calls, and all other activation was overhead due to the lack of an adequate beeper system. (Other than code pagers, our beeper system can’t be simultaneously activated, and ancillaries don’t have beepers.)
The primary nurse’s responsibilities included calling the primary team or cross-covering team and obtaining a fingerstick glucose on all patients while waiting for the team. In discussions the primary team, we learned our second important lesson: As we presented the RRT to the hospital staff, everyone was concerned about the primary team. Ensuring that a mechanism for notifying the primary team was in place and reassuring staff that the primary team would be involved emerged as essential tasks. It was also imperative to identify the chain of command.
With this need in mind, we decided the primary team would always be the captain and would, therefore, have the authority to dismiss whomever they wanted from the RRT. An ICU attending was assigned to RRT call as supervision for the ICU resident responder. At OV-UCLA, our attending is not in-house and, to date, has not been called.
Documentation
The OV-UCLA documentation team was called on to answer the following questions: How would the RRT call be documented? How would medication orders be sent to the pharmacy? How would quality indicators (QI) and data be collected on the calls?
The team’s solution involved creating a one-page, primarily check-based document. The ICU nurse who answered the X4415 telephone in the ICU would begin documentation, which included the time of the call and the chief complaint. When the RRT reached the patient, however, the documentation duties were transferred to the primary RN. All providers were to document on the same page—similar to a code sheet. The RRT nurse and the attending doctor were to check vitals and perform the physical exam, as all information was called out to the documenter.
Medications were to be verbally ordered by the doctor, then read back and verified by the nurses documenting and administering for the RRT. For the most part, medication orders were restricted to what was carried in the RRT bag. The document was eventually copied three times: The original was placed in the chart, one copy was sent to the pharmacy for a record of medication, and the other was saved for QI. The primary team was expected to write a note in the chart’s disposition and time of disposition were to be included in this message.
Equipment
The OV-UCLA equipment team had one important question to answer: What supplies did we need at the bedside?
Although equipment and medications are readily available outside the ICU, the team didn’t want to spend time looking for equipment during an RRT call. “I don’t want a quick RRT call to evolve into a three-hour scavenger hunt,” says one team member.
Because OV-UCLA does not have a 24-hour pharmacist, the group felt it essential to bring medications to the bedside to avoid delays. Our solution to this potential problem was simple. The medication box is prepared by the pharmacy and sealed with one expiration date. Once the box is opened, it is exchanged for a new sealed box. The team chose a rolling duffle to store and transport the supplies, which are compartmentalized into the following sections: infection control, medications, airway and respiratory, IV access and blood draw, and IV start. Medications include respiratory treatments, antibiotics, furosemide, nitroglycerin, metoprolol, heparin and low molecular weight heparin, naloxone, ephedrine, dopamine, glucose, glucagons, and so on. The bag is restocked upon its return to the ICU.
Because of the stress involved in maintaining emergency equipment, we opted to call the supplies a “convenience bag.” This label ensured that only the sealed medication box would require a mandatory check; the rest of the equipment would be monitored on a more informal basis. Because all equipment is available on every floor, and because any RRT call can be converted to a code blue, the team felt that this was reasonable. The committee also purchased a five-pound patient monitor that has a screen for a cardiac tracing, a pulse oximeter, a noninvasive blood pressure monitor, and a temperature probe. This monitor fits easily in a pocket of the duffle.
Education and Publicity
How would staff know to call the RRT? The OV-UCLA team, anticipating that the majority of RRT calls would be activated by the primary RNs, decided that educating all nursing staff was essential.
The hospital nursing education office trained all nurses on all shifts in a short period of time. All nursing staff were taught to use SBAR (situation, background, assessment, and recommendation) communication and to identify early warning signs.1 The importance of recognizing the early warning signs was stressed during the nursing and physician training sessions. Staff were reassured that they didn’t have to know what was wrong with the patient to know that something was wrong and that help was required.
Publicity was accomplished in a variety of ways. The facility purchased pencils in our official color—lime green—that said “Rapid Response Team X4415.” The duffle was wheeled to all nursing stations so that staff could see it. We also ordered custom green-and-white M&M candy (available at www.mms.com) labeled “RRT X4415” to give as a promotional gift when an RRT was called.
Staffing
One last question remained for our team members: Who would respond to the RRT?
The committee felt strongly that an ICU nurse, an ICU resident, and a respiratory therapist should respond. Many physicians on the team did not want a doctor to respond, mostly due to concerns over chain of command. Who would be responsible for decisions made by the RRT? What if an ICU R2 disagreed with a surgery R4? Could they write a “do not call RRT order?” Nursing, on the other hand, wanted physician response; they wanted to be able to stabilize the patient.
Standardized protocols were discussed, but the team felt that the they would unreasonably delay the start. Radiology, which has no code blue response, volunteered to respond to all calls and hand-deliver the film to a computerized viewing system. The lab volunteered to run all RRT labs—designated with a lime green sticker—as quickly as possible.
The medical staff wanted to pilot the RRT, but because we are a small facility (220 beds) and to avoid confusion we launched the RRT for all inpatients. We went live in October 2005. The original plan was to staff an ICU nurse/RRT position. This RRT RN would relieve ICU nurses for breaks to maintain staffing ratios and provide RRT coverage. Because of the omnipresent nursing shortage, however, the RRT position is often pulled and the charge nurse must cover calls. Nurses sign up for RRT overtime and get pulled for patient care duties.
Mock RRT Calls
We performed three RRT drills to determine problem areas. For the first call, we involved a physician who had been vocal about the need for an RRT. The call was for a patient with shortness of breath. Two problems occurred during this drill: The primary team was never called, and there was no overhead page. So a member of our team worked with the hospital operator on our committee and clarified our protocols.
At the second drill, the main problem was documentation. The ICU nurse was so busy documenting that he wasn’t involved with the patient. Because the expertise of the ICU nurse is essential (in fact, there are times when this RN is the most experienced person on the team) we restructured the response so that the primary nurse would document and the ICU nurse was free to provide the hands-on care required.
At the final mock RRT, the major problem was again communication; that is, everyone spoke at once. The team members were encouraged to direct all comments to the team leader and keep any other conversation to a minimum.
A Successful RRT
The following case example, which describes the successful use of our OV-UCLA’s RRT, provides an illuminating look at its effectiveness. In this case, the RRT comprised the ICU nurse, the ICU physician, and the respiratory therapist. The team carried the following equipment: a patient monitor, medications, an IV start, blood sampling tubes, a central line, oxygen masks, and suctioning equipment.
The case began when the primary nurse activated the call. The patient—a 36-year-old HIV-positive male with acute rectal bleeding—was found to have a systolic blood pressure (SBP) reading of 70 and a heart rate of 144. The patient was admitted for anal warts but was noted to have acute bright red blood per rectum. The primary physician team had been called, but had not yet arrived. The primary nurse used the bedside phone to call X4415, and the RRT arrived within three minutes.
Upon arrival, the RRT started a wide bore IV and a central line. The team then called for O-negative blood from the blood bank. The transfusion began seven minutes after the team’s arrival in the patient’s room. The patient was transferred to the ICU and was discharged to the floor the following day.
Results
In four-and-a-half months, we have had 43 calls. The warning signs that precipitated the calls include:
- Respiratory distress: 14 (resulting in eight intubations);
- Cardiac problems: six;
- Altered mental status: four;
- Hypotension: four;
- Post-procedure oversedation: three;
- Vomiting: two;
- Bleeding: two;
- Gastrointestinal: one;
- Mouth bleeding: one;
- Hypoglycemia: one; and
- Unclear etiology: five. TH
Dr. Stein is the medical director, Intensive Care Unit/SDU, at Olive View UCLA Medical Center.
References
- Bellomo R, Goldsmith D, Uchino S, et al. A prospective before-and-after trial of a medical emergency team. Med J Aust. 2003 Sep 15:179(6):283-287
- The Institute for Healthcare Improvement’s 100,000 Lives Campaign. Available at: www.ihi.org. Last accessed July 10, 2006.
- Leonard MS, Graham S, Taggart B. The human factor: effective teamwork and communication in patient strategy. In: Leonard M, Frankel A, Simmonds T, eds. Achieving safe and reliable health care strategies and solutions. 1st ed. ACHE Management Series; 2004. p.37-65.
- Schein RM, Hazday N, Pena M, et al. Clinical antecedents to in-hospital cardiopulmonary arrests. Chest. 1990;98:1388-1392.
- Franklin C, Matthew J. Developing strategies to prevent-in hospital cardiac arrest: analyzing responses of physicians and nurses in the hours before the event. Crit Care Med. 1994;22(2):244-247.
The origin of the RRT can be found in medical emergency teams (METs). METs began in Australia as a result of the realization that earlier intervention could lead to better outcomes.1 In December 2004, in response to persistent problems with patient safety, the Institute for Healthcare Improvement launched its “100,000 Lives Campaign.”2 The Institute’s key plan for saving some of these 100,000 lives was to create RRTs at every participating medical center. Participating facilities would also submit data on mortality.
Olive View-UCLA Medical Center (OV-UCLA) signed on to participate in the campaign, and part of that effort was the creation and implementation of an RRT. We joined a University Health Consortium “Commit to Action” team, which assisted us by providing support as we began the creation and implementation of the RRT. What follows is the story of how we created an RRT.
We chose team members from all disciplines that were to be part of the RRT response—both at and behind the scenes: RNs, nursing administrators, hospital administrators, ICU attendings, house staff, laboratory personnel, nursing educators, radiology technicians, and hospital operators. The group was further organized into specific teams to solve problems and present solutions. At this point we learned our first important lesson: We needed to meet individually with all inpatient department chairs to discuss the effect of RRTs.
Activation and Notification
How would the RRT call be activated—overhead or beeper? Who could call, and what would the indications be? The OV-UCLA activation and notification team decided that the RRT could be activated by any staff member. Criteria, including vital signs, mental status, or simply “concern about the patient,” were created and posted. A telephone line in the ICU (X4415) was dedicated for RRT calls, and all other activation was overhead due to the lack of an adequate beeper system. (Other than code pagers, our beeper system can’t be simultaneously activated, and ancillaries don’t have beepers.)
The primary nurse’s responsibilities included calling the primary team or cross-covering team and obtaining a fingerstick glucose on all patients while waiting for the team. In discussions the primary team, we learned our second important lesson: As we presented the RRT to the hospital staff, everyone was concerned about the primary team. Ensuring that a mechanism for notifying the primary team was in place and reassuring staff that the primary team would be involved emerged as essential tasks. It was also imperative to identify the chain of command.
With this need in mind, we decided the primary team would always be the captain and would, therefore, have the authority to dismiss whomever they wanted from the RRT. An ICU attending was assigned to RRT call as supervision for the ICU resident responder. At OV-UCLA, our attending is not in-house and, to date, has not been called.
Documentation
The OV-UCLA documentation team was called on to answer the following questions: How would the RRT call be documented? How would medication orders be sent to the pharmacy? How would quality indicators (QI) and data be collected on the calls?
The team’s solution involved creating a one-page, primarily check-based document. The ICU nurse who answered the X4415 telephone in the ICU would begin documentation, which included the time of the call and the chief complaint. When the RRT reached the patient, however, the documentation duties were transferred to the primary RN. All providers were to document on the same page—similar to a code sheet. The RRT nurse and the attending doctor were to check vitals and perform the physical exam, as all information was called out to the documenter.
Medications were to be verbally ordered by the doctor, then read back and verified by the nurses documenting and administering for the RRT. For the most part, medication orders were restricted to what was carried in the RRT bag. The document was eventually copied three times: The original was placed in the chart, one copy was sent to the pharmacy for a record of medication, and the other was saved for QI. The primary team was expected to write a note in the chart’s disposition and time of disposition were to be included in this message.
Equipment
The OV-UCLA equipment team had one important question to answer: What supplies did we need at the bedside?
Although equipment and medications are readily available outside the ICU, the team didn’t want to spend time looking for equipment during an RRT call. “I don’t want a quick RRT call to evolve into a three-hour scavenger hunt,” says one team member.
Because OV-UCLA does not have a 24-hour pharmacist, the group felt it essential to bring medications to the bedside to avoid delays. Our solution to this potential problem was simple. The medication box is prepared by the pharmacy and sealed with one expiration date. Once the box is opened, it is exchanged for a new sealed box. The team chose a rolling duffle to store and transport the supplies, which are compartmentalized into the following sections: infection control, medications, airway and respiratory, IV access and blood draw, and IV start. Medications include respiratory treatments, antibiotics, furosemide, nitroglycerin, metoprolol, heparin and low molecular weight heparin, naloxone, ephedrine, dopamine, glucose, glucagons, and so on. The bag is restocked upon its return to the ICU.
Because of the stress involved in maintaining emergency equipment, we opted to call the supplies a “convenience bag.” This label ensured that only the sealed medication box would require a mandatory check; the rest of the equipment would be monitored on a more informal basis. Because all equipment is available on every floor, and because any RRT call can be converted to a code blue, the team felt that this was reasonable. The committee also purchased a five-pound patient monitor that has a screen for a cardiac tracing, a pulse oximeter, a noninvasive blood pressure monitor, and a temperature probe. This monitor fits easily in a pocket of the duffle.
Education and Publicity
How would staff know to call the RRT? The OV-UCLA team, anticipating that the majority of RRT calls would be activated by the primary RNs, decided that educating all nursing staff was essential.
The hospital nursing education office trained all nurses on all shifts in a short period of time. All nursing staff were taught to use SBAR (situation, background, assessment, and recommendation) communication and to identify early warning signs.1 The importance of recognizing the early warning signs was stressed during the nursing and physician training sessions. Staff were reassured that they didn’t have to know what was wrong with the patient to know that something was wrong and that help was required.
Publicity was accomplished in a variety of ways. The facility purchased pencils in our official color—lime green—that said “Rapid Response Team X4415.” The duffle was wheeled to all nursing stations so that staff could see it. We also ordered custom green-and-white M&M candy (available at www.mms.com) labeled “RRT X4415” to give as a promotional gift when an RRT was called.
Staffing
One last question remained for our team members: Who would respond to the RRT?
The committee felt strongly that an ICU nurse, an ICU resident, and a respiratory therapist should respond. Many physicians on the team did not want a doctor to respond, mostly due to concerns over chain of command. Who would be responsible for decisions made by the RRT? What if an ICU R2 disagreed with a surgery R4? Could they write a “do not call RRT order?” Nursing, on the other hand, wanted physician response; they wanted to be able to stabilize the patient.
Standardized protocols were discussed, but the team felt that the they would unreasonably delay the start. Radiology, which has no code blue response, volunteered to respond to all calls and hand-deliver the film to a computerized viewing system. The lab volunteered to run all RRT labs—designated with a lime green sticker—as quickly as possible.
The medical staff wanted to pilot the RRT, but because we are a small facility (220 beds) and to avoid confusion we launched the RRT for all inpatients. We went live in October 2005. The original plan was to staff an ICU nurse/RRT position. This RRT RN would relieve ICU nurses for breaks to maintain staffing ratios and provide RRT coverage. Because of the omnipresent nursing shortage, however, the RRT position is often pulled and the charge nurse must cover calls. Nurses sign up for RRT overtime and get pulled for patient care duties.
Mock RRT Calls
We performed three RRT drills to determine problem areas. For the first call, we involved a physician who had been vocal about the need for an RRT. The call was for a patient with shortness of breath. Two problems occurred during this drill: The primary team was never called, and there was no overhead page. So a member of our team worked with the hospital operator on our committee and clarified our protocols.
At the second drill, the main problem was documentation. The ICU nurse was so busy documenting that he wasn’t involved with the patient. Because the expertise of the ICU nurse is essential (in fact, there are times when this RN is the most experienced person on the team) we restructured the response so that the primary nurse would document and the ICU nurse was free to provide the hands-on care required.
At the final mock RRT, the major problem was again communication; that is, everyone spoke at once. The team members were encouraged to direct all comments to the team leader and keep any other conversation to a minimum.
A Successful RRT
The following case example, which describes the successful use of our OV-UCLA’s RRT, provides an illuminating look at its effectiveness. In this case, the RRT comprised the ICU nurse, the ICU physician, and the respiratory therapist. The team carried the following equipment: a patient monitor, medications, an IV start, blood sampling tubes, a central line, oxygen masks, and suctioning equipment.
The case began when the primary nurse activated the call. The patient—a 36-year-old HIV-positive male with acute rectal bleeding—was found to have a systolic blood pressure (SBP) reading of 70 and a heart rate of 144. The patient was admitted for anal warts but was noted to have acute bright red blood per rectum. The primary physician team had been called, but had not yet arrived. The primary nurse used the bedside phone to call X4415, and the RRT arrived within three minutes.
Upon arrival, the RRT started a wide bore IV and a central line. The team then called for O-negative blood from the blood bank. The transfusion began seven minutes after the team’s arrival in the patient’s room. The patient was transferred to the ICU and was discharged to the floor the following day.
Results
In four-and-a-half months, we have had 43 calls. The warning signs that precipitated the calls include:
- Respiratory distress: 14 (resulting in eight intubations);
- Cardiac problems: six;
- Altered mental status: four;
- Hypotension: four;
- Post-procedure oversedation: three;
- Vomiting: two;
- Bleeding: two;
- Gastrointestinal: one;
- Mouth bleeding: one;
- Hypoglycemia: one; and
- Unclear etiology: five. TH
Dr. Stein is the medical director, Intensive Care Unit/SDU, at Olive View UCLA Medical Center.
References
- Bellomo R, Goldsmith D, Uchino S, et al. A prospective before-and-after trial of a medical emergency team. Med J Aust. 2003 Sep 15:179(6):283-287
- The Institute for Healthcare Improvement’s 100,000 Lives Campaign. Available at: www.ihi.org. Last accessed July 10, 2006.
- Leonard MS, Graham S, Taggart B. The human factor: effective teamwork and communication in patient strategy. In: Leonard M, Frankel A, Simmonds T, eds. Achieving safe and reliable health care strategies and solutions. 1st ed. ACHE Management Series; 2004. p.37-65.
- Schein RM, Hazday N, Pena M, et al. Clinical antecedents to in-hospital cardiopulmonary arrests. Chest. 1990;98:1388-1392.
- Franklin C, Matthew J. Developing strategies to prevent-in hospital cardiac arrest: analyzing responses of physicians and nurses in the hours before the event. Crit Care Med. 1994;22(2):244-247.
Doctors of the American Frontier

Discussions of the mid-19th century American physician often conjure up images of the surgeons of the Civil War who tirelessly plied their trade during battle: “During the rest of the night and early morning, he [amputated] arms below the elbow and legs below the knee in less than five minutes. The deep incision … the sweeping cut … pull back the soft parts to expose the bone … saw swiftly.”1
However, in the same period but some thousand miles west, frontier physicians faced similar battle wounds sustained in campaigns against American Indians, as well as a myriad of other duties. Some frontier physicians met these challenges with remarkable ingenuity, while others resorted to treatments later deemed quackery. They often practiced alone in the wilderness without a hospital or colleagues for support.
The first and most obvious task of a military physician on the frontier was to attend to soldiers wounded during battle. The first hurdle was reaching the soldier. In 1874, Surgeon George Miller Sternberg faced daunting challenges in aiding seriously wounded soldiers of General Oliver Otis Howard’s company after a melee with Chief Joseph’s Nez Percé tribe. As dark settled across Clearwater River, Idaho, “Surgeon George Miller Sternberg and an aide crawled out onto the battlefield looking for the wounded. They crept so close to the enemy that they could hear the Indians talking.”1 Dr. Sternberg worked tirelessly throughout the night ligating pulsing arteries and soothing the suffering soldiers with whatever means he had, from opium balls to whiskey. During the course of the evening, an American Indian sentinel spotted Dr. Sternberg’s lantern and shot it out, forcing Dr. Sternberg to continue his treatment in darkness.
In other conflicts, the frontier physician often found himself an active participant in a battle. In the Battle of the Lava Beds fought in Oregon in 1873, Dr. George Martin Kober received a gunshot wound in the arm during the course of the battle. Despite his wound he continued to “treat the wounded before he allowed Dr. Skinner to come to his relief.”1
In the Battle of Bates Creek, fought in the summer of 1874, Dr. Thomas Maghee “was the object of the direct fire of an Indian. Until, laying down his instruments for a moment, he took his carbine and killed the Indian and then returned quietly to his work.”1
When the battle concluded and the soldiers returned to camp, the physicians began to wage a fierce war with disease. Among the plagues that stalked the camps: cholera, scurvy, yellow fever, tuberculosis, and typhoid fever. On one occasion in 1874 cholera struck in the heat of the summer at Fort Riley in Kansas. The pestilence devastated the fort by swiftly taking the lives of dozens of soldiers and compelling a hundred more to desert the fort in fear. One ignorant physician attempted in vain to combat the disease by “burning barrels of pine tar beneath the open windows of the fort hospital.”1
Eventually, Dr. Sternberg conquered the outbreak by implementing a strict disinfection and isolation campaign. In the battle against scurvy, military physicians noted that the typical diet of “meat, white bread, soda biscuits, syrup, lard, and black coffee” was insufficient and often attempted to plant and harvest their own supply of vegetables to treat the vitamin C-deficient soldiers.1
The frontier physician’s duties often expanded outside of the realms of medicine because “by order of the Secretary of War they also studied weather, geography, plants, fauna, Indian customs, and antiquities.”1 In fulfilling these duties, physicians made remarkable contributions to the preservation of the history of the American West, such as Dr. James Kimball’s purchase of the autobiography of Sitting Bull. Indeed, life as a military physician on the American frontier tested the courage, durability, and ingenuity of the early American doctor. TH
John Bois is a second-year medical student at the Mayo Clinic College of Medicine, Rochester, Minn.
Reference
- Dunlop R. Doctors of the American Frontier. Garden City, New York: Doubleday & Company; 1965: 73.
Discussions of the mid-19th century American physician often conjure up images of the surgeons of the Civil War who tirelessly plied their trade during battle: “During the rest of the night and early morning, he [amputated] arms below the elbow and legs below the knee in less than five minutes. The deep incision … the sweeping cut … pull back the soft parts to expose the bone … saw swiftly.”1
However, in the same period but some thousand miles west, frontier physicians faced similar battle wounds sustained in campaigns against American Indians, as well as a myriad of other duties. Some frontier physicians met these challenges with remarkable ingenuity, while others resorted to treatments later deemed quackery. They often practiced alone in the wilderness without a hospital or colleagues for support.
The first and most obvious task of a military physician on the frontier was to attend to soldiers wounded during battle. The first hurdle was reaching the soldier. In 1874, Surgeon George Miller Sternberg faced daunting challenges in aiding seriously wounded soldiers of General Oliver Otis Howard’s company after a melee with Chief Joseph’s Nez Percé tribe. As dark settled across Clearwater River, Idaho, “Surgeon George Miller Sternberg and an aide crawled out onto the battlefield looking for the wounded. They crept so close to the enemy that they could hear the Indians talking.”1 Dr. Sternberg worked tirelessly throughout the night ligating pulsing arteries and soothing the suffering soldiers with whatever means he had, from opium balls to whiskey. During the course of the evening, an American Indian sentinel spotted Dr. Sternberg’s lantern and shot it out, forcing Dr. Sternberg to continue his treatment in darkness.
In other conflicts, the frontier physician often found himself an active participant in a battle. In the Battle of the Lava Beds fought in Oregon in 1873, Dr. George Martin Kober received a gunshot wound in the arm during the course of the battle. Despite his wound he continued to “treat the wounded before he allowed Dr. Skinner to come to his relief.”1
In the Battle of Bates Creek, fought in the summer of 1874, Dr. Thomas Maghee “was the object of the direct fire of an Indian. Until, laying down his instruments for a moment, he took his carbine and killed the Indian and then returned quietly to his work.”1
When the battle concluded and the soldiers returned to camp, the physicians began to wage a fierce war with disease. Among the plagues that stalked the camps: cholera, scurvy, yellow fever, tuberculosis, and typhoid fever. On one occasion in 1874 cholera struck in the heat of the summer at Fort Riley in Kansas. The pestilence devastated the fort by swiftly taking the lives of dozens of soldiers and compelling a hundred more to desert the fort in fear. One ignorant physician attempted in vain to combat the disease by “burning barrels of pine tar beneath the open windows of the fort hospital.”1
Eventually, Dr. Sternberg conquered the outbreak by implementing a strict disinfection and isolation campaign. In the battle against scurvy, military physicians noted that the typical diet of “meat, white bread, soda biscuits, syrup, lard, and black coffee” was insufficient and often attempted to plant and harvest their own supply of vegetables to treat the vitamin C-deficient soldiers.1
The frontier physician’s duties often expanded outside of the realms of medicine because “by order of the Secretary of War they also studied weather, geography, plants, fauna, Indian customs, and antiquities.”1 In fulfilling these duties, physicians made remarkable contributions to the preservation of the history of the American West, such as Dr. James Kimball’s purchase of the autobiography of Sitting Bull. Indeed, life as a military physician on the American frontier tested the courage, durability, and ingenuity of the early American doctor. TH
John Bois is a second-year medical student at the Mayo Clinic College of Medicine, Rochester, Minn.
Reference
- Dunlop R. Doctors of the American Frontier. Garden City, New York: Doubleday & Company; 1965: 73.
Discussions of the mid-19th century American physician often conjure up images of the surgeons of the Civil War who tirelessly plied their trade during battle: “During the rest of the night and early morning, he [amputated] arms below the elbow and legs below the knee in less than five minutes. The deep incision … the sweeping cut … pull back the soft parts to expose the bone … saw swiftly.”1
However, in the same period but some thousand miles west, frontier physicians faced similar battle wounds sustained in campaigns against American Indians, as well as a myriad of other duties. Some frontier physicians met these challenges with remarkable ingenuity, while others resorted to treatments later deemed quackery. They often practiced alone in the wilderness without a hospital or colleagues for support.
The first and most obvious task of a military physician on the frontier was to attend to soldiers wounded during battle. The first hurdle was reaching the soldier. In 1874, Surgeon George Miller Sternberg faced daunting challenges in aiding seriously wounded soldiers of General Oliver Otis Howard’s company after a melee with Chief Joseph’s Nez Percé tribe. As dark settled across Clearwater River, Idaho, “Surgeon George Miller Sternberg and an aide crawled out onto the battlefield looking for the wounded. They crept so close to the enemy that they could hear the Indians talking.”1 Dr. Sternberg worked tirelessly throughout the night ligating pulsing arteries and soothing the suffering soldiers with whatever means he had, from opium balls to whiskey. During the course of the evening, an American Indian sentinel spotted Dr. Sternberg’s lantern and shot it out, forcing Dr. Sternberg to continue his treatment in darkness.
In other conflicts, the frontier physician often found himself an active participant in a battle. In the Battle of the Lava Beds fought in Oregon in 1873, Dr. George Martin Kober received a gunshot wound in the arm during the course of the battle. Despite his wound he continued to “treat the wounded before he allowed Dr. Skinner to come to his relief.”1
In the Battle of Bates Creek, fought in the summer of 1874, Dr. Thomas Maghee “was the object of the direct fire of an Indian. Until, laying down his instruments for a moment, he took his carbine and killed the Indian and then returned quietly to his work.”1
When the battle concluded and the soldiers returned to camp, the physicians began to wage a fierce war with disease. Among the plagues that stalked the camps: cholera, scurvy, yellow fever, tuberculosis, and typhoid fever. On one occasion in 1874 cholera struck in the heat of the summer at Fort Riley in Kansas. The pestilence devastated the fort by swiftly taking the lives of dozens of soldiers and compelling a hundred more to desert the fort in fear. One ignorant physician attempted in vain to combat the disease by “burning barrels of pine tar beneath the open windows of the fort hospital.”1
Eventually, Dr. Sternberg conquered the outbreak by implementing a strict disinfection and isolation campaign. In the battle against scurvy, military physicians noted that the typical diet of “meat, white bread, soda biscuits, syrup, lard, and black coffee” was insufficient and often attempted to plant and harvest their own supply of vegetables to treat the vitamin C-deficient soldiers.1
The frontier physician’s duties often expanded outside of the realms of medicine because “by order of the Secretary of War they also studied weather, geography, plants, fauna, Indian customs, and antiquities.”1 In fulfilling these duties, physicians made remarkable contributions to the preservation of the history of the American West, such as Dr. James Kimball’s purchase of the autobiography of Sitting Bull. Indeed, life as a military physician on the American frontier tested the courage, durability, and ingenuity of the early American doctor. TH
John Bois is a second-year medical student at the Mayo Clinic College of Medicine, Rochester, Minn.
Reference
- Dunlop R. Doctors of the American Frontier. Garden City, New York: Doubleday & Company; 1965: 73.
The Yuk Factor
Despite modern wound treatment and broad-spectrum antibiotic treatment, patients with chronic wounds still exist. The appearance of antibiotic resistant bacteria, such as methicillin-resistant Staphylococcus aureus (MRSA) in the 1980s and ’90s, gave rise to a search for other remedies. One of the remedies that has been rediscovered and subsequently successfully reintroduced is maggot debridement therapy (MDT).1 The fact that more than 100 articles were published on the subject in the past two decades indicates that the use of maggots is making a strong comeback in medicine.2 In January 2004, the U.S. Food and Drug Administration (FDA) issued 510(k)#33391, allowing production and marketing of maggots as a medical device. In this article, we discuss the use of MDT in patients with a chronic wound.
A Long History of Maggot Therapy
MDT has been used in many cultures and has been known for centuries.3 Ambroise Parè is credited as the father of modern MDT. Unfortunately, no evidence can be found of Parè using maggots as a means to clean or heal wounds. The only reference is the often-cited case that occurred in 1557 at the battle of St. Quentin, when Parè observed soldiers whose wounds were covered by maggots. He mainly described the negative effects of the maggots, and, above all, believed they were spontaneously produced by the wound itself, not by the eggs of fly.4
Baron Larey (1766-1842) a famous surgeon in the army of Napoleon Bonaparte, wrote about soldiers who had larvae-infested wounds, but was frustrated that it was difficult to persuade his patients to leave the maggots in place, believing that “they promoted healing without leaving any damage.”5
The first surgeon to use MDT in patients in the hospital was the orthopedic surgeon William Baer. In the 1920s he was faced with a group of untreatable patients with severe osteomyelitis (antibiotics had not yet been discovered). He successfully treated many patients with maggots, and because of his success the therapy became regularly used in the United States.6
By 1934 more than 1,000 surgeons were using maggot therapy. Surgical Maggots were available commercially from Lederle Corporation.7 But with the introduction of antibiotics in the 1940s, the use of maggots dropped off. In the following years, case reports were published only occasionally.

The Negative Image of Maggots
A large problem of MDT is the difficulty of this type of therapy to gain acceptance in the medical community. Maggots are associated with rotting and decay. The image is of filthy, low-life creatures that are ugly and disgusting. Although a nice recent example for the general public is the scene in the movie Gladiator. The main character (played by Russell Crow) is advised to leave the maggots that spontaneously infested a wound on his shoulder in place so that the wound would heal. He leaves them in place and the wound heals without any problem, enabling Crow’s character to fight many battles.
In contrast, in an oral presentation we held recently at a Dutch scientific surgical meeting, a surgical professor in the audience said, “I will never allow those creatures in my ward.”8 This remark shows that widespread use and acceptance of MDT has not yet been reached. It seems there is still much work to do before MDT is generally accepted as a therapeutic method.
Fortunately, the negative image that seems to exist among nurses and physicians does not seem to bother patients.9 We have treated more than 100 patients in our clinic with MDT. All patients to whom we proposed MDT agreed to the therapy. All were allowed to discontinue the therapy whenever they wanted; none did. In a survey of the first 38 MDT-treated patients, 89% agreed to another session of MDT if the surgeon believed it would be beneficial, and 94% of the patients said that they would recommend it to others. This is despite the fact that the therapy was not successful in all patients (there was a below-knee of above the knee amputation-rate of 19% among patients who underwent MDT).10

Indications and Evidence
Indications and contra-indications for maggot therapy are not well defined. Some state that all kind of wounds that contain necrosis or slough can be good candidates for MDT. In our own study of 101 patients with 116 wounds treated with maggots, we had an overall success rate of 67%. (Seventy-eight out of 116 wounds had a beneficial outcome.) However, in 13 patients with septic arthritis, all wounds failed. Success rates where significantly reduced in cases of chronic limb ischemia, visible tendon or bone, and in cases of duration longer than three months before the start of MDT.11
Most physicians who start MDT use it mainly for worst-case scenarios. From our previous studies, it is clear that success rates in those patients are low. After witnessing a few failures, the physician is naturally reluctant to use it again.
What about evidence? Large randomized studies are lacking, although one containing 600 venous ulcer patients was initiated in 2004.12 There have been three randomized studies performed. Wayman, et al., have shown the cost-effectiveness of larval therapy in venous ulcers compared with hydrogel dressing.13 Contreras, et al., could not find a difference between MDT and curettage and topical silver sulfadiazine in patients with venous leg ulcers.14 At the 36th annual meeting of the European Association for the Study of Diabetes, Markevich, et al., reported on a randomized, multicenter, double-blind controlled clinical trial (n=140) for neuropathic diabetic foot lesions compared to conventional treatment. They found a significant higher percentage of granulation tissue after 10 days, compared with the hydrogel group.15 Results from large case-series indicate that MDT works and could even save limbs.2,16-18 The mechanism of action has not been unraveled yet.

Factors Influencing Effectiveness of MDT
Unfortunately, the statement made by Thomas, who said that maggot therapy works by “secreting proteolytic enzymes that break down dead tissue, turning it into a soup, which they then ingest,” still holds.19 It is known that there are mechanical effects, tissue growth effects, that direct killing of bacteria in the alimentary tract of the maggot takes place, and that maggots produce antibacterial factors.2,17,20-31
Although maggots are suitable agents for chronic wound treatment, it is likely that some wounds are more eligible than others for this type of treatment. In our opinion, all wounds that contain gangrenous or necrotic tissue with infection seem to be suited for MDT.32 Success rates of MDT reported in literature vary, but seem to be around 80% to 90%.16,17,33 In our own series, success rate is about 70%.
Patient-selection (case-mix) and method of outcome measurement play essential roles in these percentages. In our opinion, all wounds that contain necrotic tissue can be debrided effectively with MDT. However, if for example wound ischemia is the major etiologic factor, this should also be addressed. In our experience, diabetic foot, venous ulcers, traumatic ulcers, and infections after surgical procedures are all good candidates for MDT.
Absolute contraindications in our opinion are wounds close to large, uncovered blood vessels and wounds that need immediate surgical debridement (e.g., in the case of a septic patient). A relative contraindication is patients with natural of medically induced coagulopathies, but also patient preference could play a role.34 We have had very bad results with infected small joints of the foot; all wounds (n=13) eventually needed a small or large amputation.
Even the technique of application has an effect on outcome. There are two different application techniques: the free-range and the contained technique. The free-range technique is more effective in vitro and in-vivo and has become our standard application technique—not only in the outpatient department, but also in the intra-mural setting.35,36 (Figure 1, p. 16, shows a patient with a necrotic wound on the leg after radiation therapy and a surgical excision for a malignant tumor was performed.) Earlier surgical debridement combined with split skin graft failed. After four applications of maggots, the wound was free of necrosis and could be subsequently closed. (See Figure 2, p. 16.)
The contained technique is used in patients with bleeding tendencies and wounds that do not have enough healthy skin surrounding the wound; in other words, where the covering “cage” needed in case of the free-range technique can’t be applied. (This problem is shown in Figure 3, p. 16: A patient with necrotizing fasciitis of the left upper leg was treated with the contained technique—BiologiQ, Apeldoorn, Netherlands—as there is no proximal skin border. Of course, patient preference plays a role as well in the choice of application technique.37
Wound Clinic
In the Netherlands maggots can be ordered easily and are delivered within 24 hours. We started a wound clinic in 2002. First it was for MDT alone, but now the scope is broader, and we treat chronic wounds with different kind of wound therapies. We have two nurses, one nurse practitioner, one resident-surgeon, and one vascular surgeon who apply the maggots.
Patients do not need to be admitted for MDT. Fifty-nine percent of our patients are treated in the outpatient department. We are able to treat as many as 10 or 15 patients in one session, but MDT-treated patients make up only two or three patients at a time.
We found that after fast, successful biological debridement with MDT we were left with a lot of patients with red, granulating wounds that needed our attention in order to prevent relapses. In our opinion, there are many different treatment methods after MDT. Plaster casting in case of diabetic feet, secondary closure, and split skin grafting are different methods. However, other therapies like VAC-therapy and recently OASIS are promising.
At this time, all patients are prospectively followed after MDT. We are especially interested in patient selection and are now also aiming to find the ideal wound therapy after MDT. TH
Dr. Steenvoorde is a resident surgeon at Rijnland Hospital Leiderdorp, the Netherlands. van Doorn is a nurse-practitioner at Rijnland Hospital Leiderdorp. Jacobi is a senior researcher in the Medical Decision Department at Leiden University Medical Center, in the Netherlands. Dr. Oskam is a vascular surgeon at Rijnland Hospital Leiderdorp.
References
- Beasley WD, Hirst G. Making a meal of MRSA-the role of biosurgery inhospital-acquired infection. J Hosp Infect. 2004;56(1):6-9.
- Jukema GN, Menon AG, Bernards AT. et al. Amputation-sparing treatment by nature: “surgical” maggots revisited. Clin Infect Dis. 2002 Dec 15;35(12):1566-1571.
- Church JC. The traditional use of maggots in wound healing, and the development of larva therapy (biosurgery) in modern medicine. J Altern Complement Med. 1996 Winter;2(4):525-527.
- Coppi C. I dressed your wounds, God healed you—a wounded person’s psychology according to Ambroise Parè. Ostomy Wound Manage. 2005;51:62-64.
- Goldstein HI. Maggots in the treatment of wound and bone infections. J Bone Joint Surg. 1931;13:476-478.
- Baer WS. The treatment of chronic osteomyelitis with the maggot (larva of the blow fly). J Bone Joint Surg. 1931;13:438-475.
- Puckner WA. New and nonofficial remedies, surgical maggots-Lederle. J Am Med Assoc. 1932;98(5):401.
- Steenvoorde P, Doorn Lv, Jacobi CE, et al. Maggot therapy: retrospective study comparing two different application-techniques. (Dutch). Nederlands Tijdschrift voor Heelkunde. 2006;15:86.
- Contreras RJ, Fuentes SA, Karam-Orantes M, et al. Larval debridement therapy in Mexico. Wound Care Canada. 2005;3:42-46.
- Steenvoorde P, Budding TJ, Engeland Av, et al. Maggot therapy and the “yuk factor”: an issue for the patient? Wound Repair Regen. 2005 May-Jun;13(3):350-352.
- Steenvoorde P, Jacobi CA, Doorn Lv, et al. Maggot debridement therapy of infected ulcers: patient and wound factors influencing outcome. Ann Royal Coll Surg Eng. 2006.
- Raynor P, Dumville J, Cullum N. A new clinical trial of the effect of larval therapy. J Tissue Viability. 2004 Jul;14(3):104-105.
- Wayman J, Nirojogi V, Walker A, et al. The cost effectiveness of larval therapy in venous ulcers. J Tissue Viability. 2001 Jan;11(1):51.
- Contreras RJ, Fuentes SA, Arroyo ES, et al. Larval debridement therapy and infection control in venous ulcers: a comparative study. Presented at: the Second World Union of Wound Healing Societies Meeting; July 8-13, 2004.
- Markevich YO, McLeod-Roberts J, Mousley M, et al. Maggot therapy for diabetic neuropathic foot wounds: a randomized study. Presented at: the 36th Annual Meeting of the EASD; September 17-21, 2000. Ref Type: Conference Proceeding.
- Wolff H, Hansson C. Larval therapy—an effective method for ulcer debridement. Clin Exp Dermatol. 2003;28:137.
- Mumcuoglu KY, Ingber A, Gilead L, et al. Maggot therapy for the treatment of intractable wounds. Int J Dermatol. 1999 Aug;38(8):623-627.
- Courtenay M. The use of larval therapy in wound management in the UK. J Wound Care. 1999 Apr;8 (4):177-179.
- Bonn D. Maggot therapy: an alternative for wound infection. Lancet. 2000 Sep 30;356 (9236):1174.
- Robinson W. Stimulation of healing in non-healing wounds. J Bone Joint Surgery. 1935;17:267-271.
- Robinson W. Ammonium bicarbonate secreted by surgical maggots stimulates healing in purulent wounds. Am J Surg. 1940;47:111-115.
- Mumcuoglu KY, Ingber A, Gilead L, et al. Maggot therapy for the treatment of diabetic foot ulcers. Diabetes Care. 1998 Nov;21(11):2030-2031.
- Simmons S. A bactericidal principle in excretions of surgical maggots which destroys important etiological agents of pyogenic infections. J Bacteriol. 1935;30:253-267.
- Simmons S. The bactericidal properties of excretions of the maggot of Lucilia sericata. Bull Entomol Res. 1935;26:559-563.
- Mumcuoglu KY. Clinical applications for maggots in wound care. Am J Clin Dermatol. 2001;2:219-227.
- Armstrong DG, Short B, Martin BR, et al. Maggot therapy in lower extremity hospice wound care. J Am Podiatr Med Assoc. 2005;95(3):254-257.
- Robinson W, Norwood VH. The role of surgical maggots in the disinfection of osteomyelitis and other infected wounds. J Bone Joint Surgery. 1933;15:409-412.
- Robinson W, Norwood VH. Destruction of pyogenic bacteria in the alimentary tract of surgical maggots implanted in infected wounds. J Lab Clin Med. 1933;19:581-585.
- Mumcuoglu KY, Miller J, Mumcuoglu M. et al. Destruction of bacteria in the digestive tract of the maggot of Lucilia sericata (Diptera: Calliphoridae). J Med Entomol. 2001 Mar;38(2):161-166.
- Sherman RA, Hall MJ, Thomas S. Medicinal maggots: an ancient remedy for some contemporary afflictions. Annu Rev Entomol. 2000;45:55-81.
- Prete PE. Growth effects of Phaenicia sericata larval extracts on fibroblasts: mechanism for wound healing by maggot therapy. Life Sci. 1997;60(8):505-510.
- Church JCT, Courtenay M. Maggot debridement therapy for chronic wounds. Int J Low Extrem Wounds. 2002 Jun;1(2):129-134.
- Courtenay M, Church JC, Ryan TJ. Larva therapy in wound management. J R Soc Med. 2000 Feb;93:72-74.
- 34. Steenvoorde P, Oskam J. Bleeding c omplications in patients treated with maggot debridement therapy (MDT). Letter to the editor. IJLEW. 2005;4:57-58.
- Thomas S, Wynn K, Fowler T, et al. The effect of containment on the properties of sterile maggots. Br J Nurs. 2002 Jun;11(12 Suppl):S21-S22, S24, S26 passim.
- Steenvoorde P, Jacobi CE, Oskam J. Maggot debridement therapy: free-range or contained? An in-vivo study. Adv Skin Wound Care. 2005;18:430-435.
- Steenvoorde P, Oskam J. Use of larval therapy to combat infection after breast-conserving surgery. J Wound Care. 2005 May;14(5):212-213.
Despite modern wound treatment and broad-spectrum antibiotic treatment, patients with chronic wounds still exist. The appearance of antibiotic resistant bacteria, such as methicillin-resistant Staphylococcus aureus (MRSA) in the 1980s and ’90s, gave rise to a search for other remedies. One of the remedies that has been rediscovered and subsequently successfully reintroduced is maggot debridement therapy (MDT).1 The fact that more than 100 articles were published on the subject in the past two decades indicates that the use of maggots is making a strong comeback in medicine.2 In January 2004, the U.S. Food and Drug Administration (FDA) issued 510(k)#33391, allowing production and marketing of maggots as a medical device. In this article, we discuss the use of MDT in patients with a chronic wound.
A Long History of Maggot Therapy
MDT has been used in many cultures and has been known for centuries.3 Ambroise Parè is credited as the father of modern MDT. Unfortunately, no evidence can be found of Parè using maggots as a means to clean or heal wounds. The only reference is the often-cited case that occurred in 1557 at the battle of St. Quentin, when Parè observed soldiers whose wounds were covered by maggots. He mainly described the negative effects of the maggots, and, above all, believed they were spontaneously produced by the wound itself, not by the eggs of fly.4
Baron Larey (1766-1842) a famous surgeon in the army of Napoleon Bonaparte, wrote about soldiers who had larvae-infested wounds, but was frustrated that it was difficult to persuade his patients to leave the maggots in place, believing that “they promoted healing without leaving any damage.”5
The first surgeon to use MDT in patients in the hospital was the orthopedic surgeon William Baer. In the 1920s he was faced with a group of untreatable patients with severe osteomyelitis (antibiotics had not yet been discovered). He successfully treated many patients with maggots, and because of his success the therapy became regularly used in the United States.6
By 1934 more than 1,000 surgeons were using maggot therapy. Surgical Maggots were available commercially from Lederle Corporation.7 But with the introduction of antibiotics in the 1940s, the use of maggots dropped off. In the following years, case reports were published only occasionally.
The Negative Image of Maggots
A large problem of MDT is the difficulty of this type of therapy to gain acceptance in the medical community. Maggots are associated with rotting and decay. The image is of filthy, low-life creatures that are ugly and disgusting. Although a nice recent example for the general public is the scene in the movie Gladiator. The main character (played by Russell Crow) is advised to leave the maggots that spontaneously infested a wound on his shoulder in place so that the wound would heal. He leaves them in place and the wound heals without any problem, enabling Crow’s character to fight many battles.
In contrast, in an oral presentation we held recently at a Dutch scientific surgical meeting, a surgical professor in the audience said, “I will never allow those creatures in my ward.”8 This remark shows that widespread use and acceptance of MDT has not yet been reached. It seems there is still much work to do before MDT is generally accepted as a therapeutic method.
Fortunately, the negative image that seems to exist among nurses and physicians does not seem to bother patients.9 We have treated more than 100 patients in our clinic with MDT. All patients to whom we proposed MDT agreed to the therapy. All were allowed to discontinue the therapy whenever they wanted; none did. In a survey of the first 38 MDT-treated patients, 89% agreed to another session of MDT if the surgeon believed it would be beneficial, and 94% of the patients said that they would recommend it to others. This is despite the fact that the therapy was not successful in all patients (there was a below-knee of above the knee amputation-rate of 19% among patients who underwent MDT).10
Indications and Evidence
Indications and contra-indications for maggot therapy are not well defined. Some state that all kind of wounds that contain necrosis or slough can be good candidates for MDT. In our own study of 101 patients with 116 wounds treated with maggots, we had an overall success rate of 67%. (Seventy-eight out of 116 wounds had a beneficial outcome.) However, in 13 patients with septic arthritis, all wounds failed. Success rates where significantly reduced in cases of chronic limb ischemia, visible tendon or bone, and in cases of duration longer than three months before the start of MDT.11
Most physicians who start MDT use it mainly for worst-case scenarios. From our previous studies, it is clear that success rates in those patients are low. After witnessing a few failures, the physician is naturally reluctant to use it again.
What about evidence? Large randomized studies are lacking, although one containing 600 venous ulcer patients was initiated in 2004.12 There have been three randomized studies performed. Wayman, et al., have shown the cost-effectiveness of larval therapy in venous ulcers compared with hydrogel dressing.13 Contreras, et al., could not find a difference between MDT and curettage and topical silver sulfadiazine in patients with venous leg ulcers.14 At the 36th annual meeting of the European Association for the Study of Diabetes, Markevich, et al., reported on a randomized, multicenter, double-blind controlled clinical trial (n=140) for neuropathic diabetic foot lesions compared to conventional treatment. They found a significant higher percentage of granulation tissue after 10 days, compared with the hydrogel group.15 Results from large case-series indicate that MDT works and could even save limbs.2,16-18 The mechanism of action has not been unraveled yet.
Factors Influencing Effectiveness of MDT
Unfortunately, the statement made by Thomas, who said that maggot therapy works by “secreting proteolytic enzymes that break down dead tissue, turning it into a soup, which they then ingest,” still holds.19 It is known that there are mechanical effects, tissue growth effects, that direct killing of bacteria in the alimentary tract of the maggot takes place, and that maggots produce antibacterial factors.2,17,20-31
Although maggots are suitable agents for chronic wound treatment, it is likely that some wounds are more eligible than others for this type of treatment. In our opinion, all wounds that contain gangrenous or necrotic tissue with infection seem to be suited for MDT.32 Success rates of MDT reported in literature vary, but seem to be around 80% to 90%.16,17,33 In our own series, success rate is about 70%.
Patient-selection (case-mix) and method of outcome measurement play essential roles in these percentages. In our opinion, all wounds that contain necrotic tissue can be debrided effectively with MDT. However, if for example wound ischemia is the major etiologic factor, this should also be addressed. In our experience, diabetic foot, venous ulcers, traumatic ulcers, and infections after surgical procedures are all good candidates for MDT.
Absolute contraindications in our opinion are wounds close to large, uncovered blood vessels and wounds that need immediate surgical debridement (e.g., in the case of a septic patient). A relative contraindication is patients with natural of medically induced coagulopathies, but also patient preference could play a role.34 We have had very bad results with infected small joints of the foot; all wounds (n=13) eventually needed a small or large amputation.
Even the technique of application has an effect on outcome. There are two different application techniques: the free-range and the contained technique. The free-range technique is more effective in vitro and in-vivo and has become our standard application technique—not only in the outpatient department, but also in the intra-mural setting.35,36 (Figure 1, p. 16, shows a patient with a necrotic wound on the leg after radiation therapy and a surgical excision for a malignant tumor was performed.) Earlier surgical debridement combined with split skin graft failed. After four applications of maggots, the wound was free of necrosis and could be subsequently closed. (See Figure 2, p. 16.)
The contained technique is used in patients with bleeding tendencies and wounds that do not have enough healthy skin surrounding the wound; in other words, where the covering “cage” needed in case of the free-range technique can’t be applied. (This problem is shown in Figure 3, p. 16: A patient with necrotizing fasciitis of the left upper leg was treated with the contained technique—BiologiQ, Apeldoorn, Netherlands—as there is no proximal skin border. Of course, patient preference plays a role as well in the choice of application technique.37
Wound Clinic
In the Netherlands maggots can be ordered easily and are delivered within 24 hours. We started a wound clinic in 2002. First it was for MDT alone, but now the scope is broader, and we treat chronic wounds with different kind of wound therapies. We have two nurses, one nurse practitioner, one resident-surgeon, and one vascular surgeon who apply the maggots.
Patients do not need to be admitted for MDT. Fifty-nine percent of our patients are treated in the outpatient department. We are able to treat as many as 10 or 15 patients in one session, but MDT-treated patients make up only two or three patients at a time.
We found that after fast, successful biological debridement with MDT we were left with a lot of patients with red, granulating wounds that needed our attention in order to prevent relapses. In our opinion, there are many different treatment methods after MDT. Plaster casting in case of diabetic feet, secondary closure, and split skin grafting are different methods. However, other therapies like VAC-therapy and recently OASIS are promising.
At this time, all patients are prospectively followed after MDT. We are especially interested in patient selection and are now also aiming to find the ideal wound therapy after MDT. TH
Dr. Steenvoorde is a resident surgeon at Rijnland Hospital Leiderdorp, the Netherlands. van Doorn is a nurse-practitioner at Rijnland Hospital Leiderdorp. Jacobi is a senior researcher in the Medical Decision Department at Leiden University Medical Center, in the Netherlands. Dr. Oskam is a vascular surgeon at Rijnland Hospital Leiderdorp.
References
- Beasley WD, Hirst G. Making a meal of MRSA-the role of biosurgery inhospital-acquired infection. J Hosp Infect. 2004;56(1):6-9.
- Jukema GN, Menon AG, Bernards AT. et al. Amputation-sparing treatment by nature: “surgical” maggots revisited. Clin Infect Dis. 2002 Dec 15;35(12):1566-1571.
- Church JC. The traditional use of maggots in wound healing, and the development of larva therapy (biosurgery) in modern medicine. J Altern Complement Med. 1996 Winter;2(4):525-527.
- Coppi C. I dressed your wounds, God healed you—a wounded person’s psychology according to Ambroise Parè. Ostomy Wound Manage. 2005;51:62-64.
- Goldstein HI. Maggots in the treatment of wound and bone infections. J Bone Joint Surg. 1931;13:476-478.
- Baer WS. The treatment of chronic osteomyelitis with the maggot (larva of the blow fly). J Bone Joint Surg. 1931;13:438-475.
- Puckner WA. New and nonofficial remedies, surgical maggots-Lederle. J Am Med Assoc. 1932;98(5):401.
- Steenvoorde P, Doorn Lv, Jacobi CE, et al. Maggot therapy: retrospective study comparing two different application-techniques. (Dutch). Nederlands Tijdschrift voor Heelkunde. 2006;15:86.
- Contreras RJ, Fuentes SA, Karam-Orantes M, et al. Larval debridement therapy in Mexico. Wound Care Canada. 2005;3:42-46.
- Steenvoorde P, Budding TJ, Engeland Av, et al. Maggot therapy and the “yuk factor”: an issue for the patient? Wound Repair Regen. 2005 May-Jun;13(3):350-352.
- Steenvoorde P, Jacobi CA, Doorn Lv, et al. Maggot debridement therapy of infected ulcers: patient and wound factors influencing outcome. Ann Royal Coll Surg Eng. 2006.
- Raynor P, Dumville J, Cullum N. A new clinical trial of the effect of larval therapy. J Tissue Viability. 2004 Jul;14(3):104-105.
- Wayman J, Nirojogi V, Walker A, et al. The cost effectiveness of larval therapy in venous ulcers. J Tissue Viability. 2001 Jan;11(1):51.
- Contreras RJ, Fuentes SA, Arroyo ES, et al. Larval debridement therapy and infection control in venous ulcers: a comparative study. Presented at: the Second World Union of Wound Healing Societies Meeting; July 8-13, 2004.
- Markevich YO, McLeod-Roberts J, Mousley M, et al. Maggot therapy for diabetic neuropathic foot wounds: a randomized study. Presented at: the 36th Annual Meeting of the EASD; September 17-21, 2000. Ref Type: Conference Proceeding.
- Wolff H, Hansson C. Larval therapy—an effective method for ulcer debridement. Clin Exp Dermatol. 2003;28:137.
- Mumcuoglu KY, Ingber A, Gilead L, et al. Maggot therapy for the treatment of intractable wounds. Int J Dermatol. 1999 Aug;38(8):623-627.
- Courtenay M. The use of larval therapy in wound management in the UK. J Wound Care. 1999 Apr;8 (4):177-179.
- Bonn D. Maggot therapy: an alternative for wound infection. Lancet. 2000 Sep 30;356 (9236):1174.
- Robinson W. Stimulation of healing in non-healing wounds. J Bone Joint Surgery. 1935;17:267-271.
- Robinson W. Ammonium bicarbonate secreted by surgical maggots stimulates healing in purulent wounds. Am J Surg. 1940;47:111-115.
- Mumcuoglu KY, Ingber A, Gilead L, et al. Maggot therapy for the treatment of diabetic foot ulcers. Diabetes Care. 1998 Nov;21(11):2030-2031.
- Simmons S. A bactericidal principle in excretions of surgical maggots which destroys important etiological agents of pyogenic infections. J Bacteriol. 1935;30:253-267.
- Simmons S. The bactericidal properties of excretions of the maggot of Lucilia sericata. Bull Entomol Res. 1935;26:559-563.
- Mumcuoglu KY. Clinical applications for maggots in wound care. Am J Clin Dermatol. 2001;2:219-227.
- Armstrong DG, Short B, Martin BR, et al. Maggot therapy in lower extremity hospice wound care. J Am Podiatr Med Assoc. 2005;95(3):254-257.
- Robinson W, Norwood VH. The role of surgical maggots in the disinfection of osteomyelitis and other infected wounds. J Bone Joint Surgery. 1933;15:409-412.
- Robinson W, Norwood VH. Destruction of pyogenic bacteria in the alimentary tract of surgical maggots implanted in infected wounds. J Lab Clin Med. 1933;19:581-585.
- Mumcuoglu KY, Miller J, Mumcuoglu M. et al. Destruction of bacteria in the digestive tract of the maggot of Lucilia sericata (Diptera: Calliphoridae). J Med Entomol. 2001 Mar;38(2):161-166.
- Sherman RA, Hall MJ, Thomas S. Medicinal maggots: an ancient remedy for some contemporary afflictions. Annu Rev Entomol. 2000;45:55-81.
- Prete PE. Growth effects of Phaenicia sericata larval extracts on fibroblasts: mechanism for wound healing by maggot therapy. Life Sci. 1997;60(8):505-510.
- Church JCT, Courtenay M. Maggot debridement therapy for chronic wounds. Int J Low Extrem Wounds. 2002 Jun;1(2):129-134.
- Courtenay M, Church JC, Ryan TJ. Larva therapy in wound management. J R Soc Med. 2000 Feb;93:72-74.
- 34. Steenvoorde P, Oskam J. Bleeding c omplications in patients treated with maggot debridement therapy (MDT). Letter to the editor. IJLEW. 2005;4:57-58.
- Thomas S, Wynn K, Fowler T, et al. The effect of containment on the properties of sterile maggots. Br J Nurs. 2002 Jun;11(12 Suppl):S21-S22, S24, S26 passim.
- Steenvoorde P, Jacobi CE, Oskam J. Maggot debridement therapy: free-range or contained? An in-vivo study. Adv Skin Wound Care. 2005;18:430-435.
- Steenvoorde P, Oskam J. Use of larval therapy to combat infection after breast-conserving surgery. J Wound Care. 2005 May;14(5):212-213.
Despite modern wound treatment and broad-spectrum antibiotic treatment, patients with chronic wounds still exist. The appearance of antibiotic resistant bacteria, such as methicillin-resistant Staphylococcus aureus (MRSA) in the 1980s and ’90s, gave rise to a search for other remedies. One of the remedies that has been rediscovered and subsequently successfully reintroduced is maggot debridement therapy (MDT).1 The fact that more than 100 articles were published on the subject in the past two decades indicates that the use of maggots is making a strong comeback in medicine.2 In January 2004, the U.S. Food and Drug Administration (FDA) issued 510(k)#33391, allowing production and marketing of maggots as a medical device. In this article, we discuss the use of MDT in patients with a chronic wound.
A Long History of Maggot Therapy
MDT has been used in many cultures and has been known for centuries.3 Ambroise Parè is credited as the father of modern MDT. Unfortunately, no evidence can be found of Parè using maggots as a means to clean or heal wounds. The only reference is the often-cited case that occurred in 1557 at the battle of St. Quentin, when Parè observed soldiers whose wounds were covered by maggots. He mainly described the negative effects of the maggots, and, above all, believed they were spontaneously produced by the wound itself, not by the eggs of fly.4
Baron Larey (1766-1842) a famous surgeon in the army of Napoleon Bonaparte, wrote about soldiers who had larvae-infested wounds, but was frustrated that it was difficult to persuade his patients to leave the maggots in place, believing that “they promoted healing without leaving any damage.”5
The first surgeon to use MDT in patients in the hospital was the orthopedic surgeon William Baer. In the 1920s he was faced with a group of untreatable patients with severe osteomyelitis (antibiotics had not yet been discovered). He successfully treated many patients with maggots, and because of his success the therapy became regularly used in the United States.6
By 1934 more than 1,000 surgeons were using maggot therapy. Surgical Maggots were available commercially from Lederle Corporation.7 But with the introduction of antibiotics in the 1940s, the use of maggots dropped off. In the following years, case reports were published only occasionally.
The Negative Image of Maggots
A large problem of MDT is the difficulty of this type of therapy to gain acceptance in the medical community. Maggots are associated with rotting and decay. The image is of filthy, low-life creatures that are ugly and disgusting. Although a nice recent example for the general public is the scene in the movie Gladiator. The main character (played by Russell Crow) is advised to leave the maggots that spontaneously infested a wound on his shoulder in place so that the wound would heal. He leaves them in place and the wound heals without any problem, enabling Crow’s character to fight many battles.
In contrast, in an oral presentation we held recently at a Dutch scientific surgical meeting, a surgical professor in the audience said, “I will never allow those creatures in my ward.”8 This remark shows that widespread use and acceptance of MDT has not yet been reached. It seems there is still much work to do before MDT is generally accepted as a therapeutic method.
Fortunately, the negative image that seems to exist among nurses and physicians does not seem to bother patients.9 We have treated more than 100 patients in our clinic with MDT. All patients to whom we proposed MDT agreed to the therapy. All were allowed to discontinue the therapy whenever they wanted; none did. In a survey of the first 38 MDT-treated patients, 89% agreed to another session of MDT if the surgeon believed it would be beneficial, and 94% of the patients said that they would recommend it to others. This is despite the fact that the therapy was not successful in all patients (there was a below-knee of above the knee amputation-rate of 19% among patients who underwent MDT).10
Indications and Evidence
Indications and contra-indications for maggot therapy are not well defined. Some state that all kind of wounds that contain necrosis or slough can be good candidates for MDT. In our own study of 101 patients with 116 wounds treated with maggots, we had an overall success rate of 67%. (Seventy-eight out of 116 wounds had a beneficial outcome.) However, in 13 patients with septic arthritis, all wounds failed. Success rates where significantly reduced in cases of chronic limb ischemia, visible tendon or bone, and in cases of duration longer than three months before the start of MDT.11
Most physicians who start MDT use it mainly for worst-case scenarios. From our previous studies, it is clear that success rates in those patients are low. After witnessing a few failures, the physician is naturally reluctant to use it again.
What about evidence? Large randomized studies are lacking, although one containing 600 venous ulcer patients was initiated in 2004.12 There have been three randomized studies performed. Wayman, et al., have shown the cost-effectiveness of larval therapy in venous ulcers compared with hydrogel dressing.13 Contreras, et al., could not find a difference between MDT and curettage and topical silver sulfadiazine in patients with venous leg ulcers.14 At the 36th annual meeting of the European Association for the Study of Diabetes, Markevich, et al., reported on a randomized, multicenter, double-blind controlled clinical trial (n=140) for neuropathic diabetic foot lesions compared to conventional treatment. They found a significant higher percentage of granulation tissue after 10 days, compared with the hydrogel group.15 Results from large case-series indicate that MDT works and could even save limbs.2,16-18 The mechanism of action has not been unraveled yet.
Factors Influencing Effectiveness of MDT
Unfortunately, the statement made by Thomas, who said that maggot therapy works by “secreting proteolytic enzymes that break down dead tissue, turning it into a soup, which they then ingest,” still holds.19 It is known that there are mechanical effects, tissue growth effects, that direct killing of bacteria in the alimentary tract of the maggot takes place, and that maggots produce antibacterial factors.2,17,20-31
Although maggots are suitable agents for chronic wound treatment, it is likely that some wounds are more eligible than others for this type of treatment. In our opinion, all wounds that contain gangrenous or necrotic tissue with infection seem to be suited for MDT.32 Success rates of MDT reported in literature vary, but seem to be around 80% to 90%.16,17,33 In our own series, success rate is about 70%.
Patient-selection (case-mix) and method of outcome measurement play essential roles in these percentages. In our opinion, all wounds that contain necrotic tissue can be debrided effectively with MDT. However, if for example wound ischemia is the major etiologic factor, this should also be addressed. In our experience, diabetic foot, venous ulcers, traumatic ulcers, and infections after surgical procedures are all good candidates for MDT.
Absolute contraindications in our opinion are wounds close to large, uncovered blood vessels and wounds that need immediate surgical debridement (e.g., in the case of a septic patient). A relative contraindication is patients with natural of medically induced coagulopathies, but also patient preference could play a role.34 We have had very bad results with infected small joints of the foot; all wounds (n=13) eventually needed a small or large amputation.
Even the technique of application has an effect on outcome. There are two different application techniques: the free-range and the contained technique. The free-range technique is more effective in vitro and in-vivo and has become our standard application technique—not only in the outpatient department, but also in the intra-mural setting.35,36 (Figure 1, p. 16, shows a patient with a necrotic wound on the leg after radiation therapy and a surgical excision for a malignant tumor was performed.) Earlier surgical debridement combined with split skin graft failed. After four applications of maggots, the wound was free of necrosis and could be subsequently closed. (See Figure 2, p. 16.)
The contained technique is used in patients with bleeding tendencies and wounds that do not have enough healthy skin surrounding the wound; in other words, where the covering “cage” needed in case of the free-range technique can’t be applied. (This problem is shown in Figure 3, p. 16: A patient with necrotizing fasciitis of the left upper leg was treated with the contained technique—BiologiQ, Apeldoorn, Netherlands—as there is no proximal skin border. Of course, patient preference plays a role as well in the choice of application technique.37
Wound Clinic
In the Netherlands maggots can be ordered easily and are delivered within 24 hours. We started a wound clinic in 2002. First it was for MDT alone, but now the scope is broader, and we treat chronic wounds with different kind of wound therapies. We have two nurses, one nurse practitioner, one resident-surgeon, and one vascular surgeon who apply the maggots.
Patients do not need to be admitted for MDT. Fifty-nine percent of our patients are treated in the outpatient department. We are able to treat as many as 10 or 15 patients in one session, but MDT-treated patients make up only two or three patients at a time.
We found that after fast, successful biological debridement with MDT we were left with a lot of patients with red, granulating wounds that needed our attention in order to prevent relapses. In our opinion, there are many different treatment methods after MDT. Plaster casting in case of diabetic feet, secondary closure, and split skin grafting are different methods. However, other therapies like VAC-therapy and recently OASIS are promising.
At this time, all patients are prospectively followed after MDT. We are especially interested in patient selection and are now also aiming to find the ideal wound therapy after MDT. TH
Dr. Steenvoorde is a resident surgeon at Rijnland Hospital Leiderdorp, the Netherlands. van Doorn is a nurse-practitioner at Rijnland Hospital Leiderdorp. Jacobi is a senior researcher in the Medical Decision Department at Leiden University Medical Center, in the Netherlands. Dr. Oskam is a vascular surgeon at Rijnland Hospital Leiderdorp.
References
- Beasley WD, Hirst G. Making a meal of MRSA-the role of biosurgery inhospital-acquired infection. J Hosp Infect. 2004;56(1):6-9.
- Jukema GN, Menon AG, Bernards AT. et al. Amputation-sparing treatment by nature: “surgical” maggots revisited. Clin Infect Dis. 2002 Dec 15;35(12):1566-1571.
- Church JC. The traditional use of maggots in wound healing, and the development of larva therapy (biosurgery) in modern medicine. J Altern Complement Med. 1996 Winter;2(4):525-527.
- Coppi C. I dressed your wounds, God healed you—a wounded person’s psychology according to Ambroise Parè. Ostomy Wound Manage. 2005;51:62-64.
- Goldstein HI. Maggots in the treatment of wound and bone infections. J Bone Joint Surg. 1931;13:476-478.
- Baer WS. The treatment of chronic osteomyelitis with the maggot (larva of the blow fly). J Bone Joint Surg. 1931;13:438-475.
- Puckner WA. New and nonofficial remedies, surgical maggots-Lederle. J Am Med Assoc. 1932;98(5):401.
- Steenvoorde P, Doorn Lv, Jacobi CE, et al. Maggot therapy: retrospective study comparing two different application-techniques. (Dutch). Nederlands Tijdschrift voor Heelkunde. 2006;15:86.
- Contreras RJ, Fuentes SA, Karam-Orantes M, et al. Larval debridement therapy in Mexico. Wound Care Canada. 2005;3:42-46.
- Steenvoorde P, Budding TJ, Engeland Av, et al. Maggot therapy and the “yuk factor”: an issue for the patient? Wound Repair Regen. 2005 May-Jun;13(3):350-352.
- Steenvoorde P, Jacobi CA, Doorn Lv, et al. Maggot debridement therapy of infected ulcers: patient and wound factors influencing outcome. Ann Royal Coll Surg Eng. 2006.
- Raynor P, Dumville J, Cullum N. A new clinical trial of the effect of larval therapy. J Tissue Viability. 2004 Jul;14(3):104-105.
- Wayman J, Nirojogi V, Walker A, et al. The cost effectiveness of larval therapy in venous ulcers. J Tissue Viability. 2001 Jan;11(1):51.
- Contreras RJ, Fuentes SA, Arroyo ES, et al. Larval debridement therapy and infection control in venous ulcers: a comparative study. Presented at: the Second World Union of Wound Healing Societies Meeting; July 8-13, 2004.
- Markevich YO, McLeod-Roberts J, Mousley M, et al. Maggot therapy for diabetic neuropathic foot wounds: a randomized study. Presented at: the 36th Annual Meeting of the EASD; September 17-21, 2000. Ref Type: Conference Proceeding.
- Wolff H, Hansson C. Larval therapy—an effective method for ulcer debridement. Clin Exp Dermatol. 2003;28:137.
- Mumcuoglu KY, Ingber A, Gilead L, et al. Maggot therapy for the treatment of intractable wounds. Int J Dermatol. 1999 Aug;38(8):623-627.
- Courtenay M. The use of larval therapy in wound management in the UK. J Wound Care. 1999 Apr;8 (4):177-179.
- Bonn D. Maggot therapy: an alternative for wound infection. Lancet. 2000 Sep 30;356 (9236):1174.
- Robinson W. Stimulation of healing in non-healing wounds. J Bone Joint Surgery. 1935;17:267-271.
- Robinson W. Ammonium bicarbonate secreted by surgical maggots stimulates healing in purulent wounds. Am J Surg. 1940;47:111-115.
- Mumcuoglu KY, Ingber A, Gilead L, et al. Maggot therapy for the treatment of diabetic foot ulcers. Diabetes Care. 1998 Nov;21(11):2030-2031.
- Simmons S. A bactericidal principle in excretions of surgical maggots which destroys important etiological agents of pyogenic infections. J Bacteriol. 1935;30:253-267.
- Simmons S. The bactericidal properties of excretions of the maggot of Lucilia sericata. Bull Entomol Res. 1935;26:559-563.
- Mumcuoglu KY. Clinical applications for maggots in wound care. Am J Clin Dermatol. 2001;2:219-227.
- Armstrong DG, Short B, Martin BR, et al. Maggot therapy in lower extremity hospice wound care. J Am Podiatr Med Assoc. 2005;95(3):254-257.
- Robinson W, Norwood VH. The role of surgical maggots in the disinfection of osteomyelitis and other infected wounds. J Bone Joint Surgery. 1933;15:409-412.
- Robinson W, Norwood VH. Destruction of pyogenic bacteria in the alimentary tract of surgical maggots implanted in infected wounds. J Lab Clin Med. 1933;19:581-585.
- Mumcuoglu KY, Miller J, Mumcuoglu M. et al. Destruction of bacteria in the digestive tract of the maggot of Lucilia sericata (Diptera: Calliphoridae). J Med Entomol. 2001 Mar;38(2):161-166.
- Sherman RA, Hall MJ, Thomas S. Medicinal maggots: an ancient remedy for some contemporary afflictions. Annu Rev Entomol. 2000;45:55-81.
- Prete PE. Growth effects of Phaenicia sericata larval extracts on fibroblasts: mechanism for wound healing by maggot therapy. Life Sci. 1997;60(8):505-510.
- Church JCT, Courtenay M. Maggot debridement therapy for chronic wounds. Int J Low Extrem Wounds. 2002 Jun;1(2):129-134.
- Courtenay M, Church JC, Ryan TJ. Larva therapy in wound management. J R Soc Med. 2000 Feb;93:72-74.
- 34. Steenvoorde P, Oskam J. Bleeding c omplications in patients treated with maggot debridement therapy (MDT). Letter to the editor. IJLEW. 2005;4:57-58.
- Thomas S, Wynn K, Fowler T, et al. The effect of containment on the properties of sterile maggots. Br J Nurs. 2002 Jun;11(12 Suppl):S21-S22, S24, S26 passim.
- Steenvoorde P, Jacobi CE, Oskam J. Maggot debridement therapy: free-range or contained? An in-vivo study. Adv Skin Wound Care. 2005;18:430-435.
- Steenvoorde P, Oskam J. Use of larval therapy to combat infection after breast-conserving surgery. J Wound Care. 2005 May;14(5):212-213.
Pantilat Receives Endowed Chair

Increasingly, hospitals are making palliative care a priority; and more hospitalists are getting involved in providing these services and taking the lead on establishing and facilitating palliative care programs. Among the growing evidence that hospitalists are viewed as key players in the proliferation of hospital palliative care programs is the appointment of Steven Pantilat, MD, associate professor of clinical medicine, to the newly established Alan M. Kates and John M. Burnard Endowed Chair in Palliative Care at the University of California at San Francisco (UCSF).
The chair is the first palliative care chair in the University of California system and only the fifth nationwide. The endowment provides funding for salary support and efforts to build clinical, educational, research, and training components of the UCSF palliative care program. “This chair is important because hospitalists are often the main source of hospital palliative care services,” explains Dr. Pantilat. “Because I am a hospitalist, I understand the needs of these practitioners.”
Numerous Plans, Expectations
Dr. Pantilat has several expectations for what the chair will enable him to accomplish. “We hope to improve palliative care for patients, contribute to the field in terms of research and educational initiatives, and help UC advance in these areas,” he says. “Our main goal is to develop a world-class palliative care program that will advance the field in terms of education, research, and patient care and to provide the highest quality care to patients with life-threatening illness. This will provide seed money to develop educational and research programs that require some early investment when they are just ideas.”
There is a tremendous need for more and better palliative care in the hospital setting. “Patients have many needs, including management of symptoms such as shortness of breath, nausea, and fatigue,” he says. “There isn’t nearly enough research or information on these problems as compared to pain. We need more studies on the best way to treat symptoms.”
Additionally, Dr. Pantilat hopes to add to the body of literature on patient-physician communication, suggesting that hospitalists and other physicians need information about how to communicate sensitive issues such as bad news and how best to support patients and families throughout illnesses and fill their palliative care needs.
“We hope to develop and encourage more education and training on these topics,” he says. Stressing that there already are good educational programs about palliative care topics, Dr. Pantilat notes the need for more instruction specific to the unique needs of hospitalized patients and the hospitalists who care for them.
Create an Interdisciplinary System
“We need systems to provide palliative care. We also need to sensitize everyone who works in the hospital to comfort care issues,” says Dr. Pantilat, adding that there also is a need for programs and systems to ensure that patients and families will get the palliative care they need when they leave the hospital. “We need to work together to create a smooth transition from inpatient to outpatient palliative care. And we need to consider how we, as hospitalists, work with patients in the outpatient setting to ensure that someone is there to take care of them and their needs.”
Many of these needs require widespread education and training. “This grant will allow us to develop more robust and innovative educational efforts that engage ways to teach all team members about palliative care,” says Dr. Pantilat. “This will include projects such as using the Web to teach students.”
Expand the Definition
Dr. Pantilat also hopes to help expand the definition of palliative care and help people understand this as a broad concept of providing interdisciplinary care for people with terminal and chronic diseases. “An important point that we hope to emphasize is that palliative care is not just end-of-life care but something designed to improve life for people with illnesses—particularly chronic illnesses—either through the treatment of the diseases or the symptoms. It is an attempt to alleviate physical, emotional, and psychological suffering and promote the best possible quality of life,” he explains.
Helping people get “past the old limiting idea of palliative care” is another key goal. “A lot of palliative care can be provided while people are pursuing curative care,” explains Dr. Pantilat. “This is an important concept to promote.”
The Hospitalist’s Role
As a hospitalist, Dr. Pantilat also hopes to promote the growing recognition of the importance of hospitalists in palliative care programs: “The beautiful thing is that hospitalists are perfectly poised to handle palliative care programs, and with training they can become palliative care providers.”
The endowed chair reflects the importance of hospitalists in the palliative care field. “Hospitalists will be increasingly important in this area, and I hope to take a leadership role,” he says. While he is pleased and honored to have the chair at UCSF, he is confident that his work will have an impact well beyond his own university. “The chair will bring much recognition to our program but also to the field of palliative care in general and the role of hospitalists nationwide.” TH
Joanne Kaldy writes regularly for The Hospitalist.
Increasingly, hospitals are making palliative care a priority; and more hospitalists are getting involved in providing these services and taking the lead on establishing and facilitating palliative care programs. Among the growing evidence that hospitalists are viewed as key players in the proliferation of hospital palliative care programs is the appointment of Steven Pantilat, MD, associate professor of clinical medicine, to the newly established Alan M. Kates and John M. Burnard Endowed Chair in Palliative Care at the University of California at San Francisco (UCSF).
The chair is the first palliative care chair in the University of California system and only the fifth nationwide. The endowment provides funding for salary support and efforts to build clinical, educational, research, and training components of the UCSF palliative care program. “This chair is important because hospitalists are often the main source of hospital palliative care services,” explains Dr. Pantilat. “Because I am a hospitalist, I understand the needs of these practitioners.”
Numerous Plans, Expectations
Dr. Pantilat has several expectations for what the chair will enable him to accomplish. “We hope to improve palliative care for patients, contribute to the field in terms of research and educational initiatives, and help UC advance in these areas,” he says. “Our main goal is to develop a world-class palliative care program that will advance the field in terms of education, research, and patient care and to provide the highest quality care to patients with life-threatening illness. This will provide seed money to develop educational and research programs that require some early investment when they are just ideas.”
There is a tremendous need for more and better palliative care in the hospital setting. “Patients have many needs, including management of symptoms such as shortness of breath, nausea, and fatigue,” he says. “There isn’t nearly enough research or information on these problems as compared to pain. We need more studies on the best way to treat symptoms.”
Additionally, Dr. Pantilat hopes to add to the body of literature on patient-physician communication, suggesting that hospitalists and other physicians need information about how to communicate sensitive issues such as bad news and how best to support patients and families throughout illnesses and fill their palliative care needs.
“We hope to develop and encourage more education and training on these topics,” he says. Stressing that there already are good educational programs about palliative care topics, Dr. Pantilat notes the need for more instruction specific to the unique needs of hospitalized patients and the hospitalists who care for them.
Create an Interdisciplinary System
“We need systems to provide palliative care. We also need to sensitize everyone who works in the hospital to comfort care issues,” says Dr. Pantilat, adding that there also is a need for programs and systems to ensure that patients and families will get the palliative care they need when they leave the hospital. “We need to work together to create a smooth transition from inpatient to outpatient palliative care. And we need to consider how we, as hospitalists, work with patients in the outpatient setting to ensure that someone is there to take care of them and their needs.”
Many of these needs require widespread education and training. “This grant will allow us to develop more robust and innovative educational efforts that engage ways to teach all team members about palliative care,” says Dr. Pantilat. “This will include projects such as using the Web to teach students.”
Expand the Definition
Dr. Pantilat also hopes to help expand the definition of palliative care and help people understand this as a broad concept of providing interdisciplinary care for people with terminal and chronic diseases. “An important point that we hope to emphasize is that palliative care is not just end-of-life care but something designed to improve life for people with illnesses—particularly chronic illnesses—either through the treatment of the diseases or the symptoms. It is an attempt to alleviate physical, emotional, and psychological suffering and promote the best possible quality of life,” he explains.
Helping people get “past the old limiting idea of palliative care” is another key goal. “A lot of palliative care can be provided while people are pursuing curative care,” explains Dr. Pantilat. “This is an important concept to promote.”
The Hospitalist’s Role
As a hospitalist, Dr. Pantilat also hopes to promote the growing recognition of the importance of hospitalists in palliative care programs: “The beautiful thing is that hospitalists are perfectly poised to handle palliative care programs, and with training they can become palliative care providers.”
The endowed chair reflects the importance of hospitalists in the palliative care field. “Hospitalists will be increasingly important in this area, and I hope to take a leadership role,” he says. While he is pleased and honored to have the chair at UCSF, he is confident that his work will have an impact well beyond his own university. “The chair will bring much recognition to our program but also to the field of palliative care in general and the role of hospitalists nationwide.” TH
Joanne Kaldy writes regularly for The Hospitalist.
Increasingly, hospitals are making palliative care a priority; and more hospitalists are getting involved in providing these services and taking the lead on establishing and facilitating palliative care programs. Among the growing evidence that hospitalists are viewed as key players in the proliferation of hospital palliative care programs is the appointment of Steven Pantilat, MD, associate professor of clinical medicine, to the newly established Alan M. Kates and John M. Burnard Endowed Chair in Palliative Care at the University of California at San Francisco (UCSF).
The chair is the first palliative care chair in the University of California system and only the fifth nationwide. The endowment provides funding for salary support and efforts to build clinical, educational, research, and training components of the UCSF palliative care program. “This chair is important because hospitalists are often the main source of hospital palliative care services,” explains Dr. Pantilat. “Because I am a hospitalist, I understand the needs of these practitioners.”
Numerous Plans, Expectations
Dr. Pantilat has several expectations for what the chair will enable him to accomplish. “We hope to improve palliative care for patients, contribute to the field in terms of research and educational initiatives, and help UC advance in these areas,” he says. “Our main goal is to develop a world-class palliative care program that will advance the field in terms of education, research, and patient care and to provide the highest quality care to patients with life-threatening illness. This will provide seed money to develop educational and research programs that require some early investment when they are just ideas.”
There is a tremendous need for more and better palliative care in the hospital setting. “Patients have many needs, including management of symptoms such as shortness of breath, nausea, and fatigue,” he says. “There isn’t nearly enough research or information on these problems as compared to pain. We need more studies on the best way to treat symptoms.”
Additionally, Dr. Pantilat hopes to add to the body of literature on patient-physician communication, suggesting that hospitalists and other physicians need information about how to communicate sensitive issues such as bad news and how best to support patients and families throughout illnesses and fill their palliative care needs.
“We hope to develop and encourage more education and training on these topics,” he says. Stressing that there already are good educational programs about palliative care topics, Dr. Pantilat notes the need for more instruction specific to the unique needs of hospitalized patients and the hospitalists who care for them.
Create an Interdisciplinary System
“We need systems to provide palliative care. We also need to sensitize everyone who works in the hospital to comfort care issues,” says Dr. Pantilat, adding that there also is a need for programs and systems to ensure that patients and families will get the palliative care they need when they leave the hospital. “We need to work together to create a smooth transition from inpatient to outpatient palliative care. And we need to consider how we, as hospitalists, work with patients in the outpatient setting to ensure that someone is there to take care of them and their needs.”
Many of these needs require widespread education and training. “This grant will allow us to develop more robust and innovative educational efforts that engage ways to teach all team members about palliative care,” says Dr. Pantilat. “This will include projects such as using the Web to teach students.”
Expand the Definition
Dr. Pantilat also hopes to help expand the definition of palliative care and help people understand this as a broad concept of providing interdisciplinary care for people with terminal and chronic diseases. “An important point that we hope to emphasize is that palliative care is not just end-of-life care but something designed to improve life for people with illnesses—particularly chronic illnesses—either through the treatment of the diseases or the symptoms. It is an attempt to alleviate physical, emotional, and psychological suffering and promote the best possible quality of life,” he explains.
Helping people get “past the old limiting idea of palliative care” is another key goal. “A lot of palliative care can be provided while people are pursuing curative care,” explains Dr. Pantilat. “This is an important concept to promote.”
The Hospitalist’s Role
As a hospitalist, Dr. Pantilat also hopes to promote the growing recognition of the importance of hospitalists in palliative care programs: “The beautiful thing is that hospitalists are perfectly poised to handle palliative care programs, and with training they can become palliative care providers.”
The endowed chair reflects the importance of hospitalists in the palliative care field. “Hospitalists will be increasingly important in this area, and I hope to take a leadership role,” he says. While he is pleased and honored to have the chair at UCSF, he is confident that his work will have an impact well beyond his own university. “The chair will bring much recognition to our program but also to the field of palliative care in general and the role of hospitalists nationwide.” TH
Joanne Kaldy writes regularly for The Hospitalist.
Rash Judgement
A 38-year-old, healthy, incarcerated, African-American man presented with a one-and-a-half year history of an eruption in his axillae. The patient stated that the “rash” worsened with sweating but the lesions were otherwise asymptomatic.
Corticosteroid creams, antifungal creams, and oral antibiotics had not led to any improvement. The eruption progressed to involve his trunk, arms, and face. The skin exam showed hyperpigmented, firm plaques with erythematous papules in the axillae. The plaques were also present on the chest, back, and upper extremities. Verrucous papules were noted on the flexural areas of upper extremities as well as tan colored plaques at the lateral canthi of eyes. (See Figures 1-3 this page.)
CBC and serum electrolytes were normal. Lipid panel showed a cholesterol of 593 mg/dL, triglycerides 106 mg/dL, high density lipoprotein of 37 g/dL, low density lipoprotein of 535 mg/dL, and very low density lipoprotein of 21 mg/dL. A biopsy from the axilla and the umbilical area were sent for histologic examination. (See Figure 4 this page.)



What is this patient’s most likely diagnosis?
- Sarcoidosis
- Disseminated xanthomas
- Xanthoma disseminatum
- Erythema elevatum diutinum
- Necrobiosis lipoidica
Discussion
The answer is B: disseminated xanthomas. Punch biopsy from the axilla and shave biopsy from the periumbilical area both revealed localized infiltrates of lipid containing macrophages.
Xanthomas develop due to accumulation of lipid-filled macrophages and suggest an underlying disorder of lipid metabolism. Morbidity and mortality are primarily related to atherosclerosis (e.g., coronary artery disease) and pancreatitis, which occur secondarily to the increased lipid levels rather than the xanthoma itself.
In general, four clinical types of xanthomas exist: tendinous, planar, tuberous, and eruptive. A particular diagnosis cannot necessarily be made on the basis of clinical signs; however, certain types of xanthomas are more characteristic of specific hyperlipidemias. Eruptive xanthomas are found in the setting of primary or secondary hypertriglyeridemia. Tuberous xanthomas have both elevated serum cholesterol and triglycerides. This patient had plane xanthomas and xanthelasma and was especially notable for intertriginous plane xanthomas, which can be pathognomonic for homozygous familial hypercholesterolemia.
This patient’s histology from both the periumbilical area and the axilla depict the characteristic presence of vacuolated macrophages (foamy macrophages) to confirm the diagnosis as disseminated xanthoma.1-3 Sarcoidosis is a chronic idiopathic disorder characterized by noncaseating granulomas that can affect any organ system. Cutaneous sarcoidosis typically presents as asymptomatic, red-brown macules and papules affecting the face, periorbital areas, nasolabial folds, and/or extensor surfaces. Typical sarcoid lesions are characterized by the presence of circumscribed granulomas of epithelioid cells with little or no necrosis. The granulomas are characteristically referred to as “naked” due to the sparse lymphocytic infiltrate at the margins.
This patient’s histologic exam did not reveal any granulomas and localized infiltrates of lipid containing macrophages make the diagnosis of cutaneous sarcoidosis unlikely.4,5
Necrobiosis lipoidica (NL) is a cutaneous disorder that is often, but not always, associated with diabetes mellitus. NL is a disorder of collagen degeneration with a granulomatous response, thickening of blood vessel walls, and fat deposition. Patients usually present with asymptomatic shiny patches that slowly enlarge over months to years. The patient’s main complaint is the unsightly cosmetic appearance of the lesions.
Skin lesions of classic NL begin as 1- to 3-mm well-circumscribed papules or nodules that expand with an active border to become waxy, atrophic, round plaques centrally. Initially, these plaques are red-brown in color but progressively become more yellow and atrophic in appearance. Most cases of NL occur on the pretibial area, but cases have been reported on the face, scalp, trunk, and upper extremities where the diagnosis is more likely to be missed.
Although this patient’s mother had diabetes, his fasting blood glucose was well within normal limits (71 mg/dL). Histologically NL displays sclerotic collagen and obliteration of the bundle pattern, with interstitial and palisaded granulomas that involve the subcutaneous tissue and dermis. Fat containing foam cells are often present.
Although our patient’s biopsy showed fat containing foam cells, it did not have the interstitial granulomas or the sclerotic collagen. In addition, the lack of diabetes makes this diagnosis less likely.6,7
Erythema elevatum diutinum (EED) is a rare type of leukocytoclastic vasculitis characterized by red, purple, brown, or yellow papules, plaques, or nodules. These lesions are usually distributed on the extensor surfaces of the body. The lesions are usually asymptomatic but can be associated occasionally with joint pain. Clinical studies show a preference for the extensor surfaces of the hands, the wrists, the elbows, the ankles, the Achilles’ tendons, the fingers, and the toes. The buttocks, the face, and the ears as well as the palms, the soles, the legs, the forearms, and the genitals may be involved; however, the trunk is usually spared. EED is a type of necrotizing vasculitis.
In its early stages, there are no specific histologic findings that can be used to single out the diagnosis of EED from other leukocytoclastic diseases. Although the distribution and lack of symptomatology in EED is reminiscent of our patient, this patient’s lesions were more often found in the flexural areas rather than extensors. In addition, there was no necrotizing vasculitis on histology, which precludes this rare diagnosis of EED.8
Xanthoma disseminatum (XD) is a rare, benign, proliferative disorder in children and young adults characterized by xanthomatous lesions especially in the flexural folds and eyelids. Although it sounds like a disorder of lipid metabolism, it is actually a histiocytic disorder that is not associated with lipoprotein abnormalities and patients are normolipemic. Histologically, it shows mononuclear phagocyte proliferation with Touton giant cells and CD68 positivity on immunophenotyping. It is unlikely that this patient has XD despite the appropriate clinical presentation because histologically all that is found are foam cells. In addition, the patient had a definite lipoprotein abnormality while XD patients are normolipemic.9 TH
References
- Cruz PD, East C, Bergstresser P. Dermal, subcutaneous, and tendon xanthomas: diagnostic markers for specific lipoprotein disorders. J Am Acad Dermatol 1988 Jul;19(1 pt 1):95-111.
- Massengale WT, Nesbitt LT. Xanthomas. In: Bolognia JL, Jorrizo JL, Rapini RP, eds. Dermatology. Vol. 2. London: Mosby; 2003:1447-1454.
- Parker F. Xanthomas and hyperlipidemias. J Am Acad Dermatol. 1985 Jul;13 (1):1-30.
- Young RJ, 3rd, Gilson RT, Yanase D, et al. Cutaneous sarcoidosis. Int J Dermatol. 2001;40:249-253.
- English JC, Patel PJ, Greer KE. Sarcoidosis. J Am Acad Dermatol. 2001;44:725-743: quiz 744-746.
- Fitzpatrick TB, Johnson R, Wolff K, et al. Genetic, metabolic, endocrine and nutritional diseases. Color Atlas and Synopsis of Clinical Dermatology, Common and Serious Diseases. New York: McGraw-Hill; 2001:415-416.
- Lowitt MH, Dover JS. Necrobiosis lipoidica. J Am Acad Dermatol. 1991; 25:735-748.
- Yiannias JA, el-Azhary RA, Gibson LE. Erythema elevatum diutinum: a clinical and histopathologic study of 13 patients. J Am Acad Dermatol 1992 Jan;26(1):38-44.
- Alexander AS, Turner R, Uniate L, et al. Xanthoma disseminatum: a case report and literature review. Br J Radiol 2005 Feb;78(926):153-157.
A 38-year-old, healthy, incarcerated, African-American man presented with a one-and-a-half year history of an eruption in his axillae. The patient stated that the “rash” worsened with sweating but the lesions were otherwise asymptomatic.
Corticosteroid creams, antifungal creams, and oral antibiotics had not led to any improvement. The eruption progressed to involve his trunk, arms, and face. The skin exam showed hyperpigmented, firm plaques with erythematous papules in the axillae. The plaques were also present on the chest, back, and upper extremities. Verrucous papules were noted on the flexural areas of upper extremities as well as tan colored plaques at the lateral canthi of eyes. (See Figures 1-3 this page.)
CBC and serum electrolytes were normal. Lipid panel showed a cholesterol of 593 mg/dL, triglycerides 106 mg/dL, high density lipoprotein of 37 g/dL, low density lipoprotein of 535 mg/dL, and very low density lipoprotein of 21 mg/dL. A biopsy from the axilla and the umbilical area were sent for histologic examination. (See Figure 4 this page.)
What is this patient’s most likely diagnosis?
- Sarcoidosis
- Disseminated xanthomas
- Xanthoma disseminatum
- Erythema elevatum diutinum
- Necrobiosis lipoidica
Discussion
The answer is B: disseminated xanthomas. Punch biopsy from the axilla and shave biopsy from the periumbilical area both revealed localized infiltrates of lipid containing macrophages.
Xanthomas develop due to accumulation of lipid-filled macrophages and suggest an underlying disorder of lipid metabolism. Morbidity and mortality are primarily related to atherosclerosis (e.g., coronary artery disease) and pancreatitis, which occur secondarily to the increased lipid levels rather than the xanthoma itself.
In general, four clinical types of xanthomas exist: tendinous, planar, tuberous, and eruptive. A particular diagnosis cannot necessarily be made on the basis of clinical signs; however, certain types of xanthomas are more characteristic of specific hyperlipidemias. Eruptive xanthomas are found in the setting of primary or secondary hypertriglyeridemia. Tuberous xanthomas have both elevated serum cholesterol and triglycerides. This patient had plane xanthomas and xanthelasma and was especially notable for intertriginous plane xanthomas, which can be pathognomonic for homozygous familial hypercholesterolemia.
This patient’s histology from both the periumbilical area and the axilla depict the characteristic presence of vacuolated macrophages (foamy macrophages) to confirm the diagnosis as disseminated xanthoma.1-3 Sarcoidosis is a chronic idiopathic disorder characterized by noncaseating granulomas that can affect any organ system. Cutaneous sarcoidosis typically presents as asymptomatic, red-brown macules and papules affecting the face, periorbital areas, nasolabial folds, and/or extensor surfaces. Typical sarcoid lesions are characterized by the presence of circumscribed granulomas of epithelioid cells with little or no necrosis. The granulomas are characteristically referred to as “naked” due to the sparse lymphocytic infiltrate at the margins.
This patient’s histologic exam did not reveal any granulomas and localized infiltrates of lipid containing macrophages make the diagnosis of cutaneous sarcoidosis unlikely.4,5
Necrobiosis lipoidica (NL) is a cutaneous disorder that is often, but not always, associated with diabetes mellitus. NL is a disorder of collagen degeneration with a granulomatous response, thickening of blood vessel walls, and fat deposition. Patients usually present with asymptomatic shiny patches that slowly enlarge over months to years. The patient’s main complaint is the unsightly cosmetic appearance of the lesions.
Skin lesions of classic NL begin as 1- to 3-mm well-circumscribed papules or nodules that expand with an active border to become waxy, atrophic, round plaques centrally. Initially, these plaques are red-brown in color but progressively become more yellow and atrophic in appearance. Most cases of NL occur on the pretibial area, but cases have been reported on the face, scalp, trunk, and upper extremities where the diagnosis is more likely to be missed.
Although this patient’s mother had diabetes, his fasting blood glucose was well within normal limits (71 mg/dL). Histologically NL displays sclerotic collagen and obliteration of the bundle pattern, with interstitial and palisaded granulomas that involve the subcutaneous tissue and dermis. Fat containing foam cells are often present.
Although our patient’s biopsy showed fat containing foam cells, it did not have the interstitial granulomas or the sclerotic collagen. In addition, the lack of diabetes makes this diagnosis less likely.6,7
Erythema elevatum diutinum (EED) is a rare type of leukocytoclastic vasculitis characterized by red, purple, brown, or yellow papules, plaques, or nodules. These lesions are usually distributed on the extensor surfaces of the body. The lesions are usually asymptomatic but can be associated occasionally with joint pain. Clinical studies show a preference for the extensor surfaces of the hands, the wrists, the elbows, the ankles, the Achilles’ tendons, the fingers, and the toes. The buttocks, the face, and the ears as well as the palms, the soles, the legs, the forearms, and the genitals may be involved; however, the trunk is usually spared. EED is a type of necrotizing vasculitis.
In its early stages, there are no specific histologic findings that can be used to single out the diagnosis of EED from other leukocytoclastic diseases. Although the distribution and lack of symptomatology in EED is reminiscent of our patient, this patient’s lesions were more often found in the flexural areas rather than extensors. In addition, there was no necrotizing vasculitis on histology, which precludes this rare diagnosis of EED.8
Xanthoma disseminatum (XD) is a rare, benign, proliferative disorder in children and young adults characterized by xanthomatous lesions especially in the flexural folds and eyelids. Although it sounds like a disorder of lipid metabolism, it is actually a histiocytic disorder that is not associated with lipoprotein abnormalities and patients are normolipemic. Histologically, it shows mononuclear phagocyte proliferation with Touton giant cells and CD68 positivity on immunophenotyping. It is unlikely that this patient has XD despite the appropriate clinical presentation because histologically all that is found are foam cells. In addition, the patient had a definite lipoprotein abnormality while XD patients are normolipemic.9 TH
References
- Cruz PD, East C, Bergstresser P. Dermal, subcutaneous, and tendon xanthomas: diagnostic markers for specific lipoprotein disorders. J Am Acad Dermatol 1988 Jul;19(1 pt 1):95-111.
- Massengale WT, Nesbitt LT. Xanthomas. In: Bolognia JL, Jorrizo JL, Rapini RP, eds. Dermatology. Vol. 2. London: Mosby; 2003:1447-1454.
- Parker F. Xanthomas and hyperlipidemias. J Am Acad Dermatol. 1985 Jul;13 (1):1-30.
- Young RJ, 3rd, Gilson RT, Yanase D, et al. Cutaneous sarcoidosis. Int J Dermatol. 2001;40:249-253.
- English JC, Patel PJ, Greer KE. Sarcoidosis. J Am Acad Dermatol. 2001;44:725-743: quiz 744-746.
- Fitzpatrick TB, Johnson R, Wolff K, et al. Genetic, metabolic, endocrine and nutritional diseases. Color Atlas and Synopsis of Clinical Dermatology, Common and Serious Diseases. New York: McGraw-Hill; 2001:415-416.
- Lowitt MH, Dover JS. Necrobiosis lipoidica. J Am Acad Dermatol. 1991; 25:735-748.
- Yiannias JA, el-Azhary RA, Gibson LE. Erythema elevatum diutinum: a clinical and histopathologic study of 13 patients. J Am Acad Dermatol 1992 Jan;26(1):38-44.
- Alexander AS, Turner R, Uniate L, et al. Xanthoma disseminatum: a case report and literature review. Br J Radiol 2005 Feb;78(926):153-157.
A 38-year-old, healthy, incarcerated, African-American man presented with a one-and-a-half year history of an eruption in his axillae. The patient stated that the “rash” worsened with sweating but the lesions were otherwise asymptomatic.
Corticosteroid creams, antifungal creams, and oral antibiotics had not led to any improvement. The eruption progressed to involve his trunk, arms, and face. The skin exam showed hyperpigmented, firm plaques with erythematous papules in the axillae. The plaques were also present on the chest, back, and upper extremities. Verrucous papules were noted on the flexural areas of upper extremities as well as tan colored plaques at the lateral canthi of eyes. (See Figures 1-3 this page.)
CBC and serum electrolytes were normal. Lipid panel showed a cholesterol of 593 mg/dL, triglycerides 106 mg/dL, high density lipoprotein of 37 g/dL, low density lipoprotein of 535 mg/dL, and very low density lipoprotein of 21 mg/dL. A biopsy from the axilla and the umbilical area were sent for histologic examination. (See Figure 4 this page.)
What is this patient’s most likely diagnosis?
- Sarcoidosis
- Disseminated xanthomas
- Xanthoma disseminatum
- Erythema elevatum diutinum
- Necrobiosis lipoidica
Discussion
The answer is B: disseminated xanthomas. Punch biopsy from the axilla and shave biopsy from the periumbilical area both revealed localized infiltrates of lipid containing macrophages.
Xanthomas develop due to accumulation of lipid-filled macrophages and suggest an underlying disorder of lipid metabolism. Morbidity and mortality are primarily related to atherosclerosis (e.g., coronary artery disease) and pancreatitis, which occur secondarily to the increased lipid levels rather than the xanthoma itself.
In general, four clinical types of xanthomas exist: tendinous, planar, tuberous, and eruptive. A particular diagnosis cannot necessarily be made on the basis of clinical signs; however, certain types of xanthomas are more characteristic of specific hyperlipidemias. Eruptive xanthomas are found in the setting of primary or secondary hypertriglyeridemia. Tuberous xanthomas have both elevated serum cholesterol and triglycerides. This patient had plane xanthomas and xanthelasma and was especially notable for intertriginous plane xanthomas, which can be pathognomonic for homozygous familial hypercholesterolemia.
This patient’s histology from both the periumbilical area and the axilla depict the characteristic presence of vacuolated macrophages (foamy macrophages) to confirm the diagnosis as disseminated xanthoma.1-3 Sarcoidosis is a chronic idiopathic disorder characterized by noncaseating granulomas that can affect any organ system. Cutaneous sarcoidosis typically presents as asymptomatic, red-brown macules and papules affecting the face, periorbital areas, nasolabial folds, and/or extensor surfaces. Typical sarcoid lesions are characterized by the presence of circumscribed granulomas of epithelioid cells with little or no necrosis. The granulomas are characteristically referred to as “naked” due to the sparse lymphocytic infiltrate at the margins.
This patient’s histologic exam did not reveal any granulomas and localized infiltrates of lipid containing macrophages make the diagnosis of cutaneous sarcoidosis unlikely.4,5
Necrobiosis lipoidica (NL) is a cutaneous disorder that is often, but not always, associated with diabetes mellitus. NL is a disorder of collagen degeneration with a granulomatous response, thickening of blood vessel walls, and fat deposition. Patients usually present with asymptomatic shiny patches that slowly enlarge over months to years. The patient’s main complaint is the unsightly cosmetic appearance of the lesions.
Skin lesions of classic NL begin as 1- to 3-mm well-circumscribed papules or nodules that expand with an active border to become waxy, atrophic, round plaques centrally. Initially, these plaques are red-brown in color but progressively become more yellow and atrophic in appearance. Most cases of NL occur on the pretibial area, but cases have been reported on the face, scalp, trunk, and upper extremities where the diagnosis is more likely to be missed.
Although this patient’s mother had diabetes, his fasting blood glucose was well within normal limits (71 mg/dL). Histologically NL displays sclerotic collagen and obliteration of the bundle pattern, with interstitial and palisaded granulomas that involve the subcutaneous tissue and dermis. Fat containing foam cells are often present.
Although our patient’s biopsy showed fat containing foam cells, it did not have the interstitial granulomas or the sclerotic collagen. In addition, the lack of diabetes makes this diagnosis less likely.6,7
Erythema elevatum diutinum (EED) is a rare type of leukocytoclastic vasculitis characterized by red, purple, brown, or yellow papules, plaques, or nodules. These lesions are usually distributed on the extensor surfaces of the body. The lesions are usually asymptomatic but can be associated occasionally with joint pain. Clinical studies show a preference for the extensor surfaces of the hands, the wrists, the elbows, the ankles, the Achilles’ tendons, the fingers, and the toes. The buttocks, the face, and the ears as well as the palms, the soles, the legs, the forearms, and the genitals may be involved; however, the trunk is usually spared. EED is a type of necrotizing vasculitis.
In its early stages, there are no specific histologic findings that can be used to single out the diagnosis of EED from other leukocytoclastic diseases. Although the distribution and lack of symptomatology in EED is reminiscent of our patient, this patient’s lesions were more often found in the flexural areas rather than extensors. In addition, there was no necrotizing vasculitis on histology, which precludes this rare diagnosis of EED.8
Xanthoma disseminatum (XD) is a rare, benign, proliferative disorder in children and young adults characterized by xanthomatous lesions especially in the flexural folds and eyelids. Although it sounds like a disorder of lipid metabolism, it is actually a histiocytic disorder that is not associated with lipoprotein abnormalities and patients are normolipemic. Histologically, it shows mononuclear phagocyte proliferation with Touton giant cells and CD68 positivity on immunophenotyping. It is unlikely that this patient has XD despite the appropriate clinical presentation because histologically all that is found are foam cells. In addition, the patient had a definite lipoprotein abnormality while XD patients are normolipemic.9 TH
References
- Cruz PD, East C, Bergstresser P. Dermal, subcutaneous, and tendon xanthomas: diagnostic markers for specific lipoprotein disorders. J Am Acad Dermatol 1988 Jul;19(1 pt 1):95-111.
- Massengale WT, Nesbitt LT. Xanthomas. In: Bolognia JL, Jorrizo JL, Rapini RP, eds. Dermatology. Vol. 2. London: Mosby; 2003:1447-1454.
- Parker F. Xanthomas and hyperlipidemias. J Am Acad Dermatol. 1985 Jul;13 (1):1-30.
- Young RJ, 3rd, Gilson RT, Yanase D, et al. Cutaneous sarcoidosis. Int J Dermatol. 2001;40:249-253.
- English JC, Patel PJ, Greer KE. Sarcoidosis. J Am Acad Dermatol. 2001;44:725-743: quiz 744-746.
- Fitzpatrick TB, Johnson R, Wolff K, et al. Genetic, metabolic, endocrine and nutritional diseases. Color Atlas and Synopsis of Clinical Dermatology, Common and Serious Diseases. New York: McGraw-Hill; 2001:415-416.
- Lowitt MH, Dover JS. Necrobiosis lipoidica. J Am Acad Dermatol. 1991; 25:735-748.
- Yiannias JA, el-Azhary RA, Gibson LE. Erythema elevatum diutinum: a clinical and histopathologic study of 13 patients. J Am Acad Dermatol 1992 Jan;26(1):38-44.
- Alexander AS, Turner R, Uniate L, et al. Xanthoma disseminatum: a case report and literature review. Br J Radiol 2005 Feb;78(926):153-157.
Shift Perspectives
The shifts worked by a hospital medicine group can reflect its values or simply ensure adequate coverage. Either way, the shifts your group assigns can play a significant role in recruiting new hospitalists and retaining those you have. And there may be more scheduling options than you have considered.
The Most Attractive Shift Debunked
Many new hospitalists seek as much time off as possible, and there are plenty of groups catering to that desire. “Most physicians prefer time off, and seven on, seven off is attractive in recruiting new people to your practice—but it strikes me as a poisonous way to work,” says John Nelson, MD, co-founder of SHM, medical director of the hospitalist practice at Overlake Hospital in Bellevue, Wash., and author of the “Practice Management” column in The Hospitalist. Dr. Nelson acts as a consultant to hospitalist practices around the country and has written articles and given presentations on the topic of scheduling for hospital medicine groups.
Dr. Nelson understands the attractions of working seven on, seven off—particularly for young physicians. “Even seven on is not as bad as being an intern; it’s easier than they were used to in their residency,” he says. “But I worry this schedule might increase burnout and resentment of work. It’s asystole/diastole lifestyle and may not be a healthy way to organize your life or your career.”
An Alternative Scheduling Idea
Dr. Nelson has his own unique ideas of how a group’s shift assignments should work to ensure better coverage and keep hospitalists happy. His ideas are not just theories—his own group lives and works by a flexible arrangement.
Their schedule is partly dictated by a desire to keep the physicians happy and healthy. “I believe a constant mix of work and the rest of your life is best,” says Dr. Nelson. “You shouldn’t have to put the rest of your life into the seven days that you’re off.”
So Dr. Nelson’s practice allows considerable flexibility to each physician, but ensures that any given workday is shorter than 12 hours. “I think it’s better not to have a rigidly repeating schedule,” he explains.
Dr. Nelson’s group uses pagers to ensure a hospitalist is always available during coverage hours, but they don’t adhere to a strict schedule. “So many groups work specified shifts, whether it’s 10 or 12 hours, and I think there’s a better idea,” he says. “If everyone has to punch a clock, it interferes with flexibility. I would not tell doctors when to start or stop.”
Of course, as a group, someone has to be available for emergencies all the time, and physicians may need to start daily rounds to write most discharge orders by a certain time. “I have a pager on by 7 a.m., but nothing says I have to be in the hospital by 7 a.m.,” says Dr. Nelson. “It’s often in my interest to start rounding earlier than 7 a.m. so that I can finish earlier or have time for a break later in the day.”
Greater Flexibility = Better Coverage
Another benefit to moving to shorter, more flexible days is ensuring adequate coverage. “Rigidly defined shifts almost never precisely match the day’s workload,” points out Dr. Nelson. Therefore, his practice boosts staffing to cover busy periods. “My recommendation is to intentionally overstaff for the average day’s workload. When it’s busy, everyone can pitch in and work an extra one or two hours.”
If it’s not busy, one or more doctors may leave early. “This is nimble and responsive to the day-to-day workload,” says Dr. Nelson.
To move from a seven on, seven off schedule to this model, Dr. Nelson recommends that every doctor in the practice work 30 to 40 more days annually. A seven on, seven off schedule would have a physician work 182.5 days per year; if you decrease the hours per day and boost the number of working days to 220 a year, your physicians will be working the same number of hours, but in shorter days—even if the practice workload stays the same and each individual doctor’s annual productivity stays the same.
“It’s more realistic to work more days when they’re not so grueling,” says Dr. Nelson. “Plus, you have a built-in capacity to meet a sudden increase in workload. Imagine an eight-man group, where four doctors each work 12-hour shifts. Now imagine that instead of four, you get a fifth doctor to show up every day. [You can get this fifth doctor without adding staff if each doctor works more days annually.] When a day is unpredictably busy, the physicians won’t be absolutely overwhelmed. If it’s not busy, you can send someone home early. You get a lot more flexibility.”
For a hospital medicine group, implementing a flexible schedule such as this generally requires payment for production, which ties individual physicians into the economic health of their group. Compensation matches workload, allowing individual physicians to work to their values—more money or more free time.
“I think it’s better to pay on production,” says Dr. Nelson. “That way each person has the opportunity to choose. If one values money, he can volunteer to stay and work more and make more money. Each works to their own sweet spot, whereas a seven on, seven off schedule with rigidly defined shifts forces everyone to do the same thing.”
Physicians working on a flexible schedule still need to get their work finished each day, but they have more autonomy in how and when they get it done. “Doctors who work fast can go home early; physicians can decide for themselves the right balance for spending time each patient,” says Dr. Nelson. “As long as they understand there are economic consequences … and act with reasonableness. In our group, we get the work done. There’s no official start or stop time. Each of us chooses an individual work style. There are boundaries; the work needs to be done. There are costs as well, but I believe this system is healthy and liberating.” TH
Jane Jerrard regularly writes “Career Development.”
The shifts worked by a hospital medicine group can reflect its values or simply ensure adequate coverage. Either way, the shifts your group assigns can play a significant role in recruiting new hospitalists and retaining those you have. And there may be more scheduling options than you have considered.
The Most Attractive Shift Debunked
Many new hospitalists seek as much time off as possible, and there are plenty of groups catering to that desire. “Most physicians prefer time off, and seven on, seven off is attractive in recruiting new people to your practice—but it strikes me as a poisonous way to work,” says John Nelson, MD, co-founder of SHM, medical director of the hospitalist practice at Overlake Hospital in Bellevue, Wash., and author of the “Practice Management” column in The Hospitalist. Dr. Nelson acts as a consultant to hospitalist practices around the country and has written articles and given presentations on the topic of scheduling for hospital medicine groups.
Dr. Nelson understands the attractions of working seven on, seven off—particularly for young physicians. “Even seven on is not as bad as being an intern; it’s easier than they were used to in their residency,” he says. “But I worry this schedule might increase burnout and resentment of work. It’s asystole/diastole lifestyle and may not be a healthy way to organize your life or your career.”
An Alternative Scheduling Idea
Dr. Nelson has his own unique ideas of how a group’s shift assignments should work to ensure better coverage and keep hospitalists happy. His ideas are not just theories—his own group lives and works by a flexible arrangement.
Their schedule is partly dictated by a desire to keep the physicians happy and healthy. “I believe a constant mix of work and the rest of your life is best,” says Dr. Nelson. “You shouldn’t have to put the rest of your life into the seven days that you’re off.”
So Dr. Nelson’s practice allows considerable flexibility to each physician, but ensures that any given workday is shorter than 12 hours. “I think it’s better not to have a rigidly repeating schedule,” he explains.
Dr. Nelson’s group uses pagers to ensure a hospitalist is always available during coverage hours, but they don’t adhere to a strict schedule. “So many groups work specified shifts, whether it’s 10 or 12 hours, and I think there’s a better idea,” he says. “If everyone has to punch a clock, it interferes with flexibility. I would not tell doctors when to start or stop.”
Of course, as a group, someone has to be available for emergencies all the time, and physicians may need to start daily rounds to write most discharge orders by a certain time. “I have a pager on by 7 a.m., but nothing says I have to be in the hospital by 7 a.m.,” says Dr. Nelson. “It’s often in my interest to start rounding earlier than 7 a.m. so that I can finish earlier or have time for a break later in the day.”
Greater Flexibility = Better Coverage
Another benefit to moving to shorter, more flexible days is ensuring adequate coverage. “Rigidly defined shifts almost never precisely match the day’s workload,” points out Dr. Nelson. Therefore, his practice boosts staffing to cover busy periods. “My recommendation is to intentionally overstaff for the average day’s workload. When it’s busy, everyone can pitch in and work an extra one or two hours.”
If it’s not busy, one or more doctors may leave early. “This is nimble and responsive to the day-to-day workload,” says Dr. Nelson.
To move from a seven on, seven off schedule to this model, Dr. Nelson recommends that every doctor in the practice work 30 to 40 more days annually. A seven on, seven off schedule would have a physician work 182.5 days per year; if you decrease the hours per day and boost the number of working days to 220 a year, your physicians will be working the same number of hours, but in shorter days—even if the practice workload stays the same and each individual doctor’s annual productivity stays the same.
“It’s more realistic to work more days when they’re not so grueling,” says Dr. Nelson. “Plus, you have a built-in capacity to meet a sudden increase in workload. Imagine an eight-man group, where four doctors each work 12-hour shifts. Now imagine that instead of four, you get a fifth doctor to show up every day. [You can get this fifth doctor without adding staff if each doctor works more days annually.] When a day is unpredictably busy, the physicians won’t be absolutely overwhelmed. If it’s not busy, you can send someone home early. You get a lot more flexibility.”
For a hospital medicine group, implementing a flexible schedule such as this generally requires payment for production, which ties individual physicians into the economic health of their group. Compensation matches workload, allowing individual physicians to work to their values—more money or more free time.
“I think it’s better to pay on production,” says Dr. Nelson. “That way each person has the opportunity to choose. If one values money, he can volunteer to stay and work more and make more money. Each works to their own sweet spot, whereas a seven on, seven off schedule with rigidly defined shifts forces everyone to do the same thing.”
Physicians working on a flexible schedule still need to get their work finished each day, but they have more autonomy in how and when they get it done. “Doctors who work fast can go home early; physicians can decide for themselves the right balance for spending time each patient,” says Dr. Nelson. “As long as they understand there are economic consequences … and act with reasonableness. In our group, we get the work done. There’s no official start or stop time. Each of us chooses an individual work style. There are boundaries; the work needs to be done. There are costs as well, but I believe this system is healthy and liberating.” TH
Jane Jerrard regularly writes “Career Development.”
The shifts worked by a hospital medicine group can reflect its values or simply ensure adequate coverage. Either way, the shifts your group assigns can play a significant role in recruiting new hospitalists and retaining those you have. And there may be more scheduling options than you have considered.
The Most Attractive Shift Debunked
Many new hospitalists seek as much time off as possible, and there are plenty of groups catering to that desire. “Most physicians prefer time off, and seven on, seven off is attractive in recruiting new people to your practice—but it strikes me as a poisonous way to work,” says John Nelson, MD, co-founder of SHM, medical director of the hospitalist practice at Overlake Hospital in Bellevue, Wash., and author of the “Practice Management” column in The Hospitalist. Dr. Nelson acts as a consultant to hospitalist practices around the country and has written articles and given presentations on the topic of scheduling for hospital medicine groups.
Dr. Nelson understands the attractions of working seven on, seven off—particularly for young physicians. “Even seven on is not as bad as being an intern; it’s easier than they were used to in their residency,” he says. “But I worry this schedule might increase burnout and resentment of work. It’s asystole/diastole lifestyle and may not be a healthy way to organize your life or your career.”
An Alternative Scheduling Idea
Dr. Nelson has his own unique ideas of how a group’s shift assignments should work to ensure better coverage and keep hospitalists happy. His ideas are not just theories—his own group lives and works by a flexible arrangement.
Their schedule is partly dictated by a desire to keep the physicians happy and healthy. “I believe a constant mix of work and the rest of your life is best,” says Dr. Nelson. “You shouldn’t have to put the rest of your life into the seven days that you’re off.”
So Dr. Nelson’s practice allows considerable flexibility to each physician, but ensures that any given workday is shorter than 12 hours. “I think it’s better not to have a rigidly repeating schedule,” he explains.
Dr. Nelson’s group uses pagers to ensure a hospitalist is always available during coverage hours, but they don’t adhere to a strict schedule. “So many groups work specified shifts, whether it’s 10 or 12 hours, and I think there’s a better idea,” he says. “If everyone has to punch a clock, it interferes with flexibility. I would not tell doctors when to start or stop.”
Of course, as a group, someone has to be available for emergencies all the time, and physicians may need to start daily rounds to write most discharge orders by a certain time. “I have a pager on by 7 a.m., but nothing says I have to be in the hospital by 7 a.m.,” says Dr. Nelson. “It’s often in my interest to start rounding earlier than 7 a.m. so that I can finish earlier or have time for a break later in the day.”
Greater Flexibility = Better Coverage
Another benefit to moving to shorter, more flexible days is ensuring adequate coverage. “Rigidly defined shifts almost never precisely match the day’s workload,” points out Dr. Nelson. Therefore, his practice boosts staffing to cover busy periods. “My recommendation is to intentionally overstaff for the average day’s workload. When it’s busy, everyone can pitch in and work an extra one or two hours.”
If it’s not busy, one or more doctors may leave early. “This is nimble and responsive to the day-to-day workload,” says Dr. Nelson.
To move from a seven on, seven off schedule to this model, Dr. Nelson recommends that every doctor in the practice work 30 to 40 more days annually. A seven on, seven off schedule would have a physician work 182.5 days per year; if you decrease the hours per day and boost the number of working days to 220 a year, your physicians will be working the same number of hours, but in shorter days—even if the practice workload stays the same and each individual doctor’s annual productivity stays the same.
“It’s more realistic to work more days when they’re not so grueling,” says Dr. Nelson. “Plus, you have a built-in capacity to meet a sudden increase in workload. Imagine an eight-man group, where four doctors each work 12-hour shifts. Now imagine that instead of four, you get a fifth doctor to show up every day. [You can get this fifth doctor without adding staff if each doctor works more days annually.] When a day is unpredictably busy, the physicians won’t be absolutely overwhelmed. If it’s not busy, you can send someone home early. You get a lot more flexibility.”
For a hospital medicine group, implementing a flexible schedule such as this generally requires payment for production, which ties individual physicians into the economic health of their group. Compensation matches workload, allowing individual physicians to work to their values—more money or more free time.
“I think it’s better to pay on production,” says Dr. Nelson. “That way each person has the opportunity to choose. If one values money, he can volunteer to stay and work more and make more money. Each works to their own sweet spot, whereas a seven on, seven off schedule with rigidly defined shifts forces everyone to do the same thing.”
Physicians working on a flexible schedule still need to get their work finished each day, but they have more autonomy in how and when they get it done. “Doctors who work fast can go home early; physicians can decide for themselves the right balance for spending time each patient,” says Dr. Nelson. “As long as they understand there are economic consequences … and act with reasonableness. In our group, we get the work done. There’s no official start or stop time. Each of us chooses an individual work style. There are boundaries; the work needs to be done. There are costs as well, but I believe this system is healthy and liberating.” TH
Jane Jerrard regularly writes “Career Development.”
SHM Surveys Revisited
The Benchmarks Committee has had a busy 2006 so far. Many thanks to the 400-plus hospital medicine groups that completed the 2005-06 SHM survey, “The Authoritative Source on the State of Hospital Medicine,” as well as those of you who participated in the follow-up survey to clarify questions around additional revenue or supplements to program income.
We had some behind-the-scenes work on the survey. After the first pass of data analysis, it became clear that there was something amiss with the responses pertaining to the supplemental income questions. Only 47% of programs reported that they received additional income from hospitals or other sources. This seemed incompatible with what we know about current payment rates for fee-for-service work. A quick discussion took place among the committee and we decided to resurvey the group with more precise questions on exactly how finances flow into a program. As you have seen, the additional results bore out our suspicions. With the revised survey tool, 97% of the programs (when re-queried) reported receiving income above and beyond fees from direct patient care.
It was a Herculean task of digesting and formatting the data into usable form. SHM Senior Vice President Joe Miller deserves many thanks for poring through the data and creating something that all of you can use to better your programs.
Now, a few words about the recent annual meeting in Washington, DC: The work of the Benchmarks Committee was highlighted by SHM CEO Larry Wellikson, MD, in a plenary session on the first day of the meeting. An insightful panel discussion followed in which panel members Bob Wachter, MD (representing academic hospital medicine), Mary Jo Gorman, MD (corporate hospital medicine), and John Nelson, MD (community hospital medicine) gave some insightful commentary on the results of the survey and then fielded questions from the audience.
In between sessions at the conference, the committee held its annual face-to-face meeting and discussed plans for the year.
Under the guidance and editorial excellence of committee member Leslie Flores, the Benchmarks Committee continues to make strong progress with the dashboard project. As you may recall, this project will document and describe 10 commonly used dashboard metrics, including sample reports. There are plans for this material to be published as a supplement to The Hospitalist later this year.
The committee discussed the type of surveys conducted by SHM. A recommendation came out of our meeting to change from large-scale, all-encompassing, biannual surveys to smaller annual surveys. The annual survey would alternate its focus every other year between evaluating individuals’ productivity and compensation, and the characteristics of hospital medicine groups. Each survey would also have the flexibility to address specific timely questions that might focus on a specific research or hot topic of the day. The goal is to get our first trial survey out by the end of 2006, which would focus on group characteristics.
Lastly, a big thank you to our outgoing chairperson, Teresa Jones. Her hard work and organizational skills are going to be a tough act to follow.
Dr. Kealey is chair of SHM’s Benchmarks Committee
Advocacy Day Educates Lawmakers about Hospital Medicine
By Eric Siegal, MD
As reported in the SHM Meeting Reporter (see July The Hospitalist, supplement 1), SHM’s first Legislative Advocacy Day was an overwhelming success. More than 70 members from 29 states visited Capitol Hill on May 3 to educate lawmakers and their staffs about hospital medicine and SHM’s proposals to improve the quality of care in our nation’s hospitals.
Advocacy Day participants attended a morning briefing that covered procedural tips on how to have a successful meeting and the health issues currently before Congress—and SHM’s positions—before leaving for previously scheduled appointments on Capitol Hill.
Once there, hospitalists took time to educate legislators and their staff members about the fastest growing medical specialty in the United States, and then turned to SHM’s recommendations for improving the quality, safety, and cost-effectiveness of inpatient medical care.
Among the issues discussed with lawmakers: the need for more funding for the Agency for Healthcare Research and Quality (AHRQ); SHM support for federal initiatives to measure resource use and improve quality, including a CMS demonstration project to assess the contributions of hospital medicine programs to improve patient care and more efficient management of hospital resources; and the importance of gainsharing demonstration projects that focus on inpatient medical services such as those provided by hospital medicine programs.
More than 130 appointments were scheduled with House and Senate offices, many with members of Congress who sit on the key health committees with jurisdiction over Medicare as well as on committees responsible for determining funding levels for the National Institutes of Health, the CDC, and the Agency for Healthcare Research and Quality.
SHM encourages those of you who participated in Advocacy Day to thank the lawmakers and staff with whom you visited (view the sample thank-you letter and instructions online at www.hospitalmedicine.org under “Advocacy & Policy”).
Advocacy Day opened doors to congressional offices; follow-up from SHM members will keep hospital medicine’s issues before lawmakers as they vote on legislation of importance to our specialty. The more SHM members interact with members of Congress and their staff, the louder our voices and the more effective our messages. Advocacy Day is just the beginning of regular contact by hospitalists with their elected representatives in Washington.
A New Way to Get Everything SHM
SHM has launched the SHM Store, a new Internet-based marketplace that will redefine the way SHM educational products and apparel are distributed. The online store will be a convenient option for hectic lifestyles because it will be open 24 hours a day and can be accessed from anywhere there is an Internet connection.
The SHM Store is user-friendly and allows you to easily and quickly purchase the quality products and apparel that you have come to expect from SHM. Apparel and accessories include men’s and women’s wind jackets, golf shirts, scrub tops, baseball caps, and lapel pins—all with the SHM logo.
You’ll also find the most up-to-date educational materials from SHM. The 2005-2006 results of the SHM survey, “The Authoritative Source on the State of Hospital Medicine,” can be ordered in CD and print format. The Practice Management Course CD with binder is also available. This combination package includes all of the materials distributed at an onsite presentation of the course. And, last but not least, get your very own copy or additional copies of The Core Competencies in Hospital Medicine: A Framework For Curriculum Development.
The ordering process is simple. Access the SHM Store at www.hospitalmedicine.org/shmstore or navigate from www.hospitalmedicine.org and click on SHM Store. The store allows you to browse available products and descriptions. When you see something you want, select the quantity you’d like to purchase and add the items to your shopping cart. Once you have completed your shopping trip, click “Check Out.” A confirmation of your transaction will be sent to your e-mail inbox and your products will be shipped to your attention.
It’s that easy. Make sure you go online to browse the new SHM Store. If you have any questions or would like to learn more about the SHM Store, contact SHM at CustomerService@hospitalmedicine. org.
SHM, Health Groups Urge House to Boost Discretionary Funding
SHM joined more than 800 health, education, and labor organizations in writing a May 8 letter to the House leadership. Organized by the Coalition for Health Funding and the Committee on Education Funding, the letter calls on Congress to add $7 billion to the budget in discretionary funding for health, education, and labor programs. It asks lawmakers to ensure that the final allocation for the House and Senate Labor, Health and Human Services, Education Appropriations Subcommittees reflects a $7 billion increase above the President’s request for these critically important programs in FY 2007.
“While our organizations represent a wide array of domestic priorities,” the letter states, “we are united in our effort to advance the bipartisan goal of adding $7 billion in discretionary funding for health, education, labor enforcement, job training, and social services programs as the budget process moves forward. On behalf of our millions of constituents, we strongly urge you to provide at least $7 billion in additional federal support to restore funding levels to FY 2005. This is essential to sustain the well-being and prosperity of our nation.”
Agencies whose funding could be boosted by the additional spending called for in the coalition letter include the Agency for Healthcare Research and Quality, the National Institutes of Health, and the Centers for Disease Control and Prevention.
For full coverage of May 2006 advocacy and policy news, visit www.hospitalmedicine.org. TH
Dr. Siegal is chair of SHM’s Public Policy Committee.
SHM: BEHIND THE SCENES
Education and Quality Initiatives: SHM’s Heart and Soul
By Geri Barnes

This month’s SHM staff article highlights the department responsible for SHM’s education and quality initiatives. While my fellow senior managers may disagree, I believe that we are the heart and soul of SHM in meeting members’ needs. So important is this organizational focus that the Education Committee, chaired by Preetha Basaviah, MD, has its own mission, which parallels and provides detail to the organizational mission of promoting excellence in the practice of hospital medicine. And the Hospital Quality and Patient Safety Committee, chaired by Mahalakshmi Halasyamani, MD, is one of the most dynamic and prolific of SHM’s committees.
We know that members join SHM for the opportunity to effect change and network with colleagues. Equally strong is the quest for educational resources that will facilitate their efforts in improving quality inpatient care. SHM’s education plan focuses and organizes our energy on developing those resources.
SHM’s resources come in many forms. The most visible is our annual meeting. By all accounts, the 2006 annual meeting was extremely successful. It was our largest meeting to date, with almost 1,200 attendees, 99% of whom were members. That number represents more than 21% of our total membership. I wonder how many other organizations can boast of such a high percentage of member attendance at their annual meeting. The attendees actively participated in the educational sessions and the Research, Innovations, and Clinical Vignettes poster session, visited the exhibits, and networked during breaks and social events. To enhance the educational experience, we created a password-protected Web site where registrants could access the handouts for sessions they planned to attend. Because of the value of these materials, we are currently determining ways to utilize the handouts to expand our educational resources.
For several years, SHM has presented the Leadership Academy and “Best Practices in Managing a Hospital Medicine Program” course. These courses are so popular that they have become a mainstay of SHM educational programs and are offered on an annual basis. In September we will present the first Level II Leadership Academy designed to build upon and expand Leadership Academy I. Additionally, “Fundamentals in Billing and Coding” a pre-course to the University of California San Francisco “Management of the Hospitalized Patient” course will be offered in October for the first time. This outgrowth of the Best Practices course was identified as a need by attendees and other members. We anticipate that we will continue to offer these important programs for many years to come.
While we reach a significant number of hospitalists and other healthcare providers through our annual meeting and other face-to-face meetings, we reach many more through other educational and quality improvement efforts. Hospitalists, in their unique role as providers responsible for the general medical care of hospitalized patients, find themselves filling roles as key players and drivers of institutional quality improvement. To aid them in this effort, we’ve developed Web-based resource rooms designed to facilitate the implementation of a quality improvement program for specific disease state/clinical condition, including antimicrobial resistance, stroke, venous thromboembolism, and heart failure. Resource rooms on glycemic control and discharge planning are currently under development.
For most resource rooms, the key is the QI Workbook, a resource built on proven principles of quality improvement, personal experiences, and evidence-based medicine. Resources in addition to the workbook include slide sets that can be used in training sessions, “Teaching Pearls,” patient education resources, and clinical tools in the form of algorithms, order sets, and discharge planning sheets. Most of the resource rooms have online CME programs and each room has a well-developed bibliography.
What will likely prove to be SHM’s most far-reaching resource is The Core Competencies in Hospital Medicine: A Framework For Curriculum Development. Published earlier this year as a supplement to the Journal of Hospital Medicine, the Core Competencies provides a structure for professional and curricular development based on a shared understanding of the essential knowledge, skills, and attitudes expected of physicians working as hospitalists. While the target audience is the directors of hospitalist programs and fellowships and residency programs (and medical school internal medicine clerkships), imagine the number of people reached when the Core Competencies touch hospitalist students across the board. Additionally, the Core Competencies are the focal point for every educational and quality improvement initiative that we undertake. This document will continue to drive the content of each annual meeting, provide direction for the organization, and help us prioritize the development of resources rooms and other educational and quality improvement resources.
SHM is lucky to have partners who understand the importance of hospitalists as key members of the multidisciplinary team and the army that will lead the charge in implementing protocols to improve patient care. From foundations and sister associations, to government and industry, we partner with organizations that appreciate the role that hospitalists play in improving the healthcare system. The partnerships have led to the development of toolkits, resource rooms, CME modules, and other important resources. New initiatives soon to be launched are mentored implementation programs and demonstration projects that will provide us with increased knowledge of how our resources are used and identify areas in which they can be improved.
What is required on a staff level to make this happen? A commitment to do whatever it takes to get the job done. Six of us are equally dedicated to leading, managing, and supporting these efforts. In addition to me, staff members Tina Budnitz, Erica Pearson, Joy Wittnebert, Lillian Higgins, and Theresa Jones chart new ground and are actively engaged in a dynamic learning process on a daily basis. But it is our members and experts that drive this process, and we are grateful for their patience and guidance.
The Education and Quality Initiatives staff members do not work in a vacuum in the national office. We have the support and brainpower of the rest of the staff, with whom we collaborate daily. Membership and marketing, information technology, and business operations staff all play a role in our success.
What makes the national office run as a well-oiled machine? Next month you’ll hear from Steve Poitras, director, Business Operations, who is instrumental in making that happen.
Barnes is director, Education & Quality Initiatives, for SHM.
The Benchmarks Committee has had a busy 2006 so far. Many thanks to the 400-plus hospital medicine groups that completed the 2005-06 SHM survey, “The Authoritative Source on the State of Hospital Medicine,” as well as those of you who participated in the follow-up survey to clarify questions around additional revenue or supplements to program income.
We had some behind-the-scenes work on the survey. After the first pass of data analysis, it became clear that there was something amiss with the responses pertaining to the supplemental income questions. Only 47% of programs reported that they received additional income from hospitals or other sources. This seemed incompatible with what we know about current payment rates for fee-for-service work. A quick discussion took place among the committee and we decided to resurvey the group with more precise questions on exactly how finances flow into a program. As you have seen, the additional results bore out our suspicions. With the revised survey tool, 97% of the programs (when re-queried) reported receiving income above and beyond fees from direct patient care.
It was a Herculean task of digesting and formatting the data into usable form. SHM Senior Vice President Joe Miller deserves many thanks for poring through the data and creating something that all of you can use to better your programs.
Now, a few words about the recent annual meeting in Washington, DC: The work of the Benchmarks Committee was highlighted by SHM CEO Larry Wellikson, MD, in a plenary session on the first day of the meeting. An insightful panel discussion followed in which panel members Bob Wachter, MD (representing academic hospital medicine), Mary Jo Gorman, MD (corporate hospital medicine), and John Nelson, MD (community hospital medicine) gave some insightful commentary on the results of the survey and then fielded questions from the audience.
In between sessions at the conference, the committee held its annual face-to-face meeting and discussed plans for the year.
Under the guidance and editorial excellence of committee member Leslie Flores, the Benchmarks Committee continues to make strong progress with the dashboard project. As you may recall, this project will document and describe 10 commonly used dashboard metrics, including sample reports. There are plans for this material to be published as a supplement to The Hospitalist later this year.
The committee discussed the type of surveys conducted by SHM. A recommendation came out of our meeting to change from large-scale, all-encompassing, biannual surveys to smaller annual surveys. The annual survey would alternate its focus every other year between evaluating individuals’ productivity and compensation, and the characteristics of hospital medicine groups. Each survey would also have the flexibility to address specific timely questions that might focus on a specific research or hot topic of the day. The goal is to get our first trial survey out by the end of 2006, which would focus on group characteristics.
Lastly, a big thank you to our outgoing chairperson, Teresa Jones. Her hard work and organizational skills are going to be a tough act to follow.
Dr. Kealey is chair of SHM’s Benchmarks Committee
Advocacy Day Educates Lawmakers about Hospital Medicine
By Eric Siegal, MD
As reported in the SHM Meeting Reporter (see July The Hospitalist, supplement 1), SHM’s first Legislative Advocacy Day was an overwhelming success. More than 70 members from 29 states visited Capitol Hill on May 3 to educate lawmakers and their staffs about hospital medicine and SHM’s proposals to improve the quality of care in our nation’s hospitals.
Advocacy Day participants attended a morning briefing that covered procedural tips on how to have a successful meeting and the health issues currently before Congress—and SHM’s positions—before leaving for previously scheduled appointments on Capitol Hill.
Once there, hospitalists took time to educate legislators and their staff members about the fastest growing medical specialty in the United States, and then turned to SHM’s recommendations for improving the quality, safety, and cost-effectiveness of inpatient medical care.
Among the issues discussed with lawmakers: the need for more funding for the Agency for Healthcare Research and Quality (AHRQ); SHM support for federal initiatives to measure resource use and improve quality, including a CMS demonstration project to assess the contributions of hospital medicine programs to improve patient care and more efficient management of hospital resources; and the importance of gainsharing demonstration projects that focus on inpatient medical services such as those provided by hospital medicine programs.
More than 130 appointments were scheduled with House and Senate offices, many with members of Congress who sit on the key health committees with jurisdiction over Medicare as well as on committees responsible for determining funding levels for the National Institutes of Health, the CDC, and the Agency for Healthcare Research and Quality.
SHM encourages those of you who participated in Advocacy Day to thank the lawmakers and staff with whom you visited (view the sample thank-you letter and instructions online at www.hospitalmedicine.org under “Advocacy & Policy”).
Advocacy Day opened doors to congressional offices; follow-up from SHM members will keep hospital medicine’s issues before lawmakers as they vote on legislation of importance to our specialty. The more SHM members interact with members of Congress and their staff, the louder our voices and the more effective our messages. Advocacy Day is just the beginning of regular contact by hospitalists with their elected representatives in Washington.
A New Way to Get Everything SHM
SHM has launched the SHM Store, a new Internet-based marketplace that will redefine the way SHM educational products and apparel are distributed. The online store will be a convenient option for hectic lifestyles because it will be open 24 hours a day and can be accessed from anywhere there is an Internet connection.
The SHM Store is user-friendly and allows you to easily and quickly purchase the quality products and apparel that you have come to expect from SHM. Apparel and accessories include men’s and women’s wind jackets, golf shirts, scrub tops, baseball caps, and lapel pins—all with the SHM logo.
You’ll also find the most up-to-date educational materials from SHM. The 2005-2006 results of the SHM survey, “The Authoritative Source on the State of Hospital Medicine,” can be ordered in CD and print format. The Practice Management Course CD with binder is also available. This combination package includes all of the materials distributed at an onsite presentation of the course. And, last but not least, get your very own copy or additional copies of The Core Competencies in Hospital Medicine: A Framework For Curriculum Development.
The ordering process is simple. Access the SHM Store at www.hospitalmedicine.org/shmstore or navigate from www.hospitalmedicine.org and click on SHM Store. The store allows you to browse available products and descriptions. When you see something you want, select the quantity you’d like to purchase and add the items to your shopping cart. Once you have completed your shopping trip, click “Check Out.” A confirmation of your transaction will be sent to your e-mail inbox and your products will be shipped to your attention.
It’s that easy. Make sure you go online to browse the new SHM Store. If you have any questions or would like to learn more about the SHM Store, contact SHM at CustomerService@hospitalmedicine. org.
SHM, Health Groups Urge House to Boost Discretionary Funding
SHM joined more than 800 health, education, and labor organizations in writing a May 8 letter to the House leadership. Organized by the Coalition for Health Funding and the Committee on Education Funding, the letter calls on Congress to add $7 billion to the budget in discretionary funding for health, education, and labor programs. It asks lawmakers to ensure that the final allocation for the House and Senate Labor, Health and Human Services, Education Appropriations Subcommittees reflects a $7 billion increase above the President’s request for these critically important programs in FY 2007.
“While our organizations represent a wide array of domestic priorities,” the letter states, “we are united in our effort to advance the bipartisan goal of adding $7 billion in discretionary funding for health, education, labor enforcement, job training, and social services programs as the budget process moves forward. On behalf of our millions of constituents, we strongly urge you to provide at least $7 billion in additional federal support to restore funding levels to FY 2005. This is essential to sustain the well-being and prosperity of our nation.”
Agencies whose funding could be boosted by the additional spending called for in the coalition letter include the Agency for Healthcare Research and Quality, the National Institutes of Health, and the Centers for Disease Control and Prevention.
For full coverage of May 2006 advocacy and policy news, visit www.hospitalmedicine.org. TH
Dr. Siegal is chair of SHM’s Public Policy Committee.
SHM: BEHIND THE SCENES
Education and Quality Initiatives: SHM’s Heart and Soul
By Geri Barnes
This month’s SHM staff article highlights the department responsible for SHM’s education and quality initiatives. While my fellow senior managers may disagree, I believe that we are the heart and soul of SHM in meeting members’ needs. So important is this organizational focus that the Education Committee, chaired by Preetha Basaviah, MD, has its own mission, which parallels and provides detail to the organizational mission of promoting excellence in the practice of hospital medicine. And the Hospital Quality and Patient Safety Committee, chaired by Mahalakshmi Halasyamani, MD, is one of the most dynamic and prolific of SHM’s committees.
We know that members join SHM for the opportunity to effect change and network with colleagues. Equally strong is the quest for educational resources that will facilitate their efforts in improving quality inpatient care. SHM’s education plan focuses and organizes our energy on developing those resources.
SHM’s resources come in many forms. The most visible is our annual meeting. By all accounts, the 2006 annual meeting was extremely successful. It was our largest meeting to date, with almost 1,200 attendees, 99% of whom were members. That number represents more than 21% of our total membership. I wonder how many other organizations can boast of such a high percentage of member attendance at their annual meeting. The attendees actively participated in the educational sessions and the Research, Innovations, and Clinical Vignettes poster session, visited the exhibits, and networked during breaks and social events. To enhance the educational experience, we created a password-protected Web site where registrants could access the handouts for sessions they planned to attend. Because of the value of these materials, we are currently determining ways to utilize the handouts to expand our educational resources.
For several years, SHM has presented the Leadership Academy and “Best Practices in Managing a Hospital Medicine Program” course. These courses are so popular that they have become a mainstay of SHM educational programs and are offered on an annual basis. In September we will present the first Level II Leadership Academy designed to build upon and expand Leadership Academy I. Additionally, “Fundamentals in Billing and Coding” a pre-course to the University of California San Francisco “Management of the Hospitalized Patient” course will be offered in October for the first time. This outgrowth of the Best Practices course was identified as a need by attendees and other members. We anticipate that we will continue to offer these important programs for many years to come.
While we reach a significant number of hospitalists and other healthcare providers through our annual meeting and other face-to-face meetings, we reach many more through other educational and quality improvement efforts. Hospitalists, in their unique role as providers responsible for the general medical care of hospitalized patients, find themselves filling roles as key players and drivers of institutional quality improvement. To aid them in this effort, we’ve developed Web-based resource rooms designed to facilitate the implementation of a quality improvement program for specific disease state/clinical condition, including antimicrobial resistance, stroke, venous thromboembolism, and heart failure. Resource rooms on glycemic control and discharge planning are currently under development.
For most resource rooms, the key is the QI Workbook, a resource built on proven principles of quality improvement, personal experiences, and evidence-based medicine. Resources in addition to the workbook include slide sets that can be used in training sessions, “Teaching Pearls,” patient education resources, and clinical tools in the form of algorithms, order sets, and discharge planning sheets. Most of the resource rooms have online CME programs and each room has a well-developed bibliography.
What will likely prove to be SHM’s most far-reaching resource is The Core Competencies in Hospital Medicine: A Framework For Curriculum Development. Published earlier this year as a supplement to the Journal of Hospital Medicine, the Core Competencies provides a structure for professional and curricular development based on a shared understanding of the essential knowledge, skills, and attitudes expected of physicians working as hospitalists. While the target audience is the directors of hospitalist programs and fellowships and residency programs (and medical school internal medicine clerkships), imagine the number of people reached when the Core Competencies touch hospitalist students across the board. Additionally, the Core Competencies are the focal point for every educational and quality improvement initiative that we undertake. This document will continue to drive the content of each annual meeting, provide direction for the organization, and help us prioritize the development of resources rooms and other educational and quality improvement resources.
SHM is lucky to have partners who understand the importance of hospitalists as key members of the multidisciplinary team and the army that will lead the charge in implementing protocols to improve patient care. From foundations and sister associations, to government and industry, we partner with organizations that appreciate the role that hospitalists play in improving the healthcare system. The partnerships have led to the development of toolkits, resource rooms, CME modules, and other important resources. New initiatives soon to be launched are mentored implementation programs and demonstration projects that will provide us with increased knowledge of how our resources are used and identify areas in which they can be improved.
What is required on a staff level to make this happen? A commitment to do whatever it takes to get the job done. Six of us are equally dedicated to leading, managing, and supporting these efforts. In addition to me, staff members Tina Budnitz, Erica Pearson, Joy Wittnebert, Lillian Higgins, and Theresa Jones chart new ground and are actively engaged in a dynamic learning process on a daily basis. But it is our members and experts that drive this process, and we are grateful for their patience and guidance.
The Education and Quality Initiatives staff members do not work in a vacuum in the national office. We have the support and brainpower of the rest of the staff, with whom we collaborate daily. Membership and marketing, information technology, and business operations staff all play a role in our success.
What makes the national office run as a well-oiled machine? Next month you’ll hear from Steve Poitras, director, Business Operations, who is instrumental in making that happen.
Barnes is director, Education & Quality Initiatives, for SHM.
The Benchmarks Committee has had a busy 2006 so far. Many thanks to the 400-plus hospital medicine groups that completed the 2005-06 SHM survey, “The Authoritative Source on the State of Hospital Medicine,” as well as those of you who participated in the follow-up survey to clarify questions around additional revenue or supplements to program income.
We had some behind-the-scenes work on the survey. After the first pass of data analysis, it became clear that there was something amiss with the responses pertaining to the supplemental income questions. Only 47% of programs reported that they received additional income from hospitals or other sources. This seemed incompatible with what we know about current payment rates for fee-for-service work. A quick discussion took place among the committee and we decided to resurvey the group with more precise questions on exactly how finances flow into a program. As you have seen, the additional results bore out our suspicions. With the revised survey tool, 97% of the programs (when re-queried) reported receiving income above and beyond fees from direct patient care.
It was a Herculean task of digesting and formatting the data into usable form. SHM Senior Vice President Joe Miller deserves many thanks for poring through the data and creating something that all of you can use to better your programs.
Now, a few words about the recent annual meeting in Washington, DC: The work of the Benchmarks Committee was highlighted by SHM CEO Larry Wellikson, MD, in a plenary session on the first day of the meeting. An insightful panel discussion followed in which panel members Bob Wachter, MD (representing academic hospital medicine), Mary Jo Gorman, MD (corporate hospital medicine), and John Nelson, MD (community hospital medicine) gave some insightful commentary on the results of the survey and then fielded questions from the audience.
In between sessions at the conference, the committee held its annual face-to-face meeting and discussed plans for the year.
Under the guidance and editorial excellence of committee member Leslie Flores, the Benchmarks Committee continues to make strong progress with the dashboard project. As you may recall, this project will document and describe 10 commonly used dashboard metrics, including sample reports. There are plans for this material to be published as a supplement to The Hospitalist later this year.
The committee discussed the type of surveys conducted by SHM. A recommendation came out of our meeting to change from large-scale, all-encompassing, biannual surveys to smaller annual surveys. The annual survey would alternate its focus every other year between evaluating individuals’ productivity and compensation, and the characteristics of hospital medicine groups. Each survey would also have the flexibility to address specific timely questions that might focus on a specific research or hot topic of the day. The goal is to get our first trial survey out by the end of 2006, which would focus on group characteristics.
Lastly, a big thank you to our outgoing chairperson, Teresa Jones. Her hard work and organizational skills are going to be a tough act to follow.
Dr. Kealey is chair of SHM’s Benchmarks Committee
Advocacy Day Educates Lawmakers about Hospital Medicine
By Eric Siegal, MD
As reported in the SHM Meeting Reporter (see July The Hospitalist, supplement 1), SHM’s first Legislative Advocacy Day was an overwhelming success. More than 70 members from 29 states visited Capitol Hill on May 3 to educate lawmakers and their staffs about hospital medicine and SHM’s proposals to improve the quality of care in our nation’s hospitals.
Advocacy Day participants attended a morning briefing that covered procedural tips on how to have a successful meeting and the health issues currently before Congress—and SHM’s positions—before leaving for previously scheduled appointments on Capitol Hill.
Once there, hospitalists took time to educate legislators and their staff members about the fastest growing medical specialty in the United States, and then turned to SHM’s recommendations for improving the quality, safety, and cost-effectiveness of inpatient medical care.
Among the issues discussed with lawmakers: the need for more funding for the Agency for Healthcare Research and Quality (AHRQ); SHM support for federal initiatives to measure resource use and improve quality, including a CMS demonstration project to assess the contributions of hospital medicine programs to improve patient care and more efficient management of hospital resources; and the importance of gainsharing demonstration projects that focus on inpatient medical services such as those provided by hospital medicine programs.
More than 130 appointments were scheduled with House and Senate offices, many with members of Congress who sit on the key health committees with jurisdiction over Medicare as well as on committees responsible for determining funding levels for the National Institutes of Health, the CDC, and the Agency for Healthcare Research and Quality.
SHM encourages those of you who participated in Advocacy Day to thank the lawmakers and staff with whom you visited (view the sample thank-you letter and instructions online at www.hospitalmedicine.org under “Advocacy & Policy”).
Advocacy Day opened doors to congressional offices; follow-up from SHM members will keep hospital medicine’s issues before lawmakers as they vote on legislation of importance to our specialty. The more SHM members interact with members of Congress and their staff, the louder our voices and the more effective our messages. Advocacy Day is just the beginning of regular contact by hospitalists with their elected representatives in Washington.
A New Way to Get Everything SHM
SHM has launched the SHM Store, a new Internet-based marketplace that will redefine the way SHM educational products and apparel are distributed. The online store will be a convenient option for hectic lifestyles because it will be open 24 hours a day and can be accessed from anywhere there is an Internet connection.
The SHM Store is user-friendly and allows you to easily and quickly purchase the quality products and apparel that you have come to expect from SHM. Apparel and accessories include men’s and women’s wind jackets, golf shirts, scrub tops, baseball caps, and lapel pins—all with the SHM logo.
You’ll also find the most up-to-date educational materials from SHM. The 2005-2006 results of the SHM survey, “The Authoritative Source on the State of Hospital Medicine,” can be ordered in CD and print format. The Practice Management Course CD with binder is also available. This combination package includes all of the materials distributed at an onsite presentation of the course. And, last but not least, get your very own copy or additional copies of The Core Competencies in Hospital Medicine: A Framework For Curriculum Development.
The ordering process is simple. Access the SHM Store at www.hospitalmedicine.org/shmstore or navigate from www.hospitalmedicine.org and click on SHM Store. The store allows you to browse available products and descriptions. When you see something you want, select the quantity you’d like to purchase and add the items to your shopping cart. Once you have completed your shopping trip, click “Check Out.” A confirmation of your transaction will be sent to your e-mail inbox and your products will be shipped to your attention.
It’s that easy. Make sure you go online to browse the new SHM Store. If you have any questions or would like to learn more about the SHM Store, contact SHM at CustomerService@hospitalmedicine. org.
SHM, Health Groups Urge House to Boost Discretionary Funding
SHM joined more than 800 health, education, and labor organizations in writing a May 8 letter to the House leadership. Organized by the Coalition for Health Funding and the Committee on Education Funding, the letter calls on Congress to add $7 billion to the budget in discretionary funding for health, education, and labor programs. It asks lawmakers to ensure that the final allocation for the House and Senate Labor, Health and Human Services, Education Appropriations Subcommittees reflects a $7 billion increase above the President’s request for these critically important programs in FY 2007.
“While our organizations represent a wide array of domestic priorities,” the letter states, “we are united in our effort to advance the bipartisan goal of adding $7 billion in discretionary funding for health, education, labor enforcement, job training, and social services programs as the budget process moves forward. On behalf of our millions of constituents, we strongly urge you to provide at least $7 billion in additional federal support to restore funding levels to FY 2005. This is essential to sustain the well-being and prosperity of our nation.”
Agencies whose funding could be boosted by the additional spending called for in the coalition letter include the Agency for Healthcare Research and Quality, the National Institutes of Health, and the Centers for Disease Control and Prevention.
For full coverage of May 2006 advocacy and policy news, visit www.hospitalmedicine.org. TH
Dr. Siegal is chair of SHM’s Public Policy Committee.
SHM: BEHIND THE SCENES
Education and Quality Initiatives: SHM’s Heart and Soul
By Geri Barnes
This month’s SHM staff article highlights the department responsible for SHM’s education and quality initiatives. While my fellow senior managers may disagree, I believe that we are the heart and soul of SHM in meeting members’ needs. So important is this organizational focus that the Education Committee, chaired by Preetha Basaviah, MD, has its own mission, which parallels and provides detail to the organizational mission of promoting excellence in the practice of hospital medicine. And the Hospital Quality and Patient Safety Committee, chaired by Mahalakshmi Halasyamani, MD, is one of the most dynamic and prolific of SHM’s committees.
We know that members join SHM for the opportunity to effect change and network with colleagues. Equally strong is the quest for educational resources that will facilitate their efforts in improving quality inpatient care. SHM’s education plan focuses and organizes our energy on developing those resources.
SHM’s resources come in many forms. The most visible is our annual meeting. By all accounts, the 2006 annual meeting was extremely successful. It was our largest meeting to date, with almost 1,200 attendees, 99% of whom were members. That number represents more than 21% of our total membership. I wonder how many other organizations can boast of such a high percentage of member attendance at their annual meeting. The attendees actively participated in the educational sessions and the Research, Innovations, and Clinical Vignettes poster session, visited the exhibits, and networked during breaks and social events. To enhance the educational experience, we created a password-protected Web site where registrants could access the handouts for sessions they planned to attend. Because of the value of these materials, we are currently determining ways to utilize the handouts to expand our educational resources.
For several years, SHM has presented the Leadership Academy and “Best Practices in Managing a Hospital Medicine Program” course. These courses are so popular that they have become a mainstay of SHM educational programs and are offered on an annual basis. In September we will present the first Level II Leadership Academy designed to build upon and expand Leadership Academy I. Additionally, “Fundamentals in Billing and Coding” a pre-course to the University of California San Francisco “Management of the Hospitalized Patient” course will be offered in October for the first time. This outgrowth of the Best Practices course was identified as a need by attendees and other members. We anticipate that we will continue to offer these important programs for many years to come.
While we reach a significant number of hospitalists and other healthcare providers through our annual meeting and other face-to-face meetings, we reach many more through other educational and quality improvement efforts. Hospitalists, in their unique role as providers responsible for the general medical care of hospitalized patients, find themselves filling roles as key players and drivers of institutional quality improvement. To aid them in this effort, we’ve developed Web-based resource rooms designed to facilitate the implementation of a quality improvement program for specific disease state/clinical condition, including antimicrobial resistance, stroke, venous thromboembolism, and heart failure. Resource rooms on glycemic control and discharge planning are currently under development.
For most resource rooms, the key is the QI Workbook, a resource built on proven principles of quality improvement, personal experiences, and evidence-based medicine. Resources in addition to the workbook include slide sets that can be used in training sessions, “Teaching Pearls,” patient education resources, and clinical tools in the form of algorithms, order sets, and discharge planning sheets. Most of the resource rooms have online CME programs and each room has a well-developed bibliography.
What will likely prove to be SHM’s most far-reaching resource is The Core Competencies in Hospital Medicine: A Framework For Curriculum Development. Published earlier this year as a supplement to the Journal of Hospital Medicine, the Core Competencies provides a structure for professional and curricular development based on a shared understanding of the essential knowledge, skills, and attitudes expected of physicians working as hospitalists. While the target audience is the directors of hospitalist programs and fellowships and residency programs (and medical school internal medicine clerkships), imagine the number of people reached when the Core Competencies touch hospitalist students across the board. Additionally, the Core Competencies are the focal point for every educational and quality improvement initiative that we undertake. This document will continue to drive the content of each annual meeting, provide direction for the organization, and help us prioritize the development of resources rooms and other educational and quality improvement resources.
SHM is lucky to have partners who understand the importance of hospitalists as key members of the multidisciplinary team and the army that will lead the charge in implementing protocols to improve patient care. From foundations and sister associations, to government and industry, we partner with organizations that appreciate the role that hospitalists play in improving the healthcare system. The partnerships have led to the development of toolkits, resource rooms, CME modules, and other important resources. New initiatives soon to be launched are mentored implementation programs and demonstration projects that will provide us with increased knowledge of how our resources are used and identify areas in which they can be improved.
What is required on a staff level to make this happen? A commitment to do whatever it takes to get the job done. Six of us are equally dedicated to leading, managing, and supporting these efforts. In addition to me, staff members Tina Budnitz, Erica Pearson, Joy Wittnebert, Lillian Higgins, and Theresa Jones chart new ground and are actively engaged in a dynamic learning process on a daily basis. But it is our members and experts that drive this process, and we are grateful for their patience and guidance.
The Education and Quality Initiatives staff members do not work in a vacuum in the national office. We have the support and brainpower of the rest of the staff, with whom we collaborate daily. Membership and marketing, information technology, and business operations staff all play a role in our success.
What makes the national office run as a well-oiled machine? Next month you’ll hear from Steve Poitras, director, Business Operations, who is instrumental in making that happen.
Barnes is director, Education & Quality Initiatives, for SHM.
Virus Alerts
CDC Urges Awareness of Measles in Americans Returning from Germany
By Alfred Valles, resident, internal medicine, Mayo Clinic College of Medicine
The Centers for Disease Control and Prevention (CDC) has issued an alert urging American travelers to remain aware of the possibility of measles exposure. Many Americans have traveled to and from Germany for the World Cup soccer championship games. Three of the twelve hosting cities—Cologne, Dortmund, and Gelsenkirchen—are of particular concern, given the recent measles outbreaks that have been reported in those cities and their surrounding areas.
Since January 1 of this year, some 1,200 cases have been identified in or near these cities. American travelers were undoubtedly among the large crowds of people gathered to pay homage to their favorite sport, and many others will visit Germany on vacation or business, making transmission of this respiratory droplet-born pathogen a very real threat.
The CDC recommends the following precautions:
- Travelers who plan to go to Germany should check their immunization records and visit their doctors if they are not immune to measles or are not sure they are.
- People returning from Germany, especially those who went to see the World Cup, should see a healthcare provider if they develop the symptoms of measles, including a fever, a raised rash that begins on the face and spreads to the arms and legs, a cough, red eyes, or a runny nose.
- People with these symptoms should limit their contact with others.
- Clinicians seeing patients with these symptoms should inquire about travel history and immunization status.
This warning is not to be taken lightly. Approximately two of every 1,000 patients infected with measles will die of the disease. Complications such as encephalitis are of particular concern for those who are malnourished or immunosuppressed.
Remember, live virus measles vaccine given within 72 hours of exposure may prevent the disease, while immune globulin given up to six days after exposure may prevent complications of measles in those who are at risk, including pregnant women, people with weak immune systems, and children.
The World cup can be dangerous, even for non-players. For more information about the measles outbreak and travel precautions, visit www.cdc.gov.
Lymphocytic Choriomeningitis Virus: Facts and Prevention
By the Special Pathogens Branch, CDC
In May 2005, the CDC investigated a cluster of lymphocytic choriomeningitis virus (LCMV) illnesses in four solid organ transplant recipients from a common donor, three of whom died. The source of the LCMV was traced to a hamster that had recently been acquired by a member of the donor’s household. It was subsequently determined that several LCMV-infected pet rodents had originated from a single distributor, who may have distributed other infected rodents to pet stores in the northeastern and midwestern United States.1 However, the risk of contracting LCMV from rodent exposure is not limited only to this outbreak, nor is the danger confined only to patients undergoing organ transplant.
Clinicians need to be familiar with LCMV because of its potential to cause meningitis, its teratogenicity, and the risk that it may bring about serious disease in immunocompromised individuals.
LCMV is normally carried by wild house mice, but can be transmitted to laboratory and pet rodents at breeding facilities, in pet stores, and in homes. Humans become infected in one of the following ways:
- Through direct contact with the secretions or excretions of infected rodents;
- By inhalation of dust or droplets containing LCMV from rodents;
- As a result of transplacental spread from an infected pregnant woman to her fetus; and
- By receipt of an organ transplant from an infected donor.2
Among those tested, about 5% have shown serologic evidence of previous infection with LCMV.3,4 In healthy adults, LCMV is typically a nonspecific viral syndrome sometimes followed by aseptic meningitis or other neurologic signs. Patients with weakened immune systems can suffer severe, possibly fatal systemic illness.2,5 Maternal infection with LCMV during pregnancy can result in spontaneous abortion or early neonatal death, as well as in defects similar to those of other congenital infections such as toxoplasmosis and cytomegalovirus (“TORCH” infections).6-10 The proportion of developmental defects caused by LCMV is not known.
Clinicians should consider LCMV in the differential diagnosis of patients with aseptic meningitis; in cases of fetal demise or congenital defects, including congenital hydrocephalus, chorioretinitis, blindness, or mental retardation; or in recent transplant recipients who present with signs of post-transplant infection. A detailed rodent exposure history should be taken. Contact your state health department or Special Pathogens Branch, CDC (404-639-1510), for information about testing for LCMV.
Currently, there is no specific treatment for LCMV infection other than supportive care. Ribavirin inhibits LCMV multiplication in laboratory experiments but has not been tested in clinical trials.
Clinicians should counsel their patients about the risks of contracting LCMV from laboratory, pet, and wild rodents. Wild mice in the home should be controlled and removed promptly. Immunocompromised individuals and women who are pregnant or planning to become pregnant should avoid any contact with wild or pet rodents, their excretions, and their nesting materials. While a woman is pregnant, pet rodents should be housed outside the home or in a separate part of the home where other individuals can care for the pets and clean their cages. Counseling a woman already exposed to rodents during pregnancy can be challenging; for assistance, contact your state health department.
Further information about LCMV infection and its prevention, including management and prevention of rodent infestation in the home, is available from Special Pathogens Branch, CDC, at www.cdc.gov/ncidod/dvrd/spb/mnpages/dispages/lcmv.htm. For more information about diseases commonly carried by rodents, please visit www.cdc.gov/rodents. TH
References
- Centers for Disease Control and Prevention. Update: interim guidance for minimizing risk for human lymphocytic choriomeningitis virus infection associated with pet rodents. MMWR. Aug 19, 2005;54(32):799-801.
- Fischer SA, Graham MB, Kuehnert MJ, et al. Transmission of lymphocytic choriomeningitis virus by organ transplantation. N Engl J Med. 2006;354(21):2235-2249.
- Childs JE, Glass GE, Ksiazek TG, et al. Human-rodent contact and infection with lymphocytic choriomeningitis and Seoul viruses in an inner-city population. Am J Trop Med Hyg. 1991 Feb;44(2):117–121.
- Park JY, Peters CJ, Rollin PE, et al. Age distribution of lymphocytic choriomeningitis virus serum antibody in Birmingham, Alabama: evidence of a decreased risk of infection. Am J Trop Med Hyg. 1997 Jul;57(1):37–41.
- Horton J, Hotchin JE, Olson KB, et al. The effects of MP virus infection in lymphoma. Cancer Res. 1971 Aug;31(8):1066–1068.
- Barton LL, Mets MB. Congenital lymphocytic choriomeningitis virus infection: decade of rediscovery. Clin Infect Dis. 2001 Aug 1;33(3):370–374.
- Barton LL, Mets MB, Beauchamp CL. Lymphocytic choriomeningitis virus: emerging fetal teratogen. Am J Obstet Gynecol. 2002 Dec ;187(6):1715–1716.
- Wright R, Johnson D, Neumann M, et al. Congenital lymphocytic choriomeningitis virus syndrome: a disease that mimics congenital toxoplasmosis or cytomegalovirus infection. Pediatrics. 1997 Jul;100(1):E9.
- Ford-Jones EL, Ryan G . Implications for the fetus of maternal infections in pregnancy. In: Cohen J, Powderly WG, eds. Infectious Diseases, 2nd ed. New York, NY: Mosby; 2004: 709–723.
- Greenhow TL, Weintrub PS. Your diagnosis, please. Neonate with hydrocephalus. Pediatr Infect Dis J. 2003 Dec;22(12):1099, 1111–1112.
CDC Urges Awareness of Measles in Americans Returning from Germany
By Alfred Valles, resident, internal medicine, Mayo Clinic College of Medicine
The Centers for Disease Control and Prevention (CDC) has issued an alert urging American travelers to remain aware of the possibility of measles exposure. Many Americans have traveled to and from Germany for the World Cup soccer championship games. Three of the twelve hosting cities—Cologne, Dortmund, and Gelsenkirchen—are of particular concern, given the recent measles outbreaks that have been reported in those cities and their surrounding areas.
Since January 1 of this year, some 1,200 cases have been identified in or near these cities. American travelers were undoubtedly among the large crowds of people gathered to pay homage to their favorite sport, and many others will visit Germany on vacation or business, making transmission of this respiratory droplet-born pathogen a very real threat.
The CDC recommends the following precautions:
- Travelers who plan to go to Germany should check their immunization records and visit their doctors if they are not immune to measles or are not sure they are.
- People returning from Germany, especially those who went to see the World Cup, should see a healthcare provider if they develop the symptoms of measles, including a fever, a raised rash that begins on the face and spreads to the arms and legs, a cough, red eyes, or a runny nose.
- People with these symptoms should limit their contact with others.
- Clinicians seeing patients with these symptoms should inquire about travel history and immunization status.
This warning is not to be taken lightly. Approximately two of every 1,000 patients infected with measles will die of the disease. Complications such as encephalitis are of particular concern for those who are malnourished or immunosuppressed.
Remember, live virus measles vaccine given within 72 hours of exposure may prevent the disease, while immune globulin given up to six days after exposure may prevent complications of measles in those who are at risk, including pregnant women, people with weak immune systems, and children.
The World cup can be dangerous, even for non-players. For more information about the measles outbreak and travel precautions, visit www.cdc.gov.
Lymphocytic Choriomeningitis Virus: Facts and Prevention
By the Special Pathogens Branch, CDC
In May 2005, the CDC investigated a cluster of lymphocytic choriomeningitis virus (LCMV) illnesses in four solid organ transplant recipients from a common donor, three of whom died. The source of the LCMV was traced to a hamster that had recently been acquired by a member of the donor’s household. It was subsequently determined that several LCMV-infected pet rodents had originated from a single distributor, who may have distributed other infected rodents to pet stores in the northeastern and midwestern United States.1 However, the risk of contracting LCMV from rodent exposure is not limited only to this outbreak, nor is the danger confined only to patients undergoing organ transplant.
Clinicians need to be familiar with LCMV because of its potential to cause meningitis, its teratogenicity, and the risk that it may bring about serious disease in immunocompromised individuals.
LCMV is normally carried by wild house mice, but can be transmitted to laboratory and pet rodents at breeding facilities, in pet stores, and in homes. Humans become infected in one of the following ways:
- Through direct contact with the secretions or excretions of infected rodents;
- By inhalation of dust or droplets containing LCMV from rodents;
- As a result of transplacental spread from an infected pregnant woman to her fetus; and
- By receipt of an organ transplant from an infected donor.2
Among those tested, about 5% have shown serologic evidence of previous infection with LCMV.3,4 In healthy adults, LCMV is typically a nonspecific viral syndrome sometimes followed by aseptic meningitis or other neurologic signs. Patients with weakened immune systems can suffer severe, possibly fatal systemic illness.2,5 Maternal infection with LCMV during pregnancy can result in spontaneous abortion or early neonatal death, as well as in defects similar to those of other congenital infections such as toxoplasmosis and cytomegalovirus (“TORCH” infections).6-10 The proportion of developmental defects caused by LCMV is not known.
Clinicians should consider LCMV in the differential diagnosis of patients with aseptic meningitis; in cases of fetal demise or congenital defects, including congenital hydrocephalus, chorioretinitis, blindness, or mental retardation; or in recent transplant recipients who present with signs of post-transplant infection. A detailed rodent exposure history should be taken. Contact your state health department or Special Pathogens Branch, CDC (404-639-1510), for information about testing for LCMV.
Currently, there is no specific treatment for LCMV infection other than supportive care. Ribavirin inhibits LCMV multiplication in laboratory experiments but has not been tested in clinical trials.
Clinicians should counsel their patients about the risks of contracting LCMV from laboratory, pet, and wild rodents. Wild mice in the home should be controlled and removed promptly. Immunocompromised individuals and women who are pregnant or planning to become pregnant should avoid any contact with wild or pet rodents, their excretions, and their nesting materials. While a woman is pregnant, pet rodents should be housed outside the home or in a separate part of the home where other individuals can care for the pets and clean their cages. Counseling a woman already exposed to rodents during pregnancy can be challenging; for assistance, contact your state health department.
Further information about LCMV infection and its prevention, including management and prevention of rodent infestation in the home, is available from Special Pathogens Branch, CDC, at www.cdc.gov/ncidod/dvrd/spb/mnpages/dispages/lcmv.htm. For more information about diseases commonly carried by rodents, please visit www.cdc.gov/rodents. TH
References
- Centers for Disease Control and Prevention. Update: interim guidance for minimizing risk for human lymphocytic choriomeningitis virus infection associated with pet rodents. MMWR. Aug 19, 2005;54(32):799-801.
- Fischer SA, Graham MB, Kuehnert MJ, et al. Transmission of lymphocytic choriomeningitis virus by organ transplantation. N Engl J Med. 2006;354(21):2235-2249.
- Childs JE, Glass GE, Ksiazek TG, et al. Human-rodent contact and infection with lymphocytic choriomeningitis and Seoul viruses in an inner-city population. Am J Trop Med Hyg. 1991 Feb;44(2):117–121.
- Park JY, Peters CJ, Rollin PE, et al. Age distribution of lymphocytic choriomeningitis virus serum antibody in Birmingham, Alabama: evidence of a decreased risk of infection. Am J Trop Med Hyg. 1997 Jul;57(1):37–41.
- Horton J, Hotchin JE, Olson KB, et al. The effects of MP virus infection in lymphoma. Cancer Res. 1971 Aug;31(8):1066–1068.
- Barton LL, Mets MB. Congenital lymphocytic choriomeningitis virus infection: decade of rediscovery. Clin Infect Dis. 2001 Aug 1;33(3):370–374.
- Barton LL, Mets MB, Beauchamp CL. Lymphocytic choriomeningitis virus: emerging fetal teratogen. Am J Obstet Gynecol. 2002 Dec ;187(6):1715–1716.
- Wright R, Johnson D, Neumann M, et al. Congenital lymphocytic choriomeningitis virus syndrome: a disease that mimics congenital toxoplasmosis or cytomegalovirus infection. Pediatrics. 1997 Jul;100(1):E9.
- Ford-Jones EL, Ryan G . Implications for the fetus of maternal infections in pregnancy. In: Cohen J, Powderly WG, eds. Infectious Diseases, 2nd ed. New York, NY: Mosby; 2004: 709–723.
- Greenhow TL, Weintrub PS. Your diagnosis, please. Neonate with hydrocephalus. Pediatr Infect Dis J. 2003 Dec;22(12):1099, 1111–1112.
CDC Urges Awareness of Measles in Americans Returning from Germany
By Alfred Valles, resident, internal medicine, Mayo Clinic College of Medicine
The Centers for Disease Control and Prevention (CDC) has issued an alert urging American travelers to remain aware of the possibility of measles exposure. Many Americans have traveled to and from Germany for the World Cup soccer championship games. Three of the twelve hosting cities—Cologne, Dortmund, and Gelsenkirchen—are of particular concern, given the recent measles outbreaks that have been reported in those cities and their surrounding areas.
Since January 1 of this year, some 1,200 cases have been identified in or near these cities. American travelers were undoubtedly among the large crowds of people gathered to pay homage to their favorite sport, and many others will visit Germany on vacation or business, making transmission of this respiratory droplet-born pathogen a very real threat.
The CDC recommends the following precautions:
- Travelers who plan to go to Germany should check their immunization records and visit their doctors if they are not immune to measles or are not sure they are.
- People returning from Germany, especially those who went to see the World Cup, should see a healthcare provider if they develop the symptoms of measles, including a fever, a raised rash that begins on the face and spreads to the arms and legs, a cough, red eyes, or a runny nose.
- People with these symptoms should limit their contact with others.
- Clinicians seeing patients with these symptoms should inquire about travel history and immunization status.
This warning is not to be taken lightly. Approximately two of every 1,000 patients infected with measles will die of the disease. Complications such as encephalitis are of particular concern for those who are malnourished or immunosuppressed.
Remember, live virus measles vaccine given within 72 hours of exposure may prevent the disease, while immune globulin given up to six days after exposure may prevent complications of measles in those who are at risk, including pregnant women, people with weak immune systems, and children.
The World cup can be dangerous, even for non-players. For more information about the measles outbreak and travel precautions, visit www.cdc.gov.
Lymphocytic Choriomeningitis Virus: Facts and Prevention
By the Special Pathogens Branch, CDC
In May 2005, the CDC investigated a cluster of lymphocytic choriomeningitis virus (LCMV) illnesses in four solid organ transplant recipients from a common donor, three of whom died. The source of the LCMV was traced to a hamster that had recently been acquired by a member of the donor’s household. It was subsequently determined that several LCMV-infected pet rodents had originated from a single distributor, who may have distributed other infected rodents to pet stores in the northeastern and midwestern United States.1 However, the risk of contracting LCMV from rodent exposure is not limited only to this outbreak, nor is the danger confined only to patients undergoing organ transplant.
Clinicians need to be familiar with LCMV because of its potential to cause meningitis, its teratogenicity, and the risk that it may bring about serious disease in immunocompromised individuals.
LCMV is normally carried by wild house mice, but can be transmitted to laboratory and pet rodents at breeding facilities, in pet stores, and in homes. Humans become infected in one of the following ways:
- Through direct contact with the secretions or excretions of infected rodents;
- By inhalation of dust or droplets containing LCMV from rodents;
- As a result of transplacental spread from an infected pregnant woman to her fetus; and
- By receipt of an organ transplant from an infected donor.2
Among those tested, about 5% have shown serologic evidence of previous infection with LCMV.3,4 In healthy adults, LCMV is typically a nonspecific viral syndrome sometimes followed by aseptic meningitis or other neurologic signs. Patients with weakened immune systems can suffer severe, possibly fatal systemic illness.2,5 Maternal infection with LCMV during pregnancy can result in spontaneous abortion or early neonatal death, as well as in defects similar to those of other congenital infections such as toxoplasmosis and cytomegalovirus (“TORCH” infections).6-10 The proportion of developmental defects caused by LCMV is not known.
Clinicians should consider LCMV in the differential diagnosis of patients with aseptic meningitis; in cases of fetal demise or congenital defects, including congenital hydrocephalus, chorioretinitis, blindness, or mental retardation; or in recent transplant recipients who present with signs of post-transplant infection. A detailed rodent exposure history should be taken. Contact your state health department or Special Pathogens Branch, CDC (404-639-1510), for information about testing for LCMV.
Currently, there is no specific treatment for LCMV infection other than supportive care. Ribavirin inhibits LCMV multiplication in laboratory experiments but has not been tested in clinical trials.
Clinicians should counsel their patients about the risks of contracting LCMV from laboratory, pet, and wild rodents. Wild mice in the home should be controlled and removed promptly. Immunocompromised individuals and women who are pregnant or planning to become pregnant should avoid any contact with wild or pet rodents, their excretions, and their nesting materials. While a woman is pregnant, pet rodents should be housed outside the home or in a separate part of the home where other individuals can care for the pets and clean their cages. Counseling a woman already exposed to rodents during pregnancy can be challenging; for assistance, contact your state health department.
Further information about LCMV infection and its prevention, including management and prevention of rodent infestation in the home, is available from Special Pathogens Branch, CDC, at www.cdc.gov/ncidod/dvrd/spb/mnpages/dispages/lcmv.htm. For more information about diseases commonly carried by rodents, please visit www.cdc.gov/rodents. TH
References
- Centers for Disease Control and Prevention. Update: interim guidance for minimizing risk for human lymphocytic choriomeningitis virus infection associated with pet rodents. MMWR. Aug 19, 2005;54(32):799-801.
- Fischer SA, Graham MB, Kuehnert MJ, et al. Transmission of lymphocytic choriomeningitis virus by organ transplantation. N Engl J Med. 2006;354(21):2235-2249.
- Childs JE, Glass GE, Ksiazek TG, et al. Human-rodent contact and infection with lymphocytic choriomeningitis and Seoul viruses in an inner-city population. Am J Trop Med Hyg. 1991 Feb;44(2):117–121.
- Park JY, Peters CJ, Rollin PE, et al. Age distribution of lymphocytic choriomeningitis virus serum antibody in Birmingham, Alabama: evidence of a decreased risk of infection. Am J Trop Med Hyg. 1997 Jul;57(1):37–41.
- Horton J, Hotchin JE, Olson KB, et al. The effects of MP virus infection in lymphoma. Cancer Res. 1971 Aug;31(8):1066–1068.
- Barton LL, Mets MB. Congenital lymphocytic choriomeningitis virus infection: decade of rediscovery. Clin Infect Dis. 2001 Aug 1;33(3):370–374.
- Barton LL, Mets MB, Beauchamp CL. Lymphocytic choriomeningitis virus: emerging fetal teratogen. Am J Obstet Gynecol. 2002 Dec ;187(6):1715–1716.
- Wright R, Johnson D, Neumann M, et al. Congenital lymphocytic choriomeningitis virus syndrome: a disease that mimics congenital toxoplasmosis or cytomegalovirus infection. Pediatrics. 1997 Jul;100(1):E9.
- Ford-Jones EL, Ryan G . Implications for the fetus of maternal infections in pregnancy. In: Cohen J, Powderly WG, eds. Infectious Diseases, 2nd ed. New York, NY: Mosby; 2004: 709–723.
- Greenhow TL, Weintrub PS. Your diagnosis, please. Neonate with hydrocephalus. Pediatr Infect Dis J. 2003 Dec;22(12):1099, 1111–1112.