User login
Antibiotics in Early Infancy Disrupt Gut Microbiome and Increase Risk for Atopic Dermatitis
Key clinical point: Antibiotic use early in life, especially within one year of age, disrupts the gut microbiome and increases the risk for atopic dermatitis (AD) at 5 years of age.
Major finding: Children who received antibiotics during the first year of life vs later were significantly more likely to develop AD at 5 years of age (adjusted odds ratio [aOR] 1.81; P < .001), with an increased number of antibiotic courses leading to a dose-response-like increased risk for AD (1 course: aOR 1.67; P = .0044; ≥ 2 courses: aOR 2.16; P = .0030).
Study details: This study analyzed the clinical data for AD diagnosis at age 5 years of 2484 children from the prospective, general population CHILD birth cohort, which enrolled pregnant women and infants with no congenital abnormalities born at ≥ 34 weeks of gestation.
Disclosures: The CHILD Study is funded by the Canadian Institutes of Health Research, the Allergy, Genes, and Environment Network of Centres of Excellence, Debbie and Don Morrison, and others. The authors declared no conflicts of interest.
Source: Hoskinson C, Medeleanu MV, Reyna ME, et al. Antibiotics within first year are linked to infant gut microbiome disruption and elevated atopic dermatitis risk. J Allergy Clin Immunol. 2024 (Apr 24). doi: 10.1016/j.jaci.2024.03.025 Source
Key clinical point: Antibiotic use early in life, especially within one year of age, disrupts the gut microbiome and increases the risk for atopic dermatitis (AD) at 5 years of age.
Major finding: Children who received antibiotics during the first year of life vs later were significantly more likely to develop AD at 5 years of age (adjusted odds ratio [aOR] 1.81; P < .001), with an increased number of antibiotic courses leading to a dose-response-like increased risk for AD (1 course: aOR 1.67; P = .0044; ≥ 2 courses: aOR 2.16; P = .0030).
Study details: This study analyzed the clinical data for AD diagnosis at age 5 years of 2484 children from the prospective, general population CHILD birth cohort, which enrolled pregnant women and infants with no congenital abnormalities born at ≥ 34 weeks of gestation.
Disclosures: The CHILD Study is funded by the Canadian Institutes of Health Research, the Allergy, Genes, and Environment Network of Centres of Excellence, Debbie and Don Morrison, and others. The authors declared no conflicts of interest.
Source: Hoskinson C, Medeleanu MV, Reyna ME, et al. Antibiotics within first year are linked to infant gut microbiome disruption and elevated atopic dermatitis risk. J Allergy Clin Immunol. 2024 (Apr 24). doi: 10.1016/j.jaci.2024.03.025 Source
Key clinical point: Antibiotic use early in life, especially within one year of age, disrupts the gut microbiome and increases the risk for atopic dermatitis (AD) at 5 years of age.
Major finding: Children who received antibiotics during the first year of life vs later were significantly more likely to develop AD at 5 years of age (adjusted odds ratio [aOR] 1.81; P < .001), with an increased number of antibiotic courses leading to a dose-response-like increased risk for AD (1 course: aOR 1.67; P = .0044; ≥ 2 courses: aOR 2.16; P = .0030).
Study details: This study analyzed the clinical data for AD diagnosis at age 5 years of 2484 children from the prospective, general population CHILD birth cohort, which enrolled pregnant women and infants with no congenital abnormalities born at ≥ 34 weeks of gestation.
Disclosures: The CHILD Study is funded by the Canadian Institutes of Health Research, the Allergy, Genes, and Environment Network of Centres of Excellence, Debbie and Don Morrison, and others. The authors declared no conflicts of interest.
Source: Hoskinson C, Medeleanu MV, Reyna ME, et al. Antibiotics within first year are linked to infant gut microbiome disruption and elevated atopic dermatitis risk. J Allergy Clin Immunol. 2024 (Apr 24). doi: 10.1016/j.jaci.2024.03.025 Source
High-Potency Cannabis Tied to Impaired Brain Development, Psychosis, Cannabis-Use Disorder
It’s becoming clear that (CUD).
That was the message delivered by Yasmin Hurd, PhD, director of the Addiction Institute at Mount Sinai in New York, during a press briefing at the American Psychiatric Association (APA) 2024 annual meeting.
“We’re actually in historic times in that we now have highly concentrated, highly potent cannabis products that are administered in various routes,” Dr. Hurd told reporters.
Tetrahydrocannabinol (THC) concentrations in cannabis products have increased over the years, from around 2%-4% to 15%-24% now, Dr. Hurd noted.
Dr. Hurd and colleagues wrote in a commentary on the developmental trajectory of CUD published simultaneously in the American Journal of Psychiatry.
Dramatic Increase in Teen Cannabis Use
A recent study from Oregon Health & Science University showed that adolescent cannabis abuse in the United States has increased dramatically, by about 245%, since 2000.
“Drug abuse is often driven by what is in front of you,” Nora Volkow, MD, director of the National Institute on Drug Abuse, noted in an interview.
“Right now, cannabis is widely available. So, guess what? Cannabis becomes the drug that people take. Nicotine is much harder to get. It is regulated to a much greater extent than cannabis, so fewer teenagers are consuming nicotine than are consuming cannabis,” Dr. Volkow said.
Cannabis exposure during neurodevelopment has the potential to alter the endocannabinoid system, which in turn, can affect the development of neural pathways that mediate reward; emotional regulation; and multiple cognitive domains including executive functioning and decision-making, learning, abstraction, and attention — all processes central to substance use disorder and other psychiatric disorders, Dr. Hurd said at the briefing.
Dr. Volkow said that cannabis use in adolescence and young adulthood is “very concerning because that’s also the age of risk for psychosis, particularly schizophrenia, with one study showing that use of cannabis in high doses can trigger psychotic episodes, particularly among young males.”
Dr. Hurd noted that not all young people who use cannabis develop CUD, “but a significant number do,” and large-scale studies have consistently reported two main factors associated with CUD risk.
The first is age, both for the onset and frequency of use at younger age. Those who start using cannabis before age 16 years are at the highest risk for CUD. The risk for CUD also increases significantly among youth who use cannabis at least weekly, with the highest prevalence among youth who use cannabis daily. One large study linked increased frequency of use with up to a 17-fold increased risk for CUD.
The second factor consistently associated with the risk for CUD is biologic sex, with CUD rates typically higher in male individuals.
Treatment Challenges
For young people who develop CUD, access to and uptake of treatment can be challenging.
“Given that the increased potency of cannabis and cannabinoid products is expected to increase CUD risk, it is disturbing that less than 10% of youth who meet the criteria for a substance use disorder, including CUD, receive treatment,” Dr. Hurd and colleagues point out in their commentary.
Another challenge is that treatment strategies for CUD are currently limited and consist mainly of motivational enhancement and cognitive-behavioral therapies.
“Clearly new treatment strategies are needed to address the mounting challenge of CUD risk in teens and young adults,” Dr. Hurd and colleagues wrote.
Summing up, Dr. Hurd told reporters, “We now know that most psychiatric disorders have a developmental origin, and the adolescent time period is a critical window for cannabis use disorder risk.”
Yet, on a positive note, the “plasticity of the developing brain that makes it vulnerable to cannabis use disorder and psychiatric comorbidities also provides an opportunity for prevention and early intervention to change that trajectory,” Dr. Hurd said.
The changing legal landscape of cannabis — the US Drug Enforcement Agency is moving forward with plans to move marijuana from a Schedule I to a Schedule III controlled substance under the Controlled Substance Act — makes addressing these risks all the timelier.
“As states vie to leverage tax dollars from the growing cannabis industry, a significant portion of such funds must be used for early intervention/prevention strategies to reduce the impact of cannabis on the developing brain,” Dr. Hurd and colleagues wrote.
This research was supported in part by the National Institute on Drug Abuse and the National Institutes of Health. Dr. Hurd and Dr. Volkow have no relevant disclosures.
A version of this article appeared on Medscape.com.
It’s becoming clear that (CUD).
That was the message delivered by Yasmin Hurd, PhD, director of the Addiction Institute at Mount Sinai in New York, during a press briefing at the American Psychiatric Association (APA) 2024 annual meeting.
“We’re actually in historic times in that we now have highly concentrated, highly potent cannabis products that are administered in various routes,” Dr. Hurd told reporters.
Tetrahydrocannabinol (THC) concentrations in cannabis products have increased over the years, from around 2%-4% to 15%-24% now, Dr. Hurd noted.
Dr. Hurd and colleagues wrote in a commentary on the developmental trajectory of CUD published simultaneously in the American Journal of Psychiatry.
Dramatic Increase in Teen Cannabis Use
A recent study from Oregon Health & Science University showed that adolescent cannabis abuse in the United States has increased dramatically, by about 245%, since 2000.
“Drug abuse is often driven by what is in front of you,” Nora Volkow, MD, director of the National Institute on Drug Abuse, noted in an interview.
“Right now, cannabis is widely available. So, guess what? Cannabis becomes the drug that people take. Nicotine is much harder to get. It is regulated to a much greater extent than cannabis, so fewer teenagers are consuming nicotine than are consuming cannabis,” Dr. Volkow said.
Cannabis exposure during neurodevelopment has the potential to alter the endocannabinoid system, which in turn, can affect the development of neural pathways that mediate reward; emotional regulation; and multiple cognitive domains including executive functioning and decision-making, learning, abstraction, and attention — all processes central to substance use disorder and other psychiatric disorders, Dr. Hurd said at the briefing.
Dr. Volkow said that cannabis use in adolescence and young adulthood is “very concerning because that’s also the age of risk for psychosis, particularly schizophrenia, with one study showing that use of cannabis in high doses can trigger psychotic episodes, particularly among young males.”
Dr. Hurd noted that not all young people who use cannabis develop CUD, “but a significant number do,” and large-scale studies have consistently reported two main factors associated with CUD risk.
The first is age, both for the onset and frequency of use at younger age. Those who start using cannabis before age 16 years are at the highest risk for CUD. The risk for CUD also increases significantly among youth who use cannabis at least weekly, with the highest prevalence among youth who use cannabis daily. One large study linked increased frequency of use with up to a 17-fold increased risk for CUD.
The second factor consistently associated with the risk for CUD is biologic sex, with CUD rates typically higher in male individuals.
Treatment Challenges
For young people who develop CUD, access to and uptake of treatment can be challenging.
“Given that the increased potency of cannabis and cannabinoid products is expected to increase CUD risk, it is disturbing that less than 10% of youth who meet the criteria for a substance use disorder, including CUD, receive treatment,” Dr. Hurd and colleagues point out in their commentary.
Another challenge is that treatment strategies for CUD are currently limited and consist mainly of motivational enhancement and cognitive-behavioral therapies.
“Clearly new treatment strategies are needed to address the mounting challenge of CUD risk in teens and young adults,” Dr. Hurd and colleagues wrote.
Summing up, Dr. Hurd told reporters, “We now know that most psychiatric disorders have a developmental origin, and the adolescent time period is a critical window for cannabis use disorder risk.”
Yet, on a positive note, the “plasticity of the developing brain that makes it vulnerable to cannabis use disorder and psychiatric comorbidities also provides an opportunity for prevention and early intervention to change that trajectory,” Dr. Hurd said.
The changing legal landscape of cannabis — the US Drug Enforcement Agency is moving forward with plans to move marijuana from a Schedule I to a Schedule III controlled substance under the Controlled Substance Act — makes addressing these risks all the timelier.
“As states vie to leverage tax dollars from the growing cannabis industry, a significant portion of such funds must be used for early intervention/prevention strategies to reduce the impact of cannabis on the developing brain,” Dr. Hurd and colleagues wrote.
This research was supported in part by the National Institute on Drug Abuse and the National Institutes of Health. Dr. Hurd and Dr. Volkow have no relevant disclosures.
A version of this article appeared on Medscape.com.
It’s becoming clear that (CUD).
That was the message delivered by Yasmin Hurd, PhD, director of the Addiction Institute at Mount Sinai in New York, during a press briefing at the American Psychiatric Association (APA) 2024 annual meeting.
“We’re actually in historic times in that we now have highly concentrated, highly potent cannabis products that are administered in various routes,” Dr. Hurd told reporters.
Tetrahydrocannabinol (THC) concentrations in cannabis products have increased over the years, from around 2%-4% to 15%-24% now, Dr. Hurd noted.
Dr. Hurd and colleagues wrote in a commentary on the developmental trajectory of CUD published simultaneously in the American Journal of Psychiatry.
Dramatic Increase in Teen Cannabis Use
A recent study from Oregon Health & Science University showed that adolescent cannabis abuse in the United States has increased dramatically, by about 245%, since 2000.
“Drug abuse is often driven by what is in front of you,” Nora Volkow, MD, director of the National Institute on Drug Abuse, noted in an interview.
“Right now, cannabis is widely available. So, guess what? Cannabis becomes the drug that people take. Nicotine is much harder to get. It is regulated to a much greater extent than cannabis, so fewer teenagers are consuming nicotine than are consuming cannabis,” Dr. Volkow said.
Cannabis exposure during neurodevelopment has the potential to alter the endocannabinoid system, which in turn, can affect the development of neural pathways that mediate reward; emotional regulation; and multiple cognitive domains including executive functioning and decision-making, learning, abstraction, and attention — all processes central to substance use disorder and other psychiatric disorders, Dr. Hurd said at the briefing.
Dr. Volkow said that cannabis use in adolescence and young adulthood is “very concerning because that’s also the age of risk for psychosis, particularly schizophrenia, with one study showing that use of cannabis in high doses can trigger psychotic episodes, particularly among young males.”
Dr. Hurd noted that not all young people who use cannabis develop CUD, “but a significant number do,” and large-scale studies have consistently reported two main factors associated with CUD risk.
The first is age, both for the onset and frequency of use at younger age. Those who start using cannabis before age 16 years are at the highest risk for CUD. The risk for CUD also increases significantly among youth who use cannabis at least weekly, with the highest prevalence among youth who use cannabis daily. One large study linked increased frequency of use with up to a 17-fold increased risk for CUD.
The second factor consistently associated with the risk for CUD is biologic sex, with CUD rates typically higher in male individuals.
Treatment Challenges
For young people who develop CUD, access to and uptake of treatment can be challenging.
“Given that the increased potency of cannabis and cannabinoid products is expected to increase CUD risk, it is disturbing that less than 10% of youth who meet the criteria for a substance use disorder, including CUD, receive treatment,” Dr. Hurd and colleagues point out in their commentary.
Another challenge is that treatment strategies for CUD are currently limited and consist mainly of motivational enhancement and cognitive-behavioral therapies.
“Clearly new treatment strategies are needed to address the mounting challenge of CUD risk in teens and young adults,” Dr. Hurd and colleagues wrote.
Summing up, Dr. Hurd told reporters, “We now know that most psychiatric disorders have a developmental origin, and the adolescent time period is a critical window for cannabis use disorder risk.”
Yet, on a positive note, the “plasticity of the developing brain that makes it vulnerable to cannabis use disorder and psychiatric comorbidities also provides an opportunity for prevention and early intervention to change that trajectory,” Dr. Hurd said.
The changing legal landscape of cannabis — the US Drug Enforcement Agency is moving forward with plans to move marijuana from a Schedule I to a Schedule III controlled substance under the Controlled Substance Act — makes addressing these risks all the timelier.
“As states vie to leverage tax dollars from the growing cannabis industry, a significant portion of such funds must be used for early intervention/prevention strategies to reduce the impact of cannabis on the developing brain,” Dr. Hurd and colleagues wrote.
This research was supported in part by the National Institute on Drug Abuse and the National Institutes of Health. Dr. Hurd and Dr. Volkow have no relevant disclosures.
A version of this article appeared on Medscape.com.
FROM APA 2024
Follow-Up for Pediatric Depression Doubles With New Quality Initiative
TORONTO — An ambitious effort at a busy pediatrics clinic to improve follow-up in children and adolescents with a positive depression screen improved this quality metric, and it produced a fundamental change in approach.
“It was a big culture shift,” reported Landon B. Krantz, MD, a clinical fellow in the Division of General and Community Pediatrics at Cincinnati Children’s Hospital in Ohio. From a baseline position of screening, risk identification, and then referral, “we are now taking ownership of the process.”
Based on the substantial risk posed by significant levels of depression, guidelines recommend follow-up for any patient 12 years or older who has a positive screen, according to Dr. Krantz. At his center, they found only 19% had a documented follow-up within 30 days, even though timely intervention is important.
“Nearly half of suicide events in adolescents occur within 30 days after a positive PHQ-9 [9-question Patient Health Questionnaire] is completed,” said Dr. Krantz when presenting his data at the Pediatric Academic Societies annual meeting.
The issue has gained more urgency because of the substantial increase over the past several years in children presenting with depression and suicidal thoughts, according to Dr. Krantz. He said many are characterizing the upsurge as a mental health crisis in the pediatric age group.
Improving Follow-Up
. The goal at the outset was to increase the proportion to 35%.
“We know that a lot of children would receive follow-up at centers outside of our system,” said Dr. Krantz, explaining why the goal was relatively modest. Based on the likelihood that many follow-up visits would not be captured, he expected the final data would represent an underestimate.
Depression at baseline was defined as a score of 10 or higher on the PHQ-9 or any positive answer to item 9 on this screening tool, which asks specifically about thoughts of self-harm.
To be counted, follow-up had to be a documented encounter, whether by phone call, in-person visit, or telehealth visit.
“We needed patients to be checked. We did not count a prescription refill as a true follow-up,” Dr. Krantz specified.
There were numerous strategies implemented to improve follow-up, not least of which was an educational program to reinforce the importance and value of follow-up that was disseminated to clinicians in all of the participating clinics. Medical assistants were instructed to schedule a follow-up appointment for all patients who tested positive before they left the office. A target of 3 weeks was a strategy of overcorrection when so many patients were missing the initial 30-day window by just a few days.
The approach also involved an enhanced collaboration with psychologists to which patients were referred. Asking for expedited appointments when appropriate ensured that those at highest risk were prioritized, although Dr. Krantz said that this step was planned carefully to avoid overwhelming the mental health team.
“We monitored this and made sure it was not increasing the burden for psychologists from a capacity standpoint,” he said.
Other steps, like a depression action plan, which Dr. Krantz compared to an asthma action plan, were also implemented to reduce the risk of losing symptomatic patients before the chance for an effective treatment.
When compared with the 19% 30-day follow-up rate in the preintervention sample of 589 children, the 43.8% 30-day follow-up rate achieved in the 764 patients identified after implementation beat the original goal.
The improvement in follow-up was relatively consistent across all six clinics, which Dr. Krantz believes reflected a broad and shared change in a sense of responsibility for confirming that symptoms of depression were being addressed. Patients were still referred for psychological help, but referral was no longer considered enough.
“Children with mental health issues are still our patients in primary care,” said Dr. Krantz, who considers this an important change in orientation.
While the goal was to schedule patients for a follow-up at the time of a positive depression screen, Dr. Krantz described one important accommodation.
“The screen for depression was being performed in most cases during well visits, so patients and their families were not expecting to be discussing this issue,” he said. The diagnosis might be a particular surprise to parents who were not aware of any symptoms. In this case, Dr. Krantz said patients and families were given time to process the information and were contacted after a week to discuss further workup.
It is also notable that about one third of patients met the criteria for depression by answering positively to the PHQ-9 item on self-harm when they did not meet the 10 or more threshold depression score overall. In other words, these patients would have been missed without this criterion.
In the participating Cincinnati pediatric clinics, about 12%-13% of adolescents met the criteria for depression, which Dr. Krantz said is consistent with reports in the literature. He said the range is about 6%-24%.
Although outcomes were not tracked, there is evidence that early intervention for depression yields better outcomes than delayed intervention, according to Dr. Krantz. Based on approximately 600 positive screens for depression per year at his pediatric clinics, he estimated that his data predict at least 25% more patients will receive timely follow-up.
Seeking Solutions to a Growing Problem
There are several studies documenting the growing problem of adolescent depression and suicide and, for this reason, the topic is attracting a lot of attention, according to Corinna Rea, MD, MPH, a pediatrician working in the primary care center at Boston Children’s Hospital in Massachusetts.
Dr. Rea was not involved with the study, but when asked to comment, she said: “The results of this study were encouraging because we know that getting patients to care quickly is probably important.” She also agreed that referring patients with depression for care might not be enough, noting that a lot of patients do not follow up on recommendations to pursue a consultation or treatment.
“I am now involved in a project with the American Academy of Pediatrics to address this issue,” Dr. Rae said. She thinks that more work in this area is needed and agreed with Dr. Krantz that pediatricians should verify that children with depression are getting help even when other specialists are providing the treatment.
Dr. Krantz and Dr. Rae report no potential conflicts of interest.
TORONTO — An ambitious effort at a busy pediatrics clinic to improve follow-up in children and adolescents with a positive depression screen improved this quality metric, and it produced a fundamental change in approach.
“It was a big culture shift,” reported Landon B. Krantz, MD, a clinical fellow in the Division of General and Community Pediatrics at Cincinnati Children’s Hospital in Ohio. From a baseline position of screening, risk identification, and then referral, “we are now taking ownership of the process.”
Based on the substantial risk posed by significant levels of depression, guidelines recommend follow-up for any patient 12 years or older who has a positive screen, according to Dr. Krantz. At his center, they found only 19% had a documented follow-up within 30 days, even though timely intervention is important.
“Nearly half of suicide events in adolescents occur within 30 days after a positive PHQ-9 [9-question Patient Health Questionnaire] is completed,” said Dr. Krantz when presenting his data at the Pediatric Academic Societies annual meeting.
The issue has gained more urgency because of the substantial increase over the past several years in children presenting with depression and suicidal thoughts, according to Dr. Krantz. He said many are characterizing the upsurge as a mental health crisis in the pediatric age group.
Improving Follow-Up
. The goal at the outset was to increase the proportion to 35%.
“We know that a lot of children would receive follow-up at centers outside of our system,” said Dr. Krantz, explaining why the goal was relatively modest. Based on the likelihood that many follow-up visits would not be captured, he expected the final data would represent an underestimate.
Depression at baseline was defined as a score of 10 or higher on the PHQ-9 or any positive answer to item 9 on this screening tool, which asks specifically about thoughts of self-harm.
To be counted, follow-up had to be a documented encounter, whether by phone call, in-person visit, or telehealth visit.
“We needed patients to be checked. We did not count a prescription refill as a true follow-up,” Dr. Krantz specified.
There were numerous strategies implemented to improve follow-up, not least of which was an educational program to reinforce the importance and value of follow-up that was disseminated to clinicians in all of the participating clinics. Medical assistants were instructed to schedule a follow-up appointment for all patients who tested positive before they left the office. A target of 3 weeks was a strategy of overcorrection when so many patients were missing the initial 30-day window by just a few days.
The approach also involved an enhanced collaboration with psychologists to which patients were referred. Asking for expedited appointments when appropriate ensured that those at highest risk were prioritized, although Dr. Krantz said that this step was planned carefully to avoid overwhelming the mental health team.
“We monitored this and made sure it was not increasing the burden for psychologists from a capacity standpoint,” he said.
Other steps, like a depression action plan, which Dr. Krantz compared to an asthma action plan, were also implemented to reduce the risk of losing symptomatic patients before the chance for an effective treatment.
When compared with the 19% 30-day follow-up rate in the preintervention sample of 589 children, the 43.8% 30-day follow-up rate achieved in the 764 patients identified after implementation beat the original goal.
The improvement in follow-up was relatively consistent across all six clinics, which Dr. Krantz believes reflected a broad and shared change in a sense of responsibility for confirming that symptoms of depression were being addressed. Patients were still referred for psychological help, but referral was no longer considered enough.
“Children with mental health issues are still our patients in primary care,” said Dr. Krantz, who considers this an important change in orientation.
While the goal was to schedule patients for a follow-up at the time of a positive depression screen, Dr. Krantz described one important accommodation.
“The screen for depression was being performed in most cases during well visits, so patients and their families were not expecting to be discussing this issue,” he said. The diagnosis might be a particular surprise to parents who were not aware of any symptoms. In this case, Dr. Krantz said patients and families were given time to process the information and were contacted after a week to discuss further workup.
It is also notable that about one third of patients met the criteria for depression by answering positively to the PHQ-9 item on self-harm when they did not meet the 10 or more threshold depression score overall. In other words, these patients would have been missed without this criterion.
In the participating Cincinnati pediatric clinics, about 12%-13% of adolescents met the criteria for depression, which Dr. Krantz said is consistent with reports in the literature. He said the range is about 6%-24%.
Although outcomes were not tracked, there is evidence that early intervention for depression yields better outcomes than delayed intervention, according to Dr. Krantz. Based on approximately 600 positive screens for depression per year at his pediatric clinics, he estimated that his data predict at least 25% more patients will receive timely follow-up.
Seeking Solutions to a Growing Problem
There are several studies documenting the growing problem of adolescent depression and suicide and, for this reason, the topic is attracting a lot of attention, according to Corinna Rea, MD, MPH, a pediatrician working in the primary care center at Boston Children’s Hospital in Massachusetts.
Dr. Rea was not involved with the study, but when asked to comment, she said: “The results of this study were encouraging because we know that getting patients to care quickly is probably important.” She also agreed that referring patients with depression for care might not be enough, noting that a lot of patients do not follow up on recommendations to pursue a consultation or treatment.
“I am now involved in a project with the American Academy of Pediatrics to address this issue,” Dr. Rae said. She thinks that more work in this area is needed and agreed with Dr. Krantz that pediatricians should verify that children with depression are getting help even when other specialists are providing the treatment.
Dr. Krantz and Dr. Rae report no potential conflicts of interest.
TORONTO — An ambitious effort at a busy pediatrics clinic to improve follow-up in children and adolescents with a positive depression screen improved this quality metric, and it produced a fundamental change in approach.
“It was a big culture shift,” reported Landon B. Krantz, MD, a clinical fellow in the Division of General and Community Pediatrics at Cincinnati Children’s Hospital in Ohio. From a baseline position of screening, risk identification, and then referral, “we are now taking ownership of the process.”
Based on the substantial risk posed by significant levels of depression, guidelines recommend follow-up for any patient 12 years or older who has a positive screen, according to Dr. Krantz. At his center, they found only 19% had a documented follow-up within 30 days, even though timely intervention is important.
“Nearly half of suicide events in adolescents occur within 30 days after a positive PHQ-9 [9-question Patient Health Questionnaire] is completed,” said Dr. Krantz when presenting his data at the Pediatric Academic Societies annual meeting.
The issue has gained more urgency because of the substantial increase over the past several years in children presenting with depression and suicidal thoughts, according to Dr. Krantz. He said many are characterizing the upsurge as a mental health crisis in the pediatric age group.
Improving Follow-Up
. The goal at the outset was to increase the proportion to 35%.
“We know that a lot of children would receive follow-up at centers outside of our system,” said Dr. Krantz, explaining why the goal was relatively modest. Based on the likelihood that many follow-up visits would not be captured, he expected the final data would represent an underestimate.
Depression at baseline was defined as a score of 10 or higher on the PHQ-9 or any positive answer to item 9 on this screening tool, which asks specifically about thoughts of self-harm.
To be counted, follow-up had to be a documented encounter, whether by phone call, in-person visit, or telehealth visit.
“We needed patients to be checked. We did not count a prescription refill as a true follow-up,” Dr. Krantz specified.
There were numerous strategies implemented to improve follow-up, not least of which was an educational program to reinforce the importance and value of follow-up that was disseminated to clinicians in all of the participating clinics. Medical assistants were instructed to schedule a follow-up appointment for all patients who tested positive before they left the office. A target of 3 weeks was a strategy of overcorrection when so many patients were missing the initial 30-day window by just a few days.
The approach also involved an enhanced collaboration with psychologists to which patients were referred. Asking for expedited appointments when appropriate ensured that those at highest risk were prioritized, although Dr. Krantz said that this step was planned carefully to avoid overwhelming the mental health team.
“We monitored this and made sure it was not increasing the burden for psychologists from a capacity standpoint,” he said.
Other steps, like a depression action plan, which Dr. Krantz compared to an asthma action plan, were also implemented to reduce the risk of losing symptomatic patients before the chance for an effective treatment.
When compared with the 19% 30-day follow-up rate in the preintervention sample of 589 children, the 43.8% 30-day follow-up rate achieved in the 764 patients identified after implementation beat the original goal.
The improvement in follow-up was relatively consistent across all six clinics, which Dr. Krantz believes reflected a broad and shared change in a sense of responsibility for confirming that symptoms of depression were being addressed. Patients were still referred for psychological help, but referral was no longer considered enough.
“Children with mental health issues are still our patients in primary care,” said Dr. Krantz, who considers this an important change in orientation.
While the goal was to schedule patients for a follow-up at the time of a positive depression screen, Dr. Krantz described one important accommodation.
“The screen for depression was being performed in most cases during well visits, so patients and their families were not expecting to be discussing this issue,” he said. The diagnosis might be a particular surprise to parents who were not aware of any symptoms. In this case, Dr. Krantz said patients and families were given time to process the information and were contacted after a week to discuss further workup.
It is also notable that about one third of patients met the criteria for depression by answering positively to the PHQ-9 item on self-harm when they did not meet the 10 or more threshold depression score overall. In other words, these patients would have been missed without this criterion.
In the participating Cincinnati pediatric clinics, about 12%-13% of adolescents met the criteria for depression, which Dr. Krantz said is consistent with reports in the literature. He said the range is about 6%-24%.
Although outcomes were not tracked, there is evidence that early intervention for depression yields better outcomes than delayed intervention, according to Dr. Krantz. Based on approximately 600 positive screens for depression per year at his pediatric clinics, he estimated that his data predict at least 25% more patients will receive timely follow-up.
Seeking Solutions to a Growing Problem
There are several studies documenting the growing problem of adolescent depression and suicide and, for this reason, the topic is attracting a lot of attention, according to Corinna Rea, MD, MPH, a pediatrician working in the primary care center at Boston Children’s Hospital in Massachusetts.
Dr. Rea was not involved with the study, but when asked to comment, she said: “The results of this study were encouraging because we know that getting patients to care quickly is probably important.” She also agreed that referring patients with depression for care might not be enough, noting that a lot of patients do not follow up on recommendations to pursue a consultation or treatment.
“I am now involved in a project with the American Academy of Pediatrics to address this issue,” Dr. Rae said. She thinks that more work in this area is needed and agreed with Dr. Krantz that pediatricians should verify that children with depression are getting help even when other specialists are providing the treatment.
Dr. Krantz and Dr. Rae report no potential conflicts of interest.
FROM PAS 2024
Reactive Granulomatous Dermatitis: Variability of the Predominant Inflammatory Cell Type
To the Editor:
The term palisaded neutrophilic and granulomatous dermatitis (PNGD) has been proposed to encompass various conditions, including Winkelmann granuloma and superficial ulcerating rheumatoid necrobiosis. More recently, PNGD has been classified along with interstitial granulomatous dermatitis and interstitial granulomatous drug reaction under a unifying rubric of reactive granulomatous dermatitis (RGD).1-4 The diagnosis of RGD can be challenging because of a range of clinical and histopathologic features as well as variable nomenclature.1-3,5
Palisaded neutrophilic and granulomatous dermatitis classically manifests with papules and small plaques on the extensor extremities, with histopathology showing characteristic necrobiosis with both neutrophils and histiocytes.1,2,6 We report 6 cases of RGD, including an index case in which a predominance of neutrophils in the infiltrate impeded the diagnosis.
An 85-year-old woman (the index patient) presented with a several-week history of asymmetric crusted papules on the right upper extremity—3 lesions on the elbow and forearm and 1 lesion on a finger. She was an avid gardener with severe rheumatoid arthritis treated with Janus kinase (JAK) inhibitor therapy. An initial biopsy of the elbow revealed a dense infiltrate of neutrophils and sparse eosinophils within the dermis. Special stains for bacterial, fungal, and acid-fast organisms were negative.
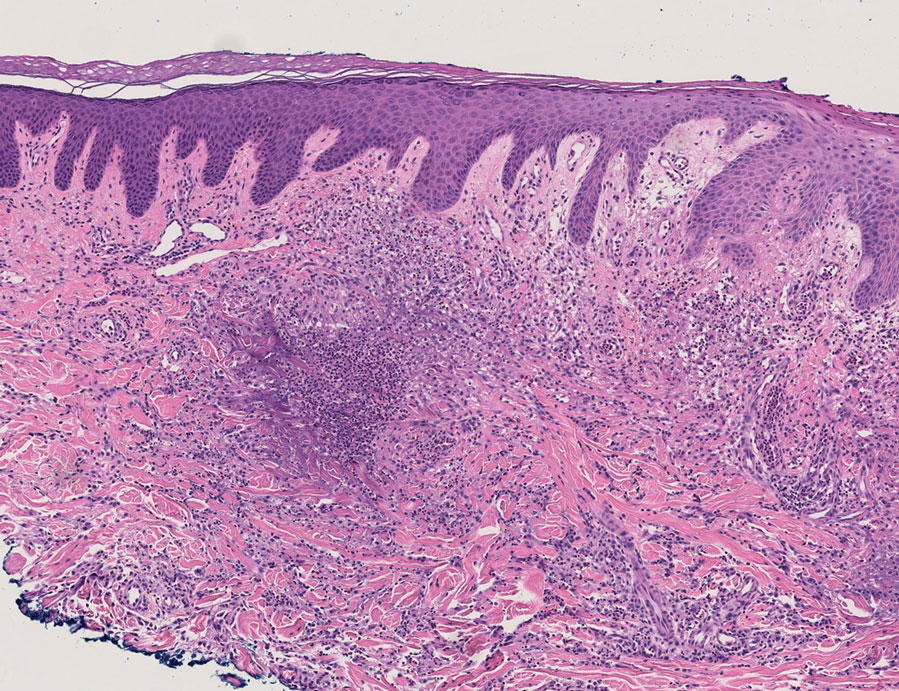
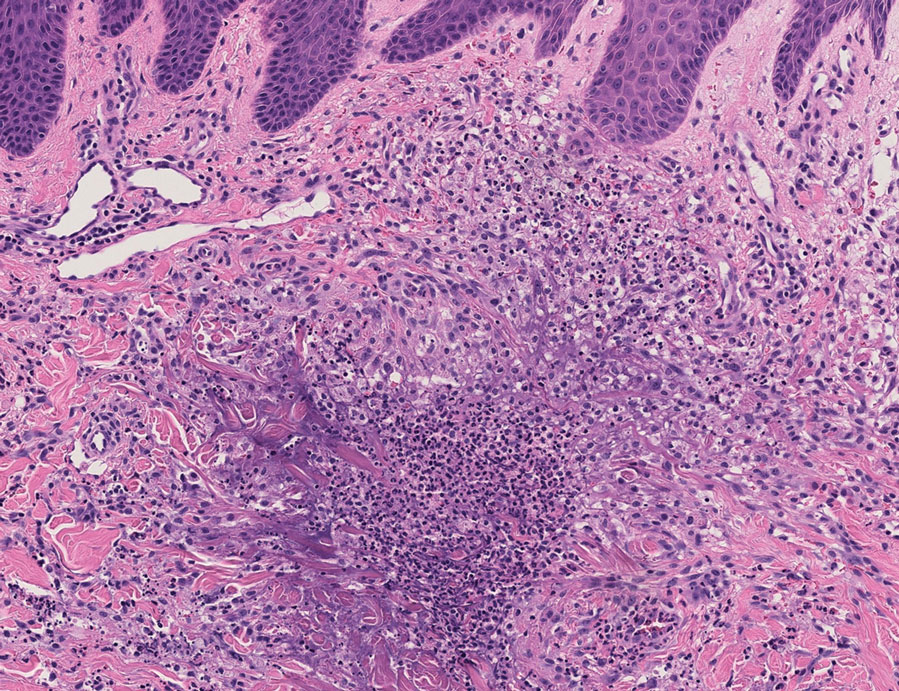
Because infection with sporotrichoid spread remained high in the differential diagnosis, the JAK inhibitor was discontinued and an antifungal agent was initiated. Given the persistence of the lesions, a subsequent biopsy of the right finger revealed scarce neutrophils and predominant histiocytes with rare foci of degenerated collagen. Sporotrichosis remained the leading diagnosis for these unilateral lesions. The patient subsequently developed additional crusted papules on the left arm (Figure 1). A biopsy of a left elbow lesion revealed palisades of histiocytes around degenerated collagen and collections of neutrophils compatible with RGD (Figures 2 and 3). Incidentally, the patient also presented with bilateral lower extremity palpable purpura, with a biopsy showing leukocytoclastic vasculitis. Antifungal therapy was discontinued and JAK inhibitor therapy resumed, with partial resolution of both the arm and right finger lesions and complete resolution of the lower extremity palpable purpura over several months.

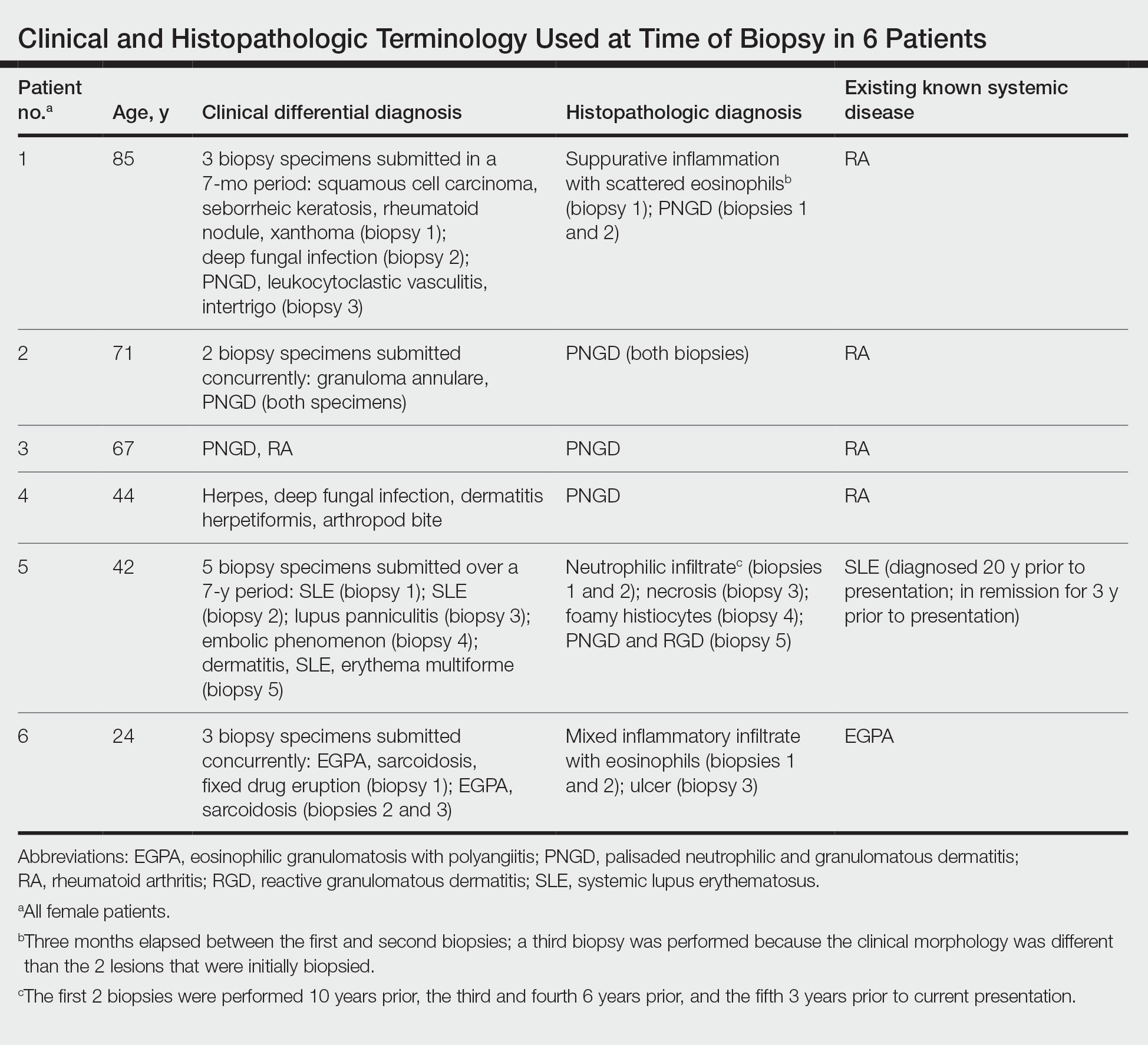
The dense neutrophilic infiltrate and asymmetric presentation seen in our index patient’s initial biopsy hindered categorization of the cutaneous findings as RGD in association with her rheumatoid arthritis rather than as an infectious process. To ascertain whether diagnosis also was difficult in other cases of RGD, we conducted a search of the Yale Dermatopathology database for the diagnosis palisaded neutrophilic and granulomatous dermatitis, a term consistently used at our institution over the past decade. This study was approved by the institutional review board of Yale University (New Haven, Connecticut), and informed consent was waived. The search covered a 10-year period; 13 patients were found. Eight patients were eliminated because further clinical information or follow-up could not be obtained, leaving 5 additional cases (Table). The 8 eliminated cases were consultations submitted to the laboratory by outside pathologists from other institutions.
In one case (patient 5), the diagnosis of RGD was delayed for 7 years from first documentation of an RGD-compatible neutrophil-predominant infiltrate (Table). In 3 other cases, PNGD was in the clinical differential diagnosis. In patient 6 with known eosinophilic granulomatosis with polyangiitis, biopsy findings included a mixed inflammatory infiltrate with eosinophils, and the clinical and histopathologic findings were deemed compatible with RGD by group consensus at Grand Rounds.
In practice, a consistent unifying nomenclature has not been achieved for RGD and the diseases it encompasses—PNGD, interstitial granulomatous dermatitis, and interstitial granulomatous drug reaction. In this small series, a diagnosis of PNGD was given in the dermatopathology report only when biopsy specimens were characterized by histiocytes, neutrophils, and necrobiosis. Histopathology reports for neutrophil-predominant, histiocyte-predominant, and eosinophil-predominant cases did not mention PNGD or RGD, though potential association with systemic disease generally was noted.
Given the variability in the predominant inflammatory cell type in these patients, adding a qualifier to the histopathologic diagnosis—“RGD, eosinophil rich,” “RGD, histiocyte rich,” or “RGD, neutrophil rich”1—would underscore the range of inflammatory cells in this entity. Employing this terminology rather than stating a solely descriptive diagnosis such as neutrophilic infiltrate, which may bias clinicians toward an infectious process, would aid in the association of a given rash with systemic disease and may prevent unnecessary tissue sampling. Indeed, 3 patients in this small series underwent more than 2 biopsies; multiple procedures might have been avoided had there been better communication about the spectrum of inflammatory cells compatible with RGD.
The inflammatory infiltrate in biopsy specimens of RGD can be solely neutrophil or histiocyte predominant or even have prominent eosinophils depending on the stage of disease. Awareness of variability in the predominant inflammatory cell in RGD may facilitate an accurate diagnosis as well as an association with any underlying autoimmune process, thereby allowing better management and treatment.1
- Rosenbach M, English JC. Reactive granulomatous dermatitis: a review of palisaded neutrophilic and granulomatous dermatitis, interstitial granulomatous dermatitis, interstitial granulomatous drug reaction, and a proposed reclassification. Dermatol Clin. 2015;33:373-387. doi:10.1016/j.det.2015.03.005
- Wanat KA, Caplan A, Messenger E, et al. Reactive granulomatous dermatitis: a useful and encompassing term. JAAD Intl. 2022;7:126-128. doi:10.1016/j.jdin.2022.03.004
- Chu P, Connolly MK, LeBoit PE. The histopathologic spectrum of palisaded neutrophilic and granulomatous dermatitis in patients with collagen vascular disease. Arch Dermatol. 1994;130:1278-1283. doi:10.1001/archderm.1994.01690100062010
- Dykman CJ, Galens GJ, Good AE. Linear subcutaneous bands in rheumatoid arthritis: an unusual form of rheumatoid granuloma. Ann Intern Med. 1965;63:134-140. doi:10.7326/0003-4819-63-1-134
- Rodríguez-Garijo N, Bielsa I, Mascaró JM Jr, et al. Reactive granulomatous dermatitis as a histological pattern including manifestations of interstitial granulomatous dermatitis and palisaded neutrophilic and granulomtous dermatitis: a study of 52 patients. J Eur Acad Dermatol Venereol. 2021;35:988-994. doi:10.1111/jdv.17010
- Kalen JE, Shokeen D, Ramos-Caro F, et al. Palisaded neutrophilic granulomatous dermatitis: spectrum of histologic findings in a single patient. JAAD Case Rep. 2017;3:425. doi:10.1016/j.jdcr.2017.06.010
To the Editor:
The term palisaded neutrophilic and granulomatous dermatitis (PNGD) has been proposed to encompass various conditions, including Winkelmann granuloma and superficial ulcerating rheumatoid necrobiosis. More recently, PNGD has been classified along with interstitial granulomatous dermatitis and interstitial granulomatous drug reaction under a unifying rubric of reactive granulomatous dermatitis (RGD).1-4 The diagnosis of RGD can be challenging because of a range of clinical and histopathologic features as well as variable nomenclature.1-3,5
Palisaded neutrophilic and granulomatous dermatitis classically manifests with papules and small plaques on the extensor extremities, with histopathology showing characteristic necrobiosis with both neutrophils and histiocytes.1,2,6 We report 6 cases of RGD, including an index case in which a predominance of neutrophils in the infiltrate impeded the diagnosis.
An 85-year-old woman (the index patient) presented with a several-week history of asymmetric crusted papules on the right upper extremity—3 lesions on the elbow and forearm and 1 lesion on a finger. She was an avid gardener with severe rheumatoid arthritis treated with Janus kinase (JAK) inhibitor therapy. An initial biopsy of the elbow revealed a dense infiltrate of neutrophils and sparse eosinophils within the dermis. Special stains for bacterial, fungal, and acid-fast organisms were negative.
Because infection with sporotrichoid spread remained high in the differential diagnosis, the JAK inhibitor was discontinued and an antifungal agent was initiated. Given the persistence of the lesions, a subsequent biopsy of the right finger revealed scarce neutrophils and predominant histiocytes with rare foci of degenerated collagen. Sporotrichosis remained the leading diagnosis for these unilateral lesions. The patient subsequently developed additional crusted papules on the left arm (Figure 1). A biopsy of a left elbow lesion revealed palisades of histiocytes around degenerated collagen and collections of neutrophils compatible with RGD (Figures 2 and 3). Incidentally, the patient also presented with bilateral lower extremity palpable purpura, with a biopsy showing leukocytoclastic vasculitis. Antifungal therapy was discontinued and JAK inhibitor therapy resumed, with partial resolution of both the arm and right finger lesions and complete resolution of the lower extremity palpable purpura over several months.
The dense neutrophilic infiltrate and asymmetric presentation seen in our index patient’s initial biopsy hindered categorization of the cutaneous findings as RGD in association with her rheumatoid arthritis rather than as an infectious process. To ascertain whether diagnosis also was difficult in other cases of RGD, we conducted a search of the Yale Dermatopathology database for the diagnosis palisaded neutrophilic and granulomatous dermatitis, a term consistently used at our institution over the past decade. This study was approved by the institutional review board of Yale University (New Haven, Connecticut), and informed consent was waived. The search covered a 10-year period; 13 patients were found. Eight patients were eliminated because further clinical information or follow-up could not be obtained, leaving 5 additional cases (Table). The 8 eliminated cases were consultations submitted to the laboratory by outside pathologists from other institutions.
In one case (patient 5), the diagnosis of RGD was delayed for 7 years from first documentation of an RGD-compatible neutrophil-predominant infiltrate (Table). In 3 other cases, PNGD was in the clinical differential diagnosis. In patient 6 with known eosinophilic granulomatosis with polyangiitis, biopsy findings included a mixed inflammatory infiltrate with eosinophils, and the clinical and histopathologic findings were deemed compatible with RGD by group consensus at Grand Rounds.
In practice, a consistent unifying nomenclature has not been achieved for RGD and the diseases it encompasses—PNGD, interstitial granulomatous dermatitis, and interstitial granulomatous drug reaction. In this small series, a diagnosis of PNGD was given in the dermatopathology report only when biopsy specimens were characterized by histiocytes, neutrophils, and necrobiosis. Histopathology reports for neutrophil-predominant, histiocyte-predominant, and eosinophil-predominant cases did not mention PNGD or RGD, though potential association with systemic disease generally was noted.
Given the variability in the predominant inflammatory cell type in these patients, adding a qualifier to the histopathologic diagnosis—“RGD, eosinophil rich,” “RGD, histiocyte rich,” or “RGD, neutrophil rich”1—would underscore the range of inflammatory cells in this entity. Employing this terminology rather than stating a solely descriptive diagnosis such as neutrophilic infiltrate, which may bias clinicians toward an infectious process, would aid in the association of a given rash with systemic disease and may prevent unnecessary tissue sampling. Indeed, 3 patients in this small series underwent more than 2 biopsies; multiple procedures might have been avoided had there been better communication about the spectrum of inflammatory cells compatible with RGD.
The inflammatory infiltrate in biopsy specimens of RGD can be solely neutrophil or histiocyte predominant or even have prominent eosinophils depending on the stage of disease. Awareness of variability in the predominant inflammatory cell in RGD may facilitate an accurate diagnosis as well as an association with any underlying autoimmune process, thereby allowing better management and treatment.1
To the Editor:
The term palisaded neutrophilic and granulomatous dermatitis (PNGD) has been proposed to encompass various conditions, including Winkelmann granuloma and superficial ulcerating rheumatoid necrobiosis. More recently, PNGD has been classified along with interstitial granulomatous dermatitis and interstitial granulomatous drug reaction under a unifying rubric of reactive granulomatous dermatitis (RGD).1-4 The diagnosis of RGD can be challenging because of a range of clinical and histopathologic features as well as variable nomenclature.1-3,5
Palisaded neutrophilic and granulomatous dermatitis classically manifests with papules and small plaques on the extensor extremities, with histopathology showing characteristic necrobiosis with both neutrophils and histiocytes.1,2,6 We report 6 cases of RGD, including an index case in which a predominance of neutrophils in the infiltrate impeded the diagnosis.
An 85-year-old woman (the index patient) presented with a several-week history of asymmetric crusted papules on the right upper extremity—3 lesions on the elbow and forearm and 1 lesion on a finger. She was an avid gardener with severe rheumatoid arthritis treated with Janus kinase (JAK) inhibitor therapy. An initial biopsy of the elbow revealed a dense infiltrate of neutrophils and sparse eosinophils within the dermis. Special stains for bacterial, fungal, and acid-fast organisms were negative.
Because infection with sporotrichoid spread remained high in the differential diagnosis, the JAK inhibitor was discontinued and an antifungal agent was initiated. Given the persistence of the lesions, a subsequent biopsy of the right finger revealed scarce neutrophils and predominant histiocytes with rare foci of degenerated collagen. Sporotrichosis remained the leading diagnosis for these unilateral lesions. The patient subsequently developed additional crusted papules on the left arm (Figure 1). A biopsy of a left elbow lesion revealed palisades of histiocytes around degenerated collagen and collections of neutrophils compatible with RGD (Figures 2 and 3). Incidentally, the patient also presented with bilateral lower extremity palpable purpura, with a biopsy showing leukocytoclastic vasculitis. Antifungal therapy was discontinued and JAK inhibitor therapy resumed, with partial resolution of both the arm and right finger lesions and complete resolution of the lower extremity palpable purpura over several months.
The dense neutrophilic infiltrate and asymmetric presentation seen in our index patient’s initial biopsy hindered categorization of the cutaneous findings as RGD in association with her rheumatoid arthritis rather than as an infectious process. To ascertain whether diagnosis also was difficult in other cases of RGD, we conducted a search of the Yale Dermatopathology database for the diagnosis palisaded neutrophilic and granulomatous dermatitis, a term consistently used at our institution over the past decade. This study was approved by the institutional review board of Yale University (New Haven, Connecticut), and informed consent was waived. The search covered a 10-year period; 13 patients were found. Eight patients were eliminated because further clinical information or follow-up could not be obtained, leaving 5 additional cases (Table). The 8 eliminated cases were consultations submitted to the laboratory by outside pathologists from other institutions.
In one case (patient 5), the diagnosis of RGD was delayed for 7 years from first documentation of an RGD-compatible neutrophil-predominant infiltrate (Table). In 3 other cases, PNGD was in the clinical differential diagnosis. In patient 6 with known eosinophilic granulomatosis with polyangiitis, biopsy findings included a mixed inflammatory infiltrate with eosinophils, and the clinical and histopathologic findings were deemed compatible with RGD by group consensus at Grand Rounds.
In practice, a consistent unifying nomenclature has not been achieved for RGD and the diseases it encompasses—PNGD, interstitial granulomatous dermatitis, and interstitial granulomatous drug reaction. In this small series, a diagnosis of PNGD was given in the dermatopathology report only when biopsy specimens were characterized by histiocytes, neutrophils, and necrobiosis. Histopathology reports for neutrophil-predominant, histiocyte-predominant, and eosinophil-predominant cases did not mention PNGD or RGD, though potential association with systemic disease generally was noted.
Given the variability in the predominant inflammatory cell type in these patients, adding a qualifier to the histopathologic diagnosis—“RGD, eosinophil rich,” “RGD, histiocyte rich,” or “RGD, neutrophil rich”1—would underscore the range of inflammatory cells in this entity. Employing this terminology rather than stating a solely descriptive diagnosis such as neutrophilic infiltrate, which may bias clinicians toward an infectious process, would aid in the association of a given rash with systemic disease and may prevent unnecessary tissue sampling. Indeed, 3 patients in this small series underwent more than 2 biopsies; multiple procedures might have been avoided had there been better communication about the spectrum of inflammatory cells compatible with RGD.
The inflammatory infiltrate in biopsy specimens of RGD can be solely neutrophil or histiocyte predominant or even have prominent eosinophils depending on the stage of disease. Awareness of variability in the predominant inflammatory cell in RGD may facilitate an accurate diagnosis as well as an association with any underlying autoimmune process, thereby allowing better management and treatment.1
- Rosenbach M, English JC. Reactive granulomatous dermatitis: a review of palisaded neutrophilic and granulomatous dermatitis, interstitial granulomatous dermatitis, interstitial granulomatous drug reaction, and a proposed reclassification. Dermatol Clin. 2015;33:373-387. doi:10.1016/j.det.2015.03.005
- Wanat KA, Caplan A, Messenger E, et al. Reactive granulomatous dermatitis: a useful and encompassing term. JAAD Intl. 2022;7:126-128. doi:10.1016/j.jdin.2022.03.004
- Chu P, Connolly MK, LeBoit PE. The histopathologic spectrum of palisaded neutrophilic and granulomatous dermatitis in patients with collagen vascular disease. Arch Dermatol. 1994;130:1278-1283. doi:10.1001/archderm.1994.01690100062010
- Dykman CJ, Galens GJ, Good AE. Linear subcutaneous bands in rheumatoid arthritis: an unusual form of rheumatoid granuloma. Ann Intern Med. 1965;63:134-140. doi:10.7326/0003-4819-63-1-134
- Rodríguez-Garijo N, Bielsa I, Mascaró JM Jr, et al. Reactive granulomatous dermatitis as a histological pattern including manifestations of interstitial granulomatous dermatitis and palisaded neutrophilic and granulomtous dermatitis: a study of 52 patients. J Eur Acad Dermatol Venereol. 2021;35:988-994. doi:10.1111/jdv.17010
- Kalen JE, Shokeen D, Ramos-Caro F, et al. Palisaded neutrophilic granulomatous dermatitis: spectrum of histologic findings in a single patient. JAAD Case Rep. 2017;3:425. doi:10.1016/j.jdcr.2017.06.010
- Rosenbach M, English JC. Reactive granulomatous dermatitis: a review of palisaded neutrophilic and granulomatous dermatitis, interstitial granulomatous dermatitis, interstitial granulomatous drug reaction, and a proposed reclassification. Dermatol Clin. 2015;33:373-387. doi:10.1016/j.det.2015.03.005
- Wanat KA, Caplan A, Messenger E, et al. Reactive granulomatous dermatitis: a useful and encompassing term. JAAD Intl. 2022;7:126-128. doi:10.1016/j.jdin.2022.03.004
- Chu P, Connolly MK, LeBoit PE. The histopathologic spectrum of palisaded neutrophilic and granulomatous dermatitis in patients with collagen vascular disease. Arch Dermatol. 1994;130:1278-1283. doi:10.1001/archderm.1994.01690100062010
- Dykman CJ, Galens GJ, Good AE. Linear subcutaneous bands in rheumatoid arthritis: an unusual form of rheumatoid granuloma. Ann Intern Med. 1965;63:134-140. doi:10.7326/0003-4819-63-1-134
- Rodríguez-Garijo N, Bielsa I, Mascaró JM Jr, et al. Reactive granulomatous dermatitis as a histological pattern including manifestations of interstitial granulomatous dermatitis and palisaded neutrophilic and granulomtous dermatitis: a study of 52 patients. J Eur Acad Dermatol Venereol. 2021;35:988-994. doi:10.1111/jdv.17010
- Kalen JE, Shokeen D, Ramos-Caro F, et al. Palisaded neutrophilic granulomatous dermatitis: spectrum of histologic findings in a single patient. JAAD Case Rep. 2017;3:425. doi:10.1016/j.jdcr.2017.06.010
Practice Points
- The term reactive granulomatous dermatitis (RGD) provides a unifying rubric for palisaded neutrophilic and granulomatous dermatitis, interstitial granulomatous dermatitis, and interstitial granulomatous drug reaction.
- Reactive granulomatous dermatitis can have a variable infiltrate that includes neutrophils, histiocytes, and/or eosinophils.
- Awareness of the variability in inflammatory cell type is important for the diagnosis of RGD.

Widespread, Long-Held Practice in Dementia Called Into Question
Hospitalized patients with dementia and dysphagia are often prescribed a “dysphagia diet,” made up of texture-modified foods and thickened liquids in an effort to reduce the risk for aspiration or other problems. However, a new study calls this widespread and long-held practice into question.
Investigators found no evidence that the use of thickened liquids reduced mortality or respiratory complications, such as pneumonia, aspiration, or choking, compared with thin-liquid diets in patients with Alzheimer’s disease and related dementias (ADRD) and dysphagia. Patients receiving thick liquids were less likely to be intubated, but they were actually more likely to have respiratory complications.
“When hospitalized patients with Alzheimer’s disease and related dementias are found to have dysphagia, our go-to solution is to use a thick liquid diet,” senior author Liron Sinvani, MD, with the Feinstein Institutes for Medical Research, Manhasset, New York, said in a news release.
“However, there is no concrete evidence that thick liquids improve health outcomes, and we also know that thick liquids can lead to decreased palatability, poor oral intake, dehydration, malnutrition, and worse quality of life,” added Dr. Sinvani, director of the geriatric hospitalist service at Northwell Health in New York.
The study was published online in JAMA Internal Medicine.
Challenging a Go-To Solution
The researchers compared outcomes in a propensity score-matched cohort of patients with ADRD and dysphagia (mean age, 86 years; 54% women) receiving mostly thick liquids versus thin liquids during their hospitalization. There were 4458 patients in each group.
They found no significant difference in hospital mortality between the thick liquids and thin liquids groups (hazard ratio [HR], 0.92; P = .46).
Patients receiving thick liquids were less likely to require intubation (odds ratio [OR], 0.66; 95% CI, 0.54-0.80) but were more likely to develop respiratory complications (OR, 1.73; 95% CI, 1.56-1.91).
The two groups did not differ significantly in terms of risk for dehydration, hospital length of stay, or rate of 30-day readmission.
“This cohort study emphasizes the need for prospective studies that evaluate whether thick liquids are associated with improved clinical outcomes in hospitalized patients with ADRD and dysphagia,” the authors wrote.
Because few patients received a Modified Barium Swallow Study at baseline, researchers were unable to confirm the presence of dysphagia or account for dysphagia severity and impairment. It’s possible that patients in the thick liquid group had more severe dysphagia than those in the thin liquid group.
Another limitation is that the type of dementia and severity were not characterized. Also, the study could not account for factors like oral hygiene, immune status, and diet adherence that could impact risks like aspiration pneumonia.
Theoretical Benefit, No Evidence
In an invited commentary on the study, Eric Widera, MD, with University of California San Francisco, noted that medicine is “littered with interventions that have become the standard of practice based on theoretical benefits without clinical evidence”.
One example is percutaneous endoscopic gastrostomy tubes for individuals with dysphagia and dementia.
“For decades, these tubes were regularly used in individuals with dementia on the assumption that bypassing the oropharyngeal route would decrease rates of aspiration and, therefore, decrease adverse outcomes like pressure ulcers, malnutrition, pneumonia, and death. However, similar to what we see with thickened liquids, evidence slowly built that this standard of practice was not evidence-based practice,” Dr. Widera wrote.
When thinking about thick liquid diets, Dr. Widera encouraged clinicians to “acknowledge the limitations of the evidence both for and against thickened-liquid diets.”
He also encouraged clinicians to “put yourself in the shoes of the patients who will be asked to adhere to this modified diet. For 12 hours, drink your tea, coffee, wine, and water as thickened liquids,” Dr. Widera suggested. “The goal is not to convince yourself never to prescribe thickened liquids, but rather to be mindful of how a thickened liquid diet affects patients’ liquid and food intake, how it changes the mouthfeel and taste of different drinks, and how it affects patients’ quality of life.”
Clinicians also should “proactively engage speech-language pathologists, but do not ask them if it is safe for a patient with dementia to eat or drink normally. Instead, ask what we can do to meet the patient’s goals and maintain quality of life given the current evidence base,” Dr. Widera wrote.
“For some, when the patient’s goals are focused on comfort, this may lead to a recommendation for thickened liquids if their use may resolve significant coughing distress after drinking thin liquids. Alternatively, even when the patient’s goals are focused on prolonging life, the risks of thickened liquids, including dehydration and decreased food and fluid intake, as well as the thin evidence for mortality improvement, will argue against their use,” Dr. Widera added.
Funding for the study was provided by grants from the National Institute on Aging and by the William S. Middleton Veteran Affairs Hospital, Madison, Wisconsin. Dr. Sinvani and Dr. Widera declared no relevant conflicts of interest.
A version of this article appeared on Medscape.com .
Hospitalized patients with dementia and dysphagia are often prescribed a “dysphagia diet,” made up of texture-modified foods and thickened liquids in an effort to reduce the risk for aspiration or other problems. However, a new study calls this widespread and long-held practice into question.
Investigators found no evidence that the use of thickened liquids reduced mortality or respiratory complications, such as pneumonia, aspiration, or choking, compared with thin-liquid diets in patients with Alzheimer’s disease and related dementias (ADRD) and dysphagia. Patients receiving thick liquids were less likely to be intubated, but they were actually more likely to have respiratory complications.
“When hospitalized patients with Alzheimer’s disease and related dementias are found to have dysphagia, our go-to solution is to use a thick liquid diet,” senior author Liron Sinvani, MD, with the Feinstein Institutes for Medical Research, Manhasset, New York, said in a news release.
“However, there is no concrete evidence that thick liquids improve health outcomes, and we also know that thick liquids can lead to decreased palatability, poor oral intake, dehydration, malnutrition, and worse quality of life,” added Dr. Sinvani, director of the geriatric hospitalist service at Northwell Health in New York.
The study was published online in JAMA Internal Medicine.
Challenging a Go-To Solution
The researchers compared outcomes in a propensity score-matched cohort of patients with ADRD and dysphagia (mean age, 86 years; 54% women) receiving mostly thick liquids versus thin liquids during their hospitalization. There were 4458 patients in each group.
They found no significant difference in hospital mortality between the thick liquids and thin liquids groups (hazard ratio [HR], 0.92; P = .46).
Patients receiving thick liquids were less likely to require intubation (odds ratio [OR], 0.66; 95% CI, 0.54-0.80) but were more likely to develop respiratory complications (OR, 1.73; 95% CI, 1.56-1.91).
The two groups did not differ significantly in terms of risk for dehydration, hospital length of stay, or rate of 30-day readmission.
“This cohort study emphasizes the need for prospective studies that evaluate whether thick liquids are associated with improved clinical outcomes in hospitalized patients with ADRD and dysphagia,” the authors wrote.
Because few patients received a Modified Barium Swallow Study at baseline, researchers were unable to confirm the presence of dysphagia or account for dysphagia severity and impairment. It’s possible that patients in the thick liquid group had more severe dysphagia than those in the thin liquid group.
Another limitation is that the type of dementia and severity were not characterized. Also, the study could not account for factors like oral hygiene, immune status, and diet adherence that could impact risks like aspiration pneumonia.
Theoretical Benefit, No Evidence
In an invited commentary on the study, Eric Widera, MD, with University of California San Francisco, noted that medicine is “littered with interventions that have become the standard of practice based on theoretical benefits without clinical evidence”.
One example is percutaneous endoscopic gastrostomy tubes for individuals with dysphagia and dementia.
“For decades, these tubes were regularly used in individuals with dementia on the assumption that bypassing the oropharyngeal route would decrease rates of aspiration and, therefore, decrease adverse outcomes like pressure ulcers, malnutrition, pneumonia, and death. However, similar to what we see with thickened liquids, evidence slowly built that this standard of practice was not evidence-based practice,” Dr. Widera wrote.
When thinking about thick liquid diets, Dr. Widera encouraged clinicians to “acknowledge the limitations of the evidence both for and against thickened-liquid diets.”
He also encouraged clinicians to “put yourself in the shoes of the patients who will be asked to adhere to this modified diet. For 12 hours, drink your tea, coffee, wine, and water as thickened liquids,” Dr. Widera suggested. “The goal is not to convince yourself never to prescribe thickened liquids, but rather to be mindful of how a thickened liquid diet affects patients’ liquid and food intake, how it changes the mouthfeel and taste of different drinks, and how it affects patients’ quality of life.”
Clinicians also should “proactively engage speech-language pathologists, but do not ask them if it is safe for a patient with dementia to eat or drink normally. Instead, ask what we can do to meet the patient’s goals and maintain quality of life given the current evidence base,” Dr. Widera wrote.
“For some, when the patient’s goals are focused on comfort, this may lead to a recommendation for thickened liquids if their use may resolve significant coughing distress after drinking thin liquids. Alternatively, even when the patient’s goals are focused on prolonging life, the risks of thickened liquids, including dehydration and decreased food and fluid intake, as well as the thin evidence for mortality improvement, will argue against their use,” Dr. Widera added.
Funding for the study was provided by grants from the National Institute on Aging and by the William S. Middleton Veteran Affairs Hospital, Madison, Wisconsin. Dr. Sinvani and Dr. Widera declared no relevant conflicts of interest.
A version of this article appeared on Medscape.com .
Hospitalized patients with dementia and dysphagia are often prescribed a “dysphagia diet,” made up of texture-modified foods and thickened liquids in an effort to reduce the risk for aspiration or other problems. However, a new study calls this widespread and long-held practice into question.
Investigators found no evidence that the use of thickened liquids reduced mortality or respiratory complications, such as pneumonia, aspiration, or choking, compared with thin-liquid diets in patients with Alzheimer’s disease and related dementias (ADRD) and dysphagia. Patients receiving thick liquids were less likely to be intubated, but they were actually more likely to have respiratory complications.
“When hospitalized patients with Alzheimer’s disease and related dementias are found to have dysphagia, our go-to solution is to use a thick liquid diet,” senior author Liron Sinvani, MD, with the Feinstein Institutes for Medical Research, Manhasset, New York, said in a news release.
“However, there is no concrete evidence that thick liquids improve health outcomes, and we also know that thick liquids can lead to decreased palatability, poor oral intake, dehydration, malnutrition, and worse quality of life,” added Dr. Sinvani, director of the geriatric hospitalist service at Northwell Health in New York.
The study was published online in JAMA Internal Medicine.
Challenging a Go-To Solution
The researchers compared outcomes in a propensity score-matched cohort of patients with ADRD and dysphagia (mean age, 86 years; 54% women) receiving mostly thick liquids versus thin liquids during their hospitalization. There were 4458 patients in each group.
They found no significant difference in hospital mortality between the thick liquids and thin liquids groups (hazard ratio [HR], 0.92; P = .46).
Patients receiving thick liquids were less likely to require intubation (odds ratio [OR], 0.66; 95% CI, 0.54-0.80) but were more likely to develop respiratory complications (OR, 1.73; 95% CI, 1.56-1.91).
The two groups did not differ significantly in terms of risk for dehydration, hospital length of stay, or rate of 30-day readmission.
“This cohort study emphasizes the need for prospective studies that evaluate whether thick liquids are associated with improved clinical outcomes in hospitalized patients with ADRD and dysphagia,” the authors wrote.
Because few patients received a Modified Barium Swallow Study at baseline, researchers were unable to confirm the presence of dysphagia or account for dysphagia severity and impairment. It’s possible that patients in the thick liquid group had more severe dysphagia than those in the thin liquid group.
Another limitation is that the type of dementia and severity were not characterized. Also, the study could not account for factors like oral hygiene, immune status, and diet adherence that could impact risks like aspiration pneumonia.
Theoretical Benefit, No Evidence
In an invited commentary on the study, Eric Widera, MD, with University of California San Francisco, noted that medicine is “littered with interventions that have become the standard of practice based on theoretical benefits without clinical evidence”.
One example is percutaneous endoscopic gastrostomy tubes for individuals with dysphagia and dementia.
“For decades, these tubes were regularly used in individuals with dementia on the assumption that bypassing the oropharyngeal route would decrease rates of aspiration and, therefore, decrease adverse outcomes like pressure ulcers, malnutrition, pneumonia, and death. However, similar to what we see with thickened liquids, evidence slowly built that this standard of practice was not evidence-based practice,” Dr. Widera wrote.
When thinking about thick liquid diets, Dr. Widera encouraged clinicians to “acknowledge the limitations of the evidence both for and against thickened-liquid diets.”
He also encouraged clinicians to “put yourself in the shoes of the patients who will be asked to adhere to this modified diet. For 12 hours, drink your tea, coffee, wine, and water as thickened liquids,” Dr. Widera suggested. “The goal is not to convince yourself never to prescribe thickened liquids, but rather to be mindful of how a thickened liquid diet affects patients’ liquid and food intake, how it changes the mouthfeel and taste of different drinks, and how it affects patients’ quality of life.”
Clinicians also should “proactively engage speech-language pathologists, but do not ask them if it is safe for a patient with dementia to eat or drink normally. Instead, ask what we can do to meet the patient’s goals and maintain quality of life given the current evidence base,” Dr. Widera wrote.
“For some, when the patient’s goals are focused on comfort, this may lead to a recommendation for thickened liquids if their use may resolve significant coughing distress after drinking thin liquids. Alternatively, even when the patient’s goals are focused on prolonging life, the risks of thickened liquids, including dehydration and decreased food and fluid intake, as well as the thin evidence for mortality improvement, will argue against their use,” Dr. Widera added.
Funding for the study was provided by grants from the National Institute on Aging and by the William S. Middleton Veteran Affairs Hospital, Madison, Wisconsin. Dr. Sinvani and Dr. Widera declared no relevant conflicts of interest.
A version of this article appeared on Medscape.com .
FROM JAMA INTERNAL MEDICINE
PCP Compensation, Part 3
In Part 2 of this series on PCP Compensation, I concluded by saying that it is possible, maybe even likely, that growing your panel size will further endanger your health. When you share this concern with your boss, based purely on economic principles, he or she should answer, “How about charging more per visit?” However, your boss knows that third-party payers are going to look askance at that simple strategy. He or she may then suggest that you make each visit worth more to justify the increased charge.

Here is where the topic of Relative Value Units (RVUs) raises its ugly head.
Before the invention of “health insurance,” when the patient paid for his or her own office visits, it was an unspoken negotiation between patient and physician that decided the value of the care.
When third-party payers first came on the scene, the value of the visit was based roughly on the time spent with the patient. Coupling time spent with value gave no credit to more experienced or skilled physicians who were more efficient at managing their patients. If, on average, it took me 10 minutes to effectively manage an ear infection and my younger associate 20 minutes, should he or she be paid twice as much as I’m paid?
But, value spent on a crude estimate of time spent was a system ripe for abuse.
I have no way of knowing what other physicians were doing, but I suspect I was not alone in factoring my own assessment of “complexity” into the calculation when deciding what to bill for a visit, giving only a passing glance at the recommended time-based definitions of short, standard, and complex visits. The payers then began demanding a more definable method of determining complexity. The result was the RVU, the labor-intensive, but no more accurate, system in which the provider must build a case to defend his or her charges.
Unfortunately, the institution of the RVU system was a major contributor to the death of the short visit. The extra work required to submit and defend the coding of any visit meant that, from a strictly clerical point of view, the short visit became as costly to the business to process as a more complex visit. The result was that every astute business consultant worth his or her salt would begin with the recommendation to “Code up!” Do whatever it takes to build your case for a more complex visit even though it may be a stretch. (It would certainly mean a lot more time-gobbling documenting.) Stop doing short visits. They are your loss leaders.
Before there were RVUs, there was a way physicians could be profitable and include short visits in their schedule. But it meant the provider had to be efficient. But patients generally don’t like going to follow-up visits they see as needless. And, more often than not, the patients are correct. However, patients love the same-day availability that an abundance of short visits in a primary care provider’s schedule can offer. The patient who knows that he or she won’t have to wait weeks or months to see the provider is far less likely to show up at a visit with a laundry list as long as their arm of problems and questions they have saved up while they were waiting to get an appointment. It used to be possible to provide efficient and profitable care by including short visits in a PCP’s schedule. Whether it can still be done under the current RVU system is unclear and probably doubtful.
In the last and final Letter in this series, we will begin with a brief look at efficiency and a PCP’s contribution to overhead before exploring the more difficult subject of defining the quality of a provider’s care and how this could relate to compensation.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
In Part 2 of this series on PCP Compensation, I concluded by saying that it is possible, maybe even likely, that growing your panel size will further endanger your health. When you share this concern with your boss, based purely on economic principles, he or she should answer, “How about charging more per visit?” However, your boss knows that third-party payers are going to look askance at that simple strategy. He or she may then suggest that you make each visit worth more to justify the increased charge.
Here is where the topic of Relative Value Units (RVUs) raises its ugly head.
Before the invention of “health insurance,” when the patient paid for his or her own office visits, it was an unspoken negotiation between patient and physician that decided the value of the care.
When third-party payers first came on the scene, the value of the visit was based roughly on the time spent with the patient. Coupling time spent with value gave no credit to more experienced or skilled physicians who were more efficient at managing their patients. If, on average, it took me 10 minutes to effectively manage an ear infection and my younger associate 20 minutes, should he or she be paid twice as much as I’m paid?
But, value spent on a crude estimate of time spent was a system ripe for abuse.
I have no way of knowing what other physicians were doing, but I suspect I was not alone in factoring my own assessment of “complexity” into the calculation when deciding what to bill for a visit, giving only a passing glance at the recommended time-based definitions of short, standard, and complex visits. The payers then began demanding a more definable method of determining complexity. The result was the RVU, the labor-intensive, but no more accurate, system in which the provider must build a case to defend his or her charges.
Unfortunately, the institution of the RVU system was a major contributor to the death of the short visit. The extra work required to submit and defend the coding of any visit meant that, from a strictly clerical point of view, the short visit became as costly to the business to process as a more complex visit. The result was that every astute business consultant worth his or her salt would begin with the recommendation to “Code up!” Do whatever it takes to build your case for a more complex visit even though it may be a stretch. (It would certainly mean a lot more time-gobbling documenting.) Stop doing short visits. They are your loss leaders.
Before there were RVUs, there was a way physicians could be profitable and include short visits in their schedule. But it meant the provider had to be efficient. But patients generally don’t like going to follow-up visits they see as needless. And, more often than not, the patients are correct. However, patients love the same-day availability that an abundance of short visits in a primary care provider’s schedule can offer. The patient who knows that he or she won’t have to wait weeks or months to see the provider is far less likely to show up at a visit with a laundry list as long as their arm of problems and questions they have saved up while they were waiting to get an appointment. It used to be possible to provide efficient and profitable care by including short visits in a PCP’s schedule. Whether it can still be done under the current RVU system is unclear and probably doubtful.
In the last and final Letter in this series, we will begin with a brief look at efficiency and a PCP’s contribution to overhead before exploring the more difficult subject of defining the quality of a provider’s care and how this could relate to compensation.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
In Part 2 of this series on PCP Compensation, I concluded by saying that it is possible, maybe even likely, that growing your panel size will further endanger your health. When you share this concern with your boss, based purely on economic principles, he or she should answer, “How about charging more per visit?” However, your boss knows that third-party payers are going to look askance at that simple strategy. He or she may then suggest that you make each visit worth more to justify the increased charge.
Here is where the topic of Relative Value Units (RVUs) raises its ugly head.
Before the invention of “health insurance,” when the patient paid for his or her own office visits, it was an unspoken negotiation between patient and physician that decided the value of the care.
When third-party payers first came on the scene, the value of the visit was based roughly on the time spent with the patient. Coupling time spent with value gave no credit to more experienced or skilled physicians who were more efficient at managing their patients. If, on average, it took me 10 minutes to effectively manage an ear infection and my younger associate 20 minutes, should he or she be paid twice as much as I’m paid?
But, value spent on a crude estimate of time spent was a system ripe for abuse.
I have no way of knowing what other physicians were doing, but I suspect I was not alone in factoring my own assessment of “complexity” into the calculation when deciding what to bill for a visit, giving only a passing glance at the recommended time-based definitions of short, standard, and complex visits. The payers then began demanding a more definable method of determining complexity. The result was the RVU, the labor-intensive, but no more accurate, system in which the provider must build a case to defend his or her charges.
Unfortunately, the institution of the RVU system was a major contributor to the death of the short visit. The extra work required to submit and defend the coding of any visit meant that, from a strictly clerical point of view, the short visit became as costly to the business to process as a more complex visit. The result was that every astute business consultant worth his or her salt would begin with the recommendation to “Code up!” Do whatever it takes to build your case for a more complex visit even though it may be a stretch. (It would certainly mean a lot more time-gobbling documenting.) Stop doing short visits. They are your loss leaders.
Before there were RVUs, there was a way physicians could be profitable and include short visits in their schedule. But it meant the provider had to be efficient. But patients generally don’t like going to follow-up visits they see as needless. And, more often than not, the patients are correct. However, patients love the same-day availability that an abundance of short visits in a primary care provider’s schedule can offer. The patient who knows that he or she won’t have to wait weeks or months to see the provider is far less likely to show up at a visit with a laundry list as long as their arm of problems and questions they have saved up while they were waiting to get an appointment. It used to be possible to provide efficient and profitable care by including short visits in a PCP’s schedule. Whether it can still be done under the current RVU system is unclear and probably doubtful.
In the last and final Letter in this series, we will begin with a brief look at efficiency and a PCP’s contribution to overhead before exploring the more difficult subject of defining the quality of a provider’s care and how this could relate to compensation.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Highly Pathogenic Avian Influenza (HPAI)
Imagine this: A 15-year-old male presents to an urgent care center with a one-day history of fever, cough, and shortness of breath. He is mildly tachypneic with bilateral scattered crackles on lung exam. A rapid test for COVID-19 and influenza is positive for influenza A — a surprising result in June.
An oxygen saturation of 90% prompts transfer to the emergency department at the local children’s hospital. The emergency medicine fellow is skeptical of the presumptive diagnosis. Influenza in the summer in a boy who had not traveled outside his small hometown in the southeastern United States? A respiratory viral panel also detected influenza A, but the specimen did not type as influenza A H1 or H3. This result prompted the laboratory technician to place a call to the ordering physician. “Does this patient have risk factors for avian flu?” the tech asked.

Highly pathogenic avian influenza (HPAI) A(H5N1) is not a new virus. It was discovered in waterfowl in China in 1996 and has since evolved into multiple clades and subclades, spreading to every continent on the globe except Oceania. It is called highly pathogenic because it kills a large number of the birds that it infects. In 2021, Clade 2.3.4.4b HPAI A(H5N1) viruses emerged in North America, causing large outbreaks in wild birds and farmed poultry populations, including backyard flocks. Sporadic infections have been identified in a diverse group of mammals, including foxes, raccoons, baby goats, bears, and harbor seals. In March of this year, HPAI A(H5N1) was detected for the first time in United States dairy cattle. As we go to press, the United States Department of Agriculture has detected HPAI A(H5N1) in dairy cattle on 36 farms in 9 states.
Human infections are rare, but often severe. Following a 1997 outbreak of HPAI A(H5N1) in Hong Kong, 18 people were infected and 6 died. Since then, more than 900 cases have been reported in humans and approximately half of these have been fatal. The spectrum of disease includes asymptomatic infection and mild disease, as occurred recently in Texas. A dairy farm worker who was exposed to dairy cattle presumed to be infected with HPAI A(H5N1) developed conjunctivitis and no other symptoms. An individual infected in Colorado in 2022 had no symptoms other than fatigue and recovered.
Human-to-human transmission was not identified with either of these cases, although very limited, non-sustained transmission has been observed in the past, usually in family members of infected people after prolonged close exposure.
Right now, most people in the United States are not at risk for HPAI A(H5N1) infection.
Careful history taking with our illustrative and hypothetical case revealed exposure to farm animals but in a state without known cases of HPAI A(H5N1) in dairy cattle. State health department officials nevertheless agreed with further testing of the patient. Some influenza diagnostic tests cleared by the US Food and Drug Administration (FDA) can detect some novel influenza A viruses such as HPAI A(H5N1) but cannot distinguish between infection with seasonal influenza A or novel influenza A viruses. Molecular assays may give an “influenza A untypeable” result, as in our case. The CDC urges further testing on these untypeable specimens at local or state public health laboratories. When HPAI A(H5N1) is suspected, a negative result on a commercially available test is not considered sufficient to exclude the possibility of infection.
Our patient was admitted to the hospital and droplet, contact, and airborne precautions were instituted along with antiviral treatment with oseltamivir. Preliminary analysis of HPAI A(H5N1) viruses predicts susceptibility to currently available antivirals. The admitting physician confirmed that the boy had received influenza vaccine in the preceding season but, unfortunately, seasonal vaccines do not protect against HPAI A(H5N1) infection.
Advice for Clinicians
Given the recent media attention and public health focus on HPAI A(H5N1), frontline clinicians may start receiving questions from patients and families and perhaps requests for testing. At this point, testing is generally recommended only for individuals with risk factors or known exposures. Healthcare providers with questions about testing are encouraged to reach out to their local or state health departments.
Public health authorities have provided recommendations for protection from HPAI. These include avoiding unprotected exposures to sick or dead wild birds, poultry, other domesticated birds, and wild or domesticated animals (including cattle). People should avoid unprotected contact with animals with suspected or confirmed HPAI A(H5N1)-virus infection or products from these animals, including raw or unpasteurized milk and raw milk products.
We can, however, reassure families that the commercial milk supply is safe. In late April, the FDA reported that HPAI viral fragments were found in one of five retail milk samples by polymerase chain reaction testing. Additional testing did not detect any live, infectious virus, indicating the effectiveness of pasteurization at inactivating the virus. Of importance to pediatricians and others pediatric clinicians, limited sampling of retail powdered infant formula and powdered milk products marketed as toddler formula revealed no viral fragments or viable virus.
The million-dollar question is whether HPAI A(H5N1) could start a new pandemic. To date, the virus has not acquired the mutations that would make it easily transmissible from person to person. If that changes and the virus does start spreading more widely, candidate vaccines that could protect against HPAI A(H5N1) have been developed and are part of the national stockpile. Let’s hope we don’t need them.
Dr. Bryant is a pediatrician specializing in infectious diseases at the University of Louisville (Ky.) and Norton Children’s Hospital, also in Louisville. She is a member of the American Academy of Pediatrics’ Committee on Infectious Diseases and the physician lead for Red Book Online. The opinions expressed in this article are her own. Dr. Bryant discloses that she has served as an investigator on clinical trials funded by Pfizer, Enanta and Gilead. Email her at [email protected]. (Also [email protected].)
Imagine this: A 15-year-old male presents to an urgent care center with a one-day history of fever, cough, and shortness of breath. He is mildly tachypneic with bilateral scattered crackles on lung exam. A rapid test for COVID-19 and influenza is positive for influenza A — a surprising result in June.
An oxygen saturation of 90% prompts transfer to the emergency department at the local children’s hospital. The emergency medicine fellow is skeptical of the presumptive diagnosis. Influenza in the summer in a boy who had not traveled outside his small hometown in the southeastern United States? A respiratory viral panel also detected influenza A, but the specimen did not type as influenza A H1 or H3. This result prompted the laboratory technician to place a call to the ordering physician. “Does this patient have risk factors for avian flu?” the tech asked.
Highly pathogenic avian influenza (HPAI) A(H5N1) is not a new virus. It was discovered in waterfowl in China in 1996 and has since evolved into multiple clades and subclades, spreading to every continent on the globe except Oceania. It is called highly pathogenic because it kills a large number of the birds that it infects. In 2021, Clade 2.3.4.4b HPAI A(H5N1) viruses emerged in North America, causing large outbreaks in wild birds and farmed poultry populations, including backyard flocks. Sporadic infections have been identified in a diverse group of mammals, including foxes, raccoons, baby goats, bears, and harbor seals. In March of this year, HPAI A(H5N1) was detected for the first time in United States dairy cattle. As we go to press, the United States Department of Agriculture has detected HPAI A(H5N1) in dairy cattle on 36 farms in 9 states.
Human infections are rare, but often severe. Following a 1997 outbreak of HPAI A(H5N1) in Hong Kong, 18 people were infected and 6 died. Since then, more than 900 cases have been reported in humans and approximately half of these have been fatal. The spectrum of disease includes asymptomatic infection and mild disease, as occurred recently in Texas. A dairy farm worker who was exposed to dairy cattle presumed to be infected with HPAI A(H5N1) developed conjunctivitis and no other symptoms. An individual infected in Colorado in 2022 had no symptoms other than fatigue and recovered.
Human-to-human transmission was not identified with either of these cases, although very limited, non-sustained transmission has been observed in the past, usually in family members of infected people after prolonged close exposure.
Right now, most people in the United States are not at risk for HPAI A(H5N1) infection.
Careful history taking with our illustrative and hypothetical case revealed exposure to farm animals but in a state without known cases of HPAI A(H5N1) in dairy cattle. State health department officials nevertheless agreed with further testing of the patient. Some influenza diagnostic tests cleared by the US Food and Drug Administration (FDA) can detect some novel influenza A viruses such as HPAI A(H5N1) but cannot distinguish between infection with seasonal influenza A or novel influenza A viruses. Molecular assays may give an “influenza A untypeable” result, as in our case. The CDC urges further testing on these untypeable specimens at local or state public health laboratories. When HPAI A(H5N1) is suspected, a negative result on a commercially available test is not considered sufficient to exclude the possibility of infection.
Our patient was admitted to the hospital and droplet, contact, and airborne precautions were instituted along with antiviral treatment with oseltamivir. Preliminary analysis of HPAI A(H5N1) viruses predicts susceptibility to currently available antivirals. The admitting physician confirmed that the boy had received influenza vaccine in the preceding season but, unfortunately, seasonal vaccines do not protect against HPAI A(H5N1) infection.
Advice for Clinicians
Given the recent media attention and public health focus on HPAI A(H5N1), frontline clinicians may start receiving questions from patients and families and perhaps requests for testing. At this point, testing is generally recommended only for individuals with risk factors or known exposures. Healthcare providers with questions about testing are encouraged to reach out to their local or state health departments.
Public health authorities have provided recommendations for protection from HPAI. These include avoiding unprotected exposures to sick or dead wild birds, poultry, other domesticated birds, and wild or domesticated animals (including cattle). People should avoid unprotected contact with animals with suspected or confirmed HPAI A(H5N1)-virus infection or products from these animals, including raw or unpasteurized milk and raw milk products.
We can, however, reassure families that the commercial milk supply is safe. In late April, the FDA reported that HPAI viral fragments were found in one of five retail milk samples by polymerase chain reaction testing. Additional testing did not detect any live, infectious virus, indicating the effectiveness of pasteurization at inactivating the virus. Of importance to pediatricians and others pediatric clinicians, limited sampling of retail powdered infant formula and powdered milk products marketed as toddler formula revealed no viral fragments or viable virus.
The million-dollar question is whether HPAI A(H5N1) could start a new pandemic. To date, the virus has not acquired the mutations that would make it easily transmissible from person to person. If that changes and the virus does start spreading more widely, candidate vaccines that could protect against HPAI A(H5N1) have been developed and are part of the national stockpile. Let’s hope we don’t need them.
Dr. Bryant is a pediatrician specializing in infectious diseases at the University of Louisville (Ky.) and Norton Children’s Hospital, also in Louisville. She is a member of the American Academy of Pediatrics’ Committee on Infectious Diseases and the physician lead for Red Book Online. The opinions expressed in this article are her own. Dr. Bryant discloses that she has served as an investigator on clinical trials funded by Pfizer, Enanta and Gilead. Email her at [email protected]. (Also [email protected].)
Imagine this: A 15-year-old male presents to an urgent care center with a one-day history of fever, cough, and shortness of breath. He is mildly tachypneic with bilateral scattered crackles on lung exam. A rapid test for COVID-19 and influenza is positive for influenza A — a surprising result in June.
An oxygen saturation of 90% prompts transfer to the emergency department at the local children’s hospital. The emergency medicine fellow is skeptical of the presumptive diagnosis. Influenza in the summer in a boy who had not traveled outside his small hometown in the southeastern United States? A respiratory viral panel also detected influenza A, but the specimen did not type as influenza A H1 or H3. This result prompted the laboratory technician to place a call to the ordering physician. “Does this patient have risk factors for avian flu?” the tech asked.
Highly pathogenic avian influenza (HPAI) A(H5N1) is not a new virus. It was discovered in waterfowl in China in 1996 and has since evolved into multiple clades and subclades, spreading to every continent on the globe except Oceania. It is called highly pathogenic because it kills a large number of the birds that it infects. In 2021, Clade 2.3.4.4b HPAI A(H5N1) viruses emerged in North America, causing large outbreaks in wild birds and farmed poultry populations, including backyard flocks. Sporadic infections have been identified in a diverse group of mammals, including foxes, raccoons, baby goats, bears, and harbor seals. In March of this year, HPAI A(H5N1) was detected for the first time in United States dairy cattle. As we go to press, the United States Department of Agriculture has detected HPAI A(H5N1) in dairy cattle on 36 farms in 9 states.
Human infections are rare, but often severe. Following a 1997 outbreak of HPAI A(H5N1) in Hong Kong, 18 people were infected and 6 died. Since then, more than 900 cases have been reported in humans and approximately half of these have been fatal. The spectrum of disease includes asymptomatic infection and mild disease, as occurred recently in Texas. A dairy farm worker who was exposed to dairy cattle presumed to be infected with HPAI A(H5N1) developed conjunctivitis and no other symptoms. An individual infected in Colorado in 2022 had no symptoms other than fatigue and recovered.
Human-to-human transmission was not identified with either of these cases, although very limited, non-sustained transmission has been observed in the past, usually in family members of infected people after prolonged close exposure.
Right now, most people in the United States are not at risk for HPAI A(H5N1) infection.
Careful history taking with our illustrative and hypothetical case revealed exposure to farm animals but in a state without known cases of HPAI A(H5N1) in dairy cattle. State health department officials nevertheless agreed with further testing of the patient. Some influenza diagnostic tests cleared by the US Food and Drug Administration (FDA) can detect some novel influenza A viruses such as HPAI A(H5N1) but cannot distinguish between infection with seasonal influenza A or novel influenza A viruses. Molecular assays may give an “influenza A untypeable” result, as in our case. The CDC urges further testing on these untypeable specimens at local or state public health laboratories. When HPAI A(H5N1) is suspected, a negative result on a commercially available test is not considered sufficient to exclude the possibility of infection.
Our patient was admitted to the hospital and droplet, contact, and airborne precautions were instituted along with antiviral treatment with oseltamivir. Preliminary analysis of HPAI A(H5N1) viruses predicts susceptibility to currently available antivirals. The admitting physician confirmed that the boy had received influenza vaccine in the preceding season but, unfortunately, seasonal vaccines do not protect against HPAI A(H5N1) infection.
Advice for Clinicians
Given the recent media attention and public health focus on HPAI A(H5N1), frontline clinicians may start receiving questions from patients and families and perhaps requests for testing. At this point, testing is generally recommended only for individuals with risk factors or known exposures. Healthcare providers with questions about testing are encouraged to reach out to their local or state health departments.
Public health authorities have provided recommendations for protection from HPAI. These include avoiding unprotected exposures to sick or dead wild birds, poultry, other domesticated birds, and wild or domesticated animals (including cattle). People should avoid unprotected contact with animals with suspected or confirmed HPAI A(H5N1)-virus infection or products from these animals, including raw or unpasteurized milk and raw milk products.
We can, however, reassure families that the commercial milk supply is safe. In late April, the FDA reported that HPAI viral fragments were found in one of five retail milk samples by polymerase chain reaction testing. Additional testing did not detect any live, infectious virus, indicating the effectiveness of pasteurization at inactivating the virus. Of importance to pediatricians and others pediatric clinicians, limited sampling of retail powdered infant formula and powdered milk products marketed as toddler formula revealed no viral fragments or viable virus.
The million-dollar question is whether HPAI A(H5N1) could start a new pandemic. To date, the virus has not acquired the mutations that would make it easily transmissible from person to person. If that changes and the virus does start spreading more widely, candidate vaccines that could protect against HPAI A(H5N1) have been developed and are part of the national stockpile. Let’s hope we don’t need them.
Dr. Bryant is a pediatrician specializing in infectious diseases at the University of Louisville (Ky.) and Norton Children’s Hospital, also in Louisville. She is a member of the American Academy of Pediatrics’ Committee on Infectious Diseases and the physician lead for Red Book Online. The opinions expressed in this article are her own. Dr. Bryant discloses that she has served as an investigator on clinical trials funded by Pfizer, Enanta and Gilead. Email her at [email protected]. (Also [email protected].)

Testosterone/CVD Risk Debate Revived by New Meta-Analysis
A new systematic literature review adds complexity to the controversy over testosterone’s relationship to risk for myocardial infarction, stroke, cardiovascular death, and all-cause mortality.
Last year, the TRAVERSE (Testosterone Replacement Therapy for Assessment of Long-term Vascular Events and Efficacy ResponSE in Hypogonadal Men) trial was the first randomized, placebo-controlled study designed and powered to determine whether testosterone therapy increased risk for major cardiovascular events in men (ages 45-80 years). Its conclusions provided reassurance that modest use of testosterone therapy short term does not increase CVD risk.
But other studies have had different conclusions and TRAVERSE left unanswered questions, so Bu B. Yeap, MBBS, PhD, an endocrinologist at the University of Western Australia in Crawley, and colleagues completed a literature review with 11 prospective cohort studies of community-dwelling men with sex steroid levels measured with mass spectrometry. Nine of the studies provided individual participation data (IPD); two used aggregate data, and all had at least 5 years of follow-up.
The findings were published in Annals of Internal Medicine .
Dr. Yeap’s team concluded that certain groups of men have higher risk for CVD events. In this study, men with very low testosterone, high luteinizing hormone (LH), or very low estradiol concentrations had higher all-cause mortality. Sex hormone–binding globulin (SHBG) concentration was positively associated and dihydrotestosterone (DHT) levels were nonlinearly associated with all-cause mortality and CVD mortality.
The testosterone level below which men had higher risk of death from any cause was 7.4 nmol/L (213 ng/dL), regardless of LH concentration, the researchers concluded, writing, “This adds to information on reference ranges based on distributions of testosterone in selected samples of healthy men.”
The link between higher SHBG concentrations and higher all-cause mortality “may be related to its role as the major binding protein for sex steroids in the circulation,” the authors wrote. “We found a U-shaped association of DHT with all-cause and CVD-related mortality risks, which were higher at lower and very high DHT concentrations. Men with very low DHT concentrations also had increased risk for incident CVD events. Further investigation into potential underlying mechanisms for these associations is warranted.”
Rigorous Methodology Adds Value
Bradley D. Anawalt, MD, with the University of Washington School of Medicine in Seattle, pointed out in an accompanying editorial that the study’s findings are particularly valuable because of the team’s rigorous methodology. The team measured testosterone with the gold standard, mass spectrometry, which can also measure DHT and estradiol more accurately than widely available commercial immunoassays, which “are inaccurate for measurement of these sex steroids in men, who typically have low serum concentrations of these two metabolites of testosterone,” Dr. Anawalt said.
Also, the researchers obtained raw data from the nine IPD studies and reanalyzed the combined data, which allows for more sophisticated analysis when combining data from multiple studies, Dr. Anawalt explained.
The main finding from the Yeap et al. study, he wrote, is that high testosterone concentrations at baseline were not linked with increased deaths from CVD or from all causes “but very low serum total testosterone concentrations at baseline were.
“It is tempting to hypothesize that testosterone therapy might have cardiovascular benefits solely in patients with very low concentrations of serum total testosterone,” Dr. Anawalt wrote.
He pointed out as particularly interesting the findings for DHT and estradiol.
“The finding that a low serum estradiol concentration is associated with higher all-cause mortality adds another reason (in addition to the adverse effects on body fat and bone health) to avoid aromatase inhibitors that are commonly taken by persons who use anabolic steroids,” he wrote. “The prospect of a U-shaped curve for the relationship between serum DHT and higher cardiovascular risk warrants further study.”
The work is funded by the Government of Western Australia and Lawley Pharmaceuticals. The authors’ and editorial writer’s conflicts of interest are listed in the full study.
A new systematic literature review adds complexity to the controversy over testosterone’s relationship to risk for myocardial infarction, stroke, cardiovascular death, and all-cause mortality.
Last year, the TRAVERSE (Testosterone Replacement Therapy for Assessment of Long-term Vascular Events and Efficacy ResponSE in Hypogonadal Men) trial was the first randomized, placebo-controlled study designed and powered to determine whether testosterone therapy increased risk for major cardiovascular events in men (ages 45-80 years). Its conclusions provided reassurance that modest use of testosterone therapy short term does not increase CVD risk.
But other studies have had different conclusions and TRAVERSE left unanswered questions, so Bu B. Yeap, MBBS, PhD, an endocrinologist at the University of Western Australia in Crawley, and colleagues completed a literature review with 11 prospective cohort studies of community-dwelling men with sex steroid levels measured with mass spectrometry. Nine of the studies provided individual participation data (IPD); two used aggregate data, and all had at least 5 years of follow-up.
The findings were published in Annals of Internal Medicine .
Dr. Yeap’s team concluded that certain groups of men have higher risk for CVD events. In this study, men with very low testosterone, high luteinizing hormone (LH), or very low estradiol concentrations had higher all-cause mortality. Sex hormone–binding globulin (SHBG) concentration was positively associated and dihydrotestosterone (DHT) levels were nonlinearly associated with all-cause mortality and CVD mortality.
The testosterone level below which men had higher risk of death from any cause was 7.4 nmol/L (213 ng/dL), regardless of LH concentration, the researchers concluded, writing, “This adds to information on reference ranges based on distributions of testosterone in selected samples of healthy men.”
The link between higher SHBG concentrations and higher all-cause mortality “may be related to its role as the major binding protein for sex steroids in the circulation,” the authors wrote. “We found a U-shaped association of DHT with all-cause and CVD-related mortality risks, which were higher at lower and very high DHT concentrations. Men with very low DHT concentrations also had increased risk for incident CVD events. Further investigation into potential underlying mechanisms for these associations is warranted.”
Rigorous Methodology Adds Value
Bradley D. Anawalt, MD, with the University of Washington School of Medicine in Seattle, pointed out in an accompanying editorial that the study’s findings are particularly valuable because of the team’s rigorous methodology. The team measured testosterone with the gold standard, mass spectrometry, which can also measure DHT and estradiol more accurately than widely available commercial immunoassays, which “are inaccurate for measurement of these sex steroids in men, who typically have low serum concentrations of these two metabolites of testosterone,” Dr. Anawalt said.
Also, the researchers obtained raw data from the nine IPD studies and reanalyzed the combined data, which allows for more sophisticated analysis when combining data from multiple studies, Dr. Anawalt explained.
The main finding from the Yeap et al. study, he wrote, is that high testosterone concentrations at baseline were not linked with increased deaths from CVD or from all causes “but very low serum total testosterone concentrations at baseline were.
“It is tempting to hypothesize that testosterone therapy might have cardiovascular benefits solely in patients with very low concentrations of serum total testosterone,” Dr. Anawalt wrote.
He pointed out as particularly interesting the findings for DHT and estradiol.
“The finding that a low serum estradiol concentration is associated with higher all-cause mortality adds another reason (in addition to the adverse effects on body fat and bone health) to avoid aromatase inhibitors that are commonly taken by persons who use anabolic steroids,” he wrote. “The prospect of a U-shaped curve for the relationship between serum DHT and higher cardiovascular risk warrants further study.”
The work is funded by the Government of Western Australia and Lawley Pharmaceuticals. The authors’ and editorial writer’s conflicts of interest are listed in the full study.
A new systematic literature review adds complexity to the controversy over testosterone’s relationship to risk for myocardial infarction, stroke, cardiovascular death, and all-cause mortality.
Last year, the TRAVERSE (Testosterone Replacement Therapy for Assessment of Long-term Vascular Events and Efficacy ResponSE in Hypogonadal Men) trial was the first randomized, placebo-controlled study designed and powered to determine whether testosterone therapy increased risk for major cardiovascular events in men (ages 45-80 years). Its conclusions provided reassurance that modest use of testosterone therapy short term does not increase CVD risk.
But other studies have had different conclusions and TRAVERSE left unanswered questions, so Bu B. Yeap, MBBS, PhD, an endocrinologist at the University of Western Australia in Crawley, and colleagues completed a literature review with 11 prospective cohort studies of community-dwelling men with sex steroid levels measured with mass spectrometry. Nine of the studies provided individual participation data (IPD); two used aggregate data, and all had at least 5 years of follow-up.
The findings were published in Annals of Internal Medicine .
Dr. Yeap’s team concluded that certain groups of men have higher risk for CVD events. In this study, men with very low testosterone, high luteinizing hormone (LH), or very low estradiol concentrations had higher all-cause mortality. Sex hormone–binding globulin (SHBG) concentration was positively associated and dihydrotestosterone (DHT) levels were nonlinearly associated with all-cause mortality and CVD mortality.
The testosterone level below which men had higher risk of death from any cause was 7.4 nmol/L (213 ng/dL), regardless of LH concentration, the researchers concluded, writing, “This adds to information on reference ranges based on distributions of testosterone in selected samples of healthy men.”
The link between higher SHBG concentrations and higher all-cause mortality “may be related to its role as the major binding protein for sex steroids in the circulation,” the authors wrote. “We found a U-shaped association of DHT with all-cause and CVD-related mortality risks, which were higher at lower and very high DHT concentrations. Men with very low DHT concentrations also had increased risk for incident CVD events. Further investigation into potential underlying mechanisms for these associations is warranted.”
Rigorous Methodology Adds Value
Bradley D. Anawalt, MD, with the University of Washington School of Medicine in Seattle, pointed out in an accompanying editorial that the study’s findings are particularly valuable because of the team’s rigorous methodology. The team measured testosterone with the gold standard, mass spectrometry, which can also measure DHT and estradiol more accurately than widely available commercial immunoassays, which “are inaccurate for measurement of these sex steroids in men, who typically have low serum concentrations of these two metabolites of testosterone,” Dr. Anawalt said.
Also, the researchers obtained raw data from the nine IPD studies and reanalyzed the combined data, which allows for more sophisticated analysis when combining data from multiple studies, Dr. Anawalt explained.
The main finding from the Yeap et al. study, he wrote, is that high testosterone concentrations at baseline were not linked with increased deaths from CVD or from all causes “but very low serum total testosterone concentrations at baseline were.
“It is tempting to hypothesize that testosterone therapy might have cardiovascular benefits solely in patients with very low concentrations of serum total testosterone,” Dr. Anawalt wrote.
He pointed out as particularly interesting the findings for DHT and estradiol.
“The finding that a low serum estradiol concentration is associated with higher all-cause mortality adds another reason (in addition to the adverse effects on body fat and bone health) to avoid aromatase inhibitors that are commonly taken by persons who use anabolic steroids,” he wrote. “The prospect of a U-shaped curve for the relationship between serum DHT and higher cardiovascular risk warrants further study.”
The work is funded by the Government of Western Australia and Lawley Pharmaceuticals. The authors’ and editorial writer’s conflicts of interest are listed in the full study.
FROM ANNALS OF INTERNAL MEDICINE
It Would Be Nice if Olive Oil Really Did Prevent Dementia
This transcript has been edited for clarity.
As you all know by now, I’m always looking out for lifestyle changes that are both pleasurable and healthy. They are hard to find, especially when it comes to diet. My kids complain about this all the time: “When you say ‘healthy food,’ you just mean yucky food.” And yes, French fries are amazing, and no, we can’t have them three times a day.
So, when I saw an article claiming that olive oil reduces the risk for dementia, I was interested. I love olive oil; I cook with it all the time. But as is always the case in the world of nutritional epidemiology, we need to be careful. There are a lot of reasons to doubt the results of this study — and one reason to believe it’s true.
The study I’m talking about is “Consumption of Olive Oil and Diet Quality and Risk of Dementia-Related Death,” appearing in JAMA Network Open and following a well-trod formula in the nutritional epidemiology space.
Nearly 100,000 participants, all healthcare workers, filled out a food frequency questionnaire every 4 years with 130 questions touching on all aspects of diet: How often do you eat bananas, bacon, olive oil? Participants were followed for more than 20 years, and if they died, the cause of death was flagged as being dementia-related or not. Over that time frame there were around 38,000 deaths, of which 4751 were due to dementia.
The rest is just statistics. The authors show that those who reported consuming more olive oil were less likely to die from dementia — about 50% less likely, if you compare those who reported eating more than 7 grams of olive oil a day with those who reported eating none.
Is It What You Eat, or What You Don’t Eat?
And we could stop there if we wanted to; I’m sure big olive oil would be happy with that. Is there such a thing as “big olive oil”? But no, we need to dig deeper here because this study has the same problems as all nutritional epidemiology studies. Number one, no one is sitting around drinking small cups of olive oil. They consume it with other foods. And it was clear from the food frequency questionnaire that people who consumed more olive oil also consumed less red meat, more fruits and vegetables, more whole grains, more butter, and less margarine. And those are just the findings reported in the paper. I suspect that people who eat more olive oil also eat more tomatoes, for example, though data this granular aren’t shown. So, it can be really hard, in studies like this, to know for sure that it’s actually the olive oil that is helpful rather than some other constituent in the diet.
The flip side of that coin presents another issue. The food you eat is also a marker of the food you don’t eat. People who ate olive oil consumed less margarine, for example. At the time of this study, margarine was still adulterated with trans-fats, which a pretty solid evidence base suggests are really bad for your vascular system. So perhaps it’s not that olive oil is particularly good for you but that something else is bad for you. In other words, simply adding olive oil to your diet without changing anything else may not do anything.
The other major problem with studies of this sort is that people don’t consume food at random. The type of person who eats a lot of olive oil is simply different from the type of person who doesn›t. For one thing, olive oil is expensive. A 25-ounce bottle of olive oil is on sale at my local supermarket right now for $11.00. A similar-sized bottle of vegetable oil goes for $4.00.
Isn’t it interesting that food that costs more money tends to be associated with better health outcomes? (I’m looking at you, red wine.) Perhaps it’s not the food; perhaps it’s the money. We aren’t provided data on household income in this study, but we can see that the heavy olive oil users were less likely to be current smokers and they got more physical activity.
Now, the authors are aware of these limitations and do their best to account for them. In multivariable models, they adjust for other stuff in the diet, and even for income (sort of; they use census tract as a proxy for income, which is really a broad brush), and still find a significant though weakened association showing a protective effect of olive oil on dementia-related death. But still — adjustment is never perfect, and the small effect size here could definitely be due to residual confounding.
Evidence More Convincing
Now, I did tell you that there is one reason to believe that this study is true, but it’s not really from this study.
It’s from the PREDIMED randomized trial.
This is nutritional epidemiology I can get behind. Published in 2018, investigators in Spain randomized around 7500 participants to receive a liter of olive oil once a week vs mixed nuts, vs small nonfood gifts, the idea here being that if you have olive oil around, you’ll use it more. And people who were randomly assigned to get the olive oil had a 30% lower rate of cardiovascular events. A secondary analysis of that study found that the rate of development of mild cognitive impairment was 65% lower in those who were randomly assigned to olive oil. That’s an impressive result.
So, there might be something to this olive oil thing, but I’m not quite ready to add it to my “pleasurable things that are still good for you” list just yet. Though it does make me wonder: Can we make French fries in the stuff?
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
As you all know by now, I’m always looking out for lifestyle changes that are both pleasurable and healthy. They are hard to find, especially when it comes to diet. My kids complain about this all the time: “When you say ‘healthy food,’ you just mean yucky food.” And yes, French fries are amazing, and no, we can’t have them three times a day.
So, when I saw an article claiming that olive oil reduces the risk for dementia, I was interested. I love olive oil; I cook with it all the time. But as is always the case in the world of nutritional epidemiology, we need to be careful. There are a lot of reasons to doubt the results of this study — and one reason to believe it’s true.
The study I’m talking about is “Consumption of Olive Oil and Diet Quality and Risk of Dementia-Related Death,” appearing in JAMA Network Open and following a well-trod formula in the nutritional epidemiology space.
Nearly 100,000 participants, all healthcare workers, filled out a food frequency questionnaire every 4 years with 130 questions touching on all aspects of diet: How often do you eat bananas, bacon, olive oil? Participants were followed for more than 20 years, and if they died, the cause of death was flagged as being dementia-related or not. Over that time frame there were around 38,000 deaths, of which 4751 were due to dementia.
The rest is just statistics. The authors show that those who reported consuming more olive oil were less likely to die from dementia — about 50% less likely, if you compare those who reported eating more than 7 grams of olive oil a day with those who reported eating none.
Is It What You Eat, or What You Don’t Eat?
And we could stop there if we wanted to; I’m sure big olive oil would be happy with that. Is there such a thing as “big olive oil”? But no, we need to dig deeper here because this study has the same problems as all nutritional epidemiology studies. Number one, no one is sitting around drinking small cups of olive oil. They consume it with other foods. And it was clear from the food frequency questionnaire that people who consumed more olive oil also consumed less red meat, more fruits and vegetables, more whole grains, more butter, and less margarine. And those are just the findings reported in the paper. I suspect that people who eat more olive oil also eat more tomatoes, for example, though data this granular aren’t shown. So, it can be really hard, in studies like this, to know for sure that it’s actually the olive oil that is helpful rather than some other constituent in the diet.
The flip side of that coin presents another issue. The food you eat is also a marker of the food you don’t eat. People who ate olive oil consumed less margarine, for example. At the time of this study, margarine was still adulterated with trans-fats, which a pretty solid evidence base suggests are really bad for your vascular system. So perhaps it’s not that olive oil is particularly good for you but that something else is bad for you. In other words, simply adding olive oil to your diet without changing anything else may not do anything.
The other major problem with studies of this sort is that people don’t consume food at random. The type of person who eats a lot of olive oil is simply different from the type of person who doesn›t. For one thing, olive oil is expensive. A 25-ounce bottle of olive oil is on sale at my local supermarket right now for $11.00. A similar-sized bottle of vegetable oil goes for $4.00.
Isn’t it interesting that food that costs more money tends to be associated with better health outcomes? (I’m looking at you, red wine.) Perhaps it’s not the food; perhaps it’s the money. We aren’t provided data on household income in this study, but we can see that the heavy olive oil users were less likely to be current smokers and they got more physical activity.
Now, the authors are aware of these limitations and do their best to account for them. In multivariable models, they adjust for other stuff in the diet, and even for income (sort of; they use census tract as a proxy for income, which is really a broad brush), and still find a significant though weakened association showing a protective effect of olive oil on dementia-related death. But still — adjustment is never perfect, and the small effect size here could definitely be due to residual confounding.
Evidence More Convincing
Now, I did tell you that there is one reason to believe that this study is true, but it’s not really from this study.
It’s from the PREDIMED randomized trial.
This is nutritional epidemiology I can get behind. Published in 2018, investigators in Spain randomized around 7500 participants to receive a liter of olive oil once a week vs mixed nuts, vs small nonfood gifts, the idea here being that if you have olive oil around, you’ll use it more. And people who were randomly assigned to get the olive oil had a 30% lower rate of cardiovascular events. A secondary analysis of that study found that the rate of development of mild cognitive impairment was 65% lower in those who were randomly assigned to olive oil. That’s an impressive result.
So, there might be something to this olive oil thing, but I’m not quite ready to add it to my “pleasurable things that are still good for you” list just yet. Though it does make me wonder: Can we make French fries in the stuff?
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
As you all know by now, I’m always looking out for lifestyle changes that are both pleasurable and healthy. They are hard to find, especially when it comes to diet. My kids complain about this all the time: “When you say ‘healthy food,’ you just mean yucky food.” And yes, French fries are amazing, and no, we can’t have them three times a day.
So, when I saw an article claiming that olive oil reduces the risk for dementia, I was interested. I love olive oil; I cook with it all the time. But as is always the case in the world of nutritional epidemiology, we need to be careful. There are a lot of reasons to doubt the results of this study — and one reason to believe it’s true.
The study I’m talking about is “Consumption of Olive Oil and Diet Quality and Risk of Dementia-Related Death,” appearing in JAMA Network Open and following a well-trod formula in the nutritional epidemiology space.
Nearly 100,000 participants, all healthcare workers, filled out a food frequency questionnaire every 4 years with 130 questions touching on all aspects of diet: How often do you eat bananas, bacon, olive oil? Participants were followed for more than 20 years, and if they died, the cause of death was flagged as being dementia-related or not. Over that time frame there were around 38,000 deaths, of which 4751 were due to dementia.
The rest is just statistics. The authors show that those who reported consuming more olive oil were less likely to die from dementia — about 50% less likely, if you compare those who reported eating more than 7 grams of olive oil a day with those who reported eating none.
Is It What You Eat, or What You Don’t Eat?
And we could stop there if we wanted to; I’m sure big olive oil would be happy with that. Is there such a thing as “big olive oil”? But no, we need to dig deeper here because this study has the same problems as all nutritional epidemiology studies. Number one, no one is sitting around drinking small cups of olive oil. They consume it with other foods. And it was clear from the food frequency questionnaire that people who consumed more olive oil also consumed less red meat, more fruits and vegetables, more whole grains, more butter, and less margarine. And those are just the findings reported in the paper. I suspect that people who eat more olive oil also eat more tomatoes, for example, though data this granular aren’t shown. So, it can be really hard, in studies like this, to know for sure that it’s actually the olive oil that is helpful rather than some other constituent in the diet.
The flip side of that coin presents another issue. The food you eat is also a marker of the food you don’t eat. People who ate olive oil consumed less margarine, for example. At the time of this study, margarine was still adulterated with trans-fats, which a pretty solid evidence base suggests are really bad for your vascular system. So perhaps it’s not that olive oil is particularly good for you but that something else is bad for you. In other words, simply adding olive oil to your diet without changing anything else may not do anything.
The other major problem with studies of this sort is that people don’t consume food at random. The type of person who eats a lot of olive oil is simply different from the type of person who doesn›t. For one thing, olive oil is expensive. A 25-ounce bottle of olive oil is on sale at my local supermarket right now for $11.00. A similar-sized bottle of vegetable oil goes for $4.00.
Isn’t it interesting that food that costs more money tends to be associated with better health outcomes? (I’m looking at you, red wine.) Perhaps it’s not the food; perhaps it’s the money. We aren’t provided data on household income in this study, but we can see that the heavy olive oil users were less likely to be current smokers and they got more physical activity.
Now, the authors are aware of these limitations and do their best to account for them. In multivariable models, they adjust for other stuff in the diet, and even for income (sort of; they use census tract as a proxy for income, which is really a broad brush), and still find a significant though weakened association showing a protective effect of olive oil on dementia-related death. But still — adjustment is never perfect, and the small effect size here could definitely be due to residual confounding.
Evidence More Convincing
Now, I did tell you that there is one reason to believe that this study is true, but it’s not really from this study.
It’s from the PREDIMED randomized trial.
This is nutritional epidemiology I can get behind. Published in 2018, investigators in Spain randomized around 7500 participants to receive a liter of olive oil once a week vs mixed nuts, vs small nonfood gifts, the idea here being that if you have olive oil around, you’ll use it more. And people who were randomly assigned to get the olive oil had a 30% lower rate of cardiovascular events. A secondary analysis of that study found that the rate of development of mild cognitive impairment was 65% lower in those who were randomly assigned to olive oil. That’s an impressive result.
So, there might be something to this olive oil thing, but I’m not quite ready to add it to my “pleasurable things that are still good for you” list just yet. Though it does make me wonder: Can we make French fries in the stuff?
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Oral Microbiome Test Could Detect Gastric Cancer Earlier
WASHINGTON, DC –
Researchers found distinct bacterial composition differences in patient samples that point to the potential for oral microbial signatures to be used as biomarkers for assessing gastric cancer risk.
“Too many patients are being diagnosed too late. There are no formal screening guidelines for gastric cancer, and more than half of patients with gastric cancer do not receive a diagnosis until their cancer is already at an advanced stage,” said Shruthi Reddy Perati, MD, a general surgery resident at Rutgers University Robert Wood Johnson School of Medicine in New Brunswick, New Jersey.
Detecting gastric cancer now generally requires an invasive procedure, such as endoscopy. Therefore, a noninvasive “swish and spit” test could be more accessible and allow for more widespread screening, Dr. Perati said at a May 8 press briefing during which her research (Abstract 949) was previewed for Digestive Disease Week® (DDW).
Gastric cancer, also known as stomach cancer, is the fourth most common cause of cancer-related death in the world. The United States can expect 26,890 new cases and 10,880 deaths from this type of cancer in 2024, the American Cancer Society estimates.
Microbial Signatures Found
Dr. Perati and colleagues collected oral rinse samples from 98 patients: 30 known to have gastric cancer , 30 with precancerous gastric conditions (pre–gastric cancer), and 38 control participants without pre-gastric or gastric cancer. Sixty-two percent were women, 32% were Hispanic, 31% had diabetes, and 18% were smokers.
The researchers analyzed the samples for alpha and beta diversity and conducted differential analysis using the framework called analysis of compositions of microbiomes.
They found distinct differences between the oral microbiomes of the healthy group and those of the groups with gastric cancer and pre–gastric cancer. In addition, the microbiomes of participants with cancer and of those with precancerous conditions were similar.
The results suggest that the microbiome changes may occur as soon as the stomach environment starts to undergo changes that can eventually turn into cancer.
“The oral microbiome may serve as a window into the composition of the stomach environment,” Dr. Perati said.
The investigators created a screening model to detect the most relevant 13 bacterial genera that differed between the control group and the gastric cancer and pre–gastric cancer groups. The tenfold cross-validation model demonstrated good ability to discriminate using bacteria alone (area under the curve [AUC], 0.74) and was further improved with the addition of clinical variables, including demographics and comorbidities (AUC, 0.91), the researchers noted.
As the investigators noted, the model’s performance improved with the addition of clinical variables, said Loren Laine, MD, professor of medicine (digestive diseases) at Yale School of Medicine and chair of DDW 2024.
An AUC of 0.74 using bacteria alone, which increased to 0.91 by adding demographics and comorbidities, “[is] starting to be really meaningful,” Dr. Laine said.
Further studies should evaluate the test’s sensitivity and specificity, Dr. Laine added.
Additional Considerations
The microbiome can vary between people and within the same individual over time. Probiotics, antibiotics, and diet can lead to changes in the microbiome, Dr. Perati said.
When asked how these changes could affect the accuracy of an oral rinse test, Dr. Perati said “it’s known that, in general, dietary modifications can have an impact on the diversity and the prevalence of certain bacteria throughout the GI tract.”
Though variance is expected, we’re hoping to see that the differences in the microbiome composition between the malignant groups and the control groups are more significant than those lower-level background changes due to dietary modifications, for example, she added.
The research is in its early days, and the results need to be validated in a larger study, Dr. Perati said.
Ninety-eight patients is “still a very small number,” said Dr. Laine, who co-moderated the press briefing. “More research is needed.”
Still, the study “has huge implications that could eventually lead to the development of noninvasive and accessible early screening for gastric cancer,” she said.
Dr. Perati and Dr. Laine reported no relevant financial relationships. The study was independently supported.
A version of this article appeared on Medscape.com.
WASHINGTON, DC –
Researchers found distinct bacterial composition differences in patient samples that point to the potential for oral microbial signatures to be used as biomarkers for assessing gastric cancer risk.
“Too many patients are being diagnosed too late. There are no formal screening guidelines for gastric cancer, and more than half of patients with gastric cancer do not receive a diagnosis until their cancer is already at an advanced stage,” said Shruthi Reddy Perati, MD, a general surgery resident at Rutgers University Robert Wood Johnson School of Medicine in New Brunswick, New Jersey.
Detecting gastric cancer now generally requires an invasive procedure, such as endoscopy. Therefore, a noninvasive “swish and spit” test could be more accessible and allow for more widespread screening, Dr. Perati said at a May 8 press briefing during which her research (Abstract 949) was previewed for Digestive Disease Week® (DDW).
Gastric cancer, also known as stomach cancer, is the fourth most common cause of cancer-related death in the world. The United States can expect 26,890 new cases and 10,880 deaths from this type of cancer in 2024, the American Cancer Society estimates.
Microbial Signatures Found
Dr. Perati and colleagues collected oral rinse samples from 98 patients: 30 known to have gastric cancer , 30 with precancerous gastric conditions (pre–gastric cancer), and 38 control participants without pre-gastric or gastric cancer. Sixty-two percent were women, 32% were Hispanic, 31% had diabetes, and 18% were smokers.
The researchers analyzed the samples for alpha and beta diversity and conducted differential analysis using the framework called analysis of compositions of microbiomes.
They found distinct differences between the oral microbiomes of the healthy group and those of the groups with gastric cancer and pre–gastric cancer. In addition, the microbiomes of participants with cancer and of those with precancerous conditions were similar.
The results suggest that the microbiome changes may occur as soon as the stomach environment starts to undergo changes that can eventually turn into cancer.
“The oral microbiome may serve as a window into the composition of the stomach environment,” Dr. Perati said.
The investigators created a screening model to detect the most relevant 13 bacterial genera that differed between the control group and the gastric cancer and pre–gastric cancer groups. The tenfold cross-validation model demonstrated good ability to discriminate using bacteria alone (area under the curve [AUC], 0.74) and was further improved with the addition of clinical variables, including demographics and comorbidities (AUC, 0.91), the researchers noted.
As the investigators noted, the model’s performance improved with the addition of clinical variables, said Loren Laine, MD, professor of medicine (digestive diseases) at Yale School of Medicine and chair of DDW 2024.
An AUC of 0.74 using bacteria alone, which increased to 0.91 by adding demographics and comorbidities, “[is] starting to be really meaningful,” Dr. Laine said.
Further studies should evaluate the test’s sensitivity and specificity, Dr. Laine added.
Additional Considerations
The microbiome can vary between people and within the same individual over time. Probiotics, antibiotics, and diet can lead to changes in the microbiome, Dr. Perati said.
When asked how these changes could affect the accuracy of an oral rinse test, Dr. Perati said “it’s known that, in general, dietary modifications can have an impact on the diversity and the prevalence of certain bacteria throughout the GI tract.”
Though variance is expected, we’re hoping to see that the differences in the microbiome composition between the malignant groups and the control groups are more significant than those lower-level background changes due to dietary modifications, for example, she added.
The research is in its early days, and the results need to be validated in a larger study, Dr. Perati said.
Ninety-eight patients is “still a very small number,” said Dr. Laine, who co-moderated the press briefing. “More research is needed.”
Still, the study “has huge implications that could eventually lead to the development of noninvasive and accessible early screening for gastric cancer,” she said.
Dr. Perati and Dr. Laine reported no relevant financial relationships. The study was independently supported.
A version of this article appeared on Medscape.com.
WASHINGTON, DC –
Researchers found distinct bacterial composition differences in patient samples that point to the potential for oral microbial signatures to be used as biomarkers for assessing gastric cancer risk.
“Too many patients are being diagnosed too late. There are no formal screening guidelines for gastric cancer, and more than half of patients with gastric cancer do not receive a diagnosis until their cancer is already at an advanced stage,” said Shruthi Reddy Perati, MD, a general surgery resident at Rutgers University Robert Wood Johnson School of Medicine in New Brunswick, New Jersey.
Detecting gastric cancer now generally requires an invasive procedure, such as endoscopy. Therefore, a noninvasive “swish and spit” test could be more accessible and allow for more widespread screening, Dr. Perati said at a May 8 press briefing during which her research (Abstract 949) was previewed for Digestive Disease Week® (DDW).
Gastric cancer, also known as stomach cancer, is the fourth most common cause of cancer-related death in the world. The United States can expect 26,890 new cases and 10,880 deaths from this type of cancer in 2024, the American Cancer Society estimates.
Microbial Signatures Found
Dr. Perati and colleagues collected oral rinse samples from 98 patients: 30 known to have gastric cancer , 30 with precancerous gastric conditions (pre–gastric cancer), and 38 control participants without pre-gastric or gastric cancer. Sixty-two percent were women, 32% were Hispanic, 31% had diabetes, and 18% were smokers.
The researchers analyzed the samples for alpha and beta diversity and conducted differential analysis using the framework called analysis of compositions of microbiomes.
They found distinct differences between the oral microbiomes of the healthy group and those of the groups with gastric cancer and pre–gastric cancer. In addition, the microbiomes of participants with cancer and of those with precancerous conditions were similar.
The results suggest that the microbiome changes may occur as soon as the stomach environment starts to undergo changes that can eventually turn into cancer.
“The oral microbiome may serve as a window into the composition of the stomach environment,” Dr. Perati said.
The investigators created a screening model to detect the most relevant 13 bacterial genera that differed between the control group and the gastric cancer and pre–gastric cancer groups. The tenfold cross-validation model demonstrated good ability to discriminate using bacteria alone (area under the curve [AUC], 0.74) and was further improved with the addition of clinical variables, including demographics and comorbidities (AUC, 0.91), the researchers noted.
As the investigators noted, the model’s performance improved with the addition of clinical variables, said Loren Laine, MD, professor of medicine (digestive diseases) at Yale School of Medicine and chair of DDW 2024.
An AUC of 0.74 using bacteria alone, which increased to 0.91 by adding demographics and comorbidities, “[is] starting to be really meaningful,” Dr. Laine said.
Further studies should evaluate the test’s sensitivity and specificity, Dr. Laine added.
Additional Considerations
The microbiome can vary between people and within the same individual over time. Probiotics, antibiotics, and diet can lead to changes in the microbiome, Dr. Perati said.
When asked how these changes could affect the accuracy of an oral rinse test, Dr. Perati said “it’s known that, in general, dietary modifications can have an impact on the diversity and the prevalence of certain bacteria throughout the GI tract.”
Though variance is expected, we’re hoping to see that the differences in the microbiome composition between the malignant groups and the control groups are more significant than those lower-level background changes due to dietary modifications, for example, she added.
The research is in its early days, and the results need to be validated in a larger study, Dr. Perati said.
Ninety-eight patients is “still a very small number,” said Dr. Laine, who co-moderated the press briefing. “More research is needed.”
Still, the study “has huge implications that could eventually lead to the development of noninvasive and accessible early screening for gastric cancer,” she said.
Dr. Perati and Dr. Laine reported no relevant financial relationships. The study was independently supported.
A version of this article appeared on Medscape.com.
AT DDW 2024