User login
Buckle fractures in children: Is urgent treatment necessary?
PURPOSE To determine whether the clinical outcome of buckle fractures in children differs between those treated acutely on the same day of trauma and those treated subacutely, and whether a change in practice patterns based on these data would result in cost savings.
METHODS In this retrospective cohort study—approved by the institutional review board—we reviewed the cases of 341 consecutive patients <18 years of age seen by the pediatric orthopedic clinic for treatment of isolated extremity buckle fractures between July 1, 2004 and August 31, 2007. Time from injury to treatment was used to divide patients into 2 groups: acute (≤1 day; n=155) and subacute treatment (>1 day; n=186). Clinical outcome at final orthopedic follow-up was recorded for each patient. We defined adverse outcome as fractures requiring manipulation, clinically apparent deformity, or functional impairment. Charge analysis compared differences in management costs for patients with buckle fractures presenting initially to the emergency department (ED) and those seen solely in the orthopedic clinic.
RESULTS No adverse outcomes were identified in either acute or subacute treatment groups. Total clinical visits did not vary (acute, 3.2 vs subacute, 3.1; P=.051). Presence of mild angulation of fractures on radiographs did not differ significantly between acute and subacute management groups at initial presentation (6.5% vs 8.6%; P=.541) or at final follow-up (12.2% vs 12.4%; P=1.0). A cost savings of approximately $3000 could have been realized for each patient referred to the ED who might otherwise have been seen subacutely in the orthopedic clinic.
CONCLUSIONS No adverse clinical outcomes resulted from subacute treatment of stable buckle fractures. Cost and time savings may be realized with subacute management of buckle fractures without affecting clinical outcome.
Next time a child in your care has a suspected fracture as a result of a fall and x-ray films reveal a buckle fracture, consider telling parents there’s no need for an urgent visit to the ED. As long as the pain is manageable, treating the injury within a day or so will likely be more convenient for the family, will cost less, and will not result in any complications for the child.
Buckle (or torus) fractures—the most common type of fracture occurring in the pediatric population and accounting for a large number of visits to primary care physicians (PCPs), EDs, and orthopedic clinics each year1 —involve impaction of bone along only 1 cortex and are therefore inherently stable.2 Even with only minimal immobilization, the overwhelming majority of buckle fractures heal without complication.3 Although many patients present directly to the ED for management of these fractures, many others present initially to their PCP, given the relatively minor nature of their symptoms and mechanism of injury.
At our institution, the radiology department and referring physician jointly triage out-patients when radiographs requested by the referring physician show evidence of a fracture. Stable and unstable fractures are referred for immediate care—in the pediatric orthopedic clinic if the clinic is open and appointments are available; otherwise in the ED for initial splinting, with follow-up in the orthopedic clinic as soon as possible.
Referral of patients with buckle fractures for same-day care in the ED may bring about unnecessary costs and inconvenience for patients and families. However, policy at our institution dictates that all fractures, including stable buckle fractures, be referred for treatment immediately, once identified.
To determine whether patients with buckle fractures can be safely counseled on the possibility of nonurgent management, we compared the clinical outcomes of pediatric buckle fractures treated acutely or subacutely. The results of our study have practical implications for the timing of treatment or referrals, and for the management of buckle fractures by appropriately trained PCPs, especially in settings where orthopedic consultation may not be readily available.
Methods
Patient selection
The Vanderbilt Children’s Hospital institutional review board approved this retrospective cohort study, with waiver of patient consent. We reviewed 1923 consecutive charts of patients who were seen in the hospital’s pediatric orthopedic clinic for stable fractures between July, 1, 2004 and August 31, 2007. We identified patients for our study population by current procedural terminology (CPT) codes for fracture care that were compatible with buckle fracture or other stable fracture management without manipulation. Applicable CPT codes included the following fracture sites: radial head/neck (24650), ulnar shaft (25530), distal radius with or without ulnar styloid (25600), metacarpal (26600), phalanx of hand or foot (26720, 28510), distal fibula (27786), and metatarsal (28470).
Inclusion and exclusion criteria. Inclusion criteria among this screened population were an isolated buckle fracture mentioned in the official radiology report or pediatric orthopedic clinical note, and age <18 years at the time of injury. We excluded patients for the following reasons: uncertain date of injury (n=67), lack of final clinical follow-up (n=59), acute manipulation of the fracture (n=10), multiple concurrent injuries (n=11), or known metabolic bone disease (n=3) or coagulopathy (n=1).
After initial patient selection, a CAQ-certified pediatric radiologist (with additional fellowship training in pediatric musculoskeletal radiology) and a board-certified orthopedic surgeon (with pediatric orthopedic fellowship training) examined available radiographic images to confirm the diagnosis of a buckle fracture. We further excluded patients whose radiographic findings did not meet criteria for isolated buckle fractures.
Study populations
The final study population consisted of 341 children with confirmed isolated buckle fractures. We assigned patients to acute or subacute treatment groups based on the length of time between injury and presentation for care. Patients were assigned to acute treatment (n=155) if they presented for care on the same day as the injury. All others first seen >1 day after documented time of injury were assigned to subacute treatment (n=186).
We determined length of time between injury and presentation based on data available in the electronic medical record. If the injury was first documented in the orthopedic clinic, we reviewed notes to determine when the patient had initially sought care, and whether from our institution, a PCP, or an outside ED. If documentation showed that initial contact with any health care professional occurred within 1 day of the injury, we assigned the patient to acute management.
Data analysis
Data collection from computerized medical records included date of injury, date of initial care, anatomic location of fracture, mechanism of injury, referring physician, whether the patient was seen initially in the ED, date of last orthopedic follow-up, number of clinical visits, and clinical outcome. Clinical outcome was judged as “good” or “poor” at the last orthopedic follow-up visit, approximately 3 to 4 weeks after injury. A poor clinical outcome could indicate a clinically apparent deformity or functional impairment, need for subacute manipulation, or refracture. We deemed 1 patient’s outcome uncertain due to an ambiguous final clinical note, and we had this case reviewed by a pediatric orthopedist. Any visit to a PCP, ED, or orthopedic clinic was included in the total number of a patient’s clinical visits.
Consulting radiologists also noted the presence and degree of fracture angulation for each patient on initial and follow-up films. Degree of angulation was rated as mild (<10°), moderate (11°-20°), or severe (>20°). Follow-up films were not available for 14 patients (5.2% of acutely treated patients; 3.2% of subacutely treated patients), as final clinical follow-up occasionally occurred outside our institution. In these cases, we relied on the clinical note to determine degree of angulation, if present.
We obtained total charges (technical and professional) for buckle fracture treatment for patients treated initially in the ED and for patients seen initially in the orthopedic clinic.
Statistical analysis
We used an independent samples t-test to compare mean patient ages, times from initial treatment to final treatment, and the numbers of clinical encounters for patients in the acute and subacute treatment groups. For the acute treatment group, time from injury to initial care, by definition, was considered “0.” For the subacute treatment group, we constructed 99.9% confidence intervals around the mean time from injury to initial care to determine whether or not they included “0.”
We used Fisher’s exact test to gauge differences in the proportions of absent or mild initial angulation, absent or mild final angulation, and the point of initial care between the acute and subacute treatment groups. We used Pearson’s chi-squared test to assess between-group differences in the distribution of fracture sites (forearm, hand/foot, or leg), mechanism of injury (fall, direct blow, other), change in angulation (none, improved, worsened), and point of entry into the health care system (PCP, ED, orthopedic clinic). We performed statistical analyses with the statistical package SPSS v15 (SPSS, Inc., Chicago, Ill).
Results
Patient characteristics
Of the 1923 pediatric patients with stable fractures seen in the orthopedic clinic at our institution during the study period, 588 had isolated buckle fractures. Of these, we excluded 151 based on predefined criteria (see Methods). After consensus review of radiographs by a pediatric orthopedist and pediatric radiologist, we excluded an additional 96 patients with inconclusive radiographs. The final study group numbered 341 pediatric patients with confirmed isolated buckle fractures.
The forearm was most commonly affected, with isolated distal radius fractures accounting for 67.7% (231/341) of all fractures, and combined radius/ulna fractures accounting for 14.7% (50/341). The most common mechanism of injury was a fall (85.9%; 293/341), usually a direct fall, with a higher percentage of patients with direct falls in the acute management group ( TABLE 1 ). Mean age and sex were not significantly different for the 2 treatment groups.
TABLE 1
Baseline characteristics of study populations
| Acute (n=155) | Subacute (n=186) | P value | |
|---|---|---|---|
| Age, y ± SD (range) | 7.9 ± 4.0 (0.9-17.8) | 7.9 ± 3.8 (1.0-16.4) | .901 |
| Male, n (%) | 79 (51.0) | 86 (46.2) | .384 |
| Site of fracture, n (%) | .022 | ||
| Forearm | 142 (91.6) | 151 (81.2) | |
| Hand or foot | 12 (7.7) | 33 (17.7) | |
| Leg | 1 (0.6) | 2 (1.1) | |
| Mechanism of injury, n (%) | .045 | ||
| Fall | 141 (90.9) | 152 (81.7) | |
| Direct blow | 5 (3.2) | 15 (8.1) | |
| Other/unknown | 9 (5.8) | 19 (10.2) | |
| SD, standard deviation. | |||
Acute vs subacute management outcomes
Of the 341 patients included in the study, 155 patients were treated acutely and 186 patients were treated subacutely. For the subacute management group, mean time between injury and treatment was 2.5±2.6 days ( TABLE 2 ). We observed no poor clinical outcomes in either acute or subacute management groups. All patients, regardless of time elapsed from injury to initial splinting, recovered without complication. The difference in number of clinical visits between the acute and subacute management groups was not significant (acute 3.2±0.5; subacute 3.1±0.5). The mean length of clinical follow-up from initial splinting to discharge from orthopedic care was higher in the acute management group (acute 32.9±17.1 days; subacute 28.9±13.4 days).
Most patients presented with non-angulated fractures, regardless of time from injury to initial presentation ( TABLE 2 ). The degree of angulation worsened in a small proportion of fractures during convalescence. The difference in initial angulation, final angulation, or change in angulation between acute and subacute management groups was not significant.
A higher proportion of patients in the acute treatment group presented directly to the ED for care, whereas a higher proportion of patients in the subacute treatment group presented to their PCP during routine working hours and were referred to the orthopedic clinic ( TABLE 2 ). For both acute and subacute management groups, we compared outcomes for patients seen initially in the ED or orthopedic clinic. No adverse outcomes occurred among any of the studied patients.
TABLE 2
Clinical outcomes did not differ between acute and subacute management groups
| Acute (n=155) | Subacute (n=186) | P value | |
|---|---|---|---|
| Time from injury to initial care, d ± SD (range) | 0 | 2.5 ± 2.6 (1-14) | <.001 |
| Good outcome, n (%) | 155 (100) | 186 (100) | 1.0 |
| Time from initial treatment to final follow-up, d ± SD (range) | 32.9 ± 17.1 (8-169) | 28.9 ± 13.4 (9-164) | .016 |
| Number of clinical encounters (primary care physician, ED, or orthopedic clinic), n ± SD (range) | 3.2 ± 0.5 (2-5) | 3.1 ± 0.5 (2-5) | .051 |
| Initial angulation, n (%) | .541 | ||
| None | 145 (93.5) | 170 (91.4) | |
| Mild (<10°) | 10 (6.5) | 16 (8.6) | |
| Final angulation, n (%) | 1.0 | ||
| None | 136 (87.7) | 163 (87.6) | |
| Mild (<10°) | 19 (12.2) | 23 (12.4) | |
| Change in angulation, n (%) | .907 | ||
| No change | 144 (92.9) | 175 (94.1) | |
| Worse | 10 (6.4) | 10 (5.4) | |
| Improved | 1 (0.6) | 1 (0.5) | |
| Point of entry to health care system, n (%) | <.001 | ||
| Primary care physician | 44 (28.4) | 115 (61.8) | |
| ED | 108 (69.7) | 54 (29.0) | |
| Orthopedic clinic | 3 (1.9) | 17 (9.1) | |
| Location of initial management, n (%) | <.001 | ||
| ED | 132 (85.2) | 81 (43.5) | |
| Orthopedic clinic | 23 (14.8) | 105 (56.4) | |
| ED, emergency department; SD, standard deviation. | |||
Charge analysis
We compared total charges (professional and technical) for managing buckle fractures initially in the ED with those initially seen in the orthopedic clinic. Total charge per patient in the ED, including subsequent follow-up in the orthopedic clinic, was $4397 ($2516, professional; $1881, technical). Total charge per patient for treatment only in the orthopedic clinic was $1426 ($918, professional; $508, technical). Total charge per patient was $2971 more for patients treated initially in the ED.
Between July 1, 2004, and August 31, 2007, 159 patients (46.6%) with buckle fractures entered the health care system through their primary care physician. Of these, 44 patients were seen acutely by the physician; 115 patients were seen on a subacute basis. Of the 44 patients seen acutely, 24 (54%) were referred directly to the ED; 20 (45%) were referred to the orthopedic clinic. Of the 115 patients seen subacutely, 27 (23%) were referred directly to the ED, and the remaining 88 (76%) were referred to the orthopedic clinic. In sum, 51 patients (32%) were seen initially by a PCP, who referred them to the ED. The cost savings with each patient seen subacutely in the orthopedic clinic was $2971, and avoiding ED treatment for all patients could have yielded a total gross savings of approximately $150,000.
Discussion
Buckle fractures are inherently stable and almost universally heal without complication.4,5 Perhaps because of the high likelihood of good outcome, there is a relative paucity of articles in the recent literature addressing the management of this common pediatric fracture. Older studies have addressed casting vs splinting and the need for follow-up, but no study has yet examined whether immediate treatment is necessary.6,7 Although some studies have noted incidentally that many children have delayed presentation for care,5 none has specifically examined the clinical or economic impact of a delay in care or the effect of subacute treatment on outcomes.
Delayed treatment does not adversely affect clinical outcome. Our study objective was to compare clinical outcomes of buckle fractures treated acutely on the same day of injury with outcomes of those treated subacutely. The 2 groups did not differ in extent or angulation of fracture at presentation. We found no difference in outcomes between the groups; all fractures healed without complication. We observed no difference in final angulation of fracture on follow-up imaging. Though our institution routinely obtains follow-up films, it is worth mentioning that the utility of repeat films in pediatric buckle fractures with minimal initial angulation has been debated.5 These data suggest that subacute treatment of a buckle fracture is a safe and reasonable option.
Non-ED treatment substantially reduces cost. One goal of efficient health care delivery is to decrease the cost and burden of care without increasing long-term morbidity and disability. Evidence suggests that families may prefer less acute management options that allow greater convenience and flexibility, provided that clinical outcomes are not compromised.8 In the case of pediatric buckle fractures, higher costs (for both the patient and the hospital) and longer wait times related to ED care may be avoided by counseling patients on the option of subacute care. Our study found that referring patients directly to the orthopedic clinic, even if this results in a delay in definitive management, leads to a reduction in health care burden without a change in clinical outcome.
Children with buckle fractures are frequently (46.6%) taken to their PCP for initial care. Many pediatricians and family physicians—especially the increasing number of physicians who have completed additional fellowship training in sports medicine—may prefer to manage buckle fractures within their practices. Many other PCPs may be practicing in communities lacking local orthopedic expertise. The results of this study provide reassurance regarding the positive outcome of buckle fractures. Furthermore, managing buckle fractures in the primary care setting may be even more cost effective than referring patients to a specialty orthopedic clinic—but additional research on this point is needed.
We do not advocate delayed imaging or treatment of suspected fractures. However, once a diagnosis of buckle fracture is confirmed radiographically, our data show that subacute treatment yields significant cost and time savings without affecting final clinical outcome.
Study limitations
This study is limited by its retrospective data collection in 1 pediatric tertiary care hospital. As current clinical practice is to treat all buckle fractures once identified, very few patients with known injury were specifically treated in a subacute fashion. We defined the subacute care group as patients who were treated >1 day from the time of injury. Because initial splinting did not occur in this group, we expect that the observed results would be similar, and no worse, compared with buckle fracture care directed by a subacute treatment algorithm.
This study examined only patients with a diagnosis of isolated buckle fracture. Non-buckle stable fractures were excluded a priori from our patient population. Although it is possible that most stable fractures (eg, nondisplaced transverse fractures, Salter-Harris I injuries) could be managed subacutely, we addressed only isolated buckle fractures.
Because of the universally positive outcomes in these cases, most of our patients had no orthopedic follow-up beyond 1 month. We are not able to comment on whether any longer-term abnormalities in function occurred. This question could be addressed through a prospective trial requiring reevaluation of each patient at a set endpoint of the study.
Although buckle fractures are inherently stable and do not present a significant risk of displacement with delayed treatment, they are nevertheless painful fractures that can be a cause of considerable anxiety for both patient and family. The goal of the physician, beyond ensuring the best medical outcome, extends to provide emotional support to the patient and family. Pain control and reassurance are therefore central to the discussion of fracture management, and are most likely the driving factor for a patient to seek urgent care. A key limitation of this study was the inability to determine differences in pain control between acute and subacute treatment. As mentioned above, a prospective study would enable the issue of pain control to be better addressed.
CORRESPONDENCE
Debbie Lee Bennett, MD, Massachusetts General Hospital, 55 Fruit Street, FND-216, Boston, MA 02114; [email protected]
(At the time this study was accepted for publication, Dr. Bennett was at Vanderbilt Children’s Hospital.)
1. Plint AC, Clifford T, Perry J, et al. Wrist buckle fractures: a survey of current practice patterns and attitudes toward immobilization. Can J Emerg Med. 2003;5:95-100.
2. England SP, Sundberg S. Management of common pediatric fractures. In: England SP, ed. Common Orthopedic Problems II. Philadelphia, Pa: WB Saunders; 1996:991–1012.
3. Van Bosse HJP, Patel RJ, Thacker M, et al. Minimalistic approach to treating wrist torus fractures. J Pediatr Orthop. 2005;25:495-500.
4. Davidson JS, Brown DJ, Barnes SN, et al. Simple treatment for torus fractures of the distal radius. J Bone Joint Surg Br. 2001;83-B:1173-1175.
5. Plint AC, Perry JJ, Tsang JLY. Pediatric wrist buckle fractures: should we just splint and go? Can J Emerg Med. 2004;6:397-401.
6. Solan MC, Rees R, Daly K. Current management of torus fractures of the distal radius. Injury. 2002;33:503-505.
7. Plint AC, Perry JJ, Correll R, et al. A randomized, controlled trial of removable splinting versus casting for wrist buckle fractures in children. Pediatrics. 2006;117:691-697.
8. Symons S, Rowsell M, Bhowal B, et al. Hospital versus home management of children with buckle fractures of the distal radius. A prospective, randomised trial. J Bone Joint Surg Br. 2001;83:556-560.
PURPOSE To determine whether the clinical outcome of buckle fractures in children differs between those treated acutely on the same day of trauma and those treated subacutely, and whether a change in practice patterns based on these data would result in cost savings.
METHODS In this retrospective cohort study—approved by the institutional review board—we reviewed the cases of 341 consecutive patients <18 years of age seen by the pediatric orthopedic clinic for treatment of isolated extremity buckle fractures between July 1, 2004 and August 31, 2007. Time from injury to treatment was used to divide patients into 2 groups: acute (≤1 day; n=155) and subacute treatment (>1 day; n=186). Clinical outcome at final orthopedic follow-up was recorded for each patient. We defined adverse outcome as fractures requiring manipulation, clinically apparent deformity, or functional impairment. Charge analysis compared differences in management costs for patients with buckle fractures presenting initially to the emergency department (ED) and those seen solely in the orthopedic clinic.
RESULTS No adverse outcomes were identified in either acute or subacute treatment groups. Total clinical visits did not vary (acute, 3.2 vs subacute, 3.1; P=.051). Presence of mild angulation of fractures on radiographs did not differ significantly between acute and subacute management groups at initial presentation (6.5% vs 8.6%; P=.541) or at final follow-up (12.2% vs 12.4%; P=1.0). A cost savings of approximately $3000 could have been realized for each patient referred to the ED who might otherwise have been seen subacutely in the orthopedic clinic.
CONCLUSIONS No adverse clinical outcomes resulted from subacute treatment of stable buckle fractures. Cost and time savings may be realized with subacute management of buckle fractures without affecting clinical outcome.
Next time a child in your care has a suspected fracture as a result of a fall and x-ray films reveal a buckle fracture, consider telling parents there’s no need for an urgent visit to the ED. As long as the pain is manageable, treating the injury within a day or so will likely be more convenient for the family, will cost less, and will not result in any complications for the child.
Buckle (or torus) fractures—the most common type of fracture occurring in the pediatric population and accounting for a large number of visits to primary care physicians (PCPs), EDs, and orthopedic clinics each year1 —involve impaction of bone along only 1 cortex and are therefore inherently stable.2 Even with only minimal immobilization, the overwhelming majority of buckle fractures heal without complication.3 Although many patients present directly to the ED for management of these fractures, many others present initially to their PCP, given the relatively minor nature of their symptoms and mechanism of injury.
At our institution, the radiology department and referring physician jointly triage out-patients when radiographs requested by the referring physician show evidence of a fracture. Stable and unstable fractures are referred for immediate care—in the pediatric orthopedic clinic if the clinic is open and appointments are available; otherwise in the ED for initial splinting, with follow-up in the orthopedic clinic as soon as possible.
Referral of patients with buckle fractures for same-day care in the ED may bring about unnecessary costs and inconvenience for patients and families. However, policy at our institution dictates that all fractures, including stable buckle fractures, be referred for treatment immediately, once identified.
To determine whether patients with buckle fractures can be safely counseled on the possibility of nonurgent management, we compared the clinical outcomes of pediatric buckle fractures treated acutely or subacutely. The results of our study have practical implications for the timing of treatment or referrals, and for the management of buckle fractures by appropriately trained PCPs, especially in settings where orthopedic consultation may not be readily available.
Methods
Patient selection
The Vanderbilt Children’s Hospital institutional review board approved this retrospective cohort study, with waiver of patient consent. We reviewed 1923 consecutive charts of patients who were seen in the hospital’s pediatric orthopedic clinic for stable fractures between July, 1, 2004 and August 31, 2007. We identified patients for our study population by current procedural terminology (CPT) codes for fracture care that were compatible with buckle fracture or other stable fracture management without manipulation. Applicable CPT codes included the following fracture sites: radial head/neck (24650), ulnar shaft (25530), distal radius with or without ulnar styloid (25600), metacarpal (26600), phalanx of hand or foot (26720, 28510), distal fibula (27786), and metatarsal (28470).
Inclusion and exclusion criteria. Inclusion criteria among this screened population were an isolated buckle fracture mentioned in the official radiology report or pediatric orthopedic clinical note, and age <18 years at the time of injury. We excluded patients for the following reasons: uncertain date of injury (n=67), lack of final clinical follow-up (n=59), acute manipulation of the fracture (n=10), multiple concurrent injuries (n=11), or known metabolic bone disease (n=3) or coagulopathy (n=1).
After initial patient selection, a CAQ-certified pediatric radiologist (with additional fellowship training in pediatric musculoskeletal radiology) and a board-certified orthopedic surgeon (with pediatric orthopedic fellowship training) examined available radiographic images to confirm the diagnosis of a buckle fracture. We further excluded patients whose radiographic findings did not meet criteria for isolated buckle fractures.
Study populations
The final study population consisted of 341 children with confirmed isolated buckle fractures. We assigned patients to acute or subacute treatment groups based on the length of time between injury and presentation for care. Patients were assigned to acute treatment (n=155) if they presented for care on the same day as the injury. All others first seen >1 day after documented time of injury were assigned to subacute treatment (n=186).
We determined length of time between injury and presentation based on data available in the electronic medical record. If the injury was first documented in the orthopedic clinic, we reviewed notes to determine when the patient had initially sought care, and whether from our institution, a PCP, or an outside ED. If documentation showed that initial contact with any health care professional occurred within 1 day of the injury, we assigned the patient to acute management.
Data analysis
Data collection from computerized medical records included date of injury, date of initial care, anatomic location of fracture, mechanism of injury, referring physician, whether the patient was seen initially in the ED, date of last orthopedic follow-up, number of clinical visits, and clinical outcome. Clinical outcome was judged as “good” or “poor” at the last orthopedic follow-up visit, approximately 3 to 4 weeks after injury. A poor clinical outcome could indicate a clinically apparent deformity or functional impairment, need for subacute manipulation, or refracture. We deemed 1 patient’s outcome uncertain due to an ambiguous final clinical note, and we had this case reviewed by a pediatric orthopedist. Any visit to a PCP, ED, or orthopedic clinic was included in the total number of a patient’s clinical visits.
Consulting radiologists also noted the presence and degree of fracture angulation for each patient on initial and follow-up films. Degree of angulation was rated as mild (<10°), moderate (11°-20°), or severe (>20°). Follow-up films were not available for 14 patients (5.2% of acutely treated patients; 3.2% of subacutely treated patients), as final clinical follow-up occasionally occurred outside our institution. In these cases, we relied on the clinical note to determine degree of angulation, if present.
We obtained total charges (technical and professional) for buckle fracture treatment for patients treated initially in the ED and for patients seen initially in the orthopedic clinic.
Statistical analysis
We used an independent samples t-test to compare mean patient ages, times from initial treatment to final treatment, and the numbers of clinical encounters for patients in the acute and subacute treatment groups. For the acute treatment group, time from injury to initial care, by definition, was considered “0.” For the subacute treatment group, we constructed 99.9% confidence intervals around the mean time from injury to initial care to determine whether or not they included “0.”
We used Fisher’s exact test to gauge differences in the proportions of absent or mild initial angulation, absent or mild final angulation, and the point of initial care between the acute and subacute treatment groups. We used Pearson’s chi-squared test to assess between-group differences in the distribution of fracture sites (forearm, hand/foot, or leg), mechanism of injury (fall, direct blow, other), change in angulation (none, improved, worsened), and point of entry into the health care system (PCP, ED, orthopedic clinic). We performed statistical analyses with the statistical package SPSS v15 (SPSS, Inc., Chicago, Ill).
Results
Patient characteristics
Of the 1923 pediatric patients with stable fractures seen in the orthopedic clinic at our institution during the study period, 588 had isolated buckle fractures. Of these, we excluded 151 based on predefined criteria (see Methods). After consensus review of radiographs by a pediatric orthopedist and pediatric radiologist, we excluded an additional 96 patients with inconclusive radiographs. The final study group numbered 341 pediatric patients with confirmed isolated buckle fractures.
The forearm was most commonly affected, with isolated distal radius fractures accounting for 67.7% (231/341) of all fractures, and combined radius/ulna fractures accounting for 14.7% (50/341). The most common mechanism of injury was a fall (85.9%; 293/341), usually a direct fall, with a higher percentage of patients with direct falls in the acute management group ( TABLE 1 ). Mean age and sex were not significantly different for the 2 treatment groups.
TABLE 1
Baseline characteristics of study populations
| Acute (n=155) | Subacute (n=186) | P value | |
|---|---|---|---|
| Age, y ± SD (range) | 7.9 ± 4.0 (0.9-17.8) | 7.9 ± 3.8 (1.0-16.4) | .901 |
| Male, n (%) | 79 (51.0) | 86 (46.2) | .384 |
| Site of fracture, n (%) | .022 | ||
| Forearm | 142 (91.6) | 151 (81.2) | |
| Hand or foot | 12 (7.7) | 33 (17.7) | |
| Leg | 1 (0.6) | 2 (1.1) | |
| Mechanism of injury, n (%) | .045 | ||
| Fall | 141 (90.9) | 152 (81.7) | |
| Direct blow | 5 (3.2) | 15 (8.1) | |
| Other/unknown | 9 (5.8) | 19 (10.2) | |
| SD, standard deviation. | |||
Acute vs subacute management outcomes
Of the 341 patients included in the study, 155 patients were treated acutely and 186 patients were treated subacutely. For the subacute management group, mean time between injury and treatment was 2.5±2.6 days ( TABLE 2 ). We observed no poor clinical outcomes in either acute or subacute management groups. All patients, regardless of time elapsed from injury to initial splinting, recovered without complication. The difference in number of clinical visits between the acute and subacute management groups was not significant (acute 3.2±0.5; subacute 3.1±0.5). The mean length of clinical follow-up from initial splinting to discharge from orthopedic care was higher in the acute management group (acute 32.9±17.1 days; subacute 28.9±13.4 days).
Most patients presented with non-angulated fractures, regardless of time from injury to initial presentation ( TABLE 2 ). The degree of angulation worsened in a small proportion of fractures during convalescence. The difference in initial angulation, final angulation, or change in angulation between acute and subacute management groups was not significant.
A higher proportion of patients in the acute treatment group presented directly to the ED for care, whereas a higher proportion of patients in the subacute treatment group presented to their PCP during routine working hours and were referred to the orthopedic clinic ( TABLE 2 ). For both acute and subacute management groups, we compared outcomes for patients seen initially in the ED or orthopedic clinic. No adverse outcomes occurred among any of the studied patients.
TABLE 2
Clinical outcomes did not differ between acute and subacute management groups
| Acute (n=155) | Subacute (n=186) | P value | |
|---|---|---|---|
| Time from injury to initial care, d ± SD (range) | 0 | 2.5 ± 2.6 (1-14) | <.001 |
| Good outcome, n (%) | 155 (100) | 186 (100) | 1.0 |
| Time from initial treatment to final follow-up, d ± SD (range) | 32.9 ± 17.1 (8-169) | 28.9 ± 13.4 (9-164) | .016 |
| Number of clinical encounters (primary care physician, ED, or orthopedic clinic), n ± SD (range) | 3.2 ± 0.5 (2-5) | 3.1 ± 0.5 (2-5) | .051 |
| Initial angulation, n (%) | .541 | ||
| None | 145 (93.5) | 170 (91.4) | |
| Mild (<10°) | 10 (6.5) | 16 (8.6) | |
| Final angulation, n (%) | 1.0 | ||
| None | 136 (87.7) | 163 (87.6) | |
| Mild (<10°) | 19 (12.2) | 23 (12.4) | |
| Change in angulation, n (%) | .907 | ||
| No change | 144 (92.9) | 175 (94.1) | |
| Worse | 10 (6.4) | 10 (5.4) | |
| Improved | 1 (0.6) | 1 (0.5) | |
| Point of entry to health care system, n (%) | <.001 | ||
| Primary care physician | 44 (28.4) | 115 (61.8) | |
| ED | 108 (69.7) | 54 (29.0) | |
| Orthopedic clinic | 3 (1.9) | 17 (9.1) | |
| Location of initial management, n (%) | <.001 | ||
| ED | 132 (85.2) | 81 (43.5) | |
| Orthopedic clinic | 23 (14.8) | 105 (56.4) | |
| ED, emergency department; SD, standard deviation. | |||
Charge analysis
We compared total charges (professional and technical) for managing buckle fractures initially in the ED with those initially seen in the orthopedic clinic. Total charge per patient in the ED, including subsequent follow-up in the orthopedic clinic, was $4397 ($2516, professional; $1881, technical). Total charge per patient for treatment only in the orthopedic clinic was $1426 ($918, professional; $508, technical). Total charge per patient was $2971 more for patients treated initially in the ED.
Between July 1, 2004, and August 31, 2007, 159 patients (46.6%) with buckle fractures entered the health care system through their primary care physician. Of these, 44 patients were seen acutely by the physician; 115 patients were seen on a subacute basis. Of the 44 patients seen acutely, 24 (54%) were referred directly to the ED; 20 (45%) were referred to the orthopedic clinic. Of the 115 patients seen subacutely, 27 (23%) were referred directly to the ED, and the remaining 88 (76%) were referred to the orthopedic clinic. In sum, 51 patients (32%) were seen initially by a PCP, who referred them to the ED. The cost savings with each patient seen subacutely in the orthopedic clinic was $2971, and avoiding ED treatment for all patients could have yielded a total gross savings of approximately $150,000.
Discussion
Buckle fractures are inherently stable and almost universally heal without complication.4,5 Perhaps because of the high likelihood of good outcome, there is a relative paucity of articles in the recent literature addressing the management of this common pediatric fracture. Older studies have addressed casting vs splinting and the need for follow-up, but no study has yet examined whether immediate treatment is necessary.6,7 Although some studies have noted incidentally that many children have delayed presentation for care,5 none has specifically examined the clinical or economic impact of a delay in care or the effect of subacute treatment on outcomes.
Delayed treatment does not adversely affect clinical outcome. Our study objective was to compare clinical outcomes of buckle fractures treated acutely on the same day of injury with outcomes of those treated subacutely. The 2 groups did not differ in extent or angulation of fracture at presentation. We found no difference in outcomes between the groups; all fractures healed without complication. We observed no difference in final angulation of fracture on follow-up imaging. Though our institution routinely obtains follow-up films, it is worth mentioning that the utility of repeat films in pediatric buckle fractures with minimal initial angulation has been debated.5 These data suggest that subacute treatment of a buckle fracture is a safe and reasonable option.
Non-ED treatment substantially reduces cost. One goal of efficient health care delivery is to decrease the cost and burden of care without increasing long-term morbidity and disability. Evidence suggests that families may prefer less acute management options that allow greater convenience and flexibility, provided that clinical outcomes are not compromised.8 In the case of pediatric buckle fractures, higher costs (for both the patient and the hospital) and longer wait times related to ED care may be avoided by counseling patients on the option of subacute care. Our study found that referring patients directly to the orthopedic clinic, even if this results in a delay in definitive management, leads to a reduction in health care burden without a change in clinical outcome.
Children with buckle fractures are frequently (46.6%) taken to their PCP for initial care. Many pediatricians and family physicians—especially the increasing number of physicians who have completed additional fellowship training in sports medicine—may prefer to manage buckle fractures within their practices. Many other PCPs may be practicing in communities lacking local orthopedic expertise. The results of this study provide reassurance regarding the positive outcome of buckle fractures. Furthermore, managing buckle fractures in the primary care setting may be even more cost effective than referring patients to a specialty orthopedic clinic—but additional research on this point is needed.
We do not advocate delayed imaging or treatment of suspected fractures. However, once a diagnosis of buckle fracture is confirmed radiographically, our data show that subacute treatment yields significant cost and time savings without affecting final clinical outcome.
Study limitations
This study is limited by its retrospective data collection in 1 pediatric tertiary care hospital. As current clinical practice is to treat all buckle fractures once identified, very few patients with known injury were specifically treated in a subacute fashion. We defined the subacute care group as patients who were treated >1 day from the time of injury. Because initial splinting did not occur in this group, we expect that the observed results would be similar, and no worse, compared with buckle fracture care directed by a subacute treatment algorithm.
This study examined only patients with a diagnosis of isolated buckle fracture. Non-buckle stable fractures were excluded a priori from our patient population. Although it is possible that most stable fractures (eg, nondisplaced transverse fractures, Salter-Harris I injuries) could be managed subacutely, we addressed only isolated buckle fractures.
Because of the universally positive outcomes in these cases, most of our patients had no orthopedic follow-up beyond 1 month. We are not able to comment on whether any longer-term abnormalities in function occurred. This question could be addressed through a prospective trial requiring reevaluation of each patient at a set endpoint of the study.
Although buckle fractures are inherently stable and do not present a significant risk of displacement with delayed treatment, they are nevertheless painful fractures that can be a cause of considerable anxiety for both patient and family. The goal of the physician, beyond ensuring the best medical outcome, extends to provide emotional support to the patient and family. Pain control and reassurance are therefore central to the discussion of fracture management, and are most likely the driving factor for a patient to seek urgent care. A key limitation of this study was the inability to determine differences in pain control between acute and subacute treatment. As mentioned above, a prospective study would enable the issue of pain control to be better addressed.
CORRESPONDENCE
Debbie Lee Bennett, MD, Massachusetts General Hospital, 55 Fruit Street, FND-216, Boston, MA 02114; [email protected]
(At the time this study was accepted for publication, Dr. Bennett was at Vanderbilt Children’s Hospital.)
PURPOSE To determine whether the clinical outcome of buckle fractures in children differs between those treated acutely on the same day of trauma and those treated subacutely, and whether a change in practice patterns based on these data would result in cost savings.
METHODS In this retrospective cohort study—approved by the institutional review board—we reviewed the cases of 341 consecutive patients <18 years of age seen by the pediatric orthopedic clinic for treatment of isolated extremity buckle fractures between July 1, 2004 and August 31, 2007. Time from injury to treatment was used to divide patients into 2 groups: acute (≤1 day; n=155) and subacute treatment (>1 day; n=186). Clinical outcome at final orthopedic follow-up was recorded for each patient. We defined adverse outcome as fractures requiring manipulation, clinically apparent deformity, or functional impairment. Charge analysis compared differences in management costs for patients with buckle fractures presenting initially to the emergency department (ED) and those seen solely in the orthopedic clinic.
RESULTS No adverse outcomes were identified in either acute or subacute treatment groups. Total clinical visits did not vary (acute, 3.2 vs subacute, 3.1; P=.051). Presence of mild angulation of fractures on radiographs did not differ significantly between acute and subacute management groups at initial presentation (6.5% vs 8.6%; P=.541) or at final follow-up (12.2% vs 12.4%; P=1.0). A cost savings of approximately $3000 could have been realized for each patient referred to the ED who might otherwise have been seen subacutely in the orthopedic clinic.
CONCLUSIONS No adverse clinical outcomes resulted from subacute treatment of stable buckle fractures. Cost and time savings may be realized with subacute management of buckle fractures without affecting clinical outcome.
Next time a child in your care has a suspected fracture as a result of a fall and x-ray films reveal a buckle fracture, consider telling parents there’s no need for an urgent visit to the ED. As long as the pain is manageable, treating the injury within a day or so will likely be more convenient for the family, will cost less, and will not result in any complications for the child.
Buckle (or torus) fractures—the most common type of fracture occurring in the pediatric population and accounting for a large number of visits to primary care physicians (PCPs), EDs, and orthopedic clinics each year1 —involve impaction of bone along only 1 cortex and are therefore inherently stable.2 Even with only minimal immobilization, the overwhelming majority of buckle fractures heal without complication.3 Although many patients present directly to the ED for management of these fractures, many others present initially to their PCP, given the relatively minor nature of their symptoms and mechanism of injury.
At our institution, the radiology department and referring physician jointly triage out-patients when radiographs requested by the referring physician show evidence of a fracture. Stable and unstable fractures are referred for immediate care—in the pediatric orthopedic clinic if the clinic is open and appointments are available; otherwise in the ED for initial splinting, with follow-up in the orthopedic clinic as soon as possible.
Referral of patients with buckle fractures for same-day care in the ED may bring about unnecessary costs and inconvenience for patients and families. However, policy at our institution dictates that all fractures, including stable buckle fractures, be referred for treatment immediately, once identified.
To determine whether patients with buckle fractures can be safely counseled on the possibility of nonurgent management, we compared the clinical outcomes of pediatric buckle fractures treated acutely or subacutely. The results of our study have practical implications for the timing of treatment or referrals, and for the management of buckle fractures by appropriately trained PCPs, especially in settings where orthopedic consultation may not be readily available.
Methods
Patient selection
The Vanderbilt Children’s Hospital institutional review board approved this retrospective cohort study, with waiver of patient consent. We reviewed 1923 consecutive charts of patients who were seen in the hospital’s pediatric orthopedic clinic for stable fractures between July, 1, 2004 and August 31, 2007. We identified patients for our study population by current procedural terminology (CPT) codes for fracture care that were compatible with buckle fracture or other stable fracture management without manipulation. Applicable CPT codes included the following fracture sites: radial head/neck (24650), ulnar shaft (25530), distal radius with or without ulnar styloid (25600), metacarpal (26600), phalanx of hand or foot (26720, 28510), distal fibula (27786), and metatarsal (28470).
Inclusion and exclusion criteria. Inclusion criteria among this screened population were an isolated buckle fracture mentioned in the official radiology report or pediatric orthopedic clinical note, and age <18 years at the time of injury. We excluded patients for the following reasons: uncertain date of injury (n=67), lack of final clinical follow-up (n=59), acute manipulation of the fracture (n=10), multiple concurrent injuries (n=11), or known metabolic bone disease (n=3) or coagulopathy (n=1).
After initial patient selection, a CAQ-certified pediatric radiologist (with additional fellowship training in pediatric musculoskeletal radiology) and a board-certified orthopedic surgeon (with pediatric orthopedic fellowship training) examined available radiographic images to confirm the diagnosis of a buckle fracture. We further excluded patients whose radiographic findings did not meet criteria for isolated buckle fractures.
Study populations
The final study population consisted of 341 children with confirmed isolated buckle fractures. We assigned patients to acute or subacute treatment groups based on the length of time between injury and presentation for care. Patients were assigned to acute treatment (n=155) if they presented for care on the same day as the injury. All others first seen >1 day after documented time of injury were assigned to subacute treatment (n=186).
We determined length of time between injury and presentation based on data available in the electronic medical record. If the injury was first documented in the orthopedic clinic, we reviewed notes to determine when the patient had initially sought care, and whether from our institution, a PCP, or an outside ED. If documentation showed that initial contact with any health care professional occurred within 1 day of the injury, we assigned the patient to acute management.
Data analysis
Data collection from computerized medical records included date of injury, date of initial care, anatomic location of fracture, mechanism of injury, referring physician, whether the patient was seen initially in the ED, date of last orthopedic follow-up, number of clinical visits, and clinical outcome. Clinical outcome was judged as “good” or “poor” at the last orthopedic follow-up visit, approximately 3 to 4 weeks after injury. A poor clinical outcome could indicate a clinically apparent deformity or functional impairment, need for subacute manipulation, or refracture. We deemed 1 patient’s outcome uncertain due to an ambiguous final clinical note, and we had this case reviewed by a pediatric orthopedist. Any visit to a PCP, ED, or orthopedic clinic was included in the total number of a patient’s clinical visits.
Consulting radiologists also noted the presence and degree of fracture angulation for each patient on initial and follow-up films. Degree of angulation was rated as mild (<10°), moderate (11°-20°), or severe (>20°). Follow-up films were not available for 14 patients (5.2% of acutely treated patients; 3.2% of subacutely treated patients), as final clinical follow-up occasionally occurred outside our institution. In these cases, we relied on the clinical note to determine degree of angulation, if present.
We obtained total charges (technical and professional) for buckle fracture treatment for patients treated initially in the ED and for patients seen initially in the orthopedic clinic.
Statistical analysis
We used an independent samples t-test to compare mean patient ages, times from initial treatment to final treatment, and the numbers of clinical encounters for patients in the acute and subacute treatment groups. For the acute treatment group, time from injury to initial care, by definition, was considered “0.” For the subacute treatment group, we constructed 99.9% confidence intervals around the mean time from injury to initial care to determine whether or not they included “0.”
We used Fisher’s exact test to gauge differences in the proportions of absent or mild initial angulation, absent or mild final angulation, and the point of initial care between the acute and subacute treatment groups. We used Pearson’s chi-squared test to assess between-group differences in the distribution of fracture sites (forearm, hand/foot, or leg), mechanism of injury (fall, direct blow, other), change in angulation (none, improved, worsened), and point of entry into the health care system (PCP, ED, orthopedic clinic). We performed statistical analyses with the statistical package SPSS v15 (SPSS, Inc., Chicago, Ill).
Results
Patient characteristics
Of the 1923 pediatric patients with stable fractures seen in the orthopedic clinic at our institution during the study period, 588 had isolated buckle fractures. Of these, we excluded 151 based on predefined criteria (see Methods). After consensus review of radiographs by a pediatric orthopedist and pediatric radiologist, we excluded an additional 96 patients with inconclusive radiographs. The final study group numbered 341 pediatric patients with confirmed isolated buckle fractures.
The forearm was most commonly affected, with isolated distal radius fractures accounting for 67.7% (231/341) of all fractures, and combined radius/ulna fractures accounting for 14.7% (50/341). The most common mechanism of injury was a fall (85.9%; 293/341), usually a direct fall, with a higher percentage of patients with direct falls in the acute management group ( TABLE 1 ). Mean age and sex were not significantly different for the 2 treatment groups.
TABLE 1
Baseline characteristics of study populations
| Acute (n=155) | Subacute (n=186) | P value | |
|---|---|---|---|
| Age, y ± SD (range) | 7.9 ± 4.0 (0.9-17.8) | 7.9 ± 3.8 (1.0-16.4) | .901 |
| Male, n (%) | 79 (51.0) | 86 (46.2) | .384 |
| Site of fracture, n (%) | .022 | ||
| Forearm | 142 (91.6) | 151 (81.2) | |
| Hand or foot | 12 (7.7) | 33 (17.7) | |
| Leg | 1 (0.6) | 2 (1.1) | |
| Mechanism of injury, n (%) | .045 | ||
| Fall | 141 (90.9) | 152 (81.7) | |
| Direct blow | 5 (3.2) | 15 (8.1) | |
| Other/unknown | 9 (5.8) | 19 (10.2) | |
| SD, standard deviation. | |||
Acute vs subacute management outcomes
Of the 341 patients included in the study, 155 patients were treated acutely and 186 patients were treated subacutely. For the subacute management group, mean time between injury and treatment was 2.5±2.6 days ( TABLE 2 ). We observed no poor clinical outcomes in either acute or subacute management groups. All patients, regardless of time elapsed from injury to initial splinting, recovered without complication. The difference in number of clinical visits between the acute and subacute management groups was not significant (acute 3.2±0.5; subacute 3.1±0.5). The mean length of clinical follow-up from initial splinting to discharge from orthopedic care was higher in the acute management group (acute 32.9±17.1 days; subacute 28.9±13.4 days).
Most patients presented with non-angulated fractures, regardless of time from injury to initial presentation ( TABLE 2 ). The degree of angulation worsened in a small proportion of fractures during convalescence. The difference in initial angulation, final angulation, or change in angulation between acute and subacute management groups was not significant.
A higher proportion of patients in the acute treatment group presented directly to the ED for care, whereas a higher proportion of patients in the subacute treatment group presented to their PCP during routine working hours and were referred to the orthopedic clinic ( TABLE 2 ). For both acute and subacute management groups, we compared outcomes for patients seen initially in the ED or orthopedic clinic. No adverse outcomes occurred among any of the studied patients.
TABLE 2
Clinical outcomes did not differ between acute and subacute management groups
| Acute (n=155) | Subacute (n=186) | P value | |
|---|---|---|---|
| Time from injury to initial care, d ± SD (range) | 0 | 2.5 ± 2.6 (1-14) | <.001 |
| Good outcome, n (%) | 155 (100) | 186 (100) | 1.0 |
| Time from initial treatment to final follow-up, d ± SD (range) | 32.9 ± 17.1 (8-169) | 28.9 ± 13.4 (9-164) | .016 |
| Number of clinical encounters (primary care physician, ED, or orthopedic clinic), n ± SD (range) | 3.2 ± 0.5 (2-5) | 3.1 ± 0.5 (2-5) | .051 |
| Initial angulation, n (%) | .541 | ||
| None | 145 (93.5) | 170 (91.4) | |
| Mild (<10°) | 10 (6.5) | 16 (8.6) | |
| Final angulation, n (%) | 1.0 | ||
| None | 136 (87.7) | 163 (87.6) | |
| Mild (<10°) | 19 (12.2) | 23 (12.4) | |
| Change in angulation, n (%) | .907 | ||
| No change | 144 (92.9) | 175 (94.1) | |
| Worse | 10 (6.4) | 10 (5.4) | |
| Improved | 1 (0.6) | 1 (0.5) | |
| Point of entry to health care system, n (%) | <.001 | ||
| Primary care physician | 44 (28.4) | 115 (61.8) | |
| ED | 108 (69.7) | 54 (29.0) | |
| Orthopedic clinic | 3 (1.9) | 17 (9.1) | |
| Location of initial management, n (%) | <.001 | ||
| ED | 132 (85.2) | 81 (43.5) | |
| Orthopedic clinic | 23 (14.8) | 105 (56.4) | |
| ED, emergency department; SD, standard deviation. | |||
Charge analysis
We compared total charges (professional and technical) for managing buckle fractures initially in the ED with those initially seen in the orthopedic clinic. Total charge per patient in the ED, including subsequent follow-up in the orthopedic clinic, was $4397 ($2516, professional; $1881, technical). Total charge per patient for treatment only in the orthopedic clinic was $1426 ($918, professional; $508, technical). Total charge per patient was $2971 more for patients treated initially in the ED.
Between July 1, 2004, and August 31, 2007, 159 patients (46.6%) with buckle fractures entered the health care system through their primary care physician. Of these, 44 patients were seen acutely by the physician; 115 patients were seen on a subacute basis. Of the 44 patients seen acutely, 24 (54%) were referred directly to the ED; 20 (45%) were referred to the orthopedic clinic. Of the 115 patients seen subacutely, 27 (23%) were referred directly to the ED, and the remaining 88 (76%) were referred to the orthopedic clinic. In sum, 51 patients (32%) were seen initially by a PCP, who referred them to the ED. The cost savings with each patient seen subacutely in the orthopedic clinic was $2971, and avoiding ED treatment for all patients could have yielded a total gross savings of approximately $150,000.
Discussion
Buckle fractures are inherently stable and almost universally heal without complication.4,5 Perhaps because of the high likelihood of good outcome, there is a relative paucity of articles in the recent literature addressing the management of this common pediatric fracture. Older studies have addressed casting vs splinting and the need for follow-up, but no study has yet examined whether immediate treatment is necessary.6,7 Although some studies have noted incidentally that many children have delayed presentation for care,5 none has specifically examined the clinical or economic impact of a delay in care or the effect of subacute treatment on outcomes.
Delayed treatment does not adversely affect clinical outcome. Our study objective was to compare clinical outcomes of buckle fractures treated acutely on the same day of injury with outcomes of those treated subacutely. The 2 groups did not differ in extent or angulation of fracture at presentation. We found no difference in outcomes between the groups; all fractures healed without complication. We observed no difference in final angulation of fracture on follow-up imaging. Though our institution routinely obtains follow-up films, it is worth mentioning that the utility of repeat films in pediatric buckle fractures with minimal initial angulation has been debated.5 These data suggest that subacute treatment of a buckle fracture is a safe and reasonable option.
Non-ED treatment substantially reduces cost. One goal of efficient health care delivery is to decrease the cost and burden of care without increasing long-term morbidity and disability. Evidence suggests that families may prefer less acute management options that allow greater convenience and flexibility, provided that clinical outcomes are not compromised.8 In the case of pediatric buckle fractures, higher costs (for both the patient and the hospital) and longer wait times related to ED care may be avoided by counseling patients on the option of subacute care. Our study found that referring patients directly to the orthopedic clinic, even if this results in a delay in definitive management, leads to a reduction in health care burden without a change in clinical outcome.
Children with buckle fractures are frequently (46.6%) taken to their PCP for initial care. Many pediatricians and family physicians—especially the increasing number of physicians who have completed additional fellowship training in sports medicine—may prefer to manage buckle fractures within their practices. Many other PCPs may be practicing in communities lacking local orthopedic expertise. The results of this study provide reassurance regarding the positive outcome of buckle fractures. Furthermore, managing buckle fractures in the primary care setting may be even more cost effective than referring patients to a specialty orthopedic clinic—but additional research on this point is needed.
We do not advocate delayed imaging or treatment of suspected fractures. However, once a diagnosis of buckle fracture is confirmed radiographically, our data show that subacute treatment yields significant cost and time savings without affecting final clinical outcome.
Study limitations
This study is limited by its retrospective data collection in 1 pediatric tertiary care hospital. As current clinical practice is to treat all buckle fractures once identified, very few patients with known injury were specifically treated in a subacute fashion. We defined the subacute care group as patients who were treated >1 day from the time of injury. Because initial splinting did not occur in this group, we expect that the observed results would be similar, and no worse, compared with buckle fracture care directed by a subacute treatment algorithm.
This study examined only patients with a diagnosis of isolated buckle fracture. Non-buckle stable fractures were excluded a priori from our patient population. Although it is possible that most stable fractures (eg, nondisplaced transverse fractures, Salter-Harris I injuries) could be managed subacutely, we addressed only isolated buckle fractures.
Because of the universally positive outcomes in these cases, most of our patients had no orthopedic follow-up beyond 1 month. We are not able to comment on whether any longer-term abnormalities in function occurred. This question could be addressed through a prospective trial requiring reevaluation of each patient at a set endpoint of the study.
Although buckle fractures are inherently stable and do not present a significant risk of displacement with delayed treatment, they are nevertheless painful fractures that can be a cause of considerable anxiety for both patient and family. The goal of the physician, beyond ensuring the best medical outcome, extends to provide emotional support to the patient and family. Pain control and reassurance are therefore central to the discussion of fracture management, and are most likely the driving factor for a patient to seek urgent care. A key limitation of this study was the inability to determine differences in pain control between acute and subacute treatment. As mentioned above, a prospective study would enable the issue of pain control to be better addressed.
CORRESPONDENCE
Debbie Lee Bennett, MD, Massachusetts General Hospital, 55 Fruit Street, FND-216, Boston, MA 02114; [email protected]
(At the time this study was accepted for publication, Dr. Bennett was at Vanderbilt Children’s Hospital.)
1. Plint AC, Clifford T, Perry J, et al. Wrist buckle fractures: a survey of current practice patterns and attitudes toward immobilization. Can J Emerg Med. 2003;5:95-100.
2. England SP, Sundberg S. Management of common pediatric fractures. In: England SP, ed. Common Orthopedic Problems II. Philadelphia, Pa: WB Saunders; 1996:991–1012.
3. Van Bosse HJP, Patel RJ, Thacker M, et al. Minimalistic approach to treating wrist torus fractures. J Pediatr Orthop. 2005;25:495-500.
4. Davidson JS, Brown DJ, Barnes SN, et al. Simple treatment for torus fractures of the distal radius. J Bone Joint Surg Br. 2001;83-B:1173-1175.
5. Plint AC, Perry JJ, Tsang JLY. Pediatric wrist buckle fractures: should we just splint and go? Can J Emerg Med. 2004;6:397-401.
6. Solan MC, Rees R, Daly K. Current management of torus fractures of the distal radius. Injury. 2002;33:503-505.
7. Plint AC, Perry JJ, Correll R, et al. A randomized, controlled trial of removable splinting versus casting for wrist buckle fractures in children. Pediatrics. 2006;117:691-697.
8. Symons S, Rowsell M, Bhowal B, et al. Hospital versus home management of children with buckle fractures of the distal radius. A prospective, randomised trial. J Bone Joint Surg Br. 2001;83:556-560.
1. Plint AC, Clifford T, Perry J, et al. Wrist buckle fractures: a survey of current practice patterns and attitudes toward immobilization. Can J Emerg Med. 2003;5:95-100.
2. England SP, Sundberg S. Management of common pediatric fractures. In: England SP, ed. Common Orthopedic Problems II. Philadelphia, Pa: WB Saunders; 1996:991–1012.
3. Van Bosse HJP, Patel RJ, Thacker M, et al. Minimalistic approach to treating wrist torus fractures. J Pediatr Orthop. 2005;25:495-500.
4. Davidson JS, Brown DJ, Barnes SN, et al. Simple treatment for torus fractures of the distal radius. J Bone Joint Surg Br. 2001;83-B:1173-1175.
5. Plint AC, Perry JJ, Tsang JLY. Pediatric wrist buckle fractures: should we just splint and go? Can J Emerg Med. 2004;6:397-401.
6. Solan MC, Rees R, Daly K. Current management of torus fractures of the distal radius. Injury. 2002;33:503-505.
7. Plint AC, Perry JJ, Correll R, et al. A randomized, controlled trial of removable splinting versus casting for wrist buckle fractures in children. Pediatrics. 2006;117:691-697.
8. Symons S, Rowsell M, Bhowal B, et al. Hospital versus home management of children with buckle fractures of the distal radius. A prospective, randomised trial. J Bone Joint Surg Br. 2001;83:556-560.
PELVIC FLOOR DYSFUNCTION
The authors report no financial relationships relevant to this article.
Overactive bladder (OAB)—urinary urgency, with or without incontinence, usually with frequency and nocturia1—is a common problem among women who seek care from an ObGyn. In fact, the condition is estimated to carry a health-care cost in excess of $12 billion annually in the United States.2
A recent community-based survey in Norway estimated the prevalence of urinary incontinence there to be 27% in women between the ages of 65 and 69 years and 35% to 40% in those 80 years or older.3 A population-based study in the United States suggested an even higher rate of urinary incontinence here: greater than 50% in women 60 years or older, with 1) urge urinary incontinence (UUI) predominating4 and 2) the prevalence particularly high among older women who are homebound or who live in a long-term care facility.5
OAB can undermine quality of life in several ways: social isolation, anxiety, poor sleep, higher risk of fracture after a fall,6 reduced ability to function, and poor self-perception. Despite these harmful effects, many women delay seeking care for OAB because they are embarrassed to talk about it with their physician.
Treatment by generalists is feasible—but there is a catch
It’s possible to treat most patients with OAB without referral to a specialist. Two common concerns, however, may set up a roadblock to successful management: the adverse effects associated with some agents and suboptimal control of symptoms.
In this Update, we review recent findings about 1) the potential that anticholinergic therapy has for impairing cognitive function in the older population of women and 2) the important role that concomitant behavioral therapy plays in the long-term success of, and patients’ satisfaction with, treatment of OAB.
Behavioral therapy for OAB: Is it worth all the effort?
Burgio KL, Locher JL, Goode PS. Combined behavioral and drug therapy for urge incontinence in older women. J Am Geriatr Soc. 2000;48:370–374.
The authors of this article followed a randomized clinical trial of older women that compared behavioral and drug therapy for OAB. In the trial, biofeedback-assisted behavioral training (comprising anorectal biofeedback, urge strategies, pelvic muscle biofeedback, and practitioner-directed review with optimization) was compared with treatment with oxybutynin, between 2.5 and 15 mg/day. Both biofeedback-assisted behavioral therapy and the drug regimen were found effective, although neither treatment provided an entirely satisfactory result for all patients. (For a brief description of what constitutes behavioral treatment, see “6 tenets of behavioral therapy for urge urinary incontinence.”)
Second phase of the trial. To determine if treatment satisfaction could be enhanced, the investigators performed a modified crossover study to determine whether combination therapy—biofeedback-assisted behavioral training plus oxybutynin—added any benefit over treatment with behavioral therapy or drug therapy alone. Eligibility was determined by age (55 years or older), demonstrated UUI for at least 3 months, and incomplete dryness or incomplete satisfaction with the outcome of 8 weeks of single-intervention treatment (with either treatment) during the initial phase of the trial.
This subgroup was offered an additional 8 weeks of combination therapy. The primary outcome measure was a reduction in the frequency of episodes of incontinence episodes as recorded by subjects in a bladder diary.
Of 197 women who participated in the original randomized clinical trial, 35—27 who completed drug therapy and 8 who completed behavioral treatment—elected to receive combination therapy. Those 35 subjects did not differ in any of the multiple baseline variables; mean age was 69.3 years (standard deviation [SD], ±7.9 years).
Among subjects originally assigned to behavioral therapy alone, overall reduction in incontinence increased from a mean of 57.5% to a mean of 88.5% after combined therapy (P=.034). Subjects originally assigned to drug therapy alone demonstrated an improvement from 72.7% reduction in incontinence to a mean 84.3% overall reduction with combined therapy (P=.001).
These data suggest that combined therapy can be more effective than behavioral therapy or drug therapy alone. The impact of this study is limited, however, by the relatively low percentage (12.7%) of patients who had received behavioral therapy and chose to add drug therapy, compared with the 41.5% who moved from drug therapy alone to add behavioral therapy.
Furthermore, subjects were self-selected: They chose to continue with an additional 8 weeks of therapy after their initial suboptimal outcome. It is possible that some subjects who were neither totally continent nor completely satisfied with initial therapy chose not to continue with the crossover segment of the trial because it posed too great a burden or because they were discouraged with the initial degree of improvement.
Generalizing these results to all older women with UUI is difficult. The authors point out, however, that, in practice, patients may be more likely than not to choose combination therapy in the hope of shortening the duration of medical therapy. Although it isn’t known whether providing combination therapy from the outset would have yielded better outcomes than either single therapy did, the authors hypothesize that initial combination therapy may result in greater improvement because patients have a high level of motivation and expectation of improvement at the beginning of treatment.
Importance of this article. The investigators demonstrated that a combination of behavioral and drug therapies can provide increased effectiveness in patients for whom each treatment alone led to suboptimal satisfaction. Furthermore, by targeting women older than 55 years, the investigators were able to demonstrate this effectiveness in a group for whom pelvic-floor training may be more difficult than it is for younger women.
It will be interesting to see if future research will 1) validate these findings and 2) determine whether combined therapy can reduce the duration of drug therapy in this older population through behavioral modification and pelvic floor reeducation.
Fluid management
This first-step therapy can involve providing a handout to the patient that details techniques she can use to monitor and control her fluid intake in a manner that addresses her problem. Among such steps:
- avoiding caffeine and artificial sweeteners
- tracking her diet to identify any other bladder irritants
- limiting fluids before times she is more likely to be incontinent—during a long drive, for example, or, in the case of nocturia, after the evening meal.
Scheduled voiding
With scheduled, or prompted, voiding, the patient empties her bladder at a set interval—usually, every 1.5 to 2 hours. If nocturia, or the more severe enuresis, is a problem, the patient can be prompted by an alarm clock or (if she is institutionalized) by nursing staff. Combining scheduled voiding with fluid management principles helps the patient avoid reaching a bladder volume at which an episode of incontinence becomes more likely.
Bladder training
This is a modification of scheduled voiding that attempts to establish a normal voiding interval in patients who have significant frequency but a small voided volume. It imposes a regimented voiding schedule that gradually (over 7 to 10 days) extends the duration between voids.
Pelvic floor-muscle exercises
The focus here is on using pelvic-floor muscles to prevent incontinence. The muscles are strengthened by having the patient perform Kegel exercises (named for Arnold H. Kegel, MD, who, in 1948, recognized the role of pelvic floor-muscle rehabilitation in the treatment of incontinence). The exercises involve simultaneous 1) contraction of the pelvic and periurethral musculature and 2) relaxation of other muscles, including abdominal muscles, which can increase pressure on the bladder.
Once the patient learns to perform Kegel exercises, she can use them to suppress urgency: Instead of hurrying to the bathroom when urgency arises, she is encouraged to sit down, relax, and contract the pelvic-floor muscles repeatedly until the urge to void diminishes. Once it does, the patient proceeds to the toilet to void normally.
Pelvic exam
By self-exam, the patient can identify and familiarize herself with her purposeful contractions of the pelvic-floor musculature and thereby strengthen those muscles with effective exercise.
Biofeedback
Direct feedback about contractions of the pelvic-floor muscles—by a display of data on a gauge or computer monitor, gathered using an intravaginal or anorectal sensor or probe—allows a patient who is exercising those muscles to better target her efforts and maximize their effectiveness.
Combining behavioral therapy and an anticholinergic medication for urge urinary incontinence may yield a superior result after either modality alone has been disappointing by the patient’s account of success.—JOHN P. JUDD, MD, AND CINDY L. AMUNDSEN, MD
Does oxybutynin for UUI further erode cognition in elderly women who are cognitively impaired?
Lackner TE, Wyman JF, McCarthy TC, Monigold M, Davey C. Randomized, placebo-controlled trial of the cognitive effect, safety, and tolerability of oral extended-release oxybutynin in cognitively impaired nursing home residents with urge urinary incontinence. J Am Geriatr Soc. 2008;56:862–870.
Although anticholinergic therapy is modestly effective against UUI in nursing home residents, past studies have suggested that such treatment can impair, or further impair, cognition in this population—a concern that may lead to underuse. This double-blinded, randomized, placebo-controlled trial compared short-term oral extended-release oxybutynin with placebo.
Consequently, the authors sought to determine the cognitive effect, safety, and tolerability of 5 mg/day oral extended-release oxybutynin (the most commonly prescribed dosage) in cognitively impaired older nursing home residents who have UUI.
Subjects were eligible if they:
- were 65 years or older
- had UUI
- lived in a nursing home longer than 3 months
- had cognitive impairment.
Women already being treated for urinary incontinence, those who had an indwelling Foley catheter or urinary retention, and those who were bed-bound or incommunicative were excluded.
Fifty women, mean age 88.6 years (SD, ±6.2), from 12 nursing home facilities, agreed to participate. They were further stratified based on the score of a Mini-Mental State Exam (MMSE): 13 had severe cognitive impairment (MMSE score, 5–10) and 37 had mild or moderate impairment (score, 11–23).
Subjects were randomized to 4 weeks’ treatment with either 5 mg/day oral extended-release oxybutynin or one placebo tablet daily. A nurse practitioner who was blinded to randomization collected all data. The Confusion Assessment Method (CAM) algorithm, MMSE, and Severe Impairment Battery (SIB) were used to assess cognitive decline. The Brief Agitation Rating Scale (BARS) assessed agitation.
No baseline differences were noted with regard to: age; demographic, functional, and neuropsychiatric characteristics; clinical factors predisposing to delirium; and serum anticholinergic activity. Adherence was similar in the treatment (97%) and placebo (97.4%) groups.
Finding: Cognitive impairment. Treatment and placebo groups in the baseline mild-or-moderate stratum (by MMSE) showed equivalent mean changes in CAM scores at all time points. Because of the small sample size, however, CAM score equivalence could not be definitively determined for the groups in the severe impairment stratum. Evaluation of mean MMSE and BARS scores showed no significant changes between groups.
Finding: Tolerability. Excellent tolerability was noted in the treatment group: 96% of subjects completed the trial (compared with 92% of the placebo group). No difference in the rate of adverse events was noted between treatment and placebo groups; of adverse events recorded, 90% were judged “mild” by the investigators. Constipation and dry mouth were most common.
Finding: Falls. More than half—54%—of subjects in both groups experienced at least one fall during the trial or during the preceding or following 3 months. Despite this, no difference in the rate of falls between the treatment and placebo groups was noted. Furthermore, regression analysis revealed no treatment or period effect on falls per month across the time of observation.
Conclusions. Treatment with 5 mg/day oral extended-release oxybutynin in older patients with some cognitive impairment is well tolerated, the study’s findings suggest, with minimal risk of further cognitive decline or delirium over the short term. The potential that long-term therapy has to harm cognitive function remains, however; data on long-term treatment are needed to illuminate that area.
The authors also address the importance of dosing, especially over time, and discuss the lower potential of newer-generation anticholinergics to produce cognitive impairment.
A limited number of articles in the medical literature address anticholinergics in an older population, specifically, and only a few of those evaluated the effects of the drugs on cognitive function. By investigating patients who had an existing cognitive impairment, the authors of this article were able to target a cohort at risk of further cognitive impairment from medication use—thereby giving further weight to their findings of no significant effect.
Main strengths and limitations of the study. The investigators used validated, standardized cognitive tests that were administered by a uniform blinded evaluator in a randomized, controlled trial. The study was limited, however, because patients were evaluated only over a relatively short period (1 month) and because the efficacy of therapy was not addressed.
Further studies of anticholinergic medications, using the same rigorous scientific approach that these investigators applied, are needed to address 1) the long-term efficacy of oxybutynin and similar agents and 2) the cognitive effects of long-term treatment in this older population.
Further impairment is unlikely over the short term when a cognitively impaired nursing home patient who has urge urinary incontinence is treated with 5 mg/day oral extended-release oxybutynin.—JOHN P. JUDD, MD, AND CINDY L. AMUNDSEN, MD
1. Abrams P, Cardozo L, Fall M, et al. The standardisation of terminology of lower urinary tract function: report from the Standardisation Sub-committee of the International Continence Society. Am J Obstet Gynecol. 2002;187:116-126.
2. Hu TW, Wagner TH, Bentkover JD, et al. Estimated economic costs of overactive bladder in the United States. Urology. 2003;61:1123-1128.
3. Hannestad YS, Rortveit G, Sandvik H, Hunskaar S. A community-based epidemiological survey of female urinary incontinence: the Norwegian EPINCONT study. Epidemiology of Incontinence in the County of Nord-Trøndelag. J Clin Epidemiol. 2000;53:1150-1157.
4. Melville JL, Katon W, Delaney K, Newton K. Urinary incontinence in US women: a population-based study. Arch Intern Med. 2005;165:537-542.
5. Fantl JA, Newman DK, Colling J, et al. Managing Acute and Chronic Urinary Incontinence. Clinical Practice Guideline. Quick Reference Guide for Clinicians, No. 2, 1996 Update. Rockville, MD: US Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research. AHCPR Pub. No. 96-0686. January 1996. Available at: http://www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=hstat6.chapter.32554. Accessed September 11, 2009.
6. Brown JS, Vittinghoff E, Wyman JF, et al. Urinary incontinence: does it increase risk for falls and fractures? Study of Osteoporotic Fractures Research Group. J Am Geriatr Soc. 2000;48:721-725.
The authors report no financial relationships relevant to this article.
Overactive bladder (OAB)—urinary urgency, with or without incontinence, usually with frequency and nocturia1—is a common problem among women who seek care from an ObGyn. In fact, the condition is estimated to carry a health-care cost in excess of $12 billion annually in the United States.2
A recent community-based survey in Norway estimated the prevalence of urinary incontinence there to be 27% in women between the ages of 65 and 69 years and 35% to 40% in those 80 years or older.3 A population-based study in the United States suggested an even higher rate of urinary incontinence here: greater than 50% in women 60 years or older, with 1) urge urinary incontinence (UUI) predominating4 and 2) the prevalence particularly high among older women who are homebound or who live in a long-term care facility.5
OAB can undermine quality of life in several ways: social isolation, anxiety, poor sleep, higher risk of fracture after a fall,6 reduced ability to function, and poor self-perception. Despite these harmful effects, many women delay seeking care for OAB because they are embarrassed to talk about it with their physician.
Treatment by generalists is feasible—but there is a catch
It’s possible to treat most patients with OAB without referral to a specialist. Two common concerns, however, may set up a roadblock to successful management: the adverse effects associated with some agents and suboptimal control of symptoms.
In this Update, we review recent findings about 1) the potential that anticholinergic therapy has for impairing cognitive function in the older population of women and 2) the important role that concomitant behavioral therapy plays in the long-term success of, and patients’ satisfaction with, treatment of OAB.
Behavioral therapy for OAB: Is it worth all the effort?
Burgio KL, Locher JL, Goode PS. Combined behavioral and drug therapy for urge incontinence in older women. J Am Geriatr Soc. 2000;48:370–374.
The authors of this article followed a randomized clinical trial of older women that compared behavioral and drug therapy for OAB. In the trial, biofeedback-assisted behavioral training (comprising anorectal biofeedback, urge strategies, pelvic muscle biofeedback, and practitioner-directed review with optimization) was compared with treatment with oxybutynin, between 2.5 and 15 mg/day. Both biofeedback-assisted behavioral therapy and the drug regimen were found effective, although neither treatment provided an entirely satisfactory result for all patients. (For a brief description of what constitutes behavioral treatment, see “6 tenets of behavioral therapy for urge urinary incontinence.”)
Second phase of the trial. To determine if treatment satisfaction could be enhanced, the investigators performed a modified crossover study to determine whether combination therapy—biofeedback-assisted behavioral training plus oxybutynin—added any benefit over treatment with behavioral therapy or drug therapy alone. Eligibility was determined by age (55 years or older), demonstrated UUI for at least 3 months, and incomplete dryness or incomplete satisfaction with the outcome of 8 weeks of single-intervention treatment (with either treatment) during the initial phase of the trial.
This subgroup was offered an additional 8 weeks of combination therapy. The primary outcome measure was a reduction in the frequency of episodes of incontinence episodes as recorded by subjects in a bladder diary.
Of 197 women who participated in the original randomized clinical trial, 35—27 who completed drug therapy and 8 who completed behavioral treatment—elected to receive combination therapy. Those 35 subjects did not differ in any of the multiple baseline variables; mean age was 69.3 years (standard deviation [SD], ±7.9 years).
Among subjects originally assigned to behavioral therapy alone, overall reduction in incontinence increased from a mean of 57.5% to a mean of 88.5% after combined therapy (P=.034). Subjects originally assigned to drug therapy alone demonstrated an improvement from 72.7% reduction in incontinence to a mean 84.3% overall reduction with combined therapy (P=.001).
These data suggest that combined therapy can be more effective than behavioral therapy or drug therapy alone. The impact of this study is limited, however, by the relatively low percentage (12.7%) of patients who had received behavioral therapy and chose to add drug therapy, compared with the 41.5% who moved from drug therapy alone to add behavioral therapy.
Furthermore, subjects were self-selected: They chose to continue with an additional 8 weeks of therapy after their initial suboptimal outcome. It is possible that some subjects who were neither totally continent nor completely satisfied with initial therapy chose not to continue with the crossover segment of the trial because it posed too great a burden or because they were discouraged with the initial degree of improvement.
Generalizing these results to all older women with UUI is difficult. The authors point out, however, that, in practice, patients may be more likely than not to choose combination therapy in the hope of shortening the duration of medical therapy. Although it isn’t known whether providing combination therapy from the outset would have yielded better outcomes than either single therapy did, the authors hypothesize that initial combination therapy may result in greater improvement because patients have a high level of motivation and expectation of improvement at the beginning of treatment.
Importance of this article. The investigators demonstrated that a combination of behavioral and drug therapies can provide increased effectiveness in patients for whom each treatment alone led to suboptimal satisfaction. Furthermore, by targeting women older than 55 years, the investigators were able to demonstrate this effectiveness in a group for whom pelvic-floor training may be more difficult than it is for younger women.
It will be interesting to see if future research will 1) validate these findings and 2) determine whether combined therapy can reduce the duration of drug therapy in this older population through behavioral modification and pelvic floor reeducation.
Fluid management
This first-step therapy can involve providing a handout to the patient that details techniques she can use to monitor and control her fluid intake in a manner that addresses her problem. Among such steps:
- avoiding caffeine and artificial sweeteners
- tracking her diet to identify any other bladder irritants
- limiting fluids before times she is more likely to be incontinent—during a long drive, for example, or, in the case of nocturia, after the evening meal.
Scheduled voiding
With scheduled, or prompted, voiding, the patient empties her bladder at a set interval—usually, every 1.5 to 2 hours. If nocturia, or the more severe enuresis, is a problem, the patient can be prompted by an alarm clock or (if she is institutionalized) by nursing staff. Combining scheduled voiding with fluid management principles helps the patient avoid reaching a bladder volume at which an episode of incontinence becomes more likely.
Bladder training
This is a modification of scheduled voiding that attempts to establish a normal voiding interval in patients who have significant frequency but a small voided volume. It imposes a regimented voiding schedule that gradually (over 7 to 10 days) extends the duration between voids.
Pelvic floor-muscle exercises
The focus here is on using pelvic-floor muscles to prevent incontinence. The muscles are strengthened by having the patient perform Kegel exercises (named for Arnold H. Kegel, MD, who, in 1948, recognized the role of pelvic floor-muscle rehabilitation in the treatment of incontinence). The exercises involve simultaneous 1) contraction of the pelvic and periurethral musculature and 2) relaxation of other muscles, including abdominal muscles, which can increase pressure on the bladder.
Once the patient learns to perform Kegel exercises, she can use them to suppress urgency: Instead of hurrying to the bathroom when urgency arises, she is encouraged to sit down, relax, and contract the pelvic-floor muscles repeatedly until the urge to void diminishes. Once it does, the patient proceeds to the toilet to void normally.
Pelvic exam
By self-exam, the patient can identify and familiarize herself with her purposeful contractions of the pelvic-floor musculature and thereby strengthen those muscles with effective exercise.
Biofeedback
Direct feedback about contractions of the pelvic-floor muscles—by a display of data on a gauge or computer monitor, gathered using an intravaginal or anorectal sensor or probe—allows a patient who is exercising those muscles to better target her efforts and maximize their effectiveness.
Combining behavioral therapy and an anticholinergic medication for urge urinary incontinence may yield a superior result after either modality alone has been disappointing by the patient’s account of success.—JOHN P. JUDD, MD, AND CINDY L. AMUNDSEN, MD
Does oxybutynin for UUI further erode cognition in elderly women who are cognitively impaired?
Lackner TE, Wyman JF, McCarthy TC, Monigold M, Davey C. Randomized, placebo-controlled trial of the cognitive effect, safety, and tolerability of oral extended-release oxybutynin in cognitively impaired nursing home residents with urge urinary incontinence. J Am Geriatr Soc. 2008;56:862–870.
Although anticholinergic therapy is modestly effective against UUI in nursing home residents, past studies have suggested that such treatment can impair, or further impair, cognition in this population—a concern that may lead to underuse. This double-blinded, randomized, placebo-controlled trial compared short-term oral extended-release oxybutynin with placebo.
Consequently, the authors sought to determine the cognitive effect, safety, and tolerability of 5 mg/day oral extended-release oxybutynin (the most commonly prescribed dosage) in cognitively impaired older nursing home residents who have UUI.
Subjects were eligible if they:
- were 65 years or older
- had UUI
- lived in a nursing home longer than 3 months
- had cognitive impairment.
Women already being treated for urinary incontinence, those who had an indwelling Foley catheter or urinary retention, and those who were bed-bound or incommunicative were excluded.
Fifty women, mean age 88.6 years (SD, ±6.2), from 12 nursing home facilities, agreed to participate. They were further stratified based on the score of a Mini-Mental State Exam (MMSE): 13 had severe cognitive impairment (MMSE score, 5–10) and 37 had mild or moderate impairment (score, 11–23).
Subjects were randomized to 4 weeks’ treatment with either 5 mg/day oral extended-release oxybutynin or one placebo tablet daily. A nurse practitioner who was blinded to randomization collected all data. The Confusion Assessment Method (CAM) algorithm, MMSE, and Severe Impairment Battery (SIB) were used to assess cognitive decline. The Brief Agitation Rating Scale (BARS) assessed agitation.
No baseline differences were noted with regard to: age; demographic, functional, and neuropsychiatric characteristics; clinical factors predisposing to delirium; and serum anticholinergic activity. Adherence was similar in the treatment (97%) and placebo (97.4%) groups.
Finding: Cognitive impairment. Treatment and placebo groups in the baseline mild-or-moderate stratum (by MMSE) showed equivalent mean changes in CAM scores at all time points. Because of the small sample size, however, CAM score equivalence could not be definitively determined for the groups in the severe impairment stratum. Evaluation of mean MMSE and BARS scores showed no significant changes between groups.
Finding: Tolerability. Excellent tolerability was noted in the treatment group: 96% of subjects completed the trial (compared with 92% of the placebo group). No difference in the rate of adverse events was noted between treatment and placebo groups; of adverse events recorded, 90% were judged “mild” by the investigators. Constipation and dry mouth were most common.
Finding: Falls. More than half—54%—of subjects in both groups experienced at least one fall during the trial or during the preceding or following 3 months. Despite this, no difference in the rate of falls between the treatment and placebo groups was noted. Furthermore, regression analysis revealed no treatment or period effect on falls per month across the time of observation.
Conclusions. Treatment with 5 mg/day oral extended-release oxybutynin in older patients with some cognitive impairment is well tolerated, the study’s findings suggest, with minimal risk of further cognitive decline or delirium over the short term. The potential that long-term therapy has to harm cognitive function remains, however; data on long-term treatment are needed to illuminate that area.
The authors also address the importance of dosing, especially over time, and discuss the lower potential of newer-generation anticholinergics to produce cognitive impairment.
A limited number of articles in the medical literature address anticholinergics in an older population, specifically, and only a few of those evaluated the effects of the drugs on cognitive function. By investigating patients who had an existing cognitive impairment, the authors of this article were able to target a cohort at risk of further cognitive impairment from medication use—thereby giving further weight to their findings of no significant effect.
Main strengths and limitations of the study. The investigators used validated, standardized cognitive tests that were administered by a uniform blinded evaluator in a randomized, controlled trial. The study was limited, however, because patients were evaluated only over a relatively short period (1 month) and because the efficacy of therapy was not addressed.
Further studies of anticholinergic medications, using the same rigorous scientific approach that these investigators applied, are needed to address 1) the long-term efficacy of oxybutynin and similar agents and 2) the cognitive effects of long-term treatment in this older population.
Further impairment is unlikely over the short term when a cognitively impaired nursing home patient who has urge urinary incontinence is treated with 5 mg/day oral extended-release oxybutynin.—JOHN P. JUDD, MD, AND CINDY L. AMUNDSEN, MD
The authors report no financial relationships relevant to this article.
Overactive bladder (OAB)—urinary urgency, with or without incontinence, usually with frequency and nocturia1—is a common problem among women who seek care from an ObGyn. In fact, the condition is estimated to carry a health-care cost in excess of $12 billion annually in the United States.2
A recent community-based survey in Norway estimated the prevalence of urinary incontinence there to be 27% in women between the ages of 65 and 69 years and 35% to 40% in those 80 years or older.3 A population-based study in the United States suggested an even higher rate of urinary incontinence here: greater than 50% in women 60 years or older, with 1) urge urinary incontinence (UUI) predominating4 and 2) the prevalence particularly high among older women who are homebound or who live in a long-term care facility.5
OAB can undermine quality of life in several ways: social isolation, anxiety, poor sleep, higher risk of fracture after a fall,6 reduced ability to function, and poor self-perception. Despite these harmful effects, many women delay seeking care for OAB because they are embarrassed to talk about it with their physician.
Treatment by generalists is feasible—but there is a catch
It’s possible to treat most patients with OAB without referral to a specialist. Two common concerns, however, may set up a roadblock to successful management: the adverse effects associated with some agents and suboptimal control of symptoms.
In this Update, we review recent findings about 1) the potential that anticholinergic therapy has for impairing cognitive function in the older population of women and 2) the important role that concomitant behavioral therapy plays in the long-term success of, and patients’ satisfaction with, treatment of OAB.
Behavioral therapy for OAB: Is it worth all the effort?
Burgio KL, Locher JL, Goode PS. Combined behavioral and drug therapy for urge incontinence in older women. J Am Geriatr Soc. 2000;48:370–374.
The authors of this article followed a randomized clinical trial of older women that compared behavioral and drug therapy for OAB. In the trial, biofeedback-assisted behavioral training (comprising anorectal biofeedback, urge strategies, pelvic muscle biofeedback, and practitioner-directed review with optimization) was compared with treatment with oxybutynin, between 2.5 and 15 mg/day. Both biofeedback-assisted behavioral therapy and the drug regimen were found effective, although neither treatment provided an entirely satisfactory result for all patients. (For a brief description of what constitutes behavioral treatment, see “6 tenets of behavioral therapy for urge urinary incontinence.”)
Second phase of the trial. To determine if treatment satisfaction could be enhanced, the investigators performed a modified crossover study to determine whether combination therapy—biofeedback-assisted behavioral training plus oxybutynin—added any benefit over treatment with behavioral therapy or drug therapy alone. Eligibility was determined by age (55 years or older), demonstrated UUI for at least 3 months, and incomplete dryness or incomplete satisfaction with the outcome of 8 weeks of single-intervention treatment (with either treatment) during the initial phase of the trial.
This subgroup was offered an additional 8 weeks of combination therapy. The primary outcome measure was a reduction in the frequency of episodes of incontinence episodes as recorded by subjects in a bladder diary.
Of 197 women who participated in the original randomized clinical trial, 35—27 who completed drug therapy and 8 who completed behavioral treatment—elected to receive combination therapy. Those 35 subjects did not differ in any of the multiple baseline variables; mean age was 69.3 years (standard deviation [SD], ±7.9 years).
Among subjects originally assigned to behavioral therapy alone, overall reduction in incontinence increased from a mean of 57.5% to a mean of 88.5% after combined therapy (P=.034). Subjects originally assigned to drug therapy alone demonstrated an improvement from 72.7% reduction in incontinence to a mean 84.3% overall reduction with combined therapy (P=.001).
These data suggest that combined therapy can be more effective than behavioral therapy or drug therapy alone. The impact of this study is limited, however, by the relatively low percentage (12.7%) of patients who had received behavioral therapy and chose to add drug therapy, compared with the 41.5% who moved from drug therapy alone to add behavioral therapy.
Furthermore, subjects were self-selected: They chose to continue with an additional 8 weeks of therapy after their initial suboptimal outcome. It is possible that some subjects who were neither totally continent nor completely satisfied with initial therapy chose not to continue with the crossover segment of the trial because it posed too great a burden or because they were discouraged with the initial degree of improvement.
Generalizing these results to all older women with UUI is difficult. The authors point out, however, that, in practice, patients may be more likely than not to choose combination therapy in the hope of shortening the duration of medical therapy. Although it isn’t known whether providing combination therapy from the outset would have yielded better outcomes than either single therapy did, the authors hypothesize that initial combination therapy may result in greater improvement because patients have a high level of motivation and expectation of improvement at the beginning of treatment.
Importance of this article. The investigators demonstrated that a combination of behavioral and drug therapies can provide increased effectiveness in patients for whom each treatment alone led to suboptimal satisfaction. Furthermore, by targeting women older than 55 years, the investigators were able to demonstrate this effectiveness in a group for whom pelvic-floor training may be more difficult than it is for younger women.
It will be interesting to see if future research will 1) validate these findings and 2) determine whether combined therapy can reduce the duration of drug therapy in this older population through behavioral modification and pelvic floor reeducation.
Fluid management
This first-step therapy can involve providing a handout to the patient that details techniques she can use to monitor and control her fluid intake in a manner that addresses her problem. Among such steps:
- avoiding caffeine and artificial sweeteners
- tracking her diet to identify any other bladder irritants
- limiting fluids before times she is more likely to be incontinent—during a long drive, for example, or, in the case of nocturia, after the evening meal.
Scheduled voiding
With scheduled, or prompted, voiding, the patient empties her bladder at a set interval—usually, every 1.5 to 2 hours. If nocturia, or the more severe enuresis, is a problem, the patient can be prompted by an alarm clock or (if she is institutionalized) by nursing staff. Combining scheduled voiding with fluid management principles helps the patient avoid reaching a bladder volume at which an episode of incontinence becomes more likely.
Bladder training
This is a modification of scheduled voiding that attempts to establish a normal voiding interval in patients who have significant frequency but a small voided volume. It imposes a regimented voiding schedule that gradually (over 7 to 10 days) extends the duration between voids.
Pelvic floor-muscle exercises
The focus here is on using pelvic-floor muscles to prevent incontinence. The muscles are strengthened by having the patient perform Kegel exercises (named for Arnold H. Kegel, MD, who, in 1948, recognized the role of pelvic floor-muscle rehabilitation in the treatment of incontinence). The exercises involve simultaneous 1) contraction of the pelvic and periurethral musculature and 2) relaxation of other muscles, including abdominal muscles, which can increase pressure on the bladder.
Once the patient learns to perform Kegel exercises, she can use them to suppress urgency: Instead of hurrying to the bathroom when urgency arises, she is encouraged to sit down, relax, and contract the pelvic-floor muscles repeatedly until the urge to void diminishes. Once it does, the patient proceeds to the toilet to void normally.
Pelvic exam
By self-exam, the patient can identify and familiarize herself with her purposeful contractions of the pelvic-floor musculature and thereby strengthen those muscles with effective exercise.
Biofeedback
Direct feedback about contractions of the pelvic-floor muscles—by a display of data on a gauge or computer monitor, gathered using an intravaginal or anorectal sensor or probe—allows a patient who is exercising those muscles to better target her efforts and maximize their effectiveness.
Combining behavioral therapy and an anticholinergic medication for urge urinary incontinence may yield a superior result after either modality alone has been disappointing by the patient’s account of success.—JOHN P. JUDD, MD, AND CINDY L. AMUNDSEN, MD
Does oxybutynin for UUI further erode cognition in elderly women who are cognitively impaired?
Lackner TE, Wyman JF, McCarthy TC, Monigold M, Davey C. Randomized, placebo-controlled trial of the cognitive effect, safety, and tolerability of oral extended-release oxybutynin in cognitively impaired nursing home residents with urge urinary incontinence. J Am Geriatr Soc. 2008;56:862–870.
Although anticholinergic therapy is modestly effective against UUI in nursing home residents, past studies have suggested that such treatment can impair, or further impair, cognition in this population—a concern that may lead to underuse. This double-blinded, randomized, placebo-controlled trial compared short-term oral extended-release oxybutynin with placebo.
Consequently, the authors sought to determine the cognitive effect, safety, and tolerability of 5 mg/day oral extended-release oxybutynin (the most commonly prescribed dosage) in cognitively impaired older nursing home residents who have UUI.
Subjects were eligible if they:
- were 65 years or older
- had UUI
- lived in a nursing home longer than 3 months
- had cognitive impairment.
Women already being treated for urinary incontinence, those who had an indwelling Foley catheter or urinary retention, and those who were bed-bound or incommunicative were excluded.
Fifty women, mean age 88.6 years (SD, ±6.2), from 12 nursing home facilities, agreed to participate. They were further stratified based on the score of a Mini-Mental State Exam (MMSE): 13 had severe cognitive impairment (MMSE score, 5–10) and 37 had mild or moderate impairment (score, 11–23).
Subjects were randomized to 4 weeks’ treatment with either 5 mg/day oral extended-release oxybutynin or one placebo tablet daily. A nurse practitioner who was blinded to randomization collected all data. The Confusion Assessment Method (CAM) algorithm, MMSE, and Severe Impairment Battery (SIB) were used to assess cognitive decline. The Brief Agitation Rating Scale (BARS) assessed agitation.
No baseline differences were noted with regard to: age; demographic, functional, and neuropsychiatric characteristics; clinical factors predisposing to delirium; and serum anticholinergic activity. Adherence was similar in the treatment (97%) and placebo (97.4%) groups.
Finding: Cognitive impairment. Treatment and placebo groups in the baseline mild-or-moderate stratum (by MMSE) showed equivalent mean changes in CAM scores at all time points. Because of the small sample size, however, CAM score equivalence could not be definitively determined for the groups in the severe impairment stratum. Evaluation of mean MMSE and BARS scores showed no significant changes between groups.
Finding: Tolerability. Excellent tolerability was noted in the treatment group: 96% of subjects completed the trial (compared with 92% of the placebo group). No difference in the rate of adverse events was noted between treatment and placebo groups; of adverse events recorded, 90% were judged “mild” by the investigators. Constipation and dry mouth were most common.
Finding: Falls. More than half—54%—of subjects in both groups experienced at least one fall during the trial or during the preceding or following 3 months. Despite this, no difference in the rate of falls between the treatment and placebo groups was noted. Furthermore, regression analysis revealed no treatment or period effect on falls per month across the time of observation.
Conclusions. Treatment with 5 mg/day oral extended-release oxybutynin in older patients with some cognitive impairment is well tolerated, the study’s findings suggest, with minimal risk of further cognitive decline or delirium over the short term. The potential that long-term therapy has to harm cognitive function remains, however; data on long-term treatment are needed to illuminate that area.
The authors also address the importance of dosing, especially over time, and discuss the lower potential of newer-generation anticholinergics to produce cognitive impairment.
A limited number of articles in the medical literature address anticholinergics in an older population, specifically, and only a few of those evaluated the effects of the drugs on cognitive function. By investigating patients who had an existing cognitive impairment, the authors of this article were able to target a cohort at risk of further cognitive impairment from medication use—thereby giving further weight to their findings of no significant effect.
Main strengths and limitations of the study. The investigators used validated, standardized cognitive tests that were administered by a uniform blinded evaluator in a randomized, controlled trial. The study was limited, however, because patients were evaluated only over a relatively short period (1 month) and because the efficacy of therapy was not addressed.
Further studies of anticholinergic medications, using the same rigorous scientific approach that these investigators applied, are needed to address 1) the long-term efficacy of oxybutynin and similar agents and 2) the cognitive effects of long-term treatment in this older population.
Further impairment is unlikely over the short term when a cognitively impaired nursing home patient who has urge urinary incontinence is treated with 5 mg/day oral extended-release oxybutynin.—JOHN P. JUDD, MD, AND CINDY L. AMUNDSEN, MD
1. Abrams P, Cardozo L, Fall M, et al. The standardisation of terminology of lower urinary tract function: report from the Standardisation Sub-committee of the International Continence Society. Am J Obstet Gynecol. 2002;187:116-126.
2. Hu TW, Wagner TH, Bentkover JD, et al. Estimated economic costs of overactive bladder in the United States. Urology. 2003;61:1123-1128.
3. Hannestad YS, Rortveit G, Sandvik H, Hunskaar S. A community-based epidemiological survey of female urinary incontinence: the Norwegian EPINCONT study. Epidemiology of Incontinence in the County of Nord-Trøndelag. J Clin Epidemiol. 2000;53:1150-1157.
4. Melville JL, Katon W, Delaney K, Newton K. Urinary incontinence in US women: a population-based study. Arch Intern Med. 2005;165:537-542.
5. Fantl JA, Newman DK, Colling J, et al. Managing Acute and Chronic Urinary Incontinence. Clinical Practice Guideline. Quick Reference Guide for Clinicians, No. 2, 1996 Update. Rockville, MD: US Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research. AHCPR Pub. No. 96-0686. January 1996. Available at: http://www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=hstat6.chapter.32554. Accessed September 11, 2009.
6. Brown JS, Vittinghoff E, Wyman JF, et al. Urinary incontinence: does it increase risk for falls and fractures? Study of Osteoporotic Fractures Research Group. J Am Geriatr Soc. 2000;48:721-725.
1. Abrams P, Cardozo L, Fall M, et al. The standardisation of terminology of lower urinary tract function: report from the Standardisation Sub-committee of the International Continence Society. Am J Obstet Gynecol. 2002;187:116-126.
2. Hu TW, Wagner TH, Bentkover JD, et al. Estimated economic costs of overactive bladder in the United States. Urology. 2003;61:1123-1128.
3. Hannestad YS, Rortveit G, Sandvik H, Hunskaar S. A community-based epidemiological survey of female urinary incontinence: the Norwegian EPINCONT study. Epidemiology of Incontinence in the County of Nord-Trøndelag. J Clin Epidemiol. 2000;53:1150-1157.
4. Melville JL, Katon W, Delaney K, Newton K. Urinary incontinence in US women: a population-based study. Arch Intern Med. 2005;165:537-542.
5. Fantl JA, Newman DK, Colling J, et al. Managing Acute and Chronic Urinary Incontinence. Clinical Practice Guideline. Quick Reference Guide for Clinicians, No. 2, 1996 Update. Rockville, MD: US Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research. AHCPR Pub. No. 96-0686. January 1996. Available at: http://www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=hstat6.chapter.32554. Accessed September 11, 2009.
6. Brown JS, Vittinghoff E, Wyman JF, et al. Urinary incontinence: does it increase risk for falls and fractures? Study of Osteoporotic Fractures Research Group. J Am Geriatr Soc. 2000;48:721-725.
Policy & Practice : Can't get enough Policy & Practice? Check out our new podcast each Monday. egmnblog.wordpress.com
Flavored Cigarettes Snubbed Out
The Food and Drug Administration has banned fruit- and candy-flavored cigarettes as part of its effort to prevent children from starting to smoke. The agency said it will act against any company that continues to make, ship, or sell such products in the United States. The tobacco control legislation approved by Congress last spring authorized the FDA to target flavored cigarettes, and the agency said it is also examining options for regulating menthol cigarettes and flavored tobacco products other than cigarettes. Almost 90% of adult smokers start the habit as teenagers, and studies have shown that 17-year-old smokers are three times as likely to use flavored cigarettes as are smokers over 25, the FDA said. “Candy and fruit flavorings have unfortunately been some of the most egregious examples of marketing tobacco products to children, and the academy supported the inclusion of this ban in the legislation,” American Academy of Pediatrics President David Tayloe Jr. said in a statement.
FDA Makes Device Grants
In an effort to have more medical devices available for children, the FDA has awarded a total of $2 million in grants to three nonprofit device consortiums. A panel of experts reviewed 16 applications for the grants, which were mandated by Congress in 2007 and will be administered by the FDA's Office of Orphan Products Development. The grants, to groups based in California, Massachusetts, and Michigan, are to encourage connections between innovators and potential manufacturers of pediatric medical devices. Each of the grant recipients will coordinate efforts of the FDA, device companies, and the National Institutes of Health to bring pediatric medical devices to market sooner. Development of medical devices for children is a challenge because of differences in size, growth, and body chemistry between age groups. As a result, availability of pediatric devices lags up to a decade behind similar devices intended for adults, according to the FDA.
Review Raps Medicaid Services
Preventive care for children and adults is lagging in Medicaid, the Government Accountability Office (GAO) found. It reported that many children covered by Medicaid are not receiving well-child checkups and that providers may not be aware that obesity-related services are covered for youngsters in the program. Most states told GAO that they have set goals for and monitored children's utilization of preventive services available and that they have taken steps to increase the number of children who received those services through Medicaid. However, the GAO study found that only 58% of children who were eligible under the program to receive a periodic screening, diagnostic, or treatment service in 2007 actually received one.
HHS Supports Health Centers
The Department of Health and Human Services has granted $25.7 million to increase and improve health and support services at public health centers, which are treating many more children than they did before the economic downturn. The federal health center system, overseen by the Health Resources and Services Administration, served more than 17 million medically needy people in 2008, up from 10 million patients in 2001, according to HHS. Since the economic downturn began, the health center patient population has grown by another million people, one-third of them children.
Obesity Counseling Found Ineffective
Primary care obesity screening followed by a series of counseling sessions failed to improve body mass index, physical activity, or nutrition in overweight or mildly obese children, a study in the British Medical Journal found. A total of 139 overweight and mildly obese children aged 5-10 years underwent four brief consultations with their physicians in Melbourne over 12 weeks. The objective was to change the children's behavior. But when compared with that of a control group after a year, the intervention group's BMI had not fallen significantly, the study found. Money might be better spent on obesity-prevention activities at the community and population levels, rather than on individual counseling by primary care physicians, the authors concluded.
HHS Awards Adoption Incentives
The Department of Health and Human Services announced the distribution of $35 million to 38 states and Puerto Rico to increase adoptions among children in foster care. Congress created the Adoptions Incentive program in 1997 as part of the Adoption and Safe Families Act, particularly to move older children and those with special needs into permanent homes. As part of the program, states can earn $4,000 for each additional adopted foster child above a baseline rate established in 2007. They receive additional payments for the adoption of foster children older than age 8 and those with special needs. States use the incentive payments to improve their programs for abused and neglected children, according to HHS.
Flavored Cigarettes Snubbed Out
The Food and Drug Administration has banned fruit- and candy-flavored cigarettes as part of its effort to prevent children from starting to smoke. The agency said it will act against any company that continues to make, ship, or sell such products in the United States. The tobacco control legislation approved by Congress last spring authorized the FDA to target flavored cigarettes, and the agency said it is also examining options for regulating menthol cigarettes and flavored tobacco products other than cigarettes. Almost 90% of adult smokers start the habit as teenagers, and studies have shown that 17-year-old smokers are three times as likely to use flavored cigarettes as are smokers over 25, the FDA said. “Candy and fruit flavorings have unfortunately been some of the most egregious examples of marketing tobacco products to children, and the academy supported the inclusion of this ban in the legislation,” American Academy of Pediatrics President David Tayloe Jr. said in a statement.
FDA Makes Device Grants
In an effort to have more medical devices available for children, the FDA has awarded a total of $2 million in grants to three nonprofit device consortiums. A panel of experts reviewed 16 applications for the grants, which were mandated by Congress in 2007 and will be administered by the FDA's Office of Orphan Products Development. The grants, to groups based in California, Massachusetts, and Michigan, are to encourage connections between innovators and potential manufacturers of pediatric medical devices. Each of the grant recipients will coordinate efforts of the FDA, device companies, and the National Institutes of Health to bring pediatric medical devices to market sooner. Development of medical devices for children is a challenge because of differences in size, growth, and body chemistry between age groups. As a result, availability of pediatric devices lags up to a decade behind similar devices intended for adults, according to the FDA.
Review Raps Medicaid Services
Preventive care for children and adults is lagging in Medicaid, the Government Accountability Office (GAO) found. It reported that many children covered by Medicaid are not receiving well-child checkups and that providers may not be aware that obesity-related services are covered for youngsters in the program. Most states told GAO that they have set goals for and monitored children's utilization of preventive services available and that they have taken steps to increase the number of children who received those services through Medicaid. However, the GAO study found that only 58% of children who were eligible under the program to receive a periodic screening, diagnostic, or treatment service in 2007 actually received one.
HHS Supports Health Centers
The Department of Health and Human Services has granted $25.7 million to increase and improve health and support services at public health centers, which are treating many more children than they did before the economic downturn. The federal health center system, overseen by the Health Resources and Services Administration, served more than 17 million medically needy people in 2008, up from 10 million patients in 2001, according to HHS. Since the economic downturn began, the health center patient population has grown by another million people, one-third of them children.
Obesity Counseling Found Ineffective
Primary care obesity screening followed by a series of counseling sessions failed to improve body mass index, physical activity, or nutrition in overweight or mildly obese children, a study in the British Medical Journal found. A total of 139 overweight and mildly obese children aged 5-10 years underwent four brief consultations with their physicians in Melbourne over 12 weeks. The objective was to change the children's behavior. But when compared with that of a control group after a year, the intervention group's BMI had not fallen significantly, the study found. Money might be better spent on obesity-prevention activities at the community and population levels, rather than on individual counseling by primary care physicians, the authors concluded.
HHS Awards Adoption Incentives
The Department of Health and Human Services announced the distribution of $35 million to 38 states and Puerto Rico to increase adoptions among children in foster care. Congress created the Adoptions Incentive program in 1997 as part of the Adoption and Safe Families Act, particularly to move older children and those with special needs into permanent homes. As part of the program, states can earn $4,000 for each additional adopted foster child above a baseline rate established in 2007. They receive additional payments for the adoption of foster children older than age 8 and those with special needs. States use the incentive payments to improve their programs for abused and neglected children, according to HHS.
Flavored Cigarettes Snubbed Out
The Food and Drug Administration has banned fruit- and candy-flavored cigarettes as part of its effort to prevent children from starting to smoke. The agency said it will act against any company that continues to make, ship, or sell such products in the United States. The tobacco control legislation approved by Congress last spring authorized the FDA to target flavored cigarettes, and the agency said it is also examining options for regulating menthol cigarettes and flavored tobacco products other than cigarettes. Almost 90% of adult smokers start the habit as teenagers, and studies have shown that 17-year-old smokers are three times as likely to use flavored cigarettes as are smokers over 25, the FDA said. “Candy and fruit flavorings have unfortunately been some of the most egregious examples of marketing tobacco products to children, and the academy supported the inclusion of this ban in the legislation,” American Academy of Pediatrics President David Tayloe Jr. said in a statement.
FDA Makes Device Grants
In an effort to have more medical devices available for children, the FDA has awarded a total of $2 million in grants to three nonprofit device consortiums. A panel of experts reviewed 16 applications for the grants, which were mandated by Congress in 2007 and will be administered by the FDA's Office of Orphan Products Development. The grants, to groups based in California, Massachusetts, and Michigan, are to encourage connections between innovators and potential manufacturers of pediatric medical devices. Each of the grant recipients will coordinate efforts of the FDA, device companies, and the National Institutes of Health to bring pediatric medical devices to market sooner. Development of medical devices for children is a challenge because of differences in size, growth, and body chemistry between age groups. As a result, availability of pediatric devices lags up to a decade behind similar devices intended for adults, according to the FDA.
Review Raps Medicaid Services
Preventive care for children and adults is lagging in Medicaid, the Government Accountability Office (GAO) found. It reported that many children covered by Medicaid are not receiving well-child checkups and that providers may not be aware that obesity-related services are covered for youngsters in the program. Most states told GAO that they have set goals for and monitored children's utilization of preventive services available and that they have taken steps to increase the number of children who received those services through Medicaid. However, the GAO study found that only 58% of children who were eligible under the program to receive a periodic screening, diagnostic, or treatment service in 2007 actually received one.
HHS Supports Health Centers
The Department of Health and Human Services has granted $25.7 million to increase and improve health and support services at public health centers, which are treating many more children than they did before the economic downturn. The federal health center system, overseen by the Health Resources and Services Administration, served more than 17 million medically needy people in 2008, up from 10 million patients in 2001, according to HHS. Since the economic downturn began, the health center patient population has grown by another million people, one-third of them children.
Obesity Counseling Found Ineffective
Primary care obesity screening followed by a series of counseling sessions failed to improve body mass index, physical activity, or nutrition in overweight or mildly obese children, a study in the British Medical Journal found. A total of 139 overweight and mildly obese children aged 5-10 years underwent four brief consultations with their physicians in Melbourne over 12 weeks. The objective was to change the children's behavior. But when compared with that of a control group after a year, the intervention group's BMI had not fallen significantly, the study found. Money might be better spent on obesity-prevention activities at the community and population levels, rather than on individual counseling by primary care physicians, the authors concluded.
HHS Awards Adoption Incentives
The Department of Health and Human Services announced the distribution of $35 million to 38 states and Puerto Rico to increase adoptions among children in foster care. Congress created the Adoptions Incentive program in 1997 as part of the Adoption and Safe Families Act, particularly to move older children and those with special needs into permanent homes. As part of the program, states can earn $4,000 for each additional adopted foster child above a baseline rate established in 2007. They receive additional payments for the adoption of foster children older than age 8 and those with special needs. States use the incentive payments to improve their programs for abused and neglected children, according to HHS.
GERD in the School-Age Child
General pediatricians can take care of a great number of children with reflux disease. I recommend a step-up approach employing lifestyle modifications and/or medication prior to specialist referral in most cases. When symptoms become more troublesome or there is no response to therapeutic interventions, consultation with a pediatric gastroenterologist may be appropriate.
Begin with a thorough patient history, which is instrumental to distinguishing gastroesophageal reflux disease (GERD) from other conditions. Family medical and medication history also are important because of compelling evidence demonstrating a family link with GERD.
Advise school-age children with GERD to eat smaller meals throughout the day and not to eat too close to bedtime. Tomato-containing products, caffeine-containing products, citrus, and—believe it or not—chocolate are commonly implicated as evoking or exacerbating symptoms of GERD. Foods with high-fat content also are associated with the disorder, as they delay the ability of the stomach to empty quickly, thus potentially worsening GERD.
Sleep disturbances may be the sole symptom for a lot of older children with reflux. Microburps or microaspirations that occur when children are supine at night wake some; they do not wake others, so keep in mind that some children might be unaware of their GERD. A good question to ask is how many pillows they sleep on at night; some children already self-manage their symptoms by elevating their upper torso at night without realizing why.
Early morning nausea also can occur after a night of continuous reflux. Therefore, the presentation of a child who says he or she routinely does not want to eat in the morning, particularly if he or she complains of nausea, raises clinical suspicion for GERD. Also, some children can report regurgitating and re-swallowing all day as they sit in class.
In addition to lifestyle changes, a trial of acid-suppressing medication, such as an H2 blocker or a proton pump inhibitor, can be tried. Limit initial treatment to 6-8 weeks for most children. If a child reports respiratory symptoms associated with GERD, consider a longer course of acid suppression therapy. It is important to discuss the specific GERD-related symptoms you expect the medication to resolve prior to initiation of therapy.
A referral to a pediatric gastroenterologist is warranted after lifestyle modifications and pharmacotherapy fail, or if symptoms return after therapy is discontinued. Sometimes patients do not improve with these interventions or they get better but you cannot get patients off the medication without symptoms returning. Also, other warning signs or symptoms such as anemia or occult blood in the stool or vomit require a referral.
Frequently, children, particularly those of school age, with GERD complain of a stomachache. However, GERD is more of a burning pain versus a cramping pain. Pain that is associated with GERD or due to another “organic” cause tends to be pain that localizes away from the belly button and is more epigastric, versus periumbilical pain, which tends to be more functional. In addition, abdominal pain that awakens children at night tends to be more organic in nature. Some children with GERD are misdiagnosed and actually have a functional GI disorder or vice versa. Definitions of pediatric functional GI disorders can aid in the differential diagnosis; these are outlined in Rome III criteria (www.romecriteria.org
There is no diagnostic test that is 100% accurate for the diagnosis of GERD. Thus, it is important to avoid too much testing or inappropriate treatment. For example, pediatricians tend to do an upper gastrointestinal series using barium and x-ray fluoroscopy, which is not good for ruling GERD in or out, but can be beneficial in identifying upper GI anatomic abnormalities. Nuclear scintigraphy can be employed to assess gastric emptying and aspiration of reflux contents.
Pediatricians can order a pH probe to ascertain the degree of acid exposure to the esophagus, although some centers require a GI consultation first. Endoscopic studies require a referral to a specialist. Specialists also may perform a newer modality called multichannel intraluminal impedance, which, when combined with the pH probe, can measure both acid reflux and nonacid or weakly acid reflux.
In a survey of 6,000 American Academy of Pediatrics members, 82% of the 1,245 responding pediatricians and pediatric specialists said they treat GERD based on clinical suspicion (J. Pediatr. Gastroenterol. Nutr. 2007;45:56-64). Such empiric therapy is still appropriate in the pediatric patient. However, there is a need for future research on the optimal therapy type, dose, and duration in these patients with clinically suspected GERD.
To promote a more standardized approach to pediatric GERD, I participated on an international committee that released an evidence-based set of definitions for reflux and GERD in the pediatric population (Am. J. Gastroenterol. 2009;104:1278-95). Additional guidance on GERD is available from the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (www.naspghan.orgwww.cdhnf.org
General pediatricians can take care of a great number of children with reflux disease. I recommend a step-up approach employing lifestyle modifications and/or medication prior to specialist referral in most cases. When symptoms become more troublesome or there is no response to therapeutic interventions, consultation with a pediatric gastroenterologist may be appropriate.
Begin with a thorough patient history, which is instrumental to distinguishing gastroesophageal reflux disease (GERD) from other conditions. Family medical and medication history also are important because of compelling evidence demonstrating a family link with GERD.
Advise school-age children with GERD to eat smaller meals throughout the day and not to eat too close to bedtime. Tomato-containing products, caffeine-containing products, citrus, and—believe it or not—chocolate are commonly implicated as evoking or exacerbating symptoms of GERD. Foods with high-fat content also are associated with the disorder, as they delay the ability of the stomach to empty quickly, thus potentially worsening GERD.
Sleep disturbances may be the sole symptom for a lot of older children with reflux. Microburps or microaspirations that occur when children are supine at night wake some; they do not wake others, so keep in mind that some children might be unaware of their GERD. A good question to ask is how many pillows they sleep on at night; some children already self-manage their symptoms by elevating their upper torso at night without realizing why.
Early morning nausea also can occur after a night of continuous reflux. Therefore, the presentation of a child who says he or she routinely does not want to eat in the morning, particularly if he or she complains of nausea, raises clinical suspicion for GERD. Also, some children can report regurgitating and re-swallowing all day as they sit in class.
In addition to lifestyle changes, a trial of acid-suppressing medication, such as an H2 blocker or a proton pump inhibitor, can be tried. Limit initial treatment to 6-8 weeks for most children. If a child reports respiratory symptoms associated with GERD, consider a longer course of acid suppression therapy. It is important to discuss the specific GERD-related symptoms you expect the medication to resolve prior to initiation of therapy.
A referral to a pediatric gastroenterologist is warranted after lifestyle modifications and pharmacotherapy fail, or if symptoms return after therapy is discontinued. Sometimes patients do not improve with these interventions or they get better but you cannot get patients off the medication without symptoms returning. Also, other warning signs or symptoms such as anemia or occult blood in the stool or vomit require a referral.
Frequently, children, particularly those of school age, with GERD complain of a stomachache. However, GERD is more of a burning pain versus a cramping pain. Pain that is associated with GERD or due to another “organic” cause tends to be pain that localizes away from the belly button and is more epigastric, versus periumbilical pain, which tends to be more functional. In addition, abdominal pain that awakens children at night tends to be more organic in nature. Some children with GERD are misdiagnosed and actually have a functional GI disorder or vice versa. Definitions of pediatric functional GI disorders can aid in the differential diagnosis; these are outlined in Rome III criteria (www.romecriteria.org
There is no diagnostic test that is 100% accurate for the diagnosis of GERD. Thus, it is important to avoid too much testing or inappropriate treatment. For example, pediatricians tend to do an upper gastrointestinal series using barium and x-ray fluoroscopy, which is not good for ruling GERD in or out, but can be beneficial in identifying upper GI anatomic abnormalities. Nuclear scintigraphy can be employed to assess gastric emptying and aspiration of reflux contents.
Pediatricians can order a pH probe to ascertain the degree of acid exposure to the esophagus, although some centers require a GI consultation first. Endoscopic studies require a referral to a specialist. Specialists also may perform a newer modality called multichannel intraluminal impedance, which, when combined with the pH probe, can measure both acid reflux and nonacid or weakly acid reflux.
In a survey of 6,000 American Academy of Pediatrics members, 82% of the 1,245 responding pediatricians and pediatric specialists said they treat GERD based on clinical suspicion (J. Pediatr. Gastroenterol. Nutr. 2007;45:56-64). Such empiric therapy is still appropriate in the pediatric patient. However, there is a need for future research on the optimal therapy type, dose, and duration in these patients with clinically suspected GERD.
To promote a more standardized approach to pediatric GERD, I participated on an international committee that released an evidence-based set of definitions for reflux and GERD in the pediatric population (Am. J. Gastroenterol. 2009;104:1278-95). Additional guidance on GERD is available from the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (www.naspghan.orgwww.cdhnf.org
General pediatricians can take care of a great number of children with reflux disease. I recommend a step-up approach employing lifestyle modifications and/or medication prior to specialist referral in most cases. When symptoms become more troublesome or there is no response to therapeutic interventions, consultation with a pediatric gastroenterologist may be appropriate.
Begin with a thorough patient history, which is instrumental to distinguishing gastroesophageal reflux disease (GERD) from other conditions. Family medical and medication history also are important because of compelling evidence demonstrating a family link with GERD.
Advise school-age children with GERD to eat smaller meals throughout the day and not to eat too close to bedtime. Tomato-containing products, caffeine-containing products, citrus, and—believe it or not—chocolate are commonly implicated as evoking or exacerbating symptoms of GERD. Foods with high-fat content also are associated with the disorder, as they delay the ability of the stomach to empty quickly, thus potentially worsening GERD.
Sleep disturbances may be the sole symptom for a lot of older children with reflux. Microburps or microaspirations that occur when children are supine at night wake some; they do not wake others, so keep in mind that some children might be unaware of their GERD. A good question to ask is how many pillows they sleep on at night; some children already self-manage their symptoms by elevating their upper torso at night without realizing why.
Early morning nausea also can occur after a night of continuous reflux. Therefore, the presentation of a child who says he or she routinely does not want to eat in the morning, particularly if he or she complains of nausea, raises clinical suspicion for GERD. Also, some children can report regurgitating and re-swallowing all day as they sit in class.
In addition to lifestyle changes, a trial of acid-suppressing medication, such as an H2 blocker or a proton pump inhibitor, can be tried. Limit initial treatment to 6-8 weeks for most children. If a child reports respiratory symptoms associated with GERD, consider a longer course of acid suppression therapy. It is important to discuss the specific GERD-related symptoms you expect the medication to resolve prior to initiation of therapy.
A referral to a pediatric gastroenterologist is warranted after lifestyle modifications and pharmacotherapy fail, or if symptoms return after therapy is discontinued. Sometimes patients do not improve with these interventions or they get better but you cannot get patients off the medication without symptoms returning. Also, other warning signs or symptoms such as anemia or occult blood in the stool or vomit require a referral.
Frequently, children, particularly those of school age, with GERD complain of a stomachache. However, GERD is more of a burning pain versus a cramping pain. Pain that is associated with GERD or due to another “organic” cause tends to be pain that localizes away from the belly button and is more epigastric, versus periumbilical pain, which tends to be more functional. In addition, abdominal pain that awakens children at night tends to be more organic in nature. Some children with GERD are misdiagnosed and actually have a functional GI disorder or vice versa. Definitions of pediatric functional GI disorders can aid in the differential diagnosis; these are outlined in Rome III criteria (www.romecriteria.org
There is no diagnostic test that is 100% accurate for the diagnosis of GERD. Thus, it is important to avoid too much testing or inappropriate treatment. For example, pediatricians tend to do an upper gastrointestinal series using barium and x-ray fluoroscopy, which is not good for ruling GERD in or out, but can be beneficial in identifying upper GI anatomic abnormalities. Nuclear scintigraphy can be employed to assess gastric emptying and aspiration of reflux contents.
Pediatricians can order a pH probe to ascertain the degree of acid exposure to the esophagus, although some centers require a GI consultation first. Endoscopic studies require a referral to a specialist. Specialists also may perform a newer modality called multichannel intraluminal impedance, which, when combined with the pH probe, can measure both acid reflux and nonacid or weakly acid reflux.
In a survey of 6,000 American Academy of Pediatrics members, 82% of the 1,245 responding pediatricians and pediatric specialists said they treat GERD based on clinical suspicion (J. Pediatr. Gastroenterol. Nutr. 2007;45:56-64). Such empiric therapy is still appropriate in the pediatric patient. However, there is a need for future research on the optimal therapy type, dose, and duration in these patients with clinically suspected GERD.
To promote a more standardized approach to pediatric GERD, I participated on an international committee that released an evidence-based set of definitions for reflux and GERD in the pediatric population (Am. J. Gastroenterol. 2009;104:1278-95). Additional guidance on GERD is available from the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (www.naspghan.orgwww.cdhnf.org
HM's Watershed Moment
John Nelson, MD, FACP, FHM, hasn't taken a medical test in more than 20 years. So when news began to spread last week that the American Board of Internal Medicine (ABIM) soon will be offering a Recognition of Focused Practice (RFP) in Hospital Medicine certification, he started to get a little nervous.
"I will lose sleep the week before I take this test," says Dr. Nelson, co-founder and past president of SHM, and a principal in the practice management firm Nelson Flores Hospital Medicine Consultants. "This exam will help identify those who see this as a career. … Boy, there is nothing like a test to demonstrate professional centeredness."
The exam, likely to be available in the fall of 2010, will identify physicians who have "maintained their internal medicine certification focused in hospital medicine," according to the ABIM Web site.
"For those individuals [whose certificate] will be expiring in 2010 or 2011, this is a viable pathway for re-certification," says Eric Holmbloe, MD, senior vice president and chief medical officer at ABIM. "Interested diplomats should be able to begin the application process in early 2010. We are feverishly working to complete the test and build the technology infrastructure. We should have more information available in about six weeks."
HM pioneers like Dr. Nelson consider the RFP designation a validation of decades-long efforts to carve a niche in medicine. The test will symbolize dedication to the specialty and provide HM physicians with professional self-regulation.
Scott Flanders, MD, FHM, president of SHM, terms the announcement a "watershed moment" for the field.
"I think this is a major, major moment for HM," says Dr. Flanders, who practices at the University of Michigan Medical Center in Ann Arbor. "We've been looking at this for a long time. This validates the field, and the belief that HM is a positive [for the field of medicine]."
Dr. Nelson couldn't agree more. "This test is the first way hospitalists will be able to show their competence," he says. "I think it's a great opportunity. This will help people take our field more seriously."
John Nelson, MD, FACP, FHM, hasn't taken a medical test in more than 20 years. So when news began to spread last week that the American Board of Internal Medicine (ABIM) soon will be offering a Recognition of Focused Practice (RFP) in Hospital Medicine certification, he started to get a little nervous.
"I will lose sleep the week before I take this test," says Dr. Nelson, co-founder and past president of SHM, and a principal in the practice management firm Nelson Flores Hospital Medicine Consultants. "This exam will help identify those who see this as a career. … Boy, there is nothing like a test to demonstrate professional centeredness."
The exam, likely to be available in the fall of 2010, will identify physicians who have "maintained their internal medicine certification focused in hospital medicine," according to the ABIM Web site.
"For those individuals [whose certificate] will be expiring in 2010 or 2011, this is a viable pathway for re-certification," says Eric Holmbloe, MD, senior vice president and chief medical officer at ABIM. "Interested diplomats should be able to begin the application process in early 2010. We are feverishly working to complete the test and build the technology infrastructure. We should have more information available in about six weeks."
HM pioneers like Dr. Nelson consider the RFP designation a validation of decades-long efforts to carve a niche in medicine. The test will symbolize dedication to the specialty and provide HM physicians with professional self-regulation.
Scott Flanders, MD, FHM, president of SHM, terms the announcement a "watershed moment" for the field.
"I think this is a major, major moment for HM," says Dr. Flanders, who practices at the University of Michigan Medical Center in Ann Arbor. "We've been looking at this for a long time. This validates the field, and the belief that HM is a positive [for the field of medicine]."
Dr. Nelson couldn't agree more. "This test is the first way hospitalists will be able to show their competence," he says. "I think it's a great opportunity. This will help people take our field more seriously."
John Nelson, MD, FACP, FHM, hasn't taken a medical test in more than 20 years. So when news began to spread last week that the American Board of Internal Medicine (ABIM) soon will be offering a Recognition of Focused Practice (RFP) in Hospital Medicine certification, he started to get a little nervous.
"I will lose sleep the week before I take this test," says Dr. Nelson, co-founder and past president of SHM, and a principal in the practice management firm Nelson Flores Hospital Medicine Consultants. "This exam will help identify those who see this as a career. … Boy, there is nothing like a test to demonstrate professional centeredness."
The exam, likely to be available in the fall of 2010, will identify physicians who have "maintained their internal medicine certification focused in hospital medicine," according to the ABIM Web site.
"For those individuals [whose certificate] will be expiring in 2010 or 2011, this is a viable pathway for re-certification," says Eric Holmbloe, MD, senior vice president and chief medical officer at ABIM. "Interested diplomats should be able to begin the application process in early 2010. We are feverishly working to complete the test and build the technology infrastructure. We should have more information available in about six weeks."
HM pioneers like Dr. Nelson consider the RFP designation a validation of decades-long efforts to carve a niche in medicine. The test will symbolize dedication to the specialty and provide HM physicians with professional self-regulation.
Scott Flanders, MD, FHM, president of SHM, terms the announcement a "watershed moment" for the field.
"I think this is a major, major moment for HM," says Dr. Flanders, who practices at the University of Michigan Medical Center in Ann Arbor. "We've been looking at this for a long time. This validates the field, and the belief that HM is a positive [for the field of medicine]."
Dr. Nelson couldn't agree more. "This test is the first way hospitalists will be able to show their competence," he says. "I think it's a great opportunity. This will help people take our field more seriously."
Social Distortion?
A presentation at last week's 13th annual Management of the Hospitalized Patient conference in San Francisco described various ways that hospitals, hospitalists, and HM groups can incorporate new social media into their practice routines.
Hospitalist Russell Cucina, MD, MS, associate medical director of information technology at the University of California at San Francisco, says some physicians mistakenly disclose unprofessional content through social networks. He points to a recent article in the Journal of the American Medical Association (2009;302(12):1309-1315), which shows some physicians inadvertently violate Health Insurance Portability and Accountability Act privacy rules by accepting e-mails from patients that contain protected personal health information.
But in many cases, hospitals and physicians use blogs, Twitter, Facebook, LinkedIn, and other networking sites to exchange information with colleagues, promote their practice in their communities, or recruit new physicians. Such organizations as the Mayo Clinic and SHM use Facebook to reach targeted audiences, while the Centers for Disease Control and Prevention (CDC) uses Twitter to quickly disseminate influenza updates. Dr. Cucina says he knows of 167 U.S. hospitals using the much-hyped Twitter, but he could not find an HM group that uses the quick-hit network. He also reports that Ozmosis and Sermo, networking sites reserved for physicians, have yet to catch on in a big way.
Christine Roed, MD, a hospitalist at El Camino Hospital in Mountain View, Calif., says she sees great potential for communicating within her small medical group and for tapping into public health information. "I also feel it might be quite overwhelming. I think we have to look quite carefully at which information sources are reliable and, in turn, advise the public," Dr. Roed says. "I think a lot of physicians don't really have time to sit down and figure out what they're going to do with these things."
A presentation at last week's 13th annual Management of the Hospitalized Patient conference in San Francisco described various ways that hospitals, hospitalists, and HM groups can incorporate new social media into their practice routines.
Hospitalist Russell Cucina, MD, MS, associate medical director of information technology at the University of California at San Francisco, says some physicians mistakenly disclose unprofessional content through social networks. He points to a recent article in the Journal of the American Medical Association (2009;302(12):1309-1315), which shows some physicians inadvertently violate Health Insurance Portability and Accountability Act privacy rules by accepting e-mails from patients that contain protected personal health information.
But in many cases, hospitals and physicians use blogs, Twitter, Facebook, LinkedIn, and other networking sites to exchange information with colleagues, promote their practice in their communities, or recruit new physicians. Such organizations as the Mayo Clinic and SHM use Facebook to reach targeted audiences, while the Centers for Disease Control and Prevention (CDC) uses Twitter to quickly disseminate influenza updates. Dr. Cucina says he knows of 167 U.S. hospitals using the much-hyped Twitter, but he could not find an HM group that uses the quick-hit network. He also reports that Ozmosis and Sermo, networking sites reserved for physicians, have yet to catch on in a big way.
Christine Roed, MD, a hospitalist at El Camino Hospital in Mountain View, Calif., says she sees great potential for communicating within her small medical group and for tapping into public health information. "I also feel it might be quite overwhelming. I think we have to look quite carefully at which information sources are reliable and, in turn, advise the public," Dr. Roed says. "I think a lot of physicians don't really have time to sit down and figure out what they're going to do with these things."
A presentation at last week's 13th annual Management of the Hospitalized Patient conference in San Francisco described various ways that hospitals, hospitalists, and HM groups can incorporate new social media into their practice routines.
Hospitalist Russell Cucina, MD, MS, associate medical director of information technology at the University of California at San Francisco, says some physicians mistakenly disclose unprofessional content through social networks. He points to a recent article in the Journal of the American Medical Association (2009;302(12):1309-1315), which shows some physicians inadvertently violate Health Insurance Portability and Accountability Act privacy rules by accepting e-mails from patients that contain protected personal health information.
But in many cases, hospitals and physicians use blogs, Twitter, Facebook, LinkedIn, and other networking sites to exchange information with colleagues, promote their practice in their communities, or recruit new physicians. Such organizations as the Mayo Clinic and SHM use Facebook to reach targeted audiences, while the Centers for Disease Control and Prevention (CDC) uses Twitter to quickly disseminate influenza updates. Dr. Cucina says he knows of 167 U.S. hospitals using the much-hyped Twitter, but he could not find an HM group that uses the quick-hit network. He also reports that Ozmosis and Sermo, networking sites reserved for physicians, have yet to catch on in a big way.
Christine Roed, MD, a hospitalist at El Camino Hospital in Mountain View, Calif., says she sees great potential for communicating within her small medical group and for tapping into public health information. "I also feel it might be quite overwhelming. I think we have to look quite carefully at which information sources are reliable and, in turn, advise the public," Dr. Roed says. "I think a lot of physicians don't really have time to sit down and figure out what they're going to do with these things."
Baucus Plan Lends Clarity to Healthcare Debate
Last week’s release of the “chairman’s mark” of the America’s Healthy Future Act from Senate Finance Committee Chairman Max Baucus (D-Mont.) opened the latest chapter in the debate over healthcare reform. Beyond the hot-button issues, several Medicare-related proposals could directly impact hospitalists. Here’s a look at four of them, with observations from Eric Siegal, MD, FHM, chair of SHM’s Public Policy Committee.
Addition of a hospital value-based purchasing (VBP) program to Medicare beginning in 2012. The program would tie incentive payments to performance on quality measures related to such conditions as heart failure, pneumonia, surgical care, and patient perceptions of care. So far, the program’s rough outlines have been well received. “We fundamentally support hospital value-based purchasing,” Dr. Siegal says. “We think it’s a necessary step in the evolution to higher-value health care in general.”
Expansion of the Physician’s Quality Reporting Initiative, with a 1% payment penalty by 2012 for nonparticipants. The bill also would direct the Centers for Medicare and Medicaid Services (CMS) to improve the appeals process and feedback mechanism. Although the Baucus plan’s “mark” doesn’t discuss transitioning to pay-for-performance, Dr. Siegal says the shift likely is inevitable. In the meantime, pay-for-reporting can encourage better outcomes through a public reporting mechanism and “grease the skids” for a pay-for-performance initiative.
Creation of a CMS Payment Innovation Center “authorized to test, evaluate, and expand different payment structures and methodologies,” with a goal of improving quality and reducing Medicare costs. Dr. Siegal says the proposal is consistent with SHM’s aims. “We have for a long time advocated for a robust capability to test new payment models and to figure out what works better than what we have right now,” he says.
Establishment of a three-year Medicare pilot called the Community Care Transitions Program. The program would spend $500 million over 10 years on efforts to reduce preventable rehospitalizations. SHM’s Project BOOST (Better Outcomes for Older Adults through Safe Transitions) likely would qualify. “We’re very positive about that,” Dr. Siegal says. “I think there is a huge amount of scrutiny now on avoidable rehospitalizations. We think BOOST is a step in the right direction, and we’d love to see greater funding to roll this out on a much larger basis.”
For more information on the current healthcare reform debate, visit SHM’s advocacy portal.
Last week’s release of the “chairman’s mark” of the America’s Healthy Future Act from Senate Finance Committee Chairman Max Baucus (D-Mont.) opened the latest chapter in the debate over healthcare reform. Beyond the hot-button issues, several Medicare-related proposals could directly impact hospitalists. Here’s a look at four of them, with observations from Eric Siegal, MD, FHM, chair of SHM’s Public Policy Committee.
Addition of a hospital value-based purchasing (VBP) program to Medicare beginning in 2012. The program would tie incentive payments to performance on quality measures related to such conditions as heart failure, pneumonia, surgical care, and patient perceptions of care. So far, the program’s rough outlines have been well received. “We fundamentally support hospital value-based purchasing,” Dr. Siegal says. “We think it’s a necessary step in the evolution to higher-value health care in general.”
Expansion of the Physician’s Quality Reporting Initiative, with a 1% payment penalty by 2012 for nonparticipants. The bill also would direct the Centers for Medicare and Medicaid Services (CMS) to improve the appeals process and feedback mechanism. Although the Baucus plan’s “mark” doesn’t discuss transitioning to pay-for-performance, Dr. Siegal says the shift likely is inevitable. In the meantime, pay-for-reporting can encourage better outcomes through a public reporting mechanism and “grease the skids” for a pay-for-performance initiative.
Creation of a CMS Payment Innovation Center “authorized to test, evaluate, and expand different payment structures and methodologies,” with a goal of improving quality and reducing Medicare costs. Dr. Siegal says the proposal is consistent with SHM’s aims. “We have for a long time advocated for a robust capability to test new payment models and to figure out what works better than what we have right now,” he says.
Establishment of a three-year Medicare pilot called the Community Care Transitions Program. The program would spend $500 million over 10 years on efforts to reduce preventable rehospitalizations. SHM’s Project BOOST (Better Outcomes for Older Adults through Safe Transitions) likely would qualify. “We’re very positive about that,” Dr. Siegal says. “I think there is a huge amount of scrutiny now on avoidable rehospitalizations. We think BOOST is a step in the right direction, and we’d love to see greater funding to roll this out on a much larger basis.”
For more information on the current healthcare reform debate, visit SHM’s advocacy portal.
Last week’s release of the “chairman’s mark” of the America’s Healthy Future Act from Senate Finance Committee Chairman Max Baucus (D-Mont.) opened the latest chapter in the debate over healthcare reform. Beyond the hot-button issues, several Medicare-related proposals could directly impact hospitalists. Here’s a look at four of them, with observations from Eric Siegal, MD, FHM, chair of SHM’s Public Policy Committee.
Addition of a hospital value-based purchasing (VBP) program to Medicare beginning in 2012. The program would tie incentive payments to performance on quality measures related to such conditions as heart failure, pneumonia, surgical care, and patient perceptions of care. So far, the program’s rough outlines have been well received. “We fundamentally support hospital value-based purchasing,” Dr. Siegal says. “We think it’s a necessary step in the evolution to higher-value health care in general.”
Expansion of the Physician’s Quality Reporting Initiative, with a 1% payment penalty by 2012 for nonparticipants. The bill also would direct the Centers for Medicare and Medicaid Services (CMS) to improve the appeals process and feedback mechanism. Although the Baucus plan’s “mark” doesn’t discuss transitioning to pay-for-performance, Dr. Siegal says the shift likely is inevitable. In the meantime, pay-for-reporting can encourage better outcomes through a public reporting mechanism and “grease the skids” for a pay-for-performance initiative.
Creation of a CMS Payment Innovation Center “authorized to test, evaluate, and expand different payment structures and methodologies,” with a goal of improving quality and reducing Medicare costs. Dr. Siegal says the proposal is consistent with SHM’s aims. “We have for a long time advocated for a robust capability to test new payment models and to figure out what works better than what we have right now,” he says.
Establishment of a three-year Medicare pilot called the Community Care Transitions Program. The program would spend $500 million over 10 years on efforts to reduce preventable rehospitalizations. SHM’s Project BOOST (Better Outcomes for Older Adults through Safe Transitions) likely would qualify. “We’re very positive about that,” Dr. Siegal says. “I think there is a huge amount of scrutiny now on avoidable rehospitalizations. We think BOOST is a step in the right direction, and we’d love to see greater funding to roll this out on a much larger basis.”
For more information on the current healthcare reform debate, visit SHM’s advocacy portal.
1,200 Satisfied Customers and Counting
Another SHM Leadership Academy just ended, with introductory and advanced courses presented at the Fontainebleau resort, complete with the backdrop of Miami Beach. These four-day courses are aimed at hospitalist leaders, and have trained more than 1,200 participants to date. The faculty includes nationally recognized experts in their respective fields, as well as experienced HM leaders.
Level I courses are designed to help new leaders in HM, and focus on communication skills, hospital business drivers, leadership, strategic planning, and conflict resolution. Harjit Bhogal, MD, a hospitalist at Johns Hopkins University School of Medicine in Baltimore, found the Level I course addressed many of the roles she has as a new hospitalist. “The session on strategic planning was interactive and extremely informative,” Dr. Bhogal says. She also says the academy is an ideal place for networking, as attendees have access to more than 100 practicing hospitalist leaders with whom to connect.
Level II takes concepts introduced in Level I and refines them. Communication and negotiation, “meta-leadership,” financial storytelling, and a leadership roundtable help more advanced leaders tackle more complex issues. The session on meta-leadership was “terrific,” according to hospitalist Darlene Tad-y, MD, of Johns Hopkins. “One of the best days I have spent as an adult learner,” she says. “Lenny [Marcus] was absolutely amazing; his walk-in-the-woods approach was a terrific method to discuss leadership.”
Many see hospitalists as the future leaders of the hospital and throughout healthcare. “In addition to helping train leaders for hospital medicine, we believe that SHM has the obligation to train hospitalists to be the next hospital CMOs and CEOs,” says Larry Wellikson, MD, FHM, CEO of SHM.
Apparently, 1,200 academy graduates agree with him.
Another SHM Leadership Academy just ended, with introductory and advanced courses presented at the Fontainebleau resort, complete with the backdrop of Miami Beach. These four-day courses are aimed at hospitalist leaders, and have trained more than 1,200 participants to date. The faculty includes nationally recognized experts in their respective fields, as well as experienced HM leaders.
Level I courses are designed to help new leaders in HM, and focus on communication skills, hospital business drivers, leadership, strategic planning, and conflict resolution. Harjit Bhogal, MD, a hospitalist at Johns Hopkins University School of Medicine in Baltimore, found the Level I course addressed many of the roles she has as a new hospitalist. “The session on strategic planning was interactive and extremely informative,” Dr. Bhogal says. She also says the academy is an ideal place for networking, as attendees have access to more than 100 practicing hospitalist leaders with whom to connect.
Level II takes concepts introduced in Level I and refines them. Communication and negotiation, “meta-leadership,” financial storytelling, and a leadership roundtable help more advanced leaders tackle more complex issues. The session on meta-leadership was “terrific,” according to hospitalist Darlene Tad-y, MD, of Johns Hopkins. “One of the best days I have spent as an adult learner,” she says. “Lenny [Marcus] was absolutely amazing; his walk-in-the-woods approach was a terrific method to discuss leadership.”
Many see hospitalists as the future leaders of the hospital and throughout healthcare. “In addition to helping train leaders for hospital medicine, we believe that SHM has the obligation to train hospitalists to be the next hospital CMOs and CEOs,” says Larry Wellikson, MD, FHM, CEO of SHM.
Apparently, 1,200 academy graduates agree with him.
Another SHM Leadership Academy just ended, with introductory and advanced courses presented at the Fontainebleau resort, complete with the backdrop of Miami Beach. These four-day courses are aimed at hospitalist leaders, and have trained more than 1,200 participants to date. The faculty includes nationally recognized experts in their respective fields, as well as experienced HM leaders.
Level I courses are designed to help new leaders in HM, and focus on communication skills, hospital business drivers, leadership, strategic planning, and conflict resolution. Harjit Bhogal, MD, a hospitalist at Johns Hopkins University School of Medicine in Baltimore, found the Level I course addressed many of the roles she has as a new hospitalist. “The session on strategic planning was interactive and extremely informative,” Dr. Bhogal says. She also says the academy is an ideal place for networking, as attendees have access to more than 100 practicing hospitalist leaders with whom to connect.
Level II takes concepts introduced in Level I and refines them. Communication and negotiation, “meta-leadership,” financial storytelling, and a leadership roundtable help more advanced leaders tackle more complex issues. The session on meta-leadership was “terrific,” according to hospitalist Darlene Tad-y, MD, of Johns Hopkins. “One of the best days I have spent as an adult learner,” she says. “Lenny [Marcus] was absolutely amazing; his walk-in-the-woods approach was a terrific method to discuss leadership.”
Many see hospitalists as the future leaders of the hospital and throughout healthcare. “In addition to helping train leaders for hospital medicine, we believe that SHM has the obligation to train hospitalists to be the next hospital CMOs and CEOs,” says Larry Wellikson, MD, FHM, CEO of SHM.
Apparently, 1,200 academy graduates agree with him.
Sleep Disruptions and Sedative Use
Adequate sleep is important for health, yet the hospital environment commonly disrupts sleep.13 Sleep improves after several days in the hospital.3, 4 Sleep deprivation increases cortisol levels5 and sleep loss of greater than 4 hours may be hyperalgesic.6 Even a few days' suppression of slow‐wave sleep worsens glucose tolerance.7 Sleep disruption may cause irritability and aggressiveness,8 impaired memory consolidation, and delirium.2
Noise may disrupt sleep. The World Health Organization recommends a maximum of 30 to 40 dBA in patients' rooms at night.9, 10 Normal conversation occurs at 60 dBA. Medical equipment alarms are about 80 dBA.
Sedative use is common in the hospital.3 Sedatives typically shorten sleep latency and suppress rapid eye movement (REM) sleep. However, some sedatives cause delirium, falls, amnesia, and confusion, particularly in the elderly.1113
Most research on sleep in hospitalized patients has been done in the critical care setting, often in sedated ventilated patients, where sleep disruption is well‐described.1416 Only a few small studies have assessed the sleep of hospitalized patients outside critical care.17, 18
A single blinded interventional trial assessed sedative use, but was a nonrandomized study.19, 20 As‐needed sedative use was measured among hospitalized elderly patients as a secondary endpoint. The intervention, known as the Hospital Elder Life Program (HELP), included a protocol with noise reduction, massage, music, and warm drinks, as well as rescheduling of medications and procedures; it resulted in a 24% reduction in as‐needed sedative use. Another trial decreased noise and reduced overnight X‐rays on a surgical unit, then measured staff and patient attitudes.21 Two interventional studies in nursing homes reduced noise and light, and/or increased daytime activity and found no effect on most objective measures of sleep.22, 23 One descriptive study found most sleep disturbances in medical‐surgical patients came from noise and sleeping in an unfamiliar bed.4
We hypothesized that an intervention designed to improve patient sleep through changes in staff behavior would decrease sedative use among unselected patients in a medical‐surgical unit. We measured sedative use as our primary endpoint as a marker for effective sleep, and because decreased sedative use is desirable. We also hypothesized that the intervention would lead to improved sleep experiences, as measured by a questionnaire and Verran Snyder‐Halpern (VSH) sleep scores as secondary endpoints.24
Materials And Methods
Study Design
This was a pre‐post study assessing the effect of the intervention on as‐needed sedative use, questionnaire responses, and sleep quality. It was an intention‐to‐treat analysis, and was blinded in terms of measurement of sedative use. The Institutional Review Board of Cambridge Health Alliance approved the study.
Setting and Patients
The site was the only medical‐surgical unit of Somerville Hospital, a small urban community teaching hospital that is part of Cambridge Health Alliance. The hospital unit was chosen for its architectural characteristics, and is organized spatially as 3 U‐shaped pods surrounding nursing workstations. Hence, patient rooms were nearly equidistant from the nurses' stations, unlike a hallway design where distant rooms are quieter. Six rooms were private; 11 were semiprivate. Most of the unit's 28 beds are used for medical patients covered by the hospitalist service. Residents see a minority of patients. A hospitalist is available around the clock. Few agency nurses are used.
Preintervention patients were recruited between April and August 2007. The intervention was planned and implemented from September 2007 to January 2008. Intervention patients were recruited between February and June 2008. The most common principle diagnoses on the unit were chest pain (11%), pneumonia (8%), congestive heart failure (CHF) (5.1%), and chronic obstructive pulmonary disease (COPD) flare (3%). Exclusion criteria ensured that no patient was ill enough to require intensive care unit (ICU)‐level care or was actively dying. All consecutive hospitalized patients on the unit on Tuesdays through Fridays were potentially eligible and invited to participate unless they met exclusion criteria. The limited days of the week ensured that technical support would be available during the intervention phase.
Exclusion criteria were: known sleep disorders; language other than English, Spanish, Portuguese, or Haitian Creole; surgery the prior day; arrival on the floor after 10 PM the prior evening; residence on the unit for more than 4 days; alcohol or drug withdrawal; end‐of‐life morphine drip; significant hearing loss; and blindness.
Study Protocol
A single investigator surveyed patients in the morning about the prior night's sleep experience. The surveys consisted of the VSH sleep scale, as well as an 8‐item questionnaire developed from informal pilot interviews with about 18 patients conducted by 1 of the investigators (M.B.) (Supporting Information Figure 1). The VSH scale is a visual analog scale using a 100‐cm line,24 which we modified with a 100‐mm line to make it easier to collect data. The questionnaire and VSH scores of patients with cognitive impairment were not included in the final analysis. Cognitive impairment was determined by diagnoses present in chart review. Surveys and consent forms were available in 4 languages and trained interpreters were used as needed. Nurses, providers, and patients were blinded to the measurement of as‐needed sedative use, and staff were unaware of which patients were study subjects.
Measurements
Nighttime administration of any medication ordered prn sleep or insomnia was measured using the pharmacy dispensing equipment (Pyxis; Cardinal Health, Dublin, OH), then verified by reviewing the patients' medication administration records. VSH sleep scores were created by measuring the distance in millimeters from the lower end of the scale (0) to the location marked.
We also tracked adherence to some aspects of the intervention. The questionnaire recorded door closing. Chart audits measured the numbers of different prescribers, and the frequency of medication orders using flexible timing.
Data Analysis
Medication use was analyzed as any as‐needed sedative use vs. none. The proportions of patients who used sedatives preintervention and postintervention were compared using a 2‐sample Z statistic, as were survey items. Mean VSH scores were compared with 2‐sample t tests. The study had greater than 80% power to detect a difference in proportion of at least 0.14 at alpha = 0.05.
Design and Implementation of the Intervention
Preintervention, routine vital signs were taken every 8 hours: 8 AM, 4 PM, and midnight. Night nurses arrived at 11 PM, and typically turned off the hallway lights, but the practice was variable and occurred at no set time.
Patients in our informal pilot interviews identified vital signs, medication administration, noise, and evening diuretic administration as disrupting their sleep. After the preintervention phase, we spent 4 months designing and implementing the intervention. We solicited opinions from staff, who identified inflexible timing of medications as disruptive. The plan was discussed at routine staff meetings of all shifts.
The intervention, called the Somerville Protocol (Figure 1) created an 8‐hour Quiet Time from 10 PM to 6 AM, when disruptions were minimized. Vital signs were taken 2 hours earlier (6 AM, 2 PM, and 10 PM); routine medication administration was avoided; and noise was reduced. As before, telemetry patients required vital signs every 4 hours. At 10 PM, hallway lights were turned off by a timer while the Lullaby by Brahms played overhead, signaling the start of Quiet Time to staff and patients. Inexpensive sound meters were installed in each nursing area. They flashed warning lights when 60 dBA was exceeded.
A physician and nurse served as champions. Educational signs were posted in the hospitalists' call room and in the nursing areas. The champions used e‐mail and detailed the intervention to staff. Because the staff played an active role in intervention planning, implementation went smoothly.
Results
During the preintervention phase, 334 patients were screened, 294 were eligible, and 54.7% of eligible subjects were enrolled (n = 161). During the intervention phase, 211 patients were screened, 188 were eligible, and 56.3% of eligible patients were enrolled (n = 106). The mean patient age was 60.6 years. The preintervention and intervention groups did not differ significantly in enrollment rate, age, gender, cognitive impairment, surgical status, or hearing deficiencies (Table 1). Over 93% of patients were nonsurgical.
| Preintervention Patients (n = 161) | Intervention Patients (n = 106) | P Values for Difference | |
|---|---|---|---|
| Mean age (years) | 59.1 | 62.95 | P = 0.146 |
| Males, n (%) | 79 (49.1%) | 46 (43.4%) | P = 0.38 |
| Hard of hearing, n (%) (self‐report) | 33/157 (21.0%) | 14/103 (13.6%) | P = 0.128 |
| English‐speaking, n (%) | 134 (83%) | 83 (78.3%) | P = 0.34 |
| Cognitive impairment, n (%) | 4 (2.5%) | 3 (2.8%) | P = 0.88 |
| Surgical patients, n (%) | 10 (6.2%) | 2 (1.8%) | P = 0.089 |
Sedative Use
Preintervention, 31.7% of patients received nighttime as‐needed sedatives, versus 16.0% of the intervention group, a 49.4% reduction (P = 0.0041; 95% confidence interval [CI]: 0.056‐0.26) (Figure 2). In patients aged 65 years or older, 38.2% received nighttime as‐needed sedatives preintervention, and 14.6% did postintervention, a 61.2% reduction (P = 0.0054; 95% CI: 0.084‐0.39).
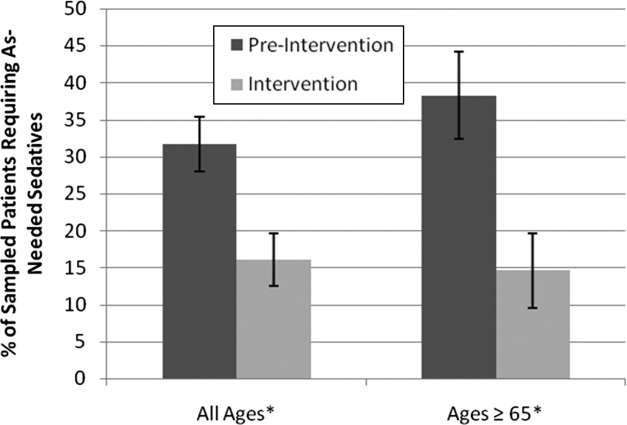
Questionnaire Results
Preintervention, hospital staff was by far the biggest factor keeping patients awake, with 42.4% of patients reporting it (Figure 3). This dropped to only 25.7% with the intervention, a 39.3% decrease (P = 0.009; 95% CI: 0.0452‐0.2765). Preintervention, 19.2% of patients selected voices as the noise most likely to bother them at night, and this dropped to 9.9% with the intervention, a 48% decrease (P = 0.045; 95% CI: 0.0074‐0.1787). No other significant differences were found.
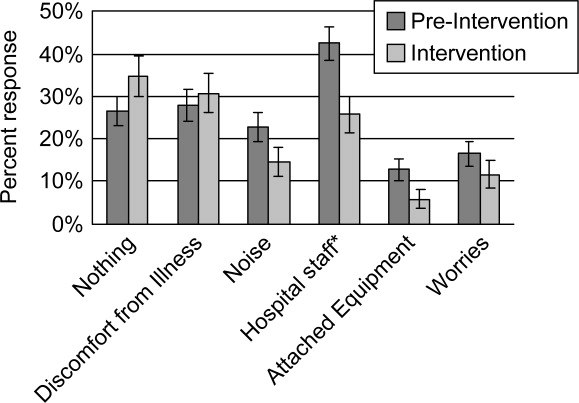
VSH Sleep Score Results
We found no improvement in any measure of the VSH sleep scale. However, 75% of our patients were unable to use the modified VSH scale, generally because they felt too ill, and were then prompted by the surveyor to choose a number between 1 and 10 that reflected their experience.
Protocol Adherence
Changes in unit routines resulted in complete adherence to the new vital signs schedule and avoidance of routine evening diuretics. The closing of patients' doors did not change. An audit of 40 charts found that the percentage of medication orders written with appropriate flexible timing increased from 82% (n = 228) to 95.5% (n = 200) (P = 0.001; 95% CI: 0.077‐0.192). From 20 to 30 different providers wrote orders during each phase.
Discussion
Our trial found that hospital staff was the factor most responsible for patient sleep disruption, and that behavioral interventions on hospital staff can reduce use of as‐needed sedatives. The only previously reported intervention to reduce sedative use, the HELP strategy, involved a complex intervention requiring extra staff, with adherence ranging from 10% to 75%.19, 20, 25 In contrast, our protocol can be easily replicated at minimal cost.
Our results are consistent with those of Freedman et al.,26 who found that noise was not the primary factor responsible for sleep disruption in ICU patients, and that staff activities were at least as important a factor. The study is also consistent with the nursing home studies in which decreases in noise and light did not improve sleep.22, 23 It refutes the study that showed that most sleep disturbance in medical‐surgical patients comes from noise and sleeping in an unfamiliar bed.4 Our results call into question the use of the VSH scale in hospitalized patients, which was designed for use in healthy subjects.
Limitations of this study were as follows: moderate size, lack of refined measures of disease severity, and, as in previous studies,19, 2123 the lack of randomized concurrent controls. Evaluation of secondary endpoints was limited by lack of validation of the questionnaire with objective observations, and inability to use the modified VSH scale. Self‐reports of sleep may correlate imperfectly with objective measures, such as polysomnography.27
A larger concurrent trial randomizing similar units at multiple hospitals would be ideal. Future research is needed to determine whether improving sleep in the hospital improves other outcomes, such as recovery times, delirium, falls, or cost.
The need to reduce as‐needed sedatives is an important safety issue and similar interventions in other hospitals may be helpful. Simple changes in staff routines and provider prescribing habits can yield significant reductions in sedative use.
Acknowledgements
The authors thank Gertrude Gavin, Steffie Woolhandler, MD, Linda Borodkin, John Brusch, MD, Patricia Crombie, Priscilla Dasse, Glen Dawson, Ben Davenny, Linda Kasten, Judith Krempin, Mark Letzeisen, Carmen Mohan, and Arun Mohan. Linda Kasten, Timothy Schmidt, and Glen Dawson provided statistical analysis. The sound meters (Yacker Trackers, Creative Toys of Colorado) were donated by John Brusch, who has no financial conflict of interest.
- ,,,.Sleep in hospitalized medical patients, Part 1: Factors affecting sleep.J Hosp Med.2008;3:473–482.
- ,.Sleep‐dependent learning and memory consolidation.Neuron.2004;44:121–133.
- ,,,,,.An assessment of quality of sleep and the use of drugs with sedating properties in hospitalized adult patients.Health Qual Life Outcomes.2004;2:17.
- ,,,.The sleep experience of medical and surgical patients.Clin Nurs Res.2003;12:159–173.
- .Metabolic and endocrine effects of sleep deprivation.Essent Psychopharmacol.2005;6:341–347.
- ,,,,.Sleep loss and REM sleep loss are hyperalgesic.Sleep.2006;29:145–151.
- ,,,.Slow‐wave sleep and the risk of type 2 diabetes in humans.Proc Natl Acad Sci USA.2008;105:1044–1049.
- .Sleep inquiry: a look with fresh eyes.Image J Nurs Sch.1993;25:249–256.
- Berglund B, Lindvall T, Schwela D, eds.Guidelines for Community Noise.World Health Organization;1999:47.
- ,,,,,.Noise levels in Johns Hopkins Hospital.J Acoust Soc Am.2005;118:3629–3645.
- .Explicit criteria for determining potentially inappropriate medication use by the elderly. An update.Arch Intern Med.1997;157:1531–1536.
- .Delirium in older persons.N Engl J Med.2006;354:1157–1165.
- ,,,,.Sedative hypnotics in older people with insomnia: meta‐analysis of risks and benefits.BMJ.2005;331:1169.
- .Sleep in acute care units.Sleep Breath.2006;10:6–15.
- ,,,,.Quantity and quality of sleep in the surgical intensive care unit: are our patients sleeping?J Trauma.2007;63:1210–1214.
- ,.Sleep in the critically ill patient.Sleep.2006;29:707–716.
- ,,.Sleep quality in hospitalized patients.J Clin Nurs.2005;14:107–113.
- ,.Interactive relationships between hospital patients' noise‐induced stress and other stress with sleep.Heart Lung.2001;30:237–243.
- ,,, et al.A multicomponent intervention to prevent delirium in hospitalized older patients.N Engl J Med.1999;340:669–676.
- ,,,,.The Hospital Elder Life Program: a model of care to prevent cognitive and functional decline in older hospitalized patients. Hospital Elder Life Program.J Am Geriatr Soc.2000;48:1697–1706.
- ,,,,.Noise control: a nursing team's approach to sleep promotion.Am J Nurs.2004;104:40–48; quiz 48‐49.
- ,,,,,.A nonpharmacological intervention to improve sleep in nursing home patients: results of a controlled clinical trial.J Am Geriatr Soc.2006;54:38–47.
- ,,,,.The nursing home at night: effects of an intervention on noise, light, and sleep.J Am Geriatr Soc.1999;47:430–438.
- ,.Instrumentation to describe subjective sleep characteristics in healthy subjects.Res Nurs Health.1987;10:155–163.
- ,,,,.The role of adherence on the effectiveness of nonpharmacologic interventions: evidence from the delirium prevention trial.Arch Intern Med.2003;163:958–964.
- ,,.Patient perception of sleep quality and etiology of sleep disruption in the intensive care unit.Am J Respir Crit Care Med.1999;159:1155–1162.
- ,,.When sleep is perceived as wakefulness: an experimental study on state perception during physiological sleep.J Sleep Res.2007;16:346–353.
Adequate sleep is important for health, yet the hospital environment commonly disrupts sleep.13 Sleep improves after several days in the hospital.3, 4 Sleep deprivation increases cortisol levels5 and sleep loss of greater than 4 hours may be hyperalgesic.6 Even a few days' suppression of slow‐wave sleep worsens glucose tolerance.7 Sleep disruption may cause irritability and aggressiveness,8 impaired memory consolidation, and delirium.2
Noise may disrupt sleep. The World Health Organization recommends a maximum of 30 to 40 dBA in patients' rooms at night.9, 10 Normal conversation occurs at 60 dBA. Medical equipment alarms are about 80 dBA.
Sedative use is common in the hospital.3 Sedatives typically shorten sleep latency and suppress rapid eye movement (REM) sleep. However, some sedatives cause delirium, falls, amnesia, and confusion, particularly in the elderly.1113
Most research on sleep in hospitalized patients has been done in the critical care setting, often in sedated ventilated patients, where sleep disruption is well‐described.1416 Only a few small studies have assessed the sleep of hospitalized patients outside critical care.17, 18
A single blinded interventional trial assessed sedative use, but was a nonrandomized study.19, 20 As‐needed sedative use was measured among hospitalized elderly patients as a secondary endpoint. The intervention, known as the Hospital Elder Life Program (HELP), included a protocol with noise reduction, massage, music, and warm drinks, as well as rescheduling of medications and procedures; it resulted in a 24% reduction in as‐needed sedative use. Another trial decreased noise and reduced overnight X‐rays on a surgical unit, then measured staff and patient attitudes.21 Two interventional studies in nursing homes reduced noise and light, and/or increased daytime activity and found no effect on most objective measures of sleep.22, 23 One descriptive study found most sleep disturbances in medical‐surgical patients came from noise and sleeping in an unfamiliar bed.4
We hypothesized that an intervention designed to improve patient sleep through changes in staff behavior would decrease sedative use among unselected patients in a medical‐surgical unit. We measured sedative use as our primary endpoint as a marker for effective sleep, and because decreased sedative use is desirable. We also hypothesized that the intervention would lead to improved sleep experiences, as measured by a questionnaire and Verran Snyder‐Halpern (VSH) sleep scores as secondary endpoints.24
Materials And Methods
Study Design
This was a pre‐post study assessing the effect of the intervention on as‐needed sedative use, questionnaire responses, and sleep quality. It was an intention‐to‐treat analysis, and was blinded in terms of measurement of sedative use. The Institutional Review Board of Cambridge Health Alliance approved the study.
Setting and Patients
The site was the only medical‐surgical unit of Somerville Hospital, a small urban community teaching hospital that is part of Cambridge Health Alliance. The hospital unit was chosen for its architectural characteristics, and is organized spatially as 3 U‐shaped pods surrounding nursing workstations. Hence, patient rooms were nearly equidistant from the nurses' stations, unlike a hallway design where distant rooms are quieter. Six rooms were private; 11 were semiprivate. Most of the unit's 28 beds are used for medical patients covered by the hospitalist service. Residents see a minority of patients. A hospitalist is available around the clock. Few agency nurses are used.
Preintervention patients were recruited between April and August 2007. The intervention was planned and implemented from September 2007 to January 2008. Intervention patients were recruited between February and June 2008. The most common principle diagnoses on the unit were chest pain (11%), pneumonia (8%), congestive heart failure (CHF) (5.1%), and chronic obstructive pulmonary disease (COPD) flare (3%). Exclusion criteria ensured that no patient was ill enough to require intensive care unit (ICU)‐level care or was actively dying. All consecutive hospitalized patients on the unit on Tuesdays through Fridays were potentially eligible and invited to participate unless they met exclusion criteria. The limited days of the week ensured that technical support would be available during the intervention phase.
Exclusion criteria were: known sleep disorders; language other than English, Spanish, Portuguese, or Haitian Creole; surgery the prior day; arrival on the floor after 10 PM the prior evening; residence on the unit for more than 4 days; alcohol or drug withdrawal; end‐of‐life morphine drip; significant hearing loss; and blindness.
Study Protocol
A single investigator surveyed patients in the morning about the prior night's sleep experience. The surveys consisted of the VSH sleep scale, as well as an 8‐item questionnaire developed from informal pilot interviews with about 18 patients conducted by 1 of the investigators (M.B.) (Supporting Information Figure 1). The VSH scale is a visual analog scale using a 100‐cm line,24 which we modified with a 100‐mm line to make it easier to collect data. The questionnaire and VSH scores of patients with cognitive impairment were not included in the final analysis. Cognitive impairment was determined by diagnoses present in chart review. Surveys and consent forms were available in 4 languages and trained interpreters were used as needed. Nurses, providers, and patients were blinded to the measurement of as‐needed sedative use, and staff were unaware of which patients were study subjects.
Measurements
Nighttime administration of any medication ordered prn sleep or insomnia was measured using the pharmacy dispensing equipment (Pyxis; Cardinal Health, Dublin, OH), then verified by reviewing the patients' medication administration records. VSH sleep scores were created by measuring the distance in millimeters from the lower end of the scale (0) to the location marked.
We also tracked adherence to some aspects of the intervention. The questionnaire recorded door closing. Chart audits measured the numbers of different prescribers, and the frequency of medication orders using flexible timing.
Data Analysis
Medication use was analyzed as any as‐needed sedative use vs. none. The proportions of patients who used sedatives preintervention and postintervention were compared using a 2‐sample Z statistic, as were survey items. Mean VSH scores were compared with 2‐sample t tests. The study had greater than 80% power to detect a difference in proportion of at least 0.14 at alpha = 0.05.
Design and Implementation of the Intervention
Preintervention, routine vital signs were taken every 8 hours: 8 AM, 4 PM, and midnight. Night nurses arrived at 11 PM, and typically turned off the hallway lights, but the practice was variable and occurred at no set time.
Patients in our informal pilot interviews identified vital signs, medication administration, noise, and evening diuretic administration as disrupting their sleep. After the preintervention phase, we spent 4 months designing and implementing the intervention. We solicited opinions from staff, who identified inflexible timing of medications as disruptive. The plan was discussed at routine staff meetings of all shifts.
The intervention, called the Somerville Protocol (Figure 1) created an 8‐hour Quiet Time from 10 PM to 6 AM, when disruptions were minimized. Vital signs were taken 2 hours earlier (6 AM, 2 PM, and 10 PM); routine medication administration was avoided; and noise was reduced. As before, telemetry patients required vital signs every 4 hours. At 10 PM, hallway lights were turned off by a timer while the Lullaby by Brahms played overhead, signaling the start of Quiet Time to staff and patients. Inexpensive sound meters were installed in each nursing area. They flashed warning lights when 60 dBA was exceeded.
A physician and nurse served as champions. Educational signs were posted in the hospitalists' call room and in the nursing areas. The champions used e‐mail and detailed the intervention to staff. Because the staff played an active role in intervention planning, implementation went smoothly.
Results
During the preintervention phase, 334 patients were screened, 294 were eligible, and 54.7% of eligible subjects were enrolled (n = 161). During the intervention phase, 211 patients were screened, 188 were eligible, and 56.3% of eligible patients were enrolled (n = 106). The mean patient age was 60.6 years. The preintervention and intervention groups did not differ significantly in enrollment rate, age, gender, cognitive impairment, surgical status, or hearing deficiencies (Table 1). Over 93% of patients were nonsurgical.
| Preintervention Patients (n = 161) | Intervention Patients (n = 106) | P Values for Difference | |
|---|---|---|---|
| Mean age (years) | 59.1 | 62.95 | P = 0.146 |
| Males, n (%) | 79 (49.1%) | 46 (43.4%) | P = 0.38 |
| Hard of hearing, n (%) (self‐report) | 33/157 (21.0%) | 14/103 (13.6%) | P = 0.128 |
| English‐speaking, n (%) | 134 (83%) | 83 (78.3%) | P = 0.34 |
| Cognitive impairment, n (%) | 4 (2.5%) | 3 (2.8%) | P = 0.88 |
| Surgical patients, n (%) | 10 (6.2%) | 2 (1.8%) | P = 0.089 |
Sedative Use
Preintervention, 31.7% of patients received nighttime as‐needed sedatives, versus 16.0% of the intervention group, a 49.4% reduction (P = 0.0041; 95% confidence interval [CI]: 0.056‐0.26) (Figure 2). In patients aged 65 years or older, 38.2% received nighttime as‐needed sedatives preintervention, and 14.6% did postintervention, a 61.2% reduction (P = 0.0054; 95% CI: 0.084‐0.39).
Questionnaire Results
Preintervention, hospital staff was by far the biggest factor keeping patients awake, with 42.4% of patients reporting it (Figure 3). This dropped to only 25.7% with the intervention, a 39.3% decrease (P = 0.009; 95% CI: 0.0452‐0.2765). Preintervention, 19.2% of patients selected voices as the noise most likely to bother them at night, and this dropped to 9.9% with the intervention, a 48% decrease (P = 0.045; 95% CI: 0.0074‐0.1787). No other significant differences were found.
VSH Sleep Score Results
We found no improvement in any measure of the VSH sleep scale. However, 75% of our patients were unable to use the modified VSH scale, generally because they felt too ill, and were then prompted by the surveyor to choose a number between 1 and 10 that reflected their experience.
Protocol Adherence
Changes in unit routines resulted in complete adherence to the new vital signs schedule and avoidance of routine evening diuretics. The closing of patients' doors did not change. An audit of 40 charts found that the percentage of medication orders written with appropriate flexible timing increased from 82% (n = 228) to 95.5% (n = 200) (P = 0.001; 95% CI: 0.077‐0.192). From 20 to 30 different providers wrote orders during each phase.
Discussion
Our trial found that hospital staff was the factor most responsible for patient sleep disruption, and that behavioral interventions on hospital staff can reduce use of as‐needed sedatives. The only previously reported intervention to reduce sedative use, the HELP strategy, involved a complex intervention requiring extra staff, with adherence ranging from 10% to 75%.19, 20, 25 In contrast, our protocol can be easily replicated at minimal cost.
Our results are consistent with those of Freedman et al.,26 who found that noise was not the primary factor responsible for sleep disruption in ICU patients, and that staff activities were at least as important a factor. The study is also consistent with the nursing home studies in which decreases in noise and light did not improve sleep.22, 23 It refutes the study that showed that most sleep disturbance in medical‐surgical patients comes from noise and sleeping in an unfamiliar bed.4 Our results call into question the use of the VSH scale in hospitalized patients, which was designed for use in healthy subjects.
Limitations of this study were as follows: moderate size, lack of refined measures of disease severity, and, as in previous studies,19, 2123 the lack of randomized concurrent controls. Evaluation of secondary endpoints was limited by lack of validation of the questionnaire with objective observations, and inability to use the modified VSH scale. Self‐reports of sleep may correlate imperfectly with objective measures, such as polysomnography.27
A larger concurrent trial randomizing similar units at multiple hospitals would be ideal. Future research is needed to determine whether improving sleep in the hospital improves other outcomes, such as recovery times, delirium, falls, or cost.
The need to reduce as‐needed sedatives is an important safety issue and similar interventions in other hospitals may be helpful. Simple changes in staff routines and provider prescribing habits can yield significant reductions in sedative use.
Acknowledgements
The authors thank Gertrude Gavin, Steffie Woolhandler, MD, Linda Borodkin, John Brusch, MD, Patricia Crombie, Priscilla Dasse, Glen Dawson, Ben Davenny, Linda Kasten, Judith Krempin, Mark Letzeisen, Carmen Mohan, and Arun Mohan. Linda Kasten, Timothy Schmidt, and Glen Dawson provided statistical analysis. The sound meters (Yacker Trackers, Creative Toys of Colorado) were donated by John Brusch, who has no financial conflict of interest.
Adequate sleep is important for health, yet the hospital environment commonly disrupts sleep.13 Sleep improves after several days in the hospital.3, 4 Sleep deprivation increases cortisol levels5 and sleep loss of greater than 4 hours may be hyperalgesic.6 Even a few days' suppression of slow‐wave sleep worsens glucose tolerance.7 Sleep disruption may cause irritability and aggressiveness,8 impaired memory consolidation, and delirium.2
Noise may disrupt sleep. The World Health Organization recommends a maximum of 30 to 40 dBA in patients' rooms at night.9, 10 Normal conversation occurs at 60 dBA. Medical equipment alarms are about 80 dBA.
Sedative use is common in the hospital.3 Sedatives typically shorten sleep latency and suppress rapid eye movement (REM) sleep. However, some sedatives cause delirium, falls, amnesia, and confusion, particularly in the elderly.1113
Most research on sleep in hospitalized patients has been done in the critical care setting, often in sedated ventilated patients, where sleep disruption is well‐described.1416 Only a few small studies have assessed the sleep of hospitalized patients outside critical care.17, 18
A single blinded interventional trial assessed sedative use, but was a nonrandomized study.19, 20 As‐needed sedative use was measured among hospitalized elderly patients as a secondary endpoint. The intervention, known as the Hospital Elder Life Program (HELP), included a protocol with noise reduction, massage, music, and warm drinks, as well as rescheduling of medications and procedures; it resulted in a 24% reduction in as‐needed sedative use. Another trial decreased noise and reduced overnight X‐rays on a surgical unit, then measured staff and patient attitudes.21 Two interventional studies in nursing homes reduced noise and light, and/or increased daytime activity and found no effect on most objective measures of sleep.22, 23 One descriptive study found most sleep disturbances in medical‐surgical patients came from noise and sleeping in an unfamiliar bed.4
We hypothesized that an intervention designed to improve patient sleep through changes in staff behavior would decrease sedative use among unselected patients in a medical‐surgical unit. We measured sedative use as our primary endpoint as a marker for effective sleep, and because decreased sedative use is desirable. We also hypothesized that the intervention would lead to improved sleep experiences, as measured by a questionnaire and Verran Snyder‐Halpern (VSH) sleep scores as secondary endpoints.24
Materials And Methods
Study Design
This was a pre‐post study assessing the effect of the intervention on as‐needed sedative use, questionnaire responses, and sleep quality. It was an intention‐to‐treat analysis, and was blinded in terms of measurement of sedative use. The Institutional Review Board of Cambridge Health Alliance approved the study.
Setting and Patients
The site was the only medical‐surgical unit of Somerville Hospital, a small urban community teaching hospital that is part of Cambridge Health Alliance. The hospital unit was chosen for its architectural characteristics, and is organized spatially as 3 U‐shaped pods surrounding nursing workstations. Hence, patient rooms were nearly equidistant from the nurses' stations, unlike a hallway design where distant rooms are quieter. Six rooms were private; 11 were semiprivate. Most of the unit's 28 beds are used for medical patients covered by the hospitalist service. Residents see a minority of patients. A hospitalist is available around the clock. Few agency nurses are used.
Preintervention patients were recruited between April and August 2007. The intervention was planned and implemented from September 2007 to January 2008. Intervention patients were recruited between February and June 2008. The most common principle diagnoses on the unit were chest pain (11%), pneumonia (8%), congestive heart failure (CHF) (5.1%), and chronic obstructive pulmonary disease (COPD) flare (3%). Exclusion criteria ensured that no patient was ill enough to require intensive care unit (ICU)‐level care or was actively dying. All consecutive hospitalized patients on the unit on Tuesdays through Fridays were potentially eligible and invited to participate unless they met exclusion criteria. The limited days of the week ensured that technical support would be available during the intervention phase.
Exclusion criteria were: known sleep disorders; language other than English, Spanish, Portuguese, or Haitian Creole; surgery the prior day; arrival on the floor after 10 PM the prior evening; residence on the unit for more than 4 days; alcohol or drug withdrawal; end‐of‐life morphine drip; significant hearing loss; and blindness.
Study Protocol
A single investigator surveyed patients in the morning about the prior night's sleep experience. The surveys consisted of the VSH sleep scale, as well as an 8‐item questionnaire developed from informal pilot interviews with about 18 patients conducted by 1 of the investigators (M.B.) (Supporting Information Figure 1). The VSH scale is a visual analog scale using a 100‐cm line,24 which we modified with a 100‐mm line to make it easier to collect data. The questionnaire and VSH scores of patients with cognitive impairment were not included in the final analysis. Cognitive impairment was determined by diagnoses present in chart review. Surveys and consent forms were available in 4 languages and trained interpreters were used as needed. Nurses, providers, and patients were blinded to the measurement of as‐needed sedative use, and staff were unaware of which patients were study subjects.
Measurements
Nighttime administration of any medication ordered prn sleep or insomnia was measured using the pharmacy dispensing equipment (Pyxis; Cardinal Health, Dublin, OH), then verified by reviewing the patients' medication administration records. VSH sleep scores were created by measuring the distance in millimeters from the lower end of the scale (0) to the location marked.
We also tracked adherence to some aspects of the intervention. The questionnaire recorded door closing. Chart audits measured the numbers of different prescribers, and the frequency of medication orders using flexible timing.
Data Analysis
Medication use was analyzed as any as‐needed sedative use vs. none. The proportions of patients who used sedatives preintervention and postintervention were compared using a 2‐sample Z statistic, as were survey items. Mean VSH scores were compared with 2‐sample t tests. The study had greater than 80% power to detect a difference in proportion of at least 0.14 at alpha = 0.05.
Design and Implementation of the Intervention
Preintervention, routine vital signs were taken every 8 hours: 8 AM, 4 PM, and midnight. Night nurses arrived at 11 PM, and typically turned off the hallway lights, but the practice was variable and occurred at no set time.
Patients in our informal pilot interviews identified vital signs, medication administration, noise, and evening diuretic administration as disrupting their sleep. After the preintervention phase, we spent 4 months designing and implementing the intervention. We solicited opinions from staff, who identified inflexible timing of medications as disruptive. The plan was discussed at routine staff meetings of all shifts.
The intervention, called the Somerville Protocol (Figure 1) created an 8‐hour Quiet Time from 10 PM to 6 AM, when disruptions were minimized. Vital signs were taken 2 hours earlier (6 AM, 2 PM, and 10 PM); routine medication administration was avoided; and noise was reduced. As before, telemetry patients required vital signs every 4 hours. At 10 PM, hallway lights were turned off by a timer while the Lullaby by Brahms played overhead, signaling the start of Quiet Time to staff and patients. Inexpensive sound meters were installed in each nursing area. They flashed warning lights when 60 dBA was exceeded.
A physician and nurse served as champions. Educational signs were posted in the hospitalists' call room and in the nursing areas. The champions used e‐mail and detailed the intervention to staff. Because the staff played an active role in intervention planning, implementation went smoothly.
Results
During the preintervention phase, 334 patients were screened, 294 were eligible, and 54.7% of eligible subjects were enrolled (n = 161). During the intervention phase, 211 patients were screened, 188 were eligible, and 56.3% of eligible patients were enrolled (n = 106). The mean patient age was 60.6 years. The preintervention and intervention groups did not differ significantly in enrollment rate, age, gender, cognitive impairment, surgical status, or hearing deficiencies (Table 1). Over 93% of patients were nonsurgical.
| Preintervention Patients (n = 161) | Intervention Patients (n = 106) | P Values for Difference | |
|---|---|---|---|
| Mean age (years) | 59.1 | 62.95 | P = 0.146 |
| Males, n (%) | 79 (49.1%) | 46 (43.4%) | P = 0.38 |
| Hard of hearing, n (%) (self‐report) | 33/157 (21.0%) | 14/103 (13.6%) | P = 0.128 |
| English‐speaking, n (%) | 134 (83%) | 83 (78.3%) | P = 0.34 |
| Cognitive impairment, n (%) | 4 (2.5%) | 3 (2.8%) | P = 0.88 |
| Surgical patients, n (%) | 10 (6.2%) | 2 (1.8%) | P = 0.089 |
Sedative Use
Preintervention, 31.7% of patients received nighttime as‐needed sedatives, versus 16.0% of the intervention group, a 49.4% reduction (P = 0.0041; 95% confidence interval [CI]: 0.056‐0.26) (Figure 2). In patients aged 65 years or older, 38.2% received nighttime as‐needed sedatives preintervention, and 14.6% did postintervention, a 61.2% reduction (P = 0.0054; 95% CI: 0.084‐0.39).
Questionnaire Results
Preintervention, hospital staff was by far the biggest factor keeping patients awake, with 42.4% of patients reporting it (Figure 3). This dropped to only 25.7% with the intervention, a 39.3% decrease (P = 0.009; 95% CI: 0.0452‐0.2765). Preintervention, 19.2% of patients selected voices as the noise most likely to bother them at night, and this dropped to 9.9% with the intervention, a 48% decrease (P = 0.045; 95% CI: 0.0074‐0.1787). No other significant differences were found.
VSH Sleep Score Results
We found no improvement in any measure of the VSH sleep scale. However, 75% of our patients were unable to use the modified VSH scale, generally because they felt too ill, and were then prompted by the surveyor to choose a number between 1 and 10 that reflected their experience.
Protocol Adherence
Changes in unit routines resulted in complete adherence to the new vital signs schedule and avoidance of routine evening diuretics. The closing of patients' doors did not change. An audit of 40 charts found that the percentage of medication orders written with appropriate flexible timing increased from 82% (n = 228) to 95.5% (n = 200) (P = 0.001; 95% CI: 0.077‐0.192). From 20 to 30 different providers wrote orders during each phase.
Discussion
Our trial found that hospital staff was the factor most responsible for patient sleep disruption, and that behavioral interventions on hospital staff can reduce use of as‐needed sedatives. The only previously reported intervention to reduce sedative use, the HELP strategy, involved a complex intervention requiring extra staff, with adherence ranging from 10% to 75%.19, 20, 25 In contrast, our protocol can be easily replicated at minimal cost.
Our results are consistent with those of Freedman et al.,26 who found that noise was not the primary factor responsible for sleep disruption in ICU patients, and that staff activities were at least as important a factor. The study is also consistent with the nursing home studies in which decreases in noise and light did not improve sleep.22, 23 It refutes the study that showed that most sleep disturbance in medical‐surgical patients comes from noise and sleeping in an unfamiliar bed.4 Our results call into question the use of the VSH scale in hospitalized patients, which was designed for use in healthy subjects.
Limitations of this study were as follows: moderate size, lack of refined measures of disease severity, and, as in previous studies,19, 2123 the lack of randomized concurrent controls. Evaluation of secondary endpoints was limited by lack of validation of the questionnaire with objective observations, and inability to use the modified VSH scale. Self‐reports of sleep may correlate imperfectly with objective measures, such as polysomnography.27
A larger concurrent trial randomizing similar units at multiple hospitals would be ideal. Future research is needed to determine whether improving sleep in the hospital improves other outcomes, such as recovery times, delirium, falls, or cost.
The need to reduce as‐needed sedatives is an important safety issue and similar interventions in other hospitals may be helpful. Simple changes in staff routines and provider prescribing habits can yield significant reductions in sedative use.
Acknowledgements
The authors thank Gertrude Gavin, Steffie Woolhandler, MD, Linda Borodkin, John Brusch, MD, Patricia Crombie, Priscilla Dasse, Glen Dawson, Ben Davenny, Linda Kasten, Judith Krempin, Mark Letzeisen, Carmen Mohan, and Arun Mohan. Linda Kasten, Timothy Schmidt, and Glen Dawson provided statistical analysis. The sound meters (Yacker Trackers, Creative Toys of Colorado) were donated by John Brusch, who has no financial conflict of interest.
- ,,,.Sleep in hospitalized medical patients, Part 1: Factors affecting sleep.J Hosp Med.2008;3:473–482.
- ,.Sleep‐dependent learning and memory consolidation.Neuron.2004;44:121–133.
- ,,,,,.An assessment of quality of sleep and the use of drugs with sedating properties in hospitalized adult patients.Health Qual Life Outcomes.2004;2:17.
- ,,,.The sleep experience of medical and surgical patients.Clin Nurs Res.2003;12:159–173.
- .Metabolic and endocrine effects of sleep deprivation.Essent Psychopharmacol.2005;6:341–347.
- ,,,,.Sleep loss and REM sleep loss are hyperalgesic.Sleep.2006;29:145–151.
- ,,,.Slow‐wave sleep and the risk of type 2 diabetes in humans.Proc Natl Acad Sci USA.2008;105:1044–1049.
- .Sleep inquiry: a look with fresh eyes.Image J Nurs Sch.1993;25:249–256.
- Berglund B, Lindvall T, Schwela D, eds.Guidelines for Community Noise.World Health Organization;1999:47.
- ,,,,,.Noise levels in Johns Hopkins Hospital.J Acoust Soc Am.2005;118:3629–3645.
- .Explicit criteria for determining potentially inappropriate medication use by the elderly. An update.Arch Intern Med.1997;157:1531–1536.
- .Delirium in older persons.N Engl J Med.2006;354:1157–1165.
- ,,,,.Sedative hypnotics in older people with insomnia: meta‐analysis of risks and benefits.BMJ.2005;331:1169.
- .Sleep in acute care units.Sleep Breath.2006;10:6–15.
- ,,,,.Quantity and quality of sleep in the surgical intensive care unit: are our patients sleeping?J Trauma.2007;63:1210–1214.
- ,.Sleep in the critically ill patient.Sleep.2006;29:707–716.
- ,,.Sleep quality in hospitalized patients.J Clin Nurs.2005;14:107–113.
- ,.Interactive relationships between hospital patients' noise‐induced stress and other stress with sleep.Heart Lung.2001;30:237–243.
- ,,, et al.A multicomponent intervention to prevent delirium in hospitalized older patients.N Engl J Med.1999;340:669–676.
- ,,,,.The Hospital Elder Life Program: a model of care to prevent cognitive and functional decline in older hospitalized patients. Hospital Elder Life Program.J Am Geriatr Soc.2000;48:1697–1706.
- ,,,,.Noise control: a nursing team's approach to sleep promotion.Am J Nurs.2004;104:40–48; quiz 48‐49.
- ,,,,,.A nonpharmacological intervention to improve sleep in nursing home patients: results of a controlled clinical trial.J Am Geriatr Soc.2006;54:38–47.
- ,,,,.The nursing home at night: effects of an intervention on noise, light, and sleep.J Am Geriatr Soc.1999;47:430–438.
- ,.Instrumentation to describe subjective sleep characteristics in healthy subjects.Res Nurs Health.1987;10:155–163.
- ,,,,.The role of adherence on the effectiveness of nonpharmacologic interventions: evidence from the delirium prevention trial.Arch Intern Med.2003;163:958–964.
- ,,.Patient perception of sleep quality and etiology of sleep disruption in the intensive care unit.Am J Respir Crit Care Med.1999;159:1155–1162.
- ,,.When sleep is perceived as wakefulness: an experimental study on state perception during physiological sleep.J Sleep Res.2007;16:346–353.
- ,,,.Sleep in hospitalized medical patients, Part 1: Factors affecting sleep.J Hosp Med.2008;3:473–482.
- ,.Sleep‐dependent learning and memory consolidation.Neuron.2004;44:121–133.
- ,,,,,.An assessment of quality of sleep and the use of drugs with sedating properties in hospitalized adult patients.Health Qual Life Outcomes.2004;2:17.
- ,,,.The sleep experience of medical and surgical patients.Clin Nurs Res.2003;12:159–173.
- .Metabolic and endocrine effects of sleep deprivation.Essent Psychopharmacol.2005;6:341–347.
- ,,,,.Sleep loss and REM sleep loss are hyperalgesic.Sleep.2006;29:145–151.
- ,,,.Slow‐wave sleep and the risk of type 2 diabetes in humans.Proc Natl Acad Sci USA.2008;105:1044–1049.
- .Sleep inquiry: a look with fresh eyes.Image J Nurs Sch.1993;25:249–256.
- Berglund B, Lindvall T, Schwela D, eds.Guidelines for Community Noise.World Health Organization;1999:47.
- ,,,,,.Noise levels in Johns Hopkins Hospital.J Acoust Soc Am.2005;118:3629–3645.
- .Explicit criteria for determining potentially inappropriate medication use by the elderly. An update.Arch Intern Med.1997;157:1531–1536.
- .Delirium in older persons.N Engl J Med.2006;354:1157–1165.
- ,,,,.Sedative hypnotics in older people with insomnia: meta‐analysis of risks and benefits.BMJ.2005;331:1169.
- .Sleep in acute care units.Sleep Breath.2006;10:6–15.
- ,,,,.Quantity and quality of sleep in the surgical intensive care unit: are our patients sleeping?J Trauma.2007;63:1210–1214.
- ,.Sleep in the critically ill patient.Sleep.2006;29:707–716.
- ,,.Sleep quality in hospitalized patients.J Clin Nurs.2005;14:107–113.
- ,.Interactive relationships between hospital patients' noise‐induced stress and other stress with sleep.Heart Lung.2001;30:237–243.
- ,,, et al.A multicomponent intervention to prevent delirium in hospitalized older patients.N Engl J Med.1999;340:669–676.
- ,,,,.The Hospital Elder Life Program: a model of care to prevent cognitive and functional decline in older hospitalized patients. Hospital Elder Life Program.J Am Geriatr Soc.2000;48:1697–1706.
- ,,,,.Noise control: a nursing team's approach to sleep promotion.Am J Nurs.2004;104:40–48; quiz 48‐49.
- ,,,,,.A nonpharmacological intervention to improve sleep in nursing home patients: results of a controlled clinical trial.J Am Geriatr Soc.2006;54:38–47.
- ,,,,.The nursing home at night: effects of an intervention on noise, light, and sleep.J Am Geriatr Soc.1999;47:430–438.
- ,.Instrumentation to describe subjective sleep characteristics in healthy subjects.Res Nurs Health.1987;10:155–163.
- ,,,,.The role of adherence on the effectiveness of nonpharmacologic interventions: evidence from the delirium prevention trial.Arch Intern Med.2003;163:958–964.
- ,,.Patient perception of sleep quality and etiology of sleep disruption in the intensive care unit.Am J Respir Crit Care Med.1999;159:1155–1162.
- ,,.When sleep is perceived as wakefulness: an experimental study on state perception during physiological sleep.J Sleep Res.2007;16:346–353.
New Jersey Cracks Down on Never Events
A landmark New Jersey law that increases public disclosure of major preventable medical errors and prohibits charges for certain medical expenses related to those mistakes has hospitalists poised to take a leadership role in patient-safety efforts.
The legislation allows the state to release hospital-specific data on 14 medical mistakes considered by the federal government to be most preventable. It also bans hospitals from charging patients or insurers for follow-up medical costs related to the errors, including pressure ulcers, DVT, and catheter-associated urinary tract infections.
“It’s hard to argue the New Jersey legislation doesn’t make sense,” says hospitalist Niraj Sehgal, MD, MPH, associate chair for quality and safety in the Department of Medicine at the University of California at San Francisco. “After all, if I had the wrong limb operated on, I certainly wouldn’t expect to pay for the subsequent care needs, and nor should our system.”
Dr. Sehgal expects more states to follow New Jersey’s lead, a likely outcome given the fact the AARP is calling the Garden State measure “a national landmark.” The legislation also dovetails with the “no pay for errors” initiative from the Centers for Medicare & Medicaid Services.
Many hospitalists think HM groups are best positioned to spearhead quality and patient-safety efforts tied to the legislation. Hospitalist Vincent Barba, MD, FACP, FHM, medical director for quality improvement with University of Medicine and Dentistry of New Jersey in Newark, says HM leaders just have to seize the opportunity.
“Be the home team,” Dr. Barba says. “Step up. Take a leading role.”
A landmark New Jersey law that increases public disclosure of major preventable medical errors and prohibits charges for certain medical expenses related to those mistakes has hospitalists poised to take a leadership role in patient-safety efforts.
The legislation allows the state to release hospital-specific data on 14 medical mistakes considered by the federal government to be most preventable. It also bans hospitals from charging patients or insurers for follow-up medical costs related to the errors, including pressure ulcers, DVT, and catheter-associated urinary tract infections.
“It’s hard to argue the New Jersey legislation doesn’t make sense,” says hospitalist Niraj Sehgal, MD, MPH, associate chair for quality and safety in the Department of Medicine at the University of California at San Francisco. “After all, if I had the wrong limb operated on, I certainly wouldn’t expect to pay for the subsequent care needs, and nor should our system.”
Dr. Sehgal expects more states to follow New Jersey’s lead, a likely outcome given the fact the AARP is calling the Garden State measure “a national landmark.” The legislation also dovetails with the “no pay for errors” initiative from the Centers for Medicare & Medicaid Services.
Many hospitalists think HM groups are best positioned to spearhead quality and patient-safety efforts tied to the legislation. Hospitalist Vincent Barba, MD, FACP, FHM, medical director for quality improvement with University of Medicine and Dentistry of New Jersey in Newark, says HM leaders just have to seize the opportunity.
“Be the home team,” Dr. Barba says. “Step up. Take a leading role.”
A landmark New Jersey law that increases public disclosure of major preventable medical errors and prohibits charges for certain medical expenses related to those mistakes has hospitalists poised to take a leadership role in patient-safety efforts.
The legislation allows the state to release hospital-specific data on 14 medical mistakes considered by the federal government to be most preventable. It also bans hospitals from charging patients or insurers for follow-up medical costs related to the errors, including pressure ulcers, DVT, and catheter-associated urinary tract infections.
“It’s hard to argue the New Jersey legislation doesn’t make sense,” says hospitalist Niraj Sehgal, MD, MPH, associate chair for quality and safety in the Department of Medicine at the University of California at San Francisco. “After all, if I had the wrong limb operated on, I certainly wouldn’t expect to pay for the subsequent care needs, and nor should our system.”
Dr. Sehgal expects more states to follow New Jersey’s lead, a likely outcome given the fact the AARP is calling the Garden State measure “a national landmark.” The legislation also dovetails with the “no pay for errors” initiative from the Centers for Medicare & Medicaid Services.
Many hospitalists think HM groups are best positioned to spearhead quality and patient-safety efforts tied to the legislation. Hospitalist Vincent Barba, MD, FACP, FHM, medical director for quality improvement with University of Medicine and Dentistry of New Jersey in Newark, says HM leaders just have to seize the opportunity.
“Be the home team,” Dr. Barba says. “Step up. Take a leading role.”