User login
Multidisciplinary teams offer key to complex deliveries
Medical practice has evolved, and will continue to do so, as we begin pushing for more personalized and better precision health care. Gone are the days of the general practitioner who attempted to treat all conditions in all patients. Health care is now so complex that not only specialists but also so-called superspecialists are needed to manage complicated cases successfully.
One of the biggest challenges, and greatest opportunities, in ob.gyn. is the need to establish a multidisciplinary health team to the address the needs of today’s patients. More than ever, we are working with patients with advanced maternal age having their first pregnancies. More than ever, we are managing patients who have preexisting diabetes and are concurrently overweight or obese. More than ever, our patients are having multiple cesarean deliveries. More than ever, our patients are hoping – perhaps even expecting – to retain their fertility after a complicated delivery. More than ever, a single patient may need the guidance and care of not just an ob.gyn. or maternal-fetal medicine subspecialist but also an endocrinologist, cardiologist, diabetologist, genetic counselor, nutritionist – the list could go on.

The emergence and continued growth of personalized and preventive medicine in the very near future will catalyze fundamental changes at many different levels in health care and health systems. The need to establish multidisciplinary care teams is already apparent in ob.gyn. but is especially necessary in helping patients who experience complicated deliveries that could jeopardize their immediate and long-term health and fertility.
This month, we have invited M. Ozhan Turan, MD, PhD, the director of fetal therapy and complex obstetric surgery at the University of Maryland, Baltimore, to discuss the use of a multidisciplinary team in the management of patients with placenta accreta and other forms of morbidly adherent placenta.
Dr. Reece, who specializes in maternal-fetal medicine, is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. Dr. Reece said he had no relevant financial disclosures. He is the medical editor of this column.
Medical practice has evolved, and will continue to do so, as we begin pushing for more personalized and better precision health care. Gone are the days of the general practitioner who attempted to treat all conditions in all patients. Health care is now so complex that not only specialists but also so-called superspecialists are needed to manage complicated cases successfully.
One of the biggest challenges, and greatest opportunities, in ob.gyn. is the need to establish a multidisciplinary health team to the address the needs of today’s patients. More than ever, we are working with patients with advanced maternal age having their first pregnancies. More than ever, we are managing patients who have preexisting diabetes and are concurrently overweight or obese. More than ever, our patients are having multiple cesarean deliveries. More than ever, our patients are hoping – perhaps even expecting – to retain their fertility after a complicated delivery. More than ever, a single patient may need the guidance and care of not just an ob.gyn. or maternal-fetal medicine subspecialist but also an endocrinologist, cardiologist, diabetologist, genetic counselor, nutritionist – the list could go on.
The emergence and continued growth of personalized and preventive medicine in the very near future will catalyze fundamental changes at many different levels in health care and health systems. The need to establish multidisciplinary care teams is already apparent in ob.gyn. but is especially necessary in helping patients who experience complicated deliveries that could jeopardize their immediate and long-term health and fertility.
This month, we have invited M. Ozhan Turan, MD, PhD, the director of fetal therapy and complex obstetric surgery at the University of Maryland, Baltimore, to discuss the use of a multidisciplinary team in the management of patients with placenta accreta and other forms of morbidly adherent placenta.
Dr. Reece, who specializes in maternal-fetal medicine, is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. Dr. Reece said he had no relevant financial disclosures. He is the medical editor of this column.
Medical practice has evolved, and will continue to do so, as we begin pushing for more personalized and better precision health care. Gone are the days of the general practitioner who attempted to treat all conditions in all patients. Health care is now so complex that not only specialists but also so-called superspecialists are needed to manage complicated cases successfully.
One of the biggest challenges, and greatest opportunities, in ob.gyn. is the need to establish a multidisciplinary health team to the address the needs of today’s patients. More than ever, we are working with patients with advanced maternal age having their first pregnancies. More than ever, we are managing patients who have preexisting diabetes and are concurrently overweight or obese. More than ever, our patients are having multiple cesarean deliveries. More than ever, our patients are hoping – perhaps even expecting – to retain their fertility after a complicated delivery. More than ever, a single patient may need the guidance and care of not just an ob.gyn. or maternal-fetal medicine subspecialist but also an endocrinologist, cardiologist, diabetologist, genetic counselor, nutritionist – the list could go on.
The emergence and continued growth of personalized and preventive medicine in the very near future will catalyze fundamental changes at many different levels in health care and health systems. The need to establish multidisciplinary care teams is already apparent in ob.gyn. but is especially necessary in helping patients who experience complicated deliveries that could jeopardize their immediate and long-term health and fertility.
This month, we have invited M. Ozhan Turan, MD, PhD, the director of fetal therapy and complex obstetric surgery at the University of Maryland, Baltimore, to discuss the use of a multidisciplinary team in the management of patients with placenta accreta and other forms of morbidly adherent placenta.
Dr. Reece, who specializes in maternal-fetal medicine, is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. Dr. Reece said he had no relevant financial disclosures. He is the medical editor of this column.
Strategies to evaluate postmenopausal bleeding
Postmenopausal bleeding is a symptom that can announce the presence of a gynecologic malignancy. In this column, we will discuss the important considerations to make in the work-up of this symptom.
Roughly 10% of women will present for evaluation of postmenopausal bleeding.1 More than a third of these women will have benign pathology, with the incidence of endometrial cancer in this group at only about 5%.2 Other gynecologic malignancies should be considered as well, including cervical, vaginal, vulvar, and more rarely, those of the fallopian tubes or ovaries.

Use of ultrasound
Ultrasound is a commonly performed initial approach to work-up because of its noninvasive nature. Transvaginal ultrasound has a high negative predictive value of 99.4%-100% in ruling out malignancy.3 Among women with postmenopausal bleeding, the risk of cancer is 7.3% if their endometrial lining is 5 mm or greater and less than 0.07% risk if their lining is 4 mm or less. Therefore, this cutoff dimension is typically used to triage patients to additional sampling.
If ultrasound is performed on postmenopausal women who are asymptomatic (no bleeding), then an endometrial stripe of greater than 11 mm is considered justification for further work-up and is associated with a 6.7% risk of endometrial cancer.4 If the ultrasound reveals intracavitary lesions, a sonohysterogram would be preferred to characterize intrauterine pathology. In fact, sonohysterography is superior to transvaginal ultrasound (with a sensitivity of 80% vs. 49%, respectively) in detecting endometrial polypoid lesions.5 Preoperative identification of an intracavitary lesion may assist in selecting the best sampling technique (blind vs. hysteroscopy-guided approach).
Endometrial sampling
If an ultrasound reveals a thickened or unevaluable endometrial stripe or if the clinician chooses to proceed directly with diagnostic confirmation, several options for endometrial sampling exist, including office-based or operative procedures, as well as blind or visually guided ones. Endometrial pipelle biopsy, D&C without hysteroscopy, endometrial lavage, and endometrial brush biopsy all constitute “blind” sampling techniques. Targeted biopsy techniques include hysteroscopy D&C and saline infusion sonohysterography–guided biopsy.
Blind D&C
Although D&C may be considered the gold standard of diagnostic sampling techniques, it should be noted that 60% of these procedures sample less than half of the endometrium.6 When used in conjunction with hysteroscopy, the sensitivity in detecting cancer is high at 97% with a specificity of 93%-100%.7
While some patients are candidates for office-based procedures, D&C often requires regional or general anesthesia and is frequently performed in a hospital-based environment or surgical center. This may be most appropriate for patients who have had failed office attempts at sampling, have multiple medical comorbidities that limit the feasibility of office-based procedures (such as morbid obesity), or have severe cervical stenosis. D&C is associated with an increased risk for uterine perforation, compared with outpatient sampling procedures.
The need to go to the operating room rather than to an ambulatory setting also may increase the costs borne by the patient. The advantages of D&C include the potential for large-volume sampling and the potentially therapeutic nature of the procedure in cases of benign pathology.
Office-based procedures
Office-based sampling techniques include those using a pipelle, those employing an endometrial brush, and those guided by saline infusion sonohysterography. If performed in the office, they require minimal or no cervical dilation, are associated with a lower risk of perforation or adverse reaction to anesthesia, and usually have lower costs for patients.
Endometrial pipelle biopsies are a very effective diagnostic tool when there is global, endometrial pathology; they have a sensitivity of 83% in confirming cancer.8 It is an inexpensive and technically straightforward technique that can be easily performed in an office setting.
However, when the endometrial lining is atrophied, alternative tools may provide superior results. Endometrial brushes have been shown to be 33% more successful in collecting adequate samples,compared with pipelles, because they sample a larger endometrial surface area.9
There is ongoing development of sampling techniques, such as endometrial lavage or the combination of saline infusion sonohysterography and endometrial biopsy.10 However, future studies regarding accuracy, cost, and patient acceptability are needed before these techniques are translated to the clinical setting.
Targeted endometrial sampling
Targeted or visually guided sampling, such as hysteroscopy, has been shown to be very accurate in identifying benign pathology, although the sensitivity of hysteroscopic diagnosis of cancer is significantly lower at approximately 50%.11 Therefore, the benefit of hysteroscopy is in complementing the blind nature of D&C by guiding sampling of intracavitary lesions, should they exist.
Hysteroscopy is safe in endometrial cancer and is not associated with upstaging the cancer from transtubal extirpation of malignant cells.12
The addition of hysteroscopy contributes some cost and equipment to the blind D&C procedure; therefore, it might be best applied in cases where there is known intracavitary pathology or inadequate prior sampling. In well-selected patients, hysteroscopy often can be used in an office setting, which improves the practicality of the procedure. Smaller and, in some cases, disposable equipment aids in the feasibility of adding visual guidance to office sampling.
Optimizing sampling
Postmenopausal women have a higher risk for sampling failure, compared with younger women. Obesity also is a risk for failed sampling.13 Cervical ripening with misoprostol may increase access to the endometrial cavity, and ultrasound guidance may decrease the risk of uterine perforation in a stenotic cervix.
Clinicians should ensure that histology results are concordant with clinical data. Discordant results should be reevaluated. For example, if an ultrasound demonstrates a thickened endometrial stripe, but the sampling reveals “scant atrophic tissue,” then there is unexplained pathology to address. Further work-up, such as more comprehensive sampling with hysteroscopy, should be considered in such cases. Additionally, persistent postmenopausal bleeding, despite a benign endometrial biopsy, should be reevaluated over time to rule out occult disease missed during prior sampling.
Clinicians are now equipped with multiple ways of obtaining clinical data, and patients have options that may decrease barriers to their care. Hysteroscopy does not improve upon D&C in the diagnosis of endometrial cancer, although it may be helpful in distinguishing and treating nonmalignant lesions.
Dr. Cotangco is a resident in the department of obstetrics and gynecology at the University of Illinois, Chicago. Dr. Rossi is an assistant professor in the division of gynecologic oncology at the University of North Carolina, Chapel Hill. They reported having no relevant financial disclosures.
References
1. Acta Obstet Gynecol Scand. 2004 Feb;83(2):203-7.
2. Menopause Int. 2010 Mar;16(1):5-8.
3. Obstet Gynecol. 2009 Aug;114(2 Pt 1):409-11.
4. Ultrasound Obstet Gynecol. 2004 Oct;24(5):558-65.
5. Ultrasound Obstet Gynecol. 2001 Aug;18(2):157-62.
6. Am J Obstet Gynecol. 2009 Jul;201(1):5-11.
7. Obstet Gynecol Clin North Am. 2000 Jun;27(2):235-44.
8. J Reprod Med. 1995 Aug;40(8):553-5.
9. BJOG. 2008 Jul;115(8):1028-36.
10. PLoS Med. 2016 Dec. doi: 10.1371/journal.pmed.1002206.
11. Arch Gynecol Obstet. 2012 Mar;285(3):839-43.
12. Am J Obstet Gynecol. 2012 Jul;207(1):71.e1-5.
13. Gynecol Oncol. 2017 Feb;144(2):324-8.
Postmenopausal bleeding is a symptom that can announce the presence of a gynecologic malignancy. In this column, we will discuss the important considerations to make in the work-up of this symptom.
Roughly 10% of women will present for evaluation of postmenopausal bleeding.1 More than a third of these women will have benign pathology, with the incidence of endometrial cancer in this group at only about 5%.2 Other gynecologic malignancies should be considered as well, including cervical, vaginal, vulvar, and more rarely, those of the fallopian tubes or ovaries.
Use of ultrasound
Ultrasound is a commonly performed initial approach to work-up because of its noninvasive nature. Transvaginal ultrasound has a high negative predictive value of 99.4%-100% in ruling out malignancy.3 Among women with postmenopausal bleeding, the risk of cancer is 7.3% if their endometrial lining is 5 mm or greater and less than 0.07% risk if their lining is 4 mm or less. Therefore, this cutoff dimension is typically used to triage patients to additional sampling.
If ultrasound is performed on postmenopausal women who are asymptomatic (no bleeding), then an endometrial stripe of greater than 11 mm is considered justification for further work-up and is associated with a 6.7% risk of endometrial cancer.4 If the ultrasound reveals intracavitary lesions, a sonohysterogram would be preferred to characterize intrauterine pathology. In fact, sonohysterography is superior to transvaginal ultrasound (with a sensitivity of 80% vs. 49%, respectively) in detecting endometrial polypoid lesions.5 Preoperative identification of an intracavitary lesion may assist in selecting the best sampling technique (blind vs. hysteroscopy-guided approach).
Endometrial sampling
If an ultrasound reveals a thickened or unevaluable endometrial stripe or if the clinician chooses to proceed directly with diagnostic confirmation, several options for endometrial sampling exist, including office-based or operative procedures, as well as blind or visually guided ones. Endometrial pipelle biopsy, D&C without hysteroscopy, endometrial lavage, and endometrial brush biopsy all constitute “blind” sampling techniques. Targeted biopsy techniques include hysteroscopy D&C and saline infusion sonohysterography–guided biopsy.
Blind D&C
Although D&C may be considered the gold standard of diagnostic sampling techniques, it should be noted that 60% of these procedures sample less than half of the endometrium.6 When used in conjunction with hysteroscopy, the sensitivity in detecting cancer is high at 97% with a specificity of 93%-100%.7
While some patients are candidates for office-based procedures, D&C often requires regional or general anesthesia and is frequently performed in a hospital-based environment or surgical center. This may be most appropriate for patients who have had failed office attempts at sampling, have multiple medical comorbidities that limit the feasibility of office-based procedures (such as morbid obesity), or have severe cervical stenosis. D&C is associated with an increased risk for uterine perforation, compared with outpatient sampling procedures.
The need to go to the operating room rather than to an ambulatory setting also may increase the costs borne by the patient. The advantages of D&C include the potential for large-volume sampling and the potentially therapeutic nature of the procedure in cases of benign pathology.
Office-based procedures
Office-based sampling techniques include those using a pipelle, those employing an endometrial brush, and those guided by saline infusion sonohysterography. If performed in the office, they require minimal or no cervical dilation, are associated with a lower risk of perforation or adverse reaction to anesthesia, and usually have lower costs for patients.
Endometrial pipelle biopsies are a very effective diagnostic tool when there is global, endometrial pathology; they have a sensitivity of 83% in confirming cancer.8 It is an inexpensive and technically straightforward technique that can be easily performed in an office setting.
However, when the endometrial lining is atrophied, alternative tools may provide superior results. Endometrial brushes have been shown to be 33% more successful in collecting adequate samples,compared with pipelles, because they sample a larger endometrial surface area.9
There is ongoing development of sampling techniques, such as endometrial lavage or the combination of saline infusion sonohysterography and endometrial biopsy.10 However, future studies regarding accuracy, cost, and patient acceptability are needed before these techniques are translated to the clinical setting.
Targeted endometrial sampling
Targeted or visually guided sampling, such as hysteroscopy, has been shown to be very accurate in identifying benign pathology, although the sensitivity of hysteroscopic diagnosis of cancer is significantly lower at approximately 50%.11 Therefore, the benefit of hysteroscopy is in complementing the blind nature of D&C by guiding sampling of intracavitary lesions, should they exist.
Hysteroscopy is safe in endometrial cancer and is not associated with upstaging the cancer from transtubal extirpation of malignant cells.12
The addition of hysteroscopy contributes some cost and equipment to the blind D&C procedure; therefore, it might be best applied in cases where there is known intracavitary pathology or inadequate prior sampling. In well-selected patients, hysteroscopy often can be used in an office setting, which improves the practicality of the procedure. Smaller and, in some cases, disposable equipment aids in the feasibility of adding visual guidance to office sampling.
Optimizing sampling
Postmenopausal women have a higher risk for sampling failure, compared with younger women. Obesity also is a risk for failed sampling.13 Cervical ripening with misoprostol may increase access to the endometrial cavity, and ultrasound guidance may decrease the risk of uterine perforation in a stenotic cervix.
Clinicians should ensure that histology results are concordant with clinical data. Discordant results should be reevaluated. For example, if an ultrasound demonstrates a thickened endometrial stripe, but the sampling reveals “scant atrophic tissue,” then there is unexplained pathology to address. Further work-up, such as more comprehensive sampling with hysteroscopy, should be considered in such cases. Additionally, persistent postmenopausal bleeding, despite a benign endometrial biopsy, should be reevaluated over time to rule out occult disease missed during prior sampling.
Clinicians are now equipped with multiple ways of obtaining clinical data, and patients have options that may decrease barriers to their care. Hysteroscopy does not improve upon D&C in the diagnosis of endometrial cancer, although it may be helpful in distinguishing and treating nonmalignant lesions.
Dr. Cotangco is a resident in the department of obstetrics and gynecology at the University of Illinois, Chicago. Dr. Rossi is an assistant professor in the division of gynecologic oncology at the University of North Carolina, Chapel Hill. They reported having no relevant financial disclosures.
References
1. Acta Obstet Gynecol Scand. 2004 Feb;83(2):203-7.
2. Menopause Int. 2010 Mar;16(1):5-8.
3. Obstet Gynecol. 2009 Aug;114(2 Pt 1):409-11.
4. Ultrasound Obstet Gynecol. 2004 Oct;24(5):558-65.
5. Ultrasound Obstet Gynecol. 2001 Aug;18(2):157-62.
6. Am J Obstet Gynecol. 2009 Jul;201(1):5-11.
7. Obstet Gynecol Clin North Am. 2000 Jun;27(2):235-44.
8. J Reprod Med. 1995 Aug;40(8):553-5.
9. BJOG. 2008 Jul;115(8):1028-36.
10. PLoS Med. 2016 Dec. doi: 10.1371/journal.pmed.1002206.
11. Arch Gynecol Obstet. 2012 Mar;285(3):839-43.
12. Am J Obstet Gynecol. 2012 Jul;207(1):71.e1-5.
13. Gynecol Oncol. 2017 Feb;144(2):324-8.
Postmenopausal bleeding is a symptom that can announce the presence of a gynecologic malignancy. In this column, we will discuss the important considerations to make in the work-up of this symptom.
Roughly 10% of women will present for evaluation of postmenopausal bleeding.1 More than a third of these women will have benign pathology, with the incidence of endometrial cancer in this group at only about 5%.2 Other gynecologic malignancies should be considered as well, including cervical, vaginal, vulvar, and more rarely, those of the fallopian tubes or ovaries.
Use of ultrasound
Ultrasound is a commonly performed initial approach to work-up because of its noninvasive nature. Transvaginal ultrasound has a high negative predictive value of 99.4%-100% in ruling out malignancy.3 Among women with postmenopausal bleeding, the risk of cancer is 7.3% if their endometrial lining is 5 mm or greater and less than 0.07% risk if their lining is 4 mm or less. Therefore, this cutoff dimension is typically used to triage patients to additional sampling.
If ultrasound is performed on postmenopausal women who are asymptomatic (no bleeding), then an endometrial stripe of greater than 11 mm is considered justification for further work-up and is associated with a 6.7% risk of endometrial cancer.4 If the ultrasound reveals intracavitary lesions, a sonohysterogram would be preferred to characterize intrauterine pathology. In fact, sonohysterography is superior to transvaginal ultrasound (with a sensitivity of 80% vs. 49%, respectively) in detecting endometrial polypoid lesions.5 Preoperative identification of an intracavitary lesion may assist in selecting the best sampling technique (blind vs. hysteroscopy-guided approach).
Endometrial sampling
If an ultrasound reveals a thickened or unevaluable endometrial stripe or if the clinician chooses to proceed directly with diagnostic confirmation, several options for endometrial sampling exist, including office-based or operative procedures, as well as blind or visually guided ones. Endometrial pipelle biopsy, D&C without hysteroscopy, endometrial lavage, and endometrial brush biopsy all constitute “blind” sampling techniques. Targeted biopsy techniques include hysteroscopy D&C and saline infusion sonohysterography–guided biopsy.
Blind D&C
Although D&C may be considered the gold standard of diagnostic sampling techniques, it should be noted that 60% of these procedures sample less than half of the endometrium.6 When used in conjunction with hysteroscopy, the sensitivity in detecting cancer is high at 97% with a specificity of 93%-100%.7
While some patients are candidates for office-based procedures, D&C often requires regional or general anesthesia and is frequently performed in a hospital-based environment or surgical center. This may be most appropriate for patients who have had failed office attempts at sampling, have multiple medical comorbidities that limit the feasibility of office-based procedures (such as morbid obesity), or have severe cervical stenosis. D&C is associated with an increased risk for uterine perforation, compared with outpatient sampling procedures.
The need to go to the operating room rather than to an ambulatory setting also may increase the costs borne by the patient. The advantages of D&C include the potential for large-volume sampling and the potentially therapeutic nature of the procedure in cases of benign pathology.
Office-based procedures
Office-based sampling techniques include those using a pipelle, those employing an endometrial brush, and those guided by saline infusion sonohysterography. If performed in the office, they require minimal or no cervical dilation, are associated with a lower risk of perforation or adverse reaction to anesthesia, and usually have lower costs for patients.
Endometrial pipelle biopsies are a very effective diagnostic tool when there is global, endometrial pathology; they have a sensitivity of 83% in confirming cancer.8 It is an inexpensive and technically straightforward technique that can be easily performed in an office setting.
However, when the endometrial lining is atrophied, alternative tools may provide superior results. Endometrial brushes have been shown to be 33% more successful in collecting adequate samples,compared with pipelles, because they sample a larger endometrial surface area.9
There is ongoing development of sampling techniques, such as endometrial lavage or the combination of saline infusion sonohysterography and endometrial biopsy.10 However, future studies regarding accuracy, cost, and patient acceptability are needed before these techniques are translated to the clinical setting.
Targeted endometrial sampling
Targeted or visually guided sampling, such as hysteroscopy, has been shown to be very accurate in identifying benign pathology, although the sensitivity of hysteroscopic diagnosis of cancer is significantly lower at approximately 50%.11 Therefore, the benefit of hysteroscopy is in complementing the blind nature of D&C by guiding sampling of intracavitary lesions, should they exist.
Hysteroscopy is safe in endometrial cancer and is not associated with upstaging the cancer from transtubal extirpation of malignant cells.12
The addition of hysteroscopy contributes some cost and equipment to the blind D&C procedure; therefore, it might be best applied in cases where there is known intracavitary pathology or inadequate prior sampling. In well-selected patients, hysteroscopy often can be used in an office setting, which improves the practicality of the procedure. Smaller and, in some cases, disposable equipment aids in the feasibility of adding visual guidance to office sampling.
Optimizing sampling
Postmenopausal women have a higher risk for sampling failure, compared with younger women. Obesity also is a risk for failed sampling.13 Cervical ripening with misoprostol may increase access to the endometrial cavity, and ultrasound guidance may decrease the risk of uterine perforation in a stenotic cervix.
Clinicians should ensure that histology results are concordant with clinical data. Discordant results should be reevaluated. For example, if an ultrasound demonstrates a thickened endometrial stripe, but the sampling reveals “scant atrophic tissue,” then there is unexplained pathology to address. Further work-up, such as more comprehensive sampling with hysteroscopy, should be considered in such cases. Additionally, persistent postmenopausal bleeding, despite a benign endometrial biopsy, should be reevaluated over time to rule out occult disease missed during prior sampling.
Clinicians are now equipped with multiple ways of obtaining clinical data, and patients have options that may decrease barriers to their care. Hysteroscopy does not improve upon D&C in the diagnosis of endometrial cancer, although it may be helpful in distinguishing and treating nonmalignant lesions.
Dr. Cotangco is a resident in the department of obstetrics and gynecology at the University of Illinois, Chicago. Dr. Rossi is an assistant professor in the division of gynecologic oncology at the University of North Carolina, Chapel Hill. They reported having no relevant financial disclosures.
References
1. Acta Obstet Gynecol Scand. 2004 Feb;83(2):203-7.
2. Menopause Int. 2010 Mar;16(1):5-8.
3. Obstet Gynecol. 2009 Aug;114(2 Pt 1):409-11.
4. Ultrasound Obstet Gynecol. 2004 Oct;24(5):558-65.
5. Ultrasound Obstet Gynecol. 2001 Aug;18(2):157-62.
6. Am J Obstet Gynecol. 2009 Jul;201(1):5-11.
7. Obstet Gynecol Clin North Am. 2000 Jun;27(2):235-44.
8. J Reprod Med. 1995 Aug;40(8):553-5.
9. BJOG. 2008 Jul;115(8):1028-36.
10. PLoS Med. 2016 Dec. doi: 10.1371/journal.pmed.1002206.
11. Arch Gynecol Obstet. 2012 Mar;285(3):839-43.
12. Am J Obstet Gynecol. 2012 Jul;207(1):71.e1-5.
13. Gynecol Oncol. 2017 Feb;144(2):324-8.
In Lewy body disease, CSF may reveal dementia risk
SAN DIEGO – In patients with Lewy body disease, cerebrospinal fluid biomarkers may predict the extent of Alzheimer’s disease pathology, according to a new postmortem analysis.
In the small prospective study, David Irwin, MD, and his colleagues at the University of Pennsylvania, Philadelphia, found that higher antemortem cerebrospinal fluid (CSF) levels of total tau (t-tau) protein and lower amyloid-beta 1-42 (Abeta 1-42) levels were associated with postmortem evidence of cerebral Alzheimer’s disease and synuclein pathology.

The findings could have prognostic indications because about 40% of LBD patients have enough Abeta 1-42 and tau tangle pathology to have a secondary diagnosis of Alzheimer’s disease, and greater Alzheimer’s disease pathology has been linked to shorter survival. It could also help individualize therapy, as LBD patients with more Alzheimer’s disease character could be expected to respond better to antisynuclein and Alzheimer’s therapies, according to Dr. Irwin, who presented the study at a poster session at the annual meeting of the American Neurological Association.
In fact, the CSF ratio of CSF t-tau/Abeta 1-42 predicted the presence or absence of Alzheimer’s disease pathology with 90% sensitivity and 100% specificity.
If the results from the small study hold up, “we can identify who has Alzheimer’s copathology and who has a more aggressive form of Lewy body disease where it’s reaching the cortex rather than being in the brain stem, and that correlates with memory loss, dementia, and other things that impair the patient’s functioning,” Dr. Irwin said in an interview.
The study was possible because the Udall Center for Parkinson’s Research at the University of Pennsylvania has an active autopsy program and a significant number of Parkinson’s disease patients who have donated their brain for research. “It’s very rare to have autopsy-confirmed samples where we can validate what we’re measuring in the spinal fluid to what is actually accumulating in the brain,” Dr. Irwin said.
The study included 24 patients with autopsy-confirmed LBD who had undergone CSF testing while they were still alive. The researchers calculated ordinal pathology scores of tau tangles, Abeta 1-42 plaques, and alpha-synuclein pathology across seven regions of the brain, producing a global pathology score for each variable. The subjects were then divided into two groups: Lewy body synuclein stages with medium to high Alzheimer’s copathology (SYN+AD, n = 10) and those with low to no Alzheimer’s copathology (SYN-AD, n = 14).
In the CSF, the researchers analyzed associations with t-tau, phosphorylated tau (p-tau), and Abeta 1-42. They found that Abeta 1-42 levels were significantly different between SYN+AD and SYN-AD patients (147.2 pg/mL vs. 231.1 pg/mL, respectively; P = .001), as were CSF t-tau levels (63.9 pg/mL vs. 36.9 pg/mL; P = .02). P-tau was not significantly different (20.2 pg/mL vs. 15.5 pg/mL; P = 0.3), which was a surprise since it “is usually the strongest correlate of tangles in the brain,” Dr. Irwin said.
A ratio of CSF t-tau/Abeta 1-42 higher than 0.30 distinguished between SYN+AD and SYN-AD (area under the curve, 0.92; 95% confidence interval, 0.7-1.0; 90% sensitivity, 100% specificity), while CSF Abeta 1-42 less than 185 pg/mL distinguished neocortical synuclein stage (AUC, 0.92; 95% CI, 0.54-0.94; 77% sensitivity, 82% specificity).
The study was funded by the National Institute of Neurological Disorders and Stroke. Dr. Irwin reported having no financial disclosures.
SAN DIEGO – In patients with Lewy body disease, cerebrospinal fluid biomarkers may predict the extent of Alzheimer’s disease pathology, according to a new postmortem analysis.
In the small prospective study, David Irwin, MD, and his colleagues at the University of Pennsylvania, Philadelphia, found that higher antemortem cerebrospinal fluid (CSF) levels of total tau (t-tau) protein and lower amyloid-beta 1-42 (Abeta 1-42) levels were associated with postmortem evidence of cerebral Alzheimer’s disease and synuclein pathology.
The findings could have prognostic indications because about 40% of LBD patients have enough Abeta 1-42 and tau tangle pathology to have a secondary diagnosis of Alzheimer’s disease, and greater Alzheimer’s disease pathology has been linked to shorter survival. It could also help individualize therapy, as LBD patients with more Alzheimer’s disease character could be expected to respond better to antisynuclein and Alzheimer’s therapies, according to Dr. Irwin, who presented the study at a poster session at the annual meeting of the American Neurological Association.
In fact, the CSF ratio of CSF t-tau/Abeta 1-42 predicted the presence or absence of Alzheimer’s disease pathology with 90% sensitivity and 100% specificity.
If the results from the small study hold up, “we can identify who has Alzheimer’s copathology and who has a more aggressive form of Lewy body disease where it’s reaching the cortex rather than being in the brain stem, and that correlates with memory loss, dementia, and other things that impair the patient’s functioning,” Dr. Irwin said in an interview.
The study was possible because the Udall Center for Parkinson’s Research at the University of Pennsylvania has an active autopsy program and a significant number of Parkinson’s disease patients who have donated their brain for research. “It’s very rare to have autopsy-confirmed samples where we can validate what we’re measuring in the spinal fluid to what is actually accumulating in the brain,” Dr. Irwin said.
The study included 24 patients with autopsy-confirmed LBD who had undergone CSF testing while they were still alive. The researchers calculated ordinal pathology scores of tau tangles, Abeta 1-42 plaques, and alpha-synuclein pathology across seven regions of the brain, producing a global pathology score for each variable. The subjects were then divided into two groups: Lewy body synuclein stages with medium to high Alzheimer’s copathology (SYN+AD, n = 10) and those with low to no Alzheimer’s copathology (SYN-AD, n = 14).
In the CSF, the researchers analyzed associations with t-tau, phosphorylated tau (p-tau), and Abeta 1-42. They found that Abeta 1-42 levels were significantly different between SYN+AD and SYN-AD patients (147.2 pg/mL vs. 231.1 pg/mL, respectively; P = .001), as were CSF t-tau levels (63.9 pg/mL vs. 36.9 pg/mL; P = .02). P-tau was not significantly different (20.2 pg/mL vs. 15.5 pg/mL; P = 0.3), which was a surprise since it “is usually the strongest correlate of tangles in the brain,” Dr. Irwin said.
A ratio of CSF t-tau/Abeta 1-42 higher than 0.30 distinguished between SYN+AD and SYN-AD (area under the curve, 0.92; 95% confidence interval, 0.7-1.0; 90% sensitivity, 100% specificity), while CSF Abeta 1-42 less than 185 pg/mL distinguished neocortical synuclein stage (AUC, 0.92; 95% CI, 0.54-0.94; 77% sensitivity, 82% specificity).
The study was funded by the National Institute of Neurological Disorders and Stroke. Dr. Irwin reported having no financial disclosures.
SAN DIEGO – In patients with Lewy body disease, cerebrospinal fluid biomarkers may predict the extent of Alzheimer’s disease pathology, according to a new postmortem analysis.
In the small prospective study, David Irwin, MD, and his colleagues at the University of Pennsylvania, Philadelphia, found that higher antemortem cerebrospinal fluid (CSF) levels of total tau (t-tau) protein and lower amyloid-beta 1-42 (Abeta 1-42) levels were associated with postmortem evidence of cerebral Alzheimer’s disease and synuclein pathology.
The findings could have prognostic indications because about 40% of LBD patients have enough Abeta 1-42 and tau tangle pathology to have a secondary diagnosis of Alzheimer’s disease, and greater Alzheimer’s disease pathology has been linked to shorter survival. It could also help individualize therapy, as LBD patients with more Alzheimer’s disease character could be expected to respond better to antisynuclein and Alzheimer’s therapies, according to Dr. Irwin, who presented the study at a poster session at the annual meeting of the American Neurological Association.
In fact, the CSF ratio of CSF t-tau/Abeta 1-42 predicted the presence or absence of Alzheimer’s disease pathology with 90% sensitivity and 100% specificity.
If the results from the small study hold up, “we can identify who has Alzheimer’s copathology and who has a more aggressive form of Lewy body disease where it’s reaching the cortex rather than being in the brain stem, and that correlates with memory loss, dementia, and other things that impair the patient’s functioning,” Dr. Irwin said in an interview.
The study was possible because the Udall Center for Parkinson’s Research at the University of Pennsylvania has an active autopsy program and a significant number of Parkinson’s disease patients who have donated their brain for research. “It’s very rare to have autopsy-confirmed samples where we can validate what we’re measuring in the spinal fluid to what is actually accumulating in the brain,” Dr. Irwin said.
The study included 24 patients with autopsy-confirmed LBD who had undergone CSF testing while they were still alive. The researchers calculated ordinal pathology scores of tau tangles, Abeta 1-42 plaques, and alpha-synuclein pathology across seven regions of the brain, producing a global pathology score for each variable. The subjects were then divided into two groups: Lewy body synuclein stages with medium to high Alzheimer’s copathology (SYN+AD, n = 10) and those with low to no Alzheimer’s copathology (SYN-AD, n = 14).
In the CSF, the researchers analyzed associations with t-tau, phosphorylated tau (p-tau), and Abeta 1-42. They found that Abeta 1-42 levels were significantly different between SYN+AD and SYN-AD patients (147.2 pg/mL vs. 231.1 pg/mL, respectively; P = .001), as were CSF t-tau levels (63.9 pg/mL vs. 36.9 pg/mL; P = .02). P-tau was not significantly different (20.2 pg/mL vs. 15.5 pg/mL; P = 0.3), which was a surprise since it “is usually the strongest correlate of tangles in the brain,” Dr. Irwin said.
A ratio of CSF t-tau/Abeta 1-42 higher than 0.30 distinguished between SYN+AD and SYN-AD (area under the curve, 0.92; 95% confidence interval, 0.7-1.0; 90% sensitivity, 100% specificity), while CSF Abeta 1-42 less than 185 pg/mL distinguished neocortical synuclein stage (AUC, 0.92; 95% CI, 0.54-0.94; 77% sensitivity, 82% specificity).
The study was funded by the National Institute of Neurological Disorders and Stroke. Dr. Irwin reported having no financial disclosures.
AT ANA 2017
Key clinical point:
Major finding: A CSF ratio of t-tau/Abeta 1-42 greater than 0.30 predicted the presence or absence of Alzheimer’s disease pathology with 90% sensitivity and 100% specificity.
Data source: Prospective study of 24 patients with Lewy body disease.
Disclosures: The study was funded by the National Institute of Neurological Disorders and Stroke. Dr. Irwin reported having no financial disclosures.
Why VADS is gaining ground in pediatrics
The miniaturization of continuous-flow ventricular assist devices has launched the era of continuous-flow VAD support in pediatric patients, and the trend may accelerate with the introduction of a continuous-flow device designed specifically for small children. In an expert opinion in the Journal of Thoracic and Cardiovascular Surgery, Iki Adachi, MD, of Baylor College of Medicine in Houston, said the emerging science of continuous-flow VADs in children promises to solve problems like device size mismatch, hospital-only VADs, and chronic therapy (J Thorac Cardiovasc Surg. 2017 Oct;154:1358-61). “With ongoing device miniaturization, enthusiasm has been growing among pediatric physicians for the use of continuous-flow VADs in children,” Dr. Adachi said. He noted the introduction of a continuous-flow device for small children, the Infant Jarvik 2015, “may further accelerate the trend.”
Dr. Adachi cited PediMACS reports that stated that more than half of the long-term devices now registered are continuous-flow devices, and that continuous-flow VADs comprised 62% of all durable VAD implants in the third quarter of 2016. “With the encouraging results recorded to date, the use of continuous-flow devices in the pediatric population is rapidly increasing,” he said.
Miniaturization has addressed the problem of size mismatch when using continuous-flow VAD devices in children, he said, noting that use of the Infant Jarvik device may be expanded even further to children as small at 8 kg or less. The PumpKIN trial(Pumps for Kids, Infants, and Neonates), which is evaluating the Infant Jarvik 2015 vs. the Berlin Heart EXCOR, could provide answers on the feasibility of continuous-flow VADs in small children.
“Based on experience with the chronic animal model, I believe that the Infant Jarvik device will properly fit the patients included in the trial,” he said.
Continuous-flow VAD in children also holds potential for managing these patients outside the hospital setting. “Outpatient management of children with continuous-flow VADs has been shown to be feasible,” he said, adding that the PediMACS registry has reported that only 45% of patients have been managed this way. “Nonetheless, with maturation of the pediatric field, outpatient management will become routine rather than the exception,” he said.
Greater use of continuous-flow VADs also may create opportunities to improve the status and suitability for transplantation of children with severe heart failure, he said. He gave as an example his group’s practice at Houston’s Texas Children’s Hospital, which is to deactivate patients on the transplant wait list for 3 months once they start continuous-flow VAD support. “A postoperative ‘grace period’ affords protected opportunities for both physical and psychological recovery,” he said. This timeout of sorts also affords the care team time to assess the myocardium for possible functional recovery.
In patients who are not good candidates for transplantation, durable continuous-flow VADs may provide chronic therapy, and in time, these patients may become suitable transplant candidates, said Dr. Adachi. “Bypassing such an unfavorable period for transplantation with prolonged VAD support may be a reasonable approach,” he said.
Patients with failing single-ventricle circulation also may benefit from VAD support, although the challenges facing this population are more profound than in other groups, Dr. Adachi said. VAD support for single-ventricle disease is sparse, but these patients require careful evaluation of the nature of their condition. “If systolic dysfunction is the predominant cause of circulatory failure, then VAD support for the failing systemic ventricle will likely improve hemodynamics,” said Dr. Adachi. VAD support also could help the patient move through the various stages of palliation.
“Again, the emphasis is not just on simply keeping the patient alive until a donor organ becomes available; rather, attention is refocused on overall health beyond survival, which may eventually affect transplantation candidacy and even post transplantation outcome,” Dr. Adachi concluded.
Dr. Adachi serves as a consultant and proctor for Berlin Heart and HeartWare, and as a consultant for the New England Research Institute related to the PumpKIN trial.
The miniaturization of continuous-flow ventricular assist devices has launched the era of continuous-flow VAD support in pediatric patients, and the trend may accelerate with the introduction of a continuous-flow device designed specifically for small children. In an expert opinion in the Journal of Thoracic and Cardiovascular Surgery, Iki Adachi, MD, of Baylor College of Medicine in Houston, said the emerging science of continuous-flow VADs in children promises to solve problems like device size mismatch, hospital-only VADs, and chronic therapy (J Thorac Cardiovasc Surg. 2017 Oct;154:1358-61). “With ongoing device miniaturization, enthusiasm has been growing among pediatric physicians for the use of continuous-flow VADs in children,” Dr. Adachi said. He noted the introduction of a continuous-flow device for small children, the Infant Jarvik 2015, “may further accelerate the trend.”
Dr. Adachi cited PediMACS reports that stated that more than half of the long-term devices now registered are continuous-flow devices, and that continuous-flow VADs comprised 62% of all durable VAD implants in the third quarter of 2016. “With the encouraging results recorded to date, the use of continuous-flow devices in the pediatric population is rapidly increasing,” he said.
Miniaturization has addressed the problem of size mismatch when using continuous-flow VAD devices in children, he said, noting that use of the Infant Jarvik device may be expanded even further to children as small at 8 kg or less. The PumpKIN trial(Pumps for Kids, Infants, and Neonates), which is evaluating the Infant Jarvik 2015 vs. the Berlin Heart EXCOR, could provide answers on the feasibility of continuous-flow VADs in small children.
“Based on experience with the chronic animal model, I believe that the Infant Jarvik device will properly fit the patients included in the trial,” he said.
Continuous-flow VAD in children also holds potential for managing these patients outside the hospital setting. “Outpatient management of children with continuous-flow VADs has been shown to be feasible,” he said, adding that the PediMACS registry has reported that only 45% of patients have been managed this way. “Nonetheless, with maturation of the pediatric field, outpatient management will become routine rather than the exception,” he said.
Greater use of continuous-flow VADs also may create opportunities to improve the status and suitability for transplantation of children with severe heart failure, he said. He gave as an example his group’s practice at Houston’s Texas Children’s Hospital, which is to deactivate patients on the transplant wait list for 3 months once they start continuous-flow VAD support. “A postoperative ‘grace period’ affords protected opportunities for both physical and psychological recovery,” he said. This timeout of sorts also affords the care team time to assess the myocardium for possible functional recovery.
In patients who are not good candidates for transplantation, durable continuous-flow VADs may provide chronic therapy, and in time, these patients may become suitable transplant candidates, said Dr. Adachi. “Bypassing such an unfavorable period for transplantation with prolonged VAD support may be a reasonable approach,” he said.
Patients with failing single-ventricle circulation also may benefit from VAD support, although the challenges facing this population are more profound than in other groups, Dr. Adachi said. VAD support for single-ventricle disease is sparse, but these patients require careful evaluation of the nature of their condition. “If systolic dysfunction is the predominant cause of circulatory failure, then VAD support for the failing systemic ventricle will likely improve hemodynamics,” said Dr. Adachi. VAD support also could help the patient move through the various stages of palliation.
“Again, the emphasis is not just on simply keeping the patient alive until a donor organ becomes available; rather, attention is refocused on overall health beyond survival, which may eventually affect transplantation candidacy and even post transplantation outcome,” Dr. Adachi concluded.
Dr. Adachi serves as a consultant and proctor for Berlin Heart and HeartWare, and as a consultant for the New England Research Institute related to the PumpKIN trial.
The miniaturization of continuous-flow ventricular assist devices has launched the era of continuous-flow VAD support in pediatric patients, and the trend may accelerate with the introduction of a continuous-flow device designed specifically for small children. In an expert opinion in the Journal of Thoracic and Cardiovascular Surgery, Iki Adachi, MD, of Baylor College of Medicine in Houston, said the emerging science of continuous-flow VADs in children promises to solve problems like device size mismatch, hospital-only VADs, and chronic therapy (J Thorac Cardiovasc Surg. 2017 Oct;154:1358-61). “With ongoing device miniaturization, enthusiasm has been growing among pediatric physicians for the use of continuous-flow VADs in children,” Dr. Adachi said. He noted the introduction of a continuous-flow device for small children, the Infant Jarvik 2015, “may further accelerate the trend.”
Dr. Adachi cited PediMACS reports that stated that more than half of the long-term devices now registered are continuous-flow devices, and that continuous-flow VADs comprised 62% of all durable VAD implants in the third quarter of 2016. “With the encouraging results recorded to date, the use of continuous-flow devices in the pediatric population is rapidly increasing,” he said.
Miniaturization has addressed the problem of size mismatch when using continuous-flow VAD devices in children, he said, noting that use of the Infant Jarvik device may be expanded even further to children as small at 8 kg or less. The PumpKIN trial(Pumps for Kids, Infants, and Neonates), which is evaluating the Infant Jarvik 2015 vs. the Berlin Heart EXCOR, could provide answers on the feasibility of continuous-flow VADs in small children.
“Based on experience with the chronic animal model, I believe that the Infant Jarvik device will properly fit the patients included in the trial,” he said.
Continuous-flow VAD in children also holds potential for managing these patients outside the hospital setting. “Outpatient management of children with continuous-flow VADs has been shown to be feasible,” he said, adding that the PediMACS registry has reported that only 45% of patients have been managed this way. “Nonetheless, with maturation of the pediatric field, outpatient management will become routine rather than the exception,” he said.
Greater use of continuous-flow VADs also may create opportunities to improve the status and suitability for transplantation of children with severe heart failure, he said. He gave as an example his group’s practice at Houston’s Texas Children’s Hospital, which is to deactivate patients on the transplant wait list for 3 months once they start continuous-flow VAD support. “A postoperative ‘grace period’ affords protected opportunities for both physical and psychological recovery,” he said. This timeout of sorts also affords the care team time to assess the myocardium for possible functional recovery.
In patients who are not good candidates for transplantation, durable continuous-flow VADs may provide chronic therapy, and in time, these patients may become suitable transplant candidates, said Dr. Adachi. “Bypassing such an unfavorable period for transplantation with prolonged VAD support may be a reasonable approach,” he said.
Patients with failing single-ventricle circulation also may benefit from VAD support, although the challenges facing this population are more profound than in other groups, Dr. Adachi said. VAD support for single-ventricle disease is sparse, but these patients require careful evaluation of the nature of their condition. “If systolic dysfunction is the predominant cause of circulatory failure, then VAD support for the failing systemic ventricle will likely improve hemodynamics,” said Dr. Adachi. VAD support also could help the patient move through the various stages of palliation.
“Again, the emphasis is not just on simply keeping the patient alive until a donor organ becomes available; rather, attention is refocused on overall health beyond survival, which may eventually affect transplantation candidacy and even post transplantation outcome,” Dr. Adachi concluded.
Dr. Adachi serves as a consultant and proctor for Berlin Heart and HeartWare, and as a consultant for the New England Research Institute related to the PumpKIN trial.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Advances in continuous-flow ventricular assist devices (VADs) promise a paradigm shift in pediatrics.
Major finding: Device miniaturization is solving problems such as size mismatch, inpatients on VADs, and chronic therapy.
Data source: Expert opinion drawing on PediMACS reports and published trials of continuous-flow VAD.
Disclosures: Dr. Adachi serves as a consultant and proctor for Berlin Heart and HeartWare and as a consultant for the New England Research Institute related to the PumpKIN trial.
Obesity-Related Cancer Is on the Rise
Overweight and obesity are associated with an increased risk of 13 types of cancer—and those cancers account for about 40% of all cancers diagnosed in 2014, according to the CDC.
The 13 cancers are meningioma, adenocarcinoma of the esophagus, multiple myeloma, kidney, uterine, ovarian, thyroid, breast, liver, gallbladder, upper stomach, pancreas, and colorectal. About 630,000 people were diagnosed with 1 of those cancers in 2014; 2 in 3 cancers were in adults aged 50 to 74 years. In 2013-2014, about 2 of every 3 American adults were overweight or obese.
Related: The Impact of Obesity on Simvastatin for Lowering LDL-C Among Veterans
Overall, the rate of new cancer cases has been on the decline since the 1990s, the report says, but increases in overweight- and obesity-related cancers “are likely slowing this progress.” Obesity-related cancers (not including colorectal cancer, which declined by 23%) increased by 7% between 2005 and 2014, while the rates of nonobesity–related cancers declined 13%.
Health care providers can help, the CDC says, by counseling patients on healthy weight and its role in cancer prevention, referring obese patients to intensive management programs and connecting patients and their families to community services that give them easier access to healthful food. The National Comprehensive Cancer Control Program (https://www.cdc.gov/cancer/ncccp/index.htm) funds cancer coalitions across the U.S., which include strategies to prevent and control overweight and obesity.
Related: The Impact of Obesity on the Recovery of Patients With Cancer
“When people ask me if there’s a cure for cancer, I say, ‘Yes, good health is the best prescription for preventing chronic diseases, including cancer,” said Lisa Richardson, MD, director of CDC’s Division of Cancer Prevention and Control. That means, she says, giving people the information they need to make healthy choices where they live, work, learn, and play.
Overweight and obesity are associated with an increased risk of 13 types of cancer—and those cancers account for about 40% of all cancers diagnosed in 2014, according to the CDC.
The 13 cancers are meningioma, adenocarcinoma of the esophagus, multiple myeloma, kidney, uterine, ovarian, thyroid, breast, liver, gallbladder, upper stomach, pancreas, and colorectal. About 630,000 people were diagnosed with 1 of those cancers in 2014; 2 in 3 cancers were in adults aged 50 to 74 years. In 2013-2014, about 2 of every 3 American adults were overweight or obese.
Related: The Impact of Obesity on Simvastatin for Lowering LDL-C Among Veterans
Overall, the rate of new cancer cases has been on the decline since the 1990s, the report says, but increases in overweight- and obesity-related cancers “are likely slowing this progress.” Obesity-related cancers (not including colorectal cancer, which declined by 23%) increased by 7% between 2005 and 2014, while the rates of nonobesity–related cancers declined 13%.
Health care providers can help, the CDC says, by counseling patients on healthy weight and its role in cancer prevention, referring obese patients to intensive management programs and connecting patients and their families to community services that give them easier access to healthful food. The National Comprehensive Cancer Control Program (https://www.cdc.gov/cancer/ncccp/index.htm) funds cancer coalitions across the U.S., which include strategies to prevent and control overweight and obesity.
Related: The Impact of Obesity on the Recovery of Patients With Cancer
“When people ask me if there’s a cure for cancer, I say, ‘Yes, good health is the best prescription for preventing chronic diseases, including cancer,” said Lisa Richardson, MD, director of CDC’s Division of Cancer Prevention and Control. That means, she says, giving people the information they need to make healthy choices where they live, work, learn, and play.
Overweight and obesity are associated with an increased risk of 13 types of cancer—and those cancers account for about 40% of all cancers diagnosed in 2014, according to the CDC.
The 13 cancers are meningioma, adenocarcinoma of the esophagus, multiple myeloma, kidney, uterine, ovarian, thyroid, breast, liver, gallbladder, upper stomach, pancreas, and colorectal. About 630,000 people were diagnosed with 1 of those cancers in 2014; 2 in 3 cancers were in adults aged 50 to 74 years. In 2013-2014, about 2 of every 3 American adults were overweight or obese.
Related: The Impact of Obesity on Simvastatin for Lowering LDL-C Among Veterans
Overall, the rate of new cancer cases has been on the decline since the 1990s, the report says, but increases in overweight- and obesity-related cancers “are likely slowing this progress.” Obesity-related cancers (not including colorectal cancer, which declined by 23%) increased by 7% between 2005 and 2014, while the rates of nonobesity–related cancers declined 13%.
Health care providers can help, the CDC says, by counseling patients on healthy weight and its role in cancer prevention, referring obese patients to intensive management programs and connecting patients and their families to community services that give them easier access to healthful food. The National Comprehensive Cancer Control Program (https://www.cdc.gov/cancer/ncccp/index.htm) funds cancer coalitions across the U.S., which include strategies to prevent and control overweight and obesity.
Related: The Impact of Obesity on the Recovery of Patients With Cancer
“When people ask me if there’s a cure for cancer, I say, ‘Yes, good health is the best prescription for preventing chronic diseases, including cancer,” said Lisa Richardson, MD, director of CDC’s Division of Cancer Prevention and Control. That means, she says, giving people the information they need to make healthy choices where they live, work, learn, and play.
Team identifies HSCs that rapidly reconstitute hematopoiesis

Researchers say they have identified a subpopulation of hematopoietic stem cells (HSCs) that immediately contributes to long-term, multilineage hematopoietic reconstitution after transplant.
These HSCs were discovered in macaques, but the cells are similar to a subset of HSCs found in humans.
The researchers found the 2 sets of cells behaved identically when tested in vitro.
The team believes their findings will increase the efficiency of future efforts for HSC transplants, gene therapies, and gene editing.
Hans-Peter Kiem, MD, PhD, of the Fred Hutchinson Cancer Research Center in Seattle, Washington, and his colleagues reported these findings in Science Translational Medicine.
The researchers performed HSC transplants in pig-tailed macaques, following hundreds of thousands of cells immediately after transplant and over the course of 7.5 years.
Previous reports had suggested that successive waves of progenitor cells expand and contract to establish the new bone marrow after transplant.
However, Dr Kiem and his colleagues homed in on a distinct group of HSCs that took hold early after transplant and went on to produce all cell lineages that constitute a complete blood system.
“These findings came as a surprise,” Dr Kiem said. “We had thought that there were multiple types of blood stem cells that take on different roles in rebuilding a blood and immune system. This population does it all.”
The population is a subset of CD34+ cells expressing CD90 and lacking CD45RA markers.
“The gold standard target cell population for stem cell gene therapy are cells with the marker CD34,” said study author Stefan Radtke, PhD, of the Fred Hutchinson Cancer Research Center.
“But we used 2 additional markers to further distinguish the population from the other blood stem cells.”
The researchers noted that the CD34+ CD45RA- CD90+ HSCs started repopulating the hematopoietic system within 10 days of being infused in macaques undergoing transplant.
A year later, the researchers found strong molecular traces of the cells, suggesting they were responsible for the ongoing maintenance of the newly transplanted system.
The team also determined the minimum numbers of CD34+ CD45RA- CD90+ HSCs that were necessary for successful transplant (defined as sustained neutrophil and platelet recovery).
And the researchers found similar gene expression profiles between macaque and human CD34+ CD45RA- CD90+ HSCs.
The team therefore believes these findings could have implications for HSC transplants in humans.
The researchers are now working to move their findings into the clinic with the hopes of integrating them in ongoing clinical trials. The team is currently looking for commercial partners. ![]()
Researchers say they have identified a subpopulation of hematopoietic stem cells (HSCs) that immediately contributes to long-term, multilineage hematopoietic reconstitution after transplant.
These HSCs were discovered in macaques, but the cells are similar to a subset of HSCs found in humans.
The researchers found the 2 sets of cells behaved identically when tested in vitro.
The team believes their findings will increase the efficiency of future efforts for HSC transplants, gene therapies, and gene editing.
Hans-Peter Kiem, MD, PhD, of the Fred Hutchinson Cancer Research Center in Seattle, Washington, and his colleagues reported these findings in Science Translational Medicine.
The researchers performed HSC transplants in pig-tailed macaques, following hundreds of thousands of cells immediately after transplant and over the course of 7.5 years.
Previous reports had suggested that successive waves of progenitor cells expand and contract to establish the new bone marrow after transplant.
However, Dr Kiem and his colleagues homed in on a distinct group of HSCs that took hold early after transplant and went on to produce all cell lineages that constitute a complete blood system.
“These findings came as a surprise,” Dr Kiem said. “We had thought that there were multiple types of blood stem cells that take on different roles in rebuilding a blood and immune system. This population does it all.”
The population is a subset of CD34+ cells expressing CD90 and lacking CD45RA markers.
“The gold standard target cell population for stem cell gene therapy are cells with the marker CD34,” said study author Stefan Radtke, PhD, of the Fred Hutchinson Cancer Research Center.
“But we used 2 additional markers to further distinguish the population from the other blood stem cells.”
The researchers noted that the CD34+ CD45RA- CD90+ HSCs started repopulating the hematopoietic system within 10 days of being infused in macaques undergoing transplant.
A year later, the researchers found strong molecular traces of the cells, suggesting they were responsible for the ongoing maintenance of the newly transplanted system.
The team also determined the minimum numbers of CD34+ CD45RA- CD90+ HSCs that were necessary for successful transplant (defined as sustained neutrophil and platelet recovery).
And the researchers found similar gene expression profiles between macaque and human CD34+ CD45RA- CD90+ HSCs.
The team therefore believes these findings could have implications for HSC transplants in humans.
The researchers are now working to move their findings into the clinic with the hopes of integrating them in ongoing clinical trials. The team is currently looking for commercial partners. ![]()
Researchers say they have identified a subpopulation of hematopoietic stem cells (HSCs) that immediately contributes to long-term, multilineage hematopoietic reconstitution after transplant.
These HSCs were discovered in macaques, but the cells are similar to a subset of HSCs found in humans.
The researchers found the 2 sets of cells behaved identically when tested in vitro.
The team believes their findings will increase the efficiency of future efforts for HSC transplants, gene therapies, and gene editing.
Hans-Peter Kiem, MD, PhD, of the Fred Hutchinson Cancer Research Center in Seattle, Washington, and his colleagues reported these findings in Science Translational Medicine.
The researchers performed HSC transplants in pig-tailed macaques, following hundreds of thousands of cells immediately after transplant and over the course of 7.5 years.
Previous reports had suggested that successive waves of progenitor cells expand and contract to establish the new bone marrow after transplant.
However, Dr Kiem and his colleagues homed in on a distinct group of HSCs that took hold early after transplant and went on to produce all cell lineages that constitute a complete blood system.
“These findings came as a surprise,” Dr Kiem said. “We had thought that there were multiple types of blood stem cells that take on different roles in rebuilding a blood and immune system. This population does it all.”
The population is a subset of CD34+ cells expressing CD90 and lacking CD45RA markers.
“The gold standard target cell population for stem cell gene therapy are cells with the marker CD34,” said study author Stefan Radtke, PhD, of the Fred Hutchinson Cancer Research Center.
“But we used 2 additional markers to further distinguish the population from the other blood stem cells.”
The researchers noted that the CD34+ CD45RA- CD90+ HSCs started repopulating the hematopoietic system within 10 days of being infused in macaques undergoing transplant.
A year later, the researchers found strong molecular traces of the cells, suggesting they were responsible for the ongoing maintenance of the newly transplanted system.
The team also determined the minimum numbers of CD34+ CD45RA- CD90+ HSCs that were necessary for successful transplant (defined as sustained neutrophil and platelet recovery).
And the researchers found similar gene expression profiles between macaque and human CD34+ CD45RA- CD90+ HSCs.
The team therefore believes these findings could have implications for HSC transplants in humans.
The researchers are now working to move their findings into the clinic with the hopes of integrating them in ongoing clinical trials. The team is currently looking for commercial partners. ![]()
FDA grants product breakthrough designation for MM

The US Food and Drug Administration (FDA) has granted breakthrough therapy designation to GSK2857916, an anti-B-cell maturation antigen (BCMA) monoclonal antibody conjugated to the cytotoxic agent monomethyl auristatin-F via a non-cleavable linker.
The designation is for GSK2857916 as monotherapy for patients with multiple myeloma (MM) who have failed at least 3 prior lines of therapy, including an anti-CD38 antibody, and who are refractory to a proteasome inhibitor and an immunomodulatory agent.
The designation is based on results from a phase 1, dose-escalation and expansion study in patients with relapsed/refractory MM, irrespective of BCMA expression (NCT02064387).
Data from this ongoing trial are scheduled to be presented December 11 in an oral presentation at the 59th Annual Meeting of the American Society of Hematology (ASH) in Atlanta, Georgia.
GSK2857916 has also received orphan drug designation from the FDA and the European Medicines Agency (EMA) as well as PRIME designation from the EMA.
About breakthrough designation
The FDA’s breakthrough designation is intended to expedite the development and review of new treatments for serious or life-threatening conditions. The designation entitles the company developing a therapy to more intensive FDA guidance on an efficient and accelerated development program, as well as eligibility for other actions to expedite FDA review, such as rolling submission and priority review.
To earn breakthrough designation, a treatment must show encouraging early clinical results demonstrating substantial improvement over available therapies with regard to a clinically significant endpoint, or it must fulfill an unmet need.
Orphan and PRIME designations
The FDA grants orphan designation to therapies intended to treat conditions that affect fewer than 200,000 people in the US. The designation qualifies a drug’s sponsor for various development incentives of the Orphan Drug Act, including tax credits for qualified clinical testing and 7 years of market exclusivity.
In Europe, sponsors who obtain orphan designation for a potential new medicine benefit from a range of incentives, including protocol assistance, access to the centralized procedure, 10 years of market exclusivity, and fee reductions.
The EMA grants PRIME designation to enhance support for the development of medicines that target an unmet medical need. The designation is based on enhanced interaction between sponsor companies and the EMA to optimize development plans and speed up evaluation so these medicines can reach patients earlier. ![]()
The US Food and Drug Administration (FDA) has granted breakthrough therapy designation to GSK2857916, an anti-B-cell maturation antigen (BCMA) monoclonal antibody conjugated to the cytotoxic agent monomethyl auristatin-F via a non-cleavable linker.
The designation is for GSK2857916 as monotherapy for patients with multiple myeloma (MM) who have failed at least 3 prior lines of therapy, including an anti-CD38 antibody, and who are refractory to a proteasome inhibitor and an immunomodulatory agent.
The designation is based on results from a phase 1, dose-escalation and expansion study in patients with relapsed/refractory MM, irrespective of BCMA expression (NCT02064387).
Data from this ongoing trial are scheduled to be presented December 11 in an oral presentation at the 59th Annual Meeting of the American Society of Hematology (ASH) in Atlanta, Georgia.
GSK2857916 has also received orphan drug designation from the FDA and the European Medicines Agency (EMA) as well as PRIME designation from the EMA.
About breakthrough designation
The FDA’s breakthrough designation is intended to expedite the development and review of new treatments for serious or life-threatening conditions. The designation entitles the company developing a therapy to more intensive FDA guidance on an efficient and accelerated development program, as well as eligibility for other actions to expedite FDA review, such as rolling submission and priority review.
To earn breakthrough designation, a treatment must show encouraging early clinical results demonstrating substantial improvement over available therapies with regard to a clinically significant endpoint, or it must fulfill an unmet need.
Orphan and PRIME designations
The FDA grants orphan designation to therapies intended to treat conditions that affect fewer than 200,000 people in the US. The designation qualifies a drug’s sponsor for various development incentives of the Orphan Drug Act, including tax credits for qualified clinical testing and 7 years of market exclusivity.
In Europe, sponsors who obtain orphan designation for a potential new medicine benefit from a range of incentives, including protocol assistance, access to the centralized procedure, 10 years of market exclusivity, and fee reductions.
The EMA grants PRIME designation to enhance support for the development of medicines that target an unmet medical need. The designation is based on enhanced interaction between sponsor companies and the EMA to optimize development plans and speed up evaluation so these medicines can reach patients earlier. ![]()
The US Food and Drug Administration (FDA) has granted breakthrough therapy designation to GSK2857916, an anti-B-cell maturation antigen (BCMA) monoclonal antibody conjugated to the cytotoxic agent monomethyl auristatin-F via a non-cleavable linker.
The designation is for GSK2857916 as monotherapy for patients with multiple myeloma (MM) who have failed at least 3 prior lines of therapy, including an anti-CD38 antibody, and who are refractory to a proteasome inhibitor and an immunomodulatory agent.
The designation is based on results from a phase 1, dose-escalation and expansion study in patients with relapsed/refractory MM, irrespective of BCMA expression (NCT02064387).
Data from this ongoing trial are scheduled to be presented December 11 in an oral presentation at the 59th Annual Meeting of the American Society of Hematology (ASH) in Atlanta, Georgia.
GSK2857916 has also received orphan drug designation from the FDA and the European Medicines Agency (EMA) as well as PRIME designation from the EMA.
About breakthrough designation
The FDA’s breakthrough designation is intended to expedite the development and review of new treatments for serious or life-threatening conditions. The designation entitles the company developing a therapy to more intensive FDA guidance on an efficient and accelerated development program, as well as eligibility for other actions to expedite FDA review, such as rolling submission and priority review.
To earn breakthrough designation, a treatment must show encouraging early clinical results demonstrating substantial improvement over available therapies with regard to a clinically significant endpoint, or it must fulfill an unmet need.
Orphan and PRIME designations
The FDA grants orphan designation to therapies intended to treat conditions that affect fewer than 200,000 people in the US. The designation qualifies a drug’s sponsor for various development incentives of the Orphan Drug Act, including tax credits for qualified clinical testing and 7 years of market exclusivity.
In Europe, sponsors who obtain orphan designation for a potential new medicine benefit from a range of incentives, including protocol assistance, access to the centralized procedure, 10 years of market exclusivity, and fee reductions.
The EMA grants PRIME designation to enhance support for the development of medicines that target an unmet medical need. The designation is based on enhanced interaction between sponsor companies and the EMA to optimize development plans and speed up evaluation so these medicines can reach patients earlier. ![]()
Cancer patients prefer computer-free interactions

SAN DIEGO—A new study suggests patients with advanced cancer may prefer doctors who do not use a computer while communicating with them.
Most of the 120 patients studied said they preferred face-to-face consultations in which a doctor used a notepad rather than a computer.
Doctors who did not use a computer were perceived as more compassionate, communicative, and professional.
These findings were presented at the 2017 Palliative and Supportive Care in Oncology Symposium (abstract 26*).
“To our knowledge, this is the only study that compares exam room interactions between people with advanced cancer and their physicians, with or without a computer present,” said study investigator Ali Haider, MD, of the University of Texas MD Anderson Cancer Center in Houston.
For this study, Dr Haider and his colleagues enrolled 120 patients with localized, recurrent, or metastatic disease. The patients’ median ECOG performance status was 2.
All patients were English speakers, they had a median age of 58 (range, 44-66), and 55% were female. Sixty-seven percent of patients were white, 18% were Hispanic, 13% were African American, and 2% were “other.” Forty-one percent of patients had completed college.
According to the Edmonton Symptom Assessment System, patients’ median pain score was 5 (range, 2-7), and their median fatigue score was 4 (range, 3-7). According to the Hospital Anxiety and Depression Scale, patients’ median anxiety score was 6 (range, 4-8), and their median depression score was 6 (range, 4-9).
The intervention
The investigators randomly assigned patients to watch different videos showing doctor-patient interactions with and without computer use. The team had filmed 4 short videos that featured actors playing the parts of doctor and patient.
All study participants were blinded to the hypothesis of the study. The actors were carefully scripted and used the same gestures, expressions, and other nonverbal communication in each video to minimize bias.
Video 1 involved Doctor A in a face-to-face consultation with just a notepad in hand, and Video 2 involved Doctor A in a consultation using a computer.
Video 3 involved Doctor B in a face-to-face consultation with just a notepad in hand, and Video 4 involved Doctor B in a consultation using a computer.
Doctors A and B looked similar, which was intended to minimize bias.
After viewing their first video, patients completed a validated questionnaire rating the doctor’s communication skills, professionalism, and compassion.
Subsequently, each group was assigned to a video topic (face-to-face or computer) they had not viewed previously featuring the doctor they had not viewed in the first video.
A follow-up questionnaire was given after this round of viewing, and the patients were also asked to rate their overall physician preference.
Results
After the first round of viewing, the patients gave better ratings to doctors (A or B) in the face-to-face videos than in the computer videos. Face-to-face doctors were rated significantly higher for compassion (P=0.0003), communication skills (P=0.0012), and professionalism (P=0.0001).
After patients had watched both videos, doctors in the face-to-face videos still had better scores for compassion, communication, and professionalism (P<0.001 for all).
Most patients (72%) said they preferred the face-to-face consultation, while 8% said they preferred the computer consultation, and 20% said they had no preference.
Dr Haider said a possible explanation for these findings is that patients with serious chronic illnesses might value undivided attention from their physicians, and patients might perceive providers using computers as more distracted or multitasking during visits.
“We know that having a good rapport with patients can be extremely beneficial for their health,” Dr Haider said. “Patients with advanced disease need the cues that come with direct interaction to help them along with their care.”
However, Dr Haider also noted that additional research is needed to confirm these results. And he said perceptions might be different in a younger population with higher computer literacy. ![]()
*Data in the abstract differ from the presentation.
SAN DIEGO—A new study suggests patients with advanced cancer may prefer doctors who do not use a computer while communicating with them.
Most of the 120 patients studied said they preferred face-to-face consultations in which a doctor used a notepad rather than a computer.
Doctors who did not use a computer were perceived as more compassionate, communicative, and professional.
These findings were presented at the 2017 Palliative and Supportive Care in Oncology Symposium (abstract 26*).
“To our knowledge, this is the only study that compares exam room interactions between people with advanced cancer and their physicians, with or without a computer present,” said study investigator Ali Haider, MD, of the University of Texas MD Anderson Cancer Center in Houston.
For this study, Dr Haider and his colleagues enrolled 120 patients with localized, recurrent, or metastatic disease. The patients’ median ECOG performance status was 2.
All patients were English speakers, they had a median age of 58 (range, 44-66), and 55% were female. Sixty-seven percent of patients were white, 18% were Hispanic, 13% were African American, and 2% were “other.” Forty-one percent of patients had completed college.
According to the Edmonton Symptom Assessment System, patients’ median pain score was 5 (range, 2-7), and their median fatigue score was 4 (range, 3-7). According to the Hospital Anxiety and Depression Scale, patients’ median anxiety score was 6 (range, 4-8), and their median depression score was 6 (range, 4-9).
The intervention
The investigators randomly assigned patients to watch different videos showing doctor-patient interactions with and without computer use. The team had filmed 4 short videos that featured actors playing the parts of doctor and patient.
All study participants were blinded to the hypothesis of the study. The actors were carefully scripted and used the same gestures, expressions, and other nonverbal communication in each video to minimize bias.
Video 1 involved Doctor A in a face-to-face consultation with just a notepad in hand, and Video 2 involved Doctor A in a consultation using a computer.
Video 3 involved Doctor B in a face-to-face consultation with just a notepad in hand, and Video 4 involved Doctor B in a consultation using a computer.
Doctors A and B looked similar, which was intended to minimize bias.
After viewing their first video, patients completed a validated questionnaire rating the doctor’s communication skills, professionalism, and compassion.
Subsequently, each group was assigned to a video topic (face-to-face or computer) they had not viewed previously featuring the doctor they had not viewed in the first video.
A follow-up questionnaire was given after this round of viewing, and the patients were also asked to rate their overall physician preference.
Results
After the first round of viewing, the patients gave better ratings to doctors (A or B) in the face-to-face videos than in the computer videos. Face-to-face doctors were rated significantly higher for compassion (P=0.0003), communication skills (P=0.0012), and professionalism (P=0.0001).
After patients had watched both videos, doctors in the face-to-face videos still had better scores for compassion, communication, and professionalism (P<0.001 for all).
Most patients (72%) said they preferred the face-to-face consultation, while 8% said they preferred the computer consultation, and 20% said they had no preference.
Dr Haider said a possible explanation for these findings is that patients with serious chronic illnesses might value undivided attention from their physicians, and patients might perceive providers using computers as more distracted or multitasking during visits.
“We know that having a good rapport with patients can be extremely beneficial for their health,” Dr Haider said. “Patients with advanced disease need the cues that come with direct interaction to help them along with their care.”
However, Dr Haider also noted that additional research is needed to confirm these results. And he said perceptions might be different in a younger population with higher computer literacy. ![]()
*Data in the abstract differ from the presentation.
SAN DIEGO—A new study suggests patients with advanced cancer may prefer doctors who do not use a computer while communicating with them.
Most of the 120 patients studied said they preferred face-to-face consultations in which a doctor used a notepad rather than a computer.
Doctors who did not use a computer were perceived as more compassionate, communicative, and professional.
These findings were presented at the 2017 Palliative and Supportive Care in Oncology Symposium (abstract 26*).
“To our knowledge, this is the only study that compares exam room interactions between people with advanced cancer and their physicians, with or without a computer present,” said study investigator Ali Haider, MD, of the University of Texas MD Anderson Cancer Center in Houston.
For this study, Dr Haider and his colleagues enrolled 120 patients with localized, recurrent, or metastatic disease. The patients’ median ECOG performance status was 2.
All patients were English speakers, they had a median age of 58 (range, 44-66), and 55% were female. Sixty-seven percent of patients were white, 18% were Hispanic, 13% were African American, and 2% were “other.” Forty-one percent of patients had completed college.
According to the Edmonton Symptom Assessment System, patients’ median pain score was 5 (range, 2-7), and their median fatigue score was 4 (range, 3-7). According to the Hospital Anxiety and Depression Scale, patients’ median anxiety score was 6 (range, 4-8), and their median depression score was 6 (range, 4-9).
The intervention
The investigators randomly assigned patients to watch different videos showing doctor-patient interactions with and without computer use. The team had filmed 4 short videos that featured actors playing the parts of doctor and patient.
All study participants were blinded to the hypothesis of the study. The actors were carefully scripted and used the same gestures, expressions, and other nonverbal communication in each video to minimize bias.
Video 1 involved Doctor A in a face-to-face consultation with just a notepad in hand, and Video 2 involved Doctor A in a consultation using a computer.
Video 3 involved Doctor B in a face-to-face consultation with just a notepad in hand, and Video 4 involved Doctor B in a consultation using a computer.
Doctors A and B looked similar, which was intended to minimize bias.
After viewing their first video, patients completed a validated questionnaire rating the doctor’s communication skills, professionalism, and compassion.
Subsequently, each group was assigned to a video topic (face-to-face or computer) they had not viewed previously featuring the doctor they had not viewed in the first video.
A follow-up questionnaire was given after this round of viewing, and the patients were also asked to rate their overall physician preference.
Results
After the first round of viewing, the patients gave better ratings to doctors (A or B) in the face-to-face videos than in the computer videos. Face-to-face doctors were rated significantly higher for compassion (P=0.0003), communication skills (P=0.0012), and professionalism (P=0.0001).
After patients had watched both videos, doctors in the face-to-face videos still had better scores for compassion, communication, and professionalism (P<0.001 for all).
Most patients (72%) said they preferred the face-to-face consultation, while 8% said they preferred the computer consultation, and 20% said they had no preference.
Dr Haider said a possible explanation for these findings is that patients with serious chronic illnesses might value undivided attention from their physicians, and patients might perceive providers using computers as more distracted or multitasking during visits.
“We know that having a good rapport with patients can be extremely beneficial for their health,” Dr Haider said. “Patients with advanced disease need the cues that come with direct interaction to help them along with their care.”
However, Dr Haider also noted that additional research is needed to confirm these results. And he said perceptions might be different in a younger population with higher computer literacy. ![]()
*Data in the abstract differ from the presentation.
Acute Management of Severe Asymptomatic Hypertension
IN THIS ARTICLE
- Patient history; what to ask
- Cardiovascular risk factors
- Disposition pathway
- Oral medications
Approximately one in three US adults, or about 75 million people, have high blood pressure (BP), which has been defined as a BP of 140/90 mm Hg or higher.1 Unfortunately, only about half (54%) of those affected have their condition under optimal control.1 From an epidemiologic standpoint, hypertension has the distinction of being the most common chronic condition in the US, affecting about 54% of persons ages 55 to 64 and about 73% of those 75 and older.2,3 It is the number one reason patients schedule office visits with physicians; it accounts for the most prescriptions; and it is a major risk factor for heart disease and stroke, as well as a significant contributor to mortality throughout the world.4
HYPERTENSIVE URGENCY VS EMERGENCY
Hypertensive urgencies and emergencies account for approximately 27% of all medical emergencies and 2% to 3% of all annual visits to the emergency department (ED).5 Hypertensive urgency, or severe asymptomatic hypertension, is a common complaint in urgent care clinics and primary care offices as well. It is often defined as a systolic BP (SBP) of ≥ 160 mm Hg and/or a diastolic BP (DBP) ≥ 100 mm Hg with no associated end-organ damage.5-7 Patients may experience hypertensive urgency if they have been noncompliant with their antihypertensive drug regimen; present with pain; have white-coat hypertension or anxiety; or use recreational drugs (eg, sympathomimetics).5,8-10
Alternatively, hypertensive emergency, also known as hypertensive crisis, is generally defined as elevated BP > 180/120 mm Hg. Equally important, it is associated with signs, symptoms, or laboratory values indicative of target end-organ damage, such as cerebrovascular accident, myocardial infarction (MI), aortic dissection, acute left ventricular failure, acute pulmonary edema, acute renal failure, acute mental status changes (hypertensive encephalopathy), and eclampsia.5,7,8,11,12
Determining appropriate management for patients with hypertensive urgency is controversial among clinicians. Practice patterns range from full screening and “rule-outs”—with prompt initiation of antihypertensive agents, regardless of whether the patient is symptomatic—to sending the patient home with minimal screening, laboratory testing, or treatment.
This article offers a guided approach to managing patients with hypertensive urgency in a logical fashion, based on risk stratification, thereby avoiding both extremes (extensive unnecessary workup or discharge without workup resulting in adverse outcomes). It is vital to differentiate between patients with hypertensive emergency, in which BP should be lowered in minutes, and patients with hypertensive urgency, in which BP can be lowered more slowly.12

PATHOPHYSIOLOGY
Normally, when BP increases, blood vessel diameter changes in response; this autoregulation serves to limit damage. However, when BP increases abruptly, the body’s ability to hemodynamically calibrate to such a rapid change is impeded, thus allowing for potential end-organ damage.5,12 The increased vascular resistance observed in many patients with hypertension appears to be an autoregulatory process that helps to maintain a normal or viable level of tissue blood flow and organ perfusion despite the increased BP, rather than a primary cause of the hypertension.13
The exact physiology of hypertensive urgencies is not clearly understood, because of the multifactorial nature of the process. One leading theory is that circulating humoral vasoconstrictors cause an abrupt increase in systemic vascular resistance, which in turn causes mechanical shear stress to the endothelial wall. This endothelial damage promotes more vasoconstriction, platelet aggregation, and activation of the renin-angiotensin-aldosterone system, which thereby increases release of angiotensin II and various cytokines.14
HISTORY AND PHYSICAL
A detailed medical history is of utmost importance in distinguishing patients who present with asymptomatic hypertensive urgency from those experiencing a hypertensive emergency. In addition, obtain a full medication list, including any nutritional supplements or illicit drugs the patient may be taking. Question the patient regarding medication adherence; some may not be taking antihypertensive agents as prescribed or may have altered the dosing frequency in an effort to extend the duration of their prescription.5,8 Table 1 lists pertinent questions to ask at presentation; the answers will dictate who needs further workup and possible admission as well as who will require screening for end-organ damage.7
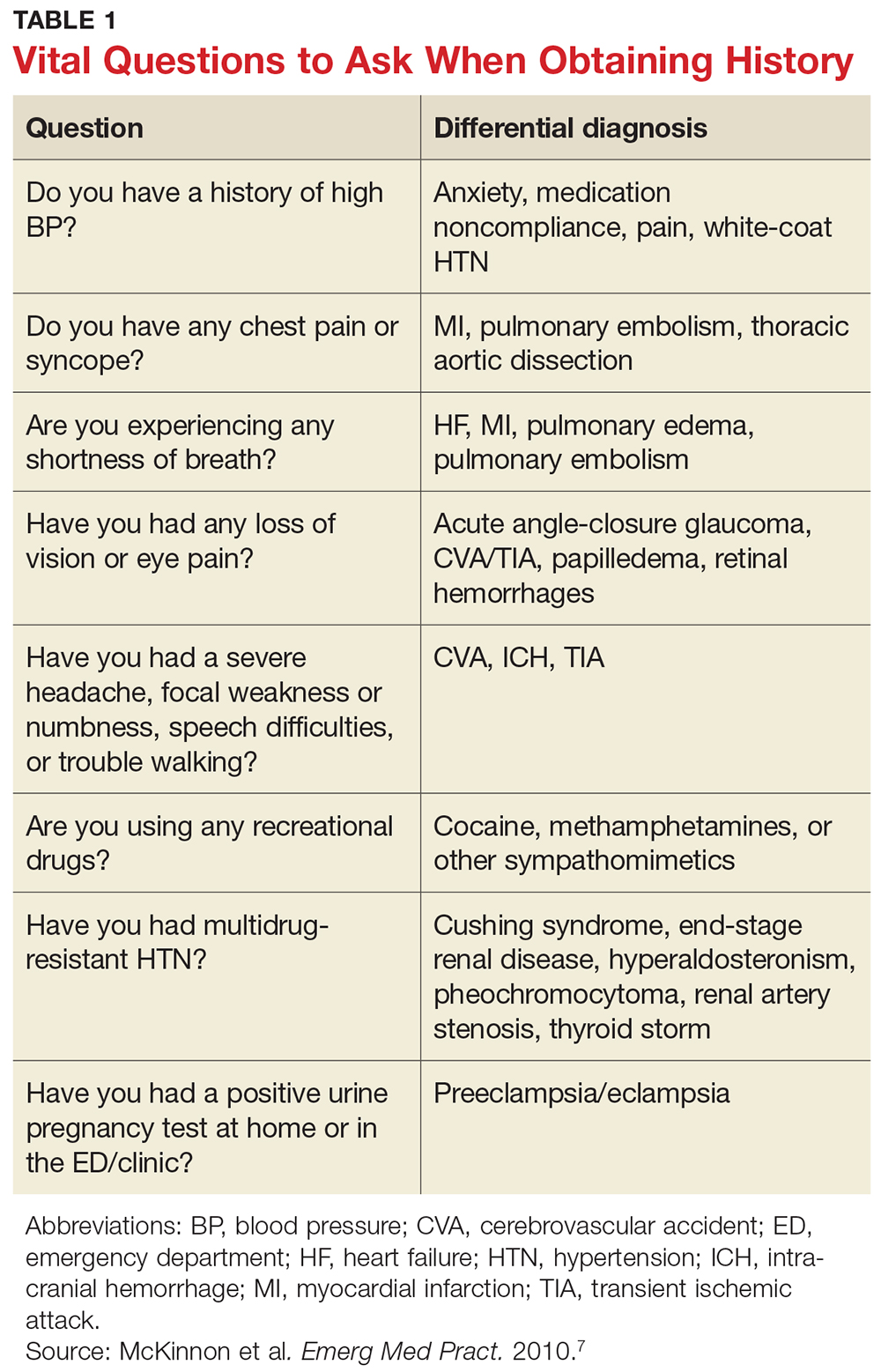
The physical exam should focus primarily on a thorough cardiopulmonary and neurologic examination, as well as funduscopic examination, if needed. A complete set of vital signs should be recorded upon the patient’s arrival to the ED or clinic and should be repeated on the opposite arm for verification. Beginning with the eyes, conduct a thorough funduscopic examination to evaluate for papilledema or hemorrhages.5 During the cardiopulmonary exam, attention should be focused on signs of congestive heart failure and/or pulmonary edema, such as increased jugular vein distension, an S3 gallop, peripheral edema, and pulmonary rales. The neurologic exam is essential in evaluating for cerebrovascular accident, transient ischemic attack, or intracranial hemorrhage. A full cranial nerve examination is necessary, in addition to motor and sensory testing, at minimum.5,9
RISK STRATIFICATION
According to the 2013 Task Force of the European Society of Hypertension (ESH) and the European Society of Cardiology (ESC), several risk factors contribute to overall cardiovascular risk in asymptomatic patients presenting with severe hypertension (see Table 2).8 This report has been monumental in linking grades of hypertension directly to cardiovascular risk factors, but it differs from that recently published by the Eighth Joint National Committee (JNC 8), which offers evidence-based guidelines for the management of high BP in the general population of adults (with some modifications for individuals with diabetes or chronic kidney disease or of black ethnicity).15
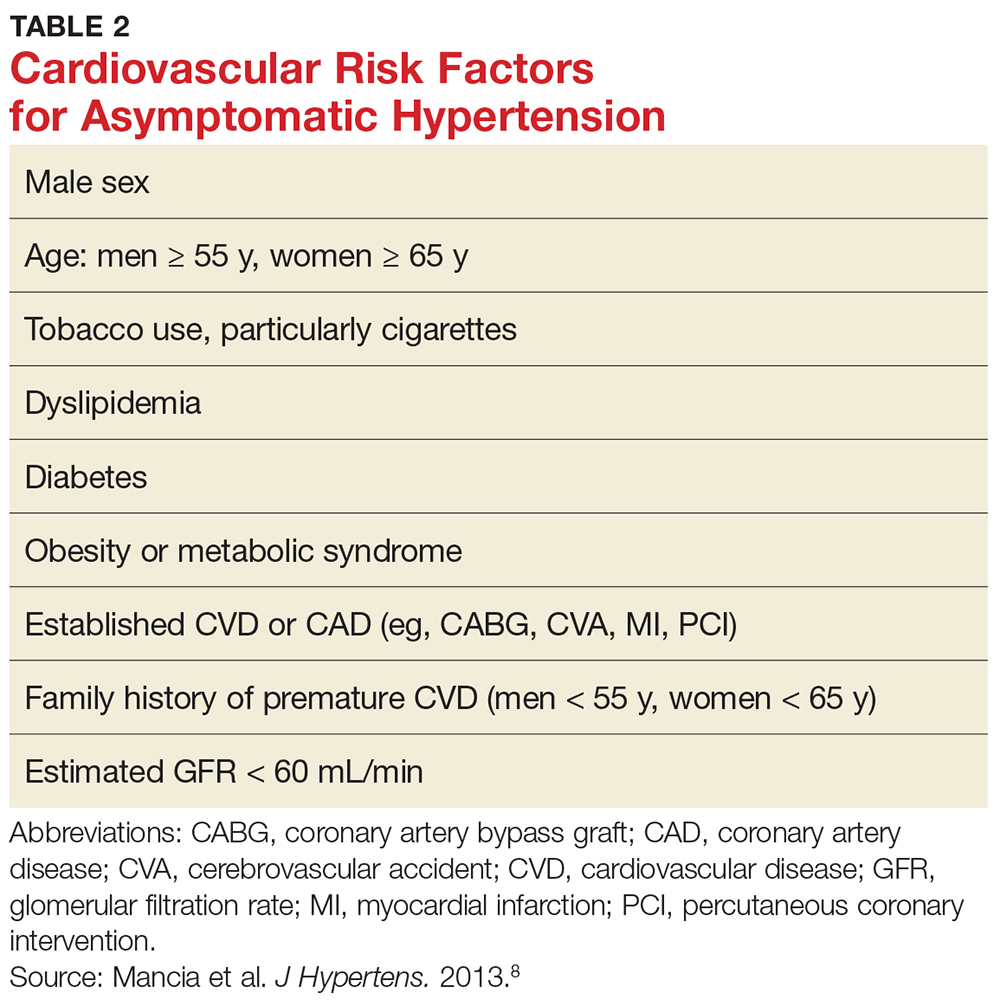
According to the ESH/ESC study, patients with one or two risk factors who have grade 1 hypertension (SBP 140-159 mm Hg) are at moderate risk for cardiovascular disease (CVD) and patients with grade 2 (SBP 160-179 mm Hg) or grade 3 (SBP ≥ 180 mm Hg) hypertension are at moderate-to-high risk and high risk, respectively.8 Patients with three or more risk factors, or who already have end-organ damage, diabetes, or chronic kidney disease, enter the high-risk category for CVD even at grade 1 hypertension.8
These cardiovascular risk factors can and should be used as guidelines for deciding who needs further screening and who may have benign causes of severe hypertension (eg, white-coat hypertension, anxiety) that can be managed safely in an outpatient setting. In the author’s opinion, patients with known cardiovascular risk factors, those with signs or symptoms of end-organ damage, and those with test results suggestive of end-organ damage should have a more immediate treatment strategy initiated.
Numerous observational studies have shown a direct relationship between systemic hypertension and CVD risk in men and women of various ages, races, and ethnicities, regardless of other risk factors for CVD.12 In patients with diabetes, uncontrolled hypertension is a strong predictor of cardiovascular morbidity and mortality and of progressive nephropathy leading to chronic kidney disease.8
SCREENING
Results from the following tests may provide useful clues in the workup of a patient with hypertensive urgency.
Basic metabolic panel. Many EDs and primary care offices offer point-of-care testing that can typically give a rapid (< 10 min) result of a basic metabolic panel. This useful, quick screening tool can identify renal failure due to chronic untreated hypertension, acute renal failure, or other disease states that cause electrolyte abnormalities such as hyperaldosteronism (hypertension with hypokalemia) or Cushing syndrome (hypertension with hypernatremia and hyperkalemia).7
Cardiac enzymes. Measurement of cardiac troponins (T or I) may provide confirmatory evidence of myocardial necrosis within two to three hours of suspected acute MI.16,17 These tests are now available in most EDs and some clinics with point-of-care testing. A variety of current guidelines advocate repeat cardiac enzyme measurements at various time points, depending on results of initial testing and concomitant risk factors. These protocols vary by facility.
ECG. Obtaining an ECG is another quick, easy, and useful way to screen patients presenting with severe hypertensive urgency. Evidence of left ventricular hypertrophy suggests an increased risk for MI, stroke, heart failure, and sudden death.7,18-20 The Cornell criteria of summing the R wave in aVL and the S wave in V3, with a cutoff of 2.8 mV in men and 2.0 mV in women, has been shown to be the best predictor of future cardiovascular mortality.7 While an isolated finding of left ventricular hypertrophy on an ECG—in and of itself—may have limited value for an individual patient, this finding coupled with other risk factors may alter the provider’s assessment.
Chest radiograph. A chest radiograph can be helpful when used in conjunction with physical exam findings that suggest pulmonary edema and cardiomegaly.7 Widened mediastinum and tortuous aorta may also be evident on chest x-ray, necessitating further workup and imaging.
Urinalysis. In a patient presenting with asymptomatic hypertensive urgency, a urine dipstick result that shows new-onset proteinuria, while not definitive for diagnosis of nephrotic syndrome, may certainly prove helpful in the patient’s workup.5,13
Urine drug screen. In patients without a history of hypertension who present with asymptomatic hypertensive urgency, the urine drug screen may ascertain exposure to cocaine, amphetamine, or phencyclidine.
Pregnancy test. A pregnancy test is essential for any female patient of childbearing age presenting to the ED, and a positive result may be concerning for preeclampsia in a hypertensive patient with no prior history of the condition.7
TREATMENT
Knowing who to treat and when is a vast area of debate among emergency and primary care providers. Patients with hypertension who have established risk factors are known to have worse outcomes than those who may be otherwise healthy. Some clinicians believe that patients presenting with hypertensive urgency should be discharged home without screening and/or treatment. However, because uncontrolled severe hypertension can lead to acute complications (eg, MI, cerebrovascular accident), in practice, many providers are unwilling to send the patient home without workup.12 The patient’s condition must be viewed in the context of the entire disease spectrum, including risk factors.
The Figure offers a disposition pathway of recommendations based on risk stratification as well as screening tools for some of the less common causes of hypertensive urgency. Regardless of the results of screening tests or the decision to treat, affected patients require close primary care follow-up. Many of these patients may need further testing and careful management of their BP medication regimen.
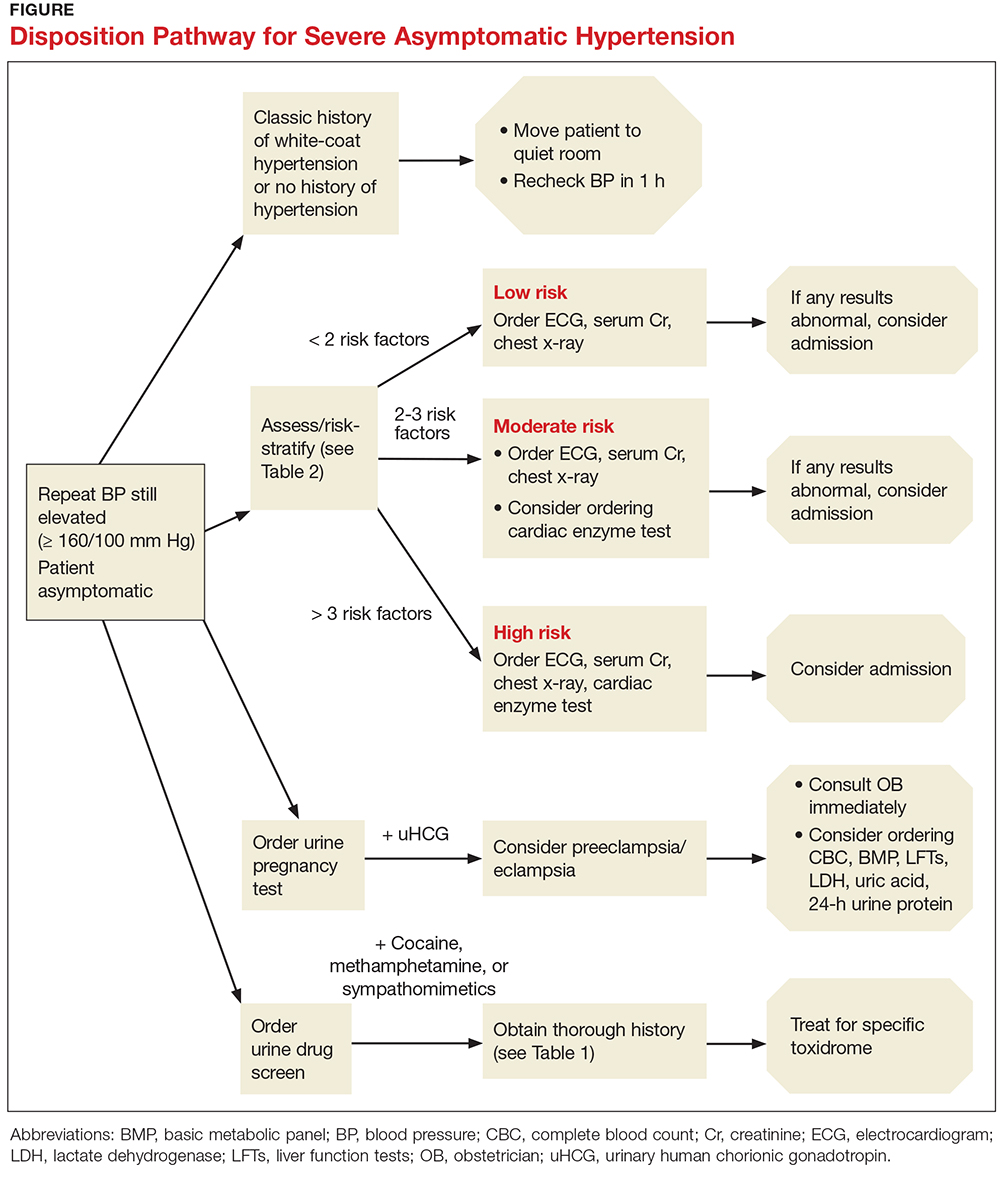
How to treat
For patients with severe asymptomatic hypertension, if the history, physical, and screening tests do not show evidence of end-organ damage, BP can be controlled within 24 to 48 hours.5,10,11,21 In adults with hypertensive urgency, the most reasonable goal is to reduce the BP to ≤ 160/100 mm Hg5-7; however, the mean arterial pressure should not be lowered by more than 25% within the first two to three hours.13
Patients at high risk for imminent neurovascular, cardiovascular, renovascular, or pulmonary events should have their BP lowered over a period of hours, not minutes. In fact, there is evidence that rapid lowering of BP in asymptomatic patients may cause adverse outcomes.6 For example, in patients with acute ischemic stroke, increases in cerebral perfusion pressure promote an increase in vascular resistance—but decreasing the cerebral perfusion pressure abruptly will thereby decrease the cerebral blood flow, potentially causing cerebral ischemia or a worsening of the stroke.9,14
Treatment options
A broad spectrum of therapeutic options has proven helpful in lowering BP over a short period of time, including oral captopril, clonidine, hydralazine, labetalol, and hydrochlorothiazide (see Table 3).7,9,12,15 Nifedipine is contraindicated because of the abrupt and often unpredictable reduction in BP and associated myocardial ischemia, especially in patients with MI or left ventricular hypertrophy.14,22,23 In cases of hypertensive urgency secondary to cocaine abuse, benzodiazepines would be the drug of choice and ß-blockers should be avoided due to the risk for coronary vasoconstriction.7
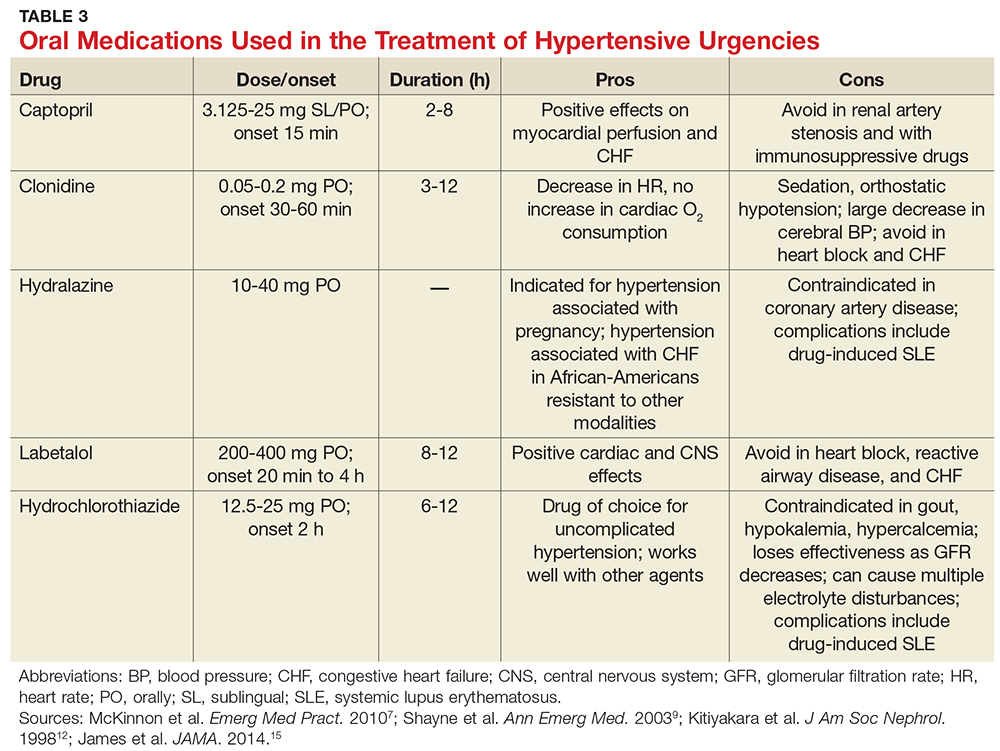
For patients with previously treated hypertension, the following options are reasonable: Increase the dose of the current antihypertensive medication; add another agent; reinstitute prior antihypertensive medications in nonadherent patients; or add a diuretic.
In patients with previously untreated hypertension, no clear evidence supports using one particular agent over another. However, initial treatment options that are generally considered safe include an ACE inhibitor, an angiotensin receptor blocker, a calcium channel blocker, or a thiazide diuretic.15 A few examples of medications within these categories include lisinopril (10 mg PO qd), losartan (50 mg PO qd), amlodipine (2.5 mg PO qd), or hydrochlorothiazide (25 mg PO qd).
Close follow-up is essential when an antihypertensive medication is started or reinstituted. Encourage the patient to reestablish care with their primary care provider (if you do not fill that role). You may need to refer the patient to a new provider or, in some cases, have the patient return to the ED for a repeat BP check.
CONCLUSION
The challenges of managing patients with hypertensive urgency are complicated by low follow-up rates with primary physicians, difficulty in obtaining referrals and follow-up for the patient, and hesitancy of providers to start patients on new BP medications. This article clarifies a well-defined algorithm for how to screen and risk-stratify patients who present to the ED or primary care office with hypertensive urgency.
1. CDC. High blood pressure fact sheet. www.cdc.gov/dhdsp/data_statistics/fact_sheets/fs_bloodpressure.htm. Accessed September 26, 2017.
2. Decker WW, Godwin SA, Hess EP, et al; American College of Emergency Physicians Clinical Policies Subcommittee (Writing Committee) on Asymptomatic Hypertension in the ED. Clinical policy: critical issues in the evaluation and management of adult patients with asymptomatic hypertension in the emergency department. Ann Emerg Med. 2006;47(3):237-249.
3. CDC. High blood pressure facts. www.cdc.gov/bloodpressure/facts.htm. Accessed October 19, 2017.
4. World Health Organization. Global Health Risks: Mortality and Burden of Disease Attributable to Selected Major Risks. Geneva, Switzerland: WHO; 2009. www.who.int/healthinfo/global_burden_disease/GlobalHealthRisks_report_full.pdf. Accessed October 19, 2017.
5. Stewart DL, Feinstein SE, Colgan R. Hypertensive urgencies and emergencies. Prim Care. 2006;33(3):613-623.
6. Wolf SJ, Lo B, Shih RD, et al; American College of Emergency Physicians Clinical Policies Committee. Clinical policy: critical issues in the evaluation and management of adult patients in the emergency department with asymptomatic elevated blood pressure. Ann Emerg Med. 2013;62(1):59-68.
7. McKinnon M, O’Neill JM. Hypertension in the emergency department: treat now, later, or not at all. Emerg Med Pract. 2010;12(6):1-22.
8. Mancia G, Fagard R, Narkiewicz K, et al. 2013 ESH/ESC Guidelines for the management of arterial hypertension: the Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens. 2013;31(7): 1281-1357.
9. Shayne PH, Pitts SR. Severely increased blood pressure in the emergency department. Ann Emerg Med. 2003;41(4): 513-529.
10. Aggarwal M, Khan IA. Hypertensive crisis: hypertensive emergencies and urgencies. Cardiol Clin. 2006;24(1):135-146.
11. Houston MC. The comparative effects of clonidine hydrochloride and nifedipine in the treatment of hypertensive crises. Am Heart J. 1998;115(1 pt 1):152-159.
12. Kitiyakara C, Guaman NJ. Malignant hypertension and hypertensive emergencies. J Am Soc Nephrol. 1998;9(1):133-142.
13. Elliott WJ. Hypertensive emergencies. Crit Care Clin. 2001;17(2):435-451.
14. Papadopoulos DP, Mourouzis I, Thomopoulos C, et al. Hypertension crisis. Blood Press. 2010;19(6):328-336.
15. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311(5):507-520.
16. Keller T, Zeller T, Peetz D, et al. Sensitive troponin I assay in early diagnosis of acute myocardial infarction. N Engl J Med. 2009;361(9):868-877.
17. Reichlin T, Hochholzer W, Bassetti S, et al. Early diagnosis of myocardial infarction with sensitive cardiac troponin assays. N Engl J Med. 2009;361(9):858-867.
18. Ghali JK, Kadakia S, Cooper RS, Liao YL. Impact of left ventricular hypertrophy on ventricular arrhythmias in the absence of coronary artery disease. J Am Coll Cardiol. 1991;17(6):1277-1282.
19. Bang CN, Soliman EZ, Simpson LM, et al. Electrocardiographic left ventricular hypertrophy predicts cardiovascular morbidity and mortality in hypertensive patients: the ALLHAT study. Am J Hypertens. 2017;30(9):914-922.
20. Hsieh BP, Pham MX, Froelicher VF. Prognostic value of electrocardiographic criteria for left ventricular hypertrophy. Am Heart J. 2005;150(1):161-167.
21. Kinsella K, Baraff LJ. Initiation of therapy for asymptomatic hypertension in the emergency department. Ann Emerg Med. 2009;54(6):791-792.
22. O’Mailia JJ, Sander GE, Giles TD. Nifedipine-associated myocardial ischemia or infarction in the treatment of hypertensive urgencies. Ann Intern Med. 1987;107(2):185-186.
23. Grossman E, Messerli FH, Grodzicki T, Kowey P. Should a moratorium be placed on sublingual nifedipine capsules given for hypertensive emergencies and pseudoemergencies? JAMA. 1996;276(16):1328-1331.
IN THIS ARTICLE
- Patient history; what to ask
- Cardiovascular risk factors
- Disposition pathway
- Oral medications
Approximately one in three US adults, or about 75 million people, have high blood pressure (BP), which has been defined as a BP of 140/90 mm Hg or higher.1 Unfortunately, only about half (54%) of those affected have their condition under optimal control.1 From an epidemiologic standpoint, hypertension has the distinction of being the most common chronic condition in the US, affecting about 54% of persons ages 55 to 64 and about 73% of those 75 and older.2,3 It is the number one reason patients schedule office visits with physicians; it accounts for the most prescriptions; and it is a major risk factor for heart disease and stroke, as well as a significant contributor to mortality throughout the world.4
HYPERTENSIVE URGENCY VS EMERGENCY
Hypertensive urgencies and emergencies account for approximately 27% of all medical emergencies and 2% to 3% of all annual visits to the emergency department (ED).5 Hypertensive urgency, or severe asymptomatic hypertension, is a common complaint in urgent care clinics and primary care offices as well. It is often defined as a systolic BP (SBP) of ≥ 160 mm Hg and/or a diastolic BP (DBP) ≥ 100 mm Hg with no associated end-organ damage.5-7 Patients may experience hypertensive urgency if they have been noncompliant with their antihypertensive drug regimen; present with pain; have white-coat hypertension or anxiety; or use recreational drugs (eg, sympathomimetics).5,8-10
Alternatively, hypertensive emergency, also known as hypertensive crisis, is generally defined as elevated BP > 180/120 mm Hg. Equally important, it is associated with signs, symptoms, or laboratory values indicative of target end-organ damage, such as cerebrovascular accident, myocardial infarction (MI), aortic dissection, acute left ventricular failure, acute pulmonary edema, acute renal failure, acute mental status changes (hypertensive encephalopathy), and eclampsia.5,7,8,11,12
Determining appropriate management for patients with hypertensive urgency is controversial among clinicians. Practice patterns range from full screening and “rule-outs”—with prompt initiation of antihypertensive agents, regardless of whether the patient is symptomatic—to sending the patient home with minimal screening, laboratory testing, or treatment.
This article offers a guided approach to managing patients with hypertensive urgency in a logical fashion, based on risk stratification, thereby avoiding both extremes (extensive unnecessary workup or discharge without workup resulting in adverse outcomes). It is vital to differentiate between patients with hypertensive emergency, in which BP should be lowered in minutes, and patients with hypertensive urgency, in which BP can be lowered more slowly.12
PATHOPHYSIOLOGY
Normally, when BP increases, blood vessel diameter changes in response; this autoregulation serves to limit damage. However, when BP increases abruptly, the body’s ability to hemodynamically calibrate to such a rapid change is impeded, thus allowing for potential end-organ damage.5,12 The increased vascular resistance observed in many patients with hypertension appears to be an autoregulatory process that helps to maintain a normal or viable level of tissue blood flow and organ perfusion despite the increased BP, rather than a primary cause of the hypertension.13
The exact physiology of hypertensive urgencies is not clearly understood, because of the multifactorial nature of the process. One leading theory is that circulating humoral vasoconstrictors cause an abrupt increase in systemic vascular resistance, which in turn causes mechanical shear stress to the endothelial wall. This endothelial damage promotes more vasoconstriction, platelet aggregation, and activation of the renin-angiotensin-aldosterone system, which thereby increases release of angiotensin II and various cytokines.14
HISTORY AND PHYSICAL
A detailed medical history is of utmost importance in distinguishing patients who present with asymptomatic hypertensive urgency from those experiencing a hypertensive emergency. In addition, obtain a full medication list, including any nutritional supplements or illicit drugs the patient may be taking. Question the patient regarding medication adherence; some may not be taking antihypertensive agents as prescribed or may have altered the dosing frequency in an effort to extend the duration of their prescription.5,8 Table 1 lists pertinent questions to ask at presentation; the answers will dictate who needs further workup and possible admission as well as who will require screening for end-organ damage.7
The physical exam should focus primarily on a thorough cardiopulmonary and neurologic examination, as well as funduscopic examination, if needed. A complete set of vital signs should be recorded upon the patient’s arrival to the ED or clinic and should be repeated on the opposite arm for verification. Beginning with the eyes, conduct a thorough funduscopic examination to evaluate for papilledema or hemorrhages.5 During the cardiopulmonary exam, attention should be focused on signs of congestive heart failure and/or pulmonary edema, such as increased jugular vein distension, an S3 gallop, peripheral edema, and pulmonary rales. The neurologic exam is essential in evaluating for cerebrovascular accident, transient ischemic attack, or intracranial hemorrhage. A full cranial nerve examination is necessary, in addition to motor and sensory testing, at minimum.5,9
RISK STRATIFICATION
According to the 2013 Task Force of the European Society of Hypertension (ESH) and the European Society of Cardiology (ESC), several risk factors contribute to overall cardiovascular risk in asymptomatic patients presenting with severe hypertension (see Table 2).8 This report has been monumental in linking grades of hypertension directly to cardiovascular risk factors, but it differs from that recently published by the Eighth Joint National Committee (JNC 8), which offers evidence-based guidelines for the management of high BP in the general population of adults (with some modifications for individuals with diabetes or chronic kidney disease or of black ethnicity).15
According to the ESH/ESC study, patients with one or two risk factors who have grade 1 hypertension (SBP 140-159 mm Hg) are at moderate risk for cardiovascular disease (CVD) and patients with grade 2 (SBP 160-179 mm Hg) or grade 3 (SBP ≥ 180 mm Hg) hypertension are at moderate-to-high risk and high risk, respectively.8 Patients with three or more risk factors, or who already have end-organ damage, diabetes, or chronic kidney disease, enter the high-risk category for CVD even at grade 1 hypertension.8
These cardiovascular risk factors can and should be used as guidelines for deciding who needs further screening and who may have benign causes of severe hypertension (eg, white-coat hypertension, anxiety) that can be managed safely in an outpatient setting. In the author’s opinion, patients with known cardiovascular risk factors, those with signs or symptoms of end-organ damage, and those with test results suggestive of end-organ damage should have a more immediate treatment strategy initiated.
Numerous observational studies have shown a direct relationship between systemic hypertension and CVD risk in men and women of various ages, races, and ethnicities, regardless of other risk factors for CVD.12 In patients with diabetes, uncontrolled hypertension is a strong predictor of cardiovascular morbidity and mortality and of progressive nephropathy leading to chronic kidney disease.8
SCREENING
Results from the following tests may provide useful clues in the workup of a patient with hypertensive urgency.
Basic metabolic panel. Many EDs and primary care offices offer point-of-care testing that can typically give a rapid (< 10 min) result of a basic metabolic panel. This useful, quick screening tool can identify renal failure due to chronic untreated hypertension, acute renal failure, or other disease states that cause electrolyte abnormalities such as hyperaldosteronism (hypertension with hypokalemia) or Cushing syndrome (hypertension with hypernatremia and hyperkalemia).7
Cardiac enzymes. Measurement of cardiac troponins (T or I) may provide confirmatory evidence of myocardial necrosis within two to three hours of suspected acute MI.16,17 These tests are now available in most EDs and some clinics with point-of-care testing. A variety of current guidelines advocate repeat cardiac enzyme measurements at various time points, depending on results of initial testing and concomitant risk factors. These protocols vary by facility.
ECG. Obtaining an ECG is another quick, easy, and useful way to screen patients presenting with severe hypertensive urgency. Evidence of left ventricular hypertrophy suggests an increased risk for MI, stroke, heart failure, and sudden death.7,18-20 The Cornell criteria of summing the R wave in aVL and the S wave in V3, with a cutoff of 2.8 mV in men and 2.0 mV in women, has been shown to be the best predictor of future cardiovascular mortality.7 While an isolated finding of left ventricular hypertrophy on an ECG—in and of itself—may have limited value for an individual patient, this finding coupled with other risk factors may alter the provider’s assessment.
Chest radiograph. A chest radiograph can be helpful when used in conjunction with physical exam findings that suggest pulmonary edema and cardiomegaly.7 Widened mediastinum and tortuous aorta may also be evident on chest x-ray, necessitating further workup and imaging.
Urinalysis. In a patient presenting with asymptomatic hypertensive urgency, a urine dipstick result that shows new-onset proteinuria, while not definitive for diagnosis of nephrotic syndrome, may certainly prove helpful in the patient’s workup.5,13
Urine drug screen. In patients without a history of hypertension who present with asymptomatic hypertensive urgency, the urine drug screen may ascertain exposure to cocaine, amphetamine, or phencyclidine.
Pregnancy test. A pregnancy test is essential for any female patient of childbearing age presenting to the ED, and a positive result may be concerning for preeclampsia in a hypertensive patient with no prior history of the condition.7
TREATMENT
Knowing who to treat and when is a vast area of debate among emergency and primary care providers. Patients with hypertension who have established risk factors are known to have worse outcomes than those who may be otherwise healthy. Some clinicians believe that patients presenting with hypertensive urgency should be discharged home without screening and/or treatment. However, because uncontrolled severe hypertension can lead to acute complications (eg, MI, cerebrovascular accident), in practice, many providers are unwilling to send the patient home without workup.12 The patient’s condition must be viewed in the context of the entire disease spectrum, including risk factors.
The Figure offers a disposition pathway of recommendations based on risk stratification as well as screening tools for some of the less common causes of hypertensive urgency. Regardless of the results of screening tests or the decision to treat, affected patients require close primary care follow-up. Many of these patients may need further testing and careful management of their BP medication regimen.
How to treat
For patients with severe asymptomatic hypertension, if the history, physical, and screening tests do not show evidence of end-organ damage, BP can be controlled within 24 to 48 hours.5,10,11,21 In adults with hypertensive urgency, the most reasonable goal is to reduce the BP to ≤ 160/100 mm Hg5-7; however, the mean arterial pressure should not be lowered by more than 25% within the first two to three hours.13
Patients at high risk for imminent neurovascular, cardiovascular, renovascular, or pulmonary events should have their BP lowered over a period of hours, not minutes. In fact, there is evidence that rapid lowering of BP in asymptomatic patients may cause adverse outcomes.6 For example, in patients with acute ischemic stroke, increases in cerebral perfusion pressure promote an increase in vascular resistance—but decreasing the cerebral perfusion pressure abruptly will thereby decrease the cerebral blood flow, potentially causing cerebral ischemia or a worsening of the stroke.9,14
Treatment options
A broad spectrum of therapeutic options has proven helpful in lowering BP over a short period of time, including oral captopril, clonidine, hydralazine, labetalol, and hydrochlorothiazide (see Table 3).7,9,12,15 Nifedipine is contraindicated because of the abrupt and often unpredictable reduction in BP and associated myocardial ischemia, especially in patients with MI or left ventricular hypertrophy.14,22,23 In cases of hypertensive urgency secondary to cocaine abuse, benzodiazepines would be the drug of choice and ß-blockers should be avoided due to the risk for coronary vasoconstriction.7
For patients with previously treated hypertension, the following options are reasonable: Increase the dose of the current antihypertensive medication; add another agent; reinstitute prior antihypertensive medications in nonadherent patients; or add a diuretic.
In patients with previously untreated hypertension, no clear evidence supports using one particular agent over another. However, initial treatment options that are generally considered safe include an ACE inhibitor, an angiotensin receptor blocker, a calcium channel blocker, or a thiazide diuretic.15 A few examples of medications within these categories include lisinopril (10 mg PO qd), losartan (50 mg PO qd), amlodipine (2.5 mg PO qd), or hydrochlorothiazide (25 mg PO qd).
Close follow-up is essential when an antihypertensive medication is started or reinstituted. Encourage the patient to reestablish care with their primary care provider (if you do not fill that role). You may need to refer the patient to a new provider or, in some cases, have the patient return to the ED for a repeat BP check.
CONCLUSION
The challenges of managing patients with hypertensive urgency are complicated by low follow-up rates with primary physicians, difficulty in obtaining referrals and follow-up for the patient, and hesitancy of providers to start patients on new BP medications. This article clarifies a well-defined algorithm for how to screen and risk-stratify patients who present to the ED or primary care office with hypertensive urgency.
IN THIS ARTICLE
- Patient history; what to ask
- Cardiovascular risk factors
- Disposition pathway
- Oral medications
Approximately one in three US adults, or about 75 million people, have high blood pressure (BP), which has been defined as a BP of 140/90 mm Hg or higher.1 Unfortunately, only about half (54%) of those affected have their condition under optimal control.1 From an epidemiologic standpoint, hypertension has the distinction of being the most common chronic condition in the US, affecting about 54% of persons ages 55 to 64 and about 73% of those 75 and older.2,3 It is the number one reason patients schedule office visits with physicians; it accounts for the most prescriptions; and it is a major risk factor for heart disease and stroke, as well as a significant contributor to mortality throughout the world.4
HYPERTENSIVE URGENCY VS EMERGENCY
Hypertensive urgencies and emergencies account for approximately 27% of all medical emergencies and 2% to 3% of all annual visits to the emergency department (ED).5 Hypertensive urgency, or severe asymptomatic hypertension, is a common complaint in urgent care clinics and primary care offices as well. It is often defined as a systolic BP (SBP) of ≥ 160 mm Hg and/or a diastolic BP (DBP) ≥ 100 mm Hg with no associated end-organ damage.5-7 Patients may experience hypertensive urgency if they have been noncompliant with their antihypertensive drug regimen; present with pain; have white-coat hypertension or anxiety; or use recreational drugs (eg, sympathomimetics).5,8-10
Alternatively, hypertensive emergency, also known as hypertensive crisis, is generally defined as elevated BP > 180/120 mm Hg. Equally important, it is associated with signs, symptoms, or laboratory values indicative of target end-organ damage, such as cerebrovascular accident, myocardial infarction (MI), aortic dissection, acute left ventricular failure, acute pulmonary edema, acute renal failure, acute mental status changes (hypertensive encephalopathy), and eclampsia.5,7,8,11,12
Determining appropriate management for patients with hypertensive urgency is controversial among clinicians. Practice patterns range from full screening and “rule-outs”—with prompt initiation of antihypertensive agents, regardless of whether the patient is symptomatic—to sending the patient home with minimal screening, laboratory testing, or treatment.
This article offers a guided approach to managing patients with hypertensive urgency in a logical fashion, based on risk stratification, thereby avoiding both extremes (extensive unnecessary workup or discharge without workup resulting in adverse outcomes). It is vital to differentiate between patients with hypertensive emergency, in which BP should be lowered in minutes, and patients with hypertensive urgency, in which BP can be lowered more slowly.12
PATHOPHYSIOLOGY
Normally, when BP increases, blood vessel diameter changes in response; this autoregulation serves to limit damage. However, when BP increases abruptly, the body’s ability to hemodynamically calibrate to such a rapid change is impeded, thus allowing for potential end-organ damage.5,12 The increased vascular resistance observed in many patients with hypertension appears to be an autoregulatory process that helps to maintain a normal or viable level of tissue blood flow and organ perfusion despite the increased BP, rather than a primary cause of the hypertension.13
The exact physiology of hypertensive urgencies is not clearly understood, because of the multifactorial nature of the process. One leading theory is that circulating humoral vasoconstrictors cause an abrupt increase in systemic vascular resistance, which in turn causes mechanical shear stress to the endothelial wall. This endothelial damage promotes more vasoconstriction, platelet aggregation, and activation of the renin-angiotensin-aldosterone system, which thereby increases release of angiotensin II and various cytokines.14
HISTORY AND PHYSICAL
A detailed medical history is of utmost importance in distinguishing patients who present with asymptomatic hypertensive urgency from those experiencing a hypertensive emergency. In addition, obtain a full medication list, including any nutritional supplements or illicit drugs the patient may be taking. Question the patient regarding medication adherence; some may not be taking antihypertensive agents as prescribed or may have altered the dosing frequency in an effort to extend the duration of their prescription.5,8 Table 1 lists pertinent questions to ask at presentation; the answers will dictate who needs further workup and possible admission as well as who will require screening for end-organ damage.7
The physical exam should focus primarily on a thorough cardiopulmonary and neurologic examination, as well as funduscopic examination, if needed. A complete set of vital signs should be recorded upon the patient’s arrival to the ED or clinic and should be repeated on the opposite arm for verification. Beginning with the eyes, conduct a thorough funduscopic examination to evaluate for papilledema or hemorrhages.5 During the cardiopulmonary exam, attention should be focused on signs of congestive heart failure and/or pulmonary edema, such as increased jugular vein distension, an S3 gallop, peripheral edema, and pulmonary rales. The neurologic exam is essential in evaluating for cerebrovascular accident, transient ischemic attack, or intracranial hemorrhage. A full cranial nerve examination is necessary, in addition to motor and sensory testing, at minimum.5,9
RISK STRATIFICATION
According to the 2013 Task Force of the European Society of Hypertension (ESH) and the European Society of Cardiology (ESC), several risk factors contribute to overall cardiovascular risk in asymptomatic patients presenting with severe hypertension (see Table 2).8 This report has been monumental in linking grades of hypertension directly to cardiovascular risk factors, but it differs from that recently published by the Eighth Joint National Committee (JNC 8), which offers evidence-based guidelines for the management of high BP in the general population of adults (with some modifications for individuals with diabetes or chronic kidney disease or of black ethnicity).15
According to the ESH/ESC study, patients with one or two risk factors who have grade 1 hypertension (SBP 140-159 mm Hg) are at moderate risk for cardiovascular disease (CVD) and patients with grade 2 (SBP 160-179 mm Hg) or grade 3 (SBP ≥ 180 mm Hg) hypertension are at moderate-to-high risk and high risk, respectively.8 Patients with three or more risk factors, or who already have end-organ damage, diabetes, or chronic kidney disease, enter the high-risk category for CVD even at grade 1 hypertension.8
These cardiovascular risk factors can and should be used as guidelines for deciding who needs further screening and who may have benign causes of severe hypertension (eg, white-coat hypertension, anxiety) that can be managed safely in an outpatient setting. In the author’s opinion, patients with known cardiovascular risk factors, those with signs or symptoms of end-organ damage, and those with test results suggestive of end-organ damage should have a more immediate treatment strategy initiated.
Numerous observational studies have shown a direct relationship between systemic hypertension and CVD risk in men and women of various ages, races, and ethnicities, regardless of other risk factors for CVD.12 In patients with diabetes, uncontrolled hypertension is a strong predictor of cardiovascular morbidity and mortality and of progressive nephropathy leading to chronic kidney disease.8
SCREENING
Results from the following tests may provide useful clues in the workup of a patient with hypertensive urgency.
Basic metabolic panel. Many EDs and primary care offices offer point-of-care testing that can typically give a rapid (< 10 min) result of a basic metabolic panel. This useful, quick screening tool can identify renal failure due to chronic untreated hypertension, acute renal failure, or other disease states that cause electrolyte abnormalities such as hyperaldosteronism (hypertension with hypokalemia) or Cushing syndrome (hypertension with hypernatremia and hyperkalemia).7
Cardiac enzymes. Measurement of cardiac troponins (T or I) may provide confirmatory evidence of myocardial necrosis within two to three hours of suspected acute MI.16,17 These tests are now available in most EDs and some clinics with point-of-care testing. A variety of current guidelines advocate repeat cardiac enzyme measurements at various time points, depending on results of initial testing and concomitant risk factors. These protocols vary by facility.
ECG. Obtaining an ECG is another quick, easy, and useful way to screen patients presenting with severe hypertensive urgency. Evidence of left ventricular hypertrophy suggests an increased risk for MI, stroke, heart failure, and sudden death.7,18-20 The Cornell criteria of summing the R wave in aVL and the S wave in V3, with a cutoff of 2.8 mV in men and 2.0 mV in women, has been shown to be the best predictor of future cardiovascular mortality.7 While an isolated finding of left ventricular hypertrophy on an ECG—in and of itself—may have limited value for an individual patient, this finding coupled with other risk factors may alter the provider’s assessment.
Chest radiograph. A chest radiograph can be helpful when used in conjunction with physical exam findings that suggest pulmonary edema and cardiomegaly.7 Widened mediastinum and tortuous aorta may also be evident on chest x-ray, necessitating further workup and imaging.
Urinalysis. In a patient presenting with asymptomatic hypertensive urgency, a urine dipstick result that shows new-onset proteinuria, while not definitive for diagnosis of nephrotic syndrome, may certainly prove helpful in the patient’s workup.5,13
Urine drug screen. In patients without a history of hypertension who present with asymptomatic hypertensive urgency, the urine drug screen may ascertain exposure to cocaine, amphetamine, or phencyclidine.
Pregnancy test. A pregnancy test is essential for any female patient of childbearing age presenting to the ED, and a positive result may be concerning for preeclampsia in a hypertensive patient with no prior history of the condition.7
TREATMENT
Knowing who to treat and when is a vast area of debate among emergency and primary care providers. Patients with hypertension who have established risk factors are known to have worse outcomes than those who may be otherwise healthy. Some clinicians believe that patients presenting with hypertensive urgency should be discharged home without screening and/or treatment. However, because uncontrolled severe hypertension can lead to acute complications (eg, MI, cerebrovascular accident), in practice, many providers are unwilling to send the patient home without workup.12 The patient’s condition must be viewed in the context of the entire disease spectrum, including risk factors.
The Figure offers a disposition pathway of recommendations based on risk stratification as well as screening tools for some of the less common causes of hypertensive urgency. Regardless of the results of screening tests or the decision to treat, affected patients require close primary care follow-up. Many of these patients may need further testing and careful management of their BP medication regimen.
How to treat
For patients with severe asymptomatic hypertension, if the history, physical, and screening tests do not show evidence of end-organ damage, BP can be controlled within 24 to 48 hours.5,10,11,21 In adults with hypertensive urgency, the most reasonable goal is to reduce the BP to ≤ 160/100 mm Hg5-7; however, the mean arterial pressure should not be lowered by more than 25% within the first two to three hours.13
Patients at high risk for imminent neurovascular, cardiovascular, renovascular, or pulmonary events should have their BP lowered over a period of hours, not minutes. In fact, there is evidence that rapid lowering of BP in asymptomatic patients may cause adverse outcomes.6 For example, in patients with acute ischemic stroke, increases in cerebral perfusion pressure promote an increase in vascular resistance—but decreasing the cerebral perfusion pressure abruptly will thereby decrease the cerebral blood flow, potentially causing cerebral ischemia or a worsening of the stroke.9,14
Treatment options
A broad spectrum of therapeutic options has proven helpful in lowering BP over a short period of time, including oral captopril, clonidine, hydralazine, labetalol, and hydrochlorothiazide (see Table 3).7,9,12,15 Nifedipine is contraindicated because of the abrupt and often unpredictable reduction in BP and associated myocardial ischemia, especially in patients with MI or left ventricular hypertrophy.14,22,23 In cases of hypertensive urgency secondary to cocaine abuse, benzodiazepines would be the drug of choice and ß-blockers should be avoided due to the risk for coronary vasoconstriction.7
For patients with previously treated hypertension, the following options are reasonable: Increase the dose of the current antihypertensive medication; add another agent; reinstitute prior antihypertensive medications in nonadherent patients; or add a diuretic.
In patients with previously untreated hypertension, no clear evidence supports using one particular agent over another. However, initial treatment options that are generally considered safe include an ACE inhibitor, an angiotensin receptor blocker, a calcium channel blocker, or a thiazide diuretic.15 A few examples of medications within these categories include lisinopril (10 mg PO qd), losartan (50 mg PO qd), amlodipine (2.5 mg PO qd), or hydrochlorothiazide (25 mg PO qd).
Close follow-up is essential when an antihypertensive medication is started or reinstituted. Encourage the patient to reestablish care with their primary care provider (if you do not fill that role). You may need to refer the patient to a new provider or, in some cases, have the patient return to the ED for a repeat BP check.
CONCLUSION
The challenges of managing patients with hypertensive urgency are complicated by low follow-up rates with primary physicians, difficulty in obtaining referrals and follow-up for the patient, and hesitancy of providers to start patients on new BP medications. This article clarifies a well-defined algorithm for how to screen and risk-stratify patients who present to the ED or primary care office with hypertensive urgency.
1. CDC. High blood pressure fact sheet. www.cdc.gov/dhdsp/data_statistics/fact_sheets/fs_bloodpressure.htm. Accessed September 26, 2017.
2. Decker WW, Godwin SA, Hess EP, et al; American College of Emergency Physicians Clinical Policies Subcommittee (Writing Committee) on Asymptomatic Hypertension in the ED. Clinical policy: critical issues in the evaluation and management of adult patients with asymptomatic hypertension in the emergency department. Ann Emerg Med. 2006;47(3):237-249.
3. CDC. High blood pressure facts. www.cdc.gov/bloodpressure/facts.htm. Accessed October 19, 2017.
4. World Health Organization. Global Health Risks: Mortality and Burden of Disease Attributable to Selected Major Risks. Geneva, Switzerland: WHO; 2009. www.who.int/healthinfo/global_burden_disease/GlobalHealthRisks_report_full.pdf. Accessed October 19, 2017.
5. Stewart DL, Feinstein SE, Colgan R. Hypertensive urgencies and emergencies. Prim Care. 2006;33(3):613-623.
6. Wolf SJ, Lo B, Shih RD, et al; American College of Emergency Physicians Clinical Policies Committee. Clinical policy: critical issues in the evaluation and management of adult patients in the emergency department with asymptomatic elevated blood pressure. Ann Emerg Med. 2013;62(1):59-68.
7. McKinnon M, O’Neill JM. Hypertension in the emergency department: treat now, later, or not at all. Emerg Med Pract. 2010;12(6):1-22.
8. Mancia G, Fagard R, Narkiewicz K, et al. 2013 ESH/ESC Guidelines for the management of arterial hypertension: the Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens. 2013;31(7): 1281-1357.
9. Shayne PH, Pitts SR. Severely increased blood pressure in the emergency department. Ann Emerg Med. 2003;41(4): 513-529.
10. Aggarwal M, Khan IA. Hypertensive crisis: hypertensive emergencies and urgencies. Cardiol Clin. 2006;24(1):135-146.
11. Houston MC. The comparative effects of clonidine hydrochloride and nifedipine in the treatment of hypertensive crises. Am Heart J. 1998;115(1 pt 1):152-159.
12. Kitiyakara C, Guaman NJ. Malignant hypertension and hypertensive emergencies. J Am Soc Nephrol. 1998;9(1):133-142.
13. Elliott WJ. Hypertensive emergencies. Crit Care Clin. 2001;17(2):435-451.
14. Papadopoulos DP, Mourouzis I, Thomopoulos C, et al. Hypertension crisis. Blood Press. 2010;19(6):328-336.
15. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311(5):507-520.
16. Keller T, Zeller T, Peetz D, et al. Sensitive troponin I assay in early diagnosis of acute myocardial infarction. N Engl J Med. 2009;361(9):868-877.
17. Reichlin T, Hochholzer W, Bassetti S, et al. Early diagnosis of myocardial infarction with sensitive cardiac troponin assays. N Engl J Med. 2009;361(9):858-867.
18. Ghali JK, Kadakia S, Cooper RS, Liao YL. Impact of left ventricular hypertrophy on ventricular arrhythmias in the absence of coronary artery disease. J Am Coll Cardiol. 1991;17(6):1277-1282.
19. Bang CN, Soliman EZ, Simpson LM, et al. Electrocardiographic left ventricular hypertrophy predicts cardiovascular morbidity and mortality in hypertensive patients: the ALLHAT study. Am J Hypertens. 2017;30(9):914-922.
20. Hsieh BP, Pham MX, Froelicher VF. Prognostic value of electrocardiographic criteria for left ventricular hypertrophy. Am Heart J. 2005;150(1):161-167.
21. Kinsella K, Baraff LJ. Initiation of therapy for asymptomatic hypertension in the emergency department. Ann Emerg Med. 2009;54(6):791-792.
22. O’Mailia JJ, Sander GE, Giles TD. Nifedipine-associated myocardial ischemia or infarction in the treatment of hypertensive urgencies. Ann Intern Med. 1987;107(2):185-186.
23. Grossman E, Messerli FH, Grodzicki T, Kowey P. Should a moratorium be placed on sublingual nifedipine capsules given for hypertensive emergencies and pseudoemergencies? JAMA. 1996;276(16):1328-1331.
1. CDC. High blood pressure fact sheet. www.cdc.gov/dhdsp/data_statistics/fact_sheets/fs_bloodpressure.htm. Accessed September 26, 2017.
2. Decker WW, Godwin SA, Hess EP, et al; American College of Emergency Physicians Clinical Policies Subcommittee (Writing Committee) on Asymptomatic Hypertension in the ED. Clinical policy: critical issues in the evaluation and management of adult patients with asymptomatic hypertension in the emergency department. Ann Emerg Med. 2006;47(3):237-249.
3. CDC. High blood pressure facts. www.cdc.gov/bloodpressure/facts.htm. Accessed October 19, 2017.
4. World Health Organization. Global Health Risks: Mortality and Burden of Disease Attributable to Selected Major Risks. Geneva, Switzerland: WHO; 2009. www.who.int/healthinfo/global_burden_disease/GlobalHealthRisks_report_full.pdf. Accessed October 19, 2017.
5. Stewart DL, Feinstein SE, Colgan R. Hypertensive urgencies and emergencies. Prim Care. 2006;33(3):613-623.
6. Wolf SJ, Lo B, Shih RD, et al; American College of Emergency Physicians Clinical Policies Committee. Clinical policy: critical issues in the evaluation and management of adult patients in the emergency department with asymptomatic elevated blood pressure. Ann Emerg Med. 2013;62(1):59-68.
7. McKinnon M, O’Neill JM. Hypertension in the emergency department: treat now, later, or not at all. Emerg Med Pract. 2010;12(6):1-22.
8. Mancia G, Fagard R, Narkiewicz K, et al. 2013 ESH/ESC Guidelines for the management of arterial hypertension: the Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens. 2013;31(7): 1281-1357.
9. Shayne PH, Pitts SR. Severely increased blood pressure in the emergency department. Ann Emerg Med. 2003;41(4): 513-529.
10. Aggarwal M, Khan IA. Hypertensive crisis: hypertensive emergencies and urgencies. Cardiol Clin. 2006;24(1):135-146.
11. Houston MC. The comparative effects of clonidine hydrochloride and nifedipine in the treatment of hypertensive crises. Am Heart J. 1998;115(1 pt 1):152-159.
12. Kitiyakara C, Guaman NJ. Malignant hypertension and hypertensive emergencies. J Am Soc Nephrol. 1998;9(1):133-142.
13. Elliott WJ. Hypertensive emergencies. Crit Care Clin. 2001;17(2):435-451.
14. Papadopoulos DP, Mourouzis I, Thomopoulos C, et al. Hypertension crisis. Blood Press. 2010;19(6):328-336.
15. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311(5):507-520.
16. Keller T, Zeller T, Peetz D, et al. Sensitive troponin I assay in early diagnosis of acute myocardial infarction. N Engl J Med. 2009;361(9):868-877.
17. Reichlin T, Hochholzer W, Bassetti S, et al. Early diagnosis of myocardial infarction with sensitive cardiac troponin assays. N Engl J Med. 2009;361(9):858-867.
18. Ghali JK, Kadakia S, Cooper RS, Liao YL. Impact of left ventricular hypertrophy on ventricular arrhythmias in the absence of coronary artery disease. J Am Coll Cardiol. 1991;17(6):1277-1282.
19. Bang CN, Soliman EZ, Simpson LM, et al. Electrocardiographic left ventricular hypertrophy predicts cardiovascular morbidity and mortality in hypertensive patients: the ALLHAT study. Am J Hypertens. 2017;30(9):914-922.
20. Hsieh BP, Pham MX, Froelicher VF. Prognostic value of electrocardiographic criteria for left ventricular hypertrophy. Am Heart J. 2005;150(1):161-167.
21. Kinsella K, Baraff LJ. Initiation of therapy for asymptomatic hypertension in the emergency department. Ann Emerg Med. 2009;54(6):791-792.
22. O’Mailia JJ, Sander GE, Giles TD. Nifedipine-associated myocardial ischemia or infarction in the treatment of hypertensive urgencies. Ann Intern Med. 1987;107(2):185-186.
23. Grossman E, Messerli FH, Grodzicki T, Kowey P. Should a moratorium be placed on sublingual nifedipine capsules given for hypertensive emergencies and pseudoemergencies? JAMA. 1996;276(16):1328-1331.

Sebum inhibition steps up against acne
In the future, topical agents that target sebum production could play a greater role in acne management.
Linda F. Stein Gold, MD, director of dermatology research at the Henry Ford Health System in Detroit highlighted several studies of these investigational therapies in a presentation on acne at the Skin Disease Education Foundation’s annual Las Vegas Dermatology Seminar.

• SB204, a topical agent that releases nitric oxide.
• DRM01, a topical sebum inhibitor that inhibits acetyl coenzyme-A carboxylase, an enzyme involved in the synthesis of fatty acids.
• Cortexolone 17a-propionate (CB-03-01) 1% cream, a topical antiandrogen.
A 4% gel formulation of SB204 once a day was compared with a vehicle, also applied topically once a day, in a pair of phase 3 randomized, multicenter pivotal trials of 2,639 patients aged 9 years and older with moderate to severe acne, Dr. Stein Gold said. At 12 weeks, the absolute change in number of noninflammatory lesions among those treated with SB204 was a reduction by 15.4 vs. 13.4 among those treated with a vehicle in one study (P = .03) and by 14.9 vs. 12.3 with a vehicle in the other study (P = .001). The absolute change in the number of inflammatory lesions among those using SB204 in the first study was not significantly different from those seen among patients using the vehicle (a reduction of 12.1 vs. 11.1, respectively) but was significant in the second study (a reduction of 12.9 vs. 10.6 for vehicle; P less than .001).
No new safety signals were observed and treatment was “generally safe and well tolerated,” with fewer than 2% of patients discontinuing treatment because of treatment-emergent adverse events, she noted.
In a phase 2 study, those treated with a 4% formulation of SB204 had a significant reduction in inflammatory and noninflammatory lesions at 12 weeks, with mild local irritation as the main adverse effect, she said (J. Drugs Dermatol. 2016 Dec 1;15[12]:1496-527). The treatment was generally safe and well tolerated, said Dr. Stein Gold, one of the study authors.
In a phase 2 randomized, multicenter, double-blind study of 108 patients with moderate or severe acne, she continued, those treated with DRM01 7.5% applied to the face twice a day for 12 weeks, those treated with DRM01 showed significant improvement across all efficacy measures at 12 weeks, including a significantly greater reduction in both inflammatory and noninflammatory lesions, and on measures of investigator’s global assessment – after 12 weeks of twice-daily treatment. Treatment was well tolerated, and no serious adverse events related to the treatment were reported, Dr. Stein Gold said.
(In October, the manufacturer, Dermira, announced that patient enrollment in two phase 3 trials of DRM01– now known as olumacostat glasaretil – in patients aged 9 years and older with facial acne had been completed.)
Phase 3 studies of cortexolone 17a-propionate (CB-03-01) 1% cream are underway, Dr. Stein Gold said.
Dr. Stein Gold disclosed relationships with multiple companies including Galderma, Leo, Novan, Valeant, Dermira, Novartis, Celgene, Allergan, Foamix, Promius, Anacor, and Medimetriks.
SDEF and this news organization are owned by the same parent company.
In the future, topical agents that target sebum production could play a greater role in acne management.
Linda F. Stein Gold, MD, director of dermatology research at the Henry Ford Health System in Detroit highlighted several studies of these investigational therapies in a presentation on acne at the Skin Disease Education Foundation’s annual Las Vegas Dermatology Seminar.
• SB204, a topical agent that releases nitric oxide.
• DRM01, a topical sebum inhibitor that inhibits acetyl coenzyme-A carboxylase, an enzyme involved in the synthesis of fatty acids.
• Cortexolone 17a-propionate (CB-03-01) 1% cream, a topical antiandrogen.
A 4% gel formulation of SB204 once a day was compared with a vehicle, also applied topically once a day, in a pair of phase 3 randomized, multicenter pivotal trials of 2,639 patients aged 9 years and older with moderate to severe acne, Dr. Stein Gold said. At 12 weeks, the absolute change in number of noninflammatory lesions among those treated with SB204 was a reduction by 15.4 vs. 13.4 among those treated with a vehicle in one study (P = .03) and by 14.9 vs. 12.3 with a vehicle in the other study (P = .001). The absolute change in the number of inflammatory lesions among those using SB204 in the first study was not significantly different from those seen among patients using the vehicle (a reduction of 12.1 vs. 11.1, respectively) but was significant in the second study (a reduction of 12.9 vs. 10.6 for vehicle; P less than .001).
No new safety signals were observed and treatment was “generally safe and well tolerated,” with fewer than 2% of patients discontinuing treatment because of treatment-emergent adverse events, she noted.
In a phase 2 study, those treated with a 4% formulation of SB204 had a significant reduction in inflammatory and noninflammatory lesions at 12 weeks, with mild local irritation as the main adverse effect, she said (J. Drugs Dermatol. 2016 Dec 1;15[12]:1496-527). The treatment was generally safe and well tolerated, said Dr. Stein Gold, one of the study authors.
In a phase 2 randomized, multicenter, double-blind study of 108 patients with moderate or severe acne, she continued, those treated with DRM01 7.5% applied to the face twice a day for 12 weeks, those treated with DRM01 showed significant improvement across all efficacy measures at 12 weeks, including a significantly greater reduction in both inflammatory and noninflammatory lesions, and on measures of investigator’s global assessment – after 12 weeks of twice-daily treatment. Treatment was well tolerated, and no serious adverse events related to the treatment were reported, Dr. Stein Gold said.
(In October, the manufacturer, Dermira, announced that patient enrollment in two phase 3 trials of DRM01– now known as olumacostat glasaretil – in patients aged 9 years and older with facial acne had been completed.)
Phase 3 studies of cortexolone 17a-propionate (CB-03-01) 1% cream are underway, Dr. Stein Gold said.
Dr. Stein Gold disclosed relationships with multiple companies including Galderma, Leo, Novan, Valeant, Dermira, Novartis, Celgene, Allergan, Foamix, Promius, Anacor, and Medimetriks.
SDEF and this news organization are owned by the same parent company.
In the future, topical agents that target sebum production could play a greater role in acne management.
Linda F. Stein Gold, MD, director of dermatology research at the Henry Ford Health System in Detroit highlighted several studies of these investigational therapies in a presentation on acne at the Skin Disease Education Foundation’s annual Las Vegas Dermatology Seminar.
• SB204, a topical agent that releases nitric oxide.
• DRM01, a topical sebum inhibitor that inhibits acetyl coenzyme-A carboxylase, an enzyme involved in the synthesis of fatty acids.
• Cortexolone 17a-propionate (CB-03-01) 1% cream, a topical antiandrogen.
A 4% gel formulation of SB204 once a day was compared with a vehicle, also applied topically once a day, in a pair of phase 3 randomized, multicenter pivotal trials of 2,639 patients aged 9 years and older with moderate to severe acne, Dr. Stein Gold said. At 12 weeks, the absolute change in number of noninflammatory lesions among those treated with SB204 was a reduction by 15.4 vs. 13.4 among those treated with a vehicle in one study (P = .03) and by 14.9 vs. 12.3 with a vehicle in the other study (P = .001). The absolute change in the number of inflammatory lesions among those using SB204 in the first study was not significantly different from those seen among patients using the vehicle (a reduction of 12.1 vs. 11.1, respectively) but was significant in the second study (a reduction of 12.9 vs. 10.6 for vehicle; P less than .001).
No new safety signals were observed and treatment was “generally safe and well tolerated,” with fewer than 2% of patients discontinuing treatment because of treatment-emergent adverse events, she noted.
In a phase 2 study, those treated with a 4% formulation of SB204 had a significant reduction in inflammatory and noninflammatory lesions at 12 weeks, with mild local irritation as the main adverse effect, she said (J. Drugs Dermatol. 2016 Dec 1;15[12]:1496-527). The treatment was generally safe and well tolerated, said Dr. Stein Gold, one of the study authors.
In a phase 2 randomized, multicenter, double-blind study of 108 patients with moderate or severe acne, she continued, those treated with DRM01 7.5% applied to the face twice a day for 12 weeks, those treated with DRM01 showed significant improvement across all efficacy measures at 12 weeks, including a significantly greater reduction in both inflammatory and noninflammatory lesions, and on measures of investigator’s global assessment – after 12 weeks of twice-daily treatment. Treatment was well tolerated, and no serious adverse events related to the treatment were reported, Dr. Stein Gold said.
(In October, the manufacturer, Dermira, announced that patient enrollment in two phase 3 trials of DRM01– now known as olumacostat glasaretil – in patients aged 9 years and older with facial acne had been completed.)
Phase 3 studies of cortexolone 17a-propionate (CB-03-01) 1% cream are underway, Dr. Stein Gold said.
Dr. Stein Gold disclosed relationships with multiple companies including Galderma, Leo, Novan, Valeant, Dermira, Novartis, Celgene, Allergan, Foamix, Promius, Anacor, and Medimetriks.
SDEF and this news organization are owned by the same parent company.
AT SDEF LAS VEGAS DERMATOLOGY SEMINAR