User login
Parsing the fine points of anxiety
Expert prescribes benzodiazepines for excessive anxiety, antidepressants for anxiety disorders
LAS VEGAS –

“People with anxiety disorders have excessive anxiety, but not everyone with excessive anxiety has a psychiatric disorder,” he said at an annual psychopharmacology update held by the Nevada Psychiatric Association. “Any anxiety above baseline can be normal. It’s not necessarily pathological. I think that’s an important point that’s easy to overlook when we’re in clinical practice, and it affects how we approach our patients.”
Anxiety can present in a variety of ways in different individuals. Panic attacks are often the primary chief complaint, and it’s common to hear complaints from family that the person is routinely seeking reassurance. In addition, tics and twitches are not unusual in people with anxiety disorder. “Some of that is brought out by anxiety itself,” said Dr. Hudak, who is a psychiatrist at the University of Pittsburgh. Sleep disturbances or other somatic complaints also are common. “They complain of racing thoughts, increased energy, and depression,” he added. “When someone complains about depression, don’t assume they have a mood disorder. The reason people with anxiety disorders complain about depression is that it really feels awful. Anxiety is incredibly dysphoric.” Physical complaints include shortness of breath, GI distress, dizziness, vague somatic complaints, and skin or gum lesions.
He went on to note that individuals with excessive anxiety virtually never lose consciousness. “The exception is blood/injection/injury phobia,” he said. “That’s the only case in which anxiety will cause loss of consciousness. It happens in virtually no other setting. Ondine’s curse while falling asleep is another symptom that only occurs with anxiety. It’s a sensation that you have to remember to breathe, and breathing is no longer automatic. There are medical conditions that cause Ondine’s curse. However, the patient who complains of Ondine’s curse as they’re falling asleep is pathognomonic for anxiety.”
Dr. Hudak said panic attacks, a discrete period of fear or discomfort, rarely last more than 30 minutes.
“I view panic attacks in three flavors,” he said. “Some people have the cardiovascular flavor with shortness of breath and heart palpitations. Some have what I call the neurological flavor, where the predominant symptoms seem to be dizziness and tingling. Other people have GI flavor, with gut pain, nausea, and diarrhea. Panic attacks are not a psychiatric disorder. It’s a qualifier for any psychiatric disorder.”
Social anxiety disorder, meanwhile, presents as two completely distinct and separate illnesses that have nothing in common with each other.
“The performance subtype of social anxiety really presents like a simple phobia,” Dr. Hudak said. “The treatment for that is really behavioral therapy and cognitive-behavioral therapy, and rarely the use of medications. The generalized type presents with intrusive, [obsessive-compulsive disorder]–like thoughts. Affected individuals describe themselves as ‘paranoid’ or feeling that they are being scrutinized. The categorical versus dimensional diagnosis is being debated.” Individuals with generalized anxiety disorder, on the other hand, have excessive and pervasive worry and anxiety present more days than not for a 6-month period. “The individual finds it difficult to control the worry,” he said. Somatic symptoms include restlessness, fatigue, difficulty concentrating, irritability, muscle tension, and insomnia. Different studies show the prevalence rate between 3% and 8%, affecting more women than men.
The medical work-up for excessive anxiety should consist of history and physical exam, complete blood count, the Chem-7 metabolic test, thyroid-stimulating hormone, and EKG if indicated. Both medications and behavioral therapy are used in the treatment of anxiety disorders. Many patients require both in order to achieve maximum treatment response. “Often, people with less severe illnesses can be managed with therapy alone,” Dr. Hudak said.
“In more severe cases, medications can help reduce symptoms to the point where therapy is easier to perform. The bottom line here is that at no time should you treat someone with an anxiety disorder with medications alone. Behavioral therapy is at least as effective as medications, and perhaps more so.”
Many trials of anxiety medications are of short duration and therefore lack evidence of long-term improvement, he said. Commonly used scales often include nonspecific items such as arousal score that can be reduced by sedating medications without improving the actual disorder. If someone has excessive anxiety that is not part of a primary anxiety disorder, Dr. Hudak typically prescribes benzodiazepines. “If someone is anxious because a loved one died, or if they’re nervous about their wedding day, or about taking a board exam, benzos can be used,” he said. “For someone who has an anxiety disorder, I virtually never use benzodiazepines. I generally use medications in the antidepressant category. I probably initiate fewer than five benzodiazepine prescriptions per year for anxiety disorder. There is also data to suggest that using benzodiazepines in patients with anxiety disorder may make cognitive-behavioral therapy more difficult.”
According to Dr. Hudak, selective serotonin reuptake inhibitors seem to have the largest evidence base in panic disorder and are first-line pharmacotherapy for both panic disorder and generalized anxiety disorder, while tricyclic antidepressants (TCAs) usually are considered a second-line therapy. “There is good data behind MAO inhibitors, and there is increasingly good data behind [selective norepinephrine reuptake inhibitors],” he said. “If someone has failed a trial of SSRIs, you may consider trying an SNRI before a TCA. However, I would try multiple SSRIs before ruling out that class of medications. I have had people fail five SSRIs and respond dramatically to the sixth SSRI.”
Dr. Hudak disclosed that he receives royalties from the Cambridge University Press.
Expert prescribes benzodiazepines for excessive anxiety, antidepressants for anxiety disorders
Expert prescribes benzodiazepines for excessive anxiety, antidepressants for anxiety disorders
LAS VEGAS –
“People with anxiety disorders have excessive anxiety, but not everyone with excessive anxiety has a psychiatric disorder,” he said at an annual psychopharmacology update held by the Nevada Psychiatric Association. “Any anxiety above baseline can be normal. It’s not necessarily pathological. I think that’s an important point that’s easy to overlook when we’re in clinical practice, and it affects how we approach our patients.”
Anxiety can present in a variety of ways in different individuals. Panic attacks are often the primary chief complaint, and it’s common to hear complaints from family that the person is routinely seeking reassurance. In addition, tics and twitches are not unusual in people with anxiety disorder. “Some of that is brought out by anxiety itself,” said Dr. Hudak, who is a psychiatrist at the University of Pittsburgh. Sleep disturbances or other somatic complaints also are common. “They complain of racing thoughts, increased energy, and depression,” he added. “When someone complains about depression, don’t assume they have a mood disorder. The reason people with anxiety disorders complain about depression is that it really feels awful. Anxiety is incredibly dysphoric.” Physical complaints include shortness of breath, GI distress, dizziness, vague somatic complaints, and skin or gum lesions.
He went on to note that individuals with excessive anxiety virtually never lose consciousness. “The exception is blood/injection/injury phobia,” he said. “That’s the only case in which anxiety will cause loss of consciousness. It happens in virtually no other setting. Ondine’s curse while falling asleep is another symptom that only occurs with anxiety. It’s a sensation that you have to remember to breathe, and breathing is no longer automatic. There are medical conditions that cause Ondine’s curse. However, the patient who complains of Ondine’s curse as they’re falling asleep is pathognomonic for anxiety.”
Dr. Hudak said panic attacks, a discrete period of fear or discomfort, rarely last more than 30 minutes.
“I view panic attacks in three flavors,” he said. “Some people have the cardiovascular flavor with shortness of breath and heart palpitations. Some have what I call the neurological flavor, where the predominant symptoms seem to be dizziness and tingling. Other people have GI flavor, with gut pain, nausea, and diarrhea. Panic attacks are not a psychiatric disorder. It’s a qualifier for any psychiatric disorder.”
Social anxiety disorder, meanwhile, presents as two completely distinct and separate illnesses that have nothing in common with each other.
“The performance subtype of social anxiety really presents like a simple phobia,” Dr. Hudak said. “The treatment for that is really behavioral therapy and cognitive-behavioral therapy, and rarely the use of medications. The generalized type presents with intrusive, [obsessive-compulsive disorder]–like thoughts. Affected individuals describe themselves as ‘paranoid’ or feeling that they are being scrutinized. The categorical versus dimensional diagnosis is being debated.” Individuals with generalized anxiety disorder, on the other hand, have excessive and pervasive worry and anxiety present more days than not for a 6-month period. “The individual finds it difficult to control the worry,” he said. Somatic symptoms include restlessness, fatigue, difficulty concentrating, irritability, muscle tension, and insomnia. Different studies show the prevalence rate between 3% and 8%, affecting more women than men.
The medical work-up for excessive anxiety should consist of history and physical exam, complete blood count, the Chem-7 metabolic test, thyroid-stimulating hormone, and EKG if indicated. Both medications and behavioral therapy are used in the treatment of anxiety disorders. Many patients require both in order to achieve maximum treatment response. “Often, people with less severe illnesses can be managed with therapy alone,” Dr. Hudak said.
“In more severe cases, medications can help reduce symptoms to the point where therapy is easier to perform. The bottom line here is that at no time should you treat someone with an anxiety disorder with medications alone. Behavioral therapy is at least as effective as medications, and perhaps more so.”
Many trials of anxiety medications are of short duration and therefore lack evidence of long-term improvement, he said. Commonly used scales often include nonspecific items such as arousal score that can be reduced by sedating medications without improving the actual disorder. If someone has excessive anxiety that is not part of a primary anxiety disorder, Dr. Hudak typically prescribes benzodiazepines. “If someone is anxious because a loved one died, or if they’re nervous about their wedding day, or about taking a board exam, benzos can be used,” he said. “For someone who has an anxiety disorder, I virtually never use benzodiazepines. I generally use medications in the antidepressant category. I probably initiate fewer than five benzodiazepine prescriptions per year for anxiety disorder. There is also data to suggest that using benzodiazepines in patients with anxiety disorder may make cognitive-behavioral therapy more difficult.”
According to Dr. Hudak, selective serotonin reuptake inhibitors seem to have the largest evidence base in panic disorder and are first-line pharmacotherapy for both panic disorder and generalized anxiety disorder, while tricyclic antidepressants (TCAs) usually are considered a second-line therapy. “There is good data behind MAO inhibitors, and there is increasingly good data behind [selective norepinephrine reuptake inhibitors],” he said. “If someone has failed a trial of SSRIs, you may consider trying an SNRI before a TCA. However, I would try multiple SSRIs before ruling out that class of medications. I have had people fail five SSRIs and respond dramatically to the sixth SSRI.”
Dr. Hudak disclosed that he receives royalties from the Cambridge University Press.
LAS VEGAS –
“People with anxiety disorders have excessive anxiety, but not everyone with excessive anxiety has a psychiatric disorder,” he said at an annual psychopharmacology update held by the Nevada Psychiatric Association. “Any anxiety above baseline can be normal. It’s not necessarily pathological. I think that’s an important point that’s easy to overlook when we’re in clinical practice, and it affects how we approach our patients.”
Anxiety can present in a variety of ways in different individuals. Panic attacks are often the primary chief complaint, and it’s common to hear complaints from family that the person is routinely seeking reassurance. In addition, tics and twitches are not unusual in people with anxiety disorder. “Some of that is brought out by anxiety itself,” said Dr. Hudak, who is a psychiatrist at the University of Pittsburgh. Sleep disturbances or other somatic complaints also are common. “They complain of racing thoughts, increased energy, and depression,” he added. “When someone complains about depression, don’t assume they have a mood disorder. The reason people with anxiety disorders complain about depression is that it really feels awful. Anxiety is incredibly dysphoric.” Physical complaints include shortness of breath, GI distress, dizziness, vague somatic complaints, and skin or gum lesions.
He went on to note that individuals with excessive anxiety virtually never lose consciousness. “The exception is blood/injection/injury phobia,” he said. “That’s the only case in which anxiety will cause loss of consciousness. It happens in virtually no other setting. Ondine’s curse while falling asleep is another symptom that only occurs with anxiety. It’s a sensation that you have to remember to breathe, and breathing is no longer automatic. There are medical conditions that cause Ondine’s curse. However, the patient who complains of Ondine’s curse as they’re falling asleep is pathognomonic for anxiety.”
Dr. Hudak said panic attacks, a discrete period of fear or discomfort, rarely last more than 30 minutes.
“I view panic attacks in three flavors,” he said. “Some people have the cardiovascular flavor with shortness of breath and heart palpitations. Some have what I call the neurological flavor, where the predominant symptoms seem to be dizziness and tingling. Other people have GI flavor, with gut pain, nausea, and diarrhea. Panic attacks are not a psychiatric disorder. It’s a qualifier for any psychiatric disorder.”
Social anxiety disorder, meanwhile, presents as two completely distinct and separate illnesses that have nothing in common with each other.
“The performance subtype of social anxiety really presents like a simple phobia,” Dr. Hudak said. “The treatment for that is really behavioral therapy and cognitive-behavioral therapy, and rarely the use of medications. The generalized type presents with intrusive, [obsessive-compulsive disorder]–like thoughts. Affected individuals describe themselves as ‘paranoid’ or feeling that they are being scrutinized. The categorical versus dimensional diagnosis is being debated.” Individuals with generalized anxiety disorder, on the other hand, have excessive and pervasive worry and anxiety present more days than not for a 6-month period. “The individual finds it difficult to control the worry,” he said. Somatic symptoms include restlessness, fatigue, difficulty concentrating, irritability, muscle tension, and insomnia. Different studies show the prevalence rate between 3% and 8%, affecting more women than men.
The medical work-up for excessive anxiety should consist of history and physical exam, complete blood count, the Chem-7 metabolic test, thyroid-stimulating hormone, and EKG if indicated. Both medications and behavioral therapy are used in the treatment of anxiety disorders. Many patients require both in order to achieve maximum treatment response. “Often, people with less severe illnesses can be managed with therapy alone,” Dr. Hudak said.
“In more severe cases, medications can help reduce symptoms to the point where therapy is easier to perform. The bottom line here is that at no time should you treat someone with an anxiety disorder with medications alone. Behavioral therapy is at least as effective as medications, and perhaps more so.”
Many trials of anxiety medications are of short duration and therefore lack evidence of long-term improvement, he said. Commonly used scales often include nonspecific items such as arousal score that can be reduced by sedating medications without improving the actual disorder. If someone has excessive anxiety that is not part of a primary anxiety disorder, Dr. Hudak typically prescribes benzodiazepines. “If someone is anxious because a loved one died, or if they’re nervous about their wedding day, or about taking a board exam, benzos can be used,” he said. “For someone who has an anxiety disorder, I virtually never use benzodiazepines. I generally use medications in the antidepressant category. I probably initiate fewer than five benzodiazepine prescriptions per year for anxiety disorder. There is also data to suggest that using benzodiazepines in patients with anxiety disorder may make cognitive-behavioral therapy more difficult.”
According to Dr. Hudak, selective serotonin reuptake inhibitors seem to have the largest evidence base in panic disorder and are first-line pharmacotherapy for both panic disorder and generalized anxiety disorder, while tricyclic antidepressants (TCAs) usually are considered a second-line therapy. “There is good data behind MAO inhibitors, and there is increasingly good data behind [selective norepinephrine reuptake inhibitors],” he said. “If someone has failed a trial of SSRIs, you may consider trying an SNRI before a TCA. However, I would try multiple SSRIs before ruling out that class of medications. I have had people fail five SSRIs and respond dramatically to the sixth SSRI.”
Dr. Hudak disclosed that he receives royalties from the Cambridge University Press.
EXPERT ANALYSIS FROM NPA 2019
Prevent burnout by tapping into passions
To fight burnout, Griffin Myers, MD, wants more out of the physicians who work at Chicago-based Oak Street Health.
Not more time, or more patients, or more codes billed – but more passion and a more meaningful professional experience, said Dr. Myers, cofounder and chief medical officer of the 42-practice group that cares for Medicare patients.
Oak Street seems to be on to something. According to the health care consultancy The Advisory Board, there are three key ways to avoid physician burnout: involve physicians in strategic decision making, recognize physicians’ contributions, and create time-limited leadership opportunities for physicians.
“What do you want to be when you grow up?”
That’s the question Dr. Myers asks physicians during job interviews. He wants to discover their personal and professional passions.
Health care leaders can’t expect physicians to prevent burnout on their own, insists Dr. Myers. “You have to change the way your organization supports clinicians.”
At Oak Street, that includes supporting physicians with medical scribes and ensuring that they aren’t bogged down with paperwork or “fighting with the fax machines,” said Dr. Myers.
Once a physician is hired at Oak Street, they’re partnered with a medical director who uses the practice’s resources to support the physician’s clinical and professional passions. Specifically, that means providing physicians with administrative time (nonpatient time) and support – both organizationally and financially – for professional development. Medical directors meet with physicians quarterly to check in and assess performance.

Take, for example, Tina Valdez, DO, an internist at Oak Street’s Englewood, Ill., location, who previously practiced at Advocate Lutheran General Hospital in Park Ridge, Ill. During the job interview process, Dr. Myers discovered that Dr. Valdez wanted to keep teaching and mentoring residents as they transitioned to attending physicians.
Dr. Myers was on board, so Dr. Valdez uses her administrative time to meet with early-career physicians on a quarterly basis.
Resident physicians are used to having a more senior physician monitor their work, Dr. Valdez noted. Without that oversight, many first-year physicians can get anxious. To support them, she leads small group discussions on topics including patient cases and ways to better work with other members of the care team, such as relying on a medical assistant to capture vital signs and conduct a thorough medication reconciliation.
In the program’s first year, 10 new physicians split into two groups for 2-hour sessions at an off-site meeting location once a quarter.
As much as early-career physicians need support, so, too, do future leaders.

When Andrea Khosropour, MD, first joined Oak Street in 2012, her mentor invested a lot of time in coaching her to become a better leader. For example, her mentor taught her the right way to have difficult conversations.
Dr. Khosropour, now a senior medical director who practices at the group’s Edgewater, Ill., location, said she finds balance at work because Oak Street gives her administrative time to attend to her management responsibilities. She also values the assistance of the medical scribes who document every patient encounter in the EHR. “That’s rare for primary care,” says Dr. Khosropour.
What qualities does Oak Street look for in its physician leaders? Dr. Myers said it starts with a physician who shares the group’s values, demonstrates clinical excellence and “scrappiness,” and has good intentions. He pointed out that Dr. Khosropour, who now oversees four practices, came to Oak Street with no experience running multiple practices.
Dr. Myers said Oak Street can grow its physicians internally as long as they share the group’s cultural values. “You can’t wait for people who already have those skills.”
Oak Street doesn’t rely on a fee-for-service model, in which physicians are paid by the volume of patients they treat. Specifically, that means 80% of its patients are in value-based contracts with private payers and the remaining patients are covered in the Medicare Shared Savings Program. About half of patients are dually eligible for Medicare and Medicaid, Dr. Myers said.
Because the group receives a set amount to manage the care of each of its attributed patients, Oak Street has the flexibility to invest in professional development, scribes, and other programs to support physicians, Dr. Myers said. That’s provided the group can successfully manage the care of their patients and keep them out of the hospital.
He advises practices that are more dependent on fee-for-service contracts to prioritize the following initiatives to prevent burnout: investing in professional development, reducing physicians’ administrative burdens, and celebrating physicians’ victories.
“Our goal is to provide the highest-quality health care employee experience possible. People will stay as long as you set that as a clear goal,” Dr. Myers said.
To fight burnout, Griffin Myers, MD, wants more out of the physicians who work at Chicago-based Oak Street Health.
Not more time, or more patients, or more codes billed – but more passion and a more meaningful professional experience, said Dr. Myers, cofounder and chief medical officer of the 42-practice group that cares for Medicare patients.
Oak Street seems to be on to something. According to the health care consultancy The Advisory Board, there are three key ways to avoid physician burnout: involve physicians in strategic decision making, recognize physicians’ contributions, and create time-limited leadership opportunities for physicians.
“What do you want to be when you grow up?”
That’s the question Dr. Myers asks physicians during job interviews. He wants to discover their personal and professional passions.
Health care leaders can’t expect physicians to prevent burnout on their own, insists Dr. Myers. “You have to change the way your organization supports clinicians.”
At Oak Street, that includes supporting physicians with medical scribes and ensuring that they aren’t bogged down with paperwork or “fighting with the fax machines,” said Dr. Myers.
Once a physician is hired at Oak Street, they’re partnered with a medical director who uses the practice’s resources to support the physician’s clinical and professional passions. Specifically, that means providing physicians with administrative time (nonpatient time) and support – both organizationally and financially – for professional development. Medical directors meet with physicians quarterly to check in and assess performance.
Take, for example, Tina Valdez, DO, an internist at Oak Street’s Englewood, Ill., location, who previously practiced at Advocate Lutheran General Hospital in Park Ridge, Ill. During the job interview process, Dr. Myers discovered that Dr. Valdez wanted to keep teaching and mentoring residents as they transitioned to attending physicians.
Dr. Myers was on board, so Dr. Valdez uses her administrative time to meet with early-career physicians on a quarterly basis.
Resident physicians are used to having a more senior physician monitor their work, Dr. Valdez noted. Without that oversight, many first-year physicians can get anxious. To support them, she leads small group discussions on topics including patient cases and ways to better work with other members of the care team, such as relying on a medical assistant to capture vital signs and conduct a thorough medication reconciliation.
In the program’s first year, 10 new physicians split into two groups for 2-hour sessions at an off-site meeting location once a quarter.
As much as early-career physicians need support, so, too, do future leaders.
When Andrea Khosropour, MD, first joined Oak Street in 2012, her mentor invested a lot of time in coaching her to become a better leader. For example, her mentor taught her the right way to have difficult conversations.
Dr. Khosropour, now a senior medical director who practices at the group’s Edgewater, Ill., location, said she finds balance at work because Oak Street gives her administrative time to attend to her management responsibilities. She also values the assistance of the medical scribes who document every patient encounter in the EHR. “That’s rare for primary care,” says Dr. Khosropour.
What qualities does Oak Street look for in its physician leaders? Dr. Myers said it starts with a physician who shares the group’s values, demonstrates clinical excellence and “scrappiness,” and has good intentions. He pointed out that Dr. Khosropour, who now oversees four practices, came to Oak Street with no experience running multiple practices.
Dr. Myers said Oak Street can grow its physicians internally as long as they share the group’s cultural values. “You can’t wait for people who already have those skills.”
Oak Street doesn’t rely on a fee-for-service model, in which physicians are paid by the volume of patients they treat. Specifically, that means 80% of its patients are in value-based contracts with private payers and the remaining patients are covered in the Medicare Shared Savings Program. About half of patients are dually eligible for Medicare and Medicaid, Dr. Myers said.
Because the group receives a set amount to manage the care of each of its attributed patients, Oak Street has the flexibility to invest in professional development, scribes, and other programs to support physicians, Dr. Myers said. That’s provided the group can successfully manage the care of their patients and keep them out of the hospital.
He advises practices that are more dependent on fee-for-service contracts to prioritize the following initiatives to prevent burnout: investing in professional development, reducing physicians’ administrative burdens, and celebrating physicians’ victories.
“Our goal is to provide the highest-quality health care employee experience possible. People will stay as long as you set that as a clear goal,” Dr. Myers said.
To fight burnout, Griffin Myers, MD, wants more out of the physicians who work at Chicago-based Oak Street Health.
Not more time, or more patients, or more codes billed – but more passion and a more meaningful professional experience, said Dr. Myers, cofounder and chief medical officer of the 42-practice group that cares for Medicare patients.
Oak Street seems to be on to something. According to the health care consultancy The Advisory Board, there are three key ways to avoid physician burnout: involve physicians in strategic decision making, recognize physicians’ contributions, and create time-limited leadership opportunities for physicians.
“What do you want to be when you grow up?”
That’s the question Dr. Myers asks physicians during job interviews. He wants to discover their personal and professional passions.
Health care leaders can’t expect physicians to prevent burnout on their own, insists Dr. Myers. “You have to change the way your organization supports clinicians.”
At Oak Street, that includes supporting physicians with medical scribes and ensuring that they aren’t bogged down with paperwork or “fighting with the fax machines,” said Dr. Myers.
Once a physician is hired at Oak Street, they’re partnered with a medical director who uses the practice’s resources to support the physician’s clinical and professional passions. Specifically, that means providing physicians with administrative time (nonpatient time) and support – both organizationally and financially – for professional development. Medical directors meet with physicians quarterly to check in and assess performance.
Take, for example, Tina Valdez, DO, an internist at Oak Street’s Englewood, Ill., location, who previously practiced at Advocate Lutheran General Hospital in Park Ridge, Ill. During the job interview process, Dr. Myers discovered that Dr. Valdez wanted to keep teaching and mentoring residents as they transitioned to attending physicians.
Dr. Myers was on board, so Dr. Valdez uses her administrative time to meet with early-career physicians on a quarterly basis.
Resident physicians are used to having a more senior physician monitor their work, Dr. Valdez noted. Without that oversight, many first-year physicians can get anxious. To support them, she leads small group discussions on topics including patient cases and ways to better work with other members of the care team, such as relying on a medical assistant to capture vital signs and conduct a thorough medication reconciliation.
In the program’s first year, 10 new physicians split into two groups for 2-hour sessions at an off-site meeting location once a quarter.
As much as early-career physicians need support, so, too, do future leaders.
When Andrea Khosropour, MD, first joined Oak Street in 2012, her mentor invested a lot of time in coaching her to become a better leader. For example, her mentor taught her the right way to have difficult conversations.
Dr. Khosropour, now a senior medical director who practices at the group’s Edgewater, Ill., location, said she finds balance at work because Oak Street gives her administrative time to attend to her management responsibilities. She also values the assistance of the medical scribes who document every patient encounter in the EHR. “That’s rare for primary care,” says Dr. Khosropour.
What qualities does Oak Street look for in its physician leaders? Dr. Myers said it starts with a physician who shares the group’s values, demonstrates clinical excellence and “scrappiness,” and has good intentions. He pointed out that Dr. Khosropour, who now oversees four practices, came to Oak Street with no experience running multiple practices.
Dr. Myers said Oak Street can grow its physicians internally as long as they share the group’s cultural values. “You can’t wait for people who already have those skills.”
Oak Street doesn’t rely on a fee-for-service model, in which physicians are paid by the volume of patients they treat. Specifically, that means 80% of its patients are in value-based contracts with private payers and the remaining patients are covered in the Medicare Shared Savings Program. About half of patients are dually eligible for Medicare and Medicaid, Dr. Myers said.
Because the group receives a set amount to manage the care of each of its attributed patients, Oak Street has the flexibility to invest in professional development, scribes, and other programs to support physicians, Dr. Myers said. That’s provided the group can successfully manage the care of their patients and keep them out of the hospital.
He advises practices that are more dependent on fee-for-service contracts to prioritize the following initiatives to prevent burnout: investing in professional development, reducing physicians’ administrative burdens, and celebrating physicians’ victories.
“Our goal is to provide the highest-quality health care employee experience possible. People will stay as long as you set that as a clear goal,” Dr. Myers said.
Primary care physician growth trails population growth
Although the total number of primary care physicians increased from 2005 to 2015, disproportionate losses across counties and general population increases have created an imbalance that may affect life expectancy, according to a study of U.S. population data and individual-level claims data linked to mortality.

“ suggesting that observed decreases in primary care physician supply may have important consequences for population health,” wrote lead author Sanjay Basu, MD, PhD, of Stanford (Calif.) University and his coauthors. The study was published online in JAMA Internal Medicine.
Dr. Basu and his colleagues gathered data from 3,142 U.S. counties, 7,144 primary care service areas, and 306 hospital referral regions over a 10-year period to determine whether primary care physician supply was correlated with changes in life expectancy and cause-specific mortality. They found that, from 2005 to 2015, the total number of primary care physicians increased from 196,014 to 204,419. However, mean primary care physician supply decreased from 46.6 per 100,000 population (95% confidence interval, 0.0-114.6 per 100,000 population) to 41.4 per 100,000 (95% CI, 0.0-108.6).
In the researchers’ fully adjusted models, an increase of 10 primary care physicians per 100,000 population was associated with a 51.5-day increase in life expectancy (95% CI, 29.5-73.5 days; 0.2% increase). This effect was more favorable than the foreseen result of a similar increase of 10 specialist physicians per 100,000 population, which was associated with a 19.2-day increase in life expectancy (95% CI, 7.0-31.3).
Almost 300 (296) counties had no primary care physicians in 2015, while 128 counties had more than 100 per 100,000 population. On average, rural areas saw a larger decrease than urban areas (–7.0 per 100,000 population vs –2.6 per 100,000 population). Primary care physician supply did not disproportionately decrease by county poverty level or racial/ethnic demographics.
The coauthors shared their study’s limitations, including the use of private insurance data to conduct individual-level analyses and the possibility for unobserved confounding. However, they also noted that their results reinforced earlier findings on primary care physician density and overall life expectancy, calling for “future investigations [to] acquire data on the quality and comprehensiveness of primary care, types of primary care physician training and service delivery offerings, and effective access rather than just supply.”
The study was supported by the National Institutes of Health; data was accessed through the Stanford Center for Population Health Sciences Data Core, which is supported by the National Center for Advancing Translational Sciences and by Stanford University. One author reported being a senior adviser at the Center for Medicare & Medicaid Innovation; another reported being an adviser to Bicycle Health. No conflicts of interest were reported.
SOURCE: Basu S et al. JAMA Intern Med. 2019 Feb 18. doi: 10.1001/jamainternmed.2018.7624.
Resolving the maldistribution of primary care physicians noted by Basu et al. will require a serious commitment to payment reform, according to Sondra Zabar, MD; Andrew Wallach, MD; and Adina Kaler, MD, of New York University.
Along with observing a steady decline in primary care interest overall, Dr. Zabar and her coauthors highlighted the lack of attraction to practicing in rural or urban areas. Among the reasons they cited are desired income, perceived workload, and level of debt. As compared to a well-run subspecialty practice, “most primary care physicians work with minimal support and can see only 2 to 3 patients per hour, and they are likely to receive lower payment than the subspecialty physician for each of those patients,” they wrote.
What solutions are there?
“Our reimbursement system needs to incentivize a realignment in the ratio between primary care and nonprimary care that is associated with the best population health such that primary care physicians no longer shoulder a disproportionate share of administrative work such as medication refills and prior authorizations,” they wrote. The problem has already been somewhat recognized by the Medicare Payment Advisory Commission and the Centers for Medicare & Medicaid Services, but more initiatives like debt forgiveness and innovative medical school curricula are needed to make a serious dent.
“To increase access to primary care, especially in underserved areas, we must align incentives to attract individuals into primary care practice, innovate primary care training, and greatly improve the primary care practice model,” they wrote. “Physician payment reform is a key to making all of this happen.”
These comments are adapted from an accompanying editorial (JAMA Intern Med. 2019 Feb 18. doi: 10.1001/jamainternmed.2018.7623 ). No conflicts of interest were reported.
Resolving the maldistribution of primary care physicians noted by Basu et al. will require a serious commitment to payment reform, according to Sondra Zabar, MD; Andrew Wallach, MD; and Adina Kaler, MD, of New York University.
Along with observing a steady decline in primary care interest overall, Dr. Zabar and her coauthors highlighted the lack of attraction to practicing in rural or urban areas. Among the reasons they cited are desired income, perceived workload, and level of debt. As compared to a well-run subspecialty practice, “most primary care physicians work with minimal support and can see only 2 to 3 patients per hour, and they are likely to receive lower payment than the subspecialty physician for each of those patients,” they wrote.
What solutions are there?
“Our reimbursement system needs to incentivize a realignment in the ratio between primary care and nonprimary care that is associated with the best population health such that primary care physicians no longer shoulder a disproportionate share of administrative work such as medication refills and prior authorizations,” they wrote. The problem has already been somewhat recognized by the Medicare Payment Advisory Commission and the Centers for Medicare & Medicaid Services, but more initiatives like debt forgiveness and innovative medical school curricula are needed to make a serious dent.
“To increase access to primary care, especially in underserved areas, we must align incentives to attract individuals into primary care practice, innovate primary care training, and greatly improve the primary care practice model,” they wrote. “Physician payment reform is a key to making all of this happen.”
These comments are adapted from an accompanying editorial (JAMA Intern Med. 2019 Feb 18. doi: 10.1001/jamainternmed.2018.7623 ). No conflicts of interest were reported.
Resolving the maldistribution of primary care physicians noted by Basu et al. will require a serious commitment to payment reform, according to Sondra Zabar, MD; Andrew Wallach, MD; and Adina Kaler, MD, of New York University.
Along with observing a steady decline in primary care interest overall, Dr. Zabar and her coauthors highlighted the lack of attraction to practicing in rural or urban areas. Among the reasons they cited are desired income, perceived workload, and level of debt. As compared to a well-run subspecialty practice, “most primary care physicians work with minimal support and can see only 2 to 3 patients per hour, and they are likely to receive lower payment than the subspecialty physician for each of those patients,” they wrote.
What solutions are there?
“Our reimbursement system needs to incentivize a realignment in the ratio between primary care and nonprimary care that is associated with the best population health such that primary care physicians no longer shoulder a disproportionate share of administrative work such as medication refills and prior authorizations,” they wrote. The problem has already been somewhat recognized by the Medicare Payment Advisory Commission and the Centers for Medicare & Medicaid Services, but more initiatives like debt forgiveness and innovative medical school curricula are needed to make a serious dent.
“To increase access to primary care, especially in underserved areas, we must align incentives to attract individuals into primary care practice, innovate primary care training, and greatly improve the primary care practice model,” they wrote. “Physician payment reform is a key to making all of this happen.”
These comments are adapted from an accompanying editorial (JAMA Intern Med. 2019 Feb 18. doi: 10.1001/jamainternmed.2018.7623 ). No conflicts of interest were reported.
Although the total number of primary care physicians increased from 2005 to 2015, disproportionate losses across counties and general population increases have created an imbalance that may affect life expectancy, according to a study of U.S. population data and individual-level claims data linked to mortality.
“ suggesting that observed decreases in primary care physician supply may have important consequences for population health,” wrote lead author Sanjay Basu, MD, PhD, of Stanford (Calif.) University and his coauthors. The study was published online in JAMA Internal Medicine.
Dr. Basu and his colleagues gathered data from 3,142 U.S. counties, 7,144 primary care service areas, and 306 hospital referral regions over a 10-year period to determine whether primary care physician supply was correlated with changes in life expectancy and cause-specific mortality. They found that, from 2005 to 2015, the total number of primary care physicians increased from 196,014 to 204,419. However, mean primary care physician supply decreased from 46.6 per 100,000 population (95% confidence interval, 0.0-114.6 per 100,000 population) to 41.4 per 100,000 (95% CI, 0.0-108.6).
In the researchers’ fully adjusted models, an increase of 10 primary care physicians per 100,000 population was associated with a 51.5-day increase in life expectancy (95% CI, 29.5-73.5 days; 0.2% increase). This effect was more favorable than the foreseen result of a similar increase of 10 specialist physicians per 100,000 population, which was associated with a 19.2-day increase in life expectancy (95% CI, 7.0-31.3).
Almost 300 (296) counties had no primary care physicians in 2015, while 128 counties had more than 100 per 100,000 population. On average, rural areas saw a larger decrease than urban areas (–7.0 per 100,000 population vs –2.6 per 100,000 population). Primary care physician supply did not disproportionately decrease by county poverty level or racial/ethnic demographics.
The coauthors shared their study’s limitations, including the use of private insurance data to conduct individual-level analyses and the possibility for unobserved confounding. However, they also noted that their results reinforced earlier findings on primary care physician density and overall life expectancy, calling for “future investigations [to] acquire data on the quality and comprehensiveness of primary care, types of primary care physician training and service delivery offerings, and effective access rather than just supply.”
The study was supported by the National Institutes of Health; data was accessed through the Stanford Center for Population Health Sciences Data Core, which is supported by the National Center for Advancing Translational Sciences and by Stanford University. One author reported being a senior adviser at the Center for Medicare & Medicaid Innovation; another reported being an adviser to Bicycle Health. No conflicts of interest were reported.
SOURCE: Basu S et al. JAMA Intern Med. 2019 Feb 18. doi: 10.1001/jamainternmed.2018.7624.
Although the total number of primary care physicians increased from 2005 to 2015, disproportionate losses across counties and general population increases have created an imbalance that may affect life expectancy, according to a study of U.S. population data and individual-level claims data linked to mortality.
“ suggesting that observed decreases in primary care physician supply may have important consequences for population health,” wrote lead author Sanjay Basu, MD, PhD, of Stanford (Calif.) University and his coauthors. The study was published online in JAMA Internal Medicine.
Dr. Basu and his colleagues gathered data from 3,142 U.S. counties, 7,144 primary care service areas, and 306 hospital referral regions over a 10-year period to determine whether primary care physician supply was correlated with changes in life expectancy and cause-specific mortality. They found that, from 2005 to 2015, the total number of primary care physicians increased from 196,014 to 204,419. However, mean primary care physician supply decreased from 46.6 per 100,000 population (95% confidence interval, 0.0-114.6 per 100,000 population) to 41.4 per 100,000 (95% CI, 0.0-108.6).
In the researchers’ fully adjusted models, an increase of 10 primary care physicians per 100,000 population was associated with a 51.5-day increase in life expectancy (95% CI, 29.5-73.5 days; 0.2% increase). This effect was more favorable than the foreseen result of a similar increase of 10 specialist physicians per 100,000 population, which was associated with a 19.2-day increase in life expectancy (95% CI, 7.0-31.3).
Almost 300 (296) counties had no primary care physicians in 2015, while 128 counties had more than 100 per 100,000 population. On average, rural areas saw a larger decrease than urban areas (–7.0 per 100,000 population vs –2.6 per 100,000 population). Primary care physician supply did not disproportionately decrease by county poverty level or racial/ethnic demographics.
The coauthors shared their study’s limitations, including the use of private insurance data to conduct individual-level analyses and the possibility for unobserved confounding. However, they also noted that their results reinforced earlier findings on primary care physician density and overall life expectancy, calling for “future investigations [to] acquire data on the quality and comprehensiveness of primary care, types of primary care physician training and service delivery offerings, and effective access rather than just supply.”
The study was supported by the National Institutes of Health; data was accessed through the Stanford Center for Population Health Sciences Data Core, which is supported by the National Center for Advancing Translational Sciences and by Stanford University. One author reported being a senior adviser at the Center for Medicare & Medicaid Innovation; another reported being an adviser to Bicycle Health. No conflicts of interest were reported.
SOURCE: Basu S et al. JAMA Intern Med. 2019 Feb 18. doi: 10.1001/jamainternmed.2018.7624.
FROM JAMA INTERNAL MEDICINE
Opportunities missed for advance care planning for elderly ICU patients
SAN DIEGO – A nationally representative survey of the problem is more pronounced among some blacks and Hispanics and those with lower net worth. The study also found that these patients see physicians an average of 20 times in the year preceding the ICU visit, which suggests that there are plenty of opportunities to put ACP in place.

“Over two-thirds were seen by a doctor in the last 2 weeks. So they’re seeing doctors, but they’re still not doing advance care planning,” said Brian Block, MD, during a presentation of the study at the Critical Care Congress sponsored by the Society of Critical Care Medicine. Dr. Block is with the University of California, San Francisco.
Lack of advance planning can put major road blocks in front of patient care in the ICU, as well as complicate communication between physicians and family members. The findings underscore the need to encourage conversations about end-of-life care between physicians and their patients – before the patients wind up in intensive care.
One audience member believes these conversations are already happening. Paul Yodice, MD, chairman of medicine at Saint Barnabas Medical Center in Livingston, N.J., suggested that physicians are attempting to engage older patients and family members in ACP, but many are unready to make decisions. “In my experience, it is happening much more frequently than is captured either in the medical record or in the research that we’ve been publishing. I’ve been a part of those conversations. Those individuals who are faced with those toughest of choices choose to delay making the decision or speaking about it further because it’s just too painful to consider, and they hold out hope of being the one to beat the odds, to have one more day,” said Dr. Yodice.
He called for further research to document whether ACP conversations are happening and to identify barriers to decisions and the means to overcome them. “A next good study would be to send out a respectful survey to the families of those who have lost people they love and ask: Has someone in the past year spoken with you or offered to have a discussion about end-of-life issues? We could get a better handle on [how often] the discussion is being had, and then find a solution,” said Dr. Yodice.
ACP can also be difficult for the provider, he added. Family members and patients, desperate for another treatment option, will often ask if there’s anything else that can be done. “In medicine, the answer almost always is ‘Well, we can try something else even though I know it’s not going to work.’ And people hold on to that, including us,” said Dr. Yodice.
The study analyzed data from a Medicare cohort of 1,109 patients who died during 2000-2013 and had an ICU admission within the last 30 days of their life. Ages were fairly evenly distributed, with 29% aged 65-74 years, 39% aged 75-84, and 32% aged 85 and over. Fifty-four percent were women, 26% were nonwhite, 42% had not completed high school, and 11% were in skilled nursing facilities.
About 35% had no ACP in 2000-2001, and that percentage gradually declined, to about 20% in 2012-2013 (slope, –1.6%/year; P = .009).
Seventeen percent of white participants had no ACP, compared with 51% of blacks and 49% of Hispanics. Net worth was also strongly associated with having ACP: The top quartile had 13% lacking ACP, compared with 43% of the bottom quartile.
The study found that 94% of patients who had no ACP had visited a health care provider in the past year. The average number of visits in the past year was 20, and 83% had seen a provider within the past 30 days.
Dr. Block did not declare a source of funding or potential conflicts. Dr. Yodice had no disclosures.
SOURCE: Block B et al. CCC48, Abstract 401.
SAN DIEGO – A nationally representative survey of the problem is more pronounced among some blacks and Hispanics and those with lower net worth. The study also found that these patients see physicians an average of 20 times in the year preceding the ICU visit, which suggests that there are plenty of opportunities to put ACP in place.
“Over two-thirds were seen by a doctor in the last 2 weeks. So they’re seeing doctors, but they’re still not doing advance care planning,” said Brian Block, MD, during a presentation of the study at the Critical Care Congress sponsored by the Society of Critical Care Medicine. Dr. Block is with the University of California, San Francisco.
Lack of advance planning can put major road blocks in front of patient care in the ICU, as well as complicate communication between physicians and family members. The findings underscore the need to encourage conversations about end-of-life care between physicians and their patients – before the patients wind up in intensive care.
One audience member believes these conversations are already happening. Paul Yodice, MD, chairman of medicine at Saint Barnabas Medical Center in Livingston, N.J., suggested that physicians are attempting to engage older patients and family members in ACP, but many are unready to make decisions. “In my experience, it is happening much more frequently than is captured either in the medical record or in the research that we’ve been publishing. I’ve been a part of those conversations. Those individuals who are faced with those toughest of choices choose to delay making the decision or speaking about it further because it’s just too painful to consider, and they hold out hope of being the one to beat the odds, to have one more day,” said Dr. Yodice.
He called for further research to document whether ACP conversations are happening and to identify barriers to decisions and the means to overcome them. “A next good study would be to send out a respectful survey to the families of those who have lost people they love and ask: Has someone in the past year spoken with you or offered to have a discussion about end-of-life issues? We could get a better handle on [how often] the discussion is being had, and then find a solution,” said Dr. Yodice.
ACP can also be difficult for the provider, he added. Family members and patients, desperate for another treatment option, will often ask if there’s anything else that can be done. “In medicine, the answer almost always is ‘Well, we can try something else even though I know it’s not going to work.’ And people hold on to that, including us,” said Dr. Yodice.
The study analyzed data from a Medicare cohort of 1,109 patients who died during 2000-2013 and had an ICU admission within the last 30 days of their life. Ages were fairly evenly distributed, with 29% aged 65-74 years, 39% aged 75-84, and 32% aged 85 and over. Fifty-four percent were women, 26% were nonwhite, 42% had not completed high school, and 11% were in skilled nursing facilities.
About 35% had no ACP in 2000-2001, and that percentage gradually declined, to about 20% in 2012-2013 (slope, –1.6%/year; P = .009).
Seventeen percent of white participants had no ACP, compared with 51% of blacks and 49% of Hispanics. Net worth was also strongly associated with having ACP: The top quartile had 13% lacking ACP, compared with 43% of the bottom quartile.
The study found that 94% of patients who had no ACP had visited a health care provider in the past year. The average number of visits in the past year was 20, and 83% had seen a provider within the past 30 days.
Dr. Block did not declare a source of funding or potential conflicts. Dr. Yodice had no disclosures.
SOURCE: Block B et al. CCC48, Abstract 401.
SAN DIEGO – A nationally representative survey of the problem is more pronounced among some blacks and Hispanics and those with lower net worth. The study also found that these patients see physicians an average of 20 times in the year preceding the ICU visit, which suggests that there are plenty of opportunities to put ACP in place.
“Over two-thirds were seen by a doctor in the last 2 weeks. So they’re seeing doctors, but they’re still not doing advance care planning,” said Brian Block, MD, during a presentation of the study at the Critical Care Congress sponsored by the Society of Critical Care Medicine. Dr. Block is with the University of California, San Francisco.
Lack of advance planning can put major road blocks in front of patient care in the ICU, as well as complicate communication between physicians and family members. The findings underscore the need to encourage conversations about end-of-life care between physicians and their patients – before the patients wind up in intensive care.
One audience member believes these conversations are already happening. Paul Yodice, MD, chairman of medicine at Saint Barnabas Medical Center in Livingston, N.J., suggested that physicians are attempting to engage older patients and family members in ACP, but many are unready to make decisions. “In my experience, it is happening much more frequently than is captured either in the medical record or in the research that we’ve been publishing. I’ve been a part of those conversations. Those individuals who are faced with those toughest of choices choose to delay making the decision or speaking about it further because it’s just too painful to consider, and they hold out hope of being the one to beat the odds, to have one more day,” said Dr. Yodice.
He called for further research to document whether ACP conversations are happening and to identify barriers to decisions and the means to overcome them. “A next good study would be to send out a respectful survey to the families of those who have lost people they love and ask: Has someone in the past year spoken with you or offered to have a discussion about end-of-life issues? We could get a better handle on [how often] the discussion is being had, and then find a solution,” said Dr. Yodice.
ACP can also be difficult for the provider, he added. Family members and patients, desperate for another treatment option, will often ask if there’s anything else that can be done. “In medicine, the answer almost always is ‘Well, we can try something else even though I know it’s not going to work.’ And people hold on to that, including us,” said Dr. Yodice.
The study analyzed data from a Medicare cohort of 1,109 patients who died during 2000-2013 and had an ICU admission within the last 30 days of their life. Ages were fairly evenly distributed, with 29% aged 65-74 years, 39% aged 75-84, and 32% aged 85 and over. Fifty-four percent were women, 26% were nonwhite, 42% had not completed high school, and 11% were in skilled nursing facilities.
About 35% had no ACP in 2000-2001, and that percentage gradually declined, to about 20% in 2012-2013 (slope, –1.6%/year; P = .009).
Seventeen percent of white participants had no ACP, compared with 51% of blacks and 49% of Hispanics. Net worth was also strongly associated with having ACP: The top quartile had 13% lacking ACP, compared with 43% of the bottom quartile.
The study found that 94% of patients who had no ACP had visited a health care provider in the past year. The average number of visits in the past year was 20, and 83% had seen a provider within the past 30 days.
Dr. Block did not declare a source of funding or potential conflicts. Dr. Yodice had no disclosures.
SOURCE: Block B et al. CCC48, Abstract 401.
REPORTING FROM CCC48
Commentary: Bias rules
Bias can be defined as a prejudice or a preformed inclination. Bias is reflective of one’s inherent mind set about any thing, concept, ideology, claim, product, person, or group of people. Since biases are well known to be inherent in human nature, one can fairly ask how important and how widespread are they and what are their effects?
Bias affects many fields including medicine. One example is the statin controversy. Some experts interpret existing data, which includes randomized controlled trials, to make a strong case that statins are harmful and do little good. In contrast, other qualified experts interpret precisely the same data to conclude that statins are miracle drugs that sharply diminish the mortality and morbidity from atherosclerosis. Again bias rules and leads to disagreement, controversy, and damaging public uncertainty.
A second examples in medicine – and there are many – is the current controversy over what constitutes the optimal treatment for patients with asymptomatic carotid stenosis. Some authorities believe no such patients should be treated invasively, while others hold the position that many should be. Still other experts opine that only a rare asymptomatic patient should undergo invasive treatment. All three groups use the same existing factual data to support their differing and sometimes totally opposite opinions. These contrasting views are reflected in articles in leading journals and differences among various guidelines from prestigious learned groups. The only explanation for their differing conclusions appears to be the fact that they are largely based on the bias of the authors of the articles or guidelines. Again, bias rules.
So these and many other examples exist in every phase of human endeavor. Biases are omnipresent and critically important in everything people do. They control our thinking, our opinions, our reasoning, our behavior, and most importantly, our decisions. They override most other forces that influence how we humans behave.
What can be done about this dominance of bias? The main safeguard against it is to recognize its controlling importance in all human thinking. Such recognition will help to offset the harmful effects of bias and encourage other, more laudable forces to influence behavior and actions. Logic is one such force. Even more important is objective interpretation of facts and a clear assessment of their validity.
Such objectivity may be difficult currently because of the overt bias expressed in our media and publications. If one doubts the influence of such bias, watch reports of the same event on CNN and Fox News. It is hard to believe the two sources are describing the same event. The same can be true of news reports in the New York Times and the Wall Street Journal. Bias often overrides objective reporting.
Somewhat surprisingly, even articles in our highly rated scientific journals are subject to the influences of bias. As in the lay press, scientific authors, reviewers, and editors all function under its spell.
By recognizing the importance, the dominance, and the universality of bias, individuals and groups can move toward neutralizing its divisive, damaging, and overall negative effects. Such recognition of bias will not eliminate it, but it would help to make the world a better place.
Dr. Veith is professor of surgery at New York University Langone Medical Center and Case Western Reserve University, Cleveland, as well as the William J. von Liebig Chair in Vascular Surgery at the Cleveland Clinic Foundation.
Bias can be defined as a prejudice or a preformed inclination. Bias is reflective of one’s inherent mind set about any thing, concept, ideology, claim, product, person, or group of people. Since biases are well known to be inherent in human nature, one can fairly ask how important and how widespread are they and what are their effects?
Bias affects many fields including medicine. One example is the statin controversy. Some experts interpret existing data, which includes randomized controlled trials, to make a strong case that statins are harmful and do little good. In contrast, other qualified experts interpret precisely the same data to conclude that statins are miracle drugs that sharply diminish the mortality and morbidity from atherosclerosis. Again bias rules and leads to disagreement, controversy, and damaging public uncertainty.
A second examples in medicine – and there are many – is the current controversy over what constitutes the optimal treatment for patients with asymptomatic carotid stenosis. Some authorities believe no such patients should be treated invasively, while others hold the position that many should be. Still other experts opine that only a rare asymptomatic patient should undergo invasive treatment. All three groups use the same existing factual data to support their differing and sometimes totally opposite opinions. These contrasting views are reflected in articles in leading journals and differences among various guidelines from prestigious learned groups. The only explanation for their differing conclusions appears to be the fact that they are largely based on the bias of the authors of the articles or guidelines. Again, bias rules.
So these and many other examples exist in every phase of human endeavor. Biases are omnipresent and critically important in everything people do. They control our thinking, our opinions, our reasoning, our behavior, and most importantly, our decisions. They override most other forces that influence how we humans behave.
What can be done about this dominance of bias? The main safeguard against it is to recognize its controlling importance in all human thinking. Such recognition will help to offset the harmful effects of bias and encourage other, more laudable forces to influence behavior and actions. Logic is one such force. Even more important is objective interpretation of facts and a clear assessment of their validity.
Such objectivity may be difficult currently because of the overt bias expressed in our media and publications. If one doubts the influence of such bias, watch reports of the same event on CNN and Fox News. It is hard to believe the two sources are describing the same event. The same can be true of news reports in the New York Times and the Wall Street Journal. Bias often overrides objective reporting.
Somewhat surprisingly, even articles in our highly rated scientific journals are subject to the influences of bias. As in the lay press, scientific authors, reviewers, and editors all function under its spell.
By recognizing the importance, the dominance, and the universality of bias, individuals and groups can move toward neutralizing its divisive, damaging, and overall negative effects. Such recognition of bias will not eliminate it, but it would help to make the world a better place.
Dr. Veith is professor of surgery at New York University Langone Medical Center and Case Western Reserve University, Cleveland, as well as the William J. von Liebig Chair in Vascular Surgery at the Cleveland Clinic Foundation.
Bias can be defined as a prejudice or a preformed inclination. Bias is reflective of one’s inherent mind set about any thing, concept, ideology, claim, product, person, or group of people. Since biases are well known to be inherent in human nature, one can fairly ask how important and how widespread are they and what are their effects?
Bias affects many fields including medicine. One example is the statin controversy. Some experts interpret existing data, which includes randomized controlled trials, to make a strong case that statins are harmful and do little good. In contrast, other qualified experts interpret precisely the same data to conclude that statins are miracle drugs that sharply diminish the mortality and morbidity from atherosclerosis. Again bias rules and leads to disagreement, controversy, and damaging public uncertainty.
A second examples in medicine – and there are many – is the current controversy over what constitutes the optimal treatment for patients with asymptomatic carotid stenosis. Some authorities believe no such patients should be treated invasively, while others hold the position that many should be. Still other experts opine that only a rare asymptomatic patient should undergo invasive treatment. All three groups use the same existing factual data to support their differing and sometimes totally opposite opinions. These contrasting views are reflected in articles in leading journals and differences among various guidelines from prestigious learned groups. The only explanation for their differing conclusions appears to be the fact that they are largely based on the bias of the authors of the articles or guidelines. Again, bias rules.
So these and many other examples exist in every phase of human endeavor. Biases are omnipresent and critically important in everything people do. They control our thinking, our opinions, our reasoning, our behavior, and most importantly, our decisions. They override most other forces that influence how we humans behave.
What can be done about this dominance of bias? The main safeguard against it is to recognize its controlling importance in all human thinking. Such recognition will help to offset the harmful effects of bias and encourage other, more laudable forces to influence behavior and actions. Logic is one such force. Even more important is objective interpretation of facts and a clear assessment of their validity.
Such objectivity may be difficult currently because of the overt bias expressed in our media and publications. If one doubts the influence of such bias, watch reports of the same event on CNN and Fox News. It is hard to believe the two sources are describing the same event. The same can be true of news reports in the New York Times and the Wall Street Journal. Bias often overrides objective reporting.
Somewhat surprisingly, even articles in our highly rated scientific journals are subject to the influences of bias. As in the lay press, scientific authors, reviewers, and editors all function under its spell.
By recognizing the importance, the dominance, and the universality of bias, individuals and groups can move toward neutralizing its divisive, damaging, and overall negative effects. Such recognition of bias will not eliminate it, but it would help to make the world a better place.
Dr. Veith is professor of surgery at New York University Langone Medical Center and Case Western Reserve University, Cleveland, as well as the William J. von Liebig Chair in Vascular Surgery at the Cleveland Clinic Foundation.
Enzalutamide boosts ADT benefit in metastatic hormone-sensitive prostate cancer
SAN FRANCISCO – Dual targeting of the androgen signaling axis in metastatic hormone-sensitive prostate cancer improves outcomes and is well tolerated, according to results of the phase 3 ARCHES trial reported at the 2019 Genitourinary Cancers Symposium sponsored by the American Society of Clinical Oncology, ASTRO, and the Society of Urologic Oncology.

“Androgen-deprivation therapy [ADT] has been the mainstay of therapy for men who present with metastatic disease for many years. But generally, progression to castration-resistant diseases is observed within approximately 3 years,” said lead investigator Andrew J. Armstrong, MD, a professor of medicine in medical oncology at Duke University, Durham, N.C.
“Thus the advent of improving outcomes with the [additional] use of early docetaxel, abiraterone, and now radiation to the primary in the face of oligometastatic disease has been shown to improve survival,” he added. “However, the most recent studies have really not studied the sequential use of docetaxel and have largely excluded patients who had had prior docetaxel chemotherapy in the hormone-sensitive setting.”
The investigators in the ARCHES trial (NCT02677896) randomized 1,150 men with metastatic hormone-sensitive prostate cancer to enzalutamide (Xtandi) plus ADT or placebo plus ADT.
With a median follow-up of 14.4 months, radiographic progression-free survival – the trial’s primary endpoint – was prolonged in the enzalutamide arm. Risk of progression or death was reduced by a relative 61% with enzalutamide versus placebo. There were also significant relative reductions in risks of other important outcomes such as time to prostate-specific antigen (PSA) progression (81% reduction), time to new antineoplastic therapy (72% reduction), and time to castration resistance (72% reduction).
Meanwhile, the enzalutamide group had somewhat more fatigue, hot flashes, and hypertension, but most of these events were grade 1 or 2. Rates of adverse events leading to treatment withdrawal were similar and low.
“Following the success of this study, all patients in the placebo group will be offered participation in an open-label extension protocol where they’ll be offered enzalutamide and the opportunity to receive a clinically beneficial treatment,” Dr. Armstrong reported.
Ready for prime time?
The ARCHES findings are probably not yet sufficient to be implemented in real-world practice, according to invited discussant Ian D. Davis, MBBS, PhD, a professor at Monash University, Melbourne.
The condition studied in the trial – metastatic hormone-sensitive prostate cancer – certainly needs treatment, but it is unclear whether radiographic progression-free survival is a meaningful endpoint, he said. “We know in the CRPC [castration-resistant prostate cancer] setting for enzalutamide in the PREVAIL study, radiographic progression-free survival was correlated with overall survival, but we haven’t actually proven that yet in the CSPC [castration-sensitive prostate cancer] setting.”
Toxicity was acceptable, but information about the efficacy of subsequent treatment is lacking. “This is where progression-free survival 2 [PFS2] information would be useful if we had it,” Dr. Davis noted. Cost-effectiveness in terms of overall survival is likewise still unknown.
“Cautiously, and I’m conscious of my conflict of interest here because I’m doing a similar trial, I’d say that the ARCHES trial should probably not yet change practice,” he said. However, he qualified that statement by pointing to recently announced results from the phase 3 TITAN trial (NCT02489318) of apalutamide (Erleada), showing significant radiographic progression-free survival and overall survival benefit in this patient population. “So we await those data with interest.”
The first interim analysis of the enzalutamide trial he is cochairing, ANZUP ENZAMET (NCT02446405), is imminent, according to Dr. Davis. “The differences here are the primary endpoint of ENZAMET is overall survival and there was an early amendment to allow concurrent docetaxel, so a significant proportion of patients on this study will have received concurrent docetaxel with enzalutamide or ADT,” he noted.
Study details
Men enrolled in ARCHES were allowed to have received prior ADT for up to 3 months or, if they had received docetaxel, for up to 6 months, Dr. Armstrong noted at the symposium.
About two-thirds each had high disease volume and had distant metastasis at their initial diagnosis. Overall, median duration of prior ADT was 1.6 months.
Radiographic progression-free survival was not reached with enzalutamide versus 19.45 months with placebo (hazard ratio, 0.39; P less than .0001). Corresponding 12-month rates were 84% and 64%. Findings were essentially the same across diverse subgroups, including among the 18% of patients who had received prior docetaxel (HR, 0.53).
Median time to PSA progression – typically one of the first indications of castration resistance – was not reached in either group, but the 12-month rate was 91% with enzalutamide versus 63% with placebo (HR, 0.19; P less than .0001), Dr. Armstrong reported. Median time to castration resistance was not reached with enzalutamide versus 13.9 months with placebo (HR, 0.28; P less than .0001).
There also were significant differences in favor of enzalutamide on the rate of achievement of undetectable PSA (68.1% vs. 17.6%; P less than .0001), the objective response rate (83.1% vs. 63.7%; P less than .0001), and the time to initiation of new antineoplastic therapy (not reached vs. 30.19 months; HR, 0.28; P less than .0001).
Quality of life was very high in both groups at study baseline and remained similarly so during follow-up. An interim analysis showed overall survival had not been reached in either group, although there was a nonsignificant trend favoring enzalutamide.
Safety was much the same, with the enzalutamide and placebo groups having similar rates of grade 3 or worse adverse events (24.3% vs. 25.6%), as well as similar rates of adverse events leading to treatment withdrawal (7.2% vs. 5.2%) and death (2.4% vs. 1.7%).
In terms of adverse events of special interest, the groups were comparable on rates of grade 3 or 4 convulsion, ischemic heart disease, falls, and fractures.
Dr. Armstrong disclosed that he has a consulting or advisory role with, receives research funding (institutional) from, and receives travel, accommodations, and/or expenses from Astellas – among other disclosures. The trial was sponsored by Astellas.
SOURCE: Armstrong AJ et al. GUCS 2019, Abstract 687.
SAN FRANCISCO – Dual targeting of the androgen signaling axis in metastatic hormone-sensitive prostate cancer improves outcomes and is well tolerated, according to results of the phase 3 ARCHES trial reported at the 2019 Genitourinary Cancers Symposium sponsored by the American Society of Clinical Oncology, ASTRO, and the Society of Urologic Oncology.
“Androgen-deprivation therapy [ADT] has been the mainstay of therapy for men who present with metastatic disease for many years. But generally, progression to castration-resistant diseases is observed within approximately 3 years,” said lead investigator Andrew J. Armstrong, MD, a professor of medicine in medical oncology at Duke University, Durham, N.C.
“Thus the advent of improving outcomes with the [additional] use of early docetaxel, abiraterone, and now radiation to the primary in the face of oligometastatic disease has been shown to improve survival,” he added. “However, the most recent studies have really not studied the sequential use of docetaxel and have largely excluded patients who had had prior docetaxel chemotherapy in the hormone-sensitive setting.”
The investigators in the ARCHES trial (NCT02677896) randomized 1,150 men with metastatic hormone-sensitive prostate cancer to enzalutamide (Xtandi) plus ADT or placebo plus ADT.
With a median follow-up of 14.4 months, radiographic progression-free survival – the trial’s primary endpoint – was prolonged in the enzalutamide arm. Risk of progression or death was reduced by a relative 61% with enzalutamide versus placebo. There were also significant relative reductions in risks of other important outcomes such as time to prostate-specific antigen (PSA) progression (81% reduction), time to new antineoplastic therapy (72% reduction), and time to castration resistance (72% reduction).
Meanwhile, the enzalutamide group had somewhat more fatigue, hot flashes, and hypertension, but most of these events were grade 1 or 2. Rates of adverse events leading to treatment withdrawal were similar and low.
“Following the success of this study, all patients in the placebo group will be offered participation in an open-label extension protocol where they’ll be offered enzalutamide and the opportunity to receive a clinically beneficial treatment,” Dr. Armstrong reported.
Ready for prime time?
The ARCHES findings are probably not yet sufficient to be implemented in real-world practice, according to invited discussant Ian D. Davis, MBBS, PhD, a professor at Monash University, Melbourne.
The condition studied in the trial – metastatic hormone-sensitive prostate cancer – certainly needs treatment, but it is unclear whether radiographic progression-free survival is a meaningful endpoint, he said. “We know in the CRPC [castration-resistant prostate cancer] setting for enzalutamide in the PREVAIL study, radiographic progression-free survival was correlated with overall survival, but we haven’t actually proven that yet in the CSPC [castration-sensitive prostate cancer] setting.”
Toxicity was acceptable, but information about the efficacy of subsequent treatment is lacking. “This is where progression-free survival 2 [PFS2] information would be useful if we had it,” Dr. Davis noted. Cost-effectiveness in terms of overall survival is likewise still unknown.
“Cautiously, and I’m conscious of my conflict of interest here because I’m doing a similar trial, I’d say that the ARCHES trial should probably not yet change practice,” he said. However, he qualified that statement by pointing to recently announced results from the phase 3 TITAN trial (NCT02489318) of apalutamide (Erleada), showing significant radiographic progression-free survival and overall survival benefit in this patient population. “So we await those data with interest.”
The first interim analysis of the enzalutamide trial he is cochairing, ANZUP ENZAMET (NCT02446405), is imminent, according to Dr. Davis. “The differences here are the primary endpoint of ENZAMET is overall survival and there was an early amendment to allow concurrent docetaxel, so a significant proportion of patients on this study will have received concurrent docetaxel with enzalutamide or ADT,” he noted.
Study details
Men enrolled in ARCHES were allowed to have received prior ADT for up to 3 months or, if they had received docetaxel, for up to 6 months, Dr. Armstrong noted at the symposium.
About two-thirds each had high disease volume and had distant metastasis at their initial diagnosis. Overall, median duration of prior ADT was 1.6 months.
Radiographic progression-free survival was not reached with enzalutamide versus 19.45 months with placebo (hazard ratio, 0.39; P less than .0001). Corresponding 12-month rates were 84% and 64%. Findings were essentially the same across diverse subgroups, including among the 18% of patients who had received prior docetaxel (HR, 0.53).
Median time to PSA progression – typically one of the first indications of castration resistance – was not reached in either group, but the 12-month rate was 91% with enzalutamide versus 63% with placebo (HR, 0.19; P less than .0001), Dr. Armstrong reported. Median time to castration resistance was not reached with enzalutamide versus 13.9 months with placebo (HR, 0.28; P less than .0001).
There also were significant differences in favor of enzalutamide on the rate of achievement of undetectable PSA (68.1% vs. 17.6%; P less than .0001), the objective response rate (83.1% vs. 63.7%; P less than .0001), and the time to initiation of new antineoplastic therapy (not reached vs. 30.19 months; HR, 0.28; P less than .0001).
Quality of life was very high in both groups at study baseline and remained similarly so during follow-up. An interim analysis showed overall survival had not been reached in either group, although there was a nonsignificant trend favoring enzalutamide.
Safety was much the same, with the enzalutamide and placebo groups having similar rates of grade 3 or worse adverse events (24.3% vs. 25.6%), as well as similar rates of adverse events leading to treatment withdrawal (7.2% vs. 5.2%) and death (2.4% vs. 1.7%).
In terms of adverse events of special interest, the groups were comparable on rates of grade 3 or 4 convulsion, ischemic heart disease, falls, and fractures.
Dr. Armstrong disclosed that he has a consulting or advisory role with, receives research funding (institutional) from, and receives travel, accommodations, and/or expenses from Astellas – among other disclosures. The trial was sponsored by Astellas.
SOURCE: Armstrong AJ et al. GUCS 2019, Abstract 687.
SAN FRANCISCO – Dual targeting of the androgen signaling axis in metastatic hormone-sensitive prostate cancer improves outcomes and is well tolerated, according to results of the phase 3 ARCHES trial reported at the 2019 Genitourinary Cancers Symposium sponsored by the American Society of Clinical Oncology, ASTRO, and the Society of Urologic Oncology.
“Androgen-deprivation therapy [ADT] has been the mainstay of therapy for men who present with metastatic disease for many years. But generally, progression to castration-resistant diseases is observed within approximately 3 years,” said lead investigator Andrew J. Armstrong, MD, a professor of medicine in medical oncology at Duke University, Durham, N.C.
“Thus the advent of improving outcomes with the [additional] use of early docetaxel, abiraterone, and now radiation to the primary in the face of oligometastatic disease has been shown to improve survival,” he added. “However, the most recent studies have really not studied the sequential use of docetaxel and have largely excluded patients who had had prior docetaxel chemotherapy in the hormone-sensitive setting.”
The investigators in the ARCHES trial (NCT02677896) randomized 1,150 men with metastatic hormone-sensitive prostate cancer to enzalutamide (Xtandi) plus ADT or placebo plus ADT.
With a median follow-up of 14.4 months, radiographic progression-free survival – the trial’s primary endpoint – was prolonged in the enzalutamide arm. Risk of progression or death was reduced by a relative 61% with enzalutamide versus placebo. There were also significant relative reductions in risks of other important outcomes such as time to prostate-specific antigen (PSA) progression (81% reduction), time to new antineoplastic therapy (72% reduction), and time to castration resistance (72% reduction).
Meanwhile, the enzalutamide group had somewhat more fatigue, hot flashes, and hypertension, but most of these events were grade 1 or 2. Rates of adverse events leading to treatment withdrawal were similar and low.
“Following the success of this study, all patients in the placebo group will be offered participation in an open-label extension protocol where they’ll be offered enzalutamide and the opportunity to receive a clinically beneficial treatment,” Dr. Armstrong reported.
Ready for prime time?
The ARCHES findings are probably not yet sufficient to be implemented in real-world practice, according to invited discussant Ian D. Davis, MBBS, PhD, a professor at Monash University, Melbourne.
The condition studied in the trial – metastatic hormone-sensitive prostate cancer – certainly needs treatment, but it is unclear whether radiographic progression-free survival is a meaningful endpoint, he said. “We know in the CRPC [castration-resistant prostate cancer] setting for enzalutamide in the PREVAIL study, radiographic progression-free survival was correlated with overall survival, but we haven’t actually proven that yet in the CSPC [castration-sensitive prostate cancer] setting.”
Toxicity was acceptable, but information about the efficacy of subsequent treatment is lacking. “This is where progression-free survival 2 [PFS2] information would be useful if we had it,” Dr. Davis noted. Cost-effectiveness in terms of overall survival is likewise still unknown.
“Cautiously, and I’m conscious of my conflict of interest here because I’m doing a similar trial, I’d say that the ARCHES trial should probably not yet change practice,” he said. However, he qualified that statement by pointing to recently announced results from the phase 3 TITAN trial (NCT02489318) of apalutamide (Erleada), showing significant radiographic progression-free survival and overall survival benefit in this patient population. “So we await those data with interest.”
The first interim analysis of the enzalutamide trial he is cochairing, ANZUP ENZAMET (NCT02446405), is imminent, according to Dr. Davis. “The differences here are the primary endpoint of ENZAMET is overall survival and there was an early amendment to allow concurrent docetaxel, so a significant proportion of patients on this study will have received concurrent docetaxel with enzalutamide or ADT,” he noted.
Study details
Men enrolled in ARCHES were allowed to have received prior ADT for up to 3 months or, if they had received docetaxel, for up to 6 months, Dr. Armstrong noted at the symposium.
About two-thirds each had high disease volume and had distant metastasis at their initial diagnosis. Overall, median duration of prior ADT was 1.6 months.
Radiographic progression-free survival was not reached with enzalutamide versus 19.45 months with placebo (hazard ratio, 0.39; P less than .0001). Corresponding 12-month rates were 84% and 64%. Findings were essentially the same across diverse subgroups, including among the 18% of patients who had received prior docetaxel (HR, 0.53).
Median time to PSA progression – typically one of the first indications of castration resistance – was not reached in either group, but the 12-month rate was 91% with enzalutamide versus 63% with placebo (HR, 0.19; P less than .0001), Dr. Armstrong reported. Median time to castration resistance was not reached with enzalutamide versus 13.9 months with placebo (HR, 0.28; P less than .0001).
There also were significant differences in favor of enzalutamide on the rate of achievement of undetectable PSA (68.1% vs. 17.6%; P less than .0001), the objective response rate (83.1% vs. 63.7%; P less than .0001), and the time to initiation of new antineoplastic therapy (not reached vs. 30.19 months; HR, 0.28; P less than .0001).
Quality of life was very high in both groups at study baseline and remained similarly so during follow-up. An interim analysis showed overall survival had not been reached in either group, although there was a nonsignificant trend favoring enzalutamide.
Safety was much the same, with the enzalutamide and placebo groups having similar rates of grade 3 or worse adverse events (24.3% vs. 25.6%), as well as similar rates of adverse events leading to treatment withdrawal (7.2% vs. 5.2%) and death (2.4% vs. 1.7%).
In terms of adverse events of special interest, the groups were comparable on rates of grade 3 or 4 convulsion, ischemic heart disease, falls, and fractures.
Dr. Armstrong disclosed that he has a consulting or advisory role with, receives research funding (institutional) from, and receives travel, accommodations, and/or expenses from Astellas – among other disclosures. The trial was sponsored by Astellas.
SOURCE: Armstrong AJ et al. GUCS 2019, Abstract 687.
REPORTING FROM GUCS 2019
The ever-evolving scope of hospitalists’ clinical services
More care ‘beyond the walls’ of the hospital
The 2018 State of Hospital Medicine (SoHM) Report provides indispensable data about the scope of clinical services routinely provided by adult and pediatric hospitalists. This year’s SoHM report reveals that a growing number of Hospital Medicine Groups (HMGs) serving adults are involved in roles beyond the inpatient medical wards, including various surgical comanagement programs, outpatient care, and post-acute care services.

The survey also compares services provided by academic and nonacademic HMGs, which remain markedly different in some areas. As the landscape of health care continues to evolve, hospitalists transform their scope of services to meet the needs of the institutions and communities they serve.
In the previous three SoHM reports, it was well established that more than 87% of adult hospital medicine groups play some role in comanaging surgical patients. In this year’s SoHM report, that role was further stratified to capture the various subspecialties represented, and to identify whether the hospitalists generally served as admitting/attending physician or consultant.
Hospitalists’ roles in comanagement are most prominent for care of orthopedic and general surgery patients, but more than 50% of surveyed HMGs reported being involved in comanagement in some capacity with neurosurgery, obstetrics, and cardiovascular surgery. Additionally, almost 95% of surveyed adult HMGs reported that they provided comanagement services for at least one other surgical specialty that was not listed in the survey.
The report also displays comanagement services provided to various medical subspecialties, including neurology, GI/liver, oncology, and more. Of the medical subspecialties represented, adult HMGs comanaged GI/liver (98.2%) and oncology (97.7%) services more often than others.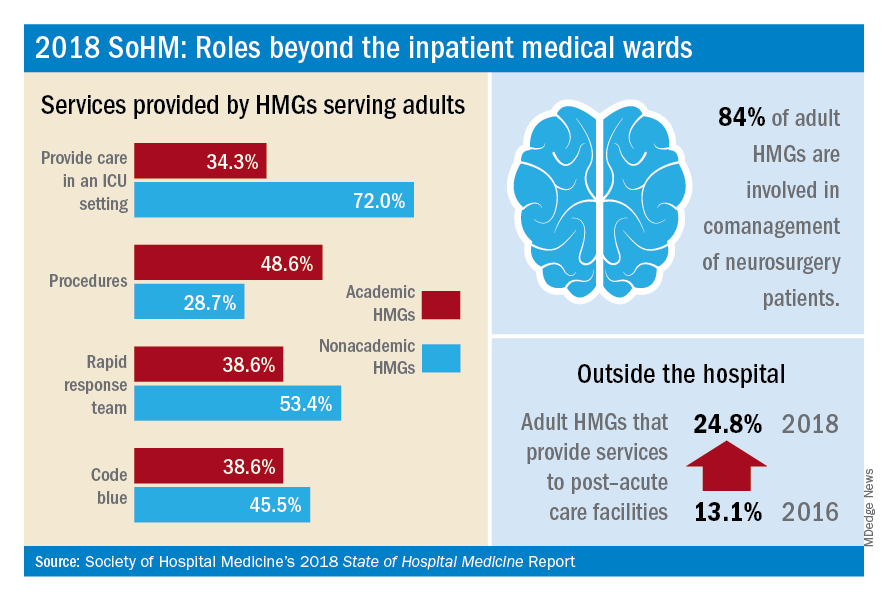
Interestingly, more HMGs are providing care for patients beyond the walls of the hospital. In the 2018 SoHM report, over 17% of surveyed HMG respondents reported providing care in an outpatient setting, representing an increase of 6.5 percentage points over 2016. Most strikingly, from 2016 to 2018, there was a 12 percentage point increase in adult HMGs reporting services provided to post-acute care facilities (from 13.1% to 24.8%).
These trends were most notable in the Midwest region where nearly 28% of HMGs provide patient care in an outpatient setting and up to 34% in post-acute care facilities. In part, this trend may result from the increased emphasis on improving transitions of care, by providing prehospital preoperative services, postdischarge follow-up encounters, or offering posthospitalization extensivist care.
Within the hospital itself, there remain striking differences in certain services provided by academic and nonacademic HMGs serving adults. Nonacademic HMGs are far more likely to cover patients in an ICU than their academic counterparts (72.0% vs. 34.3%). In contrast, academic hospitalist groups were significantly more inclined to perform procedures. However, the report also showed that there was an overall downtrend of percentage of HMGs that cover patients in an ICU or perform procedures.
As the scope of hospitalist services continues to change over time, should there be concern for scope creep? It depends on how one might view the change. As health care becomes ever more complex, high-functioning HMGs are needed to navigate it, both within and beyond the hospital. Some might consider scope evolution to be a reflection of hospitalists being recognized for their ability to provide high-quality, efficient, and comprehensive care. Hospital medicine groups will likely continue to evolve to meet the needs of an ever-changing health care environment.
Dr. Kurian is chief of the academic division of hospital medicine at Northwell Health in New York. She is a member of the SHM Practice Analysis Committee.
More care ‘beyond the walls’ of the hospital
More care ‘beyond the walls’ of the hospital
The 2018 State of Hospital Medicine (SoHM) Report provides indispensable data about the scope of clinical services routinely provided by adult and pediatric hospitalists. This year’s SoHM report reveals that a growing number of Hospital Medicine Groups (HMGs) serving adults are involved in roles beyond the inpatient medical wards, including various surgical comanagement programs, outpatient care, and post-acute care services.
The survey also compares services provided by academic and nonacademic HMGs, which remain markedly different in some areas. As the landscape of health care continues to evolve, hospitalists transform their scope of services to meet the needs of the institutions and communities they serve.
In the previous three SoHM reports, it was well established that more than 87% of adult hospital medicine groups play some role in comanaging surgical patients. In this year’s SoHM report, that role was further stratified to capture the various subspecialties represented, and to identify whether the hospitalists generally served as admitting/attending physician or consultant.
Hospitalists’ roles in comanagement are most prominent for care of orthopedic and general surgery patients, but more than 50% of surveyed HMGs reported being involved in comanagement in some capacity with neurosurgery, obstetrics, and cardiovascular surgery. Additionally, almost 95% of surveyed adult HMGs reported that they provided comanagement services for at least one other surgical specialty that was not listed in the survey.
The report also displays comanagement services provided to various medical subspecialties, including neurology, GI/liver, oncology, and more. Of the medical subspecialties represented, adult HMGs comanaged GI/liver (98.2%) and oncology (97.7%) services more often than others.
Interestingly, more HMGs are providing care for patients beyond the walls of the hospital. In the 2018 SoHM report, over 17% of surveyed HMG respondents reported providing care in an outpatient setting, representing an increase of 6.5 percentage points over 2016. Most strikingly, from 2016 to 2018, there was a 12 percentage point increase in adult HMGs reporting services provided to post-acute care facilities (from 13.1% to 24.8%).
These trends were most notable in the Midwest region where nearly 28% of HMGs provide patient care in an outpatient setting and up to 34% in post-acute care facilities. In part, this trend may result from the increased emphasis on improving transitions of care, by providing prehospital preoperative services, postdischarge follow-up encounters, or offering posthospitalization extensivist care.
Within the hospital itself, there remain striking differences in certain services provided by academic and nonacademic HMGs serving adults. Nonacademic HMGs are far more likely to cover patients in an ICU than their academic counterparts (72.0% vs. 34.3%). In contrast, academic hospitalist groups were significantly more inclined to perform procedures. However, the report also showed that there was an overall downtrend of percentage of HMGs that cover patients in an ICU or perform procedures.
As the scope of hospitalist services continues to change over time, should there be concern for scope creep? It depends on how one might view the change. As health care becomes ever more complex, high-functioning HMGs are needed to navigate it, both within and beyond the hospital. Some might consider scope evolution to be a reflection of hospitalists being recognized for their ability to provide high-quality, efficient, and comprehensive care. Hospital medicine groups will likely continue to evolve to meet the needs of an ever-changing health care environment.
Dr. Kurian is chief of the academic division of hospital medicine at Northwell Health in New York. She is a member of the SHM Practice Analysis Committee.
The 2018 State of Hospital Medicine (SoHM) Report provides indispensable data about the scope of clinical services routinely provided by adult and pediatric hospitalists. This year’s SoHM report reveals that a growing number of Hospital Medicine Groups (HMGs) serving adults are involved in roles beyond the inpatient medical wards, including various surgical comanagement programs, outpatient care, and post-acute care services.
The survey also compares services provided by academic and nonacademic HMGs, which remain markedly different in some areas. As the landscape of health care continues to evolve, hospitalists transform their scope of services to meet the needs of the institutions and communities they serve.
In the previous three SoHM reports, it was well established that more than 87% of adult hospital medicine groups play some role in comanaging surgical patients. In this year’s SoHM report, that role was further stratified to capture the various subspecialties represented, and to identify whether the hospitalists generally served as admitting/attending physician or consultant.
Hospitalists’ roles in comanagement are most prominent for care of orthopedic and general surgery patients, but more than 50% of surveyed HMGs reported being involved in comanagement in some capacity with neurosurgery, obstetrics, and cardiovascular surgery. Additionally, almost 95% of surveyed adult HMGs reported that they provided comanagement services for at least one other surgical specialty that was not listed in the survey.
The report also displays comanagement services provided to various medical subspecialties, including neurology, GI/liver, oncology, and more. Of the medical subspecialties represented, adult HMGs comanaged GI/liver (98.2%) and oncology (97.7%) services more often than others.
Interestingly, more HMGs are providing care for patients beyond the walls of the hospital. In the 2018 SoHM report, over 17% of surveyed HMG respondents reported providing care in an outpatient setting, representing an increase of 6.5 percentage points over 2016. Most strikingly, from 2016 to 2018, there was a 12 percentage point increase in adult HMGs reporting services provided to post-acute care facilities (from 13.1% to 24.8%).
These trends were most notable in the Midwest region where nearly 28% of HMGs provide patient care in an outpatient setting and up to 34% in post-acute care facilities. In part, this trend may result from the increased emphasis on improving transitions of care, by providing prehospital preoperative services, postdischarge follow-up encounters, or offering posthospitalization extensivist care.
Within the hospital itself, there remain striking differences in certain services provided by academic and nonacademic HMGs serving adults. Nonacademic HMGs are far more likely to cover patients in an ICU than their academic counterparts (72.0% vs. 34.3%). In contrast, academic hospitalist groups were significantly more inclined to perform procedures. However, the report also showed that there was an overall downtrend of percentage of HMGs that cover patients in an ICU or perform procedures.
As the scope of hospitalist services continues to change over time, should there be concern for scope creep? It depends on how one might view the change. As health care becomes ever more complex, high-functioning HMGs are needed to navigate it, both within and beyond the hospital. Some might consider scope evolution to be a reflection of hospitalists being recognized for their ability to provide high-quality, efficient, and comprehensive care. Hospital medicine groups will likely continue to evolve to meet the needs of an ever-changing health care environment.
Dr. Kurian is chief of the academic division of hospital medicine at Northwell Health in New York. She is a member of the SHM Practice Analysis Committee.
U.S. measles cases up to 159 for the year
Reported measles cases are now up to 159 for the year in the United States, according to the Centers for Disease Control and Prevention.

The most recent reporting week, which ended Feb. 21, brought another 32 cases of measles and one new outbreak of 4 cases in Illinois. The total number of outbreaks – an outbreak is defined as three or more cases – is now six, and cases have been reported in 10 states, the CDC said Feb. 25.
The majority (17) of those 32 new cases occurred in Brooklyn, one of New York state’s three outbreaks this year. The largest of the 2019 outbreaks is in Washington state, primarily in Clark County, and is up to 66 cases after 4 more were reported in the last week by the state’s department of health. The outbreaks are linked to travelers who brought the disease to the United States.
There are now two measures “advancing through the [Washington] state legislature that would bar parents from using personal or philosophical exemptions to avoid immunizing their school-age children. Both have bipartisan support despite strong antivaccination sentiment in parts of the state,” the Washington Post said on Feb. 25.
Reported measles cases are now up to 159 for the year in the United States, according to the Centers for Disease Control and Prevention.
The most recent reporting week, which ended Feb. 21, brought another 32 cases of measles and one new outbreak of 4 cases in Illinois. The total number of outbreaks – an outbreak is defined as three or more cases – is now six, and cases have been reported in 10 states, the CDC said Feb. 25.
The majority (17) of those 32 new cases occurred in Brooklyn, one of New York state’s three outbreaks this year. The largest of the 2019 outbreaks is in Washington state, primarily in Clark County, and is up to 66 cases after 4 more were reported in the last week by the state’s department of health. The outbreaks are linked to travelers who brought the disease to the United States.
There are now two measures “advancing through the [Washington] state legislature that would bar parents from using personal or philosophical exemptions to avoid immunizing their school-age children. Both have bipartisan support despite strong antivaccination sentiment in parts of the state,” the Washington Post said on Feb. 25.
Reported measles cases are now up to 159 for the year in the United States, according to the Centers for Disease Control and Prevention.
The most recent reporting week, which ended Feb. 21, brought another 32 cases of measles and one new outbreak of 4 cases in Illinois. The total number of outbreaks – an outbreak is defined as three or more cases – is now six, and cases have been reported in 10 states, the CDC said Feb. 25.
The majority (17) of those 32 new cases occurred in Brooklyn, one of New York state’s three outbreaks this year. The largest of the 2019 outbreaks is in Washington state, primarily in Clark County, and is up to 66 cases after 4 more were reported in the last week by the state’s department of health. The outbreaks are linked to travelers who brought the disease to the United States.
There are now two measures “advancing through the [Washington] state legislature that would bar parents from using personal or philosophical exemptions to avoid immunizing their school-age children. Both have bipartisan support despite strong antivaccination sentiment in parts of the state,” the Washington Post said on Feb. 25.
FDA: Safety signal emerged with higher dose of tofacitinib in RA study
the Food and Drug Administration reported.

The trial’s Data Safety and Monitoring Board identified the signal in patients taking a 10-mg dose of tofacitinib twice daily, the FDA said in a safety announcement.
Pfizer, the trial’s sponsor, took “immediate action” to transition patients in the ongoing trial from the 10-mg, twice-daily dose to 5 mg twice daily, which is the approved dose for adult patients with moderate to severe rheumatoid arthritis, the agency said. The 10-mg, twice-daily dose is approved only in the dosing regimen for patients with ulcerative colitis. Xeljanz is also approved to treat psoriatic arthritis. The 11-mg, once-daily dose of Xeljanz XR that is approved to treat rheumatoid arthritis and psoriatic arthritis was not tested in the trial.
The ongoing study was designed to assess risks of cardiovascular events, cancer, and opportunistic infections with tofacitinib 10 mg twice daily or 5 mg twice daily versus the risks in a control group treated with a tumor necrosis factor (TNF) inhibitor, according to the statement.
Patients had to be 50 years of age or older and have at least one cardiovascular risk factor to be eligible for the study, which was required by the agency in 2012 when it approved tofacitinib, the statement says.
The FDA is reviewing trial data and working with Pfizer to better understand the safety signal, its effect on patients, and how tofacitinib should be used, Janet Woodcock, MD, director of the FDA’s Center for Drug Evaluation and Research, said in a news release. The trial will continue and is expected to be completed by the end of 2019.
“The agency will take appropriate action, as warranted, to ensure patients enrolled in this and other trials are protected and that health care professionals and clinical trial researchers understand the risks associated with this use,” she added.
Health care professionals should follow tofacitinib prescribing information, monitor patients for the signs and symptoms of pulmonary embolism, and advise patients to seek medical attention immediately if they experience those signs and symptoms, according to the statement.
“We are communicating now, given the serious nature of the safety issue, to ensure that patients taking tofacitinib are aware that the FDA still believes the benefits of taking tofacitinib for its approved uses continue to outweigh the risks,” Dr. Woodcock said in the release.
While not approved in rheumatoid arthritis, the 10-mg, twice-daily dose of tofacitinib is approved in the dosing regimen for patients with ulcerative colitis, the release says.
the Food and Drug Administration reported.
The trial’s Data Safety and Monitoring Board identified the signal in patients taking a 10-mg dose of tofacitinib twice daily, the FDA said in a safety announcement.
Pfizer, the trial’s sponsor, took “immediate action” to transition patients in the ongoing trial from the 10-mg, twice-daily dose to 5 mg twice daily, which is the approved dose for adult patients with moderate to severe rheumatoid arthritis, the agency said. The 10-mg, twice-daily dose is approved only in the dosing regimen for patients with ulcerative colitis. Xeljanz is also approved to treat psoriatic arthritis. The 11-mg, once-daily dose of Xeljanz XR that is approved to treat rheumatoid arthritis and psoriatic arthritis was not tested in the trial.
The ongoing study was designed to assess risks of cardiovascular events, cancer, and opportunistic infections with tofacitinib 10 mg twice daily or 5 mg twice daily versus the risks in a control group treated with a tumor necrosis factor (TNF) inhibitor, according to the statement.
Patients had to be 50 years of age or older and have at least one cardiovascular risk factor to be eligible for the study, which was required by the agency in 2012 when it approved tofacitinib, the statement says.
The FDA is reviewing trial data and working with Pfizer to better understand the safety signal, its effect on patients, and how tofacitinib should be used, Janet Woodcock, MD, director of the FDA’s Center for Drug Evaluation and Research, said in a news release. The trial will continue and is expected to be completed by the end of 2019.
“The agency will take appropriate action, as warranted, to ensure patients enrolled in this and other trials are protected and that health care professionals and clinical trial researchers understand the risks associated with this use,” she added.
Health care professionals should follow tofacitinib prescribing information, monitor patients for the signs and symptoms of pulmonary embolism, and advise patients to seek medical attention immediately if they experience those signs and symptoms, according to the statement.
“We are communicating now, given the serious nature of the safety issue, to ensure that patients taking tofacitinib are aware that the FDA still believes the benefits of taking tofacitinib for its approved uses continue to outweigh the risks,” Dr. Woodcock said in the release.
While not approved in rheumatoid arthritis, the 10-mg, twice-daily dose of tofacitinib is approved in the dosing regimen for patients with ulcerative colitis, the release says.
the Food and Drug Administration reported.
The trial’s Data Safety and Monitoring Board identified the signal in patients taking a 10-mg dose of tofacitinib twice daily, the FDA said in a safety announcement.
Pfizer, the trial’s sponsor, took “immediate action” to transition patients in the ongoing trial from the 10-mg, twice-daily dose to 5 mg twice daily, which is the approved dose for adult patients with moderate to severe rheumatoid arthritis, the agency said. The 10-mg, twice-daily dose is approved only in the dosing regimen for patients with ulcerative colitis. Xeljanz is also approved to treat psoriatic arthritis. The 11-mg, once-daily dose of Xeljanz XR that is approved to treat rheumatoid arthritis and psoriatic arthritis was not tested in the trial.
The ongoing study was designed to assess risks of cardiovascular events, cancer, and opportunistic infections with tofacitinib 10 mg twice daily or 5 mg twice daily versus the risks in a control group treated with a tumor necrosis factor (TNF) inhibitor, according to the statement.
Patients had to be 50 years of age or older and have at least one cardiovascular risk factor to be eligible for the study, which was required by the agency in 2012 when it approved tofacitinib, the statement says.
The FDA is reviewing trial data and working with Pfizer to better understand the safety signal, its effect on patients, and how tofacitinib should be used, Janet Woodcock, MD, director of the FDA’s Center for Drug Evaluation and Research, said in a news release. The trial will continue and is expected to be completed by the end of 2019.
“The agency will take appropriate action, as warranted, to ensure patients enrolled in this and other trials are protected and that health care professionals and clinical trial researchers understand the risks associated with this use,” she added.
Health care professionals should follow tofacitinib prescribing information, monitor patients for the signs and symptoms of pulmonary embolism, and advise patients to seek medical attention immediately if they experience those signs and symptoms, according to the statement.
“We are communicating now, given the serious nature of the safety issue, to ensure that patients taking tofacitinib are aware that the FDA still believes the benefits of taking tofacitinib for its approved uses continue to outweigh the risks,” Dr. Woodcock said in the release.
While not approved in rheumatoid arthritis, the 10-mg, twice-daily dose of tofacitinib is approved in the dosing regimen for patients with ulcerative colitis, the release says.
Diabetes and the Commercial Motor Vehicle Driver
A 60-year-old man is sent by his new employer to your urgent care for a pre-employment Department of Transportation (DOT) physical to obtain clearance to drive a commercial motor vehicle. His medical history is significant for hypertension, for which he takes lisinopril. Otherwise, he is healthy, with normal vital signs. His physical exam is unremarkable, but the urine sample is notably positive for glucose. A fingerstick glucose test yields a measurement of 212 m
Commercial motor vehicle (CMV) drivers are mandated by the Federal Motor Carrier Safety Administration (FMCSA) to receive a DOT physical examination by a licensed medical examiner. To qualify to perform the exam, physician assistants, advanced practice nurses, physicians, and chiropractors must complete an educational program and pass a written certification examination.1 Subsequently, the examiners are placed on a national registry—the National Registry of Certified Medical Examiners—with the mission to improve highway safety by determining whether a CMV driver’s health meets standards and guidelines set by the FMCSA.2
Under current guidelines, a DOT physical exam for a healthy CMV driver is considered valid for a maximum of 24 months. However, some diseases and medications require frequent follow-up, which can shorten the length of time a driver can be medically cleared to operate a CMV. Furthermore, certain conditions can disqualify the driver from meeting the necessary standards required for medical certification.
This case presentation offers the opportunity to review the requirements for evaluation and certification of a CMV driver with new-onset hyperglycemia and, ultimately, diabetes. In the United States, types 1 and 2 diabetes are estimated to affect 30.3 million people.3 About 33% of CMV drivers have been diagnosed with diabetes, which is significant since research has demonstrated an increased risk for crashes in individuals with diabetes, due to potential incapacitation from hypoglycemia.4-6
Thus, for practitioners and medical examiners, it is prudent to screen and manage diabetes in CMV drivers. In fact, over the past 15 years, federal regulations have stipulated that any driver with diabetes requiring insulin for control was disqualified from this type of work.7 This standard was developed in response to the increased risk for hypoglycemic reactions with the use of insulin. However, in September 2018, the FMCSA revised this regulation, permitting individuals with a stable insulin regimen and properly controlled diabetes to be qualified to operate a CMV. As a result, for drivers requiring insulin, the treating clinician must complete a standardized form within 45 days of the DOT exam, documenting management of the patient’s diabetes.8 For drivers with diabetes who do not require insulin, determinations are made on a case-by-case basis, with discernment of the driver’s ability to manage the disease and concurrently meet other standards for qualification.
HEALTH HISTORY AND EXAMINATION
Each CMV driver completes a standard medical history form that asks about specific medications, surgeries, or medical conditions, including diabetes or blood glucose problems. Subsequently, the driver and, ultimately, the medical examiner must expand upon and discuss every “yes” response to this questionnaire.
Regarding diabetes, the examiner should determine whether the disease is controlled by diet, pills, and/or insulin, with clarification of the doses, frequency, and prescriber. In addition, the examiner should review and document glucose control, blood glucose monitoring, history of hypoglycemic episodes, and episodes of fainting, dizziness, or loss of consciousness.7
Continue to: The physical exam should focus on...
The physical exam should focus on identifying signs of complications from diabetes, such as retinopathy, nephropathy, or peripheral neuropathy. At each certification visit, the examiner should assess the patient’s height and weight, BMI, vision, hearing, blood pressure, and heart rate, and perform urinalysis to screen for proteinuria or glycosuria. A fingerstick test to obtain a random blood glucose reading is often performed in a driver with glycosuria.
Likewise, the A1C level should be documented in every patient with new-onset or known diabetes, with the recommendation from the FMCSA that a level >10% is an indicator of poor glucose control.7 It is important to note that an A1C level up to 10% is not the glycemic target recognized by the American Diabetes Association and the American Association of Clinical Endocrinologists. The FMCSA is focused more on hypoglycemic concerns than on providing management guidelines.
DETERMINING CERTIFICATION
Currently, the recertification time recommended for CMV drivers with diabetes and documented glucose control is 1 year. This is based on the assumption that the driver is under medical care with a treatment plan and that he/she is not currently experiencing any complications from the disease. Furthermore, insulin secretagogues (eg, sulfonylureas) can be used for glucose control as long as adverse effects (eg, hypoglycemia) do not interfere with safe driving. However, the FMCSA does not recommend certifying any driver who
- In the past 12 months has experienced a hypoglycemic reaction resulting in seizure; loss of consciousness; need of assistance from another person; or period of impaired cognitive function that occurred without warning.
- In the past 5 years has had recurring (≥ 2) disqualifying hypoglycemic reactions.
- Has received a formal diagnosis of peripheral neuropathy, loss of position, or pedal sensation.
- Has resting tachycardia or orthostatic hypotension.
- Has severe diabetic nephropathy requiring dialysis.
- Has severe nonproliferative or proliferative retinopathy.8
In drivers with new-onset hyperglycemia, it is appropriate for the medical examiner to refer the driver to his/her primary care provider for further testing (eg, A1C), determination of treatment, a copy of the diabetes medical standard for driving, and written opinion of the driver’s medical fitness for duty. Subsequently, the medical examiner can utilize this information from the primary care provider to determine certification for the driver. While there are no specific guidelines on the waiting period for certification, the driver should demonstrate glucose control with treatment that is adequate, effective, safe, and stable.7
Overall, while living with diabetes can be challenging, patients who demonstrate control of the disease can maintain their occupation as a CMV driver. The role of the medical examiner is to evaluate the driver’s risk to safely operate a CMV—in particular, considering the possibilities of a severe hypoglycemic episode or target organ dysfunction—whereas the clinician treating the driver’s diabetes is focused on minimizing the complications associated with hyperglycemia.
Continue to: As a reminder...
As a reminder, due to the progressive nature of the disease, recertification is recommended annually for drivers.7 Nevertheless, it is reassuring that the DOT has implemented safeguards designed to keep our citizens safe while travelling the highways and byways of the United States.
Given the patient’s elevated glucose, more information is needed to safely provide clearance for driving a CMV. The patient would be disqualified until he could provide documentation of glucose control. Therefore, this patient would benefit from a referral to his primary care provider to obtain a list of medications used to manage his disease, documentation of an A1C level <10% and no evidence of complications from diabetes, and a written opinion from the primary care provider indicating the driver is medically fit for duty. Accordingly, the primary care provider can ensure the patient demonstrates compliance in managing diabetes and can safely operate a CMV.
1. Federal Motor Carrier Safety Administration. DOT Medical Exam and Commercial Motor Vehicle Certification. www.fmcsa.dot.gov/medical/driver-medical-requirements/dot-medical-exam-and-commercial-motor-vehicle-certification. Accessed February 22, 2019.
2. Federal Motor Carrier Safety Administration. National Registry of Certified Medical Examiners. www.fmcsa.dot.gov/medical/driver-medical-requirements/national-registry-certified-medical-examiners. Accessed February 22, 2019.
3. CDC. National Diabetes Statistics Report, 2017: estimates of diabetes and its burden in the United States. www.cdc.gov/diabetes/pdfs/data/statistics/national-diabetes-statistics-report.pdf. Accessed February 22, 2019.
4. Abu Dabrh AM, Firwana B, Cowl CT, et al. Health assessment of commercial drivers: a meta-narrative systematic review. BMJ Open. 2014;4:e003434.
5. Laberge-Nadeau C, Dionne G, Maag U, et al. Medical conditions and the severity of commercial motor vehicle drivers’ road accidents. Accid Anal Prev. 1996;28:43-51.
6. Redelmeier DA, Kenshole AB, Ray JG. Motor vehicle crashes in diabetic patients with tight glycemic control: a population-based case control analysis. PLoS Med. 2009;6:e1000192.
7. Federal Motor Carrier Safety Administration. Medical Examiner Handbook. www.fmcsa.dot.gov/sites/fmcsa.dot.gov/files/docs/mission/advisory-committees/mrb/83401/fmcsamedicalexaminerhandbook.pdf. Accessed February 22, 2019.
8. Federal Motor Carrier Safety Administration. Qualifications of Drivers; Diabetes Standard. Federal Register. September 19, 2018. www.federalregister.gov/documents/2018/09/19/2018-20161/qualifications-of-drivers-diabetes-standard. Accessed February 25, 2019.
Clinician Reviews in partnership with
Shaun Lynch is an Assistant Professor and Academic Coordinator in the Department of Physician Assistant Studies at Elon University in North Carolina.
Clinician Reviews in partnership with
Shaun Lynch is an Assistant Professor and Academic Coordinator in the Department of Physician Assistant Studies at Elon University in North Carolina.
Clinician Reviews in partnership with
Shaun Lynch is an Assistant Professor and Academic Coordinator in the Department of Physician Assistant Studies at Elon University in North Carolina.
A 60-year-old man is sent by his new employer to your urgent care for a pre-employment Department of Transportation (DOT) physical to obtain clearance to drive a commercial motor vehicle. His medical history is significant for hypertension, for which he takes lisinopril. Otherwise, he is healthy, with normal vital signs. His physical exam is unremarkable, but the urine sample is notably positive for glucose. A fingerstick glucose test yields a measurement of 212 m
Commercial motor vehicle (CMV) drivers are mandated by the Federal Motor Carrier Safety Administration (FMCSA) to receive a DOT physical examination by a licensed medical examiner. To qualify to perform the exam, physician assistants, advanced practice nurses, physicians, and chiropractors must complete an educational program and pass a written certification examination.1 Subsequently, the examiners are placed on a national registry—the National Registry of Certified Medical Examiners—with the mission to improve highway safety by determining whether a CMV driver’s health meets standards and guidelines set by the FMCSA.2
Under current guidelines, a DOT physical exam for a healthy CMV driver is considered valid for a maximum of 24 months. However, some diseases and medications require frequent follow-up, which can shorten the length of time a driver can be medically cleared to operate a CMV. Furthermore, certain conditions can disqualify the driver from meeting the necessary standards required for medical certification.
This case presentation offers the opportunity to review the requirements for evaluation and certification of a CMV driver with new-onset hyperglycemia and, ultimately, diabetes. In the United States, types 1 and 2 diabetes are estimated to affect 30.3 million people.3 About 33% of CMV drivers have been diagnosed with diabetes, which is significant since research has demonstrated an increased risk for crashes in individuals with diabetes, due to potential incapacitation from hypoglycemia.4-6
Thus, for practitioners and medical examiners, it is prudent to screen and manage diabetes in CMV drivers. In fact, over the past 15 years, federal regulations have stipulated that any driver with diabetes requiring insulin for control was disqualified from this type of work.7 This standard was developed in response to the increased risk for hypoglycemic reactions with the use of insulin. However, in September 2018, the FMCSA revised this regulation, permitting individuals with a stable insulin regimen and properly controlled diabetes to be qualified to operate a CMV. As a result, for drivers requiring insulin, the treating clinician must complete a standardized form within 45 days of the DOT exam, documenting management of the patient’s diabetes.8 For drivers with diabetes who do not require insulin, determinations are made on a case-by-case basis, with discernment of the driver’s ability to manage the disease and concurrently meet other standards for qualification.
HEALTH HISTORY AND EXAMINATION
Each CMV driver completes a standard medical history form that asks about specific medications, surgeries, or medical conditions, including diabetes or blood glucose problems. Subsequently, the driver and, ultimately, the medical examiner must expand upon and discuss every “yes” response to this questionnaire.
Regarding diabetes, the examiner should determine whether the disease is controlled by diet, pills, and/or insulin, with clarification of the doses, frequency, and prescriber. In addition, the examiner should review and document glucose control, blood glucose monitoring, history of hypoglycemic episodes, and episodes of fainting, dizziness, or loss of consciousness.7
Continue to: The physical exam should focus on...
The physical exam should focus on identifying signs of complications from diabetes, such as retinopathy, nephropathy, or peripheral neuropathy. At each certification visit, the examiner should assess the patient’s height and weight, BMI, vision, hearing, blood pressure, and heart rate, and perform urinalysis to screen for proteinuria or glycosuria. A fingerstick test to obtain a random blood glucose reading is often performed in a driver with glycosuria.
Likewise, the A1C level should be documented in every patient with new-onset or known diabetes, with the recommendation from the FMCSA that a level >10% is an indicator of poor glucose control.7 It is important to note that an A1C level up to 10% is not the glycemic target recognized by the American Diabetes Association and the American Association of Clinical Endocrinologists. The FMCSA is focused more on hypoglycemic concerns than on providing management guidelines.
DETERMINING CERTIFICATION
Currently, the recertification time recommended for CMV drivers with diabetes and documented glucose control is 1 year. This is based on the assumption that the driver is under medical care with a treatment plan and that he/she is not currently experiencing any complications from the disease. Furthermore, insulin secretagogues (eg, sulfonylureas) can be used for glucose control as long as adverse effects (eg, hypoglycemia) do not interfere with safe driving. However, the FMCSA does not recommend certifying any driver who
- In the past 12 months has experienced a hypoglycemic reaction resulting in seizure; loss of consciousness; need of assistance from another person; or period of impaired cognitive function that occurred without warning.
- In the past 5 years has had recurring (≥ 2) disqualifying hypoglycemic reactions.
- Has received a formal diagnosis of peripheral neuropathy, loss of position, or pedal sensation.
- Has resting tachycardia or orthostatic hypotension.
- Has severe diabetic nephropathy requiring dialysis.
- Has severe nonproliferative or proliferative retinopathy.8
In drivers with new-onset hyperglycemia, it is appropriate for the medical examiner to refer the driver to his/her primary care provider for further testing (eg, A1C), determination of treatment, a copy of the diabetes medical standard for driving, and written opinion of the driver’s medical fitness for duty. Subsequently, the medical examiner can utilize this information from the primary care provider to determine certification for the driver. While there are no specific guidelines on the waiting period for certification, the driver should demonstrate glucose control with treatment that is adequate, effective, safe, and stable.7
Overall, while living with diabetes can be challenging, patients who demonstrate control of the disease can maintain their occupation as a CMV driver. The role of the medical examiner is to evaluate the driver’s risk to safely operate a CMV—in particular, considering the possibilities of a severe hypoglycemic episode or target organ dysfunction—whereas the clinician treating the driver’s diabetes is focused on minimizing the complications associated with hyperglycemia.
Continue to: As a reminder...
As a reminder, due to the progressive nature of the disease, recertification is recommended annually for drivers.7 Nevertheless, it is reassuring that the DOT has implemented safeguards designed to keep our citizens safe while travelling the highways and byways of the United States.
Given the patient’s elevated glucose, more information is needed to safely provide clearance for driving a CMV. The patient would be disqualified until he could provide documentation of glucose control. Therefore, this patient would benefit from a referral to his primary care provider to obtain a list of medications used to manage his disease, documentation of an A1C level <10% and no evidence of complications from diabetes, and a written opinion from the primary care provider indicating the driver is medically fit for duty. Accordingly, the primary care provider can ensure the patient demonstrates compliance in managing diabetes and can safely operate a CMV.
A 60-year-old man is sent by his new employer to your urgent care for a pre-employment Department of Transportation (DOT) physical to obtain clearance to drive a commercial motor vehicle. His medical history is significant for hypertension, for which he takes lisinopril. Otherwise, he is healthy, with normal vital signs. His physical exam is unremarkable, but the urine sample is notably positive for glucose. A fingerstick glucose test yields a measurement of 212 m
Commercial motor vehicle (CMV) drivers are mandated by the Federal Motor Carrier Safety Administration (FMCSA) to receive a DOT physical examination by a licensed medical examiner. To qualify to perform the exam, physician assistants, advanced practice nurses, physicians, and chiropractors must complete an educational program and pass a written certification examination.1 Subsequently, the examiners are placed on a national registry—the National Registry of Certified Medical Examiners—with the mission to improve highway safety by determining whether a CMV driver’s health meets standards and guidelines set by the FMCSA.2
Under current guidelines, a DOT physical exam for a healthy CMV driver is considered valid for a maximum of 24 months. However, some diseases and medications require frequent follow-up, which can shorten the length of time a driver can be medically cleared to operate a CMV. Furthermore, certain conditions can disqualify the driver from meeting the necessary standards required for medical certification.
This case presentation offers the opportunity to review the requirements for evaluation and certification of a CMV driver with new-onset hyperglycemia and, ultimately, diabetes. In the United States, types 1 and 2 diabetes are estimated to affect 30.3 million people.3 About 33% of CMV drivers have been diagnosed with diabetes, which is significant since research has demonstrated an increased risk for crashes in individuals with diabetes, due to potential incapacitation from hypoglycemia.4-6
Thus, for practitioners and medical examiners, it is prudent to screen and manage diabetes in CMV drivers. In fact, over the past 15 years, federal regulations have stipulated that any driver with diabetes requiring insulin for control was disqualified from this type of work.7 This standard was developed in response to the increased risk for hypoglycemic reactions with the use of insulin. However, in September 2018, the FMCSA revised this regulation, permitting individuals with a stable insulin regimen and properly controlled diabetes to be qualified to operate a CMV. As a result, for drivers requiring insulin, the treating clinician must complete a standardized form within 45 days of the DOT exam, documenting management of the patient’s diabetes.8 For drivers with diabetes who do not require insulin, determinations are made on a case-by-case basis, with discernment of the driver’s ability to manage the disease and concurrently meet other standards for qualification.
HEALTH HISTORY AND EXAMINATION
Each CMV driver completes a standard medical history form that asks about specific medications, surgeries, or medical conditions, including diabetes or blood glucose problems. Subsequently, the driver and, ultimately, the medical examiner must expand upon and discuss every “yes” response to this questionnaire.
Regarding diabetes, the examiner should determine whether the disease is controlled by diet, pills, and/or insulin, with clarification of the doses, frequency, and prescriber. In addition, the examiner should review and document glucose control, blood glucose monitoring, history of hypoglycemic episodes, and episodes of fainting, dizziness, or loss of consciousness.7
Continue to: The physical exam should focus on...
The physical exam should focus on identifying signs of complications from diabetes, such as retinopathy, nephropathy, or peripheral neuropathy. At each certification visit, the examiner should assess the patient’s height and weight, BMI, vision, hearing, blood pressure, and heart rate, and perform urinalysis to screen for proteinuria or glycosuria. A fingerstick test to obtain a random blood glucose reading is often performed in a driver with glycosuria.
Likewise, the A1C level should be documented in every patient with new-onset or known diabetes, with the recommendation from the FMCSA that a level >10% is an indicator of poor glucose control.7 It is important to note that an A1C level up to 10% is not the glycemic target recognized by the American Diabetes Association and the American Association of Clinical Endocrinologists. The FMCSA is focused more on hypoglycemic concerns than on providing management guidelines.
DETERMINING CERTIFICATION
Currently, the recertification time recommended for CMV drivers with diabetes and documented glucose control is 1 year. This is based on the assumption that the driver is under medical care with a treatment plan and that he/she is not currently experiencing any complications from the disease. Furthermore, insulin secretagogues (eg, sulfonylureas) can be used for glucose control as long as adverse effects (eg, hypoglycemia) do not interfere with safe driving. However, the FMCSA does not recommend certifying any driver who
- In the past 12 months has experienced a hypoglycemic reaction resulting in seizure; loss of consciousness; need of assistance from another person; or period of impaired cognitive function that occurred without warning.
- In the past 5 years has had recurring (≥ 2) disqualifying hypoglycemic reactions.
- Has received a formal diagnosis of peripheral neuropathy, loss of position, or pedal sensation.
- Has resting tachycardia or orthostatic hypotension.
- Has severe diabetic nephropathy requiring dialysis.
- Has severe nonproliferative or proliferative retinopathy.8
In drivers with new-onset hyperglycemia, it is appropriate for the medical examiner to refer the driver to his/her primary care provider for further testing (eg, A1C), determination of treatment, a copy of the diabetes medical standard for driving, and written opinion of the driver’s medical fitness for duty. Subsequently, the medical examiner can utilize this information from the primary care provider to determine certification for the driver. While there are no specific guidelines on the waiting period for certification, the driver should demonstrate glucose control with treatment that is adequate, effective, safe, and stable.7
Overall, while living with diabetes can be challenging, patients who demonstrate control of the disease can maintain their occupation as a CMV driver. The role of the medical examiner is to evaluate the driver’s risk to safely operate a CMV—in particular, considering the possibilities of a severe hypoglycemic episode or target organ dysfunction—whereas the clinician treating the driver’s diabetes is focused on minimizing the complications associated with hyperglycemia.
Continue to: As a reminder...
As a reminder, due to the progressive nature of the disease, recertification is recommended annually for drivers.7 Nevertheless, it is reassuring that the DOT has implemented safeguards designed to keep our citizens safe while travelling the highways and byways of the United States.
Given the patient’s elevated glucose, more information is needed to safely provide clearance for driving a CMV. The patient would be disqualified until he could provide documentation of glucose control. Therefore, this patient would benefit from a referral to his primary care provider to obtain a list of medications used to manage his disease, documentation of an A1C level <10% and no evidence of complications from diabetes, and a written opinion from the primary care provider indicating the driver is medically fit for duty. Accordingly, the primary care provider can ensure the patient demonstrates compliance in managing diabetes and can safely operate a CMV.
1. Federal Motor Carrier Safety Administration. DOT Medical Exam and Commercial Motor Vehicle Certification. www.fmcsa.dot.gov/medical/driver-medical-requirements/dot-medical-exam-and-commercial-motor-vehicle-certification. Accessed February 22, 2019.
2. Federal Motor Carrier Safety Administration. National Registry of Certified Medical Examiners. www.fmcsa.dot.gov/medical/driver-medical-requirements/national-registry-certified-medical-examiners. Accessed February 22, 2019.
3. CDC. National Diabetes Statistics Report, 2017: estimates of diabetes and its burden in the United States. www.cdc.gov/diabetes/pdfs/data/statistics/national-diabetes-statistics-report.pdf. Accessed February 22, 2019.
4. Abu Dabrh AM, Firwana B, Cowl CT, et al. Health assessment of commercial drivers: a meta-narrative systematic review. BMJ Open. 2014;4:e003434.
5. Laberge-Nadeau C, Dionne G, Maag U, et al. Medical conditions and the severity of commercial motor vehicle drivers’ road accidents. Accid Anal Prev. 1996;28:43-51.
6. Redelmeier DA, Kenshole AB, Ray JG. Motor vehicle crashes in diabetic patients with tight glycemic control: a population-based case control analysis. PLoS Med. 2009;6:e1000192.
7. Federal Motor Carrier Safety Administration. Medical Examiner Handbook. www.fmcsa.dot.gov/sites/fmcsa.dot.gov/files/docs/mission/advisory-committees/mrb/83401/fmcsamedicalexaminerhandbook.pdf. Accessed February 22, 2019.
8. Federal Motor Carrier Safety Administration. Qualifications of Drivers; Diabetes Standard. Federal Register. September 19, 2018. www.federalregister.gov/documents/2018/09/19/2018-20161/qualifications-of-drivers-diabetes-standard. Accessed February 25, 2019.
1. Federal Motor Carrier Safety Administration. DOT Medical Exam and Commercial Motor Vehicle Certification. www.fmcsa.dot.gov/medical/driver-medical-requirements/dot-medical-exam-and-commercial-motor-vehicle-certification. Accessed February 22, 2019.
2. Federal Motor Carrier Safety Administration. National Registry of Certified Medical Examiners. www.fmcsa.dot.gov/medical/driver-medical-requirements/national-registry-certified-medical-examiners. Accessed February 22, 2019.
3. CDC. National Diabetes Statistics Report, 2017: estimates of diabetes and its burden in the United States. www.cdc.gov/diabetes/pdfs/data/statistics/national-diabetes-statistics-report.pdf. Accessed February 22, 2019.
4. Abu Dabrh AM, Firwana B, Cowl CT, et al. Health assessment of commercial drivers: a meta-narrative systematic review. BMJ Open. 2014;4:e003434.
5. Laberge-Nadeau C, Dionne G, Maag U, et al. Medical conditions and the severity of commercial motor vehicle drivers’ road accidents. Accid Anal Prev. 1996;28:43-51.
6. Redelmeier DA, Kenshole AB, Ray JG. Motor vehicle crashes in diabetic patients with tight glycemic control: a population-based case control analysis. PLoS Med. 2009;6:e1000192.
7. Federal Motor Carrier Safety Administration. Medical Examiner Handbook. www.fmcsa.dot.gov/sites/fmcsa.dot.gov/files/docs/mission/advisory-committees/mrb/83401/fmcsamedicalexaminerhandbook.pdf. Accessed February 22, 2019.
8. Federal Motor Carrier Safety Administration. Qualifications of Drivers; Diabetes Standard. Federal Register. September 19, 2018. www.federalregister.gov/documents/2018/09/19/2018-20161/qualifications-of-drivers-diabetes-standard. Accessed February 25, 2019.
