User login
Chaplains play important part of integrated palliative care
WASHINGTON – Hospital chaplains are key partners in meeting the needs of palliative care patients and, as such, have much to offer psychiatry, according to an expert.
“I think we should work with chaplains,” Dr. Laura B. Dunn, professor of psychiatry and behavioral sciences at Stanford (Calif.) University, said in an interview at the annual meeting of the American Association for Geriatric Psychiatry. “It’s very helpful to know what they do, and for them to know what we do in terms of diagnosing and using a biopsychosocial model.”

Dr. Dunn said the relegation of chaplaincy and spiritual care in medicine has been unfortunate. After all, the level of a patient’s spiritual health is an inherent aspect of quality of life in palliative care, particularly for those over age 60 who often want help reconciling with loved ones, data collected by Dr. Dunn show. Viewing those patients in terms of their core needs rather than seeking a psychiatric diagnosis can make them more satisfied with their overall palliative care experience, she said.
How is spiritual health measured? There are few models and even fewer empirical studies, but Dr. Dunn said in addition learning how to deliver pastoral care, professional chaplains are trained to assess, intervene, and observe outcomes in spiritual health.
To begin with, spirituality is defined not in terms of “religiosity” but more as following an ethical path, similar to the idea of the Golden Rule or the ethic of reciprocity: Love your neighbor as yourself, in other words. The spiritual maturity to follow such a path requires the ability to love oneself that is balanced with a connection to others, and God, “if your belief includes God,” said Dr. Dunn, who pointed out that chaplaincy programs for atheists also exist.
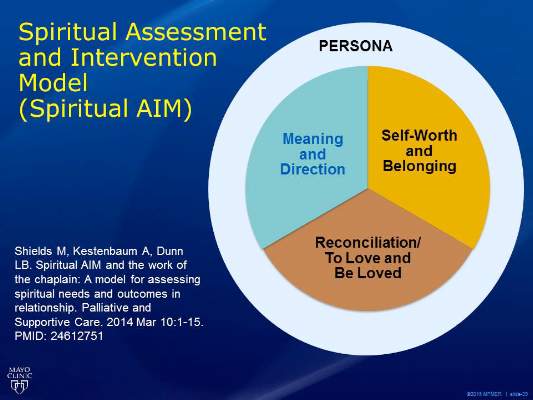
By observing a person’s behavior and conversing with him or her, paying close attention to the person’s attributions of blame, if any, and expressions of chief concerns, a chaplain will assess where on the continuum that person is in three key components of spiritual health: the need for meaning and direction, a sense of self-worth and belonging, and an ability to love and be loved. This latter component often is facilitated through seeking reconciliation when relationships are broken.
In the face of crisis, such as with terminal illness, one of those needs typically supersedes the others. This is what is known as the person’s “core spiritual need,” said Dr. Dunn, who also serves director of the university’s Geriatric Psychiatry Fellowship Training Program, and has extensive research and clinical experience evaluating and managing older adults with mood, anxiety, and cognitive disorders. As part of her research, she and her colleagues have developed a schematic called the Spiritual AIM (Spiritual Assessment and Intervention Model), which depicts those three concerns in relation to one another (Palliat Support Care. 2015 Feb;13:75-89).
Chaplains also are trained to rely on their own feelings about people, similar to the way in which psychiatrists use countertransference. “It is not intrapersonal; it is interpersonal,” Dr. Dunn said. “Healing happens in relationship, and the focus is on that relationship.”
Chaplains undergo standardized clinical pastoral training programs predicated on a combination of theological reflection and psychological theory, plus critique from professional peers and students.
“Their model is very similar to what we [geriatric psychiatrists] do when we assess a patient,” Dr. Dunn said. “We might be more structured trying to ferret out a diagnosis, but we’re assessing all the time.”
Depending on which aspect of spiritual health is most lacking, the chaplain will choose the role of either a “guide” to help with balancing the need for meaning and direction, a “valuer” to help restore feelings of worth and belonging, or a “truth-teller” who will explore with the patient ways he or she might have contributed to broken relationships, and actions the patient might take in order to heal them. This is all done within the context of an interdisciplinary team, Dr. Dunn said.
She and a team of researchers, including a chaplain, conducted a study of 31 advanced-stage adult cancer patients in an outpatient palliative care service, that measured self-reported changes in their spiritual, psychological, and physical symptoms both before and after Spiritual AIM sessions with a chaplain.
The need for balancing one of the three key components of spiritual health was determined by the chaplain to be fairly equal across the cohort, although just more than half of patients younger than 60 years of age struggled more with self-worth and belonging (P = .030). Those over 60 years were equally concerned with either reconciliation or meaning and direction (P less than .05). Two-thirds of the cohort were women, although a relationship between gender and spiritual assessment needs was not determined. Two-thirds also identified themselves as Christian, just over one-third were Jewish, and the rest identified as either Buddhist or nondenominational.
Using a variety of validated palliative care scales, such as the Edmonton Symptom Assessment Syndrome (ESAS) for physical complaints, the Center for Epidemiologic Studies Short Depression Scale, the Mini Mental Adjustment to Cancer scale (Mini-MAC), and the positive and negative RCOPE questionnaire for religious coping, among other scales, Dr. Dunn and her associates found that the change in baseline of overall spiritual health after intervention from the chaplain improved slightly in most measures. Mean baseline scores for the ESAS went from 25 to 24.4 post-intervention. The difference between baseline depression scores fell from 4.2 to 4.1.
Mini-MAC scores improved, particularly in “fighting spirit” and levels of fatalism (P = .084 and P = .036, respectively). In addition, maladaptive coping skills also improved (P = .018).The findings have helped Dr. Dunn in her work as a geriatric psychiatrist, especially when treating cancer patients, or in settings where there is not as much time for a full clinical assessment. “I think of patients in terms of their core needs and what I can do right now to help patients meet those needs.” Dr. Dunn cited, as an example, patients who feel like they don’t belong and are lonely. “If they’re in an assisted living home, can I get them to enter [the communal space]? That’s very different than thinking of them in terms only of depression.”
On Twitter @whitneymcknight
One reason chaplains are such a key part of the palliative care team is that they are seen by patients from a different perspective, Dr. Gurprit S. Lamba said. “Chaplains lend their ears, act as friends, and provide company to these patients,” Dr. Lamba said in an interview. “Discussing spiritual/religious matters helps these individuals cope better. Chaplains can provide more meaningful services with knowledge about different cultures, doctrines, and traditions, so that they can tailor their meetings accordingly.
“Studies have shown that psychiatrists are less religious and show less religious affiliation than their patients and than the population in general. As Dr. Dunn mentioned, chaplaincy programs for atheists also exist. Psychiatrists, with chaplains, can work with any individual to improve and optimize treatment. The critical part lies in assessment of patients’ religious views and spirituality along with their families’ opinions before offering meeting with chaplains.”
Dr. Lamba is a geriatric psychiatrist affiliated with BayRidge Hospital in Lynn, Mass.
One reason chaplains are such a key part of the palliative care team is that they are seen by patients from a different perspective, Dr. Gurprit S. Lamba said. “Chaplains lend their ears, act as friends, and provide company to these patients,” Dr. Lamba said in an interview. “Discussing spiritual/religious matters helps these individuals cope better. Chaplains can provide more meaningful services with knowledge about different cultures, doctrines, and traditions, so that they can tailor their meetings accordingly.
“Studies have shown that psychiatrists are less religious and show less religious affiliation than their patients and than the population in general. As Dr. Dunn mentioned, chaplaincy programs for atheists also exist. Psychiatrists, with chaplains, can work with any individual to improve and optimize treatment. The critical part lies in assessment of patients’ religious views and spirituality along with their families’ opinions before offering meeting with chaplains.”
Dr. Lamba is a geriatric psychiatrist affiliated with BayRidge Hospital in Lynn, Mass.
One reason chaplains are such a key part of the palliative care team is that they are seen by patients from a different perspective, Dr. Gurprit S. Lamba said. “Chaplains lend their ears, act as friends, and provide company to these patients,” Dr. Lamba said in an interview. “Discussing spiritual/religious matters helps these individuals cope better. Chaplains can provide more meaningful services with knowledge about different cultures, doctrines, and traditions, so that they can tailor their meetings accordingly.
“Studies have shown that psychiatrists are less religious and show less religious affiliation than their patients and than the population in general. As Dr. Dunn mentioned, chaplaincy programs for atheists also exist. Psychiatrists, with chaplains, can work with any individual to improve and optimize treatment. The critical part lies in assessment of patients’ religious views and spirituality along with their families’ opinions before offering meeting with chaplains.”
Dr. Lamba is a geriatric psychiatrist affiliated with BayRidge Hospital in Lynn, Mass.
WASHINGTON – Hospital chaplains are key partners in meeting the needs of palliative care patients and, as such, have much to offer psychiatry, according to an expert.
“I think we should work with chaplains,” Dr. Laura B. Dunn, professor of psychiatry and behavioral sciences at Stanford (Calif.) University, said in an interview at the annual meeting of the American Association for Geriatric Psychiatry. “It’s very helpful to know what they do, and for them to know what we do in terms of diagnosing and using a biopsychosocial model.”
Dr. Dunn said the relegation of chaplaincy and spiritual care in medicine has been unfortunate. After all, the level of a patient’s spiritual health is an inherent aspect of quality of life in palliative care, particularly for those over age 60 who often want help reconciling with loved ones, data collected by Dr. Dunn show. Viewing those patients in terms of their core needs rather than seeking a psychiatric diagnosis can make them more satisfied with their overall palliative care experience, she said.
How is spiritual health measured? There are few models and even fewer empirical studies, but Dr. Dunn said in addition learning how to deliver pastoral care, professional chaplains are trained to assess, intervene, and observe outcomes in spiritual health.
To begin with, spirituality is defined not in terms of “religiosity” but more as following an ethical path, similar to the idea of the Golden Rule or the ethic of reciprocity: Love your neighbor as yourself, in other words. The spiritual maturity to follow such a path requires the ability to love oneself that is balanced with a connection to others, and God, “if your belief includes God,” said Dr. Dunn, who pointed out that chaplaincy programs for atheists also exist.
By observing a person’s behavior and conversing with him or her, paying close attention to the person’s attributions of blame, if any, and expressions of chief concerns, a chaplain will assess where on the continuum that person is in three key components of spiritual health: the need for meaning and direction, a sense of self-worth and belonging, and an ability to love and be loved. This latter component often is facilitated through seeking reconciliation when relationships are broken.
In the face of crisis, such as with terminal illness, one of those needs typically supersedes the others. This is what is known as the person’s “core spiritual need,” said Dr. Dunn, who also serves director of the university’s Geriatric Psychiatry Fellowship Training Program, and has extensive research and clinical experience evaluating and managing older adults with mood, anxiety, and cognitive disorders. As part of her research, she and her colleagues have developed a schematic called the Spiritual AIM (Spiritual Assessment and Intervention Model), which depicts those three concerns in relation to one another (Palliat Support Care. 2015 Feb;13:75-89).
Chaplains also are trained to rely on their own feelings about people, similar to the way in which psychiatrists use countertransference. “It is not intrapersonal; it is interpersonal,” Dr. Dunn said. “Healing happens in relationship, and the focus is on that relationship.”
Chaplains undergo standardized clinical pastoral training programs predicated on a combination of theological reflection and psychological theory, plus critique from professional peers and students.
“Their model is very similar to what we [geriatric psychiatrists] do when we assess a patient,” Dr. Dunn said. “We might be more structured trying to ferret out a diagnosis, but we’re assessing all the time.”
Depending on which aspect of spiritual health is most lacking, the chaplain will choose the role of either a “guide” to help with balancing the need for meaning and direction, a “valuer” to help restore feelings of worth and belonging, or a “truth-teller” who will explore with the patient ways he or she might have contributed to broken relationships, and actions the patient might take in order to heal them. This is all done within the context of an interdisciplinary team, Dr. Dunn said.
She and a team of researchers, including a chaplain, conducted a study of 31 advanced-stage adult cancer patients in an outpatient palliative care service, that measured self-reported changes in their spiritual, psychological, and physical symptoms both before and after Spiritual AIM sessions with a chaplain.
The need for balancing one of the three key components of spiritual health was determined by the chaplain to be fairly equal across the cohort, although just more than half of patients younger than 60 years of age struggled more with self-worth and belonging (P = .030). Those over 60 years were equally concerned with either reconciliation or meaning and direction (P less than .05). Two-thirds of the cohort were women, although a relationship between gender and spiritual assessment needs was not determined. Two-thirds also identified themselves as Christian, just over one-third were Jewish, and the rest identified as either Buddhist or nondenominational.
Using a variety of validated palliative care scales, such as the Edmonton Symptom Assessment Syndrome (ESAS) for physical complaints, the Center for Epidemiologic Studies Short Depression Scale, the Mini Mental Adjustment to Cancer scale (Mini-MAC), and the positive and negative RCOPE questionnaire for religious coping, among other scales, Dr. Dunn and her associates found that the change in baseline of overall spiritual health after intervention from the chaplain improved slightly in most measures. Mean baseline scores for the ESAS went from 25 to 24.4 post-intervention. The difference between baseline depression scores fell from 4.2 to 4.1.
Mini-MAC scores improved, particularly in “fighting spirit” and levels of fatalism (P = .084 and P = .036, respectively). In addition, maladaptive coping skills also improved (P = .018).The findings have helped Dr. Dunn in her work as a geriatric psychiatrist, especially when treating cancer patients, or in settings where there is not as much time for a full clinical assessment. “I think of patients in terms of their core needs and what I can do right now to help patients meet those needs.” Dr. Dunn cited, as an example, patients who feel like they don’t belong and are lonely. “If they’re in an assisted living home, can I get them to enter [the communal space]? That’s very different than thinking of them in terms only of depression.”
On Twitter @whitneymcknight
WASHINGTON – Hospital chaplains are key partners in meeting the needs of palliative care patients and, as such, have much to offer psychiatry, according to an expert.
“I think we should work with chaplains,” Dr. Laura B. Dunn, professor of psychiatry and behavioral sciences at Stanford (Calif.) University, said in an interview at the annual meeting of the American Association for Geriatric Psychiatry. “It’s very helpful to know what they do, and for them to know what we do in terms of diagnosing and using a biopsychosocial model.”
Dr. Dunn said the relegation of chaplaincy and spiritual care in medicine has been unfortunate. After all, the level of a patient’s spiritual health is an inherent aspect of quality of life in palliative care, particularly for those over age 60 who often want help reconciling with loved ones, data collected by Dr. Dunn show. Viewing those patients in terms of their core needs rather than seeking a psychiatric diagnosis can make them more satisfied with their overall palliative care experience, she said.
How is spiritual health measured? There are few models and even fewer empirical studies, but Dr. Dunn said in addition learning how to deliver pastoral care, professional chaplains are trained to assess, intervene, and observe outcomes in spiritual health.
To begin with, spirituality is defined not in terms of “religiosity” but more as following an ethical path, similar to the idea of the Golden Rule or the ethic of reciprocity: Love your neighbor as yourself, in other words. The spiritual maturity to follow such a path requires the ability to love oneself that is balanced with a connection to others, and God, “if your belief includes God,” said Dr. Dunn, who pointed out that chaplaincy programs for atheists also exist.
By observing a person’s behavior and conversing with him or her, paying close attention to the person’s attributions of blame, if any, and expressions of chief concerns, a chaplain will assess where on the continuum that person is in three key components of spiritual health: the need for meaning and direction, a sense of self-worth and belonging, and an ability to love and be loved. This latter component often is facilitated through seeking reconciliation when relationships are broken.
In the face of crisis, such as with terminal illness, one of those needs typically supersedes the others. This is what is known as the person’s “core spiritual need,” said Dr. Dunn, who also serves director of the university’s Geriatric Psychiatry Fellowship Training Program, and has extensive research and clinical experience evaluating and managing older adults with mood, anxiety, and cognitive disorders. As part of her research, she and her colleagues have developed a schematic called the Spiritual AIM (Spiritual Assessment and Intervention Model), which depicts those three concerns in relation to one another (Palliat Support Care. 2015 Feb;13:75-89).
Chaplains also are trained to rely on their own feelings about people, similar to the way in which psychiatrists use countertransference. “It is not intrapersonal; it is interpersonal,” Dr. Dunn said. “Healing happens in relationship, and the focus is on that relationship.”
Chaplains undergo standardized clinical pastoral training programs predicated on a combination of theological reflection and psychological theory, plus critique from professional peers and students.
“Their model is very similar to what we [geriatric psychiatrists] do when we assess a patient,” Dr. Dunn said. “We might be more structured trying to ferret out a diagnosis, but we’re assessing all the time.”
Depending on which aspect of spiritual health is most lacking, the chaplain will choose the role of either a “guide” to help with balancing the need for meaning and direction, a “valuer” to help restore feelings of worth and belonging, or a “truth-teller” who will explore with the patient ways he or she might have contributed to broken relationships, and actions the patient might take in order to heal them. This is all done within the context of an interdisciplinary team, Dr. Dunn said.
She and a team of researchers, including a chaplain, conducted a study of 31 advanced-stage adult cancer patients in an outpatient palliative care service, that measured self-reported changes in their spiritual, psychological, and physical symptoms both before and after Spiritual AIM sessions with a chaplain.
The need for balancing one of the three key components of spiritual health was determined by the chaplain to be fairly equal across the cohort, although just more than half of patients younger than 60 years of age struggled more with self-worth and belonging (P = .030). Those over 60 years were equally concerned with either reconciliation or meaning and direction (P less than .05). Two-thirds of the cohort were women, although a relationship between gender and spiritual assessment needs was not determined. Two-thirds also identified themselves as Christian, just over one-third were Jewish, and the rest identified as either Buddhist or nondenominational.
Using a variety of validated palliative care scales, such as the Edmonton Symptom Assessment Syndrome (ESAS) for physical complaints, the Center for Epidemiologic Studies Short Depression Scale, the Mini Mental Adjustment to Cancer scale (Mini-MAC), and the positive and negative RCOPE questionnaire for religious coping, among other scales, Dr. Dunn and her associates found that the change in baseline of overall spiritual health after intervention from the chaplain improved slightly in most measures. Mean baseline scores for the ESAS went from 25 to 24.4 post-intervention. The difference between baseline depression scores fell from 4.2 to 4.1.
Mini-MAC scores improved, particularly in “fighting spirit” and levels of fatalism (P = .084 and P = .036, respectively). In addition, maladaptive coping skills also improved (P = .018).The findings have helped Dr. Dunn in her work as a geriatric psychiatrist, especially when treating cancer patients, or in settings where there is not as much time for a full clinical assessment. “I think of patients in terms of their core needs and what I can do right now to help patients meet those needs.” Dr. Dunn cited, as an example, patients who feel like they don’t belong and are lonely. “If they’re in an assisted living home, can I get them to enter [the communal space]? That’s very different than thinking of them in terms only of depression.”
On Twitter @whitneymcknight
EXPERT ANALYSIS FROM AAGP 2016

Randomized corporate clinical trials
The randomized clinical trial (RCT) has been the bulwark of the development of effective and safe medical and surgical therapy. Developed over the last half-century, they have proved the benefit and safety of new drugs and procedures and provided guidance to physicians in choosing therapeutic choices for their patients. They have replaced intuitive care that had largely directed medical care for centuries with a degree of science in making therapeutic decisions.
Although less than perfect, the RCT has been the reason for the remarkable success that we have achieved in decreasing the mortality of heart disease. This success has been driven largely by scientific altruism modified to some degree by the financial benefits of both the medical profession and the pharmaceutical industry.
As corporate hospital and third-party payers expand their role in the pattern of health care, there is the potential to make changes in how care is rendered beyond the choice of medical or surgical therapy. The expansion of care regionally and nationally provides tempting targets to modify the quality and efficacy on a large scale. It also provides potential cost-saving targets and generates corporate profits. Decisions at the corporate or administrative area in the past have been initiated on the basis of competitive costs and on intuitive decision making. The size of the market, however, provides an opportunity to test a variety of administrative plans that can lead to cost saving. These initiatives, well-meaning in their genesis, may result in patient participation in “studies” in which the patient may have a limited knowledge and benefit and uncertain risks.
RCTs demand informed consent by patients and unbiased temporal oversight by safety boards when searching for answers to questions based on contemporary knowledge. At present, there is no specific role for the patient’s voluntary and informed participation should a corporate representative initiate a “study” to answer a corporate question. Before we embark on “research” in patient care, it is imperative that we consider the principles established by RCTs. I propose two scenarios that may provide illustrative insight:
1. A nurse administrator wishes to explore the question of the cost savings achieved on a general medical ward by changing the current nurse staffing of eight professional nurses to a staffing with two professional nurses and six nursing assistants. The administrator will use personnel costs as the endpoint of the study and consider a variety of secondary issues such as the duration of time to respond to a call, sacral erythema, and wrong-dose administration, or other quality measurements.
2. The administrator of the catheterization laboratory decides to compare two catheters in the laboratory driven again by the costs of the catheters. The primary endpoint of the study will be cost savings. Secondary measurements will be time in the catheterization laboratory and postprocedure bleeding.
In both cases, the patient may or not have been informed about the research project in which they have been enrolled. In addition, there is no temporal assessment of the occurrence of adverse events that could occur during the progress of the “study” to ensure its safety. Many of the safeguards that have been developed around the RCT need to be incorporated into the design of these investigations.
This, of course, is all hypothetical, but on the other hand, it is not beyond the realm of possibility; as we move from “local care” to a system driven by anonymous personnel, it is important to obtain the consent of the patient and to establish procedures to ensure their safety.
Dr. Goldstein, medical editor of Cardiology News, is professor of medicine at Wayne State University and division head emeritus of cardiovascular medicine at Henry Ford Hospital, both in Detroit. He is on data safety monitoring committees for the National Institutes of Health and several pharmaceutical companies.
The randomized clinical trial (RCT) has been the bulwark of the development of effective and safe medical and surgical therapy. Developed over the last half-century, they have proved the benefit and safety of new drugs and procedures and provided guidance to physicians in choosing therapeutic choices for their patients. They have replaced intuitive care that had largely directed medical care for centuries with a degree of science in making therapeutic decisions.
Although less than perfect, the RCT has been the reason for the remarkable success that we have achieved in decreasing the mortality of heart disease. This success has been driven largely by scientific altruism modified to some degree by the financial benefits of both the medical profession and the pharmaceutical industry.
As corporate hospital and third-party payers expand their role in the pattern of health care, there is the potential to make changes in how care is rendered beyond the choice of medical or surgical therapy. The expansion of care regionally and nationally provides tempting targets to modify the quality and efficacy on a large scale. It also provides potential cost-saving targets and generates corporate profits. Decisions at the corporate or administrative area in the past have been initiated on the basis of competitive costs and on intuitive decision making. The size of the market, however, provides an opportunity to test a variety of administrative plans that can lead to cost saving. These initiatives, well-meaning in their genesis, may result in patient participation in “studies” in which the patient may have a limited knowledge and benefit and uncertain risks.
RCTs demand informed consent by patients and unbiased temporal oversight by safety boards when searching for answers to questions based on contemporary knowledge. At present, there is no specific role for the patient’s voluntary and informed participation should a corporate representative initiate a “study” to answer a corporate question. Before we embark on “research” in patient care, it is imperative that we consider the principles established by RCTs. I propose two scenarios that may provide illustrative insight:
1. A nurse administrator wishes to explore the question of the cost savings achieved on a general medical ward by changing the current nurse staffing of eight professional nurses to a staffing with two professional nurses and six nursing assistants. The administrator will use personnel costs as the endpoint of the study and consider a variety of secondary issues such as the duration of time to respond to a call, sacral erythema, and wrong-dose administration, or other quality measurements.
2. The administrator of the catheterization laboratory decides to compare two catheters in the laboratory driven again by the costs of the catheters. The primary endpoint of the study will be cost savings. Secondary measurements will be time in the catheterization laboratory and postprocedure bleeding.
In both cases, the patient may or not have been informed about the research project in which they have been enrolled. In addition, there is no temporal assessment of the occurrence of adverse events that could occur during the progress of the “study” to ensure its safety. Many of the safeguards that have been developed around the RCT need to be incorporated into the design of these investigations.
This, of course, is all hypothetical, but on the other hand, it is not beyond the realm of possibility; as we move from “local care” to a system driven by anonymous personnel, it is important to obtain the consent of the patient and to establish procedures to ensure their safety.
Dr. Goldstein, medical editor of Cardiology News, is professor of medicine at Wayne State University and division head emeritus of cardiovascular medicine at Henry Ford Hospital, both in Detroit. He is on data safety monitoring committees for the National Institutes of Health and several pharmaceutical companies.
The randomized clinical trial (RCT) has been the bulwark of the development of effective and safe medical and surgical therapy. Developed over the last half-century, they have proved the benefit and safety of new drugs and procedures and provided guidance to physicians in choosing therapeutic choices for their patients. They have replaced intuitive care that had largely directed medical care for centuries with a degree of science in making therapeutic decisions.
Although less than perfect, the RCT has been the reason for the remarkable success that we have achieved in decreasing the mortality of heart disease. This success has been driven largely by scientific altruism modified to some degree by the financial benefits of both the medical profession and the pharmaceutical industry.
As corporate hospital and third-party payers expand their role in the pattern of health care, there is the potential to make changes in how care is rendered beyond the choice of medical or surgical therapy. The expansion of care regionally and nationally provides tempting targets to modify the quality and efficacy on a large scale. It also provides potential cost-saving targets and generates corporate profits. Decisions at the corporate or administrative area in the past have been initiated on the basis of competitive costs and on intuitive decision making. The size of the market, however, provides an opportunity to test a variety of administrative plans that can lead to cost saving. These initiatives, well-meaning in their genesis, may result in patient participation in “studies” in which the patient may have a limited knowledge and benefit and uncertain risks.
RCTs demand informed consent by patients and unbiased temporal oversight by safety boards when searching for answers to questions based on contemporary knowledge. At present, there is no specific role for the patient’s voluntary and informed participation should a corporate representative initiate a “study” to answer a corporate question. Before we embark on “research” in patient care, it is imperative that we consider the principles established by RCTs. I propose two scenarios that may provide illustrative insight:
1. A nurse administrator wishes to explore the question of the cost savings achieved on a general medical ward by changing the current nurse staffing of eight professional nurses to a staffing with two professional nurses and six nursing assistants. The administrator will use personnel costs as the endpoint of the study and consider a variety of secondary issues such as the duration of time to respond to a call, sacral erythema, and wrong-dose administration, or other quality measurements.
2. The administrator of the catheterization laboratory decides to compare two catheters in the laboratory driven again by the costs of the catheters. The primary endpoint of the study will be cost savings. Secondary measurements will be time in the catheterization laboratory and postprocedure bleeding.
In both cases, the patient may or not have been informed about the research project in which they have been enrolled. In addition, there is no temporal assessment of the occurrence of adverse events that could occur during the progress of the “study” to ensure its safety. Many of the safeguards that have been developed around the RCT need to be incorporated into the design of these investigations.
This, of course, is all hypothetical, but on the other hand, it is not beyond the realm of possibility; as we move from “local care” to a system driven by anonymous personnel, it is important to obtain the consent of the patient and to establish procedures to ensure their safety.
Dr. Goldstein, medical editor of Cardiology News, is professor of medicine at Wayne State University and division head emeritus of cardiovascular medicine at Henry Ford Hospital, both in Detroit. He is on data safety monitoring committees for the National Institutes of Health and several pharmaceutical companies.
Tools for Diagnosing Skin Cancer Earlier: Report From the AAD Meeting
At the 74th Annual Meeting of the American Academy of Dermatology, Dr. Orit Markowitz discussed noninvasive imaging tools that can help dermatologists diagnose skin cancers earlier. She provides highlights from this session, including the use of dermoscopy and optical coherence technology to detect features of early melanoma and nonmelanoma skin cancers as well as monitor skin cancer management. A lesion that is pink clinically but shows pigment dermoscopically should be biopsied, Dr. Markowtiz advises, as it may be an early amelanotic melanoma. She also notes that noninvasive imaging tools can be used to detect residual tumor cells in treated skin that otherwise looks clinically normal.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
At the 74th Annual Meeting of the American Academy of Dermatology, Dr. Orit Markowitz discussed noninvasive imaging tools that can help dermatologists diagnose skin cancers earlier. She provides highlights from this session, including the use of dermoscopy and optical coherence technology to detect features of early melanoma and nonmelanoma skin cancers as well as monitor skin cancer management. A lesion that is pink clinically but shows pigment dermoscopically should be biopsied, Dr. Markowtiz advises, as it may be an early amelanotic melanoma. She also notes that noninvasive imaging tools can be used to detect residual tumor cells in treated skin that otherwise looks clinically normal.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
At the 74th Annual Meeting of the American Academy of Dermatology, Dr. Orit Markowitz discussed noninvasive imaging tools that can help dermatologists diagnose skin cancers earlier. She provides highlights from this session, including the use of dermoscopy and optical coherence technology to detect features of early melanoma and nonmelanoma skin cancers as well as monitor skin cancer management. A lesion that is pink clinically but shows pigment dermoscopically should be biopsied, Dr. Markowtiz advises, as it may be an early amelanotic melanoma. She also notes that noninvasive imaging tools can be used to detect residual tumor cells in treated skin that otherwise looks clinically normal.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel

The Germanwings tragedy: A look at the final report
March 24, 2016, marks 1 year since a Germanwings copilot locked the pilot out of the cockpit, then purposely crashed his plane into the French Alps, killing all those aboard the commercial airliner. You can think of it as a suicide or as a mass murder; it was both.
Initially, it was reported that the pilot had taken 10 months off from training in 2008-2009 because of depression. A full report released earlier this month by France’s Civil Aviation Safety Investigation Authority reveals that the copilot recently had resumed treatment with a psychiatrist, as well as several other physicians, without informing his employer.
According to the report, the initial episode of depression included a hospitalization. The copilot was judged to be “entirely healthy,” and communications occurred between the aviation authorities, and his psychiatrist and psychotherapist. The copilot was issued a class I, unrestricted medical certificate that allowed him to fly as long as he did not have a recurrence of depression. It would be revoked if he had either symptoms or a need for medication. The medical certificate was renewed yearly, most recently in July 2014.

In November 2014, the copilot consulted with “private physician A” and was placed on sick leave for a week. Beginning in December, the copilot saw “several private physicians” for visual difficulties and sleep disturbance. He was seen by several eye specialists who found no visual problems. On Feb. 17, 2015, the copilot saw “private physician B,” who placed him on sick leave for 8 days; he did not forward this information to Germanwings. On the same day, he saw “private physician C,” who referred him to a psychiatrist and a psychotherapist, and prescribed zopiclone, a sleep medication similar to Lunesta (eszopiclone), the report says.
On Feb. 22, 2015, the copilot returned to see “private physician C” and was placed on sick leave for 3 days. Two days later, he met with a psychiatrist and was given a prescription for mirtazapine. On March 9, “private physician D” issued a note for sick leave, which the copilot did not report to the airline. The following day, he returned to “private physician C,” who recommended hospitalization for possible psychosis. He returned to “private physician C” on March 12, 2 days later, and was given a note for sick leave – which he did not relay to Germanwings. On March 16, the treating psychiatrist prescribed escitalopram, Dominal f (a phenothiazine similar to compazine), and zolpidem. On March 18, he received a note for sick leave by “private physician E.” An email to his treating psychiatrist sometime in March also revealed that he was taking an additional dose of mirtazapine and lorazepam. In reading the list of medical contacts, one has the sense that the copilot was frantic. His remains tested positive for citalopram, mirtazapine, and zopiclone.
If I am reading the report correctly, the copilot took medical leave twice during the months preceding the crash, and copiloted flights both the day before the crash and earlier that same morning.
The aviation authority’s report noted: “The limited medical and personal data available to the safety investigation did not make it possible for an unambiguous psychiatric diagnosis to be made. In particular an interview with the copilot’s relatives and his private physicians was impossible, as they exercised their right to refuse to be interviewed.” The investigators concluded that it was likely that the copilot suffered from a psychotic depressive episode dating back to December 2014 and lasting until the tragedy.
It’s important to note that German laws are more stringent than American laws about patient privacy: Violations include criminal sanctions. What is striking from the report is that there is so little communication between the physicians, even between physician C, who referred the patient to a psychiatrist, and the treating psychiatrist. In fact, physician C recommended hospitalization, and there is no report that the psychiatrist recommended either time off or hospitalization. We don’t know if the physicians were aware of who else was treating this patient, or if the doctors even knew he was a pilot. It’s even more striking that the physicians of a dead mass murderer can simply refuse to be interviewed by aviation authorities.
When the report came out, forensic psychiatrist Paul Appelbaum tweeted, “Germanwings crash shows results of fetishing privacy when lives are at stake; I’d like to think US drs. would have reported psychotic pilot.” Please note that Dr. Appelbaum’s grammar is restricted by the 140-character limit imposed by Twitter. A tweeted discussion ensued, including Dr. Annette Hanson, over whether it would be better to hospitalize or report a pilot, and if it might be difficult to figure out whom a private psychiatrist would even report to. Dr. Hanson, who favored hospitalization, tweeted, “Creating a duty to report ‘unfitness’ apart from dangerousness could expand to other professions-liability growth.”
It does seem that in the United States, physicians treating pilots with possible psychosis and depression – serious enough to require sedating medications, time off from work, and a recommendation for hospitalization – would likely feel obligated to prevent this patient from flying an aircraft.
The issue seems complicated; if there is no way to obtain confidential treatment, those with psychiatric disorders may well go untreated, especially if those who get care risk losing their livelihoods. We do know this is the case: A survey of pilots who have inquired about the consequences of getting psychiatric care showed that the majority would forgo treatment to maintain their right to fly.
According to the French aviation report: “As an example, the Aviation Medicine Advisory Service (AMAS), a U.S.-based company providing aeromedical advice for pilots, reviewed its database of telephone inquiries from pilots between 1992 and 1997. It had received 1,200 telephone inquiries from pilots who had been diagnosed as having clinical depressions and who had been advised by their physicians to take antidepressant medications. These pilots had called AMAS to discuss the aeromedical implications of their situations. O[f] the 1,200 pilots, approximately 60% told the AMAS that they would refuse medication and continue to fly. About 15% indicated an intention to take the medications and continue their flying duties without informing the Federal Aviation Administration. And the remaining 25% said they would take sick leave, undergo the recommended treatment, and return to work when aeromedically cleared to do so. As the data were representative only of pilots who telephoned for information, the [Aerospace Medical Association] underlined the fact that the presence of depressed and untreated pilots (or treated without aeromedical supervision) was undoubtedly underreported.”
We might like to believe that psychiatric treatment would offer protection from tragedy, and that regulations that dissuade people from getting help might ultimately create more problems than they solve. In this case, the pilot was seeing a psychiatrist, and, none of his many efforts to get care prevented this suicide/mass murder. I found it interesting that there is no indication that the airline might request more information after the pilot presented two notes from outside doctors requesting sick leave, especially given his history of disabling depression. Still, without input from the physicians and the family, we will never know whether anyone had any indication that the pilot was so imminently dangerous.
Dr. Miller is a coauthor of “Shrink Rap: Three Psychiatrists Explain Their Work” (Baltimore: The Johns Hopkins University, 2011).
March 24, 2016, marks 1 year since a Germanwings copilot locked the pilot out of the cockpit, then purposely crashed his plane into the French Alps, killing all those aboard the commercial airliner. You can think of it as a suicide or as a mass murder; it was both.
Initially, it was reported that the pilot had taken 10 months off from training in 2008-2009 because of depression. A full report released earlier this month by France’s Civil Aviation Safety Investigation Authority reveals that the copilot recently had resumed treatment with a psychiatrist, as well as several other physicians, without informing his employer.
According to the report, the initial episode of depression included a hospitalization. The copilot was judged to be “entirely healthy,” and communications occurred between the aviation authorities, and his psychiatrist and psychotherapist. The copilot was issued a class I, unrestricted medical certificate that allowed him to fly as long as he did not have a recurrence of depression. It would be revoked if he had either symptoms or a need for medication. The medical certificate was renewed yearly, most recently in July 2014.
In November 2014, the copilot consulted with “private physician A” and was placed on sick leave for a week. Beginning in December, the copilot saw “several private physicians” for visual difficulties and sleep disturbance. He was seen by several eye specialists who found no visual problems. On Feb. 17, 2015, the copilot saw “private physician B,” who placed him on sick leave for 8 days; he did not forward this information to Germanwings. On the same day, he saw “private physician C,” who referred him to a psychiatrist and a psychotherapist, and prescribed zopiclone, a sleep medication similar to Lunesta (eszopiclone), the report says.
On Feb. 22, 2015, the copilot returned to see “private physician C” and was placed on sick leave for 3 days. Two days later, he met with a psychiatrist and was given a prescription for mirtazapine. On March 9, “private physician D” issued a note for sick leave, which the copilot did not report to the airline. The following day, he returned to “private physician C,” who recommended hospitalization for possible psychosis. He returned to “private physician C” on March 12, 2 days later, and was given a note for sick leave – which he did not relay to Germanwings. On March 16, the treating psychiatrist prescribed escitalopram, Dominal f (a phenothiazine similar to compazine), and zolpidem. On March 18, he received a note for sick leave by “private physician E.” An email to his treating psychiatrist sometime in March also revealed that he was taking an additional dose of mirtazapine and lorazepam. In reading the list of medical contacts, one has the sense that the copilot was frantic. His remains tested positive for citalopram, mirtazapine, and zopiclone.
If I am reading the report correctly, the copilot took medical leave twice during the months preceding the crash, and copiloted flights both the day before the crash and earlier that same morning.
The aviation authority’s report noted: “The limited medical and personal data available to the safety investigation did not make it possible for an unambiguous psychiatric diagnosis to be made. In particular an interview with the copilot’s relatives and his private physicians was impossible, as they exercised their right to refuse to be interviewed.” The investigators concluded that it was likely that the copilot suffered from a psychotic depressive episode dating back to December 2014 and lasting until the tragedy.
It’s important to note that German laws are more stringent than American laws about patient privacy: Violations include criminal sanctions. What is striking from the report is that there is so little communication between the physicians, even between physician C, who referred the patient to a psychiatrist, and the treating psychiatrist. In fact, physician C recommended hospitalization, and there is no report that the psychiatrist recommended either time off or hospitalization. We don’t know if the physicians were aware of who else was treating this patient, or if the doctors even knew he was a pilot. It’s even more striking that the physicians of a dead mass murderer can simply refuse to be interviewed by aviation authorities.
When the report came out, forensic psychiatrist Paul Appelbaum tweeted, “Germanwings crash shows results of fetishing privacy when lives are at stake; I’d like to think US drs. would have reported psychotic pilot.” Please note that Dr. Appelbaum’s grammar is restricted by the 140-character limit imposed by Twitter. A tweeted discussion ensued, including Dr. Annette Hanson, over whether it would be better to hospitalize or report a pilot, and if it might be difficult to figure out whom a private psychiatrist would even report to. Dr. Hanson, who favored hospitalization, tweeted, “Creating a duty to report ‘unfitness’ apart from dangerousness could expand to other professions-liability growth.”
It does seem that in the United States, physicians treating pilots with possible psychosis and depression – serious enough to require sedating medications, time off from work, and a recommendation for hospitalization – would likely feel obligated to prevent this patient from flying an aircraft.
The issue seems complicated; if there is no way to obtain confidential treatment, those with psychiatric disorders may well go untreated, especially if those who get care risk losing their livelihoods. We do know this is the case: A survey of pilots who have inquired about the consequences of getting psychiatric care showed that the majority would forgo treatment to maintain their right to fly.
According to the French aviation report: “As an example, the Aviation Medicine Advisory Service (AMAS), a U.S.-based company providing aeromedical advice for pilots, reviewed its database of telephone inquiries from pilots between 1992 and 1997. It had received 1,200 telephone inquiries from pilots who had been diagnosed as having clinical depressions and who had been advised by their physicians to take antidepressant medications. These pilots had called AMAS to discuss the aeromedical implications of their situations. O[f] the 1,200 pilots, approximately 60% told the AMAS that they would refuse medication and continue to fly. About 15% indicated an intention to take the medications and continue their flying duties without informing the Federal Aviation Administration. And the remaining 25% said they would take sick leave, undergo the recommended treatment, and return to work when aeromedically cleared to do so. As the data were representative only of pilots who telephoned for information, the [Aerospace Medical Association] underlined the fact that the presence of depressed and untreated pilots (or treated without aeromedical supervision) was undoubtedly underreported.”
We might like to believe that psychiatric treatment would offer protection from tragedy, and that regulations that dissuade people from getting help might ultimately create more problems than they solve. In this case, the pilot was seeing a psychiatrist, and, none of his many efforts to get care prevented this suicide/mass murder. I found it interesting that there is no indication that the airline might request more information after the pilot presented two notes from outside doctors requesting sick leave, especially given his history of disabling depression. Still, without input from the physicians and the family, we will never know whether anyone had any indication that the pilot was so imminently dangerous.
Dr. Miller is a coauthor of “Shrink Rap: Three Psychiatrists Explain Their Work” (Baltimore: The Johns Hopkins University, 2011).
March 24, 2016, marks 1 year since a Germanwings copilot locked the pilot out of the cockpit, then purposely crashed his plane into the French Alps, killing all those aboard the commercial airliner. You can think of it as a suicide or as a mass murder; it was both.
Initially, it was reported that the pilot had taken 10 months off from training in 2008-2009 because of depression. A full report released earlier this month by France’s Civil Aviation Safety Investigation Authority reveals that the copilot recently had resumed treatment with a psychiatrist, as well as several other physicians, without informing his employer.
According to the report, the initial episode of depression included a hospitalization. The copilot was judged to be “entirely healthy,” and communications occurred between the aviation authorities, and his psychiatrist and psychotherapist. The copilot was issued a class I, unrestricted medical certificate that allowed him to fly as long as he did not have a recurrence of depression. It would be revoked if he had either symptoms or a need for medication. The medical certificate was renewed yearly, most recently in July 2014.
In November 2014, the copilot consulted with “private physician A” and was placed on sick leave for a week. Beginning in December, the copilot saw “several private physicians” for visual difficulties and sleep disturbance. He was seen by several eye specialists who found no visual problems. On Feb. 17, 2015, the copilot saw “private physician B,” who placed him on sick leave for 8 days; he did not forward this information to Germanwings. On the same day, he saw “private physician C,” who referred him to a psychiatrist and a psychotherapist, and prescribed zopiclone, a sleep medication similar to Lunesta (eszopiclone), the report says.
On Feb. 22, 2015, the copilot returned to see “private physician C” and was placed on sick leave for 3 days. Two days later, he met with a psychiatrist and was given a prescription for mirtazapine. On March 9, “private physician D” issued a note for sick leave, which the copilot did not report to the airline. The following day, he returned to “private physician C,” who recommended hospitalization for possible psychosis. He returned to “private physician C” on March 12, 2 days later, and was given a note for sick leave – which he did not relay to Germanwings. On March 16, the treating psychiatrist prescribed escitalopram, Dominal f (a phenothiazine similar to compazine), and zolpidem. On March 18, he received a note for sick leave by “private physician E.” An email to his treating psychiatrist sometime in March also revealed that he was taking an additional dose of mirtazapine and lorazepam. In reading the list of medical contacts, one has the sense that the copilot was frantic. His remains tested positive for citalopram, mirtazapine, and zopiclone.
If I am reading the report correctly, the copilot took medical leave twice during the months preceding the crash, and copiloted flights both the day before the crash and earlier that same morning.
The aviation authority’s report noted: “The limited medical and personal data available to the safety investigation did not make it possible for an unambiguous psychiatric diagnosis to be made. In particular an interview with the copilot’s relatives and his private physicians was impossible, as they exercised their right to refuse to be interviewed.” The investigators concluded that it was likely that the copilot suffered from a psychotic depressive episode dating back to December 2014 and lasting until the tragedy.
It’s important to note that German laws are more stringent than American laws about patient privacy: Violations include criminal sanctions. What is striking from the report is that there is so little communication between the physicians, even between physician C, who referred the patient to a psychiatrist, and the treating psychiatrist. In fact, physician C recommended hospitalization, and there is no report that the psychiatrist recommended either time off or hospitalization. We don’t know if the physicians were aware of who else was treating this patient, or if the doctors even knew he was a pilot. It’s even more striking that the physicians of a dead mass murderer can simply refuse to be interviewed by aviation authorities.
When the report came out, forensic psychiatrist Paul Appelbaum tweeted, “Germanwings crash shows results of fetishing privacy when lives are at stake; I’d like to think US drs. would have reported psychotic pilot.” Please note that Dr. Appelbaum’s grammar is restricted by the 140-character limit imposed by Twitter. A tweeted discussion ensued, including Dr. Annette Hanson, over whether it would be better to hospitalize or report a pilot, and if it might be difficult to figure out whom a private psychiatrist would even report to. Dr. Hanson, who favored hospitalization, tweeted, “Creating a duty to report ‘unfitness’ apart from dangerousness could expand to other professions-liability growth.”
It does seem that in the United States, physicians treating pilots with possible psychosis and depression – serious enough to require sedating medications, time off from work, and a recommendation for hospitalization – would likely feel obligated to prevent this patient from flying an aircraft.
The issue seems complicated; if there is no way to obtain confidential treatment, those with psychiatric disorders may well go untreated, especially if those who get care risk losing their livelihoods. We do know this is the case: A survey of pilots who have inquired about the consequences of getting psychiatric care showed that the majority would forgo treatment to maintain their right to fly.
According to the French aviation report: “As an example, the Aviation Medicine Advisory Service (AMAS), a U.S.-based company providing aeromedical advice for pilots, reviewed its database of telephone inquiries from pilots between 1992 and 1997. It had received 1,200 telephone inquiries from pilots who had been diagnosed as having clinical depressions and who had been advised by their physicians to take antidepressant medications. These pilots had called AMAS to discuss the aeromedical implications of their situations. O[f] the 1,200 pilots, approximately 60% told the AMAS that they would refuse medication and continue to fly. About 15% indicated an intention to take the medications and continue their flying duties without informing the Federal Aviation Administration. And the remaining 25% said they would take sick leave, undergo the recommended treatment, and return to work when aeromedically cleared to do so. As the data were representative only of pilots who telephoned for information, the [Aerospace Medical Association] underlined the fact that the presence of depressed and untreated pilots (or treated without aeromedical supervision) was undoubtedly underreported.”
We might like to believe that psychiatric treatment would offer protection from tragedy, and that regulations that dissuade people from getting help might ultimately create more problems than they solve. In this case, the pilot was seeing a psychiatrist, and, none of his many efforts to get care prevented this suicide/mass murder. I found it interesting that there is no indication that the airline might request more information after the pilot presented two notes from outside doctors requesting sick leave, especially given his history of disabling depression. Still, without input from the physicians and the family, we will never know whether anyone had any indication that the pilot was so imminently dangerous.
Dr. Miller is a coauthor of “Shrink Rap: Three Psychiatrists Explain Their Work” (Baltimore: The Johns Hopkins University, 2011).

Gynecologic cancer patients underutilize advance care directives
SAN DIEGO – Fewer than half of gynecologic oncology patients surveyed at a major cancer center had completed advance care directives regarding their preferences for end-of-life care, and most of those who did had no copy of the documents in their medical records, Dr. Alaina J. Brown reported at the annual meeting of the Society of Gynecologic Oncology.
“These findings indicate there is room to improve advance directive planning documentation in our patient population,” said Dr. Brown, a fellow in gynecologic oncology and reproductive medicine at the University of Texas MD Anderson Cancer Center in Houston.

“Providers must identify and address barriers to advance care planning documentation in order to assist patients in achieving their end-of-life care goals ... I think we need to focus on educating ourselves and becoming proactive about trying to have these conversations earlier in treatment instead of when a patient is quite ill and we know that they’re going to pass away within the next week or so,” she added.
One barrier has recently been overcome by Medicare’s new policy – effective beginning this past January – of providing reimbursement for advance care planning as a separate and billable service.
In addition, Dr. Brown’s survey of 110 gynecologic oncology patients identified two significant psychological barriers to advance care planning: high levels of death anxiety and a feeling of distress that symptoms and/or treatment side effects are interfering with daily activities and relationships.
The survey showed that while 75% of the patients were familiar with advance care directives such as a living will or medical power of attorney, only 49% of subjects had actually completed those documents, and a mere 18% had a copy of an advance care directive in their medical record.
Half of the subjects had recurrent cancer, the rest were visiting the gynecologic oncology service for active surveillance. Only a minority of those with recurrent cancer had completed advance care directives.
Study participants completed two validated, self-administered questionnaire surveys: the 19-item MD Anderson Symptom Inventory (MDASI), which assesses patient-reported disease symptoms and treatment side effects during the previous 24 hours, and the 15-item Templer’s Death Anxiety Scale.
The mean MDASI Interference score, a measure of overall symptom distress and the impact of symptoms on daily life, was significantly higher in gynecologic oncology patients who hadn’t completed advance directives than in those who had. Similarly, patients who hadn’t completed advance directives scored significantly higher on the death anxiety metric.
“Patients with recurrent disease and those with increased disease symptom burden and death anxiety should be targeted for advance care planning discussions, as they may be less likely to engage in advance care planning activities,” Dr. Brown concluded.
She noted that prior research in other medical fields has shown that holding early planning discussions about end-of-life issues improves the likelihood that a patient’s final wishes will be honored, reduces utilization of hospital resources at the end of life, and reduces distress among the patient and family members. It’s important for gynecologic oncologists to step forward in this area because they are in a unique position: they often manage a cancer patient’s surgical care as well as chemotherapy and then later assist in the transition to end of life, she added.
At the conference session on palliative care where Dr. Brown presented her findings, audience members said the 49% completion rate for advance care directives that she found in her study was actually quite impressive; at many gynecologic oncology services the rates are in the 20%-25% range. The audience consensus was that much of the blame for the low rates of advance care planning documentation in their field belongs on the shoulders of gynecologic oncologists themselves.
“I would say that it’s entirely our fault,” declared session codirector Dr. Stephanie Blank of New York University.
Dr. Brown said as a result of her survey findings, she and her colleagues are working to change the institutional practice at MD Anderson such that completion of advance care directive planning directives with documentation in the medical record becomes a quality-of-care goal within the first few patient visits.
“In the past we had a social worker come to those patients who checked off a box on a form in the waiting room; now we’re trying to be more proactive about having a provider engage the patients early on,” she explained.
She reported having no financial conflicts of interest regarding her study.
SAN DIEGO – Fewer than half of gynecologic oncology patients surveyed at a major cancer center had completed advance care directives regarding their preferences for end-of-life care, and most of those who did had no copy of the documents in their medical records, Dr. Alaina J. Brown reported at the annual meeting of the Society of Gynecologic Oncology.
“These findings indicate there is room to improve advance directive planning documentation in our patient population,” said Dr. Brown, a fellow in gynecologic oncology and reproductive medicine at the University of Texas MD Anderson Cancer Center in Houston.
“Providers must identify and address barriers to advance care planning documentation in order to assist patients in achieving their end-of-life care goals ... I think we need to focus on educating ourselves and becoming proactive about trying to have these conversations earlier in treatment instead of when a patient is quite ill and we know that they’re going to pass away within the next week or so,” she added.
One barrier has recently been overcome by Medicare’s new policy – effective beginning this past January – of providing reimbursement for advance care planning as a separate and billable service.
In addition, Dr. Brown’s survey of 110 gynecologic oncology patients identified two significant psychological barriers to advance care planning: high levels of death anxiety and a feeling of distress that symptoms and/or treatment side effects are interfering with daily activities and relationships.
The survey showed that while 75% of the patients were familiar with advance care directives such as a living will or medical power of attorney, only 49% of subjects had actually completed those documents, and a mere 18% had a copy of an advance care directive in their medical record.
Half of the subjects had recurrent cancer, the rest were visiting the gynecologic oncology service for active surveillance. Only a minority of those with recurrent cancer had completed advance care directives.
Study participants completed two validated, self-administered questionnaire surveys: the 19-item MD Anderson Symptom Inventory (MDASI), which assesses patient-reported disease symptoms and treatment side effects during the previous 24 hours, and the 15-item Templer’s Death Anxiety Scale.
The mean MDASI Interference score, a measure of overall symptom distress and the impact of symptoms on daily life, was significantly higher in gynecologic oncology patients who hadn’t completed advance directives than in those who had. Similarly, patients who hadn’t completed advance directives scored significantly higher on the death anxiety metric.
“Patients with recurrent disease and those with increased disease symptom burden and death anxiety should be targeted for advance care planning discussions, as they may be less likely to engage in advance care planning activities,” Dr. Brown concluded.
She noted that prior research in other medical fields has shown that holding early planning discussions about end-of-life issues improves the likelihood that a patient’s final wishes will be honored, reduces utilization of hospital resources at the end of life, and reduces distress among the patient and family members. It’s important for gynecologic oncologists to step forward in this area because they are in a unique position: they often manage a cancer patient’s surgical care as well as chemotherapy and then later assist in the transition to end of life, she added.
At the conference session on palliative care where Dr. Brown presented her findings, audience members said the 49% completion rate for advance care directives that she found in her study was actually quite impressive; at many gynecologic oncology services the rates are in the 20%-25% range. The audience consensus was that much of the blame for the low rates of advance care planning documentation in their field belongs on the shoulders of gynecologic oncologists themselves.
“I would say that it’s entirely our fault,” declared session codirector Dr. Stephanie Blank of New York University.
Dr. Brown said as a result of her survey findings, she and her colleagues are working to change the institutional practice at MD Anderson such that completion of advance care directive planning directives with documentation in the medical record becomes a quality-of-care goal within the first few patient visits.
“In the past we had a social worker come to those patients who checked off a box on a form in the waiting room; now we’re trying to be more proactive about having a provider engage the patients early on,” she explained.
She reported having no financial conflicts of interest regarding her study.
SAN DIEGO – Fewer than half of gynecologic oncology patients surveyed at a major cancer center had completed advance care directives regarding their preferences for end-of-life care, and most of those who did had no copy of the documents in their medical records, Dr. Alaina J. Brown reported at the annual meeting of the Society of Gynecologic Oncology.
“These findings indicate there is room to improve advance directive planning documentation in our patient population,” said Dr. Brown, a fellow in gynecologic oncology and reproductive medicine at the University of Texas MD Anderson Cancer Center in Houston.
“Providers must identify and address barriers to advance care planning documentation in order to assist patients in achieving their end-of-life care goals ... I think we need to focus on educating ourselves and becoming proactive about trying to have these conversations earlier in treatment instead of when a patient is quite ill and we know that they’re going to pass away within the next week or so,” she added.
One barrier has recently been overcome by Medicare’s new policy – effective beginning this past January – of providing reimbursement for advance care planning as a separate and billable service.
In addition, Dr. Brown’s survey of 110 gynecologic oncology patients identified two significant psychological barriers to advance care planning: high levels of death anxiety and a feeling of distress that symptoms and/or treatment side effects are interfering with daily activities and relationships.
The survey showed that while 75% of the patients were familiar with advance care directives such as a living will or medical power of attorney, only 49% of subjects had actually completed those documents, and a mere 18% had a copy of an advance care directive in their medical record.
Half of the subjects had recurrent cancer, the rest were visiting the gynecologic oncology service for active surveillance. Only a minority of those with recurrent cancer had completed advance care directives.
Study participants completed two validated, self-administered questionnaire surveys: the 19-item MD Anderson Symptom Inventory (MDASI), which assesses patient-reported disease symptoms and treatment side effects during the previous 24 hours, and the 15-item Templer’s Death Anxiety Scale.
The mean MDASI Interference score, a measure of overall symptom distress and the impact of symptoms on daily life, was significantly higher in gynecologic oncology patients who hadn’t completed advance directives than in those who had. Similarly, patients who hadn’t completed advance directives scored significantly higher on the death anxiety metric.
“Patients with recurrent disease and those with increased disease symptom burden and death anxiety should be targeted for advance care planning discussions, as they may be less likely to engage in advance care planning activities,” Dr. Brown concluded.
She noted that prior research in other medical fields has shown that holding early planning discussions about end-of-life issues improves the likelihood that a patient’s final wishes will be honored, reduces utilization of hospital resources at the end of life, and reduces distress among the patient and family members. It’s important for gynecologic oncologists to step forward in this area because they are in a unique position: they often manage a cancer patient’s surgical care as well as chemotherapy and then later assist in the transition to end of life, she added.
At the conference session on palliative care where Dr. Brown presented her findings, audience members said the 49% completion rate for advance care directives that she found in her study was actually quite impressive; at many gynecologic oncology services the rates are in the 20%-25% range. The audience consensus was that much of the blame for the low rates of advance care planning documentation in their field belongs on the shoulders of gynecologic oncologists themselves.
“I would say that it’s entirely our fault,” declared session codirector Dr. Stephanie Blank of New York University.
Dr. Brown said as a result of her survey findings, she and her colleagues are working to change the institutional practice at MD Anderson such that completion of advance care directive planning directives with documentation in the medical record becomes a quality-of-care goal within the first few patient visits.
“In the past we had a social worker come to those patients who checked off a box on a form in the waiting room; now we’re trying to be more proactive about having a provider engage the patients early on,” she explained.
She reported having no financial conflicts of interest regarding her study.
AT THE ANNUAL MEETING ON WOMEN’S CANCER
Key clinical point: Gynecologic oncologists aren’t doing well at helping their patients create advance care directives in a timely way.
Major finding: Fewer than one in five gynecologic oncology patients surveyed had an advance care directive included in the medical chart.
Data source: Survey of 110 gynecologic oncology patients at a major cancer center to examine the relationship between completion of advance care directives and patients’ levels of death anxiety and symptom burden.
Disclosures: The presenter reported having no financial conflicts regarding her study, which was conducted free of commercial support.

Key Communication Tactics Highlighted in 'Everything We Say and Do'
“Everything We Say and Do” is an informational series developed by SHM’s Patient Experience Committee to provide readers with thoughtful and actionable communication tactics that have great potential to positively impact patients’ experience of care. Below is a chart of the “key communication” tactics.

“Everything We Say and Do” is an informational series developed by SHM’s Patient Experience Committee to provide readers with thoughtful and actionable communication tactics that have great potential to positively impact patients’ experience of care. Below is a chart of the “key communication” tactics.
“Everything We Say and Do” is an informational series developed by SHM’s Patient Experience Committee to provide readers with thoughtful and actionable communication tactics that have great potential to positively impact patients’ experience of care. Below is a chart of the “key communication” tactics.
CDC Released Voluntary Guidelines to Help Lower Opioid and Abuse of Painkillers
(Reuters) - Addressing a growing "epidemic" of opioid overdoses and abuse of the prescribed painkillers in the United States, the Centers for Disease Control and Prevention on Tuesday released voluntary guidelines that instruct primary care doctors to sharply deter use of the medicines for chronic pain.
"Overprescribing opioids, largely for chronic pain, is a key driver of America's drug-overdose epidemic," said CDC Director Tom Frieden. Sales of the prescription therapies have quadrupled since 1999, causing 165,000 fatal overdoses over the same period and now growing at more than 40 per day, according to the agency.
Primary care doctors who treat adults for chronic pain in outpatient settings account for nearly half of all opioid prescriptions, the CDC said. It defined chronic pain as lasting longer than three months, or past the typical time it takes for normal tissue healing.
The new guidelines recommend non-opioids, including acetaminophen and ibuprofen, as preferred therapy for chronic pain unless patients have active cancer or are receiving palliative or end-of-life care.
When opioids are used, the lowest possible dose should be prescribed to reduce risks of opioid abuse and overdose and patients should then be closely monitored, according to the CDC guidelines. The drugs should also be combined with non-drug approaches to controlling pain, like physical therapy and exercise, the agency said.
Moreover, when starting opioid therapy for chronic pain, doctors should prescribe immediate-release formulations instead of long-acting versions, the guidelines say. They recommend doctors avoid prescribing opioids with sedatives called benzodiazepines.
When prescribed for acute, or short-term pain, doctors should prescribe the lowest effective dose of immediate release opioids.
"Three days or less will often be sufficient; more than seven days will rarely be needed," the guidelines say.
Some studies suggest only 5 percent of patients prescribed opioids receive them for chronic pain, but they account for 70 percent of overall opioid prescriptions and the majority of overdoses.
For the vast majority of patients taking opioids for chronic pain, risks from the drugs will outweigh benefits, Frieden said. "The prescription overdose epidemic is doctor-driven," Frieden said, adding it can be reversed if doctors rein in their prescriptions of the painkillers.
The American College of Physicians on Tuesday said the new guidelines provide important guidance "at a time when many communities are being devastated by the adverse impact of opioid misuse."
The most widely used opioids include hydrocodone, which is the main active ingredient of Vicodin, and oxycodone, an active ingredient of OxyContin and Percocet. They are synthetic narcotics which work by binding to opioid receptors in the brain and are mostly available in pill form.
Nearly two million Americans aged 12 or older either abused or were dependent on prescription opioids in 2014, the CDC said.
Opioids also include heroin, an illegal injectable drug which has become a far cheaper alternative to oral opioids on the streets of many U.S. communities, causing many overdoses.
Other U.S. health officials on Tuesday said first responders should have wider access to naloxone, a drug that can reverse opioid overdoses.
SHM offers a safe opioid prescribing implementation guideline. The Implementation Toolkit, Reducing Adverse Drug Events related to Opioids, or RADEO, provides step-by step instructions for hospitals to implement a successful QI program to make opioid prescribing safer, with fewer adverse events, and much less likely to result in dangerous sedation, respiratory depression and death. Its scope is for hospitalized patients.
(Reuters) - Addressing a growing "epidemic" of opioid overdoses and abuse of the prescribed painkillers in the United States, the Centers for Disease Control and Prevention on Tuesday released voluntary guidelines that instruct primary care doctors to sharply deter use of the medicines for chronic pain.
"Overprescribing opioids, largely for chronic pain, is a key driver of America's drug-overdose epidemic," said CDC Director Tom Frieden. Sales of the prescription therapies have quadrupled since 1999, causing 165,000 fatal overdoses over the same period and now growing at more than 40 per day, according to the agency.
Primary care doctors who treat adults for chronic pain in outpatient settings account for nearly half of all opioid prescriptions, the CDC said. It defined chronic pain as lasting longer than three months, or past the typical time it takes for normal tissue healing.
The new guidelines recommend non-opioids, including acetaminophen and ibuprofen, as preferred therapy for chronic pain unless patients have active cancer or are receiving palliative or end-of-life care.
When opioids are used, the lowest possible dose should be prescribed to reduce risks of opioid abuse and overdose and patients should then be closely monitored, according to the CDC guidelines. The drugs should also be combined with non-drug approaches to controlling pain, like physical therapy and exercise, the agency said.
Moreover, when starting opioid therapy for chronic pain, doctors should prescribe immediate-release formulations instead of long-acting versions, the guidelines say. They recommend doctors avoid prescribing opioids with sedatives called benzodiazepines.
When prescribed for acute, or short-term pain, doctors should prescribe the lowest effective dose of immediate release opioids.
"Three days or less will often be sufficient; more than seven days will rarely be needed," the guidelines say.
Some studies suggest only 5 percent of patients prescribed opioids receive them for chronic pain, but they account for 70 percent of overall opioid prescriptions and the majority of overdoses.
For the vast majority of patients taking opioids for chronic pain, risks from the drugs will outweigh benefits, Frieden said. "The prescription overdose epidemic is doctor-driven," Frieden said, adding it can be reversed if doctors rein in their prescriptions of the painkillers.
The American College of Physicians on Tuesday said the new guidelines provide important guidance "at a time when many communities are being devastated by the adverse impact of opioid misuse."
The most widely used opioids include hydrocodone, which is the main active ingredient of Vicodin, and oxycodone, an active ingredient of OxyContin and Percocet. They are synthetic narcotics which work by binding to opioid receptors in the brain and are mostly available in pill form.
Nearly two million Americans aged 12 or older either abused or were dependent on prescription opioids in 2014, the CDC said.
Opioids also include heroin, an illegal injectable drug which has become a far cheaper alternative to oral opioids on the streets of many U.S. communities, causing many overdoses.
Other U.S. health officials on Tuesday said first responders should have wider access to naloxone, a drug that can reverse opioid overdoses.
SHM offers a safe opioid prescribing implementation guideline. The Implementation Toolkit, Reducing Adverse Drug Events related to Opioids, or RADEO, provides step-by step instructions for hospitals to implement a successful QI program to make opioid prescribing safer, with fewer adverse events, and much less likely to result in dangerous sedation, respiratory depression and death. Its scope is for hospitalized patients.
(Reuters) - Addressing a growing "epidemic" of opioid overdoses and abuse of the prescribed painkillers in the United States, the Centers for Disease Control and Prevention on Tuesday released voluntary guidelines that instruct primary care doctors to sharply deter use of the medicines for chronic pain.
"Overprescribing opioids, largely for chronic pain, is a key driver of America's drug-overdose epidemic," said CDC Director Tom Frieden. Sales of the prescription therapies have quadrupled since 1999, causing 165,000 fatal overdoses over the same period and now growing at more than 40 per day, according to the agency.
Primary care doctors who treat adults for chronic pain in outpatient settings account for nearly half of all opioid prescriptions, the CDC said. It defined chronic pain as lasting longer than three months, or past the typical time it takes for normal tissue healing.
The new guidelines recommend non-opioids, including acetaminophen and ibuprofen, as preferred therapy for chronic pain unless patients have active cancer or are receiving palliative or end-of-life care.
When opioids are used, the lowest possible dose should be prescribed to reduce risks of opioid abuse and overdose and patients should then be closely monitored, according to the CDC guidelines. The drugs should also be combined with non-drug approaches to controlling pain, like physical therapy and exercise, the agency said.
Moreover, when starting opioid therapy for chronic pain, doctors should prescribe immediate-release formulations instead of long-acting versions, the guidelines say. They recommend doctors avoid prescribing opioids with sedatives called benzodiazepines.
When prescribed for acute, or short-term pain, doctors should prescribe the lowest effective dose of immediate release opioids.
"Three days or less will often be sufficient; more than seven days will rarely be needed," the guidelines say.
Some studies suggest only 5 percent of patients prescribed opioids receive them for chronic pain, but they account for 70 percent of overall opioid prescriptions and the majority of overdoses.
For the vast majority of patients taking opioids for chronic pain, risks from the drugs will outweigh benefits, Frieden said. "The prescription overdose epidemic is doctor-driven," Frieden said, adding it can be reversed if doctors rein in their prescriptions of the painkillers.
The American College of Physicians on Tuesday said the new guidelines provide important guidance "at a time when many communities are being devastated by the adverse impact of opioid misuse."
The most widely used opioids include hydrocodone, which is the main active ingredient of Vicodin, and oxycodone, an active ingredient of OxyContin and Percocet. They are synthetic narcotics which work by binding to opioid receptors in the brain and are mostly available in pill form.
Nearly two million Americans aged 12 or older either abused or were dependent on prescription opioids in 2014, the CDC said.
Opioids also include heroin, an illegal injectable drug which has become a far cheaper alternative to oral opioids on the streets of many U.S. communities, causing many overdoses.
Other U.S. health officials on Tuesday said first responders should have wider access to naloxone, a drug that can reverse opioid overdoses.
SHM offers a safe opioid prescribing implementation guideline. The Implementation Toolkit, Reducing Adverse Drug Events related to Opioids, or RADEO, provides step-by step instructions for hospitals to implement a successful QI program to make opioid prescribing safer, with fewer adverse events, and much less likely to result in dangerous sedation, respiratory depression and death. Its scope is for hospitalized patients.
mAb gets breakthrough designation for HLH

Photo by Linda Bartlett
The US Food and Drug Administration (FDA) has granted breakthrough therapy designation to NI-0501 for the treatment of patients with primary hemophagocytic lymphohistiocytosis (HLH) who have refractory disease or recurrent/progressive disease during conventional therapy.
NI-0501 is a fully human monoclonal antibody (mAb) targeting interferon-gamma (IFNγ) that is being developed by Novimmune.
The biological activity of IFNγ, which is considered to have a pivotal pathogenic role in HLH, is neutralized by NI-0501.
“The FDA’s designation of NI-0501 as a breakthrough therapy recognizes the potential of NI-0501 to address an important unmet medical need in a disease with still high mortality, and for which there are no approved treatments,” said Novimmune Chairman and Chief Executive Officer Eduard Holdener.
The breakthrough therapy designation is intended to expedite the development and review of new therapies for serious or life threatening conditions, which have shown encouraging early clinical results demonstrating substantial improvement on a clinically significant endpoint over available therapies.
The FDA granted breakthrough designation to NI-0501 on the basis of data from a phase 2 study in children with primary HLH. Preliminary results from this study were presented at the 2015 ASH Annual Meeting.
The trial included 16 patients—8 males and 8 females. Their median age was 1.2 years (range, 0.2-13).
Two patients were receiving NI-0501 as first-line treatment, and the rest were receiving the mAb as second-line treatment. Patients had previously received dexamethasone (n=13), methylprednisone (n=2), etoposide (n=13), ATG (n=4), cyclosporine A (n=6), and “other” therapy (n=4).
NI-0501 was given at a starting dose of 1 mg/kg every 3 days, with possible dose increases guided by pharmacokinetic data and/or clinical response in each patient. The mAb was administered with dexamethasone at a dose of 5 mg/m2 to 10 mg/m2, but dexamethasone could be tapered during the treatment course.
The treatment duration ranged from 4 weeks to 8 weeks, and the follow-up period was 4 weeks.
Efficacy
One patient was excluded from the analysis due to a lymphoma diagnosis after enrollment. Two patients were still receiving treatment as of the ASH presentation, and 13 have completed treatment.
Among the patients who completed therapy, 4 had an insufficient response. Two of these patients died, and 2 proceeded to allogeneic hematopoietic stem cell transplant (HSCT) after receiving additional agents to control their disease.
Nine patients achieved a favorable response to NI-0501. Seven of these patients proceeded to HSCT, and 2 were awaiting HSCT at the time of the ASH presentation, with their disease well-controlled.
Post-transplant follow-up is still early for most patients, but 2 patients have follow-up greater than 1 year. One child died of graft-vs-host disease around day 45, but the remaining patients who went on to HSCT were still alive as of the ASH presentation.
Safety
No off-target effects of NI-0501 were observed, and none of the patients withdrew from the study for safety reasons.
There were 14 serious adverse events reported in 8 patients, but only 1 of these events was considered treatment-related.
The patient had necrotizing fasciitis following P aeruginosa skin infection, which resolved. This event was considered treatment-related by an investigator but not by the data monitoring committee or the sponsor.
Three patients had died as of the ASH presentation, but none of the deaths were related to NI-0501. Two patients died of HLH/multi-organ failure, and 1 died of graft-vs-host disease. ![]()
Photo by Linda Bartlett
The US Food and Drug Administration (FDA) has granted breakthrough therapy designation to NI-0501 for the treatment of patients with primary hemophagocytic lymphohistiocytosis (HLH) who have refractory disease or recurrent/progressive disease during conventional therapy.
NI-0501 is a fully human monoclonal antibody (mAb) targeting interferon-gamma (IFNγ) that is being developed by Novimmune.
The biological activity of IFNγ, which is considered to have a pivotal pathogenic role in HLH, is neutralized by NI-0501.
“The FDA’s designation of NI-0501 as a breakthrough therapy recognizes the potential of NI-0501 to address an important unmet medical need in a disease with still high mortality, and for which there are no approved treatments,” said Novimmune Chairman and Chief Executive Officer Eduard Holdener.
The breakthrough therapy designation is intended to expedite the development and review of new therapies for serious or life threatening conditions, which have shown encouraging early clinical results demonstrating substantial improvement on a clinically significant endpoint over available therapies.
The FDA granted breakthrough designation to NI-0501 on the basis of data from a phase 2 study in children with primary HLH. Preliminary results from this study were presented at the 2015 ASH Annual Meeting.
The trial included 16 patients—8 males and 8 females. Their median age was 1.2 years (range, 0.2-13).
Two patients were receiving NI-0501 as first-line treatment, and the rest were receiving the mAb as second-line treatment. Patients had previously received dexamethasone (n=13), methylprednisone (n=2), etoposide (n=13), ATG (n=4), cyclosporine A (n=6), and “other” therapy (n=4).
NI-0501 was given at a starting dose of 1 mg/kg every 3 days, with possible dose increases guided by pharmacokinetic data and/or clinical response in each patient. The mAb was administered with dexamethasone at a dose of 5 mg/m2 to 10 mg/m2, but dexamethasone could be tapered during the treatment course.
The treatment duration ranged from 4 weeks to 8 weeks, and the follow-up period was 4 weeks.
Efficacy
One patient was excluded from the analysis due to a lymphoma diagnosis after enrollment. Two patients were still receiving treatment as of the ASH presentation, and 13 have completed treatment.
Among the patients who completed therapy, 4 had an insufficient response. Two of these patients died, and 2 proceeded to allogeneic hematopoietic stem cell transplant (HSCT) after receiving additional agents to control their disease.
Nine patients achieved a favorable response to NI-0501. Seven of these patients proceeded to HSCT, and 2 were awaiting HSCT at the time of the ASH presentation, with their disease well-controlled.
Post-transplant follow-up is still early for most patients, but 2 patients have follow-up greater than 1 year. One child died of graft-vs-host disease around day 45, but the remaining patients who went on to HSCT were still alive as of the ASH presentation.
Safety
No off-target effects of NI-0501 were observed, and none of the patients withdrew from the study for safety reasons.
There were 14 serious adverse events reported in 8 patients, but only 1 of these events was considered treatment-related.
The patient had necrotizing fasciitis following P aeruginosa skin infection, which resolved. This event was considered treatment-related by an investigator but not by the data monitoring committee or the sponsor.
Three patients had died as of the ASH presentation, but none of the deaths were related to NI-0501. Two patients died of HLH/multi-organ failure, and 1 died of graft-vs-host disease. ![]()
Photo by Linda Bartlett
The US Food and Drug Administration (FDA) has granted breakthrough therapy designation to NI-0501 for the treatment of patients with primary hemophagocytic lymphohistiocytosis (HLH) who have refractory disease or recurrent/progressive disease during conventional therapy.
NI-0501 is a fully human monoclonal antibody (mAb) targeting interferon-gamma (IFNγ) that is being developed by Novimmune.
The biological activity of IFNγ, which is considered to have a pivotal pathogenic role in HLH, is neutralized by NI-0501.
“The FDA’s designation of NI-0501 as a breakthrough therapy recognizes the potential of NI-0501 to address an important unmet medical need in a disease with still high mortality, and for which there are no approved treatments,” said Novimmune Chairman and Chief Executive Officer Eduard Holdener.
The breakthrough therapy designation is intended to expedite the development and review of new therapies for serious or life threatening conditions, which have shown encouraging early clinical results demonstrating substantial improvement on a clinically significant endpoint over available therapies.
The FDA granted breakthrough designation to NI-0501 on the basis of data from a phase 2 study in children with primary HLH. Preliminary results from this study were presented at the 2015 ASH Annual Meeting.
The trial included 16 patients—8 males and 8 females. Their median age was 1.2 years (range, 0.2-13).
Two patients were receiving NI-0501 as first-line treatment, and the rest were receiving the mAb as second-line treatment. Patients had previously received dexamethasone (n=13), methylprednisone (n=2), etoposide (n=13), ATG (n=4), cyclosporine A (n=6), and “other” therapy (n=4).
NI-0501 was given at a starting dose of 1 mg/kg every 3 days, with possible dose increases guided by pharmacokinetic data and/or clinical response in each patient. The mAb was administered with dexamethasone at a dose of 5 mg/m2 to 10 mg/m2, but dexamethasone could be tapered during the treatment course.
The treatment duration ranged from 4 weeks to 8 weeks, and the follow-up period was 4 weeks.
Efficacy
One patient was excluded from the analysis due to a lymphoma diagnosis after enrollment. Two patients were still receiving treatment as of the ASH presentation, and 13 have completed treatment.
Among the patients who completed therapy, 4 had an insufficient response. Two of these patients died, and 2 proceeded to allogeneic hematopoietic stem cell transplant (HSCT) after receiving additional agents to control their disease.
Nine patients achieved a favorable response to NI-0501. Seven of these patients proceeded to HSCT, and 2 were awaiting HSCT at the time of the ASH presentation, with their disease well-controlled.
Post-transplant follow-up is still early for most patients, but 2 patients have follow-up greater than 1 year. One child died of graft-vs-host disease around day 45, but the remaining patients who went on to HSCT were still alive as of the ASH presentation.
Safety
No off-target effects of NI-0501 were observed, and none of the patients withdrew from the study for safety reasons.
There were 14 serious adverse events reported in 8 patients, but only 1 of these events was considered treatment-related.
The patient had necrotizing fasciitis following P aeruginosa skin infection, which resolved. This event was considered treatment-related by an investigator but not by the data monitoring committee or the sponsor.
Three patients had died as of the ASH presentation, but none of the deaths were related to NI-0501. Two patients died of HLH/multi-organ failure, and 1 died of graft-vs-host disease. ![]()
Chemo has greater impact on male fertility

Photo by Nina Matthews
Results of a large study suggest that female survivors of childhood cancer may have more luck than their male peers when it comes to conceiving a child.
Both male and female childhood cancer survivors (CCSs) reported fewer pregnancies and live births than their healthy siblings.
However, chemotherapeutic agents appeared to have a much greater impact on the fertility of male CCSs than female CCSs.
Eric Chow, MD, of the Fred Hutchinson Cancer Research Center in Seattle, Washington, and his colleagues reported these findings in The Lancet Oncology.
Previous research has shown that fertility can be compromised by several types of chemotherapy, mainly alkylating drugs. However, little is known about the dose effects on pregnancy from newer drugs, such as ifosfamide and cisplatin, in CCSs.
With this in mind, Dr Chow and his colleagues analyzed data from the Childhood Cancer Survivor Study, which tracks subjects who were diagnosed with the most common types of childhood cancer before the age of 21 and treated at 27 institutions across the US and Canada between 1970 and 1999.
Patients had been diagnosed with leukemias, lymphomas, and neuroblastoma, as well as kidney, brain, soft tissue, and bone tumors. All had survived at least 5 years after diagnosis.
The researchers examined the impact of various doses of 14 commonly used chemotherapy drugs on pregnancy and live birth in 10,938 male and female CCSs, compared with 3949 siblings.
The team specifically focused on CCSs who were treated with chemotherapy and did not receive any radiotherapy to the pelvis or the brain.
The drugs the researchers evaluated were busulfan, carboplatin, carmustine, chlorambucil, chlormethine, cisplatin, cyclophosphamide, dacarbazine, ifosfamide, lomustine, melphalan, procarbazine, temozolomide, and thiotepa.
Outcomes
Multivariable analysis showed that CCSs were significantly less likely than their siblings to have or sire a pregnancy. For male CCSs, the hazard ratio (HR) was 0.63 (P<0.0001). For female CCSs, the HR was 0.87 (P<0.0001).
CCSs were also significantly less likely to have a live birth. For male CCSs, the HR was 0.63 (P<0.0001). For female CCSs, the HR was 0.82 (P<0.0001).
The researchers noted that, overall, female CCSs were less likely to conceive and have a child when compared to their siblings, but the effect was much smaller than that observed among the men.
In addition, the difference between CCSs and siblings was more pronounced for women who delayed pregnancy until they were 30 or older, possibly because chemotherapy exposure might accelerate the natural depletion of eggs and hasten menopause.
Impact of specific drugs
In male CCSs, the reduced likelihood of siring a pregnancy was associated with upper tertile doses of cyclophosphamide (HR=0.60, P<0.0001), ifosfamide (HR=0.42, P=0.0069), procarbazine (HR=0.30, P<0.0001), and cisplatin (HR=0.56, P=0.0023).
Cyclophosphamide-equivalent dose in male CCSs was significantly associated with a decreased likelihood of siring a pregnancy per 5000 mg/m2 increments (HR=0.82, P<0.0001).
In female CCSs, the reduced likelihood of becoming pregnant was associated with busulfan—both at doses less than 450 mg/m2 (HR=0.22, P=0.020) and at doses of 450 mg/m2 or higher (HR=0.14, P=0.0051)—and with doses of lomustine at 411 mg/m2 or greater (HR=0.41, P=0.046).
Cyclophosphamide-equivalent dose in female CCSs was associated with risk only at the highest doses in analyses categorized by quartile (upper quartile vs no exposure, HR=0.85, P=0.023).
Limitations and implications
The researchers noted that a limitation of this study is that it relied on self-reported pregnancy and live birth, and some pregnancies may go unrecognized.
And although the findings are consistent with others in the field, this study did not account for other factors such as marital or cohabitation status, the intention to conceive, or length of time attempting to conceive.
The researchers also noted that, although the total number of CCSs in this study is large, the number of patients who were exposed to individual drugs varied significantly. So while the overall conclusions of the study are consistent with previous studies, more research is needed to estimate the exact risk of some less commonly used drugs.
“We think these results will be encouraging for most women who were treated with chemotherapy in childhood,” Dr Chow said. “However, I think we, as pediatric oncologists, still need to do a better job discussing fertility and fertility preservation options with patients and families upfront before starting cancer treatment.”
“In particular, all boys diagnosed post-puberty should be encouraged to bank their sperm to maximize their reproductive options in the future. The current options for post-pubertal girls remain more complicated but include oocyte and embryo cryopreservation.” ![]()
Photo by Nina Matthews
Results of a large study suggest that female survivors of childhood cancer may have more luck than their male peers when it comes to conceiving a child.
Both male and female childhood cancer survivors (CCSs) reported fewer pregnancies and live births than their healthy siblings.
However, chemotherapeutic agents appeared to have a much greater impact on the fertility of male CCSs than female CCSs.
Eric Chow, MD, of the Fred Hutchinson Cancer Research Center in Seattle, Washington, and his colleagues reported these findings in The Lancet Oncology.
Previous research has shown that fertility can be compromised by several types of chemotherapy, mainly alkylating drugs. However, little is known about the dose effects on pregnancy from newer drugs, such as ifosfamide and cisplatin, in CCSs.
With this in mind, Dr Chow and his colleagues analyzed data from the Childhood Cancer Survivor Study, which tracks subjects who were diagnosed with the most common types of childhood cancer before the age of 21 and treated at 27 institutions across the US and Canada between 1970 and 1999.
Patients had been diagnosed with leukemias, lymphomas, and neuroblastoma, as well as kidney, brain, soft tissue, and bone tumors. All had survived at least 5 years after diagnosis.
The researchers examined the impact of various doses of 14 commonly used chemotherapy drugs on pregnancy and live birth in 10,938 male and female CCSs, compared with 3949 siblings.
The team specifically focused on CCSs who were treated with chemotherapy and did not receive any radiotherapy to the pelvis or the brain.
The drugs the researchers evaluated were busulfan, carboplatin, carmustine, chlorambucil, chlormethine, cisplatin, cyclophosphamide, dacarbazine, ifosfamide, lomustine, melphalan, procarbazine, temozolomide, and thiotepa.
Outcomes
Multivariable analysis showed that CCSs were significantly less likely than their siblings to have or sire a pregnancy. For male CCSs, the hazard ratio (HR) was 0.63 (P<0.0001). For female CCSs, the HR was 0.87 (P<0.0001).
CCSs were also significantly less likely to have a live birth. For male CCSs, the HR was 0.63 (P<0.0001). For female CCSs, the HR was 0.82 (P<0.0001).
The researchers noted that, overall, female CCSs were less likely to conceive and have a child when compared to their siblings, but the effect was much smaller than that observed among the men.
In addition, the difference between CCSs and siblings was more pronounced for women who delayed pregnancy until they were 30 or older, possibly because chemotherapy exposure might accelerate the natural depletion of eggs and hasten menopause.
Impact of specific drugs
In male CCSs, the reduced likelihood of siring a pregnancy was associated with upper tertile doses of cyclophosphamide (HR=0.60, P<0.0001), ifosfamide (HR=0.42, P=0.0069), procarbazine (HR=0.30, P<0.0001), and cisplatin (HR=0.56, P=0.0023).
Cyclophosphamide-equivalent dose in male CCSs was significantly associated with a decreased likelihood of siring a pregnancy per 5000 mg/m2 increments (HR=0.82, P<0.0001).
In female CCSs, the reduced likelihood of becoming pregnant was associated with busulfan—both at doses less than 450 mg/m2 (HR=0.22, P=0.020) and at doses of 450 mg/m2 or higher (HR=0.14, P=0.0051)—and with doses of lomustine at 411 mg/m2 or greater (HR=0.41, P=0.046).
Cyclophosphamide-equivalent dose in female CCSs was associated with risk only at the highest doses in analyses categorized by quartile (upper quartile vs no exposure, HR=0.85, P=0.023).
Limitations and implications
The researchers noted that a limitation of this study is that it relied on self-reported pregnancy and live birth, and some pregnancies may go unrecognized.
And although the findings are consistent with others in the field, this study did not account for other factors such as marital or cohabitation status, the intention to conceive, or length of time attempting to conceive.
The researchers also noted that, although the total number of CCSs in this study is large, the number of patients who were exposed to individual drugs varied significantly. So while the overall conclusions of the study are consistent with previous studies, more research is needed to estimate the exact risk of some less commonly used drugs.
“We think these results will be encouraging for most women who were treated with chemotherapy in childhood,” Dr Chow said. “However, I think we, as pediatric oncologists, still need to do a better job discussing fertility and fertility preservation options with patients and families upfront before starting cancer treatment.”
“In particular, all boys diagnosed post-puberty should be encouraged to bank their sperm to maximize their reproductive options in the future. The current options for post-pubertal girls remain more complicated but include oocyte and embryo cryopreservation.” ![]()
Photo by Nina Matthews
Results of a large study suggest that female survivors of childhood cancer may have more luck than their male peers when it comes to conceiving a child.
Both male and female childhood cancer survivors (CCSs) reported fewer pregnancies and live births than their healthy siblings.
However, chemotherapeutic agents appeared to have a much greater impact on the fertility of male CCSs than female CCSs.
Eric Chow, MD, of the Fred Hutchinson Cancer Research Center in Seattle, Washington, and his colleagues reported these findings in The Lancet Oncology.
Previous research has shown that fertility can be compromised by several types of chemotherapy, mainly alkylating drugs. However, little is known about the dose effects on pregnancy from newer drugs, such as ifosfamide and cisplatin, in CCSs.
With this in mind, Dr Chow and his colleagues analyzed data from the Childhood Cancer Survivor Study, which tracks subjects who were diagnosed with the most common types of childhood cancer before the age of 21 and treated at 27 institutions across the US and Canada between 1970 and 1999.
Patients had been diagnosed with leukemias, lymphomas, and neuroblastoma, as well as kidney, brain, soft tissue, and bone tumors. All had survived at least 5 years after diagnosis.
The researchers examined the impact of various doses of 14 commonly used chemotherapy drugs on pregnancy and live birth in 10,938 male and female CCSs, compared with 3949 siblings.
The team specifically focused on CCSs who were treated with chemotherapy and did not receive any radiotherapy to the pelvis or the brain.
The drugs the researchers evaluated were busulfan, carboplatin, carmustine, chlorambucil, chlormethine, cisplatin, cyclophosphamide, dacarbazine, ifosfamide, lomustine, melphalan, procarbazine, temozolomide, and thiotepa.
Outcomes
Multivariable analysis showed that CCSs were significantly less likely than their siblings to have or sire a pregnancy. For male CCSs, the hazard ratio (HR) was 0.63 (P<0.0001). For female CCSs, the HR was 0.87 (P<0.0001).
CCSs were also significantly less likely to have a live birth. For male CCSs, the HR was 0.63 (P<0.0001). For female CCSs, the HR was 0.82 (P<0.0001).
The researchers noted that, overall, female CCSs were less likely to conceive and have a child when compared to their siblings, but the effect was much smaller than that observed among the men.
In addition, the difference between CCSs and siblings was more pronounced for women who delayed pregnancy until they were 30 or older, possibly because chemotherapy exposure might accelerate the natural depletion of eggs and hasten menopause.
Impact of specific drugs
In male CCSs, the reduced likelihood of siring a pregnancy was associated with upper tertile doses of cyclophosphamide (HR=0.60, P<0.0001), ifosfamide (HR=0.42, P=0.0069), procarbazine (HR=0.30, P<0.0001), and cisplatin (HR=0.56, P=0.0023).
Cyclophosphamide-equivalent dose in male CCSs was significantly associated with a decreased likelihood of siring a pregnancy per 5000 mg/m2 increments (HR=0.82, P<0.0001).
In female CCSs, the reduced likelihood of becoming pregnant was associated with busulfan—both at doses less than 450 mg/m2 (HR=0.22, P=0.020) and at doses of 450 mg/m2 or higher (HR=0.14, P=0.0051)—and with doses of lomustine at 411 mg/m2 or greater (HR=0.41, P=0.046).
Cyclophosphamide-equivalent dose in female CCSs was associated with risk only at the highest doses in analyses categorized by quartile (upper quartile vs no exposure, HR=0.85, P=0.023).
Limitations and implications
The researchers noted that a limitation of this study is that it relied on self-reported pregnancy and live birth, and some pregnancies may go unrecognized.
And although the findings are consistent with others in the field, this study did not account for other factors such as marital or cohabitation status, the intention to conceive, or length of time attempting to conceive.
The researchers also noted that, although the total number of CCSs in this study is large, the number of patients who were exposed to individual drugs varied significantly. So while the overall conclusions of the study are consistent with previous studies, more research is needed to estimate the exact risk of some less commonly used drugs.
“We think these results will be encouraging for most women who were treated with chemotherapy in childhood,” Dr Chow said. “However, I think we, as pediatric oncologists, still need to do a better job discussing fertility and fertility preservation options with patients and families upfront before starting cancer treatment.”
“In particular, all boys diagnosed post-puberty should be encouraged to bank their sperm to maximize their reproductive options in the future. The current options for post-pubertal girls remain more complicated but include oocyte and embryo cryopreservation.” ![]()
Flooring poses higher cancer risk than previously reported

while woman looks on
US government agencies have released a revised report on the health risks associated with formaldehyde in certain types of laminate flooring.
The new report corrects a previous error and reveals an increase in the estimated lifetime risk of cancers, including leukemias, for individuals who regularly breathe in formaldehyde from the flooring.
The report also suggests that irritation and breathing problems can result in anyone exposed to the flooring.
The report was compiled by the Agency for Toxic Substances and Disease Registry (ATSDR) and the Centers for Disease Control and Prevention’s National Center for Environmental Health (NCEH).
About the report
On March 1, 2015, the CBS news program 60 Minutes reported that an American company, Lumber Liquidators®, was selling laminate wood flooring produced in China that released elevated levels of formaldehyde.
Based on this allegation, the US Consumer Product Safety Commission (CPSC) tested laminate flooring samples manufactured in China from 2012 to 2014 that were sold at Lumber Liquidators® stores. The CPSC then requested that the NCEH and ATSDR evaluate the test results for possible health effects.
The NCEH and ATSDR published a report detailing the possible health effects on February 10, 2016. But the report was pulled on February 19, 2016, after the agencies were informed that the report’s indoor air model incorporated an incorrect value for ceiling height.
As a result, the health risks were calculated using airborne concentration estimates about 3 times lower than they should have been.
Since the discovery of the error, the NCEH and ATSDR revised the value in the model, conducted a review of the revised results, and re-evaluated the possible health implications.
In addition, the revised report has been reviewed by outside experts and experts from the CPSC, the US Environmental Protection Agency, and the US Department of Housing and Urban Development.
Results
The revised report concludes that irritation and breathing problems could occur in everyone exposed to formaldehyde in the tested flooring.
The previous report suggested such problems might only occur in sensitive groups (eg, children) and people with pre-existing health conditions (eg, asthma).
The new report also increased the estimated lifetime cancer risk from breathing the highest levels of formaldehyde from the affected flooring all day, every day for 2 years.
The previous estimate of lifetime cancer risk was 2 to 9 extra cases for every 100,000 people.
The new estimate is 6 to 30 extra cases per 100,000 people.
There is conflicting data regarding the types of cancers associated with formaldehyde exposure, but many studies have suggested that formaldehyde causes cancer of the nasopharynx, sinuses, and nasal cavity, as well as leukemia, particularly myeloid leukemia.
Recommendations
Although the revised report shows an increase in health risks associated with the flooring, the NCEH and ATSDR said their recommendations remain the same.
They recommend that people with the affected flooring:
- Reduce their exposure to formaldehyde in their homes by opening windows, running exhaust fans, avoiding use of other products containing formaldehyde, etc.
- See a doctor for ongoing health symptoms such as breathing problems or irritation of the eyes, nose, or throat
- Weigh the pros and cons of professional air testing
- Consult a professional before removing the flooring, as removing it may release more formaldehyde into the home.

while woman looks on
US government agencies have released a revised report on the health risks associated with formaldehyde in certain types of laminate flooring.
The new report corrects a previous error and reveals an increase in the estimated lifetime risk of cancers, including leukemias, for individuals who regularly breathe in formaldehyde from the flooring.
The report also suggests that irritation and breathing problems can result in anyone exposed to the flooring.
The report was compiled by the Agency for Toxic Substances and Disease Registry (ATSDR) and the Centers for Disease Control and Prevention’s National Center for Environmental Health (NCEH).
About the report
On March 1, 2015, the CBS news program 60 Minutes reported that an American company, Lumber Liquidators®, was selling laminate wood flooring produced in China that released elevated levels of formaldehyde.
Based on this allegation, the US Consumer Product Safety Commission (CPSC) tested laminate flooring samples manufactured in China from 2012 to 2014 that were sold at Lumber Liquidators® stores. The CPSC then requested that the NCEH and ATSDR evaluate the test results for possible health effects.
The NCEH and ATSDR published a report detailing the possible health effects on February 10, 2016. But the report was pulled on February 19, 2016, after the agencies were informed that the report’s indoor air model incorporated an incorrect value for ceiling height.
As a result, the health risks were calculated using airborne concentration estimates about 3 times lower than they should have been.
Since the discovery of the error, the NCEH and ATSDR revised the value in the model, conducted a review of the revised results, and re-evaluated the possible health implications.
In addition, the revised report has been reviewed by outside experts and experts from the CPSC, the US Environmental Protection Agency, and the US Department of Housing and Urban Development.
Results
The revised report concludes that irritation and breathing problems could occur in everyone exposed to formaldehyde in the tested flooring.
The previous report suggested such problems might only occur in sensitive groups (eg, children) and people with pre-existing health conditions (eg, asthma).
The new report also increased the estimated lifetime cancer risk from breathing the highest levels of formaldehyde from the affected flooring all day, every day for 2 years.
The previous estimate of lifetime cancer risk was 2 to 9 extra cases for every 100,000 people.
The new estimate is 6 to 30 extra cases per 100,000 people.
There is conflicting data regarding the types of cancers associated with formaldehyde exposure, but many studies have suggested that formaldehyde causes cancer of the nasopharynx, sinuses, and nasal cavity, as well as leukemia, particularly myeloid leukemia.
Recommendations
Although the revised report shows an increase in health risks associated with the flooring, the NCEH and ATSDR said their recommendations remain the same.
They recommend that people with the affected flooring:
- Reduce their exposure to formaldehyde in their homes by opening windows, running exhaust fans, avoiding use of other products containing formaldehyde, etc.
- See a doctor for ongoing health symptoms such as breathing problems or irritation of the eyes, nose, or throat
- Weigh the pros and cons of professional air testing
- Consult a professional before removing the flooring, as removing it may release more formaldehyde into the home.
while woman looks on
US government agencies have released a revised report on the health risks associated with formaldehyde in certain types of laminate flooring.
The new report corrects a previous error and reveals an increase in the estimated lifetime risk of cancers, including leukemias, for individuals who regularly breathe in formaldehyde from the flooring.
The report also suggests that irritation and breathing problems can result in anyone exposed to the flooring.
The report was compiled by the Agency for Toxic Substances and Disease Registry (ATSDR) and the Centers for Disease Control and Prevention’s National Center for Environmental Health (NCEH).
About the report
On March 1, 2015, the CBS news program 60 Minutes reported that an American company, Lumber Liquidators®, was selling laminate wood flooring produced in China that released elevated levels of formaldehyde.
Based on this allegation, the US Consumer Product Safety Commission (CPSC) tested laminate flooring samples manufactured in China from 2012 to 2014 that were sold at Lumber Liquidators® stores. The CPSC then requested that the NCEH and ATSDR evaluate the test results for possible health effects.
The NCEH and ATSDR published a report detailing the possible health effects on February 10, 2016. But the report was pulled on February 19, 2016, after the agencies were informed that the report’s indoor air model incorporated an incorrect value for ceiling height.
As a result, the health risks were calculated using airborne concentration estimates about 3 times lower than they should have been.
Since the discovery of the error, the NCEH and ATSDR revised the value in the model, conducted a review of the revised results, and re-evaluated the possible health implications.
In addition, the revised report has been reviewed by outside experts and experts from the CPSC, the US Environmental Protection Agency, and the US Department of Housing and Urban Development.
Results
The revised report concludes that irritation and breathing problems could occur in everyone exposed to formaldehyde in the tested flooring.
The previous report suggested such problems might only occur in sensitive groups (eg, children) and people with pre-existing health conditions (eg, asthma).
The new report also increased the estimated lifetime cancer risk from breathing the highest levels of formaldehyde from the affected flooring all day, every day for 2 years.
The previous estimate of lifetime cancer risk was 2 to 9 extra cases for every 100,000 people.
The new estimate is 6 to 30 extra cases per 100,000 people.
There is conflicting data regarding the types of cancers associated with formaldehyde exposure, but many studies have suggested that formaldehyde causes cancer of the nasopharynx, sinuses, and nasal cavity, as well as leukemia, particularly myeloid leukemia.
Recommendations
Although the revised report shows an increase in health risks associated with the flooring, the NCEH and ATSDR said their recommendations remain the same.
They recommend that people with the affected flooring:
- Reduce their exposure to formaldehyde in their homes by opening windows, running exhaust fans, avoiding use of other products containing formaldehyde, etc.
- See a doctor for ongoing health symptoms such as breathing problems or irritation of the eyes, nose, or throat
- Weigh the pros and cons of professional air testing
- Consult a professional before removing the flooring, as removing it may release more formaldehyde into the home.