User login
How much can we really do to slow age-related cognitive decline?

Flashback to 2012
It’s a whole new biosimilar world. In the April 2012 issue of GI & Hepatology News (GIHN) there was a small article on the issued Food and Drug Administration guidance on how to develop biosimilars. A biosimilar molecule must be structurally similar to the reference or originator product with the expectation that the safety and efficacy will be the same. The European Medicines Agency (EMA) established a legal framework for approving biologics in the European Union in 2003 and guidelines for approval in 2005 to 2006 with the first biosimilar approved in 2006 (somatropin [Omnitrope]).
The first monoclonal antibody biosimilar approved by the EMA was CT-P13 (infliximab-dyyb) in June 2013. There are now over 23 biosimilars approved for use in Europe. In 2012 there were no biosimilars on the market in the United States. This past year (2016) has been the year of the biosimilar with two of the four approved compounds used in inflammatory bowel disease – Inflectra (infliximab-dyyb, Hospira) April 2016 and Amjevita (adalimumab-atto, Amgen) September 2016 appearing.

The launch of these biosimilars raises a whole new series of questions. First and foremost for gastroenterologists – are the biosimilars truly similar in patients with inflammatory bowel disease? Adalimumab-atto was approved on the basis of two phase III studies in psoriasis and in rheumatoid arthritis and infliximab-dyyb was approved on the basis of studies in rheumatoid arthritis and ankylosing spondylitis. Other questions arise: 1. Can a patient who is doing well on the originator be safely switched to the biosimilar? 2. Can we use the same assays for drug monitoring? 3. Will use of biosimilars lead to a lower cost structure for patients and hospitals? 4. What are the regulations and guidelines for interchangeability? (GIHN March 2017) In the United States, development of biosimilars was slow to start but we expect to see an explosion in development of these agents in gastroenterology as the patents expire on the biologics currently in use.
Kim L. Isaacs, MD, PhD, is professor of medicine in the division of gastroenterology and hepatology at the University of North Carolina at Chapel Hill. She is codirector of the UNC Center for Inflammatory Bowel Disease. She is an Associate Editor for GI and Hepatology News.
It’s a whole new biosimilar world. In the April 2012 issue of GI & Hepatology News (GIHN) there was a small article on the issued Food and Drug Administration guidance on how to develop biosimilars. A biosimilar molecule must be structurally similar to the reference or originator product with the expectation that the safety and efficacy will be the same. The European Medicines Agency (EMA) established a legal framework for approving biologics in the European Union in 2003 and guidelines for approval in 2005 to 2006 with the first biosimilar approved in 2006 (somatropin [Omnitrope]).
The first monoclonal antibody biosimilar approved by the EMA was CT-P13 (infliximab-dyyb) in June 2013. There are now over 23 biosimilars approved for use in Europe. In 2012 there were no biosimilars on the market in the United States. This past year (2016) has been the year of the biosimilar with two of the four approved compounds used in inflammatory bowel disease – Inflectra (infliximab-dyyb, Hospira) April 2016 and Amjevita (adalimumab-atto, Amgen) September 2016 appearing.
The launch of these biosimilars raises a whole new series of questions. First and foremost for gastroenterologists – are the biosimilars truly similar in patients with inflammatory bowel disease? Adalimumab-atto was approved on the basis of two phase III studies in psoriasis and in rheumatoid arthritis and infliximab-dyyb was approved on the basis of studies in rheumatoid arthritis and ankylosing spondylitis. Other questions arise: 1. Can a patient who is doing well on the originator be safely switched to the biosimilar? 2. Can we use the same assays for drug monitoring? 3. Will use of biosimilars lead to a lower cost structure for patients and hospitals? 4. What are the regulations and guidelines for interchangeability? (GIHN March 2017) In the United States, development of biosimilars was slow to start but we expect to see an explosion in development of these agents in gastroenterology as the patents expire on the biologics currently in use.
Kim L. Isaacs, MD, PhD, is professor of medicine in the division of gastroenterology and hepatology at the University of North Carolina at Chapel Hill. She is codirector of the UNC Center for Inflammatory Bowel Disease. She is an Associate Editor for GI and Hepatology News.
It’s a whole new biosimilar world. In the April 2012 issue of GI & Hepatology News (GIHN) there was a small article on the issued Food and Drug Administration guidance on how to develop biosimilars. A biosimilar molecule must be structurally similar to the reference or originator product with the expectation that the safety and efficacy will be the same. The European Medicines Agency (EMA) established a legal framework for approving biologics in the European Union in 2003 and guidelines for approval in 2005 to 2006 with the first biosimilar approved in 2006 (somatropin [Omnitrope]).
The first monoclonal antibody biosimilar approved by the EMA was CT-P13 (infliximab-dyyb) in June 2013. There are now over 23 biosimilars approved for use in Europe. In 2012 there were no biosimilars on the market in the United States. This past year (2016) has been the year of the biosimilar with two of the four approved compounds used in inflammatory bowel disease – Inflectra (infliximab-dyyb, Hospira) April 2016 and Amjevita (adalimumab-atto, Amgen) September 2016 appearing.
The launch of these biosimilars raises a whole new series of questions. First and foremost for gastroenterologists – are the biosimilars truly similar in patients with inflammatory bowel disease? Adalimumab-atto was approved on the basis of two phase III studies in psoriasis and in rheumatoid arthritis and infliximab-dyyb was approved on the basis of studies in rheumatoid arthritis and ankylosing spondylitis. Other questions arise: 1. Can a patient who is doing well on the originator be safely switched to the biosimilar? 2. Can we use the same assays for drug monitoring? 3. Will use of biosimilars lead to a lower cost structure for patients and hospitals? 4. What are the regulations and guidelines for interchangeability? (GIHN March 2017) In the United States, development of biosimilars was slow to start but we expect to see an explosion in development of these agents in gastroenterology as the patents expire on the biologics currently in use.
Kim L. Isaacs, MD, PhD, is professor of medicine in the division of gastroenterology and hepatology at the University of North Carolina at Chapel Hill. She is codirector of the UNC Center for Inflammatory Bowel Disease. She is an Associate Editor for GI and Hepatology News.

Blazing A Trail in Medical Education
What led you to pursue a career in medical education?
Believe it or not, I pursued my path in medical education even prior to attending medical school. I was a high school teacher with a master’s in education, working during the summer of 1979 under the auspices of the Student Conservation Association at Grand Canyon National Park. Sitting on the edge of the canyon at sunset, I made the momentous decision to attend medical school, requiring attendance at a postbaccalaureate program at Columbia University. While considering medical schools, I knew that I wanted to combine my interest in education with medicine and I therefore chose to attend Case Western University School of Medicine. Since the mid-1950s, Case had been committed to innovative educational programs with a systems-based approach to the curriculum.

What do you enjoy most about working in medical education?
There are so many aspects of medical education that make work fun and rewarding. Perhaps the most rewarding is the ability to make a difference that affects the learner as well as the patients and communities that they will serve. I also enjoy the diverse experiences and opportunities in education and the ability to work with others in creative endeavors.
What are your responsibilities in a typical week?
One of the great things about a focus in education is that there never is a typical week. In the 32 years since my graduation from medical school, I have had the great fortune to fill many different roles: course director, electives director, fellowship program director, associate dean for student affairs, associate dean for undergraduate medical education, and associate dean for continuing medical education. For the past 6 years, I have been the senior associate dean for education at the University of Connecticut School of Medicine, overseeing undergraduate medical education, graduate medical education, continuing medical education, and the graduate school.
Over time I have had less interaction with students and residents as my administrative responsibilities have grown, but I know it is critical to maintain a presence with learners and I endeavor to do so in limited ways. Since our current priorities are in implementing a new curriculum and in planning for an accreditation visit, there are many days that are filled with meetings, planning, organizing, and writing. To me, the most precious responsibility is shaping a vision and bringing together a team to operationalize that vision in a collaborative and creative way, with learners, teachers, and administrators working together.
What are the different career options available for early-career GIs who are interested in medical education?
There are so many options in medical education for early-career gastroenterologists. For those working in private, group, or community practices, there are opportunities to precept students, residents, and fellows. For those working in an academic setting, opportunities abound. It is often a good idea to start within the division: get involved in teaching fellows in a clinical setting, or creating a new simulation experience or case workshop for fellows. There are opportunities to teach and supervise students. One of my first opportunities was in teaching in the physical diagnosis course. There are options to be involved in curriculum committees, admissions, CME, and to engage in educational initiatives at your institution.
The Association of American Medical Colleges has defined five areas of scholarship in education, and it is possible to get promoted to full professor – and even to attain academic tenure, as I have – if you fulfill the requirements for promotion at your institution. These areas include teaching, curriculum development, assessment, mentorship/advising, and leadership. There are also many ways to get involved in the AGA (http://www.gastro.org/trainees) and other organizations.1,2
Are there advanced training options available for those interested in medical education?
The AGA Academy of Educators (http://www.gastro.org/about/initiatives/aga-academy-of-educators)3 is a wonderful resource for networking. It has a competitive process for educational project grants as well as faculty development sessions and networking events at DDW®. There are also national leadership academies in medicine that have a focus in medical education. The Harvard Macy Institute is one such opportunity. Many medical schools have their own academies to support educators and teachers. I have been privileged to be one of the co-leaders of the AGA Future Leaders Program (http://www.gastro.org/about/initiatives/aga-future-leaders-program) and those with a niche interest in education can benefit and pursue related projects.4 One group was successful in publishing an educational article after completing the Future Leaders program.5 There are also several master’s programs for further education and training in educational theory. Some of these programs are available online or largely online, with limited requirements for onsite classes.
How do you go about finding a job in medical education?
First of all, you have to do your “day job.” In order to be a credible medical clinician-educator you must have clinical experience in patient care. It is important for the first years of your career to make sure that you have at least 70% clinical roles that can be reduced over time to accommodate advancing educational responsibilities. Get involved in teaching fellows. If you are in a practice, reach out to your local medical school or hospital to see how you might participate in educational programs. If you are in an academic setting, meet with the deans in education to express your interest and look for opportunities to get involved in an area of interest. If you are in academia, you have to make your work “count twice:” being productive in a scholarly way is not only important as a role model for learners, but it is important for you as a faculty member to grow and advance in your professional career.
It is always wise to think about when to say “yes” and when to say “no.” An important point is not to overextend yourself. Your reputation of completing tasks not only well, but on time, and thoroughly, is critical to your success. This includes making sure your learner evaluations are submitted on time, that you complete the administrative work in order to participate in CME programs, and that you honor your commitments by attending committee meetings.
What are the resources available to early-career GIs interested in medical education?
It is easy to find resources within your practice, your institution, or externally. The AGA has many resources available with a good start being the AGA Academy of Educators. Opportunities for creativity are numerous and with new advances in team-based learning, simulation, and interprofessional learning, there are new areas for involvement evolving all the time.6,7
Finally, pursuing a career in education is exciting, fun, and fulfilling. Having the opportunity to influence learners, which in turn will impact patient care, is an awesome privilege.
Dr. Rose is a professor of medicine and senior associate dean for education at the University of Connecticut School of Medicine.
References
1. Gusic M, et al. MedEdPORTAL; 2013. Available from: http://www.mededportal.org/publication/9313.
2. Gusic ME, et al. Acad Med. 2014;89(7):1006-11.
3. Pfeil SA, et al. Gastroenterology 2015;149(6):1309-14.
4. Cryer B, Rose S. Gastroenterology 2015;149:246-8.
5. Shah BJ, et al. Gastroenterology 2016;151(2):218-21.
6. Shah BJ, Rose S. Gastroenterology 2012;142:684-9.
7. Shah BJ, Rose S. AGA Perspectives 2012;April-May:20-21.
What led you to pursue a career in medical education?
Believe it or not, I pursued my path in medical education even prior to attending medical school. I was a high school teacher with a master’s in education, working during the summer of 1979 under the auspices of the Student Conservation Association at Grand Canyon National Park. Sitting on the edge of the canyon at sunset, I made the momentous decision to attend medical school, requiring attendance at a postbaccalaureate program at Columbia University. While considering medical schools, I knew that I wanted to combine my interest in education with medicine and I therefore chose to attend Case Western University School of Medicine. Since the mid-1950s, Case had been committed to innovative educational programs with a systems-based approach to the curriculum.
What do you enjoy most about working in medical education?
There are so many aspects of medical education that make work fun and rewarding. Perhaps the most rewarding is the ability to make a difference that affects the learner as well as the patients and communities that they will serve. I also enjoy the diverse experiences and opportunities in education and the ability to work with others in creative endeavors.
What are your responsibilities in a typical week?
One of the great things about a focus in education is that there never is a typical week. In the 32 years since my graduation from medical school, I have had the great fortune to fill many different roles: course director, electives director, fellowship program director, associate dean for student affairs, associate dean for undergraduate medical education, and associate dean for continuing medical education. For the past 6 years, I have been the senior associate dean for education at the University of Connecticut School of Medicine, overseeing undergraduate medical education, graduate medical education, continuing medical education, and the graduate school.
Over time I have had less interaction with students and residents as my administrative responsibilities have grown, but I know it is critical to maintain a presence with learners and I endeavor to do so in limited ways. Since our current priorities are in implementing a new curriculum and in planning for an accreditation visit, there are many days that are filled with meetings, planning, organizing, and writing. To me, the most precious responsibility is shaping a vision and bringing together a team to operationalize that vision in a collaborative and creative way, with learners, teachers, and administrators working together.
What are the different career options available for early-career GIs who are interested in medical education?
There are so many options in medical education for early-career gastroenterologists. For those working in private, group, or community practices, there are opportunities to precept students, residents, and fellows. For those working in an academic setting, opportunities abound. It is often a good idea to start within the division: get involved in teaching fellows in a clinical setting, or creating a new simulation experience or case workshop for fellows. There are opportunities to teach and supervise students. One of my first opportunities was in teaching in the physical diagnosis course. There are options to be involved in curriculum committees, admissions, CME, and to engage in educational initiatives at your institution.
The Association of American Medical Colleges has defined five areas of scholarship in education, and it is possible to get promoted to full professor – and even to attain academic tenure, as I have – if you fulfill the requirements for promotion at your institution. These areas include teaching, curriculum development, assessment, mentorship/advising, and leadership. There are also many ways to get involved in the AGA (http://www.gastro.org/trainees) and other organizations.1,2
Are there advanced training options available for those interested in medical education?
The AGA Academy of Educators (http://www.gastro.org/about/initiatives/aga-academy-of-educators)3 is a wonderful resource for networking. It has a competitive process for educational project grants as well as faculty development sessions and networking events at DDW®. There are also national leadership academies in medicine that have a focus in medical education. The Harvard Macy Institute is one such opportunity. Many medical schools have their own academies to support educators and teachers. I have been privileged to be one of the co-leaders of the AGA Future Leaders Program (http://www.gastro.org/about/initiatives/aga-future-leaders-program) and those with a niche interest in education can benefit and pursue related projects.4 One group was successful in publishing an educational article after completing the Future Leaders program.5 There are also several master’s programs for further education and training in educational theory. Some of these programs are available online or largely online, with limited requirements for onsite classes.
How do you go about finding a job in medical education?
First of all, you have to do your “day job.” In order to be a credible medical clinician-educator you must have clinical experience in patient care. It is important for the first years of your career to make sure that you have at least 70% clinical roles that can be reduced over time to accommodate advancing educational responsibilities. Get involved in teaching fellows. If you are in a practice, reach out to your local medical school or hospital to see how you might participate in educational programs. If you are in an academic setting, meet with the deans in education to express your interest and look for opportunities to get involved in an area of interest. If you are in academia, you have to make your work “count twice:” being productive in a scholarly way is not only important as a role model for learners, but it is important for you as a faculty member to grow and advance in your professional career.
It is always wise to think about when to say “yes” and when to say “no.” An important point is not to overextend yourself. Your reputation of completing tasks not only well, but on time, and thoroughly, is critical to your success. This includes making sure your learner evaluations are submitted on time, that you complete the administrative work in order to participate in CME programs, and that you honor your commitments by attending committee meetings.
What are the resources available to early-career GIs interested in medical education?
It is easy to find resources within your practice, your institution, or externally. The AGA has many resources available with a good start being the AGA Academy of Educators. Opportunities for creativity are numerous and with new advances in team-based learning, simulation, and interprofessional learning, there are new areas for involvement evolving all the time.6,7
Finally, pursuing a career in education is exciting, fun, and fulfilling. Having the opportunity to influence learners, which in turn will impact patient care, is an awesome privilege.
Dr. Rose is a professor of medicine and senior associate dean for education at the University of Connecticut School of Medicine.
References
1. Gusic M, et al. MedEdPORTAL; 2013. Available from: http://www.mededportal.org/publication/9313.
2. Gusic ME, et al. Acad Med. 2014;89(7):1006-11.
3. Pfeil SA, et al. Gastroenterology 2015;149(6):1309-14.
4. Cryer B, Rose S. Gastroenterology 2015;149:246-8.
5. Shah BJ, et al. Gastroenterology 2016;151(2):218-21.
6. Shah BJ, Rose S. Gastroenterology 2012;142:684-9.
7. Shah BJ, Rose S. AGA Perspectives 2012;April-May:20-21.
What led you to pursue a career in medical education?
Believe it or not, I pursued my path in medical education even prior to attending medical school. I was a high school teacher with a master’s in education, working during the summer of 1979 under the auspices of the Student Conservation Association at Grand Canyon National Park. Sitting on the edge of the canyon at sunset, I made the momentous decision to attend medical school, requiring attendance at a postbaccalaureate program at Columbia University. While considering medical schools, I knew that I wanted to combine my interest in education with medicine and I therefore chose to attend Case Western University School of Medicine. Since the mid-1950s, Case had been committed to innovative educational programs with a systems-based approach to the curriculum.
What do you enjoy most about working in medical education?
There are so many aspects of medical education that make work fun and rewarding. Perhaps the most rewarding is the ability to make a difference that affects the learner as well as the patients and communities that they will serve. I also enjoy the diverse experiences and opportunities in education and the ability to work with others in creative endeavors.
What are your responsibilities in a typical week?
One of the great things about a focus in education is that there never is a typical week. In the 32 years since my graduation from medical school, I have had the great fortune to fill many different roles: course director, electives director, fellowship program director, associate dean for student affairs, associate dean for undergraduate medical education, and associate dean for continuing medical education. For the past 6 years, I have been the senior associate dean for education at the University of Connecticut School of Medicine, overseeing undergraduate medical education, graduate medical education, continuing medical education, and the graduate school.
Over time I have had less interaction with students and residents as my administrative responsibilities have grown, but I know it is critical to maintain a presence with learners and I endeavor to do so in limited ways. Since our current priorities are in implementing a new curriculum and in planning for an accreditation visit, there are many days that are filled with meetings, planning, organizing, and writing. To me, the most precious responsibility is shaping a vision and bringing together a team to operationalize that vision in a collaborative and creative way, with learners, teachers, and administrators working together.
What are the different career options available for early-career GIs who are interested in medical education?
There are so many options in medical education for early-career gastroenterologists. For those working in private, group, or community practices, there are opportunities to precept students, residents, and fellows. For those working in an academic setting, opportunities abound. It is often a good idea to start within the division: get involved in teaching fellows in a clinical setting, or creating a new simulation experience or case workshop for fellows. There are opportunities to teach and supervise students. One of my first opportunities was in teaching in the physical diagnosis course. There are options to be involved in curriculum committees, admissions, CME, and to engage in educational initiatives at your institution.
The Association of American Medical Colleges has defined five areas of scholarship in education, and it is possible to get promoted to full professor – and even to attain academic tenure, as I have – if you fulfill the requirements for promotion at your institution. These areas include teaching, curriculum development, assessment, mentorship/advising, and leadership. There are also many ways to get involved in the AGA (http://www.gastro.org/trainees) and other organizations.1,2
Are there advanced training options available for those interested in medical education?
The AGA Academy of Educators (http://www.gastro.org/about/initiatives/aga-academy-of-educators)3 is a wonderful resource for networking. It has a competitive process for educational project grants as well as faculty development sessions and networking events at DDW®. There are also national leadership academies in medicine that have a focus in medical education. The Harvard Macy Institute is one such opportunity. Many medical schools have their own academies to support educators and teachers. I have been privileged to be one of the co-leaders of the AGA Future Leaders Program (http://www.gastro.org/about/initiatives/aga-future-leaders-program) and those with a niche interest in education can benefit and pursue related projects.4 One group was successful in publishing an educational article after completing the Future Leaders program.5 There are also several master’s programs for further education and training in educational theory. Some of these programs are available online or largely online, with limited requirements for onsite classes.
How do you go about finding a job in medical education?
First of all, you have to do your “day job.” In order to be a credible medical clinician-educator you must have clinical experience in patient care. It is important for the first years of your career to make sure that you have at least 70% clinical roles that can be reduced over time to accommodate advancing educational responsibilities. Get involved in teaching fellows. If you are in a practice, reach out to your local medical school or hospital to see how you might participate in educational programs. If you are in an academic setting, meet with the deans in education to express your interest and look for opportunities to get involved in an area of interest. If you are in academia, you have to make your work “count twice:” being productive in a scholarly way is not only important as a role model for learners, but it is important for you as a faculty member to grow and advance in your professional career.
It is always wise to think about when to say “yes” and when to say “no.” An important point is not to overextend yourself. Your reputation of completing tasks not only well, but on time, and thoroughly, is critical to your success. This includes making sure your learner evaluations are submitted on time, that you complete the administrative work in order to participate in CME programs, and that you honor your commitments by attending committee meetings.
What are the resources available to early-career GIs interested in medical education?
It is easy to find resources within your practice, your institution, or externally. The AGA has many resources available with a good start being the AGA Academy of Educators. Opportunities for creativity are numerous and with new advances in team-based learning, simulation, and interprofessional learning, there are new areas for involvement evolving all the time.6,7
Finally, pursuing a career in education is exciting, fun, and fulfilling. Having the opportunity to influence learners, which in turn will impact patient care, is an awesome privilege.
Dr. Rose is a professor of medicine and senior associate dean for education at the University of Connecticut School of Medicine.
References
1. Gusic M, et al. MedEdPORTAL; 2013. Available from: http://www.mededportal.org/publication/9313.
2. Gusic ME, et al. Acad Med. 2014;89(7):1006-11.
3. Pfeil SA, et al. Gastroenterology 2015;149(6):1309-14.
4. Cryer B, Rose S. Gastroenterology 2015;149:246-8.
5. Shah BJ, et al. Gastroenterology 2016;151(2):218-21.
6. Shah BJ, Rose S. Gastroenterology 2012;142:684-9.
7. Shah BJ, Rose S. AGA Perspectives 2012;April-May:20-21.
Legal Issues for the Gastroenterologist: Part I
An unfortunate fact for many physicians practicing in the United States is that they will contend with medical malpractice suits at some point in their careers. While data specific to gastroenterology malpractice claims is difficult to find,1 the Physician Insurers Association of America has reported that out of the 28 specialty fields of medicine analyzed from 1985 to 2004, gastroenterology ranked 21st in the number of claims reported2, representing about 2% of the total overall number of claims.

In 2017, JAMA Internal Medicine published additional statistical findings related to medical malpractice claims.4JAMA reported that the rate of claims paid on behalf of all physicians had declined by 55.7% between 1992 and 2014; from 20.1 per 1,000 physicians to 8.9 per 1000 physicians.4 The mean payment for the 280,368 claims reported in the National Practitioner Data Bank during this time frame was $329,565 (adjusted to 2014 dollars).4

Professional liability
Patients can allege or establish malpractice liability against a doctor based on a number of things; we will discuss a few of the most common types of liability, offer suggestions as to how you might minimize your risk of being sued, and how best to cope when you are sued.
Negligence: One of the most common theories you may be sued under is negligence. To state a negligence claim against a physician, a plaintiff must show that the doctor owed the patient a duty recognized by law, that the physician breached that duty, that the alleged breach resulted in injury to the patient, and that the patient sustained legally recognized damages as a result. In a lawsuit brought on the basis of claimed medical negligence, a patient claims that a physician, in the course of rendering treatment, failed to meet the applicable standard of care.

Contractual liability of doctor to patient: Physicians and patients can enter into express written contracts regarding the care provided. These contracts can include various treatment plans, the likelihood of success, and even the physician’s promise to cure. Traditionally, courts have respected a physician’s freedom to contract as he or she chooses. However, once a contract is formed, a plaintiff may have a cause of action for breach of contract if the outcome of the treatment is not what was promised.
Minimizing risk

Another opportunity to decrease your chances of being sued is to keep informed about recent developments in your field. Make a point to read pertinent literature, attend seminars, and do whatever is necessary to stay aware of, and to incorporate into your practice, current methods of treatment and diagnosis.
Physicians should also be cognizant of contractual liability. When discussing treatment, never guarantee results. Additionally, once a physician-patient relationship is established, you cannot withdraw from the relationship without providing adequate notice to the patient in time to obtain alternative care. Terminating the relationship without such is called abandonment, and can result in professional discipline and civil liability.

Conclusion
Before a lawsuit, and as a regular part of your practice, it is important that you thoroughly and legibly document all aspects of care provided, stay current with medical advances, and take the time to create a relationship with your patients involving quality communication. It is impossible for us to provide you with enough information to adequately prepare you for the day on which you may be sued. We nevertheless hope that following the aforementioned suggestions will be of some help.
References
1. Medical Malpractice Claims and Risk Management in Gastroenterology and Gastrointestinal Endoscopy. American Society for Gastrointestinal Endoscopy, 2017. <www.asge.org>.
2. Physician Insurers Association of America. PIAA Claim Trend Analysis: Gastroenterology, iv. Lawrenceville, N.J.: PIAA, 2004. <http://www.piaa.us>.
3. Kane C., Policy Research Perspective: Medical Liability Claim Frequency: 2007-2008 Snapshot of Physicians, American Medical Association, 2010.
4. Schaffer A.C., et al. JAMA Internal Med. 2017;177(5):710-8.
5. Dodge A.M. Wilsonville, Ore. Book Partners, Inc. 2001.
An unfortunate fact for many physicians practicing in the United States is that they will contend with medical malpractice suits at some point in their careers. While data specific to gastroenterology malpractice claims is difficult to find,1 the Physician Insurers Association of America has reported that out of the 28 specialty fields of medicine analyzed from 1985 to 2004, gastroenterology ranked 21st in the number of claims reported2, representing about 2% of the total overall number of claims.
In 2017, JAMA Internal Medicine published additional statistical findings related to medical malpractice claims.4JAMA reported that the rate of claims paid on behalf of all physicians had declined by 55.7% between 1992 and 2014; from 20.1 per 1,000 physicians to 8.9 per 1000 physicians.4 The mean payment for the 280,368 claims reported in the National Practitioner Data Bank during this time frame was $329,565 (adjusted to 2014 dollars).4
Professional liability
Patients can allege or establish malpractice liability against a doctor based on a number of things; we will discuss a few of the most common types of liability, offer suggestions as to how you might minimize your risk of being sued, and how best to cope when you are sued.
Negligence: One of the most common theories you may be sued under is negligence. To state a negligence claim against a physician, a plaintiff must show that the doctor owed the patient a duty recognized by law, that the physician breached that duty, that the alleged breach resulted in injury to the patient, and that the patient sustained legally recognized damages as a result. In a lawsuit brought on the basis of claimed medical negligence, a patient claims that a physician, in the course of rendering treatment, failed to meet the applicable standard of care.
Contractual liability of doctor to patient: Physicians and patients can enter into express written contracts regarding the care provided. These contracts can include various treatment plans, the likelihood of success, and even the physician’s promise to cure. Traditionally, courts have respected a physician’s freedom to contract as he or she chooses. However, once a contract is formed, a plaintiff may have a cause of action for breach of contract if the outcome of the treatment is not what was promised.
Minimizing risk
Another opportunity to decrease your chances of being sued is to keep informed about recent developments in your field. Make a point to read pertinent literature, attend seminars, and do whatever is necessary to stay aware of, and to incorporate into your practice, current methods of treatment and diagnosis.
Physicians should also be cognizant of contractual liability. When discussing treatment, never guarantee results. Additionally, once a physician-patient relationship is established, you cannot withdraw from the relationship without providing adequate notice to the patient in time to obtain alternative care. Terminating the relationship without such is called abandonment, and can result in professional discipline and civil liability.
Conclusion
Before a lawsuit, and as a regular part of your practice, it is important that you thoroughly and legibly document all aspects of care provided, stay current with medical advances, and take the time to create a relationship with your patients involving quality communication. It is impossible for us to provide you with enough information to adequately prepare you for the day on which you may be sued. We nevertheless hope that following the aforementioned suggestions will be of some help.
References
1. Medical Malpractice Claims and Risk Management in Gastroenterology and Gastrointestinal Endoscopy. American Society for Gastrointestinal Endoscopy, 2017. <www.asge.org>.
2. Physician Insurers Association of America. PIAA Claim Trend Analysis: Gastroenterology, iv. Lawrenceville, N.J.: PIAA, 2004. <http://www.piaa.us>.
3. Kane C., Policy Research Perspective: Medical Liability Claim Frequency: 2007-2008 Snapshot of Physicians, American Medical Association, 2010.
4. Schaffer A.C., et al. JAMA Internal Med. 2017;177(5):710-8.
5. Dodge A.M. Wilsonville, Ore. Book Partners, Inc. 2001.
An unfortunate fact for many physicians practicing in the United States is that they will contend with medical malpractice suits at some point in their careers. While data specific to gastroenterology malpractice claims is difficult to find,1 the Physician Insurers Association of America has reported that out of the 28 specialty fields of medicine analyzed from 1985 to 2004, gastroenterology ranked 21st in the number of claims reported2, representing about 2% of the total overall number of claims.
In 2017, JAMA Internal Medicine published additional statistical findings related to medical malpractice claims.4JAMA reported that the rate of claims paid on behalf of all physicians had declined by 55.7% between 1992 and 2014; from 20.1 per 1,000 physicians to 8.9 per 1000 physicians.4 The mean payment for the 280,368 claims reported in the National Practitioner Data Bank during this time frame was $329,565 (adjusted to 2014 dollars).4
Professional liability
Patients can allege or establish malpractice liability against a doctor based on a number of things; we will discuss a few of the most common types of liability, offer suggestions as to how you might minimize your risk of being sued, and how best to cope when you are sued.
Negligence: One of the most common theories you may be sued under is negligence. To state a negligence claim against a physician, a plaintiff must show that the doctor owed the patient a duty recognized by law, that the physician breached that duty, that the alleged breach resulted in injury to the patient, and that the patient sustained legally recognized damages as a result. In a lawsuit brought on the basis of claimed medical negligence, a patient claims that a physician, in the course of rendering treatment, failed to meet the applicable standard of care.
Contractual liability of doctor to patient: Physicians and patients can enter into express written contracts regarding the care provided. These contracts can include various treatment plans, the likelihood of success, and even the physician’s promise to cure. Traditionally, courts have respected a physician’s freedom to contract as he or she chooses. However, once a contract is formed, a plaintiff may have a cause of action for breach of contract if the outcome of the treatment is not what was promised.
Minimizing risk
Another opportunity to decrease your chances of being sued is to keep informed about recent developments in your field. Make a point to read pertinent literature, attend seminars, and do whatever is necessary to stay aware of, and to incorporate into your practice, current methods of treatment and diagnosis.
Physicians should also be cognizant of contractual liability. When discussing treatment, never guarantee results. Additionally, once a physician-patient relationship is established, you cannot withdraw from the relationship without providing adequate notice to the patient in time to obtain alternative care. Terminating the relationship without such is called abandonment, and can result in professional discipline and civil liability.
Conclusion
Before a lawsuit, and as a regular part of your practice, it is important that you thoroughly and legibly document all aspects of care provided, stay current with medical advances, and take the time to create a relationship with your patients involving quality communication. It is impossible for us to provide you with enough information to adequately prepare you for the day on which you may be sued. We nevertheless hope that following the aforementioned suggestions will be of some help.
References
1. Medical Malpractice Claims and Risk Management in Gastroenterology and Gastrointestinal Endoscopy. American Society for Gastrointestinal Endoscopy, 2017. <www.asge.org>.
2. Physician Insurers Association of America. PIAA Claim Trend Analysis: Gastroenterology, iv. Lawrenceville, N.J.: PIAA, 2004. <http://www.piaa.us>.
3. Kane C., Policy Research Perspective: Medical Liability Claim Frequency: 2007-2008 Snapshot of Physicians, American Medical Association, 2010.
4. Schaffer A.C., et al. JAMA Internal Med. 2017;177(5):710-8.
5. Dodge A.M. Wilsonville, Ore. Book Partners, Inc. 2001.
AGA’s 2017 Women’s Leadership Conference: Developing Skills in Advocacy and Personal Branding
The 2017 AGA Women’s Leadership Conference brought together 38 women from across the United States and Mexico for an inspiring and productive meeting. The group included 21 early-career and 17 experienced track women in GI. Among the attendees were 3 PhDs, 9 private practitioners, 1 pediatric gastroenterologist, and 25 academic gastroenterologists. We were particularly fortunate to benefit from the strong representation of AGA leadership, including Marcia Cruz-Correa, MD, PhD, AGAF (At-Large Councillor) and Deborah Proctor, MD, AGAF (Education and Training Councillor), as well as Ellen Zimmermann, MD, AGAF (Chair of the Women’s Committee) and Sheila Crowe, MD, AGAF (President, AGA Institute Governing Board).

The program included lively problem-solving sessions and a passionate discussion about negotiating skills. The latter topic was of particular interest given data indicating that pay inequity still exists. The group engaged in animated conversation about advocating for fair pay in academics and private practice.

In addition to strong mentorship, the early-career group discussed the importance of discerning one’s own individual passions. Identifying professional and personal ambitions can allow us to focus our energy and activities. We were encouraged to write down one personal and one professional goal on an annual basis. These goals can offer clarity for a range of decisions such as when to accept new responsibilities and how to structure activities and manage time at work and at home.

The AGA leaders in attendance shared inspiring stories of their own paths to leadership. These paths were not linear and it was reassuring to discover common themes of finding and developing personal strengths, identifying passions, and building areas of expertise. We learned, how once identified, strengths and passions can be connected to areas of need within a home institution or an organization such as the AGA. Dr. Zimmermann offered moving commentary about her own journey as a clinician, scientist, and mother. She encouraged those in attendance with small children to take the time to be present at home, knowing that there will be opportunities to assume leadership roles in the future. Of course, for others, the time to assume leadership roles may be now, and the Women’s Leadership Conference offered the chance to network and forge new connections within the AGA.

The second new topic was addressed in a powerful session on personal branding by Dr. Cruz-Correa. Personal branding involves identifying and communicating who one is to the world in a memorable way. Dr. Cruz-Correa emphasized that creating a personal brand is essential for leadership and critically important for advancing one’s career. Developing a personal brand should include crafting a statement of one to two sentences that considers both one’s values and the target audience. The statement should be memorable and punchy with an emphasis on solutions. Branding expands beyond indicating an area of interest; a personal brand should demonstrate consistent delivery of high-quality work. An example of a personal brand could be “Physician, fitness fanatic, and fearless foodie empowering patients and colleagues to lead healthy fulfilling lives.” An alternative might be: “Physician, teacher, empowering colleagues, advocating for patients, and evolving with the times.” Creating a personal brand that highlights action and solutions emphasizes a theme of the meeting: Follow-through after accepting responsibilities is critically important.

In summary, the 2017 AGA Women’s Leadership Conference provided an invigorating curriculum as well as many opportunities for establishing new networks of strong women in our field. Participants were charged with bringing some of the content back home, and we’re already receiving reports about these local events. Be sure to look for future content from the AGA at http://www.gastro.org/about/people/committees/womens-committee.
Acknowledgments: Dr. Garman and Dr. Alaparthi would like to offer heartfelt thanks to the AGA as well as to Celena NuQuay and Carol Brown for their support.
Dr. Garman is an assistant professor of medicine in the division of gastroenterology at Duke University, Durham, N.C. Dr. Alaparthi is managing partner of Gastroenterology Center of Connecticut and assistant clinical professor of medicine at Yale School of Medicine, Conn., and Frank Netter School of Medicine, Conn.
The 2017 AGA Women’s Leadership Conference brought together 38 women from across the United States and Mexico for an inspiring and productive meeting. The group included 21 early-career and 17 experienced track women in GI. Among the attendees were 3 PhDs, 9 private practitioners, 1 pediatric gastroenterologist, and 25 academic gastroenterologists. We were particularly fortunate to benefit from the strong representation of AGA leadership, including Marcia Cruz-Correa, MD, PhD, AGAF (At-Large Councillor) and Deborah Proctor, MD, AGAF (Education and Training Councillor), as well as Ellen Zimmermann, MD, AGAF (Chair of the Women’s Committee) and Sheila Crowe, MD, AGAF (President, AGA Institute Governing Board).
The program included lively problem-solving sessions and a passionate discussion about negotiating skills. The latter topic was of particular interest given data indicating that pay inequity still exists. The group engaged in animated conversation about advocating for fair pay in academics and private practice.
In addition to strong mentorship, the early-career group discussed the importance of discerning one’s own individual passions. Identifying professional and personal ambitions can allow us to focus our energy and activities. We were encouraged to write down one personal and one professional goal on an annual basis. These goals can offer clarity for a range of decisions such as when to accept new responsibilities and how to structure activities and manage time at work and at home.
The AGA leaders in attendance shared inspiring stories of their own paths to leadership. These paths were not linear and it was reassuring to discover common themes of finding and developing personal strengths, identifying passions, and building areas of expertise. We learned, how once identified, strengths and passions can be connected to areas of need within a home institution or an organization such as the AGA. Dr. Zimmermann offered moving commentary about her own journey as a clinician, scientist, and mother. She encouraged those in attendance with small children to take the time to be present at home, knowing that there will be opportunities to assume leadership roles in the future. Of course, for others, the time to assume leadership roles may be now, and the Women’s Leadership Conference offered the chance to network and forge new connections within the AGA.
The second new topic was addressed in a powerful session on personal branding by Dr. Cruz-Correa. Personal branding involves identifying and communicating who one is to the world in a memorable way. Dr. Cruz-Correa emphasized that creating a personal brand is essential for leadership and critically important for advancing one’s career. Developing a personal brand should include crafting a statement of one to two sentences that considers both one’s values and the target audience. The statement should be memorable and punchy with an emphasis on solutions. Branding expands beyond indicating an area of interest; a personal brand should demonstrate consistent delivery of high-quality work. An example of a personal brand could be “Physician, fitness fanatic, and fearless foodie empowering patients and colleagues to lead healthy fulfilling lives.” An alternative might be: “Physician, teacher, empowering colleagues, advocating for patients, and evolving with the times.” Creating a personal brand that highlights action and solutions emphasizes a theme of the meeting: Follow-through after accepting responsibilities is critically important.
In summary, the 2017 AGA Women’s Leadership Conference provided an invigorating curriculum as well as many opportunities for establishing new networks of strong women in our field. Participants were charged with bringing some of the content back home, and we’re already receiving reports about these local events. Be sure to look for future content from the AGA at http://www.gastro.org/about/people/committees/womens-committee.
Acknowledgments: Dr. Garman and Dr. Alaparthi would like to offer heartfelt thanks to the AGA as well as to Celena NuQuay and Carol Brown for their support.
Dr. Garman is an assistant professor of medicine in the division of gastroenterology at Duke University, Durham, N.C. Dr. Alaparthi is managing partner of Gastroenterology Center of Connecticut and assistant clinical professor of medicine at Yale School of Medicine, Conn., and Frank Netter School of Medicine, Conn.
The 2017 AGA Women’s Leadership Conference brought together 38 women from across the United States and Mexico for an inspiring and productive meeting. The group included 21 early-career and 17 experienced track women in GI. Among the attendees were 3 PhDs, 9 private practitioners, 1 pediatric gastroenterologist, and 25 academic gastroenterologists. We were particularly fortunate to benefit from the strong representation of AGA leadership, including Marcia Cruz-Correa, MD, PhD, AGAF (At-Large Councillor) and Deborah Proctor, MD, AGAF (Education and Training Councillor), as well as Ellen Zimmermann, MD, AGAF (Chair of the Women’s Committee) and Sheila Crowe, MD, AGAF (President, AGA Institute Governing Board).
The program included lively problem-solving sessions and a passionate discussion about negotiating skills. The latter topic was of particular interest given data indicating that pay inequity still exists. The group engaged in animated conversation about advocating for fair pay in academics and private practice.
In addition to strong mentorship, the early-career group discussed the importance of discerning one’s own individual passions. Identifying professional and personal ambitions can allow us to focus our energy and activities. We were encouraged to write down one personal and one professional goal on an annual basis. These goals can offer clarity for a range of decisions such as when to accept new responsibilities and how to structure activities and manage time at work and at home.
The AGA leaders in attendance shared inspiring stories of their own paths to leadership. These paths were not linear and it was reassuring to discover common themes of finding and developing personal strengths, identifying passions, and building areas of expertise. We learned, how once identified, strengths and passions can be connected to areas of need within a home institution or an organization such as the AGA. Dr. Zimmermann offered moving commentary about her own journey as a clinician, scientist, and mother. She encouraged those in attendance with small children to take the time to be present at home, knowing that there will be opportunities to assume leadership roles in the future. Of course, for others, the time to assume leadership roles may be now, and the Women’s Leadership Conference offered the chance to network and forge new connections within the AGA.
The second new topic was addressed in a powerful session on personal branding by Dr. Cruz-Correa. Personal branding involves identifying and communicating who one is to the world in a memorable way. Dr. Cruz-Correa emphasized that creating a personal brand is essential for leadership and critically important for advancing one’s career. Developing a personal brand should include crafting a statement of one to two sentences that considers both one’s values and the target audience. The statement should be memorable and punchy with an emphasis on solutions. Branding expands beyond indicating an area of interest; a personal brand should demonstrate consistent delivery of high-quality work. An example of a personal brand could be “Physician, fitness fanatic, and fearless foodie empowering patients and colleagues to lead healthy fulfilling lives.” An alternative might be: “Physician, teacher, empowering colleagues, advocating for patients, and evolving with the times.” Creating a personal brand that highlights action and solutions emphasizes a theme of the meeting: Follow-through after accepting responsibilities is critically important.
In summary, the 2017 AGA Women’s Leadership Conference provided an invigorating curriculum as well as many opportunities for establishing new networks of strong women in our field. Participants were charged with bringing some of the content back home, and we’re already receiving reports about these local events. Be sure to look for future content from the AGA at http://www.gastro.org/about/people/committees/womens-committee.
Acknowledgments: Dr. Garman and Dr. Alaparthi would like to offer heartfelt thanks to the AGA as well as to Celena NuQuay and Carol Brown for their support.
Dr. Garman is an assistant professor of medicine in the division of gastroenterology at Duke University, Durham, N.C. Dr. Alaparthi is managing partner of Gastroenterology Center of Connecticut and assistant clinical professor of medicine at Yale School of Medicine, Conn., and Frank Netter School of Medicine, Conn.
Reflux Diagnostics: Modern Techniques and Future Directions
Introduction
Chronic esophageal symptoms attributed to gastroesophageal reflux disease (GERD) are common presenting symptoms in gastroenterology, leading to high healthcare costs and adverse quality of life globally.1,2 The clinical diagnosis of GERD hinges on the presence of “troublesome” compatible typical symptoms (heartburn, acid regurgitation) or evidence of mucosal injury on endoscopy (esophagitis, Barrett’s esophagus, peptic stricture).3 With the growing availability of proton pump inhibitors (PPIs), patients and clinicians often utilize an empiric therapeutic trial of PPI as an initial test, with symptom improvement in the absence of alarm symptoms indicating a high likelihood of GERD.4 A meta-analysis of studies that used objective measures of GERD (in this case, 24-hour pH monitoring) showed that the “PPI test” has a sensitivity of 78%, but a specificity of only 54%, as a diagnostic approach to GERD symptoms.5 Apart from noncardiac chest pain, the diagnostic yield is even lower for atypical and extra-esophageal symptoms such as cough or laryngeal symptoms.6
The “nuts and bolts” of reflux testing
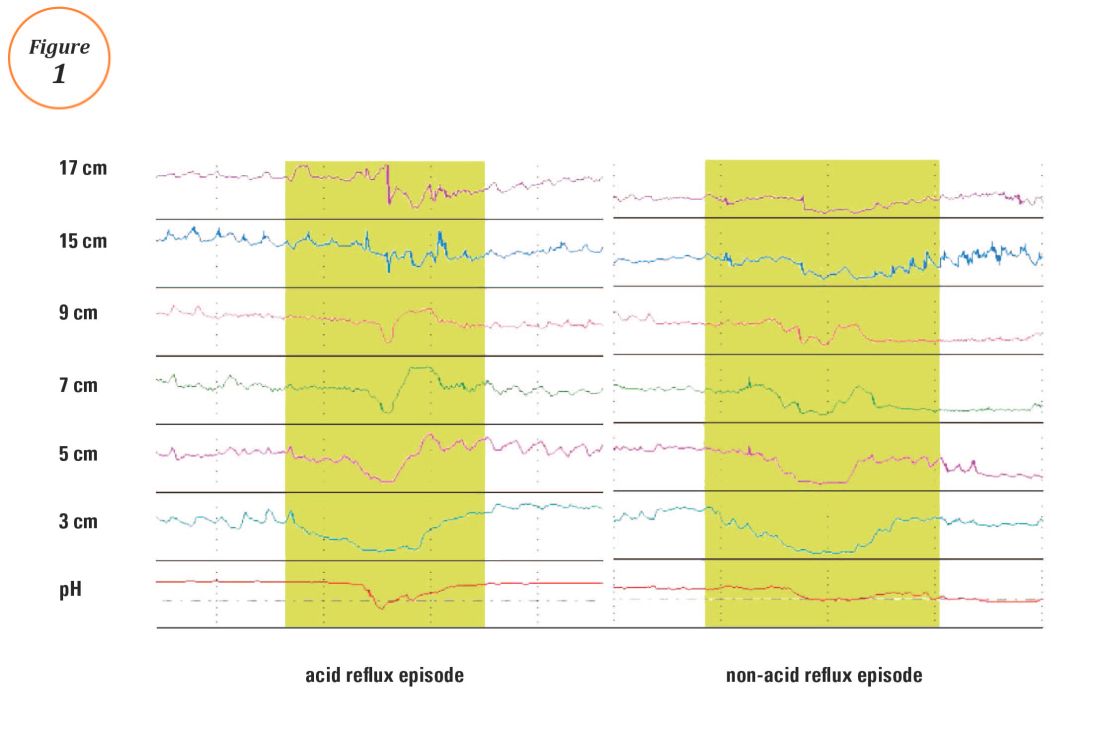
Ambulatory reflux testing assesses esophageal reflux burden and symptom-reflux association (SRA). Individual reflux events are identified as either a drop in esophageal pH to less than 4 (acid reflux events), or a sharp decrease in esophageal impedance measurements in a retrograde fashion (impedance-detected reflux events), with subsequent recovery to the baseline in each instance. Ambulatory reflux testing affords insight into three areas: 1) measurement of esophageal acid exposure time (AET); the cumulative time duration when distal esophageal pH is less than 4 at the recording site, reported as a percentage of the recording period; 2) measurement of the number of reflux events both acidic (from pH monitoring) and weakly acidic/alkaline (from impedance monitoring); and 3) quantitative evaluation of the association between reported symptom episodes and reflux events.

The SI and SAP can be calculated individually for acid-detected reflux events and for impedance-detected reflux events. Since reflux events are better detected with impedance, combined pH-impedance testing increases the yield of detecting positive SRA, especially when performed off PPI therapy.16,17 Because these indices are heavily reliant on patient reporting of symptom episodes, SRA can be overinterpreted;18 positive associations are more clinically useful than negative results in the evaluation of symptoms attributed to GERD.19 Despite these concerns, the two most consistent predictors of symptomatic outcome with antireflux therapy on pH-impedance testing are abnormal AET and positive SAP with impedance-detected reflux events.17
Testing on or off PPI?
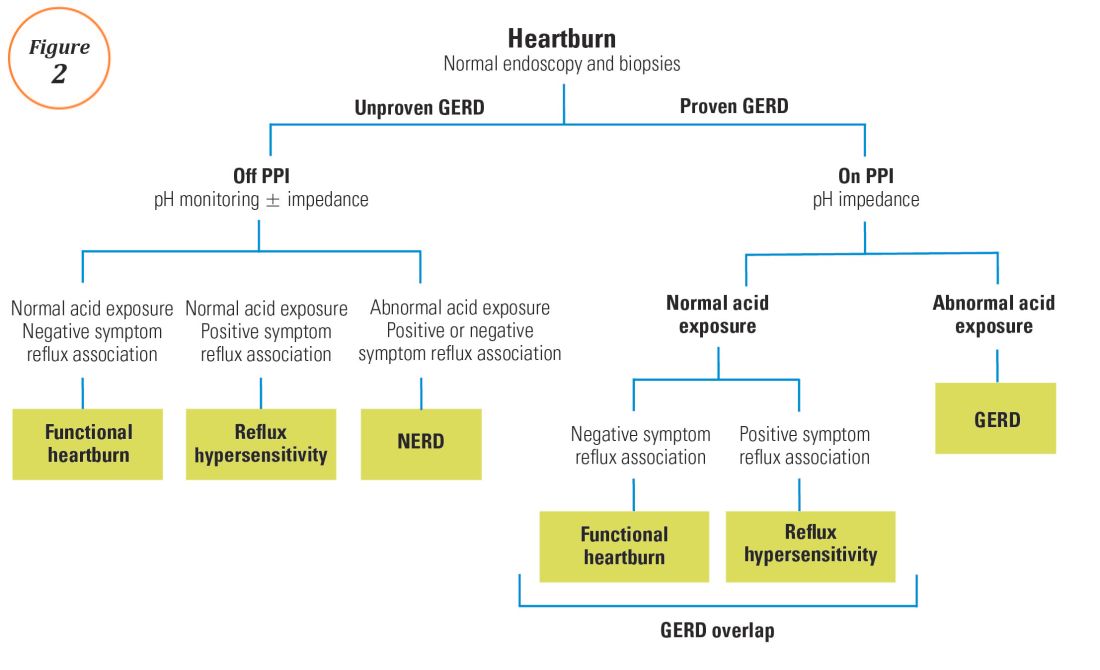
For symptoms attributable to GERD that persist despite properly administered PPI therapy, the 2013 American College of Gastroenterology guidelines suggest upper endoscopy with esophageal biopsies for typical symptoms and appropriate referrals for atypical symptoms.24 However, if these evaluations are unremarkable, reflux monitoring is recommended, with PPI status for testing guided by the pre-test probability of GERD: with a low pre-test probability of GERD, reflux testing is best performed off PPI with either pH or combined pH-impedance testing. In contrast, with a high pre-test probability of GERD, testing is best performed on PPI with combined pH-impedance testing. A similar concept is proposed in the Rome IV approach (Figure 2)23 and on GERD consensus guidelines:7 when heartburn or chest pain persists despite PPI therapy and endoscopy and esophageal biopsies are normal, evidence for GERD (past esophagitis, Barrett’s esophagus, peptic stricture, or prior positive reflux testing) prompts pH-impedance monitoring on PPI therapy (i.e., proven GERD). Those without this evidence for proven GERD (i.e., unproven GERD) are best tested off PPI, and the test utilized can be either pH alone or combined pH-impedance.
GERD phenotypes and management
The presence or absence of the two core metrics on ambulatory reflux monitoring – abnormal AET and positive SRA – can stratify symptomatic GERD patients into phenotypes that predict symptomatic improvement with antireflux therapy and guide management of symptoms (Figure 3).25,26 The presence of both abnormal AET and positive SRA suggests “strong” evidence for GERD, for which symptom improvement is likely with maximization of antireflux therapy, which can include BID PPI, baclofen (to decrease transient LES relaxations), alginates (such as Gaviscon), and consideration of endosopic or surgical antireflux procedures such as fundoplication or magnetic sphincter augmentation. Abnormal AET but negative SRA is regarded as “good” evidence for GERD, for which similar antireflux therapies can be advocated. Normal AET but positive SRA is designated as “reflux hypersensitivity,”23 with increasing proportions of patients meeting this phenotype when tested with combined pH-impedance and off PPI therapy.27 Both normal AET and negative SRA suggest equivocal evidence for GERD and the likely presence of a functional esophageal disorder, such as functional heartburn.23 For reflux hypersensitivity and especially functional esophageal disorders, antireflux therapy is unlikely to be as effective and management can include pharmacologic neuromodulation (such as tricyclic antidepressants administered at bedtime) as well as adjunctive nonpharmacologic approaches (such as stress reduction, relaxation, hypnosis, or cognitive-behavioral therapy).
The future of reflux diagnostics

Conclusions
For esophageal symptoms potentially attributable to GERD that persist despite optimized PPI therapy, esophageal testing should be undertaken, starting with endoscopy and biopsies and proceeding to ambulatory reflux monitoring with HRM. The decisions between pH testing alone versus combined pH-impedance monitoring, and between testing on or off PPI therapy, can be guided either by the pre-test probability of GERD or whether GERD has been proven or unproven in prior evaluations (Figure 2). Elevated AET and positive SRA with impedance-detected reflux events can predict the likelihood of successful management outcomes from antireflux therapy. These two core metrics can be utilized to phenotype GERD and guide management approaches for persisting symptoms (Figure 3). Novel impedance metrics (baseline mucosal impedance, postreflux swallow-induced peristaltic wave index) and markers for esophageal mucosal damage continue to be studied as potential markers for evidence of longitudinal reflux exposure.
Dr. Patel is assistant professor of medicine, division of gastroenterology, Duke University School of Medicine and the Durham Veterans Affairs Medical Center, Durham, N.C. Dr. Gyawali is professor of medicine, division of gastroenterology, Washington University School of Medicine, St. Louis, Mo.
References
1. Shaheen N.J., et al. Am J Gastroenterol. 2006;101:2128-38.
2. Patel A., Gyawali C.P.. Switzerland: Springer International, 2016.
3. Vakil N., et al. Am J Gastroenterol. 2006;101:1900-20; quiz 1943.
4. Fass R., et al. Arch Intern Med. 1999;159:2161-8.
5. Numans M.E., et al. Ann Intern Med. 2004;140:518-27.
6. Shaheen N.J., et al. Aliment Pharmacol Ther. 2011;33:225-34.
7. Roman S., et al. Neurogastroenterol Motil Mar 31. doi: 10.1111/nmo.13067. [Epub ahead of print] 2017.
8. Dellon E.S., et al. Am J Gastroenterol. 2013;108:679-92; quiz 693.
9. Pandolfino JE, Vela MF. Gastrointest Endosc. 2009;69:917-30, 930 e1.
10. Shay S., et al. Am J Gastroenterol. 2004;99:1037-43.
11. Zerbib F., et al. Clin Gastroenterol Hepatol. 2013;11:366-72.
12. Wiener G.J., et al. Am J Gastroenterol 1988;83:358-61.
13. Weusten B.L., et al. Gastroenterology. 1994;107:1741-5.
14. Ghillebert G., et al. Gut 1990;31:738-44.
15. Kushnir V.M., et al. Aliment Pharmacol Ther. 2012;35(9):1080-7.
16. Bredenoord A.J., et al. Am J Gastroenterol. 2006;101:453-9.
17. Patel A., et al. Clin Gastroenterol Hepatol. 2015;13:884-91.
18. Slaughter J.C., et al. Clin Gastroenterol Hepatol. 2011;9:868-74.
19. Kavitt R.T., et al. Am J Gastroenterol. 2012;107:1826-32.
20. Kahrilas P.J., et al. Gastroenterology 2008;135:1383-91, 1391 e1-5.
21. Kessing B.F., et al. Clin Gastroenterol Hepatol. 2011;9:1020-4.
22. Kahrilas P.J., et al. Neurogastroenterol Motil. 2015;27:160-74.
23. Aziz A, et al. Esophageal disorders. Gastroenterology 2016;150:1368-79.
24. Katz P.O., et al. Am J Gastroenterol. 2013;108:308-28; quiz 329.
25. Boeckxstaens G., et al. Gut 2014;63:1185-93.
26. Patel A., et al. Neurogastroenterol Motil. 2016;28:513-21.
27. Patel A., et al. Neurogastroenterol Motil. 2016;28:1382-90.
28. Martinucci I., et al. Neurogastroenterol Motil. 2014;26:546-55.
29. Ates F., et al. Gastroenterology 2015;148:334-43.
30. Kessing B.F., et al. Am J Gastroenterol. 2011;106:2093-7.
31. Patel A., et al. Aliment Pharmacol Ther. 2016;44:890-8.
32. Frazzoni M., et al. Neurogastroenterol Motil. 2016.
33. Frazzoni M., et al. Neurogastroenterol Motil. 2013;25:399-406, e295.
34. Vela M.F., et al. Am J Gastroenterol. 2011;106:844-50.
Introduction
Chronic esophageal symptoms attributed to gastroesophageal reflux disease (GERD) are common presenting symptoms in gastroenterology, leading to high healthcare costs and adverse quality of life globally.1,2 The clinical diagnosis of GERD hinges on the presence of “troublesome” compatible typical symptoms (heartburn, acid regurgitation) or evidence of mucosal injury on endoscopy (esophagitis, Barrett’s esophagus, peptic stricture).3 With the growing availability of proton pump inhibitors (PPIs), patients and clinicians often utilize an empiric therapeutic trial of PPI as an initial test, with symptom improvement in the absence of alarm symptoms indicating a high likelihood of GERD.4 A meta-analysis of studies that used objective measures of GERD (in this case, 24-hour pH monitoring) showed that the “PPI test” has a sensitivity of 78%, but a specificity of only 54%, as a diagnostic approach to GERD symptoms.5 Apart from noncardiac chest pain, the diagnostic yield is even lower for atypical and extra-esophageal symptoms such as cough or laryngeal symptoms.6
The “nuts and bolts” of reflux testing
Ambulatory reflux testing assesses esophageal reflux burden and symptom-reflux association (SRA). Individual reflux events are identified as either a drop in esophageal pH to less than 4 (acid reflux events), or a sharp decrease in esophageal impedance measurements in a retrograde fashion (impedance-detected reflux events), with subsequent recovery to the baseline in each instance. Ambulatory reflux testing affords insight into three areas: 1) measurement of esophageal acid exposure time (AET); the cumulative time duration when distal esophageal pH is less than 4 at the recording site, reported as a percentage of the recording period; 2) measurement of the number of reflux events both acidic (from pH monitoring) and weakly acidic/alkaline (from impedance monitoring); and 3) quantitative evaluation of the association between reported symptom episodes and reflux events.
The SI and SAP can be calculated individually for acid-detected reflux events and for impedance-detected reflux events. Since reflux events are better detected with impedance, combined pH-impedance testing increases the yield of detecting positive SRA, especially when performed off PPI therapy.16,17 Because these indices are heavily reliant on patient reporting of symptom episodes, SRA can be overinterpreted;18 positive associations are more clinically useful than negative results in the evaluation of symptoms attributed to GERD.19 Despite these concerns, the two most consistent predictors of symptomatic outcome with antireflux therapy on pH-impedance testing are abnormal AET and positive SAP with impedance-detected reflux events.17
Testing on or off PPI?
For symptoms attributable to GERD that persist despite properly administered PPI therapy, the 2013 American College of Gastroenterology guidelines suggest upper endoscopy with esophageal biopsies for typical symptoms and appropriate referrals for atypical symptoms.24 However, if these evaluations are unremarkable, reflux monitoring is recommended, with PPI status for testing guided by the pre-test probability of GERD: with a low pre-test probability of GERD, reflux testing is best performed off PPI with either pH or combined pH-impedance testing. In contrast, with a high pre-test probability of GERD, testing is best performed on PPI with combined pH-impedance testing. A similar concept is proposed in the Rome IV approach (Figure 2)23 and on GERD consensus guidelines:7 when heartburn or chest pain persists despite PPI therapy and endoscopy and esophageal biopsies are normal, evidence for GERD (past esophagitis, Barrett’s esophagus, peptic stricture, or prior positive reflux testing) prompts pH-impedance monitoring on PPI therapy (i.e., proven GERD). Those without this evidence for proven GERD (i.e., unproven GERD) are best tested off PPI, and the test utilized can be either pH alone or combined pH-impedance.
GERD phenotypes and management
The presence or absence of the two core metrics on ambulatory reflux monitoring – abnormal AET and positive SRA – can stratify symptomatic GERD patients into phenotypes that predict symptomatic improvement with antireflux therapy and guide management of symptoms (Figure 3).25,26 The presence of both abnormal AET and positive SRA suggests “strong” evidence for GERD, for which symptom improvement is likely with maximization of antireflux therapy, which can include BID PPI, baclofen (to decrease transient LES relaxations), alginates (such as Gaviscon), and consideration of endosopic or surgical antireflux procedures such as fundoplication or magnetic sphincter augmentation. Abnormal AET but negative SRA is regarded as “good” evidence for GERD, for which similar antireflux therapies can be advocated. Normal AET but positive SRA is designated as “reflux hypersensitivity,”23 with increasing proportions of patients meeting this phenotype when tested with combined pH-impedance and off PPI therapy.27 Both normal AET and negative SRA suggest equivocal evidence for GERD and the likely presence of a functional esophageal disorder, such as functional heartburn.23 For reflux hypersensitivity and especially functional esophageal disorders, antireflux therapy is unlikely to be as effective and management can include pharmacologic neuromodulation (such as tricyclic antidepressants administered at bedtime) as well as adjunctive nonpharmacologic approaches (such as stress reduction, relaxation, hypnosis, or cognitive-behavioral therapy).
The future of reflux diagnostics
Conclusions
For esophageal symptoms potentially attributable to GERD that persist despite optimized PPI therapy, esophageal testing should be undertaken, starting with endoscopy and biopsies and proceeding to ambulatory reflux monitoring with HRM. The decisions between pH testing alone versus combined pH-impedance monitoring, and between testing on or off PPI therapy, can be guided either by the pre-test probability of GERD or whether GERD has been proven or unproven in prior evaluations (Figure 2). Elevated AET and positive SRA with impedance-detected reflux events can predict the likelihood of successful management outcomes from antireflux therapy. These two core metrics can be utilized to phenotype GERD and guide management approaches for persisting symptoms (Figure 3). Novel impedance metrics (baseline mucosal impedance, postreflux swallow-induced peristaltic wave index) and markers for esophageal mucosal damage continue to be studied as potential markers for evidence of longitudinal reflux exposure.
Dr. Patel is assistant professor of medicine, division of gastroenterology, Duke University School of Medicine and the Durham Veterans Affairs Medical Center, Durham, N.C. Dr. Gyawali is professor of medicine, division of gastroenterology, Washington University School of Medicine, St. Louis, Mo.
References
1. Shaheen N.J., et al. Am J Gastroenterol. 2006;101:2128-38.
2. Patel A., Gyawali C.P.. Switzerland: Springer International, 2016.
3. Vakil N., et al. Am J Gastroenterol. 2006;101:1900-20; quiz 1943.
4. Fass R., et al. Arch Intern Med. 1999;159:2161-8.
5. Numans M.E., et al. Ann Intern Med. 2004;140:518-27.
6. Shaheen N.J., et al. Aliment Pharmacol Ther. 2011;33:225-34.
7. Roman S., et al. Neurogastroenterol Motil Mar 31. doi: 10.1111/nmo.13067. [Epub ahead of print] 2017.
8. Dellon E.S., et al. Am J Gastroenterol. 2013;108:679-92; quiz 693.
9. Pandolfino JE, Vela MF. Gastrointest Endosc. 2009;69:917-30, 930 e1.
10. Shay S., et al. Am J Gastroenterol. 2004;99:1037-43.
11. Zerbib F., et al. Clin Gastroenterol Hepatol. 2013;11:366-72.
12. Wiener G.J., et al. Am J Gastroenterol 1988;83:358-61.
13. Weusten B.L., et al. Gastroenterology. 1994;107:1741-5.
14. Ghillebert G., et al. Gut 1990;31:738-44.
15. Kushnir V.M., et al. Aliment Pharmacol Ther. 2012;35(9):1080-7.
16. Bredenoord A.J., et al. Am J Gastroenterol. 2006;101:453-9.
17. Patel A., et al. Clin Gastroenterol Hepatol. 2015;13:884-91.
18. Slaughter J.C., et al. Clin Gastroenterol Hepatol. 2011;9:868-74.
19. Kavitt R.T., et al. Am J Gastroenterol. 2012;107:1826-32.
20. Kahrilas P.J., et al. Gastroenterology 2008;135:1383-91, 1391 e1-5.
21. Kessing B.F., et al. Clin Gastroenterol Hepatol. 2011;9:1020-4.
22. Kahrilas P.J., et al. Neurogastroenterol Motil. 2015;27:160-74.
23. Aziz A, et al. Esophageal disorders. Gastroenterology 2016;150:1368-79.
24. Katz P.O., et al. Am J Gastroenterol. 2013;108:308-28; quiz 329.
25. Boeckxstaens G., et al. Gut 2014;63:1185-93.
26. Patel A., et al. Neurogastroenterol Motil. 2016;28:513-21.
27. Patel A., et al. Neurogastroenterol Motil. 2016;28:1382-90.
28. Martinucci I., et al. Neurogastroenterol Motil. 2014;26:546-55.
29. Ates F., et al. Gastroenterology 2015;148:334-43.
30. Kessing B.F., et al. Am J Gastroenterol. 2011;106:2093-7.
31. Patel A., et al. Aliment Pharmacol Ther. 2016;44:890-8.
32. Frazzoni M., et al. Neurogastroenterol Motil. 2016.
33. Frazzoni M., et al. Neurogastroenterol Motil. 2013;25:399-406, e295.
34. Vela M.F., et al. Am J Gastroenterol. 2011;106:844-50.
Introduction
Chronic esophageal symptoms attributed to gastroesophageal reflux disease (GERD) are common presenting symptoms in gastroenterology, leading to high healthcare costs and adverse quality of life globally.1,2 The clinical diagnosis of GERD hinges on the presence of “troublesome” compatible typical symptoms (heartburn, acid regurgitation) or evidence of mucosal injury on endoscopy (esophagitis, Barrett’s esophagus, peptic stricture).3 With the growing availability of proton pump inhibitors (PPIs), patients and clinicians often utilize an empiric therapeutic trial of PPI as an initial test, with symptom improvement in the absence of alarm symptoms indicating a high likelihood of GERD.4 A meta-analysis of studies that used objective measures of GERD (in this case, 24-hour pH monitoring) showed that the “PPI test” has a sensitivity of 78%, but a specificity of only 54%, as a diagnostic approach to GERD symptoms.5 Apart from noncardiac chest pain, the diagnostic yield is even lower for atypical and extra-esophageal symptoms such as cough or laryngeal symptoms.6
The “nuts and bolts” of reflux testing
Ambulatory reflux testing assesses esophageal reflux burden and symptom-reflux association (SRA). Individual reflux events are identified as either a drop in esophageal pH to less than 4 (acid reflux events), or a sharp decrease in esophageal impedance measurements in a retrograde fashion (impedance-detected reflux events), with subsequent recovery to the baseline in each instance. Ambulatory reflux testing affords insight into three areas: 1) measurement of esophageal acid exposure time (AET); the cumulative time duration when distal esophageal pH is less than 4 at the recording site, reported as a percentage of the recording period; 2) measurement of the number of reflux events both acidic (from pH monitoring) and weakly acidic/alkaline (from impedance monitoring); and 3) quantitative evaluation of the association between reported symptom episodes and reflux events.
The SI and SAP can be calculated individually for acid-detected reflux events and for impedance-detected reflux events. Since reflux events are better detected with impedance, combined pH-impedance testing increases the yield of detecting positive SRA, especially when performed off PPI therapy.16,17 Because these indices are heavily reliant on patient reporting of symptom episodes, SRA can be overinterpreted;18 positive associations are more clinically useful than negative results in the evaluation of symptoms attributed to GERD.19 Despite these concerns, the two most consistent predictors of symptomatic outcome with antireflux therapy on pH-impedance testing are abnormal AET and positive SAP with impedance-detected reflux events.17
Testing on or off PPI?
For symptoms attributable to GERD that persist despite properly administered PPI therapy, the 2013 American College of Gastroenterology guidelines suggest upper endoscopy with esophageal biopsies for typical symptoms and appropriate referrals for atypical symptoms.24 However, if these evaluations are unremarkable, reflux monitoring is recommended, with PPI status for testing guided by the pre-test probability of GERD: with a low pre-test probability of GERD, reflux testing is best performed off PPI with either pH or combined pH-impedance testing. In contrast, with a high pre-test probability of GERD, testing is best performed on PPI with combined pH-impedance testing. A similar concept is proposed in the Rome IV approach (Figure 2)23 and on GERD consensus guidelines:7 when heartburn or chest pain persists despite PPI therapy and endoscopy and esophageal biopsies are normal, evidence for GERD (past esophagitis, Barrett’s esophagus, peptic stricture, or prior positive reflux testing) prompts pH-impedance monitoring on PPI therapy (i.e., proven GERD). Those without this evidence for proven GERD (i.e., unproven GERD) are best tested off PPI, and the test utilized can be either pH alone or combined pH-impedance.
GERD phenotypes and management
The presence or absence of the two core metrics on ambulatory reflux monitoring – abnormal AET and positive SRA – can stratify symptomatic GERD patients into phenotypes that predict symptomatic improvement with antireflux therapy and guide management of symptoms (Figure 3).25,26 The presence of both abnormal AET and positive SRA suggests “strong” evidence for GERD, for which symptom improvement is likely with maximization of antireflux therapy, which can include BID PPI, baclofen (to decrease transient LES relaxations), alginates (such as Gaviscon), and consideration of endosopic or surgical antireflux procedures such as fundoplication or magnetic sphincter augmentation. Abnormal AET but negative SRA is regarded as “good” evidence for GERD, for which similar antireflux therapies can be advocated. Normal AET but positive SRA is designated as “reflux hypersensitivity,”23 with increasing proportions of patients meeting this phenotype when tested with combined pH-impedance and off PPI therapy.27 Both normal AET and negative SRA suggest equivocal evidence for GERD and the likely presence of a functional esophageal disorder, such as functional heartburn.23 For reflux hypersensitivity and especially functional esophageal disorders, antireflux therapy is unlikely to be as effective and management can include pharmacologic neuromodulation (such as tricyclic antidepressants administered at bedtime) as well as adjunctive nonpharmacologic approaches (such as stress reduction, relaxation, hypnosis, or cognitive-behavioral therapy).
The future of reflux diagnostics
Conclusions
For esophageal symptoms potentially attributable to GERD that persist despite optimized PPI therapy, esophageal testing should be undertaken, starting with endoscopy and biopsies and proceeding to ambulatory reflux monitoring with HRM. The decisions between pH testing alone versus combined pH-impedance monitoring, and between testing on or off PPI therapy, can be guided either by the pre-test probability of GERD or whether GERD has been proven or unproven in prior evaluations (Figure 2). Elevated AET and positive SRA with impedance-detected reflux events can predict the likelihood of successful management outcomes from antireflux therapy. These two core metrics can be utilized to phenotype GERD and guide management approaches for persisting symptoms (Figure 3). Novel impedance metrics (baseline mucosal impedance, postreflux swallow-induced peristaltic wave index) and markers for esophageal mucosal damage continue to be studied as potential markers for evidence of longitudinal reflux exposure.
Dr. Patel is assistant professor of medicine, division of gastroenterology, Duke University School of Medicine and the Durham Veterans Affairs Medical Center, Durham, N.C. Dr. Gyawali is professor of medicine, division of gastroenterology, Washington University School of Medicine, St. Louis, Mo.
References
1. Shaheen N.J., et al. Am J Gastroenterol. 2006;101:2128-38.
2. Patel A., Gyawali C.P.. Switzerland: Springer International, 2016.
3. Vakil N., et al. Am J Gastroenterol. 2006;101:1900-20; quiz 1943.
4. Fass R., et al. Arch Intern Med. 1999;159:2161-8.
5. Numans M.E., et al. Ann Intern Med. 2004;140:518-27.
6. Shaheen N.J., et al. Aliment Pharmacol Ther. 2011;33:225-34.
7. Roman S., et al. Neurogastroenterol Motil Mar 31. doi: 10.1111/nmo.13067. [Epub ahead of print] 2017.
8. Dellon E.S., et al. Am J Gastroenterol. 2013;108:679-92; quiz 693.
9. Pandolfino JE, Vela MF. Gastrointest Endosc. 2009;69:917-30, 930 e1.
10. Shay S., et al. Am J Gastroenterol. 2004;99:1037-43.
11. Zerbib F., et al. Clin Gastroenterol Hepatol. 2013;11:366-72.
12. Wiener G.J., et al. Am J Gastroenterol 1988;83:358-61.
13. Weusten B.L., et al. Gastroenterology. 1994;107:1741-5.
14. Ghillebert G., et al. Gut 1990;31:738-44.
15. Kushnir V.M., et al. Aliment Pharmacol Ther. 2012;35(9):1080-7.
16. Bredenoord A.J., et al. Am J Gastroenterol. 2006;101:453-9.
17. Patel A., et al. Clin Gastroenterol Hepatol. 2015;13:884-91.
18. Slaughter J.C., et al. Clin Gastroenterol Hepatol. 2011;9:868-74.
19. Kavitt R.T., et al. Am J Gastroenterol. 2012;107:1826-32.
20. Kahrilas P.J., et al. Gastroenterology 2008;135:1383-91, 1391 e1-5.
21. Kessing B.F., et al. Clin Gastroenterol Hepatol. 2011;9:1020-4.
22. Kahrilas P.J., et al. Neurogastroenterol Motil. 2015;27:160-74.
23. Aziz A, et al. Esophageal disorders. Gastroenterology 2016;150:1368-79.
24. Katz P.O., et al. Am J Gastroenterol. 2013;108:308-28; quiz 329.
25. Boeckxstaens G., et al. Gut 2014;63:1185-93.
26. Patel A., et al. Neurogastroenterol Motil. 2016;28:513-21.
27. Patel A., et al. Neurogastroenterol Motil. 2016;28:1382-90.
28. Martinucci I., et al. Neurogastroenterol Motil. 2014;26:546-55.
29. Ates F., et al. Gastroenterology 2015;148:334-43.
30. Kessing B.F., et al. Am J Gastroenterol. 2011;106:2093-7.
31. Patel A., et al. Aliment Pharmacol Ther. 2016;44:890-8.
32. Frazzoni M., et al. Neurogastroenterol Motil. 2016.
33. Frazzoni M., et al. Neurogastroenterol Motil. 2013;25:399-406, e295.
34. Vela M.F., et al. Am J Gastroenterol. 2011;106:844-50.
President’s Letter
Dear Trainees and Early-Career GIs,
As I begin my time as President of AGA, I am reflecting on other new beginnings in my career. Though time has passed, I vividly recall the excitement and uncertainty of beginning training and, subsequently, my career. It’s a career that I’ve enjoyed immensely and I hope that you will as well.

All our resources are available online at www.gastro.org and we have a suite of apps including guidelines, image challenges, DDSEP, and publications that you can download to your mobile device. You can learn more about those at www.gastro.org/mobile-offerings.
Another great resource is the AGA Community, where you can join a private online conversation with other early-career gastroenterologists. You can access a library of resources there and talk with gastroenterologists who are in the same career phase as you are. Join the conversation at community.gastro.org.
The New Gastroenterologist is the perfect place to start your professional journey and to stay on the cutting edge of the field. It provides a wealth of information you won’t find in other publications. Its unique focus promises that you’ll read content that meets your immediate needs as a trainee or early-career gastroenterologist.
On behalf of the AGA Governing Board, I wish you great success in this exciting field!
Sincerely,
Sheila E. Crowe, MD, AGAF
President, AGA Institute
Professor of Medicine and Director of Research, University of California, San Diego
Dear Trainees and Early-Career GIs,
As I begin my time as President of AGA, I am reflecting on other new beginnings in my career. Though time has passed, I vividly recall the excitement and uncertainty of beginning training and, subsequently, my career. It’s a career that I’ve enjoyed immensely and I hope that you will as well.
All our resources are available online at www.gastro.org and we have a suite of apps including guidelines, image challenges, DDSEP, and publications that you can download to your mobile device. You can learn more about those at www.gastro.org/mobile-offerings.
Another great resource is the AGA Community, where you can join a private online conversation with other early-career gastroenterologists. You can access a library of resources there and talk with gastroenterologists who are in the same career phase as you are. Join the conversation at community.gastro.org.
The New Gastroenterologist is the perfect place to start your professional journey and to stay on the cutting edge of the field. It provides a wealth of information you won’t find in other publications. Its unique focus promises that you’ll read content that meets your immediate needs as a trainee or early-career gastroenterologist.
On behalf of the AGA Governing Board, I wish you great success in this exciting field!
Sincerely,
Sheila E. Crowe, MD, AGAF
President, AGA Institute
Professor of Medicine and Director of Research, University of California, San Diego
Dear Trainees and Early-Career GIs,
As I begin my time as President of AGA, I am reflecting on other new beginnings in my career. Though time has passed, I vividly recall the excitement and uncertainty of beginning training and, subsequently, my career. It’s a career that I’ve enjoyed immensely and I hope that you will as well.
All our resources are available online at www.gastro.org and we have a suite of apps including guidelines, image challenges, DDSEP, and publications that you can download to your mobile device. You can learn more about those at www.gastro.org/mobile-offerings.
Another great resource is the AGA Community, where you can join a private online conversation with other early-career gastroenterologists. You can access a library of resources there and talk with gastroenterologists who are in the same career phase as you are. Join the conversation at community.gastro.org.
The New Gastroenterologist is the perfect place to start your professional journey and to stay on the cutting edge of the field. It provides a wealth of information you won’t find in other publications. Its unique focus promises that you’ll read content that meets your immediate needs as a trainee or early-career gastroenterologist.
On behalf of the AGA Governing Board, I wish you great success in this exciting field!
Sincerely,
Sheila E. Crowe, MD, AGAF
President, AGA Institute
Professor of Medicine and Director of Research, University of California, San Diego
Congratulations!
Dear Colleagues,
Congratulations to the new gastroenterology fellows who have just begun their fellowships and also to those who have just finished and are starting their careers. It is certainly an exciting time of year for so many! A letter from AGA President Sheila Crowe, included in this issue, details the benefits and opportunities our organization offers GIs entering practice and academia.

This issue also contains an informative perspective about pursuing a career in medical education by Suzanne Rose (University of Connecticut), an incredibly passionate educator who has dedicated her career to this endeavor. Additionally, Katherine Garman (Duke University) and Latha Alaparthi (Gastroenterology Center of Connecticut/Yale University) provide a recap of this year’s AGA Women’s Leadership conference, which brought together a large group of early-career and experienced women from many different career pathways within the field of gastroenterology.
As student loans are an issue for many, Common Bond, the AGA’s official student loan partner, highlights an early-career gastroenterologist’s experience with student loans, as well as important factors in refinancing and paying off student loans. Finally, in the first of a two-part series on medical malpractice, an experienced group of attorneys from Eckert Seamans Cherin & Mellott, LLC (Philadelphia) provide a concise overview of the basics of malpractice as well as tips to help minimize your risk of being sued.
I hope that you enjoy this issue of The New Gastroenterologist. For those in the early-career group on the AGA Community (http://community.gastro.org/), these articles will be posted to the library to further enhance access. You can also find The New Gastroenterologist online and via the free app. If you have ideas for future issues or would be interested in contributing, please e-mail either me at [email protected] or Managing Editor Ryan Farrell at [email protected].
Sincerely,
Bryson W. Katona, MD, PhD
Editor in Chief
Dr. Bryson W. Katona is an instructor of medicine in the division of gastroenterology at the University of Pennsylvania.
Dear Colleagues,
Congratulations to the new gastroenterology fellows who have just begun their fellowships and also to those who have just finished and are starting their careers. It is certainly an exciting time of year for so many! A letter from AGA President Sheila Crowe, included in this issue, details the benefits and opportunities our organization offers GIs entering practice and academia.
This issue also contains an informative perspective about pursuing a career in medical education by Suzanne Rose (University of Connecticut), an incredibly passionate educator who has dedicated her career to this endeavor. Additionally, Katherine Garman (Duke University) and Latha Alaparthi (Gastroenterology Center of Connecticut/Yale University) provide a recap of this year’s AGA Women’s Leadership conference, which brought together a large group of early-career and experienced women from many different career pathways within the field of gastroenterology.
As student loans are an issue for many, Common Bond, the AGA’s official student loan partner, highlights an early-career gastroenterologist’s experience with student loans, as well as important factors in refinancing and paying off student loans. Finally, in the first of a two-part series on medical malpractice, an experienced group of attorneys from Eckert Seamans Cherin & Mellott, LLC (Philadelphia) provide a concise overview of the basics of malpractice as well as tips to help minimize your risk of being sued.
I hope that you enjoy this issue of The New Gastroenterologist. For those in the early-career group on the AGA Community (http://community.gastro.org/), these articles will be posted to the library to further enhance access. You can also find The New Gastroenterologist online and via the free app. If you have ideas for future issues or would be interested in contributing, please e-mail either me at [email protected] or Managing Editor Ryan Farrell at [email protected].
Sincerely,
Bryson W. Katona, MD, PhD
Editor in Chief
Dr. Bryson W. Katona is an instructor of medicine in the division of gastroenterology at the University of Pennsylvania.
Dear Colleagues,
Congratulations to the new gastroenterology fellows who have just begun their fellowships and also to those who have just finished and are starting their careers. It is certainly an exciting time of year for so many! A letter from AGA President Sheila Crowe, included in this issue, details the benefits and opportunities our organization offers GIs entering practice and academia.
This issue also contains an informative perspective about pursuing a career in medical education by Suzanne Rose (University of Connecticut), an incredibly passionate educator who has dedicated her career to this endeavor. Additionally, Katherine Garman (Duke University) and Latha Alaparthi (Gastroenterology Center of Connecticut/Yale University) provide a recap of this year’s AGA Women’s Leadership conference, which brought together a large group of early-career and experienced women from many different career pathways within the field of gastroenterology.
As student loans are an issue for many, Common Bond, the AGA’s official student loan partner, highlights an early-career gastroenterologist’s experience with student loans, as well as important factors in refinancing and paying off student loans. Finally, in the first of a two-part series on medical malpractice, an experienced group of attorneys from Eckert Seamans Cherin & Mellott, LLC (Philadelphia) provide a concise overview of the basics of malpractice as well as tips to help minimize your risk of being sued.
I hope that you enjoy this issue of The New Gastroenterologist. For those in the early-career group on the AGA Community (http://community.gastro.org/), these articles will be posted to the library to further enhance access. You can also find The New Gastroenterologist online and via the free app. If you have ideas for future issues or would be interested in contributing, please e-mail either me at [email protected] or Managing Editor Ryan Farrell at [email protected].
Sincerely,
Bryson W. Katona, MD, PhD
Editor in Chief
Dr. Bryson W. Katona is an instructor of medicine in the division of gastroenterology at the University of Pennsylvania.
Minocycline may delay conversion to MS
Minocycline, an antibiotic that has immune-modulating properties and crosses the blood-brain barrier, appears to delay conversion to multiple sclerosis in patients who have an initial focal demyelinating event, according to a report published online June 1 in the New England Journal of Medicine.
Two small clinical trials involving patients with relapsing-remitting multiple sclerosis (MS) recently showed that minocycline reduces the number of lesions detected on MRI with gadolinium enhancement. So researchers led by Luanne M. Metz, MD, of the Cumming School of Medicine and the Hotchkiss Brain Institute, Calgary, Alta., conducted a randomized, double-blind, placebo-controlled trial at 12 Canadian MS clinics to determine whether the drug might delay conversion to MS after a first, clinically isolated demyelinating event, such as optic neuritis or a brainstem, cerebral, cerebellar, or myelopathy syndrome.
The primary outcome of conversion to MS within 6 months of randomization occurred in 23 (32%) patients taking minocycline, compared with 41 (59%) taking placebo – a difference that exceeded the prespecified clinically meaningful difference between the two groups. After the data were adjusted to account for the number of brain lesions at baseline, the difference in risk at 6 months was 18.5 percentage points, a magnitude of effect that is similar to what has been reported for other therapies such as interferon beta-1b, interferon beta-1a, teriflunomide, and oral cladribine.
The findings were similar in every sensitivity and subgroup analysis. All secondary outcomes, such as the decrease in mean lesion volume and the mean number of new lesions after 6 months of treatment, also favored minocycline over placebo, the investigators said (N Engl J Med. 2017 June 1. doi: 10.1056/NEJMoa1608889).
Minocycline’s neuroprotective effect persisted through 12 months of follow-up, according to a post hoc analysis, but was no longer sustained at 24 months of follow-up, they noted. In addition, post hoc analyses showed that minocycline held no significant benefit over placebo with respect to relapse or disability outcomes at either 6 months or 24 months.
This study was supported by the Multiple Sclerosis Society of Canada. Dr. Metz reported receiving grant support from Hoffmann–La Roche outside of this work; her associates reported ties to numerous industry sources.
The intriguing findings of Metz et al., together with the established safety profile and low cost of minocycline, make a compelling case for more research into the drug’s use in early MS.
However, it would be premature to begin using minocycline for MS until its benefits can be confirmed in larger and longer-term clinical trials.
Zongqi Xia, MD, PhD, is in the Program in Translational Neurology and Neuroinflammation at the Pittsburgh Institute of Neurodegenerative Diseases and at the Institute of Multiple Sclerosis Care and Research at the University of Pittsburgh. Robert M. Friedlander, MD, is in the Neuroapoptosis Laboratory and the department of neurosurgery at the University of Pittsburgh. They reported having no relevant financial disclosures. Dr. Xia and Dr. Friedlander made these remarks in an editorial accompanying Dr. Metz and colleagues’ report (N Engl J Med. 2017 June 1. doi: 10.1056/NEJMe1703230).
The intriguing findings of Metz et al., together with the established safety profile and low cost of minocycline, make a compelling case for more research into the drug’s use in early MS.
However, it would be premature to begin using minocycline for MS until its benefits can be confirmed in larger and longer-term clinical trials.
Zongqi Xia, MD, PhD, is in the Program in Translational Neurology and Neuroinflammation at the Pittsburgh Institute of Neurodegenerative Diseases and at the Institute of Multiple Sclerosis Care and Research at the University of Pittsburgh. Robert M. Friedlander, MD, is in the Neuroapoptosis Laboratory and the department of neurosurgery at the University of Pittsburgh. They reported having no relevant financial disclosures. Dr. Xia and Dr. Friedlander made these remarks in an editorial accompanying Dr. Metz and colleagues’ report (N Engl J Med. 2017 June 1. doi: 10.1056/NEJMe1703230).
The intriguing findings of Metz et al., together with the established safety profile and low cost of minocycline, make a compelling case for more research into the drug’s use in early MS.
However, it would be premature to begin using minocycline for MS until its benefits can be confirmed in larger and longer-term clinical trials.
Zongqi Xia, MD, PhD, is in the Program in Translational Neurology and Neuroinflammation at the Pittsburgh Institute of Neurodegenerative Diseases and at the Institute of Multiple Sclerosis Care and Research at the University of Pittsburgh. Robert M. Friedlander, MD, is in the Neuroapoptosis Laboratory and the department of neurosurgery at the University of Pittsburgh. They reported having no relevant financial disclosures. Dr. Xia and Dr. Friedlander made these remarks in an editorial accompanying Dr. Metz and colleagues’ report (N Engl J Med. 2017 June 1. doi: 10.1056/NEJMe1703230).
Minocycline, an antibiotic that has immune-modulating properties and crosses the blood-brain barrier, appears to delay conversion to multiple sclerosis in patients who have an initial focal demyelinating event, according to a report published online June 1 in the New England Journal of Medicine.
Two small clinical trials involving patients with relapsing-remitting multiple sclerosis (MS) recently showed that minocycline reduces the number of lesions detected on MRI with gadolinium enhancement. So researchers led by Luanne M. Metz, MD, of the Cumming School of Medicine and the Hotchkiss Brain Institute, Calgary, Alta., conducted a randomized, double-blind, placebo-controlled trial at 12 Canadian MS clinics to determine whether the drug might delay conversion to MS after a first, clinically isolated demyelinating event, such as optic neuritis or a brainstem, cerebral, cerebellar, or myelopathy syndrome.
The primary outcome of conversion to MS within 6 months of randomization occurred in 23 (32%) patients taking minocycline, compared with 41 (59%) taking placebo – a difference that exceeded the prespecified clinically meaningful difference between the two groups. After the data were adjusted to account for the number of brain lesions at baseline, the difference in risk at 6 months was 18.5 percentage points, a magnitude of effect that is similar to what has been reported for other therapies such as interferon beta-1b, interferon beta-1a, teriflunomide, and oral cladribine.
The findings were similar in every sensitivity and subgroup analysis. All secondary outcomes, such as the decrease in mean lesion volume and the mean number of new lesions after 6 months of treatment, also favored minocycline over placebo, the investigators said (N Engl J Med. 2017 June 1. doi: 10.1056/NEJMoa1608889).
Minocycline’s neuroprotective effect persisted through 12 months of follow-up, according to a post hoc analysis, but was no longer sustained at 24 months of follow-up, they noted. In addition, post hoc analyses showed that minocycline held no significant benefit over placebo with respect to relapse or disability outcomes at either 6 months or 24 months.
This study was supported by the Multiple Sclerosis Society of Canada. Dr. Metz reported receiving grant support from Hoffmann–La Roche outside of this work; her associates reported ties to numerous industry sources.
Minocycline, an antibiotic that has immune-modulating properties and crosses the blood-brain barrier, appears to delay conversion to multiple sclerosis in patients who have an initial focal demyelinating event, according to a report published online June 1 in the New England Journal of Medicine.
Two small clinical trials involving patients with relapsing-remitting multiple sclerosis (MS) recently showed that minocycline reduces the number of lesions detected on MRI with gadolinium enhancement. So researchers led by Luanne M. Metz, MD, of the Cumming School of Medicine and the Hotchkiss Brain Institute, Calgary, Alta., conducted a randomized, double-blind, placebo-controlled trial at 12 Canadian MS clinics to determine whether the drug might delay conversion to MS after a first, clinically isolated demyelinating event, such as optic neuritis or a brainstem, cerebral, cerebellar, or myelopathy syndrome.
The primary outcome of conversion to MS within 6 months of randomization occurred in 23 (32%) patients taking minocycline, compared with 41 (59%) taking placebo – a difference that exceeded the prespecified clinically meaningful difference between the two groups. After the data were adjusted to account for the number of brain lesions at baseline, the difference in risk at 6 months was 18.5 percentage points, a magnitude of effect that is similar to what has been reported for other therapies such as interferon beta-1b, interferon beta-1a, teriflunomide, and oral cladribine.
The findings were similar in every sensitivity and subgroup analysis. All secondary outcomes, such as the decrease in mean lesion volume and the mean number of new lesions after 6 months of treatment, also favored minocycline over placebo, the investigators said (N Engl J Med. 2017 June 1. doi: 10.1056/NEJMoa1608889).
Minocycline’s neuroprotective effect persisted through 12 months of follow-up, according to a post hoc analysis, but was no longer sustained at 24 months of follow-up, they noted. In addition, post hoc analyses showed that minocycline held no significant benefit over placebo with respect to relapse or disability outcomes at either 6 months or 24 months.
This study was supported by the Multiple Sclerosis Society of Canada. Dr. Metz reported receiving grant support from Hoffmann–La Roche outside of this work; her associates reported ties to numerous industry sources.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point:
Major finding: The primary outcome, conversion to MS within 6 months of randomization, occurred in 23 (32%) patients taking minocycline, compared with 41 (59%) taking placebo.
Data source: A multicenter, randomized, double-blind, placebo-controlled trial involving 142 adults treated for up to 24 months.
Disclosures: This study was supported by the Multiple Sclerosis Society of Canada. Dr. Metz reported receiving grant support from Hoffmann–La Roche outside of this work; her associates reported ties to numerous industry sources.
Practical Considerations for Moderate to Severe Asthma, Part 1: Management, Biomarkers, and When to Refer
This newsletter, Practical Considerations for Moderate to Severe Asthma, Part 1: Management, Biomarkers, and When to Refer, provides detailed guidance for nurse practitioners and physician assistants on how to identify, evaluate, and treat patients with poorly controlled, moderate to severe asthma.
Click here to read the supplement

Clinical Research Coordinator
Boys Town National Research Hospital
Boys Town, Nebraska
Kevin R. Murphy, MD
Director of Allergy, Asthma, and Pulmonary Research
Boys Town National Research Hospital
Boys Town, Nebraska
Department of Pediatrics
University of Nebraska Medical Center
Creighton University School of Medicine
Omaha, Nebraska
This newsletter, Practical Considerations for Moderate to Severe Asthma, Part 1: Management, Biomarkers, and When to Refer, provides detailed guidance for nurse practitioners and physician assistants on how to identify, evaluate, and treat patients with poorly controlled, moderate to severe asthma.
Click here to read the supplement
Clinical Research Coordinator
Boys Town National Research Hospital
Boys Town, Nebraska
Kevin R. Murphy, MD
Director of Allergy, Asthma, and Pulmonary Research
Boys Town National Research Hospital
Boys Town, Nebraska
Department of Pediatrics
University of Nebraska Medical Center
Creighton University School of Medicine
Omaha, Nebraska
This newsletter, Practical Considerations for Moderate to Severe Asthma, Part 1: Management, Biomarkers, and When to Refer, provides detailed guidance for nurse practitioners and physician assistants on how to identify, evaluate, and treat patients with poorly controlled, moderate to severe asthma.
Click here to read the supplement
Clinical Research Coordinator
Boys Town National Research Hospital
Boys Town, Nebraska
Kevin R. Murphy, MD
Director of Allergy, Asthma, and Pulmonary Research
Boys Town National Research Hospital
Boys Town, Nebraska
Department of Pediatrics
University of Nebraska Medical Center
Creighton University School of Medicine
Omaha, Nebraska
