User login
Scientific Roundtable Focuses Efforts on Leiomyosarcoma Research
Research clinicians from the US and abroad participated in a scientific research roundtable this past September to establish the most important issues facing leiomyosarcoma (LMS) research and clinical trials. The workshop, expected to be an annual event, is a joint effort of the National Leiomyosarcoma Foundation (NLMSF) and Sarcoma Patients EuroNet (SPAEN).
The roundtable’s mission is to bring together sarcoma experts for a meeting dedicated to LMS, where participants discuss the present state of LMS and the continued challenges of diagnosis and treatment. Its goal is to develop working plans to close the gaps in LMS patient care and improve LMS patient-care protocols. They also advise the NLMSF on worthy and important research projects that deserve the foundation’s future funding efforts.
Plans for roundtable meetings in 2020 and 2021 are already underway. Between the annual meetings, workgroups continue to take steps toward addressing the issues identified by the roundtable. For more information on the roundtable and NLMSF, visit: https://nlmsf.org.
Research clinicians from the US and abroad participated in a scientific research roundtable this past September to establish the most important issues facing leiomyosarcoma (LMS) research and clinical trials. The workshop, expected to be an annual event, is a joint effort of the National Leiomyosarcoma Foundation (NLMSF) and Sarcoma Patients EuroNet (SPAEN).
The roundtable’s mission is to bring together sarcoma experts for a meeting dedicated to LMS, where participants discuss the present state of LMS and the continued challenges of diagnosis and treatment. Its goal is to develop working plans to close the gaps in LMS patient care and improve LMS patient-care protocols. They also advise the NLMSF on worthy and important research projects that deserve the foundation’s future funding efforts.
Plans for roundtable meetings in 2020 and 2021 are already underway. Between the annual meetings, workgroups continue to take steps toward addressing the issues identified by the roundtable. For more information on the roundtable and NLMSF, visit: https://nlmsf.org.
Research clinicians from the US and abroad participated in a scientific research roundtable this past September to establish the most important issues facing leiomyosarcoma (LMS) research and clinical trials. The workshop, expected to be an annual event, is a joint effort of the National Leiomyosarcoma Foundation (NLMSF) and Sarcoma Patients EuroNet (SPAEN).
The roundtable’s mission is to bring together sarcoma experts for a meeting dedicated to LMS, where participants discuss the present state of LMS and the continued challenges of diagnosis and treatment. Its goal is to develop working plans to close the gaps in LMS patient care and improve LMS patient-care protocols. They also advise the NLMSF on worthy and important research projects that deserve the foundation’s future funding efforts.
Plans for roundtable meetings in 2020 and 2021 are already underway. Between the annual meetings, workgroups continue to take steps toward addressing the issues identified by the roundtable. For more information on the roundtable and NLMSF, visit: https://nlmsf.org.
State of Hospital Medicine Survey plays key role in operational decision making
Results help establish hospitalist benchmarks
The Hospitalist recently spoke with Brian Schroeder, MHA, FACHE, FHM, assistant vice president, Hospital & Emergency Medicine, at Atrium Health Medical Group in Charlotte, N.C., to discuss his participation in the State of Hospital Medicine Survey, which is distributed every other year, and how he uses the resulting report to guide important operational decisions.
Please describe your current role.
At Carolinas Hospitalist Group, we have approximately 250 providers at nearly 20 care locations across North Carolina. Along with my specialty medical director, I am responsible for the strategic growth, program development, and financial performance for our practice.
How did you first become involved with the Society of Hospital Medicine?

When I first entered the hospital medicine world in 2008, I was looking for an organization that supported our specialty. My physician leaders at the time pointed me to SHM. Since the beginning of my time as a member, I have attended the Annual Conference each year, the SHM Leadership Academy, served on an SHM committee, and participate in SHM’s multisite Leaders group. Additionally, I have served as faculty at SHM’s annual conference for 3 years – and will be presenting for the third time at HM20.
Why is it important that people participate in the State of Hospital Medicine Survey?
Participation in the survey is key for establishing benchmarks for our specialty. The more people participate (from various arenas like private groups, health system employees, and vendors), the more accurate the data. Over the past 4 years, SHM has improved the submission process of survey data – especially for practices with multiple locations.
How has the data in the report impacted important business decisions for your group?
We rely heavily on the investment/provider benchmark within the survey data. Over the years, as the investment/provider was decreasing nationally, our own investment/provider was increasing. Based on the survey, we were able to closely evaluate our staffing models at each location and determine the appropriate skill mix-to-volume ratio. Through turnover and growth, we have strategically hired advanced practice providers to align our investment more closely with the benchmark. Over the past 2 years, our investment/provider metric has decreased significantly. We were able to accomplish this while continuing to provide appropriate care to our patients. We also utilize the Report to monitor performance incentive metrics, staffing model trends, and encounter/provider ratios.
What would you tell people who are on the fence about participating in the survey – and ultimately, purchasing the finished product?
Do it! Our practice would never skip a submission year. The data produced from the survey helps us improve our clinical operations and maximize our financial affordability. The data also assists in defending staffing decisions and clinical operations change with senior leadership within the organization.
Don’t miss your chance to submit data that will build the latest snapshot of the hospital medicine specialty. The State of Hospital Medicine Survey is open now and runs through February 16, 2020. Learn more and register to participate at hospitalmedicine.org/survey.
Results help establish hospitalist benchmarks
Results help establish hospitalist benchmarks
The Hospitalist recently spoke with Brian Schroeder, MHA, FACHE, FHM, assistant vice president, Hospital & Emergency Medicine, at Atrium Health Medical Group in Charlotte, N.C., to discuss his participation in the State of Hospital Medicine Survey, which is distributed every other year, and how he uses the resulting report to guide important operational decisions.
Please describe your current role.
At Carolinas Hospitalist Group, we have approximately 250 providers at nearly 20 care locations across North Carolina. Along with my specialty medical director, I am responsible for the strategic growth, program development, and financial performance for our practice.
How did you first become involved with the Society of Hospital Medicine?
When I first entered the hospital medicine world in 2008, I was looking for an organization that supported our specialty. My physician leaders at the time pointed me to SHM. Since the beginning of my time as a member, I have attended the Annual Conference each year, the SHM Leadership Academy, served on an SHM committee, and participate in SHM’s multisite Leaders group. Additionally, I have served as faculty at SHM’s annual conference for 3 years – and will be presenting for the third time at HM20.
Why is it important that people participate in the State of Hospital Medicine Survey?
Participation in the survey is key for establishing benchmarks for our specialty. The more people participate (from various arenas like private groups, health system employees, and vendors), the more accurate the data. Over the past 4 years, SHM has improved the submission process of survey data – especially for practices with multiple locations.
How has the data in the report impacted important business decisions for your group?
We rely heavily on the investment/provider benchmark within the survey data. Over the years, as the investment/provider was decreasing nationally, our own investment/provider was increasing. Based on the survey, we were able to closely evaluate our staffing models at each location and determine the appropriate skill mix-to-volume ratio. Through turnover and growth, we have strategically hired advanced practice providers to align our investment more closely with the benchmark. Over the past 2 years, our investment/provider metric has decreased significantly. We were able to accomplish this while continuing to provide appropriate care to our patients. We also utilize the Report to monitor performance incentive metrics, staffing model trends, and encounter/provider ratios.
What would you tell people who are on the fence about participating in the survey – and ultimately, purchasing the finished product?
Do it! Our practice would never skip a submission year. The data produced from the survey helps us improve our clinical operations and maximize our financial affordability. The data also assists in defending staffing decisions and clinical operations change with senior leadership within the organization.
Don’t miss your chance to submit data that will build the latest snapshot of the hospital medicine specialty. The State of Hospital Medicine Survey is open now and runs through February 16, 2020. Learn more and register to participate at hospitalmedicine.org/survey.
The Hospitalist recently spoke with Brian Schroeder, MHA, FACHE, FHM, assistant vice president, Hospital & Emergency Medicine, at Atrium Health Medical Group in Charlotte, N.C., to discuss his participation in the State of Hospital Medicine Survey, which is distributed every other year, and how he uses the resulting report to guide important operational decisions.
Please describe your current role.
At Carolinas Hospitalist Group, we have approximately 250 providers at nearly 20 care locations across North Carolina. Along with my specialty medical director, I am responsible for the strategic growth, program development, and financial performance for our practice.
How did you first become involved with the Society of Hospital Medicine?
When I first entered the hospital medicine world in 2008, I was looking for an organization that supported our specialty. My physician leaders at the time pointed me to SHM. Since the beginning of my time as a member, I have attended the Annual Conference each year, the SHM Leadership Academy, served on an SHM committee, and participate in SHM’s multisite Leaders group. Additionally, I have served as faculty at SHM’s annual conference for 3 years – and will be presenting for the third time at HM20.
Why is it important that people participate in the State of Hospital Medicine Survey?
Participation in the survey is key for establishing benchmarks for our specialty. The more people participate (from various arenas like private groups, health system employees, and vendors), the more accurate the data. Over the past 4 years, SHM has improved the submission process of survey data – especially for practices with multiple locations.
How has the data in the report impacted important business decisions for your group?
We rely heavily on the investment/provider benchmark within the survey data. Over the years, as the investment/provider was decreasing nationally, our own investment/provider was increasing. Based on the survey, we were able to closely evaluate our staffing models at each location and determine the appropriate skill mix-to-volume ratio. Through turnover and growth, we have strategically hired advanced practice providers to align our investment more closely with the benchmark. Over the past 2 years, our investment/provider metric has decreased significantly. We were able to accomplish this while continuing to provide appropriate care to our patients. We also utilize the Report to monitor performance incentive metrics, staffing model trends, and encounter/provider ratios.
What would you tell people who are on the fence about participating in the survey – and ultimately, purchasing the finished product?
Do it! Our practice would never skip a submission year. The data produced from the survey helps us improve our clinical operations and maximize our financial affordability. The data also assists in defending staffing decisions and clinical operations change with senior leadership within the organization.
Don’t miss your chance to submit data that will build the latest snapshot of the hospital medicine specialty. The State of Hospital Medicine Survey is open now and runs through February 16, 2020. Learn more and register to participate at hospitalmedicine.org/survey.
Bimekizumab elevates psoriasis therapy
MADRID – Renowned dermatologic clinical trialist Kim A. Papp, MD, PhD, is known to pick his words carefully, and the word he uses to describe the quality of life improvement documented in psoriasis patients treated with the novel investigational humanized monoclonal antibody bimekizumab is “phenomenal.”
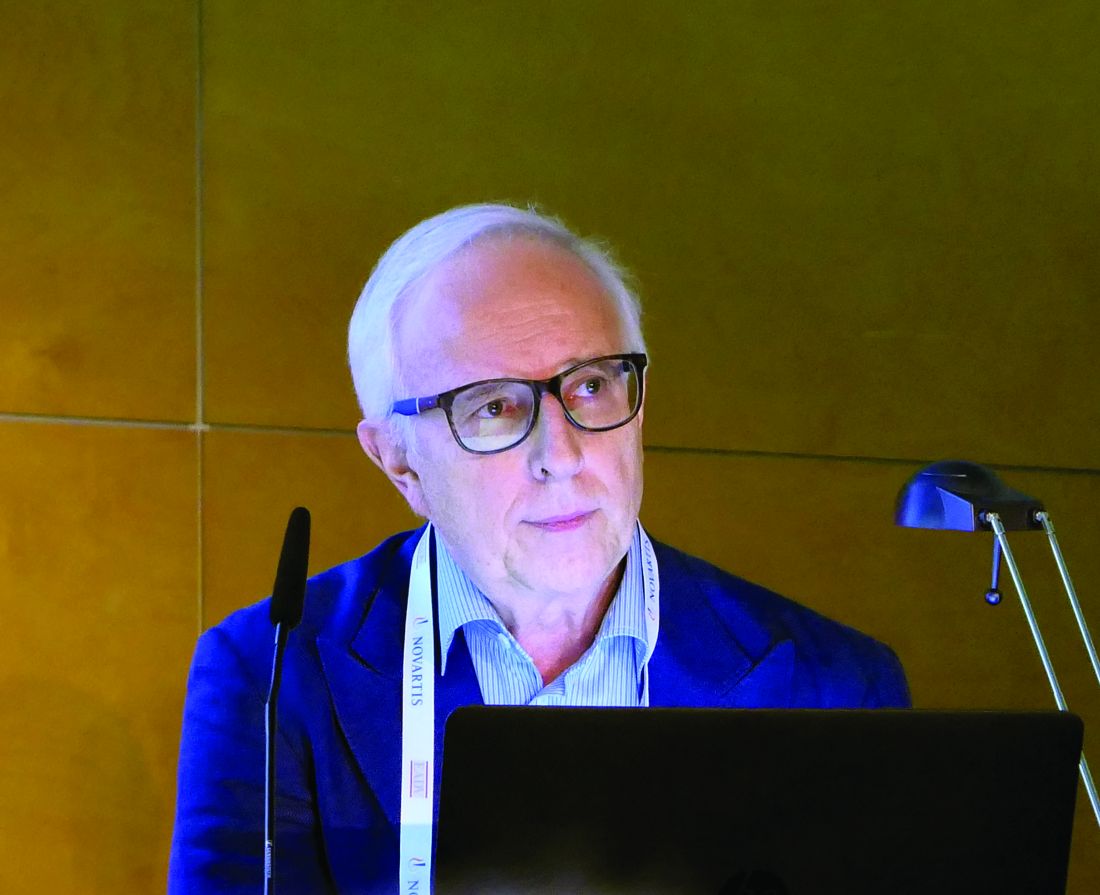
Dr. Papp was lead investigator in the previously reported phase 2b multicenter BE ABLE 1 trial, in which 250 patients with moderate to severe chronic plaque psoriasis were randomized double-blind to various doses of bimekizumab or placebo every 4 weeks for 12 weeks (J Am Acad Dermatol. 2018 Aug;79[2]:277-86.e10. doi: 10.1016/j.jaad.2018.03.037). He was also lead investigator in the 48-week phase 2b BE ABLE 2 extension study. He presented the 60-week quality-of-life BE ABLE 2 results for the first time at the annual congress of the European Academy of Dermatology and Venereology.
“Small numbers, but the results are nonetheless very compelling,” said Dr. Papp, president and founder of Probity Medical Research in Waterloo, Ont.
Bimekizumab is unique in that it selectively neutralizes both interleukin-17A and -17F, two closely related proinflammatory cytokines which, when upregulated, synergize with other proinflammatory cytokines to drive psoriasis and other immune-mediated inflammatory diseases. In contrast, secukinumab (Cosentyx) and ixekizumab (Taltz) specifically inhibit only IL-17A, and brodalumab (Siliq) targets the IL-17 receptor A. The bimekizumab clinical trials program – a work in progress – aims to demonstrate that dual neutralization of IL-17A and -17F provides a more complete therapeutic approach in psoriasis, with greater efficacy and fewer safety concerns than with current biologics, the dermatologist explained.
In BE ABLE 1, the primary endpoint of at least a 90% reduction in Psoriasis Area and Severity Index (PASI90) response was achieved at week 12 in 46%-79% of patients randomized to bimekizumab in dose-dependent fashion. Those PASI90 responses were maintained with additional treatment out to week 60 in BE ABLE 2 in 80%-100% of patients.
Dr. Papp’s focus at EADV 2019 was on the quality-of-life improvement achieved in bimekizumab-treated patients, a benefit not captured by PASI scores. For this purpose, he and coinvestigators turned to the Dermatology Life Quality Index (DLQI), measured in structured fashion every 4 weeks out to week 60.
“We often forget that even though we’re looking at the patient from the outside, what’s really important is how well they respond to our treatments internally. The DLQI is not a perfect tool, but it’s the best tool we have available. It gives us a fairly good survey of the various domains that affect patients’ day-to-day living,” he said.
In BE ABLE 1, the proportion of week-12 PASI90 responders achieving a DLQI of 0 or 1 – indicative of essentially no disease impact on quality of life – increased rapidly up until week 8. At week 12, 70%-100% of the PASI90 responders in the various treatment arms had a DLQI of 0 or 1. This quality-of-life improvement, like the PASI90 response, proved durable: When the week-12 PASI90 responders were assessed at week 60 in BE ABLE 2, 76%-93% of them had a DLQI of 0 or 1.
The improvements in quality of life correlated with clinical response. BE ABLE enrollees had an average PASI score of 19 at baseline. Overall, 79% of those with an absolute PASI score of 0 at week 12 had a DLQI of 0 or 1 at that time, as did 95% of those with a PASI of 0 at week 60. A PASI of 1 was associated with a 77% likelihood of a DLQI of 0 or 1 at week 12 and an 82% rate at week 60. In contrast, patients with an absolute PASI of 2-4 at week 12 had a 46% rate of DLQI 0/1, and those with a PASI 2-4 at week 60 had a 50% chance of having a DLQI of 0/1.
Phase 3 clinical trials of bimekizumab totaling several thousand psoriasis patients are ongoing.
The BE ABLE trials were sponsored by UCB Pharma. Dr. Papp reported serving as a consultant to and/or recipient of research grants from UCB and dozens of other pharmaceutical companies.
SOURCE: Papp KA. EADV 2019 Abstract FC02.02.
MADRID – Renowned dermatologic clinical trialist Kim A. Papp, MD, PhD, is known to pick his words carefully, and the word he uses to describe the quality of life improvement documented in psoriasis patients treated with the novel investigational humanized monoclonal antibody bimekizumab is “phenomenal.”
Dr. Papp was lead investigator in the previously reported phase 2b multicenter BE ABLE 1 trial, in which 250 patients with moderate to severe chronic plaque psoriasis were randomized double-blind to various doses of bimekizumab or placebo every 4 weeks for 12 weeks (J Am Acad Dermatol. 2018 Aug;79[2]:277-86.e10. doi: 10.1016/j.jaad.2018.03.037). He was also lead investigator in the 48-week phase 2b BE ABLE 2 extension study. He presented the 60-week quality-of-life BE ABLE 2 results for the first time at the annual congress of the European Academy of Dermatology and Venereology.
“Small numbers, but the results are nonetheless very compelling,” said Dr. Papp, president and founder of Probity Medical Research in Waterloo, Ont.
Bimekizumab is unique in that it selectively neutralizes both interleukin-17A and -17F, two closely related proinflammatory cytokines which, when upregulated, synergize with other proinflammatory cytokines to drive psoriasis and other immune-mediated inflammatory diseases. In contrast, secukinumab (Cosentyx) and ixekizumab (Taltz) specifically inhibit only IL-17A, and brodalumab (Siliq) targets the IL-17 receptor A. The bimekizumab clinical trials program – a work in progress – aims to demonstrate that dual neutralization of IL-17A and -17F provides a more complete therapeutic approach in psoriasis, with greater efficacy and fewer safety concerns than with current biologics, the dermatologist explained.
In BE ABLE 1, the primary endpoint of at least a 90% reduction in Psoriasis Area and Severity Index (PASI90) response was achieved at week 12 in 46%-79% of patients randomized to bimekizumab in dose-dependent fashion. Those PASI90 responses were maintained with additional treatment out to week 60 in BE ABLE 2 in 80%-100% of patients.
Dr. Papp’s focus at EADV 2019 was on the quality-of-life improvement achieved in bimekizumab-treated patients, a benefit not captured by PASI scores. For this purpose, he and coinvestigators turned to the Dermatology Life Quality Index (DLQI), measured in structured fashion every 4 weeks out to week 60.
“We often forget that even though we’re looking at the patient from the outside, what’s really important is how well they respond to our treatments internally. The DLQI is not a perfect tool, but it’s the best tool we have available. It gives us a fairly good survey of the various domains that affect patients’ day-to-day living,” he said.
In BE ABLE 1, the proportion of week-12 PASI90 responders achieving a DLQI of 0 or 1 – indicative of essentially no disease impact on quality of life – increased rapidly up until week 8. At week 12, 70%-100% of the PASI90 responders in the various treatment arms had a DLQI of 0 or 1. This quality-of-life improvement, like the PASI90 response, proved durable: When the week-12 PASI90 responders were assessed at week 60 in BE ABLE 2, 76%-93% of them had a DLQI of 0 or 1.
The improvements in quality of life correlated with clinical response. BE ABLE enrollees had an average PASI score of 19 at baseline. Overall, 79% of those with an absolute PASI score of 0 at week 12 had a DLQI of 0 or 1 at that time, as did 95% of those with a PASI of 0 at week 60. A PASI of 1 was associated with a 77% likelihood of a DLQI of 0 or 1 at week 12 and an 82% rate at week 60. In contrast, patients with an absolute PASI of 2-4 at week 12 had a 46% rate of DLQI 0/1, and those with a PASI 2-4 at week 60 had a 50% chance of having a DLQI of 0/1.
Phase 3 clinical trials of bimekizumab totaling several thousand psoriasis patients are ongoing.
The BE ABLE trials were sponsored by UCB Pharma. Dr. Papp reported serving as a consultant to and/or recipient of research grants from UCB and dozens of other pharmaceutical companies.
SOURCE: Papp KA. EADV 2019 Abstract FC02.02.
MADRID – Renowned dermatologic clinical trialist Kim A. Papp, MD, PhD, is known to pick his words carefully, and the word he uses to describe the quality of life improvement documented in psoriasis patients treated with the novel investigational humanized monoclonal antibody bimekizumab is “phenomenal.”
Dr. Papp was lead investigator in the previously reported phase 2b multicenter BE ABLE 1 trial, in which 250 patients with moderate to severe chronic plaque psoriasis were randomized double-blind to various doses of bimekizumab or placebo every 4 weeks for 12 weeks (J Am Acad Dermatol. 2018 Aug;79[2]:277-86.e10. doi: 10.1016/j.jaad.2018.03.037). He was also lead investigator in the 48-week phase 2b BE ABLE 2 extension study. He presented the 60-week quality-of-life BE ABLE 2 results for the first time at the annual congress of the European Academy of Dermatology and Venereology.
“Small numbers, but the results are nonetheless very compelling,” said Dr. Papp, president and founder of Probity Medical Research in Waterloo, Ont.
Bimekizumab is unique in that it selectively neutralizes both interleukin-17A and -17F, two closely related proinflammatory cytokines which, when upregulated, synergize with other proinflammatory cytokines to drive psoriasis and other immune-mediated inflammatory diseases. In contrast, secukinumab (Cosentyx) and ixekizumab (Taltz) specifically inhibit only IL-17A, and brodalumab (Siliq) targets the IL-17 receptor A. The bimekizumab clinical trials program – a work in progress – aims to demonstrate that dual neutralization of IL-17A and -17F provides a more complete therapeutic approach in psoriasis, with greater efficacy and fewer safety concerns than with current biologics, the dermatologist explained.
In BE ABLE 1, the primary endpoint of at least a 90% reduction in Psoriasis Area and Severity Index (PASI90) response was achieved at week 12 in 46%-79% of patients randomized to bimekizumab in dose-dependent fashion. Those PASI90 responses were maintained with additional treatment out to week 60 in BE ABLE 2 in 80%-100% of patients.
Dr. Papp’s focus at EADV 2019 was on the quality-of-life improvement achieved in bimekizumab-treated patients, a benefit not captured by PASI scores. For this purpose, he and coinvestigators turned to the Dermatology Life Quality Index (DLQI), measured in structured fashion every 4 weeks out to week 60.
“We often forget that even though we’re looking at the patient from the outside, what’s really important is how well they respond to our treatments internally. The DLQI is not a perfect tool, but it’s the best tool we have available. It gives us a fairly good survey of the various domains that affect patients’ day-to-day living,” he said.
In BE ABLE 1, the proportion of week-12 PASI90 responders achieving a DLQI of 0 or 1 – indicative of essentially no disease impact on quality of life – increased rapidly up until week 8. At week 12, 70%-100% of the PASI90 responders in the various treatment arms had a DLQI of 0 or 1. This quality-of-life improvement, like the PASI90 response, proved durable: When the week-12 PASI90 responders were assessed at week 60 in BE ABLE 2, 76%-93% of them had a DLQI of 0 or 1.
The improvements in quality of life correlated with clinical response. BE ABLE enrollees had an average PASI score of 19 at baseline. Overall, 79% of those with an absolute PASI score of 0 at week 12 had a DLQI of 0 or 1 at that time, as did 95% of those with a PASI of 0 at week 60. A PASI of 1 was associated with a 77% likelihood of a DLQI of 0 or 1 at week 12 and an 82% rate at week 60. In contrast, patients with an absolute PASI of 2-4 at week 12 had a 46% rate of DLQI 0/1, and those with a PASI 2-4 at week 60 had a 50% chance of having a DLQI of 0/1.
Phase 3 clinical trials of bimekizumab totaling several thousand psoriasis patients are ongoing.
The BE ABLE trials were sponsored by UCB Pharma. Dr. Papp reported serving as a consultant to and/or recipient of research grants from UCB and dozens of other pharmaceutical companies.
SOURCE: Papp KA. EADV 2019 Abstract FC02.02.
REPORTING FROM THE EADV CONGRESS
Unique T cell populations pinpointed in hepatocellular carcinoma tissue
Hepatocellular carcinoma (HCC) tissue contains several unique populations of tumor infiltrating cells, including some exhausted effector T cells that regain normal function when treated with the immunotherapy drug nivolumab, according to researchers.
The unique populations of recently activated CD4+, CD8+, and CD4-CD8 double-negative cells identified in the tumors expressed specific activation markers and inhibitor receptors, according to investigators, who have published the results of their immune profiling analyses in Cellular and Molecular Gastroenterology and Hepatology.
“Importantly, these cells expressed markers of activation and tissue residence, possibly suggesting activation within the tumor,” said Daniela Di Blasi, PhD, and the others researchers, of the University of Basel in Switzerland.
A further look at tumor histology revealed an accumulation of those activated T cells in immune-inflamed HCC, according to the investigators, who added that enumeration of specific tumor-infiltrating lymphocytes could represent “a prognostic indicator of therapy responsiveness.”
However, they advised caution in interpreting the results to date: “We are aware that the analysis described here is based on a small number of patients and that validation of its prognostic value requires ad hoc prospective studies that include more patients,” they said in their report.
The researcher’s findings were based on analysis of HCC biopsies before and after treatment with the immune checkpoint inhibitor nivolumab, nontumor liver tissue biopsies, and peripheral blood samples from 36 patients, most of whom were male, and about half of whom had cirrhosis. Investigators used multiparametric flow cytometry to characterize expression of activation markers including CD137, CD150, and ICOS, among others, as well as expression of inhibitory receptors including TIGIT and PD1.
Compared with nonneoplastic liver tissue, tumor tissue was enriched with T cells expressing the activation marker CD137 and the inhibitory receptor ICOS, indicating that HCC tumor-infiltrating lymphocytes “are different from liver-resident T cells and might have immunologic relevance,” Dr. Di Blasi and coauthors said in their report.
Further analysis revealed several cell populations unique to HCC samples, the authors said, including CD4+ T cells coexpressing ICOS and TIGIT, which tended to accumulate in tumor tissue, compared with nontumor tissue and peripheral blood mononuclear cells. Those CD4+ tumor-infiltrating T cells were functionally impaired, they added, as shown by a lack of cytokine production.
Activated CD8+ T cells likewise preferentially accumulated in tumor tissue, and most of those tumor-infiltrating cells expressed CD38 and PD1. The presence of these proliferating and functional cells may contribute to local inflammation and antitumor response, according to the investigators, who also identified two unique populations of double-negative T cells, including some that expressed CD137, which they said was a marker of recent T-cell activation.
The investigators also looked at the presence of tumor-infiltrating lymphocytes correlated to the presence of mononuclear cell infiltrate in tumor tissue. They found that immune-inflamed tumors had significantly increased proliferation of unique CD4+, CD8+, and double-negative T cell populations.
Nivolumab treatment appeared to substantially reduce the proportion of impaired CD4+ T cells, while increasing the percentage of interferon gamma–producing CD38+ CD4+ T cells and also promoting enrichment of interferon gamma–producing CD38+ CD8+ cells. Those increases in release of interferon gamma may have a positive influence on antitumor immunity via modulation of immune and tumor cell functions, according to the investigators.
Not all immune-inflamed tumors responded to nivolumab treatment, suggesting that an immune-inflamed profile is “necessary but not sufficient” for clinical response to an anti-PD1 agent, noted Dr. Di Blasi and colleagues.
Taken together, the researchers said their investigations suggest the presence of unique populations of T cells that might be providing effective anti-tumor immunity.
“These studies set the point for the identification of the tumor antigens stimulating these T cells and their possible exploitation as immunotherapeutic targets in HCC,” they concluded in the report.
The study was supported by grants from the European Research Council and the Swiss Initiative in Systems Biology, among others. Dr. Di Blasi and coauthors disclosed no conflicts of interest.
SOURCE: Di Blasi D et al. Cell Mol Gastroenterol Hepatol. 2019 Aug 22. doi: 10.1016/j.jcmgh.2019.08.004.
Immunotherapy with checkpoint inhibitors has been suggested for the treatment of hepatocellular carcinoma (HCC) and finding relevant predictors of response to immunotherapy remains one of the most challenging tasks for solid gastrointestinal cancers such as HCC where efficiency of immune therapy suggests only a moderate response so far. Recently, two randomized phase 3 trials on checkpoint inhibitors in HCC, both first-line against sorafenib (Checkmate 459) as well as second-line against placebo (KEYNOTE-240), have failed to show an overall survival benefit despite clinical benefit in some patients and a manageable side effects profile. The study by Di Blasi et al. therefore provides important insights into the immune cell composition of tumor-infiltrating lymphocytes (TILs) in HCC. In this study it was possible to identify certain cell populations within TILs that resembled recently activated tumor-specific T cells that were in an exhausted state. It was possible to reinvigorate these exhausted cell clusters and to activate IFN-delta–producing T cells with the help of checkpoint inhibitor therapy in these patients. These data suggest that the enumeration of certain immune cell infiltrates may identify patients responding to checkpoint inhibitor therapy. Another important observation from this study was that not all immune-inflamed tumors identified by immunohistochemistry (or so-called “hot tumors”) responded to checkpoint inhibitor therapy and that more sophisticated analysis of the immune infiltrates with, e.g., flow cytometry or mass cytometry seems to be necessary to understand which patients respond. Different immune cell clusters have been suggested by other research groups and further research is needed to confirm this theory and to understand which of the proposed immune cell clusters and phenotypic profiles will prove most valuable in terms of prognosis for checkpoint inhibitor therapy in HCC.
Nico Buettner, MD, and Robert Thimme, MD, are professors in the department of medicine II, Medical Center University of Freiburg, Germany. They have no conflicts of interest.
Immunotherapy with checkpoint inhibitors has been suggested for the treatment of hepatocellular carcinoma (HCC) and finding relevant predictors of response to immunotherapy remains one of the most challenging tasks for solid gastrointestinal cancers such as HCC where efficiency of immune therapy suggests only a moderate response so far. Recently, two randomized phase 3 trials on checkpoint inhibitors in HCC, both first-line against sorafenib (Checkmate 459) as well as second-line against placebo (KEYNOTE-240), have failed to show an overall survival benefit despite clinical benefit in some patients and a manageable side effects profile. The study by Di Blasi et al. therefore provides important insights into the immune cell composition of tumor-infiltrating lymphocytes (TILs) in HCC. In this study it was possible to identify certain cell populations within TILs that resembled recently activated tumor-specific T cells that were in an exhausted state. It was possible to reinvigorate these exhausted cell clusters and to activate IFN-delta–producing T cells with the help of checkpoint inhibitor therapy in these patients. These data suggest that the enumeration of certain immune cell infiltrates may identify patients responding to checkpoint inhibitor therapy. Another important observation from this study was that not all immune-inflamed tumors identified by immunohistochemistry (or so-called “hot tumors”) responded to checkpoint inhibitor therapy and that more sophisticated analysis of the immune infiltrates with, e.g., flow cytometry or mass cytometry seems to be necessary to understand which patients respond. Different immune cell clusters have been suggested by other research groups and further research is needed to confirm this theory and to understand which of the proposed immune cell clusters and phenotypic profiles will prove most valuable in terms of prognosis for checkpoint inhibitor therapy in HCC.
Nico Buettner, MD, and Robert Thimme, MD, are professors in the department of medicine II, Medical Center University of Freiburg, Germany. They have no conflicts of interest.
Immunotherapy with checkpoint inhibitors has been suggested for the treatment of hepatocellular carcinoma (HCC) and finding relevant predictors of response to immunotherapy remains one of the most challenging tasks for solid gastrointestinal cancers such as HCC where efficiency of immune therapy suggests only a moderate response so far. Recently, two randomized phase 3 trials on checkpoint inhibitors in HCC, both first-line against sorafenib (Checkmate 459) as well as second-line against placebo (KEYNOTE-240), have failed to show an overall survival benefit despite clinical benefit in some patients and a manageable side effects profile. The study by Di Blasi et al. therefore provides important insights into the immune cell composition of tumor-infiltrating lymphocytes (TILs) in HCC. In this study it was possible to identify certain cell populations within TILs that resembled recently activated tumor-specific T cells that were in an exhausted state. It was possible to reinvigorate these exhausted cell clusters and to activate IFN-delta–producing T cells with the help of checkpoint inhibitor therapy in these patients. These data suggest that the enumeration of certain immune cell infiltrates may identify patients responding to checkpoint inhibitor therapy. Another important observation from this study was that not all immune-inflamed tumors identified by immunohistochemistry (or so-called “hot tumors”) responded to checkpoint inhibitor therapy and that more sophisticated analysis of the immune infiltrates with, e.g., flow cytometry or mass cytometry seems to be necessary to understand which patients respond. Different immune cell clusters have been suggested by other research groups and further research is needed to confirm this theory and to understand which of the proposed immune cell clusters and phenotypic profiles will prove most valuable in terms of prognosis for checkpoint inhibitor therapy in HCC.
Nico Buettner, MD, and Robert Thimme, MD, are professors in the department of medicine II, Medical Center University of Freiburg, Germany. They have no conflicts of interest.
Hepatocellular carcinoma (HCC) tissue contains several unique populations of tumor infiltrating cells, including some exhausted effector T cells that regain normal function when treated with the immunotherapy drug nivolumab, according to researchers.
The unique populations of recently activated CD4+, CD8+, and CD4-CD8 double-negative cells identified in the tumors expressed specific activation markers and inhibitor receptors, according to investigators, who have published the results of their immune profiling analyses in Cellular and Molecular Gastroenterology and Hepatology.
“Importantly, these cells expressed markers of activation and tissue residence, possibly suggesting activation within the tumor,” said Daniela Di Blasi, PhD, and the others researchers, of the University of Basel in Switzerland.
A further look at tumor histology revealed an accumulation of those activated T cells in immune-inflamed HCC, according to the investigators, who added that enumeration of specific tumor-infiltrating lymphocytes could represent “a prognostic indicator of therapy responsiveness.”
However, they advised caution in interpreting the results to date: “We are aware that the analysis described here is based on a small number of patients and that validation of its prognostic value requires ad hoc prospective studies that include more patients,” they said in their report.
The researcher’s findings were based on analysis of HCC biopsies before and after treatment with the immune checkpoint inhibitor nivolumab, nontumor liver tissue biopsies, and peripheral blood samples from 36 patients, most of whom were male, and about half of whom had cirrhosis. Investigators used multiparametric flow cytometry to characterize expression of activation markers including CD137, CD150, and ICOS, among others, as well as expression of inhibitory receptors including TIGIT and PD1.
Compared with nonneoplastic liver tissue, tumor tissue was enriched with T cells expressing the activation marker CD137 and the inhibitory receptor ICOS, indicating that HCC tumor-infiltrating lymphocytes “are different from liver-resident T cells and might have immunologic relevance,” Dr. Di Blasi and coauthors said in their report.
Further analysis revealed several cell populations unique to HCC samples, the authors said, including CD4+ T cells coexpressing ICOS and TIGIT, which tended to accumulate in tumor tissue, compared with nontumor tissue and peripheral blood mononuclear cells. Those CD4+ tumor-infiltrating T cells were functionally impaired, they added, as shown by a lack of cytokine production.
Activated CD8+ T cells likewise preferentially accumulated in tumor tissue, and most of those tumor-infiltrating cells expressed CD38 and PD1. The presence of these proliferating and functional cells may contribute to local inflammation and antitumor response, according to the investigators, who also identified two unique populations of double-negative T cells, including some that expressed CD137, which they said was a marker of recent T-cell activation.
The investigators also looked at the presence of tumor-infiltrating lymphocytes correlated to the presence of mononuclear cell infiltrate in tumor tissue. They found that immune-inflamed tumors had significantly increased proliferation of unique CD4+, CD8+, and double-negative T cell populations.
Nivolumab treatment appeared to substantially reduce the proportion of impaired CD4+ T cells, while increasing the percentage of interferon gamma–producing CD38+ CD4+ T cells and also promoting enrichment of interferon gamma–producing CD38+ CD8+ cells. Those increases in release of interferon gamma may have a positive influence on antitumor immunity via modulation of immune and tumor cell functions, according to the investigators.
Not all immune-inflamed tumors responded to nivolumab treatment, suggesting that an immune-inflamed profile is “necessary but not sufficient” for clinical response to an anti-PD1 agent, noted Dr. Di Blasi and colleagues.
Taken together, the researchers said their investigations suggest the presence of unique populations of T cells that might be providing effective anti-tumor immunity.
“These studies set the point for the identification of the tumor antigens stimulating these T cells and their possible exploitation as immunotherapeutic targets in HCC,” they concluded in the report.
The study was supported by grants from the European Research Council and the Swiss Initiative in Systems Biology, among others. Dr. Di Blasi and coauthors disclosed no conflicts of interest.
SOURCE: Di Blasi D et al. Cell Mol Gastroenterol Hepatol. 2019 Aug 22. doi: 10.1016/j.jcmgh.2019.08.004.
Hepatocellular carcinoma (HCC) tissue contains several unique populations of tumor infiltrating cells, including some exhausted effector T cells that regain normal function when treated with the immunotherapy drug nivolumab, according to researchers.
The unique populations of recently activated CD4+, CD8+, and CD4-CD8 double-negative cells identified in the tumors expressed specific activation markers and inhibitor receptors, according to investigators, who have published the results of their immune profiling analyses in Cellular and Molecular Gastroenterology and Hepatology.
“Importantly, these cells expressed markers of activation and tissue residence, possibly suggesting activation within the tumor,” said Daniela Di Blasi, PhD, and the others researchers, of the University of Basel in Switzerland.
A further look at tumor histology revealed an accumulation of those activated T cells in immune-inflamed HCC, according to the investigators, who added that enumeration of specific tumor-infiltrating lymphocytes could represent “a prognostic indicator of therapy responsiveness.”
However, they advised caution in interpreting the results to date: “We are aware that the analysis described here is based on a small number of patients and that validation of its prognostic value requires ad hoc prospective studies that include more patients,” they said in their report.
The researcher’s findings were based on analysis of HCC biopsies before and after treatment with the immune checkpoint inhibitor nivolumab, nontumor liver tissue biopsies, and peripheral blood samples from 36 patients, most of whom were male, and about half of whom had cirrhosis. Investigators used multiparametric flow cytometry to characterize expression of activation markers including CD137, CD150, and ICOS, among others, as well as expression of inhibitory receptors including TIGIT and PD1.
Compared with nonneoplastic liver tissue, tumor tissue was enriched with T cells expressing the activation marker CD137 and the inhibitory receptor ICOS, indicating that HCC tumor-infiltrating lymphocytes “are different from liver-resident T cells and might have immunologic relevance,” Dr. Di Blasi and coauthors said in their report.
Further analysis revealed several cell populations unique to HCC samples, the authors said, including CD4+ T cells coexpressing ICOS and TIGIT, which tended to accumulate in tumor tissue, compared with nontumor tissue and peripheral blood mononuclear cells. Those CD4+ tumor-infiltrating T cells were functionally impaired, they added, as shown by a lack of cytokine production.
Activated CD8+ T cells likewise preferentially accumulated in tumor tissue, and most of those tumor-infiltrating cells expressed CD38 and PD1. The presence of these proliferating and functional cells may contribute to local inflammation and antitumor response, according to the investigators, who also identified two unique populations of double-negative T cells, including some that expressed CD137, which they said was a marker of recent T-cell activation.
The investigators also looked at the presence of tumor-infiltrating lymphocytes correlated to the presence of mononuclear cell infiltrate in tumor tissue. They found that immune-inflamed tumors had significantly increased proliferation of unique CD4+, CD8+, and double-negative T cell populations.
Nivolumab treatment appeared to substantially reduce the proportion of impaired CD4+ T cells, while increasing the percentage of interferon gamma–producing CD38+ CD4+ T cells and also promoting enrichment of interferon gamma–producing CD38+ CD8+ cells. Those increases in release of interferon gamma may have a positive influence on antitumor immunity via modulation of immune and tumor cell functions, according to the investigators.
Not all immune-inflamed tumors responded to nivolumab treatment, suggesting that an immune-inflamed profile is “necessary but not sufficient” for clinical response to an anti-PD1 agent, noted Dr. Di Blasi and colleagues.
Taken together, the researchers said their investigations suggest the presence of unique populations of T cells that might be providing effective anti-tumor immunity.
“These studies set the point for the identification of the tumor antigens stimulating these T cells and their possible exploitation as immunotherapeutic targets in HCC,” they concluded in the report.
The study was supported by grants from the European Research Council and the Swiss Initiative in Systems Biology, among others. Dr. Di Blasi and coauthors disclosed no conflicts of interest.
SOURCE: Di Blasi D et al. Cell Mol Gastroenterol Hepatol. 2019 Aug 22. doi: 10.1016/j.jcmgh.2019.08.004.
FROM CELLULAR AND MOLECULAR GASTROENTEROLOGY AND HEPATOLOGY
Experts in Europe issue guidance on atopic dermatitis in pregnancy
MADRID – European atopic dermatitis experts have issued formal guidance on a seriously neglected topic: treatment of the disease during pregnancy, breastfeeding, and in men planning to father children.

The impetus for the project was clear: “,” Christian Vestergaard, MD, PhD, declared at a meeting of the European Task Force on Atopic Dermatitis held in conjunction with the annual congress of the European Academy of Dermatology and Venereology.
He presented highlights of the task force’s position paper on the topic, for which he served as first author. The group’s recommendations are based on expert opinion, since randomized clinical trial literature in this area is nonexistent because of ethical concerns. But the task force, comprising a who’s who in European dermatology, drew on a wealth of collective clinical experience in this area.
“We have all of Europe involved in doing this position statement. It’s meant as what we think is proper treatment and what we can say about the different drugs,” explained Dr. Vestergaard, a dermatologist at the University of Aarhus (Denmark).
Most nonobstetricians are intimidated by atopic dermatitis (AD) in pregnancy, and are concerned about the potential for treatment-related harm to the fetus. As a consequence, they are reluctant to recommend anything beyond weak class I topical corticosteroids and emollients. That’s clearly insufficient in light of the vast scope of need, he asserted. After all, AD affects 15%-20% of all children and persists or reappears in adulthood in one out of five of them. Half of those adults are women, many of whom will at some point wish to become pregnant. And many men with AD will eventually want to father children.
A key message from the task force is that untreated AD in pregnancy potentially places the mother and fetus at risk of serious complications, including Staphylococcus aureus infection and eczema herpeticum.
“If you take one thing away from our position paper, it’s that you can use class II or III topical corticosteroids in pregnant women as first-line therapy,” Dr. Vestergaard said.
This stance contradicts a longstanding widely held concern that topical steroids in pregnancy might increase the risk of facial cleft in the offspring, a worry that has been convincingly debunked in a Cochrane systematic review of 14 studies including more than 1.6 million pregnancies. The report concluded there was no association between topical corticosteroids of any potency with preterm delivery, birth defects, or low Apgar scores (Cochrane Database Syst Rev. 2015 Oct 26. doi: 10.1002/14651858.CD007346.pub3).
The task force recommends that if class II or III topical corticosteroid use in pregnancy exceeds 200 g/month, it’s worth considering add-on UV therapy, with narrow band UVB-311 nm as the regimen of choice; it can be used liberally. UV therapy with psoralens is not advised because of a theoretical risk of mutagenicity.
Product labeling for the topical calcineurin inhibitors declares that the agents should not be used during pregnancy. However, the European task force position paper takes issue with that and declares that topical tacrolimus (Protopic) can be considered an off-label first-line therapy in pregnant women with an insufficient response to liberal use of emollients. The same holds true for breastfeeding patients with AD. Just as when topical corticosteroids are used in the nipple area, topical tacrolimus should be applied after nursing, and the nipple area should be gently cleaned before nursing.
The rationale behind recommending topical tacrolimus as a first-line treatment is that systemic absorption of the drug is trivial. Plus, observational studies of oral tacrolimus in pregnant women who have received a solid organ transplant have shown no increase in congenital malformations.
The task force recommends against the use of topical pimecrolimus (Elidel) or crisaborole (Eucrisa) in pregnancy or lactation due to lack of clinical experience in these settings, Dr. Vestergaard continued.
The task force position is that chlorhexidine and other topical antiseptics – with the notable exception of triclosan – can be used in pregnancy to prevent recurrent skin infections. Aminoglycosides should be avoided, but topical fusidic acid is a reasonable antibiotic for treatment of small areas of clinically infected atopic dermatitis in pregnancy.
Systemic therapies
If disease control is insufficient with topical therapy, it’s appropriate to engage in shared decision-making with the patient regarding systemic treatment. She needs to understand up front that the worldwide overall background stillbirth rate in the general population is about 3%, and that severe congenital malformations are present in up to 6% of all live births.
“You need to inform them that they can have systemic therapy and give birth to a child with congenital defects which have nothing to do with the medication,” noted Dr. Vestergaard.
That said, the task force recommends cyclosporine as the off-label, first-line systemic therapy in pregnancy and lactation when long-term treatment is required. This guidance is based largely upon reassuring evidence in solid organ transplant recipients.
The recommended second-line therapy is systemic corticosteroids, but it’s a qualified recommendation. Dr. Vestergaard and colleagues find that systemic corticosteroid therapy is only rarely needed in pregnant AD patients, and the task force recommendation is to limit the use to less than 2-3 weeks and no more than 0.5 mg/kg per day of prednisone. Dexamethasone is not recommended.
Azathioprine should not be started in pregnancy, according to the task force, but when no other options are available, it may be continued in women already on the drug, albeit at half of the prepregnancy dose.
Dupilumab (Dupixent) is to be avoided in pregnant women with AD until more clinical experience becomes available.
Treatment of prospective fathers with AD
The European task force recommends that topical therapies can be prescribed in prospective fathers without any special concerns. The same is true for systemic corticosteroids. Methotrexate should be halted 3 months before planned pregnancy, as is the case for mycophenolate mofetil (CellCept). Azathioprine is recommended when other options have failed. Cyclosporine is deemed a reasonable option in the treatment of men with severe AD at the time of conception if other treatments have failed; of note, neither the Food and Drug Administration nor the European regulatory agency have issued contraindications for the use of the drug in men who wish to become fathers.
Mycophenolate mofetil carries a theoretical risk of teratogenicity. The European task force recommends that men should use condoms while on the drug and for at least 90 days afterward.
Unplanned pregnancy in women on systemic therapy
The recommended course of action is to immediately stop systemic therapy, intensify appropriate topical therapy in anticipation of worsening AD, and refer the patient to an obstetrician and a teratology information center for an individualized risk assessment. Methotrexate and mycophenolate mofetil are known teratogens.
The full 16-page task force position paper was published shortly before EADV 2019 (J Eur Acad Dermatol Venereol. 2019 Sep;33[9]:1644-59).
The report was developed without commercial sponsorship. Dr. Vestergaard indicated he has received research grants from and/or serves as a consultant to eight pharmaceutical companies.
Jenny Murase, MD, is with the department of dermatology, University of California, San Francisco, and is the director of medical consultative dermatology at the Palo Alto Foundation Medical Group, Mountain View, Calif. She has served on advisory boards for Dermira, Sanofi, and UCB; performed dermatologic consulting for UpToDate and Ferndale, and given nonbranded lectures for disease state management awareness for Regeneron and UCB.
Jenny Murase, MD, is with the department of dermatology, University of California, San Francisco, and is the director of medical consultative dermatology at the Palo Alto Foundation Medical Group, Mountain View, Calif. She has served on advisory boards for Dermira, Sanofi, and UCB; performed dermatologic consulting for UpToDate and Ferndale, and given nonbranded lectures for disease state management awareness for Regeneron and UCB.
Jenny Murase, MD, is with the department of dermatology, University of California, San Francisco, and is the director of medical consultative dermatology at the Palo Alto Foundation Medical Group, Mountain View, Calif. She has served on advisory boards for Dermira, Sanofi, and UCB; performed dermatologic consulting for UpToDate and Ferndale, and given nonbranded lectures for disease state management awareness for Regeneron and UCB.
MADRID – European atopic dermatitis experts have issued formal guidance on a seriously neglected topic: treatment of the disease during pregnancy, breastfeeding, and in men planning to father children.
The impetus for the project was clear: “,” Christian Vestergaard, MD, PhD, declared at a meeting of the European Task Force on Atopic Dermatitis held in conjunction with the annual congress of the European Academy of Dermatology and Venereology.
He presented highlights of the task force’s position paper on the topic, for which he served as first author. The group’s recommendations are based on expert opinion, since randomized clinical trial literature in this area is nonexistent because of ethical concerns. But the task force, comprising a who’s who in European dermatology, drew on a wealth of collective clinical experience in this area.
“We have all of Europe involved in doing this position statement. It’s meant as what we think is proper treatment and what we can say about the different drugs,” explained Dr. Vestergaard, a dermatologist at the University of Aarhus (Denmark).
Most nonobstetricians are intimidated by atopic dermatitis (AD) in pregnancy, and are concerned about the potential for treatment-related harm to the fetus. As a consequence, they are reluctant to recommend anything beyond weak class I topical corticosteroids and emollients. That’s clearly insufficient in light of the vast scope of need, he asserted. After all, AD affects 15%-20% of all children and persists or reappears in adulthood in one out of five of them. Half of those adults are women, many of whom will at some point wish to become pregnant. And many men with AD will eventually want to father children.
A key message from the task force is that untreated AD in pregnancy potentially places the mother and fetus at risk of serious complications, including Staphylococcus aureus infection and eczema herpeticum.
“If you take one thing away from our position paper, it’s that you can use class II or III topical corticosteroids in pregnant women as first-line therapy,” Dr. Vestergaard said.
This stance contradicts a longstanding widely held concern that topical steroids in pregnancy might increase the risk of facial cleft in the offspring, a worry that has been convincingly debunked in a Cochrane systematic review of 14 studies including more than 1.6 million pregnancies. The report concluded there was no association between topical corticosteroids of any potency with preterm delivery, birth defects, or low Apgar scores (Cochrane Database Syst Rev. 2015 Oct 26. doi: 10.1002/14651858.CD007346.pub3).
The task force recommends that if class II or III topical corticosteroid use in pregnancy exceeds 200 g/month, it’s worth considering add-on UV therapy, with narrow band UVB-311 nm as the regimen of choice; it can be used liberally. UV therapy with psoralens is not advised because of a theoretical risk of mutagenicity.
Product labeling for the topical calcineurin inhibitors declares that the agents should not be used during pregnancy. However, the European task force position paper takes issue with that and declares that topical tacrolimus (Protopic) can be considered an off-label first-line therapy in pregnant women with an insufficient response to liberal use of emollients. The same holds true for breastfeeding patients with AD. Just as when topical corticosteroids are used in the nipple area, topical tacrolimus should be applied after nursing, and the nipple area should be gently cleaned before nursing.
The rationale behind recommending topical tacrolimus as a first-line treatment is that systemic absorption of the drug is trivial. Plus, observational studies of oral tacrolimus in pregnant women who have received a solid organ transplant have shown no increase in congenital malformations.
The task force recommends against the use of topical pimecrolimus (Elidel) or crisaborole (Eucrisa) in pregnancy or lactation due to lack of clinical experience in these settings, Dr. Vestergaard continued.
The task force position is that chlorhexidine and other topical antiseptics – with the notable exception of triclosan – can be used in pregnancy to prevent recurrent skin infections. Aminoglycosides should be avoided, but topical fusidic acid is a reasonable antibiotic for treatment of small areas of clinically infected atopic dermatitis in pregnancy.
Systemic therapies
If disease control is insufficient with topical therapy, it’s appropriate to engage in shared decision-making with the patient regarding systemic treatment. She needs to understand up front that the worldwide overall background stillbirth rate in the general population is about 3%, and that severe congenital malformations are present in up to 6% of all live births.
“You need to inform them that they can have systemic therapy and give birth to a child with congenital defects which have nothing to do with the medication,” noted Dr. Vestergaard.
That said, the task force recommends cyclosporine as the off-label, first-line systemic therapy in pregnancy and lactation when long-term treatment is required. This guidance is based largely upon reassuring evidence in solid organ transplant recipients.
The recommended second-line therapy is systemic corticosteroids, but it’s a qualified recommendation. Dr. Vestergaard and colleagues find that systemic corticosteroid therapy is only rarely needed in pregnant AD patients, and the task force recommendation is to limit the use to less than 2-3 weeks and no more than 0.5 mg/kg per day of prednisone. Dexamethasone is not recommended.
Azathioprine should not be started in pregnancy, according to the task force, but when no other options are available, it may be continued in women already on the drug, albeit at half of the prepregnancy dose.
Dupilumab (Dupixent) is to be avoided in pregnant women with AD until more clinical experience becomes available.
Treatment of prospective fathers with AD
The European task force recommends that topical therapies can be prescribed in prospective fathers without any special concerns. The same is true for systemic corticosteroids. Methotrexate should be halted 3 months before planned pregnancy, as is the case for mycophenolate mofetil (CellCept). Azathioprine is recommended when other options have failed. Cyclosporine is deemed a reasonable option in the treatment of men with severe AD at the time of conception if other treatments have failed; of note, neither the Food and Drug Administration nor the European regulatory agency have issued contraindications for the use of the drug in men who wish to become fathers.
Mycophenolate mofetil carries a theoretical risk of teratogenicity. The European task force recommends that men should use condoms while on the drug and for at least 90 days afterward.
Unplanned pregnancy in women on systemic therapy
The recommended course of action is to immediately stop systemic therapy, intensify appropriate topical therapy in anticipation of worsening AD, and refer the patient to an obstetrician and a teratology information center for an individualized risk assessment. Methotrexate and mycophenolate mofetil are known teratogens.
The full 16-page task force position paper was published shortly before EADV 2019 (J Eur Acad Dermatol Venereol. 2019 Sep;33[9]:1644-59).
The report was developed without commercial sponsorship. Dr. Vestergaard indicated he has received research grants from and/or serves as a consultant to eight pharmaceutical companies.
MADRID – European atopic dermatitis experts have issued formal guidance on a seriously neglected topic: treatment of the disease during pregnancy, breastfeeding, and in men planning to father children.
The impetus for the project was clear: “,” Christian Vestergaard, MD, PhD, declared at a meeting of the European Task Force on Atopic Dermatitis held in conjunction with the annual congress of the European Academy of Dermatology and Venereology.
He presented highlights of the task force’s position paper on the topic, for which he served as first author. The group’s recommendations are based on expert opinion, since randomized clinical trial literature in this area is nonexistent because of ethical concerns. But the task force, comprising a who’s who in European dermatology, drew on a wealth of collective clinical experience in this area.
“We have all of Europe involved in doing this position statement. It’s meant as what we think is proper treatment and what we can say about the different drugs,” explained Dr. Vestergaard, a dermatologist at the University of Aarhus (Denmark).
Most nonobstetricians are intimidated by atopic dermatitis (AD) in pregnancy, and are concerned about the potential for treatment-related harm to the fetus. As a consequence, they are reluctant to recommend anything beyond weak class I topical corticosteroids and emollients. That’s clearly insufficient in light of the vast scope of need, he asserted. After all, AD affects 15%-20% of all children and persists or reappears in adulthood in one out of five of them. Half of those adults are women, many of whom will at some point wish to become pregnant. And many men with AD will eventually want to father children.
A key message from the task force is that untreated AD in pregnancy potentially places the mother and fetus at risk of serious complications, including Staphylococcus aureus infection and eczema herpeticum.
“If you take one thing away from our position paper, it’s that you can use class II or III topical corticosteroids in pregnant women as first-line therapy,” Dr. Vestergaard said.
This stance contradicts a longstanding widely held concern that topical steroids in pregnancy might increase the risk of facial cleft in the offspring, a worry that has been convincingly debunked in a Cochrane systematic review of 14 studies including more than 1.6 million pregnancies. The report concluded there was no association between topical corticosteroids of any potency with preterm delivery, birth defects, or low Apgar scores (Cochrane Database Syst Rev. 2015 Oct 26. doi: 10.1002/14651858.CD007346.pub3).
The task force recommends that if class II or III topical corticosteroid use in pregnancy exceeds 200 g/month, it’s worth considering add-on UV therapy, with narrow band UVB-311 nm as the regimen of choice; it can be used liberally. UV therapy with psoralens is not advised because of a theoretical risk of mutagenicity.
Product labeling for the topical calcineurin inhibitors declares that the agents should not be used during pregnancy. However, the European task force position paper takes issue with that and declares that topical tacrolimus (Protopic) can be considered an off-label first-line therapy in pregnant women with an insufficient response to liberal use of emollients. The same holds true for breastfeeding patients with AD. Just as when topical corticosteroids are used in the nipple area, topical tacrolimus should be applied after nursing, and the nipple area should be gently cleaned before nursing.
The rationale behind recommending topical tacrolimus as a first-line treatment is that systemic absorption of the drug is trivial. Plus, observational studies of oral tacrolimus in pregnant women who have received a solid organ transplant have shown no increase in congenital malformations.
The task force recommends against the use of topical pimecrolimus (Elidel) or crisaborole (Eucrisa) in pregnancy or lactation due to lack of clinical experience in these settings, Dr. Vestergaard continued.
The task force position is that chlorhexidine and other topical antiseptics – with the notable exception of triclosan – can be used in pregnancy to prevent recurrent skin infections. Aminoglycosides should be avoided, but topical fusidic acid is a reasonable antibiotic for treatment of small areas of clinically infected atopic dermatitis in pregnancy.
Systemic therapies
If disease control is insufficient with topical therapy, it’s appropriate to engage in shared decision-making with the patient regarding systemic treatment. She needs to understand up front that the worldwide overall background stillbirth rate in the general population is about 3%, and that severe congenital malformations are present in up to 6% of all live births.
“You need to inform them that they can have systemic therapy and give birth to a child with congenital defects which have nothing to do with the medication,” noted Dr. Vestergaard.
That said, the task force recommends cyclosporine as the off-label, first-line systemic therapy in pregnancy and lactation when long-term treatment is required. This guidance is based largely upon reassuring evidence in solid organ transplant recipients.
The recommended second-line therapy is systemic corticosteroids, but it’s a qualified recommendation. Dr. Vestergaard and colleagues find that systemic corticosteroid therapy is only rarely needed in pregnant AD patients, and the task force recommendation is to limit the use to less than 2-3 weeks and no more than 0.5 mg/kg per day of prednisone. Dexamethasone is not recommended.
Azathioprine should not be started in pregnancy, according to the task force, but when no other options are available, it may be continued in women already on the drug, albeit at half of the prepregnancy dose.
Dupilumab (Dupixent) is to be avoided in pregnant women with AD until more clinical experience becomes available.
Treatment of prospective fathers with AD
The European task force recommends that topical therapies can be prescribed in prospective fathers without any special concerns. The same is true for systemic corticosteroids. Methotrexate should be halted 3 months before planned pregnancy, as is the case for mycophenolate mofetil (CellCept). Azathioprine is recommended when other options have failed. Cyclosporine is deemed a reasonable option in the treatment of men with severe AD at the time of conception if other treatments have failed; of note, neither the Food and Drug Administration nor the European regulatory agency have issued contraindications for the use of the drug in men who wish to become fathers.
Mycophenolate mofetil carries a theoretical risk of teratogenicity. The European task force recommends that men should use condoms while on the drug and for at least 90 days afterward.
Unplanned pregnancy in women on systemic therapy
The recommended course of action is to immediately stop systemic therapy, intensify appropriate topical therapy in anticipation of worsening AD, and refer the patient to an obstetrician and a teratology information center for an individualized risk assessment. Methotrexate and mycophenolate mofetil are known teratogens.
The full 16-page task force position paper was published shortly before EADV 2019 (J Eur Acad Dermatol Venereol. 2019 Sep;33[9]:1644-59).
The report was developed without commercial sponsorship. Dr. Vestergaard indicated he has received research grants from and/or serves as a consultant to eight pharmaceutical companies.
REPORTING FROM THE EADV CONGRESS
Genomic profiling of AML and MDS yields prognostic clues
ORLANDO – A genome-wide study of blood and bone marrow samples from more than 1,300 adults with myeloid disorders has both confirmed the role of known or suspected driver mutations and uncovered new associations that could inform clinical care for patients with acute myeloid leukemia and myelodysplastic syndrome.

“Integration of mutational and expression data is important to refine subytpes and constellations of mutations with prognostic significance,” Ilaria Iacobucci, PhD, of St. Jude Children’s Research Hospital in Memphis said during a late-breaking abstract session at the annual meeting of the American Society of Hematology.
Her team conducted an analysis combining full genomic sequencing and gene-expression profiles in blood and bone marrow samples from 598 adults with acute myeloid leukemia (AML) and 706 with myelodysplastic syndrome (MDS).
The goals of the study were to provide “unbiased analysis of AML and MDS by integrated genomic and transcriptome data and clinico-pathologic features and clinical outcome” and to identify and define myeloid leukemia subtypes with diagnostic, prognostic, and therapeutic significance, she said.
The median age of the MDS cohort was 73.2 years (range 23.3-93.1). According to 2016 World Health Organization criteria, 37% had a diagnosis of MDS with excess blasts, 26.3% had MDS with ring sideroblasts, 20.9% had MDS with multilineage dysplasia, 14.6% had MDS with deletion 5q, and 1.1% had unclassifiable MDS.
The median age of the AML cohort was 68 years. Of this group, 31.7% had a diagnosis of AML not otherwise specified, 29.9% had known cytogenetic alterations, 27.3% had NPM1-mutated AML, and 9.7% had RUNX1-mutated disease.
Samples from all patients underwent tumor whole-genome sequencing and whole-transcriptome sequencing.
The combined sequencing confirmed a diagnosis of AML with recurrent genetic abnormalities in 11% of cases. These patients had disease with distinct gene-expression profiles and favorable prognosis. The sequencing identified combinations of mutations in genes linked with specific AML subtypes.
For example, combinations of mutations in KIT, ZBTB7A, ASXL2, RAD21, CSF3R, and DNM2 were associated with RUNX1-RUNXT1 leukemia, whereas mutations in FLT3, DDX54, WT1, and CALR in promyelocytic leukemia/retinoic acid receptor alpha were associated with promyelocytic leukemia, and KIT and BCORL1 mutations were associated with CBFB-rearranged leukemia.
In addition to rounding up the usual genomic suspects, the investigators also identified combinations that are associated with prognosis. Notably, NPM1 mutations were found in 27.4% of AML and 1% of MDS cases, and these mutations were characterized by four gene-expression signatures that were associated with different combinations of cooperating mutations in cohesin and signaling genes, and with outcome.
They found that patients with co-occurring NPM1 and FLT3 mutations had worse prognosis than those with mutations only in NPM1, whereas patients with NPM1 mutations co-occurring with cohesin gene mutations had better outcomes.
At a briefing prior to her presentation of the data, Dr. Iacobucci explained how her group’s findings might inform treatment, including the possibility of preventing development of AML in patients with MDS.
“What we are doing, in addition to the genomic part, is also establishing a repository of patient-derived xenografts, so in this way we can have the genome information, and we can have the biological material in vivo to test different therapies,” she said.

In an interview, Andrew H. Wei, MBBS, PhD, from the Alfred Hospital in Melbourne, who was not involved in the genomic study, commented on the role of sequencing in treatment of patients with myeloid malignancies.
“I think the future is that as the leukemia evolves, our therapy will evolve along with it. Furthermore, we now have the potential to measure many of these mutations with much higher sensitivity than just whole-genome sequencing, so we can imagine a future whereby we can track and measure these mutations as they rise in the patient’s bone marrow or blood before the patients becomes sick with florid leukemia, and it gives us the potential to predictably alter our management before they become sick,” he said.
The study was supported by St. Jude Children’s Research Hospital and the Leukemia and Lymphoma Society. Dr. Iacobucci and Dr. Wei reported having no relevant disclosures.
SOURCE: Iacobucci I et al. ASH 2019, Abstract LBA-4.
ORLANDO – A genome-wide study of blood and bone marrow samples from more than 1,300 adults with myeloid disorders has both confirmed the role of known or suspected driver mutations and uncovered new associations that could inform clinical care for patients with acute myeloid leukemia and myelodysplastic syndrome.
“Integration of mutational and expression data is important to refine subytpes and constellations of mutations with prognostic significance,” Ilaria Iacobucci, PhD, of St. Jude Children’s Research Hospital in Memphis said during a late-breaking abstract session at the annual meeting of the American Society of Hematology.
Her team conducted an analysis combining full genomic sequencing and gene-expression profiles in blood and bone marrow samples from 598 adults with acute myeloid leukemia (AML) and 706 with myelodysplastic syndrome (MDS).
The goals of the study were to provide “unbiased analysis of AML and MDS by integrated genomic and transcriptome data and clinico-pathologic features and clinical outcome” and to identify and define myeloid leukemia subtypes with diagnostic, prognostic, and therapeutic significance, she said.
The median age of the MDS cohort was 73.2 years (range 23.3-93.1). According to 2016 World Health Organization criteria, 37% had a diagnosis of MDS with excess blasts, 26.3% had MDS with ring sideroblasts, 20.9% had MDS with multilineage dysplasia, 14.6% had MDS with deletion 5q, and 1.1% had unclassifiable MDS.
The median age of the AML cohort was 68 years. Of this group, 31.7% had a diagnosis of AML not otherwise specified, 29.9% had known cytogenetic alterations, 27.3% had NPM1-mutated AML, and 9.7% had RUNX1-mutated disease.
Samples from all patients underwent tumor whole-genome sequencing and whole-transcriptome sequencing.
The combined sequencing confirmed a diagnosis of AML with recurrent genetic abnormalities in 11% of cases. These patients had disease with distinct gene-expression profiles and favorable prognosis. The sequencing identified combinations of mutations in genes linked with specific AML subtypes.
For example, combinations of mutations in KIT, ZBTB7A, ASXL2, RAD21, CSF3R, and DNM2 were associated with RUNX1-RUNXT1 leukemia, whereas mutations in FLT3, DDX54, WT1, and CALR in promyelocytic leukemia/retinoic acid receptor alpha were associated with promyelocytic leukemia, and KIT and BCORL1 mutations were associated with CBFB-rearranged leukemia.
In addition to rounding up the usual genomic suspects, the investigators also identified combinations that are associated with prognosis. Notably, NPM1 mutations were found in 27.4% of AML and 1% of MDS cases, and these mutations were characterized by four gene-expression signatures that were associated with different combinations of cooperating mutations in cohesin and signaling genes, and with outcome.
They found that patients with co-occurring NPM1 and FLT3 mutations had worse prognosis than those with mutations only in NPM1, whereas patients with NPM1 mutations co-occurring with cohesin gene mutations had better outcomes.
At a briefing prior to her presentation of the data, Dr. Iacobucci explained how her group’s findings might inform treatment, including the possibility of preventing development of AML in patients with MDS.
“What we are doing, in addition to the genomic part, is also establishing a repository of patient-derived xenografts, so in this way we can have the genome information, and we can have the biological material in vivo to test different therapies,” she said.
In an interview, Andrew H. Wei, MBBS, PhD, from the Alfred Hospital in Melbourne, who was not involved in the genomic study, commented on the role of sequencing in treatment of patients with myeloid malignancies.
“I think the future is that as the leukemia evolves, our therapy will evolve along with it. Furthermore, we now have the potential to measure many of these mutations with much higher sensitivity than just whole-genome sequencing, so we can imagine a future whereby we can track and measure these mutations as they rise in the patient’s bone marrow or blood before the patients becomes sick with florid leukemia, and it gives us the potential to predictably alter our management before they become sick,” he said.
The study was supported by St. Jude Children’s Research Hospital and the Leukemia and Lymphoma Society. Dr. Iacobucci and Dr. Wei reported having no relevant disclosures.
SOURCE: Iacobucci I et al. ASH 2019, Abstract LBA-4.
ORLANDO – A genome-wide study of blood and bone marrow samples from more than 1,300 adults with myeloid disorders has both confirmed the role of known or suspected driver mutations and uncovered new associations that could inform clinical care for patients with acute myeloid leukemia and myelodysplastic syndrome.
“Integration of mutational and expression data is important to refine subytpes and constellations of mutations with prognostic significance,” Ilaria Iacobucci, PhD, of St. Jude Children’s Research Hospital in Memphis said during a late-breaking abstract session at the annual meeting of the American Society of Hematology.
Her team conducted an analysis combining full genomic sequencing and gene-expression profiles in blood and bone marrow samples from 598 adults with acute myeloid leukemia (AML) and 706 with myelodysplastic syndrome (MDS).
The goals of the study were to provide “unbiased analysis of AML and MDS by integrated genomic and transcriptome data and clinico-pathologic features and clinical outcome” and to identify and define myeloid leukemia subtypes with diagnostic, prognostic, and therapeutic significance, she said.
The median age of the MDS cohort was 73.2 years (range 23.3-93.1). According to 2016 World Health Organization criteria, 37% had a diagnosis of MDS with excess blasts, 26.3% had MDS with ring sideroblasts, 20.9% had MDS with multilineage dysplasia, 14.6% had MDS with deletion 5q, and 1.1% had unclassifiable MDS.
The median age of the AML cohort was 68 years. Of this group, 31.7% had a diagnosis of AML not otherwise specified, 29.9% had known cytogenetic alterations, 27.3% had NPM1-mutated AML, and 9.7% had RUNX1-mutated disease.
Samples from all patients underwent tumor whole-genome sequencing and whole-transcriptome sequencing.
The combined sequencing confirmed a diagnosis of AML with recurrent genetic abnormalities in 11% of cases. These patients had disease with distinct gene-expression profiles and favorable prognosis. The sequencing identified combinations of mutations in genes linked with specific AML subtypes.
For example, combinations of mutations in KIT, ZBTB7A, ASXL2, RAD21, CSF3R, and DNM2 were associated with RUNX1-RUNXT1 leukemia, whereas mutations in FLT3, DDX54, WT1, and CALR in promyelocytic leukemia/retinoic acid receptor alpha were associated with promyelocytic leukemia, and KIT and BCORL1 mutations were associated with CBFB-rearranged leukemia.
In addition to rounding up the usual genomic suspects, the investigators also identified combinations that are associated with prognosis. Notably, NPM1 mutations were found in 27.4% of AML and 1% of MDS cases, and these mutations were characterized by four gene-expression signatures that were associated with different combinations of cooperating mutations in cohesin and signaling genes, and with outcome.
They found that patients with co-occurring NPM1 and FLT3 mutations had worse prognosis than those with mutations only in NPM1, whereas patients with NPM1 mutations co-occurring with cohesin gene mutations had better outcomes.
At a briefing prior to her presentation of the data, Dr. Iacobucci explained how her group’s findings might inform treatment, including the possibility of preventing development of AML in patients with MDS.
“What we are doing, in addition to the genomic part, is also establishing a repository of patient-derived xenografts, so in this way we can have the genome information, and we can have the biological material in vivo to test different therapies,” she said.
In an interview, Andrew H. Wei, MBBS, PhD, from the Alfred Hospital in Melbourne, who was not involved in the genomic study, commented on the role of sequencing in treatment of patients with myeloid malignancies.
“I think the future is that as the leukemia evolves, our therapy will evolve along with it. Furthermore, we now have the potential to measure many of these mutations with much higher sensitivity than just whole-genome sequencing, so we can imagine a future whereby we can track and measure these mutations as they rise in the patient’s bone marrow or blood before the patients becomes sick with florid leukemia, and it gives us the potential to predictably alter our management before they become sick,” he said.
The study was supported by St. Jude Children’s Research Hospital and the Leukemia and Lymphoma Society. Dr. Iacobucci and Dr. Wei reported having no relevant disclosures.
SOURCE: Iacobucci I et al. ASH 2019, Abstract LBA-4.
REPORTING FROM ASH 2019
HRS urges consumers to direct questions about wearables’ data to clinicians
With much of the public now wearing devices on their wrists or elsewhere capable of recording a range of vital signs, including heart rate abnormalities, the Heart Rhythm Society launched a guide for American consumers about wearables and the data they collect during a session on Jan. 9 at CES 2020 in Las Vegas.

While providing a succinct but comprehensive overview of the types of wearables and the health metrics they can record, the main and recurring message of the 10-page e-pamphlet is that, when a layperson has a question or concern about their data, the best course is to consult a clinician.
The “Guidance for Wearable Health Solutions,” produced by the Heart Rhythm Society (HRS) along with the Consumer Technology Association (CTA, which presents the annual CES exhibition), cautions that “most wearables are primarily suited for fitness and wellness,” and stresses that wearables “are not a substitute for medical devices prescribed by a clinician.” And in all cases, the document advises, when questions arise about the data – including an apparently high heart rate; a reading the device identifies as abnormal; and when symptoms appear such as a rapid heart rate, dizziness, or fluttering or flopping of the heart – the response that the guidance advocates is consistent: Talk with your clinician.
“Heart Rhythm Society members are seeing more and more patients with their own data collected by wearables,” said Nassir F. Marrouche, MD, professor of medicine and director of electrophysiology at Tulane University, New Orleans, and a member of the panel that wrote the guidance document for the HRS and CTA. “Every provider is dealing with consumer wearable data. The need is important for consumers to be supported. Consumers and patients are buying over-the-counter devices and using them for diagnosis and management, with little to no guidance, and we want to help them feel supported in managing their data and understand what to do with it,” Dr. Marrouche said in an interview.
“This is a new reality in medicine; the direction of information is changing. Consumers are collecting data themselves and coming to physicians already informed. There is a new shift in how information is collected, shared, and used.” Dr. Marrouche was 1 of 5 cardiac electrophysiologists who served on the 11-member writing group.

The new document for consumers “addresses an unmet need,” and the HRS collaboration with the CTA was “a unique opportunity to develop useful guidance that supports education and empowers consumers,” said Christina Wurster, chief strategy officer for the HRS in Washington and a member of the writing panel. “The questions outlined in the document are questions our members receive daily. The document is a resource they can direct people to.”
The HRS and CTA will “partner with consumer advocacy groups and professional societies to further disseminate the document,” added Ms. Wurster. “We’ll also have a strong push on social media to reach consumer audiences and drive awareness of this new resource,” she said in an interview. In addition, HRS “has strategic partnerships with other societies and will aim to work with them for dissemination, including societies related to internal medicine, emergency medicine, cardiology, and nursing, as well as also working with patient and consumer advocacy groups to reach the public.” The CTA will also actively publicize and disseminate the guidance document through their members.
Clinical guidelines play catch-up
Ironically, the HRS has issued this guidance to the public and has told people to take their wearable-collected heart data to clinicians before the HRS or any other medical group has advised clinicians on how they should handle, interpret, and use heart rhythm data collected this way.
Presumably, many if not most of the people with questions about their heart data from wearables are asymptomatic, because symptoms are what usually drive patients with a cardiac arrhythmia to consult a physician – they don’t wait to see what their device tells them. But the best way to manage asymptomatic arrhythmias like atrial fibrillation (AFib) remains a big clinical uncertainty today, with no evidence base as a guide, although several studies exploring this question are in progress.

“There are no clear and definitive data showing that treating subclinical atrial fibrillation improves outcomes. That’s what we need, and until we get these data you won’t see strong recommendations in guidelines” to screen patients for asymptomatic AFib or other arrhythmias, said Sana M. Al-Khatib, MD, a cardiac electrophysiologist and professor of medicine at Duke University, Durham, N.C., during the 2019 American Heart Association scientific sessions in Philadelphia in a talk about wearables and guidelines.
“If you intervene with silent AFib, do you improve outcomes? That evidence is lacking,” she said. Another shortcoming of current evidence is a clear understanding of what AFib burden warrants intervention, added Dr. Al-Khatib. “We see high-rate AFib episodes recorded in patients with implanted cardiac devices [and no symptoms], and we don’t know what to do with that either.”
The closest any existing guideline from a medical society comes to currently endorsing screening for AFib by a wearable is the 2016 European Society of Cardiology’s AFib management guidelines, which give “opportunistic screening” among people aged older than 65 years a IB recommendation, but specifically for screening by taking a patient’s pulse or with a ECG recording, with no mention of the screening role for wearables (Eur Heart J. 2016 Oct 7;37[38]:2893-967), Dr. Al-Khatib noted.
The most extensive data on screening for asymptomatic AFib in an unselected population came in the recently reported results from the Apple Heart Study, which enrolled more than 419,000 people monitored by a smart watch for a median of 117 days. During this screening, 2,161 people (0.52%) received a notification of having an irregular pulse (including 3.1% of those who were aged at least 65 years), which triggered more intensive assessment with an ECG patch for a median of 13 days in 450 of the 2,161 screening positives (21%) who agreed to participate in this follow-up. Among those 450 people, the patch test identified 34% as having actual AFib (N Engl J Med. 2019 Nov 14;381[20]:1909-17). But while this study provided evidence that screening for an irregular heartbeat with a wearable can identify AFib with some level of success, the results did not address whether this approach improved short- or long-term patient outcomes.
In addition, what the Apple Heart Study results showed was that this sort of screening results in a relatively large volume of follow-up testing. Of the 2,161 participants who received an irregular pulse notification, 1,376 (64%) returned a 90-day survey. Of these, 787 (57%) reported contact with a health care provider outside the study, 28% were prescribed a new medication, 33% were recommended to see a specialist (such as a cardiologist), and 36% were recommended to have additional testing.

“The results raise the question that a lot of resources were used,” to assess patients with a positive screening result, noted Paul A. Heidenreich, MD, a cardiologist and professor of medicine at Stanford (Calif.) University who studies quality of care for patients with heart disease. He estimated that, in the Apple Heart Study, each of the more than 2,000 patients who screening positive for an irregular heartbeat and underwent subsequent assessment ran up about $700 worth of follow-up testing. But he added that, in the case of AFib, the primary intervention that many previously undiagnosed AFib patients receive is some sort of anticoagulation for stroke prevention. Moreover, because this intervention is so effective there is a lot of money to play with to make AFib screening cost effective, as judged by typical, contemporary metrics of cost efficacy that value a quality-adjusted life-year (QALY) gain as reasonable for society to pay if the cost of an incremental QALY is $50,000-$150,000.
If the benchmark is a cost that’s within $50,000/QALY, then an average follow-up cost of $116/person to assess screened positives can fall within this cost ceiling. If the benchmark is $150,000/QALY, then follow-up costs can run as high as $491/person screened, said Dr. Heidenreich during the same AHA session where Dr. Al-Khatib spoke last November.
Despite this good news for screening for AFib with a wearable from a cost-effectiveness perspective, “there is so much uncertainty regarding the benefit and the consequences of incidental findings that we need an outcomes study before widespread implementation” of this type of screening, Dr. Heidenreich concluded. “We need an outcomes study to feel comfortable” with screening. “There is a huge potential for extra care that we don’t understand.”
Dr. Marrouche agreed that collecting adequate evidence to drive changes in clinical guidelines on how to use data from wearables has lagged behind the rapid spread of wearables and the information they can produce among the American public. “Outcomes and evidence will support guidelines development, but in the meantime, we’re offering education to clinicians, patients, and consumers. Consumers own their data, and they can share them with whomever they choose.”
The document notes that people who use wearables are, in general, “enthusiastic about tracking their data, not only for their own use, but also to share” with others, often on social media websites.
“We cannot control that, but our goal in the document is focused on the clinical relevance [of the data] and to help people better understand their data and use it in a meaningful and safe way,” Dr. Marrouche said.
Dr. Marrouche has been a consultant to, advisor to, or received research support from Abbott, Biosense Webster, Biotronik, GE Healthcare, Medtronic, Preventice, Sanofi-Aventis, Siemens, and Vytronus. Ms. Wurster is an employee of the Heart Rhythm Society. Dr. Al-Khatib has been a consultant to Milestone Pharmaceuticals and Medtronic, and she has also received other financial benefits from Medtronic. Dr. Heidenreich had no disclosures,
With much of the public now wearing devices on their wrists or elsewhere capable of recording a range of vital signs, including heart rate abnormalities, the Heart Rhythm Society launched a guide for American consumers about wearables and the data they collect during a session on Jan. 9 at CES 2020 in Las Vegas.
While providing a succinct but comprehensive overview of the types of wearables and the health metrics they can record, the main and recurring message of the 10-page e-pamphlet is that, when a layperson has a question or concern about their data, the best course is to consult a clinician.
The “Guidance for Wearable Health Solutions,” produced by the Heart Rhythm Society (HRS) along with the Consumer Technology Association (CTA, which presents the annual CES exhibition), cautions that “most wearables are primarily suited for fitness and wellness,” and stresses that wearables “are not a substitute for medical devices prescribed by a clinician.” And in all cases, the document advises, when questions arise about the data – including an apparently high heart rate; a reading the device identifies as abnormal; and when symptoms appear such as a rapid heart rate, dizziness, or fluttering or flopping of the heart – the response that the guidance advocates is consistent: Talk with your clinician.
“Heart Rhythm Society members are seeing more and more patients with their own data collected by wearables,” said Nassir F. Marrouche, MD, professor of medicine and director of electrophysiology at Tulane University, New Orleans, and a member of the panel that wrote the guidance document for the HRS and CTA. “Every provider is dealing with consumer wearable data. The need is important for consumers to be supported. Consumers and patients are buying over-the-counter devices and using them for diagnosis and management, with little to no guidance, and we want to help them feel supported in managing their data and understand what to do with it,” Dr. Marrouche said in an interview.
“This is a new reality in medicine; the direction of information is changing. Consumers are collecting data themselves and coming to physicians already informed. There is a new shift in how information is collected, shared, and used.” Dr. Marrouche was 1 of 5 cardiac electrophysiologists who served on the 11-member writing group.
The new document for consumers “addresses an unmet need,” and the HRS collaboration with the CTA was “a unique opportunity to develop useful guidance that supports education and empowers consumers,” said Christina Wurster, chief strategy officer for the HRS in Washington and a member of the writing panel. “The questions outlined in the document are questions our members receive daily. The document is a resource they can direct people to.”
The HRS and CTA will “partner with consumer advocacy groups and professional societies to further disseminate the document,” added Ms. Wurster. “We’ll also have a strong push on social media to reach consumer audiences and drive awareness of this new resource,” she said in an interview. In addition, HRS “has strategic partnerships with other societies and will aim to work with them for dissemination, including societies related to internal medicine, emergency medicine, cardiology, and nursing, as well as also working with patient and consumer advocacy groups to reach the public.” The CTA will also actively publicize and disseminate the guidance document through their members.
Clinical guidelines play catch-up
Ironically, the HRS has issued this guidance to the public and has told people to take their wearable-collected heart data to clinicians before the HRS or any other medical group has advised clinicians on how they should handle, interpret, and use heart rhythm data collected this way.
Presumably, many if not most of the people with questions about their heart data from wearables are asymptomatic, because symptoms are what usually drive patients with a cardiac arrhythmia to consult a physician – they don’t wait to see what their device tells them. But the best way to manage asymptomatic arrhythmias like atrial fibrillation (AFib) remains a big clinical uncertainty today, with no evidence base as a guide, although several studies exploring this question are in progress.
“There are no clear and definitive data showing that treating subclinical atrial fibrillation improves outcomes. That’s what we need, and until we get these data you won’t see strong recommendations in guidelines” to screen patients for asymptomatic AFib or other arrhythmias, said Sana M. Al-Khatib, MD, a cardiac electrophysiologist and professor of medicine at Duke University, Durham, N.C., during the 2019 American Heart Association scientific sessions in Philadelphia in a talk about wearables and guidelines.
“If you intervene with silent AFib, do you improve outcomes? That evidence is lacking,” she said. Another shortcoming of current evidence is a clear understanding of what AFib burden warrants intervention, added Dr. Al-Khatib. “We see high-rate AFib episodes recorded in patients with implanted cardiac devices [and no symptoms], and we don’t know what to do with that either.”
The closest any existing guideline from a medical society comes to currently endorsing screening for AFib by a wearable is the 2016 European Society of Cardiology’s AFib management guidelines, which give “opportunistic screening” among people aged older than 65 years a IB recommendation, but specifically for screening by taking a patient’s pulse or with a ECG recording, with no mention of the screening role for wearables (Eur Heart J. 2016 Oct 7;37[38]:2893-967), Dr. Al-Khatib noted.
The most extensive data on screening for asymptomatic AFib in an unselected population came in the recently reported results from the Apple Heart Study, which enrolled more than 419,000 people monitored by a smart watch for a median of 117 days. During this screening, 2,161 people (0.52%) received a notification of having an irregular pulse (including 3.1% of those who were aged at least 65 years), which triggered more intensive assessment with an ECG patch for a median of 13 days in 450 of the 2,161 screening positives (21%) who agreed to participate in this follow-up. Among those 450 people, the patch test identified 34% as having actual AFib (N Engl J Med. 2019 Nov 14;381[20]:1909-17). But while this study provided evidence that screening for an irregular heartbeat with a wearable can identify AFib with some level of success, the results did not address whether this approach improved short- or long-term patient outcomes.
In addition, what the Apple Heart Study results showed was that this sort of screening results in a relatively large volume of follow-up testing. Of the 2,161 participants who received an irregular pulse notification, 1,376 (64%) returned a 90-day survey. Of these, 787 (57%) reported contact with a health care provider outside the study, 28% were prescribed a new medication, 33% were recommended to see a specialist (such as a cardiologist), and 36% were recommended to have additional testing.
“The results raise the question that a lot of resources were used,” to assess patients with a positive screening result, noted Paul A. Heidenreich, MD, a cardiologist and professor of medicine at Stanford (Calif.) University who studies quality of care for patients with heart disease. He estimated that, in the Apple Heart Study, each of the more than 2,000 patients who screening positive for an irregular heartbeat and underwent subsequent assessment ran up about $700 worth of follow-up testing. But he added that, in the case of AFib, the primary intervention that many previously undiagnosed AFib patients receive is some sort of anticoagulation for stroke prevention. Moreover, because this intervention is so effective there is a lot of money to play with to make AFib screening cost effective, as judged by typical, contemporary metrics of cost efficacy that value a quality-adjusted life-year (QALY) gain as reasonable for society to pay if the cost of an incremental QALY is $50,000-$150,000.
If the benchmark is a cost that’s within $50,000/QALY, then an average follow-up cost of $116/person to assess screened positives can fall within this cost ceiling. If the benchmark is $150,000/QALY, then follow-up costs can run as high as $491/person screened, said Dr. Heidenreich during the same AHA session where Dr. Al-Khatib spoke last November.
Despite this good news for screening for AFib with a wearable from a cost-effectiveness perspective, “there is so much uncertainty regarding the benefit and the consequences of incidental findings that we need an outcomes study before widespread implementation” of this type of screening, Dr. Heidenreich concluded. “We need an outcomes study to feel comfortable” with screening. “There is a huge potential for extra care that we don’t understand.”
Dr. Marrouche agreed that collecting adequate evidence to drive changes in clinical guidelines on how to use data from wearables has lagged behind the rapid spread of wearables and the information they can produce among the American public. “Outcomes and evidence will support guidelines development, but in the meantime, we’re offering education to clinicians, patients, and consumers. Consumers own their data, and they can share them with whomever they choose.”
The document notes that people who use wearables are, in general, “enthusiastic about tracking their data, not only for their own use, but also to share” with others, often on social media websites.
“We cannot control that, but our goal in the document is focused on the clinical relevance [of the data] and to help people better understand their data and use it in a meaningful and safe way,” Dr. Marrouche said.
Dr. Marrouche has been a consultant to, advisor to, or received research support from Abbott, Biosense Webster, Biotronik, GE Healthcare, Medtronic, Preventice, Sanofi-Aventis, Siemens, and Vytronus. Ms. Wurster is an employee of the Heart Rhythm Society. Dr. Al-Khatib has been a consultant to Milestone Pharmaceuticals and Medtronic, and she has also received other financial benefits from Medtronic. Dr. Heidenreich had no disclosures,
With much of the public now wearing devices on their wrists or elsewhere capable of recording a range of vital signs, including heart rate abnormalities, the Heart Rhythm Society launched a guide for American consumers about wearables and the data they collect during a session on Jan. 9 at CES 2020 in Las Vegas.
While providing a succinct but comprehensive overview of the types of wearables and the health metrics they can record, the main and recurring message of the 10-page e-pamphlet is that, when a layperson has a question or concern about their data, the best course is to consult a clinician.
The “Guidance for Wearable Health Solutions,” produced by the Heart Rhythm Society (HRS) along with the Consumer Technology Association (CTA, which presents the annual CES exhibition), cautions that “most wearables are primarily suited for fitness and wellness,” and stresses that wearables “are not a substitute for medical devices prescribed by a clinician.” And in all cases, the document advises, when questions arise about the data – including an apparently high heart rate; a reading the device identifies as abnormal; and when symptoms appear such as a rapid heart rate, dizziness, or fluttering or flopping of the heart – the response that the guidance advocates is consistent: Talk with your clinician.
“Heart Rhythm Society members are seeing more and more patients with their own data collected by wearables,” said Nassir F. Marrouche, MD, professor of medicine and director of electrophysiology at Tulane University, New Orleans, and a member of the panel that wrote the guidance document for the HRS and CTA. “Every provider is dealing with consumer wearable data. The need is important for consumers to be supported. Consumers and patients are buying over-the-counter devices and using them for diagnosis and management, with little to no guidance, and we want to help them feel supported in managing their data and understand what to do with it,” Dr. Marrouche said in an interview.
“This is a new reality in medicine; the direction of information is changing. Consumers are collecting data themselves and coming to physicians already informed. There is a new shift in how information is collected, shared, and used.” Dr. Marrouche was 1 of 5 cardiac electrophysiologists who served on the 11-member writing group.
The new document for consumers “addresses an unmet need,” and the HRS collaboration with the CTA was “a unique opportunity to develop useful guidance that supports education and empowers consumers,” said Christina Wurster, chief strategy officer for the HRS in Washington and a member of the writing panel. “The questions outlined in the document are questions our members receive daily. The document is a resource they can direct people to.”
The HRS and CTA will “partner with consumer advocacy groups and professional societies to further disseminate the document,” added Ms. Wurster. “We’ll also have a strong push on social media to reach consumer audiences and drive awareness of this new resource,” she said in an interview. In addition, HRS “has strategic partnerships with other societies and will aim to work with them for dissemination, including societies related to internal medicine, emergency medicine, cardiology, and nursing, as well as also working with patient and consumer advocacy groups to reach the public.” The CTA will also actively publicize and disseminate the guidance document through their members.
Clinical guidelines play catch-up
Ironically, the HRS has issued this guidance to the public and has told people to take their wearable-collected heart data to clinicians before the HRS or any other medical group has advised clinicians on how they should handle, interpret, and use heart rhythm data collected this way.
Presumably, many if not most of the people with questions about their heart data from wearables are asymptomatic, because symptoms are what usually drive patients with a cardiac arrhythmia to consult a physician – they don’t wait to see what their device tells them. But the best way to manage asymptomatic arrhythmias like atrial fibrillation (AFib) remains a big clinical uncertainty today, with no evidence base as a guide, although several studies exploring this question are in progress.
“There are no clear and definitive data showing that treating subclinical atrial fibrillation improves outcomes. That’s what we need, and until we get these data you won’t see strong recommendations in guidelines” to screen patients for asymptomatic AFib or other arrhythmias, said Sana M. Al-Khatib, MD, a cardiac electrophysiologist and professor of medicine at Duke University, Durham, N.C., during the 2019 American Heart Association scientific sessions in Philadelphia in a talk about wearables and guidelines.
“If you intervene with silent AFib, do you improve outcomes? That evidence is lacking,” she said. Another shortcoming of current evidence is a clear understanding of what AFib burden warrants intervention, added Dr. Al-Khatib. “We see high-rate AFib episodes recorded in patients with implanted cardiac devices [and no symptoms], and we don’t know what to do with that either.”
The closest any existing guideline from a medical society comes to currently endorsing screening for AFib by a wearable is the 2016 European Society of Cardiology’s AFib management guidelines, which give “opportunistic screening” among people aged older than 65 years a IB recommendation, but specifically for screening by taking a patient’s pulse or with a ECG recording, with no mention of the screening role for wearables (Eur Heart J. 2016 Oct 7;37[38]:2893-967), Dr. Al-Khatib noted.
The most extensive data on screening for asymptomatic AFib in an unselected population came in the recently reported results from the Apple Heart Study, which enrolled more than 419,000 people monitored by a smart watch for a median of 117 days. During this screening, 2,161 people (0.52%) received a notification of having an irregular pulse (including 3.1% of those who were aged at least 65 years), which triggered more intensive assessment with an ECG patch for a median of 13 days in 450 of the 2,161 screening positives (21%) who agreed to participate in this follow-up. Among those 450 people, the patch test identified 34% as having actual AFib (N Engl J Med. 2019 Nov 14;381[20]:1909-17). But while this study provided evidence that screening for an irregular heartbeat with a wearable can identify AFib with some level of success, the results did not address whether this approach improved short- or long-term patient outcomes.
In addition, what the Apple Heart Study results showed was that this sort of screening results in a relatively large volume of follow-up testing. Of the 2,161 participants who received an irregular pulse notification, 1,376 (64%) returned a 90-day survey. Of these, 787 (57%) reported contact with a health care provider outside the study, 28% were prescribed a new medication, 33% were recommended to see a specialist (such as a cardiologist), and 36% were recommended to have additional testing.
“The results raise the question that a lot of resources were used,” to assess patients with a positive screening result, noted Paul A. Heidenreich, MD, a cardiologist and professor of medicine at Stanford (Calif.) University who studies quality of care for patients with heart disease. He estimated that, in the Apple Heart Study, each of the more than 2,000 patients who screening positive for an irregular heartbeat and underwent subsequent assessment ran up about $700 worth of follow-up testing. But he added that, in the case of AFib, the primary intervention that many previously undiagnosed AFib patients receive is some sort of anticoagulation for stroke prevention. Moreover, because this intervention is so effective there is a lot of money to play with to make AFib screening cost effective, as judged by typical, contemporary metrics of cost efficacy that value a quality-adjusted life-year (QALY) gain as reasonable for society to pay if the cost of an incremental QALY is $50,000-$150,000.
If the benchmark is a cost that’s within $50,000/QALY, then an average follow-up cost of $116/person to assess screened positives can fall within this cost ceiling. If the benchmark is $150,000/QALY, then follow-up costs can run as high as $491/person screened, said Dr. Heidenreich during the same AHA session where Dr. Al-Khatib spoke last November.
Despite this good news for screening for AFib with a wearable from a cost-effectiveness perspective, “there is so much uncertainty regarding the benefit and the consequences of incidental findings that we need an outcomes study before widespread implementation” of this type of screening, Dr. Heidenreich concluded. “We need an outcomes study to feel comfortable” with screening. “There is a huge potential for extra care that we don’t understand.”
Dr. Marrouche agreed that collecting adequate evidence to drive changes in clinical guidelines on how to use data from wearables has lagged behind the rapid spread of wearables and the information they can produce among the American public. “Outcomes and evidence will support guidelines development, but in the meantime, we’re offering education to clinicians, patients, and consumers. Consumers own their data, and they can share them with whomever they choose.”
The document notes that people who use wearables are, in general, “enthusiastic about tracking their data, not only for their own use, but also to share” with others, often on social media websites.
“We cannot control that, but our goal in the document is focused on the clinical relevance [of the data] and to help people better understand their data and use it in a meaningful and safe way,” Dr. Marrouche said.
Dr. Marrouche has been a consultant to, advisor to, or received research support from Abbott, Biosense Webster, Biotronik, GE Healthcare, Medtronic, Preventice, Sanofi-Aventis, Siemens, and Vytronus. Ms. Wurster is an employee of the Heart Rhythm Society. Dr. Al-Khatib has been a consultant to Milestone Pharmaceuticals and Medtronic, and she has also received other financial benefits from Medtronic. Dr. Heidenreich had no disclosures,
Gastric electrical stimulation device may improve refractory vomiting
An implanted gastric electrical stimulation device significantly improved refractory vomiting but not quality of life in a randomized, multicenter, double-blind crossover trial of 172 patients.
After 4 months of electrical stimulation, frequency of vomiting was significantly improved from baseline in the intervention arm, compared with the control arm, in patients with both delayed (P less than .01) and normal (P = .05) gastric emptying. There was also an improvement in nausea with gastric stimulation. In contrast, there was no significant improvement in the coprimary endpoint of quality of life. Based on these findings, “a limited number of medically resistant patients may benefit from gastroelectric stimulation to relieve nausea and vomiting,” wrote Philippe Ducrotté, MD, of Rouen (France) University Hospital and associates in Gastroenterology.
High-frequency gastric electrical stimulation with the surgically implanted Enterra device is regarded as a treatment option for chronic refractory vomiting in patients with or without gastroparesis. However, only moderate evidence supports the use of this therapy, with level 1 evidence limited to a single study, according to the researchers. For the study, they enrolled 172 adults with at least 12 months of nausea or vomiting that was refractory to antiemetic or prokinetic therapy and was either idiopathic or related to type 1 or 2 diabetes mellitus or surgery (partial gastric resection or vagotomy). Symptoms “had to be severe enough to affect the general condition of the patient, including [causing] weight loss, or the need to change dietary intake to control diabetes,” said the researchers.
The study started with a 4-month run-in period, after which all patients had the device implanted and left off for one month. Patients in the intervention arm then had the device turned on and programmed at standard parameters (5 mA, 14 Hz, 330 micros, cycle on 0.1s, cycle off 5s). Both groups were assessed at 4 months, and 149 patients then crossed over to the other arm and were assessed again at 4 months. Vomiting was evaluated on a 5-point scale ranging from 0 (most severe) to 5 (symptom absent), while quality of life was assessed by means of the 36-question, self-administered Gastrointestinal Quality of Life Index (GIQLI).
During the intervention, 30.6% of patients reported at least a 1-point improvement on the vomiting frequency scale, while 53% reported no change. With the device turned off, 16.5% of patients reported an improvement in vomiting. During both phases of the trial, median vomiting frequency score was improved in the intervention arm compared with the control arm (P less than .001) in patients with (42%) and without (58%) diabetes. “Gastric emptying was not accelerated during the on period compared with the off period,” the investigators wrote.
A total of 133 (77%) patients in the study had gastroparesis. Most patients were women in their 40s who vomited several times per day. Among 45 device-related events, the most common was abdominal pain at the implantation site (62%), followed by “infectious problems” at the abdominal pouch level (36%) and hematoma (2%). Three of these events “were serious enough to prompt device removal,” the researchers wrote.
The French government funded the study. The investigators reported having no conflicts of interest. They dedicated the paper to the memory of Dr. Ducrotté, who died during the course of the study.
*This story was updated on January 13, 2020.
SOURCE: Ducrotté P et al. Gastroenterology. 2019 Oct 1. https://doi.org/10.1053/j.gastro.2019.10.018
Use of gastric electric stimulation is a controversial therapy for gastroparesis. The Enterra Gastric Electric Stimulator System received FDA approval under a Humanitarian Device Exemption in 2000 considering the device to be safe and of probable benefit. Enterra had been shown to decrease vomiting frequency in patients with medication refractory gastroparesis. Subsequent studies performed for approval for efficacy did not meet their predefined endpoint. Some physicians use this as treatment for their patients with refractory gastroparesis under the HDE and with institutional review board approval; many physicians do not.

The article by the French group brings support for gastric electric stimulation in a double blind study that showed gastric stimulation significantly reduced nausea and vomiting, both in diabetic and nondiabetic patients and in both those with delayed and normal gastric emptying.
The NIH Gastroparesis Clinical Research Consortium recently reported the symptom response with gastric stimulation for clinical care of patients with gastroparesis, compared with those who did not receive this treatment. In this observational study in multiple practice settings, 15% of patients with symptoms of gastroparesis in the NIH registry underwent gastric stimulation. Patients with more severe overall symptoms were more likely to improve symptomatically over 48 weeks, primarily because of reduction in nausea severity.
In the last 5 years, pyloromyotomy for gastroparesis has reemerged as a treatment for gastroparesis, especially when performed endoscopically (G-POEM or POP). Multiple studies, primarily single-center studies, support this treatment in improving gastroparesis symptoms and gastric emptying, though placebo-controlled studies have not been performed.
When should one perform gastric electric stimulation versus pyloromyotomy? At our center, we perform both stimulator placement and pyloromyotomy procedures in patients with refractory gastroparesis symptoms with delayed gastric emptying. We find that patients with refractory symptoms of gastroparesis undergoing stimulator placement, pyloromyotomy, or combined stimulator with pyloromyotomy each had improvement of their gastroparesis symptoms. Gastric stimulation and combined stimulator with pyloromyotomy improved nausea/vomiting, whereas pyloromyotomy alone tended to improve early satiety and postprandial fullness.
Presently, our clinical protocol for patients with refractory gastroparesis (not responding to metoclopramide, domperidone, granisetron patch, mirtazapine) is the following:
- If nausea and vomiting are particularly severe, we proceed with gastric stimulation.
- If gastric emptying is significantly delayed especially with symptoms of early satiety, patients undergo pyloromyotomy.
- If patients have significant nausea and vomiting with markedly delayed gastric emptying, patients get both stimulator placement and pyloromyotomy.
Studies are currently being performed to evaluate this type of patient-oriented management approach.
Henry P. Parkman, MD, gastroenterologist, gastroenterology section, Temple University, Philadelphia. He has no conflicts of interest.
Use of gastric electric stimulation is a controversial therapy for gastroparesis. The Enterra Gastric Electric Stimulator System received FDA approval under a Humanitarian Device Exemption in 2000 considering the device to be safe and of probable benefit. Enterra had been shown to decrease vomiting frequency in patients with medication refractory gastroparesis. Subsequent studies performed for approval for efficacy did not meet their predefined endpoint. Some physicians use this as treatment for their patients with refractory gastroparesis under the HDE and with institutional review board approval; many physicians do not.
The article by the French group brings support for gastric electric stimulation in a double blind study that showed gastric stimulation significantly reduced nausea and vomiting, both in diabetic and nondiabetic patients and in both those with delayed and normal gastric emptying.
The NIH Gastroparesis Clinical Research Consortium recently reported the symptom response with gastric stimulation for clinical care of patients with gastroparesis, compared with those who did not receive this treatment. In this observational study in multiple practice settings, 15% of patients with symptoms of gastroparesis in the NIH registry underwent gastric stimulation. Patients with more severe overall symptoms were more likely to improve symptomatically over 48 weeks, primarily because of reduction in nausea severity.
In the last 5 years, pyloromyotomy for gastroparesis has reemerged as a treatment for gastroparesis, especially when performed endoscopically (G-POEM or POP). Multiple studies, primarily single-center studies, support this treatment in improving gastroparesis symptoms and gastric emptying, though placebo-controlled studies have not been performed.
When should one perform gastric electric stimulation versus pyloromyotomy? At our center, we perform both stimulator placement and pyloromyotomy procedures in patients with refractory gastroparesis symptoms with delayed gastric emptying. We find that patients with refractory symptoms of gastroparesis undergoing stimulator placement, pyloromyotomy, or combined stimulator with pyloromyotomy each had improvement of their gastroparesis symptoms. Gastric stimulation and combined stimulator with pyloromyotomy improved nausea/vomiting, whereas pyloromyotomy alone tended to improve early satiety and postprandial fullness.
Presently, our clinical protocol for patients with refractory gastroparesis (not responding to metoclopramide, domperidone, granisetron patch, mirtazapine) is the following:
- If nausea and vomiting are particularly severe, we proceed with gastric stimulation.
- If gastric emptying is significantly delayed especially with symptoms of early satiety, patients undergo pyloromyotomy.
- If patients have significant nausea and vomiting with markedly delayed gastric emptying, patients get both stimulator placement and pyloromyotomy.
Studies are currently being performed to evaluate this type of patient-oriented management approach.
Henry P. Parkman, MD, gastroenterologist, gastroenterology section, Temple University, Philadelphia. He has no conflicts of interest.
Use of gastric electric stimulation is a controversial therapy for gastroparesis. The Enterra Gastric Electric Stimulator System received FDA approval under a Humanitarian Device Exemption in 2000 considering the device to be safe and of probable benefit. Enterra had been shown to decrease vomiting frequency in patients with medication refractory gastroparesis. Subsequent studies performed for approval for efficacy did not meet their predefined endpoint. Some physicians use this as treatment for their patients with refractory gastroparesis under the HDE and with institutional review board approval; many physicians do not.
The article by the French group brings support for gastric electric stimulation in a double blind study that showed gastric stimulation significantly reduced nausea and vomiting, both in diabetic and nondiabetic patients and in both those with delayed and normal gastric emptying.
The NIH Gastroparesis Clinical Research Consortium recently reported the symptom response with gastric stimulation for clinical care of patients with gastroparesis, compared with those who did not receive this treatment. In this observational study in multiple practice settings, 15% of patients with symptoms of gastroparesis in the NIH registry underwent gastric stimulation. Patients with more severe overall symptoms were more likely to improve symptomatically over 48 weeks, primarily because of reduction in nausea severity.
In the last 5 years, pyloromyotomy for gastroparesis has reemerged as a treatment for gastroparesis, especially when performed endoscopically (G-POEM or POP). Multiple studies, primarily single-center studies, support this treatment in improving gastroparesis symptoms and gastric emptying, though placebo-controlled studies have not been performed.
When should one perform gastric electric stimulation versus pyloromyotomy? At our center, we perform both stimulator placement and pyloromyotomy procedures in patients with refractory gastroparesis symptoms with delayed gastric emptying. We find that patients with refractory symptoms of gastroparesis undergoing stimulator placement, pyloromyotomy, or combined stimulator with pyloromyotomy each had improvement of their gastroparesis symptoms. Gastric stimulation and combined stimulator with pyloromyotomy improved nausea/vomiting, whereas pyloromyotomy alone tended to improve early satiety and postprandial fullness.
Presently, our clinical protocol for patients with refractory gastroparesis (not responding to metoclopramide, domperidone, granisetron patch, mirtazapine) is the following:
- If nausea and vomiting are particularly severe, we proceed with gastric stimulation.
- If gastric emptying is significantly delayed especially with symptoms of early satiety, patients undergo pyloromyotomy.
- If patients have significant nausea and vomiting with markedly delayed gastric emptying, patients get both stimulator placement and pyloromyotomy.
Studies are currently being performed to evaluate this type of patient-oriented management approach.
Henry P. Parkman, MD, gastroenterologist, gastroenterology section, Temple University, Philadelphia. He has no conflicts of interest.
An implanted gastric electrical stimulation device significantly improved refractory vomiting but not quality of life in a randomized, multicenter, double-blind crossover trial of 172 patients.
After 4 months of electrical stimulation, frequency of vomiting was significantly improved from baseline in the intervention arm, compared with the control arm, in patients with both delayed (P less than .01) and normal (P = .05) gastric emptying. There was also an improvement in nausea with gastric stimulation. In contrast, there was no significant improvement in the coprimary endpoint of quality of life. Based on these findings, “a limited number of medically resistant patients may benefit from gastroelectric stimulation to relieve nausea and vomiting,” wrote Philippe Ducrotté, MD, of Rouen (France) University Hospital and associates in Gastroenterology.
High-frequency gastric electrical stimulation with the surgically implanted Enterra device is regarded as a treatment option for chronic refractory vomiting in patients with or without gastroparesis. However, only moderate evidence supports the use of this therapy, with level 1 evidence limited to a single study, according to the researchers. For the study, they enrolled 172 adults with at least 12 months of nausea or vomiting that was refractory to antiemetic or prokinetic therapy and was either idiopathic or related to type 1 or 2 diabetes mellitus or surgery (partial gastric resection or vagotomy). Symptoms “had to be severe enough to affect the general condition of the patient, including [causing] weight loss, or the need to change dietary intake to control diabetes,” said the researchers.
The study started with a 4-month run-in period, after which all patients had the device implanted and left off for one month. Patients in the intervention arm then had the device turned on and programmed at standard parameters (5 mA, 14 Hz, 330 micros, cycle on 0.1s, cycle off 5s). Both groups were assessed at 4 months, and 149 patients then crossed over to the other arm and were assessed again at 4 months. Vomiting was evaluated on a 5-point scale ranging from 0 (most severe) to 5 (symptom absent), while quality of life was assessed by means of the 36-question, self-administered Gastrointestinal Quality of Life Index (GIQLI).
During the intervention, 30.6% of patients reported at least a 1-point improvement on the vomiting frequency scale, while 53% reported no change. With the device turned off, 16.5% of patients reported an improvement in vomiting. During both phases of the trial, median vomiting frequency score was improved in the intervention arm compared with the control arm (P less than .001) in patients with (42%) and without (58%) diabetes. “Gastric emptying was not accelerated during the on period compared with the off period,” the investigators wrote.
A total of 133 (77%) patients in the study had gastroparesis. Most patients were women in their 40s who vomited several times per day. Among 45 device-related events, the most common was abdominal pain at the implantation site (62%), followed by “infectious problems” at the abdominal pouch level (36%) and hematoma (2%). Three of these events “were serious enough to prompt device removal,” the researchers wrote.
The French government funded the study. The investigators reported having no conflicts of interest. They dedicated the paper to the memory of Dr. Ducrotté, who died during the course of the study.
*This story was updated on January 13, 2020.
SOURCE: Ducrotté P et al. Gastroenterology. 2019 Oct 1. https://doi.org/10.1053/j.gastro.2019.10.018
An implanted gastric electrical stimulation device significantly improved refractory vomiting but not quality of life in a randomized, multicenter, double-blind crossover trial of 172 patients.
After 4 months of electrical stimulation, frequency of vomiting was significantly improved from baseline in the intervention arm, compared with the control arm, in patients with both delayed (P less than .01) and normal (P = .05) gastric emptying. There was also an improvement in nausea with gastric stimulation. In contrast, there was no significant improvement in the coprimary endpoint of quality of life. Based on these findings, “a limited number of medically resistant patients may benefit from gastroelectric stimulation to relieve nausea and vomiting,” wrote Philippe Ducrotté, MD, of Rouen (France) University Hospital and associates in Gastroenterology.
High-frequency gastric electrical stimulation with the surgically implanted Enterra device is regarded as a treatment option for chronic refractory vomiting in patients with or without gastroparesis. However, only moderate evidence supports the use of this therapy, with level 1 evidence limited to a single study, according to the researchers. For the study, they enrolled 172 adults with at least 12 months of nausea or vomiting that was refractory to antiemetic or prokinetic therapy and was either idiopathic or related to type 1 or 2 diabetes mellitus or surgery (partial gastric resection or vagotomy). Symptoms “had to be severe enough to affect the general condition of the patient, including [causing] weight loss, or the need to change dietary intake to control diabetes,” said the researchers.
The study started with a 4-month run-in period, after which all patients had the device implanted and left off for one month. Patients in the intervention arm then had the device turned on and programmed at standard parameters (5 mA, 14 Hz, 330 micros, cycle on 0.1s, cycle off 5s). Both groups were assessed at 4 months, and 149 patients then crossed over to the other arm and were assessed again at 4 months. Vomiting was evaluated on a 5-point scale ranging from 0 (most severe) to 5 (symptom absent), while quality of life was assessed by means of the 36-question, self-administered Gastrointestinal Quality of Life Index (GIQLI).
During the intervention, 30.6% of patients reported at least a 1-point improvement on the vomiting frequency scale, while 53% reported no change. With the device turned off, 16.5% of patients reported an improvement in vomiting. During both phases of the trial, median vomiting frequency score was improved in the intervention arm compared with the control arm (P less than .001) in patients with (42%) and without (58%) diabetes. “Gastric emptying was not accelerated during the on period compared with the off period,” the investigators wrote.
A total of 133 (77%) patients in the study had gastroparesis. Most patients were women in their 40s who vomited several times per day. Among 45 device-related events, the most common was abdominal pain at the implantation site (62%), followed by “infectious problems” at the abdominal pouch level (36%) and hematoma (2%). Three of these events “were serious enough to prompt device removal,” the researchers wrote.
The French government funded the study. The investigators reported having no conflicts of interest. They dedicated the paper to the memory of Dr. Ducrotté, who died during the course of the study.
*This story was updated on January 13, 2020.
SOURCE: Ducrotté P et al. Gastroenterology. 2019 Oct 1. https://doi.org/10.1053/j.gastro.2019.10.018
FROM GASTROENTEROLOGY
ctDNA outmatches CEA for detection of colorectal cancer recurrence
For detection of recurrent colorectal cancer, circulating tumor DNA (ctDNA) may be more reliable than carcinoembryonic antigen (CEA), based on a recent Australian study.
Among 144 patients with a history of colorectal cancer, ctDNA testing offered a sensitivity of 66.0%, compared with 31.9% for CEA, reported lead author Erin L. Symonds, PhD, of Flinders University, Bedford Park, Australia, and colleagues, who noted that the two tests had comparable specificity.
According to the investigators, many patients with colorectal cancer who relapse are incurable because they have multiple unresectable metastases.
“This may be due to the poor sensitivity of the currently applied surveillance tools, with guidelines focused on radiological imaging (mostly yearly computed tomography [CT] scans) and regular blood tests for carcinoembryonic antigen (CEA),” the investigators wrote in Cancer. “There is a need to improve the timely detection of metastatic disease while it is still confined to a resectable state.”
To this end, the investigators compared ctDNA testing with CEA testing in a real-world setting. Initially, 548 patients were enrolled. The final dataset included 144 of these patients, all of whom were disease negative on CT or MRI after surgical resection or neoadjuvant therapy. Most exclusions were due to unavailability of imaging results. Circulating tumor DNA testing evaluated methylation levels of BCAT1 and IKZF1 (COLVERA test, Clinical Genomics Pty, North Ryde, New South Wales, Australia) . The LIAISON CEA test was used to measure CEA plasma concentration.
After a median follow-up of almost 4 years, 50 out of 144 patients had disease recurrence, most of which involved distant metastasis (74%). As described above, the sensitivity of ctDNA was higher than CEA by a wide and significant margin (66.0% vs. 31.9%; P less than .001). The superior sensitivity of ctDNA was observed regardless of whether recurrence was locoregional (76.9% vs. 15.4%; P = .006) or distant (62.1% vs. 38.2%; P = .044). Specificity was not statistically different between ctDNA (97.9%) and CEA (96.4%). Multivariate analysis showed that ctDNA was an independent predictor of recurrence, while CEA was not.
“In conclusion, the methylated BCAT1/IKZF1 ctDNA test is twice as sensitive as CEA for detecting recurrent CRC during the monitoring of patients after their initial treatment,” the investigators wrote.
The study was funded by the National Health and Medical Research Council, Clinical Genomics, Cancer Council SA’s Beat Cancer Project, and others. The investigators reported additional relationships with Eiken Chemical and the Commonwealth Scientific and Industrial Research Organisation.
*This story was updated on Jan. 10, 2020.
SOURCE: Symonds et al. Cancer. 2020 Jan 7. doi: 10.1002/cncr.32695.
For detection of recurrent colorectal cancer, circulating tumor DNA (ctDNA) may be more reliable than carcinoembryonic antigen (CEA), based on a recent Australian study.
Among 144 patients with a history of colorectal cancer, ctDNA testing offered a sensitivity of 66.0%, compared with 31.9% for CEA, reported lead author Erin L. Symonds, PhD, of Flinders University, Bedford Park, Australia, and colleagues, who noted that the two tests had comparable specificity.
According to the investigators, many patients with colorectal cancer who relapse are incurable because they have multiple unresectable metastases.
“This may be due to the poor sensitivity of the currently applied surveillance tools, with guidelines focused on radiological imaging (mostly yearly computed tomography [CT] scans) and regular blood tests for carcinoembryonic antigen (CEA),” the investigators wrote in Cancer. “There is a need to improve the timely detection of metastatic disease while it is still confined to a resectable state.”
To this end, the investigators compared ctDNA testing with CEA testing in a real-world setting. Initially, 548 patients were enrolled. The final dataset included 144 of these patients, all of whom were disease negative on CT or MRI after surgical resection or neoadjuvant therapy. Most exclusions were due to unavailability of imaging results. Circulating tumor DNA testing evaluated methylation levels of BCAT1 and IKZF1 (COLVERA test, Clinical Genomics Pty, North Ryde, New South Wales, Australia) . The LIAISON CEA test was used to measure CEA plasma concentration.
After a median follow-up of almost 4 years, 50 out of 144 patients had disease recurrence, most of which involved distant metastasis (74%). As described above, the sensitivity of ctDNA was higher than CEA by a wide and significant margin (66.0% vs. 31.9%; P less than .001). The superior sensitivity of ctDNA was observed regardless of whether recurrence was locoregional (76.9% vs. 15.4%; P = .006) or distant (62.1% vs. 38.2%; P = .044). Specificity was not statistically different between ctDNA (97.9%) and CEA (96.4%). Multivariate analysis showed that ctDNA was an independent predictor of recurrence, while CEA was not.
“In conclusion, the methylated BCAT1/IKZF1 ctDNA test is twice as sensitive as CEA for detecting recurrent CRC during the monitoring of patients after their initial treatment,” the investigators wrote.
The study was funded by the National Health and Medical Research Council, Clinical Genomics, Cancer Council SA’s Beat Cancer Project, and others. The investigators reported additional relationships with Eiken Chemical and the Commonwealth Scientific and Industrial Research Organisation.
*This story was updated on Jan. 10, 2020.
SOURCE: Symonds et al. Cancer. 2020 Jan 7. doi: 10.1002/cncr.32695.
For detection of recurrent colorectal cancer, circulating tumor DNA (ctDNA) may be more reliable than carcinoembryonic antigen (CEA), based on a recent Australian study.
Among 144 patients with a history of colorectal cancer, ctDNA testing offered a sensitivity of 66.0%, compared with 31.9% for CEA, reported lead author Erin L. Symonds, PhD, of Flinders University, Bedford Park, Australia, and colleagues, who noted that the two tests had comparable specificity.
According to the investigators, many patients with colorectal cancer who relapse are incurable because they have multiple unresectable metastases.
“This may be due to the poor sensitivity of the currently applied surveillance tools, with guidelines focused on radiological imaging (mostly yearly computed tomography [CT] scans) and regular blood tests for carcinoembryonic antigen (CEA),” the investigators wrote in Cancer. “There is a need to improve the timely detection of metastatic disease while it is still confined to a resectable state.”
To this end, the investigators compared ctDNA testing with CEA testing in a real-world setting. Initially, 548 patients were enrolled. The final dataset included 144 of these patients, all of whom were disease negative on CT or MRI after surgical resection or neoadjuvant therapy. Most exclusions were due to unavailability of imaging results. Circulating tumor DNA testing evaluated methylation levels of BCAT1 and IKZF1 (COLVERA test, Clinical Genomics Pty, North Ryde, New South Wales, Australia) . The LIAISON CEA test was used to measure CEA plasma concentration.
After a median follow-up of almost 4 years, 50 out of 144 patients had disease recurrence, most of which involved distant metastasis (74%). As described above, the sensitivity of ctDNA was higher than CEA by a wide and significant margin (66.0% vs. 31.9%; P less than .001). The superior sensitivity of ctDNA was observed regardless of whether recurrence was locoregional (76.9% vs. 15.4%; P = .006) or distant (62.1% vs. 38.2%; P = .044). Specificity was not statistically different between ctDNA (97.9%) and CEA (96.4%). Multivariate analysis showed that ctDNA was an independent predictor of recurrence, while CEA was not.
“In conclusion, the methylated BCAT1/IKZF1 ctDNA test is twice as sensitive as CEA for detecting recurrent CRC during the monitoring of patients after their initial treatment,” the investigators wrote.
The study was funded by the National Health and Medical Research Council, Clinical Genomics, Cancer Council SA’s Beat Cancer Project, and others. The investigators reported additional relationships with Eiken Chemical and the Commonwealth Scientific and Industrial Research Organisation.
*This story was updated on Jan. 10, 2020.
SOURCE: Symonds et al. Cancer. 2020 Jan 7. doi: 10.1002/cncr.32695.
FROM CANCER
Product update: Neuromodulation device, cystoscopy simplified, hysteroscopy seal, next immunization frontier
NEW SACRAL NEUROMODULATION DEVICE

FOR MORE INFORMATION, VISIT: https://www.axonics.com/
CERVICAL SEAL FOR HYSTEROSCOPIC DEVICES
For more information, visit: https://gynsurgicalsolutions.com/product/omni-lok/
UNIVERSAL CYSTOSCOPY SIMPLIFIED
FOR MORE INFORMATION, VISIT: https://cystosure.com/
NEXT FRONTIER IN VACCINE IMMUNIZATION

Globally, there are 410,000 cases of GBS every year. GBS is most common in newborns; women who are carriers of the GBS bacteria may pass it on to their newborns during labor and birth. An estimated 10% to 30% of pregnant women carry the GBS bacteria. The disease can manifest as sepsis, pneumonia, and meningitis, with potentially fatal outcomes for some. A maternal vaccine may prevent 231,000 infant and maternal GBS cases, says Pfizer.
According to Pfizer, RSV causes more hospitalizations each year than influenza among young children, with an estimated 33 million cases globally each year in children less than age 5 years.
FOR MORE INFORMATION, VISIT: https://www.pfizer.com/
NEW SACRAL NEUROMODULATION DEVICE
FOR MORE INFORMATION, VISIT: https://www.axonics.com/
CERVICAL SEAL FOR HYSTEROSCOPIC DEVICES
For more information, visit: https://gynsurgicalsolutions.com/product/omni-lok/
UNIVERSAL CYSTOSCOPY SIMPLIFIED
FOR MORE INFORMATION, VISIT: https://cystosure.com/
NEXT FRONTIER IN VACCINE IMMUNIZATION
Globally, there are 410,000 cases of GBS every year. GBS is most common in newborns; women who are carriers of the GBS bacteria may pass it on to their newborns during labor and birth. An estimated 10% to 30% of pregnant women carry the GBS bacteria. The disease can manifest as sepsis, pneumonia, and meningitis, with potentially fatal outcomes for some. A maternal vaccine may prevent 231,000 infant and maternal GBS cases, says Pfizer.
According to Pfizer, RSV causes more hospitalizations each year than influenza among young children, with an estimated 33 million cases globally each year in children less than age 5 years.
FOR MORE INFORMATION, VISIT: https://www.pfizer.com/
NEW SACRAL NEUROMODULATION DEVICE
FOR MORE INFORMATION, VISIT: https://www.axonics.com/
CERVICAL SEAL FOR HYSTEROSCOPIC DEVICES
For more information, visit: https://gynsurgicalsolutions.com/product/omni-lok/
UNIVERSAL CYSTOSCOPY SIMPLIFIED
FOR MORE INFORMATION, VISIT: https://cystosure.com/
NEXT FRONTIER IN VACCINE IMMUNIZATION
Globally, there are 410,000 cases of GBS every year. GBS is most common in newborns; women who are carriers of the GBS bacteria may pass it on to their newborns during labor and birth. An estimated 10% to 30% of pregnant women carry the GBS bacteria. The disease can manifest as sepsis, pneumonia, and meningitis, with potentially fatal outcomes for some. A maternal vaccine may prevent 231,000 infant and maternal GBS cases, says Pfizer.
According to Pfizer, RSV causes more hospitalizations each year than influenza among young children, with an estimated 33 million cases globally each year in children less than age 5 years.
FOR MORE INFORMATION, VISIT: https://www.pfizer.com/