User login
Poor Physical Performance May Be an Early Sign of Late-Age Dementia
Poor physical performance was linked with an increased risk of dementia in a study of individuals age 90 and older who were followed for an average of 2.6 years. After controlling for various factors, poor standing balance had the strongest association with dementia, followed by poor performance in a four-meter walk test and a handgrip test. The study findings were published online ahead of print July 5 in the Journal of the American Geriatrics Society.
“The oldest old, people aged 90 and older, represent the fastest-growing segment of society with the highest rates of dementia; however, many of the traditional risk factors of dementia lose or change their effect in this age group. Therefore, it is crucial that we identify age-specific risk and protective factors for late-age dementia,” said lead author Szofia S. Bullain, MD, an Assistant Professor of Neurology at the University of California, Irvine. “The fact that we were able to detect impairment in physical performance two to three years before the onset of dementia suggests that poor physical performance may be a risk factor for, or an early sign of, developing late-age dementia.”
Dr. Bullain and colleagues conducted a population-based, longitudinal study to examine the relationship between physical performance and dementia in individuals age 90 and older without dementia. They enrolled 176 men and 402 women without dementia from the 90+ Study. Among the total cohort of 578, the mean age was 93.3. At baseline, 54% of the participants were cognitively normal, and 46% had cognitive impairment, but no dementia.

Szofia S. Bullain, MD
Physical performance measures included a four-meter walk, five chair stands, handgrip, and standing balance. Measures were scored from zero (unable to perform) to four (best performance). The outcome was dementia, diagnosed according to DSM-IV criteria. Hazard ratios (HRs) for dementia in relation to baseline physical performance were estimated using Cox regression after adjustment for potential confounders.
Poor physical performance in most measures was associated with greater risk of incident dementia over a mean follow-up of 2.6 years (range, seven months to nine years). After controlling for potential confounders, standing balance had the strongest association with incident dementia (HR, 1.9 to 2.5), followed by four-meter walk (HR, 1.1 to 1.8) and handgrip (HR, 1.0 to 2.0). The association with five chair stands was not significant.
The researchers next plan to examine the underlying pathologic processes, which may provide clues to new preventive and treatment strategies for late-age dementia.
—Glenn S. Williams
Suggested Reading
Bullain SS, Corrada MM, Perry SM, Kawas CH. Sound body sound mind? physical performance and the risk of dementia in the oldest old: the 90+ study. J Am Geriatr Soc. 2016 July 5 [Epub ahead of print].
Poor physical performance was linked with an increased risk of dementia in a study of individuals age 90 and older who were followed for an average of 2.6 years. After controlling for various factors, poor standing balance had the strongest association with dementia, followed by poor performance in a four-meter walk test and a handgrip test. The study findings were published online ahead of print July 5 in the Journal of the American Geriatrics Society.
“The oldest old, people aged 90 and older, represent the fastest-growing segment of society with the highest rates of dementia; however, many of the traditional risk factors of dementia lose or change their effect in this age group. Therefore, it is crucial that we identify age-specific risk and protective factors for late-age dementia,” said lead author Szofia S. Bullain, MD, an Assistant Professor of Neurology at the University of California, Irvine. “The fact that we were able to detect impairment in physical performance two to three years before the onset of dementia suggests that poor physical performance may be a risk factor for, or an early sign of, developing late-age dementia.”
Dr. Bullain and colleagues conducted a population-based, longitudinal study to examine the relationship between physical performance and dementia in individuals age 90 and older without dementia. They enrolled 176 men and 402 women without dementia from the 90+ Study. Among the total cohort of 578, the mean age was 93.3. At baseline, 54% of the participants were cognitively normal, and 46% had cognitive impairment, but no dementia.
Szofia S. Bullain, MD
Physical performance measures included a four-meter walk, five chair stands, handgrip, and standing balance. Measures were scored from zero (unable to perform) to four (best performance). The outcome was dementia, diagnosed according to DSM-IV criteria. Hazard ratios (HRs) for dementia in relation to baseline physical performance were estimated using Cox regression after adjustment for potential confounders.
Poor physical performance in most measures was associated with greater risk of incident dementia over a mean follow-up of 2.6 years (range, seven months to nine years). After controlling for potential confounders, standing balance had the strongest association with incident dementia (HR, 1.9 to 2.5), followed by four-meter walk (HR, 1.1 to 1.8) and handgrip (HR, 1.0 to 2.0). The association with five chair stands was not significant.
The researchers next plan to examine the underlying pathologic processes, which may provide clues to new preventive and treatment strategies for late-age dementia.
—Glenn S. Williams
Poor physical performance was linked with an increased risk of dementia in a study of individuals age 90 and older who were followed for an average of 2.6 years. After controlling for various factors, poor standing balance had the strongest association with dementia, followed by poor performance in a four-meter walk test and a handgrip test. The study findings were published online ahead of print July 5 in the Journal of the American Geriatrics Society.
“The oldest old, people aged 90 and older, represent the fastest-growing segment of society with the highest rates of dementia; however, many of the traditional risk factors of dementia lose or change their effect in this age group. Therefore, it is crucial that we identify age-specific risk and protective factors for late-age dementia,” said lead author Szofia S. Bullain, MD, an Assistant Professor of Neurology at the University of California, Irvine. “The fact that we were able to detect impairment in physical performance two to three years before the onset of dementia suggests that poor physical performance may be a risk factor for, or an early sign of, developing late-age dementia.”
Dr. Bullain and colleagues conducted a population-based, longitudinal study to examine the relationship between physical performance and dementia in individuals age 90 and older without dementia. They enrolled 176 men and 402 women without dementia from the 90+ Study. Among the total cohort of 578, the mean age was 93.3. At baseline, 54% of the participants were cognitively normal, and 46% had cognitive impairment, but no dementia.
Szofia S. Bullain, MD
Physical performance measures included a four-meter walk, five chair stands, handgrip, and standing balance. Measures were scored from zero (unable to perform) to four (best performance). The outcome was dementia, diagnosed according to DSM-IV criteria. Hazard ratios (HRs) for dementia in relation to baseline physical performance were estimated using Cox regression after adjustment for potential confounders.
Poor physical performance in most measures was associated with greater risk of incident dementia over a mean follow-up of 2.6 years (range, seven months to nine years). After controlling for potential confounders, standing balance had the strongest association with incident dementia (HR, 1.9 to 2.5), followed by four-meter walk (HR, 1.1 to 1.8) and handgrip (HR, 1.0 to 2.0). The association with five chair stands was not significant.
The researchers next plan to examine the underlying pathologic processes, which may provide clues to new preventive and treatment strategies for late-age dementia.
—Glenn S. Williams
Suggested Reading
Bullain SS, Corrada MM, Perry SM, Kawas CH. Sound body sound mind? physical performance and the risk of dementia in the oldest old: the 90+ study. J Am Geriatr Soc. 2016 July 5 [Epub ahead of print].
Suggested Reading
Bullain SS, Corrada MM, Perry SM, Kawas CH. Sound body sound mind? physical performance and the risk of dementia in the oldest old: the 90+ study. J Am Geriatr Soc. 2016 July 5 [Epub ahead of print].

Can an Online Screening Tool Identify People With Early Parkinson’s Disease?
VANCOUVER—An algorithm that estimates a person’s risk of Parkinson’s disease based on responses to an online questionnaire may help identify people with the earliest stages of the disease, according to research described at the 68th Annual Meeting of the American Academy of Neurology. People with the highest risk scores have poorer smell, increased rates of REM sleep behavior disorder, and slower finger tapping—intermediate markers of Parkinson’s disease—compared with those with the lowest risk scores. In addition, researchers observed a significant relationship between baseline risk score and incident Parkinson’s disease at three years.
The researchers plan to evaluate the screening tool in a larger cohort, which will allow them to observe more incident cases of Parkinson’s disease and modify the algorithm to improve its strength, said Alastair Noyce, MRCP, PhD, a Parkinson’s UK Research Fellow at University College London Institute of Neurology.

Calculating Risk
Dr. Noyce and his research colleagues developed a prediction algorithm based on a systematic review of Parkinson’s disease risk factors. Factors that increase risk include family history of the disease, constipation, anxiety, depression, pesticide exposure, and head injury. Factors that decrease risk include smoking, coffee and alcohol intake, use of calcium channel blockers, and hypertension.
To evaluate the algorithm, they initiated the longitudinal PREDICT-PD study. Approximately 1,500 people enrolled, and about 1,300 of them were eligible for the study, meaning they were between the ages of 60 and 80, lived in the United Kingdom, and did not have Parkinson’s disease, movement disorders, dementia, stroke, or motor neuron disease, and did not take drugs that can cause parkinsonism. Participants answered questionnaires about motor and nonmotor features and risk factors.
Three prominent features in the Parkinson’s disease prodrome—poor smell, REM sleep behavior disorder, and slow finger tapping—were not included in the prediction algorithm. Instead, the researchers considered those features intermediate markers of Parkinson’s disease and used them to assess at baseline whether the risk stratification process was working. The investigators hypothesized that, compared with the 100 lowest-risk participants, the 100 highest-risk participants would have deficits in smell, as measured by the University of Pennsylvania Smell Identification Test (UPSIT), higher rates of REM sleep behavior disorder (RBD), as measured by the RBD Screening Questionnaire, and slower finger tapping, as measured by the bradykinesia akinesia incoordination test. “That’s exactly what we saw,” Dr. Noyce said. The differences between groups were small but statistically significant.
Participants were asked to complete the questionnaire again each year, and their risk scores were recalculated. As fewer participants completed the survey in subsequent years, researchers compared the 15% of participants with the highest risk scores versus the 15% of participants with the lowest risk scores. When they evaluated intermediate markers in year three, they again observed small but statistically significant differences between the high- and low-risk groups.
In addition, Dr. Noyce recorded video of high-, low-, and intermediate-risk participants performing motor tests in their homes. Researchers blinded to participants’ risk estimates scored them on the Unified Parkinson’s Disease Rating Scale. Depending on the definition of mild parkinsonian signs used, 20% to 30% of the high-risk group had mild parkinsonian signs, compared with 5% of the low-risk group.
Conversion to Parkinson’s Disease
Investigators plan to see if high-risk participants are more likely to convert to Parkinson’s disease over time. Seven participants so far have received independent diagnoses of Parkinson’s disease. Prior to diagnosis, the participants had heterogeneous performance on the various intermediate markers, Dr. Noyce said. For example, two of the participants had normal UPSIT scores, one participant had a borderline UPSIT score, and the remaining four had abnormal UPSIT scores. The finger tapping score “seems to be particularly useful,” he said. Several of the participants who later were diagnosed with Parkinson’s disease had low finger tapping scores.
Using Cox regression analysis, the researchers found a significant relationship between baseline risk score and incident Parkinson’s disease at three years, with a hazard ratio of 4.4. The analysis was based on a small number of incident cases, however, and the hazard ratio had wide confidence intervals, Dr. Noyce noted.
—Jake Remaly
Suggested Reading
Noyce AJ, Bestwick JP, Silveira-Moriyama L, et al. Meta-analysis of early nonmotor features and risk factors in Parkinson disease. Ann Neurol. 2012;72(6):893-901.
Noyce AJ, Bestwick JP, Silveira-Moriyama L, et al. PREDICT-PD: identifying risk of Parkinson’s disease in the community: methods and baseline results. J Neurol Neurosurg Psychiatry. 2014;85(1):31-37.
Noyce AJ, Lees AJ, Schrag AE. The prediagnostic phase of Parkinson’s disease. J Neurol Neurosurg Psychiatry. 2016;87(8):871-878.
Salat D, Noyce AJ, Schrag A, Tolosa E. Challenges of modifying disease progression in prediagnostic Parkinson’s disease. Lancet Neurol. 2016;15(6):637-648.
VANCOUVER—An algorithm that estimates a person’s risk of Parkinson’s disease based on responses to an online questionnaire may help identify people with the earliest stages of the disease, according to research described at the 68th Annual Meeting of the American Academy of Neurology. People with the highest risk scores have poorer smell, increased rates of REM sleep behavior disorder, and slower finger tapping—intermediate markers of Parkinson’s disease—compared with those with the lowest risk scores. In addition, researchers observed a significant relationship between baseline risk score and incident Parkinson’s disease at three years.
The researchers plan to evaluate the screening tool in a larger cohort, which will allow them to observe more incident cases of Parkinson’s disease and modify the algorithm to improve its strength, said Alastair Noyce, MRCP, PhD, a Parkinson’s UK Research Fellow at University College London Institute of Neurology.
Calculating Risk
Dr. Noyce and his research colleagues developed a prediction algorithm based on a systematic review of Parkinson’s disease risk factors. Factors that increase risk include family history of the disease, constipation, anxiety, depression, pesticide exposure, and head injury. Factors that decrease risk include smoking, coffee and alcohol intake, use of calcium channel blockers, and hypertension.
To evaluate the algorithm, they initiated the longitudinal PREDICT-PD study. Approximately 1,500 people enrolled, and about 1,300 of them were eligible for the study, meaning they were between the ages of 60 and 80, lived in the United Kingdom, and did not have Parkinson’s disease, movement disorders, dementia, stroke, or motor neuron disease, and did not take drugs that can cause parkinsonism. Participants answered questionnaires about motor and nonmotor features and risk factors.
Three prominent features in the Parkinson’s disease prodrome—poor smell, REM sleep behavior disorder, and slow finger tapping—were not included in the prediction algorithm. Instead, the researchers considered those features intermediate markers of Parkinson’s disease and used them to assess at baseline whether the risk stratification process was working. The investigators hypothesized that, compared with the 100 lowest-risk participants, the 100 highest-risk participants would have deficits in smell, as measured by the University of Pennsylvania Smell Identification Test (UPSIT), higher rates of REM sleep behavior disorder (RBD), as measured by the RBD Screening Questionnaire, and slower finger tapping, as measured by the bradykinesia akinesia incoordination test. “That’s exactly what we saw,” Dr. Noyce said. The differences between groups were small but statistically significant.
Participants were asked to complete the questionnaire again each year, and their risk scores were recalculated. As fewer participants completed the survey in subsequent years, researchers compared the 15% of participants with the highest risk scores versus the 15% of participants with the lowest risk scores. When they evaluated intermediate markers in year three, they again observed small but statistically significant differences between the high- and low-risk groups.
In addition, Dr. Noyce recorded video of high-, low-, and intermediate-risk participants performing motor tests in their homes. Researchers blinded to participants’ risk estimates scored them on the Unified Parkinson’s Disease Rating Scale. Depending on the definition of mild parkinsonian signs used, 20% to 30% of the high-risk group had mild parkinsonian signs, compared with 5% of the low-risk group.
Conversion to Parkinson’s Disease
Investigators plan to see if high-risk participants are more likely to convert to Parkinson’s disease over time. Seven participants so far have received independent diagnoses of Parkinson’s disease. Prior to diagnosis, the participants had heterogeneous performance on the various intermediate markers, Dr. Noyce said. For example, two of the participants had normal UPSIT scores, one participant had a borderline UPSIT score, and the remaining four had abnormal UPSIT scores. The finger tapping score “seems to be particularly useful,” he said. Several of the participants who later were diagnosed with Parkinson’s disease had low finger tapping scores.
Using Cox regression analysis, the researchers found a significant relationship between baseline risk score and incident Parkinson’s disease at three years, with a hazard ratio of 4.4. The analysis was based on a small number of incident cases, however, and the hazard ratio had wide confidence intervals, Dr. Noyce noted.
—Jake Remaly
VANCOUVER—An algorithm that estimates a person’s risk of Parkinson’s disease based on responses to an online questionnaire may help identify people with the earliest stages of the disease, according to research described at the 68th Annual Meeting of the American Academy of Neurology. People with the highest risk scores have poorer smell, increased rates of REM sleep behavior disorder, and slower finger tapping—intermediate markers of Parkinson’s disease—compared with those with the lowest risk scores. In addition, researchers observed a significant relationship between baseline risk score and incident Parkinson’s disease at three years.
The researchers plan to evaluate the screening tool in a larger cohort, which will allow them to observe more incident cases of Parkinson’s disease and modify the algorithm to improve its strength, said Alastair Noyce, MRCP, PhD, a Parkinson’s UK Research Fellow at University College London Institute of Neurology.
Calculating Risk
Dr. Noyce and his research colleagues developed a prediction algorithm based on a systematic review of Parkinson’s disease risk factors. Factors that increase risk include family history of the disease, constipation, anxiety, depression, pesticide exposure, and head injury. Factors that decrease risk include smoking, coffee and alcohol intake, use of calcium channel blockers, and hypertension.
To evaluate the algorithm, they initiated the longitudinal PREDICT-PD study. Approximately 1,500 people enrolled, and about 1,300 of them were eligible for the study, meaning they were between the ages of 60 and 80, lived in the United Kingdom, and did not have Parkinson’s disease, movement disorders, dementia, stroke, or motor neuron disease, and did not take drugs that can cause parkinsonism. Participants answered questionnaires about motor and nonmotor features and risk factors.
Three prominent features in the Parkinson’s disease prodrome—poor smell, REM sleep behavior disorder, and slow finger tapping—were not included in the prediction algorithm. Instead, the researchers considered those features intermediate markers of Parkinson’s disease and used them to assess at baseline whether the risk stratification process was working. The investigators hypothesized that, compared with the 100 lowest-risk participants, the 100 highest-risk participants would have deficits in smell, as measured by the University of Pennsylvania Smell Identification Test (UPSIT), higher rates of REM sleep behavior disorder (RBD), as measured by the RBD Screening Questionnaire, and slower finger tapping, as measured by the bradykinesia akinesia incoordination test. “That’s exactly what we saw,” Dr. Noyce said. The differences between groups were small but statistically significant.
Participants were asked to complete the questionnaire again each year, and their risk scores were recalculated. As fewer participants completed the survey in subsequent years, researchers compared the 15% of participants with the highest risk scores versus the 15% of participants with the lowest risk scores. When they evaluated intermediate markers in year three, they again observed small but statistically significant differences between the high- and low-risk groups.
In addition, Dr. Noyce recorded video of high-, low-, and intermediate-risk participants performing motor tests in their homes. Researchers blinded to participants’ risk estimates scored them on the Unified Parkinson’s Disease Rating Scale. Depending on the definition of mild parkinsonian signs used, 20% to 30% of the high-risk group had mild parkinsonian signs, compared with 5% of the low-risk group.
Conversion to Parkinson’s Disease
Investigators plan to see if high-risk participants are more likely to convert to Parkinson’s disease over time. Seven participants so far have received independent diagnoses of Parkinson’s disease. Prior to diagnosis, the participants had heterogeneous performance on the various intermediate markers, Dr. Noyce said. For example, two of the participants had normal UPSIT scores, one participant had a borderline UPSIT score, and the remaining four had abnormal UPSIT scores. The finger tapping score “seems to be particularly useful,” he said. Several of the participants who later were diagnosed with Parkinson’s disease had low finger tapping scores.
Using Cox regression analysis, the researchers found a significant relationship between baseline risk score and incident Parkinson’s disease at three years, with a hazard ratio of 4.4. The analysis was based on a small number of incident cases, however, and the hazard ratio had wide confidence intervals, Dr. Noyce noted.
—Jake Remaly
Suggested Reading
Noyce AJ, Bestwick JP, Silveira-Moriyama L, et al. Meta-analysis of early nonmotor features and risk factors in Parkinson disease. Ann Neurol. 2012;72(6):893-901.
Noyce AJ, Bestwick JP, Silveira-Moriyama L, et al. PREDICT-PD: identifying risk of Parkinson’s disease in the community: methods and baseline results. J Neurol Neurosurg Psychiatry. 2014;85(1):31-37.
Noyce AJ, Lees AJ, Schrag AE. The prediagnostic phase of Parkinson’s disease. J Neurol Neurosurg Psychiatry. 2016;87(8):871-878.
Salat D, Noyce AJ, Schrag A, Tolosa E. Challenges of modifying disease progression in prediagnostic Parkinson’s disease. Lancet Neurol. 2016;15(6):637-648.
Suggested Reading
Noyce AJ, Bestwick JP, Silveira-Moriyama L, et al. Meta-analysis of early nonmotor features and risk factors in Parkinson disease. Ann Neurol. 2012;72(6):893-901.
Noyce AJ, Bestwick JP, Silveira-Moriyama L, et al. PREDICT-PD: identifying risk of Parkinson’s disease in the community: methods and baseline results. J Neurol Neurosurg Psychiatry. 2014;85(1):31-37.
Noyce AJ, Lees AJ, Schrag AE. The prediagnostic phase of Parkinson’s disease. J Neurol Neurosurg Psychiatry. 2016;87(8):871-878.
Salat D, Noyce AJ, Schrag A, Tolosa E. Challenges of modifying disease progression in prediagnostic Parkinson’s disease. Lancet Neurol. 2016;15(6):637-648.

Sport-related concussion: How best to help young athletes
› Require athletes who sustain a concussion to wait a minimum of 7 to 10 days before returning to full unrestricted activity. C
› Ensure that any player diagnosed with concussion follows a guided return-to-play progression, supervised by an athletic trainer or physical therapist experienced in post-concussion care. C
› Advise patients who are old enough to drive not to do so for at least 24 hours after a concussion. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Each year in the United States, more than 44 million young people participate in sports activities.1 Yet the number of concussions incurred annually by children and adolescents engaged in sports and recreational play has been underestimated for years, and largely unknown.1,2
Some estimates were based solely on the number of young athletes treated in emergency departments or sports concussion clinics. Others focused only on team players of middle school or high school age, excluding younger children who were hit in the head on playgrounds or during other recreational activities. What’s more, large numbers of concussions—as many as 4 in 10 incurred by high school athletes—were never reported to a coach or medical professional.3
In a new study published in the journal Pediatrics in June, researchers used national databases and current literature to provide what they believe to be “the most accurate and precise estimate of youth concussion” thus far: Between 1.1 and 1.9 million sports- and recreation-related concussions occur among US youth ages 18 or younger annually.1
Among young people playing team sports, concussions are between 2 and 7 times more likely to occur during competitive games than in practice sessions.4-7 Boys on football and ice hockey teams have the highest rates of concussion in young athletes.For overall number of concussions, however, girls on soccer teams are second only to football players.4 Female soccer players are more likely than male soccer players to sustain concussions during equal number of hours of play.4,7
An increase in incidence. The incidence of concussion among young athletes appears to have increased in the past decade, a likely result of greater involvement in team sports, an increasing focus on safeguarding young people from the potential dangers associated with a blow to the brain, and better diagnostic techniques.4,8-10 And a recent study based on data from electronic medical records at a large regional pediatric health care network found that more than three-quarters of young people with sports-related concussions were first seen in a primary care setting.2
With this in mind, we present a comprehensive update of the evidence regarding the diagnosis and management of sport-related concussion. The recommendations we include are consistent with professional association guidelines.8-10 Although we focus on concussion in children and adolescents involved in athletic activities, the principles generally apply to patients of all ages and to concussions that may not be sports related.
Removal from play: A vital first step
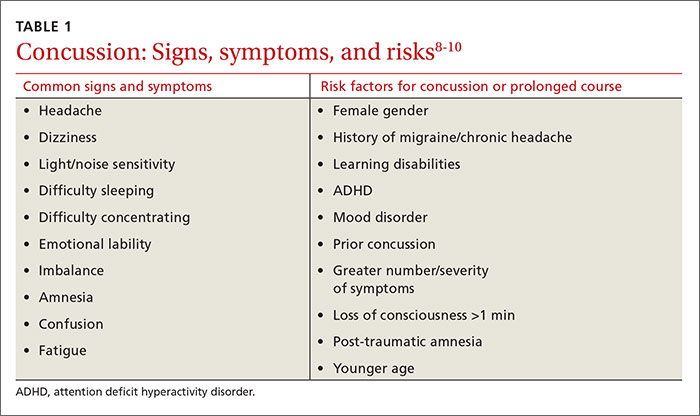
Whenever you conduct a physical exam for a young athlete, remind him or her—and the patient’s parents—that after a blow to the head, immediate removal from play is critical. Concussion is caused by a direct or indirect force to the brain that results in a transient disturbance in brain function,8-10 manifested by alterations in neurocognitive and motor function. While the signs and symptoms (TABLE 1)8-10 resolve within 10 days of injury in about 90% of cases, those who incur additional head impact within 24 hours have a higher symptom burden and prolonged recovery period.11 Even without repetitive impact, younger athletes may take longer to recover.8-10
The initial assessment
A child or adolescent who sustains a suspected concussion should be seen by a physician within 24 to 48 hours. Whether the initial assessment occurs in your office or on the sidelines of a game, it is important to confirm the time the incident occurred and the mechanism of injury.
Concussion is diagnosed by a combination of history, physical exam, and objective testing when symptoms or exam findings associated with mild brain trauma—headache, dizziness, light and/or noise sensitivity, among others—closely follow a head injury.8-10 Certain maneuvers—assessing eye movements by asking the athlete to look in various directions, for instance, then to follow a pen or finger as you move it closer to his or her face—may provoke dizziness, headache, or other symptoms of concussion that were not apparent initially.
The differential diagnosis includes cervical musculoskeletal injury, craniofacial injury, epidural and subdural hematoma, heat-related illness, uncomplicated headache and migraine, upper respiratory infection, and vertigo.8-10
Tools aid in diagnosis
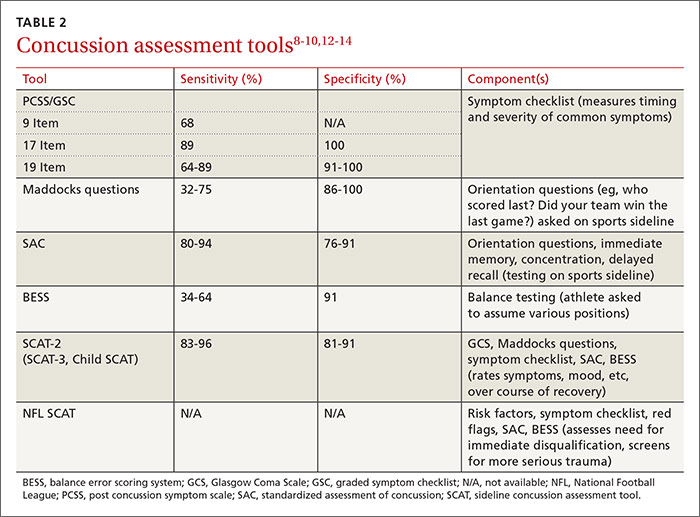
Many clinical assessment tools exist to aid in the diagnosis of concussion (TABLE 2).8-10,12-14 Any one of these tools, many of which use combinations of symptom checklists, balance exams, and cognitive assessments, may be included in your evaluation. No single tool has been found to be superior to any other.8-10 A combination of tools may improve diagnostic accuracy, but assessment tools should not be the sole basis used to diagnose or rule out concussion.
Any child or adolescent who had a blow to the head and at least one sign or symptom of concussion should be evaluated as soon as possible and assessed again later that day or the next day if any reason for concern remains.
Neuropsychological (NP) testing may involve computerized tests developed specifically for athletes. Patients may be required to react to objects that appear on a screen, for example, in a way that tests memory, performance, and reaction time. Because cognitive recovery often lags behind symptom resolution, NP testing may identify subtle brain deficits even in athletes who are asymptomatic at rest or with exercise. In general, NP testing has a sensitivity of 71% to 88% for athletes with concussion,10 but it is most beneficial when baseline test results are available. Interpretation of NP testing should be done only by qualified clinicians.
While NP testing may provide additional prognostic information, it should not alter the management of athletes who are symptomatic either at rest or with exercise.15 Nor is NP testing vital, as concussion can be accurately diagnosed and adequately managed without it.
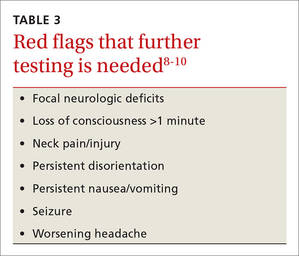
Neuroimaging, including computed tomography (CT) and magnetic resonance imaging (MRI), is often used unnecessarily in the initial assessment of a patient who sustained a possible concussion.8-10 In fact, neuroimaging should be reserved for cases in which it is necessary to rule out more serious pathology: intracranial or subdural hematoma or a craniofacial injury, for example, in patients with clinical findings that are red flags. These red flags include focal neurologic deficits, continuing nausea/vomiting, or persistent disorientation (TABLE 3),8-10 or symptoms that worsen or persist beyond a few weeks. In such cases, further evaluation—with MRI of the brain, formal NP testing, and/or referral to a neurologist, physiatrist, or other physician who specializes in concussion care—is indicated.
Concussion management: Rest is key
While there is a dearth of high-quality studies on the management of sport-related concussion across all age groups, standardized protocols for both children and adults have been adopted in most clinical settings.8-10,16,17 The protocols provide a framework for an individualized treatment plan. Yet their use among primary care physicians is inconsistent.18-20
Traditionally, concussion management begins with relative physical and cognitive rest to allow the brain time to recover.8-10 Recent randomized controlled trials have challenged this premise by suggesting that mild to moderate physical activity for post-concussion patients who are mildly symptomatic does not adversely affect recovery.21,22 These studies have significant limitations, however, and further research is needed to provide specific guidance on this aspect of concussion management before it is adopted.
Physical restrictions include organized sports, recreational activity, recess, and physical education classes. Walking is permitted unless it exacerbates symptoms. These restrictions should continue until the patient is symptom-free.
Cognitive restrictions include modifications at school and at home. Once an athlete is able to concentrate and tolerate visual and auditory stimuli, he or she may return to school. But classroom modifications should be considered, possibly including shortened school days, extra time for testing and homework, help with note taking, and restrictions from classes likely to provoke symptoms, such as computer science or music. Limiting use of mobile devices, television viewing, noisy environments, and other possible provocations may help speed symptom resolution. These restrictions, too, should remain in place until the patient is symptom-free.
Driving is often not addressed by physicians managing the care of athletes with concussion, but evidence suggests it should be. A study of patients presenting to the emergency department found that within 24 hours of a concussion diagnosis, individuals had an impaired response to traffic hazards.23,24 And Canadian clinical practice guidelines recommend that athletes with mild traumatic brain injury (TBI) avoid driving within the first 24 hours.25
While American guidelines are silent on the question of driving for this patient population, we recommend that athletes with concussion be restricted from driving and engaging in other risky complex tasks, such as welding or shop class, for at least 24 hours. For many athletes diagnosed with concussion, driving restrictions of longer duration may be necessary based on their symptom profile and neurocognitive test results. Continued dizziness or visual deficits would pose a greater risk than fatigue or short-term memory loss, for example.
Overseeing the return to play
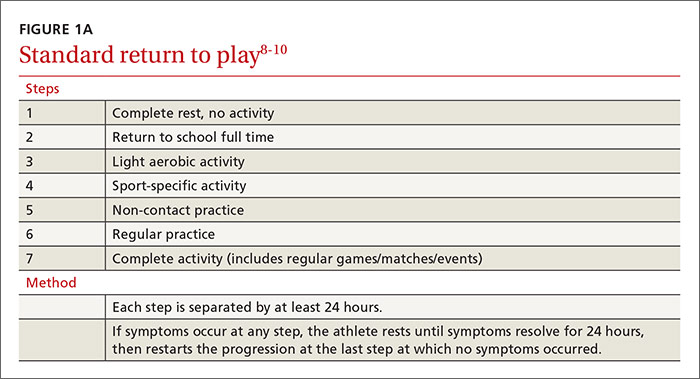
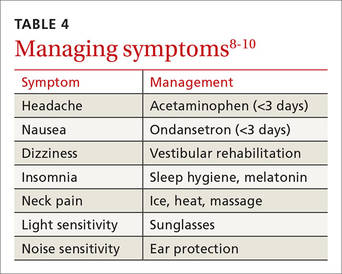
Return-to-activity progression follows a stepwise protocol, with 6 steps that the injured athlete must complete before resuming full activity (FIGURE 1A).8-10 This stepwise progression begins only when athletes are symptom free, even during provocative maneuvers; have had a normal neurologic exam, are back to school full time with no restriction; are off any medications prescribed for concussion symptoms (TABLE 4),8-10 and when neurocognitive testing, if performed, is back to baseline. If an athlete develops symptoms at any stage of the progression, rest is required until he or she remains asymptomatic for at least 24 hours. The progression is then restarted at the last stage at which the patient was symptom free.
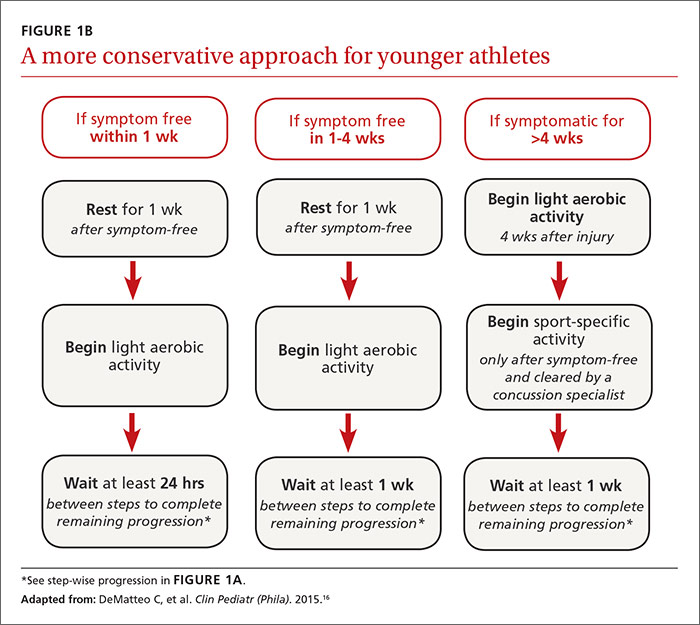
Some individualization, of course, is recommended here, too. Younger athletes and those with a prior history of concussion may require 10 days or more to complete all the steps, allowing an extra day at various steps. Neurologic maturation affects recovery time, and for younger individuals, a more conservative return-to-play protocol based on initial concussion symptom duration has been proposed (FIGURE 1B).16
Return to activity is often supervised by a certified athletic trainer at the athlete’s school. In the event that no athletic trainer is available, patients may be referred to physical therapists with experience in monitoring injured athletes.26 Anyone involved in the patient’s care, including the athlete himself, may use a symptom checklist to monitor recovery.
Although there is no evidence that the ongoing use of a symptom checklist affects the course of recovery, its use is often helpful in identifying specific symptoms that can be managed by means other than physical and cognitive rest—a sleep hygiene program for an individual with lingering difficulty sleeping, for example, or the continued application of ice, heat, and massage for persistent neck pain.
Checklist monitoring may be especially helpful for athletes whose symptoms extend beyond 10 days or who have multiple symptoms. Final clearance once all the steps have been completed requires follow-up with a health care provider.
Is a symptom-free waiting period necessary?
There is no evidence suggesting a need for a symptom-free waiting period before starting the return-to-play protocol.10,27 Because a repeat concussion is most likely within 7 to 10 days of the initial injury,8,9 however, most athletes should not return to contact play during that time frame, regardless of symptom resolution.
It is helpful to have asymptomatic athletes participate in non-contact activity before the 7 to 10 days are up, however. Doing so can help prevent deconditioning and injury upon return to contact sport, as there is evidence of increased risk of lower-extremity injury in the 90 days after concussion.28
What to tell athletes—and parents—about repetitive head trauma
There is growing concern about the long-term risks of concussion and repetitive head impact that may manifest as chronic traumatic encephalopathy (CTE) and chronic neurocognitive impairment (CNI) later in life. Indeed, some data strongly suggest—but do not definitively prove—a relationship between repetitive head injury and chronic neurodegenerative disease.8-10 You can tell worried patients or parents, however, that the majority of research on CTE and CNI has been based on professional football players.
Studies of long-term effects of soccer heading have shown conflicting results, with some finding cognitive impairment, altered postural control, and anatomic changes of the brain, while others found no effect on encephalopathy, concussion symptoms, or neurocognitive performance.29-36Here, too, most studies showing negative effects of soccer heading involved professional athletes.
Repetitive sub-concussive impact in high school football athletes has been found to induce biochemical changes to the brain,37 but the long-term effects are unknown. And, while concussion in high school athletes has been associated with short-term cognitive impairment, altered neurochemistry, and evidence of increased symptoms on baseline neurocognitive testing,8-10,38 no studies have linked concussion during middle school or high school with CNI. What’s more, a long-term (50-year) follow-up study of individuals who played football in high school found no difference in rates of neurodegenerative disease compared with age-matched controls.39
A new study of high school and college football players (mean age: 17.4 years) presented at the American Academy of Neurology 2016 Sports Concussion Conference in Chicago in July, however, found significant alterations in white matter 6 months post injury.40 The researchers compared 17 athletes with sport-related concussion with matched controls, using diffusion tensor imaging and diffusion kurtosis tensor imaging as biomarkers of brain recovery. The concussed athletes underwent MRI and symptom assessment at 24 hours, 8 days, and 6 months. The controls followed identical protocols.
At the 6-month assessment, there were no differences between the concussed group and the controls in terms of self-reported concussion symptoms, cognition, or balance. However, the concussed athletes had widespread decreased mean diffusivity compared with the controls. Despite the lack of clinical symptoms, the concussed athletes showed significant alterations in white matter “that were related to initial symptom severity ratings,” the authors concluded. These findings have implications both for determination of recovery from concussion and concussion management, they added.40
Although there is no way to eliminate all concussions, limited evidence suggests that improving athletic technique, limiting contact at practices, better enforcement of game rules, and rule changes regarding physical contact may decrease concussion risk.41-43 Many youth sports organizations have developed policies placing restrictions on head impact during practices and games. Studies are ongoing, too, to see if better headgear—or requiring helmets for soccer players—makes a difference.
CORRESPONDENCE
Ryan A. Sprouse, MD, CAQSM, 203 East Fourth Avenue, Ranson, WV 25438; [email protected].
1. Bryan MA, Rowhani-Rahbar A, Comstock RD, et al. Sports- and recreation-related concussions in US youth. Pediatrics. 2016; June 20 [Epub ahead of print].
2. Arbogast KB, Curry AE, Pfeiffer MR, et al. Point of health care entry for youth with concussion within a large pediatric care network. JAMA Pediatr. 2016; May 31 [Epub ahead of print].
3. Mihalik JK, Guskiewicz KM, Valovich McLeod TC, et al. Knowledge, attitude, and concussion-reporting behaviors among high school athletes: a preliminary study. J Ath Tr. 2013;48:645-653.
4. Marar M, McIlvain NM, Fields SK, et al. Epidemiology of concussions among United States high school athletes in 20 sports. Am J Sports Med. 2012;40:747.
5. Kontos AP, Elbin RJ, Fazio-Sumrock VC. Incidence of sports-related concussion among youth football players aged 8-12 years. J Pediatr. 2013;163:717-720.
6. Dompier TP, Kerr ZY, Marshall SW, et al. Incidence of concussion during practice and games in youth, high school, and collegiate American football players. JAMA Pediatr. 2015;169:659-665.
7. Comstock RD, Currie DW, Pierpont LA, et al. An evidence-based discussion of heading the ball and concussions in high school soccer. JAMA Pediatr. 2015;169:830-837.
8. Harmon KG, Drezner JA, Gammons M, et al. American Medical Society for Sports Medicine position statement: concussion in sport. Br J Sports Med. 2013;47:15-26.
9. McCrory P, Meeuwisse WH, Aubry M, et al. Consensus statement on concussion in sport: the 4th International Conference on Concussion in Sport held in Zurich, November 2012. Br J Sports Med. 2013;47:250-258.
10. Giza CC, Kutcher JS, Ashwal S, et al. Summary of the evidence-based guideline update: evaluation and management of concussion in sports: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2013;80:2250-2257.
11. Terwilliger VK, Pratson L, Vaughan CG, et al. Additional post-concussion impact exposure may affect recovery in adolescent athletes. J Neurotrauma. 2016;33:761-765.
12. Putukian M, Echemendia R, Dettwiler-Danspeckgruber A. Prospective clinical assessment using Sideline Concussion Assessment Tool-2 testing in the evaluation of sport-related concussion in college athletes. Clin J Sport Med. 2015;25:36-42.
13. Broglio SP, Macciocchi SN, Ferrara MS. Sensitivity of the concussion assessment battery. Neurosurgery. 2007;60:1050-1057.
14. Randolph C, McCrea M, Barr WB. Is neuropsychological testing useful in the management of sport-related concussion? J Athl Train. 2005;40:139-152.
15. Shrier I. Neuropsychological testing and concussions: a reasoned approach. Clin J Sport Med. 2012;22:211-213.
16. DeMatteo C, Stazyk K, Singh SK, et al. Development of a conservative protocol to return children and youth to activity following concussive injury. Clin Pediatr (Phila). 2015;54:152-163.
17. Broglio SP, Cantu RC, Gioia GA, et al. National Athletic Trainers Association position statement: management of sport concussion. J Athl Train. 2014;49:245-265.
18. Stoller J, Carson JD, Garel A, et al. Do family physicians, emergency department physicians, and pediatricians give consistent sport-related concussion management advice? Can Fam Physician. 2014;60:548, 550-552.
19. Lebrun CM, Mrazik M, Prasad AS, et al. Sport concussion knowledge base, clinical practices and needs for continuing medical education: a survey of family physicians and cross-border comparison. Br J Sports Med. 2013;47:54-59.
20. Zemek R, Eady K, Moreau K, et al. Knowledge of paediatric concussion among front-line primary care providers. Paediatr Child Health. 2014;19:475-480.
21. Maerlender A, Rieman W, Lichtenstein J, et al. Programmed physical exertion in recovery from sports-related concussion: a randomized pilot study. Dev Neuropsychol. 2015;40:273-278.
22. Buckley TA, Munkasy BA, Clouse BP. Acute cognitive and physical rest may not improve concussion recovery time. J Head Trauma Rehabil. 2015; July 24 [Epub ahead of print].
23. Preece MH, Horswill MS, Langlois JA, et al. The epidemiology and impact of traumatic brain injury: a brief overview. J Head Trauma Rehabil. 2006;21:375-378.
24. Baker A, Unsworth CA, Lannin NA. Fitness-to-drive after mild traumatic brain injury: mapping the time trajectory of recovery in the acute stages post injury. Accid Anal Prev. 2015;79:50-55.
25. Marshall S, Bayley M, McCullagh S, et al. Clinical practice guidelines for mild traumatic brain injury and persistent symptoms. Can Fam Physician. 2012;58:257-267.
26. Yorke AM, Littleton S, Alsalaheen BA. Concussion attitudes and beliefs, knowledge, and clinical practice: a survey of physical therapists. Phys Ther. Available at: http://dx.doi.org/10.2522/ptj.20140598. Accessed January 21, 2016.
27. McCrea M, Guskiewicz K, Randolph C, et al. Effects of a symptom-free waiting period on clinical outcome and risk of reinjury after sport-related concussion. Neurosurgery. 2009;65:876-883.
28. Brooks MA, Peterson K, Biese K, et al. Concussion increases odds of sustaining a lower extremity musculoskeletal injury after return to play among collegiate athletes. Am J Sports Med. 2016;44:742-747.
29. Witol AD, Webbe FM. Soccer heading frequency predicts neuropsychological deficits. Arch Clin Neuropsychol. 2003;18:397-417.
30. Haran FJ, Tierney R, Wright WG, et al. Acute changes in postural control after soccer heading. Int J Sports Med. 2013;34:350-354.
31. Lipton ML, Kim N, Zimmerman ME, et al. Soccer heading is associated with white matter microstructural and cognitive abnormalities. Radiology. 2013;268:850-857.
32. Jordan SE, Green GA, Galanty HL, et al. Acute and chronic brain injury in United States national team soccer players. Am J Sports Med. 1996;24:205-210.
33. Kontos AP, Dolese A, Elbin RJ, et al. Relationship of soccer heading to computerized neurocognitive performance and symptoms among female and male youth soccer players. Brain Inj. 2011;25:1234-1241.
34. Straume-Naesheim TM, Andersen TE, Dvorak J, et al. Effects of heading exposure and previous concussions on neuropsychological performance among Norwegian elite footballers. Br J Sports Med. 2005;39:70-77.
35. Stephens R, Rutherford A, Potter D, et al. Neuropsychological impairment as a consequence of football (soccer) play and football heading: a preliminary analysis and report on school students (13-16 years). Child Neuropsychol. 2005;11:513-526.
36. Stephens R, Rutherford A, Potter D, et al. Neuropsychological consequence of soccer play in adolescent UK school team soccer players. J Neuropsychiatry Clin Neurosci. 2010;22:295-303.
37. Poole VN, Breedlove EL, Shenk TE, et al. Sub-concussive hit characteristics predict deviant brain metabolism in football athletes. Dev Neuropsychol. 2015;40:12-17.
38. Mannix R, Iverson GL, Maxwell B, et al. Multiple prior concussions are associated with symptoms in high school athletes. Ann Clin Trans Neurol. 2014;1:433-438.
39. Savica R, Parisi JE, Wold LE, et al. High school football and risk of neurodegeneration: a community-based study. Mayo Clin Proc. 2012;87:335-340.
40. Lancaster M, Muftuler T, Olson D, et al. Chronic white matter changes following sport-related concussion measured by diffusion tensor and diffusion kurtosis imaging. Paper presented at: American Academy of Neurology 2016 Sports Concussion Conference; July 8-10, 2016; Chicago, Ill.
41. Kerr ZY, Yeargin SW, Valovich McLeod TC, et al. Comprehensive coach education reduces head impact exposures in American youth football. Orthop J Sports Med. 2015;3(ecollection):e232596711561545.
42. Black AM, Macpherson AK, Hagel BE, et al. Policy change eliminating body checking in non-elite ice hockey leads to a threefold reduction in injury and concussion risk in 11- and 12-year-old players. Br J Sports Med. 2016;50:55-61.
43. Council on Sports Medicine and Fitness. Tackling in youth football. Policy Statement of the American Academy of Pediatrics. Pediatrics. 2015;136:e1419-e1430.
› Require athletes who sustain a concussion to wait a minimum of 7 to 10 days before returning to full unrestricted activity. C
› Ensure that any player diagnosed with concussion follows a guided return-to-play progression, supervised by an athletic trainer or physical therapist experienced in post-concussion care. C
› Advise patients who are old enough to drive not to do so for at least 24 hours after a concussion. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Each year in the United States, more than 44 million young people participate in sports activities.1 Yet the number of concussions incurred annually by children and adolescents engaged in sports and recreational play has been underestimated for years, and largely unknown.1,2
Some estimates were based solely on the number of young athletes treated in emergency departments or sports concussion clinics. Others focused only on team players of middle school or high school age, excluding younger children who were hit in the head on playgrounds or during other recreational activities. What’s more, large numbers of concussions—as many as 4 in 10 incurred by high school athletes—were never reported to a coach or medical professional.3
In a new study published in the journal Pediatrics in June, researchers used national databases and current literature to provide what they believe to be “the most accurate and precise estimate of youth concussion” thus far: Between 1.1 and 1.9 million sports- and recreation-related concussions occur among US youth ages 18 or younger annually.1
Among young people playing team sports, concussions are between 2 and 7 times more likely to occur during competitive games than in practice sessions.4-7 Boys on football and ice hockey teams have the highest rates of concussion in young athletes.For overall number of concussions, however, girls on soccer teams are second only to football players.4 Female soccer players are more likely than male soccer players to sustain concussions during equal number of hours of play.4,7
An increase in incidence. The incidence of concussion among young athletes appears to have increased in the past decade, a likely result of greater involvement in team sports, an increasing focus on safeguarding young people from the potential dangers associated with a blow to the brain, and better diagnostic techniques.4,8-10 And a recent study based on data from electronic medical records at a large regional pediatric health care network found that more than three-quarters of young people with sports-related concussions were first seen in a primary care setting.2
With this in mind, we present a comprehensive update of the evidence regarding the diagnosis and management of sport-related concussion. The recommendations we include are consistent with professional association guidelines.8-10 Although we focus on concussion in children and adolescents involved in athletic activities, the principles generally apply to patients of all ages and to concussions that may not be sports related.
Removal from play: A vital first step
Whenever you conduct a physical exam for a young athlete, remind him or her—and the patient’s parents—that after a blow to the head, immediate removal from play is critical. Concussion is caused by a direct or indirect force to the brain that results in a transient disturbance in brain function,8-10 manifested by alterations in neurocognitive and motor function. While the signs and symptoms (TABLE 1)8-10 resolve within 10 days of injury in about 90% of cases, those who incur additional head impact within 24 hours have a higher symptom burden and prolonged recovery period.11 Even without repetitive impact, younger athletes may take longer to recover.8-10
The initial assessment
A child or adolescent who sustains a suspected concussion should be seen by a physician within 24 to 48 hours. Whether the initial assessment occurs in your office or on the sidelines of a game, it is important to confirm the time the incident occurred and the mechanism of injury.
Concussion is diagnosed by a combination of history, physical exam, and objective testing when symptoms or exam findings associated with mild brain trauma—headache, dizziness, light and/or noise sensitivity, among others—closely follow a head injury.8-10 Certain maneuvers—assessing eye movements by asking the athlete to look in various directions, for instance, then to follow a pen or finger as you move it closer to his or her face—may provoke dizziness, headache, or other symptoms of concussion that were not apparent initially.
The differential diagnosis includes cervical musculoskeletal injury, craniofacial injury, epidural and subdural hematoma, heat-related illness, uncomplicated headache and migraine, upper respiratory infection, and vertigo.8-10
Tools aid in diagnosis
Many clinical assessment tools exist to aid in the diagnosis of concussion (TABLE 2).8-10,12-14 Any one of these tools, many of which use combinations of symptom checklists, balance exams, and cognitive assessments, may be included in your evaluation. No single tool has been found to be superior to any other.8-10 A combination of tools may improve diagnostic accuracy, but assessment tools should not be the sole basis used to diagnose or rule out concussion.
Any child or adolescent who had a blow to the head and at least one sign or symptom of concussion should be evaluated as soon as possible and assessed again later that day or the next day if any reason for concern remains.
Neuropsychological (NP) testing may involve computerized tests developed specifically for athletes. Patients may be required to react to objects that appear on a screen, for example, in a way that tests memory, performance, and reaction time. Because cognitive recovery often lags behind symptom resolution, NP testing may identify subtle brain deficits even in athletes who are asymptomatic at rest or with exercise. In general, NP testing has a sensitivity of 71% to 88% for athletes with concussion,10 but it is most beneficial when baseline test results are available. Interpretation of NP testing should be done only by qualified clinicians.
While NP testing may provide additional prognostic information, it should not alter the management of athletes who are symptomatic either at rest or with exercise.15 Nor is NP testing vital, as concussion can be accurately diagnosed and adequately managed without it.
Neuroimaging, including computed tomography (CT) and magnetic resonance imaging (MRI), is often used unnecessarily in the initial assessment of a patient who sustained a possible concussion.8-10 In fact, neuroimaging should be reserved for cases in which it is necessary to rule out more serious pathology: intracranial or subdural hematoma or a craniofacial injury, for example, in patients with clinical findings that are red flags. These red flags include focal neurologic deficits, continuing nausea/vomiting, or persistent disorientation (TABLE 3),8-10 or symptoms that worsen or persist beyond a few weeks. In such cases, further evaluation—with MRI of the brain, formal NP testing, and/or referral to a neurologist, physiatrist, or other physician who specializes in concussion care—is indicated.
Concussion management: Rest is key
While there is a dearth of high-quality studies on the management of sport-related concussion across all age groups, standardized protocols for both children and adults have been adopted in most clinical settings.8-10,16,17 The protocols provide a framework for an individualized treatment plan. Yet their use among primary care physicians is inconsistent.18-20
Traditionally, concussion management begins with relative physical and cognitive rest to allow the brain time to recover.8-10 Recent randomized controlled trials have challenged this premise by suggesting that mild to moderate physical activity for post-concussion patients who are mildly symptomatic does not adversely affect recovery.21,22 These studies have significant limitations, however, and further research is needed to provide specific guidance on this aspect of concussion management before it is adopted.
Physical restrictions include organized sports, recreational activity, recess, and physical education classes. Walking is permitted unless it exacerbates symptoms. These restrictions should continue until the patient is symptom-free.
Cognitive restrictions include modifications at school and at home. Once an athlete is able to concentrate and tolerate visual and auditory stimuli, he or she may return to school. But classroom modifications should be considered, possibly including shortened school days, extra time for testing and homework, help with note taking, and restrictions from classes likely to provoke symptoms, such as computer science or music. Limiting use of mobile devices, television viewing, noisy environments, and other possible provocations may help speed symptom resolution. These restrictions, too, should remain in place until the patient is symptom-free.
Driving is often not addressed by physicians managing the care of athletes with concussion, but evidence suggests it should be. A study of patients presenting to the emergency department found that within 24 hours of a concussion diagnosis, individuals had an impaired response to traffic hazards.23,24 And Canadian clinical practice guidelines recommend that athletes with mild traumatic brain injury (TBI) avoid driving within the first 24 hours.25
While American guidelines are silent on the question of driving for this patient population, we recommend that athletes with concussion be restricted from driving and engaging in other risky complex tasks, such as welding or shop class, for at least 24 hours. For many athletes diagnosed with concussion, driving restrictions of longer duration may be necessary based on their symptom profile and neurocognitive test results. Continued dizziness or visual deficits would pose a greater risk than fatigue or short-term memory loss, for example.
Overseeing the return to play
Return-to-activity progression follows a stepwise protocol, with 6 steps that the injured athlete must complete before resuming full activity (FIGURE 1A).8-10 This stepwise progression begins only when athletes are symptom free, even during provocative maneuvers; have had a normal neurologic exam, are back to school full time with no restriction; are off any medications prescribed for concussion symptoms (TABLE 4),8-10 and when neurocognitive testing, if performed, is back to baseline. If an athlete develops symptoms at any stage of the progression, rest is required until he or she remains asymptomatic for at least 24 hours. The progression is then restarted at the last stage at which the patient was symptom free.
Some individualization, of course, is recommended here, too. Younger athletes and those with a prior history of concussion may require 10 days or more to complete all the steps, allowing an extra day at various steps. Neurologic maturation affects recovery time, and for younger individuals, a more conservative return-to-play protocol based on initial concussion symptom duration has been proposed (FIGURE 1B).16
Return to activity is often supervised by a certified athletic trainer at the athlete’s school. In the event that no athletic trainer is available, patients may be referred to physical therapists with experience in monitoring injured athletes.26 Anyone involved in the patient’s care, including the athlete himself, may use a symptom checklist to monitor recovery.
Although there is no evidence that the ongoing use of a symptom checklist affects the course of recovery, its use is often helpful in identifying specific symptoms that can be managed by means other than physical and cognitive rest—a sleep hygiene program for an individual with lingering difficulty sleeping, for example, or the continued application of ice, heat, and massage for persistent neck pain.
Checklist monitoring may be especially helpful for athletes whose symptoms extend beyond 10 days or who have multiple symptoms. Final clearance once all the steps have been completed requires follow-up with a health care provider.
Is a symptom-free waiting period necessary?
There is no evidence suggesting a need for a symptom-free waiting period before starting the return-to-play protocol.10,27 Because a repeat concussion is most likely within 7 to 10 days of the initial injury,8,9 however, most athletes should not return to contact play during that time frame, regardless of symptom resolution.
It is helpful to have asymptomatic athletes participate in non-contact activity before the 7 to 10 days are up, however. Doing so can help prevent deconditioning and injury upon return to contact sport, as there is evidence of increased risk of lower-extremity injury in the 90 days after concussion.28
What to tell athletes—and parents—about repetitive head trauma
There is growing concern about the long-term risks of concussion and repetitive head impact that may manifest as chronic traumatic encephalopathy (CTE) and chronic neurocognitive impairment (CNI) later in life. Indeed, some data strongly suggest—but do not definitively prove—a relationship between repetitive head injury and chronic neurodegenerative disease.8-10 You can tell worried patients or parents, however, that the majority of research on CTE and CNI has been based on professional football players.
Studies of long-term effects of soccer heading have shown conflicting results, with some finding cognitive impairment, altered postural control, and anatomic changes of the brain, while others found no effect on encephalopathy, concussion symptoms, or neurocognitive performance.29-36Here, too, most studies showing negative effects of soccer heading involved professional athletes.
Repetitive sub-concussive impact in high school football athletes has been found to induce biochemical changes to the brain,37 but the long-term effects are unknown. And, while concussion in high school athletes has been associated with short-term cognitive impairment, altered neurochemistry, and evidence of increased symptoms on baseline neurocognitive testing,8-10,38 no studies have linked concussion during middle school or high school with CNI. What’s more, a long-term (50-year) follow-up study of individuals who played football in high school found no difference in rates of neurodegenerative disease compared with age-matched controls.39
A new study of high school and college football players (mean age: 17.4 years) presented at the American Academy of Neurology 2016 Sports Concussion Conference in Chicago in July, however, found significant alterations in white matter 6 months post injury.40 The researchers compared 17 athletes with sport-related concussion with matched controls, using diffusion tensor imaging and diffusion kurtosis tensor imaging as biomarkers of brain recovery. The concussed athletes underwent MRI and symptom assessment at 24 hours, 8 days, and 6 months. The controls followed identical protocols.
At the 6-month assessment, there were no differences between the concussed group and the controls in terms of self-reported concussion symptoms, cognition, or balance. However, the concussed athletes had widespread decreased mean diffusivity compared with the controls. Despite the lack of clinical symptoms, the concussed athletes showed significant alterations in white matter “that were related to initial symptom severity ratings,” the authors concluded. These findings have implications both for determination of recovery from concussion and concussion management, they added.40
Although there is no way to eliminate all concussions, limited evidence suggests that improving athletic technique, limiting contact at practices, better enforcement of game rules, and rule changes regarding physical contact may decrease concussion risk.41-43 Many youth sports organizations have developed policies placing restrictions on head impact during practices and games. Studies are ongoing, too, to see if better headgear—or requiring helmets for soccer players—makes a difference.
CORRESPONDENCE
Ryan A. Sprouse, MD, CAQSM, 203 East Fourth Avenue, Ranson, WV 25438; [email protected].
› Require athletes who sustain a concussion to wait a minimum of 7 to 10 days before returning to full unrestricted activity. C
› Ensure that any player diagnosed with concussion follows a guided return-to-play progression, supervised by an athletic trainer or physical therapist experienced in post-concussion care. C
› Advise patients who are old enough to drive not to do so for at least 24 hours after a concussion. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Each year in the United States, more than 44 million young people participate in sports activities.1 Yet the number of concussions incurred annually by children and adolescents engaged in sports and recreational play has been underestimated for years, and largely unknown.1,2
Some estimates were based solely on the number of young athletes treated in emergency departments or sports concussion clinics. Others focused only on team players of middle school or high school age, excluding younger children who were hit in the head on playgrounds or during other recreational activities. What’s more, large numbers of concussions—as many as 4 in 10 incurred by high school athletes—were never reported to a coach or medical professional.3
In a new study published in the journal Pediatrics in June, researchers used national databases and current literature to provide what they believe to be “the most accurate and precise estimate of youth concussion” thus far: Between 1.1 and 1.9 million sports- and recreation-related concussions occur among US youth ages 18 or younger annually.1
Among young people playing team sports, concussions are between 2 and 7 times more likely to occur during competitive games than in practice sessions.4-7 Boys on football and ice hockey teams have the highest rates of concussion in young athletes.For overall number of concussions, however, girls on soccer teams are second only to football players.4 Female soccer players are more likely than male soccer players to sustain concussions during equal number of hours of play.4,7
An increase in incidence. The incidence of concussion among young athletes appears to have increased in the past decade, a likely result of greater involvement in team sports, an increasing focus on safeguarding young people from the potential dangers associated with a blow to the brain, and better diagnostic techniques.4,8-10 And a recent study based on data from electronic medical records at a large regional pediatric health care network found that more than three-quarters of young people with sports-related concussions were first seen in a primary care setting.2
With this in mind, we present a comprehensive update of the evidence regarding the diagnosis and management of sport-related concussion. The recommendations we include are consistent with professional association guidelines.8-10 Although we focus on concussion in children and adolescents involved in athletic activities, the principles generally apply to patients of all ages and to concussions that may not be sports related.
Removal from play: A vital first step
Whenever you conduct a physical exam for a young athlete, remind him or her—and the patient’s parents—that after a blow to the head, immediate removal from play is critical. Concussion is caused by a direct or indirect force to the brain that results in a transient disturbance in brain function,8-10 manifested by alterations in neurocognitive and motor function. While the signs and symptoms (TABLE 1)8-10 resolve within 10 days of injury in about 90% of cases, those who incur additional head impact within 24 hours have a higher symptom burden and prolonged recovery period.11 Even without repetitive impact, younger athletes may take longer to recover.8-10
The initial assessment
A child or adolescent who sustains a suspected concussion should be seen by a physician within 24 to 48 hours. Whether the initial assessment occurs in your office or on the sidelines of a game, it is important to confirm the time the incident occurred and the mechanism of injury.
Concussion is diagnosed by a combination of history, physical exam, and objective testing when symptoms or exam findings associated with mild brain trauma—headache, dizziness, light and/or noise sensitivity, among others—closely follow a head injury.8-10 Certain maneuvers—assessing eye movements by asking the athlete to look in various directions, for instance, then to follow a pen or finger as you move it closer to his or her face—may provoke dizziness, headache, or other symptoms of concussion that were not apparent initially.
The differential diagnosis includes cervical musculoskeletal injury, craniofacial injury, epidural and subdural hematoma, heat-related illness, uncomplicated headache and migraine, upper respiratory infection, and vertigo.8-10
Tools aid in diagnosis
Many clinical assessment tools exist to aid in the diagnosis of concussion (TABLE 2).8-10,12-14 Any one of these tools, many of which use combinations of symptom checklists, balance exams, and cognitive assessments, may be included in your evaluation. No single tool has been found to be superior to any other.8-10 A combination of tools may improve diagnostic accuracy, but assessment tools should not be the sole basis used to diagnose or rule out concussion.
Any child or adolescent who had a blow to the head and at least one sign or symptom of concussion should be evaluated as soon as possible and assessed again later that day or the next day if any reason for concern remains.
Neuropsychological (NP) testing may involve computerized tests developed specifically for athletes. Patients may be required to react to objects that appear on a screen, for example, in a way that tests memory, performance, and reaction time. Because cognitive recovery often lags behind symptom resolution, NP testing may identify subtle brain deficits even in athletes who are asymptomatic at rest or with exercise. In general, NP testing has a sensitivity of 71% to 88% for athletes with concussion,10 but it is most beneficial when baseline test results are available. Interpretation of NP testing should be done only by qualified clinicians.
While NP testing may provide additional prognostic information, it should not alter the management of athletes who are symptomatic either at rest or with exercise.15 Nor is NP testing vital, as concussion can be accurately diagnosed and adequately managed without it.
Neuroimaging, including computed tomography (CT) and magnetic resonance imaging (MRI), is often used unnecessarily in the initial assessment of a patient who sustained a possible concussion.8-10 In fact, neuroimaging should be reserved for cases in which it is necessary to rule out more serious pathology: intracranial or subdural hematoma or a craniofacial injury, for example, in patients with clinical findings that are red flags. These red flags include focal neurologic deficits, continuing nausea/vomiting, or persistent disorientation (TABLE 3),8-10 or symptoms that worsen or persist beyond a few weeks. In such cases, further evaluation—with MRI of the brain, formal NP testing, and/or referral to a neurologist, physiatrist, or other physician who specializes in concussion care—is indicated.
Concussion management: Rest is key
While there is a dearth of high-quality studies on the management of sport-related concussion across all age groups, standardized protocols for both children and adults have been adopted in most clinical settings.8-10,16,17 The protocols provide a framework for an individualized treatment plan. Yet their use among primary care physicians is inconsistent.18-20
Traditionally, concussion management begins with relative physical and cognitive rest to allow the brain time to recover.8-10 Recent randomized controlled trials have challenged this premise by suggesting that mild to moderate physical activity for post-concussion patients who are mildly symptomatic does not adversely affect recovery.21,22 These studies have significant limitations, however, and further research is needed to provide specific guidance on this aspect of concussion management before it is adopted.
Physical restrictions include organized sports, recreational activity, recess, and physical education classes. Walking is permitted unless it exacerbates symptoms. These restrictions should continue until the patient is symptom-free.
Cognitive restrictions include modifications at school and at home. Once an athlete is able to concentrate and tolerate visual and auditory stimuli, he or she may return to school. But classroom modifications should be considered, possibly including shortened school days, extra time for testing and homework, help with note taking, and restrictions from classes likely to provoke symptoms, such as computer science or music. Limiting use of mobile devices, television viewing, noisy environments, and other possible provocations may help speed symptom resolution. These restrictions, too, should remain in place until the patient is symptom-free.
Driving is often not addressed by physicians managing the care of athletes with concussion, but evidence suggests it should be. A study of patients presenting to the emergency department found that within 24 hours of a concussion diagnosis, individuals had an impaired response to traffic hazards.23,24 And Canadian clinical practice guidelines recommend that athletes with mild traumatic brain injury (TBI) avoid driving within the first 24 hours.25
While American guidelines are silent on the question of driving for this patient population, we recommend that athletes with concussion be restricted from driving and engaging in other risky complex tasks, such as welding or shop class, for at least 24 hours. For many athletes diagnosed with concussion, driving restrictions of longer duration may be necessary based on their symptom profile and neurocognitive test results. Continued dizziness or visual deficits would pose a greater risk than fatigue or short-term memory loss, for example.
Overseeing the return to play
Return-to-activity progression follows a stepwise protocol, with 6 steps that the injured athlete must complete before resuming full activity (FIGURE 1A).8-10 This stepwise progression begins only when athletes are symptom free, even during provocative maneuvers; have had a normal neurologic exam, are back to school full time with no restriction; are off any medications prescribed for concussion symptoms (TABLE 4),8-10 and when neurocognitive testing, if performed, is back to baseline. If an athlete develops symptoms at any stage of the progression, rest is required until he or she remains asymptomatic for at least 24 hours. The progression is then restarted at the last stage at which the patient was symptom free.
Some individualization, of course, is recommended here, too. Younger athletes and those with a prior history of concussion may require 10 days or more to complete all the steps, allowing an extra day at various steps. Neurologic maturation affects recovery time, and for younger individuals, a more conservative return-to-play protocol based on initial concussion symptom duration has been proposed (FIGURE 1B).16
Return to activity is often supervised by a certified athletic trainer at the athlete’s school. In the event that no athletic trainer is available, patients may be referred to physical therapists with experience in monitoring injured athletes.26 Anyone involved in the patient’s care, including the athlete himself, may use a symptom checklist to monitor recovery.
Although there is no evidence that the ongoing use of a symptom checklist affects the course of recovery, its use is often helpful in identifying specific symptoms that can be managed by means other than physical and cognitive rest—a sleep hygiene program for an individual with lingering difficulty sleeping, for example, or the continued application of ice, heat, and massage for persistent neck pain.
Checklist monitoring may be especially helpful for athletes whose symptoms extend beyond 10 days or who have multiple symptoms. Final clearance once all the steps have been completed requires follow-up with a health care provider.
Is a symptom-free waiting period necessary?
There is no evidence suggesting a need for a symptom-free waiting period before starting the return-to-play protocol.10,27 Because a repeat concussion is most likely within 7 to 10 days of the initial injury,8,9 however, most athletes should not return to contact play during that time frame, regardless of symptom resolution.
It is helpful to have asymptomatic athletes participate in non-contact activity before the 7 to 10 days are up, however. Doing so can help prevent deconditioning and injury upon return to contact sport, as there is evidence of increased risk of lower-extremity injury in the 90 days after concussion.28
What to tell athletes—and parents—about repetitive head trauma
There is growing concern about the long-term risks of concussion and repetitive head impact that may manifest as chronic traumatic encephalopathy (CTE) and chronic neurocognitive impairment (CNI) later in life. Indeed, some data strongly suggest—but do not definitively prove—a relationship between repetitive head injury and chronic neurodegenerative disease.8-10 You can tell worried patients or parents, however, that the majority of research on CTE and CNI has been based on professional football players.
Studies of long-term effects of soccer heading have shown conflicting results, with some finding cognitive impairment, altered postural control, and anatomic changes of the brain, while others found no effect on encephalopathy, concussion symptoms, or neurocognitive performance.29-36Here, too, most studies showing negative effects of soccer heading involved professional athletes.
Repetitive sub-concussive impact in high school football athletes has been found to induce biochemical changes to the brain,37 but the long-term effects are unknown. And, while concussion in high school athletes has been associated with short-term cognitive impairment, altered neurochemistry, and evidence of increased symptoms on baseline neurocognitive testing,8-10,38 no studies have linked concussion during middle school or high school with CNI. What’s more, a long-term (50-year) follow-up study of individuals who played football in high school found no difference in rates of neurodegenerative disease compared with age-matched controls.39
A new study of high school and college football players (mean age: 17.4 years) presented at the American Academy of Neurology 2016 Sports Concussion Conference in Chicago in July, however, found significant alterations in white matter 6 months post injury.40 The researchers compared 17 athletes with sport-related concussion with matched controls, using diffusion tensor imaging and diffusion kurtosis tensor imaging as biomarkers of brain recovery. The concussed athletes underwent MRI and symptom assessment at 24 hours, 8 days, and 6 months. The controls followed identical protocols.
At the 6-month assessment, there were no differences between the concussed group and the controls in terms of self-reported concussion symptoms, cognition, or balance. However, the concussed athletes had widespread decreased mean diffusivity compared with the controls. Despite the lack of clinical symptoms, the concussed athletes showed significant alterations in white matter “that were related to initial symptom severity ratings,” the authors concluded. These findings have implications both for determination of recovery from concussion and concussion management, they added.40
Although there is no way to eliminate all concussions, limited evidence suggests that improving athletic technique, limiting contact at practices, better enforcement of game rules, and rule changes regarding physical contact may decrease concussion risk.41-43 Many youth sports organizations have developed policies placing restrictions on head impact during practices and games. Studies are ongoing, too, to see if better headgear—or requiring helmets for soccer players—makes a difference.
CORRESPONDENCE
Ryan A. Sprouse, MD, CAQSM, 203 East Fourth Avenue, Ranson, WV 25438; [email protected].
1. Bryan MA, Rowhani-Rahbar A, Comstock RD, et al. Sports- and recreation-related concussions in US youth. Pediatrics. 2016; June 20 [Epub ahead of print].
2. Arbogast KB, Curry AE, Pfeiffer MR, et al. Point of health care entry for youth with concussion within a large pediatric care network. JAMA Pediatr. 2016; May 31 [Epub ahead of print].
3. Mihalik JK, Guskiewicz KM, Valovich McLeod TC, et al. Knowledge, attitude, and concussion-reporting behaviors among high school athletes: a preliminary study. J Ath Tr. 2013;48:645-653.
4. Marar M, McIlvain NM, Fields SK, et al. Epidemiology of concussions among United States high school athletes in 20 sports. Am J Sports Med. 2012;40:747.
5. Kontos AP, Elbin RJ, Fazio-Sumrock VC. Incidence of sports-related concussion among youth football players aged 8-12 years. J Pediatr. 2013;163:717-720.
6. Dompier TP, Kerr ZY, Marshall SW, et al. Incidence of concussion during practice and games in youth, high school, and collegiate American football players. JAMA Pediatr. 2015;169:659-665.
7. Comstock RD, Currie DW, Pierpont LA, et al. An evidence-based discussion of heading the ball and concussions in high school soccer. JAMA Pediatr. 2015;169:830-837.
8. Harmon KG, Drezner JA, Gammons M, et al. American Medical Society for Sports Medicine position statement: concussion in sport. Br J Sports Med. 2013;47:15-26.
9. McCrory P, Meeuwisse WH, Aubry M, et al. Consensus statement on concussion in sport: the 4th International Conference on Concussion in Sport held in Zurich, November 2012. Br J Sports Med. 2013;47:250-258.
10. Giza CC, Kutcher JS, Ashwal S, et al. Summary of the evidence-based guideline update: evaluation and management of concussion in sports: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2013;80:2250-2257.
11. Terwilliger VK, Pratson L, Vaughan CG, et al. Additional post-concussion impact exposure may affect recovery in adolescent athletes. J Neurotrauma. 2016;33:761-765.
12. Putukian M, Echemendia R, Dettwiler-Danspeckgruber A. Prospective clinical assessment using Sideline Concussion Assessment Tool-2 testing in the evaluation of sport-related concussion in college athletes. Clin J Sport Med. 2015;25:36-42.
13. Broglio SP, Macciocchi SN, Ferrara MS. Sensitivity of the concussion assessment battery. Neurosurgery. 2007;60:1050-1057.
14. Randolph C, McCrea M, Barr WB. Is neuropsychological testing useful in the management of sport-related concussion? J Athl Train. 2005;40:139-152.
15. Shrier I. Neuropsychological testing and concussions: a reasoned approach. Clin J Sport Med. 2012;22:211-213.
16. DeMatteo C, Stazyk K, Singh SK, et al. Development of a conservative protocol to return children and youth to activity following concussive injury. Clin Pediatr (Phila). 2015;54:152-163.
17. Broglio SP, Cantu RC, Gioia GA, et al. National Athletic Trainers Association position statement: management of sport concussion. J Athl Train. 2014;49:245-265.
18. Stoller J, Carson JD, Garel A, et al. Do family physicians, emergency department physicians, and pediatricians give consistent sport-related concussion management advice? Can Fam Physician. 2014;60:548, 550-552.
19. Lebrun CM, Mrazik M, Prasad AS, et al. Sport concussion knowledge base, clinical practices and needs for continuing medical education: a survey of family physicians and cross-border comparison. Br J Sports Med. 2013;47:54-59.
20. Zemek R, Eady K, Moreau K, et al. Knowledge of paediatric concussion among front-line primary care providers. Paediatr Child Health. 2014;19:475-480.
21. Maerlender A, Rieman W, Lichtenstein J, et al. Programmed physical exertion in recovery from sports-related concussion: a randomized pilot study. Dev Neuropsychol. 2015;40:273-278.
22. Buckley TA, Munkasy BA, Clouse BP. Acute cognitive and physical rest may not improve concussion recovery time. J Head Trauma Rehabil. 2015; July 24 [Epub ahead of print].
23. Preece MH, Horswill MS, Langlois JA, et al. The epidemiology and impact of traumatic brain injury: a brief overview. J Head Trauma Rehabil. 2006;21:375-378.
24. Baker A, Unsworth CA, Lannin NA. Fitness-to-drive after mild traumatic brain injury: mapping the time trajectory of recovery in the acute stages post injury. Accid Anal Prev. 2015;79:50-55.
25. Marshall S, Bayley M, McCullagh S, et al. Clinical practice guidelines for mild traumatic brain injury and persistent symptoms. Can Fam Physician. 2012;58:257-267.
26. Yorke AM, Littleton S, Alsalaheen BA. Concussion attitudes and beliefs, knowledge, and clinical practice: a survey of physical therapists. Phys Ther. Available at: http://dx.doi.org/10.2522/ptj.20140598. Accessed January 21, 2016.
27. McCrea M, Guskiewicz K, Randolph C, et al. Effects of a symptom-free waiting period on clinical outcome and risk of reinjury after sport-related concussion. Neurosurgery. 2009;65:876-883.
28. Brooks MA, Peterson K, Biese K, et al. Concussion increases odds of sustaining a lower extremity musculoskeletal injury after return to play among collegiate athletes. Am J Sports Med. 2016;44:742-747.
29. Witol AD, Webbe FM. Soccer heading frequency predicts neuropsychological deficits. Arch Clin Neuropsychol. 2003;18:397-417.
30. Haran FJ, Tierney R, Wright WG, et al. Acute changes in postural control after soccer heading. Int J Sports Med. 2013;34:350-354.
31. Lipton ML, Kim N, Zimmerman ME, et al. Soccer heading is associated with white matter microstructural and cognitive abnormalities. Radiology. 2013;268:850-857.
32. Jordan SE, Green GA, Galanty HL, et al. Acute and chronic brain injury in United States national team soccer players. Am J Sports Med. 1996;24:205-210.
33. Kontos AP, Dolese A, Elbin RJ, et al. Relationship of soccer heading to computerized neurocognitive performance and symptoms among female and male youth soccer players. Brain Inj. 2011;25:1234-1241.
34. Straume-Naesheim TM, Andersen TE, Dvorak J, et al. Effects of heading exposure and previous concussions on neuropsychological performance among Norwegian elite footballers. Br J Sports Med. 2005;39:70-77.
35. Stephens R, Rutherford A, Potter D, et al. Neuropsychological impairment as a consequence of football (soccer) play and football heading: a preliminary analysis and report on school students (13-16 years). Child Neuropsychol. 2005;11:513-526.
36. Stephens R, Rutherford A, Potter D, et al. Neuropsychological consequence of soccer play in adolescent UK school team soccer players. J Neuropsychiatry Clin Neurosci. 2010;22:295-303.
37. Poole VN, Breedlove EL, Shenk TE, et al. Sub-concussive hit characteristics predict deviant brain metabolism in football athletes. Dev Neuropsychol. 2015;40:12-17.
38. Mannix R, Iverson GL, Maxwell B, et al. Multiple prior concussions are associated with symptoms in high school athletes. Ann Clin Trans Neurol. 2014;1:433-438.
39. Savica R, Parisi JE, Wold LE, et al. High school football and risk of neurodegeneration: a community-based study. Mayo Clin Proc. 2012;87:335-340.
40. Lancaster M, Muftuler T, Olson D, et al. Chronic white matter changes following sport-related concussion measured by diffusion tensor and diffusion kurtosis imaging. Paper presented at: American Academy of Neurology 2016 Sports Concussion Conference; July 8-10, 2016; Chicago, Ill.
41. Kerr ZY, Yeargin SW, Valovich McLeod TC, et al. Comprehensive coach education reduces head impact exposures in American youth football. Orthop J Sports Med. 2015;3(ecollection):e232596711561545.
42. Black AM, Macpherson AK, Hagel BE, et al. Policy change eliminating body checking in non-elite ice hockey leads to a threefold reduction in injury and concussion risk in 11- and 12-year-old players. Br J Sports Med. 2016;50:55-61.
43. Council on Sports Medicine and Fitness. Tackling in youth football. Policy Statement of the American Academy of Pediatrics. Pediatrics. 2015;136:e1419-e1430.
1. Bryan MA, Rowhani-Rahbar A, Comstock RD, et al. Sports- and recreation-related concussions in US youth. Pediatrics. 2016; June 20 [Epub ahead of print].
2. Arbogast KB, Curry AE, Pfeiffer MR, et al. Point of health care entry for youth with concussion within a large pediatric care network. JAMA Pediatr. 2016; May 31 [Epub ahead of print].
3. Mihalik JK, Guskiewicz KM, Valovich McLeod TC, et al. Knowledge, attitude, and concussion-reporting behaviors among high school athletes: a preliminary study. J Ath Tr. 2013;48:645-653.
4. Marar M, McIlvain NM, Fields SK, et al. Epidemiology of concussions among United States high school athletes in 20 sports. Am J Sports Med. 2012;40:747.
5. Kontos AP, Elbin RJ, Fazio-Sumrock VC. Incidence of sports-related concussion among youth football players aged 8-12 years. J Pediatr. 2013;163:717-720.
6. Dompier TP, Kerr ZY, Marshall SW, et al. Incidence of concussion during practice and games in youth, high school, and collegiate American football players. JAMA Pediatr. 2015;169:659-665.
7. Comstock RD, Currie DW, Pierpont LA, et al. An evidence-based discussion of heading the ball and concussions in high school soccer. JAMA Pediatr. 2015;169:830-837.
8. Harmon KG, Drezner JA, Gammons M, et al. American Medical Society for Sports Medicine position statement: concussion in sport. Br J Sports Med. 2013;47:15-26.
9. McCrory P, Meeuwisse WH, Aubry M, et al. Consensus statement on concussion in sport: the 4th International Conference on Concussion in Sport held in Zurich, November 2012. Br J Sports Med. 2013;47:250-258.
10. Giza CC, Kutcher JS, Ashwal S, et al. Summary of the evidence-based guideline update: evaluation and management of concussion in sports: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2013;80:2250-2257.
11. Terwilliger VK, Pratson L, Vaughan CG, et al. Additional post-concussion impact exposure may affect recovery in adolescent athletes. J Neurotrauma. 2016;33:761-765.
12. Putukian M, Echemendia R, Dettwiler-Danspeckgruber A. Prospective clinical assessment using Sideline Concussion Assessment Tool-2 testing in the evaluation of sport-related concussion in college athletes. Clin J Sport Med. 2015;25:36-42.
13. Broglio SP, Macciocchi SN, Ferrara MS. Sensitivity of the concussion assessment battery. Neurosurgery. 2007;60:1050-1057.
14. Randolph C, McCrea M, Barr WB. Is neuropsychological testing useful in the management of sport-related concussion? J Athl Train. 2005;40:139-152.
15. Shrier I. Neuropsychological testing and concussions: a reasoned approach. Clin J Sport Med. 2012;22:211-213.
16. DeMatteo C, Stazyk K, Singh SK, et al. Development of a conservative protocol to return children and youth to activity following concussive injury. Clin Pediatr (Phila). 2015;54:152-163.
17. Broglio SP, Cantu RC, Gioia GA, et al. National Athletic Trainers Association position statement: management of sport concussion. J Athl Train. 2014;49:245-265.
18. Stoller J, Carson JD, Garel A, et al. Do family physicians, emergency department physicians, and pediatricians give consistent sport-related concussion management advice? Can Fam Physician. 2014;60:548, 550-552.
19. Lebrun CM, Mrazik M, Prasad AS, et al. Sport concussion knowledge base, clinical practices and needs for continuing medical education: a survey of family physicians and cross-border comparison. Br J Sports Med. 2013;47:54-59.
20. Zemek R, Eady K, Moreau K, et al. Knowledge of paediatric concussion among front-line primary care providers. Paediatr Child Health. 2014;19:475-480.
21. Maerlender A, Rieman W, Lichtenstein J, et al. Programmed physical exertion in recovery from sports-related concussion: a randomized pilot study. Dev Neuropsychol. 2015;40:273-278.
22. Buckley TA, Munkasy BA, Clouse BP. Acute cognitive and physical rest may not improve concussion recovery time. J Head Trauma Rehabil. 2015; July 24 [Epub ahead of print].
23. Preece MH, Horswill MS, Langlois JA, et al. The epidemiology and impact of traumatic brain injury: a brief overview. J Head Trauma Rehabil. 2006;21:375-378.
24. Baker A, Unsworth CA, Lannin NA. Fitness-to-drive after mild traumatic brain injury: mapping the time trajectory of recovery in the acute stages post injury. Accid Anal Prev. 2015;79:50-55.
25. Marshall S, Bayley M, McCullagh S, et al. Clinical practice guidelines for mild traumatic brain injury and persistent symptoms. Can Fam Physician. 2012;58:257-267.
26. Yorke AM, Littleton S, Alsalaheen BA. Concussion attitudes and beliefs, knowledge, and clinical practice: a survey of physical therapists. Phys Ther. Available at: http://dx.doi.org/10.2522/ptj.20140598. Accessed January 21, 2016.
27. McCrea M, Guskiewicz K, Randolph C, et al. Effects of a symptom-free waiting period on clinical outcome and risk of reinjury after sport-related concussion. Neurosurgery. 2009;65:876-883.
28. Brooks MA, Peterson K, Biese K, et al. Concussion increases odds of sustaining a lower extremity musculoskeletal injury after return to play among collegiate athletes. Am J Sports Med. 2016;44:742-747.
29. Witol AD, Webbe FM. Soccer heading frequency predicts neuropsychological deficits. Arch Clin Neuropsychol. 2003;18:397-417.
30. Haran FJ, Tierney R, Wright WG, et al. Acute changes in postural control after soccer heading. Int J Sports Med. 2013;34:350-354.
31. Lipton ML, Kim N, Zimmerman ME, et al. Soccer heading is associated with white matter microstructural and cognitive abnormalities. Radiology. 2013;268:850-857.
32. Jordan SE, Green GA, Galanty HL, et al. Acute and chronic brain injury in United States national team soccer players. Am J Sports Med. 1996;24:205-210.
33. Kontos AP, Dolese A, Elbin RJ, et al. Relationship of soccer heading to computerized neurocognitive performance and symptoms among female and male youth soccer players. Brain Inj. 2011;25:1234-1241.
34. Straume-Naesheim TM, Andersen TE, Dvorak J, et al. Effects of heading exposure and previous concussions on neuropsychological performance among Norwegian elite footballers. Br J Sports Med. 2005;39:70-77.
35. Stephens R, Rutherford A, Potter D, et al. Neuropsychological impairment as a consequence of football (soccer) play and football heading: a preliminary analysis and report on school students (13-16 years). Child Neuropsychol. 2005;11:513-526.
36. Stephens R, Rutherford A, Potter D, et al. Neuropsychological consequence of soccer play in adolescent UK school team soccer players. J Neuropsychiatry Clin Neurosci. 2010;22:295-303.
37. Poole VN, Breedlove EL, Shenk TE, et al. Sub-concussive hit characteristics predict deviant brain metabolism in football athletes. Dev Neuropsychol. 2015;40:12-17.
38. Mannix R, Iverson GL, Maxwell B, et al. Multiple prior concussions are associated with symptoms in high school athletes. Ann Clin Trans Neurol. 2014;1:433-438.
39. Savica R, Parisi JE, Wold LE, et al. High school football and risk of neurodegeneration: a community-based study. Mayo Clin Proc. 2012;87:335-340.
40. Lancaster M, Muftuler T, Olson D, et al. Chronic white matter changes following sport-related concussion measured by diffusion tensor and diffusion kurtosis imaging. Paper presented at: American Academy of Neurology 2016 Sports Concussion Conference; July 8-10, 2016; Chicago, Ill.
41. Kerr ZY, Yeargin SW, Valovich McLeod TC, et al. Comprehensive coach education reduces head impact exposures in American youth football. Orthop J Sports Med. 2015;3(ecollection):e232596711561545.
42. Black AM, Macpherson AK, Hagel BE, et al. Policy change eliminating body checking in non-elite ice hockey leads to a threefold reduction in injury and concussion risk in 11- and 12-year-old players. Br J Sports Med. 2016;50:55-61.
43. Council on Sports Medicine and Fitness. Tackling in youth football. Policy Statement of the American Academy of Pediatrics. Pediatrics. 2015;136:e1419-e1430.
From The Journal of Family Practice | 2016;65(8):538-544,546.
Shining a light on nonplaque psoriasis
MIAMI – People with nonplaque psoriasis could soon have their day. Some patients with nail, inverse, and genital psoriasis, for example, fail to meet traditional criteria for moderate to severe disease and therefore do not meet label indications for treatment.
That could soon change if dermatologist Abrar A. Qureshi, MD, and rheumatologist-dermatologist Joseph F. Merola, MD, have their way, according to their dual presentation at the annual meeting of the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis.

“What we’re trying to do really is go into redefining moderate to severe psoriasis. The current definition is moderate to severe plaque psoriasis,” said Dr. Qureshi, chief of dermatology at Rhode Island Hospital in Providence. “If you look at all the labels out there, it’s plaque disease.”
However, “psoriasis is poly phenotype,” Dr. Qureshi said. “This paradigm needs to change in the next few years to redefine what moderate to severe psoriasis is.” A patient with limited, nonplaque psoriasis on their elbows, one knee, or who presents only with perianal disease, for example, might not meet the traditional definition of moderate to severe psoriasis. Another patient might just have scalp disease or inverse psoriasis on a limited body area.
Currently, the Psoriasis Area and Severity Index (PASI), Physician Global Assessment (PGA) and Body Surface Area (BSA) assessments classify mild, moderate, and severe psoriasis, “with the majority of people out there in the world with mild psoriasis,” Dr. Qureshi said. A new measure called the Comprehensive Assessment of the Psoriasis Patient (CAPP) “captures more people with moderate to severe disease.”
CAPP includes a measure of plaque disease, palmoplantar, nail, scale, inverse, and genital psoriasis. “Where PASI fails, we hope the CAPP meets this unmet need,” said Dr. Merola, codirector of the Center for Skin and Related Musculoskeletal Diseases, a combined clinic at Brigham and Women’s Hospital in Boston. The two highest phenotypic scores are added to the plaque score for a final CAPP score. “It’s easy to use.”
A newly announced genital psoriasis component of CAPP measures any suprapubic, perineal, and genital involvement. Thickness, scale, and severity are included in CAPP, as well as secondary skin changes like fissuring or erosion. Then the score is equally weighted with the patient reported outcomes of pain and effect on intimacy rated on a simple visual analog scale.
Dr. Merola, Dr. Qureshi, and their colleagues collaborated on a study looking at the prevalence of nonplaque psoriasis among almost 4,000 patients (Clin Exp Dermatol. 2016;41:486-9).
“It surprised us to see such a high prevalence of inverse disease, almost 24%,” Dr. Merola said. “Many of these patients have two nonplaque phenotypes. It’s also important because it seems like there is an increased psoriatic arthritis risk.”
“The nail story and the scalp story have been out there a while, but looking at inverse disease there was a fairly high hazard ratio [2.07] for development of psoriatic arthritis.”
Proposing a polyphenotype psoriasis clinical trial
“I will end with a recommendation for a polyphenotype psoriasis clinical trial, to be really controversial,” Dr. Qureshi said. “We want to capture only the people who qualify as moderate to severe with the new measure and look at them before and after therapy.” He added participants would be “people out there in clinic who are currently not receiving treatment.”
During the Q&A, a meeting attendee asked if the investigators could recruit enough patients with nonplaque psoriasis. “We think it’s about 15%-23%,” Dr. Qureshi said. “The only type we cannot capture well is the palmoplantar phenotype because of its really low prevalence.”
MIAMI – People with nonplaque psoriasis could soon have their day. Some patients with nail, inverse, and genital psoriasis, for example, fail to meet traditional criteria for moderate to severe disease and therefore do not meet label indications for treatment.
That could soon change if dermatologist Abrar A. Qureshi, MD, and rheumatologist-dermatologist Joseph F. Merola, MD, have their way, according to their dual presentation at the annual meeting of the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis.
“What we’re trying to do really is go into redefining moderate to severe psoriasis. The current definition is moderate to severe plaque psoriasis,” said Dr. Qureshi, chief of dermatology at Rhode Island Hospital in Providence. “If you look at all the labels out there, it’s plaque disease.”
However, “psoriasis is poly phenotype,” Dr. Qureshi said. “This paradigm needs to change in the next few years to redefine what moderate to severe psoriasis is.” A patient with limited, nonplaque psoriasis on their elbows, one knee, or who presents only with perianal disease, for example, might not meet the traditional definition of moderate to severe psoriasis. Another patient might just have scalp disease or inverse psoriasis on a limited body area.
Currently, the Psoriasis Area and Severity Index (PASI), Physician Global Assessment (PGA) and Body Surface Area (BSA) assessments classify mild, moderate, and severe psoriasis, “with the majority of people out there in the world with mild psoriasis,” Dr. Qureshi said. A new measure called the Comprehensive Assessment of the Psoriasis Patient (CAPP) “captures more people with moderate to severe disease.”
CAPP includes a measure of plaque disease, palmoplantar, nail, scale, inverse, and genital psoriasis. “Where PASI fails, we hope the CAPP meets this unmet need,” said Dr. Merola, codirector of the Center for Skin and Related Musculoskeletal Diseases, a combined clinic at Brigham and Women’s Hospital in Boston. The two highest phenotypic scores are added to the plaque score for a final CAPP score. “It’s easy to use.”
A newly announced genital psoriasis component of CAPP measures any suprapubic, perineal, and genital involvement. Thickness, scale, and severity are included in CAPP, as well as secondary skin changes like fissuring or erosion. Then the score is equally weighted with the patient reported outcomes of pain and effect on intimacy rated on a simple visual analog scale.
Dr. Merola, Dr. Qureshi, and their colleagues collaborated on a study looking at the prevalence of nonplaque psoriasis among almost 4,000 patients (Clin Exp Dermatol. 2016;41:486-9).
“It surprised us to see such a high prevalence of inverse disease, almost 24%,” Dr. Merola said. “Many of these patients have two nonplaque phenotypes. It’s also important because it seems like there is an increased psoriatic arthritis risk.”
“The nail story and the scalp story have been out there a while, but looking at inverse disease there was a fairly high hazard ratio [2.07] for development of psoriatic arthritis.”
Proposing a polyphenotype psoriasis clinical trial
“I will end with a recommendation for a polyphenotype psoriasis clinical trial, to be really controversial,” Dr. Qureshi said. “We want to capture only the people who qualify as moderate to severe with the new measure and look at them before and after therapy.” He added participants would be “people out there in clinic who are currently not receiving treatment.”
During the Q&A, a meeting attendee asked if the investigators could recruit enough patients with nonplaque psoriasis. “We think it’s about 15%-23%,” Dr. Qureshi said. “The only type we cannot capture well is the palmoplantar phenotype because of its really low prevalence.”
MIAMI – People with nonplaque psoriasis could soon have their day. Some patients with nail, inverse, and genital psoriasis, for example, fail to meet traditional criteria for moderate to severe disease and therefore do not meet label indications for treatment.
That could soon change if dermatologist Abrar A. Qureshi, MD, and rheumatologist-dermatologist Joseph F. Merola, MD, have their way, according to their dual presentation at the annual meeting of the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis.
“What we’re trying to do really is go into redefining moderate to severe psoriasis. The current definition is moderate to severe plaque psoriasis,” said Dr. Qureshi, chief of dermatology at Rhode Island Hospital in Providence. “If you look at all the labels out there, it’s plaque disease.”
However, “psoriasis is poly phenotype,” Dr. Qureshi said. “This paradigm needs to change in the next few years to redefine what moderate to severe psoriasis is.” A patient with limited, nonplaque psoriasis on their elbows, one knee, or who presents only with perianal disease, for example, might not meet the traditional definition of moderate to severe psoriasis. Another patient might just have scalp disease or inverse psoriasis on a limited body area.
Currently, the Psoriasis Area and Severity Index (PASI), Physician Global Assessment (PGA) and Body Surface Area (BSA) assessments classify mild, moderate, and severe psoriasis, “with the majority of people out there in the world with mild psoriasis,” Dr. Qureshi said. A new measure called the Comprehensive Assessment of the Psoriasis Patient (CAPP) “captures more people with moderate to severe disease.”
CAPP includes a measure of plaque disease, palmoplantar, nail, scale, inverse, and genital psoriasis. “Where PASI fails, we hope the CAPP meets this unmet need,” said Dr. Merola, codirector of the Center for Skin and Related Musculoskeletal Diseases, a combined clinic at Brigham and Women’s Hospital in Boston. The two highest phenotypic scores are added to the plaque score for a final CAPP score. “It’s easy to use.”
A newly announced genital psoriasis component of CAPP measures any suprapubic, perineal, and genital involvement. Thickness, scale, and severity are included in CAPP, as well as secondary skin changes like fissuring or erosion. Then the score is equally weighted with the patient reported outcomes of pain and effect on intimacy rated on a simple visual analog scale.
Dr. Merola, Dr. Qureshi, and their colleagues collaborated on a study looking at the prevalence of nonplaque psoriasis among almost 4,000 patients (Clin Exp Dermatol. 2016;41:486-9).
“It surprised us to see such a high prevalence of inverse disease, almost 24%,” Dr. Merola said. “Many of these patients have two nonplaque phenotypes. It’s also important because it seems like there is an increased psoriatic arthritis risk.”
“The nail story and the scalp story have been out there a while, but looking at inverse disease there was a fairly high hazard ratio [2.07] for development of psoriatic arthritis.”
Proposing a polyphenotype psoriasis clinical trial
“I will end with a recommendation for a polyphenotype psoriasis clinical trial, to be really controversial,” Dr. Qureshi said. “We want to capture only the people who qualify as moderate to severe with the new measure and look at them before and after therapy.” He added participants would be “people out there in clinic who are currently not receiving treatment.”
During the Q&A, a meeting attendee asked if the investigators could recruit enough patients with nonplaque psoriasis. “We think it’s about 15%-23%,” Dr. Qureshi said. “The only type we cannot capture well is the palmoplantar phenotype because of its really low prevalence.”
AT 2016 GRAPPA ANNUAL MEETING
Key clinical point: The Comprehensive Assessment of the Psoriasis Patient measure could expand the number of patients with moderate to severe disease.
Major finding: Up to 24% of psoriasis patients can present with nonplaque psoriasis.
Data source: A study looking at the prevalence of nonplaque psoriasis among almost 4,000 patients.
Disclosures: Dr. Qureshi and Dr. Merola had no relevant disclosures.

Migraine Presentation Differs in Men and Women
SAN DIEGO—Men with migraine have fewer headache days per month, less disability, and less allodynia than women with migraine, according to research presented at the 58th Annual Scientific Meeting of the American Headache Society. “Nonetheless, migraine is disabling in men,” and physicians may be less likely to recognize migraine in men than in women, said Ann I. Scher, PhD, Professor of Preventive Medicine and Biostatistics and affiliated with Uniformed Services University of the Health Sciences in Bethesda, Maryland. In addition, men who have episodic migraine are more likely to transition from episodic to chronic migraine over one year of follow-up than women, she said.

Ann I. Scher, PhD
Despite the fact that migraine may be the most common neurologic condition in men, “the perception that migraine is a woman’s disease may contribute to migraine stigma and deny men access to diagnosis and treatment,” Dr. Scher said.
To assess sex differences in migraine, Dr. Scher and colleagues analyzed data from the Chronic Migraine Epidemiology and Outcomes (CaMEO) study. Participants completed validated online questionnaires and were broadly representative of the United States population’s demographic characteristics. Questionnaires assessed sociodemographics, headache features, headache-related disability, symptom severity, cutaneous allodynia, and treatment.
A More Severe Phenotype
The researchers included in their analysis 16,789 respondents who met modified International Classification of Headache Disorders, 3rd edition beta migraine criteria. Of the participants with migraine, 4,294 (25.6%) were men, and 12,495 (74.4%) were women. Compared with women, men were slightly older at enrollment (42.0 vs 40.8). Men and women with migraine were equally likely to be currently employed.
Women had about one more headache day per month than men (five vs four). Migraine Disability Assessment Scale (MIDAS) scores were generally lower in men than in women. For example, 15.7% of men were in the highest MIDAS disability category, compared with 24.1% of women. Significantly fewer men than women reported allodynia (32.6% vs 49.7%). A smaller proportion of men than women had chronic migraine, defined as 15 or more headache days per month (6.5% vs 9.6%). “Generally, women had a more severe phenotype than men,” Dr. Scher said.
Treatment Patterns
Men were slightly less likely than women to report currently seeing a doctor to manage their headaches (28.6% vs 31.1%). “What was striking, among those who did consult with a physician, the women were considerably more likely to receive a diagnosis of migraine,” Dr. Scher said. Researchers found that 59.2% of men received a diagnosis of migraine, compared with 77.7% of women.
Men were less likely than women to use prescription medication for headache (24.1% vs 28.2%), including acute prescription medications (16.5% vs 22.0%). About 12% of men and women used prescription preventives.
In the CaMEO study, participants completed questionnaires at baseline and at three, six, nine, and 12 months, and headache frequency was measured at each time point. Compared with women, men were at increased risk of converting to chronic migraine at all time points. This finding persisted after adjustment for various factors, including BMI, headache frequency, depression, and anxiety, Dr. Scher said. The magnitude of the hazard ratio varied at each time, however, and the researchers still are trying to determine the best way to assess the risk of converting to chronic migraine, Dr. Scher said.
The CaMEO study was funded by Allergan.
—Jake Remaly
Suggested Reading
Lipton RB, Manack Adams A, Buse DC, et al. A comparison of the Chronic Migraine Epidemiology and Outcomes (CaMEO) study and American Migraine Prevalence and Prevention (AMPP) study: demographics and headache-related disability. Headache. 2016 Jun 28 [Epub ahead of print].
SAN DIEGO—Men with migraine have fewer headache days per month, less disability, and less allodynia than women with migraine, according to research presented at the 58th Annual Scientific Meeting of the American Headache Society. “Nonetheless, migraine is disabling in men,” and physicians may be less likely to recognize migraine in men than in women, said Ann I. Scher, PhD, Professor of Preventive Medicine and Biostatistics and affiliated with Uniformed Services University of the Health Sciences in Bethesda, Maryland. In addition, men who have episodic migraine are more likely to transition from episodic to chronic migraine over one year of follow-up than women, she said.
Ann I. Scher, PhD
Despite the fact that migraine may be the most common neurologic condition in men, “the perception that migraine is a woman’s disease may contribute to migraine stigma and deny men access to diagnosis and treatment,” Dr. Scher said.
To assess sex differences in migraine, Dr. Scher and colleagues analyzed data from the Chronic Migraine Epidemiology and Outcomes (CaMEO) study. Participants completed validated online questionnaires and were broadly representative of the United States population’s demographic characteristics. Questionnaires assessed sociodemographics, headache features, headache-related disability, symptom severity, cutaneous allodynia, and treatment.
A More Severe Phenotype
The researchers included in their analysis 16,789 respondents who met modified International Classification of Headache Disorders, 3rd edition beta migraine criteria. Of the participants with migraine, 4,294 (25.6%) were men, and 12,495 (74.4%) were women. Compared with women, men were slightly older at enrollment (42.0 vs 40.8). Men and women with migraine were equally likely to be currently employed.
Women had about one more headache day per month than men (five vs four). Migraine Disability Assessment Scale (MIDAS) scores were generally lower in men than in women. For example, 15.7% of men were in the highest MIDAS disability category, compared with 24.1% of women. Significantly fewer men than women reported allodynia (32.6% vs 49.7%). A smaller proportion of men than women had chronic migraine, defined as 15 or more headache days per month (6.5% vs 9.6%). “Generally, women had a more severe phenotype than men,” Dr. Scher said.
Treatment Patterns
Men were slightly less likely than women to report currently seeing a doctor to manage their headaches (28.6% vs 31.1%). “What was striking, among those who did consult with a physician, the women were considerably more likely to receive a diagnosis of migraine,” Dr. Scher said. Researchers found that 59.2% of men received a diagnosis of migraine, compared with 77.7% of women.
Men were less likely than women to use prescription medication for headache (24.1% vs 28.2%), including acute prescription medications (16.5% vs 22.0%). About 12% of men and women used prescription preventives.
In the CaMEO study, participants completed questionnaires at baseline and at three, six, nine, and 12 months, and headache frequency was measured at each time point. Compared with women, men were at increased risk of converting to chronic migraine at all time points. This finding persisted after adjustment for various factors, including BMI, headache frequency, depression, and anxiety, Dr. Scher said. The magnitude of the hazard ratio varied at each time, however, and the researchers still are trying to determine the best way to assess the risk of converting to chronic migraine, Dr. Scher said.
The CaMEO study was funded by Allergan.
—Jake Remaly
SAN DIEGO—Men with migraine have fewer headache days per month, less disability, and less allodynia than women with migraine, according to research presented at the 58th Annual Scientific Meeting of the American Headache Society. “Nonetheless, migraine is disabling in men,” and physicians may be less likely to recognize migraine in men than in women, said Ann I. Scher, PhD, Professor of Preventive Medicine and Biostatistics and affiliated with Uniformed Services University of the Health Sciences in Bethesda, Maryland. In addition, men who have episodic migraine are more likely to transition from episodic to chronic migraine over one year of follow-up than women, she said.
Ann I. Scher, PhD
Despite the fact that migraine may be the most common neurologic condition in men, “the perception that migraine is a woman’s disease may contribute to migraine stigma and deny men access to diagnosis and treatment,” Dr. Scher said.
To assess sex differences in migraine, Dr. Scher and colleagues analyzed data from the Chronic Migraine Epidemiology and Outcomes (CaMEO) study. Participants completed validated online questionnaires and were broadly representative of the United States population’s demographic characteristics. Questionnaires assessed sociodemographics, headache features, headache-related disability, symptom severity, cutaneous allodynia, and treatment.
A More Severe Phenotype
The researchers included in their analysis 16,789 respondents who met modified International Classification of Headache Disorders, 3rd edition beta migraine criteria. Of the participants with migraine, 4,294 (25.6%) were men, and 12,495 (74.4%) were women. Compared with women, men were slightly older at enrollment (42.0 vs 40.8). Men and women with migraine were equally likely to be currently employed.
Women had about one more headache day per month than men (five vs four). Migraine Disability Assessment Scale (MIDAS) scores were generally lower in men than in women. For example, 15.7% of men were in the highest MIDAS disability category, compared with 24.1% of women. Significantly fewer men than women reported allodynia (32.6% vs 49.7%). A smaller proportion of men than women had chronic migraine, defined as 15 or more headache days per month (6.5% vs 9.6%). “Generally, women had a more severe phenotype than men,” Dr. Scher said.
Treatment Patterns
Men were slightly less likely than women to report currently seeing a doctor to manage their headaches (28.6% vs 31.1%). “What was striking, among those who did consult with a physician, the women were considerably more likely to receive a diagnosis of migraine,” Dr. Scher said. Researchers found that 59.2% of men received a diagnosis of migraine, compared with 77.7% of women.
Men were less likely than women to use prescription medication for headache (24.1% vs 28.2%), including acute prescription medications (16.5% vs 22.0%). About 12% of men and women used prescription preventives.
In the CaMEO study, participants completed questionnaires at baseline and at three, six, nine, and 12 months, and headache frequency was measured at each time point. Compared with women, men were at increased risk of converting to chronic migraine at all time points. This finding persisted after adjustment for various factors, including BMI, headache frequency, depression, and anxiety, Dr. Scher said. The magnitude of the hazard ratio varied at each time, however, and the researchers still are trying to determine the best way to assess the risk of converting to chronic migraine, Dr. Scher said.
The CaMEO study was funded by Allergan.
—Jake Remaly
Suggested Reading
Lipton RB, Manack Adams A, Buse DC, et al. A comparison of the Chronic Migraine Epidemiology and Outcomes (CaMEO) study and American Migraine Prevalence and Prevention (AMPP) study: demographics and headache-related disability. Headache. 2016 Jun 28 [Epub ahead of print].
Suggested Reading
Lipton RB, Manack Adams A, Buse DC, et al. A comparison of the Chronic Migraine Epidemiology and Outcomes (CaMEO) study and American Migraine Prevalence and Prevention (AMPP) study: demographics and headache-related disability. Headache. 2016 Jun 28 [Epub ahead of print].

Children under 6 with factor XIII deficiency had no major bleeds with recombinant product
ORLANDO –A recombinant form of factor XIII was effective at preventing serious bleeding episodes in young children with factor XIII-A subunit deficiency, a rare and serious bleeding disorder.
In a small international phase III trial, there were no major bleeding episodes among six young children treated for at least 1 year with recombinant factor XIII (rFXIII; trade name Tretten), reported Susan L. Kearney, MD, of Children’s Hospitals and Clinics of Minnesota in Minneapolis.
“Prophylaxis was effective. The annualized bleeding rate was zero and the mean trough [FXIII activity] was greater than 10%,” she said at a moderated poster session at the World Federation of Hemophilia World Congress. “We feel that recombinant factor XIII is safe and effective in pediatric subjects less than 6 years of age with congenital factor XIII-A subunit deficiency, similar to the older age cohort.”
Factor XIII-A subunit deficiency is a rare and serious heritable bleeding disorder associated with spontaneous intracranial hemorrhage and other unpredictable types of serious bleeding.
In a previous phase III trial, 77 patients, ranging in age from 7 to 60 years, received rFXIII for bleeding prophylaxis. When given monthly, the recombinant factor was effective at preventing serious bleeding in 90% of patients. The most commonly reported adverse events were headache, pain in the extremities, and injection site pain.
Based on these results, the Food and Drug Administration granted rFXIII orphan-drug designation for treatment of patients 6 and older with factor XIII-A subunit deficiency.
In the trial reported here, investigators from the United States, United Kingdom, Israel, and Denmark enrolled three boys and three girls under age 6 who had previously completed a single dose efficacy and safety study of rFXIII. The patients received intravenous rFXIII at a dose of 35 IU/kg every 28 days for a minimum of 52 weeks.
The total treatment duration ranged from 1.8 to 3.5 years, for a total of 16.6 patient years.
There were no thromboembolic events or systemic allergic reactions, the primary safety endpoint of the study. One patient experienced three incidences of atopic dermatitis, however; two serious adverse events related to head injuries from falls during play occurred in one patient, who did not experience intracranial hemorrhage.
Two adverse events were deemed to be probably or possibly related to rFXIII: a case of viral gastroenteritis affected one patient who recovered without a change in dose, and mild fluctuating lymphocytopenia seen at baseline persisted in another patient throughout the trial.
There were no inhibitory or noninhibitory antibodies to rFXIII detected in any patient during the trial, and there were no bleeding episodes requiring additional treatment. The 14 minor bleeding episodes seen in five patients did not require treatment with an FXIII-containing product, the authors noted.
“It’s a very rare disorder, but ... the phenotype is quite severe and patients are severely affected. So this product is very useful,” said Lakshmi Srivaths, MD, a pediatric hematologist at Texas Children’s Hospital in Houston. She was not involved in the study. Unlike patients with hemophilia A or B, who require frequent factor infusions, the long half-life of this product means patients need just once-a-month infusions “that change the phenotype very significantly.”
Dr. Kearney disclosed grant/research support from Novo Nordisk, which funded the study. Some coauthors reported consulting or employment with the company.
ORLANDO –A recombinant form of factor XIII was effective at preventing serious bleeding episodes in young children with factor XIII-A subunit deficiency, a rare and serious bleeding disorder.
In a small international phase III trial, there were no major bleeding episodes among six young children treated for at least 1 year with recombinant factor XIII (rFXIII; trade name Tretten), reported Susan L. Kearney, MD, of Children’s Hospitals and Clinics of Minnesota in Minneapolis.
“Prophylaxis was effective. The annualized bleeding rate was zero and the mean trough [FXIII activity] was greater than 10%,” she said at a moderated poster session at the World Federation of Hemophilia World Congress. “We feel that recombinant factor XIII is safe and effective in pediatric subjects less than 6 years of age with congenital factor XIII-A subunit deficiency, similar to the older age cohort.”
Factor XIII-A subunit deficiency is a rare and serious heritable bleeding disorder associated with spontaneous intracranial hemorrhage and other unpredictable types of serious bleeding.
In a previous phase III trial, 77 patients, ranging in age from 7 to 60 years, received rFXIII for bleeding prophylaxis. When given monthly, the recombinant factor was effective at preventing serious bleeding in 90% of patients. The most commonly reported adverse events were headache, pain in the extremities, and injection site pain.
Based on these results, the Food and Drug Administration granted rFXIII orphan-drug designation for treatment of patients 6 and older with factor XIII-A subunit deficiency.
In the trial reported here, investigators from the United States, United Kingdom, Israel, and Denmark enrolled three boys and three girls under age 6 who had previously completed a single dose efficacy and safety study of rFXIII. The patients received intravenous rFXIII at a dose of 35 IU/kg every 28 days for a minimum of 52 weeks.
The total treatment duration ranged from 1.8 to 3.5 years, for a total of 16.6 patient years.
There were no thromboembolic events or systemic allergic reactions, the primary safety endpoint of the study. One patient experienced three incidences of atopic dermatitis, however; two serious adverse events related to head injuries from falls during play occurred in one patient, who did not experience intracranial hemorrhage.
Two adverse events were deemed to be probably or possibly related to rFXIII: a case of viral gastroenteritis affected one patient who recovered without a change in dose, and mild fluctuating lymphocytopenia seen at baseline persisted in another patient throughout the trial.
There were no inhibitory or noninhibitory antibodies to rFXIII detected in any patient during the trial, and there were no bleeding episodes requiring additional treatment. The 14 minor bleeding episodes seen in five patients did not require treatment with an FXIII-containing product, the authors noted.
“It’s a very rare disorder, but ... the phenotype is quite severe and patients are severely affected. So this product is very useful,” said Lakshmi Srivaths, MD, a pediatric hematologist at Texas Children’s Hospital in Houston. She was not involved in the study. Unlike patients with hemophilia A or B, who require frequent factor infusions, the long half-life of this product means patients need just once-a-month infusions “that change the phenotype very significantly.”
Dr. Kearney disclosed grant/research support from Novo Nordisk, which funded the study. Some coauthors reported consulting or employment with the company.
ORLANDO –A recombinant form of factor XIII was effective at preventing serious bleeding episodes in young children with factor XIII-A subunit deficiency, a rare and serious bleeding disorder.
In a small international phase III trial, there were no major bleeding episodes among six young children treated for at least 1 year with recombinant factor XIII (rFXIII; trade name Tretten), reported Susan L. Kearney, MD, of Children’s Hospitals and Clinics of Minnesota in Minneapolis.
“Prophylaxis was effective. The annualized bleeding rate was zero and the mean trough [FXIII activity] was greater than 10%,” she said at a moderated poster session at the World Federation of Hemophilia World Congress. “We feel that recombinant factor XIII is safe and effective in pediatric subjects less than 6 years of age with congenital factor XIII-A subunit deficiency, similar to the older age cohort.”
Factor XIII-A subunit deficiency is a rare and serious heritable bleeding disorder associated with spontaneous intracranial hemorrhage and other unpredictable types of serious bleeding.
In a previous phase III trial, 77 patients, ranging in age from 7 to 60 years, received rFXIII for bleeding prophylaxis. When given monthly, the recombinant factor was effective at preventing serious bleeding in 90% of patients. The most commonly reported adverse events were headache, pain in the extremities, and injection site pain.
Based on these results, the Food and Drug Administration granted rFXIII orphan-drug designation for treatment of patients 6 and older with factor XIII-A subunit deficiency.
In the trial reported here, investigators from the United States, United Kingdom, Israel, and Denmark enrolled three boys and three girls under age 6 who had previously completed a single dose efficacy and safety study of rFXIII. The patients received intravenous rFXIII at a dose of 35 IU/kg every 28 days for a minimum of 52 weeks.
The total treatment duration ranged from 1.8 to 3.5 years, for a total of 16.6 patient years.
There were no thromboembolic events or systemic allergic reactions, the primary safety endpoint of the study. One patient experienced three incidences of atopic dermatitis, however; two serious adverse events related to head injuries from falls during play occurred in one patient, who did not experience intracranial hemorrhage.
Two adverse events were deemed to be probably or possibly related to rFXIII: a case of viral gastroenteritis affected one patient who recovered without a change in dose, and mild fluctuating lymphocytopenia seen at baseline persisted in another patient throughout the trial.
There were no inhibitory or noninhibitory antibodies to rFXIII detected in any patient during the trial, and there were no bleeding episodes requiring additional treatment. The 14 minor bleeding episodes seen in five patients did not require treatment with an FXIII-containing product, the authors noted.
“It’s a very rare disorder, but ... the phenotype is quite severe and patients are severely affected. So this product is very useful,” said Lakshmi Srivaths, MD, a pediatric hematologist at Texas Children’s Hospital in Houston. She was not involved in the study. Unlike patients with hemophilia A or B, who require frequent factor infusions, the long half-life of this product means patients need just once-a-month infusions “that change the phenotype very significantly.”
Dr. Kearney disclosed grant/research support from Novo Nordisk, which funded the study. Some coauthors reported consulting or employment with the company.
AT WFH 2016 WORLD CONGRESS
Key clinical point: A recombinant form of factor XIII was effective at preventing serious bleeding episodes in young children with factor XIII-A subunit deficiency.
Major finding: No bleeds occurred within a year in children with factor XIII-A subunit deficiency.
Data source: Open-label international phase III trial in three boys and three girls under age 6.
Disclosures: Dr. Kearney disclosed grant/research support from Novo Nordisk, which funded the study. Some coauthors reported consulting or employment with the company.
Why Are So Few Patients With Pharmacoresistant Epilepsy Referred to Epilepsy Centers?
VANCOUVER—Neurologists’ best chance to reduce disability in patients with pharmacoresistant epilepsy lies in early recognition of pharmacoresistance and early referral of patients to full-service epilepsy centers, according to a lecture delivered at the 68th Annual Meeting of the American Academy of Neurology (AAN).
Fewer than 1% of patients with refractory epilepsy are referred to epilepsy centers each year, and many patients are referred too late to significantly affect disability, said Jerome Engel Jr, MD, PhD, Jonathan Sinay Distinguished Professor of Neurology, Neurobiology, and Psychiatry and Biobehavioral Sciences and Director of the Seizure Disorder Center at the David Geffen School of Medicine at the University of California, Los Angeles (UCLA). Misconceptions about epilepsy centers and epilepsy surgery may be partly responsible for the dearth of referrals.
“I think a major misconception—and I have to take partial blame for this because of all the talking I’ve done about surgery in the last three decades or more—is that all epilepsy centers do is surgery. I think a common attitude among referring neurologists is, ‘My patient is not a surgical candidate or doesn’t want surgery, so there’s no reason to refer him or her to an epilepsy center,’” Dr. Engel said.
Beyond performing surgery, specialized centers can recognize pseudopharmacoresistance, diagnose nonepileptic seizures, identify specific epilepsy syndromes, and provide psychosocial support. Dr. Engel noted that, given his position as the director of an epilepsy center, his message might seem self-serving and critical of his audience, but he asked neurologists to keep an open mind. “Early, effective intervention offers the best chance to prevent irreversible psychosocial problems, a lifetime of disability, and premature death,” he said.
A Serious Burden
Refractory epilepsy can lead to developmental delays and interfere with interpersonal and vocational skills. Patients may have interictal behavioral problems, most commonly depression, or neurologic impairment. “The mortality rate for uncontrolled epilepsy is five to 10 times that of the general population, not only because of sudden unexpected death in epilepsy and accidents, but also suicide,” Dr. Engel said. Although more than 20 new antiseizure drugs have been approved in the last three decades, the percentage of patients with pharmacoresistant epilepsy has not changed.
According to the International League Against Epilepsy, a patient has drug-resistant epilepsy when he or she fails two trials of appropriate antiseizure drugs, either alone or in combination, due to inefficacy and not intolerance. Of the approximately three million people with epilepsy in the United States, about one-third have pharmacoresistant epilepsy. According to the National Association of Epilepsy Centers, about 4,000 patients are referred to epilepsy centers per year, Dr. Engel said.
The publication of evidence-based recommendations for epilepsy center referrals has not had an obvious effect on clinical practice. In 2003, Dr. Engel and colleagues in the Quality Standards Subcommittee of the AAN published a practice parameter for temporal lobe resections. Based on a randomized controlled trial and 24 case series, they concluded that surgery provides greater benefit than medical treatment, with risks that are at least comparable. The trial by Wiebe et al found that, after a year, 64% of the patients who had surgery were seizure-free, compared with 8% of patients in the medical arm. An analysis of the case series, which included 1,952 patients, yielded nearly the same results. They recommended that patients with drug-resistant temporal lobe seizures be referred to an epilepsy center, and that surgical candidates undergo surgery.
The practice parameter, however, did not lead to earlier referrals for surgery evaluations at UCLA’s epilepsy center. Haneef et al found that in the four years before publication of the practice parameter, patients’ average time from diagnosis to referral was 17 years, compared with 18.6 years in the four years after publication.
More Than Surgery
Epilepsy centers can identify pseudopharmacoresistance in patients who are not compliant in taking their medication or who are prescribed the wrong drugs or dosage. Furthermore, a third of patients admitted to epilepsy centers do not have epilepsy, Dr. Engel said. Patients’ apparent pharmacoresistance may be caused by lifestyle issues, such as substance abuse or frequent sleep deprivation, or other conditions.
Many patients, even if their condition improves, continue to have seizures and disability. “Epilepsy centers have psychologists, psychiatrists, social workers, and counselors who help patients deal with problems that are caused by their seizures,” Dr. Engel said.
Other treatments that epilepsy centers provide include experimental drug trials and stimulation techniques, such as vagus nerve stimulation, trigeminal nerve stimulation, and responsive neurostimulation. In addition, epilepsy centers can identify patients who might benefit from the ketogenic diet or modified Atkins diet.
Surgical Candidates?
Various common misconceptions about contraindications for surgery also may prevent patients from being referred to specialized centers. For instance, bilateral interictal spikes are not a contraindication for surgery because in most patients with this finding, all seizures originate from one side. A normal MRI is not a contraindication for surgery because techniques such as PET-MRI fusion and magnetoencephalography can identify epileptogenic regions that do not appear on MRI. If a patient has multiple or diffuse lesions, only one of the lesions might be epileptogenic, or if a patient has a large lesion, only part of the lesion might be epileptogenic. When an abnormality is in a primary cortex, there are ways to identify cortex that cannot be removed and still obtain good results with surgery, Dr. Engel said.
In patients with existing memory deficits, surgery typically does not worsen memory and can improve it. In patients who do not have memory deficits, however, surgery of the language-dominant temporal lobe may worsen memory, and this complication may be a concern.
Chronic psychosis is not a contraindication for surgery. “If it’s postictal psychosis, it will go away after seizures stop. If it’s interictal psychosis, a patient with schizophrenia is better off without epilepsy than with epilepsy, even if they’ll still have schizophrenia,” Dr. Engel said. An IQ less than 70 was once considered a contraindication for surgery, but that is no longer necessarily the case.
Another issue that may be increasingly common is the removal of lesions at hospitals that perform few epilepsy surgeries (ie, low-volume hospitals). “The outcomes are not as good. There’s more morbidity, and there’s mortality, which we don’t see very much in the epilepsy centers,” Dr. Engel said. In addition, many lesions are incidental findings. “You really need to demonstrate when you see a lesion that that lesion is the source of the habitual seizures,” Dr. Engel said.
In an analysis of 6,200 epilepsy surgery procedures published in the August issue of Epilepsy Research, Rolston et al observed higher rates of adverse events when low- and high-volume centers were examined together, compared with high-volume centers alone.
ERSET Outcomes
Some 100,000 to 500,000 patients with epilepsy in the US are potential surgical candidates, and about 2,000 epilepsy surgeries are performed per year. Surgical outcomes have improved over the last few decades, and new surgical techniques have been developed, including laser thermal ablation, which can be performed through a small drill hole, Dr. Engel said.
To determine whether surgery soon after failure of two antiepileptic drug trials is superior to continued medical management, Dr. Engel and colleagues conducted the Early Randomized Surgical Epilepsy Trial (ERSET), which was published in JAMA in 2012. The multicenter trial was stopped early due to slow study recruitment. It included 38 participants (ages 12 and older, 18 men) who had mesial temporal lobe epilepsy and disabling seizures for no more than two consecutive years after their two failed drug trials. Only surgical candidates were randomized. In an intent-to-treat analysis, all of the patients in the medical arm continued to have seizures, while 11 patients in the surgical arm (73%) were seizure-free during year two of follow-up. In an analysis that included only patients for whom researchers had complete data, 85% of patients in the surgical group were seizure-free. Compared with the medical treatment group, patients in the surgical group had improved quality of life. Adverse events included three episodes of status epilepticus in the medical group and a transient stroke in the surgical group. Memory decline occurred in four participants after surgery, but the sample was too small to assess the effect of treatment on cognitive function.
“All people with refractory epilepsy deserve a timely consultation at an epilepsy center,” Dr. Engel said. “Many are not refractory. Many are surgical candidates. And the remainder of them deserve psychosocial support.”
—Jake Remaly
Suggested Reading
Engel J Jr, McDermott MP, Wiebe S, et al. Early surgical therapy for drug-resistant temporal lobe epilepsy: a randomized trial. JAMA. 2012;307(9):922-930.
Engel J Jr, Wiebe S, French J, et al. Practice parameter: temporal lobe and localized neocortical resections for epilepsy: report of the Quality Standards Subcommittee of the American Academy of Neurology, in association with the American Epilepsy Society and the American Association of Neurological Surgeons. Neurology. 2003;60(4):538-547.
Haneef Z, Stern J, Dewar S, Engel J Jr. Referral pattern for epilepsy surgery after evidence-based recommendations: a retrospective study. Neurology. 2010;75(8):699-704.
Rolston JD, Englot DJ, Knowlton RC, Chang EF. Rate and complications of adult epilepsy surgery in North America: Analysis of multiple databases. Epilepsy Res. 2016;124:55-62.
VANCOUVER—Neurologists’ best chance to reduce disability in patients with pharmacoresistant epilepsy lies in early recognition of pharmacoresistance and early referral of patients to full-service epilepsy centers, according to a lecture delivered at the 68th Annual Meeting of the American Academy of Neurology (AAN).
Fewer than 1% of patients with refractory epilepsy are referred to epilepsy centers each year, and many patients are referred too late to significantly affect disability, said Jerome Engel Jr, MD, PhD, Jonathan Sinay Distinguished Professor of Neurology, Neurobiology, and Psychiatry and Biobehavioral Sciences and Director of the Seizure Disorder Center at the David Geffen School of Medicine at the University of California, Los Angeles (UCLA). Misconceptions about epilepsy centers and epilepsy surgery may be partly responsible for the dearth of referrals.
“I think a major misconception—and I have to take partial blame for this because of all the talking I’ve done about surgery in the last three decades or more—is that all epilepsy centers do is surgery. I think a common attitude among referring neurologists is, ‘My patient is not a surgical candidate or doesn’t want surgery, so there’s no reason to refer him or her to an epilepsy center,’” Dr. Engel said.
Beyond performing surgery, specialized centers can recognize pseudopharmacoresistance, diagnose nonepileptic seizures, identify specific epilepsy syndromes, and provide psychosocial support. Dr. Engel noted that, given his position as the director of an epilepsy center, his message might seem self-serving and critical of his audience, but he asked neurologists to keep an open mind. “Early, effective intervention offers the best chance to prevent irreversible psychosocial problems, a lifetime of disability, and premature death,” he said.
A Serious Burden
Refractory epilepsy can lead to developmental delays and interfere with interpersonal and vocational skills. Patients may have interictal behavioral problems, most commonly depression, or neurologic impairment. “The mortality rate for uncontrolled epilepsy is five to 10 times that of the general population, not only because of sudden unexpected death in epilepsy and accidents, but also suicide,” Dr. Engel said. Although more than 20 new antiseizure drugs have been approved in the last three decades, the percentage of patients with pharmacoresistant epilepsy has not changed.
According to the International League Against Epilepsy, a patient has drug-resistant epilepsy when he or she fails two trials of appropriate antiseizure drugs, either alone or in combination, due to inefficacy and not intolerance. Of the approximately three million people with epilepsy in the United States, about one-third have pharmacoresistant epilepsy. According to the National Association of Epilepsy Centers, about 4,000 patients are referred to epilepsy centers per year, Dr. Engel said.
The publication of evidence-based recommendations for epilepsy center referrals has not had an obvious effect on clinical practice. In 2003, Dr. Engel and colleagues in the Quality Standards Subcommittee of the AAN published a practice parameter for temporal lobe resections. Based on a randomized controlled trial and 24 case series, they concluded that surgery provides greater benefit than medical treatment, with risks that are at least comparable. The trial by Wiebe et al found that, after a year, 64% of the patients who had surgery were seizure-free, compared with 8% of patients in the medical arm. An analysis of the case series, which included 1,952 patients, yielded nearly the same results. They recommended that patients with drug-resistant temporal lobe seizures be referred to an epilepsy center, and that surgical candidates undergo surgery.
The practice parameter, however, did not lead to earlier referrals for surgery evaluations at UCLA’s epilepsy center. Haneef et al found that in the four years before publication of the practice parameter, patients’ average time from diagnosis to referral was 17 years, compared with 18.6 years in the four years after publication.
More Than Surgery
Epilepsy centers can identify pseudopharmacoresistance in patients who are not compliant in taking their medication or who are prescribed the wrong drugs or dosage. Furthermore, a third of patients admitted to epilepsy centers do not have epilepsy, Dr. Engel said. Patients’ apparent pharmacoresistance may be caused by lifestyle issues, such as substance abuse or frequent sleep deprivation, or other conditions.
Many patients, even if their condition improves, continue to have seizures and disability. “Epilepsy centers have psychologists, psychiatrists, social workers, and counselors who help patients deal with problems that are caused by their seizures,” Dr. Engel said.
Other treatments that epilepsy centers provide include experimental drug trials and stimulation techniques, such as vagus nerve stimulation, trigeminal nerve stimulation, and responsive neurostimulation. In addition, epilepsy centers can identify patients who might benefit from the ketogenic diet or modified Atkins diet.
Surgical Candidates?
Various common misconceptions about contraindications for surgery also may prevent patients from being referred to specialized centers. For instance, bilateral interictal spikes are not a contraindication for surgery because in most patients with this finding, all seizures originate from one side. A normal MRI is not a contraindication for surgery because techniques such as PET-MRI fusion and magnetoencephalography can identify epileptogenic regions that do not appear on MRI. If a patient has multiple or diffuse lesions, only one of the lesions might be epileptogenic, or if a patient has a large lesion, only part of the lesion might be epileptogenic. When an abnormality is in a primary cortex, there are ways to identify cortex that cannot be removed and still obtain good results with surgery, Dr. Engel said.
In patients with existing memory deficits, surgery typically does not worsen memory and can improve it. In patients who do not have memory deficits, however, surgery of the language-dominant temporal lobe may worsen memory, and this complication may be a concern.
Chronic psychosis is not a contraindication for surgery. “If it’s postictal psychosis, it will go away after seizures stop. If it’s interictal psychosis, a patient with schizophrenia is better off without epilepsy than with epilepsy, even if they’ll still have schizophrenia,” Dr. Engel said. An IQ less than 70 was once considered a contraindication for surgery, but that is no longer necessarily the case.
Another issue that may be increasingly common is the removal of lesions at hospitals that perform few epilepsy surgeries (ie, low-volume hospitals). “The outcomes are not as good. There’s more morbidity, and there’s mortality, which we don’t see very much in the epilepsy centers,” Dr. Engel said. In addition, many lesions are incidental findings. “You really need to demonstrate when you see a lesion that that lesion is the source of the habitual seizures,” Dr. Engel said.
In an analysis of 6,200 epilepsy surgery procedures published in the August issue of Epilepsy Research, Rolston et al observed higher rates of adverse events when low- and high-volume centers were examined together, compared with high-volume centers alone.
ERSET Outcomes
Some 100,000 to 500,000 patients with epilepsy in the US are potential surgical candidates, and about 2,000 epilepsy surgeries are performed per year. Surgical outcomes have improved over the last few decades, and new surgical techniques have been developed, including laser thermal ablation, which can be performed through a small drill hole, Dr. Engel said.
To determine whether surgery soon after failure of two antiepileptic drug trials is superior to continued medical management, Dr. Engel and colleagues conducted the Early Randomized Surgical Epilepsy Trial (ERSET), which was published in JAMA in 2012. The multicenter trial was stopped early due to slow study recruitment. It included 38 participants (ages 12 and older, 18 men) who had mesial temporal lobe epilepsy and disabling seizures for no more than two consecutive years after their two failed drug trials. Only surgical candidates were randomized. In an intent-to-treat analysis, all of the patients in the medical arm continued to have seizures, while 11 patients in the surgical arm (73%) were seizure-free during year two of follow-up. In an analysis that included only patients for whom researchers had complete data, 85% of patients in the surgical group were seizure-free. Compared with the medical treatment group, patients in the surgical group had improved quality of life. Adverse events included three episodes of status epilepticus in the medical group and a transient stroke in the surgical group. Memory decline occurred in four participants after surgery, but the sample was too small to assess the effect of treatment on cognitive function.
“All people with refractory epilepsy deserve a timely consultation at an epilepsy center,” Dr. Engel said. “Many are not refractory. Many are surgical candidates. And the remainder of them deserve psychosocial support.”
—Jake Remaly
VANCOUVER—Neurologists’ best chance to reduce disability in patients with pharmacoresistant epilepsy lies in early recognition of pharmacoresistance and early referral of patients to full-service epilepsy centers, according to a lecture delivered at the 68th Annual Meeting of the American Academy of Neurology (AAN).
Fewer than 1% of patients with refractory epilepsy are referred to epilepsy centers each year, and many patients are referred too late to significantly affect disability, said Jerome Engel Jr, MD, PhD, Jonathan Sinay Distinguished Professor of Neurology, Neurobiology, and Psychiatry and Biobehavioral Sciences and Director of the Seizure Disorder Center at the David Geffen School of Medicine at the University of California, Los Angeles (UCLA). Misconceptions about epilepsy centers and epilepsy surgery may be partly responsible for the dearth of referrals.
“I think a major misconception—and I have to take partial blame for this because of all the talking I’ve done about surgery in the last three decades or more—is that all epilepsy centers do is surgery. I think a common attitude among referring neurologists is, ‘My patient is not a surgical candidate or doesn’t want surgery, so there’s no reason to refer him or her to an epilepsy center,’” Dr. Engel said.
Beyond performing surgery, specialized centers can recognize pseudopharmacoresistance, diagnose nonepileptic seizures, identify specific epilepsy syndromes, and provide psychosocial support. Dr. Engel noted that, given his position as the director of an epilepsy center, his message might seem self-serving and critical of his audience, but he asked neurologists to keep an open mind. “Early, effective intervention offers the best chance to prevent irreversible psychosocial problems, a lifetime of disability, and premature death,” he said.
A Serious Burden
Refractory epilepsy can lead to developmental delays and interfere with interpersonal and vocational skills. Patients may have interictal behavioral problems, most commonly depression, or neurologic impairment. “The mortality rate for uncontrolled epilepsy is five to 10 times that of the general population, not only because of sudden unexpected death in epilepsy and accidents, but also suicide,” Dr. Engel said. Although more than 20 new antiseizure drugs have been approved in the last three decades, the percentage of patients with pharmacoresistant epilepsy has not changed.
According to the International League Against Epilepsy, a patient has drug-resistant epilepsy when he or she fails two trials of appropriate antiseizure drugs, either alone or in combination, due to inefficacy and not intolerance. Of the approximately three million people with epilepsy in the United States, about one-third have pharmacoresistant epilepsy. According to the National Association of Epilepsy Centers, about 4,000 patients are referred to epilepsy centers per year, Dr. Engel said.
The publication of evidence-based recommendations for epilepsy center referrals has not had an obvious effect on clinical practice. In 2003, Dr. Engel and colleagues in the Quality Standards Subcommittee of the AAN published a practice parameter for temporal lobe resections. Based on a randomized controlled trial and 24 case series, they concluded that surgery provides greater benefit than medical treatment, with risks that are at least comparable. The trial by Wiebe et al found that, after a year, 64% of the patients who had surgery were seizure-free, compared with 8% of patients in the medical arm. An analysis of the case series, which included 1,952 patients, yielded nearly the same results. They recommended that patients with drug-resistant temporal lobe seizures be referred to an epilepsy center, and that surgical candidates undergo surgery.
The practice parameter, however, did not lead to earlier referrals for surgery evaluations at UCLA’s epilepsy center. Haneef et al found that in the four years before publication of the practice parameter, patients’ average time from diagnosis to referral was 17 years, compared with 18.6 years in the four years after publication.
More Than Surgery
Epilepsy centers can identify pseudopharmacoresistance in patients who are not compliant in taking their medication or who are prescribed the wrong drugs or dosage. Furthermore, a third of patients admitted to epilepsy centers do not have epilepsy, Dr. Engel said. Patients’ apparent pharmacoresistance may be caused by lifestyle issues, such as substance abuse or frequent sleep deprivation, or other conditions.
Many patients, even if their condition improves, continue to have seizures and disability. “Epilepsy centers have psychologists, psychiatrists, social workers, and counselors who help patients deal with problems that are caused by their seizures,” Dr. Engel said.
Other treatments that epilepsy centers provide include experimental drug trials and stimulation techniques, such as vagus nerve stimulation, trigeminal nerve stimulation, and responsive neurostimulation. In addition, epilepsy centers can identify patients who might benefit from the ketogenic diet or modified Atkins diet.
Surgical Candidates?
Various common misconceptions about contraindications for surgery also may prevent patients from being referred to specialized centers. For instance, bilateral interictal spikes are not a contraindication for surgery because in most patients with this finding, all seizures originate from one side. A normal MRI is not a contraindication for surgery because techniques such as PET-MRI fusion and magnetoencephalography can identify epileptogenic regions that do not appear on MRI. If a patient has multiple or diffuse lesions, only one of the lesions might be epileptogenic, or if a patient has a large lesion, only part of the lesion might be epileptogenic. When an abnormality is in a primary cortex, there are ways to identify cortex that cannot be removed and still obtain good results with surgery, Dr. Engel said.
In patients with existing memory deficits, surgery typically does not worsen memory and can improve it. In patients who do not have memory deficits, however, surgery of the language-dominant temporal lobe may worsen memory, and this complication may be a concern.
Chronic psychosis is not a contraindication for surgery. “If it’s postictal psychosis, it will go away after seizures stop. If it’s interictal psychosis, a patient with schizophrenia is better off without epilepsy than with epilepsy, even if they’ll still have schizophrenia,” Dr. Engel said. An IQ less than 70 was once considered a contraindication for surgery, but that is no longer necessarily the case.
Another issue that may be increasingly common is the removal of lesions at hospitals that perform few epilepsy surgeries (ie, low-volume hospitals). “The outcomes are not as good. There’s more morbidity, and there’s mortality, which we don’t see very much in the epilepsy centers,” Dr. Engel said. In addition, many lesions are incidental findings. “You really need to demonstrate when you see a lesion that that lesion is the source of the habitual seizures,” Dr. Engel said.
In an analysis of 6,200 epilepsy surgery procedures published in the August issue of Epilepsy Research, Rolston et al observed higher rates of adverse events when low- and high-volume centers were examined together, compared with high-volume centers alone.
ERSET Outcomes
Some 100,000 to 500,000 patients with epilepsy in the US are potential surgical candidates, and about 2,000 epilepsy surgeries are performed per year. Surgical outcomes have improved over the last few decades, and new surgical techniques have been developed, including laser thermal ablation, which can be performed through a small drill hole, Dr. Engel said.
To determine whether surgery soon after failure of two antiepileptic drug trials is superior to continued medical management, Dr. Engel and colleagues conducted the Early Randomized Surgical Epilepsy Trial (ERSET), which was published in JAMA in 2012. The multicenter trial was stopped early due to slow study recruitment. It included 38 participants (ages 12 and older, 18 men) who had mesial temporal lobe epilepsy and disabling seizures for no more than two consecutive years after their two failed drug trials. Only surgical candidates were randomized. In an intent-to-treat analysis, all of the patients in the medical arm continued to have seizures, while 11 patients in the surgical arm (73%) were seizure-free during year two of follow-up. In an analysis that included only patients for whom researchers had complete data, 85% of patients in the surgical group were seizure-free. Compared with the medical treatment group, patients in the surgical group had improved quality of life. Adverse events included three episodes of status epilepticus in the medical group and a transient stroke in the surgical group. Memory decline occurred in four participants after surgery, but the sample was too small to assess the effect of treatment on cognitive function.
“All people with refractory epilepsy deserve a timely consultation at an epilepsy center,” Dr. Engel said. “Many are not refractory. Many are surgical candidates. And the remainder of them deserve psychosocial support.”
—Jake Remaly
Suggested Reading
Engel J Jr, McDermott MP, Wiebe S, et al. Early surgical therapy for drug-resistant temporal lobe epilepsy: a randomized trial. JAMA. 2012;307(9):922-930.
Engel J Jr, Wiebe S, French J, et al. Practice parameter: temporal lobe and localized neocortical resections for epilepsy: report of the Quality Standards Subcommittee of the American Academy of Neurology, in association with the American Epilepsy Society and the American Association of Neurological Surgeons. Neurology. 2003;60(4):538-547.
Haneef Z, Stern J, Dewar S, Engel J Jr. Referral pattern for epilepsy surgery after evidence-based recommendations: a retrospective study. Neurology. 2010;75(8):699-704.
Rolston JD, Englot DJ, Knowlton RC, Chang EF. Rate and complications of adult epilepsy surgery in North America: Analysis of multiple databases. Epilepsy Res. 2016;124:55-62.
Suggested Reading
Engel J Jr, McDermott MP, Wiebe S, et al. Early surgical therapy for drug-resistant temporal lobe epilepsy: a randomized trial. JAMA. 2012;307(9):922-930.
Engel J Jr, Wiebe S, French J, et al. Practice parameter: temporal lobe and localized neocortical resections for epilepsy: report of the Quality Standards Subcommittee of the American Academy of Neurology, in association with the American Epilepsy Society and the American Association of Neurological Surgeons. Neurology. 2003;60(4):538-547.
Haneef Z, Stern J, Dewar S, Engel J Jr. Referral pattern for epilepsy surgery after evidence-based recommendations: a retrospective study. Neurology. 2010;75(8):699-704.
Rolston JD, Englot DJ, Knowlton RC, Chang EF. Rate and complications of adult epilepsy surgery in North America: Analysis of multiple databases. Epilepsy Res. 2016;124:55-62.

ACO Insider: Not ready for an ACO? Think CPC+
The Centers for Medicare & Medicaid Services in April announced its newest initiative, Comprehensive Primary Care Plus, to target primary care practices of varying capabilities to participate in an innovative payment model designed to support the delivery of comprehensive primary care that rewards value and quality.
“Strengthening primary care is critical to an effective health care system,” said Patrick Conway, MD, CMS deputy administrator and chief medical officer. “By supporting primary care doctors and clinicians to spend time with patients, serve patients’ needs outside of the office visit, and better coordinate care with specialists, we can continue to build a health care system that results in healthier people and smarter spending of our health care dollars.”

As readers of this column know, these are also the engines of accountable care organization success. So, if you and your patient-centered medical home are not in a Medicare ACO, this gets you going on high-value activities – and pays you monthly to do it.
The rub is that once you are in the Medicare Shared Savings Program, you can’t continue with this initiative. But, it’s a great “on ramp” to prep you for ACO success. You get monthly payments instead of waiting 18 months for shared savings that you may or may not get under the Medicare Shared Savings Program.
CPC+ is an advanced primary medical home model, created from lessons learned in the Comprehensive Primary Care Initiative and the Multi-Payer Advanced Primary Care Practice Demonstration. Similar to these programs, multi-payer engagement is an essential component of the model.
In the CPC+ model, the CMS intends to nationally solicit a variety of payers committed to strengthening primary care in up to 20 regions and accept up to 5,000 practices to participate in those regions. The CPC+ program is further evidence that primary care should not only be a fundamental component to moving our health care system to one that awards clinicians based on the quality, not quantity, of care they give patients, but that payment redesign must provide flexibility to accommodate the diverse needs of primary care practices.
What to know about payment
To provide this flexibility and to attract practices of varying capabilities and levels of experience, the CPC+ program offers two tracks with different payment options, which include a monthly care management fee, comprehensive primary care payments, and performance-based incentive payments.
In track 1, the CMS will pay practices a risk-adjusted prospective monthly care management fee ($15 per beneficiary per month [PBPM] average across four risk tiers), in addition to the fee-for-service payments under the Medicare Physician Fee Schedule for activities.
In track 2, the Medicare monthly care management fees will average $28 PBPM across five risk tiers, which includes a $100 care management fee to support care for patients with the most complex needs. Instead of full Medicare fee-for-service payments for evaluation and management services, track 2 practices will receive a hybrid of reduced Medicare fee-for-service payments and up-front comprehensive primary care payments for those services.
In addition, the CMS is providing incentive payments at $2.50 PBPM for track 1 and $4 PBPM for track 2, based on practice performance on utilization metrics and quality, measured at the practice level. While these payments are prepaid at the beginning of a performance year, they are subject to recoupment if the practice does not meet thresholds for quality and utilization performance.
What to know about participation
To participate, your practice must be located within 1 of the 20 regional geographic areas selected by the CMS and must serve not only Medicare beneficiaries, but patients covered by one or more additional participating payers.
You may apply for either track 1 or track 2, but participation for the entire 5-year period will be within a single track.
All practices will be expected to deliver a set of five comprehensive primary care functions and have certified electronic health record technology capabilities. Track 2 practices will be expected to focus on a core set of advance capabilities for health information technology and must submit a letter of support from their health IT vendors. The CMS may require a track 2 applicant to participate in track 1.
Participating in the CPC+ program limits your ability to fully participate in or utilize other CMS initiatives, models, or demonstrations, however – including the Medicare Shared Savings Program and Next Generation ACO, or bill for the chronic care management fee. This is a big trade-off for practices well down the value transformation path, but an opportunity for those getting started.
Although the shift to payment for improved population health can herald the golden age of primary care, you cannot default on this opportunity through inaction. It is urgent that you choose a path to value-care delivery. CPC+ provides the ability for greater cash flow and flexibility for primary care practices to deliver high-quality, whole-person patient-centered care.
Mr. Bobbitt is head of the health law group at the Smith Anderson law firm in Raleigh, N.C. He is president of Value Health Partners, LLC, a health care strategic consulting company. He has years of experience assisting physicians to form integrated delivery systems and prepare for the value-based compensation era. Mr. Parker is a member of the health law group at Smith Anderson and works with Mr. Bobbitt to guide physicians regarding preparing for value-based care. This article is meant to be educational and does not constitute legal advice. For additional information, readers may contact the author at [email protected] or 919-821-6612.
The Centers for Medicare & Medicaid Services in April announced its newest initiative, Comprehensive Primary Care Plus, to target primary care practices of varying capabilities to participate in an innovative payment model designed to support the delivery of comprehensive primary care that rewards value and quality.
“Strengthening primary care is critical to an effective health care system,” said Patrick Conway, MD, CMS deputy administrator and chief medical officer. “By supporting primary care doctors and clinicians to spend time with patients, serve patients’ needs outside of the office visit, and better coordinate care with specialists, we can continue to build a health care system that results in healthier people and smarter spending of our health care dollars.”
As readers of this column know, these are also the engines of accountable care organization success. So, if you and your patient-centered medical home are not in a Medicare ACO, this gets you going on high-value activities – and pays you monthly to do it.
The rub is that once you are in the Medicare Shared Savings Program, you can’t continue with this initiative. But, it’s a great “on ramp” to prep you for ACO success. You get monthly payments instead of waiting 18 months for shared savings that you may or may not get under the Medicare Shared Savings Program.
CPC+ is an advanced primary medical home model, created from lessons learned in the Comprehensive Primary Care Initiative and the Multi-Payer Advanced Primary Care Practice Demonstration. Similar to these programs, multi-payer engagement is an essential component of the model.
In the CPC+ model, the CMS intends to nationally solicit a variety of payers committed to strengthening primary care in up to 20 regions and accept up to 5,000 practices to participate in those regions. The CPC+ program is further evidence that primary care should not only be a fundamental component to moving our health care system to one that awards clinicians based on the quality, not quantity, of care they give patients, but that payment redesign must provide flexibility to accommodate the diverse needs of primary care practices.
What to know about payment
To provide this flexibility and to attract practices of varying capabilities and levels of experience, the CPC+ program offers two tracks with different payment options, which include a monthly care management fee, comprehensive primary care payments, and performance-based incentive payments.
In track 1, the CMS will pay practices a risk-adjusted prospective monthly care management fee ($15 per beneficiary per month [PBPM] average across four risk tiers), in addition to the fee-for-service payments under the Medicare Physician Fee Schedule for activities.
In track 2, the Medicare monthly care management fees will average $28 PBPM across five risk tiers, which includes a $100 care management fee to support care for patients with the most complex needs. Instead of full Medicare fee-for-service payments for evaluation and management services, track 2 practices will receive a hybrid of reduced Medicare fee-for-service payments and up-front comprehensive primary care payments for those services.
In addition, the CMS is providing incentive payments at $2.50 PBPM for track 1 and $4 PBPM for track 2, based on practice performance on utilization metrics and quality, measured at the practice level. While these payments are prepaid at the beginning of a performance year, they are subject to recoupment if the practice does not meet thresholds for quality and utilization performance.
What to know about participation
To participate, your practice must be located within 1 of the 20 regional geographic areas selected by the CMS and must serve not only Medicare beneficiaries, but patients covered by one or more additional participating payers.
You may apply for either track 1 or track 2, but participation for the entire 5-year period will be within a single track.
All practices will be expected to deliver a set of five comprehensive primary care functions and have certified electronic health record technology capabilities. Track 2 practices will be expected to focus on a core set of advance capabilities for health information technology and must submit a letter of support from their health IT vendors. The CMS may require a track 2 applicant to participate in track 1.
Participating in the CPC+ program limits your ability to fully participate in or utilize other CMS initiatives, models, or demonstrations, however – including the Medicare Shared Savings Program and Next Generation ACO, or bill for the chronic care management fee. This is a big trade-off for practices well down the value transformation path, but an opportunity for those getting started.
Although the shift to payment for improved population health can herald the golden age of primary care, you cannot default on this opportunity through inaction. It is urgent that you choose a path to value-care delivery. CPC+ provides the ability for greater cash flow and flexibility for primary care practices to deliver high-quality, whole-person patient-centered care.
Mr. Bobbitt is head of the health law group at the Smith Anderson law firm in Raleigh, N.C. He is president of Value Health Partners, LLC, a health care strategic consulting company. He has years of experience assisting physicians to form integrated delivery systems and prepare for the value-based compensation era. Mr. Parker is a member of the health law group at Smith Anderson and works with Mr. Bobbitt to guide physicians regarding preparing for value-based care. This article is meant to be educational and does not constitute legal advice. For additional information, readers may contact the author at [email protected] or 919-821-6612.
The Centers for Medicare & Medicaid Services in April announced its newest initiative, Comprehensive Primary Care Plus, to target primary care practices of varying capabilities to participate in an innovative payment model designed to support the delivery of comprehensive primary care that rewards value and quality.
“Strengthening primary care is critical to an effective health care system,” said Patrick Conway, MD, CMS deputy administrator and chief medical officer. “By supporting primary care doctors and clinicians to spend time with patients, serve patients’ needs outside of the office visit, and better coordinate care with specialists, we can continue to build a health care system that results in healthier people and smarter spending of our health care dollars.”
As readers of this column know, these are also the engines of accountable care organization success. So, if you and your patient-centered medical home are not in a Medicare ACO, this gets you going on high-value activities – and pays you monthly to do it.
The rub is that once you are in the Medicare Shared Savings Program, you can’t continue with this initiative. But, it’s a great “on ramp” to prep you for ACO success. You get monthly payments instead of waiting 18 months for shared savings that you may or may not get under the Medicare Shared Savings Program.
CPC+ is an advanced primary medical home model, created from lessons learned in the Comprehensive Primary Care Initiative and the Multi-Payer Advanced Primary Care Practice Demonstration. Similar to these programs, multi-payer engagement is an essential component of the model.
In the CPC+ model, the CMS intends to nationally solicit a variety of payers committed to strengthening primary care in up to 20 regions and accept up to 5,000 practices to participate in those regions. The CPC+ program is further evidence that primary care should not only be a fundamental component to moving our health care system to one that awards clinicians based on the quality, not quantity, of care they give patients, but that payment redesign must provide flexibility to accommodate the diverse needs of primary care practices.
What to know about payment
To provide this flexibility and to attract practices of varying capabilities and levels of experience, the CPC+ program offers two tracks with different payment options, which include a monthly care management fee, comprehensive primary care payments, and performance-based incentive payments.
In track 1, the CMS will pay practices a risk-adjusted prospective monthly care management fee ($15 per beneficiary per month [PBPM] average across four risk tiers), in addition to the fee-for-service payments under the Medicare Physician Fee Schedule for activities.
In track 2, the Medicare monthly care management fees will average $28 PBPM across five risk tiers, which includes a $100 care management fee to support care for patients with the most complex needs. Instead of full Medicare fee-for-service payments for evaluation and management services, track 2 practices will receive a hybrid of reduced Medicare fee-for-service payments and up-front comprehensive primary care payments for those services.
In addition, the CMS is providing incentive payments at $2.50 PBPM for track 1 and $4 PBPM for track 2, based on practice performance on utilization metrics and quality, measured at the practice level. While these payments are prepaid at the beginning of a performance year, they are subject to recoupment if the practice does not meet thresholds for quality and utilization performance.
What to know about participation
To participate, your practice must be located within 1 of the 20 regional geographic areas selected by the CMS and must serve not only Medicare beneficiaries, but patients covered by one or more additional participating payers.
You may apply for either track 1 or track 2, but participation for the entire 5-year period will be within a single track.
All practices will be expected to deliver a set of five comprehensive primary care functions and have certified electronic health record technology capabilities. Track 2 practices will be expected to focus on a core set of advance capabilities for health information technology and must submit a letter of support from their health IT vendors. The CMS may require a track 2 applicant to participate in track 1.
Participating in the CPC+ program limits your ability to fully participate in or utilize other CMS initiatives, models, or demonstrations, however – including the Medicare Shared Savings Program and Next Generation ACO, or bill for the chronic care management fee. This is a big trade-off for practices well down the value transformation path, but an opportunity for those getting started.
Although the shift to payment for improved population health can herald the golden age of primary care, you cannot default on this opportunity through inaction. It is urgent that you choose a path to value-care delivery. CPC+ provides the ability for greater cash flow and flexibility for primary care practices to deliver high-quality, whole-person patient-centered care.
Mr. Bobbitt is head of the health law group at the Smith Anderson law firm in Raleigh, N.C. He is president of Value Health Partners, LLC, a health care strategic consulting company. He has years of experience assisting physicians to form integrated delivery systems and prepare for the value-based compensation era. Mr. Parker is a member of the health law group at Smith Anderson and works with Mr. Bobbitt to guide physicians regarding preparing for value-based care. This article is meant to be educational and does not constitute legal advice. For additional information, readers may contact the author at [email protected] or 919-821-6612.

Adding ipilimumab to chemotherapy did not boost overall survival in small-cell lung cancer
For patients with extensive-stage small-cell lung cancer, adding the anti–CTLA-4 antibody ipilimumab (Yervoy) to etoposide and platinum did not improve overall survival, compared with administering etoposide and platinum alone, investigators reported in the Journal of Clinical Oncology.
“Although exploratory in nature, chemotherapy plus ipilimumab did not demonstrate significant improvement in other endpoints, and no subgroups demonstrated greater benefit versus chemotherapy alone,” added Martin Reck, MD, of LungenClinic Grosshansdorf (Germany), and his associates.
The randomized phase III study enrolled 1,132 chemotherapy-naive patients who were randomly assigned to either chemotherapy plus ipilimumab (etoposide plus investigator’s choice of cisplatin or carboplatin during cycles one to four, and ipilimumab during cycles three to six) or to chemotherapy plus placebo (etoposide plus investigator’s choice of cisplatin or carboplatin during cycles one to four, and placebo during cycles three to six). Patients with a complete or partial response during induction could undergo prophylactic cranial irradiation before starting maintenance ipilimumab (10 mg/kg) or placebo administered every 12 weeks, the investigators reported (J Clin Oncol. 2016 July 26. doi:10.1200/JCO.2016.67.6601).
Among 954 patients who received at least one dose of study therapy, the primary endpoint, median overall survival, was 11.0 months for the ipilimumab-chemotherapy arm and 10.9 months for the placebo arm (hazard ratio, 0.9; 95% confidence interval, 0.8-1.1; P = .4). “Across most prespecified patient subgroups, hazard ratios for overall survival [also] did not seem to favor one treatment arm,” the researchers wrote.
Ipilimumab also failed to achieve a meaningful increase in median progression-free survival, compared with placebo (4.6 months and 4.4 months, respectively). There was only one complete response in the ipilimumab-chemotherapy group and none in the chemotherapy-placebo group. A total of 62% of patients achieved a partial response in each group, and the median duration of response was 4 months in the ipilimumab-chemotherapy group (95% CI, 3.3-4.2 months) versus 3.5 months (95% CI, 3.3-4.1 months) in the chemotherapy-placebo group.
There were no new or unexpected safety signals, but ipilimumab was associated with higher rates of overall and severe-grade diarrhea, colitis, and rash. The five treatment-related deaths in the ipilimumab-chemotherapy group included two from colitis, two from sepsis, and one from liver toxicity. “In the chemotherapy plus placebo arm, there were two treatment-related deaths, one resulting from sepsis and one from bone marrow suppression,” the researchers wrote. Treatment-related discontinuations also were more common with ipilimumab plus chemotherapy (18%) than with chemotherapy plus placebo (2%).
“To date, PD-1 inhibitors, alone or in combination with CTLA-4 inhibitors, show the most promise in small-cell lung cancer,” the investigators said. Multiple trials are exploring the use of these agents as maintenance therapy or in second-line settings, they added.
Bristol-Myers Squibb makes ipilimumab, funded the study, and helped collect and analyze the data. Dr. Reck disclosed financial ties to Bristol-Myers Squibb, Hoffmann-La Roche, Eli Lilly, Merck Sharp & Dohme, and several other pharmaceutical companies.
For patients with extensive-stage small-cell lung cancer, adding the anti–CTLA-4 antibody ipilimumab (Yervoy) to etoposide and platinum did not improve overall survival, compared with administering etoposide and platinum alone, investigators reported in the Journal of Clinical Oncology.
“Although exploratory in nature, chemotherapy plus ipilimumab did not demonstrate significant improvement in other endpoints, and no subgroups demonstrated greater benefit versus chemotherapy alone,” added Martin Reck, MD, of LungenClinic Grosshansdorf (Germany), and his associates.
The randomized phase III study enrolled 1,132 chemotherapy-naive patients who were randomly assigned to either chemotherapy plus ipilimumab (etoposide plus investigator’s choice of cisplatin or carboplatin during cycles one to four, and ipilimumab during cycles three to six) or to chemotherapy plus placebo (etoposide plus investigator’s choice of cisplatin or carboplatin during cycles one to four, and placebo during cycles three to six). Patients with a complete or partial response during induction could undergo prophylactic cranial irradiation before starting maintenance ipilimumab (10 mg/kg) or placebo administered every 12 weeks, the investigators reported (J Clin Oncol. 2016 July 26. doi:10.1200/JCO.2016.67.6601).
Among 954 patients who received at least one dose of study therapy, the primary endpoint, median overall survival, was 11.0 months for the ipilimumab-chemotherapy arm and 10.9 months for the placebo arm (hazard ratio, 0.9; 95% confidence interval, 0.8-1.1; P = .4). “Across most prespecified patient subgroups, hazard ratios for overall survival [also] did not seem to favor one treatment arm,” the researchers wrote.
Ipilimumab also failed to achieve a meaningful increase in median progression-free survival, compared with placebo (4.6 months and 4.4 months, respectively). There was only one complete response in the ipilimumab-chemotherapy group and none in the chemotherapy-placebo group. A total of 62% of patients achieved a partial response in each group, and the median duration of response was 4 months in the ipilimumab-chemotherapy group (95% CI, 3.3-4.2 months) versus 3.5 months (95% CI, 3.3-4.1 months) in the chemotherapy-placebo group.
There were no new or unexpected safety signals, but ipilimumab was associated with higher rates of overall and severe-grade diarrhea, colitis, and rash. The five treatment-related deaths in the ipilimumab-chemotherapy group included two from colitis, two from sepsis, and one from liver toxicity. “In the chemotherapy plus placebo arm, there were two treatment-related deaths, one resulting from sepsis and one from bone marrow suppression,” the researchers wrote. Treatment-related discontinuations also were more common with ipilimumab plus chemotherapy (18%) than with chemotherapy plus placebo (2%).
“To date, PD-1 inhibitors, alone or in combination with CTLA-4 inhibitors, show the most promise in small-cell lung cancer,” the investigators said. Multiple trials are exploring the use of these agents as maintenance therapy or in second-line settings, they added.
Bristol-Myers Squibb makes ipilimumab, funded the study, and helped collect and analyze the data. Dr. Reck disclosed financial ties to Bristol-Myers Squibb, Hoffmann-La Roche, Eli Lilly, Merck Sharp & Dohme, and several other pharmaceutical companies.
For patients with extensive-stage small-cell lung cancer, adding the anti–CTLA-4 antibody ipilimumab (Yervoy) to etoposide and platinum did not improve overall survival, compared with administering etoposide and platinum alone, investigators reported in the Journal of Clinical Oncology.
“Although exploratory in nature, chemotherapy plus ipilimumab did not demonstrate significant improvement in other endpoints, and no subgroups demonstrated greater benefit versus chemotherapy alone,” added Martin Reck, MD, of LungenClinic Grosshansdorf (Germany), and his associates.
The randomized phase III study enrolled 1,132 chemotherapy-naive patients who were randomly assigned to either chemotherapy plus ipilimumab (etoposide plus investigator’s choice of cisplatin or carboplatin during cycles one to four, and ipilimumab during cycles three to six) or to chemotherapy plus placebo (etoposide plus investigator’s choice of cisplatin or carboplatin during cycles one to four, and placebo during cycles three to six). Patients with a complete or partial response during induction could undergo prophylactic cranial irradiation before starting maintenance ipilimumab (10 mg/kg) or placebo administered every 12 weeks, the investigators reported (J Clin Oncol. 2016 July 26. doi:10.1200/JCO.2016.67.6601).
Among 954 patients who received at least one dose of study therapy, the primary endpoint, median overall survival, was 11.0 months for the ipilimumab-chemotherapy arm and 10.9 months for the placebo arm (hazard ratio, 0.9; 95% confidence interval, 0.8-1.1; P = .4). “Across most prespecified patient subgroups, hazard ratios for overall survival [also] did not seem to favor one treatment arm,” the researchers wrote.
Ipilimumab also failed to achieve a meaningful increase in median progression-free survival, compared with placebo (4.6 months and 4.4 months, respectively). There was only one complete response in the ipilimumab-chemotherapy group and none in the chemotherapy-placebo group. A total of 62% of patients achieved a partial response in each group, and the median duration of response was 4 months in the ipilimumab-chemotherapy group (95% CI, 3.3-4.2 months) versus 3.5 months (95% CI, 3.3-4.1 months) in the chemotherapy-placebo group.
There were no new or unexpected safety signals, but ipilimumab was associated with higher rates of overall and severe-grade diarrhea, colitis, and rash. The five treatment-related deaths in the ipilimumab-chemotherapy group included two from colitis, two from sepsis, and one from liver toxicity. “In the chemotherapy plus placebo arm, there were two treatment-related deaths, one resulting from sepsis and one from bone marrow suppression,” the researchers wrote. Treatment-related discontinuations also were more common with ipilimumab plus chemotherapy (18%) than with chemotherapy plus placebo (2%).
“To date, PD-1 inhibitors, alone or in combination with CTLA-4 inhibitors, show the most promise in small-cell lung cancer,” the investigators said. Multiple trials are exploring the use of these agents as maintenance therapy or in second-line settings, they added.
Bristol-Myers Squibb makes ipilimumab, funded the study, and helped collect and analyze the data. Dr. Reck disclosed financial ties to Bristol-Myers Squibb, Hoffmann-La Roche, Eli Lilly, Merck Sharp & Dohme, and several other pharmaceutical companies.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: The anti–CTLA-4 antibody ipilimumab (Yervoy) missed its primary endpoint in a trial of patients with extensive-stage small-cell lung cancer.
Major finding: The median overall survival, was 11.0 months for the ipilimumab-chemotherapy arm and 10.9 months for the placebo arm (hazard ratio, 0.9; 95% confidence interval, 0.8-1.1; P = .4).
Data source: A randomized phase III trial of 954 patients.
Disclosures: Bristol-Myers Squibb funded the study and helped collect and analyze the study results. Dr. Reck disclosed financial ties to Bristol-Myers Squibb, Hoffmann-La Roche, Eli Lilly, Merck Sharp & Dohme, and several other pharmaceutical companies.
VIDEO: Minimal disease activity criteria sought for axial spondyloarthritis
DENVER – U.S. rheumatologists plan to develop new criteria to define minimal disease activity in patients with axial spondyloarthritis to better gauge in routine clinical practice how well these patients respond to treatment.
A score on the Ankylosing Spondylitis Disease Activity Score (ASDAS) of less than 1.3 is the most commonly used measure today of minimal disease activity, but the ASDAS isn’t suitable for point-of-care assessment in routine practice because of the need for a C-reactive protein level or erythrocyte sedimentation rate.

“In the clinic, ASDAS is very difficult or next to impossible to do” because it needs CRP or ESR, which are “never available at the point of care,” Atul A. Deodhar, MD, said in an interview at the annual meeting of the Spondyloarthritis Research and Treatment Network (SPARTAN). Another limitation of ASDAS is that it focuses exclusively on musculoskeletal measures and does not take into account extra-articular manifestations of axial spondyloarthritis such as those in the eye, gastrointestinal tract, or skin.
“We would like a clinical measurement that might tell us that a patient is appropriately treated and at minimal disease activity,” said Dr. Deodhar, professor of medicine and medical director of the rheumatology clinics at Oregon Health & Science University in Portland.
As outgoing chair of SPARTAN, Dr. Deodhar introduced a proposal that SPARTAN develop new minimal disease activity criteria for patients with axial spondyloarthritis, presenting the rationale for this project at the meeting along with the incoming chair Lianne S. Gensler, MD.
“We want a way to measure disease activity at a stage that is not full remission but with enough of a reduction in disease activity to make a difference,” said Dr. Gensler, director of the Ankylosing Spondylitis Clinic at the University of California, San Francisco. Another frequently used gauge of minimal disease activity in axial spondyloarthritis, the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), is flawed by being totally based on subjective measurements without input from the attending rheumatologist, Dr. Gensler said.
The SPARTAN leadership will try to partner in this effort with the OMERACT (Outcome Measures in Rheumatology) program, the Assessment of Spondyloarthritis International Society (ASAS), or both, but if necessary SPARTAN will develop new minimal disease activity criteria on its own, Dr. Deodhar said.
Dr. Deodhar has received research support from 10 drug companies. Dr. Gensler has been a consultant to or has received research support from AbbVie, Amgen, Janssen, Novartis, and UCB.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @mitchelzoler
DENVER – U.S. rheumatologists plan to develop new criteria to define minimal disease activity in patients with axial spondyloarthritis to better gauge in routine clinical practice how well these patients respond to treatment.
A score on the Ankylosing Spondylitis Disease Activity Score (ASDAS) of less than 1.3 is the most commonly used measure today of minimal disease activity, but the ASDAS isn’t suitable for point-of-care assessment in routine practice because of the need for a C-reactive protein level or erythrocyte sedimentation rate.
“In the clinic, ASDAS is very difficult or next to impossible to do” because it needs CRP or ESR, which are “never available at the point of care,” Atul A. Deodhar, MD, said in an interview at the annual meeting of the Spondyloarthritis Research and Treatment Network (SPARTAN). Another limitation of ASDAS is that it focuses exclusively on musculoskeletal measures and does not take into account extra-articular manifestations of axial spondyloarthritis such as those in the eye, gastrointestinal tract, or skin.
“We would like a clinical measurement that might tell us that a patient is appropriately treated and at minimal disease activity,” said Dr. Deodhar, professor of medicine and medical director of the rheumatology clinics at Oregon Health & Science University in Portland.
As outgoing chair of SPARTAN, Dr. Deodhar introduced a proposal that SPARTAN develop new minimal disease activity criteria for patients with axial spondyloarthritis, presenting the rationale for this project at the meeting along with the incoming chair Lianne S. Gensler, MD.
“We want a way to measure disease activity at a stage that is not full remission but with enough of a reduction in disease activity to make a difference,” said Dr. Gensler, director of the Ankylosing Spondylitis Clinic at the University of California, San Francisco. Another frequently used gauge of minimal disease activity in axial spondyloarthritis, the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), is flawed by being totally based on subjective measurements without input from the attending rheumatologist, Dr. Gensler said.
The SPARTAN leadership will try to partner in this effort with the OMERACT (Outcome Measures in Rheumatology) program, the Assessment of Spondyloarthritis International Society (ASAS), or both, but if necessary SPARTAN will develop new minimal disease activity criteria on its own, Dr. Deodhar said.
Dr. Deodhar has received research support from 10 drug companies. Dr. Gensler has been a consultant to or has received research support from AbbVie, Amgen, Janssen, Novartis, and UCB.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @mitchelzoler
DENVER – U.S. rheumatologists plan to develop new criteria to define minimal disease activity in patients with axial spondyloarthritis to better gauge in routine clinical practice how well these patients respond to treatment.
A score on the Ankylosing Spondylitis Disease Activity Score (ASDAS) of less than 1.3 is the most commonly used measure today of minimal disease activity, but the ASDAS isn’t suitable for point-of-care assessment in routine practice because of the need for a C-reactive protein level or erythrocyte sedimentation rate.
“In the clinic, ASDAS is very difficult or next to impossible to do” because it needs CRP or ESR, which are “never available at the point of care,” Atul A. Deodhar, MD, said in an interview at the annual meeting of the Spondyloarthritis Research and Treatment Network (SPARTAN). Another limitation of ASDAS is that it focuses exclusively on musculoskeletal measures and does not take into account extra-articular manifestations of axial spondyloarthritis such as those in the eye, gastrointestinal tract, or skin.
“We would like a clinical measurement that might tell us that a patient is appropriately treated and at minimal disease activity,” said Dr. Deodhar, professor of medicine and medical director of the rheumatology clinics at Oregon Health & Science University in Portland.
As outgoing chair of SPARTAN, Dr. Deodhar introduced a proposal that SPARTAN develop new minimal disease activity criteria for patients with axial spondyloarthritis, presenting the rationale for this project at the meeting along with the incoming chair Lianne S. Gensler, MD.
“We want a way to measure disease activity at a stage that is not full remission but with enough of a reduction in disease activity to make a difference,” said Dr. Gensler, director of the Ankylosing Spondylitis Clinic at the University of California, San Francisco. Another frequently used gauge of minimal disease activity in axial spondyloarthritis, the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), is flawed by being totally based on subjective measurements without input from the attending rheumatologist, Dr. Gensler said.
The SPARTAN leadership will try to partner in this effort with the OMERACT (Outcome Measures in Rheumatology) program, the Assessment of Spondyloarthritis International Society (ASAS), or both, but if necessary SPARTAN will develop new minimal disease activity criteria on its own, Dr. Deodhar said.
Dr. Deodhar has received research support from 10 drug companies. Dr. Gensler has been a consultant to or has received research support from AbbVie, Amgen, Janssen, Novartis, and UCB.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @mitchelzoler
EXPERT ANALYSIS FROM THE 2016 SPARTAN ANNUAL MEETING
