User login
Recurrent Cerebriform Connective Tissue Nevus on the Foot of a Patient With Proteus Syndrome
To the Editor:
A 12-year-old girl presented with discomfort and walking limitation caused by cutaneous masses on the plantar aspects of the feet with associated bone abnormalities that had started as several flesh-colored papules on the plantar surface of both feet at the age of 1 year. Over time the lesions gradually enlarged and formed irregular masses, more prominently on the right foot. At the age of 6 years, surgical correction was performed due to increased walking impairment and a skin examination that suggested connective tissue nevus. The results were good. However, the local tissue overgrowth recurred after 1 year. Slowly growing lesions were found at the surgical site, which necessitated hospitalization. Her medical history was negative for other disease. There was no family history of similar skin conditions and her parents were nonconsanguineous.
Physical examination revealed malnutrition and poor development in height as well as difficulty walking. She also had moderate scoliosis with a curve to the left. Dermatological examination showed multiple reddish cerebriform hyperplasia in both plantar areas; the right side was more severely involved (Figure 1A). There was macrodactyly of 2 toes on the right foot (Figure 1B). All results of routine blood examinations were within reference range. There were no abnormalities noted in the abdominal ultrasound and cardiac examinations. Plain radiographs of the spine and feet demonstrated scoliosis and exostosis on the calcaneus and bottom of the scaphoid. Histopathologic examination of tissue from the plantar cerebriform hyperplasia revealed hyperkeratosis, slight acanthosis and papillomatosis in the epidermis, and dense collagen bands and sparse elastic fibers in the dermis (Figure 2).
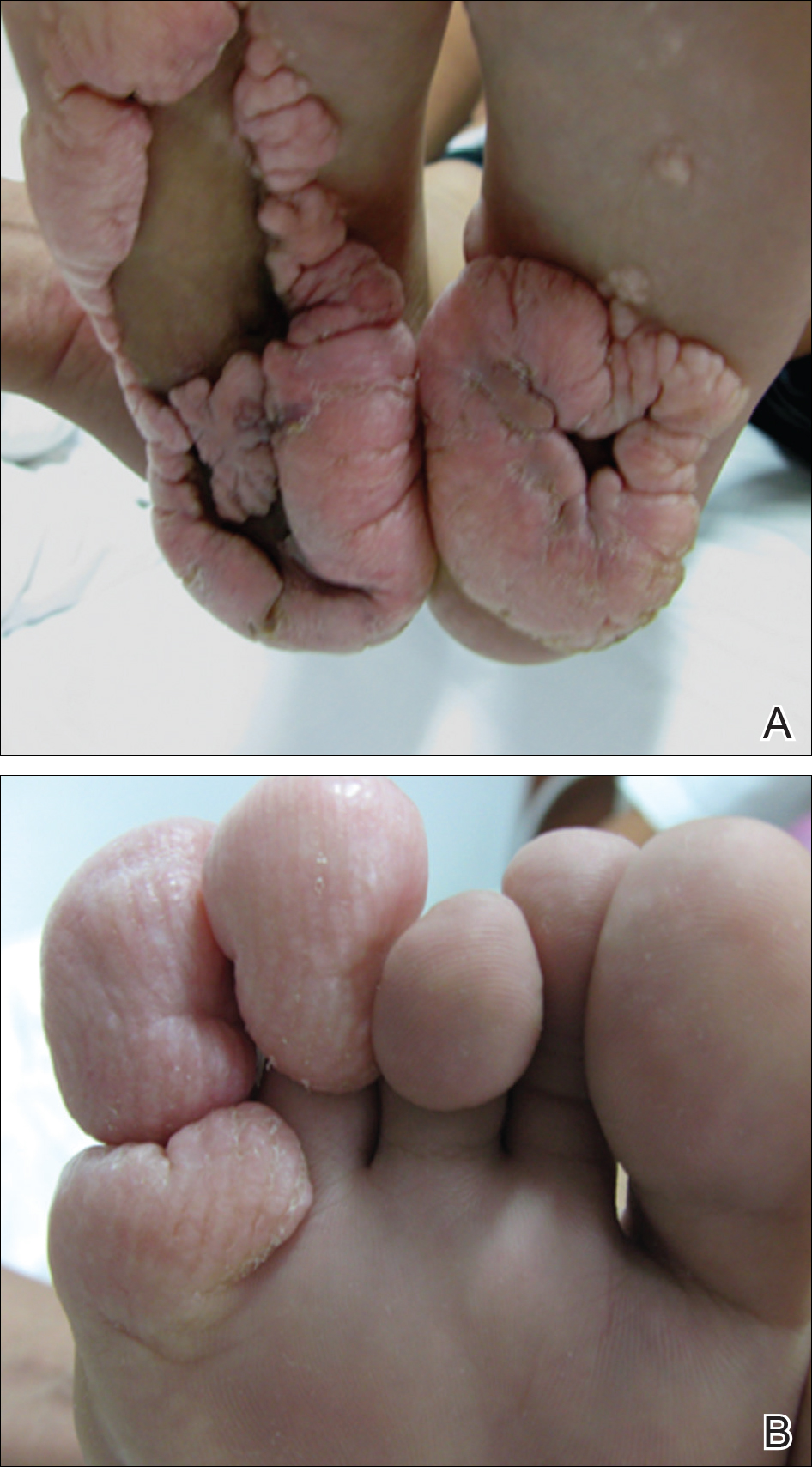

Given the clinical and radiologic manifestation, the diagnosis of Proteus syndrome (PS) was established. After taking into account the severe discomfort and the success of the first surgery, we performed a resection and full-thickness skin graft surgery once again. The feet recovered without any discomfort in daily life. The appearance of the skin graft area was normal 1 year following surgery (Figure 3). She was treated with spinal plate fixation at another institution, progressed well for 2 years, and was subsequently lost to follow-up.

Proteus syndrome is a multisystem disorder with a difficult diagnosis due to the variability of its manifestations. The worldwide incidence of this rare disorder is less than 1 per 1 million individuals, and it is thought to be caused by a somatic genetic alteration.1 Clinical characteristics include bone abnormalities, vascular malformations, dysregulation of fatty tissue, linear verrucous epidermal nevus, and cerebriform connective tissue nevus (CCTN). Although CCTN is not a common finding in patients with PS, it is considered a fairly specific sign with the greatest impact for the diagnosis of PS.2
The general feature of PS--asymmetric disproportionate overgrowth of tissues--appears at 6 to 18 months of age, which makes it challenging to diagnose disease earlier. The CCTN in our patient was present since 1 year of age.
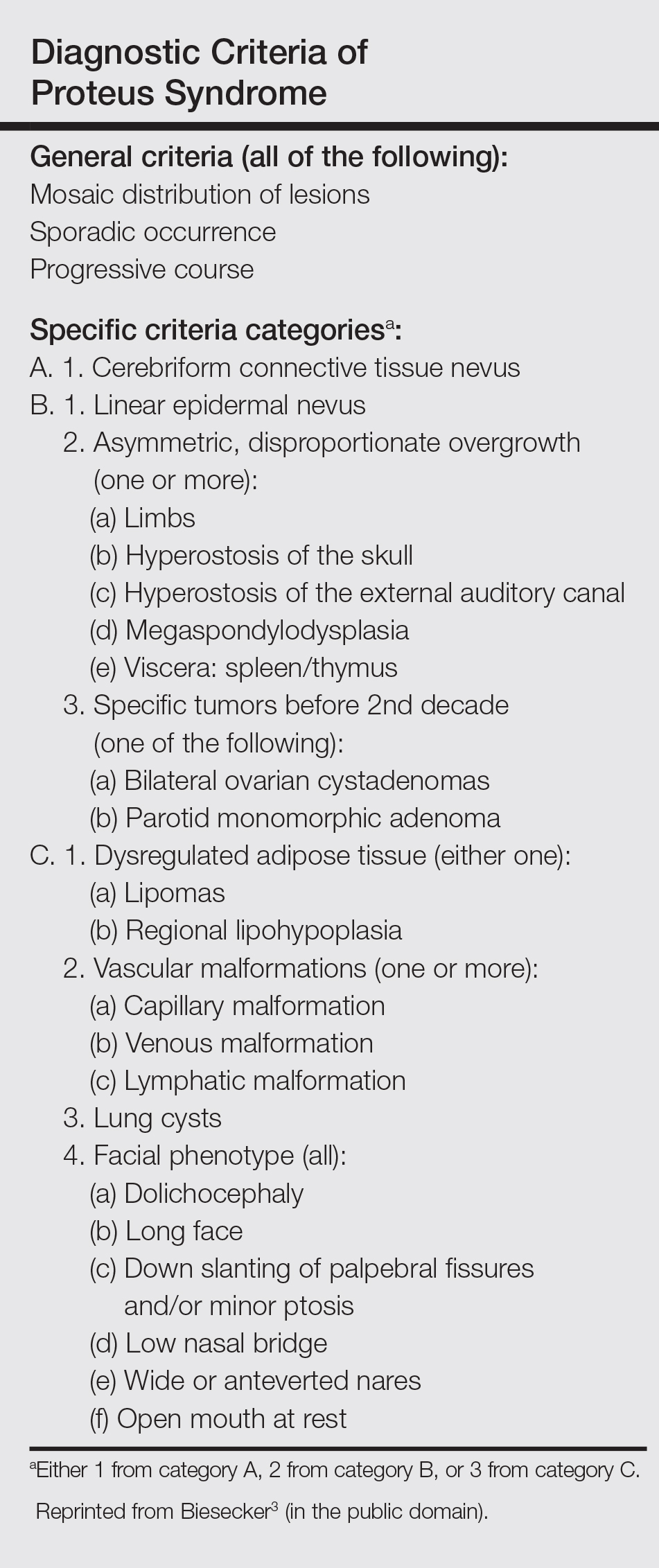
To make a diagnosis of PS, one must have all the general criteria and various specific criteria. The revised diagnostic criteria for PS are given in the Table.3 According to the diagnostic criteria, our patient fulfilled the mandatory general criteria and had plantar CCTN, epidermal nevus, and dysregulated adipose tissue. The CCTN has notable diagnostic value in mildly affected patients, as it is absent in diseases included in the differential diagnosis such as neurofibromatosis, Klippel-Trenaunay-Weber syndrome, Maffucci syndrome, and Bannayan-Riley-Ruvalcaba syndrome. Hemihyperplasia-multiple lipomatosis syndrome and CLOVES (congenital, lipomatous overgrowth, vascular malformations, epidermal nevi, and scoliosis/spinal/skeletal anomalies) syndrome also can present on the plantar surfaces, and lesions may be overgrown at birth but are softer and compressible, have wrinkles instead of deep folds, and tend to grow with the child rather than disproportionately as in PS.4
The epidermal nevi and vascular malformations generally do not spread or increase in number. In contrast, CCTN in PS grows throughout childhood but tends to remain stable in adulthood.4 Postponing surgical treatment until skin lesions stabilize appears to be the best option. However, for practical purposes, surgical intervention may be required at an earlier phase to address the severe functional and cosmetic consequences. Some patients require multiple orthopedic procedures over the ensuing years or decades to control the hyperplasia.3 New CCTN that developed from the prior surgical incision, macrodactyly of the fourth and fifth right toes, and scoliosis appeared when the patient came to our clinic for retreatment 1 year after the initial presentation. The asymmetrical and disproportionate overgrowth of tissues had moderately accelerated in that period. Considering the increasingly impaired walking, we performed a second surgery. On follow-up visits, the patient expressed improvement in daily life.
Studies had been performed to clarify the genetic bases of PS, and the somatic activating mutation in AKT1 (AKT serine/threonine kinase 1) was reported to be the cause of the disease.5,6 Germline PTEN (phosphatase and tensin homolog) mutations have been identified in some patients with overgrowth abnormalities of PS. However, given the misdiagnosis of PS with PTEN mutations and the notion that a gene alone cannot result in PS, the loss-of-function mutations of LEMD3 that have been reported in familial cutaneous collagenomas also may be related to the abnormal growth of connective and bone tissues that are typical of PS.7,8 Lindhurst et al5 concluded that PS is caused by a somatic activating mutation in AKT1, which proved the hypothesis of somatic mosaicism and implicated activation of the PI3K-AKT pathway in the characteristic clinical findings of overgrowth and tumor susceptibility in this disorder. AKT1 is activated by loss-of-function mutations in PTEN, which explains why patients with these mutations (eg, those with the segmental overgrowth, lipomatosis, arteriovenous malformation, epidermal nevus, SOLAMEN [segmental overgrowth, lipomatosis, arteriovenous malformation, and epidermal nevus] syndrome) and patients with activating mutations in AKT1 (eg, those with PS) have overlapping but distinct clinical manifestations. Molecular genetic testing may be useful to confirm the diagnosis in individuals who meet clinical criteria and to establish the diagnosis in individuals with clinical findings that are ambiguous or mild. Further studies are necessary to progress the understanding and management of PS, which will require cooperation of geneticists, surgeons, and other specialists.
- Popescu MD, Burnei G, Draghici L, et al. Proteus syndrome: a difficult diagnosis and management plan. J Med Life. 2014;7:563-566.
- Schepis C, Greco D, Siragusa M, et al. Cerebriform plantar hyperplasia: the major cutaneous feature of Proteus syndrome. Int J Dermatol. 2008;47:374-376.
- Biesecker L. The challenges of Proteus syndrome: diagnosis and management. Eur J Hum Genet. 2006;14:1151-1157.
- Beachkofsky TM, Sapp JC, Biesecker LG, et al. Progressive overgrowth of the cerebriform connective tissue nevus in patients with Proteus syndrome. J Am Acad Dermatol. 2010;63:799-804.
- Lindhurst MJ, Sapp JC, Teer JK, et al. A mosaic activating mutation in AKT1 associated with the Proteus syndrome. N Engl J Med. 2011;365:611-619.
- Wieland I, Tinschert S, Zenker M. High-level somatic mosaicism of AKT1 c.49G>A mutation in skin scrapings from epidermal nevi enables non-invasive molecular diagnosis in patients with Proteus syndrome. Am J Med Genet A. 2013;161A:889-891.
- Cohen MJ, Turner JT, Biesecker LG. Proteus syndrome: misdiagnosis with PTEN mutations. Am J Med Genet A. 2003;122A:323-324.
- Di Stefani A, Gabellini M, Ferlosio A, et al. Cerebriform plantar hyperplasia: the clinico-pathological hallmark of Proteus syndrome. Acta Derm Venereol. 2011;91:580-581.
To the Editor:
A 12-year-old girl presented with discomfort and walking limitation caused by cutaneous masses on the plantar aspects of the feet with associated bone abnormalities that had started as several flesh-colored papules on the plantar surface of both feet at the age of 1 year. Over time the lesions gradually enlarged and formed irregular masses, more prominently on the right foot. At the age of 6 years, surgical correction was performed due to increased walking impairment and a skin examination that suggested connective tissue nevus. The results were good. However, the local tissue overgrowth recurred after 1 year. Slowly growing lesions were found at the surgical site, which necessitated hospitalization. Her medical history was negative for other disease. There was no family history of similar skin conditions and her parents were nonconsanguineous.
Physical examination revealed malnutrition and poor development in height as well as difficulty walking. She also had moderate scoliosis with a curve to the left. Dermatological examination showed multiple reddish cerebriform hyperplasia in both plantar areas; the right side was more severely involved (Figure 1A). There was macrodactyly of 2 toes on the right foot (Figure 1B). All results of routine blood examinations were within reference range. There were no abnormalities noted in the abdominal ultrasound and cardiac examinations. Plain radiographs of the spine and feet demonstrated scoliosis and exostosis on the calcaneus and bottom of the scaphoid. Histopathologic examination of tissue from the plantar cerebriform hyperplasia revealed hyperkeratosis, slight acanthosis and papillomatosis in the epidermis, and dense collagen bands and sparse elastic fibers in the dermis (Figure 2).
Given the clinical and radiologic manifestation, the diagnosis of Proteus syndrome (PS) was established. After taking into account the severe discomfort and the success of the first surgery, we performed a resection and full-thickness skin graft surgery once again. The feet recovered without any discomfort in daily life. The appearance of the skin graft area was normal 1 year following surgery (Figure 3). She was treated with spinal plate fixation at another institution, progressed well for 2 years, and was subsequently lost to follow-up.
Proteus syndrome is a multisystem disorder with a difficult diagnosis due to the variability of its manifestations. The worldwide incidence of this rare disorder is less than 1 per 1 million individuals, and it is thought to be caused by a somatic genetic alteration.1 Clinical characteristics include bone abnormalities, vascular malformations, dysregulation of fatty tissue, linear verrucous epidermal nevus, and cerebriform connective tissue nevus (CCTN). Although CCTN is not a common finding in patients with PS, it is considered a fairly specific sign with the greatest impact for the diagnosis of PS.2
The general feature of PS--asymmetric disproportionate overgrowth of tissues--appears at 6 to 18 months of age, which makes it challenging to diagnose disease earlier. The CCTN in our patient was present since 1 year of age.
To make a diagnosis of PS, one must have all the general criteria and various specific criteria. The revised diagnostic criteria for PS are given in the Table.3 According to the diagnostic criteria, our patient fulfilled the mandatory general criteria and had plantar CCTN, epidermal nevus, and dysregulated adipose tissue. The CCTN has notable diagnostic value in mildly affected patients, as it is absent in diseases included in the differential diagnosis such as neurofibromatosis, Klippel-Trenaunay-Weber syndrome, Maffucci syndrome, and Bannayan-Riley-Ruvalcaba syndrome. Hemihyperplasia-multiple lipomatosis syndrome and CLOVES (congenital, lipomatous overgrowth, vascular malformations, epidermal nevi, and scoliosis/spinal/skeletal anomalies) syndrome also can present on the plantar surfaces, and lesions may be overgrown at birth but are softer and compressible, have wrinkles instead of deep folds, and tend to grow with the child rather than disproportionately as in PS.4
The epidermal nevi and vascular malformations generally do not spread or increase in number. In contrast, CCTN in PS grows throughout childhood but tends to remain stable in adulthood.4 Postponing surgical treatment until skin lesions stabilize appears to be the best option. However, for practical purposes, surgical intervention may be required at an earlier phase to address the severe functional and cosmetic consequences. Some patients require multiple orthopedic procedures over the ensuing years or decades to control the hyperplasia.3 New CCTN that developed from the prior surgical incision, macrodactyly of the fourth and fifth right toes, and scoliosis appeared when the patient came to our clinic for retreatment 1 year after the initial presentation. The asymmetrical and disproportionate overgrowth of tissues had moderately accelerated in that period. Considering the increasingly impaired walking, we performed a second surgery. On follow-up visits, the patient expressed improvement in daily life.
Studies had been performed to clarify the genetic bases of PS, and the somatic activating mutation in AKT1 (AKT serine/threonine kinase 1) was reported to be the cause of the disease.5,6 Germline PTEN (phosphatase and tensin homolog) mutations have been identified in some patients with overgrowth abnormalities of PS. However, given the misdiagnosis of PS with PTEN mutations and the notion that a gene alone cannot result in PS, the loss-of-function mutations of LEMD3 that have been reported in familial cutaneous collagenomas also may be related to the abnormal growth of connective and bone tissues that are typical of PS.7,8 Lindhurst et al5 concluded that PS is caused by a somatic activating mutation in AKT1, which proved the hypothesis of somatic mosaicism and implicated activation of the PI3K-AKT pathway in the characteristic clinical findings of overgrowth and tumor susceptibility in this disorder. AKT1 is activated by loss-of-function mutations in PTEN, which explains why patients with these mutations (eg, those with the segmental overgrowth, lipomatosis, arteriovenous malformation, epidermal nevus, SOLAMEN [segmental overgrowth, lipomatosis, arteriovenous malformation, and epidermal nevus] syndrome) and patients with activating mutations in AKT1 (eg, those with PS) have overlapping but distinct clinical manifestations. Molecular genetic testing may be useful to confirm the diagnosis in individuals who meet clinical criteria and to establish the diagnosis in individuals with clinical findings that are ambiguous or mild. Further studies are necessary to progress the understanding and management of PS, which will require cooperation of geneticists, surgeons, and other specialists.
To the Editor:
A 12-year-old girl presented with discomfort and walking limitation caused by cutaneous masses on the plantar aspects of the feet with associated bone abnormalities that had started as several flesh-colored papules on the plantar surface of both feet at the age of 1 year. Over time the lesions gradually enlarged and formed irregular masses, more prominently on the right foot. At the age of 6 years, surgical correction was performed due to increased walking impairment and a skin examination that suggested connective tissue nevus. The results were good. However, the local tissue overgrowth recurred after 1 year. Slowly growing lesions were found at the surgical site, which necessitated hospitalization. Her medical history was negative for other disease. There was no family history of similar skin conditions and her parents were nonconsanguineous.
Physical examination revealed malnutrition and poor development in height as well as difficulty walking. She also had moderate scoliosis with a curve to the left. Dermatological examination showed multiple reddish cerebriform hyperplasia in both plantar areas; the right side was more severely involved (Figure 1A). There was macrodactyly of 2 toes on the right foot (Figure 1B). All results of routine blood examinations were within reference range. There were no abnormalities noted in the abdominal ultrasound and cardiac examinations. Plain radiographs of the spine and feet demonstrated scoliosis and exostosis on the calcaneus and bottom of the scaphoid. Histopathologic examination of tissue from the plantar cerebriform hyperplasia revealed hyperkeratosis, slight acanthosis and papillomatosis in the epidermis, and dense collagen bands and sparse elastic fibers in the dermis (Figure 2).
Given the clinical and radiologic manifestation, the diagnosis of Proteus syndrome (PS) was established. After taking into account the severe discomfort and the success of the first surgery, we performed a resection and full-thickness skin graft surgery once again. The feet recovered without any discomfort in daily life. The appearance of the skin graft area was normal 1 year following surgery (Figure 3). She was treated with spinal plate fixation at another institution, progressed well for 2 years, and was subsequently lost to follow-up.
Proteus syndrome is a multisystem disorder with a difficult diagnosis due to the variability of its manifestations. The worldwide incidence of this rare disorder is less than 1 per 1 million individuals, and it is thought to be caused by a somatic genetic alteration.1 Clinical characteristics include bone abnormalities, vascular malformations, dysregulation of fatty tissue, linear verrucous epidermal nevus, and cerebriform connective tissue nevus (CCTN). Although CCTN is not a common finding in patients with PS, it is considered a fairly specific sign with the greatest impact for the diagnosis of PS.2
The general feature of PS--asymmetric disproportionate overgrowth of tissues--appears at 6 to 18 months of age, which makes it challenging to diagnose disease earlier. The CCTN in our patient was present since 1 year of age.
To make a diagnosis of PS, one must have all the general criteria and various specific criteria. The revised diagnostic criteria for PS are given in the Table.3 According to the diagnostic criteria, our patient fulfilled the mandatory general criteria and had plantar CCTN, epidermal nevus, and dysregulated adipose tissue. The CCTN has notable diagnostic value in mildly affected patients, as it is absent in diseases included in the differential diagnosis such as neurofibromatosis, Klippel-Trenaunay-Weber syndrome, Maffucci syndrome, and Bannayan-Riley-Ruvalcaba syndrome. Hemihyperplasia-multiple lipomatosis syndrome and CLOVES (congenital, lipomatous overgrowth, vascular malformations, epidermal nevi, and scoliosis/spinal/skeletal anomalies) syndrome also can present on the plantar surfaces, and lesions may be overgrown at birth but are softer and compressible, have wrinkles instead of deep folds, and tend to grow with the child rather than disproportionately as in PS.4
The epidermal nevi and vascular malformations generally do not spread or increase in number. In contrast, CCTN in PS grows throughout childhood but tends to remain stable in adulthood.4 Postponing surgical treatment until skin lesions stabilize appears to be the best option. However, for practical purposes, surgical intervention may be required at an earlier phase to address the severe functional and cosmetic consequences. Some patients require multiple orthopedic procedures over the ensuing years or decades to control the hyperplasia.3 New CCTN that developed from the prior surgical incision, macrodactyly of the fourth and fifth right toes, and scoliosis appeared when the patient came to our clinic for retreatment 1 year after the initial presentation. The asymmetrical and disproportionate overgrowth of tissues had moderately accelerated in that period. Considering the increasingly impaired walking, we performed a second surgery. On follow-up visits, the patient expressed improvement in daily life.
Studies had been performed to clarify the genetic bases of PS, and the somatic activating mutation in AKT1 (AKT serine/threonine kinase 1) was reported to be the cause of the disease.5,6 Germline PTEN (phosphatase and tensin homolog) mutations have been identified in some patients with overgrowth abnormalities of PS. However, given the misdiagnosis of PS with PTEN mutations and the notion that a gene alone cannot result in PS, the loss-of-function mutations of LEMD3 that have been reported in familial cutaneous collagenomas also may be related to the abnormal growth of connective and bone tissues that are typical of PS.7,8 Lindhurst et al5 concluded that PS is caused by a somatic activating mutation in AKT1, which proved the hypothesis of somatic mosaicism and implicated activation of the PI3K-AKT pathway in the characteristic clinical findings of overgrowth and tumor susceptibility in this disorder. AKT1 is activated by loss-of-function mutations in PTEN, which explains why patients with these mutations (eg, those with the segmental overgrowth, lipomatosis, arteriovenous malformation, epidermal nevus, SOLAMEN [segmental overgrowth, lipomatosis, arteriovenous malformation, and epidermal nevus] syndrome) and patients with activating mutations in AKT1 (eg, those with PS) have overlapping but distinct clinical manifestations. Molecular genetic testing may be useful to confirm the diagnosis in individuals who meet clinical criteria and to establish the diagnosis in individuals with clinical findings that are ambiguous or mild. Further studies are necessary to progress the understanding and management of PS, which will require cooperation of geneticists, surgeons, and other specialists.
- Popescu MD, Burnei G, Draghici L, et al. Proteus syndrome: a difficult diagnosis and management plan. J Med Life. 2014;7:563-566.
- Schepis C, Greco D, Siragusa M, et al. Cerebriform plantar hyperplasia: the major cutaneous feature of Proteus syndrome. Int J Dermatol. 2008;47:374-376.
- Biesecker L. The challenges of Proteus syndrome: diagnosis and management. Eur J Hum Genet. 2006;14:1151-1157.
- Beachkofsky TM, Sapp JC, Biesecker LG, et al. Progressive overgrowth of the cerebriform connective tissue nevus in patients with Proteus syndrome. J Am Acad Dermatol. 2010;63:799-804.
- Lindhurst MJ, Sapp JC, Teer JK, et al. A mosaic activating mutation in AKT1 associated with the Proteus syndrome. N Engl J Med. 2011;365:611-619.
- Wieland I, Tinschert S, Zenker M. High-level somatic mosaicism of AKT1 c.49G>A mutation in skin scrapings from epidermal nevi enables non-invasive molecular diagnosis in patients with Proteus syndrome. Am J Med Genet A. 2013;161A:889-891.
- Cohen MJ, Turner JT, Biesecker LG. Proteus syndrome: misdiagnosis with PTEN mutations. Am J Med Genet A. 2003;122A:323-324.
- Di Stefani A, Gabellini M, Ferlosio A, et al. Cerebriform plantar hyperplasia: the clinico-pathological hallmark of Proteus syndrome. Acta Derm Venereol. 2011;91:580-581.
- Popescu MD, Burnei G, Draghici L, et al. Proteus syndrome: a difficult diagnosis and management plan. J Med Life. 2014;7:563-566.
- Schepis C, Greco D, Siragusa M, et al. Cerebriform plantar hyperplasia: the major cutaneous feature of Proteus syndrome. Int J Dermatol. 2008;47:374-376.
- Biesecker L. The challenges of Proteus syndrome: diagnosis and management. Eur J Hum Genet. 2006;14:1151-1157.
- Beachkofsky TM, Sapp JC, Biesecker LG, et al. Progressive overgrowth of the cerebriform connective tissue nevus in patients with Proteus syndrome. J Am Acad Dermatol. 2010;63:799-804.
- Lindhurst MJ, Sapp JC, Teer JK, et al. A mosaic activating mutation in AKT1 associated with the Proteus syndrome. N Engl J Med. 2011;365:611-619.
- Wieland I, Tinschert S, Zenker M. High-level somatic mosaicism of AKT1 c.49G>A mutation in skin scrapings from epidermal nevi enables non-invasive molecular diagnosis in patients with Proteus syndrome. Am J Med Genet A. 2013;161A:889-891.
- Cohen MJ, Turner JT, Biesecker LG. Proteus syndrome: misdiagnosis with PTEN mutations. Am J Med Genet A. 2003;122A:323-324.
- Di Stefani A, Gabellini M, Ferlosio A, et al. Cerebriform plantar hyperplasia: the clinico-pathological hallmark of Proteus syndrome. Acta Derm Venereol. 2011;91:580-581.
Practice Points
- Proteus syndrome (PS) is a rare mosaic condition characterized by progressive overgrowth of skin, connective tissue, brain tissue, and other tissues.
- A somatic activating mutation of the AKT1 gene has been identified as a cause for developing PS.
- Distinct cutaneous features, including cerebriform connective tissue nevi (CCTN), epidermal nevi, vascular malformations, and adipose abnormalities, can alert the dermatologist to the underlying condition before the onset of asymmetric skeletal overgrowth.
- The CCTN in PS grows throughout childhood but tends to remain stable in adulthood. Postponing surgical treatment until skin lesions stabilize appears to be the best option. However, for practical purposes, surgical intervention may be required at an earlier phase to address the severe functional and cosmetic consequences.

Young patients suffer most from PBC
Youth is no ally when it comes to primary biliary cholangitis, according to a review of 1,990 patients in the United Kingdom–PBC cohort, the largest primary biliary cholangitis cohort in the world.
The investigators previously found that younger patients are less likely to respond to the mainstay treatment, ursodeoxycholic acid (UDCA), and more likely to eventually need a liver transplant and die from the chronic autoimmune disease. Their new study found that they also suffer most from symptoms and have the lowest quality of life.
There was a linear relationship between age and quality of life (QoL) in this study of 1,990 primary biliary cholangitis patients; people who presented at age 20 had more than a 50% chance of reporting a poor QoL, while those presenting at age 70 had less than a 30% chance.
Overall perception of primary biliary cholangitis (PBC)-related QoL and individual severity of all symptoms, as is true with UDCA response, were strongly related to the age of onset of disease, with younger presenting patients experiencing the greatest impact. Each 10-year increase in presentation age was associated with a 14% decrease in the risk of poor QoL (OR, 0.86; 95% CI, 0.75–0.98; P less than .05), after adjustment for gender, disease severity, UDCA response, and disease duration. Presentations before the age of, perhaps, 50 years signal the need for greater vigilance (Aliment Pharmacol Ther. 2016 Nov;44[10]:1039-50).
The findings challenge “the view that PBC is a relatively benign condition of typically older people with limited clinical impact.” The biology “or natural history of PBC may differ between different patient groups, with younger-presenting patients having a more aggressive or materially different form of the disease.” Alternatively, the “enhanced symptom impact in younger patients may be [due to] age-related differences in [the expectation] of chronic disease, personal coping skills, and support networks,” said Jessica Dyson, MBBS, of Newcastle University, Newcastle upon Tyne (England), and her associates.
QoL was most affected by social isolation. “Addressing and treating this single aspect could improve global quality of life significantly... Approaches could range from simple counseling to alert patients to the potential for social isolation, to the development of support groups, to the development of newer digital approaches to social networking through social media,” Dr. Dyson and her colleagues said.
Fatigue, anxiety, and depression also were especially vexing for younger patients, and could “be related to fear of the future and ability to cope, uncertainty as to disease prognosis, and frustration at limitations to life quality,” they said.
“Specifically targeting fatigue is likely to pay dividends,” but “there are currently no therapies able to do that.” However, “a more sociological approach targeting social isolation and the depression and anxiety which may accompany it are very viable approaches.” The findings should help guide future intervention trials, the team said.
QoL was assessed by the PBC-40, a 40 item questionnaire about fatigue; itch; and emotional, social, cognitive, and general symptoms. Each item is scored from 1 to 5, with higher scores indicating greater symptom severity.
The team used the results to assign patients a global QoL score from 1-5 points; scores of 1-3 indicated neutral or good QoL, while 4-5 signaled poor QoL. Overall, two-thirds of patients reported neutral/good scores, and a third had poor scores.
Meanwhile, patients doing well had a median of 18 of 50 possible points on the PBC-40 social score, while those not doing well had a median score of 34 points.
Patients in the study, 91% of whom were women, presented at a median age of 55 years, but 493 presented before the age of 50.
This research was supported by the British Medical Research Council and the National Institute for Health Research, among others. Dr. Dyson had no disclosures, but other authors reported relationships with a range of pharmaceutical companies, including Abbvie, GSK, Intercept, Novartis, and Pfizer.
Youth is no ally when it comes to primary biliary cholangitis, according to a review of 1,990 patients in the United Kingdom–PBC cohort, the largest primary biliary cholangitis cohort in the world.
The investigators previously found that younger patients are less likely to respond to the mainstay treatment, ursodeoxycholic acid (UDCA), and more likely to eventually need a liver transplant and die from the chronic autoimmune disease. Their new study found that they also suffer most from symptoms and have the lowest quality of life.
There was a linear relationship between age and quality of life (QoL) in this study of 1,990 primary biliary cholangitis patients; people who presented at age 20 had more than a 50% chance of reporting a poor QoL, while those presenting at age 70 had less than a 30% chance.
Overall perception of primary biliary cholangitis (PBC)-related QoL and individual severity of all symptoms, as is true with UDCA response, were strongly related to the age of onset of disease, with younger presenting patients experiencing the greatest impact. Each 10-year increase in presentation age was associated with a 14% decrease in the risk of poor QoL (OR, 0.86; 95% CI, 0.75–0.98; P less than .05), after adjustment for gender, disease severity, UDCA response, and disease duration. Presentations before the age of, perhaps, 50 years signal the need for greater vigilance (Aliment Pharmacol Ther. 2016 Nov;44[10]:1039-50).
The findings challenge “the view that PBC is a relatively benign condition of typically older people with limited clinical impact.” The biology “or natural history of PBC may differ between different patient groups, with younger-presenting patients having a more aggressive or materially different form of the disease.” Alternatively, the “enhanced symptom impact in younger patients may be [due to] age-related differences in [the expectation] of chronic disease, personal coping skills, and support networks,” said Jessica Dyson, MBBS, of Newcastle University, Newcastle upon Tyne (England), and her associates.
QoL was most affected by social isolation. “Addressing and treating this single aspect could improve global quality of life significantly... Approaches could range from simple counseling to alert patients to the potential for social isolation, to the development of support groups, to the development of newer digital approaches to social networking through social media,” Dr. Dyson and her colleagues said.
Fatigue, anxiety, and depression also were especially vexing for younger patients, and could “be related to fear of the future and ability to cope, uncertainty as to disease prognosis, and frustration at limitations to life quality,” they said.
“Specifically targeting fatigue is likely to pay dividends,” but “there are currently no therapies able to do that.” However, “a more sociological approach targeting social isolation and the depression and anxiety which may accompany it are very viable approaches.” The findings should help guide future intervention trials, the team said.
QoL was assessed by the PBC-40, a 40 item questionnaire about fatigue; itch; and emotional, social, cognitive, and general symptoms. Each item is scored from 1 to 5, with higher scores indicating greater symptom severity.
The team used the results to assign patients a global QoL score from 1-5 points; scores of 1-3 indicated neutral or good QoL, while 4-5 signaled poor QoL. Overall, two-thirds of patients reported neutral/good scores, and a third had poor scores.
Meanwhile, patients doing well had a median of 18 of 50 possible points on the PBC-40 social score, while those not doing well had a median score of 34 points.
Patients in the study, 91% of whom were women, presented at a median age of 55 years, but 493 presented before the age of 50.
This research was supported by the British Medical Research Council and the National Institute for Health Research, among others. Dr. Dyson had no disclosures, but other authors reported relationships with a range of pharmaceutical companies, including Abbvie, GSK, Intercept, Novartis, and Pfizer.
Youth is no ally when it comes to primary biliary cholangitis, according to a review of 1,990 patients in the United Kingdom–PBC cohort, the largest primary biliary cholangitis cohort in the world.
The investigators previously found that younger patients are less likely to respond to the mainstay treatment, ursodeoxycholic acid (UDCA), and more likely to eventually need a liver transplant and die from the chronic autoimmune disease. Their new study found that they also suffer most from symptoms and have the lowest quality of life.
There was a linear relationship between age and quality of life (QoL) in this study of 1,990 primary biliary cholangitis patients; people who presented at age 20 had more than a 50% chance of reporting a poor QoL, while those presenting at age 70 had less than a 30% chance.
Overall perception of primary biliary cholangitis (PBC)-related QoL and individual severity of all symptoms, as is true with UDCA response, were strongly related to the age of onset of disease, with younger presenting patients experiencing the greatest impact. Each 10-year increase in presentation age was associated with a 14% decrease in the risk of poor QoL (OR, 0.86; 95% CI, 0.75–0.98; P less than .05), after adjustment for gender, disease severity, UDCA response, and disease duration. Presentations before the age of, perhaps, 50 years signal the need for greater vigilance (Aliment Pharmacol Ther. 2016 Nov;44[10]:1039-50).
The findings challenge “the view that PBC is a relatively benign condition of typically older people with limited clinical impact.” The biology “or natural history of PBC may differ between different patient groups, with younger-presenting patients having a more aggressive or materially different form of the disease.” Alternatively, the “enhanced symptom impact in younger patients may be [due to] age-related differences in [the expectation] of chronic disease, personal coping skills, and support networks,” said Jessica Dyson, MBBS, of Newcastle University, Newcastle upon Tyne (England), and her associates.
QoL was most affected by social isolation. “Addressing and treating this single aspect could improve global quality of life significantly... Approaches could range from simple counseling to alert patients to the potential for social isolation, to the development of support groups, to the development of newer digital approaches to social networking through social media,” Dr. Dyson and her colleagues said.
Fatigue, anxiety, and depression also were especially vexing for younger patients, and could “be related to fear of the future and ability to cope, uncertainty as to disease prognosis, and frustration at limitations to life quality,” they said.
“Specifically targeting fatigue is likely to pay dividends,” but “there are currently no therapies able to do that.” However, “a more sociological approach targeting social isolation and the depression and anxiety which may accompany it are very viable approaches.” The findings should help guide future intervention trials, the team said.
QoL was assessed by the PBC-40, a 40 item questionnaire about fatigue; itch; and emotional, social, cognitive, and general symptoms. Each item is scored from 1 to 5, with higher scores indicating greater symptom severity.
The team used the results to assign patients a global QoL score from 1-5 points; scores of 1-3 indicated neutral or good QoL, while 4-5 signaled poor QoL. Overall, two-thirds of patients reported neutral/good scores, and a third had poor scores.
Meanwhile, patients doing well had a median of 18 of 50 possible points on the PBC-40 social score, while those not doing well had a median score of 34 points.
Patients in the study, 91% of whom were women, presented at a median age of 55 years, but 493 presented before the age of 50.
This research was supported by the British Medical Research Council and the National Institute for Health Research, among others. Dr. Dyson had no disclosures, but other authors reported relationships with a range of pharmaceutical companies, including Abbvie, GSK, Intercept, Novartis, and Pfizer.
FROM ALIMENTARY PHARMACOLOGY AND THERAPEUTICS
Key clinical point:
Major finding: There was a linear relationship between age and quality of life (QoL) in patients with primary biliary cholangitis, with younger presenting patients having the poorest QoL. Each 10-year increase in presentation age was associated with a 14% decrease in the risk of poor QoL.
Data source: Review of 1,990 patients in the United Kingdom–PBC cohort.
Disclosures: The work was funded by the British Medical Research Council and the National Institute for Health Research, among others. Dr. Dyson had no disclosures, but other authors reported relationships with a range of pharmaceutical companies, including Abbvie, GSK, Intercept, and Novartis.
Claimed missteps lead to brain damage: $53M award

Claimed missteps lead to brain damage: $53M award

At 2:00 AM, a woman at 40 weeks’ gestation went to a hospital because she felt a decrease in fetal movement. At birth, the baby was not breathing. He was rushed to the neonatal intensive care unit where he was resuscitated and placed on life support. He remained in critical care for 4 weeks. The child has cerebral palsy and cannot walk, talk, or care for himself. He will need 24-hour care for the rest of his life.
PARENT’S CLAIM:
The lawsuit cited 20 alleged missteps by physicians and nurses, including failure to: react to abnormal fetal heart-rate patterns that indicated fetal distress, perform a timely cesarean delivery, and follow a chain of command. During the 12 hours that the mother was in labor at the hospital, nurses and physicians allegedly ignored her. Although the fetal heart-rate monitor showed fetal distress, the mother continued to lie unattended. At 12:40 PM, physicians called for cesarean delivery due to fetal distress, but it took an hour for the child to be born.
The negligence of the hospital staff and delay in delivery caused hypoxia, resulting in cerebral palsy. All medical records from the hospital’s neonatal clinic show that he suffered hypoxia at birth.
HOSPITAL’S DEFENSE:
The mother and child were treated for an infection, which is a recognized cause of cerebral palsy. The child was born with normal blood oxygen levels. His injury occurred before the mother came to the hospital.
VERDICT:
A $53 million Illinois verdict was returned. The hospital applied for a mistrial based on allegedly inflammatory comments by the prosecuting attorney, but that was dismissed.
Birth trauma: $2.75M settlement
A woman had her first prenatal visit at 21 weeks’ gestation. Her advanced maternal age (39 years) and poor health history, including prior delivery of a baby with intrauterine growth restriction (IUGR), put her at risk; her prenatal care was transferred to a high-risk clinic.
At her next prenatal visit, records noted that the mother’s job required excessive standing, that she tested positive for marijuana, and that she was at risk for IUGR. Notes did not say that the mother was informed of her IUGR risk nor was a plan created for additional testing to monitor IUGR.
Ultrasonography (US) performed at 25 weeks’ gestation estimated that the baby’s weight was in the 11th- to 12th-week percentile. Amniotic fluid volume was noted as normal.
The mother missed her next appointment but returned at 28 weeks’ gestation, when she reported a headache and was found to have high blood pressure. US revealed normal fetal heart anatomy but amniotic fluid volume was noted to have decreased since the first US. The mother missed the next several appointments.
When she presented at 33 weeks’ gestation, her blood pressure was 160/97 mm Hg, fetal heart-rate tones were normal, and there was positive fetal movement. Fundal height measurement revealed a 3-cm discrepancy in date and size, suggesting a small baby, decreased amniotic fluid, or both. The ObGyn ordered testing for the next day. When a nonstress test performed from 8:44 AM to 9:10 AM was nonreassuring, the mother was ordered to immediately go to the hospital. She did not arrive at the hospital until 11:13 AM, when she was placed on fetal heart-rate monitor; test results were nonreassuring. At 11:30 AM, US revealed IUGR and oligohydramnios. An urgent cesarean delivery was performed and the baby was born at 11:56 AM.
The child’s Apgar scores were 4 and 9 at 1 and 5 minutes, respectively. The baby developed white matter brain damage and grade III and IV intraventricular hemorrhages due to hypoxia, ischemia, and metabolic acidosis. A maternal drug screen was positive for marijuana. Placental pathology revealed multiple abnormalities including placental infarcts involving approximately 50% of placental tissue, abnormal vascular changes, intervillous fibrin deposition, and chronic villitis.
At trial, the child had developmental delays, cognitive defects, learning disabilities, and breakthrough seizures.
PARENT’S CLAIM:
The mother claimed that the high-risk clinic was negligent. A plan should have been put into place at her first visit to monitor for IUGR based on her history. She was not advised of her risk of having another IUGR baby. Fundal height measurement, US to test for IUGR, or assessments of fetal heart-rate tones and fetal movement were not performed regularly. If a nonstress test had been performed earlier than 33 weeks’ gestation, she might have been admitted to the hospital for monitoring and earlier delivery, resulting in a healthier baby.
DEFENDANTS’ DEFENSE:
The mother was noncompliant and missed most of her prenatal appointments. She also continued to smoke marijuana throughout her pregnancy although she was told to stop. When the mother arrived at the prenatal clinic at 33 weeks’ gestation, tests were ordered and delivery occurred in a timely fashion. Any problems suffered by the child were a result of prematurity and damage that occurred during the 5 weeks of missed prenatal appointments.
VERDICT:
A $2.75M Missouri settlement was reached.
Who should have delivered the baby?
A mother’s prenatal care was managed by her family practitioner (FP). The mother went to the FP for induction of labor, but it was unsuccessful. Three days later, the baby was delivered by the FP and began having seizures a few minutes after birth. The child is quadriplegic and has severe cerebral palsy.
PARENTS’ CLAIM:
The FP was negligent in managing labor and delivery. She should have called an ObGyn to manage the labor. She failed to monitor fetal heart-rate tracings and failed to order an emergency cesarean delivery. The FP mismanaged the baby’s condition upon delivery and seizures started.
PHYSICIAN’S DEFENSE:
The FP properly managed the delivery and postdelivery complications. The brain injury had nothing to do with the birth; it was instead caused by a stroke disorder that occurred 3 to 7 days before delivery.
VERDICT:
A Minnesota defense verdict was returned.
Undiagnosed H1N1 influenza (swine flu) during pregnancy; mother and child die: $16.7M verdict
At 7 months’ gestation, a 27-year-old woman presented to a clinic on June 26 with a runny nose, congestion, cough, wheezing, chills, and sweats. The physician noted concern about proteinuria and that the patient reported chills and sweats, but that he was uncertain as to the symptoms’ cause. He recommended that she see her ObGyn immediately and report to the emergency department (ED) if symptoms worsened. The patient called her ObGyn to report having a temperature between 94˚F and 103˚F and taking acetaminophen. The next day, she saw a nurse practitioner in the ObGyn’s office who documented that the patient was not given antiviral medication.
On June 29, the patient was still feeling ill and went to the ED. Although a physician planned to discharge her, an ObGyn nurse recognized that the patient was too ill to leave and had her admitted.
The patient’s condition worsened overnight and she was transferred to the intensive care unit (ICU), where she was intubated and put on a ventilator. Medical notes read “as whether influenza was present was unclear…Tamiflu will be started, but the efficacy of it this late into a possible influenza episode is extremely questionable.” ICU physicians believed that the best option was to deliver the child. After the patient’s husband gave permission, the child was born by cesarean delivery. The mother never regained full consciousness and remained in a medically induced coma. She died on August 11 after the family decided to remove life support.
After being given the diagnosis of intrauterine hypoxia, the child remained in intensive care for several weeks and then was discharged home. Seven months later, the father found his daughter in bed, not breathing, which physicians believed was an episode of sudden infant death syndrome. The father performed CPR and rushed her to the hospital. Physicians tried twice to take the child off the ventilator, but she could not breathe without assistance. On February 21, life support was removed and the child died.
ESTATES’ CLAIM:
The clinic and its physician were negligent for failing to recognize that the mother had influenza; she presented with classic flu symptoms during a worldwide pandemic. In the several months before the patient’s visit, the clinic had received notices from health authorities alerting medical professionals to the dangers of H1N1 influenza, or Swine Flu. The clinic also had received, before the patient’s visit, information warning of an elevated risk of H1N1 to pregnant women, with instructions to administer oseltamivir phosphate (Tamiflu) to any pregnant woman suspected of having influenza.
DEFENDANTS’ DEFENSE:
The clinic and physician denied negligence, claiming that treatment of the mother was appropriate.
VERDICT:
A $16.7 million Washington verdict was returned.
Mother claims to being uninformed of antiepileptics’ risks
A woman with epilepsy gave birth to a child with physical and cognitive birth defects.
PARENT’S CLAIM:
The mother claimed that, although she was of child-bearing age, she had never been informed of the risk of birth defects associated with taking an antiepileptic medication. Had she known of the risk, she would not have chosen to conceive. The physicians should have prescribed a different antiepileptic drug.
DEFENDANTS’ DEFENSE:
The clinic’s physicians met the standard of care in prescribing the drug. They properly informed the mother of the risks of taking the antiepileptic drug during pregnancy. The patient was allergic to all other antiepileptic drugs available at the time, so an alternative was not available.
VERDICT:
An Illinois defense verdict was returned for the clinic.
Mother has stroke during delivery: $3M settlement
A 42-year-old woman had a hemorrhagic stroke during the delivery of her first child. She remained hospitalized for observation with a medical plan to insert a drain if her condition worsened. Initially she did well, but she then began to have episodes of decreased consciousness and loss of function and later became unresponsive. Her physicians then undertook an emergency procedure to attempt to drain blood from her brain, but the surgical measure did not prevent her from incurring significant cognitive and physical injuries.
PATIENT’S CLAIM:
The agreed-upon medical plan of treatment was not followed, resulting in severe brain damage to the patient.
DEFENDANTS’ DEFENSE:
The case was settled during the trial.
VERDICT:
A $3 million Massachusetts settlement was reached.
Did delayed cesarean cause cognitive defects?
When fetal distress was detected, the nurse called the patient’s ObGyn at 12:30 AM. The ObGyn arrived at the hospital at 12:48 AM, ordered a cesarean delivery at 12:56 AM, and the baby was born at 1:20 AM.
PARENTS’ CLAIM:
The ObGyn was negligent for not calling for the hospital’s on-duty resident physician to become involved in the case when the nurse phoned at 12:30 AM. If the ObGyn had done so, cesarean delivery would have been ordered and completed earlier, which would have averted the child’s injuries, including cognitive and physical impairments.
PHYSICIAN’S DEFENSE:
The ObGyn asserted that, based on the information provided to her, there was no reason to request the resident’s involvement. An earlier cesarean delivery was not necessary based on fetal heart-rate monitoring strip results. The ObGyn acted in a timely manner when calling for cesarean delivery. There was no concrete evidence that any alleged delay caused the child’s injuries.
VERDICT:
An Illinois defense verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Claimed missteps lead to brain damage: $53M award
At 2:00 AM, a woman at 40 weeks’ gestation went to a hospital because she felt a decrease in fetal movement. At birth, the baby was not breathing. He was rushed to the neonatal intensive care unit where he was resuscitated and placed on life support. He remained in critical care for 4 weeks. The child has cerebral palsy and cannot walk, talk, or care for himself. He will need 24-hour care for the rest of his life.
PARENT’S CLAIM:
The lawsuit cited 20 alleged missteps by physicians and nurses, including failure to: react to abnormal fetal heart-rate patterns that indicated fetal distress, perform a timely cesarean delivery, and follow a chain of command. During the 12 hours that the mother was in labor at the hospital, nurses and physicians allegedly ignored her. Although the fetal heart-rate monitor showed fetal distress, the mother continued to lie unattended. At 12:40 PM, physicians called for cesarean delivery due to fetal distress, but it took an hour for the child to be born.
The negligence of the hospital staff and delay in delivery caused hypoxia, resulting in cerebral palsy. All medical records from the hospital’s neonatal clinic show that he suffered hypoxia at birth.
HOSPITAL’S DEFENSE:
The mother and child were treated for an infection, which is a recognized cause of cerebral palsy. The child was born with normal blood oxygen levels. His injury occurred before the mother came to the hospital.
VERDICT:
A $53 million Illinois verdict was returned. The hospital applied for a mistrial based on allegedly inflammatory comments by the prosecuting attorney, but that was dismissed.
Birth trauma: $2.75M settlement
A woman had her first prenatal visit at 21 weeks’ gestation. Her advanced maternal age (39 years) and poor health history, including prior delivery of a baby with intrauterine growth restriction (IUGR), put her at risk; her prenatal care was transferred to a high-risk clinic.
At her next prenatal visit, records noted that the mother’s job required excessive standing, that she tested positive for marijuana, and that she was at risk for IUGR. Notes did not say that the mother was informed of her IUGR risk nor was a plan created for additional testing to monitor IUGR.
Ultrasonography (US) performed at 25 weeks’ gestation estimated that the baby’s weight was in the 11th- to 12th-week percentile. Amniotic fluid volume was noted as normal.
The mother missed her next appointment but returned at 28 weeks’ gestation, when she reported a headache and was found to have high blood pressure. US revealed normal fetal heart anatomy but amniotic fluid volume was noted to have decreased since the first US. The mother missed the next several appointments.
When she presented at 33 weeks’ gestation, her blood pressure was 160/97 mm Hg, fetal heart-rate tones were normal, and there was positive fetal movement. Fundal height measurement revealed a 3-cm discrepancy in date and size, suggesting a small baby, decreased amniotic fluid, or both. The ObGyn ordered testing for the next day. When a nonstress test performed from 8:44 AM to 9:10 AM was nonreassuring, the mother was ordered to immediately go to the hospital. She did not arrive at the hospital until 11:13 AM, when she was placed on fetal heart-rate monitor; test results were nonreassuring. At 11:30 AM, US revealed IUGR and oligohydramnios. An urgent cesarean delivery was performed and the baby was born at 11:56 AM.
The child’s Apgar scores were 4 and 9 at 1 and 5 minutes, respectively. The baby developed white matter brain damage and grade III and IV intraventricular hemorrhages due to hypoxia, ischemia, and metabolic acidosis. A maternal drug screen was positive for marijuana. Placental pathology revealed multiple abnormalities including placental infarcts involving approximately 50% of placental tissue, abnormal vascular changes, intervillous fibrin deposition, and chronic villitis.
At trial, the child had developmental delays, cognitive defects, learning disabilities, and breakthrough seizures.
PARENT’S CLAIM:
The mother claimed that the high-risk clinic was negligent. A plan should have been put into place at her first visit to monitor for IUGR based on her history. She was not advised of her risk of having another IUGR baby. Fundal height measurement, US to test for IUGR, or assessments of fetal heart-rate tones and fetal movement were not performed regularly. If a nonstress test had been performed earlier than 33 weeks’ gestation, she might have been admitted to the hospital for monitoring and earlier delivery, resulting in a healthier baby.
DEFENDANTS’ DEFENSE:
The mother was noncompliant and missed most of her prenatal appointments. She also continued to smoke marijuana throughout her pregnancy although she was told to stop. When the mother arrived at the prenatal clinic at 33 weeks’ gestation, tests were ordered and delivery occurred in a timely fashion. Any problems suffered by the child were a result of prematurity and damage that occurred during the 5 weeks of missed prenatal appointments.
VERDICT:
A $2.75M Missouri settlement was reached.
Who should have delivered the baby?
A mother’s prenatal care was managed by her family practitioner (FP). The mother went to the FP for induction of labor, but it was unsuccessful. Three days later, the baby was delivered by the FP and began having seizures a few minutes after birth. The child is quadriplegic and has severe cerebral palsy.
PARENTS’ CLAIM:
The FP was negligent in managing labor and delivery. She should have called an ObGyn to manage the labor. She failed to monitor fetal heart-rate tracings and failed to order an emergency cesarean delivery. The FP mismanaged the baby’s condition upon delivery and seizures started.
PHYSICIAN’S DEFENSE:
The FP properly managed the delivery and postdelivery complications. The brain injury had nothing to do with the birth; it was instead caused by a stroke disorder that occurred 3 to 7 days before delivery.
VERDICT:
A Minnesota defense verdict was returned.
Undiagnosed H1N1 influenza (swine flu) during pregnancy; mother and child die: $16.7M verdict
At 7 months’ gestation, a 27-year-old woman presented to a clinic on June 26 with a runny nose, congestion, cough, wheezing, chills, and sweats. The physician noted concern about proteinuria and that the patient reported chills and sweats, but that he was uncertain as to the symptoms’ cause. He recommended that she see her ObGyn immediately and report to the emergency department (ED) if symptoms worsened. The patient called her ObGyn to report having a temperature between 94˚F and 103˚F and taking acetaminophen. The next day, she saw a nurse practitioner in the ObGyn’s office who documented that the patient was not given antiviral medication.
On June 29, the patient was still feeling ill and went to the ED. Although a physician planned to discharge her, an ObGyn nurse recognized that the patient was too ill to leave and had her admitted.
The patient’s condition worsened overnight and she was transferred to the intensive care unit (ICU), where she was intubated and put on a ventilator. Medical notes read “as whether influenza was present was unclear…Tamiflu will be started, but the efficacy of it this late into a possible influenza episode is extremely questionable.” ICU physicians believed that the best option was to deliver the child. After the patient’s husband gave permission, the child was born by cesarean delivery. The mother never regained full consciousness and remained in a medically induced coma. She died on August 11 after the family decided to remove life support.
After being given the diagnosis of intrauterine hypoxia, the child remained in intensive care for several weeks and then was discharged home. Seven months later, the father found his daughter in bed, not breathing, which physicians believed was an episode of sudden infant death syndrome. The father performed CPR and rushed her to the hospital. Physicians tried twice to take the child off the ventilator, but she could not breathe without assistance. On February 21, life support was removed and the child died.
ESTATES’ CLAIM:
The clinic and its physician were negligent for failing to recognize that the mother had influenza; she presented with classic flu symptoms during a worldwide pandemic. In the several months before the patient’s visit, the clinic had received notices from health authorities alerting medical professionals to the dangers of H1N1 influenza, or Swine Flu. The clinic also had received, before the patient’s visit, information warning of an elevated risk of H1N1 to pregnant women, with instructions to administer oseltamivir phosphate (Tamiflu) to any pregnant woman suspected of having influenza.
DEFENDANTS’ DEFENSE:
The clinic and physician denied negligence, claiming that treatment of the mother was appropriate.
VERDICT:
A $16.7 million Washington verdict was returned.
Mother claims to being uninformed of antiepileptics’ risks
A woman with epilepsy gave birth to a child with physical and cognitive birth defects.
PARENT’S CLAIM:
The mother claimed that, although she was of child-bearing age, she had never been informed of the risk of birth defects associated with taking an antiepileptic medication. Had she known of the risk, she would not have chosen to conceive. The physicians should have prescribed a different antiepileptic drug.
DEFENDANTS’ DEFENSE:
The clinic’s physicians met the standard of care in prescribing the drug. They properly informed the mother of the risks of taking the antiepileptic drug during pregnancy. The patient was allergic to all other antiepileptic drugs available at the time, so an alternative was not available.
VERDICT:
An Illinois defense verdict was returned for the clinic.
Mother has stroke during delivery: $3M settlement
A 42-year-old woman had a hemorrhagic stroke during the delivery of her first child. She remained hospitalized for observation with a medical plan to insert a drain if her condition worsened. Initially she did well, but she then began to have episodes of decreased consciousness and loss of function and later became unresponsive. Her physicians then undertook an emergency procedure to attempt to drain blood from her brain, but the surgical measure did not prevent her from incurring significant cognitive and physical injuries.
PATIENT’S CLAIM:
The agreed-upon medical plan of treatment was not followed, resulting in severe brain damage to the patient.
DEFENDANTS’ DEFENSE:
The case was settled during the trial.
VERDICT:
A $3 million Massachusetts settlement was reached.
Did delayed cesarean cause cognitive defects?
When fetal distress was detected, the nurse called the patient’s ObGyn at 12:30 AM. The ObGyn arrived at the hospital at 12:48 AM, ordered a cesarean delivery at 12:56 AM, and the baby was born at 1:20 AM.
PARENTS’ CLAIM:
The ObGyn was negligent for not calling for the hospital’s on-duty resident physician to become involved in the case when the nurse phoned at 12:30 AM. If the ObGyn had done so, cesarean delivery would have been ordered and completed earlier, which would have averted the child’s injuries, including cognitive and physical impairments.
PHYSICIAN’S DEFENSE:
The ObGyn asserted that, based on the information provided to her, there was no reason to request the resident’s involvement. An earlier cesarean delivery was not necessary based on fetal heart-rate monitoring strip results. The ObGyn acted in a timely manner when calling for cesarean delivery. There was no concrete evidence that any alleged delay caused the child’s injuries.
VERDICT:
An Illinois defense verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Claimed missteps lead to brain damage: $53M award
At 2:00 AM, a woman at 40 weeks’ gestation went to a hospital because she felt a decrease in fetal movement. At birth, the baby was not breathing. He was rushed to the neonatal intensive care unit where he was resuscitated and placed on life support. He remained in critical care for 4 weeks. The child has cerebral palsy and cannot walk, talk, or care for himself. He will need 24-hour care for the rest of his life.
PARENT’S CLAIM:
The lawsuit cited 20 alleged missteps by physicians and nurses, including failure to: react to abnormal fetal heart-rate patterns that indicated fetal distress, perform a timely cesarean delivery, and follow a chain of command. During the 12 hours that the mother was in labor at the hospital, nurses and physicians allegedly ignored her. Although the fetal heart-rate monitor showed fetal distress, the mother continued to lie unattended. At 12:40 PM, physicians called for cesarean delivery due to fetal distress, but it took an hour for the child to be born.
The negligence of the hospital staff and delay in delivery caused hypoxia, resulting in cerebral palsy. All medical records from the hospital’s neonatal clinic show that he suffered hypoxia at birth.
HOSPITAL’S DEFENSE:
The mother and child were treated for an infection, which is a recognized cause of cerebral palsy. The child was born with normal blood oxygen levels. His injury occurred before the mother came to the hospital.
VERDICT:
A $53 million Illinois verdict was returned. The hospital applied for a mistrial based on allegedly inflammatory comments by the prosecuting attorney, but that was dismissed.
Birth trauma: $2.75M settlement
A woman had her first prenatal visit at 21 weeks’ gestation. Her advanced maternal age (39 years) and poor health history, including prior delivery of a baby with intrauterine growth restriction (IUGR), put her at risk; her prenatal care was transferred to a high-risk clinic.
At her next prenatal visit, records noted that the mother’s job required excessive standing, that she tested positive for marijuana, and that she was at risk for IUGR. Notes did not say that the mother was informed of her IUGR risk nor was a plan created for additional testing to monitor IUGR.
Ultrasonography (US) performed at 25 weeks’ gestation estimated that the baby’s weight was in the 11th- to 12th-week percentile. Amniotic fluid volume was noted as normal.
The mother missed her next appointment but returned at 28 weeks’ gestation, when she reported a headache and was found to have high blood pressure. US revealed normal fetal heart anatomy but amniotic fluid volume was noted to have decreased since the first US. The mother missed the next several appointments.
When she presented at 33 weeks’ gestation, her blood pressure was 160/97 mm Hg, fetal heart-rate tones were normal, and there was positive fetal movement. Fundal height measurement revealed a 3-cm discrepancy in date and size, suggesting a small baby, decreased amniotic fluid, or both. The ObGyn ordered testing for the next day. When a nonstress test performed from 8:44 AM to 9:10 AM was nonreassuring, the mother was ordered to immediately go to the hospital. She did not arrive at the hospital until 11:13 AM, when she was placed on fetal heart-rate monitor; test results were nonreassuring. At 11:30 AM, US revealed IUGR and oligohydramnios. An urgent cesarean delivery was performed and the baby was born at 11:56 AM.
The child’s Apgar scores were 4 and 9 at 1 and 5 minutes, respectively. The baby developed white matter brain damage and grade III and IV intraventricular hemorrhages due to hypoxia, ischemia, and metabolic acidosis. A maternal drug screen was positive for marijuana. Placental pathology revealed multiple abnormalities including placental infarcts involving approximately 50% of placental tissue, abnormal vascular changes, intervillous fibrin deposition, and chronic villitis.
At trial, the child had developmental delays, cognitive defects, learning disabilities, and breakthrough seizures.
PARENT’S CLAIM:
The mother claimed that the high-risk clinic was negligent. A plan should have been put into place at her first visit to monitor for IUGR based on her history. She was not advised of her risk of having another IUGR baby. Fundal height measurement, US to test for IUGR, or assessments of fetal heart-rate tones and fetal movement were not performed regularly. If a nonstress test had been performed earlier than 33 weeks’ gestation, she might have been admitted to the hospital for monitoring and earlier delivery, resulting in a healthier baby.
DEFENDANTS’ DEFENSE:
The mother was noncompliant and missed most of her prenatal appointments. She also continued to smoke marijuana throughout her pregnancy although she was told to stop. When the mother arrived at the prenatal clinic at 33 weeks’ gestation, tests were ordered and delivery occurred in a timely fashion. Any problems suffered by the child were a result of prematurity and damage that occurred during the 5 weeks of missed prenatal appointments.
VERDICT:
A $2.75M Missouri settlement was reached.
Who should have delivered the baby?
A mother’s prenatal care was managed by her family practitioner (FP). The mother went to the FP for induction of labor, but it was unsuccessful. Three days later, the baby was delivered by the FP and began having seizures a few minutes after birth. The child is quadriplegic and has severe cerebral palsy.
PARENTS’ CLAIM:
The FP was negligent in managing labor and delivery. She should have called an ObGyn to manage the labor. She failed to monitor fetal heart-rate tracings and failed to order an emergency cesarean delivery. The FP mismanaged the baby’s condition upon delivery and seizures started.
PHYSICIAN’S DEFENSE:
The FP properly managed the delivery and postdelivery complications. The brain injury had nothing to do with the birth; it was instead caused by a stroke disorder that occurred 3 to 7 days before delivery.
VERDICT:
A Minnesota defense verdict was returned.
Undiagnosed H1N1 influenza (swine flu) during pregnancy; mother and child die: $16.7M verdict
At 7 months’ gestation, a 27-year-old woman presented to a clinic on June 26 with a runny nose, congestion, cough, wheezing, chills, and sweats. The physician noted concern about proteinuria and that the patient reported chills and sweats, but that he was uncertain as to the symptoms’ cause. He recommended that she see her ObGyn immediately and report to the emergency department (ED) if symptoms worsened. The patient called her ObGyn to report having a temperature between 94˚F and 103˚F and taking acetaminophen. The next day, she saw a nurse practitioner in the ObGyn’s office who documented that the patient was not given antiviral medication.
On June 29, the patient was still feeling ill and went to the ED. Although a physician planned to discharge her, an ObGyn nurse recognized that the patient was too ill to leave and had her admitted.
The patient’s condition worsened overnight and she was transferred to the intensive care unit (ICU), where she was intubated and put on a ventilator. Medical notes read “as whether influenza was present was unclear…Tamiflu will be started, but the efficacy of it this late into a possible influenza episode is extremely questionable.” ICU physicians believed that the best option was to deliver the child. After the patient’s husband gave permission, the child was born by cesarean delivery. The mother never regained full consciousness and remained in a medically induced coma. She died on August 11 after the family decided to remove life support.
After being given the diagnosis of intrauterine hypoxia, the child remained in intensive care for several weeks and then was discharged home. Seven months later, the father found his daughter in bed, not breathing, which physicians believed was an episode of sudden infant death syndrome. The father performed CPR and rushed her to the hospital. Physicians tried twice to take the child off the ventilator, but she could not breathe without assistance. On February 21, life support was removed and the child died.
ESTATES’ CLAIM:
The clinic and its physician were negligent for failing to recognize that the mother had influenza; she presented with classic flu symptoms during a worldwide pandemic. In the several months before the patient’s visit, the clinic had received notices from health authorities alerting medical professionals to the dangers of H1N1 influenza, or Swine Flu. The clinic also had received, before the patient’s visit, information warning of an elevated risk of H1N1 to pregnant women, with instructions to administer oseltamivir phosphate (Tamiflu) to any pregnant woman suspected of having influenza.
DEFENDANTS’ DEFENSE:
The clinic and physician denied negligence, claiming that treatment of the mother was appropriate.
VERDICT:
A $16.7 million Washington verdict was returned.
Mother claims to being uninformed of antiepileptics’ risks
A woman with epilepsy gave birth to a child with physical and cognitive birth defects.
PARENT’S CLAIM:
The mother claimed that, although she was of child-bearing age, she had never been informed of the risk of birth defects associated with taking an antiepileptic medication. Had she known of the risk, she would not have chosen to conceive. The physicians should have prescribed a different antiepileptic drug.
DEFENDANTS’ DEFENSE:
The clinic’s physicians met the standard of care in prescribing the drug. They properly informed the mother of the risks of taking the antiepileptic drug during pregnancy. The patient was allergic to all other antiepileptic drugs available at the time, so an alternative was not available.
VERDICT:
An Illinois defense verdict was returned for the clinic.
Mother has stroke during delivery: $3M settlement
A 42-year-old woman had a hemorrhagic stroke during the delivery of her first child. She remained hospitalized for observation with a medical plan to insert a drain if her condition worsened. Initially she did well, but she then began to have episodes of decreased consciousness and loss of function and later became unresponsive. Her physicians then undertook an emergency procedure to attempt to drain blood from her brain, but the surgical measure did not prevent her from incurring significant cognitive and physical injuries.
PATIENT’S CLAIM:
The agreed-upon medical plan of treatment was not followed, resulting in severe brain damage to the patient.
DEFENDANTS’ DEFENSE:
The case was settled during the trial.
VERDICT:
A $3 million Massachusetts settlement was reached.
Did delayed cesarean cause cognitive defects?
When fetal distress was detected, the nurse called the patient’s ObGyn at 12:30 AM. The ObGyn arrived at the hospital at 12:48 AM, ordered a cesarean delivery at 12:56 AM, and the baby was born at 1:20 AM.
PARENTS’ CLAIM:
The ObGyn was negligent for not calling for the hospital’s on-duty resident physician to become involved in the case when the nurse phoned at 12:30 AM. If the ObGyn had done so, cesarean delivery would have been ordered and completed earlier, which would have averted the child’s injuries, including cognitive and physical impairments.
PHYSICIAN’S DEFENSE:
The ObGyn asserted that, based on the information provided to her, there was no reason to request the resident’s involvement. An earlier cesarean delivery was not necessary based on fetal heart-rate monitoring strip results. The ObGyn acted in a timely manner when calling for cesarean delivery. There was no concrete evidence that any alleged delay caused the child’s injuries.
VERDICT:
An Illinois defense verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
FDA Boxed Warnings
The FDA’s MedWatch program safety labeling changes for boxed warnings are compiled quarterly for drugs and therapeutic biologics where important changes have been made to the safety information. You can search these and other label changes in the Drug Safety Labeling Changes (SLC) database, where data are available to the public in downloadable and searchable formats. Boxed warnings are ordinarily used to highlight either adverse reactions so serious in proportion to the potential bene t from the drug that it is essential that it be considered in assessing the risks and bene ts of using the drug; or serious adverse reactions that can be prevented/reduced in frequency or severity by appropriate use of the drug; or FDA approved the drug with restrictions to ensure safe use because FDA concluded that the drug can be safely used only if distribution or use is restricted.
NONSTEROIDAL ANTI-INFLAMMATORY DRUGS:
Updated Warning May 2016
WARNING: RISK OF SERIOUS CARDIOVASCULAR AND GASTROINTESTINAL EVENTS
Cardiovascular Thrombotic Events
• Nonsteroidal anti-inflammatory drugs (NSAIDs) cause an increased risk of serious cardiovascular thrombotic events, including myocardial infarction and stroke, which can be fatal. This risk may occur early in treatment and may increase with duration of use.
• NSAID is contraindicated in the setting of coronary artery bypass graft surgery.
Gastrointestinal Bleeding, Ulceration, and Perforation
NSAIDs cause an increased risk of serious gastrointestinal (GI) adverse events including bleeding, ulceration, and perforation of the stomach or intestines, which can be fatal. These events can occur at any time during use and without warning symptoms. Elderly patients and patients with a prior history of peptic ulcer disease and/or GI bleeding are at greater risk for serious GI events.
JUXTAPID (lomitapide) capsules:
- Added section to warning May 2016
Prescribe Juxtapid only to patients with a clinical or laboratory diagnosis consistent with homozygous familial hypercholesterolemia (HoFH). The safety and effectiveness of Juxtapid have not been established in patients with hypercholesterolemia who do not have HoFH.
KADCYLA (ado-trastuzumab emtansine) injection, for intravenous:
- Edited and updated warning April 2016
Embryo-Fetal Toxicity: Exposure to Kadcyla during pregnancy can result in embryo-fetal harm. Advise patients of these risks and the need for effective contraception.
KYNAMRO (mipomersen sodium) solution for subcutaneous injection:
- Added section to warning May 2016
Prescribe Kynamro only to patients with a clinical or laboratory diagnosis consistent with homozygous familial hypercholesterolemia (HoFH). The safety and effectiveness of Kynamro have not been established in patients with hypercholesterolemia who do not have HoFH.
The FDA’s MedWatch program safety labeling changes for boxed warnings are compiled quarterly for drugs and therapeutic biologics where important changes have been made to the safety information. You can search these and other label changes in the Drug Safety Labeling Changes (SLC) database, where data are available to the public in downloadable and searchable formats. Boxed warnings are ordinarily used to highlight either adverse reactions so serious in proportion to the potential bene t from the drug that it is essential that it be considered in assessing the risks and bene ts of using the drug; or serious adverse reactions that can be prevented/reduced in frequency or severity by appropriate use of the drug; or FDA approved the drug with restrictions to ensure safe use because FDA concluded that the drug can be safely used only if distribution or use is restricted.
NONSTEROIDAL ANTI-INFLAMMATORY DRUGS:
Updated Warning May 2016
WARNING: RISK OF SERIOUS CARDIOVASCULAR AND GASTROINTESTINAL EVENTS
Cardiovascular Thrombotic Events
• Nonsteroidal anti-inflammatory drugs (NSAIDs) cause an increased risk of serious cardiovascular thrombotic events, including myocardial infarction and stroke, which can be fatal. This risk may occur early in treatment and may increase with duration of use.
• NSAID is contraindicated in the setting of coronary artery bypass graft surgery.
Gastrointestinal Bleeding, Ulceration, and Perforation
NSAIDs cause an increased risk of serious gastrointestinal (GI) adverse events including bleeding, ulceration, and perforation of the stomach or intestines, which can be fatal. These events can occur at any time during use and without warning symptoms. Elderly patients and patients with a prior history of peptic ulcer disease and/or GI bleeding are at greater risk for serious GI events.
JUXTAPID (lomitapide) capsules:
- Added section to warning May 2016
Prescribe Juxtapid only to patients with a clinical or laboratory diagnosis consistent with homozygous familial hypercholesterolemia (HoFH). The safety and effectiveness of Juxtapid have not been established in patients with hypercholesterolemia who do not have HoFH.
KADCYLA (ado-trastuzumab emtansine) injection, for intravenous:
- Edited and updated warning April 2016
Embryo-Fetal Toxicity: Exposure to Kadcyla during pregnancy can result in embryo-fetal harm. Advise patients of these risks and the need for effective contraception.
KYNAMRO (mipomersen sodium) solution for subcutaneous injection:
- Added section to warning May 2016
Prescribe Kynamro only to patients with a clinical or laboratory diagnosis consistent with homozygous familial hypercholesterolemia (HoFH). The safety and effectiveness of Kynamro have not been established in patients with hypercholesterolemia who do not have HoFH.
The FDA’s MedWatch program safety labeling changes for boxed warnings are compiled quarterly for drugs and therapeutic biologics where important changes have been made to the safety information. You can search these and other label changes in the Drug Safety Labeling Changes (SLC) database, where data are available to the public in downloadable and searchable formats. Boxed warnings are ordinarily used to highlight either adverse reactions so serious in proportion to the potential bene t from the drug that it is essential that it be considered in assessing the risks and bene ts of using the drug; or serious adverse reactions that can be prevented/reduced in frequency or severity by appropriate use of the drug; or FDA approved the drug with restrictions to ensure safe use because FDA concluded that the drug can be safely used only if distribution or use is restricted.
NONSTEROIDAL ANTI-INFLAMMATORY DRUGS:
Updated Warning May 2016
WARNING: RISK OF SERIOUS CARDIOVASCULAR AND GASTROINTESTINAL EVENTS
Cardiovascular Thrombotic Events
• Nonsteroidal anti-inflammatory drugs (NSAIDs) cause an increased risk of serious cardiovascular thrombotic events, including myocardial infarction and stroke, which can be fatal. This risk may occur early in treatment and may increase with duration of use.
• NSAID is contraindicated in the setting of coronary artery bypass graft surgery.
Gastrointestinal Bleeding, Ulceration, and Perforation
NSAIDs cause an increased risk of serious gastrointestinal (GI) adverse events including bleeding, ulceration, and perforation of the stomach or intestines, which can be fatal. These events can occur at any time during use and without warning symptoms. Elderly patients and patients with a prior history of peptic ulcer disease and/or GI bleeding are at greater risk for serious GI events.
JUXTAPID (lomitapide) capsules:
- Added section to warning May 2016
Prescribe Juxtapid only to patients with a clinical or laboratory diagnosis consistent with homozygous familial hypercholesterolemia (HoFH). The safety and effectiveness of Juxtapid have not been established in patients with hypercholesterolemia who do not have HoFH.
KADCYLA (ado-trastuzumab emtansine) injection, for intravenous:
- Edited and updated warning April 2016
Embryo-Fetal Toxicity: Exposure to Kadcyla during pregnancy can result in embryo-fetal harm. Advise patients of these risks and the need for effective contraception.
KYNAMRO (mipomersen sodium) solution for subcutaneous injection:
- Added section to warning May 2016
Prescribe Kynamro only to patients with a clinical or laboratory diagnosis consistent with homozygous familial hypercholesterolemia (HoFH). The safety and effectiveness of Kynamro have not been established in patients with hypercholesterolemia who do not have HoFH.
Big Health Policy Implications Loom with 2016 Election
Editor's Note: Listen to Robert Blendon talk more about the health policy implications of the 2016 election.

One thing is certain: The outcome of this year’s election will usher in profound change for the American healthcare system. It also means a great deal of uncertainty for physicians, hospital systems, insurers, patients, and healthcare providers more broadly for weeks, months, or even years to come.
The Policy Proposals
Democratic presidential nominee Hillary Clinton has vowed to keep, strengthen, and “fix” the ACA, with proposals that include allowing people to begin buying into Medicare at age 55 and eliminating the Cadillac tax, plus a vow to defend access to reproductive healthcare. Republican nominee Donald Trump has the seven-point “Healthcare Reform to Make America Great Again,” which has as its first pillar to “completely replace Obamacare.”
While Clinton’s platform is highly detailed, Trump has offered few specifics with regard to its replacement, “just a set of general principles,” says Robert Blendon, the Richard L. Menschel Professor of Public Health at Harvard T.H. Chan School of Public Health (HSPH) and a professor of health policy and political analysis at HSPH and the Harvard Kennedy School of Government. “His supporters are just not focused on what the healthcare bill of the future would look like,” he adds.
Under majority Republican leadership, “it’s absolutely clear,” Blendon says, that the party would attempt to repeal the ACA. That would mean millions of people could lose insurance coverage or face higher levels of cost-sharing, benefits would be less comprehensive, and government regulation would decrease, leading to fewer directives for physicians and providers, he says.
A Democratic sweep of the executive and legislative branches would likely bring more funding for the National Institutes of Health and the Centers for Disease Control and Prevention. It might also lead to the introduction of a government alternative insurance plan that would compete with private insurance for those under age 65, Blendon explains.
“There’d be more money spent, but there’d be much more government regulation, including discussions of Medicare price limits on certain types of drugs,” he says.
Healthcare, though, has been caught in the middle of a host of broader issues, Blendon says.
“Put very simply, you almost have three parties that are running,” he says. “You have Democratic, which is [the] more liberal-moderate party, which is basically running on a health platform that is continuing Obama’s eight years but enlarging it in a number of areas. You have the party of the Republicans strictly in the Congress, which are running as a conservative party, which is to get rid of part of the ACA, to slow Medicare costs, and very concerned with a tax cut broadly and restraining federal optional expenditures in the future.
“The third is Mr. Trump, but it’s not widely understood unless you follow European political situations a lot,” Blendon says. “Mr. Trump is actually running what would be called in Europe a nationalist party. Their issues are a bit different.”
Key components of Trump’s seven-point healthcare plan embrace some historical or current Republican policy ideas. These include using tax-free health savings accounts, allowing tax deductions for insurance premiums, and providing Medicaid block grants to states (though he has vowed not to cut overall Medicaid spending).
But Trump also breaks with the party, promising not to alter Medicare, proposing, like Clinton, to allow Medicare to negotiate pharmaceutical drug prices, and considering the idea of allowing pharmaceuticals to be imported from overseas, also like his Democratic opponent.
“I believe on the healthcare issue, he will be somewhat deferential to what the Republican leaders want their healthcare bill to look like in the future … not necessarily because that’s his particular choice but because he has a whole other agenda, which he says over and over is really important to him, and he needs the Republican leadership [to support it],” Blendon says.
How Will Things Get Done?
According to a Brookings Institution policy document published earlier this year, anyone proposing healthcare policy changes will confront “a daunting negotiation with powerful stakeholders to defend and enhance their varied interests” following the 2016 election.1
Three possible scenarios include a full Democratic president and Congress, a full Republican president and Congress, or a split presidency and Congress (including the two houses going each to the other party).
“If there is a split in the House and Senate, will things get done?” says Bradley Flansbaum, DO, MPH, MHM, a member of SHM’s Public Policy Committee. “Democrats don’t want to indicate the law has flaws and needs fixes. That admission invites the GOP to say, ‘See, it’s broken.’ Conversely, if Republicans do try to work with anyone on the other side of the aisle, they will be branded a pariah.”
One hospitalist sees Congress as the main force behind whether the ACA is kept intact.
“Congress holds the purse strings and has the control to chip away at the financial underpinnings until those toothpicks that hold up the Obamacare elephant break and it comes crashing down,” says Joshua Lenchus, DO, RPh, FACP, SFHM, a hospitalist at the University of Miami/Jackson Memorial Hospital in Florida and a member of SHM’s Public Policy Committee.
ACA Fixes?
One option Clinton has proposed is a federally administered public alternative to private insurers in the ACA marketplace, particularly as more companies leave exchanges across the country. Blendon says there is some concern over the idea’s viability since, while it could help keep pricing competitive, it might just “attract some of the sickest people because they’ll feel it provides more financial security.”
“A very high priority for a Clinton administration and a Democratic Congress [is] to get in there with a rescue team, and this is an issue of providing wraparound protection for [insurance] companies that basically end up with either older or sicker people than they had at all anticipated and some sort of a financial cushion to carry them into other years,” Blendon says.
In its policy paper, the Brookings Institution says any serious Republican idea to repeal the ACA should offer an alternative to replace the healthcare bill’s spending reductions, particularly since the Congressional Budget Office estimates repeal of the ACA would increase direct Medicare spending by $802 billion over the next decade, possibly accelerating the depletion of the program’s trust fund.1
“I think what would happen would be some amount of what the Republican leadership has talked about, some sort of a partial alternative to the ACA, and it would cover less people and less benefits, but there would be an absolute plan that they would try to have in place,” Blendon says.
But only time will tell how the election will affect hospitalists in their day-to-day work.
“Unfortunately, we’re still not at a stage that you could say to somebody, ‘This is what the next five years are going to look like; that’s how you should think about what your hospital and practice should be thinking,’” Blendon says. “You’re much more stuck with, ‘There is uncertainty here.’” TH
Kelly April Tyrrell is a freelance writer in Madison, Wis.
Reference
- Rivlin AM, Reischauer RD. Health policy issues and the 2016 presidential election. Brookings Institution website. Accessed August 31, 2016.
For Health Policy, State Races Matter, Too, in 2016

Most significant in individual states is whether to expand Medicaid. As of September 2016, 19 states had still not expanded the federal entitlement to people with incomes 138 percent above the federal poverty level.
“On a statewide level, the obvious issue of main concern to hospitalists will be Medicaid expansion,” says Joshua Lenchus, DO, RPh, FACP, SFHM, a hospitalist at the University of Miami/Jackson Memorial Hospital in Florida and a member of SHM’s Public Policy Committee. “I think as state-level elections unfold, the makeup of state legislatures will impact whether expansion happens or not.”
If Clinton is elected, states with Democratic governors are likely to expand Medicaid if they have not already done so, says Robert Blendon, the Richard L. Menschel Professor of Public Health at Harvard T.H. Chan School of Public Health (HSPH) and a professor of health policy and political analysis at HSPH and the Harvard Kennedy School of Government. He suspects conservative Republican governors might hold out longer.
“In the states that haven’t expanded Medicaid, the election of the governor and the legislature matters a great deal because if Clinton wins that means that we’re not going to repeal the [ACA], you’re not holding the line for the new Republican plan, it’s not going to be repealed in the next four years, and the question is, does your state deny the funds for the coverage and income it gets over a matter of principle?” says Blendon.
Dr. Lenchus says issues like scope-of-practice changes could impact policies for physicians in individual states as well, such that, in some states, discharge summaries following a hospital visit could be sent to nurse practitioners or physicians assistants instead of family physicians.
Bigger changes could also be on the horizon as a little-mentioned provision of the ACA, called Section 1332, becomes a possibility in 2017 if the law survives. It allows individual states to apply for waivers to eschew all or parts of the ACA in favor of plausible attempts to create customized state-level health reform.
In Colorado, this appears as a referendum in the upcoming election for universal healthcare, called ColoradoCare. In Hawaii, it is an expansion of its four-decade-old Hawaii Prepaid Health Care Act, based on employer-provided insurance combined with subsidies and limits on premium costs. Waivers must be approved by the U.S. Department of Health & Human Services and the U.S. Department of the Treasury.
Blendon believes a public option to private health insurance is most likely at the state level rather than at the federal government level under a Section 1332 waiver.
“I would expect that some number of states, particularly without enough plans coverage [as some companies leave the ACA marketplace], would argue that the states should offer a plan, which would be run by the state government and subsidized,” says Blendon.
–Kelly April Terrell
Editor's Note: Listen to Robert Blendon talk more about the health policy implications of the 2016 election.
One thing is certain: The outcome of this year’s election will usher in profound change for the American healthcare system. It also means a great deal of uncertainty for physicians, hospital systems, insurers, patients, and healthcare providers more broadly for weeks, months, or even years to come.
The Policy Proposals
Democratic presidential nominee Hillary Clinton has vowed to keep, strengthen, and “fix” the ACA, with proposals that include allowing people to begin buying into Medicare at age 55 and eliminating the Cadillac tax, plus a vow to defend access to reproductive healthcare. Republican nominee Donald Trump has the seven-point “Healthcare Reform to Make America Great Again,” which has as its first pillar to “completely replace Obamacare.”
While Clinton’s platform is highly detailed, Trump has offered few specifics with regard to its replacement, “just a set of general principles,” says Robert Blendon, the Richard L. Menschel Professor of Public Health at Harvard T.H. Chan School of Public Health (HSPH) and a professor of health policy and political analysis at HSPH and the Harvard Kennedy School of Government. “His supporters are just not focused on what the healthcare bill of the future would look like,” he adds.
Under majority Republican leadership, “it’s absolutely clear,” Blendon says, that the party would attempt to repeal the ACA. That would mean millions of people could lose insurance coverage or face higher levels of cost-sharing, benefits would be less comprehensive, and government regulation would decrease, leading to fewer directives for physicians and providers, he says.
A Democratic sweep of the executive and legislative branches would likely bring more funding for the National Institutes of Health and the Centers for Disease Control and Prevention. It might also lead to the introduction of a government alternative insurance plan that would compete with private insurance for those under age 65, Blendon explains.
“There’d be more money spent, but there’d be much more government regulation, including discussions of Medicare price limits on certain types of drugs,” he says.
Healthcare, though, has been caught in the middle of a host of broader issues, Blendon says.
“Put very simply, you almost have three parties that are running,” he says. “You have Democratic, which is [the] more liberal-moderate party, which is basically running on a health platform that is continuing Obama’s eight years but enlarging it in a number of areas. You have the party of the Republicans strictly in the Congress, which are running as a conservative party, which is to get rid of part of the ACA, to slow Medicare costs, and very concerned with a tax cut broadly and restraining federal optional expenditures in the future.
“The third is Mr. Trump, but it’s not widely understood unless you follow European political situations a lot,” Blendon says. “Mr. Trump is actually running what would be called in Europe a nationalist party. Their issues are a bit different.”
Key components of Trump’s seven-point healthcare plan embrace some historical or current Republican policy ideas. These include using tax-free health savings accounts, allowing tax deductions for insurance premiums, and providing Medicaid block grants to states (though he has vowed not to cut overall Medicaid spending).
But Trump also breaks with the party, promising not to alter Medicare, proposing, like Clinton, to allow Medicare to negotiate pharmaceutical drug prices, and considering the idea of allowing pharmaceuticals to be imported from overseas, also like his Democratic opponent.
“I believe on the healthcare issue, he will be somewhat deferential to what the Republican leaders want their healthcare bill to look like in the future … not necessarily because that’s his particular choice but because he has a whole other agenda, which he says over and over is really important to him, and he needs the Republican leadership [to support it],” Blendon says.
How Will Things Get Done?
According to a Brookings Institution policy document published earlier this year, anyone proposing healthcare policy changes will confront “a daunting negotiation with powerful stakeholders to defend and enhance their varied interests” following the 2016 election.1
Three possible scenarios include a full Democratic president and Congress, a full Republican president and Congress, or a split presidency and Congress (including the two houses going each to the other party).
“If there is a split in the House and Senate, will things get done?” says Bradley Flansbaum, DO, MPH, MHM, a member of SHM’s Public Policy Committee. “Democrats don’t want to indicate the law has flaws and needs fixes. That admission invites the GOP to say, ‘See, it’s broken.’ Conversely, if Republicans do try to work with anyone on the other side of the aisle, they will be branded a pariah.”
One hospitalist sees Congress as the main force behind whether the ACA is kept intact.
“Congress holds the purse strings and has the control to chip away at the financial underpinnings until those toothpicks that hold up the Obamacare elephant break and it comes crashing down,” says Joshua Lenchus, DO, RPh, FACP, SFHM, a hospitalist at the University of Miami/Jackson Memorial Hospital in Florida and a member of SHM’s Public Policy Committee.
ACA Fixes?
One option Clinton has proposed is a federally administered public alternative to private insurers in the ACA marketplace, particularly as more companies leave exchanges across the country. Blendon says there is some concern over the idea’s viability since, while it could help keep pricing competitive, it might just “attract some of the sickest people because they’ll feel it provides more financial security.”
“A very high priority for a Clinton administration and a Democratic Congress [is] to get in there with a rescue team, and this is an issue of providing wraparound protection for [insurance] companies that basically end up with either older or sicker people than they had at all anticipated and some sort of a financial cushion to carry them into other years,” Blendon says.
In its policy paper, the Brookings Institution says any serious Republican idea to repeal the ACA should offer an alternative to replace the healthcare bill’s spending reductions, particularly since the Congressional Budget Office estimates repeal of the ACA would increase direct Medicare spending by $802 billion over the next decade, possibly accelerating the depletion of the program’s trust fund.1
“I think what would happen would be some amount of what the Republican leadership has talked about, some sort of a partial alternative to the ACA, and it would cover less people and less benefits, but there would be an absolute plan that they would try to have in place,” Blendon says.
But only time will tell how the election will affect hospitalists in their day-to-day work.
“Unfortunately, we’re still not at a stage that you could say to somebody, ‘This is what the next five years are going to look like; that’s how you should think about what your hospital and practice should be thinking,’” Blendon says. “You’re much more stuck with, ‘There is uncertainty here.’” TH
Kelly April Tyrrell is a freelance writer in Madison, Wis.
Reference
- Rivlin AM, Reischauer RD. Health policy issues and the 2016 presidential election. Brookings Institution website. Accessed August 31, 2016.
For Health Policy, State Races Matter, Too, in 2016
Most significant in individual states is whether to expand Medicaid. As of September 2016, 19 states had still not expanded the federal entitlement to people with incomes 138 percent above the federal poverty level.
“On a statewide level, the obvious issue of main concern to hospitalists will be Medicaid expansion,” says Joshua Lenchus, DO, RPh, FACP, SFHM, a hospitalist at the University of Miami/Jackson Memorial Hospital in Florida and a member of SHM’s Public Policy Committee. “I think as state-level elections unfold, the makeup of state legislatures will impact whether expansion happens or not.”
If Clinton is elected, states with Democratic governors are likely to expand Medicaid if they have not already done so, says Robert Blendon, the Richard L. Menschel Professor of Public Health at Harvard T.H. Chan School of Public Health (HSPH) and a professor of health policy and political analysis at HSPH and the Harvard Kennedy School of Government. He suspects conservative Republican governors might hold out longer.
“In the states that haven’t expanded Medicaid, the election of the governor and the legislature matters a great deal because if Clinton wins that means that we’re not going to repeal the [ACA], you’re not holding the line for the new Republican plan, it’s not going to be repealed in the next four years, and the question is, does your state deny the funds for the coverage and income it gets over a matter of principle?” says Blendon.
Dr. Lenchus says issues like scope-of-practice changes could impact policies for physicians in individual states as well, such that, in some states, discharge summaries following a hospital visit could be sent to nurse practitioners or physicians assistants instead of family physicians.
Bigger changes could also be on the horizon as a little-mentioned provision of the ACA, called Section 1332, becomes a possibility in 2017 if the law survives. It allows individual states to apply for waivers to eschew all or parts of the ACA in favor of plausible attempts to create customized state-level health reform.
In Colorado, this appears as a referendum in the upcoming election for universal healthcare, called ColoradoCare. In Hawaii, it is an expansion of its four-decade-old Hawaii Prepaid Health Care Act, based on employer-provided insurance combined with subsidies and limits on premium costs. Waivers must be approved by the U.S. Department of Health & Human Services and the U.S. Department of the Treasury.
Blendon believes a public option to private health insurance is most likely at the state level rather than at the federal government level under a Section 1332 waiver.
“I would expect that some number of states, particularly without enough plans coverage [as some companies leave the ACA marketplace], would argue that the states should offer a plan, which would be run by the state government and subsidized,” says Blendon.
–Kelly April Terrell
Editor's Note: Listen to Robert Blendon talk more about the health policy implications of the 2016 election.
One thing is certain: The outcome of this year’s election will usher in profound change for the American healthcare system. It also means a great deal of uncertainty for physicians, hospital systems, insurers, patients, and healthcare providers more broadly for weeks, months, or even years to come.
The Policy Proposals
Democratic presidential nominee Hillary Clinton has vowed to keep, strengthen, and “fix” the ACA, with proposals that include allowing people to begin buying into Medicare at age 55 and eliminating the Cadillac tax, plus a vow to defend access to reproductive healthcare. Republican nominee Donald Trump has the seven-point “Healthcare Reform to Make America Great Again,” which has as its first pillar to “completely replace Obamacare.”
While Clinton’s platform is highly detailed, Trump has offered few specifics with regard to its replacement, “just a set of general principles,” says Robert Blendon, the Richard L. Menschel Professor of Public Health at Harvard T.H. Chan School of Public Health (HSPH) and a professor of health policy and political analysis at HSPH and the Harvard Kennedy School of Government. “His supporters are just not focused on what the healthcare bill of the future would look like,” he adds.
Under majority Republican leadership, “it’s absolutely clear,” Blendon says, that the party would attempt to repeal the ACA. That would mean millions of people could lose insurance coverage or face higher levels of cost-sharing, benefits would be less comprehensive, and government regulation would decrease, leading to fewer directives for physicians and providers, he says.
A Democratic sweep of the executive and legislative branches would likely bring more funding for the National Institutes of Health and the Centers for Disease Control and Prevention. It might also lead to the introduction of a government alternative insurance plan that would compete with private insurance for those under age 65, Blendon explains.
“There’d be more money spent, but there’d be much more government regulation, including discussions of Medicare price limits on certain types of drugs,” he says.
Healthcare, though, has been caught in the middle of a host of broader issues, Blendon says.
“Put very simply, you almost have three parties that are running,” he says. “You have Democratic, which is [the] more liberal-moderate party, which is basically running on a health platform that is continuing Obama’s eight years but enlarging it in a number of areas. You have the party of the Republicans strictly in the Congress, which are running as a conservative party, which is to get rid of part of the ACA, to slow Medicare costs, and very concerned with a tax cut broadly and restraining federal optional expenditures in the future.
“The third is Mr. Trump, but it’s not widely understood unless you follow European political situations a lot,” Blendon says. “Mr. Trump is actually running what would be called in Europe a nationalist party. Their issues are a bit different.”
Key components of Trump’s seven-point healthcare plan embrace some historical or current Republican policy ideas. These include using tax-free health savings accounts, allowing tax deductions for insurance premiums, and providing Medicaid block grants to states (though he has vowed not to cut overall Medicaid spending).
But Trump also breaks with the party, promising not to alter Medicare, proposing, like Clinton, to allow Medicare to negotiate pharmaceutical drug prices, and considering the idea of allowing pharmaceuticals to be imported from overseas, also like his Democratic opponent.
“I believe on the healthcare issue, he will be somewhat deferential to what the Republican leaders want their healthcare bill to look like in the future … not necessarily because that’s his particular choice but because he has a whole other agenda, which he says over and over is really important to him, and he needs the Republican leadership [to support it],” Blendon says.
How Will Things Get Done?
According to a Brookings Institution policy document published earlier this year, anyone proposing healthcare policy changes will confront “a daunting negotiation with powerful stakeholders to defend and enhance their varied interests” following the 2016 election.1
Three possible scenarios include a full Democratic president and Congress, a full Republican president and Congress, or a split presidency and Congress (including the two houses going each to the other party).
“If there is a split in the House and Senate, will things get done?” says Bradley Flansbaum, DO, MPH, MHM, a member of SHM’s Public Policy Committee. “Democrats don’t want to indicate the law has flaws and needs fixes. That admission invites the GOP to say, ‘See, it’s broken.’ Conversely, if Republicans do try to work with anyone on the other side of the aisle, they will be branded a pariah.”
One hospitalist sees Congress as the main force behind whether the ACA is kept intact.
“Congress holds the purse strings and has the control to chip away at the financial underpinnings until those toothpicks that hold up the Obamacare elephant break and it comes crashing down,” says Joshua Lenchus, DO, RPh, FACP, SFHM, a hospitalist at the University of Miami/Jackson Memorial Hospital in Florida and a member of SHM’s Public Policy Committee.
ACA Fixes?
One option Clinton has proposed is a federally administered public alternative to private insurers in the ACA marketplace, particularly as more companies leave exchanges across the country. Blendon says there is some concern over the idea’s viability since, while it could help keep pricing competitive, it might just “attract some of the sickest people because they’ll feel it provides more financial security.”
“A very high priority for a Clinton administration and a Democratic Congress [is] to get in there with a rescue team, and this is an issue of providing wraparound protection for [insurance] companies that basically end up with either older or sicker people than they had at all anticipated and some sort of a financial cushion to carry them into other years,” Blendon says.
In its policy paper, the Brookings Institution says any serious Republican idea to repeal the ACA should offer an alternative to replace the healthcare bill’s spending reductions, particularly since the Congressional Budget Office estimates repeal of the ACA would increase direct Medicare spending by $802 billion over the next decade, possibly accelerating the depletion of the program’s trust fund.1
“I think what would happen would be some amount of what the Republican leadership has talked about, some sort of a partial alternative to the ACA, and it would cover less people and less benefits, but there would be an absolute plan that they would try to have in place,” Blendon says.
But only time will tell how the election will affect hospitalists in their day-to-day work.
“Unfortunately, we’re still not at a stage that you could say to somebody, ‘This is what the next five years are going to look like; that’s how you should think about what your hospital and practice should be thinking,’” Blendon says. “You’re much more stuck with, ‘There is uncertainty here.’” TH
Kelly April Tyrrell is a freelance writer in Madison, Wis.
Reference
- Rivlin AM, Reischauer RD. Health policy issues and the 2016 presidential election. Brookings Institution website. Accessed August 31, 2016.
For Health Policy, State Races Matter, Too, in 2016
Most significant in individual states is whether to expand Medicaid. As of September 2016, 19 states had still not expanded the federal entitlement to people with incomes 138 percent above the federal poverty level.
“On a statewide level, the obvious issue of main concern to hospitalists will be Medicaid expansion,” says Joshua Lenchus, DO, RPh, FACP, SFHM, a hospitalist at the University of Miami/Jackson Memorial Hospital in Florida and a member of SHM’s Public Policy Committee. “I think as state-level elections unfold, the makeup of state legislatures will impact whether expansion happens or not.”
If Clinton is elected, states with Democratic governors are likely to expand Medicaid if they have not already done so, says Robert Blendon, the Richard L. Menschel Professor of Public Health at Harvard T.H. Chan School of Public Health (HSPH) and a professor of health policy and political analysis at HSPH and the Harvard Kennedy School of Government. He suspects conservative Republican governors might hold out longer.
“In the states that haven’t expanded Medicaid, the election of the governor and the legislature matters a great deal because if Clinton wins that means that we’re not going to repeal the [ACA], you’re not holding the line for the new Republican plan, it’s not going to be repealed in the next four years, and the question is, does your state deny the funds for the coverage and income it gets over a matter of principle?” says Blendon.
Dr. Lenchus says issues like scope-of-practice changes could impact policies for physicians in individual states as well, such that, in some states, discharge summaries following a hospital visit could be sent to nurse practitioners or physicians assistants instead of family physicians.
Bigger changes could also be on the horizon as a little-mentioned provision of the ACA, called Section 1332, becomes a possibility in 2017 if the law survives. It allows individual states to apply for waivers to eschew all or parts of the ACA in favor of plausible attempts to create customized state-level health reform.
In Colorado, this appears as a referendum in the upcoming election for universal healthcare, called ColoradoCare. In Hawaii, it is an expansion of its four-decade-old Hawaii Prepaid Health Care Act, based on employer-provided insurance combined with subsidies and limits on premium costs. Waivers must be approved by the U.S. Department of Health & Human Services and the U.S. Department of the Treasury.
Blendon believes a public option to private health insurance is most likely at the state level rather than at the federal government level under a Section 1332 waiver.
“I would expect that some number of states, particularly without enough plans coverage [as some companies leave the ACA marketplace], would argue that the states should offer a plan, which would be run by the state government and subsidized,” says Blendon.
–Kelly April Terrell

Team explains how MM cells alter BM to thrive

New research helps explain how multiple myeloma (MM) cells manipulate the bone marrow (BM) environment to promote disease progression.
The researchers knew that mesenchymal stem cells (MSCs) are often altered in MM in a way that favors disease progression, but the mechanisms behind this phenomenon weren’t well understood.
So the team set out to determine how and when normal MSCs evolve into tumor-promoting MSCs.
Mahmoud Dabbah, of Meir Medical Center in Kfar Saba, Israel, and his colleagues conducted this research and reported the results in the Journal of Leukocyte Biology.
The researchers cultured the MM cell lines U266 and ARP1 with MSCs from healthy donors, looking for changes in the MSCs. The team observed changes in migration and protein translation initiation.
Specifically, they found that co-culturing MSCs with MM cell lines induced an elevation in translation initiation factors eIF4E and eIF4GI as well as their regulators and targets. But these changes were reversible.
MM-conditioned MSCs had significantly elevated levels of peIF4E, total eIF4E, peIF4GI, and total eIF4GI after 3 days of co-culture with both MM cell lines (all increased about 200%, P<0.05).
In fact, levels of peIF4GI and peIF4E were significantly elevated in the MSCs within 1.5 hours of co-culture (both increased more than 250%, P<0.05).
However, when the MSCs were removed from co-culture, the levels returned to baseline within 3 to 6 hours.
MM-conditioned MSCs also showed a significant increase in migration. When cultured for 16 hours, MSC migration increased more than 400% (P<0.05).
Accordingly, the MM-conditioned MSCs expressed lower levels of microRNAs with established roles in cell migration.
The MSCs showed decreased levels of MIR-125a-5p and MIR-199b-3p after 12 hours of co-culture (a decrease of 160% to 250%, P<0.05). And this effect was maintained as long as the co-culture continued.
The researchers said their findings suggest a dynamic interaction between MM cells and the BM niche that causes profound changes in non-malignant BM constituents. They hope that future studies will reveal clinically relevant means of blocking this crosstalk to improve MM therapy.
“Our research should help identify therapeutic targets that may be used to minimize the collateral damage,” Dabbah said. “The identification of the translation initiation phase as a dialogue platform affords a potential new therapeutic target to be explored.” ![]()
New research helps explain how multiple myeloma (MM) cells manipulate the bone marrow (BM) environment to promote disease progression.
The researchers knew that mesenchymal stem cells (MSCs) are often altered in MM in a way that favors disease progression, but the mechanisms behind this phenomenon weren’t well understood.
So the team set out to determine how and when normal MSCs evolve into tumor-promoting MSCs.
Mahmoud Dabbah, of Meir Medical Center in Kfar Saba, Israel, and his colleagues conducted this research and reported the results in the Journal of Leukocyte Biology.
The researchers cultured the MM cell lines U266 and ARP1 with MSCs from healthy donors, looking for changes in the MSCs. The team observed changes in migration and protein translation initiation.
Specifically, they found that co-culturing MSCs with MM cell lines induced an elevation in translation initiation factors eIF4E and eIF4GI as well as their regulators and targets. But these changes were reversible.
MM-conditioned MSCs had significantly elevated levels of peIF4E, total eIF4E, peIF4GI, and total eIF4GI after 3 days of co-culture with both MM cell lines (all increased about 200%, P<0.05).
In fact, levels of peIF4GI and peIF4E were significantly elevated in the MSCs within 1.5 hours of co-culture (both increased more than 250%, P<0.05).
However, when the MSCs were removed from co-culture, the levels returned to baseline within 3 to 6 hours.
MM-conditioned MSCs also showed a significant increase in migration. When cultured for 16 hours, MSC migration increased more than 400% (P<0.05).
Accordingly, the MM-conditioned MSCs expressed lower levels of microRNAs with established roles in cell migration.
The MSCs showed decreased levels of MIR-125a-5p and MIR-199b-3p after 12 hours of co-culture (a decrease of 160% to 250%, P<0.05). And this effect was maintained as long as the co-culture continued.
The researchers said their findings suggest a dynamic interaction between MM cells and the BM niche that causes profound changes in non-malignant BM constituents. They hope that future studies will reveal clinically relevant means of blocking this crosstalk to improve MM therapy.
“Our research should help identify therapeutic targets that may be used to minimize the collateral damage,” Dabbah said. “The identification of the translation initiation phase as a dialogue platform affords a potential new therapeutic target to be explored.” ![]()
New research helps explain how multiple myeloma (MM) cells manipulate the bone marrow (BM) environment to promote disease progression.
The researchers knew that mesenchymal stem cells (MSCs) are often altered in MM in a way that favors disease progression, but the mechanisms behind this phenomenon weren’t well understood.
So the team set out to determine how and when normal MSCs evolve into tumor-promoting MSCs.
Mahmoud Dabbah, of Meir Medical Center in Kfar Saba, Israel, and his colleagues conducted this research and reported the results in the Journal of Leukocyte Biology.
The researchers cultured the MM cell lines U266 and ARP1 with MSCs from healthy donors, looking for changes in the MSCs. The team observed changes in migration and protein translation initiation.
Specifically, they found that co-culturing MSCs with MM cell lines induced an elevation in translation initiation factors eIF4E and eIF4GI as well as their regulators and targets. But these changes were reversible.
MM-conditioned MSCs had significantly elevated levels of peIF4E, total eIF4E, peIF4GI, and total eIF4GI after 3 days of co-culture with both MM cell lines (all increased about 200%, P<0.05).
In fact, levels of peIF4GI and peIF4E were significantly elevated in the MSCs within 1.5 hours of co-culture (both increased more than 250%, P<0.05).
However, when the MSCs were removed from co-culture, the levels returned to baseline within 3 to 6 hours.
MM-conditioned MSCs also showed a significant increase in migration. When cultured for 16 hours, MSC migration increased more than 400% (P<0.05).
Accordingly, the MM-conditioned MSCs expressed lower levels of microRNAs with established roles in cell migration.
The MSCs showed decreased levels of MIR-125a-5p and MIR-199b-3p after 12 hours of co-culture (a decrease of 160% to 250%, P<0.05). And this effect was maintained as long as the co-culture continued.
The researchers said their findings suggest a dynamic interaction between MM cells and the BM niche that causes profound changes in non-malignant BM constituents. They hope that future studies will reveal clinically relevant means of blocking this crosstalk to improve MM therapy.
“Our research should help identify therapeutic targets that may be used to minimize the collateral damage,” Dabbah said. “The identification of the translation initiation phase as a dialogue platform affords a potential new therapeutic target to be explored.” ![]()
Trial of hemophilia therapy back on

Image courtesy of NIGMS
A UK regulatory agency has lifted the hold placed on a phase 1/2 study of the gene therapy BMN 270 in patients with hemophilia A.
Dosing was suspended in this trial after the first 9 patients were enrolled, but the Medicines and Healthcare Products Regulatory Agency (MHRA) has decided the study can continue.
BioMarin Pharmaceutical Inc., the company developing BMN 270, said the trial should resume enrollment by the end of this year.
BMN 270 is a recombinant adeno-associated virus vector coding for human coagulation factor VIII (FVIII).
The phase 1/2 study of BMN 270 was designed to evaluate the safety and efficacy of the therapy in up to 15 patients with severe hemophilia A.
Results in 7 patients on this study were recently presented at the World Federation of Hemophilia 2016 World Congress.
However, after the study had enrolled 9 patients, dosing of BMN 270 was suspended due to increases in alanine aminotransferase levels that exceeded a pre-specified threshold.
Following the suspension, BioMarin reviewed safety and efficacy data on the 9 patients with the MHRA. Based on this review, the MHRA approved resumption of the study.
The agency also approved the company’s proposed amendments to the study, which included eliminating the requirement for prophylactic corticosteroids and increasing potential additional enrollment from up to 3 additional patients to up to 6 additional patients.
BioMarin said it intends to resume enrollment in the study before the end of 2016. Based on protocol amendments, 3 patients will be enrolled at a dose of 4 x 1013 vg/kg, and an additional 3 patients may be enrolled at this dose or the previously tested high dose of 6 x 1013 vg/kg.
In the up to 6 additional patients, the requirement for prophylactic corticosteroids has been removed, and the threshold for starting therapeutic corticosteroids has been increased.
BioMarin said safety and efficacy data from these patients will inform the phase 2b study expected to begin in the second half of 2017.
“We are pleased that MHRA has approved the resumption of enrollment of the BMN 270 study, as well as the study amendments,” said Hank Fuchs, MD, chief medical officer at BioMarin.
“We believe that the amendments will allow us to optimize the design of a robust phase 2b clinical trial, which potentially could support an accelerated approval by health authorities. We are grateful to the patients who are participating in this current study and are encouraged by the results so far for this phase 1/2 trial.” ![]()
Image courtesy of NIGMS
A UK regulatory agency has lifted the hold placed on a phase 1/2 study of the gene therapy BMN 270 in patients with hemophilia A.
Dosing was suspended in this trial after the first 9 patients were enrolled, but the Medicines and Healthcare Products Regulatory Agency (MHRA) has decided the study can continue.
BioMarin Pharmaceutical Inc., the company developing BMN 270, said the trial should resume enrollment by the end of this year.
BMN 270 is a recombinant adeno-associated virus vector coding for human coagulation factor VIII (FVIII).
The phase 1/2 study of BMN 270 was designed to evaluate the safety and efficacy of the therapy in up to 15 patients with severe hemophilia A.
Results in 7 patients on this study were recently presented at the World Federation of Hemophilia 2016 World Congress.
However, after the study had enrolled 9 patients, dosing of BMN 270 was suspended due to increases in alanine aminotransferase levels that exceeded a pre-specified threshold.
Following the suspension, BioMarin reviewed safety and efficacy data on the 9 patients with the MHRA. Based on this review, the MHRA approved resumption of the study.
The agency also approved the company’s proposed amendments to the study, which included eliminating the requirement for prophylactic corticosteroids and increasing potential additional enrollment from up to 3 additional patients to up to 6 additional patients.
BioMarin said it intends to resume enrollment in the study before the end of 2016. Based on protocol amendments, 3 patients will be enrolled at a dose of 4 x 1013 vg/kg, and an additional 3 patients may be enrolled at this dose or the previously tested high dose of 6 x 1013 vg/kg.
In the up to 6 additional patients, the requirement for prophylactic corticosteroids has been removed, and the threshold for starting therapeutic corticosteroids has been increased.
BioMarin said safety and efficacy data from these patients will inform the phase 2b study expected to begin in the second half of 2017.
“We are pleased that MHRA has approved the resumption of enrollment of the BMN 270 study, as well as the study amendments,” said Hank Fuchs, MD, chief medical officer at BioMarin.
“We believe that the amendments will allow us to optimize the design of a robust phase 2b clinical trial, which potentially could support an accelerated approval by health authorities. We are grateful to the patients who are participating in this current study and are encouraged by the results so far for this phase 1/2 trial.” ![]()
Image courtesy of NIGMS
A UK regulatory agency has lifted the hold placed on a phase 1/2 study of the gene therapy BMN 270 in patients with hemophilia A.
Dosing was suspended in this trial after the first 9 patients were enrolled, but the Medicines and Healthcare Products Regulatory Agency (MHRA) has decided the study can continue.
BioMarin Pharmaceutical Inc., the company developing BMN 270, said the trial should resume enrollment by the end of this year.
BMN 270 is a recombinant adeno-associated virus vector coding for human coagulation factor VIII (FVIII).
The phase 1/2 study of BMN 270 was designed to evaluate the safety and efficacy of the therapy in up to 15 patients with severe hemophilia A.
Results in 7 patients on this study were recently presented at the World Federation of Hemophilia 2016 World Congress.
However, after the study had enrolled 9 patients, dosing of BMN 270 was suspended due to increases in alanine aminotransferase levels that exceeded a pre-specified threshold.
Following the suspension, BioMarin reviewed safety and efficacy data on the 9 patients with the MHRA. Based on this review, the MHRA approved resumption of the study.
The agency also approved the company’s proposed amendments to the study, which included eliminating the requirement for prophylactic corticosteroids and increasing potential additional enrollment from up to 3 additional patients to up to 6 additional patients.
BioMarin said it intends to resume enrollment in the study before the end of 2016. Based on protocol amendments, 3 patients will be enrolled at a dose of 4 x 1013 vg/kg, and an additional 3 patients may be enrolled at this dose or the previously tested high dose of 6 x 1013 vg/kg.
In the up to 6 additional patients, the requirement for prophylactic corticosteroids has been removed, and the threshold for starting therapeutic corticosteroids has been increased.
BioMarin said safety and efficacy data from these patients will inform the phase 2b study expected to begin in the second half of 2017.
“We are pleased that MHRA has approved the resumption of enrollment of the BMN 270 study, as well as the study amendments,” said Hank Fuchs, MD, chief medical officer at BioMarin.
“We believe that the amendments will allow us to optimize the design of a robust phase 2b clinical trial, which potentially could support an accelerated approval by health authorities. We are grateful to the patients who are participating in this current study and are encouraged by the results so far for this phase 1/2 trial.” ![]()
COMP recommends orphan designation for CMV-CTLs
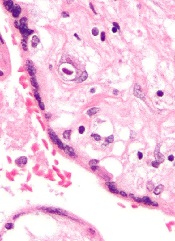
The European Medicines Agency’s Committee for Orphan Medicinal Products (COMP) is recommending orphan designation for a cytomegalovirus-specific cytotoxic T-lymphocyte product (CMV-CTLs) intended to treat CMV infection in patients with impaired cell-mediated immunity.
The CMV-CTLs are designed to find and kill cells expressing CMV.
To create CMV-CTLs, T cells are collected from the blood of third-party donors and then exposed to CMV antigens.
The resulting activated T cells are then expanded, characterized, and stored for future use in a partially HLA-matched patient.
The CMV-CTLs are being developed by Atara Biotherapeutics, Inc.
The cells are currently under investigation in a pair of phase 2 trials (NCT01646645 and NCT02136797).
Results of a phase 1 trial (published in Biology of Blood and Marrow Transplantation in 2015) suggested CMV-CTLs are safe and can clear CMV infection in patients who have undergone allogeneic hematopoietic stem cell transplant.
The trial included 17 transplant recipients with CMV viremia or clinical infection that persisted despite prolonged treatment with antiviral drugs. Fourteen of the patients had received T-cell-depleted transplants without graft-versus-host disease (GVHD) prophylaxis.
Sixteen of the patients received CMV-CTLs created using cells derived from their transplant donor, and 1 patient received cells from a third-party donor.
Fifteen patients achieved clearance of CMV viremia, including 3 of the 5 patients with overt disease and the patient who received cells from a third-party donor.
In addition, the researchers said CMV-CTLs were well-tolerated. None of the patients experienced fever, alterations in vital signs, or other toxicities during the first 48 hours of observation.
None of the patients developed manifestations of de novo acute GVHD, and GHVD did not worsen in either of the 2 patients who had GVHD prior to infusion.
About orphan designation
The COMP adopts an opinion on the granting of orphan drug designation, and that opinion is submitted to the European Commission for a final decision.
Orphan designation provides regulatory and financial incentives for companies to develop and market therapies that treat life-threatening or chronically debilitating conditions affecting no more than 5 in 10,000 people in the European Union, and where no satisfactory treatment is available.
Orphan designation provides a 10-year period of marketing exclusivity if the drug receives regulatory approval.
The designation also provides incentives for companies seeking protocol assistance from the European Medicines Agency during the product development phase and direct access to the centralized authorization procedure. ![]()
The European Medicines Agency’s Committee for Orphan Medicinal Products (COMP) is recommending orphan designation for a cytomegalovirus-specific cytotoxic T-lymphocyte product (CMV-CTLs) intended to treat CMV infection in patients with impaired cell-mediated immunity.
The CMV-CTLs are designed to find and kill cells expressing CMV.
To create CMV-CTLs, T cells are collected from the blood of third-party donors and then exposed to CMV antigens.
The resulting activated T cells are then expanded, characterized, and stored for future use in a partially HLA-matched patient.
The CMV-CTLs are being developed by Atara Biotherapeutics, Inc.
The cells are currently under investigation in a pair of phase 2 trials (NCT01646645 and NCT02136797).
Results of a phase 1 trial (published in Biology of Blood and Marrow Transplantation in 2015) suggested CMV-CTLs are safe and can clear CMV infection in patients who have undergone allogeneic hematopoietic stem cell transplant.
The trial included 17 transplant recipients with CMV viremia or clinical infection that persisted despite prolonged treatment with antiviral drugs. Fourteen of the patients had received T-cell-depleted transplants without graft-versus-host disease (GVHD) prophylaxis.
Sixteen of the patients received CMV-CTLs created using cells derived from their transplant donor, and 1 patient received cells from a third-party donor.
Fifteen patients achieved clearance of CMV viremia, including 3 of the 5 patients with overt disease and the patient who received cells from a third-party donor.
In addition, the researchers said CMV-CTLs were well-tolerated. None of the patients experienced fever, alterations in vital signs, or other toxicities during the first 48 hours of observation.
None of the patients developed manifestations of de novo acute GVHD, and GHVD did not worsen in either of the 2 patients who had GVHD prior to infusion.
About orphan designation
The COMP adopts an opinion on the granting of orphan drug designation, and that opinion is submitted to the European Commission for a final decision.
Orphan designation provides regulatory and financial incentives for companies to develop and market therapies that treat life-threatening or chronically debilitating conditions affecting no more than 5 in 10,000 people in the European Union, and where no satisfactory treatment is available.
Orphan designation provides a 10-year period of marketing exclusivity if the drug receives regulatory approval.
The designation also provides incentives for companies seeking protocol assistance from the European Medicines Agency during the product development phase and direct access to the centralized authorization procedure. ![]()
The European Medicines Agency’s Committee for Orphan Medicinal Products (COMP) is recommending orphan designation for a cytomegalovirus-specific cytotoxic T-lymphocyte product (CMV-CTLs) intended to treat CMV infection in patients with impaired cell-mediated immunity.
The CMV-CTLs are designed to find and kill cells expressing CMV.
To create CMV-CTLs, T cells are collected from the blood of third-party donors and then exposed to CMV antigens.
The resulting activated T cells are then expanded, characterized, and stored for future use in a partially HLA-matched patient.
The CMV-CTLs are being developed by Atara Biotherapeutics, Inc.
The cells are currently under investigation in a pair of phase 2 trials (NCT01646645 and NCT02136797).
Results of a phase 1 trial (published in Biology of Blood and Marrow Transplantation in 2015) suggested CMV-CTLs are safe and can clear CMV infection in patients who have undergone allogeneic hematopoietic stem cell transplant.
The trial included 17 transplant recipients with CMV viremia or clinical infection that persisted despite prolonged treatment with antiviral drugs. Fourteen of the patients had received T-cell-depleted transplants without graft-versus-host disease (GVHD) prophylaxis.
Sixteen of the patients received CMV-CTLs created using cells derived from their transplant donor, and 1 patient received cells from a third-party donor.
Fifteen patients achieved clearance of CMV viremia, including 3 of the 5 patients with overt disease and the patient who received cells from a third-party donor.
In addition, the researchers said CMV-CTLs were well-tolerated. None of the patients experienced fever, alterations in vital signs, or other toxicities during the first 48 hours of observation.
None of the patients developed manifestations of de novo acute GVHD, and GHVD did not worsen in either of the 2 patients who had GVHD prior to infusion.
About orphan designation
The COMP adopts an opinion on the granting of orphan drug designation, and that opinion is submitted to the European Commission for a final decision.
Orphan designation provides regulatory and financial incentives for companies to develop and market therapies that treat life-threatening or chronically debilitating conditions affecting no more than 5 in 10,000 people in the European Union, and where no satisfactory treatment is available.
Orphan designation provides a 10-year period of marketing exclusivity if the drug receives regulatory approval.
The designation also provides incentives for companies seeking protocol assistance from the European Medicines Agency during the product development phase and direct access to the centralized authorization procedure. ![]()
Findings could aid treatment of resistant T-ALL
(blue and purple) invaded
by leukemia cells (yellow).
Image courtesy of Edwin
Hawkins, Delfim Duarte,
and Imperial College London
Preclinical research has shed light on how certain leukemia cells survive treatment and could pave the way for better therapeutic targeting of these resistant cells.
Researchers have speculated that some leukemia cells survive treatment by hiding out in specific niches in the bone marrow.
Results of the new research, conducted in mouse models and human samples of T-cell acute lymphoblastic leukemia (T-ALL), contradict that theory.
The experiments showed that resistant T-ALL cells move rapidly through the bone marrow before, during, and after treatment, interacting with—and sometimes killing—healthy cells.
“We expected the cells that survived treatment to be sat in particular niches, but, instead, they are very active throughout the bone marrow,” said Cristina Lo Celso, PhD, of Imperial College London in the UK.
“We now know that it would be ineffective to target particular niches in the bone marrow to tackle treatment-resistant leukemia. Now that we know that the cells don’t hide, we can explore why that is and how their movement helps them to survive. Ultimately, we want to find out whether we can stop the movement and whether this could kill the treatment-resistant cells.”
Dr Lo Celso and her colleagues described these findings in a letter to Nature.
The researchers used intravital microscopy to track the movement of T-ALL cells in mice—before, during, and after treatment. Treatment consisted of dexamethasone alone, vincristine alone, or combination dexamethasone, vincristine, and L-asparaginase.
The team found that T-ALL cells moved around rapidly, not showing any preference for bone marrow subcompartments. The cells’ behavior was consistent over time—from the earliest bone marrow seeding through to treatment response and resistance.
However, the researchers noted that surviving T-ALL cells were “highly migratory” and travelled at significantly faster speeds than early infiltrating cells. In addition, resistant T-ALL cells were still capable of undergoing division at times when other T-ALL cells were dying.
The team suggested that the act of moving may help T-ALL cells to survive, possibly through short-lived interactions with other cells.
This theory was supported by the discovery that T-ALL cells actively attack osteoblasts. The researchers noted that osteoblasts are associated with hematopoietic fitness. So the loss of osteoblasts may contribute to the loss of healthy hematopoiesis observed in leukemia patients.
The team believes this insight could aid the development of treatments to safeguard the production of healthy blood cells in T-ALL patients.
“Our study supports the idea that, at least in this leukemia, new therapies should target the cancer cells themselves instead of the surrounding normal stromal cells to better eradicate the disease,” said study author Delfim Duarte, MD, a PhD student at Imperial College London.
“Our work also suggests that protecting normal stromal bone cells from the attack of leukemia cells can have wide implications in the support of healthy blood cell production,” said Edwin Hawkins, PhD, of the Walter and Eliza Hall Institute of Medical Research in Melbourne, Victoria, Australia.
“Keeping blood cell levels up would prevent anemia, infection, and bleeding.” ![]()
(blue and purple) invaded
by leukemia cells (yellow).
Image courtesy of Edwin
Hawkins, Delfim Duarte,
and Imperial College London
Preclinical research has shed light on how certain leukemia cells survive treatment and could pave the way for better therapeutic targeting of these resistant cells.
Researchers have speculated that some leukemia cells survive treatment by hiding out in specific niches in the bone marrow.
Results of the new research, conducted in mouse models and human samples of T-cell acute lymphoblastic leukemia (T-ALL), contradict that theory.
The experiments showed that resistant T-ALL cells move rapidly through the bone marrow before, during, and after treatment, interacting with—and sometimes killing—healthy cells.
“We expected the cells that survived treatment to be sat in particular niches, but, instead, they are very active throughout the bone marrow,” said Cristina Lo Celso, PhD, of Imperial College London in the UK.
“We now know that it would be ineffective to target particular niches in the bone marrow to tackle treatment-resistant leukemia. Now that we know that the cells don’t hide, we can explore why that is and how their movement helps them to survive. Ultimately, we want to find out whether we can stop the movement and whether this could kill the treatment-resistant cells.”
Dr Lo Celso and her colleagues described these findings in a letter to Nature.
The researchers used intravital microscopy to track the movement of T-ALL cells in mice—before, during, and after treatment. Treatment consisted of dexamethasone alone, vincristine alone, or combination dexamethasone, vincristine, and L-asparaginase.
The team found that T-ALL cells moved around rapidly, not showing any preference for bone marrow subcompartments. The cells’ behavior was consistent over time—from the earliest bone marrow seeding through to treatment response and resistance.
However, the researchers noted that surviving T-ALL cells were “highly migratory” and travelled at significantly faster speeds than early infiltrating cells. In addition, resistant T-ALL cells were still capable of undergoing division at times when other T-ALL cells were dying.
The team suggested that the act of moving may help T-ALL cells to survive, possibly through short-lived interactions with other cells.
This theory was supported by the discovery that T-ALL cells actively attack osteoblasts. The researchers noted that osteoblasts are associated with hematopoietic fitness. So the loss of osteoblasts may contribute to the loss of healthy hematopoiesis observed in leukemia patients.
The team believes this insight could aid the development of treatments to safeguard the production of healthy blood cells in T-ALL patients.
“Our study supports the idea that, at least in this leukemia, new therapies should target the cancer cells themselves instead of the surrounding normal stromal cells to better eradicate the disease,” said study author Delfim Duarte, MD, a PhD student at Imperial College London.
“Our work also suggests that protecting normal stromal bone cells from the attack of leukemia cells can have wide implications in the support of healthy blood cell production,” said Edwin Hawkins, PhD, of the Walter and Eliza Hall Institute of Medical Research in Melbourne, Victoria, Australia.
“Keeping blood cell levels up would prevent anemia, infection, and bleeding.” ![]()
(blue and purple) invaded
by leukemia cells (yellow).
Image courtesy of Edwin
Hawkins, Delfim Duarte,
and Imperial College London
Preclinical research has shed light on how certain leukemia cells survive treatment and could pave the way for better therapeutic targeting of these resistant cells.
Researchers have speculated that some leukemia cells survive treatment by hiding out in specific niches in the bone marrow.
Results of the new research, conducted in mouse models and human samples of T-cell acute lymphoblastic leukemia (T-ALL), contradict that theory.
The experiments showed that resistant T-ALL cells move rapidly through the bone marrow before, during, and after treatment, interacting with—and sometimes killing—healthy cells.
“We expected the cells that survived treatment to be sat in particular niches, but, instead, they are very active throughout the bone marrow,” said Cristina Lo Celso, PhD, of Imperial College London in the UK.
“We now know that it would be ineffective to target particular niches in the bone marrow to tackle treatment-resistant leukemia. Now that we know that the cells don’t hide, we can explore why that is and how their movement helps them to survive. Ultimately, we want to find out whether we can stop the movement and whether this could kill the treatment-resistant cells.”
Dr Lo Celso and her colleagues described these findings in a letter to Nature.
The researchers used intravital microscopy to track the movement of T-ALL cells in mice—before, during, and after treatment. Treatment consisted of dexamethasone alone, vincristine alone, or combination dexamethasone, vincristine, and L-asparaginase.
The team found that T-ALL cells moved around rapidly, not showing any preference for bone marrow subcompartments. The cells’ behavior was consistent over time—from the earliest bone marrow seeding through to treatment response and resistance.
However, the researchers noted that surviving T-ALL cells were “highly migratory” and travelled at significantly faster speeds than early infiltrating cells. In addition, resistant T-ALL cells were still capable of undergoing division at times when other T-ALL cells were dying.
The team suggested that the act of moving may help T-ALL cells to survive, possibly through short-lived interactions with other cells.
This theory was supported by the discovery that T-ALL cells actively attack osteoblasts. The researchers noted that osteoblasts are associated with hematopoietic fitness. So the loss of osteoblasts may contribute to the loss of healthy hematopoiesis observed in leukemia patients.
The team believes this insight could aid the development of treatments to safeguard the production of healthy blood cells in T-ALL patients.
“Our study supports the idea that, at least in this leukemia, new therapies should target the cancer cells themselves instead of the surrounding normal stromal cells to better eradicate the disease,” said study author Delfim Duarte, MD, a PhD student at Imperial College London.
“Our work also suggests that protecting normal stromal bone cells from the attack of leukemia cells can have wide implications in the support of healthy blood cell production,” said Edwin Hawkins, PhD, of the Walter and Eliza Hall Institute of Medical Research in Melbourne, Victoria, Australia.
“Keeping blood cell levels up would prevent anemia, infection, and bleeding.” ![]()
The mesh tradeoff: Lower recurrence risk vs. complicaitons
Among patients undergoing elective incisional repair of abdominal wall hernias, the use of mesh reinforcement decreases the short-term recurrence rate by 5% but increases major complications by approximately the same amount over the subsequent 5 years, Dunja Kokotovic, MB, reported at the annual clinical congress of the American College of Surgeons.
“Given the continuously increasing incidence of mesh-related complications with time, it is expected that, with even longer follow-up up than the 5 years observed in this study, mesh-related complications continue to accrue,” said Dr. Kokotovic of the Center for Surgical Science, Zealand University Hospital, Koge, Denmark. The findings of this observational registry-based cohort study were presented at the congress and simultaneously published online in JAMA (2016 Oct 17. doi: 10.1001/jama.2016.15217).
These results highlight the need to assess the long-term safety of interventions before making definitive conclusions about their benefits and widely adopting them. In the United States, manufacturers are required to demonstrate the long-term safety of drugs but not of some devices, including hernia meshes. There were approximately 190,000 such hernia repairs performed in the United States alone during the most recent year for which data are available, and mesh is estimated to have been used in at least half, Dr. Kokotovic noted.
She and her associates analyzed the 5-year outcomes for virtually all incisional hernia repairs performed in Denmark from 2007 through 2010 using data in a mandatory national registry. Their analysis included 3,242 patients (mean age, 58 years): 1,119 (34.5%) who had open mesh repair, 1,757 (54.2%) who had laparoscopic mesh repair, and 366 (11.3%) who had nonmesh repair.
The cumulative risk of reoperation for hernia recurrence was significantly lower for patients who had open mesh repair (12.3%) or laparoscopic mesh repair (10.6%) than for those who had nonmesh repair (17.1%). However, this benefit was offset by the rate of major mesh-related complications requiring surgical intervention – including surgical site infection, formation of a chronic sinus tract, late-onset intra-abdominal abscess, enterocutaneous fistula, bowel obstruction, and bowel perforation – which progressively increased over time. The cumulative incidence of such complications was 5.6% for open mesh repair and 3.7% for laparoscopic mesh repair.
This study was limited in that it was observational rather than being based on randomized data, so selection bias and imbalances among the study groups couldn’t be fully controlled for. However, two strengths of this study were that it reflects the real-world experience of an entire country and all the surgeons performing hernia repairs there, and it had 100% follow-up, the researchers said.
This study was partly funded by the Edgar Schnohr and Wife Gilberte Schnohr’s Foundation supporting independent surgical and anesthesiological research. Dr. Kokotovic reported having no relevant financial disclosures; one investigator reported receiving personal fees from Bard and Etichon for educational presentations.
These study findings suggest that the risk-benefit ratio of mesh reinforcement is not as clear as previously thought and call into question the current widespread use of mesh, even for repair of small hernias, when mesh is the norm for all incisional hernia repairs of any size.

Although the study by Kokotovic and colleagues is one of the most comprehensive long-term studies in hernia surgery, many questions remain about the optimal approach for repairing ventral hernia. To provide more rigorous data to better understand optimal approaches to this common clinical problem, surgeons will need to design large multicenter pragmatic trials with long-term follow-up.
Kamal M. F. Itani, MD, is at the VA Boston Health Care System, Boston University, West Roxbury, Mass., and Harvard Medical School in Boston. He reported having served as a research consultant to Davol 4 years ago regarding an antibiotic-coated mesh product. These remarks are excerpted from an editorial accompanying Dr. Kokotovic’s report (JAMA 2016 Oct 17. doi: 10.1001/jama.2016.15722).
These study findings suggest that the risk-benefit ratio of mesh reinforcement is not as clear as previously thought and call into question the current widespread use of mesh, even for repair of small hernias, when mesh is the norm for all incisional hernia repairs of any size.
Although the study by Kokotovic and colleagues is one of the most comprehensive long-term studies in hernia surgery, many questions remain about the optimal approach for repairing ventral hernia. To provide more rigorous data to better understand optimal approaches to this common clinical problem, surgeons will need to design large multicenter pragmatic trials with long-term follow-up.
Kamal M. F. Itani, MD, is at the VA Boston Health Care System, Boston University, West Roxbury, Mass., and Harvard Medical School in Boston. He reported having served as a research consultant to Davol 4 years ago regarding an antibiotic-coated mesh product. These remarks are excerpted from an editorial accompanying Dr. Kokotovic’s report (JAMA 2016 Oct 17. doi: 10.1001/jama.2016.15722).
These study findings suggest that the risk-benefit ratio of mesh reinforcement is not as clear as previously thought and call into question the current widespread use of mesh, even for repair of small hernias, when mesh is the norm for all incisional hernia repairs of any size.
Although the study by Kokotovic and colleagues is one of the most comprehensive long-term studies in hernia surgery, many questions remain about the optimal approach for repairing ventral hernia. To provide more rigorous data to better understand optimal approaches to this common clinical problem, surgeons will need to design large multicenter pragmatic trials with long-term follow-up.
Kamal M. F. Itani, MD, is at the VA Boston Health Care System, Boston University, West Roxbury, Mass., and Harvard Medical School in Boston. He reported having served as a research consultant to Davol 4 years ago regarding an antibiotic-coated mesh product. These remarks are excerpted from an editorial accompanying Dr. Kokotovic’s report (JAMA 2016 Oct 17. doi: 10.1001/jama.2016.15722).
Among patients undergoing elective incisional repair of abdominal wall hernias, the use of mesh reinforcement decreases the short-term recurrence rate by 5% but increases major complications by approximately the same amount over the subsequent 5 years, Dunja Kokotovic, MB, reported at the annual clinical congress of the American College of Surgeons.
“Given the continuously increasing incidence of mesh-related complications with time, it is expected that, with even longer follow-up up than the 5 years observed in this study, mesh-related complications continue to accrue,” said Dr. Kokotovic of the Center for Surgical Science, Zealand University Hospital, Koge, Denmark. The findings of this observational registry-based cohort study were presented at the congress and simultaneously published online in JAMA (2016 Oct 17. doi: 10.1001/jama.2016.15217).
These results highlight the need to assess the long-term safety of interventions before making definitive conclusions about their benefits and widely adopting them. In the United States, manufacturers are required to demonstrate the long-term safety of drugs but not of some devices, including hernia meshes. There were approximately 190,000 such hernia repairs performed in the United States alone during the most recent year for which data are available, and mesh is estimated to have been used in at least half, Dr. Kokotovic noted.
She and her associates analyzed the 5-year outcomes for virtually all incisional hernia repairs performed in Denmark from 2007 through 2010 using data in a mandatory national registry. Their analysis included 3,242 patients (mean age, 58 years): 1,119 (34.5%) who had open mesh repair, 1,757 (54.2%) who had laparoscopic mesh repair, and 366 (11.3%) who had nonmesh repair.
The cumulative risk of reoperation for hernia recurrence was significantly lower for patients who had open mesh repair (12.3%) or laparoscopic mesh repair (10.6%) than for those who had nonmesh repair (17.1%). However, this benefit was offset by the rate of major mesh-related complications requiring surgical intervention – including surgical site infection, formation of a chronic sinus tract, late-onset intra-abdominal abscess, enterocutaneous fistula, bowel obstruction, and bowel perforation – which progressively increased over time. The cumulative incidence of such complications was 5.6% for open mesh repair and 3.7% for laparoscopic mesh repair.
This study was limited in that it was observational rather than being based on randomized data, so selection bias and imbalances among the study groups couldn’t be fully controlled for. However, two strengths of this study were that it reflects the real-world experience of an entire country and all the surgeons performing hernia repairs there, and it had 100% follow-up, the researchers said.
This study was partly funded by the Edgar Schnohr and Wife Gilberte Schnohr’s Foundation supporting independent surgical and anesthesiological research. Dr. Kokotovic reported having no relevant financial disclosures; one investigator reported receiving personal fees from Bard and Etichon for educational presentations.
Among patients undergoing elective incisional repair of abdominal wall hernias, the use of mesh reinforcement decreases the short-term recurrence rate by 5% but increases major complications by approximately the same amount over the subsequent 5 years, Dunja Kokotovic, MB, reported at the annual clinical congress of the American College of Surgeons.
“Given the continuously increasing incidence of mesh-related complications with time, it is expected that, with even longer follow-up up than the 5 years observed in this study, mesh-related complications continue to accrue,” said Dr. Kokotovic of the Center for Surgical Science, Zealand University Hospital, Koge, Denmark. The findings of this observational registry-based cohort study were presented at the congress and simultaneously published online in JAMA (2016 Oct 17. doi: 10.1001/jama.2016.15217).
These results highlight the need to assess the long-term safety of interventions before making definitive conclusions about their benefits and widely adopting them. In the United States, manufacturers are required to demonstrate the long-term safety of drugs but not of some devices, including hernia meshes. There were approximately 190,000 such hernia repairs performed in the United States alone during the most recent year for which data are available, and mesh is estimated to have been used in at least half, Dr. Kokotovic noted.
She and her associates analyzed the 5-year outcomes for virtually all incisional hernia repairs performed in Denmark from 2007 through 2010 using data in a mandatory national registry. Their analysis included 3,242 patients (mean age, 58 years): 1,119 (34.5%) who had open mesh repair, 1,757 (54.2%) who had laparoscopic mesh repair, and 366 (11.3%) who had nonmesh repair.
The cumulative risk of reoperation for hernia recurrence was significantly lower for patients who had open mesh repair (12.3%) or laparoscopic mesh repair (10.6%) than for those who had nonmesh repair (17.1%). However, this benefit was offset by the rate of major mesh-related complications requiring surgical intervention – including surgical site infection, formation of a chronic sinus tract, late-onset intra-abdominal abscess, enterocutaneous fistula, bowel obstruction, and bowel perforation – which progressively increased over time. The cumulative incidence of such complications was 5.6% for open mesh repair and 3.7% for laparoscopic mesh repair.
This study was limited in that it was observational rather than being based on randomized data, so selection bias and imbalances among the study groups couldn’t be fully controlled for. However, two strengths of this study were that it reflects the real-world experience of an entire country and all the surgeons performing hernia repairs there, and it had 100% follow-up, the researchers said.
This study was partly funded by the Edgar Schnohr and Wife Gilberte Schnohr’s Foundation supporting independent surgical and anesthesiological research. Dr. Kokotovic reported having no relevant financial disclosures; one investigator reported receiving personal fees from Bard and Etichon for educational presentations.
FROM THE ACS CLINICAL CONGRESS
Key clinical point: Among patients undergoing elective incisional repair of abdominal wall hernias, the use of mesh reinforcement decreases the short-term recurrence rate by 5% but increases major complications by 5.6% over the subsequent 5 years.
Major finding: The cumulative rate of major mesh-related complications requiring surgical intervention was 5.6% for open mesh repair and 3.7% for laparoscopic mesh repair, compared with 0% for nonmesh repair.
Data source: A nationwide observational registry-based cohort study involving virtually all incisional hernia repairs (3,242) performed in Denmark from 2007 through 2010.
Disclosures: This study was partly funded by the Edgar Schnohr and Wife Gilberte Schnohr’s Foundation supporting independent surgical and anesthesiological research. Dr. Kokotovic reported having no relevant financial disclosures; one investigator reported receiving personal fees from Bard and Etichon for educational presentations.